User login
Novel oral anticoagulants best warfarin for AF in heart failure
SAN DIEGO – The novel oral anticoagulants clearly outperformed warfarin for stroke prevention and safety endpoints in patients with atrial fibrillation and comorbid heart failure in a meta-analysis of four recent landmark Phase 3 clinical trials.
Collectively the four novel oral anticoagulants (NOACs) approved for stroke prophylaxis in nonvalvular atrial fibrillation (AF) reduced the risk of stroke and systemic embolism by 14%, compared with patients randomized to warfarin. Moreover, the NOACs decreased the risks of major bleeding and intracranial bleeding by 23% and 45%, respectively, Dr. Gianluigi Savarese reported at the annual meeting of the American College of Cardiology.

“NOACs represent a valuable therapeutic option in patients with nonvalvular atrial fibrillation and heart failure,” concluded Dr. Savarese of Federico II University, Naples.
There has never been a randomized trial comparing a NOAC to warfarin specifically in patients with these dual diagnoses. In the absence of such a definitive study, the next best thing is a meta-analysis of the pivotal Phase 3 trials in which warfarin was compared to dabigatran (Pradaxa, the RE-LY study), apixaban (Eliquis, ARISTOTLE), rivaroxaban (Xarelto, ROCKET AF), and edoxaban (Savaysa, ENGAGE AF-TIMI 48).
The meta-analysis focused on a subset population of 26,384 randomized patients with AF and heart failure. It’s important to know how the NOACs stack up against warfarin in this population because symptomatic heart failure is common: indeed, it’s present in 30% of patients with AF. Patients with AF and comorbid heart failure are generally older, frailer, have more comorbidities, and are at higher risk of both stroke and bleeding, compared with AF patients without heart failure. Since heart failure is a recognized risk factor for reduced time in the therapeutic international normalized ratio (INR) range for patients on warfarin, it’s likely that warfarin-treated dual diagnosis patients would be exposed to further increased risks of stroke and bleeding, according to Dr. Savarese.
In the meta-analysis, in addition to the NOAC-treated patients’ significantly reduced risks of stroke, major bleeding, and intracranial bleeding, they showed a 12% decrease in total bleeding and an 8% reduction in cardiovascular death, compared with warfarin-treated controls, although neither of those latter two favorable trends achieved statistical significance.
The four NOACs didn’t differ significantly on any of the prespecified outcomes in the meta-analysis.
One audience member noted that while the relative risk reductions for stroke and major bleeding seen with the NOACs in the meta-analysis were large and impressive, the absolute risk reductions were actually quite small. For example, warfarin-treated controls in RE-LY, the first of the major trials, had a stroke/systemic embolism rate of 1.69%/year and a major bleeding rate of 3.4%/year (N. Engl. J. Med. 2009;361:1139-51), while controls in ENGAGE AF-TIMI 48 had annualized stroke and major bleeding rates of 1.5% and 3.4%, respectively (N. Engl. J. Med. 2013;369:2093-2104).
Dr. Savarese replied that he and his coinvestigators consider those absolute risk reductions to be clinically meaningful, especially in light of the enormous and rapidly growing number of patients with both AF and heart failure.
He reported having no financial conflicts regarding this meta-analysis, which was carried out free of commercial support.
SAN DIEGO – The novel oral anticoagulants clearly outperformed warfarin for stroke prevention and safety endpoints in patients with atrial fibrillation and comorbid heart failure in a meta-analysis of four recent landmark Phase 3 clinical trials.
Collectively the four novel oral anticoagulants (NOACs) approved for stroke prophylaxis in nonvalvular atrial fibrillation (AF) reduced the risk of stroke and systemic embolism by 14%, compared with patients randomized to warfarin. Moreover, the NOACs decreased the risks of major bleeding and intracranial bleeding by 23% and 45%, respectively, Dr. Gianluigi Savarese reported at the annual meeting of the American College of Cardiology.
“NOACs represent a valuable therapeutic option in patients with nonvalvular atrial fibrillation and heart failure,” concluded Dr. Savarese of Federico II University, Naples.
There has never been a randomized trial comparing a NOAC to warfarin specifically in patients with these dual diagnoses. In the absence of such a definitive study, the next best thing is a meta-analysis of the pivotal Phase 3 trials in which warfarin was compared to dabigatran (Pradaxa, the RE-LY study), apixaban (Eliquis, ARISTOTLE), rivaroxaban (Xarelto, ROCKET AF), and edoxaban (Savaysa, ENGAGE AF-TIMI 48).
The meta-analysis focused on a subset population of 26,384 randomized patients with AF and heart failure. It’s important to know how the NOACs stack up against warfarin in this population because symptomatic heart failure is common: indeed, it’s present in 30% of patients with AF. Patients with AF and comorbid heart failure are generally older, frailer, have more comorbidities, and are at higher risk of both stroke and bleeding, compared with AF patients without heart failure. Since heart failure is a recognized risk factor for reduced time in the therapeutic international normalized ratio (INR) range for patients on warfarin, it’s likely that warfarin-treated dual diagnosis patients would be exposed to further increased risks of stroke and bleeding, according to Dr. Savarese.
In the meta-analysis, in addition to the NOAC-treated patients’ significantly reduced risks of stroke, major bleeding, and intracranial bleeding, they showed a 12% decrease in total bleeding and an 8% reduction in cardiovascular death, compared with warfarin-treated controls, although neither of those latter two favorable trends achieved statistical significance.
The four NOACs didn’t differ significantly on any of the prespecified outcomes in the meta-analysis.
One audience member noted that while the relative risk reductions for stroke and major bleeding seen with the NOACs in the meta-analysis were large and impressive, the absolute risk reductions were actually quite small. For example, warfarin-treated controls in RE-LY, the first of the major trials, had a stroke/systemic embolism rate of 1.69%/year and a major bleeding rate of 3.4%/year (N. Engl. J. Med. 2009;361:1139-51), while controls in ENGAGE AF-TIMI 48 had annualized stroke and major bleeding rates of 1.5% and 3.4%, respectively (N. Engl. J. Med. 2013;369:2093-2104).
Dr. Savarese replied that he and his coinvestigators consider those absolute risk reductions to be clinically meaningful, especially in light of the enormous and rapidly growing number of patients with both AF and heart failure.
He reported having no financial conflicts regarding this meta-analysis, which was carried out free of commercial support.
SAN DIEGO – The novel oral anticoagulants clearly outperformed warfarin for stroke prevention and safety endpoints in patients with atrial fibrillation and comorbid heart failure in a meta-analysis of four recent landmark Phase 3 clinical trials.
Collectively the four novel oral anticoagulants (NOACs) approved for stroke prophylaxis in nonvalvular atrial fibrillation (AF) reduced the risk of stroke and systemic embolism by 14%, compared with patients randomized to warfarin. Moreover, the NOACs decreased the risks of major bleeding and intracranial bleeding by 23% and 45%, respectively, Dr. Gianluigi Savarese reported at the annual meeting of the American College of Cardiology.
“NOACs represent a valuable therapeutic option in patients with nonvalvular atrial fibrillation and heart failure,” concluded Dr. Savarese of Federico II University, Naples.
There has never been a randomized trial comparing a NOAC to warfarin specifically in patients with these dual diagnoses. In the absence of such a definitive study, the next best thing is a meta-analysis of the pivotal Phase 3 trials in which warfarin was compared to dabigatran (Pradaxa, the RE-LY study), apixaban (Eliquis, ARISTOTLE), rivaroxaban (Xarelto, ROCKET AF), and edoxaban (Savaysa, ENGAGE AF-TIMI 48).
The meta-analysis focused on a subset population of 26,384 randomized patients with AF and heart failure. It’s important to know how the NOACs stack up against warfarin in this population because symptomatic heart failure is common: indeed, it’s present in 30% of patients with AF. Patients with AF and comorbid heart failure are generally older, frailer, have more comorbidities, and are at higher risk of both stroke and bleeding, compared with AF patients without heart failure. Since heart failure is a recognized risk factor for reduced time in the therapeutic international normalized ratio (INR) range for patients on warfarin, it’s likely that warfarin-treated dual diagnosis patients would be exposed to further increased risks of stroke and bleeding, according to Dr. Savarese.
In the meta-analysis, in addition to the NOAC-treated patients’ significantly reduced risks of stroke, major bleeding, and intracranial bleeding, they showed a 12% decrease in total bleeding and an 8% reduction in cardiovascular death, compared with warfarin-treated controls, although neither of those latter two favorable trends achieved statistical significance.
The four NOACs didn’t differ significantly on any of the prespecified outcomes in the meta-analysis.
One audience member noted that while the relative risk reductions for stroke and major bleeding seen with the NOACs in the meta-analysis were large and impressive, the absolute risk reductions were actually quite small. For example, warfarin-treated controls in RE-LY, the first of the major trials, had a stroke/systemic embolism rate of 1.69%/year and a major bleeding rate of 3.4%/year (N. Engl. J. Med. 2009;361:1139-51), while controls in ENGAGE AF-TIMI 48 had annualized stroke and major bleeding rates of 1.5% and 3.4%, respectively (N. Engl. J. Med. 2013;369:2093-2104).
Dr. Savarese replied that he and his coinvestigators consider those absolute risk reductions to be clinically meaningful, especially in light of the enormous and rapidly growing number of patients with both AF and heart failure.
He reported having no financial conflicts regarding this meta-analysis, which was carried out free of commercial support.
AT ACC 15
Key clinical point: Patients with nonvalvular atrial fibrillation and heart failure clearly fare better on any of the novel oral anticoagulants than with warfarin for stroke prophylaxis.
Major finding: Dual diagnosis patients randomized to a novel oral anticoagulant had a 14% reduction in stroke/systemic embolism and a 23% decrease in major bleeding compared with those on warfarin.
Data source: This was a meta-analysis of the 26,384 patients with both atrial fibrillation and heart failure who were included in four pivotal Phase 3 clinical trials that led to approval of dabigatran, apixaban, rivaroxaban, and edoxaban.
Disclosures: The presenter reported having no financial conflicts regarding this meta-analysis, which was carried out free of commercial support.

Platelet indexes flag suspected pulmonary embolism
Levels of platelet distribution width (PDW) and mean platelet volume (MPV) were significantly higher in patients with pulmonary embolism, Dr. Jianqiang Huang and co-authors at the Department of Cardiovascular Medicine, Shantou Central Hospital in Guangdong Province, China, have reported.
A study of platelet indexes in 70 PE patients and 75 controls showed that PDW (16.40% vs. 16.00%) and MPV (9.91±1.40 fL vs. 8.84±1.68) values were significantly higher in those with PE, compared with controls. There were no significant differences in platelet count, the investigators reported.
The results indicate that measuring “MPV can increase the specificity and [positive predictive value] to improve the diagnostic value of D-dimer for PE,” the authors wrote. “Because platelet indexes are convenient to detect, clinical physicians may increase their vigilance to identify suspected PE,” they added.
Read the full article at the American Journal of Emergency Medicine: 10.1016/j.ajem.2015.02.043.
Levels of platelet distribution width (PDW) and mean platelet volume (MPV) were significantly higher in patients with pulmonary embolism, Dr. Jianqiang Huang and co-authors at the Department of Cardiovascular Medicine, Shantou Central Hospital in Guangdong Province, China, have reported.
A study of platelet indexes in 70 PE patients and 75 controls showed that PDW (16.40% vs. 16.00%) and MPV (9.91±1.40 fL vs. 8.84±1.68) values were significantly higher in those with PE, compared with controls. There were no significant differences in platelet count, the investigators reported.
The results indicate that measuring “MPV can increase the specificity and [positive predictive value] to improve the diagnostic value of D-dimer for PE,” the authors wrote. “Because platelet indexes are convenient to detect, clinical physicians may increase their vigilance to identify suspected PE,” they added.
Read the full article at the American Journal of Emergency Medicine: 10.1016/j.ajem.2015.02.043.
Levels of platelet distribution width (PDW) and mean platelet volume (MPV) were significantly higher in patients with pulmonary embolism, Dr. Jianqiang Huang and co-authors at the Department of Cardiovascular Medicine, Shantou Central Hospital in Guangdong Province, China, have reported.
A study of platelet indexes in 70 PE patients and 75 controls showed that PDW (16.40% vs. 16.00%) and MPV (9.91±1.40 fL vs. 8.84±1.68) values were significantly higher in those with PE, compared with controls. There were no significant differences in platelet count, the investigators reported.
The results indicate that measuring “MPV can increase the specificity and [positive predictive value] to improve the diagnostic value of D-dimer for PE,” the authors wrote. “Because platelet indexes are convenient to detect, clinical physicians may increase their vigilance to identify suspected PE,” they added.
Read the full article at the American Journal of Emergency Medicine: 10.1016/j.ajem.2015.02.043.
Explaining drug-resistant malaria
infecting a red blood cell
Image courtesy of St. Jude
Children’s Research Hospital
Researchers say they have identified a molecular mechanism responsible for making malaria parasites resistant to artemisinins, the leading class of antimalarial drugs.
The team found that a kinase, Plasmodium falciparum phosphatidylinositol-3-kinase (PfPI3K), and its lipid product, phosphatidylinositol-3-phosphate (PI3P), play key roles in artemisinin resistance.
So targeting PfPI3K or PI3P could potentially treat resistant Plasmodium falciparum malaria.
Alassane Mbengue, PhD, of the University of Notre Dame in Indiana, and his colleagues described this research in a letter to Nature.
“We observed that levels of [PI3P] were higher in artemisinin-resistant P falciparum than artemisinin-sensitive strains,” Dr Mbengue said. “This lipid is produced by an enzyme called PfPI3K. We found that artemisinins block this kinase from producing PI3P lipids. We also discovered that the amount of the kinase present in the parasite is controlled by the gene PfKelch13.”
“Mutation in the gene increases the kinase levels, which, in turn, increases PI3P lipid levels. The higher the level of PI3P lipids present in the parasite, the greater the level of artemisinin resistance. We also studied the lipid levels in parasites without the gene mutation and observed that when PI3P lipid levels were increased artificially, the parasites still became proportionately resistant.”
Specifically, the researchers found that increased PfPI3K was associated with the C580Y mutation in PfKelch13. The mutation reduced polyubiquitination of PfPI3K and its binding to PfKelch13, which limited proteolysis of PfPI3K and led to increased levels of both PfPI3K and PI3P.
The team found that PI3P levels were predictive of artemisinin resistance in clinical and engineered parasites. And although increases in PI3P levels induced artemisinin resistance in the absence of PfKelch13 mutations, PI3P levels were still responsive to regulation by PfKelch13.
Dr Mbengue and his colleagues said the next step for this research is to identify drugs that can kill P falciparum by preventing PfPI3K from making PI3P or disrupting the production of the kinase itself. ![]()
infecting a red blood cell
Image courtesy of St. Jude
Children’s Research Hospital
Researchers say they have identified a molecular mechanism responsible for making malaria parasites resistant to artemisinins, the leading class of antimalarial drugs.
The team found that a kinase, Plasmodium falciparum phosphatidylinositol-3-kinase (PfPI3K), and its lipid product, phosphatidylinositol-3-phosphate (PI3P), play key roles in artemisinin resistance.
So targeting PfPI3K or PI3P could potentially treat resistant Plasmodium falciparum malaria.
Alassane Mbengue, PhD, of the University of Notre Dame in Indiana, and his colleagues described this research in a letter to Nature.
“We observed that levels of [PI3P] were higher in artemisinin-resistant P falciparum than artemisinin-sensitive strains,” Dr Mbengue said. “This lipid is produced by an enzyme called PfPI3K. We found that artemisinins block this kinase from producing PI3P lipids. We also discovered that the amount of the kinase present in the parasite is controlled by the gene PfKelch13.”
“Mutation in the gene increases the kinase levels, which, in turn, increases PI3P lipid levels. The higher the level of PI3P lipids present in the parasite, the greater the level of artemisinin resistance. We also studied the lipid levels in parasites without the gene mutation and observed that when PI3P lipid levels were increased artificially, the parasites still became proportionately resistant.”
Specifically, the researchers found that increased PfPI3K was associated with the C580Y mutation in PfKelch13. The mutation reduced polyubiquitination of PfPI3K and its binding to PfKelch13, which limited proteolysis of PfPI3K and led to increased levels of both PfPI3K and PI3P.
The team found that PI3P levels were predictive of artemisinin resistance in clinical and engineered parasites. And although increases in PI3P levels induced artemisinin resistance in the absence of PfKelch13 mutations, PI3P levels were still responsive to regulation by PfKelch13.
Dr Mbengue and his colleagues said the next step for this research is to identify drugs that can kill P falciparum by preventing PfPI3K from making PI3P or disrupting the production of the kinase itself. ![]()
infecting a red blood cell
Image courtesy of St. Jude
Children’s Research Hospital
Researchers say they have identified a molecular mechanism responsible for making malaria parasites resistant to artemisinins, the leading class of antimalarial drugs.
The team found that a kinase, Plasmodium falciparum phosphatidylinositol-3-kinase (PfPI3K), and its lipid product, phosphatidylinositol-3-phosphate (PI3P), play key roles in artemisinin resistance.
So targeting PfPI3K or PI3P could potentially treat resistant Plasmodium falciparum malaria.
Alassane Mbengue, PhD, of the University of Notre Dame in Indiana, and his colleagues described this research in a letter to Nature.
“We observed that levels of [PI3P] were higher in artemisinin-resistant P falciparum than artemisinin-sensitive strains,” Dr Mbengue said. “This lipid is produced by an enzyme called PfPI3K. We found that artemisinins block this kinase from producing PI3P lipids. We also discovered that the amount of the kinase present in the parasite is controlled by the gene PfKelch13.”
“Mutation in the gene increases the kinase levels, which, in turn, increases PI3P lipid levels. The higher the level of PI3P lipids present in the parasite, the greater the level of artemisinin resistance. We also studied the lipid levels in parasites without the gene mutation and observed that when PI3P lipid levels were increased artificially, the parasites still became proportionately resistant.”
Specifically, the researchers found that increased PfPI3K was associated with the C580Y mutation in PfKelch13. The mutation reduced polyubiquitination of PfPI3K and its binding to PfKelch13, which limited proteolysis of PfPI3K and led to increased levels of both PfPI3K and PI3P.
The team found that PI3P levels were predictive of artemisinin resistance in clinical and engineered parasites. And although increases in PI3P levels induced artemisinin resistance in the absence of PfKelch13 mutations, PI3P levels were still responsive to regulation by PfKelch13.
Dr Mbengue and his colleagues said the next step for this research is to identify drugs that can kill P falciparum by preventing PfPI3K from making PI3P or disrupting the production of the kinase itself. ![]()
Point/Counterpoint: Covered stent grafts vs. drug-eluting stents for treating long superficial femoral artery occlusions
Head-to-head comparisons are lacking, but similar results have been reported
BY MICHAEL D. DAKE, M.D.
Well, at least one thing is for sure – we would not have been having this discussion a mere 10 years ago.
I remained sheepishly silent for most of my early career as well-intentioned invasive and noninvasive specialists criticized the state of evidence supporting the legitimacy of endovascular interventions as a competitive strategy to manage infrainguinal peripheral arterial disease. Good data from well-controlled randomized clinical trials were not available to make a case for endovascular therapies.

Over the recent decade and a half, however, a number of contributing factors have influenced thinking and what we now consider standard of care for symptomatic disease of the superficial femoral artery (SFA). The proposal of an “endovascular first” interventional approach has evolved to a consensually agreed upon management strategy by all interested disciplines.
This did not occur on a whim. Rather, out of the shadows of relative ignorance there slowly emerged a welcomed accumulation of a large number of publications that detail the outcomes of a wide variety of randomized trials with a range of endovascular devices. This has allowed us to enter an era where valid comparisons between interventional therapies is not only possible, but allows us to more appropriately offer care to vascular patients with more nuanced strategies. These are strategies that recognize subtleties between subgroups of individuals stratified on the basis of patient demographics and lesion characteristics in a way not appreciated prior to the recent spate of endovascular device studies.
Thus, thanks to the dedication and hard work of many, we are now at a stage where we can have meaningful dialogues on a variety of endovascular topics, such as the one at hand, and proponents can argue their perspectives armed with objective evidence to support their positions. In this discussion regarding covered stent grafts and drug-eluting stents, we wish we had even more data.
Specifically, we are missing direct head-to-head comparisons between the two devices in patients with long SFA lesions. So, what do we know?
Here are some fundamental facts: The most commonly used covered stent graft for management of femoropopliteal occlusive disease is the Viabahn endoprosthesis (W. L. Gore and Associates, Flagstaff, Ariz.). The prosthesis is composed of a self-expanding nitinol stent framework and expanded polytetrafluoroethylene (ePTFE) graft with its surface lined with a coating of covalently bound heparin (Propaten bioactive surface).The only approved drug-eluting stent with significant safety and effectiveness data available is the Zilver PTX paclitaxel-eluting, self-expanding nitinol stent (Cook Medical Inc., Bloomington, Ind.).
Now in terms of the proposition, we need to discuss the meaning of the word “long” with reference to the SFA. Just what do we consider a long SFA lesion? I think all of us could agree that an arterial stenosis or occlusion of 6 cm or less is short. Lesions between 5 cm or 6 cm to 10 cm or 12 cm in length are moderately long, and disease greater than 10 cm or 12 cm is commonly characterized as long. Segments of disease greater than 20 cm long are typically considered very long or extremely long lesions from an endovascular interventional perspective.
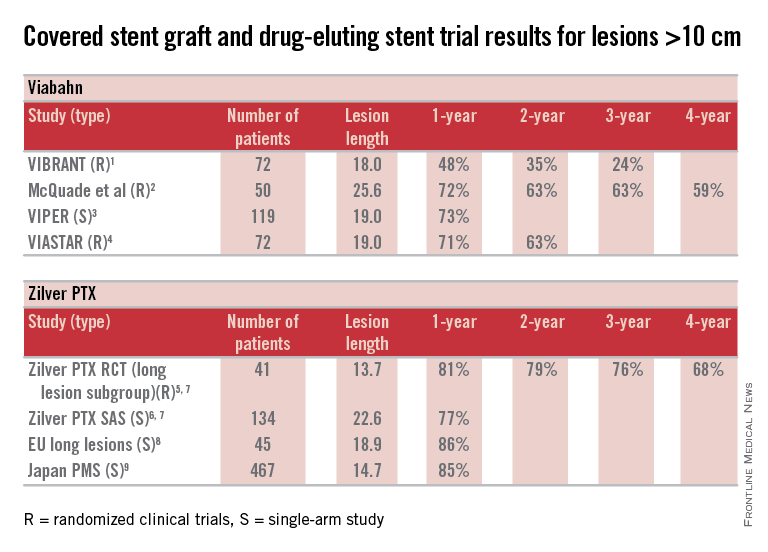
So, how can currently available trial outcomes help us? Below, I have compiled a table that includes most of the recent clinical trial data for Viabahn and Zilver PTX in patients with long SFA occlusive disease.
OK, what can we honestly say about these data besides recognizing that we are at risk when we make any conclusions based upon cross-trial comparisons? Such an accounting of results is fraught with problems, but what we can say is that the table grossly confirms the current consensus that both devices enhance the standard of care for long lesions over traditional balloon angioplasty (PTA) and bare metal stent technologies.
Beyond this, however, it is accepted that patency results with Viabahn are lesion-length immune – that is, outcomes in long and extremely long segments of disease are not very different from the patency achieved in short lesions. This is clearly different than what is traditionally found for interventions with PTA or bare metal stents. There is not enough controlled data for extremely long lesions to reach a conclusion on drug-eluting stents; however, there is an initial suggestion that they behave in a manner more similar to stent grafts than traditional devices.
Grossly, the table suggests that the midterm and available greater than 1-year patency results with Viabahn and Zilver PTX are relatively comparable. What about the price of the device? What role does it play in our selection of the current most cost-effective endovascular strategy for long SFA lesions?
In my institution Viabahn is more expensive than Zilver PTX with a relative cost premium of about 30%-50% depending on the treatment length. Of course, when treating long TASC C and D lesions any up-front difference in the costs of the devices used initially is more than made up for by any relative reduction in subsequent reinterventions.
So, there you have it. Look at the table as simply a current snapshot. In the future, we will benefit from additional trials and comparisons, not to mention better endovascular technologies to address symptomatic long SFA lesions.
Dr. Dake is the Thelma and Henry Doelger Professor of Cardiovascular Surgery at the Stanford (Calif.) School of Medicine. He disclosed that he is a member of the Peripheral Scientific Advisory Board: Abbott Vascular Member, is on the Aortic Medical Advisory Board: W. L. Gore, is a consultant for Cook Medical, Medtronic, and Surmodics Research, and receives grants/clinical trial support from W. L. Gore, Medtronic, and Novate.
References for table
1. J. Vasc. Surg. 2013;58:386-95.
2. J. Vasc. Surg. 2010;52:584-90.
3. J. Vasc. Interv. Radiol. 2013;24:165-73.
4. Cardiovasc. Interv. Radiol. 2015;38:25-32.
5. Circ. Cardiovasc. Interv. 2011;4:495-504.
6. J. Am. Coll. Cardiol. 2013;61:2417-27.
7. J. Endovasc. Ther. 2011;18:613-23.
8. Zeller T. Oral presentations. 2014.
9. Yokoi H. Oral presentations. 2014.
Covered stent grafts in the SFA are still the endovascular champion in long lesions
BY DENNIS GABLE, M.D.
There remains a continued debate among investigators as to the best modality for treatment of stenosis/occlusion of the SFA especially with the recent advent of drug-eluting technology. However, I suggest that for long lesions over 15 cm only covered stent grafts continue to outperform the competition.

If we review the numerous studies available on treatment of SFA disease, the Viabahn-covered stent device (W. L. Gore & Associates, Flagstaff, Ariz.) is by far the most studied modality. There are currently 22 independent studies available providing data on 1,473 limbs. Several of these reports are multicenter studies and many of them are prospective randomized trials. Two of the most recent are the VIPER (J. Vasc. Intervent. Radiol. 2013;24:165-73) and VIASTAR study (JACC 2013;62:1320-27).
The VIPER study prospectively enrolled 119 patients (72 with TASC II C/D disease; mean lesion length 190 mm). Primary patency was reported at 73% at 1 year but in patients with less than 20% oversizing, as is recommended by the IFU, patency as high as 88% was noted. Additionally, there was no difference in patency in smaller-diameter vessels (5 mm) versus larger-diameter vessels (6-7 mm).
In a head-to-head randomized controlled trial of Viabahn to bare metal stents (BMS), the VIASTAR study enrolled 141 patients (72 in covered stent arm; mean lesion length 190 mm). On a per protocol evaluation, the patency at 1 year was 78% and 71% on an intention-to-treat evaluation with a patency of 70% and 63% respectively at 2 years. There was no statistical difference between the two evaluations on intention to treat vs. per protocol but there was clear superiority demonstrated against BMS.
Furthermore, in a prospective, randomized, head-to-head comparison of Viabahn to prosthetic above knee femoral popliteal bypass, it was shown that there was no difference in primary or secondary patency between the two groups out to 4 years follow-up (J. Vasc. Surg. 2010;52:584-91). This included an average lesion length of 25.6 cm with a primary and secondary patency of 59% and 74% in the Viabahn group and 58% and 71% in the surgery group. When compared to a large meta-analysis for femoral popliteal bypass outcomes reported on by Bates and AbuRahma in 2004 (J. Endovasc. Ther. 2004;11[suppl. II]:II-107–27), the patency for the surgical arm with prosthetic bypass in the above Viabahn study was similar at 4 years to the 38 peer-reviewed articles Bates et al. reviewed with over 4,000 limbs. The reported primary and secondary patency at 4 years for prosthetic femoral above knee popliteal bypass was 51% and 61%, respectively in his review. Although the above Viabahn study was not powered to formally demonstrate noninferiority to surgical bypass with prosthetic, it did strongly suggest and show just that.
How do we put these data together with the Zilver data and how do we decide what is best for our patients? Some operators have expressed concern over a perceived risk for a “higher rate of amputation” or “a worse Rutherford level of ischemia on presentation” if patients with the Viabahn stent graft occlude post procedure. Commonly, this results from extrapolation of prior studies looking at results of occlusion with an ePTFE bypass. In fact, review of peer-reviewed data reveal none of the prospective studies outlined above, or those currently available, demonstrate that either of these perceptions are true and there are no published prospective data that support these fears either. In the studies listed above as well as all current prospective studies available evaluating Viabahn usage, the highest rate of amputation reported was 5% by Fisher in 2006 with all of the remaining studies reporting an amputation rate of 2% or less (when reported). Moreover, it has not been demonstrated that patients with this device present with an increased level of ischemia secondary to sudden occlusion.
There is one report used to argue against the use of the Viabahn stent graft (J. Vasc. Surg. 2008;47:967-74). This study evaluated prospectively 109 patients (71 for claudication; 38 for critical limb ischemia) treated for SFA occlusive disease (mean lesion length 15.7 cm). Only 19 of the 109 patients (17%) were treated with Viabahn (17 for claudication; 2 for critical limb ischemia). The remaining limbs were treated with various other BMS devices (n=10). The authors concluded that patients initially treated with Viabahn who presented back with occlusion had a higher chance of presenting with acute symptoms (i.e., a worse Rutherford score). The lesion length treated in the Viabahn group, however, was nearly twice as long as all the other stent platforms combined (25.4 cm vs. 13.7 cm) and there was a higher level of tibial artery deterioration with thrombosis of the BMS group, compared with the Viabahn group (7.7% vs. 5.3%). The number of Viabahn patients presenting with acute thrombosis was not defined. With the small number of limbs treated in the Viabahn group, the conclusions expressed cannot be statistically supported.
What about the in-vogue DES device?
Dr. Dake and his colleagues recently presented 5-year data on the Zilver DES platform at VIVA 2014. He reported a primary patency at 5 years of 66.4% showing superiority to angioplasty alone as well as angioplasty with provisional stenting. This study enrolled 479 patients into the randomization arm and also had a registry arm that although often included in reporting of patency, does not stand up to the scrutiny of peer review. Even though there were some patients with longer lesions, the randomized arm mean lesion length was only 66 mm, which does not compare to the published longer mean lesion length of the Viabahn device. Bosiers et al. (J. Cardiovasc. Surg. 2013 54:115-222) reviewed 135 patients treated with the Zilver device (a subgroup derived from the 787 patients enrolled in the registry data of the Zilver trial) with a mean lesion length of 226 mm. They reported 77.6% primary patency but only at 1 year. Again, however, this is registry derived data and does not have the scientific validity of a randomized trial.
So what can I conclude from these experiences? We know today that covered stent grafts have been widely used and reported on, including by Dr. Dake himself (Radiology 2000 October;217:95-104) and all appear to have had similar conclusions.
The mean lesion length treated in these studies of Viabahn is often longer than 15 cm and nearly all studies report primary patency outcomes. Zilver supporters on the other hand are prone to quote TLR which is an inferior endpoint (as recently noted in an editorial by Dr. Russell Samson (Vasc. Spec. 2015;11:2). Costs of both devices are an issue but may vary by region and institution. However, Viabahn does have the advantage of longer devices, compared with the Zilver (15 and 25 cm vs. 10 cm) so fewer devices may be required to treat long lesions. Although short lesions may be better addressed with BMS or DES, for longer SFA lesions over 12-15 cm there are very few truly comparable data that argue against the use of Viabahn.
Dr. Gable is chief of vascular and endovascular surgery at The Heart Hospital Baylor Plano (Tex.). He is also an associate medical editor for Vascular Specialist. He disclosed that he is a consultant, speaker, and receives research support from W. L. Gore and Medtronic.
Head-to-head comparisons are lacking, but similar results have been reported
BY MICHAEL D. DAKE, M.D.
Well, at least one thing is for sure – we would not have been having this discussion a mere 10 years ago.
I remained sheepishly silent for most of my early career as well-intentioned invasive and noninvasive specialists criticized the state of evidence supporting the legitimacy of endovascular interventions as a competitive strategy to manage infrainguinal peripheral arterial disease. Good data from well-controlled randomized clinical trials were not available to make a case for endovascular therapies.
Over the recent decade and a half, however, a number of contributing factors have influenced thinking and what we now consider standard of care for symptomatic disease of the superficial femoral artery (SFA). The proposal of an “endovascular first” interventional approach has evolved to a consensually agreed upon management strategy by all interested disciplines.
This did not occur on a whim. Rather, out of the shadows of relative ignorance there slowly emerged a welcomed accumulation of a large number of publications that detail the outcomes of a wide variety of randomized trials with a range of endovascular devices. This has allowed us to enter an era where valid comparisons between interventional therapies is not only possible, but allows us to more appropriately offer care to vascular patients with more nuanced strategies. These are strategies that recognize subtleties between subgroups of individuals stratified on the basis of patient demographics and lesion characteristics in a way not appreciated prior to the recent spate of endovascular device studies.
Thus, thanks to the dedication and hard work of many, we are now at a stage where we can have meaningful dialogues on a variety of endovascular topics, such as the one at hand, and proponents can argue their perspectives armed with objective evidence to support their positions. In this discussion regarding covered stent grafts and drug-eluting stents, we wish we had even more data.
Specifically, we are missing direct head-to-head comparisons between the two devices in patients with long SFA lesions. So, what do we know?
Here are some fundamental facts: The most commonly used covered stent graft for management of femoropopliteal occlusive disease is the Viabahn endoprosthesis (W. L. Gore and Associates, Flagstaff, Ariz.). The prosthesis is composed of a self-expanding nitinol stent framework and expanded polytetrafluoroethylene (ePTFE) graft with its surface lined with a coating of covalently bound heparin (Propaten bioactive surface).The only approved drug-eluting stent with significant safety and effectiveness data available is the Zilver PTX paclitaxel-eluting, self-expanding nitinol stent (Cook Medical Inc., Bloomington, Ind.).
Now in terms of the proposition, we need to discuss the meaning of the word “long” with reference to the SFA. Just what do we consider a long SFA lesion? I think all of us could agree that an arterial stenosis or occlusion of 6 cm or less is short. Lesions between 5 cm or 6 cm to 10 cm or 12 cm in length are moderately long, and disease greater than 10 cm or 12 cm is commonly characterized as long. Segments of disease greater than 20 cm long are typically considered very long or extremely long lesions from an endovascular interventional perspective.
So, how can currently available trial outcomes help us? Below, I have compiled a table that includes most of the recent clinical trial data for Viabahn and Zilver PTX in patients with long SFA occlusive disease.
OK, what can we honestly say about these data besides recognizing that we are at risk when we make any conclusions based upon cross-trial comparisons? Such an accounting of results is fraught with problems, but what we can say is that the table grossly confirms the current consensus that both devices enhance the standard of care for long lesions over traditional balloon angioplasty (PTA) and bare metal stent technologies.
Beyond this, however, it is accepted that patency results with Viabahn are lesion-length immune – that is, outcomes in long and extremely long segments of disease are not very different from the patency achieved in short lesions. This is clearly different than what is traditionally found for interventions with PTA or bare metal stents. There is not enough controlled data for extremely long lesions to reach a conclusion on drug-eluting stents; however, there is an initial suggestion that they behave in a manner more similar to stent grafts than traditional devices.
Grossly, the table suggests that the midterm and available greater than 1-year patency results with Viabahn and Zilver PTX are relatively comparable. What about the price of the device? What role does it play in our selection of the current most cost-effective endovascular strategy for long SFA lesions?
In my institution Viabahn is more expensive than Zilver PTX with a relative cost premium of about 30%-50% depending on the treatment length. Of course, when treating long TASC C and D lesions any up-front difference in the costs of the devices used initially is more than made up for by any relative reduction in subsequent reinterventions.
So, there you have it. Look at the table as simply a current snapshot. In the future, we will benefit from additional trials and comparisons, not to mention better endovascular technologies to address symptomatic long SFA lesions.
Dr. Dake is the Thelma and Henry Doelger Professor of Cardiovascular Surgery at the Stanford (Calif.) School of Medicine. He disclosed that he is a member of the Peripheral Scientific Advisory Board: Abbott Vascular Member, is on the Aortic Medical Advisory Board: W. L. Gore, is a consultant for Cook Medical, Medtronic, and Surmodics Research, and receives grants/clinical trial support from W. L. Gore, Medtronic, and Novate.
References for table
1. J. Vasc. Surg. 2013;58:386-95.
2. J. Vasc. Surg. 2010;52:584-90.
3. J. Vasc. Interv. Radiol. 2013;24:165-73.
4. Cardiovasc. Interv. Radiol. 2015;38:25-32.
5. Circ. Cardiovasc. Interv. 2011;4:495-504.
6. J. Am. Coll. Cardiol. 2013;61:2417-27.
7. J. Endovasc. Ther. 2011;18:613-23.
8. Zeller T. Oral presentations. 2014.
9. Yokoi H. Oral presentations. 2014.
Covered stent grafts in the SFA are still the endovascular champion in long lesions
BY DENNIS GABLE, M.D.
There remains a continued debate among investigators as to the best modality for treatment of stenosis/occlusion of the SFA especially with the recent advent of drug-eluting technology. However, I suggest that for long lesions over 15 cm only covered stent grafts continue to outperform the competition.
If we review the numerous studies available on treatment of SFA disease, the Viabahn-covered stent device (W. L. Gore & Associates, Flagstaff, Ariz.) is by far the most studied modality. There are currently 22 independent studies available providing data on 1,473 limbs. Several of these reports are multicenter studies and many of them are prospective randomized trials. Two of the most recent are the VIPER (J. Vasc. Intervent. Radiol. 2013;24:165-73) and VIASTAR study (JACC 2013;62:1320-27).
The VIPER study prospectively enrolled 119 patients (72 with TASC II C/D disease; mean lesion length 190 mm). Primary patency was reported at 73% at 1 year but in patients with less than 20% oversizing, as is recommended by the IFU, patency as high as 88% was noted. Additionally, there was no difference in patency in smaller-diameter vessels (5 mm) versus larger-diameter vessels (6-7 mm).
In a head-to-head randomized controlled trial of Viabahn to bare metal stents (BMS), the VIASTAR study enrolled 141 patients (72 in covered stent arm; mean lesion length 190 mm). On a per protocol evaluation, the patency at 1 year was 78% and 71% on an intention-to-treat evaluation with a patency of 70% and 63% respectively at 2 years. There was no statistical difference between the two evaluations on intention to treat vs. per protocol but there was clear superiority demonstrated against BMS.
Furthermore, in a prospective, randomized, head-to-head comparison of Viabahn to prosthetic above knee femoral popliteal bypass, it was shown that there was no difference in primary or secondary patency between the two groups out to 4 years follow-up (J. Vasc. Surg. 2010;52:584-91). This included an average lesion length of 25.6 cm with a primary and secondary patency of 59% and 74% in the Viabahn group and 58% and 71% in the surgery group. When compared to a large meta-analysis for femoral popliteal bypass outcomes reported on by Bates and AbuRahma in 2004 (J. Endovasc. Ther. 2004;11[suppl. II]:II-107–27), the patency for the surgical arm with prosthetic bypass in the above Viabahn study was similar at 4 years to the 38 peer-reviewed articles Bates et al. reviewed with over 4,000 limbs. The reported primary and secondary patency at 4 years for prosthetic femoral above knee popliteal bypass was 51% and 61%, respectively in his review. Although the above Viabahn study was not powered to formally demonstrate noninferiority to surgical bypass with prosthetic, it did strongly suggest and show just that.
How do we put these data together with the Zilver data and how do we decide what is best for our patients? Some operators have expressed concern over a perceived risk for a “higher rate of amputation” or “a worse Rutherford level of ischemia on presentation” if patients with the Viabahn stent graft occlude post procedure. Commonly, this results from extrapolation of prior studies looking at results of occlusion with an ePTFE bypass. In fact, review of peer-reviewed data reveal none of the prospective studies outlined above, or those currently available, demonstrate that either of these perceptions are true and there are no published prospective data that support these fears either. In the studies listed above as well as all current prospective studies available evaluating Viabahn usage, the highest rate of amputation reported was 5% by Fisher in 2006 with all of the remaining studies reporting an amputation rate of 2% or less (when reported). Moreover, it has not been demonstrated that patients with this device present with an increased level of ischemia secondary to sudden occlusion.
There is one report used to argue against the use of the Viabahn stent graft (J. Vasc. Surg. 2008;47:967-74). This study evaluated prospectively 109 patients (71 for claudication; 38 for critical limb ischemia) treated for SFA occlusive disease (mean lesion length 15.7 cm). Only 19 of the 109 patients (17%) were treated with Viabahn (17 for claudication; 2 for critical limb ischemia). The remaining limbs were treated with various other BMS devices (n=10). The authors concluded that patients initially treated with Viabahn who presented back with occlusion had a higher chance of presenting with acute symptoms (i.e., a worse Rutherford score). The lesion length treated in the Viabahn group, however, was nearly twice as long as all the other stent platforms combined (25.4 cm vs. 13.7 cm) and there was a higher level of tibial artery deterioration with thrombosis of the BMS group, compared with the Viabahn group (7.7% vs. 5.3%). The number of Viabahn patients presenting with acute thrombosis was not defined. With the small number of limbs treated in the Viabahn group, the conclusions expressed cannot be statistically supported.
What about the in-vogue DES device?
Dr. Dake and his colleagues recently presented 5-year data on the Zilver DES platform at VIVA 2014. He reported a primary patency at 5 years of 66.4% showing superiority to angioplasty alone as well as angioplasty with provisional stenting. This study enrolled 479 patients into the randomization arm and also had a registry arm that although often included in reporting of patency, does not stand up to the scrutiny of peer review. Even though there were some patients with longer lesions, the randomized arm mean lesion length was only 66 mm, which does not compare to the published longer mean lesion length of the Viabahn device. Bosiers et al. (J. Cardiovasc. Surg. 2013 54:115-222) reviewed 135 patients treated with the Zilver device (a subgroup derived from the 787 patients enrolled in the registry data of the Zilver trial) with a mean lesion length of 226 mm. They reported 77.6% primary patency but only at 1 year. Again, however, this is registry derived data and does not have the scientific validity of a randomized trial.
So what can I conclude from these experiences? We know today that covered stent grafts have been widely used and reported on, including by Dr. Dake himself (Radiology 2000 October;217:95-104) and all appear to have had similar conclusions.
The mean lesion length treated in these studies of Viabahn is often longer than 15 cm and nearly all studies report primary patency outcomes. Zilver supporters on the other hand are prone to quote TLR which is an inferior endpoint (as recently noted in an editorial by Dr. Russell Samson (Vasc. Spec. 2015;11:2). Costs of both devices are an issue but may vary by region and institution. However, Viabahn does have the advantage of longer devices, compared with the Zilver (15 and 25 cm vs. 10 cm) so fewer devices may be required to treat long lesions. Although short lesions may be better addressed with BMS or DES, for longer SFA lesions over 12-15 cm there are very few truly comparable data that argue against the use of Viabahn.
Dr. Gable is chief of vascular and endovascular surgery at The Heart Hospital Baylor Plano (Tex.). He is also an associate medical editor for Vascular Specialist. He disclosed that he is a consultant, speaker, and receives research support from W. L. Gore and Medtronic.
Head-to-head comparisons are lacking, but similar results have been reported
BY MICHAEL D. DAKE, M.D.
Well, at least one thing is for sure – we would not have been having this discussion a mere 10 years ago.
I remained sheepishly silent for most of my early career as well-intentioned invasive and noninvasive specialists criticized the state of evidence supporting the legitimacy of endovascular interventions as a competitive strategy to manage infrainguinal peripheral arterial disease. Good data from well-controlled randomized clinical trials were not available to make a case for endovascular therapies.
Over the recent decade and a half, however, a number of contributing factors have influenced thinking and what we now consider standard of care for symptomatic disease of the superficial femoral artery (SFA). The proposal of an “endovascular first” interventional approach has evolved to a consensually agreed upon management strategy by all interested disciplines.
This did not occur on a whim. Rather, out of the shadows of relative ignorance there slowly emerged a welcomed accumulation of a large number of publications that detail the outcomes of a wide variety of randomized trials with a range of endovascular devices. This has allowed us to enter an era where valid comparisons between interventional therapies is not only possible, but allows us to more appropriately offer care to vascular patients with more nuanced strategies. These are strategies that recognize subtleties between subgroups of individuals stratified on the basis of patient demographics and lesion characteristics in a way not appreciated prior to the recent spate of endovascular device studies.
Thus, thanks to the dedication and hard work of many, we are now at a stage where we can have meaningful dialogues on a variety of endovascular topics, such as the one at hand, and proponents can argue their perspectives armed with objective evidence to support their positions. In this discussion regarding covered stent grafts and drug-eluting stents, we wish we had even more data.
Specifically, we are missing direct head-to-head comparisons between the two devices in patients with long SFA lesions. So, what do we know?
Here are some fundamental facts: The most commonly used covered stent graft for management of femoropopliteal occlusive disease is the Viabahn endoprosthesis (W. L. Gore and Associates, Flagstaff, Ariz.). The prosthesis is composed of a self-expanding nitinol stent framework and expanded polytetrafluoroethylene (ePTFE) graft with its surface lined with a coating of covalently bound heparin (Propaten bioactive surface).The only approved drug-eluting stent with significant safety and effectiveness data available is the Zilver PTX paclitaxel-eluting, self-expanding nitinol stent (Cook Medical Inc., Bloomington, Ind.).
Now in terms of the proposition, we need to discuss the meaning of the word “long” with reference to the SFA. Just what do we consider a long SFA lesion? I think all of us could agree that an arterial stenosis or occlusion of 6 cm or less is short. Lesions between 5 cm or 6 cm to 10 cm or 12 cm in length are moderately long, and disease greater than 10 cm or 12 cm is commonly characterized as long. Segments of disease greater than 20 cm long are typically considered very long or extremely long lesions from an endovascular interventional perspective.
So, how can currently available trial outcomes help us? Below, I have compiled a table that includes most of the recent clinical trial data for Viabahn and Zilver PTX in patients with long SFA occlusive disease.
OK, what can we honestly say about these data besides recognizing that we are at risk when we make any conclusions based upon cross-trial comparisons? Such an accounting of results is fraught with problems, but what we can say is that the table grossly confirms the current consensus that both devices enhance the standard of care for long lesions over traditional balloon angioplasty (PTA) and bare metal stent technologies.
Beyond this, however, it is accepted that patency results with Viabahn are lesion-length immune – that is, outcomes in long and extremely long segments of disease are not very different from the patency achieved in short lesions. This is clearly different than what is traditionally found for interventions with PTA or bare metal stents. There is not enough controlled data for extremely long lesions to reach a conclusion on drug-eluting stents; however, there is an initial suggestion that they behave in a manner more similar to stent grafts than traditional devices.
Grossly, the table suggests that the midterm and available greater than 1-year patency results with Viabahn and Zilver PTX are relatively comparable. What about the price of the device? What role does it play in our selection of the current most cost-effective endovascular strategy for long SFA lesions?
In my institution Viabahn is more expensive than Zilver PTX with a relative cost premium of about 30%-50% depending on the treatment length. Of course, when treating long TASC C and D lesions any up-front difference in the costs of the devices used initially is more than made up for by any relative reduction in subsequent reinterventions.
So, there you have it. Look at the table as simply a current snapshot. In the future, we will benefit from additional trials and comparisons, not to mention better endovascular technologies to address symptomatic long SFA lesions.
Dr. Dake is the Thelma and Henry Doelger Professor of Cardiovascular Surgery at the Stanford (Calif.) School of Medicine. He disclosed that he is a member of the Peripheral Scientific Advisory Board: Abbott Vascular Member, is on the Aortic Medical Advisory Board: W. L. Gore, is a consultant for Cook Medical, Medtronic, and Surmodics Research, and receives grants/clinical trial support from W. L. Gore, Medtronic, and Novate.
References for table
1. J. Vasc. Surg. 2013;58:386-95.
2. J. Vasc. Surg. 2010;52:584-90.
3. J. Vasc. Interv. Radiol. 2013;24:165-73.
4. Cardiovasc. Interv. Radiol. 2015;38:25-32.
5. Circ. Cardiovasc. Interv. 2011;4:495-504.
6. J. Am. Coll. Cardiol. 2013;61:2417-27.
7. J. Endovasc. Ther. 2011;18:613-23.
8. Zeller T. Oral presentations. 2014.
9. Yokoi H. Oral presentations. 2014.
Covered stent grafts in the SFA are still the endovascular champion in long lesions
BY DENNIS GABLE, M.D.
There remains a continued debate among investigators as to the best modality for treatment of stenosis/occlusion of the SFA especially with the recent advent of drug-eluting technology. However, I suggest that for long lesions over 15 cm only covered stent grafts continue to outperform the competition.
If we review the numerous studies available on treatment of SFA disease, the Viabahn-covered stent device (W. L. Gore & Associates, Flagstaff, Ariz.) is by far the most studied modality. There are currently 22 independent studies available providing data on 1,473 limbs. Several of these reports are multicenter studies and many of them are prospective randomized trials. Two of the most recent are the VIPER (J. Vasc. Intervent. Radiol. 2013;24:165-73) and VIASTAR study (JACC 2013;62:1320-27).
The VIPER study prospectively enrolled 119 patients (72 with TASC II C/D disease; mean lesion length 190 mm). Primary patency was reported at 73% at 1 year but in patients with less than 20% oversizing, as is recommended by the IFU, patency as high as 88% was noted. Additionally, there was no difference in patency in smaller-diameter vessels (5 mm) versus larger-diameter vessels (6-7 mm).
In a head-to-head randomized controlled trial of Viabahn to bare metal stents (BMS), the VIASTAR study enrolled 141 patients (72 in covered stent arm; mean lesion length 190 mm). On a per protocol evaluation, the patency at 1 year was 78% and 71% on an intention-to-treat evaluation with a patency of 70% and 63% respectively at 2 years. There was no statistical difference between the two evaluations on intention to treat vs. per protocol but there was clear superiority demonstrated against BMS.
Furthermore, in a prospective, randomized, head-to-head comparison of Viabahn to prosthetic above knee femoral popliteal bypass, it was shown that there was no difference in primary or secondary patency between the two groups out to 4 years follow-up (J. Vasc. Surg. 2010;52:584-91). This included an average lesion length of 25.6 cm with a primary and secondary patency of 59% and 74% in the Viabahn group and 58% and 71% in the surgery group. When compared to a large meta-analysis for femoral popliteal bypass outcomes reported on by Bates and AbuRahma in 2004 (J. Endovasc. Ther. 2004;11[suppl. II]:II-107–27), the patency for the surgical arm with prosthetic bypass in the above Viabahn study was similar at 4 years to the 38 peer-reviewed articles Bates et al. reviewed with over 4,000 limbs. The reported primary and secondary patency at 4 years for prosthetic femoral above knee popliteal bypass was 51% and 61%, respectively in his review. Although the above Viabahn study was not powered to formally demonstrate noninferiority to surgical bypass with prosthetic, it did strongly suggest and show just that.
How do we put these data together with the Zilver data and how do we decide what is best for our patients? Some operators have expressed concern over a perceived risk for a “higher rate of amputation” or “a worse Rutherford level of ischemia on presentation” if patients with the Viabahn stent graft occlude post procedure. Commonly, this results from extrapolation of prior studies looking at results of occlusion with an ePTFE bypass. In fact, review of peer-reviewed data reveal none of the prospective studies outlined above, or those currently available, demonstrate that either of these perceptions are true and there are no published prospective data that support these fears either. In the studies listed above as well as all current prospective studies available evaluating Viabahn usage, the highest rate of amputation reported was 5% by Fisher in 2006 with all of the remaining studies reporting an amputation rate of 2% or less (when reported). Moreover, it has not been demonstrated that patients with this device present with an increased level of ischemia secondary to sudden occlusion.
There is one report used to argue against the use of the Viabahn stent graft (J. Vasc. Surg. 2008;47:967-74). This study evaluated prospectively 109 patients (71 for claudication; 38 for critical limb ischemia) treated for SFA occlusive disease (mean lesion length 15.7 cm). Only 19 of the 109 patients (17%) were treated with Viabahn (17 for claudication; 2 for critical limb ischemia). The remaining limbs were treated with various other BMS devices (n=10). The authors concluded that patients initially treated with Viabahn who presented back with occlusion had a higher chance of presenting with acute symptoms (i.e., a worse Rutherford score). The lesion length treated in the Viabahn group, however, was nearly twice as long as all the other stent platforms combined (25.4 cm vs. 13.7 cm) and there was a higher level of tibial artery deterioration with thrombosis of the BMS group, compared with the Viabahn group (7.7% vs. 5.3%). The number of Viabahn patients presenting with acute thrombosis was not defined. With the small number of limbs treated in the Viabahn group, the conclusions expressed cannot be statistically supported.
What about the in-vogue DES device?
Dr. Dake and his colleagues recently presented 5-year data on the Zilver DES platform at VIVA 2014. He reported a primary patency at 5 years of 66.4% showing superiority to angioplasty alone as well as angioplasty with provisional stenting. This study enrolled 479 patients into the randomization arm and also had a registry arm that although often included in reporting of patency, does not stand up to the scrutiny of peer review. Even though there were some patients with longer lesions, the randomized arm mean lesion length was only 66 mm, which does not compare to the published longer mean lesion length of the Viabahn device. Bosiers et al. (J. Cardiovasc. Surg. 2013 54:115-222) reviewed 135 patients treated with the Zilver device (a subgroup derived from the 787 patients enrolled in the registry data of the Zilver trial) with a mean lesion length of 226 mm. They reported 77.6% primary patency but only at 1 year. Again, however, this is registry derived data and does not have the scientific validity of a randomized trial.
So what can I conclude from these experiences? We know today that covered stent grafts have been widely used and reported on, including by Dr. Dake himself (Radiology 2000 October;217:95-104) and all appear to have had similar conclusions.
The mean lesion length treated in these studies of Viabahn is often longer than 15 cm and nearly all studies report primary patency outcomes. Zilver supporters on the other hand are prone to quote TLR which is an inferior endpoint (as recently noted in an editorial by Dr. Russell Samson (Vasc. Spec. 2015;11:2). Costs of both devices are an issue but may vary by region and institution. However, Viabahn does have the advantage of longer devices, compared with the Zilver (15 and 25 cm vs. 10 cm) so fewer devices may be required to treat long lesions. Although short lesions may be better addressed with BMS or DES, for longer SFA lesions over 12-15 cm there are very few truly comparable data that argue against the use of Viabahn.
Dr. Gable is chief of vascular and endovascular surgery at The Heart Hospital Baylor Plano (Tex.). He is also an associate medical editor for Vascular Specialist. He disclosed that he is a consultant, speaker, and receives research support from W. L. Gore and Medtronic.

LANDMARK STUDY: Cell-Free DNA Analysis for Down Syndrome Screening in the General Pregnancy Population
Click here to download the PDF.
To date, cell-free DNA (cfDNA) screening for fetal trisomy has been offered primarily to women at increased risk for fetal aneuploidy, but not to the general pregnancy population. Recently, the results of a large, prospective, multicenter, blinded study were published, demonstrating that the Harmony test for risk assessment of trisomy 21 (Down Syndrome) outperforms combined first trimester screening in the general pregnancy population. This supplement examines the crucial findings of cfDNA analysis for Down syndrome screening in the general pregnancy population using the Harmony test.
The Harmony Prenatal Test is developed by Ariosa Diagnostics. Ariosa Diagnostics is a laboratory certified under the Clinical Laboratory Improvement Amendments (CLIA). As with other laboratory-developed tests, this testing service has not been cleared or approved by the US FDA or any other federal regulatory agencies. Non-invasive prenatal testing (NIPT) services based on cell-free DNA analyses are not diagnostic; high-risk results should be confirmed by diagnostic testing. Data have not been submitted to or evaluated by Federal regulatory agencies and the test is not for sale as an In Vitro Diagnostic (IVD) in the US or the EU.
To view an exclusive video on the pivotal findings discussed in this supplement, click here.
Click here to download the PDF.
To date, cell-free DNA (cfDNA) screening for fetal trisomy has been offered primarily to women at increased risk for fetal aneuploidy, but not to the general pregnancy population. Recently, the results of a large, prospective, multicenter, blinded study were published, demonstrating that the Harmony test for risk assessment of trisomy 21 (Down Syndrome) outperforms combined first trimester screening in the general pregnancy population. This supplement examines the crucial findings of cfDNA analysis for Down syndrome screening in the general pregnancy population using the Harmony test.
The Harmony Prenatal Test is developed by Ariosa Diagnostics. Ariosa Diagnostics is a laboratory certified under the Clinical Laboratory Improvement Amendments (CLIA). As with other laboratory-developed tests, this testing service has not been cleared or approved by the US FDA or any other federal regulatory agencies. Non-invasive prenatal testing (NIPT) services based on cell-free DNA analyses are not diagnostic; high-risk results should be confirmed by diagnostic testing. Data have not been submitted to or evaluated by Federal regulatory agencies and the test is not for sale as an In Vitro Diagnostic (IVD) in the US or the EU.
To view an exclusive video on the pivotal findings discussed in this supplement, click here.
Click here to download the PDF.
To date, cell-free DNA (cfDNA) screening for fetal trisomy has been offered primarily to women at increased risk for fetal aneuploidy, but not to the general pregnancy population. Recently, the results of a large, prospective, multicenter, blinded study were published, demonstrating that the Harmony test for risk assessment of trisomy 21 (Down Syndrome) outperforms combined first trimester screening in the general pregnancy population. This supplement examines the crucial findings of cfDNA analysis for Down syndrome screening in the general pregnancy population using the Harmony test.
The Harmony Prenatal Test is developed by Ariosa Diagnostics. Ariosa Diagnostics is a laboratory certified under the Clinical Laboratory Improvement Amendments (CLIA). As with other laboratory-developed tests, this testing service has not been cleared or approved by the US FDA or any other federal regulatory agencies. Non-invasive prenatal testing (NIPT) services based on cell-free DNA analyses are not diagnostic; high-risk results should be confirmed by diagnostic testing. Data have not been submitted to or evaluated by Federal regulatory agencies and the test is not for sale as an In Vitro Diagnostic (IVD) in the US or the EU.
To view an exclusive video on the pivotal findings discussed in this supplement, click here.

Hybrid carotid stents eyed positively
CHICAGO – The next generation of hybrid carotid stents is slowly breathing life into the stagnant field of carotid artery stenting.
The new hybrid stents combine the flexibility of a traditional open-cell, nitinol stent with the stabilization typically offered by a closed-cell stent design. The initial clinical experience is limited, but shows promising results against embolization, Dr. Claudio Schönholzsaid at a symposium on vascular surgery sponsored by Northwestern University.

Last year, Dr. Schönholz and his colleagues at the Medical University of South Carolina in Charleston reported the first-in-man use of the investigational Gore Carotid Stent (W.L. Gore & Associates) (J. Endovasc. Thera. 2014;21:601-4).
As part of the Gore Carotid Stent Clinical Study for the Treatment of Carotid Artery Stenosis in Patients at Increased Risk for Adverse Events From Carotid Endarterectomy (SCAFFOLD) trial, the team has successfully treated another four patients with no evidence of peri- or postprocedural neurological events. This included a case with such severe high-grade stenosis and slow flow that the external carotid artery was not even visible on imaging before the stent was placed, Dr. Schönholz said.
The Food and Drug Administration recently reviewed unreleased data for the first 100 patients enrolled in SCAFFOLD and given the green light for the multicenter, 312-patient study to resume with the start of the new year, he said.Cristallo study (J. Endovasc. Ther. 2008;15:186-92).
A more recent retrospective study revealed only one minor stroke in the perioperative period and during the first 30 days in 68 patients with symptomatic carotid stenosis treated by Turkish surgeons with the Cristallo Ideale stent and a proximal protection device (MO.MA, Invatec s.r.l., Medtronic, Italy) (Int. Angiol. 2014 Nov. 14. [Epub ahead of print]).
Better patient selection, increased operator experience, and use of embolic protection devices has reduced neurological events associated with carotid artery stenting, but embolization still occurs after protection devices are removed due to plaque protrusion through the stent struts, Dr. Schönholz said. The unique design of the hybrid stents “may prevent plaque protrusion, eliminating peri- and postprocedural events,” he said.The Cristallo Ideale hybrid stent is a nitinol-based stent that has a closed-cell portion at its center and an open-cell configuration on the distal and proximal sections. In contrast, the Gore Carotid Stent has a closed-cell component throughout the entire device length that is created by placing an expanded polytetrafluoroethylene lattice with 500-micrometer pores over an open-cell frame. Once combined, both the stent frame and lattice are coated on all surfaces with Carmeda Bioactive Surface (CBAS) heparin. It’s action is limited only to the device surface and has no systemic anticoagulation effects, said Dr. Schönholz, who disclosed serving on Gore’s scientific advisory board.
The open-cell frame allows a high degree of flexibility and conformity to the native anatomy, while the stent lattice provides a high degree of plaque scaffolding that can reduce plaque prolapse, he said. The lattice also reduces the amount of emboli released during and after stent deployment and stabilizes the stent frame by resisting elongation as well as “fish-scaling,” or the misalignment of stent struts that protrude into the vessel wall, particularly when stents are deployed in tortuous anatomy.
Course director Dr. Mark K. Eskandari, chief of vascular surgery at Northwestern University in Chicago, said the results show that “carotid stenting isn’t dead yet and we can persevere. Advances in technology, both in regards to mechanical embolic protection devices and stent design systems, continue to improve the already great results of carotid artery stenting.”
CHICAGO – The next generation of hybrid carotid stents is slowly breathing life into the stagnant field of carotid artery stenting.
The new hybrid stents combine the flexibility of a traditional open-cell, nitinol stent with the stabilization typically offered by a closed-cell stent design. The initial clinical experience is limited, but shows promising results against embolization, Dr. Claudio Schönholzsaid at a symposium on vascular surgery sponsored by Northwestern University.
Last year, Dr. Schönholz and his colleagues at the Medical University of South Carolina in Charleston reported the first-in-man use of the investigational Gore Carotid Stent (W.L. Gore & Associates) (J. Endovasc. Thera. 2014;21:601-4).
As part of the Gore Carotid Stent Clinical Study for the Treatment of Carotid Artery Stenosis in Patients at Increased Risk for Adverse Events From Carotid Endarterectomy (SCAFFOLD) trial, the team has successfully treated another four patients with no evidence of peri- or postprocedural neurological events. This included a case with such severe high-grade stenosis and slow flow that the external carotid artery was not even visible on imaging before the stent was placed, Dr. Schönholz said.
The Food and Drug Administration recently reviewed unreleased data for the first 100 patients enrolled in SCAFFOLD and given the green light for the multicenter, 312-patient study to resume with the start of the new year, he said.Cristallo study (J. Endovasc. Ther. 2008;15:186-92).
A more recent retrospective study revealed only one minor stroke in the perioperative period and during the first 30 days in 68 patients with symptomatic carotid stenosis treated by Turkish surgeons with the Cristallo Ideale stent and a proximal protection device (MO.MA, Invatec s.r.l., Medtronic, Italy) (Int. Angiol. 2014 Nov. 14. [Epub ahead of print]).
Better patient selection, increased operator experience, and use of embolic protection devices has reduced neurological events associated with carotid artery stenting, but embolization still occurs after protection devices are removed due to plaque protrusion through the stent struts, Dr. Schönholz said. The unique design of the hybrid stents “may prevent plaque protrusion, eliminating peri- and postprocedural events,” he said.The Cristallo Ideale hybrid stent is a nitinol-based stent that has a closed-cell portion at its center and an open-cell configuration on the distal and proximal sections. In contrast, the Gore Carotid Stent has a closed-cell component throughout the entire device length that is created by placing an expanded polytetrafluoroethylene lattice with 500-micrometer pores over an open-cell frame. Once combined, both the stent frame and lattice are coated on all surfaces with Carmeda Bioactive Surface (CBAS) heparin. It’s action is limited only to the device surface and has no systemic anticoagulation effects, said Dr. Schönholz, who disclosed serving on Gore’s scientific advisory board.
The open-cell frame allows a high degree of flexibility and conformity to the native anatomy, while the stent lattice provides a high degree of plaque scaffolding that can reduce plaque prolapse, he said. The lattice also reduces the amount of emboli released during and after stent deployment and stabilizes the stent frame by resisting elongation as well as “fish-scaling,” or the misalignment of stent struts that protrude into the vessel wall, particularly when stents are deployed in tortuous anatomy.
Course director Dr. Mark K. Eskandari, chief of vascular surgery at Northwestern University in Chicago, said the results show that “carotid stenting isn’t dead yet and we can persevere. Advances in technology, both in regards to mechanical embolic protection devices and stent design systems, continue to improve the already great results of carotid artery stenting.”
CHICAGO – The next generation of hybrid carotid stents is slowly breathing life into the stagnant field of carotid artery stenting.
The new hybrid stents combine the flexibility of a traditional open-cell, nitinol stent with the stabilization typically offered by a closed-cell stent design. The initial clinical experience is limited, but shows promising results against embolization, Dr. Claudio Schönholzsaid at a symposium on vascular surgery sponsored by Northwestern University.
Last year, Dr. Schönholz and his colleagues at the Medical University of South Carolina in Charleston reported the first-in-man use of the investigational Gore Carotid Stent (W.L. Gore & Associates) (J. Endovasc. Thera. 2014;21:601-4).
As part of the Gore Carotid Stent Clinical Study for the Treatment of Carotid Artery Stenosis in Patients at Increased Risk for Adverse Events From Carotid Endarterectomy (SCAFFOLD) trial, the team has successfully treated another four patients with no evidence of peri- or postprocedural neurological events. This included a case with such severe high-grade stenosis and slow flow that the external carotid artery was not even visible on imaging before the stent was placed, Dr. Schönholz said.
The Food and Drug Administration recently reviewed unreleased data for the first 100 patients enrolled in SCAFFOLD and given the green light for the multicenter, 312-patient study to resume with the start of the new year, he said.Cristallo study (J. Endovasc. Ther. 2008;15:186-92).
A more recent retrospective study revealed only one minor stroke in the perioperative period and during the first 30 days in 68 patients with symptomatic carotid stenosis treated by Turkish surgeons with the Cristallo Ideale stent and a proximal protection device (MO.MA, Invatec s.r.l., Medtronic, Italy) (Int. Angiol. 2014 Nov. 14. [Epub ahead of print]).
Better patient selection, increased operator experience, and use of embolic protection devices has reduced neurological events associated with carotid artery stenting, but embolization still occurs after protection devices are removed due to plaque protrusion through the stent struts, Dr. Schönholz said. The unique design of the hybrid stents “may prevent plaque protrusion, eliminating peri- and postprocedural events,” he said.The Cristallo Ideale hybrid stent is a nitinol-based stent that has a closed-cell portion at its center and an open-cell configuration on the distal and proximal sections. In contrast, the Gore Carotid Stent has a closed-cell component throughout the entire device length that is created by placing an expanded polytetrafluoroethylene lattice with 500-micrometer pores over an open-cell frame. Once combined, both the stent frame and lattice are coated on all surfaces with Carmeda Bioactive Surface (CBAS) heparin. It’s action is limited only to the device surface and has no systemic anticoagulation effects, said Dr. Schönholz, who disclosed serving on Gore’s scientific advisory board.
The open-cell frame allows a high degree of flexibility and conformity to the native anatomy, while the stent lattice provides a high degree of plaque scaffolding that can reduce plaque prolapse, he said. The lattice also reduces the amount of emboli released during and after stent deployment and stabilizes the stent frame by resisting elongation as well as “fish-scaling,” or the misalignment of stent struts that protrude into the vessel wall, particularly when stents are deployed in tortuous anatomy.
Course director Dr. Mark K. Eskandari, chief of vascular surgery at Northwestern University in Chicago, said the results show that “carotid stenting isn’t dead yet and we can persevere. Advances in technology, both in regards to mechanical embolic protection devices and stent design systems, continue to improve the already great results of carotid artery stenting.”

Tumor sequencing fails to paint the whole picture

Image courtesy of NIGMS
Many of the genetic alterations revealed by sequencing a cancer patient’s tumor DNA are not actually associated with the cancer, according to a study published in Science Translational Medicine.
In fact, these alterations are inherited germline mutations already present in an individual’s normal cells.
To make this discovery, researchers compared DNA from tumors and normal cells in 815 patients with hematologic and solid tumor malignancies.
Almost half of the patients analyzed using tumor-only approaches had genetic alterations in their tumors that were also present in their normal cells, which suggests the alterations were “false-positive” changes not specific to the tumor.
As personalized medicine is predicated on tailoring treatments to the genetic makeup of a patient’s tumor, the high rate of false-positives uncovered in this study has implications for the accuracy of the approach when it relies on tumor-only sequencing, the researchers said.
“We knew from our pioneering whole-exome analyses of cancer patients that a significant number of the genetic alterations that were thought to be associated with tumors were also present in the inherited germline DNA,” said Siân Jones, PhD, of Personal Genome Diagnostics in Baltimore, Maryland.
“By comparing tumor DNA to DNA from normal tissue, we were able to separate out those genetic alterations that are truly tumor-specific. Accurately identifying tumor-specific alterations is essential to realizing the potential of personalized medicine to achieve better treatment outcomes.”
The researchers identified 382 genetic alterations that were potentially tumor-specific by first detecting all of the genetic changes in patients’ tumors and then eliminating those that were well-known germline alterations.
However, when the remaining alterations were compared to the genomic profiles of the patients’ germline DNA, an average of 249, or 65%, turned out to be false-positive changes that were already present in the normal cells.
The researchers also looked at the alterations in actionable genes, which have been identified as potential targets for approved or investigational cancer therapies. They found that almost half of the tumor samples (48%) had at least one false-positive mutation in an actionable gene.
The use of false-positive findings to guide personalized treatment decisions could result in a substantial number of patients receiving therapies that are not optimized for their cancer, according to the researchers. Therefore, it seems sequencing normal DNA alongside tumor DNA is essential.
In addition to selecting personalized therapies for cancer patients, sequencing normal DNA can increase the overall understanding of cancer, including finding cancer predisposition due to germline genome changes, said Victor Velculescu, MD, PhD, of Johns Hopkins University School of Medicine in Baltimore, Maryland.
In this study, the germline analyses revealed changes in cancer-related genes in 3% of the patients who had no known signs of genetically linked cancer.
“These analyses can help us find alterations in cancer-predisposing genes in ways that weren’t previously appreciated,” Dr Velculescu said.
He also acknowledged, however, that there are challenges to implementing tumor-normal DNA analyses in a clinical setting. These include the additional work and costs of sequencing and analyzing a patient’s normal tissue along with his or her tumor tissue.
Costs for tumor gene sequencing begin at several thousand dollars, which would increase if sequencing was done on DNA from normal tissue as well. And health insurance may not fully cover normal-tissue genetic sequencing. ![]()
Image courtesy of NIGMS
Many of the genetic alterations revealed by sequencing a cancer patient’s tumor DNA are not actually associated with the cancer, according to a study published in Science Translational Medicine.
In fact, these alterations are inherited germline mutations already present in an individual’s normal cells.
To make this discovery, researchers compared DNA from tumors and normal cells in 815 patients with hematologic and solid tumor malignancies.
Almost half of the patients analyzed using tumor-only approaches had genetic alterations in their tumors that were also present in their normal cells, which suggests the alterations were “false-positive” changes not specific to the tumor.
As personalized medicine is predicated on tailoring treatments to the genetic makeup of a patient’s tumor, the high rate of false-positives uncovered in this study has implications for the accuracy of the approach when it relies on tumor-only sequencing, the researchers said.
“We knew from our pioneering whole-exome analyses of cancer patients that a significant number of the genetic alterations that were thought to be associated with tumors were also present in the inherited germline DNA,” said Siân Jones, PhD, of Personal Genome Diagnostics in Baltimore, Maryland.
“By comparing tumor DNA to DNA from normal tissue, we were able to separate out those genetic alterations that are truly tumor-specific. Accurately identifying tumor-specific alterations is essential to realizing the potential of personalized medicine to achieve better treatment outcomes.”
The researchers identified 382 genetic alterations that were potentially tumor-specific by first detecting all of the genetic changes in patients’ tumors and then eliminating those that were well-known germline alterations.
However, when the remaining alterations were compared to the genomic profiles of the patients’ germline DNA, an average of 249, or 65%, turned out to be false-positive changes that were already present in the normal cells.
The researchers also looked at the alterations in actionable genes, which have been identified as potential targets for approved or investigational cancer therapies. They found that almost half of the tumor samples (48%) had at least one false-positive mutation in an actionable gene.
The use of false-positive findings to guide personalized treatment decisions could result in a substantial number of patients receiving therapies that are not optimized for their cancer, according to the researchers. Therefore, it seems sequencing normal DNA alongside tumor DNA is essential.
In addition to selecting personalized therapies for cancer patients, sequencing normal DNA can increase the overall understanding of cancer, including finding cancer predisposition due to germline genome changes, said Victor Velculescu, MD, PhD, of Johns Hopkins University School of Medicine in Baltimore, Maryland.
In this study, the germline analyses revealed changes in cancer-related genes in 3% of the patients who had no known signs of genetically linked cancer.
“These analyses can help us find alterations in cancer-predisposing genes in ways that weren’t previously appreciated,” Dr Velculescu said.
He also acknowledged, however, that there are challenges to implementing tumor-normal DNA analyses in a clinical setting. These include the additional work and costs of sequencing and analyzing a patient’s normal tissue along with his or her tumor tissue.
Costs for tumor gene sequencing begin at several thousand dollars, which would increase if sequencing was done on DNA from normal tissue as well. And health insurance may not fully cover normal-tissue genetic sequencing. ![]()
Image courtesy of NIGMS
Many of the genetic alterations revealed by sequencing a cancer patient’s tumor DNA are not actually associated with the cancer, according to a study published in Science Translational Medicine.
In fact, these alterations are inherited germline mutations already present in an individual’s normal cells.
To make this discovery, researchers compared DNA from tumors and normal cells in 815 patients with hematologic and solid tumor malignancies.
Almost half of the patients analyzed using tumor-only approaches had genetic alterations in their tumors that were also present in their normal cells, which suggests the alterations were “false-positive” changes not specific to the tumor.
As personalized medicine is predicated on tailoring treatments to the genetic makeup of a patient’s tumor, the high rate of false-positives uncovered in this study has implications for the accuracy of the approach when it relies on tumor-only sequencing, the researchers said.
“We knew from our pioneering whole-exome analyses of cancer patients that a significant number of the genetic alterations that were thought to be associated with tumors were also present in the inherited germline DNA,” said Siân Jones, PhD, of Personal Genome Diagnostics in Baltimore, Maryland.
“By comparing tumor DNA to DNA from normal tissue, we were able to separate out those genetic alterations that are truly tumor-specific. Accurately identifying tumor-specific alterations is essential to realizing the potential of personalized medicine to achieve better treatment outcomes.”
The researchers identified 382 genetic alterations that were potentially tumor-specific by first detecting all of the genetic changes in patients’ tumors and then eliminating those that were well-known germline alterations.
However, when the remaining alterations were compared to the genomic profiles of the patients’ germline DNA, an average of 249, or 65%, turned out to be false-positive changes that were already present in the normal cells.
The researchers also looked at the alterations in actionable genes, which have been identified as potential targets for approved or investigational cancer therapies. They found that almost half of the tumor samples (48%) had at least one false-positive mutation in an actionable gene.
The use of false-positive findings to guide personalized treatment decisions could result in a substantial number of patients receiving therapies that are not optimized for their cancer, according to the researchers. Therefore, it seems sequencing normal DNA alongside tumor DNA is essential.
In addition to selecting personalized therapies for cancer patients, sequencing normal DNA can increase the overall understanding of cancer, including finding cancer predisposition due to germline genome changes, said Victor Velculescu, MD, PhD, of Johns Hopkins University School of Medicine in Baltimore, Maryland.
In this study, the germline analyses revealed changes in cancer-related genes in 3% of the patients who had no known signs of genetically linked cancer.
“These analyses can help us find alterations in cancer-predisposing genes in ways that weren’t previously appreciated,” Dr Velculescu said.
He also acknowledged, however, that there are challenges to implementing tumor-normal DNA analyses in a clinical setting. These include the additional work and costs of sequencing and analyzing a patient’s normal tissue along with his or her tumor tissue.
Costs for tumor gene sequencing begin at several thousand dollars, which would increase if sequencing was done on DNA from normal tissue as well. And health insurance may not fully cover normal-tissue genetic sequencing. ![]()
Technique helps determine DLBCL subtypes

Photo by Darren Baker
A new technique can quickly and easily differentiate the two major subtypes of diffuse large B-cell lymphoma (DLBCL), researchers have reported in The Journal of Molecular Diagnostics.
The method is based on a reverse transcriptase multiplex ligation-dependent probe amplification (RT-MLPA) assay and 14 gene signatures.
It proved as accurate as the gold standard technology for identifying germinal center B-cell-like (GCB) and activated B-cell-like (ABC) DLBCL.
So the researchers believe this RT-MLPA-based assay could help clinicians evaluate a patient’s prognosis and choose the optimal therapy for a person with DLBCL.
“Differences in the progression of the disease and clinical outcomes can, at least in part, be explained by the heterogeneity of lymphoma, which can be classified into two major subtypes with different outcomes,” said study author Philippe Ruminy, PhD, of the University of Rouen in France.
“Unfortunately, these lymphomas are morphologically undistinguishable in routine diagnosis, which is a major problem for the development of targeted therapies. Furthermore, array-based gene expression profiling (GEP), which is considered the gold standard for discriminating these tumors, remains poorly transposable to routine diagnosis, and the surrogate immunohistochemical (IHC) algorithms that have been proposed are often considered poorly reliable.”
With this in mind, Dr Ruminy and his colleagues tested the RT-MLPA-based assay alongside GEP techniques in samples from 259 patients with de novo DLBCL.
The team used a series of 195 patients from a single institution to train and validate the new technique. Of these patients, 115 had a classification determined with a Veracode DASL assay, 100 had an IHC classification, and 135 had survival data. A second series of 64 patients that were previously analyzed by Affymetrix U133+2 GEP arrays served as an external validation cohort.
When the researchers looked at 50 patients randomly selected from the training cohort, they found that the RT-MLPA-based assay classified 90% of the cases within the expected subtypes (20 GCB and 25 ABC). The remaining 10% (1 GCB and 4 ABC) were considered unclassified.
In the external validation cohort, the RT-MLPA-based assay classified 80% of cases within the expected subtypes (24 ABC and 28 GCB). However, 13.8% were considered unclassified (3 GCB and 6 ABC), and 4 were misclassified.
The researchers also found the RT-MLPA-based assay was sensitive for analyzing archived formalin-fixed, paraffin-embedded (FFPE) tissue samples. A comparison of samples from paired frozen and FFPE biopsies showed that the technique correctly classified 89.3% of 28 cases.
“Because RT-MLPA requires only short cDNA fragments for the correct binding and ligation of the gene-specific oligonucleotide probes, it is less affected by the use of low RNA concentrations and RNA degradation,” Dr Ruminy said.
“It could thus be used for the retrospective analysis of archival collections and for the inclusion of patients in prospective clinical trials, because only a few institutions routinely collect frozen biopsy material.”
To evaluate the prognostic value of the assay, the researchers looked at survival in 135 treated DLBCL patients who were diagnosed between 2001 and 2011.
Patients determined to have the ABC subtype by the RT-MLPA-based assay had significantly worse progression-free survival and overall survival than patients with the GCB subtype. And the expression of several individual genes within the MLPA signature was significantly associated with prognosis (ie, high LMO2, high BCL6, and low TNFRSF13B expression).
“The robust and cost-effective RT-MLPA assay can yield results within one day and requires reagents costing less than $5 per sample,” Dr Ruminy said. “Since RT-MLPA utilizes materials and equipment that are standard in many laboratories, the process can easily be implemented for routine use.” ![]()
Photo by Darren Baker
A new technique can quickly and easily differentiate the two major subtypes of diffuse large B-cell lymphoma (DLBCL), researchers have reported in The Journal of Molecular Diagnostics.
The method is based on a reverse transcriptase multiplex ligation-dependent probe amplification (RT-MLPA) assay and 14 gene signatures.
It proved as accurate as the gold standard technology for identifying germinal center B-cell-like (GCB) and activated B-cell-like (ABC) DLBCL.
So the researchers believe this RT-MLPA-based assay could help clinicians evaluate a patient’s prognosis and choose the optimal therapy for a person with DLBCL.
“Differences in the progression of the disease and clinical outcomes can, at least in part, be explained by the heterogeneity of lymphoma, which can be classified into two major subtypes with different outcomes,” said study author Philippe Ruminy, PhD, of the University of Rouen in France.
“Unfortunately, these lymphomas are morphologically undistinguishable in routine diagnosis, which is a major problem for the development of targeted therapies. Furthermore, array-based gene expression profiling (GEP), which is considered the gold standard for discriminating these tumors, remains poorly transposable to routine diagnosis, and the surrogate immunohistochemical (IHC) algorithms that have been proposed are often considered poorly reliable.”
With this in mind, Dr Ruminy and his colleagues tested the RT-MLPA-based assay alongside GEP techniques in samples from 259 patients with de novo DLBCL.
The team used a series of 195 patients from a single institution to train and validate the new technique. Of these patients, 115 had a classification determined with a Veracode DASL assay, 100 had an IHC classification, and 135 had survival data. A second series of 64 patients that were previously analyzed by Affymetrix U133+2 GEP arrays served as an external validation cohort.
When the researchers looked at 50 patients randomly selected from the training cohort, they found that the RT-MLPA-based assay classified 90% of the cases within the expected subtypes (20 GCB and 25 ABC). The remaining 10% (1 GCB and 4 ABC) were considered unclassified.
In the external validation cohort, the RT-MLPA-based assay classified 80% of cases within the expected subtypes (24 ABC and 28 GCB). However, 13.8% were considered unclassified (3 GCB and 6 ABC), and 4 were misclassified.
The researchers also found the RT-MLPA-based assay was sensitive for analyzing archived formalin-fixed, paraffin-embedded (FFPE) tissue samples. A comparison of samples from paired frozen and FFPE biopsies showed that the technique correctly classified 89.3% of 28 cases.
“Because RT-MLPA requires only short cDNA fragments for the correct binding and ligation of the gene-specific oligonucleotide probes, it is less affected by the use of low RNA concentrations and RNA degradation,” Dr Ruminy said.
“It could thus be used for the retrospective analysis of archival collections and for the inclusion of patients in prospective clinical trials, because only a few institutions routinely collect frozen biopsy material.”
To evaluate the prognostic value of the assay, the researchers looked at survival in 135 treated DLBCL patients who were diagnosed between 2001 and 2011.
Patients determined to have the ABC subtype by the RT-MLPA-based assay had significantly worse progression-free survival and overall survival than patients with the GCB subtype. And the expression of several individual genes within the MLPA signature was significantly associated with prognosis (ie, high LMO2, high BCL6, and low TNFRSF13B expression).
“The robust and cost-effective RT-MLPA assay can yield results within one day and requires reagents costing less than $5 per sample,” Dr Ruminy said. “Since RT-MLPA utilizes materials and equipment that are standard in many laboratories, the process can easily be implemented for routine use.” ![]()
Photo by Darren Baker
A new technique can quickly and easily differentiate the two major subtypes of diffuse large B-cell lymphoma (DLBCL), researchers have reported in The Journal of Molecular Diagnostics.
The method is based on a reverse transcriptase multiplex ligation-dependent probe amplification (RT-MLPA) assay and 14 gene signatures.
It proved as accurate as the gold standard technology for identifying germinal center B-cell-like (GCB) and activated B-cell-like (ABC) DLBCL.
So the researchers believe this RT-MLPA-based assay could help clinicians evaluate a patient’s prognosis and choose the optimal therapy for a person with DLBCL.
“Differences in the progression of the disease and clinical outcomes can, at least in part, be explained by the heterogeneity of lymphoma, which can be classified into two major subtypes with different outcomes,” said study author Philippe Ruminy, PhD, of the University of Rouen in France.
“Unfortunately, these lymphomas are morphologically undistinguishable in routine diagnosis, which is a major problem for the development of targeted therapies. Furthermore, array-based gene expression profiling (GEP), which is considered the gold standard for discriminating these tumors, remains poorly transposable to routine diagnosis, and the surrogate immunohistochemical (IHC) algorithms that have been proposed are often considered poorly reliable.”
With this in mind, Dr Ruminy and his colleagues tested the RT-MLPA-based assay alongside GEP techniques in samples from 259 patients with de novo DLBCL.
The team used a series of 195 patients from a single institution to train and validate the new technique. Of these patients, 115 had a classification determined with a Veracode DASL assay, 100 had an IHC classification, and 135 had survival data. A second series of 64 patients that were previously analyzed by Affymetrix U133+2 GEP arrays served as an external validation cohort.
When the researchers looked at 50 patients randomly selected from the training cohort, they found that the RT-MLPA-based assay classified 90% of the cases within the expected subtypes (20 GCB and 25 ABC). The remaining 10% (1 GCB and 4 ABC) were considered unclassified.
In the external validation cohort, the RT-MLPA-based assay classified 80% of cases within the expected subtypes (24 ABC and 28 GCB). However, 13.8% were considered unclassified (3 GCB and 6 ABC), and 4 were misclassified.
The researchers also found the RT-MLPA-based assay was sensitive for analyzing archived formalin-fixed, paraffin-embedded (FFPE) tissue samples. A comparison of samples from paired frozen and FFPE biopsies showed that the technique correctly classified 89.3% of 28 cases.
“Because RT-MLPA requires only short cDNA fragments for the correct binding and ligation of the gene-specific oligonucleotide probes, it is less affected by the use of low RNA concentrations and RNA degradation,” Dr Ruminy said.
“It could thus be used for the retrospective analysis of archival collections and for the inclusion of patients in prospective clinical trials, because only a few institutions routinely collect frozen biopsy material.”
To evaluate the prognostic value of the assay, the researchers looked at survival in 135 treated DLBCL patients who were diagnosed between 2001 and 2011.
Patients determined to have the ABC subtype by the RT-MLPA-based assay had significantly worse progression-free survival and overall survival than patients with the GCB subtype. And the expression of several individual genes within the MLPA signature was significantly associated with prognosis (ie, high LMO2, high BCL6, and low TNFRSF13B expression).
“The robust and cost-effective RT-MLPA assay can yield results within one day and requires reagents costing less than $5 per sample,” Dr Ruminy said. “Since RT-MLPA utilizes materials and equipment that are standard in many laboratories, the process can easily be implemented for routine use.” ![]()
Team uncovers new role for macrophages

pseudopodia to engulf particles
Macrophages can substitute for dendritic cells as primers of T-cell-dependent immune responses, according to research published in Proceedings of the National Academy of Sciences.
The study showed that macrophages that function as a first line of defense in the innate immune system can also present antigens to T cells, a previously unknown role for macrophages in the induction of adaptive immune responses.
“It has been assumed until now that the dendritic cells are considered to be essentially the only cell type responsible for antigen presentation in the immune system,” said Dr Thomas Brocker, of Ludwig-Maximilians-Universität München in Germany.
“We have now discovered that macrophages can also do this job. Not only that, in certain situations, they can be more effective than dendritic cells.”
Dendritic cells present antigens to cytotoxic T lymphocytes (CTLs) if they have been directly infected, but they can also capture and display antigens from other cells. This type of indirect antigen presentation is referred to as cross-presentation.
“So, theoretically, dendritic cells could be responsible for the induction of all CTL-based responses, regardless of whether they are themselves infected or not,” Dr Brocker said. “But the significance of cross-presentation is hotly debated in the literature.”
Dr Brocker and his team used several antigens that were specifically targeted to and processed by macrophages but could not be taken up directly by dendritic cells. They were able to demonstrate that each antigen induced a normal immune response in a mouse model system, and even in a mouse strain that lacked dendritic cells altogether.
Further experiments showed the targeted macrophages were actually able to prime a more comprehensive immune reaction than cross-presenting dendritic cells. They activated T cells specific for all antigen-binding sites (epitopes) presented, whereas cross-presentation by dendritic cells stimulates only those T cells that recognize immunodominant epitopes.
“Macrophages naturally function as filters,” Dr Brocker noted. “They gobble everything up that might be harmful to the organism. And our study shows that, in contrast to cross-priming dendritic cells, they are capable of producing and presenting all T-cell-priming epitopes we tested. Macrophages therefore induce a complete immune response. These observations indicate that the significance of cross-presentation by dendritic cells has been overrated.”
He added that these findings are relevant for the development of immunization strategies.
“Preclinical trials are already underway with vaccines that are designed to activate specific sets of dendritic cells,” Dr Brocker said. “But the weak epitopes are important for a broadly directed immune response, because they can potentially recognize mutant variants of viruses, for instance.”
“Cross-priming dendritic cells fail to induce weakly antigenic epitopes, as our study shows. Our results indicate that it may make more sense to manipulate macrophages directly because they stimulate a wider-ranging immune response.” ![]()
pseudopodia to engulf particles
Macrophages can substitute for dendritic cells as primers of T-cell-dependent immune responses, according to research published in Proceedings of the National Academy of Sciences.
The study showed that macrophages that function as a first line of defense in the innate immune system can also present antigens to T cells, a previously unknown role for macrophages in the induction of adaptive immune responses.
“It has been assumed until now that the dendritic cells are considered to be essentially the only cell type responsible for antigen presentation in the immune system,” said Dr Thomas Brocker, of Ludwig-Maximilians-Universität München in Germany.
“We have now discovered that macrophages can also do this job. Not only that, in certain situations, they can be more effective than dendritic cells.”
Dendritic cells present antigens to cytotoxic T lymphocytes (CTLs) if they have been directly infected, but they can also capture and display antigens from other cells. This type of indirect antigen presentation is referred to as cross-presentation.
“So, theoretically, dendritic cells could be responsible for the induction of all CTL-based responses, regardless of whether they are themselves infected or not,” Dr Brocker said. “But the significance of cross-presentation is hotly debated in the literature.”
Dr Brocker and his team used several antigens that were specifically targeted to and processed by macrophages but could not be taken up directly by dendritic cells. They were able to demonstrate that each antigen induced a normal immune response in a mouse model system, and even in a mouse strain that lacked dendritic cells altogether.
Further experiments showed the targeted macrophages were actually able to prime a more comprehensive immune reaction than cross-presenting dendritic cells. They activated T cells specific for all antigen-binding sites (epitopes) presented, whereas cross-presentation by dendritic cells stimulates only those T cells that recognize immunodominant epitopes.
“Macrophages naturally function as filters,” Dr Brocker noted. “They gobble everything up that might be harmful to the organism. And our study shows that, in contrast to cross-priming dendritic cells, they are capable of producing and presenting all T-cell-priming epitopes we tested. Macrophages therefore induce a complete immune response. These observations indicate that the significance of cross-presentation by dendritic cells has been overrated.”
He added that these findings are relevant for the development of immunization strategies.
“Preclinical trials are already underway with vaccines that are designed to activate specific sets of dendritic cells,” Dr Brocker said. “But the weak epitopes are important for a broadly directed immune response, because they can potentially recognize mutant variants of viruses, for instance.”
“Cross-priming dendritic cells fail to induce weakly antigenic epitopes, as our study shows. Our results indicate that it may make more sense to manipulate macrophages directly because they stimulate a wider-ranging immune response.” ![]()
pseudopodia to engulf particles
Macrophages can substitute for dendritic cells as primers of T-cell-dependent immune responses, according to research published in Proceedings of the National Academy of Sciences.
The study showed that macrophages that function as a first line of defense in the innate immune system can also present antigens to T cells, a previously unknown role for macrophages in the induction of adaptive immune responses.
“It has been assumed until now that the dendritic cells are considered to be essentially the only cell type responsible for antigen presentation in the immune system,” said Dr Thomas Brocker, of Ludwig-Maximilians-Universität München in Germany.
“We have now discovered that macrophages can also do this job. Not only that, in certain situations, they can be more effective than dendritic cells.”
Dendritic cells present antigens to cytotoxic T lymphocytes (CTLs) if they have been directly infected, but they can also capture and display antigens from other cells. This type of indirect antigen presentation is referred to as cross-presentation.
“So, theoretically, dendritic cells could be responsible for the induction of all CTL-based responses, regardless of whether they are themselves infected or not,” Dr Brocker said. “But the significance of cross-presentation is hotly debated in the literature.”
Dr Brocker and his team used several antigens that were specifically targeted to and processed by macrophages but could not be taken up directly by dendritic cells. They were able to demonstrate that each antigen induced a normal immune response in a mouse model system, and even in a mouse strain that lacked dendritic cells altogether.
Further experiments showed the targeted macrophages were actually able to prime a more comprehensive immune reaction than cross-presenting dendritic cells. They activated T cells specific for all antigen-binding sites (epitopes) presented, whereas cross-presentation by dendritic cells stimulates only those T cells that recognize immunodominant epitopes.
“Macrophages naturally function as filters,” Dr Brocker noted. “They gobble everything up that might be harmful to the organism. And our study shows that, in contrast to cross-priming dendritic cells, they are capable of producing and presenting all T-cell-priming epitopes we tested. Macrophages therefore induce a complete immune response. These observations indicate that the significance of cross-presentation by dendritic cells has been overrated.”
He added that these findings are relevant for the development of immunization strategies.
“Preclinical trials are already underway with vaccines that are designed to activate specific sets of dendritic cells,” Dr Brocker said. “But the weak epitopes are important for a broadly directed immune response, because they can potentially recognize mutant variants of viruses, for instance.”
“Cross-priming dendritic cells fail to induce weakly antigenic epitopes, as our study shows. Our results indicate that it may make more sense to manipulate macrophages directly because they stimulate a wider-ranging immune response.” ![]()
RCOG releases new VTE guidelines

Photo by Nina Matthews
The Royal College of Obstetricians and Gynaecologists (RCOG) has released new guidelines for treating and preventing venous thromboembolism (VTE) during pregnancy, birth, and following delivery.
“These updated guidelines provide new evidence about risk factors for thrombosis in pregnancy and strategies that should be employed to reduce the chances of a thrombosis occurring,” said Andrew Thomson, MD, cochair of the RCOG guidelines committee.
“Furthermore, the guidelines provide updated information on the way women with a suspected thrombosis should be investigated and treated.”
VTE is uncommon in pregnancy or in the first 6 weeks postnatally, and the absolute risk of VTE is around 1 in 1000 pregnancies. It can occur at any stage in pregnancy, but the time of the highest risk is the first 6 weeks following birth, when the risk increases 20-fold.
Risk factors include previous VTE or thrombophilia, obesity, increased maternal age, immobility and long-distance travel, admission to hospital during pregnancy, and other comorbidities such as heart disease, inflammatory bowel disease, and pre-eclampsia.
Additional risk factors occurring during the first trimester of pregnancy include hyperemesis gravidarum, ovarian hyperstimulation, and in vitro fertilization pregnancy. Caesarean section is also a risk factor.
The guidelines emphasize that all women should undergo a thorough assessment for VTE in early pregnancy or prepregnancy and again intrapartum or immediately postpartum.
Any woman with risk factors should be considered for prophylactic low-molecular-weight heparin. The duration of treatment depends on the number of risk factors a woman has. It may be offered both antenatally and after the baby is born.
In addition, women with previous VTE must be offered prepregnancy counseling. A prospective management plan for VTE should also be made, including appropriate treatment to be offered as early as possible and a careful history documented.
The guidance on treating VTE focuses on the acute management of the condition and highlights the signs and symptoms, including leg pain and swelling, lower abdominal pain, shortness of breath, chest pain, coughing blood, and collapse.
Any woman presenting with signs and symptoms suggestive of VTE should be tested for the condition immediately and offered treatment with low-molecular-weight heparin.
All hospitals should have a protocol for the diagnosis of suspected VTE, with the involvement of a multidisciplinary team of obstetricians, radiologists, physicians, and hematologists.
“This guidance provides clinicians with accurate, scientific-based guidelines on the risk factors for VTE, as well as on how to prevent and treat the condition,” said guideline author Catherine Nelson-Piercy, MBBS, of Guy’s and St. Thomas’ NHS Foundation Trust in London, UK.
“It is vital that VTE is discussed with all women who are at risk, and the reasons for individual treatment recommendations must also be explained.” ![]()
Photo by Nina Matthews
The Royal College of Obstetricians and Gynaecologists (RCOG) has released new guidelines for treating and preventing venous thromboembolism (VTE) during pregnancy, birth, and following delivery.
“These updated guidelines provide new evidence about risk factors for thrombosis in pregnancy and strategies that should be employed to reduce the chances of a thrombosis occurring,” said Andrew Thomson, MD, cochair of the RCOG guidelines committee.
“Furthermore, the guidelines provide updated information on the way women with a suspected thrombosis should be investigated and treated.”
VTE is uncommon in pregnancy or in the first 6 weeks postnatally, and the absolute risk of VTE is around 1 in 1000 pregnancies. It can occur at any stage in pregnancy, but the time of the highest risk is the first 6 weeks following birth, when the risk increases 20-fold.
Risk factors include previous VTE or thrombophilia, obesity, increased maternal age, immobility and long-distance travel, admission to hospital during pregnancy, and other comorbidities such as heart disease, inflammatory bowel disease, and pre-eclampsia.
Additional risk factors occurring during the first trimester of pregnancy include hyperemesis gravidarum, ovarian hyperstimulation, and in vitro fertilization pregnancy. Caesarean section is also a risk factor.
The guidelines emphasize that all women should undergo a thorough assessment for VTE in early pregnancy or prepregnancy and again intrapartum or immediately postpartum.
Any woman with risk factors should be considered for prophylactic low-molecular-weight heparin. The duration of treatment depends on the number of risk factors a woman has. It may be offered both antenatally and after the baby is born.
In addition, women with previous VTE must be offered prepregnancy counseling. A prospective management plan for VTE should also be made, including appropriate treatment to be offered as early as possible and a careful history documented.
The guidance on treating VTE focuses on the acute management of the condition and highlights the signs and symptoms, including leg pain and swelling, lower abdominal pain, shortness of breath, chest pain, coughing blood, and collapse.
Any woman presenting with signs and symptoms suggestive of VTE should be tested for the condition immediately and offered treatment with low-molecular-weight heparin.
All hospitals should have a protocol for the diagnosis of suspected VTE, with the involvement of a multidisciplinary team of obstetricians, radiologists, physicians, and hematologists.
“This guidance provides clinicians with accurate, scientific-based guidelines on the risk factors for VTE, as well as on how to prevent and treat the condition,” said guideline author Catherine Nelson-Piercy, MBBS, of Guy’s and St. Thomas’ NHS Foundation Trust in London, UK.
“It is vital that VTE is discussed with all women who are at risk, and the reasons for individual treatment recommendations must also be explained.” ![]()
Photo by Nina Matthews
The Royal College of Obstetricians and Gynaecologists (RCOG) has released new guidelines for treating and preventing venous thromboembolism (VTE) during pregnancy, birth, and following delivery.
“These updated guidelines provide new evidence about risk factors for thrombosis in pregnancy and strategies that should be employed to reduce the chances of a thrombosis occurring,” said Andrew Thomson, MD, cochair of the RCOG guidelines committee.
“Furthermore, the guidelines provide updated information on the way women with a suspected thrombosis should be investigated and treated.”
VTE is uncommon in pregnancy or in the first 6 weeks postnatally, and the absolute risk of VTE is around 1 in 1000 pregnancies. It can occur at any stage in pregnancy, but the time of the highest risk is the first 6 weeks following birth, when the risk increases 20-fold.
Risk factors include previous VTE or thrombophilia, obesity, increased maternal age, immobility and long-distance travel, admission to hospital during pregnancy, and other comorbidities such as heart disease, inflammatory bowel disease, and pre-eclampsia.
Additional risk factors occurring during the first trimester of pregnancy include hyperemesis gravidarum, ovarian hyperstimulation, and in vitro fertilization pregnancy. Caesarean section is also a risk factor.
The guidelines emphasize that all women should undergo a thorough assessment for VTE in early pregnancy or prepregnancy and again intrapartum or immediately postpartum.
Any woman with risk factors should be considered for prophylactic low-molecular-weight heparin. The duration of treatment depends on the number of risk factors a woman has. It may be offered both antenatally and after the baby is born.
In addition, women with previous VTE must be offered prepregnancy counseling. A prospective management plan for VTE should also be made, including appropriate treatment to be offered as early as possible and a careful history documented.
The guidance on treating VTE focuses on the acute management of the condition and highlights the signs and symptoms, including leg pain and swelling, lower abdominal pain, shortness of breath, chest pain, coughing blood, and collapse.
Any woman presenting with signs and symptoms suggestive of VTE should be tested for the condition immediately and offered treatment with low-molecular-weight heparin.
All hospitals should have a protocol for the diagnosis of suspected VTE, with the involvement of a multidisciplinary team of obstetricians, radiologists, physicians, and hematologists.
“This guidance provides clinicians with accurate, scientific-based guidelines on the risk factors for VTE, as well as on how to prevent and treat the condition,” said guideline author Catherine Nelson-Piercy, MBBS, of Guy’s and St. Thomas’ NHS Foundation Trust in London, UK.
“It is vital that VTE is discussed with all women who are at risk, and the reasons for individual treatment recommendations must also be explained.” ![]()