User login
News and Views that Matter to Pediatricians
The leading independent newspaper covering news and commentary in pediatrics.
FDA Approves IL-13 inhibitor for Atopic Dermatitis
The that is not well controlled, despite treatment with topical prescription therapies.
The recommended initial starting dose of lebrikizumab consists of 500 mg (two 250 mg injections) at baseline and week 2, followed by 250 mg every 2 weeks until week 16 or later when adequate clinical response is achieved. Then, maintenance dosing is recommended with one monthly injection (250 mg every 4 weeks). Children aged 12-17 years must weigh at least 88 pounds (40 kg) to be eligible for lebrikizumab treatment.
According to a press release from Lilly, which has been developing lebrikizumab, approval was based on results from the ADvocate 1, ADvocate 2, and ADhere studies, which included over 1000 adults and children aged 12 and older with moderate to severe AD. The primary endpoint for these studies was evaluated at 16 weeks and measured clear or almost clear skin (IGA score of 0 or 1).
According to Lilly, 38% of people in ADvocate 1 and 2 who took lebrikizumab achieved clear or almost-clear skin at 16 weeks, compared with 12% of those in the placebo arm, and 10% experienced these results as early as 4 weeks. Of those treated with lebrikizumab who experienced clear or almost-clear skin at week 16, 77% maintained those results at 1 year on the once-monthly dose. In addition, on average, 43% of those on lebrikizumab experienced relief of itch at 16 weeks, compared with 12% of those on placebo, according to the press release.
The most common side effects of lebrikizumab observed in the clinical trials include eye and eyelid inflammation, such as redness, swelling, and itching; injection-site reactions; and herpes zoster (shingles).
Lebrikizumab was approved in Japan in January 2024, and by the European Commission in 2023.
A version of this article first appeared on Medscape.com.
The that is not well controlled, despite treatment with topical prescription therapies.
The recommended initial starting dose of lebrikizumab consists of 500 mg (two 250 mg injections) at baseline and week 2, followed by 250 mg every 2 weeks until week 16 or later when adequate clinical response is achieved. Then, maintenance dosing is recommended with one monthly injection (250 mg every 4 weeks). Children aged 12-17 years must weigh at least 88 pounds (40 kg) to be eligible for lebrikizumab treatment.
According to a press release from Lilly, which has been developing lebrikizumab, approval was based on results from the ADvocate 1, ADvocate 2, and ADhere studies, which included over 1000 adults and children aged 12 and older with moderate to severe AD. The primary endpoint for these studies was evaluated at 16 weeks and measured clear or almost clear skin (IGA score of 0 or 1).
According to Lilly, 38% of people in ADvocate 1 and 2 who took lebrikizumab achieved clear or almost-clear skin at 16 weeks, compared with 12% of those in the placebo arm, and 10% experienced these results as early as 4 weeks. Of those treated with lebrikizumab who experienced clear or almost-clear skin at week 16, 77% maintained those results at 1 year on the once-monthly dose. In addition, on average, 43% of those on lebrikizumab experienced relief of itch at 16 weeks, compared with 12% of those on placebo, according to the press release.
The most common side effects of lebrikizumab observed in the clinical trials include eye and eyelid inflammation, such as redness, swelling, and itching; injection-site reactions; and herpes zoster (shingles).
Lebrikizumab was approved in Japan in January 2024, and by the European Commission in 2023.
A version of this article first appeared on Medscape.com.
The that is not well controlled, despite treatment with topical prescription therapies.
The recommended initial starting dose of lebrikizumab consists of 500 mg (two 250 mg injections) at baseline and week 2, followed by 250 mg every 2 weeks until week 16 or later when adequate clinical response is achieved. Then, maintenance dosing is recommended with one monthly injection (250 mg every 4 weeks). Children aged 12-17 years must weigh at least 88 pounds (40 kg) to be eligible for lebrikizumab treatment.
According to a press release from Lilly, which has been developing lebrikizumab, approval was based on results from the ADvocate 1, ADvocate 2, and ADhere studies, which included over 1000 adults and children aged 12 and older with moderate to severe AD. The primary endpoint for these studies was evaluated at 16 weeks and measured clear or almost clear skin (IGA score of 0 or 1).
According to Lilly, 38% of people in ADvocate 1 and 2 who took lebrikizumab achieved clear or almost-clear skin at 16 weeks, compared with 12% of those in the placebo arm, and 10% experienced these results as early as 4 weeks. Of those treated with lebrikizumab who experienced clear or almost-clear skin at week 16, 77% maintained those results at 1 year on the once-monthly dose. In addition, on average, 43% of those on lebrikizumab experienced relief of itch at 16 weeks, compared with 12% of those on placebo, according to the press release.
The most common side effects of lebrikizumab observed in the clinical trials include eye and eyelid inflammation, such as redness, swelling, and itching; injection-site reactions; and herpes zoster (shingles).
Lebrikizumab was approved in Japan in January 2024, and by the European Commission in 2023.
A version of this article first appeared on Medscape.com.
A 14-Year-Old Female Presents With a Growth Under Her Toenail
BY XOCHITL LONGSTAFF, BS; ANGELINA LABIB, MD; AND DAWN EICHENFIELD, MD, PHD
Diagnosis: Subungual bony exostosis

The patient was referred to orthopedics for further evaluation and ultimately underwent excisional surgery. At her most recent follow-up visit with orthopedic surgery, her new nail was observed to be growing well.
Subungual exostosis, also known as Dupuytren’s exostosis, is a benign osteocartilaginous tumor that classically presents as a bony growth at the dorsal aspect of the distal phalanx of the great toe, near the nail bed. The pathogenesis remains unclear, but suggested etiologies include prior trauma, infection, and hereditary abnormalities.1
Clinically, lesions can be painful and may be associated with skin ulceration. The location at the dorsal distal great toe is a key distinguishing feature. Physical exam reveals a firm, fixed nodule with a hyperkeratotic smooth surface.2

Radiographic evaluation, particularly with a lateral view, is often diagnostic. The classic radiographic finding in subungual exostosis is an osseous structure connected to the distal phalanx, with a hazy periphery representing a fibrocartilage cap.
Treatment involves complete marginal excision. The complications from surgical excision are minimal, with the most common being recurrence.3 However, the recurrence rate is also generally low, around 4%.1

Ms. Longstaff is currently completing a research year as a Pediatric Clinical Research Fellow at University of California San Diego (UCSD) Rady Children’s Hospital prior to finishing her final year at the David Geffen School of Medicine at the University of California, Los Angeles. Dr. Labib is the Post-Doctoral Pediatric Clinical Research Fellow at UCSD Rady Children’s Hospital. Dr. Eichenfield is a dermatologist at Rady Children’s Hospital–San Diego and assistant clinical professor at UCSD.
References
1. Alabdullrahman LW et al. Osteochondroma. In: StatPearls [Internet]. 2024 Feb 26. https://www.ncbi.nlm.nih.gov/books/NBK544296/#.
2. DaCambra MP et al. Clin Orthop Relat Res. 2014 Apr;472(4):1251-9. doi: 10.1007/s11999-013-3345-4.
3. Womack ME et al. J Am Acad Orthop Surg Glob Res Rev. 2022 Mar 22;6(3):e21.00239. doi: 10.5435/JAAOSGlobal-D-21-00239.
BY XOCHITL LONGSTAFF, BS; ANGELINA LABIB, MD; AND DAWN EICHENFIELD, MD, PHD
Diagnosis: Subungual bony exostosis
The patient was referred to orthopedics for further evaluation and ultimately underwent excisional surgery. At her most recent follow-up visit with orthopedic surgery, her new nail was observed to be growing well.
Subungual exostosis, also known as Dupuytren’s exostosis, is a benign osteocartilaginous tumor that classically presents as a bony growth at the dorsal aspect of the distal phalanx of the great toe, near the nail bed. The pathogenesis remains unclear, but suggested etiologies include prior trauma, infection, and hereditary abnormalities.1
Clinically, lesions can be painful and may be associated with skin ulceration. The location at the dorsal distal great toe is a key distinguishing feature. Physical exam reveals a firm, fixed nodule with a hyperkeratotic smooth surface.2
Radiographic evaluation, particularly with a lateral view, is often diagnostic. The classic radiographic finding in subungual exostosis is an osseous structure connected to the distal phalanx, with a hazy periphery representing a fibrocartilage cap.
Treatment involves complete marginal excision. The complications from surgical excision are minimal, with the most common being recurrence.3 However, the recurrence rate is also generally low, around 4%.1
Ms. Longstaff is currently completing a research year as a Pediatric Clinical Research Fellow at University of California San Diego (UCSD) Rady Children’s Hospital prior to finishing her final year at the David Geffen School of Medicine at the University of California, Los Angeles. Dr. Labib is the Post-Doctoral Pediatric Clinical Research Fellow at UCSD Rady Children’s Hospital. Dr. Eichenfield is a dermatologist at Rady Children’s Hospital–San Diego and assistant clinical professor at UCSD.
References
1. Alabdullrahman LW et al. Osteochondroma. In: StatPearls [Internet]. 2024 Feb 26. https://www.ncbi.nlm.nih.gov/books/NBK544296/#.
2. DaCambra MP et al. Clin Orthop Relat Res. 2014 Apr;472(4):1251-9. doi: 10.1007/s11999-013-3345-4.
3. Womack ME et al. J Am Acad Orthop Surg Glob Res Rev. 2022 Mar 22;6(3):e21.00239. doi: 10.5435/JAAOSGlobal-D-21-00239.
BY XOCHITL LONGSTAFF, BS; ANGELINA LABIB, MD; AND DAWN EICHENFIELD, MD, PHD
Diagnosis: Subungual bony exostosis
The patient was referred to orthopedics for further evaluation and ultimately underwent excisional surgery. At her most recent follow-up visit with orthopedic surgery, her new nail was observed to be growing well.
Subungual exostosis, also known as Dupuytren’s exostosis, is a benign osteocartilaginous tumor that classically presents as a bony growth at the dorsal aspect of the distal phalanx of the great toe, near the nail bed. The pathogenesis remains unclear, but suggested etiologies include prior trauma, infection, and hereditary abnormalities.1
Clinically, lesions can be painful and may be associated with skin ulceration. The location at the dorsal distal great toe is a key distinguishing feature. Physical exam reveals a firm, fixed nodule with a hyperkeratotic smooth surface.2
Radiographic evaluation, particularly with a lateral view, is often diagnostic. The classic radiographic finding in subungual exostosis is an osseous structure connected to the distal phalanx, with a hazy periphery representing a fibrocartilage cap.
Treatment involves complete marginal excision. The complications from surgical excision are minimal, with the most common being recurrence.3 However, the recurrence rate is also generally low, around 4%.1
Ms. Longstaff is currently completing a research year as a Pediatric Clinical Research Fellow at University of California San Diego (UCSD) Rady Children’s Hospital prior to finishing her final year at the David Geffen School of Medicine at the University of California, Los Angeles. Dr. Labib is the Post-Doctoral Pediatric Clinical Research Fellow at UCSD Rady Children’s Hospital. Dr. Eichenfield is a dermatologist at Rady Children’s Hospital–San Diego and assistant clinical professor at UCSD.
References
1. Alabdullrahman LW et al. Osteochondroma. In: StatPearls [Internet]. 2024 Feb 26. https://www.ncbi.nlm.nih.gov/books/NBK544296/#.
2. DaCambra MP et al. Clin Orthop Relat Res. 2014 Apr;472(4):1251-9. doi: 10.1007/s11999-013-3345-4.
3. Womack ME et al. J Am Acad Orthop Surg Glob Res Rev. 2022 Mar 22;6(3):e21.00239. doi: 10.5435/JAAOSGlobal-D-21-00239.
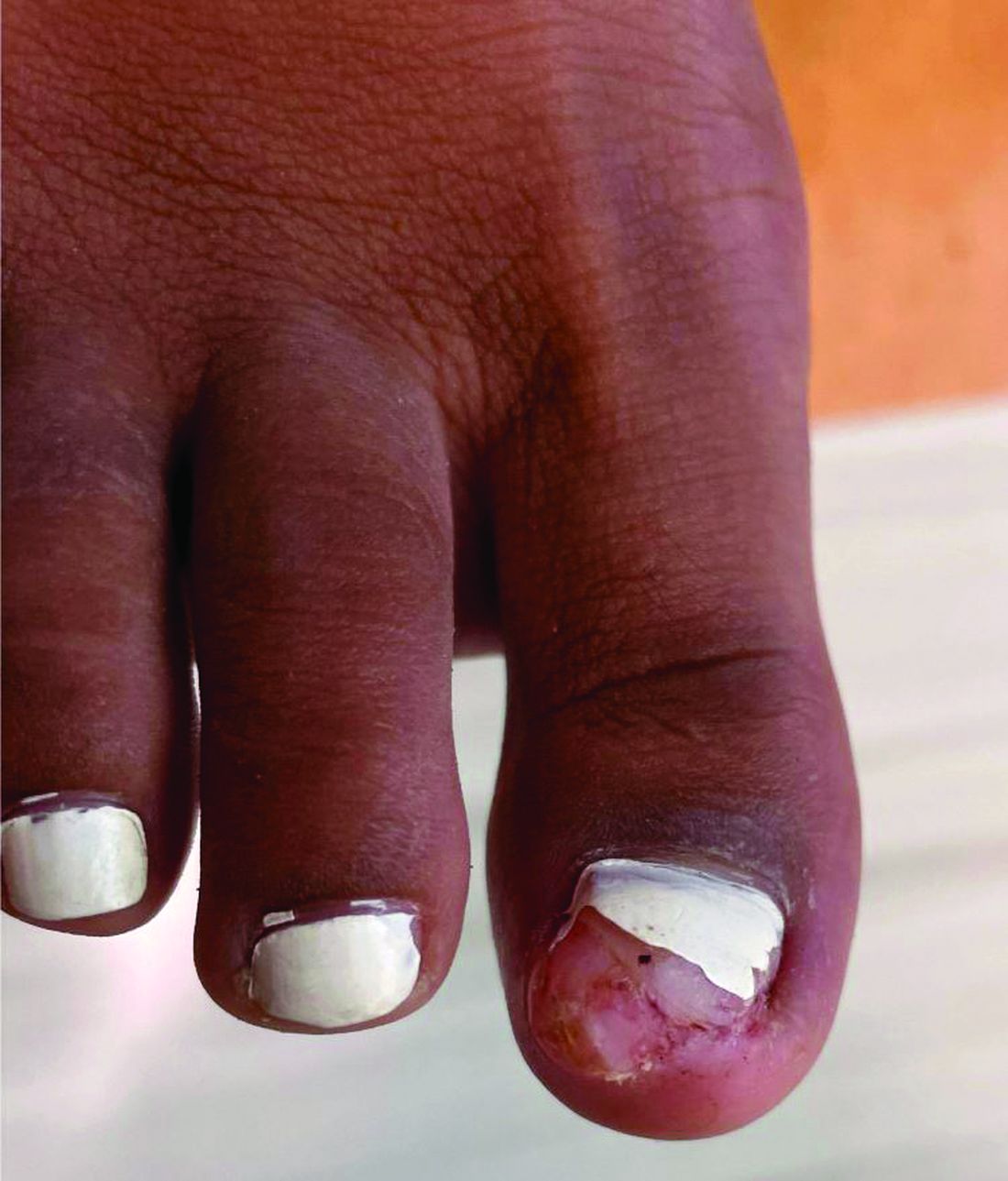
A 14-year-old healthy female presents with a painful nodule under her great toenail. The nodule had been present for 2 months and there was no preceding trauma. Three days prior to presentation, her nail cracked and bled after bumping her toe. The toe is painful to palpation. Given the associated pain, the patient visited urgent care and was prescribed cephalexin and acetaminophen.
Physical examination reveals a skin-colored subungual nodule with hypertrophic tissue originating from the nail bed of the right great toe, but no thickening of the nail plate (Figures 1-3).


Ultra-Processed Doesn’t Always Mean Bad — Here’s How to Tell
You may have been warned that ultra-processed foods can wreak havoc on your health. But not all of them are created equal.
A new study out of The Lancet Regional Health – Americas looked at different types of ultra-processed foods and found that some were even linked with lower risks of cardiovascular disease, coronary heart disease, and stroke,
“Avoiding all ultra-processed foods is not practical for most people,” said Dariush Mozaffarian, MD, a cardiologist, public health scientist, and director of the Food is Medicine Institute at Tufts University in Boston, Massachusetts. “So, it is helpful to start to understand, within the category of all processing, what food might be more or less harmful.”
Researchers analyzed food questionnaires from three large groups of US adults, with most people in their review being White and female. The study found that sugary and artificially sweetened drinks, along with processed meats, were linked to a greater risk of cardiovascular disease and coronary heart disease. But cereals, savory snacks, and yogurt and dairy-based desserts were linked to a lower risk of these diseases. Ultra-processed cereals and breads were also linked to a lower stroke risk.
The Truth About Processed Meat
Studies show that cured, salted, or smoked meats are linked to certain cancers.
“We know that sugar-sweetened beverages are associated with metabolic derangement for things like higher glucose levels, insulin resistance, visceral obesity, prediabetes, diabetes, and higher triglycerides,” said Ashish Sarraju, MD, a cardiologist with the Cleveland Clinic in Ohio. “Added sugars associated with all of those things are in turn risk factors for heart disease.” Sugar-sweetened beverages are often very high in sugar, artificial colors, and other additives, and almost “nothing beneficial” in terms of ingredients, Dr. Mozaffarian said. “They’re also consumed in very high doses, very quickly.”
Processed meats have 400% higher levels of salt, compared with unprocessed meats, said Dr. Mozaffarian. They also contain high levels of added nitrates, which are a carcinogen that could also affect the heart and blood vessels. Certain ultra-processed foods, such as bacon, are often fried at sky-high temperatures, which can trigger inflammatory compounds.
“If you put together the inflammatory effects, the salt, and the nitrates, this is a package of food that can really build to cause harm,” said Dr. Mozaffarian. The World Health Organization has also classified processed meats (bacon, ham, salami) as a group one carcinogen, he noted.
“Processed meats are typically high in saturated fats, sodium, and preservatives, which can increase blood pressure, promote inflammation, and negatively affect cholesterol levels, leading to a higher risk of coronary heart disease, said Joseph A. Daibes, DO, an interventional cardiologist at Lenox Hill Hospital, New York City. “The study underscores the importance of limiting these types of foods to reduce cardiovascular risk.”
But considering that breakfast cereals – albeit highly processed – are a top source of whole grains for Americans, it makes sense that they are linked with lower risk of heart disease, said Dr. Mozaffarian.
“They have fiber, bran, whole grains, and they also have sugar, and additives,” he said. “But on average, putting all those things together, this study suggested that the net effect is beneficial. That doesn’t mean they couldn’t be more beneficial if we made them less processed, but they don’t seem to have harm.”
The active probiotics and fermentation in yogurt can make it a healthy snack of choice, as there has been more and more research showing that fermented foods with probiotics are good for heart health and work against metabolic disease, or a cluster of conditions that can increase the risk of stroke, heart disease, and type 2 diabetes, Dr. Mozaffarian said.
Savory snacks, cereals, and yogurt and dairy-based desserts may also be less calorie dense than sugary beverages and processed meats, said Dr. Daibes.
“Additionally, the type of fat used in savory snacks and the presence of probiotics in yogurt may have neutral or even positive effects on heart health, as opposed to the harmful fats and additives found in many ultra-processed foods,” he said.
How Ultra-Processed Foods Can Harm Your Health
There are “clear and concerning links” between eating ultra-processed foods and getting heart disease, according to Dr. Daibes. “In real-life clinical practice, it’s a rather clear and straightforward relationship – the patients who tend to have poorer diets, with more ultra-processed and nutrient-barren foods, tend to have worse health outcomes, both cardiovascular and otherwise.”
Processing foods is centered on breaking down the natural structures of foods, as well as the loss of their natural nutrients, Dr. Mozaffarian explained. When you include the word “ultra,” this refers to putting in industrial additives.
“I think refined starches (such as wheat, corn, and rice) and sugars are some of the biggest harms because it leads to a big spike in blood glucose,” Dr. Mozaffarian said. “But also, those refined starches and sugars are digested so quickly in the stomach and small intestine that you starve your gut bacteria in your large intestines.”
Many “good-for-you ingredients,” such as fermentable fibers and bio-active compounds, are found in unprocessed, whole foods like fruits, vegetables, nuts, beans, and seeds, noted Dr. Mozaffarian. High levels of salt in ultra-processed foods are another cause for concern, as are other additives such as artificial flavorings, sweeteners, and thickeners.
Opting for Whole Foods
There may be people looking to eat cleaner, unprocessed foods, but high cost and a lack of access to them could create challenges. Dr. Sarraju advises his patients to simply do their best to eat foods in their whole-ingredient form and avoid prepackaged foods as much as possible.
A version of this article first appeared on WebMD.com.
You may have been warned that ultra-processed foods can wreak havoc on your health. But not all of them are created equal.
A new study out of The Lancet Regional Health – Americas looked at different types of ultra-processed foods and found that some were even linked with lower risks of cardiovascular disease, coronary heart disease, and stroke,
“Avoiding all ultra-processed foods is not practical for most people,” said Dariush Mozaffarian, MD, a cardiologist, public health scientist, and director of the Food is Medicine Institute at Tufts University in Boston, Massachusetts. “So, it is helpful to start to understand, within the category of all processing, what food might be more or less harmful.”
Researchers analyzed food questionnaires from three large groups of US adults, with most people in their review being White and female. The study found that sugary and artificially sweetened drinks, along with processed meats, were linked to a greater risk of cardiovascular disease and coronary heart disease. But cereals, savory snacks, and yogurt and dairy-based desserts were linked to a lower risk of these diseases. Ultra-processed cereals and breads were also linked to a lower stroke risk.
The Truth About Processed Meat
Studies show that cured, salted, or smoked meats are linked to certain cancers.
“We know that sugar-sweetened beverages are associated with metabolic derangement for things like higher glucose levels, insulin resistance, visceral obesity, prediabetes, diabetes, and higher triglycerides,” said Ashish Sarraju, MD, a cardiologist with the Cleveland Clinic in Ohio. “Added sugars associated with all of those things are in turn risk factors for heart disease.” Sugar-sweetened beverages are often very high in sugar, artificial colors, and other additives, and almost “nothing beneficial” in terms of ingredients, Dr. Mozaffarian said. “They’re also consumed in very high doses, very quickly.”
Processed meats have 400% higher levels of salt, compared with unprocessed meats, said Dr. Mozaffarian. They also contain high levels of added nitrates, which are a carcinogen that could also affect the heart and blood vessels. Certain ultra-processed foods, such as bacon, are often fried at sky-high temperatures, which can trigger inflammatory compounds.
“If you put together the inflammatory effects, the salt, and the nitrates, this is a package of food that can really build to cause harm,” said Dr. Mozaffarian. The World Health Organization has also classified processed meats (bacon, ham, salami) as a group one carcinogen, he noted.
“Processed meats are typically high in saturated fats, sodium, and preservatives, which can increase blood pressure, promote inflammation, and negatively affect cholesterol levels, leading to a higher risk of coronary heart disease, said Joseph A. Daibes, DO, an interventional cardiologist at Lenox Hill Hospital, New York City. “The study underscores the importance of limiting these types of foods to reduce cardiovascular risk.”
But considering that breakfast cereals – albeit highly processed – are a top source of whole grains for Americans, it makes sense that they are linked with lower risk of heart disease, said Dr. Mozaffarian.
“They have fiber, bran, whole grains, and they also have sugar, and additives,” he said. “But on average, putting all those things together, this study suggested that the net effect is beneficial. That doesn’t mean they couldn’t be more beneficial if we made them less processed, but they don’t seem to have harm.”
The active probiotics and fermentation in yogurt can make it a healthy snack of choice, as there has been more and more research showing that fermented foods with probiotics are good for heart health and work against metabolic disease, or a cluster of conditions that can increase the risk of stroke, heart disease, and type 2 diabetes, Dr. Mozaffarian said.
Savory snacks, cereals, and yogurt and dairy-based desserts may also be less calorie dense than sugary beverages and processed meats, said Dr. Daibes.
“Additionally, the type of fat used in savory snacks and the presence of probiotics in yogurt may have neutral or even positive effects on heart health, as opposed to the harmful fats and additives found in many ultra-processed foods,” he said.
How Ultra-Processed Foods Can Harm Your Health
There are “clear and concerning links” between eating ultra-processed foods and getting heart disease, according to Dr. Daibes. “In real-life clinical practice, it’s a rather clear and straightforward relationship – the patients who tend to have poorer diets, with more ultra-processed and nutrient-barren foods, tend to have worse health outcomes, both cardiovascular and otherwise.”
Processing foods is centered on breaking down the natural structures of foods, as well as the loss of their natural nutrients, Dr. Mozaffarian explained. When you include the word “ultra,” this refers to putting in industrial additives.
“I think refined starches (such as wheat, corn, and rice) and sugars are some of the biggest harms because it leads to a big spike in blood glucose,” Dr. Mozaffarian said. “But also, those refined starches and sugars are digested so quickly in the stomach and small intestine that you starve your gut bacteria in your large intestines.”
Many “good-for-you ingredients,” such as fermentable fibers and bio-active compounds, are found in unprocessed, whole foods like fruits, vegetables, nuts, beans, and seeds, noted Dr. Mozaffarian. High levels of salt in ultra-processed foods are another cause for concern, as are other additives such as artificial flavorings, sweeteners, and thickeners.
Opting for Whole Foods
There may be people looking to eat cleaner, unprocessed foods, but high cost and a lack of access to them could create challenges. Dr. Sarraju advises his patients to simply do their best to eat foods in their whole-ingredient form and avoid prepackaged foods as much as possible.
A version of this article first appeared on WebMD.com.
You may have been warned that ultra-processed foods can wreak havoc on your health. But not all of them are created equal.
A new study out of The Lancet Regional Health – Americas looked at different types of ultra-processed foods and found that some were even linked with lower risks of cardiovascular disease, coronary heart disease, and stroke,
“Avoiding all ultra-processed foods is not practical for most people,” said Dariush Mozaffarian, MD, a cardiologist, public health scientist, and director of the Food is Medicine Institute at Tufts University in Boston, Massachusetts. “So, it is helpful to start to understand, within the category of all processing, what food might be more or less harmful.”
Researchers analyzed food questionnaires from three large groups of US adults, with most people in their review being White and female. The study found that sugary and artificially sweetened drinks, along with processed meats, were linked to a greater risk of cardiovascular disease and coronary heart disease. But cereals, savory snacks, and yogurt and dairy-based desserts were linked to a lower risk of these diseases. Ultra-processed cereals and breads were also linked to a lower stroke risk.
The Truth About Processed Meat
Studies show that cured, salted, or smoked meats are linked to certain cancers.
“We know that sugar-sweetened beverages are associated with metabolic derangement for things like higher glucose levels, insulin resistance, visceral obesity, prediabetes, diabetes, and higher triglycerides,” said Ashish Sarraju, MD, a cardiologist with the Cleveland Clinic in Ohio. “Added sugars associated with all of those things are in turn risk factors for heart disease.” Sugar-sweetened beverages are often very high in sugar, artificial colors, and other additives, and almost “nothing beneficial” in terms of ingredients, Dr. Mozaffarian said. “They’re also consumed in very high doses, very quickly.”
Processed meats have 400% higher levels of salt, compared with unprocessed meats, said Dr. Mozaffarian. They also contain high levels of added nitrates, which are a carcinogen that could also affect the heart and blood vessels. Certain ultra-processed foods, such as bacon, are often fried at sky-high temperatures, which can trigger inflammatory compounds.
“If you put together the inflammatory effects, the salt, and the nitrates, this is a package of food that can really build to cause harm,” said Dr. Mozaffarian. The World Health Organization has also classified processed meats (bacon, ham, salami) as a group one carcinogen, he noted.
“Processed meats are typically high in saturated fats, sodium, and preservatives, which can increase blood pressure, promote inflammation, and negatively affect cholesterol levels, leading to a higher risk of coronary heart disease, said Joseph A. Daibes, DO, an interventional cardiologist at Lenox Hill Hospital, New York City. “The study underscores the importance of limiting these types of foods to reduce cardiovascular risk.”
But considering that breakfast cereals – albeit highly processed – are a top source of whole grains for Americans, it makes sense that they are linked with lower risk of heart disease, said Dr. Mozaffarian.
“They have fiber, bran, whole grains, and they also have sugar, and additives,” he said. “But on average, putting all those things together, this study suggested that the net effect is beneficial. That doesn’t mean they couldn’t be more beneficial if we made them less processed, but they don’t seem to have harm.”
The active probiotics and fermentation in yogurt can make it a healthy snack of choice, as there has been more and more research showing that fermented foods with probiotics are good for heart health and work against metabolic disease, or a cluster of conditions that can increase the risk of stroke, heart disease, and type 2 diabetes, Dr. Mozaffarian said.
Savory snacks, cereals, and yogurt and dairy-based desserts may also be less calorie dense than sugary beverages and processed meats, said Dr. Daibes.
“Additionally, the type of fat used in savory snacks and the presence of probiotics in yogurt may have neutral or even positive effects on heart health, as opposed to the harmful fats and additives found in many ultra-processed foods,” he said.
How Ultra-Processed Foods Can Harm Your Health
There are “clear and concerning links” between eating ultra-processed foods and getting heart disease, according to Dr. Daibes. “In real-life clinical practice, it’s a rather clear and straightforward relationship – the patients who tend to have poorer diets, with more ultra-processed and nutrient-barren foods, tend to have worse health outcomes, both cardiovascular and otherwise.”
Processing foods is centered on breaking down the natural structures of foods, as well as the loss of their natural nutrients, Dr. Mozaffarian explained. When you include the word “ultra,” this refers to putting in industrial additives.
“I think refined starches (such as wheat, corn, and rice) and sugars are some of the biggest harms because it leads to a big spike in blood glucose,” Dr. Mozaffarian said. “But also, those refined starches and sugars are digested so quickly in the stomach and small intestine that you starve your gut bacteria in your large intestines.”
Many “good-for-you ingredients,” such as fermentable fibers and bio-active compounds, are found in unprocessed, whole foods like fruits, vegetables, nuts, beans, and seeds, noted Dr. Mozaffarian. High levels of salt in ultra-processed foods are another cause for concern, as are other additives such as artificial flavorings, sweeteners, and thickeners.
Opting for Whole Foods
There may be people looking to eat cleaner, unprocessed foods, but high cost and a lack of access to them could create challenges. Dr. Sarraju advises his patients to simply do their best to eat foods in their whole-ingredient form and avoid prepackaged foods as much as possible.
A version of this article first appeared on WebMD.com.
FROM THE LANCET REGIONAL HEALTH – AMERICAS
UVA Defends Medical School Dean, Hospital CEO After Docs Call for Their Removal
The University of Virginia (UVA) is defending the CEO of its health system and its medical school dean in the wake of a very public call for their removal.
At least 128 members of the University of Virginia faculty who are employed by both the medical school and the UVA Physicians Group wrote to the UVA Board of Visitors and its peer-elected faculty leaders, expressing no confidence in K. Craig Kent, MD, CEO of UVA Health and executive vice president for health affairs, and Melina Kibbe, MD, dean of the medical school and chief health affairs officer.
Dr. Kibbe, a vascular surgeon and researcher, is also the editor in chief of JAMA Surgery.
“We call for the immediate removal of Craig Kent and Melina Kibbe,” wrote the physicians.
The letter alleged that patient safety was compromised because doctors, nurses, and other staff were pressured to abstain from reporting safety concerns and that physicians had been hired “despite concerns regarding integrity and quality.” Those who raised safety concerns faced “explicit and implicit threats and retaliation,” including delays and denials of promotion and tenure, said the letter.
The September 5 letter did not include signatures. The authors said that names were being protected, but that they would share the names with a limited audience.
UVA President Jim Ryan took issue with the notion that the signees were anonymous. He said in his own letter to medical school faculty that some of the accusations were about matters that had already been addressed or that were being worked on. As far as allegations that he was not previously aware of, “we will do our best to investigate,” he said.
The faculty who signed the letter “have besmirched the reputations of not just Melina and Craig,” wrote Mr. Ryan. “They have unfairly — and I trust unwittingly — cast a shadow over the great work of the entire health system and medical school.”
The authors claimed that reports about bullying and harassment of trainees had been “suppressed, minimized, and subsequently altered.”
And they said that spending on leadership was prioritized over addressing clinical and technical staff shortages. Whistleblowers who reported fraud were not protected, and clinicians were pressured to modify patient records to “obfuscate adverse outcomes and boost productivity metrics,” they wrote.
The 128 members of the UVA Physicians Group who signed the letter represent about 10% of the 1400 medical school faculty members.
It is not the first time that Dr. Kent has been given a vote of no confidence. In 2017, when he was the dean of the College of Medicine at the Ohio State University, Dr. Kent was accused in a “no confidence” letter from 25 physicians and faculty of helping to undermine the school’s mission and taking actions that led to resignations and early retirements of many staff, the Columbus Dispatch reported.
William G. Crutchfield Jr., a member of the UVA Health System Board, defended Dr. Kent and Dr. Kibbe in a lengthy statement shared with this news organization. He said that UVA Health’s four hospitals had received “A” ratings for safety, and that the system has a 5.1% turnover rate compared with a national average of 8.3%.
Dr. Kent and Dr. Kibbe have recruited faculty from top academic medical centers, Mr. Crutchfield wrote.
“If our work environment were so toxic, these people would not have joined our faculty,” he wrote.
Mr. Crutchfield credited Dr. Kent and Dr. Kibbe with crafting a new 10-year strategic plan and for hiring a chief strategy officer to lead the plan — a move that replaced “expensive outside consultants.”
Mr. Ryan said in his letter that his inbox “is overflowing with testimonials from some of the 1200-plus faculty who did not sign the letter, who attest that the health system today — under Melina and Craig’s leadership — is in the best shape it has ever been in, and that they have addressed changes that have needed to be made for more than two decades.”
A request to see some of these positive testimonials was not answered by press time.
Mr. Crutchfield, like Mr. Ryan, said that the letter writers were doing more harm than good.
“If a small cabal of people hiding behind anonymity can force outstanding leaders out of UVA, it will make it extremely difficult to recruit outstanding new physicians, nurses, technicians, and administrators,” he wrote.
A version of this article first appeared on Medscape.com.
The University of Virginia (UVA) is defending the CEO of its health system and its medical school dean in the wake of a very public call for their removal.
At least 128 members of the University of Virginia faculty who are employed by both the medical school and the UVA Physicians Group wrote to the UVA Board of Visitors and its peer-elected faculty leaders, expressing no confidence in K. Craig Kent, MD, CEO of UVA Health and executive vice president for health affairs, and Melina Kibbe, MD, dean of the medical school and chief health affairs officer.
Dr. Kibbe, a vascular surgeon and researcher, is also the editor in chief of JAMA Surgery.
“We call for the immediate removal of Craig Kent and Melina Kibbe,” wrote the physicians.
The letter alleged that patient safety was compromised because doctors, nurses, and other staff were pressured to abstain from reporting safety concerns and that physicians had been hired “despite concerns regarding integrity and quality.” Those who raised safety concerns faced “explicit and implicit threats and retaliation,” including delays and denials of promotion and tenure, said the letter.
The September 5 letter did not include signatures. The authors said that names were being protected, but that they would share the names with a limited audience.
UVA President Jim Ryan took issue with the notion that the signees were anonymous. He said in his own letter to medical school faculty that some of the accusations were about matters that had already been addressed or that were being worked on. As far as allegations that he was not previously aware of, “we will do our best to investigate,” he said.
The faculty who signed the letter “have besmirched the reputations of not just Melina and Craig,” wrote Mr. Ryan. “They have unfairly — and I trust unwittingly — cast a shadow over the great work of the entire health system and medical school.”
The authors claimed that reports about bullying and harassment of trainees had been “suppressed, minimized, and subsequently altered.”
And they said that spending on leadership was prioritized over addressing clinical and technical staff shortages. Whistleblowers who reported fraud were not protected, and clinicians were pressured to modify patient records to “obfuscate adverse outcomes and boost productivity metrics,” they wrote.
The 128 members of the UVA Physicians Group who signed the letter represent about 10% of the 1400 medical school faculty members.
It is not the first time that Dr. Kent has been given a vote of no confidence. In 2017, when he was the dean of the College of Medicine at the Ohio State University, Dr. Kent was accused in a “no confidence” letter from 25 physicians and faculty of helping to undermine the school’s mission and taking actions that led to resignations and early retirements of many staff, the Columbus Dispatch reported.
William G. Crutchfield Jr., a member of the UVA Health System Board, defended Dr. Kent and Dr. Kibbe in a lengthy statement shared with this news organization. He said that UVA Health’s four hospitals had received “A” ratings for safety, and that the system has a 5.1% turnover rate compared with a national average of 8.3%.
Dr. Kent and Dr. Kibbe have recruited faculty from top academic medical centers, Mr. Crutchfield wrote.
“If our work environment were so toxic, these people would not have joined our faculty,” he wrote.
Mr. Crutchfield credited Dr. Kent and Dr. Kibbe with crafting a new 10-year strategic plan and for hiring a chief strategy officer to lead the plan — a move that replaced “expensive outside consultants.”
Mr. Ryan said in his letter that his inbox “is overflowing with testimonials from some of the 1200-plus faculty who did not sign the letter, who attest that the health system today — under Melina and Craig’s leadership — is in the best shape it has ever been in, and that they have addressed changes that have needed to be made for more than two decades.”
A request to see some of these positive testimonials was not answered by press time.
Mr. Crutchfield, like Mr. Ryan, said that the letter writers were doing more harm than good.
“If a small cabal of people hiding behind anonymity can force outstanding leaders out of UVA, it will make it extremely difficult to recruit outstanding new physicians, nurses, technicians, and administrators,” he wrote.
A version of this article first appeared on Medscape.com.
The University of Virginia (UVA) is defending the CEO of its health system and its medical school dean in the wake of a very public call for their removal.
At least 128 members of the University of Virginia faculty who are employed by both the medical school and the UVA Physicians Group wrote to the UVA Board of Visitors and its peer-elected faculty leaders, expressing no confidence in K. Craig Kent, MD, CEO of UVA Health and executive vice president for health affairs, and Melina Kibbe, MD, dean of the medical school and chief health affairs officer.
Dr. Kibbe, a vascular surgeon and researcher, is also the editor in chief of JAMA Surgery.
“We call for the immediate removal of Craig Kent and Melina Kibbe,” wrote the physicians.
The letter alleged that patient safety was compromised because doctors, nurses, and other staff were pressured to abstain from reporting safety concerns and that physicians had been hired “despite concerns regarding integrity and quality.” Those who raised safety concerns faced “explicit and implicit threats and retaliation,” including delays and denials of promotion and tenure, said the letter.
The September 5 letter did not include signatures. The authors said that names were being protected, but that they would share the names with a limited audience.
UVA President Jim Ryan took issue with the notion that the signees were anonymous. He said in his own letter to medical school faculty that some of the accusations were about matters that had already been addressed or that were being worked on. As far as allegations that he was not previously aware of, “we will do our best to investigate,” he said.
The faculty who signed the letter “have besmirched the reputations of not just Melina and Craig,” wrote Mr. Ryan. “They have unfairly — and I trust unwittingly — cast a shadow over the great work of the entire health system and medical school.”
The authors claimed that reports about bullying and harassment of trainees had been “suppressed, minimized, and subsequently altered.”
And they said that spending on leadership was prioritized over addressing clinical and technical staff shortages. Whistleblowers who reported fraud were not protected, and clinicians were pressured to modify patient records to “obfuscate adverse outcomes and boost productivity metrics,” they wrote.
The 128 members of the UVA Physicians Group who signed the letter represent about 10% of the 1400 medical school faculty members.
It is not the first time that Dr. Kent has been given a vote of no confidence. In 2017, when he was the dean of the College of Medicine at the Ohio State University, Dr. Kent was accused in a “no confidence” letter from 25 physicians and faculty of helping to undermine the school’s mission and taking actions that led to resignations and early retirements of many staff, the Columbus Dispatch reported.
William G. Crutchfield Jr., a member of the UVA Health System Board, defended Dr. Kent and Dr. Kibbe in a lengthy statement shared with this news organization. He said that UVA Health’s four hospitals had received “A” ratings for safety, and that the system has a 5.1% turnover rate compared with a national average of 8.3%.
Dr. Kent and Dr. Kibbe have recruited faculty from top academic medical centers, Mr. Crutchfield wrote.
“If our work environment were so toxic, these people would not have joined our faculty,” he wrote.
Mr. Crutchfield credited Dr. Kent and Dr. Kibbe with crafting a new 10-year strategic plan and for hiring a chief strategy officer to lead the plan — a move that replaced “expensive outside consultants.”
Mr. Ryan said in his letter that his inbox “is overflowing with testimonials from some of the 1200-plus faculty who did not sign the letter, who attest that the health system today — under Melina and Craig’s leadership — is in the best shape it has ever been in, and that they have addressed changes that have needed to be made for more than two decades.”
A request to see some of these positive testimonials was not answered by press time.
Mr. Crutchfield, like Mr. Ryan, said that the letter writers were doing more harm than good.
“If a small cabal of people hiding behind anonymity can force outstanding leaders out of UVA, it will make it extremely difficult to recruit outstanding new physicians, nurses, technicians, and administrators,” he wrote.
A version of this article first appeared on Medscape.com.
The Surgeon General’s Advisory on Parental Mental Health: Implications for Pediatric Practice
As child psychiatrists and pediatricians, our mission extends beyond treating the physical health of children; it encompasses understanding the intricate web of factors that influence a child’s overall well-being. A recent advisory from U.S. Surgeon General Dr. Vivek Murthy has brought to light a critical issue that demands our attention: the declining mental health of parents and its profound impact on children. As providers who depend heavily on parental involvement to manage the needs of our pediatric patients, addressing parental mental health can be a crucial step in safeguarding the mental health of children.
The Surgeon General’s Advisory: A Call to Action
On August 28, 2024, the U.S. Surgeon General issued an advisory highlighting the significant stressors impacting parents and caregivers, and the broader implications for children’s mental health. The advisory emphasizes the bidirectional relationship between parental and child mental health, urging healthcare providers, policymakers, and communities to prioritize support for parents. It stresses that the mental health of parents is not only vital for their well-being but also plays a critical role in shaping the emotional and psychological development of their children.1
The Link Between Parental and Child Mental Health
Research shows that a parent’s mental health directly influences the child’s emotional and behavioral outcomes. Children of parents with untreated mental health conditions, such as depression, anxiety, trauma, or chronic stress, are at a significantly higher risk of developing similar conditions. This risk is mediated through various mechanisms, including genetic predisposition, compromised parent-child interactions, and exposure to adverse environments.

1. Parental Depression and Child Outcomes: Parental depression, particularly maternal depression, has been extensively studied and is strongly associated with emotional and behavioral problems in children. Children of depressed parents are more likely to experience anxiety, depression, and resulting academic difficulties. Depressed parents may struggle with consistent and positive parenting, which can disrupt the development of secure attachments and emotional regulation in children.2-4
2. Anxiety and Parenting Styles: Parental anxiety can influence parenting styles, often leading to overprotectiveness, inconsistency, or heightened criticism. These behaviors, in turn, can cultivate anxiety in children, creating a cycle that perpetuates mental health challenges across generations. Children raised in environments where anxiety is pervasive may learn to view the world as threatening, contributing to hypervigilance and stress.5
3. Impact of Chronic Stress on Parenting: Chronic stress experienced by parents, often due to financial hardship, lack of social support, or work-life imbalance, can impair their ability to engage in responsive and nurturing parenting. This, in turn, can affect children’s ability to meaningfully engage with parents to form secure attachments. Further, chronic stress can negatively impact the quality of parent-child interactions and fuel the cycle of rupture with limited opportunity for repair. The advisory stresses the need to address these systemic stressors as part of a broader public health strategy to support families.1
Implications for Pediatric Practice
Pediatricians are often the first point of contact for families navigating mental health challenges. The Surgeon General’s advisory highlights the need for pediatricians to adopt a holistic approach that considers the mental health of the entire family, not just the child. This can be challenging with the average follow-up appointment time of 16 minutes, though many of the recommendations take this logistical hurdle into consideration:
1. Screening for Parental Mental Health: Incorporating routine screening for parental mental health into pediatric visits can be a powerful tool. Questions about parental stress, depression (especially postpartum depression), and anxiety should be integrated into well-child visits, especially in families where children present with emotional or behavioral difficulties. By identifying at-risk parents early, timely referrals to mental health services can be secured.
2. Providing Resources and Referrals: Offering resources and referrals to parents who may be struggling can positively impact the entire family. This includes connecting families with mental health professionals, parenting support groups, or community resources that can alleviate stressors such as food insecurity or lack of childcare. Having a list of local mental health resources available in your practice can empower parents to seek the help they need.
3. Promoting Positive Parenting Practices: Guidance on positive parenting practices, stress management, and self-care can make a significant difference in the mental health of parents and their children. Workshops or educational materials on topics like mindfulness, managing work-life balance, and fostering healthy communication within the family can be valuable and high-yield additions to pediatric care.
4. Collaborative Care Models: Collaborative care models, where pediatricians work closely with child psychiatrists, psychologists, and social workers, can provide comprehensive support to families. This integrated approach ensures that both children and their parents receive the care they need, promoting better outcomes for the entire family unit.
Addressing Broader Systemic Issues
The advisory also calls for systemic changes that extend beyond the clinic. Policy changes such as expanding access to paid family leave, affordable childcare, and mental health services are essential to creating an environment where parents can thrive. As pediatricians, advocating for these changes at the local and national level can amplify the overall impact on families.
1. Advocating for Paid Family Leave: Paid family leave allows parents to bond with their children and attend to their own mental health needs without the added pressure of financial instability. Supporting policies that provide adequate paid leave can pave the way for a successful and healthy return to work and have long-term benefits for family health.
2. Expanding Mental Health Services: Increasing access to mental health services, especially in underserved communities, is crucial. Pediatricians can play a role by partnering with local mental health providers to offer integrated care within their practices or community settings.
3. Community Support Programs: The creation of community support programs that offer parenting classes, stress management workshops, and peer support groups can help reduce the isolation and stress that many parents feel. Pediatricians can collaborate with community organizations to promote these resources to families.
Conclusion
The Surgeon General’s advisory serves as a timely reminder of the interconnectedness of parental and child mental health. Pediatricians have a unique opportunity to influence not only the health of their pediatric patients, but also the well-being of their families. By recognizing and addressing the mental health needs of parents, we can break the cycle of stress and mental illness that affects so many families, ensuring a healthier future for the next generation.
Let us embrace this call to action and work together to create a supportive environment where all parents and children can thrive.
Dr. Richards is assistant clinical professor in the department of psychiatry and biobehavioral sciences; program director of the child and adolescent psychiatry fellowship; and associate medical director of the perinatal program at the UCLA Semel Institute for Neuroscience and Human Behavior, Los Angeles.
References
1. American Hospital Association. Surgeon General Issues Advisory on Mental Health and Well-Being of Parents. American Hospital Association. 2024 Sep 4.
2. Goodman SH, Gotlib IH. Risk for Psychopathology in the Children of Depressed Mothers: A Developmental Model for Understanding Mechanisms of Transmission. Psychol Rev. 1999;106(3):458-490. doi: 10.1037/0033-295X.106.3.458.
3. Lovejoy MC et al. Maternal Depression and Parenting Behavior: A Meta-Analytic Review. Clin Psychol Rev. 2000;20(5):561-592. doi: 10.1016/s0272-7358(98)00100-7.
4. Weissman MM et al. Offspring of Depressed Parents: 20 Years Later. Am J Psychiatry. 2006;163(6):1001-1008. doi: 10.1176/ajp.2006.163.6.1001.
5. Smith KE, Pollak SD. Early Life Stress and Development: Potential Mechanisms for Adverse Outcomes. J Neurodev Disord. 2020;12(1):3-14. doi: 10.1186/s11689-020-09337-y.
As child psychiatrists and pediatricians, our mission extends beyond treating the physical health of children; it encompasses understanding the intricate web of factors that influence a child’s overall well-being. A recent advisory from U.S. Surgeon General Dr. Vivek Murthy has brought to light a critical issue that demands our attention: the declining mental health of parents and its profound impact on children. As providers who depend heavily on parental involvement to manage the needs of our pediatric patients, addressing parental mental health can be a crucial step in safeguarding the mental health of children.
The Surgeon General’s Advisory: A Call to Action
On August 28, 2024, the U.S. Surgeon General issued an advisory highlighting the significant stressors impacting parents and caregivers, and the broader implications for children’s mental health. The advisory emphasizes the bidirectional relationship between parental and child mental health, urging healthcare providers, policymakers, and communities to prioritize support for parents. It stresses that the mental health of parents is not only vital for their well-being but also plays a critical role in shaping the emotional and psychological development of their children.1
The Link Between Parental and Child Mental Health
Research shows that a parent’s mental health directly influences the child’s emotional and behavioral outcomes. Children of parents with untreated mental health conditions, such as depression, anxiety, trauma, or chronic stress, are at a significantly higher risk of developing similar conditions. This risk is mediated through various mechanisms, including genetic predisposition, compromised parent-child interactions, and exposure to adverse environments.
1. Parental Depression and Child Outcomes: Parental depression, particularly maternal depression, has been extensively studied and is strongly associated with emotional and behavioral problems in children. Children of depressed parents are more likely to experience anxiety, depression, and resulting academic difficulties. Depressed parents may struggle with consistent and positive parenting, which can disrupt the development of secure attachments and emotional regulation in children.2-4
2. Anxiety and Parenting Styles: Parental anxiety can influence parenting styles, often leading to overprotectiveness, inconsistency, or heightened criticism. These behaviors, in turn, can cultivate anxiety in children, creating a cycle that perpetuates mental health challenges across generations. Children raised in environments where anxiety is pervasive may learn to view the world as threatening, contributing to hypervigilance and stress.5
3. Impact of Chronic Stress on Parenting: Chronic stress experienced by parents, often due to financial hardship, lack of social support, or work-life imbalance, can impair their ability to engage in responsive and nurturing parenting. This, in turn, can affect children’s ability to meaningfully engage with parents to form secure attachments. Further, chronic stress can negatively impact the quality of parent-child interactions and fuel the cycle of rupture with limited opportunity for repair. The advisory stresses the need to address these systemic stressors as part of a broader public health strategy to support families.1
Implications for Pediatric Practice
Pediatricians are often the first point of contact for families navigating mental health challenges. The Surgeon General’s advisory highlights the need for pediatricians to adopt a holistic approach that considers the mental health of the entire family, not just the child. This can be challenging with the average follow-up appointment time of 16 minutes, though many of the recommendations take this logistical hurdle into consideration:
1. Screening for Parental Mental Health: Incorporating routine screening for parental mental health into pediatric visits can be a powerful tool. Questions about parental stress, depression (especially postpartum depression), and anxiety should be integrated into well-child visits, especially in families where children present with emotional or behavioral difficulties. By identifying at-risk parents early, timely referrals to mental health services can be secured.
2. Providing Resources and Referrals: Offering resources and referrals to parents who may be struggling can positively impact the entire family. This includes connecting families with mental health professionals, parenting support groups, or community resources that can alleviate stressors such as food insecurity or lack of childcare. Having a list of local mental health resources available in your practice can empower parents to seek the help they need.
3. Promoting Positive Parenting Practices: Guidance on positive parenting practices, stress management, and self-care can make a significant difference in the mental health of parents and their children. Workshops or educational materials on topics like mindfulness, managing work-life balance, and fostering healthy communication within the family can be valuable and high-yield additions to pediatric care.
4. Collaborative Care Models: Collaborative care models, where pediatricians work closely with child psychiatrists, psychologists, and social workers, can provide comprehensive support to families. This integrated approach ensures that both children and their parents receive the care they need, promoting better outcomes for the entire family unit.
Addressing Broader Systemic Issues
The advisory also calls for systemic changes that extend beyond the clinic. Policy changes such as expanding access to paid family leave, affordable childcare, and mental health services are essential to creating an environment where parents can thrive. As pediatricians, advocating for these changes at the local and national level can amplify the overall impact on families.
1. Advocating for Paid Family Leave: Paid family leave allows parents to bond with their children and attend to their own mental health needs without the added pressure of financial instability. Supporting policies that provide adequate paid leave can pave the way for a successful and healthy return to work and have long-term benefits for family health.
2. Expanding Mental Health Services: Increasing access to mental health services, especially in underserved communities, is crucial. Pediatricians can play a role by partnering with local mental health providers to offer integrated care within their practices or community settings.
3. Community Support Programs: The creation of community support programs that offer parenting classes, stress management workshops, and peer support groups can help reduce the isolation and stress that many parents feel. Pediatricians can collaborate with community organizations to promote these resources to families.
Conclusion
The Surgeon General’s advisory serves as a timely reminder of the interconnectedness of parental and child mental health. Pediatricians have a unique opportunity to influence not only the health of their pediatric patients, but also the well-being of their families. By recognizing and addressing the mental health needs of parents, we can break the cycle of stress and mental illness that affects so many families, ensuring a healthier future for the next generation.
Let us embrace this call to action and work together to create a supportive environment where all parents and children can thrive.
Dr. Richards is assistant clinical professor in the department of psychiatry and biobehavioral sciences; program director of the child and adolescent psychiatry fellowship; and associate medical director of the perinatal program at the UCLA Semel Institute for Neuroscience and Human Behavior, Los Angeles.
References
1. American Hospital Association. Surgeon General Issues Advisory on Mental Health and Well-Being of Parents. American Hospital Association. 2024 Sep 4.
2. Goodman SH, Gotlib IH. Risk for Psychopathology in the Children of Depressed Mothers: A Developmental Model for Understanding Mechanisms of Transmission. Psychol Rev. 1999;106(3):458-490. doi: 10.1037/0033-295X.106.3.458.
3. Lovejoy MC et al. Maternal Depression and Parenting Behavior: A Meta-Analytic Review. Clin Psychol Rev. 2000;20(5):561-592. doi: 10.1016/s0272-7358(98)00100-7.
4. Weissman MM et al. Offspring of Depressed Parents: 20 Years Later. Am J Psychiatry. 2006;163(6):1001-1008. doi: 10.1176/ajp.2006.163.6.1001.
5. Smith KE, Pollak SD. Early Life Stress and Development: Potential Mechanisms for Adverse Outcomes. J Neurodev Disord. 2020;12(1):3-14. doi: 10.1186/s11689-020-09337-y.
As child psychiatrists and pediatricians, our mission extends beyond treating the physical health of children; it encompasses understanding the intricate web of factors that influence a child’s overall well-being. A recent advisory from U.S. Surgeon General Dr. Vivek Murthy has brought to light a critical issue that demands our attention: the declining mental health of parents and its profound impact on children. As providers who depend heavily on parental involvement to manage the needs of our pediatric patients, addressing parental mental health can be a crucial step in safeguarding the mental health of children.
The Surgeon General’s Advisory: A Call to Action
On August 28, 2024, the U.S. Surgeon General issued an advisory highlighting the significant stressors impacting parents and caregivers, and the broader implications for children’s mental health. The advisory emphasizes the bidirectional relationship between parental and child mental health, urging healthcare providers, policymakers, and communities to prioritize support for parents. It stresses that the mental health of parents is not only vital for their well-being but also plays a critical role in shaping the emotional and psychological development of their children.1
The Link Between Parental and Child Mental Health
Research shows that a parent’s mental health directly influences the child’s emotional and behavioral outcomes. Children of parents with untreated mental health conditions, such as depression, anxiety, trauma, or chronic stress, are at a significantly higher risk of developing similar conditions. This risk is mediated through various mechanisms, including genetic predisposition, compromised parent-child interactions, and exposure to adverse environments.
1. Parental Depression and Child Outcomes: Parental depression, particularly maternal depression, has been extensively studied and is strongly associated with emotional and behavioral problems in children. Children of depressed parents are more likely to experience anxiety, depression, and resulting academic difficulties. Depressed parents may struggle with consistent and positive parenting, which can disrupt the development of secure attachments and emotional regulation in children.2-4
2. Anxiety and Parenting Styles: Parental anxiety can influence parenting styles, often leading to overprotectiveness, inconsistency, or heightened criticism. These behaviors, in turn, can cultivate anxiety in children, creating a cycle that perpetuates mental health challenges across generations. Children raised in environments where anxiety is pervasive may learn to view the world as threatening, contributing to hypervigilance and stress.5
3. Impact of Chronic Stress on Parenting: Chronic stress experienced by parents, often due to financial hardship, lack of social support, or work-life imbalance, can impair their ability to engage in responsive and nurturing parenting. This, in turn, can affect children’s ability to meaningfully engage with parents to form secure attachments. Further, chronic stress can negatively impact the quality of parent-child interactions and fuel the cycle of rupture with limited opportunity for repair. The advisory stresses the need to address these systemic stressors as part of a broader public health strategy to support families.1
Implications for Pediatric Practice
Pediatricians are often the first point of contact for families navigating mental health challenges. The Surgeon General’s advisory highlights the need for pediatricians to adopt a holistic approach that considers the mental health of the entire family, not just the child. This can be challenging with the average follow-up appointment time of 16 minutes, though many of the recommendations take this logistical hurdle into consideration:
1. Screening for Parental Mental Health: Incorporating routine screening for parental mental health into pediatric visits can be a powerful tool. Questions about parental stress, depression (especially postpartum depression), and anxiety should be integrated into well-child visits, especially in families where children present with emotional or behavioral difficulties. By identifying at-risk parents early, timely referrals to mental health services can be secured.
2. Providing Resources and Referrals: Offering resources and referrals to parents who may be struggling can positively impact the entire family. This includes connecting families with mental health professionals, parenting support groups, or community resources that can alleviate stressors such as food insecurity or lack of childcare. Having a list of local mental health resources available in your practice can empower parents to seek the help they need.
3. Promoting Positive Parenting Practices: Guidance on positive parenting practices, stress management, and self-care can make a significant difference in the mental health of parents and their children. Workshops or educational materials on topics like mindfulness, managing work-life balance, and fostering healthy communication within the family can be valuable and high-yield additions to pediatric care.
4. Collaborative Care Models: Collaborative care models, where pediatricians work closely with child psychiatrists, psychologists, and social workers, can provide comprehensive support to families. This integrated approach ensures that both children and their parents receive the care they need, promoting better outcomes for the entire family unit.
Addressing Broader Systemic Issues
The advisory also calls for systemic changes that extend beyond the clinic. Policy changes such as expanding access to paid family leave, affordable childcare, and mental health services are essential to creating an environment where parents can thrive. As pediatricians, advocating for these changes at the local and national level can amplify the overall impact on families.
1. Advocating for Paid Family Leave: Paid family leave allows parents to bond with their children and attend to their own mental health needs without the added pressure of financial instability. Supporting policies that provide adequate paid leave can pave the way for a successful and healthy return to work and have long-term benefits for family health.
2. Expanding Mental Health Services: Increasing access to mental health services, especially in underserved communities, is crucial. Pediatricians can play a role by partnering with local mental health providers to offer integrated care within their practices or community settings.
3. Community Support Programs: The creation of community support programs that offer parenting classes, stress management workshops, and peer support groups can help reduce the isolation and stress that many parents feel. Pediatricians can collaborate with community organizations to promote these resources to families.
Conclusion
The Surgeon General’s advisory serves as a timely reminder of the interconnectedness of parental and child mental health. Pediatricians have a unique opportunity to influence not only the health of their pediatric patients, but also the well-being of their families. By recognizing and addressing the mental health needs of parents, we can break the cycle of stress and mental illness that affects so many families, ensuring a healthier future for the next generation.
Let us embrace this call to action and work together to create a supportive environment where all parents and children can thrive.
Dr. Richards is assistant clinical professor in the department of psychiatry and biobehavioral sciences; program director of the child and adolescent psychiatry fellowship; and associate medical director of the perinatal program at the UCLA Semel Institute for Neuroscience and Human Behavior, Los Angeles.
References
1. American Hospital Association. Surgeon General Issues Advisory on Mental Health and Well-Being of Parents. American Hospital Association. 2024 Sep 4.
2. Goodman SH, Gotlib IH. Risk for Psychopathology in the Children of Depressed Mothers: A Developmental Model for Understanding Mechanisms of Transmission. Psychol Rev. 1999;106(3):458-490. doi: 10.1037/0033-295X.106.3.458.
3. Lovejoy MC et al. Maternal Depression and Parenting Behavior: A Meta-Analytic Review. Clin Psychol Rev. 2000;20(5):561-592. doi: 10.1016/s0272-7358(98)00100-7.
4. Weissman MM et al. Offspring of Depressed Parents: 20 Years Later. Am J Psychiatry. 2006;163(6):1001-1008. doi: 10.1176/ajp.2006.163.6.1001.
5. Smith KE, Pollak SD. Early Life Stress and Development: Potential Mechanisms for Adverse Outcomes. J Neurodev Disord. 2020;12(1):3-14. doi: 10.1186/s11689-020-09337-y.
The Silent Exodus: Are Nurse Practitioners and Physician Assistants Quiet Quitting?
While she cared deeply about her work, Melissa Adams*, a family nurse practitioner (NP) in Madison, Alabama, was being frequently triple-booked, didn’t feel respected by her office manager, and started to worry about becoming burned out. When she sought help, “the administration was tone-deaf,” she said. “When I asked about what I could do to prevent burnout, they sent me an article about it. It was clear to me that asking for respite from triple-booking and asking to be respected by my office manager wasn’t being heard ... so I thought, ‘how do I fly under the radar and get by with what I can?’ ” That meant focusing on patient care and refusing to take on additional responsibilities, like training new hires or working with students.
“You’re overworked and underpaid, and you start giving less and less of yourself,” Ms. Adams said in an interview.
Quiet quitting, defined as performing only the assigned tasks of the job without making any extra effort or going the proverbial extra mile, has gained attention in the press in recent years. A Gallup poll found that about 50% of the workforce were “quiet quitters” or disengaged.
It may be even more prevalent in healthcare, where a recent survey found that 57% of frontline medical staff, including NPs and physician assistants (PAs), report being disengaged at work.
The Causes of Quiet Quitting
Potential causes of quiet quitting among PAs and NPs include:
- Unrealistic care expectations. Ms. Adams said.
- Lack of trust or respect. Physicians don’t always respect the role that PAs and NPs play in a practice.
- Dissatisfaction with leadership or administration. There’s often a feeling that the PA or NP isn’t “heard” or appreciated.
- Dissatisfaction with pay or working conditions.
- Moral injury. “There’s no way to escape being morally injured when you work with an at-risk population,” said Ms. Adams. “You may see someone who has 20-24 determinants of health, and you’re expected to schlep them through in 8 minutes — you know you’re not able to do what they need.”
What Quiet Quitting Looks Like
Terri Smith*, an NP at an academic medical center outpatient clinic in rural Vermont, said that, while she feels appreciated by her patients and her team, there’s poor communication from the administration, which has caused her to quietly quit.
“I stopped saying ‘yes’ to all the normal committee work and the extra stuff that used to add a lot to my professional enjoyment,” she said. “The last couple of years, my whole motto is to nod and smile when administration says to do something — to put your head down and take care of your patients.”
While the term “quiet quitting” may be new, the issue is not, said Bridget Roberts, PhD, a healthcare executive who ran a large physician’s group of 100 healthcare providers in Jacksonville, Florida, for a decade. “Quiet quitting is a fancy title for employees who are completely disengaged,” said Dr. Roberts. “When they’re on the way out, they ‘check the box’. That’s not a new thing.”
“Typically, the first thing you see is a lot of frustration in that they aren’t able to complete the tasks they have at hand,” said Rebecca Day, PMNHP, a doctoral-educated NP and director of nursing practice at a Federally Qualified Health Center in Corbin, Kentucky. “Staff may be overworked and not have enough time to do what’s required of them with patient care as well as the paperwork required behind the scenes. It [quiet quitting] is doing just enough to get by, but shortcutting as much as they can to try to save some time.”
Addressing Quiet Quitting
Those kinds of shortcuts may affect patients, admits Ms. Smith. “I do think it starts to seep into patient care,” she said. “And that really doesn’t feel good ... at our institution, I’m not just an NP — I’m the nurse, the doctor, the secretary — I’m everybody, and for the last year, almost every single day in clinic, I’m apologizing [to a patient] because we can’t do something.”
Watching for this frustration can help alert administrators to NPs and PAs who may be “checking out” at work. Open lines of communication can help you address the issue. “Ask questions like ‘What could we do differently to make your day easier?’” said Dr. Roberts. Understanding the day-to-day issues NPs and PAs face at work can help in developing a plan to address disengagement.
When Dr. Day sees quiet quitting at her practice, she talks with the advance practice provider about what’s causing the issue. “’Are you overworked? Are you understaffed? Are there problems at home? Do you feel you’re receiving inadequate pay?’ ” she said. “The first thing to do is address that and find mutual ground on the issues…deal with the person as a person and then go back and deal with the person as an employee. If your staff isn’t happy, your clinic isn’t going to be productive.”
Finally, while reasons for quiet quitting may vary, cultivating a collaborative atmosphere where NPs and PAs feel appreciated and valued can help reduce the risk for quiet quitting. “Get to know your advanced practice providers,” said Ms. Adams. “Understand their strengths and what they’re about. It’s not an ‘us vs them’ ... there is a lot more commonality when we approach it that way.” Respect for the integral role that NPs and PAs play in your practice can help reduce the risk for quiet quitting — and help provide better patient care.
*Names have been changed.
A version of this article first appeared on Medscape.com.
While she cared deeply about her work, Melissa Adams*, a family nurse practitioner (NP) in Madison, Alabama, was being frequently triple-booked, didn’t feel respected by her office manager, and started to worry about becoming burned out. When she sought help, “the administration was tone-deaf,” she said. “When I asked about what I could do to prevent burnout, they sent me an article about it. It was clear to me that asking for respite from triple-booking and asking to be respected by my office manager wasn’t being heard ... so I thought, ‘how do I fly under the radar and get by with what I can?’ ” That meant focusing on patient care and refusing to take on additional responsibilities, like training new hires or working with students.
“You’re overworked and underpaid, and you start giving less and less of yourself,” Ms. Adams said in an interview.
Quiet quitting, defined as performing only the assigned tasks of the job without making any extra effort or going the proverbial extra mile, has gained attention in the press in recent years. A Gallup poll found that about 50% of the workforce were “quiet quitters” or disengaged.
It may be even more prevalent in healthcare, where a recent survey found that 57% of frontline medical staff, including NPs and physician assistants (PAs), report being disengaged at work.
The Causes of Quiet Quitting
Potential causes of quiet quitting among PAs and NPs include:
- Unrealistic care expectations. Ms. Adams said.
- Lack of trust or respect. Physicians don’t always respect the role that PAs and NPs play in a practice.
- Dissatisfaction with leadership or administration. There’s often a feeling that the PA or NP isn’t “heard” or appreciated.
- Dissatisfaction with pay or working conditions.
- Moral injury. “There’s no way to escape being morally injured when you work with an at-risk population,” said Ms. Adams. “You may see someone who has 20-24 determinants of health, and you’re expected to schlep them through in 8 minutes — you know you’re not able to do what they need.”
What Quiet Quitting Looks Like
Terri Smith*, an NP at an academic medical center outpatient clinic in rural Vermont, said that, while she feels appreciated by her patients and her team, there’s poor communication from the administration, which has caused her to quietly quit.
“I stopped saying ‘yes’ to all the normal committee work and the extra stuff that used to add a lot to my professional enjoyment,” she said. “The last couple of years, my whole motto is to nod and smile when administration says to do something — to put your head down and take care of your patients.”
While the term “quiet quitting” may be new, the issue is not, said Bridget Roberts, PhD, a healthcare executive who ran a large physician’s group of 100 healthcare providers in Jacksonville, Florida, for a decade. “Quiet quitting is a fancy title for employees who are completely disengaged,” said Dr. Roberts. “When they’re on the way out, they ‘check the box’. That’s not a new thing.”
“Typically, the first thing you see is a lot of frustration in that they aren’t able to complete the tasks they have at hand,” said Rebecca Day, PMNHP, a doctoral-educated NP and director of nursing practice at a Federally Qualified Health Center in Corbin, Kentucky. “Staff may be overworked and not have enough time to do what’s required of them with patient care as well as the paperwork required behind the scenes. It [quiet quitting] is doing just enough to get by, but shortcutting as much as they can to try to save some time.”
Addressing Quiet Quitting
Those kinds of shortcuts may affect patients, admits Ms. Smith. “I do think it starts to seep into patient care,” she said. “And that really doesn’t feel good ... at our institution, I’m not just an NP — I’m the nurse, the doctor, the secretary — I’m everybody, and for the last year, almost every single day in clinic, I’m apologizing [to a patient] because we can’t do something.”
Watching for this frustration can help alert administrators to NPs and PAs who may be “checking out” at work. Open lines of communication can help you address the issue. “Ask questions like ‘What could we do differently to make your day easier?’” said Dr. Roberts. Understanding the day-to-day issues NPs and PAs face at work can help in developing a plan to address disengagement.
When Dr. Day sees quiet quitting at her practice, she talks with the advance practice provider about what’s causing the issue. “’Are you overworked? Are you understaffed? Are there problems at home? Do you feel you’re receiving inadequate pay?’ ” she said. “The first thing to do is address that and find mutual ground on the issues…deal with the person as a person and then go back and deal with the person as an employee. If your staff isn’t happy, your clinic isn’t going to be productive.”
Finally, while reasons for quiet quitting may vary, cultivating a collaborative atmosphere where NPs and PAs feel appreciated and valued can help reduce the risk for quiet quitting. “Get to know your advanced practice providers,” said Ms. Adams. “Understand their strengths and what they’re about. It’s not an ‘us vs them’ ... there is a lot more commonality when we approach it that way.” Respect for the integral role that NPs and PAs play in your practice can help reduce the risk for quiet quitting — and help provide better patient care.
*Names have been changed.
A version of this article first appeared on Medscape.com.
While she cared deeply about her work, Melissa Adams*, a family nurse practitioner (NP) in Madison, Alabama, was being frequently triple-booked, didn’t feel respected by her office manager, and started to worry about becoming burned out. When she sought help, “the administration was tone-deaf,” she said. “When I asked about what I could do to prevent burnout, they sent me an article about it. It was clear to me that asking for respite from triple-booking and asking to be respected by my office manager wasn’t being heard ... so I thought, ‘how do I fly under the radar and get by with what I can?’ ” That meant focusing on patient care and refusing to take on additional responsibilities, like training new hires or working with students.
“You’re overworked and underpaid, and you start giving less and less of yourself,” Ms. Adams said in an interview.
Quiet quitting, defined as performing only the assigned tasks of the job without making any extra effort or going the proverbial extra mile, has gained attention in the press in recent years. A Gallup poll found that about 50% of the workforce were “quiet quitters” or disengaged.
It may be even more prevalent in healthcare, where a recent survey found that 57% of frontline medical staff, including NPs and physician assistants (PAs), report being disengaged at work.
The Causes of Quiet Quitting
Potential causes of quiet quitting among PAs and NPs include:
- Unrealistic care expectations. Ms. Adams said.
- Lack of trust or respect. Physicians don’t always respect the role that PAs and NPs play in a practice.
- Dissatisfaction with leadership or administration. There’s often a feeling that the PA or NP isn’t “heard” or appreciated.
- Dissatisfaction with pay or working conditions.
- Moral injury. “There’s no way to escape being morally injured when you work with an at-risk population,” said Ms. Adams. “You may see someone who has 20-24 determinants of health, and you’re expected to schlep them through in 8 minutes — you know you’re not able to do what they need.”
What Quiet Quitting Looks Like
Terri Smith*, an NP at an academic medical center outpatient clinic in rural Vermont, said that, while she feels appreciated by her patients and her team, there’s poor communication from the administration, which has caused her to quietly quit.
“I stopped saying ‘yes’ to all the normal committee work and the extra stuff that used to add a lot to my professional enjoyment,” she said. “The last couple of years, my whole motto is to nod and smile when administration says to do something — to put your head down and take care of your patients.”
While the term “quiet quitting” may be new, the issue is not, said Bridget Roberts, PhD, a healthcare executive who ran a large physician’s group of 100 healthcare providers in Jacksonville, Florida, for a decade. “Quiet quitting is a fancy title for employees who are completely disengaged,” said Dr. Roberts. “When they’re on the way out, they ‘check the box’. That’s not a new thing.”
“Typically, the first thing you see is a lot of frustration in that they aren’t able to complete the tasks they have at hand,” said Rebecca Day, PMNHP, a doctoral-educated NP and director of nursing practice at a Federally Qualified Health Center in Corbin, Kentucky. “Staff may be overworked and not have enough time to do what’s required of them with patient care as well as the paperwork required behind the scenes. It [quiet quitting] is doing just enough to get by, but shortcutting as much as they can to try to save some time.”
Addressing Quiet Quitting
Those kinds of shortcuts may affect patients, admits Ms. Smith. “I do think it starts to seep into patient care,” she said. “And that really doesn’t feel good ... at our institution, I’m not just an NP — I’m the nurse, the doctor, the secretary — I’m everybody, and for the last year, almost every single day in clinic, I’m apologizing [to a patient] because we can’t do something.”
Watching for this frustration can help alert administrators to NPs and PAs who may be “checking out” at work. Open lines of communication can help you address the issue. “Ask questions like ‘What could we do differently to make your day easier?’” said Dr. Roberts. Understanding the day-to-day issues NPs and PAs face at work can help in developing a plan to address disengagement.
When Dr. Day sees quiet quitting at her practice, she talks with the advance practice provider about what’s causing the issue. “’Are you overworked? Are you understaffed? Are there problems at home? Do you feel you’re receiving inadequate pay?’ ” she said. “The first thing to do is address that and find mutual ground on the issues…deal with the person as a person and then go back and deal with the person as an employee. If your staff isn’t happy, your clinic isn’t going to be productive.”
Finally, while reasons for quiet quitting may vary, cultivating a collaborative atmosphere where NPs and PAs feel appreciated and valued can help reduce the risk for quiet quitting. “Get to know your advanced practice providers,” said Ms. Adams. “Understand their strengths and what they’re about. It’s not an ‘us vs them’ ... there is a lot more commonality when we approach it that way.” Respect for the integral role that NPs and PAs play in your practice can help reduce the risk for quiet quitting — and help provide better patient care.
*Names have been changed.
A version of this article first appeared on Medscape.com.
Baby-Led Weaning
I first heard the term “baby-led weaning” about 20 years ago, which turns out was just a few years after the concept was introduced to the public by a public health/midwife in Britain. Starting infants on solid foods when they could feed themselves didn’t sound as off-the-wall to me as it did to most other folks, but I chose not to include it in my list of standard recommendations at the 4- and 6-month well child visits. If any parent had asked me my opinion I would have told them to give it a try with a few specific cautions about what and how. But, I don’t recall any parents asking me. The ones who knew me well or had read, or at least heard about, my book on picky eating must have already figured out what my answer would be. The parents who didn’t know me may have been afraid I would tell them it was a crazy idea.
Twelve years ago I retired from office practice and hadn’t heard a peep about baby-led weaning until last week when I encountered a story in The New York Times. It appears that while I have been reveling in my post-practice existence, baby-led weaning has become a “thing.” As the author of the article observed: “The concept seems to appeal to millennials who favor parenting philosophies that prioritize child autonomy.”

Baby-led weaning’s traction has been so robust that the largest manufacturer of baby food in this country has been labeling some of its products “baby-led friendly since 2021.” There are several online businesses that have tapped into the growing market. One offers a very detailed free directory that lists almost any edible you can imagine with recommendations of when and how they can be presented in a safe and appealing matter to little hand feeders. Of course the company has also figured out a way to monetize the product.
Not surprisingly the American Academy of Pediatrics (AAP) has remained silent on baby-led weaning. However, in The New York Times article, Dr. Mark R. Corkins, chair of the AAP nutrition committee, is quoted as describing baby-led weaning is “a social media–driven invention.”
While I was interested to learn about the concept’s growth and commercialization, I was troubled to find that like co-sleeping, sleep training, and exclusive breastfeeding, baby-led weaning has become one of those angst-producing topics that is torturing new parents who live every day in fear that they “aren’t doing it right.” We pediatricians might deserve a small dose of blame for not vigorously emphasizing that there are numerous ways to skin that cat known as parenting. However, social media websites and Mom chat rooms are probably more responsible for creating an atmosphere in which parents are afraid of being ostracized for the decisions they have made in good faith whether it is about weaning or when to start toilet training.
In isolated cultures, weaning a baby to solids was probably never a topic for discussion or debate. New parents did what their parents did, or more likely a child’s grandmother advised or took over the process herself. The child was fed what the rest of the family ate. If it was something the infant could handle himself you gave it to him. If not you mashed it up or maybe you chewed it for him into a consistency he could manage.
However, most new parents have become so distanced from their own parents’ childrearing practices geographically, temporally, and philosophically, that they must rely on folks like us and others whom they believe are, or at least claim to be, experts. Young adults are no longer hesitant to cross ethnic thresholds when they decide to be co-parents, meaning that any remnant of family tradition is either diluted or lost outright. In the void created by this abandonment of tradition, corporations were happy to step in with easy-to-prepare baby food that lacks in nutritional and dietary variety. Baby-led weaning is just one more logical step in the metamorphosis of our society’s infant feeding patterns.
I still have no problem with baby-led weaning as an option for parents, particularly if with just a click of a mouse they can access safe and healthy advice to make up for generations of grandmotherly experience acquired over hundreds of years. However,
It is one thing when parents hoping to encourage the process of self-feeding offer their infants an edible that may not be in the family’s usual diet. However, it is a totally different matter when a family allows itself to become dietary contortionists to a accommodate a 4-year-old whose diet consists of a monotonous rotation of three pasta shapes topped with grated Parmesan cheese, and on a good day a raw carrot slice or two. Parents living in this nutritional wasteland may have given up on managing their children’s pickiness, and may find it is less stressful to join the child and eat a few forkfuls of pasta to preserve some semblance of a family dinner. Then after the child has been put to bed they have their own balanced meal.
Almost by definition family meals are a compromise. Even adults without children negotiate often unspoken menu patterns with their partners. “This evening we’ll have your favorite, I may have my favorite next week.”
Most parents of young children understand that their diet may be a bit heavier on pasta than they might prefer and a little less varied when it comes to vegetables. It is just part of the deal. However, when mealtimes become totally dictated by the pickiness of a child there is a problem. While a poorly structured child-led family diet may be nutritionally deficient, the bigger problem is that it is expensive in time and labor, two resources usually in short supply in young families.
Theoretically, infants who have led their own weaning are more likely to have been introduced to a broad variety of flavors and textures and this may carry them into childhood as more adventuresome eaters. Picky eating can be managed successfully and result in a family that can enjoy the psychological and emotional benefits of nutritionally balanced family meals, but it requires a combination of parental courage and patience.
It is unclear exactly how we got into a situation in which a generation of parents makes things more difficult for themselves by favoring practices that overemphasize child autonomy. It may be that the parents had suffered under autocratic parents themselves, or more likely they have read too many novels or watched too many movies and TV shows in which the parents were portrayed as overbearing or controlling. Or, it may simply be that they haven’t had enough exposure to young children to realize that they all benefit from clear limits to a varying degree.
In the process of watching tens of thousands of parents, it has become clear to me that those who are the most successful are leaders and that they lead primarily by example. They have learned to be masters in the art of deception by creating a safe environment with sensible limits while at the same time fostering an atmosphere in which the child sees himself as participating in the process.
The biblical prophet Isaiah (11:6-9) in his description of how things will be different after the Lord acts to help his people predicts: “and a little child shall lead them.” This prediction fits nicely as the last in a string of crazy situations that includes a wolf living with a lamb and a leopard lying down with a calf.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
I first heard the term “baby-led weaning” about 20 years ago, which turns out was just a few years after the concept was introduced to the public by a public health/midwife in Britain. Starting infants on solid foods when they could feed themselves didn’t sound as off-the-wall to me as it did to most other folks, but I chose not to include it in my list of standard recommendations at the 4- and 6-month well child visits. If any parent had asked me my opinion I would have told them to give it a try with a few specific cautions about what and how. But, I don’t recall any parents asking me. The ones who knew me well or had read, or at least heard about, my book on picky eating must have already figured out what my answer would be. The parents who didn’t know me may have been afraid I would tell them it was a crazy idea.
Twelve years ago I retired from office practice and hadn’t heard a peep about baby-led weaning until last week when I encountered a story in The New York Times. It appears that while I have been reveling in my post-practice existence, baby-led weaning has become a “thing.” As the author of the article observed: “The concept seems to appeal to millennials who favor parenting philosophies that prioritize child autonomy.”
Baby-led weaning’s traction has been so robust that the largest manufacturer of baby food in this country has been labeling some of its products “baby-led friendly since 2021.” There are several online businesses that have tapped into the growing market. One offers a very detailed free directory that lists almost any edible you can imagine with recommendations of when and how they can be presented in a safe and appealing matter to little hand feeders. Of course the company has also figured out a way to monetize the product.
Not surprisingly the American Academy of Pediatrics (AAP) has remained silent on baby-led weaning. However, in The New York Times article, Dr. Mark R. Corkins, chair of the AAP nutrition committee, is quoted as describing baby-led weaning is “a social media–driven invention.”
While I was interested to learn about the concept’s growth and commercialization, I was troubled to find that like co-sleeping, sleep training, and exclusive breastfeeding, baby-led weaning has become one of those angst-producing topics that is torturing new parents who live every day in fear that they “aren’t doing it right.” We pediatricians might deserve a small dose of blame for not vigorously emphasizing that there are numerous ways to skin that cat known as parenting. However, social media websites and Mom chat rooms are probably more responsible for creating an atmosphere in which parents are afraid of being ostracized for the decisions they have made in good faith whether it is about weaning or when to start toilet training.
In isolated cultures, weaning a baby to solids was probably never a topic for discussion or debate. New parents did what their parents did, or more likely a child’s grandmother advised or took over the process herself. The child was fed what the rest of the family ate. If it was something the infant could handle himself you gave it to him. If not you mashed it up or maybe you chewed it for him into a consistency he could manage.
However, most new parents have become so distanced from their own parents’ childrearing practices geographically, temporally, and philosophically, that they must rely on folks like us and others whom they believe are, or at least claim to be, experts. Young adults are no longer hesitant to cross ethnic thresholds when they decide to be co-parents, meaning that any remnant of family tradition is either diluted or lost outright. In the void created by this abandonment of tradition, corporations were happy to step in with easy-to-prepare baby food that lacks in nutritional and dietary variety. Baby-led weaning is just one more logical step in the metamorphosis of our society’s infant feeding patterns.
I still have no problem with baby-led weaning as an option for parents, particularly if with just a click of a mouse they can access safe and healthy advice to make up for generations of grandmotherly experience acquired over hundreds of years. However,
It is one thing when parents hoping to encourage the process of self-feeding offer their infants an edible that may not be in the family’s usual diet. However, it is a totally different matter when a family allows itself to become dietary contortionists to a accommodate a 4-year-old whose diet consists of a monotonous rotation of three pasta shapes topped with grated Parmesan cheese, and on a good day a raw carrot slice or two. Parents living in this nutritional wasteland may have given up on managing their children’s pickiness, and may find it is less stressful to join the child and eat a few forkfuls of pasta to preserve some semblance of a family dinner. Then after the child has been put to bed they have their own balanced meal.
Almost by definition family meals are a compromise. Even adults without children negotiate often unspoken menu patterns with their partners. “This evening we’ll have your favorite, I may have my favorite next week.”
Most parents of young children understand that their diet may be a bit heavier on pasta than they might prefer and a little less varied when it comes to vegetables. It is just part of the deal. However, when mealtimes become totally dictated by the pickiness of a child there is a problem. While a poorly structured child-led family diet may be nutritionally deficient, the bigger problem is that it is expensive in time and labor, two resources usually in short supply in young families.
Theoretically, infants who have led their own weaning are more likely to have been introduced to a broad variety of flavors and textures and this may carry them into childhood as more adventuresome eaters. Picky eating can be managed successfully and result in a family that can enjoy the psychological and emotional benefits of nutritionally balanced family meals, but it requires a combination of parental courage and patience.
It is unclear exactly how we got into a situation in which a generation of parents makes things more difficult for themselves by favoring practices that overemphasize child autonomy. It may be that the parents had suffered under autocratic parents themselves, or more likely they have read too many novels or watched too many movies and TV shows in which the parents were portrayed as overbearing or controlling. Or, it may simply be that they haven’t had enough exposure to young children to realize that they all benefit from clear limits to a varying degree.
In the process of watching tens of thousands of parents, it has become clear to me that those who are the most successful are leaders and that they lead primarily by example. They have learned to be masters in the art of deception by creating a safe environment with sensible limits while at the same time fostering an atmosphere in which the child sees himself as participating in the process.
The biblical prophet Isaiah (11:6-9) in his description of how things will be different after the Lord acts to help his people predicts: “and a little child shall lead them.” This prediction fits nicely as the last in a string of crazy situations that includes a wolf living with a lamb and a leopard lying down with a calf.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
I first heard the term “baby-led weaning” about 20 years ago, which turns out was just a few years after the concept was introduced to the public by a public health/midwife in Britain. Starting infants on solid foods when they could feed themselves didn’t sound as off-the-wall to me as it did to most other folks, but I chose not to include it in my list of standard recommendations at the 4- and 6-month well child visits. If any parent had asked me my opinion I would have told them to give it a try with a few specific cautions about what and how. But, I don’t recall any parents asking me. The ones who knew me well or had read, or at least heard about, my book on picky eating must have already figured out what my answer would be. The parents who didn’t know me may have been afraid I would tell them it was a crazy idea.
Twelve years ago I retired from office practice and hadn’t heard a peep about baby-led weaning until last week when I encountered a story in The New York Times. It appears that while I have been reveling in my post-practice existence, baby-led weaning has become a “thing.” As the author of the article observed: “The concept seems to appeal to millennials who favor parenting philosophies that prioritize child autonomy.”
Baby-led weaning’s traction has been so robust that the largest manufacturer of baby food in this country has been labeling some of its products “baby-led friendly since 2021.” There are several online businesses that have tapped into the growing market. One offers a very detailed free directory that lists almost any edible you can imagine with recommendations of when and how they can be presented in a safe and appealing matter to little hand feeders. Of course the company has also figured out a way to monetize the product.
Not surprisingly the American Academy of Pediatrics (AAP) has remained silent on baby-led weaning. However, in The New York Times article, Dr. Mark R. Corkins, chair of the AAP nutrition committee, is quoted as describing baby-led weaning is “a social media–driven invention.”
While I was interested to learn about the concept’s growth and commercialization, I was troubled to find that like co-sleeping, sleep training, and exclusive breastfeeding, baby-led weaning has become one of those angst-producing topics that is torturing new parents who live every day in fear that they “aren’t doing it right.” We pediatricians might deserve a small dose of blame for not vigorously emphasizing that there are numerous ways to skin that cat known as parenting. However, social media websites and Mom chat rooms are probably more responsible for creating an atmosphere in which parents are afraid of being ostracized for the decisions they have made in good faith whether it is about weaning or when to start toilet training.
In isolated cultures, weaning a baby to solids was probably never a topic for discussion or debate. New parents did what their parents did, or more likely a child’s grandmother advised or took over the process herself. The child was fed what the rest of the family ate. If it was something the infant could handle himself you gave it to him. If not you mashed it up or maybe you chewed it for him into a consistency he could manage.
However, most new parents have become so distanced from their own parents’ childrearing practices geographically, temporally, and philosophically, that they must rely on folks like us and others whom they believe are, or at least claim to be, experts. Young adults are no longer hesitant to cross ethnic thresholds when they decide to be co-parents, meaning that any remnant of family tradition is either diluted or lost outright. In the void created by this abandonment of tradition, corporations were happy to step in with easy-to-prepare baby food that lacks in nutritional and dietary variety. Baby-led weaning is just one more logical step in the metamorphosis of our society’s infant feeding patterns.
I still have no problem with baby-led weaning as an option for parents, particularly if with just a click of a mouse they can access safe and healthy advice to make up for generations of grandmotherly experience acquired over hundreds of years. However,
It is one thing when parents hoping to encourage the process of self-feeding offer their infants an edible that may not be in the family’s usual diet. However, it is a totally different matter when a family allows itself to become dietary contortionists to a accommodate a 4-year-old whose diet consists of a monotonous rotation of three pasta shapes topped with grated Parmesan cheese, and on a good day a raw carrot slice or two. Parents living in this nutritional wasteland may have given up on managing their children’s pickiness, and may find it is less stressful to join the child and eat a few forkfuls of pasta to preserve some semblance of a family dinner. Then after the child has been put to bed they have their own balanced meal.
Almost by definition family meals are a compromise. Even adults without children negotiate often unspoken menu patterns with their partners. “This evening we’ll have your favorite, I may have my favorite next week.”
Most parents of young children understand that their diet may be a bit heavier on pasta than they might prefer and a little less varied when it comes to vegetables. It is just part of the deal. However, when mealtimes become totally dictated by the pickiness of a child there is a problem. While a poorly structured child-led family diet may be nutritionally deficient, the bigger problem is that it is expensive in time and labor, two resources usually in short supply in young families.
Theoretically, infants who have led their own weaning are more likely to have been introduced to a broad variety of flavors and textures and this may carry them into childhood as more adventuresome eaters. Picky eating can be managed successfully and result in a family that can enjoy the psychological and emotional benefits of nutritionally balanced family meals, but it requires a combination of parental courage and patience.
It is unclear exactly how we got into a situation in which a generation of parents makes things more difficult for themselves by favoring practices that overemphasize child autonomy. It may be that the parents had suffered under autocratic parents themselves, or more likely they have read too many novels or watched too many movies and TV shows in which the parents were portrayed as overbearing or controlling. Or, it may simply be that they haven’t had enough exposure to young children to realize that they all benefit from clear limits to a varying degree.
In the process of watching tens of thousands of parents, it has become clear to me that those who are the most successful are leaders and that they lead primarily by example. They have learned to be masters in the art of deception by creating a safe environment with sensible limits while at the same time fostering an atmosphere in which the child sees himself as participating in the process.
The biblical prophet Isaiah (11:6-9) in his description of how things will be different after the Lord acts to help his people predicts: “and a little child shall lead them.” This prediction fits nicely as the last in a string of crazy situations that includes a wolf living with a lamb and a leopard lying down with a calf.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Can Antihistamines Trigger Seizures in Young Kids?
TOPLINE:
new research shows. The risk appears to be most pronounced in children aged 6-24 months.
METHODOLOGY:
- Researchers in Korea used a self-controlled case-crossover design to assess the risk for seizures associated with prescriptions of first-generation antihistamines.
- They analyzed data from 11,729 children who had a seizure event (an emergency department visit with a diagnosis of epilepsy, status epilepticus, or convulsion) and had previously received a prescription for a first-generation antihistamine, including chlorpheniramine maleate, mequitazine, oxatomide, piprinhydrinate, or hydroxyzine hydrochloride.
- Prescriptions during the 15 days before a seizure were considered to have been received during a hazard period, whereas earlier prescriptions were considered to have been received during a control period.
- The researchers excluded patients with febrile seizures.
TAKEAWAY:
- In an adjusted analysis, a prescription for an antihistamine during the hazard period was associated with a 22% higher risk for seizures in children (adjusted odds ratio, 1.22; 95% CI, 1.13-1.31).
- The seizure risk was significant in children aged 6-24 months, with an adjusted odds ratio of 1.49 (95% CI, 1.31-1.70).
- For older children, the risk was not statistically significant.
IN PRACTICE:
“The study underscores a substantial increase in seizure risk associated with antihistamine prescription among children aged 6-24 months,” the authors of the study wrote. “We are not aware of any other studies that have pointed out the increased risk of seizures with first-generation antihistamines in this particular age group. ... The benefits and risks of antihistamine use should always be carefully considered, especially when prescribing H1 antihistamines to vulnerable infants.”
The findings raise a host of questions for clinicians, including how a “relatively small risk” should translate into practice, and whether the risk may be attenuated with newer antihistamines, wrote Frank Max Charles Besag, MB, ChB, with East London NHS Foundation Trust in England, in an editorial accompanying the study. “It would be reasonable to inform families that at least one study has suggested a relatively small increase in the risk of seizures with first-generation antihistamines, adding that there are still too few data to draw any firm conclusions and also providing families with the information on what to do if the child were to have a seizure.”
SOURCE:
Seonkyeong Rhie, MD, and Man Yong Han, MD, both with the Department of Pediatrics at CHA University School of Medicine, in Seongnam, South Korea, were the corresponding authors on the study. The research was published online in JAMA Network Open.
LIMITATIONS:
The researchers did not have details about seizure symptoms, did not include children seen in outpatient clinics, and were unable to verify the actual intake of the prescribed antihistamines. Although second-generation antihistamines may be less likely to cross the blood-brain barrier, one newer medication, desloratadine, has been associated with seizures.
DISCLOSURES:
The study was supported by grants from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute, the Ministry of Health and Welfare, Republic of Korea.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
new research shows. The risk appears to be most pronounced in children aged 6-24 months.
METHODOLOGY:
- Researchers in Korea used a self-controlled case-crossover design to assess the risk for seizures associated with prescriptions of first-generation antihistamines.
- They analyzed data from 11,729 children who had a seizure event (an emergency department visit with a diagnosis of epilepsy, status epilepticus, or convulsion) and had previously received a prescription for a first-generation antihistamine, including chlorpheniramine maleate, mequitazine, oxatomide, piprinhydrinate, or hydroxyzine hydrochloride.
- Prescriptions during the 15 days before a seizure were considered to have been received during a hazard period, whereas earlier prescriptions were considered to have been received during a control period.
- The researchers excluded patients with febrile seizures.
TAKEAWAY:
- In an adjusted analysis, a prescription for an antihistamine during the hazard period was associated with a 22% higher risk for seizures in children (adjusted odds ratio, 1.22; 95% CI, 1.13-1.31).
- The seizure risk was significant in children aged 6-24 months, with an adjusted odds ratio of 1.49 (95% CI, 1.31-1.70).
- For older children, the risk was not statistically significant.
IN PRACTICE:
“The study underscores a substantial increase in seizure risk associated with antihistamine prescription among children aged 6-24 months,” the authors of the study wrote. “We are not aware of any other studies that have pointed out the increased risk of seizures with first-generation antihistamines in this particular age group. ... The benefits and risks of antihistamine use should always be carefully considered, especially when prescribing H1 antihistamines to vulnerable infants.”
The findings raise a host of questions for clinicians, including how a “relatively small risk” should translate into practice, and whether the risk may be attenuated with newer antihistamines, wrote Frank Max Charles Besag, MB, ChB, with East London NHS Foundation Trust in England, in an editorial accompanying the study. “It would be reasonable to inform families that at least one study has suggested a relatively small increase in the risk of seizures with first-generation antihistamines, adding that there are still too few data to draw any firm conclusions and also providing families with the information on what to do if the child were to have a seizure.”
SOURCE:
Seonkyeong Rhie, MD, and Man Yong Han, MD, both with the Department of Pediatrics at CHA University School of Medicine, in Seongnam, South Korea, were the corresponding authors on the study. The research was published online in JAMA Network Open.
LIMITATIONS:
The researchers did not have details about seizure symptoms, did not include children seen in outpatient clinics, and were unable to verify the actual intake of the prescribed antihistamines. Although second-generation antihistamines may be less likely to cross the blood-brain barrier, one newer medication, desloratadine, has been associated with seizures.
DISCLOSURES:
The study was supported by grants from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute, the Ministry of Health and Welfare, Republic of Korea.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
new research shows. The risk appears to be most pronounced in children aged 6-24 months.
METHODOLOGY:
- Researchers in Korea used a self-controlled case-crossover design to assess the risk for seizures associated with prescriptions of first-generation antihistamines.
- They analyzed data from 11,729 children who had a seizure event (an emergency department visit with a diagnosis of epilepsy, status epilepticus, or convulsion) and had previously received a prescription for a first-generation antihistamine, including chlorpheniramine maleate, mequitazine, oxatomide, piprinhydrinate, or hydroxyzine hydrochloride.
- Prescriptions during the 15 days before a seizure were considered to have been received during a hazard period, whereas earlier prescriptions were considered to have been received during a control period.
- The researchers excluded patients with febrile seizures.
TAKEAWAY:
- In an adjusted analysis, a prescription for an antihistamine during the hazard period was associated with a 22% higher risk for seizures in children (adjusted odds ratio, 1.22; 95% CI, 1.13-1.31).
- The seizure risk was significant in children aged 6-24 months, with an adjusted odds ratio of 1.49 (95% CI, 1.31-1.70).
- For older children, the risk was not statistically significant.
IN PRACTICE:
“The study underscores a substantial increase in seizure risk associated with antihistamine prescription among children aged 6-24 months,” the authors of the study wrote. “We are not aware of any other studies that have pointed out the increased risk of seizures with first-generation antihistamines in this particular age group. ... The benefits and risks of antihistamine use should always be carefully considered, especially when prescribing H1 antihistamines to vulnerable infants.”
The findings raise a host of questions for clinicians, including how a “relatively small risk” should translate into practice, and whether the risk may be attenuated with newer antihistamines, wrote Frank Max Charles Besag, MB, ChB, with East London NHS Foundation Trust in England, in an editorial accompanying the study. “It would be reasonable to inform families that at least one study has suggested a relatively small increase in the risk of seizures with first-generation antihistamines, adding that there are still too few data to draw any firm conclusions and also providing families with the information on what to do if the child were to have a seizure.”
SOURCE:
Seonkyeong Rhie, MD, and Man Yong Han, MD, both with the Department of Pediatrics at CHA University School of Medicine, in Seongnam, South Korea, were the corresponding authors on the study. The research was published online in JAMA Network Open.
LIMITATIONS:
The researchers did not have details about seizure symptoms, did not include children seen in outpatient clinics, and were unable to verify the actual intake of the prescribed antihistamines. Although second-generation antihistamines may be less likely to cross the blood-brain barrier, one newer medication, desloratadine, has been associated with seizures.
DISCLOSURES:
The study was supported by grants from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute, the Ministry of Health and Welfare, Republic of Korea.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Blood Eosinophil Counts Might Predict Childhood Asthma, Treatment Response
VIENNA — Simply relying on clinical symptoms is insufficient to predict which children with wheezing will develop asthma and respond to treatments.
Sejal Saglani, MD, PhD, a professor of pediatric respiratory medicine at the National Heart and Lung Institute, Imperial College, London, England, said that preschool wheezing has long-term adverse consequences through to adulthood. “We need to prevent that downward trajectory of low lung function,” she said, presenting the latest research in the field at the annual European Respiratory Society International Congress.
Wheezing affects up to one third of all infants and preschool children, with one third developing asthma later in life. “It’s important to identify those kids because then we can treat them with the right medication,” said Mariëlle W.H. Pijnenburg, MD, PhD, a pulmonary specialist at Erasmus University Rotterdam in the Netherlands.
“We cannot just use clinical phenotype to decide what treatment a child should get. We need to run tests to identify the endotype of preschool wheeze and intervene appropriately,” Dr. Saglani added.
Eosinophilia as a Biomarker for Predicting Exacerbations and Steroid Responsiveness
In a cluster analysis, Dr. Saglani and colleagues classified preschool children with wheezing into two main subgroups: Those who experience frequent exacerbations and those who experience sporadic attacks. Frequent exacerbators were more likely to develop asthma, use asthma medications, and show signs of reduced lung function and airway inflammation, such as higher fractional exhaled nitric oxide and allergic sensitization. “Severe and frequent exacerbators are the kids that get in trouble,” she said. “They’re the ones we must identify at preschool age and really try to minimize their exacerbations.”
Research has shown that eosinophilia is a valuable biomarker in predicting both asthma exacerbations and responsiveness to inhaled corticosteroids. Children with elevated blood eosinophils are more likely to experience frequent and severe exacerbations. These children often demonstrate an inflammatory profile more responsive to corticosteroids, making eosinophilia a predictor of treatment success. Children with eosinophilia are also more likely to have underlying allergic sensitizations, which further supports the use of corticosteroids as part of their management strategy.
Dr. Saglani said a simple blood test can provide a window into the child’s inflammatory status, allowing physicians to make more targeted and personalized treatment plans.
Traditionally, identifying eosinophilia required venipuncture and laboratory analysis, which can be time consuming and impractical in a busy clinical setting. Dr. Saglani’s research group is developing a point-of-care test designed to quickly and efficiently measure blood eosinophil levels in children with asthma or wheezing symptoms from a finger-prick test. Preliminary data presented at the congress show that children with higher eosinophil counts in the clinic were more likely to experience an asthma attack within 3 months.
“The problem is the majority of the children we see are either not atopic or do not have high blood eosinophils. What are we going to do with those?”
How to Treat Those Who Don’t Have Eosinophilia
Most children with wheezing are not atopic and do not exhibit eosinophilic inflammation, and these children may not respond as effectively to corticosteroids. How to treat them remains the “1-billion-dollar question,” Dr. Saglani said.
Respiratory syncytial virus and rhinovirus play a crucial role in triggering wheezing episodes in these children. Research has shown that viral-induced wheezing is a common feature in this phenotype, and repeated viral infections can lead to an increased severity and frequency of exacerbations. However, there are currently no effective antiviral therapies or vaccines for rhinovirus, which limits the ability to address the viral component of the disease directly.
Up to 50% of children with severe, recurrent wheezing also have bacterial pathogens like Moraxella catarrhalis and Haemophilus influenzae in their lower airways. For these children, addressing the bacterial infection is the best treatment option to mitigate the wheezing. “We now have something that we can target with antibiotics for those who don’t respond to corticosteroids,” Dr. Saglani said.
Dr. Pijnenburg said that this body of research is helping pulmonary specialists and general pediatricians navigate the complexity of childhood wheezing beyond phenotyping and symptoms. “We need to dive more deeply into those kids with preschool wheezing to see what’s happening in their lungs.”
Dr. Pijnenburg and Dr. Saglani reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
VIENNA — Simply relying on clinical symptoms is insufficient to predict which children with wheezing will develop asthma and respond to treatments.
Sejal Saglani, MD, PhD, a professor of pediatric respiratory medicine at the National Heart and Lung Institute, Imperial College, London, England, said that preschool wheezing has long-term adverse consequences through to adulthood. “We need to prevent that downward trajectory of low lung function,” she said, presenting the latest research in the field at the annual European Respiratory Society International Congress.
Wheezing affects up to one third of all infants and preschool children, with one third developing asthma later in life. “It’s important to identify those kids because then we can treat them with the right medication,” said Mariëlle W.H. Pijnenburg, MD, PhD, a pulmonary specialist at Erasmus University Rotterdam in the Netherlands.
“We cannot just use clinical phenotype to decide what treatment a child should get. We need to run tests to identify the endotype of preschool wheeze and intervene appropriately,” Dr. Saglani added.
Eosinophilia as a Biomarker for Predicting Exacerbations and Steroid Responsiveness
In a cluster analysis, Dr. Saglani and colleagues classified preschool children with wheezing into two main subgroups: Those who experience frequent exacerbations and those who experience sporadic attacks. Frequent exacerbators were more likely to develop asthma, use asthma medications, and show signs of reduced lung function and airway inflammation, such as higher fractional exhaled nitric oxide and allergic sensitization. “Severe and frequent exacerbators are the kids that get in trouble,” she said. “They’re the ones we must identify at preschool age and really try to minimize their exacerbations.”
Research has shown that eosinophilia is a valuable biomarker in predicting both asthma exacerbations and responsiveness to inhaled corticosteroids. Children with elevated blood eosinophils are more likely to experience frequent and severe exacerbations. These children often demonstrate an inflammatory profile more responsive to corticosteroids, making eosinophilia a predictor of treatment success. Children with eosinophilia are also more likely to have underlying allergic sensitizations, which further supports the use of corticosteroids as part of their management strategy.
Dr. Saglani said a simple blood test can provide a window into the child’s inflammatory status, allowing physicians to make more targeted and personalized treatment plans.
Traditionally, identifying eosinophilia required venipuncture and laboratory analysis, which can be time consuming and impractical in a busy clinical setting. Dr. Saglani’s research group is developing a point-of-care test designed to quickly and efficiently measure blood eosinophil levels in children with asthma or wheezing symptoms from a finger-prick test. Preliminary data presented at the congress show that children with higher eosinophil counts in the clinic were more likely to experience an asthma attack within 3 months.
“The problem is the majority of the children we see are either not atopic or do not have high blood eosinophils. What are we going to do with those?”
How to Treat Those Who Don’t Have Eosinophilia
Most children with wheezing are not atopic and do not exhibit eosinophilic inflammation, and these children may not respond as effectively to corticosteroids. How to treat them remains the “1-billion-dollar question,” Dr. Saglani said.
Respiratory syncytial virus and rhinovirus play a crucial role in triggering wheezing episodes in these children. Research has shown that viral-induced wheezing is a common feature in this phenotype, and repeated viral infections can lead to an increased severity and frequency of exacerbations. However, there are currently no effective antiviral therapies or vaccines for rhinovirus, which limits the ability to address the viral component of the disease directly.
Up to 50% of children with severe, recurrent wheezing also have bacterial pathogens like Moraxella catarrhalis and Haemophilus influenzae in their lower airways. For these children, addressing the bacterial infection is the best treatment option to mitigate the wheezing. “We now have something that we can target with antibiotics for those who don’t respond to corticosteroids,” Dr. Saglani said.
Dr. Pijnenburg said that this body of research is helping pulmonary specialists and general pediatricians navigate the complexity of childhood wheezing beyond phenotyping and symptoms. “We need to dive more deeply into those kids with preschool wheezing to see what’s happening in their lungs.”
Dr. Pijnenburg and Dr. Saglani reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
VIENNA — Simply relying on clinical symptoms is insufficient to predict which children with wheezing will develop asthma and respond to treatments.
Sejal Saglani, MD, PhD, a professor of pediatric respiratory medicine at the National Heart and Lung Institute, Imperial College, London, England, said that preschool wheezing has long-term adverse consequences through to adulthood. “We need to prevent that downward trajectory of low lung function,” she said, presenting the latest research in the field at the annual European Respiratory Society International Congress.
Wheezing affects up to one third of all infants and preschool children, with one third developing asthma later in life. “It’s important to identify those kids because then we can treat them with the right medication,” said Mariëlle W.H. Pijnenburg, MD, PhD, a pulmonary specialist at Erasmus University Rotterdam in the Netherlands.
“We cannot just use clinical phenotype to decide what treatment a child should get. We need to run tests to identify the endotype of preschool wheeze and intervene appropriately,” Dr. Saglani added.
Eosinophilia as a Biomarker for Predicting Exacerbations and Steroid Responsiveness
In a cluster analysis, Dr. Saglani and colleagues classified preschool children with wheezing into two main subgroups: Those who experience frequent exacerbations and those who experience sporadic attacks. Frequent exacerbators were more likely to develop asthma, use asthma medications, and show signs of reduced lung function and airway inflammation, such as higher fractional exhaled nitric oxide and allergic sensitization. “Severe and frequent exacerbators are the kids that get in trouble,” she said. “They’re the ones we must identify at preschool age and really try to minimize their exacerbations.”
Research has shown that eosinophilia is a valuable biomarker in predicting both asthma exacerbations and responsiveness to inhaled corticosteroids. Children with elevated blood eosinophils are more likely to experience frequent and severe exacerbations. These children often demonstrate an inflammatory profile more responsive to corticosteroids, making eosinophilia a predictor of treatment success. Children with eosinophilia are also more likely to have underlying allergic sensitizations, which further supports the use of corticosteroids as part of their management strategy.
Dr. Saglani said a simple blood test can provide a window into the child’s inflammatory status, allowing physicians to make more targeted and personalized treatment plans.
Traditionally, identifying eosinophilia required venipuncture and laboratory analysis, which can be time consuming and impractical in a busy clinical setting. Dr. Saglani’s research group is developing a point-of-care test designed to quickly and efficiently measure blood eosinophil levels in children with asthma or wheezing symptoms from a finger-prick test. Preliminary data presented at the congress show that children with higher eosinophil counts in the clinic were more likely to experience an asthma attack within 3 months.
“The problem is the majority of the children we see are either not atopic or do not have high blood eosinophils. What are we going to do with those?”
How to Treat Those Who Don’t Have Eosinophilia
Most children with wheezing are not atopic and do not exhibit eosinophilic inflammation, and these children may not respond as effectively to corticosteroids. How to treat them remains the “1-billion-dollar question,” Dr. Saglani said.
Respiratory syncytial virus and rhinovirus play a crucial role in triggering wheezing episodes in these children. Research has shown that viral-induced wheezing is a common feature in this phenotype, and repeated viral infections can lead to an increased severity and frequency of exacerbations. However, there are currently no effective antiviral therapies or vaccines for rhinovirus, which limits the ability to address the viral component of the disease directly.
Up to 50% of children with severe, recurrent wheezing also have bacterial pathogens like Moraxella catarrhalis and Haemophilus influenzae in their lower airways. For these children, addressing the bacterial infection is the best treatment option to mitigate the wheezing. “We now have something that we can target with antibiotics for those who don’t respond to corticosteroids,” Dr. Saglani said.
Dr. Pijnenburg said that this body of research is helping pulmonary specialists and general pediatricians navigate the complexity of childhood wheezing beyond phenotyping and symptoms. “We need to dive more deeply into those kids with preschool wheezing to see what’s happening in their lungs.”
Dr. Pijnenburg and Dr. Saglani reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
New COVID-19 Vaccines That Target KP.2 Variant Available
New COVID-19 vaccines formulated for better protection against the currently circulating variants have been approved by the US Food and Drug Administration.
The COVID vaccines available this fall have been updated to better match the currently circulating COVID strains, said William Schaffner, MD, professor of medicine in the Division of Infectious Diseases at Vanderbilt University, Nashville, Tennessee, in an interview.
“The Pfizer and Moderna vaccines — both mRNA vaccines — target the KP.2 variant, while the Novavax vaccine targets the JN.1 variant, which is a predecessor to KP.2,” said Dr. Schaffner, who also serves as a spokesperson for the National Foundation for Infectious Diseases. “The Novavax vaccine is a protein adjuvant vaccine made in a more traditional fashion and may appeal to those who remain hesitant about receiving an mRNA vaccine,” he explained. However, , he said.
Who Needs It?
“The CDC’s Advisory Committee on Immunization Practices (ACIP) continues to recommend that everyone in the United States who is age 6 months and older receive the updated COVID vaccine this fall, along with influenza vaccine,” Dr. Schaffner said.
“This was not a surprise because COVID will produce a sizable winter outbreak,” he predicted. Although older people and those who have chronic medical conditions such as heart or lung disease, diabetes, or other immunocompromising conditions suffer the most serious impact of COVID, he said. “The virus can strike anyone, even the young and healthy.” The risk for long COVID persists as well, he pointed out.
The ACIP recommendation is endorsed by the American Academy of Pediatrics and other professional organizations, Dr. Shaffner said.
A frequently asked question is whether the COVID and flu vaccines can be given at the same time, and the answer is yes, according to a statement from the Centers for Disease Control and Prevention (CDC).
“The optimal time to be vaccinated is late September and anytime during October in order to get the benefit of protection through the winter,” Dr. Schaffner said.
As with earlier versions of the COVID-19 vaccine, side effects vary from person to person. Reported side effects of the updated vaccine are similar to those seen with earlier versions and may include injection site pain, redness and swelling, fatigue, headache, muscle pain, chills, nausea, and fever, but most of these are short-lived, according to the CDC.
Clinical Guidance
The CDC’s clinical guidance for COVID-19 vaccination outlines more specific guidance for vaccination based on age, vaccination history, and immunocompromised status and will be updated as needed.
A notable difference in the latest guidance is the recommendation of only one shot for adults aged 65 years and older who are NOT moderately or severely immunocompromised. For those who are moderately or severely immunocompromised, the CDC recommends two to three doses of the same brand of vaccine.
Dr. Schaffner strongly encouraged clinicians to recommend the COVID-19 vaccination for all eligible patients. “COVID is a nasty virus that can cause serious disease in anyone,” and protection from previous vaccination or prior infection has likely waned, he said.
Dr. Schaffner also encouraged healthcare professionals and their families to lead by example. “We should all be vaccinated and let our patients know that we are vaccinated and that we want all our patents to be protected,” he said.
The updated COVID-19 vaccination recommendations have become much simpler for clinicians and patients, with a single messenger RNA (mRNA) vaccine required for anyone older than 5 years, said David J. Cennimo, MD, associate professor of medicine and pediatrics in the Division of Infectious Disease at Rutgers New Jersey Medical School, Newark, New Jersey, in an interview.
“The recommendations are a bit more complex for children under 5 years old receiving their first vaccination; they require two to three doses depending on the brand,” he said. “It is important to review the latest recommendations to plan the doses with the correct interval timing. Considering the doses may be 3-4 weeks apart, start early,” he advised.
One-Time Dosing
Although the updated mRNA vaccine is currently recommended as a one-time dose, Dr. Cennimo said he can envision a scenario later in the season when a second dose is recommended for the elderly and those at high risk for severe illness. Dr. Cennimo said that he strongly agrees with the recommendations that everyone aged 6 months and older receive an updated COVID-19 vaccine. Older age remains the prime risk factor, but anyone can become infected, he said.
Predicting a prime time to get vaccinated is tricky because no one knows when the expected rise in winter cases will occur, said Dr. Cennimo.
“We know from years of flu vaccine data that some number of people who delay the vaccine will never return and will miss protection,” he said. Therefore, delaying vaccination is not recommended. Dr. Cennimo plans to follow his habit of getting vaccinated in early October. “I anticipate the maximal effectiveness of the vaccine will carry me through the winter,” he said.
Data support the safety and effectiveness for both flu and COVID vaccines if they are given together, and some research on earlier versions of COVID vaccines suggested that receiving flu and COVID vaccines together might increase the antibody response against COVID, but similar studies of the updated version have not been done, Dr. Cennimo said.
Clinicians may have to overcome the barrier of COVID fatigue to encourage vaccination, Dr. Cennimo said. Many people say they “want it to be over,” he said, but SARS-CoV-2, established as a viral respiratory infection, shows no signs of disappearing. In addition, new data continue to show higher mortality associated with COVID-19 than with influenza, he said.
“We need to explain to our patients that COVID-19 is still here and is still dangerous. The yearly influenza vaccination campaigns should have established and normalized the idea of an updated vaccine targeted for the season’s predicated strains is expected,” he emphasized. “We now have years of safety data behind these vaccines, and we need to make a strong recommendation for this protection,” he said.
COVID-19 vaccines are covered by private insurance, as well as by Medicare and Medicaid, according to the CDC. Vaccination for uninsured children is covered through the Vaccines for Children Program.
A version of this article first appeared on Medscape.com.
New COVID-19 vaccines formulated for better protection against the currently circulating variants have been approved by the US Food and Drug Administration.
The COVID vaccines available this fall have been updated to better match the currently circulating COVID strains, said William Schaffner, MD, professor of medicine in the Division of Infectious Diseases at Vanderbilt University, Nashville, Tennessee, in an interview.
“The Pfizer and Moderna vaccines — both mRNA vaccines — target the KP.2 variant, while the Novavax vaccine targets the JN.1 variant, which is a predecessor to KP.2,” said Dr. Schaffner, who also serves as a spokesperson for the National Foundation for Infectious Diseases. “The Novavax vaccine is a protein adjuvant vaccine made in a more traditional fashion and may appeal to those who remain hesitant about receiving an mRNA vaccine,” he explained. However, , he said.
Who Needs It?
“The CDC’s Advisory Committee on Immunization Practices (ACIP) continues to recommend that everyone in the United States who is age 6 months and older receive the updated COVID vaccine this fall, along with influenza vaccine,” Dr. Schaffner said.
“This was not a surprise because COVID will produce a sizable winter outbreak,” he predicted. Although older people and those who have chronic medical conditions such as heart or lung disease, diabetes, or other immunocompromising conditions suffer the most serious impact of COVID, he said. “The virus can strike anyone, even the young and healthy.” The risk for long COVID persists as well, he pointed out.
The ACIP recommendation is endorsed by the American Academy of Pediatrics and other professional organizations, Dr. Shaffner said.
A frequently asked question is whether the COVID and flu vaccines can be given at the same time, and the answer is yes, according to a statement from the Centers for Disease Control and Prevention (CDC).
“The optimal time to be vaccinated is late September and anytime during October in order to get the benefit of protection through the winter,” Dr. Schaffner said.
As with earlier versions of the COVID-19 vaccine, side effects vary from person to person. Reported side effects of the updated vaccine are similar to those seen with earlier versions and may include injection site pain, redness and swelling, fatigue, headache, muscle pain, chills, nausea, and fever, but most of these are short-lived, according to the CDC.
Clinical Guidance
The CDC’s clinical guidance for COVID-19 vaccination outlines more specific guidance for vaccination based on age, vaccination history, and immunocompromised status and will be updated as needed.
A notable difference in the latest guidance is the recommendation of only one shot for adults aged 65 years and older who are NOT moderately or severely immunocompromised. For those who are moderately or severely immunocompromised, the CDC recommends two to three doses of the same brand of vaccine.
Dr. Schaffner strongly encouraged clinicians to recommend the COVID-19 vaccination for all eligible patients. “COVID is a nasty virus that can cause serious disease in anyone,” and protection from previous vaccination or prior infection has likely waned, he said.
Dr. Schaffner also encouraged healthcare professionals and their families to lead by example. “We should all be vaccinated and let our patients know that we are vaccinated and that we want all our patents to be protected,” he said.
The updated COVID-19 vaccination recommendations have become much simpler for clinicians and patients, with a single messenger RNA (mRNA) vaccine required for anyone older than 5 years, said David J. Cennimo, MD, associate professor of medicine and pediatrics in the Division of Infectious Disease at Rutgers New Jersey Medical School, Newark, New Jersey, in an interview.
“The recommendations are a bit more complex for children under 5 years old receiving their first vaccination; they require two to three doses depending on the brand,” he said. “It is important to review the latest recommendations to plan the doses with the correct interval timing. Considering the doses may be 3-4 weeks apart, start early,” he advised.
One-Time Dosing
Although the updated mRNA vaccine is currently recommended as a one-time dose, Dr. Cennimo said he can envision a scenario later in the season when a second dose is recommended for the elderly and those at high risk for severe illness. Dr. Cennimo said that he strongly agrees with the recommendations that everyone aged 6 months and older receive an updated COVID-19 vaccine. Older age remains the prime risk factor, but anyone can become infected, he said.
Predicting a prime time to get vaccinated is tricky because no one knows when the expected rise in winter cases will occur, said Dr. Cennimo.
“We know from years of flu vaccine data that some number of people who delay the vaccine will never return and will miss protection,” he said. Therefore, delaying vaccination is not recommended. Dr. Cennimo plans to follow his habit of getting vaccinated in early October. “I anticipate the maximal effectiveness of the vaccine will carry me through the winter,” he said.
Data support the safety and effectiveness for both flu and COVID vaccines if they are given together, and some research on earlier versions of COVID vaccines suggested that receiving flu and COVID vaccines together might increase the antibody response against COVID, but similar studies of the updated version have not been done, Dr. Cennimo said.
Clinicians may have to overcome the barrier of COVID fatigue to encourage vaccination, Dr. Cennimo said. Many people say they “want it to be over,” he said, but SARS-CoV-2, established as a viral respiratory infection, shows no signs of disappearing. In addition, new data continue to show higher mortality associated with COVID-19 than with influenza, he said.
“We need to explain to our patients that COVID-19 is still here and is still dangerous. The yearly influenza vaccination campaigns should have established and normalized the idea of an updated vaccine targeted for the season’s predicated strains is expected,” he emphasized. “We now have years of safety data behind these vaccines, and we need to make a strong recommendation for this protection,” he said.
COVID-19 vaccines are covered by private insurance, as well as by Medicare and Medicaid, according to the CDC. Vaccination for uninsured children is covered through the Vaccines for Children Program.
A version of this article first appeared on Medscape.com.
New COVID-19 vaccines formulated for better protection against the currently circulating variants have been approved by the US Food and Drug Administration.
The COVID vaccines available this fall have been updated to better match the currently circulating COVID strains, said William Schaffner, MD, professor of medicine in the Division of Infectious Diseases at Vanderbilt University, Nashville, Tennessee, in an interview.
“The Pfizer and Moderna vaccines — both mRNA vaccines — target the KP.2 variant, while the Novavax vaccine targets the JN.1 variant, which is a predecessor to KP.2,” said Dr. Schaffner, who also serves as a spokesperson for the National Foundation for Infectious Diseases. “The Novavax vaccine is a protein adjuvant vaccine made in a more traditional fashion and may appeal to those who remain hesitant about receiving an mRNA vaccine,” he explained. However, , he said.
Who Needs It?
“The CDC’s Advisory Committee on Immunization Practices (ACIP) continues to recommend that everyone in the United States who is age 6 months and older receive the updated COVID vaccine this fall, along with influenza vaccine,” Dr. Schaffner said.
“This was not a surprise because COVID will produce a sizable winter outbreak,” he predicted. Although older people and those who have chronic medical conditions such as heart or lung disease, diabetes, or other immunocompromising conditions suffer the most serious impact of COVID, he said. “The virus can strike anyone, even the young and healthy.” The risk for long COVID persists as well, he pointed out.
The ACIP recommendation is endorsed by the American Academy of Pediatrics and other professional organizations, Dr. Shaffner said.
A frequently asked question is whether the COVID and flu vaccines can be given at the same time, and the answer is yes, according to a statement from the Centers for Disease Control and Prevention (CDC).
“The optimal time to be vaccinated is late September and anytime during October in order to get the benefit of protection through the winter,” Dr. Schaffner said.
As with earlier versions of the COVID-19 vaccine, side effects vary from person to person. Reported side effects of the updated vaccine are similar to those seen with earlier versions and may include injection site pain, redness and swelling, fatigue, headache, muscle pain, chills, nausea, and fever, but most of these are short-lived, according to the CDC.
Clinical Guidance
The CDC’s clinical guidance for COVID-19 vaccination outlines more specific guidance for vaccination based on age, vaccination history, and immunocompromised status and will be updated as needed.
A notable difference in the latest guidance is the recommendation of only one shot for adults aged 65 years and older who are NOT moderately or severely immunocompromised. For those who are moderately or severely immunocompromised, the CDC recommends two to three doses of the same brand of vaccine.
Dr. Schaffner strongly encouraged clinicians to recommend the COVID-19 vaccination for all eligible patients. “COVID is a nasty virus that can cause serious disease in anyone,” and protection from previous vaccination or prior infection has likely waned, he said.
Dr. Schaffner also encouraged healthcare professionals and their families to lead by example. “We should all be vaccinated and let our patients know that we are vaccinated and that we want all our patents to be protected,” he said.
The updated COVID-19 vaccination recommendations have become much simpler for clinicians and patients, with a single messenger RNA (mRNA) vaccine required for anyone older than 5 years, said David J. Cennimo, MD, associate professor of medicine and pediatrics in the Division of Infectious Disease at Rutgers New Jersey Medical School, Newark, New Jersey, in an interview.
“The recommendations are a bit more complex for children under 5 years old receiving their first vaccination; they require two to three doses depending on the brand,” he said. “It is important to review the latest recommendations to plan the doses with the correct interval timing. Considering the doses may be 3-4 weeks apart, start early,” he advised.
One-Time Dosing
Although the updated mRNA vaccine is currently recommended as a one-time dose, Dr. Cennimo said he can envision a scenario later in the season when a second dose is recommended for the elderly and those at high risk for severe illness. Dr. Cennimo said that he strongly agrees with the recommendations that everyone aged 6 months and older receive an updated COVID-19 vaccine. Older age remains the prime risk factor, but anyone can become infected, he said.
Predicting a prime time to get vaccinated is tricky because no one knows when the expected rise in winter cases will occur, said Dr. Cennimo.
“We know from years of flu vaccine data that some number of people who delay the vaccine will never return and will miss protection,” he said. Therefore, delaying vaccination is not recommended. Dr. Cennimo plans to follow his habit of getting vaccinated in early October. “I anticipate the maximal effectiveness of the vaccine will carry me through the winter,” he said.
Data support the safety and effectiveness for both flu and COVID vaccines if they are given together, and some research on earlier versions of COVID vaccines suggested that receiving flu and COVID vaccines together might increase the antibody response against COVID, but similar studies of the updated version have not been done, Dr. Cennimo said.
Clinicians may have to overcome the barrier of COVID fatigue to encourage vaccination, Dr. Cennimo said. Many people say they “want it to be over,” he said, but SARS-CoV-2, established as a viral respiratory infection, shows no signs of disappearing. In addition, new data continue to show higher mortality associated with COVID-19 than with influenza, he said.
“We need to explain to our patients that COVID-19 is still here and is still dangerous. The yearly influenza vaccination campaigns should have established and normalized the idea of an updated vaccine targeted for the season’s predicated strains is expected,” he emphasized. “We now have years of safety data behind these vaccines, and we need to make a strong recommendation for this protection,” he said.
COVID-19 vaccines are covered by private insurance, as well as by Medicare and Medicaid, according to the CDC. Vaccination for uninsured children is covered through the Vaccines for Children Program.
A version of this article first appeared on Medscape.com.