User login
Emotional eating tied to risk of diastolic dysfunction
Eating in response to stress – known as emotional eating – was significantly associated with several markers of long-term cardiovascular damage, based on data from 1,109 individuals.
“We know diet plays a huge role in cardiovascular disease, but we have focused a lot of work on what you eat, not on what makes you eat” – the current study did exactly that, Martha Gulati, MD, who wasn’t involved in the study, said in an interview.

“Emotional eaters consume food to satisfy their brains rather than their stomachs,” study investigator Nicolas Girerd, MD, of the National Institute of Health and Medical Research (INSERM) and a cardiologist at the University Hospital of Nancy (France), wrote in a press release accompanying the study.
Diet plays a role in the development of cardiovascular disease (CVD), but the impact of eating behavior on long-term cardiovascular health remains unclear, wrote Dr. Girerd and colleagues. Previous research has yielded three common psychological dimensions for eating behavior: emotional eating, restrained eating, and external eating.
Both emotional eating and restrained eating have been linked to cardiovascular disease risk, the researchers noted. “Because of previous findings, we hypothesized that [emotional and/or restrained dimensions of eating behavior] are positively associated with cardiovascular damages, as well as with CV risk factors, such as metabolic syndrome,” they wrote.
In a study published in the European Journal of Preventive Cardiology, the researchers reviewed data from 916 adults and 193 adolescents who were participants in the STANISLAS (Suivi Temporaire Annuel Non-Invasif de la Santé des Lorrains Assurés Sociaux), a longitudinal familial cohort in France. Cardiovascular data were collected at four medical visits as part of a full clinical examination between 1993 and 2016, with one visit every 5-10 years. Roughly one-third (31.0%) of the adults were overweight, 7.9% were obese, and 2.7% were underweight. The median age of the adults at the second visit was 44.7 years; the median age of the adolescent group was 15.2 years.
The primary outcome of cardiovascular damage was measured at the fourth visit. Eating behavior was assessed during the second visit using the Dutch Eating Behaviour Questionnaire (DEBQ), and participants were identified as emotional eaters, restrained eaters, or external eaters.
Among the adults, emotional eating was associated with a 38% increased risk of diastolic dysfunction (odds ratio, 1.38; P = .02), over an average follow-up of 13 years, and this association was mediated by stress in 32% of cases. Emotional eating also was positively linked with a higher carotid-femoral pulse-wave velocity (cfPWV-beta), indicative of increased arterial stiffness. However, none of the three dimensions of eating behavior was associated with cardiovascular damage among the adolescents. In addition, none of the eating-behavior dimensions was tied to metabolic syndrome in the adult group (this association was not measured in the adolescents).
Energy intake had no apparent impact on any associations between eating behavior and CVD measures, Dr. Girerd said in the press release. “We might expect that emotional eaters would consume high-calorie foods, which would in turn lead to cardiovascular problems, but this was not the case. One explanation is that we measured average calorie intake and emotional eaters may binge when stressed and then eat less at other times,” and that the resulting “yo-yo” pattern might negatively affect the heart and blood vessels more than stable food intake, he said.
The study findings were limited by several factors, including the observational design that prevented conclusions of causality, the researchers noted. Other limitations included the use of a nonvalidated scale to measure stress, the lack of data on physical activity, and the use of a mainly healthy population in a limited geographic area, which may limit generalizability, they said.
More research is needed in other contexts and larger cohorts, but the results were strengthened by the large study population and the complete data on eating behaviors and detailed health information, they wrote. The results support previous studies and suggest that patients with emotional eating behavior could benefit from emotion regulation skills training, including cognitive, behavioral, psychological, and interpersonal therapies used in other areas, and from pharmacological treatments, the researchers concluded.
The current study offers a unique and important perspective on the relationship between diet and cardiovascular disease, Dr. Gulati, director of preventive cardiology at the Smidt Heart Institute at Cedars-Sinai Medical Center, Los Angeles, told this news organization.
“Examining eating behavior and its relationship with cardiovascular effects in healthy individuals in this prospective way is quite interesting,” said Dr. Gulati, who was not involved in the study.
The researchers examined healthy people at baseline, inquired about their eating habits, and found that emotional eaters “have evidence of cardiovascular changes when compared with the other groups of eaters, after controlling for other risk factors that are associated with cardiovascular disease when following them for 13 years,” said Dr. Gulati, who was recently named Anita Dann Friedman Endowed Chair in Women’s Cardiovascular Medicine and Research at Cedars-Sinai. “This same finding wasn’t seen in adolescents, but this is probably because they are younger, and the effects aren’t seen. That is reassuring, because it means that the more we address eating behaviors, the more likely we are to reduce their effects to the heart,” she noted.
“This study is important because usually, as cardiologists or anyone in medicine, how we assess diet is by assessment of what food people eat; we don’t usually ask about what triggers them to eat,” Dr. Gulati said. “Eating behaviors based on their triggers ultimately affect food choice and food quantity, and help us understand weight changes during a lifetime,” she said.
“I think we don’t have the data to know that an eating behavior would be able to affect cardiac function,” said Dr. Gulati, “but I think we all might hypothesize that emotional eating may be associated with abnormal diastolic function simply through eating high-density food and weight gain.”
The current study did not show a relationship between eating behavior and metabolic syndrome, in contrast with prior studies, Dr. Gulati noted. However, “the authors report that the association between eating behaviors and diastolic dysfunction was mediated through the stress level,” Dr. Gulati said. “It is important to note that this European population was healthy at baseline, and also relatively healthy 13 years later, which makes these findings even more profound.”
Dr. Gulati said that she agrees with the study authors on the need to assess diet and eating behaviors when assessing cardiovascular risk in patient. “Diet assessment as part of prevention is central, but we should ask not only ‘what do you eat,’ but also ‘what makes you eat,’ ” she said.
More research is needed in other populations, Dr. Gulati added. The current study population was healthy at baseline and follow-up. Studies are needed in cohorts in the United States and in the developing world to see how the results might differ; as well as in rural America or in “food deserts” where food choices are limited.
Another research topic is the interplay between eating behaviors and social determinants of health, in terms of their effect on cardiovascular function, Dr. Gulati said, “and it will be valuable to follow this cohort further to see how these eating behaviors and these intermediate measures translate into cardiovascular outcomes.” Future studies should also examine whether the changes in cardiac function are reversible by interventions to modify eating behavior, particularly emotional eating, she said.
Supporters of the study included the Regional University Hospital Center of Nancy, the French Ministry of Solidarity and Health, and a public grant overseen by the French National Research Agency. The researchers had no financial conflicts to disclose.
Dr. Gulati, who serves on the editorial advisory board of MDedge Cardiology, had no financial conflicts to disclose.
Eating in response to stress – known as emotional eating – was significantly associated with several markers of long-term cardiovascular damage, based on data from 1,109 individuals.
“We know diet plays a huge role in cardiovascular disease, but we have focused a lot of work on what you eat, not on what makes you eat” – the current study did exactly that, Martha Gulati, MD, who wasn’t involved in the study, said in an interview.
“Emotional eaters consume food to satisfy their brains rather than their stomachs,” study investigator Nicolas Girerd, MD, of the National Institute of Health and Medical Research (INSERM) and a cardiologist at the University Hospital of Nancy (France), wrote in a press release accompanying the study.
Diet plays a role in the development of cardiovascular disease (CVD), but the impact of eating behavior on long-term cardiovascular health remains unclear, wrote Dr. Girerd and colleagues. Previous research has yielded three common psychological dimensions for eating behavior: emotional eating, restrained eating, and external eating.
Both emotional eating and restrained eating have been linked to cardiovascular disease risk, the researchers noted. “Because of previous findings, we hypothesized that [emotional and/or restrained dimensions of eating behavior] are positively associated with cardiovascular damages, as well as with CV risk factors, such as metabolic syndrome,” they wrote.
In a study published in the European Journal of Preventive Cardiology, the researchers reviewed data from 916 adults and 193 adolescents who were participants in the STANISLAS (Suivi Temporaire Annuel Non-Invasif de la Santé des Lorrains Assurés Sociaux), a longitudinal familial cohort in France. Cardiovascular data were collected at four medical visits as part of a full clinical examination between 1993 and 2016, with one visit every 5-10 years. Roughly one-third (31.0%) of the adults were overweight, 7.9% were obese, and 2.7% were underweight. The median age of the adults at the second visit was 44.7 years; the median age of the adolescent group was 15.2 years.
The primary outcome of cardiovascular damage was measured at the fourth visit. Eating behavior was assessed during the second visit using the Dutch Eating Behaviour Questionnaire (DEBQ), and participants were identified as emotional eaters, restrained eaters, or external eaters.
Among the adults, emotional eating was associated with a 38% increased risk of diastolic dysfunction (odds ratio, 1.38; P = .02), over an average follow-up of 13 years, and this association was mediated by stress in 32% of cases. Emotional eating also was positively linked with a higher carotid-femoral pulse-wave velocity (cfPWV-beta), indicative of increased arterial stiffness. However, none of the three dimensions of eating behavior was associated with cardiovascular damage among the adolescents. In addition, none of the eating-behavior dimensions was tied to metabolic syndrome in the adult group (this association was not measured in the adolescents).
Energy intake had no apparent impact on any associations between eating behavior and CVD measures, Dr. Girerd said in the press release. “We might expect that emotional eaters would consume high-calorie foods, which would in turn lead to cardiovascular problems, but this was not the case. One explanation is that we measured average calorie intake and emotional eaters may binge when stressed and then eat less at other times,” and that the resulting “yo-yo” pattern might negatively affect the heart and blood vessels more than stable food intake, he said.
The study findings were limited by several factors, including the observational design that prevented conclusions of causality, the researchers noted. Other limitations included the use of a nonvalidated scale to measure stress, the lack of data on physical activity, and the use of a mainly healthy population in a limited geographic area, which may limit generalizability, they said.
More research is needed in other contexts and larger cohorts, but the results were strengthened by the large study population and the complete data on eating behaviors and detailed health information, they wrote. The results support previous studies and suggest that patients with emotional eating behavior could benefit from emotion regulation skills training, including cognitive, behavioral, psychological, and interpersonal therapies used in other areas, and from pharmacological treatments, the researchers concluded.
The current study offers a unique and important perspective on the relationship between diet and cardiovascular disease, Dr. Gulati, director of preventive cardiology at the Smidt Heart Institute at Cedars-Sinai Medical Center, Los Angeles, told this news organization.
“Examining eating behavior and its relationship with cardiovascular effects in healthy individuals in this prospective way is quite interesting,” said Dr. Gulati, who was not involved in the study.
The researchers examined healthy people at baseline, inquired about their eating habits, and found that emotional eaters “have evidence of cardiovascular changes when compared with the other groups of eaters, after controlling for other risk factors that are associated with cardiovascular disease when following them for 13 years,” said Dr. Gulati, who was recently named Anita Dann Friedman Endowed Chair in Women’s Cardiovascular Medicine and Research at Cedars-Sinai. “This same finding wasn’t seen in adolescents, but this is probably because they are younger, and the effects aren’t seen. That is reassuring, because it means that the more we address eating behaviors, the more likely we are to reduce their effects to the heart,” she noted.
“This study is important because usually, as cardiologists or anyone in medicine, how we assess diet is by assessment of what food people eat; we don’t usually ask about what triggers them to eat,” Dr. Gulati said. “Eating behaviors based on their triggers ultimately affect food choice and food quantity, and help us understand weight changes during a lifetime,” she said.
“I think we don’t have the data to know that an eating behavior would be able to affect cardiac function,” said Dr. Gulati, “but I think we all might hypothesize that emotional eating may be associated with abnormal diastolic function simply through eating high-density food and weight gain.”
The current study did not show a relationship between eating behavior and metabolic syndrome, in contrast with prior studies, Dr. Gulati noted. However, “the authors report that the association between eating behaviors and diastolic dysfunction was mediated through the stress level,” Dr. Gulati said. “It is important to note that this European population was healthy at baseline, and also relatively healthy 13 years later, which makes these findings even more profound.”
Dr. Gulati said that she agrees with the study authors on the need to assess diet and eating behaviors when assessing cardiovascular risk in patient. “Diet assessment as part of prevention is central, but we should ask not only ‘what do you eat,’ but also ‘what makes you eat,’ ” she said.
More research is needed in other populations, Dr. Gulati added. The current study population was healthy at baseline and follow-up. Studies are needed in cohorts in the United States and in the developing world to see how the results might differ; as well as in rural America or in “food deserts” where food choices are limited.
Another research topic is the interplay between eating behaviors and social determinants of health, in terms of their effect on cardiovascular function, Dr. Gulati said, “and it will be valuable to follow this cohort further to see how these eating behaviors and these intermediate measures translate into cardiovascular outcomes.” Future studies should also examine whether the changes in cardiac function are reversible by interventions to modify eating behavior, particularly emotional eating, she said.
Supporters of the study included the Regional University Hospital Center of Nancy, the French Ministry of Solidarity and Health, and a public grant overseen by the French National Research Agency. The researchers had no financial conflicts to disclose.
Dr. Gulati, who serves on the editorial advisory board of MDedge Cardiology, had no financial conflicts to disclose.
Eating in response to stress – known as emotional eating – was significantly associated with several markers of long-term cardiovascular damage, based on data from 1,109 individuals.
“We know diet plays a huge role in cardiovascular disease, but we have focused a lot of work on what you eat, not on what makes you eat” – the current study did exactly that, Martha Gulati, MD, who wasn’t involved in the study, said in an interview.
“Emotional eaters consume food to satisfy their brains rather than their stomachs,” study investigator Nicolas Girerd, MD, of the National Institute of Health and Medical Research (INSERM) and a cardiologist at the University Hospital of Nancy (France), wrote in a press release accompanying the study.
Diet plays a role in the development of cardiovascular disease (CVD), but the impact of eating behavior on long-term cardiovascular health remains unclear, wrote Dr. Girerd and colleagues. Previous research has yielded three common psychological dimensions for eating behavior: emotional eating, restrained eating, and external eating.
Both emotional eating and restrained eating have been linked to cardiovascular disease risk, the researchers noted. “Because of previous findings, we hypothesized that [emotional and/or restrained dimensions of eating behavior] are positively associated with cardiovascular damages, as well as with CV risk factors, such as metabolic syndrome,” they wrote.
In a study published in the European Journal of Preventive Cardiology, the researchers reviewed data from 916 adults and 193 adolescents who were participants in the STANISLAS (Suivi Temporaire Annuel Non-Invasif de la Santé des Lorrains Assurés Sociaux), a longitudinal familial cohort in France. Cardiovascular data were collected at four medical visits as part of a full clinical examination between 1993 and 2016, with one visit every 5-10 years. Roughly one-third (31.0%) of the adults were overweight, 7.9% were obese, and 2.7% were underweight. The median age of the adults at the second visit was 44.7 years; the median age of the adolescent group was 15.2 years.
The primary outcome of cardiovascular damage was measured at the fourth visit. Eating behavior was assessed during the second visit using the Dutch Eating Behaviour Questionnaire (DEBQ), and participants were identified as emotional eaters, restrained eaters, or external eaters.
Among the adults, emotional eating was associated with a 38% increased risk of diastolic dysfunction (odds ratio, 1.38; P = .02), over an average follow-up of 13 years, and this association was mediated by stress in 32% of cases. Emotional eating also was positively linked with a higher carotid-femoral pulse-wave velocity (cfPWV-beta), indicative of increased arterial stiffness. However, none of the three dimensions of eating behavior was associated with cardiovascular damage among the adolescents. In addition, none of the eating-behavior dimensions was tied to metabolic syndrome in the adult group (this association was not measured in the adolescents).
Energy intake had no apparent impact on any associations between eating behavior and CVD measures, Dr. Girerd said in the press release. “We might expect that emotional eaters would consume high-calorie foods, which would in turn lead to cardiovascular problems, but this was not the case. One explanation is that we measured average calorie intake and emotional eaters may binge when stressed and then eat less at other times,” and that the resulting “yo-yo” pattern might negatively affect the heart and blood vessels more than stable food intake, he said.
The study findings were limited by several factors, including the observational design that prevented conclusions of causality, the researchers noted. Other limitations included the use of a nonvalidated scale to measure stress, the lack of data on physical activity, and the use of a mainly healthy population in a limited geographic area, which may limit generalizability, they said.
More research is needed in other contexts and larger cohorts, but the results were strengthened by the large study population and the complete data on eating behaviors and detailed health information, they wrote. The results support previous studies and suggest that patients with emotional eating behavior could benefit from emotion regulation skills training, including cognitive, behavioral, psychological, and interpersonal therapies used in other areas, and from pharmacological treatments, the researchers concluded.
The current study offers a unique and important perspective on the relationship between diet and cardiovascular disease, Dr. Gulati, director of preventive cardiology at the Smidt Heart Institute at Cedars-Sinai Medical Center, Los Angeles, told this news organization.
“Examining eating behavior and its relationship with cardiovascular effects in healthy individuals in this prospective way is quite interesting,” said Dr. Gulati, who was not involved in the study.
The researchers examined healthy people at baseline, inquired about their eating habits, and found that emotional eaters “have evidence of cardiovascular changes when compared with the other groups of eaters, after controlling for other risk factors that are associated with cardiovascular disease when following them for 13 years,” said Dr. Gulati, who was recently named Anita Dann Friedman Endowed Chair in Women’s Cardiovascular Medicine and Research at Cedars-Sinai. “This same finding wasn’t seen in adolescents, but this is probably because they are younger, and the effects aren’t seen. That is reassuring, because it means that the more we address eating behaviors, the more likely we are to reduce their effects to the heart,” she noted.
“This study is important because usually, as cardiologists or anyone in medicine, how we assess diet is by assessment of what food people eat; we don’t usually ask about what triggers them to eat,” Dr. Gulati said. “Eating behaviors based on their triggers ultimately affect food choice and food quantity, and help us understand weight changes during a lifetime,” she said.
“I think we don’t have the data to know that an eating behavior would be able to affect cardiac function,” said Dr. Gulati, “but I think we all might hypothesize that emotional eating may be associated with abnormal diastolic function simply through eating high-density food and weight gain.”
The current study did not show a relationship between eating behavior and metabolic syndrome, in contrast with prior studies, Dr. Gulati noted. However, “the authors report that the association between eating behaviors and diastolic dysfunction was mediated through the stress level,” Dr. Gulati said. “It is important to note that this European population was healthy at baseline, and also relatively healthy 13 years later, which makes these findings even more profound.”
Dr. Gulati said that she agrees with the study authors on the need to assess diet and eating behaviors when assessing cardiovascular risk in patient. “Diet assessment as part of prevention is central, but we should ask not only ‘what do you eat,’ but also ‘what makes you eat,’ ” she said.
More research is needed in other populations, Dr. Gulati added. The current study population was healthy at baseline and follow-up. Studies are needed in cohorts in the United States and in the developing world to see how the results might differ; as well as in rural America or in “food deserts” where food choices are limited.
Another research topic is the interplay between eating behaviors and social determinants of health, in terms of their effect on cardiovascular function, Dr. Gulati said, “and it will be valuable to follow this cohort further to see how these eating behaviors and these intermediate measures translate into cardiovascular outcomes.” Future studies should also examine whether the changes in cardiac function are reversible by interventions to modify eating behavior, particularly emotional eating, she said.
Supporters of the study included the Regional University Hospital Center of Nancy, the French Ministry of Solidarity and Health, and a public grant overseen by the French National Research Agency. The researchers had no financial conflicts to disclose.
Dr. Gulati, who serves on the editorial advisory board of MDedge Cardiology, had no financial conflicts to disclose.
FROM THE EUROPEAN JOURNAL OF PREVENTIVE CARDIOLOGY
Will your smartphone be the next doctor’s office?
A fingertip pressed against a phone’s camera lens can measure a heart rate. The microphone, kept by the bedside, can screen for sleep apnea. Even the speaker is being tapped, to monitor breathing using sonar technology.
In the best of this new world, the data is conveyed remotely to a medical professional for the convenience and comfort of the patient or, in some cases, to support a clinician without the need for costly hardware.
But using smartphones as diagnostic tools is a work in progress, experts say. Although doctors and their patients have found some real-world success in deploying the phone as a medical device, the overall potential remains unfulfilled and uncertain.
Smartphones come packed with sensors capable of monitoring a patient’s vital signs. They can help assess people for concussions, watch for atrial fibrillation, and conduct mental health wellness checks, to name the uses of a few nascent applications.
Companies and researchers eager to find medical applications for smartphone technology are tapping into modern phones’ built-in cameras and light sensors; microphones; accelerometers, which detect body movements; gyroscopes; and even speakers. The apps then use artificial intelligence software to analyze the collected sights and sounds to create an easy connection between patients and physicians. Earning potential and marketability are evidenced by the more than 350,000 digital health products available in app stores, according to a Grand View Research report.
“It’s very hard to put devices into the patient home or in the hospital, but everybody is just walking around with a cellphone that has a network connection,” said Dr. Andrew Gostine, CEO of the sensor network company Artisight. Most Americans own a smartphone, including more than 60% of people 65 and over, an increase from just 13% a decade ago, according the Pew Research Center. The COVID-19 pandemic has also pushed people to become more comfortable with virtual care.
Some of these products have sought FDA clearance to be marketed as a medical device. That way, if patients must pay to use the software, health insurers are more likely to cover at least part of the cost. Other products are designated as exempt from this regulatory process, placed in the same clinical classification as a Band-Aid. But how the agency handles AI and machine learning–based medical devices is still being adjusted to reflect software’s adaptive nature.
Ensuring accuracy and clinical validation is crucial to securing buy-in from health care providers. And many tools still need fine-tuning, said Eugene Yang, MD, a professor of medicine at the University of Washington, Seattle. Currently, Dr. Yang is testing contactless measurement of blood pressure, heart rate, and oxygen saturation gleaned remotely via Zoom camera footage of a patient’s face.
Judging these new technologies is difficult because they rely on algorithms built by machine learning and artificial intelligence to collect data, rather than the physical tools typically used in hospitals. So researchers cannot “compare apples to apples” with medical industry standards, Dr. Yang said. Failure to build in such assurances undermines the technology’s ultimate goals of easing costs and access because a doctor still must verify results.
“False positives and false negatives lead to more testing and more cost to the health care system,” he said.
Big tech companies like Google have heavily invested in researching this kind of technology, catering to clinicians and in-home caregivers, as well as consumers. Currently, in the Google Fit app, users can check their heart rate by placing their finger on the rear-facing camera lens or track their breathing rate using the front-facing camera.
“If you took the sensor out of the phone and out of a clinical device, they are probably the same thing,” said Shwetak Patel, director of health technologies at Google and a professor of electrical and computer engineering at the University of Washington.
Google’s research uses machine learning and computer vision, a field within AI based on information from visual inputs like videos or images. So instead of using a blood pressure cuff, for example, the algorithm can interpret slight visual changes to the body that serve as proxies and biosignals for a patient’s blood pressure, Mr. Patel said.
Google is also investigating the effectiveness of the built-in microphone for detecting heartbeats and murmurs and using the camera to preserve eyesight by screening for diabetic eye disease, according to information the company published last year.
The tech giant recently purchased Sound Life Sciences, a Seattle startup with an FDA-cleared sonar technology app. It uses a smart device’s speaker to bounce inaudible pulses off a patient’s body to identify movement and monitor breathing.
Binah.ai, based in Israel, is another company using the smartphone camera to calculate vital signs. Its software looks at the region around the eyes, where the skin is a bit thinner, and analyzes the light reflecting off blood vessels back to the lens. The company is wrapping up a U.S. clinical trial and marketing its wellness app directly to insurers and other health companies, said company spokesperson Mona Popilian-Yona.
The applications even reach into disciplines such as optometry and mental health:
- With the microphone, Canary Speech uses the same underlying technology as Amazon’s Alexa to analyze patients’ voices for mental health conditions. The software can integrate with telemedicine appointments and allow clinicians to screen for anxiety and depression using a library of vocal biomarkers and predictive analytics, said Henry O’Connell, the company’s CEO.
- Australia-based ResApp Health last year for its iPhone app that screens for moderate to severe obstructive sleep apnea by listening to breathing and snoring. SleepCheckRx, which will require a prescription, is minimally invasive compared with sleep studies currently used to diagnose sleep apnea. Those can cost thousands of dollars and require an array of tests.
- Brightlamp’s Reflex app is a clinical decision support tool for helping manage concussions and vision rehabilitation, among other things. Using an iPad’s or iPhone’s camera, the mobile app measures how a person’s pupils react to changes in light. Through machine learning analysis, the imagery gives practitioners data points for evaluating patients. Brightlamp sells directly to health care providers and is being used in more than 230 clinics. Clinicians pay a $400 standard annual fee per account, which is currently not covered by insurance. The Department of Defense has an ongoing clinical trial using Reflex.
In some cases, such as with the Reflex app, the data is processed directly on the phone – rather than in the cloud, Brightlamp CEO Kurtis Sluss said. By processing everything on the device, the app avoids running into privacy issues, as streaming data elsewhere requires patient consent.
But algorithms need to be trained and tested by collecting reams of data, and that is an ongoing process.
Researchers, for example, have found that some computer vision applications, like heart rate or blood pressure monitoring, can be less accurate for darker skin. Studies are underway to find better solutions.
Small algorithm glitches can also produce false alarms and frighten patients enough to keep widespread adoption out of reach. For example, Apple’s new car-crash detection feature, available on both the latest iPhone and Apple Watch, was set off when people were riding roller coasters and automatically dialed 911.
“We’re not there yet,” Dr. Yang said. “That’s the bottom line.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
A fingertip pressed against a phone’s camera lens can measure a heart rate. The microphone, kept by the bedside, can screen for sleep apnea. Even the speaker is being tapped, to monitor breathing using sonar technology.
In the best of this new world, the data is conveyed remotely to a medical professional for the convenience and comfort of the patient or, in some cases, to support a clinician without the need for costly hardware.
But using smartphones as diagnostic tools is a work in progress, experts say. Although doctors and their patients have found some real-world success in deploying the phone as a medical device, the overall potential remains unfulfilled and uncertain.
Smartphones come packed with sensors capable of monitoring a patient’s vital signs. They can help assess people for concussions, watch for atrial fibrillation, and conduct mental health wellness checks, to name the uses of a few nascent applications.
Companies and researchers eager to find medical applications for smartphone technology are tapping into modern phones’ built-in cameras and light sensors; microphones; accelerometers, which detect body movements; gyroscopes; and even speakers. The apps then use artificial intelligence software to analyze the collected sights and sounds to create an easy connection between patients and physicians. Earning potential and marketability are evidenced by the more than 350,000 digital health products available in app stores, according to a Grand View Research report.
“It’s very hard to put devices into the patient home or in the hospital, but everybody is just walking around with a cellphone that has a network connection,” said Dr. Andrew Gostine, CEO of the sensor network company Artisight. Most Americans own a smartphone, including more than 60% of people 65 and over, an increase from just 13% a decade ago, according the Pew Research Center. The COVID-19 pandemic has also pushed people to become more comfortable with virtual care.
Some of these products have sought FDA clearance to be marketed as a medical device. That way, if patients must pay to use the software, health insurers are more likely to cover at least part of the cost. Other products are designated as exempt from this regulatory process, placed in the same clinical classification as a Band-Aid. But how the agency handles AI and machine learning–based medical devices is still being adjusted to reflect software’s adaptive nature.
Ensuring accuracy and clinical validation is crucial to securing buy-in from health care providers. And many tools still need fine-tuning, said Eugene Yang, MD, a professor of medicine at the University of Washington, Seattle. Currently, Dr. Yang is testing contactless measurement of blood pressure, heart rate, and oxygen saturation gleaned remotely via Zoom camera footage of a patient’s face.
Judging these new technologies is difficult because they rely on algorithms built by machine learning and artificial intelligence to collect data, rather than the physical tools typically used in hospitals. So researchers cannot “compare apples to apples” with medical industry standards, Dr. Yang said. Failure to build in such assurances undermines the technology’s ultimate goals of easing costs and access because a doctor still must verify results.
“False positives and false negatives lead to more testing and more cost to the health care system,” he said.
Big tech companies like Google have heavily invested in researching this kind of technology, catering to clinicians and in-home caregivers, as well as consumers. Currently, in the Google Fit app, users can check their heart rate by placing their finger on the rear-facing camera lens or track their breathing rate using the front-facing camera.
“If you took the sensor out of the phone and out of a clinical device, they are probably the same thing,” said Shwetak Patel, director of health technologies at Google and a professor of electrical and computer engineering at the University of Washington.
Google’s research uses machine learning and computer vision, a field within AI based on information from visual inputs like videos or images. So instead of using a blood pressure cuff, for example, the algorithm can interpret slight visual changes to the body that serve as proxies and biosignals for a patient’s blood pressure, Mr. Patel said.
Google is also investigating the effectiveness of the built-in microphone for detecting heartbeats and murmurs and using the camera to preserve eyesight by screening for diabetic eye disease, according to information the company published last year.
The tech giant recently purchased Sound Life Sciences, a Seattle startup with an FDA-cleared sonar technology app. It uses a smart device’s speaker to bounce inaudible pulses off a patient’s body to identify movement and monitor breathing.
Binah.ai, based in Israel, is another company using the smartphone camera to calculate vital signs. Its software looks at the region around the eyes, where the skin is a bit thinner, and analyzes the light reflecting off blood vessels back to the lens. The company is wrapping up a U.S. clinical trial and marketing its wellness app directly to insurers and other health companies, said company spokesperson Mona Popilian-Yona.
The applications even reach into disciplines such as optometry and mental health:
- With the microphone, Canary Speech uses the same underlying technology as Amazon’s Alexa to analyze patients’ voices for mental health conditions. The software can integrate with telemedicine appointments and allow clinicians to screen for anxiety and depression using a library of vocal biomarkers and predictive analytics, said Henry O’Connell, the company’s CEO.
- Australia-based ResApp Health last year for its iPhone app that screens for moderate to severe obstructive sleep apnea by listening to breathing and snoring. SleepCheckRx, which will require a prescription, is minimally invasive compared with sleep studies currently used to diagnose sleep apnea. Those can cost thousands of dollars and require an array of tests.
- Brightlamp’s Reflex app is a clinical decision support tool for helping manage concussions and vision rehabilitation, among other things. Using an iPad’s or iPhone’s camera, the mobile app measures how a person’s pupils react to changes in light. Through machine learning analysis, the imagery gives practitioners data points for evaluating patients. Brightlamp sells directly to health care providers and is being used in more than 230 clinics. Clinicians pay a $400 standard annual fee per account, which is currently not covered by insurance. The Department of Defense has an ongoing clinical trial using Reflex.
In some cases, such as with the Reflex app, the data is processed directly on the phone – rather than in the cloud, Brightlamp CEO Kurtis Sluss said. By processing everything on the device, the app avoids running into privacy issues, as streaming data elsewhere requires patient consent.
But algorithms need to be trained and tested by collecting reams of data, and that is an ongoing process.
Researchers, for example, have found that some computer vision applications, like heart rate or blood pressure monitoring, can be less accurate for darker skin. Studies are underway to find better solutions.
Small algorithm glitches can also produce false alarms and frighten patients enough to keep widespread adoption out of reach. For example, Apple’s new car-crash detection feature, available on both the latest iPhone and Apple Watch, was set off when people were riding roller coasters and automatically dialed 911.
“We’re not there yet,” Dr. Yang said. “That’s the bottom line.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
A fingertip pressed against a phone’s camera lens can measure a heart rate. The microphone, kept by the bedside, can screen for sleep apnea. Even the speaker is being tapped, to monitor breathing using sonar technology.
In the best of this new world, the data is conveyed remotely to a medical professional for the convenience and comfort of the patient or, in some cases, to support a clinician without the need for costly hardware.
But using smartphones as diagnostic tools is a work in progress, experts say. Although doctors and their patients have found some real-world success in deploying the phone as a medical device, the overall potential remains unfulfilled and uncertain.
Smartphones come packed with sensors capable of monitoring a patient’s vital signs. They can help assess people for concussions, watch for atrial fibrillation, and conduct mental health wellness checks, to name the uses of a few nascent applications.
Companies and researchers eager to find medical applications for smartphone technology are tapping into modern phones’ built-in cameras and light sensors; microphones; accelerometers, which detect body movements; gyroscopes; and even speakers. The apps then use artificial intelligence software to analyze the collected sights and sounds to create an easy connection between patients and physicians. Earning potential and marketability are evidenced by the more than 350,000 digital health products available in app stores, according to a Grand View Research report.
“It’s very hard to put devices into the patient home or in the hospital, but everybody is just walking around with a cellphone that has a network connection,” said Dr. Andrew Gostine, CEO of the sensor network company Artisight. Most Americans own a smartphone, including more than 60% of people 65 and over, an increase from just 13% a decade ago, according the Pew Research Center. The COVID-19 pandemic has also pushed people to become more comfortable with virtual care.
Some of these products have sought FDA clearance to be marketed as a medical device. That way, if patients must pay to use the software, health insurers are more likely to cover at least part of the cost. Other products are designated as exempt from this regulatory process, placed in the same clinical classification as a Band-Aid. But how the agency handles AI and machine learning–based medical devices is still being adjusted to reflect software’s adaptive nature.
Ensuring accuracy and clinical validation is crucial to securing buy-in from health care providers. And many tools still need fine-tuning, said Eugene Yang, MD, a professor of medicine at the University of Washington, Seattle. Currently, Dr. Yang is testing contactless measurement of blood pressure, heart rate, and oxygen saturation gleaned remotely via Zoom camera footage of a patient’s face.
Judging these new technologies is difficult because they rely on algorithms built by machine learning and artificial intelligence to collect data, rather than the physical tools typically used in hospitals. So researchers cannot “compare apples to apples” with medical industry standards, Dr. Yang said. Failure to build in such assurances undermines the technology’s ultimate goals of easing costs and access because a doctor still must verify results.
“False positives and false negatives lead to more testing and more cost to the health care system,” he said.
Big tech companies like Google have heavily invested in researching this kind of technology, catering to clinicians and in-home caregivers, as well as consumers. Currently, in the Google Fit app, users can check their heart rate by placing their finger on the rear-facing camera lens or track their breathing rate using the front-facing camera.
“If you took the sensor out of the phone and out of a clinical device, they are probably the same thing,” said Shwetak Patel, director of health technologies at Google and a professor of electrical and computer engineering at the University of Washington.
Google’s research uses machine learning and computer vision, a field within AI based on information from visual inputs like videos or images. So instead of using a blood pressure cuff, for example, the algorithm can interpret slight visual changes to the body that serve as proxies and biosignals for a patient’s blood pressure, Mr. Patel said.
Google is also investigating the effectiveness of the built-in microphone for detecting heartbeats and murmurs and using the camera to preserve eyesight by screening for diabetic eye disease, according to information the company published last year.
The tech giant recently purchased Sound Life Sciences, a Seattle startup with an FDA-cleared sonar technology app. It uses a smart device’s speaker to bounce inaudible pulses off a patient’s body to identify movement and monitor breathing.
Binah.ai, based in Israel, is another company using the smartphone camera to calculate vital signs. Its software looks at the region around the eyes, where the skin is a bit thinner, and analyzes the light reflecting off blood vessels back to the lens. The company is wrapping up a U.S. clinical trial and marketing its wellness app directly to insurers and other health companies, said company spokesperson Mona Popilian-Yona.
The applications even reach into disciplines such as optometry and mental health:
- With the microphone, Canary Speech uses the same underlying technology as Amazon’s Alexa to analyze patients’ voices for mental health conditions. The software can integrate with telemedicine appointments and allow clinicians to screen for anxiety and depression using a library of vocal biomarkers and predictive analytics, said Henry O’Connell, the company’s CEO.
- Australia-based ResApp Health last year for its iPhone app that screens for moderate to severe obstructive sleep apnea by listening to breathing and snoring. SleepCheckRx, which will require a prescription, is minimally invasive compared with sleep studies currently used to diagnose sleep apnea. Those can cost thousands of dollars and require an array of tests.
- Brightlamp’s Reflex app is a clinical decision support tool for helping manage concussions and vision rehabilitation, among other things. Using an iPad’s or iPhone’s camera, the mobile app measures how a person’s pupils react to changes in light. Through machine learning analysis, the imagery gives practitioners data points for evaluating patients. Brightlamp sells directly to health care providers and is being used in more than 230 clinics. Clinicians pay a $400 standard annual fee per account, which is currently not covered by insurance. The Department of Defense has an ongoing clinical trial using Reflex.
In some cases, such as with the Reflex app, the data is processed directly on the phone – rather than in the cloud, Brightlamp CEO Kurtis Sluss said. By processing everything on the device, the app avoids running into privacy issues, as streaming data elsewhere requires patient consent.
But algorithms need to be trained and tested by collecting reams of data, and that is an ongoing process.
Researchers, for example, have found that some computer vision applications, like heart rate or blood pressure monitoring, can be less accurate for darker skin. Studies are underway to find better solutions.
Small algorithm glitches can also produce false alarms and frighten patients enough to keep widespread adoption out of reach. For example, Apple’s new car-crash detection feature, available on both the latest iPhone and Apple Watch, was set off when people were riding roller coasters and automatically dialed 911.
“We’re not there yet,” Dr. Yang said. “That’s the bottom line.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Brain differences suggest therapeutic targets in Takotsubo
A new study has identified differences in the brain present in patients with the cardiac disorder Takotsubo syndrome versus control scans, which may lead to new therapeutic targets.
Takotsubo syndrome is an acute heart failure cardiomyopathy mimicking an acute myocardial infarction in its presentation, but on investigation, no obstructive coronary disease is present. The syndrome, which mainly affects women, typically occurs in the aftermath of intense emotional or physical stress and has become known as “broken heart syndrome.”
The mechanism by which emotional processing in the context of stress leads to significant cardiac injury and acute left ventricular dysfunction is not understood. So, the current study examined both structural and functional effects in the brain in patients with Takotsubo syndrome to shed more light on the issue.
“The abnormalities in the thalamus-amygdala-insula and basal ganglia support the concept of involvement of higher-level function centers in Takotsubo syndrome, and interventions aimed at modulating these may be of benefit,” the authors conclude.
The study was published online in JACC: Heart Failure.
Lead author Hilal Khan, MB BCh, BAO, from the University of Aberdeen (Scotland), explained to this news organization that patients with Takotsubo syndrome have a substantial drop in heart function and show an apical ballooning of the heart.
It is a relatively newly defined condition and was first described in 1990 in Japan, and so named because the heart was thought to resemble the Takotsubo pot used by Japanese fishermen to trap octopus.
Although uncommon, the condition is not rare. Dr. Khan estimates that about 1 in 20 women with suspected MI turn out to have Takotsubo syndrome, with cases increasing in times of global stress such as in the recent pandemic.
While patients tend to recover in a few weeks and the pumping function of the heart usually returns to normal, there are some long-term cardiac complications including a reduction in global longitudinal strain, and patients have similar long-term outcomes as those with MI.
“It is believed that these cardiac changes may be triggered by changes in the brain caused by emotional stress, so we wanted to look at this more closely,” Dr. Khan said.
There have been a couple of studies published previously looking at brain changes in Takotsubo syndrome, but they haven’t reported patients in the acute stage of the condition and they haven’t compared the patients to controls, he noted.
For the current study, the researchers looked at brain scans for 25 acute Takotsubo patients and in 25 controls matched for age, gender, comorbidities, and medications. All the patients and controls were examined using the same MRI scanner in the same hospital.
“This is the largest structural and functional brain study of acute Takotsubo syndrome patients compared with matched control subjects,” Dr. Khan said.
The researchers looked at many different factors including brain volume in different regions, cortical thickness, small-vessel disease, and functional and structural connectivity to try and obtain a complete holistic view of the brain.
Key findings were that patients with Takotsubo syndrome had smaller brain volumes, compared with matched controls, driven by a reduction in brain surface area. In contrast, the insula and thalamus regions were larger.
“A reduction in brain volume could be caused by inflammation; this is often seen in depression,” Dr. Khan commented.
The researchers also found that certain areas of the brain had a reduction in functional connectivity, particularly the thalamus – the central autonomic area of the brain, which regulates the autonomic nervous system – and also the insula region, which is also involved in the autonomic regulation of the heart.
They suggest that there may be a loss of parasympathetic inhibition in Takotsubo syndrome, which would fit the theory that Takotsubo brings with it a surge of catecholamines, which could injure the heart.
Reduced functional connectivity was also seen in parts of the basal ganglia, abnormalities of which have been associated with an increased risk of both arrhythmias, and in the amygdala, similar to patients with a tendency to catastrophize events.
The other observation was that there appeared to be an increase in structural connectivity in certain areas of the brain.
“Structural pathways seem to be increased but functional connectivity was reduced, so while physical pathways are enhanced, they don’t seem to be doing anything,” Dr. Khan said. “We don’t know why this occurs, or if this has happened over time and made the brain and heart more vulnerable in some way.”
One possibility is that ,under a significant emotional stress, the brain may divert function from some areas to others to be able to cope, and that this results in reduced functioning in areas of the brain responsible for regulating the heart, Dr. Khan suggested.
“We believe this study confirms that the brain is involved in Takotsubo syndrome, and we have identified markers in the brain that may be contributing to the condition,” he said.
The researchers are planning to further study these markers and whether it might be possible to modulate these changes with various interventions such as exercise or mindfulness.
“We believe there is some interface between the brain changes and the impact on the heart. We don’t think it is just the release of catecholamines that causes damage to the heart. We think there is something else happening as well,” Dr. Khan commented.
It is also possible that the hearts of patients with Takotsubo syndrome are predisposed in some way and more vulnerable to this condition occurring.
“It will be important to obtain a greater understanding of the triggers and identify people who may be vulnerable,” Dr. Khan noted. “Around 10% of individuals who experience Takotsubo syndrome will have a recurrence, so we need to try and develop preventative strategies to reduce this.”
He suggested that possible preventive or therapeutic approaches may involve interventions such as exercise or mindfulness.
This work was supported by National Health Service Grampian Endowment. The authors report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new study has identified differences in the brain present in patients with the cardiac disorder Takotsubo syndrome versus control scans, which may lead to new therapeutic targets.
Takotsubo syndrome is an acute heart failure cardiomyopathy mimicking an acute myocardial infarction in its presentation, but on investigation, no obstructive coronary disease is present. The syndrome, which mainly affects women, typically occurs in the aftermath of intense emotional or physical stress and has become known as “broken heart syndrome.”
The mechanism by which emotional processing in the context of stress leads to significant cardiac injury and acute left ventricular dysfunction is not understood. So, the current study examined both structural and functional effects in the brain in patients with Takotsubo syndrome to shed more light on the issue.
“The abnormalities in the thalamus-amygdala-insula and basal ganglia support the concept of involvement of higher-level function centers in Takotsubo syndrome, and interventions aimed at modulating these may be of benefit,” the authors conclude.
The study was published online in JACC: Heart Failure.
Lead author Hilal Khan, MB BCh, BAO, from the University of Aberdeen (Scotland), explained to this news organization that patients with Takotsubo syndrome have a substantial drop in heart function and show an apical ballooning of the heart.
It is a relatively newly defined condition and was first described in 1990 in Japan, and so named because the heart was thought to resemble the Takotsubo pot used by Japanese fishermen to trap octopus.
Although uncommon, the condition is not rare. Dr. Khan estimates that about 1 in 20 women with suspected MI turn out to have Takotsubo syndrome, with cases increasing in times of global stress such as in the recent pandemic.
While patients tend to recover in a few weeks and the pumping function of the heart usually returns to normal, there are some long-term cardiac complications including a reduction in global longitudinal strain, and patients have similar long-term outcomes as those with MI.
“It is believed that these cardiac changes may be triggered by changes in the brain caused by emotional stress, so we wanted to look at this more closely,” Dr. Khan said.
There have been a couple of studies published previously looking at brain changes in Takotsubo syndrome, but they haven’t reported patients in the acute stage of the condition and they haven’t compared the patients to controls, he noted.
For the current study, the researchers looked at brain scans for 25 acute Takotsubo patients and in 25 controls matched for age, gender, comorbidities, and medications. All the patients and controls were examined using the same MRI scanner in the same hospital.
“This is the largest structural and functional brain study of acute Takotsubo syndrome patients compared with matched control subjects,” Dr. Khan said.
The researchers looked at many different factors including brain volume in different regions, cortical thickness, small-vessel disease, and functional and structural connectivity to try and obtain a complete holistic view of the brain.
Key findings were that patients with Takotsubo syndrome had smaller brain volumes, compared with matched controls, driven by a reduction in brain surface area. In contrast, the insula and thalamus regions were larger.
“A reduction in brain volume could be caused by inflammation; this is often seen in depression,” Dr. Khan commented.
The researchers also found that certain areas of the brain had a reduction in functional connectivity, particularly the thalamus – the central autonomic area of the brain, which regulates the autonomic nervous system – and also the insula region, which is also involved in the autonomic regulation of the heart.
They suggest that there may be a loss of parasympathetic inhibition in Takotsubo syndrome, which would fit the theory that Takotsubo brings with it a surge of catecholamines, which could injure the heart.
Reduced functional connectivity was also seen in parts of the basal ganglia, abnormalities of which have been associated with an increased risk of both arrhythmias, and in the amygdala, similar to patients with a tendency to catastrophize events.
The other observation was that there appeared to be an increase in structural connectivity in certain areas of the brain.
“Structural pathways seem to be increased but functional connectivity was reduced, so while physical pathways are enhanced, they don’t seem to be doing anything,” Dr. Khan said. “We don’t know why this occurs, or if this has happened over time and made the brain and heart more vulnerable in some way.”
One possibility is that ,under a significant emotional stress, the brain may divert function from some areas to others to be able to cope, and that this results in reduced functioning in areas of the brain responsible for regulating the heart, Dr. Khan suggested.
“We believe this study confirms that the brain is involved in Takotsubo syndrome, and we have identified markers in the brain that may be contributing to the condition,” he said.
The researchers are planning to further study these markers and whether it might be possible to modulate these changes with various interventions such as exercise or mindfulness.
“We believe there is some interface between the brain changes and the impact on the heart. We don’t think it is just the release of catecholamines that causes damage to the heart. We think there is something else happening as well,” Dr. Khan commented.
It is also possible that the hearts of patients with Takotsubo syndrome are predisposed in some way and more vulnerable to this condition occurring.
“It will be important to obtain a greater understanding of the triggers and identify people who may be vulnerable,” Dr. Khan noted. “Around 10% of individuals who experience Takotsubo syndrome will have a recurrence, so we need to try and develop preventative strategies to reduce this.”
He suggested that possible preventive or therapeutic approaches may involve interventions such as exercise or mindfulness.
This work was supported by National Health Service Grampian Endowment. The authors report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new study has identified differences in the brain present in patients with the cardiac disorder Takotsubo syndrome versus control scans, which may lead to new therapeutic targets.
Takotsubo syndrome is an acute heart failure cardiomyopathy mimicking an acute myocardial infarction in its presentation, but on investigation, no obstructive coronary disease is present. The syndrome, which mainly affects women, typically occurs in the aftermath of intense emotional or physical stress and has become known as “broken heart syndrome.”
The mechanism by which emotional processing in the context of stress leads to significant cardiac injury and acute left ventricular dysfunction is not understood. So, the current study examined both structural and functional effects in the brain in patients with Takotsubo syndrome to shed more light on the issue.
“The abnormalities in the thalamus-amygdala-insula and basal ganglia support the concept of involvement of higher-level function centers in Takotsubo syndrome, and interventions aimed at modulating these may be of benefit,” the authors conclude.
The study was published online in JACC: Heart Failure.
Lead author Hilal Khan, MB BCh, BAO, from the University of Aberdeen (Scotland), explained to this news organization that patients with Takotsubo syndrome have a substantial drop in heart function and show an apical ballooning of the heart.
It is a relatively newly defined condition and was first described in 1990 in Japan, and so named because the heart was thought to resemble the Takotsubo pot used by Japanese fishermen to trap octopus.
Although uncommon, the condition is not rare. Dr. Khan estimates that about 1 in 20 women with suspected MI turn out to have Takotsubo syndrome, with cases increasing in times of global stress such as in the recent pandemic.
While patients tend to recover in a few weeks and the pumping function of the heart usually returns to normal, there are some long-term cardiac complications including a reduction in global longitudinal strain, and patients have similar long-term outcomes as those with MI.
“It is believed that these cardiac changes may be triggered by changes in the brain caused by emotional stress, so we wanted to look at this more closely,” Dr. Khan said.
There have been a couple of studies published previously looking at brain changes in Takotsubo syndrome, but they haven’t reported patients in the acute stage of the condition and they haven’t compared the patients to controls, he noted.
For the current study, the researchers looked at brain scans for 25 acute Takotsubo patients and in 25 controls matched for age, gender, comorbidities, and medications. All the patients and controls were examined using the same MRI scanner in the same hospital.
“This is the largest structural and functional brain study of acute Takotsubo syndrome patients compared with matched control subjects,” Dr. Khan said.
The researchers looked at many different factors including brain volume in different regions, cortical thickness, small-vessel disease, and functional and structural connectivity to try and obtain a complete holistic view of the brain.
Key findings were that patients with Takotsubo syndrome had smaller brain volumes, compared with matched controls, driven by a reduction in brain surface area. In contrast, the insula and thalamus regions were larger.
“A reduction in brain volume could be caused by inflammation; this is often seen in depression,” Dr. Khan commented.
The researchers also found that certain areas of the brain had a reduction in functional connectivity, particularly the thalamus – the central autonomic area of the brain, which regulates the autonomic nervous system – and also the insula region, which is also involved in the autonomic regulation of the heart.
They suggest that there may be a loss of parasympathetic inhibition in Takotsubo syndrome, which would fit the theory that Takotsubo brings with it a surge of catecholamines, which could injure the heart.
Reduced functional connectivity was also seen in parts of the basal ganglia, abnormalities of which have been associated with an increased risk of both arrhythmias, and in the amygdala, similar to patients with a tendency to catastrophize events.
The other observation was that there appeared to be an increase in structural connectivity in certain areas of the brain.
“Structural pathways seem to be increased but functional connectivity was reduced, so while physical pathways are enhanced, they don’t seem to be doing anything,” Dr. Khan said. “We don’t know why this occurs, or if this has happened over time and made the brain and heart more vulnerable in some way.”
One possibility is that ,under a significant emotional stress, the brain may divert function from some areas to others to be able to cope, and that this results in reduced functioning in areas of the brain responsible for regulating the heart, Dr. Khan suggested.
“We believe this study confirms that the brain is involved in Takotsubo syndrome, and we have identified markers in the brain that may be contributing to the condition,” he said.
The researchers are planning to further study these markers and whether it might be possible to modulate these changes with various interventions such as exercise or mindfulness.
“We believe there is some interface between the brain changes and the impact on the heart. We don’t think it is just the release of catecholamines that causes damage to the heart. We think there is something else happening as well,” Dr. Khan commented.
It is also possible that the hearts of patients with Takotsubo syndrome are predisposed in some way and more vulnerable to this condition occurring.
“It will be important to obtain a greater understanding of the triggers and identify people who may be vulnerable,” Dr. Khan noted. “Around 10% of individuals who experience Takotsubo syndrome will have a recurrence, so we need to try and develop preventative strategies to reduce this.”
He suggested that possible preventive or therapeutic approaches may involve interventions such as exercise or mindfulness.
This work was supported by National Health Service Grampian Endowment. The authors report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JACC: HEART FAILURE
Simulation-based training effective for transesophageal echo
Simulation-based teaching of transesophageal echocardiography (TEE) improved cardiology fellows’ knowledge, skills, and comfort with the procedure, compared with traditional training, a new study shows.
“TEE learning may be hampered by the lack of availability of teachers and equipment and by the need for esophageal intubation, which is semi-invasive,” Augustin Coisne, MD, PhD, of the Cardiovascular Research Foundation in New York, said in an interview. “In this setting, simulation emerges as a key educational tool, but we were lacking evidence supporting simulation-based educational programs.”
Fellows in the simulation group achieved higher theoretical test scores and practical test scores after the training than did those in the traditional group.
Furthermore, Dr. Coisne said, “the results of the subgroup analyses were surprising and unexpected. The effect of the simulation-based training was greater among fellows at the beginning of fellowship – i.e., 2 years or less of training – in both theoretical and practical tests and in women [versus men] for the theoretical test.”
Their results, from the randomized SIMULATOR study, were published online in JAMA Cardiology.
More ready, more confident
The researchers randomly assigned 324 cardiology fellows (mean age, 26.4 years; about 30% women) inexperienced in TEE from 42 French university centers to TEE training with or without simulation support. Both groups participated in traditional didactic training using e-learning with an online course that is compulsory for all cardiology fellows in France.
The simulation group also participated in two 2-hour teaching sessions using a TEE simulator.
Each fellow completed a theoretical and a practical test prior to training to assess their baseline TEE level and again 3 months after the end of the training program. A TEE simulator (U/S Mentor Simulator; 3D Systems Simbionix) was used for all tests, and 24 certified echocardiography teachers served as both trainers and raters.
The theoretical tests included 20 online video-based questions to evaluate recognition of standard TEE views, normal anatomy, and some pathological cases. Fellows had 90 seconds to choose the best answer for each question from five multiple-choice options.
For the practical tests, fellows had 3 minutes to familiarize themselves with the handling of the simulator, without specific training and before the probe introduction.
They were asked to show 10 basic views on the simulator and had a maximum of 1 minute for each view.
The coprimary outcomes were the scores in the final theoretical and practical tests. TEE duration and the fellows’ self-assessment of their proficiency were also evaluated.
At baseline, the theoretical and practical test scores were similar between the groups (33.0 for the simulator group vs. 32.5 for the traditional group, and 44.2 vs. 46.1, respectively).
After training, the fellows in the simulation group had higher theoretical and practical test scores than those in the traditional group (47.2% vs. 38.3% and 74.5% vs. 59.0%, respectively).
Score changes were consistently higher when the pretraining scores were lower, an association that was stronger in the simulation group.
Dr. Coisne noted that subgroup analyses showed that the effectiveness of the simulation training was greater when performed at the beginning of the fellowship. On the theoretical test, the point increase was 11.9 for the simulation group versus 4.25 points for the traditional training group; for the practical test, the increases were 24.0 points versus 10.1 points.
After training, it took significantly less time for the simulation group to complete a TEE than it did the traditional group (8.3 vs. 9.4 minutes).
Furthermore, simulation group fellows reported that they felt more ready (mean score, 3.0 vs. 1.7) and more confident (mean score, 3.3 vs. 2.4) about performing a TEE alone after training.
“The simulation approach is definitively scalable to every institution,” Dr. Coisne said. “However, a medico-economic analysis should be interesting because the cost of the simulator and its maintenance might be a limitation to spread simulation-based teaching. The possibility for smaller hospitals to pool their financial input to share a TEE simulator could be considered to increase its cost-effectiveness.”
Real-world outcomes required
Commenting on the study, S. Justin Szawlewicz, MD, chair of cardiovascular medicine at Deborah Heart and Lung Center in Brown Mills, N.J., pointed out that the authors indicated that the number of TEEs performed by the trainees was not collected.
“This would be useful information to determine if those who received simulator training sought out and performed more TEEs, and also to determine if cardiology trainees in France perform a similar number of TEEs as cardiology trainees in the United States.”
In addition, he said, “the 4 hours of simulator training in TEE is extra education and experience that the standard trainees didn’t get. Would 4 extra hours of standard training didactics also improve trainees’ scores?”
Noting that the fellows’ ability to perform TEE in real patients was not assessed, Dr. Szawlewicz said, “a study could be designed that evaluated TEE images from real patients to see if trainees receiving simulator training performed better, more comprehensive and efficient TEEs than standard training.”
Nevertheless, he concluded, “Four hours of simulator training appears to improve TEE knowledge and skills. This is something we would consider at our institution.”
Like Dr. Szawlewicz, Michael Spooner, MD, MBA, of Mercy One North Iowa Heart Center in Mason City, and Kathryn Bertlacher, MD, of the University of Pittsburgh Medical Center, noted in a related editorial, “data are not provided about change in the learner’s behavior or performance on an actual TEE after the course, nor are there data about clinical outcomes such as patient safety or completeness of subsequent TEEs.
“This limitation, which is a limitation of most of the existing TEE simulation literature, is a high bar to cross,” they concluded. “Reaching this bar will require studies such as this to provide foundational understanding.”
Twin-Medical provided the TEE simulators. No relevant conflicts of interest were disclosed.
A version of this article first appeared on Medscape.com.
Simulation-based teaching of transesophageal echocardiography (TEE) improved cardiology fellows’ knowledge, skills, and comfort with the procedure, compared with traditional training, a new study shows.
“TEE learning may be hampered by the lack of availability of teachers and equipment and by the need for esophageal intubation, which is semi-invasive,” Augustin Coisne, MD, PhD, of the Cardiovascular Research Foundation in New York, said in an interview. “In this setting, simulation emerges as a key educational tool, but we were lacking evidence supporting simulation-based educational programs.”
Fellows in the simulation group achieved higher theoretical test scores and practical test scores after the training than did those in the traditional group.
Furthermore, Dr. Coisne said, “the results of the subgroup analyses were surprising and unexpected. The effect of the simulation-based training was greater among fellows at the beginning of fellowship – i.e., 2 years or less of training – in both theoretical and practical tests and in women [versus men] for the theoretical test.”
Their results, from the randomized SIMULATOR study, were published online in JAMA Cardiology.
More ready, more confident
The researchers randomly assigned 324 cardiology fellows (mean age, 26.4 years; about 30% women) inexperienced in TEE from 42 French university centers to TEE training with or without simulation support. Both groups participated in traditional didactic training using e-learning with an online course that is compulsory for all cardiology fellows in France.
The simulation group also participated in two 2-hour teaching sessions using a TEE simulator.
Each fellow completed a theoretical and a practical test prior to training to assess their baseline TEE level and again 3 months after the end of the training program. A TEE simulator (U/S Mentor Simulator; 3D Systems Simbionix) was used for all tests, and 24 certified echocardiography teachers served as both trainers and raters.
The theoretical tests included 20 online video-based questions to evaluate recognition of standard TEE views, normal anatomy, and some pathological cases. Fellows had 90 seconds to choose the best answer for each question from five multiple-choice options.
For the practical tests, fellows had 3 minutes to familiarize themselves with the handling of the simulator, without specific training and before the probe introduction.
They were asked to show 10 basic views on the simulator and had a maximum of 1 minute for each view.
The coprimary outcomes were the scores in the final theoretical and practical tests. TEE duration and the fellows’ self-assessment of their proficiency were also evaluated.
At baseline, the theoretical and practical test scores were similar between the groups (33.0 for the simulator group vs. 32.5 for the traditional group, and 44.2 vs. 46.1, respectively).
After training, the fellows in the simulation group had higher theoretical and practical test scores than those in the traditional group (47.2% vs. 38.3% and 74.5% vs. 59.0%, respectively).
Score changes were consistently higher when the pretraining scores were lower, an association that was stronger in the simulation group.
Dr. Coisne noted that subgroup analyses showed that the effectiveness of the simulation training was greater when performed at the beginning of the fellowship. On the theoretical test, the point increase was 11.9 for the simulation group versus 4.25 points for the traditional training group; for the practical test, the increases were 24.0 points versus 10.1 points.
After training, it took significantly less time for the simulation group to complete a TEE than it did the traditional group (8.3 vs. 9.4 minutes).
Furthermore, simulation group fellows reported that they felt more ready (mean score, 3.0 vs. 1.7) and more confident (mean score, 3.3 vs. 2.4) about performing a TEE alone after training.
“The simulation approach is definitively scalable to every institution,” Dr. Coisne said. “However, a medico-economic analysis should be interesting because the cost of the simulator and its maintenance might be a limitation to spread simulation-based teaching. The possibility for smaller hospitals to pool their financial input to share a TEE simulator could be considered to increase its cost-effectiveness.”
Real-world outcomes required
Commenting on the study, S. Justin Szawlewicz, MD, chair of cardiovascular medicine at Deborah Heart and Lung Center in Brown Mills, N.J., pointed out that the authors indicated that the number of TEEs performed by the trainees was not collected.
“This would be useful information to determine if those who received simulator training sought out and performed more TEEs, and also to determine if cardiology trainees in France perform a similar number of TEEs as cardiology trainees in the United States.”
In addition, he said, “the 4 hours of simulator training in TEE is extra education and experience that the standard trainees didn’t get. Would 4 extra hours of standard training didactics also improve trainees’ scores?”
Noting that the fellows’ ability to perform TEE in real patients was not assessed, Dr. Szawlewicz said, “a study could be designed that evaluated TEE images from real patients to see if trainees receiving simulator training performed better, more comprehensive and efficient TEEs than standard training.”
Nevertheless, he concluded, “Four hours of simulator training appears to improve TEE knowledge and skills. This is something we would consider at our institution.”
Like Dr. Szawlewicz, Michael Spooner, MD, MBA, of Mercy One North Iowa Heart Center in Mason City, and Kathryn Bertlacher, MD, of the University of Pittsburgh Medical Center, noted in a related editorial, “data are not provided about change in the learner’s behavior or performance on an actual TEE after the course, nor are there data about clinical outcomes such as patient safety or completeness of subsequent TEEs.
“This limitation, which is a limitation of most of the existing TEE simulation literature, is a high bar to cross,” they concluded. “Reaching this bar will require studies such as this to provide foundational understanding.”
Twin-Medical provided the TEE simulators. No relevant conflicts of interest were disclosed.
A version of this article first appeared on Medscape.com.
Simulation-based teaching of transesophageal echocardiography (TEE) improved cardiology fellows’ knowledge, skills, and comfort with the procedure, compared with traditional training, a new study shows.
“TEE learning may be hampered by the lack of availability of teachers and equipment and by the need for esophageal intubation, which is semi-invasive,” Augustin Coisne, MD, PhD, of the Cardiovascular Research Foundation in New York, said in an interview. “In this setting, simulation emerges as a key educational tool, but we were lacking evidence supporting simulation-based educational programs.”
Fellows in the simulation group achieved higher theoretical test scores and practical test scores after the training than did those in the traditional group.
Furthermore, Dr. Coisne said, “the results of the subgroup analyses were surprising and unexpected. The effect of the simulation-based training was greater among fellows at the beginning of fellowship – i.e., 2 years or less of training – in both theoretical and practical tests and in women [versus men] for the theoretical test.”
Their results, from the randomized SIMULATOR study, were published online in JAMA Cardiology.
More ready, more confident
The researchers randomly assigned 324 cardiology fellows (mean age, 26.4 years; about 30% women) inexperienced in TEE from 42 French university centers to TEE training with or without simulation support. Both groups participated in traditional didactic training using e-learning with an online course that is compulsory for all cardiology fellows in France.
The simulation group also participated in two 2-hour teaching sessions using a TEE simulator.
Each fellow completed a theoretical and a practical test prior to training to assess their baseline TEE level and again 3 months after the end of the training program. A TEE simulator (U/S Mentor Simulator; 3D Systems Simbionix) was used for all tests, and 24 certified echocardiography teachers served as both trainers and raters.
The theoretical tests included 20 online video-based questions to evaluate recognition of standard TEE views, normal anatomy, and some pathological cases. Fellows had 90 seconds to choose the best answer for each question from five multiple-choice options.
For the practical tests, fellows had 3 minutes to familiarize themselves with the handling of the simulator, without specific training and before the probe introduction.
They were asked to show 10 basic views on the simulator and had a maximum of 1 minute for each view.
The coprimary outcomes were the scores in the final theoretical and practical tests. TEE duration and the fellows’ self-assessment of their proficiency were also evaluated.
At baseline, the theoretical and practical test scores were similar between the groups (33.0 for the simulator group vs. 32.5 for the traditional group, and 44.2 vs. 46.1, respectively).
After training, the fellows in the simulation group had higher theoretical and practical test scores than those in the traditional group (47.2% vs. 38.3% and 74.5% vs. 59.0%, respectively).
Score changes were consistently higher when the pretraining scores were lower, an association that was stronger in the simulation group.
Dr. Coisne noted that subgroup analyses showed that the effectiveness of the simulation training was greater when performed at the beginning of the fellowship. On the theoretical test, the point increase was 11.9 for the simulation group versus 4.25 points for the traditional training group; for the practical test, the increases were 24.0 points versus 10.1 points.
After training, it took significantly less time for the simulation group to complete a TEE than it did the traditional group (8.3 vs. 9.4 minutes).
Furthermore, simulation group fellows reported that they felt more ready (mean score, 3.0 vs. 1.7) and more confident (mean score, 3.3 vs. 2.4) about performing a TEE alone after training.
“The simulation approach is definitively scalable to every institution,” Dr. Coisne said. “However, a medico-economic analysis should be interesting because the cost of the simulator and its maintenance might be a limitation to spread simulation-based teaching. The possibility for smaller hospitals to pool their financial input to share a TEE simulator could be considered to increase its cost-effectiveness.”
Real-world outcomes required
Commenting on the study, S. Justin Szawlewicz, MD, chair of cardiovascular medicine at Deborah Heart and Lung Center in Brown Mills, N.J., pointed out that the authors indicated that the number of TEEs performed by the trainees was not collected.
“This would be useful information to determine if those who received simulator training sought out and performed more TEEs, and also to determine if cardiology trainees in France perform a similar number of TEEs as cardiology trainees in the United States.”
In addition, he said, “the 4 hours of simulator training in TEE is extra education and experience that the standard trainees didn’t get. Would 4 extra hours of standard training didactics also improve trainees’ scores?”
Noting that the fellows’ ability to perform TEE in real patients was not assessed, Dr. Szawlewicz said, “a study could be designed that evaluated TEE images from real patients to see if trainees receiving simulator training performed better, more comprehensive and efficient TEEs than standard training.”
Nevertheless, he concluded, “Four hours of simulator training appears to improve TEE knowledge and skills. This is something we would consider at our institution.”
Like Dr. Szawlewicz, Michael Spooner, MD, MBA, of Mercy One North Iowa Heart Center in Mason City, and Kathryn Bertlacher, MD, of the University of Pittsburgh Medical Center, noted in a related editorial, “data are not provided about change in the learner’s behavior or performance on an actual TEE after the course, nor are there data about clinical outcomes such as patient safety or completeness of subsequent TEEs.
“This limitation, which is a limitation of most of the existing TEE simulation literature, is a high bar to cross,” they concluded. “Reaching this bar will require studies such as this to provide foundational understanding.”
Twin-Medical provided the TEE simulators. No relevant conflicts of interest were disclosed.
A version of this article first appeared on Medscape.com.
FROM JAMA CARDIOLOGY
Evolocumab’s LDL lowering surpassed inclisiran’s in ORION-3
Patients who received an injection of inclisiran (Leqvio), a small interfering RNA (siRNA) agent, every 6 months for as long as 4 years safely maintained about a 45% reduction from baseline in their level of low-density lipoprotein cholesterol (LDL-C) in an open-label extension study with 382 patients.
In addition to providing the longest reported treatment experience with inclisiran, which received Food and Drug Administration marketing approval a little over a year ago, the results also suggest with the most definitive evidence to date that inclisiran is less effective for lowering LDL-C, compared with a class of medications that reduce LDL-C by a related but distinct mechanism: antibodies that directly inhibit activity of the proprotein convertase subtilisin/kexin type 9 (PCSK9) enzyme, a drug class that includes alirocumab (Praluent) and evolocumab (Repatha). Inclisiran cuts PCSK9 activity by blocking this enzyme’s gene transcription in liver cells thereby interfering with PCSK9 production.

Results from this study, the ORION-3 trial, provide “the first prospective long-term evaluation of the durability and safety of an siRNA-based therapy to provide clinically meaningful reductions in LDL cholesterol with a convenient dosing schedule,” wrote Kausik K. Ray, MD, and coauthors in a report in The Lancet Diabetes & Endocrinology.
The findings “provide assurance that siRNA-based therapies are safe and have the potential to provide a convenient approach to managing” LDL-C, wrote Dr. Ray, a cardiologist and professor of public health at Imperial College London, and his associates.
Evolocumab surpasses inclisiran in crossover cohort
The new data from ORION-3 study included findings from 92 patients first treated with evolocumab injections every 2 weeks for a year, an intervention that lowered their LDL-C levels by an average of about 60%, compared with their pretreatment level. ORION-3’s study design then crossed these patients to treatment with injections of inclisiran twice a year during 3 further years of follow-up, during which their average LDL levels reset to a roughly 45% drop from baseline, a potentially clinically meaningful difference, commented Robert S. Rosenson, MD, a lipid management specialist who was not involved in the ORION-3 study.
“This is the first evidence that compared the two classes” within a single study, thereby avoiding a problematic cross-study comparison. “That’s why the data are important. They underscore that the monoclonal antibodies are more effective for lowering LDL-C,” compared with inclisiran, said Dr. Rosenson, professor and director of cardiometabolic disorders at the Icahn School of Medicine at Mount Sinai in New York.
The findings “confirm in a trial that the PCSK9 monoclonal antibodies are indeed more potent,” he said in an interview.
But Dr. Rosenson acknowledged that, while this analysis used data on patients treated with evolocumab and then switched to inclisiran collected prospectively in a single study, it has the limitation of involving a comparison that was not prespecified. The primary goal of the evolocumab-to-inclisiran switch included in ORION-3 was to assess the ease, safety, and efficacy of a switch to inclisiran from treatment with a PCSK9 antibody and was not intended to compare the two drug classes.
The roughly 15% absolute difference in LDL-C lowering between the two tested drug classes can have substantial clinical implications for patients who start treatment with highly elevated levels of LDL-C, more than 190 mg/dL, because they have heterozygous familial hypercholesterolemia, are unable to take a statin because of intolerance, or both. The difference in LDL-C reduction with an antibody or with inclisiran could mean the difference between whether or not a patient like this achieves their LDL-C goal level, Dr. Rosenson explained.
Inclisiran’s upside
On the other hand, inclisiran has a couple of important advantages. First, its mechanism of action means that effective treatment involves one injection every 6 months following a patient’s first two injections at onset and after 90 days, with all injections administered in a clinician’s office. In contrast, both of the monoclonal antibodies require injections every other week, a schedule that depends on patient self-injections using prefilled syringes obtained from a pharmacy.

Twice-a-year dosing by a clinician can be a major attraction because it helps ensure treatment compliance, aids patients with physical or psychological limitations to self-injection, reduces the pill burden for patients who require multiple medications, and facilitates frequent travelers who would otherwise need to carry syringes with them on trips, Dr. Rosenson noted.
The second big advantage of office-based administration of inclisiran for U.S. Medicare patients is that the treatment is billed under a patient’s part B coverage, usually resulting in easier coverage and a significantly lower patient co-pay, compared with Medicare’s coverage for a pharmacy-dispensed agent, which is covered under Medicare part D. “Part B coverage is financially more doable” for most Medicare patients, said Dr. Rosenson.
The administration schedule for inclisiran as well as its superior Medicare coverage makes the agent “transformative” for LDL-C lowering in patients for whom treatment delivery, frequency, and payment are issues, he said.
Inclisiran uptake modest after FDA approval
Despite these pluses, uptake of inclisiran has been modest since it received U.S. marketing approval in December 2021. In its most recent quarterly financial filing, in October 2022, Novartis reported total worldwide income from inclisiran (Leqvio) of $70 million during the first 9 months of 2022, although a Novartis spokesperson noted that the company has seen “positive trends in uptake” over the course of 2022. Inclisiran is labeled as an “adjunct to diet and maximally tolerated statin therapy for the treatment of adults with heterozygous familial hypercholesterolemia or clinical atherosclerotic cardiovascular disease who require additional lowering” of LDL-C.
During 2022, inclisiran uptake lagged because of the usual problems that slow the introduction of new drugs and new drug classes, especially ones that require dosing by a clinician. Months were spent waiting for billing codes to roll out, for clinical staffs to incorporate inclisiran injections into their routines, and for commercial insurers to get up to speed on their coverage, Dr. Rosenson said.
Also, a key step for widespread uptake of a new medication for improving cardiovascular disease outcomes – results from phase 3 studies that document safety and efficacy for these outcomes – remains several years off. The ORION-4 trial and the VICTORION-2P trial, each assessing the impact of inclisiran on cardiovascular disease events in roughly 15,000 people, will need about another 3-4 years before their results become available.
Professional medical societies that issue cardiovascular-disease management guidelines “prefer agents with proven benefits in phase 3 trials,” Dr. Rosenson noted.
Hence, the most recent update to U.S. LDL-C–management guidelines, released in the second half of 2022 by the American College of Cardiology as an Expert Consensus Decision Pathway, said this about the current role for inclisiran: “At the present time, a PCSK9 monoclonal antibody is preferred as the initial PCSK9 inhibitor of choice in view of its demonstrated safety, efficacy, and benefits for cardiovascular outcomes in the FOURIER [for evolocumab] and ODYSSEY Outcomes [for alirocumab] trials. The ORION-4 and VICTORION-2P cardiovascular outcomes trials with inclisiran are currently underway, and their completion is anticipated in 2026 and 2027, respectively. In view of the twice-yearly dosing regimen, inclisiran may be considered in patients with demonstrated poor adherence to PCSK9 monoclonal antibodies. Patients with adverse effects from both PSCK9 monoclonal antibodies or those who may be unable to self-inject may also be considered for therapy with inclisiran.”
ORION-3 extended the ORION-1 trial
The ORION-1 study was a phase 2 placebo-controlled, dose-ranging safety and efficacy assessment of inclisiran that gave patients two injections of the drug, at day zero and 90 days, and followed them for an additional 120 days (210 days total follow-up duration), and in some cases for as long as 360 days total. Of the 370 patients who received inclisiran in ORION-1, 290 agreed to continue inclisiran in the open-label extension, ORION-3. ORION-1 also included 127 patients randomized to initial placebo treatment, and 92 of these patients agreed to continue in ORION-3 and became the patients initially treated with evolocumab injections every other week for 1 year followed by initiation of an inclisiran regimen.
The primary outcome of ORION-3 was the change in LDL-C from baseline (the ORION-1 baseline) after 210 days of receiving inclisiran in ORION-3 (or a total of roughly 570 days after the start of ORION-1). The primary endpoint showed that, at day 210 of ORION-3 the average reduction in LDL-C from the original baseline level was 47.5%.
But a “more important” outcome, said Dr. Ray when he first reported the ORION-3 results during the American Heart Association scientific sessions in Chicago in November 2022, was that, overall, during 4 years on inclisiran this cohort showed an average cut in LDL-C from baseline of about 45% that consistently remained at this level throughout the 4 years of treatment.
“This provides us with an idea of what happens with chronic inclisiran dosing,” Dr. Ray explained. “There was no loss of biological efficacy, and we achieved these clinically meaningful, time-averaged reductions with a good safety profile. The great thing is that when patients get their injections [every 6 months] you see a consistent LDL-C reduction. A twice-annual injection is an opportunity to redesign” the way patients receive preventive cardiology care and treatment to lower LDL-C, Dr Ray said.
ORION-1 was sponsored by The Medicines Company. ORION-3 was sponsored by Novartis (which acquired The Medicines Company). Dr. Ray has received consulting fees, personal fees, and research grants from Novartis, as well as consulting fees and research grants from Amgen, the company that markets evolocumab (Repatha), and research grants from Regeneron, the company that markets alirocumab (Praluent). He has also received consulting fee, personal fees, and research grants from numerous other companies. Dr. Rosenson has been a consultant to and has received research funding from Amgen, Novartis, and Regeneron, and he has received speaking fees from Amgen and Regeneron, and has ties to several other pharmaceutical companies.
This article was updated on 1/26/2023.
Patients who received an injection of inclisiran (Leqvio), a small interfering RNA (siRNA) agent, every 6 months for as long as 4 years safely maintained about a 45% reduction from baseline in their level of low-density lipoprotein cholesterol (LDL-C) in an open-label extension study with 382 patients.
In addition to providing the longest reported treatment experience with inclisiran, which received Food and Drug Administration marketing approval a little over a year ago, the results also suggest with the most definitive evidence to date that inclisiran is less effective for lowering LDL-C, compared with a class of medications that reduce LDL-C by a related but distinct mechanism: antibodies that directly inhibit activity of the proprotein convertase subtilisin/kexin type 9 (PCSK9) enzyme, a drug class that includes alirocumab (Praluent) and evolocumab (Repatha). Inclisiran cuts PCSK9 activity by blocking this enzyme’s gene transcription in liver cells thereby interfering with PCSK9 production.
Results from this study, the ORION-3 trial, provide “the first prospective long-term evaluation of the durability and safety of an siRNA-based therapy to provide clinically meaningful reductions in LDL cholesterol with a convenient dosing schedule,” wrote Kausik K. Ray, MD, and coauthors in a report in The Lancet Diabetes & Endocrinology.
The findings “provide assurance that siRNA-based therapies are safe and have the potential to provide a convenient approach to managing” LDL-C, wrote Dr. Ray, a cardiologist and professor of public health at Imperial College London, and his associates.
Evolocumab surpasses inclisiran in crossover cohort
The new data from ORION-3 study included findings from 92 patients first treated with evolocumab injections every 2 weeks for a year, an intervention that lowered their LDL-C levels by an average of about 60%, compared with their pretreatment level. ORION-3’s study design then crossed these patients to treatment with injections of inclisiran twice a year during 3 further years of follow-up, during which their average LDL levels reset to a roughly 45% drop from baseline, a potentially clinically meaningful difference, commented Robert S. Rosenson, MD, a lipid management specialist who was not involved in the ORION-3 study.
“This is the first evidence that compared the two classes” within a single study, thereby avoiding a problematic cross-study comparison. “That’s why the data are important. They underscore that the monoclonal antibodies are more effective for lowering LDL-C,” compared with inclisiran, said Dr. Rosenson, professor and director of cardiometabolic disorders at the Icahn School of Medicine at Mount Sinai in New York.
The findings “confirm in a trial that the PCSK9 monoclonal antibodies are indeed more potent,” he said in an interview.
But Dr. Rosenson acknowledged that, while this analysis used data on patients treated with evolocumab and then switched to inclisiran collected prospectively in a single study, it has the limitation of involving a comparison that was not prespecified. The primary goal of the evolocumab-to-inclisiran switch included in ORION-3 was to assess the ease, safety, and efficacy of a switch to inclisiran from treatment with a PCSK9 antibody and was not intended to compare the two drug classes.
The roughly 15% absolute difference in LDL-C lowering between the two tested drug classes can have substantial clinical implications for patients who start treatment with highly elevated levels of LDL-C, more than 190 mg/dL, because they have heterozygous familial hypercholesterolemia, are unable to take a statin because of intolerance, or both. The difference in LDL-C reduction with an antibody or with inclisiran could mean the difference between whether or not a patient like this achieves their LDL-C goal level, Dr. Rosenson explained.
Inclisiran’s upside
On the other hand, inclisiran has a couple of important advantages. First, its mechanism of action means that effective treatment involves one injection every 6 months following a patient’s first two injections at onset and after 90 days, with all injections administered in a clinician’s office. In contrast, both of the monoclonal antibodies require injections every other week, a schedule that depends on patient self-injections using prefilled syringes obtained from a pharmacy.
Twice-a-year dosing by a clinician can be a major attraction because it helps ensure treatment compliance, aids patients with physical or psychological limitations to self-injection, reduces the pill burden for patients who require multiple medications, and facilitates frequent travelers who would otherwise need to carry syringes with them on trips, Dr. Rosenson noted.
The second big advantage of office-based administration of inclisiran for U.S. Medicare patients is that the treatment is billed under a patient’s part B coverage, usually resulting in easier coverage and a significantly lower patient co-pay, compared with Medicare’s coverage for a pharmacy-dispensed agent, which is covered under Medicare part D. “Part B coverage is financially more doable” for most Medicare patients, said Dr. Rosenson.
The administration schedule for inclisiran as well as its superior Medicare coverage makes the agent “transformative” for LDL-C lowering in patients for whom treatment delivery, frequency, and payment are issues, he said.
Inclisiran uptake modest after FDA approval
Despite these pluses, uptake of inclisiran has been modest since it received U.S. marketing approval in December 2021. In its most recent quarterly financial filing, in October 2022, Novartis reported total worldwide income from inclisiran (Leqvio) of $70 million during the first 9 months of 2022, although a Novartis spokesperson noted that the company has seen “positive trends in uptake” over the course of 2022. Inclisiran is labeled as an “adjunct to diet and maximally tolerated statin therapy for the treatment of adults with heterozygous familial hypercholesterolemia or clinical atherosclerotic cardiovascular disease who require additional lowering” of LDL-C.
During 2022, inclisiran uptake lagged because of the usual problems that slow the introduction of new drugs and new drug classes, especially ones that require dosing by a clinician. Months were spent waiting for billing codes to roll out, for clinical staffs to incorporate inclisiran injections into their routines, and for commercial insurers to get up to speed on their coverage, Dr. Rosenson said.
Also, a key step for widespread uptake of a new medication for improving cardiovascular disease outcomes – results from phase 3 studies that document safety and efficacy for these outcomes – remains several years off. The ORION-4 trial and the VICTORION-2P trial, each assessing the impact of inclisiran on cardiovascular disease events in roughly 15,000 people, will need about another 3-4 years before their results become available.
Professional medical societies that issue cardiovascular-disease management guidelines “prefer agents with proven benefits in phase 3 trials,” Dr. Rosenson noted.
Hence, the most recent update to U.S. LDL-C–management guidelines, released in the second half of 2022 by the American College of Cardiology as an Expert Consensus Decision Pathway, said this about the current role for inclisiran: “At the present time, a PCSK9 monoclonal antibody is preferred as the initial PCSK9 inhibitor of choice in view of its demonstrated safety, efficacy, and benefits for cardiovascular outcomes in the FOURIER [for evolocumab] and ODYSSEY Outcomes [for alirocumab] trials. The ORION-4 and VICTORION-2P cardiovascular outcomes trials with inclisiran are currently underway, and their completion is anticipated in 2026 and 2027, respectively. In view of the twice-yearly dosing regimen, inclisiran may be considered in patients with demonstrated poor adherence to PCSK9 monoclonal antibodies. Patients with adverse effects from both PSCK9 monoclonal antibodies or those who may be unable to self-inject may also be considered for therapy with inclisiran.”
ORION-3 extended the ORION-1 trial
The ORION-1 study was a phase 2 placebo-controlled, dose-ranging safety and efficacy assessment of inclisiran that gave patients two injections of the drug, at day zero and 90 days, and followed them for an additional 120 days (210 days total follow-up duration), and in some cases for as long as 360 days total. Of the 370 patients who received inclisiran in ORION-1, 290 agreed to continue inclisiran in the open-label extension, ORION-3. ORION-1 also included 127 patients randomized to initial placebo treatment, and 92 of these patients agreed to continue in ORION-3 and became the patients initially treated with evolocumab injections every other week for 1 year followed by initiation of an inclisiran regimen.
The primary outcome of ORION-3 was the change in LDL-C from baseline (the ORION-1 baseline) after 210 days of receiving inclisiran in ORION-3 (or a total of roughly 570 days after the start of ORION-1). The primary endpoint showed that, at day 210 of ORION-3 the average reduction in LDL-C from the original baseline level was 47.5%.
But a “more important” outcome, said Dr. Ray when he first reported the ORION-3 results during the American Heart Association scientific sessions in Chicago in November 2022, was that, overall, during 4 years on inclisiran this cohort showed an average cut in LDL-C from baseline of about 45% that consistently remained at this level throughout the 4 years of treatment.
“This provides us with an idea of what happens with chronic inclisiran dosing,” Dr. Ray explained. “There was no loss of biological efficacy, and we achieved these clinically meaningful, time-averaged reductions with a good safety profile. The great thing is that when patients get their injections [every 6 months] you see a consistent LDL-C reduction. A twice-annual injection is an opportunity to redesign” the way patients receive preventive cardiology care and treatment to lower LDL-C, Dr Ray said.
ORION-1 was sponsored by The Medicines Company. ORION-3 was sponsored by Novartis (which acquired The Medicines Company). Dr. Ray has received consulting fees, personal fees, and research grants from Novartis, as well as consulting fees and research grants from Amgen, the company that markets evolocumab (Repatha), and research grants from Regeneron, the company that markets alirocumab (Praluent). He has also received consulting fee, personal fees, and research grants from numerous other companies. Dr. Rosenson has been a consultant to and has received research funding from Amgen, Novartis, and Regeneron, and he has received speaking fees from Amgen and Regeneron, and has ties to several other pharmaceutical companies.
This article was updated on 1/26/2023.
Patients who received an injection of inclisiran (Leqvio), a small interfering RNA (siRNA) agent, every 6 months for as long as 4 years safely maintained about a 45% reduction from baseline in their level of low-density lipoprotein cholesterol (LDL-C) in an open-label extension study with 382 patients.
In addition to providing the longest reported treatment experience with inclisiran, which received Food and Drug Administration marketing approval a little over a year ago, the results also suggest with the most definitive evidence to date that inclisiran is less effective for lowering LDL-C, compared with a class of medications that reduce LDL-C by a related but distinct mechanism: antibodies that directly inhibit activity of the proprotein convertase subtilisin/kexin type 9 (PCSK9) enzyme, a drug class that includes alirocumab (Praluent) and evolocumab (Repatha). Inclisiran cuts PCSK9 activity by blocking this enzyme’s gene transcription in liver cells thereby interfering with PCSK9 production.
Results from this study, the ORION-3 trial, provide “the first prospective long-term evaluation of the durability and safety of an siRNA-based therapy to provide clinically meaningful reductions in LDL cholesterol with a convenient dosing schedule,” wrote Kausik K. Ray, MD, and coauthors in a report in The Lancet Diabetes & Endocrinology.
The findings “provide assurance that siRNA-based therapies are safe and have the potential to provide a convenient approach to managing” LDL-C, wrote Dr. Ray, a cardiologist and professor of public health at Imperial College London, and his associates.
Evolocumab surpasses inclisiran in crossover cohort
The new data from ORION-3 study included findings from 92 patients first treated with evolocumab injections every 2 weeks for a year, an intervention that lowered their LDL-C levels by an average of about 60%, compared with their pretreatment level. ORION-3’s study design then crossed these patients to treatment with injections of inclisiran twice a year during 3 further years of follow-up, during which their average LDL levels reset to a roughly 45% drop from baseline, a potentially clinically meaningful difference, commented Robert S. Rosenson, MD, a lipid management specialist who was not involved in the ORION-3 study.
“This is the first evidence that compared the two classes” within a single study, thereby avoiding a problematic cross-study comparison. “That’s why the data are important. They underscore that the monoclonal antibodies are more effective for lowering LDL-C,” compared with inclisiran, said Dr. Rosenson, professor and director of cardiometabolic disorders at the Icahn School of Medicine at Mount Sinai in New York.
The findings “confirm in a trial that the PCSK9 monoclonal antibodies are indeed more potent,” he said in an interview.
But Dr. Rosenson acknowledged that, while this analysis used data on patients treated with evolocumab and then switched to inclisiran collected prospectively in a single study, it has the limitation of involving a comparison that was not prespecified. The primary goal of the evolocumab-to-inclisiran switch included in ORION-3 was to assess the ease, safety, and efficacy of a switch to inclisiran from treatment with a PCSK9 antibody and was not intended to compare the two drug classes.
The roughly 15% absolute difference in LDL-C lowering between the two tested drug classes can have substantial clinical implications for patients who start treatment with highly elevated levels of LDL-C, more than 190 mg/dL, because they have heterozygous familial hypercholesterolemia, are unable to take a statin because of intolerance, or both. The difference in LDL-C reduction with an antibody or with inclisiran could mean the difference between whether or not a patient like this achieves their LDL-C goal level, Dr. Rosenson explained.
Inclisiran’s upside
On the other hand, inclisiran has a couple of important advantages. First, its mechanism of action means that effective treatment involves one injection every 6 months following a patient’s first two injections at onset and after 90 days, with all injections administered in a clinician’s office. In contrast, both of the monoclonal antibodies require injections every other week, a schedule that depends on patient self-injections using prefilled syringes obtained from a pharmacy.
Twice-a-year dosing by a clinician can be a major attraction because it helps ensure treatment compliance, aids patients with physical or psychological limitations to self-injection, reduces the pill burden for patients who require multiple medications, and facilitates frequent travelers who would otherwise need to carry syringes with them on trips, Dr. Rosenson noted.
The second big advantage of office-based administration of inclisiran for U.S. Medicare patients is that the treatment is billed under a patient’s part B coverage, usually resulting in easier coverage and a significantly lower patient co-pay, compared with Medicare’s coverage for a pharmacy-dispensed agent, which is covered under Medicare part D. “Part B coverage is financially more doable” for most Medicare patients, said Dr. Rosenson.
The administration schedule for inclisiran as well as its superior Medicare coverage makes the agent “transformative” for LDL-C lowering in patients for whom treatment delivery, frequency, and payment are issues, he said.
Inclisiran uptake modest after FDA approval
Despite these pluses, uptake of inclisiran has been modest since it received U.S. marketing approval in December 2021. In its most recent quarterly financial filing, in October 2022, Novartis reported total worldwide income from inclisiran (Leqvio) of $70 million during the first 9 months of 2022, although a Novartis spokesperson noted that the company has seen “positive trends in uptake” over the course of 2022. Inclisiran is labeled as an “adjunct to diet and maximally tolerated statin therapy for the treatment of adults with heterozygous familial hypercholesterolemia or clinical atherosclerotic cardiovascular disease who require additional lowering” of LDL-C.
During 2022, inclisiran uptake lagged because of the usual problems that slow the introduction of new drugs and new drug classes, especially ones that require dosing by a clinician. Months were spent waiting for billing codes to roll out, for clinical staffs to incorporate inclisiran injections into their routines, and for commercial insurers to get up to speed on their coverage, Dr. Rosenson said.
Also, a key step for widespread uptake of a new medication for improving cardiovascular disease outcomes – results from phase 3 studies that document safety and efficacy for these outcomes – remains several years off. The ORION-4 trial and the VICTORION-2P trial, each assessing the impact of inclisiran on cardiovascular disease events in roughly 15,000 people, will need about another 3-4 years before their results become available.
Professional medical societies that issue cardiovascular-disease management guidelines “prefer agents with proven benefits in phase 3 trials,” Dr. Rosenson noted.
Hence, the most recent update to U.S. LDL-C–management guidelines, released in the second half of 2022 by the American College of Cardiology as an Expert Consensus Decision Pathway, said this about the current role for inclisiran: “At the present time, a PCSK9 monoclonal antibody is preferred as the initial PCSK9 inhibitor of choice in view of its demonstrated safety, efficacy, and benefits for cardiovascular outcomes in the FOURIER [for evolocumab] and ODYSSEY Outcomes [for alirocumab] trials. The ORION-4 and VICTORION-2P cardiovascular outcomes trials with inclisiran are currently underway, and their completion is anticipated in 2026 and 2027, respectively. In view of the twice-yearly dosing regimen, inclisiran may be considered in patients with demonstrated poor adherence to PCSK9 monoclonal antibodies. Patients with adverse effects from both PSCK9 monoclonal antibodies or those who may be unable to self-inject may also be considered for therapy with inclisiran.”
ORION-3 extended the ORION-1 trial
The ORION-1 study was a phase 2 placebo-controlled, dose-ranging safety and efficacy assessment of inclisiran that gave patients two injections of the drug, at day zero and 90 days, and followed them for an additional 120 days (210 days total follow-up duration), and in some cases for as long as 360 days total. Of the 370 patients who received inclisiran in ORION-1, 290 agreed to continue inclisiran in the open-label extension, ORION-3. ORION-1 also included 127 patients randomized to initial placebo treatment, and 92 of these patients agreed to continue in ORION-3 and became the patients initially treated with evolocumab injections every other week for 1 year followed by initiation of an inclisiran regimen.
The primary outcome of ORION-3 was the change in LDL-C from baseline (the ORION-1 baseline) after 210 days of receiving inclisiran in ORION-3 (or a total of roughly 570 days after the start of ORION-1). The primary endpoint showed that, at day 210 of ORION-3 the average reduction in LDL-C from the original baseline level was 47.5%.
But a “more important” outcome, said Dr. Ray when he first reported the ORION-3 results during the American Heart Association scientific sessions in Chicago in November 2022, was that, overall, during 4 years on inclisiran this cohort showed an average cut in LDL-C from baseline of about 45% that consistently remained at this level throughout the 4 years of treatment.
“This provides us with an idea of what happens with chronic inclisiran dosing,” Dr. Ray explained. “There was no loss of biological efficacy, and we achieved these clinically meaningful, time-averaged reductions with a good safety profile. The great thing is that when patients get their injections [every 6 months] you see a consistent LDL-C reduction. A twice-annual injection is an opportunity to redesign” the way patients receive preventive cardiology care and treatment to lower LDL-C, Dr Ray said.
ORION-1 was sponsored by The Medicines Company. ORION-3 was sponsored by Novartis (which acquired The Medicines Company). Dr. Ray has received consulting fees, personal fees, and research grants from Novartis, as well as consulting fees and research grants from Amgen, the company that markets evolocumab (Repatha), and research grants from Regeneron, the company that markets alirocumab (Praluent). He has also received consulting fee, personal fees, and research grants from numerous other companies. Dr. Rosenson has been a consultant to and has received research funding from Amgen, Novartis, and Regeneron, and he has received speaking fees from Amgen and Regeneron, and has ties to several other pharmaceutical companies.
This article was updated on 1/26/2023.
FROM THE LANCET DIABETES & ENDOCRINOLOGY
Possible bivalent vaccine link to strokes in people over 65
who got the shot, the Centers for Disease Control and Prevention and the Food and Drug Administration said in a joint news release.
The release did not recommend people change their vaccine practices, saying the database finding probably did not represent a “true clinical risk.” The CDC said everybody, including people over 65, should stay up to date on their COVID vaccines, including the bivalent booster.
The news release said the Vaccine Safety Datalink (VSD), “a near real-time surveillance system,” raised a safety concern about the Pfizer/BioNTech booster.
“Rapid-response investigation of the signal in the VSD raised a question of whether people 65 and older who have received the Pfizer-BioNTech COVID-19 Vaccine, Bivalent were more likely to have an ischemic stroke in the 21 days following vaccination compared with days 22-44 following vaccination,” the news release said.
Ischemic strokes are blockages of blood to the brain, often caused by blood clots.
“Although the totality of the data currently suggests that it is very unlikely that the signal in VSD (Vaccine Safety Datalink) represents a true clinical risk, we believe it is important to share this information with the public, as we have in the past, when one of our safety monitoring systems detects a signal,” the release said.
No higher likelihood of strokes linked to the Pfizer bivalent vaccine had been found by Pfizer/BioNTech, the Department of Veterans Affairs, the Vaccine Adverse Event Reporting System maintained by the CDC and the FDA, or other agencies that monitor reactions of vaccines, the news release said. No safety issues about strokes have been identified with the Moderna bivalent vaccine.
CNN, citing a CDC official, reported that about 550,000 seniors who got Pfizer bivalent boosters were tracked by the VSD, and 130 of them had strokes within 3 weeks of getting the shot. None of those 130 people died, CNN said. The official spoke on the condition of anonymity because they weren’t authorized to share the data.
The issue will be discussed at the January meeting of the FDA’s Vaccines and Related Biological Products Advisory Committee.
In a joint statement, Pfizer and BioNTech said: “Neither Pfizer and BioNTech nor the CDC or FDA have observed similar findings across numerous other monitoring systems in the U.S. and globally and there is no evidence to conclude that ischemic stroke is associated with the use of the companies’ COVID-19 vaccines.”
Bivalent boosters contain two strains of vaccine – one to protect against the original COVID-19 virus and another targeting Omicron subvariants.
A version of this article first appeared on WebMD.com.
who got the shot, the Centers for Disease Control and Prevention and the Food and Drug Administration said in a joint news release.
The release did not recommend people change their vaccine practices, saying the database finding probably did not represent a “true clinical risk.” The CDC said everybody, including people over 65, should stay up to date on their COVID vaccines, including the bivalent booster.
The news release said the Vaccine Safety Datalink (VSD), “a near real-time surveillance system,” raised a safety concern about the Pfizer/BioNTech booster.
“Rapid-response investigation of the signal in the VSD raised a question of whether people 65 and older who have received the Pfizer-BioNTech COVID-19 Vaccine, Bivalent were more likely to have an ischemic stroke in the 21 days following vaccination compared with days 22-44 following vaccination,” the news release said.
Ischemic strokes are blockages of blood to the brain, often caused by blood clots.
“Although the totality of the data currently suggests that it is very unlikely that the signal in VSD (Vaccine Safety Datalink) represents a true clinical risk, we believe it is important to share this information with the public, as we have in the past, when one of our safety monitoring systems detects a signal,” the release said.
No higher likelihood of strokes linked to the Pfizer bivalent vaccine had been found by Pfizer/BioNTech, the Department of Veterans Affairs, the Vaccine Adverse Event Reporting System maintained by the CDC and the FDA, or other agencies that monitor reactions of vaccines, the news release said. No safety issues about strokes have been identified with the Moderna bivalent vaccine.
CNN, citing a CDC official, reported that about 550,000 seniors who got Pfizer bivalent boosters were tracked by the VSD, and 130 of them had strokes within 3 weeks of getting the shot. None of those 130 people died, CNN said. The official spoke on the condition of anonymity because they weren’t authorized to share the data.
The issue will be discussed at the January meeting of the FDA’s Vaccines and Related Biological Products Advisory Committee.
In a joint statement, Pfizer and BioNTech said: “Neither Pfizer and BioNTech nor the CDC or FDA have observed similar findings across numerous other monitoring systems in the U.S. and globally and there is no evidence to conclude that ischemic stroke is associated with the use of the companies’ COVID-19 vaccines.”
Bivalent boosters contain two strains of vaccine – one to protect against the original COVID-19 virus and another targeting Omicron subvariants.
A version of this article first appeared on WebMD.com.
who got the shot, the Centers for Disease Control and Prevention and the Food and Drug Administration said in a joint news release.
The release did not recommend people change their vaccine practices, saying the database finding probably did not represent a “true clinical risk.” The CDC said everybody, including people over 65, should stay up to date on their COVID vaccines, including the bivalent booster.
The news release said the Vaccine Safety Datalink (VSD), “a near real-time surveillance system,” raised a safety concern about the Pfizer/BioNTech booster.
“Rapid-response investigation of the signal in the VSD raised a question of whether people 65 and older who have received the Pfizer-BioNTech COVID-19 Vaccine, Bivalent were more likely to have an ischemic stroke in the 21 days following vaccination compared with days 22-44 following vaccination,” the news release said.
Ischemic strokes are blockages of blood to the brain, often caused by blood clots.
“Although the totality of the data currently suggests that it is very unlikely that the signal in VSD (Vaccine Safety Datalink) represents a true clinical risk, we believe it is important to share this information with the public, as we have in the past, when one of our safety monitoring systems detects a signal,” the release said.
No higher likelihood of strokes linked to the Pfizer bivalent vaccine had been found by Pfizer/BioNTech, the Department of Veterans Affairs, the Vaccine Adverse Event Reporting System maintained by the CDC and the FDA, or other agencies that monitor reactions of vaccines, the news release said. No safety issues about strokes have been identified with the Moderna bivalent vaccine.
CNN, citing a CDC official, reported that about 550,000 seniors who got Pfizer bivalent boosters were tracked by the VSD, and 130 of them had strokes within 3 weeks of getting the shot. None of those 130 people died, CNN said. The official spoke on the condition of anonymity because they weren’t authorized to share the data.
The issue will be discussed at the January meeting of the FDA’s Vaccines and Related Biological Products Advisory Committee.
In a joint statement, Pfizer and BioNTech said: “Neither Pfizer and BioNTech nor the CDC or FDA have observed similar findings across numerous other monitoring systems in the U.S. and globally and there is no evidence to conclude that ischemic stroke is associated with the use of the companies’ COVID-19 vaccines.”
Bivalent boosters contain two strains of vaccine – one to protect against the original COVID-19 virus and another targeting Omicron subvariants.
A version of this article first appeared on WebMD.com.
Cardiac Adverse Events Following COVID-19 Vaccination in Patients With Prior Vaccine-Associated Myocarditis
Vaccinations have substantially reduced morbidity and mortality from many infectious diseases. Despite the clear value of vaccinations in public health, efforts to better understand adverse events (AEs) following immunization are important to sustain public trust and vaccine confidence. Noninfectious inflammation of the heart may manifest as myocarditis or pericarditis, or occasionally, with shared signs and symptoms of each, as myopericarditis. This is a rare AE following some immunizations. Vaccine-associated myocarditis, pericarditis, or myopericarditis (VAMP) has been most clearly associated with smallpox vaccines and mRNA COVID-19 vaccines.1-6 Although extremely rare, VAMP also has been associated with other vaccines.7,8 Limited information exists to guide shared clinical decision making on COVID-19 vaccination in persons with a history of VAMP. It is unknown whether individuals with a history of VAMP are at higher risk for developing a recurrence or experiencing a more severe outcome following COVID-19 vaccination.
Methods
As part of the collaborative public health mission with the Centers for Disease Control and Prevention (CDC) for enhanced vaccine AE surveillance, the Defense Health Agency Immunization Healthcare Division (IHD) maintains a clinical database of service members and beneficiaries referred for suspected AEs following immunizations. A review of all AEs following immunization cases in this database from January 1, 2003, through February 28, 2022, identified individuals meeting the following criteria: (a) VAMP prior to receipt of COVID-19 vaccine; (b) receipt of COVID-19 vaccine in 2021; and (c) medical documentation in available electronic health records sufficient to describe health status at least 30 days following COVID-19 vaccination.9 If medical entries suggested cardiac symptoms following a COVID-19 vaccine, additional information was sought to verify VAMP based on current published criteria.10,11 Both the initial VAMP cases and the suspected COVID-19 VAMP cases were adjudicated by a team of vaccine experts and specialists in immunology, cardiology, and preventive medicine.
This retrospective review was approved and conducted in accordance with the Walter Reed National Military Medical Center Institutional Review Board protocol #20664. All individuals with recurrent VAMP consented to share their health records and clinical details.
Results
Among 9260 cases in the IHD database, 431 met the case definition for VAMP. 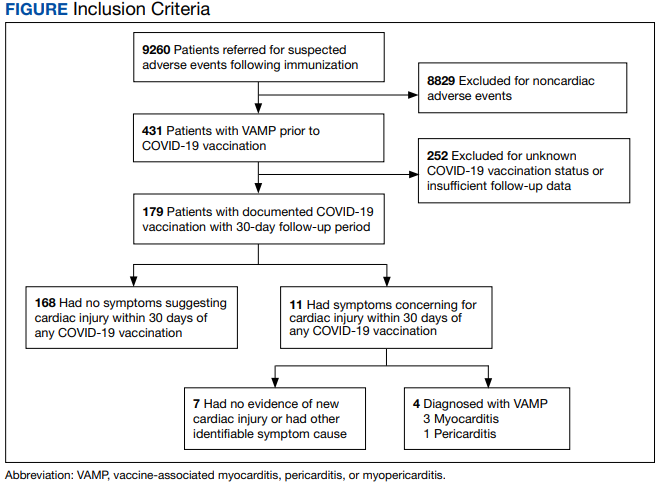
Among the 179 patients included in this analysis, 171 (96%) were male. Their median age was 39 years at the time of COVID-19 vaccination.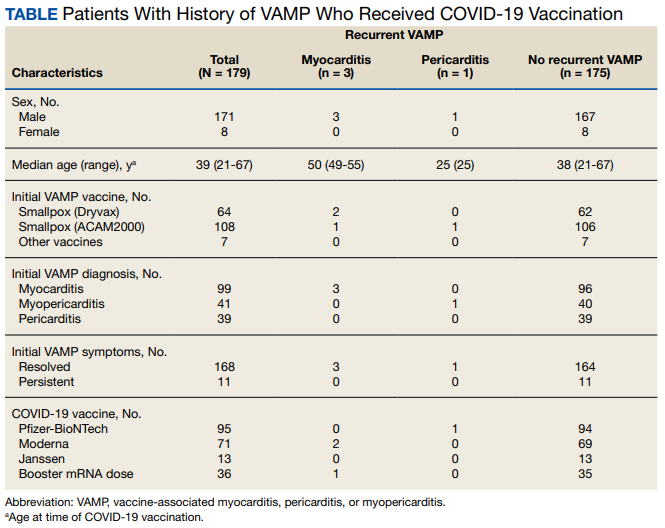
Within 1 month of receipt of any COVID-19 vaccine, 11 individuals had documented symptoms suggesting cardiac involvement, specifically, chest pain, palpitations, or dyspnea. After cardiac evaluation, 4 patients met the criteria for VAMP after COVID-19 vaccination.10,11 Seven patients either did not meet the criteria for VAMP or had alternative causes for their symptoms.
Two men aged 49 and 50 years with a history of vaccine-associated myocarditis following smallpox vaccination (Dryvax and ACAM2000) developed myocarditis 3 days after their second dose of the Moderna vaccine. One of these patients received a Pfizer-BioNTech booster 10 months later with no recurrence of symptoms. A 55-year-old man with a history of vaccine-associated myocarditis following Dryvax vaccination developed myocarditis 2 days after his Pfizer-BioNTech booster. None of the patients who developed post-COVID-19 VAMP reported residual symptoms from their initial VAMP episode, which occurred 12 to 18 years earlier. All were hospitalized briefly for observation and had complete symptom resolution within 6 weeks.
A 25-year-old man developed pericarditis 4 days after his second Pfizer-BioNTech vaccination. His previous ACAM2000 vaccine-associated myocarditis occurred 3 years earlier, with no residual symptoms. Of note, he had a mild COVID-19 infection 78 days before the onset of his pericarditis. After the onset of his COVID-19 vaccine-associated pericarditis, he continued to experience transient bouts of chest pressure and exertional dyspnea that resolved within 7 months of onset.
The median interval between COVID-19 vaccine doses in those who developed post-COVID-19 VAMP was within the recommended mRNA vaccine dosing intervals of 3 to 4 weeks and was consistent with the median mRNA vaccine dosing intervals among the entire cohort.
Due to the small cohort size and other limitations of this study, the suggested rate of cardiac injury in this review (4 cases in 179 persons, or 2.2%) is an imprecise estimate of risk in a small population (95% CI, 0.1%-4.4%). While this rate may seem higher than expected within the general population after COVID-19 vaccination, it is lower than the estimated lifetime risk of recurrent myocarditis from any cause.6,12
Discussion
To our knowledge, this is the first report describing cardiac outcomes after COVID-19 vaccination among a cohort of individuals with prior history of VAMP. Four cases of COVID-19 VAMP were identified among 179 patients with previous VAMP. All cases had experienced VAMP after the smallpox vaccine several years earlier, with complete resolution of symptoms. Three cases presented with recurrent VAMP after their second dose of an mRNA COVID-19 vaccine, and one after an mRNA booster dose. All fully recovered over the course of several months.
Myocarditis is a heterogeneous inflammatory injury with diverse, sometimes idiopathic, etiologies.13 In contrast to infection-related cardiac injury, prior reports of vaccine-associated myocarditis have suggested a hypersensitivity reaction characterized by patchy eosinophilic infiltrates, a benign clinical course, and good prognosis.2,3
There are several common features between VAMP after smallpox and COVID-19 vaccination. Cases occur predominantly in young men. The onset of symptoms after smallpox vaccine (mean, 10 days) and after mRNA COVID-19 vaccine (mean, 3 days) appears to correspond to the timing of peak postvaccination pro-inflammatory cytokine elevation.14 While all VAMP cases are serious events, the majority of patients appear to have a relatively benign clinical course with rapid and full recovery.13
Patients who have experienced an inflammatory cardiac injury may be at higher risk for recurrence, but quantifying risk of this rare phenomenon is challenging. Cases of VAMP after the COVID-19 vaccine have occasionally been reported in patients with previous cardiac injury unrelated to vaccination.15-17 The cases presented here represent the first report of recurrent VAMP following prior non-COVID-19 vaccinations.
Most patients with prior VAMP in this cohort did not experience cardiac-suggestive symptoms following COVID-19 vaccination. Among 11 patients who developed symptoms, 3 had confirmed myocarditis and 1 had confirmed pericarditis. The clinical course for these patients with recurrent VAMP was observed to be no different in severity or duration from those who experience new-onset VAMP.4 All other patients not meeting criteria for VAMP or having alternative explanations for their symptoms also had a benign clinical course. Nonetheless, of the study cohort of 179, recurrent VAMP was diagnosed in 4 of the 11 who developed cardiac-suggestive symptoms following COVID-19 vaccination. The importance of cardiac evaluation should be emphasized for any patient presenting with chest pain, dyspnea, or other cardiac-suggestive symptoms following vaccination.
Strengths and Limitations
The strength of this review of VAMP recurrence associated with COVID-19 vaccination derives from our large and unique longitudinal database of VAMP among current and prior service members. Additionally, the IHD’s ongoing enhanced vaccine AEs surveillance provides the opportunity to contact patients and review their electronic health records over an extended interval of time.
When interpreting this report’s implications, limitations inherent to any retrospective case review should be considered. The cohort of cases of prior VAMP included primarily healthy, fit, young service members; this population is not representative of the general population. The cohort included prior VAMP cases that generally occurred after smallpox vaccination. Experiences after smallpox vaccine may not apply to cardiac injury from other vaccines or etiologies. By the nature of this review, the population studied at the time of COVID-19 vaccination was somewhat older than those most likely to develop an initial bout of VAMP.2 This review was limited by information available in the electronic health records of a small number of patients. Subclinical cases of VAMP and cases without adequate clinical evaluation also could not be included.
Conclusions
Noninfectious inflammation of the heart (myocarditis, pericarditis, or myopericarditis) is a rare AE following certain vaccines, especially live replicating smallpox vaccine and mRNA COVID-19 vaccines. In this observational analysis, the majority of patients with previous VAMP successfully received a COVID-19 vaccine without recurrence. The 4 patients who were identified with recurrent VAMP following COVID-19 vaccination all recovered with supportive care. While the CDC endorses that individuals with a history of infectious myocarditis may receive COVID-19 vaccine after symptoms have resolved, there is currently insufficient safety data regarding COVID-19 vaccination of those with prior non-COVID-19 VAMP or following subsequent COVID-19 vaccination in those with prior VAMP related to COVID-19.10 For these individuals, COVID-19 vaccination is a precaution.10 Although insufficient to determine a precise level of risk, this report does provide data on which to base the CDC-recommended shared decision-making counseling of these patients. More research is needed to better define factors that increase risk for, or protection from, immune-mediated AEs following immunization, including VAMP. While benefits of vaccination have clearly outweighed risks during the COVID-19 pandemic, such research may optimize future vaccine recommendations.18
1. Decker MD, Garman PM, Hughes H, et al. Enhanced safety surveillance study of ACAM2000 smallpox vaccine among US military service members. Vaccine. 2021;39(39):5541-5547. doi:10.1016/j.vaccine.2021.08.041
2. Engler RJ, Nelson MR, Collins LC Jr, et al. A prospective study of the incidence of myocarditis/pericarditis and new onset cardiac symptoms following smallpox and influenza vaccination. PLoS One. 2015;10(3):e0118283. doi:10.1371/journal.pone.0118283
3. Faix DJ, Gordon DM, Perry LN, et al. Prospective safety surveillance study of ACAM2000 smallpox vaccine in deploying military personnel. Vaccine. 2020;38(46):7323-7330. doi:10.1016/j.vaccine.2020.09.037
4. Montgomery J, Ryan M, Engler R, et al. Myocarditis following immunization with mRNA COVID-19 vaccines in members of the US military. JAMA Cardiol. 2021;6(10):1202-1206. doi:10.1001/jamacardio.2021.2833
5. Witberg G, Barda N, Hoss S, et al. Myocarditis after Covid-19 vaccination in a large health care organization. N Engl J Med. 2021;385(23):2132-2139. doi:10.1056/NEJMoa2110737
6. Oster ME, Shay DK, Su JR, et al. Myocarditis cases reported after mRNA-based COVID-19 vaccination in the US from December 2020 to August 2021. JAMA. 2022;327(4):331-340. doi:10.1001/jama.2021.24110
7. Su JR, McNeil MM, Welsh KJ, et al. Myopericarditis after vaccination, Vaccine Adverse Event Reporting System (VAERS), 1990-2018. Vaccine. 2021;39(5):839-845. doi:10.1016/j.vaccine.2020.12.046
8. Mei R, Raschi E, Forcesi E, Diemberger I, De Ponti F, Poluzzi E. Myocarditis and pericarditis after immunization: gaining insights through the Vaccine Adverse Event Reporting System. Int J Cardiol. 2018;273:183-186. doi:10.1016/j.ijcard.2018.09.054
9. Centers for Disease Control and Prevention (CDC). Update: cardiac-related events during the civilian smallpox vaccination program—United States, 2003. MMWR Morb Mortal Wkly Rep. 2003;52(21):492-496.
10. Gargano JW, Wallace M, Hadler SC, et al. Use of mRNA COVID-19 vaccine after reports of myocarditis among vaccine recipients: update from the Advisory Committee on Immunization Practices—United States, June 2021. MMWR Morb Mortal Wkly Rep. 2021;70(27):977-982. doi:10.15585/mmwr.mm7027e2
11. Sexson Tejtel SK, Munoz FM, Al-Ammouri I, et al. Myocarditis and pericarditis: case definition and guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine. 2022;40(10):1499-1511. doi:10.1016/j.vaccine.2021.11.074
12. Sagar S, Liu PP, Cooper LT Jr. Myocarditis. Lancet. 2012;379(9817):738-747. doi:10.1016/S0140-6736(11) 60648-X
13. Heymans S, Cooper LT. Myocarditis after COVID-19 mRNA vaccination: clinical observations and potential mechanisms. Nat Rev Cardiol. 2022;19(2):75-77. doi:10.1038/s41569-021-00662-w
14. Cohen JI, Hohman P, Fulton R, et al. Kinetics of serum cytokines after primary or repeat vaccination with the smallpox vaccine. J Infect Dis. 2010;201(8):1183-1191. doi:10.1086/651453
15. Minocha PK, Better D, Singh RK, Hoque T. Recurrence of acute myocarditis temporally associated with receipt of the mRNA COVID-19 vaccine in an adolescent male. J Pediatr. 2021;238:321-323. doi:10.1016/j.jpeds.2021.06.035
16. Umei TC, Kishino Y, Watanabe K, et al. Recurrence of myopericarditis following mRNA COVID-19 vaccination in a male adolescent. CJC Open. 2022;4(3):350-352. doi:10.1016/j.cjco.2021.12.002
17. Pasha MA, Isaac S, Khan Z. Recurrent myocarditis following COVID-19 infection and the mRNA vaccine. Cureus. 2022;14(7):e26650. doi:10.7759/cureus.26650
18. Block JP, Boehmer TK, Forrest CB, et al. Cardiac complications after SARS-CoV-2 infection and mRNA COVID-19 vaccination—PCORnet, United States, January 2021-January 2022. MMWR Morb Mortal Wkly Rep. 2022;71(14):517-523. Published 2022 Apr 8. doi:10.15585/mmwr.mm7114e1
Vaccinations have substantially reduced morbidity and mortality from many infectious diseases. Despite the clear value of vaccinations in public health, efforts to better understand adverse events (AEs) following immunization are important to sustain public trust and vaccine confidence. Noninfectious inflammation of the heart may manifest as myocarditis or pericarditis, or occasionally, with shared signs and symptoms of each, as myopericarditis. This is a rare AE following some immunizations. Vaccine-associated myocarditis, pericarditis, or myopericarditis (VAMP) has been most clearly associated with smallpox vaccines and mRNA COVID-19 vaccines.1-6 Although extremely rare, VAMP also has been associated with other vaccines.7,8 Limited information exists to guide shared clinical decision making on COVID-19 vaccination in persons with a history of VAMP. It is unknown whether individuals with a history of VAMP are at higher risk for developing a recurrence or experiencing a more severe outcome following COVID-19 vaccination.
Methods
As part of the collaborative public health mission with the Centers for Disease Control and Prevention (CDC) for enhanced vaccine AE surveillance, the Defense Health Agency Immunization Healthcare Division (IHD) maintains a clinical database of service members and beneficiaries referred for suspected AEs following immunizations. A review of all AEs following immunization cases in this database from January 1, 2003, through February 28, 2022, identified individuals meeting the following criteria: (a) VAMP prior to receipt of COVID-19 vaccine; (b) receipt of COVID-19 vaccine in 2021; and (c) medical documentation in available electronic health records sufficient to describe health status at least 30 days following COVID-19 vaccination.9 If medical entries suggested cardiac symptoms following a COVID-19 vaccine, additional information was sought to verify VAMP based on current published criteria.10,11 Both the initial VAMP cases and the suspected COVID-19 VAMP cases were adjudicated by a team of vaccine experts and specialists in immunology, cardiology, and preventive medicine.
This retrospective review was approved and conducted in accordance with the Walter Reed National Military Medical Center Institutional Review Board protocol #20664. All individuals with recurrent VAMP consented to share their health records and clinical details.
Results
Among 9260 cases in the IHD database, 431 met the case definition for VAMP.
Among the 179 patients included in this analysis, 171 (96%) were male. Their median age was 39 years at the time of COVID-19 vaccination.
Within 1 month of receipt of any COVID-19 vaccine, 11 individuals had documented symptoms suggesting cardiac involvement, specifically, chest pain, palpitations, or dyspnea. After cardiac evaluation, 4 patients met the criteria for VAMP after COVID-19 vaccination.10,11 Seven patients either did not meet the criteria for VAMP or had alternative causes for their symptoms.
Two men aged 49 and 50 years with a history of vaccine-associated myocarditis following smallpox vaccination (Dryvax and ACAM2000) developed myocarditis 3 days after their second dose of the Moderna vaccine. One of these patients received a Pfizer-BioNTech booster 10 months later with no recurrence of symptoms. A 55-year-old man with a history of vaccine-associated myocarditis following Dryvax vaccination developed myocarditis 2 days after his Pfizer-BioNTech booster. None of the patients who developed post-COVID-19 VAMP reported residual symptoms from their initial VAMP episode, which occurred 12 to 18 years earlier. All were hospitalized briefly for observation and had complete symptom resolution within 6 weeks.
A 25-year-old man developed pericarditis 4 days after his second Pfizer-BioNTech vaccination. His previous ACAM2000 vaccine-associated myocarditis occurred 3 years earlier, with no residual symptoms. Of note, he had a mild COVID-19 infection 78 days before the onset of his pericarditis. After the onset of his COVID-19 vaccine-associated pericarditis, he continued to experience transient bouts of chest pressure and exertional dyspnea that resolved within 7 months of onset.
The median interval between COVID-19 vaccine doses in those who developed post-COVID-19 VAMP was within the recommended mRNA vaccine dosing intervals of 3 to 4 weeks and was consistent with the median mRNA vaccine dosing intervals among the entire cohort.
Due to the small cohort size and other limitations of this study, the suggested rate of cardiac injury in this review (4 cases in 179 persons, or 2.2%) is an imprecise estimate of risk in a small population (95% CI, 0.1%-4.4%). While this rate may seem higher than expected within the general population after COVID-19 vaccination, it is lower than the estimated lifetime risk of recurrent myocarditis from any cause.6,12
Discussion
To our knowledge, this is the first report describing cardiac outcomes after COVID-19 vaccination among a cohort of individuals with prior history of VAMP. Four cases of COVID-19 VAMP were identified among 179 patients with previous VAMP. All cases had experienced VAMP after the smallpox vaccine several years earlier, with complete resolution of symptoms. Three cases presented with recurrent VAMP after their second dose of an mRNA COVID-19 vaccine, and one after an mRNA booster dose. All fully recovered over the course of several months.
Myocarditis is a heterogeneous inflammatory injury with diverse, sometimes idiopathic, etiologies.13 In contrast to infection-related cardiac injury, prior reports of vaccine-associated myocarditis have suggested a hypersensitivity reaction characterized by patchy eosinophilic infiltrates, a benign clinical course, and good prognosis.2,3
There are several common features between VAMP after smallpox and COVID-19 vaccination. Cases occur predominantly in young men. The onset of symptoms after smallpox vaccine (mean, 10 days) and after mRNA COVID-19 vaccine (mean, 3 days) appears to correspond to the timing of peak postvaccination pro-inflammatory cytokine elevation.14 While all VAMP cases are serious events, the majority of patients appear to have a relatively benign clinical course with rapid and full recovery.13
Patients who have experienced an inflammatory cardiac injury may be at higher risk for recurrence, but quantifying risk of this rare phenomenon is challenging. Cases of VAMP after the COVID-19 vaccine have occasionally been reported in patients with previous cardiac injury unrelated to vaccination.15-17 The cases presented here represent the first report of recurrent VAMP following prior non-COVID-19 vaccinations.
Most patients with prior VAMP in this cohort did not experience cardiac-suggestive symptoms following COVID-19 vaccination. Among 11 patients who developed symptoms, 3 had confirmed myocarditis and 1 had confirmed pericarditis. The clinical course for these patients with recurrent VAMP was observed to be no different in severity or duration from those who experience new-onset VAMP.4 All other patients not meeting criteria for VAMP or having alternative explanations for their symptoms also had a benign clinical course. Nonetheless, of the study cohort of 179, recurrent VAMP was diagnosed in 4 of the 11 who developed cardiac-suggestive symptoms following COVID-19 vaccination. The importance of cardiac evaluation should be emphasized for any patient presenting with chest pain, dyspnea, or other cardiac-suggestive symptoms following vaccination.
Strengths and Limitations
The strength of this review of VAMP recurrence associated with COVID-19 vaccination derives from our large and unique longitudinal database of VAMP among current and prior service members. Additionally, the IHD’s ongoing enhanced vaccine AEs surveillance provides the opportunity to contact patients and review their electronic health records over an extended interval of time.
When interpreting this report’s implications, limitations inherent to any retrospective case review should be considered. The cohort of cases of prior VAMP included primarily healthy, fit, young service members; this population is not representative of the general population. The cohort included prior VAMP cases that generally occurred after smallpox vaccination. Experiences after smallpox vaccine may not apply to cardiac injury from other vaccines or etiologies. By the nature of this review, the population studied at the time of COVID-19 vaccination was somewhat older than those most likely to develop an initial bout of VAMP.2 This review was limited by information available in the electronic health records of a small number of patients. Subclinical cases of VAMP and cases without adequate clinical evaluation also could not be included.
Conclusions
Noninfectious inflammation of the heart (myocarditis, pericarditis, or myopericarditis) is a rare AE following certain vaccines, especially live replicating smallpox vaccine and mRNA COVID-19 vaccines. In this observational analysis, the majority of patients with previous VAMP successfully received a COVID-19 vaccine without recurrence. The 4 patients who were identified with recurrent VAMP following COVID-19 vaccination all recovered with supportive care. While the CDC endorses that individuals with a history of infectious myocarditis may receive COVID-19 vaccine after symptoms have resolved, there is currently insufficient safety data regarding COVID-19 vaccination of those with prior non-COVID-19 VAMP or following subsequent COVID-19 vaccination in those with prior VAMP related to COVID-19.10 For these individuals, COVID-19 vaccination is a precaution.10 Although insufficient to determine a precise level of risk, this report does provide data on which to base the CDC-recommended shared decision-making counseling of these patients. More research is needed to better define factors that increase risk for, or protection from, immune-mediated AEs following immunization, including VAMP. While benefits of vaccination have clearly outweighed risks during the COVID-19 pandemic, such research may optimize future vaccine recommendations.18
Vaccinations have substantially reduced morbidity and mortality from many infectious diseases. Despite the clear value of vaccinations in public health, efforts to better understand adverse events (AEs) following immunization are important to sustain public trust and vaccine confidence. Noninfectious inflammation of the heart may manifest as myocarditis or pericarditis, or occasionally, with shared signs and symptoms of each, as myopericarditis. This is a rare AE following some immunizations. Vaccine-associated myocarditis, pericarditis, or myopericarditis (VAMP) has been most clearly associated with smallpox vaccines and mRNA COVID-19 vaccines.1-6 Although extremely rare, VAMP also has been associated with other vaccines.7,8 Limited information exists to guide shared clinical decision making on COVID-19 vaccination in persons with a history of VAMP. It is unknown whether individuals with a history of VAMP are at higher risk for developing a recurrence or experiencing a more severe outcome following COVID-19 vaccination.
Methods
As part of the collaborative public health mission with the Centers for Disease Control and Prevention (CDC) for enhanced vaccine AE surveillance, the Defense Health Agency Immunization Healthcare Division (IHD) maintains a clinical database of service members and beneficiaries referred for suspected AEs following immunizations. A review of all AEs following immunization cases in this database from January 1, 2003, through February 28, 2022, identified individuals meeting the following criteria: (a) VAMP prior to receipt of COVID-19 vaccine; (b) receipt of COVID-19 vaccine in 2021; and (c) medical documentation in available electronic health records sufficient to describe health status at least 30 days following COVID-19 vaccination.9 If medical entries suggested cardiac symptoms following a COVID-19 vaccine, additional information was sought to verify VAMP based on current published criteria.10,11 Both the initial VAMP cases and the suspected COVID-19 VAMP cases were adjudicated by a team of vaccine experts and specialists in immunology, cardiology, and preventive medicine.
This retrospective review was approved and conducted in accordance with the Walter Reed National Military Medical Center Institutional Review Board protocol #20664. All individuals with recurrent VAMP consented to share their health records and clinical details.
Results
Among 9260 cases in the IHD database, 431 met the case definition for VAMP.
Among the 179 patients included in this analysis, 171 (96%) were male. Their median age was 39 years at the time of COVID-19 vaccination.
Within 1 month of receipt of any COVID-19 vaccine, 11 individuals had documented symptoms suggesting cardiac involvement, specifically, chest pain, palpitations, or dyspnea. After cardiac evaluation, 4 patients met the criteria for VAMP after COVID-19 vaccination.10,11 Seven patients either did not meet the criteria for VAMP or had alternative causes for their symptoms.
Two men aged 49 and 50 years with a history of vaccine-associated myocarditis following smallpox vaccination (Dryvax and ACAM2000) developed myocarditis 3 days after their second dose of the Moderna vaccine. One of these patients received a Pfizer-BioNTech booster 10 months later with no recurrence of symptoms. A 55-year-old man with a history of vaccine-associated myocarditis following Dryvax vaccination developed myocarditis 2 days after his Pfizer-BioNTech booster. None of the patients who developed post-COVID-19 VAMP reported residual symptoms from their initial VAMP episode, which occurred 12 to 18 years earlier. All were hospitalized briefly for observation and had complete symptom resolution within 6 weeks.
A 25-year-old man developed pericarditis 4 days after his second Pfizer-BioNTech vaccination. His previous ACAM2000 vaccine-associated myocarditis occurred 3 years earlier, with no residual symptoms. Of note, he had a mild COVID-19 infection 78 days before the onset of his pericarditis. After the onset of his COVID-19 vaccine-associated pericarditis, he continued to experience transient bouts of chest pressure and exertional dyspnea that resolved within 7 months of onset.
The median interval between COVID-19 vaccine doses in those who developed post-COVID-19 VAMP was within the recommended mRNA vaccine dosing intervals of 3 to 4 weeks and was consistent with the median mRNA vaccine dosing intervals among the entire cohort.
Due to the small cohort size and other limitations of this study, the suggested rate of cardiac injury in this review (4 cases in 179 persons, or 2.2%) is an imprecise estimate of risk in a small population (95% CI, 0.1%-4.4%). While this rate may seem higher than expected within the general population after COVID-19 vaccination, it is lower than the estimated lifetime risk of recurrent myocarditis from any cause.6,12
Discussion
To our knowledge, this is the first report describing cardiac outcomes after COVID-19 vaccination among a cohort of individuals with prior history of VAMP. Four cases of COVID-19 VAMP were identified among 179 patients with previous VAMP. All cases had experienced VAMP after the smallpox vaccine several years earlier, with complete resolution of symptoms. Three cases presented with recurrent VAMP after their second dose of an mRNA COVID-19 vaccine, and one after an mRNA booster dose. All fully recovered over the course of several months.
Myocarditis is a heterogeneous inflammatory injury with diverse, sometimes idiopathic, etiologies.13 In contrast to infection-related cardiac injury, prior reports of vaccine-associated myocarditis have suggested a hypersensitivity reaction characterized by patchy eosinophilic infiltrates, a benign clinical course, and good prognosis.2,3
There are several common features between VAMP after smallpox and COVID-19 vaccination. Cases occur predominantly in young men. The onset of symptoms after smallpox vaccine (mean, 10 days) and after mRNA COVID-19 vaccine (mean, 3 days) appears to correspond to the timing of peak postvaccination pro-inflammatory cytokine elevation.14 While all VAMP cases are serious events, the majority of patients appear to have a relatively benign clinical course with rapid and full recovery.13
Patients who have experienced an inflammatory cardiac injury may be at higher risk for recurrence, but quantifying risk of this rare phenomenon is challenging. Cases of VAMP after the COVID-19 vaccine have occasionally been reported in patients with previous cardiac injury unrelated to vaccination.15-17 The cases presented here represent the first report of recurrent VAMP following prior non-COVID-19 vaccinations.
Most patients with prior VAMP in this cohort did not experience cardiac-suggestive symptoms following COVID-19 vaccination. Among 11 patients who developed symptoms, 3 had confirmed myocarditis and 1 had confirmed pericarditis. The clinical course for these patients with recurrent VAMP was observed to be no different in severity or duration from those who experience new-onset VAMP.4 All other patients not meeting criteria for VAMP or having alternative explanations for their symptoms also had a benign clinical course. Nonetheless, of the study cohort of 179, recurrent VAMP was diagnosed in 4 of the 11 who developed cardiac-suggestive symptoms following COVID-19 vaccination. The importance of cardiac evaluation should be emphasized for any patient presenting with chest pain, dyspnea, or other cardiac-suggestive symptoms following vaccination.
Strengths and Limitations
The strength of this review of VAMP recurrence associated with COVID-19 vaccination derives from our large and unique longitudinal database of VAMP among current and prior service members. Additionally, the IHD’s ongoing enhanced vaccine AEs surveillance provides the opportunity to contact patients and review their electronic health records over an extended interval of time.
When interpreting this report’s implications, limitations inherent to any retrospective case review should be considered. The cohort of cases of prior VAMP included primarily healthy, fit, young service members; this population is not representative of the general population. The cohort included prior VAMP cases that generally occurred after smallpox vaccination. Experiences after smallpox vaccine may not apply to cardiac injury from other vaccines or etiologies. By the nature of this review, the population studied at the time of COVID-19 vaccination was somewhat older than those most likely to develop an initial bout of VAMP.2 This review was limited by information available in the electronic health records of a small number of patients. Subclinical cases of VAMP and cases without adequate clinical evaluation also could not be included.
Conclusions
Noninfectious inflammation of the heart (myocarditis, pericarditis, or myopericarditis) is a rare AE following certain vaccines, especially live replicating smallpox vaccine and mRNA COVID-19 vaccines. In this observational analysis, the majority of patients with previous VAMP successfully received a COVID-19 vaccine without recurrence. The 4 patients who were identified with recurrent VAMP following COVID-19 vaccination all recovered with supportive care. While the CDC endorses that individuals with a history of infectious myocarditis may receive COVID-19 vaccine after symptoms have resolved, there is currently insufficient safety data regarding COVID-19 vaccination of those with prior non-COVID-19 VAMP or following subsequent COVID-19 vaccination in those with prior VAMP related to COVID-19.10 For these individuals, COVID-19 vaccination is a precaution.10 Although insufficient to determine a precise level of risk, this report does provide data on which to base the CDC-recommended shared decision-making counseling of these patients. More research is needed to better define factors that increase risk for, or protection from, immune-mediated AEs following immunization, including VAMP. While benefits of vaccination have clearly outweighed risks during the COVID-19 pandemic, such research may optimize future vaccine recommendations.18
1. Decker MD, Garman PM, Hughes H, et al. Enhanced safety surveillance study of ACAM2000 smallpox vaccine among US military service members. Vaccine. 2021;39(39):5541-5547. doi:10.1016/j.vaccine.2021.08.041
2. Engler RJ, Nelson MR, Collins LC Jr, et al. A prospective study of the incidence of myocarditis/pericarditis and new onset cardiac symptoms following smallpox and influenza vaccination. PLoS One. 2015;10(3):e0118283. doi:10.1371/journal.pone.0118283
3. Faix DJ, Gordon DM, Perry LN, et al. Prospective safety surveillance study of ACAM2000 smallpox vaccine in deploying military personnel. Vaccine. 2020;38(46):7323-7330. doi:10.1016/j.vaccine.2020.09.037
4. Montgomery J, Ryan M, Engler R, et al. Myocarditis following immunization with mRNA COVID-19 vaccines in members of the US military. JAMA Cardiol. 2021;6(10):1202-1206. doi:10.1001/jamacardio.2021.2833
5. Witberg G, Barda N, Hoss S, et al. Myocarditis after Covid-19 vaccination in a large health care organization. N Engl J Med. 2021;385(23):2132-2139. doi:10.1056/NEJMoa2110737
6. Oster ME, Shay DK, Su JR, et al. Myocarditis cases reported after mRNA-based COVID-19 vaccination in the US from December 2020 to August 2021. JAMA. 2022;327(4):331-340. doi:10.1001/jama.2021.24110
7. Su JR, McNeil MM, Welsh KJ, et al. Myopericarditis after vaccination, Vaccine Adverse Event Reporting System (VAERS), 1990-2018. Vaccine. 2021;39(5):839-845. doi:10.1016/j.vaccine.2020.12.046
8. Mei R, Raschi E, Forcesi E, Diemberger I, De Ponti F, Poluzzi E. Myocarditis and pericarditis after immunization: gaining insights through the Vaccine Adverse Event Reporting System. Int J Cardiol. 2018;273:183-186. doi:10.1016/j.ijcard.2018.09.054
9. Centers for Disease Control and Prevention (CDC). Update: cardiac-related events during the civilian smallpox vaccination program—United States, 2003. MMWR Morb Mortal Wkly Rep. 2003;52(21):492-496.
10. Gargano JW, Wallace M, Hadler SC, et al. Use of mRNA COVID-19 vaccine after reports of myocarditis among vaccine recipients: update from the Advisory Committee on Immunization Practices—United States, June 2021. MMWR Morb Mortal Wkly Rep. 2021;70(27):977-982. doi:10.15585/mmwr.mm7027e2
11. Sexson Tejtel SK, Munoz FM, Al-Ammouri I, et al. Myocarditis and pericarditis: case definition and guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine. 2022;40(10):1499-1511. doi:10.1016/j.vaccine.2021.11.074
12. Sagar S, Liu PP, Cooper LT Jr. Myocarditis. Lancet. 2012;379(9817):738-747. doi:10.1016/S0140-6736(11) 60648-X
13. Heymans S, Cooper LT. Myocarditis after COVID-19 mRNA vaccination: clinical observations and potential mechanisms. Nat Rev Cardiol. 2022;19(2):75-77. doi:10.1038/s41569-021-00662-w
14. Cohen JI, Hohman P, Fulton R, et al. Kinetics of serum cytokines after primary or repeat vaccination with the smallpox vaccine. J Infect Dis. 2010;201(8):1183-1191. doi:10.1086/651453
15. Minocha PK, Better D, Singh RK, Hoque T. Recurrence of acute myocarditis temporally associated with receipt of the mRNA COVID-19 vaccine in an adolescent male. J Pediatr. 2021;238:321-323. doi:10.1016/j.jpeds.2021.06.035
16. Umei TC, Kishino Y, Watanabe K, et al. Recurrence of myopericarditis following mRNA COVID-19 vaccination in a male adolescent. CJC Open. 2022;4(3):350-352. doi:10.1016/j.cjco.2021.12.002
17. Pasha MA, Isaac S, Khan Z. Recurrent myocarditis following COVID-19 infection and the mRNA vaccine. Cureus. 2022;14(7):e26650. doi:10.7759/cureus.26650
18. Block JP, Boehmer TK, Forrest CB, et al. Cardiac complications after SARS-CoV-2 infection and mRNA COVID-19 vaccination—PCORnet, United States, January 2021-January 2022. MMWR Morb Mortal Wkly Rep. 2022;71(14):517-523. Published 2022 Apr 8. doi:10.15585/mmwr.mm7114e1
1. Decker MD, Garman PM, Hughes H, et al. Enhanced safety surveillance study of ACAM2000 smallpox vaccine among US military service members. Vaccine. 2021;39(39):5541-5547. doi:10.1016/j.vaccine.2021.08.041
2. Engler RJ, Nelson MR, Collins LC Jr, et al. A prospective study of the incidence of myocarditis/pericarditis and new onset cardiac symptoms following smallpox and influenza vaccination. PLoS One. 2015;10(3):e0118283. doi:10.1371/journal.pone.0118283
3. Faix DJ, Gordon DM, Perry LN, et al. Prospective safety surveillance study of ACAM2000 smallpox vaccine in deploying military personnel. Vaccine. 2020;38(46):7323-7330. doi:10.1016/j.vaccine.2020.09.037
4. Montgomery J, Ryan M, Engler R, et al. Myocarditis following immunization with mRNA COVID-19 vaccines in members of the US military. JAMA Cardiol. 2021;6(10):1202-1206. doi:10.1001/jamacardio.2021.2833
5. Witberg G, Barda N, Hoss S, et al. Myocarditis after Covid-19 vaccination in a large health care organization. N Engl J Med. 2021;385(23):2132-2139. doi:10.1056/NEJMoa2110737
6. Oster ME, Shay DK, Su JR, et al. Myocarditis cases reported after mRNA-based COVID-19 vaccination in the US from December 2020 to August 2021. JAMA. 2022;327(4):331-340. doi:10.1001/jama.2021.24110
7. Su JR, McNeil MM, Welsh KJ, et al. Myopericarditis after vaccination, Vaccine Adverse Event Reporting System (VAERS), 1990-2018. Vaccine. 2021;39(5):839-845. doi:10.1016/j.vaccine.2020.12.046
8. Mei R, Raschi E, Forcesi E, Diemberger I, De Ponti F, Poluzzi E. Myocarditis and pericarditis after immunization: gaining insights through the Vaccine Adverse Event Reporting System. Int J Cardiol. 2018;273:183-186. doi:10.1016/j.ijcard.2018.09.054
9. Centers for Disease Control and Prevention (CDC). Update: cardiac-related events during the civilian smallpox vaccination program—United States, 2003. MMWR Morb Mortal Wkly Rep. 2003;52(21):492-496.
10. Gargano JW, Wallace M, Hadler SC, et al. Use of mRNA COVID-19 vaccine after reports of myocarditis among vaccine recipients: update from the Advisory Committee on Immunization Practices—United States, June 2021. MMWR Morb Mortal Wkly Rep. 2021;70(27):977-982. doi:10.15585/mmwr.mm7027e2
11. Sexson Tejtel SK, Munoz FM, Al-Ammouri I, et al. Myocarditis and pericarditis: case definition and guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine. 2022;40(10):1499-1511. doi:10.1016/j.vaccine.2021.11.074
12. Sagar S, Liu PP, Cooper LT Jr. Myocarditis. Lancet. 2012;379(9817):738-747. doi:10.1016/S0140-6736(11) 60648-X
13. Heymans S, Cooper LT. Myocarditis after COVID-19 mRNA vaccination: clinical observations and potential mechanisms. Nat Rev Cardiol. 2022;19(2):75-77. doi:10.1038/s41569-021-00662-w
14. Cohen JI, Hohman P, Fulton R, et al. Kinetics of serum cytokines after primary or repeat vaccination with the smallpox vaccine. J Infect Dis. 2010;201(8):1183-1191. doi:10.1086/651453
15. Minocha PK, Better D, Singh RK, Hoque T. Recurrence of acute myocarditis temporally associated with receipt of the mRNA COVID-19 vaccine in an adolescent male. J Pediatr. 2021;238:321-323. doi:10.1016/j.jpeds.2021.06.035
16. Umei TC, Kishino Y, Watanabe K, et al. Recurrence of myopericarditis following mRNA COVID-19 vaccination in a male adolescent. CJC Open. 2022;4(3):350-352. doi:10.1016/j.cjco.2021.12.002
17. Pasha MA, Isaac S, Khan Z. Recurrent myocarditis following COVID-19 infection and the mRNA vaccine. Cureus. 2022;14(7):e26650. doi:10.7759/cureus.26650
18. Block JP, Boehmer TK, Forrest CB, et al. Cardiac complications after SARS-CoV-2 infection and mRNA COVID-19 vaccination—PCORnet, United States, January 2021-January 2022. MMWR Morb Mortal Wkly Rep. 2022;71(14):517-523. Published 2022 Apr 8. doi:10.15585/mmwr.mm7114e1
Can siRNA improve compliance in patients with hypertension?
Many approaches have been explored in recent years to make life easier for patients living with chronic conditions that require them to take daily medication: subcutaneous implantable devices, nanogels, and, more specifically in the case of hypertension, renal denervation or small interfering RNA (siRNA) with a long half-life.
It’s siRNA that Michel Azizi, MD, PhD, head of the blood pressure clinic at Georges Pompidou European Hospital (HEGP) in Paris, discussed at the International Meeting of the French Society of Hypertension.
These small molecules have already shown their worth in treating rare diseases such as transthyretin amyloidosis. More recently, treating hypercholesterolemia with the PCSK9 inhibitor inclisiran has proven effective. “One subcutaneous injection of inclisiran reduces LDL cholesterol by 50% for a period of 210 days,” said Dr. Azizi.
The benefit of a new therapeutic siRNA – zilebesiran, administered subcutaneously – in treating hypertension is currently the subject of a phase II clinical trial.
This is a double-stranded RNA. One of the strands is linked to a sugar, N-acetylgalactosamine (GalNAc), which protects these highly fragile siRNA and binds with a very strong affinity in the liver. The second strand binds to a specific area of the RNA to prevent synthesis of the precursor peptide of angiotensin, angiotensinogen. The resulting effect is suppression of the production of angiotensin I and II, which leads to a long-lasting lowering of blood pressure.
Lasting efficacy
Phase I studies with zilebesiran have demonstrated a long-term effect, with a reduction of greater than 90% in circulating angiotensinogen over 6 months after a single subcutaneous dose (800 mg). The peak in reduction of circulating angiotensinogen occurs after approximately 3 weeks.
“It’s extremely powerful,” said Dr. Azizi.
Lasting reductions in blood pressure have also been observed, with 24-hour ambulatory blood pressure monitoring showing a reduction in systolic BP of greater than 15 mm Hg 8 weeks after administration of a single dose of zilebesiran (800 mg).
Zilebesiran was also well tolerated, with only mild to moderate reactions at the site of the injection (n = 5/56) and no serious treatment-related adverse events, hypotension, or significant changes in kidney or liver function.
“In terms of benefits, the effect is ongoing. Zilebesiran leads to reduced medication use and causes less variability in blood pressure response. Nevertheless, interfering RNA acts slowly, meaning that zilebesiran would not be suitable for people presenting with a hypertensive crisis. The fact that it blocks the renin-angiotensin system [RAS] for a very long period of time also poses the question of how to reverse its hypotensive effects,” said Dr. Azizi.
Unanswered questions
The lasting RAS antagonist and blood pressure–lowering effects pose a potential safety problem in circumstances involving patients in a state of hypovolemia and hypotension who require rapid blood pressure–raising interventions to prevent morbidity and mortality.
In recent studies, Estrellita Uijl et al. have thus examined strategies to counteract the blood pressure–lowering effect of siRNA in spontaneously hypertensive rats.
Fludrocortisone and a high-salt diet were both successful in gradually increasing blood pressure, which returned to its baseline levels on days 5 and 7, respectively. Yet this rate of response would be wholly inadequate in an urgent clinical situation.
However, midodrine could not reduce blood pressure to normal levels, whether administered subcutaneously or orally.
A rapid and short-lasting increase in blood pressure was observed with bolus doses of vasopressors, but clinically, these would need to be administered intravenously to achieve a lasting effect. Such administration would require hospitalization, close monitoring, and the use of human resources and additional health care provisions.
Encouragingly, the laboratory that created this molecule, Alnylam Pharmaceuticals, has come up with an antidote: Reversir. It is a GalNAc-conjugated, single-stranded, high-affinity oligonucleotide complementary to the zilebesiran strand that achieves effective reversal of siRNA activity in 24 hours.
In the future, after the phase 2 trials have been completed, whether or not zilebesiran reduces the incidence of cardiovascular events and mortality remains to be seen. But as for Dr. Azizi, the director of HEGP’s blood pressure clinic in Paris, he has no doubt that “this approach is about to shake up how we treat patients in the cardiovascular field.”
On the horizon
Zilebesiran is being studied in phase 2 trials in patients with mild to moderate hypertension not taking antihypertensive drugs (KARDIA-1: 375 patients; double-blind, placebo-controlled, five-arm trial; zilebesiran at 150, 300, and 600 mg twice per year and 300 mg once every 3 months) and in patients whose blood pressure is not controlled (KARDIA-2: 800 patients; initial open-label start-up period of 4 weeks with indapamide/amlodipine/olmesartan, followed by a double-blind, placebo-controlled study over 6 months, then an open-label extension study for up to 12 additional months; zilebesiran at 600 mg on the first day of the initial double-blind period, then every 6 months during the open-label extension period).
This article was translated from the Medscape French edition and a version appeared on Medscape.com.
Many approaches have been explored in recent years to make life easier for patients living with chronic conditions that require them to take daily medication: subcutaneous implantable devices, nanogels, and, more specifically in the case of hypertension, renal denervation or small interfering RNA (siRNA) with a long half-life.
It’s siRNA that Michel Azizi, MD, PhD, head of the blood pressure clinic at Georges Pompidou European Hospital (HEGP) in Paris, discussed at the International Meeting of the French Society of Hypertension.
These small molecules have already shown their worth in treating rare diseases such as transthyretin amyloidosis. More recently, treating hypercholesterolemia with the PCSK9 inhibitor inclisiran has proven effective. “One subcutaneous injection of inclisiran reduces LDL cholesterol by 50% for a period of 210 days,” said Dr. Azizi.
The benefit of a new therapeutic siRNA – zilebesiran, administered subcutaneously – in treating hypertension is currently the subject of a phase II clinical trial.
This is a double-stranded RNA. One of the strands is linked to a sugar, N-acetylgalactosamine (GalNAc), which protects these highly fragile siRNA and binds with a very strong affinity in the liver. The second strand binds to a specific area of the RNA to prevent synthesis of the precursor peptide of angiotensin, angiotensinogen. The resulting effect is suppression of the production of angiotensin I and II, which leads to a long-lasting lowering of blood pressure.
Lasting efficacy
Phase I studies with zilebesiran have demonstrated a long-term effect, with a reduction of greater than 90% in circulating angiotensinogen over 6 months after a single subcutaneous dose (800 mg). The peak in reduction of circulating angiotensinogen occurs after approximately 3 weeks.
“It’s extremely powerful,” said Dr. Azizi.
Lasting reductions in blood pressure have also been observed, with 24-hour ambulatory blood pressure monitoring showing a reduction in systolic BP of greater than 15 mm Hg 8 weeks after administration of a single dose of zilebesiran (800 mg).
Zilebesiran was also well tolerated, with only mild to moderate reactions at the site of the injection (n = 5/56) and no serious treatment-related adverse events, hypotension, or significant changes in kidney or liver function.
“In terms of benefits, the effect is ongoing. Zilebesiran leads to reduced medication use and causes less variability in blood pressure response. Nevertheless, interfering RNA acts slowly, meaning that zilebesiran would not be suitable for people presenting with a hypertensive crisis. The fact that it blocks the renin-angiotensin system [RAS] for a very long period of time also poses the question of how to reverse its hypotensive effects,” said Dr. Azizi.
Unanswered questions
The lasting RAS antagonist and blood pressure–lowering effects pose a potential safety problem in circumstances involving patients in a state of hypovolemia and hypotension who require rapid blood pressure–raising interventions to prevent morbidity and mortality.
In recent studies, Estrellita Uijl et al. have thus examined strategies to counteract the blood pressure–lowering effect of siRNA in spontaneously hypertensive rats.
Fludrocortisone and a high-salt diet were both successful in gradually increasing blood pressure, which returned to its baseline levels on days 5 and 7, respectively. Yet this rate of response would be wholly inadequate in an urgent clinical situation.
However, midodrine could not reduce blood pressure to normal levels, whether administered subcutaneously or orally.
A rapid and short-lasting increase in blood pressure was observed with bolus doses of vasopressors, but clinically, these would need to be administered intravenously to achieve a lasting effect. Such administration would require hospitalization, close monitoring, and the use of human resources and additional health care provisions.
Encouragingly, the laboratory that created this molecule, Alnylam Pharmaceuticals, has come up with an antidote: Reversir. It is a GalNAc-conjugated, single-stranded, high-affinity oligonucleotide complementary to the zilebesiran strand that achieves effective reversal of siRNA activity in 24 hours.
In the future, after the phase 2 trials have been completed, whether or not zilebesiran reduces the incidence of cardiovascular events and mortality remains to be seen. But as for Dr. Azizi, the director of HEGP’s blood pressure clinic in Paris, he has no doubt that “this approach is about to shake up how we treat patients in the cardiovascular field.”
On the horizon
Zilebesiran is being studied in phase 2 trials in patients with mild to moderate hypertension not taking antihypertensive drugs (KARDIA-1: 375 patients; double-blind, placebo-controlled, five-arm trial; zilebesiran at 150, 300, and 600 mg twice per year and 300 mg once every 3 months) and in patients whose blood pressure is not controlled (KARDIA-2: 800 patients; initial open-label start-up period of 4 weeks with indapamide/amlodipine/olmesartan, followed by a double-blind, placebo-controlled study over 6 months, then an open-label extension study for up to 12 additional months; zilebesiran at 600 mg on the first day of the initial double-blind period, then every 6 months during the open-label extension period).
This article was translated from the Medscape French edition and a version appeared on Medscape.com.
Many approaches have been explored in recent years to make life easier for patients living with chronic conditions that require them to take daily medication: subcutaneous implantable devices, nanogels, and, more specifically in the case of hypertension, renal denervation or small interfering RNA (siRNA) with a long half-life.
It’s siRNA that Michel Azizi, MD, PhD, head of the blood pressure clinic at Georges Pompidou European Hospital (HEGP) in Paris, discussed at the International Meeting of the French Society of Hypertension.
These small molecules have already shown their worth in treating rare diseases such as transthyretin amyloidosis. More recently, treating hypercholesterolemia with the PCSK9 inhibitor inclisiran has proven effective. “One subcutaneous injection of inclisiran reduces LDL cholesterol by 50% for a period of 210 days,” said Dr. Azizi.
The benefit of a new therapeutic siRNA – zilebesiran, administered subcutaneously – in treating hypertension is currently the subject of a phase II clinical trial.
This is a double-stranded RNA. One of the strands is linked to a sugar, N-acetylgalactosamine (GalNAc), which protects these highly fragile siRNA and binds with a very strong affinity in the liver. The second strand binds to a specific area of the RNA to prevent synthesis of the precursor peptide of angiotensin, angiotensinogen. The resulting effect is suppression of the production of angiotensin I and II, which leads to a long-lasting lowering of blood pressure.
Lasting efficacy
Phase I studies with zilebesiran have demonstrated a long-term effect, with a reduction of greater than 90% in circulating angiotensinogen over 6 months after a single subcutaneous dose (800 mg). The peak in reduction of circulating angiotensinogen occurs after approximately 3 weeks.
“It’s extremely powerful,” said Dr. Azizi.
Lasting reductions in blood pressure have also been observed, with 24-hour ambulatory blood pressure monitoring showing a reduction in systolic BP of greater than 15 mm Hg 8 weeks after administration of a single dose of zilebesiran (800 mg).
Zilebesiran was also well tolerated, with only mild to moderate reactions at the site of the injection (n = 5/56) and no serious treatment-related adverse events, hypotension, or significant changes in kidney or liver function.
“In terms of benefits, the effect is ongoing. Zilebesiran leads to reduced medication use and causes less variability in blood pressure response. Nevertheless, interfering RNA acts slowly, meaning that zilebesiran would not be suitable for people presenting with a hypertensive crisis. The fact that it blocks the renin-angiotensin system [RAS] for a very long period of time also poses the question of how to reverse its hypotensive effects,” said Dr. Azizi.
Unanswered questions
The lasting RAS antagonist and blood pressure–lowering effects pose a potential safety problem in circumstances involving patients in a state of hypovolemia and hypotension who require rapid blood pressure–raising interventions to prevent morbidity and mortality.
In recent studies, Estrellita Uijl et al. have thus examined strategies to counteract the blood pressure–lowering effect of siRNA in spontaneously hypertensive rats.
Fludrocortisone and a high-salt diet were both successful in gradually increasing blood pressure, which returned to its baseline levels on days 5 and 7, respectively. Yet this rate of response would be wholly inadequate in an urgent clinical situation.
However, midodrine could not reduce blood pressure to normal levels, whether administered subcutaneously or orally.
A rapid and short-lasting increase in blood pressure was observed with bolus doses of vasopressors, but clinically, these would need to be administered intravenously to achieve a lasting effect. Such administration would require hospitalization, close monitoring, and the use of human resources and additional health care provisions.
Encouragingly, the laboratory that created this molecule, Alnylam Pharmaceuticals, has come up with an antidote: Reversir. It is a GalNAc-conjugated, single-stranded, high-affinity oligonucleotide complementary to the zilebesiran strand that achieves effective reversal of siRNA activity in 24 hours.
In the future, after the phase 2 trials have been completed, whether or not zilebesiran reduces the incidence of cardiovascular events and mortality remains to be seen. But as for Dr. Azizi, the director of HEGP’s blood pressure clinic in Paris, he has no doubt that “this approach is about to shake up how we treat patients in the cardiovascular field.”
On the horizon
Zilebesiran is being studied in phase 2 trials in patients with mild to moderate hypertension not taking antihypertensive drugs (KARDIA-1: 375 patients; double-blind, placebo-controlled, five-arm trial; zilebesiran at 150, 300, and 600 mg twice per year and 300 mg once every 3 months) and in patients whose blood pressure is not controlled (KARDIA-2: 800 patients; initial open-label start-up period of 4 weeks with indapamide/amlodipine/olmesartan, followed by a double-blind, placebo-controlled study over 6 months, then an open-label extension study for up to 12 additional months; zilebesiran at 600 mg on the first day of the initial double-blind period, then every 6 months during the open-label extension period).
This article was translated from the Medscape French edition and a version appeared on Medscape.com.
AT INTERNATIONAL MEETING OF THE FRENCH SOCIETY OF HYPERTENSION
Atrial failure or insufficiency: A new syndrome
Atrial dysfunction, widely considered a marker or consequence of other heart diseases, is a relevant clinical entity, which is why it is justified to define atrial failure or insufficiency as “a new syndrome that all cardiologists should be aware of,” said Adrián Baranchuk, MD, PhD, professor of medicine at Queen’s University, Kingston, Ont., during the 2022 48th Argentine Congress of Cardiology in Buenos Aires.
“The atria are like the heart’s silly sisters and can fail just like the ventricle fails. Understanding their function and dysfunction helps us to understand heart failure. And as electrophysiologists and clinical cardiologists, we have to embrace this concept and understand it in depth,” Dr. Baranchuk, president-elect of the Inter-American Society of Cardiology, said in an interview.
The specialist first proposed atrial failure as an entity or syndrome in early 2020 in an article in the Journal of the American College of Cardiology. His four collaborators included the experienced Eugene Braunwald, MD, from Brigham and Women’s Hospital, Boston, and Antoni Bayés de Luna, PhD, from the department of medicine of the autonomous University of Barcelona.
Pathology despite function
“In many patients with heart failure, the pump function is preserved, but what causes the pathology? For the last 5-10 years, attention has been focused on the ventricle: whether it contracts poorly or whether it contracts properly and relaxes poorly. However, we have also seen patients in whom the ventricle contracts properly and relaxes properly. Where else can we look? We started looking at atrial contraction, especially the left atrium,” recalled Dr. Baranchuk.
He and his colleagues proposed the following consensus definition of atrial failure or insufficiency: any atrial dysfunction (anatomical, mechanical, electrical, and rheological, including blood homeostasis) that causes impaired function, heart symptoms, and a worsening of quality of life (or life expectancy) in the absence of significant valvular or ventricular abnormalities.
In his presentation, recorded and projected by video from Canada, Dr. Baranchuk pointed out that there are two large groups of causes of atrial failure: one that has to do with electrical disorders of atrial and interatrial contraction and another related to the progressive development of fibrosis, which gradually leads to dyssynchrony in interatrial contraction, pump failure, and impaired atrial function as a reservoir and as a conduit.
“In turn, these mechanisms trigger neurohormonal alterations that perpetuate atrial failure, so it is not just a matter of progressive fibrosis, which is very difficult to treat, but also of constant neurohormonal activation that guarantees that these phenomena never resolve,” said Dr. Baranchuk. The manifestations or end point of this cascade of events are the known ones: stroke, ischemia, and heart failure.
New entity necessary?
Defining atrial failure or insufficiency as a clinical entity not only restores the hierarchy of the atria in cardiac function, which was already postulated by William Harvey in 1628, but also enables new lines of research that would eventually allow timely preventive interventions.
One key is early recognition of partial or total interatrial block by analyzing the characteristics of the P wave on the electrocardiogram, which could serve to prevent progression to atrial fibrillation. Left atrial enlargement can also be detected by echocardiography.
“When the contractile impairment is severe and you are in atrial fibrillation, all that remains is to apply patches. The strategy is to correct risk factors beforehand, such as high blood pressure, sleep apnea, or high-dose alcohol consumption, as well as tirelessly searching for atrial fibrillation, with Holter electrocardiograms, continuous monitoring devices, such as Apple Watch, KardiaMobile, or an implantable loop recorder,” Dr. Baranchuk said in an interview.
Two ongoing or planned studies, ARCADIA and AMIABLE, will seek to determine whether anticoagulation in patients with elevated cardiovascular risk scores and any of these atrial disorders that have not yet led to atrial fibrillation could reduce the incidence of stroke.
The strategy has a rational basis. In a subanalysis of raw data from the NAVIGATE ESUS study in patients with embolic stroke of unknown cause, Dr. Baranchuk estimated that the presence of interatrial block was a tenfold higher predictor of the risk of experiencing a second stroke. Another 2018 observational study in which he participated found that in outpatients with heart failure, advanced interatrial block approximately tripled the risk of developing atrial fibrillation and ischemic stroke.
For Dr. Baranchuk, other questions that still need to be answered include whether drugs used for heart failure with preserved ejection fraction can be useful in primary atrial failure or whether specific drugs can be repositioned or developed to suppress or slow the process of fibrosis. “From generating the clinical concept, many lines of research are enabled.”
“The concept of atrial failure is very interesting and opens our eyes to treatments,” another speaker at the session, Alejo Tronconi, MD, a cardiologist and electrophysiologist at the Cardiovascular Institute of the South, Cipolletti, Argentina, said in an interview.
“It is necessary to cut circuits that have been extensively studied in heart failure models, and now we are beginning to see their participation in atrial dysfunction,” he said.
Dr. Baranchuk and Dr. Tronconi declared no relevant financial conflict of interest.
A version of this article first appeared on Medscape.com.
Atrial dysfunction, widely considered a marker or consequence of other heart diseases, is a relevant clinical entity, which is why it is justified to define atrial failure or insufficiency as “a new syndrome that all cardiologists should be aware of,” said Adrián Baranchuk, MD, PhD, professor of medicine at Queen’s University, Kingston, Ont., during the 2022 48th Argentine Congress of Cardiology in Buenos Aires.
“The atria are like the heart’s silly sisters and can fail just like the ventricle fails. Understanding their function and dysfunction helps us to understand heart failure. And as electrophysiologists and clinical cardiologists, we have to embrace this concept and understand it in depth,” Dr. Baranchuk, president-elect of the Inter-American Society of Cardiology, said in an interview.
The specialist first proposed atrial failure as an entity or syndrome in early 2020 in an article in the Journal of the American College of Cardiology. His four collaborators included the experienced Eugene Braunwald, MD, from Brigham and Women’s Hospital, Boston, and Antoni Bayés de Luna, PhD, from the department of medicine of the autonomous University of Barcelona.
Pathology despite function
“In many patients with heart failure, the pump function is preserved, but what causes the pathology? For the last 5-10 years, attention has been focused on the ventricle: whether it contracts poorly or whether it contracts properly and relaxes poorly. However, we have also seen patients in whom the ventricle contracts properly and relaxes properly. Where else can we look? We started looking at atrial contraction, especially the left atrium,” recalled Dr. Baranchuk.
He and his colleagues proposed the following consensus definition of atrial failure or insufficiency: any atrial dysfunction (anatomical, mechanical, electrical, and rheological, including blood homeostasis) that causes impaired function, heart symptoms, and a worsening of quality of life (or life expectancy) in the absence of significant valvular or ventricular abnormalities.
In his presentation, recorded and projected by video from Canada, Dr. Baranchuk pointed out that there are two large groups of causes of atrial failure: one that has to do with electrical disorders of atrial and interatrial contraction and another related to the progressive development of fibrosis, which gradually leads to dyssynchrony in interatrial contraction, pump failure, and impaired atrial function as a reservoir and as a conduit.
“In turn, these mechanisms trigger neurohormonal alterations that perpetuate atrial failure, so it is not just a matter of progressive fibrosis, which is very difficult to treat, but also of constant neurohormonal activation that guarantees that these phenomena never resolve,” said Dr. Baranchuk. The manifestations or end point of this cascade of events are the known ones: stroke, ischemia, and heart failure.
New entity necessary?
Defining atrial failure or insufficiency as a clinical entity not only restores the hierarchy of the atria in cardiac function, which was already postulated by William Harvey in 1628, but also enables new lines of research that would eventually allow timely preventive interventions.
One key is early recognition of partial or total interatrial block by analyzing the characteristics of the P wave on the electrocardiogram, which could serve to prevent progression to atrial fibrillation. Left atrial enlargement can also be detected by echocardiography.
“When the contractile impairment is severe and you are in atrial fibrillation, all that remains is to apply patches. The strategy is to correct risk factors beforehand, such as high blood pressure, sleep apnea, or high-dose alcohol consumption, as well as tirelessly searching for atrial fibrillation, with Holter electrocardiograms, continuous monitoring devices, such as Apple Watch, KardiaMobile, or an implantable loop recorder,” Dr. Baranchuk said in an interview.
Two ongoing or planned studies, ARCADIA and AMIABLE, will seek to determine whether anticoagulation in patients with elevated cardiovascular risk scores and any of these atrial disorders that have not yet led to atrial fibrillation could reduce the incidence of stroke.
The strategy has a rational basis. In a subanalysis of raw data from the NAVIGATE ESUS study in patients with embolic stroke of unknown cause, Dr. Baranchuk estimated that the presence of interatrial block was a tenfold higher predictor of the risk of experiencing a second stroke. Another 2018 observational study in which he participated found that in outpatients with heart failure, advanced interatrial block approximately tripled the risk of developing atrial fibrillation and ischemic stroke.
For Dr. Baranchuk, other questions that still need to be answered include whether drugs used for heart failure with preserved ejection fraction can be useful in primary atrial failure or whether specific drugs can be repositioned or developed to suppress or slow the process of fibrosis. “From generating the clinical concept, many lines of research are enabled.”
“The concept of atrial failure is very interesting and opens our eyes to treatments,” another speaker at the session, Alejo Tronconi, MD, a cardiologist and electrophysiologist at the Cardiovascular Institute of the South, Cipolletti, Argentina, said in an interview.
“It is necessary to cut circuits that have been extensively studied in heart failure models, and now we are beginning to see their participation in atrial dysfunction,” he said.
Dr. Baranchuk and Dr. Tronconi declared no relevant financial conflict of interest.
A version of this article first appeared on Medscape.com.
Atrial dysfunction, widely considered a marker or consequence of other heart diseases, is a relevant clinical entity, which is why it is justified to define atrial failure or insufficiency as “a new syndrome that all cardiologists should be aware of,” said Adrián Baranchuk, MD, PhD, professor of medicine at Queen’s University, Kingston, Ont., during the 2022 48th Argentine Congress of Cardiology in Buenos Aires.
“The atria are like the heart’s silly sisters and can fail just like the ventricle fails. Understanding their function and dysfunction helps us to understand heart failure. And as electrophysiologists and clinical cardiologists, we have to embrace this concept and understand it in depth,” Dr. Baranchuk, president-elect of the Inter-American Society of Cardiology, said in an interview.
The specialist first proposed atrial failure as an entity or syndrome in early 2020 in an article in the Journal of the American College of Cardiology. His four collaborators included the experienced Eugene Braunwald, MD, from Brigham and Women’s Hospital, Boston, and Antoni Bayés de Luna, PhD, from the department of medicine of the autonomous University of Barcelona.
Pathology despite function
“In many patients with heart failure, the pump function is preserved, but what causes the pathology? For the last 5-10 years, attention has been focused on the ventricle: whether it contracts poorly or whether it contracts properly and relaxes poorly. However, we have also seen patients in whom the ventricle contracts properly and relaxes properly. Where else can we look? We started looking at atrial contraction, especially the left atrium,” recalled Dr. Baranchuk.
He and his colleagues proposed the following consensus definition of atrial failure or insufficiency: any atrial dysfunction (anatomical, mechanical, electrical, and rheological, including blood homeostasis) that causes impaired function, heart symptoms, and a worsening of quality of life (or life expectancy) in the absence of significant valvular or ventricular abnormalities.
In his presentation, recorded and projected by video from Canada, Dr. Baranchuk pointed out that there are two large groups of causes of atrial failure: one that has to do with electrical disorders of atrial and interatrial contraction and another related to the progressive development of fibrosis, which gradually leads to dyssynchrony in interatrial contraction, pump failure, and impaired atrial function as a reservoir and as a conduit.
“In turn, these mechanisms trigger neurohormonal alterations that perpetuate atrial failure, so it is not just a matter of progressive fibrosis, which is very difficult to treat, but also of constant neurohormonal activation that guarantees that these phenomena never resolve,” said Dr. Baranchuk. The manifestations or end point of this cascade of events are the known ones: stroke, ischemia, and heart failure.
New entity necessary?
Defining atrial failure or insufficiency as a clinical entity not only restores the hierarchy of the atria in cardiac function, which was already postulated by William Harvey in 1628, but also enables new lines of research that would eventually allow timely preventive interventions.
One key is early recognition of partial or total interatrial block by analyzing the characteristics of the P wave on the electrocardiogram, which could serve to prevent progression to atrial fibrillation. Left atrial enlargement can also be detected by echocardiography.
“When the contractile impairment is severe and you are in atrial fibrillation, all that remains is to apply patches. The strategy is to correct risk factors beforehand, such as high blood pressure, sleep apnea, or high-dose alcohol consumption, as well as tirelessly searching for atrial fibrillation, with Holter electrocardiograms, continuous monitoring devices, such as Apple Watch, KardiaMobile, or an implantable loop recorder,” Dr. Baranchuk said in an interview.
Two ongoing or planned studies, ARCADIA and AMIABLE, will seek to determine whether anticoagulation in patients with elevated cardiovascular risk scores and any of these atrial disorders that have not yet led to atrial fibrillation could reduce the incidence of stroke.
The strategy has a rational basis. In a subanalysis of raw data from the NAVIGATE ESUS study in patients with embolic stroke of unknown cause, Dr. Baranchuk estimated that the presence of interatrial block was a tenfold higher predictor of the risk of experiencing a second stroke. Another 2018 observational study in which he participated found that in outpatients with heart failure, advanced interatrial block approximately tripled the risk of developing atrial fibrillation and ischemic stroke.
For Dr. Baranchuk, other questions that still need to be answered include whether drugs used for heart failure with preserved ejection fraction can be useful in primary atrial failure or whether specific drugs can be repositioned or developed to suppress or slow the process of fibrosis. “From generating the clinical concept, many lines of research are enabled.”
“The concept of atrial failure is very interesting and opens our eyes to treatments,” another speaker at the session, Alejo Tronconi, MD, a cardiologist and electrophysiologist at the Cardiovascular Institute of the South, Cipolletti, Argentina, said in an interview.
“It is necessary to cut circuits that have been extensively studied in heart failure models, and now we are beginning to see their participation in atrial dysfunction,” he said.
Dr. Baranchuk and Dr. Tronconi declared no relevant financial conflict of interest.
A version of this article first appeared on Medscape.com.
What is the optimal pad position in transcutaneous pacing?
Transvenous pacing is typically the most effective therapy for unstable bradycardia but it is invasive, takes some time to perform, and is a procedure for which many acute care physicians lack comfort and significant experience. Transcutaneous pacing (TCP), on the other hand, is fast, easy to perform, and tends to be well tolerated by most patients when they receive appropriate doses of analgesia.
Unfortunately, TCP often fails to produce electrical or, more importantly, mechanical capture. Oftentimes when capture initially fails, the electrical current is increased in hopes of gaining capture but much to the discomfort of the patient. Increased body mass index can contribute to failure to capture, but what about TCP pad position? Despite recommendations for TCP in the United States and European resuscitation guidelines for many years, until now, no studies have evaluated optimal pad position for TCP. As a result, the default position for most clinicians using TCP has been the anterior-lateral (AL) position on the chest wall.
A study published in October 2022 compared the common AL position (anterior pad placed at the right upper chest and lateral pad placed over the left lower rib cage at the mid-axillary line) with the anterior-posterior (AP) position (anterior pad placed on the left chest over the apex of the heart and the posterior pad on the left mid-back area approximating the level of the mid-portion of the heart). The AP position has become more commonly used in defibrillating arrested hearts because it more accurately sends the current through the left ventricle. The concern with the AL position, especially in patients with large body habitus, is that the vector of the current may partially or entirely miss the left ventricle.
Moayedi and colleagues hypothesized that optimal TCP should employ pad placement that is similar to that used during optimal defibrillation attempts. They conducted a study comparing AL versus AP position during TCP and published their results in two parts, which will be discussed together.
The investigators evaluated 20 patients (6 women, 14 men) who had elective cardioversion of atrial fibrillation in the electrophysiology lab (Resuscitation. 2022 Dec;181:140-6). After successful cardioversion to sinus rhythm, the cardioversion pads were removed, and two new sets of pacer pads were placed on the patients’ chests. Pads were placed in both the AL and the AP positions, as previously described. Starting at a current output of 40 mA, the output was slowly increased on one set of pads until mechanical capture was obtained at the same rate as the pacer setting for at least 10 seconds. Pacing was then discontinued, but then the process was repeated using the second set of pads. The order in which the positions were tested (that is, AL tested first vs. AP tested first) was alternated. If capture was not obtained by 140 mA (the pacer’s maximum output), failure to capture was documented. Both positions were tested in all patients except for three cases where the second position was not tested because of inadequate analgesia.
The investigators found that 8 in 19 (42%) of the AL trials and 14 in 18 (78%) of the AP trials successfully captured. For the 17 participants who completed both trials, both positions captured in 8 in 17 (47%). AP but not AL was captured in 5 in 17 (29%); AL but not AP was captured in 0 cases. Neither position captured in 4 in 17 (24%). Of note, there was no association between successful capture and body mass index, chest circumference, or chest diameter. The AP position was more successful in both women and men, compared with the AL position. The investigators also found that, among the successful trials, the AP position tended to capture at lower currents than the AL position (93 mA vs. 126 mA).
In summary
TCP is a potentially lifesaving intervention in the treatment of patients with unstable bradycardia. Many of us who have attempted to perform TCP on unstable patients have frequently been disappointed with the results. In retrospect, however, I can recall that each time I have attempted this procedure, it has been using pads placed in the AL position.
Now for the first time we have data indicating that the standard AL position may be suboptimal, compared with the AP position. The study by Moayedi and colleagues is small, but the results are compelling, and the AP pad placement intuitively makes more sense. By using the AP pad placement, which provides greater likelihood of electrical current passing through the left ventricle, we should expect a greater likelihood of successful capture during attempts at TCP. In addition, we may anticipate lower analgesia needs if the AP position requires less current for success. Kudos to Moayedi and colleagues for performing a novel study of a critical procedure in acute care medicine.
Amal Mattu, MD, is a professor, vice chair of education, and codirector of the emergency cardiology fellowship in the department of emergency medicine at the University of Maryland, Baltimore. He had no disclosures. A version of this article first appeared on Medscape.com.
Transvenous pacing is typically the most effective therapy for unstable bradycardia but it is invasive, takes some time to perform, and is a procedure for which many acute care physicians lack comfort and significant experience. Transcutaneous pacing (TCP), on the other hand, is fast, easy to perform, and tends to be well tolerated by most patients when they receive appropriate doses of analgesia.
Unfortunately, TCP often fails to produce electrical or, more importantly, mechanical capture. Oftentimes when capture initially fails, the electrical current is increased in hopes of gaining capture but much to the discomfort of the patient. Increased body mass index can contribute to failure to capture, but what about TCP pad position? Despite recommendations for TCP in the United States and European resuscitation guidelines for many years, until now, no studies have evaluated optimal pad position for TCP. As a result, the default position for most clinicians using TCP has been the anterior-lateral (AL) position on the chest wall.
A study published in October 2022 compared the common AL position (anterior pad placed at the right upper chest and lateral pad placed over the left lower rib cage at the mid-axillary line) with the anterior-posterior (AP) position (anterior pad placed on the left chest over the apex of the heart and the posterior pad on the left mid-back area approximating the level of the mid-portion of the heart). The AP position has become more commonly used in defibrillating arrested hearts because it more accurately sends the current through the left ventricle. The concern with the AL position, especially in patients with large body habitus, is that the vector of the current may partially or entirely miss the left ventricle.
Moayedi and colleagues hypothesized that optimal TCP should employ pad placement that is similar to that used during optimal defibrillation attempts. They conducted a study comparing AL versus AP position during TCP and published their results in two parts, which will be discussed together.
The investigators evaluated 20 patients (6 women, 14 men) who had elective cardioversion of atrial fibrillation in the electrophysiology lab (Resuscitation. 2022 Dec;181:140-6). After successful cardioversion to sinus rhythm, the cardioversion pads were removed, and two new sets of pacer pads were placed on the patients’ chests. Pads were placed in both the AL and the AP positions, as previously described. Starting at a current output of 40 mA, the output was slowly increased on one set of pads until mechanical capture was obtained at the same rate as the pacer setting for at least 10 seconds. Pacing was then discontinued, but then the process was repeated using the second set of pads. The order in which the positions were tested (that is, AL tested first vs. AP tested first) was alternated. If capture was not obtained by 140 mA (the pacer’s maximum output), failure to capture was documented. Both positions were tested in all patients except for three cases where the second position was not tested because of inadequate analgesia.
The investigators found that 8 in 19 (42%) of the AL trials and 14 in 18 (78%) of the AP trials successfully captured. For the 17 participants who completed both trials, both positions captured in 8 in 17 (47%). AP but not AL was captured in 5 in 17 (29%); AL but not AP was captured in 0 cases. Neither position captured in 4 in 17 (24%). Of note, there was no association between successful capture and body mass index, chest circumference, or chest diameter. The AP position was more successful in both women and men, compared with the AL position. The investigators also found that, among the successful trials, the AP position tended to capture at lower currents than the AL position (93 mA vs. 126 mA).
In summary
TCP is a potentially lifesaving intervention in the treatment of patients with unstable bradycardia. Many of us who have attempted to perform TCP on unstable patients have frequently been disappointed with the results. In retrospect, however, I can recall that each time I have attempted this procedure, it has been using pads placed in the AL position.
Now for the first time we have data indicating that the standard AL position may be suboptimal, compared with the AP position. The study by Moayedi and colleagues is small, but the results are compelling, and the AP pad placement intuitively makes more sense. By using the AP pad placement, which provides greater likelihood of electrical current passing through the left ventricle, we should expect a greater likelihood of successful capture during attempts at TCP. In addition, we may anticipate lower analgesia needs if the AP position requires less current for success. Kudos to Moayedi and colleagues for performing a novel study of a critical procedure in acute care medicine.
Amal Mattu, MD, is a professor, vice chair of education, and codirector of the emergency cardiology fellowship in the department of emergency medicine at the University of Maryland, Baltimore. He had no disclosures. A version of this article first appeared on Medscape.com.
Transvenous pacing is typically the most effective therapy for unstable bradycardia but it is invasive, takes some time to perform, and is a procedure for which many acute care physicians lack comfort and significant experience. Transcutaneous pacing (TCP), on the other hand, is fast, easy to perform, and tends to be well tolerated by most patients when they receive appropriate doses of analgesia.
Unfortunately, TCP often fails to produce electrical or, more importantly, mechanical capture. Oftentimes when capture initially fails, the electrical current is increased in hopes of gaining capture but much to the discomfort of the patient. Increased body mass index can contribute to failure to capture, but what about TCP pad position? Despite recommendations for TCP in the United States and European resuscitation guidelines for many years, until now, no studies have evaluated optimal pad position for TCP. As a result, the default position for most clinicians using TCP has been the anterior-lateral (AL) position on the chest wall.
A study published in October 2022 compared the common AL position (anterior pad placed at the right upper chest and lateral pad placed over the left lower rib cage at the mid-axillary line) with the anterior-posterior (AP) position (anterior pad placed on the left chest over the apex of the heart and the posterior pad on the left mid-back area approximating the level of the mid-portion of the heart). The AP position has become more commonly used in defibrillating arrested hearts because it more accurately sends the current through the left ventricle. The concern with the AL position, especially in patients with large body habitus, is that the vector of the current may partially or entirely miss the left ventricle.
Moayedi and colleagues hypothesized that optimal TCP should employ pad placement that is similar to that used during optimal defibrillation attempts. They conducted a study comparing AL versus AP position during TCP and published their results in two parts, which will be discussed together.
The investigators evaluated 20 patients (6 women, 14 men) who had elective cardioversion of atrial fibrillation in the electrophysiology lab (Resuscitation. 2022 Dec;181:140-6). After successful cardioversion to sinus rhythm, the cardioversion pads were removed, and two new sets of pacer pads were placed on the patients’ chests. Pads were placed in both the AL and the AP positions, as previously described. Starting at a current output of 40 mA, the output was slowly increased on one set of pads until mechanical capture was obtained at the same rate as the pacer setting for at least 10 seconds. Pacing was then discontinued, but then the process was repeated using the second set of pads. The order in which the positions were tested (that is, AL tested first vs. AP tested first) was alternated. If capture was not obtained by 140 mA (the pacer’s maximum output), failure to capture was documented. Both positions were tested in all patients except for three cases where the second position was not tested because of inadequate analgesia.
The investigators found that 8 in 19 (42%) of the AL trials and 14 in 18 (78%) of the AP trials successfully captured. For the 17 participants who completed both trials, both positions captured in 8 in 17 (47%). AP but not AL was captured in 5 in 17 (29%); AL but not AP was captured in 0 cases. Neither position captured in 4 in 17 (24%). Of note, there was no association between successful capture and body mass index, chest circumference, or chest diameter. The AP position was more successful in both women and men, compared with the AL position. The investigators also found that, among the successful trials, the AP position tended to capture at lower currents than the AL position (93 mA vs. 126 mA).
In summary
TCP is a potentially lifesaving intervention in the treatment of patients with unstable bradycardia. Many of us who have attempted to perform TCP on unstable patients have frequently been disappointed with the results. In retrospect, however, I can recall that each time I have attempted this procedure, it has been using pads placed in the AL position.
Now for the first time we have data indicating that the standard AL position may be suboptimal, compared with the AP position. The study by Moayedi and colleagues is small, but the results are compelling, and the AP pad placement intuitively makes more sense. By using the AP pad placement, which provides greater likelihood of electrical current passing through the left ventricle, we should expect a greater likelihood of successful capture during attempts at TCP. In addition, we may anticipate lower analgesia needs if the AP position requires less current for success. Kudos to Moayedi and colleagues for performing a novel study of a critical procedure in acute care medicine.
Amal Mattu, MD, is a professor, vice chair of education, and codirector of the emergency cardiology fellowship in the department of emergency medicine at the University of Maryland, Baltimore. He had no disclosures. A version of this article first appeared on Medscape.com.