User login
Pregnancy risks elevated in women with chronic pancreatitis
TOPLINE:
METHODOLOGY:
- A retrospective analysis of hospital discharge records from the National Inpatient Sample database between 2009 and 2019 was conducted.
- The sample included 3,094 pregnancies with chronic pancreatitis and roughly 40.8 million pregnancies without this condition.
- The study focused on primary maternal outcomes and primary perinatal outcomes in pregnancies affected by chronic pancreatitis after accounting for relevant covariates.
TAKEAWAY:
- Chronic pancreatitis pregnancies had elevated rates of gestational diabetes (adjusted odds ratio, 1.63), gestational hypertensive complications (aOR, 2.48), preterm labor (aOR, 3.10), and small size for gestational age (aOR, 2.40).
- Women with chronic pancreatitis and a history of renal failure were more prone to gestational hypertensive complications (aOR, 20.09).
- Women with alcohol-induced chronic pancreatitis had a 17-fold higher risk for fetal death (aOR, 17.15).
- Pregnancies with chronic pancreatitis were associated with longer hospital stays and higher hospital costs.
IN PRACTICE:
“Our study provides novel insights into the impact of chronic pancreatitis on maternal and fetal health. The implications of our findings are critical for health care professionals, particularly those involved in preconception counseling. Pregnant women with chronic pancreatitis should be under the care of a multidisciplinary team of health care providers,” the authors advise.
SOURCE:
The study was led by Chengu Niu, MD, with Rochester General Hospital, Rochester, N.Y. It was published online July 18 in Digestive and Liver Disease. The study had no specific funding.
LIMITATIONS:
The authors note potential inaccuracies because of coding in the National Inpatient Sample database, a lack of detailed information regarding medication use, and a lack of follow-up clinical information. The findings are specific to the United States and may not be applicable to other countries.
DISCLOSURES:
The authors have no relevant disclosures.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- A retrospective analysis of hospital discharge records from the National Inpatient Sample database between 2009 and 2019 was conducted.
- The sample included 3,094 pregnancies with chronic pancreatitis and roughly 40.8 million pregnancies without this condition.
- The study focused on primary maternal outcomes and primary perinatal outcomes in pregnancies affected by chronic pancreatitis after accounting for relevant covariates.
TAKEAWAY:
- Chronic pancreatitis pregnancies had elevated rates of gestational diabetes (adjusted odds ratio, 1.63), gestational hypertensive complications (aOR, 2.48), preterm labor (aOR, 3.10), and small size for gestational age (aOR, 2.40).
- Women with chronic pancreatitis and a history of renal failure were more prone to gestational hypertensive complications (aOR, 20.09).
- Women with alcohol-induced chronic pancreatitis had a 17-fold higher risk for fetal death (aOR, 17.15).
- Pregnancies with chronic pancreatitis were associated with longer hospital stays and higher hospital costs.
IN PRACTICE:
“Our study provides novel insights into the impact of chronic pancreatitis on maternal and fetal health. The implications of our findings are critical for health care professionals, particularly those involved in preconception counseling. Pregnant women with chronic pancreatitis should be under the care of a multidisciplinary team of health care providers,” the authors advise.
SOURCE:
The study was led by Chengu Niu, MD, with Rochester General Hospital, Rochester, N.Y. It was published online July 18 in Digestive and Liver Disease. The study had no specific funding.
LIMITATIONS:
The authors note potential inaccuracies because of coding in the National Inpatient Sample database, a lack of detailed information regarding medication use, and a lack of follow-up clinical information. The findings are specific to the United States and may not be applicable to other countries.
DISCLOSURES:
The authors have no relevant disclosures.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- A retrospective analysis of hospital discharge records from the National Inpatient Sample database between 2009 and 2019 was conducted.
- The sample included 3,094 pregnancies with chronic pancreatitis and roughly 40.8 million pregnancies without this condition.
- The study focused on primary maternal outcomes and primary perinatal outcomes in pregnancies affected by chronic pancreatitis after accounting for relevant covariates.
TAKEAWAY:
- Chronic pancreatitis pregnancies had elevated rates of gestational diabetes (adjusted odds ratio, 1.63), gestational hypertensive complications (aOR, 2.48), preterm labor (aOR, 3.10), and small size for gestational age (aOR, 2.40).
- Women with chronic pancreatitis and a history of renal failure were more prone to gestational hypertensive complications (aOR, 20.09).
- Women with alcohol-induced chronic pancreatitis had a 17-fold higher risk for fetal death (aOR, 17.15).
- Pregnancies with chronic pancreatitis were associated with longer hospital stays and higher hospital costs.
IN PRACTICE:
“Our study provides novel insights into the impact of chronic pancreatitis on maternal and fetal health. The implications of our findings are critical for health care professionals, particularly those involved in preconception counseling. Pregnant women with chronic pancreatitis should be under the care of a multidisciplinary team of health care providers,” the authors advise.
SOURCE:
The study was led by Chengu Niu, MD, with Rochester General Hospital, Rochester, N.Y. It was published online July 18 in Digestive and Liver Disease. The study had no specific funding.
LIMITATIONS:
The authors note potential inaccuracies because of coding in the National Inpatient Sample database, a lack of detailed information regarding medication use, and a lack of follow-up clinical information. The findings are specific to the United States and may not be applicable to other countries.
DISCLOSURES:
The authors have no relevant disclosures.
A version of this article appeared on Medscape.com.
Statins post PCI: Moderate intensity plus ezetimibe may be preferable
, suggests a “real-world” cohort study that is consistent with trial evidence.
In the observational study with more than 273,000 patients who received percutaneous coronary intervention (PCI) with drug-eluting stents (DES), risk for a broad composite clinical primary endpoint fell by one-fourth (P < .001) among those put on the two-drug regimen with a moderate-intensity statin, compared with those getting a high-intensity statin alone.
The dual-agent approach was also associated with a 15% drop in statin discontinuation and a 20% reduced risk for new-onset diabetes requiring medication (P < .001 for both benefits), reported investigators in the Journal of the American College of Cardiology.
The study’s primary endpoint – a composite of cardiovascular (CV) death, myocardial infarction (MI), coronary revascularization, heart failure (HF) hospitalization, or nonfatal stroke at 3 years – replicated that of the randomized RACING trial conducted by many of the same researchers and published about a year ago in The Lancet.
RACING demonstrated that ezetimibe plus a moderate-intensity statin could be as effective as a high-intensity statin in patients with CV disease, “but have fewer side effects and better compliance,” Myeong-Ki Hong, MD, PhD, Severance Hospital, Yonsei University, Seoul, South Korea, said in an interview.
Dr. Hong is senior author on the current observational study based on the CONNECT-DES registry, which compared rosuvastatin 10 mg/day plus ezetimibe 10 mg/day – used in RACING – with rosuvastatin 20 mg/day in a nationwide cohort of 72,050 patients.
“As we know, populations who are enrolled in randomized studies do not sufficiently represent real patients in practice,” he observed, “so we wanted to evaluate the generalizability of the RACING results in daily clinical practice.”
Deepak L. Bhatt, MD, said he likes studies that look at whether clinical trial results “play out in the real world,” as this one did. “They have largely replicated the results of the RACING trial,” suggesting the approach using a moderate-intensity statin “is the way to go,” Dr. Bhatt of Mount Sinai Health System, New York, who was not affiliated with the current report, said in an interview. “In fact, the moderate-intensity combination regimen was actually better in this study.”
He said the observed reduction in new-onset diabetes with the moderate-intensity statin approach is also important. “There is a link between high-dose statins and diabetes. So, if given the choice, if you can get the benefits from a cardiovascular perspective with a lower risk of diabetes, it makes sense to use the combination therapy.”
Dr. Bhatt said he had been using high-intensity statin monotherapy in his high-risk patients, but RACING made him reconsider the value of moderate-dose statin combination therapy. “Going with lower doses of two drugs instead of high doses of one drug minimizes side effects and, in some cases, can even enhance efficacy – so this is not an unreasonable paradigm.”
In the current cohort study of patients prescribed rosuvastatin after DES implantation, 10,794 received rosuvastatin 10 mg/day plus ezetimibe 10 mg/day, and 61,256 were put on rosuvastatin 20 mg/day.
Hazard ratio risk reductions with the dual-agent lipid-lowering therapy approach, compared with high-intensity statin monotherapy, were more favorable for the primary composite clinical endpoint and important secondary events:
- HR, 0.75; 95% confidence interval, 0.70-0.79; P < .001) for CV death, MI, coronary artery revascularization, HF, or stroke at 3 years.
- HR, 0.85; 95% CI, 0.78-0.94; P = .001) for statin discontinuation.
- HR, 0.80; 95% CI, 0.72-0.88; P < .001) for new-onset diabetes requiring medication.
But HRs for rhabdomyolysis, cholecystectomy, or a new cancer diagnosis did not indicate significant differences between the two groups.
“Now that there is evidence to support the favorable clinical outcomes of combination lipid-lowering therapy with moderate-intensity statin plus ezetimibe” for secondary prevention from both RACING and a study reflecting daily clinical practice, Dr. Hong said, “physicians may feel more comfortable with this approach.”
The registry analysis “is remarkable not only for validating the results of the RACING trial in routine clinical practice in a high-risk secondary prevention population, but also for its innovative methodology,” states an accompanying editorial by Ori Ben-Yehuda, MD, Sulpizio Cardiovascular Center, University of California, San Diego.
Use of such a large single-payer database in their study “affords even greater external validity to the findings, complementing the internal validity of the randomized RACING trial,” Dr. Ben-Yehuda writes.
The rationale for combination therapy is strong, but additional data would be helpful, particularly for informing guidelines, he continues. “A pragmatic trial randomizing a broad racial and ethnic group of patients to low-dose statin,” such as a starting dose of 10 mg/day atorvastatin or 5 mg/day rosuvastatin “plus ezetimibe vs. high-intensity statin alone would provide much needed data to help guide lipid-lowering therapy for millions of patients and hopefully increase persistence on therapy.”
The study was supported by the Cardiovascular Research Center, Seoul, South Korea. Dr. Hong and Dr. Ben-Yehuda have disclosed no relevant financial relationships. Dr. Bhatt has previously disclosed grants and/or personal fees from many companies; personal fees from WebMD and other publications or organizations; and having other relationships with Medscape Cardiology and other publications or organizations.
A version of this article appeared on Medscape.com.
, suggests a “real-world” cohort study that is consistent with trial evidence.
In the observational study with more than 273,000 patients who received percutaneous coronary intervention (PCI) with drug-eluting stents (DES), risk for a broad composite clinical primary endpoint fell by one-fourth (P < .001) among those put on the two-drug regimen with a moderate-intensity statin, compared with those getting a high-intensity statin alone.
The dual-agent approach was also associated with a 15% drop in statin discontinuation and a 20% reduced risk for new-onset diabetes requiring medication (P < .001 for both benefits), reported investigators in the Journal of the American College of Cardiology.
The study’s primary endpoint – a composite of cardiovascular (CV) death, myocardial infarction (MI), coronary revascularization, heart failure (HF) hospitalization, or nonfatal stroke at 3 years – replicated that of the randomized RACING trial conducted by many of the same researchers and published about a year ago in The Lancet.
RACING demonstrated that ezetimibe plus a moderate-intensity statin could be as effective as a high-intensity statin in patients with CV disease, “but have fewer side effects and better compliance,” Myeong-Ki Hong, MD, PhD, Severance Hospital, Yonsei University, Seoul, South Korea, said in an interview.
Dr. Hong is senior author on the current observational study based on the CONNECT-DES registry, which compared rosuvastatin 10 mg/day plus ezetimibe 10 mg/day – used in RACING – with rosuvastatin 20 mg/day in a nationwide cohort of 72,050 patients.
“As we know, populations who are enrolled in randomized studies do not sufficiently represent real patients in practice,” he observed, “so we wanted to evaluate the generalizability of the RACING results in daily clinical practice.”
Deepak L. Bhatt, MD, said he likes studies that look at whether clinical trial results “play out in the real world,” as this one did. “They have largely replicated the results of the RACING trial,” suggesting the approach using a moderate-intensity statin “is the way to go,” Dr. Bhatt of Mount Sinai Health System, New York, who was not affiliated with the current report, said in an interview. “In fact, the moderate-intensity combination regimen was actually better in this study.”
He said the observed reduction in new-onset diabetes with the moderate-intensity statin approach is also important. “There is a link between high-dose statins and diabetes. So, if given the choice, if you can get the benefits from a cardiovascular perspective with a lower risk of diabetes, it makes sense to use the combination therapy.”
Dr. Bhatt said he had been using high-intensity statin monotherapy in his high-risk patients, but RACING made him reconsider the value of moderate-dose statin combination therapy. “Going with lower doses of two drugs instead of high doses of one drug minimizes side effects and, in some cases, can even enhance efficacy – so this is not an unreasonable paradigm.”
In the current cohort study of patients prescribed rosuvastatin after DES implantation, 10,794 received rosuvastatin 10 mg/day plus ezetimibe 10 mg/day, and 61,256 were put on rosuvastatin 20 mg/day.
Hazard ratio risk reductions with the dual-agent lipid-lowering therapy approach, compared with high-intensity statin monotherapy, were more favorable for the primary composite clinical endpoint and important secondary events:
- HR, 0.75; 95% confidence interval, 0.70-0.79; P < .001) for CV death, MI, coronary artery revascularization, HF, or stroke at 3 years.
- HR, 0.85; 95% CI, 0.78-0.94; P = .001) for statin discontinuation.
- HR, 0.80; 95% CI, 0.72-0.88; P < .001) for new-onset diabetes requiring medication.
But HRs for rhabdomyolysis, cholecystectomy, or a new cancer diagnosis did not indicate significant differences between the two groups.
“Now that there is evidence to support the favorable clinical outcomes of combination lipid-lowering therapy with moderate-intensity statin plus ezetimibe” for secondary prevention from both RACING and a study reflecting daily clinical practice, Dr. Hong said, “physicians may feel more comfortable with this approach.”
The registry analysis “is remarkable not only for validating the results of the RACING trial in routine clinical practice in a high-risk secondary prevention population, but also for its innovative methodology,” states an accompanying editorial by Ori Ben-Yehuda, MD, Sulpizio Cardiovascular Center, University of California, San Diego.
Use of such a large single-payer database in their study “affords even greater external validity to the findings, complementing the internal validity of the randomized RACING trial,” Dr. Ben-Yehuda writes.
The rationale for combination therapy is strong, but additional data would be helpful, particularly for informing guidelines, he continues. “A pragmatic trial randomizing a broad racial and ethnic group of patients to low-dose statin,” such as a starting dose of 10 mg/day atorvastatin or 5 mg/day rosuvastatin “plus ezetimibe vs. high-intensity statin alone would provide much needed data to help guide lipid-lowering therapy for millions of patients and hopefully increase persistence on therapy.”
The study was supported by the Cardiovascular Research Center, Seoul, South Korea. Dr. Hong and Dr. Ben-Yehuda have disclosed no relevant financial relationships. Dr. Bhatt has previously disclosed grants and/or personal fees from many companies; personal fees from WebMD and other publications or organizations; and having other relationships with Medscape Cardiology and other publications or organizations.
A version of this article appeared on Medscape.com.
, suggests a “real-world” cohort study that is consistent with trial evidence.
In the observational study with more than 273,000 patients who received percutaneous coronary intervention (PCI) with drug-eluting stents (DES), risk for a broad composite clinical primary endpoint fell by one-fourth (P < .001) among those put on the two-drug regimen with a moderate-intensity statin, compared with those getting a high-intensity statin alone.
The dual-agent approach was also associated with a 15% drop in statin discontinuation and a 20% reduced risk for new-onset diabetes requiring medication (P < .001 for both benefits), reported investigators in the Journal of the American College of Cardiology.
The study’s primary endpoint – a composite of cardiovascular (CV) death, myocardial infarction (MI), coronary revascularization, heart failure (HF) hospitalization, or nonfatal stroke at 3 years – replicated that of the randomized RACING trial conducted by many of the same researchers and published about a year ago in The Lancet.
RACING demonstrated that ezetimibe plus a moderate-intensity statin could be as effective as a high-intensity statin in patients with CV disease, “but have fewer side effects and better compliance,” Myeong-Ki Hong, MD, PhD, Severance Hospital, Yonsei University, Seoul, South Korea, said in an interview.
Dr. Hong is senior author on the current observational study based on the CONNECT-DES registry, which compared rosuvastatin 10 mg/day plus ezetimibe 10 mg/day – used in RACING – with rosuvastatin 20 mg/day in a nationwide cohort of 72,050 patients.
“As we know, populations who are enrolled in randomized studies do not sufficiently represent real patients in practice,” he observed, “so we wanted to evaluate the generalizability of the RACING results in daily clinical practice.”
Deepak L. Bhatt, MD, said he likes studies that look at whether clinical trial results “play out in the real world,” as this one did. “They have largely replicated the results of the RACING trial,” suggesting the approach using a moderate-intensity statin “is the way to go,” Dr. Bhatt of Mount Sinai Health System, New York, who was not affiliated with the current report, said in an interview. “In fact, the moderate-intensity combination regimen was actually better in this study.”
He said the observed reduction in new-onset diabetes with the moderate-intensity statin approach is also important. “There is a link between high-dose statins and diabetes. So, if given the choice, if you can get the benefits from a cardiovascular perspective with a lower risk of diabetes, it makes sense to use the combination therapy.”
Dr. Bhatt said he had been using high-intensity statin monotherapy in his high-risk patients, but RACING made him reconsider the value of moderate-dose statin combination therapy. “Going with lower doses of two drugs instead of high doses of one drug minimizes side effects and, in some cases, can even enhance efficacy – so this is not an unreasonable paradigm.”
In the current cohort study of patients prescribed rosuvastatin after DES implantation, 10,794 received rosuvastatin 10 mg/day plus ezetimibe 10 mg/day, and 61,256 were put on rosuvastatin 20 mg/day.
Hazard ratio risk reductions with the dual-agent lipid-lowering therapy approach, compared with high-intensity statin monotherapy, were more favorable for the primary composite clinical endpoint and important secondary events:
- HR, 0.75; 95% confidence interval, 0.70-0.79; P < .001) for CV death, MI, coronary artery revascularization, HF, or stroke at 3 years.
- HR, 0.85; 95% CI, 0.78-0.94; P = .001) for statin discontinuation.
- HR, 0.80; 95% CI, 0.72-0.88; P < .001) for new-onset diabetes requiring medication.
But HRs for rhabdomyolysis, cholecystectomy, or a new cancer diagnosis did not indicate significant differences between the two groups.
“Now that there is evidence to support the favorable clinical outcomes of combination lipid-lowering therapy with moderate-intensity statin plus ezetimibe” for secondary prevention from both RACING and a study reflecting daily clinical practice, Dr. Hong said, “physicians may feel more comfortable with this approach.”
The registry analysis “is remarkable not only for validating the results of the RACING trial in routine clinical practice in a high-risk secondary prevention population, but also for its innovative methodology,” states an accompanying editorial by Ori Ben-Yehuda, MD, Sulpizio Cardiovascular Center, University of California, San Diego.
Use of such a large single-payer database in their study “affords even greater external validity to the findings, complementing the internal validity of the randomized RACING trial,” Dr. Ben-Yehuda writes.
The rationale for combination therapy is strong, but additional data would be helpful, particularly for informing guidelines, he continues. “A pragmatic trial randomizing a broad racial and ethnic group of patients to low-dose statin,” such as a starting dose of 10 mg/day atorvastatin or 5 mg/day rosuvastatin “plus ezetimibe vs. high-intensity statin alone would provide much needed data to help guide lipid-lowering therapy for millions of patients and hopefully increase persistence on therapy.”
The study was supported by the Cardiovascular Research Center, Seoul, South Korea. Dr. Hong and Dr. Ben-Yehuda have disclosed no relevant financial relationships. Dr. Bhatt has previously disclosed grants and/or personal fees from many companies; personal fees from WebMD and other publications or organizations; and having other relationships with Medscape Cardiology and other publications or organizations.
A version of this article appeared on Medscape.com.
FROM JACC
New guidelines on diabetes-related laboratory testing
The document, titled, “Guidelines and recommendations for laboratory analysis in the diagnosis and management of diabetes mellitus,” is primarily aimed at both laboratory professionals and clinicians involved in diabetes care.
The guidance is focused “on the practical aspects of care in order to assist with decisions regarding the use or interpretation of laboratory tests while screening, diagnosing, or monitoring patients with diabetes,” wrote David B. Sacks, MBChB, chief of the clinical chemistry service at the National Institutes of Health (NIH), Bethesda, Md., and coauthors. It was published online in both Clinical Chemistry and Diabetes Care, including the guidelines and executive summary.
Coauthor M. Sue Kirkman, MD, of the University of North Carolina, Chapel Hill, said in an interview: “One objective of the guidelines is to increase clinicians’ understanding of the strengths and limitations of tests done in a laboratory and also at the point of care, or in daily life, by people with diabetes.”
The evidence-based recommendations, an update of prior versions published in 2011 and 2002, are meant as a supplement to the ADA Standards of Care in Diabetes and do not address aspects of clinical management, she stressed.
Addition of advice on CGM
A significant addition since 2011 is detailed information regarding the use of real-time continuous glucose monitoring (CGM), with a “strong” recommendation based on a “high” level of evidence for use in teens and adults with type 1 diabetes who meet certain criteria, and lower-grade advice to use real-time or intermittently scanned CGM in other populations, including children with diabetes, pregnant women with type 1 diabetes, and adults with type 2 diabetes taking insulin.
The document also reminds clinicians to consider test limitations, Dr. Kirkman pointed out.
“We do a lot of testing in screening, diagnosis, and monitoring of diabetes and its complications, yet for many clinicians we think that any result we get – or that a patient gets from home testing – is perfect. We often don’t think about the accuracy or precision of some tests, things that might interfere with the result, intra-individual variation of the test, or how one test may compare to a test of higher accuracy,” she said.
One example is a recommendation to collect blood samples for glucose analysis in tubes containing a rapidly effective inhibitor of glycolysis such as a granulated citrate buffer. If unavailable, the sample tube should be placed immediately into an ice water slurry and centrifuged within 15-30 minutes to remove the cells.
Without those measures, “red cells in blood sitting in the test tube continue to break down glucose, so the concentration of glucose will start to fall very soon. ... How the specimen is handled makes a huge difference in the result,” Dr. Kirkman emphasized.
Another is the recommendation of a confirmatory test when diagnosing diabetes, regardless of the initial test used (A1c, fasting glucose, or oral glucose tolerance test). “There is large intra-individual variation of fasting glucose and even larger for 2-hour glucose on the oral glucose tolerance test. ... This means if you do the test one week and then repeat it the next day or a week later, the results will be quite different. This is a reason why confirmation of an abnormal test is important. Yet many times this isn’t done,” she noted.
Other “strong” recommendations based on “high” evidence levels include:
- Fasting glucose should be measured in venous plasma when used to establish the diagnosis of diabetes, with a diagnostic cutoff of > 7.0 mmol/L (> 126 mg/dL) for diabetes.
- Frequent blood glucose monitoring is recommended for all people with diabetes treated with intensive insulin regimens (with multiple daily injections or insulin pump therapy) and who are not using CGM.
- Routine use of blood glucose monitoring is not recommended for people with type 2 diabetes who are treated with diet and/or oral agents alone.
- Treatment goals should be based on ADA recommendations, i.e., A1c < 7% (< 53 mmol/mol) if it can be achieved without significant hypoglycemia or other adverse treatment effects, with higher targets for special populations.
- Annual testing for albuminuria should begin in pubertal or postpubertal individuals 5 years after diagnosis of type 1 diabetes and at time of diagnosis of type 2 diabetes, regardless of treatment.
- Urine albumin should be measured annually in adults with diabetes using morning spot urine albumin-to-creatinine ratio.
Other guidance in the document pertains to use of ketone testing, genetic markers, autoimmune markers, and C-peptide.
According to Dr. Sacks, “It’s important to measure accurately, but it’s also very important to communicate the relevance to clinicians and to listen to them and share information. ... Patient care is a team effort.”
Dr. Sachs has reported receiving funding from the NIH. Dr. Kirkman has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The document, titled, “Guidelines and recommendations for laboratory analysis in the diagnosis and management of diabetes mellitus,” is primarily aimed at both laboratory professionals and clinicians involved in diabetes care.
The guidance is focused “on the practical aspects of care in order to assist with decisions regarding the use or interpretation of laboratory tests while screening, diagnosing, or monitoring patients with diabetes,” wrote David B. Sacks, MBChB, chief of the clinical chemistry service at the National Institutes of Health (NIH), Bethesda, Md., and coauthors. It was published online in both Clinical Chemistry and Diabetes Care, including the guidelines and executive summary.
Coauthor M. Sue Kirkman, MD, of the University of North Carolina, Chapel Hill, said in an interview: “One objective of the guidelines is to increase clinicians’ understanding of the strengths and limitations of tests done in a laboratory and also at the point of care, or in daily life, by people with diabetes.”
The evidence-based recommendations, an update of prior versions published in 2011 and 2002, are meant as a supplement to the ADA Standards of Care in Diabetes and do not address aspects of clinical management, she stressed.
Addition of advice on CGM
A significant addition since 2011 is detailed information regarding the use of real-time continuous glucose monitoring (CGM), with a “strong” recommendation based on a “high” level of evidence for use in teens and adults with type 1 diabetes who meet certain criteria, and lower-grade advice to use real-time or intermittently scanned CGM in other populations, including children with diabetes, pregnant women with type 1 diabetes, and adults with type 2 diabetes taking insulin.
The document also reminds clinicians to consider test limitations, Dr. Kirkman pointed out.
“We do a lot of testing in screening, diagnosis, and monitoring of diabetes and its complications, yet for many clinicians we think that any result we get – or that a patient gets from home testing – is perfect. We often don’t think about the accuracy or precision of some tests, things that might interfere with the result, intra-individual variation of the test, or how one test may compare to a test of higher accuracy,” she said.
One example is a recommendation to collect blood samples for glucose analysis in tubes containing a rapidly effective inhibitor of glycolysis such as a granulated citrate buffer. If unavailable, the sample tube should be placed immediately into an ice water slurry and centrifuged within 15-30 minutes to remove the cells.
Without those measures, “red cells in blood sitting in the test tube continue to break down glucose, so the concentration of glucose will start to fall very soon. ... How the specimen is handled makes a huge difference in the result,” Dr. Kirkman emphasized.
Another is the recommendation of a confirmatory test when diagnosing diabetes, regardless of the initial test used (A1c, fasting glucose, or oral glucose tolerance test). “There is large intra-individual variation of fasting glucose and even larger for 2-hour glucose on the oral glucose tolerance test. ... This means if you do the test one week and then repeat it the next day or a week later, the results will be quite different. This is a reason why confirmation of an abnormal test is important. Yet many times this isn’t done,” she noted.
Other “strong” recommendations based on “high” evidence levels include:
- Fasting glucose should be measured in venous plasma when used to establish the diagnosis of diabetes, with a diagnostic cutoff of > 7.0 mmol/L (> 126 mg/dL) for diabetes.
- Frequent blood glucose monitoring is recommended for all people with diabetes treated with intensive insulin regimens (with multiple daily injections or insulin pump therapy) and who are not using CGM.
- Routine use of blood glucose monitoring is not recommended for people with type 2 diabetes who are treated with diet and/or oral agents alone.
- Treatment goals should be based on ADA recommendations, i.e., A1c < 7% (< 53 mmol/mol) if it can be achieved without significant hypoglycemia or other adverse treatment effects, with higher targets for special populations.
- Annual testing for albuminuria should begin in pubertal or postpubertal individuals 5 years after diagnosis of type 1 diabetes and at time of diagnosis of type 2 diabetes, regardless of treatment.
- Urine albumin should be measured annually in adults with diabetes using morning spot urine albumin-to-creatinine ratio.
Other guidance in the document pertains to use of ketone testing, genetic markers, autoimmune markers, and C-peptide.
According to Dr. Sacks, “It’s important to measure accurately, but it’s also very important to communicate the relevance to clinicians and to listen to them and share information. ... Patient care is a team effort.”
Dr. Sachs has reported receiving funding from the NIH. Dr. Kirkman has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The document, titled, “Guidelines and recommendations for laboratory analysis in the diagnosis and management of diabetes mellitus,” is primarily aimed at both laboratory professionals and clinicians involved in diabetes care.
The guidance is focused “on the practical aspects of care in order to assist with decisions regarding the use or interpretation of laboratory tests while screening, diagnosing, or monitoring patients with diabetes,” wrote David B. Sacks, MBChB, chief of the clinical chemistry service at the National Institutes of Health (NIH), Bethesda, Md., and coauthors. It was published online in both Clinical Chemistry and Diabetes Care, including the guidelines and executive summary.
Coauthor M. Sue Kirkman, MD, of the University of North Carolina, Chapel Hill, said in an interview: “One objective of the guidelines is to increase clinicians’ understanding of the strengths and limitations of tests done in a laboratory and also at the point of care, or in daily life, by people with diabetes.”
The evidence-based recommendations, an update of prior versions published in 2011 and 2002, are meant as a supplement to the ADA Standards of Care in Diabetes and do not address aspects of clinical management, she stressed.
Addition of advice on CGM
A significant addition since 2011 is detailed information regarding the use of real-time continuous glucose monitoring (CGM), with a “strong” recommendation based on a “high” level of evidence for use in teens and adults with type 1 diabetes who meet certain criteria, and lower-grade advice to use real-time or intermittently scanned CGM in other populations, including children with diabetes, pregnant women with type 1 diabetes, and adults with type 2 diabetes taking insulin.
The document also reminds clinicians to consider test limitations, Dr. Kirkman pointed out.
“We do a lot of testing in screening, diagnosis, and monitoring of diabetes and its complications, yet for many clinicians we think that any result we get – or that a patient gets from home testing – is perfect. We often don’t think about the accuracy or precision of some tests, things that might interfere with the result, intra-individual variation of the test, or how one test may compare to a test of higher accuracy,” she said.
One example is a recommendation to collect blood samples for glucose analysis in tubes containing a rapidly effective inhibitor of glycolysis such as a granulated citrate buffer. If unavailable, the sample tube should be placed immediately into an ice water slurry and centrifuged within 15-30 minutes to remove the cells.
Without those measures, “red cells in blood sitting in the test tube continue to break down glucose, so the concentration of glucose will start to fall very soon. ... How the specimen is handled makes a huge difference in the result,” Dr. Kirkman emphasized.
Another is the recommendation of a confirmatory test when diagnosing diabetes, regardless of the initial test used (A1c, fasting glucose, or oral glucose tolerance test). “There is large intra-individual variation of fasting glucose and even larger for 2-hour glucose on the oral glucose tolerance test. ... This means if you do the test one week and then repeat it the next day or a week later, the results will be quite different. This is a reason why confirmation of an abnormal test is important. Yet many times this isn’t done,” she noted.
Other “strong” recommendations based on “high” evidence levels include:
- Fasting glucose should be measured in venous plasma when used to establish the diagnosis of diabetes, with a diagnostic cutoff of > 7.0 mmol/L (> 126 mg/dL) for diabetes.
- Frequent blood glucose monitoring is recommended for all people with diabetes treated with intensive insulin regimens (with multiple daily injections or insulin pump therapy) and who are not using CGM.
- Routine use of blood glucose monitoring is not recommended for people with type 2 diabetes who are treated with diet and/or oral agents alone.
- Treatment goals should be based on ADA recommendations, i.e., A1c < 7% (< 53 mmol/mol) if it can be achieved without significant hypoglycemia or other adverse treatment effects, with higher targets for special populations.
- Annual testing for albuminuria should begin in pubertal or postpubertal individuals 5 years after diagnosis of type 1 diabetes and at time of diagnosis of type 2 diabetes, regardless of treatment.
- Urine albumin should be measured annually in adults with diabetes using morning spot urine albumin-to-creatinine ratio.
Other guidance in the document pertains to use of ketone testing, genetic markers, autoimmune markers, and C-peptide.
According to Dr. Sacks, “It’s important to measure accurately, but it’s also very important to communicate the relevance to clinicians and to listen to them and share information. ... Patient care is a team effort.”
Dr. Sachs has reported receiving funding from the NIH. Dr. Kirkman has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CLINICAL CHEMISTRY AND DIABETES CARE
Vegetarian diets can improve high-risk cardiovascular disease
, a meta-analysis of randomized controlled trials shows.

“To the best of our knowledge, this meta-analysis is the first that generates evidence from randomized controlled trials to assess the association of vegetarian diets with outcomes in people affected by cardiovascular diseases,” report the authors. The study was published online in JAMA Network Open.
“The greatest improvements in hemoglobin A1c and low-density lipoprotein cholesterol (LDL-C) were observed in individuals with type 2 diabetes and people at high risk of cardiovascular disease, highlighting the potential protective and synergistic effects of vegetarian diets for the primary prevention of cardiovascular disease,” they say.
Poor diet is well-established as increasing the morbidity and mortality associated with cardiovascular disease; however, although data has linked vegetarian diets to cardiovascular disease prevention in the general population, research on the effectiveness of such diets in people at high risk of cardiovascular disease is lacking.
“To the best of our knowledge, no meta-analysis of randomized controlled trials has been conducted to investigate the association of vegetarian diets with outcomes among people with CVD – indeed, research here has primarily focused on observational studies,” writes Tian Wang, RD, and colleagues at the University of Sydney.
Greater decreases in LDL-C, A1c, and body weight with vegetarian diets
For the meta-analysis, researchers identified 20 randomized controlled trials involving vegetarian diets that included 1,878 adults with or at a high risk of cardiovascular disease and included measurements of LDL-C, A1c, or systolic blood pressure.
The studies were conducted in the United States, Asia, Europe, and New Zealand between 1990 and 2021. Sample sizes ranged from 12 to 291 participants.
The mean range age of participants was 28-64 years. Studies included patients with cardiovascular disease (four studies), diabetes (seven studies), and those with at least two cardiovascular risk factors (nine studies).
The mean duration of the dietary intervention was 25.4 weeks (range 2-24 months). The most commonly prescribed diets were vegan (plant-based foods only), lacto-ovo-vegetarian (excluded meat, poultry, seafood, and dairy products, but allowed eggs), and lacto-vegetarian (same as previous but allowed dairy products).
Overall, those who consumed a vegetarian diet for an average of 6 months, versus comparison diets, had significantly greater decreases in LDL-C (6.6 mg/dL beyond the reduction achieved with standard therapy); A1c (0.24%); and body weight (3.4 kg), but the reduction in systolic blood pressure (0.1 mmHg) was not significantly greater.
Assessment of the overall certainty of evidence evaluated using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) tool showed a moderate level of evidence for reductions in LDL-C and A1c with the vegetarian diet.
Lacto-ovo vegetarian diets were associated with the greatest reduction in LDL-C (14.1 mg/dL); however, four out of the five trials restricted energy intake.
Of note, vegetarian diets were most effective for achieving glycemic control among people with type 2 diabetes and leading to improvements in weight among those at high risk of cardiovascular disease as well as those with type 2 diabetes.
The effects “suggest that vegetarian diets might have a synergistic [or at least nonantagonistic] use in potentiating the effects of optimal drug therapy in the prevention and treatment of a range of cardiometabolic diseases,” the authors write.
Although previous studies have shown similar improvements associated with a vegetarian diet, most studies did not stratify populations based on disease status, type of vegetarian diet, or comparison diet, the authors note.
The lack of improvement in systolic blood pressure is consistent with previous meta-analyses of vegetarian diets in general and suggests that salt intake may be the more important factor for those measures.
“[The meta-analysis] suggests that diet quality plays a major role in lowering blood pressure independent of animal food consumption, as the DASH [Dietary Approaches to Stop Hypertension] ... trial demonstrated,” the authors note.
Decreases in medication dose with vegetarian diet
Although most patients were taking medications to manage hypertension, hyperglycemia, and/or dyslipidemia at trial enrollment in as many as eight of the studies, the vegetarian diet intervention resulted in a decrease in medication dose.
In fact, medication use could obscure the favorable effects of vegetarian diets, which could have a larger effect size, the authors speculate.
“This hypothesis is supported by two randomized controlled trials in our meta-analysis that required patients not to take medication that could influence cardiometabolic outcomes, [and] these studies significantly improved systolic blood pressure and LDL-C,” they write.
Not all vegetarian diets are healthy
Although there are numerous variations in vegetarian diets, ranging from vegan diets that eliminate all animal food to pesco-vegetarian diets that allow fish or seafood, most that are well-balanced can provide health benefits including lower saturated fat, L-carnitine, and choline (precursors of the atherogenic TMAO), and other benefits that might explain the improvements seen in the meta-analysis.
The diets may also be high in dietary fiber, mono- and polyunsaturated fatty acids, potassium, magnesium, and phytochemical, and have lower glycemic index scores.
Of note, 12 studies in the meta-analysis emphasized low-fat content, which the authors speculate may have contributed to the improvements observed in LDC-C.
Specifically, lacto-ovo vegetarian diets were associated with the greatest reduction in LDL-C (–14.1 mg/dL); however, four out of five of the trials restricted energy intake, which could have also played a role in improvements.
Importantly, not all vegetarian diets are healthy, and the authors caution about some that allow, for instance, deep-fried foods rich in trans-fatty acids and salt, such as tempura vegetables, potentially increasing the risk of type 2 diabetes and coronary heart disease.
They note that “more than one-third of the studies included in our meta-analysis did not emphasize the importance of consuming minimally processed plant-based whole foods.”
Overall, however, the fact that the greatest improvements in A1c and LDL-C were seen in patients with type 2 diabetes and those at high risk of CVD “highlight[s] the potential protective and synergistic effects of vegetarian diets for the primary prevention of CVD.”
A version of this article first appeared on Medscape.com.
, a meta-analysis of randomized controlled trials shows.
“To the best of our knowledge, this meta-analysis is the first that generates evidence from randomized controlled trials to assess the association of vegetarian diets with outcomes in people affected by cardiovascular diseases,” report the authors. The study was published online in JAMA Network Open.
“The greatest improvements in hemoglobin A1c and low-density lipoprotein cholesterol (LDL-C) were observed in individuals with type 2 diabetes and people at high risk of cardiovascular disease, highlighting the potential protective and synergistic effects of vegetarian diets for the primary prevention of cardiovascular disease,” they say.
Poor diet is well-established as increasing the morbidity and mortality associated with cardiovascular disease; however, although data has linked vegetarian diets to cardiovascular disease prevention in the general population, research on the effectiveness of such diets in people at high risk of cardiovascular disease is lacking.
“To the best of our knowledge, no meta-analysis of randomized controlled trials has been conducted to investigate the association of vegetarian diets with outcomes among people with CVD – indeed, research here has primarily focused on observational studies,” writes Tian Wang, RD, and colleagues at the University of Sydney.
Greater decreases in LDL-C, A1c, and body weight with vegetarian diets
For the meta-analysis, researchers identified 20 randomized controlled trials involving vegetarian diets that included 1,878 adults with or at a high risk of cardiovascular disease and included measurements of LDL-C, A1c, or systolic blood pressure.
The studies were conducted in the United States, Asia, Europe, and New Zealand between 1990 and 2021. Sample sizes ranged from 12 to 291 participants.
The mean range age of participants was 28-64 years. Studies included patients with cardiovascular disease (four studies), diabetes (seven studies), and those with at least two cardiovascular risk factors (nine studies).
The mean duration of the dietary intervention was 25.4 weeks (range 2-24 months). The most commonly prescribed diets were vegan (plant-based foods only), lacto-ovo-vegetarian (excluded meat, poultry, seafood, and dairy products, but allowed eggs), and lacto-vegetarian (same as previous but allowed dairy products).
Overall, those who consumed a vegetarian diet for an average of 6 months, versus comparison diets, had significantly greater decreases in LDL-C (6.6 mg/dL beyond the reduction achieved with standard therapy); A1c (0.24%); and body weight (3.4 kg), but the reduction in systolic blood pressure (0.1 mmHg) was not significantly greater.
Assessment of the overall certainty of evidence evaluated using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) tool showed a moderate level of evidence for reductions in LDL-C and A1c with the vegetarian diet.
Lacto-ovo vegetarian diets were associated with the greatest reduction in LDL-C (14.1 mg/dL); however, four out of the five trials restricted energy intake.
Of note, vegetarian diets were most effective for achieving glycemic control among people with type 2 diabetes and leading to improvements in weight among those at high risk of cardiovascular disease as well as those with type 2 diabetes.
The effects “suggest that vegetarian diets might have a synergistic [or at least nonantagonistic] use in potentiating the effects of optimal drug therapy in the prevention and treatment of a range of cardiometabolic diseases,” the authors write.
Although previous studies have shown similar improvements associated with a vegetarian diet, most studies did not stratify populations based on disease status, type of vegetarian diet, or comparison diet, the authors note.
The lack of improvement in systolic blood pressure is consistent with previous meta-analyses of vegetarian diets in general and suggests that salt intake may be the more important factor for those measures.
“[The meta-analysis] suggests that diet quality plays a major role in lowering blood pressure independent of animal food consumption, as the DASH [Dietary Approaches to Stop Hypertension] ... trial demonstrated,” the authors note.
Decreases in medication dose with vegetarian diet
Although most patients were taking medications to manage hypertension, hyperglycemia, and/or dyslipidemia at trial enrollment in as many as eight of the studies, the vegetarian diet intervention resulted in a decrease in medication dose.
In fact, medication use could obscure the favorable effects of vegetarian diets, which could have a larger effect size, the authors speculate.
“This hypothesis is supported by two randomized controlled trials in our meta-analysis that required patients not to take medication that could influence cardiometabolic outcomes, [and] these studies significantly improved systolic blood pressure and LDL-C,” they write.
Not all vegetarian diets are healthy
Although there are numerous variations in vegetarian diets, ranging from vegan diets that eliminate all animal food to pesco-vegetarian diets that allow fish or seafood, most that are well-balanced can provide health benefits including lower saturated fat, L-carnitine, and choline (precursors of the atherogenic TMAO), and other benefits that might explain the improvements seen in the meta-analysis.
The diets may also be high in dietary fiber, mono- and polyunsaturated fatty acids, potassium, magnesium, and phytochemical, and have lower glycemic index scores.
Of note, 12 studies in the meta-analysis emphasized low-fat content, which the authors speculate may have contributed to the improvements observed in LDC-C.
Specifically, lacto-ovo vegetarian diets were associated with the greatest reduction in LDL-C (–14.1 mg/dL); however, four out of five of the trials restricted energy intake, which could have also played a role in improvements.
Importantly, not all vegetarian diets are healthy, and the authors caution about some that allow, for instance, deep-fried foods rich in trans-fatty acids and salt, such as tempura vegetables, potentially increasing the risk of type 2 diabetes and coronary heart disease.
They note that “more than one-third of the studies included in our meta-analysis did not emphasize the importance of consuming minimally processed plant-based whole foods.”
Overall, however, the fact that the greatest improvements in A1c and LDL-C were seen in patients with type 2 diabetes and those at high risk of CVD “highlight[s] the potential protective and synergistic effects of vegetarian diets for the primary prevention of CVD.”
A version of this article first appeared on Medscape.com.
, a meta-analysis of randomized controlled trials shows.
“To the best of our knowledge, this meta-analysis is the first that generates evidence from randomized controlled trials to assess the association of vegetarian diets with outcomes in people affected by cardiovascular diseases,” report the authors. The study was published online in JAMA Network Open.
“The greatest improvements in hemoglobin A1c and low-density lipoprotein cholesterol (LDL-C) were observed in individuals with type 2 diabetes and people at high risk of cardiovascular disease, highlighting the potential protective and synergistic effects of vegetarian diets for the primary prevention of cardiovascular disease,” they say.
Poor diet is well-established as increasing the morbidity and mortality associated with cardiovascular disease; however, although data has linked vegetarian diets to cardiovascular disease prevention in the general population, research on the effectiveness of such diets in people at high risk of cardiovascular disease is lacking.
“To the best of our knowledge, no meta-analysis of randomized controlled trials has been conducted to investigate the association of vegetarian diets with outcomes among people with CVD – indeed, research here has primarily focused on observational studies,” writes Tian Wang, RD, and colleagues at the University of Sydney.
Greater decreases in LDL-C, A1c, and body weight with vegetarian diets
For the meta-analysis, researchers identified 20 randomized controlled trials involving vegetarian diets that included 1,878 adults with or at a high risk of cardiovascular disease and included measurements of LDL-C, A1c, or systolic blood pressure.
The studies were conducted in the United States, Asia, Europe, and New Zealand between 1990 and 2021. Sample sizes ranged from 12 to 291 participants.
The mean range age of participants was 28-64 years. Studies included patients with cardiovascular disease (four studies), diabetes (seven studies), and those with at least two cardiovascular risk factors (nine studies).
The mean duration of the dietary intervention was 25.4 weeks (range 2-24 months). The most commonly prescribed diets were vegan (plant-based foods only), lacto-ovo-vegetarian (excluded meat, poultry, seafood, and dairy products, but allowed eggs), and lacto-vegetarian (same as previous but allowed dairy products).
Overall, those who consumed a vegetarian diet for an average of 6 months, versus comparison diets, had significantly greater decreases in LDL-C (6.6 mg/dL beyond the reduction achieved with standard therapy); A1c (0.24%); and body weight (3.4 kg), but the reduction in systolic blood pressure (0.1 mmHg) was not significantly greater.
Assessment of the overall certainty of evidence evaluated using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) tool showed a moderate level of evidence for reductions in LDL-C and A1c with the vegetarian diet.
Lacto-ovo vegetarian diets were associated with the greatest reduction in LDL-C (14.1 mg/dL); however, four out of the five trials restricted energy intake.
Of note, vegetarian diets were most effective for achieving glycemic control among people with type 2 diabetes and leading to improvements in weight among those at high risk of cardiovascular disease as well as those with type 2 diabetes.
The effects “suggest that vegetarian diets might have a synergistic [or at least nonantagonistic] use in potentiating the effects of optimal drug therapy in the prevention and treatment of a range of cardiometabolic diseases,” the authors write.
Although previous studies have shown similar improvements associated with a vegetarian diet, most studies did not stratify populations based on disease status, type of vegetarian diet, or comparison diet, the authors note.
The lack of improvement in systolic blood pressure is consistent with previous meta-analyses of vegetarian diets in general and suggests that salt intake may be the more important factor for those measures.
“[The meta-analysis] suggests that diet quality plays a major role in lowering blood pressure independent of animal food consumption, as the DASH [Dietary Approaches to Stop Hypertension] ... trial demonstrated,” the authors note.
Decreases in medication dose with vegetarian diet
Although most patients were taking medications to manage hypertension, hyperglycemia, and/or dyslipidemia at trial enrollment in as many as eight of the studies, the vegetarian diet intervention resulted in a decrease in medication dose.
In fact, medication use could obscure the favorable effects of vegetarian diets, which could have a larger effect size, the authors speculate.
“This hypothesis is supported by two randomized controlled trials in our meta-analysis that required patients not to take medication that could influence cardiometabolic outcomes, [and] these studies significantly improved systolic blood pressure and LDL-C,” they write.
Not all vegetarian diets are healthy
Although there are numerous variations in vegetarian diets, ranging from vegan diets that eliminate all animal food to pesco-vegetarian diets that allow fish or seafood, most that are well-balanced can provide health benefits including lower saturated fat, L-carnitine, and choline (precursors of the atherogenic TMAO), and other benefits that might explain the improvements seen in the meta-analysis.
The diets may also be high in dietary fiber, mono- and polyunsaturated fatty acids, potassium, magnesium, and phytochemical, and have lower glycemic index scores.
Of note, 12 studies in the meta-analysis emphasized low-fat content, which the authors speculate may have contributed to the improvements observed in LDC-C.
Specifically, lacto-ovo vegetarian diets were associated with the greatest reduction in LDL-C (–14.1 mg/dL); however, four out of five of the trials restricted energy intake, which could have also played a role in improvements.
Importantly, not all vegetarian diets are healthy, and the authors caution about some that allow, for instance, deep-fried foods rich in trans-fatty acids and salt, such as tempura vegetables, potentially increasing the risk of type 2 diabetes and coronary heart disease.
They note that “more than one-third of the studies included in our meta-analysis did not emphasize the importance of consuming minimally processed plant-based whole foods.”
Overall, however, the fact that the greatest improvements in A1c and LDL-C were seen in patients with type 2 diabetes and those at high risk of CVD “highlight[s] the potential protective and synergistic effects of vegetarian diets for the primary prevention of CVD.”
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
SGLT2 inhibitors linked with fewer gout flares in diabetes
TOPLINE:
compared with matched patients treated with a dipeptidyl peptidase–4 (DPP-4) inhibitor.
METHODOLOGY:
- The study used observational data collected from the entire population of British Columbia that included 15,067 adults with both gout and type 2 diabetes in 2014-2020.
- The group included 8,318 patients who initiated an SGLT2 inhibitor and 6,749 patients who initiated a DPP-4 inhibitor during the study period after at least 1 year of continuous enrollment.
- Using propensity-score matching, 4,075 matched pairs were identified, where one person initiated an SGLT2 inhibitor and the other started a DPP-4 inhibitor.
- Primary outcome was recurrent gout flare counts during follow-up that required an ED visit, hospital admission, or an outpatient visit for a gout flare coupled with appropriate treatment, tallied from the first day of drug receipt until June 30, 2022, with an average follow-up of 1.6 years.
- Secondary endpoints included the incidence of myocardial infarction and stroke.
TAKEAWAY:
- Total gout-flare rates after SGLT2 inhibitor initiation were 52.4/1000 person-years and after DPP-4 inhibitor initiation were 79.7/1,000 person-years, an adjusted rate ratio of 0.66, a reduction significantly linked with SGLT2 inhibitor use.
- For flares that required an ED visit or hospitalization, initiation of an SGLT2 inhibitor was linked with a significant, reduced aRR of 0.52, compared with DPP-4 inhibitor initiation.
- The flare-rate reduction linked with SGLT2 inhibitor use was consistent regardless of sex, age, baseline diuretic use, prior treatment with a urate-lowering agent, and baseline gout intensity.
- SGLT2 inhibitor initiation was also significantly linked with an adjusted reduced hazard ratio of 0.69 in the incidence of myocardial infarction, compared with DPP-4 inhibitor initiation, but stroke incidence was not significantly different between the groups.
IN PRACTICE:
These findings suggest that SGLT2 inhibitors could have a much-needed ability to simultaneously reduce the burden of recurrent gout flares and coronary sequelae in patients with gout and type 2 diabetes, indicating that “SGLT2 inhibitors may offer distinct benefits,” making the drug class “a particularly attractive addition to current urate-lowering therapies,” the researchers write.
SOURCE:
The study was primarily conducted by researchers at Massachusetts General Hospital in Boston. The study was published online July 24 in Annals of Internal Medicine.
LIMITATIONS:
The data used in the study did not include gout flares that did not require medical attention and did not include laboratory findings for study participants. Because the data were observational the findings may be susceptible to unmeasured confounding.
DISCLOSURES:
The study received no commercial funding. One author has reported receiving consulting fees from ANI and LG Chem.
A version of this article first appeared on Medscape.com.
TOPLINE:
compared with matched patients treated with a dipeptidyl peptidase–4 (DPP-4) inhibitor.
METHODOLOGY:
- The study used observational data collected from the entire population of British Columbia that included 15,067 adults with both gout and type 2 diabetes in 2014-2020.
- The group included 8,318 patients who initiated an SGLT2 inhibitor and 6,749 patients who initiated a DPP-4 inhibitor during the study period after at least 1 year of continuous enrollment.
- Using propensity-score matching, 4,075 matched pairs were identified, where one person initiated an SGLT2 inhibitor and the other started a DPP-4 inhibitor.
- Primary outcome was recurrent gout flare counts during follow-up that required an ED visit, hospital admission, or an outpatient visit for a gout flare coupled with appropriate treatment, tallied from the first day of drug receipt until June 30, 2022, with an average follow-up of 1.6 years.
- Secondary endpoints included the incidence of myocardial infarction and stroke.
TAKEAWAY:
- Total gout-flare rates after SGLT2 inhibitor initiation were 52.4/1000 person-years and after DPP-4 inhibitor initiation were 79.7/1,000 person-years, an adjusted rate ratio of 0.66, a reduction significantly linked with SGLT2 inhibitor use.
- For flares that required an ED visit or hospitalization, initiation of an SGLT2 inhibitor was linked with a significant, reduced aRR of 0.52, compared with DPP-4 inhibitor initiation.
- The flare-rate reduction linked with SGLT2 inhibitor use was consistent regardless of sex, age, baseline diuretic use, prior treatment with a urate-lowering agent, and baseline gout intensity.
- SGLT2 inhibitor initiation was also significantly linked with an adjusted reduced hazard ratio of 0.69 in the incidence of myocardial infarction, compared with DPP-4 inhibitor initiation, but stroke incidence was not significantly different between the groups.
IN PRACTICE:
These findings suggest that SGLT2 inhibitors could have a much-needed ability to simultaneously reduce the burden of recurrent gout flares and coronary sequelae in patients with gout and type 2 diabetes, indicating that “SGLT2 inhibitors may offer distinct benefits,” making the drug class “a particularly attractive addition to current urate-lowering therapies,” the researchers write.
SOURCE:
The study was primarily conducted by researchers at Massachusetts General Hospital in Boston. The study was published online July 24 in Annals of Internal Medicine.
LIMITATIONS:
The data used in the study did not include gout flares that did not require medical attention and did not include laboratory findings for study participants. Because the data were observational the findings may be susceptible to unmeasured confounding.
DISCLOSURES:
The study received no commercial funding. One author has reported receiving consulting fees from ANI and LG Chem.
A version of this article first appeared on Medscape.com.
TOPLINE:
compared with matched patients treated with a dipeptidyl peptidase–4 (DPP-4) inhibitor.
METHODOLOGY:
- The study used observational data collected from the entire population of British Columbia that included 15,067 adults with both gout and type 2 diabetes in 2014-2020.
- The group included 8,318 patients who initiated an SGLT2 inhibitor and 6,749 patients who initiated a DPP-4 inhibitor during the study period after at least 1 year of continuous enrollment.
- Using propensity-score matching, 4,075 matched pairs were identified, where one person initiated an SGLT2 inhibitor and the other started a DPP-4 inhibitor.
- Primary outcome was recurrent gout flare counts during follow-up that required an ED visit, hospital admission, or an outpatient visit for a gout flare coupled with appropriate treatment, tallied from the first day of drug receipt until June 30, 2022, with an average follow-up of 1.6 years.
- Secondary endpoints included the incidence of myocardial infarction and stroke.
TAKEAWAY:
- Total gout-flare rates after SGLT2 inhibitor initiation were 52.4/1000 person-years and after DPP-4 inhibitor initiation were 79.7/1,000 person-years, an adjusted rate ratio of 0.66, a reduction significantly linked with SGLT2 inhibitor use.
- For flares that required an ED visit or hospitalization, initiation of an SGLT2 inhibitor was linked with a significant, reduced aRR of 0.52, compared with DPP-4 inhibitor initiation.
- The flare-rate reduction linked with SGLT2 inhibitor use was consistent regardless of sex, age, baseline diuretic use, prior treatment with a urate-lowering agent, and baseline gout intensity.
- SGLT2 inhibitor initiation was also significantly linked with an adjusted reduced hazard ratio of 0.69 in the incidence of myocardial infarction, compared with DPP-4 inhibitor initiation, but stroke incidence was not significantly different between the groups.
IN PRACTICE:
These findings suggest that SGLT2 inhibitors could have a much-needed ability to simultaneously reduce the burden of recurrent gout flares and coronary sequelae in patients with gout and type 2 diabetes, indicating that “SGLT2 inhibitors may offer distinct benefits,” making the drug class “a particularly attractive addition to current urate-lowering therapies,” the researchers write.
SOURCE:
The study was primarily conducted by researchers at Massachusetts General Hospital in Boston. The study was published online July 24 in Annals of Internal Medicine.
LIMITATIONS:
The data used in the study did not include gout flares that did not require medical attention and did not include laboratory findings for study participants. Because the data were observational the findings may be susceptible to unmeasured confounding.
DISCLOSURES:
The study received no commercial funding. One author has reported receiving consulting fees from ANI and LG Chem.
A version of this article first appeared on Medscape.com.
FROM ANNALS OF INTERNAL MEDICINE
Intermittent fasting vs. calorie counting for weight loss
BOSTON –
For the study, 57 overweight and obese participants with type 2 diabetes were randomly assigned to three different groups: The first group ate between noon and 8 p.m., the second was asked to reduce caloric intake by 25% of maintenance calories, and the third, a control group, continued eating normally.
The calorie-restriction group tracked intake on MyFitnessPal, an app that logs the calorie content of different foods. Both the intermittent-fasting and calorie-restriction groups were assigned a dietitian to help with adherence.
After 6 months, participants in the intermittent-fasting group lost about 4.3% of body weight – the equivalent of 10 pounds of weight loss for a person weighing 230 pounds – whereas participants in the calorie-restriction group lost about 2.5% of body weight.
The difference between the two groups was not significant, so one approach isn’t necessarily better than the other for weight loss.
“Let’s not think of this as an approach that’s better than calorie restriction,” William Yancy, MD, MHS, an internist and weight management specialist at Duke Lifestyle and Weight Management Center, Durham, N.C., said in an interview. “It’s an alternative approach to calorie restriction.”
Participants’ willingness to adhere to the diet likely accounted for the percentage difference between the groups, study author Vasiliki Pavlou, RDN, told this news organization. Ms. Pavlou presented the findings at the Nutrition 2023 conference.
“People that have type 2 diabetes, they’ve already been to the doctor, they’ve already been told to count calories,” said Ms. Pavlou, a doctoral student at the University of Illinois at Chicago. “There were many weeks where they came to us with nothing on MyFitnessPal and we’d have to encourage them to start tracking again.”
The intermittent-fasting group adhered to the eating time window 6 out of 7 days of the week, with a 1-hour grace period for the noon-to-8-p.m. window. In comparison, one-third of the calorie-restriction group didn’t stay within 200 calories of the goal, according to Ms. Pavlou.
That meant the fasting group cut about 100 calories more per day than the calorie-restriction group, which was reflected in their weight loss, Ms. Pavlou said.
A1c levels dropped by about 1% in both the intermittent-fasting and calorie-restriction groups – a meaningful decrease, said Dr. Yancy. “I think a 0.5% difference would have some clinical significance in terms of complications from diabetes,” he said. “So 1% would be even more clinically meaningful.”
However, fewer participants taking insulin in the calorie-restriction group could explain the difference, according to Ms. Pavlou. “Usually, when someone goes on insulin, their pancreas is already not functioning as well,” she said. “And it’s way harder to see improvements in their A1c and glycemic control.”
Up to 90% of people with type 2 diabetes are overweight or obese. Weight loss is one of the major components of type 2 diabetes care, according to the American Diabetes Association, and studies have shown that even a 5% reduction in body weight can reduce blood glucose concentration and A1c. Some studies suggest diabetes remission can occur after a 10% loss in body weight, but Dr. Yancy said it depends on the person.
“It depends on the individual, their metabolic situation, how long they’ve had diabetes, what kind of approach they’re following, maybe what medicines they’re taking,” Dr. Yancy said. “There’s a lot of different factors involved in remission.”
The study cohort generally had advanced diabetes and was taking a mix of medications, so the results might not be applicable to people with a more recent diabetes diagnosis, according to Ms. Pavlou.
Dr. Yancy said intermittent fasting could work well for the right person. The success of the approach could depend on a person’s eating habits and whether their meals usually fall outside the time-restricted window, or it could depend on how well a person follows rules, according to Dr. Yancy.
“Some people might not eat much after 8 o’clock, and some people might skip breakfast,” Dr. Yancy said. “And if that’s the case, then it’s not going to make a big impact on their weight probably.”
Medication is also an important consideration. Not eating can be dangerous for patients taking short-acting insulin or sulfonylureas, according to Dr. Yancy.
Ms. Pavlou said these findings show intermittent fasting is another option for patients with type 2 diabetes trying to lose weight. “If you’ve tried calorie counting, that’s not working for you or if you’re kind of burnt out, this is something else that you could try,” she said.
“We have a lot of patients that need to lose weight, and we have patients who respond differently to different approaches,” said Dr. Yancy. “So having various approaches is really valuable.”
The manuscript is currently under review at JAMA Internal Medicine, said Ms. Pavlou.
A version of this article appeared on Medscape.com.
BOSTON –
For the study, 57 overweight and obese participants with type 2 diabetes were randomly assigned to three different groups: The first group ate between noon and 8 p.m., the second was asked to reduce caloric intake by 25% of maintenance calories, and the third, a control group, continued eating normally.
The calorie-restriction group tracked intake on MyFitnessPal, an app that logs the calorie content of different foods. Both the intermittent-fasting and calorie-restriction groups were assigned a dietitian to help with adherence.
After 6 months, participants in the intermittent-fasting group lost about 4.3% of body weight – the equivalent of 10 pounds of weight loss for a person weighing 230 pounds – whereas participants in the calorie-restriction group lost about 2.5% of body weight.
The difference between the two groups was not significant, so one approach isn’t necessarily better than the other for weight loss.
“Let’s not think of this as an approach that’s better than calorie restriction,” William Yancy, MD, MHS, an internist and weight management specialist at Duke Lifestyle and Weight Management Center, Durham, N.C., said in an interview. “It’s an alternative approach to calorie restriction.”
Participants’ willingness to adhere to the diet likely accounted for the percentage difference between the groups, study author Vasiliki Pavlou, RDN, told this news organization. Ms. Pavlou presented the findings at the Nutrition 2023 conference.
“People that have type 2 diabetes, they’ve already been to the doctor, they’ve already been told to count calories,” said Ms. Pavlou, a doctoral student at the University of Illinois at Chicago. “There were many weeks where they came to us with nothing on MyFitnessPal and we’d have to encourage them to start tracking again.”
The intermittent-fasting group adhered to the eating time window 6 out of 7 days of the week, with a 1-hour grace period for the noon-to-8-p.m. window. In comparison, one-third of the calorie-restriction group didn’t stay within 200 calories of the goal, according to Ms. Pavlou.
That meant the fasting group cut about 100 calories more per day than the calorie-restriction group, which was reflected in their weight loss, Ms. Pavlou said.
A1c levels dropped by about 1% in both the intermittent-fasting and calorie-restriction groups – a meaningful decrease, said Dr. Yancy. “I think a 0.5% difference would have some clinical significance in terms of complications from diabetes,” he said. “So 1% would be even more clinically meaningful.”
However, fewer participants taking insulin in the calorie-restriction group could explain the difference, according to Ms. Pavlou. “Usually, when someone goes on insulin, their pancreas is already not functioning as well,” she said. “And it’s way harder to see improvements in their A1c and glycemic control.”
Up to 90% of people with type 2 diabetes are overweight or obese. Weight loss is one of the major components of type 2 diabetes care, according to the American Diabetes Association, and studies have shown that even a 5% reduction in body weight can reduce blood glucose concentration and A1c. Some studies suggest diabetes remission can occur after a 10% loss in body weight, but Dr. Yancy said it depends on the person.
“It depends on the individual, their metabolic situation, how long they’ve had diabetes, what kind of approach they’re following, maybe what medicines they’re taking,” Dr. Yancy said. “There’s a lot of different factors involved in remission.”
The study cohort generally had advanced diabetes and was taking a mix of medications, so the results might not be applicable to people with a more recent diabetes diagnosis, according to Ms. Pavlou.
Dr. Yancy said intermittent fasting could work well for the right person. The success of the approach could depend on a person’s eating habits and whether their meals usually fall outside the time-restricted window, or it could depend on how well a person follows rules, according to Dr. Yancy.
“Some people might not eat much after 8 o’clock, and some people might skip breakfast,” Dr. Yancy said. “And if that’s the case, then it’s not going to make a big impact on their weight probably.”
Medication is also an important consideration. Not eating can be dangerous for patients taking short-acting insulin or sulfonylureas, according to Dr. Yancy.
Ms. Pavlou said these findings show intermittent fasting is another option for patients with type 2 diabetes trying to lose weight. “If you’ve tried calorie counting, that’s not working for you or if you’re kind of burnt out, this is something else that you could try,” she said.
“We have a lot of patients that need to lose weight, and we have patients who respond differently to different approaches,” said Dr. Yancy. “So having various approaches is really valuable.”
The manuscript is currently under review at JAMA Internal Medicine, said Ms. Pavlou.
A version of this article appeared on Medscape.com.
BOSTON –
For the study, 57 overweight and obese participants with type 2 diabetes were randomly assigned to three different groups: The first group ate between noon and 8 p.m., the second was asked to reduce caloric intake by 25% of maintenance calories, and the third, a control group, continued eating normally.
The calorie-restriction group tracked intake on MyFitnessPal, an app that logs the calorie content of different foods. Both the intermittent-fasting and calorie-restriction groups were assigned a dietitian to help with adherence.
After 6 months, participants in the intermittent-fasting group lost about 4.3% of body weight – the equivalent of 10 pounds of weight loss for a person weighing 230 pounds – whereas participants in the calorie-restriction group lost about 2.5% of body weight.
The difference between the two groups was not significant, so one approach isn’t necessarily better than the other for weight loss.
“Let’s not think of this as an approach that’s better than calorie restriction,” William Yancy, MD, MHS, an internist and weight management specialist at Duke Lifestyle and Weight Management Center, Durham, N.C., said in an interview. “It’s an alternative approach to calorie restriction.”
Participants’ willingness to adhere to the diet likely accounted for the percentage difference between the groups, study author Vasiliki Pavlou, RDN, told this news organization. Ms. Pavlou presented the findings at the Nutrition 2023 conference.
“People that have type 2 diabetes, they’ve already been to the doctor, they’ve already been told to count calories,” said Ms. Pavlou, a doctoral student at the University of Illinois at Chicago. “There were many weeks where they came to us with nothing on MyFitnessPal and we’d have to encourage them to start tracking again.”
The intermittent-fasting group adhered to the eating time window 6 out of 7 days of the week, with a 1-hour grace period for the noon-to-8-p.m. window. In comparison, one-third of the calorie-restriction group didn’t stay within 200 calories of the goal, according to Ms. Pavlou.
That meant the fasting group cut about 100 calories more per day than the calorie-restriction group, which was reflected in their weight loss, Ms. Pavlou said.
A1c levels dropped by about 1% in both the intermittent-fasting and calorie-restriction groups – a meaningful decrease, said Dr. Yancy. “I think a 0.5% difference would have some clinical significance in terms of complications from diabetes,” he said. “So 1% would be even more clinically meaningful.”
However, fewer participants taking insulin in the calorie-restriction group could explain the difference, according to Ms. Pavlou. “Usually, when someone goes on insulin, their pancreas is already not functioning as well,” she said. “And it’s way harder to see improvements in their A1c and glycemic control.”
Up to 90% of people with type 2 diabetes are overweight or obese. Weight loss is one of the major components of type 2 diabetes care, according to the American Diabetes Association, and studies have shown that even a 5% reduction in body weight can reduce blood glucose concentration and A1c. Some studies suggest diabetes remission can occur after a 10% loss in body weight, but Dr. Yancy said it depends on the person.
“It depends on the individual, their metabolic situation, how long they’ve had diabetes, what kind of approach they’re following, maybe what medicines they’re taking,” Dr. Yancy said. “There’s a lot of different factors involved in remission.”
The study cohort generally had advanced diabetes and was taking a mix of medications, so the results might not be applicable to people with a more recent diabetes diagnosis, according to Ms. Pavlou.
Dr. Yancy said intermittent fasting could work well for the right person. The success of the approach could depend on a person’s eating habits and whether their meals usually fall outside the time-restricted window, or it could depend on how well a person follows rules, according to Dr. Yancy.
“Some people might not eat much after 8 o’clock, and some people might skip breakfast,” Dr. Yancy said. “And if that’s the case, then it’s not going to make a big impact on their weight probably.”
Medication is also an important consideration. Not eating can be dangerous for patients taking short-acting insulin or sulfonylureas, according to Dr. Yancy.
Ms. Pavlou said these findings show intermittent fasting is another option for patients with type 2 diabetes trying to lose weight. “If you’ve tried calorie counting, that’s not working for you or if you’re kind of burnt out, this is something else that you could try,” she said.
“We have a lot of patients that need to lose weight, and we have patients who respond differently to different approaches,” said Dr. Yancy. “So having various approaches is really valuable.”
The manuscript is currently under review at JAMA Internal Medicine, said Ms. Pavlou.
A version of this article appeared on Medscape.com.
AT NUTRITION 2023
Does use of continuous or flash glucose monitors decrease hypoglycemia episodes in T2D?
Evidence summary
Continuous glucose monitoring: Nonsignificant reductions in event rates
A 2021 multicenter RCT (N = 175) evaluated CGM effectiveness in patients with basal insulin–treated T2D.1 Patients (mean age, 57 years; mean A1C, 9.1%) wore a blinded CGM device for baseline glucose measurement (minimum of 168 hours) before being randomly assigned to either CGM (n = 116) or traditional blood glucose monitoring (BGM; n = 59). At 8-month follow-up, patients in the BGM group again had blinded sensors placed. A significant reduction in hypoglycemia duration was observed for the CGM group vs the BGM group at 8 months for glucose values < 70 mg/mL (adjusted mean difference [aMD] = –0.24%; 95% CI, –0.42 to –0.05) and < 54 mg/dL (aMD = –0.10%; 95% CI, –0.15 to –0.04). A nonsignificant decrease in severe hypoglycemic events requiring resuscitative assistance occurred for BGM (2%) vs CGM (1%) patients. Study limitations included virtual visits due to COVID-19 and a short follow-up period.
A 2022 multicenter prospective study (N = 174) examined CGM effects on hypoglycemia frequency and severity in adults with T2D.2 Patients with insulin-requiring T2D (mean age, 61 years; mean A1C, 8.0%) participated in a 12-month study with 6 months of self-monitored blood glucose (SMBG) followed by 6 months of CGM use. The primary outcome was the rate of severe hypoglycemic events. A nonsignificant decrease was observed in the CGM group compared to the SMBG group for hypoglycemic event rate, per participant per 6-month period (relative risk [RR] = 0.43; 95% CI, 0.07-2.64). Four moderate hypoglycemic adverse events occurred in the SMBG phase vs 2 in the CGM phase. Financial support by the study sponsor decreases the study’s validity.
A 2021 prospective study (N = 90) evaluated the use of CGM to improve glycemic control.3 Patients younger than 66 years with insulin-treated T2D and an A1C > 7.5% participated in a 7-day blinded CGM cycle every 4 months for 1 year. A nonsignificant decrease in hypoglycemia duration was observed for glucose values < 70 mg/dL and < 54 mg/dL at 12 months. No change in hypoglycemic event rate was seen with the use of CGM. Funding by the device manufacturer was a limitation of this study.
Flash glucose monitoring: Mixed results on hypoglycemia events
A 2019 open-label RCT (N = 82) assessed the effectiveness of FGM on diabetes control.4 Patients with insulin-treated T2D were randomly assigned to the intervention or standard-care groups. The intervention group (n = 46; mean age, 66 years; mean A1C, 8.3%) used the FGM system for 10 weeks, while the standard-care group (n = 36; mean age, 70 years; mean A1C, 8.9%) maintained use of their glucometers. Both groups received similar types and duration of counseling. Treatment satisfaction was the primary outcome; total hypoglycemic events was a secondary outcome. No significant difference in the number of hypoglycemic episodes was observed between the intervention and control groups at 55 to 70 mg/dL (RR = 0.79; 95% CI, 0.44-1.4) or < 54 mg/dL (RR = 1.27; 95% CI, 0.38-4.2). No adverse events of severe hypoglycemia occurred during the study. Funding by the device manufacturer was a limitation of this study.
A 2017 open-label, multicenter RCT (N = 224) assessed FGM efficacy.5 Adults (mean age, 59 years; mean A1C, 8.8%) with T2D on intensive insulin therapy were randomized to FGM (n = 149) or SMBG (n = 75) after a 14-day masked baseline period. The 6-month treatment phase was unblinded. The duration of hypoglycemic events (glucose values < 70 mg/dL and < 55 mg/dL) was obtained from the sensors. Compared to the SMBG group, the FGM group spent 43% less time at < 70 mg/dL (aMD = –0.47 ± 0.13 h/d; P = .0006) and 53% less time at < 55 mg/dL (aMD = –0.22 ± 0.068 h/d; P = .0014). Hypoglycemic event rates significantly decreased by 28% (aMD = –0.16 ± 0.065; P = 0.016) and 44% (aMD = –0.12 ± 0.037; P = .0017) for glucose levels < 70 mg/dL and < 55 mg/dL, respectively. A nonsignificant difference occurred in severe hypoglycemic events requiring third-party assistance for the FGM (2%) vs control (1%) groups. Involvement of the device manufacturer and unblinded group allocations are study limitations.
A 2021 single-arm, multicenter prospective study looked at the impact of FGM on glycemic control in adults with insulin-treated T2D (N = 90; mean age, 64 years; mean A1C, 7.5%).6 After a 14-day baseline period consisting of masked sensor readings paired with self-monitored fingerstick tests, participants were followed for 11 weeks using the sensor to monitor glucose levels. The primary outcome was amount of time spent in hypoglycemia (< 70 mg/dL), with secondary outcomes including time and events in hypoglycemia (< 70, < 55, or < 45 mg/dL). No significant decrease in hypoglycemia duration or hypoglycemic event rates at < 70, < 55, or < 45 mg/dL was observed for FGM compared to baseline. Adverse events were observed in 64% of participants; 94% of the events were hypoglycemia related. Serious adverse events were reported for 5.3% of participants. The single-arm study format, lack of generalizability due to the single-race study population, and sponsor support were study limitations.
Editor’s takeaway
This reasonably good evidence shows a decrease in measured or monitored hypoglycemia, a disease-oriented outcome, but it did not reach statistical significance for symptomatic hypoglycemia (1% vs 2%), a patient-oriented outcome. Nevertheless, in patients reporting symptomatic hypoglycemia, a continuous or flash glucose monitor may allow for more aggressive glucose control.
1. Martens T, Beck RW, Bailey R, et al. Effect of continuous glucose monitoring on glycemic control in patients with type 2 diabetes treated with basal insulin: a randomized clinical trial. JAMA. 2021;325:2262-2272. doi: 10.1001/jama.2021.7444
2. Beck SE, Kelly C, Price DA. Non-adjunctive continuous glucose monitoring for control of hypoglycaemia (COACH): results of a post-approval observational study. Diabet Med. 2022;39:e14739. doi: 10.1111/dme.14739
3. Ribeiro RT, Andrade R, Nascimento do O D, et al. Impact of blinded retrospective continuous glucose monitoring on clinical decision making and glycemic control in persons with type 2 diabetes on insulin therapy. Nutr Metab Cardiovasc Dis. 2021;31:1267-1275. doi: 10.1016/j.numecd.2020.12.024
4. Yaron M, Roitman E, Aharon-Hananel G, et al. Effect of flash glucose monitoring technology on glycemic control and treatment satisfaction in patients with type 2 diabetes. Diabetes Care. 2019;42:1178-1184. doi: 10.2337/dc18-0166
5. Haak T, Hanaire H, Ajjan R, et al. Flash glucose-sensing technology as a replacement for blood glucose monitoring for the management of insulin-treated type 2 diabetes: a multicenter, open-label randomized controlled trial. Diabetes Ther. 2017;8:55-73. doi: 10.1007/s13300-016-0223-6
6. Ogawa W, Hirota Y, Osonoi T, et al. Effect of the FreeStyle Libre™ flash glucose monitoring system on glycemic control in individuals with type 2 diabetes treated with basal-bolus insulin therapy: an open label, prospective, multicenter trial in Japan. J Diabetes Investig. 2021;12:82-90. doi: 10.1111/jdi.13327
Evidence summary
Continuous glucose monitoring: Nonsignificant reductions in event rates
A 2021 multicenter RCT (N = 175) evaluated CGM effectiveness in patients with basal insulin–treated T2D.1 Patients (mean age, 57 years; mean A1C, 9.1%) wore a blinded CGM device for baseline glucose measurement (minimum of 168 hours) before being randomly assigned to either CGM (n = 116) or traditional blood glucose monitoring (BGM; n = 59). At 8-month follow-up, patients in the BGM group again had blinded sensors placed. A significant reduction in hypoglycemia duration was observed for the CGM group vs the BGM group at 8 months for glucose values < 70 mg/mL (adjusted mean difference [aMD] = –0.24%; 95% CI, –0.42 to –0.05) and < 54 mg/dL (aMD = –0.10%; 95% CI, –0.15 to –0.04). A nonsignificant decrease in severe hypoglycemic events requiring resuscitative assistance occurred for BGM (2%) vs CGM (1%) patients. Study limitations included virtual visits due to COVID-19 and a short follow-up period.
A 2022 multicenter prospective study (N = 174) examined CGM effects on hypoglycemia frequency and severity in adults with T2D.2 Patients with insulin-requiring T2D (mean age, 61 years; mean A1C, 8.0%) participated in a 12-month study with 6 months of self-monitored blood glucose (SMBG) followed by 6 months of CGM use. The primary outcome was the rate of severe hypoglycemic events. A nonsignificant decrease was observed in the CGM group compared to the SMBG group for hypoglycemic event rate, per participant per 6-month period (relative risk [RR] = 0.43; 95% CI, 0.07-2.64). Four moderate hypoglycemic adverse events occurred in the SMBG phase vs 2 in the CGM phase. Financial support by the study sponsor decreases the study’s validity.
A 2021 prospective study (N = 90) evaluated the use of CGM to improve glycemic control.3 Patients younger than 66 years with insulin-treated T2D and an A1C > 7.5% participated in a 7-day blinded CGM cycle every 4 months for 1 year. A nonsignificant decrease in hypoglycemia duration was observed for glucose values < 70 mg/dL and < 54 mg/dL at 12 months. No change in hypoglycemic event rate was seen with the use of CGM. Funding by the device manufacturer was a limitation of this study.
Flash glucose monitoring: Mixed results on hypoglycemia events
A 2019 open-label RCT (N = 82) assessed the effectiveness of FGM on diabetes control.4 Patients with insulin-treated T2D were randomly assigned to the intervention or standard-care groups. The intervention group (n = 46; mean age, 66 years; mean A1C, 8.3%) used the FGM system for 10 weeks, while the standard-care group (n = 36; mean age, 70 years; mean A1C, 8.9%) maintained use of their glucometers. Both groups received similar types and duration of counseling. Treatment satisfaction was the primary outcome; total hypoglycemic events was a secondary outcome. No significant difference in the number of hypoglycemic episodes was observed between the intervention and control groups at 55 to 70 mg/dL (RR = 0.79; 95% CI, 0.44-1.4) or < 54 mg/dL (RR = 1.27; 95% CI, 0.38-4.2). No adverse events of severe hypoglycemia occurred during the study. Funding by the device manufacturer was a limitation of this study.
A 2017 open-label, multicenter RCT (N = 224) assessed FGM efficacy.5 Adults (mean age, 59 years; mean A1C, 8.8%) with T2D on intensive insulin therapy were randomized to FGM (n = 149) or SMBG (n = 75) after a 14-day masked baseline period. The 6-month treatment phase was unblinded. The duration of hypoglycemic events (glucose values < 70 mg/dL and < 55 mg/dL) was obtained from the sensors. Compared to the SMBG group, the FGM group spent 43% less time at < 70 mg/dL (aMD = –0.47 ± 0.13 h/d; P = .0006) and 53% less time at < 55 mg/dL (aMD = –0.22 ± 0.068 h/d; P = .0014). Hypoglycemic event rates significantly decreased by 28% (aMD = –0.16 ± 0.065; P = 0.016) and 44% (aMD = –0.12 ± 0.037; P = .0017) for glucose levels < 70 mg/dL and < 55 mg/dL, respectively. A nonsignificant difference occurred in severe hypoglycemic events requiring third-party assistance for the FGM (2%) vs control (1%) groups. Involvement of the device manufacturer and unblinded group allocations are study limitations.
A 2021 single-arm, multicenter prospective study looked at the impact of FGM on glycemic control in adults with insulin-treated T2D (N = 90; mean age, 64 years; mean A1C, 7.5%).6 After a 14-day baseline period consisting of masked sensor readings paired with self-monitored fingerstick tests, participants were followed for 11 weeks using the sensor to monitor glucose levels. The primary outcome was amount of time spent in hypoglycemia (< 70 mg/dL), with secondary outcomes including time and events in hypoglycemia (< 70, < 55, or < 45 mg/dL). No significant decrease in hypoglycemia duration or hypoglycemic event rates at < 70, < 55, or < 45 mg/dL was observed for FGM compared to baseline. Adverse events were observed in 64% of participants; 94% of the events were hypoglycemia related. Serious adverse events were reported for 5.3% of participants. The single-arm study format, lack of generalizability due to the single-race study population, and sponsor support were study limitations.
Editor’s takeaway
This reasonably good evidence shows a decrease in measured or monitored hypoglycemia, a disease-oriented outcome, but it did not reach statistical significance for symptomatic hypoglycemia (1% vs 2%), a patient-oriented outcome. Nevertheless, in patients reporting symptomatic hypoglycemia, a continuous or flash glucose monitor may allow for more aggressive glucose control.
Evidence summary
Continuous glucose monitoring: Nonsignificant reductions in event rates
A 2021 multicenter RCT (N = 175) evaluated CGM effectiveness in patients with basal insulin–treated T2D.1 Patients (mean age, 57 years; mean A1C, 9.1%) wore a blinded CGM device for baseline glucose measurement (minimum of 168 hours) before being randomly assigned to either CGM (n = 116) or traditional blood glucose monitoring (BGM; n = 59). At 8-month follow-up, patients in the BGM group again had blinded sensors placed. A significant reduction in hypoglycemia duration was observed for the CGM group vs the BGM group at 8 months for glucose values < 70 mg/mL (adjusted mean difference [aMD] = –0.24%; 95% CI, –0.42 to –0.05) and < 54 mg/dL (aMD = –0.10%; 95% CI, –0.15 to –0.04). A nonsignificant decrease in severe hypoglycemic events requiring resuscitative assistance occurred for BGM (2%) vs CGM (1%) patients. Study limitations included virtual visits due to COVID-19 and a short follow-up period.
A 2022 multicenter prospective study (N = 174) examined CGM effects on hypoglycemia frequency and severity in adults with T2D.2 Patients with insulin-requiring T2D (mean age, 61 years; mean A1C, 8.0%) participated in a 12-month study with 6 months of self-monitored blood glucose (SMBG) followed by 6 months of CGM use. The primary outcome was the rate of severe hypoglycemic events. A nonsignificant decrease was observed in the CGM group compared to the SMBG group for hypoglycemic event rate, per participant per 6-month period (relative risk [RR] = 0.43; 95% CI, 0.07-2.64). Four moderate hypoglycemic adverse events occurred in the SMBG phase vs 2 in the CGM phase. Financial support by the study sponsor decreases the study’s validity.
A 2021 prospective study (N = 90) evaluated the use of CGM to improve glycemic control.3 Patients younger than 66 years with insulin-treated T2D and an A1C > 7.5% participated in a 7-day blinded CGM cycle every 4 months for 1 year. A nonsignificant decrease in hypoglycemia duration was observed for glucose values < 70 mg/dL and < 54 mg/dL at 12 months. No change in hypoglycemic event rate was seen with the use of CGM. Funding by the device manufacturer was a limitation of this study.
Flash glucose monitoring: Mixed results on hypoglycemia events
A 2019 open-label RCT (N = 82) assessed the effectiveness of FGM on diabetes control.4 Patients with insulin-treated T2D were randomly assigned to the intervention or standard-care groups. The intervention group (n = 46; mean age, 66 years; mean A1C, 8.3%) used the FGM system for 10 weeks, while the standard-care group (n = 36; mean age, 70 years; mean A1C, 8.9%) maintained use of their glucometers. Both groups received similar types and duration of counseling. Treatment satisfaction was the primary outcome; total hypoglycemic events was a secondary outcome. No significant difference in the number of hypoglycemic episodes was observed between the intervention and control groups at 55 to 70 mg/dL (RR = 0.79; 95% CI, 0.44-1.4) or < 54 mg/dL (RR = 1.27; 95% CI, 0.38-4.2). No adverse events of severe hypoglycemia occurred during the study. Funding by the device manufacturer was a limitation of this study.
A 2017 open-label, multicenter RCT (N = 224) assessed FGM efficacy.5 Adults (mean age, 59 years; mean A1C, 8.8%) with T2D on intensive insulin therapy were randomized to FGM (n = 149) or SMBG (n = 75) after a 14-day masked baseline period. The 6-month treatment phase was unblinded. The duration of hypoglycemic events (glucose values < 70 mg/dL and < 55 mg/dL) was obtained from the sensors. Compared to the SMBG group, the FGM group spent 43% less time at < 70 mg/dL (aMD = –0.47 ± 0.13 h/d; P = .0006) and 53% less time at < 55 mg/dL (aMD = –0.22 ± 0.068 h/d; P = .0014). Hypoglycemic event rates significantly decreased by 28% (aMD = –0.16 ± 0.065; P = 0.016) and 44% (aMD = –0.12 ± 0.037; P = .0017) for glucose levels < 70 mg/dL and < 55 mg/dL, respectively. A nonsignificant difference occurred in severe hypoglycemic events requiring third-party assistance for the FGM (2%) vs control (1%) groups. Involvement of the device manufacturer and unblinded group allocations are study limitations.
A 2021 single-arm, multicenter prospective study looked at the impact of FGM on glycemic control in adults with insulin-treated T2D (N = 90; mean age, 64 years; mean A1C, 7.5%).6 After a 14-day baseline period consisting of masked sensor readings paired with self-monitored fingerstick tests, participants were followed for 11 weeks using the sensor to monitor glucose levels. The primary outcome was amount of time spent in hypoglycemia (< 70 mg/dL), with secondary outcomes including time and events in hypoglycemia (< 70, < 55, or < 45 mg/dL). No significant decrease in hypoglycemia duration or hypoglycemic event rates at < 70, < 55, or < 45 mg/dL was observed for FGM compared to baseline. Adverse events were observed in 64% of participants; 94% of the events were hypoglycemia related. Serious adverse events were reported for 5.3% of participants. The single-arm study format, lack of generalizability due to the single-race study population, and sponsor support were study limitations.
Editor’s takeaway
This reasonably good evidence shows a decrease in measured or monitored hypoglycemia, a disease-oriented outcome, but it did not reach statistical significance for symptomatic hypoglycemia (1% vs 2%), a patient-oriented outcome. Nevertheless, in patients reporting symptomatic hypoglycemia, a continuous or flash glucose monitor may allow for more aggressive glucose control.
1. Martens T, Beck RW, Bailey R, et al. Effect of continuous glucose monitoring on glycemic control in patients with type 2 diabetes treated with basal insulin: a randomized clinical trial. JAMA. 2021;325:2262-2272. doi: 10.1001/jama.2021.7444
2. Beck SE, Kelly C, Price DA. Non-adjunctive continuous glucose monitoring for control of hypoglycaemia (COACH): results of a post-approval observational study. Diabet Med. 2022;39:e14739. doi: 10.1111/dme.14739
3. Ribeiro RT, Andrade R, Nascimento do O D, et al. Impact of blinded retrospective continuous glucose monitoring on clinical decision making and glycemic control in persons with type 2 diabetes on insulin therapy. Nutr Metab Cardiovasc Dis. 2021;31:1267-1275. doi: 10.1016/j.numecd.2020.12.024
4. Yaron M, Roitman E, Aharon-Hananel G, et al. Effect of flash glucose monitoring technology on glycemic control and treatment satisfaction in patients with type 2 diabetes. Diabetes Care. 2019;42:1178-1184. doi: 10.2337/dc18-0166
5. Haak T, Hanaire H, Ajjan R, et al. Flash glucose-sensing technology as a replacement for blood glucose monitoring for the management of insulin-treated type 2 diabetes: a multicenter, open-label randomized controlled trial. Diabetes Ther. 2017;8:55-73. doi: 10.1007/s13300-016-0223-6
6. Ogawa W, Hirota Y, Osonoi T, et al. Effect of the FreeStyle Libre™ flash glucose monitoring system on glycemic control in individuals with type 2 diabetes treated with basal-bolus insulin therapy: an open label, prospective, multicenter trial in Japan. J Diabetes Investig. 2021;12:82-90. doi: 10.1111/jdi.13327
1. Martens T, Beck RW, Bailey R, et al. Effect of continuous glucose monitoring on glycemic control in patients with type 2 diabetes treated with basal insulin: a randomized clinical trial. JAMA. 2021;325:2262-2272. doi: 10.1001/jama.2021.7444
2. Beck SE, Kelly C, Price DA. Non-adjunctive continuous glucose monitoring for control of hypoglycaemia (COACH): results of a post-approval observational study. Diabet Med. 2022;39:e14739. doi: 10.1111/dme.14739
3. Ribeiro RT, Andrade R, Nascimento do O D, et al. Impact of blinded retrospective continuous glucose monitoring on clinical decision making and glycemic control in persons with type 2 diabetes on insulin therapy. Nutr Metab Cardiovasc Dis. 2021;31:1267-1275. doi: 10.1016/j.numecd.2020.12.024
4. Yaron M, Roitman E, Aharon-Hananel G, et al. Effect of flash glucose monitoring technology on glycemic control and treatment satisfaction in patients with type 2 diabetes. Diabetes Care. 2019;42:1178-1184. doi: 10.2337/dc18-0166
5. Haak T, Hanaire H, Ajjan R, et al. Flash glucose-sensing technology as a replacement for blood glucose monitoring for the management of insulin-treated type 2 diabetes: a multicenter, open-label randomized controlled trial. Diabetes Ther. 2017;8:55-73. doi: 10.1007/s13300-016-0223-6
6. Ogawa W, Hirota Y, Osonoi T, et al. Effect of the FreeStyle Libre™ flash glucose monitoring system on glycemic control in individuals with type 2 diabetes treated with basal-bolus insulin therapy: an open label, prospective, multicenter trial in Japan. J Diabetes Investig. 2021;12:82-90. doi: 10.1111/jdi.13327
EVIDENCE-BASED REVIEW:
NO. In adults with insulin-treated type 2 diabetes (T2D), continuous glucose monitoring (CGM) and flash glucose monitoring (FGM) do not decrease symptomatic hypoglycemia episodes (strength of recommendation [SOR], B) but do lower time in hypoglycemia (SOR, C; disease-oriented evidence).
CGM, in which glucose levels are sent automatically in numeric and graphic format to a patient’s smart device for their potential action, did not change the hypoglycemic event rate (SOR, B; 2 prospective studies). CGM significantly reduced hypoglycemia duration in an 8-month randomized controlled trial (RCT; SOR, C) but not in a 1-year prospective study (SOR, C).
FGM, in which glucose levels are sent on demand to a device, did not significantly reduce hypoglycemic episodes (SOR, B; 1 small RCT and 1 prospective study). Hypoglycemia duration was reduced significantly with FGM in a 6-month RCT (SOR, B) but not in a 1-year prospective study (SOR, B).

An Atypical Discussion of the Link Between Metabolic Syndrome and Type 2 Diabetes—and the Use of Precision Medicine to Treat the Whole Patient
Metabolic syndrome, type 2 diabetes mellitus (T2DM), and the “diabetes syndrome,” are interrelated, serious health conditions that share common risk factors and mechanisms. While they are each distinct conditions, a significant association exists between them, with metabolic syndrome often being considered a precursor to the development of typical T2DM.
Metabolic syndrome is a cluster of individual metabolic abnormalities that includes a combination of risk factors such as abdominal obesity, high blood pressure, elevated insulin levels, high triglyceride levels, and low levels of high-density lipoprotein (HDL) cholesterol related to genes and epigenetic changes associated with insulin resistance. These risk factors increase the likelihood of developing cardiovascular diseases, such as heart disease and stroke, and, when combined with significant damage to β -cell function and the influence of concordant environmental precipitants, result in hyperglycemia/overt diabetes—classically defined as T2DM.
It is estimated that there will be a staggering 3.1 billion people living with T2DM by 2050, according to a recent article in The Lancet. This devastating number will place a heavy burden on the health care system.
However, this typical pathophysiologic definition of T2DM is imprecise. Twenty percent of patients with T2DM have islet-cell antibodies that are typical of the immune destruction of β-cells in patients with type 1 diabetes mellitus (T1DM). Furthermore, approximately 40% of patients with T1DM have insulin resistance.
Thus, to better understand and distinguish the disease processes unique to each individual, we have defined a new beta cell classification for all forms of diabetes mellitus (DM). In this classification, there are 4 common pathophysiologic causes of all DM (including classic T2DM), with resultant damage to the β-cells (ie, genetic and epigenetic changes, inflammation, an abnormal environment, and insulin resistance), which results in 11 mechanisms of hyperglycemia, represented as “the egregious eleven” in Figure 1.
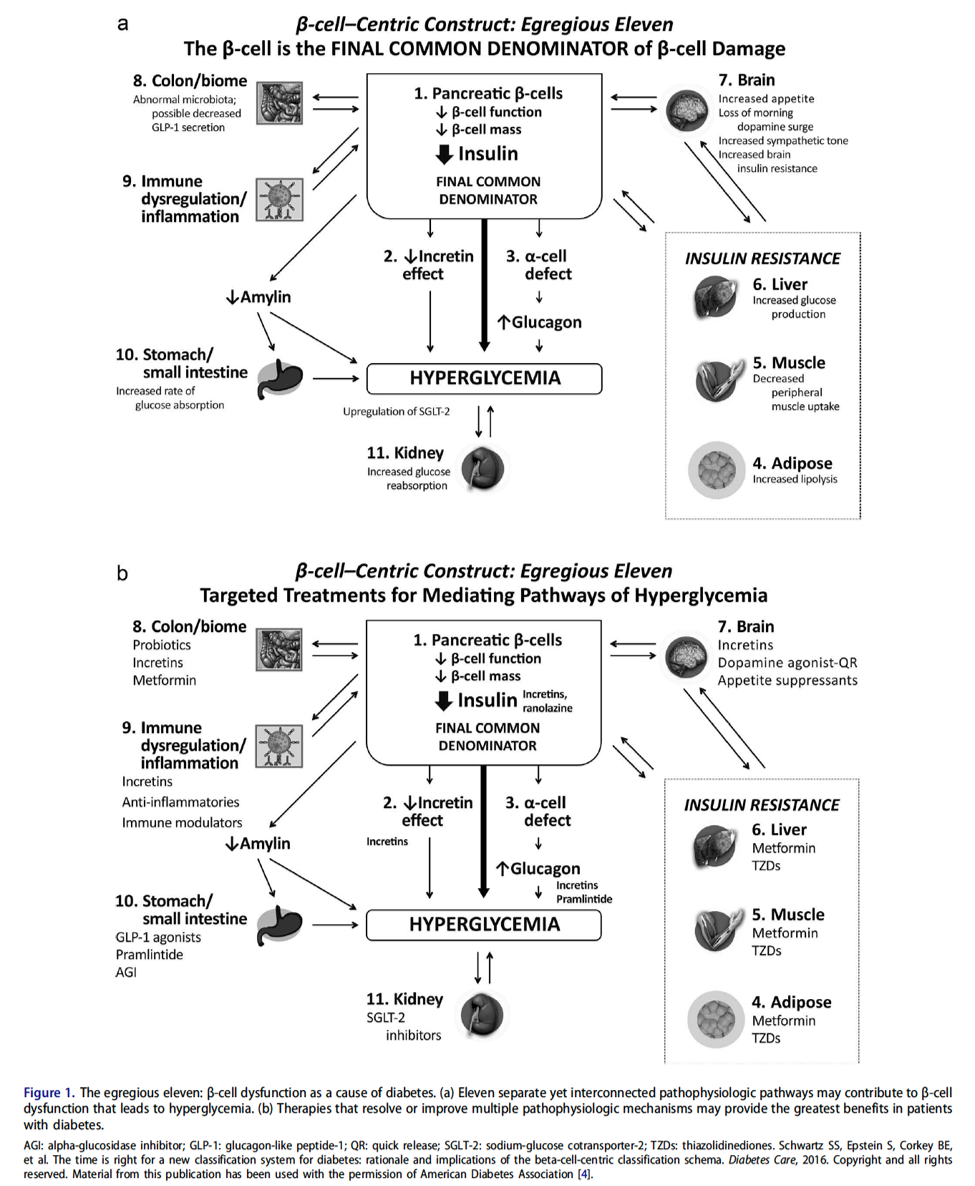
Additionally, Figure 2 illustrates the association between overlapping genes/epigenetic changes responsible for DM and the increased susceptibility to developing various microvascular complications commonly observed in all forms of DM, including classic T2DM. These complications, now recognized as components of the diabetes syndrome, encompass a range of conditions with shared interrelated pathophysiologic mechanisms, such as arteriosclerotic vascular disease (ASVD), dementia, some cancers, nonalcoholic fatty liver disease or nonalcoholic steatohepatitis (NAFLD/NASH), or psoriasis.
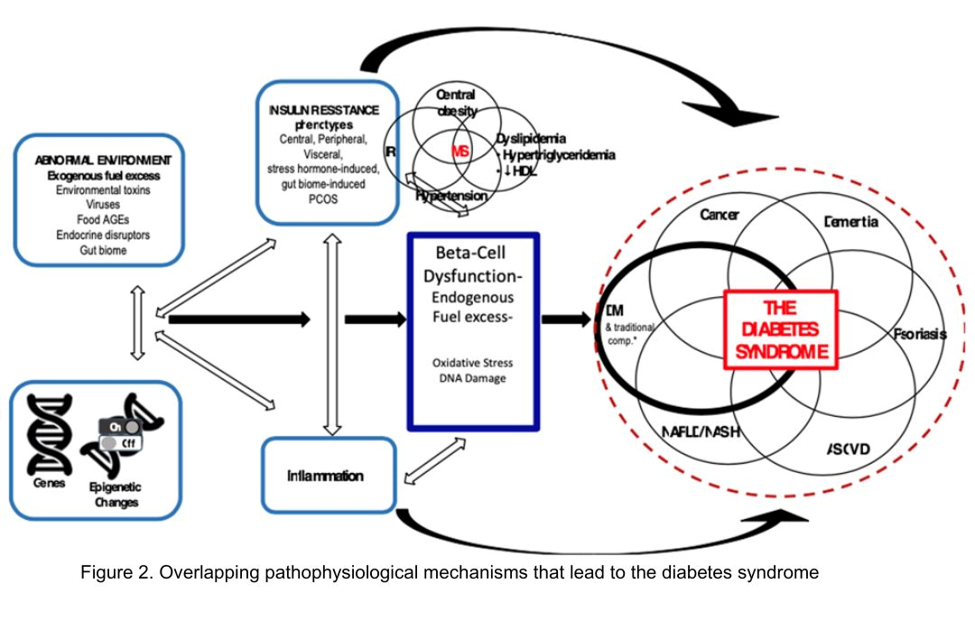
The likelihood of developing a specific type of DM, with classic complications or associated conditions, is contingent on an individual’s genes, epigenetic factors, inflammation, insulin resistance, and environmental exposures over time. It has now been postulated that these factors can be identified in a particular individual by a set of genomics, metabolomics, proteomics, and markers of these processes.
This more precise approach has the added benefit of giving rise to a more accurate individualization of therapy—precision medicine.
Precision medicine is an approach to healthcare that considers an individual's specific characteristics, such as genetic makeup, lifestyle, and environmental factors, to tailor medical treatments and interventions. In the context of this discussion on T2DM, precision medicine’s goal is to provide targeted therapies and interventions based on an individual's unique -omic profile to improve treatment outcomes and minimize side effects. An additional benefit of precision medicine use in diabetes syndrome is giving the diabetes specialist the opportunity to treat the whole patient, looking for complications and associated conditions earlier via defining the presence or absence of various markers of their individual pathophysiology. Additionally, we have come to recognize that many of the medications for treating T2DM (eg, glucagon-like peptide 1 receptor agonists [GLP-1 RA], dipeptidyl peptidase 4 inhibitors [DPP-4 inhibitors], sodium-glucose cotransporter-2 inhibitors [SGLT-2 inhibitors], metformin, Cycloset [bromocriptine mesylate]) can offer other benefits for the patient—treating not only multiple mechanisms of hyperglycemia (the egregious eleven: use the fewest number of agents in combination to treat the most number of mechanisms of hyperglycemia) but also recognize that they can prevent and treat the complications and associated conditions of the diabetes syndrome: cardiovascular, renal, liver, some cancers, psoriasis, and dementia.
The classic link between metabolic syndrome and T2DM is important to consider when applying precision medicine approaches to the management of T2DM. Here are some examples of how precision medicine is being applied in the management of T2DM:
Genetic testing: Genetic testing can help identify specific genetic variants or mutations that may influence an individual's risk of developing T2DM or their response to certain medications. By understanding a person's genetic predisposition, clinicians can make more informed decisions about treatment options and develop personalized strategies for their patients.
Pharmacogenomics: Certain genetic variations can impact how a person metabolizes and responds to specific diabetes medications. By analyzing an individual's genetic profile, medications that are more likely to be effective and have fewer adverse effects for that patient may be selected.
Continuous glucose monitoring (CGM): CGM devices provide real-time information about an individual’s blood glucose levels, allowing for more precise management of diabetes. By continuously monitoring glucose levels, patterns can be identified, allowing for adjustments to medication dosages, dietary recommendations, and lifestyle modifications on an individualized basis.
Lifestyle interventions: Precision medicine also recognizes that lifestyle factors play a crucial role in the development and management of T2DM. Lifestyle interventions, such as diet and exercise plans, based on an individual's preferences, metabolic profile, and response to different interventions can be personalized (ie, some individuals may benefit more from a low-carbohydrate diet, while others may respond better to a Mediterranean-style diet).
Predictive modeling and risk stratification: Precision medicine leverages data analytics and predictive modeling to assess an individual's risk of developing complications associated with T2DM. By analyzing various factors such as medical history, genetics, lifestyle, and biomarkers, individuals who are at a higher risk of developing complications can be identified, and their treatment plans can be tailored accordingly. Precision medicine enables early identification of individuals who are at a higher risk of developing T2DM based on their metabolic syndrome status.
In summary, precision medicine for T2DM considers the link between metabolic syndrome and diabetes syndrome to develop personalized approaches for prevention, early intervention, and treatment. By understanding an individual's metabolic and genetic profile, targeted strategies to optimize management and improve outcomes for patients with metabolic syndrome and those at risk of developing diabetes can be implemented.
It is important to note that while precision medicine holds promise in improving diabetes management, it is still an evolving field, and its widespread implementation is not yet fully realized. Collaboration between clinicians, researchers, and technological advancements will continue to drive the progress of precision medicine in T2DM management.
Metabolic syndrome, type 2 diabetes mellitus (T2DM), and the “diabetes syndrome,” are interrelated, serious health conditions that share common risk factors and mechanisms. While they are each distinct conditions, a significant association exists between them, with metabolic syndrome often being considered a precursor to the development of typical T2DM.
Metabolic syndrome is a cluster of individual metabolic abnormalities that includes a combination of risk factors such as abdominal obesity, high blood pressure, elevated insulin levels, high triglyceride levels, and low levels of high-density lipoprotein (HDL) cholesterol related to genes and epigenetic changes associated with insulin resistance. These risk factors increase the likelihood of developing cardiovascular diseases, such as heart disease and stroke, and, when combined with significant damage to β -cell function and the influence of concordant environmental precipitants, result in hyperglycemia/overt diabetes—classically defined as T2DM.
It is estimated that there will be a staggering 3.1 billion people living with T2DM by 2050, according to a recent article in The Lancet. This devastating number will place a heavy burden on the health care system.
However, this typical pathophysiologic definition of T2DM is imprecise. Twenty percent of patients with T2DM have islet-cell antibodies that are typical of the immune destruction of β-cells in patients with type 1 diabetes mellitus (T1DM). Furthermore, approximately 40% of patients with T1DM have insulin resistance.
Thus, to better understand and distinguish the disease processes unique to each individual, we have defined a new beta cell classification for all forms of diabetes mellitus (DM). In this classification, there are 4 common pathophysiologic causes of all DM (including classic T2DM), with resultant damage to the β-cells (ie, genetic and epigenetic changes, inflammation, an abnormal environment, and insulin resistance), which results in 11 mechanisms of hyperglycemia, represented as “the egregious eleven” in Figure 1.
Additionally, Figure 2 illustrates the association between overlapping genes/epigenetic changes responsible for DM and the increased susceptibility to developing various microvascular complications commonly observed in all forms of DM, including classic T2DM. These complications, now recognized as components of the diabetes syndrome, encompass a range of conditions with shared interrelated pathophysiologic mechanisms, such as arteriosclerotic vascular disease (ASVD), dementia, some cancers, nonalcoholic fatty liver disease or nonalcoholic steatohepatitis (NAFLD/NASH), or psoriasis.
The likelihood of developing a specific type of DM, with classic complications or associated conditions, is contingent on an individual’s genes, epigenetic factors, inflammation, insulin resistance, and environmental exposures over time. It has now been postulated that these factors can be identified in a particular individual by a set of genomics, metabolomics, proteomics, and markers of these processes.
This more precise approach has the added benefit of giving rise to a more accurate individualization of therapy—precision medicine.
Precision medicine is an approach to healthcare that considers an individual's specific characteristics, such as genetic makeup, lifestyle, and environmental factors, to tailor medical treatments and interventions. In the context of this discussion on T2DM, precision medicine’s goal is to provide targeted therapies and interventions based on an individual's unique -omic profile to improve treatment outcomes and minimize side effects. An additional benefit of precision medicine use in diabetes syndrome is giving the diabetes specialist the opportunity to treat the whole patient, looking for complications and associated conditions earlier via defining the presence or absence of various markers of their individual pathophysiology. Additionally, we have come to recognize that many of the medications for treating T2DM (eg, glucagon-like peptide 1 receptor agonists [GLP-1 RA], dipeptidyl peptidase 4 inhibitors [DPP-4 inhibitors], sodium-glucose cotransporter-2 inhibitors [SGLT-2 inhibitors], metformin, Cycloset [bromocriptine mesylate]) can offer other benefits for the patient—treating not only multiple mechanisms of hyperglycemia (the egregious eleven: use the fewest number of agents in combination to treat the most number of mechanisms of hyperglycemia) but also recognize that they can prevent and treat the complications and associated conditions of the diabetes syndrome: cardiovascular, renal, liver, some cancers, psoriasis, and dementia.
The classic link between metabolic syndrome and T2DM is important to consider when applying precision medicine approaches to the management of T2DM. Here are some examples of how precision medicine is being applied in the management of T2DM:
Genetic testing: Genetic testing can help identify specific genetic variants or mutations that may influence an individual's risk of developing T2DM or their response to certain medications. By understanding a person's genetic predisposition, clinicians can make more informed decisions about treatment options and develop personalized strategies for their patients.
Pharmacogenomics: Certain genetic variations can impact how a person metabolizes and responds to specific diabetes medications. By analyzing an individual's genetic profile, medications that are more likely to be effective and have fewer adverse effects for that patient may be selected.
Continuous glucose monitoring (CGM): CGM devices provide real-time information about an individual’s blood glucose levels, allowing for more precise management of diabetes. By continuously monitoring glucose levels, patterns can be identified, allowing for adjustments to medication dosages, dietary recommendations, and lifestyle modifications on an individualized basis.
Lifestyle interventions: Precision medicine also recognizes that lifestyle factors play a crucial role in the development and management of T2DM. Lifestyle interventions, such as diet and exercise plans, based on an individual's preferences, metabolic profile, and response to different interventions can be personalized (ie, some individuals may benefit more from a low-carbohydrate diet, while others may respond better to a Mediterranean-style diet).
Predictive modeling and risk stratification: Precision medicine leverages data analytics and predictive modeling to assess an individual's risk of developing complications associated with T2DM. By analyzing various factors such as medical history, genetics, lifestyle, and biomarkers, individuals who are at a higher risk of developing complications can be identified, and their treatment plans can be tailored accordingly. Precision medicine enables early identification of individuals who are at a higher risk of developing T2DM based on their metabolic syndrome status.
In summary, precision medicine for T2DM considers the link between metabolic syndrome and diabetes syndrome to develop personalized approaches for prevention, early intervention, and treatment. By understanding an individual's metabolic and genetic profile, targeted strategies to optimize management and improve outcomes for patients with metabolic syndrome and those at risk of developing diabetes can be implemented.
It is important to note that while precision medicine holds promise in improving diabetes management, it is still an evolving field, and its widespread implementation is not yet fully realized. Collaboration between clinicians, researchers, and technological advancements will continue to drive the progress of precision medicine in T2DM management.
Metabolic syndrome, type 2 diabetes mellitus (T2DM), and the “diabetes syndrome,” are interrelated, serious health conditions that share common risk factors and mechanisms. While they are each distinct conditions, a significant association exists between them, with metabolic syndrome often being considered a precursor to the development of typical T2DM.
Metabolic syndrome is a cluster of individual metabolic abnormalities that includes a combination of risk factors such as abdominal obesity, high blood pressure, elevated insulin levels, high triglyceride levels, and low levels of high-density lipoprotein (HDL) cholesterol related to genes and epigenetic changes associated with insulin resistance. These risk factors increase the likelihood of developing cardiovascular diseases, such as heart disease and stroke, and, when combined with significant damage to β -cell function and the influence of concordant environmental precipitants, result in hyperglycemia/overt diabetes—classically defined as T2DM.
It is estimated that there will be a staggering 3.1 billion people living with T2DM by 2050, according to a recent article in The Lancet. This devastating number will place a heavy burden on the health care system.
However, this typical pathophysiologic definition of T2DM is imprecise. Twenty percent of patients with T2DM have islet-cell antibodies that are typical of the immune destruction of β-cells in patients with type 1 diabetes mellitus (T1DM). Furthermore, approximately 40% of patients with T1DM have insulin resistance.
Thus, to better understand and distinguish the disease processes unique to each individual, we have defined a new beta cell classification for all forms of diabetes mellitus (DM). In this classification, there are 4 common pathophysiologic causes of all DM (including classic T2DM), with resultant damage to the β-cells (ie, genetic and epigenetic changes, inflammation, an abnormal environment, and insulin resistance), which results in 11 mechanisms of hyperglycemia, represented as “the egregious eleven” in Figure 1.
Additionally, Figure 2 illustrates the association between overlapping genes/epigenetic changes responsible for DM and the increased susceptibility to developing various microvascular complications commonly observed in all forms of DM, including classic T2DM. These complications, now recognized as components of the diabetes syndrome, encompass a range of conditions with shared interrelated pathophysiologic mechanisms, such as arteriosclerotic vascular disease (ASVD), dementia, some cancers, nonalcoholic fatty liver disease or nonalcoholic steatohepatitis (NAFLD/NASH), or psoriasis.
The likelihood of developing a specific type of DM, with classic complications or associated conditions, is contingent on an individual’s genes, epigenetic factors, inflammation, insulin resistance, and environmental exposures over time. It has now been postulated that these factors can be identified in a particular individual by a set of genomics, metabolomics, proteomics, and markers of these processes.
This more precise approach has the added benefit of giving rise to a more accurate individualization of therapy—precision medicine.
Precision medicine is an approach to healthcare that considers an individual's specific characteristics, such as genetic makeup, lifestyle, and environmental factors, to tailor medical treatments and interventions. In the context of this discussion on T2DM, precision medicine’s goal is to provide targeted therapies and interventions based on an individual's unique -omic profile to improve treatment outcomes and minimize side effects. An additional benefit of precision medicine use in diabetes syndrome is giving the diabetes specialist the opportunity to treat the whole patient, looking for complications and associated conditions earlier via defining the presence or absence of various markers of their individual pathophysiology. Additionally, we have come to recognize that many of the medications for treating T2DM (eg, glucagon-like peptide 1 receptor agonists [GLP-1 RA], dipeptidyl peptidase 4 inhibitors [DPP-4 inhibitors], sodium-glucose cotransporter-2 inhibitors [SGLT-2 inhibitors], metformin, Cycloset [bromocriptine mesylate]) can offer other benefits for the patient—treating not only multiple mechanisms of hyperglycemia (the egregious eleven: use the fewest number of agents in combination to treat the most number of mechanisms of hyperglycemia) but also recognize that they can prevent and treat the complications and associated conditions of the diabetes syndrome: cardiovascular, renal, liver, some cancers, psoriasis, and dementia.
The classic link between metabolic syndrome and T2DM is important to consider when applying precision medicine approaches to the management of T2DM. Here are some examples of how precision medicine is being applied in the management of T2DM:
Genetic testing: Genetic testing can help identify specific genetic variants or mutations that may influence an individual's risk of developing T2DM or their response to certain medications. By understanding a person's genetic predisposition, clinicians can make more informed decisions about treatment options and develop personalized strategies for their patients.
Pharmacogenomics: Certain genetic variations can impact how a person metabolizes and responds to specific diabetes medications. By analyzing an individual's genetic profile, medications that are more likely to be effective and have fewer adverse effects for that patient may be selected.
Continuous glucose monitoring (CGM): CGM devices provide real-time information about an individual’s blood glucose levels, allowing for more precise management of diabetes. By continuously monitoring glucose levels, patterns can be identified, allowing for adjustments to medication dosages, dietary recommendations, and lifestyle modifications on an individualized basis.
Lifestyle interventions: Precision medicine also recognizes that lifestyle factors play a crucial role in the development and management of T2DM. Lifestyle interventions, such as diet and exercise plans, based on an individual's preferences, metabolic profile, and response to different interventions can be personalized (ie, some individuals may benefit more from a low-carbohydrate diet, while others may respond better to a Mediterranean-style diet).
Predictive modeling and risk stratification: Precision medicine leverages data analytics and predictive modeling to assess an individual's risk of developing complications associated with T2DM. By analyzing various factors such as medical history, genetics, lifestyle, and biomarkers, individuals who are at a higher risk of developing complications can be identified, and their treatment plans can be tailored accordingly. Precision medicine enables early identification of individuals who are at a higher risk of developing T2DM based on their metabolic syndrome status.
In summary, precision medicine for T2DM considers the link between metabolic syndrome and diabetes syndrome to develop personalized approaches for prevention, early intervention, and treatment. By understanding an individual's metabolic and genetic profile, targeted strategies to optimize management and improve outcomes for patients with metabolic syndrome and those at risk of developing diabetes can be implemented.
It is important to note that while precision medicine holds promise in improving diabetes management, it is still an evolving field, and its widespread implementation is not yet fully realized. Collaboration between clinicians, researchers, and technological advancements will continue to drive the progress of precision medicine in T2DM management.
How a heat wave affects glycemic control
TOPLINE:
, according to research published online May 17 in Science of The Total Environment.
METHODOLOGY:
Researchers in Spain analyzed data from 2,701 adults with type 1 diabetes who had been using intermittently scanned continuous glucose monitoring (CGM) devices during a 2022 heat wave (July 9-26) and 14 days after. Extreme heat claimed nearly 62,000 lives across Europe in the summer of 2022.
TAKEAWAY:
Time in range (between 70 mg/dL and 180 mg/dL of interstitial glucose) decreased by 4%, from 60.8% during the heat wave to 54.8% after (P < .001).
Patients who scanned their CGM results the most during the heat wave (more than 13 scans per day) scanned less often after the weather broke (1.8 fewer scans per day) and experienced the biggest drop in time in range (−5.4%).
More patients met all time-in-range recommendations during the heat wave (10.6% vs. 8.4%, P < .001).
IN PRACTICE:
“We hypothesized that people with diabetes, who are highly vulnerable, have more time for self-management as they spend more time indoors,” study author Jesús Moreno Fernández, MD, PhD, said in an interview. “During the COVID-19 pandemic, something similar was observed among people with diabetes.”
SOURCE:
Moreno Fernández, with the department of endocrinology and nutrition at Ciudad Real General University Hospital in Spain, is the study’s lead author.
LIMITATIONS:
The CGM data were anonymized, so researchers could not examine how individual patient factors like sex, education, or treatment type may have influenced outcomes. Temperatures remained higher than usual even after the heat wave. Worsening glycemic control could be interpreted as a lag effect of prolonged heat exposure, the researchers note.
DISCLOSURES:
The authors reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
, according to research published online May 17 in Science of The Total Environment.
METHODOLOGY:
Researchers in Spain analyzed data from 2,701 adults with type 1 diabetes who had been using intermittently scanned continuous glucose monitoring (CGM) devices during a 2022 heat wave (July 9-26) and 14 days after. Extreme heat claimed nearly 62,000 lives across Europe in the summer of 2022.
TAKEAWAY:
Time in range (between 70 mg/dL and 180 mg/dL of interstitial glucose) decreased by 4%, from 60.8% during the heat wave to 54.8% after (P < .001).
Patients who scanned their CGM results the most during the heat wave (more than 13 scans per day) scanned less often after the weather broke (1.8 fewer scans per day) and experienced the biggest drop in time in range (−5.4%).
More patients met all time-in-range recommendations during the heat wave (10.6% vs. 8.4%, P < .001).
IN PRACTICE:
“We hypothesized that people with diabetes, who are highly vulnerable, have more time for self-management as they spend more time indoors,” study author Jesús Moreno Fernández, MD, PhD, said in an interview. “During the COVID-19 pandemic, something similar was observed among people with diabetes.”
SOURCE:
Moreno Fernández, with the department of endocrinology and nutrition at Ciudad Real General University Hospital in Spain, is the study’s lead author.
LIMITATIONS:
The CGM data were anonymized, so researchers could not examine how individual patient factors like sex, education, or treatment type may have influenced outcomes. Temperatures remained higher than usual even after the heat wave. Worsening glycemic control could be interpreted as a lag effect of prolonged heat exposure, the researchers note.
DISCLOSURES:
The authors reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
, according to research published online May 17 in Science of The Total Environment.
METHODOLOGY:
Researchers in Spain analyzed data from 2,701 adults with type 1 diabetes who had been using intermittently scanned continuous glucose monitoring (CGM) devices during a 2022 heat wave (July 9-26) and 14 days after. Extreme heat claimed nearly 62,000 lives across Europe in the summer of 2022.
TAKEAWAY:
Time in range (between 70 mg/dL and 180 mg/dL of interstitial glucose) decreased by 4%, from 60.8% during the heat wave to 54.8% after (P < .001).
Patients who scanned their CGM results the most during the heat wave (more than 13 scans per day) scanned less often after the weather broke (1.8 fewer scans per day) and experienced the biggest drop in time in range (−5.4%).
More patients met all time-in-range recommendations during the heat wave (10.6% vs. 8.4%, P < .001).
IN PRACTICE:
“We hypothesized that people with diabetes, who are highly vulnerable, have more time for self-management as they spend more time indoors,” study author Jesús Moreno Fernández, MD, PhD, said in an interview. “During the COVID-19 pandemic, something similar was observed among people with diabetes.”
SOURCE:
Moreno Fernández, with the department of endocrinology and nutrition at Ciudad Real General University Hospital in Spain, is the study’s lead author.
LIMITATIONS:
The CGM data were anonymized, so researchers could not examine how individual patient factors like sex, education, or treatment type may have influenced outcomes. Temperatures remained higher than usual even after the heat wave. Worsening glycemic control could be interpreted as a lag effect of prolonged heat exposure, the researchers note.
DISCLOSURES:
The authors reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM SCIENCE OF THE TOTAL ENVIRONMENT
Goodbye, finger sticks; hello, CGMs
Nearly 90% of diabetes management in the United States is provided by primary care clinicians; diabetes is the fifth most common reason for a primary care visit. State-of-the-art technology such as continuous glucose monitors (CGMs) will inevitably transform the management of diabetes in primary care. Clinicians and staff must be ready to educate, counsel, and support primary care patients in the use of CGMs.
CGMs (also called glucose sensors) are small, minimally invasive devices that attach to the skin of the upper arm or trunk. A tiny electrode in the subcutaneous space prompts an enzyme reaction that measures the interstitial (rather than blood) glucose concentration, typically every 5 minutes. The results are displayed on an accompanying reader or transmitted to an app on the user’s mobile phone.
CGMs could eliminate the need for finger-stick blood glucose testing, which until now, has been the much-despised gold standard for self-monitoring of glucose levels in diabetes. Despite being relatively inexpensive and accurate, finger-stick glucose tests are inconvenient and often painful. But of greater significance is this downside: Finger-stick monitoring reveals the patient’s blood glucose concentration at a single point in time, which can be difficult to interpret. Is the blood glucose rising or falling? Multiple finger-stick tests are required to determine the trend of a patient’s glucose levels or the response to food or exercise.
In contrast, the graphic display from a CGM sensor is more like a movie, telling a story as it unfolds. Uninterrupted data provide valuable feedback to patients about the effects of diet, physical activity, stress, or pain on their glucose levels. And for the first time, it’s easy to determine the proportion of time the patient spends in or out of the target glucose range.
Incorporating new technology into your practice may seem like a burden, but the reward is better information that leads to better management of diabetes. If you’re new to glucose sensors, many excellent resources are available to learn how to use them.
I recommend starting with a website called diabeteswise.org, which has both a patient-facing and clinician-facing version. This unbranded site serves as a kind of Consumer Reports for diabetes technology, allowing both patients and professionals to compare and contrast currently available CGM devices.
DiabetesWisePro has information ranging from CGM device fundamentals and best practices to CGM prescribing and reimbursement.
Clinical Diabetes also provides multiple tools to help incorporate these devices into primary care clinical practice, including:
• Continuous Glucose Monitoring: Optimizing Diabetes Care (CME course).
• Diabetes Technology in Primary Care.
The next article in this series will cover two types of CGMs used in primary care: professional and personal devices.
Dr. Shubrook is a professor in the department of primary care, Touro University California College of Osteopathic Medicine, Vallejo, Calif., and director of diabetes services, Solano County Family Health Services, Fairfield, Calif. He disclosed ties with Abbott, Astra Zeneca, Bayer, Nevro, and Novo Nordisk.
A version of this article first appeared on Medscape.com.
Nearly 90% of diabetes management in the United States is provided by primary care clinicians; diabetes is the fifth most common reason for a primary care visit. State-of-the-art technology such as continuous glucose monitors (CGMs) will inevitably transform the management of diabetes in primary care. Clinicians and staff must be ready to educate, counsel, and support primary care patients in the use of CGMs.
CGMs (also called glucose sensors) are small, minimally invasive devices that attach to the skin of the upper arm or trunk. A tiny electrode in the subcutaneous space prompts an enzyme reaction that measures the interstitial (rather than blood) glucose concentration, typically every 5 minutes. The results are displayed on an accompanying reader or transmitted to an app on the user’s mobile phone.
CGMs could eliminate the need for finger-stick blood glucose testing, which until now, has been the much-despised gold standard for self-monitoring of glucose levels in diabetes. Despite being relatively inexpensive and accurate, finger-stick glucose tests are inconvenient and often painful. But of greater significance is this downside: Finger-stick monitoring reveals the patient’s blood glucose concentration at a single point in time, which can be difficult to interpret. Is the blood glucose rising or falling? Multiple finger-stick tests are required to determine the trend of a patient’s glucose levels or the response to food or exercise.
In contrast, the graphic display from a CGM sensor is more like a movie, telling a story as it unfolds. Uninterrupted data provide valuable feedback to patients about the effects of diet, physical activity, stress, or pain on their glucose levels. And for the first time, it’s easy to determine the proportion of time the patient spends in or out of the target glucose range.
Incorporating new technology into your practice may seem like a burden, but the reward is better information that leads to better management of diabetes. If you’re new to glucose sensors, many excellent resources are available to learn how to use them.
I recommend starting with a website called diabeteswise.org, which has both a patient-facing and clinician-facing version. This unbranded site serves as a kind of Consumer Reports for diabetes technology, allowing both patients and professionals to compare and contrast currently available CGM devices.
DiabetesWisePro has information ranging from CGM device fundamentals and best practices to CGM prescribing and reimbursement.
Clinical Diabetes also provides multiple tools to help incorporate these devices into primary care clinical practice, including:
• Continuous Glucose Monitoring: Optimizing Diabetes Care (CME course).
• Diabetes Technology in Primary Care.
The next article in this series will cover two types of CGMs used in primary care: professional and personal devices.
Dr. Shubrook is a professor in the department of primary care, Touro University California College of Osteopathic Medicine, Vallejo, Calif., and director of diabetes services, Solano County Family Health Services, Fairfield, Calif. He disclosed ties with Abbott, Astra Zeneca, Bayer, Nevro, and Novo Nordisk.
A version of this article first appeared on Medscape.com.
Nearly 90% of diabetes management in the United States is provided by primary care clinicians; diabetes is the fifth most common reason for a primary care visit. State-of-the-art technology such as continuous glucose monitors (CGMs) will inevitably transform the management of diabetes in primary care. Clinicians and staff must be ready to educate, counsel, and support primary care patients in the use of CGMs.
CGMs (also called glucose sensors) are small, minimally invasive devices that attach to the skin of the upper arm or trunk. A tiny electrode in the subcutaneous space prompts an enzyme reaction that measures the interstitial (rather than blood) glucose concentration, typically every 5 minutes. The results are displayed on an accompanying reader or transmitted to an app on the user’s mobile phone.
CGMs could eliminate the need for finger-stick blood glucose testing, which until now, has been the much-despised gold standard for self-monitoring of glucose levels in diabetes. Despite being relatively inexpensive and accurate, finger-stick glucose tests are inconvenient and often painful. But of greater significance is this downside: Finger-stick monitoring reveals the patient’s blood glucose concentration at a single point in time, which can be difficult to interpret. Is the blood glucose rising or falling? Multiple finger-stick tests are required to determine the trend of a patient’s glucose levels or the response to food or exercise.
In contrast, the graphic display from a CGM sensor is more like a movie, telling a story as it unfolds. Uninterrupted data provide valuable feedback to patients about the effects of diet, physical activity, stress, or pain on their glucose levels. And for the first time, it’s easy to determine the proportion of time the patient spends in or out of the target glucose range.
Incorporating new technology into your practice may seem like a burden, but the reward is better information that leads to better management of diabetes. If you’re new to glucose sensors, many excellent resources are available to learn how to use them.
I recommend starting with a website called diabeteswise.org, which has both a patient-facing and clinician-facing version. This unbranded site serves as a kind of Consumer Reports for diabetes technology, allowing both patients and professionals to compare and contrast currently available CGM devices.
DiabetesWisePro has information ranging from CGM device fundamentals and best practices to CGM prescribing and reimbursement.
Clinical Diabetes also provides multiple tools to help incorporate these devices into primary care clinical practice, including:
• Continuous Glucose Monitoring: Optimizing Diabetes Care (CME course).
• Diabetes Technology in Primary Care.
The next article in this series will cover two types of CGMs used in primary care: professional and personal devices.
Dr. Shubrook is a professor in the department of primary care, Touro University California College of Osteopathic Medicine, Vallejo, Calif., and director of diabetes services, Solano County Family Health Services, Fairfield, Calif. He disclosed ties with Abbott, Astra Zeneca, Bayer, Nevro, and Novo Nordisk.
A version of this article first appeared on Medscape.com.