User login
Emerging Cataract Surgery Practice Patterns in the Veterans Health Administration
The rates of cataract surgery, the most commonly performed ophthalmic procedure in the U.S., have increased in the past few decades with an estimated rate of 1,100 surgeries per 100,000 people in 2011.1,2 Several emerging practices have the potential to radically impact the efficacy, safety, and cost of cataract surgery.3-5 These practices include femtosecond laser-assisted cataract surgery, intracameral antibiotics, and bilateral same-day cataract surgery.
The femtosecond laser is capable of producing precise incisions in the cornea for access by surgical instruments and reduction of astigmatism. Laser pulses also can create a perfectly round incision of the anterior lens capsule, which surrounds and supports the crystalline lens, and make incisions into the cataractous lens to facilitate disassembly for easy removal of fragments.
Placement of antibiotics internally into the anterior chamber, the space between the crystalline lens and the posterior cornea (intracameral space), is a more direct method to prevent bacterial infection within the eye (endophthalmitis), compared with current external methods, including injections under the conjunctiva (subconjunctival) and/or use of antibiotic drops directly onto the eye surface (topical).6
Routine cataract surgery is typically staged, with a period of time between sequential surgeries of 1 week or more to allow for observation of infection (delayed sequential surgery). In view of the very low rate of infection and the impact of staged surgery on patients, including additional visits and copays, some surgeons have begun to perform bilateral surgery (immediate sequential bilateral surgery, using separate patient safety checklists, surgical preps, instruments, and medications) on the same day for patients with significant cataracts in both eyes to promote rapid restoration of binocular vision as well reduce the number of patient visits.
The extent of adaptation of femtosecond laser surgery, intracameral antibiotics, and immediate sequential bilateral surgery in the U.S. is currently unknown.7,8 To provide an updated snapshot of these cataract surgery practices, the authors report on the results of a brief survey administered to ophthalmology section chiefs in the VHA, the largest integrated health care system and the largest provider of health care training in the U.S.
Methods
Following institutional review board approval from the Providence VA Medical Center, the office of the National Program Director of VA Ophthalmology provided a list of all VHA ophthalmology section chiefs and their contact information. The study targeted section chiefs because they are responsible for all eye surgery performed at their respective VAMCs. The survey queried the section chiefs on femtosecond laser-assisted cataract surgery, intracameral antibiotics, immediate sequential bilateral cataract surgery, and resident training at their institutions (Table).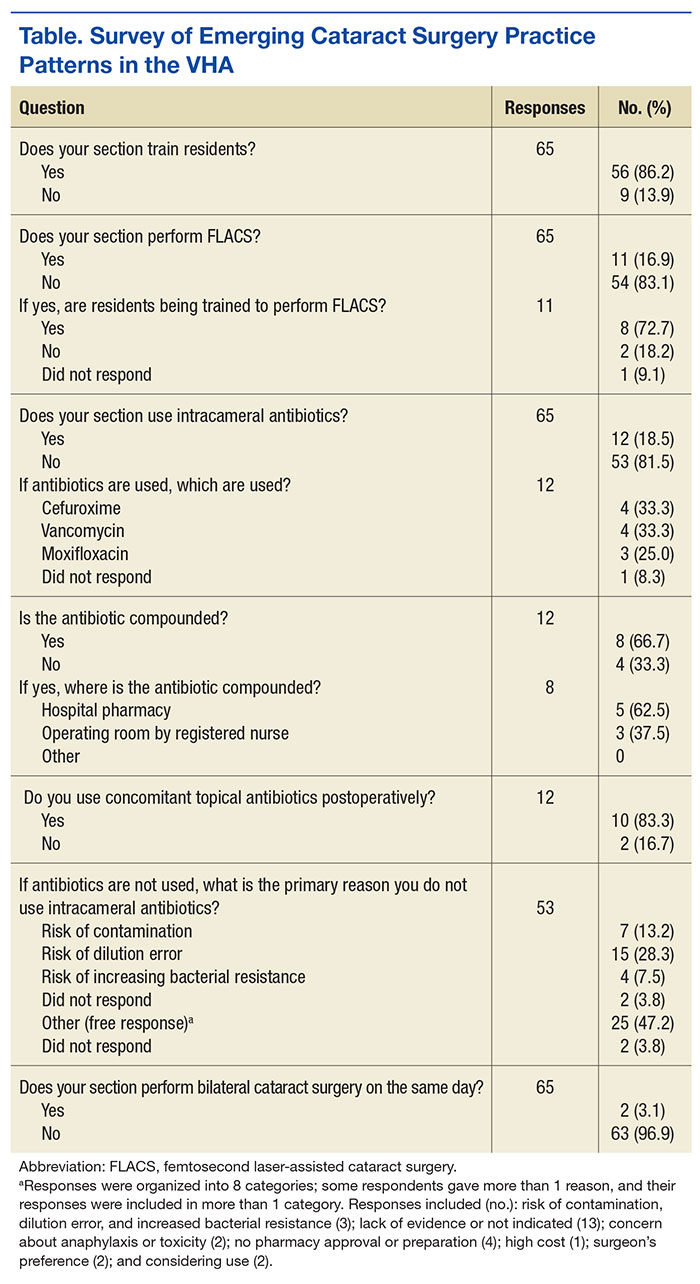
The survey was administered using the web-based Research Electronic Data Capture (REDCap) software.9 The initial survey was e-mailed in April 2015, followed by 2 reminder e-mails 1 week apart and then 2 phone calls 1 week apart to nonresponders.
The survey responses were stored anonymously in the REDCap database and analyzed using descriptive statistics.
Results
The original list from the office of the National Program Director included 114 ophthalmology section chiefs (excluding one of the authors). After follow-up phone calls, 9 individuals were identified who were not ophthalmologists (eg, optometrists or nonophthalmic surgeons) or who were incorrectly listed as section chiefs, and 9 were duplicates from institutions that were represented twice on the contact list. These 18 individuals, none of whom had responded to the survey, were removed from the eligible sample. Hence, the analysis included 86% (95/111) of the VAMCs where cataract surgery is performed.10 Sixty-five responses were received for an overall response rate of 68% (65/96), including 1 ophthalmologist who responded to the survey twice.
Most section chiefs (86%, 56/65) trained ophthalmology residents at their respective medical centers (Table). Eleven VAMCs (17%) offered femtosecond laser-assisted cataract surgery; 8 of those 11 (73%) also offered resident training in this surgery. At 12 VAMCs (18%), cataract surgeons used intracameral antibiotics, which included vancomycin (4), cefuroxime (4), moxifloxacin (3), and unspecified (1); at 10 of these VAMCs (83%), surgeons used intracameral and postoperative topical antibiotics concomitantly; 8 VAMCs (67%) compounded the intracameral antibiotics—either in the hospital pharmacy (5) or within the operating room (3). The 2 most common reasons cited for not using intracameral antibiotics were risk of dilution error (28%; 15/53) and a lack of evidence for use (25%; 13/53). Only 2 medical centers (3.1%) offered immediate sequential bilateral cataract surgery.
Discussion
This survey provides updated information on the role of emerging cataract surgery practices in the VHA. These trends may impact future U.S. cataract surgery practice patterns given the large number of ophthalmology residents who receive training in the VHA.
Only 17% of VAMCs offered femtosecond laser-assisted cataract surgery. Reasons for this low rate may include (a) the high cost of the femtosecond laser units (the lowest average cost of a laser is $400,000, while the average costs of services can be $40,000 or more per year); and (b) the lack of evidence that a femtosecond laser improves cataract surgery outcomes relative to standard phacoemulsification.4,11-15 Another potential barrier to procurement of femtosecond lasers is the emphasis within VHA to increase access to care for the many newly enrolled veterans, which this technology does not address. However, most of the VAMCs with a femtosecond laser unit offered resident training in this technique, confirming early reports on the potential for incorporating femtosecond laser-assisted cataract surgery into ophthalmic graduate medical education.16
In 2007, the multicenter, prospective, randomized European Society of Cataract and Refractive Surgery Endophthalmitis Study demonstrated that intracameral cefuroxime was associated with a 5-fold decrease in the risk of postoperative endophthalmitis.17 In 2011, a statement from the American Society of Cataract and Refractive Surgery (ASCRS) Cataract Clinical Committee noted that the method of antibiotic prophylaxis with the strongest evidence base is “a direct intracameral bolus at the conclusion of surgery.”18 However, surgeons used intracameral antibiotics in only 19% of VAMCs. Although this is a higher rate than those reported in older surveys of VHA ophthalmologists (14%)7 and ASCRS members (15%), it is still significantly lower than the 74% reported in a recent survey of the European Society of Cataract and Refractive Surgeons.3,8
The most common reasons given for not using intracameral antibiotics included risk of a dilution error when preparing the antibiotics and lack of evidence supporting their effectiveness. Less common reasons included risk of contamination, lack of pharmacy approval, and increasing bacterial resistance to commonly used antibiotics. Most of these concerns have been previously cited as barriers to the adoption of intracameral antibiotics.19 The availability of a prepackaged intracameral antibiotic (eg, cefuroxime in Europe) would help address the risks of compounding dilution errors and contamination in the U.S.6 The publication of 3 large observational studies in 2016 has also significantly strengthened the evidence base supporting the use of intracameral antibiotics.20-22
Only 2 VAMCs (3%) offered immediate sequential bilateral cataract surgery. The advocates of this practice have touted its potential cost savings, patient convenience, and the opportunity for more rapid visual rehabilitation.23 Recently, several multicenter, randomized clinical trials have reported similar refractive outcomes, complication rates, and patient satisfaction for immediate and delayed bilateral cataract surgery.24,25 Hence, it is possible that rates of immediate sequential bilateral cataract surgery may increase in the VHA over the next few years.
Strengths/Limitations
A strength of this survey is its high response rate (67.7%), which exceeds the 53% and 33% rates reported in previous surveys of cataract surgery practice patterns among VHA ophthalmologistsand ASCRS members, respectively.7,8 Another strength is lack of financial incentive for adaptation of any new practices by VHA surgeons, suggesting that these decisions have been made to improve patient safety, quality of care, and/or resident education. A limitation of this study is that its findings may not be generalizable to ophthalmologists practicing in the private sector or in teaching hospitals outside the VHA.
Conclusion
This study suggests that femtosecond laser-assisted cataract surgery, intracameral antibiotics, and immediate sequential bilateral cataract surgery have limited roles in VHA cataract surgery. More research and clinical experience are needed to understand the barriers to more widespread acceptance and to assess the impact of these emerging practices on cataract surgery in the U.S.
1. Lindstrom R. Thoughts on cataract surgery: 2015. http://www.reviewofophthalmology.com/content/t/surgical_education/c/53422/. Published March 9, 2015. Accessed June 23, 2016.
2. Gollogly HE, Hodge DO, St Sauver JL, Erie JC. Increasing incidence of cataract surgery: population-based study. J Cataract Refract Surg. 2013;39(9):1383-1389.
3. Barry P. Adoption of intracameral antibiotic prophylaxis of endophthalmitis following cataract surgery: update on the ESCRS Endophthalmitis Study. J Cataract Refract Surg. 2014;40(1):138-142.
4. Quiñones A, Gleitsmann K, Freeman M, et al. Benefits and Harms of Femtosecond Laser Assisted Cataract Surgery: A Systematic Review. VA-ESP Project #05-225; 2013. Washington, DC: Department of Veterans Affairs; 2013.
5. Naseri A, McLeod S. Benefits of and barriers to immediate sequential cataract surgery. JAMA Ophthalmol. 2014;132(11):1362-1363.
6. Brage-Mele R, Chang DF, Henderson BA, Mamalis N, Talley-Rostov A, Vasavada A; ASCRS Clinical Cataract Committee. Intracameral antibiotics: safety, efficacy, and preparation. J Cataract Refract Surg. 2014;40(12):2134-2142.
7. Greenberg PB, Havnaer A, Oetting TA, Garcia-Ferrer FJ. Cataract surgery practice patterns in the United States Veterans Health Administration. J Cataract Refract Surg. 2012;38(4):705-709.
8. Chang DF, Braga-Mele R, Mamalis N, et al; ASCRS Clinical Cataract Committee. Prophylaxis of postoperative endophthalmitis after cataract surgery: results of the 2007 ASCRS member survey. J Cataract Refract Surg. 2007;33(10):1801-1805.
9. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377-381.
10. French DD, Margo CE, Campbell RR. Do ophthalmology training programs affect corrective procedure rates after cataract surgery? Am J Med Qual. 2013;28(3):250-255.
11. Donaldson KE, Braga-Mele R, Cabot F, et al; ASCRS Refractive Cataract Surgery Subcommittee. Femtosecond laser-assisted cataract surgery. J Cataract Refract Surg. 2013;39(11):1753-1763.
12. Abouzeid H, Ferrini W. Femtosecond-laser assisted cataract surgery: a review. Acta Ophthalmol. 2014;92(7):597-603.
13. Chen H, Hyatt T, Afshari N. Visual and refractive outcomes of laser cataract surgery. Curr Opin Ophthalmol. 2014;25(1):49-53.
14. Yu Y, Chen X, Hua H, Wu M, Lai K, Yao K. Comparative outcomes of femtosecond laser-assisted cataract surgery and manual phacoemusification: a six-month follow-up. Clin Experiment Ophthalmol. 2016;44(6):472-480.
15. Ewe SY, Abell RG, Oakley CL, et al. A comparative cohort study of visual outcomes in femtosecond laser-assisted versus phacoemulsification cataract surgery. Ophthalmology. 2016;123(1):178-182.
16. Cohen MN, Intili A, Ni N, Blecher MH. Femtosecond laser-assisted cataract surgery in residency training. Curr Opin Ophthalmol. 2015;26(1):56-60.
17. Endophthalmitis Study Group, European Society of Cataract & Refractive Surgeons. Prophylaxis of postoperative endophthalmitis following cataract surgery: results of the ESCRS multicenter study and identification of risk factors. J Cataract Refract Surg. 2007;33(6):978-988.
18. Packer M, Chang DF, Dewey SH, et al; ASCRS Cataract Clinical Committee. Prevention, diagnosis, and management of acute postoperative bacterial endophthalmitis. J Cataract Refract Surg. 2011;37(9):1699-1714.
19. Schimel AM, Alfonso EC, Flynn HW Jr. Endophthalmitis prophylaxis for cataract surgery: are intracameral antibiotics necessary? JAMA Ophthalmol. 2014;132(11):1269-1270.
20. Herrinton LJ, Shorstein NH, Paschal JF, et al. Comparative effectiveness of antibiotic prophylaxis in cataract surgery. Ophthalmology. 2016;123(2):287-294.
21. Haripriya A, Chang DF, Namburar S, Smita A, Ravindran RD. Efficacy of intracameral moxifloxacin endophthalmitis prophylaxis at Aravind Eye Hospital. Ophthalmology. 2016;123(2):302-308.
22. Jabbarvand M, Hashemian H, Khodaparast M, Jouhari M, Tabatabaei A, Rezaei S. Endophthalmitis occurring after cataract surgery: outcomes of more than 480 000 cataract surgeries, epidemiologic features, and risk factors. Ophthalmology. 2016;123(2):295-301.
23. Neel ST. A cost and policy analysis comparing immediate sequential cataract surgery and delayed sequential cataract surgery from the physician perspective in the United States. JAMA Ophthalmol. 2014;132(11):1359-1362.
24. Sarikkola AU, Uusitalo RJ, Hellstedt T, Ess SL, Leivo T, Kivelä T. Simultaneous bilateral versus sequential bilateral cataract surgery: Helsinki Simultaneous Bilateral Cataract Surgery Study Report 1. J Cataract Refract Surg. 2011;37(6):992-1002.
25. Serrano-Aguilar P, Ramallo-Fariña Y, Cabrera-Hernández JM, et al. Immediately sequential versus delayed sequential bilateral cataract surgery: safety and effectiveness. J Cataract Refract Surg. 2012;38(10):1734-1742.
The rates of cataract surgery, the most commonly performed ophthalmic procedure in the U.S., have increased in the past few decades with an estimated rate of 1,100 surgeries per 100,000 people in 2011.1,2 Several emerging practices have the potential to radically impact the efficacy, safety, and cost of cataract surgery.3-5 These practices include femtosecond laser-assisted cataract surgery, intracameral antibiotics, and bilateral same-day cataract surgery.
The femtosecond laser is capable of producing precise incisions in the cornea for access by surgical instruments and reduction of astigmatism. Laser pulses also can create a perfectly round incision of the anterior lens capsule, which surrounds and supports the crystalline lens, and make incisions into the cataractous lens to facilitate disassembly for easy removal of fragments.
Placement of antibiotics internally into the anterior chamber, the space between the crystalline lens and the posterior cornea (intracameral space), is a more direct method to prevent bacterial infection within the eye (endophthalmitis), compared with current external methods, including injections under the conjunctiva (subconjunctival) and/or use of antibiotic drops directly onto the eye surface (topical).6
Routine cataract surgery is typically staged, with a period of time between sequential surgeries of 1 week or more to allow for observation of infection (delayed sequential surgery). In view of the very low rate of infection and the impact of staged surgery on patients, including additional visits and copays, some surgeons have begun to perform bilateral surgery (immediate sequential bilateral surgery, using separate patient safety checklists, surgical preps, instruments, and medications) on the same day for patients with significant cataracts in both eyes to promote rapid restoration of binocular vision as well reduce the number of patient visits.
The extent of adaptation of femtosecond laser surgery, intracameral antibiotics, and immediate sequential bilateral surgery in the U.S. is currently unknown.7,8 To provide an updated snapshot of these cataract surgery practices, the authors report on the results of a brief survey administered to ophthalmology section chiefs in the VHA, the largest integrated health care system and the largest provider of health care training in the U.S.
Methods
Following institutional review board approval from the Providence VA Medical Center, the office of the National Program Director of VA Ophthalmology provided a list of all VHA ophthalmology section chiefs and their contact information. The study targeted section chiefs because they are responsible for all eye surgery performed at their respective VAMCs. The survey queried the section chiefs on femtosecond laser-assisted cataract surgery, intracameral antibiotics, immediate sequential bilateral cataract surgery, and resident training at their institutions (Table).
The survey was administered using the web-based Research Electronic Data Capture (REDCap) software.9 The initial survey was e-mailed in April 2015, followed by 2 reminder e-mails 1 week apart and then 2 phone calls 1 week apart to nonresponders.
The survey responses were stored anonymously in the REDCap database and analyzed using descriptive statistics.
Results
The original list from the office of the National Program Director included 114 ophthalmology section chiefs (excluding one of the authors). After follow-up phone calls, 9 individuals were identified who were not ophthalmologists (eg, optometrists or nonophthalmic surgeons) or who were incorrectly listed as section chiefs, and 9 were duplicates from institutions that were represented twice on the contact list. These 18 individuals, none of whom had responded to the survey, were removed from the eligible sample. Hence, the analysis included 86% (95/111) of the VAMCs where cataract surgery is performed.10 Sixty-five responses were received for an overall response rate of 68% (65/96), including 1 ophthalmologist who responded to the survey twice.
Most section chiefs (86%, 56/65) trained ophthalmology residents at their respective medical centers (Table). Eleven VAMCs (17%) offered femtosecond laser-assisted cataract surgery; 8 of those 11 (73%) also offered resident training in this surgery. At 12 VAMCs (18%), cataract surgeons used intracameral antibiotics, which included vancomycin (4), cefuroxime (4), moxifloxacin (3), and unspecified (1); at 10 of these VAMCs (83%), surgeons used intracameral and postoperative topical antibiotics concomitantly; 8 VAMCs (67%) compounded the intracameral antibiotics—either in the hospital pharmacy (5) or within the operating room (3). The 2 most common reasons cited for not using intracameral antibiotics were risk of dilution error (28%; 15/53) and a lack of evidence for use (25%; 13/53). Only 2 medical centers (3.1%) offered immediate sequential bilateral cataract surgery.
Discussion
This survey provides updated information on the role of emerging cataract surgery practices in the VHA. These trends may impact future U.S. cataract surgery practice patterns given the large number of ophthalmology residents who receive training in the VHA.
Only 17% of VAMCs offered femtosecond laser-assisted cataract surgery. Reasons for this low rate may include (a) the high cost of the femtosecond laser units (the lowest average cost of a laser is $400,000, while the average costs of services can be $40,000 or more per year); and (b) the lack of evidence that a femtosecond laser improves cataract surgery outcomes relative to standard phacoemulsification.4,11-15 Another potential barrier to procurement of femtosecond lasers is the emphasis within VHA to increase access to care for the many newly enrolled veterans, which this technology does not address. However, most of the VAMCs with a femtosecond laser unit offered resident training in this technique, confirming early reports on the potential for incorporating femtosecond laser-assisted cataract surgery into ophthalmic graduate medical education.16
In 2007, the multicenter, prospective, randomized European Society of Cataract and Refractive Surgery Endophthalmitis Study demonstrated that intracameral cefuroxime was associated with a 5-fold decrease in the risk of postoperative endophthalmitis.17 In 2011, a statement from the American Society of Cataract and Refractive Surgery (ASCRS) Cataract Clinical Committee noted that the method of antibiotic prophylaxis with the strongest evidence base is “a direct intracameral bolus at the conclusion of surgery.”18 However, surgeons used intracameral antibiotics in only 19% of VAMCs. Although this is a higher rate than those reported in older surveys of VHA ophthalmologists (14%)7 and ASCRS members (15%), it is still significantly lower than the 74% reported in a recent survey of the European Society of Cataract and Refractive Surgeons.3,8
The most common reasons given for not using intracameral antibiotics included risk of a dilution error when preparing the antibiotics and lack of evidence supporting their effectiveness. Less common reasons included risk of contamination, lack of pharmacy approval, and increasing bacterial resistance to commonly used antibiotics. Most of these concerns have been previously cited as barriers to the adoption of intracameral antibiotics.19 The availability of a prepackaged intracameral antibiotic (eg, cefuroxime in Europe) would help address the risks of compounding dilution errors and contamination in the U.S.6 The publication of 3 large observational studies in 2016 has also significantly strengthened the evidence base supporting the use of intracameral antibiotics.20-22
Only 2 VAMCs (3%) offered immediate sequential bilateral cataract surgery. The advocates of this practice have touted its potential cost savings, patient convenience, and the opportunity for more rapid visual rehabilitation.23 Recently, several multicenter, randomized clinical trials have reported similar refractive outcomes, complication rates, and patient satisfaction for immediate and delayed bilateral cataract surgery.24,25 Hence, it is possible that rates of immediate sequential bilateral cataract surgery may increase in the VHA over the next few years.
Strengths/Limitations
A strength of this survey is its high response rate (67.7%), which exceeds the 53% and 33% rates reported in previous surveys of cataract surgery practice patterns among VHA ophthalmologistsand ASCRS members, respectively.7,8 Another strength is lack of financial incentive for adaptation of any new practices by VHA surgeons, suggesting that these decisions have been made to improve patient safety, quality of care, and/or resident education. A limitation of this study is that its findings may not be generalizable to ophthalmologists practicing in the private sector or in teaching hospitals outside the VHA.
Conclusion
This study suggests that femtosecond laser-assisted cataract surgery, intracameral antibiotics, and immediate sequential bilateral cataract surgery have limited roles in VHA cataract surgery. More research and clinical experience are needed to understand the barriers to more widespread acceptance and to assess the impact of these emerging practices on cataract surgery in the U.S.
The rates of cataract surgery, the most commonly performed ophthalmic procedure in the U.S., have increased in the past few decades with an estimated rate of 1,100 surgeries per 100,000 people in 2011.1,2 Several emerging practices have the potential to radically impact the efficacy, safety, and cost of cataract surgery.3-5 These practices include femtosecond laser-assisted cataract surgery, intracameral antibiotics, and bilateral same-day cataract surgery.
The femtosecond laser is capable of producing precise incisions in the cornea for access by surgical instruments and reduction of astigmatism. Laser pulses also can create a perfectly round incision of the anterior lens capsule, which surrounds and supports the crystalline lens, and make incisions into the cataractous lens to facilitate disassembly for easy removal of fragments.
Placement of antibiotics internally into the anterior chamber, the space between the crystalline lens and the posterior cornea (intracameral space), is a more direct method to prevent bacterial infection within the eye (endophthalmitis), compared with current external methods, including injections under the conjunctiva (subconjunctival) and/or use of antibiotic drops directly onto the eye surface (topical).6
Routine cataract surgery is typically staged, with a period of time between sequential surgeries of 1 week or more to allow for observation of infection (delayed sequential surgery). In view of the very low rate of infection and the impact of staged surgery on patients, including additional visits and copays, some surgeons have begun to perform bilateral surgery (immediate sequential bilateral surgery, using separate patient safety checklists, surgical preps, instruments, and medications) on the same day for patients with significant cataracts in both eyes to promote rapid restoration of binocular vision as well reduce the number of patient visits.
The extent of adaptation of femtosecond laser surgery, intracameral antibiotics, and immediate sequential bilateral surgery in the U.S. is currently unknown.7,8 To provide an updated snapshot of these cataract surgery practices, the authors report on the results of a brief survey administered to ophthalmology section chiefs in the VHA, the largest integrated health care system and the largest provider of health care training in the U.S.
Methods
Following institutional review board approval from the Providence VA Medical Center, the office of the National Program Director of VA Ophthalmology provided a list of all VHA ophthalmology section chiefs and their contact information. The study targeted section chiefs because they are responsible for all eye surgery performed at their respective VAMCs. The survey queried the section chiefs on femtosecond laser-assisted cataract surgery, intracameral antibiotics, immediate sequential bilateral cataract surgery, and resident training at their institutions (Table).
The survey was administered using the web-based Research Electronic Data Capture (REDCap) software.9 The initial survey was e-mailed in April 2015, followed by 2 reminder e-mails 1 week apart and then 2 phone calls 1 week apart to nonresponders.
The survey responses were stored anonymously in the REDCap database and analyzed using descriptive statistics.
Results
The original list from the office of the National Program Director included 114 ophthalmology section chiefs (excluding one of the authors). After follow-up phone calls, 9 individuals were identified who were not ophthalmologists (eg, optometrists or nonophthalmic surgeons) or who were incorrectly listed as section chiefs, and 9 were duplicates from institutions that were represented twice on the contact list. These 18 individuals, none of whom had responded to the survey, were removed from the eligible sample. Hence, the analysis included 86% (95/111) of the VAMCs where cataract surgery is performed.10 Sixty-five responses were received for an overall response rate of 68% (65/96), including 1 ophthalmologist who responded to the survey twice.
Most section chiefs (86%, 56/65) trained ophthalmology residents at their respective medical centers (Table). Eleven VAMCs (17%) offered femtosecond laser-assisted cataract surgery; 8 of those 11 (73%) also offered resident training in this surgery. At 12 VAMCs (18%), cataract surgeons used intracameral antibiotics, which included vancomycin (4), cefuroxime (4), moxifloxacin (3), and unspecified (1); at 10 of these VAMCs (83%), surgeons used intracameral and postoperative topical antibiotics concomitantly; 8 VAMCs (67%) compounded the intracameral antibiotics—either in the hospital pharmacy (5) or within the operating room (3). The 2 most common reasons cited for not using intracameral antibiotics were risk of dilution error (28%; 15/53) and a lack of evidence for use (25%; 13/53). Only 2 medical centers (3.1%) offered immediate sequential bilateral cataract surgery.
Discussion
This survey provides updated information on the role of emerging cataract surgery practices in the VHA. These trends may impact future U.S. cataract surgery practice patterns given the large number of ophthalmology residents who receive training in the VHA.
Only 17% of VAMCs offered femtosecond laser-assisted cataract surgery. Reasons for this low rate may include (a) the high cost of the femtosecond laser units (the lowest average cost of a laser is $400,000, while the average costs of services can be $40,000 or more per year); and (b) the lack of evidence that a femtosecond laser improves cataract surgery outcomes relative to standard phacoemulsification.4,11-15 Another potential barrier to procurement of femtosecond lasers is the emphasis within VHA to increase access to care for the many newly enrolled veterans, which this technology does not address. However, most of the VAMCs with a femtosecond laser unit offered resident training in this technique, confirming early reports on the potential for incorporating femtosecond laser-assisted cataract surgery into ophthalmic graduate medical education.16
In 2007, the multicenter, prospective, randomized European Society of Cataract and Refractive Surgery Endophthalmitis Study demonstrated that intracameral cefuroxime was associated with a 5-fold decrease in the risk of postoperative endophthalmitis.17 In 2011, a statement from the American Society of Cataract and Refractive Surgery (ASCRS) Cataract Clinical Committee noted that the method of antibiotic prophylaxis with the strongest evidence base is “a direct intracameral bolus at the conclusion of surgery.”18 However, surgeons used intracameral antibiotics in only 19% of VAMCs. Although this is a higher rate than those reported in older surveys of VHA ophthalmologists (14%)7 and ASCRS members (15%), it is still significantly lower than the 74% reported in a recent survey of the European Society of Cataract and Refractive Surgeons.3,8
The most common reasons given for not using intracameral antibiotics included risk of a dilution error when preparing the antibiotics and lack of evidence supporting their effectiveness. Less common reasons included risk of contamination, lack of pharmacy approval, and increasing bacterial resistance to commonly used antibiotics. Most of these concerns have been previously cited as barriers to the adoption of intracameral antibiotics.19 The availability of a prepackaged intracameral antibiotic (eg, cefuroxime in Europe) would help address the risks of compounding dilution errors and contamination in the U.S.6 The publication of 3 large observational studies in 2016 has also significantly strengthened the evidence base supporting the use of intracameral antibiotics.20-22
Only 2 VAMCs (3%) offered immediate sequential bilateral cataract surgery. The advocates of this practice have touted its potential cost savings, patient convenience, and the opportunity for more rapid visual rehabilitation.23 Recently, several multicenter, randomized clinical trials have reported similar refractive outcomes, complication rates, and patient satisfaction for immediate and delayed bilateral cataract surgery.24,25 Hence, it is possible that rates of immediate sequential bilateral cataract surgery may increase in the VHA over the next few years.
Strengths/Limitations
A strength of this survey is its high response rate (67.7%), which exceeds the 53% and 33% rates reported in previous surveys of cataract surgery practice patterns among VHA ophthalmologistsand ASCRS members, respectively.7,8 Another strength is lack of financial incentive for adaptation of any new practices by VHA surgeons, suggesting that these decisions have been made to improve patient safety, quality of care, and/or resident education. A limitation of this study is that its findings may not be generalizable to ophthalmologists practicing in the private sector or in teaching hospitals outside the VHA.
Conclusion
This study suggests that femtosecond laser-assisted cataract surgery, intracameral antibiotics, and immediate sequential bilateral cataract surgery have limited roles in VHA cataract surgery. More research and clinical experience are needed to understand the barriers to more widespread acceptance and to assess the impact of these emerging practices on cataract surgery in the U.S.
1. Lindstrom R. Thoughts on cataract surgery: 2015. http://www.reviewofophthalmology.com/content/t/surgical_education/c/53422/. Published March 9, 2015. Accessed June 23, 2016.
2. Gollogly HE, Hodge DO, St Sauver JL, Erie JC. Increasing incidence of cataract surgery: population-based study. J Cataract Refract Surg. 2013;39(9):1383-1389.
3. Barry P. Adoption of intracameral antibiotic prophylaxis of endophthalmitis following cataract surgery: update on the ESCRS Endophthalmitis Study. J Cataract Refract Surg. 2014;40(1):138-142.
4. Quiñones A, Gleitsmann K, Freeman M, et al. Benefits and Harms of Femtosecond Laser Assisted Cataract Surgery: A Systematic Review. VA-ESP Project #05-225; 2013. Washington, DC: Department of Veterans Affairs; 2013.
5. Naseri A, McLeod S. Benefits of and barriers to immediate sequential cataract surgery. JAMA Ophthalmol. 2014;132(11):1362-1363.
6. Brage-Mele R, Chang DF, Henderson BA, Mamalis N, Talley-Rostov A, Vasavada A; ASCRS Clinical Cataract Committee. Intracameral antibiotics: safety, efficacy, and preparation. J Cataract Refract Surg. 2014;40(12):2134-2142.
7. Greenberg PB, Havnaer A, Oetting TA, Garcia-Ferrer FJ. Cataract surgery practice patterns in the United States Veterans Health Administration. J Cataract Refract Surg. 2012;38(4):705-709.
8. Chang DF, Braga-Mele R, Mamalis N, et al; ASCRS Clinical Cataract Committee. Prophylaxis of postoperative endophthalmitis after cataract surgery: results of the 2007 ASCRS member survey. J Cataract Refract Surg. 2007;33(10):1801-1805.
9. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377-381.
10. French DD, Margo CE, Campbell RR. Do ophthalmology training programs affect corrective procedure rates after cataract surgery? Am J Med Qual. 2013;28(3):250-255.
11. Donaldson KE, Braga-Mele R, Cabot F, et al; ASCRS Refractive Cataract Surgery Subcommittee. Femtosecond laser-assisted cataract surgery. J Cataract Refract Surg. 2013;39(11):1753-1763.
12. Abouzeid H, Ferrini W. Femtosecond-laser assisted cataract surgery: a review. Acta Ophthalmol. 2014;92(7):597-603.
13. Chen H, Hyatt T, Afshari N. Visual and refractive outcomes of laser cataract surgery. Curr Opin Ophthalmol. 2014;25(1):49-53.
14. Yu Y, Chen X, Hua H, Wu M, Lai K, Yao K. Comparative outcomes of femtosecond laser-assisted cataract surgery and manual phacoemusification: a six-month follow-up. Clin Experiment Ophthalmol. 2016;44(6):472-480.
15. Ewe SY, Abell RG, Oakley CL, et al. A comparative cohort study of visual outcomes in femtosecond laser-assisted versus phacoemulsification cataract surgery. Ophthalmology. 2016;123(1):178-182.
16. Cohen MN, Intili A, Ni N, Blecher MH. Femtosecond laser-assisted cataract surgery in residency training. Curr Opin Ophthalmol. 2015;26(1):56-60.
17. Endophthalmitis Study Group, European Society of Cataract & Refractive Surgeons. Prophylaxis of postoperative endophthalmitis following cataract surgery: results of the ESCRS multicenter study and identification of risk factors. J Cataract Refract Surg. 2007;33(6):978-988.
18. Packer M, Chang DF, Dewey SH, et al; ASCRS Cataract Clinical Committee. Prevention, diagnosis, and management of acute postoperative bacterial endophthalmitis. J Cataract Refract Surg. 2011;37(9):1699-1714.
19. Schimel AM, Alfonso EC, Flynn HW Jr. Endophthalmitis prophylaxis for cataract surgery: are intracameral antibiotics necessary? JAMA Ophthalmol. 2014;132(11):1269-1270.
20. Herrinton LJ, Shorstein NH, Paschal JF, et al. Comparative effectiveness of antibiotic prophylaxis in cataract surgery. Ophthalmology. 2016;123(2):287-294.
21. Haripriya A, Chang DF, Namburar S, Smita A, Ravindran RD. Efficacy of intracameral moxifloxacin endophthalmitis prophylaxis at Aravind Eye Hospital. Ophthalmology. 2016;123(2):302-308.
22. Jabbarvand M, Hashemian H, Khodaparast M, Jouhari M, Tabatabaei A, Rezaei S. Endophthalmitis occurring after cataract surgery: outcomes of more than 480 000 cataract surgeries, epidemiologic features, and risk factors. Ophthalmology. 2016;123(2):295-301.
23. Neel ST. A cost and policy analysis comparing immediate sequential cataract surgery and delayed sequential cataract surgery from the physician perspective in the United States. JAMA Ophthalmol. 2014;132(11):1359-1362.
24. Sarikkola AU, Uusitalo RJ, Hellstedt T, Ess SL, Leivo T, Kivelä T. Simultaneous bilateral versus sequential bilateral cataract surgery: Helsinki Simultaneous Bilateral Cataract Surgery Study Report 1. J Cataract Refract Surg. 2011;37(6):992-1002.
25. Serrano-Aguilar P, Ramallo-Fariña Y, Cabrera-Hernández JM, et al. Immediately sequential versus delayed sequential bilateral cataract surgery: safety and effectiveness. J Cataract Refract Surg. 2012;38(10):1734-1742.
1. Lindstrom R. Thoughts on cataract surgery: 2015. http://www.reviewofophthalmology.com/content/t/surgical_education/c/53422/. Published March 9, 2015. Accessed June 23, 2016.
2. Gollogly HE, Hodge DO, St Sauver JL, Erie JC. Increasing incidence of cataract surgery: population-based study. J Cataract Refract Surg. 2013;39(9):1383-1389.
3. Barry P. Adoption of intracameral antibiotic prophylaxis of endophthalmitis following cataract surgery: update on the ESCRS Endophthalmitis Study. J Cataract Refract Surg. 2014;40(1):138-142.
4. Quiñones A, Gleitsmann K, Freeman M, et al. Benefits and Harms of Femtosecond Laser Assisted Cataract Surgery: A Systematic Review. VA-ESP Project #05-225; 2013. Washington, DC: Department of Veterans Affairs; 2013.
5. Naseri A, McLeod S. Benefits of and barriers to immediate sequential cataract surgery. JAMA Ophthalmol. 2014;132(11):1362-1363.
6. Brage-Mele R, Chang DF, Henderson BA, Mamalis N, Talley-Rostov A, Vasavada A; ASCRS Clinical Cataract Committee. Intracameral antibiotics: safety, efficacy, and preparation. J Cataract Refract Surg. 2014;40(12):2134-2142.
7. Greenberg PB, Havnaer A, Oetting TA, Garcia-Ferrer FJ. Cataract surgery practice patterns in the United States Veterans Health Administration. J Cataract Refract Surg. 2012;38(4):705-709.
8. Chang DF, Braga-Mele R, Mamalis N, et al; ASCRS Clinical Cataract Committee. Prophylaxis of postoperative endophthalmitis after cataract surgery: results of the 2007 ASCRS member survey. J Cataract Refract Surg. 2007;33(10):1801-1805.
9. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377-381.
10. French DD, Margo CE, Campbell RR. Do ophthalmology training programs affect corrective procedure rates after cataract surgery? Am J Med Qual. 2013;28(3):250-255.
11. Donaldson KE, Braga-Mele R, Cabot F, et al; ASCRS Refractive Cataract Surgery Subcommittee. Femtosecond laser-assisted cataract surgery. J Cataract Refract Surg. 2013;39(11):1753-1763.
12. Abouzeid H, Ferrini W. Femtosecond-laser assisted cataract surgery: a review. Acta Ophthalmol. 2014;92(7):597-603.
13. Chen H, Hyatt T, Afshari N. Visual and refractive outcomes of laser cataract surgery. Curr Opin Ophthalmol. 2014;25(1):49-53.
14. Yu Y, Chen X, Hua H, Wu M, Lai K, Yao K. Comparative outcomes of femtosecond laser-assisted cataract surgery and manual phacoemusification: a six-month follow-up. Clin Experiment Ophthalmol. 2016;44(6):472-480.
15. Ewe SY, Abell RG, Oakley CL, et al. A comparative cohort study of visual outcomes in femtosecond laser-assisted versus phacoemulsification cataract surgery. Ophthalmology. 2016;123(1):178-182.
16. Cohen MN, Intili A, Ni N, Blecher MH. Femtosecond laser-assisted cataract surgery in residency training. Curr Opin Ophthalmol. 2015;26(1):56-60.
17. Endophthalmitis Study Group, European Society of Cataract & Refractive Surgeons. Prophylaxis of postoperative endophthalmitis following cataract surgery: results of the ESCRS multicenter study and identification of risk factors. J Cataract Refract Surg. 2007;33(6):978-988.
18. Packer M, Chang DF, Dewey SH, et al; ASCRS Cataract Clinical Committee. Prevention, diagnosis, and management of acute postoperative bacterial endophthalmitis. J Cataract Refract Surg. 2011;37(9):1699-1714.
19. Schimel AM, Alfonso EC, Flynn HW Jr. Endophthalmitis prophylaxis for cataract surgery: are intracameral antibiotics necessary? JAMA Ophthalmol. 2014;132(11):1269-1270.
20. Herrinton LJ, Shorstein NH, Paschal JF, et al. Comparative effectiveness of antibiotic prophylaxis in cataract surgery. Ophthalmology. 2016;123(2):287-294.
21. Haripriya A, Chang DF, Namburar S, Smita A, Ravindran RD. Efficacy of intracameral moxifloxacin endophthalmitis prophylaxis at Aravind Eye Hospital. Ophthalmology. 2016;123(2):302-308.
22. Jabbarvand M, Hashemian H, Khodaparast M, Jouhari M, Tabatabaei A, Rezaei S. Endophthalmitis occurring after cataract surgery: outcomes of more than 480 000 cataract surgeries, epidemiologic features, and risk factors. Ophthalmology. 2016;123(2):295-301.
23. Neel ST. A cost and policy analysis comparing immediate sequential cataract surgery and delayed sequential cataract surgery from the physician perspective in the United States. JAMA Ophthalmol. 2014;132(11):1359-1362.
24. Sarikkola AU, Uusitalo RJ, Hellstedt T, Ess SL, Leivo T, Kivelä T. Simultaneous bilateral versus sequential bilateral cataract surgery: Helsinki Simultaneous Bilateral Cataract Surgery Study Report 1. J Cataract Refract Surg. 2011;37(6):992-1002.
25. Serrano-Aguilar P, Ramallo-Fariña Y, Cabrera-Hernández JM, et al. Immediately sequential versus delayed sequential bilateral cataract surgery: safety and effectiveness. J Cataract Refract Surg. 2012;38(10):1734-1742.

Combo could provide cure for CML, team says

Preclinical research suggests that combining a BCL2 inhibitor with a BCR-ABL tyrosine kinase inhibitor (TKI) can eradicate leukemia stem cells (LSCs) in chronic myeloid leukemia (CML).
In mouse models of CML, combining the TKI nilotinib with the BCL2 inhibitor venetoclax enhanced antileukemic activity and decreased numbers of long-term LSCs.
The 2-drug combination exhibited similar activity in samples from patients with blast crisis CML.
“Our results demonstrate that . . . employing combined blockade of BCL-2 and BCR-ABL has the potential for curing CML and significantly improving outcomes for patients with blast crisis, and, as such, warrants clinical testing,” said Michael Andreeff, MD, of the University of Texas MD Anderson Cancer Center in Houston.
Dr Andreeff and his colleagues reported these results in Science Translational Medicine. The study was funded by National Institutes of Health, the Paul and Mary Haas Chair in Genetics, and Abbvie Inc., the company developing venetoclax.
The researchers noted that, although BCR-ABL TKIs have proven effective against CML, they rarely eliminate CML stem cells.
“It is believed that TKIs do not eliminate residual stem cells because they are not dependent on BCR-ABL signaling,” said study author Bing Carter, PhD, also of MD Anderson Cancer Center. “Hence, cures of CML with TKIs are rare.”
Dr Carter has worked for several years on eliminating residual CML stem cells, which could mean CML patients would no longer require long-term treatment with TKIs. Based on the current study, she and her colleagues believe that combining a TKI with a BCL-2 inhibitor may be a solution.
The researchers found that targeting both BCL-2 and BCR-ABL with venetoclax and nilotinib, respectively, exerted “potent antileukemic activity” and prolonged survival in BCR-ABL transgenic mice.
After stopping treatment, the median survival was 34.5 days for control mice, 70 days for mice treated with nilotinib alone (P=0.2146), 115 days for mice treated with venetoclax alone (P=0.0079), and 168 days for mice treated with nilotinib and venetoclax in combination (P=0.0002).
Subsequent experiments in mice showed that nilotinib alone did not significantly affect the frequency of long-term LSCs, although venetoclax alone did. Treatment with both drugs reduced the frequency of long-term LSCs even more than venetoclax alone.
Finally, the researchers tested venetoclax, nilotinib, and the combination in cells from 6 patients with blast crisis CML, all of whom had failed treatment with at least 1 TKI.
The team found that venetoclax and nilotinib had a synergistic apoptotic effect on bulk and stem/progenitor CML cells.
The researchers said these results suggest that combined inhibition of BCL-2 and BCR-ABL tyrosine kinase has the potential to significantly improve the depth of response and cure rates of chronic phase and blast crisis CML.
“This combination strategy may also apply to other malignancies that depend on kinase signaling for progression and maintenance,” Dr Andreeff added. ![]()
Preclinical research suggests that combining a BCL2 inhibitor with a BCR-ABL tyrosine kinase inhibitor (TKI) can eradicate leukemia stem cells (LSCs) in chronic myeloid leukemia (CML).
In mouse models of CML, combining the TKI nilotinib with the BCL2 inhibitor venetoclax enhanced antileukemic activity and decreased numbers of long-term LSCs.
The 2-drug combination exhibited similar activity in samples from patients with blast crisis CML.
“Our results demonstrate that . . . employing combined blockade of BCL-2 and BCR-ABL has the potential for curing CML and significantly improving outcomes for patients with blast crisis, and, as such, warrants clinical testing,” said Michael Andreeff, MD, of the University of Texas MD Anderson Cancer Center in Houston.
Dr Andreeff and his colleagues reported these results in Science Translational Medicine. The study was funded by National Institutes of Health, the Paul and Mary Haas Chair in Genetics, and Abbvie Inc., the company developing venetoclax.
The researchers noted that, although BCR-ABL TKIs have proven effective against CML, they rarely eliminate CML stem cells.
“It is believed that TKIs do not eliminate residual stem cells because they are not dependent on BCR-ABL signaling,” said study author Bing Carter, PhD, also of MD Anderson Cancer Center. “Hence, cures of CML with TKIs are rare.”
Dr Carter has worked for several years on eliminating residual CML stem cells, which could mean CML patients would no longer require long-term treatment with TKIs. Based on the current study, she and her colleagues believe that combining a TKI with a BCL-2 inhibitor may be a solution.
The researchers found that targeting both BCL-2 and BCR-ABL with venetoclax and nilotinib, respectively, exerted “potent antileukemic activity” and prolonged survival in BCR-ABL transgenic mice.
After stopping treatment, the median survival was 34.5 days for control mice, 70 days for mice treated with nilotinib alone (P=0.2146), 115 days for mice treated with venetoclax alone (P=0.0079), and 168 days for mice treated with nilotinib and venetoclax in combination (P=0.0002).
Subsequent experiments in mice showed that nilotinib alone did not significantly affect the frequency of long-term LSCs, although venetoclax alone did. Treatment with both drugs reduced the frequency of long-term LSCs even more than venetoclax alone.
Finally, the researchers tested venetoclax, nilotinib, and the combination in cells from 6 patients with blast crisis CML, all of whom had failed treatment with at least 1 TKI.
The team found that venetoclax and nilotinib had a synergistic apoptotic effect on bulk and stem/progenitor CML cells.
The researchers said these results suggest that combined inhibition of BCL-2 and BCR-ABL tyrosine kinase has the potential to significantly improve the depth of response and cure rates of chronic phase and blast crisis CML.
“This combination strategy may also apply to other malignancies that depend on kinase signaling for progression and maintenance,” Dr Andreeff added. ![]()
Preclinical research suggests that combining a BCL2 inhibitor with a BCR-ABL tyrosine kinase inhibitor (TKI) can eradicate leukemia stem cells (LSCs) in chronic myeloid leukemia (CML).
In mouse models of CML, combining the TKI nilotinib with the BCL2 inhibitor venetoclax enhanced antileukemic activity and decreased numbers of long-term LSCs.
The 2-drug combination exhibited similar activity in samples from patients with blast crisis CML.
“Our results demonstrate that . . . employing combined blockade of BCL-2 and BCR-ABL has the potential for curing CML and significantly improving outcomes for patients with blast crisis, and, as such, warrants clinical testing,” said Michael Andreeff, MD, of the University of Texas MD Anderson Cancer Center in Houston.
Dr Andreeff and his colleagues reported these results in Science Translational Medicine. The study was funded by National Institutes of Health, the Paul and Mary Haas Chair in Genetics, and Abbvie Inc., the company developing venetoclax.
The researchers noted that, although BCR-ABL TKIs have proven effective against CML, they rarely eliminate CML stem cells.
“It is believed that TKIs do not eliminate residual stem cells because they are not dependent on BCR-ABL signaling,” said study author Bing Carter, PhD, also of MD Anderson Cancer Center. “Hence, cures of CML with TKIs are rare.”
Dr Carter has worked for several years on eliminating residual CML stem cells, which could mean CML patients would no longer require long-term treatment with TKIs. Based on the current study, she and her colleagues believe that combining a TKI with a BCL-2 inhibitor may be a solution.
The researchers found that targeting both BCL-2 and BCR-ABL with venetoclax and nilotinib, respectively, exerted “potent antileukemic activity” and prolonged survival in BCR-ABL transgenic mice.
After stopping treatment, the median survival was 34.5 days for control mice, 70 days for mice treated with nilotinib alone (P=0.2146), 115 days for mice treated with venetoclax alone (P=0.0079), and 168 days for mice treated with nilotinib and venetoclax in combination (P=0.0002).
Subsequent experiments in mice showed that nilotinib alone did not significantly affect the frequency of long-term LSCs, although venetoclax alone did. Treatment with both drugs reduced the frequency of long-term LSCs even more than venetoclax alone.
Finally, the researchers tested venetoclax, nilotinib, and the combination in cells from 6 patients with blast crisis CML, all of whom had failed treatment with at least 1 TKI.
The team found that venetoclax and nilotinib had a synergistic apoptotic effect on bulk and stem/progenitor CML cells.
The researchers said these results suggest that combined inhibition of BCL-2 and BCR-ABL tyrosine kinase has the potential to significantly improve the depth of response and cure rates of chronic phase and blast crisis CML.
“This combination strategy may also apply to other malignancies that depend on kinase signaling for progression and maintenance,” Dr Andreeff added. ![]()
Blood sample collection, storage impacts protein levels

Photo by Graham Colm
Factors related to blood sample collection and storage can have a substantial impact on the biomolecular composition of the sample, according to research published in EBioMedicine.
The study showed that freezer storage time and the month and season during which a blood sample is collected can affect protein concentrations.
In fact, researchers said these factors should be considered covariates of the same importance as the sample provider’s age or gender.
“This discovery will change the way the entire world works with biobank blood,” said study author Stefan Enroth, PhD, of Uppsala University in Sweden.
“All research on, and analysis of, biobank blood going forward should also take into account what we have discovered—namely, the time aspect. It is completely new.”
As part of their research on uterine cancer, Dr Enroth and his colleagues looked at plasma samples collected from 1988 to 2014. There were 380 samples from 106 women between the ages of 29 and 73.
The researchers looked at the duration of sample storage, the women’s chronological age at sample collection, and the season and month of the year the sample was collected, assessing the impact of these factors on the abundance levels of 108 proteins.
When studying the impact of storage time, the researchers used only samples from 50-year-old women in order to isolate the time effect. The team found that storage time affected 18 proteins and explained 4.8% to 34.9% of the variance observed.
The women’s chronological age at the time of sample collection, after the adjustment for storage time, affected 70 proteins and explained 1.1% to 33.5% of the variance.
“We suspected that we’d find an influence from storage time, but we thought it would be much less,” said study author Ulf Gyllensten, PhD, of Uppsala University.
“It has now been demonstrated that storage time can be a factor at least as important as the age of the individual at sampling.”
The other major finding of the study is that protein levels vary depending on the season or month in which the samples were taken.
The researchers said results in the month analysis corresponded with the seasonal analysis, so they hypothesized that sunlight hours at the time of sampling could explain some of the variance they observed in plasma protein abundance levels.
The team found the number of sunlight hours affected 36 proteins and explained up to 4.5% of the variance observed after adjusting for storage time and age.
The researchers said these results suggest that information on the sample handling history should be regarded as “equally prominent covariates” as age or gender. Therefore, the information should be included in epidemiological studies involving protein levels. ![]()
Photo by Graham Colm
Factors related to blood sample collection and storage can have a substantial impact on the biomolecular composition of the sample, according to research published in EBioMedicine.
The study showed that freezer storage time and the month and season during which a blood sample is collected can affect protein concentrations.
In fact, researchers said these factors should be considered covariates of the same importance as the sample provider’s age or gender.
“This discovery will change the way the entire world works with biobank blood,” said study author Stefan Enroth, PhD, of Uppsala University in Sweden.
“All research on, and analysis of, biobank blood going forward should also take into account what we have discovered—namely, the time aspect. It is completely new.”
As part of their research on uterine cancer, Dr Enroth and his colleagues looked at plasma samples collected from 1988 to 2014. There were 380 samples from 106 women between the ages of 29 and 73.
The researchers looked at the duration of sample storage, the women’s chronological age at sample collection, and the season and month of the year the sample was collected, assessing the impact of these factors on the abundance levels of 108 proteins.
When studying the impact of storage time, the researchers used only samples from 50-year-old women in order to isolate the time effect. The team found that storage time affected 18 proteins and explained 4.8% to 34.9% of the variance observed.
The women’s chronological age at the time of sample collection, after the adjustment for storage time, affected 70 proteins and explained 1.1% to 33.5% of the variance.
“We suspected that we’d find an influence from storage time, but we thought it would be much less,” said study author Ulf Gyllensten, PhD, of Uppsala University.
“It has now been demonstrated that storage time can be a factor at least as important as the age of the individual at sampling.”
The other major finding of the study is that protein levels vary depending on the season or month in which the samples were taken.
The researchers said results in the month analysis corresponded with the seasonal analysis, so they hypothesized that sunlight hours at the time of sampling could explain some of the variance they observed in plasma protein abundance levels.
The team found the number of sunlight hours affected 36 proteins and explained up to 4.5% of the variance observed after adjusting for storage time and age.
The researchers said these results suggest that information on the sample handling history should be regarded as “equally prominent covariates” as age or gender. Therefore, the information should be included in epidemiological studies involving protein levels. ![]()
Photo by Graham Colm
Factors related to blood sample collection and storage can have a substantial impact on the biomolecular composition of the sample, according to research published in EBioMedicine.
The study showed that freezer storage time and the month and season during which a blood sample is collected can affect protein concentrations.
In fact, researchers said these factors should be considered covariates of the same importance as the sample provider’s age or gender.
“This discovery will change the way the entire world works with biobank blood,” said study author Stefan Enroth, PhD, of Uppsala University in Sweden.
“All research on, and analysis of, biobank blood going forward should also take into account what we have discovered—namely, the time aspect. It is completely new.”
As part of their research on uterine cancer, Dr Enroth and his colleagues looked at plasma samples collected from 1988 to 2014. There were 380 samples from 106 women between the ages of 29 and 73.
The researchers looked at the duration of sample storage, the women’s chronological age at sample collection, and the season and month of the year the sample was collected, assessing the impact of these factors on the abundance levels of 108 proteins.
When studying the impact of storage time, the researchers used only samples from 50-year-old women in order to isolate the time effect. The team found that storage time affected 18 proteins and explained 4.8% to 34.9% of the variance observed.
The women’s chronological age at the time of sample collection, after the adjustment for storage time, affected 70 proteins and explained 1.1% to 33.5% of the variance.
“We suspected that we’d find an influence from storage time, but we thought it would be much less,” said study author Ulf Gyllensten, PhD, of Uppsala University.
“It has now been demonstrated that storage time can be a factor at least as important as the age of the individual at sampling.”
The other major finding of the study is that protein levels vary depending on the season or month in which the samples were taken.
The researchers said results in the month analysis corresponded with the seasonal analysis, so they hypothesized that sunlight hours at the time of sampling could explain some of the variance they observed in plasma protein abundance levels.
The team found the number of sunlight hours affected 36 proteins and explained up to 4.5% of the variance observed after adjusting for storage time and age.
The researchers said these results suggest that information on the sample handling history should be regarded as “equally prominent covariates” as age or gender. Therefore, the information should be included in epidemiological studies involving protein levels. ![]()
Change may improve efficacy of malaria vaccine

Photo by Caitlin Kleiboer
Results of a phase 2 trial suggest that changing the dosing schedule can improve the efficacy of the malaria vaccine candidate RTS,S/AS01 (Mosquirix).
Researchers tested RTS,S/AS01 in 46 malaria-naïve US adults, using the controlled human malaria infection model (CHMI).
About 87% of subjects who received the modified dosing regimen were protected from malaria, compared to 63% of subjects who received the standard dosing schedule.
Jason Regules, MD, of the US Army Medical Research Institute of Infectious Diseases in Frederick, Maryland, and his colleagues reported these results in the Journal of Infectious Diseases.
The study was funded by GlaxoSmithKline, the US Military Infectious Disease Research Program, and the PATH Malaria Vaccine Initiative. RTS,S/AS01 is being developed by GlaxoSmithKline and the PATH Malaria Vaccine Initiative.
RTS,S/AS01 has been tested in trials of young children in Africa, and early results seemed promising. But long-term follow-up in a phase 2 study and a phase 3 study suggested the vaccine’s efficacy wanes over time.
Therefore, Dr Regules and his colleagues sought to determine if a novel immunization schedule—specifically, delaying RTS,S/AS01 administration and reducing dosage of the third vaccination, as well as any following booster dose—would significantly increase the vaccine’s ability to protect against infection.
The researchers evaluated RTS,S/AS01 in 46 malaria-naïve adults. First, the team immunized the subjects according to 2 regimens:
- A 0-, 1-, 7-month schedule with a fractional third dose (Fx017M)
- A 0-, 1-, 2-month schedule (012M, the current standard).
Following the third vaccination, subjects were exposed to malaria-causing parasites using CHMI, and the researchers evaluated the extent to which each regimen protected against infection.
During follow-up, the team assessed the efficacy of an additional fractional dose, or booster, in protecting against a second CHMI.
Twenty-six of the 30 subjects—86.7%—who received the Fx017M regimen and 10 of the 16—62.5%—who received the 012M regimen were protected from infection following the first CHMI.
In addition to providing more protection from malaria infection, the Fx017M regimen delayed infection longer than the 012M regimen.
About 90% of the Fx017M group who received a fourth fractional booster dose and underwent the second CHMI were protected from infection.
Four out of 5 subjects from both vaccination groups who were infected during the first CHMI were protected against the second, after receiving the fourth (fractional) dose of RTS,S/AS01.
The subjects did not report any serious health events as a result of receiving the vaccinations, and no safety concerns were associated with reducing dosages.
“With these results in hand, we are planning additional studies in the United States and Africa that will seek to further refine the dosing and schedule for maximum impact and to see whether these early stage results in American adults will translate into similarly high efficacy in sub-Saharan Africa, a region that bears much of the malaria disease burden,” said study author Ashley J. Birkett, PhD, director of PATH’s Malaria Vaccine Initiative.
“The results of these planned studies won’t be available for several years, however. It therefore remains critical that the pilot implementation for the recommended pediatric regimen of RTS,S/AS01, being led by the World Health Organization, moves forward as soon as possible. We need to help protect as many children as we can, as soon as we can, while we continue to pursue eradication—the only truly sustainable solution to malaria.” ![]()
Photo by Caitlin Kleiboer
Results of a phase 2 trial suggest that changing the dosing schedule can improve the efficacy of the malaria vaccine candidate RTS,S/AS01 (Mosquirix).
Researchers tested RTS,S/AS01 in 46 malaria-naïve US adults, using the controlled human malaria infection model (CHMI).
About 87% of subjects who received the modified dosing regimen were protected from malaria, compared to 63% of subjects who received the standard dosing schedule.
Jason Regules, MD, of the US Army Medical Research Institute of Infectious Diseases in Frederick, Maryland, and his colleagues reported these results in the Journal of Infectious Diseases.
The study was funded by GlaxoSmithKline, the US Military Infectious Disease Research Program, and the PATH Malaria Vaccine Initiative. RTS,S/AS01 is being developed by GlaxoSmithKline and the PATH Malaria Vaccine Initiative.
RTS,S/AS01 has been tested in trials of young children in Africa, and early results seemed promising. But long-term follow-up in a phase 2 study and a phase 3 study suggested the vaccine’s efficacy wanes over time.
Therefore, Dr Regules and his colleagues sought to determine if a novel immunization schedule—specifically, delaying RTS,S/AS01 administration and reducing dosage of the third vaccination, as well as any following booster dose—would significantly increase the vaccine’s ability to protect against infection.
The researchers evaluated RTS,S/AS01 in 46 malaria-naïve adults. First, the team immunized the subjects according to 2 regimens:
- A 0-, 1-, 7-month schedule with a fractional third dose (Fx017M)
- A 0-, 1-, 2-month schedule (012M, the current standard).
Following the third vaccination, subjects were exposed to malaria-causing parasites using CHMI, and the researchers evaluated the extent to which each regimen protected against infection.
During follow-up, the team assessed the efficacy of an additional fractional dose, or booster, in protecting against a second CHMI.
Twenty-six of the 30 subjects—86.7%—who received the Fx017M regimen and 10 of the 16—62.5%—who received the 012M regimen were protected from infection following the first CHMI.
In addition to providing more protection from malaria infection, the Fx017M regimen delayed infection longer than the 012M regimen.
About 90% of the Fx017M group who received a fourth fractional booster dose and underwent the second CHMI were protected from infection.
Four out of 5 subjects from both vaccination groups who were infected during the first CHMI were protected against the second, after receiving the fourth (fractional) dose of RTS,S/AS01.
The subjects did not report any serious health events as a result of receiving the vaccinations, and no safety concerns were associated with reducing dosages.
“With these results in hand, we are planning additional studies in the United States and Africa that will seek to further refine the dosing and schedule for maximum impact and to see whether these early stage results in American adults will translate into similarly high efficacy in sub-Saharan Africa, a region that bears much of the malaria disease burden,” said study author Ashley J. Birkett, PhD, director of PATH’s Malaria Vaccine Initiative.
“The results of these planned studies won’t be available for several years, however. It therefore remains critical that the pilot implementation for the recommended pediatric regimen of RTS,S/AS01, being led by the World Health Organization, moves forward as soon as possible. We need to help protect as many children as we can, as soon as we can, while we continue to pursue eradication—the only truly sustainable solution to malaria.” ![]()
Photo by Caitlin Kleiboer
Results of a phase 2 trial suggest that changing the dosing schedule can improve the efficacy of the malaria vaccine candidate RTS,S/AS01 (Mosquirix).
Researchers tested RTS,S/AS01 in 46 malaria-naïve US adults, using the controlled human malaria infection model (CHMI).
About 87% of subjects who received the modified dosing regimen were protected from malaria, compared to 63% of subjects who received the standard dosing schedule.
Jason Regules, MD, of the US Army Medical Research Institute of Infectious Diseases in Frederick, Maryland, and his colleagues reported these results in the Journal of Infectious Diseases.
The study was funded by GlaxoSmithKline, the US Military Infectious Disease Research Program, and the PATH Malaria Vaccine Initiative. RTS,S/AS01 is being developed by GlaxoSmithKline and the PATH Malaria Vaccine Initiative.
RTS,S/AS01 has been tested in trials of young children in Africa, and early results seemed promising. But long-term follow-up in a phase 2 study and a phase 3 study suggested the vaccine’s efficacy wanes over time.
Therefore, Dr Regules and his colleagues sought to determine if a novel immunization schedule—specifically, delaying RTS,S/AS01 administration and reducing dosage of the third vaccination, as well as any following booster dose—would significantly increase the vaccine’s ability to protect against infection.
The researchers evaluated RTS,S/AS01 in 46 malaria-naïve adults. First, the team immunized the subjects according to 2 regimens:
- A 0-, 1-, 7-month schedule with a fractional third dose (Fx017M)
- A 0-, 1-, 2-month schedule (012M, the current standard).
Following the third vaccination, subjects were exposed to malaria-causing parasites using CHMI, and the researchers evaluated the extent to which each regimen protected against infection.
During follow-up, the team assessed the efficacy of an additional fractional dose, or booster, in protecting against a second CHMI.
Twenty-six of the 30 subjects—86.7%—who received the Fx017M regimen and 10 of the 16—62.5%—who received the 012M regimen were protected from infection following the first CHMI.
In addition to providing more protection from malaria infection, the Fx017M regimen delayed infection longer than the 012M regimen.
About 90% of the Fx017M group who received a fourth fractional booster dose and underwent the second CHMI were protected from infection.
Four out of 5 subjects from both vaccination groups who were infected during the first CHMI were protected against the second, after receiving the fourth (fractional) dose of RTS,S/AS01.
The subjects did not report any serious health events as a result of receiving the vaccinations, and no safety concerns were associated with reducing dosages.
“With these results in hand, we are planning additional studies in the United States and Africa that will seek to further refine the dosing and schedule for maximum impact and to see whether these early stage results in American adults will translate into similarly high efficacy in sub-Saharan Africa, a region that bears much of the malaria disease burden,” said study author Ashley J. Birkett, PhD, director of PATH’s Malaria Vaccine Initiative.
“The results of these planned studies won’t be available for several years, however. It therefore remains critical that the pilot implementation for the recommended pediatric regimen of RTS,S/AS01, being led by the World Health Organization, moves forward as soon as possible. We need to help protect as many children as we can, as soon as we can, while we continue to pursue eradication—the only truly sustainable solution to malaria.” ![]()
How AML suppresses hematopoiesis

Exosomes shed by acute myeloid leukemia (AML) cells carry microRNAs that directly impair hematopoiesis, according to preclinical research published in Science Signaling.
Previous research suggested that AML exosomes can suppress residual hematopoietic stem and progenitor cell (HSPC) function indirectly through stromal reprogramming of niche retention factors.
The new study indicates that AML exosomes can block hematopoiesis by delivering microRNAs that directly suppress blood production when taken up by HSPCs.
Noah Hornick, of Oregon Health & Science University in Portland, and his colleagues conducted this study, isolating exosomes from cultures of human AML cells and from the plasma of mice with AML.
The researchers found these exosomes were enriched in 2 microRNAs—miR-150 and miR-155.
When cultured with HSPCs, the exosomes suppressed the expression of the transcription factor c-MYB, which is involved in HSPC proliferation and differentiation.
Blocking the function of miR-155 prevented AML cells or their exosomes from reducing c-MYB abundance and inhibiting the proliferation of cultured HSPCs.
Using a method called RISC-Trap, the researchers identified other targets of microRNAs in AML exosomes, from which they predicted protein networks that could be disrupted in cells taking up the exosomes.
The team said this study suggests that interfering with exosome-delivered microRNAs in the bone marrow or restoring the abundance of their targets may enhance AML patients’ ability to produce healthy blood cells. ![]()
Exosomes shed by acute myeloid leukemia (AML) cells carry microRNAs that directly impair hematopoiesis, according to preclinical research published in Science Signaling.
Previous research suggested that AML exosomes can suppress residual hematopoietic stem and progenitor cell (HSPC) function indirectly through stromal reprogramming of niche retention factors.
The new study indicates that AML exosomes can block hematopoiesis by delivering microRNAs that directly suppress blood production when taken up by HSPCs.
Noah Hornick, of Oregon Health & Science University in Portland, and his colleagues conducted this study, isolating exosomes from cultures of human AML cells and from the plasma of mice with AML.
The researchers found these exosomes were enriched in 2 microRNAs—miR-150 and miR-155.
When cultured with HSPCs, the exosomes suppressed the expression of the transcription factor c-MYB, which is involved in HSPC proliferation and differentiation.
Blocking the function of miR-155 prevented AML cells or their exosomes from reducing c-MYB abundance and inhibiting the proliferation of cultured HSPCs.
Using a method called RISC-Trap, the researchers identified other targets of microRNAs in AML exosomes, from which they predicted protein networks that could be disrupted in cells taking up the exosomes.
The team said this study suggests that interfering with exosome-delivered microRNAs in the bone marrow or restoring the abundance of their targets may enhance AML patients’ ability to produce healthy blood cells. ![]()
Exosomes shed by acute myeloid leukemia (AML) cells carry microRNAs that directly impair hematopoiesis, according to preclinical research published in Science Signaling.
Previous research suggested that AML exosomes can suppress residual hematopoietic stem and progenitor cell (HSPC) function indirectly through stromal reprogramming of niche retention factors.
The new study indicates that AML exosomes can block hematopoiesis by delivering microRNAs that directly suppress blood production when taken up by HSPCs.
Noah Hornick, of Oregon Health & Science University in Portland, and his colleagues conducted this study, isolating exosomes from cultures of human AML cells and from the plasma of mice with AML.
The researchers found these exosomes were enriched in 2 microRNAs—miR-150 and miR-155.
When cultured with HSPCs, the exosomes suppressed the expression of the transcription factor c-MYB, which is involved in HSPC proliferation and differentiation.
Blocking the function of miR-155 prevented AML cells or their exosomes from reducing c-MYB abundance and inhibiting the proliferation of cultured HSPCs.
Using a method called RISC-Trap, the researchers identified other targets of microRNAs in AML exosomes, from which they predicted protein networks that could be disrupted in cells taking up the exosomes.
The team said this study suggests that interfering with exosome-delivered microRNAs in the bone marrow or restoring the abundance of their targets may enhance AML patients’ ability to produce healthy blood cells. ![]()
Patients With Difficult Personalities
Much has been written about the importance of the doctor‐patient relationship, with a positive therapeutic alliance being associated with both improvement in patient healthcare outcomes and physician job satisfaction.[1, 2] However, some patients severely test their physician's ability to provide needed care. These patients can rankle even experienced clinicians, leaving them feeling frustrated and ineffectual while consuming disproportionate amounts of clinical time. Although these disruptive acts may feel volitional and purposeful to the clinicians attempting to provide care, they may stem from a dysfunctional personality structure. Personality disorders are pervasive patterns of maladaptive behaviors, thoughts, and emotions that often go unrecognized and can wreak havoc in the patient's interpersonal life.[3] These inflexible patterns of managing the world can be disruptive when an individual is admitted to the hospital, causing distress for both the patient who lacks the skills to deal with the expectations of the hospital environment and the treatment team who can feel ill equipped to manage such behaviors.[4, 5] Here, we discuss personality disorders, how they can manifest in the hospital setting, and interventions to assist both the individual and the team.
Although personality disorders come in a variety of forms, central to all is interpersonal disarray with difficulty forming and maintaining acceptable relationships with others. In the hospital setting, the patient needs to be able to relate to, and cooperate with, a myriad of different care providers all while under some degree of physical and emotional distress. This can be destabilizing even for those without personality issues. For those with personality disorders, it is nearly inevitable that conflict will arise. Although true prevalence rates can be difficult to ascertain due to diagnostic challenges, surveys have found 4% to 15% of the population are affected by at least 1 personality disorder.[6] The prevalence is thought to be even higher among those seeking healthcare services, with researchers suggesting that 1 in 4 primary care patients meet criteria for a personality disorder.[6, 7]
Having a personality disorder has implications for an individual's healthcare outcomes. Studies in the United Kingdom have shown that those with a personality disorder have a life expectancy nearly 2 decades shorter than the general population.[8] Although suicide and homicide account for part of this, they also have increased risk of a number of health issues, including obesity, metabolic syndrome, cardiovascular disease, and sleep disorders.[9] In addition to lifestyle factors such as drinking and drug use, it has been suggested that dysfunctional personality structures may interfere with the ability to access and utilize care, leading to higher morbidity and mortality.[7]
In addition to impacting their own life, individuals with personality disorders have a tendency to disrupt the environment around them. They often elicit strong emotional responses from others that can range from a desire to help and protect to frustration and a sense of loathing.[10] The presence of a personality disorder often comes to light in the hospital when the patient is feeling vulnerable and acts out, evoking strong responses from team members. In the literature, patients with personality disorders are frequently referred to as a difficult or even hateful.[11] These individuals can be emotionally draining to care for, and the team must manage their own divergent responses in addition to the patient's disruptive behavior. Understanding personality disorders as a mental illness and using behavioral interventions can help to ease these interactions.
PERSONALITY DISORDERS: AN OVERVIEW
Personality disorders are characterized by persistent patterns of emotional reactivity, interpersonal interactions, and ways of perceiving the world that are inflexible and maladaptive and lead to significant distress and dysfunction.[3, 7] These disorders are notable for the interactive nature of the diagnosis; rather than being completely dependent on the individual's symptoms, a significant component of identification depends on how these individuals relate to others.[7] Although the trajectory can change over time, personality disorders are generally pervasive across the lifetime of an individual, beginning in adolescence or early adulthood.[7, 12] Personality disorders are divided into 3 clusters (Table 1).
| Personality Disorders | Features | Possible Manifestations in the Hospital |
|---|---|---|
| Cluster A | Odd and eccentric, socially avoidant |
Mistrust of medical staff and treatments offered Hostility toward treatment team Accusations of exploitation and harm without reasonable evidence General sense from the team that something is off |
| Paranoid | Highly suspicious of others; interpret malice where none was intended | |
| Schizoid | Minimal social relationships; limited emotional range | |
| Schizotypal | Eccentric behavior and magical thinking; uncomfortable with close relationships | |
| Cluster B | Emotionally labile and impulsive |
Splitting of the team, clear favorite providers and hated providers Extremes of emotion with responses out of proportion to the situation Rapid escalation when they perceive their needs not being met Evoke a strong emotional response from the team, taking up time out of proportion to their medical illness Help‐rejecting behavior Fear of abandonment manifesting as escalation of behavior around discharge |
| Antisocial | Frequent disregard for rights of others | |
| Borderline | Impulsive with volatile interpersonal relationships | |
| Histrionic | Disproportionate emotionality with engagement seeking | |
| Narcissistic | Grandiose, seeks admiration | |
| Cluster C | Anxious and neurotic |
Resistance to participating in their own care Frequent demands on the staff Particular, sometimes seemingly illogical, preferences regarding their care or other aspects of their stay |
| Avoidant | Socially fearful with feelings of inadequacy | |
| Dependent | Need to be taken care of, often manifesting as clinging and obsequious behavior | |
| Obsessive‐compulsive | Preoccupied by orderliness and control, but without actual obsessions or compulsions |
Cluster A
Those falling into cluster A, which includes paranoid, schizoid, and schizotypal personality disorders, are odd and eccentric and often avoid social engagement[3]; these individuals have few friends or associates and do not care to make more. At times, their unusual thinking can be difficult to differentiate from primary psychotic disorders like schizophrenia.
Cluster B
Cluster B is most heavily studied, consisting of antisocial, borderline, histrionic, and narcissistic personality disorders. These individuals share a high degree of emotional lability and erratic behavior.[3] Frequently, their tendency toward impulsive and self‐destructive behaviors can result in the need for medical care.
Cluster C
Cluster C includes avoidant, dependent, and obsessive‐compulsive personality disorders. These individuals are often anxious and fearful. Like individuals in Cluster A, they have few friends; unlike Cluster A, they long for friendships but struggle to make them. On the inpatient unit, these individuals may have trouble engaging in needed care, relying heavily on others to have their needs met or may be very particular about how their care is administered.
NEUROPHYSIOLOGY
Personality disorders are the product of complex interactions between genes and environment. These disorders are highly heritable, with 55% to 72% heritability across the 3 clusters.[13, 14, 15] Studies have implicated alterations in the serotonin system as playing a role in the underlying pathophysiology, which may contribute to the emotional dysregulation.[16, 17, 18] Neuroimaging has shown alterations in regions of the brain related to emotional reactivity and the processing of social interactions, suggesting neural mechanisms behind these individuals' difficulty with interpersonal relationships.[19, 20, 21, 22]
IDENTIFICATION OF PERSONALITY DISORDERS
These disorders are under‐recognized due, at least in part, to difficulty in making the diagnosis.[7] With 10 different personality disorders, many with overlapping characteristics, establishing a specific diagnosis can be time consuming, and a single individual may fit multiple different personality disorders.[7] Although self‐report surveys and structured interviews exist, these are often time consuming or inaccurate.[7] It is unlikely to be practical to make a diagnosis of a specific personality disorder while in the hospital. Instead, the focus should be placed on identifying impaired personality structures that interfere with interpersonal relationships and thereby disrupt the course of treatment. Consider a personality disorder if any of the following features are present:
- The patient elicits a strong emotional reaction from providers; these may vary markedly between providers.
- The patient's emotional responses may appear disproportionate to the inciting event.
- The patient is on a number of different psychiatric medications with little relief of symptoms.
- The patient takes up a disproportionate amount of the providers' time.
- The patient externalizes blame, seeing others as the source of discomfort or distress and therefore sees others as the solution.
Once identified, steps can be taken to help both the team and the patient.
BEHAVIORAL INTERVENTIONS
The first line of intervention for individuals with dysfunctional personality structures is behavioral, changing the way the team and patient interact (Table 2). Such interventions have long been the cornerstone of treatment for these individuals.[23] The preponderance of the research has focused on cluster B, and specifically individuals with borderline personality disorder, and applying these principles more broadly is largely based on expert opinion.
| Clinical Examples and Behavioral Interventions | ||
|---|---|---|
| Background | Situation | Response |
| Cluster A: Mr. A is a 75‐year‐old man transferred from his small town after a myocardial infarction. Although he has improved medically, he repeatedly expresses distrust and dissatisfaction with his doctors. He refuses to go to a skilled nursing facility but will not work with physical therapy to discharge home. He lives alone and has worked as a cattle rancher all his life. | Mr. A repeatedly accuses his team of being in this for the money. At times he mutters about government conspiracies. |
Check the team's emotions and reinforce desired behaviors and move past negative ones: Recognize paranoia as part of the illness. Rather than confront the paranoia, ignore this behavior as long as it is not directly interfering with care. |
| Cluster B: Ms. B is a 22‐year‐old woman admitted after a car accident resulting in multiple fractures. The pain service is consulted due to her ever‐increasing need for opiates. When the team first meets her, she is bright, effusing, Thank you for coming! My other doctors have no idea how to control my pain. She starts crying, I just can't do this anymore. Midway through the conversation, she offers, I can tell you are the best doctors I've had. Finally, I have someone who understands. Later, the pain team receives numerous pages that the patient is demanding to see them. The following day she is furious at the team for not keeping your promises. Nursing complains about her unwillingness to cooperate with dressing changes, insisting she only work with certain people, Because they understand me. | Ms. B is frequently insulting staff in a demanding and at times threatening manner. |
Reinforce desired behaviors and move past negative ones: Interact in a neutral manner to avoid reinforcing the disruptive behavior. If she becomes threatening or insulting, label the behavior and give her 1 opportunity to stop. Cursing upsets me. It's hard for me to help someone when they're cursing at me. This wording separates the behavior from the person. If she is able to calm herself, thank her (to reinforce this behavior) and offer to help. If she continues to escalate, you can say, You seem to be upset. I'll come back when it is a better time. Withdrawal of social contact can be a powerful tool. Return after a brief period to see if she has been able to calm down and, if so, re‐engage. Re‐engagement is key to reinforce calm, socially acceptable behavior. Check the team's emotions: Recognize patients with challenging behaviors can place a strong emotional toll on the team, particularly nursing staff who must frequently interact with these patients. Offer support to all members of the team to ensure appropriate patient care. |
| Ms. B is crying inconsolably, saying, I just can't stand being in the hospital anymore. They won't give me the pain meds I need. |
Offer validation and reinforce desired behaviors and move past negative ones: Offer empathy but then move to skill building. I can see you are upset. Is there anything that helps you when you are feeling this way? If the patient is unable to come up with anything feasible, offer her choices, such as walking with her around the unit or listening to music. |
|
| Cluster C: Mr. C is a 57‐year‐old man admitted for hyperosmolar hyperglycemic state. His condition has now stabilized, but when the nutritionist attempts to meet with him, he says he has a migraine. Later, when the diabetes nurse comes to discuss his insulin regimen, he is too tired to learn anything. When she persists, he listens, but repeatedly says, I'm never going to be able to do this and is unwilling to participate further. He repeatedly uses his call button, asking for help to the bathroom, despite being ambulatory previously. He talks for extended periods with nursing staff, sharing his fears about his inability to care for himself and his concerns that this will happen again. | Mr. C is repeatedly pressing his nurse call button multiple times throughout the day for seemingly trivial requests. |
Establish parameters: Mr. C is seeking contact with others. Have nursing arrange a regular schedule for checking in on the patient, such as every hour between 10 to and 10 after the hour. These visits can be kept brief, but offer a structure for the patient and encourage him or her to bundle their requests. Caregivers may also consider having Mr. C sit by the nurse's station to increase social interaction. Keep the message consistent: Work to maintain increased social contact across nursing shifts. |
Check the Team's Emotions
Managing patients with personality disorders begins by recognizing that these individuals evoke strong responses from even the most seasoned professional.[10, 11, 24, 25] Reactions toward people with personality disorders can range from a need to care for and protect the patient to feelings of futility or contempt.[10] Referred to as countertransference, these unconscious emotional reactions are common, but can interfere with medical care.[26] Given the increased understanding of the importance of team cohesion in patient care,[27] part of treating an individual with a personality disorder involves recognizing and managing the responses elicited amongst all members of the team. The disparate feelings among team members, which may be driven by different patient behaviors with different people, can lead to a variety of responses including overinvolvement, withdrawal, or even aggression.[28] Recognizing and discussing these differing reactions can help maintain team cohesion and support appropriate patient care.
Offer Empathy and Validation
Patients with personality disorders were often raised in invalidating environments and their ongoing intense emotional reactions can lead to perpetuation of invalidating responses from their caregivers.[29] They are accustomed to eliciting a defensive response from others and can be deliberately provocative, as these intense emotional interactions are comfortable territory, keeping providers feeling off balance and under attack. Instead, offering an empathic response can de‐escalate situations and is associated with the lowest level of invoked anger in patients.[30] Empathy can take the form of validation by acknowledging a person's feelings, thoughts, and emotions as legitimate, even if others may not fully understand or agree with them. As extreme as a patient's response may seem, he or she is genuinely experiencing these feelings and beliefs. Validation includes listening nonjudgmentally, objectively naming emotions the patient is experiencing, and conveying that the patient's response makes sense within the context of the situation.[31] This can include acknowledging the patient's level of distress, saying things such as, I can see you are really frustrated or I am concerned that what I just said has been upsetting. Empathy is more than words; it is the ability to see a situation from someone else's point of view. An empathic approach acknowledges the patient's intense emotional response to the challenges of hospitalization without frustration and judgment. Maintaining an empathicor even simply neutralstance can avoid a power struggle and also improves the therapeutic alliance with the patient.[32]
Establish Parameters but Pick the Battles
Individuals with personality disorders have trouble perceiving social boundaries. Even trained mental health professionals find this difficult to navigate.[33] The provider's first response is often to establish rigid boundaries. However, rigid rules can lead to power struggles between patients and providers, with limits being perceived as punitive. Instead of a list of rules, the creation of boundaries requires a thoughtful, practical establishment of parameters for both the individual and staff.[34] This may include guidelines for frequent, predictable nursing checks on the patient so that attention is provided on a time‐contingent rather than behavior‐contingent basis. If the patient remains dysregulated after a brief attempt to problem solve a nonemergent issue, staff can walk away with the comment that they will return within a specified period of time when things are calmer. If the patient is able to engage in the problem‐solving process, this has the advantage of generating a plan both can agree with while supporting more effective skills in the patient. Rather than a list of stringent rules, consider what is truly necessary for patient safety and well‐being.
Keep the Message Consistent
Hospital care involves many moving parts; nursing staff, the primary team, support staff, and consultants all interact with the patient throughout the day, sometimes providing conflicting messages. Although the typical patient can tolerate this, those with personality disorders have trouble dealing with the inconsistency, and this can exacerbate other problems. Carefully consider potentially contentious issues, such dosing of pain medications and benzodiazepines, and ensure that the team offers a consistent plan.[34] Ideally, meet with the patient as a team, including nursing, to convey a unified message.
Reinforce Desired Behaviors and Move Past Maladaptive Ones
Often in the life of a person with a personality disorder, their interpersonal interactions are negative. These patients are accustomed to negotiating a chaotic world. When not acting out, the patient may receive less attention while nursing and physician attention is appropriately distributed to other patients. Inadvertently, this reinforces using provocative behavior to get attention. Instead, if the patient is not demanding attention, providers should take the opportunity to provide positive reinforcement for calm behavior. This can be done by establishing a routine menu of interactions with the patient that occur when they are not acting in a disruptive manner; this avoids engagement being contingent on negative behaviors.[4] For example, having a nonillness‐related conversation during a dressing change or offering the patient a snack after a positive (or neutral) interaction can reinforce desirable behaviors. In contrast, when patients exhibit disruptive or inappropriate behaviors, the caregiver should respond by removing what the patient seeks, usually engagement, with a neutral attitude to avoid reinforcing the behavior: You seem upset. I'll come back when you feel better. By not reinforcing maladaptive behaviors, caregivers can decrease or extinguish such behaviors over time.[29] If the situation is nonemergent, the caregiver should briefly acknowledge the patient's distress and then focus on possible solutions: I can see you are really upset right now. What helps you in these situations? This both validates the patient's emotional state and encourages him or her to engage in problem solving around his or her distress.[29] If the patient is unable to identify a coping strategy in the moment, suggesting possibilities, such as walking around the unit or listening to music, can help the patient move past their intense emotions while also encouraging skill building.
PHARMACOLOGICAL INTERVENTIONS
Although there are no Food and Drug Administrationapproved medications for treatment of personality disorders, there is limited evidence for use of pharmacological interventions to address particular features of these disorders, such as impulsivity, affective dysregulation, or cognitiveperceptual symptoms.[35] Antipsychotics can be helpful in treating cognitive disturbances such as paranoia and dissociation that some of these patients experience.[35] Antidepressants may have a relatively small effect on anxiety and anger.[35] Mood stabilizers are shown to have a positive impact on impulsivity, anger, anxiety, and depressed mood.[35] However, medication should be used with caution, as polypharmacy is a significant problem with these patients and may have limited utility. Up to 40% of patients with borderline personality disorder take 3 or more psychotropic medications, many of which can have significant side effects,[36] and 1 in 3 are prescribed benzodiazepines despite a lack of evidence and potential for abuse.[37] Thus, although medications may offer an opportunity to target specific symptoms, the focus of management for patients with personality disorders should be behavioral rather than pharmacological.
CONSIDER A CONSULT
Patients with personality disorders can be very difficult to treat, and it may be necessary to consult psychiatry. There are a number of situations in which a formal psychiatric consultation is indicated (Table 3). Patients with personality disorders, particularly cluster B, may present for treatment after harming themselves or others.[38] A psychiatric consultation can provide a formal risk assessment, help with behavior and medication management while the patient is hospitalized, and determine whether follow‐up psychiatric care is appropriate.[39] The psychiatry team can also offer a more complete diagnostic formulation, including screening for disorders that often co‐occur with personality disorders, such as depression and anxiety, and recommend treatment options.[39] In addition, if initial attempts at behavioral interventions are ineffectual, a psychiatric consult may be able to provide additional guidance in behavioral modifications.[40] This is especially appropriate if the patient's behaviors are interfering with medical care. A psychiatric consult can also provide additional support around issues of countertransference that can arise when managing patients with dysfunctional personality structures.[41, 42]
| Safety assessment in a patient who has threatened or engaged in self‐harming behavior or harm to others |
| Diagnostic clarification, particularly when there is concern for a co‐occurring psychiatric illness |
| Creation of a more complex behavioral plan |
| Facilitation of interdisciplinary discussion and problem‐solving around patients with challenging behaviors |
| Assistance with establishment of outpatient psychiatric care when appropriate |
As with all interventions, the psychiatric consult is not without its side effects. Regardless of personality structure, it is not uncommon for patients to be initially opposed to engaging with psychiatry.[43] Individuals with personality disorders can be particularly susceptible to a rupture of the therapeutic alliance,[44] and calling a psychiatric consult can affect the therapeutic relationship with the primary team, as the patient may feel that others are judging them and can also be part of a greater theme of help rejecting.[11] However, this rupture may be repaired as the patient comes to see the psychiatry team as an ally. Even for patients who refuse to engage with the consult‐liaison team, there may be a benefit to a consult, as the consultants can offer strategies to the primary team and help establish a plan of care to facilitate ongoing treatment of the patient's medical needs without direct contact with the patient. These situations illustrate that a psychiatric consult cannot be done in isolation and requires collaboration with the primary team, nurses, and other support staff for interventions to be effective.
CONCLUSIONS
In his now famous speech Dr. Francis W. Peabody gave to Harvard Medical School he noted that [T]he secret of the care of the patient is caring for the patient.[45] Patients with a dysfunctional personality structure can make this task difficult. They can appear to reject the very help we have to offer, divide the team, absorb great amounts of time, and evoke strong feelings of frustration and resentment. However, by understanding that the way in which they interact with the world is in part the product of biology and upbringing, we can better recognize how ill these individuals can be. Just as a patient with diabetes requires management of his blood glucose when admitted for pneumonia, those with personality disorders require management of their mental illness while their other medical conditions are addressed.
Although personality disorders can seem intractable, studies have shown that, like many chronic illnesses, the severity can wax and wane over time with remissions and relapses. Notably, rates of remission for borderline personality disorder at 10 years are comparable to those for major depressive disorder, bipolar disorder, and panic disorder, with lower rates of relapse even without specific treatment, suggesting they are not entirely intractable.[46] However, the stress of hospitalization can easily exacerbate the symptoms of a personality disorder. By providing an empathic approach that addresses the emotional responses of the team while also reinforcing positive behaviors of the patient, the hospital stay can be an opportunity for these individuals to get needed support and develop new skills while also having their physical needs addressed.
Disclosures: Nothing to report.
- , . The effects of trust in physician on self‐efficacy, adherence and diabetes outcomes. Soc Sci Med. 2009;68(6):1060–1068.
- , , , et al. The physician‐patient working alliance. Patient Educ Couns. 2007;66(1):29–36.
- Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, VA: American Psychiatric Association; 2013.
- , , . The borderline patient on the med‐surg unit. Am J Nursing. 1988;88(12):1644–1650.
- , , . “Difficult” patient? Or does he have a personality disorder? J Fam Pract. 2014;63(12):697–703.
- , , , et al. Prevalence, correlates, and disability of personality disorders in the United States: results from the national epidemiologic survey on alcohol and related conditions. J Clin Psychiatry. 2004;65(7):948–958.
- , , . Classification, assessment, prevalence, and effect of personality disorder. Lancet. 2015;385(9969):717–726.
- , , , , , . Life expectancy at birth and all‐cause mortality among people with personality disorder. J Psychosom Res. 2012;73(2):104–107.
- , , , . A systematic review of personality disorders and health outcomes. Can Psychol. 2015;56(2):168–190.
- , , , . Patient personality and therapist response: an empirical investigation. Am J Psychiatry. 2014;171(1):102–108.
- . Taking care of the hateful patient. N Engl J Med. 1978;298(16):883–887.
- , , . Personality disorder across the life course. Lancet. 2015;385(9969):727–734.
- , , , , . The heritability of cluster A personality disorders assessed by both personal interview and questionnaire. Psychol Med. 2007;37(5):655–665.
- , , , et al. The heritability of avoidant and dependent personality disorder assessed by personal interview and questionnaire. Acta Psychiatr Scand. 2012;126(6):448–457.
- , , , , , . The heritability of Cluster B personality disorders assessed both by personal interview and questionnaire. J Pers Disord. 2012;26(6):848–866.
- , , . Association between genetic polymorphisms in the serotonergic system and comorbid personality disorders among patients with first‐episode depression. J Pers Disord. 2014;28(3):365–378.
- , , , et al. Tryptophan‐hydroxylase 2 haplotype association with borderline personality disorder and aggression in a sample of patients with personality disorders and healthy controls. J Psychiatr Res. 2010;44(15):1075–1081.
- , , , et al. Monoamine oxidase A gene promoter methylation and transcriptional downregulation in an offender population with antisocial personality disorder. Br J Psychiatry. 2015;206(3):216–222.
- , , , et al. Regional cortical thinning may be a biological marker for borderline personality disorder. Acta Psychiatr Scand. 2014;130(3):193–204.
- , , . Empathy and social problem solving in alcohol dependence, mood disorders and selected personality disorders. Neurosci Biobehav Rev. 2013;37(3):448–470.
- , , , . Changes in low‐frequency fluctuations in patients with antisocial personality disorder revealed by resting‐state functional MRI. PLoS One. 2014;9(3):e89790.
- , . Prefrontal structural and functional brain imaging findings in antisocial, violent, and psychopathic individuals: a meta‐analysis. Psychiatry Res. 2009;174(2):81–88.
- , , . Treatment of personality disorder. Lancet. 2015;385(9969):735–743.
- . Management of the borderline patient on a medical or surgical ward: the psychiatric consultant's role. Int J Psychiatry Med. 1975;6(3):337–348.
- , , , et al. The attitudes of psychiatric hospital staff toward hospitalization and treatment of patients with borderline personality disorder. BMC Psychiatry. 2015;15:2.
- , , , . The hateful physician: the role of affect bias in the care of the psychiatric patient in the ED. Am J Emerg Med. 2014;32(5):483–485.
- , , , et al. Relationships within inpatient physician housestaff teams and their association with hospitalized patient outcomes. J Hosp Med. 2014;9(12):764–771.
- . Countertransference in the nurse‐patient relationship: a review of the literature. J Adv Nurs. 1998;28(2):391–397.
- , , , , . Mechanisms of change in dialectical behavior therapy: theoretical and empirical observations. J Clin Psychol. 2006;62(4):459–480.
- , , , . The relationship between nurses' limit‐setting styles and anger in psychiatric inpatients. Psychiatr Serv. 1995;46(6):609–613.
- , , , , , . Attachment disorganization and borderline patients' metacognitive responses to therapists' expressed understanding of their states of mind: a pilot study. Psychother Res. 2008;18(1):28–36.
- , , . Narcissistic personality disorder: diagnostic and clinical challenges. Am J Psychiatry. 2015;172(5):415–422.
- , . An evaluation of the difficulties and attitudes mental health professionals experience with people with personality disorders. J Psychiatr Ment Health Nurs. 2016;23(1):22–36.
- , . Nursing care of personality disorders in the medical surgery setting. Nurs Clin North Am. 1998;33(1):173–186.
- , , , , . Effectiveness of pharmacotherapy for severe personality disorders: meta‐analyses of randomized controlled trials. J Clin Psychiatry. 2010;71(1):14–25.
- , , , . Mental health service utilization by borderline personality disorder patients and Axis II comparison subjects followed prospectively for 6 years. J Clin Psychiatry. 2004;65(1):28–36.
- , , , , . The use of psychotropic medication in patients with emotionally unstable personality disorder under the care of UK mental health services. J Clin Psychiatry. 2015;76(4):e512–e518.
- , , , , . Prevalence and characteristics of cluster B personality disorder in a consultation‐liaison psychiatry practice. Int J Psychiatry Clin Pract. 2015;19(1):65–70.
- , , , et al. The Academy of Psychosomatic Medicine practice guidelines for psychiatric consultation in the general medical setting. The Academy of Psychosomatic Medicine. Psychosomatics. 1998;39(4):S8–S30.
- , , . Interventions in consultation/liaison psychiatry. Part I: Patterns of recommendations. Gen Hosp Psychiatry. 1990;12(4):213–220.
- , , . Psychodynamics in medically ill patients. Harv Rev Psychiatry. 2009;17(6):389–397.
- . Patient dynamics, staff burnout, and consultation‐liaison psychiatry. Physician Exec. 1991;17(5):37–40.
- , . Facilitating patient acceptance of a psychiatric referral. Arch Intern Med. 1985;145(1):73–75.
- . The therapeutic alliance in the treatment of personality disorders. J Psychiatr Pract. 2005;11(2):73–87.
- . Dr. Francis w. Peabody, we need you. Tex Heart Inst J. 2011;38(4):327–328; discussion 328–329.
- , , , et al. Ten‐year course of borderline personality disorder: psychopathology and function from the Collaborative Longitudinal Personality Disorders study. Arch Gen Psychiatry. 2011;68(8):827–837.
Much has been written about the importance of the doctor‐patient relationship, with a positive therapeutic alliance being associated with both improvement in patient healthcare outcomes and physician job satisfaction.[1, 2] However, some patients severely test their physician's ability to provide needed care. These patients can rankle even experienced clinicians, leaving them feeling frustrated and ineffectual while consuming disproportionate amounts of clinical time. Although these disruptive acts may feel volitional and purposeful to the clinicians attempting to provide care, they may stem from a dysfunctional personality structure. Personality disorders are pervasive patterns of maladaptive behaviors, thoughts, and emotions that often go unrecognized and can wreak havoc in the patient's interpersonal life.[3] These inflexible patterns of managing the world can be disruptive when an individual is admitted to the hospital, causing distress for both the patient who lacks the skills to deal with the expectations of the hospital environment and the treatment team who can feel ill equipped to manage such behaviors.[4, 5] Here, we discuss personality disorders, how they can manifest in the hospital setting, and interventions to assist both the individual and the team.
Although personality disorders come in a variety of forms, central to all is interpersonal disarray with difficulty forming and maintaining acceptable relationships with others. In the hospital setting, the patient needs to be able to relate to, and cooperate with, a myriad of different care providers all while under some degree of physical and emotional distress. This can be destabilizing even for those without personality issues. For those with personality disorders, it is nearly inevitable that conflict will arise. Although true prevalence rates can be difficult to ascertain due to diagnostic challenges, surveys have found 4% to 15% of the population are affected by at least 1 personality disorder.[6] The prevalence is thought to be even higher among those seeking healthcare services, with researchers suggesting that 1 in 4 primary care patients meet criteria for a personality disorder.[6, 7]
Having a personality disorder has implications for an individual's healthcare outcomes. Studies in the United Kingdom have shown that those with a personality disorder have a life expectancy nearly 2 decades shorter than the general population.[8] Although suicide and homicide account for part of this, they also have increased risk of a number of health issues, including obesity, metabolic syndrome, cardiovascular disease, and sleep disorders.[9] In addition to lifestyle factors such as drinking and drug use, it has been suggested that dysfunctional personality structures may interfere with the ability to access and utilize care, leading to higher morbidity and mortality.[7]
In addition to impacting their own life, individuals with personality disorders have a tendency to disrupt the environment around them. They often elicit strong emotional responses from others that can range from a desire to help and protect to frustration and a sense of loathing.[10] The presence of a personality disorder often comes to light in the hospital when the patient is feeling vulnerable and acts out, evoking strong responses from team members. In the literature, patients with personality disorders are frequently referred to as a difficult or even hateful.[11] These individuals can be emotionally draining to care for, and the team must manage their own divergent responses in addition to the patient's disruptive behavior. Understanding personality disorders as a mental illness and using behavioral interventions can help to ease these interactions.
PERSONALITY DISORDERS: AN OVERVIEW
Personality disorders are characterized by persistent patterns of emotional reactivity, interpersonal interactions, and ways of perceiving the world that are inflexible and maladaptive and lead to significant distress and dysfunction.[3, 7] These disorders are notable for the interactive nature of the diagnosis; rather than being completely dependent on the individual's symptoms, a significant component of identification depends on how these individuals relate to others.[7] Although the trajectory can change over time, personality disorders are generally pervasive across the lifetime of an individual, beginning in adolescence or early adulthood.[7, 12] Personality disorders are divided into 3 clusters (Table 1).
| Personality Disorders | Features | Possible Manifestations in the Hospital |
|---|---|---|
| Cluster A | Odd and eccentric, socially avoidant |
Mistrust of medical staff and treatments offered Hostility toward treatment team Accusations of exploitation and harm without reasonable evidence General sense from the team that something is off |
| Paranoid | Highly suspicious of others; interpret malice where none was intended | |
| Schizoid | Minimal social relationships; limited emotional range | |
| Schizotypal | Eccentric behavior and magical thinking; uncomfortable with close relationships | |
| Cluster B | Emotionally labile and impulsive |
Splitting of the team, clear favorite providers and hated providers Extremes of emotion with responses out of proportion to the situation Rapid escalation when they perceive their needs not being met Evoke a strong emotional response from the team, taking up time out of proportion to their medical illness Help‐rejecting behavior Fear of abandonment manifesting as escalation of behavior around discharge |
| Antisocial | Frequent disregard for rights of others | |
| Borderline | Impulsive with volatile interpersonal relationships | |
| Histrionic | Disproportionate emotionality with engagement seeking | |
| Narcissistic | Grandiose, seeks admiration | |
| Cluster C | Anxious and neurotic |
Resistance to participating in their own care Frequent demands on the staff Particular, sometimes seemingly illogical, preferences regarding their care or other aspects of their stay |
| Avoidant | Socially fearful with feelings of inadequacy | |
| Dependent | Need to be taken care of, often manifesting as clinging and obsequious behavior | |
| Obsessive‐compulsive | Preoccupied by orderliness and control, but without actual obsessions or compulsions |
Cluster A
Those falling into cluster A, which includes paranoid, schizoid, and schizotypal personality disorders, are odd and eccentric and often avoid social engagement[3]; these individuals have few friends or associates and do not care to make more. At times, their unusual thinking can be difficult to differentiate from primary psychotic disorders like schizophrenia.
Cluster B
Cluster B is most heavily studied, consisting of antisocial, borderline, histrionic, and narcissistic personality disorders. These individuals share a high degree of emotional lability and erratic behavior.[3] Frequently, their tendency toward impulsive and self‐destructive behaviors can result in the need for medical care.
Cluster C
Cluster C includes avoidant, dependent, and obsessive‐compulsive personality disorders. These individuals are often anxious and fearful. Like individuals in Cluster A, they have few friends; unlike Cluster A, they long for friendships but struggle to make them. On the inpatient unit, these individuals may have trouble engaging in needed care, relying heavily on others to have their needs met or may be very particular about how their care is administered.
NEUROPHYSIOLOGY
Personality disorders are the product of complex interactions between genes and environment. These disorders are highly heritable, with 55% to 72% heritability across the 3 clusters.[13, 14, 15] Studies have implicated alterations in the serotonin system as playing a role in the underlying pathophysiology, which may contribute to the emotional dysregulation.[16, 17, 18] Neuroimaging has shown alterations in regions of the brain related to emotional reactivity and the processing of social interactions, suggesting neural mechanisms behind these individuals' difficulty with interpersonal relationships.[19, 20, 21, 22]
IDENTIFICATION OF PERSONALITY DISORDERS
These disorders are under‐recognized due, at least in part, to difficulty in making the diagnosis.[7] With 10 different personality disorders, many with overlapping characteristics, establishing a specific diagnosis can be time consuming, and a single individual may fit multiple different personality disorders.[7] Although self‐report surveys and structured interviews exist, these are often time consuming or inaccurate.[7] It is unlikely to be practical to make a diagnosis of a specific personality disorder while in the hospital. Instead, the focus should be placed on identifying impaired personality structures that interfere with interpersonal relationships and thereby disrupt the course of treatment. Consider a personality disorder if any of the following features are present:
- The patient elicits a strong emotional reaction from providers; these may vary markedly between providers.
- The patient's emotional responses may appear disproportionate to the inciting event.
- The patient is on a number of different psychiatric medications with little relief of symptoms.
- The patient takes up a disproportionate amount of the providers' time.
- The patient externalizes blame, seeing others as the source of discomfort or distress and therefore sees others as the solution.
Once identified, steps can be taken to help both the team and the patient.
BEHAVIORAL INTERVENTIONS
The first line of intervention for individuals with dysfunctional personality structures is behavioral, changing the way the team and patient interact (Table 2). Such interventions have long been the cornerstone of treatment for these individuals.[23] The preponderance of the research has focused on cluster B, and specifically individuals with borderline personality disorder, and applying these principles more broadly is largely based on expert opinion.
| Clinical Examples and Behavioral Interventions | ||
|---|---|---|
| Background | Situation | Response |
| Cluster A: Mr. A is a 75‐year‐old man transferred from his small town after a myocardial infarction. Although he has improved medically, he repeatedly expresses distrust and dissatisfaction with his doctors. He refuses to go to a skilled nursing facility but will not work with physical therapy to discharge home. He lives alone and has worked as a cattle rancher all his life. | Mr. A repeatedly accuses his team of being in this for the money. At times he mutters about government conspiracies. |
Check the team's emotions and reinforce desired behaviors and move past negative ones: Recognize paranoia as part of the illness. Rather than confront the paranoia, ignore this behavior as long as it is not directly interfering with care. |
| Cluster B: Ms. B is a 22‐year‐old woman admitted after a car accident resulting in multiple fractures. The pain service is consulted due to her ever‐increasing need for opiates. When the team first meets her, she is bright, effusing, Thank you for coming! My other doctors have no idea how to control my pain. She starts crying, I just can't do this anymore. Midway through the conversation, she offers, I can tell you are the best doctors I've had. Finally, I have someone who understands. Later, the pain team receives numerous pages that the patient is demanding to see them. The following day she is furious at the team for not keeping your promises. Nursing complains about her unwillingness to cooperate with dressing changes, insisting she only work with certain people, Because they understand me. | Ms. B is frequently insulting staff in a demanding and at times threatening manner. |
Reinforce desired behaviors and move past negative ones: Interact in a neutral manner to avoid reinforcing the disruptive behavior. If she becomes threatening or insulting, label the behavior and give her 1 opportunity to stop. Cursing upsets me. It's hard for me to help someone when they're cursing at me. This wording separates the behavior from the person. If she is able to calm herself, thank her (to reinforce this behavior) and offer to help. If she continues to escalate, you can say, You seem to be upset. I'll come back when it is a better time. Withdrawal of social contact can be a powerful tool. Return after a brief period to see if she has been able to calm down and, if so, re‐engage. Re‐engagement is key to reinforce calm, socially acceptable behavior. Check the team's emotions: Recognize patients with challenging behaviors can place a strong emotional toll on the team, particularly nursing staff who must frequently interact with these patients. Offer support to all members of the team to ensure appropriate patient care. |
| Ms. B is crying inconsolably, saying, I just can't stand being in the hospital anymore. They won't give me the pain meds I need. |
Offer validation and reinforce desired behaviors and move past negative ones: Offer empathy but then move to skill building. I can see you are upset. Is there anything that helps you when you are feeling this way? If the patient is unable to come up with anything feasible, offer her choices, such as walking with her around the unit or listening to music. |
|
| Cluster C: Mr. C is a 57‐year‐old man admitted for hyperosmolar hyperglycemic state. His condition has now stabilized, but when the nutritionist attempts to meet with him, he says he has a migraine. Later, when the diabetes nurse comes to discuss his insulin regimen, he is too tired to learn anything. When she persists, he listens, but repeatedly says, I'm never going to be able to do this and is unwilling to participate further. He repeatedly uses his call button, asking for help to the bathroom, despite being ambulatory previously. He talks for extended periods with nursing staff, sharing his fears about his inability to care for himself and his concerns that this will happen again. | Mr. C is repeatedly pressing his nurse call button multiple times throughout the day for seemingly trivial requests. |
Establish parameters: Mr. C is seeking contact with others. Have nursing arrange a regular schedule for checking in on the patient, such as every hour between 10 to and 10 after the hour. These visits can be kept brief, but offer a structure for the patient and encourage him or her to bundle their requests. Caregivers may also consider having Mr. C sit by the nurse's station to increase social interaction. Keep the message consistent: Work to maintain increased social contact across nursing shifts. |
Check the Team's Emotions
Managing patients with personality disorders begins by recognizing that these individuals evoke strong responses from even the most seasoned professional.[10, 11, 24, 25] Reactions toward people with personality disorders can range from a need to care for and protect the patient to feelings of futility or contempt.[10] Referred to as countertransference, these unconscious emotional reactions are common, but can interfere with medical care.[26] Given the increased understanding of the importance of team cohesion in patient care,[27] part of treating an individual with a personality disorder involves recognizing and managing the responses elicited amongst all members of the team. The disparate feelings among team members, which may be driven by different patient behaviors with different people, can lead to a variety of responses including overinvolvement, withdrawal, or even aggression.[28] Recognizing and discussing these differing reactions can help maintain team cohesion and support appropriate patient care.
Offer Empathy and Validation
Patients with personality disorders were often raised in invalidating environments and their ongoing intense emotional reactions can lead to perpetuation of invalidating responses from their caregivers.[29] They are accustomed to eliciting a defensive response from others and can be deliberately provocative, as these intense emotional interactions are comfortable territory, keeping providers feeling off balance and under attack. Instead, offering an empathic response can de‐escalate situations and is associated with the lowest level of invoked anger in patients.[30] Empathy can take the form of validation by acknowledging a person's feelings, thoughts, and emotions as legitimate, even if others may not fully understand or agree with them. As extreme as a patient's response may seem, he or she is genuinely experiencing these feelings and beliefs. Validation includes listening nonjudgmentally, objectively naming emotions the patient is experiencing, and conveying that the patient's response makes sense within the context of the situation.[31] This can include acknowledging the patient's level of distress, saying things such as, I can see you are really frustrated or I am concerned that what I just said has been upsetting. Empathy is more than words; it is the ability to see a situation from someone else's point of view. An empathic approach acknowledges the patient's intense emotional response to the challenges of hospitalization without frustration and judgment. Maintaining an empathicor even simply neutralstance can avoid a power struggle and also improves the therapeutic alliance with the patient.[32]
Establish Parameters but Pick the Battles
Individuals with personality disorders have trouble perceiving social boundaries. Even trained mental health professionals find this difficult to navigate.[33] The provider's first response is often to establish rigid boundaries. However, rigid rules can lead to power struggles between patients and providers, with limits being perceived as punitive. Instead of a list of rules, the creation of boundaries requires a thoughtful, practical establishment of parameters for both the individual and staff.[34] This may include guidelines for frequent, predictable nursing checks on the patient so that attention is provided on a time‐contingent rather than behavior‐contingent basis. If the patient remains dysregulated after a brief attempt to problem solve a nonemergent issue, staff can walk away with the comment that they will return within a specified period of time when things are calmer. If the patient is able to engage in the problem‐solving process, this has the advantage of generating a plan both can agree with while supporting more effective skills in the patient. Rather than a list of stringent rules, consider what is truly necessary for patient safety and well‐being.
Keep the Message Consistent
Hospital care involves many moving parts; nursing staff, the primary team, support staff, and consultants all interact with the patient throughout the day, sometimes providing conflicting messages. Although the typical patient can tolerate this, those with personality disorders have trouble dealing with the inconsistency, and this can exacerbate other problems. Carefully consider potentially contentious issues, such dosing of pain medications and benzodiazepines, and ensure that the team offers a consistent plan.[34] Ideally, meet with the patient as a team, including nursing, to convey a unified message.
Reinforce Desired Behaviors and Move Past Maladaptive Ones
Often in the life of a person with a personality disorder, their interpersonal interactions are negative. These patients are accustomed to negotiating a chaotic world. When not acting out, the patient may receive less attention while nursing and physician attention is appropriately distributed to other patients. Inadvertently, this reinforces using provocative behavior to get attention. Instead, if the patient is not demanding attention, providers should take the opportunity to provide positive reinforcement for calm behavior. This can be done by establishing a routine menu of interactions with the patient that occur when they are not acting in a disruptive manner; this avoids engagement being contingent on negative behaviors.[4] For example, having a nonillness‐related conversation during a dressing change or offering the patient a snack after a positive (or neutral) interaction can reinforce desirable behaviors. In contrast, when patients exhibit disruptive or inappropriate behaviors, the caregiver should respond by removing what the patient seeks, usually engagement, with a neutral attitude to avoid reinforcing the behavior: You seem upset. I'll come back when you feel better. By not reinforcing maladaptive behaviors, caregivers can decrease or extinguish such behaviors over time.[29] If the situation is nonemergent, the caregiver should briefly acknowledge the patient's distress and then focus on possible solutions: I can see you are really upset right now. What helps you in these situations? This both validates the patient's emotional state and encourages him or her to engage in problem solving around his or her distress.[29] If the patient is unable to identify a coping strategy in the moment, suggesting possibilities, such as walking around the unit or listening to music, can help the patient move past their intense emotions while also encouraging skill building.
PHARMACOLOGICAL INTERVENTIONS
Although there are no Food and Drug Administrationapproved medications for treatment of personality disorders, there is limited evidence for use of pharmacological interventions to address particular features of these disorders, such as impulsivity, affective dysregulation, or cognitiveperceptual symptoms.[35] Antipsychotics can be helpful in treating cognitive disturbances such as paranoia and dissociation that some of these patients experience.[35] Antidepressants may have a relatively small effect on anxiety and anger.[35] Mood stabilizers are shown to have a positive impact on impulsivity, anger, anxiety, and depressed mood.[35] However, medication should be used with caution, as polypharmacy is a significant problem with these patients and may have limited utility. Up to 40% of patients with borderline personality disorder take 3 or more psychotropic medications, many of which can have significant side effects,[36] and 1 in 3 are prescribed benzodiazepines despite a lack of evidence and potential for abuse.[37] Thus, although medications may offer an opportunity to target specific symptoms, the focus of management for patients with personality disorders should be behavioral rather than pharmacological.
CONSIDER A CONSULT
Patients with personality disorders can be very difficult to treat, and it may be necessary to consult psychiatry. There are a number of situations in which a formal psychiatric consultation is indicated (Table 3). Patients with personality disorders, particularly cluster B, may present for treatment after harming themselves or others.[38] A psychiatric consultation can provide a formal risk assessment, help with behavior and medication management while the patient is hospitalized, and determine whether follow‐up psychiatric care is appropriate.[39] The psychiatry team can also offer a more complete diagnostic formulation, including screening for disorders that often co‐occur with personality disorders, such as depression and anxiety, and recommend treatment options.[39] In addition, if initial attempts at behavioral interventions are ineffectual, a psychiatric consult may be able to provide additional guidance in behavioral modifications.[40] This is especially appropriate if the patient's behaviors are interfering with medical care. A psychiatric consult can also provide additional support around issues of countertransference that can arise when managing patients with dysfunctional personality structures.[41, 42]
| Safety assessment in a patient who has threatened or engaged in self‐harming behavior or harm to others |
| Diagnostic clarification, particularly when there is concern for a co‐occurring psychiatric illness |
| Creation of a more complex behavioral plan |
| Facilitation of interdisciplinary discussion and problem‐solving around patients with challenging behaviors |
| Assistance with establishment of outpatient psychiatric care when appropriate |
As with all interventions, the psychiatric consult is not without its side effects. Regardless of personality structure, it is not uncommon for patients to be initially opposed to engaging with psychiatry.[43] Individuals with personality disorders can be particularly susceptible to a rupture of the therapeutic alliance,[44] and calling a psychiatric consult can affect the therapeutic relationship with the primary team, as the patient may feel that others are judging them and can also be part of a greater theme of help rejecting.[11] However, this rupture may be repaired as the patient comes to see the psychiatry team as an ally. Even for patients who refuse to engage with the consult‐liaison team, there may be a benefit to a consult, as the consultants can offer strategies to the primary team and help establish a plan of care to facilitate ongoing treatment of the patient's medical needs without direct contact with the patient. These situations illustrate that a psychiatric consult cannot be done in isolation and requires collaboration with the primary team, nurses, and other support staff for interventions to be effective.
CONCLUSIONS
In his now famous speech Dr. Francis W. Peabody gave to Harvard Medical School he noted that [T]he secret of the care of the patient is caring for the patient.[45] Patients with a dysfunctional personality structure can make this task difficult. They can appear to reject the very help we have to offer, divide the team, absorb great amounts of time, and evoke strong feelings of frustration and resentment. However, by understanding that the way in which they interact with the world is in part the product of biology and upbringing, we can better recognize how ill these individuals can be. Just as a patient with diabetes requires management of his blood glucose when admitted for pneumonia, those with personality disorders require management of their mental illness while their other medical conditions are addressed.
Although personality disorders can seem intractable, studies have shown that, like many chronic illnesses, the severity can wax and wane over time with remissions and relapses. Notably, rates of remission for borderline personality disorder at 10 years are comparable to those for major depressive disorder, bipolar disorder, and panic disorder, with lower rates of relapse even without specific treatment, suggesting they are not entirely intractable.[46] However, the stress of hospitalization can easily exacerbate the symptoms of a personality disorder. By providing an empathic approach that addresses the emotional responses of the team while also reinforcing positive behaviors of the patient, the hospital stay can be an opportunity for these individuals to get needed support and develop new skills while also having their physical needs addressed.
Disclosures: Nothing to report.
Much has been written about the importance of the doctor‐patient relationship, with a positive therapeutic alliance being associated with both improvement in patient healthcare outcomes and physician job satisfaction.[1, 2] However, some patients severely test their physician's ability to provide needed care. These patients can rankle even experienced clinicians, leaving them feeling frustrated and ineffectual while consuming disproportionate amounts of clinical time. Although these disruptive acts may feel volitional and purposeful to the clinicians attempting to provide care, they may stem from a dysfunctional personality structure. Personality disorders are pervasive patterns of maladaptive behaviors, thoughts, and emotions that often go unrecognized and can wreak havoc in the patient's interpersonal life.[3] These inflexible patterns of managing the world can be disruptive when an individual is admitted to the hospital, causing distress for both the patient who lacks the skills to deal with the expectations of the hospital environment and the treatment team who can feel ill equipped to manage such behaviors.[4, 5] Here, we discuss personality disorders, how they can manifest in the hospital setting, and interventions to assist both the individual and the team.
Although personality disorders come in a variety of forms, central to all is interpersonal disarray with difficulty forming and maintaining acceptable relationships with others. In the hospital setting, the patient needs to be able to relate to, and cooperate with, a myriad of different care providers all while under some degree of physical and emotional distress. This can be destabilizing even for those without personality issues. For those with personality disorders, it is nearly inevitable that conflict will arise. Although true prevalence rates can be difficult to ascertain due to diagnostic challenges, surveys have found 4% to 15% of the population are affected by at least 1 personality disorder.[6] The prevalence is thought to be even higher among those seeking healthcare services, with researchers suggesting that 1 in 4 primary care patients meet criteria for a personality disorder.[6, 7]
Having a personality disorder has implications for an individual's healthcare outcomes. Studies in the United Kingdom have shown that those with a personality disorder have a life expectancy nearly 2 decades shorter than the general population.[8] Although suicide and homicide account for part of this, they also have increased risk of a number of health issues, including obesity, metabolic syndrome, cardiovascular disease, and sleep disorders.[9] In addition to lifestyle factors such as drinking and drug use, it has been suggested that dysfunctional personality structures may interfere with the ability to access and utilize care, leading to higher morbidity and mortality.[7]
In addition to impacting their own life, individuals with personality disorders have a tendency to disrupt the environment around them. They often elicit strong emotional responses from others that can range from a desire to help and protect to frustration and a sense of loathing.[10] The presence of a personality disorder often comes to light in the hospital when the patient is feeling vulnerable and acts out, evoking strong responses from team members. In the literature, patients with personality disorders are frequently referred to as a difficult or even hateful.[11] These individuals can be emotionally draining to care for, and the team must manage their own divergent responses in addition to the patient's disruptive behavior. Understanding personality disorders as a mental illness and using behavioral interventions can help to ease these interactions.
PERSONALITY DISORDERS: AN OVERVIEW
Personality disorders are characterized by persistent patterns of emotional reactivity, interpersonal interactions, and ways of perceiving the world that are inflexible and maladaptive and lead to significant distress and dysfunction.[3, 7] These disorders are notable for the interactive nature of the diagnosis; rather than being completely dependent on the individual's symptoms, a significant component of identification depends on how these individuals relate to others.[7] Although the trajectory can change over time, personality disorders are generally pervasive across the lifetime of an individual, beginning in adolescence or early adulthood.[7, 12] Personality disorders are divided into 3 clusters (Table 1).
| Personality Disorders | Features | Possible Manifestations in the Hospital |
|---|---|---|
| Cluster A | Odd and eccentric, socially avoidant |
Mistrust of medical staff and treatments offered Hostility toward treatment team Accusations of exploitation and harm without reasonable evidence General sense from the team that something is off |
| Paranoid | Highly suspicious of others; interpret malice where none was intended | |
| Schizoid | Minimal social relationships; limited emotional range | |
| Schizotypal | Eccentric behavior and magical thinking; uncomfortable with close relationships | |
| Cluster B | Emotionally labile and impulsive |
Splitting of the team, clear favorite providers and hated providers Extremes of emotion with responses out of proportion to the situation Rapid escalation when they perceive their needs not being met Evoke a strong emotional response from the team, taking up time out of proportion to their medical illness Help‐rejecting behavior Fear of abandonment manifesting as escalation of behavior around discharge |
| Antisocial | Frequent disregard for rights of others | |
| Borderline | Impulsive with volatile interpersonal relationships | |
| Histrionic | Disproportionate emotionality with engagement seeking | |
| Narcissistic | Grandiose, seeks admiration | |
| Cluster C | Anxious and neurotic |
Resistance to participating in their own care Frequent demands on the staff Particular, sometimes seemingly illogical, preferences regarding their care or other aspects of their stay |
| Avoidant | Socially fearful with feelings of inadequacy | |
| Dependent | Need to be taken care of, often manifesting as clinging and obsequious behavior | |
| Obsessive‐compulsive | Preoccupied by orderliness and control, but without actual obsessions or compulsions |
Cluster A
Those falling into cluster A, which includes paranoid, schizoid, and schizotypal personality disorders, are odd and eccentric and often avoid social engagement[3]; these individuals have few friends or associates and do not care to make more. At times, their unusual thinking can be difficult to differentiate from primary psychotic disorders like schizophrenia.
Cluster B
Cluster B is most heavily studied, consisting of antisocial, borderline, histrionic, and narcissistic personality disorders. These individuals share a high degree of emotional lability and erratic behavior.[3] Frequently, their tendency toward impulsive and self‐destructive behaviors can result in the need for medical care.
Cluster C
Cluster C includes avoidant, dependent, and obsessive‐compulsive personality disorders. These individuals are often anxious and fearful. Like individuals in Cluster A, they have few friends; unlike Cluster A, they long for friendships but struggle to make them. On the inpatient unit, these individuals may have trouble engaging in needed care, relying heavily on others to have their needs met or may be very particular about how their care is administered.
NEUROPHYSIOLOGY
Personality disorders are the product of complex interactions between genes and environment. These disorders are highly heritable, with 55% to 72% heritability across the 3 clusters.[13, 14, 15] Studies have implicated alterations in the serotonin system as playing a role in the underlying pathophysiology, which may contribute to the emotional dysregulation.[16, 17, 18] Neuroimaging has shown alterations in regions of the brain related to emotional reactivity and the processing of social interactions, suggesting neural mechanisms behind these individuals' difficulty with interpersonal relationships.[19, 20, 21, 22]
IDENTIFICATION OF PERSONALITY DISORDERS
These disorders are under‐recognized due, at least in part, to difficulty in making the diagnosis.[7] With 10 different personality disorders, many with overlapping characteristics, establishing a specific diagnosis can be time consuming, and a single individual may fit multiple different personality disorders.[7] Although self‐report surveys and structured interviews exist, these are often time consuming or inaccurate.[7] It is unlikely to be practical to make a diagnosis of a specific personality disorder while in the hospital. Instead, the focus should be placed on identifying impaired personality structures that interfere with interpersonal relationships and thereby disrupt the course of treatment. Consider a personality disorder if any of the following features are present:
- The patient elicits a strong emotional reaction from providers; these may vary markedly between providers.
- The patient's emotional responses may appear disproportionate to the inciting event.
- The patient is on a number of different psychiatric medications with little relief of symptoms.
- The patient takes up a disproportionate amount of the providers' time.
- The patient externalizes blame, seeing others as the source of discomfort or distress and therefore sees others as the solution.
Once identified, steps can be taken to help both the team and the patient.
BEHAVIORAL INTERVENTIONS
The first line of intervention for individuals with dysfunctional personality structures is behavioral, changing the way the team and patient interact (Table 2). Such interventions have long been the cornerstone of treatment for these individuals.[23] The preponderance of the research has focused on cluster B, and specifically individuals with borderline personality disorder, and applying these principles more broadly is largely based on expert opinion.
| Clinical Examples and Behavioral Interventions | ||
|---|---|---|
| Background | Situation | Response |
| Cluster A: Mr. A is a 75‐year‐old man transferred from his small town after a myocardial infarction. Although he has improved medically, he repeatedly expresses distrust and dissatisfaction with his doctors. He refuses to go to a skilled nursing facility but will not work with physical therapy to discharge home. He lives alone and has worked as a cattle rancher all his life. | Mr. A repeatedly accuses his team of being in this for the money. At times he mutters about government conspiracies. |
Check the team's emotions and reinforce desired behaviors and move past negative ones: Recognize paranoia as part of the illness. Rather than confront the paranoia, ignore this behavior as long as it is not directly interfering with care. |
| Cluster B: Ms. B is a 22‐year‐old woman admitted after a car accident resulting in multiple fractures. The pain service is consulted due to her ever‐increasing need for opiates. When the team first meets her, she is bright, effusing, Thank you for coming! My other doctors have no idea how to control my pain. She starts crying, I just can't do this anymore. Midway through the conversation, she offers, I can tell you are the best doctors I've had. Finally, I have someone who understands. Later, the pain team receives numerous pages that the patient is demanding to see them. The following day she is furious at the team for not keeping your promises. Nursing complains about her unwillingness to cooperate with dressing changes, insisting she only work with certain people, Because they understand me. | Ms. B is frequently insulting staff in a demanding and at times threatening manner. |
Reinforce desired behaviors and move past negative ones: Interact in a neutral manner to avoid reinforcing the disruptive behavior. If she becomes threatening or insulting, label the behavior and give her 1 opportunity to stop. Cursing upsets me. It's hard for me to help someone when they're cursing at me. This wording separates the behavior from the person. If she is able to calm herself, thank her (to reinforce this behavior) and offer to help. If she continues to escalate, you can say, You seem to be upset. I'll come back when it is a better time. Withdrawal of social contact can be a powerful tool. Return after a brief period to see if she has been able to calm down and, if so, re‐engage. Re‐engagement is key to reinforce calm, socially acceptable behavior. Check the team's emotions: Recognize patients with challenging behaviors can place a strong emotional toll on the team, particularly nursing staff who must frequently interact with these patients. Offer support to all members of the team to ensure appropriate patient care. |
| Ms. B is crying inconsolably, saying, I just can't stand being in the hospital anymore. They won't give me the pain meds I need. |
Offer validation and reinforce desired behaviors and move past negative ones: Offer empathy but then move to skill building. I can see you are upset. Is there anything that helps you when you are feeling this way? If the patient is unable to come up with anything feasible, offer her choices, such as walking with her around the unit or listening to music. |
|
| Cluster C: Mr. C is a 57‐year‐old man admitted for hyperosmolar hyperglycemic state. His condition has now stabilized, but when the nutritionist attempts to meet with him, he says he has a migraine. Later, when the diabetes nurse comes to discuss his insulin regimen, he is too tired to learn anything. When she persists, he listens, but repeatedly says, I'm never going to be able to do this and is unwilling to participate further. He repeatedly uses his call button, asking for help to the bathroom, despite being ambulatory previously. He talks for extended periods with nursing staff, sharing his fears about his inability to care for himself and his concerns that this will happen again. | Mr. C is repeatedly pressing his nurse call button multiple times throughout the day for seemingly trivial requests. |
Establish parameters: Mr. C is seeking contact with others. Have nursing arrange a regular schedule for checking in on the patient, such as every hour between 10 to and 10 after the hour. These visits can be kept brief, but offer a structure for the patient and encourage him or her to bundle their requests. Caregivers may also consider having Mr. C sit by the nurse's station to increase social interaction. Keep the message consistent: Work to maintain increased social contact across nursing shifts. |
Check the Team's Emotions
Managing patients with personality disorders begins by recognizing that these individuals evoke strong responses from even the most seasoned professional.[10, 11, 24, 25] Reactions toward people with personality disorders can range from a need to care for and protect the patient to feelings of futility or contempt.[10] Referred to as countertransference, these unconscious emotional reactions are common, but can interfere with medical care.[26] Given the increased understanding of the importance of team cohesion in patient care,[27] part of treating an individual with a personality disorder involves recognizing and managing the responses elicited amongst all members of the team. The disparate feelings among team members, which may be driven by different patient behaviors with different people, can lead to a variety of responses including overinvolvement, withdrawal, or even aggression.[28] Recognizing and discussing these differing reactions can help maintain team cohesion and support appropriate patient care.
Offer Empathy and Validation
Patients with personality disorders were often raised in invalidating environments and their ongoing intense emotional reactions can lead to perpetuation of invalidating responses from their caregivers.[29] They are accustomed to eliciting a defensive response from others and can be deliberately provocative, as these intense emotional interactions are comfortable territory, keeping providers feeling off balance and under attack. Instead, offering an empathic response can de‐escalate situations and is associated with the lowest level of invoked anger in patients.[30] Empathy can take the form of validation by acknowledging a person's feelings, thoughts, and emotions as legitimate, even if others may not fully understand or agree with them. As extreme as a patient's response may seem, he or she is genuinely experiencing these feelings and beliefs. Validation includes listening nonjudgmentally, objectively naming emotions the patient is experiencing, and conveying that the patient's response makes sense within the context of the situation.[31] This can include acknowledging the patient's level of distress, saying things such as, I can see you are really frustrated or I am concerned that what I just said has been upsetting. Empathy is more than words; it is the ability to see a situation from someone else's point of view. An empathic approach acknowledges the patient's intense emotional response to the challenges of hospitalization without frustration and judgment. Maintaining an empathicor even simply neutralstance can avoid a power struggle and also improves the therapeutic alliance with the patient.[32]
Establish Parameters but Pick the Battles
Individuals with personality disorders have trouble perceiving social boundaries. Even trained mental health professionals find this difficult to navigate.[33] The provider's first response is often to establish rigid boundaries. However, rigid rules can lead to power struggles between patients and providers, with limits being perceived as punitive. Instead of a list of rules, the creation of boundaries requires a thoughtful, practical establishment of parameters for both the individual and staff.[34] This may include guidelines for frequent, predictable nursing checks on the patient so that attention is provided on a time‐contingent rather than behavior‐contingent basis. If the patient remains dysregulated after a brief attempt to problem solve a nonemergent issue, staff can walk away with the comment that they will return within a specified period of time when things are calmer. If the patient is able to engage in the problem‐solving process, this has the advantage of generating a plan both can agree with while supporting more effective skills in the patient. Rather than a list of stringent rules, consider what is truly necessary for patient safety and well‐being.
Keep the Message Consistent
Hospital care involves many moving parts; nursing staff, the primary team, support staff, and consultants all interact with the patient throughout the day, sometimes providing conflicting messages. Although the typical patient can tolerate this, those with personality disorders have trouble dealing with the inconsistency, and this can exacerbate other problems. Carefully consider potentially contentious issues, such dosing of pain medications and benzodiazepines, and ensure that the team offers a consistent plan.[34] Ideally, meet with the patient as a team, including nursing, to convey a unified message.
Reinforce Desired Behaviors and Move Past Maladaptive Ones
Often in the life of a person with a personality disorder, their interpersonal interactions are negative. These patients are accustomed to negotiating a chaotic world. When not acting out, the patient may receive less attention while nursing and physician attention is appropriately distributed to other patients. Inadvertently, this reinforces using provocative behavior to get attention. Instead, if the patient is not demanding attention, providers should take the opportunity to provide positive reinforcement for calm behavior. This can be done by establishing a routine menu of interactions with the patient that occur when they are not acting in a disruptive manner; this avoids engagement being contingent on negative behaviors.[4] For example, having a nonillness‐related conversation during a dressing change or offering the patient a snack after a positive (or neutral) interaction can reinforce desirable behaviors. In contrast, when patients exhibit disruptive or inappropriate behaviors, the caregiver should respond by removing what the patient seeks, usually engagement, with a neutral attitude to avoid reinforcing the behavior: You seem upset. I'll come back when you feel better. By not reinforcing maladaptive behaviors, caregivers can decrease or extinguish such behaviors over time.[29] If the situation is nonemergent, the caregiver should briefly acknowledge the patient's distress and then focus on possible solutions: I can see you are really upset right now. What helps you in these situations? This both validates the patient's emotional state and encourages him or her to engage in problem solving around his or her distress.[29] If the patient is unable to identify a coping strategy in the moment, suggesting possibilities, such as walking around the unit or listening to music, can help the patient move past their intense emotions while also encouraging skill building.
PHARMACOLOGICAL INTERVENTIONS
Although there are no Food and Drug Administrationapproved medications for treatment of personality disorders, there is limited evidence for use of pharmacological interventions to address particular features of these disorders, such as impulsivity, affective dysregulation, or cognitiveperceptual symptoms.[35] Antipsychotics can be helpful in treating cognitive disturbances such as paranoia and dissociation that some of these patients experience.[35] Antidepressants may have a relatively small effect on anxiety and anger.[35] Mood stabilizers are shown to have a positive impact on impulsivity, anger, anxiety, and depressed mood.[35] However, medication should be used with caution, as polypharmacy is a significant problem with these patients and may have limited utility. Up to 40% of patients with borderline personality disorder take 3 or more psychotropic medications, many of which can have significant side effects,[36] and 1 in 3 are prescribed benzodiazepines despite a lack of evidence and potential for abuse.[37] Thus, although medications may offer an opportunity to target specific symptoms, the focus of management for patients with personality disorders should be behavioral rather than pharmacological.
CONSIDER A CONSULT
Patients with personality disorders can be very difficult to treat, and it may be necessary to consult psychiatry. There are a number of situations in which a formal psychiatric consultation is indicated (Table 3). Patients with personality disorders, particularly cluster B, may present for treatment after harming themselves or others.[38] A psychiatric consultation can provide a formal risk assessment, help with behavior and medication management while the patient is hospitalized, and determine whether follow‐up psychiatric care is appropriate.[39] The psychiatry team can also offer a more complete diagnostic formulation, including screening for disorders that often co‐occur with personality disorders, such as depression and anxiety, and recommend treatment options.[39] In addition, if initial attempts at behavioral interventions are ineffectual, a psychiatric consult may be able to provide additional guidance in behavioral modifications.[40] This is especially appropriate if the patient's behaviors are interfering with medical care. A psychiatric consult can also provide additional support around issues of countertransference that can arise when managing patients with dysfunctional personality structures.[41, 42]
| Safety assessment in a patient who has threatened or engaged in self‐harming behavior or harm to others |
| Diagnostic clarification, particularly when there is concern for a co‐occurring psychiatric illness |
| Creation of a more complex behavioral plan |
| Facilitation of interdisciplinary discussion and problem‐solving around patients with challenging behaviors |
| Assistance with establishment of outpatient psychiatric care when appropriate |
As with all interventions, the psychiatric consult is not without its side effects. Regardless of personality structure, it is not uncommon for patients to be initially opposed to engaging with psychiatry.[43] Individuals with personality disorders can be particularly susceptible to a rupture of the therapeutic alliance,[44] and calling a psychiatric consult can affect the therapeutic relationship with the primary team, as the patient may feel that others are judging them and can also be part of a greater theme of help rejecting.[11] However, this rupture may be repaired as the patient comes to see the psychiatry team as an ally. Even for patients who refuse to engage with the consult‐liaison team, there may be a benefit to a consult, as the consultants can offer strategies to the primary team and help establish a plan of care to facilitate ongoing treatment of the patient's medical needs without direct contact with the patient. These situations illustrate that a psychiatric consult cannot be done in isolation and requires collaboration with the primary team, nurses, and other support staff for interventions to be effective.
CONCLUSIONS
In his now famous speech Dr. Francis W. Peabody gave to Harvard Medical School he noted that [T]he secret of the care of the patient is caring for the patient.[45] Patients with a dysfunctional personality structure can make this task difficult. They can appear to reject the very help we have to offer, divide the team, absorb great amounts of time, and evoke strong feelings of frustration and resentment. However, by understanding that the way in which they interact with the world is in part the product of biology and upbringing, we can better recognize how ill these individuals can be. Just as a patient with diabetes requires management of his blood glucose when admitted for pneumonia, those with personality disorders require management of their mental illness while their other medical conditions are addressed.
Although personality disorders can seem intractable, studies have shown that, like many chronic illnesses, the severity can wax and wane over time with remissions and relapses. Notably, rates of remission for borderline personality disorder at 10 years are comparable to those for major depressive disorder, bipolar disorder, and panic disorder, with lower rates of relapse even without specific treatment, suggesting they are not entirely intractable.[46] However, the stress of hospitalization can easily exacerbate the symptoms of a personality disorder. By providing an empathic approach that addresses the emotional responses of the team while also reinforcing positive behaviors of the patient, the hospital stay can be an opportunity for these individuals to get needed support and develop new skills while also having their physical needs addressed.
Disclosures: Nothing to report.
- , . The effects of trust in physician on self‐efficacy, adherence and diabetes outcomes. Soc Sci Med. 2009;68(6):1060–1068.
- , , , et al. The physician‐patient working alliance. Patient Educ Couns. 2007;66(1):29–36.
- Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, VA: American Psychiatric Association; 2013.
- , , . The borderline patient on the med‐surg unit. Am J Nursing. 1988;88(12):1644–1650.
- , , . “Difficult” patient? Or does he have a personality disorder? J Fam Pract. 2014;63(12):697–703.
- , , , et al. Prevalence, correlates, and disability of personality disorders in the United States: results from the national epidemiologic survey on alcohol and related conditions. J Clin Psychiatry. 2004;65(7):948–958.
- , , . Classification, assessment, prevalence, and effect of personality disorder. Lancet. 2015;385(9969):717–726.
- , , , , , . Life expectancy at birth and all‐cause mortality among people with personality disorder. J Psychosom Res. 2012;73(2):104–107.
- , , , . A systematic review of personality disorders and health outcomes. Can Psychol. 2015;56(2):168–190.
- , , , . Patient personality and therapist response: an empirical investigation. Am J Psychiatry. 2014;171(1):102–108.
- . Taking care of the hateful patient. N Engl J Med. 1978;298(16):883–887.
- , , . Personality disorder across the life course. Lancet. 2015;385(9969):727–734.
- , , , , . The heritability of cluster A personality disorders assessed by both personal interview and questionnaire. Psychol Med. 2007;37(5):655–665.
- , , , et al. The heritability of avoidant and dependent personality disorder assessed by personal interview and questionnaire. Acta Psychiatr Scand. 2012;126(6):448–457.
- , , , , , . The heritability of Cluster B personality disorders assessed both by personal interview and questionnaire. J Pers Disord. 2012;26(6):848–866.
- , , . Association between genetic polymorphisms in the serotonergic system and comorbid personality disorders among patients with first‐episode depression. J Pers Disord. 2014;28(3):365–378.
- , , , et al. Tryptophan‐hydroxylase 2 haplotype association with borderline personality disorder and aggression in a sample of patients with personality disorders and healthy controls. J Psychiatr Res. 2010;44(15):1075–1081.
- , , , et al. Monoamine oxidase A gene promoter methylation and transcriptional downregulation in an offender population with antisocial personality disorder. Br J Psychiatry. 2015;206(3):216–222.
- , , , et al. Regional cortical thinning may be a biological marker for borderline personality disorder. Acta Psychiatr Scand. 2014;130(3):193–204.
- , , . Empathy and social problem solving in alcohol dependence, mood disorders and selected personality disorders. Neurosci Biobehav Rev. 2013;37(3):448–470.
- , , , . Changes in low‐frequency fluctuations in patients with antisocial personality disorder revealed by resting‐state functional MRI. PLoS One. 2014;9(3):e89790.
- , . Prefrontal structural and functional brain imaging findings in antisocial, violent, and psychopathic individuals: a meta‐analysis. Psychiatry Res. 2009;174(2):81–88.
- , , . Treatment of personality disorder. Lancet. 2015;385(9969):735–743.
- . Management of the borderline patient on a medical or surgical ward: the psychiatric consultant's role. Int J Psychiatry Med. 1975;6(3):337–348.
- , , , et al. The attitudes of psychiatric hospital staff toward hospitalization and treatment of patients with borderline personality disorder. BMC Psychiatry. 2015;15:2.
- , , , . The hateful physician: the role of affect bias in the care of the psychiatric patient in the ED. Am J Emerg Med. 2014;32(5):483–485.
- , , , et al. Relationships within inpatient physician housestaff teams and their association with hospitalized patient outcomes. J Hosp Med. 2014;9(12):764–771.
- . Countertransference in the nurse‐patient relationship: a review of the literature. J Adv Nurs. 1998;28(2):391–397.
- , , , , . Mechanisms of change in dialectical behavior therapy: theoretical and empirical observations. J Clin Psychol. 2006;62(4):459–480.
- , , , . The relationship between nurses' limit‐setting styles and anger in psychiatric inpatients. Psychiatr Serv. 1995;46(6):609–613.
- , , , , , . Attachment disorganization and borderline patients' metacognitive responses to therapists' expressed understanding of their states of mind: a pilot study. Psychother Res. 2008;18(1):28–36.
- , , . Narcissistic personality disorder: diagnostic and clinical challenges. Am J Psychiatry. 2015;172(5):415–422.
- , . An evaluation of the difficulties and attitudes mental health professionals experience with people with personality disorders. J Psychiatr Ment Health Nurs. 2016;23(1):22–36.
- , . Nursing care of personality disorders in the medical surgery setting. Nurs Clin North Am. 1998;33(1):173–186.
- , , , , . Effectiveness of pharmacotherapy for severe personality disorders: meta‐analyses of randomized controlled trials. J Clin Psychiatry. 2010;71(1):14–25.
- , , , . Mental health service utilization by borderline personality disorder patients and Axis II comparison subjects followed prospectively for 6 years. J Clin Psychiatry. 2004;65(1):28–36.
- , , , , . The use of psychotropic medication in patients with emotionally unstable personality disorder under the care of UK mental health services. J Clin Psychiatry. 2015;76(4):e512–e518.
- , , , , . Prevalence and characteristics of cluster B personality disorder in a consultation‐liaison psychiatry practice. Int J Psychiatry Clin Pract. 2015;19(1):65–70.
- , , , et al. The Academy of Psychosomatic Medicine practice guidelines for psychiatric consultation in the general medical setting. The Academy of Psychosomatic Medicine. Psychosomatics. 1998;39(4):S8–S30.
- , , . Interventions in consultation/liaison psychiatry. Part I: Patterns of recommendations. Gen Hosp Psychiatry. 1990;12(4):213–220.
- , , . Psychodynamics in medically ill patients. Harv Rev Psychiatry. 2009;17(6):389–397.
- . Patient dynamics, staff burnout, and consultation‐liaison psychiatry. Physician Exec. 1991;17(5):37–40.
- , . Facilitating patient acceptance of a psychiatric referral. Arch Intern Med. 1985;145(1):73–75.
- . The therapeutic alliance in the treatment of personality disorders. J Psychiatr Pract. 2005;11(2):73–87.
- . Dr. Francis w. Peabody, we need you. Tex Heart Inst J. 2011;38(4):327–328; discussion 328–329.
- , , , et al. Ten‐year course of borderline personality disorder: psychopathology and function from the Collaborative Longitudinal Personality Disorders study. Arch Gen Psychiatry. 2011;68(8):827–837.
- , . The effects of trust in physician on self‐efficacy, adherence and diabetes outcomes. Soc Sci Med. 2009;68(6):1060–1068.
- , , , et al. The physician‐patient working alliance. Patient Educ Couns. 2007;66(1):29–36.
- Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, VA: American Psychiatric Association; 2013.
- , , . The borderline patient on the med‐surg unit. Am J Nursing. 1988;88(12):1644–1650.
- , , . “Difficult” patient? Or does he have a personality disorder? J Fam Pract. 2014;63(12):697–703.
- , , , et al. Prevalence, correlates, and disability of personality disorders in the United States: results from the national epidemiologic survey on alcohol and related conditions. J Clin Psychiatry. 2004;65(7):948–958.
- , , . Classification, assessment, prevalence, and effect of personality disorder. Lancet. 2015;385(9969):717–726.
- , , , , , . Life expectancy at birth and all‐cause mortality among people with personality disorder. J Psychosom Res. 2012;73(2):104–107.
- , , , . A systematic review of personality disorders and health outcomes. Can Psychol. 2015;56(2):168–190.
- , , , . Patient personality and therapist response: an empirical investigation. Am J Psychiatry. 2014;171(1):102–108.
- . Taking care of the hateful patient. N Engl J Med. 1978;298(16):883–887.
- , , . Personality disorder across the life course. Lancet. 2015;385(9969):727–734.
- , , , , . The heritability of cluster A personality disorders assessed by both personal interview and questionnaire. Psychol Med. 2007;37(5):655–665.
- , , , et al. The heritability of avoidant and dependent personality disorder assessed by personal interview and questionnaire. Acta Psychiatr Scand. 2012;126(6):448–457.
- , , , , , . The heritability of Cluster B personality disorders assessed both by personal interview and questionnaire. J Pers Disord. 2012;26(6):848–866.
- , , . Association between genetic polymorphisms in the serotonergic system and comorbid personality disorders among patients with first‐episode depression. J Pers Disord. 2014;28(3):365–378.
- , , , et al. Tryptophan‐hydroxylase 2 haplotype association with borderline personality disorder and aggression in a sample of patients with personality disorders and healthy controls. J Psychiatr Res. 2010;44(15):1075–1081.
- , , , et al. Monoamine oxidase A gene promoter methylation and transcriptional downregulation in an offender population with antisocial personality disorder. Br J Psychiatry. 2015;206(3):216–222.
- , , , et al. Regional cortical thinning may be a biological marker for borderline personality disorder. Acta Psychiatr Scand. 2014;130(3):193–204.
- , , . Empathy and social problem solving in alcohol dependence, mood disorders and selected personality disorders. Neurosci Biobehav Rev. 2013;37(3):448–470.
- , , , . Changes in low‐frequency fluctuations in patients with antisocial personality disorder revealed by resting‐state functional MRI. PLoS One. 2014;9(3):e89790.
- , . Prefrontal structural and functional brain imaging findings in antisocial, violent, and psychopathic individuals: a meta‐analysis. Psychiatry Res. 2009;174(2):81–88.
- , , . Treatment of personality disorder. Lancet. 2015;385(9969):735–743.
- . Management of the borderline patient on a medical or surgical ward: the psychiatric consultant's role. Int J Psychiatry Med. 1975;6(3):337–348.
- , , , et al. The attitudes of psychiatric hospital staff toward hospitalization and treatment of patients with borderline personality disorder. BMC Psychiatry. 2015;15:2.
- , , , . The hateful physician: the role of affect bias in the care of the psychiatric patient in the ED. Am J Emerg Med. 2014;32(5):483–485.
- , , , et al. Relationships within inpatient physician housestaff teams and their association with hospitalized patient outcomes. J Hosp Med. 2014;9(12):764–771.
- . Countertransference in the nurse‐patient relationship: a review of the literature. J Adv Nurs. 1998;28(2):391–397.
- , , , , . Mechanisms of change in dialectical behavior therapy: theoretical and empirical observations. J Clin Psychol. 2006;62(4):459–480.
- , , , . The relationship between nurses' limit‐setting styles and anger in psychiatric inpatients. Psychiatr Serv. 1995;46(6):609–613.
- , , , , , . Attachment disorganization and borderline patients' metacognitive responses to therapists' expressed understanding of their states of mind: a pilot study. Psychother Res. 2008;18(1):28–36.
- , , . Narcissistic personality disorder: diagnostic and clinical challenges. Am J Psychiatry. 2015;172(5):415–422.
- , . An evaluation of the difficulties and attitudes mental health professionals experience with people with personality disorders. J Psychiatr Ment Health Nurs. 2016;23(1):22–36.
- , . Nursing care of personality disorders in the medical surgery setting. Nurs Clin North Am. 1998;33(1):173–186.
- , , , , . Effectiveness of pharmacotherapy for severe personality disorders: meta‐analyses of randomized controlled trials. J Clin Psychiatry. 2010;71(1):14–25.
- , , , . Mental health service utilization by borderline personality disorder patients and Axis II comparison subjects followed prospectively for 6 years. J Clin Psychiatry. 2004;65(1):28–36.
- , , , , . The use of psychotropic medication in patients with emotionally unstable personality disorder under the care of UK mental health services. J Clin Psychiatry. 2015;76(4):e512–e518.
- , , , , . Prevalence and characteristics of cluster B personality disorder in a consultation‐liaison psychiatry practice. Int J Psychiatry Clin Pract. 2015;19(1):65–70.
- , , , et al. The Academy of Psychosomatic Medicine practice guidelines for psychiatric consultation in the general medical setting. The Academy of Psychosomatic Medicine. Psychosomatics. 1998;39(4):S8–S30.
- , , . Interventions in consultation/liaison psychiatry. Part I: Patterns of recommendations. Gen Hosp Psychiatry. 1990;12(4):213–220.
- , , . Psychodynamics in medically ill patients. Harv Rev Psychiatry. 2009;17(6):389–397.
- . Patient dynamics, staff burnout, and consultation‐liaison psychiatry. Physician Exec. 1991;17(5):37–40.
- , . Facilitating patient acceptance of a psychiatric referral. Arch Intern Med. 1985;145(1):73–75.
- . The therapeutic alliance in the treatment of personality disorders. J Psychiatr Pract. 2005;11(2):73–87.
- . Dr. Francis w. Peabody, we need you. Tex Heart Inst J. 2011;38(4):327–328; discussion 328–329.
- , , , et al. Ten‐year course of borderline personality disorder: psychopathology and function from the Collaborative Longitudinal Personality Disorders study. Arch Gen Psychiatry. 2011;68(8):827–837.
Challenge of Personality Disorders
All practicing hospitalists encounter challenging patient situations that stem from issues beyond medical illness. Those situations include the patient who demands to talk with the doctor repeatedly disregarding the lack of urgency, or the patient who, despite seeing multiple well‐regarded specialists, attempts to split the healthcare team by generating unwarranted praise or criticism toward individual caregivers.
Although these patients may be labeled difficult, hateful, or simply a unique patient‐management opportunity, effective care requires a more nuanced understanding of a possible underlying personality disorder that adversely affects the patientphysician relationship. In this issue of the Journal of Hospital Medicine, Riddle et al. provide an important review that outlines a framework for identifying the likely presence of a personality disorder along with practical advice for how to manage these patients.[1] As the authors point out, personality disorders are relatively common among patients seeking medical care but are challenging to diagnose, particularly in the setting of superimposed medical illness. Common to all personality disorders are difficulties forming and maintaining positive relationships with others such that care providers find themselves feeling frustrated, fearful, or inadequate. Inpatient providers typically receive very little training in how to care for patients with personality disorders.
The approach of avoiding collaborative teaching rounds, driven perhaps by a need for time efficiency, deprives learners of the chance to reflect on effective interactions with these patients.
Personality disorders result from genetic predisposition, complex brain dysfunction, and environmental influences. Social determinants also play a role, although limited social networks may simultaneously be a result of a personality disorder and a contributing factor.[2] Although there is a temptation to view personality disorders separate from medical conditions such as diabetes mellitus, diagnosing a personality disorder is far more complicated than simply checking a glycosylated hemoglobin. As Riddle et al. suggest, making a specific diagnosis from the list of 10 personality disorders is challenging in the hospital setting, even for experienced psychiatrists. Given the danger of propagating a diagnosis unabated and unquestioned through the electronic medical record, the attending hospitalist should be reluctant to include a diagnosis such as borderline personality disorder or histrionic personality disorder in the patient problem list without input from experts. Instead, it is useful to document the specific behaviors that are impacting patient care during this episode of illness.
We are concerned about the impact of personality disorders on a number of aspects of patient care, and these are areas that are potentially fertile ground for scholarship and research.
EFFECT ON THE PATIENT EXPERIENCE
Patients with personality disorders may have difficulty assessing the severity of their own medical illnesses. Educating patients on the meaning and value of recovery may be helpful in establishing appropriate expectations of care,[3] although it is equally important to assess the value of illness from the patient's perspective. As Riddle et al. point out, the goal for the hospitalist team is to mitigate the negative impact of adverse behavior on overall care. A recent pilot study of smartphone applications for use by patients with borderline personality disorder might have utility in the inpatient setting.[4] These types of innovations provide opportunities for hospitalist research in the care of patients with personality disorders.
EFFECT OF PERSONALITY DISORDERS ON TEAM‐BASED CLINICAL CARE
A recent observational study published in the Journal of Hospital Medicine identified several important attributes of a high‐functioning inpatient care team.[5] The findings reinforced the concept that patient care is a social activity. To provide high‐quality care, a high‐functioning partnership between team members is required. Riddle et al. point out that patients with personality traits and disorders can negatively impact the relationship among care team members. The hospitalist may be tempted to leave the nursing staff to handle the unwanted communication with the patient. This strategy is maladaptive and creates friction between the hospitalist and the nursing staff. In addition, it reduces an opportunity to recognize important real‐time changes in patients' clinical status that may adversely affect patient outcomes.
EFFECT ON DIAGNOSTIC REASONING
Clinical and diagnostic reasoning plays a central role in patient care. Hospitalists must identify key elements from empirical data and formulate their problem representation to assist in planning the next diagnostic and treatment plans. The medical literature regarding the effect of providing care to patients with maladaptive personality structures is limited. Recent literature investigating the effect of negative patient attributes on diagnostic reasoning suggests that caring for disruptive patients, such as those with maladaptive personality structures, adversely impacts the diagnostic reasoning process. In other words, we are more likely to make cognitive errors when faced with patients who foster a negative feeling. When given vignettes of the same diagnosis but prefaced with patient characteristics that would affect their likeability, trainees of both family practice and internal medicine made significantly fewer correct diagnoses in patients who were given negative connotation, such as overly demanding, a trait not uncommonly seen in patients with personality disorders/traits.[6] The diagnosis rate was more pronounced with complex cases. It is theorized that our cognitive reasoning and use of illness scripts can overcome maladaptive behavior when it comes to common presentations of common illness. However, more complex or atypical presentations require a higher level of diagnostic reasoning that may be impacted by patients who have maladaptive behaviors. The authors hypothesize a resource depletion of mental energy as a result of managing these patients.
EFFECT ON PHYSICIAN WELL‐BEING
Patients with personality disorders require increased time from healthcare providers. Burnout is a major issue for internists.[7] Any provider who has cared for patients with personality disorders can attest to the effects on emotional energy, although this effect deserves study. Without adequate coping strategies by care providers, we run the risk of depleting both our empathy and our mental resources, all of which can negatively affect patient experience and outcomes. The coping strategies that are described by Riddle et al. should be helpful in mitigating the anticipated challenges of caring for these patients and improve both our diagnostic reasoning and care‐provider resiliency.
There is still much to be learned about the long‐term effects of maladaptive personality structures on patient outcomes. We believe that is imperative to have the skills to recognize our patients with maladaptive personality traits and how the care of these patients poses challenges on the functioning of the interdisciplinary care team. Without the advanced training to make the challenging diagnosis of a personality disorder during an acute inpatient stay, it is recommended that hospitalists document the specific behaviors that are impacting patient care and the care team. It is our hope that effective coping strategies can lead to reduced risk of diagnostic errors and bolster the resiliency of the hospitalist.
Disclosure
Nothing to report.
- , , , . When personality is the problem: managing patients with difficulty personalities on the acute care unit. J Hosp Med. 2016;11(12):873–878.
- , . An examination of social network quality and composition in women with and without borderline personality disorder [published online June 27, 2016]. Personal Disord. doi:10.1037/per0000201.
- , , , et al. Values as determinant of meaning among patients with psychiatric disorders in the perspective of recovery [published online June 8, 2016]. Sci Rep. doi:10.1038/srep27617.
- , , , et al. EMOTEO: a smartphone application for monitoring and reducing aversive tension in borderline personality disorder patients, a pilot study [published online July 21, 2016]. Perspect Psychiatr Care. doi:10.1111/ppc12178.
- , , , et al. Relationships within inpatient physician housestaff teams and their association with hospitalized patient outcomes. J Hosp Med. 2014;9(12):764–771.
- , , , et al. Why patients' disruptive behaviours impair diagnostic reasoning: a randomised experiment [published online March 7, 2016]. BMJ Qual Saf. doi:10.1136/bmjqs-2015-005065.
- , , , . A national comparison of burnout and work‐life balance among internal medicine hospitalists and outpatient general internists. J Hosp Med. 2014;9(3):176–181.
All practicing hospitalists encounter challenging patient situations that stem from issues beyond medical illness. Those situations include the patient who demands to talk with the doctor repeatedly disregarding the lack of urgency, or the patient who, despite seeing multiple well‐regarded specialists, attempts to split the healthcare team by generating unwarranted praise or criticism toward individual caregivers.
Although these patients may be labeled difficult, hateful, or simply a unique patient‐management opportunity, effective care requires a more nuanced understanding of a possible underlying personality disorder that adversely affects the patientphysician relationship. In this issue of the Journal of Hospital Medicine, Riddle et al. provide an important review that outlines a framework for identifying the likely presence of a personality disorder along with practical advice for how to manage these patients.[1] As the authors point out, personality disorders are relatively common among patients seeking medical care but are challenging to diagnose, particularly in the setting of superimposed medical illness. Common to all personality disorders are difficulties forming and maintaining positive relationships with others such that care providers find themselves feeling frustrated, fearful, or inadequate. Inpatient providers typically receive very little training in how to care for patients with personality disorders.
The approach of avoiding collaborative teaching rounds, driven perhaps by a need for time efficiency, deprives learners of the chance to reflect on effective interactions with these patients.
Personality disorders result from genetic predisposition, complex brain dysfunction, and environmental influences. Social determinants also play a role, although limited social networks may simultaneously be a result of a personality disorder and a contributing factor.[2] Although there is a temptation to view personality disorders separate from medical conditions such as diabetes mellitus, diagnosing a personality disorder is far more complicated than simply checking a glycosylated hemoglobin. As Riddle et al. suggest, making a specific diagnosis from the list of 10 personality disorders is challenging in the hospital setting, even for experienced psychiatrists. Given the danger of propagating a diagnosis unabated and unquestioned through the electronic medical record, the attending hospitalist should be reluctant to include a diagnosis such as borderline personality disorder or histrionic personality disorder in the patient problem list without input from experts. Instead, it is useful to document the specific behaviors that are impacting patient care during this episode of illness.
We are concerned about the impact of personality disorders on a number of aspects of patient care, and these are areas that are potentially fertile ground for scholarship and research.
EFFECT ON THE PATIENT EXPERIENCE
Patients with personality disorders may have difficulty assessing the severity of their own medical illnesses. Educating patients on the meaning and value of recovery may be helpful in establishing appropriate expectations of care,[3] although it is equally important to assess the value of illness from the patient's perspective. As Riddle et al. point out, the goal for the hospitalist team is to mitigate the negative impact of adverse behavior on overall care. A recent pilot study of smartphone applications for use by patients with borderline personality disorder might have utility in the inpatient setting.[4] These types of innovations provide opportunities for hospitalist research in the care of patients with personality disorders.
EFFECT OF PERSONALITY DISORDERS ON TEAM‐BASED CLINICAL CARE
A recent observational study published in the Journal of Hospital Medicine identified several important attributes of a high‐functioning inpatient care team.[5] The findings reinforced the concept that patient care is a social activity. To provide high‐quality care, a high‐functioning partnership between team members is required. Riddle et al. point out that patients with personality traits and disorders can negatively impact the relationship among care team members. The hospitalist may be tempted to leave the nursing staff to handle the unwanted communication with the patient. This strategy is maladaptive and creates friction between the hospitalist and the nursing staff. In addition, it reduces an opportunity to recognize important real‐time changes in patients' clinical status that may adversely affect patient outcomes.
EFFECT ON DIAGNOSTIC REASONING
Clinical and diagnostic reasoning plays a central role in patient care. Hospitalists must identify key elements from empirical data and formulate their problem representation to assist in planning the next diagnostic and treatment plans. The medical literature regarding the effect of providing care to patients with maladaptive personality structures is limited. Recent literature investigating the effect of negative patient attributes on diagnostic reasoning suggests that caring for disruptive patients, such as those with maladaptive personality structures, adversely impacts the diagnostic reasoning process. In other words, we are more likely to make cognitive errors when faced with patients who foster a negative feeling. When given vignettes of the same diagnosis but prefaced with patient characteristics that would affect their likeability, trainees of both family practice and internal medicine made significantly fewer correct diagnoses in patients who were given negative connotation, such as overly demanding, a trait not uncommonly seen in patients with personality disorders/traits.[6] The diagnosis rate was more pronounced with complex cases. It is theorized that our cognitive reasoning and use of illness scripts can overcome maladaptive behavior when it comes to common presentations of common illness. However, more complex or atypical presentations require a higher level of diagnostic reasoning that may be impacted by patients who have maladaptive behaviors. The authors hypothesize a resource depletion of mental energy as a result of managing these patients.
EFFECT ON PHYSICIAN WELL‐BEING
Patients with personality disorders require increased time from healthcare providers. Burnout is a major issue for internists.[7] Any provider who has cared for patients with personality disorders can attest to the effects on emotional energy, although this effect deserves study. Without adequate coping strategies by care providers, we run the risk of depleting both our empathy and our mental resources, all of which can negatively affect patient experience and outcomes. The coping strategies that are described by Riddle et al. should be helpful in mitigating the anticipated challenges of caring for these patients and improve both our diagnostic reasoning and care‐provider resiliency.
There is still much to be learned about the long‐term effects of maladaptive personality structures on patient outcomes. We believe that is imperative to have the skills to recognize our patients with maladaptive personality traits and how the care of these patients poses challenges on the functioning of the interdisciplinary care team. Without the advanced training to make the challenging diagnosis of a personality disorder during an acute inpatient stay, it is recommended that hospitalists document the specific behaviors that are impacting patient care and the care team. It is our hope that effective coping strategies can lead to reduced risk of diagnostic errors and bolster the resiliency of the hospitalist.
Disclosure
Nothing to report.
All practicing hospitalists encounter challenging patient situations that stem from issues beyond medical illness. Those situations include the patient who demands to talk with the doctor repeatedly disregarding the lack of urgency, or the patient who, despite seeing multiple well‐regarded specialists, attempts to split the healthcare team by generating unwarranted praise or criticism toward individual caregivers.
Although these patients may be labeled difficult, hateful, or simply a unique patient‐management opportunity, effective care requires a more nuanced understanding of a possible underlying personality disorder that adversely affects the patientphysician relationship. In this issue of the Journal of Hospital Medicine, Riddle et al. provide an important review that outlines a framework for identifying the likely presence of a personality disorder along with practical advice for how to manage these patients.[1] As the authors point out, personality disorders are relatively common among patients seeking medical care but are challenging to diagnose, particularly in the setting of superimposed medical illness. Common to all personality disorders are difficulties forming and maintaining positive relationships with others such that care providers find themselves feeling frustrated, fearful, or inadequate. Inpatient providers typically receive very little training in how to care for patients with personality disorders.
The approach of avoiding collaborative teaching rounds, driven perhaps by a need for time efficiency, deprives learners of the chance to reflect on effective interactions with these patients.
Personality disorders result from genetic predisposition, complex brain dysfunction, and environmental influences. Social determinants also play a role, although limited social networks may simultaneously be a result of a personality disorder and a contributing factor.[2] Although there is a temptation to view personality disorders separate from medical conditions such as diabetes mellitus, diagnosing a personality disorder is far more complicated than simply checking a glycosylated hemoglobin. As Riddle et al. suggest, making a specific diagnosis from the list of 10 personality disorders is challenging in the hospital setting, even for experienced psychiatrists. Given the danger of propagating a diagnosis unabated and unquestioned through the electronic medical record, the attending hospitalist should be reluctant to include a diagnosis such as borderline personality disorder or histrionic personality disorder in the patient problem list without input from experts. Instead, it is useful to document the specific behaviors that are impacting patient care during this episode of illness.
We are concerned about the impact of personality disorders on a number of aspects of patient care, and these are areas that are potentially fertile ground for scholarship and research.
EFFECT ON THE PATIENT EXPERIENCE
Patients with personality disorders may have difficulty assessing the severity of their own medical illnesses. Educating patients on the meaning and value of recovery may be helpful in establishing appropriate expectations of care,[3] although it is equally important to assess the value of illness from the patient's perspective. As Riddle et al. point out, the goal for the hospitalist team is to mitigate the negative impact of adverse behavior on overall care. A recent pilot study of smartphone applications for use by patients with borderline personality disorder might have utility in the inpatient setting.[4] These types of innovations provide opportunities for hospitalist research in the care of patients with personality disorders.
EFFECT OF PERSONALITY DISORDERS ON TEAM‐BASED CLINICAL CARE
A recent observational study published in the Journal of Hospital Medicine identified several important attributes of a high‐functioning inpatient care team.[5] The findings reinforced the concept that patient care is a social activity. To provide high‐quality care, a high‐functioning partnership between team members is required. Riddle et al. point out that patients with personality traits and disorders can negatively impact the relationship among care team members. The hospitalist may be tempted to leave the nursing staff to handle the unwanted communication with the patient. This strategy is maladaptive and creates friction between the hospitalist and the nursing staff. In addition, it reduces an opportunity to recognize important real‐time changes in patients' clinical status that may adversely affect patient outcomes.
EFFECT ON DIAGNOSTIC REASONING
Clinical and diagnostic reasoning plays a central role in patient care. Hospitalists must identify key elements from empirical data and formulate their problem representation to assist in planning the next diagnostic and treatment plans. The medical literature regarding the effect of providing care to patients with maladaptive personality structures is limited. Recent literature investigating the effect of negative patient attributes on diagnostic reasoning suggests that caring for disruptive patients, such as those with maladaptive personality structures, adversely impacts the diagnostic reasoning process. In other words, we are more likely to make cognitive errors when faced with patients who foster a negative feeling. When given vignettes of the same diagnosis but prefaced with patient characteristics that would affect their likeability, trainees of both family practice and internal medicine made significantly fewer correct diagnoses in patients who were given negative connotation, such as overly demanding, a trait not uncommonly seen in patients with personality disorders/traits.[6] The diagnosis rate was more pronounced with complex cases. It is theorized that our cognitive reasoning and use of illness scripts can overcome maladaptive behavior when it comes to common presentations of common illness. However, more complex or atypical presentations require a higher level of diagnostic reasoning that may be impacted by patients who have maladaptive behaviors. The authors hypothesize a resource depletion of mental energy as a result of managing these patients.
EFFECT ON PHYSICIAN WELL‐BEING
Patients with personality disorders require increased time from healthcare providers. Burnout is a major issue for internists.[7] Any provider who has cared for patients with personality disorders can attest to the effects on emotional energy, although this effect deserves study. Without adequate coping strategies by care providers, we run the risk of depleting both our empathy and our mental resources, all of which can negatively affect patient experience and outcomes. The coping strategies that are described by Riddle et al. should be helpful in mitigating the anticipated challenges of caring for these patients and improve both our diagnostic reasoning and care‐provider resiliency.
There is still much to be learned about the long‐term effects of maladaptive personality structures on patient outcomes. We believe that is imperative to have the skills to recognize our patients with maladaptive personality traits and how the care of these patients poses challenges on the functioning of the interdisciplinary care team. Without the advanced training to make the challenging diagnosis of a personality disorder during an acute inpatient stay, it is recommended that hospitalists document the specific behaviors that are impacting patient care and the care team. It is our hope that effective coping strategies can lead to reduced risk of diagnostic errors and bolster the resiliency of the hospitalist.
Disclosure
Nothing to report.
- , , , . When personality is the problem: managing patients with difficulty personalities on the acute care unit. J Hosp Med. 2016;11(12):873–878.
- , . An examination of social network quality and composition in women with and without borderline personality disorder [published online June 27, 2016]. Personal Disord. doi:10.1037/per0000201.
- , , , et al. Values as determinant of meaning among patients with psychiatric disorders in the perspective of recovery [published online June 8, 2016]. Sci Rep. doi:10.1038/srep27617.
- , , , et al. EMOTEO: a smartphone application for monitoring and reducing aversive tension in borderline personality disorder patients, a pilot study [published online July 21, 2016]. Perspect Psychiatr Care. doi:10.1111/ppc12178.
- , , , et al. Relationships within inpatient physician housestaff teams and their association with hospitalized patient outcomes. J Hosp Med. 2014;9(12):764–771.
- , , , et al. Why patients' disruptive behaviours impair diagnostic reasoning: a randomised experiment [published online March 7, 2016]. BMJ Qual Saf. doi:10.1136/bmjqs-2015-005065.
- , , , . A national comparison of burnout and work‐life balance among internal medicine hospitalists and outpatient general internists. J Hosp Med. 2014;9(3):176–181.
- , , , . When personality is the problem: managing patients with difficulty personalities on the acute care unit. J Hosp Med. 2016;11(12):873–878.
- , . An examination of social network quality and composition in women with and without borderline personality disorder [published online June 27, 2016]. Personal Disord. doi:10.1037/per0000201.
- , , , et al. Values as determinant of meaning among patients with psychiatric disorders in the perspective of recovery [published online June 8, 2016]. Sci Rep. doi:10.1038/srep27617.
- , , , et al. EMOTEO: a smartphone application for monitoring and reducing aversive tension in borderline personality disorder patients, a pilot study [published online July 21, 2016]. Perspect Psychiatr Care. doi:10.1111/ppc12178.
- , , , et al. Relationships within inpatient physician housestaff teams and their association with hospitalized patient outcomes. J Hosp Med. 2014;9(12):764–771.
- , , , et al. Why patients' disruptive behaviours impair diagnostic reasoning: a randomised experiment [published online March 7, 2016]. BMJ Qual Saf. doi:10.1136/bmjqs-2015-005065.
- , , , . A national comparison of burnout and work‐life balance among internal medicine hospitalists and outpatient general internists. J Hosp Med. 2014;9(3):176–181.
Another infant with Zika-related birth defect born in the United States
The first new case of a live-born infant with Zika virus–related birth defects in almost a month was reported during the week ending Sept. 1, bringing the U.S. total to 18 so far, according to the Centers for Disease Control and Prevention.
The infant was born in one of the 50 states or the District of Columbia and is the first case of a Zika-related birth defect reported since the week ending Aug. 4. The CDC is not reporting state- or territorial-level data to protect the privacy of affected women and children. There were no new Zika-related pregnancy losses for the week of Sept. 1, so the total remains at six for the states, D.C., and the territories, the CDC reported Sept. 8.
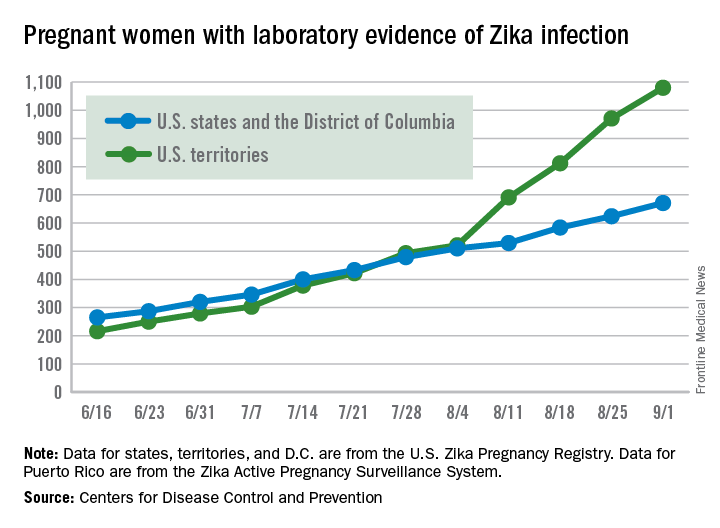
The number of pregnant women with any laboratory evidence of Zika infection increased by 156 during the week ending Sept. 1: 47 new cases in the states/D.C. and 109 new cases in the territories. The total number of pregnant women with Zika for 2016 is now 1,751, the CDC said.
For 2015-2016, there have been 18,833 cases reported in the entire U.S. population: 2,964 in the states/D.C. (all but 44 were travel associated) and 15,869 in the territories. All but 60 cases in the territories were locally acquired, and 98% have occurred in Puerto Rico, the CDC also reported Sept. 8.
The figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
Zika-related birth defects recorded by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
The first new case of a live-born infant with Zika virus–related birth defects in almost a month was reported during the week ending Sept. 1, bringing the U.S. total to 18 so far, according to the Centers for Disease Control and Prevention.
The infant was born in one of the 50 states or the District of Columbia and is the first case of a Zika-related birth defect reported since the week ending Aug. 4. The CDC is not reporting state- or territorial-level data to protect the privacy of affected women and children. There were no new Zika-related pregnancy losses for the week of Sept. 1, so the total remains at six for the states, D.C., and the territories, the CDC reported Sept. 8.
The number of pregnant women with any laboratory evidence of Zika infection increased by 156 during the week ending Sept. 1: 47 new cases in the states/D.C. and 109 new cases in the territories. The total number of pregnant women with Zika for 2016 is now 1,751, the CDC said.
For 2015-2016, there have been 18,833 cases reported in the entire U.S. population: 2,964 in the states/D.C. (all but 44 were travel associated) and 15,869 in the territories. All but 60 cases in the territories were locally acquired, and 98% have occurred in Puerto Rico, the CDC also reported Sept. 8.
The figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
Zika-related birth defects recorded by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
The first new case of a live-born infant with Zika virus–related birth defects in almost a month was reported during the week ending Sept. 1, bringing the U.S. total to 18 so far, according to the Centers for Disease Control and Prevention.
The infant was born in one of the 50 states or the District of Columbia and is the first case of a Zika-related birth defect reported since the week ending Aug. 4. The CDC is not reporting state- or territorial-level data to protect the privacy of affected women and children. There were no new Zika-related pregnancy losses for the week of Sept. 1, so the total remains at six for the states, D.C., and the territories, the CDC reported Sept. 8.
The number of pregnant women with any laboratory evidence of Zika infection increased by 156 during the week ending Sept. 1: 47 new cases in the states/D.C. and 109 new cases in the territories. The total number of pregnant women with Zika for 2016 is now 1,751, the CDC said.
For 2015-2016, there have been 18,833 cases reported in the entire U.S. population: 2,964 in the states/D.C. (all but 44 were travel associated) and 15,869 in the territories. All but 60 cases in the territories were locally acquired, and 98% have occurred in Puerto Rico, the CDC also reported Sept. 8.
The figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
Zika-related birth defects recorded by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
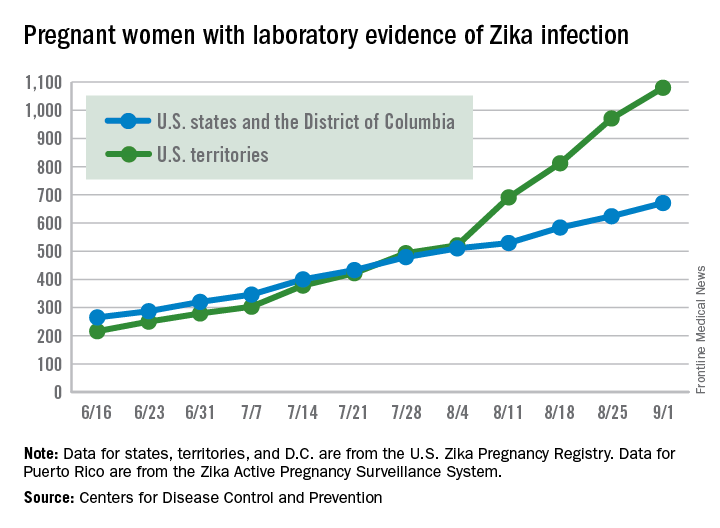
CMS offers lower-stress reporting options for MACRA in 2017
Physicians will have options for when they can start meeting the requirements for the Merit-based Incentive Payment System (MIPS) track under regulations that implement the Medicare Access and CHIP Reauthorization Act.
The options are designed to allow physicians a variety of ways to get started with the new Quality Payment Program – the term CMS has given the MACRA-legislated reforms – and provide more limited ways to participate in 2017.

Option 1: Test the quality payment program in 2017 by submitting data without facing any negative payment adjustments. This will give physicians the year to make sure their processes are in place and ready for broader participation in 2018 and beyond.
Option 2: Delay the start of the performance period and participate for just part of 2017. Depending on how long a physician delays reporting quality information back to CMS, they could still qualify for a smaller bonus payment.
Option 3: Participate for the entire calendar year as called for by the law and be eligible for the full participation bonuses.
Option 4: For those who qualify, participate in an Advanced Alternative Payment Model (APM) beginning next year.
The final regulations for implementing MACRA will be released on Nov. 1, CMS Acting Administrator Andy Slavitt wrote in a blog post published Sept. 8.
“However you choose to participate in 2017, we will have resources available to assist you and walk you through what needs to be done,” Mr. Slavitt wrote.
Physicians will have options for when they can start meeting the requirements for the Merit-based Incentive Payment System (MIPS) track under regulations that implement the Medicare Access and CHIP Reauthorization Act.
The options are designed to allow physicians a variety of ways to get started with the new Quality Payment Program – the term CMS has given the MACRA-legislated reforms – and provide more limited ways to participate in 2017.
Option 1: Test the quality payment program in 2017 by submitting data without facing any negative payment adjustments. This will give physicians the year to make sure their processes are in place and ready for broader participation in 2018 and beyond.
Option 2: Delay the start of the performance period and participate for just part of 2017. Depending on how long a physician delays reporting quality information back to CMS, they could still qualify for a smaller bonus payment.
Option 3: Participate for the entire calendar year as called for by the law and be eligible for the full participation bonuses.
Option 4: For those who qualify, participate in an Advanced Alternative Payment Model (APM) beginning next year.
The final regulations for implementing MACRA will be released on Nov. 1, CMS Acting Administrator Andy Slavitt wrote in a blog post published Sept. 8.
“However you choose to participate in 2017, we will have resources available to assist you and walk you through what needs to be done,” Mr. Slavitt wrote.
Physicians will have options for when they can start meeting the requirements for the Merit-based Incentive Payment System (MIPS) track under regulations that implement the Medicare Access and CHIP Reauthorization Act.
The options are designed to allow physicians a variety of ways to get started with the new Quality Payment Program – the term CMS has given the MACRA-legislated reforms – and provide more limited ways to participate in 2017.
Option 1: Test the quality payment program in 2017 by submitting data without facing any negative payment adjustments. This will give physicians the year to make sure their processes are in place and ready for broader participation in 2018 and beyond.
Option 2: Delay the start of the performance period and participate for just part of 2017. Depending on how long a physician delays reporting quality information back to CMS, they could still qualify for a smaller bonus payment.
Option 3: Participate for the entire calendar year as called for by the law and be eligible for the full participation bonuses.
Option 4: For those who qualify, participate in an Advanced Alternative Payment Model (APM) beginning next year.
The final regulations for implementing MACRA will be released on Nov. 1, CMS Acting Administrator Andy Slavitt wrote in a blog post published Sept. 8.
“However you choose to participate in 2017, we will have resources available to assist you and walk you through what needs to be done,” Mr. Slavitt wrote.

The EHR Report: Seeing through a glass, darkly
Recently, we were invited to take part in an case presentation focused on a young female patient. The reason for our specific invitation was because a key component in the patient’s case was centered on her electronic health record. This kind of story was not new to us – in fact, stories like these are becoming almost common everywhere. But this particular conference promised to be very special, because the patient herself was asked to take an active role and present the story from a unique perspective – her own.
Seated on stage in a hospital gown and accompanied by her I.V. pole, the patient related a 4-month history of symptoms. She had obviously told the story dozens of times – through seemingly endless encounters – to her primary physician, hospital residents, medical students, emergency physicians, and just about anyone else who would lend an ear. Listening to her share her story with a large audience while still a patient in the hospital was incredibly powerful; it was difficult not to become emotional with her as she welled up with tears. She told a complex, though very coherent tale that included her past medical and family histories, her employment, her hobbies, and her unusual signs and symptoms as they developed over an extended period of time. When the patient was done, her case was presented from another perspective: the way it was recorded in her electronic record. For a brief moment, those seated in the audience were confused. Then the theme of the conference became evident – these were completely different stories.

This was no case of mistaken identity or registration error. The chart presented at the conference did belong to the patient, but the story told by the chart was wrong. Reading through the chart, it would be easy to come away with the same sense as her care team; this must simply be a common illness that wasn’t responding to conventional treatment. Encounter after encounter, a new plan was devised to address the presumed diagnosis. But the patient’s telling of the history barely mentioned any symptoms related to that diagnosis. Her version focused more on how her life was affected, how she could no longer take care of her daughter, how she could no longer exercise (which she did avidly), and how she was sinking deeper into despair and losing hope. Woven through all of this were the historical details and seemingly obvious physical manifestations that might easily disclose the real cause of her symptoms. A few basic questions about her family history would also reveal multiple immediate family members who suffered from the same disease! But even if these questions had been asked, and even if the story had been heard, the image in the mirror – her chart – did not reflect an accurate understanding of the patient.
We often solicit comments from readers, and the response is alway encouraging. It is clear that our colleagues in the medical community feel a strong sense of obligation to their patients and care deeply for maintaining the sanctity of the physician-patient relationship. However, many feel the electronic health record has become a barrier to developing and nurturing that relationship, standing in the way understanding their stories. One poignant letter from a cardiologist in Florida, Eugene H. Eisman, MD, does a beautiful job in crystallizing this sentiment. Dr. Eisman writes:
“Many of my patients end up hospitalized where I do not have privileges. Almost every attending is attentive enough to send me a discharge summary. These, however, are EHR-generated. The patient may have been hospitalized for 3 days, yet the summary is seven pages long. It is filled with total nonsense, such as whether the patient had traveled to North Africa (even though he was hospitalized with a fractured hip while skiing in Colorado). The attending has managed to cut and paste reports of every chest film and CBC, and I have pages of normal studies. The final diagnosis and discharge medications are difficult to find in this morass of words. I cannot force myself to read this document, and it is thrown into his chart after a cursory glance. Yet, I can’t sleep at night. Is there buried in this seven-page document a discovery of malignancy, etc.?”
Dr. Eisman’s words are powerful because they reveal an oft-overlooked truth about modern medical records. The patient’s chart, once considered a sacred text containing the key inflection points in a patient’s story, has become merely a filing cabinet in which to stuff every piece of data about the patient, no matter how mundane or trivial. No thought need be put into preserving the important details, because now absolutely every detail can be included. We have become so overloaded with the unimportant, that we may lose the truly critical in this sea of information. It has become, therefore, imperative that physicians rediscover the patient in their story, and not rely solely on the poor reflection we may find in their chart.
Thousands of years ago, the apostle Paul wrote that “we see now as through a glass, darkly.” Borrowing from his original meaning, these ancient words have been quoted throughout literature to describe an “incomplete understanding,” often mixed with a state of despair. Today, we might think of the electronic record as the glass – or mirror – reflecting the patient’s story. Ironically, in spite of having more information than ever, the image we see may be incomplete, and possibly even wrong altogether. While the amount of available data may at first glance appear enlightening, the reflection in the glass may be rather dark indeed.
Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is also a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. An avid programmer, he has published software for handheld devices in partnership with national organizations, and he is always looking for new ways to bring evidence-based medicine to the point of care. Neil Skolnik, MD, is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University, Philadelphia. He is also editor-in-chief of Redi-Reference Inc., a software company that creates mobile apps.
Recently, we were invited to take part in an case presentation focused on a young female patient. The reason for our specific invitation was because a key component in the patient’s case was centered on her electronic health record. This kind of story was not new to us – in fact, stories like these are becoming almost common everywhere. But this particular conference promised to be very special, because the patient herself was asked to take an active role and present the story from a unique perspective – her own.
Seated on stage in a hospital gown and accompanied by her I.V. pole, the patient related a 4-month history of symptoms. She had obviously told the story dozens of times – through seemingly endless encounters – to her primary physician, hospital residents, medical students, emergency physicians, and just about anyone else who would lend an ear. Listening to her share her story with a large audience while still a patient in the hospital was incredibly powerful; it was difficult not to become emotional with her as she welled up with tears. She told a complex, though very coherent tale that included her past medical and family histories, her employment, her hobbies, and her unusual signs and symptoms as they developed over an extended period of time. When the patient was done, her case was presented from another perspective: the way it was recorded in her electronic record. For a brief moment, those seated in the audience were confused. Then the theme of the conference became evident – these were completely different stories.
This was no case of mistaken identity or registration error. The chart presented at the conference did belong to the patient, but the story told by the chart was wrong. Reading through the chart, it would be easy to come away with the same sense as her care team; this must simply be a common illness that wasn’t responding to conventional treatment. Encounter after encounter, a new plan was devised to address the presumed diagnosis. But the patient’s telling of the history barely mentioned any symptoms related to that diagnosis. Her version focused more on how her life was affected, how she could no longer take care of her daughter, how she could no longer exercise (which she did avidly), and how she was sinking deeper into despair and losing hope. Woven through all of this were the historical details and seemingly obvious physical manifestations that might easily disclose the real cause of her symptoms. A few basic questions about her family history would also reveal multiple immediate family members who suffered from the same disease! But even if these questions had been asked, and even if the story had been heard, the image in the mirror – her chart – did not reflect an accurate understanding of the patient.
We often solicit comments from readers, and the response is alway encouraging. It is clear that our colleagues in the medical community feel a strong sense of obligation to their patients and care deeply for maintaining the sanctity of the physician-patient relationship. However, many feel the electronic health record has become a barrier to developing and nurturing that relationship, standing in the way understanding their stories. One poignant letter from a cardiologist in Florida, Eugene H. Eisman, MD, does a beautiful job in crystallizing this sentiment. Dr. Eisman writes:
“Many of my patients end up hospitalized where I do not have privileges. Almost every attending is attentive enough to send me a discharge summary. These, however, are EHR-generated. The patient may have been hospitalized for 3 days, yet the summary is seven pages long. It is filled with total nonsense, such as whether the patient had traveled to North Africa (even though he was hospitalized with a fractured hip while skiing in Colorado). The attending has managed to cut and paste reports of every chest film and CBC, and I have pages of normal studies. The final diagnosis and discharge medications are difficult to find in this morass of words. I cannot force myself to read this document, and it is thrown into his chart after a cursory glance. Yet, I can’t sleep at night. Is there buried in this seven-page document a discovery of malignancy, etc.?”
Dr. Eisman’s words are powerful because they reveal an oft-overlooked truth about modern medical records. The patient’s chart, once considered a sacred text containing the key inflection points in a patient’s story, has become merely a filing cabinet in which to stuff every piece of data about the patient, no matter how mundane or trivial. No thought need be put into preserving the important details, because now absolutely every detail can be included. We have become so overloaded with the unimportant, that we may lose the truly critical in this sea of information. It has become, therefore, imperative that physicians rediscover the patient in their story, and not rely solely on the poor reflection we may find in their chart.
Thousands of years ago, the apostle Paul wrote that “we see now as through a glass, darkly.” Borrowing from his original meaning, these ancient words have been quoted throughout literature to describe an “incomplete understanding,” often mixed with a state of despair. Today, we might think of the electronic record as the glass – or mirror – reflecting the patient’s story. Ironically, in spite of having more information than ever, the image we see may be incomplete, and possibly even wrong altogether. While the amount of available data may at first glance appear enlightening, the reflection in the glass may be rather dark indeed.
Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is also a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. An avid programmer, he has published software for handheld devices in partnership with national organizations, and he is always looking for new ways to bring evidence-based medicine to the point of care. Neil Skolnik, MD, is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University, Philadelphia. He is also editor-in-chief of Redi-Reference Inc., a software company that creates mobile apps.
Recently, we were invited to take part in an case presentation focused on a young female patient. The reason for our specific invitation was because a key component in the patient’s case was centered on her electronic health record. This kind of story was not new to us – in fact, stories like these are becoming almost common everywhere. But this particular conference promised to be very special, because the patient herself was asked to take an active role and present the story from a unique perspective – her own.
Seated on stage in a hospital gown and accompanied by her I.V. pole, the patient related a 4-month history of symptoms. She had obviously told the story dozens of times – through seemingly endless encounters – to her primary physician, hospital residents, medical students, emergency physicians, and just about anyone else who would lend an ear. Listening to her share her story with a large audience while still a patient in the hospital was incredibly powerful; it was difficult not to become emotional with her as she welled up with tears. She told a complex, though very coherent tale that included her past medical and family histories, her employment, her hobbies, and her unusual signs and symptoms as they developed over an extended period of time. When the patient was done, her case was presented from another perspective: the way it was recorded in her electronic record. For a brief moment, those seated in the audience were confused. Then the theme of the conference became evident – these were completely different stories.
This was no case of mistaken identity or registration error. The chart presented at the conference did belong to the patient, but the story told by the chart was wrong. Reading through the chart, it would be easy to come away with the same sense as her care team; this must simply be a common illness that wasn’t responding to conventional treatment. Encounter after encounter, a new plan was devised to address the presumed diagnosis. But the patient’s telling of the history barely mentioned any symptoms related to that diagnosis. Her version focused more on how her life was affected, how she could no longer take care of her daughter, how she could no longer exercise (which she did avidly), and how she was sinking deeper into despair and losing hope. Woven through all of this were the historical details and seemingly obvious physical manifestations that might easily disclose the real cause of her symptoms. A few basic questions about her family history would also reveal multiple immediate family members who suffered from the same disease! But even if these questions had been asked, and even if the story had been heard, the image in the mirror – her chart – did not reflect an accurate understanding of the patient.
We often solicit comments from readers, and the response is alway encouraging. It is clear that our colleagues in the medical community feel a strong sense of obligation to their patients and care deeply for maintaining the sanctity of the physician-patient relationship. However, many feel the electronic health record has become a barrier to developing and nurturing that relationship, standing in the way understanding their stories. One poignant letter from a cardiologist in Florida, Eugene H. Eisman, MD, does a beautiful job in crystallizing this sentiment. Dr. Eisman writes:
“Many of my patients end up hospitalized where I do not have privileges. Almost every attending is attentive enough to send me a discharge summary. These, however, are EHR-generated. The patient may have been hospitalized for 3 days, yet the summary is seven pages long. It is filled with total nonsense, such as whether the patient had traveled to North Africa (even though he was hospitalized with a fractured hip while skiing in Colorado). The attending has managed to cut and paste reports of every chest film and CBC, and I have pages of normal studies. The final diagnosis and discharge medications are difficult to find in this morass of words. I cannot force myself to read this document, and it is thrown into his chart after a cursory glance. Yet, I can’t sleep at night. Is there buried in this seven-page document a discovery of malignancy, etc.?”
Dr. Eisman’s words are powerful because they reveal an oft-overlooked truth about modern medical records. The patient’s chart, once considered a sacred text containing the key inflection points in a patient’s story, has become merely a filing cabinet in which to stuff every piece of data about the patient, no matter how mundane or trivial. No thought need be put into preserving the important details, because now absolutely every detail can be included. We have become so overloaded with the unimportant, that we may lose the truly critical in this sea of information. It has become, therefore, imperative that physicians rediscover the patient in their story, and not rely solely on the poor reflection we may find in their chart.
Thousands of years ago, the apostle Paul wrote that “we see now as through a glass, darkly.” Borrowing from his original meaning, these ancient words have been quoted throughout literature to describe an “incomplete understanding,” often mixed with a state of despair. Today, we might think of the electronic record as the glass – or mirror – reflecting the patient’s story. Ironically, in spite of having more information than ever, the image we see may be incomplete, and possibly even wrong altogether. While the amount of available data may at first glance appear enlightening, the reflection in the glass may be rather dark indeed.
Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is also a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. An avid programmer, he has published software for handheld devices in partnership with national organizations, and he is always looking for new ways to bring evidence-based medicine to the point of care. Neil Skolnik, MD, is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University, Philadelphia. He is also editor-in-chief of Redi-Reference Inc., a software company that creates mobile apps.
