User login
Why Hospitalists Should Embrace Population Health
Population health focuses on the specific health needs of an individual within a defined population.
“In order to truly measure a patient’s health outcomes and identify best practices, providers must evaluate a group of people with similar health needs,” explains Joseph Damore, vice president of population health management for Charlotte-N.C.-based Premier, Inc. “Once we understand a population’s outcomes, we can then target the individual.”

Fundamentally, population health is about individualized care and intervening earlier in order to get a better outcome based on what generally works for the population. It’s also about identifying populations that need specific, targeted care, such as diabetic and oncology patients.
Back in 2003, David A. Kindig MD, PhD, and Greg Stoddart, PhD, defined population health as “the health outcomes of a group of individuals, including the distribution of such outcomes within the group.”1
In order to achieve population health, according to Nick Fitterman, MD, SFHM, vice chair of hospital medicine for the Hofstra North Shore-LIJ School of Medicine in Hempstead, N.Y., “it is necessary to reduce health inequities or disparities among different populations due to, among other factors, the social determinants of health, which include social, environmental, cultural, and physical factors.”
Even though the concept of population health emerged more than 25 years ago, Dr. Fitterman points out that, until recently, the U.S. healthcare system has looked at an individual’s episodic illness rather than at population health, which focuses on wellness, prevention, and coordinated care across the continuum.

Marianne McPherson, PhD, MS, senior director of programs, research, and evaluation for the National Institute for Children’s Health Quality in Boston, says it is important for hospitalists to focus on both the patient and the population.
“You need to understand the particular factors facing the patient in front of you and understand that that individual is a product of a variety of different circumstances,” she says. “If you only look at an individual’s health, you can miss important trends across a group of patients within a population or community.
“By looking at both the individual and entire population, you can provide the most effective healthcare and health promotion.”
Government Spearheads Initiatives

With passage of the Patient Protection and Affordable Care Act (ACA) of 2010, the U.S. government helped accelerate the movement toward population health. According to Joshua D. Lenchus, DO, RPh, FACP, SFHM, a veteran hospitalist, president of Jackson Health System Medical Staff, and associate professor of clinical medicine and anesthesiology at the University of Miami Miller School of Medicine, the act’s provisions aim to improve the quality of care and create accountable care organizations (ACOs).
“The idea was to provide patients with insurance coverage, which would improve the access to care of which they were previously deprived,” he says. “With better access, they may receive quality healthcare and the identification and mitigation of disease at an early stage, thereby reducing overall healthcare costs, with the commensurate benefit of a healthy patient population.
“Of course, this is fraught with naïveté, because it explicitly dismisses nonmedical health determinants (i.e., socioeconomic status, education, literacy rate, transportation availability, employment status, individual patient responsibility, and so forth).”
Now, with ACOs, a hospital or healthcare system can manage patient risk with a potential financial gain—if they manage it well. The government shifts the episodic cost of care to an ACO, charges it with achieving health outcome metrics, and allows it to reap the reward of doing so in a cost-effective manner. More risk equals more reward, potentially. But to affect positive change in patient outcomes (e.g. health) in this manner requires acknowledging such external determinants. Hospitals, hospitalists, and physician leaders must seriously consider health determinants and how they impact patients if they are going to adequately address population health.

David Nash, MD, MBA, founding dean of the Jefferson College of Population Health at Thomas Jefferson University in Philadelphia, sees the ACA as the major driver of population health, with the payment structure moving from a world of volume to one of value.
“It’s all about demonstrating an improvement in the population’s health,” he says.
In January 2015, U.S. Department of Health and Human Services Secretary Sylvia Mathews Burwell announced that by 2018, 50 cents of every Medicare dollar will be attached to some measure of outcome.2
“So this move, from volume to value, will be the underpinning of the entire population health movement,” Dr. Nash says, “and we will be rewarded based on an improvement in a population’s health, instead of rewards for using resources on a per person basis.”
What’s a Hospitalist to Do?
Hospitalists typically are focused on inpatient care, managing a patient stay and coordinating discharge. Population health is an area, experts say, where hospitalists can extend their expertise in patient care and take a leadership role beyond the hospital.
“Hospitalists need to be aware of population health, embrace it, and help to develop structures within their programs that allow them to more closely partner with social services and case managers,” Dr. Fitterman says. “[You can] coordinate this type of care.”
Listen to more of our interview with Dr. Fitterman.
Dr. Lenchus agrees, noting that hospitalists intersect with population health most at discharge.
“The time point during which we must reconcile our discharge plan with the realities of the patient’s everyday life,” he says. “As we encourage an increasingly active lifestyle, we must pause to ascertain whether or not the patient lives in a neighborhood that is safe for outdoor activity.
As better nutrition is suggested, we must understand that the cost of a meal at a fast food chain is likely cheaper than one at a health food store. And, when arranging for a follow-up appointment, we must account for the bus schedule if a patient depends on that mode of transportation, as well as the potential to be released from work if employed.
“All of these external health determinants play a significant role in patients’ ability to adhere to instructions. Failure to [consider them in the discharge plan] will inevitably result in worsened health outcomes for the patient, and possibly hospital readmission.”
Hospitalists should be aware of the community-based organizations and services that exist, maintaining a working knowledge of who can provide volunteers, aid, food, and clothing to patients in need.
“Hospitalists should help lead or coordinate efforts to catalog these services in a community in which we practice, so we can steer patients toward these facilities,” Dr. Fitterman says. “In the past, we would treat acute medical issues and walk away. Now we need to be involved in patients’ needs, and those of their families.”
Establish a Team
A team-based approach is key to improving patient outcomes upon discharge, Dr. Lenchus says. Hospitalists should interact with social workers and case managers in anticipation of discharge; include the pharmacist in discharge medication counseling sessions. Are there relevant pharmaceutical industry-sponsored programs that can help the patient obtain prescription medications? Does the patient already qualify for some assistance? If the patient is insured, is the medication being prescribed on the formulary, or can it be modified so that it is covered? Could a generic version be prescribed? Does the patient understand the reason for hospitalization, have a follow-up appointment, and know how to take his medications?
Dr. Nash sees physicians as the team captains; physicians know how the system works, because they see it up close every day. The team includes key personnel, such as nurse practitioners, physician assistants, pharmacists, patient navigators, social workers, and patient educators.
“A physician, who might be a hospitalist, ideally will have additional training in both leadership and in population health,” Dr. Nash says.
He also encourages hospitalists to become patient advocates and educators, even though this is not their traditional role.
“They can do a lot to help a hospitalized patient face their challenges,” he says. “Encourage patients to stop smoking, go on a diet, and exercise. When a physician engages in this conversation, it aids in a patient’s ability to tackle challenges.”
For hospitalists who already feel overstretched with demands and overwhelmed with taking on the task of managing population health, Dr. McPherson suggests they learn more about the trend by studying it as part of their continuing education requirements. In addition, many hospitals have a department dedicated to patient safety or quality assurance.
“Ask how they can help the hospital to provide better patient care,” Dr. McPherson says. “Ask patients about their concerns or those of their neighbors. You may start to see trends.”
For example, if you suspect a trend of children who live in a certain housing development having difficulty breathing, try to find out if other hospital units are aware of this. Also try to ascertain whether or not any community groups connected to the hospital are already working to make the housing safer.
Population Health Challenges
The transition to being accountable for the health of a population will most likely be challenging for all providers. It involves significant risk, especially during the transition period, when an organization must live in both worlds (fee-for-service and value-based payment), says Damore, Premier’s vice president of population health management. He says it also requires:
- Enlightened and supportive leadership;
- Information technology to analyze claims and other infrastructure;
- New care management programs to coordinate care across the continuum;
- Agreements that align payment with population health management; and
- Skills and ability to transform a culture to a new value-based model.
To overcome the challenge of incorporating population health, Dr. McPherson suggests hospitals look to their large network of peers and learn from those already doing this, rather than reinventing the wheel. Look for champions to spearhead such initiatives.
“Identify folks who are already oriented in this direction and took steps in this vein,” she says.
Time and money are potential concerns, especially if embarking on a population health initiative will be an additional expense.
“A potential solution would be to look at ways to shift the focus, so that population health becomes integral to proper patient care, from promoting health and well-being to treating illness,” Dr. McPherson says. For example, by minimizing environmentally associated risks, hospitalists might be able to decrease the number of admissions, which will result in a return on your investment and improve population health.
Population health is here to stay, as payment models shift from fee-for-service to the value-based model. Hospitalists should embrace the movement and spearhead initiatives to get others on board. A hospital-wide team approach is advised. And, to save time and money, seek guidance from others who have already been successful. TH
Karen Appold is a medical writer in Pennsylvania.
References
1. Kindig D, Stoddart G. What is population health? Am J Public Health. 2003:93(3):380-383. doi: 10.2105/AJPH.93.3.380
2. Mathews Burwell S. Progress towards achieving better care, smarter spending, healthier people. U.S. Department of Health and Human Services website. January 26, 2015. Available at: http://www.hhs.gov/blog/2015/01/26/progress-towards-better-care-smarter-spending-healthier-people.html. Accessed November 8, 2015.
A Population’s Health Isn’t Just about Healthcare
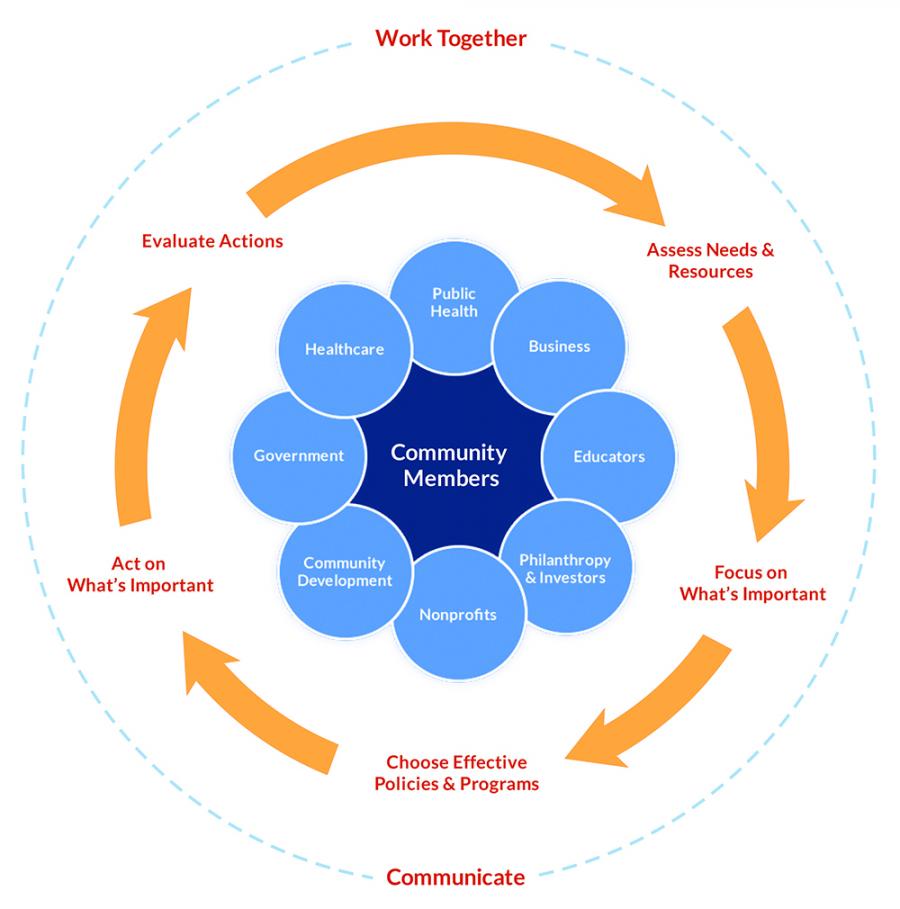
Improvement in population health requires action on multiple determinants, including medical care, health behaviors, and the social and physical environments; therefore, no single entity can be held accountable for achieving improved outcomes. Medical organizations, the government, schools, businesses, and community organizations all need to make substantial changes in how they approach health and allocate resources.1
“Community organizations have important roles, such as social services and urban planning, and businesses need to understand that they have to invest in their communities if they want a healthy future workforce,” says David A. Kindig MD, PhD, emeritus professor of population health sciences at the University of Wisconsin Madison School of Medicine and Public Health. “Everyone has a role to play.”

Healthcare organizations need to reach beyond their traditional roles to support these interventions.
“It is a team sport in 2015,” Dr. Kindig says. “For many decades, medical care was considered the most prominent factor for a population’s health. Of course it remains so, but from a population health perspective, these other factors are equally or even more important.”
According to county health rankings and roadmaps compiled for the entire United States by the University of Wisconsin, the following factors play a role in population health: clinical care, 20%; health behaviors (e.g. tobacco use, diet and exercise, sexual activity), 30%; social and economic factors (e.g. jobs, education, and social support), 40%; and physical environment (i.e., air and water quality, housing, and transit), 10%.2
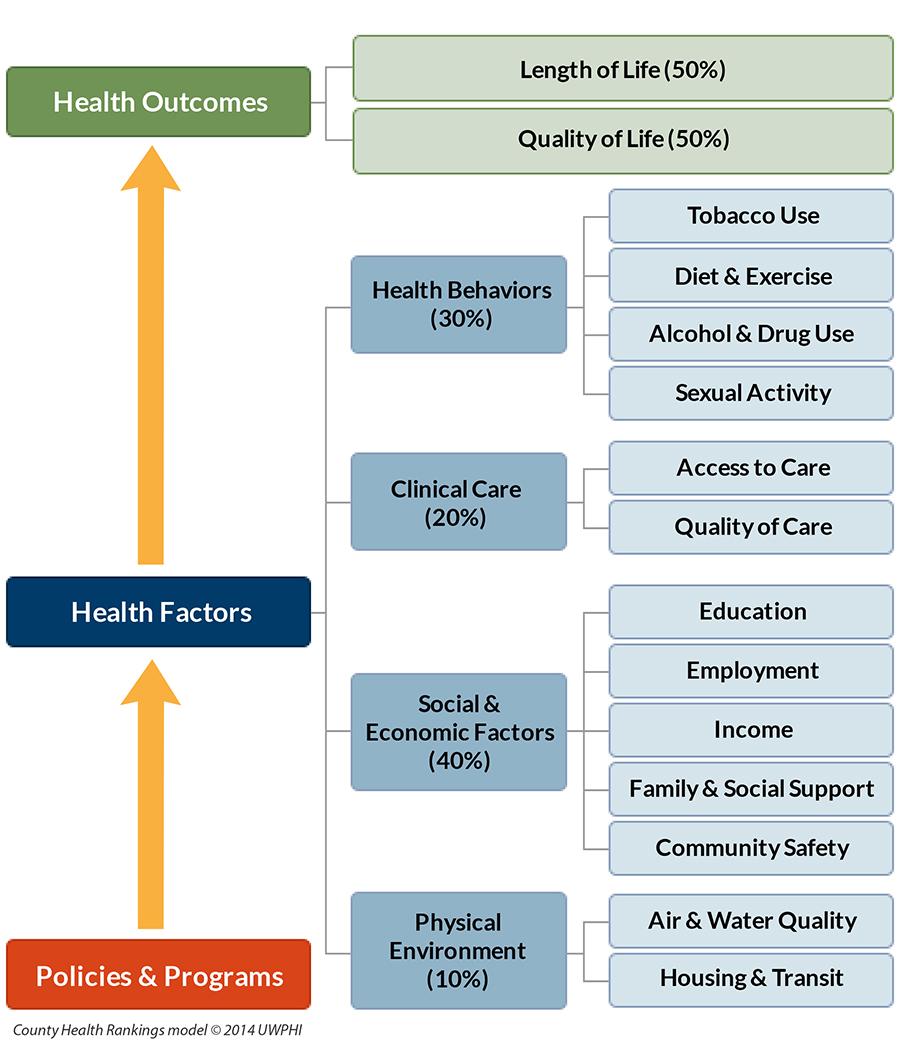
The bottom line is that most determinants of health (80%) are nonclinical.
“Social determinants are the principal driver of well-being,” says David Nash, MD, MBA, founding dean of the Jefferson College of Population Health at Thomas Jefferson University in Philadelphia. “It’s mostly about what someone does every day to stay healthy.” TH
References
1. Kindig DA, Isham G. Population health improvement: a community health business model that engages partners in all sectors. Front Health Serv Manage. 2014;30(4):3-20.
2. Our approach. County Health Rankings & Roadmaps website. Available at: http://www.countyhealthrankings.org/our-approach. Accessed November 8, 2015.
Population health focuses on the specific health needs of an individual within a defined population.
“In order to truly measure a patient’s health outcomes and identify best practices, providers must evaluate a group of people with similar health needs,” explains Joseph Damore, vice president of population health management for Charlotte-N.C.-based Premier, Inc. “Once we understand a population’s outcomes, we can then target the individual.”
Fundamentally, population health is about individualized care and intervening earlier in order to get a better outcome based on what generally works for the population. It’s also about identifying populations that need specific, targeted care, such as diabetic and oncology patients.
Back in 2003, David A. Kindig MD, PhD, and Greg Stoddart, PhD, defined population health as “the health outcomes of a group of individuals, including the distribution of such outcomes within the group.”1
In order to achieve population health, according to Nick Fitterman, MD, SFHM, vice chair of hospital medicine for the Hofstra North Shore-LIJ School of Medicine in Hempstead, N.Y., “it is necessary to reduce health inequities or disparities among different populations due to, among other factors, the social determinants of health, which include social, environmental, cultural, and physical factors.”
Even though the concept of population health emerged more than 25 years ago, Dr. Fitterman points out that, until recently, the U.S. healthcare system has looked at an individual’s episodic illness rather than at population health, which focuses on wellness, prevention, and coordinated care across the continuum.
Marianne McPherson, PhD, MS, senior director of programs, research, and evaluation for the National Institute for Children’s Health Quality in Boston, says it is important for hospitalists to focus on both the patient and the population.
“You need to understand the particular factors facing the patient in front of you and understand that that individual is a product of a variety of different circumstances,” she says. “If you only look at an individual’s health, you can miss important trends across a group of patients within a population or community.
“By looking at both the individual and entire population, you can provide the most effective healthcare and health promotion.”
Government Spearheads Initiatives
With passage of the Patient Protection and Affordable Care Act (ACA) of 2010, the U.S. government helped accelerate the movement toward population health. According to Joshua D. Lenchus, DO, RPh, FACP, SFHM, a veteran hospitalist, president of Jackson Health System Medical Staff, and associate professor of clinical medicine and anesthesiology at the University of Miami Miller School of Medicine, the act’s provisions aim to improve the quality of care and create accountable care organizations (ACOs).
“The idea was to provide patients with insurance coverage, which would improve the access to care of which they were previously deprived,” he says. “With better access, they may receive quality healthcare and the identification and mitigation of disease at an early stage, thereby reducing overall healthcare costs, with the commensurate benefit of a healthy patient population.
“Of course, this is fraught with naïveté, because it explicitly dismisses nonmedical health determinants (i.e., socioeconomic status, education, literacy rate, transportation availability, employment status, individual patient responsibility, and so forth).”
Now, with ACOs, a hospital or healthcare system can manage patient risk with a potential financial gain—if they manage it well. The government shifts the episodic cost of care to an ACO, charges it with achieving health outcome metrics, and allows it to reap the reward of doing so in a cost-effective manner. More risk equals more reward, potentially. But to affect positive change in patient outcomes (e.g. health) in this manner requires acknowledging such external determinants. Hospitals, hospitalists, and physician leaders must seriously consider health determinants and how they impact patients if they are going to adequately address population health.
David Nash, MD, MBA, founding dean of the Jefferson College of Population Health at Thomas Jefferson University in Philadelphia, sees the ACA as the major driver of population health, with the payment structure moving from a world of volume to one of value.
“It’s all about demonstrating an improvement in the population’s health,” he says.
In January 2015, U.S. Department of Health and Human Services Secretary Sylvia Mathews Burwell announced that by 2018, 50 cents of every Medicare dollar will be attached to some measure of outcome.2
“So this move, from volume to value, will be the underpinning of the entire population health movement,” Dr. Nash says, “and we will be rewarded based on an improvement in a population’s health, instead of rewards for using resources on a per person basis.”
What’s a Hospitalist to Do?
Hospitalists typically are focused on inpatient care, managing a patient stay and coordinating discharge. Population health is an area, experts say, where hospitalists can extend their expertise in patient care and take a leadership role beyond the hospital.
“Hospitalists need to be aware of population health, embrace it, and help to develop structures within their programs that allow them to more closely partner with social services and case managers,” Dr. Fitterman says. “[You can] coordinate this type of care.”
Listen to more of our interview with Dr. Fitterman.
Dr. Lenchus agrees, noting that hospitalists intersect with population health most at discharge.
“The time point during which we must reconcile our discharge plan with the realities of the patient’s everyday life,” he says. “As we encourage an increasingly active lifestyle, we must pause to ascertain whether or not the patient lives in a neighborhood that is safe for outdoor activity.
As better nutrition is suggested, we must understand that the cost of a meal at a fast food chain is likely cheaper than one at a health food store. And, when arranging for a follow-up appointment, we must account for the bus schedule if a patient depends on that mode of transportation, as well as the potential to be released from work if employed.
“All of these external health determinants play a significant role in patients’ ability to adhere to instructions. Failure to [consider them in the discharge plan] will inevitably result in worsened health outcomes for the patient, and possibly hospital readmission.”
Hospitalists should be aware of the community-based organizations and services that exist, maintaining a working knowledge of who can provide volunteers, aid, food, and clothing to patients in need.
“Hospitalists should help lead or coordinate efforts to catalog these services in a community in which we practice, so we can steer patients toward these facilities,” Dr. Fitterman says. “In the past, we would treat acute medical issues and walk away. Now we need to be involved in patients’ needs, and those of their families.”
Establish a Team
A team-based approach is key to improving patient outcomes upon discharge, Dr. Lenchus says. Hospitalists should interact with social workers and case managers in anticipation of discharge; include the pharmacist in discharge medication counseling sessions. Are there relevant pharmaceutical industry-sponsored programs that can help the patient obtain prescription medications? Does the patient already qualify for some assistance? If the patient is insured, is the medication being prescribed on the formulary, or can it be modified so that it is covered? Could a generic version be prescribed? Does the patient understand the reason for hospitalization, have a follow-up appointment, and know how to take his medications?
Dr. Nash sees physicians as the team captains; physicians know how the system works, because they see it up close every day. The team includes key personnel, such as nurse practitioners, physician assistants, pharmacists, patient navigators, social workers, and patient educators.
“A physician, who might be a hospitalist, ideally will have additional training in both leadership and in population health,” Dr. Nash says.
He also encourages hospitalists to become patient advocates and educators, even though this is not their traditional role.
“They can do a lot to help a hospitalized patient face their challenges,” he says. “Encourage patients to stop smoking, go on a diet, and exercise. When a physician engages in this conversation, it aids in a patient’s ability to tackle challenges.”
For hospitalists who already feel overstretched with demands and overwhelmed with taking on the task of managing population health, Dr. McPherson suggests they learn more about the trend by studying it as part of their continuing education requirements. In addition, many hospitals have a department dedicated to patient safety or quality assurance.
“Ask how they can help the hospital to provide better patient care,” Dr. McPherson says. “Ask patients about their concerns or those of their neighbors. You may start to see trends.”
For example, if you suspect a trend of children who live in a certain housing development having difficulty breathing, try to find out if other hospital units are aware of this. Also try to ascertain whether or not any community groups connected to the hospital are already working to make the housing safer.
Population Health Challenges
The transition to being accountable for the health of a population will most likely be challenging for all providers. It involves significant risk, especially during the transition period, when an organization must live in both worlds (fee-for-service and value-based payment), says Damore, Premier’s vice president of population health management. He says it also requires:
- Enlightened and supportive leadership;
- Information technology to analyze claims and other infrastructure;
- New care management programs to coordinate care across the continuum;
- Agreements that align payment with population health management; and
- Skills and ability to transform a culture to a new value-based model.
To overcome the challenge of incorporating population health, Dr. McPherson suggests hospitals look to their large network of peers and learn from those already doing this, rather than reinventing the wheel. Look for champions to spearhead such initiatives.
“Identify folks who are already oriented in this direction and took steps in this vein,” she says.
Time and money are potential concerns, especially if embarking on a population health initiative will be an additional expense.
“A potential solution would be to look at ways to shift the focus, so that population health becomes integral to proper patient care, from promoting health and well-being to treating illness,” Dr. McPherson says. For example, by minimizing environmentally associated risks, hospitalists might be able to decrease the number of admissions, which will result in a return on your investment and improve population health.
Population health is here to stay, as payment models shift from fee-for-service to the value-based model. Hospitalists should embrace the movement and spearhead initiatives to get others on board. A hospital-wide team approach is advised. And, to save time and money, seek guidance from others who have already been successful. TH
Karen Appold is a medical writer in Pennsylvania.
References
1. Kindig D, Stoddart G. What is population health? Am J Public Health. 2003:93(3):380-383. doi: 10.2105/AJPH.93.3.380
2. Mathews Burwell S. Progress towards achieving better care, smarter spending, healthier people. U.S. Department of Health and Human Services website. January 26, 2015. Available at: http://www.hhs.gov/blog/2015/01/26/progress-towards-better-care-smarter-spending-healthier-people.html. Accessed November 8, 2015.
A Population’s Health Isn’t Just about Healthcare
Improvement in population health requires action on multiple determinants, including medical care, health behaviors, and the social and physical environments; therefore, no single entity can be held accountable for achieving improved outcomes. Medical organizations, the government, schools, businesses, and community organizations all need to make substantial changes in how they approach health and allocate resources.1
“Community organizations have important roles, such as social services and urban planning, and businesses need to understand that they have to invest in their communities if they want a healthy future workforce,” says David A. Kindig MD, PhD, emeritus professor of population health sciences at the University of Wisconsin Madison School of Medicine and Public Health. “Everyone has a role to play.”
Healthcare organizations need to reach beyond their traditional roles to support these interventions.
“It is a team sport in 2015,” Dr. Kindig says. “For many decades, medical care was considered the most prominent factor for a population’s health. Of course it remains so, but from a population health perspective, these other factors are equally or even more important.”
According to county health rankings and roadmaps compiled for the entire United States by the University of Wisconsin, the following factors play a role in population health: clinical care, 20%; health behaviors (e.g. tobacco use, diet and exercise, sexual activity), 30%; social and economic factors (e.g. jobs, education, and social support), 40%; and physical environment (i.e., air and water quality, housing, and transit), 10%.2
The bottom line is that most determinants of health (80%) are nonclinical.
“Social determinants are the principal driver of well-being,” says David Nash, MD, MBA, founding dean of the Jefferson College of Population Health at Thomas Jefferson University in Philadelphia. “It’s mostly about what someone does every day to stay healthy.” TH
References
1. Kindig DA, Isham G. Population health improvement: a community health business model that engages partners in all sectors. Front Health Serv Manage. 2014;30(4):3-20.
2. Our approach. County Health Rankings & Roadmaps website. Available at: http://www.countyhealthrankings.org/our-approach. Accessed November 8, 2015.
Population health focuses on the specific health needs of an individual within a defined population.
“In order to truly measure a patient’s health outcomes and identify best practices, providers must evaluate a group of people with similar health needs,” explains Joseph Damore, vice president of population health management for Charlotte-N.C.-based Premier, Inc. “Once we understand a population’s outcomes, we can then target the individual.”
Fundamentally, population health is about individualized care and intervening earlier in order to get a better outcome based on what generally works for the population. It’s also about identifying populations that need specific, targeted care, such as diabetic and oncology patients.
Back in 2003, David A. Kindig MD, PhD, and Greg Stoddart, PhD, defined population health as “the health outcomes of a group of individuals, including the distribution of such outcomes within the group.”1
In order to achieve population health, according to Nick Fitterman, MD, SFHM, vice chair of hospital medicine for the Hofstra North Shore-LIJ School of Medicine in Hempstead, N.Y., “it is necessary to reduce health inequities or disparities among different populations due to, among other factors, the social determinants of health, which include social, environmental, cultural, and physical factors.”
Even though the concept of population health emerged more than 25 years ago, Dr. Fitterman points out that, until recently, the U.S. healthcare system has looked at an individual’s episodic illness rather than at population health, which focuses on wellness, prevention, and coordinated care across the continuum.
Marianne McPherson, PhD, MS, senior director of programs, research, and evaluation for the National Institute for Children’s Health Quality in Boston, says it is important for hospitalists to focus on both the patient and the population.
“You need to understand the particular factors facing the patient in front of you and understand that that individual is a product of a variety of different circumstances,” she says. “If you only look at an individual’s health, you can miss important trends across a group of patients within a population or community.
“By looking at both the individual and entire population, you can provide the most effective healthcare and health promotion.”
Government Spearheads Initiatives
With passage of the Patient Protection and Affordable Care Act (ACA) of 2010, the U.S. government helped accelerate the movement toward population health. According to Joshua D. Lenchus, DO, RPh, FACP, SFHM, a veteran hospitalist, president of Jackson Health System Medical Staff, and associate professor of clinical medicine and anesthesiology at the University of Miami Miller School of Medicine, the act’s provisions aim to improve the quality of care and create accountable care organizations (ACOs).
“The idea was to provide patients with insurance coverage, which would improve the access to care of which they were previously deprived,” he says. “With better access, they may receive quality healthcare and the identification and mitigation of disease at an early stage, thereby reducing overall healthcare costs, with the commensurate benefit of a healthy patient population.
“Of course, this is fraught with naïveté, because it explicitly dismisses nonmedical health determinants (i.e., socioeconomic status, education, literacy rate, transportation availability, employment status, individual patient responsibility, and so forth).”
Now, with ACOs, a hospital or healthcare system can manage patient risk with a potential financial gain—if they manage it well. The government shifts the episodic cost of care to an ACO, charges it with achieving health outcome metrics, and allows it to reap the reward of doing so in a cost-effective manner. More risk equals more reward, potentially. But to affect positive change in patient outcomes (e.g. health) in this manner requires acknowledging such external determinants. Hospitals, hospitalists, and physician leaders must seriously consider health determinants and how they impact patients if they are going to adequately address population health.
David Nash, MD, MBA, founding dean of the Jefferson College of Population Health at Thomas Jefferson University in Philadelphia, sees the ACA as the major driver of population health, with the payment structure moving from a world of volume to one of value.
“It’s all about demonstrating an improvement in the population’s health,” he says.
In January 2015, U.S. Department of Health and Human Services Secretary Sylvia Mathews Burwell announced that by 2018, 50 cents of every Medicare dollar will be attached to some measure of outcome.2
“So this move, from volume to value, will be the underpinning of the entire population health movement,” Dr. Nash says, “and we will be rewarded based on an improvement in a population’s health, instead of rewards for using resources on a per person basis.”
What’s a Hospitalist to Do?
Hospitalists typically are focused on inpatient care, managing a patient stay and coordinating discharge. Population health is an area, experts say, where hospitalists can extend their expertise in patient care and take a leadership role beyond the hospital.
“Hospitalists need to be aware of population health, embrace it, and help to develop structures within their programs that allow them to more closely partner with social services and case managers,” Dr. Fitterman says. “[You can] coordinate this type of care.”
Listen to more of our interview with Dr. Fitterman.
Dr. Lenchus agrees, noting that hospitalists intersect with population health most at discharge.
“The time point during which we must reconcile our discharge plan with the realities of the patient’s everyday life,” he says. “As we encourage an increasingly active lifestyle, we must pause to ascertain whether or not the patient lives in a neighborhood that is safe for outdoor activity.
As better nutrition is suggested, we must understand that the cost of a meal at a fast food chain is likely cheaper than one at a health food store. And, when arranging for a follow-up appointment, we must account for the bus schedule if a patient depends on that mode of transportation, as well as the potential to be released from work if employed.
“All of these external health determinants play a significant role in patients’ ability to adhere to instructions. Failure to [consider them in the discharge plan] will inevitably result in worsened health outcomes for the patient, and possibly hospital readmission.”
Hospitalists should be aware of the community-based organizations and services that exist, maintaining a working knowledge of who can provide volunteers, aid, food, and clothing to patients in need.
“Hospitalists should help lead or coordinate efforts to catalog these services in a community in which we practice, so we can steer patients toward these facilities,” Dr. Fitterman says. “In the past, we would treat acute medical issues and walk away. Now we need to be involved in patients’ needs, and those of their families.”
Establish a Team
A team-based approach is key to improving patient outcomes upon discharge, Dr. Lenchus says. Hospitalists should interact with social workers and case managers in anticipation of discharge; include the pharmacist in discharge medication counseling sessions. Are there relevant pharmaceutical industry-sponsored programs that can help the patient obtain prescription medications? Does the patient already qualify for some assistance? If the patient is insured, is the medication being prescribed on the formulary, or can it be modified so that it is covered? Could a generic version be prescribed? Does the patient understand the reason for hospitalization, have a follow-up appointment, and know how to take his medications?
Dr. Nash sees physicians as the team captains; physicians know how the system works, because they see it up close every day. The team includes key personnel, such as nurse practitioners, physician assistants, pharmacists, patient navigators, social workers, and patient educators.
“A physician, who might be a hospitalist, ideally will have additional training in both leadership and in population health,” Dr. Nash says.
He also encourages hospitalists to become patient advocates and educators, even though this is not their traditional role.
“They can do a lot to help a hospitalized patient face their challenges,” he says. “Encourage patients to stop smoking, go on a diet, and exercise. When a physician engages in this conversation, it aids in a patient’s ability to tackle challenges.”
For hospitalists who already feel overstretched with demands and overwhelmed with taking on the task of managing population health, Dr. McPherson suggests they learn more about the trend by studying it as part of their continuing education requirements. In addition, many hospitals have a department dedicated to patient safety or quality assurance.
“Ask how they can help the hospital to provide better patient care,” Dr. McPherson says. “Ask patients about their concerns or those of their neighbors. You may start to see trends.”
For example, if you suspect a trend of children who live in a certain housing development having difficulty breathing, try to find out if other hospital units are aware of this. Also try to ascertain whether or not any community groups connected to the hospital are already working to make the housing safer.
Population Health Challenges
The transition to being accountable for the health of a population will most likely be challenging for all providers. It involves significant risk, especially during the transition period, when an organization must live in both worlds (fee-for-service and value-based payment), says Damore, Premier’s vice president of population health management. He says it also requires:
- Enlightened and supportive leadership;
- Information technology to analyze claims and other infrastructure;
- New care management programs to coordinate care across the continuum;
- Agreements that align payment with population health management; and
- Skills and ability to transform a culture to a new value-based model.
To overcome the challenge of incorporating population health, Dr. McPherson suggests hospitals look to their large network of peers and learn from those already doing this, rather than reinventing the wheel. Look for champions to spearhead such initiatives.
“Identify folks who are already oriented in this direction and took steps in this vein,” she says.
Time and money are potential concerns, especially if embarking on a population health initiative will be an additional expense.
“A potential solution would be to look at ways to shift the focus, so that population health becomes integral to proper patient care, from promoting health and well-being to treating illness,” Dr. McPherson says. For example, by minimizing environmentally associated risks, hospitalists might be able to decrease the number of admissions, which will result in a return on your investment and improve population health.
Population health is here to stay, as payment models shift from fee-for-service to the value-based model. Hospitalists should embrace the movement and spearhead initiatives to get others on board. A hospital-wide team approach is advised. And, to save time and money, seek guidance from others who have already been successful. TH
Karen Appold is a medical writer in Pennsylvania.
References
1. Kindig D, Stoddart G. What is population health? Am J Public Health. 2003:93(3):380-383. doi: 10.2105/AJPH.93.3.380
2. Mathews Burwell S. Progress towards achieving better care, smarter spending, healthier people. U.S. Department of Health and Human Services website. January 26, 2015. Available at: http://www.hhs.gov/blog/2015/01/26/progress-towards-better-care-smarter-spending-healthier-people.html. Accessed November 8, 2015.
A Population’s Health Isn’t Just about Healthcare
Improvement in population health requires action on multiple determinants, including medical care, health behaviors, and the social and physical environments; therefore, no single entity can be held accountable for achieving improved outcomes. Medical organizations, the government, schools, businesses, and community organizations all need to make substantial changes in how they approach health and allocate resources.1
“Community organizations have important roles, such as social services and urban planning, and businesses need to understand that they have to invest in their communities if they want a healthy future workforce,” says David A. Kindig MD, PhD, emeritus professor of population health sciences at the University of Wisconsin Madison School of Medicine and Public Health. “Everyone has a role to play.”
Healthcare organizations need to reach beyond their traditional roles to support these interventions.
“It is a team sport in 2015,” Dr. Kindig says. “For many decades, medical care was considered the most prominent factor for a population’s health. Of course it remains so, but from a population health perspective, these other factors are equally or even more important.”
According to county health rankings and roadmaps compiled for the entire United States by the University of Wisconsin, the following factors play a role in population health: clinical care, 20%; health behaviors (e.g. tobacco use, diet and exercise, sexual activity), 30%; social and economic factors (e.g. jobs, education, and social support), 40%; and physical environment (i.e., air and water quality, housing, and transit), 10%.2
The bottom line is that most determinants of health (80%) are nonclinical.
“Social determinants are the principal driver of well-being,” says David Nash, MD, MBA, founding dean of the Jefferson College of Population Health at Thomas Jefferson University in Philadelphia. “It’s mostly about what someone does every day to stay healthy.” TH
References
1. Kindig DA, Isham G. Population health improvement: a community health business model that engages partners in all sectors. Front Health Serv Manage. 2014;30(4):3-20.
2. Our approach. County Health Rankings & Roadmaps website. Available at: http://www.countyhealthrankings.org/our-approach. Accessed November 8, 2015.

Population Health Prevails at Two Institutions
Population health—a movement to improve the health of an entire population—is a growing trend driven by the U.S. government. Many health systems are already on board, as healthcare shifts from a fee-for-service system to a value-based system.
One group of Premier Health hospitals and health systems has been collaborating since 2011 to build capabilities to become clinically integrated care networks that are accountable for the health of defined populations within their communities, according to Joseph Damore, vice president of population health management for the Charlotte, N.C-based company.
Damore says Premier has developed a comprehensive framework for the activities and capabilities necessary for successful population health management. Building blocks include:
- Patient-centered foundation (greater patient engagement and involvement in clinical decisions);
- Health home (a primary care medical home);
- High-value network (a set of providers who deliver quality care at an efficient price and whose performance is measured in the areas of cost, quality, and satisfaction);
- Payer partnership (care delivery network providers working with payers to create aligned financial incentives consistent with providing high-value care);
- Population health data management (collecting, analyzing, and reporting data covering all of the care the network’s patient population receives); and
- Network leadership (systematic governance and administration) focused on improving health, managing and coordinating care, and managing per capita cost.
“We’re also working with health systems on initiatives to establish patient-centered foundations and medical homes and create clinically integrated networks, providing our members with a direct roadmap to follow to successfully transition to this new value-based model,” Damore says.
At Jackson Memorial Hospital, one of the nation’s largest safety net hospitals, managing population health is ingrained in staff from day one. Nonetheless, Joshua D. Lenchus, DO, RPh, FACP, SFHM, president of Jackson Health System Medical Staff, says there are opportunities for improvement.
“A more team-based, collaborative approach is being piloted on some floors of our hospital, with specific physician groups,” he says. “Armed with the knowledge of these interventions, we can work on bolstering the pearls and rectifying the pitfalls as we move forward.
“One of our biggest obstacles to success is our patients’ general socioeconomic status.”
A current initiative at Jackson includes piloting a physician-led, multidisciplinary approach to address some of the health determinants. Furthermore, the health system is building additional satellite community clinics and urgent care centers, as it attempts to address disease earlier in the process. Additionally, there is a renewed emphasis on reinforcing the primary care infrastructure to facilitate patient appointment needs, Dr. Lenchus says. TH
Population health—a movement to improve the health of an entire population—is a growing trend driven by the U.S. government. Many health systems are already on board, as healthcare shifts from a fee-for-service system to a value-based system.
One group of Premier Health hospitals and health systems has been collaborating since 2011 to build capabilities to become clinically integrated care networks that are accountable for the health of defined populations within their communities, according to Joseph Damore, vice president of population health management for the Charlotte, N.C-based company.
Damore says Premier has developed a comprehensive framework for the activities and capabilities necessary for successful population health management. Building blocks include:
- Patient-centered foundation (greater patient engagement and involvement in clinical decisions);
- Health home (a primary care medical home);
- High-value network (a set of providers who deliver quality care at an efficient price and whose performance is measured in the areas of cost, quality, and satisfaction);
- Payer partnership (care delivery network providers working with payers to create aligned financial incentives consistent with providing high-value care);
- Population health data management (collecting, analyzing, and reporting data covering all of the care the network’s patient population receives); and
- Network leadership (systematic governance and administration) focused on improving health, managing and coordinating care, and managing per capita cost.
“We’re also working with health systems on initiatives to establish patient-centered foundations and medical homes and create clinically integrated networks, providing our members with a direct roadmap to follow to successfully transition to this new value-based model,” Damore says.
At Jackson Memorial Hospital, one of the nation’s largest safety net hospitals, managing population health is ingrained in staff from day one. Nonetheless, Joshua D. Lenchus, DO, RPh, FACP, SFHM, president of Jackson Health System Medical Staff, says there are opportunities for improvement.
“A more team-based, collaborative approach is being piloted on some floors of our hospital, with specific physician groups,” he says. “Armed with the knowledge of these interventions, we can work on bolstering the pearls and rectifying the pitfalls as we move forward.
“One of our biggest obstacles to success is our patients’ general socioeconomic status.”
A current initiative at Jackson includes piloting a physician-led, multidisciplinary approach to address some of the health determinants. Furthermore, the health system is building additional satellite community clinics and urgent care centers, as it attempts to address disease earlier in the process. Additionally, there is a renewed emphasis on reinforcing the primary care infrastructure to facilitate patient appointment needs, Dr. Lenchus says. TH
Population health—a movement to improve the health of an entire population—is a growing trend driven by the U.S. government. Many health systems are already on board, as healthcare shifts from a fee-for-service system to a value-based system.
One group of Premier Health hospitals and health systems has been collaborating since 2011 to build capabilities to become clinically integrated care networks that are accountable for the health of defined populations within their communities, according to Joseph Damore, vice president of population health management for the Charlotte, N.C-based company.
Damore says Premier has developed a comprehensive framework for the activities and capabilities necessary for successful population health management. Building blocks include:
- Patient-centered foundation (greater patient engagement and involvement in clinical decisions);
- Health home (a primary care medical home);
- High-value network (a set of providers who deliver quality care at an efficient price and whose performance is measured in the areas of cost, quality, and satisfaction);
- Payer partnership (care delivery network providers working with payers to create aligned financial incentives consistent with providing high-value care);
- Population health data management (collecting, analyzing, and reporting data covering all of the care the network’s patient population receives); and
- Network leadership (systematic governance and administration) focused on improving health, managing and coordinating care, and managing per capita cost.
“We’re also working with health systems on initiatives to establish patient-centered foundations and medical homes and create clinically integrated networks, providing our members with a direct roadmap to follow to successfully transition to this new value-based model,” Damore says.
At Jackson Memorial Hospital, one of the nation’s largest safety net hospitals, managing population health is ingrained in staff from day one. Nonetheless, Joshua D. Lenchus, DO, RPh, FACP, SFHM, president of Jackson Health System Medical Staff, says there are opportunities for improvement.
“A more team-based, collaborative approach is being piloted on some floors of our hospital, with specific physician groups,” he says. “Armed with the knowledge of these interventions, we can work on bolstering the pearls and rectifying the pitfalls as we move forward.
“One of our biggest obstacles to success is our patients’ general socioeconomic status.”
A current initiative at Jackson includes piloting a physician-led, multidisciplinary approach to address some of the health determinants. Furthermore, the health system is building additional satellite community clinics and urgent care centers, as it attempts to address disease earlier in the process. Additionally, there is a renewed emphasis on reinforcing the primary care infrastructure to facilitate patient appointment needs, Dr. Lenchus says. TH
Team discovers virus linked to HCV

Photo by Daniel Gay
Researchers have discovered a bloodborne virus, known as human pegivirus 2 (HPgV-2), in patients with hepatitis C virus (HCV).
The team identified 8 complete strains of HPgV-2 and noted that the virus was only found in patients who tested positive for HCV RNA. However, it’s not clear if HPgV-2 causes hepatitis.
Charles Chiu, MD, PhD, of the University of California San Francisco, and his colleagues described their discovery of HPgV-2 in PLOS Pathogens.
The team identified the virus by sequencing plasma from an HCV-infected patient with multiple bloodborne exposures who died from sepsis of unknown etiology.
They said HPgV-2 is “highly divergent,” sharing less than 32% amino acid identity with its nearest relatives, rodent and bat pegiviruses.
After their initial discovery, the researchers screened an additional 2440 plasma samples and found 11 HPgV-2 RNA-positive samples.
All 12 HPgV-2 RNA-positive cases were found in patients who tested positive for HCV RNA, including 2 patients who were also infected with HIV.
The researchers performed longitudinal sampling in 2 patients and found that active HPgV-2 infection can persist in blood for at least 7 weeks, despite the presence of virus-specific antibodies.
The team also identified 1 patient with HPgV-2 and HCV RNA who was seronegative for both viruses. They said this suggests a high likelihood of simultaneous acquisition of HCV and HPgV-2 infection from an acute co-transmission event.
“Based on our findings, our team used the genetic makeup of the virus to develop both a molecular test for detecting it in the bloodstream and an antibody test for determining an immune response to the virus,” said John Hackett Jr, PhD, of Abbott Laboratories, Inc. in Abbott Park, Illinois.
“Our next step is to explore whether this new virus can cause disease, and if so, work with blood banks to continue to help safeguard the world’s blood supply against these types of new viruses. Research such as this is ultimately focused on unlocking new technologies that hold the potential for significant improvements to the practice of healthcare.” ![]()
Photo by Daniel Gay
Researchers have discovered a bloodborne virus, known as human pegivirus 2 (HPgV-2), in patients with hepatitis C virus (HCV).
The team identified 8 complete strains of HPgV-2 and noted that the virus was only found in patients who tested positive for HCV RNA. However, it’s not clear if HPgV-2 causes hepatitis.
Charles Chiu, MD, PhD, of the University of California San Francisco, and his colleagues described their discovery of HPgV-2 in PLOS Pathogens.
The team identified the virus by sequencing plasma from an HCV-infected patient with multiple bloodborne exposures who died from sepsis of unknown etiology.
They said HPgV-2 is “highly divergent,” sharing less than 32% amino acid identity with its nearest relatives, rodent and bat pegiviruses.
After their initial discovery, the researchers screened an additional 2440 plasma samples and found 11 HPgV-2 RNA-positive samples.
All 12 HPgV-2 RNA-positive cases were found in patients who tested positive for HCV RNA, including 2 patients who were also infected with HIV.
The researchers performed longitudinal sampling in 2 patients and found that active HPgV-2 infection can persist in blood for at least 7 weeks, despite the presence of virus-specific antibodies.
The team also identified 1 patient with HPgV-2 and HCV RNA who was seronegative for both viruses. They said this suggests a high likelihood of simultaneous acquisition of HCV and HPgV-2 infection from an acute co-transmission event.
“Based on our findings, our team used the genetic makeup of the virus to develop both a molecular test for detecting it in the bloodstream and an antibody test for determining an immune response to the virus,” said John Hackett Jr, PhD, of Abbott Laboratories, Inc. in Abbott Park, Illinois.
“Our next step is to explore whether this new virus can cause disease, and if so, work with blood banks to continue to help safeguard the world’s blood supply against these types of new viruses. Research such as this is ultimately focused on unlocking new technologies that hold the potential for significant improvements to the practice of healthcare.” ![]()
Photo by Daniel Gay
Researchers have discovered a bloodborne virus, known as human pegivirus 2 (HPgV-2), in patients with hepatitis C virus (HCV).
The team identified 8 complete strains of HPgV-2 and noted that the virus was only found in patients who tested positive for HCV RNA. However, it’s not clear if HPgV-2 causes hepatitis.
Charles Chiu, MD, PhD, of the University of California San Francisco, and his colleagues described their discovery of HPgV-2 in PLOS Pathogens.
The team identified the virus by sequencing plasma from an HCV-infected patient with multiple bloodborne exposures who died from sepsis of unknown etiology.
They said HPgV-2 is “highly divergent,” sharing less than 32% amino acid identity with its nearest relatives, rodent and bat pegiviruses.
After their initial discovery, the researchers screened an additional 2440 plasma samples and found 11 HPgV-2 RNA-positive samples.
All 12 HPgV-2 RNA-positive cases were found in patients who tested positive for HCV RNA, including 2 patients who were also infected with HIV.
The researchers performed longitudinal sampling in 2 patients and found that active HPgV-2 infection can persist in blood for at least 7 weeks, despite the presence of virus-specific antibodies.
The team also identified 1 patient with HPgV-2 and HCV RNA who was seronegative for both viruses. They said this suggests a high likelihood of simultaneous acquisition of HCV and HPgV-2 infection from an acute co-transmission event.
“Based on our findings, our team used the genetic makeup of the virus to develop both a molecular test for detecting it in the bloodstream and an antibody test for determining an immune response to the virus,” said John Hackett Jr, PhD, of Abbott Laboratories, Inc. in Abbott Park, Illinois.
“Our next step is to explore whether this new virus can cause disease, and if so, work with blood banks to continue to help safeguard the world’s blood supply against these types of new viruses. Research such as this is ultimately focused on unlocking new technologies that hold the potential for significant improvements to the practice of healthcare.” ![]()
2016 Directory of VA and DoD Facilities
Click here to access the 2016 Directory of VA and DoD Facilities Digital Edition
Table of Contents
- Letter From the Publisher
- Explanatory Notes and Abbreviation Key
- Veterans Integrated Service Network (VISN) Guide / MyVA Regions Guide
- Department of Veterans Affairs Health Care Facilities
- TRICARE Region Guide
- Department of Defense Health Care Facilities
Click here to access the 2016 Directory of VA and DoD Facilities Digital Edition
Table of Contents
- Letter From the Publisher
- Explanatory Notes and Abbreviation Key
- Veterans Integrated Service Network (VISN) Guide / MyVA Regions Guide
- Department of Veterans Affairs Health Care Facilities
- TRICARE Region Guide
- Department of Defense Health Care Facilities
Click here to access the 2016 Directory of VA and DoD Facilities Digital Edition
Table of Contents
- Letter From the Publisher
- Explanatory Notes and Abbreviation Key
- Veterans Integrated Service Network (VISN) Guide / MyVA Regions Guide
- Department of Veterans Affairs Health Care Facilities
- TRICARE Region Guide
- Department of Defense Health Care Facilities
Hepatitis C virus infection linked to cardiovascular death, disease, and stroke
Patients with hepatitis C virus (HCV) infection face a significantly increased risk of cardiovascular death, subclinical carotid thickening and atherosclerosis, and cerebrocardiovascular events, especially when they also have diabetes and hypertension, according to a systematic review and meta-analysis of 22 studies published in the January issue of Gastroenterology.
“To our knowledge, our meta-analysis clearly highlights, for the first time, that HCV infection increases the risk of cardiovascular disease-related mortality,” wrote Dr. Salvatore Petta and his associates at the University of Palermo, Italy. “We [also] found a twofold higher risk of subclinical carotid plaques among HCV-infected individuals compared to uninfected controls, without significant heterogeneity among studies, as well as an increased risk of carotid thickening. We observed a slightly significant increase in cerebrocardiovascular events among HCV-infected patients, despite the high heterogeneity among studies that was mostly related to the prevalence of diabetes mellitus and hypertension.”
A number of observational studies have reported cardiovascular outcomes in HCV-infected patients, but results have been “ambiguous,” Dr. Petta and his colleagues said. For their meta-analysis, they searched PubMed, Medline, EMBASE, the Cochrane Library, and reference lists of articles to identify studies published through July 2015 that either compared cardiovascular disease between HCV-infected and uninfected patients, or evaluated the prevalence of HCV infection among patients with cardiovascular disease. This literature search identified 12 case-control studies and 10 cohort studies. Outcome measures included carotid atherosclerosis (nine studies), intima media thickness (eight studies), coronary artery disease (seven studies), stroke (six studies), and cardiovascular mortality (three studies) (Gastroenterology. 2015 Sep 18. doi: 10.1053/j.gastro.2015.09.00).In the pooled analysis, the odds of cardiovascular death were 65% higher in HCV-infected patients, compared with uninfected individuals (95% confidence interval for this increase, 1.07%-2.56%). Compared with controls, HCV-infected patients also were at higher risk of carotid plaques (odds ratio, 2.27; 95% CI, 1.76-2.94), especially when they were smokers (P = .02). HCV infection also significantly increased the odds of carotid artery intima-media thickening (OR, 1.20; 95% CI, 1.03-1.40), and cerebrocardiovascular events (OR, 1.30; 95% CI, 1.10-1.55). However, subgroup analyses showed that HCV infection only increased the likelihood of cerebrocardiovascular events in populations with a more than 10% prevalence of diabetes or a more than 20% prevalence of hypertension (OR, 1.71; P less than .001 for both subgroup analyses).
Because the studies of cerebrocardiovascular events were heterogeneous, the researchers also stratified them by study design and by the average age of patients. Pooled odds ratios for the link between HCV infection and cerebrocardiovascular events remained significant at 1.21 for the cohort studies, 2.01 for the case-control studies, 2.46 among patients who averaged more than 50 years of age, and 1.35 among younger patients.
The Egger test for publication bias showed that the literature search was unlikely to have overlooked studies in terms of any of the outcome measures, the investigators noted. “From a clinical standpoint, the results of our meta-analysis suggest that HCV infection increases cardiovascular risk, particularly for individuals who already have cardiovascular risk factors, such as diabetes and hypertension,” they concluded. “Although effective and safe oral antiviral regimens are available, more information is needed to confirm whether anti-HCV medications will decrease cardiovascular risk, as suggested in some studies.”
The researchers reported having no funding sources or conflicts of interest.
Source: American Gastroenterological Association
Patients with hepatitis C virus (HCV) infection face a significantly increased risk of cardiovascular death, subclinical carotid thickening and atherosclerosis, and cerebrocardiovascular events, especially when they also have diabetes and hypertension, according to a systematic review and meta-analysis of 22 studies published in the January issue of Gastroenterology.
“To our knowledge, our meta-analysis clearly highlights, for the first time, that HCV infection increases the risk of cardiovascular disease-related mortality,” wrote Dr. Salvatore Petta and his associates at the University of Palermo, Italy. “We [also] found a twofold higher risk of subclinical carotid plaques among HCV-infected individuals compared to uninfected controls, without significant heterogeneity among studies, as well as an increased risk of carotid thickening. We observed a slightly significant increase in cerebrocardiovascular events among HCV-infected patients, despite the high heterogeneity among studies that was mostly related to the prevalence of diabetes mellitus and hypertension.”
A number of observational studies have reported cardiovascular outcomes in HCV-infected patients, but results have been “ambiguous,” Dr. Petta and his colleagues said. For their meta-analysis, they searched PubMed, Medline, EMBASE, the Cochrane Library, and reference lists of articles to identify studies published through July 2015 that either compared cardiovascular disease between HCV-infected and uninfected patients, or evaluated the prevalence of HCV infection among patients with cardiovascular disease. This literature search identified 12 case-control studies and 10 cohort studies. Outcome measures included carotid atherosclerosis (nine studies), intima media thickness (eight studies), coronary artery disease (seven studies), stroke (six studies), and cardiovascular mortality (three studies) (Gastroenterology. 2015 Sep 18. doi: 10.1053/j.gastro.2015.09.00).In the pooled analysis, the odds of cardiovascular death were 65% higher in HCV-infected patients, compared with uninfected individuals (95% confidence interval for this increase, 1.07%-2.56%). Compared with controls, HCV-infected patients also were at higher risk of carotid plaques (odds ratio, 2.27; 95% CI, 1.76-2.94), especially when they were smokers (P = .02). HCV infection also significantly increased the odds of carotid artery intima-media thickening (OR, 1.20; 95% CI, 1.03-1.40), and cerebrocardiovascular events (OR, 1.30; 95% CI, 1.10-1.55). However, subgroup analyses showed that HCV infection only increased the likelihood of cerebrocardiovascular events in populations with a more than 10% prevalence of diabetes or a more than 20% prevalence of hypertension (OR, 1.71; P less than .001 for both subgroup analyses).
Because the studies of cerebrocardiovascular events were heterogeneous, the researchers also stratified them by study design and by the average age of patients. Pooled odds ratios for the link between HCV infection and cerebrocardiovascular events remained significant at 1.21 for the cohort studies, 2.01 for the case-control studies, 2.46 among patients who averaged more than 50 years of age, and 1.35 among younger patients.
The Egger test for publication bias showed that the literature search was unlikely to have overlooked studies in terms of any of the outcome measures, the investigators noted. “From a clinical standpoint, the results of our meta-analysis suggest that HCV infection increases cardiovascular risk, particularly for individuals who already have cardiovascular risk factors, such as diabetes and hypertension,” they concluded. “Although effective and safe oral antiviral regimens are available, more information is needed to confirm whether anti-HCV medications will decrease cardiovascular risk, as suggested in some studies.”
The researchers reported having no funding sources or conflicts of interest.
Source: American Gastroenterological Association
Patients with hepatitis C virus (HCV) infection face a significantly increased risk of cardiovascular death, subclinical carotid thickening and atherosclerosis, and cerebrocardiovascular events, especially when they also have diabetes and hypertension, according to a systematic review and meta-analysis of 22 studies published in the January issue of Gastroenterology.
“To our knowledge, our meta-analysis clearly highlights, for the first time, that HCV infection increases the risk of cardiovascular disease-related mortality,” wrote Dr. Salvatore Petta and his associates at the University of Palermo, Italy. “We [also] found a twofold higher risk of subclinical carotid plaques among HCV-infected individuals compared to uninfected controls, without significant heterogeneity among studies, as well as an increased risk of carotid thickening. We observed a slightly significant increase in cerebrocardiovascular events among HCV-infected patients, despite the high heterogeneity among studies that was mostly related to the prevalence of diabetes mellitus and hypertension.”
A number of observational studies have reported cardiovascular outcomes in HCV-infected patients, but results have been “ambiguous,” Dr. Petta and his colleagues said. For their meta-analysis, they searched PubMed, Medline, EMBASE, the Cochrane Library, and reference lists of articles to identify studies published through July 2015 that either compared cardiovascular disease between HCV-infected and uninfected patients, or evaluated the prevalence of HCV infection among patients with cardiovascular disease. This literature search identified 12 case-control studies and 10 cohort studies. Outcome measures included carotid atherosclerosis (nine studies), intima media thickness (eight studies), coronary artery disease (seven studies), stroke (six studies), and cardiovascular mortality (three studies) (Gastroenterology. 2015 Sep 18. doi: 10.1053/j.gastro.2015.09.00).In the pooled analysis, the odds of cardiovascular death were 65% higher in HCV-infected patients, compared with uninfected individuals (95% confidence interval for this increase, 1.07%-2.56%). Compared with controls, HCV-infected patients also were at higher risk of carotid plaques (odds ratio, 2.27; 95% CI, 1.76-2.94), especially when they were smokers (P = .02). HCV infection also significantly increased the odds of carotid artery intima-media thickening (OR, 1.20; 95% CI, 1.03-1.40), and cerebrocardiovascular events (OR, 1.30; 95% CI, 1.10-1.55). However, subgroup analyses showed that HCV infection only increased the likelihood of cerebrocardiovascular events in populations with a more than 10% prevalence of diabetes or a more than 20% prevalence of hypertension (OR, 1.71; P less than .001 for both subgroup analyses).
Because the studies of cerebrocardiovascular events were heterogeneous, the researchers also stratified them by study design and by the average age of patients. Pooled odds ratios for the link between HCV infection and cerebrocardiovascular events remained significant at 1.21 for the cohort studies, 2.01 for the case-control studies, 2.46 among patients who averaged more than 50 years of age, and 1.35 among younger patients.
The Egger test for publication bias showed that the literature search was unlikely to have overlooked studies in terms of any of the outcome measures, the investigators noted. “From a clinical standpoint, the results of our meta-analysis suggest that HCV infection increases cardiovascular risk, particularly for individuals who already have cardiovascular risk factors, such as diabetes and hypertension,” they concluded. “Although effective and safe oral antiviral regimens are available, more information is needed to confirm whether anti-HCV medications will decrease cardiovascular risk, as suggested in some studies.”
The researchers reported having no funding sources or conflicts of interest.
Source: American Gastroenterological Association
FROM GASTROENTEROLOGY
Key clinical point: Patients with HCV infection are at increased risk of cardiovascular death, stroke, and subclinical carotid atherosclerosis and thickening.
Major finding: The pooled odds of cardiovascular death were 65% higher among infected, compared with uninfected individuals.
Data source: A systematic review and meta-analysis of 22 observational studies.
Disclosures: The researchers reported having no funding sources or conflicts of interest.
Nonalcoholic fatty liver disease linked to liver cancer without cirrhosis
About 13% of U.S. veterans with hepatocellular carcinoma had no evidence of preexisting cirrhosis, according to a report published in the January issue of Clinical Gastroenterology and Hepatology.
“The main risk factors for this entity were nonalcoholic fatty liver disease [NAFLD] or metabolic syndrome” – not hepatitis C virus infection [HCV], HBV [hepatitis B virus] infection, or alcohol abuse, said Dr. Sahil Mittal of the Michael E. DeBakey Veterans Affairs Medical Center and Baylor College of Medicine in Houston. Screening all patients with NAFLD for hepatocellular carcinoma [HCC] is impractical, so studies should seek “actionable risk factors” or biomarkers that reliably identify NAFLD patients who are at particular risk of HCC, wrote Dr. Mittal and his coinvestigators.
Researchers have debated whether chronic HCV infection or alcohol abuse can lead to HCC in the absence of cirrhosis, while at least one study has shown that NAFLD can predispose patients to this disease entity (Arch Pathol Lab Med. 2008;132:1761-6).
But few studies have systematically examined risk factors for HCC without cirrhosis in the general population, the investigators said. Therefore, they randomly selected 1,500 patients from the U.S. Veterans Affairs system who were diagnosed with HCC between 2005 and 2010 on the basis of histopathology or established imaging criteria (Hepatology 2005;42:1208-36).
They reviewed complete medical records for these patients, and classified those who did not have cirrhosis according to the quality of supporting histology, laboratory, and imaging data (Clin Gastroenterol Hepatol. 2015. doi: 0.1016/j.cgh.2015.07.019).
In all, 3% of the cohort had level 1 (“highest-quality”) evidence for not having cirrhosis, while another 10% had level 2 evidence for no cirrhosis, the investigators said. “Compared with HCC in the presence of cirrhosis, these patients were more likely to have metabolic syndrome or NAFLD or no identifiable risk factor, and less likely to have alcohol abuse or HCV infection,” they added. Only two-thirds of NAFLD patients with HCC had cirrhosis, compared with 91% of patients with chronic HCV infection, 92% of HCV-infected patients, and 88% of patients with an alcohol use disorder. Notably, the odds of HCC in the absence of cirrhosis were more than five times higher when patients had NAFLD (odds ratio [OR], 5.4; 95% confidence interval [CI], 3.4-8.5) or metabolic syndrome (OR, 5.0; 95% CI, 3.1-7.8) compared with HCV infection.
Patients with cirrhosis often go unscreened for HCC even though they are at greatest risk of this cancer. Therefore, trying to screen all patients with NAFLD for HCC would be “logistically impractical,” particularly when the absolute risk of HCC in noncirrhotic patients is unknown and no one has examined the best ways to screen this population, the investigators said. Instead, clinicians could prioritize screening and treating NAFLD patients for diabetes mellitus and obesity, both of which are associated with HCC. “There is evidence to suggest that metformin reduces the risk of HCC among diabetics,” they added. “Studies of these and other risk factors of HCC among NAFLD patients with and without cirrhosis are needed.”
Most patients in the study were male, potentially limiting the generalizability of the findings, the researchers noted.
The National Cancer Institute, the Houston Veterans Affairs Health Services Research and Development Center of Excellence, the Michael E. DeBakey Veterans Affairs Medical Center, and the Dan Duncan Cancer Center funded the study. The researchers had no disclosures.
Source: American Gastroenterological Association
About 13% of U.S. veterans with hepatocellular carcinoma had no evidence of preexisting cirrhosis, according to a report published in the January issue of Clinical Gastroenterology and Hepatology.
“The main risk factors for this entity were nonalcoholic fatty liver disease [NAFLD] or metabolic syndrome” – not hepatitis C virus infection [HCV], HBV [hepatitis B virus] infection, or alcohol abuse, said Dr. Sahil Mittal of the Michael E. DeBakey Veterans Affairs Medical Center and Baylor College of Medicine in Houston. Screening all patients with NAFLD for hepatocellular carcinoma [HCC] is impractical, so studies should seek “actionable risk factors” or biomarkers that reliably identify NAFLD patients who are at particular risk of HCC, wrote Dr. Mittal and his coinvestigators.
Researchers have debated whether chronic HCV infection or alcohol abuse can lead to HCC in the absence of cirrhosis, while at least one study has shown that NAFLD can predispose patients to this disease entity (Arch Pathol Lab Med. 2008;132:1761-6).
But few studies have systematically examined risk factors for HCC without cirrhosis in the general population, the investigators said. Therefore, they randomly selected 1,500 patients from the U.S. Veterans Affairs system who were diagnosed with HCC between 2005 and 2010 on the basis of histopathology or established imaging criteria (Hepatology 2005;42:1208-36).
They reviewed complete medical records for these patients, and classified those who did not have cirrhosis according to the quality of supporting histology, laboratory, and imaging data (Clin Gastroenterol Hepatol. 2015. doi: 0.1016/j.cgh.2015.07.019).
In all, 3% of the cohort had level 1 (“highest-quality”) evidence for not having cirrhosis, while another 10% had level 2 evidence for no cirrhosis, the investigators said. “Compared with HCC in the presence of cirrhosis, these patients were more likely to have metabolic syndrome or NAFLD or no identifiable risk factor, and less likely to have alcohol abuse or HCV infection,” they added. Only two-thirds of NAFLD patients with HCC had cirrhosis, compared with 91% of patients with chronic HCV infection, 92% of HCV-infected patients, and 88% of patients with an alcohol use disorder. Notably, the odds of HCC in the absence of cirrhosis were more than five times higher when patients had NAFLD (odds ratio [OR], 5.4; 95% confidence interval [CI], 3.4-8.5) or metabolic syndrome (OR, 5.0; 95% CI, 3.1-7.8) compared with HCV infection.
Patients with cirrhosis often go unscreened for HCC even though they are at greatest risk of this cancer. Therefore, trying to screen all patients with NAFLD for HCC would be “logistically impractical,” particularly when the absolute risk of HCC in noncirrhotic patients is unknown and no one has examined the best ways to screen this population, the investigators said. Instead, clinicians could prioritize screening and treating NAFLD patients for diabetes mellitus and obesity, both of which are associated with HCC. “There is evidence to suggest that metformin reduces the risk of HCC among diabetics,” they added. “Studies of these and other risk factors of HCC among NAFLD patients with and without cirrhosis are needed.”
Most patients in the study were male, potentially limiting the generalizability of the findings, the researchers noted.
The National Cancer Institute, the Houston Veterans Affairs Health Services Research and Development Center of Excellence, the Michael E. DeBakey Veterans Affairs Medical Center, and the Dan Duncan Cancer Center funded the study. The researchers had no disclosures.
Source: American Gastroenterological Association
About 13% of U.S. veterans with hepatocellular carcinoma had no evidence of preexisting cirrhosis, according to a report published in the January issue of Clinical Gastroenterology and Hepatology.
“The main risk factors for this entity were nonalcoholic fatty liver disease [NAFLD] or metabolic syndrome” – not hepatitis C virus infection [HCV], HBV [hepatitis B virus] infection, or alcohol abuse, said Dr. Sahil Mittal of the Michael E. DeBakey Veterans Affairs Medical Center and Baylor College of Medicine in Houston. Screening all patients with NAFLD for hepatocellular carcinoma [HCC] is impractical, so studies should seek “actionable risk factors” or biomarkers that reliably identify NAFLD patients who are at particular risk of HCC, wrote Dr. Mittal and his coinvestigators.
Researchers have debated whether chronic HCV infection or alcohol abuse can lead to HCC in the absence of cirrhosis, while at least one study has shown that NAFLD can predispose patients to this disease entity (Arch Pathol Lab Med. 2008;132:1761-6).
But few studies have systematically examined risk factors for HCC without cirrhosis in the general population, the investigators said. Therefore, they randomly selected 1,500 patients from the U.S. Veterans Affairs system who were diagnosed with HCC between 2005 and 2010 on the basis of histopathology or established imaging criteria (Hepatology 2005;42:1208-36).
They reviewed complete medical records for these patients, and classified those who did not have cirrhosis according to the quality of supporting histology, laboratory, and imaging data (Clin Gastroenterol Hepatol. 2015. doi: 0.1016/j.cgh.2015.07.019).
In all, 3% of the cohort had level 1 (“highest-quality”) evidence for not having cirrhosis, while another 10% had level 2 evidence for no cirrhosis, the investigators said. “Compared with HCC in the presence of cirrhosis, these patients were more likely to have metabolic syndrome or NAFLD or no identifiable risk factor, and less likely to have alcohol abuse or HCV infection,” they added. Only two-thirds of NAFLD patients with HCC had cirrhosis, compared with 91% of patients with chronic HCV infection, 92% of HCV-infected patients, and 88% of patients with an alcohol use disorder. Notably, the odds of HCC in the absence of cirrhosis were more than five times higher when patients had NAFLD (odds ratio [OR], 5.4; 95% confidence interval [CI], 3.4-8.5) or metabolic syndrome (OR, 5.0; 95% CI, 3.1-7.8) compared with HCV infection.
Patients with cirrhosis often go unscreened for HCC even though they are at greatest risk of this cancer. Therefore, trying to screen all patients with NAFLD for HCC would be “logistically impractical,” particularly when the absolute risk of HCC in noncirrhotic patients is unknown and no one has examined the best ways to screen this population, the investigators said. Instead, clinicians could prioritize screening and treating NAFLD patients for diabetes mellitus and obesity, both of which are associated with HCC. “There is evidence to suggest that metformin reduces the risk of HCC among diabetics,” they added. “Studies of these and other risk factors of HCC among NAFLD patients with and without cirrhosis are needed.”
Most patients in the study were male, potentially limiting the generalizability of the findings, the researchers noted.
The National Cancer Institute, the Houston Veterans Affairs Health Services Research and Development Center of Excellence, the Michael E. DeBakey Veterans Affairs Medical Center, and the Dan Duncan Cancer Center funded the study. The researchers had no disclosures.
Source: American Gastroenterological Association
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Key clinical point: Nonalcoholic fatty liver disease and metabolic syndrome are risk factors for hepatocellular carcinoma in the absence of cirrhosis.
Major finding: Patients with these diseases were more than five times as likely to develop noncirrhotic HCC compared with patients with chronic hepatitis C virus infection.
Data source: A study of 1,500 randomly selected U.S. veterans diagnosed with HCC between 2005 and 2010.
Disclosures: The National Cancer Institute, the Houston Veterans Affairs Health Services Research and Development Center of Excellence, the Michael E. DeBakey Veterans Affairs Medical Center, and the Dan Duncan Cancer Center funded the study. The researchers had no disclosures.
Study lays groundwork for autologous nerve cell transplantation in Hirschsprung disease
Neural progenitor cells from the proximal colons of patients with Hirschsprung disease divided and formed neurons and glia in their own distal aganglionic colon tissue, according to a study published in the January issue of Cellular and Molecular Gastroenterology and Hepatology.
The approach could lead to “a promising therapeutic strategy” for Hirschsprung disease, because autologous transplantation of nerve progenitor cells would prevent immune rejection, said Dr. Benjamin Rollo of Murdoch Children’s Research Institute in Victoria, Australia, and his associates. But they cautioned against reading too much into their findings, “as there are distributional hurdles to surmount” before cell therapy can be used alone or in combination with surgery.
Hirschsprung disease is a congenital disorder in which embryonic neural crest cells fail to form the distal part of the enteric nervous system. The resulting lack of bowel motility leads to severe constipation and potentially fatal megacolon. Treatment involves surgically resecting the aganglionic distal bowel and anastomosing the normal proximal bowel to the anorectum, but this approach itself can cause constipation as well as fecal soiling, the investigators noted (Cell Molec Gastroenterol Hepatol. 2015 Oct. 22 [doi: 10.1016/j.jcmgh.2015.09.007]).
For the study, they harvested tissue from the proximal (neuronal) and distal (aneuronal) margins of resection of the colons of 31 infants and children with Hirschsprung disease. They cultured cells from the myenteric plexus of the proximal colon, and separated out nerve cells by using flow cytometry for the p75 neural crest marker. To test whether these nerve cells could colonize aganglionic colon, they co-cultured them with aneural avian embryo gut and with patients’ own aneuronal colon muscle. In addition, they co-cultured embryonic mouse enteric nernous system cells with human aneuronal colon muscle. They used quantitative reverse transcriptase PCR and several other standard laboratory techniques to detect cellular markers and mitosis.
Ganglia from the patients’ proximal colons expressed the neural crest markers p75, SOX10, and HNK1, as well as several neuronal, neurite, and glial markers, the researchers reported. The proximal colon specimens also contained ENS progenitor cells, which were SOX10-positive but lacked neuronal or glial markers. The progenitor cells comprised less than 5% of all cells from the proximal colon, but proliferated fourfold more after supplementation with CHIR-99021, a selective inhibitor of glycogen synthase kinase 3. They successfully colonized avian aneural embryonic gut and autologous postnatal aneuronal colon tissue, and the latter also was colonized successfully by mouse enteric neural crest cells.
The study “fulfilled three key requirements” for transplantation – harvesting enteric nervous system cells from the proximal colons of patients with Hirschsprung disease; confirming that postnatal aneuronal colon tissue could support an enteric nervous system; and showing that enteric nervous system–derived cells could colonize both embryonic gut and autologous postnatal colon tissue, said the researchers. More work is needed to sufficiently expand embryonic neural crest stem or progenitor cells and transplant them over a large area of colon, although supplementation with growth factors and use of elastic polymer substrates might help, they added.
The National Health and Medical Research Council, Murdoch Children’s Research Institute, Graham Burke and Yvonne Spencer, the Federation of Chinese Associations, Fonds du Service de chirurgie pédiatrique et de Perfectionnement du CHUV, Fondation SICPA, and Société Académique Vaudoise funded the study. The researchers disclosed no conflicts of interest.
Hirschsprung disease results from a failure of complete neural crest cell migration into the distal colon. Current therapy relies on surgical resection of the aganglionic distal colon. However, for many children, particularly those with large aganglionic segments, surgery often fails to completely normalize function.
One therapeutic approach might be to transplant new enteric neural cells into the aganglionic colon. This has been partially accomplished in rodent and avian models. However, it is not known if human smooth muscle can be colonized or if human postnatal enteric nervous system cells are capable of migration, expansion, and differentiation.
Rollo et al. show that human postnatal enteric nervous system cells isolated from the proximal, i.e., ganglionic, margin of Hirschsprung disease resection specimens can migrate and spread to colonize aganglionic smooth muscle from the distal margin of the same specimen. Remarkably, the transplanted cells differentiated into neurons and glia and formed normal-appearing neural structures.
Many questions remain. If neural cells isolated from the proximal margin can migrate ex vivo, why didn’t they migrate during in utero development? Do the transplanted cells restore normal motility, which requires a complex series of events that must be precisely orchestrated?
Nevertheless, the demonstration that human postnatal neural cells can be isolated from surgical specimens and used to colonize aganglionic smooth muscle suggests that it may be possible to conserve and restore motility and, potentially, to successfully treat Hirschprung disease patients without the need for surgery.
Marion France, Ph.D., is a postdoctoral research fellow at Brigham and Women’s Hospital and Harvard Medical School, Boston. She has no conflicts of interest.
Hirschsprung disease results from a failure of complete neural crest cell migration into the distal colon. Current therapy relies on surgical resection of the aganglionic distal colon. However, for many children, particularly those with large aganglionic segments, surgery often fails to completely normalize function.
One therapeutic approach might be to transplant new enteric neural cells into the aganglionic colon. This has been partially accomplished in rodent and avian models. However, it is not known if human smooth muscle can be colonized or if human postnatal enteric nervous system cells are capable of migration, expansion, and differentiation.
Rollo et al. show that human postnatal enteric nervous system cells isolated from the proximal, i.e., ganglionic, margin of Hirschsprung disease resection specimens can migrate and spread to colonize aganglionic smooth muscle from the distal margin of the same specimen. Remarkably, the transplanted cells differentiated into neurons and glia and formed normal-appearing neural structures.
Many questions remain. If neural cells isolated from the proximal margin can migrate ex vivo, why didn’t they migrate during in utero development? Do the transplanted cells restore normal motility, which requires a complex series of events that must be precisely orchestrated?
Nevertheless, the demonstration that human postnatal neural cells can be isolated from surgical specimens and used to colonize aganglionic smooth muscle suggests that it may be possible to conserve and restore motility and, potentially, to successfully treat Hirschprung disease patients without the need for surgery.
Marion France, Ph.D., is a postdoctoral research fellow at Brigham and Women’s Hospital and Harvard Medical School, Boston. She has no conflicts of interest.
Hirschsprung disease results from a failure of complete neural crest cell migration into the distal colon. Current therapy relies on surgical resection of the aganglionic distal colon. However, for many children, particularly those with large aganglionic segments, surgery often fails to completely normalize function.
One therapeutic approach might be to transplant new enteric neural cells into the aganglionic colon. This has been partially accomplished in rodent and avian models. However, it is not known if human smooth muscle can be colonized or if human postnatal enteric nervous system cells are capable of migration, expansion, and differentiation.
Rollo et al. show that human postnatal enteric nervous system cells isolated from the proximal, i.e., ganglionic, margin of Hirschsprung disease resection specimens can migrate and spread to colonize aganglionic smooth muscle from the distal margin of the same specimen. Remarkably, the transplanted cells differentiated into neurons and glia and formed normal-appearing neural structures.
Many questions remain. If neural cells isolated from the proximal margin can migrate ex vivo, why didn’t they migrate during in utero development? Do the transplanted cells restore normal motility, which requires a complex series of events that must be precisely orchestrated?
Nevertheless, the demonstration that human postnatal neural cells can be isolated from surgical specimens and used to colonize aganglionic smooth muscle suggests that it may be possible to conserve and restore motility and, potentially, to successfully treat Hirschprung disease patients without the need for surgery.
Marion France, Ph.D., is a postdoctoral research fellow at Brigham and Women’s Hospital and Harvard Medical School, Boston. She has no conflicts of interest.
Neural progenitor cells from the proximal colons of patients with Hirschsprung disease divided and formed neurons and glia in their own distal aganglionic colon tissue, according to a study published in the January issue of Cellular and Molecular Gastroenterology and Hepatology.
The approach could lead to “a promising therapeutic strategy” for Hirschsprung disease, because autologous transplantation of nerve progenitor cells would prevent immune rejection, said Dr. Benjamin Rollo of Murdoch Children’s Research Institute in Victoria, Australia, and his associates. But they cautioned against reading too much into their findings, “as there are distributional hurdles to surmount” before cell therapy can be used alone or in combination with surgery.
Hirschsprung disease is a congenital disorder in which embryonic neural crest cells fail to form the distal part of the enteric nervous system. The resulting lack of bowel motility leads to severe constipation and potentially fatal megacolon. Treatment involves surgically resecting the aganglionic distal bowel and anastomosing the normal proximal bowel to the anorectum, but this approach itself can cause constipation as well as fecal soiling, the investigators noted (Cell Molec Gastroenterol Hepatol. 2015 Oct. 22 [doi: 10.1016/j.jcmgh.2015.09.007]).
For the study, they harvested tissue from the proximal (neuronal) and distal (aneuronal) margins of resection of the colons of 31 infants and children with Hirschsprung disease. They cultured cells from the myenteric plexus of the proximal colon, and separated out nerve cells by using flow cytometry for the p75 neural crest marker. To test whether these nerve cells could colonize aganglionic colon, they co-cultured them with aneural avian embryo gut and with patients’ own aneuronal colon muscle. In addition, they co-cultured embryonic mouse enteric nernous system cells with human aneuronal colon muscle. They used quantitative reverse transcriptase PCR and several other standard laboratory techniques to detect cellular markers and mitosis.
Ganglia from the patients’ proximal colons expressed the neural crest markers p75, SOX10, and HNK1, as well as several neuronal, neurite, and glial markers, the researchers reported. The proximal colon specimens also contained ENS progenitor cells, which were SOX10-positive but lacked neuronal or glial markers. The progenitor cells comprised less than 5% of all cells from the proximal colon, but proliferated fourfold more after supplementation with CHIR-99021, a selective inhibitor of glycogen synthase kinase 3. They successfully colonized avian aneural embryonic gut and autologous postnatal aneuronal colon tissue, and the latter also was colonized successfully by mouse enteric neural crest cells.
The study “fulfilled three key requirements” for transplantation – harvesting enteric nervous system cells from the proximal colons of patients with Hirschsprung disease; confirming that postnatal aneuronal colon tissue could support an enteric nervous system; and showing that enteric nervous system–derived cells could colonize both embryonic gut and autologous postnatal colon tissue, said the researchers. More work is needed to sufficiently expand embryonic neural crest stem or progenitor cells and transplant them over a large area of colon, although supplementation with growth factors and use of elastic polymer substrates might help, they added.
The National Health and Medical Research Council, Murdoch Children’s Research Institute, Graham Burke and Yvonne Spencer, the Federation of Chinese Associations, Fonds du Service de chirurgie pédiatrique et de Perfectionnement du CHUV, Fondation SICPA, and Société Académique Vaudoise funded the study. The researchers disclosed no conflicts of interest.
Neural progenitor cells from the proximal colons of patients with Hirschsprung disease divided and formed neurons and glia in their own distal aganglionic colon tissue, according to a study published in the January issue of Cellular and Molecular Gastroenterology and Hepatology.
The approach could lead to “a promising therapeutic strategy” for Hirschsprung disease, because autologous transplantation of nerve progenitor cells would prevent immune rejection, said Dr. Benjamin Rollo of Murdoch Children’s Research Institute in Victoria, Australia, and his associates. But they cautioned against reading too much into their findings, “as there are distributional hurdles to surmount” before cell therapy can be used alone or in combination with surgery.
Hirschsprung disease is a congenital disorder in which embryonic neural crest cells fail to form the distal part of the enteric nervous system. The resulting lack of bowel motility leads to severe constipation and potentially fatal megacolon. Treatment involves surgically resecting the aganglionic distal bowel and anastomosing the normal proximal bowel to the anorectum, but this approach itself can cause constipation as well as fecal soiling, the investigators noted (Cell Molec Gastroenterol Hepatol. 2015 Oct. 22 [doi: 10.1016/j.jcmgh.2015.09.007]).
For the study, they harvested tissue from the proximal (neuronal) and distal (aneuronal) margins of resection of the colons of 31 infants and children with Hirschsprung disease. They cultured cells from the myenteric plexus of the proximal colon, and separated out nerve cells by using flow cytometry for the p75 neural crest marker. To test whether these nerve cells could colonize aganglionic colon, they co-cultured them with aneural avian embryo gut and with patients’ own aneuronal colon muscle. In addition, they co-cultured embryonic mouse enteric nernous system cells with human aneuronal colon muscle. They used quantitative reverse transcriptase PCR and several other standard laboratory techniques to detect cellular markers and mitosis.
Ganglia from the patients’ proximal colons expressed the neural crest markers p75, SOX10, and HNK1, as well as several neuronal, neurite, and glial markers, the researchers reported. The proximal colon specimens also contained ENS progenitor cells, which were SOX10-positive but lacked neuronal or glial markers. The progenitor cells comprised less than 5% of all cells from the proximal colon, but proliferated fourfold more after supplementation with CHIR-99021, a selective inhibitor of glycogen synthase kinase 3. They successfully colonized avian aneural embryonic gut and autologous postnatal aneuronal colon tissue, and the latter also was colonized successfully by mouse enteric neural crest cells.
The study “fulfilled three key requirements” for transplantation – harvesting enteric nervous system cells from the proximal colons of patients with Hirschsprung disease; confirming that postnatal aneuronal colon tissue could support an enteric nervous system; and showing that enteric nervous system–derived cells could colonize both embryonic gut and autologous postnatal colon tissue, said the researchers. More work is needed to sufficiently expand embryonic neural crest stem or progenitor cells and transplant them over a large area of colon, although supplementation with growth factors and use of elastic polymer substrates might help, they added.
The National Health and Medical Research Council, Murdoch Children’s Research Institute, Graham Burke and Yvonne Spencer, the Federation of Chinese Associations, Fonds du Service de chirurgie pédiatrique et de Perfectionnement du CHUV, Fondation SICPA, and Société Académique Vaudoise funded the study. The researchers disclosed no conflicts of interest.
FROM CELLULAR AND MOLECULAR GASTROENTEROLOGY AND HEPATOLOGY
Key clinical point: A preclinical study took several key steps toward autologous transplantation of nerve progenitor cells to treat Hirschsprung disease.
Major finding: Neural progenitor cells from the proximal colons of patients with Hirschsprung disease divided and formed neurons and glia in their own distal aganglionic colon tissue.
Data source: Flow cytometry, reverse transcriptase-PCR, immunohistochemistry, and cell culture of proximal (neuronal) and distal (aneuronal) colon tissue from 31 affected patients, and co-culture with avian embryonic gut and mouse enteric nervous system cells.
Disclosures: The National Health and Medical Research Council, Murdoch Children’s Research Institute, Graham Burke and Yvonne Spencer, the Federation of Chinese Associations, Fonds du Service de chirurgie pédiatrique et de Perfectionnement du CHUV, Fondation SICPA, and Société Académique Vaudoise funded the study. The researchers disclosed no conflicts of interest.
PPIs caused remission in about half of esophageal eosinophilia cases
About half of patients with symptomatic esophageal eosinophilia achieved complete clinical and histologic remission on proton pump inhibitors (PPIs), according to a systematic review and meta-analysis of 33 studies.
“Our results support the concept of PPIs as first-line therapy in both children and adults,” Dr. Alfredo Lucendo of the Servicio de Salud de Castillo–La Mancha, Hospital General de Tomelloso, Albacete, Spain, and his associates wrote in the January issue of Clinical Gastroenterology and Hepatology. “Other effective alternatives, such as dietary or topical steroid therapy, likely might be set aside as second-line treatment, owing to long-term safety concerns (topical steroid therapy) and impairment of quality of life and nutritional inadequacy (dietary interventions).”

The study also confirmed that esophageal pH monitoring does not accurately predict therapeutic response to PPI therapy. “The performance of this test before histologic reevaluation on PPI therapy should be discouraged,” according to the researchers (Clin Gastroenterol Hepatol. 2015. [doi:10.1016/j.cgh.2015.07.041]). Eosinophilic esophagitis was first described as a distinct disorder about 20 years ago, but only recently was understood to be the most common cause of chronic esophageal symptoms among children and young adults. Some cases are now known to respond to PPI therapy, but reported remission rates have varied depending on study design and patient population, the investigators said. In addition, no one had systematically reviewed studies of PPI-responsive esophageal eosinophilia for quality or to determine the optimal type of PPI, dose, or treatment duration.
Therefore, the investigators searched MEDLINE, EMBASE, SCOPUS, and abstracts from the annual meetings of the American Gastroenterological Association, the American College of Gastroenterology, and United European Gastroenterology, identifying 33 studies of 619 patients with symptomatic esophageal eosinophilia. Eleven of the studies were prospective, of which only two were randomized controlled trials. The researchers defined a histologic response as less than 15 eosinophils per high-powered frame after PPI therapy. “Missing data regarding PPI therapy were common and prevented us from drawing conclusions on the most effective PPI drug and doses,” they said. In addition, most studies lacked structured or objective survey tools or other measures of clinical improvement, making it impossible to rule out self-adapted coping strategies as a main cause of improvement over time.
With those caveats in mind, about 61% of patients in the pooled analysis had a clinical response to PPI therapy (95% confidence interval, 48%-72%), and half achieved clinical and histologic remission (95% CI, 42%-59%), the investigators reported. Therapy was somewhat more effective when administered twice a day instead of once daily, when clinicians used esophageal pH monitoring, and when studies were prospective instead of retrospective, but the differences were not significant. Nor did therapeutic response significantly differ based on the age of patients, type of report, or quality of the study.
The overall findings “should be interpreted with caution because of poor-quality evidence, heterogeneity, and publication bias,” the researchers said. Prospective studies are needed to examine the best PPI, dose, and dosing interval to use in an initial trial in the clinic; to clarify long-term effects and dosing strategies; to assess the ability of PPIs to reverse fibrotic esophageal remodeling; and to examine the effects of the CYP2C19 genotype on clinical and histologic response, they added. “More quality evidence on pediatric PPI-responsive eosinophilic esophagitis is needed urgently,” they emphasized.
The authors reported no funding sources and had no disclosures.
Proton pump inhibitor–responsive esophageal eosinophilia (PPI-REE) is a condition in which patients have symptoms of esophageal dysfunction (often dysphagia or heartburn), biopsies with at least 15 eosinophils per high-power field (eos/hpf), and symptomatic and histologic resolution after a PPI trial, typically at twice-daily dosing. Currently, PPI-REE and eosinophilic esophagitis (EoE) overlap substantially, but in the most recent guidelines, they are still considered to be distinct entities. PPI-REE was first reported almost 10 years ago, and since then multiple prospective and retrospective studies in both children and adults have further characterized it. The study by Dr. Lucendo and colleagues, a comprehensive and rigorously conducted systematic review and meta-analysis of 33 studies accounting for 619 patients, found that just over 50% of patients with esophageal eosinophilia had histologic remission (less than 15 eos/hpf) and just over 60% had symptomatic improvement after PPI use. Moreover, similar responses were seen whether or not there was pathologic acid exposure on pH testing.

|
| Dr. Evan S. Dellon |
While there was heterogeneity between studies on meta-analysis, there are several important messages from this study. First, PPI-REE is commonly seen in patients with esophageal eosinophilia, and is not always simply due to reflux. Second, PPIs have a potent antieosinophil effect in these patients. Interestingly, novel acid-independent mechanisms for this anti-inflammatory action recently have been described in other studies. Third, a PPI trial remains important prior to confirming the diagnosis of EoE, and PPIs should be considered the first-line treatment when esophageal eosinophilia is identified. However, it bears emphasizing that all esophageal eosinophilia is not due to EoE. If a patient responds to the PPI trial, there is no clear need to move toward topical steroid or dietary elimination therapy specifically for EoE, and starting multiple antieosinophil treatments concomitantly precludes determining which is most effective. In the future, understanding which patients with esophageal eosinophilia will most benefit from a PPI trial will be important, as we are currently unable to predict this from clinical, endoscopic, and histologic factors. Future studies and guidelines will also need to address whether EoE and PPI-REE are distinct diseases or manifestations of the same underlying process.
Dr. Evan S. Dellon, MPH, is associate professor of medicine and epidemiology at the Center for Esophageal Diseases and Swallowing, division of gastroenterology and hepatology, University of North Carolina School of Medicine at Chapel Hill. He has received research funding from Meritage, Miraca, Receptos, and Regeneron and consulted for Aptalis, Banner, Novartis, Receptos, Regeneron, and Roche.
Proton pump inhibitor–responsive esophageal eosinophilia (PPI-REE) is a condition in which patients have symptoms of esophageal dysfunction (often dysphagia or heartburn), biopsies with at least 15 eosinophils per high-power field (eos/hpf), and symptomatic and histologic resolution after a PPI trial, typically at twice-daily dosing. Currently, PPI-REE and eosinophilic esophagitis (EoE) overlap substantially, but in the most recent guidelines, they are still considered to be distinct entities. PPI-REE was first reported almost 10 years ago, and since then multiple prospective and retrospective studies in both children and adults have further characterized it. The study by Dr. Lucendo and colleagues, a comprehensive and rigorously conducted systematic review and meta-analysis of 33 studies accounting for 619 patients, found that just over 50% of patients with esophageal eosinophilia had histologic remission (less than 15 eos/hpf) and just over 60% had symptomatic improvement after PPI use. Moreover, similar responses were seen whether or not there was pathologic acid exposure on pH testing.
|
|
| Dr. Evan S. Dellon |
While there was heterogeneity between studies on meta-analysis, there are several important messages from this study. First, PPI-REE is commonly seen in patients with esophageal eosinophilia, and is not always simply due to reflux. Second, PPIs have a potent antieosinophil effect in these patients. Interestingly, novel acid-independent mechanisms for this anti-inflammatory action recently have been described in other studies. Third, a PPI trial remains important prior to confirming the diagnosis of EoE, and PPIs should be considered the first-line treatment when esophageal eosinophilia is identified. However, it bears emphasizing that all esophageal eosinophilia is not due to EoE. If a patient responds to the PPI trial, there is no clear need to move toward topical steroid or dietary elimination therapy specifically for EoE, and starting multiple antieosinophil treatments concomitantly precludes determining which is most effective. In the future, understanding which patients with esophageal eosinophilia will most benefit from a PPI trial will be important, as we are currently unable to predict this from clinical, endoscopic, and histologic factors. Future studies and guidelines will also need to address whether EoE and PPI-REE are distinct diseases or manifestations of the same underlying process.
Dr. Evan S. Dellon, MPH, is associate professor of medicine and epidemiology at the Center for Esophageal Diseases and Swallowing, division of gastroenterology and hepatology, University of North Carolina School of Medicine at Chapel Hill. He has received research funding from Meritage, Miraca, Receptos, and Regeneron and consulted for Aptalis, Banner, Novartis, Receptos, Regeneron, and Roche.
Proton pump inhibitor–responsive esophageal eosinophilia (PPI-REE) is a condition in which patients have symptoms of esophageal dysfunction (often dysphagia or heartburn), biopsies with at least 15 eosinophils per high-power field (eos/hpf), and symptomatic and histologic resolution after a PPI trial, typically at twice-daily dosing. Currently, PPI-REE and eosinophilic esophagitis (EoE) overlap substantially, but in the most recent guidelines, they are still considered to be distinct entities. PPI-REE was first reported almost 10 years ago, and since then multiple prospective and retrospective studies in both children and adults have further characterized it. The study by Dr. Lucendo and colleagues, a comprehensive and rigorously conducted systematic review and meta-analysis of 33 studies accounting for 619 patients, found that just over 50% of patients with esophageal eosinophilia had histologic remission (less than 15 eos/hpf) and just over 60% had symptomatic improvement after PPI use. Moreover, similar responses were seen whether or not there was pathologic acid exposure on pH testing.
|
|
| Dr. Evan S. Dellon |
While there was heterogeneity between studies on meta-analysis, there are several important messages from this study. First, PPI-REE is commonly seen in patients with esophageal eosinophilia, and is not always simply due to reflux. Second, PPIs have a potent antieosinophil effect in these patients. Interestingly, novel acid-independent mechanisms for this anti-inflammatory action recently have been described in other studies. Third, a PPI trial remains important prior to confirming the diagnosis of EoE, and PPIs should be considered the first-line treatment when esophageal eosinophilia is identified. However, it bears emphasizing that all esophageal eosinophilia is not due to EoE. If a patient responds to the PPI trial, there is no clear need to move toward topical steroid or dietary elimination therapy specifically for EoE, and starting multiple antieosinophil treatments concomitantly precludes determining which is most effective. In the future, understanding which patients with esophageal eosinophilia will most benefit from a PPI trial will be important, as we are currently unable to predict this from clinical, endoscopic, and histologic factors. Future studies and guidelines will also need to address whether EoE and PPI-REE are distinct diseases or manifestations of the same underlying process.
Dr. Evan S. Dellon, MPH, is associate professor of medicine and epidemiology at the Center for Esophageal Diseases and Swallowing, division of gastroenterology and hepatology, University of North Carolina School of Medicine at Chapel Hill. He has received research funding from Meritage, Miraca, Receptos, and Regeneron and consulted for Aptalis, Banner, Novartis, Receptos, Regeneron, and Roche.
About half of patients with symptomatic esophageal eosinophilia achieved complete clinical and histologic remission on proton pump inhibitors (PPIs), according to a systematic review and meta-analysis of 33 studies.
“Our results support the concept of PPIs as first-line therapy in both children and adults,” Dr. Alfredo Lucendo of the Servicio de Salud de Castillo–La Mancha, Hospital General de Tomelloso, Albacete, Spain, and his associates wrote in the January issue of Clinical Gastroenterology and Hepatology. “Other effective alternatives, such as dietary or topical steroid therapy, likely might be set aside as second-line treatment, owing to long-term safety concerns (topical steroid therapy) and impairment of quality of life and nutritional inadequacy (dietary interventions).”
The study also confirmed that esophageal pH monitoring does not accurately predict therapeutic response to PPI therapy. “The performance of this test before histologic reevaluation on PPI therapy should be discouraged,” according to the researchers (Clin Gastroenterol Hepatol. 2015. [doi:10.1016/j.cgh.2015.07.041]). Eosinophilic esophagitis was first described as a distinct disorder about 20 years ago, but only recently was understood to be the most common cause of chronic esophageal symptoms among children and young adults. Some cases are now known to respond to PPI therapy, but reported remission rates have varied depending on study design and patient population, the investigators said. In addition, no one had systematically reviewed studies of PPI-responsive esophageal eosinophilia for quality or to determine the optimal type of PPI, dose, or treatment duration.
Therefore, the investigators searched MEDLINE, EMBASE, SCOPUS, and abstracts from the annual meetings of the American Gastroenterological Association, the American College of Gastroenterology, and United European Gastroenterology, identifying 33 studies of 619 patients with symptomatic esophageal eosinophilia. Eleven of the studies were prospective, of which only two were randomized controlled trials. The researchers defined a histologic response as less than 15 eosinophils per high-powered frame after PPI therapy. “Missing data regarding PPI therapy were common and prevented us from drawing conclusions on the most effective PPI drug and doses,” they said. In addition, most studies lacked structured or objective survey tools or other measures of clinical improvement, making it impossible to rule out self-adapted coping strategies as a main cause of improvement over time.
With those caveats in mind, about 61% of patients in the pooled analysis had a clinical response to PPI therapy (95% confidence interval, 48%-72%), and half achieved clinical and histologic remission (95% CI, 42%-59%), the investigators reported. Therapy was somewhat more effective when administered twice a day instead of once daily, when clinicians used esophageal pH monitoring, and when studies were prospective instead of retrospective, but the differences were not significant. Nor did therapeutic response significantly differ based on the age of patients, type of report, or quality of the study.
The overall findings “should be interpreted with caution because of poor-quality evidence, heterogeneity, and publication bias,” the researchers said. Prospective studies are needed to examine the best PPI, dose, and dosing interval to use in an initial trial in the clinic; to clarify long-term effects and dosing strategies; to assess the ability of PPIs to reverse fibrotic esophageal remodeling; and to examine the effects of the CYP2C19 genotype on clinical and histologic response, they added. “More quality evidence on pediatric PPI-responsive eosinophilic esophagitis is needed urgently,” they emphasized.
The authors reported no funding sources and had no disclosures.
About half of patients with symptomatic esophageal eosinophilia achieved complete clinical and histologic remission on proton pump inhibitors (PPIs), according to a systematic review and meta-analysis of 33 studies.
“Our results support the concept of PPIs as first-line therapy in both children and adults,” Dr. Alfredo Lucendo of the Servicio de Salud de Castillo–La Mancha, Hospital General de Tomelloso, Albacete, Spain, and his associates wrote in the January issue of Clinical Gastroenterology and Hepatology. “Other effective alternatives, such as dietary or topical steroid therapy, likely might be set aside as second-line treatment, owing to long-term safety concerns (topical steroid therapy) and impairment of quality of life and nutritional inadequacy (dietary interventions).”
The study also confirmed that esophageal pH monitoring does not accurately predict therapeutic response to PPI therapy. “The performance of this test before histologic reevaluation on PPI therapy should be discouraged,” according to the researchers (Clin Gastroenterol Hepatol. 2015. [doi:10.1016/j.cgh.2015.07.041]). Eosinophilic esophagitis was first described as a distinct disorder about 20 years ago, but only recently was understood to be the most common cause of chronic esophageal symptoms among children and young adults. Some cases are now known to respond to PPI therapy, but reported remission rates have varied depending on study design and patient population, the investigators said. In addition, no one had systematically reviewed studies of PPI-responsive esophageal eosinophilia for quality or to determine the optimal type of PPI, dose, or treatment duration.
Therefore, the investigators searched MEDLINE, EMBASE, SCOPUS, and abstracts from the annual meetings of the American Gastroenterological Association, the American College of Gastroenterology, and United European Gastroenterology, identifying 33 studies of 619 patients with symptomatic esophageal eosinophilia. Eleven of the studies were prospective, of which only two were randomized controlled trials. The researchers defined a histologic response as less than 15 eosinophils per high-powered frame after PPI therapy. “Missing data regarding PPI therapy were common and prevented us from drawing conclusions on the most effective PPI drug and doses,” they said. In addition, most studies lacked structured or objective survey tools or other measures of clinical improvement, making it impossible to rule out self-adapted coping strategies as a main cause of improvement over time.
With those caveats in mind, about 61% of patients in the pooled analysis had a clinical response to PPI therapy (95% confidence interval, 48%-72%), and half achieved clinical and histologic remission (95% CI, 42%-59%), the investigators reported. Therapy was somewhat more effective when administered twice a day instead of once daily, when clinicians used esophageal pH monitoring, and when studies were prospective instead of retrospective, but the differences were not significant. Nor did therapeutic response significantly differ based on the age of patients, type of report, or quality of the study.
The overall findings “should be interpreted with caution because of poor-quality evidence, heterogeneity, and publication bias,” the researchers said. Prospective studies are needed to examine the best PPI, dose, and dosing interval to use in an initial trial in the clinic; to clarify long-term effects and dosing strategies; to assess the ability of PPIs to reverse fibrotic esophageal remodeling; and to examine the effects of the CYP2C19 genotype on clinical and histologic response, they added. “More quality evidence on pediatric PPI-responsive eosinophilic esophagitis is needed urgently,” they emphasized.
The authors reported no funding sources and had no disclosures.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Key clinical point: Proton pump inhibitors should be considered in the first-line treatment of esophageal eosinophilia.
Major finding: Half of patients achieved clinical and histologic remission after a trial of PPIs.
Data source: Meta-analysis of 33 studies of 619 patients with symptomatic esophageal eosinophilia indicative of eosinophilic esophagitis.
Disclosures: The authors reported no funding sources and had no disclosures.

Measure found significant variations in outpatient colonoscopy quality
Facilities that performed outpatient colonoscopies varied significantly in terms of subsequent unplanned hospital visits, even after patient-level risk factors were adjusted for, according to a Medicare claims analysis reported in the January issue of Gastroenterology.
This first-in-kind quality measure will help “make transparent the full range of adverse events requiring hospital care that patients experience post-[colonoscopy], inform patient choice, create incentives for improved care, and assist providers’ quality improvement efforts, wrote Dr. Isuru Ranasinghe of Yale–New Haven (Conn.) Hospital and his associates. Preventing unplanned hospitals visits after colonoscopy could also help improve patient outcomes and cut health care costs, they added.

More than 90% of colonoscopies occur in outpatient settings, where it is difficult to follow-up and track serious adverse events such as colonic perforation or gastrointestinal bleeding. Furthermore, there are no publicly available quality reports of providers or facilities that perform outpatient colonoscopies. To help fill that gap, the researchers tracked unplanned hospital visits within 7 days after colonoscopy as part of an outpatient quality initiative by the Centers for Medicare & Medicaid Services. The analysis included 20% of Medicare outpatient colonoscopy claims in 2010, which amounted to 331,880 colonoscopies performed at 8,140 facilities (Gastroenterology 2015 [doi: 10.1053/j.gastro.2015.09.009]).
In 2010, there were 16.3 unplanned hospital visits for every 1,000 Medicare claims for outpatient colonoscopies, which equated to 27,000 such visits nationwide, the investigators said. Patients who were older than 85 years were significantly more likely to have an unplanned hospital visit than were patients aged 65-69 years (odds ratio, 1.87; 95% confidence interval, 1.54-2.28). The other most significant predictors included having an electrolyte or acid/base imbalance (OR, 1.43) or a psychiatric disorder (OR, 1.34). After adjusting for these factors, unplanned admission rates varied significantly among facilities in all four states with available data, including New York, California, Florida, and Nebraska, the researchers said.
These findings might not apply to patients who are too young to be enrolled in Medicare, which “is important, as most colonoscopies are performed among patients aged less than 65 years, although older patients are more likely to suffer adverse events,” Dr. Ranasinghe and his associates noted. The study also did not assess deaths, the one-third of GI bleeding events that occur more than a week after colonoscopy, or the various factors that might affect quality of care, such as type of anesthesia, polypectomy technique, and access to follow-up care. “The goal of the measure is to reveal the opportunity for improvement, and to prompt facilities to examine their practices in depth to identify ways to lower hospital visit rates to the level achieved by the best providers,” the researchers emphasized.
The work was supported by the Centers for Medicare & Medicaid Services, the National Health and Medical Research Council, the National Heart Foundation of Australia, the National Institute on Aging, the American Federation for Aging Research. Dr. Ranasinghe and nine coinvestigators reported working under contract with CMS to develop and maintain performance measures. Three coinvestigators reported financial relationships with AbbVie, qMed, Pentax, Olympus, Myriad Genetics, UnitedHealth, Medtronic, and Johnson & Johnson.
Source: American Gastroenterological Association
As part of the Centers for Medicare & Medicaid Services initiative to develop outpatient quality measures, Dr. Ranasinghe and his colleagues designed a risk-adjusted measure to capture serious adverse events characterized by unplanned hospitalization within 7 days after colonoscopy.
While no measure is perfect, this measure captures many important adverse outcomes after colonoscopy. Their methods carefully excluded hospitalizations that were elective or could be attributable to other conditions. This is an important quality measure because the endoscopist is often unaware of hospitalizations that occur post colonoscopy (Arch Intern Med. 2010;170:1752-7), and therefore cannot target quality improvement (QI) efforts at preventing such unplanned outcomes.

|
| Dr. Jeremy Adler |
This measure can be calculated from available data without chart audit and will fulfill CMS reporting requirements. However, it will be important to keep in mind that it was developed for patients 65 years and older, and may not be applicable to younger patients. Furthermore, to make this measure meaningful, it should be used to improve quality, not just assess quality.
The authors demonstrated that they were able to identify practices that were outliers, even when risk adjusted and adjusted for practice volume. This could allow practices to become self-aware and provide benchmarks against which to compare and improve their performance.
However, one major limitation to using this measure for QI is that the Healthcare Cost and Utilization Project only provides updated data yearly, after a substantial time lag, making it unsuitable for short-term or rapid-cycle QI efforts. In order for individual practices to target their improvement efforts, they would need to review their own local postcolonoscopy hospitalization data as an outcome measure more frequently. They could then review each case in depth to learn details that could further help target improvement efforts.
Dr. Jeremy Adler, M.Sc. is assistant professor, division of pediatric gastroenterology and Child Health Evaluation and Research Unit, University of Michigan, Ann Arbor. He has no conflicts of interest.
As part of the Centers for Medicare & Medicaid Services initiative to develop outpatient quality measures, Dr. Ranasinghe and his colleagues designed a risk-adjusted measure to capture serious adverse events characterized by unplanned hospitalization within 7 days after colonoscopy.
While no measure is perfect, this measure captures many important adverse outcomes after colonoscopy. Their methods carefully excluded hospitalizations that were elective or could be attributable to other conditions. This is an important quality measure because the endoscopist is often unaware of hospitalizations that occur post colonoscopy (Arch Intern Med. 2010;170:1752-7), and therefore cannot target quality improvement (QI) efforts at preventing such unplanned outcomes.
|
|
| Dr. Jeremy Adler |
This measure can be calculated from available data without chart audit and will fulfill CMS reporting requirements. However, it will be important to keep in mind that it was developed for patients 65 years and older, and may not be applicable to younger patients. Furthermore, to make this measure meaningful, it should be used to improve quality, not just assess quality.
The authors demonstrated that they were able to identify practices that were outliers, even when risk adjusted and adjusted for practice volume. This could allow practices to become self-aware and provide benchmarks against which to compare and improve their performance.
However, one major limitation to using this measure for QI is that the Healthcare Cost and Utilization Project only provides updated data yearly, after a substantial time lag, making it unsuitable for short-term or rapid-cycle QI efforts. In order for individual practices to target their improvement efforts, they would need to review their own local postcolonoscopy hospitalization data as an outcome measure more frequently. They could then review each case in depth to learn details that could further help target improvement efforts.
Dr. Jeremy Adler, M.Sc. is assistant professor, division of pediatric gastroenterology and Child Health Evaluation and Research Unit, University of Michigan, Ann Arbor. He has no conflicts of interest.
As part of the Centers for Medicare & Medicaid Services initiative to develop outpatient quality measures, Dr. Ranasinghe and his colleagues designed a risk-adjusted measure to capture serious adverse events characterized by unplanned hospitalization within 7 days after colonoscopy.
While no measure is perfect, this measure captures many important adverse outcomes after colonoscopy. Their methods carefully excluded hospitalizations that were elective or could be attributable to other conditions. This is an important quality measure because the endoscopist is often unaware of hospitalizations that occur post colonoscopy (Arch Intern Med. 2010;170:1752-7), and therefore cannot target quality improvement (QI) efforts at preventing such unplanned outcomes.
|
|
| Dr. Jeremy Adler |
This measure can be calculated from available data without chart audit and will fulfill CMS reporting requirements. However, it will be important to keep in mind that it was developed for patients 65 years and older, and may not be applicable to younger patients. Furthermore, to make this measure meaningful, it should be used to improve quality, not just assess quality.
The authors demonstrated that they were able to identify practices that were outliers, even when risk adjusted and adjusted for practice volume. This could allow practices to become self-aware and provide benchmarks against which to compare and improve their performance.
However, one major limitation to using this measure for QI is that the Healthcare Cost and Utilization Project only provides updated data yearly, after a substantial time lag, making it unsuitable for short-term or rapid-cycle QI efforts. In order for individual practices to target their improvement efforts, they would need to review their own local postcolonoscopy hospitalization data as an outcome measure more frequently. They could then review each case in depth to learn details that could further help target improvement efforts.
Dr. Jeremy Adler, M.Sc. is assistant professor, division of pediatric gastroenterology and Child Health Evaluation and Research Unit, University of Michigan, Ann Arbor. He has no conflicts of interest.
Facilities that performed outpatient colonoscopies varied significantly in terms of subsequent unplanned hospital visits, even after patient-level risk factors were adjusted for, according to a Medicare claims analysis reported in the January issue of Gastroenterology.
This first-in-kind quality measure will help “make transparent the full range of adverse events requiring hospital care that patients experience post-[colonoscopy], inform patient choice, create incentives for improved care, and assist providers’ quality improvement efforts, wrote Dr. Isuru Ranasinghe of Yale–New Haven (Conn.) Hospital and his associates. Preventing unplanned hospitals visits after colonoscopy could also help improve patient outcomes and cut health care costs, they added.
More than 90% of colonoscopies occur in outpatient settings, where it is difficult to follow-up and track serious adverse events such as colonic perforation or gastrointestinal bleeding. Furthermore, there are no publicly available quality reports of providers or facilities that perform outpatient colonoscopies. To help fill that gap, the researchers tracked unplanned hospital visits within 7 days after colonoscopy as part of an outpatient quality initiative by the Centers for Medicare & Medicaid Services. The analysis included 20% of Medicare outpatient colonoscopy claims in 2010, which amounted to 331,880 colonoscopies performed at 8,140 facilities (Gastroenterology 2015 [doi: 10.1053/j.gastro.2015.09.009]).
In 2010, there were 16.3 unplanned hospital visits for every 1,000 Medicare claims for outpatient colonoscopies, which equated to 27,000 such visits nationwide, the investigators said. Patients who were older than 85 years were significantly more likely to have an unplanned hospital visit than were patients aged 65-69 years (odds ratio, 1.87; 95% confidence interval, 1.54-2.28). The other most significant predictors included having an electrolyte or acid/base imbalance (OR, 1.43) or a psychiatric disorder (OR, 1.34). After adjusting for these factors, unplanned admission rates varied significantly among facilities in all four states with available data, including New York, California, Florida, and Nebraska, the researchers said.
These findings might not apply to patients who are too young to be enrolled in Medicare, which “is important, as most colonoscopies are performed among patients aged less than 65 years, although older patients are more likely to suffer adverse events,” Dr. Ranasinghe and his associates noted. The study also did not assess deaths, the one-third of GI bleeding events that occur more than a week after colonoscopy, or the various factors that might affect quality of care, such as type of anesthesia, polypectomy technique, and access to follow-up care. “The goal of the measure is to reveal the opportunity for improvement, and to prompt facilities to examine their practices in depth to identify ways to lower hospital visit rates to the level achieved by the best providers,” the researchers emphasized.
The work was supported by the Centers for Medicare & Medicaid Services, the National Health and Medical Research Council, the National Heart Foundation of Australia, the National Institute on Aging, the American Federation for Aging Research. Dr. Ranasinghe and nine coinvestigators reported working under contract with CMS to develop and maintain performance measures. Three coinvestigators reported financial relationships with AbbVie, qMed, Pentax, Olympus, Myriad Genetics, UnitedHealth, Medtronic, and Johnson & Johnson.
Source: American Gastroenterological Association
Facilities that performed outpatient colonoscopies varied significantly in terms of subsequent unplanned hospital visits, even after patient-level risk factors were adjusted for, according to a Medicare claims analysis reported in the January issue of Gastroenterology.
This first-in-kind quality measure will help “make transparent the full range of adverse events requiring hospital care that patients experience post-[colonoscopy], inform patient choice, create incentives for improved care, and assist providers’ quality improvement efforts, wrote Dr. Isuru Ranasinghe of Yale–New Haven (Conn.) Hospital and his associates. Preventing unplanned hospitals visits after colonoscopy could also help improve patient outcomes and cut health care costs, they added.
More than 90% of colonoscopies occur in outpatient settings, where it is difficult to follow-up and track serious adverse events such as colonic perforation or gastrointestinal bleeding. Furthermore, there are no publicly available quality reports of providers or facilities that perform outpatient colonoscopies. To help fill that gap, the researchers tracked unplanned hospital visits within 7 days after colonoscopy as part of an outpatient quality initiative by the Centers for Medicare & Medicaid Services. The analysis included 20% of Medicare outpatient colonoscopy claims in 2010, which amounted to 331,880 colonoscopies performed at 8,140 facilities (Gastroenterology 2015 [doi: 10.1053/j.gastro.2015.09.009]).
In 2010, there were 16.3 unplanned hospital visits for every 1,000 Medicare claims for outpatient colonoscopies, which equated to 27,000 such visits nationwide, the investigators said. Patients who were older than 85 years were significantly more likely to have an unplanned hospital visit than were patients aged 65-69 years (odds ratio, 1.87; 95% confidence interval, 1.54-2.28). The other most significant predictors included having an electrolyte or acid/base imbalance (OR, 1.43) or a psychiatric disorder (OR, 1.34). After adjusting for these factors, unplanned admission rates varied significantly among facilities in all four states with available data, including New York, California, Florida, and Nebraska, the researchers said.
These findings might not apply to patients who are too young to be enrolled in Medicare, which “is important, as most colonoscopies are performed among patients aged less than 65 years, although older patients are more likely to suffer adverse events,” Dr. Ranasinghe and his associates noted. The study also did not assess deaths, the one-third of GI bleeding events that occur more than a week after colonoscopy, or the various factors that might affect quality of care, such as type of anesthesia, polypectomy technique, and access to follow-up care. “The goal of the measure is to reveal the opportunity for improvement, and to prompt facilities to examine their practices in depth to identify ways to lower hospital visit rates to the level achieved by the best providers,” the researchers emphasized.
The work was supported by the Centers for Medicare & Medicaid Services, the National Health and Medical Research Council, the National Heart Foundation of Australia, the National Institute on Aging, the American Federation for Aging Research. Dr. Ranasinghe and nine coinvestigators reported working under contract with CMS to develop and maintain performance measures. Three coinvestigators reported financial relationships with AbbVie, qMed, Pentax, Olympus, Myriad Genetics, UnitedHealth, Medtronic, and Johnson & Johnson.
Source: American Gastroenterological Association
FROM GASTROENTEROLOGY
Key clinical point: Researchers validated a new measure to evaluate the quality of outpatient colonoscopies.
Major finding: Risk-adjusted rates of these visits varied significantly among health care facilities in all four states with available data.
Data source: An analysis of 20% of Medicare outpatient colonoscopy claims in 2010, which included 331,880 procedures performed at 8,140 facilities.
Disclosures: The work was supported by the Centers for Medicare & Medicaid Services, the National Health and Medical Research Council, the National Heart Foundation of Australia, the National Institute on Aging, and the American Federation for Aging Research. Dr. Ranasinghe and nine coinvestigators reported working under contract with CMS to develop and maintain performance measures. Three coinvestigators reported financial relationships with AbbVie, gMed, Pentax, Olympus, Myriad Genetics, UnitedHealth, Medtronic, and Johnson & Johnson.

Malpractice Counsel: Allergic Reaction Versus Anaphylaxis
Allergic Reaction Versus Anaphylaxis
A 34-year-old woman presented to ED with complaints of an allergic reaction, the onset of which began approximately 1 hour prior. The patient did not know what might have caused her symptoms. She complained of hives and itching all over; she denied difficulty swallowing, wheezing, and shortness of breath. Her medical history was unremarkable. She was on no medications, and she denied any alcohol or tobacco use. She had no known medication or food allergies.
Physical examination revealed a woman in mild discomfort, secondary to generalized itching. Her vital signs, including pulse oximetry, were normal. There was no swelling of the face, lips, or oropharynx. The lungs were clear to auscultation bilaterally. The heart and abdominal examinations were normal. Examination of the skin revealed diffuse urticaria without petechiae or purpura.
The emergency physician (EP) ordered 125 mg of methylprednisolone sodium succinate and 25 mg of diphenhydramine intravenously (IV). After approximately 1 hour, the hives and itching decreased and the patient felt improved. She was diagnosed with an allergic reaction and discharged home with a prescription for diphenhydramine and a methylprednisolone dose pack.

The following day, the patient collapsed at home and emergency medical services was called. Unfortunately, the patient could not be resuscitated and was pronounced dead at the scene. An autopsy revealed the patient had died from anaphylaxis and laryngeal edema, with an extremely elevated tryptase level of 200 ng/mL (normal, <11.5 ng/mL).
The patient’s family sued the EP for failure to diagnose and treat anaphylaxis, failure to treat with epinephrine, and failure to admit the patient to the hospital. The defense claimed the patient did not present with anaphylaxis, but rather simply a worsening of the hives and angioedema, and that the treatment provided was appropriate. The jury found in favor of the defendants.
Discussion
It does not appear the patient presented with anaphylaxis on the first visit, but may have had it on the second visit. In 2004, the National Institutes of Allergy and Infectious Disease (NIAID) panel and the Food Allergy and Anaphylaxis Network (FAAN) developed criteria for the diagnosis of anaphylaxis.1 According to the criteria, anaphylaxis is likely when any one of the following three criteria are present: (1) acute onset of symptoms involving the skin or mucosa (eg, pruritus, hives, angioedema), and either respiratory compromise (eg, dyspnea, wheezing, stridor, hypoxia) or hypotension/end-organ dysfunction (eg, syncope, incontinence); (2) two or more symptoms (eg, respiratory compromise, hypotension/end-organ dysfunction, persistent gastrointestinal [GI] symptoms such as vomiting, diarrhea, or crampy abdominal pain) that occur rapidly after exposure involving the skin or mucosa; or (3) hypotension from a known allergen to the patient. The accuracy of these criteria has been retrospectively evaluated in an ED study, and found to have a 97% sensitivity and an 82% specificity.2 The negative predictive value was good at 98%, but the positive predictive value was only 69%.2
When a patient presents with minimal or subtle symptoms, anaphylaxis can be a very difficult diagnosis to make in the ED early on in the process. While no EP will miss the diagnosis in a patient with hives, hypotension, and wheezing, it can be easy to miss when the predominant symptoms are GI, such as nausea, vomiting, or diarrhea. In addition, the differential diagnosis for the presentation of anaphylaxis in the ED can be extremely broad and include vasovagal reaction, asthma attack, myocardial infarction, gastroenteritis, panic attack, or airway obstruction.
Due to the nature of emergency medicine, EPs must consider multiple etiologies before determining an evaluation and management plan. While recognizing there are limitations to the NIAID/FAAN criteria, EPs should be aware of them. We are very good at treating these types of symptoms with antihistamines and steroids; however, we frequently fail to give epinephrine when indicated. It is important to remember that epinephrine is the first-line treatment for anaphylaxis—not corticosteroids or antihistamines.3
Reasons for not administering epinephrine are multiple. First, as discussed above, if the diagnosis of anaphylaxis is not considered, the EP is not going to administer the drug of choice. Secondly, EPs have been taught to have a healthy respect for epinephrine and its effects, especially in older patients. Due to this cautious approach, epinephrine is frequently not given to patients with mild symptoms or to those who present early in the course of disease.
Emergency physicians have experience giving epinephrine subcutaneously, but not nearly as much with the intramuscular (IM) route. This is important, because an IM injection in the anterolateral thigh is the recommended location for the treatment of anaphylaxis. The dose should be weight based (0.01 mg/kg) to a maximum of 0.5 mg. This dose can be given every 5 to 15 minutes as necessary to control symptoms.3 The dosing is important to remember, since many EDs stock only autoinjectable epinephrine devices for use in anaphylaxis. These autoinjectors only contain 0.3 mg of epinephrine, so some patients may be underdosed if used.
In the management of allergic reactions and anaphylaxis, EPs frequently administer antihistamines and corticosteroids. While there is no direct evidence to support their use in the management of anaphylaxis, theoretical benefits do exist.3 This, combined with the excellent medication safety profile and lack of serious side effects, make these two medication classes appropriate for use in the ED.
- Allergic Reaction Versus Anaphylaxis
- Manivannan V, Decker WW, Stead LG, Li JT, Campbell RL. National Institute of Allergy and Infectious Disease and Food Allergy and Anaphylaxis Network criteria for anaphylaxis. Int J Emerg Med. 2009;2(1):3-5.
- Campbell RL, Hagan JB, Manivannan V, et al. Evaluation of National Institute of Allergy and Infectious Diseases/Food Allergy and Anaphylaxis Network criteria for the diagnosis of anaphylaxis in emergency department patients. J Allergy Clin Immunol. 2012;129(3):748-752.
- Campbell RL, Li JT, Nicklas RA, Sadosty AT; Members of the Joint Task Force; Practice Parameter Workgroup. Emergency department diagnosis and treatment of anaphylaxis: a practice parameter. Ann Allergy Asthma Immunol. 2014;113(6):599-608.
Allergic Reaction Versus Anaphylaxis
A 34-year-old woman presented to ED with complaints of an allergic reaction, the onset of which began approximately 1 hour prior. The patient did not know what might have caused her symptoms. She complained of hives and itching all over; she denied difficulty swallowing, wheezing, and shortness of breath. Her medical history was unremarkable. She was on no medications, and she denied any alcohol or tobacco use. She had no known medication or food allergies.
Physical examination revealed a woman in mild discomfort, secondary to generalized itching. Her vital signs, including pulse oximetry, were normal. There was no swelling of the face, lips, or oropharynx. The lungs were clear to auscultation bilaterally. The heart and abdominal examinations were normal. Examination of the skin revealed diffuse urticaria without petechiae or purpura.
The emergency physician (EP) ordered 125 mg of methylprednisolone sodium succinate and 25 mg of diphenhydramine intravenously (IV). After approximately 1 hour, the hives and itching decreased and the patient felt improved. She was diagnosed with an allergic reaction and discharged home with a prescription for diphenhydramine and a methylprednisolone dose pack.
The following day, the patient collapsed at home and emergency medical services was called. Unfortunately, the patient could not be resuscitated and was pronounced dead at the scene. An autopsy revealed the patient had died from anaphylaxis and laryngeal edema, with an extremely elevated tryptase level of 200 ng/mL (normal, <11.5 ng/mL).
The patient’s family sued the EP for failure to diagnose and treat anaphylaxis, failure to treat with epinephrine, and failure to admit the patient to the hospital. The defense claimed the patient did not present with anaphylaxis, but rather simply a worsening of the hives and angioedema, and that the treatment provided was appropriate. The jury found in favor of the defendants.
Discussion
It does not appear the patient presented with anaphylaxis on the first visit, but may have had it on the second visit. In 2004, the National Institutes of Allergy and Infectious Disease (NIAID) panel and the Food Allergy and Anaphylaxis Network (FAAN) developed criteria for the diagnosis of anaphylaxis.1 According to the criteria, anaphylaxis is likely when any one of the following three criteria are present: (1) acute onset of symptoms involving the skin or mucosa (eg, pruritus, hives, angioedema), and either respiratory compromise (eg, dyspnea, wheezing, stridor, hypoxia) or hypotension/end-organ dysfunction (eg, syncope, incontinence); (2) two or more symptoms (eg, respiratory compromise, hypotension/end-organ dysfunction, persistent gastrointestinal [GI] symptoms such as vomiting, diarrhea, or crampy abdominal pain) that occur rapidly after exposure involving the skin or mucosa; or (3) hypotension from a known allergen to the patient. The accuracy of these criteria has been retrospectively evaluated in an ED study, and found to have a 97% sensitivity and an 82% specificity.2 The negative predictive value was good at 98%, but the positive predictive value was only 69%.2
When a patient presents with minimal or subtle symptoms, anaphylaxis can be a very difficult diagnosis to make in the ED early on in the process. While no EP will miss the diagnosis in a patient with hives, hypotension, and wheezing, it can be easy to miss when the predominant symptoms are GI, such as nausea, vomiting, or diarrhea. In addition, the differential diagnosis for the presentation of anaphylaxis in the ED can be extremely broad and include vasovagal reaction, asthma attack, myocardial infarction, gastroenteritis, panic attack, or airway obstruction.
Due to the nature of emergency medicine, EPs must consider multiple etiologies before determining an evaluation and management plan. While recognizing there are limitations to the NIAID/FAAN criteria, EPs should be aware of them. We are very good at treating these types of symptoms with antihistamines and steroids; however, we frequently fail to give epinephrine when indicated. It is important to remember that epinephrine is the first-line treatment for anaphylaxis—not corticosteroids or antihistamines.3
Reasons for not administering epinephrine are multiple. First, as discussed above, if the diagnosis of anaphylaxis is not considered, the EP is not going to administer the drug of choice. Secondly, EPs have been taught to have a healthy respect for epinephrine and its effects, especially in older patients. Due to this cautious approach, epinephrine is frequently not given to patients with mild symptoms or to those who present early in the course of disease.
Emergency physicians have experience giving epinephrine subcutaneously, but not nearly as much with the intramuscular (IM) route. This is important, because an IM injection in the anterolateral thigh is the recommended location for the treatment of anaphylaxis. The dose should be weight based (0.01 mg/kg) to a maximum of 0.5 mg. This dose can be given every 5 to 15 minutes as necessary to control symptoms.3 The dosing is important to remember, since many EDs stock only autoinjectable epinephrine devices for use in anaphylaxis. These autoinjectors only contain 0.3 mg of epinephrine, so some patients may be underdosed if used.
In the management of allergic reactions and anaphylaxis, EPs frequently administer antihistamines and corticosteroids. While there is no direct evidence to support their use in the management of anaphylaxis, theoretical benefits do exist.3 This, combined with the excellent medication safety profile and lack of serious side effects, make these two medication classes appropriate for use in the ED.
Allergic Reaction Versus Anaphylaxis
A 34-year-old woman presented to ED with complaints of an allergic reaction, the onset of which began approximately 1 hour prior. The patient did not know what might have caused her symptoms. She complained of hives and itching all over; she denied difficulty swallowing, wheezing, and shortness of breath. Her medical history was unremarkable. She was on no medications, and she denied any alcohol or tobacco use. She had no known medication or food allergies.
Physical examination revealed a woman in mild discomfort, secondary to generalized itching. Her vital signs, including pulse oximetry, were normal. There was no swelling of the face, lips, or oropharynx. The lungs were clear to auscultation bilaterally. The heart and abdominal examinations were normal. Examination of the skin revealed diffuse urticaria without petechiae or purpura.
The emergency physician (EP) ordered 125 mg of methylprednisolone sodium succinate and 25 mg of diphenhydramine intravenously (IV). After approximately 1 hour, the hives and itching decreased and the patient felt improved. She was diagnosed with an allergic reaction and discharged home with a prescription for diphenhydramine and a methylprednisolone dose pack.
The following day, the patient collapsed at home and emergency medical services was called. Unfortunately, the patient could not be resuscitated and was pronounced dead at the scene. An autopsy revealed the patient had died from anaphylaxis and laryngeal edema, with an extremely elevated tryptase level of 200 ng/mL (normal, <11.5 ng/mL).
The patient’s family sued the EP for failure to diagnose and treat anaphylaxis, failure to treat with epinephrine, and failure to admit the patient to the hospital. The defense claimed the patient did not present with anaphylaxis, but rather simply a worsening of the hives and angioedema, and that the treatment provided was appropriate. The jury found in favor of the defendants.
Discussion
It does not appear the patient presented with anaphylaxis on the first visit, but may have had it on the second visit. In 2004, the National Institutes of Allergy and Infectious Disease (NIAID) panel and the Food Allergy and Anaphylaxis Network (FAAN) developed criteria for the diagnosis of anaphylaxis.1 According to the criteria, anaphylaxis is likely when any one of the following three criteria are present: (1) acute onset of symptoms involving the skin or mucosa (eg, pruritus, hives, angioedema), and either respiratory compromise (eg, dyspnea, wheezing, stridor, hypoxia) or hypotension/end-organ dysfunction (eg, syncope, incontinence); (2) two or more symptoms (eg, respiratory compromise, hypotension/end-organ dysfunction, persistent gastrointestinal [GI] symptoms such as vomiting, diarrhea, or crampy abdominal pain) that occur rapidly after exposure involving the skin or mucosa; or (3) hypotension from a known allergen to the patient. The accuracy of these criteria has been retrospectively evaluated in an ED study, and found to have a 97% sensitivity and an 82% specificity.2 The negative predictive value was good at 98%, but the positive predictive value was only 69%.2
When a patient presents with minimal or subtle symptoms, anaphylaxis can be a very difficult diagnosis to make in the ED early on in the process. While no EP will miss the diagnosis in a patient with hives, hypotension, and wheezing, it can be easy to miss when the predominant symptoms are GI, such as nausea, vomiting, or diarrhea. In addition, the differential diagnosis for the presentation of anaphylaxis in the ED can be extremely broad and include vasovagal reaction, asthma attack, myocardial infarction, gastroenteritis, panic attack, or airway obstruction.
Due to the nature of emergency medicine, EPs must consider multiple etiologies before determining an evaluation and management plan. While recognizing there are limitations to the NIAID/FAAN criteria, EPs should be aware of them. We are very good at treating these types of symptoms with antihistamines and steroids; however, we frequently fail to give epinephrine when indicated. It is important to remember that epinephrine is the first-line treatment for anaphylaxis—not corticosteroids or antihistamines.3
Reasons for not administering epinephrine are multiple. First, as discussed above, if the diagnosis of anaphylaxis is not considered, the EP is not going to administer the drug of choice. Secondly, EPs have been taught to have a healthy respect for epinephrine and its effects, especially in older patients. Due to this cautious approach, epinephrine is frequently not given to patients with mild symptoms or to those who present early in the course of disease.
Emergency physicians have experience giving epinephrine subcutaneously, but not nearly as much with the intramuscular (IM) route. This is important, because an IM injection in the anterolateral thigh is the recommended location for the treatment of anaphylaxis. The dose should be weight based (0.01 mg/kg) to a maximum of 0.5 mg. This dose can be given every 5 to 15 minutes as necessary to control symptoms.3 The dosing is important to remember, since many EDs stock only autoinjectable epinephrine devices for use in anaphylaxis. These autoinjectors only contain 0.3 mg of epinephrine, so some patients may be underdosed if used.
In the management of allergic reactions and anaphylaxis, EPs frequently administer antihistamines and corticosteroids. While there is no direct evidence to support their use in the management of anaphylaxis, theoretical benefits do exist.3 This, combined with the excellent medication safety profile and lack of serious side effects, make these two medication classes appropriate for use in the ED.
- Allergic Reaction Versus Anaphylaxis
- Manivannan V, Decker WW, Stead LG, Li JT, Campbell RL. National Institute of Allergy and Infectious Disease and Food Allergy and Anaphylaxis Network criteria for anaphylaxis. Int J Emerg Med. 2009;2(1):3-5.
- Campbell RL, Hagan JB, Manivannan V, et al. Evaluation of National Institute of Allergy and Infectious Diseases/Food Allergy and Anaphylaxis Network criteria for the diagnosis of anaphylaxis in emergency department patients. J Allergy Clin Immunol. 2012;129(3):748-752.
- Campbell RL, Li JT, Nicklas RA, Sadosty AT; Members of the Joint Task Force; Practice Parameter Workgroup. Emergency department diagnosis and treatment of anaphylaxis: a practice parameter. Ann Allergy Asthma Immunol. 2014;113(6):599-608.
- Allergic Reaction Versus Anaphylaxis
- Manivannan V, Decker WW, Stead LG, Li JT, Campbell RL. National Institute of Allergy and Infectious Disease and Food Allergy and Anaphylaxis Network criteria for anaphylaxis. Int J Emerg Med. 2009;2(1):3-5.
- Campbell RL, Hagan JB, Manivannan V, et al. Evaluation of National Institute of Allergy and Infectious Diseases/Food Allergy and Anaphylaxis Network criteria for the diagnosis of anaphylaxis in emergency department patients. J Allergy Clin Immunol. 2012;129(3):748-752.
- Campbell RL, Li JT, Nicklas RA, Sadosty AT; Members of the Joint Task Force; Practice Parameter Workgroup. Emergency department diagnosis and treatment of anaphylaxis: a practice parameter. Ann Allergy Asthma Immunol. 2014;113(6):599-608.
