User login
A remote mountain bike crash forces a doctor to take knife in hand
It started as a mountain biking excursion with two friends. When we drove into the trailhead parking lot, we saw several emergency vehicles. Then a helicopter passed overhead.
Half a mile down the trail, we encountered another police officer. He asked if we would be willing to go back to get an oxygen tank from the ambulance and carry it out to the scene. The three of us turned around, went back to the parking lot and were able to snag a tank of oxygen. We put it in a backpack and biked out again.
We found the scene about a mile down the trail. An adult male was lying on his back in the dirt after a crash. His eyes were closed and he wasn’t moving except for occasional breaths. Six emergency medical personnel huddled around him, one assisting breaths with a bag mask. I didn’t introduce myself initially. I just listened to hear what was happening.
They were debating the dose of medication to give him in order to intubate. I knew the answer to that question, so I introduced myself. They were happy to have somebody else to assist.
They already had an IV in place and quite a lot of supplies. They administered the meds and the paramedic attempted to intubate through the mouth. Within a few seconds, she pulled the intubating blade out and said, “I’m not going to be able to get this. His tongue is too big.”
I took the blade myself and kneeled at the head of the victim. I made three attempts at intubating, and each time couldn’t view the landmarks. I wasn’t sure if his tongue was too large or if there was some traumatic injury. To make it more difficult, a lot of secretions clogged the airway. The paramedics had a portable suction, which was somewhat functional, but I still couldn’t visualize the landmarks.
I started asking about alternative methods of establishing an airway. They had an i-gel, which is a supraglottic device that goes into the back of the mouth. So, we placed it. But when we attached the bag, air still wasn’t getting into the lungs.
We removed it and put the bag mask back on. Now I was worried. We were having difficulty keeping his oxygen above 90%. I examined the chest and abdomen again. I was wondering if perhaps he was having some gastric distention, which can result from prolonged bagging, but that didn’t seem to be the case.
Bagging became progressively more difficult, and the oxygen slowly trended down through the 80s. Then the 70s. Heart rate dropped below 60 beats per minute. The trajectory was obvious.
That’s when I asked if they had the tools for a surgical airway.
No one thought the question was crazy. In fact, they pulled out a scalpel from an equipment bag.
But now I had to actually do it. I knelt next to the patient, trying to palpate the front of the neck to identify the correct location to cut. I had difficulty finding the appropriate landmarks there as well. Frustrating.
I glanced at the monitor. O2 was now in the 60s. Later the paramedic told me the heart rate was down to 30.
One of the medics looked me in the eye and said, “We’ve got to do something. The time is now.” That helped me snap out of it and act. I made my large vertical incision on the front of the victim’s neck, which of course resulted in quite a bit of bleeding.
My two friends, who were watching, later told me this was the moment the intensity of the scene really increased (it was already pretty intense for me, thanks).
Next, I made the horizontal stab incision. Then I probed with my finger, but it seems the incision hadn’t reached the trachea. I had to make the stab much deeper than I would’ve thought.
And then air bubbled out through the blood. A paramedic was ready with the ET tube in hand and she put it through the incision. We attached the bag. We had air movement into the lungs, and within minutes the oxygen came up.
Not long after, the flight paramedics from the helicopter showed up, having jogged a mile through the woods. They seemed rather surprised to find a patient with a cricothyrotomy. We filled them in on the situation. Now we had to get the patient out of the woods (literally and figuratively).
The emergency responders had a really great transport device: A litter with one big wheel underneath in the middle so we could roll the patient down the mountain bike trail over rocks relatively safely. One person’s job was to hold the tube as we went since we didn’t have suture to hold it in place.
We got back to the parking lot and loaded him into the ambulance, which drove another mile to the helicopter, which then had to take him a hundred miles to the hospital.
To be honest, I thought the prognosis was poor. I suspected he had an intercranial bleed slowly squeezing his brain (that later turned out to not be the case). Even though we had established an airway, it took us so long to get him to the ambulance.
The director of the local EMS called me that evening and said the patient had made it to the hospital. I had never been a part of anything with this intensity. I definitely lost sleep over it. Partly just from the uncertainty of not knowing what the outcome would be. But also second-guessing if I had done everything that I could have.
The story doesn’t quite end there, however.
A week later, a friend of the patient called me. He had recovered well and was going to be discharged from the hospital. He’d chosen to share the story with the media, and the local TV station was going to interview him. They had asked if I would agree to be interviewed.
After the local news story ran, it was kind of a media blitz. In came numerous media requests. But honestly, the portrayal of the story made me feel really weird. It was overly dramatized and not entirely accurate. It really didn’t sit well with me.
Friends all over the country saw the story, and here’s what they got from the coverage:
I was biking behind the patient when he crashed.
I had my own tools. Even the patient himself was told I used my own blade to make the incision.
The true story is what I just told you: A half-dozen emergency medical personnel were already there when I arrived. It was a combination of all of us – together – in the right place at the right time.
A month later, the patient and his family drove to the city where I live to take me out to lunch. It was emotional. There were plenty of tears. His wife and daughter were expressing a lot of gratitude and had some gifts for me. I was able to get his version of the story and learned some details. He had facial trauma in the past with some reconstruction. I realized that perhaps those anatomical changes affected my ability to do the intubation.
I hope to never again have to do this outside of the hospital. But I suppose I’m more prepared than ever now. I’ve reviewed my cricothyrotomy technique many times since then.
I was trained as a family doctor and did clinic and hospital medicine for several years. It was only in 2020 that I transitioned to doing emergency medicine work in a rural hospital. So, 2 years earlier, I’m not sure I would’ve been able to do what I did that day. To me, it was almost symbolic of the transition of my practice to emergency medicine.
I’m still in touch with the patient. We’ve talked about biking together. That hasn’t happened yet, but it may very well happen someday.
Jesse Coenen, MD, is an emergency medicine physician at Hayward Area Memorial Hospital in Hayward, Wisc.
A version of this article first appeared on Medscape.com.
It started as a mountain biking excursion with two friends. When we drove into the trailhead parking lot, we saw several emergency vehicles. Then a helicopter passed overhead.
Half a mile down the trail, we encountered another police officer. He asked if we would be willing to go back to get an oxygen tank from the ambulance and carry it out to the scene. The three of us turned around, went back to the parking lot and were able to snag a tank of oxygen. We put it in a backpack and biked out again.
We found the scene about a mile down the trail. An adult male was lying on his back in the dirt after a crash. His eyes were closed and he wasn’t moving except for occasional breaths. Six emergency medical personnel huddled around him, one assisting breaths with a bag mask. I didn’t introduce myself initially. I just listened to hear what was happening.
They were debating the dose of medication to give him in order to intubate. I knew the answer to that question, so I introduced myself. They were happy to have somebody else to assist.
They already had an IV in place and quite a lot of supplies. They administered the meds and the paramedic attempted to intubate through the mouth. Within a few seconds, she pulled the intubating blade out and said, “I’m not going to be able to get this. His tongue is too big.”
I took the blade myself and kneeled at the head of the victim. I made three attempts at intubating, and each time couldn’t view the landmarks. I wasn’t sure if his tongue was too large or if there was some traumatic injury. To make it more difficult, a lot of secretions clogged the airway. The paramedics had a portable suction, which was somewhat functional, but I still couldn’t visualize the landmarks.
I started asking about alternative methods of establishing an airway. They had an i-gel, which is a supraglottic device that goes into the back of the mouth. So, we placed it. But when we attached the bag, air still wasn’t getting into the lungs.
We removed it and put the bag mask back on. Now I was worried. We were having difficulty keeping his oxygen above 90%. I examined the chest and abdomen again. I was wondering if perhaps he was having some gastric distention, which can result from prolonged bagging, but that didn’t seem to be the case.
Bagging became progressively more difficult, and the oxygen slowly trended down through the 80s. Then the 70s. Heart rate dropped below 60 beats per minute. The trajectory was obvious.
That’s when I asked if they had the tools for a surgical airway.
No one thought the question was crazy. In fact, they pulled out a scalpel from an equipment bag.
But now I had to actually do it. I knelt next to the patient, trying to palpate the front of the neck to identify the correct location to cut. I had difficulty finding the appropriate landmarks there as well. Frustrating.
I glanced at the monitor. O2 was now in the 60s. Later the paramedic told me the heart rate was down to 30.
One of the medics looked me in the eye and said, “We’ve got to do something. The time is now.” That helped me snap out of it and act. I made my large vertical incision on the front of the victim’s neck, which of course resulted in quite a bit of bleeding.
My two friends, who were watching, later told me this was the moment the intensity of the scene really increased (it was already pretty intense for me, thanks).
Next, I made the horizontal stab incision. Then I probed with my finger, but it seems the incision hadn’t reached the trachea. I had to make the stab much deeper than I would’ve thought.
And then air bubbled out through the blood. A paramedic was ready with the ET tube in hand and she put it through the incision. We attached the bag. We had air movement into the lungs, and within minutes the oxygen came up.
Not long after, the flight paramedics from the helicopter showed up, having jogged a mile through the woods. They seemed rather surprised to find a patient with a cricothyrotomy. We filled them in on the situation. Now we had to get the patient out of the woods (literally and figuratively).
The emergency responders had a really great transport device: A litter with one big wheel underneath in the middle so we could roll the patient down the mountain bike trail over rocks relatively safely. One person’s job was to hold the tube as we went since we didn’t have suture to hold it in place.
We got back to the parking lot and loaded him into the ambulance, which drove another mile to the helicopter, which then had to take him a hundred miles to the hospital.
To be honest, I thought the prognosis was poor. I suspected he had an intercranial bleed slowly squeezing his brain (that later turned out to not be the case). Even though we had established an airway, it took us so long to get him to the ambulance.
The director of the local EMS called me that evening and said the patient had made it to the hospital. I had never been a part of anything with this intensity. I definitely lost sleep over it. Partly just from the uncertainty of not knowing what the outcome would be. But also second-guessing if I had done everything that I could have.
The story doesn’t quite end there, however.
A week later, a friend of the patient called me. He had recovered well and was going to be discharged from the hospital. He’d chosen to share the story with the media, and the local TV station was going to interview him. They had asked if I would agree to be interviewed.
After the local news story ran, it was kind of a media blitz. In came numerous media requests. But honestly, the portrayal of the story made me feel really weird. It was overly dramatized and not entirely accurate. It really didn’t sit well with me.
Friends all over the country saw the story, and here’s what they got from the coverage:
I was biking behind the patient when he crashed.
I had my own tools. Even the patient himself was told I used my own blade to make the incision.
The true story is what I just told you: A half-dozen emergency medical personnel were already there when I arrived. It was a combination of all of us – together – in the right place at the right time.
A month later, the patient and his family drove to the city where I live to take me out to lunch. It was emotional. There were plenty of tears. His wife and daughter were expressing a lot of gratitude and had some gifts for me. I was able to get his version of the story and learned some details. He had facial trauma in the past with some reconstruction. I realized that perhaps those anatomical changes affected my ability to do the intubation.
I hope to never again have to do this outside of the hospital. But I suppose I’m more prepared than ever now. I’ve reviewed my cricothyrotomy technique many times since then.
I was trained as a family doctor and did clinic and hospital medicine for several years. It was only in 2020 that I transitioned to doing emergency medicine work in a rural hospital. So, 2 years earlier, I’m not sure I would’ve been able to do what I did that day. To me, it was almost symbolic of the transition of my practice to emergency medicine.
I’m still in touch with the patient. We’ve talked about biking together. That hasn’t happened yet, but it may very well happen someday.
Jesse Coenen, MD, is an emergency medicine physician at Hayward Area Memorial Hospital in Hayward, Wisc.
A version of this article first appeared on Medscape.com.
It started as a mountain biking excursion with two friends. When we drove into the trailhead parking lot, we saw several emergency vehicles. Then a helicopter passed overhead.
Half a mile down the trail, we encountered another police officer. He asked if we would be willing to go back to get an oxygen tank from the ambulance and carry it out to the scene. The three of us turned around, went back to the parking lot and were able to snag a tank of oxygen. We put it in a backpack and biked out again.
We found the scene about a mile down the trail. An adult male was lying on his back in the dirt after a crash. His eyes were closed and he wasn’t moving except for occasional breaths. Six emergency medical personnel huddled around him, one assisting breaths with a bag mask. I didn’t introduce myself initially. I just listened to hear what was happening.
They were debating the dose of medication to give him in order to intubate. I knew the answer to that question, so I introduced myself. They were happy to have somebody else to assist.
They already had an IV in place and quite a lot of supplies. They administered the meds and the paramedic attempted to intubate through the mouth. Within a few seconds, she pulled the intubating blade out and said, “I’m not going to be able to get this. His tongue is too big.”
I took the blade myself and kneeled at the head of the victim. I made three attempts at intubating, and each time couldn’t view the landmarks. I wasn’t sure if his tongue was too large or if there was some traumatic injury. To make it more difficult, a lot of secretions clogged the airway. The paramedics had a portable suction, which was somewhat functional, but I still couldn’t visualize the landmarks.
I started asking about alternative methods of establishing an airway. They had an i-gel, which is a supraglottic device that goes into the back of the mouth. So, we placed it. But when we attached the bag, air still wasn’t getting into the lungs.
We removed it and put the bag mask back on. Now I was worried. We were having difficulty keeping his oxygen above 90%. I examined the chest and abdomen again. I was wondering if perhaps he was having some gastric distention, which can result from prolonged bagging, but that didn’t seem to be the case.
Bagging became progressively more difficult, and the oxygen slowly trended down through the 80s. Then the 70s. Heart rate dropped below 60 beats per minute. The trajectory was obvious.
That’s when I asked if they had the tools for a surgical airway.
No one thought the question was crazy. In fact, they pulled out a scalpel from an equipment bag.
But now I had to actually do it. I knelt next to the patient, trying to palpate the front of the neck to identify the correct location to cut. I had difficulty finding the appropriate landmarks there as well. Frustrating.
I glanced at the monitor. O2 was now in the 60s. Later the paramedic told me the heart rate was down to 30.
One of the medics looked me in the eye and said, “We’ve got to do something. The time is now.” That helped me snap out of it and act. I made my large vertical incision on the front of the victim’s neck, which of course resulted in quite a bit of bleeding.
My two friends, who were watching, later told me this was the moment the intensity of the scene really increased (it was already pretty intense for me, thanks).
Next, I made the horizontal stab incision. Then I probed with my finger, but it seems the incision hadn’t reached the trachea. I had to make the stab much deeper than I would’ve thought.
And then air bubbled out through the blood. A paramedic was ready with the ET tube in hand and she put it through the incision. We attached the bag. We had air movement into the lungs, and within minutes the oxygen came up.
Not long after, the flight paramedics from the helicopter showed up, having jogged a mile through the woods. They seemed rather surprised to find a patient with a cricothyrotomy. We filled them in on the situation. Now we had to get the patient out of the woods (literally and figuratively).
The emergency responders had a really great transport device: A litter with one big wheel underneath in the middle so we could roll the patient down the mountain bike trail over rocks relatively safely. One person’s job was to hold the tube as we went since we didn’t have suture to hold it in place.
We got back to the parking lot and loaded him into the ambulance, which drove another mile to the helicopter, which then had to take him a hundred miles to the hospital.
To be honest, I thought the prognosis was poor. I suspected he had an intercranial bleed slowly squeezing his brain (that later turned out to not be the case). Even though we had established an airway, it took us so long to get him to the ambulance.
The director of the local EMS called me that evening and said the patient had made it to the hospital. I had never been a part of anything with this intensity. I definitely lost sleep over it. Partly just from the uncertainty of not knowing what the outcome would be. But also second-guessing if I had done everything that I could have.
The story doesn’t quite end there, however.
A week later, a friend of the patient called me. He had recovered well and was going to be discharged from the hospital. He’d chosen to share the story with the media, and the local TV station was going to interview him. They had asked if I would agree to be interviewed.
After the local news story ran, it was kind of a media blitz. In came numerous media requests. But honestly, the portrayal of the story made me feel really weird. It was overly dramatized and not entirely accurate. It really didn’t sit well with me.
Friends all over the country saw the story, and here’s what they got from the coverage:
I was biking behind the patient when he crashed.
I had my own tools. Even the patient himself was told I used my own blade to make the incision.
The true story is what I just told you: A half-dozen emergency medical personnel were already there when I arrived. It was a combination of all of us – together – in the right place at the right time.
A month later, the patient and his family drove to the city where I live to take me out to lunch. It was emotional. There were plenty of tears. His wife and daughter were expressing a lot of gratitude and had some gifts for me. I was able to get his version of the story and learned some details. He had facial trauma in the past with some reconstruction. I realized that perhaps those anatomical changes affected my ability to do the intubation.
I hope to never again have to do this outside of the hospital. But I suppose I’m more prepared than ever now. I’ve reviewed my cricothyrotomy technique many times since then.
I was trained as a family doctor and did clinic and hospital medicine for several years. It was only in 2020 that I transitioned to doing emergency medicine work in a rural hospital. So, 2 years earlier, I’m not sure I would’ve been able to do what I did that day. To me, it was almost symbolic of the transition of my practice to emergency medicine.
I’m still in touch with the patient. We’ve talked about biking together. That hasn’t happened yet, but it may very well happen someday.
Jesse Coenen, MD, is an emergency medicine physician at Hayward Area Memorial Hospital in Hayward, Wisc.
A version of this article first appeared on Medscape.com.
Arkansas cardiologist pays $900K to settle false claims allegations
in violation of the False Claims Act.
As part of the settlement, Dr. Tauth will enter into an integrity agreement with the U.S. Department of Health & Human Services, according to a news release from Henry Leventis, U.S. attorney for the Middle District of Tennessee.
“Health care fraud is a top priority of this office. We will aggressively pursue all those who are involved in fraud against government programs,” Mr. Leventis said.
Dr. Tauth formerly treated patients at National Park Medical Center (NPMC) in Hot Springs. The alleged false claims were submitted from September 2013 through August 2019.
The settlement with Dr. Tauth, aged 60, follows a November 2019 voluntary disclosure of the alleged false claims by Brentwood, Tenn.–based Lifepoint Health, which acquired NPMC and Hot Springs Cardiology Associates in November 2018.
NPMC and Hot Springs Cardiology entered into a settlement in October 2020 for the alleged violations and agreed to pay roughly $14.6 million, which includes over $9 million in restitution, according to the news release.
NPMC CEO Scott Smith said NPMC is “committed to maintaining high standards of integrity, legal compliance, and quality care for our patients. We regularly monitor our processes, procedures, and reporting and actively self-report concerns to regulators to ensure we are upholding these standards across our organization.”
“We are proud that our hospital took the appropriate steps to promptly self-report and finalize a settlement with the government for a swift resolution more than 2 years ago,” Mr. Smith said.
Dr. Tauth, however, maintains that the allegations made by NPMC are false.
“I am pleased to have reached a settlement agreement with the Department of Justice regarding allegations brought to them by my former employer, National Park Medical Center,” he said in a statement.
“The settlement agreement specifically states that it is not ‘an admission of liability’ by me, and I remain steadfast in my position that the allegations made by my former employer are false and without merit,” Dr. Tauth added.
He further stated that he has “chosen to enter into the settlement agreement because the legal process initiated by National Park’s allegations has been emotionally and financially damaging to me and my family in the extreme, and a settlement puts an end to the delays, uncertainties, inconveniences, and expenses of protracted litigation. Settlement is in the best interests of my family, my patients, and my medical practice.”
Dr. Tauth said he is “extremely grateful for the support I have received from my patients, medical staff, colleagues, friends, and family during this difficult time, and I look forward to providing high-quality cardiac care in the greater Hot Springs community for many years to come.”
A version of this article first appeared on Medscape.com.
in violation of the False Claims Act.
As part of the settlement, Dr. Tauth will enter into an integrity agreement with the U.S. Department of Health & Human Services, according to a news release from Henry Leventis, U.S. attorney for the Middle District of Tennessee.
“Health care fraud is a top priority of this office. We will aggressively pursue all those who are involved in fraud against government programs,” Mr. Leventis said.
Dr. Tauth formerly treated patients at National Park Medical Center (NPMC) in Hot Springs. The alleged false claims were submitted from September 2013 through August 2019.
The settlement with Dr. Tauth, aged 60, follows a November 2019 voluntary disclosure of the alleged false claims by Brentwood, Tenn.–based Lifepoint Health, which acquired NPMC and Hot Springs Cardiology Associates in November 2018.
NPMC and Hot Springs Cardiology entered into a settlement in October 2020 for the alleged violations and agreed to pay roughly $14.6 million, which includes over $9 million in restitution, according to the news release.
NPMC CEO Scott Smith said NPMC is “committed to maintaining high standards of integrity, legal compliance, and quality care for our patients. We regularly monitor our processes, procedures, and reporting and actively self-report concerns to regulators to ensure we are upholding these standards across our organization.”
“We are proud that our hospital took the appropriate steps to promptly self-report and finalize a settlement with the government for a swift resolution more than 2 years ago,” Mr. Smith said.
Dr. Tauth, however, maintains that the allegations made by NPMC are false.
“I am pleased to have reached a settlement agreement with the Department of Justice regarding allegations brought to them by my former employer, National Park Medical Center,” he said in a statement.
“The settlement agreement specifically states that it is not ‘an admission of liability’ by me, and I remain steadfast in my position that the allegations made by my former employer are false and without merit,” Dr. Tauth added.
He further stated that he has “chosen to enter into the settlement agreement because the legal process initiated by National Park’s allegations has been emotionally and financially damaging to me and my family in the extreme, and a settlement puts an end to the delays, uncertainties, inconveniences, and expenses of protracted litigation. Settlement is in the best interests of my family, my patients, and my medical practice.”
Dr. Tauth said he is “extremely grateful for the support I have received from my patients, medical staff, colleagues, friends, and family during this difficult time, and I look forward to providing high-quality cardiac care in the greater Hot Springs community for many years to come.”
A version of this article first appeared on Medscape.com.
in violation of the False Claims Act.
As part of the settlement, Dr. Tauth will enter into an integrity agreement with the U.S. Department of Health & Human Services, according to a news release from Henry Leventis, U.S. attorney for the Middle District of Tennessee.
“Health care fraud is a top priority of this office. We will aggressively pursue all those who are involved in fraud against government programs,” Mr. Leventis said.
Dr. Tauth formerly treated patients at National Park Medical Center (NPMC) in Hot Springs. The alleged false claims were submitted from September 2013 through August 2019.
The settlement with Dr. Tauth, aged 60, follows a November 2019 voluntary disclosure of the alleged false claims by Brentwood, Tenn.–based Lifepoint Health, which acquired NPMC and Hot Springs Cardiology Associates in November 2018.
NPMC and Hot Springs Cardiology entered into a settlement in October 2020 for the alleged violations and agreed to pay roughly $14.6 million, which includes over $9 million in restitution, according to the news release.
NPMC CEO Scott Smith said NPMC is “committed to maintaining high standards of integrity, legal compliance, and quality care for our patients. We regularly monitor our processes, procedures, and reporting and actively self-report concerns to regulators to ensure we are upholding these standards across our organization.”
“We are proud that our hospital took the appropriate steps to promptly self-report and finalize a settlement with the government for a swift resolution more than 2 years ago,” Mr. Smith said.
Dr. Tauth, however, maintains that the allegations made by NPMC are false.
“I am pleased to have reached a settlement agreement with the Department of Justice regarding allegations brought to them by my former employer, National Park Medical Center,” he said in a statement.
“The settlement agreement specifically states that it is not ‘an admission of liability’ by me, and I remain steadfast in my position that the allegations made by my former employer are false and without merit,” Dr. Tauth added.
He further stated that he has “chosen to enter into the settlement agreement because the legal process initiated by National Park’s allegations has been emotionally and financially damaging to me and my family in the extreme, and a settlement puts an end to the delays, uncertainties, inconveniences, and expenses of protracted litigation. Settlement is in the best interests of my family, my patients, and my medical practice.”
Dr. Tauth said he is “extremely grateful for the support I have received from my patients, medical staff, colleagues, friends, and family during this difficult time, and I look forward to providing high-quality cardiac care in the greater Hot Springs community for many years to come.”
A version of this article first appeared on Medscape.com.
Does EPA lower CV risk? REDUCE-IT revisited
The prescription product (Vascepa), consisting of a “highly purified” form of the omega-3 acid eicosapentaenoic acid (EPA), was heralded in 2018 (N Engl J Med. 2019;380:11-22) as ushering in “the dawn of a new era” in cardiovascular disease (CVD) prevention that “should definitely change practice going forward,” according to REDUCE-IT’s lead author Deepak L. Bhatt, MD, formerly of Brigham and Women’s Hospital in Boston and now director of the Mount Sinai Heart Center in New York.
However, skeptics questioned why the results differed from most previous trials of fish oil that showed no benefit. Was it caused by the high dose of EPA: 4 g/daily versus 1 g daily in earlier trials with fish oil capsules? Was it the different formulation of purified EPA versus more common combinations of EPA plus docosahexaenoic acid (DHA)? Or, as suggested by Steven Nissen, MD, chief academic officer of Cleveland Clinic’s Heart and Vascular Institute and others, was it caused by the negative effects of the mineral oil placebo, given the significant increases in LDL cholesterol and high-sensitivity C-reactive protein (hsCRP) seen in the control group?
‘Not all omega-3s created equal’
Dr. Bhatt recently said in an interview: “I think there’s confusion in the field. It’s a challenge when just one drug in a class looks good and everything else in that class looks bad. That in itself can breed some skepticism. Also, not everyone always embraces advances. Some people have other reasons to impugn datasets; for example, it could be because they are running competing trials with competing drugs.”
REDUCE-IT enrolled more than 8,000 patients at high CV risk despite statin treatment, and randomly assigned them to 2 g of EPA twice daily or the mineral oil placebo. Although the results showed a 25% reduction in the rate of CV events in the EPA group, there was also an increased risk of atrial fibrillation among those taking EPA after a median of 4.9 years follow-up.
Dr. Bhatt noted that Amarin, which manufactures Vascepa, is essentially a one-drug company, and its stock price is dependent on the product. When the trial results were released, he said, “there were people in the investor world that wanted the stock price to go up or wanted it to go down, and they were alternately hyping or disparaging the data in both cases, sometimes inappropriately and excessively, which created noise around the science.”
The fact is, he said, “not all omega-3 fatty acids are created equal. There are differences between supplements and prescription medicines, and within the prescription medicines, differences between pure EPA and the mixtures of EPA and DHA.”
Dr. Bhatt added that other trials also showed positive results. He pointed to the JELIS trial, published in 2007, which showed a 19% reduction in major adverse CV events with a 1.8-g daily EPA dose.
More recently, RESPECT-EPA was presented at the 2022 annual meeting of the American Heart Association. That study had methodological issues and was underpowered, but it did suggest a possible benefit of EPA in reducing CV events in patients with chronic coronary artery disease who were taking statins. “Looking at the totality of evidence, I think it’s quite clear there’s CV benefit,” Dr. Bhatt said.
Placebo effects?
Concerns about the mineral oil placebo cast doubt on that benefit. Table 4 of the supplement accompanying REDUCE-IT’s publication in the New England Journal of Medicine shows significant increases of non–HDL cholesterol, LDL cholesterol, apolipoprotein B, and hsCRP in the control group.
Jane Armitage, MBBS, a professor of clinical trials and epidemiology, clinical trial service unit at Oxford University (England), said in an interview: “I was surprised by the backlash and at the time felt that it was unlikely that the mineral oil was the problem. But the size of benefit was still out of kilter.”
“Two further pieces of evidence have influenced my thoughts since then,” she said. One is the lack of effect of high doses of fish oils in the STRENGTH trial. STRENGTH tested 4 g of omega-3 oil containing a mixture of EPA and DHA and found no benefit in statin-treated, high-risk patients.
“The amount of EPA [was] substantially less than given in REDUCE-IT,” Armitage said, “but it seems to me that in a similar hypertriglyceridemic population, if the effect were due to the EPA, you would have seen some impact in STRENGTH – and none was seen.”
“The other piece of evidence is in a paper by Paul Ridker, MD, et al. on the changes in biomarkers during REDUCE-IT,” she said. “Several inflammatory biomarkers associated with atherosclerosis rose during the study among those allocated mineral oil, but remained largely unchanged in the EPA group. This is in contrast to what is seen with these biomarkers in other large trials, where no changes were seen in the placebo groups, and once again raises the possibility that the apparent benefits of EPA may be related to hazard from the mineral oil.”
Still room for benefit?
Based largely on the results of REDUCE-IT, Vascepa is currently approved by the Food and Drug Administration as an adjunctive therapy to lower the risk for CV events among adults with elevated triglyceride levels (≥ 150 mg/dL). Patients must also have either established CVD or diabetes and two or more additional CV risk factors and are advised to continue physical activity and maintain a healthy diet.
Dr. Nissen, the principal author of the STRENGTH trial, said in an interview, “REDUCE-IT is an outlier. Other trials of omega-3 fatty acids, some of them very large, showed no benefits, and a meta-analysis of nearly 78,000 patients showed no beneficial effects. In this context,” he said, “the large ‘benefit’ observed in REDUCE-IT doesn’t make any sense.”
Dr. Nissen noted that a secondary analysis of STRENGTH further showed that higher plasma EPA levels did not reduce CV outcomes. He also highlighted the elevated risk of atrial fibrillation with EPA. “We need to see another study comparing EPA to a neutral comparator such as corn oil, which had no significant effect on lipid or inflammatory biomarkers in STRENGTH,” he said. “Without such a trial, the results of REDUCE-IT cannot be accepted as definitive.”
Dr. Ridker, the lead author of the REDUCE-IT substudy that found biomarker changes with the mineral oil placebo, said in an interview: “Is it possible that EPA is an outstanding drug? Absolutely, and I continue to think it useful for our very high-risk, secondary-prevention patients when we are running out of options.”
“But,” said Dr. Ridker, who is a professor at Harvard Medical School, Boston, and director of the Center for Cardiovascular Disease Prevention at Brigham and Women’s, “the reality ... is that ongoing uncertainties need resolution.” Like Dr. Nissen, he thinks the best way to resolve these uncertainties is through a second trial using a fully neutral comparator. “I am hopeful that the U.S. National Institutes of Health will see fit to undertake such an endeavor, perhaps with support from industry partners.”
Although Dr. Armitage is no longer in clinical practice, when asked how she might use EPA, she said it might be reasonable for patients who meet the prescribing criteria and remain high risk after all other risk factors have been addressed. She added that, although EPA is approved in the United Kingdom, she doesn’t think it is being widely prescribed.
Salim S. Virani, MD, PhD, a professor in the Sections of Cardiology and Cardiovascular Research at Baylor College of Medicine who has published articles about REDUCE-IT and on the eligibility and cost of EPA in the Veterans Affairs system, said in an interview: “In my personal opinion, clinicians [should] first optimize diet and lifestyle and work on secondary causes, as they play a very big role in hypertriglyceridemia.” He also recommended optimizing LDL-C levels because of “consistent data showing that LDL [cholesterol] control leads to significant reduction in atherosclerotic CVD events.”
“Once these two steps are taken and triglycerides still remain elevated,” he said, “then adding EPA in patients with established atherosclerotic CVD or those with diabetes plus other CV risk factors may be a reasonable option to further lower residual atherosclerotic CVD risk.”
Clinical inertia?
Dr. Bhatt acknowledged that, despite the benefit of EPA in the context of REDUCE-IT, “a few issues stand in the way of prescribing, particularly in the U.S.”
Vascepa’s manufacturer Amarin lost a patent challenge in the United States, enabling the relatively early introduction of multiple generics. “They’ve lost interest in the U.S. because there are three generics.”
“The sad truth is, if there isn’t a drug rep saying, ‘hey, look at this new data,’ there’s clinical inertia,” said Dr. Bhatt. He believes that the lack of marketing will hurt awareness among physicians and “ultimately hurt patients because they won’t get the drug.”
Cost is also an issue, Dr. Bhatt affirmed. Vascepa has significant out-of-pocket costs for many patients, as do some of the generics. Currently, the branded product costs about $300 per month without insurance, according to drugs.com; prices for generics vary widely, running anywhere from $82 to $200 or more.
Despite these challenges, he noted that many guidelines around the world have already changed to reflect the data, including the American Diabetes Association and the U.S. National Lipid Association.
Will there be another trial of EPA with a neutral placebo? Dr. Bhatt believes it’s not going to happen. “The company that funded REDUCE-IT is struggling just to stay alive, and another investigator-funded trial like RESPECT EPA would probably be underpowered and not move the needle much.”
Dr. Virani agreed that while it would be best to test EPA against a fully inert placebo, “whether there is enough appetite to fund such a large trial remains a big question.”
Meanwhile, Dr. Bhatt said, “EPA is not for everybody, but for the high-risk patients who meet the stringent inclusion criteria of REDUCE-IT, I think clinicians should at least consider use of EPA in a way consistent with the U.S. FDA label, the Canadian label, and the label in parts of Europe where the drug is being introduced.”
A version of this article first appeared on Medscape.com.
The prescription product (Vascepa), consisting of a “highly purified” form of the omega-3 acid eicosapentaenoic acid (EPA), was heralded in 2018 (N Engl J Med. 2019;380:11-22) as ushering in “the dawn of a new era” in cardiovascular disease (CVD) prevention that “should definitely change practice going forward,” according to REDUCE-IT’s lead author Deepak L. Bhatt, MD, formerly of Brigham and Women’s Hospital in Boston and now director of the Mount Sinai Heart Center in New York.
However, skeptics questioned why the results differed from most previous trials of fish oil that showed no benefit. Was it caused by the high dose of EPA: 4 g/daily versus 1 g daily in earlier trials with fish oil capsules? Was it the different formulation of purified EPA versus more common combinations of EPA plus docosahexaenoic acid (DHA)? Or, as suggested by Steven Nissen, MD, chief academic officer of Cleveland Clinic’s Heart and Vascular Institute and others, was it caused by the negative effects of the mineral oil placebo, given the significant increases in LDL cholesterol and high-sensitivity C-reactive protein (hsCRP) seen in the control group?
‘Not all omega-3s created equal’
Dr. Bhatt recently said in an interview: “I think there’s confusion in the field. It’s a challenge when just one drug in a class looks good and everything else in that class looks bad. That in itself can breed some skepticism. Also, not everyone always embraces advances. Some people have other reasons to impugn datasets; for example, it could be because they are running competing trials with competing drugs.”
REDUCE-IT enrolled more than 8,000 patients at high CV risk despite statin treatment, and randomly assigned them to 2 g of EPA twice daily or the mineral oil placebo. Although the results showed a 25% reduction in the rate of CV events in the EPA group, there was also an increased risk of atrial fibrillation among those taking EPA after a median of 4.9 years follow-up.
Dr. Bhatt noted that Amarin, which manufactures Vascepa, is essentially a one-drug company, and its stock price is dependent on the product. When the trial results were released, he said, “there were people in the investor world that wanted the stock price to go up or wanted it to go down, and they were alternately hyping or disparaging the data in both cases, sometimes inappropriately and excessively, which created noise around the science.”
The fact is, he said, “not all omega-3 fatty acids are created equal. There are differences between supplements and prescription medicines, and within the prescription medicines, differences between pure EPA and the mixtures of EPA and DHA.”
Dr. Bhatt added that other trials also showed positive results. He pointed to the JELIS trial, published in 2007, which showed a 19% reduction in major adverse CV events with a 1.8-g daily EPA dose.
More recently, RESPECT-EPA was presented at the 2022 annual meeting of the American Heart Association. That study had methodological issues and was underpowered, but it did suggest a possible benefit of EPA in reducing CV events in patients with chronic coronary artery disease who were taking statins. “Looking at the totality of evidence, I think it’s quite clear there’s CV benefit,” Dr. Bhatt said.
Placebo effects?
Concerns about the mineral oil placebo cast doubt on that benefit. Table 4 of the supplement accompanying REDUCE-IT’s publication in the New England Journal of Medicine shows significant increases of non–HDL cholesterol, LDL cholesterol, apolipoprotein B, and hsCRP in the control group.
Jane Armitage, MBBS, a professor of clinical trials and epidemiology, clinical trial service unit at Oxford University (England), said in an interview: “I was surprised by the backlash and at the time felt that it was unlikely that the mineral oil was the problem. But the size of benefit was still out of kilter.”
“Two further pieces of evidence have influenced my thoughts since then,” she said. One is the lack of effect of high doses of fish oils in the STRENGTH trial. STRENGTH tested 4 g of omega-3 oil containing a mixture of EPA and DHA and found no benefit in statin-treated, high-risk patients.
“The amount of EPA [was] substantially less than given in REDUCE-IT,” Armitage said, “but it seems to me that in a similar hypertriglyceridemic population, if the effect were due to the EPA, you would have seen some impact in STRENGTH – and none was seen.”
“The other piece of evidence is in a paper by Paul Ridker, MD, et al. on the changes in biomarkers during REDUCE-IT,” she said. “Several inflammatory biomarkers associated with atherosclerosis rose during the study among those allocated mineral oil, but remained largely unchanged in the EPA group. This is in contrast to what is seen with these biomarkers in other large trials, where no changes were seen in the placebo groups, and once again raises the possibility that the apparent benefits of EPA may be related to hazard from the mineral oil.”
Still room for benefit?
Based largely on the results of REDUCE-IT, Vascepa is currently approved by the Food and Drug Administration as an adjunctive therapy to lower the risk for CV events among adults with elevated triglyceride levels (≥ 150 mg/dL). Patients must also have either established CVD or diabetes and two or more additional CV risk factors and are advised to continue physical activity and maintain a healthy diet.
Dr. Nissen, the principal author of the STRENGTH trial, said in an interview, “REDUCE-IT is an outlier. Other trials of omega-3 fatty acids, some of them very large, showed no benefits, and a meta-analysis of nearly 78,000 patients showed no beneficial effects. In this context,” he said, “the large ‘benefit’ observed in REDUCE-IT doesn’t make any sense.”
Dr. Nissen noted that a secondary analysis of STRENGTH further showed that higher plasma EPA levels did not reduce CV outcomes. He also highlighted the elevated risk of atrial fibrillation with EPA. “We need to see another study comparing EPA to a neutral comparator such as corn oil, which had no significant effect on lipid or inflammatory biomarkers in STRENGTH,” he said. “Without such a trial, the results of REDUCE-IT cannot be accepted as definitive.”
Dr. Ridker, the lead author of the REDUCE-IT substudy that found biomarker changes with the mineral oil placebo, said in an interview: “Is it possible that EPA is an outstanding drug? Absolutely, and I continue to think it useful for our very high-risk, secondary-prevention patients when we are running out of options.”
“But,” said Dr. Ridker, who is a professor at Harvard Medical School, Boston, and director of the Center for Cardiovascular Disease Prevention at Brigham and Women’s, “the reality ... is that ongoing uncertainties need resolution.” Like Dr. Nissen, he thinks the best way to resolve these uncertainties is through a second trial using a fully neutral comparator. “I am hopeful that the U.S. National Institutes of Health will see fit to undertake such an endeavor, perhaps with support from industry partners.”
Although Dr. Armitage is no longer in clinical practice, when asked how she might use EPA, she said it might be reasonable for patients who meet the prescribing criteria and remain high risk after all other risk factors have been addressed. She added that, although EPA is approved in the United Kingdom, she doesn’t think it is being widely prescribed.
Salim S. Virani, MD, PhD, a professor in the Sections of Cardiology and Cardiovascular Research at Baylor College of Medicine who has published articles about REDUCE-IT and on the eligibility and cost of EPA in the Veterans Affairs system, said in an interview: “In my personal opinion, clinicians [should] first optimize diet and lifestyle and work on secondary causes, as they play a very big role in hypertriglyceridemia.” He also recommended optimizing LDL-C levels because of “consistent data showing that LDL [cholesterol] control leads to significant reduction in atherosclerotic CVD events.”
“Once these two steps are taken and triglycerides still remain elevated,” he said, “then adding EPA in patients with established atherosclerotic CVD or those with diabetes plus other CV risk factors may be a reasonable option to further lower residual atherosclerotic CVD risk.”
Clinical inertia?
Dr. Bhatt acknowledged that, despite the benefit of EPA in the context of REDUCE-IT, “a few issues stand in the way of prescribing, particularly in the U.S.”
Vascepa’s manufacturer Amarin lost a patent challenge in the United States, enabling the relatively early introduction of multiple generics. “They’ve lost interest in the U.S. because there are three generics.”
“The sad truth is, if there isn’t a drug rep saying, ‘hey, look at this new data,’ there’s clinical inertia,” said Dr. Bhatt. He believes that the lack of marketing will hurt awareness among physicians and “ultimately hurt patients because they won’t get the drug.”
Cost is also an issue, Dr. Bhatt affirmed. Vascepa has significant out-of-pocket costs for many patients, as do some of the generics. Currently, the branded product costs about $300 per month without insurance, according to drugs.com; prices for generics vary widely, running anywhere from $82 to $200 or more.
Despite these challenges, he noted that many guidelines around the world have already changed to reflect the data, including the American Diabetes Association and the U.S. National Lipid Association.
Will there be another trial of EPA with a neutral placebo? Dr. Bhatt believes it’s not going to happen. “The company that funded REDUCE-IT is struggling just to stay alive, and another investigator-funded trial like RESPECT EPA would probably be underpowered and not move the needle much.”
Dr. Virani agreed that while it would be best to test EPA against a fully inert placebo, “whether there is enough appetite to fund such a large trial remains a big question.”
Meanwhile, Dr. Bhatt said, “EPA is not for everybody, but for the high-risk patients who meet the stringent inclusion criteria of REDUCE-IT, I think clinicians should at least consider use of EPA in a way consistent with the U.S. FDA label, the Canadian label, and the label in parts of Europe where the drug is being introduced.”
A version of this article first appeared on Medscape.com.
The prescription product (Vascepa), consisting of a “highly purified” form of the omega-3 acid eicosapentaenoic acid (EPA), was heralded in 2018 (N Engl J Med. 2019;380:11-22) as ushering in “the dawn of a new era” in cardiovascular disease (CVD) prevention that “should definitely change practice going forward,” according to REDUCE-IT’s lead author Deepak L. Bhatt, MD, formerly of Brigham and Women’s Hospital in Boston and now director of the Mount Sinai Heart Center in New York.
However, skeptics questioned why the results differed from most previous trials of fish oil that showed no benefit. Was it caused by the high dose of EPA: 4 g/daily versus 1 g daily in earlier trials with fish oil capsules? Was it the different formulation of purified EPA versus more common combinations of EPA plus docosahexaenoic acid (DHA)? Or, as suggested by Steven Nissen, MD, chief academic officer of Cleveland Clinic’s Heart and Vascular Institute and others, was it caused by the negative effects of the mineral oil placebo, given the significant increases in LDL cholesterol and high-sensitivity C-reactive protein (hsCRP) seen in the control group?
‘Not all omega-3s created equal’
Dr. Bhatt recently said in an interview: “I think there’s confusion in the field. It’s a challenge when just one drug in a class looks good and everything else in that class looks bad. That in itself can breed some skepticism. Also, not everyone always embraces advances. Some people have other reasons to impugn datasets; for example, it could be because they are running competing trials with competing drugs.”
REDUCE-IT enrolled more than 8,000 patients at high CV risk despite statin treatment, and randomly assigned them to 2 g of EPA twice daily or the mineral oil placebo. Although the results showed a 25% reduction in the rate of CV events in the EPA group, there was also an increased risk of atrial fibrillation among those taking EPA after a median of 4.9 years follow-up.
Dr. Bhatt noted that Amarin, which manufactures Vascepa, is essentially a one-drug company, and its stock price is dependent on the product. When the trial results were released, he said, “there were people in the investor world that wanted the stock price to go up or wanted it to go down, and they were alternately hyping or disparaging the data in both cases, sometimes inappropriately and excessively, which created noise around the science.”
The fact is, he said, “not all omega-3 fatty acids are created equal. There are differences between supplements and prescription medicines, and within the prescription medicines, differences between pure EPA and the mixtures of EPA and DHA.”
Dr. Bhatt added that other trials also showed positive results. He pointed to the JELIS trial, published in 2007, which showed a 19% reduction in major adverse CV events with a 1.8-g daily EPA dose.
More recently, RESPECT-EPA was presented at the 2022 annual meeting of the American Heart Association. That study had methodological issues and was underpowered, but it did suggest a possible benefit of EPA in reducing CV events in patients with chronic coronary artery disease who were taking statins. “Looking at the totality of evidence, I think it’s quite clear there’s CV benefit,” Dr. Bhatt said.
Placebo effects?
Concerns about the mineral oil placebo cast doubt on that benefit. Table 4 of the supplement accompanying REDUCE-IT’s publication in the New England Journal of Medicine shows significant increases of non–HDL cholesterol, LDL cholesterol, apolipoprotein B, and hsCRP in the control group.
Jane Armitage, MBBS, a professor of clinical trials and epidemiology, clinical trial service unit at Oxford University (England), said in an interview: “I was surprised by the backlash and at the time felt that it was unlikely that the mineral oil was the problem. But the size of benefit was still out of kilter.”
“Two further pieces of evidence have influenced my thoughts since then,” she said. One is the lack of effect of high doses of fish oils in the STRENGTH trial. STRENGTH tested 4 g of omega-3 oil containing a mixture of EPA and DHA and found no benefit in statin-treated, high-risk patients.
“The amount of EPA [was] substantially less than given in REDUCE-IT,” Armitage said, “but it seems to me that in a similar hypertriglyceridemic population, if the effect were due to the EPA, you would have seen some impact in STRENGTH – and none was seen.”
“The other piece of evidence is in a paper by Paul Ridker, MD, et al. on the changes in biomarkers during REDUCE-IT,” she said. “Several inflammatory biomarkers associated with atherosclerosis rose during the study among those allocated mineral oil, but remained largely unchanged in the EPA group. This is in contrast to what is seen with these biomarkers in other large trials, where no changes were seen in the placebo groups, and once again raises the possibility that the apparent benefits of EPA may be related to hazard from the mineral oil.”
Still room for benefit?
Based largely on the results of REDUCE-IT, Vascepa is currently approved by the Food and Drug Administration as an adjunctive therapy to lower the risk for CV events among adults with elevated triglyceride levels (≥ 150 mg/dL). Patients must also have either established CVD or diabetes and two or more additional CV risk factors and are advised to continue physical activity and maintain a healthy diet.
Dr. Nissen, the principal author of the STRENGTH trial, said in an interview, “REDUCE-IT is an outlier. Other trials of omega-3 fatty acids, some of them very large, showed no benefits, and a meta-analysis of nearly 78,000 patients showed no beneficial effects. In this context,” he said, “the large ‘benefit’ observed in REDUCE-IT doesn’t make any sense.”
Dr. Nissen noted that a secondary analysis of STRENGTH further showed that higher plasma EPA levels did not reduce CV outcomes. He also highlighted the elevated risk of atrial fibrillation with EPA. “We need to see another study comparing EPA to a neutral comparator such as corn oil, which had no significant effect on lipid or inflammatory biomarkers in STRENGTH,” he said. “Without such a trial, the results of REDUCE-IT cannot be accepted as definitive.”
Dr. Ridker, the lead author of the REDUCE-IT substudy that found biomarker changes with the mineral oil placebo, said in an interview: “Is it possible that EPA is an outstanding drug? Absolutely, and I continue to think it useful for our very high-risk, secondary-prevention patients when we are running out of options.”
“But,” said Dr. Ridker, who is a professor at Harvard Medical School, Boston, and director of the Center for Cardiovascular Disease Prevention at Brigham and Women’s, “the reality ... is that ongoing uncertainties need resolution.” Like Dr. Nissen, he thinks the best way to resolve these uncertainties is through a second trial using a fully neutral comparator. “I am hopeful that the U.S. National Institutes of Health will see fit to undertake such an endeavor, perhaps with support from industry partners.”
Although Dr. Armitage is no longer in clinical practice, when asked how she might use EPA, she said it might be reasonable for patients who meet the prescribing criteria and remain high risk after all other risk factors have been addressed. She added that, although EPA is approved in the United Kingdom, she doesn’t think it is being widely prescribed.
Salim S. Virani, MD, PhD, a professor in the Sections of Cardiology and Cardiovascular Research at Baylor College of Medicine who has published articles about REDUCE-IT and on the eligibility and cost of EPA in the Veterans Affairs system, said in an interview: “In my personal opinion, clinicians [should] first optimize diet and lifestyle and work on secondary causes, as they play a very big role in hypertriglyceridemia.” He also recommended optimizing LDL-C levels because of “consistent data showing that LDL [cholesterol] control leads to significant reduction in atherosclerotic CVD events.”
“Once these two steps are taken and triglycerides still remain elevated,” he said, “then adding EPA in patients with established atherosclerotic CVD or those with diabetes plus other CV risk factors may be a reasonable option to further lower residual atherosclerotic CVD risk.”
Clinical inertia?
Dr. Bhatt acknowledged that, despite the benefit of EPA in the context of REDUCE-IT, “a few issues stand in the way of prescribing, particularly in the U.S.”
Vascepa’s manufacturer Amarin lost a patent challenge in the United States, enabling the relatively early introduction of multiple generics. “They’ve lost interest in the U.S. because there are three generics.”
“The sad truth is, if there isn’t a drug rep saying, ‘hey, look at this new data,’ there’s clinical inertia,” said Dr. Bhatt. He believes that the lack of marketing will hurt awareness among physicians and “ultimately hurt patients because they won’t get the drug.”
Cost is also an issue, Dr. Bhatt affirmed. Vascepa has significant out-of-pocket costs for many patients, as do some of the generics. Currently, the branded product costs about $300 per month without insurance, according to drugs.com; prices for generics vary widely, running anywhere from $82 to $200 or more.
Despite these challenges, he noted that many guidelines around the world have already changed to reflect the data, including the American Diabetes Association and the U.S. National Lipid Association.
Will there be another trial of EPA with a neutral placebo? Dr. Bhatt believes it’s not going to happen. “The company that funded REDUCE-IT is struggling just to stay alive, and another investigator-funded trial like RESPECT EPA would probably be underpowered and not move the needle much.”
Dr. Virani agreed that while it would be best to test EPA against a fully inert placebo, “whether there is enough appetite to fund such a large trial remains a big question.”
Meanwhile, Dr. Bhatt said, “EPA is not for everybody, but for the high-risk patients who meet the stringent inclusion criteria of REDUCE-IT, I think clinicians should at least consider use of EPA in a way consistent with the U.S. FDA label, the Canadian label, and the label in parts of Europe where the drug is being introduced.”
A version of this article first appeared on Medscape.com.
PPI use in type 2 diabetes links with cardiovascular events
Among people with type 2 diabetes who self-reported regularly using a proton pump inhibitor (PPI), the incidence of cardiovascular disease (CVD) events as well as all-cause death was significantly increased in a study of more than 19,000 people with type 2 diabetes in a prospective U.K. database.
During median follow-up of about 11 years, regular use of a PPI by people with type 2 diabetes was significantly linked with a 27% relative increase in the incidence of coronary artery disease, compared with nonuse of a PPI, after full adjustment for potential confounding variables.
The results also show PPI use was significantly linked after full adjustment with a 34% relative increase in MI, a 35% relative increase in heart failure, and a 30% relative increase in all-cause death, say a team of Chinese researchers in a recent report in the Journal of Clinical Endocrinology and Metabolism.
PPIs are a medication class widely used in both over-the-counter and prescription formulations to reduce acid production in the stomach and to treat gastroesophageal reflux disease and other acid-related disorders. The PPI class includes such widely used agents as esomeprazole (Nexium), lansoprazole (Prevacid), and omeprazole (Prilosec).
The analyses in this report, which used data collected in the UK Biobank, are “rigorous,” and the findings of “a modest elevation of CVD risk are consistent with a growing number of observational studies in populations with and without diabetes,” commented Mary R. Rooney, PhD, an epidemiologist at Johns Hopkins University, Baltimore, who focuses on diabetes and cardiovascular diseases.
Prior observational reports
For example, a report from a prospective, observational study of more than 4300 U.S. residents published in 2021 that Dr. Rooney coauthored documented that cumulative PPI exposure for more than 5 years was significantly linked with a twofold increase in the rate of CVD events, compared with people who did not use a PPI. (This analysis did not examine a possible effect of diabetes status.)
And in a separate prospective, observational study of more than 1,000 Australians with type 2 diabetes, initiation of PPI treatment was significantly linked with a 3.6-fold increased incidence of CVD events, compared with PPI nonuse.
However, Dr. Rooney cautioned that the role of PPI use in raising CVD events “is still an unresolved question. It is too soon to tell if PPI use in people with diabetes should trigger additional caution.” Findings are needed from prospective, randomized trials to determine more definitively whether PPIs play a causal role in the incidence of CVD events, she said in an interview.
U.S. practice often results in unwarranted prolongation of PPI treatment, said the authors of an editorial that accompanied the 2021 report by Dr. Rooney and coauthors.
Long-term PPI use threatens harm
“The practice of initiating stress ulcer prophylaxis [by administering a PPI] in critical care is common,” wrote the authors of the 2021 editorial, Nitin Malik, MD, and William S. Weintraub, MD. “Although it is data driven and well intentioned, the possibility of causing harm – if it is continued on a long-term basis after resolution of the acute illness – is palpable.”
The new analyses using UK Biobank data included 19,229 adults with type 2 diabetes and no preexisting coronary artery disease, MI, heart failure, or stroke. The cohort included 15,954 people (83%) who did not report using a PPI and 3,275 who currently used PPIs regularly. Study limitations include self-report as the only verification of PPI use and lack of information on type of PPI, dose size, or use duration.
The findings remained consistent in several sensitivity analyses, including a propensity score–matched analysis and after further adjustment for use of histamine2 receptor antagonists, a drug class with indications similar to those for PPIs.
The authors of the report speculated that mechanisms that might link PPI use and increased CVD and mortality risk could include changes to the gut microbiota and possible interactions between PPIs and antiplatelet agents.
The study received no commercial funding. The authors and Dr. Rooney disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Among people with type 2 diabetes who self-reported regularly using a proton pump inhibitor (PPI), the incidence of cardiovascular disease (CVD) events as well as all-cause death was significantly increased in a study of more than 19,000 people with type 2 diabetes in a prospective U.K. database.
During median follow-up of about 11 years, regular use of a PPI by people with type 2 diabetes was significantly linked with a 27% relative increase in the incidence of coronary artery disease, compared with nonuse of a PPI, after full adjustment for potential confounding variables.
The results also show PPI use was significantly linked after full adjustment with a 34% relative increase in MI, a 35% relative increase in heart failure, and a 30% relative increase in all-cause death, say a team of Chinese researchers in a recent report in the Journal of Clinical Endocrinology and Metabolism.
PPIs are a medication class widely used in both over-the-counter and prescription formulations to reduce acid production in the stomach and to treat gastroesophageal reflux disease and other acid-related disorders. The PPI class includes such widely used agents as esomeprazole (Nexium), lansoprazole (Prevacid), and omeprazole (Prilosec).
The analyses in this report, which used data collected in the UK Biobank, are “rigorous,” and the findings of “a modest elevation of CVD risk are consistent with a growing number of observational studies in populations with and without diabetes,” commented Mary R. Rooney, PhD, an epidemiologist at Johns Hopkins University, Baltimore, who focuses on diabetes and cardiovascular diseases.
Prior observational reports
For example, a report from a prospective, observational study of more than 4300 U.S. residents published in 2021 that Dr. Rooney coauthored documented that cumulative PPI exposure for more than 5 years was significantly linked with a twofold increase in the rate of CVD events, compared with people who did not use a PPI. (This analysis did not examine a possible effect of diabetes status.)
And in a separate prospective, observational study of more than 1,000 Australians with type 2 diabetes, initiation of PPI treatment was significantly linked with a 3.6-fold increased incidence of CVD events, compared with PPI nonuse.
However, Dr. Rooney cautioned that the role of PPI use in raising CVD events “is still an unresolved question. It is too soon to tell if PPI use in people with diabetes should trigger additional caution.” Findings are needed from prospective, randomized trials to determine more definitively whether PPIs play a causal role in the incidence of CVD events, she said in an interview.
U.S. practice often results in unwarranted prolongation of PPI treatment, said the authors of an editorial that accompanied the 2021 report by Dr. Rooney and coauthors.
Long-term PPI use threatens harm
“The practice of initiating stress ulcer prophylaxis [by administering a PPI] in critical care is common,” wrote the authors of the 2021 editorial, Nitin Malik, MD, and William S. Weintraub, MD. “Although it is data driven and well intentioned, the possibility of causing harm – if it is continued on a long-term basis after resolution of the acute illness – is palpable.”
The new analyses using UK Biobank data included 19,229 adults with type 2 diabetes and no preexisting coronary artery disease, MI, heart failure, or stroke. The cohort included 15,954 people (83%) who did not report using a PPI and 3,275 who currently used PPIs regularly. Study limitations include self-report as the only verification of PPI use and lack of information on type of PPI, dose size, or use duration.
The findings remained consistent in several sensitivity analyses, including a propensity score–matched analysis and after further adjustment for use of histamine2 receptor antagonists, a drug class with indications similar to those for PPIs.
The authors of the report speculated that mechanisms that might link PPI use and increased CVD and mortality risk could include changes to the gut microbiota and possible interactions between PPIs and antiplatelet agents.
The study received no commercial funding. The authors and Dr. Rooney disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Among people with type 2 diabetes who self-reported regularly using a proton pump inhibitor (PPI), the incidence of cardiovascular disease (CVD) events as well as all-cause death was significantly increased in a study of more than 19,000 people with type 2 diabetes in a prospective U.K. database.
During median follow-up of about 11 years, regular use of a PPI by people with type 2 diabetes was significantly linked with a 27% relative increase in the incidence of coronary artery disease, compared with nonuse of a PPI, after full adjustment for potential confounding variables.
The results also show PPI use was significantly linked after full adjustment with a 34% relative increase in MI, a 35% relative increase in heart failure, and a 30% relative increase in all-cause death, say a team of Chinese researchers in a recent report in the Journal of Clinical Endocrinology and Metabolism.
PPIs are a medication class widely used in both over-the-counter and prescription formulations to reduce acid production in the stomach and to treat gastroesophageal reflux disease and other acid-related disorders. The PPI class includes such widely used agents as esomeprazole (Nexium), lansoprazole (Prevacid), and omeprazole (Prilosec).
The analyses in this report, which used data collected in the UK Biobank, are “rigorous,” and the findings of “a modest elevation of CVD risk are consistent with a growing number of observational studies in populations with and without diabetes,” commented Mary R. Rooney, PhD, an epidemiologist at Johns Hopkins University, Baltimore, who focuses on diabetes and cardiovascular diseases.
Prior observational reports
For example, a report from a prospective, observational study of more than 4300 U.S. residents published in 2021 that Dr. Rooney coauthored documented that cumulative PPI exposure for more than 5 years was significantly linked with a twofold increase in the rate of CVD events, compared with people who did not use a PPI. (This analysis did not examine a possible effect of diabetes status.)
And in a separate prospective, observational study of more than 1,000 Australians with type 2 diabetes, initiation of PPI treatment was significantly linked with a 3.6-fold increased incidence of CVD events, compared with PPI nonuse.
However, Dr. Rooney cautioned that the role of PPI use in raising CVD events “is still an unresolved question. It is too soon to tell if PPI use in people with diabetes should trigger additional caution.” Findings are needed from prospective, randomized trials to determine more definitively whether PPIs play a causal role in the incidence of CVD events, she said in an interview.
U.S. practice often results in unwarranted prolongation of PPI treatment, said the authors of an editorial that accompanied the 2021 report by Dr. Rooney and coauthors.
Long-term PPI use threatens harm
“The practice of initiating stress ulcer prophylaxis [by administering a PPI] in critical care is common,” wrote the authors of the 2021 editorial, Nitin Malik, MD, and William S. Weintraub, MD. “Although it is data driven and well intentioned, the possibility of causing harm – if it is continued on a long-term basis after resolution of the acute illness – is palpable.”
The new analyses using UK Biobank data included 19,229 adults with type 2 diabetes and no preexisting coronary artery disease, MI, heart failure, or stroke. The cohort included 15,954 people (83%) who did not report using a PPI and 3,275 who currently used PPIs regularly. Study limitations include self-report as the only verification of PPI use and lack of information on type of PPI, dose size, or use duration.
The findings remained consistent in several sensitivity analyses, including a propensity score–matched analysis and after further adjustment for use of histamine2 receptor antagonists, a drug class with indications similar to those for PPIs.
The authors of the report speculated that mechanisms that might link PPI use and increased CVD and mortality risk could include changes to the gut microbiota and possible interactions between PPIs and antiplatelet agents.
The study received no commercial funding. The authors and Dr. Rooney disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL ENDOCRINOLOGY AND METABOLISM
Frail ADHF patients benefit more from early rehab
Patients with acute decompensated heart failure who were frail at baseline improved more with targeted, early physical rehabilitation than those who were prefrail, a new analysis of the REHAB-HF study suggests.
“The robust response to the intervention by frail patients exceeded our expectations,” Gordon R. Reeves, MD, PT, of Novant Health Heart and Vascular Institute, Charlotte, N.C., told this news organization. “The effect size from improvement in physical function among frail patients was very large, with at least four times the minimal meaningful improvement, based on the Short Physical Performance Battery (SPPB).”
Furthermore, the interaction between baseline frailty status and treatment in REHAB-HF was such that a 2.6-fold larger improvement in SPPB was seen among frail versus prefrail patients.
However, Dr. Reeves noted, “We need to further evaluate safety and efficacy as it relates to adverse clinical events. Specifically, we observed a numerically higher number of deaths with the REHAB-HF intervention, which warrants further investigation before the intervention is implemented in clinical practice.”
The study was published online in JAMA Cardiology.
Interpret with caution
Dr. Reeves and colleagues conducted a prespecified secondary analysis of the previously published Therapy in Older Acute Heart Failure Patients (REHAB-HF) trial, a multicenter, randomized controlled trial that showed that a 3-month early, transitional, tailored, multidomain physical rehabilitation intervention improved physical function and quality of life (QoL), compared with usual care. The secondary analysis aimed to evaluate whether baseline frailty altered the benefits of the intervention or was associated with risk of adverse outcomes.
According to Dr. Reeves, REHAB-HF differs from more traditional cardiac rehab programs in several ways.
- The intervention targets patients with acute HF, including HF with preserved ejection fraction (HFpEF). Medicare policy limits standard cardiac rehabilitation in HF to long-term patients with HF with reduced ejection fraction (HFrEF) only who have been stabilized for 6 weeks or longer after a recent hospitalization.
- It addresses multiple physical function domains, including balance, mobility, functional strength, and endurance. Standard cardiac rehab is primarily focused on endurance training, which can result in injuries and falls if deficits in balance, mobility, and strength are not addressed first.
- It is delivered one to one rather than in a group setting and primarily by physical therapists who are experts in the rehabilitation of medically complex patients.
- It is transitional, beginning in the hospital, then moving to the outpatient setting, then to home and includes a home assessment.
For the analysis, the Fried phenotype model was used to assess baseline frailty across five domains: unintentional weight loss during the past year; self-reported exhaustion; grip strength; slowness, as assessed by gait speed; and low physical activity, as assessed by the Short Form-12 Physical Composite Score.
At the baseline visit, patients were categorized as frail if they met three or more of these criteria. They were categorized as prefrail if they met one or two criteria and as nonfrail if they met none of the criteria. Because of the small number of nonfrail participants, the analysis included only frail and prefrail participants.
The analysis included 337 participants (mean age, 72; 54%, women; 50%, Black). At baseline, 57% were frail, and 43% were prefrail.
A significant interaction was seen between baseline frailty and the intervention for the primary trial endpoint of overall SPPB score, with a 2.6-fold larger improvement in SPPB among frail (2.1) versus prefrail (0.8) patients.
Trends favored a larger intervention effect size, with significant improvement among frail versus prefrail participants for 6-minute walk distance, QoL, and the geriatric depression score.
“However, we must interpret these findings with caution,” the authors write. “The REHAB-HF trial was not adequately powered to determine the effect of the intervention on clinical events.” This plus the number of deaths “underscore the need for additional research, including prospective clinical trials, investigating the effect of physical function interventions on clinical events among frail patients with HF.”
To address this need, the researchers recently launched a larger clinical trial, called REHAB-HFpEF, which is powered to assess the impact of the intervention on clinical events, according to Dr. Reeves. “As the name implies,” he said, “this trial is focused on older patients recently hospitalized with HFpEF, who, [compared with HFrEF] also showed a more robust response to the intervention, with worse physical function and very high prevalence of frailty near the time of hospital discharge.”
‘Never too old or sick to benefit’
Jonathan H. Whiteson, MD, vice chair of clinical operations and medical director of cardiac and pulmonary rehabilitation at NYU Langone Health’s Rusk Rehabilitation, said, “We have seen in clinical practice and in other (non–heart failure) clinical areas that frail older patients do improve proportionally more than younger and less frail patients with rehabilitation programs. Encouragingly, this very much supports the practice that patients are never too old or too sick to benefit from an individualized multidisciplinary rehabilitation program.”
However, he noted, “patients had to be independent with basic activities of daily living to be included in the study,” so many frail, elderly patients with heart failure who are not independent were not included in the study. It also wasn’t clear whether patients who received postacute care at a rehab facility before going home were included in the trial.
Furthermore, he said, outcomes over 1 to 5 years are needed to understand the long-term impact of the intervention.
On the other hand, he added, the fact that about half of participants were Black and were women is a “tremendous strength.”
“Repeating this study in population groups at high risk for frailty with different diagnoses, such as chronic lung diseases, interstitial lung diseases, chronic kidney disease, and rheumatologic disorders will further support the value of rehabilitation in improving patient health, function, quality of life, and reducing rehospitalizations and health care costs,” Dr. Whiteson concluded.
The study was supported by grants from the National Key R&D program. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Patients with acute decompensated heart failure who were frail at baseline improved more with targeted, early physical rehabilitation than those who were prefrail, a new analysis of the REHAB-HF study suggests.
“The robust response to the intervention by frail patients exceeded our expectations,” Gordon R. Reeves, MD, PT, of Novant Health Heart and Vascular Institute, Charlotte, N.C., told this news organization. “The effect size from improvement in physical function among frail patients was very large, with at least four times the minimal meaningful improvement, based on the Short Physical Performance Battery (SPPB).”
Furthermore, the interaction between baseline frailty status and treatment in REHAB-HF was such that a 2.6-fold larger improvement in SPPB was seen among frail versus prefrail patients.
However, Dr. Reeves noted, “We need to further evaluate safety and efficacy as it relates to adverse clinical events. Specifically, we observed a numerically higher number of deaths with the REHAB-HF intervention, which warrants further investigation before the intervention is implemented in clinical practice.”
The study was published online in JAMA Cardiology.
Interpret with caution
Dr. Reeves and colleagues conducted a prespecified secondary analysis of the previously published Therapy in Older Acute Heart Failure Patients (REHAB-HF) trial, a multicenter, randomized controlled trial that showed that a 3-month early, transitional, tailored, multidomain physical rehabilitation intervention improved physical function and quality of life (QoL), compared with usual care. The secondary analysis aimed to evaluate whether baseline frailty altered the benefits of the intervention or was associated with risk of adverse outcomes.
According to Dr. Reeves, REHAB-HF differs from more traditional cardiac rehab programs in several ways.
- The intervention targets patients with acute HF, including HF with preserved ejection fraction (HFpEF). Medicare policy limits standard cardiac rehabilitation in HF to long-term patients with HF with reduced ejection fraction (HFrEF) only who have been stabilized for 6 weeks or longer after a recent hospitalization.
- It addresses multiple physical function domains, including balance, mobility, functional strength, and endurance. Standard cardiac rehab is primarily focused on endurance training, which can result in injuries and falls if deficits in balance, mobility, and strength are not addressed first.
- It is delivered one to one rather than in a group setting and primarily by physical therapists who are experts in the rehabilitation of medically complex patients.
- It is transitional, beginning in the hospital, then moving to the outpatient setting, then to home and includes a home assessment.
For the analysis, the Fried phenotype model was used to assess baseline frailty across five domains: unintentional weight loss during the past year; self-reported exhaustion; grip strength; slowness, as assessed by gait speed; and low physical activity, as assessed by the Short Form-12 Physical Composite Score.
At the baseline visit, patients were categorized as frail if they met three or more of these criteria. They were categorized as prefrail if they met one or two criteria and as nonfrail if they met none of the criteria. Because of the small number of nonfrail participants, the analysis included only frail and prefrail participants.
The analysis included 337 participants (mean age, 72; 54%, women; 50%, Black). At baseline, 57% were frail, and 43% were prefrail.
A significant interaction was seen between baseline frailty and the intervention for the primary trial endpoint of overall SPPB score, with a 2.6-fold larger improvement in SPPB among frail (2.1) versus prefrail (0.8) patients.
Trends favored a larger intervention effect size, with significant improvement among frail versus prefrail participants for 6-minute walk distance, QoL, and the geriatric depression score.
“However, we must interpret these findings with caution,” the authors write. “The REHAB-HF trial was not adequately powered to determine the effect of the intervention on clinical events.” This plus the number of deaths “underscore the need for additional research, including prospective clinical trials, investigating the effect of physical function interventions on clinical events among frail patients with HF.”
To address this need, the researchers recently launched a larger clinical trial, called REHAB-HFpEF, which is powered to assess the impact of the intervention on clinical events, according to Dr. Reeves. “As the name implies,” he said, “this trial is focused on older patients recently hospitalized with HFpEF, who, [compared with HFrEF] also showed a more robust response to the intervention, with worse physical function and very high prevalence of frailty near the time of hospital discharge.”
‘Never too old or sick to benefit’
Jonathan H. Whiteson, MD, vice chair of clinical operations and medical director of cardiac and pulmonary rehabilitation at NYU Langone Health’s Rusk Rehabilitation, said, “We have seen in clinical practice and in other (non–heart failure) clinical areas that frail older patients do improve proportionally more than younger and less frail patients with rehabilitation programs. Encouragingly, this very much supports the practice that patients are never too old or too sick to benefit from an individualized multidisciplinary rehabilitation program.”
However, he noted, “patients had to be independent with basic activities of daily living to be included in the study,” so many frail, elderly patients with heart failure who are not independent were not included in the study. It also wasn’t clear whether patients who received postacute care at a rehab facility before going home were included in the trial.
Furthermore, he said, outcomes over 1 to 5 years are needed to understand the long-term impact of the intervention.
On the other hand, he added, the fact that about half of participants were Black and were women is a “tremendous strength.”
“Repeating this study in population groups at high risk for frailty with different diagnoses, such as chronic lung diseases, interstitial lung diseases, chronic kidney disease, and rheumatologic disorders will further support the value of rehabilitation in improving patient health, function, quality of life, and reducing rehospitalizations and health care costs,” Dr. Whiteson concluded.
The study was supported by grants from the National Key R&D program. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Patients with acute decompensated heart failure who were frail at baseline improved more with targeted, early physical rehabilitation than those who were prefrail, a new analysis of the REHAB-HF study suggests.
“The robust response to the intervention by frail patients exceeded our expectations,” Gordon R. Reeves, MD, PT, of Novant Health Heart and Vascular Institute, Charlotte, N.C., told this news organization. “The effect size from improvement in physical function among frail patients was very large, with at least four times the minimal meaningful improvement, based on the Short Physical Performance Battery (SPPB).”
Furthermore, the interaction between baseline frailty status and treatment in REHAB-HF was such that a 2.6-fold larger improvement in SPPB was seen among frail versus prefrail patients.
However, Dr. Reeves noted, “We need to further evaluate safety and efficacy as it relates to adverse clinical events. Specifically, we observed a numerically higher number of deaths with the REHAB-HF intervention, which warrants further investigation before the intervention is implemented in clinical practice.”
The study was published online in JAMA Cardiology.
Interpret with caution
Dr. Reeves and colleagues conducted a prespecified secondary analysis of the previously published Therapy in Older Acute Heart Failure Patients (REHAB-HF) trial, a multicenter, randomized controlled trial that showed that a 3-month early, transitional, tailored, multidomain physical rehabilitation intervention improved physical function and quality of life (QoL), compared with usual care. The secondary analysis aimed to evaluate whether baseline frailty altered the benefits of the intervention or was associated with risk of adverse outcomes.
According to Dr. Reeves, REHAB-HF differs from more traditional cardiac rehab programs in several ways.
- The intervention targets patients with acute HF, including HF with preserved ejection fraction (HFpEF). Medicare policy limits standard cardiac rehabilitation in HF to long-term patients with HF with reduced ejection fraction (HFrEF) only who have been stabilized for 6 weeks or longer after a recent hospitalization.
- It addresses multiple physical function domains, including balance, mobility, functional strength, and endurance. Standard cardiac rehab is primarily focused on endurance training, which can result in injuries and falls if deficits in balance, mobility, and strength are not addressed first.
- It is delivered one to one rather than in a group setting and primarily by physical therapists who are experts in the rehabilitation of medically complex patients.
- It is transitional, beginning in the hospital, then moving to the outpatient setting, then to home and includes a home assessment.
For the analysis, the Fried phenotype model was used to assess baseline frailty across five domains: unintentional weight loss during the past year; self-reported exhaustion; grip strength; slowness, as assessed by gait speed; and low physical activity, as assessed by the Short Form-12 Physical Composite Score.
At the baseline visit, patients were categorized as frail if they met three or more of these criteria. They were categorized as prefrail if they met one or two criteria and as nonfrail if they met none of the criteria. Because of the small number of nonfrail participants, the analysis included only frail and prefrail participants.
The analysis included 337 participants (mean age, 72; 54%, women; 50%, Black). At baseline, 57% were frail, and 43% were prefrail.
A significant interaction was seen between baseline frailty and the intervention for the primary trial endpoint of overall SPPB score, with a 2.6-fold larger improvement in SPPB among frail (2.1) versus prefrail (0.8) patients.
Trends favored a larger intervention effect size, with significant improvement among frail versus prefrail participants for 6-minute walk distance, QoL, and the geriatric depression score.
“However, we must interpret these findings with caution,” the authors write. “The REHAB-HF trial was not adequately powered to determine the effect of the intervention on clinical events.” This plus the number of deaths “underscore the need for additional research, including prospective clinical trials, investigating the effect of physical function interventions on clinical events among frail patients with HF.”
To address this need, the researchers recently launched a larger clinical trial, called REHAB-HFpEF, which is powered to assess the impact of the intervention on clinical events, according to Dr. Reeves. “As the name implies,” he said, “this trial is focused on older patients recently hospitalized with HFpEF, who, [compared with HFrEF] also showed a more robust response to the intervention, with worse physical function and very high prevalence of frailty near the time of hospital discharge.”
‘Never too old or sick to benefit’
Jonathan H. Whiteson, MD, vice chair of clinical operations and medical director of cardiac and pulmonary rehabilitation at NYU Langone Health’s Rusk Rehabilitation, said, “We have seen in clinical practice and in other (non–heart failure) clinical areas that frail older patients do improve proportionally more than younger and less frail patients with rehabilitation programs. Encouragingly, this very much supports the practice that patients are never too old or too sick to benefit from an individualized multidisciplinary rehabilitation program.”
However, he noted, “patients had to be independent with basic activities of daily living to be included in the study,” so many frail, elderly patients with heart failure who are not independent were not included in the study. It also wasn’t clear whether patients who received postacute care at a rehab facility before going home were included in the trial.
Furthermore, he said, outcomes over 1 to 5 years are needed to understand the long-term impact of the intervention.
On the other hand, he added, the fact that about half of participants were Black and were women is a “tremendous strength.”
“Repeating this study in population groups at high risk for frailty with different diagnoses, such as chronic lung diseases, interstitial lung diseases, chronic kidney disease, and rheumatologic disorders will further support the value of rehabilitation in improving patient health, function, quality of life, and reducing rehospitalizations and health care costs,” Dr. Whiteson concluded.
The study was supported by grants from the National Key R&D program. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Some BP meds tied to significantly lower risk for dementia, Alzheimer’s
Antihypertensive medications that stimulate rather than inhibit type 2 and 4 angiotensin II receptors can lower the rate of dementia among new users of these medications, new research suggests.
Results from a cohort study of more than 57,000 older Medicare beneficiaries showed that the initiation of antihypertensives that stimulate the receptors was linked to a 16% lower risk for incident Alzheimer’s disease and related dementia (ADRD) and an 18% lower risk for vascular dementia compared with those that inhibit the receptors.
“Achieving appropriate blood pressure control is essential for maximizing brain health, and this promising research suggests certain antihypertensives could yield brain benefit compared to others,” lead study author Zachary A. Marcum, PharmD, PhD, associate professor, University of Washington School of Pharmacy, Seattle, told this news organization.
The findings were published online in JAMA Network Open.
Medicare beneficiaries
Previous observational studies showed that antihypertensive medications that stimulate type 2 and 4 angiotensin II receptors, in comparison with those that don’t, were associated with lower rates of dementia. However, those studies included individuals with prevalent hypertension and were relatively small.
The new retrospective cohort study included a random sample of 57,773 Medicare beneficiaries aged at least 65 years with new-onset hypertension. The mean age of participants was 73.8 years, 62.9% were women, and 86.9% were White.
Over the course of the study, some participants filled at least one prescription for a stimulating angiotensin II receptor type 2 and 4, such as angiotensin II receptor type 1 blockers, dihydropyridine calcium channel blockers, and thiazide diuretics.
Others participants filled a prescription for an inhibiting type 2 and 4 angiotensin II receptors, including angiotensin-converting enzyme (ACE) inhibitors, beta-blockers, and nondihydropyridine calcium channel blockers.
“All these medications lower blood pressure, but they do it in different ways,” said Dr. Marcum.
The researchers were interested in the varying activity of these drugs at the type 2 and 4 angiotensin II receptors.
For each 30-day interval, they categorized beneficiaries into four groups: a stimulating medication group (n = 4,879) consisting of individuals mostly taking stimulating antihypertensives; an inhibiting medication group (n = 10,303) that mostly included individuals prescribed this type of antihypertensive; a mixed group (n = 2,179) that included a combination of the first two classifications; and a nonuser group (n = 40,413) of individuals who were not using either type of drug.
The primary outcome was time to first occurrence of ADRD. The secondary outcome was time to first occurrence of vascular dementia.
Researchers controlled for cardiovascular risk factors and sociodemographic characteristics, such as age, sex, race/ethnicity, and receipt of low-income subsidy.
Unanswered questions
After adjustments, results showed that initiation of an antihypertensive medication regimen that exclusively stimulates, rather than inhibits, type 2 and 4 angiotensin II receptors was associated with a 16% lower risk for incident ADRD over a follow-up of just under 7 years (hazard ratio, 0.84; 95% confidence interval, 0.79-0.90; P < .001).
The mixed regimen was also associated with statistically significant (P = .001) reduced odds of ADRD compared with the inhibiting medications.
As for vascular dementia, use of stimulating vs. inhibiting medications was associated with an 18% lower risk (HR, 0.82; 95% CI, 0.69-0.96; P = .02).
Again, use of the mixed regimen was associated with reduced risk of vascular dementia compared with the inhibiting medications (P = .03).
A variety of potential mechanisms might explain the superiority of stimulating agents when it comes to dementia risk, said Dr. Marcum. These could include, for example, increased blood flow to the brain and reduced amyloid.
“But more mechanistic work is needed as well as evaluation of dose responses, because that’s not something we looked at in this study,” Dr. Marcum said. “There are still a lot of unanswered questions.”
Stimulators instead of inhibitors?
The results of the current analysis come on the heels of some previous work showing the benefits of lowering blood pressure. For example, the Systolic Blood Pressure Intervention Trial (SPRINT) showed that targeting a systolic blood pressure below 120 mm Hg significantly reduces risk for heart disease, stroke, and death from these diseases.
But in contrast to previous research, the current study included only beneficiaries with incident hypertension and new use of antihypertensive medications, and it adjusted for time-varying confounding.
Prescribing stimulating instead of inhibiting treatments could make a difference at the population level, Dr. Marcum noted.
“If we could shift the prescribing a little bit from inhibiting to stimulating, that could possibly reduce dementia risk,” he said.
However, “we’re not suggesting [that all patients] have their regimen switched,” he added.
That’s because inhibiting medications still have an important place in the antihypertensive treatment armamentarium, Dr. Marcum noted. As an example, beta-blockers are used post heart attack.
As well, factors such as cost and side effects should be taken into consideration when prescribing an antihypertensive drug.
The new results could be used to set up a comparison in a future randomized controlled trial that would provide the strongest evidence for estimating causal effects of treatments, said Dr. Marcum.
‘More convincing’
Carlos G. Santos-Gallego, MD, Icahn School of Medicine at Mount Sinai, New York, said the study is “more convincing” than previous related research, as it has a larger sample size and a longer follow-up.

“And the exquisite statistical analysis gives more robustness, more solidity, to the hypothesis that drugs that stimulate type 2 and 4 angiotensin II receptors might be protective for dementia,” said Dr. Santos-Gallego, who was not involved with the research.
However, he noted that the retrospective study had some limitations, including the underdiagnosis of dementia. “The diagnosis of dementia is, honestly, very poorly done in the clinical setting,” he said.
As well, the study could be subject to “confounding by indication,” Dr. Santos-Gallego said. “There could be a third variable, another confounding factor, that’s responsible both for the dementia and for the prescription of these drugs,” he added.
For example, he noted that comorbidities such as atrial fibrillation, myocardial infarction, and heart failure might increase the risk of dementia.
He agreed with the investigators that a randomized clinical trial would address these limitations. “All comorbidities would be equally shared” in the randomized groups, and all participants would be given “a specific test for dementia at the same time,” Dr. Santos-Gallego said.
Still, he noted that the new results are in keeping with hypertension guidelines that recommend stimulating drugs.
“This trial definitely shows that the current hypertension guidelines are good treatment for our patients, not only to control blood pressure and not only to prevent infarction to prevent stroke but also to prevent dementia,” said Dr. Santos-Gallego.
Also commenting for this news organization, Heather Snyder, PhD, vice president of medical and scientific relations at the Alzheimer’s Association, said the new data provide “clarity” on why previous research had differing results on the effect of antihypertensives on cognition.
Among the caveats of this new analysis is that “it’s unclear if the demographics in this study are fully representative of Medicare beneficiaries,” said Dr. Snyder.
She, too, said a clinical trial is important “to understand if there is a preventative and/or treatment potential in the medications that stimulate type 2 and 4 angiotensin II receptors.”
The study received funding from the National Institute on Aging. Dr. Marcum and Dr. Santos-Gallego have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Antihypertensive medications that stimulate rather than inhibit type 2 and 4 angiotensin II receptors can lower the rate of dementia among new users of these medications, new research suggests.
Results from a cohort study of more than 57,000 older Medicare beneficiaries showed that the initiation of antihypertensives that stimulate the receptors was linked to a 16% lower risk for incident Alzheimer’s disease and related dementia (ADRD) and an 18% lower risk for vascular dementia compared with those that inhibit the receptors.
“Achieving appropriate blood pressure control is essential for maximizing brain health, and this promising research suggests certain antihypertensives could yield brain benefit compared to others,” lead study author Zachary A. Marcum, PharmD, PhD, associate professor, University of Washington School of Pharmacy, Seattle, told this news organization.
The findings were published online in JAMA Network Open.
Medicare beneficiaries
Previous observational studies showed that antihypertensive medications that stimulate type 2 and 4 angiotensin II receptors, in comparison with those that don’t, were associated with lower rates of dementia. However, those studies included individuals with prevalent hypertension and were relatively small.
The new retrospective cohort study included a random sample of 57,773 Medicare beneficiaries aged at least 65 years with new-onset hypertension. The mean age of participants was 73.8 years, 62.9% were women, and 86.9% were White.
Over the course of the study, some participants filled at least one prescription for a stimulating angiotensin II receptor type 2 and 4, such as angiotensin II receptor type 1 blockers, dihydropyridine calcium channel blockers, and thiazide diuretics.
Others participants filled a prescription for an inhibiting type 2 and 4 angiotensin II receptors, including angiotensin-converting enzyme (ACE) inhibitors, beta-blockers, and nondihydropyridine calcium channel blockers.
“All these medications lower blood pressure, but they do it in different ways,” said Dr. Marcum.
The researchers were interested in the varying activity of these drugs at the type 2 and 4 angiotensin II receptors.
For each 30-day interval, they categorized beneficiaries into four groups: a stimulating medication group (n = 4,879) consisting of individuals mostly taking stimulating antihypertensives; an inhibiting medication group (n = 10,303) that mostly included individuals prescribed this type of antihypertensive; a mixed group (n = 2,179) that included a combination of the first two classifications; and a nonuser group (n = 40,413) of individuals who were not using either type of drug.
The primary outcome was time to first occurrence of ADRD. The secondary outcome was time to first occurrence of vascular dementia.
Researchers controlled for cardiovascular risk factors and sociodemographic characteristics, such as age, sex, race/ethnicity, and receipt of low-income subsidy.
Unanswered questions
After adjustments, results showed that initiation of an antihypertensive medication regimen that exclusively stimulates, rather than inhibits, type 2 and 4 angiotensin II receptors was associated with a 16% lower risk for incident ADRD over a follow-up of just under 7 years (hazard ratio, 0.84; 95% confidence interval, 0.79-0.90; P < .001).
The mixed regimen was also associated with statistically significant (P = .001) reduced odds of ADRD compared with the inhibiting medications.
As for vascular dementia, use of stimulating vs. inhibiting medications was associated with an 18% lower risk (HR, 0.82; 95% CI, 0.69-0.96; P = .02).
Again, use of the mixed regimen was associated with reduced risk of vascular dementia compared with the inhibiting medications (P = .03).
A variety of potential mechanisms might explain the superiority of stimulating agents when it comes to dementia risk, said Dr. Marcum. These could include, for example, increased blood flow to the brain and reduced amyloid.
“But more mechanistic work is needed as well as evaluation of dose responses, because that’s not something we looked at in this study,” Dr. Marcum said. “There are still a lot of unanswered questions.”
Stimulators instead of inhibitors?
The results of the current analysis come on the heels of some previous work showing the benefits of lowering blood pressure. For example, the Systolic Blood Pressure Intervention Trial (SPRINT) showed that targeting a systolic blood pressure below 120 mm Hg significantly reduces risk for heart disease, stroke, and death from these diseases.
But in contrast to previous research, the current study included only beneficiaries with incident hypertension and new use of antihypertensive medications, and it adjusted for time-varying confounding.
Prescribing stimulating instead of inhibiting treatments could make a difference at the population level, Dr. Marcum noted.
“If we could shift the prescribing a little bit from inhibiting to stimulating, that could possibly reduce dementia risk,” he said.
However, “we’re not suggesting [that all patients] have their regimen switched,” he added.
That’s because inhibiting medications still have an important place in the antihypertensive treatment armamentarium, Dr. Marcum noted. As an example, beta-blockers are used post heart attack.
As well, factors such as cost and side effects should be taken into consideration when prescribing an antihypertensive drug.
The new results could be used to set up a comparison in a future randomized controlled trial that would provide the strongest evidence for estimating causal effects of treatments, said Dr. Marcum.
‘More convincing’
Carlos G. Santos-Gallego, MD, Icahn School of Medicine at Mount Sinai, New York, said the study is “more convincing” than previous related research, as it has a larger sample size and a longer follow-up.
“And the exquisite statistical analysis gives more robustness, more solidity, to the hypothesis that drugs that stimulate type 2 and 4 angiotensin II receptors might be protective for dementia,” said Dr. Santos-Gallego, who was not involved with the research.
However, he noted that the retrospective study had some limitations, including the underdiagnosis of dementia. “The diagnosis of dementia is, honestly, very poorly done in the clinical setting,” he said.
As well, the study could be subject to “confounding by indication,” Dr. Santos-Gallego said. “There could be a third variable, another confounding factor, that’s responsible both for the dementia and for the prescription of these drugs,” he added.
For example, he noted that comorbidities such as atrial fibrillation, myocardial infarction, and heart failure might increase the risk of dementia.
He agreed with the investigators that a randomized clinical trial would address these limitations. “All comorbidities would be equally shared” in the randomized groups, and all participants would be given “a specific test for dementia at the same time,” Dr. Santos-Gallego said.
Still, he noted that the new results are in keeping with hypertension guidelines that recommend stimulating drugs.
“This trial definitely shows that the current hypertension guidelines are good treatment for our patients, not only to control blood pressure and not only to prevent infarction to prevent stroke but also to prevent dementia,” said Dr. Santos-Gallego.
Also commenting for this news organization, Heather Snyder, PhD, vice president of medical and scientific relations at the Alzheimer’s Association, said the new data provide “clarity” on why previous research had differing results on the effect of antihypertensives on cognition.
Among the caveats of this new analysis is that “it’s unclear if the demographics in this study are fully representative of Medicare beneficiaries,” said Dr. Snyder.
She, too, said a clinical trial is important “to understand if there is a preventative and/or treatment potential in the medications that stimulate type 2 and 4 angiotensin II receptors.”
The study received funding from the National Institute on Aging. Dr. Marcum and Dr. Santos-Gallego have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Antihypertensive medications that stimulate rather than inhibit type 2 and 4 angiotensin II receptors can lower the rate of dementia among new users of these medications, new research suggests.
Results from a cohort study of more than 57,000 older Medicare beneficiaries showed that the initiation of antihypertensives that stimulate the receptors was linked to a 16% lower risk for incident Alzheimer’s disease and related dementia (ADRD) and an 18% lower risk for vascular dementia compared with those that inhibit the receptors.
“Achieving appropriate blood pressure control is essential for maximizing brain health, and this promising research suggests certain antihypertensives could yield brain benefit compared to others,” lead study author Zachary A. Marcum, PharmD, PhD, associate professor, University of Washington School of Pharmacy, Seattle, told this news organization.
The findings were published online in JAMA Network Open.
Medicare beneficiaries
Previous observational studies showed that antihypertensive medications that stimulate type 2 and 4 angiotensin II receptors, in comparison with those that don’t, were associated with lower rates of dementia. However, those studies included individuals with prevalent hypertension and were relatively small.
The new retrospective cohort study included a random sample of 57,773 Medicare beneficiaries aged at least 65 years with new-onset hypertension. The mean age of participants was 73.8 years, 62.9% were women, and 86.9% were White.
Over the course of the study, some participants filled at least one prescription for a stimulating angiotensin II receptor type 2 and 4, such as angiotensin II receptor type 1 blockers, dihydropyridine calcium channel blockers, and thiazide diuretics.
Others participants filled a prescription for an inhibiting type 2 and 4 angiotensin II receptors, including angiotensin-converting enzyme (ACE) inhibitors, beta-blockers, and nondihydropyridine calcium channel blockers.
“All these medications lower blood pressure, but they do it in different ways,” said Dr. Marcum.
The researchers were interested in the varying activity of these drugs at the type 2 and 4 angiotensin II receptors.
For each 30-day interval, they categorized beneficiaries into four groups: a stimulating medication group (n = 4,879) consisting of individuals mostly taking stimulating antihypertensives; an inhibiting medication group (n = 10,303) that mostly included individuals prescribed this type of antihypertensive; a mixed group (n = 2,179) that included a combination of the first two classifications; and a nonuser group (n = 40,413) of individuals who were not using either type of drug.
The primary outcome was time to first occurrence of ADRD. The secondary outcome was time to first occurrence of vascular dementia.
Researchers controlled for cardiovascular risk factors and sociodemographic characteristics, such as age, sex, race/ethnicity, and receipt of low-income subsidy.
Unanswered questions
After adjustments, results showed that initiation of an antihypertensive medication regimen that exclusively stimulates, rather than inhibits, type 2 and 4 angiotensin II receptors was associated with a 16% lower risk for incident ADRD over a follow-up of just under 7 years (hazard ratio, 0.84; 95% confidence interval, 0.79-0.90; P < .001).
The mixed regimen was also associated with statistically significant (P = .001) reduced odds of ADRD compared with the inhibiting medications.
As for vascular dementia, use of stimulating vs. inhibiting medications was associated with an 18% lower risk (HR, 0.82; 95% CI, 0.69-0.96; P = .02).
Again, use of the mixed regimen was associated with reduced risk of vascular dementia compared with the inhibiting medications (P = .03).
A variety of potential mechanisms might explain the superiority of stimulating agents when it comes to dementia risk, said Dr. Marcum. These could include, for example, increased blood flow to the brain and reduced amyloid.
“But more mechanistic work is needed as well as evaluation of dose responses, because that’s not something we looked at in this study,” Dr. Marcum said. “There are still a lot of unanswered questions.”
Stimulators instead of inhibitors?
The results of the current analysis come on the heels of some previous work showing the benefits of lowering blood pressure. For example, the Systolic Blood Pressure Intervention Trial (SPRINT) showed that targeting a systolic blood pressure below 120 mm Hg significantly reduces risk for heart disease, stroke, and death from these diseases.
But in contrast to previous research, the current study included only beneficiaries with incident hypertension and new use of antihypertensive medications, and it adjusted for time-varying confounding.
Prescribing stimulating instead of inhibiting treatments could make a difference at the population level, Dr. Marcum noted.
“If we could shift the prescribing a little bit from inhibiting to stimulating, that could possibly reduce dementia risk,” he said.
However, “we’re not suggesting [that all patients] have their regimen switched,” he added.
That’s because inhibiting medications still have an important place in the antihypertensive treatment armamentarium, Dr. Marcum noted. As an example, beta-blockers are used post heart attack.
As well, factors such as cost and side effects should be taken into consideration when prescribing an antihypertensive drug.
The new results could be used to set up a comparison in a future randomized controlled trial that would provide the strongest evidence for estimating causal effects of treatments, said Dr. Marcum.
‘More convincing’
Carlos G. Santos-Gallego, MD, Icahn School of Medicine at Mount Sinai, New York, said the study is “more convincing” than previous related research, as it has a larger sample size and a longer follow-up.
“And the exquisite statistical analysis gives more robustness, more solidity, to the hypothesis that drugs that stimulate type 2 and 4 angiotensin II receptors might be protective for dementia,” said Dr. Santos-Gallego, who was not involved with the research.
However, he noted that the retrospective study had some limitations, including the underdiagnosis of dementia. “The diagnosis of dementia is, honestly, very poorly done in the clinical setting,” he said.
As well, the study could be subject to “confounding by indication,” Dr. Santos-Gallego said. “There could be a third variable, another confounding factor, that’s responsible both for the dementia and for the prescription of these drugs,” he added.
For example, he noted that comorbidities such as atrial fibrillation, myocardial infarction, and heart failure might increase the risk of dementia.
He agreed with the investigators that a randomized clinical trial would address these limitations. “All comorbidities would be equally shared” in the randomized groups, and all participants would be given “a specific test for dementia at the same time,” Dr. Santos-Gallego said.
Still, he noted that the new results are in keeping with hypertension guidelines that recommend stimulating drugs.
“This trial definitely shows that the current hypertension guidelines are good treatment for our patients, not only to control blood pressure and not only to prevent infarction to prevent stroke but also to prevent dementia,” said Dr. Santos-Gallego.
Also commenting for this news organization, Heather Snyder, PhD, vice president of medical and scientific relations at the Alzheimer’s Association, said the new data provide “clarity” on why previous research had differing results on the effect of antihypertensives on cognition.
Among the caveats of this new analysis is that “it’s unclear if the demographics in this study are fully representative of Medicare beneficiaries,” said Dr. Snyder.
She, too, said a clinical trial is important “to understand if there is a preventative and/or treatment potential in the medications that stimulate type 2 and 4 angiotensin II receptors.”
The study received funding from the National Institute on Aging. Dr. Marcum and Dr. Santos-Gallego have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
LDL cholesterol triglycerides ‘robust’ ASCVD risk marker
High levels of triglyceride molecules in LDL cholesterol are “robustly” linked with an increased risk of atherosclerotic cardiovascular disease, according to a study that used two different methods in two separate cohorts from a large European population study plus a meta-analysis to verify the results.
“There have been some studies in the past, as you can see from our meta-analysis, that found a similar association, but I don’t think most people are convinced that there is really this relationship, and certainly I was not convinced,” lead investigator Børge G. Nordestgaard, MD, DMSc, professor at the University of Copenhagen, said in an interview.

The study enrolled 68,290 patients from the Copenhagen General Population study; 38,081 were assigned to direct automated assay to measure their LDL triglycerides and 30,208 had nuclear magnetic resonance (NMR) spectroscopy. Median follow-up was 3 and 9.2 years for the respective cohorts.
LDL triglycerides carry higher ASCVD risk
In the automated assay group, each 0.1-mmol/L (9 mg/dL)–higher direct LDL triglycerides carried a 22%-38% higher risk for the following outcomes: ASCVD (hazard ratio, 1.26; 95% confidence interval, 1.17-1.35); ischemic heart disease (HR, 1.27; 95% CI, 1.16-1.39); myocardial infarction (HR, 1.28; 95% CI, 1.11-1.48); ischemic stroke (HR, 1.22; 95% CI, 1.08-1.38); and peripheral artery disease (HR, 1.38; 95% CI, 1.21-1.58).
In the group that had NMR spectroscopy to measure LDL triglycerides, risks were similar, ranging from HRs of 1.13 (95% CI, 1.05-1.23) for ischemic stroke to 1.41 (95% CI, 1.31-1.52) for myocardial infarction. The investigators noted that apolipoprotein B levels didn’t entirely explain these results.
The meta-analysis included 18 studies that evaluated varying cardiovascular disease outcomes. It compared random-effects risk ratios for the highest quartile vs. the lowest quartile of LDL triglycerides. They were 1.50 (95% CI, 1.35-1.66) for ASCVD (four studies, 71,526 individuals, 8,576 events); 1.62 (95% CI, 1.37-1.93) for ischemic heart disease (six studies, 107,538 individuals, 9,734 events); 1.30 (95% CI, 1.13-1.49) for ischemic stroke (four studies, 78,026 individuals, 4,273 events); and 1.53 (95% CI, 1.29-1.81) for peripheral artery disease (four studies, 107,511 individuals, 1,848 events). The study was published online in the Journal of the American College of Cardiology.
Results confirm hypothesis the study sought to disprove
The purpose of the study was to actually disprove the hypothesis that the study ended up confirming, Dr. Nordestgaard said. “When we started this study, my idea was that we wanted to show that LDL triglyceride was not related to these diseases, because that didn’t make sense to me,” he said. “I’m so used to the thinking that the cholesterol content of these particles drive atherosclerosis and therefore atherosclerotic cardiovascular disease.”
He noted that LDL can carry both cholesterol and triglycerides, and that larger remnant lipoproteins can carry a substantial amount of triglycerides and a lesser amount of cholesterol. “Those remnants actually transfer into LDL, so they somewhat bring the triglycerides molecules into LDL,” Dr. Nordestgaard said.
The direct automated assay test used in the study to measure LDL triglycerides is not approved for use in the United States by the Food and Drug Administration, according to Denka, the manufacturer of the test.
The use of the Copenhagen General Population Study cohorts is a strength of the study because it has 100% follow-up with all patients, Dr. Nordestgaard said. The meta-analysis is another strength. “So we can show real clearly, not only in our two prospective studies, but also added to the former ones in the literature: All say exactly the same thing: High LDL triglycerides carry a high risk for ASCVD and its components.”
A limitation Dr. Nordestgaard acknowledged: The study doesn’t explain the causal relationship between high LDL triglycerides and ASCVD. But the study provides “very sound evidence that there’s a relationship,” he added. The study population was also a White, Danish population that lacked ethnic and racial diversity.
Next step is finding a treatment
The Danish study essentially confirms what the Atherosclerosis Risk in Community Study (ARIC) found with regard to LDL triglycerides, said Christie M. Ballantyne, MD, chief of cardiology at Baylor College of Medicine in Houston, and an ARIC investigator.

This study is the “first step” to coming up with a test to identify risk, he said. “These data are pretty convincing, when you throw in the data in this study plus all the meta-analyses data, that LDL triglycerides, when they’re elevated, identify individuals at increased risk for an atherosclerotic cardiovascular event.”
The next step, he said, is coming up with a treatment for people with elevated HDL triglyceride. “That’s where we don’t have as much data because this test hasn’t been used. I’m pretty sure that statins are going to work fine for these people, because they lower LDL cholesterol and they also lower triglycerides, and some of the data have shown already that they reduce the LDL remnant,” Dr. Ballantyne said.
The Danish study provides enough of a basis for pursuing future studies to better understand the effect of statins on LDL triglyceride levels, Dr. Ballantyne added.
The study received funding from the Novo Nordisk Foundation and the Danish Heart Foundation, along with institutional support. Dr. Nordestgaard has no relevant disclosures. Dr. Ballantyne disclosed receiving research support from Denka.
High levels of triglyceride molecules in LDL cholesterol are “robustly” linked with an increased risk of atherosclerotic cardiovascular disease, according to a study that used two different methods in two separate cohorts from a large European population study plus a meta-analysis to verify the results.
“There have been some studies in the past, as you can see from our meta-analysis, that found a similar association, but I don’t think most people are convinced that there is really this relationship, and certainly I was not convinced,” lead investigator Børge G. Nordestgaard, MD, DMSc, professor at the University of Copenhagen, said in an interview.
The study enrolled 68,290 patients from the Copenhagen General Population study; 38,081 were assigned to direct automated assay to measure their LDL triglycerides and 30,208 had nuclear magnetic resonance (NMR) spectroscopy. Median follow-up was 3 and 9.2 years for the respective cohorts.
LDL triglycerides carry higher ASCVD risk
In the automated assay group, each 0.1-mmol/L (9 mg/dL)–higher direct LDL triglycerides carried a 22%-38% higher risk for the following outcomes: ASCVD (hazard ratio, 1.26; 95% confidence interval, 1.17-1.35); ischemic heart disease (HR, 1.27; 95% CI, 1.16-1.39); myocardial infarction (HR, 1.28; 95% CI, 1.11-1.48); ischemic stroke (HR, 1.22; 95% CI, 1.08-1.38); and peripheral artery disease (HR, 1.38; 95% CI, 1.21-1.58).
In the group that had NMR spectroscopy to measure LDL triglycerides, risks were similar, ranging from HRs of 1.13 (95% CI, 1.05-1.23) for ischemic stroke to 1.41 (95% CI, 1.31-1.52) for myocardial infarction. The investigators noted that apolipoprotein B levels didn’t entirely explain these results.
The meta-analysis included 18 studies that evaluated varying cardiovascular disease outcomes. It compared random-effects risk ratios for the highest quartile vs. the lowest quartile of LDL triglycerides. They were 1.50 (95% CI, 1.35-1.66) for ASCVD (four studies, 71,526 individuals, 8,576 events); 1.62 (95% CI, 1.37-1.93) for ischemic heart disease (six studies, 107,538 individuals, 9,734 events); 1.30 (95% CI, 1.13-1.49) for ischemic stroke (four studies, 78,026 individuals, 4,273 events); and 1.53 (95% CI, 1.29-1.81) for peripheral artery disease (four studies, 107,511 individuals, 1,848 events). The study was published online in the Journal of the American College of Cardiology.
Results confirm hypothesis the study sought to disprove
The purpose of the study was to actually disprove the hypothesis that the study ended up confirming, Dr. Nordestgaard said. “When we started this study, my idea was that we wanted to show that LDL triglyceride was not related to these diseases, because that didn’t make sense to me,” he said. “I’m so used to the thinking that the cholesterol content of these particles drive atherosclerosis and therefore atherosclerotic cardiovascular disease.”
He noted that LDL can carry both cholesterol and triglycerides, and that larger remnant lipoproteins can carry a substantial amount of triglycerides and a lesser amount of cholesterol. “Those remnants actually transfer into LDL, so they somewhat bring the triglycerides molecules into LDL,” Dr. Nordestgaard said.
The direct automated assay test used in the study to measure LDL triglycerides is not approved for use in the United States by the Food and Drug Administration, according to Denka, the manufacturer of the test.
The use of the Copenhagen General Population Study cohorts is a strength of the study because it has 100% follow-up with all patients, Dr. Nordestgaard said. The meta-analysis is another strength. “So we can show real clearly, not only in our two prospective studies, but also added to the former ones in the literature: All say exactly the same thing: High LDL triglycerides carry a high risk for ASCVD and its components.”
A limitation Dr. Nordestgaard acknowledged: The study doesn’t explain the causal relationship between high LDL triglycerides and ASCVD. But the study provides “very sound evidence that there’s a relationship,” he added. The study population was also a White, Danish population that lacked ethnic and racial diversity.
Next step is finding a treatment
The Danish study essentially confirms what the Atherosclerosis Risk in Community Study (ARIC) found with regard to LDL triglycerides, said Christie M. Ballantyne, MD, chief of cardiology at Baylor College of Medicine in Houston, and an ARIC investigator.
This study is the “first step” to coming up with a test to identify risk, he said. “These data are pretty convincing, when you throw in the data in this study plus all the meta-analyses data, that LDL triglycerides, when they’re elevated, identify individuals at increased risk for an atherosclerotic cardiovascular event.”
The next step, he said, is coming up with a treatment for people with elevated HDL triglyceride. “That’s where we don’t have as much data because this test hasn’t been used. I’m pretty sure that statins are going to work fine for these people, because they lower LDL cholesterol and they also lower triglycerides, and some of the data have shown already that they reduce the LDL remnant,” Dr. Ballantyne said.
The Danish study provides enough of a basis for pursuing future studies to better understand the effect of statins on LDL triglyceride levels, Dr. Ballantyne added.
The study received funding from the Novo Nordisk Foundation and the Danish Heart Foundation, along with institutional support. Dr. Nordestgaard has no relevant disclosures. Dr. Ballantyne disclosed receiving research support from Denka.
High levels of triglyceride molecules in LDL cholesterol are “robustly” linked with an increased risk of atherosclerotic cardiovascular disease, according to a study that used two different methods in two separate cohorts from a large European population study plus a meta-analysis to verify the results.
“There have been some studies in the past, as you can see from our meta-analysis, that found a similar association, but I don’t think most people are convinced that there is really this relationship, and certainly I was not convinced,” lead investigator Børge G. Nordestgaard, MD, DMSc, professor at the University of Copenhagen, said in an interview.
The study enrolled 68,290 patients from the Copenhagen General Population study; 38,081 were assigned to direct automated assay to measure their LDL triglycerides and 30,208 had nuclear magnetic resonance (NMR) spectroscopy. Median follow-up was 3 and 9.2 years for the respective cohorts.
LDL triglycerides carry higher ASCVD risk
In the automated assay group, each 0.1-mmol/L (9 mg/dL)–higher direct LDL triglycerides carried a 22%-38% higher risk for the following outcomes: ASCVD (hazard ratio, 1.26; 95% confidence interval, 1.17-1.35); ischemic heart disease (HR, 1.27; 95% CI, 1.16-1.39); myocardial infarction (HR, 1.28; 95% CI, 1.11-1.48); ischemic stroke (HR, 1.22; 95% CI, 1.08-1.38); and peripheral artery disease (HR, 1.38; 95% CI, 1.21-1.58).
In the group that had NMR spectroscopy to measure LDL triglycerides, risks were similar, ranging from HRs of 1.13 (95% CI, 1.05-1.23) for ischemic stroke to 1.41 (95% CI, 1.31-1.52) for myocardial infarction. The investigators noted that apolipoprotein B levels didn’t entirely explain these results.
The meta-analysis included 18 studies that evaluated varying cardiovascular disease outcomes. It compared random-effects risk ratios for the highest quartile vs. the lowest quartile of LDL triglycerides. They were 1.50 (95% CI, 1.35-1.66) for ASCVD (four studies, 71,526 individuals, 8,576 events); 1.62 (95% CI, 1.37-1.93) for ischemic heart disease (six studies, 107,538 individuals, 9,734 events); 1.30 (95% CI, 1.13-1.49) for ischemic stroke (four studies, 78,026 individuals, 4,273 events); and 1.53 (95% CI, 1.29-1.81) for peripheral artery disease (four studies, 107,511 individuals, 1,848 events). The study was published online in the Journal of the American College of Cardiology.
Results confirm hypothesis the study sought to disprove
The purpose of the study was to actually disprove the hypothesis that the study ended up confirming, Dr. Nordestgaard said. “When we started this study, my idea was that we wanted to show that LDL triglyceride was not related to these diseases, because that didn’t make sense to me,” he said. “I’m so used to the thinking that the cholesterol content of these particles drive atherosclerosis and therefore atherosclerotic cardiovascular disease.”
He noted that LDL can carry both cholesterol and triglycerides, and that larger remnant lipoproteins can carry a substantial amount of triglycerides and a lesser amount of cholesterol. “Those remnants actually transfer into LDL, so they somewhat bring the triglycerides molecules into LDL,” Dr. Nordestgaard said.
The direct automated assay test used in the study to measure LDL triglycerides is not approved for use in the United States by the Food and Drug Administration, according to Denka, the manufacturer of the test.
The use of the Copenhagen General Population Study cohorts is a strength of the study because it has 100% follow-up with all patients, Dr. Nordestgaard said. The meta-analysis is another strength. “So we can show real clearly, not only in our two prospective studies, but also added to the former ones in the literature: All say exactly the same thing: High LDL triglycerides carry a high risk for ASCVD and its components.”
A limitation Dr. Nordestgaard acknowledged: The study doesn’t explain the causal relationship between high LDL triglycerides and ASCVD. But the study provides “very sound evidence that there’s a relationship,” he added. The study population was also a White, Danish population that lacked ethnic and racial diversity.
Next step is finding a treatment
The Danish study essentially confirms what the Atherosclerosis Risk in Community Study (ARIC) found with regard to LDL triglycerides, said Christie M. Ballantyne, MD, chief of cardiology at Baylor College of Medicine in Houston, and an ARIC investigator.
This study is the “first step” to coming up with a test to identify risk, he said. “These data are pretty convincing, when you throw in the data in this study plus all the meta-analyses data, that LDL triglycerides, when they’re elevated, identify individuals at increased risk for an atherosclerotic cardiovascular event.”
The next step, he said, is coming up with a treatment for people with elevated HDL triglyceride. “That’s where we don’t have as much data because this test hasn’t been used. I’m pretty sure that statins are going to work fine for these people, because they lower LDL cholesterol and they also lower triglycerides, and some of the data have shown already that they reduce the LDL remnant,” Dr. Ballantyne said.
The Danish study provides enough of a basis for pursuing future studies to better understand the effect of statins on LDL triglyceride levels, Dr. Ballantyne added.
The study received funding from the Novo Nordisk Foundation and the Danish Heart Foundation, along with institutional support. Dr. Nordestgaard has no relevant disclosures. Dr. Ballantyne disclosed receiving research support from Denka.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Spikes out: A COVID mystery
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
To date, it has been a mystery, like “Glass Onion.” And in the spirit of all the great mysteries, to get to the bottom of this, we’ll need to round up the usual suspects.
Appearing in Circulation, a new study does a great job of systematically evaluating multiple hypotheses linking vaccination to myocarditis, and eliminating them, Poirot-style, one by one until only one remains. We’ll get there.
But first, let’s review the suspects. Why do the mRNA vaccines cause myocarditis in a small subset of people?
There are a few leading candidates.
Number one: antibody responses. There are two flavors here. The quantitative hypothesis suggests that some people simply generate too many antibodies to the vaccine, leading to increased inflammation and heart damage.
The qualitative hypothesis suggests that maybe it’s the nature of the antibodies generated rather than the amount; they might cross-react with some protein on the surface of heart cells for instance.
Or maybe it is driven by T-cell responses, which, of course, are independent of antibody levels.
There’s the idea that myocarditis is due to excessive cytokine release – sort of like what we see in the multisystem inflammatory syndrome in children.
Or it could be due to the viral antigens themselves – the spike protein the mRNA codes for that is generated after vaccination.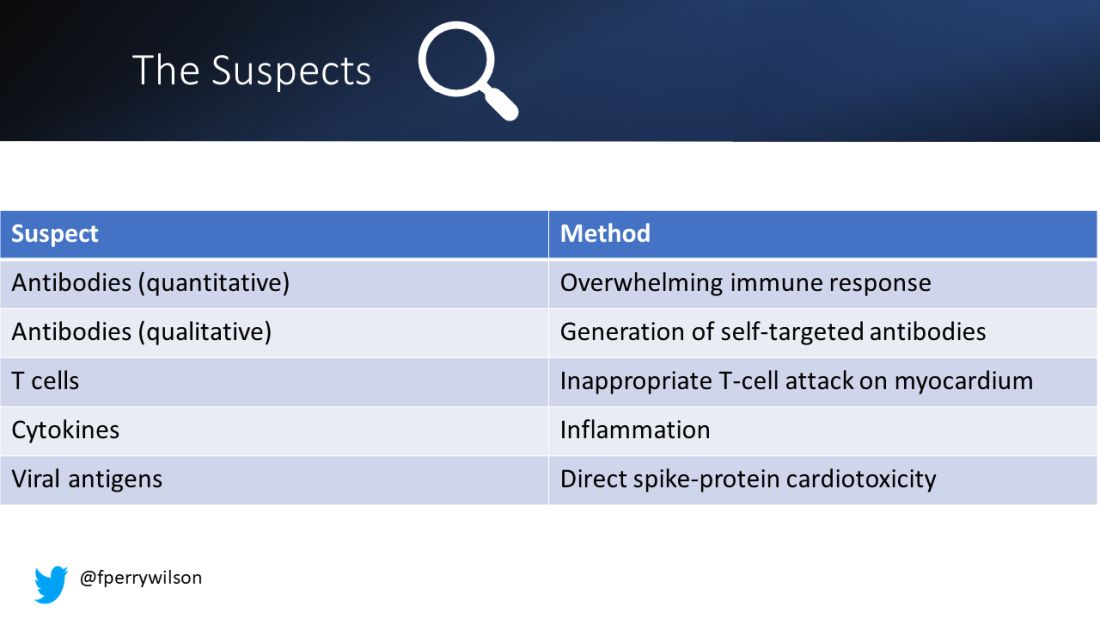
To tease all these possibilities apart, researchers led by Lael Yonker at Mass General performed a case-control study. Sixteen children with postvaccine myocarditis were matched by age to 45 control children who had been vaccinated without complications.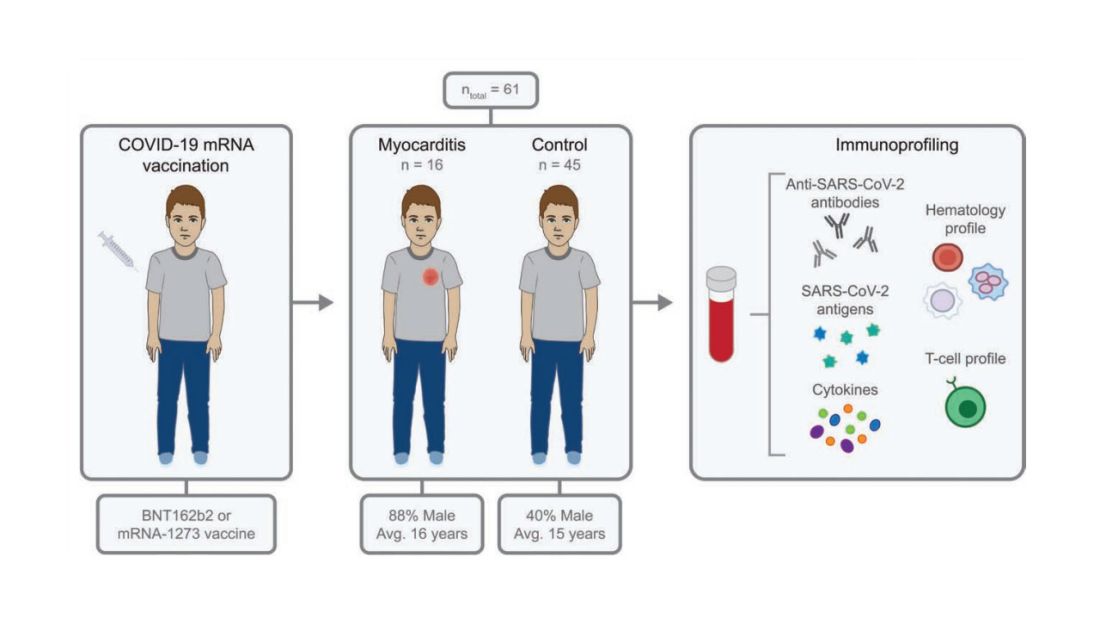
The matching was OK, but as you can see here, there were more boys in the myocarditis group, and the time from vaccination was a bit shorter in that group as well. We’ll keep that in mind as we go through the results.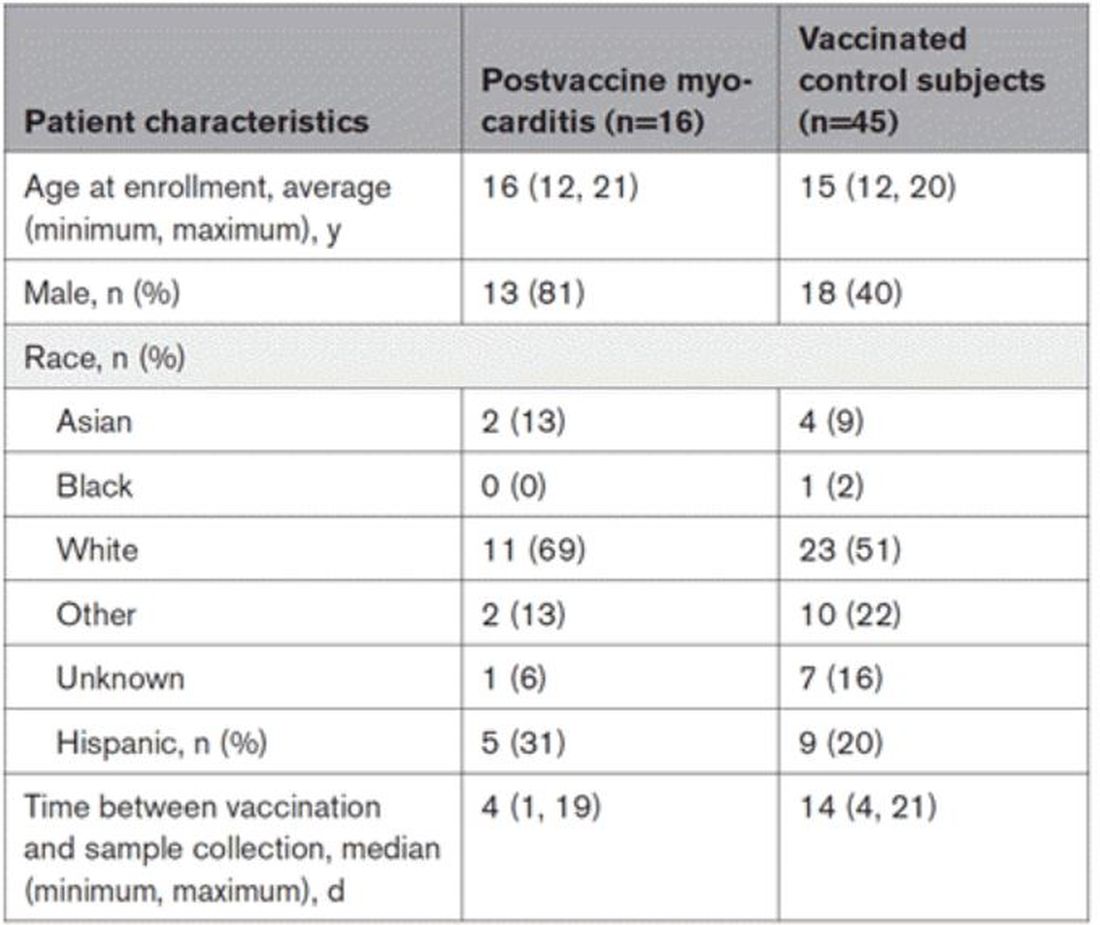
OK, let’s start eliminating suspects.
First, quantitative antibodies. Seems unlikely. Absolute antibody titers were really no different in the myocarditis vs. the control group.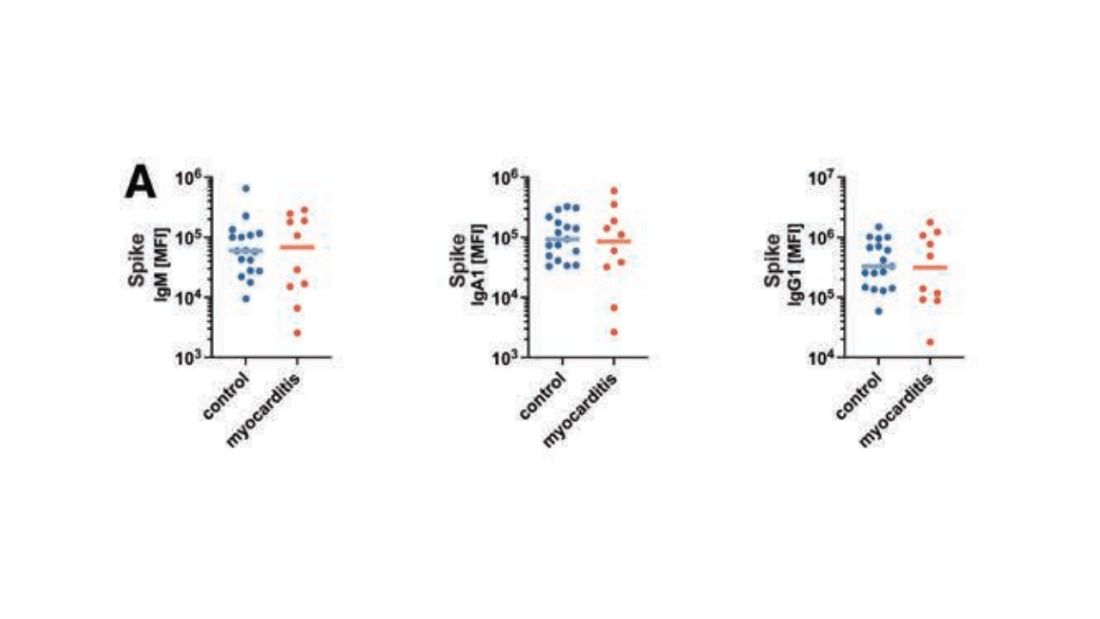
What about the quality of the antibodies? Would the kids with myocarditis have more self-recognizing antibodies present? It doesn’t appear so. Autoantibody levels were similar in the two groups.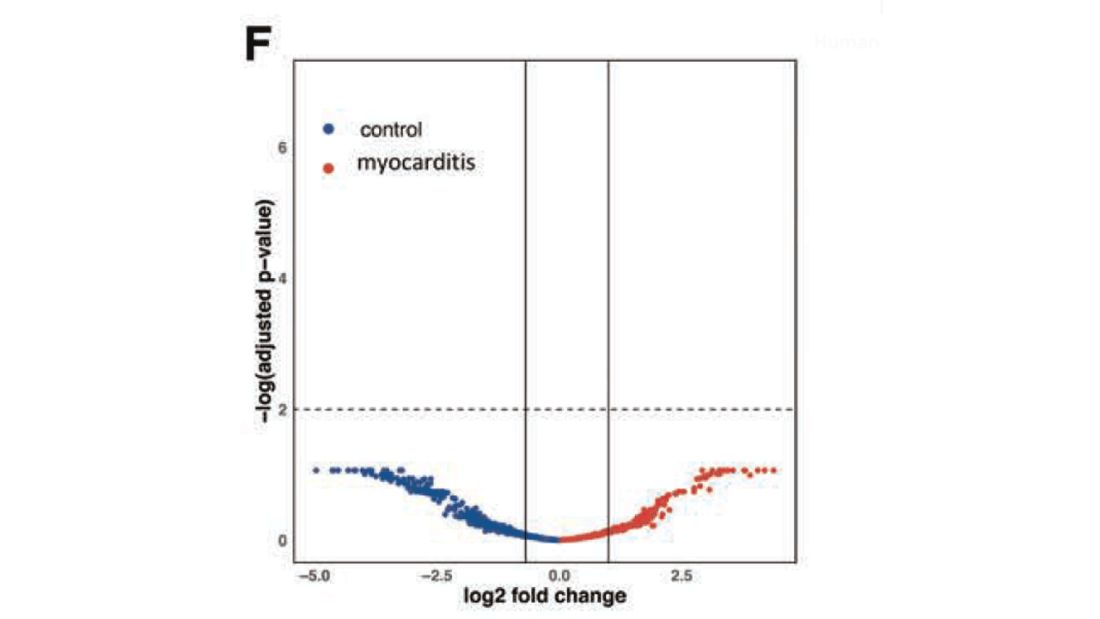
Take antibodies off the list.
T-cell responses come next, and, again, no major differences here, save for one specific T-cell subtype that was moderately elevated in the myocarditis group. Not what I would call a smoking gun, frankly.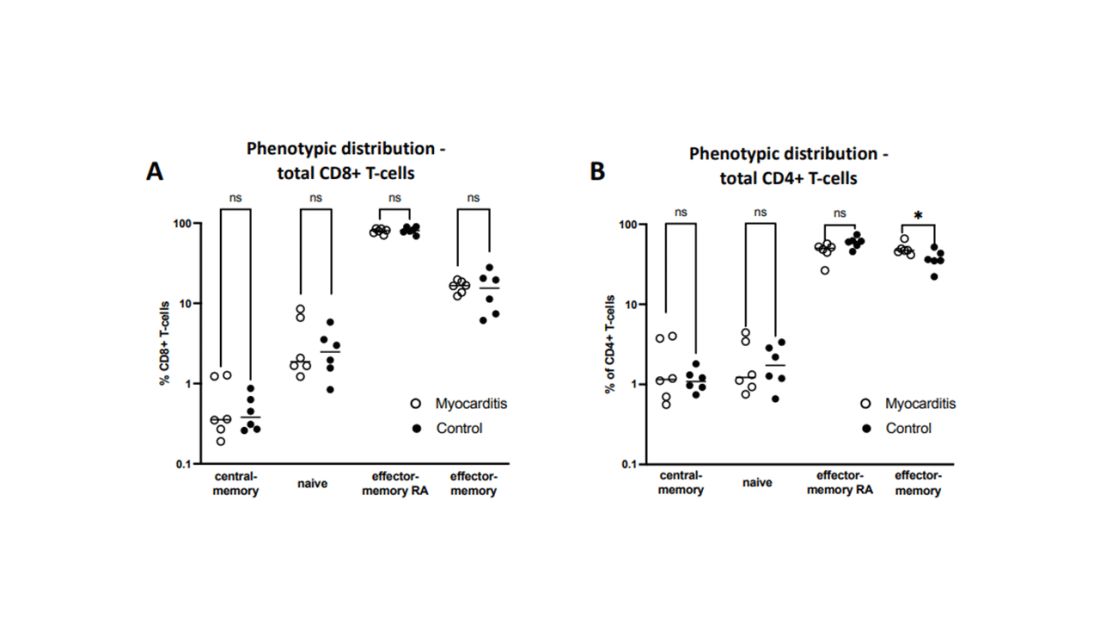
Cytokines give us a bit more to chew on. Levels of interleukin (IL)-8, IL-6, tumor necrosis factor (TNF)-alpha, and IL-10 were all substantially higher in the kids with myocarditis.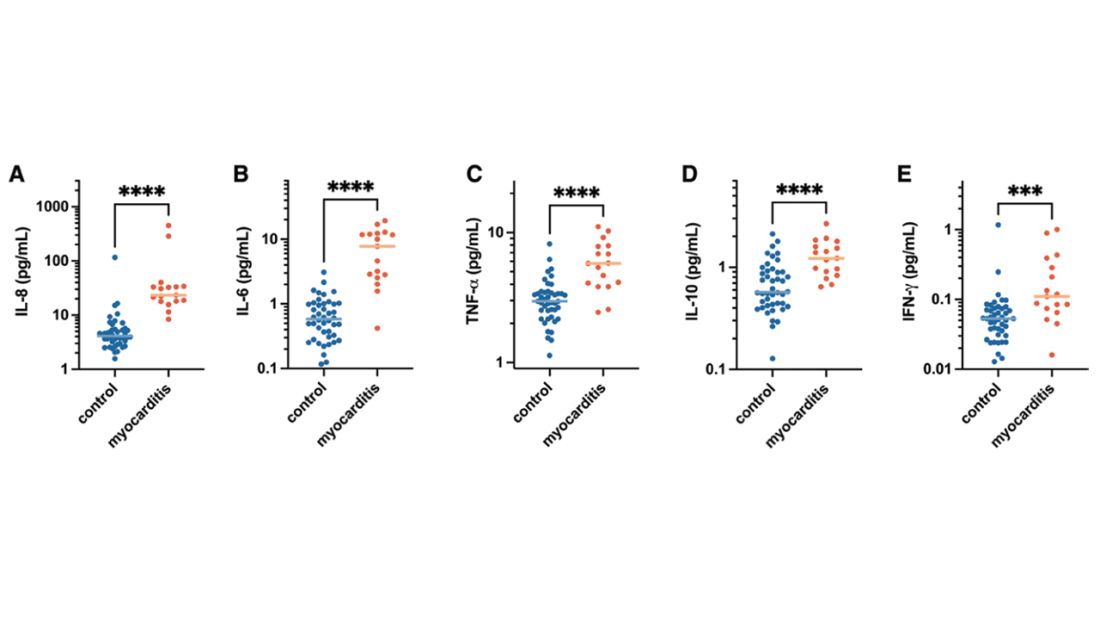
But the thing about cytokines is that they are not particularly specific. OK, kids with myocarditis have more systemic inflammation than kids without; that’s not really surprising. It still leaves us with the question of what is causing all this inflammation? Who is the arch-villain? The kingpin? The don?
It’s the analyses of antigens – the protein products of vaccination – that may hold the key here.
In 12 out of 16 kids with myocarditis, the researchers were able to measure free spike protein in the blood – that is to say spike protein, not bound by antispike antibodies.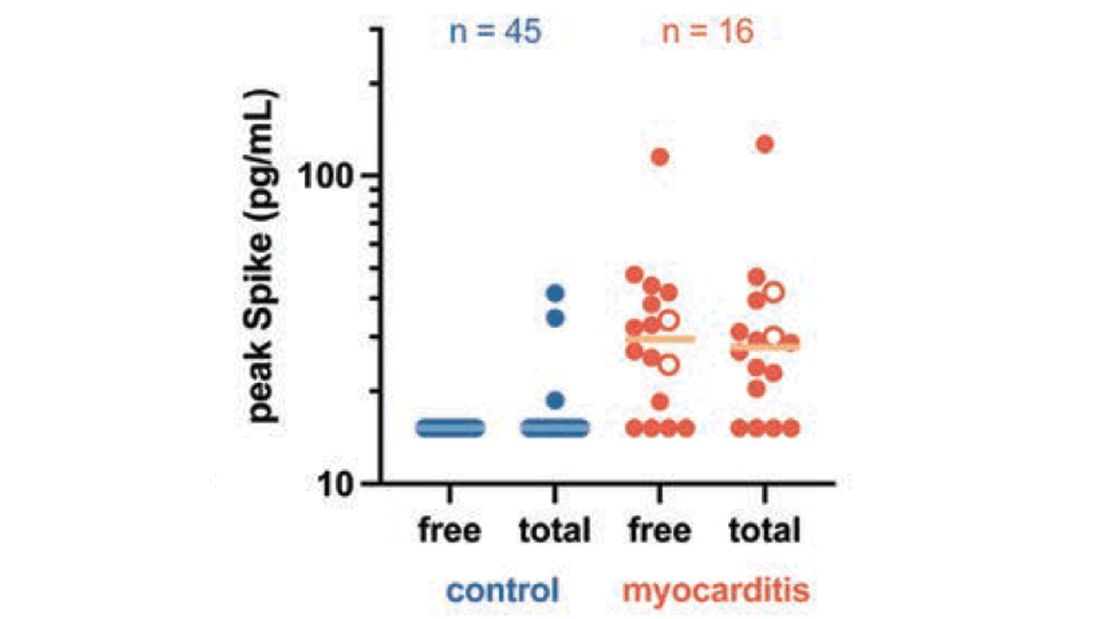
These free spikes were present in – wait for it – zero of the 45 control patients. That makes spike protein itself our prime suspect. J’accuse free spike protein!
Of course, all good detectives need to wrap up the case with a good story: How was it all done?
And here’s where we could use Agatha Christie’s help. How could this all work? The vaccine gets injected; mRNA is taken up into cells, where spike protein is generated and released, generating antibody and T-cell responses all the while. Those responses rapidly clear that spike protein from the system – this has been demonstrated in multiple studies – in adults, at least. But in some small number of people, apparently, spike protein is not cleared. Why? It makes no damn sense. Compels me, though. Some have suggested that inadvertent intravenous injection of vaccine, compared with the appropriate intramuscular route, might distribute the vaccine to sites with less immune surveillance. But that is definitely not proven yet.
We are on the path for sure, but this is, as Benoit Blanc would say, a twisted web – and we are not finished untangling it. Not yet.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here. He tweets @fperrywilson and his new book, “How Medicine Works and When It Doesn’t,” is available for preorder now. He reports no conflicts of interest.
A version of this article first appeared on Medscape.com.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
To date, it has been a mystery, like “Glass Onion.” And in the spirit of all the great mysteries, to get to the bottom of this, we’ll need to round up the usual suspects.
Appearing in Circulation, a new study does a great job of systematically evaluating multiple hypotheses linking vaccination to myocarditis, and eliminating them, Poirot-style, one by one until only one remains. We’ll get there.
But first, let’s review the suspects. Why do the mRNA vaccines cause myocarditis in a small subset of people?
There are a few leading candidates.
Number one: antibody responses. There are two flavors here. The quantitative hypothesis suggests that some people simply generate too many antibodies to the vaccine, leading to increased inflammation and heart damage.
The qualitative hypothesis suggests that maybe it’s the nature of the antibodies generated rather than the amount; they might cross-react with some protein on the surface of heart cells for instance.
Or maybe it is driven by T-cell responses, which, of course, are independent of antibody levels.
There’s the idea that myocarditis is due to excessive cytokine release – sort of like what we see in the multisystem inflammatory syndrome in children.
Or it could be due to the viral antigens themselves – the spike protein the mRNA codes for that is generated after vaccination.
To tease all these possibilities apart, researchers led by Lael Yonker at Mass General performed a case-control study. Sixteen children with postvaccine myocarditis were matched by age to 45 control children who had been vaccinated without complications.
The matching was OK, but as you can see here, there were more boys in the myocarditis group, and the time from vaccination was a bit shorter in that group as well. We’ll keep that in mind as we go through the results.
OK, let’s start eliminating suspects.
First, quantitative antibodies. Seems unlikely. Absolute antibody titers were really no different in the myocarditis vs. the control group.
What about the quality of the antibodies? Would the kids with myocarditis have more self-recognizing antibodies present? It doesn’t appear so. Autoantibody levels were similar in the two groups.
Take antibodies off the list.
T-cell responses come next, and, again, no major differences here, save for one specific T-cell subtype that was moderately elevated in the myocarditis group. Not what I would call a smoking gun, frankly.
Cytokines give us a bit more to chew on. Levels of interleukin (IL)-8, IL-6, tumor necrosis factor (TNF)-alpha, and IL-10 were all substantially higher in the kids with myocarditis.
But the thing about cytokines is that they are not particularly specific. OK, kids with myocarditis have more systemic inflammation than kids without; that’s not really surprising. It still leaves us with the question of what is causing all this inflammation? Who is the arch-villain? The kingpin? The don?
It’s the analyses of antigens – the protein products of vaccination – that may hold the key here.
In 12 out of 16 kids with myocarditis, the researchers were able to measure free spike protein in the blood – that is to say spike protein, not bound by antispike antibodies.
These free spikes were present in – wait for it – zero of the 45 control patients. That makes spike protein itself our prime suspect. J’accuse free spike protein!
Of course, all good detectives need to wrap up the case with a good story: How was it all done?
And here’s where we could use Agatha Christie’s help. How could this all work? The vaccine gets injected; mRNA is taken up into cells, where spike protein is generated and released, generating antibody and T-cell responses all the while. Those responses rapidly clear that spike protein from the system – this has been demonstrated in multiple studies – in adults, at least. But in some small number of people, apparently, spike protein is not cleared. Why? It makes no damn sense. Compels me, though. Some have suggested that inadvertent intravenous injection of vaccine, compared with the appropriate intramuscular route, might distribute the vaccine to sites with less immune surveillance. But that is definitely not proven yet.
We are on the path for sure, but this is, as Benoit Blanc would say, a twisted web – and we are not finished untangling it. Not yet.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here. He tweets @fperrywilson and his new book, “How Medicine Works and When It Doesn’t,” is available for preorder now. He reports no conflicts of interest.
A version of this article first appeared on Medscape.com.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
To date, it has been a mystery, like “Glass Onion.” And in the spirit of all the great mysteries, to get to the bottom of this, we’ll need to round up the usual suspects.
Appearing in Circulation, a new study does a great job of systematically evaluating multiple hypotheses linking vaccination to myocarditis, and eliminating them, Poirot-style, one by one until only one remains. We’ll get there.
But first, let’s review the suspects. Why do the mRNA vaccines cause myocarditis in a small subset of people?
There are a few leading candidates.
Number one: antibody responses. There are two flavors here. The quantitative hypothesis suggests that some people simply generate too many antibodies to the vaccine, leading to increased inflammation and heart damage.
The qualitative hypothesis suggests that maybe it’s the nature of the antibodies generated rather than the amount; they might cross-react with some protein on the surface of heart cells for instance.
Or maybe it is driven by T-cell responses, which, of course, are independent of antibody levels.
There’s the idea that myocarditis is due to excessive cytokine release – sort of like what we see in the multisystem inflammatory syndrome in children.
Or it could be due to the viral antigens themselves – the spike protein the mRNA codes for that is generated after vaccination.
To tease all these possibilities apart, researchers led by Lael Yonker at Mass General performed a case-control study. Sixteen children with postvaccine myocarditis were matched by age to 45 control children who had been vaccinated without complications.
The matching was OK, but as you can see here, there were more boys in the myocarditis group, and the time from vaccination was a bit shorter in that group as well. We’ll keep that in mind as we go through the results.
OK, let’s start eliminating suspects.
First, quantitative antibodies. Seems unlikely. Absolute antibody titers were really no different in the myocarditis vs. the control group.
What about the quality of the antibodies? Would the kids with myocarditis have more self-recognizing antibodies present? It doesn’t appear so. Autoantibody levels were similar in the two groups.
Take antibodies off the list.
T-cell responses come next, and, again, no major differences here, save for one specific T-cell subtype that was moderately elevated in the myocarditis group. Not what I would call a smoking gun, frankly.
Cytokines give us a bit more to chew on. Levels of interleukin (IL)-8, IL-6, tumor necrosis factor (TNF)-alpha, and IL-10 were all substantially higher in the kids with myocarditis.
But the thing about cytokines is that they are not particularly specific. OK, kids with myocarditis have more systemic inflammation than kids without; that’s not really surprising. It still leaves us with the question of what is causing all this inflammation? Who is the arch-villain? The kingpin? The don?
It’s the analyses of antigens – the protein products of vaccination – that may hold the key here.
In 12 out of 16 kids with myocarditis, the researchers were able to measure free spike protein in the blood – that is to say spike protein, not bound by antispike antibodies.
These free spikes were present in – wait for it – zero of the 45 control patients. That makes spike protein itself our prime suspect. J’accuse free spike protein!
Of course, all good detectives need to wrap up the case with a good story: How was it all done?
And here’s where we could use Agatha Christie’s help. How could this all work? The vaccine gets injected; mRNA is taken up into cells, where spike protein is generated and released, generating antibody and T-cell responses all the while. Those responses rapidly clear that spike protein from the system – this has been demonstrated in multiple studies – in adults, at least. But in some small number of people, apparently, spike protein is not cleared. Why? It makes no damn sense. Compels me, though. Some have suggested that inadvertent intravenous injection of vaccine, compared with the appropriate intramuscular route, might distribute the vaccine to sites with less immune surveillance. But that is definitely not proven yet.
We are on the path for sure, but this is, as Benoit Blanc would say, a twisted web – and we are not finished untangling it. Not yet.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here. He tweets @fperrywilson and his new book, “How Medicine Works and When It Doesn’t,” is available for preorder now. He reports no conflicts of interest.
A version of this article first appeared on Medscape.com.
Atrial fibrillation: Sex differences and modifiable risk factors
This transcript has been edited for clarity.
Hello. This is Dr. JoAnn Manson, professor of medicine at Harvard Medical School and Brigham and Women’s Hospital.
We looked at these questions in our vitamin D and omega-3 trial VITAL in an ancillary study called VITAL Rhythm, led by Dr. Christine Albert at Cedars-Sinai. And this particular project was led by Dr. Hasan Siddiqi at Vanderbilt.
As you know, AF is the most common arrhythmia in the world, and it’s burgeoning in numbers, primarily because of the aging of the population. It’s also a major cause of stroke, heart failure, and cardiovascular mortality. Although women are known to have lower rates of AF than men, they’re also known to have a higher risk for cardiovascular complications and sequelae, such as higher risk for stroke and CVD mortality. Therefore, we thought that understanding sex differences in risk and modifiable risk factors for AF that could reduce the burden of disease would be important.
It’s known that greater height is a risk factor for AF, but the extent to which it explains the differences in AF risk between men and women isn’t really known. So we looked at these questions in the VITAL cohort. VITAL has more than 25,000 participants. It’s a large, diverse, nationwide cohort. About 51% are women, and all are aged 50 years or older, with a mean age of 67. All were free of known clinical cardiovascular disease at the start of the study.
AF reports were confirmed by medical records and also supplemented by Medicare CMS linkage for fuller ascertainment of outcomes. We had 900 incident cases of AF in the study, and we did see that women were less likely to be diagnosed with AF. They had a 32% lower risk – strongly statistically significant compared with men, with a P < .001. Women were also more likely to be symptomatic: About 77% of women vs. 63% of men had symptoms prior to or at diagnosis.
It was very interesting that adjustment for height eliminated the lower risk for AF in women compared with men. After accounting for height, there was not only no reduction in risk for AF among the women, there was actually a reversal of the association so that there was a slightly higher risk for AF in the women. Other risk factors for AF in the cohort included older age, higher body mass index, hypertension, and higher consumption of alcohol. We did not see an association between diabetes and higher risk for AF. We also saw no clear association with physical activity, although very strenuous physical activity has been linked to AF in some other studies.
We looked at the interventions of vitamin D (2,000 IU/day) and omega-3 fatty acids (460 mg/day of EPA and 380 mg/day of DHA) and found no association with AF, although some other studies have seen increased risk for AF with higher doses of the marine omega-3s > 1 g/day and certainly at doses of 4 g/day. So overall, the findings highlight the fact that many of the risk factors for AF do seem to be modifiable, and it is really important to identify and try to reduce these risk factors in order to reduce the burden of AF. This may be particularly important in women because women are more likely to have stroke and cardiovascular mortality in these adverse cardiovascular outcomes.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello. This is Dr. JoAnn Manson, professor of medicine at Harvard Medical School and Brigham and Women’s Hospital.
We looked at these questions in our vitamin D and omega-3 trial VITAL in an ancillary study called VITAL Rhythm, led by Dr. Christine Albert at Cedars-Sinai. And this particular project was led by Dr. Hasan Siddiqi at Vanderbilt.
As you know, AF is the most common arrhythmia in the world, and it’s burgeoning in numbers, primarily because of the aging of the population. It’s also a major cause of stroke, heart failure, and cardiovascular mortality. Although women are known to have lower rates of AF than men, they’re also known to have a higher risk for cardiovascular complications and sequelae, such as higher risk for stroke and CVD mortality. Therefore, we thought that understanding sex differences in risk and modifiable risk factors for AF that could reduce the burden of disease would be important.
It’s known that greater height is a risk factor for AF, but the extent to which it explains the differences in AF risk between men and women isn’t really known. So we looked at these questions in the VITAL cohort. VITAL has more than 25,000 participants. It’s a large, diverse, nationwide cohort. About 51% are women, and all are aged 50 years or older, with a mean age of 67. All were free of known clinical cardiovascular disease at the start of the study.
AF reports were confirmed by medical records and also supplemented by Medicare CMS linkage for fuller ascertainment of outcomes. We had 900 incident cases of AF in the study, and we did see that women were less likely to be diagnosed with AF. They had a 32% lower risk – strongly statistically significant compared with men, with a P < .001. Women were also more likely to be symptomatic: About 77% of women vs. 63% of men had symptoms prior to or at diagnosis.
It was very interesting that adjustment for height eliminated the lower risk for AF in women compared with men. After accounting for height, there was not only no reduction in risk for AF among the women, there was actually a reversal of the association so that there was a slightly higher risk for AF in the women. Other risk factors for AF in the cohort included older age, higher body mass index, hypertension, and higher consumption of alcohol. We did not see an association between diabetes and higher risk for AF. We also saw no clear association with physical activity, although very strenuous physical activity has been linked to AF in some other studies.
We looked at the interventions of vitamin D (2,000 IU/day) and omega-3 fatty acids (460 mg/day of EPA and 380 mg/day of DHA) and found no association with AF, although some other studies have seen increased risk for AF with higher doses of the marine omega-3s > 1 g/day and certainly at doses of 4 g/day. So overall, the findings highlight the fact that many of the risk factors for AF do seem to be modifiable, and it is really important to identify and try to reduce these risk factors in order to reduce the burden of AF. This may be particularly important in women because women are more likely to have stroke and cardiovascular mortality in these adverse cardiovascular outcomes.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello. This is Dr. JoAnn Manson, professor of medicine at Harvard Medical School and Brigham and Women’s Hospital.
We looked at these questions in our vitamin D and omega-3 trial VITAL in an ancillary study called VITAL Rhythm, led by Dr. Christine Albert at Cedars-Sinai. And this particular project was led by Dr. Hasan Siddiqi at Vanderbilt.
As you know, AF is the most common arrhythmia in the world, and it’s burgeoning in numbers, primarily because of the aging of the population. It’s also a major cause of stroke, heart failure, and cardiovascular mortality. Although women are known to have lower rates of AF than men, they’re also known to have a higher risk for cardiovascular complications and sequelae, such as higher risk for stroke and CVD mortality. Therefore, we thought that understanding sex differences in risk and modifiable risk factors for AF that could reduce the burden of disease would be important.
It’s known that greater height is a risk factor for AF, but the extent to which it explains the differences in AF risk between men and women isn’t really known. So we looked at these questions in the VITAL cohort. VITAL has more than 25,000 participants. It’s a large, diverse, nationwide cohort. About 51% are women, and all are aged 50 years or older, with a mean age of 67. All were free of known clinical cardiovascular disease at the start of the study.
AF reports were confirmed by medical records and also supplemented by Medicare CMS linkage for fuller ascertainment of outcomes. We had 900 incident cases of AF in the study, and we did see that women were less likely to be diagnosed with AF. They had a 32% lower risk – strongly statistically significant compared with men, with a P < .001. Women were also more likely to be symptomatic: About 77% of women vs. 63% of men had symptoms prior to or at diagnosis.
It was very interesting that adjustment for height eliminated the lower risk for AF in women compared with men. After accounting for height, there was not only no reduction in risk for AF among the women, there was actually a reversal of the association so that there was a slightly higher risk for AF in the women. Other risk factors for AF in the cohort included older age, higher body mass index, hypertension, and higher consumption of alcohol. We did not see an association between diabetes and higher risk for AF. We also saw no clear association with physical activity, although very strenuous physical activity has been linked to AF in some other studies.
We looked at the interventions of vitamin D (2,000 IU/day) and omega-3 fatty acids (460 mg/day of EPA and 380 mg/day of DHA) and found no association with AF, although some other studies have seen increased risk for AF with higher doses of the marine omega-3s > 1 g/day and certainly at doses of 4 g/day. So overall, the findings highlight the fact that many of the risk factors for AF do seem to be modifiable, and it is really important to identify and try to reduce these risk factors in order to reduce the burden of AF. This may be particularly important in women because women are more likely to have stroke and cardiovascular mortality in these adverse cardiovascular outcomes.
A version of this article first appeared on Medscape.com.
Little-used fitness measure could be key to exercise results
A new study out of Brigham Young University, Provo, Utah, suggests doctors could take that initiative to the next level, prescribing exercise plans that result in a specific health outcome; say, lowering your blood pressure or losing weight.
“The findings of this study, and others, suggest that we should be able to more consistently and accurately prescribe exercise like medicine,” says senior study author Jayson Gifford, PhD, an exercise sciences professor at BYU.
These exercise prescriptions would be tailored to patients based on a largely ignored fitness measure called critical power, or maximum steady state – the fastest you can go while maintaining a pace you can sustain for a long time.
By crafting workouts around critical power instead of the more frequently used VO2 max (maximum effort), we could more accurately predict health outcomes, just as we can with medicine, the researchers wrote in the Journal of Applied Physiology.
“We’ve known for centuries that exercise is part of the way to develop a healthy and long life,” says Jordan Metzl, MD, a sports medicine doctor at the Hospital for Special Surgery in New York and author of The Exercise Cure. “But it’s only in the past 70 years that we’ve recognized the medicinal value of exercise.”
Dr. Metzl, who was not involved in the study, helped develop an annual seminar at Cornell Medical School teaching medical students ways to prescribe exercise that go beyond the “30 minutes per day” cookie-cutter advice. Still, doctors and other health care professionals often struggle to prescribe exercise to prevent or treat disease. And a recent study from Oxford found that when doctors do give weight loss advice, it’s often vague and hard for patients to use.
“The drug of movement is one of the safest and most effective forms of preventive health,” says Dr. Metzl. “We need to get the medical community fully engaged in prescribing exercise for their patients.”
This study suggests that a focus on critical power could be key in making that happen.
What the research found
In the study, 22 adults completed 8 weeks of either moderate-intensity training or high-intensity interval training (HIIT). The intensity levels specified in both plans were based on VO2 max. So, the people in the study trained at given percentages of their VO2 max.
Both groups saw improvements in endurance, but results varied greatly from person to person. Those mixed results could be explained by individual differences in critical power.
“Improvement was much more correlated with the percentage of critical powers the individuals worked at rather than the percentage of their VO2max, like exercise physiologists have thought for years,” says lead study author Jessica Collins, a researcher at Brigham Young University.
Not only that but several subjects who did not improve their VO2 max did see an increase in critical power and endurance.
“People tend to only focus on VO2 max,” Dr. Gifford says. “Many might see the lack of increase in VO2 max for some people and conclude that the training was ineffective. I personally believe that a lot of potentially useful therapies have been ruled out because of an almost exclusive focus on VO2 max.”
Turns out, critical power varies a lot from person to person, even among those with similar VO2 maxes.
“Let’s say you and Jessica had the same VO2 max,” explains Dr. Gifford. “If we had you both going at 70% of [your VO2 max], it could be above your maximum steady state, which would make it really hard for you. And it could be below her maximum steady state, which would make it easy for her.”
This means you are each stressing your body differently, and that stress is what triggers improvements in fitness and endurance.
“Below critical power, the metabolic stressors are well-managed and maintained at elevated-but-steady levels,” Dr. Gifford says. “Above critical power, the metabolic stressors are produced so fast that they cannot be controlled, and consistently accrue until reaching very high levels that cause failure.”
Knowing your critical power means you can predict how those stressors will build up, and you can tailor an exercise program that provides just the right stressor “dose” for you, Dr. Gifford says.
Such programs could be used for rehab patients recovering from a heart attack or from lung disease, Dr. Gifford suggests. Or they could help older adults improve endurance and physical function, Ms. Collins notes.
But first, researchers must confirm these results by programming workouts based on people’s critical power and seeing how much different measures improve.
How to find your critical power
Critical power is not new, but exercise physiologists and medical professionals have largely ignored it because it’s not easy to measure.
“People generally train off VO2 max or maximum heart rate, which is even less precise,” Dr. Gifford says.
Finding people’s critical power in the study involved multiple timed trials and calculating the relationship between speed/power and time, Dr. Gifford explains.
But for a rough measure of your critical power, you could use an app that measures functional threshold power (FTP), something Dr. Gifford refers to as the “Walmart version” of critical power. “It’s not exactly the same, but it’s close,” he says. (The app Strava features FTP as well as a pretty sophisticated power analysis.)
Or skip the tech and go by feel. If you’re below your critical power, “it’s going to be challenging, but you’ll feel under control,” Dr. Gifford says. Above your critical power, “your breathing and heart rate will continuously climb until you fail in about 2 to 15 minutes, depending on how far above you are.” Still, you don’t need to know your critical power to start exercising, Ms. Collins notes.
“The beauty of exercise is that it is such a powerful drug that you can see benefits without fine-tuning the workout this way,” Dr. Gifford explains. “I would hate for this to become a barrier to exercising. The important thing is to do something.”
A version of this article first appeared on WebMD.com.
A new study out of Brigham Young University, Provo, Utah, suggests doctors could take that initiative to the next level, prescribing exercise plans that result in a specific health outcome; say, lowering your blood pressure or losing weight.
“The findings of this study, and others, suggest that we should be able to more consistently and accurately prescribe exercise like medicine,” says senior study author Jayson Gifford, PhD, an exercise sciences professor at BYU.
These exercise prescriptions would be tailored to patients based on a largely ignored fitness measure called critical power, or maximum steady state – the fastest you can go while maintaining a pace you can sustain for a long time.
By crafting workouts around critical power instead of the more frequently used VO2 max (maximum effort), we could more accurately predict health outcomes, just as we can with medicine, the researchers wrote in the Journal of Applied Physiology.
“We’ve known for centuries that exercise is part of the way to develop a healthy and long life,” says Jordan Metzl, MD, a sports medicine doctor at the Hospital for Special Surgery in New York and author of The Exercise Cure. “But it’s only in the past 70 years that we’ve recognized the medicinal value of exercise.”
Dr. Metzl, who was not involved in the study, helped develop an annual seminar at Cornell Medical School teaching medical students ways to prescribe exercise that go beyond the “30 minutes per day” cookie-cutter advice. Still, doctors and other health care professionals often struggle to prescribe exercise to prevent or treat disease. And a recent study from Oxford found that when doctors do give weight loss advice, it’s often vague and hard for patients to use.
“The drug of movement is one of the safest and most effective forms of preventive health,” says Dr. Metzl. “We need to get the medical community fully engaged in prescribing exercise for their patients.”
This study suggests that a focus on critical power could be key in making that happen.
What the research found
In the study, 22 adults completed 8 weeks of either moderate-intensity training or high-intensity interval training (HIIT). The intensity levels specified in both plans were based on VO2 max. So, the people in the study trained at given percentages of their VO2 max.
Both groups saw improvements in endurance, but results varied greatly from person to person. Those mixed results could be explained by individual differences in critical power.
“Improvement was much more correlated with the percentage of critical powers the individuals worked at rather than the percentage of their VO2max, like exercise physiologists have thought for years,” says lead study author Jessica Collins, a researcher at Brigham Young University.
Not only that but several subjects who did not improve their VO2 max did see an increase in critical power and endurance.
“People tend to only focus on VO2 max,” Dr. Gifford says. “Many might see the lack of increase in VO2 max for some people and conclude that the training was ineffective. I personally believe that a lot of potentially useful therapies have been ruled out because of an almost exclusive focus on VO2 max.”
Turns out, critical power varies a lot from person to person, even among those with similar VO2 maxes.
“Let’s say you and Jessica had the same VO2 max,” explains Dr. Gifford. “If we had you both going at 70% of [your VO2 max], it could be above your maximum steady state, which would make it really hard for you. And it could be below her maximum steady state, which would make it easy for her.”
This means you are each stressing your body differently, and that stress is what triggers improvements in fitness and endurance.
“Below critical power, the metabolic stressors are well-managed and maintained at elevated-but-steady levels,” Dr. Gifford says. “Above critical power, the metabolic stressors are produced so fast that they cannot be controlled, and consistently accrue until reaching very high levels that cause failure.”
Knowing your critical power means you can predict how those stressors will build up, and you can tailor an exercise program that provides just the right stressor “dose” for you, Dr. Gifford says.
Such programs could be used for rehab patients recovering from a heart attack or from lung disease, Dr. Gifford suggests. Or they could help older adults improve endurance and physical function, Ms. Collins notes.
But first, researchers must confirm these results by programming workouts based on people’s critical power and seeing how much different measures improve.
How to find your critical power
Critical power is not new, but exercise physiologists and medical professionals have largely ignored it because it’s not easy to measure.
“People generally train off VO2 max or maximum heart rate, which is even less precise,” Dr. Gifford says.
Finding people’s critical power in the study involved multiple timed trials and calculating the relationship between speed/power and time, Dr. Gifford explains.
But for a rough measure of your critical power, you could use an app that measures functional threshold power (FTP), something Dr. Gifford refers to as the “Walmart version” of critical power. “It’s not exactly the same, but it’s close,” he says. (The app Strava features FTP as well as a pretty sophisticated power analysis.)
Or skip the tech and go by feel. If you’re below your critical power, “it’s going to be challenging, but you’ll feel under control,” Dr. Gifford says. Above your critical power, “your breathing and heart rate will continuously climb until you fail in about 2 to 15 minutes, depending on how far above you are.” Still, you don’t need to know your critical power to start exercising, Ms. Collins notes.
“The beauty of exercise is that it is such a powerful drug that you can see benefits without fine-tuning the workout this way,” Dr. Gifford explains. “I would hate for this to become a barrier to exercising. The important thing is to do something.”
A version of this article first appeared on WebMD.com.
A new study out of Brigham Young University, Provo, Utah, suggests doctors could take that initiative to the next level, prescribing exercise plans that result in a specific health outcome; say, lowering your blood pressure or losing weight.
“The findings of this study, and others, suggest that we should be able to more consistently and accurately prescribe exercise like medicine,” says senior study author Jayson Gifford, PhD, an exercise sciences professor at BYU.
These exercise prescriptions would be tailored to patients based on a largely ignored fitness measure called critical power, or maximum steady state – the fastest you can go while maintaining a pace you can sustain for a long time.
By crafting workouts around critical power instead of the more frequently used VO2 max (maximum effort), we could more accurately predict health outcomes, just as we can with medicine, the researchers wrote in the Journal of Applied Physiology.
“We’ve known for centuries that exercise is part of the way to develop a healthy and long life,” says Jordan Metzl, MD, a sports medicine doctor at the Hospital for Special Surgery in New York and author of The Exercise Cure. “But it’s only in the past 70 years that we’ve recognized the medicinal value of exercise.”
Dr. Metzl, who was not involved in the study, helped develop an annual seminar at Cornell Medical School teaching medical students ways to prescribe exercise that go beyond the “30 minutes per day” cookie-cutter advice. Still, doctors and other health care professionals often struggle to prescribe exercise to prevent or treat disease. And a recent study from Oxford found that when doctors do give weight loss advice, it’s often vague and hard for patients to use.
“The drug of movement is one of the safest and most effective forms of preventive health,” says Dr. Metzl. “We need to get the medical community fully engaged in prescribing exercise for their patients.”
This study suggests that a focus on critical power could be key in making that happen.
What the research found
In the study, 22 adults completed 8 weeks of either moderate-intensity training or high-intensity interval training (HIIT). The intensity levels specified in both plans were based on VO2 max. So, the people in the study trained at given percentages of their VO2 max.
Both groups saw improvements in endurance, but results varied greatly from person to person. Those mixed results could be explained by individual differences in critical power.
“Improvement was much more correlated with the percentage of critical powers the individuals worked at rather than the percentage of their VO2max, like exercise physiologists have thought for years,” says lead study author Jessica Collins, a researcher at Brigham Young University.
Not only that but several subjects who did not improve their VO2 max did see an increase in critical power and endurance.
“People tend to only focus on VO2 max,” Dr. Gifford says. “Many might see the lack of increase in VO2 max for some people and conclude that the training was ineffective. I personally believe that a lot of potentially useful therapies have been ruled out because of an almost exclusive focus on VO2 max.”
Turns out, critical power varies a lot from person to person, even among those with similar VO2 maxes.
“Let’s say you and Jessica had the same VO2 max,” explains Dr. Gifford. “If we had you both going at 70% of [your VO2 max], it could be above your maximum steady state, which would make it really hard for you. And it could be below her maximum steady state, which would make it easy for her.”
This means you are each stressing your body differently, and that stress is what triggers improvements in fitness and endurance.
“Below critical power, the metabolic stressors are well-managed and maintained at elevated-but-steady levels,” Dr. Gifford says. “Above critical power, the metabolic stressors are produced so fast that they cannot be controlled, and consistently accrue until reaching very high levels that cause failure.”
Knowing your critical power means you can predict how those stressors will build up, and you can tailor an exercise program that provides just the right stressor “dose” for you, Dr. Gifford says.
Such programs could be used for rehab patients recovering from a heart attack or from lung disease, Dr. Gifford suggests. Or they could help older adults improve endurance and physical function, Ms. Collins notes.
But first, researchers must confirm these results by programming workouts based on people’s critical power and seeing how much different measures improve.
How to find your critical power
Critical power is not new, but exercise physiologists and medical professionals have largely ignored it because it’s not easy to measure.
“People generally train off VO2 max or maximum heart rate, which is even less precise,” Dr. Gifford says.
Finding people’s critical power in the study involved multiple timed trials and calculating the relationship between speed/power and time, Dr. Gifford explains.
But for a rough measure of your critical power, you could use an app that measures functional threshold power (FTP), something Dr. Gifford refers to as the “Walmart version” of critical power. “It’s not exactly the same, but it’s close,” he says. (The app Strava features FTP as well as a pretty sophisticated power analysis.)
Or skip the tech and go by feel. If you’re below your critical power, “it’s going to be challenging, but you’ll feel under control,” Dr. Gifford says. Above your critical power, “your breathing and heart rate will continuously climb until you fail in about 2 to 15 minutes, depending on how far above you are.” Still, you don’t need to know your critical power to start exercising, Ms. Collins notes.
“The beauty of exercise is that it is such a powerful drug that you can see benefits without fine-tuning the workout this way,” Dr. Gifford explains. “I would hate for this to become a barrier to exercising. The important thing is to do something.”
A version of this article first appeared on WebMD.com.
FROM THE JOURNAL OF APPLIED PHYSIOLOGY