User login
Pinterest as a marketing tool
My wife and I recently (and successfully) had our kitchen and bathrooms remodeled. It wouldn’t have been possible without Pinterest.
For the uninitiated, Pinterest is a wildly popular social media site that allows users to find, share, and organize images called "pins." Pinterest launched in September 2010, and today it has more than 70 million active users. It’s one of the fastest-growing social media sites in history, and it ranks as one of the Top 50 most-visited websites in the United States.
In a previous column about Pinterest, I mentioned several reasons why it’s important for your medical practice. More than 80% of Pinterest users are female, and, according to the U.S. Department of Labor, women make 80% of health care decisions for their families. Therefore, Pinterest could be a persuasive marketing tool for physicians looking to expand their practices. Pinterest also can be an effective platform to share patient stories, to introduce your practice and staff to the public, and to show before and after images of medical procedures.
New research from Vision Critical, the world’s leading provider of Insight Communities, discovered a surprising new finding about Pinterest (published in the July-August 2013 issue of Harvard Business Review).
The researchers examined "showrooming," a phenomenon whereby shoppers visit actual stores to examine merchandise before purchasing it online. They say the threat is so intense to brick-and-mortar stores that at least one merchant has begun charging people to browse in his store! Their research, however, shows much less of a threat. Of the 3,000 social media users they surveyed, only 26% reported "regularly engaging in showrooming."
What they found more surprising was that 41% of respondents said that practice "reverse showrooming;" that is, they browse online first then purchase the product in a store. That’s exactly what my wife did when choosing and purchasing our new furniture, lighting fixtures, wallpaper, paint, and more.
This led me to contemplate how "reverse showrooming" might help a physician market his or her medical practice. First, understand that Pinterest relies on aspirational messaging. Marketers use images that tap into our desires, wants, and dreams. Pinterest typically represents our idealized selves – the fashion-forward woman, the perfect garden wedding, the sublime oceanfront hotel room. Pinterest is about the version of you that you want to become. The you with flawless skin, lustrous hair, and smooth thighs.
Pinterest can be a powerful marketing tool for dermatologists, particularly cosmetic dermatologists. Consider the Pinterest customer base: Data show that 83% of Pinterest users are female and 45% are aged 35-54 years. Consumers turn to Pinterest largely for fashion and beauty, DIY projects, home design, inspiration, education, humor, and product recommendations. In fact, Pinterest has become the No. 1 traffic driver to websites of women’s lifestyle magazines.
You can use Pinterest to drive traffic to your office website, where people can book appointments or buy products online. Although no formal data exist for physician referrals from Pinterest, the study showed that the social-to-sale purchasing power was 17% for hair and beauty products and women’s and men’s apparel.
How can Pinterest help you market your practice and encourage "pinners" to "reverse showroom" into your office? Let’s use the example of a cosmetic surgeon who is seeking to expand her patient base and promote her organic skincare product line.
Pinterest users are more likely to purchase items that are easy to find. So, if they’re looking for an organic sunscreen, and they click through the Pinterest image the doctor posted and land on her website where they can buy it, then they’ll be more apt to do so. Research shows that the likelihood of a purchase increases by an additional 34% when there are existing reviews and recommendations for the product, and 30% when there are product details provided.
Pins don’t have to be strictly medical; consider more purely social boards that relate to your specialty, such as the following examples:
Family practice doctors could use Pinterest for wellness promotion, with boards for spreading happiness, healthy recipes, and habits of healthy families. Oncologists could use Pinterest to share inspirational patient testimonials, best foods for chemotherapy patients, and support for caregivers. Ob.gyns could use Pinterest as an outreach tool for expectant and new moms with boards for breast-feeding tutorials, fashionable maternity clothing, and cool baby gear.
Pinterest has proven to deliver value to businesses. With the above recommendations, you can quickly and cost-effectively add this platform to your marketing and patient relationship efforts.
Dr. Jeffrey Benabio is a partner physician in the department of dermatology of the Southern California Permanente Group in San Diego and a volunteer clinical assistant professor at the University of California, San Diego. Dr. Benabio is @Dermdoc on Twitter.
My wife and I recently (and successfully) had our kitchen and bathrooms remodeled. It wouldn’t have been possible without Pinterest.
For the uninitiated, Pinterest is a wildly popular social media site that allows users to find, share, and organize images called "pins." Pinterest launched in September 2010, and today it has more than 70 million active users. It’s one of the fastest-growing social media sites in history, and it ranks as one of the Top 50 most-visited websites in the United States.
In a previous column about Pinterest, I mentioned several reasons why it’s important for your medical practice. More than 80% of Pinterest users are female, and, according to the U.S. Department of Labor, women make 80% of health care decisions for their families. Therefore, Pinterest could be a persuasive marketing tool for physicians looking to expand their practices. Pinterest also can be an effective platform to share patient stories, to introduce your practice and staff to the public, and to show before and after images of medical procedures.
New research from Vision Critical, the world’s leading provider of Insight Communities, discovered a surprising new finding about Pinterest (published in the July-August 2013 issue of Harvard Business Review).
The researchers examined "showrooming," a phenomenon whereby shoppers visit actual stores to examine merchandise before purchasing it online. They say the threat is so intense to brick-and-mortar stores that at least one merchant has begun charging people to browse in his store! Their research, however, shows much less of a threat. Of the 3,000 social media users they surveyed, only 26% reported "regularly engaging in showrooming."
What they found more surprising was that 41% of respondents said that practice "reverse showrooming;" that is, they browse online first then purchase the product in a store. That’s exactly what my wife did when choosing and purchasing our new furniture, lighting fixtures, wallpaper, paint, and more.
This led me to contemplate how "reverse showrooming" might help a physician market his or her medical practice. First, understand that Pinterest relies on aspirational messaging. Marketers use images that tap into our desires, wants, and dreams. Pinterest typically represents our idealized selves – the fashion-forward woman, the perfect garden wedding, the sublime oceanfront hotel room. Pinterest is about the version of you that you want to become. The you with flawless skin, lustrous hair, and smooth thighs.
Pinterest can be a powerful marketing tool for dermatologists, particularly cosmetic dermatologists. Consider the Pinterest customer base: Data show that 83% of Pinterest users are female and 45% are aged 35-54 years. Consumers turn to Pinterest largely for fashion and beauty, DIY projects, home design, inspiration, education, humor, and product recommendations. In fact, Pinterest has become the No. 1 traffic driver to websites of women’s lifestyle magazines.
You can use Pinterest to drive traffic to your office website, where people can book appointments or buy products online. Although no formal data exist for physician referrals from Pinterest, the study showed that the social-to-sale purchasing power was 17% for hair and beauty products and women’s and men’s apparel.
How can Pinterest help you market your practice and encourage "pinners" to "reverse showroom" into your office? Let’s use the example of a cosmetic surgeon who is seeking to expand her patient base and promote her organic skincare product line.
Pinterest users are more likely to purchase items that are easy to find. So, if they’re looking for an organic sunscreen, and they click through the Pinterest image the doctor posted and land on her website where they can buy it, then they’ll be more apt to do so. Research shows that the likelihood of a purchase increases by an additional 34% when there are existing reviews and recommendations for the product, and 30% when there are product details provided.
Pins don’t have to be strictly medical; consider more purely social boards that relate to your specialty, such as the following examples:
Family practice doctors could use Pinterest for wellness promotion, with boards for spreading happiness, healthy recipes, and habits of healthy families. Oncologists could use Pinterest to share inspirational patient testimonials, best foods for chemotherapy patients, and support for caregivers. Ob.gyns could use Pinterest as an outreach tool for expectant and new moms with boards for breast-feeding tutorials, fashionable maternity clothing, and cool baby gear.
Pinterest has proven to deliver value to businesses. With the above recommendations, you can quickly and cost-effectively add this platform to your marketing and patient relationship efforts.
Dr. Jeffrey Benabio is a partner physician in the department of dermatology of the Southern California Permanente Group in San Diego and a volunteer clinical assistant professor at the University of California, San Diego. Dr. Benabio is @Dermdoc on Twitter.
My wife and I recently (and successfully) had our kitchen and bathrooms remodeled. It wouldn’t have been possible without Pinterest.
For the uninitiated, Pinterest is a wildly popular social media site that allows users to find, share, and organize images called "pins." Pinterest launched in September 2010, and today it has more than 70 million active users. It’s one of the fastest-growing social media sites in history, and it ranks as one of the Top 50 most-visited websites in the United States.
In a previous column about Pinterest, I mentioned several reasons why it’s important for your medical practice. More than 80% of Pinterest users are female, and, according to the U.S. Department of Labor, women make 80% of health care decisions for their families. Therefore, Pinterest could be a persuasive marketing tool for physicians looking to expand their practices. Pinterest also can be an effective platform to share patient stories, to introduce your practice and staff to the public, and to show before and after images of medical procedures.
New research from Vision Critical, the world’s leading provider of Insight Communities, discovered a surprising new finding about Pinterest (published in the July-August 2013 issue of Harvard Business Review).
The researchers examined "showrooming," a phenomenon whereby shoppers visit actual stores to examine merchandise before purchasing it online. They say the threat is so intense to brick-and-mortar stores that at least one merchant has begun charging people to browse in his store! Their research, however, shows much less of a threat. Of the 3,000 social media users they surveyed, only 26% reported "regularly engaging in showrooming."
What they found more surprising was that 41% of respondents said that practice "reverse showrooming;" that is, they browse online first then purchase the product in a store. That’s exactly what my wife did when choosing and purchasing our new furniture, lighting fixtures, wallpaper, paint, and more.
This led me to contemplate how "reverse showrooming" might help a physician market his or her medical practice. First, understand that Pinterest relies on aspirational messaging. Marketers use images that tap into our desires, wants, and dreams. Pinterest typically represents our idealized selves – the fashion-forward woman, the perfect garden wedding, the sublime oceanfront hotel room. Pinterest is about the version of you that you want to become. The you with flawless skin, lustrous hair, and smooth thighs.
Pinterest can be a powerful marketing tool for dermatologists, particularly cosmetic dermatologists. Consider the Pinterest customer base: Data show that 83% of Pinterest users are female and 45% are aged 35-54 years. Consumers turn to Pinterest largely for fashion and beauty, DIY projects, home design, inspiration, education, humor, and product recommendations. In fact, Pinterest has become the No. 1 traffic driver to websites of women’s lifestyle magazines.
You can use Pinterest to drive traffic to your office website, where people can book appointments or buy products online. Although no formal data exist for physician referrals from Pinterest, the study showed that the social-to-sale purchasing power was 17% for hair and beauty products and women’s and men’s apparel.
How can Pinterest help you market your practice and encourage "pinners" to "reverse showroom" into your office? Let’s use the example of a cosmetic surgeon who is seeking to expand her patient base and promote her organic skincare product line.
Pinterest users are more likely to purchase items that are easy to find. So, if they’re looking for an organic sunscreen, and they click through the Pinterest image the doctor posted and land on her website where they can buy it, then they’ll be more apt to do so. Research shows that the likelihood of a purchase increases by an additional 34% when there are existing reviews and recommendations for the product, and 30% when there are product details provided.
Pins don’t have to be strictly medical; consider more purely social boards that relate to your specialty, such as the following examples:
Family practice doctors could use Pinterest for wellness promotion, with boards for spreading happiness, healthy recipes, and habits of healthy families. Oncologists could use Pinterest to share inspirational patient testimonials, best foods for chemotherapy patients, and support for caregivers. Ob.gyns could use Pinterest as an outreach tool for expectant and new moms with boards for breast-feeding tutorials, fashionable maternity clothing, and cool baby gear.
Pinterest has proven to deliver value to businesses. With the above recommendations, you can quickly and cost-effectively add this platform to your marketing and patient relationship efforts.
Dr. Jeffrey Benabio is a partner physician in the department of dermatology of the Southern California Permanente Group in San Diego and a volunteer clinical assistant professor at the University of California, San Diego. Dr. Benabio is @Dermdoc on Twitter.

Accentuate the positive in your online presence
Have you ever run across a negative or even malicious comment about you or your practice on the web, in full view of the world? You’re certainly not alone.
Chances are it was on one of those doctor rating sites, whose supposedly "objective" evaluations are anything but fair or accurate. One curmudgeon, angry about something that usually has nothing to do with your clinical skills, can use his First Amendment–protected right to trash you unfairly, as thousands of satisfied patients remain silent.
What to do? You could hire one of the many companies in the rapidly burgeoning field of online reputation management, but that can cost hundreds to thousands of dollars per month for monitoring and intervention, and there are no guarantees of success.
A better solution is to generate your own search results – positive ones – that will overwhelm any negative comments that search engines might find. Start with the social networking sites. However you feel about networking, there’s no getting around the fact that personal pages on Facebook, LinkedIn, and Twitter rank very high on major search engines. (Some consultants say a favorable LinkedIn profile is particularly helpful because of that site’s reputation as a "professional" network.) Your community activities, charitable work, interesting hobbies – anything that casts you in a favorable light – need to be mentioned prominently in your network profiles.
You can also use Google’s profiling tool (google.com/profiles) to create a sterling bio, complete with links to URLs, photos, and anything else that shows you in the best possible light. And your Google profile will be at or near the top of any Google search.
Wikipedia articles go to the top of most searches, so if you’re notable enough to merit mention in one – or to have one of your own – see that it is updated regularly. You can’t do that yourself, however; Wikipedia’s conflict-of-interest rules forbid writing or editing content about yourself. Someone with a "neutral point of view" will have to do it.
If you don’t yet have a website, now would be a good time. As I’ve discussed many times, a professionally-designed site will be far more attractive and polished than anything you could build yourself. Furthermore, an experienced designer will employ "search engine optimization" (SEO), meaning that content will be created in a way that is readily visible to search engine users.
Leave design and SEO to the pros, but don’t delegate the content itself. As captain of the ship, you are responsible for all the facts and opinions on your site. And remember that once it’s online, it’s online forever. Consider the ramifications of anything you post on any site (yours or others) before hitting the "send" button. "The most damaging item about you," one consultant told me, "could well be something you posted yourself." Just ask any of several prominent politicians who have sabotaged their careers online.
That said; don’t be shy about creating content. Make your (noncontroversial) opinions known on Facebook and Twitter. If social networks are not your thing, add a blog to your website and write about what you know, and what interests you. If you have expertise in a particular field, write about that.
Incidentally, if the URL for your website is not your name, you should also register your name as a separate domain name, if only to be sure that a trickster – or someone with the same name and a bad reputation – doesn’t get it.
Set up an RSS news feed for yourself so you’ll know immediately anytime your name pops up in news or gossip sites, or on blogs. If something untrue is posted about you, take action. Reputable news sites and blogs have their own reputations to protect, and so can usually be persuaded to correct anything that is demonstrably false. Try to get the error removed entirely, or corrected within the original article. An erratum on the last page of the next edition will be ignored, and will leave the false information online, intact.
Unfair comments on doctor rating sites are unlikely to be removed unless they are blatantly libelous, but there is nothing wrong with encouraging happy patients to write favorable reviews. Turnabout is fair play.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He holds teaching positions at several hospitals and has delivered more than 500 academic speaking presentations. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Skin & Allergy News.
Have you ever run across a negative or even malicious comment about you or your practice on the web, in full view of the world? You’re certainly not alone.
Chances are it was on one of those doctor rating sites, whose supposedly "objective" evaluations are anything but fair or accurate. One curmudgeon, angry about something that usually has nothing to do with your clinical skills, can use his First Amendment–protected right to trash you unfairly, as thousands of satisfied patients remain silent.
What to do? You could hire one of the many companies in the rapidly burgeoning field of online reputation management, but that can cost hundreds to thousands of dollars per month for monitoring and intervention, and there are no guarantees of success.
A better solution is to generate your own search results – positive ones – that will overwhelm any negative comments that search engines might find. Start with the social networking sites. However you feel about networking, there’s no getting around the fact that personal pages on Facebook, LinkedIn, and Twitter rank very high on major search engines. (Some consultants say a favorable LinkedIn profile is particularly helpful because of that site’s reputation as a "professional" network.) Your community activities, charitable work, interesting hobbies – anything that casts you in a favorable light – need to be mentioned prominently in your network profiles.
You can also use Google’s profiling tool (google.com/profiles) to create a sterling bio, complete with links to URLs, photos, and anything else that shows you in the best possible light. And your Google profile will be at or near the top of any Google search.
Wikipedia articles go to the top of most searches, so if you’re notable enough to merit mention in one – or to have one of your own – see that it is updated regularly. You can’t do that yourself, however; Wikipedia’s conflict-of-interest rules forbid writing or editing content about yourself. Someone with a "neutral point of view" will have to do it.
If you don’t yet have a website, now would be a good time. As I’ve discussed many times, a professionally-designed site will be far more attractive and polished than anything you could build yourself. Furthermore, an experienced designer will employ "search engine optimization" (SEO), meaning that content will be created in a way that is readily visible to search engine users.
Leave design and SEO to the pros, but don’t delegate the content itself. As captain of the ship, you are responsible for all the facts and opinions on your site. And remember that once it’s online, it’s online forever. Consider the ramifications of anything you post on any site (yours or others) before hitting the "send" button. "The most damaging item about you," one consultant told me, "could well be something you posted yourself." Just ask any of several prominent politicians who have sabotaged their careers online.
That said; don’t be shy about creating content. Make your (noncontroversial) opinions known on Facebook and Twitter. If social networks are not your thing, add a blog to your website and write about what you know, and what interests you. If you have expertise in a particular field, write about that.
Incidentally, if the URL for your website is not your name, you should also register your name as a separate domain name, if only to be sure that a trickster – or someone with the same name and a bad reputation – doesn’t get it.
Set up an RSS news feed for yourself so you’ll know immediately anytime your name pops up in news or gossip sites, or on blogs. If something untrue is posted about you, take action. Reputable news sites and blogs have their own reputations to protect, and so can usually be persuaded to correct anything that is demonstrably false. Try to get the error removed entirely, or corrected within the original article. An erratum on the last page of the next edition will be ignored, and will leave the false information online, intact.
Unfair comments on doctor rating sites are unlikely to be removed unless they are blatantly libelous, but there is nothing wrong with encouraging happy patients to write favorable reviews. Turnabout is fair play.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He holds teaching positions at several hospitals and has delivered more than 500 academic speaking presentations. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Skin & Allergy News.
Have you ever run across a negative or even malicious comment about you or your practice on the web, in full view of the world? You’re certainly not alone.
Chances are it was on one of those doctor rating sites, whose supposedly "objective" evaluations are anything but fair or accurate. One curmudgeon, angry about something that usually has nothing to do with your clinical skills, can use his First Amendment–protected right to trash you unfairly, as thousands of satisfied patients remain silent.
What to do? You could hire one of the many companies in the rapidly burgeoning field of online reputation management, but that can cost hundreds to thousands of dollars per month for monitoring and intervention, and there are no guarantees of success.
A better solution is to generate your own search results – positive ones – that will overwhelm any negative comments that search engines might find. Start with the social networking sites. However you feel about networking, there’s no getting around the fact that personal pages on Facebook, LinkedIn, and Twitter rank very high on major search engines. (Some consultants say a favorable LinkedIn profile is particularly helpful because of that site’s reputation as a "professional" network.) Your community activities, charitable work, interesting hobbies – anything that casts you in a favorable light – need to be mentioned prominently in your network profiles.
You can also use Google’s profiling tool (google.com/profiles) to create a sterling bio, complete with links to URLs, photos, and anything else that shows you in the best possible light. And your Google profile will be at or near the top of any Google search.
Wikipedia articles go to the top of most searches, so if you’re notable enough to merit mention in one – or to have one of your own – see that it is updated regularly. You can’t do that yourself, however; Wikipedia’s conflict-of-interest rules forbid writing or editing content about yourself. Someone with a "neutral point of view" will have to do it.
If you don’t yet have a website, now would be a good time. As I’ve discussed many times, a professionally-designed site will be far more attractive and polished than anything you could build yourself. Furthermore, an experienced designer will employ "search engine optimization" (SEO), meaning that content will be created in a way that is readily visible to search engine users.
Leave design and SEO to the pros, but don’t delegate the content itself. As captain of the ship, you are responsible for all the facts and opinions on your site. And remember that once it’s online, it’s online forever. Consider the ramifications of anything you post on any site (yours or others) before hitting the "send" button. "The most damaging item about you," one consultant told me, "could well be something you posted yourself." Just ask any of several prominent politicians who have sabotaged their careers online.
That said; don’t be shy about creating content. Make your (noncontroversial) opinions known on Facebook and Twitter. If social networks are not your thing, add a blog to your website and write about what you know, and what interests you. If you have expertise in a particular field, write about that.
Incidentally, if the URL for your website is not your name, you should also register your name as a separate domain name, if only to be sure that a trickster – or someone with the same name and a bad reputation – doesn’t get it.
Set up an RSS news feed for yourself so you’ll know immediately anytime your name pops up in news or gossip sites, or on blogs. If something untrue is posted about you, take action. Reputable news sites and blogs have their own reputations to protect, and so can usually be persuaded to correct anything that is demonstrably false. Try to get the error removed entirely, or corrected within the original article. An erratum on the last page of the next edition will be ignored, and will leave the false information online, intact.
Unfair comments on doctor rating sites are unlikely to be removed unless they are blatantly libelous, but there is nothing wrong with encouraging happy patients to write favorable reviews. Turnabout is fair play.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He holds teaching positions at several hospitals and has delivered more than 500 academic speaking presentations. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Skin & Allergy News.

Hereditary cancer syndromes
Obstetrician-gynecologists play a unique role in screening women for various malignancies, including breast, colon, and cervical carcinoma. Although less common, genetic syndromes also can affect the female reproductive tract; therefore, knowledge of the screening guidelines for the most common genetic syndromes – hereditary breast and ovarian cancer syndrome, hereditary nonpolyposis colorectal cancer syndrome, and Cowden syndrome – is important.
Hereditary breast and ovarian cancer syndrome
Caused by autosomal-dominant deletions in the BRCA1/2 genes, the lifetime risk of ovarian cancer in patients with a BRCA1 and BRCA2 mutation is 39%-46% and 12%-20%, respectively. Although not proven to improve detection or survival, the American College of Obstetricians and Gynecologists (ACOG) and National Comprehensive Cancer Network (NCCN) guidelines recommend that women with BRCA1/2 mutations should undergo screening with transvaginal ultrasonography and CA125 every 6 months beginning between ages 30-35 years or 5-10 years prior to the age of the youngest affected family member. For patients who have not completed childbearing, a recent meta-analysis showed that use of oral contraceptives was associated with a decreased risk of ovarian cancer in patients with BRCA1/2 (J. Clin. Oncol. 2013;31:4188-98). Once childbearing has been completed or at the age of 40 years, a risk-reducing bilateral salpingo-oophorectomy (BSO) should be strongly considered (Gynecol. Oncol. 2009;113:6-11; Obstet. Gynecol. 2011;117:742-6).
In addition, patients with BRCA 1/2 mutations carry a 65%-74% lifetime risk of developing breast cancer (Gynecol. Oncol. 2009;113:6-11).ACOG recommends that these women begin screening for breast cancer at the age of 25 years through semiannual self-breast exams as well as annual mammography and breast MRI or sooner if a family member’s cancer was diagnosed prior to this age. Chemoprevention with tamoxifen also has been shown to reduce the risk of breast cancer in patients with BRCA2 disease, but is less effective for BRCA1 patients. Prophylactic mastectomy has the ability to reduce a woman’s risk of developing breast cancer by 90%-95%.
Hereditary nonpolyposis colorectal cancer syndrome
Another autosomal-dominant disorder, hereditary nonpolyposis colorectal cancer (HNPCC) syndrome arises as a result of a genetic defect in DNA mismatch repair mechanisms. Colon cancer is the most common malignancy associated with this syndrome, with a 70% risk by the age of 70 years (JAMA 2006;296:1507-17). Other associated cancers include those of the urinary tract, hepatobiliary tract, small intestine, skin, and brain, but strong supportive data are lacking. Beginning at age 20-25 years (or 10 years before the age of the youngest family member to develop colon cancer), a colonoscopy is recommended every 1-2 years. Annual urinalysis with cytology is advocated by some as a screening test for urinary tract cancers.
Patients with HNPCC have up to a 60% lifetime risk of endometrial cancer and a 10% risk of ovarian cancer (Int. J. Cancer 1999;81:214-8; Hum. Mol. Gene. 1997;6:105-10). The American Cancer Society recommends an endometrial biopsy and transvaginal ultrasonography annually between 30-35 years of age (JAMA 2006;296:1507-17). Schmeler et al. compared outcomes among 315 women with mismatch repair defects, 61 of whom underwent risk-reducing hysterectomy and BSO. With an average follow-up of greater than 7 years, none of the patients who underwent surgery developed cancer, while 33% of those who did not have surgery developed endometrial cancer and 5.5% developed ovarian cancer (N. Engl. J. Med. 2006;354:261-9). Because of these data, risk-reducing surgery at the age of 35 should be considered.
Cowden Syndrome
Cowden Syndrome, caused by an autosomal-dominant mutation in the PTEN gene, is associated with an up to 10% lifetime risk of endometrial cancer and a 50% risk of breast cancer (Obstet. Gynecol. Clin. N. Am. 2010;37:109-33). The NCCN notes that data are limited, but discussion of endometrial cancer symptoms should be encouraged (NCCN Guidelines Version 4, 2013). Annual endometrial sampling and ultrasound should be considered in woman aged 35-40 years or 10 years earlier than the youngest affected family member (Obstet. Gynecol. Clin. N. Am. 2010;37:109-33). Screening for breast cancer should include annual mammography and breast MRI starting between age 30-35 years or earlier depending on family history, per the NCCN guidelines.
It is important to note that additional genetic syndromes can have repercussions on the female genital tract, including the Li-Fraumeni (ovarian cancer), the Peutz-Jeghers (sex cord–stromal tumors of the ovary, granulosa cell tumors), and the Ollier (granulosa cell tumors) syndromes; unfortunately, screening guidelines for these rare syndromes have not been well studied (JAMA 2006;296:1507-17).
Dr. Schuler is a gynecologic oncologist at Good Samaritan Hospital in Cincinnati. Dr. Gehrig is professor and director of gynecologic oncology at the University of North Carolina at Chapel Hill. Dr. Gehrig and Dr. Schuler said they had no relevant financial disclosures.
Obstetrician-gynecologists play a unique role in screening women for various malignancies, including breast, colon, and cervical carcinoma. Although less common, genetic syndromes also can affect the female reproductive tract; therefore, knowledge of the screening guidelines for the most common genetic syndromes – hereditary breast and ovarian cancer syndrome, hereditary nonpolyposis colorectal cancer syndrome, and Cowden syndrome – is important.
Hereditary breast and ovarian cancer syndrome
Caused by autosomal-dominant deletions in the BRCA1/2 genes, the lifetime risk of ovarian cancer in patients with a BRCA1 and BRCA2 mutation is 39%-46% and 12%-20%, respectively. Although not proven to improve detection or survival, the American College of Obstetricians and Gynecologists (ACOG) and National Comprehensive Cancer Network (NCCN) guidelines recommend that women with BRCA1/2 mutations should undergo screening with transvaginal ultrasonography and CA125 every 6 months beginning between ages 30-35 years or 5-10 years prior to the age of the youngest affected family member. For patients who have not completed childbearing, a recent meta-analysis showed that use of oral contraceptives was associated with a decreased risk of ovarian cancer in patients with BRCA1/2 (J. Clin. Oncol. 2013;31:4188-98). Once childbearing has been completed or at the age of 40 years, a risk-reducing bilateral salpingo-oophorectomy (BSO) should be strongly considered (Gynecol. Oncol. 2009;113:6-11; Obstet. Gynecol. 2011;117:742-6).
In addition, patients with BRCA 1/2 mutations carry a 65%-74% lifetime risk of developing breast cancer (Gynecol. Oncol. 2009;113:6-11).ACOG recommends that these women begin screening for breast cancer at the age of 25 years through semiannual self-breast exams as well as annual mammography and breast MRI or sooner if a family member’s cancer was diagnosed prior to this age. Chemoprevention with tamoxifen also has been shown to reduce the risk of breast cancer in patients with BRCA2 disease, but is less effective for BRCA1 patients. Prophylactic mastectomy has the ability to reduce a woman’s risk of developing breast cancer by 90%-95%.
Hereditary nonpolyposis colorectal cancer syndrome
Another autosomal-dominant disorder, hereditary nonpolyposis colorectal cancer (HNPCC) syndrome arises as a result of a genetic defect in DNA mismatch repair mechanisms. Colon cancer is the most common malignancy associated with this syndrome, with a 70% risk by the age of 70 years (JAMA 2006;296:1507-17). Other associated cancers include those of the urinary tract, hepatobiliary tract, small intestine, skin, and brain, but strong supportive data are lacking. Beginning at age 20-25 years (or 10 years before the age of the youngest family member to develop colon cancer), a colonoscopy is recommended every 1-2 years. Annual urinalysis with cytology is advocated by some as a screening test for urinary tract cancers.
Patients with HNPCC have up to a 60% lifetime risk of endometrial cancer and a 10% risk of ovarian cancer (Int. J. Cancer 1999;81:214-8; Hum. Mol. Gene. 1997;6:105-10). The American Cancer Society recommends an endometrial biopsy and transvaginal ultrasonography annually between 30-35 years of age (JAMA 2006;296:1507-17). Schmeler et al. compared outcomes among 315 women with mismatch repair defects, 61 of whom underwent risk-reducing hysterectomy and BSO. With an average follow-up of greater than 7 years, none of the patients who underwent surgery developed cancer, while 33% of those who did not have surgery developed endometrial cancer and 5.5% developed ovarian cancer (N. Engl. J. Med. 2006;354:261-9). Because of these data, risk-reducing surgery at the age of 35 should be considered.
Cowden Syndrome
Cowden Syndrome, caused by an autosomal-dominant mutation in the PTEN gene, is associated with an up to 10% lifetime risk of endometrial cancer and a 50% risk of breast cancer (Obstet. Gynecol. Clin. N. Am. 2010;37:109-33). The NCCN notes that data are limited, but discussion of endometrial cancer symptoms should be encouraged (NCCN Guidelines Version 4, 2013). Annual endometrial sampling and ultrasound should be considered in woman aged 35-40 years or 10 years earlier than the youngest affected family member (Obstet. Gynecol. Clin. N. Am. 2010;37:109-33). Screening for breast cancer should include annual mammography and breast MRI starting between age 30-35 years or earlier depending on family history, per the NCCN guidelines.
It is important to note that additional genetic syndromes can have repercussions on the female genital tract, including the Li-Fraumeni (ovarian cancer), the Peutz-Jeghers (sex cord–stromal tumors of the ovary, granulosa cell tumors), and the Ollier (granulosa cell tumors) syndromes; unfortunately, screening guidelines for these rare syndromes have not been well studied (JAMA 2006;296:1507-17).
Dr. Schuler is a gynecologic oncologist at Good Samaritan Hospital in Cincinnati. Dr. Gehrig is professor and director of gynecologic oncology at the University of North Carolina at Chapel Hill. Dr. Gehrig and Dr. Schuler said they had no relevant financial disclosures.
Obstetrician-gynecologists play a unique role in screening women for various malignancies, including breast, colon, and cervical carcinoma. Although less common, genetic syndromes also can affect the female reproductive tract; therefore, knowledge of the screening guidelines for the most common genetic syndromes – hereditary breast and ovarian cancer syndrome, hereditary nonpolyposis colorectal cancer syndrome, and Cowden syndrome – is important.
Hereditary breast and ovarian cancer syndrome
Caused by autosomal-dominant deletions in the BRCA1/2 genes, the lifetime risk of ovarian cancer in patients with a BRCA1 and BRCA2 mutation is 39%-46% and 12%-20%, respectively. Although not proven to improve detection or survival, the American College of Obstetricians and Gynecologists (ACOG) and National Comprehensive Cancer Network (NCCN) guidelines recommend that women with BRCA1/2 mutations should undergo screening with transvaginal ultrasonography and CA125 every 6 months beginning between ages 30-35 years or 5-10 years prior to the age of the youngest affected family member. For patients who have not completed childbearing, a recent meta-analysis showed that use of oral contraceptives was associated with a decreased risk of ovarian cancer in patients with BRCA1/2 (J. Clin. Oncol. 2013;31:4188-98). Once childbearing has been completed or at the age of 40 years, a risk-reducing bilateral salpingo-oophorectomy (BSO) should be strongly considered (Gynecol. Oncol. 2009;113:6-11; Obstet. Gynecol. 2011;117:742-6).
In addition, patients with BRCA 1/2 mutations carry a 65%-74% lifetime risk of developing breast cancer (Gynecol. Oncol. 2009;113:6-11).ACOG recommends that these women begin screening for breast cancer at the age of 25 years through semiannual self-breast exams as well as annual mammography and breast MRI or sooner if a family member’s cancer was diagnosed prior to this age. Chemoprevention with tamoxifen also has been shown to reduce the risk of breast cancer in patients with BRCA2 disease, but is less effective for BRCA1 patients. Prophylactic mastectomy has the ability to reduce a woman’s risk of developing breast cancer by 90%-95%.
Hereditary nonpolyposis colorectal cancer syndrome
Another autosomal-dominant disorder, hereditary nonpolyposis colorectal cancer (HNPCC) syndrome arises as a result of a genetic defect in DNA mismatch repair mechanisms. Colon cancer is the most common malignancy associated with this syndrome, with a 70% risk by the age of 70 years (JAMA 2006;296:1507-17). Other associated cancers include those of the urinary tract, hepatobiliary tract, small intestine, skin, and brain, but strong supportive data are lacking. Beginning at age 20-25 years (or 10 years before the age of the youngest family member to develop colon cancer), a colonoscopy is recommended every 1-2 years. Annual urinalysis with cytology is advocated by some as a screening test for urinary tract cancers.
Patients with HNPCC have up to a 60% lifetime risk of endometrial cancer and a 10% risk of ovarian cancer (Int. J. Cancer 1999;81:214-8; Hum. Mol. Gene. 1997;6:105-10). The American Cancer Society recommends an endometrial biopsy and transvaginal ultrasonography annually between 30-35 years of age (JAMA 2006;296:1507-17). Schmeler et al. compared outcomes among 315 women with mismatch repair defects, 61 of whom underwent risk-reducing hysterectomy and BSO. With an average follow-up of greater than 7 years, none of the patients who underwent surgery developed cancer, while 33% of those who did not have surgery developed endometrial cancer and 5.5% developed ovarian cancer (N. Engl. J. Med. 2006;354:261-9). Because of these data, risk-reducing surgery at the age of 35 should be considered.
Cowden Syndrome
Cowden Syndrome, caused by an autosomal-dominant mutation in the PTEN gene, is associated with an up to 10% lifetime risk of endometrial cancer and a 50% risk of breast cancer (Obstet. Gynecol. Clin. N. Am. 2010;37:109-33). The NCCN notes that data are limited, but discussion of endometrial cancer symptoms should be encouraged (NCCN Guidelines Version 4, 2013). Annual endometrial sampling and ultrasound should be considered in woman aged 35-40 years or 10 years earlier than the youngest affected family member (Obstet. Gynecol. Clin. N. Am. 2010;37:109-33). Screening for breast cancer should include annual mammography and breast MRI starting between age 30-35 years or earlier depending on family history, per the NCCN guidelines.
It is important to note that additional genetic syndromes can have repercussions on the female genital tract, including the Li-Fraumeni (ovarian cancer), the Peutz-Jeghers (sex cord–stromal tumors of the ovary, granulosa cell tumors), and the Ollier (granulosa cell tumors) syndromes; unfortunately, screening guidelines for these rare syndromes have not been well studied (JAMA 2006;296:1507-17).
Dr. Schuler is a gynecologic oncologist at Good Samaritan Hospital in Cincinnati. Dr. Gehrig is professor and director of gynecologic oncology at the University of North Carolina at Chapel Hill. Dr. Gehrig and Dr. Schuler said they had no relevant financial disclosures.

You've got mail
As a parent, I hate how you have to sign kids up for camps way before summer even starts. What 12-year-old can really answer whether he’d rather go indoor skydiving or learn SCUBA when he’s still trying to build a cardboard suit of armor for Social Studies? (A suit that would prove equally useless for skydiving, SCUBA, or understanding the role of economic subjugation in feudal societies.) However, if we don’t act in time, the only spots left will be in that engineering camp he attended last year, the one where they built the same catapult over and over again. At least if he ends up there, he’ll have just the right armor.
Joint attention
It’s hard to explain to a kid that just because something is legal doesn’t meant it’s good for you. After all, no one has outlawed large sugary sodas, tequila, or Miley Cyrus. So, with two states now allowing recreational use of marijuana, I find it just the teeniest bit alarming that a new study confirms that marijuana use can lead to permanent brain damage in young adults. On the up side, once your brain has been impaired by smoking pot, you could care less.
Dr. Hans Breiter and his colleagues obtained high-resolution (“High.” Heh!) MRI scans of the brains of recreational marijuana users between the ages of 18 and 25 years, then analyzed the volume and composition of their brains, compared with matched controls, with particular attention to brain regions responsible for regulating emotion and motivation. (For those of you who are still motivated, those are the nucleus accumbens and the amygdala. For the rest of you...“high-resolution.” Heh!)
Dr. Breiter explained, "What we're seeing is changes in people who are 18-25 in core brain regions that you never, ever want to fool around with. Our hypothesis from this early work is that these changes may be an early sign of what later becomes amotivation, where people aren't focused on their goals." Of course, marijuana advocates may have a different take on things. Some people “suffer amotivational symptoms.” Some just “abide.”
Mother’s little helper
Doesn’t it seem unfair that toddlers can’t use the same coping skills as adults do? Being little presents all sorts of stresses, but small children can’t go for a run, they can’t drink alcohol, heck, they can’t even yell at their subordinates. But there is one thing they can do, and new research shows that the crankier children are, the more they indulge: watching mindless television. I’d explain more, but my show is on.
Okay, commercial break. Dr. Jenny Radesky and her colleagues evaluated data from 7,450 children in the Early Childhood Longitudinal Study–Birth Cohort, attempting to correlate measures of emotional self-regulation with hours spent in front of a screen. As it turns out, kids who were especially fussy at ages 9 months and 24 months spent more time watching videos than did their calmer peers. The authors fail to document whether their parents drank more.
The study also did not address cause and effect: Do children with poor emotional regulation get stuck in front of screens to calm them down, or does increased screen time prevent kids from building more advanced coping mechanisms? I became so perplexed reading this study that I had to watch an episode of The Golden Girls. It relaxes me: Every time someone says “Blanche,” I take a shot.
Tipping the scales
The vaccine-autism myth is like the pediatric version of the Sewer Gator: It started with a study that has been flushed down the toilet, yet no amount of evidence will convince some people that it’s not real, and it grows more dangerous every day. The only difference is that the Sewer Gator never actually killed a child. In the midst of outbreaks of measles, mumps, and whooping cough, I was not reassured to read a new Harris Poll reporting that 1 in 3 parents still believe that vaccines can cause autism. At least the existence of the Sewer Gator has not been definitively disproven by 23 studies.
Before we waste any more energy fighting this misconception, however, we have to acknowledge what we’re up against. According to the National Science Foundation’s annual survey, fewer than 40% of Americans believe in the Big Bang, fewer than 50% believe in evolution, and 26% of Americans think the sun revolves around the earth. And we’re hoping that 95% of Americans will understand the epidemiology of infectious diseases and the fetal origins of autism spectrum disorders. Right. If you need me, I’ll be watching The Golden Girls, wearing cardboard armor.
David L. Hill, M.D., FAAP is the author of Dad to Dad: Parenting Like a Pro (AAP Publishing, 2012). He is also vice president of Cape Fear Pediatrics in Wilmington, N.C., and adjunct assistant professor of pediatrics at the University of North Carolina at Chapel Hill. He serves as Program Director for the AAP Council on Communications and Media and as an executive committee member of the North Carolina Pediatric Society. He has recorded commentaries for NPR's All Things Considered and provided content for various print, television, and Internet outlets.
As a parent, I hate how you have to sign kids up for camps way before summer even starts. What 12-year-old can really answer whether he’d rather go indoor skydiving or learn SCUBA when he’s still trying to build a cardboard suit of armor for Social Studies? (A suit that would prove equally useless for skydiving, SCUBA, or understanding the role of economic subjugation in feudal societies.) However, if we don’t act in time, the only spots left will be in that engineering camp he attended last year, the one where they built the same catapult over and over again. At least if he ends up there, he’ll have just the right armor.
Joint attention
It’s hard to explain to a kid that just because something is legal doesn’t meant it’s good for you. After all, no one has outlawed large sugary sodas, tequila, or Miley Cyrus. So, with two states now allowing recreational use of marijuana, I find it just the teeniest bit alarming that a new study confirms that marijuana use can lead to permanent brain damage in young adults. On the up side, once your brain has been impaired by smoking pot, you could care less.
Dr. Hans Breiter and his colleagues obtained high-resolution (“High.” Heh!) MRI scans of the brains of recreational marijuana users between the ages of 18 and 25 years, then analyzed the volume and composition of their brains, compared with matched controls, with particular attention to brain regions responsible for regulating emotion and motivation. (For those of you who are still motivated, those are the nucleus accumbens and the amygdala. For the rest of you...“high-resolution.” Heh!)
Dr. Breiter explained, "What we're seeing is changes in people who are 18-25 in core brain regions that you never, ever want to fool around with. Our hypothesis from this early work is that these changes may be an early sign of what later becomes amotivation, where people aren't focused on their goals." Of course, marijuana advocates may have a different take on things. Some people “suffer amotivational symptoms.” Some just “abide.”
Mother’s little helper
Doesn’t it seem unfair that toddlers can’t use the same coping skills as adults do? Being little presents all sorts of stresses, but small children can’t go for a run, they can’t drink alcohol, heck, they can’t even yell at their subordinates. But there is one thing they can do, and new research shows that the crankier children are, the more they indulge: watching mindless television. I’d explain more, but my show is on.
Okay, commercial break. Dr. Jenny Radesky and her colleagues evaluated data from 7,450 children in the Early Childhood Longitudinal Study–Birth Cohort, attempting to correlate measures of emotional self-regulation with hours spent in front of a screen. As it turns out, kids who were especially fussy at ages 9 months and 24 months spent more time watching videos than did their calmer peers. The authors fail to document whether their parents drank more.
The study also did not address cause and effect: Do children with poor emotional regulation get stuck in front of screens to calm them down, or does increased screen time prevent kids from building more advanced coping mechanisms? I became so perplexed reading this study that I had to watch an episode of The Golden Girls. It relaxes me: Every time someone says “Blanche,” I take a shot.
Tipping the scales
The vaccine-autism myth is like the pediatric version of the Sewer Gator: It started with a study that has been flushed down the toilet, yet no amount of evidence will convince some people that it’s not real, and it grows more dangerous every day. The only difference is that the Sewer Gator never actually killed a child. In the midst of outbreaks of measles, mumps, and whooping cough, I was not reassured to read a new Harris Poll reporting that 1 in 3 parents still believe that vaccines can cause autism. At least the existence of the Sewer Gator has not been definitively disproven by 23 studies.
Before we waste any more energy fighting this misconception, however, we have to acknowledge what we’re up against. According to the National Science Foundation’s annual survey, fewer than 40% of Americans believe in the Big Bang, fewer than 50% believe in evolution, and 26% of Americans think the sun revolves around the earth. And we’re hoping that 95% of Americans will understand the epidemiology of infectious diseases and the fetal origins of autism spectrum disorders. Right. If you need me, I’ll be watching The Golden Girls, wearing cardboard armor.
David L. Hill, M.D., FAAP is the author of Dad to Dad: Parenting Like a Pro (AAP Publishing, 2012). He is also vice president of Cape Fear Pediatrics in Wilmington, N.C., and adjunct assistant professor of pediatrics at the University of North Carolina at Chapel Hill. He serves as Program Director for the AAP Council on Communications and Media and as an executive committee member of the North Carolina Pediatric Society. He has recorded commentaries for NPR's All Things Considered and provided content for various print, television, and Internet outlets.
As a parent, I hate how you have to sign kids up for camps way before summer even starts. What 12-year-old can really answer whether he’d rather go indoor skydiving or learn SCUBA when he’s still trying to build a cardboard suit of armor for Social Studies? (A suit that would prove equally useless for skydiving, SCUBA, or understanding the role of economic subjugation in feudal societies.) However, if we don’t act in time, the only spots left will be in that engineering camp he attended last year, the one where they built the same catapult over and over again. At least if he ends up there, he’ll have just the right armor.
Joint attention
It’s hard to explain to a kid that just because something is legal doesn’t meant it’s good for you. After all, no one has outlawed large sugary sodas, tequila, or Miley Cyrus. So, with two states now allowing recreational use of marijuana, I find it just the teeniest bit alarming that a new study confirms that marijuana use can lead to permanent brain damage in young adults. On the up side, once your brain has been impaired by smoking pot, you could care less.
Dr. Hans Breiter and his colleagues obtained high-resolution (“High.” Heh!) MRI scans of the brains of recreational marijuana users between the ages of 18 and 25 years, then analyzed the volume and composition of their brains, compared with matched controls, with particular attention to brain regions responsible for regulating emotion and motivation. (For those of you who are still motivated, those are the nucleus accumbens and the amygdala. For the rest of you...“high-resolution.” Heh!)
Dr. Breiter explained, "What we're seeing is changes in people who are 18-25 in core brain regions that you never, ever want to fool around with. Our hypothesis from this early work is that these changes may be an early sign of what later becomes amotivation, where people aren't focused on their goals." Of course, marijuana advocates may have a different take on things. Some people “suffer amotivational symptoms.” Some just “abide.”
Mother’s little helper
Doesn’t it seem unfair that toddlers can’t use the same coping skills as adults do? Being little presents all sorts of stresses, but small children can’t go for a run, they can’t drink alcohol, heck, they can’t even yell at their subordinates. But there is one thing they can do, and new research shows that the crankier children are, the more they indulge: watching mindless television. I’d explain more, but my show is on.
Okay, commercial break. Dr. Jenny Radesky and her colleagues evaluated data from 7,450 children in the Early Childhood Longitudinal Study–Birth Cohort, attempting to correlate measures of emotional self-regulation with hours spent in front of a screen. As it turns out, kids who were especially fussy at ages 9 months and 24 months spent more time watching videos than did their calmer peers. The authors fail to document whether their parents drank more.
The study also did not address cause and effect: Do children with poor emotional regulation get stuck in front of screens to calm them down, or does increased screen time prevent kids from building more advanced coping mechanisms? I became so perplexed reading this study that I had to watch an episode of The Golden Girls. It relaxes me: Every time someone says “Blanche,” I take a shot.
Tipping the scales
The vaccine-autism myth is like the pediatric version of the Sewer Gator: It started with a study that has been flushed down the toilet, yet no amount of evidence will convince some people that it’s not real, and it grows more dangerous every day. The only difference is that the Sewer Gator never actually killed a child. In the midst of outbreaks of measles, mumps, and whooping cough, I was not reassured to read a new Harris Poll reporting that 1 in 3 parents still believe that vaccines can cause autism. At least the existence of the Sewer Gator has not been definitively disproven by 23 studies.
Before we waste any more energy fighting this misconception, however, we have to acknowledge what we’re up against. According to the National Science Foundation’s annual survey, fewer than 40% of Americans believe in the Big Bang, fewer than 50% believe in evolution, and 26% of Americans think the sun revolves around the earth. And we’re hoping that 95% of Americans will understand the epidemiology of infectious diseases and the fetal origins of autism spectrum disorders. Right. If you need me, I’ll be watching The Golden Girls, wearing cardboard armor.
David L. Hill, M.D., FAAP is the author of Dad to Dad: Parenting Like a Pro (AAP Publishing, 2012). He is also vice president of Cape Fear Pediatrics in Wilmington, N.C., and adjunct assistant professor of pediatrics at the University of North Carolina at Chapel Hill. He serves as Program Director for the AAP Council on Communications and Media and as an executive committee member of the North Carolina Pediatric Society. He has recorded commentaries for NPR's All Things Considered and provided content for various print, television, and Internet outlets.
Antitrust issues in health care (Part I)
This article introduces United States antitrust laws and discusses their application in health care. Part 2 will summarize major court decisions covering that subject.
Question: Antitrust laws:
A. Are based in part on the physician-patient trust relationship.
B. Prohibit anticompetitive behavior.
C. Regulate business activities but not professional services.
D. A, B, and C are correct.
E. B and C are correct.
Answer: B. Economic interests are best served in a freely competitive marketplace. Trade restraints such as price fixing and monopolization tend to promote inefficiency and increase profit for the perpetrators, at the expense of consumer welfare.
Accordingly, Congress enacted the Sherman Antitrust Act way back in 1890 to promote competition and outlaw unreasonable restraint of trade. Additional laws prohibit mergers that substantially lessen competition, price discrimination, and unfair trade practices. Collectively, these are known as the antitrust laws, the term reflecting their initial purpose to prevent commercial traders from forming anticompetitive groups or "trusts."
The Department of Justice (DOJ), the Federal Trade Commission (FTC), and their state counterparts enforce these laws, which have nothing whatsoever to do with the doctor-patient trust relationship.
Section I of the Sherman Act, the paramount antitrust statute, declares that "Every contract, combination in the form of trust or otherwise, or conspiracy, in restraint of trade or commerce among the several States, or with foreign nations, is declared to be illegal." Section II stipulates, "Every person who shall monopolize, or attempt to monopolize, or combine or conspire with any other person or persons, to monopolize any part of the trade or commerce among the several States, or with foreign nations, shall be deemed guilty of a felony."
Other important laws are Sections 4 and 7 of the Clayton Antitrust Act and Section 5(a)(1) of the Federal Trade Commission Act, which outlaws "unfair methods of competition in or affecting commerce ... " Additionally, all states have their own antitrust statutes, which in some cases may be more restrictive than the federal laws are.
These laws initially targeted anticompetitive business practices. In 1975, the U.S. Supreme Court declared that there was to be no "learned profession" exemption, although special considerations may apply.1 However, activities of state government officials and employees are exempt from antitrust scrutiny under the so-called "state action doctrine," which confers immunity if an exemption is clearly articulated and affirmatively expressed as state policy, and there is active state supervision of the conduct in question.
Antitrust issues are ubiquitous in health care, and fall into seven major categories: 1) price fixing; 2) boycotts; 3) market division; 4) monopolization; 5) joint ventures; 6) exclusive contracts, and 7) peer review.
1. Price fixing. An agreement to fix prices is the most egregious example of anticompetitive conduct, so much so that the courts will use a per se analysis, i.e., without need to consider other factors, to arrive at its decision. Price fixing does not require any party to show market dominance or power, and its presence can be inferred from circumstances and agreements, which can be either oral or written.
For example, physician fee schedules or guidelines by a medical association would constitute price fixing. Even an agreement to fix maximum prices, as opposed to minimum prices, has been ruled illegal. At a practical level, physicians should avoid sharing pricing information with anyone, especially with colleagues, unless strict FTC "safety zone" criteria are satisfied.
2. Boycotts. Group boycotts are usually per se illegal, but in the health care industry, a rule of reason analysis is frequently used. Courts will look at the circumstances and purpose of the boycott, its pro- and anti-competitive effects, and whether there are other less restrictive ways to achieve the purported goal.
Affiliating physicians face this risk when forming alliances, as boycott questions may arise when a doctor is inappropriately excluded, which deprives him/her from earning a living in the relevant market.
A related controversial issue is the unionization of doctors. Unionization protects labor rights, especially those of medical residents, and offers greater parity in collective bargaining. On the other hand, the danger is in tying a physician’s obligations to the interests of other workers who may not share the same ethical commitment to patients.2
Strikes by doctors are likely to interfere with patient care, raise serious ethical questions, and may also be in violation of antitrust laws although boycotts for sociopolitical and noncommercial reasons are not specifically prohibited.
3. Market division. Agreements to restrict competition by dividing or allocating territories or patients are illegal per se under the Sherman Act.
4. Monopolization. Section 2 of the Sherman Act prohibits monopolization and attempts to monopolize. Examples are predatory pricing, long-term exclusive contracts, and refusal to deal. Mergers and acquisitions may substantially lessen competition with the tendency to create a monopoly, and they are subject to Section 7 of the Clayton Act. Proof of monopolization requires an inquiry into the relevant product and geographic markets (usually greater than 50%-60% market share), and regularly requires an economist’s expertise at trial.
As a general proposition, restraint of trade and monopolistic charges are difficult to prove. Monopoly through "the exercise of skill, foresight, and industry" does not constitute monopolizing conduct.
5. Joint ventures. The two main ways physicians form network joint ventures are: 1) join together in an entity with shared financial risks and clinical integration, and 2) join a looser network without integration to simply facilitate the flow of information for contracting purposes between physicians and other payers, the so-called messenger method.
Many health delivery systems involve joint venture agreements among practitioners or groups of health professionals and health care institutions, e.g., physician hospital organizations (PHOs), independent practice associations (IPAs), and preferred physician organization (PPOs). Physicians and physician practice groups may become targets if their attempted efforts at joint ventures are deemed to be a pretext for price fixing or otherwise anticompetitive.
The DOJ and FTC have promulgated guidelines regarding joint venture structures and will perform a review of the proposal upon request.3
However, under Obamacare, which promotes the efficient integration of health services through competition such as accountable care organizations, these guidelines are likely to be revised in the near future.
6. Exclusive contracts. Many hospitals have exclusive contracts with health professionals such as radiologists, anesthesiologists, and pathologists. Patients using the facility may be forced to use the services of these providers ("tying arrangement"). If the hospital does not possess requisite market power, or force the acceptance of the service, such agreements may pass antitrust scrutiny.
7. Peer review. The Health Care Quality Improvement Act (42 U.S.C. §§ 1101 et seq.) immunizes physicians and others performing peer review activities from federal antitrust claims so long as peer review was carried out: 1) in reasonable belief that the action was in furtherance of quality health care; 2) after reasonable effort to obtain the facts; 3) after an adequate notice and hearing procedure; 4) in reasonable belief that the action was warranted; and 5) any adverse outcome was reported to the National Practitioners’ Data Bank.
A doctor who is judged wanting in peer review occasionally asserts a discriminatory or anticompetitive intent, and may file a retaliatory lawsuit. One caveat: Peer review deliberations are always held in strict confidence. Disparaging a doctor under review in an unrelated forum constitutes a violation of the peer review process, which risks nullification of discovery protection and antitrust immunity.
Antitrust problems are highly fact dependent and analytically complex, and therefore require counsel with special expertise and experience. Issues are surprisingly prevalent and may be counterintuitive, affecting not only parties in joint ventures and mergers, but also the solo office or hospital practitioner. Matters of medical staffing, joint purchasing, information exchange, managed care negotiation, peer review and price agreements are some examples.
Penalties are severe, and may cover more than simple cease and desist orders. Some behavior constitutes criminality punishable by prison terms, though this is rare in the health care arena.
More often, the guilty parties face heavy monetary fines from both governmental officials as well as private litigants who can join in the lawsuit and stand to benefit from awards of treble damages and attorneys’ fees.
References:
1. Goldfarb v. Virginia State Bar 421 U.S. 773, 1975.
2. Code of Medical Ethics, AMA, 9.025, 2012-2013 edition.
3. Statements of Antitrust Enforcement Policy in Health Care. Department of Justice and Federal Trade Commission (1996).
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii. This article is meant to be educational and does not constitute medical, ethical or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, "Medical Malpractice: Understanding the Law, Managing the Risk," and his 2012 Halsbury treatise, "Medical Negligence and Professional Misconduct." For additional information, readers may contact the author at [email protected].
This article introduces United States antitrust laws and discusses their application in health care. Part 2 will summarize major court decisions covering that subject.
Question: Antitrust laws:
A. Are based in part on the physician-patient trust relationship.
B. Prohibit anticompetitive behavior.
C. Regulate business activities but not professional services.
D. A, B, and C are correct.
E. B and C are correct.
Answer: B. Economic interests are best served in a freely competitive marketplace. Trade restraints such as price fixing and monopolization tend to promote inefficiency and increase profit for the perpetrators, at the expense of consumer welfare.
Accordingly, Congress enacted the Sherman Antitrust Act way back in 1890 to promote competition and outlaw unreasonable restraint of trade. Additional laws prohibit mergers that substantially lessen competition, price discrimination, and unfair trade practices. Collectively, these are known as the antitrust laws, the term reflecting their initial purpose to prevent commercial traders from forming anticompetitive groups or "trusts."
The Department of Justice (DOJ), the Federal Trade Commission (FTC), and their state counterparts enforce these laws, which have nothing whatsoever to do with the doctor-patient trust relationship.
Section I of the Sherman Act, the paramount antitrust statute, declares that "Every contract, combination in the form of trust or otherwise, or conspiracy, in restraint of trade or commerce among the several States, or with foreign nations, is declared to be illegal." Section II stipulates, "Every person who shall monopolize, or attempt to monopolize, or combine or conspire with any other person or persons, to monopolize any part of the trade or commerce among the several States, or with foreign nations, shall be deemed guilty of a felony."
Other important laws are Sections 4 and 7 of the Clayton Antitrust Act and Section 5(a)(1) of the Federal Trade Commission Act, which outlaws "unfair methods of competition in or affecting commerce ... " Additionally, all states have their own antitrust statutes, which in some cases may be more restrictive than the federal laws are.
These laws initially targeted anticompetitive business practices. In 1975, the U.S. Supreme Court declared that there was to be no "learned profession" exemption, although special considerations may apply.1 However, activities of state government officials and employees are exempt from antitrust scrutiny under the so-called "state action doctrine," which confers immunity if an exemption is clearly articulated and affirmatively expressed as state policy, and there is active state supervision of the conduct in question.
Antitrust issues are ubiquitous in health care, and fall into seven major categories: 1) price fixing; 2) boycotts; 3) market division; 4) monopolization; 5) joint ventures; 6) exclusive contracts, and 7) peer review.
1. Price fixing. An agreement to fix prices is the most egregious example of anticompetitive conduct, so much so that the courts will use a per se analysis, i.e., without need to consider other factors, to arrive at its decision. Price fixing does not require any party to show market dominance or power, and its presence can be inferred from circumstances and agreements, which can be either oral or written.
For example, physician fee schedules or guidelines by a medical association would constitute price fixing. Even an agreement to fix maximum prices, as opposed to minimum prices, has been ruled illegal. At a practical level, physicians should avoid sharing pricing information with anyone, especially with colleagues, unless strict FTC "safety zone" criteria are satisfied.
2. Boycotts. Group boycotts are usually per se illegal, but in the health care industry, a rule of reason analysis is frequently used. Courts will look at the circumstances and purpose of the boycott, its pro- and anti-competitive effects, and whether there are other less restrictive ways to achieve the purported goal.
Affiliating physicians face this risk when forming alliances, as boycott questions may arise when a doctor is inappropriately excluded, which deprives him/her from earning a living in the relevant market.
A related controversial issue is the unionization of doctors. Unionization protects labor rights, especially those of medical residents, and offers greater parity in collective bargaining. On the other hand, the danger is in tying a physician’s obligations to the interests of other workers who may not share the same ethical commitment to patients.2
Strikes by doctors are likely to interfere with patient care, raise serious ethical questions, and may also be in violation of antitrust laws although boycotts for sociopolitical and noncommercial reasons are not specifically prohibited.
3. Market division. Agreements to restrict competition by dividing or allocating territories or patients are illegal per se under the Sherman Act.
4. Monopolization. Section 2 of the Sherman Act prohibits monopolization and attempts to monopolize. Examples are predatory pricing, long-term exclusive contracts, and refusal to deal. Mergers and acquisitions may substantially lessen competition with the tendency to create a monopoly, and they are subject to Section 7 of the Clayton Act. Proof of monopolization requires an inquiry into the relevant product and geographic markets (usually greater than 50%-60% market share), and regularly requires an economist’s expertise at trial.
As a general proposition, restraint of trade and monopolistic charges are difficult to prove. Monopoly through "the exercise of skill, foresight, and industry" does not constitute monopolizing conduct.
5. Joint ventures. The two main ways physicians form network joint ventures are: 1) join together in an entity with shared financial risks and clinical integration, and 2) join a looser network without integration to simply facilitate the flow of information for contracting purposes between physicians and other payers, the so-called messenger method.
Many health delivery systems involve joint venture agreements among practitioners or groups of health professionals and health care institutions, e.g., physician hospital organizations (PHOs), independent practice associations (IPAs), and preferred physician organization (PPOs). Physicians and physician practice groups may become targets if their attempted efforts at joint ventures are deemed to be a pretext for price fixing or otherwise anticompetitive.
The DOJ and FTC have promulgated guidelines regarding joint venture structures and will perform a review of the proposal upon request.3
However, under Obamacare, which promotes the efficient integration of health services through competition such as accountable care organizations, these guidelines are likely to be revised in the near future.
6. Exclusive contracts. Many hospitals have exclusive contracts with health professionals such as radiologists, anesthesiologists, and pathologists. Patients using the facility may be forced to use the services of these providers ("tying arrangement"). If the hospital does not possess requisite market power, or force the acceptance of the service, such agreements may pass antitrust scrutiny.
7. Peer review. The Health Care Quality Improvement Act (42 U.S.C. §§ 1101 et seq.) immunizes physicians and others performing peer review activities from federal antitrust claims so long as peer review was carried out: 1) in reasonable belief that the action was in furtherance of quality health care; 2) after reasonable effort to obtain the facts; 3) after an adequate notice and hearing procedure; 4) in reasonable belief that the action was warranted; and 5) any adverse outcome was reported to the National Practitioners’ Data Bank.
A doctor who is judged wanting in peer review occasionally asserts a discriminatory or anticompetitive intent, and may file a retaliatory lawsuit. One caveat: Peer review deliberations are always held in strict confidence. Disparaging a doctor under review in an unrelated forum constitutes a violation of the peer review process, which risks nullification of discovery protection and antitrust immunity.
Antitrust problems are highly fact dependent and analytically complex, and therefore require counsel with special expertise and experience. Issues are surprisingly prevalent and may be counterintuitive, affecting not only parties in joint ventures and mergers, but also the solo office or hospital practitioner. Matters of medical staffing, joint purchasing, information exchange, managed care negotiation, peer review and price agreements are some examples.
Penalties are severe, and may cover more than simple cease and desist orders. Some behavior constitutes criminality punishable by prison terms, though this is rare in the health care arena.
More often, the guilty parties face heavy monetary fines from both governmental officials as well as private litigants who can join in the lawsuit and stand to benefit from awards of treble damages and attorneys’ fees.
References:
1. Goldfarb v. Virginia State Bar 421 U.S. 773, 1975.
2. Code of Medical Ethics, AMA, 9.025, 2012-2013 edition.
3. Statements of Antitrust Enforcement Policy in Health Care. Department of Justice and Federal Trade Commission (1996).
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii. This article is meant to be educational and does not constitute medical, ethical or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, "Medical Malpractice: Understanding the Law, Managing the Risk," and his 2012 Halsbury treatise, "Medical Negligence and Professional Misconduct." For additional information, readers may contact the author at [email protected].
This article introduces United States antitrust laws and discusses their application in health care. Part 2 will summarize major court decisions covering that subject.
Question: Antitrust laws:
A. Are based in part on the physician-patient trust relationship.
B. Prohibit anticompetitive behavior.
C. Regulate business activities but not professional services.
D. A, B, and C are correct.
E. B and C are correct.
Answer: B. Economic interests are best served in a freely competitive marketplace. Trade restraints such as price fixing and monopolization tend to promote inefficiency and increase profit for the perpetrators, at the expense of consumer welfare.
Accordingly, Congress enacted the Sherman Antitrust Act way back in 1890 to promote competition and outlaw unreasonable restraint of trade. Additional laws prohibit mergers that substantially lessen competition, price discrimination, and unfair trade practices. Collectively, these are known as the antitrust laws, the term reflecting their initial purpose to prevent commercial traders from forming anticompetitive groups or "trusts."
The Department of Justice (DOJ), the Federal Trade Commission (FTC), and their state counterparts enforce these laws, which have nothing whatsoever to do with the doctor-patient trust relationship.
Section I of the Sherman Act, the paramount antitrust statute, declares that "Every contract, combination in the form of trust or otherwise, or conspiracy, in restraint of trade or commerce among the several States, or with foreign nations, is declared to be illegal." Section II stipulates, "Every person who shall monopolize, or attempt to monopolize, or combine or conspire with any other person or persons, to monopolize any part of the trade or commerce among the several States, or with foreign nations, shall be deemed guilty of a felony."
Other important laws are Sections 4 and 7 of the Clayton Antitrust Act and Section 5(a)(1) of the Federal Trade Commission Act, which outlaws "unfair methods of competition in or affecting commerce ... " Additionally, all states have their own antitrust statutes, which in some cases may be more restrictive than the federal laws are.
These laws initially targeted anticompetitive business practices. In 1975, the U.S. Supreme Court declared that there was to be no "learned profession" exemption, although special considerations may apply.1 However, activities of state government officials and employees are exempt from antitrust scrutiny under the so-called "state action doctrine," which confers immunity if an exemption is clearly articulated and affirmatively expressed as state policy, and there is active state supervision of the conduct in question.
Antitrust issues are ubiquitous in health care, and fall into seven major categories: 1) price fixing; 2) boycotts; 3) market division; 4) monopolization; 5) joint ventures; 6) exclusive contracts, and 7) peer review.
1. Price fixing. An agreement to fix prices is the most egregious example of anticompetitive conduct, so much so that the courts will use a per se analysis, i.e., without need to consider other factors, to arrive at its decision. Price fixing does not require any party to show market dominance or power, and its presence can be inferred from circumstances and agreements, which can be either oral or written.
For example, physician fee schedules or guidelines by a medical association would constitute price fixing. Even an agreement to fix maximum prices, as opposed to minimum prices, has been ruled illegal. At a practical level, physicians should avoid sharing pricing information with anyone, especially with colleagues, unless strict FTC "safety zone" criteria are satisfied.
2. Boycotts. Group boycotts are usually per se illegal, but in the health care industry, a rule of reason analysis is frequently used. Courts will look at the circumstances and purpose of the boycott, its pro- and anti-competitive effects, and whether there are other less restrictive ways to achieve the purported goal.
Affiliating physicians face this risk when forming alliances, as boycott questions may arise when a doctor is inappropriately excluded, which deprives him/her from earning a living in the relevant market.
A related controversial issue is the unionization of doctors. Unionization protects labor rights, especially those of medical residents, and offers greater parity in collective bargaining. On the other hand, the danger is in tying a physician’s obligations to the interests of other workers who may not share the same ethical commitment to patients.2
Strikes by doctors are likely to interfere with patient care, raise serious ethical questions, and may also be in violation of antitrust laws although boycotts for sociopolitical and noncommercial reasons are not specifically prohibited.
3. Market division. Agreements to restrict competition by dividing or allocating territories or patients are illegal per se under the Sherman Act.
4. Monopolization. Section 2 of the Sherman Act prohibits monopolization and attempts to monopolize. Examples are predatory pricing, long-term exclusive contracts, and refusal to deal. Mergers and acquisitions may substantially lessen competition with the tendency to create a monopoly, and they are subject to Section 7 of the Clayton Act. Proof of monopolization requires an inquiry into the relevant product and geographic markets (usually greater than 50%-60% market share), and regularly requires an economist’s expertise at trial.
As a general proposition, restraint of trade and monopolistic charges are difficult to prove. Monopoly through "the exercise of skill, foresight, and industry" does not constitute monopolizing conduct.
5. Joint ventures. The two main ways physicians form network joint ventures are: 1) join together in an entity with shared financial risks and clinical integration, and 2) join a looser network without integration to simply facilitate the flow of information for contracting purposes between physicians and other payers, the so-called messenger method.
Many health delivery systems involve joint venture agreements among practitioners or groups of health professionals and health care institutions, e.g., physician hospital organizations (PHOs), independent practice associations (IPAs), and preferred physician organization (PPOs). Physicians and physician practice groups may become targets if their attempted efforts at joint ventures are deemed to be a pretext for price fixing or otherwise anticompetitive.
The DOJ and FTC have promulgated guidelines regarding joint venture structures and will perform a review of the proposal upon request.3
However, under Obamacare, which promotes the efficient integration of health services through competition such as accountable care organizations, these guidelines are likely to be revised in the near future.
6. Exclusive contracts. Many hospitals have exclusive contracts with health professionals such as radiologists, anesthesiologists, and pathologists. Patients using the facility may be forced to use the services of these providers ("tying arrangement"). If the hospital does not possess requisite market power, or force the acceptance of the service, such agreements may pass antitrust scrutiny.
7. Peer review. The Health Care Quality Improvement Act (42 U.S.C. §§ 1101 et seq.) immunizes physicians and others performing peer review activities from federal antitrust claims so long as peer review was carried out: 1) in reasonable belief that the action was in furtherance of quality health care; 2) after reasonable effort to obtain the facts; 3) after an adequate notice and hearing procedure; 4) in reasonable belief that the action was warranted; and 5) any adverse outcome was reported to the National Practitioners’ Data Bank.
A doctor who is judged wanting in peer review occasionally asserts a discriminatory or anticompetitive intent, and may file a retaliatory lawsuit. One caveat: Peer review deliberations are always held in strict confidence. Disparaging a doctor under review in an unrelated forum constitutes a violation of the peer review process, which risks nullification of discovery protection and antitrust immunity.
Antitrust problems are highly fact dependent and analytically complex, and therefore require counsel with special expertise and experience. Issues are surprisingly prevalent and may be counterintuitive, affecting not only parties in joint ventures and mergers, but also the solo office or hospital practitioner. Matters of medical staffing, joint purchasing, information exchange, managed care negotiation, peer review and price agreements are some examples.
Penalties are severe, and may cover more than simple cease and desist orders. Some behavior constitutes criminality punishable by prison terms, though this is rare in the health care arena.
More often, the guilty parties face heavy monetary fines from both governmental officials as well as private litigants who can join in the lawsuit and stand to benefit from awards of treble damages and attorneys’ fees.
References:
1. Goldfarb v. Virginia State Bar 421 U.S. 773, 1975.
2. Code of Medical Ethics, AMA, 9.025, 2012-2013 edition.
3. Statements of Antitrust Enforcement Policy in Health Care. Department of Justice and Federal Trade Commission (1996).
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii. This article is meant to be educational and does not constitute medical, ethical or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, "Medical Malpractice: Understanding the Law, Managing the Risk," and his 2012 Halsbury treatise, "Medical Negligence and Professional Misconduct." For additional information, readers may contact the author at [email protected].

Difficult to teach when you have a small practice
Recently, my alma mater, Creighton University, approached me to teach medical students. Sadly, I told them no.
I enjoy teaching. Medical students and residents always lift my spirits. I think I’m a good neurologist, with a decent grasp of practical issues (esoteric ones, not so much), and I like sharing it with those starting out on this road.
So why did I tell them no? It’s quite simple: I can’t afford it.
Solo practice in medicine is an "eat what you kill" world. You try to see patients, dictate notes, review tests, answer questions, and refill meds in a continuous blur from start to finish.
Teaching – at least worthwhile teaching – takes time. Questions have to be answered, take-home points explained, and exam findings pointed out. The last time I did routine teaching (2001), it added 1-2 hours to the end of each day. I had to make up the office work on weekends, which didn’t sit well with my family.
The alternative is to schedule extra time on teaching days – like an open 30 minutes twice a day – to compensate, but the problem with that is then you have empty time where you aren’t seeing patients and, hence, not making money. In a small practice on a thin margin, cash flow is critical and can’t be ignored.
It doesn’t seem fair to ask medical students and residents to pay, say, $500 a week to cover that time. Their tuition is high enough as it is.
Of course, the program they pay tuition to doesn’t offer a stipend to cover this, either. I don’t know why. I’m not privy to their finances, but I assume they’re facing the same challenges I am. I’m not greedy. I’m just trying to make ends meet.
This bothers me because I think I’m a good teacher. Back when I did it more, in my early days of solo practice (before reality kicked in), electives with me got high ratings from those who took them. I liked sharing my personal knowledge and experience with the next generation of doctors, and I hope those who were there gained something from it.
But the current nature of the education system makes that impossible and limits teaching primarily to academic practices or those large enough to absorb the loss through other means. That is sad because small practitioners have a lot to contribute, too.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Recently, my alma mater, Creighton University, approached me to teach medical students. Sadly, I told them no.
I enjoy teaching. Medical students and residents always lift my spirits. I think I’m a good neurologist, with a decent grasp of practical issues (esoteric ones, not so much), and I like sharing it with those starting out on this road.
So why did I tell them no? It’s quite simple: I can’t afford it.
Solo practice in medicine is an "eat what you kill" world. You try to see patients, dictate notes, review tests, answer questions, and refill meds in a continuous blur from start to finish.
Teaching – at least worthwhile teaching – takes time. Questions have to be answered, take-home points explained, and exam findings pointed out. The last time I did routine teaching (2001), it added 1-2 hours to the end of each day. I had to make up the office work on weekends, which didn’t sit well with my family.
The alternative is to schedule extra time on teaching days – like an open 30 minutes twice a day – to compensate, but the problem with that is then you have empty time where you aren’t seeing patients and, hence, not making money. In a small practice on a thin margin, cash flow is critical and can’t be ignored.
It doesn’t seem fair to ask medical students and residents to pay, say, $500 a week to cover that time. Their tuition is high enough as it is.
Of course, the program they pay tuition to doesn’t offer a stipend to cover this, either. I don’t know why. I’m not privy to their finances, but I assume they’re facing the same challenges I am. I’m not greedy. I’m just trying to make ends meet.
This bothers me because I think I’m a good teacher. Back when I did it more, in my early days of solo practice (before reality kicked in), electives with me got high ratings from those who took them. I liked sharing my personal knowledge and experience with the next generation of doctors, and I hope those who were there gained something from it.
But the current nature of the education system makes that impossible and limits teaching primarily to academic practices or those large enough to absorb the loss through other means. That is sad because small practitioners have a lot to contribute, too.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Recently, my alma mater, Creighton University, approached me to teach medical students. Sadly, I told them no.
I enjoy teaching. Medical students and residents always lift my spirits. I think I’m a good neurologist, with a decent grasp of practical issues (esoteric ones, not so much), and I like sharing it with those starting out on this road.
So why did I tell them no? It’s quite simple: I can’t afford it.
Solo practice in medicine is an "eat what you kill" world. You try to see patients, dictate notes, review tests, answer questions, and refill meds in a continuous blur from start to finish.
Teaching – at least worthwhile teaching – takes time. Questions have to be answered, take-home points explained, and exam findings pointed out. The last time I did routine teaching (2001), it added 1-2 hours to the end of each day. I had to make up the office work on weekends, which didn’t sit well with my family.
The alternative is to schedule extra time on teaching days – like an open 30 minutes twice a day – to compensate, but the problem with that is then you have empty time where you aren’t seeing patients and, hence, not making money. In a small practice on a thin margin, cash flow is critical and can’t be ignored.
It doesn’t seem fair to ask medical students and residents to pay, say, $500 a week to cover that time. Their tuition is high enough as it is.
Of course, the program they pay tuition to doesn’t offer a stipend to cover this, either. I don’t know why. I’m not privy to their finances, but I assume they’re facing the same challenges I am. I’m not greedy. I’m just trying to make ends meet.
This bothers me because I think I’m a good teacher. Back when I did it more, in my early days of solo practice (before reality kicked in), electives with me got high ratings from those who took them. I liked sharing my personal knowledge and experience with the next generation of doctors, and I hope those who were there gained something from it.
But the current nature of the education system makes that impossible and limits teaching primarily to academic practices or those large enough to absorb the loss through other means. That is sad because small practitioners have a lot to contribute, too.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.

A tragic transition of care
The story:
JR is a 32-year-old woman with a medical history of juvenile diabetes mellitus and end-stage renal disease on intermittent hemodialysis for the past 2 years. She was admitted to the hospital with shortness of breath and was found to have a large right-sided pleural effusion with loculations. Antibiotics were initiated. On hospital day 2 she underwent a video-assisted thoracoscopy for drainage, lysis of adhesions, and placement of two chest tubes. After returning to the floor from the postanesthesia care unit, JR had difficulty achieving adequate pain control despite a hydromorphone patient-controlled analgesic pump. Additional "as needed" intravenous morphine was ordered for relief. Before going home, the attending internist checked in on JR and discontinued her intravenous fluids (D5 half-normal saline), but wrote to resume her long-acting insulin later that same evening.
At approximately 7:30 p.m., JR was found by the nurse barely breathing. Her pupils were pinpoint and her respiratory rate was only 5 breaths per minute. A code blue was called and a hospitalist responded. A combination of epinephrine, atropine, and naloxone led to a return of consciousness, and JR was never intubated. In fact, the code sheet reflected that after the naloxone, JR was now fully awake, crying, and complaining of right-sided pain.

JR subsequently complained of nausea and began to vomit. Prior to transferring her to the intensive care unit, the hospitalist placed a nasogastric tube and made JR nil per os. To complete JR’s transfer to the ICU, the hospitalist contacted a critical care attending to give report, and then wrote "holding" ICU admission orders.
JR remained on the regular nursing floor for another hour as the ICU prepared for her arrival. Just prior to leaving the floor, JR’s nurse gave her 13 units of glargine insulin as ordered earlier that afternoon by the attending internist.
JR underwent a standard admission assessment upon her arrival at the ICU. The hospitalist "holding admission orders" included regular blood glucose checks and regular insulin coverage on a sliding scale. At midnight, JR’s blood glucose was over 250 mg/dL, and she was administered 6 units of regular insulin. At 5 a.m., another blood glucose was obtained and was recorded as 114 mg/dL. At 7:45 a.m., the new day shift ICU nurse did a complete assessment and noted that JR was lethargic with slurred speech. The critical care consultant rounded on JR at approximately 10 a.m. and also noted a change in mental status. Thirty minutes later, JR became unresponsive to verbal or tactile stimuli. A point-of-care blood glucose was performed and found to be 10 mg/dL. JR was subsequently intubated, but she never regained consciousness again.
She lived for another 2 months before her family decided to stop her dialysis and she passed away.
Complaint:
The family was upset to learn that JR suffered irreversible brain injury from low blood sugar. JR had been a diabetic on insulin all of her life, and the family couldn’t understand how such a thing could happen under the watchful eye of doctors and nurses.
The complaint alleged that there was an egregious failure with respect to communication between the attending physician, the floor nurse, the hospitalist, and the critical care consultant. Specific to the hospitalist, the complaint alleged that the "holding admission orders" should have included intravenous fluids with dextrose and/or explicit instructions to not give the glargine insulin as ordered earlier that same day.
The complaint was also disparaging of the critical care consultant for not recognizing the hypoglycemia earlier, given the mental status changes that JR exhibited.
Scientific principles:
Hypoglycemia can produce a myriad of neurologic signs and symptoms, but usually presents with symptoms of increased epinephrine release (e.g., tremor, diaphoresis) followed by neurologic symptoms that include generalized seizures, bizarre behavior, coma, and focal deficits. In acute severe hypoglycemia, a bolus of 25-50 grams of dextrose should be administered intravenously, followed by a continuous dextrose infusion. Blood glucose concentrations should be measured hourly. Reversal of neurologic symptoms may lag behind normalization of glucose levels.
Complaint rebuttal and discussion
All the health care providers thought their actions were reasonable in this case.
At the time that the attending internist wrote to resume JR’s glargine and stop the dextrose-containing intravenous fluids, JR was awake and was planning to have a light dinner. The floor nurse who gave the glargine later that night testified that she had a valid order to administer the medication.
The hospitalist testified that he was there to respond to emergencies, and that he transferred care of JR to the critical care consultant by verbal report. The critical care consultant acknowledged the verbal handoff from the hospitalist, but doubts there was any discussion regarding JR’s diabetes and was adamant that she was not responsible for JR receiving two doses of insulin (glargine and regular insulin) via the orders of two other physicians before she even had the opportunity to see the patient. The critical care consultant also testified that JR’s mental status change was nonspecific and was reasonably due to the pain medications she was receiving.
The plaintiffs countered with the reality that JR, a 32-year-old woman, died from low blood sugar because she received insulin when she wasn’t allowed to eat or drink – all at the hands of the medical team.
Conclusion:
Much of the attention regarding safe transitions of care is focused on the hospital discharge. Yet discontinuity within hospital walls is frequently associated with medical errors, and communication problems represent the largest category for hospital sentinel events.
The Joint Commission, the World Health Organization, the Institute of Medicine and the National Quality Foundation have all published white paper recommendations regarding the need to improve medical handoffs. Most hospitalists probably see this case as a "system error," and sure enough following this event the hospital overhauled its policies and procedures as they related to ICU transfers. But in the world of medical malpractice, the "system" doesn’t face the jury in litigation.
Although the attending internist was eventually dropped from this case, the hospital, the critical care consultant, and the hospitalist all settled with the plaintiff for an undisclosed amount.
Dr. Michota is director of academic affairs in the hospital medicine department at the Cleveland Clinic and medical editor of Hospitalist News. He has been involved in peer review both within and outside the legal system.
The story:
JR is a 32-year-old woman with a medical history of juvenile diabetes mellitus and end-stage renal disease on intermittent hemodialysis for the past 2 years. She was admitted to the hospital with shortness of breath and was found to have a large right-sided pleural effusion with loculations. Antibiotics were initiated. On hospital day 2 she underwent a video-assisted thoracoscopy for drainage, lysis of adhesions, and placement of two chest tubes. After returning to the floor from the postanesthesia care unit, JR had difficulty achieving adequate pain control despite a hydromorphone patient-controlled analgesic pump. Additional "as needed" intravenous morphine was ordered for relief. Before going home, the attending internist checked in on JR and discontinued her intravenous fluids (D5 half-normal saline), but wrote to resume her long-acting insulin later that same evening.
At approximately 7:30 p.m., JR was found by the nurse barely breathing. Her pupils were pinpoint and her respiratory rate was only 5 breaths per minute. A code blue was called and a hospitalist responded. A combination of epinephrine, atropine, and naloxone led to a return of consciousness, and JR was never intubated. In fact, the code sheet reflected that after the naloxone, JR was now fully awake, crying, and complaining of right-sided pain.
JR subsequently complained of nausea and began to vomit. Prior to transferring her to the intensive care unit, the hospitalist placed a nasogastric tube and made JR nil per os. To complete JR’s transfer to the ICU, the hospitalist contacted a critical care attending to give report, and then wrote "holding" ICU admission orders.
JR remained on the regular nursing floor for another hour as the ICU prepared for her arrival. Just prior to leaving the floor, JR’s nurse gave her 13 units of glargine insulin as ordered earlier that afternoon by the attending internist.
JR underwent a standard admission assessment upon her arrival at the ICU. The hospitalist "holding admission orders" included regular blood glucose checks and regular insulin coverage on a sliding scale. At midnight, JR’s blood glucose was over 250 mg/dL, and she was administered 6 units of regular insulin. At 5 a.m., another blood glucose was obtained and was recorded as 114 mg/dL. At 7:45 a.m., the new day shift ICU nurse did a complete assessment and noted that JR was lethargic with slurred speech. The critical care consultant rounded on JR at approximately 10 a.m. and also noted a change in mental status. Thirty minutes later, JR became unresponsive to verbal or tactile stimuli. A point-of-care blood glucose was performed and found to be 10 mg/dL. JR was subsequently intubated, but she never regained consciousness again.
She lived for another 2 months before her family decided to stop her dialysis and she passed away.
Complaint:
The family was upset to learn that JR suffered irreversible brain injury from low blood sugar. JR had been a diabetic on insulin all of her life, and the family couldn’t understand how such a thing could happen under the watchful eye of doctors and nurses.
The complaint alleged that there was an egregious failure with respect to communication between the attending physician, the floor nurse, the hospitalist, and the critical care consultant. Specific to the hospitalist, the complaint alleged that the "holding admission orders" should have included intravenous fluids with dextrose and/or explicit instructions to not give the glargine insulin as ordered earlier that same day.
The complaint was also disparaging of the critical care consultant for not recognizing the hypoglycemia earlier, given the mental status changes that JR exhibited.
Scientific principles:
Hypoglycemia can produce a myriad of neurologic signs and symptoms, but usually presents with symptoms of increased epinephrine release (e.g., tremor, diaphoresis) followed by neurologic symptoms that include generalized seizures, bizarre behavior, coma, and focal deficits. In acute severe hypoglycemia, a bolus of 25-50 grams of dextrose should be administered intravenously, followed by a continuous dextrose infusion. Blood glucose concentrations should be measured hourly. Reversal of neurologic symptoms may lag behind normalization of glucose levels.
Complaint rebuttal and discussion
All the health care providers thought their actions were reasonable in this case.
At the time that the attending internist wrote to resume JR’s glargine and stop the dextrose-containing intravenous fluids, JR was awake and was planning to have a light dinner. The floor nurse who gave the glargine later that night testified that she had a valid order to administer the medication.
The hospitalist testified that he was there to respond to emergencies, and that he transferred care of JR to the critical care consultant by verbal report. The critical care consultant acknowledged the verbal handoff from the hospitalist, but doubts there was any discussion regarding JR’s diabetes and was adamant that she was not responsible for JR receiving two doses of insulin (glargine and regular insulin) via the orders of two other physicians before she even had the opportunity to see the patient. The critical care consultant also testified that JR’s mental status change was nonspecific and was reasonably due to the pain medications she was receiving.
The plaintiffs countered with the reality that JR, a 32-year-old woman, died from low blood sugar because she received insulin when she wasn’t allowed to eat or drink – all at the hands of the medical team.
Conclusion:
Much of the attention regarding safe transitions of care is focused on the hospital discharge. Yet discontinuity within hospital walls is frequently associated with medical errors, and communication problems represent the largest category for hospital sentinel events.
The Joint Commission, the World Health Organization, the Institute of Medicine and the National Quality Foundation have all published white paper recommendations regarding the need to improve medical handoffs. Most hospitalists probably see this case as a "system error," and sure enough following this event the hospital overhauled its policies and procedures as they related to ICU transfers. But in the world of medical malpractice, the "system" doesn’t face the jury in litigation.
Although the attending internist was eventually dropped from this case, the hospital, the critical care consultant, and the hospitalist all settled with the plaintiff for an undisclosed amount.
Dr. Michota is director of academic affairs in the hospital medicine department at the Cleveland Clinic and medical editor of Hospitalist News. He has been involved in peer review both within and outside the legal system.
The story:
JR is a 32-year-old woman with a medical history of juvenile diabetes mellitus and end-stage renal disease on intermittent hemodialysis for the past 2 years. She was admitted to the hospital with shortness of breath and was found to have a large right-sided pleural effusion with loculations. Antibiotics were initiated. On hospital day 2 she underwent a video-assisted thoracoscopy for drainage, lysis of adhesions, and placement of two chest tubes. After returning to the floor from the postanesthesia care unit, JR had difficulty achieving adequate pain control despite a hydromorphone patient-controlled analgesic pump. Additional "as needed" intravenous morphine was ordered for relief. Before going home, the attending internist checked in on JR and discontinued her intravenous fluids (D5 half-normal saline), but wrote to resume her long-acting insulin later that same evening.
At approximately 7:30 p.m., JR was found by the nurse barely breathing. Her pupils were pinpoint and her respiratory rate was only 5 breaths per minute. A code blue was called and a hospitalist responded. A combination of epinephrine, atropine, and naloxone led to a return of consciousness, and JR was never intubated. In fact, the code sheet reflected that after the naloxone, JR was now fully awake, crying, and complaining of right-sided pain.
JR subsequently complained of nausea and began to vomit. Prior to transferring her to the intensive care unit, the hospitalist placed a nasogastric tube and made JR nil per os. To complete JR’s transfer to the ICU, the hospitalist contacted a critical care attending to give report, and then wrote "holding" ICU admission orders.
JR remained on the regular nursing floor for another hour as the ICU prepared for her arrival. Just prior to leaving the floor, JR’s nurse gave her 13 units of glargine insulin as ordered earlier that afternoon by the attending internist.
JR underwent a standard admission assessment upon her arrival at the ICU. The hospitalist "holding admission orders" included regular blood glucose checks and regular insulin coverage on a sliding scale. At midnight, JR’s blood glucose was over 250 mg/dL, and she was administered 6 units of regular insulin. At 5 a.m., another blood glucose was obtained and was recorded as 114 mg/dL. At 7:45 a.m., the new day shift ICU nurse did a complete assessment and noted that JR was lethargic with slurred speech. The critical care consultant rounded on JR at approximately 10 a.m. and also noted a change in mental status. Thirty minutes later, JR became unresponsive to verbal or tactile stimuli. A point-of-care blood glucose was performed and found to be 10 mg/dL. JR was subsequently intubated, but she never regained consciousness again.
She lived for another 2 months before her family decided to stop her dialysis and she passed away.
Complaint:
The family was upset to learn that JR suffered irreversible brain injury from low blood sugar. JR had been a diabetic on insulin all of her life, and the family couldn’t understand how such a thing could happen under the watchful eye of doctors and nurses.
The complaint alleged that there was an egregious failure with respect to communication between the attending physician, the floor nurse, the hospitalist, and the critical care consultant. Specific to the hospitalist, the complaint alleged that the "holding admission orders" should have included intravenous fluids with dextrose and/or explicit instructions to not give the glargine insulin as ordered earlier that same day.
The complaint was also disparaging of the critical care consultant for not recognizing the hypoglycemia earlier, given the mental status changes that JR exhibited.
Scientific principles:
Hypoglycemia can produce a myriad of neurologic signs and symptoms, but usually presents with symptoms of increased epinephrine release (e.g., tremor, diaphoresis) followed by neurologic symptoms that include generalized seizures, bizarre behavior, coma, and focal deficits. In acute severe hypoglycemia, a bolus of 25-50 grams of dextrose should be administered intravenously, followed by a continuous dextrose infusion. Blood glucose concentrations should be measured hourly. Reversal of neurologic symptoms may lag behind normalization of glucose levels.
Complaint rebuttal and discussion
All the health care providers thought their actions were reasonable in this case.
At the time that the attending internist wrote to resume JR’s glargine and stop the dextrose-containing intravenous fluids, JR was awake and was planning to have a light dinner. The floor nurse who gave the glargine later that night testified that she had a valid order to administer the medication.
The hospitalist testified that he was there to respond to emergencies, and that he transferred care of JR to the critical care consultant by verbal report. The critical care consultant acknowledged the verbal handoff from the hospitalist, but doubts there was any discussion regarding JR’s diabetes and was adamant that she was not responsible for JR receiving two doses of insulin (glargine and regular insulin) via the orders of two other physicians before she even had the opportunity to see the patient. The critical care consultant also testified that JR’s mental status change was nonspecific and was reasonably due to the pain medications she was receiving.
The plaintiffs countered with the reality that JR, a 32-year-old woman, died from low blood sugar because she received insulin when she wasn’t allowed to eat or drink – all at the hands of the medical team.
Conclusion:
Much of the attention regarding safe transitions of care is focused on the hospital discharge. Yet discontinuity within hospital walls is frequently associated with medical errors, and communication problems represent the largest category for hospital sentinel events.
The Joint Commission, the World Health Organization, the Institute of Medicine and the National Quality Foundation have all published white paper recommendations regarding the need to improve medical handoffs. Most hospitalists probably see this case as a "system error," and sure enough following this event the hospital overhauled its policies and procedures as they related to ICU transfers. But in the world of medical malpractice, the "system" doesn’t face the jury in litigation.
Although the attending internist was eventually dropped from this case, the hospital, the critical care consultant, and the hospitalist all settled with the plaintiff for an undisclosed amount.
Dr. Michota is director of academic affairs in the hospital medicine department at the Cleveland Clinic and medical editor of Hospitalist News. He has been involved in peer review both within and outside the legal system.

A new paradigm for preeclampsia
That preeclampsia is a growing problem, and one of the most significant causes of maternal-fetal morbidity and mortality today, is what drove the American College of Obstetricians and Gynecologists (ACOG) to convene a task force on hypertension in pregnancy in 2011. Indeed, the incidence of preeclampsia has increased approximately 10% over the last 3 decades in the United States, such that approximately 5%-7% of all pregnant women will develop the disorder.
The specific etiology of preeclampsia remains unclear, but the reasons for the increased incidence likely include the rise in delayed childbearing, the increased use of assisted reproductive technology, a rise in the number of twins, and the obesity pandemic.
Epidemiologically, older women with their first pregnancy are at higher risk of developing preeclampsia, whether or not they use assisted reproductive technology (ART). The not-infrequent use of ART among older women, namely IVF, has a compounding effect. So too, does the incidence of twinning. While we fortunately are seeing a lower rate of higher-order multiple gestations associated with IVF than we did in the 1990s, the incidence of twinning has increased dramatically. Women with multiple gestations of any order are at higher risk of developing preeclampsia.

The obesity pandemic is widely believed to be the most modifiable risk factor for preeclampsia. If we can help women to achieve a body mass index (BMI) that is as close to optimal as possible prior to conception, we will likely see significant reductions in the incidence of hypertensive disorders.
Prompt diagnosis of preeclampsia is critical, and on this front, ACOG\'s Task Force on Hypertension in Pregnancy report of 2013 sets forth an important new paradigm for thinking about the disorder and establishing its presence.
Managing preeclampsia remains challenging, however, as there are many areas in which evidence for guiding therapy and management is still insufficient. ACOG’s task force set out to review available data and to attempt to provide clarity on the management of preeclampsia as well as its diagnosis. This was no easy task, and in their culminating report, which lists 60 distinct recommendations, the task force clearly acknowledges the weak evidence base, giving relatively few of their recommendations top marks for both the quality of evidence and their strength of recommendation.
The report appropriately reminds us that there are few if any prescriptions or protocols when it comes to managing preeclampsia. My main concern with the task force’s coverage of management involves their recommendations that magnesium sulfate be used to treat patients with eclampsia and those with preeclampsia with severe features, but not necessarily those without severe features. Patients can progress so rapidly that unless every woman with preeclampsia is vigilantly scrutinized during labor and post delivery – a difficult, if not impossible, task – the window of opportunity to prevent convulsions through the use of magnesium sulfate may well be missed.
ACOG’s new terminology, definitions
Importantly, ACOG’s Task Force on Hypertension in Pregnancy report emphasizes that preeclampsia is an evolving, dynamic, and multisystemic process. It recommends elimination of the terms "mild" and "severe" preeclampsia and encourages the use of new terminology, pushing us to think instead of preeclampsia as being a disorder with or without "severe features." According to the report, a diagnosis of "mild preeclampsia" applies only at the moment at which the diagnosis is established, making the phrase misleading.
Physicians and other providers who have long been in practice will have a hard time ridding their vocabulary of the terms mild and severe preeclampsia, but the intent of the recommendation – to foster appreciation of preeclampsia as an evolving disease – is important and should become entrenched in our approach to hypertension in pregnancy.
The report also downgrades the role of proteinuria in the diagnosis of preeclampsia. Proteinuria is defined as the excretion of 300 mg or more of protein in a 24-hour urine collection or a urine protein/creatinine ratio of at least 0.3 mg/dL. Although proteinuria may indeed be a primary diagnostic finding, it should not be required in order to make the diagnosis of preeclampsia if other severe features are present.
As described in the report, severe features of preeclampsia may include thrombocytopenia (platelet count less than 100,000/microliter), impaired liver function, a rise in serum creatinine indicating progressive renal insufficiency (a serum creatinine concentration greater than 1.1 mg/dL or a doubling of the serum creatinine concentration in the absence of other renal disease), central nervous system disturbances, pulmonary edema, and persistently high elevations in blood pressure (a systolic blood pressure of 160 mm Hg or higher or a diastolic reading of 110 mm Hg or higher on two occasions at least 4 hours apart).
The document states, in other words, that to establish preeclampsia, equal weight should be given to any of these so-called severe features – even in the absence of proteinuria – when they occur along with new-onset hypertension at 20 weeks’ gestation or beyond. (The blood pressure criteria stipulate hypertension as a systolic blood pressure of 140 mm Hg or higher and a diastolic of 90 mm Hg or higher, taken on at least two occasions 4 hours apart.)
This new approach to diagnosing preeclampsia is a major change. It reflects what the ACOG document rightly calls a "minimal relationship" between the quantity of urinary protein and maternal and fetal outcomes in preeclampsia, as well as the fact that preeclampsia may quickly evolve. We need these broader criteria and lower thresholds so that we will not miss patients who might present atypically, with proteinuria not yet a significant finding, but with disease quickly developing.
Another helpful change is the removal of significant fetal growth restriction (less than the fifth percentile) as a diagnostic feature for traditionally coined "severe preeclampsia." Fetal growth restriction is not included in ACOG’s recommended list of severe features of preeclampsia. This is a helpful clarification that should prevent potentially unnecessary deliveries. The problems of fetal growth restriction (FGR) and preeclampsia should be considered and managed separately, with the option of expectant management considered with respect to each entity alone, as opposed to the finding of FGR driving a diagnosis of severe preeclampsia and thus delivery within 48 hours.
Where evidence is strongest
ACOG’s report contains 60 distinct recommendations covering hypertensive disorders in pregnancy, but only 6 of these recommendations are graded as both "strong" and based on "high-quality" evidence. (A "strong" recommendation is one that the task force considered so well supported by the literature that it is applicable to "virtually all patients.")
The remaining recommendations are either graded as "qualified" or are based on evidence that is rated as "very low," "low," or "moderate," or some combination of the "qualified" grade and a quality-of-evidence ranking below "high."
The task force utilized a strategy developed by the Grading of Recommendations Assessment, Development and Evaluation Working Group that rates the quality of evidence based largely on what’s called "confidence in estimates of effect." Under this approach, randomized, controlled trials are important but may still be considered flawed and observational studies are usually but not necessarily classified as low quality.
The small number of strong, high-quality recommendations in the ACOG report reflects the fact that, despite advances in our understanding of preeclampsia, there are many areas in which we lack good evidence from randomized, controlled trials. Importantly, the task force emphasizes that it offers recommendations and not prescriptions, and that sound clinical judgment remains a key part of patient management.
The six strong recommendations in the report that are based on high-quality evidence are as follows:
• The administration of vitamin C or vitamin E to prevent preeclampsia is not recommended.
• Women with severe preeclampsia who are being expectantly managed at 34 weeks’ or less of gestation should receive corticosteroids for the benefit of accelerating fetal lung maturation.
• Women who have chronic hypertension with superimposed preeclampsia and are being expectantly managed at 34 weeks’ or less of gestation also should have corticosteroids administered for the purpose of accelerating fetal lung maturation.
• For women with eclampsia, the administration of parenteral magnesium sulfate is recommended.
• For women with severe preeclampsia, the administration of intrapartum-postpartum magnesium sulfate to prevent eclampsia is recommended.
• For women with HELLP (hemolysis, elevated liver enzymes, low platelet count) syndrome who are before the gestational age of fetal viability, delivery should be undertaken shortly after initial maternal stabilization.
My take
Contrary to former recommendations, the task force’s new recommendations suggest that use of magnesium sulfate for preeclampsia without severe features (formerly called "mild preeclampsia") may not be needed. Although magnesium sulfate may not be warranted in every case, patients can progress so rapidly from having no severe symptoms to developing severe symptoms that it is difficult if not impossible to parse out who would or would not benefit from treatment. If we try to do so, we run the great risk of not providing the necessary medication to our patients, thereby increasing the chances of maternal morbidity and mortality.
In our institution, we continue to use magnesium sulfate intrapartum and post partum for every patient with a diagnosis of preeclampsia, whether or not she has severe features. Without high-quality evidence to the contrary, I do not believe that we should alter the former recommendation that magnesium sulfate be used in all cases of preeclampsia. We administer the agent for 24 hours post partum because studies looking at a 48-hour window have shown that most patients who have an eclamptic seizure within 48 hours after delivery will actually experience it within the first 24 hours.
There is a remaining conundrum. We know that approximately 50% of postpartum seizures occur more than 48 hours post delivery. It is vital, therefore, that patients who have hypertensive disorders during pregnancy be educated about the signs and symptoms of postpartum preeclampsia and be given clear directions about how to contact their provider if any signs or symptoms – such as headache, visual disturbances, and right-upper-quadrant pain – are noticed. Patients who are discharged with blood pressures that are still elevated (but not enough to require hospitalization) should be seen again within 72 hours or a week for an evaluation of their blood pressure. The threshold in our practices for arranging earlier postpartum visits, moreover, should be set very low for these women.
The need for patient education is mentioned in the ACOG report, which says, "It is suggested that health care providers convey information about preeclampsia in the context of prenatal care and postpartum care using proven health care communication practices."
The wording of the recommendation as well as its "qualified" strength and the designation of a "low" quality of evidence should not detract from the importance of the message that patient education is a key to successful recognition and management of preeclampsia. The awareness of and knowledge about postpartum preeclampsia have been shown in recent research to be disappointingly low. We need to do better.
With respect to prevention, there are two strategies that, despite not having strong recommendations and/or the backing of high-quality evidence, are still considered to be effective. One is the use of daily low-dose aspirin (60-80 mg) in women with a history of early-onset preeclampsia and preterm delivery prior to 34 weeks’ of gestation. The other is calcium supplementation for women who have an inadequate daily intake of calcium, although this practice has less relevance in the United States than in the developing world.
The goal of low-dose aspirin is really to reduce the likelihood of severe preeclampsia recurring. Almost half of patients with a history of preeclampsia will not develop the disorder in a subsequent pregnancy (without aspirin therapy), so the reduction in the incidence of preeclampsia with low-dose aspirin is unlikely to be significant. However, as aspirin therapy is a relatively benign and inexpensive intervention, it is worth considering. Indeed, meta-analyses of women in randomized trials of low-dose aspirin for preeclampsia prevention have shown small reductions in the incidence and morbidity of preeclampsia, without any evidence of adverse effects.
[Notably, the U.S. Preventive Services Task Force said in a draft recommendation statement issued in April that it recommends low-dose aspirin use after 12 weeks of pregnancy in women who are at high risk for preeclampsia. (See accompanying story.)]
Over the years a variety of predictive strategies – for predicting early-onset preeclampsia in particular – have been proposed and researched, including various biomarkers, blood tests, and imaging studies. These are all worthwhile endeavors at the research level, but for any screening strategy to be implemented there must be an effective intervention. At the current time, our only effective intervention is delivery based on clinical findings.
On the other end of the spectrum, it is clear today that preeclampsia is associated with later-life cardiovascular disease in women. It is only in the last 5-10 years that research findings have come to the fore and that we have thought about preeclampsia as a marker for increased disease risk, just as we did starting several decades ago with gestational diabetes and the risk of future type 2 diabetes.
ACOG’s task force suggests yearly assessment of blood pressure, lipids, fasting blood glucose, and BMI in women with a medical history of preeclampsia who delivered preterm or who have a history of recurrent preeclampsia. The recommendation is "qualified," with a low quality of evidence, and contains a cautionary footnote stating that "the value and appropriate timing of assessment is not yet established."
Indeed, the next step in research will be to follow patients with preeclampsia longitudinally and determine whether or not interventional strategies can be devised to reduce the cardiovascular risk to baseline or, ideally below baseline, in these patients. Until we have such information, we should still recognize that this group of patients may be at higher risk for cardiovascular disease later in life, and, at the very least, be even more vigilant about adhering to regular health maintenance examinations.
Dr. John T. Repke is professor and chair of obstetrics and gynecology at Pennsylvania State University, Hershey, and has published extensively on hypertension in pregnancy. Dr. Repke said he has no relevant financial disclosures.
That preeclampsia is a growing problem, and one of the most significant causes of maternal-fetal morbidity and mortality today, is what drove the American College of Obstetricians and Gynecologists (ACOG) to convene a task force on hypertension in pregnancy in 2011. Indeed, the incidence of preeclampsia has increased approximately 10% over the last 3 decades in the United States, such that approximately 5%-7% of all pregnant women will develop the disorder.
The specific etiology of preeclampsia remains unclear, but the reasons for the increased incidence likely include the rise in delayed childbearing, the increased use of assisted reproductive technology, a rise in the number of twins, and the obesity pandemic.
Epidemiologically, older women with their first pregnancy are at higher risk of developing preeclampsia, whether or not they use assisted reproductive technology (ART). The not-infrequent use of ART among older women, namely IVF, has a compounding effect. So too, does the incidence of twinning. While we fortunately are seeing a lower rate of higher-order multiple gestations associated with IVF than we did in the 1990s, the incidence of twinning has increased dramatically. Women with multiple gestations of any order are at higher risk of developing preeclampsia.
The obesity pandemic is widely believed to be the most modifiable risk factor for preeclampsia. If we can help women to achieve a body mass index (BMI) that is as close to optimal as possible prior to conception, we will likely see significant reductions in the incidence of hypertensive disorders.
Prompt diagnosis of preeclampsia is critical, and on this front, ACOG\'s Task Force on Hypertension in Pregnancy report of 2013 sets forth an important new paradigm for thinking about the disorder and establishing its presence.
Managing preeclampsia remains challenging, however, as there are many areas in which evidence for guiding therapy and management is still insufficient. ACOG’s task force set out to review available data and to attempt to provide clarity on the management of preeclampsia as well as its diagnosis. This was no easy task, and in their culminating report, which lists 60 distinct recommendations, the task force clearly acknowledges the weak evidence base, giving relatively few of their recommendations top marks for both the quality of evidence and their strength of recommendation.
The report appropriately reminds us that there are few if any prescriptions or protocols when it comes to managing preeclampsia. My main concern with the task force’s coverage of management involves their recommendations that magnesium sulfate be used to treat patients with eclampsia and those with preeclampsia with severe features, but not necessarily those without severe features. Patients can progress so rapidly that unless every woman with preeclampsia is vigilantly scrutinized during labor and post delivery – a difficult, if not impossible, task – the window of opportunity to prevent convulsions through the use of magnesium sulfate may well be missed.
ACOG’s new terminology, definitions
Importantly, ACOG’s Task Force on Hypertension in Pregnancy report emphasizes that preeclampsia is an evolving, dynamic, and multisystemic process. It recommends elimination of the terms "mild" and "severe" preeclampsia and encourages the use of new terminology, pushing us to think instead of preeclampsia as being a disorder with or without "severe features." According to the report, a diagnosis of "mild preeclampsia" applies only at the moment at which the diagnosis is established, making the phrase misleading.
Physicians and other providers who have long been in practice will have a hard time ridding their vocabulary of the terms mild and severe preeclampsia, but the intent of the recommendation – to foster appreciation of preeclampsia as an evolving disease – is important and should become entrenched in our approach to hypertension in pregnancy.
The report also downgrades the role of proteinuria in the diagnosis of preeclampsia. Proteinuria is defined as the excretion of 300 mg or more of protein in a 24-hour urine collection or a urine protein/creatinine ratio of at least 0.3 mg/dL. Although proteinuria may indeed be a primary diagnostic finding, it should not be required in order to make the diagnosis of preeclampsia if other severe features are present.
As described in the report, severe features of preeclampsia may include thrombocytopenia (platelet count less than 100,000/microliter), impaired liver function, a rise in serum creatinine indicating progressive renal insufficiency (a serum creatinine concentration greater than 1.1 mg/dL or a doubling of the serum creatinine concentration in the absence of other renal disease), central nervous system disturbances, pulmonary edema, and persistently high elevations in blood pressure (a systolic blood pressure of 160 mm Hg or higher or a diastolic reading of 110 mm Hg or higher on two occasions at least 4 hours apart).
The document states, in other words, that to establish preeclampsia, equal weight should be given to any of these so-called severe features – even in the absence of proteinuria – when they occur along with new-onset hypertension at 20 weeks’ gestation or beyond. (The blood pressure criteria stipulate hypertension as a systolic blood pressure of 140 mm Hg or higher and a diastolic of 90 mm Hg or higher, taken on at least two occasions 4 hours apart.)
This new approach to diagnosing preeclampsia is a major change. It reflects what the ACOG document rightly calls a "minimal relationship" between the quantity of urinary protein and maternal and fetal outcomes in preeclampsia, as well as the fact that preeclampsia may quickly evolve. We need these broader criteria and lower thresholds so that we will not miss patients who might present atypically, with proteinuria not yet a significant finding, but with disease quickly developing.
Another helpful change is the removal of significant fetal growth restriction (less than the fifth percentile) as a diagnostic feature for traditionally coined "severe preeclampsia." Fetal growth restriction is not included in ACOG’s recommended list of severe features of preeclampsia. This is a helpful clarification that should prevent potentially unnecessary deliveries. The problems of fetal growth restriction (FGR) and preeclampsia should be considered and managed separately, with the option of expectant management considered with respect to each entity alone, as opposed to the finding of FGR driving a diagnosis of severe preeclampsia and thus delivery within 48 hours.
Where evidence is strongest
ACOG’s report contains 60 distinct recommendations covering hypertensive disorders in pregnancy, but only 6 of these recommendations are graded as both "strong" and based on "high-quality" evidence. (A "strong" recommendation is one that the task force considered so well supported by the literature that it is applicable to "virtually all patients.")
The remaining recommendations are either graded as "qualified" or are based on evidence that is rated as "very low," "low," or "moderate," or some combination of the "qualified" grade and a quality-of-evidence ranking below "high."
The task force utilized a strategy developed by the Grading of Recommendations Assessment, Development and Evaluation Working Group that rates the quality of evidence based largely on what’s called "confidence in estimates of effect." Under this approach, randomized, controlled trials are important but may still be considered flawed and observational studies are usually but not necessarily classified as low quality.
The small number of strong, high-quality recommendations in the ACOG report reflects the fact that, despite advances in our understanding of preeclampsia, there are many areas in which we lack good evidence from randomized, controlled trials. Importantly, the task force emphasizes that it offers recommendations and not prescriptions, and that sound clinical judgment remains a key part of patient management.
The six strong recommendations in the report that are based on high-quality evidence are as follows:
• The administration of vitamin C or vitamin E to prevent preeclampsia is not recommended.
• Women with severe preeclampsia who are being expectantly managed at 34 weeks’ or less of gestation should receive corticosteroids for the benefit of accelerating fetal lung maturation.
• Women who have chronic hypertension with superimposed preeclampsia and are being expectantly managed at 34 weeks’ or less of gestation also should have corticosteroids administered for the purpose of accelerating fetal lung maturation.
• For women with eclampsia, the administration of parenteral magnesium sulfate is recommended.
• For women with severe preeclampsia, the administration of intrapartum-postpartum magnesium sulfate to prevent eclampsia is recommended.
• For women with HELLP (hemolysis, elevated liver enzymes, low platelet count) syndrome who are before the gestational age of fetal viability, delivery should be undertaken shortly after initial maternal stabilization.
My take
Contrary to former recommendations, the task force’s new recommendations suggest that use of magnesium sulfate for preeclampsia without severe features (formerly called "mild preeclampsia") may not be needed. Although magnesium sulfate may not be warranted in every case, patients can progress so rapidly from having no severe symptoms to developing severe symptoms that it is difficult if not impossible to parse out who would or would not benefit from treatment. If we try to do so, we run the great risk of not providing the necessary medication to our patients, thereby increasing the chances of maternal morbidity and mortality.
In our institution, we continue to use magnesium sulfate intrapartum and post partum for every patient with a diagnosis of preeclampsia, whether or not she has severe features. Without high-quality evidence to the contrary, I do not believe that we should alter the former recommendation that magnesium sulfate be used in all cases of preeclampsia. We administer the agent for 24 hours post partum because studies looking at a 48-hour window have shown that most patients who have an eclamptic seizure within 48 hours after delivery will actually experience it within the first 24 hours.
There is a remaining conundrum. We know that approximately 50% of postpartum seizures occur more than 48 hours post delivery. It is vital, therefore, that patients who have hypertensive disorders during pregnancy be educated about the signs and symptoms of postpartum preeclampsia and be given clear directions about how to contact their provider if any signs or symptoms – such as headache, visual disturbances, and right-upper-quadrant pain – are noticed. Patients who are discharged with blood pressures that are still elevated (but not enough to require hospitalization) should be seen again within 72 hours or a week for an evaluation of their blood pressure. The threshold in our practices for arranging earlier postpartum visits, moreover, should be set very low for these women.
The need for patient education is mentioned in the ACOG report, which says, "It is suggested that health care providers convey information about preeclampsia in the context of prenatal care and postpartum care using proven health care communication practices."
The wording of the recommendation as well as its "qualified" strength and the designation of a "low" quality of evidence should not detract from the importance of the message that patient education is a key to successful recognition and management of preeclampsia. The awareness of and knowledge about postpartum preeclampsia have been shown in recent research to be disappointingly low. We need to do better.
With respect to prevention, there are two strategies that, despite not having strong recommendations and/or the backing of high-quality evidence, are still considered to be effective. One is the use of daily low-dose aspirin (60-80 mg) in women with a history of early-onset preeclampsia and preterm delivery prior to 34 weeks’ of gestation. The other is calcium supplementation for women who have an inadequate daily intake of calcium, although this practice has less relevance in the United States than in the developing world.
The goal of low-dose aspirin is really to reduce the likelihood of severe preeclampsia recurring. Almost half of patients with a history of preeclampsia will not develop the disorder in a subsequent pregnancy (without aspirin therapy), so the reduction in the incidence of preeclampsia with low-dose aspirin is unlikely to be significant. However, as aspirin therapy is a relatively benign and inexpensive intervention, it is worth considering. Indeed, meta-analyses of women in randomized trials of low-dose aspirin for preeclampsia prevention have shown small reductions in the incidence and morbidity of preeclampsia, without any evidence of adverse effects.
[Notably, the U.S. Preventive Services Task Force said in a draft recommendation statement issued in April that it recommends low-dose aspirin use after 12 weeks of pregnancy in women who are at high risk for preeclampsia. (See accompanying story.)]
Over the years a variety of predictive strategies – for predicting early-onset preeclampsia in particular – have been proposed and researched, including various biomarkers, blood tests, and imaging studies. These are all worthwhile endeavors at the research level, but for any screening strategy to be implemented there must be an effective intervention. At the current time, our only effective intervention is delivery based on clinical findings.
On the other end of the spectrum, it is clear today that preeclampsia is associated with later-life cardiovascular disease in women. It is only in the last 5-10 years that research findings have come to the fore and that we have thought about preeclampsia as a marker for increased disease risk, just as we did starting several decades ago with gestational diabetes and the risk of future type 2 diabetes.
ACOG’s task force suggests yearly assessment of blood pressure, lipids, fasting blood glucose, and BMI in women with a medical history of preeclampsia who delivered preterm or who have a history of recurrent preeclampsia. The recommendation is "qualified," with a low quality of evidence, and contains a cautionary footnote stating that "the value and appropriate timing of assessment is not yet established."
Indeed, the next step in research will be to follow patients with preeclampsia longitudinally and determine whether or not interventional strategies can be devised to reduce the cardiovascular risk to baseline or, ideally below baseline, in these patients. Until we have such information, we should still recognize that this group of patients may be at higher risk for cardiovascular disease later in life, and, at the very least, be even more vigilant about adhering to regular health maintenance examinations.
Dr. John T. Repke is professor and chair of obstetrics and gynecology at Pennsylvania State University, Hershey, and has published extensively on hypertension in pregnancy. Dr. Repke said he has no relevant financial disclosures.
That preeclampsia is a growing problem, and one of the most significant causes of maternal-fetal morbidity and mortality today, is what drove the American College of Obstetricians and Gynecologists (ACOG) to convene a task force on hypertension in pregnancy in 2011. Indeed, the incidence of preeclampsia has increased approximately 10% over the last 3 decades in the United States, such that approximately 5%-7% of all pregnant women will develop the disorder.
The specific etiology of preeclampsia remains unclear, but the reasons for the increased incidence likely include the rise in delayed childbearing, the increased use of assisted reproductive technology, a rise in the number of twins, and the obesity pandemic.
Epidemiologically, older women with their first pregnancy are at higher risk of developing preeclampsia, whether or not they use assisted reproductive technology (ART). The not-infrequent use of ART among older women, namely IVF, has a compounding effect. So too, does the incidence of twinning. While we fortunately are seeing a lower rate of higher-order multiple gestations associated with IVF than we did in the 1990s, the incidence of twinning has increased dramatically. Women with multiple gestations of any order are at higher risk of developing preeclampsia.
The obesity pandemic is widely believed to be the most modifiable risk factor for preeclampsia. If we can help women to achieve a body mass index (BMI) that is as close to optimal as possible prior to conception, we will likely see significant reductions in the incidence of hypertensive disorders.
Prompt diagnosis of preeclampsia is critical, and on this front, ACOG\'s Task Force on Hypertension in Pregnancy report of 2013 sets forth an important new paradigm for thinking about the disorder and establishing its presence.
Managing preeclampsia remains challenging, however, as there are many areas in which evidence for guiding therapy and management is still insufficient. ACOG’s task force set out to review available data and to attempt to provide clarity on the management of preeclampsia as well as its diagnosis. This was no easy task, and in their culminating report, which lists 60 distinct recommendations, the task force clearly acknowledges the weak evidence base, giving relatively few of their recommendations top marks for both the quality of evidence and their strength of recommendation.
The report appropriately reminds us that there are few if any prescriptions or protocols when it comes to managing preeclampsia. My main concern with the task force’s coverage of management involves their recommendations that magnesium sulfate be used to treat patients with eclampsia and those with preeclampsia with severe features, but not necessarily those without severe features. Patients can progress so rapidly that unless every woman with preeclampsia is vigilantly scrutinized during labor and post delivery – a difficult, if not impossible, task – the window of opportunity to prevent convulsions through the use of magnesium sulfate may well be missed.
ACOG’s new terminology, definitions
Importantly, ACOG’s Task Force on Hypertension in Pregnancy report emphasizes that preeclampsia is an evolving, dynamic, and multisystemic process. It recommends elimination of the terms "mild" and "severe" preeclampsia and encourages the use of new terminology, pushing us to think instead of preeclampsia as being a disorder with or without "severe features." According to the report, a diagnosis of "mild preeclampsia" applies only at the moment at which the diagnosis is established, making the phrase misleading.
Physicians and other providers who have long been in practice will have a hard time ridding their vocabulary of the terms mild and severe preeclampsia, but the intent of the recommendation – to foster appreciation of preeclampsia as an evolving disease – is important and should become entrenched in our approach to hypertension in pregnancy.
The report also downgrades the role of proteinuria in the diagnosis of preeclampsia. Proteinuria is defined as the excretion of 300 mg or more of protein in a 24-hour urine collection or a urine protein/creatinine ratio of at least 0.3 mg/dL. Although proteinuria may indeed be a primary diagnostic finding, it should not be required in order to make the diagnosis of preeclampsia if other severe features are present.
As described in the report, severe features of preeclampsia may include thrombocytopenia (platelet count less than 100,000/microliter), impaired liver function, a rise in serum creatinine indicating progressive renal insufficiency (a serum creatinine concentration greater than 1.1 mg/dL or a doubling of the serum creatinine concentration in the absence of other renal disease), central nervous system disturbances, pulmonary edema, and persistently high elevations in blood pressure (a systolic blood pressure of 160 mm Hg or higher or a diastolic reading of 110 mm Hg or higher on two occasions at least 4 hours apart).
The document states, in other words, that to establish preeclampsia, equal weight should be given to any of these so-called severe features – even in the absence of proteinuria – when they occur along with new-onset hypertension at 20 weeks’ gestation or beyond. (The blood pressure criteria stipulate hypertension as a systolic blood pressure of 140 mm Hg or higher and a diastolic of 90 mm Hg or higher, taken on at least two occasions 4 hours apart.)
This new approach to diagnosing preeclampsia is a major change. It reflects what the ACOG document rightly calls a "minimal relationship" between the quantity of urinary protein and maternal and fetal outcomes in preeclampsia, as well as the fact that preeclampsia may quickly evolve. We need these broader criteria and lower thresholds so that we will not miss patients who might present atypically, with proteinuria not yet a significant finding, but with disease quickly developing.
Another helpful change is the removal of significant fetal growth restriction (less than the fifth percentile) as a diagnostic feature for traditionally coined "severe preeclampsia." Fetal growth restriction is not included in ACOG’s recommended list of severe features of preeclampsia. This is a helpful clarification that should prevent potentially unnecessary deliveries. The problems of fetal growth restriction (FGR) and preeclampsia should be considered and managed separately, with the option of expectant management considered with respect to each entity alone, as opposed to the finding of FGR driving a diagnosis of severe preeclampsia and thus delivery within 48 hours.
Where evidence is strongest
ACOG’s report contains 60 distinct recommendations covering hypertensive disorders in pregnancy, but only 6 of these recommendations are graded as both "strong" and based on "high-quality" evidence. (A "strong" recommendation is one that the task force considered so well supported by the literature that it is applicable to "virtually all patients.")
The remaining recommendations are either graded as "qualified" or are based on evidence that is rated as "very low," "low," or "moderate," or some combination of the "qualified" grade and a quality-of-evidence ranking below "high."
The task force utilized a strategy developed by the Grading of Recommendations Assessment, Development and Evaluation Working Group that rates the quality of evidence based largely on what’s called "confidence in estimates of effect." Under this approach, randomized, controlled trials are important but may still be considered flawed and observational studies are usually but not necessarily classified as low quality.
The small number of strong, high-quality recommendations in the ACOG report reflects the fact that, despite advances in our understanding of preeclampsia, there are many areas in which we lack good evidence from randomized, controlled trials. Importantly, the task force emphasizes that it offers recommendations and not prescriptions, and that sound clinical judgment remains a key part of patient management.
The six strong recommendations in the report that are based on high-quality evidence are as follows:
• The administration of vitamin C or vitamin E to prevent preeclampsia is not recommended.
• Women with severe preeclampsia who are being expectantly managed at 34 weeks’ or less of gestation should receive corticosteroids for the benefit of accelerating fetal lung maturation.
• Women who have chronic hypertension with superimposed preeclampsia and are being expectantly managed at 34 weeks’ or less of gestation also should have corticosteroids administered for the purpose of accelerating fetal lung maturation.
• For women with eclampsia, the administration of parenteral magnesium sulfate is recommended.
• For women with severe preeclampsia, the administration of intrapartum-postpartum magnesium sulfate to prevent eclampsia is recommended.
• For women with HELLP (hemolysis, elevated liver enzymes, low platelet count) syndrome who are before the gestational age of fetal viability, delivery should be undertaken shortly after initial maternal stabilization.
My take
Contrary to former recommendations, the task force’s new recommendations suggest that use of magnesium sulfate for preeclampsia without severe features (formerly called "mild preeclampsia") may not be needed. Although magnesium sulfate may not be warranted in every case, patients can progress so rapidly from having no severe symptoms to developing severe symptoms that it is difficult if not impossible to parse out who would or would not benefit from treatment. If we try to do so, we run the great risk of not providing the necessary medication to our patients, thereby increasing the chances of maternal morbidity and mortality.
In our institution, we continue to use magnesium sulfate intrapartum and post partum for every patient with a diagnosis of preeclampsia, whether or not she has severe features. Without high-quality evidence to the contrary, I do not believe that we should alter the former recommendation that magnesium sulfate be used in all cases of preeclampsia. We administer the agent for 24 hours post partum because studies looking at a 48-hour window have shown that most patients who have an eclamptic seizure within 48 hours after delivery will actually experience it within the first 24 hours.
There is a remaining conundrum. We know that approximately 50% of postpartum seizures occur more than 48 hours post delivery. It is vital, therefore, that patients who have hypertensive disorders during pregnancy be educated about the signs and symptoms of postpartum preeclampsia and be given clear directions about how to contact their provider if any signs or symptoms – such as headache, visual disturbances, and right-upper-quadrant pain – are noticed. Patients who are discharged with blood pressures that are still elevated (but not enough to require hospitalization) should be seen again within 72 hours or a week for an evaluation of their blood pressure. The threshold in our practices for arranging earlier postpartum visits, moreover, should be set very low for these women.
The need for patient education is mentioned in the ACOG report, which says, "It is suggested that health care providers convey information about preeclampsia in the context of prenatal care and postpartum care using proven health care communication practices."
The wording of the recommendation as well as its "qualified" strength and the designation of a "low" quality of evidence should not detract from the importance of the message that patient education is a key to successful recognition and management of preeclampsia. The awareness of and knowledge about postpartum preeclampsia have been shown in recent research to be disappointingly low. We need to do better.
With respect to prevention, there are two strategies that, despite not having strong recommendations and/or the backing of high-quality evidence, are still considered to be effective. One is the use of daily low-dose aspirin (60-80 mg) in women with a history of early-onset preeclampsia and preterm delivery prior to 34 weeks’ of gestation. The other is calcium supplementation for women who have an inadequate daily intake of calcium, although this practice has less relevance in the United States than in the developing world.
The goal of low-dose aspirin is really to reduce the likelihood of severe preeclampsia recurring. Almost half of patients with a history of preeclampsia will not develop the disorder in a subsequent pregnancy (without aspirin therapy), so the reduction in the incidence of preeclampsia with low-dose aspirin is unlikely to be significant. However, as aspirin therapy is a relatively benign and inexpensive intervention, it is worth considering. Indeed, meta-analyses of women in randomized trials of low-dose aspirin for preeclampsia prevention have shown small reductions in the incidence and morbidity of preeclampsia, without any evidence of adverse effects.
[Notably, the U.S. Preventive Services Task Force said in a draft recommendation statement issued in April that it recommends low-dose aspirin use after 12 weeks of pregnancy in women who are at high risk for preeclampsia. (See accompanying story.)]
Over the years a variety of predictive strategies – for predicting early-onset preeclampsia in particular – have been proposed and researched, including various biomarkers, blood tests, and imaging studies. These are all worthwhile endeavors at the research level, but for any screening strategy to be implemented there must be an effective intervention. At the current time, our only effective intervention is delivery based on clinical findings.
On the other end of the spectrum, it is clear today that preeclampsia is associated with later-life cardiovascular disease in women. It is only in the last 5-10 years that research findings have come to the fore and that we have thought about preeclampsia as a marker for increased disease risk, just as we did starting several decades ago with gestational diabetes and the risk of future type 2 diabetes.
ACOG’s task force suggests yearly assessment of blood pressure, lipids, fasting blood glucose, and BMI in women with a medical history of preeclampsia who delivered preterm or who have a history of recurrent preeclampsia. The recommendation is "qualified," with a low quality of evidence, and contains a cautionary footnote stating that "the value and appropriate timing of assessment is not yet established."
Indeed, the next step in research will be to follow patients with preeclampsia longitudinally and determine whether or not interventional strategies can be devised to reduce the cardiovascular risk to baseline or, ideally below baseline, in these patients. Until we have such information, we should still recognize that this group of patients may be at higher risk for cardiovascular disease later in life, and, at the very least, be even more vigilant about adhering to regular health maintenance examinations.
Dr. John T. Repke is professor and chair of obstetrics and gynecology at Pennsylvania State University, Hershey, and has published extensively on hypertension in pregnancy. Dr. Repke said he has no relevant financial disclosures.
JNC 8: Not So Great?

The previous set of official recommendations for hypertension management was published way back in 2003. So the practice community has waited very patiently for an updated set of guidelines. The previous guidelines were known as JNC 7, referring to the seventh iteration of recommendations emanating from a group of big-time hypertension experts known as the Joint National Committee (JNC). All the JNC reports have been sponsored by the National Institutes of Health (NIH), and hence, had a high degree of visibility and credibility. However, many practitioners felt that cost considerations mitigating in favor of inexpensive drugs, such as thiazide diuretics, unfairly colored and distorted the JNC 7 recommendations.
In the interest of full disclosure, I should point out that I was one of the many Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) investigators who produced an influential study result that indeed seemed to favor diuretics over the newer and more expensive antihypertensive therapies. So JNC 7 was received with some suspicion that saving money might have taken precedence over optimal therapeutic management.
Many new studies relevant to hypertension goals and preferred antihypertensive therapies have come out in the years since JNC 7 first appeared. So there was a lot of anticipation that these more recent studies would inform and modify some of the existing JNC recommendations. This sort of speculation was all very fair and reasonable. But then something quite unanticipated happened. The JNC 8 experts met and discussed recommendations, but no guidelines emerged. Literally, years went by, and the recommendations that were expected as JNC 8 instead became known as JNC Wait and then JNC Late.
Then the NIH decided that it didn’t want to be in the guideline-issuing business any longer. The NIH outsourced its lipid guidelines, which had previously been known as the NCEP (National Cholesterol Education Panel) recommendations, to a joint committee of the American Heart Association and the American College of Cardiology. The hypertension experts who had met as the JNC 8 group were similarly cut loose from formal NIH sponsorship. This action was not because the NIH was unhappy with their work, but rather because the NIH had simply decided that it no longer wanted to sponsor any clinical recommendations of any sort.
So what to do? Having finally reached consensus after years of meetings, the JNC 8 experts found themselves without an official sponsor. So they decided to take a page from rock star Prince’s playbook, and they published their recommendations as “the Panel Members Appointed to the Eighth Joint National Committee.” This move was a bit awkward, to say the least, but it was certainly preferable to leaving the fruits of their extensive labors unavailable to the practice community.
Apart from all these distractions, what has generated the most controversy has been the actual guidelines for the management of patients with hypertension who are aged 60 years or older. This is a pretty sizable chunk of the total population with hypertension, since the prevalence of elevated blood pressure increases dramatically with age. And this is also the population whose consequences of inadequately controlled hypertension are the most severe. The majority of strokes occur in those over the age of 60, as do most of the myocardial infarctions and cases of new-onset heart failure.
This group truly has a lot at stake when it comes to hypertension control or lack thereof. And I have to tell you, it’s a group I identify with. I saw 60 in the rearview mirror several years back, and I’ve been on antihypertensive therapy since my late thirties. Consequently, I am following this discussion very closely for both professional and personal reasons.
The JNC 8 authors recommended against initiating antihypertensive therapy in patients over the age of 60 unless their blood pressure was over 150/90 mm Hg, which represents a loosening of the earlier recommendations to start drug treatment at the lower systolic level of 140 mm Hg. Also, the new goal for antihypertensive therapy in this age group is simply to achieve a systolic pressure of ≤ 150 mm Hg, instead of the previous goal of under 140 mm Hg.
I am of two minds about this relaxation of the blood pressure goals. On the one hand, I acknowledge that the recommendations are evidence based, at least in the sense that no incontrovertible data exist to refute this more relaxed goal. There are simply not any credible studies out there that demonstrate better results when the systolic goal is 140 mm Hg rather than 150 mm Hg. It doesn’t mean that it might not be true—140 might really be better than 150—it simply means that the issue has not been studied in any clinical trial. So from a purist, evidence-based standpoint, I can accept that the new recommendation is perfectly valid from a scientific point of view.
But the part of me that values the art of medicine as well as the science is profoundly troubled by this lockstep scientific purity. What I am extremely concerned about is the possibility that the practice community will misinterpret the recommendations and take them as a mandate to loosen blood pressure control in those over age 60. If the target is just to get the systolic below 150 mm Hg, some may conclude that a pressure of 160 or even 165 is “close enough for government work,” to use the convenient phrase that dogs us federal employees. This would be a misinterpretation of the guidelines’ actual recommendation, but nonetheless, a very understandable and almost predictable one. Given that the practice community has never done a bang-up job of getting patients to the goals previously recommended, is it really the time to relax those guidelines and run the risk of even less blood pressure control?
I have to reluctantly conclude that the pseudo JNC 8 guidelines are not so great, at least for hypertensive patients over age 60. Although I cannot quibble with the strict scientific underpinning of the guidelines, they seem very likely to lead to a setback in hypertension control. We may see more heart attacks, strokes, heart failure, and renal failure if practitioners take the new guidelines as license to be less vigilant in treating elevated blood pressure. Treating elevated blood pressure is the low-hanging fruit for most primary care providers, and discouraging them from plucking that fruit from the tree is clearly a step in the wrong direction.
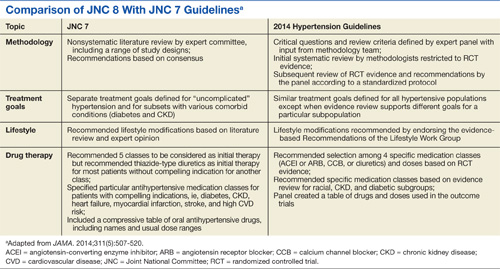
Author disclosures
The author reports no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the author and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
The previous set of official recommendations for hypertension management was published way back in 2003. So the practice community has waited very patiently for an updated set of guidelines. The previous guidelines were known as JNC 7, referring to the seventh iteration of recommendations emanating from a group of big-time hypertension experts known as the Joint National Committee (JNC). All the JNC reports have been sponsored by the National Institutes of Health (NIH), and hence, had a high degree of visibility and credibility. However, many practitioners felt that cost considerations mitigating in favor of inexpensive drugs, such as thiazide diuretics, unfairly colored and distorted the JNC 7 recommendations.
In the interest of full disclosure, I should point out that I was one of the many Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) investigators who produced an influential study result that indeed seemed to favor diuretics over the newer and more expensive antihypertensive therapies. So JNC 7 was received with some suspicion that saving money might have taken precedence over optimal therapeutic management.
Many new studies relevant to hypertension goals and preferred antihypertensive therapies have come out in the years since JNC 7 first appeared. So there was a lot of anticipation that these more recent studies would inform and modify some of the existing JNC recommendations. This sort of speculation was all very fair and reasonable. But then something quite unanticipated happened. The JNC 8 experts met and discussed recommendations, but no guidelines emerged. Literally, years went by, and the recommendations that were expected as JNC 8 instead became known as JNC Wait and then JNC Late.
Then the NIH decided that it didn’t want to be in the guideline-issuing business any longer. The NIH outsourced its lipid guidelines, which had previously been known as the NCEP (National Cholesterol Education Panel) recommendations, to a joint committee of the American Heart Association and the American College of Cardiology. The hypertension experts who had met as the JNC 8 group were similarly cut loose from formal NIH sponsorship. This action was not because the NIH was unhappy with their work, but rather because the NIH had simply decided that it no longer wanted to sponsor any clinical recommendations of any sort.
So what to do? Having finally reached consensus after years of meetings, the JNC 8 experts found themselves without an official sponsor. So they decided to take a page from rock star Prince’s playbook, and they published their recommendations as “the Panel Members Appointed to the Eighth Joint National Committee.” This move was a bit awkward, to say the least, but it was certainly preferable to leaving the fruits of their extensive labors unavailable to the practice community.
Apart from all these distractions, what has generated the most controversy has been the actual guidelines for the management of patients with hypertension who are aged 60 years or older. This is a pretty sizable chunk of the total population with hypertension, since the prevalence of elevated blood pressure increases dramatically with age. And this is also the population whose consequences of inadequately controlled hypertension are the most severe. The majority of strokes occur in those over the age of 60, as do most of the myocardial infarctions and cases of new-onset heart failure.
This group truly has a lot at stake when it comes to hypertension control or lack thereof. And I have to tell you, it’s a group I identify with. I saw 60 in the rearview mirror several years back, and I’ve been on antihypertensive therapy since my late thirties. Consequently, I am following this discussion very closely for both professional and personal reasons.
The JNC 8 authors recommended against initiating antihypertensive therapy in patients over the age of 60 unless their blood pressure was over 150/90 mm Hg, which represents a loosening of the earlier recommendations to start drug treatment at the lower systolic level of 140 mm Hg. Also, the new goal for antihypertensive therapy in this age group is simply to achieve a systolic pressure of ≤ 150 mm Hg, instead of the previous goal of under 140 mm Hg.
I am of two minds about this relaxation of the blood pressure goals. On the one hand, I acknowledge that the recommendations are evidence based, at least in the sense that no incontrovertible data exist to refute this more relaxed goal. There are simply not any credible studies out there that demonstrate better results when the systolic goal is 140 mm Hg rather than 150 mm Hg. It doesn’t mean that it might not be true—140 might really be better than 150—it simply means that the issue has not been studied in any clinical trial. So from a purist, evidence-based standpoint, I can accept that the new recommendation is perfectly valid from a scientific point of view.
But the part of me that values the art of medicine as well as the science is profoundly troubled by this lockstep scientific purity. What I am extremely concerned about is the possibility that the practice community will misinterpret the recommendations and take them as a mandate to loosen blood pressure control in those over age 60. If the target is just to get the systolic below 150 mm Hg, some may conclude that a pressure of 160 or even 165 is “close enough for government work,” to use the convenient phrase that dogs us federal employees. This would be a misinterpretation of the guidelines’ actual recommendation, but nonetheless, a very understandable and almost predictable one. Given that the practice community has never done a bang-up job of getting patients to the goals previously recommended, is it really the time to relax those guidelines and run the risk of even less blood pressure control?
I have to reluctantly conclude that the pseudo JNC 8 guidelines are not so great, at least for hypertensive patients over age 60. Although I cannot quibble with the strict scientific underpinning of the guidelines, they seem very likely to lead to a setback in hypertension control. We may see more heart attacks, strokes, heart failure, and renal failure if practitioners take the new guidelines as license to be less vigilant in treating elevated blood pressure. Treating elevated blood pressure is the low-hanging fruit for most primary care providers, and discouraging them from plucking that fruit from the tree is clearly a step in the wrong direction.
Author disclosures
The author reports no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the author and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
The previous set of official recommendations for hypertension management was published way back in 2003. So the practice community has waited very patiently for an updated set of guidelines. The previous guidelines were known as JNC 7, referring to the seventh iteration of recommendations emanating from a group of big-time hypertension experts known as the Joint National Committee (JNC). All the JNC reports have been sponsored by the National Institutes of Health (NIH), and hence, had a high degree of visibility and credibility. However, many practitioners felt that cost considerations mitigating in favor of inexpensive drugs, such as thiazide diuretics, unfairly colored and distorted the JNC 7 recommendations.
In the interest of full disclosure, I should point out that I was one of the many Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) investigators who produced an influential study result that indeed seemed to favor diuretics over the newer and more expensive antihypertensive therapies. So JNC 7 was received with some suspicion that saving money might have taken precedence over optimal therapeutic management.
Many new studies relevant to hypertension goals and preferred antihypertensive therapies have come out in the years since JNC 7 first appeared. So there was a lot of anticipation that these more recent studies would inform and modify some of the existing JNC recommendations. This sort of speculation was all very fair and reasonable. But then something quite unanticipated happened. The JNC 8 experts met and discussed recommendations, but no guidelines emerged. Literally, years went by, and the recommendations that were expected as JNC 8 instead became known as JNC Wait and then JNC Late.
Then the NIH decided that it didn’t want to be in the guideline-issuing business any longer. The NIH outsourced its lipid guidelines, which had previously been known as the NCEP (National Cholesterol Education Panel) recommendations, to a joint committee of the American Heart Association and the American College of Cardiology. The hypertension experts who had met as the JNC 8 group were similarly cut loose from formal NIH sponsorship. This action was not because the NIH was unhappy with their work, but rather because the NIH had simply decided that it no longer wanted to sponsor any clinical recommendations of any sort.
So what to do? Having finally reached consensus after years of meetings, the JNC 8 experts found themselves without an official sponsor. So they decided to take a page from rock star Prince’s playbook, and they published their recommendations as “the Panel Members Appointed to the Eighth Joint National Committee.” This move was a bit awkward, to say the least, but it was certainly preferable to leaving the fruits of their extensive labors unavailable to the practice community.
Apart from all these distractions, what has generated the most controversy has been the actual guidelines for the management of patients with hypertension who are aged 60 years or older. This is a pretty sizable chunk of the total population with hypertension, since the prevalence of elevated blood pressure increases dramatically with age. And this is also the population whose consequences of inadequately controlled hypertension are the most severe. The majority of strokes occur in those over the age of 60, as do most of the myocardial infarctions and cases of new-onset heart failure.
This group truly has a lot at stake when it comes to hypertension control or lack thereof. And I have to tell you, it’s a group I identify with. I saw 60 in the rearview mirror several years back, and I’ve been on antihypertensive therapy since my late thirties. Consequently, I am following this discussion very closely for both professional and personal reasons.
The JNC 8 authors recommended against initiating antihypertensive therapy in patients over the age of 60 unless their blood pressure was over 150/90 mm Hg, which represents a loosening of the earlier recommendations to start drug treatment at the lower systolic level of 140 mm Hg. Also, the new goal for antihypertensive therapy in this age group is simply to achieve a systolic pressure of ≤ 150 mm Hg, instead of the previous goal of under 140 mm Hg.
I am of two minds about this relaxation of the blood pressure goals. On the one hand, I acknowledge that the recommendations are evidence based, at least in the sense that no incontrovertible data exist to refute this more relaxed goal. There are simply not any credible studies out there that demonstrate better results when the systolic goal is 140 mm Hg rather than 150 mm Hg. It doesn’t mean that it might not be true—140 might really be better than 150—it simply means that the issue has not been studied in any clinical trial. So from a purist, evidence-based standpoint, I can accept that the new recommendation is perfectly valid from a scientific point of view.
But the part of me that values the art of medicine as well as the science is profoundly troubled by this lockstep scientific purity. What I am extremely concerned about is the possibility that the practice community will misinterpret the recommendations and take them as a mandate to loosen blood pressure control in those over age 60. If the target is just to get the systolic below 150 mm Hg, some may conclude that a pressure of 160 or even 165 is “close enough for government work,” to use the convenient phrase that dogs us federal employees. This would be a misinterpretation of the guidelines’ actual recommendation, but nonetheless, a very understandable and almost predictable one. Given that the practice community has never done a bang-up job of getting patients to the goals previously recommended, is it really the time to relax those guidelines and run the risk of even less blood pressure control?
I have to reluctantly conclude that the pseudo JNC 8 guidelines are not so great, at least for hypertensive patients over age 60. Although I cannot quibble with the strict scientific underpinning of the guidelines, they seem very likely to lead to a setback in hypertension control. We may see more heart attacks, strokes, heart failure, and renal failure if practitioners take the new guidelines as license to be less vigilant in treating elevated blood pressure. Treating elevated blood pressure is the low-hanging fruit for most primary care providers, and discouraging them from plucking that fruit from the tree is clearly a step in the wrong direction.
Author disclosures
The author reports no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the author and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Reinventing the role of the gynecologist
The time is now to change office gynecologic care.
Scientific advances in cervical surveillance enable women to be screened later in life, less frequently, and more efficiently than ever before. The American Congress of Obstetricians and Gynecologists recommends that screening start at age 21, then continue at 3-year intervals until age 30, if the results are normal. At age 30, cotesting for human papillomavirus enables the screening interval to be extended to 5 years, if the results are normal. Screening endpoints may be reached upon removal of the cervix (if there is no history of cervical intraepithelial neoplasia [CIN] II or greater) or by age 65 (if there is adequate negative screening and no history of CIN II or greater in the past 20 years).

In November 2009, the U.S. Preventive Services Task Force (USPSTF) released the statement that the current evidence is insufficient to assess the additional benefits and harms of the clinical breast exam beyond those of the screening mammogram.
The ACOG Committee Opinion #534, entitled "The Well-Women Visit," was published in August 2012. This document states: "An annual pelvic examination seems logical, but also lacks data to support a specific time frame of frequency of such examinations. The decision whether or not to perform a complete pelvic examination at the time of the periodic health examination for the asymptomatic patient should be a shared decision after a discussion between the patient and her health care provider."
The recent recommendation for dual-energy x-ray absorptiometry scans state that with a normal result, the testing interval may be extended to 15 years.
The traditional "annual exam" must change or office gynecology may run the risk of becoming obsolete.
Epidemiologic data from the Centers for Disease Control & Prevention show that the most common cause of death in women is cardiovascular disease (23.5%), followed by cancer (22.6%). Obesity continues to plague the United States, and is more common in women than in men, and most common in African American women.
In the past, gynecologists have significantly impacted public health through our vigilant use of the Pap smear. Today, we have the opportunity to lead the charge in cardiovascular disease prevention, genetics screenings for cancer risk, lifestyle intervention to begin the fight against obesity, and fulfillment of the mandate to educate reproductive age women about the benefits of long-acting reversible contraception.
Certainly ob.gyns. are adept in the art of obtaining a family history. With the ever-changing opportunities in the expanding world of genetic testing, it is incumbent upon ob.gyns. to guide our at-risk patients to a genetic counselor. Positive outcomes will lead to more vigilant testing, and at best cancer prevention, or at the least, a diagnosis prior to advanced stages. Negative results will limit unnecessary testing and relieve patient anxiety.
We must find novel and effective tools to help our patients begin to wage war on obesity. We may start by listing the body mass index for every patient in every chart, and discussing weight as a health concern, which is no different from how we address hypertension.
Recent data reveal that prematurity, preeclampsia, placental abruption, and gestational diabetes are harbingers of cardiovascular risk. In addition, the Dallas Heart Study found that "women who have two to three live births have a lower rate of subclinical atherosclerosis when compared to women that have either never delivered a live baby or those that have delivered four or more children." These obstetrically derived data place the ob.gyn. in a unique position to identify possible cardiovascular risk potentially years before there is clinical disease. Our patients also should be queried about familial cardiac risk factors such as stroke, myocardial infarction, and early cardiac death (defined as cardiac death in a first-degree male relative younger than 55 years of age or in a first-degree female relative younger than 65 years of age).
We propose that ob.gyns. adopt a hybrid ob.gyn. approach to the algorithm accepted by the American College of Cardiology/American Heart Association Global Cardiovascular Risk Calculator (which can be found in the Apple app store). The calculation is based on race, age, systolic blood pressure, total cholesterol, high-density lipoprotein cholesterol, diabetes, smoking, and current use of blood pressure medication. If your patient is 40 years of age or older and her global score is 7.5% or greater for a cardiovascular event in 10 years, your patient should be considered for aggressive risk factor modification. If the score is less than 7.5% with a family history of cardiovascular disease in the same patient, additional testing should be considered to further risk stratify the patient.
In addition, if the risk assessment shows the score is less than 7.5% and your patient has a personal history of preeclampsia, preterm delivery, placental abruption, gestational diabetes mellitus, polycystic ovarian syndrome, or metabolic syndrome, or a family history of early cardiac death, she should be considered for aggressive risk factor modification in conjunction with management by a medical provider with expertise in cardiovascular disease prevention.
Although the 10-year risk assessment cannot be calculated for women less than 40 years of age, a lifetime cardiovascular risk can be calculated using the app. Thus for women less than 40 years of age with a lifetime cardiovascular risk of greater than 45%, we recommend aggressive risk factor modification. For women less than 40 years of age with a lifetime cardiovascular risk that does not exceed 45%, with a personal history of preeclampsia, preterm delivery, placental abruption, gestational diabetes mellitus, polycystic ovarian syndrome, or metabolic syndrome, or a family history of early cardiac death, aggressive risk factor modification should be considered in conjunction with management by a medical provider with expertise in cardiovascular disease prevention.
Once we assess risk and fully understand the metabolism of our patients, we can educate them about the pathophysiology of vascular disease and its prevention, with a focus on stress management, nutritional prudence, and appropriate exercise.
It is critical that patients understand that they are at risk for a future cardiovascular event and that their risk is real and quantifiable. This represents a paradigm shift not only in gynecologic care but also cardiac care. Too often patients adjust their behavior with their first cardiac event, be that angina or a myocardial infarction. We now have the opportunity to provide our patients the opportunity to modify their lives in their reproductive years, and thus significantly reduce their chance of ever experiencing a cardiac event.
As providers of women’s health, we must evolve to meet the needs of our patients. We have the opportunity to provide early intervention to reduce the most common causes of morbidity and mortality among our patients.
Dr. Jaspan is chairman of the department of obstetrics and gynecology at the Einstein Health Care Network and associate professor of obstetrics and gynecology at Thomas Jefferson University in Philadelphia. Dr. Shipon is cofounder of the Heart Center of Philadelphia at Jefferson and director of cardiovascular rehabilitation at Jefferson University Hospitals and Methodist Hospital in Philadelphia. Dr. Jaspan and Dr. Shipon said they had no relevant financial disclosures.
The time is now to change office gynecologic care.
Scientific advances in cervical surveillance enable women to be screened later in life, less frequently, and more efficiently than ever before. The American Congress of Obstetricians and Gynecologists recommends that screening start at age 21, then continue at 3-year intervals until age 30, if the results are normal. At age 30, cotesting for human papillomavirus enables the screening interval to be extended to 5 years, if the results are normal. Screening endpoints may be reached upon removal of the cervix (if there is no history of cervical intraepithelial neoplasia [CIN] II or greater) or by age 65 (if there is adequate negative screening and no history of CIN II or greater in the past 20 years).
In November 2009, the U.S. Preventive Services Task Force (USPSTF) released the statement that the current evidence is insufficient to assess the additional benefits and harms of the clinical breast exam beyond those of the screening mammogram.
The ACOG Committee Opinion #534, entitled "The Well-Women Visit," was published in August 2012. This document states: "An annual pelvic examination seems logical, but also lacks data to support a specific time frame of frequency of such examinations. The decision whether or not to perform a complete pelvic examination at the time of the periodic health examination for the asymptomatic patient should be a shared decision after a discussion between the patient and her health care provider."
The recent recommendation for dual-energy x-ray absorptiometry scans state that with a normal result, the testing interval may be extended to 15 years.
The traditional "annual exam" must change or office gynecology may run the risk of becoming obsolete.
Epidemiologic data from the Centers for Disease Control & Prevention show that the most common cause of death in women is cardiovascular disease (23.5%), followed by cancer (22.6%). Obesity continues to plague the United States, and is more common in women than in men, and most common in African American women.
In the past, gynecologists have significantly impacted public health through our vigilant use of the Pap smear. Today, we have the opportunity to lead the charge in cardiovascular disease prevention, genetics screenings for cancer risk, lifestyle intervention to begin the fight against obesity, and fulfillment of the mandate to educate reproductive age women about the benefits of long-acting reversible contraception.
Certainly ob.gyns. are adept in the art of obtaining a family history. With the ever-changing opportunities in the expanding world of genetic testing, it is incumbent upon ob.gyns. to guide our at-risk patients to a genetic counselor. Positive outcomes will lead to more vigilant testing, and at best cancer prevention, or at the least, a diagnosis prior to advanced stages. Negative results will limit unnecessary testing and relieve patient anxiety.
We must find novel and effective tools to help our patients begin to wage war on obesity. We may start by listing the body mass index for every patient in every chart, and discussing weight as a health concern, which is no different from how we address hypertension.
Recent data reveal that prematurity, preeclampsia, placental abruption, and gestational diabetes are harbingers of cardiovascular risk. In addition, the Dallas Heart Study found that "women who have two to three live births have a lower rate of subclinical atherosclerosis when compared to women that have either never delivered a live baby or those that have delivered four or more children." These obstetrically derived data place the ob.gyn. in a unique position to identify possible cardiovascular risk potentially years before there is clinical disease. Our patients also should be queried about familial cardiac risk factors such as stroke, myocardial infarction, and early cardiac death (defined as cardiac death in a first-degree male relative younger than 55 years of age or in a first-degree female relative younger than 65 years of age).
We propose that ob.gyns. adopt a hybrid ob.gyn. approach to the algorithm accepted by the American College of Cardiology/American Heart Association Global Cardiovascular Risk Calculator (which can be found in the Apple app store). The calculation is based on race, age, systolic blood pressure, total cholesterol, high-density lipoprotein cholesterol, diabetes, smoking, and current use of blood pressure medication. If your patient is 40 years of age or older and her global score is 7.5% or greater for a cardiovascular event in 10 years, your patient should be considered for aggressive risk factor modification. If the score is less than 7.5% with a family history of cardiovascular disease in the same patient, additional testing should be considered to further risk stratify the patient.
In addition, if the risk assessment shows the score is less than 7.5% and your patient has a personal history of preeclampsia, preterm delivery, placental abruption, gestational diabetes mellitus, polycystic ovarian syndrome, or metabolic syndrome, or a family history of early cardiac death, she should be considered for aggressive risk factor modification in conjunction with management by a medical provider with expertise in cardiovascular disease prevention.
Although the 10-year risk assessment cannot be calculated for women less than 40 years of age, a lifetime cardiovascular risk can be calculated using the app. Thus for women less than 40 years of age with a lifetime cardiovascular risk of greater than 45%, we recommend aggressive risk factor modification. For women less than 40 years of age with a lifetime cardiovascular risk that does not exceed 45%, with a personal history of preeclampsia, preterm delivery, placental abruption, gestational diabetes mellitus, polycystic ovarian syndrome, or metabolic syndrome, or a family history of early cardiac death, aggressive risk factor modification should be considered in conjunction with management by a medical provider with expertise in cardiovascular disease prevention.
Once we assess risk and fully understand the metabolism of our patients, we can educate them about the pathophysiology of vascular disease and its prevention, with a focus on stress management, nutritional prudence, and appropriate exercise.
It is critical that patients understand that they are at risk for a future cardiovascular event and that their risk is real and quantifiable. This represents a paradigm shift not only in gynecologic care but also cardiac care. Too often patients adjust their behavior with their first cardiac event, be that angina or a myocardial infarction. We now have the opportunity to provide our patients the opportunity to modify their lives in their reproductive years, and thus significantly reduce their chance of ever experiencing a cardiac event.
As providers of women’s health, we must evolve to meet the needs of our patients. We have the opportunity to provide early intervention to reduce the most common causes of morbidity and mortality among our patients.
Dr. Jaspan is chairman of the department of obstetrics and gynecology at the Einstein Health Care Network and associate professor of obstetrics and gynecology at Thomas Jefferson University in Philadelphia. Dr. Shipon is cofounder of the Heart Center of Philadelphia at Jefferson and director of cardiovascular rehabilitation at Jefferson University Hospitals and Methodist Hospital in Philadelphia. Dr. Jaspan and Dr. Shipon said they had no relevant financial disclosures.
The time is now to change office gynecologic care.
Scientific advances in cervical surveillance enable women to be screened later in life, less frequently, and more efficiently than ever before. The American Congress of Obstetricians and Gynecologists recommends that screening start at age 21, then continue at 3-year intervals until age 30, if the results are normal. At age 30, cotesting for human papillomavirus enables the screening interval to be extended to 5 years, if the results are normal. Screening endpoints may be reached upon removal of the cervix (if there is no history of cervical intraepithelial neoplasia [CIN] II or greater) or by age 65 (if there is adequate negative screening and no history of CIN II or greater in the past 20 years).
In November 2009, the U.S. Preventive Services Task Force (USPSTF) released the statement that the current evidence is insufficient to assess the additional benefits and harms of the clinical breast exam beyond those of the screening mammogram.
The ACOG Committee Opinion #534, entitled "The Well-Women Visit," was published in August 2012. This document states: "An annual pelvic examination seems logical, but also lacks data to support a specific time frame of frequency of such examinations. The decision whether or not to perform a complete pelvic examination at the time of the periodic health examination for the asymptomatic patient should be a shared decision after a discussion between the patient and her health care provider."
The recent recommendation for dual-energy x-ray absorptiometry scans state that with a normal result, the testing interval may be extended to 15 years.
The traditional "annual exam" must change or office gynecology may run the risk of becoming obsolete.
Epidemiologic data from the Centers for Disease Control & Prevention show that the most common cause of death in women is cardiovascular disease (23.5%), followed by cancer (22.6%). Obesity continues to plague the United States, and is more common in women than in men, and most common in African American women.
In the past, gynecologists have significantly impacted public health through our vigilant use of the Pap smear. Today, we have the opportunity to lead the charge in cardiovascular disease prevention, genetics screenings for cancer risk, lifestyle intervention to begin the fight against obesity, and fulfillment of the mandate to educate reproductive age women about the benefits of long-acting reversible contraception.
Certainly ob.gyns. are adept in the art of obtaining a family history. With the ever-changing opportunities in the expanding world of genetic testing, it is incumbent upon ob.gyns. to guide our at-risk patients to a genetic counselor. Positive outcomes will lead to more vigilant testing, and at best cancer prevention, or at the least, a diagnosis prior to advanced stages. Negative results will limit unnecessary testing and relieve patient anxiety.
We must find novel and effective tools to help our patients begin to wage war on obesity. We may start by listing the body mass index for every patient in every chart, and discussing weight as a health concern, which is no different from how we address hypertension.
Recent data reveal that prematurity, preeclampsia, placental abruption, and gestational diabetes are harbingers of cardiovascular risk. In addition, the Dallas Heart Study found that "women who have two to three live births have a lower rate of subclinical atherosclerosis when compared to women that have either never delivered a live baby or those that have delivered four or more children." These obstetrically derived data place the ob.gyn. in a unique position to identify possible cardiovascular risk potentially years before there is clinical disease. Our patients also should be queried about familial cardiac risk factors such as stroke, myocardial infarction, and early cardiac death (defined as cardiac death in a first-degree male relative younger than 55 years of age or in a first-degree female relative younger than 65 years of age).
We propose that ob.gyns. adopt a hybrid ob.gyn. approach to the algorithm accepted by the American College of Cardiology/American Heart Association Global Cardiovascular Risk Calculator (which can be found in the Apple app store). The calculation is based on race, age, systolic blood pressure, total cholesterol, high-density lipoprotein cholesterol, diabetes, smoking, and current use of blood pressure medication. If your patient is 40 years of age or older and her global score is 7.5% or greater for a cardiovascular event in 10 years, your patient should be considered for aggressive risk factor modification. If the score is less than 7.5% with a family history of cardiovascular disease in the same patient, additional testing should be considered to further risk stratify the patient.
In addition, if the risk assessment shows the score is less than 7.5% and your patient has a personal history of preeclampsia, preterm delivery, placental abruption, gestational diabetes mellitus, polycystic ovarian syndrome, or metabolic syndrome, or a family history of early cardiac death, she should be considered for aggressive risk factor modification in conjunction with management by a medical provider with expertise in cardiovascular disease prevention.
Although the 10-year risk assessment cannot be calculated for women less than 40 years of age, a lifetime cardiovascular risk can be calculated using the app. Thus for women less than 40 years of age with a lifetime cardiovascular risk of greater than 45%, we recommend aggressive risk factor modification. For women less than 40 years of age with a lifetime cardiovascular risk that does not exceed 45%, with a personal history of preeclampsia, preterm delivery, placental abruption, gestational diabetes mellitus, polycystic ovarian syndrome, or metabolic syndrome, or a family history of early cardiac death, aggressive risk factor modification should be considered in conjunction with management by a medical provider with expertise in cardiovascular disease prevention.
Once we assess risk and fully understand the metabolism of our patients, we can educate them about the pathophysiology of vascular disease and its prevention, with a focus on stress management, nutritional prudence, and appropriate exercise.
It is critical that patients understand that they are at risk for a future cardiovascular event and that their risk is real and quantifiable. This represents a paradigm shift not only in gynecologic care but also cardiac care. Too often patients adjust their behavior with their first cardiac event, be that angina or a myocardial infarction. We now have the opportunity to provide our patients the opportunity to modify their lives in their reproductive years, and thus significantly reduce their chance of ever experiencing a cardiac event.
As providers of women’s health, we must evolve to meet the needs of our patients. We have the opportunity to provide early intervention to reduce the most common causes of morbidity and mortality among our patients.
Dr. Jaspan is chairman of the department of obstetrics and gynecology at the Einstein Health Care Network and associate professor of obstetrics and gynecology at Thomas Jefferson University in Philadelphia. Dr. Shipon is cofounder of the Heart Center of Philadelphia at Jefferson and director of cardiovascular rehabilitation at Jefferson University Hospitals and Methodist Hospital in Philadelphia. Dr. Jaspan and Dr. Shipon said they had no relevant financial disclosures.
