User login
Night Owls May Be at Greater Risk for T2D, Beyond Lifestyle
MADRID — research presented at the annual meeting of the European Association for the Study of Diabetes suggested.
In the study, night owls were almost 50% more likely to develop T2D than those who went to sleep earlier.
“The magnitude of this risk was more than I expected, [although] residual confounding may have occurred,” said Jeroen van der Velde, PhD, Leiden University Medical Center in the Netherlands, who presented the study.
“Late chronotype has previously been associated with unhealthy lifestyle and overweight or obesity and, subsequently, cardiometabolic diseases,” he said in an interview. However, although the current study found that individuals with late chronotypes did indeed have larger waists and more visceral fat, “we (and others) believe that lifestyle cannot fully explain the relation between late chronotype and metabolic disorders.”
“In addition,” he noted, “previous studies that observed that late chronotype is associated with overweight or obesity mainly focused on body mass index [BMI]. However, BMI alone does not provide accurate information regarding fat distribution in the body. People with similar BMI may have different underlying fat distribution, and this may be more relevant than BMI for metabolic risk.”
The researchers examined associations between chronotype and BMI, waist circumference, visceral fat, liver fat, and the risk for T2D in a middle-aged population from the Netherlands Epidemiology of Obesity study. Among the 5026 participants, the mean age was 56 years, 54% were women, and mean BMI was 30.
Using data from the study, the study investigators calculated the midpoint of sleep (MPS) and divided participants into three chronotypes: Early MPS < 2:30 PM (20% of participants); intermediate MPS 2:30–4:00 PM (reference category; 60% of participants); and late MPS ≥ 4:00 PM (20% of participants). BMI and waist circumference were measured in all participants, and visceral fat and liver fat were measured in 1576 participants using MRI scans and MR spectroscopy, respectively.
During a median follow-up of 6.6 years, 225 participants were diagnosed with T2D. After adjustment for age, sex, education, physical activity, smoking, alcohol intake, diet quality, sleep quality and duration, and total body fat, participants with a late chronotype had a 46% increased risk for T2D.
Further, those with a late chronotype had 0.7 higher BMI, 1.9-cm larger waist circumference, 7 cm2 more visceral fat, and 14% more liver fat.
Body Clock Out of Sync?
“Late chronotype was associated with increased ectopic body fat and with an increased risk of T2D independent of lifestyle factors and is an emerging risk factor for metabolic diseases,” the researchers concluded.
“A likely explanation is that the circadian rhythm or body clock in late chronotypes is out of sync with the work and social schedules followed by society,” Dr. van der Velde suggested. “This can lead to circadian misalignment, which we know can lead to metabolic disturbances and ultimately type 2 diabetes.”
Might trying to adjust chronotype earlier in life have an effect on risk?
“Chronotype, as measured via midpoint of sleep, does change a lot in the first 30 years or so in life,” he said. “After that it seems to stabilize. I suppose that if you adapt an intermediate or early chronotype around the age of 30 years, this will help to maintain an earlier chronotype later in life, although we cannot answer this from our study.”
Nevertheless, with respect to T2D risk, “chronotype is likely only part of the puzzle,” he noted.
“People with late chronotypes typically eat late in the evening, and this has also been associated with adverse metabolic effects. At this stage, we do not know if a person changes his/her chronotype that this will also lead to metabolic improvements. More research is needed before we can make recommendations regarding chronotype and timing of other lifestyle behaviors.”
Commenting on the study, Gianluca Iacobellis, MD, PhD, director of the University of Miami Hospital Diabetes Service, Coral Gables, Florida, said: “Interesting data. Altering the physiological circadian rhythm can affect the complex hormonal system — including cortisol, ghrelin, leptin, and serotonin — that regulates insulin sensitivity, glucose, and blood pressure control. The night owl may become more insulin resistant and therefore at higher risk of developing diabetes.”
Like Dr. van der Velde, he noted that “late sleep may be associated with night binging that can cause weight gain and ultimately obesity, further increasing the risk of diabetes.”
Dr. Iacobellis’s group recently showed that vital exhaustion, which is characterized by fatigue and loss of vigor, is associated with a higher cardiovascular risk for and markers of visceral adiposity.
“Abnormal circadian rhythms can be easily associated with vital exhaustion,” he said. Therefore, night owls with more visceral than peripheral fat accumulation might also be at higher cardiometabolic risk through that mechanism.
“However environmental factors and family history can play an important role too,” he added.
Regardless of the mechanisms involved, “preventive actions should be taken to educate teenagers and individuals at higher risk to have healthy sleep habits,” Dr. Iacobellis concluded.
No information regarding funding was provided; Dr. van der Velde and Dr. Iacobellis reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
MADRID — research presented at the annual meeting of the European Association for the Study of Diabetes suggested.
In the study, night owls were almost 50% more likely to develop T2D than those who went to sleep earlier.
“The magnitude of this risk was more than I expected, [although] residual confounding may have occurred,” said Jeroen van der Velde, PhD, Leiden University Medical Center in the Netherlands, who presented the study.
“Late chronotype has previously been associated with unhealthy lifestyle and overweight or obesity and, subsequently, cardiometabolic diseases,” he said in an interview. However, although the current study found that individuals with late chronotypes did indeed have larger waists and more visceral fat, “we (and others) believe that lifestyle cannot fully explain the relation between late chronotype and metabolic disorders.”
“In addition,” he noted, “previous studies that observed that late chronotype is associated with overweight or obesity mainly focused on body mass index [BMI]. However, BMI alone does not provide accurate information regarding fat distribution in the body. People with similar BMI may have different underlying fat distribution, and this may be more relevant than BMI for metabolic risk.”
The researchers examined associations between chronotype and BMI, waist circumference, visceral fat, liver fat, and the risk for T2D in a middle-aged population from the Netherlands Epidemiology of Obesity study. Among the 5026 participants, the mean age was 56 years, 54% were women, and mean BMI was 30.
Using data from the study, the study investigators calculated the midpoint of sleep (MPS) and divided participants into three chronotypes: Early MPS < 2:30 PM (20% of participants); intermediate MPS 2:30–4:00 PM (reference category; 60% of participants); and late MPS ≥ 4:00 PM (20% of participants). BMI and waist circumference were measured in all participants, and visceral fat and liver fat were measured in 1576 participants using MRI scans and MR spectroscopy, respectively.
During a median follow-up of 6.6 years, 225 participants were diagnosed with T2D. After adjustment for age, sex, education, physical activity, smoking, alcohol intake, diet quality, sleep quality and duration, and total body fat, participants with a late chronotype had a 46% increased risk for T2D.
Further, those with a late chronotype had 0.7 higher BMI, 1.9-cm larger waist circumference, 7 cm2 more visceral fat, and 14% more liver fat.
Body Clock Out of Sync?
“Late chronotype was associated with increased ectopic body fat and with an increased risk of T2D independent of lifestyle factors and is an emerging risk factor for metabolic diseases,” the researchers concluded.
“A likely explanation is that the circadian rhythm or body clock in late chronotypes is out of sync with the work and social schedules followed by society,” Dr. van der Velde suggested. “This can lead to circadian misalignment, which we know can lead to metabolic disturbances and ultimately type 2 diabetes.”
Might trying to adjust chronotype earlier in life have an effect on risk?
“Chronotype, as measured via midpoint of sleep, does change a lot in the first 30 years or so in life,” he said. “After that it seems to stabilize. I suppose that if you adapt an intermediate or early chronotype around the age of 30 years, this will help to maintain an earlier chronotype later in life, although we cannot answer this from our study.”
Nevertheless, with respect to T2D risk, “chronotype is likely only part of the puzzle,” he noted.
“People with late chronotypes typically eat late in the evening, and this has also been associated with adverse metabolic effects. At this stage, we do not know if a person changes his/her chronotype that this will also lead to metabolic improvements. More research is needed before we can make recommendations regarding chronotype and timing of other lifestyle behaviors.”
Commenting on the study, Gianluca Iacobellis, MD, PhD, director of the University of Miami Hospital Diabetes Service, Coral Gables, Florida, said: “Interesting data. Altering the physiological circadian rhythm can affect the complex hormonal system — including cortisol, ghrelin, leptin, and serotonin — that regulates insulin sensitivity, glucose, and blood pressure control. The night owl may become more insulin resistant and therefore at higher risk of developing diabetes.”
Like Dr. van der Velde, he noted that “late sleep may be associated with night binging that can cause weight gain and ultimately obesity, further increasing the risk of diabetes.”
Dr. Iacobellis’s group recently showed that vital exhaustion, which is characterized by fatigue and loss of vigor, is associated with a higher cardiovascular risk for and markers of visceral adiposity.
“Abnormal circadian rhythms can be easily associated with vital exhaustion,” he said. Therefore, night owls with more visceral than peripheral fat accumulation might also be at higher cardiometabolic risk through that mechanism.
“However environmental factors and family history can play an important role too,” he added.
Regardless of the mechanisms involved, “preventive actions should be taken to educate teenagers and individuals at higher risk to have healthy sleep habits,” Dr. Iacobellis concluded.
No information regarding funding was provided; Dr. van der Velde and Dr. Iacobellis reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
MADRID — research presented at the annual meeting of the European Association for the Study of Diabetes suggested.
In the study, night owls were almost 50% more likely to develop T2D than those who went to sleep earlier.
“The magnitude of this risk was more than I expected, [although] residual confounding may have occurred,” said Jeroen van der Velde, PhD, Leiden University Medical Center in the Netherlands, who presented the study.
“Late chronotype has previously been associated with unhealthy lifestyle and overweight or obesity and, subsequently, cardiometabolic diseases,” he said in an interview. However, although the current study found that individuals with late chronotypes did indeed have larger waists and more visceral fat, “we (and others) believe that lifestyle cannot fully explain the relation between late chronotype and metabolic disorders.”
“In addition,” he noted, “previous studies that observed that late chronotype is associated with overweight or obesity mainly focused on body mass index [BMI]. However, BMI alone does not provide accurate information regarding fat distribution in the body. People with similar BMI may have different underlying fat distribution, and this may be more relevant than BMI for metabolic risk.”
The researchers examined associations between chronotype and BMI, waist circumference, visceral fat, liver fat, and the risk for T2D in a middle-aged population from the Netherlands Epidemiology of Obesity study. Among the 5026 participants, the mean age was 56 years, 54% were women, and mean BMI was 30.
Using data from the study, the study investigators calculated the midpoint of sleep (MPS) and divided participants into three chronotypes: Early MPS < 2:30 PM (20% of participants); intermediate MPS 2:30–4:00 PM (reference category; 60% of participants); and late MPS ≥ 4:00 PM (20% of participants). BMI and waist circumference were measured in all participants, and visceral fat and liver fat were measured in 1576 participants using MRI scans and MR spectroscopy, respectively.
During a median follow-up of 6.6 years, 225 participants were diagnosed with T2D. After adjustment for age, sex, education, physical activity, smoking, alcohol intake, diet quality, sleep quality and duration, and total body fat, participants with a late chronotype had a 46% increased risk for T2D.
Further, those with a late chronotype had 0.7 higher BMI, 1.9-cm larger waist circumference, 7 cm2 more visceral fat, and 14% more liver fat.
Body Clock Out of Sync?
“Late chronotype was associated with increased ectopic body fat and with an increased risk of T2D independent of lifestyle factors and is an emerging risk factor for metabolic diseases,” the researchers concluded.
“A likely explanation is that the circadian rhythm or body clock in late chronotypes is out of sync with the work and social schedules followed by society,” Dr. van der Velde suggested. “This can lead to circadian misalignment, which we know can lead to metabolic disturbances and ultimately type 2 diabetes.”
Might trying to adjust chronotype earlier in life have an effect on risk?
“Chronotype, as measured via midpoint of sleep, does change a lot in the first 30 years or so in life,” he said. “After that it seems to stabilize. I suppose that if you adapt an intermediate or early chronotype around the age of 30 years, this will help to maintain an earlier chronotype later in life, although we cannot answer this from our study.”
Nevertheless, with respect to T2D risk, “chronotype is likely only part of the puzzle,” he noted.
“People with late chronotypes typically eat late in the evening, and this has also been associated with adverse metabolic effects. At this stage, we do not know if a person changes his/her chronotype that this will also lead to metabolic improvements. More research is needed before we can make recommendations regarding chronotype and timing of other lifestyle behaviors.”
Commenting on the study, Gianluca Iacobellis, MD, PhD, director of the University of Miami Hospital Diabetes Service, Coral Gables, Florida, said: “Interesting data. Altering the physiological circadian rhythm can affect the complex hormonal system — including cortisol, ghrelin, leptin, and serotonin — that regulates insulin sensitivity, glucose, and blood pressure control. The night owl may become more insulin resistant and therefore at higher risk of developing diabetes.”
Like Dr. van der Velde, he noted that “late sleep may be associated with night binging that can cause weight gain and ultimately obesity, further increasing the risk of diabetes.”
Dr. Iacobellis’s group recently showed that vital exhaustion, which is characterized by fatigue and loss of vigor, is associated with a higher cardiovascular risk for and markers of visceral adiposity.
“Abnormal circadian rhythms can be easily associated with vital exhaustion,” he said. Therefore, night owls with more visceral than peripheral fat accumulation might also be at higher cardiometabolic risk through that mechanism.
“However environmental factors and family history can play an important role too,” he added.
Regardless of the mechanisms involved, “preventive actions should be taken to educate teenagers and individuals at higher risk to have healthy sleep habits,” Dr. Iacobellis concluded.
No information regarding funding was provided; Dr. van der Velde and Dr. Iacobellis reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM EASD 2024
Will Tirzepatide Vials Help Patients? Endos Weigh in
Tirzepatide (Zepbound) is not in shortage for now, but the weight loss drug has remained inaccessible to people without insurance coverage who can’t afford to pay out of pocket. Now, its manufacturer, Eli Lilly, has introduced a new formulation it says will “significantly expand” the supply. But not all endocrinologists are enthusiastic.
As of August 27, LillyDirect made 2.5-mg and 5-mg single-dose vials of tirzepatide available to self-pay patients with an on-label electronic prescription. Lilly’s announcement said the single-dose vials “are priced at a 50% or greater discount compared to the list price of all other incretin (glucagon-like peptide 1 receptor agonists or GLP-1) medicines for obesity.”
For a 4-week supply of the weekly injections, the discount at LillyDirect translates to $399 for a 2.5-mg single-dose vial ($99.75 per vial) and $549 for the 5-mg dose ($137.25 per vial), which the company noted was “in line with the Zepbound savings program for noncovered individuals.” (The new direct single-dose prescriptions cannot be filled at community or retail pharmacies.)
“In a clinical study, the 5-mg maintenance dose helped patients achieve an average of 15% weight loss after 72 weeks of treatment and has been a powerful tool for millions of people with obesity looking to lose weight and keep it off,” according to the announcement.
The clinical study, which is not named or referenced in the announcement, is SURMOUNT-1, a Lilly spokesperson said in an interview. Yet, that study also found that patients achieved an average weight loss of 19.5% with 10-mg doses and 20.9% with 15-mg doses of tirzepatide. Furthermore, the percentage of participants achieving body weight reductions of ≥ 5% was 85% (5 mg), 89% (10 mg), and 91% (15 mg), showing the benefits of higher doses.
And there’s the rub.
‘Only Two Different Doses’
Anne Peters, MD, a professor of clinical medicine and a clinical scholar at the University of Southern California, Los Angeles, said in an interview: “My concern is, they’re only providing two different doses, 2.5 mg and 5 mg. You get somebody on it, and then they still have to go back to the traditional pens. I’m very opposed to getting patients connected to a medication they can’t then continue to take.
“Now we have starter doses that are easy to come by,” she said. “But the problem isn’t starting. The problem for all of these patients is chronic continuation of the right dose of the drug, and out-of-pocket costs become exorbitantly higher when they have to self-purchase the pens for the higher doses.
“Yes, the 5-mg dose has benefits, but not the same as higher doses,” she continued. “I have nobody for whom 5 mg is the right dose. They have to take more, sometimes within a month or 2 of starting, in order to achieve the kind of weight loss they need.”
If their insurance doesn’t cover the drug, “what are they going to do to stay on 5 mg? Or pay a crapload of money to buy three of the 5-mg doses to reach a higher dose?”
Michael Weintraub, MD, clinical assistant professor in the Department of Medicine, Division of Endocrinology, Diabetes, and Metabolism at New York University Grossman School of Medicine in New York City, said that, “for many, this lower monthly cost is attainable and is a significant advancement in increasing access. For others, however, an out-of-pocket monthly cost of $349-549 for a chronic medication is still unaffordable.”
And like Dr. Peters, he said, “some patients do not lose a clinically significant amount of weight with 2.5 mg or 5 mg and require higher doses. There is no way of prescribing a higher dose of Zepbound vials, so patients would have to resort to the higher-dose auto-injector pens that are still double the price.”
A Lilly spokesperson countered in a comment: “Offering Zepbound single-dose vials in higher dosage strengths could increase the potential for dose splitting, which is not contemplated by the FDA [Food and Drug Adminstration]–approved label and may pose patient safety risks.”
But Dr. Peters wondered: “Wouldn’t dose splitting of a known-to-be-pure compound be better than getting it at a compounding pharmacy that lacks purity/safety? The one message from all of this is that patients need to know what they’re getting into. They’re starting a drug that can help with weight loss, but they’re going to be on a sub-max dose. And a higher dose is going to be double the price.”
In addition, said Robert F. Kushner, MD, a professor at Northwestern University Feinberg School of Medicine in Chicago, Illinois, “for the lower-dose vials, instead of administering the drug with a self-auto-injection pen, patients will need to use a needle and syringe and draw up the dose from a vial. This will take a higher skill level and health literacy that may be challenging for some patients. Patients may need additional training on how to use this new formulation. That will take additional time and resources, such as a demonstration in the office or referral to video.”
The Lilly news release noted that “patients can also purchase ancillary supplies, like syringes and needles, and will have access to important patient-friendly instructional materials on correctly administering the medicine via needle and syringe.”
Protection From Compounders?
According to the Lilly spokesperson, the launch of Zepbound vials “furthers our commitment to helping patients avoid the risks associated with compounded products by providing patients another option for access to genuine Lilly medicine.”
Indeed, said Jaime Almandoz, MD, medical director of the Weight Wellness Program and associate professor of internal medicine at the University of Texas Southwestern Medical Center in Dallas, “The introduction of Zepbound/tirzepatide in single-dose vials should improve access to evidence-based obesity treatments, reducing potential risks associated with compounded additives and eliminating the need for patients to calculate correct medication doses,” which have led to accidental overdoses of compounded semaglutide.
Lilly’s spokesperson added: “We have taken multiple steps — including publishing an open letter and launching lilly.com/real-medicine — to warn the public about the risks posed by the proliferation of counterfeit, fake, unsafe, or untested knockoffs of Lilly’s genuine medicines.”
But whether these steps are strong enough to overcome the realities of cost and the need for affordable higher doses remains to be seen.
Scott Brunner, CEO of the Alliance for Pharmacy Compounding, said in a statement that the new version of Zepbound “is great news for patients. It’s a much more rational and care-focused response to the remarkable demand for their drug than the lawsuits and cease-and-desist letters Lilly has been raining down on compounding pharmacies.”
“For 20 months now,” he continued,
Dr. Almandoz affirmed: “Everyone wants to see improved access to evidence-based obesity care. It’s crucial to ensure patients receive the most appropriate interventions, whether it is lifestyle changes, medications, or bariatric surgery,” he said. “There are resources available, [including his recent paper], for nutrition and lifestyle modifications specifically for patients taking obesity medications, which can help clinicians guide their patients toward better health.”
Dr. Almandoz is a member of advisory boards and consults for: Novo Nordisk, Eli Lilly, and Boehringer Ingelheim. Dr. Kushner is an adviser to Eli Lilly and Novo Nordisk. Dr. Peters and Dr. Weintraub declared no competing interests.
A version of this article appeared on Medscape.com.
Tirzepatide (Zepbound) is not in shortage for now, but the weight loss drug has remained inaccessible to people without insurance coverage who can’t afford to pay out of pocket. Now, its manufacturer, Eli Lilly, has introduced a new formulation it says will “significantly expand” the supply. But not all endocrinologists are enthusiastic.
As of August 27, LillyDirect made 2.5-mg and 5-mg single-dose vials of tirzepatide available to self-pay patients with an on-label electronic prescription. Lilly’s announcement said the single-dose vials “are priced at a 50% or greater discount compared to the list price of all other incretin (glucagon-like peptide 1 receptor agonists or GLP-1) medicines for obesity.”
For a 4-week supply of the weekly injections, the discount at LillyDirect translates to $399 for a 2.5-mg single-dose vial ($99.75 per vial) and $549 for the 5-mg dose ($137.25 per vial), which the company noted was “in line with the Zepbound savings program for noncovered individuals.” (The new direct single-dose prescriptions cannot be filled at community or retail pharmacies.)
“In a clinical study, the 5-mg maintenance dose helped patients achieve an average of 15% weight loss after 72 weeks of treatment and has been a powerful tool for millions of people with obesity looking to lose weight and keep it off,” according to the announcement.
The clinical study, which is not named or referenced in the announcement, is SURMOUNT-1, a Lilly spokesperson said in an interview. Yet, that study also found that patients achieved an average weight loss of 19.5% with 10-mg doses and 20.9% with 15-mg doses of tirzepatide. Furthermore, the percentage of participants achieving body weight reductions of ≥ 5% was 85% (5 mg), 89% (10 mg), and 91% (15 mg), showing the benefits of higher doses.
And there’s the rub.
‘Only Two Different Doses’
Anne Peters, MD, a professor of clinical medicine and a clinical scholar at the University of Southern California, Los Angeles, said in an interview: “My concern is, they’re only providing two different doses, 2.5 mg and 5 mg. You get somebody on it, and then they still have to go back to the traditional pens. I’m very opposed to getting patients connected to a medication they can’t then continue to take.
“Now we have starter doses that are easy to come by,” she said. “But the problem isn’t starting. The problem for all of these patients is chronic continuation of the right dose of the drug, and out-of-pocket costs become exorbitantly higher when they have to self-purchase the pens for the higher doses.
“Yes, the 5-mg dose has benefits, but not the same as higher doses,” she continued. “I have nobody for whom 5 mg is the right dose. They have to take more, sometimes within a month or 2 of starting, in order to achieve the kind of weight loss they need.”
If their insurance doesn’t cover the drug, “what are they going to do to stay on 5 mg? Or pay a crapload of money to buy three of the 5-mg doses to reach a higher dose?”
Michael Weintraub, MD, clinical assistant professor in the Department of Medicine, Division of Endocrinology, Diabetes, and Metabolism at New York University Grossman School of Medicine in New York City, said that, “for many, this lower monthly cost is attainable and is a significant advancement in increasing access. For others, however, an out-of-pocket monthly cost of $349-549 for a chronic medication is still unaffordable.”
And like Dr. Peters, he said, “some patients do not lose a clinically significant amount of weight with 2.5 mg or 5 mg and require higher doses. There is no way of prescribing a higher dose of Zepbound vials, so patients would have to resort to the higher-dose auto-injector pens that are still double the price.”
A Lilly spokesperson countered in a comment: “Offering Zepbound single-dose vials in higher dosage strengths could increase the potential for dose splitting, which is not contemplated by the FDA [Food and Drug Adminstration]–approved label and may pose patient safety risks.”
But Dr. Peters wondered: “Wouldn’t dose splitting of a known-to-be-pure compound be better than getting it at a compounding pharmacy that lacks purity/safety? The one message from all of this is that patients need to know what they’re getting into. They’re starting a drug that can help with weight loss, but they’re going to be on a sub-max dose. And a higher dose is going to be double the price.”
In addition, said Robert F. Kushner, MD, a professor at Northwestern University Feinberg School of Medicine in Chicago, Illinois, “for the lower-dose vials, instead of administering the drug with a self-auto-injection pen, patients will need to use a needle and syringe and draw up the dose from a vial. This will take a higher skill level and health literacy that may be challenging for some patients. Patients may need additional training on how to use this new formulation. That will take additional time and resources, such as a demonstration in the office or referral to video.”
The Lilly news release noted that “patients can also purchase ancillary supplies, like syringes and needles, and will have access to important patient-friendly instructional materials on correctly administering the medicine via needle and syringe.”
Protection From Compounders?
According to the Lilly spokesperson, the launch of Zepbound vials “furthers our commitment to helping patients avoid the risks associated with compounded products by providing patients another option for access to genuine Lilly medicine.”
Indeed, said Jaime Almandoz, MD, medical director of the Weight Wellness Program and associate professor of internal medicine at the University of Texas Southwestern Medical Center in Dallas, “The introduction of Zepbound/tirzepatide in single-dose vials should improve access to evidence-based obesity treatments, reducing potential risks associated with compounded additives and eliminating the need for patients to calculate correct medication doses,” which have led to accidental overdoses of compounded semaglutide.
Lilly’s spokesperson added: “We have taken multiple steps — including publishing an open letter and launching lilly.com/real-medicine — to warn the public about the risks posed by the proliferation of counterfeit, fake, unsafe, or untested knockoffs of Lilly’s genuine medicines.”
But whether these steps are strong enough to overcome the realities of cost and the need for affordable higher doses remains to be seen.
Scott Brunner, CEO of the Alliance for Pharmacy Compounding, said in a statement that the new version of Zepbound “is great news for patients. It’s a much more rational and care-focused response to the remarkable demand for their drug than the lawsuits and cease-and-desist letters Lilly has been raining down on compounding pharmacies.”
“For 20 months now,” he continued,
Dr. Almandoz affirmed: “Everyone wants to see improved access to evidence-based obesity care. It’s crucial to ensure patients receive the most appropriate interventions, whether it is lifestyle changes, medications, or bariatric surgery,” he said. “There are resources available, [including his recent paper], for nutrition and lifestyle modifications specifically for patients taking obesity medications, which can help clinicians guide their patients toward better health.”
Dr. Almandoz is a member of advisory boards and consults for: Novo Nordisk, Eli Lilly, and Boehringer Ingelheim. Dr. Kushner is an adviser to Eli Lilly and Novo Nordisk. Dr. Peters and Dr. Weintraub declared no competing interests.
A version of this article appeared on Medscape.com.
Tirzepatide (Zepbound) is not in shortage for now, but the weight loss drug has remained inaccessible to people without insurance coverage who can’t afford to pay out of pocket. Now, its manufacturer, Eli Lilly, has introduced a new formulation it says will “significantly expand” the supply. But not all endocrinologists are enthusiastic.
As of August 27, LillyDirect made 2.5-mg and 5-mg single-dose vials of tirzepatide available to self-pay patients with an on-label electronic prescription. Lilly’s announcement said the single-dose vials “are priced at a 50% or greater discount compared to the list price of all other incretin (glucagon-like peptide 1 receptor agonists or GLP-1) medicines for obesity.”
For a 4-week supply of the weekly injections, the discount at LillyDirect translates to $399 for a 2.5-mg single-dose vial ($99.75 per vial) and $549 for the 5-mg dose ($137.25 per vial), which the company noted was “in line with the Zepbound savings program for noncovered individuals.” (The new direct single-dose prescriptions cannot be filled at community or retail pharmacies.)
“In a clinical study, the 5-mg maintenance dose helped patients achieve an average of 15% weight loss after 72 weeks of treatment and has been a powerful tool for millions of people with obesity looking to lose weight and keep it off,” according to the announcement.
The clinical study, which is not named or referenced in the announcement, is SURMOUNT-1, a Lilly spokesperson said in an interview. Yet, that study also found that patients achieved an average weight loss of 19.5% with 10-mg doses and 20.9% with 15-mg doses of tirzepatide. Furthermore, the percentage of participants achieving body weight reductions of ≥ 5% was 85% (5 mg), 89% (10 mg), and 91% (15 mg), showing the benefits of higher doses.
And there’s the rub.
‘Only Two Different Doses’
Anne Peters, MD, a professor of clinical medicine and a clinical scholar at the University of Southern California, Los Angeles, said in an interview: “My concern is, they’re only providing two different doses, 2.5 mg and 5 mg. You get somebody on it, and then they still have to go back to the traditional pens. I’m very opposed to getting patients connected to a medication they can’t then continue to take.
“Now we have starter doses that are easy to come by,” she said. “But the problem isn’t starting. The problem for all of these patients is chronic continuation of the right dose of the drug, and out-of-pocket costs become exorbitantly higher when they have to self-purchase the pens for the higher doses.
“Yes, the 5-mg dose has benefits, but not the same as higher doses,” she continued. “I have nobody for whom 5 mg is the right dose. They have to take more, sometimes within a month or 2 of starting, in order to achieve the kind of weight loss they need.”
If their insurance doesn’t cover the drug, “what are they going to do to stay on 5 mg? Or pay a crapload of money to buy three of the 5-mg doses to reach a higher dose?”
Michael Weintraub, MD, clinical assistant professor in the Department of Medicine, Division of Endocrinology, Diabetes, and Metabolism at New York University Grossman School of Medicine in New York City, said that, “for many, this lower monthly cost is attainable and is a significant advancement in increasing access. For others, however, an out-of-pocket monthly cost of $349-549 for a chronic medication is still unaffordable.”
And like Dr. Peters, he said, “some patients do not lose a clinically significant amount of weight with 2.5 mg or 5 mg and require higher doses. There is no way of prescribing a higher dose of Zepbound vials, so patients would have to resort to the higher-dose auto-injector pens that are still double the price.”
A Lilly spokesperson countered in a comment: “Offering Zepbound single-dose vials in higher dosage strengths could increase the potential for dose splitting, which is not contemplated by the FDA [Food and Drug Adminstration]–approved label and may pose patient safety risks.”
But Dr. Peters wondered: “Wouldn’t dose splitting of a known-to-be-pure compound be better than getting it at a compounding pharmacy that lacks purity/safety? The one message from all of this is that patients need to know what they’re getting into. They’re starting a drug that can help with weight loss, but they’re going to be on a sub-max dose. And a higher dose is going to be double the price.”
In addition, said Robert F. Kushner, MD, a professor at Northwestern University Feinberg School of Medicine in Chicago, Illinois, “for the lower-dose vials, instead of administering the drug with a self-auto-injection pen, patients will need to use a needle and syringe and draw up the dose from a vial. This will take a higher skill level and health literacy that may be challenging for some patients. Patients may need additional training on how to use this new formulation. That will take additional time and resources, such as a demonstration in the office or referral to video.”
The Lilly news release noted that “patients can also purchase ancillary supplies, like syringes and needles, and will have access to important patient-friendly instructional materials on correctly administering the medicine via needle and syringe.”
Protection From Compounders?
According to the Lilly spokesperson, the launch of Zepbound vials “furthers our commitment to helping patients avoid the risks associated with compounded products by providing patients another option for access to genuine Lilly medicine.”
Indeed, said Jaime Almandoz, MD, medical director of the Weight Wellness Program and associate professor of internal medicine at the University of Texas Southwestern Medical Center in Dallas, “The introduction of Zepbound/tirzepatide in single-dose vials should improve access to evidence-based obesity treatments, reducing potential risks associated with compounded additives and eliminating the need for patients to calculate correct medication doses,” which have led to accidental overdoses of compounded semaglutide.
Lilly’s spokesperson added: “We have taken multiple steps — including publishing an open letter and launching lilly.com/real-medicine — to warn the public about the risks posed by the proliferation of counterfeit, fake, unsafe, or untested knockoffs of Lilly’s genuine medicines.”
But whether these steps are strong enough to overcome the realities of cost and the need for affordable higher doses remains to be seen.
Scott Brunner, CEO of the Alliance for Pharmacy Compounding, said in a statement that the new version of Zepbound “is great news for patients. It’s a much more rational and care-focused response to the remarkable demand for their drug than the lawsuits and cease-and-desist letters Lilly has been raining down on compounding pharmacies.”
“For 20 months now,” he continued,
Dr. Almandoz affirmed: “Everyone wants to see improved access to evidence-based obesity care. It’s crucial to ensure patients receive the most appropriate interventions, whether it is lifestyle changes, medications, or bariatric surgery,” he said. “There are resources available, [including his recent paper], for nutrition and lifestyle modifications specifically for patients taking obesity medications, which can help clinicians guide their patients toward better health.”
Dr. Almandoz is a member of advisory boards and consults for: Novo Nordisk, Eli Lilly, and Boehringer Ingelheim. Dr. Kushner is an adviser to Eli Lilly and Novo Nordisk. Dr. Peters and Dr. Weintraub declared no competing interests.
A version of this article appeared on Medscape.com.
Time-Restricted Eating Fails for Weight Loss and Glucose Homeostasis
, a small randomized controlled trial found.
The results suggested that any effects of TRE on weight observed in prior studies may be due to reductions in caloric intake and not timing, according to Nisa M. Maruthur, MD, MHS, of the Division of General Internal Medicine at the Johns Hopkins School of Medicine in Baltimore, and colleagues.
Published in Annals of Internal Medicine, the 12-week trial randomly assigned 41 adults aged 18-69 years with obesity and prediabetes or diet-controlled diabetes 1:1 as follows: To TRE, involving a 10-hour eating window with 80% of calories consumed before 1 PM, or to UEP, involving a ≤ 16-hour window, with at least 50% of calories consumed after 5 PM. The regimen in each group was based on the OmniHeart unsaturated fat diet and the SPICE study.
“The diet was similar to the DASH [Dietary Approaches to Stop Hypertension] diet for hypertension and maybe a bit higher in unsaturated fat and micronutrients,” said study co-author Scott J. Pilla, MD, MHS, an assistant professor of medicine at the Johns Hopkins Bloomberg School of Public Health, Baltimore, in an interview. For each participant, macro- and micronutrient content remained constant throughout the study period, with total calories individually determined at baseline and ranging from 1600 to 3500 kcal/d. “That differs from some TRE studies in which calories were adjusted according to whether participants lost or gained weight,” he said. “This was a purely mechanistic study to determine the impact of time of eating alone with no change in calories.”

Although the current findings revealed no weight loss advantage, some evidence suggests that limiting the food consumption window to 4-10 hours naturally reduces energy intake by approximately 200-550 calories per day and can result in a loss of 3%-5% of baseline body weight for 2-12 months. In addition, TRE has been shown to improve metabolic risk factors, such as insulin resistance, blood pressure, and triglyceride concentrations — but not in this study.
The Cohort
The mean age was 59 years, 93% of patients were women, and 93% were Black. The mean body mass index was 36, and the mean baseline weight was 96.2 kg — 95.6 kg in the TRE group and 103.7 kg in the UEP group.
At 12 weeks, weight decreased comparably by 2.3 kg (95% CI, 1.0-3.5) in the TRE group and by 2.6 kg (95% CI, 1.5-3.7) in the UEP group. Change in glycemic measures did not differ between the two groups.
Interestingly, self-reporting questionnaires revealed a slight reduction in physical activity in the TRE group, an effect that requires further study. “We don’t know why but anecdotally, some TRE participants said they tended to go to bed earlier,” Dr. Pilla said. Earlier bedtimes may put an end sooner to the daily eating pattern.
Subanalyses of the data are ongoing and will be published later.
“In the context of several clinical trials that suggest a benefit of TRE, our findings suggest that if or when TRE interventions induce weight loss, it is likely in part due to a reduction in energy intake, and therefore, clinicians can counsel patients that TRE may help them lose weight by decreasing their caloric intake,” the authors wrote.
In an accompanying editorial, Krista A. Varady, PhD, and Vanessa M. Oddo, PhD, of the Department of Kinesiology and Nutrition at the University of Illinois–Chicago, said the study results have important clinical implications. “Many patients stop following standard-care diets (such as daily calorie restriction) because they become frustrated with having to monitor food intake vigilantly each day,” they wrote.

Although TRE is no more effective than other diet interventions for weight reduction, it offers a simplified approach to treat obesity by omitting the need for calorie counting. “TRE bypasses this requirement simply by allowing participants to ‘watch the clock’ instead of monitoring calories, while still producing weight loss,” they wrote.
The straightforward nature of this diet makes it well suited for remote delivery, which can reduce the scheduling and financial barriers associated with inpatient visits, they added. “Moreover, TRE does not require the purchase of expensive food products and allows a person to continue consuming familiar foods, making it a high accessible diet for lower-resource populations.”
Gastroenterologists and Obesity
Of late, support has grown for gastroenterologists to become actively involved in obesity treatment — even to “take ownership” of this field.
In a 2023 article in Gut, Michael Camilleri, MD, AGAF, a gastroenterologist at the Mayo Clinic in Rochester, Minnesota, made the case for the natural fit between gastrointestinal (GI) specialists and obesity management. He noted that obesity is a significant risk factor for GI, pancreatic, and liver diseases. It can even affect inflammatory bowel disease.

“Treating obesity starting when patients present in gastroenterology and hepatology clinics has potential to impact serious consequences of obesity such as cardiovascular risks,” he wrote.
Gastroenterologists already treat GI conditions with pharmacologic and surgical interventions that can also be used to treat obesity and improve glycemic control. These include pancreatic lipase inhibitors and incretin, bariatric endoscopy and surgery, and combination therapies targeting metabolic problems.
This study was supported by the American Heart Association.
Dr. Maruthur reported receiving royalties from a virtual diabetes prevention program. Dr. Pilla reported receiving travel, advisory, and speaker fees from the American Diabetes Association. Numerous authors reported receiving grants from government and nonprofit research funding organizations. Dr. Varady disclosed having no competing interests. Dr. Odda reported receiving research support and honoraria from government nonprofit funding organizations.
A version of this article first appeared on Medscape.com.
, a small randomized controlled trial found.
The results suggested that any effects of TRE on weight observed in prior studies may be due to reductions in caloric intake and not timing, according to Nisa M. Maruthur, MD, MHS, of the Division of General Internal Medicine at the Johns Hopkins School of Medicine in Baltimore, and colleagues.
Published in Annals of Internal Medicine, the 12-week trial randomly assigned 41 adults aged 18-69 years with obesity and prediabetes or diet-controlled diabetes 1:1 as follows: To TRE, involving a 10-hour eating window with 80% of calories consumed before 1 PM, or to UEP, involving a ≤ 16-hour window, with at least 50% of calories consumed after 5 PM. The regimen in each group was based on the OmniHeart unsaturated fat diet and the SPICE study.
“The diet was similar to the DASH [Dietary Approaches to Stop Hypertension] diet for hypertension and maybe a bit higher in unsaturated fat and micronutrients,” said study co-author Scott J. Pilla, MD, MHS, an assistant professor of medicine at the Johns Hopkins Bloomberg School of Public Health, Baltimore, in an interview. For each participant, macro- and micronutrient content remained constant throughout the study period, with total calories individually determined at baseline and ranging from 1600 to 3500 kcal/d. “That differs from some TRE studies in which calories were adjusted according to whether participants lost or gained weight,” he said. “This was a purely mechanistic study to determine the impact of time of eating alone with no change in calories.”
Although the current findings revealed no weight loss advantage, some evidence suggests that limiting the food consumption window to 4-10 hours naturally reduces energy intake by approximately 200-550 calories per day and can result in a loss of 3%-5% of baseline body weight for 2-12 months. In addition, TRE has been shown to improve metabolic risk factors, such as insulin resistance, blood pressure, and triglyceride concentrations — but not in this study.
The Cohort
The mean age was 59 years, 93% of patients were women, and 93% were Black. The mean body mass index was 36, and the mean baseline weight was 96.2 kg — 95.6 kg in the TRE group and 103.7 kg in the UEP group.
At 12 weeks, weight decreased comparably by 2.3 kg (95% CI, 1.0-3.5) in the TRE group and by 2.6 kg (95% CI, 1.5-3.7) in the UEP group. Change in glycemic measures did not differ between the two groups.
Interestingly, self-reporting questionnaires revealed a slight reduction in physical activity in the TRE group, an effect that requires further study. “We don’t know why but anecdotally, some TRE participants said they tended to go to bed earlier,” Dr. Pilla said. Earlier bedtimes may put an end sooner to the daily eating pattern.
Subanalyses of the data are ongoing and will be published later.
“In the context of several clinical trials that suggest a benefit of TRE, our findings suggest that if or when TRE interventions induce weight loss, it is likely in part due to a reduction in energy intake, and therefore, clinicians can counsel patients that TRE may help them lose weight by decreasing their caloric intake,” the authors wrote.
In an accompanying editorial, Krista A. Varady, PhD, and Vanessa M. Oddo, PhD, of the Department of Kinesiology and Nutrition at the University of Illinois–Chicago, said the study results have important clinical implications. “Many patients stop following standard-care diets (such as daily calorie restriction) because they become frustrated with having to monitor food intake vigilantly each day,” they wrote.
Although TRE is no more effective than other diet interventions for weight reduction, it offers a simplified approach to treat obesity by omitting the need for calorie counting. “TRE bypasses this requirement simply by allowing participants to ‘watch the clock’ instead of monitoring calories, while still producing weight loss,” they wrote.
The straightforward nature of this diet makes it well suited for remote delivery, which can reduce the scheduling and financial barriers associated with inpatient visits, they added. “Moreover, TRE does not require the purchase of expensive food products and allows a person to continue consuming familiar foods, making it a high accessible diet for lower-resource populations.”
Gastroenterologists and Obesity
Of late, support has grown for gastroenterologists to become actively involved in obesity treatment — even to “take ownership” of this field.
In a 2023 article in Gut, Michael Camilleri, MD, AGAF, a gastroenterologist at the Mayo Clinic in Rochester, Minnesota, made the case for the natural fit between gastrointestinal (GI) specialists and obesity management. He noted that obesity is a significant risk factor for GI, pancreatic, and liver diseases. It can even affect inflammatory bowel disease.
“Treating obesity starting when patients present in gastroenterology and hepatology clinics has potential to impact serious consequences of obesity such as cardiovascular risks,” he wrote.
Gastroenterologists already treat GI conditions with pharmacologic and surgical interventions that can also be used to treat obesity and improve glycemic control. These include pancreatic lipase inhibitors and incretin, bariatric endoscopy and surgery, and combination therapies targeting metabolic problems.
This study was supported by the American Heart Association.
Dr. Maruthur reported receiving royalties from a virtual diabetes prevention program. Dr. Pilla reported receiving travel, advisory, and speaker fees from the American Diabetes Association. Numerous authors reported receiving grants from government and nonprofit research funding organizations. Dr. Varady disclosed having no competing interests. Dr. Odda reported receiving research support and honoraria from government nonprofit funding organizations.
A version of this article first appeared on Medscape.com.
, a small randomized controlled trial found.
The results suggested that any effects of TRE on weight observed in prior studies may be due to reductions in caloric intake and not timing, according to Nisa M. Maruthur, MD, MHS, of the Division of General Internal Medicine at the Johns Hopkins School of Medicine in Baltimore, and colleagues.
Published in Annals of Internal Medicine, the 12-week trial randomly assigned 41 adults aged 18-69 years with obesity and prediabetes or diet-controlled diabetes 1:1 as follows: To TRE, involving a 10-hour eating window with 80% of calories consumed before 1 PM, or to UEP, involving a ≤ 16-hour window, with at least 50% of calories consumed after 5 PM. The regimen in each group was based on the OmniHeart unsaturated fat diet and the SPICE study.
“The diet was similar to the DASH [Dietary Approaches to Stop Hypertension] diet for hypertension and maybe a bit higher in unsaturated fat and micronutrients,” said study co-author Scott J. Pilla, MD, MHS, an assistant professor of medicine at the Johns Hopkins Bloomberg School of Public Health, Baltimore, in an interview. For each participant, macro- and micronutrient content remained constant throughout the study period, with total calories individually determined at baseline and ranging from 1600 to 3500 kcal/d. “That differs from some TRE studies in which calories were adjusted according to whether participants lost or gained weight,” he said. “This was a purely mechanistic study to determine the impact of time of eating alone with no change in calories.”
Although the current findings revealed no weight loss advantage, some evidence suggests that limiting the food consumption window to 4-10 hours naturally reduces energy intake by approximately 200-550 calories per day and can result in a loss of 3%-5% of baseline body weight for 2-12 months. In addition, TRE has been shown to improve metabolic risk factors, such as insulin resistance, blood pressure, and triglyceride concentrations — but not in this study.
The Cohort
The mean age was 59 years, 93% of patients were women, and 93% were Black. The mean body mass index was 36, and the mean baseline weight was 96.2 kg — 95.6 kg in the TRE group and 103.7 kg in the UEP group.
At 12 weeks, weight decreased comparably by 2.3 kg (95% CI, 1.0-3.5) in the TRE group and by 2.6 kg (95% CI, 1.5-3.7) in the UEP group. Change in glycemic measures did not differ between the two groups.
Interestingly, self-reporting questionnaires revealed a slight reduction in physical activity in the TRE group, an effect that requires further study. “We don’t know why but anecdotally, some TRE participants said they tended to go to bed earlier,” Dr. Pilla said. Earlier bedtimes may put an end sooner to the daily eating pattern.
Subanalyses of the data are ongoing and will be published later.
“In the context of several clinical trials that suggest a benefit of TRE, our findings suggest that if or when TRE interventions induce weight loss, it is likely in part due to a reduction in energy intake, and therefore, clinicians can counsel patients that TRE may help them lose weight by decreasing their caloric intake,” the authors wrote.
In an accompanying editorial, Krista A. Varady, PhD, and Vanessa M. Oddo, PhD, of the Department of Kinesiology and Nutrition at the University of Illinois–Chicago, said the study results have important clinical implications. “Many patients stop following standard-care diets (such as daily calorie restriction) because they become frustrated with having to monitor food intake vigilantly each day,” they wrote.
Although TRE is no more effective than other diet interventions for weight reduction, it offers a simplified approach to treat obesity by omitting the need for calorie counting. “TRE bypasses this requirement simply by allowing participants to ‘watch the clock’ instead of monitoring calories, while still producing weight loss,” they wrote.
The straightforward nature of this diet makes it well suited for remote delivery, which can reduce the scheduling and financial barriers associated with inpatient visits, they added. “Moreover, TRE does not require the purchase of expensive food products and allows a person to continue consuming familiar foods, making it a high accessible diet for lower-resource populations.”
Gastroenterologists and Obesity
Of late, support has grown for gastroenterologists to become actively involved in obesity treatment — even to “take ownership” of this field.
In a 2023 article in Gut, Michael Camilleri, MD, AGAF, a gastroenterologist at the Mayo Clinic in Rochester, Minnesota, made the case for the natural fit between gastrointestinal (GI) specialists and obesity management. He noted that obesity is a significant risk factor for GI, pancreatic, and liver diseases. It can even affect inflammatory bowel disease.
“Treating obesity starting when patients present in gastroenterology and hepatology clinics has potential to impact serious consequences of obesity such as cardiovascular risks,” he wrote.
Gastroenterologists already treat GI conditions with pharmacologic and surgical interventions that can also be used to treat obesity and improve glycemic control. These include pancreatic lipase inhibitors and incretin, bariatric endoscopy and surgery, and combination therapies targeting metabolic problems.
This study was supported by the American Heart Association.
Dr. Maruthur reported receiving royalties from a virtual diabetes prevention program. Dr. Pilla reported receiving travel, advisory, and speaker fees from the American Diabetes Association. Numerous authors reported receiving grants from government and nonprofit research funding organizations. Dr. Varady disclosed having no competing interests. Dr. Odda reported receiving research support and honoraria from government nonprofit funding organizations.
A version of this article first appeared on Medscape.com.
Thyroid Resistance Ups Mortality in Euthyroid CKD Patients
TOPLINE:
An impaired central sensitivity to thyroid hormone may be associated with an increased risk for death in patients with chronic kidney disease (CKD) and normal thyroid function.
METHODOLOGY:
- Previous studies have shown that abnormal levels of thyroid-stimulating hormone (TSH) are associated with a higher mortality risk in patients with CKD, but whether the risk extends to those with normal thyroid function remains controversial.
- Researchers investigated the association between central sensitivity to thyroid hormone and the risk for all-cause mortality in 1303 euthyroid patients with CKD (mean age, 60 years; 59% women) from the National Health and Nutrition Examination Survey database (2007-2012).
- All participants had CKD stages I-IV, defined as an estimated glomerular filtration rate < 60 mL/min/1.73 m2 and/or a urinary albumin to urinary creatinine ratio ≥ 30 mg/g.
- The central sensitivity to thyroid hormone was primarily evaluated using a new central thyroid hormone resistance index, the Thyroid Feedback Quantile–based Index (TFQI), using free thyroxine and TSH concentrations.
- The participants were followed for a median duration of 115 months, during which 503 died.
TAKEAWAY:
- Patients with CKD who died during the follow-up period had a significantly higher TFQI (P < .001) than those who survived.
- The rates of all-cause mortality increased from 26.61% in the lowest TFQI tertile to 40.89% in the highest tertile (P = .001).
- A per unit increase in the TFQI was associated with a 40% increased risk for all-cause mortality (hazard ratio, 1.40; 95% CI, 1.10-1.79).
- This association between TFQI level and all-cause mortality persisted in all subgroups stratified by age, gender, race, body mass index, hypertension, diabetes, cardiovascular diseases, and CKD stages.
IN PRACTICE:
“Our study demonstrates that impaired sensitivity to thyroid hormone might be associated with all-cause mortality in CKD patients with normal thyroid function, independent of other traditional risk factors and comorbidities,” the authors wrote.
SOURCE:
This study was led by Qichao Yang and Ru Dong, Department of Endocrinology, Affiliated Wujin Hospital of Jiangsu University, Changzhou, China, and was published online on August 6, 2024, in BMC Public Health.
LIMITATIONS:
Thyroid function was measured only at baseline, and the changes in thyroid function over time were not measured. The study excluded people on thyroid hormone replacement therapy but did not consider other medication use that might have affected thyroid function, such as beta-blockers, steroids, and amiodarone. Thyroid-related antibodies, metabolic syndrome, and nonalcoholic fatty liver disease were not included in the analysis as possible confounding factors. The US-based sample requires further validation.
DISCLOSURES:
The study was supported by the Changzhou Health Commission. The authors declared no competing interests.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
An impaired central sensitivity to thyroid hormone may be associated with an increased risk for death in patients with chronic kidney disease (CKD) and normal thyroid function.
METHODOLOGY:
- Previous studies have shown that abnormal levels of thyroid-stimulating hormone (TSH) are associated with a higher mortality risk in patients with CKD, but whether the risk extends to those with normal thyroid function remains controversial.
- Researchers investigated the association between central sensitivity to thyroid hormone and the risk for all-cause mortality in 1303 euthyroid patients with CKD (mean age, 60 years; 59% women) from the National Health and Nutrition Examination Survey database (2007-2012).
- All participants had CKD stages I-IV, defined as an estimated glomerular filtration rate < 60 mL/min/1.73 m2 and/or a urinary albumin to urinary creatinine ratio ≥ 30 mg/g.
- The central sensitivity to thyroid hormone was primarily evaluated using a new central thyroid hormone resistance index, the Thyroid Feedback Quantile–based Index (TFQI), using free thyroxine and TSH concentrations.
- The participants were followed for a median duration of 115 months, during which 503 died.
TAKEAWAY:
- Patients with CKD who died during the follow-up period had a significantly higher TFQI (P < .001) than those who survived.
- The rates of all-cause mortality increased from 26.61% in the lowest TFQI tertile to 40.89% in the highest tertile (P = .001).
- A per unit increase in the TFQI was associated with a 40% increased risk for all-cause mortality (hazard ratio, 1.40; 95% CI, 1.10-1.79).
- This association between TFQI level and all-cause mortality persisted in all subgroups stratified by age, gender, race, body mass index, hypertension, diabetes, cardiovascular diseases, and CKD stages.
IN PRACTICE:
“Our study demonstrates that impaired sensitivity to thyroid hormone might be associated with all-cause mortality in CKD patients with normal thyroid function, independent of other traditional risk factors and comorbidities,” the authors wrote.
SOURCE:
This study was led by Qichao Yang and Ru Dong, Department of Endocrinology, Affiliated Wujin Hospital of Jiangsu University, Changzhou, China, and was published online on August 6, 2024, in BMC Public Health.
LIMITATIONS:
Thyroid function was measured only at baseline, and the changes in thyroid function over time were not measured. The study excluded people on thyroid hormone replacement therapy but did not consider other medication use that might have affected thyroid function, such as beta-blockers, steroids, and amiodarone. Thyroid-related antibodies, metabolic syndrome, and nonalcoholic fatty liver disease were not included in the analysis as possible confounding factors. The US-based sample requires further validation.
DISCLOSURES:
The study was supported by the Changzhou Health Commission. The authors declared no competing interests.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
An impaired central sensitivity to thyroid hormone may be associated with an increased risk for death in patients with chronic kidney disease (CKD) and normal thyroid function.
METHODOLOGY:
- Previous studies have shown that abnormal levels of thyroid-stimulating hormone (TSH) are associated with a higher mortality risk in patients with CKD, but whether the risk extends to those with normal thyroid function remains controversial.
- Researchers investigated the association between central sensitivity to thyroid hormone and the risk for all-cause mortality in 1303 euthyroid patients with CKD (mean age, 60 years; 59% women) from the National Health and Nutrition Examination Survey database (2007-2012).
- All participants had CKD stages I-IV, defined as an estimated glomerular filtration rate < 60 mL/min/1.73 m2 and/or a urinary albumin to urinary creatinine ratio ≥ 30 mg/g.
- The central sensitivity to thyroid hormone was primarily evaluated using a new central thyroid hormone resistance index, the Thyroid Feedback Quantile–based Index (TFQI), using free thyroxine and TSH concentrations.
- The participants were followed for a median duration of 115 months, during which 503 died.
TAKEAWAY:
- Patients with CKD who died during the follow-up period had a significantly higher TFQI (P < .001) than those who survived.
- The rates of all-cause mortality increased from 26.61% in the lowest TFQI tertile to 40.89% in the highest tertile (P = .001).
- A per unit increase in the TFQI was associated with a 40% increased risk for all-cause mortality (hazard ratio, 1.40; 95% CI, 1.10-1.79).
- This association between TFQI level and all-cause mortality persisted in all subgroups stratified by age, gender, race, body mass index, hypertension, diabetes, cardiovascular diseases, and CKD stages.
IN PRACTICE:
“Our study demonstrates that impaired sensitivity to thyroid hormone might be associated with all-cause mortality in CKD patients with normal thyroid function, independent of other traditional risk factors and comorbidities,” the authors wrote.
SOURCE:
This study was led by Qichao Yang and Ru Dong, Department of Endocrinology, Affiliated Wujin Hospital of Jiangsu University, Changzhou, China, and was published online on August 6, 2024, in BMC Public Health.
LIMITATIONS:
Thyroid function was measured only at baseline, and the changes in thyroid function over time were not measured. The study excluded people on thyroid hormone replacement therapy but did not consider other medication use that might have affected thyroid function, such as beta-blockers, steroids, and amiodarone. Thyroid-related antibodies, metabolic syndrome, and nonalcoholic fatty liver disease were not included in the analysis as possible confounding factors. The US-based sample requires further validation.
DISCLOSURES:
The study was supported by the Changzhou Health Commission. The authors declared no competing interests.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
High Breast Cancer Risk With Menopausal Hormone Therapy & Strong Family History
TOPLINE:
These women have a striking cumulative risk of developing breast cancer (age, 50-80 years) of 22.4%, according to a new modelling study of UK women.
METHODOLOGY:
This was a modeling study integrating two data-sets of UK women: the BOADICEA dataset of age-specific breast cancer risk with family history and the Collaborative Group on Hormonal Factors in Breast Cancer, which covers relative risk for breast cancer with different types and durations of MHT.
Four different breast cancer family history profiles were:
- “Average” family history of breast cancer has unknown affected family members;
- “Modest” family history comprises a single first-degree relative with breast cancer at the age of 60 years.
- “Intermediate” family history comprises a single first-degree relative who developed breast cancer at the age of 40 years.
- “Strong” family history comprises two first-degree relatives who developed breast cancer at the age of 50 years.
TAKEAWAY:
- The lowest risk category: “Average” family history with no MHT use has a cumulative breast cancer risk (age, 50-80 years) of 9.8% and a risk of dying from breast cancer of 1.7%. These risks rise with 5 years’ exposure to MHT (age, 50-55 years) to 11.0% and 1.8%, respectively.
- The highest risk category: “Strong” family history with no MHT use has a cumulative breast cancer risk (age, 50-80 years) of 19.6% and a risk of dying from breast cancer of 3.2%. These risks rise with 5 years’ exposure to MHT (age, 50-55 years) to 22.4% and 3.5%, respectively.
IN PRACTICE:
The authors concluded that, “These integrated data will enable more accurate estimates of absolute and attributable risk associated with MHT exposure for women with a family history of breast cancer, informing shared decision-making.”
SOURCE:
The lead author is Catherine Huntley of the Institute of Cancer Research, London, England. The study appeared in the British Journal of General Practice.
LIMITATIONS:
Limitations included modeling study that did not directly measure individuals with combined risks.
DISCLOSURES:
The study was funded by several sources including Cancer Research UK. The authors reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
These women have a striking cumulative risk of developing breast cancer (age, 50-80 years) of 22.4%, according to a new modelling study of UK women.
METHODOLOGY:
This was a modeling study integrating two data-sets of UK women: the BOADICEA dataset of age-specific breast cancer risk with family history and the Collaborative Group on Hormonal Factors in Breast Cancer, which covers relative risk for breast cancer with different types and durations of MHT.
Four different breast cancer family history profiles were:
- “Average” family history of breast cancer has unknown affected family members;
- “Modest” family history comprises a single first-degree relative with breast cancer at the age of 60 years.
- “Intermediate” family history comprises a single first-degree relative who developed breast cancer at the age of 40 years.
- “Strong” family history comprises two first-degree relatives who developed breast cancer at the age of 50 years.
TAKEAWAY:
- The lowest risk category: “Average” family history with no MHT use has a cumulative breast cancer risk (age, 50-80 years) of 9.8% and a risk of dying from breast cancer of 1.7%. These risks rise with 5 years’ exposure to MHT (age, 50-55 years) to 11.0% and 1.8%, respectively.
- The highest risk category: “Strong” family history with no MHT use has a cumulative breast cancer risk (age, 50-80 years) of 19.6% and a risk of dying from breast cancer of 3.2%. These risks rise with 5 years’ exposure to MHT (age, 50-55 years) to 22.4% and 3.5%, respectively.
IN PRACTICE:
The authors concluded that, “These integrated data will enable more accurate estimates of absolute and attributable risk associated with MHT exposure for women with a family history of breast cancer, informing shared decision-making.”
SOURCE:
The lead author is Catherine Huntley of the Institute of Cancer Research, London, England. The study appeared in the British Journal of General Practice.
LIMITATIONS:
Limitations included modeling study that did not directly measure individuals with combined risks.
DISCLOSURES:
The study was funded by several sources including Cancer Research UK. The authors reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
These women have a striking cumulative risk of developing breast cancer (age, 50-80 years) of 22.4%, according to a new modelling study of UK women.
METHODOLOGY:
This was a modeling study integrating two data-sets of UK women: the BOADICEA dataset of age-specific breast cancer risk with family history and the Collaborative Group on Hormonal Factors in Breast Cancer, which covers relative risk for breast cancer with different types and durations of MHT.
Four different breast cancer family history profiles were:
- “Average” family history of breast cancer has unknown affected family members;
- “Modest” family history comprises a single first-degree relative with breast cancer at the age of 60 years.
- “Intermediate” family history comprises a single first-degree relative who developed breast cancer at the age of 40 years.
- “Strong” family history comprises two first-degree relatives who developed breast cancer at the age of 50 years.
TAKEAWAY:
- The lowest risk category: “Average” family history with no MHT use has a cumulative breast cancer risk (age, 50-80 years) of 9.8% and a risk of dying from breast cancer of 1.7%. These risks rise with 5 years’ exposure to MHT (age, 50-55 years) to 11.0% and 1.8%, respectively.
- The highest risk category: “Strong” family history with no MHT use has a cumulative breast cancer risk (age, 50-80 years) of 19.6% and a risk of dying from breast cancer of 3.2%. These risks rise with 5 years’ exposure to MHT (age, 50-55 years) to 22.4% and 3.5%, respectively.
IN PRACTICE:
The authors concluded that, “These integrated data will enable more accurate estimates of absolute and attributable risk associated with MHT exposure for women with a family history of breast cancer, informing shared decision-making.”
SOURCE:
The lead author is Catherine Huntley of the Institute of Cancer Research, London, England. The study appeared in the British Journal of General Practice.
LIMITATIONS:
Limitations included modeling study that did not directly measure individuals with combined risks.
DISCLOSURES:
The study was funded by several sources including Cancer Research UK. The authors reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Breast Cancer Hormone Therapy May Protect Against Dementia
TOPLINE:
with the greatest benefit seen in younger Black women.
METHODOLOGY:
- Hormone-modulating therapy is widely used to treat hormone receptor–positive breast cancer, but the cognitive effects of the treatment, including a potential link to dementia, remain unclear.
- To investigate, researchers used the SEER-Medicare linked database to identify women aged 65 years or older with breast cancer who did and did not receive hormone-modulating therapy within 3 years following their diagnosis.
- The researchers excluded women with preexisting Alzheimer’s disease/dementia diagnoses or those who had received hormone-modulating therapy before their breast cancer diagnosis.
- Analyses were adjusted for demographic, sociocultural, and clinical variables, and subgroup analyses evaluated the impact of age, race, and type of hormone-modulating therapy on Alzheimer’s disease/dementia risk.
TAKEAWAY:
- Among the 18,808 women included in the analysis, 66% received hormone-modulating therapy and 34% did not. During the mean follow-up of 12 years, 24% of hormone-modulating therapy users and 28% of nonusers developed Alzheimer’s disease/dementia.
- Overall, hormone-modulating therapy use (vs nonuse) was associated with a significant 7% lower risk for Alzheimer’s disease/dementia (hazard ratio [HR], 0.93; P = .005), with notable age and racial differences.
- Hormone-modulating therapy use was associated with a 24% lower risk for Alzheimer’s disease/dementia in Black women aged 65-74 years (HR, 0.76), but that protective effect decreased to 19% in Black women aged 75 years or older (HR, 0.81). White women aged 65-74 years who received hormone-modulating therapy (vs those who did not) had an 11% lower risk for Alzheimer’s disease/dementia (HR, 0.89), but the association disappeared among those aged 75 years or older (HR, 0.96; 95% CI, 0.90-1.02). Other races demonstrated no significant association between hormone-modulating therapy use and Alzheimer’s disease/dementia.
- Overall, the use of an aromatase inhibitor or a selective estrogen receptor modulator was associated with a significantly lower risk for Alzheimer’s disease/dementia (HR, 0.93 and HR, 0.89, respectively).
IN PRACTICE:
Overall, the retrospective study found that “hormone therapy was associated with protection against [Alzheimer’s/dementia] in women aged 65 years or older with newly diagnosed breast cancer,” with the decrease in risk relatively greater for Black women and women younger than 75 years, the authors concluded.
“The results highlight the critical need for personalized breast cancer treatment plans that are tailored to the individual characteristics of each patient, particularly given the significantly higher likelihood (two to three times more) of Black women developing [Alzheimer’s/dementia], compared with their White counterparts,” the researchers added.
SOURCE:
The study, with first author Chao Cai, PhD, Department of Clinical Pharmacy and Outcomes Sciences, University of South Carolina, Columbia, was published online on July 16 in JAMA Network Open.
LIMITATIONS:
The study included only women aged 65 years or older, limiting generalizability to younger women. The dataset lacked genetic information and laboratory data related to dementia. The duration of hormone-modulating therapy use beyond 3 years and specific formulations were not assessed. Potential confounders such as variations in chemotherapy, radiation, and surgery were not fully addressed.
DISCLOSURES:
Support for the study was provided by the National Institutes of Health; Carolina Center on Alzheimer’s Disease and Minority Research pilot project; and the Dean’s Faculty Advancement Fund, University of Pittsburgh, Pennsylvania. The authors reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
TOPLINE:
with the greatest benefit seen in younger Black women.
METHODOLOGY:
- Hormone-modulating therapy is widely used to treat hormone receptor–positive breast cancer, but the cognitive effects of the treatment, including a potential link to dementia, remain unclear.
- To investigate, researchers used the SEER-Medicare linked database to identify women aged 65 years or older with breast cancer who did and did not receive hormone-modulating therapy within 3 years following their diagnosis.
- The researchers excluded women with preexisting Alzheimer’s disease/dementia diagnoses or those who had received hormone-modulating therapy before their breast cancer diagnosis.
- Analyses were adjusted for demographic, sociocultural, and clinical variables, and subgroup analyses evaluated the impact of age, race, and type of hormone-modulating therapy on Alzheimer’s disease/dementia risk.
TAKEAWAY:
- Among the 18,808 women included in the analysis, 66% received hormone-modulating therapy and 34% did not. During the mean follow-up of 12 years, 24% of hormone-modulating therapy users and 28% of nonusers developed Alzheimer’s disease/dementia.
- Overall, hormone-modulating therapy use (vs nonuse) was associated with a significant 7% lower risk for Alzheimer’s disease/dementia (hazard ratio [HR], 0.93; P = .005), with notable age and racial differences.
- Hormone-modulating therapy use was associated with a 24% lower risk for Alzheimer’s disease/dementia in Black women aged 65-74 years (HR, 0.76), but that protective effect decreased to 19% in Black women aged 75 years or older (HR, 0.81). White women aged 65-74 years who received hormone-modulating therapy (vs those who did not) had an 11% lower risk for Alzheimer’s disease/dementia (HR, 0.89), but the association disappeared among those aged 75 years or older (HR, 0.96; 95% CI, 0.90-1.02). Other races demonstrated no significant association between hormone-modulating therapy use and Alzheimer’s disease/dementia.
- Overall, the use of an aromatase inhibitor or a selective estrogen receptor modulator was associated with a significantly lower risk for Alzheimer’s disease/dementia (HR, 0.93 and HR, 0.89, respectively).
IN PRACTICE:
Overall, the retrospective study found that “hormone therapy was associated with protection against [Alzheimer’s/dementia] in women aged 65 years or older with newly diagnosed breast cancer,” with the decrease in risk relatively greater for Black women and women younger than 75 years, the authors concluded.
“The results highlight the critical need for personalized breast cancer treatment plans that are tailored to the individual characteristics of each patient, particularly given the significantly higher likelihood (two to three times more) of Black women developing [Alzheimer’s/dementia], compared with their White counterparts,” the researchers added.
SOURCE:
The study, with first author Chao Cai, PhD, Department of Clinical Pharmacy and Outcomes Sciences, University of South Carolina, Columbia, was published online on July 16 in JAMA Network Open.
LIMITATIONS:
The study included only women aged 65 years or older, limiting generalizability to younger women. The dataset lacked genetic information and laboratory data related to dementia. The duration of hormone-modulating therapy use beyond 3 years and specific formulations were not assessed. Potential confounders such as variations in chemotherapy, radiation, and surgery were not fully addressed.
DISCLOSURES:
Support for the study was provided by the National Institutes of Health; Carolina Center on Alzheimer’s Disease and Minority Research pilot project; and the Dean’s Faculty Advancement Fund, University of Pittsburgh, Pennsylvania. The authors reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
TOPLINE:
with the greatest benefit seen in younger Black women.
METHODOLOGY:
- Hormone-modulating therapy is widely used to treat hormone receptor–positive breast cancer, but the cognitive effects of the treatment, including a potential link to dementia, remain unclear.
- To investigate, researchers used the SEER-Medicare linked database to identify women aged 65 years or older with breast cancer who did and did not receive hormone-modulating therapy within 3 years following their diagnosis.
- The researchers excluded women with preexisting Alzheimer’s disease/dementia diagnoses or those who had received hormone-modulating therapy before their breast cancer diagnosis.
- Analyses were adjusted for demographic, sociocultural, and clinical variables, and subgroup analyses evaluated the impact of age, race, and type of hormone-modulating therapy on Alzheimer’s disease/dementia risk.
TAKEAWAY:
- Among the 18,808 women included in the analysis, 66% received hormone-modulating therapy and 34% did not. During the mean follow-up of 12 years, 24% of hormone-modulating therapy users and 28% of nonusers developed Alzheimer’s disease/dementia.
- Overall, hormone-modulating therapy use (vs nonuse) was associated with a significant 7% lower risk for Alzheimer’s disease/dementia (hazard ratio [HR], 0.93; P = .005), with notable age and racial differences.
- Hormone-modulating therapy use was associated with a 24% lower risk for Alzheimer’s disease/dementia in Black women aged 65-74 years (HR, 0.76), but that protective effect decreased to 19% in Black women aged 75 years or older (HR, 0.81). White women aged 65-74 years who received hormone-modulating therapy (vs those who did not) had an 11% lower risk for Alzheimer’s disease/dementia (HR, 0.89), but the association disappeared among those aged 75 years or older (HR, 0.96; 95% CI, 0.90-1.02). Other races demonstrated no significant association between hormone-modulating therapy use and Alzheimer’s disease/dementia.
- Overall, the use of an aromatase inhibitor or a selective estrogen receptor modulator was associated with a significantly lower risk for Alzheimer’s disease/dementia (HR, 0.93 and HR, 0.89, respectively).
IN PRACTICE:
Overall, the retrospective study found that “hormone therapy was associated with protection against [Alzheimer’s/dementia] in women aged 65 years or older with newly diagnosed breast cancer,” with the decrease in risk relatively greater for Black women and women younger than 75 years, the authors concluded.
“The results highlight the critical need for personalized breast cancer treatment plans that are tailored to the individual characteristics of each patient, particularly given the significantly higher likelihood (two to three times more) of Black women developing [Alzheimer’s/dementia], compared with their White counterparts,” the researchers added.
SOURCE:
The study, with first author Chao Cai, PhD, Department of Clinical Pharmacy and Outcomes Sciences, University of South Carolina, Columbia, was published online on July 16 in JAMA Network Open.
LIMITATIONS:
The study included only women aged 65 years or older, limiting generalizability to younger women. The dataset lacked genetic information and laboratory data related to dementia. The duration of hormone-modulating therapy use beyond 3 years and specific formulations were not assessed. Potential confounders such as variations in chemotherapy, radiation, and surgery were not fully addressed.
DISCLOSURES:
Support for the study was provided by the National Institutes of Health; Carolina Center on Alzheimer’s Disease and Minority Research pilot project; and the Dean’s Faculty Advancement Fund, University of Pittsburgh, Pennsylvania. The authors reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
How Do Plant-Based Foods Reduce Type 2 Diabetes Risk?
TOPLINE:
especially in individuals with obesity or premenopausal women.
METHODOLOGY:
- Lignans, polyphenolic compounds abundant in plant-based foods, are the primary dietary source of phytoestrogens in Western diets and are associated with a reduced risk for cardiometabolic conditions, but the relative associations of individual lignans with T2D are unknown.
- Researchers assessed the associations between the risk for T2D and the intake of total and four primary lignans using the data of 201,111 participants (mean age, 44.7 years; 80.2% women; 96.7% White individuals) from three large prospective US cohorts with over 30 years of follow-up, as well as the association between lignan intake and hemoglobin A1c in 496 participants from the Men’s Lifestyle Validation Study (MLVS).
- For the three large cohorts, lignan intake (total, secoisolariciresinol, matairesinol, pinoresinol, and lariciresinol) was assessed using a validated food frequency questionnaire updated every 2-4 years and categorized into quintiles. For MLVS, diet was assessed by two sets of 7-day diet records and presented as percentage changes in A1c for linear increases in lignan intake.
- Incident T2D was confirmed using diagnostic tests, symptoms, hypoglycemic medication, elevated glucose by several measures.
TAKEAWAY:
- Across the three cohorts, 20,291 cases of T2D were recorded in the full follow-up.
- Higher intakes of total and individual ligands, except for lariciresinol, were associated with about 8%-27% lower T2D incidents (approximate hazard ratio [HR], 0.72-0.93)
- Of the individual lignans, secoisolariciresinol (but not others) showed a significant inverse association with the risk for T2D among those with a body mass index ≥ 30 (HR, 0.75; 95% CI, 0.71-0.79) and premenopausal women (HR, 0.67; 95% CI, 0.65-0.69).
- The dietary intake of lignans assessed using the 7-day diet records in MLVS was associated with lower levels of A1c (percentage changes ranging from −0.92% to −1.50%.
IN PRACTICE:
“Our findings underscore the importance of a healthy plant-based diet rich in lignan-containing foods, including flaxseed products, whole grains, and coffee for the primary prevention of T2D,” the authors wrote.
SOURCE:
The study, led by Siyue Wang, PhD, Department of Nutrition, Harvard TH Chan School of Public Health, Boston, Massachusetts, and the School of Public Health, Peking University, Beijing, China, was published online in JAMA Network Open.
LIMITATIONS:
The study’s limitations include the potential for measurement errors in dietary assessments. Flax seed, the most concentrated source of lignans, was not assessed until midway through the three large cohort follow-ups, and this may have resulted in misclassification of the intake levels of secoisolariciresinol. The lack of diversity in the socioeconomic status and race within the population may restrict the generalizability of the findings. Despite making multivariable adjustments, residual confounding cannot be fully ruled out.
DISCLOSURES:
The three cohort studies were supported by grants from the National Institutes of Health. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
especially in individuals with obesity or premenopausal women.
METHODOLOGY:
- Lignans, polyphenolic compounds abundant in plant-based foods, are the primary dietary source of phytoestrogens in Western diets and are associated with a reduced risk for cardiometabolic conditions, but the relative associations of individual lignans with T2D are unknown.
- Researchers assessed the associations between the risk for T2D and the intake of total and four primary lignans using the data of 201,111 participants (mean age, 44.7 years; 80.2% women; 96.7% White individuals) from three large prospective US cohorts with over 30 years of follow-up, as well as the association between lignan intake and hemoglobin A1c in 496 participants from the Men’s Lifestyle Validation Study (MLVS).
- For the three large cohorts, lignan intake (total, secoisolariciresinol, matairesinol, pinoresinol, and lariciresinol) was assessed using a validated food frequency questionnaire updated every 2-4 years and categorized into quintiles. For MLVS, diet was assessed by two sets of 7-day diet records and presented as percentage changes in A1c for linear increases in lignan intake.
- Incident T2D was confirmed using diagnostic tests, symptoms, hypoglycemic medication, elevated glucose by several measures.
TAKEAWAY:
- Across the three cohorts, 20,291 cases of T2D were recorded in the full follow-up.
- Higher intakes of total and individual ligands, except for lariciresinol, were associated with about 8%-27% lower T2D incidents (approximate hazard ratio [HR], 0.72-0.93)
- Of the individual lignans, secoisolariciresinol (but not others) showed a significant inverse association with the risk for T2D among those with a body mass index ≥ 30 (HR, 0.75; 95% CI, 0.71-0.79) and premenopausal women (HR, 0.67; 95% CI, 0.65-0.69).
- The dietary intake of lignans assessed using the 7-day diet records in MLVS was associated with lower levels of A1c (percentage changes ranging from −0.92% to −1.50%.
IN PRACTICE:
“Our findings underscore the importance of a healthy plant-based diet rich in lignan-containing foods, including flaxseed products, whole grains, and coffee for the primary prevention of T2D,” the authors wrote.
SOURCE:
The study, led by Siyue Wang, PhD, Department of Nutrition, Harvard TH Chan School of Public Health, Boston, Massachusetts, and the School of Public Health, Peking University, Beijing, China, was published online in JAMA Network Open.
LIMITATIONS:
The study’s limitations include the potential for measurement errors in dietary assessments. Flax seed, the most concentrated source of lignans, was not assessed until midway through the three large cohort follow-ups, and this may have resulted in misclassification of the intake levels of secoisolariciresinol. The lack of diversity in the socioeconomic status and race within the population may restrict the generalizability of the findings. Despite making multivariable adjustments, residual confounding cannot be fully ruled out.
DISCLOSURES:
The three cohort studies were supported by grants from the National Institutes of Health. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
especially in individuals with obesity or premenopausal women.
METHODOLOGY:
- Lignans, polyphenolic compounds abundant in plant-based foods, are the primary dietary source of phytoestrogens in Western diets and are associated with a reduced risk for cardiometabolic conditions, but the relative associations of individual lignans with T2D are unknown.
- Researchers assessed the associations between the risk for T2D and the intake of total and four primary lignans using the data of 201,111 participants (mean age, 44.7 years; 80.2% women; 96.7% White individuals) from three large prospective US cohorts with over 30 years of follow-up, as well as the association between lignan intake and hemoglobin A1c in 496 participants from the Men’s Lifestyle Validation Study (MLVS).
- For the three large cohorts, lignan intake (total, secoisolariciresinol, matairesinol, pinoresinol, and lariciresinol) was assessed using a validated food frequency questionnaire updated every 2-4 years and categorized into quintiles. For MLVS, diet was assessed by two sets of 7-day diet records and presented as percentage changes in A1c for linear increases in lignan intake.
- Incident T2D was confirmed using diagnostic tests, symptoms, hypoglycemic medication, elevated glucose by several measures.
TAKEAWAY:
- Across the three cohorts, 20,291 cases of T2D were recorded in the full follow-up.
- Higher intakes of total and individual ligands, except for lariciresinol, were associated with about 8%-27% lower T2D incidents (approximate hazard ratio [HR], 0.72-0.93)
- Of the individual lignans, secoisolariciresinol (but not others) showed a significant inverse association with the risk for T2D among those with a body mass index ≥ 30 (HR, 0.75; 95% CI, 0.71-0.79) and premenopausal women (HR, 0.67; 95% CI, 0.65-0.69).
- The dietary intake of lignans assessed using the 7-day diet records in MLVS was associated with lower levels of A1c (percentage changes ranging from −0.92% to −1.50%.
IN PRACTICE:
“Our findings underscore the importance of a healthy plant-based diet rich in lignan-containing foods, including flaxseed products, whole grains, and coffee for the primary prevention of T2D,” the authors wrote.
SOURCE:
The study, led by Siyue Wang, PhD, Department of Nutrition, Harvard TH Chan School of Public Health, Boston, Massachusetts, and the School of Public Health, Peking University, Beijing, China, was published online in JAMA Network Open.
LIMITATIONS:
The study’s limitations include the potential for measurement errors in dietary assessments. Flax seed, the most concentrated source of lignans, was not assessed until midway through the three large cohort follow-ups, and this may have resulted in misclassification of the intake levels of secoisolariciresinol. The lack of diversity in the socioeconomic status and race within the population may restrict the generalizability of the findings. Despite making multivariable adjustments, residual confounding cannot be fully ruled out.
DISCLOSURES:
The three cohort studies were supported by grants from the National Institutes of Health. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Men, Women, & Exercise: How Metabolism Differs
TOPLINE:
METHODOLOGY:
- By stimulating skeletal muscle, exercise can help prevent muscle loss associated with weight loss and improve insulin sensitivity and glucose control in type 2 diabetes, but biological sex-based differences have been reported for many measures.
- This study of sedentary men and women evaluated the molecular differences in skeletal muscle in response to a training program.
- Researchers collected muscle biopsies from 16 women and nine men with overweight or obesity (average age, 30 years) at three time points — baseline, after the first exercise session, and after the last session at the end of training.
- Training involved 1 hour of moderate to intense endurance exercise under supervision (30 minutes cycling on an ergometer and 30 minutes walking on a treadmill) thrice a week for 8 weeks.
- The biopsies were profiled for patterns of three sets of omics data — DNA methylation for insight into genes switched on and off (epigenomics), RNA molecules transcribed from genes (transcriptomics), and proteins (proteomics).
TAKEAWAY:
- At baseline, sex-specific differences were observed most tellingly in 120 proteins and also in DNA methylation sites of 16,012 genes and in 1366 RNA transcripts.
- Men displayed a higher abundance of glycolysis-related proteins and other fast-twitch fiber–type proteins, which are involved in the processing of glucose, while women showed more proteins responsible for regulating fatty acid metabolism.
- The response to the first exercise session differed between men and women, with the cellular stress response upregulated predominantly in men.
- The 8-week exercise training mitigated these sex-specific differences in the skeletal muscle, leading to an upregulation of mitochondrial proteins responsible for substrate oxidation and ATP generation in both men and women.
IN PRACTICE:
“This is important because the increased capacity after exercise to use glucose and lipids for energy production is generally regarded as key to prevent type 2 diabetes,” study leader Professor Cora Weigert from the University of Tübingen, Germany, said in a news release from the meeting organizers. “While initial response of skeletal muscles to exercise differs between females and males, repeated exercise appears to cancel out these differences and trigger beneficial metabolic changes in both sexes,” she added.
SOURCE:
The study was led by Simon I. Dreher, PhD, Institute for Clinical Chemistry and Pathobiochemistry, Department for Diagnostic Laboratory Medicine, Tübingen, Germany. It was published on August 15, 2024, as an early release from the annual meeting of the European Association for the Study of Diabetes 2024, Madrid, September 9-13.
LIMITATIONS:
This abstract did not discuss any limitations.
DISCLOSURES:
The authors did not disclose any funding information. The authors declared no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- By stimulating skeletal muscle, exercise can help prevent muscle loss associated with weight loss and improve insulin sensitivity and glucose control in type 2 diabetes, but biological sex-based differences have been reported for many measures.
- This study of sedentary men and women evaluated the molecular differences in skeletal muscle in response to a training program.
- Researchers collected muscle biopsies from 16 women and nine men with overweight or obesity (average age, 30 years) at three time points — baseline, after the first exercise session, and after the last session at the end of training.
- Training involved 1 hour of moderate to intense endurance exercise under supervision (30 minutes cycling on an ergometer and 30 minutes walking on a treadmill) thrice a week for 8 weeks.
- The biopsies were profiled for patterns of three sets of omics data — DNA methylation for insight into genes switched on and off (epigenomics), RNA molecules transcribed from genes (transcriptomics), and proteins (proteomics).
TAKEAWAY:
- At baseline, sex-specific differences were observed most tellingly in 120 proteins and also in DNA methylation sites of 16,012 genes and in 1366 RNA transcripts.
- Men displayed a higher abundance of glycolysis-related proteins and other fast-twitch fiber–type proteins, which are involved in the processing of glucose, while women showed more proteins responsible for regulating fatty acid metabolism.
- The response to the first exercise session differed between men and women, with the cellular stress response upregulated predominantly in men.
- The 8-week exercise training mitigated these sex-specific differences in the skeletal muscle, leading to an upregulation of mitochondrial proteins responsible for substrate oxidation and ATP generation in both men and women.
IN PRACTICE:
“This is important because the increased capacity after exercise to use glucose and lipids for energy production is generally regarded as key to prevent type 2 diabetes,” study leader Professor Cora Weigert from the University of Tübingen, Germany, said in a news release from the meeting organizers. “While initial response of skeletal muscles to exercise differs between females and males, repeated exercise appears to cancel out these differences and trigger beneficial metabolic changes in both sexes,” she added.
SOURCE:
The study was led by Simon I. Dreher, PhD, Institute for Clinical Chemistry and Pathobiochemistry, Department for Diagnostic Laboratory Medicine, Tübingen, Germany. It was published on August 15, 2024, as an early release from the annual meeting of the European Association for the Study of Diabetes 2024, Madrid, September 9-13.
LIMITATIONS:
This abstract did not discuss any limitations.
DISCLOSURES:
The authors did not disclose any funding information. The authors declared no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- By stimulating skeletal muscle, exercise can help prevent muscle loss associated with weight loss and improve insulin sensitivity and glucose control in type 2 diabetes, but biological sex-based differences have been reported for many measures.
- This study of sedentary men and women evaluated the molecular differences in skeletal muscle in response to a training program.
- Researchers collected muscle biopsies from 16 women and nine men with overweight or obesity (average age, 30 years) at three time points — baseline, after the first exercise session, and after the last session at the end of training.
- Training involved 1 hour of moderate to intense endurance exercise under supervision (30 minutes cycling on an ergometer and 30 minutes walking on a treadmill) thrice a week for 8 weeks.
- The biopsies were profiled for patterns of three sets of omics data — DNA methylation for insight into genes switched on and off (epigenomics), RNA molecules transcribed from genes (transcriptomics), and proteins (proteomics).
TAKEAWAY:
- At baseline, sex-specific differences were observed most tellingly in 120 proteins and also in DNA methylation sites of 16,012 genes and in 1366 RNA transcripts.
- Men displayed a higher abundance of glycolysis-related proteins and other fast-twitch fiber–type proteins, which are involved in the processing of glucose, while women showed more proteins responsible for regulating fatty acid metabolism.
- The response to the first exercise session differed between men and women, with the cellular stress response upregulated predominantly in men.
- The 8-week exercise training mitigated these sex-specific differences in the skeletal muscle, leading to an upregulation of mitochondrial proteins responsible for substrate oxidation and ATP generation in both men and women.
IN PRACTICE:
“This is important because the increased capacity after exercise to use glucose and lipids for energy production is generally regarded as key to prevent type 2 diabetes,” study leader Professor Cora Weigert from the University of Tübingen, Germany, said in a news release from the meeting organizers. “While initial response of skeletal muscles to exercise differs between females and males, repeated exercise appears to cancel out these differences and trigger beneficial metabolic changes in both sexes,” she added.
SOURCE:
The study was led by Simon I. Dreher, PhD, Institute for Clinical Chemistry and Pathobiochemistry, Department for Diagnostic Laboratory Medicine, Tübingen, Germany. It was published on August 15, 2024, as an early release from the annual meeting of the European Association for the Study of Diabetes 2024, Madrid, September 9-13.
LIMITATIONS:
This abstract did not discuss any limitations.
DISCLOSURES:
The authors did not disclose any funding information. The authors declared no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
A Step-by-Step Guide for Diagnosing Cushing Syndrome
“Moon face” is a term that’s become popular on social media, used to describe people with unusually round faces who are purported to have high levels of cortisol. But the term “moon face” isn’t new. It was actually coined in the 1930s by neurosurgeon Harvey Cushing, MD, who identified patients with a constellation of clinical characteristics — a condition that came to bear his name — which included rapidly developing facial adiposity. And indeed, elevated cortisol is a hallmark feature of Cushing syndrome (CS), but there are other reasons for elevated cortisol and other manifestations of CS.
Today, the term “moon face” has been replaced with “round face,” which is considered more encompassing and culturally sensitive, said Maria Fleseriu, MD, professor of medicine and neurological surgery and director of the Pituitary Center at Oregon Health and Science University in Portland, Oregon.
Facial roundness can lead clinicians to be suspicious that their patient is experiencing CS. But because a round face is associated with several other conditions, it’s important to be familiar with its particular presentation in CS, as well as how to diagnose and treat CS.
Pathophysiology of CS
Dr. Fleseriu defined CS as “prolonged nonphysiologic increase in cortisol, due either to exogenous use of steroids (oral, topical, or inhaled) or to excess endogenous cortisol production.” She added that it’s important “to always exclude exogenous causes before conducting a further workup to determine the type and cause of cortisol excess.”
Dr. Fleseriu said. Other causes of CS are ectopic (caused by neuroendocrine tumors) or adrenal. CS affects primarily females and typically has an onset between ages 20 and 50 years, depending on the CS type.
Diagnosis of CS is “substantially delayed for most patients, due to metabolic syndrome phenotypic overlap and lack of a single pathognomonic symptom,” according to Dr. Fleseriu.
An accurate diagnosis should be on the basis of signs and symptoms, biochemical screening, other laboratory testing, and diagnostic imaging.
Look for Clinical Signs and Symptoms of CS
“CS mostly presents as a combination of two or more features,” Dr. Fleseriu stated. These include increased fat pads (in the face, neck, and trunk), skin changes, signs of protein catabolism, growth retardation and body weight increase in children, and metabolic dysregulations (Table).
“Biochemical screening should be performed in patients with a combination of symptoms, and therefore an increased pretest probability for CS,” Dr. Fleseriu advised.
A CS diagnosis requires not only biochemical confirmation of hypercortisolemia but also determination of the underlying cause of the excess endogenous cortisol production. This is a key step, as the management of CS is specific to its etiology.
Elevated plasma cortisol alone is insufficient for diagnosing CS, as several conditions can be associated with physiologic, nonneoplastic endogenous hypercortisolemia, according to the 2021 updated CS guidelines for which Dr. Fleseriu served as a coauthor. These include depression, alcohol dependence, glucocorticoid resistance, obesity, diabetes, pregnancy, prolonged physical exertion, malnutrition, and cortisol-binding globulin excess.
The diagnosis begins with the following screening tests:
- Late-night salivary cortisol (LNSC) to assess an abnormal circadian rhythm
According to the 2021 guideline, this is “based on the assumption that patients with CS lose the normal circadian nadir of cortisol secretion.”
- Overnight 1-mg dexamethasone suppression test (DST) to assess impaired glucocorticoid feedback
The authors noted that in healthy individuals, a supraphysiologic dexamethasone dose inhibits vasopressin and adrenocorticotropic hormone (ACTH) secretion, leading to decreased cortisol concentration. Cortisol concentrations of < 1-8 μg/dL in the morning (after administration of the dexamethasone between 11 p.m. and midnight) are considered “normal,” and a negative result “strongly predicts” the absence of CS. But false-positive and false-negative results can occur. Thus, “it is imperative that first-line testing is elected on the basis of physiologic conditions and drug intake — for example, use of CYP2A4/5 inhibitors or stimulators and oral estrogen — as well as laboratory quality control measure, and special attention to night shift workers,” Dr. Fleseriu emphasized.
- A 24-hour urinary free cortisol (UFC) test to assess increased bioavailable cortisol
The guideline encourages conducting several 24-hour urine collections to account for intra-patient variability.
Dr. Fleseriu recommended utilizing at least two of the three screening tests, all of which have reasonable sensitivity and specificity.
“Two normal test results usually exclude the presence of CS, except in rare cyclic CS,” she added.
Conduct Additional Laboratory Testing
Additional laboratory abnormalities suggestive of CS include:
- Increased leukocytes with decreased lymphocytes, eosinophils, monocytes, and basophils
- Elevated glucose and insulin levels
- Hypokalemia
- Increased triglycerides and total cholesterol levels
- Elevated liver enzymes
- Changes in activated thromboplastin time and plasma concentrations of pro- and anticoagulant factors
- Hypercalciuria, hypocalcemia (rare), hypophosphatemia, decreased phosphate maximum resorption, and increased alkaline phosphatase activity
Dr. Fleseriu noted that, in most cases, a final CS diagnosis can be reached after confirmation of biochemical hypercortisolism, which is done after an initial positive screening test.
She added that plasma ACTH levels are “instrumental” in distinguishing ACTH-depending forms of CS — such as Cushing disease and ectopic CS — from adrenal cases. Bilateral inferior petrosal sinus sampling is necessary in ACTH-dependent CS.
Utilize Diagnostic Imaging
There are several diagnostic imaging techniques that localize the origin of the hypercortisolism, thus informing the course of treatment.
- Pituitary MRI to detect corticotropin-secreting corticotroph adenomas, which are typically small lesions (< 6 mm in diameter)
- CT evaluation of the neck, thoracic cavity, and abdomen to diagnose ectopic CS, including lung neuroendocrine tumors and bronchial neuroendocrine tumors
- Cervical and thyroid ultrasonography to identify primary or metastatic medullary thyroid carcinoma, and PET scans, which have greater sensitivity in detecting tumors, compared with CT scans
- Contrast-enhanced CT scans to detect adrenal adenomas and adrenocortical carcinomas
Management of CS
“The primary aim of treatment is eucortisolemia, and in those with endogenous CS, complete surgical resection of the underlying tumor is the primary method,” Dr. Fleseriu said.
It’s critical to monitor for biochemical remission following surgery, utilizing 24-hour UFC, LNSC, and DST “because clinical manifestations may lag behind biochemical evidence.”
In Cushing disease, almost half of patients will have either persistent or recurrent hypercortisolemia after surgery. In those cases, individualized adjuvant treatments are recommended. These include repeat surgery, bilateral adrenalectomy, radiation, or medical treatments, including pituitary-directed drugs, adrenal steroidogenesis inhibitors, or glucocorticoid receptor-blocking agents. The last two groups are used for other types of CS.
Dr. Fleseriu pointed out that CS is “associated with increased metabolic, cardiovascular, psychiatric, infectious, and musculoskeletal morbidity, which are only partially reversible with successful [CS] treatment.” These comorbidities need to be addressed via individualized therapies. Moreover, long-term mortality is increased in all forms of CS. Thus, patients require lifelong follow-up to detect recurrence at an early stage and to treat comorbidities.
“It is likely that delayed diagnosis might explain the long-term consequences of CS, including increased morbidity and mortality despite remission,” she said.
Familiarity with the presenting signs and symptoms of CS and ordering recommended screening and confirmatory tests will enable appropriate management of the condition, leading to better outcomes.
Dr. Fleseriu reported receiving research grants from Sparrow Pharmaceuticals to Oregon Health and Science University as principal investigator and receiving occasional fees for scientific consulting/advisory boards from Sparrow Pharmaceuticals, Recordati Rare Diseases Inc., and Xeris Biopharma Holdings Inc.
A version of this article first appeared on Medscape.com.
“Moon face” is a term that’s become popular on social media, used to describe people with unusually round faces who are purported to have high levels of cortisol. But the term “moon face” isn’t new. It was actually coined in the 1930s by neurosurgeon Harvey Cushing, MD, who identified patients with a constellation of clinical characteristics — a condition that came to bear his name — which included rapidly developing facial adiposity. And indeed, elevated cortisol is a hallmark feature of Cushing syndrome (CS), but there are other reasons for elevated cortisol and other manifestations of CS.
Today, the term “moon face” has been replaced with “round face,” which is considered more encompassing and culturally sensitive, said Maria Fleseriu, MD, professor of medicine and neurological surgery and director of the Pituitary Center at Oregon Health and Science University in Portland, Oregon.
Facial roundness can lead clinicians to be suspicious that their patient is experiencing CS. But because a round face is associated with several other conditions, it’s important to be familiar with its particular presentation in CS, as well as how to diagnose and treat CS.
Pathophysiology of CS
Dr. Fleseriu defined CS as “prolonged nonphysiologic increase in cortisol, due either to exogenous use of steroids (oral, topical, or inhaled) or to excess endogenous cortisol production.” She added that it’s important “to always exclude exogenous causes before conducting a further workup to determine the type and cause of cortisol excess.”
Dr. Fleseriu said. Other causes of CS are ectopic (caused by neuroendocrine tumors) or adrenal. CS affects primarily females and typically has an onset between ages 20 and 50 years, depending on the CS type.
Diagnosis of CS is “substantially delayed for most patients, due to metabolic syndrome phenotypic overlap and lack of a single pathognomonic symptom,” according to Dr. Fleseriu.
An accurate diagnosis should be on the basis of signs and symptoms, biochemical screening, other laboratory testing, and diagnostic imaging.
Look for Clinical Signs and Symptoms of CS
“CS mostly presents as a combination of two or more features,” Dr. Fleseriu stated. These include increased fat pads (in the face, neck, and trunk), skin changes, signs of protein catabolism, growth retardation and body weight increase in children, and metabolic dysregulations (Table).
“Biochemical screening should be performed in patients with a combination of symptoms, and therefore an increased pretest probability for CS,” Dr. Fleseriu advised.
A CS diagnosis requires not only biochemical confirmation of hypercortisolemia but also determination of the underlying cause of the excess endogenous cortisol production. This is a key step, as the management of CS is specific to its etiology.
Elevated plasma cortisol alone is insufficient for diagnosing CS, as several conditions can be associated with physiologic, nonneoplastic endogenous hypercortisolemia, according to the 2021 updated CS guidelines for which Dr. Fleseriu served as a coauthor. These include depression, alcohol dependence, glucocorticoid resistance, obesity, diabetes, pregnancy, prolonged physical exertion, malnutrition, and cortisol-binding globulin excess.
The diagnosis begins with the following screening tests:
- Late-night salivary cortisol (LNSC) to assess an abnormal circadian rhythm
According to the 2021 guideline, this is “based on the assumption that patients with CS lose the normal circadian nadir of cortisol secretion.”
- Overnight 1-mg dexamethasone suppression test (DST) to assess impaired glucocorticoid feedback
The authors noted that in healthy individuals, a supraphysiologic dexamethasone dose inhibits vasopressin and adrenocorticotropic hormone (ACTH) secretion, leading to decreased cortisol concentration. Cortisol concentrations of < 1-8 μg/dL in the morning (after administration of the dexamethasone between 11 p.m. and midnight) are considered “normal,” and a negative result “strongly predicts” the absence of CS. But false-positive and false-negative results can occur. Thus, “it is imperative that first-line testing is elected on the basis of physiologic conditions and drug intake — for example, use of CYP2A4/5 inhibitors or stimulators and oral estrogen — as well as laboratory quality control measure, and special attention to night shift workers,” Dr. Fleseriu emphasized.
- A 24-hour urinary free cortisol (UFC) test to assess increased bioavailable cortisol
The guideline encourages conducting several 24-hour urine collections to account for intra-patient variability.
Dr. Fleseriu recommended utilizing at least two of the three screening tests, all of which have reasonable sensitivity and specificity.
“Two normal test results usually exclude the presence of CS, except in rare cyclic CS,” she added.
Conduct Additional Laboratory Testing
Additional laboratory abnormalities suggestive of CS include:
- Increased leukocytes with decreased lymphocytes, eosinophils, monocytes, and basophils
- Elevated glucose and insulin levels
- Hypokalemia
- Increased triglycerides and total cholesterol levels
- Elevated liver enzymes
- Changes in activated thromboplastin time and plasma concentrations of pro- and anticoagulant factors
- Hypercalciuria, hypocalcemia (rare), hypophosphatemia, decreased phosphate maximum resorption, and increased alkaline phosphatase activity
Dr. Fleseriu noted that, in most cases, a final CS diagnosis can be reached after confirmation of biochemical hypercortisolism, which is done after an initial positive screening test.
She added that plasma ACTH levels are “instrumental” in distinguishing ACTH-depending forms of CS — such as Cushing disease and ectopic CS — from adrenal cases. Bilateral inferior petrosal sinus sampling is necessary in ACTH-dependent CS.
Utilize Diagnostic Imaging
There are several diagnostic imaging techniques that localize the origin of the hypercortisolism, thus informing the course of treatment.
- Pituitary MRI to detect corticotropin-secreting corticotroph adenomas, which are typically small lesions (< 6 mm in diameter)
- CT evaluation of the neck, thoracic cavity, and abdomen to diagnose ectopic CS, including lung neuroendocrine tumors and bronchial neuroendocrine tumors
- Cervical and thyroid ultrasonography to identify primary or metastatic medullary thyroid carcinoma, and PET scans, which have greater sensitivity in detecting tumors, compared with CT scans
- Contrast-enhanced CT scans to detect adrenal adenomas and adrenocortical carcinomas
Management of CS
“The primary aim of treatment is eucortisolemia, and in those with endogenous CS, complete surgical resection of the underlying tumor is the primary method,” Dr. Fleseriu said.
It’s critical to monitor for biochemical remission following surgery, utilizing 24-hour UFC, LNSC, and DST “because clinical manifestations may lag behind biochemical evidence.”
In Cushing disease, almost half of patients will have either persistent or recurrent hypercortisolemia after surgery. In those cases, individualized adjuvant treatments are recommended. These include repeat surgery, bilateral adrenalectomy, radiation, or medical treatments, including pituitary-directed drugs, adrenal steroidogenesis inhibitors, or glucocorticoid receptor-blocking agents. The last two groups are used for other types of CS.
Dr. Fleseriu pointed out that CS is “associated with increased metabolic, cardiovascular, psychiatric, infectious, and musculoskeletal morbidity, which are only partially reversible with successful [CS] treatment.” These comorbidities need to be addressed via individualized therapies. Moreover, long-term mortality is increased in all forms of CS. Thus, patients require lifelong follow-up to detect recurrence at an early stage and to treat comorbidities.
“It is likely that delayed diagnosis might explain the long-term consequences of CS, including increased morbidity and mortality despite remission,” she said.
Familiarity with the presenting signs and symptoms of CS and ordering recommended screening and confirmatory tests will enable appropriate management of the condition, leading to better outcomes.
Dr. Fleseriu reported receiving research grants from Sparrow Pharmaceuticals to Oregon Health and Science University as principal investigator and receiving occasional fees for scientific consulting/advisory boards from Sparrow Pharmaceuticals, Recordati Rare Diseases Inc., and Xeris Biopharma Holdings Inc.
A version of this article first appeared on Medscape.com.
“Moon face” is a term that’s become popular on social media, used to describe people with unusually round faces who are purported to have high levels of cortisol. But the term “moon face” isn’t new. It was actually coined in the 1930s by neurosurgeon Harvey Cushing, MD, who identified patients with a constellation of clinical characteristics — a condition that came to bear his name — which included rapidly developing facial adiposity. And indeed, elevated cortisol is a hallmark feature of Cushing syndrome (CS), but there are other reasons for elevated cortisol and other manifestations of CS.
Today, the term “moon face” has been replaced with “round face,” which is considered more encompassing and culturally sensitive, said Maria Fleseriu, MD, professor of medicine and neurological surgery and director of the Pituitary Center at Oregon Health and Science University in Portland, Oregon.
Facial roundness can lead clinicians to be suspicious that their patient is experiencing CS. But because a round face is associated with several other conditions, it’s important to be familiar with its particular presentation in CS, as well as how to diagnose and treat CS.
Pathophysiology of CS
Dr. Fleseriu defined CS as “prolonged nonphysiologic increase in cortisol, due either to exogenous use of steroids (oral, topical, or inhaled) or to excess endogenous cortisol production.” She added that it’s important “to always exclude exogenous causes before conducting a further workup to determine the type and cause of cortisol excess.”
Dr. Fleseriu said. Other causes of CS are ectopic (caused by neuroendocrine tumors) or adrenal. CS affects primarily females and typically has an onset between ages 20 and 50 years, depending on the CS type.
Diagnosis of CS is “substantially delayed for most patients, due to metabolic syndrome phenotypic overlap and lack of a single pathognomonic symptom,” according to Dr. Fleseriu.
An accurate diagnosis should be on the basis of signs and symptoms, biochemical screening, other laboratory testing, and diagnostic imaging.
Look for Clinical Signs and Symptoms of CS
“CS mostly presents as a combination of two or more features,” Dr. Fleseriu stated. These include increased fat pads (in the face, neck, and trunk), skin changes, signs of protein catabolism, growth retardation and body weight increase in children, and metabolic dysregulations (Table).
“Biochemical screening should be performed in patients with a combination of symptoms, and therefore an increased pretest probability for CS,” Dr. Fleseriu advised.
A CS diagnosis requires not only biochemical confirmation of hypercortisolemia but also determination of the underlying cause of the excess endogenous cortisol production. This is a key step, as the management of CS is specific to its etiology.
Elevated plasma cortisol alone is insufficient for diagnosing CS, as several conditions can be associated with physiologic, nonneoplastic endogenous hypercortisolemia, according to the 2021 updated CS guidelines for which Dr. Fleseriu served as a coauthor. These include depression, alcohol dependence, glucocorticoid resistance, obesity, diabetes, pregnancy, prolonged physical exertion, malnutrition, and cortisol-binding globulin excess.
The diagnosis begins with the following screening tests:
- Late-night salivary cortisol (LNSC) to assess an abnormal circadian rhythm
According to the 2021 guideline, this is “based on the assumption that patients with CS lose the normal circadian nadir of cortisol secretion.”
- Overnight 1-mg dexamethasone suppression test (DST) to assess impaired glucocorticoid feedback
The authors noted that in healthy individuals, a supraphysiologic dexamethasone dose inhibits vasopressin and adrenocorticotropic hormone (ACTH) secretion, leading to decreased cortisol concentration. Cortisol concentrations of < 1-8 μg/dL in the morning (after administration of the dexamethasone between 11 p.m. and midnight) are considered “normal,” and a negative result “strongly predicts” the absence of CS. But false-positive and false-negative results can occur. Thus, “it is imperative that first-line testing is elected on the basis of physiologic conditions and drug intake — for example, use of CYP2A4/5 inhibitors or stimulators and oral estrogen — as well as laboratory quality control measure, and special attention to night shift workers,” Dr. Fleseriu emphasized.
- A 24-hour urinary free cortisol (UFC) test to assess increased bioavailable cortisol
The guideline encourages conducting several 24-hour urine collections to account for intra-patient variability.
Dr. Fleseriu recommended utilizing at least two of the three screening tests, all of which have reasonable sensitivity and specificity.
“Two normal test results usually exclude the presence of CS, except in rare cyclic CS,” she added.
Conduct Additional Laboratory Testing
Additional laboratory abnormalities suggestive of CS include:
- Increased leukocytes with decreased lymphocytes, eosinophils, monocytes, and basophils
- Elevated glucose and insulin levels
- Hypokalemia
- Increased triglycerides and total cholesterol levels
- Elevated liver enzymes
- Changes in activated thromboplastin time and plasma concentrations of pro- and anticoagulant factors
- Hypercalciuria, hypocalcemia (rare), hypophosphatemia, decreased phosphate maximum resorption, and increased alkaline phosphatase activity
Dr. Fleseriu noted that, in most cases, a final CS diagnosis can be reached after confirmation of biochemical hypercortisolism, which is done after an initial positive screening test.
She added that plasma ACTH levels are “instrumental” in distinguishing ACTH-depending forms of CS — such as Cushing disease and ectopic CS — from adrenal cases. Bilateral inferior petrosal sinus sampling is necessary in ACTH-dependent CS.
Utilize Diagnostic Imaging
There are several diagnostic imaging techniques that localize the origin of the hypercortisolism, thus informing the course of treatment.
- Pituitary MRI to detect corticotropin-secreting corticotroph adenomas, which are typically small lesions (< 6 mm in diameter)
- CT evaluation of the neck, thoracic cavity, and abdomen to diagnose ectopic CS, including lung neuroendocrine tumors and bronchial neuroendocrine tumors
- Cervical and thyroid ultrasonography to identify primary or metastatic medullary thyroid carcinoma, and PET scans, which have greater sensitivity in detecting tumors, compared with CT scans
- Contrast-enhanced CT scans to detect adrenal adenomas and adrenocortical carcinomas
Management of CS
“The primary aim of treatment is eucortisolemia, and in those with endogenous CS, complete surgical resection of the underlying tumor is the primary method,” Dr. Fleseriu said.
It’s critical to monitor for biochemical remission following surgery, utilizing 24-hour UFC, LNSC, and DST “because clinical manifestations may lag behind biochemical evidence.”
In Cushing disease, almost half of patients will have either persistent or recurrent hypercortisolemia after surgery. In those cases, individualized adjuvant treatments are recommended. These include repeat surgery, bilateral adrenalectomy, radiation, or medical treatments, including pituitary-directed drugs, adrenal steroidogenesis inhibitors, or glucocorticoid receptor-blocking agents. The last two groups are used for other types of CS.
Dr. Fleseriu pointed out that CS is “associated with increased metabolic, cardiovascular, psychiatric, infectious, and musculoskeletal morbidity, which are only partially reversible with successful [CS] treatment.” These comorbidities need to be addressed via individualized therapies. Moreover, long-term mortality is increased in all forms of CS. Thus, patients require lifelong follow-up to detect recurrence at an early stage and to treat comorbidities.
“It is likely that delayed diagnosis might explain the long-term consequences of CS, including increased morbidity and mortality despite remission,” she said.
Familiarity with the presenting signs and symptoms of CS and ordering recommended screening and confirmatory tests will enable appropriate management of the condition, leading to better outcomes.
Dr. Fleseriu reported receiving research grants from Sparrow Pharmaceuticals to Oregon Health and Science University as principal investigator and receiving occasional fees for scientific consulting/advisory boards from Sparrow Pharmaceuticals, Recordati Rare Diseases Inc., and Xeris Biopharma Holdings Inc.
A version of this article first appeared on Medscape.com.
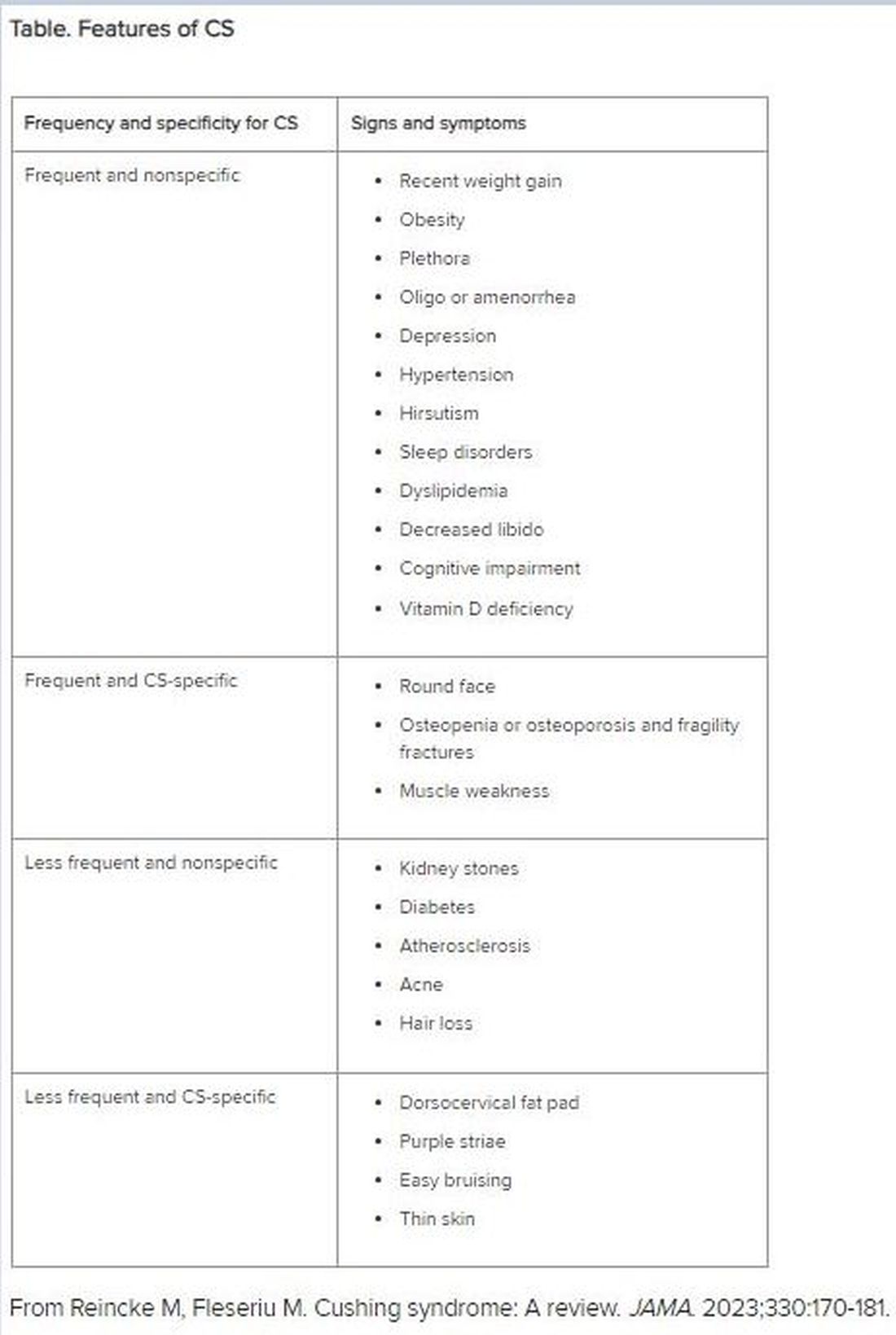
Patients With Immune-Mediated Inflammatory Diseases, Type 2 Diabetes Reap GLP-1 Receptor Agonist Benefits, Too
TOPLINE:
Compared with dipeptidyl peptidase 4 (DPP-4) inhibitors, glucagon-like peptide 1 receptor agonists (GLP-1 RAs) are associated with a lower risk for all-cause mortality and major adverse cardiovascular events (MACE) in patients with immune-mediated inflammatory diseases (IMIDs) and type 2 diabetes (T2D).
METHODOLOGY:
- GLP-1 RAs reduce the risk for all-cause mortality, cardiovascular mortality, and stroke in patients with diabetes. However, previous trials have excluded those with IMIDs, leaving a gap in understanding the cardioprotective effects of GLP-1 RAs in this population.
- Researchers conducted a population-based cohort study to assess if patients with an IMID derive greater benefits from GLP-1 RAs than DPP-4 inhibitors.
- They used administrative health data from British Columbia, Canada, to include 10,855 patients with IMIDs (rheumatoid arthritis, psoriatic disease, ankylosing spondylitis, inflammatory bowel disease, or systemic autoimmune rheumatic disease) and T2D who initiated either GLP-1 RA (n = 3570) or DPP-4 inhibitor (n = 7285).
- The mean follow-up was 1.46 and 1.88 years in the GLP-1 RA and DPP-4 inhibitor cohorts, respectively.
- The primary outcome was all-cause mortality, and the secondary outcome was MACE, including cardiovascular death, myocardial infarction, and ischemic stroke.
TAKEAWAY:
- The risk for all-cause mortality was 52% lower in patients who initiated GLP-1 RAs than in those who initiated DPP-4 inhibitors (weighted hazard ratio [HR], 0.48; 95% CI, 0.31-0.75).
- Additionally, patients initiating DPP-4 inhibitors.
- In the subgroup of patients with GLP-1 RAs had a significantly lower risk for MACE (weighted HR, 0.66; 95% CI, 0.50-0.88), particularly myocardial infarction (weighted HR, 0.62; 95% CI, 0.40-0.96), than those initiating rheumatoid arthritis and T2D, those who initiated GLP-1 RAs had a 55% lower risk for all-cause mortality and 61% lower risk for MACE than those who initiated DPP-4 inhibitors.
IN PRACTICE:
“This corresponds to nine fewer deaths and 11 fewer MACE per 1000 person-years, respectively, supporting the hypothesis that these agents have a cardioprotective effect in this high-risk population,” the authors wrote.
SOURCE:
This study was led by Derin Karacabeyli, MD, Division of Rheumatology, Department of Medicine, University of British Columbia, Vancouver, Canada, and was published online on August 8, 2024, in PLOS ONE.
LIMITATIONS:
The study’s dependence on administrative health data might have resulted in incomplete capture of comorbidities, particularly obesity. The mean follow-up period was relatively short, which might have limited the long-term applicability of these findings. The accuracy of the case definitions for IMIDs and T2D, according to International Classification of Diseases codes, could not be fully ascertained.
DISCLOSURES:
The study was supported by grants from the Canadian Institutes of Health Research. Two authors declared receiving research support, consulting fees, or participating in advisory boards outside the submitted work.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Compared with dipeptidyl peptidase 4 (DPP-4) inhibitors, glucagon-like peptide 1 receptor agonists (GLP-1 RAs) are associated with a lower risk for all-cause mortality and major adverse cardiovascular events (MACE) in patients with immune-mediated inflammatory diseases (IMIDs) and type 2 diabetes (T2D).
METHODOLOGY:
- GLP-1 RAs reduce the risk for all-cause mortality, cardiovascular mortality, and stroke in patients with diabetes. However, previous trials have excluded those with IMIDs, leaving a gap in understanding the cardioprotective effects of GLP-1 RAs in this population.
- Researchers conducted a population-based cohort study to assess if patients with an IMID derive greater benefits from GLP-1 RAs than DPP-4 inhibitors.
- They used administrative health data from British Columbia, Canada, to include 10,855 patients with IMIDs (rheumatoid arthritis, psoriatic disease, ankylosing spondylitis, inflammatory bowel disease, or systemic autoimmune rheumatic disease) and T2D who initiated either GLP-1 RA (n = 3570) or DPP-4 inhibitor (n = 7285).
- The mean follow-up was 1.46 and 1.88 years in the GLP-1 RA and DPP-4 inhibitor cohorts, respectively.
- The primary outcome was all-cause mortality, and the secondary outcome was MACE, including cardiovascular death, myocardial infarction, and ischemic stroke.
TAKEAWAY:
- The risk for all-cause mortality was 52% lower in patients who initiated GLP-1 RAs than in those who initiated DPP-4 inhibitors (weighted hazard ratio [HR], 0.48; 95% CI, 0.31-0.75).
- Additionally, patients initiating DPP-4 inhibitors.
- In the subgroup of patients with GLP-1 RAs had a significantly lower risk for MACE (weighted HR, 0.66; 95% CI, 0.50-0.88), particularly myocardial infarction (weighted HR, 0.62; 95% CI, 0.40-0.96), than those initiating rheumatoid arthritis and T2D, those who initiated GLP-1 RAs had a 55% lower risk for all-cause mortality and 61% lower risk for MACE than those who initiated DPP-4 inhibitors.
IN PRACTICE:
“This corresponds to nine fewer deaths and 11 fewer MACE per 1000 person-years, respectively, supporting the hypothesis that these agents have a cardioprotective effect in this high-risk population,” the authors wrote.
SOURCE:
This study was led by Derin Karacabeyli, MD, Division of Rheumatology, Department of Medicine, University of British Columbia, Vancouver, Canada, and was published online on August 8, 2024, in PLOS ONE.
LIMITATIONS:
The study’s dependence on administrative health data might have resulted in incomplete capture of comorbidities, particularly obesity. The mean follow-up period was relatively short, which might have limited the long-term applicability of these findings. The accuracy of the case definitions for IMIDs and T2D, according to International Classification of Diseases codes, could not be fully ascertained.
DISCLOSURES:
The study was supported by grants from the Canadian Institutes of Health Research. Two authors declared receiving research support, consulting fees, or participating in advisory boards outside the submitted work.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Compared with dipeptidyl peptidase 4 (DPP-4) inhibitors, glucagon-like peptide 1 receptor agonists (GLP-1 RAs) are associated with a lower risk for all-cause mortality and major adverse cardiovascular events (MACE) in patients with immune-mediated inflammatory diseases (IMIDs) and type 2 diabetes (T2D).
METHODOLOGY:
- GLP-1 RAs reduce the risk for all-cause mortality, cardiovascular mortality, and stroke in patients with diabetes. However, previous trials have excluded those with IMIDs, leaving a gap in understanding the cardioprotective effects of GLP-1 RAs in this population.
- Researchers conducted a population-based cohort study to assess if patients with an IMID derive greater benefits from GLP-1 RAs than DPP-4 inhibitors.
- They used administrative health data from British Columbia, Canada, to include 10,855 patients with IMIDs (rheumatoid arthritis, psoriatic disease, ankylosing spondylitis, inflammatory bowel disease, or systemic autoimmune rheumatic disease) and T2D who initiated either GLP-1 RA (n = 3570) or DPP-4 inhibitor (n = 7285).
- The mean follow-up was 1.46 and 1.88 years in the GLP-1 RA and DPP-4 inhibitor cohorts, respectively.
- The primary outcome was all-cause mortality, and the secondary outcome was MACE, including cardiovascular death, myocardial infarction, and ischemic stroke.
TAKEAWAY:
- The risk for all-cause mortality was 52% lower in patients who initiated GLP-1 RAs than in those who initiated DPP-4 inhibitors (weighted hazard ratio [HR], 0.48; 95% CI, 0.31-0.75).
- Additionally, patients initiating DPP-4 inhibitors.
- In the subgroup of patients with GLP-1 RAs had a significantly lower risk for MACE (weighted HR, 0.66; 95% CI, 0.50-0.88), particularly myocardial infarction (weighted HR, 0.62; 95% CI, 0.40-0.96), than those initiating rheumatoid arthritis and T2D, those who initiated GLP-1 RAs had a 55% lower risk for all-cause mortality and 61% lower risk for MACE than those who initiated DPP-4 inhibitors.
IN PRACTICE:
“This corresponds to nine fewer deaths and 11 fewer MACE per 1000 person-years, respectively, supporting the hypothesis that these agents have a cardioprotective effect in this high-risk population,” the authors wrote.
SOURCE:
This study was led by Derin Karacabeyli, MD, Division of Rheumatology, Department of Medicine, University of British Columbia, Vancouver, Canada, and was published online on August 8, 2024, in PLOS ONE.
LIMITATIONS:
The study’s dependence on administrative health data might have resulted in incomplete capture of comorbidities, particularly obesity. The mean follow-up period was relatively short, which might have limited the long-term applicability of these findings. The accuracy of the case definitions for IMIDs and T2D, according to International Classification of Diseases codes, could not be fully ascertained.
DISCLOSURES:
The study was supported by grants from the Canadian Institutes of Health Research. Two authors declared receiving research support, consulting fees, or participating in advisory boards outside the submitted work.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.