User login
Religion and LGBTQ identities
JB is a 15-year-old female who presents to your office for a wellness check. Mom is concerned because she has seemed more depressed and withdrawn over the past few months. During the confidential portion of your visit, JB discloses that, while she has had boyfriends in the past, she is realizing that she is romantically and sexually attracted to females. Many members of her religious faith, which she is strongly connected to, believe that homosexuality is a sin. She has been secretly researching therapies to help her “not be gay” and asks you for advice.
Adolescence is a time of rapid growth and development. Two important developmental tasks of adolescence are to establish key aspects of identity and identify meaningful moral standards, values, and belief systems.1 For some LGBTQ adolescents, these tasks can become more complicated when the value system or religious faith in which they were raised views homosexuality or gender nonconformity as a sin.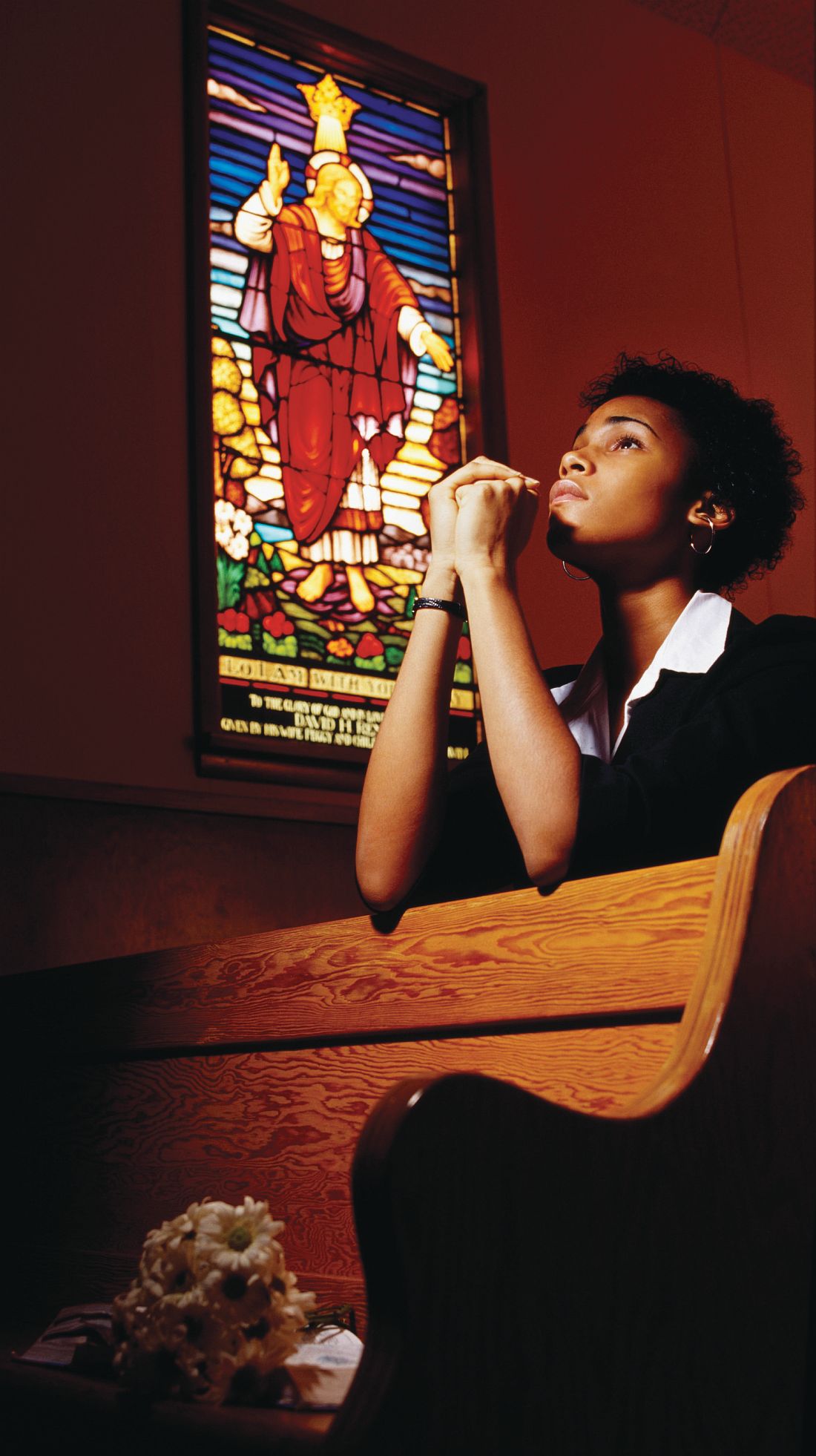
- Identifying as lesbian, gay, bisexual, or transgender is normal, just different.
- LGBT people exist in almost every faith group across the country.
- Many religious groups have wrestled with homosexuality, gender identity, and religion and decided to be more welcoming to LGBT communities.
- Within most faiths, there are many interpretations of religious texts, such as the Bible and the Koran, on all issues, including homosexuality.
- While every religion has different teachings, almost all religions advocate love and compassion.
- Clergy and other faith leaders can be a source of support. However, every faith community is different and may not always be supportive. Safely investigate your individual community’s approach. You have the right to question and explore your faith, sexuality, and/or gender identity and reconcile these in a way that is true to you.
- Remember this is your journey. You get to decide the path and the pace.
- Recognize that this may involve working for change within your community or it may mean leaving it.
- Referral for “conversion” or “reparative therapy” is never indicated. Such therapy is not effective and may be harmful to LGBTQ individuals by increasing internalized stigma, distress, and depression.

Dr. Chelvakumar is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at the Ohio State University, both in Columbus. She has no relevant financial disclosures. Email her at [email protected].
Spirituality resources
- LGBTQ and Religion: Your Relationship with Religion is Completely Up to You, the FAQ Page by the Trevor Project, a national organization that provides crisis intervention and suicide prevention resources to LGBTQ young people ages 13-24 years. www.thetrevorproject.org/pages/lgbtq-and-religion
- Faith in Our Families: Parents, Families and Friends Talk About Religion and Homosexuality, a resource from PFLAG (Parents, Families, and Friends of Lesbians and Gays). www.pflag.org/sites/default/files/Faith%20In%20Our%20Families.pdf
- LGBT Center UNC Chapel Hill: Religion and Spirituality, a page with a link to nondenominational and denomination-specific resources with various religious and spiritual communities’ beliefs regarding faith and LGBTQIA+ (Lesbian, Gay, Bisexual, Transgender, Queer, Intersex, Asexual). lgbtq.unc.edu/resources/exploring-identities/religion-and-spirituality
- HRC: Explore Religion and Faith, a Human Rights Campaign page containing links to resources on religion and faith. It also has links to the Coming Home Series, guides aimed at those who hope to lead their faith communities toward a more welcoming stance and those seeking a path back to beloved traditions. www.hrc.org/explore/topic/religion-faith
References
1. Raising teens: A synthesis or research and a foundation for action. (Boston: Center for Health Communication, Harvard School of Public Health, 2001).
2. Faith in Our Families: Parents, Families and Friends Talk About Religion and Homosexuality (Washington, D.C.: Parents, Families and Friends of Lesbians and Gays, 1997)
3. Pediatrics. 2013 Jul;132(1):198-203.
4. The Health of Lesbian, Gay, Bisexual, and Transgender People: Building a Foundation for Better Understanding. (Washington, D.C.: National Academies Press, 2011)
5. Coming Home: To Faith, to Spirit, to Self. Pamphlet by the Human Rights Campaign.
JB is a 15-year-old female who presents to your office for a wellness check. Mom is concerned because she has seemed more depressed and withdrawn over the past few months. During the confidential portion of your visit, JB discloses that, while she has had boyfriends in the past, she is realizing that she is romantically and sexually attracted to females. Many members of her religious faith, which she is strongly connected to, believe that homosexuality is a sin. She has been secretly researching therapies to help her “not be gay” and asks you for advice.
Adolescence is a time of rapid growth and development. Two important developmental tasks of adolescence are to establish key aspects of identity and identify meaningful moral standards, values, and belief systems.1 For some LGBTQ adolescents, these tasks can become more complicated when the value system or religious faith in which they were raised views homosexuality or gender nonconformity as a sin.
- Identifying as lesbian, gay, bisexual, or transgender is normal, just different.
- LGBT people exist in almost every faith group across the country.
- Many religious groups have wrestled with homosexuality, gender identity, and religion and decided to be more welcoming to LGBT communities.
- Within most faiths, there are many interpretations of religious texts, such as the Bible and the Koran, on all issues, including homosexuality.
- While every religion has different teachings, almost all religions advocate love and compassion.
- Clergy and other faith leaders can be a source of support. However, every faith community is different and may not always be supportive. Safely investigate your individual community’s approach. You have the right to question and explore your faith, sexuality, and/or gender identity and reconcile these in a way that is true to you.
- Remember this is your journey. You get to decide the path and the pace.
- Recognize that this may involve working for change within your community or it may mean leaving it.
- Referral for “conversion” or “reparative therapy” is never indicated. Such therapy is not effective and may be harmful to LGBTQ individuals by increasing internalized stigma, distress, and depression.
Dr. Chelvakumar is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at the Ohio State University, both in Columbus. She has no relevant financial disclosures. Email her at [email protected].
Spirituality resources
- LGBTQ and Religion: Your Relationship with Religion is Completely Up to You, the FAQ Page by the Trevor Project, a national organization that provides crisis intervention and suicide prevention resources to LGBTQ young people ages 13-24 years. www.thetrevorproject.org/pages/lgbtq-and-religion
- Faith in Our Families: Parents, Families and Friends Talk About Religion and Homosexuality, a resource from PFLAG (Parents, Families, and Friends of Lesbians and Gays). www.pflag.org/sites/default/files/Faith%20In%20Our%20Families.pdf
- LGBT Center UNC Chapel Hill: Religion and Spirituality, a page with a link to nondenominational and denomination-specific resources with various religious and spiritual communities’ beliefs regarding faith and LGBTQIA+ (Lesbian, Gay, Bisexual, Transgender, Queer, Intersex, Asexual). lgbtq.unc.edu/resources/exploring-identities/religion-and-spirituality
- HRC: Explore Religion and Faith, a Human Rights Campaign page containing links to resources on religion and faith. It also has links to the Coming Home Series, guides aimed at those who hope to lead their faith communities toward a more welcoming stance and those seeking a path back to beloved traditions. www.hrc.org/explore/topic/religion-faith
References
1. Raising teens: A synthesis or research and a foundation for action. (Boston: Center for Health Communication, Harvard School of Public Health, 2001).
2. Faith in Our Families: Parents, Families and Friends Talk About Religion and Homosexuality (Washington, D.C.: Parents, Families and Friends of Lesbians and Gays, 1997)
3. Pediatrics. 2013 Jul;132(1):198-203.
4. The Health of Lesbian, Gay, Bisexual, and Transgender People: Building a Foundation for Better Understanding. (Washington, D.C.: National Academies Press, 2011)
5. Coming Home: To Faith, to Spirit, to Self. Pamphlet by the Human Rights Campaign.
JB is a 15-year-old female who presents to your office for a wellness check. Mom is concerned because she has seemed more depressed and withdrawn over the past few months. During the confidential portion of your visit, JB discloses that, while she has had boyfriends in the past, she is realizing that she is romantically and sexually attracted to females. Many members of her religious faith, which she is strongly connected to, believe that homosexuality is a sin. She has been secretly researching therapies to help her “not be gay” and asks you for advice.
Adolescence is a time of rapid growth and development. Two important developmental tasks of adolescence are to establish key aspects of identity and identify meaningful moral standards, values, and belief systems.1 For some LGBTQ adolescents, these tasks can become more complicated when the value system or religious faith in which they were raised views homosexuality or gender nonconformity as a sin.
- Identifying as lesbian, gay, bisexual, or transgender is normal, just different.
- LGBT people exist in almost every faith group across the country.
- Many religious groups have wrestled with homosexuality, gender identity, and religion and decided to be more welcoming to LGBT communities.
- Within most faiths, there are many interpretations of religious texts, such as the Bible and the Koran, on all issues, including homosexuality.
- While every religion has different teachings, almost all religions advocate love and compassion.
- Clergy and other faith leaders can be a source of support. However, every faith community is different and may not always be supportive. Safely investigate your individual community’s approach. You have the right to question and explore your faith, sexuality, and/or gender identity and reconcile these in a way that is true to you.
- Remember this is your journey. You get to decide the path and the pace.
- Recognize that this may involve working for change within your community or it may mean leaving it.
- Referral for “conversion” or “reparative therapy” is never indicated. Such therapy is not effective and may be harmful to LGBTQ individuals by increasing internalized stigma, distress, and depression.
Dr. Chelvakumar is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at the Ohio State University, both in Columbus. She has no relevant financial disclosures. Email her at [email protected].
Spirituality resources
- LGBTQ and Religion: Your Relationship with Religion is Completely Up to You, the FAQ Page by the Trevor Project, a national organization that provides crisis intervention and suicide prevention resources to LGBTQ young people ages 13-24 years. www.thetrevorproject.org/pages/lgbtq-and-religion
- Faith in Our Families: Parents, Families and Friends Talk About Religion and Homosexuality, a resource from PFLAG (Parents, Families, and Friends of Lesbians and Gays). www.pflag.org/sites/default/files/Faith%20In%20Our%20Families.pdf
- LGBT Center UNC Chapel Hill: Religion and Spirituality, a page with a link to nondenominational and denomination-specific resources with various religious and spiritual communities’ beliefs regarding faith and LGBTQIA+ (Lesbian, Gay, Bisexual, Transgender, Queer, Intersex, Asexual). lgbtq.unc.edu/resources/exploring-identities/religion-and-spirituality
- HRC: Explore Religion and Faith, a Human Rights Campaign page containing links to resources on religion and faith. It also has links to the Coming Home Series, guides aimed at those who hope to lead their faith communities toward a more welcoming stance and those seeking a path back to beloved traditions. www.hrc.org/explore/topic/religion-faith
References
1. Raising teens: A synthesis or research and a foundation for action. (Boston: Center for Health Communication, Harvard School of Public Health, 2001).
2. Faith in Our Families: Parents, Families and Friends Talk About Religion and Homosexuality (Washington, D.C.: Parents, Families and Friends of Lesbians and Gays, 1997)
3. Pediatrics. 2013 Jul;132(1):198-203.
4. The Health of Lesbian, Gay, Bisexual, and Transgender People: Building a Foundation for Better Understanding. (Washington, D.C.: National Academies Press, 2011)
5. Coming Home: To Faith, to Spirit, to Self. Pamphlet by the Human Rights Campaign.
Do you talk about marijuana with your patients?
Do you talk about marijuana with your patients?
In medical school, I had a roommate. He was a smart law school graduate, good looking, outgoing, had lots of friends, was funny, and he was a great cook.

I should tell you another thing about my friend: He was a heavy, daily user of marijuana.
I believe that most of us, at a certain point of our lives, have met someone like my friend. The combination of a high-stress lifestyle, high self-expectations, and lack of appropriate skills to tackle life’s obstacles when encountered with failure frequently leads to addiction or a behavioral problem. In most cases, that will cause a pathological relationship with an outside substance or stimuli (Internet overuse/shopping too much/overeating or drinking, and so on).
Living a life filled with severe trauma and pain, especially at a developmental stage, often leads to an addiction. We frequently see people escape to the sweet narcotic-induced sleep via opioid abuse. On the other hand, for people who did not suffer trauma and are highly functional, marijuana offers a means of emotional detachment from pain, in its different form, and existential depression. That is the main benefit my patients who live with marijuana addiction get.
My friend serves as a rather stereotypical – and some may say – subjective, simplistic example of what is becoming more and more common in our society. I’m willing to bet that a good number of clinicians who read this have a similar example in mind.
With its intoxication state perceived as benign and the limited medicinal advantages, marijuana rapidly is gaining more and more legitimacy in the eyes of the general public (Addict Behav. 2008 Mar;33:397-411), (Monitoring the Future: National Results on Drug Use: 1975-2016). The risk of addiction is perceived as negligible and often nonexistent.
Almost no one knows about the potential risk of addiction (around 9%) (Drug Alcohol Depend. 2011;115:120-30). No one knows about about tolerance and withdrawal states – or about the real risk of psychosis (N Engl J Med. 2014 Jun 5;370:2219-27) or about the possible risk of schizophrenia in vulnerable populations (Schizophr Res. 2016 Mar;171:[1-3]:62-7). No one talks about the fact that it’s often used with tobacco. (How many times have you been told during history taking that a patient doesn’t smoke tobacco, only to find that in drug history he smokes 3-5 joints with tobacco daily?)
[polldaddy:9796432]
Throughout my journey in the psychiatric world (studying and working on three different continents) another typical marijuana user is the patient living with chronic mental illness. My Israeli mentor often complained about not having a single “clean” patient with schizophrenia anymore. I now see the same phenomena in Philadelphia and was also exposed to the same reality in Europe during medical school.
As physicians, and especially as psychiatrists, I believe we are obligated to educate our patients by telling them about the risks in their behaviors. Educating patients about marijuana in today’s atmosphere can be a very important preventive measure, and awareness is an important step toward change.
The current generation of psychiatrists is dealing with an opioid epidemic. Let’s educate ourselves and our patients so this current epidemic won’t be followed by another, severe cannabis epidemic.
Dr. Shilo is a second-year PGY in the department of psychiatry at Einstein Medical Center, Philadelphia.
Do you talk about marijuana with your patients?
In medical school, I had a roommate. He was a smart law school graduate, good looking, outgoing, had lots of friends, was funny, and he was a great cook.
I should tell you another thing about my friend: He was a heavy, daily user of marijuana.
I believe that most of us, at a certain point of our lives, have met someone like my friend. The combination of a high-stress lifestyle, high self-expectations, and lack of appropriate skills to tackle life’s obstacles when encountered with failure frequently leads to addiction or a behavioral problem. In most cases, that will cause a pathological relationship with an outside substance or stimuli (Internet overuse/shopping too much/overeating or drinking, and so on).
Living a life filled with severe trauma and pain, especially at a developmental stage, often leads to an addiction. We frequently see people escape to the sweet narcotic-induced sleep via opioid abuse. On the other hand, for people who did not suffer trauma and are highly functional, marijuana offers a means of emotional detachment from pain, in its different form, and existential depression. That is the main benefit my patients who live with marijuana addiction get.
My friend serves as a rather stereotypical – and some may say – subjective, simplistic example of what is becoming more and more common in our society. I’m willing to bet that a good number of clinicians who read this have a similar example in mind.
With its intoxication state perceived as benign and the limited medicinal advantages, marijuana rapidly is gaining more and more legitimacy in the eyes of the general public (Addict Behav. 2008 Mar;33:397-411), (Monitoring the Future: National Results on Drug Use: 1975-2016). The risk of addiction is perceived as negligible and often nonexistent.
Almost no one knows about the potential risk of addiction (around 9%) (Drug Alcohol Depend. 2011;115:120-30). No one knows about about tolerance and withdrawal states – or about the real risk of psychosis (N Engl J Med. 2014 Jun 5;370:2219-27) or about the possible risk of schizophrenia in vulnerable populations (Schizophr Res. 2016 Mar;171:[1-3]:62-7). No one talks about the fact that it’s often used with tobacco. (How many times have you been told during history taking that a patient doesn’t smoke tobacco, only to find that in drug history he smokes 3-5 joints with tobacco daily?)
[polldaddy:9796432]
Throughout my journey in the psychiatric world (studying and working on three different continents) another typical marijuana user is the patient living with chronic mental illness. My Israeli mentor often complained about not having a single “clean” patient with schizophrenia anymore. I now see the same phenomena in Philadelphia and was also exposed to the same reality in Europe during medical school.
As physicians, and especially as psychiatrists, I believe we are obligated to educate our patients by telling them about the risks in their behaviors. Educating patients about marijuana in today’s atmosphere can be a very important preventive measure, and awareness is an important step toward change.
The current generation of psychiatrists is dealing with an opioid epidemic. Let’s educate ourselves and our patients so this current epidemic won’t be followed by another, severe cannabis epidemic.
Dr. Shilo is a second-year PGY in the department of psychiatry at Einstein Medical Center, Philadelphia.
Do you talk about marijuana with your patients?
In medical school, I had a roommate. He was a smart law school graduate, good looking, outgoing, had lots of friends, was funny, and he was a great cook.
I should tell you another thing about my friend: He was a heavy, daily user of marijuana.
I believe that most of us, at a certain point of our lives, have met someone like my friend. The combination of a high-stress lifestyle, high self-expectations, and lack of appropriate skills to tackle life’s obstacles when encountered with failure frequently leads to addiction or a behavioral problem. In most cases, that will cause a pathological relationship with an outside substance or stimuli (Internet overuse/shopping too much/overeating or drinking, and so on).
Living a life filled with severe trauma and pain, especially at a developmental stage, often leads to an addiction. We frequently see people escape to the sweet narcotic-induced sleep via opioid abuse. On the other hand, for people who did not suffer trauma and are highly functional, marijuana offers a means of emotional detachment from pain, in its different form, and existential depression. That is the main benefit my patients who live with marijuana addiction get.
My friend serves as a rather stereotypical – and some may say – subjective, simplistic example of what is becoming more and more common in our society. I’m willing to bet that a good number of clinicians who read this have a similar example in mind.
With its intoxication state perceived as benign and the limited medicinal advantages, marijuana rapidly is gaining more and more legitimacy in the eyes of the general public (Addict Behav. 2008 Mar;33:397-411), (Monitoring the Future: National Results on Drug Use: 1975-2016). The risk of addiction is perceived as negligible and often nonexistent.
Almost no one knows about the potential risk of addiction (around 9%) (Drug Alcohol Depend. 2011;115:120-30). No one knows about about tolerance and withdrawal states – or about the real risk of psychosis (N Engl J Med. 2014 Jun 5;370:2219-27) or about the possible risk of schizophrenia in vulnerable populations (Schizophr Res. 2016 Mar;171:[1-3]:62-7). No one talks about the fact that it’s often used with tobacco. (How many times have you been told during history taking that a patient doesn’t smoke tobacco, only to find that in drug history he smokes 3-5 joints with tobacco daily?)
[polldaddy:9796432]
Throughout my journey in the psychiatric world (studying and working on three different continents) another typical marijuana user is the patient living with chronic mental illness. My Israeli mentor often complained about not having a single “clean” patient with schizophrenia anymore. I now see the same phenomena in Philadelphia and was also exposed to the same reality in Europe during medical school.
As physicians, and especially as psychiatrists, I believe we are obligated to educate our patients by telling them about the risks in their behaviors. Educating patients about marijuana in today’s atmosphere can be a very important preventive measure, and awareness is an important step toward change.
The current generation of psychiatrists is dealing with an opioid epidemic. Let’s educate ourselves and our patients so this current epidemic won’t be followed by another, severe cannabis epidemic.
Dr. Shilo is a second-year PGY in the department of psychiatry at Einstein Medical Center, Philadelphia.
Lupus classification criteria need input from dermatologists
Editor’s note: This commentary relates to the story, “ New classification system for systemic lupus erythematosus moves forward .”
The ACR/EULAR committee that is developing new classification criteria for systemic lupus erythematosus (SLE) has done the field a service by releasing its draft version in a presentation at the recent EULAR meeting. Releasing the draft version facilitates comments before the new classification criteria become finalized.
Many in the derm-rheum field, ourselves included, classify patients with skin-predominant lupus as lupus, but the new draft classification would place a significant percentage of these patients outside of lupus.
The presentation by Dr. Johnson at EULAR stated, “... a patient can’t be classified on skin findings alone. There is concern that skin findings by themselves may not be lupus, but something else, and some people even consider that cutaneous and systemic lupus are two different things.”
Abundant data indicate instead that lupus is a spectrum that includes skin-predominant lupus. For example, the histology is identical between discoid lupus erythematosus whether or not there is SLE. Moreover, we and others have published significant rates of progression of cutaneous lupus erythematosus (CLE) to SLE. By not viewing CLE in the lupus spectrum, we have a false sense that the patients won’t progress to SLE, yet many of them do.
Importantly, patients respond similarly to therapies when they have either CLE or SLE, so removing this subset of lupus hurts their inclusion in trials and access to new treatments.
When criteria are devised by one group without input from experts who see a specific subset of the disease, that is also a problem. We went down that path in dermatomyositis and missed a lot of patients with the disease when criteria were devised that said the patient had to have muscle involvement. Those criteria have now finally been revised as the ACR/EULAR myositis criteria.
We and others from the derm-rheum community would be happy to speak with the ACR/EULAR committee about these concerns.
Victoria P. Werth, MD, is professor of medicine and dermatology at the University of Pennsylvania, Philadelphia. Joseph F. Merola, MD, is codirector of the Center for Skin and Related Musculoskeletal Diseases at Brigham and Women’s Hospital, Boston. Andrew G. Franks, MD, is a clinical professor in the departments of medicine and dermatology at New York University. Benjamin F. Chong, MD, is an assistant professor of dermatology at the University of Texas, Dallas.
Editor’s note: This commentary relates to the story, “ New classification system for systemic lupus erythematosus moves forward .”
The ACR/EULAR committee that is developing new classification criteria for systemic lupus erythematosus (SLE) has done the field a service by releasing its draft version in a presentation at the recent EULAR meeting. Releasing the draft version facilitates comments before the new classification criteria become finalized.
Many in the derm-rheum field, ourselves included, classify patients with skin-predominant lupus as lupus, but the new draft classification would place a significant percentage of these patients outside of lupus.
The presentation by Dr. Johnson at EULAR stated, “... a patient can’t be classified on skin findings alone. There is concern that skin findings by themselves may not be lupus, but something else, and some people even consider that cutaneous and systemic lupus are two different things.”
Abundant data indicate instead that lupus is a spectrum that includes skin-predominant lupus. For example, the histology is identical between discoid lupus erythematosus whether or not there is SLE. Moreover, we and others have published significant rates of progression of cutaneous lupus erythematosus (CLE) to SLE. By not viewing CLE in the lupus spectrum, we have a false sense that the patients won’t progress to SLE, yet many of them do.
Importantly, patients respond similarly to therapies when they have either CLE or SLE, so removing this subset of lupus hurts their inclusion in trials and access to new treatments.
When criteria are devised by one group without input from experts who see a specific subset of the disease, that is also a problem. We went down that path in dermatomyositis and missed a lot of patients with the disease when criteria were devised that said the patient had to have muscle involvement. Those criteria have now finally been revised as the ACR/EULAR myositis criteria.
We and others from the derm-rheum community would be happy to speak with the ACR/EULAR committee about these concerns.
Victoria P. Werth, MD, is professor of medicine and dermatology at the University of Pennsylvania, Philadelphia. Joseph F. Merola, MD, is codirector of the Center for Skin and Related Musculoskeletal Diseases at Brigham and Women’s Hospital, Boston. Andrew G. Franks, MD, is a clinical professor in the departments of medicine and dermatology at New York University. Benjamin F. Chong, MD, is an assistant professor of dermatology at the University of Texas, Dallas.
Editor’s note: This commentary relates to the story, “ New classification system for systemic lupus erythematosus moves forward .”
The ACR/EULAR committee that is developing new classification criteria for systemic lupus erythematosus (SLE) has done the field a service by releasing its draft version in a presentation at the recent EULAR meeting. Releasing the draft version facilitates comments before the new classification criteria become finalized.
Many in the derm-rheum field, ourselves included, classify patients with skin-predominant lupus as lupus, but the new draft classification would place a significant percentage of these patients outside of lupus.
The presentation by Dr. Johnson at EULAR stated, “... a patient can’t be classified on skin findings alone. There is concern that skin findings by themselves may not be lupus, but something else, and some people even consider that cutaneous and systemic lupus are two different things.”
Abundant data indicate instead that lupus is a spectrum that includes skin-predominant lupus. For example, the histology is identical between discoid lupus erythematosus whether or not there is SLE. Moreover, we and others have published significant rates of progression of cutaneous lupus erythematosus (CLE) to SLE. By not viewing CLE in the lupus spectrum, we have a false sense that the patients won’t progress to SLE, yet many of them do.
Importantly, patients respond similarly to therapies when they have either CLE or SLE, so removing this subset of lupus hurts their inclusion in trials and access to new treatments.
When criteria are devised by one group without input from experts who see a specific subset of the disease, that is also a problem. We went down that path in dermatomyositis and missed a lot of patients with the disease when criteria were devised that said the patient had to have muscle involvement. Those criteria have now finally been revised as the ACR/EULAR myositis criteria.
We and others from the derm-rheum community would be happy to speak with the ACR/EULAR committee about these concerns.
Victoria P. Werth, MD, is professor of medicine and dermatology at the University of Pennsylvania, Philadelphia. Joseph F. Merola, MD, is codirector of the Center for Skin and Related Musculoskeletal Diseases at Brigham and Women’s Hospital, Boston. Andrew G. Franks, MD, is a clinical professor in the departments of medicine and dermatology at New York University. Benjamin F. Chong, MD, is an assistant professor of dermatology at the University of Texas, Dallas.
Lupus classification criteria effort is going in the wrong direction
Editor’s note: This commentary relates to the story, “New classification system for systemic lupus erythematosus moves forward.”
While work to develop a new set of lupus classification criteria more suitable for clinical research is important, the Lupus Foundation of America believes the current work is going in the wrong direction.
Increasingly, key opinion leaders understand lupus to be a spectrum of disease, and there is ample justification of this from scientific evidence (Nat Rev Rheumatol. 2015;11[7]:385-6) The criteria being worked on by ACR and EULAR draws upon an archaic concept with the musty name of “systemic lupus erythematosus,” which relies on a 19th century approach to categorizing disease by counting the signs and symptoms instead of by modern concepts of pathophysiology and prognostic severity. This imposes a homogeneity on the population that simply does not exist. Attempts to re-order obsolescent arrays of organs and autoantibodies to classify lupus will be futile, especially if the aim is to improve the rationale for clinical trial recruitment. Recent clinical trials and modern immunologic methods have already demonstrated, beyond a doubt, that subsets of patients, definable by gene expression patterns or state of the art pharmacodynamic responses, do or do not respond to individual targeted treatments. We now know that patients who require different treatments may well share many of their symptoms in many of the same organs, and this fact defies the outmoded, abacus-based approach to disease classification.
We are concerned that redefining SLE by weighting all disease in one organ as more or less impactful than all disease in another organ flies in the face of current scientific knowledge. If this is the direction in which the effort is going, there is the potential for a negative impact on drug development, clinical care, and access to treatment. The term itself, “SLE,” interferes with selecting appropriate lupus patients for participation in trials. Many people have moderate and even severe lupus syndromes who do not meet enough criteria to be labeled “SLE” (for example, immune thrombocytopenia, hemolytic anemia, discoid lupus, or subacute cutaneous lupus, which can cause severe rashes covering wide areas of the body). In this iteration, assigning less weight to cutaneous lupus as currently proposed is not just problematic, it will set the field back.
By not viewing cutaneous lupus as part of the lupus spectrum, we develop a false sense that this subset of people with lupus will not progress to “SLE,” yet many of them do. Even those who do not later develop features in other organs besides the skin may have more severe disease than other patients who do. Minimizing the “score” for cutaneous lupus will lead to individuals who carry a significant burden of disease being barred from trials, and from access to the treatments they need, once approved.
Conversely, people who do meet criteria for “SLE” under any algorithm, past or present, may have a range of severity, from very severe to very mild. The very mild patients (who may have, in their lifetime met the multiorgan criteria) are entering trials in large numbers and contributing to the high placebo responses which have stopped many promising investigational treatments from further development. Additionally, the common misuse of the current classification criteria as diagnostic criteria has become an unacceptable norm in the lupus community. This leads us to believe that new criteria will continue to be misused, further disenfranchising a huge segment of the population who have lupus from access to state-of-the-art research and care.
Advancing the development new classification criteria deserves a wider discussion among the field’s stakeholders, particularly those with expertise in clinical trial outcomes and the clinical care of the full spectrum of lupus patients.
Sandra C. Raymond is CEO and President, Leslie M. Hanrahan is VP of Education and Research, and Joan Merrill, MD, is the Chief Adviser for Clinical Development at the Lupus Foundation of America. Dr. Merrill is also the Oklahoma Medical Research Foundation Professor of Medicine at the University of Oklahoma, Oklahoma City.
Editor’s note: This commentary relates to the story, “New classification system for systemic lupus erythematosus moves forward.”
While work to develop a new set of lupus classification criteria more suitable for clinical research is important, the Lupus Foundation of America believes the current work is going in the wrong direction.
Increasingly, key opinion leaders understand lupus to be a spectrum of disease, and there is ample justification of this from scientific evidence (Nat Rev Rheumatol. 2015;11[7]:385-6) The criteria being worked on by ACR and EULAR draws upon an archaic concept with the musty name of “systemic lupus erythematosus,” which relies on a 19th century approach to categorizing disease by counting the signs and symptoms instead of by modern concepts of pathophysiology and prognostic severity. This imposes a homogeneity on the population that simply does not exist. Attempts to re-order obsolescent arrays of organs and autoantibodies to classify lupus will be futile, especially if the aim is to improve the rationale for clinical trial recruitment. Recent clinical trials and modern immunologic methods have already demonstrated, beyond a doubt, that subsets of patients, definable by gene expression patterns or state of the art pharmacodynamic responses, do or do not respond to individual targeted treatments. We now know that patients who require different treatments may well share many of their symptoms in many of the same organs, and this fact defies the outmoded, abacus-based approach to disease classification.
We are concerned that redefining SLE by weighting all disease in one organ as more or less impactful than all disease in another organ flies in the face of current scientific knowledge. If this is the direction in which the effort is going, there is the potential for a negative impact on drug development, clinical care, and access to treatment. The term itself, “SLE,” interferes with selecting appropriate lupus patients for participation in trials. Many people have moderate and even severe lupus syndromes who do not meet enough criteria to be labeled “SLE” (for example, immune thrombocytopenia, hemolytic anemia, discoid lupus, or subacute cutaneous lupus, which can cause severe rashes covering wide areas of the body). In this iteration, assigning less weight to cutaneous lupus as currently proposed is not just problematic, it will set the field back.
By not viewing cutaneous lupus as part of the lupus spectrum, we develop a false sense that this subset of people with lupus will not progress to “SLE,” yet many of them do. Even those who do not later develop features in other organs besides the skin may have more severe disease than other patients who do. Minimizing the “score” for cutaneous lupus will lead to individuals who carry a significant burden of disease being barred from trials, and from access to the treatments they need, once approved.
Conversely, people who do meet criteria for “SLE” under any algorithm, past or present, may have a range of severity, from very severe to very mild. The very mild patients (who may have, in their lifetime met the multiorgan criteria) are entering trials in large numbers and contributing to the high placebo responses which have stopped many promising investigational treatments from further development. Additionally, the common misuse of the current classification criteria as diagnostic criteria has become an unacceptable norm in the lupus community. This leads us to believe that new criteria will continue to be misused, further disenfranchising a huge segment of the population who have lupus from access to state-of-the-art research and care.
Advancing the development new classification criteria deserves a wider discussion among the field’s stakeholders, particularly those with expertise in clinical trial outcomes and the clinical care of the full spectrum of lupus patients.
Sandra C. Raymond is CEO and President, Leslie M. Hanrahan is VP of Education and Research, and Joan Merrill, MD, is the Chief Adviser for Clinical Development at the Lupus Foundation of America. Dr. Merrill is also the Oklahoma Medical Research Foundation Professor of Medicine at the University of Oklahoma, Oklahoma City.
Editor’s note: This commentary relates to the story, “New classification system for systemic lupus erythematosus moves forward.”
While work to develop a new set of lupus classification criteria more suitable for clinical research is important, the Lupus Foundation of America believes the current work is going in the wrong direction.
Increasingly, key opinion leaders understand lupus to be a spectrum of disease, and there is ample justification of this from scientific evidence (Nat Rev Rheumatol. 2015;11[7]:385-6) The criteria being worked on by ACR and EULAR draws upon an archaic concept with the musty name of “systemic lupus erythematosus,” which relies on a 19th century approach to categorizing disease by counting the signs and symptoms instead of by modern concepts of pathophysiology and prognostic severity. This imposes a homogeneity on the population that simply does not exist. Attempts to re-order obsolescent arrays of organs and autoantibodies to classify lupus will be futile, especially if the aim is to improve the rationale for clinical trial recruitment. Recent clinical trials and modern immunologic methods have already demonstrated, beyond a doubt, that subsets of patients, definable by gene expression patterns or state of the art pharmacodynamic responses, do or do not respond to individual targeted treatments. We now know that patients who require different treatments may well share many of their symptoms in many of the same organs, and this fact defies the outmoded, abacus-based approach to disease classification.
We are concerned that redefining SLE by weighting all disease in one organ as more or less impactful than all disease in another organ flies in the face of current scientific knowledge. If this is the direction in which the effort is going, there is the potential for a negative impact on drug development, clinical care, and access to treatment. The term itself, “SLE,” interferes with selecting appropriate lupus patients for participation in trials. Many people have moderate and even severe lupus syndromes who do not meet enough criteria to be labeled “SLE” (for example, immune thrombocytopenia, hemolytic anemia, discoid lupus, or subacute cutaneous lupus, which can cause severe rashes covering wide areas of the body). In this iteration, assigning less weight to cutaneous lupus as currently proposed is not just problematic, it will set the field back.
By not viewing cutaneous lupus as part of the lupus spectrum, we develop a false sense that this subset of people with lupus will not progress to “SLE,” yet many of them do. Even those who do not later develop features in other organs besides the skin may have more severe disease than other patients who do. Minimizing the “score” for cutaneous lupus will lead to individuals who carry a significant burden of disease being barred from trials, and from access to the treatments they need, once approved.
Conversely, people who do meet criteria for “SLE” under any algorithm, past or present, may have a range of severity, from very severe to very mild. The very mild patients (who may have, in their lifetime met the multiorgan criteria) are entering trials in large numbers and contributing to the high placebo responses which have stopped many promising investigational treatments from further development. Additionally, the common misuse of the current classification criteria as diagnostic criteria has become an unacceptable norm in the lupus community. This leads us to believe that new criteria will continue to be misused, further disenfranchising a huge segment of the population who have lupus from access to state-of-the-art research and care.
Advancing the development new classification criteria deserves a wider discussion among the field’s stakeholders, particularly those with expertise in clinical trial outcomes and the clinical care of the full spectrum of lupus patients.
Sandra C. Raymond is CEO and President, Leslie M. Hanrahan is VP of Education and Research, and Joan Merrill, MD, is the Chief Adviser for Clinical Development at the Lupus Foundation of America. Dr. Merrill is also the Oklahoma Medical Research Foundation Professor of Medicine at the University of Oklahoma, Oklahoma City.
Lupus classification criteria effort is going in the wrong direction
Editor’s note: This commentary relates to the story, “New classification system for systemic lupus erythematosus moves forward.”
While work to develop a new set of lupus classification criteria more suitable for clinical research is important, the Lupus Foundation of America believes the current work is going in the wrong direction.
Increasingly, key opinion leaders understand lupus to be a spectrum of disease, and there is ample justification of this from scientific evidence (Nat Rev Rheumatol. 2015;11[7]:385-6) The criteria being worked on by ACR and EULAR draws upon an archaic concept with the musty name of “systemic lupus erythematosus,” which relies on a 19th century approach to categorizing disease by counting the signs and symptoms instead of by modern concepts of pathophysiology and prognostic severity. This imposes a homogeneity on the population that simply does not exist. Attempts to re-order obsolescent arrays of organs and autoantibodies to classify lupus will be futile, especially if the aim is to improve the rationale for clinical trial recruitment. Recent clinical trials and modern immunologic methods have already demonstrated, beyond a doubt, that subsets of patients, definable by gene expression patterns or state-of-the-art pharmacodynamic responses, do or do not respond to individual targeted treatments. We now know that patients who require different treatments may well share many of their symptoms in many of the same organs, and this fact defies the outmoded, abacus-based approach to disease classification.
We are concerned that redefining SLE by weighting all disease in one organ as more or less impactful than all disease in another organ flies in the face of current scientific knowledge. If this is the direction in which the effort is going, there is the potential for a negative impact on drug development, clinical care, and access to treatment. The term itself, “SLE,” interferes with selecting appropriate lupus patients for participation in trials. Many people have moderate and even severe lupus syndromes who do not meet enough criteria to be labeled “SLE” (for example, immune thrombocytopenia, hemolytic anemia, discoid lupus, or subacute cutaneous lupus, which can cause severe rashes covering wide areas of the body). In this iteration, assigning less weight to cutaneous lupus as currently proposed is not just problematic; it will set the field back.
By not viewing cutaneous lupus as part of the lupus spectrum, we develop a false sense that this subset of people with lupus will not progress to “SLE,” yet many of them do. Even those who do not later develop features in other organs besides the skin may have more severe disease than other patients who do. Minimizing the “score” for cutaneous lupus will lead to individuals who carry a significant burden of disease being barred from trials, and from access to the treatments they need, once approved.
Conversely, people who do meet criteria for “SLE” under any algorithm, past or present, may have a range of severity, from very severe to very mild. The very mild patients (who may have, in their lifetime, met the multiorgan criteria) are entering trials in large numbers and contributing to the high placebo responses which have stopped many promising investigational treatments from further development. Additionally, the common misuse of the current classification criteria as diagnostic criteria has become an unacceptable norm in the lupus community. This leads us to believe that new criteria will continue to be misused, further disenfranchising a huge segment of the population who have lupus from access to state-of-the-art research and care.
Advancing the development of new classification criteria deserves a wider discussion among the field’s stakeholders, particularly those with expertise in clinical trial outcomes and the clinical care of the full spectrum of lupus patients.
Sandra C. Raymond is CEO and President, Leslie M. Hanrahan is VP of Education and Research, and Joan Merrill, MD, is the Chief Adviser for Clinical Development at the Lupus Foundation of America. Dr. Merrill is also the Oklahoma Medical Research Foundation Professor of Medicine at the University of Oklahoma, Oklahoma City.
Editor’s note: This commentary relates to the story, “New classification system for systemic lupus erythematosus moves forward.”
While work to develop a new set of lupus classification criteria more suitable for clinical research is important, the Lupus Foundation of America believes the current work is going in the wrong direction.
Increasingly, key opinion leaders understand lupus to be a spectrum of disease, and there is ample justification of this from scientific evidence (Nat Rev Rheumatol. 2015;11[7]:385-6) The criteria being worked on by ACR and EULAR draws upon an archaic concept with the musty name of “systemic lupus erythematosus,” which relies on a 19th century approach to categorizing disease by counting the signs and symptoms instead of by modern concepts of pathophysiology and prognostic severity. This imposes a homogeneity on the population that simply does not exist. Attempts to re-order obsolescent arrays of organs and autoantibodies to classify lupus will be futile, especially if the aim is to improve the rationale for clinical trial recruitment. Recent clinical trials and modern immunologic methods have already demonstrated, beyond a doubt, that subsets of patients, definable by gene expression patterns or state-of-the-art pharmacodynamic responses, do or do not respond to individual targeted treatments. We now know that patients who require different treatments may well share many of their symptoms in many of the same organs, and this fact defies the outmoded, abacus-based approach to disease classification.
We are concerned that redefining SLE by weighting all disease in one organ as more or less impactful than all disease in another organ flies in the face of current scientific knowledge. If this is the direction in which the effort is going, there is the potential for a negative impact on drug development, clinical care, and access to treatment. The term itself, “SLE,” interferes with selecting appropriate lupus patients for participation in trials. Many people have moderate and even severe lupus syndromes who do not meet enough criteria to be labeled “SLE” (for example, immune thrombocytopenia, hemolytic anemia, discoid lupus, or subacute cutaneous lupus, which can cause severe rashes covering wide areas of the body). In this iteration, assigning less weight to cutaneous lupus as currently proposed is not just problematic; it will set the field back.
By not viewing cutaneous lupus as part of the lupus spectrum, we develop a false sense that this subset of people with lupus will not progress to “SLE,” yet many of them do. Even those who do not later develop features in other organs besides the skin may have more severe disease than other patients who do. Minimizing the “score” for cutaneous lupus will lead to individuals who carry a significant burden of disease being barred from trials, and from access to the treatments they need, once approved.
Conversely, people who do meet criteria for “SLE” under any algorithm, past or present, may have a range of severity, from very severe to very mild. The very mild patients (who may have, in their lifetime, met the multiorgan criteria) are entering trials in large numbers and contributing to the high placebo responses which have stopped many promising investigational treatments from further development. Additionally, the common misuse of the current classification criteria as diagnostic criteria has become an unacceptable norm in the lupus community. This leads us to believe that new criteria will continue to be misused, further disenfranchising a huge segment of the population who have lupus from access to state-of-the-art research and care.
Advancing the development of new classification criteria deserves a wider discussion among the field’s stakeholders, particularly those with expertise in clinical trial outcomes and the clinical care of the full spectrum of lupus patients.
Sandra C. Raymond is CEO and President, Leslie M. Hanrahan is VP of Education and Research, and Joan Merrill, MD, is the Chief Adviser for Clinical Development at the Lupus Foundation of America. Dr. Merrill is also the Oklahoma Medical Research Foundation Professor of Medicine at the University of Oklahoma, Oklahoma City.
Editor’s note: This commentary relates to the story, “New classification system for systemic lupus erythematosus moves forward.”
While work to develop a new set of lupus classification criteria more suitable for clinical research is important, the Lupus Foundation of America believes the current work is going in the wrong direction.
Increasingly, key opinion leaders understand lupus to be a spectrum of disease, and there is ample justification of this from scientific evidence (Nat Rev Rheumatol. 2015;11[7]:385-6) The criteria being worked on by ACR and EULAR draws upon an archaic concept with the musty name of “systemic lupus erythematosus,” which relies on a 19th century approach to categorizing disease by counting the signs and symptoms instead of by modern concepts of pathophysiology and prognostic severity. This imposes a homogeneity on the population that simply does not exist. Attempts to re-order obsolescent arrays of organs and autoantibodies to classify lupus will be futile, especially if the aim is to improve the rationale for clinical trial recruitment. Recent clinical trials and modern immunologic methods have already demonstrated, beyond a doubt, that subsets of patients, definable by gene expression patterns or state-of-the-art pharmacodynamic responses, do or do not respond to individual targeted treatments. We now know that patients who require different treatments may well share many of their symptoms in many of the same organs, and this fact defies the outmoded, abacus-based approach to disease classification.
We are concerned that redefining SLE by weighting all disease in one organ as more or less impactful than all disease in another organ flies in the face of current scientific knowledge. If this is the direction in which the effort is going, there is the potential for a negative impact on drug development, clinical care, and access to treatment. The term itself, “SLE,” interferes with selecting appropriate lupus patients for participation in trials. Many people have moderate and even severe lupus syndromes who do not meet enough criteria to be labeled “SLE” (for example, immune thrombocytopenia, hemolytic anemia, discoid lupus, or subacute cutaneous lupus, which can cause severe rashes covering wide areas of the body). In this iteration, assigning less weight to cutaneous lupus as currently proposed is not just problematic; it will set the field back.
By not viewing cutaneous lupus as part of the lupus spectrum, we develop a false sense that this subset of people with lupus will not progress to “SLE,” yet many of them do. Even those who do not later develop features in other organs besides the skin may have more severe disease than other patients who do. Minimizing the “score” for cutaneous lupus will lead to individuals who carry a significant burden of disease being barred from trials, and from access to the treatments they need, once approved.
Conversely, people who do meet criteria for “SLE” under any algorithm, past or present, may have a range of severity, from very severe to very mild. The very mild patients (who may have, in their lifetime, met the multiorgan criteria) are entering trials in large numbers and contributing to the high placebo responses which have stopped many promising investigational treatments from further development. Additionally, the common misuse of the current classification criteria as diagnostic criteria has become an unacceptable norm in the lupus community. This leads us to believe that new criteria will continue to be misused, further disenfranchising a huge segment of the population who have lupus from access to state-of-the-art research and care.
Advancing the development of new classification criteria deserves a wider discussion among the field’s stakeholders, particularly those with expertise in clinical trial outcomes and the clinical care of the full spectrum of lupus patients.
Sandra C. Raymond is CEO and President, Leslie M. Hanrahan is VP of Education and Research, and Joan Merrill, MD, is the Chief Adviser for Clinical Development at the Lupus Foundation of America. Dr. Merrill is also the Oklahoma Medical Research Foundation Professor of Medicine at the University of Oklahoma, Oklahoma City.
Lupus classification criteria need input from dermatologists
Editor’s note: This commentary relates to the story, “ New classification system for systemic lupus erythematosus moves forward .”
The ACR/EULAR committee that is developing new classification criteria for systemic lupus erythematosus (SLE) has done the field a service by releasing its draft version in a presentation at the recent EULAR meeting. Releasing the draft version facilitates comments before the new classification criteria become finalized.
Many in the derm-rheum field, ourselves included, classify patients with skin-predominant lupus as lupus, but the new draft classification would place a significant percentage of these patients outside of lupus.
The presentation by Dr. Johnson at EULAR stated, “... a patient can’t be classified on skin findings alone. There is concern that skin findings by themselves may not be lupus, but something else, and some people even consider that cutaneous and systemic lupus are two different things.”
Abundant data indicate instead that lupus is a spectrum that includes skin-predominant lupus. For example, the histology is identical between discoid lupus erythematosus whether or not there is SLE. Moreover, we and others have published significant rates of progression of cutaneous lupus erythematosus (CLE) to SLE. By not viewing CLE in the lupus spectrum, we have a false sense that the patients won’t progress to SLE, yet many of them do.
Importantly, patients respond similarly to therapies when they have either CLE or SLE, so removing this subset of lupus hurts their inclusion in trials and access to new treatments.
When criteria are devised by one group without input from experts who see a specific subset of the disease, that is also a problem. We went down that path in dermatomyositis and missed a lot of patients with the disease when criteria were devised that said the patient had to have muscle involvement. Those criteria have now finally been revised as the ACR/EULAR myositis criteria.
We and others from the derm-rheum community would be happy to speak with the ACR/EULAR committee about these concerns.
Victoria P. Werth, MD, is professor of medicine and dermatology at the University of Pennsylvania, Philadelphia. Joseph F. Merola, MD, is codirector of the Center for Skin and Related Musculoskeletal Diseases at Brigham and Women’s Hospital, Boston. Andrew G. Franks, MD, is a clinical professor in the departments of medicine and dermatology at New York University. Benjamin F. Chong, MD, is an assistant professor of dermatology at the University of Texas, Dallas.
Editor’s note: This commentary relates to the story, “ New classification system for systemic lupus erythematosus moves forward .”
The ACR/EULAR committee that is developing new classification criteria for systemic lupus erythematosus (SLE) has done the field a service by releasing its draft version in a presentation at the recent EULAR meeting. Releasing the draft version facilitates comments before the new classification criteria become finalized.
Many in the derm-rheum field, ourselves included, classify patients with skin-predominant lupus as lupus, but the new draft classification would place a significant percentage of these patients outside of lupus.
The presentation by Dr. Johnson at EULAR stated, “... a patient can’t be classified on skin findings alone. There is concern that skin findings by themselves may not be lupus, but something else, and some people even consider that cutaneous and systemic lupus are two different things.”
Abundant data indicate instead that lupus is a spectrum that includes skin-predominant lupus. For example, the histology is identical between discoid lupus erythematosus whether or not there is SLE. Moreover, we and others have published significant rates of progression of cutaneous lupus erythematosus (CLE) to SLE. By not viewing CLE in the lupus spectrum, we have a false sense that the patients won’t progress to SLE, yet many of them do.
Importantly, patients respond similarly to therapies when they have either CLE or SLE, so removing this subset of lupus hurts their inclusion in trials and access to new treatments.
When criteria are devised by one group without input from experts who see a specific subset of the disease, that is also a problem. We went down that path in dermatomyositis and missed a lot of patients with the disease when criteria were devised that said the patient had to have muscle involvement. Those criteria have now finally been revised as the ACR/EULAR myositis criteria.
We and others from the derm-rheum community would be happy to speak with the ACR/EULAR committee about these concerns.
Victoria P. Werth, MD, is professor of medicine and dermatology at the University of Pennsylvania, Philadelphia. Joseph F. Merola, MD, is codirector of the Center for Skin and Related Musculoskeletal Diseases at Brigham and Women’s Hospital, Boston. Andrew G. Franks, MD, is a clinical professor in the departments of medicine and dermatology at New York University. Benjamin F. Chong, MD, is an assistant professor of dermatology at the University of Texas, Dallas.
Editor’s note: This commentary relates to the story, “ New classification system for systemic lupus erythematosus moves forward .”
The ACR/EULAR committee that is developing new classification criteria for systemic lupus erythematosus (SLE) has done the field a service by releasing its draft version in a presentation at the recent EULAR meeting. Releasing the draft version facilitates comments before the new classification criteria become finalized.
Many in the derm-rheum field, ourselves included, classify patients with skin-predominant lupus as lupus, but the new draft classification would place a significant percentage of these patients outside of lupus.
The presentation by Dr. Johnson at EULAR stated, “... a patient can’t be classified on skin findings alone. There is concern that skin findings by themselves may not be lupus, but something else, and some people even consider that cutaneous and systemic lupus are two different things.”
Abundant data indicate instead that lupus is a spectrum that includes skin-predominant lupus. For example, the histology is identical between discoid lupus erythematosus whether or not there is SLE. Moreover, we and others have published significant rates of progression of cutaneous lupus erythematosus (CLE) to SLE. By not viewing CLE in the lupus spectrum, we have a false sense that the patients won’t progress to SLE, yet many of them do.
Importantly, patients respond similarly to therapies when they have either CLE or SLE, so removing this subset of lupus hurts their inclusion in trials and access to new treatments.
When criteria are devised by one group without input from experts who see a specific subset of the disease, that is also a problem. We went down that path in dermatomyositis and missed a lot of patients with the disease when criteria were devised that said the patient had to have muscle involvement. Those criteria have now finally been revised as the ACR/EULAR myositis criteria.
We and others from the derm-rheum community would be happy to speak with the ACR/EULAR committee about these concerns.
Victoria P. Werth, MD, is professor of medicine and dermatology at the University of Pennsylvania, Philadelphia. Joseph F. Merola, MD, is codirector of the Center for Skin and Related Musculoskeletal Diseases at Brigham and Women’s Hospital, Boston. Andrew G. Franks, MD, is a clinical professor in the departments of medicine and dermatology at New York University. Benjamin F. Chong, MD, is an assistant professor of dermatology at the University of Texas, Dallas.
Small community hospitals need antibiotic stewardship programs
Antibiotic use and misuse is driving drug resistance. Each year in the United States, at least 2 million people become infected with bacteria that are resistant to antibiotics, and at least 23,000 people die each year as a result of these infections, according to the Centers for Disease Control and Prevention.
Over 70% of U.S. hospitals are small community hospitals with 200 beds or fewer; however, our understanding of antibiotic use in these facilities is extremely limited. Most of the existing data on antibiotic use rates come from larger academic medical centers. Describing antibiotic usage patterns in small facilities is a high priority, given they constitute the majority of acute care hospitals and national antibiotic stewardship is forthcoming.
Intermountain has a long history of antibiotic use measurements and digital data support. All facilities use an electronic medical record system that transmits data to a centralized enterprise data warehouse. Since 2011, antibiotic use reports have been collected from the data system and submitted to the CDC’s National Healthcare and Safety Network Antimicrobial Use (NHSN AU) module.
Using data from the NHSN AU module from January 2011 through December 2013, we calculated monthly and 3-year antibiotic use rates for each facility, care unit type, and antibiotic category. Data included in the NHSN AU modules include:
• Patient care location.
• Facility-wide antibiotic use.
• Use of individual antibiotics.
• Classes of antibiotics.
• Days of therapy.
• Patient-day data.
Antibiotic agents were categorized into five groups based on antibiotic spectrum and ability to treat multidrug-resistant organisms (MDROs). Category one antibiotics are narrower-spectrum agents, and category five antibiotics are the broadest-spectrum antibiotics or associated with treating MDROs. Categories four and five were classified as broad-spectrum antibiotics. Hospital care units were categorized as intensive care, medical/surgical, pediatric, or miscellaneous.
Antibiotic use rates, expressed as days of therapy per 1,000 patient-days (DOT/1000PD), were calculated for each small community hospital and compared with rates in large community hospitals. Negative-binomial regression was used to relate antibiotic use.
The key findings of the study include:
• Total antibiotic use rates varied widely across the 15 small community hospitals and were similar to rates in four large community hospitals.
• The proportion of patient-days spent in the respective care unit types varied substantially within small community hospitals and had a large impact on facility-level antibiotic use rates.
• Broad-spectrum antibiotics accounted for 26% of use in small community hospitals, similar to the proportion in large community hospitals.
• Significant predictors of antibiotic use include case mix index, proportion of patient-days in specific care unit types, and season.
• Small community hospitals need to become a focus of antibiotic stewardship efforts.
All hospitals in 2017 are required to have an antibiotic stewardship program in place according to Joint Commission guidelines. Small community hospitals in the United States face significant challenges meeting the national antibiotic stewardship requirements. These challenges include: limited access to infectious diseases physician and/or pharmacist leadership, limited information technology support, and lack of antibiotic guidance.
In order to holistically address the growing problem of antibiotic-resistant bacteria, the infectious disease community must respond to antibiotic use in ALL hospitals, not just the large academic medical facilities. Small hospitals are least likely to have stewardship programs even though antibiotic usage patterns are similar to larger facilities. We need to bring stewardship support to ALL hospitals, but the challenges come in knowing how to do that.
To address the challenges, researchers at Intermountain Healthcare are currently conducting a study to identify recommendations that will help build antibiotic stewardship programs for these facilities.
Eddie Stenehjem, MD, is an infectious disease physician and researcher at Intermountain Medical Center, Salt Lake City, the flagship facility for the Intermountain Healthcare system.
Antibiotic use and misuse is driving drug resistance. Each year in the United States, at least 2 million people become infected with bacteria that are resistant to antibiotics, and at least 23,000 people die each year as a result of these infections, according to the Centers for Disease Control and Prevention.
Over 70% of U.S. hospitals are small community hospitals with 200 beds or fewer; however, our understanding of antibiotic use in these facilities is extremely limited. Most of the existing data on antibiotic use rates come from larger academic medical centers. Describing antibiotic usage patterns in small facilities is a high priority, given they constitute the majority of acute care hospitals and national antibiotic stewardship is forthcoming.
Intermountain has a long history of antibiotic use measurements and digital data support. All facilities use an electronic medical record system that transmits data to a centralized enterprise data warehouse. Since 2011, antibiotic use reports have been collected from the data system and submitted to the CDC’s National Healthcare and Safety Network Antimicrobial Use (NHSN AU) module.
Using data from the NHSN AU module from January 2011 through December 2013, we calculated monthly and 3-year antibiotic use rates for each facility, care unit type, and antibiotic category. Data included in the NHSN AU modules include:
• Patient care location.
• Facility-wide antibiotic use.
• Use of individual antibiotics.
• Classes of antibiotics.
• Days of therapy.
• Patient-day data.
Antibiotic agents were categorized into five groups based on antibiotic spectrum and ability to treat multidrug-resistant organisms (MDROs). Category one antibiotics are narrower-spectrum agents, and category five antibiotics are the broadest-spectrum antibiotics or associated with treating MDROs. Categories four and five were classified as broad-spectrum antibiotics. Hospital care units were categorized as intensive care, medical/surgical, pediatric, or miscellaneous.
Antibiotic use rates, expressed as days of therapy per 1,000 patient-days (DOT/1000PD), were calculated for each small community hospital and compared with rates in large community hospitals. Negative-binomial regression was used to relate antibiotic use.
The key findings of the study include:
• Total antibiotic use rates varied widely across the 15 small community hospitals and were similar to rates in four large community hospitals.
• The proportion of patient-days spent in the respective care unit types varied substantially within small community hospitals and had a large impact on facility-level antibiotic use rates.
• Broad-spectrum antibiotics accounted for 26% of use in small community hospitals, similar to the proportion in large community hospitals.
• Significant predictors of antibiotic use include case mix index, proportion of patient-days in specific care unit types, and season.
• Small community hospitals need to become a focus of antibiotic stewardship efforts.
All hospitals in 2017 are required to have an antibiotic stewardship program in place according to Joint Commission guidelines. Small community hospitals in the United States face significant challenges meeting the national antibiotic stewardship requirements. These challenges include: limited access to infectious diseases physician and/or pharmacist leadership, limited information technology support, and lack of antibiotic guidance.
In order to holistically address the growing problem of antibiotic-resistant bacteria, the infectious disease community must respond to antibiotic use in ALL hospitals, not just the large academic medical facilities. Small hospitals are least likely to have stewardship programs even though antibiotic usage patterns are similar to larger facilities. We need to bring stewardship support to ALL hospitals, but the challenges come in knowing how to do that.
To address the challenges, researchers at Intermountain Healthcare are currently conducting a study to identify recommendations that will help build antibiotic stewardship programs for these facilities.
Eddie Stenehjem, MD, is an infectious disease physician and researcher at Intermountain Medical Center, Salt Lake City, the flagship facility for the Intermountain Healthcare system.
Antibiotic use and misuse is driving drug resistance. Each year in the United States, at least 2 million people become infected with bacteria that are resistant to antibiotics, and at least 23,000 people die each year as a result of these infections, according to the Centers for Disease Control and Prevention.
Over 70% of U.S. hospitals are small community hospitals with 200 beds or fewer; however, our understanding of antibiotic use in these facilities is extremely limited. Most of the existing data on antibiotic use rates come from larger academic medical centers. Describing antibiotic usage patterns in small facilities is a high priority, given they constitute the majority of acute care hospitals and national antibiotic stewardship is forthcoming.
Intermountain has a long history of antibiotic use measurements and digital data support. All facilities use an electronic medical record system that transmits data to a centralized enterprise data warehouse. Since 2011, antibiotic use reports have been collected from the data system and submitted to the CDC’s National Healthcare and Safety Network Antimicrobial Use (NHSN AU) module.
Using data from the NHSN AU module from January 2011 through December 2013, we calculated monthly and 3-year antibiotic use rates for each facility, care unit type, and antibiotic category. Data included in the NHSN AU modules include:
• Patient care location.
• Facility-wide antibiotic use.
• Use of individual antibiotics.
• Classes of antibiotics.
• Days of therapy.
• Patient-day data.
Antibiotic agents were categorized into five groups based on antibiotic spectrum and ability to treat multidrug-resistant organisms (MDROs). Category one antibiotics are narrower-spectrum agents, and category five antibiotics are the broadest-spectrum antibiotics or associated with treating MDROs. Categories four and five were classified as broad-spectrum antibiotics. Hospital care units were categorized as intensive care, medical/surgical, pediatric, or miscellaneous.
Antibiotic use rates, expressed as days of therapy per 1,000 patient-days (DOT/1000PD), were calculated for each small community hospital and compared with rates in large community hospitals. Negative-binomial regression was used to relate antibiotic use.
The key findings of the study include:
• Total antibiotic use rates varied widely across the 15 small community hospitals and were similar to rates in four large community hospitals.
• The proportion of patient-days spent in the respective care unit types varied substantially within small community hospitals and had a large impact on facility-level antibiotic use rates.
• Broad-spectrum antibiotics accounted for 26% of use in small community hospitals, similar to the proportion in large community hospitals.
• Significant predictors of antibiotic use include case mix index, proportion of patient-days in specific care unit types, and season.
• Small community hospitals need to become a focus of antibiotic stewardship efforts.
All hospitals in 2017 are required to have an antibiotic stewardship program in place according to Joint Commission guidelines. Small community hospitals in the United States face significant challenges meeting the national antibiotic stewardship requirements. These challenges include: limited access to infectious diseases physician and/or pharmacist leadership, limited information technology support, and lack of antibiotic guidance.
In order to holistically address the growing problem of antibiotic-resistant bacteria, the infectious disease community must respond to antibiotic use in ALL hospitals, not just the large academic medical facilities. Small hospitals are least likely to have stewardship programs even though antibiotic usage patterns are similar to larger facilities. We need to bring stewardship support to ALL hospitals, but the challenges come in knowing how to do that.
To address the challenges, researchers at Intermountain Healthcare are currently conducting a study to identify recommendations that will help build antibiotic stewardship programs for these facilities.
Eddie Stenehjem, MD, is an infectious disease physician and researcher at Intermountain Medical Center, Salt Lake City, the flagship facility for the Intermountain Healthcare system.
Release nears for revised U.S. hypertension guidelines
Authoritative U.S. guidelines for managing high blood pressure have traveled a rocky and serpentine path ever since the expert group originally constituted as the Eighth Joint National Committee (JNC 8) released its controversial report in early 2014, when it relaxed the target blood pressure for most adults aged 60-79 years from less than 140 mm Hg to under 150/90 mm Hg (JAMA. 2014 Feb 5;3311[5]:507-20). A few months before those recommendations came out, the National Heart, Lung, and Blood Institute, which since 1977 had organized seven preceding iterations of U.S. blood pressure guidelines, handed off oversight of the project and any future updates to the American Heart Association, the American College of Cardiology, and the American Society of Hypertension. A year later, an expert panel organized by those three groups reset the blood pressure target for most U.S. adults with coronary artery disease back to a pressure of less than 140/90 mm Hg (Hypertension. 2015 Jun;65[6]:1372-1407), and that has been the prevailing U.S. standard in the 2-plus years since.
A few months later, in September 2015, data from the SPRINT trial in more than 9,000 patients with high cardiovascular risk first came out and showed that treating to a target systolic blood pressure of less than 120 mm Hg led to a significant 25% reduction in cardiovascular disease events, compared with controls treated to a systolic pressure of less than 140 mm Hg (N Engl J Med. 2015 Nov 26;373[22]:2103-16). Ever since, the big question surrounding blood pressure targets in U.S. practice has been, when would new official guidelines emerge that took the SPRINT findings into consideration? It now looks like it will finally happen in September 2017.
That’s when the ASH and the AHA’s Hypertension Council will for the first time hold a joint annual meeting, after many years when each organization had its own, individual annual meeting. The ASH’s traditional spring meeting didn’t happen this year; early fall has traditionally been when the AHA’s Hypertension Council meets.
The Council’s posted preliminary program for the September meeting showed, as of late July, an opening session the morning of September 14 called a “Review of AHA Scientific Statement 2017.” On the ASH’s website is a virtual flier for a session the afternoon of September 15 on the “2017 Guidelines for Adult and Pediatric Hypertension.”

“I know that something will be discussed on September 14,” he told me recently. “I am not sure the full report will be ready then, but I think something will be presented that will at least describe the ‘attitude’ of the guidelines, if not the whole report. There will be more presented at the AHA Sessions in November.” Of course, there will also be “an accompanying evidence document describing the studies and evidence that generated the report, but I don’t know the release date,” he added.
Some of the suspense is already gone from the new guidelines, because the punch line – the new target blood pressure to treat toward for most U.S. adults with hypertension – is already known to be less than 130/80 mm Hg. That was the treatment goal set in April in updated guidelines for treating patients with heart failure by a panel of the ACC, the AHA, and the Heart Failure Society of America (J Am Coll Cardiol. 2017 Apr 30. doi: 10.1016/j.jacc.2017.04.025). Among the heart failure patients subject to this blood pressure target are adults with stage A heart failure, which the panel defined as any adult diagnosed with hypertension, as well as those with diabetes, coronary artery disease, or other risk factors that clearly predispose patients to develop heart failure.
Last April, the heart failure panel’s vice-chair, Mariell Jessup, MD, told me that the group chose a treatment target of less than 130/80 mm Hg to “harmonize” with the target that the hypertension guideline group had already selected.
So, in truth, an official U.S. hypertension treatment target of less than 130/80 mm Hg is already on the books for clinicians to follow that’s endorsed by the ACC and AHA. Unless the hypertension group throws a real curve ball its target will be identical.
But just knowing this lower target leaves important questions unanswered that presumably the hypertension panel will address. Questions like the best drug combinations to use to get blood pressures this low, and how aggressively to treat older patients with comorbidities who may need upward of four drugs to achieve a systolic blood pressure in this target range.
“I suspect some will say that the heart failure guidelines are for patients with heart failure, and thus the hypertension guidelines will complement them,” said Dr. Lackland. On the other hand, the SPRINT evidence is so persuasive that at least “some physicians will move to 130/80 mm Hg” readily, he predicted. “Others will probably wait and see, and some will wait even longer for follow-up comments” to come out.
Dr. Lackland also stressed the usual caveat about any medical guideline, that both the heart failure and hypertension statements simply give clinicians the recommended approach but “should not override clinical judgment for specific patients.”
But before the medical community can embrace or question the new hypertension guidelines it needs to at least see them. That finally seems ready to happen in September, and perhaps in November too.
[email protected]
On Twitter @mitchelzoler
Authoritative U.S. guidelines for managing high blood pressure have traveled a rocky and serpentine path ever since the expert group originally constituted as the Eighth Joint National Committee (JNC 8) released its controversial report in early 2014, when it relaxed the target blood pressure for most adults aged 60-79 years from less than 140 mm Hg to under 150/90 mm Hg (JAMA. 2014 Feb 5;3311[5]:507-20). A few months before those recommendations came out, the National Heart, Lung, and Blood Institute, which since 1977 had organized seven preceding iterations of U.S. blood pressure guidelines, handed off oversight of the project and any future updates to the American Heart Association, the American College of Cardiology, and the American Society of Hypertension. A year later, an expert panel organized by those three groups reset the blood pressure target for most U.S. adults with coronary artery disease back to a pressure of less than 140/90 mm Hg (Hypertension. 2015 Jun;65[6]:1372-1407), and that has been the prevailing U.S. standard in the 2-plus years since.
A few months later, in September 2015, data from the SPRINT trial in more than 9,000 patients with high cardiovascular risk first came out and showed that treating to a target systolic blood pressure of less than 120 mm Hg led to a significant 25% reduction in cardiovascular disease events, compared with controls treated to a systolic pressure of less than 140 mm Hg (N Engl J Med. 2015 Nov 26;373[22]:2103-16). Ever since, the big question surrounding blood pressure targets in U.S. practice has been, when would new official guidelines emerge that took the SPRINT findings into consideration? It now looks like it will finally happen in September 2017.
That’s when the ASH and the AHA’s Hypertension Council will for the first time hold a joint annual meeting, after many years when each organization had its own, individual annual meeting. The ASH’s traditional spring meeting didn’t happen this year; early fall has traditionally been when the AHA’s Hypertension Council meets.
The Council’s posted preliminary program for the September meeting showed, as of late July, an opening session the morning of September 14 called a “Review of AHA Scientific Statement 2017.” On the ASH’s website is a virtual flier for a session the afternoon of September 15 on the “2017 Guidelines for Adult and Pediatric Hypertension.”
“I know that something will be discussed on September 14,” he told me recently. “I am not sure the full report will be ready then, but I think something will be presented that will at least describe the ‘attitude’ of the guidelines, if not the whole report. There will be more presented at the AHA Sessions in November.” Of course, there will also be “an accompanying evidence document describing the studies and evidence that generated the report, but I don’t know the release date,” he added.
Some of the suspense is already gone from the new guidelines, because the punch line – the new target blood pressure to treat toward for most U.S. adults with hypertension – is already known to be less than 130/80 mm Hg. That was the treatment goal set in April in updated guidelines for treating patients with heart failure by a panel of the ACC, the AHA, and the Heart Failure Society of America (J Am Coll Cardiol. 2017 Apr 30. doi: 10.1016/j.jacc.2017.04.025). Among the heart failure patients subject to this blood pressure target are adults with stage A heart failure, which the panel defined as any adult diagnosed with hypertension, as well as those with diabetes, coronary artery disease, or other risk factors that clearly predispose patients to develop heart failure.
Last April, the heart failure panel’s vice-chair, Mariell Jessup, MD, told me that the group chose a treatment target of less than 130/80 mm Hg to “harmonize” with the target that the hypertension guideline group had already selected.
So, in truth, an official U.S. hypertension treatment target of less than 130/80 mm Hg is already on the books for clinicians to follow that’s endorsed by the ACC and AHA. Unless the hypertension group throws a real curve ball its target will be identical.
But just knowing this lower target leaves important questions unanswered that presumably the hypertension panel will address. Questions like the best drug combinations to use to get blood pressures this low, and how aggressively to treat older patients with comorbidities who may need upward of four drugs to achieve a systolic blood pressure in this target range.
“I suspect some will say that the heart failure guidelines are for patients with heart failure, and thus the hypertension guidelines will complement them,” said Dr. Lackland. On the other hand, the SPRINT evidence is so persuasive that at least “some physicians will move to 130/80 mm Hg” readily, he predicted. “Others will probably wait and see, and some will wait even longer for follow-up comments” to come out.
Dr. Lackland also stressed the usual caveat about any medical guideline, that both the heart failure and hypertension statements simply give clinicians the recommended approach but “should not override clinical judgment for specific patients.”
But before the medical community can embrace or question the new hypertension guidelines it needs to at least see them. That finally seems ready to happen in September, and perhaps in November too.
[email protected]
On Twitter @mitchelzoler
Authoritative U.S. guidelines for managing high blood pressure have traveled a rocky and serpentine path ever since the expert group originally constituted as the Eighth Joint National Committee (JNC 8) released its controversial report in early 2014, when it relaxed the target blood pressure for most adults aged 60-79 years from less than 140 mm Hg to under 150/90 mm Hg (JAMA. 2014 Feb 5;3311[5]:507-20). A few months before those recommendations came out, the National Heart, Lung, and Blood Institute, which since 1977 had organized seven preceding iterations of U.S. blood pressure guidelines, handed off oversight of the project and any future updates to the American Heart Association, the American College of Cardiology, and the American Society of Hypertension. A year later, an expert panel organized by those three groups reset the blood pressure target for most U.S. adults with coronary artery disease back to a pressure of less than 140/90 mm Hg (Hypertension. 2015 Jun;65[6]:1372-1407), and that has been the prevailing U.S. standard in the 2-plus years since.
A few months later, in September 2015, data from the SPRINT trial in more than 9,000 patients with high cardiovascular risk first came out and showed that treating to a target systolic blood pressure of less than 120 mm Hg led to a significant 25% reduction in cardiovascular disease events, compared with controls treated to a systolic pressure of less than 140 mm Hg (N Engl J Med. 2015 Nov 26;373[22]:2103-16). Ever since, the big question surrounding blood pressure targets in U.S. practice has been, when would new official guidelines emerge that took the SPRINT findings into consideration? It now looks like it will finally happen in September 2017.
That’s when the ASH and the AHA’s Hypertension Council will for the first time hold a joint annual meeting, after many years when each organization had its own, individual annual meeting. The ASH’s traditional spring meeting didn’t happen this year; early fall has traditionally been when the AHA’s Hypertension Council meets.
The Council’s posted preliminary program for the September meeting showed, as of late July, an opening session the morning of September 14 called a “Review of AHA Scientific Statement 2017.” On the ASH’s website is a virtual flier for a session the afternoon of September 15 on the “2017 Guidelines for Adult and Pediatric Hypertension.”
“I know that something will be discussed on September 14,” he told me recently. “I am not sure the full report will be ready then, but I think something will be presented that will at least describe the ‘attitude’ of the guidelines, if not the whole report. There will be more presented at the AHA Sessions in November.” Of course, there will also be “an accompanying evidence document describing the studies and evidence that generated the report, but I don’t know the release date,” he added.
Some of the suspense is already gone from the new guidelines, because the punch line – the new target blood pressure to treat toward for most U.S. adults with hypertension – is already known to be less than 130/80 mm Hg. That was the treatment goal set in April in updated guidelines for treating patients with heart failure by a panel of the ACC, the AHA, and the Heart Failure Society of America (J Am Coll Cardiol. 2017 Apr 30. doi: 10.1016/j.jacc.2017.04.025). Among the heart failure patients subject to this blood pressure target are adults with stage A heart failure, which the panel defined as any adult diagnosed with hypertension, as well as those with diabetes, coronary artery disease, or other risk factors that clearly predispose patients to develop heart failure.
Last April, the heart failure panel’s vice-chair, Mariell Jessup, MD, told me that the group chose a treatment target of less than 130/80 mm Hg to “harmonize” with the target that the hypertension guideline group had already selected.
So, in truth, an official U.S. hypertension treatment target of less than 130/80 mm Hg is already on the books for clinicians to follow that’s endorsed by the ACC and AHA. Unless the hypertension group throws a real curve ball its target will be identical.
But just knowing this lower target leaves important questions unanswered that presumably the hypertension panel will address. Questions like the best drug combinations to use to get blood pressures this low, and how aggressively to treat older patients with comorbidities who may need upward of four drugs to achieve a systolic blood pressure in this target range.
“I suspect some will say that the heart failure guidelines are for patients with heart failure, and thus the hypertension guidelines will complement them,” said Dr. Lackland. On the other hand, the SPRINT evidence is so persuasive that at least “some physicians will move to 130/80 mm Hg” readily, he predicted. “Others will probably wait and see, and some will wait even longer for follow-up comments” to come out.
Dr. Lackland also stressed the usual caveat about any medical guideline, that both the heart failure and hypertension statements simply give clinicians the recommended approach but “should not override clinical judgment for specific patients.”
But before the medical community can embrace or question the new hypertension guidelines it needs to at least see them. That finally seems ready to happen in September, and perhaps in November too.
[email protected]
On Twitter @mitchelzoler
The VA Is in Critical Condition, but What Is the Prognosis?
In his first ever—and perhaps the first ever state of the VA—speech delivered on May 30, 2017, VA Secretary David J. Shulkin, MD, reported to the nation and Congress that “the VA is still in critical condition.” This medical metaphor reflects Dr. Shulkin’s distinction of being the only physician ever to hold this cabinet-level post.
For anyone in health care, such a reference immediately calls forth a variety of associations—most of them serious concerns for the status of the VA and whether it will survive. In this editorial, I will expand on this metaphor and explore its meaning for the future of the VA.
Dr. Shulkin extended the metaphor when he said that the “VA requires intensive care.” For clinicians, this remark tells us that the VA is either seriously ill or injured. Yet there is hope because the chief doctor of the VA reassures us that the patient—the largest health care system in the country—is improving. This improvement from critical care to intensive care status informs us that the VA was very sick, maybe even dying, during the previous administration in which Dr. Shulkin served as VA’s Under Secretary for Health.
Dr. Shulkin, a general internist who still sees primary care patients at the VA, gave us a diagnosis of the VA’s most serious symptoms: a lack of access to timely care, a high rate of veteran suicides, an inability to enforce employee accountability, multiple obstacles to hiring and retaining qualified staff, an unacceptable quality of care at some VAMCs, and a backlog of disability claims due to inefficient processing.
Dr. Shulkin also gave us a broad idea of his goal for care, “We are taking immediate and decisive steps stabilizing the organization.” But the more I thought about this impressive speech, the more I wondered, What is the VA’s actual diagnosis?
Several of the many news commentaries analyzing Shulkin’s State of the VA speech suggested possible etiologies. According to the Public Broadcasting Service (PBS), “In a ‘State of the VA’ report, Shulkin, a physician, issued a blunt diagnosis: ‘There is a lot of work to do.’” Astute clinicians will immediately recognize that PBS is right about the secretary’s honesty regarding the magnitude of the task facing him.
He was not providing a diagnosis as much as offering an indirect assessment of the patient’s condition. “A lot of work,” although not a diagnosis, is a colloquial description of the treatment plan that the secretary further outlined in his report. Like any good treatment plan, there is a direct correlation between the major symptoms of the disorder and the therapies that Dr. Shulkin prescribed.
The Secretary recommended and the President signed the Department of Veterans Affairs Accountability and Whistleblower Protection Act of 2017 on June 23, 2017, to make it easier to discipline and terminate VA employees who may be keeping the VA organization ill or at least preventing it from getting better. He also prescribed continued and even higher dose infusions of community care to treat the central access problem. In addition, Dr. Shulkin ordered that the most effective available interventions be used for suicide prevention, enhancement of the overall quality of care, and to improve accountability.
Even with the most efficacious treatments, a high-functioning intensive care unit needs state-of-theart technology and equipment. In a long-awaited announcement, Dr. Shulkin reported on June 5 that of 2 competing modalities to revive the VA’s ailing electronic health record system—the brain of our critical care patient—rather than repair the moribund CPRS, the VA will receive a transplant of the DoD MHS Genesis. Critical care, especially when delivered in a combat zone, requires difficult triage decisions. The secretary has made similar tough resource allocation decisions, determining that some of the VA’s oldest and most debilitated facilities will not be sustained in their present form.
I am near the end of this editorial and still do not have a diagnosis. Pundits, politicians, and policy specialists all have their differential diagnosis as well as veterans groups and VA employees.“Bloated bureaucracy” is the diagnosis from many of these VA critics. Dr. Shulkin proposed a remedy for this disease: He plans to consolidate the VA headquarters.
Even more important, for those who believe the VA should not have a DNR but be allowed to recover, what does the physician who holds the VA’s life in his hands believe is the prognosis for this 86-year-old institution? Dr. Shulkin expressed the hope that the VA can recover its health, saying he is “confident that we will be able turn VA into the organization veterans and their families deserve, and one that America can take pride in.” The most vehement of VA’s opponents would say that pouring additional millions of dollars into such a moribund entity is futile care. Yet the secretary and thousands of VA patients, staff, and supporters believe that the agency that President Lincoln created at the end of the bloodiest war in U.S. history still has value and can be restored to meaningful service for those who have, who are, and who will place their lives on the line for their country.
In his first ever—and perhaps the first ever state of the VA—speech delivered on May 30, 2017, VA Secretary David J. Shulkin, MD, reported to the nation and Congress that “the VA is still in critical condition.” This medical metaphor reflects Dr. Shulkin’s distinction of being the only physician ever to hold this cabinet-level post.
For anyone in health care, such a reference immediately calls forth a variety of associations—most of them serious concerns for the status of the VA and whether it will survive. In this editorial, I will expand on this metaphor and explore its meaning for the future of the VA.
Dr. Shulkin extended the metaphor when he said that the “VA requires intensive care.” For clinicians, this remark tells us that the VA is either seriously ill or injured. Yet there is hope because the chief doctor of the VA reassures us that the patient—the largest health care system in the country—is improving. This improvement from critical care to intensive care status informs us that the VA was very sick, maybe even dying, during the previous administration in which Dr. Shulkin served as VA’s Under Secretary for Health.
Dr. Shulkin, a general internist who still sees primary care patients at the VA, gave us a diagnosis of the VA’s most serious symptoms: a lack of access to timely care, a high rate of veteran suicides, an inability to enforce employee accountability, multiple obstacles to hiring and retaining qualified staff, an unacceptable quality of care at some VAMCs, and a backlog of disability claims due to inefficient processing.
Dr. Shulkin also gave us a broad idea of his goal for care, “We are taking immediate and decisive steps stabilizing the organization.” But the more I thought about this impressive speech, the more I wondered, What is the VA’s actual diagnosis?
Several of the many news commentaries analyzing Shulkin’s State of the VA speech suggested possible etiologies. According to the Public Broadcasting Service (PBS), “In a ‘State of the VA’ report, Shulkin, a physician, issued a blunt diagnosis: ‘There is a lot of work to do.’” Astute clinicians will immediately recognize that PBS is right about the secretary’s honesty regarding the magnitude of the task facing him.
He was not providing a diagnosis as much as offering an indirect assessment of the patient’s condition. “A lot of work,” although not a diagnosis, is a colloquial description of the treatment plan that the secretary further outlined in his report. Like any good treatment plan, there is a direct correlation between the major symptoms of the disorder and the therapies that Dr. Shulkin prescribed.
The Secretary recommended and the President signed the Department of Veterans Affairs Accountability and Whistleblower Protection Act of 2017 on June 23, 2017, to make it easier to discipline and terminate VA employees who may be keeping the VA organization ill or at least preventing it from getting better. He also prescribed continued and even higher dose infusions of community care to treat the central access problem. In addition, Dr. Shulkin ordered that the most effective available interventions be used for suicide prevention, enhancement of the overall quality of care, and to improve accountability.
Even with the most efficacious treatments, a high-functioning intensive care unit needs state-of-theart technology and equipment. In a long-awaited announcement, Dr. Shulkin reported on June 5 that of 2 competing modalities to revive the VA’s ailing electronic health record system—the brain of our critical care patient—rather than repair the moribund CPRS, the VA will receive a transplant of the DoD MHS Genesis. Critical care, especially when delivered in a combat zone, requires difficult triage decisions. The secretary has made similar tough resource allocation decisions, determining that some of the VA’s oldest and most debilitated facilities will not be sustained in their present form.
I am near the end of this editorial and still do not have a diagnosis. Pundits, politicians, and policy specialists all have their differential diagnosis as well as veterans groups and VA employees.“Bloated bureaucracy” is the diagnosis from many of these VA critics. Dr. Shulkin proposed a remedy for this disease: He plans to consolidate the VA headquarters.
Even more important, for those who believe the VA should not have a DNR but be allowed to recover, what does the physician who holds the VA’s life in his hands believe is the prognosis for this 86-year-old institution? Dr. Shulkin expressed the hope that the VA can recover its health, saying he is “confident that we will be able turn VA into the organization veterans and their families deserve, and one that America can take pride in.” The most vehement of VA’s opponents would say that pouring additional millions of dollars into such a moribund entity is futile care. Yet the secretary and thousands of VA patients, staff, and supporters believe that the agency that President Lincoln created at the end of the bloodiest war in U.S. history still has value and can be restored to meaningful service for those who have, who are, and who will place their lives on the line for their country.
In his first ever—and perhaps the first ever state of the VA—speech delivered on May 30, 2017, VA Secretary David J. Shulkin, MD, reported to the nation and Congress that “the VA is still in critical condition.” This medical metaphor reflects Dr. Shulkin’s distinction of being the only physician ever to hold this cabinet-level post.
For anyone in health care, such a reference immediately calls forth a variety of associations—most of them serious concerns for the status of the VA and whether it will survive. In this editorial, I will expand on this metaphor and explore its meaning for the future of the VA.
Dr. Shulkin extended the metaphor when he said that the “VA requires intensive care.” For clinicians, this remark tells us that the VA is either seriously ill or injured. Yet there is hope because the chief doctor of the VA reassures us that the patient—the largest health care system in the country—is improving. This improvement from critical care to intensive care status informs us that the VA was very sick, maybe even dying, during the previous administration in which Dr. Shulkin served as VA’s Under Secretary for Health.
Dr. Shulkin, a general internist who still sees primary care patients at the VA, gave us a diagnosis of the VA’s most serious symptoms: a lack of access to timely care, a high rate of veteran suicides, an inability to enforce employee accountability, multiple obstacles to hiring and retaining qualified staff, an unacceptable quality of care at some VAMCs, and a backlog of disability claims due to inefficient processing.
Dr. Shulkin also gave us a broad idea of his goal for care, “We are taking immediate and decisive steps stabilizing the organization.” But the more I thought about this impressive speech, the more I wondered, What is the VA’s actual diagnosis?
Several of the many news commentaries analyzing Shulkin’s State of the VA speech suggested possible etiologies. According to the Public Broadcasting Service (PBS), “In a ‘State of the VA’ report, Shulkin, a physician, issued a blunt diagnosis: ‘There is a lot of work to do.’” Astute clinicians will immediately recognize that PBS is right about the secretary’s honesty regarding the magnitude of the task facing him.
He was not providing a diagnosis as much as offering an indirect assessment of the patient’s condition. “A lot of work,” although not a diagnosis, is a colloquial description of the treatment plan that the secretary further outlined in his report. Like any good treatment plan, there is a direct correlation between the major symptoms of the disorder and the therapies that Dr. Shulkin prescribed.
The Secretary recommended and the President signed the Department of Veterans Affairs Accountability and Whistleblower Protection Act of 2017 on June 23, 2017, to make it easier to discipline and terminate VA employees who may be keeping the VA organization ill or at least preventing it from getting better. He also prescribed continued and even higher dose infusions of community care to treat the central access problem. In addition, Dr. Shulkin ordered that the most effective available interventions be used for suicide prevention, enhancement of the overall quality of care, and to improve accountability.
Even with the most efficacious treatments, a high-functioning intensive care unit needs state-of-theart technology and equipment. In a long-awaited announcement, Dr. Shulkin reported on June 5 that of 2 competing modalities to revive the VA’s ailing electronic health record system—the brain of our critical care patient—rather than repair the moribund CPRS, the VA will receive a transplant of the DoD MHS Genesis. Critical care, especially when delivered in a combat zone, requires difficult triage decisions. The secretary has made similar tough resource allocation decisions, determining that some of the VA’s oldest and most debilitated facilities will not be sustained in their present form.
I am near the end of this editorial and still do not have a diagnosis. Pundits, politicians, and policy specialists all have their differential diagnosis as well as veterans groups and VA employees.“Bloated bureaucracy” is the diagnosis from many of these VA critics. Dr. Shulkin proposed a remedy for this disease: He plans to consolidate the VA headquarters.
Even more important, for those who believe the VA should not have a DNR but be allowed to recover, what does the physician who holds the VA’s life in his hands believe is the prognosis for this 86-year-old institution? Dr. Shulkin expressed the hope that the VA can recover its health, saying he is “confident that we will be able turn VA into the organization veterans and their families deserve, and one that America can take pride in.” The most vehement of VA’s opponents would say that pouring additional millions of dollars into such a moribund entity is futile care. Yet the secretary and thousands of VA patients, staff, and supporters believe that the agency that President Lincoln created at the end of the bloodiest war in U.S. history still has value and can be restored to meaningful service for those who have, who are, and who will place their lives on the line for their country.

The surgical sky may not be falling
Unlike Dr. Elsey (“Surgery can be demanding work: Grit needed,” Letter to the Editor, May 2017, p. 6) and many others in various surgical publications, I have NOT enjoyed recent discussions about my generation’s perceived lack of readiness for independent practice following general surgery residency. Having been subjected to another round this month of “Why The Surgical Sky Is Falling,” I would like to take a moment to offer a different viewpoint.
I graduated from Tufts Medical Center’s general surgery residency in June 2014. After taking the written board exams, I started practice in a hospital-based group in Maine that same summer. My partners, both with 20+ years of experience, instituted a probationary period for observation of skill (ostensibly, and with good-natured teasing, to ensure I would not harm their patients, though I suspect such a thing is fairly universal for a new grad to receive institutional privileges), and, after convincing them I was not a reckless maniac, within a few months I was “on my own” in the operating room. I relied heavily on colleagues those first 18 months in practice, and ,if they ever grew weary of my asking advice about hemorrhoids, biliary colic, and diverticular disease, they never displayed perceptible annoyance. They were, and are, the best mentors I could have had.

Metrics and studies that rely on resident self-evaluation – and conversely, ones that rely on “objective” identification of resident strengths and weaknesses by faculty – are subject to the very bias that has dominated this argument for years. If you tell us we are not good enough or lacking in some capacity, often enough, we inevitably will start to believe it. Then, you will reinforce that same belief in your perception of us, which drives the wedge further into an increasingly irreconcilable situation.
I had a decent self-opinion of my surgical skill as a chief resident, but, on any given day, the number I would have assigned to my own “readiness” for independence would have varied greatly for any number of reasons. I did not contend with much in the way of spirited discouragement or admonishment regarding my skill progression over 5 years, but, in keeping with the “gritty” surgical personality espoused by Dr. Elsey in his letter, I’m not sure I would have let that stop me. Honestly though, it’s impossible to say how it would have affected my confidence to leave residency straight for attendinghood had I been subjected to daily thrashings over 5 years regarding my lack of attending-level skill.
It seems to me, some of the current teaching generation has displayed an inability to connect with their pupils. The majority of surgical residents in 2017 are millennials, and the “good old ways” of effective teaching through guilt, embarrassment, and punitive action will not work. Browbeaters need not apply, for you already have lost this war. For better or worse, educators must find a way to engage these residents on a positive emotional level at the same time as they engage on a higher intellectual plane.
Before the coffee spurts across your OR lounge and the surgical hats start flying fast and furious, let me clarify: In no way do I support the notion that general surgery residents should be coddled, pampered, or emotionally shielded from the gut-wrenching difficulty of practicing surgery. It was imperative in my education that I learned how to be wrong, how to admit it, and how to take ownership of my actions, whether right or wrong. Thankfully, I had a few good examples in Boston, and I’ll never forget the impact they made on my education. But, those lessons were reinforced in a way that made me WANT to weave them into the fabric of my surgical life. Never a heavy-handed dictum; without ego or audience; lacking the morose condescension associated with “those giants” of classical surgical training – what I received in my training was a whole-person engagement that fulfilled my desire to succeed and allowed me the room to grow up as an adult learner without feeling too akin to a 16-year-old, grounded and without car keys, when I had the audacity to make a mistake. Some tried this tack, but my grit won. Somewhere in Lawrenceville, Ga., I hope Dr. Elsey is smiling.
Those who taught best in my residency did so by example. They did it by letting me drive the ship, by giving credit when I did well, by educating when I did not. They did it by making me understand a patient is not a statistic, that you can be honest and kind and a giver of hope all at the same time and that a true surgeon does not need to brag and boast about her accomplishments, nor does he imperiously tear down those lower than himself on the “hierarchy.” The best of the best at Tufts Medical Center showed me what it means when a good person sits in an exam room with a hurting human being and starts the healing process with a kind smile, a gentle touch, words of reassurance, and confidence in his ability to change that patient’s life for the better.
Could it be that we need more of that – and less devotion to metrics – in surgical education? What might training become if we focus entirely on the patient and stop worrying about how the statistics make us all look? What would happen if educators traded nostalgia for engagement with their pupils? It may just be me, but all that sounds suspiciously ... old school, no?
So, before I have to choke down another article explaining how my contemporaries and I represent a kind of global warming to the long-established surgical polar ice caps, let me assure you that at least one young whippersnapper made it out of modern (read: postduty hours) surgical training and actually found a little success – and more than a bit of professional satisfaction – in the unforgiving world of independent general surgery by adhering to the same principles that guided Zollinger and DeBakey, Graham and Fisher: Do what is right for the patient, every single time, to the very best of your God-given and man-made ability. Those are some time-tested lessons I am very proud to have learned.
And, if you want the real story about my 3 years in practice, talk to my partners here in Maine. There is no critique quite like daily proximity. For what it’s worth, they have tolerated me splendidly.
Dr. Crosslin is a general surgeon practicing in Rockport, Maine, and an FACS Initiate, October 2017.
Unlike Dr. Elsey (“Surgery can be demanding work: Grit needed,” Letter to the Editor, May 2017, p. 6) and many others in various surgical publications, I have NOT enjoyed recent discussions about my generation’s perceived lack of readiness for independent practice following general surgery residency. Having been subjected to another round this month of “Why The Surgical Sky Is Falling,” I would like to take a moment to offer a different viewpoint.
I graduated from Tufts Medical Center’s general surgery residency in June 2014. After taking the written board exams, I started practice in a hospital-based group in Maine that same summer. My partners, both with 20+ years of experience, instituted a probationary period for observation of skill (ostensibly, and with good-natured teasing, to ensure I would not harm their patients, though I suspect such a thing is fairly universal for a new grad to receive institutional privileges), and, after convincing them I was not a reckless maniac, within a few months I was “on my own” in the operating room. I relied heavily on colleagues those first 18 months in practice, and ,if they ever grew weary of my asking advice about hemorrhoids, biliary colic, and diverticular disease, they never displayed perceptible annoyance. They were, and are, the best mentors I could have had.
Metrics and studies that rely on resident self-evaluation – and conversely, ones that rely on “objective” identification of resident strengths and weaknesses by faculty – are subject to the very bias that has dominated this argument for years. If you tell us we are not good enough or lacking in some capacity, often enough, we inevitably will start to believe it. Then, you will reinforce that same belief in your perception of us, which drives the wedge further into an increasingly irreconcilable situation.
I had a decent self-opinion of my surgical skill as a chief resident, but, on any given day, the number I would have assigned to my own “readiness” for independence would have varied greatly for any number of reasons. I did not contend with much in the way of spirited discouragement or admonishment regarding my skill progression over 5 years, but, in keeping with the “gritty” surgical personality espoused by Dr. Elsey in his letter, I’m not sure I would have let that stop me. Honestly though, it’s impossible to say how it would have affected my confidence to leave residency straight for attendinghood had I been subjected to daily thrashings over 5 years regarding my lack of attending-level skill.
It seems to me, some of the current teaching generation has displayed an inability to connect with their pupils. The majority of surgical residents in 2017 are millennials, and the “good old ways” of effective teaching through guilt, embarrassment, and punitive action will not work. Browbeaters need not apply, for you already have lost this war. For better or worse, educators must find a way to engage these residents on a positive emotional level at the same time as they engage on a higher intellectual plane.
Before the coffee spurts across your OR lounge and the surgical hats start flying fast and furious, let me clarify: In no way do I support the notion that general surgery residents should be coddled, pampered, or emotionally shielded from the gut-wrenching difficulty of practicing surgery. It was imperative in my education that I learned how to be wrong, how to admit it, and how to take ownership of my actions, whether right or wrong. Thankfully, I had a few good examples in Boston, and I’ll never forget the impact they made on my education. But, those lessons were reinforced in a way that made me WANT to weave them into the fabric of my surgical life. Never a heavy-handed dictum; without ego or audience; lacking the morose condescension associated with “those giants” of classical surgical training – what I received in my training was a whole-person engagement that fulfilled my desire to succeed and allowed me the room to grow up as an adult learner without feeling too akin to a 16-year-old, grounded and without car keys, when I had the audacity to make a mistake. Some tried this tack, but my grit won. Somewhere in Lawrenceville, Ga., I hope Dr. Elsey is smiling.
Those who taught best in my residency did so by example. They did it by letting me drive the ship, by giving credit when I did well, by educating when I did not. They did it by making me understand a patient is not a statistic, that you can be honest and kind and a giver of hope all at the same time and that a true surgeon does not need to brag and boast about her accomplishments, nor does he imperiously tear down those lower than himself on the “hierarchy.” The best of the best at Tufts Medical Center showed me what it means when a good person sits in an exam room with a hurting human being and starts the healing process with a kind smile, a gentle touch, words of reassurance, and confidence in his ability to change that patient’s life for the better.
Could it be that we need more of that – and less devotion to metrics – in surgical education? What might training become if we focus entirely on the patient and stop worrying about how the statistics make us all look? What would happen if educators traded nostalgia for engagement with their pupils? It may just be me, but all that sounds suspiciously ... old school, no?
So, before I have to choke down another article explaining how my contemporaries and I represent a kind of global warming to the long-established surgical polar ice caps, let me assure you that at least one young whippersnapper made it out of modern (read: postduty hours) surgical training and actually found a little success – and more than a bit of professional satisfaction – in the unforgiving world of independent general surgery by adhering to the same principles that guided Zollinger and DeBakey, Graham and Fisher: Do what is right for the patient, every single time, to the very best of your God-given and man-made ability. Those are some time-tested lessons I am very proud to have learned.
And, if you want the real story about my 3 years in practice, talk to my partners here in Maine. There is no critique quite like daily proximity. For what it’s worth, they have tolerated me splendidly.
Dr. Crosslin is a general surgeon practicing in Rockport, Maine, and an FACS Initiate, October 2017.
Unlike Dr. Elsey (“Surgery can be demanding work: Grit needed,” Letter to the Editor, May 2017, p. 6) and many others in various surgical publications, I have NOT enjoyed recent discussions about my generation’s perceived lack of readiness for independent practice following general surgery residency. Having been subjected to another round this month of “Why The Surgical Sky Is Falling,” I would like to take a moment to offer a different viewpoint.
I graduated from Tufts Medical Center’s general surgery residency in June 2014. After taking the written board exams, I started practice in a hospital-based group in Maine that same summer. My partners, both with 20+ years of experience, instituted a probationary period for observation of skill (ostensibly, and with good-natured teasing, to ensure I would not harm their patients, though I suspect such a thing is fairly universal for a new grad to receive institutional privileges), and, after convincing them I was not a reckless maniac, within a few months I was “on my own” in the operating room. I relied heavily on colleagues those first 18 months in practice, and ,if they ever grew weary of my asking advice about hemorrhoids, biliary colic, and diverticular disease, they never displayed perceptible annoyance. They were, and are, the best mentors I could have had.
Metrics and studies that rely on resident self-evaluation – and conversely, ones that rely on “objective” identification of resident strengths and weaknesses by faculty – are subject to the very bias that has dominated this argument for years. If you tell us we are not good enough or lacking in some capacity, often enough, we inevitably will start to believe it. Then, you will reinforce that same belief in your perception of us, which drives the wedge further into an increasingly irreconcilable situation.
I had a decent self-opinion of my surgical skill as a chief resident, but, on any given day, the number I would have assigned to my own “readiness” for independence would have varied greatly for any number of reasons. I did not contend with much in the way of spirited discouragement or admonishment regarding my skill progression over 5 years, but, in keeping with the “gritty” surgical personality espoused by Dr. Elsey in his letter, I’m not sure I would have let that stop me. Honestly though, it’s impossible to say how it would have affected my confidence to leave residency straight for attendinghood had I been subjected to daily thrashings over 5 years regarding my lack of attending-level skill.
It seems to me, some of the current teaching generation has displayed an inability to connect with their pupils. The majority of surgical residents in 2017 are millennials, and the “good old ways” of effective teaching through guilt, embarrassment, and punitive action will not work. Browbeaters need not apply, for you already have lost this war. For better or worse, educators must find a way to engage these residents on a positive emotional level at the same time as they engage on a higher intellectual plane.
Before the coffee spurts across your OR lounge and the surgical hats start flying fast and furious, let me clarify: In no way do I support the notion that general surgery residents should be coddled, pampered, or emotionally shielded from the gut-wrenching difficulty of practicing surgery. It was imperative in my education that I learned how to be wrong, how to admit it, and how to take ownership of my actions, whether right or wrong. Thankfully, I had a few good examples in Boston, and I’ll never forget the impact they made on my education. But, those lessons were reinforced in a way that made me WANT to weave them into the fabric of my surgical life. Never a heavy-handed dictum; without ego or audience; lacking the morose condescension associated with “those giants” of classical surgical training – what I received in my training was a whole-person engagement that fulfilled my desire to succeed and allowed me the room to grow up as an adult learner without feeling too akin to a 16-year-old, grounded and without car keys, when I had the audacity to make a mistake. Some tried this tack, but my grit won. Somewhere in Lawrenceville, Ga., I hope Dr. Elsey is smiling.
Those who taught best in my residency did so by example. They did it by letting me drive the ship, by giving credit when I did well, by educating when I did not. They did it by making me understand a patient is not a statistic, that you can be honest and kind and a giver of hope all at the same time and that a true surgeon does not need to brag and boast about her accomplishments, nor does he imperiously tear down those lower than himself on the “hierarchy.” The best of the best at Tufts Medical Center showed me what it means when a good person sits in an exam room with a hurting human being and starts the healing process with a kind smile, a gentle touch, words of reassurance, and confidence in his ability to change that patient’s life for the better.
Could it be that we need more of that – and less devotion to metrics – in surgical education? What might training become if we focus entirely on the patient and stop worrying about how the statistics make us all look? What would happen if educators traded nostalgia for engagement with their pupils? It may just be me, but all that sounds suspiciously ... old school, no?
So, before I have to choke down another article explaining how my contemporaries and I represent a kind of global warming to the long-established surgical polar ice caps, let me assure you that at least one young whippersnapper made it out of modern (read: postduty hours) surgical training and actually found a little success – and more than a bit of professional satisfaction – in the unforgiving world of independent general surgery by adhering to the same principles that guided Zollinger and DeBakey, Graham and Fisher: Do what is right for the patient, every single time, to the very best of your God-given and man-made ability. Those are some time-tested lessons I am very proud to have learned.
And, if you want the real story about my 3 years in practice, talk to my partners here in Maine. There is no critique quite like daily proximity. For what it’s worth, they have tolerated me splendidly.
Dr. Crosslin is a general surgeon practicing in Rockport, Maine, and an FACS Initiate, October 2017.
