User login
Pediatric mental illness dx, drug prescribing vary widely
A lack of psychiatrists only partially accounted for substantial variations in rates of mental illness diagnosis and prescriptions for psychotropic medications in practices nationwide, a study has shown.
Although a lack of available specialty care was associated with significantly higher odds of a diagnosis or prescription, the colocation of mental health professionals or percentage of children in foster care treated in a practice did not fully explain the differences.
Among 294,748 children aged 4-18 years, seen one or more times in 43 primary care practices nationwide, 15% received a mental health diagnosis between Jan. 1, 2009, and June 30, 2014. Psychotropic medications were prescribed to 14%, reported lead researcher Stephanie L. Mayne of the center for pediatric clinical effectiveness at the the Children’s Hospital of Philadelphia (Pediatrics. 2016 doi: 10.1542/peds.2015-2974).
The most common diagnosis was attention-deficit/hyperactivity disorder at a rate of between 1% and 16%. Differences in other diagnoses “were smaller, but still meaningful” at ranges of 1%-8% for anxiety, 0%-5% for depression, 0.2%-3% for autism, 0%-3% for conduct disorder, and 0%-2% for oppositional-defiant disorder. Bipolar disorder was “uncommon” at less than 1%, Ms. Mayne and her associates reported.
The rate of children receiving any psychotropic medication was between 4% and 26%, while the proportion of patients receiving two or more medication classes ranged between 1% and 12%. Prescription rates for specific medication classes also varied at between 4% and 18% for stimulants, 1% and 12% for antidepressants, 0.1% and 8% for alpha-agonists, and 0.1% and 5% for second-generation antipsychotics.
“Primary care providers’ level of agreement with current guidelines, perceived self-efficacy in diagnosing or treating particular conditions, training, relationships with schools, and reimbursement from insurers might affect prescribing practices,” Ms. Mayne and her associates wrote.
“Even with colocation, barriers such as financial differences in reimbursement for medical and mental health services, difficulties with information sharing, differing expertise, and limited hours may impede integration,” they commented.
Dr. Alexander G. Fiks is an investigator for Pfizer; the other researchers said they had no relevant financial disclosures. This study was funded by the National Institutes of Health and the National Institute of Child Health and Human Development under the Best Pharmaceuticals for Children Act.
On Twitter @whitneymcknight
The integration of mental health services into primary care is an important strategy for increasing access. Future studies that investigate variations in mental health care seen in the primary care setting can help us better understand the quality of this care and consistency with published guidelines.

|
Dr. Lee Savio Beers |
Increased education and support for primary care physicians is essential, as they are at the front lines of providing care to children with mental and behavioral health concerns. However, working together with specialty mental health providers is also important, as they are important partners in the early identification, diagnosis, and treatment of mental disorders.
Education and consultation models such as Child Psychiatry Access Programs can significantly improve a primary care physician’s capacity to care for children with mental health concerns in the medical home, and arrange for appropriate specialty mental health treatment when indicated.
Dr. Lee Savio Beers is the medical director for municipal and regional affairs for the Child Health Advocacy Institute at Children’s National Medical Center, the director of the Washington, D.C., Mental Health Access in Pediatrics (DC MAP) program, and an assistant professor of pediatrics at George Washington University, all in Washington. She had no relevant financial disclosures.
The integration of mental health services into primary care is an important strategy for increasing access. Future studies that investigate variations in mental health care seen in the primary care setting can help us better understand the quality of this care and consistency with published guidelines.
|
|
Dr. Lee Savio Beers |
Increased education and support for primary care physicians is essential, as they are at the front lines of providing care to children with mental and behavioral health concerns. However, working together with specialty mental health providers is also important, as they are important partners in the early identification, diagnosis, and treatment of mental disorders.
Education and consultation models such as Child Psychiatry Access Programs can significantly improve a primary care physician’s capacity to care for children with mental health concerns in the medical home, and arrange for appropriate specialty mental health treatment when indicated.
Dr. Lee Savio Beers is the medical director for municipal and regional affairs for the Child Health Advocacy Institute at Children’s National Medical Center, the director of the Washington, D.C., Mental Health Access in Pediatrics (DC MAP) program, and an assistant professor of pediatrics at George Washington University, all in Washington. She had no relevant financial disclosures.
The integration of mental health services into primary care is an important strategy for increasing access. Future studies that investigate variations in mental health care seen in the primary care setting can help us better understand the quality of this care and consistency with published guidelines.
|
|
Dr. Lee Savio Beers |
Increased education and support for primary care physicians is essential, as they are at the front lines of providing care to children with mental and behavioral health concerns. However, working together with specialty mental health providers is also important, as they are important partners in the early identification, diagnosis, and treatment of mental disorders.
Education and consultation models such as Child Psychiatry Access Programs can significantly improve a primary care physician’s capacity to care for children with mental health concerns in the medical home, and arrange for appropriate specialty mental health treatment when indicated.
Dr. Lee Savio Beers is the medical director for municipal and regional affairs for the Child Health Advocacy Institute at Children’s National Medical Center, the director of the Washington, D.C., Mental Health Access in Pediatrics (DC MAP) program, and an assistant professor of pediatrics at George Washington University, all in Washington. She had no relevant financial disclosures.
A lack of psychiatrists only partially accounted for substantial variations in rates of mental illness diagnosis and prescriptions for psychotropic medications in practices nationwide, a study has shown.
Although a lack of available specialty care was associated with significantly higher odds of a diagnosis or prescription, the colocation of mental health professionals or percentage of children in foster care treated in a practice did not fully explain the differences.
Among 294,748 children aged 4-18 years, seen one or more times in 43 primary care practices nationwide, 15% received a mental health diagnosis between Jan. 1, 2009, and June 30, 2014. Psychotropic medications were prescribed to 14%, reported lead researcher Stephanie L. Mayne of the center for pediatric clinical effectiveness at the the Children’s Hospital of Philadelphia (Pediatrics. 2016 doi: 10.1542/peds.2015-2974).
The most common diagnosis was attention-deficit/hyperactivity disorder at a rate of between 1% and 16%. Differences in other diagnoses “were smaller, but still meaningful” at ranges of 1%-8% for anxiety, 0%-5% for depression, 0.2%-3% for autism, 0%-3% for conduct disorder, and 0%-2% for oppositional-defiant disorder. Bipolar disorder was “uncommon” at less than 1%, Ms. Mayne and her associates reported.
The rate of children receiving any psychotropic medication was between 4% and 26%, while the proportion of patients receiving two or more medication classes ranged between 1% and 12%. Prescription rates for specific medication classes also varied at between 4% and 18% for stimulants, 1% and 12% for antidepressants, 0.1% and 8% for alpha-agonists, and 0.1% and 5% for second-generation antipsychotics.
“Primary care providers’ level of agreement with current guidelines, perceived self-efficacy in diagnosing or treating particular conditions, training, relationships with schools, and reimbursement from insurers might affect prescribing practices,” Ms. Mayne and her associates wrote.
“Even with colocation, barriers such as financial differences in reimbursement for medical and mental health services, difficulties with information sharing, differing expertise, and limited hours may impede integration,” they commented.
Dr. Alexander G. Fiks is an investigator for Pfizer; the other researchers said they had no relevant financial disclosures. This study was funded by the National Institutes of Health and the National Institute of Child Health and Human Development under the Best Pharmaceuticals for Children Act.
On Twitter @whitneymcknight
A lack of psychiatrists only partially accounted for substantial variations in rates of mental illness diagnosis and prescriptions for psychotropic medications in practices nationwide, a study has shown.
Although a lack of available specialty care was associated with significantly higher odds of a diagnosis or prescription, the colocation of mental health professionals or percentage of children in foster care treated in a practice did not fully explain the differences.
Among 294,748 children aged 4-18 years, seen one or more times in 43 primary care practices nationwide, 15% received a mental health diagnosis between Jan. 1, 2009, and June 30, 2014. Psychotropic medications were prescribed to 14%, reported lead researcher Stephanie L. Mayne of the center for pediatric clinical effectiveness at the the Children’s Hospital of Philadelphia (Pediatrics. 2016 doi: 10.1542/peds.2015-2974).
The most common diagnosis was attention-deficit/hyperactivity disorder at a rate of between 1% and 16%. Differences in other diagnoses “were smaller, but still meaningful” at ranges of 1%-8% for anxiety, 0%-5% for depression, 0.2%-3% for autism, 0%-3% for conduct disorder, and 0%-2% for oppositional-defiant disorder. Bipolar disorder was “uncommon” at less than 1%, Ms. Mayne and her associates reported.
The rate of children receiving any psychotropic medication was between 4% and 26%, while the proportion of patients receiving two or more medication classes ranged between 1% and 12%. Prescription rates for specific medication classes also varied at between 4% and 18% for stimulants, 1% and 12% for antidepressants, 0.1% and 8% for alpha-agonists, and 0.1% and 5% for second-generation antipsychotics.
“Primary care providers’ level of agreement with current guidelines, perceived self-efficacy in diagnosing or treating particular conditions, training, relationships with schools, and reimbursement from insurers might affect prescribing practices,” Ms. Mayne and her associates wrote.
“Even with colocation, barriers such as financial differences in reimbursement for medical and mental health services, difficulties with information sharing, differing expertise, and limited hours may impede integration,” they commented.
Dr. Alexander G. Fiks is an investigator for Pfizer; the other researchers said they had no relevant financial disclosures. This study was funded by the National Institutes of Health and the National Institute of Child Health and Human Development under the Best Pharmaceuticals for Children Act.
On Twitter @whitneymcknight
FROM PEDIATRICS
Key clinical point: A lack of psychiatrists only partially accounted for substantial variations in rates of mental illness diagnosis and prescriptions for psychotropic medications given in practices nationwide, a study has shown.
Major finding: Nationwide, 15% of pediatric patients received a mental health diagnosis, and 14% were prescribed psychotropic medications in primary care, regardless of colocated mental health services.
Data source: A retrospective study of electronic health records for 294,748 patients aged 4-18 years.
Disclosures: Dr. Alexander G. Fiks is an investigator for Pfizer; the other researchers said they had no relevant financial disclosures. This study was funded by the National Institutes of Health and the National Institute of Child Health and Human Development under the Best Pharmaceuticals for Children Act.

Kidney Stones? It’s Time to Rethink Those Meds
PRACTICE CHANGER
Do not prescribe tamsulosin or nifedipine for stone expulsion in patients with ureteral stones that are ≤ 10 mm.1
Strength of recommendation
A: Based on a high-quality randomized controlled trial (RCT).1
Bob Z, age 48, presents to the emergency department (ED) with unspecified groin pain. CT of the kidney, ureter, and bladder (CT KUB) finds evidence of a single ureteral stone measuring 8 mm. He’s prescribed medication for the pain and discharged. The day after his ED visit, he comes to your office to discuss further treatment options. Should you prescribe tamsulosin or nifedipine to help him pass the stone?
The most recent National Health and Nutrition Examination Survey found kidney stones affect 8.8% of the population.2 Outpatient therapy is indicated for patients with ureteric colic secondary to stones ≤ 10 mm who do not have uncontrolled pain, impaired kidney function, or severe infection. Routine outpatient care includes oral hydration, antiemetics, and pain medications.
Medical expulsive therapy (MET) is also used to facilitate stone passage. MET is increasingly becoming part of routine care; use of MET in kidney stone patients in the United States has grown from 14% in 2009 to 64% in 2012.3,4
The joint European Association of Urology/American Urological Association Nephrolithiasis Guideline Panel supports the use of MET.5 Meta-analyses of multiple RCTs suggest that an α-blocker (tamsulosin) or a calcium channel blocker (nifedipine) can reduce pain and lead to quicker stone passage and a higher rate of eventual stone passage when compared to placebo or observation.6,7 However, these reviews included small, heterogeneous studies with a high or unclear risk for bias.
Continue for the study summary >>
STUDY SUMMARY
MET doesn’t increase the rate of stone passage
The SUSPEND (Spontaneous Urinary Stone Passage ENabled by Drugs) trial1 was a multicenter RCT designed to determine the effectiveness of tamsulosin or nifedipine as MET for patients ages 18 to 65 with a single ureteric stone measuring ≤ 10 mm on CT KUB, which has 98% diagnostic accuracy.8 (Stones > 10 mm typically require surgery or lithotripsy.)
In this RCT, 1,167 adults were randomized to take tamsulosin (0.4 mg/d), nifedipine (30 mg/d), or placebo for four weeks or until the stone spontaneously passed, whichever came first. The participants, clinicians, and research staff were blinded to treatment assignment. The primary outcome was the proportion of participants who spontaneously passed their stone, as indicated in patient self-reported questionnaires and case-report forms completed by researchers. Secondary outcomes were time to stone passage and pain as assessed by analgesic use and a visual analogue scale (VAS).
At four weeks, 1,136 (97%) of the randomized participants had data available for analysis. The proportion of participants who passed their stone did not differ between MET and placebo; 80% of the placebo group (303 of 379 participants) passed the stone, compared with 81% (307 of 378) of the tamsulosin group and 80% (304 of 379) of the nifedipine group. The odds ratio (OR) for MET vs placebo was 1.04 (95% confidence interval [CI], 0.77 to 1.43) and the OR for tamsulosin vs nifedipine was 1.07 (95% CI, 0.74 to 1.53). These findings did not change with further subgroup analysis, including by sex, stone size (≤ 5 mm vs > 5 mm), or stone location.
There were no differences between groups in time to stone passage as measured by clinical report and confirmed by imaging. Time to passage of stone was available for 237 (21% of) participants. The mean days to stone passage was 15.9 (n = 84) for placebo, 16.5 (n = 79) for tamsulosin, and 16.2 (n = 74) for nifedipine, with a MET vs placebo difference of 0.5 days (95% CI, –2.9 to 3.9; P = .78). Sensitivity analysis accounting for bias from missing data did not change this outcome.
No differences in analgesic use or pain. Self-reported use of pain medication during the first four weeks was similar between groups: 59% (placebo patients), 56% (tamsulosin), and 56% (nifedipine). The mean days of pain medication use was 10.5 for placebo, 11.6 for tamsulosin, and 10.7 for nifedipine, with a MET vs placebo difference of 0.6 days (95% CI, –1.6 to 2.8; P = .45).
There was no difference between groups in the VAS pain score at four weeks. The MET vs placebo difference was 0.0 (95% CI, –0.4 to 0.4; P = .96) and the mean VAS pain score was 1.2 for placebo, 1.0 for tamsulosin, and 1.3 for nifedipine.
WHAT’S NEW
This large RCT contradicts results from previous meta-analyses
The SUSPEND study is the first large, multicenter RCT of MET with tamsulosin or nifedipine for kidney stones that used patient-oriented outcomes to find no benefit for stone expulsion, analgesic use, or reported pain compared to placebo. The discrepancy with prior meta-analyses is not unusual. Up to one-third of meta-analyses that show positive outcomes of a therapy are subsequently altered by the inclusion of results from a single, large, well-designed, multicenter RCT.9
Continue for caveats >>
CAVEATS
This trial included fewer women than previous studies
The SUSPEND study included a smaller proportion of women than previously published case series due to a need for a diagnostic CT KUB, which excluded more women than men due to radiation concerns. However, the proportion of women was balanced across all groups in this trial, and there was no evidence that sex impacted the efficacy of treatment for the primary outcome.1
CHALLENGES TO IMPLEMENTATION
We see no challenges to the implementation of this recommendation.
References
1. Pickard R, Starr K, MacLennan G, et al. Medical expulsive therapy in adults with ureteric colic: a multicentre, randomised, placebo-controlled trial. Lancet. 2015;386:341-349.
2. Scales CD Jr, Smith AC, Hanley JM, et al. Prevalence of kidney stones in the United States. Eur Urol. 2012;62:160-165.
3. Fwu CW, Eggers PW, Kimmel PL, et al. Emergency department visits, use of imaging, and drugs for urolithiasis have increased in the United States. Kidney Int. 2013;89:479-486.
4. Bagga H, Appa A, Wang R, et al. 2257 medical expulsion therapy is underutilized in women presenting to an emergency department with acute urinary stone disease. J Urol. 2013; 189:e925-e926.
5. Preminger GM, Tiselius HG, Assimos DG, et al; American Urological Association Education and Research, Inc; European Association of Urology. 2007 Guideline for the management of ureteral calculi. Eur Urol. 2007;52:1610-1631.
6. Campschroer T, Zhu Y, Duijvesz D, et al. Alpha-blockers as medical expulsive therapy for ureteral stones. Cochrane Database Syst Rev. 2014;4:CD008509.
7. Seitz C, Liatsikos E, Porpiglia F, et al. Medical therapy to facilitate the passage of stones: what is the evidence? Eur Urol. 2009;56:455-471.
8. Worster A, Preyra I, Weaver B, et al. The accuracy of noncontrast helical computed tomography versus intravenous pyelography in the diagnosis of suspected acute urolithiasis: a meta-analysis. Ann Emerg Med. 2002;40: 280-286.
9. LeLorier J, Gregoire G, Benhaddad A, et al. Discrepancies between meta-analyses and subsequent large randomized, controlled trials. N Engl J Med. 1997;337:536-542.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2016. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2016;65(2):118-120.
PRACTICE CHANGER
Do not prescribe tamsulosin or nifedipine for stone expulsion in patients with ureteral stones that are ≤ 10 mm.1
Strength of recommendation
A: Based on a high-quality randomized controlled trial (RCT).1
Bob Z, age 48, presents to the emergency department (ED) with unspecified groin pain. CT of the kidney, ureter, and bladder (CT KUB) finds evidence of a single ureteral stone measuring 8 mm. He’s prescribed medication for the pain and discharged. The day after his ED visit, he comes to your office to discuss further treatment options. Should you prescribe tamsulosin or nifedipine to help him pass the stone?
The most recent National Health and Nutrition Examination Survey found kidney stones affect 8.8% of the population.2 Outpatient therapy is indicated for patients with ureteric colic secondary to stones ≤ 10 mm who do not have uncontrolled pain, impaired kidney function, or severe infection. Routine outpatient care includes oral hydration, antiemetics, and pain medications.
Medical expulsive therapy (MET) is also used to facilitate stone passage. MET is increasingly becoming part of routine care; use of MET in kidney stone patients in the United States has grown from 14% in 2009 to 64% in 2012.3,4
The joint European Association of Urology/American Urological Association Nephrolithiasis Guideline Panel supports the use of MET.5 Meta-analyses of multiple RCTs suggest that an α-blocker (tamsulosin) or a calcium channel blocker (nifedipine) can reduce pain and lead to quicker stone passage and a higher rate of eventual stone passage when compared to placebo or observation.6,7 However, these reviews included small, heterogeneous studies with a high or unclear risk for bias.
Continue for the study summary >>
STUDY SUMMARY
MET doesn’t increase the rate of stone passage
The SUSPEND (Spontaneous Urinary Stone Passage ENabled by Drugs) trial1 was a multicenter RCT designed to determine the effectiveness of tamsulosin or nifedipine as MET for patients ages 18 to 65 with a single ureteric stone measuring ≤ 10 mm on CT KUB, which has 98% diagnostic accuracy.8 (Stones > 10 mm typically require surgery or lithotripsy.)
In this RCT, 1,167 adults were randomized to take tamsulosin (0.4 mg/d), nifedipine (30 mg/d), or placebo for four weeks or until the stone spontaneously passed, whichever came first. The participants, clinicians, and research staff were blinded to treatment assignment. The primary outcome was the proportion of participants who spontaneously passed their stone, as indicated in patient self-reported questionnaires and case-report forms completed by researchers. Secondary outcomes were time to stone passage and pain as assessed by analgesic use and a visual analogue scale (VAS).
At four weeks, 1,136 (97%) of the randomized participants had data available for analysis. The proportion of participants who passed their stone did not differ between MET and placebo; 80% of the placebo group (303 of 379 participants) passed the stone, compared with 81% (307 of 378) of the tamsulosin group and 80% (304 of 379) of the nifedipine group. The odds ratio (OR) for MET vs placebo was 1.04 (95% confidence interval [CI], 0.77 to 1.43) and the OR for tamsulosin vs nifedipine was 1.07 (95% CI, 0.74 to 1.53). These findings did not change with further subgroup analysis, including by sex, stone size (≤ 5 mm vs > 5 mm), or stone location.
There were no differences between groups in time to stone passage as measured by clinical report and confirmed by imaging. Time to passage of stone was available for 237 (21% of) participants. The mean days to stone passage was 15.9 (n = 84) for placebo, 16.5 (n = 79) for tamsulosin, and 16.2 (n = 74) for nifedipine, with a MET vs placebo difference of 0.5 days (95% CI, –2.9 to 3.9; P = .78). Sensitivity analysis accounting for bias from missing data did not change this outcome.
No differences in analgesic use or pain. Self-reported use of pain medication during the first four weeks was similar between groups: 59% (placebo patients), 56% (tamsulosin), and 56% (nifedipine). The mean days of pain medication use was 10.5 for placebo, 11.6 for tamsulosin, and 10.7 for nifedipine, with a MET vs placebo difference of 0.6 days (95% CI, –1.6 to 2.8; P = .45).
There was no difference between groups in the VAS pain score at four weeks. The MET vs placebo difference was 0.0 (95% CI, –0.4 to 0.4; P = .96) and the mean VAS pain score was 1.2 for placebo, 1.0 for tamsulosin, and 1.3 for nifedipine.
WHAT’S NEW
This large RCT contradicts results from previous meta-analyses
The SUSPEND study is the first large, multicenter RCT of MET with tamsulosin or nifedipine for kidney stones that used patient-oriented outcomes to find no benefit for stone expulsion, analgesic use, or reported pain compared to placebo. The discrepancy with prior meta-analyses is not unusual. Up to one-third of meta-analyses that show positive outcomes of a therapy are subsequently altered by the inclusion of results from a single, large, well-designed, multicenter RCT.9
Continue for caveats >>
CAVEATS
This trial included fewer women than previous studies
The SUSPEND study included a smaller proportion of women than previously published case series due to a need for a diagnostic CT KUB, which excluded more women than men due to radiation concerns. However, the proportion of women was balanced across all groups in this trial, and there was no evidence that sex impacted the efficacy of treatment for the primary outcome.1
CHALLENGES TO IMPLEMENTATION
We see no challenges to the implementation of this recommendation.
References
1. Pickard R, Starr K, MacLennan G, et al. Medical expulsive therapy in adults with ureteric colic: a multicentre, randomised, placebo-controlled trial. Lancet. 2015;386:341-349.
2. Scales CD Jr, Smith AC, Hanley JM, et al. Prevalence of kidney stones in the United States. Eur Urol. 2012;62:160-165.
3. Fwu CW, Eggers PW, Kimmel PL, et al. Emergency department visits, use of imaging, and drugs for urolithiasis have increased in the United States. Kidney Int. 2013;89:479-486.
4. Bagga H, Appa A, Wang R, et al. 2257 medical expulsion therapy is underutilized in women presenting to an emergency department with acute urinary stone disease. J Urol. 2013; 189:e925-e926.
5. Preminger GM, Tiselius HG, Assimos DG, et al; American Urological Association Education and Research, Inc; European Association of Urology. 2007 Guideline for the management of ureteral calculi. Eur Urol. 2007;52:1610-1631.
6. Campschroer T, Zhu Y, Duijvesz D, et al. Alpha-blockers as medical expulsive therapy for ureteral stones. Cochrane Database Syst Rev. 2014;4:CD008509.
7. Seitz C, Liatsikos E, Porpiglia F, et al. Medical therapy to facilitate the passage of stones: what is the evidence? Eur Urol. 2009;56:455-471.
8. Worster A, Preyra I, Weaver B, et al. The accuracy of noncontrast helical computed tomography versus intravenous pyelography in the diagnosis of suspected acute urolithiasis: a meta-analysis. Ann Emerg Med. 2002;40: 280-286.
9. LeLorier J, Gregoire G, Benhaddad A, et al. Discrepancies between meta-analyses and subsequent large randomized, controlled trials. N Engl J Med. 1997;337:536-542.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2016. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2016;65(2):118-120.
PRACTICE CHANGER
Do not prescribe tamsulosin or nifedipine for stone expulsion in patients with ureteral stones that are ≤ 10 mm.1
Strength of recommendation
A: Based on a high-quality randomized controlled trial (RCT).1
Bob Z, age 48, presents to the emergency department (ED) with unspecified groin pain. CT of the kidney, ureter, and bladder (CT KUB) finds evidence of a single ureteral stone measuring 8 mm. He’s prescribed medication for the pain and discharged. The day after his ED visit, he comes to your office to discuss further treatment options. Should you prescribe tamsulosin or nifedipine to help him pass the stone?
The most recent National Health and Nutrition Examination Survey found kidney stones affect 8.8% of the population.2 Outpatient therapy is indicated for patients with ureteric colic secondary to stones ≤ 10 mm who do not have uncontrolled pain, impaired kidney function, or severe infection. Routine outpatient care includes oral hydration, antiemetics, and pain medications.
Medical expulsive therapy (MET) is also used to facilitate stone passage. MET is increasingly becoming part of routine care; use of MET in kidney stone patients in the United States has grown from 14% in 2009 to 64% in 2012.3,4
The joint European Association of Urology/American Urological Association Nephrolithiasis Guideline Panel supports the use of MET.5 Meta-analyses of multiple RCTs suggest that an α-blocker (tamsulosin) or a calcium channel blocker (nifedipine) can reduce pain and lead to quicker stone passage and a higher rate of eventual stone passage when compared to placebo or observation.6,7 However, these reviews included small, heterogeneous studies with a high or unclear risk for bias.
Continue for the study summary >>
STUDY SUMMARY
MET doesn’t increase the rate of stone passage
The SUSPEND (Spontaneous Urinary Stone Passage ENabled by Drugs) trial1 was a multicenter RCT designed to determine the effectiveness of tamsulosin or nifedipine as MET for patients ages 18 to 65 with a single ureteric stone measuring ≤ 10 mm on CT KUB, which has 98% diagnostic accuracy.8 (Stones > 10 mm typically require surgery or lithotripsy.)
In this RCT, 1,167 adults were randomized to take tamsulosin (0.4 mg/d), nifedipine (30 mg/d), or placebo for four weeks or until the stone spontaneously passed, whichever came first. The participants, clinicians, and research staff were blinded to treatment assignment. The primary outcome was the proportion of participants who spontaneously passed their stone, as indicated in patient self-reported questionnaires and case-report forms completed by researchers. Secondary outcomes were time to stone passage and pain as assessed by analgesic use and a visual analogue scale (VAS).
At four weeks, 1,136 (97%) of the randomized participants had data available for analysis. The proportion of participants who passed their stone did not differ between MET and placebo; 80% of the placebo group (303 of 379 participants) passed the stone, compared with 81% (307 of 378) of the tamsulosin group and 80% (304 of 379) of the nifedipine group. The odds ratio (OR) for MET vs placebo was 1.04 (95% confidence interval [CI], 0.77 to 1.43) and the OR for tamsulosin vs nifedipine was 1.07 (95% CI, 0.74 to 1.53). These findings did not change with further subgroup analysis, including by sex, stone size (≤ 5 mm vs > 5 mm), or stone location.
There were no differences between groups in time to stone passage as measured by clinical report and confirmed by imaging. Time to passage of stone was available for 237 (21% of) participants. The mean days to stone passage was 15.9 (n = 84) for placebo, 16.5 (n = 79) for tamsulosin, and 16.2 (n = 74) for nifedipine, with a MET vs placebo difference of 0.5 days (95% CI, –2.9 to 3.9; P = .78). Sensitivity analysis accounting for bias from missing data did not change this outcome.
No differences in analgesic use or pain. Self-reported use of pain medication during the first four weeks was similar between groups: 59% (placebo patients), 56% (tamsulosin), and 56% (nifedipine). The mean days of pain medication use was 10.5 for placebo, 11.6 for tamsulosin, and 10.7 for nifedipine, with a MET vs placebo difference of 0.6 days (95% CI, –1.6 to 2.8; P = .45).
There was no difference between groups in the VAS pain score at four weeks. The MET vs placebo difference was 0.0 (95% CI, –0.4 to 0.4; P = .96) and the mean VAS pain score was 1.2 for placebo, 1.0 for tamsulosin, and 1.3 for nifedipine.
WHAT’S NEW
This large RCT contradicts results from previous meta-analyses
The SUSPEND study is the first large, multicenter RCT of MET with tamsulosin or nifedipine for kidney stones that used patient-oriented outcomes to find no benefit for stone expulsion, analgesic use, or reported pain compared to placebo. The discrepancy with prior meta-analyses is not unusual. Up to one-third of meta-analyses that show positive outcomes of a therapy are subsequently altered by the inclusion of results from a single, large, well-designed, multicenter RCT.9
Continue for caveats >>
CAVEATS
This trial included fewer women than previous studies
The SUSPEND study included a smaller proportion of women than previously published case series due to a need for a diagnostic CT KUB, which excluded more women than men due to radiation concerns. However, the proportion of women was balanced across all groups in this trial, and there was no evidence that sex impacted the efficacy of treatment for the primary outcome.1
CHALLENGES TO IMPLEMENTATION
We see no challenges to the implementation of this recommendation.
References
1. Pickard R, Starr K, MacLennan G, et al. Medical expulsive therapy in adults with ureteric colic: a multicentre, randomised, placebo-controlled trial. Lancet. 2015;386:341-349.
2. Scales CD Jr, Smith AC, Hanley JM, et al. Prevalence of kidney stones in the United States. Eur Urol. 2012;62:160-165.
3. Fwu CW, Eggers PW, Kimmel PL, et al. Emergency department visits, use of imaging, and drugs for urolithiasis have increased in the United States. Kidney Int. 2013;89:479-486.
4. Bagga H, Appa A, Wang R, et al. 2257 medical expulsion therapy is underutilized in women presenting to an emergency department with acute urinary stone disease. J Urol. 2013; 189:e925-e926.
5. Preminger GM, Tiselius HG, Assimos DG, et al; American Urological Association Education and Research, Inc; European Association of Urology. 2007 Guideline for the management of ureteral calculi. Eur Urol. 2007;52:1610-1631.
6. Campschroer T, Zhu Y, Duijvesz D, et al. Alpha-blockers as medical expulsive therapy for ureteral stones. Cochrane Database Syst Rev. 2014;4:CD008509.
7. Seitz C, Liatsikos E, Porpiglia F, et al. Medical therapy to facilitate the passage of stones: what is the evidence? Eur Urol. 2009;56:455-471.
8. Worster A, Preyra I, Weaver B, et al. The accuracy of noncontrast helical computed tomography versus intravenous pyelography in the diagnosis of suspected acute urolithiasis: a meta-analysis. Ann Emerg Med. 2002;40: 280-286.
9. LeLorier J, Gregoire G, Benhaddad A, et al. Discrepancies between meta-analyses and subsequent large randomized, controlled trials. N Engl J Med. 1997;337:536-542.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2016. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2016;65(2):118-120.
Managing endometriosis to prevent ovarian cancer
Endometriosis is a common condition, occurring in this country in 1 of 10 women of reproductive age. An association between endometriosis and subsequent ovarian carcinoma has been reported for decades, yet it is only recently that our knowledge has deepened enough to support more rational methods for preventing the malignancy.
Each year, approximately 22,000 new cases of ovarian cancer are diagnosed. The lifetime risk of developing this malignancy is low, but it is the deadliest of the gynecologic malignancies, with diagnosis usually made in advanced stages when prognosis is poor.

Endometriosis shows some characteristics of malignancy, such as the development of local and distant foci, and attachment to and invasion of other tissues with subsequent damage to these tissues. Endometriosis also is characterized by recurrent, unregulated cell proliferation and estrogen-dependent growth.
Our attempts during the past 2 decades to detect ovarian carcinoma at the early stages through a combined screening modality involving transvaginal ultrasound and a test for the serum level of cancer antigen 125 have failed to provide any survival benefit or even any measurable reduction in morbidity. Today, early-stage ovarian carcinoma, which has a 5-year survival rate of more than 90%, is diagnosed in only a minority of women.
There is good news, however. In recent years our insight into the pathophysiology of ovarian cancer has deepened, providing us with a new paradigm for ovarian cancer pathogenesis that divides ovarian epithelial carcinoma into two distinct types with distinct molecular profiles – one which originates largely in the distal portion of the fallopian tube and the other which traces back to endometriosis.
This new paradigm strengthens and helps to explain the reported association between endometriosis and ovarian cancer. It also has important clinical implications for current practice. While we have much more to learn about the etiology of endometriosis and the causes of malignant transformation, our current knowledge provides a strong rationale for identification and close monitoring of some patients with endometriosis deemed at risk for ovarian cancer, risk-reducing medical management, earlier and more meticulous surgical treatment, and close monitoring.
By combining this new approach to endometriosis with consideration of salpingectomy after completion of childbearing, we have an unprecedented opportunity to reduce the incidence of epithelial ovarian cancer.
Dual pathogenesis
The majority of ovarian cancers are of epithelial origin and fall into four histologic categories: serous, endometrioid, clear cell, and mucinous. In recent years, we have gained a deeper understanding of the pathogenesis of ovarian carcinoma, with an array of epidemiologic, histologic, and molecular data showing us that epithelial ovarian cancers are also of two distinct types (Am J Obstet Gynecol. 2015 Sep;213[3]:262-7).
One of these types, a high-grade serous carcinoma, appears to arise in many cases in the epithelium of the fallopian tube. The other type of tumor is a low-grade carcinoma – particularly of the endometrioid and clear cell histologic subtypes – that originates largely from ovarian endometriotic lesions or from borderline serous tumors in the case of serous histology.
The majority of diagnosed stage 1 ovarian cancers are carcinomas of this low-grade type and not high-grade serous carcinomas. In a study of 76 consecutive stage 1 carcinomas, investigators found that ovarian endometriosis was present in 40 of the 76 cases. More than two-thirds of the 76 cases (71%) were nonserous cancers, and almost all of these cases were associated with endometriosis based on histologic examination (Fertil Steril. 2007 Oct;88[4]:906-10).
This study was among the first to show that the majority of stage 1 ovarian carcinomas are not high-grade serous carcinomas, but rather nonserous, primarily endometrioid and clear cell, cancers. The research demonstrated that endometriosis should be viewed as a potential precursor lesion to specific subtypes of ovarian cancer.
The malignant transformation of endometriosis was first suggested by Dr. J. A. Sampson in 1925, and a number of studies – in addition to the 2007 landmark study – have since described ovarian cancer arising from endometriosis, based on the frequent co-occurrence in surgical specimens.
Most recently, a study from the Ovarian Cancer Association Consortium (OCAC) found that women who reported a history of endometriosis had a significantly higher risk of developing ovarian cancer than the general population (odds ratio, 1.46).
Investigators of this critical study pooled data from 13 ovarian cancer case-control studies involving more than 13,226 controls and 7,911 women with invasive epithelial ovarian cancer – 818 (6.2%) and 738 (9.3%) of whom, respectively, reported a history of endometriosis. Specifically, they determined that self-reported endometriosis was associated with a 3.05-fold increased risk for clear cell invasive ovarian cancer and a 2.04-fold increased risk of endometrioid ovarian cancer.
Moreover, a significant association between preexisting endometriosis and low-grade serous invasive ovarian cancer (OR, 2.11) was demonstrated, while no association was found between endometriosis and the risk of high-grade serous invasive ovarian cancer (Lancet Oncol. 2012 Apr;13[4]:385-94).
A second recently published report – a meta-analysis of 20 case-control and 15 cohort studies published between 1990 and 2012 and involving more than 444,000 patients – found that endometriosis increased cancer risk in case-control or two-arm cohort studies by 27% (relative risk, 1.265) and by approximately 80% in single-arm cohort studies (standard incidence ratio, 1.797). Endometrioid and clear cell carcinomas were more common in endometriosis-associated ovarian cancer, while serous carcinoma was less frequent (Br J Cancer. 2014 Apr 2;110[7]:1878-90).
Findings of both of these large studies have served to clarify the association between endometriosis and specific histologic subtypes and suggested that there are important differences in the pathogenesis of low-grade and high-grade serous ovarian carcinomas.
Clinical implications
It is not clear what causes malignant transformation or what predisposes some patients with endometriosis to develop ovarian cancer, but the risk likely involves genetic and epigenetic influences as well as immunologic, inflammatory, and hormonal factors.
The molecular profiles of the main two types of ovarian cancer are different: While the majority of high-grade serous ovarian tumors are characterized by TP53 mutations, the low-grade carcinomas are characterized by a variety of mutations, including KRAS, BRAF, ERBB2, CTNNB1, and BCL2 mutations.
There currently are not enough data to recommend genetic screening tests in patients with endometriosis, but our hope is that we eventually will be able to screen for “high-risk” endometriotic lesions by testing for genes specific to various histologic subtypes of low-grade ovarian cancer, or by finding and utilizing other biomarkers.

In the meantime, we believe it is important to more thoroughly treat endometriosis and to identify and follow women with a history of the condition, especially those with a long-standing history, those with a history of endometriosis associated with infertility, and those with ovarian endometrioma. Each of these factors predisposes patients to a higher risk of malignant transformation.
Complete surgical resection of all visible endometriosis is the most effective treatment and will afford the best cancer prevention, even in women who are asymptomatic. In a recent Swedish national registry case-control study, women who underwent radical surgical excision of all visible endometriosis were significantly less likely (OR, 0.30) to develop ovarian cancer (Acta Obstet Gynecol Scand. 2013 May;92[5]:546-54).
Suppressive hormonal therapy is another treatment option for patients with no interest in conceiving. Most large endometriomas are functional ovarian cysts that have been invaded by cortical ovarian endometriosis or by small primary endometriomas (J Reprod Med. 1992 Sep;37[9]:771-6).
While hormonal therapy will not always result in complete regression of endometriotic lesions, it will decrease the recurrence rate of endometriomas and can be considered for long-term prevention of potentially premalignant lesions. It is most effective when it follows surgical excision of endometriomas and associated endometriosis.
A patient who has completed childbearing at the time of surgical resection may be offered bilateral salpingectomy, regardless of menopausal status. Salpingectomy in both average and high-risk populations (e.g., BRCA 1/2 carriers) not only prevents high-grade serous carcinoma by eliminating the site of origin, but also may decrease the risk of endometrioid and clear cell carcinoma by blocking the passageway that enables the flow of endometrium and factors that induce inflammation. It is estimated that the procedure reduces the risk of ovarian cancer by 40%.
Interestingly, tubal ligation has historically been shown to decrease the risk of ovarian cancer, and recent data have shown that the risk of endometrioid and clear cell carcinoma is cut even more than the risk of high-grade serous carcinoma (Int J Epidemiol. 2013 Apr;42[2]:579-89).
The Society of Gynecologic Oncology recommends that risk-reducing salpingectomy be considered at the time of hysterectomy or other abdominal or pelvic surgery, and in lieu of tubal ligation. The American College of Obstetricians and Gynecologists similarly has stated that prophylactic salpingectomy may offer clinicians the opportunity to prevent ovarian cancer in their patients. Salpingectomy is an important option for all patients, but is especially important when the fallopian tubes are found to be damaged by endometriosis and/or pelvic inflammatory disease. When imaging studies show that endometriomas are present and resection is not performed, pelvic ultrasound should become part of the patient’s routine examination.
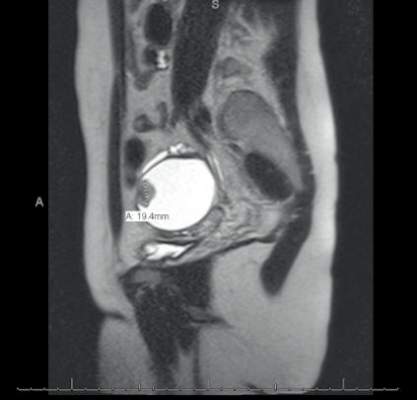
Most endometriomas have a homogeneous appearance; any significant increase in size or a change in the homogeneous cystic characteristics to a more heterogeneous appearance with mural components should raise suspicion about malignant change.
It can be difficult to detect relatively small endocystic components with ultrasound, so if there is any doubt about whether there is some heterogeneous consistency, an MRI should be performed. MRI is showing more promise in detecting malignant change. Hyperdense mural nodules within the ovary and rapid growth of an endometrioma have both been associated with malignant transformation and can be seen on these images.
In a cohort study comparing MRI findings of 10 patients with ovarian adenocarcinoma to 10 patients with benign endometriomas, investigators found mural nodules in all 10 malignancies but in only three of the benign cases (AJR Am J Roentgenol. 2000 Nov;175[5]:1423-30).
Long-term follow-up is necessary to understand the timeline of transformation in patients with mural nodules. This together with increasing knowledge of molecular events underpinning evolution of endometriosis will lead to better screening and preventive strategies.
Dr. Nezhat is the director of minimally invasive gynecologic surgery and robotics at Winthrop University Hospital in Mineola, N.Y., and an adjunct professor of obstetrics, gynecology, and reproductive medicine at the State University of New York at Stony Brook. He reported having no financial disclosures.
Endometriosis is a common condition, occurring in this country in 1 of 10 women of reproductive age. An association between endometriosis and subsequent ovarian carcinoma has been reported for decades, yet it is only recently that our knowledge has deepened enough to support more rational methods for preventing the malignancy.
Each year, approximately 22,000 new cases of ovarian cancer are diagnosed. The lifetime risk of developing this malignancy is low, but it is the deadliest of the gynecologic malignancies, with diagnosis usually made in advanced stages when prognosis is poor.
Endometriosis shows some characteristics of malignancy, such as the development of local and distant foci, and attachment to and invasion of other tissues with subsequent damage to these tissues. Endometriosis also is characterized by recurrent, unregulated cell proliferation and estrogen-dependent growth.
Our attempts during the past 2 decades to detect ovarian carcinoma at the early stages through a combined screening modality involving transvaginal ultrasound and a test for the serum level of cancer antigen 125 have failed to provide any survival benefit or even any measurable reduction in morbidity. Today, early-stage ovarian carcinoma, which has a 5-year survival rate of more than 90%, is diagnosed in only a minority of women.
There is good news, however. In recent years our insight into the pathophysiology of ovarian cancer has deepened, providing us with a new paradigm for ovarian cancer pathogenesis that divides ovarian epithelial carcinoma into two distinct types with distinct molecular profiles – one which originates largely in the distal portion of the fallopian tube and the other which traces back to endometriosis.
This new paradigm strengthens and helps to explain the reported association between endometriosis and ovarian cancer. It also has important clinical implications for current practice. While we have much more to learn about the etiology of endometriosis and the causes of malignant transformation, our current knowledge provides a strong rationale for identification and close monitoring of some patients with endometriosis deemed at risk for ovarian cancer, risk-reducing medical management, earlier and more meticulous surgical treatment, and close monitoring.
By combining this new approach to endometriosis with consideration of salpingectomy after completion of childbearing, we have an unprecedented opportunity to reduce the incidence of epithelial ovarian cancer.
Dual pathogenesis
The majority of ovarian cancers are of epithelial origin and fall into four histologic categories: serous, endometrioid, clear cell, and mucinous. In recent years, we have gained a deeper understanding of the pathogenesis of ovarian carcinoma, with an array of epidemiologic, histologic, and molecular data showing us that epithelial ovarian cancers are also of two distinct types (Am J Obstet Gynecol. 2015 Sep;213[3]:262-7).
One of these types, a high-grade serous carcinoma, appears to arise in many cases in the epithelium of the fallopian tube. The other type of tumor is a low-grade carcinoma – particularly of the endometrioid and clear cell histologic subtypes – that originates largely from ovarian endometriotic lesions or from borderline serous tumors in the case of serous histology.
The majority of diagnosed stage 1 ovarian cancers are carcinomas of this low-grade type and not high-grade serous carcinomas. In a study of 76 consecutive stage 1 carcinomas, investigators found that ovarian endometriosis was present in 40 of the 76 cases. More than two-thirds of the 76 cases (71%) were nonserous cancers, and almost all of these cases were associated with endometriosis based on histologic examination (Fertil Steril. 2007 Oct;88[4]:906-10).
This study was among the first to show that the majority of stage 1 ovarian carcinomas are not high-grade serous carcinomas, but rather nonserous, primarily endometrioid and clear cell, cancers. The research demonstrated that endometriosis should be viewed as a potential precursor lesion to specific subtypes of ovarian cancer.
The malignant transformation of endometriosis was first suggested by Dr. J. A. Sampson in 1925, and a number of studies – in addition to the 2007 landmark study – have since described ovarian cancer arising from endometriosis, based on the frequent co-occurrence in surgical specimens.
Most recently, a study from the Ovarian Cancer Association Consortium (OCAC) found that women who reported a history of endometriosis had a significantly higher risk of developing ovarian cancer than the general population (odds ratio, 1.46).
Investigators of this critical study pooled data from 13 ovarian cancer case-control studies involving more than 13,226 controls and 7,911 women with invasive epithelial ovarian cancer – 818 (6.2%) and 738 (9.3%) of whom, respectively, reported a history of endometriosis. Specifically, they determined that self-reported endometriosis was associated with a 3.05-fold increased risk for clear cell invasive ovarian cancer and a 2.04-fold increased risk of endometrioid ovarian cancer.
Moreover, a significant association between preexisting endometriosis and low-grade serous invasive ovarian cancer (OR, 2.11) was demonstrated, while no association was found between endometriosis and the risk of high-grade serous invasive ovarian cancer (Lancet Oncol. 2012 Apr;13[4]:385-94).
A second recently published report – a meta-analysis of 20 case-control and 15 cohort studies published between 1990 and 2012 and involving more than 444,000 patients – found that endometriosis increased cancer risk in case-control or two-arm cohort studies by 27% (relative risk, 1.265) and by approximately 80% in single-arm cohort studies (standard incidence ratio, 1.797). Endometrioid and clear cell carcinomas were more common in endometriosis-associated ovarian cancer, while serous carcinoma was less frequent (Br J Cancer. 2014 Apr 2;110[7]:1878-90).
Findings of both of these large studies have served to clarify the association between endometriosis and specific histologic subtypes and suggested that there are important differences in the pathogenesis of low-grade and high-grade serous ovarian carcinomas.
Clinical implications
It is not clear what causes malignant transformation or what predisposes some patients with endometriosis to develop ovarian cancer, but the risk likely involves genetic and epigenetic influences as well as immunologic, inflammatory, and hormonal factors.
The molecular profiles of the main two types of ovarian cancer are different: While the majority of high-grade serous ovarian tumors are characterized by TP53 mutations, the low-grade carcinomas are characterized by a variety of mutations, including KRAS, BRAF, ERBB2, CTNNB1, and BCL2 mutations.
There currently are not enough data to recommend genetic screening tests in patients with endometriosis, but our hope is that we eventually will be able to screen for “high-risk” endometriotic lesions by testing for genes specific to various histologic subtypes of low-grade ovarian cancer, or by finding and utilizing other biomarkers.
In the meantime, we believe it is important to more thoroughly treat endometriosis and to identify and follow women with a history of the condition, especially those with a long-standing history, those with a history of endometriosis associated with infertility, and those with ovarian endometrioma. Each of these factors predisposes patients to a higher risk of malignant transformation.
Complete surgical resection of all visible endometriosis is the most effective treatment and will afford the best cancer prevention, even in women who are asymptomatic. In a recent Swedish national registry case-control study, women who underwent radical surgical excision of all visible endometriosis were significantly less likely (OR, 0.30) to develop ovarian cancer (Acta Obstet Gynecol Scand. 2013 May;92[5]:546-54).
Suppressive hormonal therapy is another treatment option for patients with no interest in conceiving. Most large endometriomas are functional ovarian cysts that have been invaded by cortical ovarian endometriosis or by small primary endometriomas (J Reprod Med. 1992 Sep;37[9]:771-6).
While hormonal therapy will not always result in complete regression of endometriotic lesions, it will decrease the recurrence rate of endometriomas and can be considered for long-term prevention of potentially premalignant lesions. It is most effective when it follows surgical excision of endometriomas and associated endometriosis.
A patient who has completed childbearing at the time of surgical resection may be offered bilateral salpingectomy, regardless of menopausal status. Salpingectomy in both average and high-risk populations (e.g., BRCA 1/2 carriers) not only prevents high-grade serous carcinoma by eliminating the site of origin, but also may decrease the risk of endometrioid and clear cell carcinoma by blocking the passageway that enables the flow of endometrium and factors that induce inflammation. It is estimated that the procedure reduces the risk of ovarian cancer by 40%.
Interestingly, tubal ligation has historically been shown to decrease the risk of ovarian cancer, and recent data have shown that the risk of endometrioid and clear cell carcinoma is cut even more than the risk of high-grade serous carcinoma (Int J Epidemiol. 2013 Apr;42[2]:579-89).
The Society of Gynecologic Oncology recommends that risk-reducing salpingectomy be considered at the time of hysterectomy or other abdominal or pelvic surgery, and in lieu of tubal ligation. The American College of Obstetricians and Gynecologists similarly has stated that prophylactic salpingectomy may offer clinicians the opportunity to prevent ovarian cancer in their patients. Salpingectomy is an important option for all patients, but is especially important when the fallopian tubes are found to be damaged by endometriosis and/or pelvic inflammatory disease. When imaging studies show that endometriomas are present and resection is not performed, pelvic ultrasound should become part of the patient’s routine examination.
Most endometriomas have a homogeneous appearance; any significant increase in size or a change in the homogeneous cystic characteristics to a more heterogeneous appearance with mural components should raise suspicion about malignant change.
It can be difficult to detect relatively small endocystic components with ultrasound, so if there is any doubt about whether there is some heterogeneous consistency, an MRI should be performed. MRI is showing more promise in detecting malignant change. Hyperdense mural nodules within the ovary and rapid growth of an endometrioma have both been associated with malignant transformation and can be seen on these images.
In a cohort study comparing MRI findings of 10 patients with ovarian adenocarcinoma to 10 patients with benign endometriomas, investigators found mural nodules in all 10 malignancies but in only three of the benign cases (AJR Am J Roentgenol. 2000 Nov;175[5]:1423-30).
Long-term follow-up is necessary to understand the timeline of transformation in patients with mural nodules. This together with increasing knowledge of molecular events underpinning evolution of endometriosis will lead to better screening and preventive strategies.
Dr. Nezhat is the director of minimally invasive gynecologic surgery and robotics at Winthrop University Hospital in Mineola, N.Y., and an adjunct professor of obstetrics, gynecology, and reproductive medicine at the State University of New York at Stony Brook. He reported having no financial disclosures.
Endometriosis is a common condition, occurring in this country in 1 of 10 women of reproductive age. An association between endometriosis and subsequent ovarian carcinoma has been reported for decades, yet it is only recently that our knowledge has deepened enough to support more rational methods for preventing the malignancy.
Each year, approximately 22,000 new cases of ovarian cancer are diagnosed. The lifetime risk of developing this malignancy is low, but it is the deadliest of the gynecologic malignancies, with diagnosis usually made in advanced stages when prognosis is poor.
Endometriosis shows some characteristics of malignancy, such as the development of local and distant foci, and attachment to and invasion of other tissues with subsequent damage to these tissues. Endometriosis also is characterized by recurrent, unregulated cell proliferation and estrogen-dependent growth.
Our attempts during the past 2 decades to detect ovarian carcinoma at the early stages through a combined screening modality involving transvaginal ultrasound and a test for the serum level of cancer antigen 125 have failed to provide any survival benefit or even any measurable reduction in morbidity. Today, early-stage ovarian carcinoma, which has a 5-year survival rate of more than 90%, is diagnosed in only a minority of women.
There is good news, however. In recent years our insight into the pathophysiology of ovarian cancer has deepened, providing us with a new paradigm for ovarian cancer pathogenesis that divides ovarian epithelial carcinoma into two distinct types with distinct molecular profiles – one which originates largely in the distal portion of the fallopian tube and the other which traces back to endometriosis.
This new paradigm strengthens and helps to explain the reported association between endometriosis and ovarian cancer. It also has important clinical implications for current practice. While we have much more to learn about the etiology of endometriosis and the causes of malignant transformation, our current knowledge provides a strong rationale for identification and close monitoring of some patients with endometriosis deemed at risk for ovarian cancer, risk-reducing medical management, earlier and more meticulous surgical treatment, and close monitoring.
By combining this new approach to endometriosis with consideration of salpingectomy after completion of childbearing, we have an unprecedented opportunity to reduce the incidence of epithelial ovarian cancer.
Dual pathogenesis
The majority of ovarian cancers are of epithelial origin and fall into four histologic categories: serous, endometrioid, clear cell, and mucinous. In recent years, we have gained a deeper understanding of the pathogenesis of ovarian carcinoma, with an array of epidemiologic, histologic, and molecular data showing us that epithelial ovarian cancers are also of two distinct types (Am J Obstet Gynecol. 2015 Sep;213[3]:262-7).
One of these types, a high-grade serous carcinoma, appears to arise in many cases in the epithelium of the fallopian tube. The other type of tumor is a low-grade carcinoma – particularly of the endometrioid and clear cell histologic subtypes – that originates largely from ovarian endometriotic lesions or from borderline serous tumors in the case of serous histology.
The majority of diagnosed stage 1 ovarian cancers are carcinomas of this low-grade type and not high-grade serous carcinomas. In a study of 76 consecutive stage 1 carcinomas, investigators found that ovarian endometriosis was present in 40 of the 76 cases. More than two-thirds of the 76 cases (71%) were nonserous cancers, and almost all of these cases were associated with endometriosis based on histologic examination (Fertil Steril. 2007 Oct;88[4]:906-10).
This study was among the first to show that the majority of stage 1 ovarian carcinomas are not high-grade serous carcinomas, but rather nonserous, primarily endometrioid and clear cell, cancers. The research demonstrated that endometriosis should be viewed as a potential precursor lesion to specific subtypes of ovarian cancer.
The malignant transformation of endometriosis was first suggested by Dr. J. A. Sampson in 1925, and a number of studies – in addition to the 2007 landmark study – have since described ovarian cancer arising from endometriosis, based on the frequent co-occurrence in surgical specimens.
Most recently, a study from the Ovarian Cancer Association Consortium (OCAC) found that women who reported a history of endometriosis had a significantly higher risk of developing ovarian cancer than the general population (odds ratio, 1.46).
Investigators of this critical study pooled data from 13 ovarian cancer case-control studies involving more than 13,226 controls and 7,911 women with invasive epithelial ovarian cancer – 818 (6.2%) and 738 (9.3%) of whom, respectively, reported a history of endometriosis. Specifically, they determined that self-reported endometriosis was associated with a 3.05-fold increased risk for clear cell invasive ovarian cancer and a 2.04-fold increased risk of endometrioid ovarian cancer.
Moreover, a significant association between preexisting endometriosis and low-grade serous invasive ovarian cancer (OR, 2.11) was demonstrated, while no association was found between endometriosis and the risk of high-grade serous invasive ovarian cancer (Lancet Oncol. 2012 Apr;13[4]:385-94).
A second recently published report – a meta-analysis of 20 case-control and 15 cohort studies published between 1990 and 2012 and involving more than 444,000 patients – found that endometriosis increased cancer risk in case-control or two-arm cohort studies by 27% (relative risk, 1.265) and by approximately 80% in single-arm cohort studies (standard incidence ratio, 1.797). Endometrioid and clear cell carcinomas were more common in endometriosis-associated ovarian cancer, while serous carcinoma was less frequent (Br J Cancer. 2014 Apr 2;110[7]:1878-90).
Findings of both of these large studies have served to clarify the association between endometriosis and specific histologic subtypes and suggested that there are important differences in the pathogenesis of low-grade and high-grade serous ovarian carcinomas.
Clinical implications
It is not clear what causes malignant transformation or what predisposes some patients with endometriosis to develop ovarian cancer, but the risk likely involves genetic and epigenetic influences as well as immunologic, inflammatory, and hormonal factors.
The molecular profiles of the main two types of ovarian cancer are different: While the majority of high-grade serous ovarian tumors are characterized by TP53 mutations, the low-grade carcinomas are characterized by a variety of mutations, including KRAS, BRAF, ERBB2, CTNNB1, and BCL2 mutations.
There currently are not enough data to recommend genetic screening tests in patients with endometriosis, but our hope is that we eventually will be able to screen for “high-risk” endometriotic lesions by testing for genes specific to various histologic subtypes of low-grade ovarian cancer, or by finding and utilizing other biomarkers.
In the meantime, we believe it is important to more thoroughly treat endometriosis and to identify and follow women with a history of the condition, especially those with a long-standing history, those with a history of endometriosis associated with infertility, and those with ovarian endometrioma. Each of these factors predisposes patients to a higher risk of malignant transformation.
Complete surgical resection of all visible endometriosis is the most effective treatment and will afford the best cancer prevention, even in women who are asymptomatic. In a recent Swedish national registry case-control study, women who underwent radical surgical excision of all visible endometriosis were significantly less likely (OR, 0.30) to develop ovarian cancer (Acta Obstet Gynecol Scand. 2013 May;92[5]:546-54).
Suppressive hormonal therapy is another treatment option for patients with no interest in conceiving. Most large endometriomas are functional ovarian cysts that have been invaded by cortical ovarian endometriosis or by small primary endometriomas (J Reprod Med. 1992 Sep;37[9]:771-6).
While hormonal therapy will not always result in complete regression of endometriotic lesions, it will decrease the recurrence rate of endometriomas and can be considered for long-term prevention of potentially premalignant lesions. It is most effective when it follows surgical excision of endometriomas and associated endometriosis.
A patient who has completed childbearing at the time of surgical resection may be offered bilateral salpingectomy, regardless of menopausal status. Salpingectomy in both average and high-risk populations (e.g., BRCA 1/2 carriers) not only prevents high-grade serous carcinoma by eliminating the site of origin, but also may decrease the risk of endometrioid and clear cell carcinoma by blocking the passageway that enables the flow of endometrium and factors that induce inflammation. It is estimated that the procedure reduces the risk of ovarian cancer by 40%.
Interestingly, tubal ligation has historically been shown to decrease the risk of ovarian cancer, and recent data have shown that the risk of endometrioid and clear cell carcinoma is cut even more than the risk of high-grade serous carcinoma (Int J Epidemiol. 2013 Apr;42[2]:579-89).
The Society of Gynecologic Oncology recommends that risk-reducing salpingectomy be considered at the time of hysterectomy or other abdominal or pelvic surgery, and in lieu of tubal ligation. The American College of Obstetricians and Gynecologists similarly has stated that prophylactic salpingectomy may offer clinicians the opportunity to prevent ovarian cancer in their patients. Salpingectomy is an important option for all patients, but is especially important when the fallopian tubes are found to be damaged by endometriosis and/or pelvic inflammatory disease. When imaging studies show that endometriomas are present and resection is not performed, pelvic ultrasound should become part of the patient’s routine examination.
Most endometriomas have a homogeneous appearance; any significant increase in size or a change in the homogeneous cystic characteristics to a more heterogeneous appearance with mural components should raise suspicion about malignant change.
It can be difficult to detect relatively small endocystic components with ultrasound, so if there is any doubt about whether there is some heterogeneous consistency, an MRI should be performed. MRI is showing more promise in detecting malignant change. Hyperdense mural nodules within the ovary and rapid growth of an endometrioma have both been associated with malignant transformation and can be seen on these images.
In a cohort study comparing MRI findings of 10 patients with ovarian adenocarcinoma to 10 patients with benign endometriomas, investigators found mural nodules in all 10 malignancies but in only three of the benign cases (AJR Am J Roentgenol. 2000 Nov;175[5]:1423-30).
Long-term follow-up is necessary to understand the timeline of transformation in patients with mural nodules. This together with increasing knowledge of molecular events underpinning evolution of endometriosis will lead to better screening and preventive strategies.
Dr. Nezhat is the director of minimally invasive gynecologic surgery and robotics at Winthrop University Hospital in Mineola, N.Y., and an adjunct professor of obstetrics, gynecology, and reproductive medicine at the State University of New York at Stony Brook. He reported having no financial disclosures.

The impact of endometriosis on ovarian cancer
During an ob.gyn. rotation, a medical student quickly learns the risks related to endometriosis; that is, pelvic pain, abnormal uterine bleeding, and infertility. With more experience, the young practitioner realizes the concern of unopposed estrogen therapy in patients with a history of endometriosis (i.e., cancer).
Now, in this excellent discussion by Dr. Farr Nezhat, for the current edition of the Master Class in Gynecologic Surgery, he describes the risk of endometriosis and ovarian cancer. Not only does Dr. Nezhat present data revealing the increased association between ovarian cancer and endometriosis, but he goes on to describe the usual type of epithelial ovarian cancer that is noted in the patient with endometriosis.

Dr. Nezhat describes women who appear to be predisposed to malignant transformation and provides current recommendations to lower the risk of malignancy in patients with endometriosis. This includes complete surgical resection of endometriosis, routine ultrasound/MRI if endometriosis is not resected, suppressive hormonal therapy, and bilateral salpingectomy. Moreover, Dr. Nezhat looks to the future and the possibility of genetic screening tests.
Dr. Nezhat is board certified in gynecologic oncology and is world renowned for his work with advanced laparoscopic and robotic surgery for the treatment of gynecologic cancers and complex benign conditions. He is the director of minimally invasive gynecologic surgery and robotics at Winthrop University Hospital in Mineola, N.Y., and an adjunct professor of obstetrics, gynecology, and reproductive medicine at State University of New York at Stony Brook.
His main areas of interest and research include early detection and treatment of early and advanced ovarian cancer, as well as cancer arising in endometriosis. Dr. Nezhat has authored and coauthored more than 200 medical and scientific manuscripts and book chapters.
Dr. Miller is a clinical associate professor at the University of Illinois at Chicago, and a past president of the AAGL and the International Society for Gynecologic Endoscopy (ISGE). He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville and Schaumburg, Ill.; director of minimally invasive gynecologic surgery and the director of the AAGL/Society of Reproductive Surgery fellowship in minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill.; and the medical editor of this column, Master Class. Dr. Miller reported having no financial disclosures relevant to this column.
During an ob.gyn. rotation, a medical student quickly learns the risks related to endometriosis; that is, pelvic pain, abnormal uterine bleeding, and infertility. With more experience, the young practitioner realizes the concern of unopposed estrogen therapy in patients with a history of endometriosis (i.e., cancer).
Now, in this excellent discussion by Dr. Farr Nezhat, for the current edition of the Master Class in Gynecologic Surgery, he describes the risk of endometriosis and ovarian cancer. Not only does Dr. Nezhat present data revealing the increased association between ovarian cancer and endometriosis, but he goes on to describe the usual type of epithelial ovarian cancer that is noted in the patient with endometriosis.
Dr. Nezhat describes women who appear to be predisposed to malignant transformation and provides current recommendations to lower the risk of malignancy in patients with endometriosis. This includes complete surgical resection of endometriosis, routine ultrasound/MRI if endometriosis is not resected, suppressive hormonal therapy, and bilateral salpingectomy. Moreover, Dr. Nezhat looks to the future and the possibility of genetic screening tests.
Dr. Nezhat is board certified in gynecologic oncology and is world renowned for his work with advanced laparoscopic and robotic surgery for the treatment of gynecologic cancers and complex benign conditions. He is the director of minimally invasive gynecologic surgery and robotics at Winthrop University Hospital in Mineola, N.Y., and an adjunct professor of obstetrics, gynecology, and reproductive medicine at State University of New York at Stony Brook.
His main areas of interest and research include early detection and treatment of early and advanced ovarian cancer, as well as cancer arising in endometriosis. Dr. Nezhat has authored and coauthored more than 200 medical and scientific manuscripts and book chapters.
Dr. Miller is a clinical associate professor at the University of Illinois at Chicago, and a past president of the AAGL and the International Society for Gynecologic Endoscopy (ISGE). He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville and Schaumburg, Ill.; director of minimally invasive gynecologic surgery and the director of the AAGL/Society of Reproductive Surgery fellowship in minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill.; and the medical editor of this column, Master Class. Dr. Miller reported having no financial disclosures relevant to this column.
During an ob.gyn. rotation, a medical student quickly learns the risks related to endometriosis; that is, pelvic pain, abnormal uterine bleeding, and infertility. With more experience, the young practitioner realizes the concern of unopposed estrogen therapy in patients with a history of endometriosis (i.e., cancer).
Now, in this excellent discussion by Dr. Farr Nezhat, for the current edition of the Master Class in Gynecologic Surgery, he describes the risk of endometriosis and ovarian cancer. Not only does Dr. Nezhat present data revealing the increased association between ovarian cancer and endometriosis, but he goes on to describe the usual type of epithelial ovarian cancer that is noted in the patient with endometriosis.
Dr. Nezhat describes women who appear to be predisposed to malignant transformation and provides current recommendations to lower the risk of malignancy in patients with endometriosis. This includes complete surgical resection of endometriosis, routine ultrasound/MRI if endometriosis is not resected, suppressive hormonal therapy, and bilateral salpingectomy. Moreover, Dr. Nezhat looks to the future and the possibility of genetic screening tests.
Dr. Nezhat is board certified in gynecologic oncology and is world renowned for his work with advanced laparoscopic and robotic surgery for the treatment of gynecologic cancers and complex benign conditions. He is the director of minimally invasive gynecologic surgery and robotics at Winthrop University Hospital in Mineola, N.Y., and an adjunct professor of obstetrics, gynecology, and reproductive medicine at State University of New York at Stony Brook.
His main areas of interest and research include early detection and treatment of early and advanced ovarian cancer, as well as cancer arising in endometriosis. Dr. Nezhat has authored and coauthored more than 200 medical and scientific manuscripts and book chapters.
Dr. Miller is a clinical associate professor at the University of Illinois at Chicago, and a past president of the AAGL and the International Society for Gynecologic Endoscopy (ISGE). He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville and Schaumburg, Ill.; director of minimally invasive gynecologic surgery and the director of the AAGL/Society of Reproductive Surgery fellowship in minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill.; and the medical editor of this column, Master Class. Dr. Miller reported having no financial disclosures relevant to this column.

High-grade cervical dysplasia in pregnancy
Cervical intraepithelial neoplasia (CIN) describes a precancerous lesion of the squamous epithelium of the ectocervix. The cervical cancer screening paradigm in the United States begins with collection of cervical cytology with a Pap smear, frequently in conjunction with human papillomavirus testing. Abnormalities will frequently lead to colposcopy with directed biopsy, which can result in a diagnosis of CIN. There are different grades of severity within CIN, which aids in making treatment recommendations.
Pregnancy is a convenient time to capture women for cervical cancer screening, given the increased contact with health care providers. Routine guidelines should be followed for screening women who are pregnant, as collection of cervical cytology and human papillomavirus (HPV) cotesting is safe.

In women who have been found to have abnormal cytology, CIN or malignancy has been identified in up to 19% of cases (Am J Obstet Gynecol. 2004 Jul;191[1]:105-13). High-grade lesions identified in pregnant women create a unique management dilemma.
Terminology
The Bethesda system describes colposcopic abnormalities as CIN and divides premalignant lesions into grades from 1 to 3 with the highest grade representing more worrisome lesions. CIN2 has been found to have poor reproducibility and likely represents a mix of low- and high-grade lesions. In addition, there is concern that HPV-associated lesions of the lower anogenital tract have incongruent terminology among different specialties that may not accurately represent the current understanding of HPV pathogenesis.
In 2012, the Lower Anogenital Squamous Terminology (LAST) project of the College of American Pathologists and the American Society for Colposcopy and Cervical Pathology (ASCCP) advocated for consistent terminology across all lower anogenital tract lesions with HPV, including CIN (Int J Gynecol Pathol. 2013 Jan;32[1]:76-115).
With this new terminology, CIN1 is referred to as low-grade squamous intraepithelial lesion (LSIL). CIN2 is characterized by its p16 immunostaining; lesions that are p16 negative are considered LSIL, while those that are positive are considered HSIL (high-grade squamous intraepithelial lesion). While this staining is not universally performed, physicians will start seeing p16 staining results with increasing frequency on their cervical biopsies. CIN3 lesions are referred to as HSIL.

Given the current understanding of HPV-mediated disease, and a commitment to represent the most up-to-date information, the LAST project terminology of HSIL to represent previously identified CIN2 and CIN3 lesions will be used for the remainder of this text.
Diagnosis
There is little data on the natural history of HSIL diagnosed after colposcopy, as most women get some form of therapy. The information that is available suggests that in patients with untreated HSIL, the cumulative incidence of malignancy is as high as 30% at 30 years (Lancet Oncol. 2008 May;9[5]:425-34). Treatment recommendations for excision are aimed at addressing this alarming number; however, care must be individualized, especially in the setting of pregnancy.
If abnormal cervical cytology is obtained on routine screening, appropriate patients should be referred for colposcopic exam. Physicians performing colposcopy should be familiar with the physiologic effects of pregnancy that can obscure the exam, including the increased cervical mucus production, prominence of endocervical glands, and increased vascularity.
Colposcopic-directed ectocervical biopsies have been found to be safe in pregnancy, and these women should be provided the same care as those who are not pregnant (Obstet Gynecol. 1993 Jun;81[6]:915-8). Endocervical sampling and endometrial sampling should not be performed, however, and physicians should remain dedicated to checking pregnancy tests prior to colposcopy.

HSIL cytology should prompt a biopsy in pregnancy; a decision to skip the biopsy and perform an excisional procedure in this setting is not recommended regardless of patient or gestational age. If LSIL (CIN1) is noted on biopsy, reevaluation post partum should be strongly considered, unless a suspicious lesion was felt to be inadequately biopsied.
Management
Managing HSIL in pregnancy focuses on diagnosis and excluding malignancy, while treatment can be reserved for the postpartum period. When choosing a management option, consider individual patient factors such as colposcopic appearance of the lesion, gestational age, and access to health care.
If HSIL is noted on colposcopic-directed biopsy, consider one of several options. The most conservative approach is reevaluation with cytology and colposcopy 6 weeks post partum. This is an option for patients who do not have a colposcopic exam that was concerning for an invasive lesion, were able to be adequately biopsied, and will reliably return for follow-up. Many physicians feel more comfortable with repeat cytology and colposcopy in 3 months from the original biopsy. The most aggressive management would include an excisional procedure during pregnancy.
There are varying rates of regression of biopsy-proven HSIL in pregnancy ranging from 34% to 70% (Obstet Gynecol. 1999 Mar;93[3]:359-62; Acta Obstet Gynecol Scand. 2006;85[9]:1134-7; Reprod Sci. 2009 Nov;16[11]:1034-9). Out of more than 200 patients across these three studies, just two patients were diagnosed with an invasive lesion post partum. Given the low likelihood of progression during pregnancy and the high rate of regression, an excisional procedure should be considered only in cases where there is concern about invasive carcinoma.
In cases where an invasive lesion is suspected, consider an an excisional procedure. While there is some evidence that performing a laser excisional procedure early in pregnancy (18 weeks and earlier) can be safely done, that is not the most common management strategy in the United States (Tumori. 1998 Sep-Oct;84[5]:567-70; Int J Gynecol Cancer. 2007 Jan-Feb;17[1]:127-31). In this circumstance, referral to a gynecologic oncologist is warranted where consideration can be made for performing a cold knife conization. Physicians should be aware of the increased risk of bleeding with this procedure in pregnancy and the potential for preterm birth. There is little literature to guide counseling regarding these risks, and the decision to perform an excisional procedure should be made with a multidisciplinary team (Arch Gynecol Obstet. 2016 Jan 4. doi: 10.1007/s00404-015-3980-y).
The see-and-treat paradigm is not recommended in pregnancy. Those patients with poor follow-up should still undergo colposcopic-directed biopsies prior to any excisional procedure.
Treatment recommendations in pregnancy should be made on the basis of careful consideration of individual patient factors, with strong consideration of repeat testing with cytology and colposcopy prior to an excision procedure.
Dr. Sullivan is a fellow in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. Dr. Gehrig is professor and director of gynecologic oncology at the university. Dr. Sullivan and Dr. Gehrig reported having no relevant financial disclosures. Email them at [email protected].
Cervical intraepithelial neoplasia (CIN) describes a precancerous lesion of the squamous epithelium of the ectocervix. The cervical cancer screening paradigm in the United States begins with collection of cervical cytology with a Pap smear, frequently in conjunction with human papillomavirus testing. Abnormalities will frequently lead to colposcopy with directed biopsy, which can result in a diagnosis of CIN. There are different grades of severity within CIN, which aids in making treatment recommendations.
Pregnancy is a convenient time to capture women for cervical cancer screening, given the increased contact with health care providers. Routine guidelines should be followed for screening women who are pregnant, as collection of cervical cytology and human papillomavirus (HPV) cotesting is safe.
In women who have been found to have abnormal cytology, CIN or malignancy has been identified in up to 19% of cases (Am J Obstet Gynecol. 2004 Jul;191[1]:105-13). High-grade lesions identified in pregnant women create a unique management dilemma.
Terminology
The Bethesda system describes colposcopic abnormalities as CIN and divides premalignant lesions into grades from 1 to 3 with the highest grade representing more worrisome lesions. CIN2 has been found to have poor reproducibility and likely represents a mix of low- and high-grade lesions. In addition, there is concern that HPV-associated lesions of the lower anogenital tract have incongruent terminology among different specialties that may not accurately represent the current understanding of HPV pathogenesis.
In 2012, the Lower Anogenital Squamous Terminology (LAST) project of the College of American Pathologists and the American Society for Colposcopy and Cervical Pathology (ASCCP) advocated for consistent terminology across all lower anogenital tract lesions with HPV, including CIN (Int J Gynecol Pathol. 2013 Jan;32[1]:76-115).
With this new terminology, CIN1 is referred to as low-grade squamous intraepithelial lesion (LSIL). CIN2 is characterized by its p16 immunostaining; lesions that are p16 negative are considered LSIL, while those that are positive are considered HSIL (high-grade squamous intraepithelial lesion). While this staining is not universally performed, physicians will start seeing p16 staining results with increasing frequency on their cervical biopsies. CIN3 lesions are referred to as HSIL.
Given the current understanding of HPV-mediated disease, and a commitment to represent the most up-to-date information, the LAST project terminology of HSIL to represent previously identified CIN2 and CIN3 lesions will be used for the remainder of this text.
Diagnosis
There is little data on the natural history of HSIL diagnosed after colposcopy, as most women get some form of therapy. The information that is available suggests that in patients with untreated HSIL, the cumulative incidence of malignancy is as high as 30% at 30 years (Lancet Oncol. 2008 May;9[5]:425-34). Treatment recommendations for excision are aimed at addressing this alarming number; however, care must be individualized, especially in the setting of pregnancy.
If abnormal cervical cytology is obtained on routine screening, appropriate patients should be referred for colposcopic exam. Physicians performing colposcopy should be familiar with the physiologic effects of pregnancy that can obscure the exam, including the increased cervical mucus production, prominence of endocervical glands, and increased vascularity.
Colposcopic-directed ectocervical biopsies have been found to be safe in pregnancy, and these women should be provided the same care as those who are not pregnant (Obstet Gynecol. 1993 Jun;81[6]:915-8). Endocervical sampling and endometrial sampling should not be performed, however, and physicians should remain dedicated to checking pregnancy tests prior to colposcopy.
HSIL cytology should prompt a biopsy in pregnancy; a decision to skip the biopsy and perform an excisional procedure in this setting is not recommended regardless of patient or gestational age. If LSIL (CIN1) is noted on biopsy, reevaluation post partum should be strongly considered, unless a suspicious lesion was felt to be inadequately biopsied.
Management
Managing HSIL in pregnancy focuses on diagnosis and excluding malignancy, while treatment can be reserved for the postpartum period. When choosing a management option, consider individual patient factors such as colposcopic appearance of the lesion, gestational age, and access to health care.
If HSIL is noted on colposcopic-directed biopsy, consider one of several options. The most conservative approach is reevaluation with cytology and colposcopy 6 weeks post partum. This is an option for patients who do not have a colposcopic exam that was concerning for an invasive lesion, were able to be adequately biopsied, and will reliably return for follow-up. Many physicians feel more comfortable with repeat cytology and colposcopy in 3 months from the original biopsy. The most aggressive management would include an excisional procedure during pregnancy.
There are varying rates of regression of biopsy-proven HSIL in pregnancy ranging from 34% to 70% (Obstet Gynecol. 1999 Mar;93[3]:359-62; Acta Obstet Gynecol Scand. 2006;85[9]:1134-7; Reprod Sci. 2009 Nov;16[11]:1034-9). Out of more than 200 patients across these three studies, just two patients were diagnosed with an invasive lesion post partum. Given the low likelihood of progression during pregnancy and the high rate of regression, an excisional procedure should be considered only in cases where there is concern about invasive carcinoma.
In cases where an invasive lesion is suspected, consider an an excisional procedure. While there is some evidence that performing a laser excisional procedure early in pregnancy (18 weeks and earlier) can be safely done, that is not the most common management strategy in the United States (Tumori. 1998 Sep-Oct;84[5]:567-70; Int J Gynecol Cancer. 2007 Jan-Feb;17[1]:127-31). In this circumstance, referral to a gynecologic oncologist is warranted where consideration can be made for performing a cold knife conization. Physicians should be aware of the increased risk of bleeding with this procedure in pregnancy and the potential for preterm birth. There is little literature to guide counseling regarding these risks, and the decision to perform an excisional procedure should be made with a multidisciplinary team (Arch Gynecol Obstet. 2016 Jan 4. doi: 10.1007/s00404-015-3980-y).
The see-and-treat paradigm is not recommended in pregnancy. Those patients with poor follow-up should still undergo colposcopic-directed biopsies prior to any excisional procedure.
Treatment recommendations in pregnancy should be made on the basis of careful consideration of individual patient factors, with strong consideration of repeat testing with cytology and colposcopy prior to an excision procedure.
Dr. Sullivan is a fellow in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. Dr. Gehrig is professor and director of gynecologic oncology at the university. Dr. Sullivan and Dr. Gehrig reported having no relevant financial disclosures. Email them at [email protected].
Cervical intraepithelial neoplasia (CIN) describes a precancerous lesion of the squamous epithelium of the ectocervix. The cervical cancer screening paradigm in the United States begins with collection of cervical cytology with a Pap smear, frequently in conjunction with human papillomavirus testing. Abnormalities will frequently lead to colposcopy with directed biopsy, which can result in a diagnosis of CIN. There are different grades of severity within CIN, which aids in making treatment recommendations.
Pregnancy is a convenient time to capture women for cervical cancer screening, given the increased contact with health care providers. Routine guidelines should be followed for screening women who are pregnant, as collection of cervical cytology and human papillomavirus (HPV) cotesting is safe.
In women who have been found to have abnormal cytology, CIN or malignancy has been identified in up to 19% of cases (Am J Obstet Gynecol. 2004 Jul;191[1]:105-13). High-grade lesions identified in pregnant women create a unique management dilemma.
Terminology
The Bethesda system describes colposcopic abnormalities as CIN and divides premalignant lesions into grades from 1 to 3 with the highest grade representing more worrisome lesions. CIN2 has been found to have poor reproducibility and likely represents a mix of low- and high-grade lesions. In addition, there is concern that HPV-associated lesions of the lower anogenital tract have incongruent terminology among different specialties that may not accurately represent the current understanding of HPV pathogenesis.
In 2012, the Lower Anogenital Squamous Terminology (LAST) project of the College of American Pathologists and the American Society for Colposcopy and Cervical Pathology (ASCCP) advocated for consistent terminology across all lower anogenital tract lesions with HPV, including CIN (Int J Gynecol Pathol. 2013 Jan;32[1]:76-115).
With this new terminology, CIN1 is referred to as low-grade squamous intraepithelial lesion (LSIL). CIN2 is characterized by its p16 immunostaining; lesions that are p16 negative are considered LSIL, while those that are positive are considered HSIL (high-grade squamous intraepithelial lesion). While this staining is not universally performed, physicians will start seeing p16 staining results with increasing frequency on their cervical biopsies. CIN3 lesions are referred to as HSIL.
Given the current understanding of HPV-mediated disease, and a commitment to represent the most up-to-date information, the LAST project terminology of HSIL to represent previously identified CIN2 and CIN3 lesions will be used for the remainder of this text.
Diagnosis
There is little data on the natural history of HSIL diagnosed after colposcopy, as most women get some form of therapy. The information that is available suggests that in patients with untreated HSIL, the cumulative incidence of malignancy is as high as 30% at 30 years (Lancet Oncol. 2008 May;9[5]:425-34). Treatment recommendations for excision are aimed at addressing this alarming number; however, care must be individualized, especially in the setting of pregnancy.
If abnormal cervical cytology is obtained on routine screening, appropriate patients should be referred for colposcopic exam. Physicians performing colposcopy should be familiar with the physiologic effects of pregnancy that can obscure the exam, including the increased cervical mucus production, prominence of endocervical glands, and increased vascularity.
Colposcopic-directed ectocervical biopsies have been found to be safe in pregnancy, and these women should be provided the same care as those who are not pregnant (Obstet Gynecol. 1993 Jun;81[6]:915-8). Endocervical sampling and endometrial sampling should not be performed, however, and physicians should remain dedicated to checking pregnancy tests prior to colposcopy.
HSIL cytology should prompt a biopsy in pregnancy; a decision to skip the biopsy and perform an excisional procedure in this setting is not recommended regardless of patient or gestational age. If LSIL (CIN1) is noted on biopsy, reevaluation post partum should be strongly considered, unless a suspicious lesion was felt to be inadequately biopsied.
Management
Managing HSIL in pregnancy focuses on diagnosis and excluding malignancy, while treatment can be reserved for the postpartum period. When choosing a management option, consider individual patient factors such as colposcopic appearance of the lesion, gestational age, and access to health care.
If HSIL is noted on colposcopic-directed biopsy, consider one of several options. The most conservative approach is reevaluation with cytology and colposcopy 6 weeks post partum. This is an option for patients who do not have a colposcopic exam that was concerning for an invasive lesion, were able to be adequately biopsied, and will reliably return for follow-up. Many physicians feel more comfortable with repeat cytology and colposcopy in 3 months from the original biopsy. The most aggressive management would include an excisional procedure during pregnancy.
There are varying rates of regression of biopsy-proven HSIL in pregnancy ranging from 34% to 70% (Obstet Gynecol. 1999 Mar;93[3]:359-62; Acta Obstet Gynecol Scand. 2006;85[9]:1134-7; Reprod Sci. 2009 Nov;16[11]:1034-9). Out of more than 200 patients across these three studies, just two patients were diagnosed with an invasive lesion post partum. Given the low likelihood of progression during pregnancy and the high rate of regression, an excisional procedure should be considered only in cases where there is concern about invasive carcinoma.
In cases where an invasive lesion is suspected, consider an an excisional procedure. While there is some evidence that performing a laser excisional procedure early in pregnancy (18 weeks and earlier) can be safely done, that is not the most common management strategy in the United States (Tumori. 1998 Sep-Oct;84[5]:567-70; Int J Gynecol Cancer. 2007 Jan-Feb;17[1]:127-31). In this circumstance, referral to a gynecologic oncologist is warranted where consideration can be made for performing a cold knife conization. Physicians should be aware of the increased risk of bleeding with this procedure in pregnancy and the potential for preterm birth. There is little literature to guide counseling regarding these risks, and the decision to perform an excisional procedure should be made with a multidisciplinary team (Arch Gynecol Obstet. 2016 Jan 4. doi: 10.1007/s00404-015-3980-y).
The see-and-treat paradigm is not recommended in pregnancy. Those patients with poor follow-up should still undergo colposcopic-directed biopsies prior to any excisional procedure.
Treatment recommendations in pregnancy should be made on the basis of careful consideration of individual patient factors, with strong consideration of repeat testing with cytology and colposcopy prior to an excision procedure.
Dr. Sullivan is a fellow in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. Dr. Gehrig is professor and director of gynecologic oncology at the university. Dr. Sullivan and Dr. Gehrig reported having no relevant financial disclosures. Email them at [email protected].

AIMS65 Score Helps Predict Inpatient Mortality in Acute Upper Gastrointestinal Bleed
Clinical question: Does AIMS65 risk stratification score predict inpatient mortality in patients with acute upper gastrointestinal bleed (UGIB)?

Background: Acute UGIB is associated with significant morbidity and mortality, which makes it crucial to identify high-risk patients early. Several prognostic algorithms such as Glasgow-Blatchford (GBS) and pre-endoscopy (pre-RS) and post-endoscopy (post-RS) Rockall scores are available to triage such patients. The goal of this study was to validate AIMS65 score as a predictor of inpatient mortality in patients with acute UGIB compared to these other prognostic scores.
Study Design: Retrospective, cohort study.
Setting: Tertiary-care center in Australia, January 2010 to June 2013.
Synopsis: Using ICD-10 diagnosis codes, investigators identified 424 patients with UGIB requiring endoscopy. All patients were risk-stratified using AIMS65, GBS, pre-RS, and post-RS. The AIMS65 score was found to be superior in predicting inpatient mortality compared to GBS and pre-RS scores and statistically superior to all other scores in predicting need for ICU admission.
In addition to being a single-center, retrospective study, other limitations include the use of ICD-10 codes to identify patients. Further prospective studies are needed to further validate the AIMS65 in acute UGIB.
Bottom line: AIMS65 is a simple and useful tool in predicting inpatient mortality in patients with acute UGIB. However, its applicability in making clinical decisions remains unclear.
Citation: Robertson M, Majumdar A, Boyapati R, et al. Risk stratification in acute upper GI bleeding: comparison of the AIMS65 score with the Glasgow-Blatchford and Rockall scoring systems [published online ahead of print October 16, 2015]. Gastrointest Endosc. doi:10.1016/j.gie.2015.10.021.
Clinical question: Does AIMS65 risk stratification score predict inpatient mortality in patients with acute upper gastrointestinal bleed (UGIB)?
Background: Acute UGIB is associated with significant morbidity and mortality, which makes it crucial to identify high-risk patients early. Several prognostic algorithms such as Glasgow-Blatchford (GBS) and pre-endoscopy (pre-RS) and post-endoscopy (post-RS) Rockall scores are available to triage such patients. The goal of this study was to validate AIMS65 score as a predictor of inpatient mortality in patients with acute UGIB compared to these other prognostic scores.
Study Design: Retrospective, cohort study.
Setting: Tertiary-care center in Australia, January 2010 to June 2013.
Synopsis: Using ICD-10 diagnosis codes, investigators identified 424 patients with UGIB requiring endoscopy. All patients were risk-stratified using AIMS65, GBS, pre-RS, and post-RS. The AIMS65 score was found to be superior in predicting inpatient mortality compared to GBS and pre-RS scores and statistically superior to all other scores in predicting need for ICU admission.
In addition to being a single-center, retrospective study, other limitations include the use of ICD-10 codes to identify patients. Further prospective studies are needed to further validate the AIMS65 in acute UGIB.
Bottom line: AIMS65 is a simple and useful tool in predicting inpatient mortality in patients with acute UGIB. However, its applicability in making clinical decisions remains unclear.
Citation: Robertson M, Majumdar A, Boyapati R, et al. Risk stratification in acute upper GI bleeding: comparison of the AIMS65 score with the Glasgow-Blatchford and Rockall scoring systems [published online ahead of print October 16, 2015]. Gastrointest Endosc. doi:10.1016/j.gie.2015.10.021.
Clinical question: Does AIMS65 risk stratification score predict inpatient mortality in patients with acute upper gastrointestinal bleed (UGIB)?
Background: Acute UGIB is associated with significant morbidity and mortality, which makes it crucial to identify high-risk patients early. Several prognostic algorithms such as Glasgow-Blatchford (GBS) and pre-endoscopy (pre-RS) and post-endoscopy (post-RS) Rockall scores are available to triage such patients. The goal of this study was to validate AIMS65 score as a predictor of inpatient mortality in patients with acute UGIB compared to these other prognostic scores.
Study Design: Retrospective, cohort study.
Setting: Tertiary-care center in Australia, January 2010 to June 2013.
Synopsis: Using ICD-10 diagnosis codes, investigators identified 424 patients with UGIB requiring endoscopy. All patients were risk-stratified using AIMS65, GBS, pre-RS, and post-RS. The AIMS65 score was found to be superior in predicting inpatient mortality compared to GBS and pre-RS scores and statistically superior to all other scores in predicting need for ICU admission.
In addition to being a single-center, retrospective study, other limitations include the use of ICD-10 codes to identify patients. Further prospective studies are needed to further validate the AIMS65 in acute UGIB.
Bottom line: AIMS65 is a simple and useful tool in predicting inpatient mortality in patients with acute UGIB. However, its applicability in making clinical decisions remains unclear.
Citation: Robertson M, Majumdar A, Boyapati R, et al. Risk stratification in acute upper GI bleeding: comparison of the AIMS65 score with the Glasgow-Blatchford and Rockall scoring systems [published online ahead of print October 16, 2015]. Gastrointest Endosc. doi:10.1016/j.gie.2015.10.021.

VTE risk varies with hormone therapy

Image by Andre E.X. Brown
Results of a case-control study indicate that estrogen-only hormone therapy carries a lower risk of venous thromboembolism (VTE) than combined estrogen-progestogen therapy.
The study also suggests the type of progestogen a patient receives does not significantly impact the risk of VTE, but the route of administration for estrogen does.
Annica Bergendal, MD, PhD, of Karolinska Institutet in Stockholm, Sweden, and her colleagues reported these findings in Menopause.
The study was conducted in Sweden between 2003 and 2009. It included 838 women with VTE and 891 age-matched control subjects.
Analyses suggested the risk of VTE was almost 2-fold higher in women currently on hormone therapy than in those not taking hormones. The odds ratio (OR)—which was adjusted for smoking, body mass index, and immobilization—was 1.72 (95% CI 1.34-2.20).
Women who took combined estrogen-progestogen therapy had nearly 3 times the VTE risk of those who took no hormones (OR 2.85, 95% CI 2.08-3.90), but the risk was much lower for women who took estrogen alone (OR 1.31, 95% CI 0.78-2.21).
The risk of VTE with combined estrogen-progestogen treatment was about double that of estrogen alone (OR 2.18, 95% CI 1.21-3.92).
Researchers have wondered whether the type of progestogen used makes a difference in the risk of VTE, but this study didn’t show any significant difference in risk between 2 commonly used progestogens.
When oral estrogen was combined with progestogen, the risk of VTE was somewhat, but not significantly, higher among users of medroxyprogesterone acetate (OR 2.94, 95% CI 1.67-5.36) than among users of norethisterone acetate (OR 2.29, 95% CI 1.50-3.40).
On the other hand, the way estrogen was delivered appeared to impact the risk of VTE, with oral estrogen conferring the highest risk.
When the researchers used transdermal estrogen—given alone—as reference, they observed an increased risk of VTE associated with oral estrogen alone (OR 1.84, 95% CI 0.62-5.52).
And when the researchers used locally (vaginally) administered estrogen alone as reference, they saw an increased risk of VTE associated with oral estrogen alone (OR 2.64, 95% CI 1.30-5.38).
Among women using combined estrogen-progestogen treatment, with transdermal estrogen as a reference, there was an increase in VTE risk associated with oral estrogen (OR 2.21, 95% CI 0.88-5.60).
“This study adds to our knowledge that transdermal estrogen therapies are safer than oral, and that different estrogen or progestogen combinations may have different risks,” said JoAnn V. Pinkerton, MD, executive director of the North American Menopause Society, who was not involved in this study.
“The lack of blood clots with transdermal estrogen and with vaginal estrogen is very reassuring for women who need to continue taking hormones as they age, when risk of blood clots increases.” ![]()
Image by Andre E.X. Brown
Results of a case-control study indicate that estrogen-only hormone therapy carries a lower risk of venous thromboembolism (VTE) than combined estrogen-progestogen therapy.
The study also suggests the type of progestogen a patient receives does not significantly impact the risk of VTE, but the route of administration for estrogen does.
Annica Bergendal, MD, PhD, of Karolinska Institutet in Stockholm, Sweden, and her colleagues reported these findings in Menopause.
The study was conducted in Sweden between 2003 and 2009. It included 838 women with VTE and 891 age-matched control subjects.
Analyses suggested the risk of VTE was almost 2-fold higher in women currently on hormone therapy than in those not taking hormones. The odds ratio (OR)—which was adjusted for smoking, body mass index, and immobilization—was 1.72 (95% CI 1.34-2.20).
Women who took combined estrogen-progestogen therapy had nearly 3 times the VTE risk of those who took no hormones (OR 2.85, 95% CI 2.08-3.90), but the risk was much lower for women who took estrogen alone (OR 1.31, 95% CI 0.78-2.21).
The risk of VTE with combined estrogen-progestogen treatment was about double that of estrogen alone (OR 2.18, 95% CI 1.21-3.92).
Researchers have wondered whether the type of progestogen used makes a difference in the risk of VTE, but this study didn’t show any significant difference in risk between 2 commonly used progestogens.
When oral estrogen was combined with progestogen, the risk of VTE was somewhat, but not significantly, higher among users of medroxyprogesterone acetate (OR 2.94, 95% CI 1.67-5.36) than among users of norethisterone acetate (OR 2.29, 95% CI 1.50-3.40).
On the other hand, the way estrogen was delivered appeared to impact the risk of VTE, with oral estrogen conferring the highest risk.
When the researchers used transdermal estrogen—given alone—as reference, they observed an increased risk of VTE associated with oral estrogen alone (OR 1.84, 95% CI 0.62-5.52).
And when the researchers used locally (vaginally) administered estrogen alone as reference, they saw an increased risk of VTE associated with oral estrogen alone (OR 2.64, 95% CI 1.30-5.38).
Among women using combined estrogen-progestogen treatment, with transdermal estrogen as a reference, there was an increase in VTE risk associated with oral estrogen (OR 2.21, 95% CI 0.88-5.60).
“This study adds to our knowledge that transdermal estrogen therapies are safer than oral, and that different estrogen or progestogen combinations may have different risks,” said JoAnn V. Pinkerton, MD, executive director of the North American Menopause Society, who was not involved in this study.
“The lack of blood clots with transdermal estrogen and with vaginal estrogen is very reassuring for women who need to continue taking hormones as they age, when risk of blood clots increases.” ![]()
Image by Andre E.X. Brown
Results of a case-control study indicate that estrogen-only hormone therapy carries a lower risk of venous thromboembolism (VTE) than combined estrogen-progestogen therapy.
The study also suggests the type of progestogen a patient receives does not significantly impact the risk of VTE, but the route of administration for estrogen does.
Annica Bergendal, MD, PhD, of Karolinska Institutet in Stockholm, Sweden, and her colleagues reported these findings in Menopause.
The study was conducted in Sweden between 2003 and 2009. It included 838 women with VTE and 891 age-matched control subjects.
Analyses suggested the risk of VTE was almost 2-fold higher in women currently on hormone therapy than in those not taking hormones. The odds ratio (OR)—which was adjusted for smoking, body mass index, and immobilization—was 1.72 (95% CI 1.34-2.20).
Women who took combined estrogen-progestogen therapy had nearly 3 times the VTE risk of those who took no hormones (OR 2.85, 95% CI 2.08-3.90), but the risk was much lower for women who took estrogen alone (OR 1.31, 95% CI 0.78-2.21).
The risk of VTE with combined estrogen-progestogen treatment was about double that of estrogen alone (OR 2.18, 95% CI 1.21-3.92).
Researchers have wondered whether the type of progestogen used makes a difference in the risk of VTE, but this study didn’t show any significant difference in risk between 2 commonly used progestogens.
When oral estrogen was combined with progestogen, the risk of VTE was somewhat, but not significantly, higher among users of medroxyprogesterone acetate (OR 2.94, 95% CI 1.67-5.36) than among users of norethisterone acetate (OR 2.29, 95% CI 1.50-3.40).
On the other hand, the way estrogen was delivered appeared to impact the risk of VTE, with oral estrogen conferring the highest risk.
When the researchers used transdermal estrogen—given alone—as reference, they observed an increased risk of VTE associated with oral estrogen alone (OR 1.84, 95% CI 0.62-5.52).
And when the researchers used locally (vaginally) administered estrogen alone as reference, they saw an increased risk of VTE associated with oral estrogen alone (OR 2.64, 95% CI 1.30-5.38).
Among women using combined estrogen-progestogen treatment, with transdermal estrogen as a reference, there was an increase in VTE risk associated with oral estrogen (OR 2.21, 95% CI 0.88-5.60).
“This study adds to our knowledge that transdermal estrogen therapies are safer than oral, and that different estrogen or progestogen combinations may have different risks,” said JoAnn V. Pinkerton, MD, executive director of the North American Menopause Society, who was not involved in this study.
“The lack of blood clots with transdermal estrogen and with vaginal estrogen is very reassuring for women who need to continue taking hormones as they age, when risk of blood clots increases.” ![]()
Study implicates circular RNAs in leukemia, other cancers

Image courtesy of The Armed
Forces Institute of Pathology
A class of circular RNAs may play a key role in the development and progression of certain leukemias and other cancers, according to research published in Cell.
Investigators found that cancer-associated chromosomal translocations give rise to fusion circular RNAs (f-circRNAs).
And these f-circRNAs aid cellular transformation, promote cell viability, confer treatment resistance, and exhibit tumor-promoting properties in vivo.
“Cancer is essentially a disease of mutated or broken genes, so that motivated us to examine whether circular RNAs, like proteins, can be affected by these chromosomal breaks,” said study author Pier Paolo Pandolfi, MD, PhD, of Beth Israel Deaconess Medical Center in Boston, Massachusetts.
“Our work paves the way to discovering many more of these unusual RNAs and how they contribute to cancer, which could reveal new mechanisms and druggable pathways involved in tumor progression.”
Curious about the possibility of circular RNAs contributing to cancer, Dr Pandolfi and his colleagues set out to see if they could detect relevant changes in tumors known to harbor distinct fusion proteins.
The team examined acute promyelocytic leukemia, which often carries a translocation between the PML and RARα genes, and acute myeloid leukemia, which can harbor a translocation between the MLL and AF9 genes.
The investigators found f-circRNAs corresponding to different exons associated with the PML-RARα gene fusion and the MLL-AF9 gene fusion. Normally, multiple circular RNAs can be generated from a single gene, so the team was not surprised to find different f-circRNAs emerging from the same fusion gene.
Dr Pandolfi and his colleagues also uncovered f-circRNAs in solid tumors—in Ewing sarcoma and lung cancer.
The team identified the f-circRNAs using 2 distinct methods—PCR-based amplification and sequencing-based approaches. They said this suggests f-circRNAs are bona fide biological entities, rather than experimental artifacts.
“Our ability to readily detect these fusion-circular RNAs—and their normal, non-fused counterparts—will be enhanced by advances in sequencing technology and analytic methods,” said study author Jlenia Guarnerio, PhD, also of Beth Israel Deaconess Medical Center.
“Indeed, as we look ahead to cataloguing them comprehensively across all cancers and to deeply understanding their mechanisms of action, we will need to propel these new methodologies even further.”
To determine whether f-circRNAs play a functional role in cancer, the investigators introduced the RNAs into cells. This caused the cells to increase their proliferation and tendency to overgrow—features shared by tumor cells.
On the other hand, when the team blocked f-circRNA activity, the cells’ normal behaviors were restored.
Dr Pandolfi and his colleagues also conducted experiments using a mouse model of leukemia. They focused on a specific f-circRNA associated with the MLL-AF9 fusion gene, called f-circM9.
Although f-circM9 could not trigger leukemia on its own, it appeared to work with other cancer-promoting signals—such as the MLL-AF9 fusion protein—to cause leukemia.
Additional experiments suggested that f-circM9 may also help tumor cells persist despite treatment with anticancer drugs.
“These results are particularly exciting because they suggest that drugs directed at fusion-circular RNAs could be a powerful strategy to pursue for future therapeutic development in cancer,” Dr Pandolfi said.
“[However,] our knowledge of circular RNAs is really in its infancy. We know that, normally, they can bind proteins as well as DNA and microRNAs, but much more needs to be done to understand how fusion-circular RNAs work. We have only scratched the surface of these RNAs and their roles in cancer and other diseases.” ![]()
Image courtesy of The Armed
Forces Institute of Pathology
A class of circular RNAs may play a key role in the development and progression of certain leukemias and other cancers, according to research published in Cell.
Investigators found that cancer-associated chromosomal translocations give rise to fusion circular RNAs (f-circRNAs).
And these f-circRNAs aid cellular transformation, promote cell viability, confer treatment resistance, and exhibit tumor-promoting properties in vivo.
“Cancer is essentially a disease of mutated or broken genes, so that motivated us to examine whether circular RNAs, like proteins, can be affected by these chromosomal breaks,” said study author Pier Paolo Pandolfi, MD, PhD, of Beth Israel Deaconess Medical Center in Boston, Massachusetts.
“Our work paves the way to discovering many more of these unusual RNAs and how they contribute to cancer, which could reveal new mechanisms and druggable pathways involved in tumor progression.”
Curious about the possibility of circular RNAs contributing to cancer, Dr Pandolfi and his colleagues set out to see if they could detect relevant changes in tumors known to harbor distinct fusion proteins.
The team examined acute promyelocytic leukemia, which often carries a translocation between the PML and RARα genes, and acute myeloid leukemia, which can harbor a translocation between the MLL and AF9 genes.
The investigators found f-circRNAs corresponding to different exons associated with the PML-RARα gene fusion and the MLL-AF9 gene fusion. Normally, multiple circular RNAs can be generated from a single gene, so the team was not surprised to find different f-circRNAs emerging from the same fusion gene.
Dr Pandolfi and his colleagues also uncovered f-circRNAs in solid tumors—in Ewing sarcoma and lung cancer.
The team identified the f-circRNAs using 2 distinct methods—PCR-based amplification and sequencing-based approaches. They said this suggests f-circRNAs are bona fide biological entities, rather than experimental artifacts.
“Our ability to readily detect these fusion-circular RNAs—and their normal, non-fused counterparts—will be enhanced by advances in sequencing technology and analytic methods,” said study author Jlenia Guarnerio, PhD, also of Beth Israel Deaconess Medical Center.
“Indeed, as we look ahead to cataloguing them comprehensively across all cancers and to deeply understanding their mechanisms of action, we will need to propel these new methodologies even further.”
To determine whether f-circRNAs play a functional role in cancer, the investigators introduced the RNAs into cells. This caused the cells to increase their proliferation and tendency to overgrow—features shared by tumor cells.
On the other hand, when the team blocked f-circRNA activity, the cells’ normal behaviors were restored.
Dr Pandolfi and his colleagues also conducted experiments using a mouse model of leukemia. They focused on a specific f-circRNA associated with the MLL-AF9 fusion gene, called f-circM9.
Although f-circM9 could not trigger leukemia on its own, it appeared to work with other cancer-promoting signals—such as the MLL-AF9 fusion protein—to cause leukemia.
Additional experiments suggested that f-circM9 may also help tumor cells persist despite treatment with anticancer drugs.
“These results are particularly exciting because they suggest that drugs directed at fusion-circular RNAs could be a powerful strategy to pursue for future therapeutic development in cancer,” Dr Pandolfi said.
“[However,] our knowledge of circular RNAs is really in its infancy. We know that, normally, they can bind proteins as well as DNA and microRNAs, but much more needs to be done to understand how fusion-circular RNAs work. We have only scratched the surface of these RNAs and their roles in cancer and other diseases.” ![]()
Image courtesy of The Armed
Forces Institute of Pathology
A class of circular RNAs may play a key role in the development and progression of certain leukemias and other cancers, according to research published in Cell.
Investigators found that cancer-associated chromosomal translocations give rise to fusion circular RNAs (f-circRNAs).
And these f-circRNAs aid cellular transformation, promote cell viability, confer treatment resistance, and exhibit tumor-promoting properties in vivo.
“Cancer is essentially a disease of mutated or broken genes, so that motivated us to examine whether circular RNAs, like proteins, can be affected by these chromosomal breaks,” said study author Pier Paolo Pandolfi, MD, PhD, of Beth Israel Deaconess Medical Center in Boston, Massachusetts.
“Our work paves the way to discovering many more of these unusual RNAs and how they contribute to cancer, which could reveal new mechanisms and druggable pathways involved in tumor progression.”
Curious about the possibility of circular RNAs contributing to cancer, Dr Pandolfi and his colleagues set out to see if they could detect relevant changes in tumors known to harbor distinct fusion proteins.
The team examined acute promyelocytic leukemia, which often carries a translocation between the PML and RARα genes, and acute myeloid leukemia, which can harbor a translocation between the MLL and AF9 genes.
The investigators found f-circRNAs corresponding to different exons associated with the PML-RARα gene fusion and the MLL-AF9 gene fusion. Normally, multiple circular RNAs can be generated from a single gene, so the team was not surprised to find different f-circRNAs emerging from the same fusion gene.
Dr Pandolfi and his colleagues also uncovered f-circRNAs in solid tumors—in Ewing sarcoma and lung cancer.
The team identified the f-circRNAs using 2 distinct methods—PCR-based amplification and sequencing-based approaches. They said this suggests f-circRNAs are bona fide biological entities, rather than experimental artifacts.
“Our ability to readily detect these fusion-circular RNAs—and their normal, non-fused counterparts—will be enhanced by advances in sequencing technology and analytic methods,” said study author Jlenia Guarnerio, PhD, also of Beth Israel Deaconess Medical Center.
“Indeed, as we look ahead to cataloguing them comprehensively across all cancers and to deeply understanding their mechanisms of action, we will need to propel these new methodologies even further.”
To determine whether f-circRNAs play a functional role in cancer, the investigators introduced the RNAs into cells. This caused the cells to increase their proliferation and tendency to overgrow—features shared by tumor cells.
On the other hand, when the team blocked f-circRNA activity, the cells’ normal behaviors were restored.
Dr Pandolfi and his colleagues also conducted experiments using a mouse model of leukemia. They focused on a specific f-circRNA associated with the MLL-AF9 fusion gene, called f-circM9.
Although f-circM9 could not trigger leukemia on its own, it appeared to work with other cancer-promoting signals—such as the MLL-AF9 fusion protein—to cause leukemia.
Additional experiments suggested that f-circM9 may also help tumor cells persist despite treatment with anticancer drugs.
“These results are particularly exciting because they suggest that drugs directed at fusion-circular RNAs could be a powerful strategy to pursue for future therapeutic development in cancer,” Dr Pandolfi said.
“[However,] our knowledge of circular RNAs is really in its infancy. We know that, normally, they can bind proteins as well as DNA and microRNAs, but much more needs to be done to understand how fusion-circular RNAs work. We have only scratched the surface of these RNAs and their roles in cancer and other diseases.” ![]()
FDA grants product orphan designation for AML

Image by Lance Liotta
The US Food and Drug Administration (FDA) has granted orphan designation for the radioimmunoconjugate Iomab-B to be used as a conditioning agent for patients with relapsed or refractory acute myeloid leukemia (AML) who are undergoing hematopoietic stem cell transplant (HSCT).
Iomab-B is a radioimmunoconjugate consisting of BC8, a novel murine monoclonal antibody, and the radioisotope iodine-131.
BC8 targets CD45, a pan-leukocytic antigen widely expressed on white blood cells. This makes BC8 potentially useful in targeting white blood cells in preparation for HSCT.
When labeled with radioactive isotopes, BC8 carries radioactivity directly to the site of cancerous growth and bone marrow, while avoiding the effects of radiation on most healthy tissues, according to Actinium Pharmaceuticals, Inc., the company developing Iomab-B.
Actinium said Iomab-B has been tested as a myeloconditioning/myeloablative agent in more than 250 patients with incurable hematologic malignancies.
The company has released data from a phase 1/2 trial of Iomab-B in patients with relapsed/refractory AML who are older than 50.
The data show that patients who received Iomab-B before HSCT (n=27) had higher rates of survival at 1 and 2 years than patients who underwent HSCT with conventional myeloablative conditioning (n=10) or chemotherapy (n=61).
One-year survival rates were 30% in the Iomab-B arm and 10% each in the conventional conditioning and chemotherapy arms. Two-year survival rates were 19%, 0%, and 0%, respectively.
Now, Actinium is planning a phase 3 trial of Iomab-B in relapsed/refractory AML patients over the age of 55.
About orphan designation
The FDA grants orphan designation to drugs intended to treat diseases or conditions affecting fewer than 200,000 patients in the US.
The designation provides the drug’s sponsor with various development incentives, including opportunities to apply for research-related tax credits and grant funding, assistance in designing clinical trials, and 7 years of US market exclusivity if the drug is approved. ![]()
Image by Lance Liotta
The US Food and Drug Administration (FDA) has granted orphan designation for the radioimmunoconjugate Iomab-B to be used as a conditioning agent for patients with relapsed or refractory acute myeloid leukemia (AML) who are undergoing hematopoietic stem cell transplant (HSCT).
Iomab-B is a radioimmunoconjugate consisting of BC8, a novel murine monoclonal antibody, and the radioisotope iodine-131.
BC8 targets CD45, a pan-leukocytic antigen widely expressed on white blood cells. This makes BC8 potentially useful in targeting white blood cells in preparation for HSCT.
When labeled with radioactive isotopes, BC8 carries radioactivity directly to the site of cancerous growth and bone marrow, while avoiding the effects of radiation on most healthy tissues, according to Actinium Pharmaceuticals, Inc., the company developing Iomab-B.
Actinium said Iomab-B has been tested as a myeloconditioning/myeloablative agent in more than 250 patients with incurable hematologic malignancies.
The company has released data from a phase 1/2 trial of Iomab-B in patients with relapsed/refractory AML who are older than 50.
The data show that patients who received Iomab-B before HSCT (n=27) had higher rates of survival at 1 and 2 years than patients who underwent HSCT with conventional myeloablative conditioning (n=10) or chemotherapy (n=61).
One-year survival rates were 30% in the Iomab-B arm and 10% each in the conventional conditioning and chemotherapy arms. Two-year survival rates were 19%, 0%, and 0%, respectively.
Now, Actinium is planning a phase 3 trial of Iomab-B in relapsed/refractory AML patients over the age of 55.
About orphan designation
The FDA grants orphan designation to drugs intended to treat diseases or conditions affecting fewer than 200,000 patients in the US.
The designation provides the drug’s sponsor with various development incentives, including opportunities to apply for research-related tax credits and grant funding, assistance in designing clinical trials, and 7 years of US market exclusivity if the drug is approved. ![]()
Image by Lance Liotta
The US Food and Drug Administration (FDA) has granted orphan designation for the radioimmunoconjugate Iomab-B to be used as a conditioning agent for patients with relapsed or refractory acute myeloid leukemia (AML) who are undergoing hematopoietic stem cell transplant (HSCT).
Iomab-B is a radioimmunoconjugate consisting of BC8, a novel murine monoclonal antibody, and the radioisotope iodine-131.
BC8 targets CD45, a pan-leukocytic antigen widely expressed on white blood cells. This makes BC8 potentially useful in targeting white blood cells in preparation for HSCT.
When labeled with radioactive isotopes, BC8 carries radioactivity directly to the site of cancerous growth and bone marrow, while avoiding the effects of radiation on most healthy tissues, according to Actinium Pharmaceuticals, Inc., the company developing Iomab-B.
Actinium said Iomab-B has been tested as a myeloconditioning/myeloablative agent in more than 250 patients with incurable hematologic malignancies.
The company has released data from a phase 1/2 trial of Iomab-B in patients with relapsed/refractory AML who are older than 50.
The data show that patients who received Iomab-B before HSCT (n=27) had higher rates of survival at 1 and 2 years than patients who underwent HSCT with conventional myeloablative conditioning (n=10) or chemotherapy (n=61).
One-year survival rates were 30% in the Iomab-B arm and 10% each in the conventional conditioning and chemotherapy arms. Two-year survival rates were 19%, 0%, and 0%, respectively.
Now, Actinium is planning a phase 3 trial of Iomab-B in relapsed/refractory AML patients over the age of 55.
About orphan designation
The FDA grants orphan designation to drugs intended to treat diseases or conditions affecting fewer than 200,000 patients in the US.
The designation provides the drug’s sponsor with various development incentives, including opportunities to apply for research-related tax credits and grant funding, assistance in designing clinical trials, and 7 years of US market exclusivity if the drug is approved. ![]()
Drug bests placebo in iron deficiency anemia trial

Top-line results from a phase 3 trial suggest the oral, iron-based drug ferric citrate is more effective than placebo for treating iron deficiency anemia in adults with stage 3-5, non-dialysis-dependent chronic kidney disease.
Fifty-two percent of patients who received ferric citrate achieved at least a 1 g/dL increase in hemoglobin over a 16-week period, compared to 19% of patients who received placebo.
Researchers said the safety profile of ferric citrate in this trial was consistent with that in previous studies.
Keryx Biopharmaceuticals, Inc., the company developing ferric citrate, recently announced these results.
Patients and treatment
In this phase 3 study, researchers compared treatment with ferric citrate to placebo in 234 patients who previously had not adequately responded to or tolerated current oral iron therapies. The patients were not allowed to receive any iron (intravenous or oral) or erythropoiesis-stimulating agents during this study.
The patients were randomized 1:1 to receive ferric citrate (n=117) or placebo (n=115). Two patients in the placebo arm discontinued the study and were not included in the efficacy analysis. One discontinued after randomization prior to receiving placebo, and the other discontinued after taking a dose of placebo but before having laboratory values drawn.
The study had a 16-week, randomized, double-blind, placebo-controlled efficacy period, followed by an 8-week, open-label safety extension period. During the extension period, all patients remaining in the study, including the placebo arm, received ferric citrate.
During the efficacy period, ferric citrate was administered at a starting dose of 3 tablets per day, with food, and could be titrated every 4 weeks by an additional 3 tablets, for up to 12 tablets per day. The mean dose of ferric citrate was 5 tablets per day.
Baseline laboratory values were similar between the treatment arms. The mean hemoglobin was 10.4 g/dL in both arms.
The mean transferrin saturation was 20.2% in the ferric citrate arm and 19.6% in the placebo arm. The mean ferritin was 85.9 ng/mL and 81.7 ng/mL, respectively. And the mean serum phosphate was 4.2 mg/dL and 4.1 mg/dL, respectively.
Efficacy results
The study achieved its primary endpoint, with 52.1% (61/117) of patients who received ferric citrate achieving a 1g/dL or greater rise in hemoglobin at any time point during the 16-week efficacy period, compared to 19.1% (22/115) of patients in the placebo arm (P<0.001).
The researchers also observed significant differences in all pre-specified secondary efficacy endpoints.
The mean change in hemoglobin was 0.75 g/dL in the ferric citrate arm and -0.08 g/dL in the placebo arm (P<0.001). The mean change in transferrin saturation was 17.8% and -0.6%, respectively (P<0.001).
The mean change in ferritin was 162.5 ng/mL and -7.7 ng/mL, respectively (P<0.001). And the mean change in serum phosphate was -0.43 mg/dL and -0.22 mg/dL, respectively (P=0.02).
The proportion of patients with a durable response during the efficacy period was 48.7% in the ferric citrate arm and 14.8% in the placebo arm (P<0.001).
A durable response was defined as a mean change in hemoglobin from baseline of at least 0.75 g/dL over any 4-week time period during the efficacy period, provided that an increase of at least 1.0 g/dL had occurred during that 4-week period.
Safety results
During the efficacy period, the majority of adverse events (AEs) were mild to moderate. The most common AEs—in the ferric citrate and placebo arms, respectively—were diarrhea (20.5% vs 16.4%), constipation (18.8% vs 12.9%), discolored feces (14.5% vs 0%), and nausea (11.1% vs 2.6%).
Hypophosphatemia was reported in 4 patients—1 in the ferric citrate arm and 3 in the placebo arm.
Twenty-six percent (31/117) of ferric citrate-treated patients and 30% (35/116) of patients receiving placebo discontinued treatment during the efficacy period. Twelve patients treated with ferric citrate discontinued due to an AE, as did 10 patients who received placebo.
During the efficacy period, the rate of serious AEs was balanced between the ferric citrate and placebo arms, at 12% and 10%, respectively. None of the serious AEs were deemed drug-related.
Over the course of the study, there were 2 deaths reported. Both occurred in patients receiving ferric citrate, but neither were considered drug-related. ![]()
Top-line results from a phase 3 trial suggest the oral, iron-based drug ferric citrate is more effective than placebo for treating iron deficiency anemia in adults with stage 3-5, non-dialysis-dependent chronic kidney disease.
Fifty-two percent of patients who received ferric citrate achieved at least a 1 g/dL increase in hemoglobin over a 16-week period, compared to 19% of patients who received placebo.
Researchers said the safety profile of ferric citrate in this trial was consistent with that in previous studies.
Keryx Biopharmaceuticals, Inc., the company developing ferric citrate, recently announced these results.
Patients and treatment
In this phase 3 study, researchers compared treatment with ferric citrate to placebo in 234 patients who previously had not adequately responded to or tolerated current oral iron therapies. The patients were not allowed to receive any iron (intravenous or oral) or erythropoiesis-stimulating agents during this study.
The patients were randomized 1:1 to receive ferric citrate (n=117) or placebo (n=115). Two patients in the placebo arm discontinued the study and were not included in the efficacy analysis. One discontinued after randomization prior to receiving placebo, and the other discontinued after taking a dose of placebo but before having laboratory values drawn.
The study had a 16-week, randomized, double-blind, placebo-controlled efficacy period, followed by an 8-week, open-label safety extension period. During the extension period, all patients remaining in the study, including the placebo arm, received ferric citrate.
During the efficacy period, ferric citrate was administered at a starting dose of 3 tablets per day, with food, and could be titrated every 4 weeks by an additional 3 tablets, for up to 12 tablets per day. The mean dose of ferric citrate was 5 tablets per day.
Baseline laboratory values were similar between the treatment arms. The mean hemoglobin was 10.4 g/dL in both arms.
The mean transferrin saturation was 20.2% in the ferric citrate arm and 19.6% in the placebo arm. The mean ferritin was 85.9 ng/mL and 81.7 ng/mL, respectively. And the mean serum phosphate was 4.2 mg/dL and 4.1 mg/dL, respectively.
Efficacy results
The study achieved its primary endpoint, with 52.1% (61/117) of patients who received ferric citrate achieving a 1g/dL or greater rise in hemoglobin at any time point during the 16-week efficacy period, compared to 19.1% (22/115) of patients in the placebo arm (P<0.001).
The researchers also observed significant differences in all pre-specified secondary efficacy endpoints.
The mean change in hemoglobin was 0.75 g/dL in the ferric citrate arm and -0.08 g/dL in the placebo arm (P<0.001). The mean change in transferrin saturation was 17.8% and -0.6%, respectively (P<0.001).
The mean change in ferritin was 162.5 ng/mL and -7.7 ng/mL, respectively (P<0.001). And the mean change in serum phosphate was -0.43 mg/dL and -0.22 mg/dL, respectively (P=0.02).
The proportion of patients with a durable response during the efficacy period was 48.7% in the ferric citrate arm and 14.8% in the placebo arm (P<0.001).
A durable response was defined as a mean change in hemoglobin from baseline of at least 0.75 g/dL over any 4-week time period during the efficacy period, provided that an increase of at least 1.0 g/dL had occurred during that 4-week period.
Safety results
During the efficacy period, the majority of adverse events (AEs) were mild to moderate. The most common AEs—in the ferric citrate and placebo arms, respectively—were diarrhea (20.5% vs 16.4%), constipation (18.8% vs 12.9%), discolored feces (14.5% vs 0%), and nausea (11.1% vs 2.6%).
Hypophosphatemia was reported in 4 patients—1 in the ferric citrate arm and 3 in the placebo arm.
Twenty-six percent (31/117) of ferric citrate-treated patients and 30% (35/116) of patients receiving placebo discontinued treatment during the efficacy period. Twelve patients treated with ferric citrate discontinued due to an AE, as did 10 patients who received placebo.
During the efficacy period, the rate of serious AEs was balanced between the ferric citrate and placebo arms, at 12% and 10%, respectively. None of the serious AEs were deemed drug-related.
Over the course of the study, there were 2 deaths reported. Both occurred in patients receiving ferric citrate, but neither were considered drug-related. ![]()
Top-line results from a phase 3 trial suggest the oral, iron-based drug ferric citrate is more effective than placebo for treating iron deficiency anemia in adults with stage 3-5, non-dialysis-dependent chronic kidney disease.
Fifty-two percent of patients who received ferric citrate achieved at least a 1 g/dL increase in hemoglobin over a 16-week period, compared to 19% of patients who received placebo.
Researchers said the safety profile of ferric citrate in this trial was consistent with that in previous studies.
Keryx Biopharmaceuticals, Inc., the company developing ferric citrate, recently announced these results.
Patients and treatment
In this phase 3 study, researchers compared treatment with ferric citrate to placebo in 234 patients who previously had not adequately responded to or tolerated current oral iron therapies. The patients were not allowed to receive any iron (intravenous or oral) or erythropoiesis-stimulating agents during this study.
The patients were randomized 1:1 to receive ferric citrate (n=117) or placebo (n=115). Two patients in the placebo arm discontinued the study and were not included in the efficacy analysis. One discontinued after randomization prior to receiving placebo, and the other discontinued after taking a dose of placebo but before having laboratory values drawn.
The study had a 16-week, randomized, double-blind, placebo-controlled efficacy period, followed by an 8-week, open-label safety extension period. During the extension period, all patients remaining in the study, including the placebo arm, received ferric citrate.
During the efficacy period, ferric citrate was administered at a starting dose of 3 tablets per day, with food, and could be titrated every 4 weeks by an additional 3 tablets, for up to 12 tablets per day. The mean dose of ferric citrate was 5 tablets per day.
Baseline laboratory values were similar between the treatment arms. The mean hemoglobin was 10.4 g/dL in both arms.
The mean transferrin saturation was 20.2% in the ferric citrate arm and 19.6% in the placebo arm. The mean ferritin was 85.9 ng/mL and 81.7 ng/mL, respectively. And the mean serum phosphate was 4.2 mg/dL and 4.1 mg/dL, respectively.
Efficacy results
The study achieved its primary endpoint, with 52.1% (61/117) of patients who received ferric citrate achieving a 1g/dL or greater rise in hemoglobin at any time point during the 16-week efficacy period, compared to 19.1% (22/115) of patients in the placebo arm (P<0.001).
The researchers also observed significant differences in all pre-specified secondary efficacy endpoints.
The mean change in hemoglobin was 0.75 g/dL in the ferric citrate arm and -0.08 g/dL in the placebo arm (P<0.001). The mean change in transferrin saturation was 17.8% and -0.6%, respectively (P<0.001).
The mean change in ferritin was 162.5 ng/mL and -7.7 ng/mL, respectively (P<0.001). And the mean change in serum phosphate was -0.43 mg/dL and -0.22 mg/dL, respectively (P=0.02).
The proportion of patients with a durable response during the efficacy period was 48.7% in the ferric citrate arm and 14.8% in the placebo arm (P<0.001).
A durable response was defined as a mean change in hemoglobin from baseline of at least 0.75 g/dL over any 4-week time period during the efficacy period, provided that an increase of at least 1.0 g/dL had occurred during that 4-week period.
Safety results
During the efficacy period, the majority of adverse events (AEs) were mild to moderate. The most common AEs—in the ferric citrate and placebo arms, respectively—were diarrhea (20.5% vs 16.4%), constipation (18.8% vs 12.9%), discolored feces (14.5% vs 0%), and nausea (11.1% vs 2.6%).
Hypophosphatemia was reported in 4 patients—1 in the ferric citrate arm and 3 in the placebo arm.
Twenty-six percent (31/117) of ferric citrate-treated patients and 30% (35/116) of patients receiving placebo discontinued treatment during the efficacy period. Twelve patients treated with ferric citrate discontinued due to an AE, as did 10 patients who received placebo.
During the efficacy period, the rate of serious AEs was balanced between the ferric citrate and placebo arms, at 12% and 10%, respectively. None of the serious AEs were deemed drug-related.
Over the course of the study, there were 2 deaths reported. Both occurred in patients receiving ferric citrate, but neither were considered drug-related. ![]()