User login
California Dreamin’
Project BOOST, SHM’s popular mentorship program designed to help hospitals reduce readmissions, is headed to the most populous state in the country. In a joint venture with the California HealthCare Foundation, Project BOOST (Better Outcomes for Older Adults through Safe Transitions) will launch a groundbreaking, two-year program in 20 hospitals in the Golden State.
The California HealthCare Founda-tion will cover almost half of the $28,000 in tuition costs for each hospital accepted into the collaborative program. Individual sites will be responsible for the other $14,500.
In year one, hospitals will begin improving their discharge procedures using Project BOOST’s toolkit and one-on-one mentorships with leaders in the field. The second year of the project will focus on training additional mentors in California. The foundation has committed not only to improving outcomes in the first 20 sites, but also building a sustainable infrastructure that will allow gains to quickly spread throughout the state.
Recruiting for the California sites has just begun. Potential applicants can visit www.hospitalmedicine.org/boost for more information.
“California is a microcosm for the challenges and opportunities for hospitalized care in our healthcare system,” says Janet Nagamine, RN, MD, SFHM, program leader for the California BOOST program and an SHM board member. “We are very excited to work with the California HealthCare Foundation, one of the state’s leaders in healthcare quality improvement. … Their support will help California’s hospitals and primary-care physicians [PCPs] safely transition patients from hospital to home during that vulnerable period.”

Project BOOST’s Continued Expansion
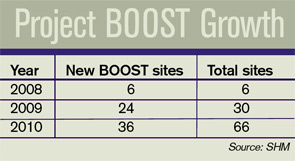
The California program will be SHM’s largest state-specific program to date, representing the fourth wave of BOOST’s continued expansion. With the support of the John A. Hartford Foundation, the program began with six pilot sites throughout the country in 2008. In 2009, Hartford funded 24 additional sites.
In January, SHM, the University of Michigan, and Blue Cross Blue Shield of Michigan announced the first state-specific Project BOOST program. The three organizations announced Michigan’s 14 participating sites in May.
Two other hospital sites began implementing Project BOOST on a tuition-based model in May.
Readmission Challenge
Most hospitalists are intimately familiar with the challenges involved with transitions of care. Research in the April 2009 New England Journal of Medicine by Stephen F. Jencks, MD, MPH, Mark V. Williams, MD, FHM, and Eric A. Coleman, MD, MPH, indicates that 1 in 5 hospitalized patients is readmitted to the hospital within a month of their discharge.1
Balancing the three-legged stool of communication between the hospitalist, PCP, and patient can be demanding. For the individual hospitalist or PCP, it requires intense attention to detail, strong communication skills, and patience. For hospitals, safe transitions require a systemic, team-based approach.
But the alternative—continued or increased readmissions after discharge—is even more taxing. The study found that unplanned readmissions cost Medicare $17.4 billion each year, making estimates of the total cost even higher.1
Looking beyond the costs directly associated with readmissions, the study’s authors see the issue as a potential vital sign that could assess overall healthcare quality. “Although the readmission rate is often presented as a measure of the performance of hospitals, it may also be a useful indicator of the performance of our healthcare system,” they write.
The Approach: Gain Traction, Results
Rather than forcing a one-size-fits-all process on every hospital site, Project BOOST provides individual hospitals with the capacity and experience necessary to implement processes that best fit their unique situation.
Project BOOST sites participate in a two-pronged program consisting of a yearlong, one-on-one mentorship with the leaders in the field. It begins with an intensive, two-day conference and the Project BOOST toolkit.
The toolkit includes printed materials and a new DVD for use by hospitalists and other care providers to facilitate communication with patients and caregivers during discharge.
New case studies published by SHM document some of the program’s earliest successes.
At Piedmont Hospital, a 481-bed acute-care hospital near Atlanta, the full implementation of Project BOOST in one hospital unit has improved many of its “vital signs” in comparison with units that have not implemented BOOST, including decreased length of stay and lower 30-day readmissions (see “Piedmont Hospital: Project BOOST unit vs. regular hospital units,” p. 6).
For St. Mary’s Medical Center, a 582-bed community teaching hospital in St. Louis, hospitalists implementing Project BOOST made a major difference in just three months:
Not only did the Project BOOST unit nearly halve 30-day readmissions (7% from 12%), but the program also increased patient satisfaction, to 68% from 52%.
BOOSTing into the Future
Project BOOST benefits haven’t been limited to program sites and their patients. New innovations from the mentored implementation program have led to resources that all hospitals can use.
SHM recently introduced a new DVD and curriculum package that teaches nurses and discharge planners to use the “teachback” method to communicate with patients during the discharge process. It helps ensure that patients fully understand their care plans and post-discharge instructions.
The teachback package is available at the SHM online store (www.hospitalmedicine.org); it is $85 for SHM members and $125 for nonmembers.
SHM has also launched a BOOST data center and a BOOST community site. The data center enables sites to enter, track, and benchmark key outcomes, which can then be evaluated against comparison units at their own hospitals, BOOST averages, and subsets of hospitals with similar characteristics. The BOOST community site facilitates the sharing of ideas and documents between BOOST hospitals.
New funding approaches will help Project BOOST to continue to reach more hospitals. Since its inception, third parties have provided financial resources for the program.
Now, SHM is offering a tuition-based model, open to hospitals nationwide, which is set to begin this fall.
SHM is accepting applications at www.hospitalmedicine.org/boost. TH
Brendon Shank is a freelance writer based in Philadelphia.
Reference
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Eng J Med. 2009:360:1418-1428.
Project BOOST, SHM’s popular mentorship program designed to help hospitals reduce readmissions, is headed to the most populous state in the country. In a joint venture with the California HealthCare Foundation, Project BOOST (Better Outcomes for Older Adults through Safe Transitions) will launch a groundbreaking, two-year program in 20 hospitals in the Golden State.
The California HealthCare Founda-tion will cover almost half of the $28,000 in tuition costs for each hospital accepted into the collaborative program. Individual sites will be responsible for the other $14,500.
In year one, hospitals will begin improving their discharge procedures using Project BOOST’s toolkit and one-on-one mentorships with leaders in the field. The second year of the project will focus on training additional mentors in California. The foundation has committed not only to improving outcomes in the first 20 sites, but also building a sustainable infrastructure that will allow gains to quickly spread throughout the state.
Recruiting for the California sites has just begun. Potential applicants can visit www.hospitalmedicine.org/boost for more information.
“California is a microcosm for the challenges and opportunities for hospitalized care in our healthcare system,” says Janet Nagamine, RN, MD, SFHM, program leader for the California BOOST program and an SHM board member. “We are very excited to work with the California HealthCare Foundation, one of the state’s leaders in healthcare quality improvement. … Their support will help California’s hospitals and primary-care physicians [PCPs] safely transition patients from hospital to home during that vulnerable period.”
Project BOOST’s Continued Expansion
The California program will be SHM’s largest state-specific program to date, representing the fourth wave of BOOST’s continued expansion. With the support of the John A. Hartford Foundation, the program began with six pilot sites throughout the country in 2008. In 2009, Hartford funded 24 additional sites.
In January, SHM, the University of Michigan, and Blue Cross Blue Shield of Michigan announced the first state-specific Project BOOST program. The three organizations announced Michigan’s 14 participating sites in May.
Two other hospital sites began implementing Project BOOST on a tuition-based model in May.
Readmission Challenge
Most hospitalists are intimately familiar with the challenges involved with transitions of care. Research in the April 2009 New England Journal of Medicine by Stephen F. Jencks, MD, MPH, Mark V. Williams, MD, FHM, and Eric A. Coleman, MD, MPH, indicates that 1 in 5 hospitalized patients is readmitted to the hospital within a month of their discharge.1
Balancing the three-legged stool of communication between the hospitalist, PCP, and patient can be demanding. For the individual hospitalist or PCP, it requires intense attention to detail, strong communication skills, and patience. For hospitals, safe transitions require a systemic, team-based approach.
But the alternative—continued or increased readmissions after discharge—is even more taxing. The study found that unplanned readmissions cost Medicare $17.4 billion each year, making estimates of the total cost even higher.1
Looking beyond the costs directly associated with readmissions, the study’s authors see the issue as a potential vital sign that could assess overall healthcare quality. “Although the readmission rate is often presented as a measure of the performance of hospitals, it may also be a useful indicator of the performance of our healthcare system,” they write.
The Approach: Gain Traction, Results
Rather than forcing a one-size-fits-all process on every hospital site, Project BOOST provides individual hospitals with the capacity and experience necessary to implement processes that best fit their unique situation.
Project BOOST sites participate in a two-pronged program consisting of a yearlong, one-on-one mentorship with the leaders in the field. It begins with an intensive, two-day conference and the Project BOOST toolkit.
The toolkit includes printed materials and a new DVD for use by hospitalists and other care providers to facilitate communication with patients and caregivers during discharge.
New case studies published by SHM document some of the program’s earliest successes.
At Piedmont Hospital, a 481-bed acute-care hospital near Atlanta, the full implementation of Project BOOST in one hospital unit has improved many of its “vital signs” in comparison with units that have not implemented BOOST, including decreased length of stay and lower 30-day readmissions (see “Piedmont Hospital: Project BOOST unit vs. regular hospital units,” p. 6).
For St. Mary’s Medical Center, a 582-bed community teaching hospital in St. Louis, hospitalists implementing Project BOOST made a major difference in just three months:
Not only did the Project BOOST unit nearly halve 30-day readmissions (7% from 12%), but the program also increased patient satisfaction, to 68% from 52%.
BOOSTing into the Future
Project BOOST benefits haven’t been limited to program sites and their patients. New innovations from the mentored implementation program have led to resources that all hospitals can use.
SHM recently introduced a new DVD and curriculum package that teaches nurses and discharge planners to use the “teachback” method to communicate with patients during the discharge process. It helps ensure that patients fully understand their care plans and post-discharge instructions.
The teachback package is available at the SHM online store (www.hospitalmedicine.org); it is $85 for SHM members and $125 for nonmembers.
SHM has also launched a BOOST data center and a BOOST community site. The data center enables sites to enter, track, and benchmark key outcomes, which can then be evaluated against comparison units at their own hospitals, BOOST averages, and subsets of hospitals with similar characteristics. The BOOST community site facilitates the sharing of ideas and documents between BOOST hospitals.
New funding approaches will help Project BOOST to continue to reach more hospitals. Since its inception, third parties have provided financial resources for the program.
Now, SHM is offering a tuition-based model, open to hospitals nationwide, which is set to begin this fall.
SHM is accepting applications at www.hospitalmedicine.org/boost. TH
Brendon Shank is a freelance writer based in Philadelphia.
Reference
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Eng J Med. 2009:360:1418-1428.
Project BOOST, SHM’s popular mentorship program designed to help hospitals reduce readmissions, is headed to the most populous state in the country. In a joint venture with the California HealthCare Foundation, Project BOOST (Better Outcomes for Older Adults through Safe Transitions) will launch a groundbreaking, two-year program in 20 hospitals in the Golden State.
The California HealthCare Founda-tion will cover almost half of the $28,000 in tuition costs for each hospital accepted into the collaborative program. Individual sites will be responsible for the other $14,500.
In year one, hospitals will begin improving their discharge procedures using Project BOOST’s toolkit and one-on-one mentorships with leaders in the field. The second year of the project will focus on training additional mentors in California. The foundation has committed not only to improving outcomes in the first 20 sites, but also building a sustainable infrastructure that will allow gains to quickly spread throughout the state.
Recruiting for the California sites has just begun. Potential applicants can visit www.hospitalmedicine.org/boost for more information.
“California is a microcosm for the challenges and opportunities for hospitalized care in our healthcare system,” says Janet Nagamine, RN, MD, SFHM, program leader for the California BOOST program and an SHM board member. “We are very excited to work with the California HealthCare Foundation, one of the state’s leaders in healthcare quality improvement. … Their support will help California’s hospitals and primary-care physicians [PCPs] safely transition patients from hospital to home during that vulnerable period.”
Project BOOST’s Continued Expansion
The California program will be SHM’s largest state-specific program to date, representing the fourth wave of BOOST’s continued expansion. With the support of the John A. Hartford Foundation, the program began with six pilot sites throughout the country in 2008. In 2009, Hartford funded 24 additional sites.
In January, SHM, the University of Michigan, and Blue Cross Blue Shield of Michigan announced the first state-specific Project BOOST program. The three organizations announced Michigan’s 14 participating sites in May.
Two other hospital sites began implementing Project BOOST on a tuition-based model in May.
Readmission Challenge
Most hospitalists are intimately familiar with the challenges involved with transitions of care. Research in the April 2009 New England Journal of Medicine by Stephen F. Jencks, MD, MPH, Mark V. Williams, MD, FHM, and Eric A. Coleman, MD, MPH, indicates that 1 in 5 hospitalized patients is readmitted to the hospital within a month of their discharge.1
Balancing the three-legged stool of communication between the hospitalist, PCP, and patient can be demanding. For the individual hospitalist or PCP, it requires intense attention to detail, strong communication skills, and patience. For hospitals, safe transitions require a systemic, team-based approach.
But the alternative—continued or increased readmissions after discharge—is even more taxing. The study found that unplanned readmissions cost Medicare $17.4 billion each year, making estimates of the total cost even higher.1
Looking beyond the costs directly associated with readmissions, the study’s authors see the issue as a potential vital sign that could assess overall healthcare quality. “Although the readmission rate is often presented as a measure of the performance of hospitals, it may also be a useful indicator of the performance of our healthcare system,” they write.
The Approach: Gain Traction, Results
Rather than forcing a one-size-fits-all process on every hospital site, Project BOOST provides individual hospitals with the capacity and experience necessary to implement processes that best fit their unique situation.
Project BOOST sites participate in a two-pronged program consisting of a yearlong, one-on-one mentorship with the leaders in the field. It begins with an intensive, two-day conference and the Project BOOST toolkit.
The toolkit includes printed materials and a new DVD for use by hospitalists and other care providers to facilitate communication with patients and caregivers during discharge.
New case studies published by SHM document some of the program’s earliest successes.
At Piedmont Hospital, a 481-bed acute-care hospital near Atlanta, the full implementation of Project BOOST in one hospital unit has improved many of its “vital signs” in comparison with units that have not implemented BOOST, including decreased length of stay and lower 30-day readmissions (see “Piedmont Hospital: Project BOOST unit vs. regular hospital units,” p. 6).
For St. Mary’s Medical Center, a 582-bed community teaching hospital in St. Louis, hospitalists implementing Project BOOST made a major difference in just three months:
Not only did the Project BOOST unit nearly halve 30-day readmissions (7% from 12%), but the program also increased patient satisfaction, to 68% from 52%.
BOOSTing into the Future
Project BOOST benefits haven’t been limited to program sites and their patients. New innovations from the mentored implementation program have led to resources that all hospitals can use.
SHM recently introduced a new DVD and curriculum package that teaches nurses and discharge planners to use the “teachback” method to communicate with patients during the discharge process. It helps ensure that patients fully understand their care plans and post-discharge instructions.
The teachback package is available at the SHM online store (www.hospitalmedicine.org); it is $85 for SHM members and $125 for nonmembers.
SHM has also launched a BOOST data center and a BOOST community site. The data center enables sites to enter, track, and benchmark key outcomes, which can then be evaluated against comparison units at their own hospitals, BOOST averages, and subsets of hospitals with similar characteristics. The BOOST community site facilitates the sharing of ideas and documents between BOOST hospitals.
New funding approaches will help Project BOOST to continue to reach more hospitals. Since its inception, third parties have provided financial resources for the program.
Now, SHM is offering a tuition-based model, open to hospitals nationwide, which is set to begin this fall.
SHM is accepting applications at www.hospitalmedicine.org/boost. TH
Brendon Shank is a freelance writer based in Philadelphia.
Reference
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Eng J Med. 2009:360:1418-1428.
Market Watch
New Drugs, Indications, Dosage Forms, and Approval Recommendations
- Acetaminophen intravenous (Ofirmev) received a complete response letter in February from the FDA related to facility manufacturing deficiencies. The FDA did not cite any safety or efficacy issues and is not requiring any additional studies to be done prior to approval.1 The third-party manufacturer has submitted its response to the FDA and is ready to resubmit their new drug application (NDA) for this agent. It is being investigated to treat fever and pain in adults and children.2
- Ciprofloxacin dry powder inhaler (DPI) has received orphan drug status from the FDA for treating pulmonary infections in cystic fibrosis (CF) patients.3,4 It is in clinical trials to determine if it can improve pulmonary function in CF patients with Pseudomonas aeruginosa infections.
- Carglumic acid (Carbaglu) has been approved by the FDA to treat the metabolic disorder N-acetylglutamate synthetase (NAGS) deficiency.5 NAGS deficiency is an extremely rare genetic disorder that presents shortly after birth. It results in hyperammonemia, and can be fatal if not rapidly detected and managed. Carglumic acid treats the hyperammonemia within three days, with a lowering of the ammonia level within 24 hours. In clinical trials, a small number of patients (n=23) received the drug from six months to 21 years; the majority of patients were able to maintain normal ammonia levels long-term with continued treatment. It is recommended that carglumic acid only be administered by physicians who have experience dealing with metabolic disorders. The starting dose is between 100 mg/kg/day and 250 mg/kg/day for treatment of acute hyperammonemia. Using other agents to lower the ammonia level during acute episodes is recommended. Dosing should be based on the ammonia level and the patient’s symptoms.
- CK-2017357 has received orphan drug status for treating amyotrophic lateral sclerosis (ALS), or Lou Gehrig’s disease.6
- Desirudin injection (Iprivask), a direct thrombin inhibitor, has been approved by the FDA for the prevention of DVT.7 In clinical trials, it was superior to enoxaparin and unfractionated heparin for preventing proximal DVT and prevention of major venous thromboembolic events following elective hip replacement surgery. Desirudin is administered as a fixed subcutaneous dose. It does not cause thrombocytopenia, is relatively short-acting, and is easy to monitor. Some of the adverse reactions in clinical trials were thrombosis, hypotension, lower-extremity edema, fever, decreased hemoglobin level, and hematuria.8 Also known as Revasc, this medication has been available in Europe for more than 10 years.
- Doxepin tablets (Silenor) have been approved by the FDA for the treatment of short-term and chronic insomnia distinguished by difficulty with sleep maintenance in adults and elderly patients.9 Sleep maintenance includes difficulty staying asleep, waking up too much or too early, and not being able to fall back asleep. In clinical trials, adverse reactions were similar to placebo, there was a low-therapy discontinuation rate, and no evidence of amnesia, tolerance, or complex sleep behaviors such as sleep eating or sleep driving.10 It will be available in 3-mg and 6-mg tablets. It is not designated as a controlled substance.
- GVAX pancreas vaccine has received orphan drug status as a potential treatment for pancreatic cancer.11 It also is being investigated for other cancers, including those of the breast and for leukemias.
- Ritonavir (Norvir) has been approved by the FDA in a new formulation, which is heat-stable and can be stored at room temperature rather than in the refrigerator.12 The rate of drug absorption with the new formulation is different but does not require a dosage change.
- Somatropin [rDNA origin] prefilled injection pen (Norditropin FlexPro) has been approved by the FDA to treat adults and children with growth hormone disorders.13 The pen has an audible click and does not require any reconstitution or cartridge loading. After initial use, the pen can be left at room temperature for up to three weeks without worry of drug degradation.
Pipeline
- Agalsidase (Replagal) has received fast-track status from the FDA for treating Fabry disease.14 It is an enzyme replacement therapy.
- Exenatide LAR (Bydureon), the once-weekly version of exenatide (Byetta), is in final discussions at the FDA. The FDA has asked for additional information related to the product label, risk mitigation, and manufacturing, which the manufacturer is addressing.15
- Insulin powder for inhalation, ultra-rapid-acting (Afrezza), has been reviewed by the FDA, and the agency has requested additional information related to safety and labeling.16
- A combination therapy of saxagliptin/metformin has been submitted to the FDA as a once-daily treatment of Type 2 diabetes mellitus as an adjunct to diet in adults who cannot adequately control their diabetes on metformin monotherapy, or in treatment-naïve patients.17
- Vilanterol/fluticasone is a combination of the inhaled corticosteroid fluticasone and the long-acting beta-agonist (LABA) vilanterol, which is currently in Phase 3 clinical trials for treating asthma.18 The trial will compare the combination’s efficacy and safety to fluticasone/salmeterol (Advair). TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Cadence pharmaceuticals receives complete response letter from FDA for intravenous acetaminophen NDA. Cadence Pharmaceuticals website. Available at: http://cadx.client.shareholder.com/releasedetail.cfm?ReleaseID=444303. Accessed March 23, 2010.
- Cadence pharmaceuticals reports fourth quarter and full year 2009 financial results. Cadence Pharmaceuticals website. Available at: http://files.shareholder.com/downloads/CADX/874963043x0x359109/1cf00f72-0872-4d4e-b27d-bde1c03d625a/CADX_News_2010_3_15_General_Releases.pdf. Accessed March 23, 2010.
- Bayer lung infection drug gets orphan status. Forbes website. Available at: http://www.forbes.com/feeds/ap/2010/03/11/business-energy-us-bayer-healthcare-orphan-drug_7427368.html. Accessed March 23, 2010.
- FDA grants orphan status for Bayer’s ciprofloxacin for cystic fibrosis. The Pharma Letter website. Available at: http://www.thepharmaletter.com/file/4e4fb33313eddf122cdb730e3ea71840/fda-grants-orphan-status-for-bayers-ciprofloxacin-for-cystic-fibrosis.html. Accessed March 23, 2010.
- Burgess S. FDA approves drug to treat condition that causes elevated ammonia levels. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm205150.htm. Accessed March 23, 2010.
- UPDATE 1: Cytokinetics’ Lou Gehrig’s drug gets orphan status. Reuters website. Available at: http://www.reuters.com/assets/print?aid=USSGE6290J820100310. Accessed March 23, 2010.
- Iprivask available for prevention of deep vein thrombosis. Monthly Prescribing Reference website. Available at: http://www.empr.com/iprivask-available-for-prevention-of-deep-vein-thrombosis/article/164779/. Accessed March 23, 2010.
- First direct thrombin inhibitor for DVT prevention now available from Canyon Pharmaceuticals. Canyon Pharmaceuticals website. Available at: http://www.canyonpharma.com/newsexpand.aspx?id=7. Accessed March 23, 2010.
- FDA approves Silenor. Drugs.com website. Available at: http://www.drugs.com/newdrugs/somaxon-announces-fda-approval-silenor-doxepin-insomnia-2070.html?printable=1. Accessed March 23, 2010.
- UPDATE 1: Somaxon gets FDA nod for insomnia drug, shares soar. Reuters website. Available at: http://www.reuters.com/assets/print?aid=USSGE62H0KI20100318. Accessed March 21, 2010.
- BioSante announces FDA orphan drug designation for GVAX pancreatic cancer vaccine. The New York Times website. Available at: http://markets.on.nytimes.com/research/stocks/news/press_release.asp?docTag=201003150755BIZWIRE_USPRX____BW5298&feedID=600&press_symbol=64917. Accessed March 23, 2010.
- Abbott receives U.S. FDA approval for heat-stable Norvir (ritonavir) tablets. Abbott website. Available at: http://www.abbott.com/global/url/pressRelease/en_US/60.5:5/Press_Release_0820.htm. Accessed March 23, 2010.
- Novo Nordisk receives FDA approval for Norditropin FlexPro for growth hormone treatment. Novo Nordisk website. Available at: http://press.novonordisk-us.com/index.php?s=43&item=239. Accessed March 23, 2010.
- Dane L. Shire receives FDA fast-track designation for Replagal. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=97AF48EBA7054EF0857F055877E82B2C&logRowId=352323. Accessed March 23, 2010.
- Amylin shares up on FDA response for diabetes drug. Forbes website. Available at: http://www.forbes.com/feeds/ap/2010/03/15/business-health-care-us-amylin-mover_7435579.html. Accessed March 23, 2010.
- Russell J. MannKind drug fails to win FDA approval. Los Angeles Business Journal website. Available at: http://labusinessjournal.com/article.asp?aid=4998235.0597195.1894204.8500584.7421642.713. Accessed March 23, 2010.
- U.S. Food and Drug Administration accepts NDA for once-daily fixed dose combination of Onglyza (saxagliptin) and extended-release metformin for the treatment of type 2 diabetes mellitus in adults. AstraZeneca website. Available at: http://www.astrazeneca-us.com/about-astrazeneca-us/newsroom/product/8804120?itemId=8804120#. Accessed March 23, 2010.
- Dennis M. GlaxoSmithKline begins late-stage clinical programme for asthma drug Relovair. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=E256469FBD8F4A2F80C5DD3E844CC1E1&logRowId=356423. Accessed March 23, 2010.
New Drugs, Indications, Dosage Forms, and Approval Recommendations
- Acetaminophen intravenous (Ofirmev) received a complete response letter in February from the FDA related to facility manufacturing deficiencies. The FDA did not cite any safety or efficacy issues and is not requiring any additional studies to be done prior to approval.1 The third-party manufacturer has submitted its response to the FDA and is ready to resubmit their new drug application (NDA) for this agent. It is being investigated to treat fever and pain in adults and children.2
- Ciprofloxacin dry powder inhaler (DPI) has received orphan drug status from the FDA for treating pulmonary infections in cystic fibrosis (CF) patients.3,4 It is in clinical trials to determine if it can improve pulmonary function in CF patients with Pseudomonas aeruginosa infections.
- Carglumic acid (Carbaglu) has been approved by the FDA to treat the metabolic disorder N-acetylglutamate synthetase (NAGS) deficiency.5 NAGS deficiency is an extremely rare genetic disorder that presents shortly after birth. It results in hyperammonemia, and can be fatal if not rapidly detected and managed. Carglumic acid treats the hyperammonemia within three days, with a lowering of the ammonia level within 24 hours. In clinical trials, a small number of patients (n=23) received the drug from six months to 21 years; the majority of patients were able to maintain normal ammonia levels long-term with continued treatment. It is recommended that carglumic acid only be administered by physicians who have experience dealing with metabolic disorders. The starting dose is between 100 mg/kg/day and 250 mg/kg/day for treatment of acute hyperammonemia. Using other agents to lower the ammonia level during acute episodes is recommended. Dosing should be based on the ammonia level and the patient’s symptoms.
- CK-2017357 has received orphan drug status for treating amyotrophic lateral sclerosis (ALS), or Lou Gehrig’s disease.6
- Desirudin injection (Iprivask), a direct thrombin inhibitor, has been approved by the FDA for the prevention of DVT.7 In clinical trials, it was superior to enoxaparin and unfractionated heparin for preventing proximal DVT and prevention of major venous thromboembolic events following elective hip replacement surgery. Desirudin is administered as a fixed subcutaneous dose. It does not cause thrombocytopenia, is relatively short-acting, and is easy to monitor. Some of the adverse reactions in clinical trials were thrombosis, hypotension, lower-extremity edema, fever, decreased hemoglobin level, and hematuria.8 Also known as Revasc, this medication has been available in Europe for more than 10 years.
- Doxepin tablets (Silenor) have been approved by the FDA for the treatment of short-term and chronic insomnia distinguished by difficulty with sleep maintenance in adults and elderly patients.9 Sleep maintenance includes difficulty staying asleep, waking up too much or too early, and not being able to fall back asleep. In clinical trials, adverse reactions were similar to placebo, there was a low-therapy discontinuation rate, and no evidence of amnesia, tolerance, or complex sleep behaviors such as sleep eating or sleep driving.10 It will be available in 3-mg and 6-mg tablets. It is not designated as a controlled substance.
- GVAX pancreas vaccine has received orphan drug status as a potential treatment for pancreatic cancer.11 It also is being investigated for other cancers, including those of the breast and for leukemias.
- Ritonavir (Norvir) has been approved by the FDA in a new formulation, which is heat-stable and can be stored at room temperature rather than in the refrigerator.12 The rate of drug absorption with the new formulation is different but does not require a dosage change.
- Somatropin [rDNA origin] prefilled injection pen (Norditropin FlexPro) has been approved by the FDA to treat adults and children with growth hormone disorders.13 The pen has an audible click and does not require any reconstitution or cartridge loading. After initial use, the pen can be left at room temperature for up to three weeks without worry of drug degradation.
Pipeline
- Agalsidase (Replagal) has received fast-track status from the FDA for treating Fabry disease.14 It is an enzyme replacement therapy.
- Exenatide LAR (Bydureon), the once-weekly version of exenatide (Byetta), is in final discussions at the FDA. The FDA has asked for additional information related to the product label, risk mitigation, and manufacturing, which the manufacturer is addressing.15
- Insulin powder for inhalation, ultra-rapid-acting (Afrezza), has been reviewed by the FDA, and the agency has requested additional information related to safety and labeling.16
- A combination therapy of saxagliptin/metformin has been submitted to the FDA as a once-daily treatment of Type 2 diabetes mellitus as an adjunct to diet in adults who cannot adequately control their diabetes on metformin monotherapy, or in treatment-naïve patients.17
- Vilanterol/fluticasone is a combination of the inhaled corticosteroid fluticasone and the long-acting beta-agonist (LABA) vilanterol, which is currently in Phase 3 clinical trials for treating asthma.18 The trial will compare the combination’s efficacy and safety to fluticasone/salmeterol (Advair). TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Cadence pharmaceuticals receives complete response letter from FDA for intravenous acetaminophen NDA. Cadence Pharmaceuticals website. Available at: http://cadx.client.shareholder.com/releasedetail.cfm?ReleaseID=444303. Accessed March 23, 2010.
- Cadence pharmaceuticals reports fourth quarter and full year 2009 financial results. Cadence Pharmaceuticals website. Available at: http://files.shareholder.com/downloads/CADX/874963043x0x359109/1cf00f72-0872-4d4e-b27d-bde1c03d625a/CADX_News_2010_3_15_General_Releases.pdf. Accessed March 23, 2010.
- Bayer lung infection drug gets orphan status. Forbes website. Available at: http://www.forbes.com/feeds/ap/2010/03/11/business-energy-us-bayer-healthcare-orphan-drug_7427368.html. Accessed March 23, 2010.
- FDA grants orphan status for Bayer’s ciprofloxacin for cystic fibrosis. The Pharma Letter website. Available at: http://www.thepharmaletter.com/file/4e4fb33313eddf122cdb730e3ea71840/fda-grants-orphan-status-for-bayers-ciprofloxacin-for-cystic-fibrosis.html. Accessed March 23, 2010.
- Burgess S. FDA approves drug to treat condition that causes elevated ammonia levels. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm205150.htm. Accessed March 23, 2010.
- UPDATE 1: Cytokinetics’ Lou Gehrig’s drug gets orphan status. Reuters website. Available at: http://www.reuters.com/assets/print?aid=USSGE6290J820100310. Accessed March 23, 2010.
- Iprivask available for prevention of deep vein thrombosis. Monthly Prescribing Reference website. Available at: http://www.empr.com/iprivask-available-for-prevention-of-deep-vein-thrombosis/article/164779/. Accessed March 23, 2010.
- First direct thrombin inhibitor for DVT prevention now available from Canyon Pharmaceuticals. Canyon Pharmaceuticals website. Available at: http://www.canyonpharma.com/newsexpand.aspx?id=7. Accessed March 23, 2010.
- FDA approves Silenor. Drugs.com website. Available at: http://www.drugs.com/newdrugs/somaxon-announces-fda-approval-silenor-doxepin-insomnia-2070.html?printable=1. Accessed March 23, 2010.
- UPDATE 1: Somaxon gets FDA nod for insomnia drug, shares soar. Reuters website. Available at: http://www.reuters.com/assets/print?aid=USSGE62H0KI20100318. Accessed March 21, 2010.
- BioSante announces FDA orphan drug designation for GVAX pancreatic cancer vaccine. The New York Times website. Available at: http://markets.on.nytimes.com/research/stocks/news/press_release.asp?docTag=201003150755BIZWIRE_USPRX____BW5298&feedID=600&press_symbol=64917. Accessed March 23, 2010.
- Abbott receives U.S. FDA approval for heat-stable Norvir (ritonavir) tablets. Abbott website. Available at: http://www.abbott.com/global/url/pressRelease/en_US/60.5:5/Press_Release_0820.htm. Accessed March 23, 2010.
- Novo Nordisk receives FDA approval for Norditropin FlexPro for growth hormone treatment. Novo Nordisk website. Available at: http://press.novonordisk-us.com/index.php?s=43&item=239. Accessed March 23, 2010.
- Dane L. Shire receives FDA fast-track designation for Replagal. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=97AF48EBA7054EF0857F055877E82B2C&logRowId=352323. Accessed March 23, 2010.
- Amylin shares up on FDA response for diabetes drug. Forbes website. Available at: http://www.forbes.com/feeds/ap/2010/03/15/business-health-care-us-amylin-mover_7435579.html. Accessed March 23, 2010.
- Russell J. MannKind drug fails to win FDA approval. Los Angeles Business Journal website. Available at: http://labusinessjournal.com/article.asp?aid=4998235.0597195.1894204.8500584.7421642.713. Accessed March 23, 2010.
- U.S. Food and Drug Administration accepts NDA for once-daily fixed dose combination of Onglyza (saxagliptin) and extended-release metformin for the treatment of type 2 diabetes mellitus in adults. AstraZeneca website. Available at: http://www.astrazeneca-us.com/about-astrazeneca-us/newsroom/product/8804120?itemId=8804120#. Accessed March 23, 2010.
- Dennis M. GlaxoSmithKline begins late-stage clinical programme for asthma drug Relovair. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=E256469FBD8F4A2F80C5DD3E844CC1E1&logRowId=356423. Accessed March 23, 2010.
New Drugs, Indications, Dosage Forms, and Approval Recommendations
- Acetaminophen intravenous (Ofirmev) received a complete response letter in February from the FDA related to facility manufacturing deficiencies. The FDA did not cite any safety or efficacy issues and is not requiring any additional studies to be done prior to approval.1 The third-party manufacturer has submitted its response to the FDA and is ready to resubmit their new drug application (NDA) for this agent. It is being investigated to treat fever and pain in adults and children.2
- Ciprofloxacin dry powder inhaler (DPI) has received orphan drug status from the FDA for treating pulmonary infections in cystic fibrosis (CF) patients.3,4 It is in clinical trials to determine if it can improve pulmonary function in CF patients with Pseudomonas aeruginosa infections.
- Carglumic acid (Carbaglu) has been approved by the FDA to treat the metabolic disorder N-acetylglutamate synthetase (NAGS) deficiency.5 NAGS deficiency is an extremely rare genetic disorder that presents shortly after birth. It results in hyperammonemia, and can be fatal if not rapidly detected and managed. Carglumic acid treats the hyperammonemia within three days, with a lowering of the ammonia level within 24 hours. In clinical trials, a small number of patients (n=23) received the drug from six months to 21 years; the majority of patients were able to maintain normal ammonia levels long-term with continued treatment. It is recommended that carglumic acid only be administered by physicians who have experience dealing with metabolic disorders. The starting dose is between 100 mg/kg/day and 250 mg/kg/day for treatment of acute hyperammonemia. Using other agents to lower the ammonia level during acute episodes is recommended. Dosing should be based on the ammonia level and the patient’s symptoms.
- CK-2017357 has received orphan drug status for treating amyotrophic lateral sclerosis (ALS), or Lou Gehrig’s disease.6
- Desirudin injection (Iprivask), a direct thrombin inhibitor, has been approved by the FDA for the prevention of DVT.7 In clinical trials, it was superior to enoxaparin and unfractionated heparin for preventing proximal DVT and prevention of major venous thromboembolic events following elective hip replacement surgery. Desirudin is administered as a fixed subcutaneous dose. It does not cause thrombocytopenia, is relatively short-acting, and is easy to monitor. Some of the adverse reactions in clinical trials were thrombosis, hypotension, lower-extremity edema, fever, decreased hemoglobin level, and hematuria.8 Also known as Revasc, this medication has been available in Europe for more than 10 years.
- Doxepin tablets (Silenor) have been approved by the FDA for the treatment of short-term and chronic insomnia distinguished by difficulty with sleep maintenance in adults and elderly patients.9 Sleep maintenance includes difficulty staying asleep, waking up too much or too early, and not being able to fall back asleep. In clinical trials, adverse reactions were similar to placebo, there was a low-therapy discontinuation rate, and no evidence of amnesia, tolerance, or complex sleep behaviors such as sleep eating or sleep driving.10 It will be available in 3-mg and 6-mg tablets. It is not designated as a controlled substance.
- GVAX pancreas vaccine has received orphan drug status as a potential treatment for pancreatic cancer.11 It also is being investigated for other cancers, including those of the breast and for leukemias.
- Ritonavir (Norvir) has been approved by the FDA in a new formulation, which is heat-stable and can be stored at room temperature rather than in the refrigerator.12 The rate of drug absorption with the new formulation is different but does not require a dosage change.
- Somatropin [rDNA origin] prefilled injection pen (Norditropin FlexPro) has been approved by the FDA to treat adults and children with growth hormone disorders.13 The pen has an audible click and does not require any reconstitution or cartridge loading. After initial use, the pen can be left at room temperature for up to three weeks without worry of drug degradation.
Pipeline
- Agalsidase (Replagal) has received fast-track status from the FDA for treating Fabry disease.14 It is an enzyme replacement therapy.
- Exenatide LAR (Bydureon), the once-weekly version of exenatide (Byetta), is in final discussions at the FDA. The FDA has asked for additional information related to the product label, risk mitigation, and manufacturing, which the manufacturer is addressing.15
- Insulin powder for inhalation, ultra-rapid-acting (Afrezza), has been reviewed by the FDA, and the agency has requested additional information related to safety and labeling.16
- A combination therapy of saxagliptin/metformin has been submitted to the FDA as a once-daily treatment of Type 2 diabetes mellitus as an adjunct to diet in adults who cannot adequately control their diabetes on metformin monotherapy, or in treatment-naïve patients.17
- Vilanterol/fluticasone is a combination of the inhaled corticosteroid fluticasone and the long-acting beta-agonist (LABA) vilanterol, which is currently in Phase 3 clinical trials for treating asthma.18 The trial will compare the combination’s efficacy and safety to fluticasone/salmeterol (Advair). TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Cadence pharmaceuticals receives complete response letter from FDA for intravenous acetaminophen NDA. Cadence Pharmaceuticals website. Available at: http://cadx.client.shareholder.com/releasedetail.cfm?ReleaseID=444303. Accessed March 23, 2010.
- Cadence pharmaceuticals reports fourth quarter and full year 2009 financial results. Cadence Pharmaceuticals website. Available at: http://files.shareholder.com/downloads/CADX/874963043x0x359109/1cf00f72-0872-4d4e-b27d-bde1c03d625a/CADX_News_2010_3_15_General_Releases.pdf. Accessed March 23, 2010.
- Bayer lung infection drug gets orphan status. Forbes website. Available at: http://www.forbes.com/feeds/ap/2010/03/11/business-energy-us-bayer-healthcare-orphan-drug_7427368.html. Accessed March 23, 2010.
- FDA grants orphan status for Bayer’s ciprofloxacin for cystic fibrosis. The Pharma Letter website. Available at: http://www.thepharmaletter.com/file/4e4fb33313eddf122cdb730e3ea71840/fda-grants-orphan-status-for-bayers-ciprofloxacin-for-cystic-fibrosis.html. Accessed March 23, 2010.
- Burgess S. FDA approves drug to treat condition that causes elevated ammonia levels. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm205150.htm. Accessed March 23, 2010.
- UPDATE 1: Cytokinetics’ Lou Gehrig’s drug gets orphan status. Reuters website. Available at: http://www.reuters.com/assets/print?aid=USSGE6290J820100310. Accessed March 23, 2010.
- Iprivask available for prevention of deep vein thrombosis. Monthly Prescribing Reference website. Available at: http://www.empr.com/iprivask-available-for-prevention-of-deep-vein-thrombosis/article/164779/. Accessed March 23, 2010.
- First direct thrombin inhibitor for DVT prevention now available from Canyon Pharmaceuticals. Canyon Pharmaceuticals website. Available at: http://www.canyonpharma.com/newsexpand.aspx?id=7. Accessed March 23, 2010.
- FDA approves Silenor. Drugs.com website. Available at: http://www.drugs.com/newdrugs/somaxon-announces-fda-approval-silenor-doxepin-insomnia-2070.html?printable=1. Accessed March 23, 2010.
- UPDATE 1: Somaxon gets FDA nod for insomnia drug, shares soar. Reuters website. Available at: http://www.reuters.com/assets/print?aid=USSGE62H0KI20100318. Accessed March 21, 2010.
- BioSante announces FDA orphan drug designation for GVAX pancreatic cancer vaccine. The New York Times website. Available at: http://markets.on.nytimes.com/research/stocks/news/press_release.asp?docTag=201003150755BIZWIRE_USPRX____BW5298&feedID=600&press_symbol=64917. Accessed March 23, 2010.
- Abbott receives U.S. FDA approval for heat-stable Norvir (ritonavir) tablets. Abbott website. Available at: http://www.abbott.com/global/url/pressRelease/en_US/60.5:5/Press_Release_0820.htm. Accessed March 23, 2010.
- Novo Nordisk receives FDA approval for Norditropin FlexPro for growth hormone treatment. Novo Nordisk website. Available at: http://press.novonordisk-us.com/index.php?s=43&item=239. Accessed March 23, 2010.
- Dane L. Shire receives FDA fast-track designation for Replagal. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=97AF48EBA7054EF0857F055877E82B2C&logRowId=352323. Accessed March 23, 2010.
- Amylin shares up on FDA response for diabetes drug. Forbes website. Available at: http://www.forbes.com/feeds/ap/2010/03/15/business-health-care-us-amylin-mover_7435579.html. Accessed March 23, 2010.
- Russell J. MannKind drug fails to win FDA approval. Los Angeles Business Journal website. Available at: http://labusinessjournal.com/article.asp?aid=4998235.0597195.1894204.8500584.7421642.713. Accessed March 23, 2010.
- U.S. Food and Drug Administration accepts NDA for once-daily fixed dose combination of Onglyza (saxagliptin) and extended-release metformin for the treatment of type 2 diabetes mellitus in adults. AstraZeneca website. Available at: http://www.astrazeneca-us.com/about-astrazeneca-us/newsroom/product/8804120?itemId=8804120#. Accessed March 23, 2010.
- Dennis M. GlaxoSmithKline begins late-stage clinical programme for asthma drug Relovair. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=E256469FBD8F4A2F80C5DD3E844CC1E1&logRowId=356423. Accessed March 23, 2010.
In the Literature
In This Edition
Literature at a Glance
A guide to this month’s studies
- Effect of restrictive antibiotic policies on dosing timeliness
- Desired consultation format and content
- Risk of cancer associated with CT imaging
- Bleeding, mortality with aspirin after peptic ulcer bleed
- Diagnosis of lung cancer after pneumonia
- Outcomes associated with hyponatremia
- Patient awareness, interest in inpatient medication list
- Monoclonal antibodies in C. difficile
Restrictive Antimicrobial Policy Delays Administration
Clinical question: Does the approval process for restricted on-formulary antimicrobials cause a significant delay in their administration?
Background: Widespread and often unwarranted, antimicrobial use in the hospital lends itself to the development of microbial resistance and increases overall costs. To curb such practices, many hospitals require subspecialty approval prior to dispensing select broad-spectrum antimicrobials. Though shown to improve outcomes, the impact of the approval process on the timeliness of antimicrobial administration remains to be seen.
Study design: Retrospective cohort study.
Setting: Tertiary-care university hospital.
Synopsis: The study included 3,251 inpatients with computerized orders for a “stat” first dose of any of 24 pre-selected, parenteral antimicrobials. Time lag (more than one hour, and more than two hours) to nursing documentation of drug administration was separately analyzed for restricted and unrestricted antimicrobials.
Delay of more than one hour was significantly higher for restricted antimicrobials with an odds ratio of 1.49 (95% CI; 1.23-1.82), while the odds ratio for a delay of more than two hours was 1.78 (95% CI, 1.39-2.21). Also, for restricted antimicrobials, the percentage of orders delayed for more than one hour was significantly different between daytime and nighttime (when the first dose was exempt from pre-approval) orders: 46.1% versus 38.8% (P<0.001). For unrestricted drugs, delay was uniform irrespective of time of day (36.4% of daytime and 36.6% of nighttime orders were delayed more than one hour). The effect of delay in drug administration on patient outcomes was not evaluated.
Though the approval process aims in part to affect resistance patterns and overall costs, this research highlights the need to minimize the delay in administration and probably skip the approval for the first dose in critically ill patients.
Bottom line: Antibiotic approval processes can delay their administration in hospitalized patients, but the effect of this delay on patient outcomes is not yet known.
Citation: Winters BD, Thiemann DR, Brotman DJ. Impact of a restrictive antimicrobial policy on the process and timing of antimicrobial administration. J Hosp Med. 2010;5(1):E41-45.
Physicians Uphold Tenets of Effective Consultation while Highlighting Some Newer Viewpoints
Clinical question: What key features of a consultation are most desirable for physicians?
Background: With new changes in healthcare delivery, the standardization offered by the electronic health record (EHR) system will undoubtedly be confronted by the heterogeneity of clinical consultations. Determination of the various characteristics considered essential for a consultation can help standardize the processes and improve the quality of communication.
Study design: Opinion surveys with a 16-question, Web-based questionnaire about inpatient consultations.
Setting: Four Minnesota teaching hospitals affiliated with the University of Minnesota.
Synopsis: This study surveyed 651 physicians, mostly from general medicine and pediatrics (30% in-training; 54% were more than five years out of training). The response rate to the survey was 50% (323). Responses were analyzed separately for physicians predominantly requesting consultations (requesters) and those predominantly providing them (consultants).
Regarding the consultation request, the majority of consultants preferred a precise consult question (94%), contact information of the ordering provider (68%), and the urgency of consultation (66%), with telephonic communication for emergent consults (75%). Responses were similar regardless of practice site, specialty, or experience.
Regarding the consultation, more requesters desired verbal communication over written advice alone: Sixty-six percent preferred to have the rationale of the recommendations explained. They also preferred a separate recommendations section (48%) with bulleted suggestions (69%) at the top or bottom of the note (74%). Emphasis was placed on specificity of drug names, dose, and duration of therapy (80%), along with alternative options (76%). Most requesters desired a clear “signoff” note when appropriate, with a follow-up plan (74%) or scheduled appointments (44%).
Bottom line: For consultations, the majority of physicians prefer an explanation of medical decision-making, a crisp recommendation section, and specific directions for follow-up.
Citation: Boulware DR, Dekarske AS, Filice GA. Physician preferences for elements of effective consultations. J Gen Intern Med. 2010;25(1):25-30.
CT Scanning Could Be Related to a Future Risk of Cancer at a Population Level
Clinical question: Does the accelerated use of CT scans increase the future risk for radiation-related cancer?
Background: Computed tomography (CT) has come through as a powerful diagnostic and interventional imaging modality at the cost of higher radiation exposures. The potential cancer risk is minimal at an individual level; however, CT technology is used in more than 70 million scans annually. This volume can translate into a significant number of future cancers in the population.
Study design: Indirect risk modeling based on CT scan frequencies and radiation risk models.
Synopsis: Annual frequencies of CT scans (age- and sex-specific) were extracted from insurance claims. The study included 57 million scans, of which 30% were performed in adults 35 to 54 years old. The majority of scans were in females (60%).
Age-specific cancer risk for each CT scan type was estimated through published radiation risk models and national surveys. The projected number of incident cancers per 10,000 scans was highest for chest or abdominal CT angiography (CTA) and whole-body CT. Incidence was higher for females.
The CT scan frequencies were combined with the cancer risk, and it was estimated that approximately 29,000 (95% UL, 15,000-45,000) future cancers could be related to the exposure from CT scans. Uncertainty limits (UL), an estimation of the total error of measurement, accounted for statistical and subjective uncertainties. The risk was dependent on the radiation dose (chest CTA) and frequency of use (abdomen/pelvis followed by chest and head). The most common cancers were lung, colon, and leukemia.
Two-thirds of the projected cancers were in females and attributable to the higher frequency of scans in women coupled with their dual risk of breast and lung cancer with chest radiation. The results provide potential study targets for risk-reduction efforts.
Bottom line: CTA of the chest, abdomen, or pelvis could be related to risk of future cancers, especially in middle-aged females.
Citation: Berrington de González A, Mahesh M, Kim KP, et al. Projected cancer risks from computed tomographic scans performed in the United States in 2007. Arch Intern Med. 2009;169(22):2071-2077.
Early Resumption of Low-Dose Aspirin after Peptic Ulcer Bleeding Might Be Beneficial
Clinical question: Is it safe to restart aspirin after acute gastrointestinal (GI) bleeding in patients with cardiovascular or cerebrovascular disease?
Background: The increasing cardiovascular burden in the aging population has indirectly increased aspirin-related peptic ulcer bleeding. Proton-pump inhibitors (PPI) have shown promise in reducing recurrent GI bleeding in non-aspirin-related cases. It is unclear if this protective effect applies to patients on aspirin and, if so, if aspirin resumption after endoscopic treatment is safe.
Study design: Parallel, randomized, placebo-controlled, noninferiority trial.
Setting: Single tertiary endoscopy center in Hong Kong.
Synopsis: One hundred fifty-six patients with aspirin-related peptic ulcer bleeding were selected for the study. After successful endoscopic treatment and 72 hours on pantoprazole infusion, the patients were started on oral pantoprazole for the duration of the study (eight weeks). Patients were equally randomized to receive low-dose aspirin (80 mg/d) or placebo. Primary outcome was recurrent bleeding within 30 days. Secondary outcomes included eight-week all-cause mortality, cause-specific mortality, and recurrence of cardiovascular events.
The aspirin group had a 50% higher risk of recurrent bleeding within 30 days compared with placebo (10.3% vs. 5.4%). However, for the secondary endpoints, aspirin had lower all-cause mortality (1.3% vs. 12.9%), which was not related to increased GI bleeding. On the other hand, discontinuation of aspirin and use of PPI in the placebo group did not prevent mortality related to GI complications.
The small numbers restrict interpretation of the mortality rates but offer support to the fact that the cardioprotective effects of aspirin outweigh its potential for GI bleeding. It is to be noted that these results cannot be extrapolated to higher doses of aspirin.
Bottom line: Early resumption of aspirin after successful treatment of peptic ulcer bleeding might increase the risk of rebleeding but potentially decreases overall mortality.
Citation: Sung JJ, Lau JY, Ching JY, et al. Continuation of low-dose aspirin therapy in peptic ulcer bleeding: a randomized trial. Ann Intern Med. 2010;152(1):1-9.
A Substantial Number of Elderly Patients with Pneumonia Have Pulmonary Malignancy
Clinical question: What is the incidence of, and risk factors for, diagnosis of lung cancer after discharge for pneumonia?
Background: Pneumonia-related admissions in elderly individuals have increased by nearly 20% during the past two decades. Based on the risk profile of this age group, many physicians recommend follow-up chest imaging after pneumonia to ensure resolution and exclude underlying malignancy. However, this practice is not backed by substantial evidence.
Study design: Retrospective cohort study from administrative databases of the VA system.
Setting: Veteran Affairs (VA) Health Care System.
Synopsis: More than 40,000 patients (older than 65, 98.1% male) hospitalized for pneumonia were included in the study. These patients had no pneumonia in the preceding year and did not carry a diagnosis of lung cancer. During the follow-up period of up to five years, a significant proportion (9.2%) of these patients were diagnosed with pulmonary malignancy.
Pertinent factors associated with increased risk of diagnosis included active tobacco use, COPD, and prior nonpulmonary malignancy. Interestingly, stroke, diabetes, dementia, and heart failure were associated with a lower risk of diagnosis, likely due to early mortality from these diseases prior to diagnosis of lung cancer.
Mean time to diagnosis was 297 days, with just 27% diagnosed within 30 days. On mortality analysis, 12.9% (n=5270) of the patients died within 30 days and 20.7% (n=8451) within 90 days. Thus, a period of surveillance of 30 to 90 days following pneumonia, especially in patients with risk factors, could be beneficial.
This study was limited due to the shortcomings of database analyses. Also, the predominantly male, elderly, veteran population restricts extrapolation to the general population.
Bottom line: Patients with risk factors for lung cancer might benefit from surveillance chest imaging after hospitalization for pneumonia to rule out an underlying malignancy.
Citation: Mortensen EM, Copeland LA, Pugh MJ, et al. Diagnosis of pulmonary malignancy after hospitalization for pneumonia. Am J Med. 2010:123(1):66-71.
Hospital-Associated Hyponatremia of Any Severity Adversely Impacts Mortality and Financial Metrics
Clinical question: Does hyponatremia during a hospitalization prophesize a worse outcome?
Study design: Retrospective cohort study from 2002-2007.
Setting: Urban academic medical center.
Synopsis: This study included 53,236 adults based on the presence of admission or subsequent hyponatremia (defined as [Na+] <138 mEq/L). The patients were classified as community-acquired (CAH=37.9%), hospital-aggravated (5.7%), or hospital-acquired hyponatremia (HAH=38.2%).
Across all subgroups, all types of hyponatremia were independently associated with worse primary outcomes, including an increase in hospital mortality (CAH 52%, HAH 66%), prolongation of hospital stay, and discharge to a facility. Also, for the same [Na+], HAH had significantly increased mortality compared with CAH. Though the elderly were more prone to develop hyponatremia, patients younger than 65 had worse outcomes.
The severity of hyponatremia prognosticated adverse outcomes. The liberal definition of hyponatremia, as opposed to the current standard of <135 mEq/L, explains the large numbers in prevalence. However, even mild hyponatremia (133 mEq/L to 137) was linked to poor outcomes (adjusted OR 1.34; CI 1.18-1.51).
The study weaknesses include the use of administrative codes to identify comorbidities, less applicability to outpatient setting, and lack of evaluation of outcomes postdischarge. However, the robust numbers do establish inpatient hyponatremia as a marker of worse outcomes.
Bottom line: Inpatient hyponatremia of any severity is a marker of increased mortality and excessive financial burden.
Citation: Wald R, Jaber BL, Price LL, Upadhyay A, Madias NE. Impact of hospital-associated hyponatremia on selected outcomes. Arch Intern Med. 2010;170(3):294-302.
Patients Lack Awareness and Prefer to Be Updated Regarding Their Inpatient Medications
Clinical question: Is patient knowledge of their medications deficient, and does this reflect a lack of desire to be involved in the medication reconciliation process?
Background: Medication errors remain a significant healthcare problem due to their potential to increase morbidity. For medication administration errors, apart from the dispensing pharmacist and the nurses, patients could be the final checkpoint to ensure medication safety. However, their awareness and enthusiasm to participate has not been adequately assessed in the literature.
Study design: A cross-sectional study using individual surveys to assess awareness and attitudes regarding inpatient medications.
Setting: Single tertiary-care academic teaching hospital.
Synopsis: Fifty cognitively intact adult patients were consented for the study. Of these, 54% provided an accurate recollection of their outpatient medications. When they were surveyed regarding inpatient medications, 96% omitted at least one medication, with the average of 6.8 medication omissions. This was noted to correlate with age >65 years. Also, 44% erroneously presumed they were on a medication while they were in the hospital, even though they weren’t.
When attitudes were surveyed, most of the patients would have preferred to get an inpatient medication list (78%) with the goal of improving their satisfaction (81%) and reducing errors (94%). Also, no association was found between patients’ errors of omission and their reported desire to be involved in the medication safety process.
This small study was limited to cognitively intact patients only. Also, the relatively younger age might cause an overestimation of patient interest in participation. However, the results highlight key medication reconciliation issues. Although patient involvement is desirable, a systematic program of educating them about their medications would be required to make their feedback effective and useful.
Bottom line: Healthy patients might be unaware of their exact hospital medications but prefer to be kept in the loop.
Citation: Cumbler E, Wald H, Kutner J. Lack of patient knowledge regarding hospital medications. J Hosp Med. 2010;5(2):83-86.
Monoclonal Antibodies against Clostridium difficile Toxins Prevent Recurrence
Clinical question: Are human monoclonal antibodies against C. difficile toxin A (CDA1) and B (CDB1) effective in preventing recurrence of C. diff infection (CDI)?
Background: Widespread use of antibiotics, coupled with the emergence of the hypervirulent (B1/NAP1/027) strain of C. diff, has altered the epidemiology of CDI. Even with effective treatment regimens, there is an escalation in severity, treatment failures, and recurrences. Antibodies against the C. diff toxins are being evaluated as the next frontier in treatment of CDI.
Study design: Phase 2 randomized, double-blind, placebo-controlled trial.
Setting: Thirty study centers in Canada and the U.S.
Synopsis: Two hundred patients with laboratory documented CDI on standard therapy with either metronidazole or vancomycin were randomized to receive a single IV infusion of combined monoclonal antibodies against CDA1 and CDB1 (n=101) or a normal saline placebo infusion (n=99). Patients were followed for 84 days with daily stool counts and intermittent blood samples for immunogenicity analysis.
The primary endpoint of recurrence of laboratory-proven C. diff diarrhea was significantly lower in the monoclonal antibody group (7% vs. 25% in placebo. 95% CI, 7-29; P <0.001). In a subgroup analysis of the epidemic BI/NAP1/027 strain, this favorable association persisted (8% vs. 32%). Recurrence in the antibody group was seen more in elderly patients hospitalized with a higher severity of underlying disease.
Secondary endpoints relating to the initial episode of CDI including treatment failure, severity of diarrhea, and duration to resolution were not significantly different between the two groups. Fewer accounts of serious adverse events were documented in the antibody group (18 patients vs. 28 patients in placebo, P=0.09), and immunogenicity was not detected in any patient.
Bottom line: Monoclonal antibody infusion against C. diff toxins reduces recurrence of infection, even with a hypervirulent (B1/NAP1/027) strain, without any significant adverse events.
Citation: Lowy I, Molrine DC, Leav BA, et al. Treatment with monoclonal antibodies against Clostridium difficile toxins. N Engl J Med. 2010; 362(3):197-205. TH
PEDIATRIC HM LITERATURE
By Mark Shen, MD

Rectal Colonization with S. aureus Associated with Skin Abscesses
Clinical question: Is rectal colonization with Staphylococcus aureus more strongly associated with staphylococcal skin abscesses than nasal colonization?
Background: Staphylococcal skin and soft tissue infections have dramatically increased in recent years. While increased rates of nasal colonization with S. aureus have also been noted, a strong association with skin infections in children has not been established. The relationship between staphylococcal colonization of other body sites and skin infection is unknown.
Study design: Prospective cohort study.
Setting: Tertiary-care hospital in Buffalo, N.Y.
Synopsis: Sixty children, 0 to 18 years of age, requiring surgical drainage of S. aureus skin abscesses and 90 children undergoing other surgical procedures were enrolled consecutively. Rectal, nasal, and abscess (if applicable) cultures were obtained on all patients. Enrollment ceased when notably different rates of rectal colonization were recorded.
Rectal cultures were significantly more likely to be positive in the abscess group than the control group (47% vs. 1%; P<0.0001), while rates of nasal colonization were similar (27% vs. 21%; P=0.44). Abscess isolates were identical to rectal isolates in 88% of cases and nasal isolates in 75% of cases.
Other findings included a 60% prevalence of methicillin-resistant S. aureus (MRSA) in the abscess group. Fifty-nine of the 60 abscess isolates contained Panton-Valentine leukocidin genes; 57 were pulsed-field type USA300; and all 60 contained the staphylococcal cassette chromosome mec type IVa.
Given this representative sample of community-associated staphylococcal disease, these findings suggest that a focus on nasal carriage of S. aureus might be misguided.
Bottom Line: Rectal colonization with S. aureus better predicts skin abscess isolate than nasal carriage.
Citation: Faden H, Lesse AJ, Trask J, et al. Importance of colonization site in the current epidemic of staphylococcal skin abscesses. Pediatrics. 2010;125(3):e618-e624.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Effect of restrictive antibiotic policies on dosing timeliness
- Desired consultation format and content
- Risk of cancer associated with CT imaging
- Bleeding, mortality with aspirin after peptic ulcer bleed
- Diagnosis of lung cancer after pneumonia
- Outcomes associated with hyponatremia
- Patient awareness, interest in inpatient medication list
- Monoclonal antibodies in C. difficile
Restrictive Antimicrobial Policy Delays Administration
Clinical question: Does the approval process for restricted on-formulary antimicrobials cause a significant delay in their administration?
Background: Widespread and often unwarranted, antimicrobial use in the hospital lends itself to the development of microbial resistance and increases overall costs. To curb such practices, many hospitals require subspecialty approval prior to dispensing select broad-spectrum antimicrobials. Though shown to improve outcomes, the impact of the approval process on the timeliness of antimicrobial administration remains to be seen.
Study design: Retrospective cohort study.
Setting: Tertiary-care university hospital.
Synopsis: The study included 3,251 inpatients with computerized orders for a “stat” first dose of any of 24 pre-selected, parenteral antimicrobials. Time lag (more than one hour, and more than two hours) to nursing documentation of drug administration was separately analyzed for restricted and unrestricted antimicrobials.
Delay of more than one hour was significantly higher for restricted antimicrobials with an odds ratio of 1.49 (95% CI; 1.23-1.82), while the odds ratio for a delay of more than two hours was 1.78 (95% CI, 1.39-2.21). Also, for restricted antimicrobials, the percentage of orders delayed for more than one hour was significantly different between daytime and nighttime (when the first dose was exempt from pre-approval) orders: 46.1% versus 38.8% (P<0.001). For unrestricted drugs, delay was uniform irrespective of time of day (36.4% of daytime and 36.6% of nighttime orders were delayed more than one hour). The effect of delay in drug administration on patient outcomes was not evaluated.
Though the approval process aims in part to affect resistance patterns and overall costs, this research highlights the need to minimize the delay in administration and probably skip the approval for the first dose in critically ill patients.
Bottom line: Antibiotic approval processes can delay their administration in hospitalized patients, but the effect of this delay on patient outcomes is not yet known.
Citation: Winters BD, Thiemann DR, Brotman DJ. Impact of a restrictive antimicrobial policy on the process and timing of antimicrobial administration. J Hosp Med. 2010;5(1):E41-45.
Physicians Uphold Tenets of Effective Consultation while Highlighting Some Newer Viewpoints
Clinical question: What key features of a consultation are most desirable for physicians?
Background: With new changes in healthcare delivery, the standardization offered by the electronic health record (EHR) system will undoubtedly be confronted by the heterogeneity of clinical consultations. Determination of the various characteristics considered essential for a consultation can help standardize the processes and improve the quality of communication.
Study design: Opinion surveys with a 16-question, Web-based questionnaire about inpatient consultations.
Setting: Four Minnesota teaching hospitals affiliated with the University of Minnesota.
Synopsis: This study surveyed 651 physicians, mostly from general medicine and pediatrics (30% in-training; 54% were more than five years out of training). The response rate to the survey was 50% (323). Responses were analyzed separately for physicians predominantly requesting consultations (requesters) and those predominantly providing them (consultants).
Regarding the consultation request, the majority of consultants preferred a precise consult question (94%), contact information of the ordering provider (68%), and the urgency of consultation (66%), with telephonic communication for emergent consults (75%). Responses were similar regardless of practice site, specialty, or experience.
Regarding the consultation, more requesters desired verbal communication over written advice alone: Sixty-six percent preferred to have the rationale of the recommendations explained. They also preferred a separate recommendations section (48%) with bulleted suggestions (69%) at the top or bottom of the note (74%). Emphasis was placed on specificity of drug names, dose, and duration of therapy (80%), along with alternative options (76%). Most requesters desired a clear “signoff” note when appropriate, with a follow-up plan (74%) or scheduled appointments (44%).
Bottom line: For consultations, the majority of physicians prefer an explanation of medical decision-making, a crisp recommendation section, and specific directions for follow-up.
Citation: Boulware DR, Dekarske AS, Filice GA. Physician preferences for elements of effective consultations. J Gen Intern Med. 2010;25(1):25-30.
CT Scanning Could Be Related to a Future Risk of Cancer at a Population Level
Clinical question: Does the accelerated use of CT scans increase the future risk for radiation-related cancer?
Background: Computed tomography (CT) has come through as a powerful diagnostic and interventional imaging modality at the cost of higher radiation exposures. The potential cancer risk is minimal at an individual level; however, CT technology is used in more than 70 million scans annually. This volume can translate into a significant number of future cancers in the population.
Study design: Indirect risk modeling based on CT scan frequencies and radiation risk models.
Synopsis: Annual frequencies of CT scans (age- and sex-specific) were extracted from insurance claims. The study included 57 million scans, of which 30% were performed in adults 35 to 54 years old. The majority of scans were in females (60%).
Age-specific cancer risk for each CT scan type was estimated through published radiation risk models and national surveys. The projected number of incident cancers per 10,000 scans was highest for chest or abdominal CT angiography (CTA) and whole-body CT. Incidence was higher for females.
The CT scan frequencies were combined with the cancer risk, and it was estimated that approximately 29,000 (95% UL, 15,000-45,000) future cancers could be related to the exposure from CT scans. Uncertainty limits (UL), an estimation of the total error of measurement, accounted for statistical and subjective uncertainties. The risk was dependent on the radiation dose (chest CTA) and frequency of use (abdomen/pelvis followed by chest and head). The most common cancers were lung, colon, and leukemia.
Two-thirds of the projected cancers were in females and attributable to the higher frequency of scans in women coupled with their dual risk of breast and lung cancer with chest radiation. The results provide potential study targets for risk-reduction efforts.
Bottom line: CTA of the chest, abdomen, or pelvis could be related to risk of future cancers, especially in middle-aged females.
Citation: Berrington de González A, Mahesh M, Kim KP, et al. Projected cancer risks from computed tomographic scans performed in the United States in 2007. Arch Intern Med. 2009;169(22):2071-2077.
Early Resumption of Low-Dose Aspirin after Peptic Ulcer Bleeding Might Be Beneficial
Clinical question: Is it safe to restart aspirin after acute gastrointestinal (GI) bleeding in patients with cardiovascular or cerebrovascular disease?
Background: The increasing cardiovascular burden in the aging population has indirectly increased aspirin-related peptic ulcer bleeding. Proton-pump inhibitors (PPI) have shown promise in reducing recurrent GI bleeding in non-aspirin-related cases. It is unclear if this protective effect applies to patients on aspirin and, if so, if aspirin resumption after endoscopic treatment is safe.
Study design: Parallel, randomized, placebo-controlled, noninferiority trial.
Setting: Single tertiary endoscopy center in Hong Kong.
Synopsis: One hundred fifty-six patients with aspirin-related peptic ulcer bleeding were selected for the study. After successful endoscopic treatment and 72 hours on pantoprazole infusion, the patients were started on oral pantoprazole for the duration of the study (eight weeks). Patients were equally randomized to receive low-dose aspirin (80 mg/d) or placebo. Primary outcome was recurrent bleeding within 30 days. Secondary outcomes included eight-week all-cause mortality, cause-specific mortality, and recurrence of cardiovascular events.
The aspirin group had a 50% higher risk of recurrent bleeding within 30 days compared with placebo (10.3% vs. 5.4%). However, for the secondary endpoints, aspirin had lower all-cause mortality (1.3% vs. 12.9%), which was not related to increased GI bleeding. On the other hand, discontinuation of aspirin and use of PPI in the placebo group did not prevent mortality related to GI complications.
The small numbers restrict interpretation of the mortality rates but offer support to the fact that the cardioprotective effects of aspirin outweigh its potential for GI bleeding. It is to be noted that these results cannot be extrapolated to higher doses of aspirin.
Bottom line: Early resumption of aspirin after successful treatment of peptic ulcer bleeding might increase the risk of rebleeding but potentially decreases overall mortality.
Citation: Sung JJ, Lau JY, Ching JY, et al. Continuation of low-dose aspirin therapy in peptic ulcer bleeding: a randomized trial. Ann Intern Med. 2010;152(1):1-9.
A Substantial Number of Elderly Patients with Pneumonia Have Pulmonary Malignancy
Clinical question: What is the incidence of, and risk factors for, diagnosis of lung cancer after discharge for pneumonia?
Background: Pneumonia-related admissions in elderly individuals have increased by nearly 20% during the past two decades. Based on the risk profile of this age group, many physicians recommend follow-up chest imaging after pneumonia to ensure resolution and exclude underlying malignancy. However, this practice is not backed by substantial evidence.
Study design: Retrospective cohort study from administrative databases of the VA system.
Setting: Veteran Affairs (VA) Health Care System.
Synopsis: More than 40,000 patients (older than 65, 98.1% male) hospitalized for pneumonia were included in the study. These patients had no pneumonia in the preceding year and did not carry a diagnosis of lung cancer. During the follow-up period of up to five years, a significant proportion (9.2%) of these patients were diagnosed with pulmonary malignancy.
Pertinent factors associated with increased risk of diagnosis included active tobacco use, COPD, and prior nonpulmonary malignancy. Interestingly, stroke, diabetes, dementia, and heart failure were associated with a lower risk of diagnosis, likely due to early mortality from these diseases prior to diagnosis of lung cancer.
Mean time to diagnosis was 297 days, with just 27% diagnosed within 30 days. On mortality analysis, 12.9% (n=5270) of the patients died within 30 days and 20.7% (n=8451) within 90 days. Thus, a period of surveillance of 30 to 90 days following pneumonia, especially in patients with risk factors, could be beneficial.
This study was limited due to the shortcomings of database analyses. Also, the predominantly male, elderly, veteran population restricts extrapolation to the general population.
Bottom line: Patients with risk factors for lung cancer might benefit from surveillance chest imaging after hospitalization for pneumonia to rule out an underlying malignancy.
Citation: Mortensen EM, Copeland LA, Pugh MJ, et al. Diagnosis of pulmonary malignancy after hospitalization for pneumonia. Am J Med. 2010:123(1):66-71.
Hospital-Associated Hyponatremia of Any Severity Adversely Impacts Mortality and Financial Metrics
Clinical question: Does hyponatremia during a hospitalization prophesize a worse outcome?
Study design: Retrospective cohort study from 2002-2007.
Setting: Urban academic medical center.
Synopsis: This study included 53,236 adults based on the presence of admission or subsequent hyponatremia (defined as [Na+] <138 mEq/L). The patients were classified as community-acquired (CAH=37.9%), hospital-aggravated (5.7%), or hospital-acquired hyponatremia (HAH=38.2%).
Across all subgroups, all types of hyponatremia were independently associated with worse primary outcomes, including an increase in hospital mortality (CAH 52%, HAH 66%), prolongation of hospital stay, and discharge to a facility. Also, for the same [Na+], HAH had significantly increased mortality compared with CAH. Though the elderly were more prone to develop hyponatremia, patients younger than 65 had worse outcomes.
The severity of hyponatremia prognosticated adverse outcomes. The liberal definition of hyponatremia, as opposed to the current standard of <135 mEq/L, explains the large numbers in prevalence. However, even mild hyponatremia (133 mEq/L to 137) was linked to poor outcomes (adjusted OR 1.34; CI 1.18-1.51).
The study weaknesses include the use of administrative codes to identify comorbidities, less applicability to outpatient setting, and lack of evaluation of outcomes postdischarge. However, the robust numbers do establish inpatient hyponatremia as a marker of worse outcomes.
Bottom line: Inpatient hyponatremia of any severity is a marker of increased mortality and excessive financial burden.
Citation: Wald R, Jaber BL, Price LL, Upadhyay A, Madias NE. Impact of hospital-associated hyponatremia on selected outcomes. Arch Intern Med. 2010;170(3):294-302.
Patients Lack Awareness and Prefer to Be Updated Regarding Their Inpatient Medications
Clinical question: Is patient knowledge of their medications deficient, and does this reflect a lack of desire to be involved in the medication reconciliation process?
Background: Medication errors remain a significant healthcare problem due to their potential to increase morbidity. For medication administration errors, apart from the dispensing pharmacist and the nurses, patients could be the final checkpoint to ensure medication safety. However, their awareness and enthusiasm to participate has not been adequately assessed in the literature.
Study design: A cross-sectional study using individual surveys to assess awareness and attitudes regarding inpatient medications.
Setting: Single tertiary-care academic teaching hospital.
Synopsis: Fifty cognitively intact adult patients were consented for the study. Of these, 54% provided an accurate recollection of their outpatient medications. When they were surveyed regarding inpatient medications, 96% omitted at least one medication, with the average of 6.8 medication omissions. This was noted to correlate with age >65 years. Also, 44% erroneously presumed they were on a medication while they were in the hospital, even though they weren’t.
When attitudes were surveyed, most of the patients would have preferred to get an inpatient medication list (78%) with the goal of improving their satisfaction (81%) and reducing errors (94%). Also, no association was found between patients’ errors of omission and their reported desire to be involved in the medication safety process.
This small study was limited to cognitively intact patients only. Also, the relatively younger age might cause an overestimation of patient interest in participation. However, the results highlight key medication reconciliation issues. Although patient involvement is desirable, a systematic program of educating them about their medications would be required to make their feedback effective and useful.
Bottom line: Healthy patients might be unaware of their exact hospital medications but prefer to be kept in the loop.
Citation: Cumbler E, Wald H, Kutner J. Lack of patient knowledge regarding hospital medications. J Hosp Med. 2010;5(2):83-86.
Monoclonal Antibodies against Clostridium difficile Toxins Prevent Recurrence
Clinical question: Are human monoclonal antibodies against C. difficile toxin A (CDA1) and B (CDB1) effective in preventing recurrence of C. diff infection (CDI)?
Background: Widespread use of antibiotics, coupled with the emergence of the hypervirulent (B1/NAP1/027) strain of C. diff, has altered the epidemiology of CDI. Even with effective treatment regimens, there is an escalation in severity, treatment failures, and recurrences. Antibodies against the C. diff toxins are being evaluated as the next frontier in treatment of CDI.
Study design: Phase 2 randomized, double-blind, placebo-controlled trial.
Setting: Thirty study centers in Canada and the U.S.
Synopsis: Two hundred patients with laboratory documented CDI on standard therapy with either metronidazole or vancomycin were randomized to receive a single IV infusion of combined monoclonal antibodies against CDA1 and CDB1 (n=101) or a normal saline placebo infusion (n=99). Patients were followed for 84 days with daily stool counts and intermittent blood samples for immunogenicity analysis.
The primary endpoint of recurrence of laboratory-proven C. diff diarrhea was significantly lower in the monoclonal antibody group (7% vs. 25% in placebo. 95% CI, 7-29; P <0.001). In a subgroup analysis of the epidemic BI/NAP1/027 strain, this favorable association persisted (8% vs. 32%). Recurrence in the antibody group was seen more in elderly patients hospitalized with a higher severity of underlying disease.
Secondary endpoints relating to the initial episode of CDI including treatment failure, severity of diarrhea, and duration to resolution were not significantly different between the two groups. Fewer accounts of serious adverse events were documented in the antibody group (18 patients vs. 28 patients in placebo, P=0.09), and immunogenicity was not detected in any patient.
Bottom line: Monoclonal antibody infusion against C. diff toxins reduces recurrence of infection, even with a hypervirulent (B1/NAP1/027) strain, without any significant adverse events.
Citation: Lowy I, Molrine DC, Leav BA, et al. Treatment with monoclonal antibodies against Clostridium difficile toxins. N Engl J Med. 2010; 362(3):197-205. TH
PEDIATRIC HM LITERATURE
By Mark Shen, MD
Rectal Colonization with S. aureus Associated with Skin Abscesses
Clinical question: Is rectal colonization with Staphylococcus aureus more strongly associated with staphylococcal skin abscesses than nasal colonization?
Background: Staphylococcal skin and soft tissue infections have dramatically increased in recent years. While increased rates of nasal colonization with S. aureus have also been noted, a strong association with skin infections in children has not been established. The relationship between staphylococcal colonization of other body sites and skin infection is unknown.
Study design: Prospective cohort study.
Setting: Tertiary-care hospital in Buffalo, N.Y.
Synopsis: Sixty children, 0 to 18 years of age, requiring surgical drainage of S. aureus skin abscesses and 90 children undergoing other surgical procedures were enrolled consecutively. Rectal, nasal, and abscess (if applicable) cultures were obtained on all patients. Enrollment ceased when notably different rates of rectal colonization were recorded.
Rectal cultures were significantly more likely to be positive in the abscess group than the control group (47% vs. 1%; P<0.0001), while rates of nasal colonization were similar (27% vs. 21%; P=0.44). Abscess isolates were identical to rectal isolates in 88% of cases and nasal isolates in 75% of cases.
Other findings included a 60% prevalence of methicillin-resistant S. aureus (MRSA) in the abscess group. Fifty-nine of the 60 abscess isolates contained Panton-Valentine leukocidin genes; 57 were pulsed-field type USA300; and all 60 contained the staphylococcal cassette chromosome mec type IVa.
Given this representative sample of community-associated staphylococcal disease, these findings suggest that a focus on nasal carriage of S. aureus might be misguided.
Bottom Line: Rectal colonization with S. aureus better predicts skin abscess isolate than nasal carriage.
Citation: Faden H, Lesse AJ, Trask J, et al. Importance of colonization site in the current epidemic of staphylococcal skin abscesses. Pediatrics. 2010;125(3):e618-e624.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Effect of restrictive antibiotic policies on dosing timeliness
- Desired consultation format and content
- Risk of cancer associated with CT imaging
- Bleeding, mortality with aspirin after peptic ulcer bleed
- Diagnosis of lung cancer after pneumonia
- Outcomes associated with hyponatremia
- Patient awareness, interest in inpatient medication list
- Monoclonal antibodies in C. difficile
Restrictive Antimicrobial Policy Delays Administration
Clinical question: Does the approval process for restricted on-formulary antimicrobials cause a significant delay in their administration?
Background: Widespread and often unwarranted, antimicrobial use in the hospital lends itself to the development of microbial resistance and increases overall costs. To curb such practices, many hospitals require subspecialty approval prior to dispensing select broad-spectrum antimicrobials. Though shown to improve outcomes, the impact of the approval process on the timeliness of antimicrobial administration remains to be seen.
Study design: Retrospective cohort study.
Setting: Tertiary-care university hospital.
Synopsis: The study included 3,251 inpatients with computerized orders for a “stat” first dose of any of 24 pre-selected, parenteral antimicrobials. Time lag (more than one hour, and more than two hours) to nursing documentation of drug administration was separately analyzed for restricted and unrestricted antimicrobials.
Delay of more than one hour was significantly higher for restricted antimicrobials with an odds ratio of 1.49 (95% CI; 1.23-1.82), while the odds ratio for a delay of more than two hours was 1.78 (95% CI, 1.39-2.21). Also, for restricted antimicrobials, the percentage of orders delayed for more than one hour was significantly different between daytime and nighttime (when the first dose was exempt from pre-approval) orders: 46.1% versus 38.8% (P<0.001). For unrestricted drugs, delay was uniform irrespective of time of day (36.4% of daytime and 36.6% of nighttime orders were delayed more than one hour). The effect of delay in drug administration on patient outcomes was not evaluated.
Though the approval process aims in part to affect resistance patterns and overall costs, this research highlights the need to minimize the delay in administration and probably skip the approval for the first dose in critically ill patients.
Bottom line: Antibiotic approval processes can delay their administration in hospitalized patients, but the effect of this delay on patient outcomes is not yet known.
Citation: Winters BD, Thiemann DR, Brotman DJ. Impact of a restrictive antimicrobial policy on the process and timing of antimicrobial administration. J Hosp Med. 2010;5(1):E41-45.
Physicians Uphold Tenets of Effective Consultation while Highlighting Some Newer Viewpoints
Clinical question: What key features of a consultation are most desirable for physicians?
Background: With new changes in healthcare delivery, the standardization offered by the electronic health record (EHR) system will undoubtedly be confronted by the heterogeneity of clinical consultations. Determination of the various characteristics considered essential for a consultation can help standardize the processes and improve the quality of communication.
Study design: Opinion surveys with a 16-question, Web-based questionnaire about inpatient consultations.
Setting: Four Minnesota teaching hospitals affiliated with the University of Minnesota.
Synopsis: This study surveyed 651 physicians, mostly from general medicine and pediatrics (30% in-training; 54% were more than five years out of training). The response rate to the survey was 50% (323). Responses were analyzed separately for physicians predominantly requesting consultations (requesters) and those predominantly providing them (consultants).
Regarding the consultation request, the majority of consultants preferred a precise consult question (94%), contact information of the ordering provider (68%), and the urgency of consultation (66%), with telephonic communication for emergent consults (75%). Responses were similar regardless of practice site, specialty, or experience.
Regarding the consultation, more requesters desired verbal communication over written advice alone: Sixty-six percent preferred to have the rationale of the recommendations explained. They also preferred a separate recommendations section (48%) with bulleted suggestions (69%) at the top or bottom of the note (74%). Emphasis was placed on specificity of drug names, dose, and duration of therapy (80%), along with alternative options (76%). Most requesters desired a clear “signoff” note when appropriate, with a follow-up plan (74%) or scheduled appointments (44%).
Bottom line: For consultations, the majority of physicians prefer an explanation of medical decision-making, a crisp recommendation section, and specific directions for follow-up.
Citation: Boulware DR, Dekarske AS, Filice GA. Physician preferences for elements of effective consultations. J Gen Intern Med. 2010;25(1):25-30.
CT Scanning Could Be Related to a Future Risk of Cancer at a Population Level
Clinical question: Does the accelerated use of CT scans increase the future risk for radiation-related cancer?
Background: Computed tomography (CT) has come through as a powerful diagnostic and interventional imaging modality at the cost of higher radiation exposures. The potential cancer risk is minimal at an individual level; however, CT technology is used in more than 70 million scans annually. This volume can translate into a significant number of future cancers in the population.
Study design: Indirect risk modeling based on CT scan frequencies and radiation risk models.
Synopsis: Annual frequencies of CT scans (age- and sex-specific) were extracted from insurance claims. The study included 57 million scans, of which 30% were performed in adults 35 to 54 years old. The majority of scans were in females (60%).
Age-specific cancer risk for each CT scan type was estimated through published radiation risk models and national surveys. The projected number of incident cancers per 10,000 scans was highest for chest or abdominal CT angiography (CTA) and whole-body CT. Incidence was higher for females.
The CT scan frequencies were combined with the cancer risk, and it was estimated that approximately 29,000 (95% UL, 15,000-45,000) future cancers could be related to the exposure from CT scans. Uncertainty limits (UL), an estimation of the total error of measurement, accounted for statistical and subjective uncertainties. The risk was dependent on the radiation dose (chest CTA) and frequency of use (abdomen/pelvis followed by chest and head). The most common cancers were lung, colon, and leukemia.
Two-thirds of the projected cancers were in females and attributable to the higher frequency of scans in women coupled with their dual risk of breast and lung cancer with chest radiation. The results provide potential study targets for risk-reduction efforts.
Bottom line: CTA of the chest, abdomen, or pelvis could be related to risk of future cancers, especially in middle-aged females.
Citation: Berrington de González A, Mahesh M, Kim KP, et al. Projected cancer risks from computed tomographic scans performed in the United States in 2007. Arch Intern Med. 2009;169(22):2071-2077.
Early Resumption of Low-Dose Aspirin after Peptic Ulcer Bleeding Might Be Beneficial
Clinical question: Is it safe to restart aspirin after acute gastrointestinal (GI) bleeding in patients with cardiovascular or cerebrovascular disease?
Background: The increasing cardiovascular burden in the aging population has indirectly increased aspirin-related peptic ulcer bleeding. Proton-pump inhibitors (PPI) have shown promise in reducing recurrent GI bleeding in non-aspirin-related cases. It is unclear if this protective effect applies to patients on aspirin and, if so, if aspirin resumption after endoscopic treatment is safe.
Study design: Parallel, randomized, placebo-controlled, noninferiority trial.
Setting: Single tertiary endoscopy center in Hong Kong.
Synopsis: One hundred fifty-six patients with aspirin-related peptic ulcer bleeding were selected for the study. After successful endoscopic treatment and 72 hours on pantoprazole infusion, the patients were started on oral pantoprazole for the duration of the study (eight weeks). Patients were equally randomized to receive low-dose aspirin (80 mg/d) or placebo. Primary outcome was recurrent bleeding within 30 days. Secondary outcomes included eight-week all-cause mortality, cause-specific mortality, and recurrence of cardiovascular events.
The aspirin group had a 50% higher risk of recurrent bleeding within 30 days compared with placebo (10.3% vs. 5.4%). However, for the secondary endpoints, aspirin had lower all-cause mortality (1.3% vs. 12.9%), which was not related to increased GI bleeding. On the other hand, discontinuation of aspirin and use of PPI in the placebo group did not prevent mortality related to GI complications.
The small numbers restrict interpretation of the mortality rates but offer support to the fact that the cardioprotective effects of aspirin outweigh its potential for GI bleeding. It is to be noted that these results cannot be extrapolated to higher doses of aspirin.
Bottom line: Early resumption of aspirin after successful treatment of peptic ulcer bleeding might increase the risk of rebleeding but potentially decreases overall mortality.
Citation: Sung JJ, Lau JY, Ching JY, et al. Continuation of low-dose aspirin therapy in peptic ulcer bleeding: a randomized trial. Ann Intern Med. 2010;152(1):1-9.
A Substantial Number of Elderly Patients with Pneumonia Have Pulmonary Malignancy
Clinical question: What is the incidence of, and risk factors for, diagnosis of lung cancer after discharge for pneumonia?
Background: Pneumonia-related admissions in elderly individuals have increased by nearly 20% during the past two decades. Based on the risk profile of this age group, many physicians recommend follow-up chest imaging after pneumonia to ensure resolution and exclude underlying malignancy. However, this practice is not backed by substantial evidence.
Study design: Retrospective cohort study from administrative databases of the VA system.
Setting: Veteran Affairs (VA) Health Care System.
Synopsis: More than 40,000 patients (older than 65, 98.1% male) hospitalized for pneumonia were included in the study. These patients had no pneumonia in the preceding year and did not carry a diagnosis of lung cancer. During the follow-up period of up to five years, a significant proportion (9.2%) of these patients were diagnosed with pulmonary malignancy.
Pertinent factors associated with increased risk of diagnosis included active tobacco use, COPD, and prior nonpulmonary malignancy. Interestingly, stroke, diabetes, dementia, and heart failure were associated with a lower risk of diagnosis, likely due to early mortality from these diseases prior to diagnosis of lung cancer.
Mean time to diagnosis was 297 days, with just 27% diagnosed within 30 days. On mortality analysis, 12.9% (n=5270) of the patients died within 30 days and 20.7% (n=8451) within 90 days. Thus, a period of surveillance of 30 to 90 days following pneumonia, especially in patients with risk factors, could be beneficial.
This study was limited due to the shortcomings of database analyses. Also, the predominantly male, elderly, veteran population restricts extrapolation to the general population.
Bottom line: Patients with risk factors for lung cancer might benefit from surveillance chest imaging after hospitalization for pneumonia to rule out an underlying malignancy.
Citation: Mortensen EM, Copeland LA, Pugh MJ, et al. Diagnosis of pulmonary malignancy after hospitalization for pneumonia. Am J Med. 2010:123(1):66-71.
Hospital-Associated Hyponatremia of Any Severity Adversely Impacts Mortality and Financial Metrics
Clinical question: Does hyponatremia during a hospitalization prophesize a worse outcome?
Study design: Retrospective cohort study from 2002-2007.
Setting: Urban academic medical center.
Synopsis: This study included 53,236 adults based on the presence of admission or subsequent hyponatremia (defined as [Na+] <138 mEq/L). The patients were classified as community-acquired (CAH=37.9%), hospital-aggravated (5.7%), or hospital-acquired hyponatremia (HAH=38.2%).
Across all subgroups, all types of hyponatremia were independently associated with worse primary outcomes, including an increase in hospital mortality (CAH 52%, HAH 66%), prolongation of hospital stay, and discharge to a facility. Also, for the same [Na+], HAH had significantly increased mortality compared with CAH. Though the elderly were more prone to develop hyponatremia, patients younger than 65 had worse outcomes.
The severity of hyponatremia prognosticated adverse outcomes. The liberal definition of hyponatremia, as opposed to the current standard of <135 mEq/L, explains the large numbers in prevalence. However, even mild hyponatremia (133 mEq/L to 137) was linked to poor outcomes (adjusted OR 1.34; CI 1.18-1.51).
The study weaknesses include the use of administrative codes to identify comorbidities, less applicability to outpatient setting, and lack of evaluation of outcomes postdischarge. However, the robust numbers do establish inpatient hyponatremia as a marker of worse outcomes.
Bottom line: Inpatient hyponatremia of any severity is a marker of increased mortality and excessive financial burden.
Citation: Wald R, Jaber BL, Price LL, Upadhyay A, Madias NE. Impact of hospital-associated hyponatremia on selected outcomes. Arch Intern Med. 2010;170(3):294-302.
Patients Lack Awareness and Prefer to Be Updated Regarding Their Inpatient Medications
Clinical question: Is patient knowledge of their medications deficient, and does this reflect a lack of desire to be involved in the medication reconciliation process?
Background: Medication errors remain a significant healthcare problem due to their potential to increase morbidity. For medication administration errors, apart from the dispensing pharmacist and the nurses, patients could be the final checkpoint to ensure medication safety. However, their awareness and enthusiasm to participate has not been adequately assessed in the literature.
Study design: A cross-sectional study using individual surveys to assess awareness and attitudes regarding inpatient medications.
Setting: Single tertiary-care academic teaching hospital.
Synopsis: Fifty cognitively intact adult patients were consented for the study. Of these, 54% provided an accurate recollection of their outpatient medications. When they were surveyed regarding inpatient medications, 96% omitted at least one medication, with the average of 6.8 medication omissions. This was noted to correlate with age >65 years. Also, 44% erroneously presumed they were on a medication while they were in the hospital, even though they weren’t.
When attitudes were surveyed, most of the patients would have preferred to get an inpatient medication list (78%) with the goal of improving their satisfaction (81%) and reducing errors (94%). Also, no association was found between patients’ errors of omission and their reported desire to be involved in the medication safety process.
This small study was limited to cognitively intact patients only. Also, the relatively younger age might cause an overestimation of patient interest in participation. However, the results highlight key medication reconciliation issues. Although patient involvement is desirable, a systematic program of educating them about their medications would be required to make their feedback effective and useful.
Bottom line: Healthy patients might be unaware of their exact hospital medications but prefer to be kept in the loop.
Citation: Cumbler E, Wald H, Kutner J. Lack of patient knowledge regarding hospital medications. J Hosp Med. 2010;5(2):83-86.
Monoclonal Antibodies against Clostridium difficile Toxins Prevent Recurrence
Clinical question: Are human monoclonal antibodies against C. difficile toxin A (CDA1) and B (CDB1) effective in preventing recurrence of C. diff infection (CDI)?
Background: Widespread use of antibiotics, coupled with the emergence of the hypervirulent (B1/NAP1/027) strain of C. diff, has altered the epidemiology of CDI. Even with effective treatment regimens, there is an escalation in severity, treatment failures, and recurrences. Antibodies against the C. diff toxins are being evaluated as the next frontier in treatment of CDI.
Study design: Phase 2 randomized, double-blind, placebo-controlled trial.
Setting: Thirty study centers in Canada and the U.S.
Synopsis: Two hundred patients with laboratory documented CDI on standard therapy with either metronidazole or vancomycin were randomized to receive a single IV infusion of combined monoclonal antibodies against CDA1 and CDB1 (n=101) or a normal saline placebo infusion (n=99). Patients were followed for 84 days with daily stool counts and intermittent blood samples for immunogenicity analysis.
The primary endpoint of recurrence of laboratory-proven C. diff diarrhea was significantly lower in the monoclonal antibody group (7% vs. 25% in placebo. 95% CI, 7-29; P <0.001). In a subgroup analysis of the epidemic BI/NAP1/027 strain, this favorable association persisted (8% vs. 32%). Recurrence in the antibody group was seen more in elderly patients hospitalized with a higher severity of underlying disease.
Secondary endpoints relating to the initial episode of CDI including treatment failure, severity of diarrhea, and duration to resolution were not significantly different between the two groups. Fewer accounts of serious adverse events were documented in the antibody group (18 patients vs. 28 patients in placebo, P=0.09), and immunogenicity was not detected in any patient.
Bottom line: Monoclonal antibody infusion against C. diff toxins reduces recurrence of infection, even with a hypervirulent (B1/NAP1/027) strain, without any significant adverse events.
Citation: Lowy I, Molrine DC, Leav BA, et al. Treatment with monoclonal antibodies against Clostridium difficile toxins. N Engl J Med. 2010; 362(3):197-205. TH
PEDIATRIC HM LITERATURE
By Mark Shen, MD
Rectal Colonization with S. aureus Associated with Skin Abscesses
Clinical question: Is rectal colonization with Staphylococcus aureus more strongly associated with staphylococcal skin abscesses than nasal colonization?
Background: Staphylococcal skin and soft tissue infections have dramatically increased in recent years. While increased rates of nasal colonization with S. aureus have also been noted, a strong association with skin infections in children has not been established. The relationship between staphylococcal colonization of other body sites and skin infection is unknown.
Study design: Prospective cohort study.
Setting: Tertiary-care hospital in Buffalo, N.Y.
Synopsis: Sixty children, 0 to 18 years of age, requiring surgical drainage of S. aureus skin abscesses and 90 children undergoing other surgical procedures were enrolled consecutively. Rectal, nasal, and abscess (if applicable) cultures were obtained on all patients. Enrollment ceased when notably different rates of rectal colonization were recorded.
Rectal cultures were significantly more likely to be positive in the abscess group than the control group (47% vs. 1%; P<0.0001), while rates of nasal colonization were similar (27% vs. 21%; P=0.44). Abscess isolates were identical to rectal isolates in 88% of cases and nasal isolates in 75% of cases.
Other findings included a 60% prevalence of methicillin-resistant S. aureus (MRSA) in the abscess group. Fifty-nine of the 60 abscess isolates contained Panton-Valentine leukocidin genes; 57 were pulsed-field type USA300; and all 60 contained the staphylococcal cassette chromosome mec type IVa.
Given this representative sample of community-associated staphylococcal disease, these findings suggest that a focus on nasal carriage of S. aureus might be misguided.
Bottom Line: Rectal colonization with S. aureus better predicts skin abscess isolate than nasal carriage.
Citation: Faden H, Lesse AJ, Trask J, et al. Importance of colonization site in the current epidemic of staphylococcal skin abscesses. Pediatrics. 2010;125(3):e618-e624.
Observation Care
Many conditions once treated during an “inpatient” hospital stay are currently treated during an “observation” stay (OBS). Although the care remains the same, physician billing is different and requires close attention to admission details for effective charge capture.
Let’s take a look at a typical OBS scenario. A 65-year-old female with longstanding diabetes presents to the ED at 10 p.m. with palpitations, lightheadedness, mild disorientation, and elevated blood sugar. The hospitalist admits the patient to observation, treats her for dehydration, and discharges her the next day. Before billing, the hospitalist should consider the following factors.
Physician of Record
The attending of record writes the orders to admit the patient to observation; indicates the reason for the stay; outlines the plan of care; and manages the patient during the stay. The attending reports the initial patient encounter with the most appropriate initial observation-care code, as reflected by the documentation:1
- 99218: Initial observation care, requiring both a detailed or comprehensive history and exam, and straightforward/low-complexity medical decision-making. Usually, the problem(s) is of low severity.
- 99219: Initial observation care, requiring both a comprehensive history and exam, and moderate-complexity medical decision-making. Usually, the problem(s) is of moderate severity.
- 99220: Initial observation care, requiring both a comprehensive history and exam, and high-complexity medical decision-making. Usually, the problem(s) is of high severity.
While other physicians (e.g., specialists) might be involved in the patient’s care, only the attending physician reports codes 99218-99220. Specialists typically are called to an OBS case for their opinion or advice but do not function as the attending of record. Billing for the specialist (consultation) service depends upon the payor.
For a non-Medicare patient who pays for consultation codes, the specialist reports an outpatient consultation code (99241-99245) for the appropriately documented service. Conversely, Medicare no longer recognizes consultation codes, and specialists must report either a new patient visit code (99201-99205) or established patient visit code (99212-99215) for Medicare beneficiaries.
Selection of the new or established patient codes follows the “three-year rule”: A “new patient” has not received any face-to-face services (e.g., visit or procedure) in any location from any physician within the same group and same specialty within the past three years.2 There could be occasion when a hospitalist is not the attending of record but is asked to provide their opinion, and must report one of the “non-OBS” codes.
The attending of record is permitted to report a discharge service as long as this service occurs on a calendar day different from the admission service (as in the listed scenario). The attending documents the face-to-face discharge service and any pertinent clinical details, and reports 99217 (observation-care discharge-day management).
Length of Stay
Observation-care services typically do not exceed 24 hours and two calendar days. Observation care for more than 48 hours without inpatient admission is not considered medically necessary but might be payable after medical review. Should the OBS stay span more than two calendar days (as might be the case with “downgraded” hospitalizations), hospitalists should report established patient visit codes (99212-99215) for the calendar day(s) between the admission service (99218-99220) and the discharge service (99217).3 The physician must provide and document a face-to-face encounter on each date of service for which a claim was submitted.
A more likely occurrence is the admission and discharge from OBS on the same calendar date. The attending of record reports the code that corresponds to the patient’s length of stay (LOS). If the total LOS is less than eight hours, the attending only reports standard OBS codes (99218-99220). The hospitalist does not separately report the OBS discharge service (99217), even though the documentation must reflect the attending discharge order and corresponding discharge plan. If the total duration of the patient’s stay lasts more than eight hours and does not overlap two calendar days, the attending reports the same-day admit/discharge codes:1
- 99234: Observation or inpatient care, same date admission and discharge, requiring both a detailed or comprehensive history and exam, and straightforward or low-complexity medical decision-making. Usually the presenting problem(s) is of low severity.
- 99235: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and moderate-complexity medical decision-making. Usually the presenting problem(s) is of moderate severity.
- 99236: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and high-complexity medical decision-making. Usually the presenting problem(s) is of high severity.
OBS discharge service (99217) is not separately reported with 99234-99236 because these codes are valued to include the discharge component (e.g., the comprehensive service, 99236 [4.26 wRVU, $211], is equivalent to its components, 99220 [2.99 wRVU, $148] and 99217 [1.28 wRVU, $68]). The attending must document the total duration of the stay, as well as the face-to-face service and the corresponding details of each service component (i.e., both an admission and discharge note).3TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010:11-16.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.7A. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8C. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8D. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 1, Section 50.3. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c01.pdf. Accessed May 12, 2010.
Many conditions once treated during an “inpatient” hospital stay are currently treated during an “observation” stay (OBS). Although the care remains the same, physician billing is different and requires close attention to admission details for effective charge capture.
Let’s take a look at a typical OBS scenario. A 65-year-old female with longstanding diabetes presents to the ED at 10 p.m. with palpitations, lightheadedness, mild disorientation, and elevated blood sugar. The hospitalist admits the patient to observation, treats her for dehydration, and discharges her the next day. Before billing, the hospitalist should consider the following factors.
Physician of Record
The attending of record writes the orders to admit the patient to observation; indicates the reason for the stay; outlines the plan of care; and manages the patient during the stay. The attending reports the initial patient encounter with the most appropriate initial observation-care code, as reflected by the documentation:1
- 99218: Initial observation care, requiring both a detailed or comprehensive history and exam, and straightforward/low-complexity medical decision-making. Usually, the problem(s) is of low severity.
- 99219: Initial observation care, requiring both a comprehensive history and exam, and moderate-complexity medical decision-making. Usually, the problem(s) is of moderate severity.
- 99220: Initial observation care, requiring both a comprehensive history and exam, and high-complexity medical decision-making. Usually, the problem(s) is of high severity.
While other physicians (e.g., specialists) might be involved in the patient’s care, only the attending physician reports codes 99218-99220. Specialists typically are called to an OBS case for their opinion or advice but do not function as the attending of record. Billing for the specialist (consultation) service depends upon the payor.
For a non-Medicare patient who pays for consultation codes, the specialist reports an outpatient consultation code (99241-99245) for the appropriately documented service. Conversely, Medicare no longer recognizes consultation codes, and specialists must report either a new patient visit code (99201-99205) or established patient visit code (99212-99215) for Medicare beneficiaries.
Selection of the new or established patient codes follows the “three-year rule”: A “new patient” has not received any face-to-face services (e.g., visit or procedure) in any location from any physician within the same group and same specialty within the past three years.2 There could be occasion when a hospitalist is not the attending of record but is asked to provide their opinion, and must report one of the “non-OBS” codes.
The attending of record is permitted to report a discharge service as long as this service occurs on a calendar day different from the admission service (as in the listed scenario). The attending documents the face-to-face discharge service and any pertinent clinical details, and reports 99217 (observation-care discharge-day management).
Length of Stay
Observation-care services typically do not exceed 24 hours and two calendar days. Observation care for more than 48 hours without inpatient admission is not considered medically necessary but might be payable after medical review. Should the OBS stay span more than two calendar days (as might be the case with “downgraded” hospitalizations), hospitalists should report established patient visit codes (99212-99215) for the calendar day(s) between the admission service (99218-99220) and the discharge service (99217).3 The physician must provide and document a face-to-face encounter on each date of service for which a claim was submitted.
A more likely occurrence is the admission and discharge from OBS on the same calendar date. The attending of record reports the code that corresponds to the patient’s length of stay (LOS). If the total LOS is less than eight hours, the attending only reports standard OBS codes (99218-99220). The hospitalist does not separately report the OBS discharge service (99217), even though the documentation must reflect the attending discharge order and corresponding discharge plan. If the total duration of the patient’s stay lasts more than eight hours and does not overlap two calendar days, the attending reports the same-day admit/discharge codes:1
- 99234: Observation or inpatient care, same date admission and discharge, requiring both a detailed or comprehensive history and exam, and straightforward or low-complexity medical decision-making. Usually the presenting problem(s) is of low severity.
- 99235: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and moderate-complexity medical decision-making. Usually the presenting problem(s) is of moderate severity.
- 99236: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and high-complexity medical decision-making. Usually the presenting problem(s) is of high severity.
OBS discharge service (99217) is not separately reported with 99234-99236 because these codes are valued to include the discharge component (e.g., the comprehensive service, 99236 [4.26 wRVU, $211], is equivalent to its components, 99220 [2.99 wRVU, $148] and 99217 [1.28 wRVU, $68]). The attending must document the total duration of the stay, as well as the face-to-face service and the corresponding details of each service component (i.e., both an admission and discharge note).3TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010:11-16.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.7A. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8C. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8D. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 1, Section 50.3. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c01.pdf. Accessed May 12, 2010.
Many conditions once treated during an “inpatient” hospital stay are currently treated during an “observation” stay (OBS). Although the care remains the same, physician billing is different and requires close attention to admission details for effective charge capture.
Let’s take a look at a typical OBS scenario. A 65-year-old female with longstanding diabetes presents to the ED at 10 p.m. with palpitations, lightheadedness, mild disorientation, and elevated blood sugar. The hospitalist admits the patient to observation, treats her for dehydration, and discharges her the next day. Before billing, the hospitalist should consider the following factors.
Physician of Record
The attending of record writes the orders to admit the patient to observation; indicates the reason for the stay; outlines the plan of care; and manages the patient during the stay. The attending reports the initial patient encounter with the most appropriate initial observation-care code, as reflected by the documentation:1
- 99218: Initial observation care, requiring both a detailed or comprehensive history and exam, and straightforward/low-complexity medical decision-making. Usually, the problem(s) is of low severity.
- 99219: Initial observation care, requiring both a comprehensive history and exam, and moderate-complexity medical decision-making. Usually, the problem(s) is of moderate severity.
- 99220: Initial observation care, requiring both a comprehensive history and exam, and high-complexity medical decision-making. Usually, the problem(s) is of high severity.
While other physicians (e.g., specialists) might be involved in the patient’s care, only the attending physician reports codes 99218-99220. Specialists typically are called to an OBS case for their opinion or advice but do not function as the attending of record. Billing for the specialist (consultation) service depends upon the payor.
For a non-Medicare patient who pays for consultation codes, the specialist reports an outpatient consultation code (99241-99245) for the appropriately documented service. Conversely, Medicare no longer recognizes consultation codes, and specialists must report either a new patient visit code (99201-99205) or established patient visit code (99212-99215) for Medicare beneficiaries.
Selection of the new or established patient codes follows the “three-year rule”: A “new patient” has not received any face-to-face services (e.g., visit or procedure) in any location from any physician within the same group and same specialty within the past three years.2 There could be occasion when a hospitalist is not the attending of record but is asked to provide their opinion, and must report one of the “non-OBS” codes.
The attending of record is permitted to report a discharge service as long as this service occurs on a calendar day different from the admission service (as in the listed scenario). The attending documents the face-to-face discharge service and any pertinent clinical details, and reports 99217 (observation-care discharge-day management).
Length of Stay
Observation-care services typically do not exceed 24 hours and two calendar days. Observation care for more than 48 hours without inpatient admission is not considered medically necessary but might be payable after medical review. Should the OBS stay span more than two calendar days (as might be the case with “downgraded” hospitalizations), hospitalists should report established patient visit codes (99212-99215) for the calendar day(s) between the admission service (99218-99220) and the discharge service (99217).3 The physician must provide and document a face-to-face encounter on each date of service for which a claim was submitted.
A more likely occurrence is the admission and discharge from OBS on the same calendar date. The attending of record reports the code that corresponds to the patient’s length of stay (LOS). If the total LOS is less than eight hours, the attending only reports standard OBS codes (99218-99220). The hospitalist does not separately report the OBS discharge service (99217), even though the documentation must reflect the attending discharge order and corresponding discharge plan. If the total duration of the patient’s stay lasts more than eight hours and does not overlap two calendar days, the attending reports the same-day admit/discharge codes:1
- 99234: Observation or inpatient care, same date admission and discharge, requiring both a detailed or comprehensive history and exam, and straightforward or low-complexity medical decision-making. Usually the presenting problem(s) is of low severity.
- 99235: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and moderate-complexity medical decision-making. Usually the presenting problem(s) is of moderate severity.
- 99236: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and high-complexity medical decision-making. Usually the presenting problem(s) is of high severity.
OBS discharge service (99217) is not separately reported with 99234-99236 because these codes are valued to include the discharge component (e.g., the comprehensive service, 99236 [4.26 wRVU, $211], is equivalent to its components, 99220 [2.99 wRVU, $148] and 99217 [1.28 wRVU, $68]). The attending must document the total duration of the stay, as well as the face-to-face service and the corresponding details of each service component (i.e., both an admission and discharge note).3TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010:11-16.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.7A. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8C. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8D. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 1, Section 50.3. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c01.pdf. Accessed May 12, 2010.
What Is the Most Cost- Effective Evaluation for a First Syncopal Episode?
Case
A 71-year-old woman is admitted after losing consciousness and falling at home. Her history is significant for hypertension, bilateral internal carotid artery stenoses, chronic kidney disease, and diabetes. Resting vital signs are normal. Cardiac, pulmonary, and neurologic exams are unremarkable, as is an electrocardiogram (ECG). She was noted to have a small scalp laceration. Noncontrast CT of the head demonstrates a small occipital subdural bleed thought to be a result of her fall.

What is the most cost-effective evaluation for this patient admitted with suspected first syncopal episode?
Overview
Syncope is defined as sudden, self-terminating loss of consciousness. The final common pathway of all causes of syncope is global cerebral hypoperfusion—specifically, hypoperfusion of the reticular activating system. The differential diagnosis of syncopal loss of consciousness includes neurally mediated (e.g., vasovagal) syncope, orthostatic hypotension, cardiac arrhythmias, structural heart disease, and cerebrovascular disease.
Among young, otherwise healthy people, neurally mediated syncope, which has a relatively benign prognosis, is by far the most common etiology, while in older patients, primary cardiac causes are more common. Nonsyncopal mechanisms, such as seizure and hypoglycemia, should also be considered in the differential diagnosis of transient loss of consciousness (see Table 1, p. 19).1
Syncope is a common problem, accounting for 1% to 2% of ED visits in the U.S.2 The primary objective for evaluation is identification of individuals at increased risk of death due to associated conditions, especially cardiac conditions such as structural heart disease; myocardial ischemia and infarction (MI); Wolff-Parkinson-White, Brugada, or long QT syndromes; and polymorphic ventricular tachycardia.3 True syncope can be associated with other concerning causes, such as aortic stenosis, aortic dissection, and massive pulmonary embolus, as well as arrhythmias from underlying cardiac disease.4
Review of the Data
History: A detailed history and physical examination reveals the cause in 50% of syncopal episodes. Key factors include the account of third-party observers, although it is important to note that tonic-clonic movements can be associated with the global cerebral hypoperfusion of syncope as well as with seizure.4 History of dyspnea, chest pain, or palpitations argue for a primary cardiac or pulmonary cause.
Among patients who endorse a history of palpitations, the sensation of rapid and regular pulsations in the neck points very strongly toward an AV-nodal re-entrant tachycardia, because the carotid pulse and cannon A wave arrive simultaneously in the neck.5 Postictal confusion and focal neurologic exam findings suggest a neurologic rather than syncopal cause, although there are exceptions, and the relationship between seizure and impaired myocardial perfusion is complex.
One factor shown to be significantly associated with a cardiac cause for episodic syncope is family history of sudden cardiac death.4
Physical exam: A thorough general and neurologic exam is critical in evaluation of a first syncopal episode. Supine and standing blood pressure and heart rate should be measured, waiting at least one minute (and by some protocols up to three minutes) after the patient stands up to record standing vitals. Measurement of sitting vitals is not necessary. Neither postural hypotension nor tachycardia are sensitive for hypovolemia in normal volunteers, but a 30-point increase in heart rate is more than 99% specific; a 20-point drop in systolic blood pressure (SBP) is less so.5 A difference of more than 20 mmHg between systolic arm pressures in an individual with chest pain suggests aortic dissection.
Other findings useful in diagnosis of syncope include signs of aortic stenosis, pulmonary hypertension, and myxoma. Absent aortic component of S2, a late-peaking or prolonged murmur, sustained apical impulse, and delayed carotid upstroke (“pulsus tardus”) strongly support the presence of severe aortic stenosis. Absence of a palpable pulmonic component of S2 argues strongly against significant pulmonary hypertension.
There are few physical exam findings reliably seen in pulmonary embolism, but the presence of tachycardia is reliably seen about 80% of the time.4 Although atrial myxoma is associated with a characteristic “tumor plop” heard in early diastole, the finding is not common.5
Diagnostic studies: In a recent observational study of more than 2,000 adults older than 65 hospitalized after a syncopal episode, cardiac enzymes, electroencephalography, CT scan of the head, and carotid ultrasonography determined the etiology of syncope in less than 1% of cases. Inpatient monitoring on telemetry was helpful about 5% of the time. On the other hand, postural vital signs contributed to the diagnosis more than 20% of the time, at a fraction of the cost of these other diagnostics (see Table 2, above).6
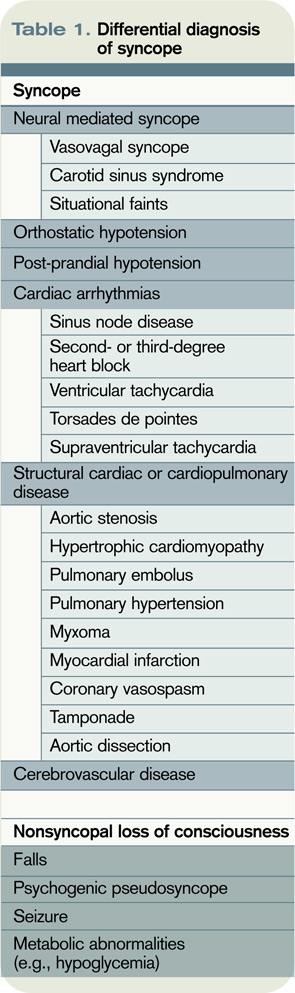
The role of transthoracic echocardiogram (echo) is more controversial. It does seem clear, however, that echo is more likely to be diagnostic in adults older than 60, in the presence of a heart murmur on physical exam or with an abnormal ECG.7 Although it demonstrated an arrhythmia that determined the etiology of syncope in only 3% of cases in this study, ECG is still routinely recommended; it is relatively inexpensive, risk-free, and can reveal abnormalities, including bundle-branch block, prior MI, and nonsustained ventricular tachycardia, which may be associated with cardiovascular comorbidities.4
Although the diagnostic tests above are of limited utility in uncovering the cause of syncopal episodes, they may be helpful when history or physical examination suggests a specific cause. For example, in individuals presenting with syncope who have lateralizing neurologic signs or symptoms or carotid bruits, carotid ultrasound is an appropriate diagnostic tool. In a retrospective analysis of 140 older adults who underwent carotid ultrasonography as part of a syncope evaluation, carotid lesions were identified in just 2% of subjects.8 These lesions were not thought to have been the primary etiology of syncope but did prompt additional evaluation or intervention.
Among older individuals or individuals with known heart disease, longer-term cardiac monitoring might be appropriate. The method of cardiac monitoring should be guided by the frequency of episodes. For events occurring daily, Holter monitoring is appropriate. For events occurring at least monthly, an event monitor is appropriate.
For less frequent events, the clinician can consider an implantable loop recorder (ILR).3 In a study of 167 individuals without a clear cause of syncope after initial evaluation, diagnosis was achieved in 90% of patients after one year of monitoring by ILR.9
Among individuals in whom the etiology remains unclear, tilt-table testing is often considered. This modality remains controversial and is unlikely to establish a diagnosis in individuals with an otherwise normal evaluation.3 Electrophysiologic testing is of similarly low yield in individuals with otherwise normal evaluation and is generally not recommended, except in individuals with known heart disease, including history of MI, congestive heart failure (CHF), and pre-excitation.10
Diagnostic algorithms: Algorithm-driven diagnostic protocols for evaluation of syncope do exist, but they are generally based on expert consensus opinion rather than large-scale studies. There are evidence-based syncope risk scores under development, but definitive validation is forthcoming. Examination of two such protocols is provided here.
The San Francisco Syncope Rule is among the most well-known algorithms, and predicts adverse outcomes at seven days. The study cohort included 684 patients presenting with syncope to an academic ED. Adverse outcomes, including death, myocardial infarction, arrhythmia, pulmonary embolus, stroke, subarachnoid hemorrhage, ED return, or hospitalization at seven days, were identified. History of CHF, hematocrit less than 30%, ECG abnormality, shortness of breath, and SBP less than 90 mmHg at presentation were associated with increased risk of an adverse outcome. If any of these findings is present, a patient is considered at high risk for adverse outcome at one week.2 The rule is simple to use; however, external validation has been controversial.
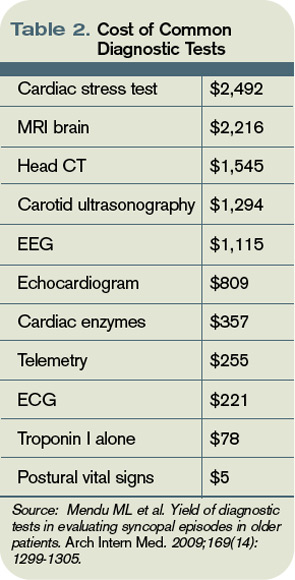
In another risk-prediction study—a large multicenter study of patients older than 60—age greater than 90 years, male sex, history of arrhythmia, SBP greater than 160 mm Hg, ECG abnormality, and elevated troponin I were used to construct a score for risk stratification.11 Specific ECG abnormalities included nonsinus rhythm, heart rate less than 40 beats per minute, evidence of acute or chronic ischemic heart disease, prolonged QRS or QT, left or right ventricular hypertrophy, left-axis deviation, and bundle-branch block. Notably, in this older cohort, CHF (specifically, systolic dysfunction with ejection fraction less than 40%) was not significantly associated with risk of adverse event at 30 days. Study authors stratified participants into low- (score ≤0), intermediate- (score 1-2), and high-risk groups (score >2), with 30-day risk of an adverse event ranging from 2.5% to 20%.
One caveat to the interpretation of these data is the fact that even in the “low risk” group, risk of adverse event was still 2.5%, a figure that many clinicians might consider intolerably high.11 This risk score has not been externally validated.
Back to the Case
Our patient was admitted to the inpatient medicine service. She was monitored overnight on telemetry without evidence of arrhythmia. Collateral history revealed new use of multiple antihypertensives prescribed by outside providers, including both atenolol and propranolol. Her subdural hematoma was managed conservatively and she remained free of neurologic deficits. On discharge, her hypertension regimen was simplified. She was referred for outpatient stress echocardiogram.
Bottom Line
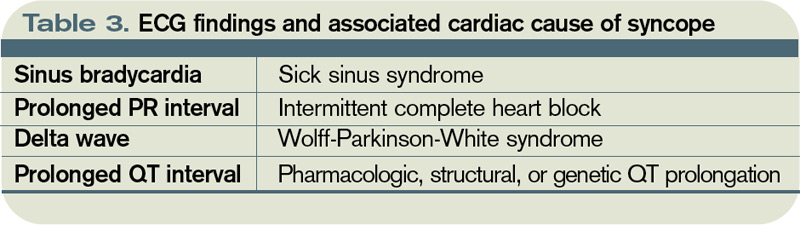
Detailed history and physical exam, including postural vital signs, should form the backbone of the routine evaluation of syncope. An ECG is a critical—and inexpensive—initial diagnostic test, while inpatient telemetry, although a routine component of inpatient evaluation, is expensive and relatively low-yield. Risk prediction rules might ultimately help guide admission decisions and inpatient workup, but definitive external validation of these rules has yet to be accomplished. TH
Dr. Wander is a resident in the Department of Medicine at the University of Washington School of Medicine in Seattle. Dr. Best is an assistant professor of medicine in the Division of General Internal Medicine at the University of Washington School of Medicine.
References
- Jhanjee R, Can I, Benditt DG. Syncope. Dis Mon. 2009;55(9):532-585.
- Quinn JV, Stiell IG, McDermott DA, Sellers KL, Kohn MA, Wells GA. Derivation of the San Francisco Syncope Rule to predict patients with short-term serious outcomes. Ann Emerg Med. 2004;43(2):224-232.
- Strickberger SA, Benson DW, Biaggioni I, et al. AHA/ACCF Scientific Statement on the evaluation of syncope: from the American Heart Association Councils on Clinical Cardiology, Cardiovascular Nursing, Cardiovascular Disease in the Young, and Stroke, and the Quality of Care and Outcomes Research Interdisciplinary Working Group; and the American College of Cardiology Foundation: in collaboration with the Heart Rhythm Society: endorsed by the American Autonomic Society. Circulation. 2006;113(2):316-327.
- Linzer M, Yang EH, Estes NA 3rd, Wang P, Vorperian VR, Kapoor WN. Diagnosing syncope. Part 1: Value of history, physical examination, and electrocardiography. Clinical Efficacy Assessment Project of the American College of Physicians. Ann Intern Med. 1997;126(12):989-996.
- McGee S. Evidence-Based Physical Diagnosis. Saunders; 2001.
- Mendu ML, McAvay G, Lampert R, Stoehr J, Tinetti ME. Yield of diagnostic tests in evaluating syncopal episodes in older patients. Arch Intern Med. 2009;169(14):1299-1305.
- Panther R, Mahmood S, Gal R. Echocardiography in the diagnostic evaluation of syncope. J Am Soc Echocardiogr. 1998;11(3):294-298.
- Schnipper JL, Ackerman RH, Krier JB, Honour M. Diagnostic yield and utility of neurovascular ultrasonography in the evaluation of patients with syncope. Mayo Clin Proc. 2005;80(4):480-488.
- Assar MD, Krahn AD, Klein GJ, Yee R, Skanes AC. Optimal duration of monitoring in patients with unexplained syncope. Am J Cardiol. 2003;92(10):1231-1233.
- Linzer M, Yang EH, Estes NA 3rd, Wang P, Vorperian VR, Kapoor WN. Diagnosing syncope. Part 2: Unexplained syncope. Clinical Efficacy Assessment Project of the American College of Physicians. Ann Intern Med. 1997;127(1):76-86.
- Sun BC, Derose SF, Liang LJ, et al. Predictors of 30-day serious events in older patients with syncope. Ann Emerg Med. 2009;54(6):769-778.e1-5.
Case
A 71-year-old woman is admitted after losing consciousness and falling at home. Her history is significant for hypertension, bilateral internal carotid artery stenoses, chronic kidney disease, and diabetes. Resting vital signs are normal. Cardiac, pulmonary, and neurologic exams are unremarkable, as is an electrocardiogram (ECG). She was noted to have a small scalp laceration. Noncontrast CT of the head demonstrates a small occipital subdural bleed thought to be a result of her fall.
What is the most cost-effective evaluation for this patient admitted with suspected first syncopal episode?
Overview
Syncope is defined as sudden, self-terminating loss of consciousness. The final common pathway of all causes of syncope is global cerebral hypoperfusion—specifically, hypoperfusion of the reticular activating system. The differential diagnosis of syncopal loss of consciousness includes neurally mediated (e.g., vasovagal) syncope, orthostatic hypotension, cardiac arrhythmias, structural heart disease, and cerebrovascular disease.
Among young, otherwise healthy people, neurally mediated syncope, which has a relatively benign prognosis, is by far the most common etiology, while in older patients, primary cardiac causes are more common. Nonsyncopal mechanisms, such as seizure and hypoglycemia, should also be considered in the differential diagnosis of transient loss of consciousness (see Table 1, p. 19).1
Syncope is a common problem, accounting for 1% to 2% of ED visits in the U.S.2 The primary objective for evaluation is identification of individuals at increased risk of death due to associated conditions, especially cardiac conditions such as structural heart disease; myocardial ischemia and infarction (MI); Wolff-Parkinson-White, Brugada, or long QT syndromes; and polymorphic ventricular tachycardia.3 True syncope can be associated with other concerning causes, such as aortic stenosis, aortic dissection, and massive pulmonary embolus, as well as arrhythmias from underlying cardiac disease.4
Review of the Data
History: A detailed history and physical examination reveals the cause in 50% of syncopal episodes. Key factors include the account of third-party observers, although it is important to note that tonic-clonic movements can be associated with the global cerebral hypoperfusion of syncope as well as with seizure.4 History of dyspnea, chest pain, or palpitations argue for a primary cardiac or pulmonary cause.
Among patients who endorse a history of palpitations, the sensation of rapid and regular pulsations in the neck points very strongly toward an AV-nodal re-entrant tachycardia, because the carotid pulse and cannon A wave arrive simultaneously in the neck.5 Postictal confusion and focal neurologic exam findings suggest a neurologic rather than syncopal cause, although there are exceptions, and the relationship between seizure and impaired myocardial perfusion is complex.
One factor shown to be significantly associated with a cardiac cause for episodic syncope is family history of sudden cardiac death.4
Physical exam: A thorough general and neurologic exam is critical in evaluation of a first syncopal episode. Supine and standing blood pressure and heart rate should be measured, waiting at least one minute (and by some protocols up to three minutes) after the patient stands up to record standing vitals. Measurement of sitting vitals is not necessary. Neither postural hypotension nor tachycardia are sensitive for hypovolemia in normal volunteers, but a 30-point increase in heart rate is more than 99% specific; a 20-point drop in systolic blood pressure (SBP) is less so.5 A difference of more than 20 mmHg between systolic arm pressures in an individual with chest pain suggests aortic dissection.
Other findings useful in diagnosis of syncope include signs of aortic stenosis, pulmonary hypertension, and myxoma. Absent aortic component of S2, a late-peaking or prolonged murmur, sustained apical impulse, and delayed carotid upstroke (“pulsus tardus”) strongly support the presence of severe aortic stenosis. Absence of a palpable pulmonic component of S2 argues strongly against significant pulmonary hypertension.
There are few physical exam findings reliably seen in pulmonary embolism, but the presence of tachycardia is reliably seen about 80% of the time.4 Although atrial myxoma is associated with a characteristic “tumor plop” heard in early diastole, the finding is not common.5
Diagnostic studies: In a recent observational study of more than 2,000 adults older than 65 hospitalized after a syncopal episode, cardiac enzymes, electroencephalography, CT scan of the head, and carotid ultrasonography determined the etiology of syncope in less than 1% of cases. Inpatient monitoring on telemetry was helpful about 5% of the time. On the other hand, postural vital signs contributed to the diagnosis more than 20% of the time, at a fraction of the cost of these other diagnostics (see Table 2, above).6
The role of transthoracic echocardiogram (echo) is more controversial. It does seem clear, however, that echo is more likely to be diagnostic in adults older than 60, in the presence of a heart murmur on physical exam or with an abnormal ECG.7 Although it demonstrated an arrhythmia that determined the etiology of syncope in only 3% of cases in this study, ECG is still routinely recommended; it is relatively inexpensive, risk-free, and can reveal abnormalities, including bundle-branch block, prior MI, and nonsustained ventricular tachycardia, which may be associated with cardiovascular comorbidities.4
Although the diagnostic tests above are of limited utility in uncovering the cause of syncopal episodes, they may be helpful when history or physical examination suggests a specific cause. For example, in individuals presenting with syncope who have lateralizing neurologic signs or symptoms or carotid bruits, carotid ultrasound is an appropriate diagnostic tool. In a retrospective analysis of 140 older adults who underwent carotid ultrasonography as part of a syncope evaluation, carotid lesions were identified in just 2% of subjects.8 These lesions were not thought to have been the primary etiology of syncope but did prompt additional evaluation or intervention.
Among older individuals or individuals with known heart disease, longer-term cardiac monitoring might be appropriate. The method of cardiac monitoring should be guided by the frequency of episodes. For events occurring daily, Holter monitoring is appropriate. For events occurring at least monthly, an event monitor is appropriate.
For less frequent events, the clinician can consider an implantable loop recorder (ILR).3 In a study of 167 individuals without a clear cause of syncope after initial evaluation, diagnosis was achieved in 90% of patients after one year of monitoring by ILR.9
Among individuals in whom the etiology remains unclear, tilt-table testing is often considered. This modality remains controversial and is unlikely to establish a diagnosis in individuals with an otherwise normal evaluation.3 Electrophysiologic testing is of similarly low yield in individuals with otherwise normal evaluation and is generally not recommended, except in individuals with known heart disease, including history of MI, congestive heart failure (CHF), and pre-excitation.10
Diagnostic algorithms: Algorithm-driven diagnostic protocols for evaluation of syncope do exist, but they are generally based on expert consensus opinion rather than large-scale studies. There are evidence-based syncope risk scores under development, but definitive validation is forthcoming. Examination of two such protocols is provided here.
The San Francisco Syncope Rule is among the most well-known algorithms, and predicts adverse outcomes at seven days. The study cohort included 684 patients presenting with syncope to an academic ED. Adverse outcomes, including death, myocardial infarction, arrhythmia, pulmonary embolus, stroke, subarachnoid hemorrhage, ED return, or hospitalization at seven days, were identified. History of CHF, hematocrit less than 30%, ECG abnormality, shortness of breath, and SBP less than 90 mmHg at presentation were associated with increased risk of an adverse outcome. If any of these findings is present, a patient is considered at high risk for adverse outcome at one week.2 The rule is simple to use; however, external validation has been controversial.
In another risk-prediction study—a large multicenter study of patients older than 60—age greater than 90 years, male sex, history of arrhythmia, SBP greater than 160 mm Hg, ECG abnormality, and elevated troponin I were used to construct a score for risk stratification.11 Specific ECG abnormalities included nonsinus rhythm, heart rate less than 40 beats per minute, evidence of acute or chronic ischemic heart disease, prolonged QRS or QT, left or right ventricular hypertrophy, left-axis deviation, and bundle-branch block. Notably, in this older cohort, CHF (specifically, systolic dysfunction with ejection fraction less than 40%) was not significantly associated with risk of adverse event at 30 days. Study authors stratified participants into low- (score ≤0), intermediate- (score 1-2), and high-risk groups (score >2), with 30-day risk of an adverse event ranging from 2.5% to 20%.
One caveat to the interpretation of these data is the fact that even in the “low risk” group, risk of adverse event was still 2.5%, a figure that many clinicians might consider intolerably high.11 This risk score has not been externally validated.
Back to the Case
Our patient was admitted to the inpatient medicine service. She was monitored overnight on telemetry without evidence of arrhythmia. Collateral history revealed new use of multiple antihypertensives prescribed by outside providers, including both atenolol and propranolol. Her subdural hematoma was managed conservatively and she remained free of neurologic deficits. On discharge, her hypertension regimen was simplified. She was referred for outpatient stress echocardiogram.
Bottom Line
Detailed history and physical exam, including postural vital signs, should form the backbone of the routine evaluation of syncope. An ECG is a critical—and inexpensive—initial diagnostic test, while inpatient telemetry, although a routine component of inpatient evaluation, is expensive and relatively low-yield. Risk prediction rules might ultimately help guide admission decisions and inpatient workup, but definitive external validation of these rules has yet to be accomplished. TH
Dr. Wander is a resident in the Department of Medicine at the University of Washington School of Medicine in Seattle. Dr. Best is an assistant professor of medicine in the Division of General Internal Medicine at the University of Washington School of Medicine.
References
- Jhanjee R, Can I, Benditt DG. Syncope. Dis Mon. 2009;55(9):532-585.
- Quinn JV, Stiell IG, McDermott DA, Sellers KL, Kohn MA, Wells GA. Derivation of the San Francisco Syncope Rule to predict patients with short-term serious outcomes. Ann Emerg Med. 2004;43(2):224-232.
- Strickberger SA, Benson DW, Biaggioni I, et al. AHA/ACCF Scientific Statement on the evaluation of syncope: from the American Heart Association Councils on Clinical Cardiology, Cardiovascular Nursing, Cardiovascular Disease in the Young, and Stroke, and the Quality of Care and Outcomes Research Interdisciplinary Working Group; and the American College of Cardiology Foundation: in collaboration with the Heart Rhythm Society: endorsed by the American Autonomic Society. Circulation. 2006;113(2):316-327.
- Linzer M, Yang EH, Estes NA 3rd, Wang P, Vorperian VR, Kapoor WN. Diagnosing syncope. Part 1: Value of history, physical examination, and electrocardiography. Clinical Efficacy Assessment Project of the American College of Physicians. Ann Intern Med. 1997;126(12):989-996.
- McGee S. Evidence-Based Physical Diagnosis. Saunders; 2001.
- Mendu ML, McAvay G, Lampert R, Stoehr J, Tinetti ME. Yield of diagnostic tests in evaluating syncopal episodes in older patients. Arch Intern Med. 2009;169(14):1299-1305.
- Panther R, Mahmood S, Gal R. Echocardiography in the diagnostic evaluation of syncope. J Am Soc Echocardiogr. 1998;11(3):294-298.
- Schnipper JL, Ackerman RH, Krier JB, Honour M. Diagnostic yield and utility of neurovascular ultrasonography in the evaluation of patients with syncope. Mayo Clin Proc. 2005;80(4):480-488.
- Assar MD, Krahn AD, Klein GJ, Yee R, Skanes AC. Optimal duration of monitoring in patients with unexplained syncope. Am J Cardiol. 2003;92(10):1231-1233.
- Linzer M, Yang EH, Estes NA 3rd, Wang P, Vorperian VR, Kapoor WN. Diagnosing syncope. Part 2: Unexplained syncope. Clinical Efficacy Assessment Project of the American College of Physicians. Ann Intern Med. 1997;127(1):76-86.
- Sun BC, Derose SF, Liang LJ, et al. Predictors of 30-day serious events in older patients with syncope. Ann Emerg Med. 2009;54(6):769-778.e1-5.
Case
A 71-year-old woman is admitted after losing consciousness and falling at home. Her history is significant for hypertension, bilateral internal carotid artery stenoses, chronic kidney disease, and diabetes. Resting vital signs are normal. Cardiac, pulmonary, and neurologic exams are unremarkable, as is an electrocardiogram (ECG). She was noted to have a small scalp laceration. Noncontrast CT of the head demonstrates a small occipital subdural bleed thought to be a result of her fall.
What is the most cost-effective evaluation for this patient admitted with suspected first syncopal episode?
Overview
Syncope is defined as sudden, self-terminating loss of consciousness. The final common pathway of all causes of syncope is global cerebral hypoperfusion—specifically, hypoperfusion of the reticular activating system. The differential diagnosis of syncopal loss of consciousness includes neurally mediated (e.g., vasovagal) syncope, orthostatic hypotension, cardiac arrhythmias, structural heart disease, and cerebrovascular disease.
Among young, otherwise healthy people, neurally mediated syncope, which has a relatively benign prognosis, is by far the most common etiology, while in older patients, primary cardiac causes are more common. Nonsyncopal mechanisms, such as seizure and hypoglycemia, should also be considered in the differential diagnosis of transient loss of consciousness (see Table 1, p. 19).1
Syncope is a common problem, accounting for 1% to 2% of ED visits in the U.S.2 The primary objective for evaluation is identification of individuals at increased risk of death due to associated conditions, especially cardiac conditions such as structural heart disease; myocardial ischemia and infarction (MI); Wolff-Parkinson-White, Brugada, or long QT syndromes; and polymorphic ventricular tachycardia.3 True syncope can be associated with other concerning causes, such as aortic stenosis, aortic dissection, and massive pulmonary embolus, as well as arrhythmias from underlying cardiac disease.4
Review of the Data
History: A detailed history and physical examination reveals the cause in 50% of syncopal episodes. Key factors include the account of third-party observers, although it is important to note that tonic-clonic movements can be associated with the global cerebral hypoperfusion of syncope as well as with seizure.4 History of dyspnea, chest pain, or palpitations argue for a primary cardiac or pulmonary cause.
Among patients who endorse a history of palpitations, the sensation of rapid and regular pulsations in the neck points very strongly toward an AV-nodal re-entrant tachycardia, because the carotid pulse and cannon A wave arrive simultaneously in the neck.5 Postictal confusion and focal neurologic exam findings suggest a neurologic rather than syncopal cause, although there are exceptions, and the relationship between seizure and impaired myocardial perfusion is complex.
One factor shown to be significantly associated with a cardiac cause for episodic syncope is family history of sudden cardiac death.4
Physical exam: A thorough general and neurologic exam is critical in evaluation of a first syncopal episode. Supine and standing blood pressure and heart rate should be measured, waiting at least one minute (and by some protocols up to three minutes) after the patient stands up to record standing vitals. Measurement of sitting vitals is not necessary. Neither postural hypotension nor tachycardia are sensitive for hypovolemia in normal volunteers, but a 30-point increase in heart rate is more than 99% specific; a 20-point drop in systolic blood pressure (SBP) is less so.5 A difference of more than 20 mmHg between systolic arm pressures in an individual with chest pain suggests aortic dissection.
Other findings useful in diagnosis of syncope include signs of aortic stenosis, pulmonary hypertension, and myxoma. Absent aortic component of S2, a late-peaking or prolonged murmur, sustained apical impulse, and delayed carotid upstroke (“pulsus tardus”) strongly support the presence of severe aortic stenosis. Absence of a palpable pulmonic component of S2 argues strongly against significant pulmonary hypertension.
There are few physical exam findings reliably seen in pulmonary embolism, but the presence of tachycardia is reliably seen about 80% of the time.4 Although atrial myxoma is associated with a characteristic “tumor plop” heard in early diastole, the finding is not common.5
Diagnostic studies: In a recent observational study of more than 2,000 adults older than 65 hospitalized after a syncopal episode, cardiac enzymes, electroencephalography, CT scan of the head, and carotid ultrasonography determined the etiology of syncope in less than 1% of cases. Inpatient monitoring on telemetry was helpful about 5% of the time. On the other hand, postural vital signs contributed to the diagnosis more than 20% of the time, at a fraction of the cost of these other diagnostics (see Table 2, above).6
The role of transthoracic echocardiogram (echo) is more controversial. It does seem clear, however, that echo is more likely to be diagnostic in adults older than 60, in the presence of a heart murmur on physical exam or with an abnormal ECG.7 Although it demonstrated an arrhythmia that determined the etiology of syncope in only 3% of cases in this study, ECG is still routinely recommended; it is relatively inexpensive, risk-free, and can reveal abnormalities, including bundle-branch block, prior MI, and nonsustained ventricular tachycardia, which may be associated with cardiovascular comorbidities.4
Although the diagnostic tests above are of limited utility in uncovering the cause of syncopal episodes, they may be helpful when history or physical examination suggests a specific cause. For example, in individuals presenting with syncope who have lateralizing neurologic signs or symptoms or carotid bruits, carotid ultrasound is an appropriate diagnostic tool. In a retrospective analysis of 140 older adults who underwent carotid ultrasonography as part of a syncope evaluation, carotid lesions were identified in just 2% of subjects.8 These lesions were not thought to have been the primary etiology of syncope but did prompt additional evaluation or intervention.
Among older individuals or individuals with known heart disease, longer-term cardiac monitoring might be appropriate. The method of cardiac monitoring should be guided by the frequency of episodes. For events occurring daily, Holter monitoring is appropriate. For events occurring at least monthly, an event monitor is appropriate.
For less frequent events, the clinician can consider an implantable loop recorder (ILR).3 In a study of 167 individuals without a clear cause of syncope after initial evaluation, diagnosis was achieved in 90% of patients after one year of monitoring by ILR.9
Among individuals in whom the etiology remains unclear, tilt-table testing is often considered. This modality remains controversial and is unlikely to establish a diagnosis in individuals with an otherwise normal evaluation.3 Electrophysiologic testing is of similarly low yield in individuals with otherwise normal evaluation and is generally not recommended, except in individuals with known heart disease, including history of MI, congestive heart failure (CHF), and pre-excitation.10
Diagnostic algorithms: Algorithm-driven diagnostic protocols for evaluation of syncope do exist, but they are generally based on expert consensus opinion rather than large-scale studies. There are evidence-based syncope risk scores under development, but definitive validation is forthcoming. Examination of two such protocols is provided here.
The San Francisco Syncope Rule is among the most well-known algorithms, and predicts adverse outcomes at seven days. The study cohort included 684 patients presenting with syncope to an academic ED. Adverse outcomes, including death, myocardial infarction, arrhythmia, pulmonary embolus, stroke, subarachnoid hemorrhage, ED return, or hospitalization at seven days, were identified. History of CHF, hematocrit less than 30%, ECG abnormality, shortness of breath, and SBP less than 90 mmHg at presentation were associated with increased risk of an adverse outcome. If any of these findings is present, a patient is considered at high risk for adverse outcome at one week.2 The rule is simple to use; however, external validation has been controversial.
In another risk-prediction study—a large multicenter study of patients older than 60—age greater than 90 years, male sex, history of arrhythmia, SBP greater than 160 mm Hg, ECG abnormality, and elevated troponin I were used to construct a score for risk stratification.11 Specific ECG abnormalities included nonsinus rhythm, heart rate less than 40 beats per minute, evidence of acute or chronic ischemic heart disease, prolonged QRS or QT, left or right ventricular hypertrophy, left-axis deviation, and bundle-branch block. Notably, in this older cohort, CHF (specifically, systolic dysfunction with ejection fraction less than 40%) was not significantly associated with risk of adverse event at 30 days. Study authors stratified participants into low- (score ≤0), intermediate- (score 1-2), and high-risk groups (score >2), with 30-day risk of an adverse event ranging from 2.5% to 20%.
One caveat to the interpretation of these data is the fact that even in the “low risk” group, risk of adverse event was still 2.5%, a figure that many clinicians might consider intolerably high.11 This risk score has not been externally validated.
Back to the Case
Our patient was admitted to the inpatient medicine service. She was monitored overnight on telemetry without evidence of arrhythmia. Collateral history revealed new use of multiple antihypertensives prescribed by outside providers, including both atenolol and propranolol. Her subdural hematoma was managed conservatively and she remained free of neurologic deficits. On discharge, her hypertension regimen was simplified. She was referred for outpatient stress echocardiogram.
Bottom Line
Detailed history and physical exam, including postural vital signs, should form the backbone of the routine evaluation of syncope. An ECG is a critical—and inexpensive—initial diagnostic test, while inpatient telemetry, although a routine component of inpatient evaluation, is expensive and relatively low-yield. Risk prediction rules might ultimately help guide admission decisions and inpatient workup, but definitive external validation of these rules has yet to be accomplished. TH
Dr. Wander is a resident in the Department of Medicine at the University of Washington School of Medicine in Seattle. Dr. Best is an assistant professor of medicine in the Division of General Internal Medicine at the University of Washington School of Medicine.
References
- Jhanjee R, Can I, Benditt DG. Syncope. Dis Mon. 2009;55(9):532-585.
- Quinn JV, Stiell IG, McDermott DA, Sellers KL, Kohn MA, Wells GA. Derivation of the San Francisco Syncope Rule to predict patients with short-term serious outcomes. Ann Emerg Med. 2004;43(2):224-232.
- Strickberger SA, Benson DW, Biaggioni I, et al. AHA/ACCF Scientific Statement on the evaluation of syncope: from the American Heart Association Councils on Clinical Cardiology, Cardiovascular Nursing, Cardiovascular Disease in the Young, and Stroke, and the Quality of Care and Outcomes Research Interdisciplinary Working Group; and the American College of Cardiology Foundation: in collaboration with the Heart Rhythm Society: endorsed by the American Autonomic Society. Circulation. 2006;113(2):316-327.
- Linzer M, Yang EH, Estes NA 3rd, Wang P, Vorperian VR, Kapoor WN. Diagnosing syncope. Part 1: Value of history, physical examination, and electrocardiography. Clinical Efficacy Assessment Project of the American College of Physicians. Ann Intern Med. 1997;126(12):989-996.
- McGee S. Evidence-Based Physical Diagnosis. Saunders; 2001.
- Mendu ML, McAvay G, Lampert R, Stoehr J, Tinetti ME. Yield of diagnostic tests in evaluating syncopal episodes in older patients. Arch Intern Med. 2009;169(14):1299-1305.
- Panther R, Mahmood S, Gal R. Echocardiography in the diagnostic evaluation of syncope. J Am Soc Echocardiogr. 1998;11(3):294-298.
- Schnipper JL, Ackerman RH, Krier JB, Honour M. Diagnostic yield and utility of neurovascular ultrasonography in the evaluation of patients with syncope. Mayo Clin Proc. 2005;80(4):480-488.
- Assar MD, Krahn AD, Klein GJ, Yee R, Skanes AC. Optimal duration of monitoring in patients with unexplained syncope. Am J Cardiol. 2003;92(10):1231-1233.
- Linzer M, Yang EH, Estes NA 3rd, Wang P, Vorperian VR, Kapoor WN. Diagnosing syncope. Part 2: Unexplained syncope. Clinical Efficacy Assessment Project of the American College of Physicians. Ann Intern Med. 1997;127(1):76-86.
- Sun BC, Derose SF, Liang LJ, et al. Predictors of 30-day serious events in older patients with syncope. Ann Emerg Med. 2009;54(6):769-778.e1-5.
Controlling Emesis: Evolving Challenges, Novel Strategies

Continued research over the past 25 years has led to steady progress in the management of nausea and vomiting among patients with cancer undergoing emetogenic chemotherapy, radiation therapy, or surgery. This review of antiemetic therapy discusses the evolution and improvement in treatment options available, the identification of risk factors for acute and delayed nausea and vomiting, and the development of alternative drug delivery systems and their impact on patient compliance and convenience.
Continued research over the past 25 years has led to steady progress in the management of nausea and vomiting among patients with cancer undergoing emetogenic chemotherapy, radiation therapy, or surgery. This review of antiemetic therapy discusses the evolution and improvement in treatment options available, the identification of risk factors for acute and delayed nausea and vomiting, and the development of alternative drug delivery systems and their impact on patient compliance and convenience.
Continued research over the past 25 years has led to steady progress in the management of nausea and vomiting among patients with cancer undergoing emetogenic chemotherapy, radiation therapy, or surgery. This review of antiemetic therapy discusses the evolution and improvement in treatment options available, the identification of risk factors for acute and delayed nausea and vomiting, and the development of alternative drug delivery systems and their impact on patient compliance and convenience.
Continued research over the past 25 years has led to steady progress in the management of nausea and vomiting among patients with cancer undergoing emetogenic chemotherapy, radiation therapy, or surgery. This review of antiemetic therapy discusses the evolution and improvement in treatment options available, the identification of risk factors for acute and delayed nausea and vomiting, and the development of alternative drug delivery systems and their impact on patient compliance and convenience.

Rule Proposes Electronic Prescription of Controlled Substances, Doesn’t Scrap Pen-and-Paper Method

Is it true that the Drug Enforcement Administration (DEA) is going to allow doctors to prescribe controlled drugs electronically?
Will I still be able to prescribe on my prescription pads, or is this big government forcing me to use a computer for prescriptions?
J. Hockenstein, DO
Des Moines, Iowa
Dr. Hospitalist responds: On March 31, the DEA published in the Federal Register an interim final rule regarding the “electronic prescription for controlled substances.” (View the entire rule at www.gpoaccess.gov/fr.) The DEA is seeking comment on the proposed rule for the next 60 days. Some of us might remember that the DEA proposed a similar rule for electronic prescribing in June 2008, but that rule did not meet the security requirements already in place at federal healthcare facilities.
Under the current system, providers can create prescriptions electronically, but the prescription has to be printed on paper. The new rule proposes a system of true electronic prescribing; data can be transmitted electronically from the hospital or doctor’s office to the pharmacy without the use of a printer or fax.
This proposed rule does not eliminate the traditional method of paper and pen for prescriptions but allows providers the voluntary option of prescribing controlled substances electronically. This proposed rule also allows pharmacies to receive, dispense, and archive these electronic prescriptions.
For those providers who choose to prescribe electronically, there will be specific requirements to prevent diversion and maintain privacy. Providers must utilize software that meets the rule’s specific requirements. For example, the software system will require a two-step process to authenticate the prescribing provider. These measures might include a password, a token, or the use of biometric identifier (e.g., fingerprint or handprint). For some of us, this might sound space-aged, but such biometric systems are commonplace in other industries. For example, I provided my fingerprint as part of the test center security system when I checked in for my American Board of Internal Medicine (ABIM) recertification examination.
There are several other issues with the proposed rule that one should consider. The new proposal does not affect the existing rule regarding emergency prescriptions. The current law allows physicians to prescribe a Schedule II controlled substance by telephone and the pharmacist to dispense this substance, provided that the amount being dispensed is limited to what is reasonably required during the emergency time period and that the provider provides a hard copy of the prescription to the pharmacist within seven days of the telephone prescription. Under the proposed rule, providers will still be able to prescribe Schedule II substances by telephone under emergency situations but will have the option of providing an electronic copy of the prescription, rather than a paper one, within seven days.
There are other components of the proposed rule that could change your practice. The rule clearly states that an electronic prescription cannot be changed after transmission and that any change to the content of the prescription will render it invalid. This might be important in a handful of situations. For example, if the provider electronically prescribes a brand-name drug, the pharmacist would not be able to make a generic substitution.
Another component of the proposed rule is that it precludes the printing of an electronic prescription, which already has been transmitted and precludes the electronic transmission of a prescription that already has been printed. This situation might arise if the electronic prescription did not transmit due to a computer problem. The provider would not be able to print or fax a copy of the electronic prescription.
The proposed rule has the potential to reduce medical errors, reduce prescription forgeries, and help providers and hospitals integrate their medical records. True electronic prescribing is long overdue. In the future, I envision hospitalists prescribing from their handheld devices.
The key to success, like any computerized system, will be the ability to keep the system running and continuously maintaining and upgrading security measures. For more information regarding electronic prescriptions for controlled substances, visit www.DEAdiversion.usdoj.gov. TH
Is it true that the Drug Enforcement Administration (DEA) is going to allow doctors to prescribe controlled drugs electronically?
Will I still be able to prescribe on my prescription pads, or is this big government forcing me to use a computer for prescriptions?
J. Hockenstein, DO
Des Moines, Iowa
Dr. Hospitalist responds: On March 31, the DEA published in the Federal Register an interim final rule regarding the “electronic prescription for controlled substances.” (View the entire rule at www.gpoaccess.gov/fr.) The DEA is seeking comment on the proposed rule for the next 60 days. Some of us might remember that the DEA proposed a similar rule for electronic prescribing in June 2008, but that rule did not meet the security requirements already in place at federal healthcare facilities.
Under the current system, providers can create prescriptions electronically, but the prescription has to be printed on paper. The new rule proposes a system of true electronic prescribing; data can be transmitted electronically from the hospital or doctor’s office to the pharmacy without the use of a printer or fax.
This proposed rule does not eliminate the traditional method of paper and pen for prescriptions but allows providers the voluntary option of prescribing controlled substances electronically. This proposed rule also allows pharmacies to receive, dispense, and archive these electronic prescriptions.
For those providers who choose to prescribe electronically, there will be specific requirements to prevent diversion and maintain privacy. Providers must utilize software that meets the rule’s specific requirements. For example, the software system will require a two-step process to authenticate the prescribing provider. These measures might include a password, a token, or the use of biometric identifier (e.g., fingerprint or handprint). For some of us, this might sound space-aged, but such biometric systems are commonplace in other industries. For example, I provided my fingerprint as part of the test center security system when I checked in for my American Board of Internal Medicine (ABIM) recertification examination.
There are several other issues with the proposed rule that one should consider. The new proposal does not affect the existing rule regarding emergency prescriptions. The current law allows physicians to prescribe a Schedule II controlled substance by telephone and the pharmacist to dispense this substance, provided that the amount being dispensed is limited to what is reasonably required during the emergency time period and that the provider provides a hard copy of the prescription to the pharmacist within seven days of the telephone prescription. Under the proposed rule, providers will still be able to prescribe Schedule II substances by telephone under emergency situations but will have the option of providing an electronic copy of the prescription, rather than a paper one, within seven days.
There are other components of the proposed rule that could change your practice. The rule clearly states that an electronic prescription cannot be changed after transmission and that any change to the content of the prescription will render it invalid. This might be important in a handful of situations. For example, if the provider electronically prescribes a brand-name drug, the pharmacist would not be able to make a generic substitution.
Another component of the proposed rule is that it precludes the printing of an electronic prescription, which already has been transmitted and precludes the electronic transmission of a prescription that already has been printed. This situation might arise if the electronic prescription did not transmit due to a computer problem. The provider would not be able to print or fax a copy of the electronic prescription.
The proposed rule has the potential to reduce medical errors, reduce prescription forgeries, and help providers and hospitals integrate their medical records. True electronic prescribing is long overdue. In the future, I envision hospitalists prescribing from their handheld devices.
The key to success, like any computerized system, will be the ability to keep the system running and continuously maintaining and upgrading security measures. For more information regarding electronic prescriptions for controlled substances, visit www.DEAdiversion.usdoj.gov. TH
Is it true that the Drug Enforcement Administration (DEA) is going to allow doctors to prescribe controlled drugs electronically?
Will I still be able to prescribe on my prescription pads, or is this big government forcing me to use a computer for prescriptions?
J. Hockenstein, DO
Des Moines, Iowa
Dr. Hospitalist responds: On March 31, the DEA published in the Federal Register an interim final rule regarding the “electronic prescription for controlled substances.” (View the entire rule at www.gpoaccess.gov/fr.) The DEA is seeking comment on the proposed rule for the next 60 days. Some of us might remember that the DEA proposed a similar rule for electronic prescribing in June 2008, but that rule did not meet the security requirements already in place at federal healthcare facilities.
Under the current system, providers can create prescriptions electronically, but the prescription has to be printed on paper. The new rule proposes a system of true electronic prescribing; data can be transmitted electronically from the hospital or doctor’s office to the pharmacy without the use of a printer or fax.
This proposed rule does not eliminate the traditional method of paper and pen for prescriptions but allows providers the voluntary option of prescribing controlled substances electronically. This proposed rule also allows pharmacies to receive, dispense, and archive these electronic prescriptions.
For those providers who choose to prescribe electronically, there will be specific requirements to prevent diversion and maintain privacy. Providers must utilize software that meets the rule’s specific requirements. For example, the software system will require a two-step process to authenticate the prescribing provider. These measures might include a password, a token, or the use of biometric identifier (e.g., fingerprint or handprint). For some of us, this might sound space-aged, but such biometric systems are commonplace in other industries. For example, I provided my fingerprint as part of the test center security system when I checked in for my American Board of Internal Medicine (ABIM) recertification examination.
There are several other issues with the proposed rule that one should consider. The new proposal does not affect the existing rule regarding emergency prescriptions. The current law allows physicians to prescribe a Schedule II controlled substance by telephone and the pharmacist to dispense this substance, provided that the amount being dispensed is limited to what is reasonably required during the emergency time period and that the provider provides a hard copy of the prescription to the pharmacist within seven days of the telephone prescription. Under the proposed rule, providers will still be able to prescribe Schedule II substances by telephone under emergency situations but will have the option of providing an electronic copy of the prescription, rather than a paper one, within seven days.
There are other components of the proposed rule that could change your practice. The rule clearly states that an electronic prescription cannot be changed after transmission and that any change to the content of the prescription will render it invalid. This might be important in a handful of situations. For example, if the provider electronically prescribes a brand-name drug, the pharmacist would not be able to make a generic substitution.
Another component of the proposed rule is that it precludes the printing of an electronic prescription, which already has been transmitted and precludes the electronic transmission of a prescription that already has been printed. This situation might arise if the electronic prescription did not transmit due to a computer problem. The provider would not be able to print or fax a copy of the electronic prescription.
The proposed rule has the potential to reduce medical errors, reduce prescription forgeries, and help providers and hospitals integrate their medical records. True electronic prescribing is long overdue. In the future, I envision hospitalists prescribing from their handheld devices.
The key to success, like any computerized system, will be the ability to keep the system running and continuously maintaining and upgrading security measures. For more information regarding electronic prescriptions for controlled substances, visit www.DEAdiversion.usdoj.gov. TH
A randomized phase III trial of BIBW 2992 versus chemotherapy as first-line treatment for stage IIIB/IV adenocarcinoma of the lung harboring an epidermal growth factor receptor-activating mutation

LUX-Lung 3, an ongoing randomized, multicenter, open-label phase III trial, compares single-agent BIBW 2992 (afatinib) with standard pemetrexed/cisplatin chemotherapy as first-line treatment of stage IIIB/IV adenocarcinoma of the lung with epidermal growth factor receptor (EGFR)-activating mutations. BIBW 2992 is an investigational, orally administered irreversible EGFR-1 and human epidermal growth factor receptor-2 (HER2) tyrosine kinase inhibitor (TKI). The current trial (LUX-Lung 3) will randomize 330 patients in a 2:1 ratio to receive either BIBW 2992 or chemotherapy with pemetrexed/cisplatin. Patients will receive either BIBW 2992 at a starting dose of 40 mg once daily continuously or pemetrexed (500 mg/m² IV) and cisplatin (75 mg/m²) on day 1 of 21-day cycles. Patients will receive 6 cycles of chemotherapy unless unacceptable toxicity occurs. BIBW 2992 will be given continuously until disease progression occurs. The primary endpoint is progression-free survival (PFS). Secondary endpoints include objective response, disease control assessed using Response Evaluation Criteria in Solid Tumors (RECIST) criteria, and overall survival. Oncologists may obtain information on how to enroll patients from the National Institutes of Health’s Web site (www.clinicaltrials.gov/ct2/show/NCT00949650).
LUX-Lung 3, an ongoing randomized, multicenter, open-label phase III trial, compares single-agent BIBW 2992 (afatinib) with standard pemetrexed/cisplatin chemotherapy as first-line treatment of stage IIIB/IV adenocarcinoma of the lung with epidermal growth factor receptor (EGFR)-activating mutations. BIBW 2992 is an investigational, orally administered irreversible EGFR-1 and human epidermal growth factor receptor-2 (HER2) tyrosine kinase inhibitor (TKI). The current trial (LUX-Lung 3) will randomize 330 patients in a 2:1 ratio to receive either BIBW 2992 or chemotherapy with pemetrexed/cisplatin. Patients will receive either BIBW 2992 at a starting dose of 40 mg once daily continuously or pemetrexed (500 mg/m² IV) and cisplatin (75 mg/m²) on day 1 of 21-day cycles. Patients will receive 6 cycles of chemotherapy unless unacceptable toxicity occurs. BIBW 2992 will be given continuously until disease progression occurs. The primary endpoint is progression-free survival (PFS). Secondary endpoints include objective response, disease control assessed using Response Evaluation Criteria in Solid Tumors (RECIST) criteria, and overall survival. Oncologists may obtain information on how to enroll patients from the National Institutes of Health’s Web site (www.clinicaltrials.gov/ct2/show/NCT00949650).
LUX-Lung 3, an ongoing randomized, multicenter, open-label phase III trial, compares single-agent BIBW 2992 (afatinib) with standard pemetrexed/cisplatin chemotherapy as first-line treatment of stage IIIB/IV adenocarcinoma of the lung with epidermal growth factor receptor (EGFR)-activating mutations. BIBW 2992 is an investigational, orally administered irreversible EGFR-1 and human epidermal growth factor receptor-2 (HER2) tyrosine kinase inhibitor (TKI). The current trial (LUX-Lung 3) will randomize 330 patients in a 2:1 ratio to receive either BIBW 2992 or chemotherapy with pemetrexed/cisplatin. Patients will receive either BIBW 2992 at a starting dose of 40 mg once daily continuously or pemetrexed (500 mg/m² IV) and cisplatin (75 mg/m²) on day 1 of 21-day cycles. Patients will receive 6 cycles of chemotherapy unless unacceptable toxicity occurs. BIBW 2992 will be given continuously until disease progression occurs. The primary endpoint is progression-free survival (PFS). Secondary endpoints include objective response, disease control assessed using Response Evaluation Criteria in Solid Tumors (RECIST) criteria, and overall survival. Oncologists may obtain information on how to enroll patients from the National Institutes of Health’s Web site (www.clinicaltrials.gov/ct2/show/NCT00949650).
LUX-Lung 3, an ongoing randomized, multicenter, open-label phase III trial, compares single-agent BIBW 2992 (afatinib) with standard pemetrexed/cisplatin chemotherapy as first-line treatment of stage IIIB/IV adenocarcinoma of the lung with epidermal growth factor receptor (EGFR)-activating mutations.

National Champions

It’s unfortunate that medical organizations such as SHM do not have the equivalent of a national championship or a Super Bowl. If there was, given what SHM has accomplished in the past 13 years, there is no question that SHM would have won it.
So as my first act as SHM president, I hereby declare the Society of Hospital Medicine the national champions of physician organizations.
With that out of the way, now comes the hard part: because the only thing harder than winning a championship is keeping it. For with success comes the temptation to rest. The struggle to achieve success is about outward comparisons. But having achieved success, the perspective of the champion must shift if it is to be sustained. For in the mind of the champion, the perspective is internal, and the measure of competition is about besting oneself. For a champion such as SHM, future success will be measured solely upon an internal inventory of what we do well . . . and what could be done better. Allow me to make this more tangible.
Continued Growth and Inclusion
Our membership continues to grow. And with 10,000 members, it would be easy to rest. But given that there are 30,000 hospitalists, it would be convenient to ignore the question we have to answer: “Where are the other 20,000?”
Would they not benefit from our attention to quality and patient safety? SHM, like no other organization, has built an infrastructure of empowerment, particularly with respect to advancing the goals of quality and patient safety. It is not merely a self-serving goal to recruit these 20,000 hospitalists to SHM; in your heart, you have to believe that their time with SHM would improve the care of their patients. I am confident that Brian Curtis, Manoj Matthews, and their respective Membership and Chapter Support committees will be instrumental as we work toward this goal.
As we grow, for our colleagues in pediatrics, family medicine, the nonphysician providers, and practice administrators, will we make the right decision to maintain the “big tent” that has defined SHM’s success? Quality is quality, regardless of specialty, and the principles of improving a healthcare system that is safe and patient-centered apply to us all.
But as we continue to grow, sustaining the big tent will become increasingly difficult to maintain. Even so, it must remain our priority. Erin Stucky, Bob Harrington, Jeannette Kalupa, Ajay Kharbanda, and their respective teams will be central in preserving this important goal.
At HM10, our annual meeting, attendance topped out at more than 2,500 participants, and the quality of the programming has never been stronger. But there are new challenges that come with this success. Can we sustain the intimacy—the personal attention—necessary for networking and collaboration as the annual meeting continues to grow? There are homogenous messages that do, and will continue to, speak to us all.
But heterogeneity persists in hospitalist systems, and the ability to network with other hospitalists around these unique issues has been an incredibly valuable service of the national meeting. Yet as the meeting grows, it will become increasingly difficult to network hospitalists with similar needs. Preserving the intimacy of the annual meeting, despite its growing size, must be our goal. Dan Dressler, Jeff Glasheen, Mike Pistoria, and the Annual Meeting Committee will be tasked with finding creative solutions to achieving this goal.
Technology = Solutions
At the heart of the solution to both challenges is Kendall Rogers and his Information Technology team. IT sustains meaningful communication in the face of growth, and I believe this to be a central solution. However, the tasks for our IT team are not merely internal. Our profession is at the very beginning of a sharp upward slope on the IT curve, and IT will play an increasing role in patient care.
Technology should be the servant of the people, not the other way around. The unanticipated consequence of more IT has been the temptation to depersonalize patient care in lieu of practicing medicine via computer. IT unquestionably makes healthcare more efficient, but it has the equal prospect of making it less patient-centered; no efficiency is worth that.
Our goal as a society must be to take a leadership role in ensuring that the efficiencies brought about by IT leverage more time to spend with our patients, and empower systems solutions that prevent medical errors. SHM must be positioned so that we have a meaningful voice in advocating for health IT solutions that enable the hospitalist to meet PQRI standards, and to empower the hospitalist to be a leader in the advocacy of appropriate IT solutions that advance, not deter, our mission of quality care. At no time should a computer screen replace the provider’s time at the bedside with the patient; we must be the leaders in preserving this central tenet of patient-centered care.
One Voice—Credible, Unified, Patient-Focused
Hospitalists have spent a decade trying to a get a voice in the legislative discussion. Now that we have a voice in the national healthcare conversation, we must speak with credibility. And the measure of our credibility will be grounded in fidelity to our core mission: preserving what is best for the patient. We cannot succumb, as so many other organizations have done, to merely advocating what is best for SHM. If we do, our time at the table will be short.
Finding the balance between what is best for hospitalists without compromising what is best for the patient will be our challenge. Eric Siegal, Pat Torcson, Kirk Matthews, and their respective Advocacy, Practice Analysis, and Performance and Standards committees will be at the heart of this solution. But through it all, we must not be afraid of confronting the tough issues. Whatever might come with value-based purchasing, bundling, or PQRI, we must have a voice in designing legislation that not only ensures the welfare of the hospitalized patient, but also the sustainability of the hospitalist who is central to that care.
For if we are who we say we are, one is synonymous with the other.
Quality Remains Job No. 1
Perhaps the biggest challenge facing us is heterogeneity. Thanks to SHM’s mentored implementation programs, there is an increasing number of high-performance hospitalist teams. But we are only as strong as our weakest link, and our success will be ignored in light of our weakness until we can ensure, from a quality perspective, homogeneity across all hospital groups. Tex Landis, Steve Deitelzweig, and their respective Practice Management and Practice Analysis committees will be central to finding this solution.
SHM’s biannual hospitalist survey has partnered with industry leader MGMA, and as such, we have gained great credibility in leveraging the results of the survey with the C-suite. But surveys are only as good as the questions that are asked, and SHM must continue its role in collaborating with MGMA to ensure that we are asking the right questions. We need to know what defines the highest-performing teams, and we must find creative solutions to bring every hospitalist team to that same standard of quality by adopting the best practices of our strongest groups.
But at the heart of it all is quality: SHM’s universal mandate is that hospitalists ensure safe, timely, efficient, equitable, and patient-centered care. The leadership of Vikas Parekh and the Education Committee, and Nasim Afsarmanesh, Andrew Dunn, Kevin O’Leary, Greg Maynard and their respective Quality committees, will be central to the advancement of this mandate.
But this mandate must not go unsupported. Each hospitalist group must not be tasked with reinventing the wheel with each QI project, and each hospitalist group must not suffer from the same mistakes. Imagine a day when SHM becomes the repository of QI projects, enabling one hospitalist group to search a database to find QI projects designed and executed by other groups of similar size and character. It is an ambitious goal, but it is a measure that will ensure that all hospitalists can prosper from the success of our colleagues. It will close the heterogeneity gap and ensure that in five years’ time, if there is a hospitalist who does not engage in QI, it is not because they didn’t know how.
Properly designed, such a database could enable hospitalists to create and complete the Practice Improvement Module (PIM) for the American Board of Internal Medicine’s Focused Practice in Hospital Medicine Maintenance of Certification, and empower hospitalists to meet PQRI requirements.
Train Generation Next
As we make all of these advances, we must not lose sight of the importance of a balance between “production” and “production capacity.” For SHM to be a true leader in hospital quality, we must become more than reactionary. Via “user-inspired research,” we must produce new knowledge that improves the practice of us all. And we must address the “hole in the boat.”
Despite our success in improving the understanding of quality with our current membership, I fear we are losing ground: Each year, 10,000 new practitioners leave their residency having been inadequately trained in the principles of quality and patient safety. To make meaningful changes in healthcare quality, we have to fulfill our call to become the stewards of this training, ensuring that the next generations of physicians will be more adept in the fundamentals of quality and patient safety than we were. Jeff Glasheen, David Meltzer, Lorenz DiFrancesco, Paul Grant, Greg Seymann, and the Academic, Research, Pipeline, and Early Career Hospitalists teams will be tasked with this important legacy.
And so we come to a defining moment in SHM’s history. Will SHM be a one-and-done champion? Or will it be defined as a legacy?
Less ambitious goals and visions are certainly more comfortable, but it is not the spirit that has brought us this far. I doubt that the legendary figures of hospital medicine—John Nelson, Win Whitcomb, Bob Wachter, Larry Wellikson, et al—dreamed of a day when SHM would be “OK.” I suspect even our success as an organization is not enough for them, and personally, it’s not enough for me, either.
So digest this as an ambitious strategy that only a champion would be brave enough to design. No team wins without coaching, but no team wins on coaching alone. It will take all of us to make meaningful execution of this strategy a reality. Yes, we are the champions. Now, let’s play like it. TH
Dr. Wiese is president of SHM.
It’s unfortunate that medical organizations such as SHM do not have the equivalent of a national championship or a Super Bowl. If there was, given what SHM has accomplished in the past 13 years, there is no question that SHM would have won it.
So as my first act as SHM president, I hereby declare the Society of Hospital Medicine the national champions of physician organizations.
With that out of the way, now comes the hard part: because the only thing harder than winning a championship is keeping it. For with success comes the temptation to rest. The struggle to achieve success is about outward comparisons. But having achieved success, the perspective of the champion must shift if it is to be sustained. For in the mind of the champion, the perspective is internal, and the measure of competition is about besting oneself. For a champion such as SHM, future success will be measured solely upon an internal inventory of what we do well . . . and what could be done better. Allow me to make this more tangible.
Continued Growth and Inclusion
Our membership continues to grow. And with 10,000 members, it would be easy to rest. But given that there are 30,000 hospitalists, it would be convenient to ignore the question we have to answer: “Where are the other 20,000?”
Would they not benefit from our attention to quality and patient safety? SHM, like no other organization, has built an infrastructure of empowerment, particularly with respect to advancing the goals of quality and patient safety. It is not merely a self-serving goal to recruit these 20,000 hospitalists to SHM; in your heart, you have to believe that their time with SHM would improve the care of their patients. I am confident that Brian Curtis, Manoj Matthews, and their respective Membership and Chapter Support committees will be instrumental as we work toward this goal.
As we grow, for our colleagues in pediatrics, family medicine, the nonphysician providers, and practice administrators, will we make the right decision to maintain the “big tent” that has defined SHM’s success? Quality is quality, regardless of specialty, and the principles of improving a healthcare system that is safe and patient-centered apply to us all.
But as we continue to grow, sustaining the big tent will become increasingly difficult to maintain. Even so, it must remain our priority. Erin Stucky, Bob Harrington, Jeannette Kalupa, Ajay Kharbanda, and their respective teams will be central in preserving this important goal.
At HM10, our annual meeting, attendance topped out at more than 2,500 participants, and the quality of the programming has never been stronger. But there are new challenges that come with this success. Can we sustain the intimacy—the personal attention—necessary for networking and collaboration as the annual meeting continues to grow? There are homogenous messages that do, and will continue to, speak to us all.
But heterogeneity persists in hospitalist systems, and the ability to network with other hospitalists around these unique issues has been an incredibly valuable service of the national meeting. Yet as the meeting grows, it will become increasingly difficult to network hospitalists with similar needs. Preserving the intimacy of the annual meeting, despite its growing size, must be our goal. Dan Dressler, Jeff Glasheen, Mike Pistoria, and the Annual Meeting Committee will be tasked with finding creative solutions to achieving this goal.
Technology = Solutions
At the heart of the solution to both challenges is Kendall Rogers and his Information Technology team. IT sustains meaningful communication in the face of growth, and I believe this to be a central solution. However, the tasks for our IT team are not merely internal. Our profession is at the very beginning of a sharp upward slope on the IT curve, and IT will play an increasing role in patient care.
Technology should be the servant of the people, not the other way around. The unanticipated consequence of more IT has been the temptation to depersonalize patient care in lieu of practicing medicine via computer. IT unquestionably makes healthcare more efficient, but it has the equal prospect of making it less patient-centered; no efficiency is worth that.
Our goal as a society must be to take a leadership role in ensuring that the efficiencies brought about by IT leverage more time to spend with our patients, and empower systems solutions that prevent medical errors. SHM must be positioned so that we have a meaningful voice in advocating for health IT solutions that enable the hospitalist to meet PQRI standards, and to empower the hospitalist to be a leader in the advocacy of appropriate IT solutions that advance, not deter, our mission of quality care. At no time should a computer screen replace the provider’s time at the bedside with the patient; we must be the leaders in preserving this central tenet of patient-centered care.
One Voice—Credible, Unified, Patient-Focused
Hospitalists have spent a decade trying to a get a voice in the legislative discussion. Now that we have a voice in the national healthcare conversation, we must speak with credibility. And the measure of our credibility will be grounded in fidelity to our core mission: preserving what is best for the patient. We cannot succumb, as so many other organizations have done, to merely advocating what is best for SHM. If we do, our time at the table will be short.
Finding the balance between what is best for hospitalists without compromising what is best for the patient will be our challenge. Eric Siegal, Pat Torcson, Kirk Matthews, and their respective Advocacy, Practice Analysis, and Performance and Standards committees will be at the heart of this solution. But through it all, we must not be afraid of confronting the tough issues. Whatever might come with value-based purchasing, bundling, or PQRI, we must have a voice in designing legislation that not only ensures the welfare of the hospitalized patient, but also the sustainability of the hospitalist who is central to that care.
For if we are who we say we are, one is synonymous with the other.
Quality Remains Job No. 1
Perhaps the biggest challenge facing us is heterogeneity. Thanks to SHM’s mentored implementation programs, there is an increasing number of high-performance hospitalist teams. But we are only as strong as our weakest link, and our success will be ignored in light of our weakness until we can ensure, from a quality perspective, homogeneity across all hospital groups. Tex Landis, Steve Deitelzweig, and their respective Practice Management and Practice Analysis committees will be central to finding this solution.
SHM’s biannual hospitalist survey has partnered with industry leader MGMA, and as such, we have gained great credibility in leveraging the results of the survey with the C-suite. But surveys are only as good as the questions that are asked, and SHM must continue its role in collaborating with MGMA to ensure that we are asking the right questions. We need to know what defines the highest-performing teams, and we must find creative solutions to bring every hospitalist team to that same standard of quality by adopting the best practices of our strongest groups.
But at the heart of it all is quality: SHM’s universal mandate is that hospitalists ensure safe, timely, efficient, equitable, and patient-centered care. The leadership of Vikas Parekh and the Education Committee, and Nasim Afsarmanesh, Andrew Dunn, Kevin O’Leary, Greg Maynard and their respective Quality committees, will be central to the advancement of this mandate.
But this mandate must not go unsupported. Each hospitalist group must not be tasked with reinventing the wheel with each QI project, and each hospitalist group must not suffer from the same mistakes. Imagine a day when SHM becomes the repository of QI projects, enabling one hospitalist group to search a database to find QI projects designed and executed by other groups of similar size and character. It is an ambitious goal, but it is a measure that will ensure that all hospitalists can prosper from the success of our colleagues. It will close the heterogeneity gap and ensure that in five years’ time, if there is a hospitalist who does not engage in QI, it is not because they didn’t know how.
Properly designed, such a database could enable hospitalists to create and complete the Practice Improvement Module (PIM) for the American Board of Internal Medicine’s Focused Practice in Hospital Medicine Maintenance of Certification, and empower hospitalists to meet PQRI requirements.
Train Generation Next
As we make all of these advances, we must not lose sight of the importance of a balance between “production” and “production capacity.” For SHM to be a true leader in hospital quality, we must become more than reactionary. Via “user-inspired research,” we must produce new knowledge that improves the practice of us all. And we must address the “hole in the boat.”
Despite our success in improving the understanding of quality with our current membership, I fear we are losing ground: Each year, 10,000 new practitioners leave their residency having been inadequately trained in the principles of quality and patient safety. To make meaningful changes in healthcare quality, we have to fulfill our call to become the stewards of this training, ensuring that the next generations of physicians will be more adept in the fundamentals of quality and patient safety than we were. Jeff Glasheen, David Meltzer, Lorenz DiFrancesco, Paul Grant, Greg Seymann, and the Academic, Research, Pipeline, and Early Career Hospitalists teams will be tasked with this important legacy.
And so we come to a defining moment in SHM’s history. Will SHM be a one-and-done champion? Or will it be defined as a legacy?
Less ambitious goals and visions are certainly more comfortable, but it is not the spirit that has brought us this far. I doubt that the legendary figures of hospital medicine—John Nelson, Win Whitcomb, Bob Wachter, Larry Wellikson, et al—dreamed of a day when SHM would be “OK.” I suspect even our success as an organization is not enough for them, and personally, it’s not enough for me, either.
So digest this as an ambitious strategy that only a champion would be brave enough to design. No team wins without coaching, but no team wins on coaching alone. It will take all of us to make meaningful execution of this strategy a reality. Yes, we are the champions. Now, let’s play like it. TH
Dr. Wiese is president of SHM.
It’s unfortunate that medical organizations such as SHM do not have the equivalent of a national championship or a Super Bowl. If there was, given what SHM has accomplished in the past 13 years, there is no question that SHM would have won it.
So as my first act as SHM president, I hereby declare the Society of Hospital Medicine the national champions of physician organizations.
With that out of the way, now comes the hard part: because the only thing harder than winning a championship is keeping it. For with success comes the temptation to rest. The struggle to achieve success is about outward comparisons. But having achieved success, the perspective of the champion must shift if it is to be sustained. For in the mind of the champion, the perspective is internal, and the measure of competition is about besting oneself. For a champion such as SHM, future success will be measured solely upon an internal inventory of what we do well . . . and what could be done better. Allow me to make this more tangible.
Continued Growth and Inclusion
Our membership continues to grow. And with 10,000 members, it would be easy to rest. But given that there are 30,000 hospitalists, it would be convenient to ignore the question we have to answer: “Where are the other 20,000?”
Would they not benefit from our attention to quality and patient safety? SHM, like no other organization, has built an infrastructure of empowerment, particularly with respect to advancing the goals of quality and patient safety. It is not merely a self-serving goal to recruit these 20,000 hospitalists to SHM; in your heart, you have to believe that their time with SHM would improve the care of their patients. I am confident that Brian Curtis, Manoj Matthews, and their respective Membership and Chapter Support committees will be instrumental as we work toward this goal.
As we grow, for our colleagues in pediatrics, family medicine, the nonphysician providers, and practice administrators, will we make the right decision to maintain the “big tent” that has defined SHM’s success? Quality is quality, regardless of specialty, and the principles of improving a healthcare system that is safe and patient-centered apply to us all.
But as we continue to grow, sustaining the big tent will become increasingly difficult to maintain. Even so, it must remain our priority. Erin Stucky, Bob Harrington, Jeannette Kalupa, Ajay Kharbanda, and their respective teams will be central in preserving this important goal.
At HM10, our annual meeting, attendance topped out at more than 2,500 participants, and the quality of the programming has never been stronger. But there are new challenges that come with this success. Can we sustain the intimacy—the personal attention—necessary for networking and collaboration as the annual meeting continues to grow? There are homogenous messages that do, and will continue to, speak to us all.
But heterogeneity persists in hospitalist systems, and the ability to network with other hospitalists around these unique issues has been an incredibly valuable service of the national meeting. Yet as the meeting grows, it will become increasingly difficult to network hospitalists with similar needs. Preserving the intimacy of the annual meeting, despite its growing size, must be our goal. Dan Dressler, Jeff Glasheen, Mike Pistoria, and the Annual Meeting Committee will be tasked with finding creative solutions to achieving this goal.
Technology = Solutions
At the heart of the solution to both challenges is Kendall Rogers and his Information Technology team. IT sustains meaningful communication in the face of growth, and I believe this to be a central solution. However, the tasks for our IT team are not merely internal. Our profession is at the very beginning of a sharp upward slope on the IT curve, and IT will play an increasing role in patient care.
Technology should be the servant of the people, not the other way around. The unanticipated consequence of more IT has been the temptation to depersonalize patient care in lieu of practicing medicine via computer. IT unquestionably makes healthcare more efficient, but it has the equal prospect of making it less patient-centered; no efficiency is worth that.
Our goal as a society must be to take a leadership role in ensuring that the efficiencies brought about by IT leverage more time to spend with our patients, and empower systems solutions that prevent medical errors. SHM must be positioned so that we have a meaningful voice in advocating for health IT solutions that enable the hospitalist to meet PQRI standards, and to empower the hospitalist to be a leader in the advocacy of appropriate IT solutions that advance, not deter, our mission of quality care. At no time should a computer screen replace the provider’s time at the bedside with the patient; we must be the leaders in preserving this central tenet of patient-centered care.
One Voice—Credible, Unified, Patient-Focused
Hospitalists have spent a decade trying to a get a voice in the legislative discussion. Now that we have a voice in the national healthcare conversation, we must speak with credibility. And the measure of our credibility will be grounded in fidelity to our core mission: preserving what is best for the patient. We cannot succumb, as so many other organizations have done, to merely advocating what is best for SHM. If we do, our time at the table will be short.
Finding the balance between what is best for hospitalists without compromising what is best for the patient will be our challenge. Eric Siegal, Pat Torcson, Kirk Matthews, and their respective Advocacy, Practice Analysis, and Performance and Standards committees will be at the heart of this solution. But through it all, we must not be afraid of confronting the tough issues. Whatever might come with value-based purchasing, bundling, or PQRI, we must have a voice in designing legislation that not only ensures the welfare of the hospitalized patient, but also the sustainability of the hospitalist who is central to that care.
For if we are who we say we are, one is synonymous with the other.
Quality Remains Job No. 1
Perhaps the biggest challenge facing us is heterogeneity. Thanks to SHM’s mentored implementation programs, there is an increasing number of high-performance hospitalist teams. But we are only as strong as our weakest link, and our success will be ignored in light of our weakness until we can ensure, from a quality perspective, homogeneity across all hospital groups. Tex Landis, Steve Deitelzweig, and their respective Practice Management and Practice Analysis committees will be central to finding this solution.
SHM’s biannual hospitalist survey has partnered with industry leader MGMA, and as such, we have gained great credibility in leveraging the results of the survey with the C-suite. But surveys are only as good as the questions that are asked, and SHM must continue its role in collaborating with MGMA to ensure that we are asking the right questions. We need to know what defines the highest-performing teams, and we must find creative solutions to bring every hospitalist team to that same standard of quality by adopting the best practices of our strongest groups.
But at the heart of it all is quality: SHM’s universal mandate is that hospitalists ensure safe, timely, efficient, equitable, and patient-centered care. The leadership of Vikas Parekh and the Education Committee, and Nasim Afsarmanesh, Andrew Dunn, Kevin O’Leary, Greg Maynard and their respective Quality committees, will be central to the advancement of this mandate.
But this mandate must not go unsupported. Each hospitalist group must not be tasked with reinventing the wheel with each QI project, and each hospitalist group must not suffer from the same mistakes. Imagine a day when SHM becomes the repository of QI projects, enabling one hospitalist group to search a database to find QI projects designed and executed by other groups of similar size and character. It is an ambitious goal, but it is a measure that will ensure that all hospitalists can prosper from the success of our colleagues. It will close the heterogeneity gap and ensure that in five years’ time, if there is a hospitalist who does not engage in QI, it is not because they didn’t know how.
Properly designed, such a database could enable hospitalists to create and complete the Practice Improvement Module (PIM) for the American Board of Internal Medicine’s Focused Practice in Hospital Medicine Maintenance of Certification, and empower hospitalists to meet PQRI requirements.
Train Generation Next
As we make all of these advances, we must not lose sight of the importance of a balance between “production” and “production capacity.” For SHM to be a true leader in hospital quality, we must become more than reactionary. Via “user-inspired research,” we must produce new knowledge that improves the practice of us all. And we must address the “hole in the boat.”
Despite our success in improving the understanding of quality with our current membership, I fear we are losing ground: Each year, 10,000 new practitioners leave their residency having been inadequately trained in the principles of quality and patient safety. To make meaningful changes in healthcare quality, we have to fulfill our call to become the stewards of this training, ensuring that the next generations of physicians will be more adept in the fundamentals of quality and patient safety than we were. Jeff Glasheen, David Meltzer, Lorenz DiFrancesco, Paul Grant, Greg Seymann, and the Academic, Research, Pipeline, and Early Career Hospitalists teams will be tasked with this important legacy.
And so we come to a defining moment in SHM’s history. Will SHM be a one-and-done champion? Or will it be defined as a legacy?
Less ambitious goals and visions are certainly more comfortable, but it is not the spirit that has brought us this far. I doubt that the legendary figures of hospital medicine—John Nelson, Win Whitcomb, Bob Wachter, Larry Wellikson, et al—dreamed of a day when SHM would be “OK.” I suspect even our success as an organization is not enough for them, and personally, it’s not enough for me, either.
So digest this as an ambitious strategy that only a champion would be brave enough to design. No team wins without coaching, but no team wins on coaching alone. It will take all of us to make meaningful execution of this strategy a reality. Yes, we are the champions. Now, let’s play like it. TH
Dr. Wiese is president of SHM.
Hospitalist Salary Spike

In case you haven’t seen it, the latest national survey data on hospitalist production, compensation, and other metrics was released in June.
Just as the Masters golf tournament is promoted as “a tradition like no other,” the combined SHM-MGMA (Medical Group Management Association) survey is without peer. Prior to this year, MGMA and SHM conducted separate surveys annually and biannually, respectively. The organizations chose to do a combined survey to take advantage of MGMA’s size and expertise in survey work (they’ve been conducting an annual survey of every specialty in medicine for decades) as well as SHM’s database of hospitalists and knowledge of the issues unique to HM.
If you want the most reliable data, this is the source you should use. I freely acknowledge my potential conflict of interest, which stems from my history with SHM (as a cofounder of SHM, I feel like a proud parent eager to trumpet all its accomplishments), and my consulting partner, Leslie Flores, was in charge of the survey process and data analysis for SHM. You should consider other sources of hospitalist data that might be available to you, but unless you have an unusually robust local or regional survey, the SHM-MGMA data will be the most valuable.
It’s Just a Survey
This survey provides the best national data, but like all such surveys, it has limitations. First, survey respondents vary in their diligence and accuracy in reporting their own data. It is even likely that some might “sanitize” or adjust the data they report in an effort, usually misguided, to provide a more accurate picture of their practice or cover up what might be for them an embarrassing issue. There is a process in place to catch outlier and inconsistent data submitted by a practice, and such practices are questioned to ensure accurate reporting and clear up any confusion or errors. But even that process is imperfect. There isn’t a team of auditors sent to “look at the books” to independently verify the accuracy of the data reported by each practice; that would be too costly, time-consuming, and even intimidating or annoying to be practical. So keep in mind that there is clearly some unavoidable “noise” or contamination in the data.
People sometimes say “SHM [or MGMA] says that ‘X’ is the right number of encounters for a hospitalist in a year,” where X is a number taken from the survey. Don’t make this mistake. I think it is misleading to think of the survey as establishing optimal or “right” benchmarks for any metric.
In fact, I think of benchmarks being something other than just survey numbers; instead, they’re well-considered data points derived from research showing what is optimal. The average glycohemoglobin of diabetics in the U.S. isn’t a desirable benchmark or goal, but the glycohemoglobin shown by research to be associated with the lowest risk of diabetic complications is. Keep this in mind when thinking about the survey results. There are little or no robust and generalizable research data regarding hospitalist productivity and compensation targets associated with the best performance.
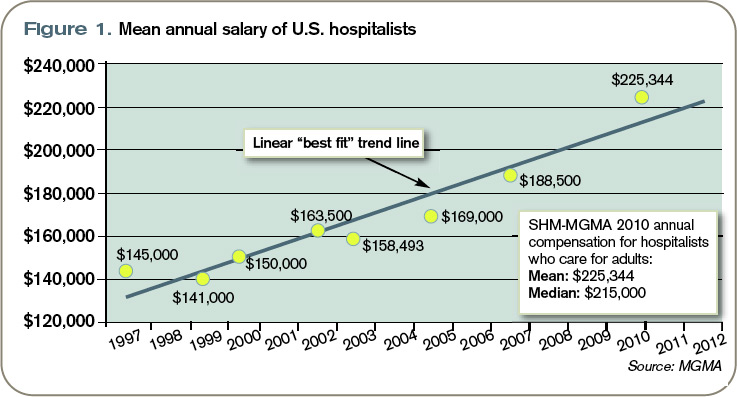
Hospitalist Incomes Surge
Let’s look at one data point: mean salary. The data points in Figure 1 (left) are the average salary going back to the first year the SHM survey was conducted. Note that all historical data points are from the SHM survey only, and thus represent a different population of respondents than the 2010 SHM-MGMA data point. It is important to remember this when looking at any trended hospitalist data.
Perhaps most importantly, previous SHM survey numbers included a significant proportion of academic hospitalist practices, which were largely unrepresented in the new SHM-MGMA survey data because SHM and MGMA will be conducting a separate survey of academic hospitalist practices in the fall.
Since academic hospitalists tend to earn less—and have lower overall productivity—than hospitalists in other settings, their absence from this survey likely results in greater increases in average compensation and production than would otherwise have been the case.
Beginning in about 2001, MGMA began reporting hospitalist compensation, but I have left those numbers off of this figure. And since about 2002, SHM has separated data for hospitalists who care for adults versus those that care for children; when separate data were available, this figure shows the compensation for hospitalists who care for adults and excludes pediatric hospitalists.
Note that the compensation figures include all salary elements, including a “base” or fixed component, productivity component, quality bonus, etc. The numbers exclude such benefits as the cost of health insurance or matching retirement plan contributions.
Inflation and a trend of increased hospitalist productivity are two reasons that hospitalist compensation has been increasing, but neither explains more than a portion of the increase in salary. (According to computational-knowledge engine WolframAlpha.com, inflation in the U.S. averaged 2.3% per year from 1997 to 2002. I’ll talk more about trends in hospitalist productivity in a future column.) I think the principal reason for the rising trend in our pay is “market forces,” primarily demand for hospitalists that has exceeded the supply.
What the Future Holds
It is interesting to speculate whether the historical trend line will accurately predict future increases in salary. At some point, forces will have to “bend the curve” so that it climbs more slowly. It could look like a curve reaching asymptote.
It is anyone’s guess when that might start to happen, but there are two developments over the last couple of years that suggest it might be coming: In some markets, the demand for hospitalists has been met and new candidates can’t find positions, so salaries in those markets might start to level off. And, unlike a few years ago, hospitalists are now competing with nearly every other physician specialty to get financial support from their hospitals, so hospitalists might find their hospital has less money available for them.
But the really big—and unknown—variable that could increase or decrease future hospitalist salaries is the effect of any further national healthcare reform legislation. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
In case you haven’t seen it, the latest national survey data on hospitalist production, compensation, and other metrics was released in June.
Just as the Masters golf tournament is promoted as “a tradition like no other,” the combined SHM-MGMA (Medical Group Management Association) survey is without peer. Prior to this year, MGMA and SHM conducted separate surveys annually and biannually, respectively. The organizations chose to do a combined survey to take advantage of MGMA’s size and expertise in survey work (they’ve been conducting an annual survey of every specialty in medicine for decades) as well as SHM’s database of hospitalists and knowledge of the issues unique to HM.
If you want the most reliable data, this is the source you should use. I freely acknowledge my potential conflict of interest, which stems from my history with SHM (as a cofounder of SHM, I feel like a proud parent eager to trumpet all its accomplishments), and my consulting partner, Leslie Flores, was in charge of the survey process and data analysis for SHM. You should consider other sources of hospitalist data that might be available to you, but unless you have an unusually robust local or regional survey, the SHM-MGMA data will be the most valuable.
It’s Just a Survey
This survey provides the best national data, but like all such surveys, it has limitations. First, survey respondents vary in their diligence and accuracy in reporting their own data. It is even likely that some might “sanitize” or adjust the data they report in an effort, usually misguided, to provide a more accurate picture of their practice or cover up what might be for them an embarrassing issue. There is a process in place to catch outlier and inconsistent data submitted by a practice, and such practices are questioned to ensure accurate reporting and clear up any confusion or errors. But even that process is imperfect. There isn’t a team of auditors sent to “look at the books” to independently verify the accuracy of the data reported by each practice; that would be too costly, time-consuming, and even intimidating or annoying to be practical. So keep in mind that there is clearly some unavoidable “noise” or contamination in the data.
People sometimes say “SHM [or MGMA] says that ‘X’ is the right number of encounters for a hospitalist in a year,” where X is a number taken from the survey. Don’t make this mistake. I think it is misleading to think of the survey as establishing optimal or “right” benchmarks for any metric.
In fact, I think of benchmarks being something other than just survey numbers; instead, they’re well-considered data points derived from research showing what is optimal. The average glycohemoglobin of diabetics in the U.S. isn’t a desirable benchmark or goal, but the glycohemoglobin shown by research to be associated with the lowest risk of diabetic complications is. Keep this in mind when thinking about the survey results. There are little or no robust and generalizable research data regarding hospitalist productivity and compensation targets associated with the best performance.
Hospitalist Incomes Surge
Let’s look at one data point: mean salary. The data points in Figure 1 (left) are the average salary going back to the first year the SHM survey was conducted. Note that all historical data points are from the SHM survey only, and thus represent a different population of respondents than the 2010 SHM-MGMA data point. It is important to remember this when looking at any trended hospitalist data.
Perhaps most importantly, previous SHM survey numbers included a significant proportion of academic hospitalist practices, which were largely unrepresented in the new SHM-MGMA survey data because SHM and MGMA will be conducting a separate survey of academic hospitalist practices in the fall.
Since academic hospitalists tend to earn less—and have lower overall productivity—than hospitalists in other settings, their absence from this survey likely results in greater increases in average compensation and production than would otherwise have been the case.
Beginning in about 2001, MGMA began reporting hospitalist compensation, but I have left those numbers off of this figure. And since about 2002, SHM has separated data for hospitalists who care for adults versus those that care for children; when separate data were available, this figure shows the compensation for hospitalists who care for adults and excludes pediatric hospitalists.
Note that the compensation figures include all salary elements, including a “base” or fixed component, productivity component, quality bonus, etc. The numbers exclude such benefits as the cost of health insurance or matching retirement plan contributions.
Inflation and a trend of increased hospitalist productivity are two reasons that hospitalist compensation has been increasing, but neither explains more than a portion of the increase in salary. (According to computational-knowledge engine WolframAlpha.com, inflation in the U.S. averaged 2.3% per year from 1997 to 2002. I’ll talk more about trends in hospitalist productivity in a future column.) I think the principal reason for the rising trend in our pay is “market forces,” primarily demand for hospitalists that has exceeded the supply.
What the Future Holds
It is interesting to speculate whether the historical trend line will accurately predict future increases in salary. At some point, forces will have to “bend the curve” so that it climbs more slowly. It could look like a curve reaching asymptote.
It is anyone’s guess when that might start to happen, but there are two developments over the last couple of years that suggest it might be coming: In some markets, the demand for hospitalists has been met and new candidates can’t find positions, so salaries in those markets might start to level off. And, unlike a few years ago, hospitalists are now competing with nearly every other physician specialty to get financial support from their hospitals, so hospitalists might find their hospital has less money available for them.
But the really big—and unknown—variable that could increase or decrease future hospitalist salaries is the effect of any further national healthcare reform legislation. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
In case you haven’t seen it, the latest national survey data on hospitalist production, compensation, and other metrics was released in June.
Just as the Masters golf tournament is promoted as “a tradition like no other,” the combined SHM-MGMA (Medical Group Management Association) survey is without peer. Prior to this year, MGMA and SHM conducted separate surveys annually and biannually, respectively. The organizations chose to do a combined survey to take advantage of MGMA’s size and expertise in survey work (they’ve been conducting an annual survey of every specialty in medicine for decades) as well as SHM’s database of hospitalists and knowledge of the issues unique to HM.
If you want the most reliable data, this is the source you should use. I freely acknowledge my potential conflict of interest, which stems from my history with SHM (as a cofounder of SHM, I feel like a proud parent eager to trumpet all its accomplishments), and my consulting partner, Leslie Flores, was in charge of the survey process and data analysis for SHM. You should consider other sources of hospitalist data that might be available to you, but unless you have an unusually robust local or regional survey, the SHM-MGMA data will be the most valuable.
It’s Just a Survey
This survey provides the best national data, but like all such surveys, it has limitations. First, survey respondents vary in their diligence and accuracy in reporting their own data. It is even likely that some might “sanitize” or adjust the data they report in an effort, usually misguided, to provide a more accurate picture of their practice or cover up what might be for them an embarrassing issue. There is a process in place to catch outlier and inconsistent data submitted by a practice, and such practices are questioned to ensure accurate reporting and clear up any confusion or errors. But even that process is imperfect. There isn’t a team of auditors sent to “look at the books” to independently verify the accuracy of the data reported by each practice; that would be too costly, time-consuming, and even intimidating or annoying to be practical. So keep in mind that there is clearly some unavoidable “noise” or contamination in the data.
People sometimes say “SHM [or MGMA] says that ‘X’ is the right number of encounters for a hospitalist in a year,” where X is a number taken from the survey. Don’t make this mistake. I think it is misleading to think of the survey as establishing optimal or “right” benchmarks for any metric.
In fact, I think of benchmarks being something other than just survey numbers; instead, they’re well-considered data points derived from research showing what is optimal. The average glycohemoglobin of diabetics in the U.S. isn’t a desirable benchmark or goal, but the glycohemoglobin shown by research to be associated with the lowest risk of diabetic complications is. Keep this in mind when thinking about the survey results. There are little or no robust and generalizable research data regarding hospitalist productivity and compensation targets associated with the best performance.
Hospitalist Incomes Surge
Let’s look at one data point: mean salary. The data points in Figure 1 (left) are the average salary going back to the first year the SHM survey was conducted. Note that all historical data points are from the SHM survey only, and thus represent a different population of respondents than the 2010 SHM-MGMA data point. It is important to remember this when looking at any trended hospitalist data.
Perhaps most importantly, previous SHM survey numbers included a significant proportion of academic hospitalist practices, which were largely unrepresented in the new SHM-MGMA survey data because SHM and MGMA will be conducting a separate survey of academic hospitalist practices in the fall.
Since academic hospitalists tend to earn less—and have lower overall productivity—than hospitalists in other settings, their absence from this survey likely results in greater increases in average compensation and production than would otherwise have been the case.
Beginning in about 2001, MGMA began reporting hospitalist compensation, but I have left those numbers off of this figure. And since about 2002, SHM has separated data for hospitalists who care for adults versus those that care for children; when separate data were available, this figure shows the compensation for hospitalists who care for adults and excludes pediatric hospitalists.
Note that the compensation figures include all salary elements, including a “base” or fixed component, productivity component, quality bonus, etc. The numbers exclude such benefits as the cost of health insurance or matching retirement plan contributions.
Inflation and a trend of increased hospitalist productivity are two reasons that hospitalist compensation has been increasing, but neither explains more than a portion of the increase in salary. (According to computational-knowledge engine WolframAlpha.com, inflation in the U.S. averaged 2.3% per year from 1997 to 2002. I’ll talk more about trends in hospitalist productivity in a future column.) I think the principal reason for the rising trend in our pay is “market forces,” primarily demand for hospitalists that has exceeded the supply.
What the Future Holds
It is interesting to speculate whether the historical trend line will accurately predict future increases in salary. At some point, forces will have to “bend the curve” so that it climbs more slowly. It could look like a curve reaching asymptote.
It is anyone’s guess when that might start to happen, but there are two developments over the last couple of years that suggest it might be coming: In some markets, the demand for hospitalists has been met and new candidates can’t find positions, so salaries in those markets might start to level off. And, unlike a few years ago, hospitalists are now competing with nearly every other physician specialty to get financial support from their hospitals, so hospitalists might find their hospital has less money available for them.
But the really big—and unknown—variable that could increase or decrease future hospitalist salaries is the effect of any further national healthcare reform legislation. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.