User login
Molecular Imaging of ER Status in Breast Cancer: A Preclinical Study
Background: Currently there are no FDA-approved imaging biomarkers capable of accurately identifying and quantitatively differentiating estrogen receptor (ER) status in breast cancer. The current preclinical study evaluated the ability of a Ga-68 positron emission tomography (PET) imaging biomarker and the analogous Lu-177 theranostic peptide construct to target and determine the status of ER expression.
Methods: Five human breast cancer cell line xenograft models were established in severe combined immunodeficiency mice. Western blot analysis confirmed the BB2r expression. The BB2r antagonist peptide construct was radiolabeled with Ga-68 and Lu-177, using fully automated radiochemistry labeling techniques. Pharmacokinetic, micro-SPECT/CT, and micro-PET/CT studies were performed.
Results: Pharmacokinetic studies confirmed that the Lu-177 construct targeted BB2r positive tissue in ER+ tumor xenograft models to a much greater extent than in ER- tumor xenograft models. In contrast, the ER-tumor xenografts demonstrated low initial uptake, followed by nearly complete washout from all tumor tissue within 24-hours after injection. The variances in tracer uptake by the tumor tissue correlated with BB2r expression via western blot analysis. Ga-68 micro-PET/CT data also correlated with the Lu-177 pharma-cokinetic studies, demonstrating visualization of BB2r+ tumor tissue with trends in standardized uptake values correlating directly with BB2r expression and ER status.
Conclusions: In summary, our study demonstrates selective tumor targeting for both a Ga-68 PET imaging biomarker and a Lu-177 theranostic agent in all breast cancer models studied. The Ga-68 PET SUV data suggest that PET imaging with this tracer or an analog of this tracer may have the potential to noninvasively differentiate ER status in vivo. Further studies are required involving an expanded panel of human cell lines and correlation with BB2 receptor expression/ER status obtained from biopsy data to confirm the potential validity of this finding.
Background: Currently there are no FDA-approved imaging biomarkers capable of accurately identifying and quantitatively differentiating estrogen receptor (ER) status in breast cancer. The current preclinical study evaluated the ability of a Ga-68 positron emission tomography (PET) imaging biomarker and the analogous Lu-177 theranostic peptide construct to target and determine the status of ER expression.
Methods: Five human breast cancer cell line xenograft models were established in severe combined immunodeficiency mice. Western blot analysis confirmed the BB2r expression. The BB2r antagonist peptide construct was radiolabeled with Ga-68 and Lu-177, using fully automated radiochemistry labeling techniques. Pharmacokinetic, micro-SPECT/CT, and micro-PET/CT studies were performed.
Results: Pharmacokinetic studies confirmed that the Lu-177 construct targeted BB2r positive tissue in ER+ tumor xenograft models to a much greater extent than in ER- tumor xenograft models. In contrast, the ER-tumor xenografts demonstrated low initial uptake, followed by nearly complete washout from all tumor tissue within 24-hours after injection. The variances in tracer uptake by the tumor tissue correlated with BB2r expression via western blot analysis. Ga-68 micro-PET/CT data also correlated with the Lu-177 pharma-cokinetic studies, demonstrating visualization of BB2r+ tumor tissue with trends in standardized uptake values correlating directly with BB2r expression and ER status.
Conclusions: In summary, our study demonstrates selective tumor targeting for both a Ga-68 PET imaging biomarker and a Lu-177 theranostic agent in all breast cancer models studied. The Ga-68 PET SUV data suggest that PET imaging with this tracer or an analog of this tracer may have the potential to noninvasively differentiate ER status in vivo. Further studies are required involving an expanded panel of human cell lines and correlation with BB2 receptor expression/ER status obtained from biopsy data to confirm the potential validity of this finding.
Background: Currently there are no FDA-approved imaging biomarkers capable of accurately identifying and quantitatively differentiating estrogen receptor (ER) status in breast cancer. The current preclinical study evaluated the ability of a Ga-68 positron emission tomography (PET) imaging biomarker and the analogous Lu-177 theranostic peptide construct to target and determine the status of ER expression.
Methods: Five human breast cancer cell line xenograft models were established in severe combined immunodeficiency mice. Western blot analysis confirmed the BB2r expression. The BB2r antagonist peptide construct was radiolabeled with Ga-68 and Lu-177, using fully automated radiochemistry labeling techniques. Pharmacokinetic, micro-SPECT/CT, and micro-PET/CT studies were performed.
Results: Pharmacokinetic studies confirmed that the Lu-177 construct targeted BB2r positive tissue in ER+ tumor xenograft models to a much greater extent than in ER- tumor xenograft models. In contrast, the ER-tumor xenografts demonstrated low initial uptake, followed by nearly complete washout from all tumor tissue within 24-hours after injection. The variances in tracer uptake by the tumor tissue correlated with BB2r expression via western blot analysis. Ga-68 micro-PET/CT data also correlated with the Lu-177 pharma-cokinetic studies, demonstrating visualization of BB2r+ tumor tissue with trends in standardized uptake values correlating directly with BB2r expression and ER status.
Conclusions: In summary, our study demonstrates selective tumor targeting for both a Ga-68 PET imaging biomarker and a Lu-177 theranostic agent in all breast cancer models studied. The Ga-68 PET SUV data suggest that PET imaging with this tracer or an analog of this tracer may have the potential to noninvasively differentiate ER status in vivo. Further studies are required involving an expanded panel of human cell lines and correlation with BB2 receptor expression/ER status obtained from biopsy data to confirm the potential validity of this finding.
Compared to Open Repair, EVAR Reduces Mortality up to 3 Years
NEW YORK - Endovascular repair (EVAR) of abdominal aortic aneurysms (AAAs) is associated with an initial survival advantage over open repair, according to a study of "real-world" data from California.
However, the difference disappears in the long term, researchers report in JAMA Surgery, online September 2.
Dr. David C. Chang of Harvard Medical School in Boston said by email that the study "highlights the importance of looking at real-world data in evaluating surgical options. Clinically, our study found that the survival advantage for EVAR repairs is maintained until 3 years, after which mortality was higher for patients who had EVAR repairs."
The team studied more than 23,000 patients who underwent AAA repair between 2001 and 2009. Just over half had EVAR while the remaining patients underwent open repair. Median follow-up was for three years.
EVAR was associated with improved 30-day all-cause mortality (1.54% vs. 4.74%) and significantly improved survival until three years postoperatively. After that mortality rose, and the researchers found no difference in long-term mortality for the entire cohort after adjusting for confounders (hazard ratio, 0.99; p=0.64).
EVAR was linked with a significantly higher rate of reinterventions and AAA late ruptures. At five years, for instance, the reintervention rate was 6.59% in the EVAR group vs. 1.48% in the open group.
"This is different from data from clinical trials," Dr. Chang pointed out. "The short-term survival advantage of EVAR from clinical trials data likely eroded as patient risk factors exact their toll over time. These are real-world issues and concerns that are often not captured in idealized clinical trials."
Senior author Dr. Samuel E. Wilson, of the University of California-Irvine Medical Center, added by email that EVAR is safer than the open procedure, which it has replaced. The mortality advantage last for three years, "then other morbidity, especially effects of smoking, even out survival."
Dr. Chang went on to note that "our use of data from the State of California also has an important policy implication: That many states actually have better and more complete population data than the federal government when it comes to healthcare quality. While research and policies related to healthcare quality are driven mostly by the federal government
currently (through Medicare), the federal government has limited data on patient care outside of Medicare."
"Therefore," Dr. Chang concluded, "an argument can be made that the federal government should delegate healthcare research and quality improvement responsibilities to individual states, and support state-level efforts to examine and improve healthcare quality. Healthcare, like politics, is all local."
In an accompanying editorial, Drs. Jamie E. Anderson and James W. Holcroft, of the University of California Davis Medical Center, Sacramento, observe that the study "offers a glimpse into the future of population-based health services research methods."
In a joint email, they said, "Harnessing information already captured for patient care or billing purposes to advance medical research makes sense."
NEW YORK - Endovascular repair (EVAR) of abdominal aortic aneurysms (AAAs) is associated with an initial survival advantage over open repair, according to a study of "real-world" data from California.
However, the difference disappears in the long term, researchers report in JAMA Surgery, online September 2.
Dr. David C. Chang of Harvard Medical School in Boston said by email that the study "highlights the importance of looking at real-world data in evaluating surgical options. Clinically, our study found that the survival advantage for EVAR repairs is maintained until 3 years, after which mortality was higher for patients who had EVAR repairs."
The team studied more than 23,000 patients who underwent AAA repair between 2001 and 2009. Just over half had EVAR while the remaining patients underwent open repair. Median follow-up was for three years.
EVAR was associated with improved 30-day all-cause mortality (1.54% vs. 4.74%) and significantly improved survival until three years postoperatively. After that mortality rose, and the researchers found no difference in long-term mortality for the entire cohort after adjusting for confounders (hazard ratio, 0.99; p=0.64).
EVAR was linked with a significantly higher rate of reinterventions and AAA late ruptures. At five years, for instance, the reintervention rate was 6.59% in the EVAR group vs. 1.48% in the open group.
"This is different from data from clinical trials," Dr. Chang pointed out. "The short-term survival advantage of EVAR from clinical trials data likely eroded as patient risk factors exact their toll over time. These are real-world issues and concerns that are often not captured in idealized clinical trials."
Senior author Dr. Samuel E. Wilson, of the University of California-Irvine Medical Center, added by email that EVAR is safer than the open procedure, which it has replaced. The mortality advantage last for three years, "then other morbidity, especially effects of smoking, even out survival."
Dr. Chang went on to note that "our use of data from the State of California also has an important policy implication: That many states actually have better and more complete population data than the federal government when it comes to healthcare quality. While research and policies related to healthcare quality are driven mostly by the federal government
currently (through Medicare), the federal government has limited data on patient care outside of Medicare."
"Therefore," Dr. Chang concluded, "an argument can be made that the federal government should delegate healthcare research and quality improvement responsibilities to individual states, and support state-level efforts to examine and improve healthcare quality. Healthcare, like politics, is all local."
In an accompanying editorial, Drs. Jamie E. Anderson and James W. Holcroft, of the University of California Davis Medical Center, Sacramento, observe that the study "offers a glimpse into the future of population-based health services research methods."
In a joint email, they said, "Harnessing information already captured for patient care or billing purposes to advance medical research makes sense."
NEW YORK - Endovascular repair (EVAR) of abdominal aortic aneurysms (AAAs) is associated with an initial survival advantage over open repair, according to a study of "real-world" data from California.
However, the difference disappears in the long term, researchers report in JAMA Surgery, online September 2.
Dr. David C. Chang of Harvard Medical School in Boston said by email that the study "highlights the importance of looking at real-world data in evaluating surgical options. Clinically, our study found that the survival advantage for EVAR repairs is maintained until 3 years, after which mortality was higher for patients who had EVAR repairs."
The team studied more than 23,000 patients who underwent AAA repair between 2001 and 2009. Just over half had EVAR while the remaining patients underwent open repair. Median follow-up was for three years.
EVAR was associated with improved 30-day all-cause mortality (1.54% vs. 4.74%) and significantly improved survival until three years postoperatively. After that mortality rose, and the researchers found no difference in long-term mortality for the entire cohort after adjusting for confounders (hazard ratio, 0.99; p=0.64).
EVAR was linked with a significantly higher rate of reinterventions and AAA late ruptures. At five years, for instance, the reintervention rate was 6.59% in the EVAR group vs. 1.48% in the open group.
"This is different from data from clinical trials," Dr. Chang pointed out. "The short-term survival advantage of EVAR from clinical trials data likely eroded as patient risk factors exact their toll over time. These are real-world issues and concerns that are often not captured in idealized clinical trials."
Senior author Dr. Samuel E. Wilson, of the University of California-Irvine Medical Center, added by email that EVAR is safer than the open procedure, which it has replaced. The mortality advantage last for three years, "then other morbidity, especially effects of smoking, even out survival."
Dr. Chang went on to note that "our use of data from the State of California also has an important policy implication: That many states actually have better and more complete population data than the federal government when it comes to healthcare quality. While research and policies related to healthcare quality are driven mostly by the federal government
currently (through Medicare), the federal government has limited data on patient care outside of Medicare."
"Therefore," Dr. Chang concluded, "an argument can be made that the federal government should delegate healthcare research and quality improvement responsibilities to individual states, and support state-level efforts to examine and improve healthcare quality. Healthcare, like politics, is all local."
In an accompanying editorial, Drs. Jamie E. Anderson and James W. Holcroft, of the University of California Davis Medical Center, Sacramento, observe that the study "offers a glimpse into the future of population-based health services research methods."
In a joint email, they said, "Harnessing information already captured for patient care or billing purposes to advance medical research makes sense."
First-line BV can produce high response rate in older HL patients

Photo from Business Wire
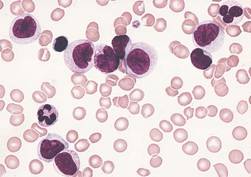
First-line treatment with brentuximab vedotin (BV) can produce a high response rate in older Hodgkin lymphoma (HL) patients who are unfit for chemotherapy, according to research published in Blood.
In this small study, single-agent BV produced an overall response rate of 92% and a complete response rate of 73%.
However, the drug also produced a high rate of peripheral sensory neuropathy (78%), which was the most common adverse event.
This phase 2 trial is the first to assess BV as front-line treatment. The study was funded by Seattle Genetics, Inc., which is developing BV in collaboration with Takeda Pharmaceutical Company.
Andres Forero-Torres, MD, of the University of Alabama at Birmingham, and his colleagues conducted the research, enrolling 27 HL patients (ages 64 to 92) in the trial.
The patients were either ineligible for conventional chemotherapy or declined treatment after receiving information about its risks.
They received 1.8 mg/kg of intravenous BV every 3 weeks for up to 16 doses. Those who benefitted from the drug could continue beyond this time period until disease progression, unacceptable toxicity, or study closure.
Patients received a median of 8 cycles, with 4 patients completing 16 cycles and 1 patient completing 23 cycles.
Peripheral neuropathy was the primary adverse event leading to dose modifications. Fourteen patients (52%) had dose delays, typically lasting a week (range, 1 to 3). But 11 patients (41%) had permanent dose reductions to 1.2 mg/kg.
Safety
All 27 patients were evaluable for safety, and all experienced at least 1 adverse event. The most commonly reported events were peripheral sensory neuropathy (n=21, 78%), fatigue (n=12, 44%), and nausea (n=12, 44%).
Treatment-emergent grade 3 adverse events included peripheral sensory neuropathy (n=7, 26%), rash (n=2, 7%), urinary tract infection (n=1, 4%), and maculopapular rash (n=1, 4%)
There were 2 grade 4 events—hyperuricemia and drug hypersensitivity to anesthesia—considered unrelated to BV.
Efficacy
Twenty-six patients were evaluable for efficacy. One patient was found to have nodular lymphocyte predominant HL and was therefore excluded.
The overall response rate was 92%. Nineteen patients had a complete response, 5 had a partial response, and 2 had stable disease.
The median duration of response was about 9.1 months (range, 2.8 to 20.9+ months).
The median progression-free survival was 10.5 months (range, 2.6+ to 22.3+ months), and the median overall survival had not been reached at the time of analysis (range, 4.6+ to 24.9+ months).
“While we observed promising responses,” Dr Forero-Torres said, “the next step is to evaluate this drug in combination with additional chemotherapy or immunotherapies that might allow us to prolong the response without relapse.” ![]()
Photo from Business Wire
First-line treatment with brentuximab vedotin (BV) can produce a high response rate in older Hodgkin lymphoma (HL) patients who are unfit for chemotherapy, according to research published in Blood.
In this small study, single-agent BV produced an overall response rate of 92% and a complete response rate of 73%.
However, the drug also produced a high rate of peripheral sensory neuropathy (78%), which was the most common adverse event.
This phase 2 trial is the first to assess BV as front-line treatment. The study was funded by Seattle Genetics, Inc., which is developing BV in collaboration with Takeda Pharmaceutical Company.
Andres Forero-Torres, MD, of the University of Alabama at Birmingham, and his colleagues conducted the research, enrolling 27 HL patients (ages 64 to 92) in the trial.
The patients were either ineligible for conventional chemotherapy or declined treatment after receiving information about its risks.
They received 1.8 mg/kg of intravenous BV every 3 weeks for up to 16 doses. Those who benefitted from the drug could continue beyond this time period until disease progression, unacceptable toxicity, or study closure.
Patients received a median of 8 cycles, with 4 patients completing 16 cycles and 1 patient completing 23 cycles.
Peripheral neuropathy was the primary adverse event leading to dose modifications. Fourteen patients (52%) had dose delays, typically lasting a week (range, 1 to 3). But 11 patients (41%) had permanent dose reductions to 1.2 mg/kg.
Safety
All 27 patients were evaluable for safety, and all experienced at least 1 adverse event. The most commonly reported events were peripheral sensory neuropathy (n=21, 78%), fatigue (n=12, 44%), and nausea (n=12, 44%).
Treatment-emergent grade 3 adverse events included peripheral sensory neuropathy (n=7, 26%), rash (n=2, 7%), urinary tract infection (n=1, 4%), and maculopapular rash (n=1, 4%)
There were 2 grade 4 events—hyperuricemia and drug hypersensitivity to anesthesia—considered unrelated to BV.
Efficacy
Twenty-six patients were evaluable for efficacy. One patient was found to have nodular lymphocyte predominant HL and was therefore excluded.
The overall response rate was 92%. Nineteen patients had a complete response, 5 had a partial response, and 2 had stable disease.
The median duration of response was about 9.1 months (range, 2.8 to 20.9+ months).
The median progression-free survival was 10.5 months (range, 2.6+ to 22.3+ months), and the median overall survival had not been reached at the time of analysis (range, 4.6+ to 24.9+ months).
“While we observed promising responses,” Dr Forero-Torres said, “the next step is to evaluate this drug in combination with additional chemotherapy or immunotherapies that might allow us to prolong the response without relapse.” ![]()
Photo from Business Wire
First-line treatment with brentuximab vedotin (BV) can produce a high response rate in older Hodgkin lymphoma (HL) patients who are unfit for chemotherapy, according to research published in Blood.
In this small study, single-agent BV produced an overall response rate of 92% and a complete response rate of 73%.
However, the drug also produced a high rate of peripheral sensory neuropathy (78%), which was the most common adverse event.
This phase 2 trial is the first to assess BV as front-line treatment. The study was funded by Seattle Genetics, Inc., which is developing BV in collaboration with Takeda Pharmaceutical Company.
Andres Forero-Torres, MD, of the University of Alabama at Birmingham, and his colleagues conducted the research, enrolling 27 HL patients (ages 64 to 92) in the trial.
The patients were either ineligible for conventional chemotherapy or declined treatment after receiving information about its risks.
They received 1.8 mg/kg of intravenous BV every 3 weeks for up to 16 doses. Those who benefitted from the drug could continue beyond this time period until disease progression, unacceptable toxicity, or study closure.
Patients received a median of 8 cycles, with 4 patients completing 16 cycles and 1 patient completing 23 cycles.
Peripheral neuropathy was the primary adverse event leading to dose modifications. Fourteen patients (52%) had dose delays, typically lasting a week (range, 1 to 3). But 11 patients (41%) had permanent dose reductions to 1.2 mg/kg.
Safety
All 27 patients were evaluable for safety, and all experienced at least 1 adverse event. The most commonly reported events were peripheral sensory neuropathy (n=21, 78%), fatigue (n=12, 44%), and nausea (n=12, 44%).
Treatment-emergent grade 3 adverse events included peripheral sensory neuropathy (n=7, 26%), rash (n=2, 7%), urinary tract infection (n=1, 4%), and maculopapular rash (n=1, 4%)
There were 2 grade 4 events—hyperuricemia and drug hypersensitivity to anesthesia—considered unrelated to BV.
Efficacy
Twenty-six patients were evaluable for efficacy. One patient was found to have nodular lymphocyte predominant HL and was therefore excluded.
The overall response rate was 92%. Nineteen patients had a complete response, 5 had a partial response, and 2 had stable disease.
The median duration of response was about 9.1 months (range, 2.8 to 20.9+ months).
The median progression-free survival was 10.5 months (range, 2.6+ to 22.3+ months), and the median overall survival had not been reached at the time of analysis (range, 4.6+ to 24.9+ months).
“While we observed promising responses,” Dr Forero-Torres said, “the next step is to evaluate this drug in combination with additional chemotherapy or immunotherapies that might allow us to prolong the response without relapse.” ![]()
Readmissions due to infection after HSCT

Photo courtesy of the CDC
SAN DIEGO—A retrospective study has provided insight into hospital readmissions related to opportunistic infection following hematopoietic stem cell transplant (HSCT).
Of the roughly 4200 HSCT recipients studied, 26% were readmitted to the hospital due to opportunistic infection.
About 1 in 3 infection-related readmissions were due to double-stranded DNA (dsDNA) viral infections, and cytomegalovirus (CMV) infections were the most common.
Nearly half of the dsDNA viral infections occurred within the first month of HSCT discharge.
These findings were presented at ICAAC/ICC 2015 (poster T-1360). The study was sponsored by Chimerix, Inc.
Investigators searched the Premier hospital database for patients who underwent HSCT between January 2009 and September 2013. The team identified 4393 patients with a mean age of 50.4 years. Most were adults (91.2%), most were male (57.9%), and most received an autologous HSCT (63.2%).
About 42% (n=1841) of patients had a diagnostic code for opportunistic infection in their HSCT discharge records. Overall, 7.3% (n=319) of patients had dsDNA virus infections, including 13.4% (n=216) of patients who received an allogeneic HSCT.
One hundred and fifty-seven patients died during HSCT hospitalization, leaving 4236 patients evaluable for readmission analysis.
In all, 37.7% (n=1595) of the surviving patients were readmitted to the hospital for any reason during the 12 months after HSCT discharge. And 65.6% of the readmissions occurred within the first 3 months of HSCT discharge.
Readmissions were most frequently related to opportunistic infections (25.8%, n=1091), followed by graft-versus-host disease (13.7%, n=579), renal impairment (11.1%, n=470), and neutropenia (10.0%, n=422).
The investigators noted that patients may have had multiple readmissions or readmission with multiple diagnoses.
Of the hospital readmissions related to opportunistic infections, 32.0% (n=349) were related to dsDNA virus infections. This included CMV (65.9%, n=230), BK virus (13.8%, n=48), adenovirus (5.2%, n=18), and other dsDNA virus infections (32.7%, n=114).
Patients may have experienced more than one viral infection, so the number of hospital readmissions related to each dsDNA virus was not mutually exclusive.
Readmission within the first month of HSCT discharge occurred in 41.8% of patients with any dsDNA virus infection, 49.6% with CMV infection, and 56.3% with BK virus infection. More than half (55.6%) of readmissions related to adenovirus infection occurred within the first 3 months of HSCT discharge.
Taking these results together, the investigators concluded that hospital readmissions related to opportunistic infections were relatively common among HSCT recipients. So strategies that minimize the risks of these infections might have significant clinical and economic advantages. ![]()
Photo courtesy of the CDC
SAN DIEGO—A retrospective study has provided insight into hospital readmissions related to opportunistic infection following hematopoietic stem cell transplant (HSCT).
Of the roughly 4200 HSCT recipients studied, 26% were readmitted to the hospital due to opportunistic infection.
About 1 in 3 infection-related readmissions were due to double-stranded DNA (dsDNA) viral infections, and cytomegalovirus (CMV) infections were the most common.
Nearly half of the dsDNA viral infections occurred within the first month of HSCT discharge.
These findings were presented at ICAAC/ICC 2015 (poster T-1360). The study was sponsored by Chimerix, Inc.
Investigators searched the Premier hospital database for patients who underwent HSCT between January 2009 and September 2013. The team identified 4393 patients with a mean age of 50.4 years. Most were adults (91.2%), most were male (57.9%), and most received an autologous HSCT (63.2%).
About 42% (n=1841) of patients had a diagnostic code for opportunistic infection in their HSCT discharge records. Overall, 7.3% (n=319) of patients had dsDNA virus infections, including 13.4% (n=216) of patients who received an allogeneic HSCT.
One hundred and fifty-seven patients died during HSCT hospitalization, leaving 4236 patients evaluable for readmission analysis.
In all, 37.7% (n=1595) of the surviving patients were readmitted to the hospital for any reason during the 12 months after HSCT discharge. And 65.6% of the readmissions occurred within the first 3 months of HSCT discharge.
Readmissions were most frequently related to opportunistic infections (25.8%, n=1091), followed by graft-versus-host disease (13.7%, n=579), renal impairment (11.1%, n=470), and neutropenia (10.0%, n=422).
The investigators noted that patients may have had multiple readmissions or readmission with multiple diagnoses.
Of the hospital readmissions related to opportunistic infections, 32.0% (n=349) were related to dsDNA virus infections. This included CMV (65.9%, n=230), BK virus (13.8%, n=48), adenovirus (5.2%, n=18), and other dsDNA virus infections (32.7%, n=114).
Patients may have experienced more than one viral infection, so the number of hospital readmissions related to each dsDNA virus was not mutually exclusive.
Readmission within the first month of HSCT discharge occurred in 41.8% of patients with any dsDNA virus infection, 49.6% with CMV infection, and 56.3% with BK virus infection. More than half (55.6%) of readmissions related to adenovirus infection occurred within the first 3 months of HSCT discharge.
Taking these results together, the investigators concluded that hospital readmissions related to opportunistic infections were relatively common among HSCT recipients. So strategies that minimize the risks of these infections might have significant clinical and economic advantages. ![]()
Photo courtesy of the CDC
SAN DIEGO—A retrospective study has provided insight into hospital readmissions related to opportunistic infection following hematopoietic stem cell transplant (HSCT).
Of the roughly 4200 HSCT recipients studied, 26% were readmitted to the hospital due to opportunistic infection.
About 1 in 3 infection-related readmissions were due to double-stranded DNA (dsDNA) viral infections, and cytomegalovirus (CMV) infections were the most common.
Nearly half of the dsDNA viral infections occurred within the first month of HSCT discharge.
These findings were presented at ICAAC/ICC 2015 (poster T-1360). The study was sponsored by Chimerix, Inc.
Investigators searched the Premier hospital database for patients who underwent HSCT between January 2009 and September 2013. The team identified 4393 patients with a mean age of 50.4 years. Most were adults (91.2%), most were male (57.9%), and most received an autologous HSCT (63.2%).
About 42% (n=1841) of patients had a diagnostic code for opportunistic infection in their HSCT discharge records. Overall, 7.3% (n=319) of patients had dsDNA virus infections, including 13.4% (n=216) of patients who received an allogeneic HSCT.
One hundred and fifty-seven patients died during HSCT hospitalization, leaving 4236 patients evaluable for readmission analysis.
In all, 37.7% (n=1595) of the surviving patients were readmitted to the hospital for any reason during the 12 months after HSCT discharge. And 65.6% of the readmissions occurred within the first 3 months of HSCT discharge.
Readmissions were most frequently related to opportunistic infections (25.8%, n=1091), followed by graft-versus-host disease (13.7%, n=579), renal impairment (11.1%, n=470), and neutropenia (10.0%, n=422).
The investigators noted that patients may have had multiple readmissions or readmission with multiple diagnoses.
Of the hospital readmissions related to opportunistic infections, 32.0% (n=349) were related to dsDNA virus infections. This included CMV (65.9%, n=230), BK virus (13.8%, n=48), adenovirus (5.2%, n=18), and other dsDNA virus infections (32.7%, n=114).
Patients may have experienced more than one viral infection, so the number of hospital readmissions related to each dsDNA virus was not mutually exclusive.
Readmission within the first month of HSCT discharge occurred in 41.8% of patients with any dsDNA virus infection, 49.6% with CMV infection, and 56.3% with BK virus infection. More than half (55.6%) of readmissions related to adenovirus infection occurred within the first 3 months of HSCT discharge.
Taking these results together, the investigators concluded that hospital readmissions related to opportunistic infections were relatively common among HSCT recipients. So strategies that minimize the risks of these infections might have significant clinical and economic advantages. ![]()
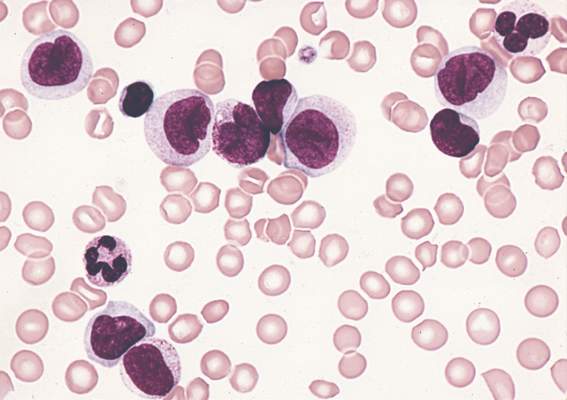
mAb gets priority review as maintenance in CLL

Photo by Linda Bartlett
The US Food and Drug Administration (FDA) has granted priority review for an application for ofatumumab (Arzerra) as maintenance therapy in
patients with relapsed chronic lymphocytic leukemia (CLL).
The FDA grants priority review to investigational therapies that, if approved, may offer significant improvements in the treatment, prevention, or diagnosis of a serious condition.
The designation shortens the review period from 10 months to 6 months.
Ofatumumab is a human monoclonal antibody (mAb) designed to target CD20 on the surface of CLL cells and normal B lymphocytes.
The mAb is already FDA-approved to treat patients with CLL that is refractory to fludarabine and alemtuzumab. Ofatumumab is also approved for use in combination with chlorambucil to treat previously untreated patients with CLL for whom fludarabine-based therapy is considered inappropriate.
The FDA said it aims to complete its review of the application for ofatumumab as maintenance therapy in relapsed CLL by January 21, 2016.
PROLONG trial
The application for ofatumumab as maintenance is based on interim results from the phase 3 PROLONG (OMB112517) trial, which were presented at ASH 2014.
In this trial, researchers compared ofatumumab maintenance to no further treatment in patients with a complete or partial response after second-
or third-line treatment for CLL.
Interim results suggested that ofatumumab significantly improves progression-free survival but not overall survival.
The median progression-free survival was about 29 months in patients who received ofatumumab and about 15 months for patients who did not receive
maintenance (P<0.0001).
There was no significant difference in the median overall survival, which was not reached in either treatment arm.
Ofatumumab development
Ofatumumab is approved in more than 50 countries worldwide as monotherapy for CLL patients who are refractory to fludarabine and alemtuzumab.
In the European Union, ofatumumab is approved for use in combination with chlorambucil or bendamustine to treat CLL patients who have not received prior therapy and who are not eligible for fludarabine-based therapy.
Ofatumumab is not approved anywhere in the world as maintenance therapy for relapsed CLL. The drug is being developed by Genmab and Novartis. ![]()
Photo by Linda Bartlett
The US Food and Drug Administration (FDA) has granted priority review for an application for ofatumumab (Arzerra) as maintenance therapy in
patients with relapsed chronic lymphocytic leukemia (CLL).
The FDA grants priority review to investigational therapies that, if approved, may offer significant improvements in the treatment, prevention, or diagnosis of a serious condition.
The designation shortens the review period from 10 months to 6 months.
Ofatumumab is a human monoclonal antibody (mAb) designed to target CD20 on the surface of CLL cells and normal B lymphocytes.
The mAb is already FDA-approved to treat patients with CLL that is refractory to fludarabine and alemtuzumab. Ofatumumab is also approved for use in combination with chlorambucil to treat previously untreated patients with CLL for whom fludarabine-based therapy is considered inappropriate.
The FDA said it aims to complete its review of the application for ofatumumab as maintenance therapy in relapsed CLL by January 21, 2016.
PROLONG trial
The application for ofatumumab as maintenance is based on interim results from the phase 3 PROLONG (OMB112517) trial, which were presented at ASH 2014.
In this trial, researchers compared ofatumumab maintenance to no further treatment in patients with a complete or partial response after second-
or third-line treatment for CLL.
Interim results suggested that ofatumumab significantly improves progression-free survival but not overall survival.
The median progression-free survival was about 29 months in patients who received ofatumumab and about 15 months for patients who did not receive
maintenance (P<0.0001).
There was no significant difference in the median overall survival, which was not reached in either treatment arm.
Ofatumumab development
Ofatumumab is approved in more than 50 countries worldwide as monotherapy for CLL patients who are refractory to fludarabine and alemtuzumab.
In the European Union, ofatumumab is approved for use in combination with chlorambucil or bendamustine to treat CLL patients who have not received prior therapy and who are not eligible for fludarabine-based therapy.
Ofatumumab is not approved anywhere in the world as maintenance therapy for relapsed CLL. The drug is being developed by Genmab and Novartis. ![]()
Photo by Linda Bartlett
The US Food and Drug Administration (FDA) has granted priority review for an application for ofatumumab (Arzerra) as maintenance therapy in
patients with relapsed chronic lymphocytic leukemia (CLL).
The FDA grants priority review to investigational therapies that, if approved, may offer significant improvements in the treatment, prevention, or diagnosis of a serious condition.
The designation shortens the review period from 10 months to 6 months.
Ofatumumab is a human monoclonal antibody (mAb) designed to target CD20 on the surface of CLL cells and normal B lymphocytes.
The mAb is already FDA-approved to treat patients with CLL that is refractory to fludarabine and alemtuzumab. Ofatumumab is also approved for use in combination with chlorambucil to treat previously untreated patients with CLL for whom fludarabine-based therapy is considered inappropriate.
The FDA said it aims to complete its review of the application for ofatumumab as maintenance therapy in relapsed CLL by January 21, 2016.
PROLONG trial
The application for ofatumumab as maintenance is based on interim results from the phase 3 PROLONG (OMB112517) trial, which were presented at ASH 2014.
In this trial, researchers compared ofatumumab maintenance to no further treatment in patients with a complete or partial response after second-
or third-line treatment for CLL.
Interim results suggested that ofatumumab significantly improves progression-free survival but not overall survival.
The median progression-free survival was about 29 months in patients who received ofatumumab and about 15 months for patients who did not receive
maintenance (P<0.0001).
There was no significant difference in the median overall survival, which was not reached in either treatment arm.
Ofatumumab development
Ofatumumab is approved in more than 50 countries worldwide as monotherapy for CLL patients who are refractory to fludarabine and alemtuzumab.
In the European Union, ofatumumab is approved for use in combination with chlorambucil or bendamustine to treat CLL patients who have not received prior therapy and who are not eligible for fludarabine-based therapy.
Ofatumumab is not approved anywhere in the world as maintenance therapy for relapsed CLL. The drug is being developed by Genmab and Novartis. ![]()
CDK inhibitor active against lymphoma too

HOUSTON—Preclinical data suggest the second-generation cyclin-dependent kinase (CDK) inhibitor CYC065 is active against lymphomas as well as leukemias.
Previous research showed that CYC065 can fight acute myeloid leukemia (AML) in vitro and in vivo.
New research shows that CYC065 can decrease cell viability in a range of B-cell lymphoma cell lines, and the drug synergizes with both venetoclax and cytarabine.
Sheelagh Frame, PhD, and her colleagues presented these results at the SOHO 2015 Annual Meeting (poster 213). All of the investigators involved in the research are employees of Cyclacel Ltd., the company developing CYC065.
The investigators analyzed the anticancer activity of CYC065 in a range of cell lines and found that CYC065 induced apoptosis by inhibiting the expression of CDK9-dependent oncogenic transcripts, including Mcl-1, c-Myc, Hoxa9, and Meis1.
Results in AML
Experiments in the AML-MLL cell line MOLM-13 showed that short pulses of CYC065 (6 hours), rather than continuous treatment, were sufficient to achieve maximal cytotoxicity.
CYC065 induced apoptosis, in a dose-dependent manner, in other AML cell lines as well, including EOL-1 (MLL-PTD), MV4-11 (MLL-AF4, FLT3-ITD, and trisomy chr 8), HL60 (Myc amplified), and Kasumi-1.
The investigators noted that AML cell lines with MLL rearrangements were especially sensitive to CYC065, and the reliance of AML on Mcl-1 confers sensitivity to CYC065.
They also found evidence to suggest that Bak and Bcl-xL levels may be predictive of CYC065 response in AML. Cell lines that were less sensitive to treatment had high levels of Bcl-xL and negligible levels of Bak.
B-cell lymphomas
In B-cell lymphoma cell lines, the investigators observed a dose-dependent reduction in cell viability after CYC065 treatment (8-hour pulses).
CYC065 proved most effective in cell lines without genomic alterations associated with poor prognosis (HT and U-698-M) and in cell lines with Myc rearrangements (SU-DHL-8 and WILL-1).
The drug also decreased cell viability—but to a lesser degree—in cell lines with Bcl-2 rearrangements (SU-DHL-4 and U2932) and in double-hit lymphoma cell lines (MAVER-1, RI-1, SC-1, and SU-DHL-10).
The investigators therefore theorized that combining CYC065 with a Bcl-2 inhibitor might prove more effective in these cell lines.
CYC065 in combination
CYC065 synergized with the Bcl-2 inhibitor venetoclax in all B-cell lymphoma cell lines tested. The drugs were “strongly synergistic” in U2932 and RI-1 cell lines but simply “synergistic” in SU-CHL-4 and MAVER-1 cell lines.
CYC065 also synergized with cytarabine to fight AML. The combination proved synergistic at a range of doses in the HL60 and MV4-11 cell lines.
Considering these results together, the investigators concluded that CYC065 has shown potential for treating a range of leukemias and lymphomas with unmet clinical need, including MLL-rearranged leukemia and Myc-driven lymphoma.
And the drug might prove effective in combination with standard cytotoxic agents or agents targeting apoptotic regulators. ![]()
HOUSTON—Preclinical data suggest the second-generation cyclin-dependent kinase (CDK) inhibitor CYC065 is active against lymphomas as well as leukemias.
Previous research showed that CYC065 can fight acute myeloid leukemia (AML) in vitro and in vivo.
New research shows that CYC065 can decrease cell viability in a range of B-cell lymphoma cell lines, and the drug synergizes with both venetoclax and cytarabine.
Sheelagh Frame, PhD, and her colleagues presented these results at the SOHO 2015 Annual Meeting (poster 213). All of the investigators involved in the research are employees of Cyclacel Ltd., the company developing CYC065.
The investigators analyzed the anticancer activity of CYC065 in a range of cell lines and found that CYC065 induced apoptosis by inhibiting the expression of CDK9-dependent oncogenic transcripts, including Mcl-1, c-Myc, Hoxa9, and Meis1.
Results in AML
Experiments in the AML-MLL cell line MOLM-13 showed that short pulses of CYC065 (6 hours), rather than continuous treatment, were sufficient to achieve maximal cytotoxicity.
CYC065 induced apoptosis, in a dose-dependent manner, in other AML cell lines as well, including EOL-1 (MLL-PTD), MV4-11 (MLL-AF4, FLT3-ITD, and trisomy chr 8), HL60 (Myc amplified), and Kasumi-1.
The investigators noted that AML cell lines with MLL rearrangements were especially sensitive to CYC065, and the reliance of AML on Mcl-1 confers sensitivity to CYC065.
They also found evidence to suggest that Bak and Bcl-xL levels may be predictive of CYC065 response in AML. Cell lines that were less sensitive to treatment had high levels of Bcl-xL and negligible levels of Bak.
B-cell lymphomas
In B-cell lymphoma cell lines, the investigators observed a dose-dependent reduction in cell viability after CYC065 treatment (8-hour pulses).
CYC065 proved most effective in cell lines without genomic alterations associated with poor prognosis (HT and U-698-M) and in cell lines with Myc rearrangements (SU-DHL-8 and WILL-1).
The drug also decreased cell viability—but to a lesser degree—in cell lines with Bcl-2 rearrangements (SU-DHL-4 and U2932) and in double-hit lymphoma cell lines (MAVER-1, RI-1, SC-1, and SU-DHL-10).
The investigators therefore theorized that combining CYC065 with a Bcl-2 inhibitor might prove more effective in these cell lines.
CYC065 in combination
CYC065 synergized with the Bcl-2 inhibitor venetoclax in all B-cell lymphoma cell lines tested. The drugs were “strongly synergistic” in U2932 and RI-1 cell lines but simply “synergistic” in SU-CHL-4 and MAVER-1 cell lines.
CYC065 also synergized with cytarabine to fight AML. The combination proved synergistic at a range of doses in the HL60 and MV4-11 cell lines.
Considering these results together, the investigators concluded that CYC065 has shown potential for treating a range of leukemias and lymphomas with unmet clinical need, including MLL-rearranged leukemia and Myc-driven lymphoma.
And the drug might prove effective in combination with standard cytotoxic agents or agents targeting apoptotic regulators. ![]()
HOUSTON—Preclinical data suggest the second-generation cyclin-dependent kinase (CDK) inhibitor CYC065 is active against lymphomas as well as leukemias.
Previous research showed that CYC065 can fight acute myeloid leukemia (AML) in vitro and in vivo.
New research shows that CYC065 can decrease cell viability in a range of B-cell lymphoma cell lines, and the drug synergizes with both venetoclax and cytarabine.
Sheelagh Frame, PhD, and her colleagues presented these results at the SOHO 2015 Annual Meeting (poster 213). All of the investigators involved in the research are employees of Cyclacel Ltd., the company developing CYC065.
The investigators analyzed the anticancer activity of CYC065 in a range of cell lines and found that CYC065 induced apoptosis by inhibiting the expression of CDK9-dependent oncogenic transcripts, including Mcl-1, c-Myc, Hoxa9, and Meis1.
Results in AML
Experiments in the AML-MLL cell line MOLM-13 showed that short pulses of CYC065 (6 hours), rather than continuous treatment, were sufficient to achieve maximal cytotoxicity.
CYC065 induced apoptosis, in a dose-dependent manner, in other AML cell lines as well, including EOL-1 (MLL-PTD), MV4-11 (MLL-AF4, FLT3-ITD, and trisomy chr 8), HL60 (Myc amplified), and Kasumi-1.
The investigators noted that AML cell lines with MLL rearrangements were especially sensitive to CYC065, and the reliance of AML on Mcl-1 confers sensitivity to CYC065.
They also found evidence to suggest that Bak and Bcl-xL levels may be predictive of CYC065 response in AML. Cell lines that were less sensitive to treatment had high levels of Bcl-xL and negligible levels of Bak.
B-cell lymphomas
In B-cell lymphoma cell lines, the investigators observed a dose-dependent reduction in cell viability after CYC065 treatment (8-hour pulses).
CYC065 proved most effective in cell lines without genomic alterations associated with poor prognosis (HT and U-698-M) and in cell lines with Myc rearrangements (SU-DHL-8 and WILL-1).
The drug also decreased cell viability—but to a lesser degree—in cell lines with Bcl-2 rearrangements (SU-DHL-4 and U2932) and in double-hit lymphoma cell lines (MAVER-1, RI-1, SC-1, and SU-DHL-10).
The investigators therefore theorized that combining CYC065 with a Bcl-2 inhibitor might prove more effective in these cell lines.
CYC065 in combination
CYC065 synergized with the Bcl-2 inhibitor venetoclax in all B-cell lymphoma cell lines tested. The drugs were “strongly synergistic” in U2932 and RI-1 cell lines but simply “synergistic” in SU-CHL-4 and MAVER-1 cell lines.
CYC065 also synergized with cytarabine to fight AML. The combination proved synergistic at a range of doses in the HL60 and MV4-11 cell lines.
Considering these results together, the investigators concluded that CYC065 has shown potential for treating a range of leukemias and lymphomas with unmet clinical need, including MLL-rearranged leukemia and Myc-driven lymphoma.
And the drug might prove effective in combination with standard cytotoxic agents or agents targeting apoptotic regulators. ![]()
Mandatory prescriber training now available for flibanserin
Physicians can now complete the training and paperwork required to prescribe flibanserin (Addyi, Sprout Pharmaceuticals), a new centrally acting, nonhormonal daily medication that treats female hypoactive sexual desire disorder.
The Food and Drug Administration’s August 2015 approval of flibanserin came with a required REMS(Risk Evaluation and Mitigation Strategy ) to address safety concerns.
Flibanserin, which the FDA had twice previously declined to approve, has an increased risk for syncope and hypotension with alcohol and moderate or strong CYP3A4 inhibitors, such as proton pump inhibitors, selective serotonin reuptake inhibitors, benzodiazepines, and antifungals. Flibanserin taken alone also caused hypotension and syncope in a few patients during clinical trials.
The REMS addresses these risks by requiring all prescribers to complete training and a knowledge assessment about flibanserin’s risks and to enroll in a REMS certification program for the drug. Prescribers must also review a patient-provider agreement form with patients and have both parties sign before prescribing flibanserin.

Outpatient pharmacies must designate a representative to complete training and knowledge assessment, train their staff, and counsel every patient receiving flibanserin to abstain from alcohol. Inpatient pharmacies have similar training requirements and may not dispense flibanserin for outpatient use.
Flibanserin is approved for treatment of acquired, generalized hypoactive sexual desire disorder in premenopausal women only. It is a medication that is meant to be taken on a chronic basis, acting as a mixed agonist/antagonist for dopamine and serotonin receptors. In clinical trials, it showed a statistically significant, but modest improvement in reported sexual desire and the number of sexually satisfying events per month.
The certification materials are available online at www.Addyi.com. To complete the certification process, prescribers and pharmacists should fax the completed knowledge assessment and enrollment forms to 844-694-3373 or email scanned copies to [email protected].
On Twitter @karioakes
Physicians can now complete the training and paperwork required to prescribe flibanserin (Addyi, Sprout Pharmaceuticals), a new centrally acting, nonhormonal daily medication that treats female hypoactive sexual desire disorder.
The Food and Drug Administration’s August 2015 approval of flibanserin came with a required REMS(Risk Evaluation and Mitigation Strategy ) to address safety concerns.
Flibanserin, which the FDA had twice previously declined to approve, has an increased risk for syncope and hypotension with alcohol and moderate or strong CYP3A4 inhibitors, such as proton pump inhibitors, selective serotonin reuptake inhibitors, benzodiazepines, and antifungals. Flibanserin taken alone also caused hypotension and syncope in a few patients during clinical trials.
The REMS addresses these risks by requiring all prescribers to complete training and a knowledge assessment about flibanserin’s risks and to enroll in a REMS certification program for the drug. Prescribers must also review a patient-provider agreement form with patients and have both parties sign before prescribing flibanserin.
Outpatient pharmacies must designate a representative to complete training and knowledge assessment, train their staff, and counsel every patient receiving flibanserin to abstain from alcohol. Inpatient pharmacies have similar training requirements and may not dispense flibanserin for outpatient use.
Flibanserin is approved for treatment of acquired, generalized hypoactive sexual desire disorder in premenopausal women only. It is a medication that is meant to be taken on a chronic basis, acting as a mixed agonist/antagonist for dopamine and serotonin receptors. In clinical trials, it showed a statistically significant, but modest improvement in reported sexual desire and the number of sexually satisfying events per month.
The certification materials are available online at www.Addyi.com. To complete the certification process, prescribers and pharmacists should fax the completed knowledge assessment and enrollment forms to 844-694-3373 or email scanned copies to [email protected].
On Twitter @karioakes
Physicians can now complete the training and paperwork required to prescribe flibanserin (Addyi, Sprout Pharmaceuticals), a new centrally acting, nonhormonal daily medication that treats female hypoactive sexual desire disorder.
The Food and Drug Administration’s August 2015 approval of flibanserin came with a required REMS(Risk Evaluation and Mitigation Strategy ) to address safety concerns.
Flibanserin, which the FDA had twice previously declined to approve, has an increased risk for syncope and hypotension with alcohol and moderate or strong CYP3A4 inhibitors, such as proton pump inhibitors, selective serotonin reuptake inhibitors, benzodiazepines, and antifungals. Flibanserin taken alone also caused hypotension and syncope in a few patients during clinical trials.
The REMS addresses these risks by requiring all prescribers to complete training and a knowledge assessment about flibanserin’s risks and to enroll in a REMS certification program for the drug. Prescribers must also review a patient-provider agreement form with patients and have both parties sign before prescribing flibanserin.
Outpatient pharmacies must designate a representative to complete training and knowledge assessment, train their staff, and counsel every patient receiving flibanserin to abstain from alcohol. Inpatient pharmacies have similar training requirements and may not dispense flibanserin for outpatient use.
Flibanserin is approved for treatment of acquired, generalized hypoactive sexual desire disorder in premenopausal women only. It is a medication that is meant to be taken on a chronic basis, acting as a mixed agonist/antagonist for dopamine and serotonin receptors. In clinical trials, it showed a statistically significant, but modest improvement in reported sexual desire and the number of sexually satisfying events per month.
The certification materials are available online at www.Addyi.com. To complete the certification process, prescribers and pharmacists should fax the completed knowledge assessment and enrollment forms to 844-694-3373 or email scanned copies to [email protected].
On Twitter @karioakes

Advances in AML understanding could translate to improved therapy
An understanding of the various molecular differences between acute myeloid leukemia (AML) particles is guiding the search for new drug combinations targeting a variety of AML cellular processes, according to research published in the New England Journal of Medicine.
After a brief overview of disease classification and prognostic factors for AML, the authors, led by Dr. Hartmut Döhner of University Hospital Ulm in Germany, described a number of new treatment strategies. These approaches include directly addressing mutant proteins by targeting mutation-specific dependencies, developing inhibitors that could cut down on the occurrence of mutations in receptor tyrosine kinase genes, and developing new epigenetic therapies based on targeting specific mutant metabolic enzymes such as IDH1 and IDH2.
Other strategies, such as antibody therapy that focuses on the development of new monoclonal antibodies targeting CD33, and new formulations of older cytotoxic agents, also are being developed or are in clinical trial stages; however, many of these developments have not yet been translated into clinical practice, the researchers noted.
“New compounds hold promise to improve treatment outcomes; however, it is unlikely that any of these compounds, when used as single agents, will cure the disease. A major challenge will be to identify predictors for a response to specific agents, which will allow for the rational design of combinatorial therapies,” they wrote.
Dr. Döhner and a coauthor disclosed ties with several pharmaceutical companies.
Read the article here.
An understanding of the various molecular differences between acute myeloid leukemia (AML) particles is guiding the search for new drug combinations targeting a variety of AML cellular processes, according to research published in the New England Journal of Medicine.
After a brief overview of disease classification and prognostic factors for AML, the authors, led by Dr. Hartmut Döhner of University Hospital Ulm in Germany, described a number of new treatment strategies. These approaches include directly addressing mutant proteins by targeting mutation-specific dependencies, developing inhibitors that could cut down on the occurrence of mutations in receptor tyrosine kinase genes, and developing new epigenetic therapies based on targeting specific mutant metabolic enzymes such as IDH1 and IDH2.
Other strategies, such as antibody therapy that focuses on the development of new monoclonal antibodies targeting CD33, and new formulations of older cytotoxic agents, also are being developed or are in clinical trial stages; however, many of these developments have not yet been translated into clinical practice, the researchers noted.
“New compounds hold promise to improve treatment outcomes; however, it is unlikely that any of these compounds, when used as single agents, will cure the disease. A major challenge will be to identify predictors for a response to specific agents, which will allow for the rational design of combinatorial therapies,” they wrote.
Dr. Döhner and a coauthor disclosed ties with several pharmaceutical companies.
Read the article here.
An understanding of the various molecular differences between acute myeloid leukemia (AML) particles is guiding the search for new drug combinations targeting a variety of AML cellular processes, according to research published in the New England Journal of Medicine.
After a brief overview of disease classification and prognostic factors for AML, the authors, led by Dr. Hartmut Döhner of University Hospital Ulm in Germany, described a number of new treatment strategies. These approaches include directly addressing mutant proteins by targeting mutation-specific dependencies, developing inhibitors that could cut down on the occurrence of mutations in receptor tyrosine kinase genes, and developing new epigenetic therapies based on targeting specific mutant metabolic enzymes such as IDH1 and IDH2.
Other strategies, such as antibody therapy that focuses on the development of new monoclonal antibodies targeting CD33, and new formulations of older cytotoxic agents, also are being developed or are in clinical trial stages; however, many of these developments have not yet been translated into clinical practice, the researchers noted.
“New compounds hold promise to improve treatment outcomes; however, it is unlikely that any of these compounds, when used as single agents, will cure the disease. A major challenge will be to identify predictors for a response to specific agents, which will allow for the rational design of combinatorial therapies,” they wrote.
Dr. Döhner and a coauthor disclosed ties with several pharmaceutical companies.
Read the article here.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Pain Control in Patients With Bone Metastases
Background: Pain due to bone metastases represents a common source of cancer-related morbidity. Not all patients who develop bone metastases develop pain. It is a subjective experience unique to each patient. We conducted a quality assessment project at the Providence VA Medical Center (PVAMC) to characterize the problem of pain due to bone metastases.
Methods: All veterans with bone metastases seen by the oncology service during 2011 to 2013 at the PVAMC were included. Pain scores were assessed from each outpatient visit. Scores ranged from 0 to10 with 0 to 3 considered mild pain, 4 to 6 moderate pain, and 7 to 10 severe pain. If veterans were found to have severe pain, then their charts were reviewed for the interventions undertaken and whether pain was brought to a more acceptable score.
Results: Sixty-nine veterans with bone metastases were included. Fifty-one percent experienced severe pain. Of those experiencing severe pain, 46% had lung cancer and 37% had prostate cancer. Ninety-four percent of veterans with lung cancer and bone metastases experienced severe pain. Of those veterans with severe pain, 94% were prescribed narcotics, 83% enrolled in hospice, 66% received palliative care, and 63% received radiation therapy. Eleven veterans in total were admitted to the hospital for pain control. It took a median of 25 days to reduce pain to a score of 3. Overall the median time from onset of severe pain to death was 80 days. For veterans with lung cancer, the median time to death was 63 days compared with 371 days in veterans with prostate cancer.
Conclusions: Many veterans with bone metastases experince severe pain. This project demonstrated that the majority of lung cancer patients reported extreme pain from their bone metastases, and the median time from severe pain onset to death was about 2 months. Early and aggressive pain control and palliative or hospice care may be particularly beneficial for these patients. In the future, we will seek to shorten the duration of time to adequate pain control through a quality improvement project.
Background: Pain due to bone metastases represents a common source of cancer-related morbidity. Not all patients who develop bone metastases develop pain. It is a subjective experience unique to each patient. We conducted a quality assessment project at the Providence VA Medical Center (PVAMC) to characterize the problem of pain due to bone metastases.
Methods: All veterans with bone metastases seen by the oncology service during 2011 to 2013 at the PVAMC were included. Pain scores were assessed from each outpatient visit. Scores ranged from 0 to10 with 0 to 3 considered mild pain, 4 to 6 moderate pain, and 7 to 10 severe pain. If veterans were found to have severe pain, then their charts were reviewed for the interventions undertaken and whether pain was brought to a more acceptable score.
Results: Sixty-nine veterans with bone metastases were included. Fifty-one percent experienced severe pain. Of those experiencing severe pain, 46% had lung cancer and 37% had prostate cancer. Ninety-four percent of veterans with lung cancer and bone metastases experienced severe pain. Of those veterans with severe pain, 94% were prescribed narcotics, 83% enrolled in hospice, 66% received palliative care, and 63% received radiation therapy. Eleven veterans in total were admitted to the hospital for pain control. It took a median of 25 days to reduce pain to a score of 3. Overall the median time from onset of severe pain to death was 80 days. For veterans with lung cancer, the median time to death was 63 days compared with 371 days in veterans with prostate cancer.
Conclusions: Many veterans with bone metastases experince severe pain. This project demonstrated that the majority of lung cancer patients reported extreme pain from their bone metastases, and the median time from severe pain onset to death was about 2 months. Early and aggressive pain control and palliative or hospice care may be particularly beneficial for these patients. In the future, we will seek to shorten the duration of time to adequate pain control through a quality improvement project.
Background: Pain due to bone metastases represents a common source of cancer-related morbidity. Not all patients who develop bone metastases develop pain. It is a subjective experience unique to each patient. We conducted a quality assessment project at the Providence VA Medical Center (PVAMC) to characterize the problem of pain due to bone metastases.
Methods: All veterans with bone metastases seen by the oncology service during 2011 to 2013 at the PVAMC were included. Pain scores were assessed from each outpatient visit. Scores ranged from 0 to10 with 0 to 3 considered mild pain, 4 to 6 moderate pain, and 7 to 10 severe pain. If veterans were found to have severe pain, then their charts were reviewed for the interventions undertaken and whether pain was brought to a more acceptable score.
Results: Sixty-nine veterans with bone metastases were included. Fifty-one percent experienced severe pain. Of those experiencing severe pain, 46% had lung cancer and 37% had prostate cancer. Ninety-four percent of veterans with lung cancer and bone metastases experienced severe pain. Of those veterans with severe pain, 94% were prescribed narcotics, 83% enrolled in hospice, 66% received palliative care, and 63% received radiation therapy. Eleven veterans in total were admitted to the hospital for pain control. It took a median of 25 days to reduce pain to a score of 3. Overall the median time from onset of severe pain to death was 80 days. For veterans with lung cancer, the median time to death was 63 days compared with 371 days in veterans with prostate cancer.
Conclusions: Many veterans with bone metastases experince severe pain. This project demonstrated that the majority of lung cancer patients reported extreme pain from their bone metastases, and the median time from severe pain onset to death was about 2 months. Early and aggressive pain control and palliative or hospice care may be particularly beneficial for these patients. In the future, we will seek to shorten the duration of time to adequate pain control through a quality improvement project.
Patterns of Failure and Survival Analysis of Advanced Tonsillar Cancer Treated With IMRT Radiation Therapy and Chemotherapy and Implications of HPV-Positive Tumors in Management
Purpose/Objectives: To evaluate the outcomes of patients with tonsillar cancer treated at G.V. Sonny Montgomery VA Medical Center between 2006 and 2014 and to compare survival and patterns of failure between human papillomavirus (HPV)-positive tonsillar cancer and HPV-negative tonsillar cancer.
Methods: There were 70 patients with biopsy proven squamous cell carcinoma of the tonsil in the retrospective review. Sixty-one of 70 patients had stage III/IV disease. Forty-seven of 70 patients had their HPV status evaluated. There were 22 HPV-positive and 25 HPV-negative patients. The majority of patients were treated with concurrent chemoradiotherapy, consisting of either weekly cisplatin 45 mg/m2 or weekly cetuximab 400 mg/m2 loading dose and 250 mg/m2 once a week for 7 weeks. Radiation therapy was given using intensity modulated radiation therapy to 70 Gy at 2 Gy per fraction over 7 weeks. The median radiation dose was 70 Gy. We evaluated the outcomes, including loco-regional failure, distant metastases, and survival. Rates were estimated by Kaplan-Meier method, and comparisons between HPV groups were evaluated using the Fisher exact test for categorical variables and Kruskal-Wallis test. Intermediate risk was defined as having ≥ 10 pack-years smoking history in the HPV-positive group (11 patients) and < 10 pack-years in the HPV-negative group (5 patients).
Results: Follow-up ranged from 14 to 88 months (median 22 mo). Overall survival (OS) for the entire group was 68% at 3 years with a disease-free survival (DFS) rate of 56%. At 3 years, the OS and DFS were 73% and 59% in the HPV-positive group and 50% and 50%, respectively, in the HPV-negative group. In the HPV-positive group, the failure rate was 2/11(16%) in the low-risk group and 8/11 (72%) in the intermediate-risk group. Six of 11 (55%) of the failures in the HPV-positive intermediate-risk group were local. Failure in the HPV-negative group was 3/5 (60%) in the intermediate-risk group and 12/20 (60%) in the high-risk group.
Conclusions: The results for the entire tonsillar group were comparable with that found in published literature. Patients with HPV-positive tumors had improved OS compared with HPV-negative tonsillar cancer, although not statistically significant due to small numbers.
Purpose/Objectives: To evaluate the outcomes of patients with tonsillar cancer treated at G.V. Sonny Montgomery VA Medical Center between 2006 and 2014 and to compare survival and patterns of failure between human papillomavirus (HPV)-positive tonsillar cancer and HPV-negative tonsillar cancer.
Methods: There were 70 patients with biopsy proven squamous cell carcinoma of the tonsil in the retrospective review. Sixty-one of 70 patients had stage III/IV disease. Forty-seven of 70 patients had their HPV status evaluated. There were 22 HPV-positive and 25 HPV-negative patients. The majority of patients were treated with concurrent chemoradiotherapy, consisting of either weekly cisplatin 45 mg/m2 or weekly cetuximab 400 mg/m2 loading dose and 250 mg/m2 once a week for 7 weeks. Radiation therapy was given using intensity modulated radiation therapy to 70 Gy at 2 Gy per fraction over 7 weeks. The median radiation dose was 70 Gy. We evaluated the outcomes, including loco-regional failure, distant metastases, and survival. Rates were estimated by Kaplan-Meier method, and comparisons between HPV groups were evaluated using the Fisher exact test for categorical variables and Kruskal-Wallis test. Intermediate risk was defined as having ≥ 10 pack-years smoking history in the HPV-positive group (11 patients) and < 10 pack-years in the HPV-negative group (5 patients).
Results: Follow-up ranged from 14 to 88 months (median 22 mo). Overall survival (OS) for the entire group was 68% at 3 years with a disease-free survival (DFS) rate of 56%. At 3 years, the OS and DFS were 73% and 59% in the HPV-positive group and 50% and 50%, respectively, in the HPV-negative group. In the HPV-positive group, the failure rate was 2/11(16%) in the low-risk group and 8/11 (72%) in the intermediate-risk group. Six of 11 (55%) of the failures in the HPV-positive intermediate-risk group were local. Failure in the HPV-negative group was 3/5 (60%) in the intermediate-risk group and 12/20 (60%) in the high-risk group.
Conclusions: The results for the entire tonsillar group were comparable with that found in published literature. Patients with HPV-positive tumors had improved OS compared with HPV-negative tonsillar cancer, although not statistically significant due to small numbers.
Purpose/Objectives: To evaluate the outcomes of patients with tonsillar cancer treated at G.V. Sonny Montgomery VA Medical Center between 2006 and 2014 and to compare survival and patterns of failure between human papillomavirus (HPV)-positive tonsillar cancer and HPV-negative tonsillar cancer.
Methods: There were 70 patients with biopsy proven squamous cell carcinoma of the tonsil in the retrospective review. Sixty-one of 70 patients had stage III/IV disease. Forty-seven of 70 patients had their HPV status evaluated. There were 22 HPV-positive and 25 HPV-negative patients. The majority of patients were treated with concurrent chemoradiotherapy, consisting of either weekly cisplatin 45 mg/m2 or weekly cetuximab 400 mg/m2 loading dose and 250 mg/m2 once a week for 7 weeks. Radiation therapy was given using intensity modulated radiation therapy to 70 Gy at 2 Gy per fraction over 7 weeks. The median radiation dose was 70 Gy. We evaluated the outcomes, including loco-regional failure, distant metastases, and survival. Rates were estimated by Kaplan-Meier method, and comparisons between HPV groups were evaluated using the Fisher exact test for categorical variables and Kruskal-Wallis test. Intermediate risk was defined as having ≥ 10 pack-years smoking history in the HPV-positive group (11 patients) and < 10 pack-years in the HPV-negative group (5 patients).
Results: Follow-up ranged from 14 to 88 months (median 22 mo). Overall survival (OS) for the entire group was 68% at 3 years with a disease-free survival (DFS) rate of 56%. At 3 years, the OS and DFS were 73% and 59% in the HPV-positive group and 50% and 50%, respectively, in the HPV-negative group. In the HPV-positive group, the failure rate was 2/11(16%) in the low-risk group and 8/11 (72%) in the intermediate-risk group. Six of 11 (55%) of the failures in the HPV-positive intermediate-risk group were local. Failure in the HPV-negative group was 3/5 (60%) in the intermediate-risk group and 12/20 (60%) in the high-risk group.
Conclusions: The results for the entire tonsillar group were comparable with that found in published literature. Patients with HPV-positive tumors had improved OS compared with HPV-negative tonsillar cancer, although not statistically significant due to small numbers.