User login
Analgesia for the Body, Mind, and Soul: It’s Complicated
Cancer pain wasn’t on my mind when I carved out time this week to attend Cottage Health System’s psychiatric grand rounds entitled, “Dueling Diagnosis: Complicated Pain and Substance Use Disorders,” in Santa Barbara. But the lecture by Dr. Jerry Lerner, chief of pain medicine at Arizona’s Sierra Tucson residential treatment center, soon had me thinking about the many levels of pain suffered by patients diagnosed with cancer and other organic diseases.
Ironically, the oncology community has struggled for years against the erroneous belief among patients and family members that effectively managing cancer pain will make addicts of patients once they’re cured. It’s simply not true, of course, but the barriers to effective cancer pain management are vast, multifactorial, and deeply held, as documented by the International Association for the Study of Pain.
As they say in the pain medicine world, it’s complicated.

And becoming even more so, it would seem.
A growing epidemic of prescription painkiller abuse, especially among young adults, will mean that a growing number of cancer patients arrive at our doorsteps already grappling with pre-existing addictions to opioids. The past decade has seen a 400% increase in substance disorders arising from prescription painkiller use, resulting in an overdose rate that today outpaces deaths from heroin and cocaine combined, according to the Centers for Disease Control and Prevention.
Dr. Lerner outlined a delicate strategy for treating moderate to severe pain in patients with preexisting addiction or dependency problems. Any pain at a 6 or above on a 0-10 pain scale must be treated medically, he said, or attempts at treating the substance problem will be undermined by a diminishment of therapeutic trust and a lack of “attendance, attention, and intention.”
On the other hand, pain is more than the mere presence of nerve signals to the brain because of compromised tissue.
Long-term opioid use can create hyperalgesia, a condition where the body is actually more sensitized to pain, Dr. Lerner explained. “Things that didn’t hurt before, hurt,” he said.
With 1 in 20 Americans over the age of 12 years – an estimated 12 million people – diverting and using prescription painkillers “nonmedically,” chances are that many present and future cancer patients will present to oncologists already resistant to the relief such medications might offer for cancer-related pain.
Dr. Lerner emphasized as well that pain of all kinds is influenced not only by physical biological events (tumor growth, for example), but by other factors as well: inflammation (sometimes activated or exacerbated by stress and fear), hypersensitivity from overactivity of the sympathetic nervous system, unresolved emotional trauma, and dysfunctional relationships.
He views each of these as “tumblers” in the combination lock that must be cracked to adequately treat pain, be it the result of a broken bone, a tumor, or a body-wide pain syndrome of unknown origin.
With most cancer patients, the physical source of pain is clear, and no preexisting painkiller addiction will interfere with the action of appropriately prescribed analgesics. Still, the evidence is growing that pain is a multisystemic, multifactorial challenge, felt more acutely in the face of fear or stress, so the wise guidance of those who treat “Dueling Diagnoses” will add value to the treatment of cancer pain, even in the most straightforward of cases.
Dr. Freed is a psychologist in Santa Barbara, Calif., and a medical journalist.
Cancer pain wasn’t on my mind when I carved out time this week to attend Cottage Health System’s psychiatric grand rounds entitled, “Dueling Diagnosis: Complicated Pain and Substance Use Disorders,” in Santa Barbara. But the lecture by Dr. Jerry Lerner, chief of pain medicine at Arizona’s Sierra Tucson residential treatment center, soon had me thinking about the many levels of pain suffered by patients diagnosed with cancer and other organic diseases.
Ironically, the oncology community has struggled for years against the erroneous belief among patients and family members that effectively managing cancer pain will make addicts of patients once they’re cured. It’s simply not true, of course, but the barriers to effective cancer pain management are vast, multifactorial, and deeply held, as documented by the International Association for the Study of Pain.
As they say in the pain medicine world, it’s complicated.
And becoming even more so, it would seem.
A growing epidemic of prescription painkiller abuse, especially among young adults, will mean that a growing number of cancer patients arrive at our doorsteps already grappling with pre-existing addictions to opioids. The past decade has seen a 400% increase in substance disorders arising from prescription painkiller use, resulting in an overdose rate that today outpaces deaths from heroin and cocaine combined, according to the Centers for Disease Control and Prevention.
Dr. Lerner outlined a delicate strategy for treating moderate to severe pain in patients with preexisting addiction or dependency problems. Any pain at a 6 or above on a 0-10 pain scale must be treated medically, he said, or attempts at treating the substance problem will be undermined by a diminishment of therapeutic trust and a lack of “attendance, attention, and intention.”
On the other hand, pain is more than the mere presence of nerve signals to the brain because of compromised tissue.
Long-term opioid use can create hyperalgesia, a condition where the body is actually more sensitized to pain, Dr. Lerner explained. “Things that didn’t hurt before, hurt,” he said.
With 1 in 20 Americans over the age of 12 years – an estimated 12 million people – diverting and using prescription painkillers “nonmedically,” chances are that many present and future cancer patients will present to oncologists already resistant to the relief such medications might offer for cancer-related pain.
Dr. Lerner emphasized as well that pain of all kinds is influenced not only by physical biological events (tumor growth, for example), but by other factors as well: inflammation (sometimes activated or exacerbated by stress and fear), hypersensitivity from overactivity of the sympathetic nervous system, unresolved emotional trauma, and dysfunctional relationships.
He views each of these as “tumblers” in the combination lock that must be cracked to adequately treat pain, be it the result of a broken bone, a tumor, or a body-wide pain syndrome of unknown origin.
With most cancer patients, the physical source of pain is clear, and no preexisting painkiller addiction will interfere with the action of appropriately prescribed analgesics. Still, the evidence is growing that pain is a multisystemic, multifactorial challenge, felt more acutely in the face of fear or stress, so the wise guidance of those who treat “Dueling Diagnoses” will add value to the treatment of cancer pain, even in the most straightforward of cases.
Dr. Freed is a psychologist in Santa Barbara, Calif., and a medical journalist.
Cancer pain wasn’t on my mind when I carved out time this week to attend Cottage Health System’s psychiatric grand rounds entitled, “Dueling Diagnosis: Complicated Pain and Substance Use Disorders,” in Santa Barbara. But the lecture by Dr. Jerry Lerner, chief of pain medicine at Arizona’s Sierra Tucson residential treatment center, soon had me thinking about the many levels of pain suffered by patients diagnosed with cancer and other organic diseases.
Ironically, the oncology community has struggled for years against the erroneous belief among patients and family members that effectively managing cancer pain will make addicts of patients once they’re cured. It’s simply not true, of course, but the barriers to effective cancer pain management are vast, multifactorial, and deeply held, as documented by the International Association for the Study of Pain.
As they say in the pain medicine world, it’s complicated.
And becoming even more so, it would seem.
A growing epidemic of prescription painkiller abuse, especially among young adults, will mean that a growing number of cancer patients arrive at our doorsteps already grappling with pre-existing addictions to opioids. The past decade has seen a 400% increase in substance disorders arising from prescription painkiller use, resulting in an overdose rate that today outpaces deaths from heroin and cocaine combined, according to the Centers for Disease Control and Prevention.
Dr. Lerner outlined a delicate strategy for treating moderate to severe pain in patients with preexisting addiction or dependency problems. Any pain at a 6 or above on a 0-10 pain scale must be treated medically, he said, or attempts at treating the substance problem will be undermined by a diminishment of therapeutic trust and a lack of “attendance, attention, and intention.”
On the other hand, pain is more than the mere presence of nerve signals to the brain because of compromised tissue.
Long-term opioid use can create hyperalgesia, a condition where the body is actually more sensitized to pain, Dr. Lerner explained. “Things that didn’t hurt before, hurt,” he said.
With 1 in 20 Americans over the age of 12 years – an estimated 12 million people – diverting and using prescription painkillers “nonmedically,” chances are that many present and future cancer patients will present to oncologists already resistant to the relief such medications might offer for cancer-related pain.
Dr. Lerner emphasized as well that pain of all kinds is influenced not only by physical biological events (tumor growth, for example), but by other factors as well: inflammation (sometimes activated or exacerbated by stress and fear), hypersensitivity from overactivity of the sympathetic nervous system, unresolved emotional trauma, and dysfunctional relationships.
He views each of these as “tumblers” in the combination lock that must be cracked to adequately treat pain, be it the result of a broken bone, a tumor, or a body-wide pain syndrome of unknown origin.
With most cancer patients, the physical source of pain is clear, and no preexisting painkiller addiction will interfere with the action of appropriately prescribed analgesics. Still, the evidence is growing that pain is a multisystemic, multifactorial challenge, felt more acutely in the face of fear or stress, so the wise guidance of those who treat “Dueling Diagnoses” will add value to the treatment of cancer pain, even in the most straightforward of cases.
Dr. Freed is a psychologist in Santa Barbara, Calif., and a medical journalist.

Tips to Facing Difficult Patient Conversations
At the eighth annual Chicago Supportive Oncology Conference, we spoke with Dr. Anthony Back about talking to patients about the cost of care and whether the costs are worth it. Dr. Back stressed that it is crucial for cost to be a part of the decision making process, and not a separate stand-alone issue. He added that it is the physician who should take the lead in initiating this discussion.
Dr. Back is a professor in the Department of Medicine, Division of Oncology at the University of Washington's School of Medicine and a medical oncologist with the Seattle Cancer Care Alliance in Seattle, Washington.
At the eighth annual Chicago Supportive Oncology Conference, we spoke with Dr. Anthony Back about talking to patients about the cost of care and whether the costs are worth it. Dr. Back stressed that it is crucial for cost to be a part of the decision making process, and not a separate stand-alone issue. He added that it is the physician who should take the lead in initiating this discussion.
Dr. Back is a professor in the Department of Medicine, Division of Oncology at the University of Washington's School of Medicine and a medical oncologist with the Seattle Cancer Care Alliance in Seattle, Washington.
At the eighth annual Chicago Supportive Oncology Conference, we spoke with Dr. Anthony Back about talking to patients about the cost of care and whether the costs are worth it. Dr. Back stressed that it is crucial for cost to be a part of the decision making process, and not a separate stand-alone issue. He added that it is the physician who should take the lead in initiating this discussion.
Dr. Back is a professor in the Department of Medicine, Division of Oncology at the University of Washington's School of Medicine and a medical oncologist with the Seattle Cancer Care Alliance in Seattle, Washington.
End-of-Life Care Can Bring on Challenges for Hospitalists
How do you cope with a family that wants you to "do everything" for their seriously ill loved one? This dilemma was one of the topics explored at the Management of the Hospitalized Patient conference held last month at the University of California at San Francisco (UCSF).
"We don't actually know what 'everything' means to the family, not without probing into a range of possible meanings," said presenter Steve Pantilat, MD, FACP, SFHM, hospitalist and director of the palliative-care service at UCSF Medical Center. "The family may not have a clear understanding of what 'everything' entails, including mechanical ventilation or cardio-pulmonary resuscitation. I prefer to ask, 'How were you hoping we could help?' The answer can provide a great deal of insight."
In spite of various tools to aid decisions, prognosis is inherently uncertain, said co-presenter Matthew Gonzales, MD, assistant professor of hospital medicine and palliative care at UCSF Medical Center. "We use the Palliative Performance Scale [PDF]."
The family might not trust the hospitalist’s prognosis, especially when meeting the doctor for the first time in a stressful situation, and there might be disagreements within the family about the course of treatment, Dr. Gonzales said. Cultural differences also come into play.
"I have started to ask, 'How do you decide these questions in your family?' because of the differences within a cultural group," Dr. Pantilat said. "If they talk about hoping for a miracle, I probe the meaning of 'miracle' to them. Physicians can't work on the basis of miracles; they have to practice medicine. And you should resist getting drawn into a religious debate. That's a loser for the physician."
Visit our website for more information about palliative care.
How do you cope with a family that wants you to "do everything" for their seriously ill loved one? This dilemma was one of the topics explored at the Management of the Hospitalized Patient conference held last month at the University of California at San Francisco (UCSF).
"We don't actually know what 'everything' means to the family, not without probing into a range of possible meanings," said presenter Steve Pantilat, MD, FACP, SFHM, hospitalist and director of the palliative-care service at UCSF Medical Center. "The family may not have a clear understanding of what 'everything' entails, including mechanical ventilation or cardio-pulmonary resuscitation. I prefer to ask, 'How were you hoping we could help?' The answer can provide a great deal of insight."
In spite of various tools to aid decisions, prognosis is inherently uncertain, said co-presenter Matthew Gonzales, MD, assistant professor of hospital medicine and palliative care at UCSF Medical Center. "We use the Palliative Performance Scale [PDF]."
The family might not trust the hospitalist’s prognosis, especially when meeting the doctor for the first time in a stressful situation, and there might be disagreements within the family about the course of treatment, Dr. Gonzales said. Cultural differences also come into play.
"I have started to ask, 'How do you decide these questions in your family?' because of the differences within a cultural group," Dr. Pantilat said. "If they talk about hoping for a miracle, I probe the meaning of 'miracle' to them. Physicians can't work on the basis of miracles; they have to practice medicine. And you should resist getting drawn into a religious debate. That's a loser for the physician."
Visit our website for more information about palliative care.
How do you cope with a family that wants you to "do everything" for their seriously ill loved one? This dilemma was one of the topics explored at the Management of the Hospitalized Patient conference held last month at the University of California at San Francisco (UCSF).
"We don't actually know what 'everything' means to the family, not without probing into a range of possible meanings," said presenter Steve Pantilat, MD, FACP, SFHM, hospitalist and director of the palliative-care service at UCSF Medical Center. "The family may not have a clear understanding of what 'everything' entails, including mechanical ventilation or cardio-pulmonary resuscitation. I prefer to ask, 'How were you hoping we could help?' The answer can provide a great deal of insight."
In spite of various tools to aid decisions, prognosis is inherently uncertain, said co-presenter Matthew Gonzales, MD, assistant professor of hospital medicine and palliative care at UCSF Medical Center. "We use the Palliative Performance Scale [PDF]."
The family might not trust the hospitalist’s prognosis, especially when meeting the doctor for the first time in a stressful situation, and there might be disagreements within the family about the course of treatment, Dr. Gonzales said. Cultural differences also come into play.
"I have started to ask, 'How do you decide these questions in your family?' because of the differences within a cultural group," Dr. Pantilat said. "If they talk about hoping for a miracle, I probe the meaning of 'miracle' to them. Physicians can't work on the basis of miracles; they have to practice medicine. And you should resist getting drawn into a religious debate. That's a loser for the physician."
Visit our website for more information about palliative care.
Earlier End-of-Life Talks Deter Aggressive Care of Terminal Cancer Patients
Patients with stage IV lung or colorectal cancer who had end-of-life discussions with caregivers before the last 30 days of life were significantly less likely to receive aggressive care in their final days and more likely to get hospice care and to enter hospice earlier, a study of 1,231 patients found.
Nearly half received some kind of aggressive care in their last 30 days (47%), including chemotherapy in the last 14 days (16%), ICU care in the last 30 days (6%), and/or acute hospital-based care in the last 30 days of life (40%), Dr. Jennifer W. Mack and her associates reported.
Multiple current guidelines recommend starting end-of-life care planning for patients with incurable cancer early in the course of the disease while patients are relatively stable, not when they are acutely deteriorating.
Many physicians in the study postponed the discussion until the final month of life, and many patients didn’t remember or didn’t recognize the end-of-life discussions. Discussions that were documented in charts were not associated with less-aggressive care or greater hospice use, if patients or their surrogates said no end-of-life discussions took place.
Eighty-eight percent of patients in the current study had end-of-life discussions. Twenty-three percent of the discussion were reported by patients or their surrogates in interviews but not documented in records, 17% were documented in medical records but not reported by patients or surrogates, and 48% were both reported and documented.
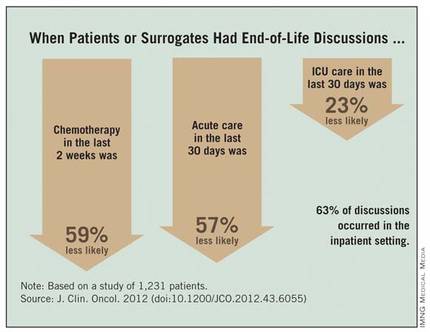
Among the 794 patients with end-of-life discussions documented in medical records, 39% took place in the last 30 days of life, 63% happened in the inpatient setting, and 40% included an oncologist. Fifty-eight percent of patients entered hospice care, which started in the last 7 days of life for 15% of them, reported Dr. Mack, a pediatric oncologist at the Dana-Farber Cancer Institute and Harvard Medical School, Boston.
The study was published online Nov. 13, 2012 by the Journal of Clinical Oncology (doi:10.1200/JCO.2012.43.6055).
Chemotherapy in the last 2 weeks of life was 59% less likely, acute care in the last 30 days was 57% less likely, and ICU care in the last 30 days was 23% less likely when patients or surrogates reported having end-of-life discussions.
Patients Followed 15 Months After Diagnosis
Patients whose first end-of-life discussion happened while they were hospitalized were more than twice as likely to get any kind of aggressive care at the end of life and three times more likely to get acute care or ICU care in the last 30 days and to have hospice care start within the last week before death.

Having a medical oncologist present at the first end-of-life discussion increased the odds of having chemotherapy in the last 2 weeks of life by 48%, decreased the odds of ICU care in the last 30 days by 56%, increased the likelihood of hospice care by 43%, and doubled the chance of hospice care starting in the last 7 days of life. All of these odds ratios were significant after controlling for other factors.
Data came from a larger cohort of 2,155 patients with stage IV lung or colorectal cancer receiving care in HMOs or Veterans Affairs medical centers in five states. All were followed for 15 months after diagnosis in the Cancer Care Outcomes Research and Surveillance Consortium.
An earlier analysis by the same investigators showed that 87% of the 1,470 patients who died and 41% of the 685 still alive by the end of follow-up had end-of-life care discussions, but oncologists documented end-of-life discussions with only 27% of their patients, suggesting that most discussions were with non-oncologists. Among those who died, documented discussions took place a median of 33 days before death (Ann. Intern. Med. 2012;156:204-10).
"Our previous study on this database found that most physicians do have end-of-life discussions before death, but most occur near the end of life," Dr. Mack said in an interview.
The current study analyzed data for 1,231 of the patients who died but who lived at least 1 month after diagnosis, in order to assess whether the timing of discussions influenced end-of-life care. "Besides the fact that that seems like logical practice, there really wasn’t a clear evidence base that that affects care," she said.
Patients were significantly less likely to say they’d had an end-of-life discussion if they were unmarried, black or non-white Hispanic, or not in an HMO.
Start Talks Closer to Diagnosis
When discussions don’t begin until the last 30 days of life, the end-of-life period usually is already underway, the investigators noted. Physicians should consider moving end-of-life care discussions closer to diagnosis, they suggested, while patients are relatively well and have time to plan for what’s ahead.
"It’s something that any physician can do," but some previous studies report that physicians are reluctant to start end-of-life discussions early because these are emotionally difficult conversations, they worry about taking away hope, and they are concerned about the psychological impact on patients – though there is no clear evidence that it does have psychological consequences for patients, Dr. Mack said.
"It’s a compassionate instinct," she said. "Being in the room with a family when I deliver this kind of news, that emotional impact is right in front of me. I believe there are bigger consequences" from not discussing end-of-life care, such as perpetuating false hopes and asking people to make decisions about what’s ahead without a clear picture of the situation, she added.
The conversation should take place more than once because patient preferences may change over time and patients need time to process the information and their thoughts about it, Dr. Mack said.
Ask Patients What They Hear
Further work is needed on why some documented end-of-life discussions were not reported by patients/surrogates. "Every physician can relate to this, that sometimes we have conversations but they’re not heard or understood by patients," she said. "It reminds me that I need to ask patients what they’re taking away from these conversations and use that to guide me going forward."
That finding echoes two recent large, population-based studies that found many patients with terminal cancer mistakenly think that palliative chemotherapy or radiation will cure their disease.
Some previous studies suggest that patients dying of cancer increasingly are receiving aggressive care at the end of life and that this trend may be modifiable. Cross-sectional studies that assessed one point in time between diagnosis and death have shown that many patients don’t have end-of-life discussions, but these studies probably missed discussions closer to death, Dr. Mack noted.
Other studies have reported an association between having end-of-life discussions and reduced intensity in care. The current study was longitudinal and is one of the first to look at the effects of the timing of these discussions and other factors.
Most patients who realize that they are dying do not want aggressive care, previous studies have shown. Other studies report that less-aggressive end-of-life care is easier on family members and less expensive.
Guidelines from the National Comprehensive Cancer Network, the National Consensus Project for Quality Palliative Care, the American Society of Clinical Oncology, and the American College of Physicians and American Society of Internal Medicine recommend beginning end-of-life discussions early for patients with incurable cancer.
When investigators conducted secondary analyses that excluded patients from Veterans Affairs sites or excluded interviews with patient surrogates, the findings were similar to results of the main analysis.
In the current analysis, 82% of patients had lung cancer, and the rest had colorectal cancer.
Future research on this topic could take many paths, Dr. Mack suggested, including implementing routine early discussions and seeing whether that alters the intensity of final care. Much more could be learned about the quality of discussions between physicians and patients. The current study had no data on discussions led by nurses or social workers or that took place among family members without a medical provider present.
"We’re also interested in looking at a longer trajectory of end-of-life decision making" for patients with incurable cancer – from diagnosis to death, she said.
Dr. Mack and her associates reported having no financial disclosures.
This is an important study that documents the fact that early discussions about end-of-life care for patients with stage IV cancer are associated with decreased intensity of care at the end of life, and that the timing of the initiation of these discussions is very important and should happen earlier than it does much of the time.
This is not the first study to show that this communication is associated with decreased intensity of care (JAMA 2008;300:1665-73). However, this is an important study because it is the first to document that early discussions are important (prior to the last 30 days of life).

|
|
Moving end-of-life discussions closer to diagnosis definitely is realistic and the way this should occur. However, it is not an "either-or" situation. Early discussions don’t mean that later discussions aren’t necessary and important. Early discussions set the frame and make it easier to have later discussions if/when patients get worse.
There is a need for physicians to improve communication to make sure patients or their surrogates understand end-of-life discussions. Our challenge now is to find successful ways to teach these communication skills to physicians and help physicians implement these discussions in clinical practice. It is not useful to tell physicians to have these discussions if they haven’t been trained to do it well, and we don’t create systems that make it practical and feasible.
When the Obama administration tried to implement a policy of paying physicians to conduct advance care planning on an annual basis through Medicare, Sarah Palin and others used the "death panel" scare tactics to defeat this important effort. We need to change the public discussion to be more aware of the importance of early and regular discussions about advance care planning.
We also need research to figure out how best to implement "earlier discussions" in clinical practice and to identify the long-term consequences of such a practice.
Dr. J. Randall Curtis is director of the University of Washington Palliative Care Center of Excellence and head of Pulmonary and Critical Care Medicine at Harborview Medical Center, Seattle. He provided these comments in an interview. Dr. Curtis reported having no financial disclosures.
This is an important study that documents the fact that early discussions about end-of-life care for patients with stage IV cancer are associated with decreased intensity of care at the end of life, and that the timing of the initiation of these discussions is very important and should happen earlier than it does much of the time.
This is not the first study to show that this communication is associated with decreased intensity of care (JAMA 2008;300:1665-73). However, this is an important study because it is the first to document that early discussions are important (prior to the last 30 days of life).
|
|
|
Moving end-of-life discussions closer to diagnosis definitely is realistic and the way this should occur. However, it is not an "either-or" situation. Early discussions don’t mean that later discussions aren’t necessary and important. Early discussions set the frame and make it easier to have later discussions if/when patients get worse.
There is a need for physicians to improve communication to make sure patients or their surrogates understand end-of-life discussions. Our challenge now is to find successful ways to teach these communication skills to physicians and help physicians implement these discussions in clinical practice. It is not useful to tell physicians to have these discussions if they haven’t been trained to do it well, and we don’t create systems that make it practical and feasible.
When the Obama administration tried to implement a policy of paying physicians to conduct advance care planning on an annual basis through Medicare, Sarah Palin and others used the "death panel" scare tactics to defeat this important effort. We need to change the public discussion to be more aware of the importance of early and regular discussions about advance care planning.
We also need research to figure out how best to implement "earlier discussions" in clinical practice and to identify the long-term consequences of such a practice.
Dr. J. Randall Curtis is director of the University of Washington Palliative Care Center of Excellence and head of Pulmonary and Critical Care Medicine at Harborview Medical Center, Seattle. He provided these comments in an interview. Dr. Curtis reported having no financial disclosures.
This is an important study that documents the fact that early discussions about end-of-life care for patients with stage IV cancer are associated with decreased intensity of care at the end of life, and that the timing of the initiation of these discussions is very important and should happen earlier than it does much of the time.
This is not the first study to show that this communication is associated with decreased intensity of care (JAMA 2008;300:1665-73). However, this is an important study because it is the first to document that early discussions are important (prior to the last 30 days of life).
|
|
|
Moving end-of-life discussions closer to diagnosis definitely is realistic and the way this should occur. However, it is not an "either-or" situation. Early discussions don’t mean that later discussions aren’t necessary and important. Early discussions set the frame and make it easier to have later discussions if/when patients get worse.
There is a need for physicians to improve communication to make sure patients or their surrogates understand end-of-life discussions. Our challenge now is to find successful ways to teach these communication skills to physicians and help physicians implement these discussions in clinical practice. It is not useful to tell physicians to have these discussions if they haven’t been trained to do it well, and we don’t create systems that make it practical and feasible.
When the Obama administration tried to implement a policy of paying physicians to conduct advance care planning on an annual basis through Medicare, Sarah Palin and others used the "death panel" scare tactics to defeat this important effort. We need to change the public discussion to be more aware of the importance of early and regular discussions about advance care planning.
We also need research to figure out how best to implement "earlier discussions" in clinical practice and to identify the long-term consequences of such a practice.
Dr. J. Randall Curtis is director of the University of Washington Palliative Care Center of Excellence and head of Pulmonary and Critical Care Medicine at Harborview Medical Center, Seattle. He provided these comments in an interview. Dr. Curtis reported having no financial disclosures.
Patients with stage IV lung or colorectal cancer who had end-of-life discussions with caregivers before the last 30 days of life were significantly less likely to receive aggressive care in their final days and more likely to get hospice care and to enter hospice earlier, a study of 1,231 patients found.
Nearly half received some kind of aggressive care in their last 30 days (47%), including chemotherapy in the last 14 days (16%), ICU care in the last 30 days (6%), and/or acute hospital-based care in the last 30 days of life (40%), Dr. Jennifer W. Mack and her associates reported.
Multiple current guidelines recommend starting end-of-life care planning for patients with incurable cancer early in the course of the disease while patients are relatively stable, not when they are acutely deteriorating.
Many physicians in the study postponed the discussion until the final month of life, and many patients didn’t remember or didn’t recognize the end-of-life discussions. Discussions that were documented in charts were not associated with less-aggressive care or greater hospice use, if patients or their surrogates said no end-of-life discussions took place.
Eighty-eight percent of patients in the current study had end-of-life discussions. Twenty-three percent of the discussion were reported by patients or their surrogates in interviews but not documented in records, 17% were documented in medical records but not reported by patients or surrogates, and 48% were both reported and documented.
Among the 794 patients with end-of-life discussions documented in medical records, 39% took place in the last 30 days of life, 63% happened in the inpatient setting, and 40% included an oncologist. Fifty-eight percent of patients entered hospice care, which started in the last 7 days of life for 15% of them, reported Dr. Mack, a pediatric oncologist at the Dana-Farber Cancer Institute and Harvard Medical School, Boston.
The study was published online Nov. 13, 2012 by the Journal of Clinical Oncology (doi:10.1200/JCO.2012.43.6055).
Chemotherapy in the last 2 weeks of life was 59% less likely, acute care in the last 30 days was 57% less likely, and ICU care in the last 30 days was 23% less likely when patients or surrogates reported having end-of-life discussions.
Patients Followed 15 Months After Diagnosis
Patients whose first end-of-life discussion happened while they were hospitalized were more than twice as likely to get any kind of aggressive care at the end of life and three times more likely to get acute care or ICU care in the last 30 days and to have hospice care start within the last week before death.
Having a medical oncologist present at the first end-of-life discussion increased the odds of having chemotherapy in the last 2 weeks of life by 48%, decreased the odds of ICU care in the last 30 days by 56%, increased the likelihood of hospice care by 43%, and doubled the chance of hospice care starting in the last 7 days of life. All of these odds ratios were significant after controlling for other factors.
Data came from a larger cohort of 2,155 patients with stage IV lung or colorectal cancer receiving care in HMOs or Veterans Affairs medical centers in five states. All were followed for 15 months after diagnosis in the Cancer Care Outcomes Research and Surveillance Consortium.
An earlier analysis by the same investigators showed that 87% of the 1,470 patients who died and 41% of the 685 still alive by the end of follow-up had end-of-life care discussions, but oncologists documented end-of-life discussions with only 27% of their patients, suggesting that most discussions were with non-oncologists. Among those who died, documented discussions took place a median of 33 days before death (Ann. Intern. Med. 2012;156:204-10).
"Our previous study on this database found that most physicians do have end-of-life discussions before death, but most occur near the end of life," Dr. Mack said in an interview.
The current study analyzed data for 1,231 of the patients who died but who lived at least 1 month after diagnosis, in order to assess whether the timing of discussions influenced end-of-life care. "Besides the fact that that seems like logical practice, there really wasn’t a clear evidence base that that affects care," she said.
Patients were significantly less likely to say they’d had an end-of-life discussion if they were unmarried, black or non-white Hispanic, or not in an HMO.
Start Talks Closer to Diagnosis
When discussions don’t begin until the last 30 days of life, the end-of-life period usually is already underway, the investigators noted. Physicians should consider moving end-of-life care discussions closer to diagnosis, they suggested, while patients are relatively well and have time to plan for what’s ahead.
"It’s something that any physician can do," but some previous studies report that physicians are reluctant to start end-of-life discussions early because these are emotionally difficult conversations, they worry about taking away hope, and they are concerned about the psychological impact on patients – though there is no clear evidence that it does have psychological consequences for patients, Dr. Mack said.
"It’s a compassionate instinct," she said. "Being in the room with a family when I deliver this kind of news, that emotional impact is right in front of me. I believe there are bigger consequences" from not discussing end-of-life care, such as perpetuating false hopes and asking people to make decisions about what’s ahead without a clear picture of the situation, she added.
The conversation should take place more than once because patient preferences may change over time and patients need time to process the information and their thoughts about it, Dr. Mack said.
Ask Patients What They Hear
Further work is needed on why some documented end-of-life discussions were not reported by patients/surrogates. "Every physician can relate to this, that sometimes we have conversations but they’re not heard or understood by patients," she said. "It reminds me that I need to ask patients what they’re taking away from these conversations and use that to guide me going forward."
That finding echoes two recent large, population-based studies that found many patients with terminal cancer mistakenly think that palliative chemotherapy or radiation will cure their disease.
Some previous studies suggest that patients dying of cancer increasingly are receiving aggressive care at the end of life and that this trend may be modifiable. Cross-sectional studies that assessed one point in time between diagnosis and death have shown that many patients don’t have end-of-life discussions, but these studies probably missed discussions closer to death, Dr. Mack noted.
Other studies have reported an association between having end-of-life discussions and reduced intensity in care. The current study was longitudinal and is one of the first to look at the effects of the timing of these discussions and other factors.
Most patients who realize that they are dying do not want aggressive care, previous studies have shown. Other studies report that less-aggressive end-of-life care is easier on family members and less expensive.
Guidelines from the National Comprehensive Cancer Network, the National Consensus Project for Quality Palliative Care, the American Society of Clinical Oncology, and the American College of Physicians and American Society of Internal Medicine recommend beginning end-of-life discussions early for patients with incurable cancer.
When investigators conducted secondary analyses that excluded patients from Veterans Affairs sites or excluded interviews with patient surrogates, the findings were similar to results of the main analysis.
In the current analysis, 82% of patients had lung cancer, and the rest had colorectal cancer.
Future research on this topic could take many paths, Dr. Mack suggested, including implementing routine early discussions and seeing whether that alters the intensity of final care. Much more could be learned about the quality of discussions between physicians and patients. The current study had no data on discussions led by nurses or social workers or that took place among family members without a medical provider present.
"We’re also interested in looking at a longer trajectory of end-of-life decision making" for patients with incurable cancer – from diagnosis to death, she said.
Dr. Mack and her associates reported having no financial disclosures.
Patients with stage IV lung or colorectal cancer who had end-of-life discussions with caregivers before the last 30 days of life were significantly less likely to receive aggressive care in their final days and more likely to get hospice care and to enter hospice earlier, a study of 1,231 patients found.
Nearly half received some kind of aggressive care in their last 30 days (47%), including chemotherapy in the last 14 days (16%), ICU care in the last 30 days (6%), and/or acute hospital-based care in the last 30 days of life (40%), Dr. Jennifer W. Mack and her associates reported.
Multiple current guidelines recommend starting end-of-life care planning for patients with incurable cancer early in the course of the disease while patients are relatively stable, not when they are acutely deteriorating.
Many physicians in the study postponed the discussion until the final month of life, and many patients didn’t remember or didn’t recognize the end-of-life discussions. Discussions that were documented in charts were not associated with less-aggressive care or greater hospice use, if patients or their surrogates said no end-of-life discussions took place.
Eighty-eight percent of patients in the current study had end-of-life discussions. Twenty-three percent of the discussion were reported by patients or their surrogates in interviews but not documented in records, 17% were documented in medical records but not reported by patients or surrogates, and 48% were both reported and documented.
Among the 794 patients with end-of-life discussions documented in medical records, 39% took place in the last 30 days of life, 63% happened in the inpatient setting, and 40% included an oncologist. Fifty-eight percent of patients entered hospice care, which started in the last 7 days of life for 15% of them, reported Dr. Mack, a pediatric oncologist at the Dana-Farber Cancer Institute and Harvard Medical School, Boston.
The study was published online Nov. 13, 2012 by the Journal of Clinical Oncology (doi:10.1200/JCO.2012.43.6055).
Chemotherapy in the last 2 weeks of life was 59% less likely, acute care in the last 30 days was 57% less likely, and ICU care in the last 30 days was 23% less likely when patients or surrogates reported having end-of-life discussions.
Patients Followed 15 Months After Diagnosis
Patients whose first end-of-life discussion happened while they were hospitalized were more than twice as likely to get any kind of aggressive care at the end of life and three times more likely to get acute care or ICU care in the last 30 days and to have hospice care start within the last week before death.
Having a medical oncologist present at the first end-of-life discussion increased the odds of having chemotherapy in the last 2 weeks of life by 48%, decreased the odds of ICU care in the last 30 days by 56%, increased the likelihood of hospice care by 43%, and doubled the chance of hospice care starting in the last 7 days of life. All of these odds ratios were significant after controlling for other factors.
Data came from a larger cohort of 2,155 patients with stage IV lung or colorectal cancer receiving care in HMOs or Veterans Affairs medical centers in five states. All were followed for 15 months after diagnosis in the Cancer Care Outcomes Research and Surveillance Consortium.
An earlier analysis by the same investigators showed that 87% of the 1,470 patients who died and 41% of the 685 still alive by the end of follow-up had end-of-life care discussions, but oncologists documented end-of-life discussions with only 27% of their patients, suggesting that most discussions were with non-oncologists. Among those who died, documented discussions took place a median of 33 days before death (Ann. Intern. Med. 2012;156:204-10).
"Our previous study on this database found that most physicians do have end-of-life discussions before death, but most occur near the end of life," Dr. Mack said in an interview.
The current study analyzed data for 1,231 of the patients who died but who lived at least 1 month after diagnosis, in order to assess whether the timing of discussions influenced end-of-life care. "Besides the fact that that seems like logical practice, there really wasn’t a clear evidence base that that affects care," she said.
Patients were significantly less likely to say they’d had an end-of-life discussion if they were unmarried, black or non-white Hispanic, or not in an HMO.
Start Talks Closer to Diagnosis
When discussions don’t begin until the last 30 days of life, the end-of-life period usually is already underway, the investigators noted. Physicians should consider moving end-of-life care discussions closer to diagnosis, they suggested, while patients are relatively well and have time to plan for what’s ahead.
"It’s something that any physician can do," but some previous studies report that physicians are reluctant to start end-of-life discussions early because these are emotionally difficult conversations, they worry about taking away hope, and they are concerned about the psychological impact on patients – though there is no clear evidence that it does have psychological consequences for patients, Dr. Mack said.
"It’s a compassionate instinct," she said. "Being in the room with a family when I deliver this kind of news, that emotional impact is right in front of me. I believe there are bigger consequences" from not discussing end-of-life care, such as perpetuating false hopes and asking people to make decisions about what’s ahead without a clear picture of the situation, she added.
The conversation should take place more than once because patient preferences may change over time and patients need time to process the information and their thoughts about it, Dr. Mack said.
Ask Patients What They Hear
Further work is needed on why some documented end-of-life discussions were not reported by patients/surrogates. "Every physician can relate to this, that sometimes we have conversations but they’re not heard or understood by patients," she said. "It reminds me that I need to ask patients what they’re taking away from these conversations and use that to guide me going forward."
That finding echoes two recent large, population-based studies that found many patients with terminal cancer mistakenly think that palliative chemotherapy or radiation will cure their disease.
Some previous studies suggest that patients dying of cancer increasingly are receiving aggressive care at the end of life and that this trend may be modifiable. Cross-sectional studies that assessed one point in time between diagnosis and death have shown that many patients don’t have end-of-life discussions, but these studies probably missed discussions closer to death, Dr. Mack noted.
Other studies have reported an association between having end-of-life discussions and reduced intensity in care. The current study was longitudinal and is one of the first to look at the effects of the timing of these discussions and other factors.
Most patients who realize that they are dying do not want aggressive care, previous studies have shown. Other studies report that less-aggressive end-of-life care is easier on family members and less expensive.
Guidelines from the National Comprehensive Cancer Network, the National Consensus Project for Quality Palliative Care, the American Society of Clinical Oncology, and the American College of Physicians and American Society of Internal Medicine recommend beginning end-of-life discussions early for patients with incurable cancer.
When investigators conducted secondary analyses that excluded patients from Veterans Affairs sites or excluded interviews with patient surrogates, the findings were similar to results of the main analysis.
In the current analysis, 82% of patients had lung cancer, and the rest had colorectal cancer.
Future research on this topic could take many paths, Dr. Mack suggested, including implementing routine early discussions and seeing whether that alters the intensity of final care. Much more could be learned about the quality of discussions between physicians and patients. The current study had no data on discussions led by nurses or social workers or that took place among family members without a medical provider present.
"We’re also interested in looking at a longer trajectory of end-of-life decision making" for patients with incurable cancer – from diagnosis to death, she said.
Dr. Mack and her associates reported having no financial disclosures.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Major Finding: Chemotherapy in the last 2 weeks of life was 59% less likely, acute care in the last 30 days was 57% less likely, and ICU care in the last 30 days was 23% less likely when patients or their surrogates reported having end-of-life discussions.
Data Source: This was a longitudinal study of 1,231 patients with stage IV lung or colorectal cancer at HMOs or Veterans Affairs sites in five states.
Disclosures: Dr. Mack and her associates reported having no financial disclosures.

Experts: Palliative Care Lowers Costs
It is very common for health care professionals to want to shy away from those difficult conversations with patients when caring for them throughout their cancer treatment.
At the eighth annual Chicago Supportive Oncology Conference, Thomas J. Smith, M.D., Director of Palliative Care for Johns Hopkins Medicine and the Hopkins’ Sidney Kimmel Comprehensive Cancer Center, offered practical insight on the economics of integrating palliative care.
When it comes to discussing patient preferences for end-of-life and treatment decisions, Dr. Smith said: "People do want this information; it won't make [them] depressed; it won’t take away their hope; it won’t make them die sooner. We can give realistic forecasts for survival. It is always culturally appropriate to ask, 'How much do you know about your illness?' "
Is it possible to provide the best in care while "bending the cost curve" by having open and honest discussions with your patients? Absolutely, said Dr. Smith, because "we are asking [them] what is important to them." (See the commentary, "Talking with Patients about Dying,” by Dr. Smith and Dan L. Longo, M.D.; N Engl J Med 2012;367:1651-2.)
It is very common for health care professionals to want to shy away from those difficult conversations with patients when caring for them throughout their cancer treatment.
At the eighth annual Chicago Supportive Oncology Conference, Thomas J. Smith, M.D., Director of Palliative Care for Johns Hopkins Medicine and the Hopkins’ Sidney Kimmel Comprehensive Cancer Center, offered practical insight on the economics of integrating palliative care.
When it comes to discussing patient preferences for end-of-life and treatment decisions, Dr. Smith said: "People do want this information; it won't make [them] depressed; it won’t take away their hope; it won’t make them die sooner. We can give realistic forecasts for survival. It is always culturally appropriate to ask, 'How much do you know about your illness?' "
Is it possible to provide the best in care while "bending the cost curve" by having open and honest discussions with your patients? Absolutely, said Dr. Smith, because "we are asking [them] what is important to them." (See the commentary, "Talking with Patients about Dying,” by Dr. Smith and Dan L. Longo, M.D.; N Engl J Med 2012;367:1651-2.)
It is very common for health care professionals to want to shy away from those difficult conversations with patients when caring for them throughout their cancer treatment.
At the eighth annual Chicago Supportive Oncology Conference, Thomas J. Smith, M.D., Director of Palliative Care for Johns Hopkins Medicine and the Hopkins’ Sidney Kimmel Comprehensive Cancer Center, offered practical insight on the economics of integrating palliative care.
When it comes to discussing patient preferences for end-of-life and treatment decisions, Dr. Smith said: "People do want this information; it won't make [them] depressed; it won’t take away their hope; it won’t make them die sooner. We can give realistic forecasts for survival. It is always culturally appropriate to ask, 'How much do you know about your illness?' "
Is it possible to provide the best in care while "bending the cost curve" by having open and honest discussions with your patients? Absolutely, said Dr. Smith, because "we are asking [them] what is important to them." (See the commentary, "Talking with Patients about Dying,” by Dr. Smith and Dan L. Longo, M.D.; N Engl J Med 2012;367:1651-2.)

Palliative Care Teams in 65% of Hospitals
Portion of hospitals that had palliative-care teams in 2010, according to the latest tally from the Center to Advance Palliative Care at Mount Sinai School of Medicine in New York City (www.capc.org), an increase of 148.5% from 2000. Hospitals of 300-plus beds are more likely to have a palliative-care team than those with fewer than 300 beds (87.9% vs. 56.5%).
Portion of hospitals that had palliative-care teams in 2010, according to the latest tally from the Center to Advance Palliative Care at Mount Sinai School of Medicine in New York City (www.capc.org), an increase of 148.5% from 2000. Hospitals of 300-plus beds are more likely to have a palliative-care team than those with fewer than 300 beds (87.9% vs. 56.5%).
Portion of hospitals that had palliative-care teams in 2010, according to the latest tally from the Center to Advance Palliative Care at Mount Sinai School of Medicine in New York City (www.capc.org), an increase of 148.5% from 2000. Hospitals of 300-plus beds are more likely to have a palliative-care team than those with fewer than 300 beds (87.9% vs. 56.5%).
Medical Coding: Hospice Care vs. Palliative Care
Hospice care” and “palliative care” are not synonymous terms. Hospice care is defined as a comprehensive set of services (see “Hospice Coverage,” below) identified and coordinated by an interdisciplinary group to provide for the physical, psychosocial, spiritual, and emotional needs of a terminally ill patient and/or family members, as delineated in a specific patient plan of care.1 Palliative care is defined as patient- and family-centered care that optimizes quality of life by anticipating, preventing, and treating suffering. Palliative care throughout the continuum of illness involves addressing physical, intellectual, emotional, social, and spiritual needs, and facilitates patient autonomy, access to information, and choice.1
As an approach, hospice care of terminally ill individuals involves palliative care (relief of pain and uncomfortable symptoms), and emphasizes maintaining the patient at home with family and friends as long as possible. Hospice services can be provided in a home, center, skilled-nursing facility, or hospital setting. In contrast, palliative-care services can be provided during hospice care, or coincide with care that is focused on a cure.
Many hospitalists provide both hospice care and palliative-care services to their patients. Different factors affect how to report these services. These programs can be quite costly, as they involve several team members and a substantial amount of time delivering these services. Capturing services appropriately and obtaining reimbursement to help continue program initiatives are significant issues.
Hospice Care
When a patient enrolls in hospice, all rights to Medicare Part B payments are waived during the benefit period involving professional services related to the treatment and management of the terminal illness. Payment is made through the Part A benefit for the associated costs of daily care and the services provided by the hospice-employed physician. An exception occurs for professional services of an independent attending physician who is not an employee of the designated hospice and does not receive compensation from the hospice for those services. The “attending physician” for hospice services must be an individual who is a doctor of medicine or osteopathy, or a nurse practitioner identified by the individual, at the time they elect hospice coverage, as having the most significant role in the determination and delivery of their medical care.2
Patients often receive hospice in the hospital setting, where the hospitalist manages the patient’s daily care. If the hospitalist is designated as the “attending physician” for hospice services, the visits should be reported to Medicare Part B with modifier GV (e.g. 99232-GV).3 This will allow for separate payment to the hospitalist (the independent attending physician), while the hospice agency maintains its daily-care rate. Reporting services absent this modifier will result in denial.
In some cases, the hospitalist is not identified as the “attending physician” for hospice services but occasionally provides care related to the terminal illness. This situation proves most difficult. Although the hospitalist might be the most accessible physician to the staff and is putting the patient’s needs first, reimbursement is unlikely. Regulations stipulate that patients must not see independent physicians other than their “attending physician” for care related to their terminal illness unless the hospice arranges it. When the service is related to the hospice patient’s terminal illness but was furnished by someone other than the designated “attending physician,” this “other physician” must look to the hospice for payment.3
Nonhospice Palliative Care
Members of the palliative-care team often are called to provide management options to assist in reducing pain and suffering. When the palliative-care specialist is asked to provide opinions or advice, the initial service may qualify as a consultation for those payors that still recognize these codes. However, all of the requirements4 must be met in order to report the service as an inpatient consultation (99251-99255):3
- There must be a written request from a qualified healthcare provider who is involved in the patient’s care (e.g. physician, resident, nurse practitioner); this may be documented as a physician order or in the assessment/plan of the requesting provider’s progress note. Standing orders for consultation are not permitted.
- The requesting provider should clearly and accurately identify the reason for consult request to support the medical necessity of the service.
- The palliative-care physician renders and documents the service.
- The palliative-care physician reports his or her findings to the requesting physician via written communication; because the requesting physician and the consultant share a common inpatient medical record, the consultant’s inpatient progress note satisfies the “written report” requirement.
Consider the nature of the request when reporting a consultation. If the request demonstrates the need for opinions or advice from the palliative-care specialist, the service can be reported as a consultation. If the indication cites “medical management” or “palliative management,” payors are less likely to consider the service as a consultation because the physician is not seeking opinions or advice from the consultant to incorporate into his or her own plan of care for the patient and would rather the consultant just take over that portion of patient care. When consultations do not meet the requirements, subsequent hospital care services should be reported (99231-99233).3
The requesting physician can be in the same or a different provider group as the consultant. The consultant must possess expertise in an area that is beyond that of the requesting provider. Because most hospitalists carry a specialty designation of internal medicine (physician specialty code 11), hospitalists providing palliative-care services can distinguish themselves by their own code (physician specialty code 17, hospice and palliative care).5 Payor concerns arise when physicians of the same designated specialty submit a claim for the same patient on the same date. The payor is likely to pay the first claim received and deny the second claim received pending review of documentation. If this occurs, submit a copy of both progress notes for the date in question to distinguish the services provided. The payor may still require that both encounters be reported as one cumulative service under one physician.
Consultations are not an option for Medicare beneficiaries. Hospitalists providing palliative care can report initial hospital care codes (99221-99223) for their first encounter with the patient.3 This is only acceptable when no other hospitalist from the group has reported initial hospital care during the patient stay, unless the palliative-care hospitalist carries the corresponding designation (i.e. enrolled with Medicare as physician specialty code 17). Without this separate designation, the palliative-care hospitalist can only report subsequent hospital care codes (99231-99233) as the patient was seen previously by a hospitalist in the same group.3
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- U.S. Government Printing Office. Electronic Code of Federal Regulations: Title 42: Public Health, Part 418: Hospice Care, §418.3. June 2012. U.S. Government Printing Office website. Available at: http://ecfr.gpoaccess.gov/cgi/t/text/text-idx?c=ecfr&sid=818258235647b14d2961ad30fa3e68e6&rgn=div5&view=text&node=42:3.0.1.1.5&idno=42#42:3.0.1.1.5.1.3.3. Accessed June 23, 2012.
- Centers for Medicare & Medicaid Services. Medicare Claims Processing Manual: Chapter 11: processing hospice claims. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c11.pdf. Accessed June 23, 2012.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011.
- American Medical Association. Consultation services and transfer of care. American Medical Association website. Available at: http://www.ama-assn.org/resources/doc/cpt/cpt-consultation-services.pdf. Accessed June 23, 2012.
- Centers for Medicare & Medicaid Services. Medicare Claims Processing Manual: Chapter 26: completing and processing form CMS-1500 data set. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c26.pdf. Accessed June 23, 2012. Department of Health and Human Services.
- Hospice Payment System: payment system fact sheet series. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/hospice_pay_sys_fs.pdf. Accessed June 23, 2012.
Hospice care” and “palliative care” are not synonymous terms. Hospice care is defined as a comprehensive set of services (see “Hospice Coverage,” below) identified and coordinated by an interdisciplinary group to provide for the physical, psychosocial, spiritual, and emotional needs of a terminally ill patient and/or family members, as delineated in a specific patient plan of care.1 Palliative care is defined as patient- and family-centered care that optimizes quality of life by anticipating, preventing, and treating suffering. Palliative care throughout the continuum of illness involves addressing physical, intellectual, emotional, social, and spiritual needs, and facilitates patient autonomy, access to information, and choice.1
As an approach, hospice care of terminally ill individuals involves palliative care (relief of pain and uncomfortable symptoms), and emphasizes maintaining the patient at home with family and friends as long as possible. Hospice services can be provided in a home, center, skilled-nursing facility, or hospital setting. In contrast, palliative-care services can be provided during hospice care, or coincide with care that is focused on a cure.
Many hospitalists provide both hospice care and palliative-care services to their patients. Different factors affect how to report these services. These programs can be quite costly, as they involve several team members and a substantial amount of time delivering these services. Capturing services appropriately and obtaining reimbursement to help continue program initiatives are significant issues.
Hospice Care
When a patient enrolls in hospice, all rights to Medicare Part B payments are waived during the benefit period involving professional services related to the treatment and management of the terminal illness. Payment is made through the Part A benefit for the associated costs of daily care and the services provided by the hospice-employed physician. An exception occurs for professional services of an independent attending physician who is not an employee of the designated hospice and does not receive compensation from the hospice for those services. The “attending physician” for hospice services must be an individual who is a doctor of medicine or osteopathy, or a nurse practitioner identified by the individual, at the time they elect hospice coverage, as having the most significant role in the determination and delivery of their medical care.2
Patients often receive hospice in the hospital setting, where the hospitalist manages the patient’s daily care. If the hospitalist is designated as the “attending physician” for hospice services, the visits should be reported to Medicare Part B with modifier GV (e.g. 99232-GV).3 This will allow for separate payment to the hospitalist (the independent attending physician), while the hospice agency maintains its daily-care rate. Reporting services absent this modifier will result in denial.
In some cases, the hospitalist is not identified as the “attending physician” for hospice services but occasionally provides care related to the terminal illness. This situation proves most difficult. Although the hospitalist might be the most accessible physician to the staff and is putting the patient’s needs first, reimbursement is unlikely. Regulations stipulate that patients must not see independent physicians other than their “attending physician” for care related to their terminal illness unless the hospice arranges it. When the service is related to the hospice patient’s terminal illness but was furnished by someone other than the designated “attending physician,” this “other physician” must look to the hospice for payment.3
Nonhospice Palliative Care
Members of the palliative-care team often are called to provide management options to assist in reducing pain and suffering. When the palliative-care specialist is asked to provide opinions or advice, the initial service may qualify as a consultation for those payors that still recognize these codes. However, all of the requirements4 must be met in order to report the service as an inpatient consultation (99251-99255):3
- There must be a written request from a qualified healthcare provider who is involved in the patient’s care (e.g. physician, resident, nurse practitioner); this may be documented as a physician order or in the assessment/plan of the requesting provider’s progress note. Standing orders for consultation are not permitted.
- The requesting provider should clearly and accurately identify the reason for consult request to support the medical necessity of the service.
- The palliative-care physician renders and documents the service.
- The palliative-care physician reports his or her findings to the requesting physician via written communication; because the requesting physician and the consultant share a common inpatient medical record, the consultant’s inpatient progress note satisfies the “written report” requirement.
Consider the nature of the request when reporting a consultation. If the request demonstrates the need for opinions or advice from the palliative-care specialist, the service can be reported as a consultation. If the indication cites “medical management” or “palliative management,” payors are less likely to consider the service as a consultation because the physician is not seeking opinions or advice from the consultant to incorporate into his or her own plan of care for the patient and would rather the consultant just take over that portion of patient care. When consultations do not meet the requirements, subsequent hospital care services should be reported (99231-99233).3
The requesting physician can be in the same or a different provider group as the consultant. The consultant must possess expertise in an area that is beyond that of the requesting provider. Because most hospitalists carry a specialty designation of internal medicine (physician specialty code 11), hospitalists providing palliative-care services can distinguish themselves by their own code (physician specialty code 17, hospice and palliative care).5 Payor concerns arise when physicians of the same designated specialty submit a claim for the same patient on the same date. The payor is likely to pay the first claim received and deny the second claim received pending review of documentation. If this occurs, submit a copy of both progress notes for the date in question to distinguish the services provided. The payor may still require that both encounters be reported as one cumulative service under one physician.
Consultations are not an option for Medicare beneficiaries. Hospitalists providing palliative care can report initial hospital care codes (99221-99223) for their first encounter with the patient.3 This is only acceptable when no other hospitalist from the group has reported initial hospital care during the patient stay, unless the palliative-care hospitalist carries the corresponding designation (i.e. enrolled with Medicare as physician specialty code 17). Without this separate designation, the palliative-care hospitalist can only report subsequent hospital care codes (99231-99233) as the patient was seen previously by a hospitalist in the same group.3
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- U.S. Government Printing Office. Electronic Code of Federal Regulations: Title 42: Public Health, Part 418: Hospice Care, §418.3. June 2012. U.S. Government Printing Office website. Available at: http://ecfr.gpoaccess.gov/cgi/t/text/text-idx?c=ecfr&sid=818258235647b14d2961ad30fa3e68e6&rgn=div5&view=text&node=42:3.0.1.1.5&idno=42#42:3.0.1.1.5.1.3.3. Accessed June 23, 2012.
- Centers for Medicare & Medicaid Services. Medicare Claims Processing Manual: Chapter 11: processing hospice claims. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c11.pdf. Accessed June 23, 2012.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011.
- American Medical Association. Consultation services and transfer of care. American Medical Association website. Available at: http://www.ama-assn.org/resources/doc/cpt/cpt-consultation-services.pdf. Accessed June 23, 2012.
- Centers for Medicare & Medicaid Services. Medicare Claims Processing Manual: Chapter 26: completing and processing form CMS-1500 data set. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c26.pdf. Accessed June 23, 2012. Department of Health and Human Services.
- Hospice Payment System: payment system fact sheet series. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/hospice_pay_sys_fs.pdf. Accessed June 23, 2012.
Hospice care” and “palliative care” are not synonymous terms. Hospice care is defined as a comprehensive set of services (see “Hospice Coverage,” below) identified and coordinated by an interdisciplinary group to provide for the physical, psychosocial, spiritual, and emotional needs of a terminally ill patient and/or family members, as delineated in a specific patient plan of care.1 Palliative care is defined as patient- and family-centered care that optimizes quality of life by anticipating, preventing, and treating suffering. Palliative care throughout the continuum of illness involves addressing physical, intellectual, emotional, social, and spiritual needs, and facilitates patient autonomy, access to information, and choice.1
As an approach, hospice care of terminally ill individuals involves palliative care (relief of pain and uncomfortable symptoms), and emphasizes maintaining the patient at home with family and friends as long as possible. Hospice services can be provided in a home, center, skilled-nursing facility, or hospital setting. In contrast, palliative-care services can be provided during hospice care, or coincide with care that is focused on a cure.
Many hospitalists provide both hospice care and palliative-care services to their patients. Different factors affect how to report these services. These programs can be quite costly, as they involve several team members and a substantial amount of time delivering these services. Capturing services appropriately and obtaining reimbursement to help continue program initiatives are significant issues.
Hospice Care
When a patient enrolls in hospice, all rights to Medicare Part B payments are waived during the benefit period involving professional services related to the treatment and management of the terminal illness. Payment is made through the Part A benefit for the associated costs of daily care and the services provided by the hospice-employed physician. An exception occurs for professional services of an independent attending physician who is not an employee of the designated hospice and does not receive compensation from the hospice for those services. The “attending physician” for hospice services must be an individual who is a doctor of medicine or osteopathy, or a nurse practitioner identified by the individual, at the time they elect hospice coverage, as having the most significant role in the determination and delivery of their medical care.2
Patients often receive hospice in the hospital setting, where the hospitalist manages the patient’s daily care. If the hospitalist is designated as the “attending physician” for hospice services, the visits should be reported to Medicare Part B with modifier GV (e.g. 99232-GV).3 This will allow for separate payment to the hospitalist (the independent attending physician), while the hospice agency maintains its daily-care rate. Reporting services absent this modifier will result in denial.
In some cases, the hospitalist is not identified as the “attending physician” for hospice services but occasionally provides care related to the terminal illness. This situation proves most difficult. Although the hospitalist might be the most accessible physician to the staff and is putting the patient’s needs first, reimbursement is unlikely. Regulations stipulate that patients must not see independent physicians other than their “attending physician” for care related to their terminal illness unless the hospice arranges it. When the service is related to the hospice patient’s terminal illness but was furnished by someone other than the designated “attending physician,” this “other physician” must look to the hospice for payment.3
Nonhospice Palliative Care
Members of the palliative-care team often are called to provide management options to assist in reducing pain and suffering. When the palliative-care specialist is asked to provide opinions or advice, the initial service may qualify as a consultation for those payors that still recognize these codes. However, all of the requirements4 must be met in order to report the service as an inpatient consultation (99251-99255):3
- There must be a written request from a qualified healthcare provider who is involved in the patient’s care (e.g. physician, resident, nurse practitioner); this may be documented as a physician order or in the assessment/plan of the requesting provider’s progress note. Standing orders for consultation are not permitted.
- The requesting provider should clearly and accurately identify the reason for consult request to support the medical necessity of the service.
- The palliative-care physician renders and documents the service.
- The palliative-care physician reports his or her findings to the requesting physician via written communication; because the requesting physician and the consultant share a common inpatient medical record, the consultant’s inpatient progress note satisfies the “written report” requirement.
Consider the nature of the request when reporting a consultation. If the request demonstrates the need for opinions or advice from the palliative-care specialist, the service can be reported as a consultation. If the indication cites “medical management” or “palliative management,” payors are less likely to consider the service as a consultation because the physician is not seeking opinions or advice from the consultant to incorporate into his or her own plan of care for the patient and would rather the consultant just take over that portion of patient care. When consultations do not meet the requirements, subsequent hospital care services should be reported (99231-99233).3
The requesting physician can be in the same or a different provider group as the consultant. The consultant must possess expertise in an area that is beyond that of the requesting provider. Because most hospitalists carry a specialty designation of internal medicine (physician specialty code 11), hospitalists providing palliative-care services can distinguish themselves by their own code (physician specialty code 17, hospice and palliative care).5 Payor concerns arise when physicians of the same designated specialty submit a claim for the same patient on the same date. The payor is likely to pay the first claim received and deny the second claim received pending review of documentation. If this occurs, submit a copy of both progress notes for the date in question to distinguish the services provided. The payor may still require that both encounters be reported as one cumulative service under one physician.
Consultations are not an option for Medicare beneficiaries. Hospitalists providing palliative care can report initial hospital care codes (99221-99223) for their first encounter with the patient.3 This is only acceptable when no other hospitalist from the group has reported initial hospital care during the patient stay, unless the palliative-care hospitalist carries the corresponding designation (i.e. enrolled with Medicare as physician specialty code 17). Without this separate designation, the palliative-care hospitalist can only report subsequent hospital care codes (99231-99233) as the patient was seen previously by a hospitalist in the same group.3
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- U.S. Government Printing Office. Electronic Code of Federal Regulations: Title 42: Public Health, Part 418: Hospice Care, §418.3. June 2012. U.S. Government Printing Office website. Available at: http://ecfr.gpoaccess.gov/cgi/t/text/text-idx?c=ecfr&sid=818258235647b14d2961ad30fa3e68e6&rgn=div5&view=text&node=42:3.0.1.1.5&idno=42#42:3.0.1.1.5.1.3.3. Accessed June 23, 2012.
- Centers for Medicare & Medicaid Services. Medicare Claims Processing Manual: Chapter 11: processing hospice claims. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c11.pdf. Accessed June 23, 2012.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011.
- American Medical Association. Consultation services and transfer of care. American Medical Association website. Available at: http://www.ama-assn.org/resources/doc/cpt/cpt-consultation-services.pdf. Accessed June 23, 2012.
- Centers for Medicare & Medicaid Services. Medicare Claims Processing Manual: Chapter 26: completing and processing form CMS-1500 data set. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c26.pdf. Accessed June 23, 2012. Department of Health and Human Services.
- Hospice Payment System: payment system fact sheet series. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/hospice_pay_sys_fs.pdf. Accessed June 23, 2012.
A Palliative Care Coordination Program for Veterans With Advanced Cancer
50 Practical Medication Tips at End of Life
Patients with a life-limiting illness frequently experience pain and other symptoms. It is important to pay close attention when medication therapy is used to manage these symptoms. Occasionally, practitioners need to be creative in selecting, dosing, administering, and discontinuing medications at the end of life because of the patient’s changing health care needs.
In the video below, Dr. Kathryn Walker and Dr. Lynn McPherson of the University of Maryland discuss the role of the pharmacist in the hospital and hospice settings, as well as a few of their favorite medication tips and tricks in end-of-life care.
This article offers practical end-of-life medication tips including, but not limited to, medication administration; guidance on how to increase and decrease doses; medication selection for difficult to-treat patients; alternative dosage formulations; routes of medication administration; debridement medication regimens; and appropriate drug therapy selection. Dr. McPherson and Dr. Walker discuss how to deal with changing the goals of care for your dying patients and their families. They offer suggestions on how to integrate some helpful end-of-life medication tips into your practice.
*For a PDF of the full article, click on the link to the left of this introduction.
Patients with a life-limiting illness frequently experience pain and other symptoms. It is important to pay close attention when medication therapy is used to manage these symptoms. Occasionally, practitioners need to be creative in selecting, dosing, administering, and discontinuing medications at the end of life because of the patient’s changing health care needs.
In the video below, Dr. Kathryn Walker and Dr. Lynn McPherson of the University of Maryland discuss the role of the pharmacist in the hospital and hospice settings, as well as a few of their favorite medication tips and tricks in end-of-life care.
This article offers practical end-of-life medication tips including, but not limited to, medication administration; guidance on how to increase and decrease doses; medication selection for difficult to-treat patients; alternative dosage formulations; routes of medication administration; debridement medication regimens; and appropriate drug therapy selection. Dr. McPherson and Dr. Walker discuss how to deal with changing the goals of care for your dying patients and their families. They offer suggestions on how to integrate some helpful end-of-life medication tips into your practice.
*For a PDF of the full article, click on the link to the left of this introduction.
Patients with a life-limiting illness frequently experience pain and other symptoms. It is important to pay close attention when medication therapy is used to manage these symptoms. Occasionally, practitioners need to be creative in selecting, dosing, administering, and discontinuing medications at the end of life because of the patient’s changing health care needs.
In the video below, Dr. Kathryn Walker and Dr. Lynn McPherson of the University of Maryland discuss the role of the pharmacist in the hospital and hospice settings, as well as a few of their favorite medication tips and tricks in end-of-life care.
This article offers practical end-of-life medication tips including, but not limited to, medication administration; guidance on how to increase and decrease doses; medication selection for difficult to-treat patients; alternative dosage formulations; routes of medication administration; debridement medication regimens; and appropriate drug therapy selection. Dr. McPherson and Dr. Walker discuss how to deal with changing the goals of care for your dying patients and their families. They offer suggestions on how to integrate some helpful end-of-life medication tips into your practice.
*For a PDF of the full article, click on the link to the left of this introduction.
Inappropriate Medications for the Elderly: Three Big Offenders
ESTES PARK, COLO. – Topping Dr. Jeffrey I. Wallace’s pantheon of peeves in prescribing for the elderly are:
• Megestrol acetate (Megace): These are widely prescribed in older patients who aren’t eating well and are experiencing failure to thrive. But the randomized trials with 6- to 12-month followup clearly show that any modest benefit achieved in terms of weight gain takes 2-3 months of therapy. And megestrol acetate is a progestational agent associated with increased risk of thrombotic events and a possible increase in mortality.
"The data on Megace really look terrible. I much prefer using mirtazapine to increase appetite in a patient with even a hint of depression. I’d probably use medical marijuana in the form of Marinol [dronabinol] before I’d use Megace," declared Dr. Wallace at an update in internal medicine sponsored by the University of Colorado, Denver, where he is a professor of medicine.
• Oral iron more than once daily: "I see patients in the nursing homes all the time who’ve been discharged from the hospital by the surgeons on T.I.D. (three times a day) iron," according to the geriatrician.
Absorption of iron is an active process occurring in the duodenum and jejunum. By taking once-daily iron, a patient gets roughly 75% of all the iron that can possibly be absorbed in a day. Moving up to B.I.D. iron, that figure rises to 90%, and T.I.D. dosing bumps up another 5%.
"So each time, I get a little more iron absorbed. The problem is I get a lot more GI side effects. Most of the geriatric patients I see after they get out of the hospital aren’t feeling good already – and now I’m going to make them constipated and give them some dyspepsia and decreased appetite? It’s just not worth it; you don’t get much more bang for the buck. I’m pretty much a stickler to always take the iron down to once a day," he said.
A tip: Oral iron requires an acid environment to be absorbed well. A patient who has had a GI bleed or is at increased risk because of chronic NSAID therapy is likely to be on a proton pump inhibitor, which will interfere with iron absorption. "Have the patient take the iron with some orange juice or vitamin C to help absorption. The data isn’t all that good that it makes much difference, but it’s worth a try," according to the geriatrician.
• Muscle relaxants: These medications are sedating; cause anticholinergic side effects and are linked to an increased risk of falls; and are of questionable efficacy.
"It used to be that if you were 65 or 70 [years old] and came to the ED with back pain, everyone walked out of there with Flexeril [cyclobenzaprine] or some variant thereof. Our ED at the university pretty much doesn’t hand out muscle relaxants anymore. They’re not really pain pills; the data are terrible in terms of helping pain. For run-of-the-mill back pain, I’d rather give an older patient an opiate than a muscle relaxant. So unless you have a definitive muscle spasm, treat the pain with pain pills," he urged at the conference.
He reported having no financial conflicts.
ESTES PARK, COLO. – Topping Dr. Jeffrey I. Wallace’s pantheon of peeves in prescribing for the elderly are:
• Megestrol acetate (Megace): These are widely prescribed in older patients who aren’t eating well and are experiencing failure to thrive. But the randomized trials with 6- to 12-month followup clearly show that any modest benefit achieved in terms of weight gain takes 2-3 months of therapy. And megestrol acetate is a progestational agent associated with increased risk of thrombotic events and a possible increase in mortality.
"The data on Megace really look terrible. I much prefer using mirtazapine to increase appetite in a patient with even a hint of depression. I’d probably use medical marijuana in the form of Marinol [dronabinol] before I’d use Megace," declared Dr. Wallace at an update in internal medicine sponsored by the University of Colorado, Denver, where he is a professor of medicine.
• Oral iron more than once daily: "I see patients in the nursing homes all the time who’ve been discharged from the hospital by the surgeons on T.I.D. (three times a day) iron," according to the geriatrician.
Absorption of iron is an active process occurring in the duodenum and jejunum. By taking once-daily iron, a patient gets roughly 75% of all the iron that can possibly be absorbed in a day. Moving up to B.I.D. iron, that figure rises to 90%, and T.I.D. dosing bumps up another 5%.
"So each time, I get a little more iron absorbed. The problem is I get a lot more GI side effects. Most of the geriatric patients I see after they get out of the hospital aren’t feeling good already – and now I’m going to make them constipated and give them some dyspepsia and decreased appetite? It’s just not worth it; you don’t get much more bang for the buck. I’m pretty much a stickler to always take the iron down to once a day," he said.
A tip: Oral iron requires an acid environment to be absorbed well. A patient who has had a GI bleed or is at increased risk because of chronic NSAID therapy is likely to be on a proton pump inhibitor, which will interfere with iron absorption. "Have the patient take the iron with some orange juice or vitamin C to help absorption. The data isn’t all that good that it makes much difference, but it’s worth a try," according to the geriatrician.
• Muscle relaxants: These medications are sedating; cause anticholinergic side effects and are linked to an increased risk of falls; and are of questionable efficacy.
"It used to be that if you were 65 or 70 [years old] and came to the ED with back pain, everyone walked out of there with Flexeril [cyclobenzaprine] or some variant thereof. Our ED at the university pretty much doesn’t hand out muscle relaxants anymore. They’re not really pain pills; the data are terrible in terms of helping pain. For run-of-the-mill back pain, I’d rather give an older patient an opiate than a muscle relaxant. So unless you have a definitive muscle spasm, treat the pain with pain pills," he urged at the conference.
He reported having no financial conflicts.
ESTES PARK, COLO. – Topping Dr. Jeffrey I. Wallace’s pantheon of peeves in prescribing for the elderly are:
• Megestrol acetate (Megace): These are widely prescribed in older patients who aren’t eating well and are experiencing failure to thrive. But the randomized trials with 6- to 12-month followup clearly show that any modest benefit achieved in terms of weight gain takes 2-3 months of therapy. And megestrol acetate is a progestational agent associated with increased risk of thrombotic events and a possible increase in mortality.
"The data on Megace really look terrible. I much prefer using mirtazapine to increase appetite in a patient with even a hint of depression. I’d probably use medical marijuana in the form of Marinol [dronabinol] before I’d use Megace," declared Dr. Wallace at an update in internal medicine sponsored by the University of Colorado, Denver, where he is a professor of medicine.
• Oral iron more than once daily: "I see patients in the nursing homes all the time who’ve been discharged from the hospital by the surgeons on T.I.D. (three times a day) iron," according to the geriatrician.
Absorption of iron is an active process occurring in the duodenum and jejunum. By taking once-daily iron, a patient gets roughly 75% of all the iron that can possibly be absorbed in a day. Moving up to B.I.D. iron, that figure rises to 90%, and T.I.D. dosing bumps up another 5%.
"So each time, I get a little more iron absorbed. The problem is I get a lot more GI side effects. Most of the geriatric patients I see after they get out of the hospital aren’t feeling good already – and now I’m going to make them constipated and give them some dyspepsia and decreased appetite? It’s just not worth it; you don’t get much more bang for the buck. I’m pretty much a stickler to always take the iron down to once a day," he said.
A tip: Oral iron requires an acid environment to be absorbed well. A patient who has had a GI bleed or is at increased risk because of chronic NSAID therapy is likely to be on a proton pump inhibitor, which will interfere with iron absorption. "Have the patient take the iron with some orange juice or vitamin C to help absorption. The data isn’t all that good that it makes much difference, but it’s worth a try," according to the geriatrician.
• Muscle relaxants: These medications are sedating; cause anticholinergic side effects and are linked to an increased risk of falls; and are of questionable efficacy.
"It used to be that if you were 65 or 70 [years old] and came to the ED with back pain, everyone walked out of there with Flexeril [cyclobenzaprine] or some variant thereof. Our ED at the university pretty much doesn’t hand out muscle relaxants anymore. They’re not really pain pills; the data are terrible in terms of helping pain. For run-of-the-mill back pain, I’d rather give an older patient an opiate than a muscle relaxant. So unless you have a definitive muscle spasm, treat the pain with pain pills," he urged at the conference.
He reported having no financial conflicts.
EXPERT ANALYSIS FROM AN UPDATE IN INTERNAL MEDICINE SPONSORED BY THE UNIVERSITIY OF COLORADO