User login
Proteus mirabilis: Isolating a Cause of Kidney Stones
The incidence of kidney stones in the United States is as high as 11% among men and 6% among women.1 This translates into a 1-in-11 risk nationwide, with white men being at greater risk than any other cohort. However, for those patients with high-risk medical issues, such as metabolic syndrome, chronic indwelling urinary catheters, frequent catheterization, and/or recurrent urinary tract infections (UTIs), kidney stones are even more common.2 Often, the cause of the stones in at-risk patients is an infection. The most frequent source of UTIs is Escherichia coli, but more complicated infections are often caused by Proteus mirabilis.3 Seventy percent of the stones resulting from UTIs are attributed to P mirabilis.4
In 2008, a group of microbiology researchers led by Melanie Pearson, PhD, were able to isolate the genome sequence of P mirabilis.5Proteus is a gram-negative enteric bacterium that is often found in complicated UTIs. Proteus is more common among patients with the aforementioned high-risk medical issues and is a particularly common cause of UTIs in the nursing home population (particularly in residents with indwelling catheters).3 It is also a potential cause of kidney stones.
While calcium stones are the most common type of stones,1 infections, though uncommon, are a secondary source. Stones resulting from infection are imminently treatable; the difficulty is in isolating the source of the infection. Proteus is a particularly toxic, difficult-to treat bacterium that can become resistant to antibiotics.3Proteus produces the enzyme urease, which can reduce the acidity of the urine, allowing stones to form. Once stone formation begins, bacteria can sequester within the stone, making them less susceptible to antibiotic treatment.
Proteus often seems to occur randomly. It has been found as a cause of kidney stones, for example, in a patient who four months earlier underwent transurethral resection of the prostate.7Proteus has been reported in a nursing home patient with dementia but no known risk factors.8Proteus can cause a pyelonephritis to coalesce into a stone; this complicates what is already an insult to the urinary tract and makes treatment all the more complicated.9
Pearson’s group from the University of Michigan has spent the past 10 years sequencing the Proteus bacterium in order to try to gain a foothold in the fight against the infection and the kidney stones it can produce. In 2014 they published their findings on the fimbriae of the Proteus organism.10 Fimbriae are small pili, or adherence factors, found on the surface of a bacterium (more often on gram-negative bacteria than on gram-positive bacteria), which allow the bacteria to attach to urinary tract tissue and prevent them from being easily dislodged.11 Pearson’s group also found that the fimbriae of the Proteus bacterium are more numerous than those of other bacteria, allowing Proteus to more easily attach to tissue than, say, Salmonella enterica.5 Thus, Proteus is more likely than other uropathogenic agents to cause a kidney stone, in part because of the “stickiness” of its many fimbriae.
While stones with an infectious cause are less common than others, they are a danger to our most fragile patients. Thus, when an infectious kidney stone forms, it will require aggressive treatment and a hard-hitting plan to minimize recurrence. Proteus is an especially virulent organism that will require all our resources to overcome it.
REFERENCES
1. Scales CD Jr, Smith AC, Hanley JM, Saigal CS; Urologic Diseases in America Project. Prevalence of kidney stones in the United States. Eur Urol. 2012;62(1):160-165.
2. National Kidney Foundation. Diet and kidney stones. kidney.org/atoz/content/diet.cfm. Accessed October 1, 2104.
3. University of Michigan Health System. Bacterium that causes kidney stones and complicated urinary tract infections gives up its genetic secrets (2006). ScienceDaily. sciencedaily.com/releases/2006/05/060524125023.htm. Accessed October 1, 2014.
4. Torzewska A, Budzyńska A, Białczak-Kokot M, Różalski A. In vitro studies of epithelium-associated crystallization caused by uropathogens during urinary calculi development. Microb Pathog. 2014;71-72:25-31.
5. Pearson MM, Sebaihia M, Churcher C, et al. Complete genome sequence of uropathogenic Proteus mirabilis, a master of both adherence and motility. J Bacteriol. 2008;190(11):4027-4037.
6. Wells CG, Chandrashekar KB, Jyothirmayi GN, et al. Kidney stones: current diagnosis and management. Clinician Reviews. 2012;22(2):31-37.
7. Rowe CM, Ghei M, Adamska E. Moans, groans and renal stones: an interesting case of abdominal pain. BMJ Case Rep. 2013 Nov 4.
8. Chew R, Thomas S, Mantha ML, et al. Large urate cystolith associated with Proteus urinary tract infection. Kidney Int. 2012;81(8):802.
9. Shields J, Maxwell AP. Acute pyelonephritis can have serious complications. Practitioner. 2010;254(1728):19, 21, 23-24.
10. Kuan L, Schaffer JN, Zouzias CD, Pearson MM. Characterization of 17 chaperone-usher fimbriae encoded by Proteus mirabilis reveals strong conservation. J Med Microbiol. 2014;63(pt 7):911-922.
11. Proft T, Baker EN. Pili in Gram-negative and Gram-positive bacteria: structure, assembly and their role in disease. Cell Mol Life Sci. 2009;66(4):613-635.
The incidence of kidney stones in the United States is as high as 11% among men and 6% among women.1 This translates into a 1-in-11 risk nationwide, with white men being at greater risk than any other cohort. However, for those patients with high-risk medical issues, such as metabolic syndrome, chronic indwelling urinary catheters, frequent catheterization, and/or recurrent urinary tract infections (UTIs), kidney stones are even more common.2 Often, the cause of the stones in at-risk patients is an infection. The most frequent source of UTIs is Escherichia coli, but more complicated infections are often caused by Proteus mirabilis.3 Seventy percent of the stones resulting from UTIs are attributed to P mirabilis.4
In 2008, a group of microbiology researchers led by Melanie Pearson, PhD, were able to isolate the genome sequence of P mirabilis.5Proteus is a gram-negative enteric bacterium that is often found in complicated UTIs. Proteus is more common among patients with the aforementioned high-risk medical issues and is a particularly common cause of UTIs in the nursing home population (particularly in residents with indwelling catheters).3 It is also a potential cause of kidney stones.
While calcium stones are the most common type of stones,1 infections, though uncommon, are a secondary source. Stones resulting from infection are imminently treatable; the difficulty is in isolating the source of the infection. Proteus is a particularly toxic, difficult-to treat bacterium that can become resistant to antibiotics.3Proteus produces the enzyme urease, which can reduce the acidity of the urine, allowing stones to form. Once stone formation begins, bacteria can sequester within the stone, making them less susceptible to antibiotic treatment.
Proteus often seems to occur randomly. It has been found as a cause of kidney stones, for example, in a patient who four months earlier underwent transurethral resection of the prostate.7Proteus has been reported in a nursing home patient with dementia but no known risk factors.8Proteus can cause a pyelonephritis to coalesce into a stone; this complicates what is already an insult to the urinary tract and makes treatment all the more complicated.9
Pearson’s group from the University of Michigan has spent the past 10 years sequencing the Proteus bacterium in order to try to gain a foothold in the fight against the infection and the kidney stones it can produce. In 2014 they published their findings on the fimbriae of the Proteus organism.10 Fimbriae are small pili, or adherence factors, found on the surface of a bacterium (more often on gram-negative bacteria than on gram-positive bacteria), which allow the bacteria to attach to urinary tract tissue and prevent them from being easily dislodged.11 Pearson’s group also found that the fimbriae of the Proteus bacterium are more numerous than those of other bacteria, allowing Proteus to more easily attach to tissue than, say, Salmonella enterica.5 Thus, Proteus is more likely than other uropathogenic agents to cause a kidney stone, in part because of the “stickiness” of its many fimbriae.
While stones with an infectious cause are less common than others, they are a danger to our most fragile patients. Thus, when an infectious kidney stone forms, it will require aggressive treatment and a hard-hitting plan to minimize recurrence. Proteus is an especially virulent organism that will require all our resources to overcome it.
REFERENCES
1. Scales CD Jr, Smith AC, Hanley JM, Saigal CS; Urologic Diseases in America Project. Prevalence of kidney stones in the United States. Eur Urol. 2012;62(1):160-165.
2. National Kidney Foundation. Diet and kidney stones. kidney.org/atoz/content/diet.cfm. Accessed October 1, 2104.
3. University of Michigan Health System. Bacterium that causes kidney stones and complicated urinary tract infections gives up its genetic secrets (2006). ScienceDaily. sciencedaily.com/releases/2006/05/060524125023.htm. Accessed October 1, 2014.
4. Torzewska A, Budzyńska A, Białczak-Kokot M, Różalski A. In vitro studies of epithelium-associated crystallization caused by uropathogens during urinary calculi development. Microb Pathog. 2014;71-72:25-31.
5. Pearson MM, Sebaihia M, Churcher C, et al. Complete genome sequence of uropathogenic Proteus mirabilis, a master of both adherence and motility. J Bacteriol. 2008;190(11):4027-4037.
6. Wells CG, Chandrashekar KB, Jyothirmayi GN, et al. Kidney stones: current diagnosis and management. Clinician Reviews. 2012;22(2):31-37.
7. Rowe CM, Ghei M, Adamska E. Moans, groans and renal stones: an interesting case of abdominal pain. BMJ Case Rep. 2013 Nov 4.
8. Chew R, Thomas S, Mantha ML, et al. Large urate cystolith associated with Proteus urinary tract infection. Kidney Int. 2012;81(8):802.
9. Shields J, Maxwell AP. Acute pyelonephritis can have serious complications. Practitioner. 2010;254(1728):19, 21, 23-24.
10. Kuan L, Schaffer JN, Zouzias CD, Pearson MM. Characterization of 17 chaperone-usher fimbriae encoded by Proteus mirabilis reveals strong conservation. J Med Microbiol. 2014;63(pt 7):911-922.
11. Proft T, Baker EN. Pili in Gram-negative and Gram-positive bacteria: structure, assembly and their role in disease. Cell Mol Life Sci. 2009;66(4):613-635.
The incidence of kidney stones in the United States is as high as 11% among men and 6% among women.1 This translates into a 1-in-11 risk nationwide, with white men being at greater risk than any other cohort. However, for those patients with high-risk medical issues, such as metabolic syndrome, chronic indwelling urinary catheters, frequent catheterization, and/or recurrent urinary tract infections (UTIs), kidney stones are even more common.2 Often, the cause of the stones in at-risk patients is an infection. The most frequent source of UTIs is Escherichia coli, but more complicated infections are often caused by Proteus mirabilis.3 Seventy percent of the stones resulting from UTIs are attributed to P mirabilis.4
In 2008, a group of microbiology researchers led by Melanie Pearson, PhD, were able to isolate the genome sequence of P mirabilis.5Proteus is a gram-negative enteric bacterium that is often found in complicated UTIs. Proteus is more common among patients with the aforementioned high-risk medical issues and is a particularly common cause of UTIs in the nursing home population (particularly in residents with indwelling catheters).3 It is also a potential cause of kidney stones.
While calcium stones are the most common type of stones,1 infections, though uncommon, are a secondary source. Stones resulting from infection are imminently treatable; the difficulty is in isolating the source of the infection. Proteus is a particularly toxic, difficult-to treat bacterium that can become resistant to antibiotics.3Proteus produces the enzyme urease, which can reduce the acidity of the urine, allowing stones to form. Once stone formation begins, bacteria can sequester within the stone, making them less susceptible to antibiotic treatment.
Proteus often seems to occur randomly. It has been found as a cause of kidney stones, for example, in a patient who four months earlier underwent transurethral resection of the prostate.7Proteus has been reported in a nursing home patient with dementia but no known risk factors.8Proteus can cause a pyelonephritis to coalesce into a stone; this complicates what is already an insult to the urinary tract and makes treatment all the more complicated.9
Pearson’s group from the University of Michigan has spent the past 10 years sequencing the Proteus bacterium in order to try to gain a foothold in the fight against the infection and the kidney stones it can produce. In 2014 they published their findings on the fimbriae of the Proteus organism.10 Fimbriae are small pili, or adherence factors, found on the surface of a bacterium (more often on gram-negative bacteria than on gram-positive bacteria), which allow the bacteria to attach to urinary tract tissue and prevent them from being easily dislodged.11 Pearson’s group also found that the fimbriae of the Proteus bacterium are more numerous than those of other bacteria, allowing Proteus to more easily attach to tissue than, say, Salmonella enterica.5 Thus, Proteus is more likely than other uropathogenic agents to cause a kidney stone, in part because of the “stickiness” of its many fimbriae.
While stones with an infectious cause are less common than others, they are a danger to our most fragile patients. Thus, when an infectious kidney stone forms, it will require aggressive treatment and a hard-hitting plan to minimize recurrence. Proteus is an especially virulent organism that will require all our resources to overcome it.
REFERENCES
1. Scales CD Jr, Smith AC, Hanley JM, Saigal CS; Urologic Diseases in America Project. Prevalence of kidney stones in the United States. Eur Urol. 2012;62(1):160-165.
2. National Kidney Foundation. Diet and kidney stones. kidney.org/atoz/content/diet.cfm. Accessed October 1, 2104.
3. University of Michigan Health System. Bacterium that causes kidney stones and complicated urinary tract infections gives up its genetic secrets (2006). ScienceDaily. sciencedaily.com/releases/2006/05/060524125023.htm. Accessed October 1, 2014.
4. Torzewska A, Budzyńska A, Białczak-Kokot M, Różalski A. In vitro studies of epithelium-associated crystallization caused by uropathogens during urinary calculi development. Microb Pathog. 2014;71-72:25-31.
5. Pearson MM, Sebaihia M, Churcher C, et al. Complete genome sequence of uropathogenic Proteus mirabilis, a master of both adherence and motility. J Bacteriol. 2008;190(11):4027-4037.
6. Wells CG, Chandrashekar KB, Jyothirmayi GN, et al. Kidney stones: current diagnosis and management. Clinician Reviews. 2012;22(2):31-37.
7. Rowe CM, Ghei M, Adamska E. Moans, groans and renal stones: an interesting case of abdominal pain. BMJ Case Rep. 2013 Nov 4.
8. Chew R, Thomas S, Mantha ML, et al. Large urate cystolith associated with Proteus urinary tract infection. Kidney Int. 2012;81(8):802.
9. Shields J, Maxwell AP. Acute pyelonephritis can have serious complications. Practitioner. 2010;254(1728):19, 21, 23-24.
10. Kuan L, Schaffer JN, Zouzias CD, Pearson MM. Characterization of 17 chaperone-usher fimbriae encoded by Proteus mirabilis reveals strong conservation. J Med Microbiol. 2014;63(pt 7):911-922.
11. Proft T, Baker EN. Pili in Gram-negative and Gram-positive bacteria: structure, assembly and their role in disease. Cell Mol Life Sci. 2009;66(4):613-635.
Breaking News: Kidney Stones and Heart Disease
Kidney stones are found in 11% of the population and are more than twice as common in men as in women.1 Patients with underlying metabolic conditions (ie, obesity, diabetes, hypertension, hyperuricemia, hypercholesterolemia, hypertension, chronic kidney disease) are much more likely than others to have kidney stones. This is also a population at increased risk for cardiac disease. So if a patient has both kidney stones and heart disease, is kidney stone disease a cause or effect of heart disease? Or are the causes of heart disease also the causes of kidney stones?
For many years, professionals thought the population affected by kidney stones was also the group with risk factors for heart disease—that the metabolic conditions were found in both groups, but that the stones were not meaningful: The finding of kidney stones in the cardiac patient was an incidental, and slightly interesting, finding. Yet a study published recently in the American Journal of Kidney Disease has turned this concept on its head.2 Liu and associates have done a meta-analysis of studies involving more than 3.5 million patients to explain exactly how kidney stones are related to cardiac disease.
In 1973, Westlund reported that patients who had kidney stones were just as likely to have had a myocardial infarction (MI).3 He was unable to identify an increased risk for MI in stone formers in his all-male cohort. In 1976, Elmfeldt and colleagues reported twice as many MIs in study subjects with kidney stones as in patients without stones.4 However, that same year, Ljunghall and Hedstrand were unable to find a correlation between kidney stones and heart disease in middle-aged men.5 Recently, Rule et al, using a 10,800-member study cohort of Minnesota residents, did show a 31% increased incidence of MI in patients with kidney stones.6
Liu and his group decided to try to answer this question once and for all. Using a graded system that examined studies of kidney stone patients who also showed signs of cardiac disease, they performed a meta-analysis comparing 50,000 patients with kidney stones and more than 3.5 million controls (patients without kidney stones). Controlling for the standard risk factors within this group (eg, age, gender, BMI, medication use, diabetes, smoking, alcohol use), the investigators identified kidney stones as a separate identifiable risk factor for cardiac disease.
In fact, Liu’s study team was able to quantify exactly how much greater a risk for cardiac disease exists in a kidney stone patient.2 Using a multivariate outcomes data plot and defining cardiac disease using hard endpoints (fatal or nonfatal MI or coronary revascularization), the researchers found a 19% increase in cardiac disease among the kidney stone patients.7 When the endpoint used was cerebrovascular accident (CVA), patients with kidney stones had a 40% higher rate of stroke.
However, the real shock came when Liu and colleagues looked at the risk factors by gender. Quite simply, women with kidney stones had a higher rate of cardiac disease and stroke than men. In totality, the increased risk for cardiac disease and stroke for a male stone patient was not statistically significant. But in female stone patients, a 40% higher rate of stroke and a 31% higher rate of cardiac disease was discovered. This explains the huge disparity in previous studies. The increased risk for cardiac disease in the kidney stone patient is borne solely by the females of the population!2
Thus, we need to aggressively evaluate and treat our female patients for heart disease when they present with kidney stones. Just as the woman’s symptoms of MI are not “classic,” and one needs to consider gender when evaluating for MI, so do we need to consider gender in the kidney stone patient.8
Next time your patient is a woman with a kidney stone, remember to raise cardiac issues with her. The MI you prevent may be in my mother or my sister.
REFERENCES
1. Wells CG, Chandrashekar KB, Jyothirmayi GN, et al. Kidney stones: current diagnosis and management. Clinician Reviews. 2012;22(2):31-37.
2. Liu Y, Li S, Zeng Z, et al. Kidney stones and cardiovascular risk: a meta-analysis of cohort studies. Am J Kidney Dis. 2014;64(3):402-410.
3. Westlund K. Urolithiasis and coronary heart disease: a note on association. Am J Epidemiol. 1973;97(3):167-172.
4. Elmfeldt D, Vedin A, Wilhelmsson C, et al. Morbidity in representative male survivors of myocardial infarction compared to representative population samples. J Chronic Dis. 1976;29(4):221-231.
5. Ljunghall S, Hedstrand H. Renal stones and coronary heart disease. Acta Med Scand. 1976;199(6):481-485.
6. Rule AD, Roger VL, Melton LJ 3rd, et al. Kidney stones associate with increased risk for myocardial infarction. J Am Soc Nephrol. 2010;21(10):1641-1644.
7. Kidney stones linked to coronary heart disease, stroke [press release]. New York, NY: National Kidney Foundation; September 1, 2014. www.kidney.org/news/kidney-stones-linked-coronary-heart-disease-stroke. Accessed September 30, 2014.
8. McSweeney JC, Cody M, O’Sullivan P, et al. Women’s early warning symptoms of acute myocardial infarction. Circulation. 2003;108(21):2619-2623.
Kidney stones are found in 11% of the population and are more than twice as common in men as in women.1 Patients with underlying metabolic conditions (ie, obesity, diabetes, hypertension, hyperuricemia, hypercholesterolemia, hypertension, chronic kidney disease) are much more likely than others to have kidney stones. This is also a population at increased risk for cardiac disease. So if a patient has both kidney stones and heart disease, is kidney stone disease a cause or effect of heart disease? Or are the causes of heart disease also the causes of kidney stones?
For many years, professionals thought the population affected by kidney stones was also the group with risk factors for heart disease—that the metabolic conditions were found in both groups, but that the stones were not meaningful: The finding of kidney stones in the cardiac patient was an incidental, and slightly interesting, finding. Yet a study published recently in the American Journal of Kidney Disease has turned this concept on its head.2 Liu and associates have done a meta-analysis of studies involving more than 3.5 million patients to explain exactly how kidney stones are related to cardiac disease.
In 1973, Westlund reported that patients who had kidney stones were just as likely to have had a myocardial infarction (MI).3 He was unable to identify an increased risk for MI in stone formers in his all-male cohort. In 1976, Elmfeldt and colleagues reported twice as many MIs in study subjects with kidney stones as in patients without stones.4 However, that same year, Ljunghall and Hedstrand were unable to find a correlation between kidney stones and heart disease in middle-aged men.5 Recently, Rule et al, using a 10,800-member study cohort of Minnesota residents, did show a 31% increased incidence of MI in patients with kidney stones.6
Liu and his group decided to try to answer this question once and for all. Using a graded system that examined studies of kidney stone patients who also showed signs of cardiac disease, they performed a meta-analysis comparing 50,000 patients with kidney stones and more than 3.5 million controls (patients without kidney stones). Controlling for the standard risk factors within this group (eg, age, gender, BMI, medication use, diabetes, smoking, alcohol use), the investigators identified kidney stones as a separate identifiable risk factor for cardiac disease.
In fact, Liu’s study team was able to quantify exactly how much greater a risk for cardiac disease exists in a kidney stone patient.2 Using a multivariate outcomes data plot and defining cardiac disease using hard endpoints (fatal or nonfatal MI or coronary revascularization), the researchers found a 19% increase in cardiac disease among the kidney stone patients.7 When the endpoint used was cerebrovascular accident (CVA), patients with kidney stones had a 40% higher rate of stroke.
However, the real shock came when Liu and colleagues looked at the risk factors by gender. Quite simply, women with kidney stones had a higher rate of cardiac disease and stroke than men. In totality, the increased risk for cardiac disease and stroke for a male stone patient was not statistically significant. But in female stone patients, a 40% higher rate of stroke and a 31% higher rate of cardiac disease was discovered. This explains the huge disparity in previous studies. The increased risk for cardiac disease in the kidney stone patient is borne solely by the females of the population!2
Thus, we need to aggressively evaluate and treat our female patients for heart disease when they present with kidney stones. Just as the woman’s symptoms of MI are not “classic,” and one needs to consider gender when evaluating for MI, so do we need to consider gender in the kidney stone patient.8
Next time your patient is a woman with a kidney stone, remember to raise cardiac issues with her. The MI you prevent may be in my mother or my sister.
REFERENCES
1. Wells CG, Chandrashekar KB, Jyothirmayi GN, et al. Kidney stones: current diagnosis and management. Clinician Reviews. 2012;22(2):31-37.
2. Liu Y, Li S, Zeng Z, et al. Kidney stones and cardiovascular risk: a meta-analysis of cohort studies. Am J Kidney Dis. 2014;64(3):402-410.
3. Westlund K. Urolithiasis and coronary heart disease: a note on association. Am J Epidemiol. 1973;97(3):167-172.
4. Elmfeldt D, Vedin A, Wilhelmsson C, et al. Morbidity in representative male survivors of myocardial infarction compared to representative population samples. J Chronic Dis. 1976;29(4):221-231.
5. Ljunghall S, Hedstrand H. Renal stones and coronary heart disease. Acta Med Scand. 1976;199(6):481-485.
6. Rule AD, Roger VL, Melton LJ 3rd, et al. Kidney stones associate with increased risk for myocardial infarction. J Am Soc Nephrol. 2010;21(10):1641-1644.
7. Kidney stones linked to coronary heart disease, stroke [press release]. New York, NY: National Kidney Foundation; September 1, 2014. www.kidney.org/news/kidney-stones-linked-coronary-heart-disease-stroke. Accessed September 30, 2014.
8. McSweeney JC, Cody M, O’Sullivan P, et al. Women’s early warning symptoms of acute myocardial infarction. Circulation. 2003;108(21):2619-2623.
Kidney stones are found in 11% of the population and are more than twice as common in men as in women.1 Patients with underlying metabolic conditions (ie, obesity, diabetes, hypertension, hyperuricemia, hypercholesterolemia, hypertension, chronic kidney disease) are much more likely than others to have kidney stones. This is also a population at increased risk for cardiac disease. So if a patient has both kidney stones and heart disease, is kidney stone disease a cause or effect of heart disease? Or are the causes of heart disease also the causes of kidney stones?
For many years, professionals thought the population affected by kidney stones was also the group with risk factors for heart disease—that the metabolic conditions were found in both groups, but that the stones were not meaningful: The finding of kidney stones in the cardiac patient was an incidental, and slightly interesting, finding. Yet a study published recently in the American Journal of Kidney Disease has turned this concept on its head.2 Liu and associates have done a meta-analysis of studies involving more than 3.5 million patients to explain exactly how kidney stones are related to cardiac disease.
In 1973, Westlund reported that patients who had kidney stones were just as likely to have had a myocardial infarction (MI).3 He was unable to identify an increased risk for MI in stone formers in his all-male cohort. In 1976, Elmfeldt and colleagues reported twice as many MIs in study subjects with kidney stones as in patients without stones.4 However, that same year, Ljunghall and Hedstrand were unable to find a correlation between kidney stones and heart disease in middle-aged men.5 Recently, Rule et al, using a 10,800-member study cohort of Minnesota residents, did show a 31% increased incidence of MI in patients with kidney stones.6
Liu and his group decided to try to answer this question once and for all. Using a graded system that examined studies of kidney stone patients who also showed signs of cardiac disease, they performed a meta-analysis comparing 50,000 patients with kidney stones and more than 3.5 million controls (patients without kidney stones). Controlling for the standard risk factors within this group (eg, age, gender, BMI, medication use, diabetes, smoking, alcohol use), the investigators identified kidney stones as a separate identifiable risk factor for cardiac disease.
In fact, Liu’s study team was able to quantify exactly how much greater a risk for cardiac disease exists in a kidney stone patient.2 Using a multivariate outcomes data plot and defining cardiac disease using hard endpoints (fatal or nonfatal MI or coronary revascularization), the researchers found a 19% increase in cardiac disease among the kidney stone patients.7 When the endpoint used was cerebrovascular accident (CVA), patients with kidney stones had a 40% higher rate of stroke.
However, the real shock came when Liu and colleagues looked at the risk factors by gender. Quite simply, women with kidney stones had a higher rate of cardiac disease and stroke than men. In totality, the increased risk for cardiac disease and stroke for a male stone patient was not statistically significant. But in female stone patients, a 40% higher rate of stroke and a 31% higher rate of cardiac disease was discovered. This explains the huge disparity in previous studies. The increased risk for cardiac disease in the kidney stone patient is borne solely by the females of the population!2
Thus, we need to aggressively evaluate and treat our female patients for heart disease when they present with kidney stones. Just as the woman’s symptoms of MI are not “classic,” and one needs to consider gender when evaluating for MI, so do we need to consider gender in the kidney stone patient.8
Next time your patient is a woman with a kidney stone, remember to raise cardiac issues with her. The MI you prevent may be in my mother or my sister.
REFERENCES
1. Wells CG, Chandrashekar KB, Jyothirmayi GN, et al. Kidney stones: current diagnosis and management. Clinician Reviews. 2012;22(2):31-37.
2. Liu Y, Li S, Zeng Z, et al. Kidney stones and cardiovascular risk: a meta-analysis of cohort studies. Am J Kidney Dis. 2014;64(3):402-410.
3. Westlund K. Urolithiasis and coronary heart disease: a note on association. Am J Epidemiol. 1973;97(3):167-172.
4. Elmfeldt D, Vedin A, Wilhelmsson C, et al. Morbidity in representative male survivors of myocardial infarction compared to representative population samples. J Chronic Dis. 1976;29(4):221-231.
5. Ljunghall S, Hedstrand H. Renal stones and coronary heart disease. Acta Med Scand. 1976;199(6):481-485.
6. Rule AD, Roger VL, Melton LJ 3rd, et al. Kidney stones associate with increased risk for myocardial infarction. J Am Soc Nephrol. 2010;21(10):1641-1644.
7. Kidney stones linked to coronary heart disease, stroke [press release]. New York, NY: National Kidney Foundation; September 1, 2014. www.kidney.org/news/kidney-stones-linked-coronary-heart-disease-stroke. Accessed September 30, 2014.
8. McSweeney JC, Cody M, O’Sullivan P, et al. Women’s early warning symptoms of acute myocardial infarction. Circulation. 2003;108(21):2619-2623.
ROKS: The Kidney Stone Calculator
Each year in the United States alone, more than half a million patients are seen in emergency departments with kidney stones. This translates to a stone incidence of 9% of all males and 6% of all females over the lifespan, or 1 in 11 people.1 Of these, 53% will have another stone during their lifetime.2 Since kidney stones are extremely painful and can cause permanent kidney damage, the ability to predict which patients are likely to have a stone recurrence is extremely valuable. Recently, an online calculator has been developed that can help clinicians predict which first-time kidney stone patients are in the “worrisome” group and which are less likely to have a recurrence.3
Kidney stones (nephrolithiasis) are increasingly common in males, those between ages 30 and 50, and those with certain underlying medical conditions, such as hypertension, diabetes, and gout, as well as those with a history of bariatric surgery.4 A family history of stone formation is also predictive.
Since more than half of patients will have a second episode of kidney stones, the ability to identify and aggressively treat at-risk patients is vital. Using a data set of clinical characteristics from more than 2,000 first-time kidney stone patients from Olmsted County, Minnesota, and following these patients longitudinally for more than 20 years, Rule et al identified patients who had a second episode of kidney stones—as well as the characteristics associated with stone recurrence.5 They then developed a multivariate calculator, the ROKS nomogram, which can be used after a patient’s first episode of kidney stones to predict the likelihood of stone recurrence at 2, 5, and 10 years.3 The authors of the ROKS stone calculator were inspired by the World Health Organization’s FRAX calculator, which predicts 10-year fracture probability.5,6
Rule et al identified 11 risk factors that they incorporated into the ROKS calculator. These include, but are not limited to, age, sex, race, family history, hematuria, presence of uric acid stones, and characteristics of the position of the initial stone in the pelvis. Not surprisingly, Rule et al found the kidney stone recurrence rate greatest in younger males who were white and had a family history of stones.
Minnesota, it should be noted, is an area of the country where summers are cooler; since people in warmer climates are at increased risk for kidney stones (particularly during the summer months), it is possible that the ROKS calculator would be even more useful in the South or Southwest than in the original study setting.5
A free, downloadable app of the ROKS calculator is available at the QxMD app “Calculate” (iOS: http://qx.md/qx, Android: http://qx.md/android, or web-based http://qxmd.com/ROKS).
Any episode of kidney stones increases the risk for chronic kidney disease and/or kidney failure.7 The absolute risk increase, though small, is present; any preventive measures one can offer at-risk patients is valuable. These range from increasing fluids and acidifying the urine to adding medications, including thiazide diuretics and allopurinol, to reduce stone formation. Unfortunately, only 3% of all first-time kidney stone patients are currently treated with medication to prevent a second episode.3 This creates an unnecessary risk for complications in a significant number of patients. By identifying members of the stone population who are likely to have a second event, clinicians can reduce the risk for recurrence.
Close monitoring of a patient with a significant stone history is vital. The ROKS calculator will allow practitioners to identify patients at increased risk for recurrent kidney stones and treat them aggressively—reducing the associated kidney damage and pain.
References
1. Scales CD Jr, Smith AC, Hanley JM, Saigal CS. Urologic Diseases in America Project: prevalence of kidney stones in the United States. Eur Urol. 2012;62:160-165.
2. Ljunghall S. Incidence of upper urinary tract stones. Miner Electrolyte Metab. 1987;13(4):220-227.
3. Rule AD, Lieske JC, Li X, et al. The ROKS Nomogram for Predicting a Second Symptomatic Stone Episode. J Am Soc Nephrol. 2014 Aug 7. [Epub ahead of print]
4. National Kidney Foundation. Kidney stones: how common are kidney stones? www.kidney.org/atoz/content/kidneystones.cfm. Accessed September 24, 2014.
5. Eisner BH, Goldfarb DS. A Nomogram for the Prediction of Kidney Stone Recurrence. J Am Soc Nephrol. 2014 Aug 7. [Epub ahead of print]
6. Kanis JA on behalf of the World Health Organization Scientific Group (2007). Assessment of osteoporosis at the primary healthcare level: report of a WHO Scientific Group. www.iofbonehealth.org/sites/default/files/WHO_Technical_Report-2007.pdf. Accessed September 26, 2014.
7. Alexander RT, Hemmelgarn BR, Wiebe N, et al. Kidney stones and kidney function loss: a cohort study. BMJ. 2012;345:e5287.
Each year in the United States alone, more than half a million patients are seen in emergency departments with kidney stones. This translates to a stone incidence of 9% of all males and 6% of all females over the lifespan, or 1 in 11 people.1 Of these, 53% will have another stone during their lifetime.2 Since kidney stones are extremely painful and can cause permanent kidney damage, the ability to predict which patients are likely to have a stone recurrence is extremely valuable. Recently, an online calculator has been developed that can help clinicians predict which first-time kidney stone patients are in the “worrisome” group and which are less likely to have a recurrence.3
Kidney stones (nephrolithiasis) are increasingly common in males, those between ages 30 and 50, and those with certain underlying medical conditions, such as hypertension, diabetes, and gout, as well as those with a history of bariatric surgery.4 A family history of stone formation is also predictive.
Since more than half of patients will have a second episode of kidney stones, the ability to identify and aggressively treat at-risk patients is vital. Using a data set of clinical characteristics from more than 2,000 first-time kidney stone patients from Olmsted County, Minnesota, and following these patients longitudinally for more than 20 years, Rule et al identified patients who had a second episode of kidney stones—as well as the characteristics associated with stone recurrence.5 They then developed a multivariate calculator, the ROKS nomogram, which can be used after a patient’s first episode of kidney stones to predict the likelihood of stone recurrence at 2, 5, and 10 years.3 The authors of the ROKS stone calculator were inspired by the World Health Organization’s FRAX calculator, which predicts 10-year fracture probability.5,6
Rule et al identified 11 risk factors that they incorporated into the ROKS calculator. These include, but are not limited to, age, sex, race, family history, hematuria, presence of uric acid stones, and characteristics of the position of the initial stone in the pelvis. Not surprisingly, Rule et al found the kidney stone recurrence rate greatest in younger males who were white and had a family history of stones.
Minnesota, it should be noted, is an area of the country where summers are cooler; since people in warmer climates are at increased risk for kidney stones (particularly during the summer months), it is possible that the ROKS calculator would be even more useful in the South or Southwest than in the original study setting.5
A free, downloadable app of the ROKS calculator is available at the QxMD app “Calculate” (iOS: http://qx.md/qx, Android: http://qx.md/android, or web-based http://qxmd.com/ROKS).
Any episode of kidney stones increases the risk for chronic kidney disease and/or kidney failure.7 The absolute risk increase, though small, is present; any preventive measures one can offer at-risk patients is valuable. These range from increasing fluids and acidifying the urine to adding medications, including thiazide diuretics and allopurinol, to reduce stone formation. Unfortunately, only 3% of all first-time kidney stone patients are currently treated with medication to prevent a second episode.3 This creates an unnecessary risk for complications in a significant number of patients. By identifying members of the stone population who are likely to have a second event, clinicians can reduce the risk for recurrence.
Close monitoring of a patient with a significant stone history is vital. The ROKS calculator will allow practitioners to identify patients at increased risk for recurrent kidney stones and treat them aggressively—reducing the associated kidney damage and pain.
References
1. Scales CD Jr, Smith AC, Hanley JM, Saigal CS. Urologic Diseases in America Project: prevalence of kidney stones in the United States. Eur Urol. 2012;62:160-165.
2. Ljunghall S. Incidence of upper urinary tract stones. Miner Electrolyte Metab. 1987;13(4):220-227.
3. Rule AD, Lieske JC, Li X, et al. The ROKS Nomogram for Predicting a Second Symptomatic Stone Episode. J Am Soc Nephrol. 2014 Aug 7. [Epub ahead of print]
4. National Kidney Foundation. Kidney stones: how common are kidney stones? www.kidney.org/atoz/content/kidneystones.cfm. Accessed September 24, 2014.
5. Eisner BH, Goldfarb DS. A Nomogram for the Prediction of Kidney Stone Recurrence. J Am Soc Nephrol. 2014 Aug 7. [Epub ahead of print]
6. Kanis JA on behalf of the World Health Organization Scientific Group (2007). Assessment of osteoporosis at the primary healthcare level: report of a WHO Scientific Group. www.iofbonehealth.org/sites/default/files/WHO_Technical_Report-2007.pdf. Accessed September 26, 2014.
7. Alexander RT, Hemmelgarn BR, Wiebe N, et al. Kidney stones and kidney function loss: a cohort study. BMJ. 2012;345:e5287.
Each year in the United States alone, more than half a million patients are seen in emergency departments with kidney stones. This translates to a stone incidence of 9% of all males and 6% of all females over the lifespan, or 1 in 11 people.1 Of these, 53% will have another stone during their lifetime.2 Since kidney stones are extremely painful and can cause permanent kidney damage, the ability to predict which patients are likely to have a stone recurrence is extremely valuable. Recently, an online calculator has been developed that can help clinicians predict which first-time kidney stone patients are in the “worrisome” group and which are less likely to have a recurrence.3
Kidney stones (nephrolithiasis) are increasingly common in males, those between ages 30 and 50, and those with certain underlying medical conditions, such as hypertension, diabetes, and gout, as well as those with a history of bariatric surgery.4 A family history of stone formation is also predictive.
Since more than half of patients will have a second episode of kidney stones, the ability to identify and aggressively treat at-risk patients is vital. Using a data set of clinical characteristics from more than 2,000 first-time kidney stone patients from Olmsted County, Minnesota, and following these patients longitudinally for more than 20 years, Rule et al identified patients who had a second episode of kidney stones—as well as the characteristics associated with stone recurrence.5 They then developed a multivariate calculator, the ROKS nomogram, which can be used after a patient’s first episode of kidney stones to predict the likelihood of stone recurrence at 2, 5, and 10 years.3 The authors of the ROKS stone calculator were inspired by the World Health Organization’s FRAX calculator, which predicts 10-year fracture probability.5,6
Rule et al identified 11 risk factors that they incorporated into the ROKS calculator. These include, but are not limited to, age, sex, race, family history, hematuria, presence of uric acid stones, and characteristics of the position of the initial stone in the pelvis. Not surprisingly, Rule et al found the kidney stone recurrence rate greatest in younger males who were white and had a family history of stones.
Minnesota, it should be noted, is an area of the country where summers are cooler; since people in warmer climates are at increased risk for kidney stones (particularly during the summer months), it is possible that the ROKS calculator would be even more useful in the South or Southwest than in the original study setting.5
A free, downloadable app of the ROKS calculator is available at the QxMD app “Calculate” (iOS: http://qx.md/qx, Android: http://qx.md/android, or web-based http://qxmd.com/ROKS).
Any episode of kidney stones increases the risk for chronic kidney disease and/or kidney failure.7 The absolute risk increase, though small, is present; any preventive measures one can offer at-risk patients is valuable. These range from increasing fluids and acidifying the urine to adding medications, including thiazide diuretics and allopurinol, to reduce stone formation. Unfortunately, only 3% of all first-time kidney stone patients are currently treated with medication to prevent a second episode.3 This creates an unnecessary risk for complications in a significant number of patients. By identifying members of the stone population who are likely to have a second event, clinicians can reduce the risk for recurrence.
Close monitoring of a patient with a significant stone history is vital. The ROKS calculator will allow practitioners to identify patients at increased risk for recurrent kidney stones and treat them aggressively—reducing the associated kidney damage and pain.
References
1. Scales CD Jr, Smith AC, Hanley JM, Saigal CS. Urologic Diseases in America Project: prevalence of kidney stones in the United States. Eur Urol. 2012;62:160-165.
2. Ljunghall S. Incidence of upper urinary tract stones. Miner Electrolyte Metab. 1987;13(4):220-227.
3. Rule AD, Lieske JC, Li X, et al. The ROKS Nomogram for Predicting a Second Symptomatic Stone Episode. J Am Soc Nephrol. 2014 Aug 7. [Epub ahead of print]
4. National Kidney Foundation. Kidney stones: how common are kidney stones? www.kidney.org/atoz/content/kidneystones.cfm. Accessed September 24, 2014.
5. Eisner BH, Goldfarb DS. A Nomogram for the Prediction of Kidney Stone Recurrence. J Am Soc Nephrol. 2014 Aug 7. [Epub ahead of print]
6. Kanis JA on behalf of the World Health Organization Scientific Group (2007). Assessment of osteoporosis at the primary healthcare level: report of a WHO Scientific Group. www.iofbonehealth.org/sites/default/files/WHO_Technical_Report-2007.pdf. Accessed September 26, 2014.
7. Alexander RT, Hemmelgarn BR, Wiebe N, et al. Kidney stones and kidney function loss: a cohort study. BMJ. 2012;345:e5287.
What Are the Types of Kidney Stones?
By age 70, 11% of men and 6% of women in the United States will have had at least one occurrence of kidney stones (nephrolithiasis).1,2 This translates to a nationwide incidence rate of one in 11. More than 50% of those affected by kidney stones will experience a recurrence.3
Treatments for kidney stones, though available, are underutilized; only 3% of patients are treated after their first occurrence.3 Since treatment depends on the composition of the initial stone, identification is essential. Once the stone type is identified, treatment can be directed at the metabolic abnormality that caused the stone’s formation.
There are five types of stones: calcium-based, struvite, uric-acid, cystine, and the problematic “mixed.” The most common is the calcium-based stone, which accounts for nearly 80% of identified stones.3,4 It is not the amount of calcium in the diet that usually causes a stone but rather the calcium excreted by the kidney collecting system.
One of the first recommendations for treatment of a calcium-based stone is a low-salt diet.4 Extra urinary sodium excretion (as a result of excess consumption) will increase calcium excretion in the urine. Decreasing salt in the diet will reduce sodium in the urine and, by extension, calcium as well. If conservative dietary changes are insufficient, a thiazide diuretic may be prescribed. (At present, a randomized clinical trial assessing treatment with oral potassium vs thiazides vs allopurinol for calcium-based stones is underway. Data from this trial will direct prevention strategies for calcium-based stones in the future.)
Uric acid stones can occur if the urine contains a high level of purine as a result of acidic foods in the diet. This usually means a diet rich in meats, shellfish, and high-purine foods (the same ones that can trigger gout).5 Control of the diet, alkalization of the urine, and/or treatment of the underlying high serum uric acid levels with allopurinol are the current recommended treatments.6
Struvite stones are caused by kidney infections. Many require long-term low-dose antibiotics in order to reduce reoccurrence.6 It is vital to know if a stone is struvite, since the treatment is significantly different from that for other types of stones.
Cystine stones result from a genetic disorder (cystinuria) that affects an amino acid. Often, these types of stones are seen in younger patients, and any teen who presents with kidney stones should undergo a work-up for the genetic abnormality. (See Zuber K. Woman, 26, with kidney stones. Clinician Reviews. 2011;21(3):8-10.)
When a patient complains of severe, colicky abdominal pain, hematuria, or a sharp pain in the back or flank, the thought of kidney stones must be front and center. Evaluation incudes both serum testing and CT.5,7 Abdominal plain films and/or an intravenous pyelogram were considered state of the art in the 1980s and 1990s, but helical CT has become the scan of choice since it allows for measurement of the size, position, and level of obstruction. Helical CTs are increasingly available nationwide—and a sensitivity of 95% to 100% makes them the preferred method of evalution.5,8
REFERENCES
1. Scales CD Jr, Smith AC, Hanley JM, Saigal CS. Urologic Diseases in America Project: Prevalence of kidney stones in the United States. Eur Urol. 2012;62:160-165.
2. Worcester EM, Coe FL. Calcium kidney stones. N Engl J Med. 2010;363:954-963.
3. Rule A, Lieske JC, Li X, et al. The ROKS Nomogram for Predicting a Second Symptomatic Stone Episode. J Am Soc Nephrol. 2014 Aug 7; [Epub ahead of print].
4. National Kidney Foundation. Diet and kidney stones. www.kidney.org/atoz/content/diet.cfm. Accessed September 9, 2104.
5. Jackman SV, Potter SR, Regan F, Jarrett TW. Plain abdominal x-ray versus computerized tomography screening: sensitivity for stone localization after nonenhanced spiral computerized tomography. J Urol. 2000;164(2):308-310.
6. Lipkin ME, Preminger GM. Demystifying the medical management of nephrolithiasis. Rev Urol. 2011;13(1):34-38.
7. National Institute of Diabetes and Digestive and Kidney Diseases. Kidney stones in adults: what are the types of kidney stones? http://kidney.niddk.nih.gov/KUDiseases/pubs/stonesadults/index.aspx#types. Accessed September 9, 2014.
8. Harrington K, Torreggiani W. CT analysis of renal stone composition: a novel and noninvasive method to analyse stones. Ir Med J. 2014;107(3):69.
By age 70, 11% of men and 6% of women in the United States will have had at least one occurrence of kidney stones (nephrolithiasis).1,2 This translates to a nationwide incidence rate of one in 11. More than 50% of those affected by kidney stones will experience a recurrence.3
Treatments for kidney stones, though available, are underutilized; only 3% of patients are treated after their first occurrence.3 Since treatment depends on the composition of the initial stone, identification is essential. Once the stone type is identified, treatment can be directed at the metabolic abnormality that caused the stone’s formation.
There are five types of stones: calcium-based, struvite, uric-acid, cystine, and the problematic “mixed.” The most common is the calcium-based stone, which accounts for nearly 80% of identified stones.3,4 It is not the amount of calcium in the diet that usually causes a stone but rather the calcium excreted by the kidney collecting system.
One of the first recommendations for treatment of a calcium-based stone is a low-salt diet.4 Extra urinary sodium excretion (as a result of excess consumption) will increase calcium excretion in the urine. Decreasing salt in the diet will reduce sodium in the urine and, by extension, calcium as well. If conservative dietary changes are insufficient, a thiazide diuretic may be prescribed. (At present, a randomized clinical trial assessing treatment with oral potassium vs thiazides vs allopurinol for calcium-based stones is underway. Data from this trial will direct prevention strategies for calcium-based stones in the future.)
Uric acid stones can occur if the urine contains a high level of purine as a result of acidic foods in the diet. This usually means a diet rich in meats, shellfish, and high-purine foods (the same ones that can trigger gout).5 Control of the diet, alkalization of the urine, and/or treatment of the underlying high serum uric acid levels with allopurinol are the current recommended treatments.6
Struvite stones are caused by kidney infections. Many require long-term low-dose antibiotics in order to reduce reoccurrence.6 It is vital to know if a stone is struvite, since the treatment is significantly different from that for other types of stones.
Cystine stones result from a genetic disorder (cystinuria) that affects an amino acid. Often, these types of stones are seen in younger patients, and any teen who presents with kidney stones should undergo a work-up for the genetic abnormality. (See Zuber K. Woman, 26, with kidney stones. Clinician Reviews. 2011;21(3):8-10.)
When a patient complains of severe, colicky abdominal pain, hematuria, or a sharp pain in the back or flank, the thought of kidney stones must be front and center. Evaluation incudes both serum testing and CT.5,7 Abdominal plain films and/or an intravenous pyelogram were considered state of the art in the 1980s and 1990s, but helical CT has become the scan of choice since it allows for measurement of the size, position, and level of obstruction. Helical CTs are increasingly available nationwide—and a sensitivity of 95% to 100% makes them the preferred method of evalution.5,8
REFERENCES
1. Scales CD Jr, Smith AC, Hanley JM, Saigal CS. Urologic Diseases in America Project: Prevalence of kidney stones in the United States. Eur Urol. 2012;62:160-165.
2. Worcester EM, Coe FL. Calcium kidney stones. N Engl J Med. 2010;363:954-963.
3. Rule A, Lieske JC, Li X, et al. The ROKS Nomogram for Predicting a Second Symptomatic Stone Episode. J Am Soc Nephrol. 2014 Aug 7; [Epub ahead of print].
4. National Kidney Foundation. Diet and kidney stones. www.kidney.org/atoz/content/diet.cfm. Accessed September 9, 2104.
5. Jackman SV, Potter SR, Regan F, Jarrett TW. Plain abdominal x-ray versus computerized tomography screening: sensitivity for stone localization after nonenhanced spiral computerized tomography. J Urol. 2000;164(2):308-310.
6. Lipkin ME, Preminger GM. Demystifying the medical management of nephrolithiasis. Rev Urol. 2011;13(1):34-38.
7. National Institute of Diabetes and Digestive and Kidney Diseases. Kidney stones in adults: what are the types of kidney stones? http://kidney.niddk.nih.gov/KUDiseases/pubs/stonesadults/index.aspx#types. Accessed September 9, 2014.
8. Harrington K, Torreggiani W. CT analysis of renal stone composition: a novel and noninvasive method to analyse stones. Ir Med J. 2014;107(3):69.
By age 70, 11% of men and 6% of women in the United States will have had at least one occurrence of kidney stones (nephrolithiasis).1,2 This translates to a nationwide incidence rate of one in 11. More than 50% of those affected by kidney stones will experience a recurrence.3
Treatments for kidney stones, though available, are underutilized; only 3% of patients are treated after their first occurrence.3 Since treatment depends on the composition of the initial stone, identification is essential. Once the stone type is identified, treatment can be directed at the metabolic abnormality that caused the stone’s formation.
There are five types of stones: calcium-based, struvite, uric-acid, cystine, and the problematic “mixed.” The most common is the calcium-based stone, which accounts for nearly 80% of identified stones.3,4 It is not the amount of calcium in the diet that usually causes a stone but rather the calcium excreted by the kidney collecting system.
One of the first recommendations for treatment of a calcium-based stone is a low-salt diet.4 Extra urinary sodium excretion (as a result of excess consumption) will increase calcium excretion in the urine. Decreasing salt in the diet will reduce sodium in the urine and, by extension, calcium as well. If conservative dietary changes are insufficient, a thiazide diuretic may be prescribed. (At present, a randomized clinical trial assessing treatment with oral potassium vs thiazides vs allopurinol for calcium-based stones is underway. Data from this trial will direct prevention strategies for calcium-based stones in the future.)
Uric acid stones can occur if the urine contains a high level of purine as a result of acidic foods in the diet. This usually means a diet rich in meats, shellfish, and high-purine foods (the same ones that can trigger gout).5 Control of the diet, alkalization of the urine, and/or treatment of the underlying high serum uric acid levels with allopurinol are the current recommended treatments.6
Struvite stones are caused by kidney infections. Many require long-term low-dose antibiotics in order to reduce reoccurrence.6 It is vital to know if a stone is struvite, since the treatment is significantly different from that for other types of stones.
Cystine stones result from a genetic disorder (cystinuria) that affects an amino acid. Often, these types of stones are seen in younger patients, and any teen who presents with kidney stones should undergo a work-up for the genetic abnormality. (See Zuber K. Woman, 26, with kidney stones. Clinician Reviews. 2011;21(3):8-10.)
When a patient complains of severe, colicky abdominal pain, hematuria, or a sharp pain in the back or flank, the thought of kidney stones must be front and center. Evaluation incudes both serum testing and CT.5,7 Abdominal plain films and/or an intravenous pyelogram were considered state of the art in the 1980s and 1990s, but helical CT has become the scan of choice since it allows for measurement of the size, position, and level of obstruction. Helical CTs are increasingly available nationwide—and a sensitivity of 95% to 100% makes them the preferred method of evalution.5,8
REFERENCES
1. Scales CD Jr, Smith AC, Hanley JM, Saigal CS. Urologic Diseases in America Project: Prevalence of kidney stones in the United States. Eur Urol. 2012;62:160-165.
2. Worcester EM, Coe FL. Calcium kidney stones. N Engl J Med. 2010;363:954-963.
3. Rule A, Lieske JC, Li X, et al. The ROKS Nomogram for Predicting a Second Symptomatic Stone Episode. J Am Soc Nephrol. 2014 Aug 7; [Epub ahead of print].
4. National Kidney Foundation. Diet and kidney stones. www.kidney.org/atoz/content/diet.cfm. Accessed September 9, 2104.
5. Jackman SV, Potter SR, Regan F, Jarrett TW. Plain abdominal x-ray versus computerized tomography screening: sensitivity for stone localization after nonenhanced spiral computerized tomography. J Urol. 2000;164(2):308-310.
6. Lipkin ME, Preminger GM. Demystifying the medical management of nephrolithiasis. Rev Urol. 2011;13(1):34-38.
7. National Institute of Diabetes and Digestive and Kidney Diseases. Kidney stones in adults: what are the types of kidney stones? http://kidney.niddk.nih.gov/KUDiseases/pubs/stonesadults/index.aspx#types. Accessed September 9, 2014.
8. Harrington K, Torreggiani W. CT analysis of renal stone composition: a novel and noninvasive method to analyse stones. Ir Med J. 2014;107(3):69.
The Not-So-Common Stone
Kidney stones (nephrolithiasis), seen in 11% of all Americans, may increase patients’ risk for chronic kidney disease (CKD), although current research findings are insufficient to support a well-established relationship.1,2 Actually, CKD may have a protective effect against the formation of calcium-based stones (which account for about 80% of all stones), since the CKD-affected kidney may fail to concentrate and excrete calcium. However, this effect is often offset by metabolic syndrome, diabetes, and hypertension—all of which increase the risk for calcium-based stones.4,5 Heredity is also a factor.
After calcium-based stones, the most common types are struvite, uric acid, cysteine, and “mixed” stones. Not so common are the hereditary stones associated with four relatively rare conditions: primary hyperoxaluria (PH), adenine phosphoribosyltransferase (APRT) deficiency, cystinuria, and Dent’s disease. According to the NIH Rare Diseases Clinical Research Network, only 524 patients with these conditions are enrolled in the Mayo Clinic–based Rare Kidney Stone Consortium, indicating the orphan status of these illnesses.6
Patients with PH are born with an autosomal recessive error of glyoxylate metabolism that results in an overproduction of calcium oxalate.7 The oxalate is deposited in various organs—most often the kidneys, in the form of kidney stones. PH can occur in infants; parents are often alerted by rust spots in diapers, caused by passage of small stones.
There are three types of PH: PH1, PH2, and PH3. PH1 and PH2 account for approximately 90% of cases.8 In PH1, the genetic error is linked to an insufficient or absent liver enzyme. About 50% of children with PH1 will develop end-stage renal disease by young adulthood.9 One of the suggested treatments is liver transplantation, because replacing the diseased kidney alone would not spare the newly transplanted kidney from the same fate: a shower of stones from the liver. For patients with PH2 (which is generally less severe than PH1), kidney transplantation alone is often effective.10 In patients with any type of PH, high fluid intake is recommended.
Like PH, APRT/2,8-DHA crystalluria is an autosomal recessive disorder, one that researchers consider underrecognized and underdiagnosed. The majority of cases have been reported from Japan, France, and Iceland.11 Often the stones are misidentified as uric acid or xanthine stones. Patients with APRT deficiency present with a range of symptoms—from stone disease to full kidney failure.12 Treatment components include administration of allopurinol (a purine analog), increased fluid intake, a mildly purine-restricted diet, and extracorporeal shock-wave lithotripsy, when indicated.13
Cystinuria is found in 1% to 2% of patients with kidney stones but about 5% of children with stones14; it most often presents in early childhood. Patients have impaired renal cysteine transport, which leads to stone formation.15 Before it became possible to identify the genes responsible for cystinuria, patients were classified according to cystine excretion levels. Treatment includes high fluid intake, mild restriction of protein and sodium, alkalinization of urine, and use of medications including penicillamine and captopril.16,17
The rare stone-producing illness Dent’s disease is an X-linked recessive condition that can lead to hypercalciuria, stones, CKD, and rickets.18 It usually presents in childhood, often in children who fail to thrive, and is associated with mutations of at least two genes (accounting for different disease types). Low-molecular-weight proteinuria is almost always present, but renal failure is relatively uncommon. Thiazide therapy has been found effective in treating the hypercalciuria associated with Dent’s disease, and addition of an ACE inhibitor may be helpful in patients with cystinosis.19
Kidney stones should be suspected in children with a family history of stones and symptoms such as hematuria, flank or abdominal pain, and/or urinary symptoms (dysuria, urinary tract infection). Genetic testing and counseling is frequently advised for these children and their families, as the correct diagnosis guides appropriate treatment.
References
1. Scales CD Jr, Smith AC, Hanley JM, Saigal CS. Urologic Diseases in America Project: Prevalence of kidney stones in the United States. Eur Urol. 2012;62:160-165.
2. Worcester EM, Coe FL. Calcium kidney stones. N Engl J Med. 2010;363:954-963.
3. Rule AD, Krambeck AE, Lieske JC. Chronic kidney disease in kidney stone formers. Clin J Am Soc Nephrol. 2011;6(8):2069-2075.
4. Teichman JM. Clinical practice. Acute renal colic from ureteral calculus. N Engl J Med. 2004;350(7):684-693.
5. National Institute of Diabetes and Digestive and Kidney Diseases. Kidney stones in adults: what are the types of kidney stones? http://kidney.niddk.nih.gov/KUDiseases/pubs/stonesadults/index.aspx. Accessed September 29, 2014.
6. Nazzal L. Spotlight on RDCRN consortia: the Rare Kidney Stone Consortium. http://rarediseasesnetwork.org/spotlight/April2013/RKSC. Accessed September 26, 2014.
7. Hoppe B. An update on primary hyperoxaluria. Nat Rev Nephrol. 2012;8(8):467-475.
8. Hoppe B, Langman CB. A United States survey on diagnosis, treatment, and outcome of primary hyperoxaluria. Pediatr Nephrol. 2003;18(10):986-991.
9. Harambat J, Farque S, Acquaviva C. Genotype-phenotype correlation in primary hyperoxaluria type 1: the p.Gly170Arg AGXT mutation is associated with a better outcome. Kidney Int. 2010;77(5):443-449.
10. Bergstralh EJ, Monico CG, Lieske JC. Transplantation outcomes in primary hyperoxaluria. Am J Transplant. 2010;10(11):2493-2501.
11. Rare Clinical Diseases Research Network. Diseases in depth: adenine phosphoribosyltransferase (APRT) deficiency. www.rarediseasesnetwork.org/RKSC/professional/APRT/index.htm. Accessed September 29, 2014.
12. Edvardsson V, Palsson R. Adenine phosphoribosyltransferase deficiency and 2,8-dihydroxyadeninuria. In: Moriwaki Y, ed. Genetic Errors Associated with Purine and Pyrimidine Metabolism in Humans: Diagnosis and Treatment. Kerala, India: Research Signpost; 2006:79-93.
13. Edvardsson V, Palsson R, Olafsson I, et al. Clinical features and genotype of adenine phosphoribosyltransferase deficiency in Iceland. Am J Kidney Dis. 2001;38(3):473-480.
14. Stapleton FB. Childhood stones. Endocrinol Metab Clin North Am. 2002;31(4):1001-1015.
15. Mattoo A, Goldfarb DS. Cystinuria. Semin Nephrol. 2008;28(2):181-191.
16. Goldfarb DS, Coe FL, Asplin JR. Urinary cystine excretion and capacity in patients with cystinuria. Kidney Int. 2006;69(6):1041-1047.
17. Perazella MA, Buller GK. Successful treatment of cystinuria with captopril. Am J Kidney Dis. 1993;21(5):504-507.
18. Devuyst O, Thakker RV. Dent’s disease. Orphanet J Rare Dis. 2010;5:28.
19. Ludwig M, Utsch B, Monnens LA. Recent advances in understanding the clinical and genetic heterogeneity of Dent’s disease. Nephrol Dial Transplant. 2006;21(10):2708-2717.
Kidney stones (nephrolithiasis), seen in 11% of all Americans, may increase patients’ risk for chronic kidney disease (CKD), although current research findings are insufficient to support a well-established relationship.1,2 Actually, CKD may have a protective effect against the formation of calcium-based stones (which account for about 80% of all stones), since the CKD-affected kidney may fail to concentrate and excrete calcium. However, this effect is often offset by metabolic syndrome, diabetes, and hypertension—all of which increase the risk for calcium-based stones.4,5 Heredity is also a factor.
After calcium-based stones, the most common types are struvite, uric acid, cysteine, and “mixed” stones. Not so common are the hereditary stones associated with four relatively rare conditions: primary hyperoxaluria (PH), adenine phosphoribosyltransferase (APRT) deficiency, cystinuria, and Dent’s disease. According to the NIH Rare Diseases Clinical Research Network, only 524 patients with these conditions are enrolled in the Mayo Clinic–based Rare Kidney Stone Consortium, indicating the orphan status of these illnesses.6
Patients with PH are born with an autosomal recessive error of glyoxylate metabolism that results in an overproduction of calcium oxalate.7 The oxalate is deposited in various organs—most often the kidneys, in the form of kidney stones. PH can occur in infants; parents are often alerted by rust spots in diapers, caused by passage of small stones.
There are three types of PH: PH1, PH2, and PH3. PH1 and PH2 account for approximately 90% of cases.8 In PH1, the genetic error is linked to an insufficient or absent liver enzyme. About 50% of children with PH1 will develop end-stage renal disease by young adulthood.9 One of the suggested treatments is liver transplantation, because replacing the diseased kidney alone would not spare the newly transplanted kidney from the same fate: a shower of stones from the liver. For patients with PH2 (which is generally less severe than PH1), kidney transplantation alone is often effective.10 In patients with any type of PH, high fluid intake is recommended.
Like PH, APRT/2,8-DHA crystalluria is an autosomal recessive disorder, one that researchers consider underrecognized and underdiagnosed. The majority of cases have been reported from Japan, France, and Iceland.11 Often the stones are misidentified as uric acid or xanthine stones. Patients with APRT deficiency present with a range of symptoms—from stone disease to full kidney failure.12 Treatment components include administration of allopurinol (a purine analog), increased fluid intake, a mildly purine-restricted diet, and extracorporeal shock-wave lithotripsy, when indicated.13
Cystinuria is found in 1% to 2% of patients with kidney stones but about 5% of children with stones14; it most often presents in early childhood. Patients have impaired renal cysteine transport, which leads to stone formation.15 Before it became possible to identify the genes responsible for cystinuria, patients were classified according to cystine excretion levels. Treatment includes high fluid intake, mild restriction of protein and sodium, alkalinization of urine, and use of medications including penicillamine and captopril.16,17
The rare stone-producing illness Dent’s disease is an X-linked recessive condition that can lead to hypercalciuria, stones, CKD, and rickets.18 It usually presents in childhood, often in children who fail to thrive, and is associated with mutations of at least two genes (accounting for different disease types). Low-molecular-weight proteinuria is almost always present, but renal failure is relatively uncommon. Thiazide therapy has been found effective in treating the hypercalciuria associated with Dent’s disease, and addition of an ACE inhibitor may be helpful in patients with cystinosis.19
Kidney stones should be suspected in children with a family history of stones and symptoms such as hematuria, flank or abdominal pain, and/or urinary symptoms (dysuria, urinary tract infection). Genetic testing and counseling is frequently advised for these children and their families, as the correct diagnosis guides appropriate treatment.
References
1. Scales CD Jr, Smith AC, Hanley JM, Saigal CS. Urologic Diseases in America Project: Prevalence of kidney stones in the United States. Eur Urol. 2012;62:160-165.
2. Worcester EM, Coe FL. Calcium kidney stones. N Engl J Med. 2010;363:954-963.
3. Rule AD, Krambeck AE, Lieske JC. Chronic kidney disease in kidney stone formers. Clin J Am Soc Nephrol. 2011;6(8):2069-2075.
4. Teichman JM. Clinical practice. Acute renal colic from ureteral calculus. N Engl J Med. 2004;350(7):684-693.
5. National Institute of Diabetes and Digestive and Kidney Diseases. Kidney stones in adults: what are the types of kidney stones? http://kidney.niddk.nih.gov/KUDiseases/pubs/stonesadults/index.aspx. Accessed September 29, 2014.
6. Nazzal L. Spotlight on RDCRN consortia: the Rare Kidney Stone Consortium. http://rarediseasesnetwork.org/spotlight/April2013/RKSC. Accessed September 26, 2014.
7. Hoppe B. An update on primary hyperoxaluria. Nat Rev Nephrol. 2012;8(8):467-475.
8. Hoppe B, Langman CB. A United States survey on diagnosis, treatment, and outcome of primary hyperoxaluria. Pediatr Nephrol. 2003;18(10):986-991.
9. Harambat J, Farque S, Acquaviva C. Genotype-phenotype correlation in primary hyperoxaluria type 1: the p.Gly170Arg AGXT mutation is associated with a better outcome. Kidney Int. 2010;77(5):443-449.
10. Bergstralh EJ, Monico CG, Lieske JC. Transplantation outcomes in primary hyperoxaluria. Am J Transplant. 2010;10(11):2493-2501.
11. Rare Clinical Diseases Research Network. Diseases in depth: adenine phosphoribosyltransferase (APRT) deficiency. www.rarediseasesnetwork.org/RKSC/professional/APRT/index.htm. Accessed September 29, 2014.
12. Edvardsson V, Palsson R. Adenine phosphoribosyltransferase deficiency and 2,8-dihydroxyadeninuria. In: Moriwaki Y, ed. Genetic Errors Associated with Purine and Pyrimidine Metabolism in Humans: Diagnosis and Treatment. Kerala, India: Research Signpost; 2006:79-93.
13. Edvardsson V, Palsson R, Olafsson I, et al. Clinical features and genotype of adenine phosphoribosyltransferase deficiency in Iceland. Am J Kidney Dis. 2001;38(3):473-480.
14. Stapleton FB. Childhood stones. Endocrinol Metab Clin North Am. 2002;31(4):1001-1015.
15. Mattoo A, Goldfarb DS. Cystinuria. Semin Nephrol. 2008;28(2):181-191.
16. Goldfarb DS, Coe FL, Asplin JR. Urinary cystine excretion and capacity in patients with cystinuria. Kidney Int. 2006;69(6):1041-1047.
17. Perazella MA, Buller GK. Successful treatment of cystinuria with captopril. Am J Kidney Dis. 1993;21(5):504-507.
18. Devuyst O, Thakker RV. Dent’s disease. Orphanet J Rare Dis. 2010;5:28.
19. Ludwig M, Utsch B, Monnens LA. Recent advances in understanding the clinical and genetic heterogeneity of Dent’s disease. Nephrol Dial Transplant. 2006;21(10):2708-2717.
Kidney stones (nephrolithiasis), seen in 11% of all Americans, may increase patients’ risk for chronic kidney disease (CKD), although current research findings are insufficient to support a well-established relationship.1,2 Actually, CKD may have a protective effect against the formation of calcium-based stones (which account for about 80% of all stones), since the CKD-affected kidney may fail to concentrate and excrete calcium. However, this effect is often offset by metabolic syndrome, diabetes, and hypertension—all of which increase the risk for calcium-based stones.4,5 Heredity is also a factor.
After calcium-based stones, the most common types are struvite, uric acid, cysteine, and “mixed” stones. Not so common are the hereditary stones associated with four relatively rare conditions: primary hyperoxaluria (PH), adenine phosphoribosyltransferase (APRT) deficiency, cystinuria, and Dent’s disease. According to the NIH Rare Diseases Clinical Research Network, only 524 patients with these conditions are enrolled in the Mayo Clinic–based Rare Kidney Stone Consortium, indicating the orphan status of these illnesses.6
Patients with PH are born with an autosomal recessive error of glyoxylate metabolism that results in an overproduction of calcium oxalate.7 The oxalate is deposited in various organs—most often the kidneys, in the form of kidney stones. PH can occur in infants; parents are often alerted by rust spots in diapers, caused by passage of small stones.
There are three types of PH: PH1, PH2, and PH3. PH1 and PH2 account for approximately 90% of cases.8 In PH1, the genetic error is linked to an insufficient or absent liver enzyme. About 50% of children with PH1 will develop end-stage renal disease by young adulthood.9 One of the suggested treatments is liver transplantation, because replacing the diseased kidney alone would not spare the newly transplanted kidney from the same fate: a shower of stones from the liver. For patients with PH2 (which is generally less severe than PH1), kidney transplantation alone is often effective.10 In patients with any type of PH, high fluid intake is recommended.
Like PH, APRT/2,8-DHA crystalluria is an autosomal recessive disorder, one that researchers consider underrecognized and underdiagnosed. The majority of cases have been reported from Japan, France, and Iceland.11 Often the stones are misidentified as uric acid or xanthine stones. Patients with APRT deficiency present with a range of symptoms—from stone disease to full kidney failure.12 Treatment components include administration of allopurinol (a purine analog), increased fluid intake, a mildly purine-restricted diet, and extracorporeal shock-wave lithotripsy, when indicated.13
Cystinuria is found in 1% to 2% of patients with kidney stones but about 5% of children with stones14; it most often presents in early childhood. Patients have impaired renal cysteine transport, which leads to stone formation.15 Before it became possible to identify the genes responsible for cystinuria, patients were classified according to cystine excretion levels. Treatment includes high fluid intake, mild restriction of protein and sodium, alkalinization of urine, and use of medications including penicillamine and captopril.16,17
The rare stone-producing illness Dent’s disease is an X-linked recessive condition that can lead to hypercalciuria, stones, CKD, and rickets.18 It usually presents in childhood, often in children who fail to thrive, and is associated with mutations of at least two genes (accounting for different disease types). Low-molecular-weight proteinuria is almost always present, but renal failure is relatively uncommon. Thiazide therapy has been found effective in treating the hypercalciuria associated with Dent’s disease, and addition of an ACE inhibitor may be helpful in patients with cystinosis.19
Kidney stones should be suspected in children with a family history of stones and symptoms such as hematuria, flank or abdominal pain, and/or urinary symptoms (dysuria, urinary tract infection). Genetic testing and counseling is frequently advised for these children and their families, as the correct diagnosis guides appropriate treatment.
References
1. Scales CD Jr, Smith AC, Hanley JM, Saigal CS. Urologic Diseases in America Project: Prevalence of kidney stones in the United States. Eur Urol. 2012;62:160-165.
2. Worcester EM, Coe FL. Calcium kidney stones. N Engl J Med. 2010;363:954-963.
3. Rule AD, Krambeck AE, Lieske JC. Chronic kidney disease in kidney stone formers. Clin J Am Soc Nephrol. 2011;6(8):2069-2075.
4. Teichman JM. Clinical practice. Acute renal colic from ureteral calculus. N Engl J Med. 2004;350(7):684-693.
5. National Institute of Diabetes and Digestive and Kidney Diseases. Kidney stones in adults: what are the types of kidney stones? http://kidney.niddk.nih.gov/KUDiseases/pubs/stonesadults/index.aspx. Accessed September 29, 2014.
6. Nazzal L. Spotlight on RDCRN consortia: the Rare Kidney Stone Consortium. http://rarediseasesnetwork.org/spotlight/April2013/RKSC. Accessed September 26, 2014.
7. Hoppe B. An update on primary hyperoxaluria. Nat Rev Nephrol. 2012;8(8):467-475.
8. Hoppe B, Langman CB. A United States survey on diagnosis, treatment, and outcome of primary hyperoxaluria. Pediatr Nephrol. 2003;18(10):986-991.
9. Harambat J, Farque S, Acquaviva C. Genotype-phenotype correlation in primary hyperoxaluria type 1: the p.Gly170Arg AGXT mutation is associated with a better outcome. Kidney Int. 2010;77(5):443-449.
10. Bergstralh EJ, Monico CG, Lieske JC. Transplantation outcomes in primary hyperoxaluria. Am J Transplant. 2010;10(11):2493-2501.
11. Rare Clinical Diseases Research Network. Diseases in depth: adenine phosphoribosyltransferase (APRT) deficiency. www.rarediseasesnetwork.org/RKSC/professional/APRT/index.htm. Accessed September 29, 2014.
12. Edvardsson V, Palsson R. Adenine phosphoribosyltransferase deficiency and 2,8-dihydroxyadeninuria. In: Moriwaki Y, ed. Genetic Errors Associated with Purine and Pyrimidine Metabolism in Humans: Diagnosis and Treatment. Kerala, India: Research Signpost; 2006:79-93.
13. Edvardsson V, Palsson R, Olafsson I, et al. Clinical features and genotype of adenine phosphoribosyltransferase deficiency in Iceland. Am J Kidney Dis. 2001;38(3):473-480.
14. Stapleton FB. Childhood stones. Endocrinol Metab Clin North Am. 2002;31(4):1001-1015.
15. Mattoo A, Goldfarb DS. Cystinuria. Semin Nephrol. 2008;28(2):181-191.
16. Goldfarb DS, Coe FL, Asplin JR. Urinary cystine excretion and capacity in patients with cystinuria. Kidney Int. 2006;69(6):1041-1047.
17. Perazella MA, Buller GK. Successful treatment of cystinuria with captopril. Am J Kidney Dis. 1993;21(5):504-507.
18. Devuyst O, Thakker RV. Dent’s disease. Orphanet J Rare Dis. 2010;5:28.
19. Ludwig M, Utsch B, Monnens LA. Recent advances in understanding the clinical and genetic heterogeneity of Dent’s disease. Nephrol Dial Transplant. 2006;21(10):2708-2717.
Hot & Bothered About Kidney Stones
The long lazy days of summer are ending: The warm evenings, the iced tea, the sounds of kids playing at the pool being overshadowed by the loud moans of the patient with kidney stones ….
Kidney stones (nephrolithiasis) are collections of crystals that coalesce into a hard ball and can lodge in any location of the urinary collecting systems. More than half a million patients seen in US emergency departments each year will receive a diagnosis of nephrolithiasis.1
But the problem is much more common in the summer, thanks to the double whammy of heat and humidity.2-4 Research indicates that it is not geographic area but instead the effects of climate that impact stone incidence.5 As climate change occurs, it is expected that the incidence of kidney stones will rise.
There is a “stone belt” that covers the southern portion of the United States (see Figure). As reported in Kidney International, this area is growing due to climate change and is expected to reach as far north as Nebraska, Illinois, Pennsylvania, and Oregon by 2095. Thus, the incidence of stone formation will increase throughout the 21st century in many parts of the US.6
Kidney stones are more common in men than in women and in white than in nonwhite persons (by three to four times). Peak incidence occurs between ages 20 and 50.1 Heat plays a greater role in the increased incidence of stone formation in men for unknown reasons.6
Stones that lodge in the ureter or the calyces of the kidney will often cause obstruction. When the flow of urine is obstructed, infection, loss of kidney function, and chronic permanent damage can result. Thus, decreasing the incidence of stones is vital at any time of the year—but most significant during the summer.
All patients with a history of stones require fluid hydration, up to 2.5 L/d, with extra intake during the heat of summer.7 Patients who travel to hot, humid regions must be encouraged to increase fluid consumption. Often, foreign travel can be problematic due to a decrease in access to clean drinking water and/or lavatory facilities. It is incumbent upon the practitioner to review risk for kidney stones with patients who plan to travel to warm areas.
As the summer season closes and school starts, this is a perfect time to review the causes, treatment, and most importantly, the methods to decrease recurrent kidney stone formation with patients. Each incident of stone formation for our patients can translate to an increased incidence of chronic kidney disease and a 50% risk for another stone during their lifetime.1
REFERENCES
1. National Kidney Foundation. Kidney stones. www.kidney.org/atoz/content/kidneystones.cfm. Accessed September 10, 2014.
2.Schade GR, Faerber GJ. Urinary tract stones. Prim Care. 2010;37(3):565-581, ix.
3. Pearle MS, Calhoun E, Curhan GC. Urolithiasis. In: Litwin MS, Saigal CS, eds. Urologic Diseases in America. National Institute of Diabetes and Digestive and Kidney Diseases. 2007:281-320. http://kidney.niddk.nih.gov/statistics/uda/Urologic_Diseases_in_America.pdf. Accessed September 10, 2014.
4. Romero V, Akpinar H, Assimos DG. Kidney stones: a global picture of prevalence, incidence and associated risk factors. Rev Urol. 2010;12(2-3):e86-e96.
5. Eisner BH, Sheth S, Herrick B, et al. The effects of ambient temperature, humidity and season of year on urine composition in patients with nephrolithiasis. BJU Int. 2012;110(11c):E1014–E1017.
6. Fakheri RJ, Goldfarb DS. Ambient temperature as a contributor to kidney stone formation: Implications of global warming. Kidney Int. 2011;79:1178–1185.
7. Lipkin ME, Preminger GM. Demystifying the medical management of nephrolithiasis. Rev Urol. 2011;13(1):34-38.
The long lazy days of summer are ending: The warm evenings, the iced tea, the sounds of kids playing at the pool being overshadowed by the loud moans of the patient with kidney stones ….
Kidney stones (nephrolithiasis) are collections of crystals that coalesce into a hard ball and can lodge in any location of the urinary collecting systems. More than half a million patients seen in US emergency departments each year will receive a diagnosis of nephrolithiasis.1
But the problem is much more common in the summer, thanks to the double whammy of heat and humidity.2-4 Research indicates that it is not geographic area but instead the effects of climate that impact stone incidence.5 As climate change occurs, it is expected that the incidence of kidney stones will rise.
There is a “stone belt” that covers the southern portion of the United States (see Figure). As reported in Kidney International, this area is growing due to climate change and is expected to reach as far north as Nebraska, Illinois, Pennsylvania, and Oregon by 2095. Thus, the incidence of stone formation will increase throughout the 21st century in many parts of the US.6
Kidney stones are more common in men than in women and in white than in nonwhite persons (by three to four times). Peak incidence occurs between ages 20 and 50.1 Heat plays a greater role in the increased incidence of stone formation in men for unknown reasons.6
Stones that lodge in the ureter or the calyces of the kidney will often cause obstruction. When the flow of urine is obstructed, infection, loss of kidney function, and chronic permanent damage can result. Thus, decreasing the incidence of stones is vital at any time of the year—but most significant during the summer.
All patients with a history of stones require fluid hydration, up to 2.5 L/d, with extra intake during the heat of summer.7 Patients who travel to hot, humid regions must be encouraged to increase fluid consumption. Often, foreign travel can be problematic due to a decrease in access to clean drinking water and/or lavatory facilities. It is incumbent upon the practitioner to review risk for kidney stones with patients who plan to travel to warm areas.
As the summer season closes and school starts, this is a perfect time to review the causes, treatment, and most importantly, the methods to decrease recurrent kidney stone formation with patients. Each incident of stone formation for our patients can translate to an increased incidence of chronic kidney disease and a 50% risk for another stone during their lifetime.1
REFERENCES
1. National Kidney Foundation. Kidney stones. www.kidney.org/atoz/content/kidneystones.cfm. Accessed September 10, 2014.
2.Schade GR, Faerber GJ. Urinary tract stones. Prim Care. 2010;37(3):565-581, ix.
3. Pearle MS, Calhoun E, Curhan GC. Urolithiasis. In: Litwin MS, Saigal CS, eds. Urologic Diseases in America. National Institute of Diabetes and Digestive and Kidney Diseases. 2007:281-320. http://kidney.niddk.nih.gov/statistics/uda/Urologic_Diseases_in_America.pdf. Accessed September 10, 2014.
4. Romero V, Akpinar H, Assimos DG. Kidney stones: a global picture of prevalence, incidence and associated risk factors. Rev Urol. 2010;12(2-3):e86-e96.
5. Eisner BH, Sheth S, Herrick B, et al. The effects of ambient temperature, humidity and season of year on urine composition in patients with nephrolithiasis. BJU Int. 2012;110(11c):E1014–E1017.
6. Fakheri RJ, Goldfarb DS. Ambient temperature as a contributor to kidney stone formation: Implications of global warming. Kidney Int. 2011;79:1178–1185.
7. Lipkin ME, Preminger GM. Demystifying the medical management of nephrolithiasis. Rev Urol. 2011;13(1):34-38.
The long lazy days of summer are ending: The warm evenings, the iced tea, the sounds of kids playing at the pool being overshadowed by the loud moans of the patient with kidney stones ….
Kidney stones (nephrolithiasis) are collections of crystals that coalesce into a hard ball and can lodge in any location of the urinary collecting systems. More than half a million patients seen in US emergency departments each year will receive a diagnosis of nephrolithiasis.1
But the problem is much more common in the summer, thanks to the double whammy of heat and humidity.2-4 Research indicates that it is not geographic area but instead the effects of climate that impact stone incidence.5 As climate change occurs, it is expected that the incidence of kidney stones will rise.
There is a “stone belt” that covers the southern portion of the United States (see Figure). As reported in Kidney International, this area is growing due to climate change and is expected to reach as far north as Nebraska, Illinois, Pennsylvania, and Oregon by 2095. Thus, the incidence of stone formation will increase throughout the 21st century in many parts of the US.6
Kidney stones are more common in men than in women and in white than in nonwhite persons (by three to four times). Peak incidence occurs between ages 20 and 50.1 Heat plays a greater role in the increased incidence of stone formation in men for unknown reasons.6
Stones that lodge in the ureter or the calyces of the kidney will often cause obstruction. When the flow of urine is obstructed, infection, loss of kidney function, and chronic permanent damage can result. Thus, decreasing the incidence of stones is vital at any time of the year—but most significant during the summer.
All patients with a history of stones require fluid hydration, up to 2.5 L/d, with extra intake during the heat of summer.7 Patients who travel to hot, humid regions must be encouraged to increase fluid consumption. Often, foreign travel can be problematic due to a decrease in access to clean drinking water and/or lavatory facilities. It is incumbent upon the practitioner to review risk for kidney stones with patients who plan to travel to warm areas.
As the summer season closes and school starts, this is a perfect time to review the causes, treatment, and most importantly, the methods to decrease recurrent kidney stone formation with patients. Each incident of stone formation for our patients can translate to an increased incidence of chronic kidney disease and a 50% risk for another stone during their lifetime.1
REFERENCES
1. National Kidney Foundation. Kidney stones. www.kidney.org/atoz/content/kidneystones.cfm. Accessed September 10, 2014.
2.Schade GR, Faerber GJ. Urinary tract stones. Prim Care. 2010;37(3):565-581, ix.
3. Pearle MS, Calhoun E, Curhan GC. Urolithiasis. In: Litwin MS, Saigal CS, eds. Urologic Diseases in America. National Institute of Diabetes and Digestive and Kidney Diseases. 2007:281-320. http://kidney.niddk.nih.gov/statistics/uda/Urologic_Diseases_in_America.pdf. Accessed September 10, 2014.
4. Romero V, Akpinar H, Assimos DG. Kidney stones: a global picture of prevalence, incidence and associated risk factors. Rev Urol. 2010;12(2-3):e86-e96.
5. Eisner BH, Sheth S, Herrick B, et al. The effects of ambient temperature, humidity and season of year on urine composition in patients with nephrolithiasis. BJU Int. 2012;110(11c):E1014–E1017.
6. Fakheri RJ, Goldfarb DS. Ambient temperature as a contributor to kidney stone formation: Implications of global warming. Kidney Int. 2011;79:1178–1185.
7. Lipkin ME, Preminger GM. Demystifying the medical management of nephrolithiasis. Rev Urol. 2011;13(1):34-38.
2014 Update on sexual dysfunction
Since the last installment of this Update on Sexual Dysfunction, three new drugs have been added to the armamentarium for menopausal symptoms and dyspareunia:
- paroxetine 7.5 mg (Brisdelle)
- conjugated estrogens and bazedoxifene (Duavee)
- ospemifene (Osphena).
In this article, I present a case-based approach to incorporating these drugs into practice and restoring sexual function in the setting of vulvovaginal atrophy and dyspareunia. As is often the case, decision-making requires sifting through multiple layers of information.
How to “tease out” the problem and help the patient regain sexual function
Simon JA, Portman DJ, Kazempour K, Mekonnen H, Bhaskar S, Lippman J. Safety profile of paroxetine 7.5 mg in women with moderate-to-severe vasomotor symptoms. Obstet Gynecol. 2014;123(suppl 1):132S–133S.
Conjugated estrogens/bazedoxifene (Duavee) for menopausal symptoms and prevention of osteoporosis. Med Lett Drugs Ther. 2014;56(1441):33–34.
DeGregorio MW, Zerbe RL, Wurz GT. Ospemifene: a first-in-class, non-hormonal selective estrogen receptor modulator approved for the treatment of dyspareunia associated with vulvar and vaginal atrophy [published online ahead of print August 1, 2014]. Steroids. doi:10.1016/j.steroids.2014.07.012.
Goldstein SR, Archer DF, Simon JA, Constantine G. Endometrial safety of ospemifene and the ability of transvaginal ultrasonography to detect small changes in endometrial thickness. Obstet Gynecol. 2014;123(suppl 1):96S–97S.
CASE: LOW DESIRE AND DISCOMFORT DURING INTERCOURSE
Your 58-year-old patient, G2P2, mentions during her annual visit that she’s not that interested in sex anymore. Her children are grown, she’s been happily married for 28 years, and she enjoys her job and denies any symptoms of depression. She says her relationship with her husband is good and, aside from her low desire, she has no worries about the marriage. Her only medication is paroxetine 7.5 mg/day (Brisdelle) for management of her moderate hot flashes, which she initiated at her last annual visit. She reports improvement in her sleep and menopausal symptoms as a result. She has an intact uterus.
You perform a pelvic exam and find atrophic vulva and vagina with mild erythema, and thinned epithelium. When you ask if she has experienced any discomfort, she reports that she needs to use lubrication for intercourse and that, even with lubrication, she has pain upon penetration and a burning sensation that continues throughout intercourse. She also reports that it seems to take her much longer to achieve arousal than in the past, and she often fails to reach orgasm.
How would you manage this patient?
As always, begin with the history
The transition to menopause creates multiple layers of potential symptoms and problems for our patients, and sometimes medical therapy can generate additional ones.
In a patient reporting the onset of low desire and dyspareunia, you would want to first consider her medication history, despite the clear evidence of vaginal atrophy. Begin by asking whether she is taking any new medications prescribed by another provider. In some cases, antihypertensive drugs, psychotropic agents, and other medications can affect sexual function.
This patient has been taking Brisdelle for 1 year and is happy with its effect on her sleep and hot flashes. Simon and colleagues found this nonhormonal agent for moderate to severe vasomotor symptoms to produce no notable effects in weight, libido, or sleep, compared with placebo.
Nevertheless, in this case, because selective serotonin reuptake inhibitors (SSRIs) such as paroxetine can affect arousal and orgasm, it is unclear whether the ultra-low dose of paroxetine she is taking is contributing to her problems. If you were to discontinue the drug to find out, her vasomotor symptoms and sleep disruption would likely recur.
Your decision-making is important here and should involve the patient in an extensive discussion. If there is not enough time for this discussion at the current visit, schedule a follow-up to address her issues fully.
Vulvovaginal atrophy has its own timeline
In many cases, vasomotor symptoms such as hot flashes occur years before the skin begins to atrophy in the vulva and vagina, particularly in women who enter menopause naturally. Among menopausal women who continue to have intercourse on a regular basis, however, these skin changes often are much less troublesome than they are for women who have sex more rarely.
In this patient, one possible scenario is that paroxetine caused a slight reduction in sexual interest, and the frequency of intercourse went down as a result. In women who have little or no intercourse, the vagina begins to shrink and the tissues lose elasticity. This patient may have been undergoing the natural process of menopause, and that process may have been compounded by a decrease in the frequency of sex.
If you were to discontinue the paroxetine, it would still be necessary to treat the vulvovaginal skin and work on manual techniques to gently dilate the introitus.
Option 1: Systemic hormone therapy
Systemic estrogen is the most effective treatment for menopausal vasomotor symptoms, reducing hot flashes by 50% to 100% within 4 weeks of initiation. However, because our patient has an intact uterus, any systemic estrogen she opts to use must be opposed by a progestin for safety reasons.
In terms of estrogen, her options are oral or nonoral formulations. Not only would estrogen manage our patient’s hot flashes but, over time, it would improve her sexual problems and atrophy, which might or might not improve her current complaint of low desire. You likely would need to add a short regimen of topical estrogen and perhaps even a dilator to restore her sexual function completely, however.
Since our patient chose the nonhormonal agent Brisdelle to manage her menopausal symptoms, she may be worried about the increased risk of breast cancer associated with use of a progestin in combination with estrogen. One hormonal option now available that eliminates the need for a progestin is conjugated estrogens and bazedoxefine (Duavee). Bazedoxefine is a third-
generation selective estrogen receptor modulator (SERM). This drug has estrogen-like effects on bone and antiestrogen effects on the uterus.
Duavee is indicated for use in women with a uterus for treatment of:
- moderate to severe vasomotor symptoms of menopause
- prevention of postmenopausal osteoporosis.
Among the risks are an increased risk of venous thromboembolism (VTE) and stroke. It is not approved specifically for the treatment of dyspareunia.
Another hormonal option is ospemifene (Osphena), an estrogen agonist/antagonist indicated for the treatment of moderate to severe dyspareunia in menopausal women. Among the drugs in its class, such as tamoxifen and raloxifene, ospemifene is the only agent that maintains a full estrogenic effect on vaginal tissues. Its risks include VTE and stroke.
Although the labeling includes a warning about the risk of endometrial hyperplasia associated with its use, Goldstein and colleagues found no significant difference in the rate of endometrial thickening greater than 5 mm between women taking ospemifene and those taking placebo after 1 year of daily oral treatment. No carcinomas were found in either group.
Option 2: Local estrogen
If our patient declines all systemic hormone therapy, the topical approach should resolve her vulvovaginal symptoms, and she could continue taking Brisdelle for her menopausal symptoms. Vaginal estrogen would address the skin problems, provided the patient applies it correctly. Many women are afraid to use estrogen creams and compensate by applying them only to the vulva, thinking that, by limiting their use to external tissues, they are avoiding any associated risks.
If she opts for the local approach, this patient should be encouraged to use transvaginal estrogen in small doses to increase the elasticity of the vulvovaginal tissue, even though it may require daily use for a week or two to improve her symptoms, after which once- or twice-weekly administration should suffice.
The use of low-dose vaginal cream for a short duration is unlikely to increase her risks in any way.
Local estrogen is available as a tablet, cream, or ring.
Option 3: A nonhormonal approach
If the patient refuses any hormonal agent—even topical estrogen—I would recommend the use of silicone-based lubricants and a dilator and prescribe more frequent penetration to increase elasticity and reduce pain.
Brisdelle could be continued to address her menopausal symptoms.
Don’t overlook behavioral techniques
Before this patient leaves your office with the option of her choice, a bit of counseling is necessary to instruct her about methods of restoring full sexual function.
Pain is a powerful aversive stimulus. This patient clearly states that she has had less frequent intercourse as a result of dyspareunia. It is not unusual for patients to develop a “habit” of avoidance in response to the behavior that causes their pain.
One recommendation is to talk to this patient about putting sex back into her life by encouraging her to increase sexual activity without penetration until she begins to arouse easily again. Arousal produces physiologic effects, increasing the caliber and length of the vagina as well as lubrication. The use of fingers or dilators may help restore caliber.
The patient can be encouraged to engage in snuggling and cuddling to regain those activities without the fear of pain associated with penetration. Follow-up after 2 weeks of this therapy can confirm the restoration of tissue elasticity, and the green light can be given for penetration to begin again. Couples can be encouraged to plan a “honeymoon weekend” and put some fun back into their sex lives so that this phase of healing doesn’t become an onerous task.
CASE RESOLVED After a discussion of her options, the patient chooses to stick with Brisdelle and use behavioral therapy alone to resolve her dyspareunia. At her follow-up visit 2 weeks later, she reports that she has enjoyed the period of pain-free “sex” and feels ready to add penetration into her activities.
You encourage her to continue sexual intercourse on a regular, relatively frequent basis to prevent a recurrence of dyspareunia. She continues to use silicone-based lubricants.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.

Barbara S. Levy, MD
Dr. Levy is Vice President of Health Policy for the American College of Obstetricians and Gynecologists.
The author reports no financial relationships relevant to this article.
Barbara S. Levy, MD
Dr. Levy is Vice President of Health Policy for the American College of Obstetricians and Gynecologists.
The author reports no financial relationships relevant to this article.
Barbara S. Levy, MD
Dr. Levy is Vice President of Health Policy for the American College of Obstetricians and Gynecologists.
The author reports no financial relationships relevant to this article.
Since the last installment of this Update on Sexual Dysfunction, three new drugs have been added to the armamentarium for menopausal symptoms and dyspareunia:
- paroxetine 7.5 mg (Brisdelle)
- conjugated estrogens and bazedoxifene (Duavee)
- ospemifene (Osphena).
In this article, I present a case-based approach to incorporating these drugs into practice and restoring sexual function in the setting of vulvovaginal atrophy and dyspareunia. As is often the case, decision-making requires sifting through multiple layers of information.
How to “tease out” the problem and help the patient regain sexual function
Simon JA, Portman DJ, Kazempour K, Mekonnen H, Bhaskar S, Lippman J. Safety profile of paroxetine 7.5 mg in women with moderate-to-severe vasomotor symptoms. Obstet Gynecol. 2014;123(suppl 1):132S–133S.
Conjugated estrogens/bazedoxifene (Duavee) for menopausal symptoms and prevention of osteoporosis. Med Lett Drugs Ther. 2014;56(1441):33–34.
DeGregorio MW, Zerbe RL, Wurz GT. Ospemifene: a first-in-class, non-hormonal selective estrogen receptor modulator approved for the treatment of dyspareunia associated with vulvar and vaginal atrophy [published online ahead of print August 1, 2014]. Steroids. doi:10.1016/j.steroids.2014.07.012.
Goldstein SR, Archer DF, Simon JA, Constantine G. Endometrial safety of ospemifene and the ability of transvaginal ultrasonography to detect small changes in endometrial thickness. Obstet Gynecol. 2014;123(suppl 1):96S–97S.
CASE: LOW DESIRE AND DISCOMFORT DURING INTERCOURSE
Your 58-year-old patient, G2P2, mentions during her annual visit that she’s not that interested in sex anymore. Her children are grown, she’s been happily married for 28 years, and she enjoys her job and denies any symptoms of depression. She says her relationship with her husband is good and, aside from her low desire, she has no worries about the marriage. Her only medication is paroxetine 7.5 mg/day (Brisdelle) for management of her moderate hot flashes, which she initiated at her last annual visit. She reports improvement in her sleep and menopausal symptoms as a result. She has an intact uterus.
You perform a pelvic exam and find atrophic vulva and vagina with mild erythema, and thinned epithelium. When you ask if she has experienced any discomfort, she reports that she needs to use lubrication for intercourse and that, even with lubrication, she has pain upon penetration and a burning sensation that continues throughout intercourse. She also reports that it seems to take her much longer to achieve arousal than in the past, and she often fails to reach orgasm.
How would you manage this patient?
As always, begin with the history
The transition to menopause creates multiple layers of potential symptoms and problems for our patients, and sometimes medical therapy can generate additional ones.
In a patient reporting the onset of low desire and dyspareunia, you would want to first consider her medication history, despite the clear evidence of vaginal atrophy. Begin by asking whether she is taking any new medications prescribed by another provider. In some cases, antihypertensive drugs, psychotropic agents, and other medications can affect sexual function.
This patient has been taking Brisdelle for 1 year and is happy with its effect on her sleep and hot flashes. Simon and colleagues found this nonhormonal agent for moderate to severe vasomotor symptoms to produce no notable effects in weight, libido, or sleep, compared with placebo.
Nevertheless, in this case, because selective serotonin reuptake inhibitors (SSRIs) such as paroxetine can affect arousal and orgasm, it is unclear whether the ultra-low dose of paroxetine she is taking is contributing to her problems. If you were to discontinue the drug to find out, her vasomotor symptoms and sleep disruption would likely recur.
Your decision-making is important here and should involve the patient in an extensive discussion. If there is not enough time for this discussion at the current visit, schedule a follow-up to address her issues fully.
Vulvovaginal atrophy has its own timeline
In many cases, vasomotor symptoms such as hot flashes occur years before the skin begins to atrophy in the vulva and vagina, particularly in women who enter menopause naturally. Among menopausal women who continue to have intercourse on a regular basis, however, these skin changes often are much less troublesome than they are for women who have sex more rarely.
In this patient, one possible scenario is that paroxetine caused a slight reduction in sexual interest, and the frequency of intercourse went down as a result. In women who have little or no intercourse, the vagina begins to shrink and the tissues lose elasticity. This patient may have been undergoing the natural process of menopause, and that process may have been compounded by a decrease in the frequency of sex.
If you were to discontinue the paroxetine, it would still be necessary to treat the vulvovaginal skin and work on manual techniques to gently dilate the introitus.
Option 1: Systemic hormone therapy
Systemic estrogen is the most effective treatment for menopausal vasomotor symptoms, reducing hot flashes by 50% to 100% within 4 weeks of initiation. However, because our patient has an intact uterus, any systemic estrogen she opts to use must be opposed by a progestin for safety reasons.
In terms of estrogen, her options are oral or nonoral formulations. Not only would estrogen manage our patient’s hot flashes but, over time, it would improve her sexual problems and atrophy, which might or might not improve her current complaint of low desire. You likely would need to add a short regimen of topical estrogen and perhaps even a dilator to restore her sexual function completely, however.
Since our patient chose the nonhormonal agent Brisdelle to manage her menopausal symptoms, she may be worried about the increased risk of breast cancer associated with use of a progestin in combination with estrogen. One hormonal option now available that eliminates the need for a progestin is conjugated estrogens and bazedoxefine (Duavee). Bazedoxefine is a third-
generation selective estrogen receptor modulator (SERM). This drug has estrogen-like effects on bone and antiestrogen effects on the uterus.
Duavee is indicated for use in women with a uterus for treatment of:
- moderate to severe vasomotor symptoms of menopause
- prevention of postmenopausal osteoporosis.
Among the risks are an increased risk of venous thromboembolism (VTE) and stroke. It is not approved specifically for the treatment of dyspareunia.
Another hormonal option is ospemifene (Osphena), an estrogen agonist/antagonist indicated for the treatment of moderate to severe dyspareunia in menopausal women. Among the drugs in its class, such as tamoxifen and raloxifene, ospemifene is the only agent that maintains a full estrogenic effect on vaginal tissues. Its risks include VTE and stroke.
Although the labeling includes a warning about the risk of endometrial hyperplasia associated with its use, Goldstein and colleagues found no significant difference in the rate of endometrial thickening greater than 5 mm between women taking ospemifene and those taking placebo after 1 year of daily oral treatment. No carcinomas were found in either group.
Option 2: Local estrogen
If our patient declines all systemic hormone therapy, the topical approach should resolve her vulvovaginal symptoms, and she could continue taking Brisdelle for her menopausal symptoms. Vaginal estrogen would address the skin problems, provided the patient applies it correctly. Many women are afraid to use estrogen creams and compensate by applying them only to the vulva, thinking that, by limiting their use to external tissues, they are avoiding any associated risks.
If she opts for the local approach, this patient should be encouraged to use transvaginal estrogen in small doses to increase the elasticity of the vulvovaginal tissue, even though it may require daily use for a week or two to improve her symptoms, after which once- or twice-weekly administration should suffice.
The use of low-dose vaginal cream for a short duration is unlikely to increase her risks in any way.
Local estrogen is available as a tablet, cream, or ring.
Option 3: A nonhormonal approach
If the patient refuses any hormonal agent—even topical estrogen—I would recommend the use of silicone-based lubricants and a dilator and prescribe more frequent penetration to increase elasticity and reduce pain.
Brisdelle could be continued to address her menopausal symptoms.
Don’t overlook behavioral techniques
Before this patient leaves your office with the option of her choice, a bit of counseling is necessary to instruct her about methods of restoring full sexual function.
Pain is a powerful aversive stimulus. This patient clearly states that she has had less frequent intercourse as a result of dyspareunia. It is not unusual for patients to develop a “habit” of avoidance in response to the behavior that causes their pain.
One recommendation is to talk to this patient about putting sex back into her life by encouraging her to increase sexual activity without penetration until she begins to arouse easily again. Arousal produces physiologic effects, increasing the caliber and length of the vagina as well as lubrication. The use of fingers or dilators may help restore caliber.
The patient can be encouraged to engage in snuggling and cuddling to regain those activities without the fear of pain associated with penetration. Follow-up after 2 weeks of this therapy can confirm the restoration of tissue elasticity, and the green light can be given for penetration to begin again. Couples can be encouraged to plan a “honeymoon weekend” and put some fun back into their sex lives so that this phase of healing doesn’t become an onerous task.
CASE RESOLVED After a discussion of her options, the patient chooses to stick with Brisdelle and use behavioral therapy alone to resolve her dyspareunia. At her follow-up visit 2 weeks later, she reports that she has enjoyed the period of pain-free “sex” and feels ready to add penetration into her activities.
You encourage her to continue sexual intercourse on a regular, relatively frequent basis to prevent a recurrence of dyspareunia. She continues to use silicone-based lubricants.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Since the last installment of this Update on Sexual Dysfunction, three new drugs have been added to the armamentarium for menopausal symptoms and dyspareunia:
- paroxetine 7.5 mg (Brisdelle)
- conjugated estrogens and bazedoxifene (Duavee)
- ospemifene (Osphena).
In this article, I present a case-based approach to incorporating these drugs into practice and restoring sexual function in the setting of vulvovaginal atrophy and dyspareunia. As is often the case, decision-making requires sifting through multiple layers of information.
How to “tease out” the problem and help the patient regain sexual function
Simon JA, Portman DJ, Kazempour K, Mekonnen H, Bhaskar S, Lippman J. Safety profile of paroxetine 7.5 mg in women with moderate-to-severe vasomotor symptoms. Obstet Gynecol. 2014;123(suppl 1):132S–133S.
Conjugated estrogens/bazedoxifene (Duavee) for menopausal symptoms and prevention of osteoporosis. Med Lett Drugs Ther. 2014;56(1441):33–34.
DeGregorio MW, Zerbe RL, Wurz GT. Ospemifene: a first-in-class, non-hormonal selective estrogen receptor modulator approved for the treatment of dyspareunia associated with vulvar and vaginal atrophy [published online ahead of print August 1, 2014]. Steroids. doi:10.1016/j.steroids.2014.07.012.
Goldstein SR, Archer DF, Simon JA, Constantine G. Endometrial safety of ospemifene and the ability of transvaginal ultrasonography to detect small changes in endometrial thickness. Obstet Gynecol. 2014;123(suppl 1):96S–97S.
CASE: LOW DESIRE AND DISCOMFORT DURING INTERCOURSE
Your 58-year-old patient, G2P2, mentions during her annual visit that she’s not that interested in sex anymore. Her children are grown, she’s been happily married for 28 years, and she enjoys her job and denies any symptoms of depression. She says her relationship with her husband is good and, aside from her low desire, she has no worries about the marriage. Her only medication is paroxetine 7.5 mg/day (Brisdelle) for management of her moderate hot flashes, which she initiated at her last annual visit. She reports improvement in her sleep and menopausal symptoms as a result. She has an intact uterus.
You perform a pelvic exam and find atrophic vulva and vagina with mild erythema, and thinned epithelium. When you ask if she has experienced any discomfort, she reports that she needs to use lubrication for intercourse and that, even with lubrication, she has pain upon penetration and a burning sensation that continues throughout intercourse. She also reports that it seems to take her much longer to achieve arousal than in the past, and she often fails to reach orgasm.
How would you manage this patient?
As always, begin with the history
The transition to menopause creates multiple layers of potential symptoms and problems for our patients, and sometimes medical therapy can generate additional ones.
In a patient reporting the onset of low desire and dyspareunia, you would want to first consider her medication history, despite the clear evidence of vaginal atrophy. Begin by asking whether she is taking any new medications prescribed by another provider. In some cases, antihypertensive drugs, psychotropic agents, and other medications can affect sexual function.
This patient has been taking Brisdelle for 1 year and is happy with its effect on her sleep and hot flashes. Simon and colleagues found this nonhormonal agent for moderate to severe vasomotor symptoms to produce no notable effects in weight, libido, or sleep, compared with placebo.
Nevertheless, in this case, because selective serotonin reuptake inhibitors (SSRIs) such as paroxetine can affect arousal and orgasm, it is unclear whether the ultra-low dose of paroxetine she is taking is contributing to her problems. If you were to discontinue the drug to find out, her vasomotor symptoms and sleep disruption would likely recur.
Your decision-making is important here and should involve the patient in an extensive discussion. If there is not enough time for this discussion at the current visit, schedule a follow-up to address her issues fully.
Vulvovaginal atrophy has its own timeline
In many cases, vasomotor symptoms such as hot flashes occur years before the skin begins to atrophy in the vulva and vagina, particularly in women who enter menopause naturally. Among menopausal women who continue to have intercourse on a regular basis, however, these skin changes often are much less troublesome than they are for women who have sex more rarely.
In this patient, one possible scenario is that paroxetine caused a slight reduction in sexual interest, and the frequency of intercourse went down as a result. In women who have little or no intercourse, the vagina begins to shrink and the tissues lose elasticity. This patient may have been undergoing the natural process of menopause, and that process may have been compounded by a decrease in the frequency of sex.
If you were to discontinue the paroxetine, it would still be necessary to treat the vulvovaginal skin and work on manual techniques to gently dilate the introitus.
Option 1: Systemic hormone therapy
Systemic estrogen is the most effective treatment for menopausal vasomotor symptoms, reducing hot flashes by 50% to 100% within 4 weeks of initiation. However, because our patient has an intact uterus, any systemic estrogen she opts to use must be opposed by a progestin for safety reasons.
In terms of estrogen, her options are oral or nonoral formulations. Not only would estrogen manage our patient’s hot flashes but, over time, it would improve her sexual problems and atrophy, which might or might not improve her current complaint of low desire. You likely would need to add a short regimen of topical estrogen and perhaps even a dilator to restore her sexual function completely, however.
Since our patient chose the nonhormonal agent Brisdelle to manage her menopausal symptoms, she may be worried about the increased risk of breast cancer associated with use of a progestin in combination with estrogen. One hormonal option now available that eliminates the need for a progestin is conjugated estrogens and bazedoxefine (Duavee). Bazedoxefine is a third-
generation selective estrogen receptor modulator (SERM). This drug has estrogen-like effects on bone and antiestrogen effects on the uterus.
Duavee is indicated for use in women with a uterus for treatment of:
- moderate to severe vasomotor symptoms of menopause
- prevention of postmenopausal osteoporosis.
Among the risks are an increased risk of venous thromboembolism (VTE) and stroke. It is not approved specifically for the treatment of dyspareunia.
Another hormonal option is ospemifene (Osphena), an estrogen agonist/antagonist indicated for the treatment of moderate to severe dyspareunia in menopausal women. Among the drugs in its class, such as tamoxifen and raloxifene, ospemifene is the only agent that maintains a full estrogenic effect on vaginal tissues. Its risks include VTE and stroke.
Although the labeling includes a warning about the risk of endometrial hyperplasia associated with its use, Goldstein and colleagues found no significant difference in the rate of endometrial thickening greater than 5 mm between women taking ospemifene and those taking placebo after 1 year of daily oral treatment. No carcinomas were found in either group.
Option 2: Local estrogen
If our patient declines all systemic hormone therapy, the topical approach should resolve her vulvovaginal symptoms, and she could continue taking Brisdelle for her menopausal symptoms. Vaginal estrogen would address the skin problems, provided the patient applies it correctly. Many women are afraid to use estrogen creams and compensate by applying them only to the vulva, thinking that, by limiting their use to external tissues, they are avoiding any associated risks.
If she opts for the local approach, this patient should be encouraged to use transvaginal estrogen in small doses to increase the elasticity of the vulvovaginal tissue, even though it may require daily use for a week or two to improve her symptoms, after which once- or twice-weekly administration should suffice.
The use of low-dose vaginal cream for a short duration is unlikely to increase her risks in any way.
Local estrogen is available as a tablet, cream, or ring.
Option 3: A nonhormonal approach
If the patient refuses any hormonal agent—even topical estrogen—I would recommend the use of silicone-based lubricants and a dilator and prescribe more frequent penetration to increase elasticity and reduce pain.
Brisdelle could be continued to address her menopausal symptoms.
Don’t overlook behavioral techniques
Before this patient leaves your office with the option of her choice, a bit of counseling is necessary to instruct her about methods of restoring full sexual function.
Pain is a powerful aversive stimulus. This patient clearly states that she has had less frequent intercourse as a result of dyspareunia. It is not unusual for patients to develop a “habit” of avoidance in response to the behavior that causes their pain.
One recommendation is to talk to this patient about putting sex back into her life by encouraging her to increase sexual activity without penetration until she begins to arouse easily again. Arousal produces physiologic effects, increasing the caliber and length of the vagina as well as lubrication. The use of fingers or dilators may help restore caliber.
The patient can be encouraged to engage in snuggling and cuddling to regain those activities without the fear of pain associated with penetration. Follow-up after 2 weeks of this therapy can confirm the restoration of tissue elasticity, and the green light can be given for penetration to begin again. Couples can be encouraged to plan a “honeymoon weekend” and put some fun back into their sex lives so that this phase of healing doesn’t become an onerous task.
CASE RESOLVED After a discussion of her options, the patient chooses to stick with Brisdelle and use behavioral therapy alone to resolve her dyspareunia. At her follow-up visit 2 weeks later, she reports that she has enjoyed the period of pain-free “sex” and feels ready to add penetration into her activities.
You encourage her to continue sexual intercourse on a regular, relatively frequent basis to prevent a recurrence of dyspareunia. She continues to use silicone-based lubricants.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Experience Tells in Hip Arthroplasty
For total hip arthroplasty success, is there a magic number for a surgeon to surpass? According to researchers from University of Toronto and Women’s College Hospital, both in Toronto, Canada, that number is 35. The researchers found that patients whose surgeons had performed ≤ 35 such procedures in the year before had a 48% higher risk of dislocation and 44% higher risk of early revision.
The analysis covered 37,881 people who received their first primary total hip arthroplasty during 2002 to 2009 and were followed for ≥ 2 years after surgery. Researchers found that the main outcomes included surgical complications, such as venous thromboembolism, death within 90 days, and infection. Other complications included dislocation, periprosthetic fracture, and revision within 2 years. The procedures were performed by 350 surgeons, with 19 years median experience and a median annual volume of 55 procedures.
As the surgeon’s yearly volume of hip arthroplasty procedures rose, the researchers saw a “noticeable decrease” in likelihood of dislocation and revision, but the relation was not linear. Surgeons with extremely low volumes had predicted rates of dislocation of about 4%, with a drop in likelihood to about 2% at 25 to 50 procedures a year. After that point, the relative improvement in complication rates in relation to volume attenuated, but the trend of decreasing risk continued downward. That trend indicates that increased surgeon volume continues to have a beneficial impact, albeit less pronounced, the researchers conclude.
The effects on thromboembolism, death, infection, and periprosthetic fracture did not show an obvious association between surgeon volume and risk of complication. That conclusion is consistent with the current knowledge about the risk factors for those complications, which have more to do with patient factors, such as gender and frailty, the researchers say.
The researchers also note that their novel method of using a spline to visually describe the relationship between surgeon volume and complications allowed them to select a cut point with “more confidence than in previous studies.” That method, they believe, could be applied easily to other procedures to optimize health care delivery.
Source
Ravi B, Jenkinson R, Austin PC, et al. BMJ. 2014;348:g3284.
doi: 10.1136/bmj.g3284.
For total hip arthroplasty success, is there a magic number for a surgeon to surpass? According to researchers from University of Toronto and Women’s College Hospital, both in Toronto, Canada, that number is 35. The researchers found that patients whose surgeons had performed ≤ 35 such procedures in the year before had a 48% higher risk of dislocation and 44% higher risk of early revision.
The analysis covered 37,881 people who received their first primary total hip arthroplasty during 2002 to 2009 and were followed for ≥ 2 years after surgery. Researchers found that the main outcomes included surgical complications, such as venous thromboembolism, death within 90 days, and infection. Other complications included dislocation, periprosthetic fracture, and revision within 2 years. The procedures were performed by 350 surgeons, with 19 years median experience and a median annual volume of 55 procedures.
As the surgeon’s yearly volume of hip arthroplasty procedures rose, the researchers saw a “noticeable decrease” in likelihood of dislocation and revision, but the relation was not linear. Surgeons with extremely low volumes had predicted rates of dislocation of about 4%, with a drop in likelihood to about 2% at 25 to 50 procedures a year. After that point, the relative improvement in complication rates in relation to volume attenuated, but the trend of decreasing risk continued downward. That trend indicates that increased surgeon volume continues to have a beneficial impact, albeit less pronounced, the researchers conclude.
The effects on thromboembolism, death, infection, and periprosthetic fracture did not show an obvious association between surgeon volume and risk of complication. That conclusion is consistent with the current knowledge about the risk factors for those complications, which have more to do with patient factors, such as gender and frailty, the researchers say.
The researchers also note that their novel method of using a spline to visually describe the relationship between surgeon volume and complications allowed them to select a cut point with “more confidence than in previous studies.” That method, they believe, could be applied easily to other procedures to optimize health care delivery.
Source
Ravi B, Jenkinson R, Austin PC, et al. BMJ. 2014;348:g3284.
doi: 10.1136/bmj.g3284.
For total hip arthroplasty success, is there a magic number for a surgeon to surpass? According to researchers from University of Toronto and Women’s College Hospital, both in Toronto, Canada, that number is 35. The researchers found that patients whose surgeons had performed ≤ 35 such procedures in the year before had a 48% higher risk of dislocation and 44% higher risk of early revision.
The analysis covered 37,881 people who received their first primary total hip arthroplasty during 2002 to 2009 and were followed for ≥ 2 years after surgery. Researchers found that the main outcomes included surgical complications, such as venous thromboembolism, death within 90 days, and infection. Other complications included dislocation, periprosthetic fracture, and revision within 2 years. The procedures were performed by 350 surgeons, with 19 years median experience and a median annual volume of 55 procedures.
As the surgeon’s yearly volume of hip arthroplasty procedures rose, the researchers saw a “noticeable decrease” in likelihood of dislocation and revision, but the relation was not linear. Surgeons with extremely low volumes had predicted rates of dislocation of about 4%, with a drop in likelihood to about 2% at 25 to 50 procedures a year. After that point, the relative improvement in complication rates in relation to volume attenuated, but the trend of decreasing risk continued downward. That trend indicates that increased surgeon volume continues to have a beneficial impact, albeit less pronounced, the researchers conclude.
The effects on thromboembolism, death, infection, and periprosthetic fracture did not show an obvious association between surgeon volume and risk of complication. That conclusion is consistent with the current knowledge about the risk factors for those complications, which have more to do with patient factors, such as gender and frailty, the researchers say.
The researchers also note that their novel method of using a spline to visually describe the relationship between surgeon volume and complications allowed them to select a cut point with “more confidence than in previous studies.” That method, they believe, could be applied easily to other procedures to optimize health care delivery.
Source
Ravi B, Jenkinson R, Austin PC, et al. BMJ. 2014;348:g3284.
doi: 10.1136/bmj.g3284.
Approach to the Limping Child
The child with limp represents a common scenario in the pediatric ED. Evaluation of such patients may be difficult due to vague clinical histories and nonspecific physical examination findings. The differential diagnosis is broad and includes mild self-limited processes (eg, toxic synovitis), as well as potentially limb and life-threatening etiologies (eg, osteomyelitis, malignancy). Careful attention to historical clues and a focused physical examination are often suggestive of a diagnosis, but laboratory and radiographic studies are necessary in most cases.
While trauma is the most common source of limp in children, infectious, inflammatory, and anatomic causes are also frequently encountered. This review focuses on several of the most important etiologies of limp in children: toxic synovitis, septic arthritis, osteomyelitis, Perthes disease, slipped capital femoral epiphysis (SCFE), and Osgood-Schlatter disease.
Case Presentation
Kailey, a 28-month-old girl, was brought to the ED by her parents, who stated that their child “isn’t walking right.” They noted that their daughter’s right leg had been bothering her for about a week, but that the limp had become more noticeable. Aside from a cold a week before presentation, both parents stated that the child has been healthy; they also denied any trauma or systemic symptoms such as rash, weight loss, vomiting, or diarrhea. The mother believed Kailey may have had a low-grade fever earlier in the week. There were no sick contacts at home, but the child did attend daycare.
On examination, Kailey was well-appearing on her mother’s lap. Her vital signs were unremarkable and she was afebrile. She was able to bear weight on the right leg but walked with a slightly antalgic gait, which became more apparent when she was asked to run across the room to her mother. Her right leg was normal appearing on examination with normal reflexes; however, the child appeared to wince when passively ranging her right hip and right knee joint. The emergency physician (EP) was not able to determine any particular areas of point tenderness. The remainder of the examination, including neurological and musculoskeletal examinations, was normal.
Regarding further history, the child’s parents informed the EP that they had taken their daughter to an urgent care clinic earlier in the week. X-rays taken of the girl’s right knee and hip at this visit were both normal; however, the girl’s limp had been getting worse.
Overview
Limp is a common presenting complaint in the pediatric ED, and its evaluation is often challenging as the clinical course of limp in a child varies from benign and self-limited to serious and limb-threatening. However, with careful attention to the history and physical examination, appropriate laboratory evaluation, and focused imaging studies, a diagnosis can be made in most cases and treatment initiated. Of paramount importance for clinicians is to remember that limp in a child nearly always represents an organic disease.1,2
While trauma is the most common cause of limp in children, infectious, inflammatory, and anatomic processes are other potential etiologies. A clue to the diagnosis may also be inferred from the patient’s age, as certain conditions such as fracture, Perthes disease, and transient synovitis are seen in younger children, while SCFE and Osgood-Schlatter are more common in children older than 10 years of age. Other serious conditions such as septic hip or osteomyelitis may be encountered at any age.
Initial Management
A thorough history and physical examination provide the basis for subsequent laboratory and radiographic testing of children presenting with a limp. The duration and localization of symptoms should be elicited; traumatic or infectious causes are more common among those presenting with acute (<2 weeks) complaints. The presence of systemic symptoms (eg, fever, weight loss, chills, rashes, recurrent arthralgias) increases the likelihood of underlying oncologic or rheumatologic process. Examination of the child begins with a full physical examination to uncover other possible etiologic clues such as other involved joints (juvenile idiopathic arthritis), signs of old bruising (nonaccidental trauma), firm lymph nodes (malignancy), abdominal pain (eg, appendicitis, psoas abscess, constipation), or limb-length discrepancy (developmental dysplasia of the hip).
Focused assessment of the limp itself involves watching the child walk or run; different variations of limp may also offer a clue to the diagnosis. An antalgic gait simply refers to one in which the affected leg spends less time in the weight-bearing stage, and it is most commonly seen with infection and trauma. Trendelenburg gait, frequently seen with SCFE and Perthes disease, is characterized by a downward tilt of the pelvis away from the affected side while the affected leg is bearing weight.
In many cases, it may be difficult to accurately characterize a limp due to a patient’s pain or lack of compliance. Evaluation of any limp should also focus on the joint above and below the child’s apparent main source of pain. This is particularly true of knee complaints as referred pain from the hip may often present as isolated thigh or knee pain. Areas of point tenderness, erythema, joint effusion, and warmth strongly point to an infectious source but are frequently absent early in disease presentation. While swelling and severe pain with passive movement of a joint indicate septic arthritis, limitation of joint movement at the hip can be seen with SCFE and Perthes disease.
Laboratory Studies
In most children presenting with limp, extensive laboratory testing is not needed for the diagnosis but is helpful when infectious, oncologic, and rheumatologic causes are considered. Inflammatory markers such as the erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) are elevated in most acute infectious processes. A complete blood count (CBC) should also be obtained in cases of suspected infection to evaluate the white blood cell count (WBC). Due to the high prevalence of joint infections and postinfectious processes caused by group A streptococcus (GAS), an antistreptolysin titer (ASO), throat culture, and rapid streptococcal antigen swab should be considered. If infection is suspected and a joint effusion is present, cell counts, gram stain, and culture from the synovial fluid should be sent to assist with diagnosis and antibiotic management. If a child appears septic, a blood culture should be obtained as well. With suspected osteomyelitis, cultures of the bone should be taken in the operating room in addition to a peripheral blood culture. Ideally, antibiotics should be withheld until cultures are sent unless the child appears acutely ill.
Diagnostic Imaging

Toxic Synovitis and Septic Arthritis
Clinicians may have difficulty differentiating between toxic synovitis (also known as transient synovitis) and septic arthritis of the hip in pediatric patients. In both toxic synovitis and septic arthritis, the child is unable to bear weight on the affected side, and ultrasound may demonstrate effusion.3,4
Toxic synovitis is thought to be a viral or postviral phenomenon, though the exact agent responsible for initiating the inflammatory cascade is not known. It has a relatively benign course and generally responds over 3 to 10 days to rest and nonsteroidal anti-inflammatory drugs (NSAIDs).5,6
Septic arthritis, however, is a serious infection with the capacity to cause permanent joint damage as well as spread into the blood or bone. Staphylococcal and streptococcal bacteria, including GAS and methicillin-resistant staphylococcus aureus (MRSA) are the most common causes of septic arthritis in the pediatric population.7 However, Kingella kingae, a gram-negative organism, is an increasingly recognized cause of septic arthritis in children younger than 3 years of age. Commonly found in the posterior pharynx, Kingella is very difficult to culture but may be detected by polymerase chain reaction (PCR) assays.8 The spectrum of GAS-related joint infections ranges from a postinfectious type that may be indistinguishable from toxic synovitis (but with evidence of recent GAS pharyngitis) to typical bacterial septic arthritis.9
Multiple clinical prediction rules and algorithms have been developed to assist with the management of these cases. The Kocher criteria, which include history of fever >101.3˚F, nonweight-bearing status, ESR >40 mm/hour, and WBC >12,000 cells/mm3 were found to be independent clinical predictors for the differentiation between transient arthritis and septic arthritis. Children with none of the risk factors had a 0.2% chance of septic arthritis while those with two risk factors had a 40% chance of septic arthritis. Subsequent validation studies among pediatric populations with a lower prevalence of septic arthritis found the positive predictive values to be lower; nevertheless, the Kocher criteria remain useful in guiding management.3,4
If a diagnosis of septic arthritis remains a consideration after the history, physical examination, and plain radiography, laboratory studies should be obtained, including a CBC, ESR, CRP, blood culture, rapid streptococcal assay, throat culture, and ASO titer. An ultrasound should also be performed to assess for the presence of a hip effusion.
Elevated inflammatory markers (ESR >40 mm/hour, CRP >20 mg/L, WBC >12,000 cells/mm3) and an effusion should prompt orthopedic consultation and arthrocentesis for synovial fluid-cell counts, gram stain, and culture. Synovial fluid WBC counts >50,000 cells/mm3 or a positive gram stain or culture is diagnostic of septic arthritis and requires treatment with intravenous (IV) antibiotics and likely operative intervention. The absence of an effusion on ultrasound, synovial fluid WBC counts <50,000 cells/mm3, and inflammatory markers that are not significantly elevated indicate an alternative diagnosis such as toxic synovitis. However, there may be cases in which the diagnosis is not clear due to ambiguous laboratory values from the blood or synovial fluid; in these cases the decision to proceed with IV antibiotics must be made in consultation with an orthopedist.10
Empiric antibiotic therapy in patients with septic arthritis should take into account the prevalence of MRSA in the community. Clindamycin is a popular choice due to its high oral bioavailability, which facilitates transition to a home regimen. Vancomycin is another option and can be reserved for more severely ill children. Empiric coverage for suspected septic arthritis in children younger than 3 years of age should also include an anti-gram negative agent, such as a cephalosporin, to treat Kingella.7
Osteomyelitis
Acute osteomyelitis is a common cause of limp among children and is usually caused by the hematogenous spread of bacteria. Staphylococcus aureus, including MRSA, is responsible for up to 90% of cases of osteomyelitis, though recent studies have identified Kingella as an etiologic agent among children younger age 3 years.7 The highly vascular metaphysis of the tibia and femur in children can become infected during times of otherwise asymptomatic bacteremia in healthy patients.8 Among younger children with less well-developed anatomic separation between the bone and joint space, it is possible for infection to spread into the joint space. Younger children with osteomyelitis may present with poorly localized pain with or without systemic symptoms; older children and those with more advanced disease may describe point tenderness on the bone. In many cases it may be difficult clinically to distinguish osteomyelitis from septic arthritis; excessive pain with passive range of motion of the joint is more indicative of septic arthritis.

Ideally, antibiotic therapy should be deferred until cultures from the site of infection are obtained operatively or via aspiration. The local staphylococcus aureus resistance pattern should guide empiric antibiotic therapy. With the rise of MRSA, clindamycin has become first-line therapy with vancomycin as an alternative for severely-ill or clindamycin-allergic patients. For children younger than 3 years of age with a more subacute presentation, the possibility of Kingella infection should be considered and treated with a cephalosporin. Some children with osteomyelitis will require operative debridement, though
many can be treated with antibiotics alone. The standard duration of antibiotic treatment is 4 to 6 weeks, with transition to an oral regimen once the patient is afebrile with downtrending inflammatory markers.7,8,11
Perthes Disease
Perthes disease (also called Legg-Calve-Perthes disease) is an idiopathic process that involves avascular necrosis and revascularization of the blood supply of the femoral head. The condition is most common in children ages 3 to 12 years and has a 4:1 male to female predominance. The remodeling takes place over the course of 2 to 4 years. During this process, the epiphysis of the femoral head is weakened and undergoes irreversible deformation that, if uncorrected, will persist throughout life. Severe degenerative arthritis may result and ultimately require hip replacement.12
Perthes disease typically presents as a subacute limp, sometimes with referred pain to the groin, thigh, or knee of the affected side. Range of motion of the hip may be limited, particularly in abduction and internal rotation. Plain films demonstrate necrotic avascular areas of the distal femoral head during active disease; after the remodeling process is complete, the femoral head often shows residual deformities. Magnetic resonance imaging is useful in cases in which plain film findings are subtle, particularly early in the course of the disease.12,13
Management of Perthes disease depends on the age of the child and clinical factors such as radiographic progression and range of motion of the hip. The goal of therapy is to limit damage to the femoral head during the revascularization process. In children younger than 5 years of age, nonsurgical management with an abduction splint to keep the femoral head contained and protected within the acetabulum may be used. Surgical osteotomies are used in older and more severely affected children to artificially contain the femoral head during the healing process.13
Slipped Capital Femoral Epiphysis
A common cause of limp among older children, the average age of presentation for SCFE is 13.5 years for boys and 12 years for girls. This condition occurs when the proximal femoral epiphysis slides posteriorly and inferiorly relative to the metaphysis. Epidemiological studies have established a connection between SCFE and obesity. Although the precise pathogenesis remains unknown, it is hypothesized that increased mechanical forces during a time of rapid pubertal growth lead to weakness at the physis. Among children who develop SCFE outside of the usual age distribution, endocrinopathies such as hypothyroidism, hypogonadism, and panhypopituitarism are often discovered.14
As with Perthes disease, SCFE may present as a chronic, subacute, or acute limp with referred pain to the groin, thigh, or knee. The patient with SCFE often has severe pain with internal rotation of the affected hip and will hold the hip in obligatory external rotation if it is flexed. Patients unable to bear weight on the affected side have unstable SCFE.
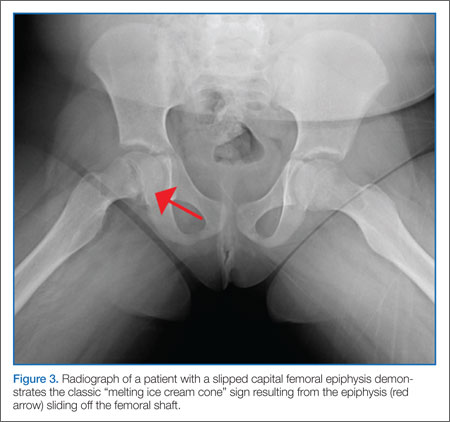
All patients with SCFE should be made nonweight bearing on the affected hip to prevent further slippage of the epiphysis. Definitive treatment involves in-situ fixation of the femoral neck with the proximal femoral epiphysis. Close orthopedic follow up is essential as roughly 50% of children with unilateral SCFE will go on to develop SCFE in the contralateral hip. Long-term complications of SCFE include osteonecrosis, joint space narrowing, and osteoarthritis.14,15
Osgood-Schlatter Disease
Osgood-Schlatter disease is a relatively benign cause of limp that is thought to occur due to repetitive trauma to the secondary ossification center tibial tubercle. Over time, the strong pull of the quadriceps muscle group on the patellar tendon causes a chronic avulsion at the site of the patellar tendon insertion on the tibial tuberosity. It most commonly develops in early puberty from ages 9 to 14 years. Affected children develop tenderness over the tibial tuberosity that is made worse with activity. On examination, pain can be elicited by having the child extend the knee against resistance or kneel. Lateral radiographs of the knee may be normal or demonstrate swelling, irregularity, or elevation of the tibial tubercle. Treatment consists of NSAIDs, ice, and physical therapy; activity restriction is generally unnecessary. Most cases resolve over 6 to 18 months as the growth plate at the secondary ossification center ossifies.16
Case Conclusion
Initial examination confirmed the presence of a limp; the differential in this age group includes toxic synovitis, septic arthritis, and osteomyelitis. Although Kailey appeared relatively well on examination, her history of recent fever and the worsening symptoms over the past week were concerning. The workup began with plain films of the pelvis and the right knee because of the possibility of referred pain and the lack of localizing signs on examination. In addition, laboratory evaluation was performed, including CBC, CRP, and ESR. Due to her young age, a rapid streptococcal assay, throat culture, or an ASO titer was not necessary.
Plain films of the pelvis and the right knee were normal. The patient’s WBC was unremarkable, but her ESR was 50 mm/hour and CRP was 25 mg/L. Given these elevated inflammatory markers, ultrasound of the right hip was ordered, which revealed a small effusion. An orthopedic specialist was consulted, who performed a sedated joint aspiration. Cell counts from the joint aspirate were sent for evaluation, as well as culture, gram stain, and a PCR for Kingella.
After joint aspiration, Kailey was admitted to the hospital overnight and was started on empiric treatment with IV clindamycin and ceftriaxone. The synovial fluid gram stain was negative, but the WBC was 65,000 cells/mm3. Over the next several days, her inflammatory markers trended downward, she remained afebrile, and her gait slowly improved. The synovial fluid culture remained negative, but the PCR was positive for Kingella. Kailey was discharged on hospital day 3 with a 21-day course of oral cephalexin.
Dr Kane is a fellow in the department of pediatrics, division of pediatric emergency medicine, Vanderbilt Children’s Hospital, Nashville, Tennessee. Dr McMorrow is an assistant professor of emergency medicine and assistant professor of pediatrics, department of pediatrics, division of pediatric emergency medicine, Vanderbilt Children’s Hospital, Nashville, Tennessee.
- Smith E, Anderson M, Foster H. The child with a limp: a symptom and not a diagnosis. Arch Dis Child Educ Pract Ed. 2012;97(5):185-193.
- Leung AK, Lemay JF. The limping child. J Pediatr Health Care. 2004;18(5):219-223.
- Taekema HC, Landham PR, Maconochie I. Towards evidence based medicine for paediatricians. Distinguishing between transient synovitis and septic arthritis in the limping child: how useful are clinical prediction tools? Arch Dis Child. 2009;94(2):167,168.
- Luhmann SJ, Jones A, Schootman M, Gordon JE, Schoenecker PL, Luhmann JD. Differentiation between septic arthritis and transient synovitis of the hip in children with clinical prediction algorithms. J Bone Joint Surg Am. 2004;86-A(5):956-962.
- Do TT. Transient synovitis as a cause of painful limps in children. Curr Opin Pediatr. 2000;12(1):48-51.
- Nouri A, Walmsley D, Pruszczynski B, Synder M. Transient synovitis of the hip: a comprehensive review. J Pediatr Orthop B. 2014;23(1):32-36.
- Thomsen I, Creech CB. Advances in the diagnosis and management of pediatric osteomyelitis. Curr Infect Dis Rep. 2011;13(5):451-460.
- Dodwell ER. Osteomyelitis and septic arthritis in children: current concepts. Curr Opin Pediatr. 2013;25(1):58-63.
- Mignemi ME, Martus JE, Bracikowski AC, Lovejoy SA, Mencio GA, Schoenecker JG. The spectrum of group A streptococcal joint pathology in the acute care setting. Pediatr Emerg Care. 2012;28(11):
1185-1189. - Rutz E, Spoerri M. Septic arthritis of the paediatric hip - A review of current diagnostic approaches and therapeutic concepts. Acta Orthop Belg. 2013;79(2):123-134.
- Harik NS, Smeltzer MS. Management of acute hematogenous osteomyelitis in children. Expert Rev Anti Infect Ther. 2010;8(2):175-181.
- Shah H. Perthes disease: evaluation and management. Orthop Clin North Am. 2014;45(1):87-97.
- Nelitz M, Lippacher S, Krauspe R, Reichel H. Perthes disease: current principles of diagnosis
and treatment. Dtsch Arztebl Int. 2009;106(31-32):517-523. - Novais EN, Millis MB. Slipped capital femoral epiphysis: prevalence, pathogenesis, and natural history. Clin Orthop Relat Res. 2012;470(12):3432-3438.
- Peck D. Slipped capital femoral epiphysis: diagnosis and management. Am Fam Physician. 2010;82(3):258-262.
- Gholve PA, Scher DM, Khakharia S, Widmann RF, Green DW. Osgood Schlatter syndrome. Curr Opin Pediatr. 2007;19(1):44-50.
The child with limp represents a common scenario in the pediatric ED. Evaluation of such patients may be difficult due to vague clinical histories and nonspecific physical examination findings. The differential diagnosis is broad and includes mild self-limited processes (eg, toxic synovitis), as well as potentially limb and life-threatening etiologies (eg, osteomyelitis, malignancy). Careful attention to historical clues and a focused physical examination are often suggestive of a diagnosis, but laboratory and radiographic studies are necessary in most cases.
While trauma is the most common source of limp in children, infectious, inflammatory, and anatomic causes are also frequently encountered. This review focuses on several of the most important etiologies of limp in children: toxic synovitis, septic arthritis, osteomyelitis, Perthes disease, slipped capital femoral epiphysis (SCFE), and Osgood-Schlatter disease.
Case Presentation
Kailey, a 28-month-old girl, was brought to the ED by her parents, who stated that their child “isn’t walking right.” They noted that their daughter’s right leg had been bothering her for about a week, but that the limp had become more noticeable. Aside from a cold a week before presentation, both parents stated that the child has been healthy; they also denied any trauma or systemic symptoms such as rash, weight loss, vomiting, or diarrhea. The mother believed Kailey may have had a low-grade fever earlier in the week. There were no sick contacts at home, but the child did attend daycare.
On examination, Kailey was well-appearing on her mother’s lap. Her vital signs were unremarkable and she was afebrile. She was able to bear weight on the right leg but walked with a slightly antalgic gait, which became more apparent when she was asked to run across the room to her mother. Her right leg was normal appearing on examination with normal reflexes; however, the child appeared to wince when passively ranging her right hip and right knee joint. The emergency physician (EP) was not able to determine any particular areas of point tenderness. The remainder of the examination, including neurological and musculoskeletal examinations, was normal.
Regarding further history, the child’s parents informed the EP that they had taken their daughter to an urgent care clinic earlier in the week. X-rays taken of the girl’s right knee and hip at this visit were both normal; however, the girl’s limp had been getting worse.
Overview
Limp is a common presenting complaint in the pediatric ED, and its evaluation is often challenging as the clinical course of limp in a child varies from benign and self-limited to serious and limb-threatening. However, with careful attention to the history and physical examination, appropriate laboratory evaluation, and focused imaging studies, a diagnosis can be made in most cases and treatment initiated. Of paramount importance for clinicians is to remember that limp in a child nearly always represents an organic disease.1,2
While trauma is the most common cause of limp in children, infectious, inflammatory, and anatomic processes are other potential etiologies. A clue to the diagnosis may also be inferred from the patient’s age, as certain conditions such as fracture, Perthes disease, and transient synovitis are seen in younger children, while SCFE and Osgood-Schlatter are more common in children older than 10 years of age. Other serious conditions such as septic hip or osteomyelitis may be encountered at any age.
Initial Management
A thorough history and physical examination provide the basis for subsequent laboratory and radiographic testing of children presenting with a limp. The duration and localization of symptoms should be elicited; traumatic or infectious causes are more common among those presenting with acute (<2 weeks) complaints. The presence of systemic symptoms (eg, fever, weight loss, chills, rashes, recurrent arthralgias) increases the likelihood of underlying oncologic or rheumatologic process. Examination of the child begins with a full physical examination to uncover other possible etiologic clues such as other involved joints (juvenile idiopathic arthritis), signs of old bruising (nonaccidental trauma), firm lymph nodes (malignancy), abdominal pain (eg, appendicitis, psoas abscess, constipation), or limb-length discrepancy (developmental dysplasia of the hip).
Focused assessment of the limp itself involves watching the child walk or run; different variations of limp may also offer a clue to the diagnosis. An antalgic gait simply refers to one in which the affected leg spends less time in the weight-bearing stage, and it is most commonly seen with infection and trauma. Trendelenburg gait, frequently seen with SCFE and Perthes disease, is characterized by a downward tilt of the pelvis away from the affected side while the affected leg is bearing weight.
In many cases, it may be difficult to accurately characterize a limp due to a patient’s pain or lack of compliance. Evaluation of any limp should also focus on the joint above and below the child’s apparent main source of pain. This is particularly true of knee complaints as referred pain from the hip may often present as isolated thigh or knee pain. Areas of point tenderness, erythema, joint effusion, and warmth strongly point to an infectious source but are frequently absent early in disease presentation. While swelling and severe pain with passive movement of a joint indicate septic arthritis, limitation of joint movement at the hip can be seen with SCFE and Perthes disease.
Laboratory Studies
In most children presenting with limp, extensive laboratory testing is not needed for the diagnosis but is helpful when infectious, oncologic, and rheumatologic causes are considered. Inflammatory markers such as the erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) are elevated in most acute infectious processes. A complete blood count (CBC) should also be obtained in cases of suspected infection to evaluate the white blood cell count (WBC). Due to the high prevalence of joint infections and postinfectious processes caused by group A streptococcus (GAS), an antistreptolysin titer (ASO), throat culture, and rapid streptococcal antigen swab should be considered. If infection is suspected and a joint effusion is present, cell counts, gram stain, and culture from the synovial fluid should be sent to assist with diagnosis and antibiotic management. If a child appears septic, a blood culture should be obtained as well. With suspected osteomyelitis, cultures of the bone should be taken in the operating room in addition to a peripheral blood culture. Ideally, antibiotics should be withheld until cultures are sent unless the child appears acutely ill.
Diagnostic Imaging
Toxic Synovitis and Septic Arthritis
Clinicians may have difficulty differentiating between toxic synovitis (also known as transient synovitis) and septic arthritis of the hip in pediatric patients. In both toxic synovitis and septic arthritis, the child is unable to bear weight on the affected side, and ultrasound may demonstrate effusion.3,4
Toxic synovitis is thought to be a viral or postviral phenomenon, though the exact agent responsible for initiating the inflammatory cascade is not known. It has a relatively benign course and generally responds over 3 to 10 days to rest and nonsteroidal anti-inflammatory drugs (NSAIDs).5,6
Septic arthritis, however, is a serious infection with the capacity to cause permanent joint damage as well as spread into the blood or bone. Staphylococcal and streptococcal bacteria, including GAS and methicillin-resistant staphylococcus aureus (MRSA) are the most common causes of septic arthritis in the pediatric population.7 However, Kingella kingae, a gram-negative organism, is an increasingly recognized cause of septic arthritis in children younger than 3 years of age. Commonly found in the posterior pharynx, Kingella is very difficult to culture but may be detected by polymerase chain reaction (PCR) assays.8 The spectrum of GAS-related joint infections ranges from a postinfectious type that may be indistinguishable from toxic synovitis (but with evidence of recent GAS pharyngitis) to typical bacterial septic arthritis.9
Multiple clinical prediction rules and algorithms have been developed to assist with the management of these cases. The Kocher criteria, which include history of fever >101.3˚F, nonweight-bearing status, ESR >40 mm/hour, and WBC >12,000 cells/mm3 were found to be independent clinical predictors for the differentiation between transient arthritis and septic arthritis. Children with none of the risk factors had a 0.2% chance of septic arthritis while those with two risk factors had a 40% chance of septic arthritis. Subsequent validation studies among pediatric populations with a lower prevalence of septic arthritis found the positive predictive values to be lower; nevertheless, the Kocher criteria remain useful in guiding management.3,4
If a diagnosis of septic arthritis remains a consideration after the history, physical examination, and plain radiography, laboratory studies should be obtained, including a CBC, ESR, CRP, blood culture, rapid streptococcal assay, throat culture, and ASO titer. An ultrasound should also be performed to assess for the presence of a hip effusion.
Elevated inflammatory markers (ESR >40 mm/hour, CRP >20 mg/L, WBC >12,000 cells/mm3) and an effusion should prompt orthopedic consultation and arthrocentesis for synovial fluid-cell counts, gram stain, and culture. Synovial fluid WBC counts >50,000 cells/mm3 or a positive gram stain or culture is diagnostic of septic arthritis and requires treatment with intravenous (IV) antibiotics and likely operative intervention. The absence of an effusion on ultrasound, synovial fluid WBC counts <50,000 cells/mm3, and inflammatory markers that are not significantly elevated indicate an alternative diagnosis such as toxic synovitis. However, there may be cases in which the diagnosis is not clear due to ambiguous laboratory values from the blood or synovial fluid; in these cases the decision to proceed with IV antibiotics must be made in consultation with an orthopedist.10
Empiric antibiotic therapy in patients with septic arthritis should take into account the prevalence of MRSA in the community. Clindamycin is a popular choice due to its high oral bioavailability, which facilitates transition to a home regimen. Vancomycin is another option and can be reserved for more severely ill children. Empiric coverage for suspected septic arthritis in children younger than 3 years of age should also include an anti-gram negative agent, such as a cephalosporin, to treat Kingella.7
Osteomyelitis
Acute osteomyelitis is a common cause of limp among children and is usually caused by the hematogenous spread of bacteria. Staphylococcus aureus, including MRSA, is responsible for up to 90% of cases of osteomyelitis, though recent studies have identified Kingella as an etiologic agent among children younger age 3 years.7 The highly vascular metaphysis of the tibia and femur in children can become infected during times of otherwise asymptomatic bacteremia in healthy patients.8 Among younger children with less well-developed anatomic separation between the bone and joint space, it is possible for infection to spread into the joint space. Younger children with osteomyelitis may present with poorly localized pain with or without systemic symptoms; older children and those with more advanced disease may describe point tenderness on the bone. In many cases it may be difficult clinically to distinguish osteomyelitis from septic arthritis; excessive pain with passive range of motion of the joint is more indicative of septic arthritis.
Ideally, antibiotic therapy should be deferred until cultures from the site of infection are obtained operatively or via aspiration. The local staphylococcus aureus resistance pattern should guide empiric antibiotic therapy. With the rise of MRSA, clindamycin has become first-line therapy with vancomycin as an alternative for severely-ill or clindamycin-allergic patients. For children younger than 3 years of age with a more subacute presentation, the possibility of Kingella infection should be considered and treated with a cephalosporin. Some children with osteomyelitis will require operative debridement, though
many can be treated with antibiotics alone. The standard duration of antibiotic treatment is 4 to 6 weeks, with transition to an oral regimen once the patient is afebrile with downtrending inflammatory markers.7,8,11
Perthes Disease
Perthes disease (also called Legg-Calve-Perthes disease) is an idiopathic process that involves avascular necrosis and revascularization of the blood supply of the femoral head. The condition is most common in children ages 3 to 12 years and has a 4:1 male to female predominance. The remodeling takes place over the course of 2 to 4 years. During this process, the epiphysis of the femoral head is weakened and undergoes irreversible deformation that, if uncorrected, will persist throughout life. Severe degenerative arthritis may result and ultimately require hip replacement.12
Perthes disease typically presents as a subacute limp, sometimes with referred pain to the groin, thigh, or knee of the affected side. Range of motion of the hip may be limited, particularly in abduction and internal rotation. Plain films demonstrate necrotic avascular areas of the distal femoral head during active disease; after the remodeling process is complete, the femoral head often shows residual deformities. Magnetic resonance imaging is useful in cases in which plain film findings are subtle, particularly early in the course of the disease.12,13
Management of Perthes disease depends on the age of the child and clinical factors such as radiographic progression and range of motion of the hip. The goal of therapy is to limit damage to the femoral head during the revascularization process. In children younger than 5 years of age, nonsurgical management with an abduction splint to keep the femoral head contained and protected within the acetabulum may be used. Surgical osteotomies are used in older and more severely affected children to artificially contain the femoral head during the healing process.13
Slipped Capital Femoral Epiphysis
A common cause of limp among older children, the average age of presentation for SCFE is 13.5 years for boys and 12 years for girls. This condition occurs when the proximal femoral epiphysis slides posteriorly and inferiorly relative to the metaphysis. Epidemiological studies have established a connection between SCFE and obesity. Although the precise pathogenesis remains unknown, it is hypothesized that increased mechanical forces during a time of rapid pubertal growth lead to weakness at the physis. Among children who develop SCFE outside of the usual age distribution, endocrinopathies such as hypothyroidism, hypogonadism, and panhypopituitarism are often discovered.14
As with Perthes disease, SCFE may present as a chronic, subacute, or acute limp with referred pain to the groin, thigh, or knee. The patient with SCFE often has severe pain with internal rotation of the affected hip and will hold the hip in obligatory external rotation if it is flexed. Patients unable to bear weight on the affected side have unstable SCFE.
All patients with SCFE should be made nonweight bearing on the affected hip to prevent further slippage of the epiphysis. Definitive treatment involves in-situ fixation of the femoral neck with the proximal femoral epiphysis. Close orthopedic follow up is essential as roughly 50% of children with unilateral SCFE will go on to develop SCFE in the contralateral hip. Long-term complications of SCFE include osteonecrosis, joint space narrowing, and osteoarthritis.14,15
Osgood-Schlatter Disease
Osgood-Schlatter disease is a relatively benign cause of limp that is thought to occur due to repetitive trauma to the secondary ossification center tibial tubercle. Over time, the strong pull of the quadriceps muscle group on the patellar tendon causes a chronic avulsion at the site of the patellar tendon insertion on the tibial tuberosity. It most commonly develops in early puberty from ages 9 to 14 years. Affected children develop tenderness over the tibial tuberosity that is made worse with activity. On examination, pain can be elicited by having the child extend the knee against resistance or kneel. Lateral radiographs of the knee may be normal or demonstrate swelling, irregularity, or elevation of the tibial tubercle. Treatment consists of NSAIDs, ice, and physical therapy; activity restriction is generally unnecessary. Most cases resolve over 6 to 18 months as the growth plate at the secondary ossification center ossifies.16
Case Conclusion
Initial examination confirmed the presence of a limp; the differential in this age group includes toxic synovitis, septic arthritis, and osteomyelitis. Although Kailey appeared relatively well on examination, her history of recent fever and the worsening symptoms over the past week were concerning. The workup began with plain films of the pelvis and the right knee because of the possibility of referred pain and the lack of localizing signs on examination. In addition, laboratory evaluation was performed, including CBC, CRP, and ESR. Due to her young age, a rapid streptococcal assay, throat culture, or an ASO titer was not necessary.
Plain films of the pelvis and the right knee were normal. The patient’s WBC was unremarkable, but her ESR was 50 mm/hour and CRP was 25 mg/L. Given these elevated inflammatory markers, ultrasound of the right hip was ordered, which revealed a small effusion. An orthopedic specialist was consulted, who performed a sedated joint aspiration. Cell counts from the joint aspirate were sent for evaluation, as well as culture, gram stain, and a PCR for Kingella.
After joint aspiration, Kailey was admitted to the hospital overnight and was started on empiric treatment with IV clindamycin and ceftriaxone. The synovial fluid gram stain was negative, but the WBC was 65,000 cells/mm3. Over the next several days, her inflammatory markers trended downward, she remained afebrile, and her gait slowly improved. The synovial fluid culture remained negative, but the PCR was positive for Kingella. Kailey was discharged on hospital day 3 with a 21-day course of oral cephalexin.
Dr Kane is a fellow in the department of pediatrics, division of pediatric emergency medicine, Vanderbilt Children’s Hospital, Nashville, Tennessee. Dr McMorrow is an assistant professor of emergency medicine and assistant professor of pediatrics, department of pediatrics, division of pediatric emergency medicine, Vanderbilt Children’s Hospital, Nashville, Tennessee.
The child with limp represents a common scenario in the pediatric ED. Evaluation of such patients may be difficult due to vague clinical histories and nonspecific physical examination findings. The differential diagnosis is broad and includes mild self-limited processes (eg, toxic synovitis), as well as potentially limb and life-threatening etiologies (eg, osteomyelitis, malignancy). Careful attention to historical clues and a focused physical examination are often suggestive of a diagnosis, but laboratory and radiographic studies are necessary in most cases.
While trauma is the most common source of limp in children, infectious, inflammatory, and anatomic causes are also frequently encountered. This review focuses on several of the most important etiologies of limp in children: toxic synovitis, septic arthritis, osteomyelitis, Perthes disease, slipped capital femoral epiphysis (SCFE), and Osgood-Schlatter disease.
Case Presentation
Kailey, a 28-month-old girl, was brought to the ED by her parents, who stated that their child “isn’t walking right.” They noted that their daughter’s right leg had been bothering her for about a week, but that the limp had become more noticeable. Aside from a cold a week before presentation, both parents stated that the child has been healthy; they also denied any trauma or systemic symptoms such as rash, weight loss, vomiting, or diarrhea. The mother believed Kailey may have had a low-grade fever earlier in the week. There were no sick contacts at home, but the child did attend daycare.
On examination, Kailey was well-appearing on her mother’s lap. Her vital signs were unremarkable and she was afebrile. She was able to bear weight on the right leg but walked with a slightly antalgic gait, which became more apparent when she was asked to run across the room to her mother. Her right leg was normal appearing on examination with normal reflexes; however, the child appeared to wince when passively ranging her right hip and right knee joint. The emergency physician (EP) was not able to determine any particular areas of point tenderness. The remainder of the examination, including neurological and musculoskeletal examinations, was normal.
Regarding further history, the child’s parents informed the EP that they had taken their daughter to an urgent care clinic earlier in the week. X-rays taken of the girl’s right knee and hip at this visit were both normal; however, the girl’s limp had been getting worse.
Overview
Limp is a common presenting complaint in the pediatric ED, and its evaluation is often challenging as the clinical course of limp in a child varies from benign and self-limited to serious and limb-threatening. However, with careful attention to the history and physical examination, appropriate laboratory evaluation, and focused imaging studies, a diagnosis can be made in most cases and treatment initiated. Of paramount importance for clinicians is to remember that limp in a child nearly always represents an organic disease.1,2
While trauma is the most common cause of limp in children, infectious, inflammatory, and anatomic processes are other potential etiologies. A clue to the diagnosis may also be inferred from the patient’s age, as certain conditions such as fracture, Perthes disease, and transient synovitis are seen in younger children, while SCFE and Osgood-Schlatter are more common in children older than 10 years of age. Other serious conditions such as septic hip or osteomyelitis may be encountered at any age.
Initial Management
A thorough history and physical examination provide the basis for subsequent laboratory and radiographic testing of children presenting with a limp. The duration and localization of symptoms should be elicited; traumatic or infectious causes are more common among those presenting with acute (<2 weeks) complaints. The presence of systemic symptoms (eg, fever, weight loss, chills, rashes, recurrent arthralgias) increases the likelihood of underlying oncologic or rheumatologic process. Examination of the child begins with a full physical examination to uncover other possible etiologic clues such as other involved joints (juvenile idiopathic arthritis), signs of old bruising (nonaccidental trauma), firm lymph nodes (malignancy), abdominal pain (eg, appendicitis, psoas abscess, constipation), or limb-length discrepancy (developmental dysplasia of the hip).
Focused assessment of the limp itself involves watching the child walk or run; different variations of limp may also offer a clue to the diagnosis. An antalgic gait simply refers to one in which the affected leg spends less time in the weight-bearing stage, and it is most commonly seen with infection and trauma. Trendelenburg gait, frequently seen with SCFE and Perthes disease, is characterized by a downward tilt of the pelvis away from the affected side while the affected leg is bearing weight.
In many cases, it may be difficult to accurately characterize a limp due to a patient’s pain or lack of compliance. Evaluation of any limp should also focus on the joint above and below the child’s apparent main source of pain. This is particularly true of knee complaints as referred pain from the hip may often present as isolated thigh or knee pain. Areas of point tenderness, erythema, joint effusion, and warmth strongly point to an infectious source but are frequently absent early in disease presentation. While swelling and severe pain with passive movement of a joint indicate septic arthritis, limitation of joint movement at the hip can be seen with SCFE and Perthes disease.
Laboratory Studies
In most children presenting with limp, extensive laboratory testing is not needed for the diagnosis but is helpful when infectious, oncologic, and rheumatologic causes are considered. Inflammatory markers such as the erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) are elevated in most acute infectious processes. A complete blood count (CBC) should also be obtained in cases of suspected infection to evaluate the white blood cell count (WBC). Due to the high prevalence of joint infections and postinfectious processes caused by group A streptococcus (GAS), an antistreptolysin titer (ASO), throat culture, and rapid streptococcal antigen swab should be considered. If infection is suspected and a joint effusion is present, cell counts, gram stain, and culture from the synovial fluid should be sent to assist with diagnosis and antibiotic management. If a child appears septic, a blood culture should be obtained as well. With suspected osteomyelitis, cultures of the bone should be taken in the operating room in addition to a peripheral blood culture. Ideally, antibiotics should be withheld until cultures are sent unless the child appears acutely ill.
Diagnostic Imaging
Toxic Synovitis and Septic Arthritis
Clinicians may have difficulty differentiating between toxic synovitis (also known as transient synovitis) and septic arthritis of the hip in pediatric patients. In both toxic synovitis and septic arthritis, the child is unable to bear weight on the affected side, and ultrasound may demonstrate effusion.3,4
Toxic synovitis is thought to be a viral or postviral phenomenon, though the exact agent responsible for initiating the inflammatory cascade is not known. It has a relatively benign course and generally responds over 3 to 10 days to rest and nonsteroidal anti-inflammatory drugs (NSAIDs).5,6
Septic arthritis, however, is a serious infection with the capacity to cause permanent joint damage as well as spread into the blood or bone. Staphylococcal and streptococcal bacteria, including GAS and methicillin-resistant staphylococcus aureus (MRSA) are the most common causes of septic arthritis in the pediatric population.7 However, Kingella kingae, a gram-negative organism, is an increasingly recognized cause of septic arthritis in children younger than 3 years of age. Commonly found in the posterior pharynx, Kingella is very difficult to culture but may be detected by polymerase chain reaction (PCR) assays.8 The spectrum of GAS-related joint infections ranges from a postinfectious type that may be indistinguishable from toxic synovitis (but with evidence of recent GAS pharyngitis) to typical bacterial septic arthritis.9
Multiple clinical prediction rules and algorithms have been developed to assist with the management of these cases. The Kocher criteria, which include history of fever >101.3˚F, nonweight-bearing status, ESR >40 mm/hour, and WBC >12,000 cells/mm3 were found to be independent clinical predictors for the differentiation between transient arthritis and septic arthritis. Children with none of the risk factors had a 0.2% chance of septic arthritis while those with two risk factors had a 40% chance of septic arthritis. Subsequent validation studies among pediatric populations with a lower prevalence of septic arthritis found the positive predictive values to be lower; nevertheless, the Kocher criteria remain useful in guiding management.3,4
If a diagnosis of septic arthritis remains a consideration after the history, physical examination, and plain radiography, laboratory studies should be obtained, including a CBC, ESR, CRP, blood culture, rapid streptococcal assay, throat culture, and ASO titer. An ultrasound should also be performed to assess for the presence of a hip effusion.
Elevated inflammatory markers (ESR >40 mm/hour, CRP >20 mg/L, WBC >12,000 cells/mm3) and an effusion should prompt orthopedic consultation and arthrocentesis for synovial fluid-cell counts, gram stain, and culture. Synovial fluid WBC counts >50,000 cells/mm3 or a positive gram stain or culture is diagnostic of septic arthritis and requires treatment with intravenous (IV) antibiotics and likely operative intervention. The absence of an effusion on ultrasound, synovial fluid WBC counts <50,000 cells/mm3, and inflammatory markers that are not significantly elevated indicate an alternative diagnosis such as toxic synovitis. However, there may be cases in which the diagnosis is not clear due to ambiguous laboratory values from the blood or synovial fluid; in these cases the decision to proceed with IV antibiotics must be made in consultation with an orthopedist.10
Empiric antibiotic therapy in patients with septic arthritis should take into account the prevalence of MRSA in the community. Clindamycin is a popular choice due to its high oral bioavailability, which facilitates transition to a home regimen. Vancomycin is another option and can be reserved for more severely ill children. Empiric coverage for suspected septic arthritis in children younger than 3 years of age should also include an anti-gram negative agent, such as a cephalosporin, to treat Kingella.7
Osteomyelitis
Acute osteomyelitis is a common cause of limp among children and is usually caused by the hematogenous spread of bacteria. Staphylococcus aureus, including MRSA, is responsible for up to 90% of cases of osteomyelitis, though recent studies have identified Kingella as an etiologic agent among children younger age 3 years.7 The highly vascular metaphysis of the tibia and femur in children can become infected during times of otherwise asymptomatic bacteremia in healthy patients.8 Among younger children with less well-developed anatomic separation between the bone and joint space, it is possible for infection to spread into the joint space. Younger children with osteomyelitis may present with poorly localized pain with or without systemic symptoms; older children and those with more advanced disease may describe point tenderness on the bone. In many cases it may be difficult clinically to distinguish osteomyelitis from septic arthritis; excessive pain with passive range of motion of the joint is more indicative of septic arthritis.
Ideally, antibiotic therapy should be deferred until cultures from the site of infection are obtained operatively or via aspiration. The local staphylococcus aureus resistance pattern should guide empiric antibiotic therapy. With the rise of MRSA, clindamycin has become first-line therapy with vancomycin as an alternative for severely-ill or clindamycin-allergic patients. For children younger than 3 years of age with a more subacute presentation, the possibility of Kingella infection should be considered and treated with a cephalosporin. Some children with osteomyelitis will require operative debridement, though
many can be treated with antibiotics alone. The standard duration of antibiotic treatment is 4 to 6 weeks, with transition to an oral regimen once the patient is afebrile with downtrending inflammatory markers.7,8,11
Perthes Disease
Perthes disease (also called Legg-Calve-Perthes disease) is an idiopathic process that involves avascular necrosis and revascularization of the blood supply of the femoral head. The condition is most common in children ages 3 to 12 years and has a 4:1 male to female predominance. The remodeling takes place over the course of 2 to 4 years. During this process, the epiphysis of the femoral head is weakened and undergoes irreversible deformation that, if uncorrected, will persist throughout life. Severe degenerative arthritis may result and ultimately require hip replacement.12
Perthes disease typically presents as a subacute limp, sometimes with referred pain to the groin, thigh, or knee of the affected side. Range of motion of the hip may be limited, particularly in abduction and internal rotation. Plain films demonstrate necrotic avascular areas of the distal femoral head during active disease; after the remodeling process is complete, the femoral head often shows residual deformities. Magnetic resonance imaging is useful in cases in which plain film findings are subtle, particularly early in the course of the disease.12,13
Management of Perthes disease depends on the age of the child and clinical factors such as radiographic progression and range of motion of the hip. The goal of therapy is to limit damage to the femoral head during the revascularization process. In children younger than 5 years of age, nonsurgical management with an abduction splint to keep the femoral head contained and protected within the acetabulum may be used. Surgical osteotomies are used in older and more severely affected children to artificially contain the femoral head during the healing process.13
Slipped Capital Femoral Epiphysis
A common cause of limp among older children, the average age of presentation for SCFE is 13.5 years for boys and 12 years for girls. This condition occurs when the proximal femoral epiphysis slides posteriorly and inferiorly relative to the metaphysis. Epidemiological studies have established a connection between SCFE and obesity. Although the precise pathogenesis remains unknown, it is hypothesized that increased mechanical forces during a time of rapid pubertal growth lead to weakness at the physis. Among children who develop SCFE outside of the usual age distribution, endocrinopathies such as hypothyroidism, hypogonadism, and panhypopituitarism are often discovered.14
As with Perthes disease, SCFE may present as a chronic, subacute, or acute limp with referred pain to the groin, thigh, or knee. The patient with SCFE often has severe pain with internal rotation of the affected hip and will hold the hip in obligatory external rotation if it is flexed. Patients unable to bear weight on the affected side have unstable SCFE.
All patients with SCFE should be made nonweight bearing on the affected hip to prevent further slippage of the epiphysis. Definitive treatment involves in-situ fixation of the femoral neck with the proximal femoral epiphysis. Close orthopedic follow up is essential as roughly 50% of children with unilateral SCFE will go on to develop SCFE in the contralateral hip. Long-term complications of SCFE include osteonecrosis, joint space narrowing, and osteoarthritis.14,15
Osgood-Schlatter Disease
Osgood-Schlatter disease is a relatively benign cause of limp that is thought to occur due to repetitive trauma to the secondary ossification center tibial tubercle. Over time, the strong pull of the quadriceps muscle group on the patellar tendon causes a chronic avulsion at the site of the patellar tendon insertion on the tibial tuberosity. It most commonly develops in early puberty from ages 9 to 14 years. Affected children develop tenderness over the tibial tuberosity that is made worse with activity. On examination, pain can be elicited by having the child extend the knee against resistance or kneel. Lateral radiographs of the knee may be normal or demonstrate swelling, irregularity, or elevation of the tibial tubercle. Treatment consists of NSAIDs, ice, and physical therapy; activity restriction is generally unnecessary. Most cases resolve over 6 to 18 months as the growth plate at the secondary ossification center ossifies.16
Case Conclusion
Initial examination confirmed the presence of a limp; the differential in this age group includes toxic synovitis, septic arthritis, and osteomyelitis. Although Kailey appeared relatively well on examination, her history of recent fever and the worsening symptoms over the past week were concerning. The workup began with plain films of the pelvis and the right knee because of the possibility of referred pain and the lack of localizing signs on examination. In addition, laboratory evaluation was performed, including CBC, CRP, and ESR. Due to her young age, a rapid streptococcal assay, throat culture, or an ASO titer was not necessary.
Plain films of the pelvis and the right knee were normal. The patient’s WBC was unremarkable, but her ESR was 50 mm/hour and CRP was 25 mg/L. Given these elevated inflammatory markers, ultrasound of the right hip was ordered, which revealed a small effusion. An orthopedic specialist was consulted, who performed a sedated joint aspiration. Cell counts from the joint aspirate were sent for evaluation, as well as culture, gram stain, and a PCR for Kingella.
After joint aspiration, Kailey was admitted to the hospital overnight and was started on empiric treatment with IV clindamycin and ceftriaxone. The synovial fluid gram stain was negative, but the WBC was 65,000 cells/mm3. Over the next several days, her inflammatory markers trended downward, she remained afebrile, and her gait slowly improved. The synovial fluid culture remained negative, but the PCR was positive for Kingella. Kailey was discharged on hospital day 3 with a 21-day course of oral cephalexin.
Dr Kane is a fellow in the department of pediatrics, division of pediatric emergency medicine, Vanderbilt Children’s Hospital, Nashville, Tennessee. Dr McMorrow is an assistant professor of emergency medicine and assistant professor of pediatrics, department of pediatrics, division of pediatric emergency medicine, Vanderbilt Children’s Hospital, Nashville, Tennessee.
- Smith E, Anderson M, Foster H. The child with a limp: a symptom and not a diagnosis. Arch Dis Child Educ Pract Ed. 2012;97(5):185-193.
- Leung AK, Lemay JF. The limping child. J Pediatr Health Care. 2004;18(5):219-223.
- Taekema HC, Landham PR, Maconochie I. Towards evidence based medicine for paediatricians. Distinguishing between transient synovitis and septic arthritis in the limping child: how useful are clinical prediction tools? Arch Dis Child. 2009;94(2):167,168.
- Luhmann SJ, Jones A, Schootman M, Gordon JE, Schoenecker PL, Luhmann JD. Differentiation between septic arthritis and transient synovitis of the hip in children with clinical prediction algorithms. J Bone Joint Surg Am. 2004;86-A(5):956-962.
- Do TT. Transient synovitis as a cause of painful limps in children. Curr Opin Pediatr. 2000;12(1):48-51.
- Nouri A, Walmsley D, Pruszczynski B, Synder M. Transient synovitis of the hip: a comprehensive review. J Pediatr Orthop B. 2014;23(1):32-36.
- Thomsen I, Creech CB. Advances in the diagnosis and management of pediatric osteomyelitis. Curr Infect Dis Rep. 2011;13(5):451-460.
- Dodwell ER. Osteomyelitis and septic arthritis in children: current concepts. Curr Opin Pediatr. 2013;25(1):58-63.
- Mignemi ME, Martus JE, Bracikowski AC, Lovejoy SA, Mencio GA, Schoenecker JG. The spectrum of group A streptococcal joint pathology in the acute care setting. Pediatr Emerg Care. 2012;28(11):
1185-1189. - Rutz E, Spoerri M. Septic arthritis of the paediatric hip - A review of current diagnostic approaches and therapeutic concepts. Acta Orthop Belg. 2013;79(2):123-134.
- Harik NS, Smeltzer MS. Management of acute hematogenous osteomyelitis in children. Expert Rev Anti Infect Ther. 2010;8(2):175-181.
- Shah H. Perthes disease: evaluation and management. Orthop Clin North Am. 2014;45(1):87-97.
- Nelitz M, Lippacher S, Krauspe R, Reichel H. Perthes disease: current principles of diagnosis
and treatment. Dtsch Arztebl Int. 2009;106(31-32):517-523. - Novais EN, Millis MB. Slipped capital femoral epiphysis: prevalence, pathogenesis, and natural history. Clin Orthop Relat Res. 2012;470(12):3432-3438.
- Peck D. Slipped capital femoral epiphysis: diagnosis and management. Am Fam Physician. 2010;82(3):258-262.
- Gholve PA, Scher DM, Khakharia S, Widmann RF, Green DW. Osgood Schlatter syndrome. Curr Opin Pediatr. 2007;19(1):44-50.
- Smith E, Anderson M, Foster H. The child with a limp: a symptom and not a diagnosis. Arch Dis Child Educ Pract Ed. 2012;97(5):185-193.
- Leung AK, Lemay JF. The limping child. J Pediatr Health Care. 2004;18(5):219-223.
- Taekema HC, Landham PR, Maconochie I. Towards evidence based medicine for paediatricians. Distinguishing between transient synovitis and septic arthritis in the limping child: how useful are clinical prediction tools? Arch Dis Child. 2009;94(2):167,168.
- Luhmann SJ, Jones A, Schootman M, Gordon JE, Schoenecker PL, Luhmann JD. Differentiation between septic arthritis and transient synovitis of the hip in children with clinical prediction algorithms. J Bone Joint Surg Am. 2004;86-A(5):956-962.
- Do TT. Transient synovitis as a cause of painful limps in children. Curr Opin Pediatr. 2000;12(1):48-51.
- Nouri A, Walmsley D, Pruszczynski B, Synder M. Transient synovitis of the hip: a comprehensive review. J Pediatr Orthop B. 2014;23(1):32-36.
- Thomsen I, Creech CB. Advances in the diagnosis and management of pediatric osteomyelitis. Curr Infect Dis Rep. 2011;13(5):451-460.
- Dodwell ER. Osteomyelitis and septic arthritis in children: current concepts. Curr Opin Pediatr. 2013;25(1):58-63.
- Mignemi ME, Martus JE, Bracikowski AC, Lovejoy SA, Mencio GA, Schoenecker JG. The spectrum of group A streptococcal joint pathology in the acute care setting. Pediatr Emerg Care. 2012;28(11):
1185-1189. - Rutz E, Spoerri M. Septic arthritis of the paediatric hip - A review of current diagnostic approaches and therapeutic concepts. Acta Orthop Belg. 2013;79(2):123-134.
- Harik NS, Smeltzer MS. Management of acute hematogenous osteomyelitis in children. Expert Rev Anti Infect Ther. 2010;8(2):175-181.
- Shah H. Perthes disease: evaluation and management. Orthop Clin North Am. 2014;45(1):87-97.
- Nelitz M, Lippacher S, Krauspe R, Reichel H. Perthes disease: current principles of diagnosis
and treatment. Dtsch Arztebl Int. 2009;106(31-32):517-523. - Novais EN, Millis MB. Slipped capital femoral epiphysis: prevalence, pathogenesis, and natural history. Clin Orthop Relat Res. 2012;470(12):3432-3438.
- Peck D. Slipped capital femoral epiphysis: diagnosis and management. Am Fam Physician. 2010;82(3):258-262.
- Gholve PA, Scher DM, Khakharia S, Widmann RF, Green DW. Osgood Schlatter syndrome. Curr Opin Pediatr. 2007;19(1):44-50.

Four Fracture Patterns Unique to Pediatric Patients
Case 1
A 2-year-old girl presented to the ED with arm pain. Her mother stated that her daughter was playing with a 5-year-old sibling when she heard the child cry- out in pain and noticed she was holding her right arm by her side, not wanting to move it. Neither child gave a reliable story of the injury.
Nursemaid’s Elbow
Nursemaid’s elbow, also known as pulled elbow, subluxation of the radial head, and most recently annular ligament displacement, is a common injury in children younger than age 6 years. One study estimates that the condition represented about 1% of injury-related ED visits in 2005.1
Patients with nursemaid’s elbow typically present holding the injured arm at their side, slightly flexed and pronated. These patients appear relatively comfortable until moved actively or passively. The classic history of nursemaid’s elbow includes a traction mechanism, with the child being pulled up by one arm or being grabbed by the arm suddenly to keep him or her out of harm’s way.2 Due to the laxity of connective tissues in children of this age, the head of the radius slips out of the annular ligament causing acute pain and decreased function.
Nursemaid’s elbow is usually diagnosed by history and examination alone, with special consideration to the mechanism of injury. There is rarely swelling or bruising.3 Passive flexion and extension at the elbow may be normal, but rotational maneuvers can be painful or fully resisted.
Reduction Techniques
In 2012, Cochrane updated its earlier review on nursemaid’s elbow and in 2013 followed up with an article in Pediatrics in Review.3,4 Each covered research on reduction techniques, summarizing studies comparing supination-flexion (SF) versus hyperpronation (HP) as the initial reduction maneuver. Given that these maneuvers are difficult to camouflage, studies tend to be pseudorandomized with assessment by a nonblinded healthcare provider, decreasing the strength of the studies. In the Cochrane review, four different trials that included 379 children under age 7 years were selected for the review. In all four studies, pronation was found to have the least chance of failed first attempt, the chosen outcome for this meta-analysis. The risk ratio of failure of reduction for pronation was 0.45 (95% confidence interval [CI], 0.28-0.73).
There is some data supporting hyperpronation to be less painful as well; however, the Cochrane reviewers felt there may have been reporting bias.4 Since the time of each of these reviews, another study comprised of 150 children was conducted and also favored similar practice styles, as the hyperpronation maneuver had 95% success rate on first attempt versus 68% first-time success with supination and flexion.5
Complications and Recurrence
In a small study aimed at identifying recurrence rates for nursemaid’s elbow, Teach and Schultzman6 studied 93 children for 1 year after probable or definite diagnosis of nursemaid’s elbow. Of these children, 23.7% had recurrent radial head subluxation. Children younger than age 2 years were found to have a relative risk of 2.6 (95% CI, 1.04-6.30) for one or more recurrences when compared to children older than age 2 years.
While the great majority of children with nursemaid’s elbow do not need referral to an orthopedist, those with two or more occurrences should be considered for referral to a specialist.
Case 2
A 6-year-old boy was presented to the ED by his father, who had placed the boy’s arm in a home-made sling. The child tearfully told the provider that he fell trying to catch himself after tripping over the house pet.
FOOSH Injury
The above case depicts a very common presentation in the ED—the so-called “FOOSH” (fall onto an outstretched hand) injury. This type of injury occurs with such frequency in both adults and children that it is one of the only injury patterns with a commonly used acronym. The bony injuries seen with FOOSH in children, however, have a different pattern than those in adults.
Pediatric fractures are unique due to the difference in the structure of the bones themselves. A child’s bones are more elastic than an adult’s bones, allowing them to bow and bend before they fracture.7 Despite this malleability, pediatric bones have been noted to have a thicker periosteum. For this reason, compression or impact may interrupt the periosteal sleeve, minimally yielding an incomplete interruption of the cortex unilaterally.

One fracture pattern commonly seen in children is the torus fracture. This type of fracture is also referred to as a buckle fracture as the bone cortex on radiographic imaging appears “buckled” as a result of the compressive forces on that side of the bone (Figure 1). Since the bone itself is minimally affected, these fractures are quite stable and not at risk for complications.
In comparison, a greenstick fracture, also unique to the pediatric population, is one in which the cortex shows plastic deformity on the side of the force or impact but is interrupted on the opposite side due to the tension of the impact itself. Greenstick fractures are frequently angulated and may require reduction for anatomic alignment, but long-term complications are typically minimal. These fracture patterns are distinguished from complete fractures (as seen in adults), which are quite unstable and generally require surgical intervention.
Of note, the location of pediatric forearm fractures varies with age as well. Diaphyseal fractures are more common in prepubescent children, whereas the highest incidence of physeal injuries occurs during large growth spurts, particularly throughout adolescence.7
Management
The remodeling potential of pediatric bones also makes management unique. Pediatric orthopedic literature has well-studied acceptable angles and degrees of appropriate displacement based largely on the age of the patient and proximity to a growth plate. Knowledge of these is imperative for definitive care of such fractures but is beyond the scope of this review.
Traditional treatment of pediatric forearm fractures includes immobilization of various types and duration to minimize pain and deformity while producing the best possible outcome. Several recent studies have aimed to determine best practice for the different fracture types with the goal of producing best alignment and return to function while decreasing cost, discomfort, and number of physician visits. Another concern among healthcare providers is the risk of refracture, which in buckle fractures is estimated at approximately 2% with a median time of 8 to 16 weeks after the initial injury.7
A 2010 review by Kennedy et al8 sought to determine if the refracture rate was affected by the technique used to immobilize torus fractures. The five studies used in this review had no reports of refracture in the 443 patients included in analysis, though only one of the studies (Plint et al) followed patients for more than 6 weeks.8,9 In this study, 75 patients were randomized to either a plaster removable splint or full below-elbow cast for 3 weeks; thereafter, they were followed for 6 months, during which time none experienced refracture.9
Another outcome from the same study assessed the ability of the patient to use the affected arm in the recovery period. While those in removable splints scored better during and immediately after cast removal, no differences were present after 1 week. Not surprisingly, families preferred the soft bandages or a removable splint for treatment.
Case 3
A 13-year-old boy presented to the ED with right ankle pain and difficulty bearing weight. He stated that he was playing basketball when he “rolled” his right ankle coming down from a rebound.
Ankle Fractures
Ankle fractures are among the most common acute injuries of the lower extremity in children, accounting for approximately 5% of pediatric fractures and 15% of physeal injuries.10 Ankle fractures also account for up to 40% of all injuries to the skeletally immature athlete.10,11 More specifically, distal fibular physeal fractures are the most common types of pediatric ankle fracture; however, they are associated with a relatively low risk for long-term complications. In contrast, distal tibial physeal fractures are associated with a higher risk for long-term complications.12,13
Presentation and Evaluation
Typically, patients presenting with ankle fractures are too sore to bear weight, and swelling and ecchymosis can be identified anterior to the ankle. In addition, there may be diffuse tenderness throughout the ankle and point tenderness may be induced on the anterolateral aspect of the distal tibia.14 A complete evaluation of the entire lower extremity should be conducted before assuming that the injury is confined to the ankle, especially in children younger than age 5 years and/or who are nonverbal.10 When evaluating an ankle fracture, in general, orthopedic consultation should be obtained for children with neurovascular compromise, open fractures, and/or Salter-Harris III, IV, and V fractures.
The juvenile Tillaux fracture represents a Salter-Harris III physeal injury that involves the anterolateral portion of the tibia. It usually occurs in children between ages 12 and 14 years as they approach skeletal maturity and who have a partially fused tibial physis. The common mechanism of injury is inversion of the ankle with the foot pointed away from the midline (supination with external rotation). This leads to avulsion of the lateral tibial epiphysis that is attached to the anterior inferior tibiofibular ligament. The uninvolved medial portion of the epiphysis is closed.10
Radiographic Imaging

Three radiographic views should be obtained in the evaluation of pediatric ankle injuries as Tillaux fractures or other subtle injuries could be easily missed if only two views are obtained. Interpretation of the radiographs must be correlated with the physical examination.10 The fracture line is usually best seen on a mortise view (Figure 2). Computed tomography (CT) is warranted in cases in which displacement greater than 2 mm is suspected because it better defines fracture displacement and can aid in surgical planning.14 Because of its sensitivity in detecting fractures displaced more than 2 mm, CT is now the preferred imaging modality in the assessment of juvenile Tillaux fractures.15
Definitive Management
There are two important goals when treating children with ankle fractures—achieving a satisfactory reduction and avoiding physeal arrest so as to minimize the risks of angular deformity, early arthrosis, leg-length inequality, and joint stiffness.11 Juvenile Tillaux fractures with greater than 2 mm of displacement require orthopedic consultation for closed or open reduction. Closed reduction is attempted by internally rotating the foot and applying direct pressure over the anterolateral tibia. If necessary, percutaneous pins can be used for stabilization of the reduction. If closed reduction is unsuccessful, open reduction is required. Care must be taken to assure no displacement occurs after casting; this requires weekly X-ray evaluation for the first 2 weeks.12
Patients with nondisplaced Salter-Harris III fractures are treated with long-leg casting for 4 weeks with conversion to a short-leg cast or boot for an additional 4 weeks. Patients should anticipate 8 weeks of nonweight-bearing. The patient is allowed to remove the boot for range-of-motion exercises but must remain nonweight-bearing for the first 2 weeks.14
Case 4
A 3-year-old previously healthy girl presented to the ED with a limp and difficulty bearing weight. Her mother reported that the child was playing in the yard when she caught her foot on a tree root, stumbled, and fell down. Since the incident, the child has been tearful, limping, and refusing to walk.
Tibial Fractures
Tibial fractures are among the most frequent types of orthopedic injuries in young children, with only femur and forearm fractures having a higher incidence of occurrence. Tibial fractures account for up to 15% of long bone fractures in children and adolescents.16,17 The mechanism of injury varies depending on the patient’s age. In young children, the most common cause of injury is from a seemingly minor twisting around a fixed foot or from a minor fall. In older children and adults, high-energy motor vehicle accidents and sports-related injuries are more common causes.
Fractures of the tibial shaft are typically short oblique or transverse fractures of the middle or distal third of the shaft. Thirty percent of tibial shaft fractures are associated with fractures of the fibula.16
Toddler’s Fracture
The term toddler’s fracture refers to a nondisplaced oblique fracture of the tibial shaft without concomitant fibular fracture. It usually results from an indirect rotational or twisting force applied to the foot and lower leg.16-18 More specifically, the term describes a specialized case of spiral fracture of the distal tibia in patients aged 9 months to 3 years, when weight-bearing is just beginning.19,20 Such injuries commonly occur when a toddler stumbles and falls, or attempts to extricate the foot from between the bars of a crib. Often, however, the mechanism is minimal or unknown.18 Of those injuries that are witnessed, most caregivers report a minor twisting mechanism. Most children with toddler’s fracture are younger than age 6 years. Sixty-three of 76 such fractures reported by Dunbar et al17,19 occurred in children younger than 2.5 years of age. Toddler’s fractures occur more often in boys than girls, and in the right leg more often than the left. Most children will give a history of tripping or twisting their ankle.17
Evaluating the Toddler
Toddlers can be challenging patients as they can not relate history and are often uncooperative on examination. A child may present with a limp, diminished movement of the affected limb, or refuse to bear weight without a distinct history of injury. The onset of limping or refusal to bear weight after minor trauma, or without an obvious injury in a young ambulatory child, warrants a detailed examination looking for tenderness over the tibia, along with radiographic evaluation to rule out a toddler’s fracture.
The examination of the patient is rarely impressive as there is little swelling and bruising with most toddlers’ fractures. A complete clinical history is needed, including a detailed description of any observed traumatic event to exclude the existence of other injuries.
When no traumatic event is observed or an inconsistent history is provided, the physician should obtain a detailed social history, including a list of the child’s most recent caregivers and contacts.16 Because of mild clinical symptoms and frequent lack of a history of injury in this patient population, presentation for evaluation may be delayed. In such cases, by the time the extremity is examined, the fracture has begun to heal. This healing phase may be accompanied by periosteal new bone and, in the absence of a history, may erroneously suggest other, more ominous conditions such as osteomylelitis or tumor.17,18
Consideration of Abuse
Although tibial shaft fractures are rarely found in abused children, diagnosis of child abuse must be considered in cases where a tibial fracture is discovered in the nonambulatory child; his or her clinical history is inconsistent with the injury; and/or there are other physical findings suggestive of abuse. Investigation for suspected nonaccidental trauma includes a thorough physical examination, skeletal survey, and evaluation by social services personnel.16
Radiographic Imaging
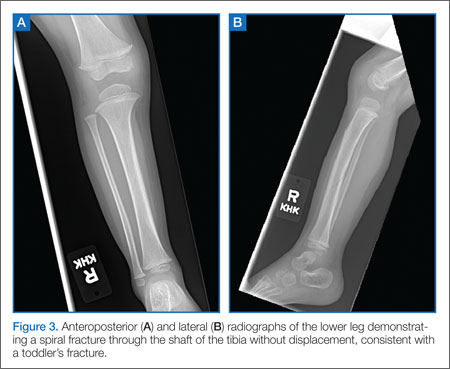
Quality anteroposterior (AP) or lateral radiographs of the affected leg may show a hairline fracture, but these can easily be missed on initial plain films in almost a third of patients.21 An internal oblique view can aid in identifying nondisplaced toddler fractures.17 The AP view is the best view for observing the nondisplaced spiral fracture along the distal tibia (Figure 3).6 Occasionally, a fracture line is not identified on initial plain films and the first evidence of fracture becomes apparent on X-ray when new periosteal bone forms 7 to 10 days after the initial injury.
Definitive Treatment
Children with a classic history for a toddler’s fracture and an inability to bear weight should be immobilized with a long-leg splint or cast—even when X-rays are negative—until a definitive diagnosis can be made. Such fractures usually become visible on X-ray 7 to 10 days after injury as a result of new bone growth.22
When definitive diagnosis of a toddler’s fracture is made on plain radiographs, the child should either be immobilized in a long-leg splint with referral to an orthopedist within 5 to 7 days, or immediately casted.16
Conclusion
Fractures in both children and adults are among the most common injury-related presentations to the ED. Based on the structure and increased elasticity of bone in the pediatric patient, there are several fracture patterns unique to this population. Appropriate evaluation, diagnosis, and management in the ED helps to maximize and ensure long-term function and healing while minimizing trauma to the patient.
Dr McBride is an associate professor of pediatrics and pediatric emergency medicine, Wake Forest Baptist Health, Brenner Children’s Hospital, Winston-Salem, North Carolina.
Dr Sutton is a pediatric resident, Wake Forest Baptist Health, Brenner Children’s Hospital, Winston-Salem, North Carolina.
- Brown D. Emergency department visits for nursemaid’s elbow in the United States, 2005-2006. Orthop Nurs. 2009;28(4):161,162.
- Hardy RH. Pulled elbow. J R Coll Gen Pract. 1978;28(189):224-226.
- Browner EA. Nursemaid’s elbow (annular ligament displacement). Pediatr Rev. 2013;34(8):366,367.
- Krul M, van der Wouden JC,van Suijlekom-Smit LW, Koes BM. Manipulative interventions for reducing pulled elbow in young children. Cochrane Database of Syst Rev. 2012;1:CD007759.
- Gunaydin YK, Katirci Y, Duymaz H, et al. Comparison of success and pain levels of supination-flexion and hyperpronation maneuvers in childhood nursemaid’s elbow cases. Am J Emerg Med. 2013;31(7):1078-1081.
- Teach SJ, Schutzman SA. Prospective study of recurrent radial head subluxation. Arch Pediatr Adolesc Med. 1996;150(2):164-166.
- Dolan M and Waters PM. Fractures and dislocations of the forearm, wrist, and hand. In: Green NE, Swiontkowski MF, eds. Skeletal Trauma in Children. 4th ed. Philadephia, PA: Saunders Elsevier; 2009:159-206.
- Kennedy SA, Slobogean GP, Mulpuri K. Does degree of immobilization influence refracture rate in the forearm buckle fracture? J Pediatr Orthop B. 2010;19(1):77-81.
- Plint AC, Perry JJ, Correll R, Gaboury I, Lawtown L. A randomized, controlled trial of removable splinting versus casting for wrist buckle fractures in children. Pediatrics. 2006;117(3):691-697.
- Kay RM, Matthys GA. Pediatric ankle fractures: evaluation and treatment. J Am Acad Orthop Surg. 2001;9(4):268-278.
- Marsh JS, Daigneault JP. Ankle injuries in the pediatric population. Curr Opin Pediatr. 2000;12(1):52-60
- Cummings RJ. Distal tibial and fibular fractures. In: Beaty JH, Kasser JR, eds. Rockwood and Wilkins’ Fractures in Children. 6th ed. Pennsylvania, PA: Lippincott Williams & Wilkins; 2006:1096-1104.
- Boutis K, Willan AR, Babyn P, Narayanan UG, Alman B, Schuh S. A randomized, controlled trial of a removable brace versus casting in children with low-risk ankle fractures. Pediatrics. 2007;119(6):1256-1263.
- Wuerz TH, Gurd DP. Pediatric physeal ankle fracture. J Am Acad Orthop Surg. 2013;21(4):234-244.
- Horn BD, Crisci K, Krug M, Pizzutillo PD, MacEwen GD. Radiologic evaluation of juvenile Tillaux fractures of the distal tibia. J Pediatr Orthop. 2001;21(2):162-164.
- Mashru RP, Herman MJ, Pizzutillo PD. Tibial shaft fractures in children and adolescents. J Am Acad Orthop Surg. 2005;139(5):345-352.
- Heinrich SD, Mooney JF. Fractures of the shaft of the tibia and fibula. In: Beaty JH, Kasser JR, eds. Rockwood and Wilkins’ Fractures in Children. 6th ed. Pennsylvania, PA: Lippincott Williams & Wilkins; 2006:1063,1064.
- John SD, Moorthy CS, Swischuk LE. Expanding the concept of the toddler’s fracture. Radiographics. 1997;17(2):367-376.
- Dunbar JS, Owen HF, Nogrady MB, McLeese R. Obscure tibial fracture of infants—the toddlers’ fracture. J Can Assoc Radiol 1964;15:136-144.
- Tenenbein M, Reed MH, Black GB. The toddler’s fracture revisited. Am J Emerg Med. 1990;8(3):208-211.
- Shravat BP, Harrop SN, Kane TP. Toddler’s fracture. J Accid Emerg Med. 1996;13(1):59-61.
- Halsey MF, Finzel KC, Carrion WV, Haralabatos SS, Gruber MA, Meinhard BP. Toddler’s fracture: presumptive diagnosis and treatment. J Pediatr Orthop. 2001;21(2):152-156.
Case 1
A 2-year-old girl presented to the ED with arm pain. Her mother stated that her daughter was playing with a 5-year-old sibling when she heard the child cry- out in pain and noticed she was holding her right arm by her side, not wanting to move it. Neither child gave a reliable story of the injury.
Nursemaid’s Elbow
Nursemaid’s elbow, also known as pulled elbow, subluxation of the radial head, and most recently annular ligament displacement, is a common injury in children younger than age 6 years. One study estimates that the condition represented about 1% of injury-related ED visits in 2005.1
Patients with nursemaid’s elbow typically present holding the injured arm at their side, slightly flexed and pronated. These patients appear relatively comfortable until moved actively or passively. The classic history of nursemaid’s elbow includes a traction mechanism, with the child being pulled up by one arm or being grabbed by the arm suddenly to keep him or her out of harm’s way.2 Due to the laxity of connective tissues in children of this age, the head of the radius slips out of the annular ligament causing acute pain and decreased function.
Nursemaid’s elbow is usually diagnosed by history and examination alone, with special consideration to the mechanism of injury. There is rarely swelling or bruising.3 Passive flexion and extension at the elbow may be normal, but rotational maneuvers can be painful or fully resisted.
Reduction Techniques
In 2012, Cochrane updated its earlier review on nursemaid’s elbow and in 2013 followed up with an article in Pediatrics in Review.3,4 Each covered research on reduction techniques, summarizing studies comparing supination-flexion (SF) versus hyperpronation (HP) as the initial reduction maneuver. Given that these maneuvers are difficult to camouflage, studies tend to be pseudorandomized with assessment by a nonblinded healthcare provider, decreasing the strength of the studies. In the Cochrane review, four different trials that included 379 children under age 7 years were selected for the review. In all four studies, pronation was found to have the least chance of failed first attempt, the chosen outcome for this meta-analysis. The risk ratio of failure of reduction for pronation was 0.45 (95% confidence interval [CI], 0.28-0.73).
There is some data supporting hyperpronation to be less painful as well; however, the Cochrane reviewers felt there may have been reporting bias.4 Since the time of each of these reviews, another study comprised of 150 children was conducted and also favored similar practice styles, as the hyperpronation maneuver had 95% success rate on first attempt versus 68% first-time success with supination and flexion.5
Complications and Recurrence
In a small study aimed at identifying recurrence rates for nursemaid’s elbow, Teach and Schultzman6 studied 93 children for 1 year after probable or definite diagnosis of nursemaid’s elbow. Of these children, 23.7% had recurrent radial head subluxation. Children younger than age 2 years were found to have a relative risk of 2.6 (95% CI, 1.04-6.30) for one or more recurrences when compared to children older than age 2 years.
While the great majority of children with nursemaid’s elbow do not need referral to an orthopedist, those with two or more occurrences should be considered for referral to a specialist.
Case 2
A 6-year-old boy was presented to the ED by his father, who had placed the boy’s arm in a home-made sling. The child tearfully told the provider that he fell trying to catch himself after tripping over the house pet.
FOOSH Injury
The above case depicts a very common presentation in the ED—the so-called “FOOSH” (fall onto an outstretched hand) injury. This type of injury occurs with such frequency in both adults and children that it is one of the only injury patterns with a commonly used acronym. The bony injuries seen with FOOSH in children, however, have a different pattern than those in adults.
Pediatric fractures are unique due to the difference in the structure of the bones themselves. A child’s bones are more elastic than an adult’s bones, allowing them to bow and bend before they fracture.7 Despite this malleability, pediatric bones have been noted to have a thicker periosteum. For this reason, compression or impact may interrupt the periosteal sleeve, minimally yielding an incomplete interruption of the cortex unilaterally.
One fracture pattern commonly seen in children is the torus fracture. This type of fracture is also referred to as a buckle fracture as the bone cortex on radiographic imaging appears “buckled” as a result of the compressive forces on that side of the bone (Figure 1). Since the bone itself is minimally affected, these fractures are quite stable and not at risk for complications.
In comparison, a greenstick fracture, also unique to the pediatric population, is one in which the cortex shows plastic deformity on the side of the force or impact but is interrupted on the opposite side due to the tension of the impact itself. Greenstick fractures are frequently angulated and may require reduction for anatomic alignment, but long-term complications are typically minimal. These fracture patterns are distinguished from complete fractures (as seen in adults), which are quite unstable and generally require surgical intervention.
Of note, the location of pediatric forearm fractures varies with age as well. Diaphyseal fractures are more common in prepubescent children, whereas the highest incidence of physeal injuries occurs during large growth spurts, particularly throughout adolescence.7
Management
The remodeling potential of pediatric bones also makes management unique. Pediatric orthopedic literature has well-studied acceptable angles and degrees of appropriate displacement based largely on the age of the patient and proximity to a growth plate. Knowledge of these is imperative for definitive care of such fractures but is beyond the scope of this review.
Traditional treatment of pediatric forearm fractures includes immobilization of various types and duration to minimize pain and deformity while producing the best possible outcome. Several recent studies have aimed to determine best practice for the different fracture types with the goal of producing best alignment and return to function while decreasing cost, discomfort, and number of physician visits. Another concern among healthcare providers is the risk of refracture, which in buckle fractures is estimated at approximately 2% with a median time of 8 to 16 weeks after the initial injury.7
A 2010 review by Kennedy et al8 sought to determine if the refracture rate was affected by the technique used to immobilize torus fractures. The five studies used in this review had no reports of refracture in the 443 patients included in analysis, though only one of the studies (Plint et al) followed patients for more than 6 weeks.8,9 In this study, 75 patients were randomized to either a plaster removable splint or full below-elbow cast for 3 weeks; thereafter, they were followed for 6 months, during which time none experienced refracture.9
Another outcome from the same study assessed the ability of the patient to use the affected arm in the recovery period. While those in removable splints scored better during and immediately after cast removal, no differences were present after 1 week. Not surprisingly, families preferred the soft bandages or a removable splint for treatment.
Case 3
A 13-year-old boy presented to the ED with right ankle pain and difficulty bearing weight. He stated that he was playing basketball when he “rolled” his right ankle coming down from a rebound.
Ankle Fractures
Ankle fractures are among the most common acute injuries of the lower extremity in children, accounting for approximately 5% of pediatric fractures and 15% of physeal injuries.10 Ankle fractures also account for up to 40% of all injuries to the skeletally immature athlete.10,11 More specifically, distal fibular physeal fractures are the most common types of pediatric ankle fracture; however, they are associated with a relatively low risk for long-term complications. In contrast, distal tibial physeal fractures are associated with a higher risk for long-term complications.12,13
Presentation and Evaluation
Typically, patients presenting with ankle fractures are too sore to bear weight, and swelling and ecchymosis can be identified anterior to the ankle. In addition, there may be diffuse tenderness throughout the ankle and point tenderness may be induced on the anterolateral aspect of the distal tibia.14 A complete evaluation of the entire lower extremity should be conducted before assuming that the injury is confined to the ankle, especially in children younger than age 5 years and/or who are nonverbal.10 When evaluating an ankle fracture, in general, orthopedic consultation should be obtained for children with neurovascular compromise, open fractures, and/or Salter-Harris III, IV, and V fractures.
The juvenile Tillaux fracture represents a Salter-Harris III physeal injury that involves the anterolateral portion of the tibia. It usually occurs in children between ages 12 and 14 years as they approach skeletal maturity and who have a partially fused tibial physis. The common mechanism of injury is inversion of the ankle with the foot pointed away from the midline (supination with external rotation). This leads to avulsion of the lateral tibial epiphysis that is attached to the anterior inferior tibiofibular ligament. The uninvolved medial portion of the epiphysis is closed.10
Radiographic Imaging
Three radiographic views should be obtained in the evaluation of pediatric ankle injuries as Tillaux fractures or other subtle injuries could be easily missed if only two views are obtained. Interpretation of the radiographs must be correlated with the physical examination.10 The fracture line is usually best seen on a mortise view (Figure 2). Computed tomography (CT) is warranted in cases in which displacement greater than 2 mm is suspected because it better defines fracture displacement and can aid in surgical planning.14 Because of its sensitivity in detecting fractures displaced more than 2 mm, CT is now the preferred imaging modality in the assessment of juvenile Tillaux fractures.15
Definitive Management
There are two important goals when treating children with ankle fractures—achieving a satisfactory reduction and avoiding physeal arrest so as to minimize the risks of angular deformity, early arthrosis, leg-length inequality, and joint stiffness.11 Juvenile Tillaux fractures with greater than 2 mm of displacement require orthopedic consultation for closed or open reduction. Closed reduction is attempted by internally rotating the foot and applying direct pressure over the anterolateral tibia. If necessary, percutaneous pins can be used for stabilization of the reduction. If closed reduction is unsuccessful, open reduction is required. Care must be taken to assure no displacement occurs after casting; this requires weekly X-ray evaluation for the first 2 weeks.12
Patients with nondisplaced Salter-Harris III fractures are treated with long-leg casting for 4 weeks with conversion to a short-leg cast or boot for an additional 4 weeks. Patients should anticipate 8 weeks of nonweight-bearing. The patient is allowed to remove the boot for range-of-motion exercises but must remain nonweight-bearing for the first 2 weeks.14
Case 4
A 3-year-old previously healthy girl presented to the ED with a limp and difficulty bearing weight. Her mother reported that the child was playing in the yard when she caught her foot on a tree root, stumbled, and fell down. Since the incident, the child has been tearful, limping, and refusing to walk.
Tibial Fractures
Tibial fractures are among the most frequent types of orthopedic injuries in young children, with only femur and forearm fractures having a higher incidence of occurrence. Tibial fractures account for up to 15% of long bone fractures in children and adolescents.16,17 The mechanism of injury varies depending on the patient’s age. In young children, the most common cause of injury is from a seemingly minor twisting around a fixed foot or from a minor fall. In older children and adults, high-energy motor vehicle accidents and sports-related injuries are more common causes.
Fractures of the tibial shaft are typically short oblique or transverse fractures of the middle or distal third of the shaft. Thirty percent of tibial shaft fractures are associated with fractures of the fibula.16
Toddler’s Fracture
The term toddler’s fracture refers to a nondisplaced oblique fracture of the tibial shaft without concomitant fibular fracture. It usually results from an indirect rotational or twisting force applied to the foot and lower leg.16-18 More specifically, the term describes a specialized case of spiral fracture of the distal tibia in patients aged 9 months to 3 years, when weight-bearing is just beginning.19,20 Such injuries commonly occur when a toddler stumbles and falls, or attempts to extricate the foot from between the bars of a crib. Often, however, the mechanism is minimal or unknown.18 Of those injuries that are witnessed, most caregivers report a minor twisting mechanism. Most children with toddler’s fracture are younger than age 6 years. Sixty-three of 76 such fractures reported by Dunbar et al17,19 occurred in children younger than 2.5 years of age. Toddler’s fractures occur more often in boys than girls, and in the right leg more often than the left. Most children will give a history of tripping or twisting their ankle.17
Evaluating the Toddler
Toddlers can be challenging patients as they can not relate history and are often uncooperative on examination. A child may present with a limp, diminished movement of the affected limb, or refuse to bear weight without a distinct history of injury. The onset of limping or refusal to bear weight after minor trauma, or without an obvious injury in a young ambulatory child, warrants a detailed examination looking for tenderness over the tibia, along with radiographic evaluation to rule out a toddler’s fracture.
The examination of the patient is rarely impressive as there is little swelling and bruising with most toddlers’ fractures. A complete clinical history is needed, including a detailed description of any observed traumatic event to exclude the existence of other injuries.
When no traumatic event is observed or an inconsistent history is provided, the physician should obtain a detailed social history, including a list of the child’s most recent caregivers and contacts.16 Because of mild clinical symptoms and frequent lack of a history of injury in this patient population, presentation for evaluation may be delayed. In such cases, by the time the extremity is examined, the fracture has begun to heal. This healing phase may be accompanied by periosteal new bone and, in the absence of a history, may erroneously suggest other, more ominous conditions such as osteomylelitis or tumor.17,18
Consideration of Abuse
Although tibial shaft fractures are rarely found in abused children, diagnosis of child abuse must be considered in cases where a tibial fracture is discovered in the nonambulatory child; his or her clinical history is inconsistent with the injury; and/or there are other physical findings suggestive of abuse. Investigation for suspected nonaccidental trauma includes a thorough physical examination, skeletal survey, and evaluation by social services personnel.16
Radiographic Imaging
Quality anteroposterior (AP) or lateral radiographs of the affected leg may show a hairline fracture, but these can easily be missed on initial plain films in almost a third of patients.21 An internal oblique view can aid in identifying nondisplaced toddler fractures.17 The AP view is the best view for observing the nondisplaced spiral fracture along the distal tibia (Figure 3).6 Occasionally, a fracture line is not identified on initial plain films and the first evidence of fracture becomes apparent on X-ray when new periosteal bone forms 7 to 10 days after the initial injury.
Definitive Treatment
Children with a classic history for a toddler’s fracture and an inability to bear weight should be immobilized with a long-leg splint or cast—even when X-rays are negative—until a definitive diagnosis can be made. Such fractures usually become visible on X-ray 7 to 10 days after injury as a result of new bone growth.22
When definitive diagnosis of a toddler’s fracture is made on plain radiographs, the child should either be immobilized in a long-leg splint with referral to an orthopedist within 5 to 7 days, or immediately casted.16
Conclusion
Fractures in both children and adults are among the most common injury-related presentations to the ED. Based on the structure and increased elasticity of bone in the pediatric patient, there are several fracture patterns unique to this population. Appropriate evaluation, diagnosis, and management in the ED helps to maximize and ensure long-term function and healing while minimizing trauma to the patient.
Dr McBride is an associate professor of pediatrics and pediatric emergency medicine, Wake Forest Baptist Health, Brenner Children’s Hospital, Winston-Salem, North Carolina.
Dr Sutton is a pediatric resident, Wake Forest Baptist Health, Brenner Children’s Hospital, Winston-Salem, North Carolina.
Case 1
A 2-year-old girl presented to the ED with arm pain. Her mother stated that her daughter was playing with a 5-year-old sibling when she heard the child cry- out in pain and noticed she was holding her right arm by her side, not wanting to move it. Neither child gave a reliable story of the injury.
Nursemaid’s Elbow
Nursemaid’s elbow, also known as pulled elbow, subluxation of the radial head, and most recently annular ligament displacement, is a common injury in children younger than age 6 years. One study estimates that the condition represented about 1% of injury-related ED visits in 2005.1
Patients with nursemaid’s elbow typically present holding the injured arm at their side, slightly flexed and pronated. These patients appear relatively comfortable until moved actively or passively. The classic history of nursemaid’s elbow includes a traction mechanism, with the child being pulled up by one arm or being grabbed by the arm suddenly to keep him or her out of harm’s way.2 Due to the laxity of connective tissues in children of this age, the head of the radius slips out of the annular ligament causing acute pain and decreased function.
Nursemaid’s elbow is usually diagnosed by history and examination alone, with special consideration to the mechanism of injury. There is rarely swelling or bruising.3 Passive flexion and extension at the elbow may be normal, but rotational maneuvers can be painful or fully resisted.
Reduction Techniques
In 2012, Cochrane updated its earlier review on nursemaid’s elbow and in 2013 followed up with an article in Pediatrics in Review.3,4 Each covered research on reduction techniques, summarizing studies comparing supination-flexion (SF) versus hyperpronation (HP) as the initial reduction maneuver. Given that these maneuvers are difficult to camouflage, studies tend to be pseudorandomized with assessment by a nonblinded healthcare provider, decreasing the strength of the studies. In the Cochrane review, four different trials that included 379 children under age 7 years were selected for the review. In all four studies, pronation was found to have the least chance of failed first attempt, the chosen outcome for this meta-analysis. The risk ratio of failure of reduction for pronation was 0.45 (95% confidence interval [CI], 0.28-0.73).
There is some data supporting hyperpronation to be less painful as well; however, the Cochrane reviewers felt there may have been reporting bias.4 Since the time of each of these reviews, another study comprised of 150 children was conducted and also favored similar practice styles, as the hyperpronation maneuver had 95% success rate on first attempt versus 68% first-time success with supination and flexion.5
Complications and Recurrence
In a small study aimed at identifying recurrence rates for nursemaid’s elbow, Teach and Schultzman6 studied 93 children for 1 year after probable or definite diagnosis of nursemaid’s elbow. Of these children, 23.7% had recurrent radial head subluxation. Children younger than age 2 years were found to have a relative risk of 2.6 (95% CI, 1.04-6.30) for one or more recurrences when compared to children older than age 2 years.
While the great majority of children with nursemaid’s elbow do not need referral to an orthopedist, those with two or more occurrences should be considered for referral to a specialist.
Case 2
A 6-year-old boy was presented to the ED by his father, who had placed the boy’s arm in a home-made sling. The child tearfully told the provider that he fell trying to catch himself after tripping over the house pet.
FOOSH Injury
The above case depicts a very common presentation in the ED—the so-called “FOOSH” (fall onto an outstretched hand) injury. This type of injury occurs with such frequency in both adults and children that it is one of the only injury patterns with a commonly used acronym. The bony injuries seen with FOOSH in children, however, have a different pattern than those in adults.
Pediatric fractures are unique due to the difference in the structure of the bones themselves. A child’s bones are more elastic than an adult’s bones, allowing them to bow and bend before they fracture.7 Despite this malleability, pediatric bones have been noted to have a thicker periosteum. For this reason, compression or impact may interrupt the periosteal sleeve, minimally yielding an incomplete interruption of the cortex unilaterally.
One fracture pattern commonly seen in children is the torus fracture. This type of fracture is also referred to as a buckle fracture as the bone cortex on radiographic imaging appears “buckled” as a result of the compressive forces on that side of the bone (Figure 1). Since the bone itself is minimally affected, these fractures are quite stable and not at risk for complications.
In comparison, a greenstick fracture, also unique to the pediatric population, is one in which the cortex shows plastic deformity on the side of the force or impact but is interrupted on the opposite side due to the tension of the impact itself. Greenstick fractures are frequently angulated and may require reduction for anatomic alignment, but long-term complications are typically minimal. These fracture patterns are distinguished from complete fractures (as seen in adults), which are quite unstable and generally require surgical intervention.
Of note, the location of pediatric forearm fractures varies with age as well. Diaphyseal fractures are more common in prepubescent children, whereas the highest incidence of physeal injuries occurs during large growth spurts, particularly throughout adolescence.7
Management
The remodeling potential of pediatric bones also makes management unique. Pediatric orthopedic literature has well-studied acceptable angles and degrees of appropriate displacement based largely on the age of the patient and proximity to a growth plate. Knowledge of these is imperative for definitive care of such fractures but is beyond the scope of this review.
Traditional treatment of pediatric forearm fractures includes immobilization of various types and duration to minimize pain and deformity while producing the best possible outcome. Several recent studies have aimed to determine best practice for the different fracture types with the goal of producing best alignment and return to function while decreasing cost, discomfort, and number of physician visits. Another concern among healthcare providers is the risk of refracture, which in buckle fractures is estimated at approximately 2% with a median time of 8 to 16 weeks after the initial injury.7
A 2010 review by Kennedy et al8 sought to determine if the refracture rate was affected by the technique used to immobilize torus fractures. The five studies used in this review had no reports of refracture in the 443 patients included in analysis, though only one of the studies (Plint et al) followed patients for more than 6 weeks.8,9 In this study, 75 patients were randomized to either a plaster removable splint or full below-elbow cast for 3 weeks; thereafter, they were followed for 6 months, during which time none experienced refracture.9
Another outcome from the same study assessed the ability of the patient to use the affected arm in the recovery period. While those in removable splints scored better during and immediately after cast removal, no differences were present after 1 week. Not surprisingly, families preferred the soft bandages or a removable splint for treatment.
Case 3
A 13-year-old boy presented to the ED with right ankle pain and difficulty bearing weight. He stated that he was playing basketball when he “rolled” his right ankle coming down from a rebound.
Ankle Fractures
Ankle fractures are among the most common acute injuries of the lower extremity in children, accounting for approximately 5% of pediatric fractures and 15% of physeal injuries.10 Ankle fractures also account for up to 40% of all injuries to the skeletally immature athlete.10,11 More specifically, distal fibular physeal fractures are the most common types of pediatric ankle fracture; however, they are associated with a relatively low risk for long-term complications. In contrast, distal tibial physeal fractures are associated with a higher risk for long-term complications.12,13
Presentation and Evaluation
Typically, patients presenting with ankle fractures are too sore to bear weight, and swelling and ecchymosis can be identified anterior to the ankle. In addition, there may be diffuse tenderness throughout the ankle and point tenderness may be induced on the anterolateral aspect of the distal tibia.14 A complete evaluation of the entire lower extremity should be conducted before assuming that the injury is confined to the ankle, especially in children younger than age 5 years and/or who are nonverbal.10 When evaluating an ankle fracture, in general, orthopedic consultation should be obtained for children with neurovascular compromise, open fractures, and/or Salter-Harris III, IV, and V fractures.
The juvenile Tillaux fracture represents a Salter-Harris III physeal injury that involves the anterolateral portion of the tibia. It usually occurs in children between ages 12 and 14 years as they approach skeletal maturity and who have a partially fused tibial physis. The common mechanism of injury is inversion of the ankle with the foot pointed away from the midline (supination with external rotation). This leads to avulsion of the lateral tibial epiphysis that is attached to the anterior inferior tibiofibular ligament. The uninvolved medial portion of the epiphysis is closed.10
Radiographic Imaging
Three radiographic views should be obtained in the evaluation of pediatric ankle injuries as Tillaux fractures or other subtle injuries could be easily missed if only two views are obtained. Interpretation of the radiographs must be correlated with the physical examination.10 The fracture line is usually best seen on a mortise view (Figure 2). Computed tomography (CT) is warranted in cases in which displacement greater than 2 mm is suspected because it better defines fracture displacement and can aid in surgical planning.14 Because of its sensitivity in detecting fractures displaced more than 2 mm, CT is now the preferred imaging modality in the assessment of juvenile Tillaux fractures.15
Definitive Management
There are two important goals when treating children with ankle fractures—achieving a satisfactory reduction and avoiding physeal arrest so as to minimize the risks of angular deformity, early arthrosis, leg-length inequality, and joint stiffness.11 Juvenile Tillaux fractures with greater than 2 mm of displacement require orthopedic consultation for closed or open reduction. Closed reduction is attempted by internally rotating the foot and applying direct pressure over the anterolateral tibia. If necessary, percutaneous pins can be used for stabilization of the reduction. If closed reduction is unsuccessful, open reduction is required. Care must be taken to assure no displacement occurs after casting; this requires weekly X-ray evaluation for the first 2 weeks.12
Patients with nondisplaced Salter-Harris III fractures are treated with long-leg casting for 4 weeks with conversion to a short-leg cast or boot for an additional 4 weeks. Patients should anticipate 8 weeks of nonweight-bearing. The patient is allowed to remove the boot for range-of-motion exercises but must remain nonweight-bearing for the first 2 weeks.14
Case 4
A 3-year-old previously healthy girl presented to the ED with a limp and difficulty bearing weight. Her mother reported that the child was playing in the yard when she caught her foot on a tree root, stumbled, and fell down. Since the incident, the child has been tearful, limping, and refusing to walk.
Tibial Fractures
Tibial fractures are among the most frequent types of orthopedic injuries in young children, with only femur and forearm fractures having a higher incidence of occurrence. Tibial fractures account for up to 15% of long bone fractures in children and adolescents.16,17 The mechanism of injury varies depending on the patient’s age. In young children, the most common cause of injury is from a seemingly minor twisting around a fixed foot or from a minor fall. In older children and adults, high-energy motor vehicle accidents and sports-related injuries are more common causes.
Fractures of the tibial shaft are typically short oblique or transverse fractures of the middle or distal third of the shaft. Thirty percent of tibial shaft fractures are associated with fractures of the fibula.16
Toddler’s Fracture
The term toddler’s fracture refers to a nondisplaced oblique fracture of the tibial shaft without concomitant fibular fracture. It usually results from an indirect rotational or twisting force applied to the foot and lower leg.16-18 More specifically, the term describes a specialized case of spiral fracture of the distal tibia in patients aged 9 months to 3 years, when weight-bearing is just beginning.19,20 Such injuries commonly occur when a toddler stumbles and falls, or attempts to extricate the foot from between the bars of a crib. Often, however, the mechanism is minimal or unknown.18 Of those injuries that are witnessed, most caregivers report a minor twisting mechanism. Most children with toddler’s fracture are younger than age 6 years. Sixty-three of 76 such fractures reported by Dunbar et al17,19 occurred in children younger than 2.5 years of age. Toddler’s fractures occur more often in boys than girls, and in the right leg more often than the left. Most children will give a history of tripping or twisting their ankle.17
Evaluating the Toddler
Toddlers can be challenging patients as they can not relate history and are often uncooperative on examination. A child may present with a limp, diminished movement of the affected limb, or refuse to bear weight without a distinct history of injury. The onset of limping or refusal to bear weight after minor trauma, or without an obvious injury in a young ambulatory child, warrants a detailed examination looking for tenderness over the tibia, along with radiographic evaluation to rule out a toddler’s fracture.
The examination of the patient is rarely impressive as there is little swelling and bruising with most toddlers’ fractures. A complete clinical history is needed, including a detailed description of any observed traumatic event to exclude the existence of other injuries.
When no traumatic event is observed or an inconsistent history is provided, the physician should obtain a detailed social history, including a list of the child’s most recent caregivers and contacts.16 Because of mild clinical symptoms and frequent lack of a history of injury in this patient population, presentation for evaluation may be delayed. In such cases, by the time the extremity is examined, the fracture has begun to heal. This healing phase may be accompanied by periosteal new bone and, in the absence of a history, may erroneously suggest other, more ominous conditions such as osteomylelitis or tumor.17,18
Consideration of Abuse
Although tibial shaft fractures are rarely found in abused children, diagnosis of child abuse must be considered in cases where a tibial fracture is discovered in the nonambulatory child; his or her clinical history is inconsistent with the injury; and/or there are other physical findings suggestive of abuse. Investigation for suspected nonaccidental trauma includes a thorough physical examination, skeletal survey, and evaluation by social services personnel.16
Radiographic Imaging
Quality anteroposterior (AP) or lateral radiographs of the affected leg may show a hairline fracture, but these can easily be missed on initial plain films in almost a third of patients.21 An internal oblique view can aid in identifying nondisplaced toddler fractures.17 The AP view is the best view for observing the nondisplaced spiral fracture along the distal tibia (Figure 3).6 Occasionally, a fracture line is not identified on initial plain films and the first evidence of fracture becomes apparent on X-ray when new periosteal bone forms 7 to 10 days after the initial injury.
Definitive Treatment
Children with a classic history for a toddler’s fracture and an inability to bear weight should be immobilized with a long-leg splint or cast—even when X-rays are negative—until a definitive diagnosis can be made. Such fractures usually become visible on X-ray 7 to 10 days after injury as a result of new bone growth.22
When definitive diagnosis of a toddler’s fracture is made on plain radiographs, the child should either be immobilized in a long-leg splint with referral to an orthopedist within 5 to 7 days, or immediately casted.16
Conclusion
Fractures in both children and adults are among the most common injury-related presentations to the ED. Based on the structure and increased elasticity of bone in the pediatric patient, there are several fracture patterns unique to this population. Appropriate evaluation, diagnosis, and management in the ED helps to maximize and ensure long-term function and healing while minimizing trauma to the patient.
Dr McBride is an associate professor of pediatrics and pediatric emergency medicine, Wake Forest Baptist Health, Brenner Children’s Hospital, Winston-Salem, North Carolina.
Dr Sutton is a pediatric resident, Wake Forest Baptist Health, Brenner Children’s Hospital, Winston-Salem, North Carolina.
- Brown D. Emergency department visits for nursemaid’s elbow in the United States, 2005-2006. Orthop Nurs. 2009;28(4):161,162.
- Hardy RH. Pulled elbow. J R Coll Gen Pract. 1978;28(189):224-226.
- Browner EA. Nursemaid’s elbow (annular ligament displacement). Pediatr Rev. 2013;34(8):366,367.
- Krul M, van der Wouden JC,van Suijlekom-Smit LW, Koes BM. Manipulative interventions for reducing pulled elbow in young children. Cochrane Database of Syst Rev. 2012;1:CD007759.
- Gunaydin YK, Katirci Y, Duymaz H, et al. Comparison of success and pain levels of supination-flexion and hyperpronation maneuvers in childhood nursemaid’s elbow cases. Am J Emerg Med. 2013;31(7):1078-1081.
- Teach SJ, Schutzman SA. Prospective study of recurrent radial head subluxation. Arch Pediatr Adolesc Med. 1996;150(2):164-166.
- Dolan M and Waters PM. Fractures and dislocations of the forearm, wrist, and hand. In: Green NE, Swiontkowski MF, eds. Skeletal Trauma in Children. 4th ed. Philadephia, PA: Saunders Elsevier; 2009:159-206.
- Kennedy SA, Slobogean GP, Mulpuri K. Does degree of immobilization influence refracture rate in the forearm buckle fracture? J Pediatr Orthop B. 2010;19(1):77-81.
- Plint AC, Perry JJ, Correll R, Gaboury I, Lawtown L. A randomized, controlled trial of removable splinting versus casting for wrist buckle fractures in children. Pediatrics. 2006;117(3):691-697.
- Kay RM, Matthys GA. Pediatric ankle fractures: evaluation and treatment. J Am Acad Orthop Surg. 2001;9(4):268-278.
- Marsh JS, Daigneault JP. Ankle injuries in the pediatric population. Curr Opin Pediatr. 2000;12(1):52-60
- Cummings RJ. Distal tibial and fibular fractures. In: Beaty JH, Kasser JR, eds. Rockwood and Wilkins’ Fractures in Children. 6th ed. Pennsylvania, PA: Lippincott Williams & Wilkins; 2006:1096-1104.
- Boutis K, Willan AR, Babyn P, Narayanan UG, Alman B, Schuh S. A randomized, controlled trial of a removable brace versus casting in children with low-risk ankle fractures. Pediatrics. 2007;119(6):1256-1263.
- Wuerz TH, Gurd DP. Pediatric physeal ankle fracture. J Am Acad Orthop Surg. 2013;21(4):234-244.
- Horn BD, Crisci K, Krug M, Pizzutillo PD, MacEwen GD. Radiologic evaluation of juvenile Tillaux fractures of the distal tibia. J Pediatr Orthop. 2001;21(2):162-164.
- Mashru RP, Herman MJ, Pizzutillo PD. Tibial shaft fractures in children and adolescents. J Am Acad Orthop Surg. 2005;139(5):345-352.
- Heinrich SD, Mooney JF. Fractures of the shaft of the tibia and fibula. In: Beaty JH, Kasser JR, eds. Rockwood and Wilkins’ Fractures in Children. 6th ed. Pennsylvania, PA: Lippincott Williams & Wilkins; 2006:1063,1064.
- John SD, Moorthy CS, Swischuk LE. Expanding the concept of the toddler’s fracture. Radiographics. 1997;17(2):367-376.
- Dunbar JS, Owen HF, Nogrady MB, McLeese R. Obscure tibial fracture of infants—the toddlers’ fracture. J Can Assoc Radiol 1964;15:136-144.
- Tenenbein M, Reed MH, Black GB. The toddler’s fracture revisited. Am J Emerg Med. 1990;8(3):208-211.
- Shravat BP, Harrop SN, Kane TP. Toddler’s fracture. J Accid Emerg Med. 1996;13(1):59-61.
- Halsey MF, Finzel KC, Carrion WV, Haralabatos SS, Gruber MA, Meinhard BP. Toddler’s fracture: presumptive diagnosis and treatment. J Pediatr Orthop. 2001;21(2):152-156.
- Brown D. Emergency department visits for nursemaid’s elbow in the United States, 2005-2006. Orthop Nurs. 2009;28(4):161,162.
- Hardy RH. Pulled elbow. J R Coll Gen Pract. 1978;28(189):224-226.
- Browner EA. Nursemaid’s elbow (annular ligament displacement). Pediatr Rev. 2013;34(8):366,367.
- Krul M, van der Wouden JC,van Suijlekom-Smit LW, Koes BM. Manipulative interventions for reducing pulled elbow in young children. Cochrane Database of Syst Rev. 2012;1:CD007759.
- Gunaydin YK, Katirci Y, Duymaz H, et al. Comparison of success and pain levels of supination-flexion and hyperpronation maneuvers in childhood nursemaid’s elbow cases. Am J Emerg Med. 2013;31(7):1078-1081.
- Teach SJ, Schutzman SA. Prospective study of recurrent radial head subluxation. Arch Pediatr Adolesc Med. 1996;150(2):164-166.
- Dolan M and Waters PM. Fractures and dislocations of the forearm, wrist, and hand. In: Green NE, Swiontkowski MF, eds. Skeletal Trauma in Children. 4th ed. Philadephia, PA: Saunders Elsevier; 2009:159-206.
- Kennedy SA, Slobogean GP, Mulpuri K. Does degree of immobilization influence refracture rate in the forearm buckle fracture? J Pediatr Orthop B. 2010;19(1):77-81.
- Plint AC, Perry JJ, Correll R, Gaboury I, Lawtown L. A randomized, controlled trial of removable splinting versus casting for wrist buckle fractures in children. Pediatrics. 2006;117(3):691-697.
- Kay RM, Matthys GA. Pediatric ankle fractures: evaluation and treatment. J Am Acad Orthop Surg. 2001;9(4):268-278.
- Marsh JS, Daigneault JP. Ankle injuries in the pediatric population. Curr Opin Pediatr. 2000;12(1):52-60
- Cummings RJ. Distal tibial and fibular fractures. In: Beaty JH, Kasser JR, eds. Rockwood and Wilkins’ Fractures in Children. 6th ed. Pennsylvania, PA: Lippincott Williams & Wilkins; 2006:1096-1104.
- Boutis K, Willan AR, Babyn P, Narayanan UG, Alman B, Schuh S. A randomized, controlled trial of a removable brace versus casting in children with low-risk ankle fractures. Pediatrics. 2007;119(6):1256-1263.
- Wuerz TH, Gurd DP. Pediatric physeal ankle fracture. J Am Acad Orthop Surg. 2013;21(4):234-244.
- Horn BD, Crisci K, Krug M, Pizzutillo PD, MacEwen GD. Radiologic evaluation of juvenile Tillaux fractures of the distal tibia. J Pediatr Orthop. 2001;21(2):162-164.
- Mashru RP, Herman MJ, Pizzutillo PD. Tibial shaft fractures in children and adolescents. J Am Acad Orthop Surg. 2005;139(5):345-352.
- Heinrich SD, Mooney JF. Fractures of the shaft of the tibia and fibula. In: Beaty JH, Kasser JR, eds. Rockwood and Wilkins’ Fractures in Children. 6th ed. Pennsylvania, PA: Lippincott Williams & Wilkins; 2006:1063,1064.
- John SD, Moorthy CS, Swischuk LE. Expanding the concept of the toddler’s fracture. Radiographics. 1997;17(2):367-376.
- Dunbar JS, Owen HF, Nogrady MB, McLeese R. Obscure tibial fracture of infants—the toddlers’ fracture. J Can Assoc Radiol 1964;15:136-144.
- Tenenbein M, Reed MH, Black GB. The toddler’s fracture revisited. Am J Emerg Med. 1990;8(3):208-211.
- Shravat BP, Harrop SN, Kane TP. Toddler’s fracture. J Accid Emerg Med. 1996;13(1):59-61.
- Halsey MF, Finzel KC, Carrion WV, Haralabatos SS, Gruber MA, Meinhard BP. Toddler’s fracture: presumptive diagnosis and treatment. J Pediatr Orthop. 2001;21(2):152-156.

{kind=link}