User login
Pitfalls in Prescribing for the Elderly
ESTES PARK, COLO. – As a geriatrician with several decades of experience, Dr. Jeffrey I. Wallace is particularly loath to see three things prescribed in older patients: megestrol acetate, oral iron more than once daily, or muscle relaxants.
While he considers those three prescriptions to be especially egregious because the at-best tiny potential benefits are so clearly overshadowed by the sizeable downside risks, other agents on his personal ‘just say no’ list for the elderly include chronic NSAIDs, benzodiazepines, chronic proton pump inhibitors, sedating antihistamines, and first-generation tricyclic antidepressants, said Dr. Wallace at an update in internal medicine sponsored by the University of Colorado, Denver, where he is a professor of medicine.
Learn more about three of the most popular, inappropriate prescriptions for the elderly.
Those agents, with the sole exception of more-than-once-daily oral iron, are among the 53 medications or medication classes included on the recently overhauled Beers list of potentially inappropriate medications in older adults published by the American Geriatrics Society (2012 [doi:10.1111/j.1532-5415.2012.03923.x]). Dr. Wallace has some issues with the list.

"My problem with the Beers list is that most of us have some patients taking a drug that’s on that list because they didn’t respond to the first three drugs we used, yet we can’t get rid of the Beers list drug because they really need treatment. And I’m telling you, there are quality assurance measures that will ding us for that," the physician explained.
He has similar reservations about the STOPP/START criteria developed by an expert panel in Ireland (Int. J. Clin. Pharmacol. Ther. 2008; 46:72-83) and the Healthcare Effectiveness Data and Information Set (HEDIS) list.
"It’s good to be aware of what’s on those lists – the attorneys are aware of them – but if a drug you’re using is on a list and it’s your fourth choice because the first three didn’t work, then you should feel OK," he continued.
Rather than slavishly trying to steer clear of drugs on the Beers or other "potentially inappropriate drug" lists, Dr. Wallace’s preference in his own daily medical practice is to incorporate the "Good Palliative–Geriatric Practice" algorithm (Arch. Intern. Med. 2010;170:1648-54). This tool, developed by Israeli geriatricians in an effort to reduce rampant polypharmacy and inappropriate medications in the elderly, challenges the clinician at multiple points to consider whether an individual patient really needs to be on a particular drug at a given dose. The algorithm has been shown in multiple small controlled trials to improve key outcomes, including hospitalization and mortality.
For example, in a study of 190 patients on a baseline average of 7.1 drugs at six Israeli nursing homes, application of the algorithm in 119 patients led to discontinuation of an average of 2.8 drugs each. The 1-year rates of acute hospitalization and mortality were 12% and 21%, respectively, in the group where the algorithm was applied, compared with 30% and 45% in the control group, making the point that when it comes to prescribing for the elderly, less is often more (Isr. Med. Assoc. J. 2007;9:430-4).
More recently, a study in 70 Israeli geriatric outpatients on an average of 7.7 medications at baseline showed that application of the Good Palliative–Geriatric Practice algorithm resulted in discontinuation of an average of 4.9 drugs, with no significant increase in morbidity or mortality during a mean follow-up of 19 months. A total of 88% of patients who discontinued drugs reported a global improvement in their health (Arch. Intern. Med. 2010;170:1648-54).
Dr. Wallace tries hard to limit older patients to a maximum of six drugs. It can be tough because so many elderly patients have multiple comorbid conditions. But studies show that when elderly patients are on more than six medications, the rate of adverse drug reactions shoots up exponentially. With eight drugs, the chance of a drug-drug interaction is nearly 100%.
Interestingly, he noted, a landmark national study of emergency hospitalizations for adverse drug reactions in the elderly found that only 1.2% of the admissions involved drugs considered high risk because they were on the 2003 version of the Beers criteria or the HEDIS list. Two-thirds of all adverse drug reactions severe enough to lead to hospitalization after an emergency department (ED) visit involved warfarin, diabetes medications, or oral antiplatelet agents (N. Engl. J. Med. 2011;365:2002-12).
An annual or semiannual office visit devoted specifically to a medications review by the patient’s primary care physician or a skilled pharmacist is an excellent way to optimize therapy. Drug plans are willing to pay for it.
An acute hospitalization or trip to the ED provides a good opportunity for another physician to take a critical look at an older patient’s medications.
"I used to get cranky when a hospitalist would take one of my patients who I’ve been taking care of for 10 years and say, ‘Gee, Wallace – this is a dumb drug for this patient; I’m stopping the Fosamax.’ I’d reply, ‘I know the patient; don’t mess with him.’ But more and more, as I look at the literature, I’m thinking that when a patient is in the hospital or the ED, it’s a great time to cut back. I would urge those of you who are hospitalists to do that for reasons of adherence and safety. The data are out there to support you. Just let us know what you’ve done," the geriatrician said.
One of the key means of reducing polypharmacy in the elderly involves avoidance of what’s been called "the prescribing cascade." This cascade occurs when an adverse effect of one drug gets misinterpreted as a new medical condition, for which a second drug is dutifully prescribed.
"This happens all the time," according to Dr. Wallace.
Examples: A patient on hydrochlorothiazide experiences rising uric acid levels, is diagnosed with gout, and put on allopurinol; had he simply been switched to another antihypertensive agent, he’d still be on one drug instead of two for two diseases. Or a patient on chronic daily NSAID therapy develops rising blood pressure as a drug side effect, gets labeled hypertensive, and goes on antihypertensive medications. Or a patient on donepezil or another cholesterase inhibitor reports an increased frequency of urination because of the drug’s effects on the bladder; in response, tolterodine is prescribed.
Three years ago, the cholinesterase inhibitors used in treating dementia were linked to a previously unrecognized increased risk of bradycardia. In a large Canadian study, these medications were associated with a 69% increased rate of emergency department visits for symptomatic bradycardia, a 76% increase in syncope, a 49% greater likelihood of permanent pacemaker implantation, and an 18% increased risk of hip fracture (Arch. Intern. Med. 169: 867-73).
"We didn’t know about this until 2009. I grew up using donepezil in the 1990s when I was a fellow. We were using it all the time and no one thought about bradycardia. It wasn’t in our differential," Dr. Wallace recalled. "I’m sure patients passed out and got pacemakers as an unrecognized drug side effect. My question is this: We think we’re smart, but what else do we not know, especially with newer agents coming along?"
Dr. Wallace reported having no financial conflicts.
ESTES PARK, COLO. – As a geriatrician with several decades of experience, Dr. Jeffrey I. Wallace is particularly loath to see three things prescribed in older patients: megestrol acetate, oral iron more than once daily, or muscle relaxants.
While he considers those three prescriptions to be especially egregious because the at-best tiny potential benefits are so clearly overshadowed by the sizeable downside risks, other agents on his personal ‘just say no’ list for the elderly include chronic NSAIDs, benzodiazepines, chronic proton pump inhibitors, sedating antihistamines, and first-generation tricyclic antidepressants, said Dr. Wallace at an update in internal medicine sponsored by the University of Colorado, Denver, where he is a professor of medicine.
Learn more about three of the most popular, inappropriate prescriptions for the elderly.
Those agents, with the sole exception of more-than-once-daily oral iron, are among the 53 medications or medication classes included on the recently overhauled Beers list of potentially inappropriate medications in older adults published by the American Geriatrics Society (2012 [doi:10.1111/j.1532-5415.2012.03923.x]). Dr. Wallace has some issues with the list.
"My problem with the Beers list is that most of us have some patients taking a drug that’s on that list because they didn’t respond to the first three drugs we used, yet we can’t get rid of the Beers list drug because they really need treatment. And I’m telling you, there are quality assurance measures that will ding us for that," the physician explained.
He has similar reservations about the STOPP/START criteria developed by an expert panel in Ireland (Int. J. Clin. Pharmacol. Ther. 2008; 46:72-83) and the Healthcare Effectiveness Data and Information Set (HEDIS) list.
"It’s good to be aware of what’s on those lists – the attorneys are aware of them – but if a drug you’re using is on a list and it’s your fourth choice because the first three didn’t work, then you should feel OK," he continued.
Rather than slavishly trying to steer clear of drugs on the Beers or other "potentially inappropriate drug" lists, Dr. Wallace’s preference in his own daily medical practice is to incorporate the "Good Palliative–Geriatric Practice" algorithm (Arch. Intern. Med. 2010;170:1648-54). This tool, developed by Israeli geriatricians in an effort to reduce rampant polypharmacy and inappropriate medications in the elderly, challenges the clinician at multiple points to consider whether an individual patient really needs to be on a particular drug at a given dose. The algorithm has been shown in multiple small controlled trials to improve key outcomes, including hospitalization and mortality.
For example, in a study of 190 patients on a baseline average of 7.1 drugs at six Israeli nursing homes, application of the algorithm in 119 patients led to discontinuation of an average of 2.8 drugs each. The 1-year rates of acute hospitalization and mortality were 12% and 21%, respectively, in the group where the algorithm was applied, compared with 30% and 45% in the control group, making the point that when it comes to prescribing for the elderly, less is often more (Isr. Med. Assoc. J. 2007;9:430-4).
More recently, a study in 70 Israeli geriatric outpatients on an average of 7.7 medications at baseline showed that application of the Good Palliative–Geriatric Practice algorithm resulted in discontinuation of an average of 4.9 drugs, with no significant increase in morbidity or mortality during a mean follow-up of 19 months. A total of 88% of patients who discontinued drugs reported a global improvement in their health (Arch. Intern. Med. 2010;170:1648-54).
Dr. Wallace tries hard to limit older patients to a maximum of six drugs. It can be tough because so many elderly patients have multiple comorbid conditions. But studies show that when elderly patients are on more than six medications, the rate of adverse drug reactions shoots up exponentially. With eight drugs, the chance of a drug-drug interaction is nearly 100%.
Interestingly, he noted, a landmark national study of emergency hospitalizations for adverse drug reactions in the elderly found that only 1.2% of the admissions involved drugs considered high risk because they were on the 2003 version of the Beers criteria or the HEDIS list. Two-thirds of all adverse drug reactions severe enough to lead to hospitalization after an emergency department (ED) visit involved warfarin, diabetes medications, or oral antiplatelet agents (N. Engl. J. Med. 2011;365:2002-12).
An annual or semiannual office visit devoted specifically to a medications review by the patient’s primary care physician or a skilled pharmacist is an excellent way to optimize therapy. Drug plans are willing to pay for it.
An acute hospitalization or trip to the ED provides a good opportunity for another physician to take a critical look at an older patient’s medications.
"I used to get cranky when a hospitalist would take one of my patients who I’ve been taking care of for 10 years and say, ‘Gee, Wallace – this is a dumb drug for this patient; I’m stopping the Fosamax.’ I’d reply, ‘I know the patient; don’t mess with him.’ But more and more, as I look at the literature, I’m thinking that when a patient is in the hospital or the ED, it’s a great time to cut back. I would urge those of you who are hospitalists to do that for reasons of adherence and safety. The data are out there to support you. Just let us know what you’ve done," the geriatrician said.
One of the key means of reducing polypharmacy in the elderly involves avoidance of what’s been called "the prescribing cascade." This cascade occurs when an adverse effect of one drug gets misinterpreted as a new medical condition, for which a second drug is dutifully prescribed.
"This happens all the time," according to Dr. Wallace.
Examples: A patient on hydrochlorothiazide experiences rising uric acid levels, is diagnosed with gout, and put on allopurinol; had he simply been switched to another antihypertensive agent, he’d still be on one drug instead of two for two diseases. Or a patient on chronic daily NSAID therapy develops rising blood pressure as a drug side effect, gets labeled hypertensive, and goes on antihypertensive medications. Or a patient on donepezil or another cholesterase inhibitor reports an increased frequency of urination because of the drug’s effects on the bladder; in response, tolterodine is prescribed.
Three years ago, the cholinesterase inhibitors used in treating dementia were linked to a previously unrecognized increased risk of bradycardia. In a large Canadian study, these medications were associated with a 69% increased rate of emergency department visits for symptomatic bradycardia, a 76% increase in syncope, a 49% greater likelihood of permanent pacemaker implantation, and an 18% increased risk of hip fracture (Arch. Intern. Med. 169: 867-73).
"We didn’t know about this until 2009. I grew up using donepezil in the 1990s when I was a fellow. We were using it all the time and no one thought about bradycardia. It wasn’t in our differential," Dr. Wallace recalled. "I’m sure patients passed out and got pacemakers as an unrecognized drug side effect. My question is this: We think we’re smart, but what else do we not know, especially with newer agents coming along?"
Dr. Wallace reported having no financial conflicts.
ESTES PARK, COLO. – As a geriatrician with several decades of experience, Dr. Jeffrey I. Wallace is particularly loath to see three things prescribed in older patients: megestrol acetate, oral iron more than once daily, or muscle relaxants.
While he considers those three prescriptions to be especially egregious because the at-best tiny potential benefits are so clearly overshadowed by the sizeable downside risks, other agents on his personal ‘just say no’ list for the elderly include chronic NSAIDs, benzodiazepines, chronic proton pump inhibitors, sedating antihistamines, and first-generation tricyclic antidepressants, said Dr. Wallace at an update in internal medicine sponsored by the University of Colorado, Denver, where he is a professor of medicine.
Learn more about three of the most popular, inappropriate prescriptions for the elderly.
Those agents, with the sole exception of more-than-once-daily oral iron, are among the 53 medications or medication classes included on the recently overhauled Beers list of potentially inappropriate medications in older adults published by the American Geriatrics Society (2012 [doi:10.1111/j.1532-5415.2012.03923.x]). Dr. Wallace has some issues with the list.
"My problem with the Beers list is that most of us have some patients taking a drug that’s on that list because they didn’t respond to the first three drugs we used, yet we can’t get rid of the Beers list drug because they really need treatment. And I’m telling you, there are quality assurance measures that will ding us for that," the physician explained.
He has similar reservations about the STOPP/START criteria developed by an expert panel in Ireland (Int. J. Clin. Pharmacol. Ther. 2008; 46:72-83) and the Healthcare Effectiveness Data and Information Set (HEDIS) list.
"It’s good to be aware of what’s on those lists – the attorneys are aware of them – but if a drug you’re using is on a list and it’s your fourth choice because the first three didn’t work, then you should feel OK," he continued.
Rather than slavishly trying to steer clear of drugs on the Beers or other "potentially inappropriate drug" lists, Dr. Wallace’s preference in his own daily medical practice is to incorporate the "Good Palliative–Geriatric Practice" algorithm (Arch. Intern. Med. 2010;170:1648-54). This tool, developed by Israeli geriatricians in an effort to reduce rampant polypharmacy and inappropriate medications in the elderly, challenges the clinician at multiple points to consider whether an individual patient really needs to be on a particular drug at a given dose. The algorithm has been shown in multiple small controlled trials to improve key outcomes, including hospitalization and mortality.
For example, in a study of 190 patients on a baseline average of 7.1 drugs at six Israeli nursing homes, application of the algorithm in 119 patients led to discontinuation of an average of 2.8 drugs each. The 1-year rates of acute hospitalization and mortality were 12% and 21%, respectively, in the group where the algorithm was applied, compared with 30% and 45% in the control group, making the point that when it comes to prescribing for the elderly, less is often more (Isr. Med. Assoc. J. 2007;9:430-4).
More recently, a study in 70 Israeli geriatric outpatients on an average of 7.7 medications at baseline showed that application of the Good Palliative–Geriatric Practice algorithm resulted in discontinuation of an average of 4.9 drugs, with no significant increase in morbidity or mortality during a mean follow-up of 19 months. A total of 88% of patients who discontinued drugs reported a global improvement in their health (Arch. Intern. Med. 2010;170:1648-54).
Dr. Wallace tries hard to limit older patients to a maximum of six drugs. It can be tough because so many elderly patients have multiple comorbid conditions. But studies show that when elderly patients are on more than six medications, the rate of adverse drug reactions shoots up exponentially. With eight drugs, the chance of a drug-drug interaction is nearly 100%.
Interestingly, he noted, a landmark national study of emergency hospitalizations for adverse drug reactions in the elderly found that only 1.2% of the admissions involved drugs considered high risk because they were on the 2003 version of the Beers criteria or the HEDIS list. Two-thirds of all adverse drug reactions severe enough to lead to hospitalization after an emergency department (ED) visit involved warfarin, diabetes medications, or oral antiplatelet agents (N. Engl. J. Med. 2011;365:2002-12).
An annual or semiannual office visit devoted specifically to a medications review by the patient’s primary care physician or a skilled pharmacist is an excellent way to optimize therapy. Drug plans are willing to pay for it.
An acute hospitalization or trip to the ED provides a good opportunity for another physician to take a critical look at an older patient’s medications.
"I used to get cranky when a hospitalist would take one of my patients who I’ve been taking care of for 10 years and say, ‘Gee, Wallace – this is a dumb drug for this patient; I’m stopping the Fosamax.’ I’d reply, ‘I know the patient; don’t mess with him.’ But more and more, as I look at the literature, I’m thinking that when a patient is in the hospital or the ED, it’s a great time to cut back. I would urge those of you who are hospitalists to do that for reasons of adherence and safety. The data are out there to support you. Just let us know what you’ve done," the geriatrician said.
One of the key means of reducing polypharmacy in the elderly involves avoidance of what’s been called "the prescribing cascade." This cascade occurs when an adverse effect of one drug gets misinterpreted as a new medical condition, for which a second drug is dutifully prescribed.
"This happens all the time," according to Dr. Wallace.
Examples: A patient on hydrochlorothiazide experiences rising uric acid levels, is diagnosed with gout, and put on allopurinol; had he simply been switched to another antihypertensive agent, he’d still be on one drug instead of two for two diseases. Or a patient on chronic daily NSAID therapy develops rising blood pressure as a drug side effect, gets labeled hypertensive, and goes on antihypertensive medications. Or a patient on donepezil or another cholesterase inhibitor reports an increased frequency of urination because of the drug’s effects on the bladder; in response, tolterodine is prescribed.
Three years ago, the cholinesterase inhibitors used in treating dementia were linked to a previously unrecognized increased risk of bradycardia. In a large Canadian study, these medications were associated with a 69% increased rate of emergency department visits for symptomatic bradycardia, a 76% increase in syncope, a 49% greater likelihood of permanent pacemaker implantation, and an 18% increased risk of hip fracture (Arch. Intern. Med. 169: 867-73).
"We didn’t know about this until 2009. I grew up using donepezil in the 1990s when I was a fellow. We were using it all the time and no one thought about bradycardia. It wasn’t in our differential," Dr. Wallace recalled. "I’m sure patients passed out and got pacemakers as an unrecognized drug side effect. My question is this: We think we’re smart, but what else do we not know, especially with newer agents coming along?"
Dr. Wallace reported having no financial conflicts.
EXPERT ANALYSIS FROM AN UPDATE IN INTERNAL MEDICINE SPONSORED BY THE UNIVERSITY OF COLORADO
Changing How We Prescribe Antipsychotics for Dementia
The vast majority of patients with Alzheimer’s disease will show agitation, delusion, and other disruptive behaviors during the course of their illnesses. These behaviors cause suffering and distress for patients and for caregivers and families, often diminishing quality of life and making care more difficult.
The behaviors are variable and hard to classify. The phenotypes are often unstable and overlapping. We may diagnose depression when we see apathy and aggression when we see psychomotor agitation. The term "agitation" commonly subsumes a wide range of behaviors.
Because certain phenotypes improve with certain drugs across psychiatric disorders – for example, antipsychotics for delusions in both schizophrenia and mood disorder – we often assume that the behavioral phenotypes seen in dementia, such as depression or delusions, will also improve with antidepressants and antipsychotics as they do in other disorders.
Patients with dementia receive psychotropic medications to try and control these behaviors. But are antipsychotics the best choice? Are they effective and safe? The Food and Drug Administration and clinical researchers agree: These drugs are largely ineffective and are associated with significant adverse events in patients with dementia.
Antipsychotics have been advocated for disruptive behavior in dementia since their inception. Manufacturers promoted this use into the mid-1980s, even as concern mounted about their overuse. For example, a 1956 journal advertisement pictured an elderly man aggressively raising his cane, his daughter on the phone to his physician asking, "What can you do for Pop?" The tag line touted Thorazine [chlorpromazine] "for the prompt control of the agitated, belligerent senile."
The Federal Nursing Home Reform Act was enacted in 1987 (OBRA ’87), and regulations were established in 1991. It required, in part, restriction, justification, and monitoring of antipsychotics to address their potential unnecessary and inappropriate use as chemical restraints.
The advent of atypical antipsychotics in the early 1990s – risperidone (Risperdal) in particular – led to their promotion for treating aggression and psychosis in dementia. It’s fair to say as well that atypicals were enthusiastically adopted by physicians as alternatives to conventional antipsychotics; they were viewed as different, safer, less sedative, and had fewer motor system effects than did the first generation antipsychotics. Indeed, advertisements from 1998 depicted an elderly woman entitled "Hostile outside. ... Fragile inside," calling Risperdal the most prescribed antipsychotic in long-term care, improving a "broad range of psychotic symptoms," and having few adverse events. The advertisements were remarkably similar to the Thorazine advertisements 40 years earlier.
By the early 2000s, reports of increased cardiovascular events and stroke surfaced. In 2003, the drugs began to carry a warning of cerebrovascular events, including stroke, in elderly patients with dementia-related psychosis. In 2005, this was followed by a black box warning: "Elderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death," adding that the drugs were "not approved for the treatment of dementia-related psychosis." The latter phrase expressed the FDA’s view that there was insufficient randomized controlled trials evidence of benefit for this indication.
Efficacy of antipsychotics from controlled clinical trials is indeed marginal. Many trials yielded insignificant outcomes, and those that were significant showed only a few points difference on scales of uncertain clinical significance. Notably, when the trials are statistically combined, there is no efficacy evidence for olanzapine (Zyprexa) or quetiapine (Seroquel) and only slight evidence for risperidone and aripiprazole (Abilify), but adverse events with these drugs are considerable, compared with placebo. A characteristic of the trials is that both the drug and placebo groups improve considerably and to such an extent that any statistically significant effect for antipsychotics is marginal or incremental over placebo.
The warnings, however, generated only a relatively small change in prescribing patterns. Risperidone use decreased somewhat, but quetiapine use increased, all the more remarkable because of the lack of efficacy data and the very low quetiapine doses that are used clinically (Arch. Gen. Psychiatry 2011;68:190-7). A 2007 look at Canadian prescribing rates showed a substantial and highly variable amount of antipsychotic use in nursing homes. Rates ranged from 20% to 44%, suggesting that we are not all clear on how to use them (Arch. Intern. Med. 2007;167:676-83).
A recent retrospective study enumerates the risks for death that antipsychotics pose for Alzheimer’s patients. In a large cohort of elderly veterans with dementia, the death rate per 100 person-years was 46 for haloperidol, 27 for olanzapine and risperidone, and 19 for quetiapine, rates that are noticeable in busy practices (Am. J. Psychiatry 2012;169:71-9).
Lawyers and state departments of justice have entered the picture as well with malpractice pleadings and enforcement against elder abuse, questioning whether we physicians are doing our job in protecting patients. Pharmaceutical companies have been sued, prosecuted, settled, and pled to criminal and civil offenses involving past misleading or fraudulent promotion of the drugs. Companies have paid out billions, with the latest being Johnson & Johnson’s anticipated $2.2 billion settlement over misleading marketing claims for risperidone.
Antipsychotics, when used appropriately and for a short time, can be effective for some. But, in general, they are most commonly used chronically. The continuing long-term prescribing of these drugs underlines the need to be able to treat behavioral disorders.
We need to examine how we treat dementia patients with disruptive behaviors and what we are doing with these medications, and consider alternatives. If we don’t, patients may continue to be harmed and to a greater extent than we think. We can do better in treating behavioral symptoms.
Dr. Schneider is a professor of psychiatry, neurology, and gerontology at the University of Southern California, Los Angeles. He is also director of the university’s Alzheimer’s Disease Research and Clinical Center. Dr. Schneider reports being an editor on the Cochrane Collaboration Dementia and Cognitive Improvement Group, which oversees systematic reviews of drugs for cognitive impairment and dementia. He has multiple financial relationships with a number of companies that manufacturer drugs for Alzheimer’s disease.
The vast majority of patients with Alzheimer’s disease will show agitation, delusion, and other disruptive behaviors during the course of their illnesses. These behaviors cause suffering and distress for patients and for caregivers and families, often diminishing quality of life and making care more difficult.
The behaviors are variable and hard to classify. The phenotypes are often unstable and overlapping. We may diagnose depression when we see apathy and aggression when we see psychomotor agitation. The term "agitation" commonly subsumes a wide range of behaviors.
Because certain phenotypes improve with certain drugs across psychiatric disorders – for example, antipsychotics for delusions in both schizophrenia and mood disorder – we often assume that the behavioral phenotypes seen in dementia, such as depression or delusions, will also improve with antidepressants and antipsychotics as they do in other disorders.
Patients with dementia receive psychotropic medications to try and control these behaviors. But are antipsychotics the best choice? Are they effective and safe? The Food and Drug Administration and clinical researchers agree: These drugs are largely ineffective and are associated with significant adverse events in patients with dementia.
Antipsychotics have been advocated for disruptive behavior in dementia since their inception. Manufacturers promoted this use into the mid-1980s, even as concern mounted about their overuse. For example, a 1956 journal advertisement pictured an elderly man aggressively raising his cane, his daughter on the phone to his physician asking, "What can you do for Pop?" The tag line touted Thorazine [chlorpromazine] "for the prompt control of the agitated, belligerent senile."
The Federal Nursing Home Reform Act was enacted in 1987 (OBRA ’87), and regulations were established in 1991. It required, in part, restriction, justification, and monitoring of antipsychotics to address their potential unnecessary and inappropriate use as chemical restraints.
The advent of atypical antipsychotics in the early 1990s – risperidone (Risperdal) in particular – led to their promotion for treating aggression and psychosis in dementia. It’s fair to say as well that atypicals were enthusiastically adopted by physicians as alternatives to conventional antipsychotics; they were viewed as different, safer, less sedative, and had fewer motor system effects than did the first generation antipsychotics. Indeed, advertisements from 1998 depicted an elderly woman entitled "Hostile outside. ... Fragile inside," calling Risperdal the most prescribed antipsychotic in long-term care, improving a "broad range of psychotic symptoms," and having few adverse events. The advertisements were remarkably similar to the Thorazine advertisements 40 years earlier.
By the early 2000s, reports of increased cardiovascular events and stroke surfaced. In 2003, the drugs began to carry a warning of cerebrovascular events, including stroke, in elderly patients with dementia-related psychosis. In 2005, this was followed by a black box warning: "Elderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death," adding that the drugs were "not approved for the treatment of dementia-related psychosis." The latter phrase expressed the FDA’s view that there was insufficient randomized controlled trials evidence of benefit for this indication.
Efficacy of antipsychotics from controlled clinical trials is indeed marginal. Many trials yielded insignificant outcomes, and those that were significant showed only a few points difference on scales of uncertain clinical significance. Notably, when the trials are statistically combined, there is no efficacy evidence for olanzapine (Zyprexa) or quetiapine (Seroquel) and only slight evidence for risperidone and aripiprazole (Abilify), but adverse events with these drugs are considerable, compared with placebo. A characteristic of the trials is that both the drug and placebo groups improve considerably and to such an extent that any statistically significant effect for antipsychotics is marginal or incremental over placebo.
The warnings, however, generated only a relatively small change in prescribing patterns. Risperidone use decreased somewhat, but quetiapine use increased, all the more remarkable because of the lack of efficacy data and the very low quetiapine doses that are used clinically (Arch. Gen. Psychiatry 2011;68:190-7). A 2007 look at Canadian prescribing rates showed a substantial and highly variable amount of antipsychotic use in nursing homes. Rates ranged from 20% to 44%, suggesting that we are not all clear on how to use them (Arch. Intern. Med. 2007;167:676-83).
A recent retrospective study enumerates the risks for death that antipsychotics pose for Alzheimer’s patients. In a large cohort of elderly veterans with dementia, the death rate per 100 person-years was 46 for haloperidol, 27 for olanzapine and risperidone, and 19 for quetiapine, rates that are noticeable in busy practices (Am. J. Psychiatry 2012;169:71-9).
Lawyers and state departments of justice have entered the picture as well with malpractice pleadings and enforcement against elder abuse, questioning whether we physicians are doing our job in protecting patients. Pharmaceutical companies have been sued, prosecuted, settled, and pled to criminal and civil offenses involving past misleading or fraudulent promotion of the drugs. Companies have paid out billions, with the latest being Johnson & Johnson’s anticipated $2.2 billion settlement over misleading marketing claims for risperidone.
Antipsychotics, when used appropriately and for a short time, can be effective for some. But, in general, they are most commonly used chronically. The continuing long-term prescribing of these drugs underlines the need to be able to treat behavioral disorders.
We need to examine how we treat dementia patients with disruptive behaviors and what we are doing with these medications, and consider alternatives. If we don’t, patients may continue to be harmed and to a greater extent than we think. We can do better in treating behavioral symptoms.
Dr. Schneider is a professor of psychiatry, neurology, and gerontology at the University of Southern California, Los Angeles. He is also director of the university’s Alzheimer’s Disease Research and Clinical Center. Dr. Schneider reports being an editor on the Cochrane Collaboration Dementia and Cognitive Improvement Group, which oversees systematic reviews of drugs for cognitive impairment and dementia. He has multiple financial relationships with a number of companies that manufacturer drugs for Alzheimer’s disease.
The vast majority of patients with Alzheimer’s disease will show agitation, delusion, and other disruptive behaviors during the course of their illnesses. These behaviors cause suffering and distress for patients and for caregivers and families, often diminishing quality of life and making care more difficult.
The behaviors are variable and hard to classify. The phenotypes are often unstable and overlapping. We may diagnose depression when we see apathy and aggression when we see psychomotor agitation. The term "agitation" commonly subsumes a wide range of behaviors.
Because certain phenotypes improve with certain drugs across psychiatric disorders – for example, antipsychotics for delusions in both schizophrenia and mood disorder – we often assume that the behavioral phenotypes seen in dementia, such as depression or delusions, will also improve with antidepressants and antipsychotics as they do in other disorders.
Patients with dementia receive psychotropic medications to try and control these behaviors. But are antipsychotics the best choice? Are they effective and safe? The Food and Drug Administration and clinical researchers agree: These drugs are largely ineffective and are associated with significant adverse events in patients with dementia.
Antipsychotics have been advocated for disruptive behavior in dementia since their inception. Manufacturers promoted this use into the mid-1980s, even as concern mounted about their overuse. For example, a 1956 journal advertisement pictured an elderly man aggressively raising his cane, his daughter on the phone to his physician asking, "What can you do for Pop?" The tag line touted Thorazine [chlorpromazine] "for the prompt control of the agitated, belligerent senile."
The Federal Nursing Home Reform Act was enacted in 1987 (OBRA ’87), and regulations were established in 1991. It required, in part, restriction, justification, and monitoring of antipsychotics to address their potential unnecessary and inappropriate use as chemical restraints.
The advent of atypical antipsychotics in the early 1990s – risperidone (Risperdal) in particular – led to their promotion for treating aggression and psychosis in dementia. It’s fair to say as well that atypicals were enthusiastically adopted by physicians as alternatives to conventional antipsychotics; they were viewed as different, safer, less sedative, and had fewer motor system effects than did the first generation antipsychotics. Indeed, advertisements from 1998 depicted an elderly woman entitled "Hostile outside. ... Fragile inside," calling Risperdal the most prescribed antipsychotic in long-term care, improving a "broad range of psychotic symptoms," and having few adverse events. The advertisements were remarkably similar to the Thorazine advertisements 40 years earlier.
By the early 2000s, reports of increased cardiovascular events and stroke surfaced. In 2003, the drugs began to carry a warning of cerebrovascular events, including stroke, in elderly patients with dementia-related psychosis. In 2005, this was followed by a black box warning: "Elderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death," adding that the drugs were "not approved for the treatment of dementia-related psychosis." The latter phrase expressed the FDA’s view that there was insufficient randomized controlled trials evidence of benefit for this indication.
Efficacy of antipsychotics from controlled clinical trials is indeed marginal. Many trials yielded insignificant outcomes, and those that were significant showed only a few points difference on scales of uncertain clinical significance. Notably, when the trials are statistically combined, there is no efficacy evidence for olanzapine (Zyprexa) or quetiapine (Seroquel) and only slight evidence for risperidone and aripiprazole (Abilify), but adverse events with these drugs are considerable, compared with placebo. A characteristic of the trials is that both the drug and placebo groups improve considerably and to such an extent that any statistically significant effect for antipsychotics is marginal or incremental over placebo.
The warnings, however, generated only a relatively small change in prescribing patterns. Risperidone use decreased somewhat, but quetiapine use increased, all the more remarkable because of the lack of efficacy data and the very low quetiapine doses that are used clinically (Arch. Gen. Psychiatry 2011;68:190-7). A 2007 look at Canadian prescribing rates showed a substantial and highly variable amount of antipsychotic use in nursing homes. Rates ranged from 20% to 44%, suggesting that we are not all clear on how to use them (Arch. Intern. Med. 2007;167:676-83).
A recent retrospective study enumerates the risks for death that antipsychotics pose for Alzheimer’s patients. In a large cohort of elderly veterans with dementia, the death rate per 100 person-years was 46 for haloperidol, 27 for olanzapine and risperidone, and 19 for quetiapine, rates that are noticeable in busy practices (Am. J. Psychiatry 2012;169:71-9).
Lawyers and state departments of justice have entered the picture as well with malpractice pleadings and enforcement against elder abuse, questioning whether we physicians are doing our job in protecting patients. Pharmaceutical companies have been sued, prosecuted, settled, and pled to criminal and civil offenses involving past misleading or fraudulent promotion of the drugs. Companies have paid out billions, with the latest being Johnson & Johnson’s anticipated $2.2 billion settlement over misleading marketing claims for risperidone.
Antipsychotics, when used appropriately and for a short time, can be effective for some. But, in general, they are most commonly used chronically. The continuing long-term prescribing of these drugs underlines the need to be able to treat behavioral disorders.
We need to examine how we treat dementia patients with disruptive behaviors and what we are doing with these medications, and consider alternatives. If we don’t, patients may continue to be harmed and to a greater extent than we think. We can do better in treating behavioral symptoms.
Dr. Schneider is a professor of psychiatry, neurology, and gerontology at the University of Southern California, Los Angeles. He is also director of the university’s Alzheimer’s Disease Research and Clinical Center. Dr. Schneider reports being an editor on the Cochrane Collaboration Dementia and Cognitive Improvement Group, which oversees systematic reviews of drugs for cognitive impairment and dementia. He has multiple financial relationships with a number of companies that manufacturer drugs for Alzheimer’s disease.
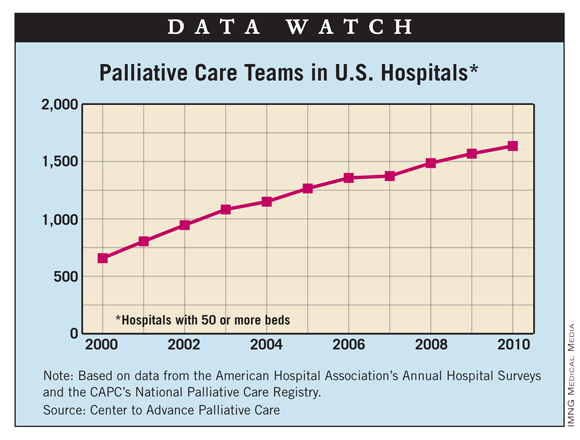
More Hospitals House Palliative Care Teams
The number of U.S. hospitals with palliative care teams increased for the 10th consecutive year, according to a new analysis from the Center to Advance Palliative Care.
In 2010, the last year for which data are available, there were 1,635 palliative care teams in hospitals – an increase of 4.3% over 2009 and an increase of 148.5% since 2000. In 2010, almost 66% of hospitals had a palliative care team, compared with 24.5% in 2000, the CAPC reported.

By region, the South had a much lower prevalence of hospitals with palliative care teams (53%) than the rest of the country: Northeast (76%), Midwest (75%), and West (71%). In terms of hospital size, those with 300 or more beds had an 88% prevalence of palliative care teams, compared with 57% for hospitals with 50-299 beds, the CAPC said.
The analysis – based mainly on data from the American Hospital Association and supplemented by data from the CAPC’s National Palliative Care Registry – excluded hospitals with less than 50 beds and those that are controlled by the federal government, such as Veterans Affairs hospitals.
The number of U.S. hospitals with palliative care teams increased for the 10th consecutive year, according to a new analysis from the Center to Advance Palliative Care.
In 2010, the last year for which data are available, there were 1,635 palliative care teams in hospitals – an increase of 4.3% over 2009 and an increase of 148.5% since 2000. In 2010, almost 66% of hospitals had a palliative care team, compared with 24.5% in 2000, the CAPC reported.
By region, the South had a much lower prevalence of hospitals with palliative care teams (53%) than the rest of the country: Northeast (76%), Midwest (75%), and West (71%). In terms of hospital size, those with 300 or more beds had an 88% prevalence of palliative care teams, compared with 57% for hospitals with 50-299 beds, the CAPC said.
The analysis – based mainly on data from the American Hospital Association and supplemented by data from the CAPC’s National Palliative Care Registry – excluded hospitals with less than 50 beds and those that are controlled by the federal government, such as Veterans Affairs hospitals.
The number of U.S. hospitals with palliative care teams increased for the 10th consecutive year, according to a new analysis from the Center to Advance Palliative Care.
In 2010, the last year for which data are available, there were 1,635 palliative care teams in hospitals – an increase of 4.3% over 2009 and an increase of 148.5% since 2000. In 2010, almost 66% of hospitals had a palliative care team, compared with 24.5% in 2000, the CAPC reported.
By region, the South had a much lower prevalence of hospitals with palliative care teams (53%) than the rest of the country: Northeast (76%), Midwest (75%), and West (71%). In terms of hospital size, those with 300 or more beds had an 88% prevalence of palliative care teams, compared with 57% for hospitals with 50-299 beds, the CAPC said.
The analysis – based mainly on data from the American Hospital Association and supplemented by data from the CAPC’s National Palliative Care Registry – excluded hospitals with less than 50 beds and those that are controlled by the federal government, such as Veterans Affairs hospitals.
Palliative-Care-Focused Hospitalist Appreciates Training the Next Generation

Chithra Perumalswami, MD, knew early on what she wanted to do with her life. As a teenager, she volunteered in an ED and with a hospice group, volunteerism that continued throughout her education. When she graduated from high school, she was tapped for Brown University’s Program in Liberal Medical Education, which calls itself the only baccalaureate-MD program in the Ivy League. And though she eventually turned down the offer, she pursued dual majors in cellular and molecular biology and English at the University of Michigan, where she earned her medical degree in 2004 and completed her residency.
In 2009, she participated in the Palliative Care Education and Practice Program at Harvard Medical School in Boston, a two-week post-graduate course aimed at professional development for physicians dedicated to careers in palliative-care education. “I really found that there were just so many aspects to caring for a patient as a palliative-care specialist and as a hospitalist that really strike at the heart of what being a doctor is,” says Dr. Perumalswami, assistant professor of medicine in the Division of Hospital Medicine at Northwestern Memorial Hospital in Chicago and one of four new members of Team Hospitalist. “I think it’s been an interest I’ve always had. During my residency training, I definitely experienced quite a few patient cases where I felt that we really needed to help patients and their families, and I didn’t necessarily have the best skill set to do that until I had more experience and more training.”
Dr. Perumalswami now wants to get better at her craft.
“As an academic hospitalist, it’s not just about doing research and writing papers and seeing papers,” she says, “but it’s also developing those leadership skills and helping that become an integral part of the educational experience.”
Question: What drew you to a career in HM?
Answer: I chose a career in academic hospital medicine primarily because I enjoy taking care of acutely ill, hospitalized, adult patients. I also really enjoy teaching medical students, residents, and fellows, and I enjoy doing that in the hospital setting. I think that there’s great satisfaction from taking care of a patient from admission to discharge.… I enjoyed every aspect of internal medicine, and when I graduated, I thought I could choose a subspecialty, but I felt that my skills and my expertise was really in taking care of the hospitalized patient.
Q: You have sought out extra training in palliative care and pain management. How has that impacted your career?
A: It’s not something that I necessarily started out thinking that I would specialize in, but the more I took care of hospitalized patients, the more I realized that we actually take care of a fair number of patients who have really complex symptom needs, and also really have a lot of needs with regard to recognizing when their prognosis is poor and understanding what their options are, if they’re even amenable to a palliative approach. I really felt that that was a skill that I needed to fine-tune. So I ended up gaining enough clinical experience and participating with hospice patients to the point where that’s really supplemented my hospitalist career, because what I found is that it’s made me a better hospitalist, and being a hospitalist has made me a better palliative-care doc.
Q: Working in academia, there’s no way to escape talk of the duty-hour rules recently put in place. What’s your view on the issue?
A: My view is that the work hours are here to stay. I think that there are some definite benefits that we’ve gained from having work hours. I’d say first and foremost of those gains is public trust. I think most physicians will tell you that they don’t want a physician who’s in the 36th hour of their day taking care of them when we know that studies actually can demonstrate that when you’ve been awake that long, that your cognitive abilities decline.
Q: But?
A: I think we have a lot of challenges, though, because a lot of things require creative solutions. And I think the first on that list is education, because that’s the first thing that I think has the potential to drop to the bottom of the list.
Q: In terms of HM’s growth, as you see residents coming through your program, how popular do you think the model is going to be with them moving forward?
A: I do, actually, because as an academic hospitalist, I’ve had several medical students and residents tell me, “Watching you, I think that I want to go into this field.” Or they’ll say, “What do you think about doing this for a year or two?” Or, “What do you think about subspecializing, and then being a hospitalist?” And my answer to all of them is it’s a dynamic specialty, and if you’re up for creating change and being a leader, it’s a good field, because we need people in a lot of different buckets, so to speak. We need people who have done other things in their career to contribute to our field.
Q: How do you prepare trainees for all the challenges coming down the pike?
A: A lot of the people who are doing work in medical education are starting to look to other fields to see if there are other models that we can adapt, or that we can somehow absorb into our practice. I think that there are some parts of our education which are not really formalized early on, but I think we have a lot to learn from organizational behavior circles, and systems that actually look at teams and leadership.
Q: What do the next five to 10 years hold for you?
A: All physician leaders have to stay somewhat in the clinical world. I think if you lose sight of that, you can’t be a very effective leader, or a very effective agent for change. Because part of my work is with palliative care, and I really feel that it’s affected my work as a hospitalist in a positive way, I don’t think I ever see myself leaving the clinical world completely. But I do see myself becoming, ideally, more involved with leadership and more involved with helping to train the next set of leaders.
Q: What do you see as SHM’s role specific to academic HM?
A: HM is changing the way healthcare is delivered in the U.S., and I think having an organization to represent us is vital to our success in other arenas of change—including healthcare policy and innovative care models. I see SHM as a large umbrella group, of which academic HM is one part. Academic hospitalists are increasingly involved in the education of future generations of physicians, and are uniquely poised for facilitating cascading leadership. The traditional, hierarchical model of attending-fellow-resident-medical student is shifting, and academic hospitalists are well-suited to study and explore this leadership structure and how it affects patient care, feedback, and mentoring.
Richard Quinn is a freelance writer based in New Jersey.
Chithra Perumalswami, MD, knew early on what she wanted to do with her life. As a teenager, she volunteered in an ED and with a hospice group, volunteerism that continued throughout her education. When she graduated from high school, she was tapped for Brown University’s Program in Liberal Medical Education, which calls itself the only baccalaureate-MD program in the Ivy League. And though she eventually turned down the offer, she pursued dual majors in cellular and molecular biology and English at the University of Michigan, where she earned her medical degree in 2004 and completed her residency.
In 2009, she participated in the Palliative Care Education and Practice Program at Harvard Medical School in Boston, a two-week post-graduate course aimed at professional development for physicians dedicated to careers in palliative-care education. “I really found that there were just so many aspects to caring for a patient as a palliative-care specialist and as a hospitalist that really strike at the heart of what being a doctor is,” says Dr. Perumalswami, assistant professor of medicine in the Division of Hospital Medicine at Northwestern Memorial Hospital in Chicago and one of four new members of Team Hospitalist. “I think it’s been an interest I’ve always had. During my residency training, I definitely experienced quite a few patient cases where I felt that we really needed to help patients and their families, and I didn’t necessarily have the best skill set to do that until I had more experience and more training.”
Dr. Perumalswami now wants to get better at her craft.
“As an academic hospitalist, it’s not just about doing research and writing papers and seeing papers,” she says, “but it’s also developing those leadership skills and helping that become an integral part of the educational experience.”
Question: What drew you to a career in HM?
Answer: I chose a career in academic hospital medicine primarily because I enjoy taking care of acutely ill, hospitalized, adult patients. I also really enjoy teaching medical students, residents, and fellows, and I enjoy doing that in the hospital setting. I think that there’s great satisfaction from taking care of a patient from admission to discharge.… I enjoyed every aspect of internal medicine, and when I graduated, I thought I could choose a subspecialty, but I felt that my skills and my expertise was really in taking care of the hospitalized patient.
Q: You have sought out extra training in palliative care and pain management. How has that impacted your career?
A: It’s not something that I necessarily started out thinking that I would specialize in, but the more I took care of hospitalized patients, the more I realized that we actually take care of a fair number of patients who have really complex symptom needs, and also really have a lot of needs with regard to recognizing when their prognosis is poor and understanding what their options are, if they’re even amenable to a palliative approach. I really felt that that was a skill that I needed to fine-tune. So I ended up gaining enough clinical experience and participating with hospice patients to the point where that’s really supplemented my hospitalist career, because what I found is that it’s made me a better hospitalist, and being a hospitalist has made me a better palliative-care doc.
Q: Working in academia, there’s no way to escape talk of the duty-hour rules recently put in place. What’s your view on the issue?
A: My view is that the work hours are here to stay. I think that there are some definite benefits that we’ve gained from having work hours. I’d say first and foremost of those gains is public trust. I think most physicians will tell you that they don’t want a physician who’s in the 36th hour of their day taking care of them when we know that studies actually can demonstrate that when you’ve been awake that long, that your cognitive abilities decline.
Q: But?
A: I think we have a lot of challenges, though, because a lot of things require creative solutions. And I think the first on that list is education, because that’s the first thing that I think has the potential to drop to the bottom of the list.
Q: In terms of HM’s growth, as you see residents coming through your program, how popular do you think the model is going to be with them moving forward?
A: I do, actually, because as an academic hospitalist, I’ve had several medical students and residents tell me, “Watching you, I think that I want to go into this field.” Or they’ll say, “What do you think about doing this for a year or two?” Or, “What do you think about subspecializing, and then being a hospitalist?” And my answer to all of them is it’s a dynamic specialty, and if you’re up for creating change and being a leader, it’s a good field, because we need people in a lot of different buckets, so to speak. We need people who have done other things in their career to contribute to our field.
Q: How do you prepare trainees for all the challenges coming down the pike?
A: A lot of the people who are doing work in medical education are starting to look to other fields to see if there are other models that we can adapt, or that we can somehow absorb into our practice. I think that there are some parts of our education which are not really formalized early on, but I think we have a lot to learn from organizational behavior circles, and systems that actually look at teams and leadership.
Q: What do the next five to 10 years hold for you?
A: All physician leaders have to stay somewhat in the clinical world. I think if you lose sight of that, you can’t be a very effective leader, or a very effective agent for change. Because part of my work is with palliative care, and I really feel that it’s affected my work as a hospitalist in a positive way, I don’t think I ever see myself leaving the clinical world completely. But I do see myself becoming, ideally, more involved with leadership and more involved with helping to train the next set of leaders.
Q: What do you see as SHM’s role specific to academic HM?
A: HM is changing the way healthcare is delivered in the U.S., and I think having an organization to represent us is vital to our success in other arenas of change—including healthcare policy and innovative care models. I see SHM as a large umbrella group, of which academic HM is one part. Academic hospitalists are increasingly involved in the education of future generations of physicians, and are uniquely poised for facilitating cascading leadership. The traditional, hierarchical model of attending-fellow-resident-medical student is shifting, and academic hospitalists are well-suited to study and explore this leadership structure and how it affects patient care, feedback, and mentoring.
Richard Quinn is a freelance writer based in New Jersey.
Chithra Perumalswami, MD, knew early on what she wanted to do with her life. As a teenager, she volunteered in an ED and with a hospice group, volunteerism that continued throughout her education. When she graduated from high school, she was tapped for Brown University’s Program in Liberal Medical Education, which calls itself the only baccalaureate-MD program in the Ivy League. And though she eventually turned down the offer, she pursued dual majors in cellular and molecular biology and English at the University of Michigan, where she earned her medical degree in 2004 and completed her residency.
In 2009, she participated in the Palliative Care Education and Practice Program at Harvard Medical School in Boston, a two-week post-graduate course aimed at professional development for physicians dedicated to careers in palliative-care education. “I really found that there were just so many aspects to caring for a patient as a palliative-care specialist and as a hospitalist that really strike at the heart of what being a doctor is,” says Dr. Perumalswami, assistant professor of medicine in the Division of Hospital Medicine at Northwestern Memorial Hospital in Chicago and one of four new members of Team Hospitalist. “I think it’s been an interest I’ve always had. During my residency training, I definitely experienced quite a few patient cases where I felt that we really needed to help patients and their families, and I didn’t necessarily have the best skill set to do that until I had more experience and more training.”
Dr. Perumalswami now wants to get better at her craft.
“As an academic hospitalist, it’s not just about doing research and writing papers and seeing papers,” she says, “but it’s also developing those leadership skills and helping that become an integral part of the educational experience.”
Question: What drew you to a career in HM?
Answer: I chose a career in academic hospital medicine primarily because I enjoy taking care of acutely ill, hospitalized, adult patients. I also really enjoy teaching medical students, residents, and fellows, and I enjoy doing that in the hospital setting. I think that there’s great satisfaction from taking care of a patient from admission to discharge.… I enjoyed every aspect of internal medicine, and when I graduated, I thought I could choose a subspecialty, but I felt that my skills and my expertise was really in taking care of the hospitalized patient.
Q: You have sought out extra training in palliative care and pain management. How has that impacted your career?
A: It’s not something that I necessarily started out thinking that I would specialize in, but the more I took care of hospitalized patients, the more I realized that we actually take care of a fair number of patients who have really complex symptom needs, and also really have a lot of needs with regard to recognizing when their prognosis is poor and understanding what their options are, if they’re even amenable to a palliative approach. I really felt that that was a skill that I needed to fine-tune. So I ended up gaining enough clinical experience and participating with hospice patients to the point where that’s really supplemented my hospitalist career, because what I found is that it’s made me a better hospitalist, and being a hospitalist has made me a better palliative-care doc.
Q: Working in academia, there’s no way to escape talk of the duty-hour rules recently put in place. What’s your view on the issue?
A: My view is that the work hours are here to stay. I think that there are some definite benefits that we’ve gained from having work hours. I’d say first and foremost of those gains is public trust. I think most physicians will tell you that they don’t want a physician who’s in the 36th hour of their day taking care of them when we know that studies actually can demonstrate that when you’ve been awake that long, that your cognitive abilities decline.
Q: But?
A: I think we have a lot of challenges, though, because a lot of things require creative solutions. And I think the first on that list is education, because that’s the first thing that I think has the potential to drop to the bottom of the list.
Q: In terms of HM’s growth, as you see residents coming through your program, how popular do you think the model is going to be with them moving forward?
A: I do, actually, because as an academic hospitalist, I’ve had several medical students and residents tell me, “Watching you, I think that I want to go into this field.” Or they’ll say, “What do you think about doing this for a year or two?” Or, “What do you think about subspecializing, and then being a hospitalist?” And my answer to all of them is it’s a dynamic specialty, and if you’re up for creating change and being a leader, it’s a good field, because we need people in a lot of different buckets, so to speak. We need people who have done other things in their career to contribute to our field.
Q: How do you prepare trainees for all the challenges coming down the pike?
A: A lot of the people who are doing work in medical education are starting to look to other fields to see if there are other models that we can adapt, or that we can somehow absorb into our practice. I think that there are some parts of our education which are not really formalized early on, but I think we have a lot to learn from organizational behavior circles, and systems that actually look at teams and leadership.
Q: What do the next five to 10 years hold for you?
A: All physician leaders have to stay somewhat in the clinical world. I think if you lose sight of that, you can’t be a very effective leader, or a very effective agent for change. Because part of my work is with palliative care, and I really feel that it’s affected my work as a hospitalist in a positive way, I don’t think I ever see myself leaving the clinical world completely. But I do see myself becoming, ideally, more involved with leadership and more involved with helping to train the next set of leaders.
Q: What do you see as SHM’s role specific to academic HM?
A: HM is changing the way healthcare is delivered in the U.S., and I think having an organization to represent us is vital to our success in other arenas of change—including healthcare policy and innovative care models. I see SHM as a large umbrella group, of which academic HM is one part. Academic hospitalists are increasingly involved in the education of future generations of physicians, and are uniquely poised for facilitating cascading leadership. The traditional, hierarchical model of attending-fellow-resident-medical student is shifting, and academic hospitalists are well-suited to study and explore this leadership structure and how it affects patient care, feedback, and mentoring.
Richard Quinn is a freelance writer based in New Jersey.
Pain Scales: What to Ponder When Making Your Pick
SAN DIEGO – Of the many scales at a clinician’s disposal to measure acute pain, the three most commonly used are the Numerical Rating Scale, the Verbal Rating Scale, and the Visual Analog Scale, Dr. Jeffrey A. Stone said at the annual meeting of the Society of Neurointerventional Surgery.
"All of these scales have been shown to be statistically reliable and valid," said Dr. Stone, associate professor of neurointerventional surgery in the radiology department at the Mayo Clinic, Jacksonville, Fla. In his clinical experience, most patients prefer the Numerical Rating Scale (NRS) and the Verbal Rating Scale (VRS) because they are easy to use. "The other advantage is that these can be conducted by telephone or electronic diaries," he said.

The NRS is a familiar and commonly used 0-10 scale, where 0 = no pain, 1-3 = mild pain, 4-6 = moderate pain, and 7-10 = severe pain. "If patients tell you, ‘I’m a 5 out of 10,’ that can be difficult to gauge, particularly in the elderly," Dr. Stone said. "The VRS, a four-scale system ranging from no pain up to severe pain, is somewhat simpler and correlates well with the NRS."
With the Visual Analog Scale, patients are asked to make a vertical slash on a 100-mm line to denote their level of pain. "I use this scale a lot, but it can be cumbersome, particularly with follow-up," he said.
Factors to consider in the backdrop of pain intensity include rescue analgesics, which may be prescribed by other physicians for sleep or anxiety, or may be used to prevent pain from increased activity or to treat unrelated pain. "Another factor is concomitant pain treatments, such as acupuncture and chiropractic treatments," Dr. Stone said. "In addition, patients enrolled in the placebo group of a clinical trial are generally expected to have more pain medication use compared with those in an efficacious treatment group."
Other distinct components of pain include pain sensation and pain affect. Pain sensation "is the quality of the pain, such as burning, throbbing, or sharp pain versus dull pain," Dr. Stone said. "There are also temporal aspects to pain, such as variability of intensity over time; time to onset of meaningful pain relief; durability of pain relief; and the frequency, duration, and intensity of pain episodes. Pain affect is the mental distress caused by the pain."
Global pain assessments for pain sensation and pain affect include a modification of the McGill Pain Questionnaire (MPQ), known as the short-form MPQ, and the Brief Pain Inventory (BPI), which was adapted from the Wisconsin Brief Pain Questionnaire. The short-form MPQ contains 15 sensory and affective descriptors, while the BPI "does a much better job measuring the temporal aspect of pain and is often used in conjunction with the short-form MPQ," Dr. Stone said.
Two other core pain outcome domains are physical function and emotional function. Effective outcome measures for these domains include the Oswestry Disability Index (ODI), the Short Form-36 (SF-36), the Roland-Morris Disability Questionnaire (RMQ) and the Pain Disability Index (PDI).
The ODI, a 10-item questionnaire, "has been used in many pain trials," he said. "It looks at pain intensity but also other things such as lifting, the ability to walk, social life, sexual activity, and sleep cycle. It is a very accurate way to look at a patient’s global disability from pain."
He described the SF-36 as "a little bit more cumbersome for patients to complete" in measuring physical and emotional function. This tool provides an eight-scale profile of functional health and well-being scores, as well as a psychometric-based physical and mental health summary.
The 24-item RMQ consists of yes/no questions intended to measure self-perceived disability, while the 7-question PDI measures pain interference in physical and psychosocial role performance.
In a later interview, Dr. Stone said that the NRS, VRS, and VAS instruments can be used in hospitalized patients. Outcome measures such as the ODI and the RMQ "would not be very useful, as they ask many functional questions such as sex life [and] activity level, which would not be applicable to a hospitalized patient."
Dr. Stone said that he had no relevant financial disclosures to make.
SAN DIEGO – Of the many scales at a clinician’s disposal to measure acute pain, the three most commonly used are the Numerical Rating Scale, the Verbal Rating Scale, and the Visual Analog Scale, Dr. Jeffrey A. Stone said at the annual meeting of the Society of Neurointerventional Surgery.
"All of these scales have been shown to be statistically reliable and valid," said Dr. Stone, associate professor of neurointerventional surgery in the radiology department at the Mayo Clinic, Jacksonville, Fla. In his clinical experience, most patients prefer the Numerical Rating Scale (NRS) and the Verbal Rating Scale (VRS) because they are easy to use. "The other advantage is that these can be conducted by telephone or electronic diaries," he said.
The NRS is a familiar and commonly used 0-10 scale, where 0 = no pain, 1-3 = mild pain, 4-6 = moderate pain, and 7-10 = severe pain. "If patients tell you, ‘I’m a 5 out of 10,’ that can be difficult to gauge, particularly in the elderly," Dr. Stone said. "The VRS, a four-scale system ranging from no pain up to severe pain, is somewhat simpler and correlates well with the NRS."
With the Visual Analog Scale, patients are asked to make a vertical slash on a 100-mm line to denote their level of pain. "I use this scale a lot, but it can be cumbersome, particularly with follow-up," he said.
Factors to consider in the backdrop of pain intensity include rescue analgesics, which may be prescribed by other physicians for sleep or anxiety, or may be used to prevent pain from increased activity or to treat unrelated pain. "Another factor is concomitant pain treatments, such as acupuncture and chiropractic treatments," Dr. Stone said. "In addition, patients enrolled in the placebo group of a clinical trial are generally expected to have more pain medication use compared with those in an efficacious treatment group."
Other distinct components of pain include pain sensation and pain affect. Pain sensation "is the quality of the pain, such as burning, throbbing, or sharp pain versus dull pain," Dr. Stone said. "There are also temporal aspects to pain, such as variability of intensity over time; time to onset of meaningful pain relief; durability of pain relief; and the frequency, duration, and intensity of pain episodes. Pain affect is the mental distress caused by the pain."
Global pain assessments for pain sensation and pain affect include a modification of the McGill Pain Questionnaire (MPQ), known as the short-form MPQ, and the Brief Pain Inventory (BPI), which was adapted from the Wisconsin Brief Pain Questionnaire. The short-form MPQ contains 15 sensory and affective descriptors, while the BPI "does a much better job measuring the temporal aspect of pain and is often used in conjunction with the short-form MPQ," Dr. Stone said.
Two other core pain outcome domains are physical function and emotional function. Effective outcome measures for these domains include the Oswestry Disability Index (ODI), the Short Form-36 (SF-36), the Roland-Morris Disability Questionnaire (RMQ) and the Pain Disability Index (PDI).
The ODI, a 10-item questionnaire, "has been used in many pain trials," he said. "It looks at pain intensity but also other things such as lifting, the ability to walk, social life, sexual activity, and sleep cycle. It is a very accurate way to look at a patient’s global disability from pain."
He described the SF-36 as "a little bit more cumbersome for patients to complete" in measuring physical and emotional function. This tool provides an eight-scale profile of functional health and well-being scores, as well as a psychometric-based physical and mental health summary.
The 24-item RMQ consists of yes/no questions intended to measure self-perceived disability, while the 7-question PDI measures pain interference in physical and psychosocial role performance.
In a later interview, Dr. Stone said that the NRS, VRS, and VAS instruments can be used in hospitalized patients. Outcome measures such as the ODI and the RMQ "would not be very useful, as they ask many functional questions such as sex life [and] activity level, which would not be applicable to a hospitalized patient."
Dr. Stone said that he had no relevant financial disclosures to make.
SAN DIEGO – Of the many scales at a clinician’s disposal to measure acute pain, the three most commonly used are the Numerical Rating Scale, the Verbal Rating Scale, and the Visual Analog Scale, Dr. Jeffrey A. Stone said at the annual meeting of the Society of Neurointerventional Surgery.
"All of these scales have been shown to be statistically reliable and valid," said Dr. Stone, associate professor of neurointerventional surgery in the radiology department at the Mayo Clinic, Jacksonville, Fla. In his clinical experience, most patients prefer the Numerical Rating Scale (NRS) and the Verbal Rating Scale (VRS) because they are easy to use. "The other advantage is that these can be conducted by telephone or electronic diaries," he said.
The NRS is a familiar and commonly used 0-10 scale, where 0 = no pain, 1-3 = mild pain, 4-6 = moderate pain, and 7-10 = severe pain. "If patients tell you, ‘I’m a 5 out of 10,’ that can be difficult to gauge, particularly in the elderly," Dr. Stone said. "The VRS, a four-scale system ranging from no pain up to severe pain, is somewhat simpler and correlates well with the NRS."
With the Visual Analog Scale, patients are asked to make a vertical slash on a 100-mm line to denote their level of pain. "I use this scale a lot, but it can be cumbersome, particularly with follow-up," he said.
Factors to consider in the backdrop of pain intensity include rescue analgesics, which may be prescribed by other physicians for sleep or anxiety, or may be used to prevent pain from increased activity or to treat unrelated pain. "Another factor is concomitant pain treatments, such as acupuncture and chiropractic treatments," Dr. Stone said. "In addition, patients enrolled in the placebo group of a clinical trial are generally expected to have more pain medication use compared with those in an efficacious treatment group."
Other distinct components of pain include pain sensation and pain affect. Pain sensation "is the quality of the pain, such as burning, throbbing, or sharp pain versus dull pain," Dr. Stone said. "There are also temporal aspects to pain, such as variability of intensity over time; time to onset of meaningful pain relief; durability of pain relief; and the frequency, duration, and intensity of pain episodes. Pain affect is the mental distress caused by the pain."
Global pain assessments for pain sensation and pain affect include a modification of the McGill Pain Questionnaire (MPQ), known as the short-form MPQ, and the Brief Pain Inventory (BPI), which was adapted from the Wisconsin Brief Pain Questionnaire. The short-form MPQ contains 15 sensory and affective descriptors, while the BPI "does a much better job measuring the temporal aspect of pain and is often used in conjunction with the short-form MPQ," Dr. Stone said.
Two other core pain outcome domains are physical function and emotional function. Effective outcome measures for these domains include the Oswestry Disability Index (ODI), the Short Form-36 (SF-36), the Roland-Morris Disability Questionnaire (RMQ) and the Pain Disability Index (PDI).
The ODI, a 10-item questionnaire, "has been used in many pain trials," he said. "It looks at pain intensity but also other things such as lifting, the ability to walk, social life, sexual activity, and sleep cycle. It is a very accurate way to look at a patient’s global disability from pain."
He described the SF-36 as "a little bit more cumbersome for patients to complete" in measuring physical and emotional function. This tool provides an eight-scale profile of functional health and well-being scores, as well as a psychometric-based physical and mental health summary.
The 24-item RMQ consists of yes/no questions intended to measure self-perceived disability, while the 7-question PDI measures pain interference in physical and psychosocial role performance.
In a later interview, Dr. Stone said that the NRS, VRS, and VAS instruments can be used in hospitalized patients. Outcome measures such as the ODI and the RMQ "would not be very useful, as they ask many functional questions such as sex life [and] activity level, which would not be applicable to a hospitalized patient."
Dr. Stone said that he had no relevant financial disclosures to make.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE SOCIETY OF NEUROINTERVENTIONAL SURGERY

Isotretinoin Quells EGFR Inhibitor-Related Rash
ORLANDO – Oral isotretinoin holds potential as a bridge therapy for cancer patients who develop severe rashes during treatment, according to Dr. Milan J. Anadkat.
Dermatologists can play an integral role here. "Most oncologists see these patients first, and most oncologists are not enrolled in the iPledge program," said Dr. Anadkat of the division of dermatology at Washington University in St. Louis.
He noted that all treatment options are off label because there are no Food and Drug Administration–approved agents to treat chemotherapy-related cutaneous toxicities.
Getting patients through rashes that occur within a week or two of beginning targeted chemotherapy is important, as patients who develop the greatest reactions tend to have cancers that respond best to treatment, said Dr. Anadkat at the annual meeting of the Florida Society of Dermatology and Dermatologic Surgery. For this reason, the management of these patients is more complicated than simple drug cessation.
"The problem with just taking them off the drug is that they have cancer. Ultimately, the big goal here is treating the cancer, not avoiding the rash," he said.
Tetracycline or doxycycline can also reduce the severity of the rash, but the timing of administration is important. Better outcomes are associated with prophylaxis that is timed with the initiation of EGFR (epidermal growth factor receptor) inhibitors (Cancer 2008;113:847-53). "Waiting for the rash to appear is not the time to give it. It makes a difference if you give at day 0, not in terms of incidence but in the severity of the rash," he said.
Educate patients that the rash typically appears in an estimated 60%-90% of people within 8-10 days of EGFR inhibitor initiation, with a peak presentation at 2-4 weeks. "Bridging them through with something as effective as isotretinoin is useful," said Dr. Anadkat.
The rash generally appears on the face and upper trunk, but be careful not to confuse the presentation with a photo-exposure phenomenon.
Although some oncologists will describe the skin eruptions as "acnelike," histology will show mixed inflammatory infiltrate and follicular rupture. For this reason, "topical acne medications do very little," Dr. Anadkat said. Also, rule out infection, except when patients present with pustules on their arms, legs, or other non–EGFR receptor areas.
EGFR inhibitors can cause inflammatory alopecia, eyelash trichomegaly, and periungual and nail alterations.
About one in six patients will develop periungual or nail abnormalities, typically on their first finger or toe. These effects can be painful, Dr. Anadkat said. Culture is mandatory to rule out superinfection.
Again, the approach is to get patients through the adverse events with petroleum jelly, high-dose topical steroids, or oral tetracyclines. "Tumor markers are going down; [oncologists] are not going to want to stop chemotherapy for a painful thumb or toe," he said. "I recommend antimicrobial soaks with bleach or vinegar to prevent paronychia superinfection."
Dry, itchy skin is another concern with long-term EGFR inhibitor treatment. Histology shows "stark differences" in the stratum corneum. "This is the No. 1 side effect for patients on long-term EGFR – 3 months or longer; [it is] not a grade 3 or higher toxicity, but it is annoying."
Investigators compared oral minocycline and topical tazarotene prophylaxis in a study of 48 patients with cetuximab associated rash (J. Clin. Oncol. 2007:25:5390-6). Although oral minocycline was associated with reduced lesion counts, topical tazarotene yielded no significant benefit. "Again, this is not acne," Dr. Anadkat said.
He disclosed being a consultant or speaker for AstraZeneca, Bristol-Myers Squibb, Eisai, Genentech, and ImClone regarding strategies for managing skin toxicities from chemotherapy. He has never prescribed chemotherapy agents.
ORLANDO – Oral isotretinoin holds potential as a bridge therapy for cancer patients who develop severe rashes during treatment, according to Dr. Milan J. Anadkat.
Dermatologists can play an integral role here. "Most oncologists see these patients first, and most oncologists are not enrolled in the iPledge program," said Dr. Anadkat of the division of dermatology at Washington University in St. Louis.
He noted that all treatment options are off label because there are no Food and Drug Administration–approved agents to treat chemotherapy-related cutaneous toxicities.
Getting patients through rashes that occur within a week or two of beginning targeted chemotherapy is important, as patients who develop the greatest reactions tend to have cancers that respond best to treatment, said Dr. Anadkat at the annual meeting of the Florida Society of Dermatology and Dermatologic Surgery. For this reason, the management of these patients is more complicated than simple drug cessation.
"The problem with just taking them off the drug is that they have cancer. Ultimately, the big goal here is treating the cancer, not avoiding the rash," he said.
Tetracycline or doxycycline can also reduce the severity of the rash, but the timing of administration is important. Better outcomes are associated with prophylaxis that is timed with the initiation of EGFR (epidermal growth factor receptor) inhibitors (Cancer 2008;113:847-53). "Waiting for the rash to appear is not the time to give it. It makes a difference if you give at day 0, not in terms of incidence but in the severity of the rash," he said.
Educate patients that the rash typically appears in an estimated 60%-90% of people within 8-10 days of EGFR inhibitor initiation, with a peak presentation at 2-4 weeks. "Bridging them through with something as effective as isotretinoin is useful," said Dr. Anadkat.
The rash generally appears on the face and upper trunk, but be careful not to confuse the presentation with a photo-exposure phenomenon.
Although some oncologists will describe the skin eruptions as "acnelike," histology will show mixed inflammatory infiltrate and follicular rupture. For this reason, "topical acne medications do very little," Dr. Anadkat said. Also, rule out infection, except when patients present with pustules on their arms, legs, or other non–EGFR receptor areas.
EGFR inhibitors can cause inflammatory alopecia, eyelash trichomegaly, and periungual and nail alterations.
About one in six patients will develop periungual or nail abnormalities, typically on their first finger or toe. These effects can be painful, Dr. Anadkat said. Culture is mandatory to rule out superinfection.
Again, the approach is to get patients through the adverse events with petroleum jelly, high-dose topical steroids, or oral tetracyclines. "Tumor markers are going down; [oncologists] are not going to want to stop chemotherapy for a painful thumb or toe," he said. "I recommend antimicrobial soaks with bleach or vinegar to prevent paronychia superinfection."
Dry, itchy skin is another concern with long-term EGFR inhibitor treatment. Histology shows "stark differences" in the stratum corneum. "This is the No. 1 side effect for patients on long-term EGFR – 3 months or longer; [it is] not a grade 3 or higher toxicity, but it is annoying."
Investigators compared oral minocycline and topical tazarotene prophylaxis in a study of 48 patients with cetuximab associated rash (J. Clin. Oncol. 2007:25:5390-6). Although oral minocycline was associated with reduced lesion counts, topical tazarotene yielded no significant benefit. "Again, this is not acne," Dr. Anadkat said.
He disclosed being a consultant or speaker for AstraZeneca, Bristol-Myers Squibb, Eisai, Genentech, and ImClone regarding strategies for managing skin toxicities from chemotherapy. He has never prescribed chemotherapy agents.
ORLANDO – Oral isotretinoin holds potential as a bridge therapy for cancer patients who develop severe rashes during treatment, according to Dr. Milan J. Anadkat.
Dermatologists can play an integral role here. "Most oncologists see these patients first, and most oncologists are not enrolled in the iPledge program," said Dr. Anadkat of the division of dermatology at Washington University in St. Louis.
He noted that all treatment options are off label because there are no Food and Drug Administration–approved agents to treat chemotherapy-related cutaneous toxicities.
Getting patients through rashes that occur within a week or two of beginning targeted chemotherapy is important, as patients who develop the greatest reactions tend to have cancers that respond best to treatment, said Dr. Anadkat at the annual meeting of the Florida Society of Dermatology and Dermatologic Surgery. For this reason, the management of these patients is more complicated than simple drug cessation.
"The problem with just taking them off the drug is that they have cancer. Ultimately, the big goal here is treating the cancer, not avoiding the rash," he said.
Tetracycline or doxycycline can also reduce the severity of the rash, but the timing of administration is important. Better outcomes are associated with prophylaxis that is timed with the initiation of EGFR (epidermal growth factor receptor) inhibitors (Cancer 2008;113:847-53). "Waiting for the rash to appear is not the time to give it. It makes a difference if you give at day 0, not in terms of incidence but in the severity of the rash," he said.
Educate patients that the rash typically appears in an estimated 60%-90% of people within 8-10 days of EGFR inhibitor initiation, with a peak presentation at 2-4 weeks. "Bridging them through with something as effective as isotretinoin is useful," said Dr. Anadkat.
The rash generally appears on the face and upper trunk, but be careful not to confuse the presentation with a photo-exposure phenomenon.
Although some oncologists will describe the skin eruptions as "acnelike," histology will show mixed inflammatory infiltrate and follicular rupture. For this reason, "topical acne medications do very little," Dr. Anadkat said. Also, rule out infection, except when patients present with pustules on their arms, legs, or other non–EGFR receptor areas.
EGFR inhibitors can cause inflammatory alopecia, eyelash trichomegaly, and periungual and nail alterations.
About one in six patients will develop periungual or nail abnormalities, typically on their first finger or toe. These effects can be painful, Dr. Anadkat said. Culture is mandatory to rule out superinfection.
Again, the approach is to get patients through the adverse events with petroleum jelly, high-dose topical steroids, or oral tetracyclines. "Tumor markers are going down; [oncologists] are not going to want to stop chemotherapy for a painful thumb or toe," he said. "I recommend antimicrobial soaks with bleach or vinegar to prevent paronychia superinfection."
Dry, itchy skin is another concern with long-term EGFR inhibitor treatment. Histology shows "stark differences" in the stratum corneum. "This is the No. 1 side effect for patients on long-term EGFR – 3 months or longer; [it is] not a grade 3 or higher toxicity, but it is annoying."
Investigators compared oral minocycline and topical tazarotene prophylaxis in a study of 48 patients with cetuximab associated rash (J. Clin. Oncol. 2007:25:5390-6). Although oral minocycline was associated with reduced lesion counts, topical tazarotene yielded no significant benefit. "Again, this is not acne," Dr. Anadkat said.
He disclosed being a consultant or speaker for AstraZeneca, Bristol-Myers Squibb, Eisai, Genentech, and ImClone regarding strategies for managing skin toxicities from chemotherapy. He has never prescribed chemotherapy agents.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE FLORIDA SOCIETY OF DERMATOLOGY AND DERMATOLOGIC SURGERY
Estimating End-of-Life for Hospitalized Patients
Quotes from the Field

We cannot rely solely on a tool to make decisions. The tool is a decision aid.
Alvin H. Moss, MD, FAAHPM
Professor of medicine in the nephrology section and director of the Center for Health Ethics and Law at West Virginia University School of Medicine in Morgantown

Predictions really apply to groups of people, not individuals.
J. Randall Curtis, MD, MPH
Professor and section head in the division of pulmonary and critical care medicine at the University of Washington’s Harborview Medical Center in Seattle

if you ask a physician to provide you with his or her impression of a patient progression, we generally tend to overestimate how well they’re doing.
JoAnn Wood, MD, MSEd, MHA
Hospitalist and division director of general internal medicine at the University of Arkansas for Medical Sciences in Little Rock

Patients feel that you’re almost abandoning them, that there’s something you’re withholding.
Ann Sheehy
Director of the hospitalist service at University of Wisconsin Medical Center in Madison

Telling patients there is a 20% chance that they might die in the next year isn’t usually enough to change their thinking.
David Casarett, MD, MA
Associate professor of medicine at the University of Pennsylvania and chief medical officer of Penn-Wissahickon Hospice in Philadelphia
End-of-life conversations are common in hospital medicine, and Caitlin Foxley, MD, FHM, is no stranger to their nuance. She offers patients and loved ones as much factual information as she can. And regardless of their preference—aggressive treatment, comfort care, something in between—it’s ultimately their choice, not hers. But no matter what, she will ensure the patient’s pain remains under control.
“The way I practice is to allow my patients to make the end-of-life decision that is in accordance with their wishes, and not simply push the least expensive one on them,” says Dr. Foxley, medical director of IMI Hospitalists and hospital service chief of internal medicine at Nebraska Medical Center in Omaha. However, she adds, “most people, given accurate information in a compassionate manner, would choose to die at home, and not in an ICU on a ventilator, with chemo and pressers going through a central line.”
Although hospitalists differ in their approaches to end-of-life discussions, most agree that the majority of critically ill patients want to know their prognosis. Tested end-of-life prediction tools can help physicians provide realistic ranges for patients and families (see “Helpful End-of-Life Prediction Tools,” p. 39). Armed with this insight, they can hope to deliver better and more cost-effective end-of-life care.
Nonetheless, “we cannot rely solely on a tool to make decisions,” says Alvin H. Moss, MD, FAAHPM, professor of medicine in the nephrology section and director of the Center for Health Ethics and Law at West Virginia University School of Medicine in Morgantown. “The tool is a decision aid.”
Clinicians still need to help patients and families identify their treatment goals while determining which life-sustaining options they would or wouldn’t want to pursue, Dr. Moss says. That conversation would include an estimated prognosis of survival.
“If you try to prognosticate a specific length of time, you will be wrong,” says Steven Z. Pantilat, MD, FACP, SFHM, professor of clinical medicine and director of the palliative care program at the University of California San Francisco Medical Center. “You can give patients a lot of useful information by speaking in ranges.”
But it’s important to also convey the inherent uncertainty of any prognosis, considering that a very sick patient might suffer a sudden decline. For this reason, even the best prognostic indicators aren’t exact, Dr. Pantilat cautions. A prediction tool could forecast a 20% chance of six-month survival on the day before a patient’s death in the ICU.
“Predictions really apply to groups of people, not individuals,” says J. Randall Curtis, MD, MPH, professor and section head in the division of pulmonary and critical care medicine at the University of Washington’s Harborview Medical Center in Seattle. Physicians can’t possibly know whether someone will fall into the 95% of patients who die or the 5% of patients who beat the odds.
“It’s never certain that a patient is not going to survive,” says Dr. Curtis, who is director of the Harborview/University of Washington End-of-Life Care Research Program. While patients are less likely to request aggressive care in light of a poor prognosis, some will elect intensive treatment in hopes of defying even the grimmest statistics.
More Medical Tests and Procedures
In the U.S., it’s much more common for patients to receive life-saving treatments than in other countries. The expectation is that expensive medical technology can always prolong life.1
“A lot of patients have that mentality,” says Ann Sheehy, MD, MS, director of the hospitalist service at University of Wisconsin Medical Center in Madison. “That makes it harder to have the discussion with patients that there isn’t something else we can do.” Patients feel “that you’re almost abandoning them, that there’s something you’re withholding.”
The widespread assumption that more medical tests and procedures lead to better outcomes goes hand in hand with the misperception that sufficiently controlling pain and other symptoms draws death closer. As a result, many patients end up dying with distressing symptoms in the hospital instead of peacefully at home.1
As physicians, Dr. Sheehy points out, “We don’t do a good job of saying, ‘This care probably is not going to help you or that it will leave you with a very bad quality of life in the end.’” But projections are far from perfect.
“Telling patients there is a 20% chance that they might die in the next year isn’t usually enough to change their thinking. Nor is it enough to justify withholding treatment,” says David Casarett, MD, MA, associate professor of medicine at the University of Pennsylvania and chief medical officer of Penn-Wissahickon Hospice in Philadelphia.
What prognostic information can do is play an important part in guiding appropriate screening and preventive health measures. For example, if a male patient has a 50% chance of dying within four years, it doesn’t make sense to screen for prostate cancer, a slow-growing malignancy that often takes years to develop. This protocol may also apply to cancer screenings, as well as treatments for diabetes, high blood pressure, or high cholesterol, Dr. Casarett says.
End-of-Life Conversations
By not taking a patient’s prognosis into account, many clinical decisions are not fully informed. In physicians’ clinical practice and training, there tends to be less emphasis on estimating prognosis than on diagnosing and treating illness. This is particularly significant in older adults with competing chronic conditions and diminished life expectancy.2
“Many physicians have not been trained in how to have these conversations, which is something we’re trying to change,” says Dr. Curtis, the pulmonary and critical care specialist at the University of Washington. “This is very emotionally difficult for patients and families, and therefore, it can also be emotionally difficult for physicians.”
Starting this summer, medical residents at Cooper University Hospital in Camden, N.J., will have mandated exposure to palliative care. The rotation, lasting from two to four weeks, will occur in their second year of training, says Mark Angelo, MD, FACP, director of palliative medicine.
Residents will accompany the palliative-care team for an intensive period of time to learn about different techniques for symptom control and to observe end-of-life conversations, which often elicit patients’ angst, depression, and physiologic and spiritual unrest.
“We already have residents rotating with us now in the palliative-care program, and everybody is very struck by how honest patients want you to be,” Dr. Angelo says. “It certainly is devastating, and we understand that. But it does give patients the opportunity to reorganize their lives and to prioritize a number of issues, including medical treatment.”
Some patients opt to spend more time with their grandchildren rather than stay in the hospital. Others prefer to eat and drink whatever they want. Many terminally ill Hispanic patients in the Camden area travel to Latin America, where they were born, or they invite relatives to visit them here, Dr. Angelo says.
While it’s difficult to accept finality, “there’s a certain amount of freedom that comes with that,” he says. “If someone has a prognosis of two months, they may make very different decisions than someone who has a prognosis of two years.”
Physicians tend to be overly optimistic, notes JoAnn Wood, MD, MSEd, MHA, a hospitalist and division director of general internal medicine at the University of Arkansas for Medical Sciences in Little Rock. “The data suggest that, if you ask a physician to provide you with his or her impression of a patient progression, we generally tend to overestimate how well they’re doing,” particularly with cancer patients, Dr. Wood says. “Physicians don’t choose this line of work to facilitate people’s dying.”

When Doing Less Is More
End-of-life prediction tools enable clinicians to keep their expectations of a patient’s survival grounded in reality. And in many hospitals, palliative-care providers are available to lend their expertise. “The field of palliative medicine has taken a lot of strides,” Dr. Wood says, “in helping us to seeing that dying is something that can be done well, just like living can be done well.”
In fact, growing evidence indicates that treating a patient’s discomfort is linked to improvement in physical status and might even increase survival.3 What this means is that, at the end of life, sometimes doing less is actually more. And if patients request less medical care, physicians should honor those desires.4,5
Dr. Pantilat, the UCSF palliative-care expert, suggests asking open-ended questions to get at the heart of a patient’s wishes. For instance: “‘When you look to the future, what do you hope will happen?’ Or ‘When you think of life ahead, what worries you the most?’” The responses guide physicians in devising a plan of care that is consistent with a patient’s values. Having these discussions sooner rather than later is best for everyone involved, Dr. Pantilat says. Unfortunately, that’s not what usually happens.
About half of the more than 40% of Americans who die annually under hospice care do so within two weeks after being admitted. In such a short timeframe, even the most skilled experts are limited in what they can do, according to the National Hospice and Palliative Care Organization. To reverse this trend, Dr. Pantilat recommends that physicians consider making referrals to palliative care much earlier, whenever they sense that a patient may have a year or less to live.
Providing palliative care can be done in conjunction with life-prolonging therapies or as the central focus. The goal is to prevent and relieve suffering and to ensure the best possible quality of life for patients and their families, regardless of disease stage or the need for other treatments. Such care is suitable for patients with cancer, heart conditions, liver or renal failure, Alzheimer’s disease, spinal cord injuries, and a number of other illnesses, according to the National Consensus Project for Quality Palliative Care.

—Caitlin Foxley, MD, FHM, medical director, IMI Hospitalists, hospital service chief of internal medicine, Nebraska Medical Center, Omaha
Planning Ahead
In Arkansas, Dr. Wood typically turns to the hospital’s palliative-care team in end-of-life situations, asking its members to join in a conference with the patient and family. The team typically consists of a nurse, social worker and chaplain who can address various concerns. An employee from the medical billing department participates if necessary.
“Physicians should never assume that they understand the healthcare system, because it’s incredibly complicated,” Dr. Wood says, adding that she doesn’t pretend to be an expert in Medicare, Medicaid, or private insurance reimbursement issues.
Helping patients with advanced care planning can minimize difficulties later. Most patients who die in hospitals are admitted with end-stage disease, and most spend time in the ICU with mechanical ventilation. Physicians often are unaware of patients’ preferences, and this could lead to misunderstandings, especially in the ICU setting, where prognoses can shift quickly. One study showed that, in order for some of these patients to die, clinicians and families generally had to decide explicitly to strive toward less-than-completely-aggressive care.1
“We’re trying to make sure that patients and families have an opportunity to do advanced-care planning,” Dr. Curtis says. Talking with them about their values and goals is essential for clinicians to understand their preferences.
Part of this involves crafting advanced-care directives. One such directive would be a power of attorney for healthcare, in which a patient states who is authorized to make decisions if he or she becomes unable to do so. This is particularly important for patients who select someone other than whom their state’s law would normally designate.
Another document—the living will—allows patients to specify their own preferences for end-of-life care. Yet “it’s often very difficult to know exactly what decisions will need to be made,” Dr. Curtis says. “Those documents are rarely determinative.” Even when a patient stipulates his or her wishes against “extraordinary life-sustaining measures, it still leaves a lot for interpretation.”
Some patients may spell out more clearly whether they wouldn’t want tube-feeding, CPR, or ventilation. This can be prescribed in written and signed Physician Orders for Life-Sustaining Treatment (POLST).

—Steven Z. Pantilat, MD, FACP, professor of clinical medicine, director of the palliative-care program, University of California San Francisco Medical Center
Educating the Public
End-of-life discussions also pose a threat of litigation. “It takes a significant amount of time, often during a very busy day, to sit down with a patient and family members to bring up an issue that will undoubtedly raise many questions, some of which are impossible to answer,” says Dr. Foxley, the hospitalist service chief in Omaha. “I’m sure many physicians are uncomfortable with the tears that are shed.”
When Dr. Foxley recently advised a patient’s family that aggressive care would be futile, they directed their anger toward her. Their loved one died, despite the intensive treatment. It’s just one example of many in which Dr. Foxley has witnessed how high-tech medical treatments can incur astronomical hospital bills after just a few days while doing little—if anything—helpful for the patient.
“We have a lot of work to do to educate the public about the dying process,” she says, adding that the entire burden shouldn’t fall on physicians, and that patients should inform family members of their end-of-life wishes. “We are all going to die someday, and we all need to think about how and where we want to be when it happens, if we have any choice in it.”
Susan Kreimer is a freelance medical writer based in New York.
Helpful End-of-Life Prediction Tools

APACHE II (Acute Physiology and Chronic Health Evaluation II)
A severity-of-disease classification system and one of several ICU scoring systems, it is applied within 24 hours of patient admission. An integer score from 0 to 71 is computed based on several measurements; higher scores correspond to more severe disease and a higher risk of death. http://clincalc.com/IcuMortality/APACHEII.aspx
SOFA (Sequential Organ Failure Assessment)
SOFA tracks a patient’s status during an ICU stay. This scoring system determines the extent of a person’s organ function or rate of failure. The overall score is based on scores of the respiratory, cardiovascular, hepatic, coagulation, renal, and neurological systems. http://www.sfar.org/scores2/sofa2.html
The Karnofsky Performance Scale Index
This tool allows patients to be classified by functional impairment. It compares effectiveness of different therapies and assesses the prognosis in individual patients. The lower the Karnofsky score, the worse the survival outlook for most serious illnesses. http://www.hospicepatients.org/karnofsky.html
PPS (Palliative Performance Scale)
First introduced in 1996 as a tool for performance status in palliative care, the PPS uses five observer-rated domains correlated to the Karnofsky index (100-0). PPS is used in many countries and is translated into many languages. http://supportforhome.wordpress.com/2011/06/15/palliative-performance-scale/
The BODE Index
BODE helps predict mortality from chronic obstructive pulmonary disease (COPD) after diagnosis. Presumably, a higher BODE score correlates with an increased risk of death. http://copd.about.com/od/copdbasics/a/BODEIndex.htm
The Charlson Comorbidity Index
This index predicts the 10-year mortality for a patient who might have a range of comorbid conditions, such as heart disease, AIDS, or cancer (a total of 22 conditions). Each condition is assigned a score, depending on the risk of dying associated with the condition. http://www.medal.org/OnlineCalculators/ch1/ch1.13/ch1.13.01.php
Hemodialysis Mortality Predictor
This online calculator estimates prognosis in end-stage renal disease patients using an integrated model that incorporates the patient age, serum albumin, comorbidities, and clinician assessment of the patient’s likelihood of being dead within a year. http://touchcalc.com/calculators/sq
—Susan Kreimer
References
- Walling AM, Asch SM, Lorenz KA, et al. The quality of care provided to hospitalized patients at the end of life. Arch Intern Med. 2010;170(12):1057-1063.
- Yourman LC, Lee SJ, Schonberg MA, Widera EW, Smith AK. Prognostic indices for older adults: a systematic review. JAMA. 2012;307(2):182-192.
- Grudzen C, Grady D. Improving care at the end of life. Arch Intern Med. 2011;171(13):1202.
- Grudzen C. At the end of life, sometimes less is more. Arch Intern Med. 2011;171(13):1201.
- Bale PW. Honoring patients’ wishes for less health care. Arch Intern Med. 2011;171(13):1200.
Quotes from the Field
We cannot rely solely on a tool to make decisions. The tool is a decision aid.
Alvin H. Moss, MD, FAAHPM
Professor of medicine in the nephrology section and director of the Center for Health Ethics and Law at West Virginia University School of Medicine in Morgantown
Predictions really apply to groups of people, not individuals.
J. Randall Curtis, MD, MPH
Professor and section head in the division of pulmonary and critical care medicine at the University of Washington’s Harborview Medical Center in Seattle
if you ask a physician to provide you with his or her impression of a patient progression, we generally tend to overestimate how well they’re doing.
JoAnn Wood, MD, MSEd, MHA
Hospitalist and division director of general internal medicine at the University of Arkansas for Medical Sciences in Little Rock
Patients feel that you’re almost abandoning them, that there’s something you’re withholding.
Ann Sheehy
Director of the hospitalist service at University of Wisconsin Medical Center in Madison
Telling patients there is a 20% chance that they might die in the next year isn’t usually enough to change their thinking.
David Casarett, MD, MA
Associate professor of medicine at the University of Pennsylvania and chief medical officer of Penn-Wissahickon Hospice in Philadelphia
End-of-life conversations are common in hospital medicine, and Caitlin Foxley, MD, FHM, is no stranger to their nuance. She offers patients and loved ones as much factual information as she can. And regardless of their preference—aggressive treatment, comfort care, something in between—it’s ultimately their choice, not hers. But no matter what, she will ensure the patient’s pain remains under control.
“The way I practice is to allow my patients to make the end-of-life decision that is in accordance with their wishes, and not simply push the least expensive one on them,” says Dr. Foxley, medical director of IMI Hospitalists and hospital service chief of internal medicine at Nebraska Medical Center in Omaha. However, she adds, “most people, given accurate information in a compassionate manner, would choose to die at home, and not in an ICU on a ventilator, with chemo and pressers going through a central line.”
Although hospitalists differ in their approaches to end-of-life discussions, most agree that the majority of critically ill patients want to know their prognosis. Tested end-of-life prediction tools can help physicians provide realistic ranges for patients and families (see “Helpful End-of-Life Prediction Tools,” p. 39). Armed with this insight, they can hope to deliver better and more cost-effective end-of-life care.
Nonetheless, “we cannot rely solely on a tool to make decisions,” says Alvin H. Moss, MD, FAAHPM, professor of medicine in the nephrology section and director of the Center for Health Ethics and Law at West Virginia University School of Medicine in Morgantown. “The tool is a decision aid.”
Clinicians still need to help patients and families identify their treatment goals while determining which life-sustaining options they would or wouldn’t want to pursue, Dr. Moss says. That conversation would include an estimated prognosis of survival.
“If you try to prognosticate a specific length of time, you will be wrong,” says Steven Z. Pantilat, MD, FACP, SFHM, professor of clinical medicine and director of the palliative care program at the University of California San Francisco Medical Center. “You can give patients a lot of useful information by speaking in ranges.”
But it’s important to also convey the inherent uncertainty of any prognosis, considering that a very sick patient might suffer a sudden decline. For this reason, even the best prognostic indicators aren’t exact, Dr. Pantilat cautions. A prediction tool could forecast a 20% chance of six-month survival on the day before a patient’s death in the ICU.
“Predictions really apply to groups of people, not individuals,” says J. Randall Curtis, MD, MPH, professor and section head in the division of pulmonary and critical care medicine at the University of Washington’s Harborview Medical Center in Seattle. Physicians can’t possibly know whether someone will fall into the 95% of patients who die or the 5% of patients who beat the odds.
“It’s never certain that a patient is not going to survive,” says Dr. Curtis, who is director of the Harborview/University of Washington End-of-Life Care Research Program. While patients are less likely to request aggressive care in light of a poor prognosis, some will elect intensive treatment in hopes of defying even the grimmest statistics.
More Medical Tests and Procedures
In the U.S., it’s much more common for patients to receive life-saving treatments than in other countries. The expectation is that expensive medical technology can always prolong life.1
“A lot of patients have that mentality,” says Ann Sheehy, MD, MS, director of the hospitalist service at University of Wisconsin Medical Center in Madison. “That makes it harder to have the discussion with patients that there isn’t something else we can do.” Patients feel “that you’re almost abandoning them, that there’s something you’re withholding.”
The widespread assumption that more medical tests and procedures lead to better outcomes goes hand in hand with the misperception that sufficiently controlling pain and other symptoms draws death closer. As a result, many patients end up dying with distressing symptoms in the hospital instead of peacefully at home.1
As physicians, Dr. Sheehy points out, “We don’t do a good job of saying, ‘This care probably is not going to help you or that it will leave you with a very bad quality of life in the end.’” But projections are far from perfect.
“Telling patients there is a 20% chance that they might die in the next year isn’t usually enough to change their thinking. Nor is it enough to justify withholding treatment,” says David Casarett, MD, MA, associate professor of medicine at the University of Pennsylvania and chief medical officer of Penn-Wissahickon Hospice in Philadelphia.
What prognostic information can do is play an important part in guiding appropriate screening and preventive health measures. For example, if a male patient has a 50% chance of dying within four years, it doesn’t make sense to screen for prostate cancer, a slow-growing malignancy that often takes years to develop. This protocol may also apply to cancer screenings, as well as treatments for diabetes, high blood pressure, or high cholesterol, Dr. Casarett says.
End-of-Life Conversations
By not taking a patient’s prognosis into account, many clinical decisions are not fully informed. In physicians’ clinical practice and training, there tends to be less emphasis on estimating prognosis than on diagnosing and treating illness. This is particularly significant in older adults with competing chronic conditions and diminished life expectancy.2
“Many physicians have not been trained in how to have these conversations, which is something we’re trying to change,” says Dr. Curtis, the pulmonary and critical care specialist at the University of Washington. “This is very emotionally difficult for patients and families, and therefore, it can also be emotionally difficult for physicians.”
Starting this summer, medical residents at Cooper University Hospital in Camden, N.J., will have mandated exposure to palliative care. The rotation, lasting from two to four weeks, will occur in their second year of training, says Mark Angelo, MD, FACP, director of palliative medicine.
Residents will accompany the palliative-care team for an intensive period of time to learn about different techniques for symptom control and to observe end-of-life conversations, which often elicit patients’ angst, depression, and physiologic and spiritual unrest.
“We already have residents rotating with us now in the palliative-care program, and everybody is very struck by how honest patients want you to be,” Dr. Angelo says. “It certainly is devastating, and we understand that. But it does give patients the opportunity to reorganize their lives and to prioritize a number of issues, including medical treatment.”
Some patients opt to spend more time with their grandchildren rather than stay in the hospital. Others prefer to eat and drink whatever they want. Many terminally ill Hispanic patients in the Camden area travel to Latin America, where they were born, or they invite relatives to visit them here, Dr. Angelo says.
While it’s difficult to accept finality, “there’s a certain amount of freedom that comes with that,” he says. “If someone has a prognosis of two months, they may make very different decisions than someone who has a prognosis of two years.”
Physicians tend to be overly optimistic, notes JoAnn Wood, MD, MSEd, MHA, a hospitalist and division director of general internal medicine at the University of Arkansas for Medical Sciences in Little Rock. “The data suggest that, if you ask a physician to provide you with his or her impression of a patient progression, we generally tend to overestimate how well they’re doing,” particularly with cancer patients, Dr. Wood says. “Physicians don’t choose this line of work to facilitate people’s dying.”
When Doing Less Is More
End-of-life prediction tools enable clinicians to keep their expectations of a patient’s survival grounded in reality. And in many hospitals, palliative-care providers are available to lend their expertise. “The field of palliative medicine has taken a lot of strides,” Dr. Wood says, “in helping us to seeing that dying is something that can be done well, just like living can be done well.”
In fact, growing evidence indicates that treating a patient’s discomfort is linked to improvement in physical status and might even increase survival.3 What this means is that, at the end of life, sometimes doing less is actually more. And if patients request less medical care, physicians should honor those desires.4,5
Dr. Pantilat, the UCSF palliative-care expert, suggests asking open-ended questions to get at the heart of a patient’s wishes. For instance: “‘When you look to the future, what do you hope will happen?’ Or ‘When you think of life ahead, what worries you the most?’” The responses guide physicians in devising a plan of care that is consistent with a patient’s values. Having these discussions sooner rather than later is best for everyone involved, Dr. Pantilat says. Unfortunately, that’s not what usually happens.
About half of the more than 40% of Americans who die annually under hospice care do so within two weeks after being admitted. In such a short timeframe, even the most skilled experts are limited in what they can do, according to the National Hospice and Palliative Care Organization. To reverse this trend, Dr. Pantilat recommends that physicians consider making referrals to palliative care much earlier, whenever they sense that a patient may have a year or less to live.
Providing palliative care can be done in conjunction with life-prolonging therapies or as the central focus. The goal is to prevent and relieve suffering and to ensure the best possible quality of life for patients and their families, regardless of disease stage or the need for other treatments. Such care is suitable for patients with cancer, heart conditions, liver or renal failure, Alzheimer’s disease, spinal cord injuries, and a number of other illnesses, according to the National Consensus Project for Quality Palliative Care.
—Caitlin Foxley, MD, FHM, medical director, IMI Hospitalists, hospital service chief of internal medicine, Nebraska Medical Center, Omaha
Planning Ahead
In Arkansas, Dr. Wood typically turns to the hospital’s palliative-care team in end-of-life situations, asking its members to join in a conference with the patient and family. The team typically consists of a nurse, social worker and chaplain who can address various concerns. An employee from the medical billing department participates if necessary.
“Physicians should never assume that they understand the healthcare system, because it’s incredibly complicated,” Dr. Wood says, adding that she doesn’t pretend to be an expert in Medicare, Medicaid, or private insurance reimbursement issues.
Helping patients with advanced care planning can minimize difficulties later. Most patients who die in hospitals are admitted with end-stage disease, and most spend time in the ICU with mechanical ventilation. Physicians often are unaware of patients’ preferences, and this could lead to misunderstandings, especially in the ICU setting, where prognoses can shift quickly. One study showed that, in order for some of these patients to die, clinicians and families generally had to decide explicitly to strive toward less-than-completely-aggressive care.1
“We’re trying to make sure that patients and families have an opportunity to do advanced-care planning,” Dr. Curtis says. Talking with them about their values and goals is essential for clinicians to understand their preferences.
Part of this involves crafting advanced-care directives. One such directive would be a power of attorney for healthcare, in which a patient states who is authorized to make decisions if he or she becomes unable to do so. This is particularly important for patients who select someone other than whom their state’s law would normally designate.
Another document—the living will—allows patients to specify their own preferences for end-of-life care. Yet “it’s often very difficult to know exactly what decisions will need to be made,” Dr. Curtis says. “Those documents are rarely determinative.” Even when a patient stipulates his or her wishes against “extraordinary life-sustaining measures, it still leaves a lot for interpretation.”
Some patients may spell out more clearly whether they wouldn’t want tube-feeding, CPR, or ventilation. This can be prescribed in written and signed Physician Orders for Life-Sustaining Treatment (POLST).
—Steven Z. Pantilat, MD, FACP, professor of clinical medicine, director of the palliative-care program, University of California San Francisco Medical Center
Educating the Public
End-of-life discussions also pose a threat of litigation. “It takes a significant amount of time, often during a very busy day, to sit down with a patient and family members to bring up an issue that will undoubtedly raise many questions, some of which are impossible to answer,” says Dr. Foxley, the hospitalist service chief in Omaha. “I’m sure many physicians are uncomfortable with the tears that are shed.”
When Dr. Foxley recently advised a patient’s family that aggressive care would be futile, they directed their anger toward her. Their loved one died, despite the intensive treatment. It’s just one example of many in which Dr. Foxley has witnessed how high-tech medical treatments can incur astronomical hospital bills after just a few days while doing little—if anything—helpful for the patient.
“We have a lot of work to do to educate the public about the dying process,” she says, adding that the entire burden shouldn’t fall on physicians, and that patients should inform family members of their end-of-life wishes. “We are all going to die someday, and we all need to think about how and where we want to be when it happens, if we have any choice in it.”
Susan Kreimer is a freelance medical writer based in New York.
Helpful End-of-Life Prediction Tools
APACHE II (Acute Physiology and Chronic Health Evaluation II)
A severity-of-disease classification system and one of several ICU scoring systems, it is applied within 24 hours of patient admission. An integer score from 0 to 71 is computed based on several measurements; higher scores correspond to more severe disease and a higher risk of death. http://clincalc.com/IcuMortality/APACHEII.aspx
SOFA (Sequential Organ Failure Assessment)
SOFA tracks a patient’s status during an ICU stay. This scoring system determines the extent of a person’s organ function or rate of failure. The overall score is based on scores of the respiratory, cardiovascular, hepatic, coagulation, renal, and neurological systems. http://www.sfar.org/scores2/sofa2.html
The Karnofsky Performance Scale Index
This tool allows patients to be classified by functional impairment. It compares effectiveness of different therapies and assesses the prognosis in individual patients. The lower the Karnofsky score, the worse the survival outlook for most serious illnesses. http://www.hospicepatients.org/karnofsky.html
PPS (Palliative Performance Scale)
First introduced in 1996 as a tool for performance status in palliative care, the PPS uses five observer-rated domains correlated to the Karnofsky index (100-0). PPS is used in many countries and is translated into many languages. http://supportforhome.wordpress.com/2011/06/15/palliative-performance-scale/
The BODE Index
BODE helps predict mortality from chronic obstructive pulmonary disease (COPD) after diagnosis. Presumably, a higher BODE score correlates with an increased risk of death. http://copd.about.com/od/copdbasics/a/BODEIndex.htm
The Charlson Comorbidity Index
This index predicts the 10-year mortality for a patient who might have a range of comorbid conditions, such as heart disease, AIDS, or cancer (a total of 22 conditions). Each condition is assigned a score, depending on the risk of dying associated with the condition. http://www.medal.org/OnlineCalculators/ch1/ch1.13/ch1.13.01.php
Hemodialysis Mortality Predictor
This online calculator estimates prognosis in end-stage renal disease patients using an integrated model that incorporates the patient age, serum albumin, comorbidities, and clinician assessment of the patient’s likelihood of being dead within a year. http://touchcalc.com/calculators/sq
—Susan Kreimer
References
- Walling AM, Asch SM, Lorenz KA, et al. The quality of care provided to hospitalized patients at the end of life. Arch Intern Med. 2010;170(12):1057-1063.
- Yourman LC, Lee SJ, Schonberg MA, Widera EW, Smith AK. Prognostic indices for older adults: a systematic review. JAMA. 2012;307(2):182-192.
- Grudzen C, Grady D. Improving care at the end of life. Arch Intern Med. 2011;171(13):1202.
- Grudzen C. At the end of life, sometimes less is more. Arch Intern Med. 2011;171(13):1201.
- Bale PW. Honoring patients’ wishes for less health care. Arch Intern Med. 2011;171(13):1200.
Quotes from the Field
We cannot rely solely on a tool to make decisions. The tool is a decision aid.
Alvin H. Moss, MD, FAAHPM
Professor of medicine in the nephrology section and director of the Center for Health Ethics and Law at West Virginia University School of Medicine in Morgantown
Predictions really apply to groups of people, not individuals.
J. Randall Curtis, MD, MPH
Professor and section head in the division of pulmonary and critical care medicine at the University of Washington’s Harborview Medical Center in Seattle
if you ask a physician to provide you with his or her impression of a patient progression, we generally tend to overestimate how well they’re doing.
JoAnn Wood, MD, MSEd, MHA
Hospitalist and division director of general internal medicine at the University of Arkansas for Medical Sciences in Little Rock
Patients feel that you’re almost abandoning them, that there’s something you’re withholding.
Ann Sheehy
Director of the hospitalist service at University of Wisconsin Medical Center in Madison
Telling patients there is a 20% chance that they might die in the next year isn’t usually enough to change their thinking.
David Casarett, MD, MA
Associate professor of medicine at the University of Pennsylvania and chief medical officer of Penn-Wissahickon Hospice in Philadelphia
End-of-life conversations are common in hospital medicine, and Caitlin Foxley, MD, FHM, is no stranger to their nuance. She offers patients and loved ones as much factual information as she can. And regardless of their preference—aggressive treatment, comfort care, something in between—it’s ultimately their choice, not hers. But no matter what, she will ensure the patient’s pain remains under control.
“The way I practice is to allow my patients to make the end-of-life decision that is in accordance with their wishes, and not simply push the least expensive one on them,” says Dr. Foxley, medical director of IMI Hospitalists and hospital service chief of internal medicine at Nebraska Medical Center in Omaha. However, she adds, “most people, given accurate information in a compassionate manner, would choose to die at home, and not in an ICU on a ventilator, with chemo and pressers going through a central line.”
Although hospitalists differ in their approaches to end-of-life discussions, most agree that the majority of critically ill patients want to know their prognosis. Tested end-of-life prediction tools can help physicians provide realistic ranges for patients and families (see “Helpful End-of-Life Prediction Tools,” p. 39). Armed with this insight, they can hope to deliver better and more cost-effective end-of-life care.
Nonetheless, “we cannot rely solely on a tool to make decisions,” says Alvin H. Moss, MD, FAAHPM, professor of medicine in the nephrology section and director of the Center for Health Ethics and Law at West Virginia University School of Medicine in Morgantown. “The tool is a decision aid.”
Clinicians still need to help patients and families identify their treatment goals while determining which life-sustaining options they would or wouldn’t want to pursue, Dr. Moss says. That conversation would include an estimated prognosis of survival.
“If you try to prognosticate a specific length of time, you will be wrong,” says Steven Z. Pantilat, MD, FACP, SFHM, professor of clinical medicine and director of the palliative care program at the University of California San Francisco Medical Center. “You can give patients a lot of useful information by speaking in ranges.”
But it’s important to also convey the inherent uncertainty of any prognosis, considering that a very sick patient might suffer a sudden decline. For this reason, even the best prognostic indicators aren’t exact, Dr. Pantilat cautions. A prediction tool could forecast a 20% chance of six-month survival on the day before a patient’s death in the ICU.
“Predictions really apply to groups of people, not individuals,” says J. Randall Curtis, MD, MPH, professor and section head in the division of pulmonary and critical care medicine at the University of Washington’s Harborview Medical Center in Seattle. Physicians can’t possibly know whether someone will fall into the 95% of patients who die or the 5% of patients who beat the odds.
“It’s never certain that a patient is not going to survive,” says Dr. Curtis, who is director of the Harborview/University of Washington End-of-Life Care Research Program. While patients are less likely to request aggressive care in light of a poor prognosis, some will elect intensive treatment in hopes of defying even the grimmest statistics.
More Medical Tests and Procedures
In the U.S., it’s much more common for patients to receive life-saving treatments than in other countries. The expectation is that expensive medical technology can always prolong life.1
“A lot of patients have that mentality,” says Ann Sheehy, MD, MS, director of the hospitalist service at University of Wisconsin Medical Center in Madison. “That makes it harder to have the discussion with patients that there isn’t something else we can do.” Patients feel “that you’re almost abandoning them, that there’s something you’re withholding.”
The widespread assumption that more medical tests and procedures lead to better outcomes goes hand in hand with the misperception that sufficiently controlling pain and other symptoms draws death closer. As a result, many patients end up dying with distressing symptoms in the hospital instead of peacefully at home.1
As physicians, Dr. Sheehy points out, “We don’t do a good job of saying, ‘This care probably is not going to help you or that it will leave you with a very bad quality of life in the end.’” But projections are far from perfect.
“Telling patients there is a 20% chance that they might die in the next year isn’t usually enough to change their thinking. Nor is it enough to justify withholding treatment,” says David Casarett, MD, MA, associate professor of medicine at the University of Pennsylvania and chief medical officer of Penn-Wissahickon Hospice in Philadelphia.
What prognostic information can do is play an important part in guiding appropriate screening and preventive health measures. For example, if a male patient has a 50% chance of dying within four years, it doesn’t make sense to screen for prostate cancer, a slow-growing malignancy that often takes years to develop. This protocol may also apply to cancer screenings, as well as treatments for diabetes, high blood pressure, or high cholesterol, Dr. Casarett says.
End-of-Life Conversations
By not taking a patient’s prognosis into account, many clinical decisions are not fully informed. In physicians’ clinical practice and training, there tends to be less emphasis on estimating prognosis than on diagnosing and treating illness. This is particularly significant in older adults with competing chronic conditions and diminished life expectancy.2
“Many physicians have not been trained in how to have these conversations, which is something we’re trying to change,” says Dr. Curtis, the pulmonary and critical care specialist at the University of Washington. “This is very emotionally difficult for patients and families, and therefore, it can also be emotionally difficult for physicians.”
Starting this summer, medical residents at Cooper University Hospital in Camden, N.J., will have mandated exposure to palliative care. The rotation, lasting from two to four weeks, will occur in their second year of training, says Mark Angelo, MD, FACP, director of palliative medicine.
Residents will accompany the palliative-care team for an intensive period of time to learn about different techniques for symptom control and to observe end-of-life conversations, which often elicit patients’ angst, depression, and physiologic and spiritual unrest.
“We already have residents rotating with us now in the palliative-care program, and everybody is very struck by how honest patients want you to be,” Dr. Angelo says. “It certainly is devastating, and we understand that. But it does give patients the opportunity to reorganize their lives and to prioritize a number of issues, including medical treatment.”
Some patients opt to spend more time with their grandchildren rather than stay in the hospital. Others prefer to eat and drink whatever they want. Many terminally ill Hispanic patients in the Camden area travel to Latin America, where they were born, or they invite relatives to visit them here, Dr. Angelo says.
While it’s difficult to accept finality, “there’s a certain amount of freedom that comes with that,” he says. “If someone has a prognosis of two months, they may make very different decisions than someone who has a prognosis of two years.”
Physicians tend to be overly optimistic, notes JoAnn Wood, MD, MSEd, MHA, a hospitalist and division director of general internal medicine at the University of Arkansas for Medical Sciences in Little Rock. “The data suggest that, if you ask a physician to provide you with his or her impression of a patient progression, we generally tend to overestimate how well they’re doing,” particularly with cancer patients, Dr. Wood says. “Physicians don’t choose this line of work to facilitate people’s dying.”
When Doing Less Is More
End-of-life prediction tools enable clinicians to keep their expectations of a patient’s survival grounded in reality. And in many hospitals, palliative-care providers are available to lend their expertise. “The field of palliative medicine has taken a lot of strides,” Dr. Wood says, “in helping us to seeing that dying is something that can be done well, just like living can be done well.”
In fact, growing evidence indicates that treating a patient’s discomfort is linked to improvement in physical status and might even increase survival.3 What this means is that, at the end of life, sometimes doing less is actually more. And if patients request less medical care, physicians should honor those desires.4,5
Dr. Pantilat, the UCSF palliative-care expert, suggests asking open-ended questions to get at the heart of a patient’s wishes. For instance: “‘When you look to the future, what do you hope will happen?’ Or ‘When you think of life ahead, what worries you the most?’” The responses guide physicians in devising a plan of care that is consistent with a patient’s values. Having these discussions sooner rather than later is best for everyone involved, Dr. Pantilat says. Unfortunately, that’s not what usually happens.
About half of the more than 40% of Americans who die annually under hospice care do so within two weeks after being admitted. In such a short timeframe, even the most skilled experts are limited in what they can do, according to the National Hospice and Palliative Care Organization. To reverse this trend, Dr. Pantilat recommends that physicians consider making referrals to palliative care much earlier, whenever they sense that a patient may have a year or less to live.
Providing palliative care can be done in conjunction with life-prolonging therapies or as the central focus. The goal is to prevent and relieve suffering and to ensure the best possible quality of life for patients and their families, regardless of disease stage or the need for other treatments. Such care is suitable for patients with cancer, heart conditions, liver or renal failure, Alzheimer’s disease, spinal cord injuries, and a number of other illnesses, according to the National Consensus Project for Quality Palliative Care.
—Caitlin Foxley, MD, FHM, medical director, IMI Hospitalists, hospital service chief of internal medicine, Nebraska Medical Center, Omaha
Planning Ahead
In Arkansas, Dr. Wood typically turns to the hospital’s palliative-care team in end-of-life situations, asking its members to join in a conference with the patient and family. The team typically consists of a nurse, social worker and chaplain who can address various concerns. An employee from the medical billing department participates if necessary.
“Physicians should never assume that they understand the healthcare system, because it’s incredibly complicated,” Dr. Wood says, adding that she doesn’t pretend to be an expert in Medicare, Medicaid, or private insurance reimbursement issues.
Helping patients with advanced care planning can minimize difficulties later. Most patients who die in hospitals are admitted with end-stage disease, and most spend time in the ICU with mechanical ventilation. Physicians often are unaware of patients’ preferences, and this could lead to misunderstandings, especially in the ICU setting, where prognoses can shift quickly. One study showed that, in order for some of these patients to die, clinicians and families generally had to decide explicitly to strive toward less-than-completely-aggressive care.1
“We’re trying to make sure that patients and families have an opportunity to do advanced-care planning,” Dr. Curtis says. Talking with them about their values and goals is essential for clinicians to understand their preferences.
Part of this involves crafting advanced-care directives. One such directive would be a power of attorney for healthcare, in which a patient states who is authorized to make decisions if he or she becomes unable to do so. This is particularly important for patients who select someone other than whom their state’s law would normally designate.
Another document—the living will—allows patients to specify their own preferences for end-of-life care. Yet “it’s often very difficult to know exactly what decisions will need to be made,” Dr. Curtis says. “Those documents are rarely determinative.” Even when a patient stipulates his or her wishes against “extraordinary life-sustaining measures, it still leaves a lot for interpretation.”
Some patients may spell out more clearly whether they wouldn’t want tube-feeding, CPR, or ventilation. This can be prescribed in written and signed Physician Orders for Life-Sustaining Treatment (POLST).
—Steven Z. Pantilat, MD, FACP, professor of clinical medicine, director of the palliative-care program, University of California San Francisco Medical Center
Educating the Public
End-of-life discussions also pose a threat of litigation. “It takes a significant amount of time, often during a very busy day, to sit down with a patient and family members to bring up an issue that will undoubtedly raise many questions, some of which are impossible to answer,” says Dr. Foxley, the hospitalist service chief in Omaha. “I’m sure many physicians are uncomfortable with the tears that are shed.”
When Dr. Foxley recently advised a patient’s family that aggressive care would be futile, they directed their anger toward her. Their loved one died, despite the intensive treatment. It’s just one example of many in which Dr. Foxley has witnessed how high-tech medical treatments can incur astronomical hospital bills after just a few days while doing little—if anything—helpful for the patient.
“We have a lot of work to do to educate the public about the dying process,” she says, adding that the entire burden shouldn’t fall on physicians, and that patients should inform family members of their end-of-life wishes. “We are all going to die someday, and we all need to think about how and where we want to be when it happens, if we have any choice in it.”
Susan Kreimer is a freelance medical writer based in New York.
Helpful End-of-Life Prediction Tools
APACHE II (Acute Physiology and Chronic Health Evaluation II)
A severity-of-disease classification system and one of several ICU scoring systems, it is applied within 24 hours of patient admission. An integer score from 0 to 71 is computed based on several measurements; higher scores correspond to more severe disease and a higher risk of death. http://clincalc.com/IcuMortality/APACHEII.aspx
SOFA (Sequential Organ Failure Assessment)
SOFA tracks a patient’s status during an ICU stay. This scoring system determines the extent of a person’s organ function or rate of failure. The overall score is based on scores of the respiratory, cardiovascular, hepatic, coagulation, renal, and neurological systems. http://www.sfar.org/scores2/sofa2.html
The Karnofsky Performance Scale Index
This tool allows patients to be classified by functional impairment. It compares effectiveness of different therapies and assesses the prognosis in individual patients. The lower the Karnofsky score, the worse the survival outlook for most serious illnesses. http://www.hospicepatients.org/karnofsky.html
PPS (Palliative Performance Scale)
First introduced in 1996 as a tool for performance status in palliative care, the PPS uses five observer-rated domains correlated to the Karnofsky index (100-0). PPS is used in many countries and is translated into many languages. http://supportforhome.wordpress.com/2011/06/15/palliative-performance-scale/
The BODE Index
BODE helps predict mortality from chronic obstructive pulmonary disease (COPD) after diagnosis. Presumably, a higher BODE score correlates with an increased risk of death. http://copd.about.com/od/copdbasics/a/BODEIndex.htm
The Charlson Comorbidity Index
This index predicts the 10-year mortality for a patient who might have a range of comorbid conditions, such as heart disease, AIDS, or cancer (a total of 22 conditions). Each condition is assigned a score, depending on the risk of dying associated with the condition. http://www.medal.org/OnlineCalculators/ch1/ch1.13/ch1.13.01.php
Hemodialysis Mortality Predictor
This online calculator estimates prognosis in end-stage renal disease patients using an integrated model that incorporates the patient age, serum albumin, comorbidities, and clinician assessment of the patient’s likelihood of being dead within a year. http://touchcalc.com/calculators/sq
—Susan Kreimer
References
- Walling AM, Asch SM, Lorenz KA, et al. The quality of care provided to hospitalized patients at the end of life. Arch Intern Med. 2010;170(12):1057-1063.
- Yourman LC, Lee SJ, Schonberg MA, Widera EW, Smith AK. Prognostic indices for older adults: a systematic review. JAMA. 2012;307(2):182-192.
- Grudzen C, Grady D. Improving care at the end of life. Arch Intern Med. 2011;171(13):1202.
- Grudzen C. At the end of life, sometimes less is more. Arch Intern Med. 2011;171(13):1201.
- Bale PW. Honoring patients’ wishes for less health care. Arch Intern Med. 2011;171(13):1200.
Washington Post Blasts Proliferation of ESAs for Anemia
Anemia drugs sold under the brand names of Procrit, Aranesp, and Epogen come under new and scathing scrutiny in an exclusive report published July 20 in the Washington Post.
The investigative article by Peter Whoriskey alleges that pharmaceutical giants Amgen and Johnson & Johnson "wildly overstated" benefits while understating potentially lethal side effects of these erythropoiesis-stimulating agents (ESAs).
While safety trials required by the Food and Drug Administration lagged for more than a decade, the companies successfully lobbied for a payment system that rewarded physicians for giving large doses of their high-priced drugs, according to the report.
Use of the drugs declined in recent years after studies showed higher mortality rates in patients given ESAs. Epoetin-alfa (Procrit and Epogen) and darbepoetin alfa (Aranesp) are used to treat anemia in patients undergoing cancer chemotherapy or dialysis for chronic kidney disease.
Anemia drugs sold under the brand names of Procrit, Aranesp, and Epogen come under new and scathing scrutiny in an exclusive report published July 20 in the Washington Post.
The investigative article by Peter Whoriskey alleges that pharmaceutical giants Amgen and Johnson & Johnson "wildly overstated" benefits while understating potentially lethal side effects of these erythropoiesis-stimulating agents (ESAs).
While safety trials required by the Food and Drug Administration lagged for more than a decade, the companies successfully lobbied for a payment system that rewarded physicians for giving large doses of their high-priced drugs, according to the report.
Use of the drugs declined in recent years after studies showed higher mortality rates in patients given ESAs. Epoetin-alfa (Procrit and Epogen) and darbepoetin alfa (Aranesp) are used to treat anemia in patients undergoing cancer chemotherapy or dialysis for chronic kidney disease.
Anemia drugs sold under the brand names of Procrit, Aranesp, and Epogen come under new and scathing scrutiny in an exclusive report published July 20 in the Washington Post.
The investigative article by Peter Whoriskey alleges that pharmaceutical giants Amgen and Johnson & Johnson "wildly overstated" benefits while understating potentially lethal side effects of these erythropoiesis-stimulating agents (ESAs).
While safety trials required by the Food and Drug Administration lagged for more than a decade, the companies successfully lobbied for a payment system that rewarded physicians for giving large doses of their high-priced drugs, according to the report.
Use of the drugs declined in recent years after studies showed higher mortality rates in patients given ESAs. Epoetin-alfa (Procrit and Epogen) and darbepoetin alfa (Aranesp) are used to treat anemia in patients undergoing cancer chemotherapy or dialysis for chronic kidney disease.
FDA Approves REMS for Long-Acting Opioids
A risk evaluation and mitigation strategy for extended-release and long-acting opioid medications has received Food and Drug Administration approval.
The move has been anticipated as an important element in an attempt to stem the swelling tide of abuse, misuse, and overdose of these prescription drugs while assuring continued access to the highly potent analgesics for patients with moderate to severe persistent pain, Dr. Margaret A. Hamburg said in a media briefing.
The new safety measures, which pertain to approximately 30 currently available medications, will require the manufacturers of the drugs to make FDA-approved education materials available to prescribers no later than March 1, 2013, via development grants to continuing education providers who will develop and deliver the training, said Dr. Hamburg, commissioner of the FDA. In addition, the risk evaluation and mitigation strategy (REMS) will include the distribution of a patient counseling leaflet to prescribers regarding the safe and effective use of the drugs; an updated, single-page medication guide for consumers, an implementation plan, and periodic assessments to evaluate the impact of the program on the safe use of these products, which the FDA will review and use to tweak the program as needed, she said.
"It is important to note that we are focusing on extended-release and long-acting opioid medications ... because these have very specific safety problems that have to be addressed very carefully," according to Dr. John Jenkins, director of the Office of New Drugs within the FDA’s Center for Drug Evaluation and Research. These drugs, including hydromorphone, oxycodone, morphine, oxymorphone, methadone, transdermal fentanyl, and transdermal buprenorphine, "can cause problems even when prescribed appropriately."
The prescriber education component of the REMS will include information regarding the risks and benefits of opioid therapy for individual patients, choosing patients appropriately, patient management and monitoring, and patient counseling, Dr. Jenkins explained. It will also include guidance on the potential for misuse, abuse, and addition, as well as recognizing evidence for these outcomes. The updated medication guide and patient counseling document will include information on how to safely use, store, and dispose of these analgesics, specific instructions for recognizing the signs of potential overdose and advice for preventing accidental exposure to family and household visitors, he said.
With respect to the assessment and auditing component of the program, the FDA has established goals, which the manufacturers are expected to achieve, for the percentage of prescribers who complete the training and for assessing prescribers’ understanding of the risk information. Participation in the educational programs is not mandatory for prescribers, Dr. Hamburg stated. The assessments are also required to evaluate whether the [REMS] adversely affect patient access to these drugs, she said. "Patients in pain must have continued assess to medications they need," she added.
The new REMS program is one component of a multiagency, national strategy unveiled by the White House in 2011 to address prescription drug abuse, "which is this country’s fastest-growing drug problem," said Dr. Hamburg, noting that opioid overdoses in particular were the cause of approximately 15,000 deaths among Americans in 2008 and nearly 16,000 in 2009. Called Epidemic: Responding to America's Prescription Drug Abuse Crisis, the national plan suggests expansion of state-based prescription drug-monitoring programs; seeks creation of recommendations for convenient and environmentally responsible ways to dispose of unused medications; and calls for legislative action to reduce "doctor shopping" and "pill mills."
In the absence of the legislative changes needed to fulfill the comprehensive White House plan, the REMS "is an important and timely step by FDA to supplement prescriber training and consumer information," R. Gil Kerlikowske, director of the White House Office of National Drug Control Policy, said during the telebriefing.
A risk evaluation and mitigation strategy for extended-release and long-acting opioid medications has received Food and Drug Administration approval.
The move has been anticipated as an important element in an attempt to stem the swelling tide of abuse, misuse, and overdose of these prescription drugs while assuring continued access to the highly potent analgesics for patients with moderate to severe persistent pain, Dr. Margaret A. Hamburg said in a media briefing.
The new safety measures, which pertain to approximately 30 currently available medications, will require the manufacturers of the drugs to make FDA-approved education materials available to prescribers no later than March 1, 2013, via development grants to continuing education providers who will develop and deliver the training, said Dr. Hamburg, commissioner of the FDA. In addition, the risk evaluation and mitigation strategy (REMS) will include the distribution of a patient counseling leaflet to prescribers regarding the safe and effective use of the drugs; an updated, single-page medication guide for consumers, an implementation plan, and periodic assessments to evaluate the impact of the program on the safe use of these products, which the FDA will review and use to tweak the program as needed, she said.
"It is important to note that we are focusing on extended-release and long-acting opioid medications ... because these have very specific safety problems that have to be addressed very carefully," according to Dr. John Jenkins, director of the Office of New Drugs within the FDA’s Center for Drug Evaluation and Research. These drugs, including hydromorphone, oxycodone, morphine, oxymorphone, methadone, transdermal fentanyl, and transdermal buprenorphine, "can cause problems even when prescribed appropriately."
The prescriber education component of the REMS will include information regarding the risks and benefits of opioid therapy for individual patients, choosing patients appropriately, patient management and monitoring, and patient counseling, Dr. Jenkins explained. It will also include guidance on the potential for misuse, abuse, and addition, as well as recognizing evidence for these outcomes. The updated medication guide and patient counseling document will include information on how to safely use, store, and dispose of these analgesics, specific instructions for recognizing the signs of potential overdose and advice for preventing accidental exposure to family and household visitors, he said.
With respect to the assessment and auditing component of the program, the FDA has established goals, which the manufacturers are expected to achieve, for the percentage of prescribers who complete the training and for assessing prescribers’ understanding of the risk information. Participation in the educational programs is not mandatory for prescribers, Dr. Hamburg stated. The assessments are also required to evaluate whether the [REMS] adversely affect patient access to these drugs, she said. "Patients in pain must have continued assess to medications they need," she added.
The new REMS program is one component of a multiagency, national strategy unveiled by the White House in 2011 to address prescription drug abuse, "which is this country’s fastest-growing drug problem," said Dr. Hamburg, noting that opioid overdoses in particular were the cause of approximately 15,000 deaths among Americans in 2008 and nearly 16,000 in 2009. Called Epidemic: Responding to America's Prescription Drug Abuse Crisis, the national plan suggests expansion of state-based prescription drug-monitoring programs; seeks creation of recommendations for convenient and environmentally responsible ways to dispose of unused medications; and calls for legislative action to reduce "doctor shopping" and "pill mills."
In the absence of the legislative changes needed to fulfill the comprehensive White House plan, the REMS "is an important and timely step by FDA to supplement prescriber training and consumer information," R. Gil Kerlikowske, director of the White House Office of National Drug Control Policy, said during the telebriefing.
A risk evaluation and mitigation strategy for extended-release and long-acting opioid medications has received Food and Drug Administration approval.
The move has been anticipated as an important element in an attempt to stem the swelling tide of abuse, misuse, and overdose of these prescription drugs while assuring continued access to the highly potent analgesics for patients with moderate to severe persistent pain, Dr. Margaret A. Hamburg said in a media briefing.
The new safety measures, which pertain to approximately 30 currently available medications, will require the manufacturers of the drugs to make FDA-approved education materials available to prescribers no later than March 1, 2013, via development grants to continuing education providers who will develop and deliver the training, said Dr. Hamburg, commissioner of the FDA. In addition, the risk evaluation and mitigation strategy (REMS) will include the distribution of a patient counseling leaflet to prescribers regarding the safe and effective use of the drugs; an updated, single-page medication guide for consumers, an implementation plan, and periodic assessments to evaluate the impact of the program on the safe use of these products, which the FDA will review and use to tweak the program as needed, she said.
"It is important to note that we are focusing on extended-release and long-acting opioid medications ... because these have very specific safety problems that have to be addressed very carefully," according to Dr. John Jenkins, director of the Office of New Drugs within the FDA’s Center for Drug Evaluation and Research. These drugs, including hydromorphone, oxycodone, morphine, oxymorphone, methadone, transdermal fentanyl, and transdermal buprenorphine, "can cause problems even when prescribed appropriately."
The prescriber education component of the REMS will include information regarding the risks and benefits of opioid therapy for individual patients, choosing patients appropriately, patient management and monitoring, and patient counseling, Dr. Jenkins explained. It will also include guidance on the potential for misuse, abuse, and addition, as well as recognizing evidence for these outcomes. The updated medication guide and patient counseling document will include information on how to safely use, store, and dispose of these analgesics, specific instructions for recognizing the signs of potential overdose and advice for preventing accidental exposure to family and household visitors, he said.
With respect to the assessment and auditing component of the program, the FDA has established goals, which the manufacturers are expected to achieve, for the percentage of prescribers who complete the training and for assessing prescribers’ understanding of the risk information. Participation in the educational programs is not mandatory for prescribers, Dr. Hamburg stated. The assessments are also required to evaluate whether the [REMS] adversely affect patient access to these drugs, she said. "Patients in pain must have continued assess to medications they need," she added.
The new REMS program is one component of a multiagency, national strategy unveiled by the White House in 2011 to address prescription drug abuse, "which is this country’s fastest-growing drug problem," said Dr. Hamburg, noting that opioid overdoses in particular were the cause of approximately 15,000 deaths among Americans in 2008 and nearly 16,000 in 2009. Called Epidemic: Responding to America's Prescription Drug Abuse Crisis, the national plan suggests expansion of state-based prescription drug-monitoring programs; seeks creation of recommendations for convenient and environmentally responsible ways to dispose of unused medications; and calls for legislative action to reduce "doctor shopping" and "pill mills."
In the absence of the legislative changes needed to fulfill the comprehensive White House plan, the REMS "is an important and timely step by FDA to supplement prescriber training and consumer information," R. Gil Kerlikowske, director of the White House Office of National Drug Control Policy, said during the telebriefing.
Awareness Is Top Weapon Against Delirium
I expect that [insert patient name here] will have a hospital stay measured in a period of days. During that time we will do our best to prevent complications of hospitalization, which include things such as blood clots and infections. We will also do our best to quickly recognize and treat those complications that do occur such as confusion or pain." This is a conversation I have with the majority of patients’ families when their medically complicated loved one is hospitalized.
I was certain that one gentleman, who has esophageal cancer with metastasis to the spine causing cord compression, would suffer from delirium during his hospital stay. His advanced age, multiple comorbidities, urgent surgery, intensive-care unit stay, and the medications he required to control his pain -- which initially included a fentanyl PCA (patient-controlled analgesia) and was later augmented by a ketamine infusion -- all seemed to put him at high risk for this. Yet, even during his time on our ketamine protocol he had clear and appropriate conversations with our team.

Another elderly woman, with previously undiagnosed dementia, was living at home with family assistance until coming to the hospital after suffering from a fall at home. During her hospital course she experienced side effects of pain medications and also developed a urinary tract infection. The delirium that ensued was severe. She required ICU admission because of the intense nursing supervision she needed to keep her out of physical restraints.
Eventually, when it was appropriate, she was discharged to a skilled nursing facility rather than home because of the persistent cognitive problems she was experiencing. The emergency room physician who called me about the admission anticipated that the patient could return home less than 24 hours after coming in. She left the hospital almost 2 weeks later.
Delirium in hospitalized patients is a common problem. Its presence is often partnered with extended lengths of stay, escalation of care, and poorer outcomes. Once it occurs, we turn to screening tools and treatment protocols that evidence has shown to be useful. Therefore, it should come as no surprise that a hospital’s approach to delirium management is now recognized as a quality-of-care marker.
Two new studies highlight the impact of delirium and provide a new tool for predicting this condition. They expand our body of knowledge, and one of them may even empower us to possibly head off delirium before it occurs.

The first study is a prospective cohort enrolled between 1991 and 2006 into a patient registry for Alzheimer’s disease (AD). Participants were over the age of 65 years with a clinical diagnosis of AD in this community setting, which included 771 patients. Databases identified those who were hospitalized, experienced delirium, died, or were institutionalized. Cognitive decline was also evaluated and based upon a validated test score.
Forty-eight percent (n = 367) were hospitalized and 25% (n = 194) developed delirium. Patients who did not experience delirium in the hospital had an increased risk of death or requiring institutionalization (relative risks of 4.7 and 6.9, respectively). An even more dramatic increase in risk was noted in those with delirium (RRs of 5.4 and 9.3). Delirium was associated with 6% of deaths, 15% of institutionalizations, and 21% of cognitive declines in hospitalized patients with AD.
This is the first time the relative contributions of hospitalizations and episodes of delirium to adverse outcomes for AD patients have been evaluated. The investigators’ goal of observing outcomes for at least 1 year clearly shows that hospitalization is a danger to this patient population and that the outcomes are worse for those with delirium. At least one in eight patients with AD will have an adverse event or death from hospitalization. This clinical cohort was created by merging multiple databases, so incomplete medical records were a problem. Two other aspects of the study are worth noting. As this study was nonrandomized, the hospitalized patients had lower baseline cognitive function than those who avoided admission. Also, ethnic minorities made up only 5% of the study population and therefore do not represent the U.S. Alzheimer’s community in that regard.
The second work is a multicenter observational study. This entailed the development of the Prediction of Delirium in ICU Patients (PRE-DELIRIC) model in a prospective cohort of 1,613 patients, a temporal validation in a second prospective cohort in the same hospital using 549 patients, and external validation with a total of 894 patients in four separate hospitals.

The PRE-DELIRIC model contains 10 risk factors: age, APACHE-II (Acute Physiology and Chronic Health Evaluation) score, admission group (consisting of medical, surgical, trauma, and neurological patients), coma, infection, metabolic acidosis, use of sedating medications, morphine use, blood urea nitrogen levels, and urgent admission. The main outcome measured was development of delirium within the ICU. The model’s ability to predict delirium was compared with that of ICU physicians and nurses to independently predicting delirium within 24 hours of admission.
The model’s area under receiver operating characteristics curve (AUROC) was 0.85 pooled across three cohorts (0.87, 0.86, and 0.84 for the first, second, and third cohorts, respectively). The AUROC for both physicians’ and nurses’ predictions of delirium was 0.59. Providers’ predictive accuracy did not differ by level of clinical experience.
PRE-DELIRIC is the first predictive model published for the ICU population experiencing delirium. Study design makes sense for the intention. It is important to note that patients with a history of alcohol abuse and dementia were excluded. It was felt that their risk for developing delirium is high even without consideration of other factors.
The model clearly outperformed the physicians and nurses, who were equally inferior when it came to predicting delirium. It also appears that this could be an area of medicine where experience is not accompanied by improved accuracy. More experienced clinicians fared no better than their greener colleagues. Limitations included a varied case mix from multiple specialties and inclusion of risk factors that were not based on their systematic review for those associated with delirium.
Both of these studies move us forward. The first should heighten our level of awareness that hospitalization with delirium is a major marker for undesired outcomes. It also should prompt proactive communication with our AD patients’ families about expectations in this scenario. The second should help create a mindset of predicting and preventing delirium rather than our current model, which is to screen and then treat.
Dr. Bekanich is with the department of medicine and is medical director of palliative care at Seton Healthcare in Austin, Tex. To respond to this commentary, e-mail [email protected].
I expect that [insert patient name here] will have a hospital stay measured in a period of days. During that time we will do our best to prevent complications of hospitalization, which include things such as blood clots and infections. We will also do our best to quickly recognize and treat those complications that do occur such as confusion or pain." This is a conversation I have with the majority of patients’ families when their medically complicated loved one is hospitalized.
I was certain that one gentleman, who has esophageal cancer with metastasis to the spine causing cord compression, would suffer from delirium during his hospital stay. His advanced age, multiple comorbidities, urgent surgery, intensive-care unit stay, and the medications he required to control his pain -- which initially included a fentanyl PCA (patient-controlled analgesia) and was later augmented by a ketamine infusion -- all seemed to put him at high risk for this. Yet, even during his time on our ketamine protocol he had clear and appropriate conversations with our team.
Another elderly woman, with previously undiagnosed dementia, was living at home with family assistance until coming to the hospital after suffering from a fall at home. During her hospital course she experienced side effects of pain medications and also developed a urinary tract infection. The delirium that ensued was severe. She required ICU admission because of the intense nursing supervision she needed to keep her out of physical restraints.
Eventually, when it was appropriate, she was discharged to a skilled nursing facility rather than home because of the persistent cognitive problems she was experiencing. The emergency room physician who called me about the admission anticipated that the patient could return home less than 24 hours after coming in. She left the hospital almost 2 weeks later.
Delirium in hospitalized patients is a common problem. Its presence is often partnered with extended lengths of stay, escalation of care, and poorer outcomes. Once it occurs, we turn to screening tools and treatment protocols that evidence has shown to be useful. Therefore, it should come as no surprise that a hospital’s approach to delirium management is now recognized as a quality-of-care marker.
Two new studies highlight the impact of delirium and provide a new tool for predicting this condition. They expand our body of knowledge, and one of them may even empower us to possibly head off delirium before it occurs.
The first study is a prospective cohort enrolled between 1991 and 2006 into a patient registry for Alzheimer’s disease (AD). Participants were over the age of 65 years with a clinical diagnosis of AD in this community setting, which included 771 patients. Databases identified those who were hospitalized, experienced delirium, died, or were institutionalized. Cognitive decline was also evaluated and based upon a validated test score.
Forty-eight percent (n = 367) were hospitalized and 25% (n = 194) developed delirium. Patients who did not experience delirium in the hospital had an increased risk of death or requiring institutionalization (relative risks of 4.7 and 6.9, respectively). An even more dramatic increase in risk was noted in those with delirium (RRs of 5.4 and 9.3). Delirium was associated with 6% of deaths, 15% of institutionalizations, and 21% of cognitive declines in hospitalized patients with AD.
This is the first time the relative contributions of hospitalizations and episodes of delirium to adverse outcomes for AD patients have been evaluated. The investigators’ goal of observing outcomes for at least 1 year clearly shows that hospitalization is a danger to this patient population and that the outcomes are worse for those with delirium. At least one in eight patients with AD will have an adverse event or death from hospitalization. This clinical cohort was created by merging multiple databases, so incomplete medical records were a problem. Two other aspects of the study are worth noting. As this study was nonrandomized, the hospitalized patients had lower baseline cognitive function than those who avoided admission. Also, ethnic minorities made up only 5% of the study population and therefore do not represent the U.S. Alzheimer’s community in that regard.
The second work is a multicenter observational study. This entailed the development of the Prediction of Delirium in ICU Patients (PRE-DELIRIC) model in a prospective cohort of 1,613 patients, a temporal validation in a second prospective cohort in the same hospital using 549 patients, and external validation with a total of 894 patients in four separate hospitals.
The PRE-DELIRIC model contains 10 risk factors: age, APACHE-II (Acute Physiology and Chronic Health Evaluation) score, admission group (consisting of medical, surgical, trauma, and neurological patients), coma, infection, metabolic acidosis, use of sedating medications, morphine use, blood urea nitrogen levels, and urgent admission. The main outcome measured was development of delirium within the ICU. The model’s ability to predict delirium was compared with that of ICU physicians and nurses to independently predicting delirium within 24 hours of admission.
The model’s area under receiver operating characteristics curve (AUROC) was 0.85 pooled across three cohorts (0.87, 0.86, and 0.84 for the first, second, and third cohorts, respectively). The AUROC for both physicians’ and nurses’ predictions of delirium was 0.59. Providers’ predictive accuracy did not differ by level of clinical experience.
PRE-DELIRIC is the first predictive model published for the ICU population experiencing delirium. Study design makes sense for the intention. It is important to note that patients with a history of alcohol abuse and dementia were excluded. It was felt that their risk for developing delirium is high even without consideration of other factors.
The model clearly outperformed the physicians and nurses, who were equally inferior when it came to predicting delirium. It also appears that this could be an area of medicine where experience is not accompanied by improved accuracy. More experienced clinicians fared no better than their greener colleagues. Limitations included a varied case mix from multiple specialties and inclusion of risk factors that were not based on their systematic review for those associated with delirium.
Both of these studies move us forward. The first should heighten our level of awareness that hospitalization with delirium is a major marker for undesired outcomes. It also should prompt proactive communication with our AD patients’ families about expectations in this scenario. The second should help create a mindset of predicting and preventing delirium rather than our current model, which is to screen and then treat.
Dr. Bekanich is with the department of medicine and is medical director of palliative care at Seton Healthcare in Austin, Tex. To respond to this commentary, e-mail [email protected].
I expect that [insert patient name here] will have a hospital stay measured in a period of days. During that time we will do our best to prevent complications of hospitalization, which include things such as blood clots and infections. We will also do our best to quickly recognize and treat those complications that do occur such as confusion or pain." This is a conversation I have with the majority of patients’ families when their medically complicated loved one is hospitalized.
I was certain that one gentleman, who has esophageal cancer with metastasis to the spine causing cord compression, would suffer from delirium during his hospital stay. His advanced age, multiple comorbidities, urgent surgery, intensive-care unit stay, and the medications he required to control his pain -- which initially included a fentanyl PCA (patient-controlled analgesia) and was later augmented by a ketamine infusion -- all seemed to put him at high risk for this. Yet, even during his time on our ketamine protocol he had clear and appropriate conversations with our team.
Another elderly woman, with previously undiagnosed dementia, was living at home with family assistance until coming to the hospital after suffering from a fall at home. During her hospital course she experienced side effects of pain medications and also developed a urinary tract infection. The delirium that ensued was severe. She required ICU admission because of the intense nursing supervision she needed to keep her out of physical restraints.
Eventually, when it was appropriate, she was discharged to a skilled nursing facility rather than home because of the persistent cognitive problems she was experiencing. The emergency room physician who called me about the admission anticipated that the patient could return home less than 24 hours after coming in. She left the hospital almost 2 weeks later.
Delirium in hospitalized patients is a common problem. Its presence is often partnered with extended lengths of stay, escalation of care, and poorer outcomes. Once it occurs, we turn to screening tools and treatment protocols that evidence has shown to be useful. Therefore, it should come as no surprise that a hospital’s approach to delirium management is now recognized as a quality-of-care marker.
Two new studies highlight the impact of delirium and provide a new tool for predicting this condition. They expand our body of knowledge, and one of them may even empower us to possibly head off delirium before it occurs.
The first study is a prospective cohort enrolled between 1991 and 2006 into a patient registry for Alzheimer’s disease (AD). Participants were over the age of 65 years with a clinical diagnosis of AD in this community setting, which included 771 patients. Databases identified those who were hospitalized, experienced delirium, died, or were institutionalized. Cognitive decline was also evaluated and based upon a validated test score.
Forty-eight percent (n = 367) were hospitalized and 25% (n = 194) developed delirium. Patients who did not experience delirium in the hospital had an increased risk of death or requiring institutionalization (relative risks of 4.7 and 6.9, respectively). An even more dramatic increase in risk was noted in those with delirium (RRs of 5.4 and 9.3). Delirium was associated with 6% of deaths, 15% of institutionalizations, and 21% of cognitive declines in hospitalized patients with AD.
This is the first time the relative contributions of hospitalizations and episodes of delirium to adverse outcomes for AD patients have been evaluated. The investigators’ goal of observing outcomes for at least 1 year clearly shows that hospitalization is a danger to this patient population and that the outcomes are worse for those with delirium. At least one in eight patients with AD will have an adverse event or death from hospitalization. This clinical cohort was created by merging multiple databases, so incomplete medical records were a problem. Two other aspects of the study are worth noting. As this study was nonrandomized, the hospitalized patients had lower baseline cognitive function than those who avoided admission. Also, ethnic minorities made up only 5% of the study population and therefore do not represent the U.S. Alzheimer’s community in that regard.
The second work is a multicenter observational study. This entailed the development of the Prediction of Delirium in ICU Patients (PRE-DELIRIC) model in a prospective cohort of 1,613 patients, a temporal validation in a second prospective cohort in the same hospital using 549 patients, and external validation with a total of 894 patients in four separate hospitals.
The PRE-DELIRIC model contains 10 risk factors: age, APACHE-II (Acute Physiology and Chronic Health Evaluation) score, admission group (consisting of medical, surgical, trauma, and neurological patients), coma, infection, metabolic acidosis, use of sedating medications, morphine use, blood urea nitrogen levels, and urgent admission. The main outcome measured was development of delirium within the ICU. The model’s ability to predict delirium was compared with that of ICU physicians and nurses to independently predicting delirium within 24 hours of admission.
The model’s area under receiver operating characteristics curve (AUROC) was 0.85 pooled across three cohorts (0.87, 0.86, and 0.84 for the first, second, and third cohorts, respectively). The AUROC for both physicians’ and nurses’ predictions of delirium was 0.59. Providers’ predictive accuracy did not differ by level of clinical experience.
PRE-DELIRIC is the first predictive model published for the ICU population experiencing delirium. Study design makes sense for the intention. It is important to note that patients with a history of alcohol abuse and dementia were excluded. It was felt that their risk for developing delirium is high even without consideration of other factors.
The model clearly outperformed the physicians and nurses, who were equally inferior when it came to predicting delirium. It also appears that this could be an area of medicine where experience is not accompanied by improved accuracy. More experienced clinicians fared no better than their greener colleagues. Limitations included a varied case mix from multiple specialties and inclusion of risk factors that were not based on their systematic review for those associated with delirium.
Both of these studies move us forward. The first should heighten our level of awareness that hospitalization with delirium is a major marker for undesired outcomes. It also should prompt proactive communication with our AD patients’ families about expectations in this scenario. The second should help create a mindset of predicting and preventing delirium rather than our current model, which is to screen and then treat.
Dr. Bekanich is with the department of medicine and is medical director of palliative care at Seton Healthcare in Austin, Tex. To respond to this commentary, e-mail [email protected].