User login
Photobiomodulation: Evaluation in a wide range of medical specialties underway
according to Juanita J. Anders, PhD.

During the annual conference of the American Society for Laser Medicine and Surgery, Dr. Anders, professor of anatomy, physiology, and genetics at the Uniformed Services University of the Health Sciences, Bethesda, Md., defined photobiomodulation (PBM) as the mechanism by which nonionizing optical radiation in the visible and near-infrared spectral range is absorbed by endogenous chromophores to elicit photophysical and photochemical events at various biological scales. Photobiomodulation therapy (PBMT) involves the use of light sources including lasers, LEDs, and broadband light, that emit visible and/or near-infrared light to cause physiological changes in cells and tissues and result in therapeutic benefits.
In dermatology, LED light therapy devices are commonly used for PBMT in wavelengths that range from blue (415 nm) and red (633 nm) to near infrared (830 nm). “Often, when PBMT is referred to by dermatologists it’s called LED therapy or LED light therapy,” Dr. Anders noted. “Some people are under the impression that this is different from PBMT. But remember: It’s not the device that’s producing the photons that is clinically relevant, but it’s the photons themselves. In both cases, the same radiances and fluence ranges are being used and the mechanisms are the same, so it’s all PBMT.”
The therapy is used to treat a wide variety of medical and aesthetic disorders including acne vulgaris, psoriasis, burns, and wound healing. It has also been used in conjunction with surgical aesthetic and resurfacing procedures and has been reported to reduce erythema, edema, bruising, and days to healing. It’s been shown that PBMT stimulates fibroblast proliferation, collagen synthesis, and extracellular matrix resulting in lifting and tightening lax skin.
According to Dr. Anders, French dermatologists Linda Fouque, MD, and Michele Pelletier, MD, performed a series of in vivo and in vitro studies in which they tested the effects of yellow and red light for skin rejuvenation when used individually or in combination. “They found that fibroblasts and keratinocytes in vitro had great improvement in their morphology both with the yellow and red light, but the best improvement was seen with combination therapy,” Dr. Anders said. “This held true in their work looking at epidermal and dermal markers in the skin, where they found the best up-regulation in protein synthesis of such markers as collagens and fibronectin were produced when a combination wavelength light was used.”
Oral mucositis and pain
PBMT is also being used to treat oral mucositis (OM), a common adverse response to chemotherapy and/or radiation therapy, which causes pain, difficulty in swallowing and eating, and oral ulceration, and often interrupts the course of treatments. Authors of a recently published review on the risks and benefits of PBMT concluded that there is consistent evidence from a small number of high-quality studies that PBMT can help prevent the development of cancer therapy–induced OM, reduce pain intensity, as well as promote healing, and enhance patient quality of life.
“They also cautioned that, due to the limited long-term follow-up of patients, there is still concern for the potential long-term risks of PBMT in cancer cell mutation and amplification,” Dr. Anders said. “They advised that PBMT should be used carefully when the irradiation beam is in the direction of the tumor zone.”
Using PBMT for modulation of pain is another area of active research. Based on work from the laboratory of Dr. Anders and others, there are two methods to modulate pain. The first is to target tissue at irradiances below 100 mW/cm2.
“In my laboratory, based on in vivo preclinical animal models of neuropathic pain, we used a 980-nm wavelength laser at 43.25 mW/cm2 transcutaneously delivered to the level of the nerve for 20 seconds,” said Dr. Anders, who is a past president of the ASLMS. “Essentially, we found that the pain was modulated by reducing sensitivity to mechanical stimulation and also by causing an anti-inflammatory shift in microglial and macrophage phenotype in the dorsal root ganglion and spinal cord of affected segments.”
The second way to modulate pain, she continued, is to target tissue at irradiances above 250 mW/cm2. She and her colleagues have conducted in vitro and in vivo studies, which indicate that treatment with an irradiance/fluence rate at 270 mW/cm2 or higher at the nerve can rapidly block pain transmission.
“In vitro, we found that if we used an 810-nm wavelength light at 300 mW/cm2, we got a disruption of microtubules in the DRG neurons in culture, specifically the small neurons, the nociceptive fibers, but we did not affect the proprioceptive fibers unless we increased the length of the treatment,” she said. “We essentially found the same thing in vivo in a rodent model of neuropathic pain.”
In a pilot study, Dr. Anders and coauthors examined the efficacy of laser irradiation of the dorsal root ganglion of the second lumbar spinal nerve for patients with chronic back pain.
They found that PBMT effectively reduced back pain equal to the effects of lidocaine.
Based on these two irradiation approaches of targeting tissue, Dr. Anders recommends that a combination therapy be used to modulate neuropathic pain going forward. “This approach would involve the initial use of a high-irradiance treatment [at least 250 mW/cm2] at the nerve to block the pain transmission,” she said. “That treatment would be followed by a series of low-irradiance treatments [10-100 mW/cm2] along the course of the involved nerve to alter chronic pathology and inflammation.”
Potential applications in neurology
Dr. Anders also discussed research efforts under way involving transcranial PBMT: the delivery of near-infrared light through the tissues of the scalp and skull to targeted brain regions to treat neurologic injuries and disorders. “There have been some exciting results in preclinical animal work and in small clinical pilot work that show that there could be possible beneficial effects in Parkinson’s disease, Alzheimer’s disease, depression, and improvement in cognition and memory after a brain injury, such as a TBI,” she said.
“Initially, though, there were a lot of questions about whether you could really deliver light to the brain through the scalp. In my laboratory, we used slices of nonfixed brain and found that the sulci within the human brain act as light-wave guides. We used an 808-nm near-infrared wavelength of light, so that the light could penetrate more deeply.” Using nonfixed cadaver heads, where the light was applied at the scalp surface, Dr. Anders and colleagues were able to measure photons down to the depth of 4 cm. “It’s generally agreed now, though, that it’s to a maximum depth of 2.5-3 cm that enough photons are delivered that would cause a beneficial therapeutic effect,” she said.
Dr. Anders disclosed that she has received equipment from LiteCure, grant funding from the Department of Defense, and that she holds advisory board roles with LiteCure and Neurothera. She has also served in leadership roles for the Optical Society and holds intellectual property rights for the Henry M. Jackson Foundation for the Advancement of Military Medicine.
according to Juanita J. Anders, PhD.
During the annual conference of the American Society for Laser Medicine and Surgery, Dr. Anders, professor of anatomy, physiology, and genetics at the Uniformed Services University of the Health Sciences, Bethesda, Md., defined photobiomodulation (PBM) as the mechanism by which nonionizing optical radiation in the visible and near-infrared spectral range is absorbed by endogenous chromophores to elicit photophysical and photochemical events at various biological scales. Photobiomodulation therapy (PBMT) involves the use of light sources including lasers, LEDs, and broadband light, that emit visible and/or near-infrared light to cause physiological changes in cells and tissues and result in therapeutic benefits.
In dermatology, LED light therapy devices are commonly used for PBMT in wavelengths that range from blue (415 nm) and red (633 nm) to near infrared (830 nm). “Often, when PBMT is referred to by dermatologists it’s called LED therapy or LED light therapy,” Dr. Anders noted. “Some people are under the impression that this is different from PBMT. But remember: It’s not the device that’s producing the photons that is clinically relevant, but it’s the photons themselves. In both cases, the same radiances and fluence ranges are being used and the mechanisms are the same, so it’s all PBMT.”
The therapy is used to treat a wide variety of medical and aesthetic disorders including acne vulgaris, psoriasis, burns, and wound healing. It has also been used in conjunction with surgical aesthetic and resurfacing procedures and has been reported to reduce erythema, edema, bruising, and days to healing. It’s been shown that PBMT stimulates fibroblast proliferation, collagen synthesis, and extracellular matrix resulting in lifting and tightening lax skin.
According to Dr. Anders, French dermatologists Linda Fouque, MD, and Michele Pelletier, MD, performed a series of in vivo and in vitro studies in which they tested the effects of yellow and red light for skin rejuvenation when used individually or in combination. “They found that fibroblasts and keratinocytes in vitro had great improvement in their morphology both with the yellow and red light, but the best improvement was seen with combination therapy,” Dr. Anders said. “This held true in their work looking at epidermal and dermal markers in the skin, where they found the best up-regulation in protein synthesis of such markers as collagens and fibronectin were produced when a combination wavelength light was used.”
Oral mucositis and pain
PBMT is also being used to treat oral mucositis (OM), a common adverse response to chemotherapy and/or radiation therapy, which causes pain, difficulty in swallowing and eating, and oral ulceration, and often interrupts the course of treatments. Authors of a recently published review on the risks and benefits of PBMT concluded that there is consistent evidence from a small number of high-quality studies that PBMT can help prevent the development of cancer therapy–induced OM, reduce pain intensity, as well as promote healing, and enhance patient quality of life.
“They also cautioned that, due to the limited long-term follow-up of patients, there is still concern for the potential long-term risks of PBMT in cancer cell mutation and amplification,” Dr. Anders said. “They advised that PBMT should be used carefully when the irradiation beam is in the direction of the tumor zone.”
Using PBMT for modulation of pain is another area of active research. Based on work from the laboratory of Dr. Anders and others, there are two methods to modulate pain. The first is to target tissue at irradiances below 100 mW/cm2.
“In my laboratory, based on in vivo preclinical animal models of neuropathic pain, we used a 980-nm wavelength laser at 43.25 mW/cm2 transcutaneously delivered to the level of the nerve for 20 seconds,” said Dr. Anders, who is a past president of the ASLMS. “Essentially, we found that the pain was modulated by reducing sensitivity to mechanical stimulation and also by causing an anti-inflammatory shift in microglial and macrophage phenotype in the dorsal root ganglion and spinal cord of affected segments.”
The second way to modulate pain, she continued, is to target tissue at irradiances above 250 mW/cm2. She and her colleagues have conducted in vitro and in vivo studies, which indicate that treatment with an irradiance/fluence rate at 270 mW/cm2 or higher at the nerve can rapidly block pain transmission.
“In vitro, we found that if we used an 810-nm wavelength light at 300 mW/cm2, we got a disruption of microtubules in the DRG neurons in culture, specifically the small neurons, the nociceptive fibers, but we did not affect the proprioceptive fibers unless we increased the length of the treatment,” she said. “We essentially found the same thing in vivo in a rodent model of neuropathic pain.”
In a pilot study, Dr. Anders and coauthors examined the efficacy of laser irradiation of the dorsal root ganglion of the second lumbar spinal nerve for patients with chronic back pain.
They found that PBMT effectively reduced back pain equal to the effects of lidocaine.
Based on these two irradiation approaches of targeting tissue, Dr. Anders recommends that a combination therapy be used to modulate neuropathic pain going forward. “This approach would involve the initial use of a high-irradiance treatment [at least 250 mW/cm2] at the nerve to block the pain transmission,” she said. “That treatment would be followed by a series of low-irradiance treatments [10-100 mW/cm2] along the course of the involved nerve to alter chronic pathology and inflammation.”
Potential applications in neurology
Dr. Anders also discussed research efforts under way involving transcranial PBMT: the delivery of near-infrared light through the tissues of the scalp and skull to targeted brain regions to treat neurologic injuries and disorders. “There have been some exciting results in preclinical animal work and in small clinical pilot work that show that there could be possible beneficial effects in Parkinson’s disease, Alzheimer’s disease, depression, and improvement in cognition and memory after a brain injury, such as a TBI,” she said.
“Initially, though, there were a lot of questions about whether you could really deliver light to the brain through the scalp. In my laboratory, we used slices of nonfixed brain and found that the sulci within the human brain act as light-wave guides. We used an 808-nm near-infrared wavelength of light, so that the light could penetrate more deeply.” Using nonfixed cadaver heads, where the light was applied at the scalp surface, Dr. Anders and colleagues were able to measure photons down to the depth of 4 cm. “It’s generally agreed now, though, that it’s to a maximum depth of 2.5-3 cm that enough photons are delivered that would cause a beneficial therapeutic effect,” she said.
Dr. Anders disclosed that she has received equipment from LiteCure, grant funding from the Department of Defense, and that she holds advisory board roles with LiteCure and Neurothera. She has also served in leadership roles for the Optical Society and holds intellectual property rights for the Henry M. Jackson Foundation for the Advancement of Military Medicine.
according to Juanita J. Anders, PhD.
During the annual conference of the American Society for Laser Medicine and Surgery, Dr. Anders, professor of anatomy, physiology, and genetics at the Uniformed Services University of the Health Sciences, Bethesda, Md., defined photobiomodulation (PBM) as the mechanism by which nonionizing optical radiation in the visible and near-infrared spectral range is absorbed by endogenous chromophores to elicit photophysical and photochemical events at various biological scales. Photobiomodulation therapy (PBMT) involves the use of light sources including lasers, LEDs, and broadband light, that emit visible and/or near-infrared light to cause physiological changes in cells and tissues and result in therapeutic benefits.
In dermatology, LED light therapy devices are commonly used for PBMT in wavelengths that range from blue (415 nm) and red (633 nm) to near infrared (830 nm). “Often, when PBMT is referred to by dermatologists it’s called LED therapy or LED light therapy,” Dr. Anders noted. “Some people are under the impression that this is different from PBMT. But remember: It’s not the device that’s producing the photons that is clinically relevant, but it’s the photons themselves. In both cases, the same radiances and fluence ranges are being used and the mechanisms are the same, so it’s all PBMT.”
The therapy is used to treat a wide variety of medical and aesthetic disorders including acne vulgaris, psoriasis, burns, and wound healing. It has also been used in conjunction with surgical aesthetic and resurfacing procedures and has been reported to reduce erythema, edema, bruising, and days to healing. It’s been shown that PBMT stimulates fibroblast proliferation, collagen synthesis, and extracellular matrix resulting in lifting and tightening lax skin.
According to Dr. Anders, French dermatologists Linda Fouque, MD, and Michele Pelletier, MD, performed a series of in vivo and in vitro studies in which they tested the effects of yellow and red light for skin rejuvenation when used individually or in combination. “They found that fibroblasts and keratinocytes in vitro had great improvement in their morphology both with the yellow and red light, but the best improvement was seen with combination therapy,” Dr. Anders said. “This held true in their work looking at epidermal and dermal markers in the skin, where they found the best up-regulation in protein synthesis of such markers as collagens and fibronectin were produced when a combination wavelength light was used.”
Oral mucositis and pain
PBMT is also being used to treat oral mucositis (OM), a common adverse response to chemotherapy and/or radiation therapy, which causes pain, difficulty in swallowing and eating, and oral ulceration, and often interrupts the course of treatments. Authors of a recently published review on the risks and benefits of PBMT concluded that there is consistent evidence from a small number of high-quality studies that PBMT can help prevent the development of cancer therapy–induced OM, reduce pain intensity, as well as promote healing, and enhance patient quality of life.
“They also cautioned that, due to the limited long-term follow-up of patients, there is still concern for the potential long-term risks of PBMT in cancer cell mutation and amplification,” Dr. Anders said. “They advised that PBMT should be used carefully when the irradiation beam is in the direction of the tumor zone.”
Using PBMT for modulation of pain is another area of active research. Based on work from the laboratory of Dr. Anders and others, there are two methods to modulate pain. The first is to target tissue at irradiances below 100 mW/cm2.
“In my laboratory, based on in vivo preclinical animal models of neuropathic pain, we used a 980-nm wavelength laser at 43.25 mW/cm2 transcutaneously delivered to the level of the nerve for 20 seconds,” said Dr. Anders, who is a past president of the ASLMS. “Essentially, we found that the pain was modulated by reducing sensitivity to mechanical stimulation and also by causing an anti-inflammatory shift in microglial and macrophage phenotype in the dorsal root ganglion and spinal cord of affected segments.”
The second way to modulate pain, she continued, is to target tissue at irradiances above 250 mW/cm2. She and her colleagues have conducted in vitro and in vivo studies, which indicate that treatment with an irradiance/fluence rate at 270 mW/cm2 or higher at the nerve can rapidly block pain transmission.
“In vitro, we found that if we used an 810-nm wavelength light at 300 mW/cm2, we got a disruption of microtubules in the DRG neurons in culture, specifically the small neurons, the nociceptive fibers, but we did not affect the proprioceptive fibers unless we increased the length of the treatment,” she said. “We essentially found the same thing in vivo in a rodent model of neuropathic pain.”
In a pilot study, Dr. Anders and coauthors examined the efficacy of laser irradiation of the dorsal root ganglion of the second lumbar spinal nerve for patients with chronic back pain.
They found that PBMT effectively reduced back pain equal to the effects of lidocaine.
Based on these two irradiation approaches of targeting tissue, Dr. Anders recommends that a combination therapy be used to modulate neuropathic pain going forward. “This approach would involve the initial use of a high-irradiance treatment [at least 250 mW/cm2] at the nerve to block the pain transmission,” she said. “That treatment would be followed by a series of low-irradiance treatments [10-100 mW/cm2] along the course of the involved nerve to alter chronic pathology and inflammation.”
Potential applications in neurology
Dr. Anders also discussed research efforts under way involving transcranial PBMT: the delivery of near-infrared light through the tissues of the scalp and skull to targeted brain regions to treat neurologic injuries and disorders. “There have been some exciting results in preclinical animal work and in small clinical pilot work that show that there could be possible beneficial effects in Parkinson’s disease, Alzheimer’s disease, depression, and improvement in cognition and memory after a brain injury, such as a TBI,” she said.
“Initially, though, there were a lot of questions about whether you could really deliver light to the brain through the scalp. In my laboratory, we used slices of nonfixed brain and found that the sulci within the human brain act as light-wave guides. We used an 808-nm near-infrared wavelength of light, so that the light could penetrate more deeply.” Using nonfixed cadaver heads, where the light was applied at the scalp surface, Dr. Anders and colleagues were able to measure photons down to the depth of 4 cm. “It’s generally agreed now, though, that it’s to a maximum depth of 2.5-3 cm that enough photons are delivered that would cause a beneficial therapeutic effect,” she said.
Dr. Anders disclosed that she has received equipment from LiteCure, grant funding from the Department of Defense, and that she holds advisory board roles with LiteCure and Neurothera. She has also served in leadership roles for the Optical Society and holds intellectual property rights for the Henry M. Jackson Foundation for the Advancement of Military Medicine.
FROM ASLMS 2021
The aducanumab revolution
The approval was hailed by advocacy groups and some practitioners as a victory for patients and families, as the drug – the first anti-Alzheimer’s agent to reach the market in 18 years – is a potentially disease-modifying therapy, which acts to clear amyloid plaques from the brain.
But several prominent Alzheimer’s researchers lambasted the agency’s decision, citing unclear evidence of benefit, trials that did not meet their primary endpoints, and reliance on a post hoc analysis of a high-dose subgroup of patients in a halted trial to argue that aducanumab (Aduhelm, Biogen, and Eisai), slowed cognitive and functional decline by 22% on one measure. In November 2020, 10 of 11 members of an independent FDA advisory committee voted against aducanumab’s approval, citing holes in the data and concerns about the quality of the evidence. After the agency went on to approve anyway, three members of that committee resigned in protest.
The FDA decision on aducanumab was made using the agency’s accelerated approval pathway, which allows for the use of a surrogate endpoint – in this case imaging that showed amyloid clearance from the brain – to predict clinical benefit. But amyloid clearance, which a number of experimental antiamyloid antibodies have been shown capable of, has not been definitively linked to clinical benefit. Aducanumab, which is delivered by monthly intravenous infusion, will be marketed pending results from a phase 4 clinical trial, which the manufacturer has nearly a decade to complete. The drug’s price was announced at $56,000 per year, underscoring concern over its modest-at-best benefits.
Clinicians prescribing aducanumab must obtain magnetic resonance imaging at baseline and repeatedly during the course of treatment to detect brain edema and microhemorrhages, which occurred in a third of high-dose patients in clinical trials. Beyond this, there are few restrictions. The FDA label allows for its use in any patient deemed to have Alzheimer’s disease, without stipulations as to disease stage or evidence of brain amyloid. Payers, of course, are likely to restrict use to certain patient groups, and to require evidence of amyloid positivity. The FDA offered no guidance on when treatment should be ceased, leaving payers to make that call as well. Whatever aducanumab’s value and role turns out to be, the first-in-class treatment for Alzheimer’s disease is likely to have a major impact on how patients are assessed and treated in the coming years, and embolden manufactures of similar agents to seek FDA approval.
This news organization reached out to researchers, advocates, and specialists in the community to learn how they see this change playing out.
Fielding broad interest
Maria C. Carrillo, PhD, chief science officer of the Alzheimer’s Association, which was a strong proponent of aducanumab’s approval, acknowledged in an interview that the months to come are likely to be confusing for practitioners and families alike as the drug makes its way into community practices.

“We understand that off the bat millions of Americans will not have access to this tomorrow, but over time that will build. And the physician community, the specialists most likely to be prescribing this, over the next few years will even expand further,” Dr. Carrillo said.
For now, those specialists are mostly just struggling to respond responsibly to a deluge of inquiries from patients and their families.
“I’ve gotten like 20 calls in the just the past 2 days,” said neurologist Philip R. Delio, MD, who practices in Santa Barbara, Calif. “This is a longstanding issue that physicians have with patients’ access to information. Patients are getting information about a drug which isn’t available yet. They don’t know that it’s not ready to be sold. They don’t necessarily realize that a biopharma company won’t go into production until the FDA approves the drug.”

Many patients, Dr. Delio said, are aware of the controversy surrounding aducanumab and eager to hear their neurologist’s opinion. “I have tried to let them know that I want to see the trial data and to better understand the FDA’s rationale in approving it. I always caution patients that the devil will be in the details.”
While aducanumab’s label gives physicians remarkably wide latitude in whom to treat, clinicians say that until payers weigh in, the label is all but meaningless. Neurologist Douglas Scharre, MD, of the Ohio State University Wexner Medical Center, and a site investigator on a trial of aducanumab, said that he and his colleagues at the university’s memory center have tried to anticipate who might be deemed eligible by triaging calls.

Dr. Scharre and colleagues have been working under the assumption that payers will support aducanumab only for patients like those who seemed to benefit in the trials – people with mild cognitive impairment (MCI) or in the earliest stages of dementia with evidence of brain amyloid.
“I don’t want to fill up our new patient slots with people who are not even appropriate for this drug,” Dr. Scharre said. “We have a call center, and we have a few triage questions. After that a nurse practitioner collects some more data, and there’s a review process. Only then do we decide whether that person could be a candidate. If we deem that they are, we will want them in and to order an amyloid PET” – a type of brain scan that is seldom used outside research settings and not reimbursed by Medicare.
Dr. Scharre predicts that regardless of payer limitations, “there will be people hounding for the drug who are not appropriate for the drug. There will be very wealthy people who will want to pay for tests and get it no matter what.” Another concern, he said, was that having poorly selected patients on the drug could make definitive trial results even more elusive.
“The label the way it’s written is not going to help the drug in phase 4 trials,” he said. “It’s good to have real-world patient data, but if you have all these people in your cohort who are too early or too late, you won’t have good results.”
The challenge of delivery
Intravenous infusions are new to Alzheimer’s disease and pose all sorts of logistical hurdles. The Alzheimer’s Association’s Dr. Carrillo described the situation as “manageable,” noting that infusions are standard of care for many diseases, and that neurologists now have more than 15 years’ experience with them for multiple sclerosis.
Still, most clinicians treating Alzheimer’s disease in the community – neurologists, geriatricians, psychiatrists, and primary care physicians – do not have infusion centers in their practices. Virtually none have experience with or access to PET-amyloid, or with screening for amyloid-related imaging abnormalities–edema (ARIA-e) on MRI, as required by the FDA.
“I contacted the hospital infusion center we use and said I could end up sending five or six patients a week, can you handle this? They only have so many chairs,” Dr. Delio said. “I am one neurologist in a local community, and I might have 50 candidates for this drug. That’s a lot for them.” Patients with cognitive impairment are also difficult to infuse and may need to be treated at home, he noted.
“MRIs are easy enough to do,” Dr. Delio said. “But do we know what ARIA-e looks like on imaging? You’d have to talk to the radiologists – this is another element of uncertainty. Do we even know what we’re looking for with these scans? Will we recognize this?”
Neurologist Jeffrey L. Cummings, MD, ScD, of the University of Nevada, Las Vegas, a vocal proponent of aducanumab and lead author of a May 2021 paper defending the evidence for it, acknowledged that the field was unprepared for a wide-scale adoption of infusions in dementia treatment, pointing to a Rand Corporation study from 2017 that warned that screening, diagnosis, and availability of infusion chairs would have to be drastically scaled up to meet demand.

“There are few clinicians who know how to identify MCI, too few imaging centers, too few radiologists who know how to identify ARIA-e on MRI, so all of these things will be required to be put into place. The label doesn’t specify any of this, but good clinical practice will require that, and getting this up and running will take 18 to 24 months,” Dr. Cummings said.
Neurologist David S. Knopman, MD, of the Mayo Clinic in Rochester, Minn., a leading critic of the evidence for aducanumab who recently resigned his position on the independent committee that advises the FDA on neurology drugs, said that for large research institutions like his that have served as trial sites, the transition to offering PET-amyloid, MRI, and infusions in clinical practice will be easier.
“We have all this because this is what we do every day. And we have a very extensive understanding of MCI and mild dementia staging,” Dr. Knopman said. “But the amount of infrastructure that is implied by this, and all the extra steps it would take, would be a real challenge for people in general neurology practice.”
In addition to routine use of PET-amyloid and MRI screening for ARIA-e, Dr. Knopman said, clinicians will have to provide genetic screening and counseling before administering aducanumab, as clinical trials showed that treated patients have a higher risk of developing ARIA-e if they have APOE4, a risk variant for Alzheimer’s disease. “And that has real implications for the families and the children of patients,” he said.
Uncertainty over costs
Aducanumab’s true costs, to patients and to taxpayers, remain unknown. The $56,000 per year currently cited by its manufacturer “doesn’t count the PET scans and MRIs,” Dr. Knopman noted. “We’re probably pushing $100,00 a year for the first year of treatment.”
Most of that expense will likely be borne by Medicare, he said, and if not, “that will exacerbate existing health care disparities. People who can pay out of pocket are a pretty limited group.”
Dr. Scharre agreed that the costs of treatment were concerning, and that “at least you should be able to narrow it down and hopefully just use health care dollars for people who might stand to benefit,” he said – namely patients in an earlier stage of disease.
The Alzheimer’s Association’s Dr. Carrillo declined to address the high price of aducanumab or its implications, saying only that the association is “very invested in all aspects of access including covering costs associated with the drug and the rest of treatment.”
Access also means “infrastructure, access to physicians to diagnose, access to diagnostics,” Dr. Carrillo said.
Dr. Cummings said aducanumab’s price would likely come down through negotiations with the Centers for Medicare & Medicaid Services, copayments, and bulk purchases.
The FDA has offered no guidance on how long treatment with aducanumab should last, or what should prompt withdrawal of treatment, meaning that patients could, in theory, stay on it to the end of their lives – raising costs further.
Critics have also noted that a built-in financial incentive under Medicare Part B, which covers infusion drugs, could result in overprescription of aducanumab. Under Medicare Part B, prescribing physicians are reimbursed 6% of a drug’s average sales price.
Geriatricians wary
On social media and in the lay press, geriatricians have been among the most outspoken opponents of the FDA decision and the Alzheimer’s Association’s advocacy of aducanumab.
Eric Widera, MD, a geriatrician at the University of California, San Francisco, said that the specialty might be less likely than others to embrace aducanumab. “I think part of the reasons geriatricians don’t make a lot of money is they have strong commitment to their values,” Dr. Widera said.

The American Geriatrics Society opposed the drug’s approval, citing concerns about evidence, side effects, and cost. “Additional considerations are the unintended consequences of overstressing Medicare’s limited financial reserves, and of challenging health care systems … to divert precious resources to an expensive treatment of uncertain value,” the society’s president, Peter Hollmann, MD, and chief executive officer, Nancy E. Lundebjerg, wrote in a June 2 letter to the FDA.
Dr. Widera said the approval was likely to undermine confidence in the FDA and in the Alzheimer’s Association, which receives significant funding from drug manufacturers, including Biogen and Eisai. “There’s a lot of reasons that the Geriatrics Society could have done what the Alzheimer’s Association did, and yet they came out against it, which I applaud.”
Dr. Widera pointed to a study showing that dementia patients were less likely to be on an antidementia drug if they were treated by a geriatrician, compared with a psychiatrist or a neurologist. But whether the specialty will prove as cautious with aducanumab remains to be seen. Some geriatricians will be tempted to open lucrative infusion centers, he predicted.
What is especially worrisome, Dr. Widera said, is that aducanumab’s label offers no guidance as to when to withdraw treatment. “We’ll probably see something similar to what happened with the cholinesterase inhibitors” – the class of marginally effective antidementia drugs that includes donepezil (Aricept, Pfizer) and rivastigmine (Exelon, Novartis). “No one thinks about deprescribing them. People are prescribed them even in their last months of life. There is no reason to think these infusions won’t be continued for a very long time, well beyond how long people were dosed in the trials.”
“Taking care of someone with dementia is hard enough,” Dr. Widera added. “We can’t even get normal support in the home for someone with dementia. But we are more than happy to throw money to Biogen for a drug they have not yet showed benefit for. Hopefully in 5 years we’ll have a drug that actually works,” Dr. Widera said. “After 5 years of giving this to people at $50,000 a year.”
A fractured research community
Ever since October 2019, when Biogen and Eisai announced that despite two trials halted for futility, they would go ahead and seek FDA approval for aducanumab, the Alzheimer’s research community has been bitterly divided over the drug and the FDA’s accelerated approval process.
Top researchers published critical editorials in journals, with some eventually taking their case to major newspapers as well. The Alzheimer’s Association’s position on the drug has clashed with that of many researchers whose work it supports.
“The Alzheimer’s community has been wonderfully collegial – we all have a common purpose,” Dr. Cummings said. “Now we have people taking extreme positions and I’m hoping this will not result in a permanent fracturing of the community.”
Chief among the critics’ concerns is that the FDA decision ratified the use of antiamyloid therapies based on biomarker evidence, opening the door for makers of similar drugs – those still under development or even those whose development has been halted – to seek approval on weak evidence of clinical benefit.
Whether the approval will chill research into drugs targeting pathways other than amyloid is uncertain.
Dr. Cummings said he felt that while the aducanumab decision would spur other manufacturers of antiamyloid drugs to seek accelerated approval, other classes of Alzheimer’s therapies in development also stand to get a boost. Many Alzheimer’s experts believe that a combination of drugs targeting different elements of the disease pathway – not just amyloid – will be needed in the long run.
Dr. Scharre said that the buzz over aducanumab’s approval will have at least one concrete benefit: people getting into doctors’ offices sooner.
“The people who come into our memory centers represent only a fraction of people walking around with MCI – there are people out there who may have heard that it’s normal aging; they have decreased insight; there’s denial, there’s embarrassment – there’s hundreds of reasons people avoid getting seen,” he said.
“Perhaps they come in and learn that they don’t have any degenerative process but their thyroid is out of whack, or there’s something else causing cognitive impairment. And if they do have a degenerative process, they’ll have time to start [aducanumab], and hopefully get to see a reduction in the decline.”
Dr. Knopman was a site investigator for the Biogen aducanumab trials and has consulted for Samus Therapeutics, Third Rock, Roche, and Alzeca Biosciences. A former member of the FDA’s Peripheral and Central Nervous System Drugs Advisory Committee, he was recused from the Nov. 6, 2020, meeting that voted against aducanumab. Dr. Cummings has consulted for Biogen, Eisai, and other manufacturers. Dr. Scharre reports financial relationships with Biogen, Brain Test, Acadia, and Vascular Scientific. Dr. Widera has no disclosures. Dr. Delio is a speaker for Gore Medical, Allergan, and Biohaven Pharmaceuticals.
The approval was hailed by advocacy groups and some practitioners as a victory for patients and families, as the drug – the first anti-Alzheimer’s agent to reach the market in 18 years – is a potentially disease-modifying therapy, which acts to clear amyloid plaques from the brain.
But several prominent Alzheimer’s researchers lambasted the agency’s decision, citing unclear evidence of benefit, trials that did not meet their primary endpoints, and reliance on a post hoc analysis of a high-dose subgroup of patients in a halted trial to argue that aducanumab (Aduhelm, Biogen, and Eisai), slowed cognitive and functional decline by 22% on one measure. In November 2020, 10 of 11 members of an independent FDA advisory committee voted against aducanumab’s approval, citing holes in the data and concerns about the quality of the evidence. After the agency went on to approve anyway, three members of that committee resigned in protest.
The FDA decision on aducanumab was made using the agency’s accelerated approval pathway, which allows for the use of a surrogate endpoint – in this case imaging that showed amyloid clearance from the brain – to predict clinical benefit. But amyloid clearance, which a number of experimental antiamyloid antibodies have been shown capable of, has not been definitively linked to clinical benefit. Aducanumab, which is delivered by monthly intravenous infusion, will be marketed pending results from a phase 4 clinical trial, which the manufacturer has nearly a decade to complete. The drug’s price was announced at $56,000 per year, underscoring concern over its modest-at-best benefits.
Clinicians prescribing aducanumab must obtain magnetic resonance imaging at baseline and repeatedly during the course of treatment to detect brain edema and microhemorrhages, which occurred in a third of high-dose patients in clinical trials. Beyond this, there are few restrictions. The FDA label allows for its use in any patient deemed to have Alzheimer’s disease, without stipulations as to disease stage or evidence of brain amyloid. Payers, of course, are likely to restrict use to certain patient groups, and to require evidence of amyloid positivity. The FDA offered no guidance on when treatment should be ceased, leaving payers to make that call as well. Whatever aducanumab’s value and role turns out to be, the first-in-class treatment for Alzheimer’s disease is likely to have a major impact on how patients are assessed and treated in the coming years, and embolden manufactures of similar agents to seek FDA approval.
This news organization reached out to researchers, advocates, and specialists in the community to learn how they see this change playing out.
Fielding broad interest
Maria C. Carrillo, PhD, chief science officer of the Alzheimer’s Association, which was a strong proponent of aducanumab’s approval, acknowledged in an interview that the months to come are likely to be confusing for practitioners and families alike as the drug makes its way into community practices.
“We understand that off the bat millions of Americans will not have access to this tomorrow, but over time that will build. And the physician community, the specialists most likely to be prescribing this, over the next few years will even expand further,” Dr. Carrillo said.
For now, those specialists are mostly just struggling to respond responsibly to a deluge of inquiries from patients and their families.
“I’ve gotten like 20 calls in the just the past 2 days,” said neurologist Philip R. Delio, MD, who practices in Santa Barbara, Calif. “This is a longstanding issue that physicians have with patients’ access to information. Patients are getting information about a drug which isn’t available yet. They don’t know that it’s not ready to be sold. They don’t necessarily realize that a biopharma company won’t go into production until the FDA approves the drug.”
Many patients, Dr. Delio said, are aware of the controversy surrounding aducanumab and eager to hear their neurologist’s opinion. “I have tried to let them know that I want to see the trial data and to better understand the FDA’s rationale in approving it. I always caution patients that the devil will be in the details.”
While aducanumab’s label gives physicians remarkably wide latitude in whom to treat, clinicians say that until payers weigh in, the label is all but meaningless. Neurologist Douglas Scharre, MD, of the Ohio State University Wexner Medical Center, and a site investigator on a trial of aducanumab, said that he and his colleagues at the university’s memory center have tried to anticipate who might be deemed eligible by triaging calls.
Dr. Scharre and colleagues have been working under the assumption that payers will support aducanumab only for patients like those who seemed to benefit in the trials – people with mild cognitive impairment (MCI) or in the earliest stages of dementia with evidence of brain amyloid.
“I don’t want to fill up our new patient slots with people who are not even appropriate for this drug,” Dr. Scharre said. “We have a call center, and we have a few triage questions. After that a nurse practitioner collects some more data, and there’s a review process. Only then do we decide whether that person could be a candidate. If we deem that they are, we will want them in and to order an amyloid PET” – a type of brain scan that is seldom used outside research settings and not reimbursed by Medicare.
Dr. Scharre predicts that regardless of payer limitations, “there will be people hounding for the drug who are not appropriate for the drug. There will be very wealthy people who will want to pay for tests and get it no matter what.” Another concern, he said, was that having poorly selected patients on the drug could make definitive trial results even more elusive.
“The label the way it’s written is not going to help the drug in phase 4 trials,” he said. “It’s good to have real-world patient data, but if you have all these people in your cohort who are too early or too late, you won’t have good results.”
The challenge of delivery
Intravenous infusions are new to Alzheimer’s disease and pose all sorts of logistical hurdles. The Alzheimer’s Association’s Dr. Carrillo described the situation as “manageable,” noting that infusions are standard of care for many diseases, and that neurologists now have more than 15 years’ experience with them for multiple sclerosis.
Still, most clinicians treating Alzheimer’s disease in the community – neurologists, geriatricians, psychiatrists, and primary care physicians – do not have infusion centers in their practices. Virtually none have experience with or access to PET-amyloid, or with screening for amyloid-related imaging abnormalities–edema (ARIA-e) on MRI, as required by the FDA.
“I contacted the hospital infusion center we use and said I could end up sending five or six patients a week, can you handle this? They only have so many chairs,” Dr. Delio said. “I am one neurologist in a local community, and I might have 50 candidates for this drug. That’s a lot for them.” Patients with cognitive impairment are also difficult to infuse and may need to be treated at home, he noted.
“MRIs are easy enough to do,” Dr. Delio said. “But do we know what ARIA-e looks like on imaging? You’d have to talk to the radiologists – this is another element of uncertainty. Do we even know what we’re looking for with these scans? Will we recognize this?”
Neurologist Jeffrey L. Cummings, MD, ScD, of the University of Nevada, Las Vegas, a vocal proponent of aducanumab and lead author of a May 2021 paper defending the evidence for it, acknowledged that the field was unprepared for a wide-scale adoption of infusions in dementia treatment, pointing to a Rand Corporation study from 2017 that warned that screening, diagnosis, and availability of infusion chairs would have to be drastically scaled up to meet demand.
“There are few clinicians who know how to identify MCI, too few imaging centers, too few radiologists who know how to identify ARIA-e on MRI, so all of these things will be required to be put into place. The label doesn’t specify any of this, but good clinical practice will require that, and getting this up and running will take 18 to 24 months,” Dr. Cummings said.
Neurologist David S. Knopman, MD, of the Mayo Clinic in Rochester, Minn., a leading critic of the evidence for aducanumab who recently resigned his position on the independent committee that advises the FDA on neurology drugs, said that for large research institutions like his that have served as trial sites, the transition to offering PET-amyloid, MRI, and infusions in clinical practice will be easier.
“We have all this because this is what we do every day. And we have a very extensive understanding of MCI and mild dementia staging,” Dr. Knopman said. “But the amount of infrastructure that is implied by this, and all the extra steps it would take, would be a real challenge for people in general neurology practice.”
In addition to routine use of PET-amyloid and MRI screening for ARIA-e, Dr. Knopman said, clinicians will have to provide genetic screening and counseling before administering aducanumab, as clinical trials showed that treated patients have a higher risk of developing ARIA-e if they have APOE4, a risk variant for Alzheimer’s disease. “And that has real implications for the families and the children of patients,” he said.
Uncertainty over costs
Aducanumab’s true costs, to patients and to taxpayers, remain unknown. The $56,000 per year currently cited by its manufacturer “doesn’t count the PET scans and MRIs,” Dr. Knopman noted. “We’re probably pushing $100,00 a year for the first year of treatment.”
Most of that expense will likely be borne by Medicare, he said, and if not, “that will exacerbate existing health care disparities. People who can pay out of pocket are a pretty limited group.”
Dr. Scharre agreed that the costs of treatment were concerning, and that “at least you should be able to narrow it down and hopefully just use health care dollars for people who might stand to benefit,” he said – namely patients in an earlier stage of disease.
The Alzheimer’s Association’s Dr. Carrillo declined to address the high price of aducanumab or its implications, saying only that the association is “very invested in all aspects of access including covering costs associated with the drug and the rest of treatment.”
Access also means “infrastructure, access to physicians to diagnose, access to diagnostics,” Dr. Carrillo said.
Dr. Cummings said aducanumab’s price would likely come down through negotiations with the Centers for Medicare & Medicaid Services, copayments, and bulk purchases.
The FDA has offered no guidance on how long treatment with aducanumab should last, or what should prompt withdrawal of treatment, meaning that patients could, in theory, stay on it to the end of their lives – raising costs further.
Critics have also noted that a built-in financial incentive under Medicare Part B, which covers infusion drugs, could result in overprescription of aducanumab. Under Medicare Part B, prescribing physicians are reimbursed 6% of a drug’s average sales price.
Geriatricians wary
On social media and in the lay press, geriatricians have been among the most outspoken opponents of the FDA decision and the Alzheimer’s Association’s advocacy of aducanumab.
Eric Widera, MD, a geriatrician at the University of California, San Francisco, said that the specialty might be less likely than others to embrace aducanumab. “I think part of the reasons geriatricians don’t make a lot of money is they have strong commitment to their values,” Dr. Widera said.
The American Geriatrics Society opposed the drug’s approval, citing concerns about evidence, side effects, and cost. “Additional considerations are the unintended consequences of overstressing Medicare’s limited financial reserves, and of challenging health care systems … to divert precious resources to an expensive treatment of uncertain value,” the society’s president, Peter Hollmann, MD, and chief executive officer, Nancy E. Lundebjerg, wrote in a June 2 letter to the FDA.
Dr. Widera said the approval was likely to undermine confidence in the FDA and in the Alzheimer’s Association, which receives significant funding from drug manufacturers, including Biogen and Eisai. “There’s a lot of reasons that the Geriatrics Society could have done what the Alzheimer’s Association did, and yet they came out against it, which I applaud.”
Dr. Widera pointed to a study showing that dementia patients were less likely to be on an antidementia drug if they were treated by a geriatrician, compared with a psychiatrist or a neurologist. But whether the specialty will prove as cautious with aducanumab remains to be seen. Some geriatricians will be tempted to open lucrative infusion centers, he predicted.
What is especially worrisome, Dr. Widera said, is that aducanumab’s label offers no guidance as to when to withdraw treatment. “We’ll probably see something similar to what happened with the cholinesterase inhibitors” – the class of marginally effective antidementia drugs that includes donepezil (Aricept, Pfizer) and rivastigmine (Exelon, Novartis). “No one thinks about deprescribing them. People are prescribed them even in their last months of life. There is no reason to think these infusions won’t be continued for a very long time, well beyond how long people were dosed in the trials.”
“Taking care of someone with dementia is hard enough,” Dr. Widera added. “We can’t even get normal support in the home for someone with dementia. But we are more than happy to throw money to Biogen for a drug they have not yet showed benefit for. Hopefully in 5 years we’ll have a drug that actually works,” Dr. Widera said. “After 5 years of giving this to people at $50,000 a year.”
A fractured research community
Ever since October 2019, when Biogen and Eisai announced that despite two trials halted for futility, they would go ahead and seek FDA approval for aducanumab, the Alzheimer’s research community has been bitterly divided over the drug and the FDA’s accelerated approval process.
Top researchers published critical editorials in journals, with some eventually taking their case to major newspapers as well. The Alzheimer’s Association’s position on the drug has clashed with that of many researchers whose work it supports.
“The Alzheimer’s community has been wonderfully collegial – we all have a common purpose,” Dr. Cummings said. “Now we have people taking extreme positions and I’m hoping this will not result in a permanent fracturing of the community.”
Chief among the critics’ concerns is that the FDA decision ratified the use of antiamyloid therapies based on biomarker evidence, opening the door for makers of similar drugs – those still under development or even those whose development has been halted – to seek approval on weak evidence of clinical benefit.
Whether the approval will chill research into drugs targeting pathways other than amyloid is uncertain.
Dr. Cummings said he felt that while the aducanumab decision would spur other manufacturers of antiamyloid drugs to seek accelerated approval, other classes of Alzheimer’s therapies in development also stand to get a boost. Many Alzheimer’s experts believe that a combination of drugs targeting different elements of the disease pathway – not just amyloid – will be needed in the long run.
Dr. Scharre said that the buzz over aducanumab’s approval will have at least one concrete benefit: people getting into doctors’ offices sooner.
“The people who come into our memory centers represent only a fraction of people walking around with MCI – there are people out there who may have heard that it’s normal aging; they have decreased insight; there’s denial, there’s embarrassment – there’s hundreds of reasons people avoid getting seen,” he said.
“Perhaps they come in and learn that they don’t have any degenerative process but their thyroid is out of whack, or there’s something else causing cognitive impairment. And if they do have a degenerative process, they’ll have time to start [aducanumab], and hopefully get to see a reduction in the decline.”
Dr. Knopman was a site investigator for the Biogen aducanumab trials and has consulted for Samus Therapeutics, Third Rock, Roche, and Alzeca Biosciences. A former member of the FDA’s Peripheral and Central Nervous System Drugs Advisory Committee, he was recused from the Nov. 6, 2020, meeting that voted against aducanumab. Dr. Cummings has consulted for Biogen, Eisai, and other manufacturers. Dr. Scharre reports financial relationships with Biogen, Brain Test, Acadia, and Vascular Scientific. Dr. Widera has no disclosures. Dr. Delio is a speaker for Gore Medical, Allergan, and Biohaven Pharmaceuticals.
The approval was hailed by advocacy groups and some practitioners as a victory for patients and families, as the drug – the first anti-Alzheimer’s agent to reach the market in 18 years – is a potentially disease-modifying therapy, which acts to clear amyloid plaques from the brain.
But several prominent Alzheimer’s researchers lambasted the agency’s decision, citing unclear evidence of benefit, trials that did not meet their primary endpoints, and reliance on a post hoc analysis of a high-dose subgroup of patients in a halted trial to argue that aducanumab (Aduhelm, Biogen, and Eisai), slowed cognitive and functional decline by 22% on one measure. In November 2020, 10 of 11 members of an independent FDA advisory committee voted against aducanumab’s approval, citing holes in the data and concerns about the quality of the evidence. After the agency went on to approve anyway, three members of that committee resigned in protest.
The FDA decision on aducanumab was made using the agency’s accelerated approval pathway, which allows for the use of a surrogate endpoint – in this case imaging that showed amyloid clearance from the brain – to predict clinical benefit. But amyloid clearance, which a number of experimental antiamyloid antibodies have been shown capable of, has not been definitively linked to clinical benefit. Aducanumab, which is delivered by monthly intravenous infusion, will be marketed pending results from a phase 4 clinical trial, which the manufacturer has nearly a decade to complete. The drug’s price was announced at $56,000 per year, underscoring concern over its modest-at-best benefits.
Clinicians prescribing aducanumab must obtain magnetic resonance imaging at baseline and repeatedly during the course of treatment to detect brain edema and microhemorrhages, which occurred in a third of high-dose patients in clinical trials. Beyond this, there are few restrictions. The FDA label allows for its use in any patient deemed to have Alzheimer’s disease, without stipulations as to disease stage or evidence of brain amyloid. Payers, of course, are likely to restrict use to certain patient groups, and to require evidence of amyloid positivity. The FDA offered no guidance on when treatment should be ceased, leaving payers to make that call as well. Whatever aducanumab’s value and role turns out to be, the first-in-class treatment for Alzheimer’s disease is likely to have a major impact on how patients are assessed and treated in the coming years, and embolden manufactures of similar agents to seek FDA approval.
This news organization reached out to researchers, advocates, and specialists in the community to learn how they see this change playing out.
Fielding broad interest
Maria C. Carrillo, PhD, chief science officer of the Alzheimer’s Association, which was a strong proponent of aducanumab’s approval, acknowledged in an interview that the months to come are likely to be confusing for practitioners and families alike as the drug makes its way into community practices.
“We understand that off the bat millions of Americans will not have access to this tomorrow, but over time that will build. And the physician community, the specialists most likely to be prescribing this, over the next few years will even expand further,” Dr. Carrillo said.
For now, those specialists are mostly just struggling to respond responsibly to a deluge of inquiries from patients and their families.
“I’ve gotten like 20 calls in the just the past 2 days,” said neurologist Philip R. Delio, MD, who practices in Santa Barbara, Calif. “This is a longstanding issue that physicians have with patients’ access to information. Patients are getting information about a drug which isn’t available yet. They don’t know that it’s not ready to be sold. They don’t necessarily realize that a biopharma company won’t go into production until the FDA approves the drug.”
Many patients, Dr. Delio said, are aware of the controversy surrounding aducanumab and eager to hear their neurologist’s opinion. “I have tried to let them know that I want to see the trial data and to better understand the FDA’s rationale in approving it. I always caution patients that the devil will be in the details.”
While aducanumab’s label gives physicians remarkably wide latitude in whom to treat, clinicians say that until payers weigh in, the label is all but meaningless. Neurologist Douglas Scharre, MD, of the Ohio State University Wexner Medical Center, and a site investigator on a trial of aducanumab, said that he and his colleagues at the university’s memory center have tried to anticipate who might be deemed eligible by triaging calls.
Dr. Scharre and colleagues have been working under the assumption that payers will support aducanumab only for patients like those who seemed to benefit in the trials – people with mild cognitive impairment (MCI) or in the earliest stages of dementia with evidence of brain amyloid.
“I don’t want to fill up our new patient slots with people who are not even appropriate for this drug,” Dr. Scharre said. “We have a call center, and we have a few triage questions. After that a nurse practitioner collects some more data, and there’s a review process. Only then do we decide whether that person could be a candidate. If we deem that they are, we will want them in and to order an amyloid PET” – a type of brain scan that is seldom used outside research settings and not reimbursed by Medicare.
Dr. Scharre predicts that regardless of payer limitations, “there will be people hounding for the drug who are not appropriate for the drug. There will be very wealthy people who will want to pay for tests and get it no matter what.” Another concern, he said, was that having poorly selected patients on the drug could make definitive trial results even more elusive.
“The label the way it’s written is not going to help the drug in phase 4 trials,” he said. “It’s good to have real-world patient data, but if you have all these people in your cohort who are too early or too late, you won’t have good results.”
The challenge of delivery
Intravenous infusions are new to Alzheimer’s disease and pose all sorts of logistical hurdles. The Alzheimer’s Association’s Dr. Carrillo described the situation as “manageable,” noting that infusions are standard of care for many diseases, and that neurologists now have more than 15 years’ experience with them for multiple sclerosis.
Still, most clinicians treating Alzheimer’s disease in the community – neurologists, geriatricians, psychiatrists, and primary care physicians – do not have infusion centers in their practices. Virtually none have experience with or access to PET-amyloid, or with screening for amyloid-related imaging abnormalities–edema (ARIA-e) on MRI, as required by the FDA.
“I contacted the hospital infusion center we use and said I could end up sending five or six patients a week, can you handle this? They only have so many chairs,” Dr. Delio said. “I am one neurologist in a local community, and I might have 50 candidates for this drug. That’s a lot for them.” Patients with cognitive impairment are also difficult to infuse and may need to be treated at home, he noted.
“MRIs are easy enough to do,” Dr. Delio said. “But do we know what ARIA-e looks like on imaging? You’d have to talk to the radiologists – this is another element of uncertainty. Do we even know what we’re looking for with these scans? Will we recognize this?”
Neurologist Jeffrey L. Cummings, MD, ScD, of the University of Nevada, Las Vegas, a vocal proponent of aducanumab and lead author of a May 2021 paper defending the evidence for it, acknowledged that the field was unprepared for a wide-scale adoption of infusions in dementia treatment, pointing to a Rand Corporation study from 2017 that warned that screening, diagnosis, and availability of infusion chairs would have to be drastically scaled up to meet demand.
“There are few clinicians who know how to identify MCI, too few imaging centers, too few radiologists who know how to identify ARIA-e on MRI, so all of these things will be required to be put into place. The label doesn’t specify any of this, but good clinical practice will require that, and getting this up and running will take 18 to 24 months,” Dr. Cummings said.
Neurologist David S. Knopman, MD, of the Mayo Clinic in Rochester, Minn., a leading critic of the evidence for aducanumab who recently resigned his position on the independent committee that advises the FDA on neurology drugs, said that for large research institutions like his that have served as trial sites, the transition to offering PET-amyloid, MRI, and infusions in clinical practice will be easier.
“We have all this because this is what we do every day. And we have a very extensive understanding of MCI and mild dementia staging,” Dr. Knopman said. “But the amount of infrastructure that is implied by this, and all the extra steps it would take, would be a real challenge for people in general neurology practice.”
In addition to routine use of PET-amyloid and MRI screening for ARIA-e, Dr. Knopman said, clinicians will have to provide genetic screening and counseling before administering aducanumab, as clinical trials showed that treated patients have a higher risk of developing ARIA-e if they have APOE4, a risk variant for Alzheimer’s disease. “And that has real implications for the families and the children of patients,” he said.
Uncertainty over costs
Aducanumab’s true costs, to patients and to taxpayers, remain unknown. The $56,000 per year currently cited by its manufacturer “doesn’t count the PET scans and MRIs,” Dr. Knopman noted. “We’re probably pushing $100,00 a year for the first year of treatment.”
Most of that expense will likely be borne by Medicare, he said, and if not, “that will exacerbate existing health care disparities. People who can pay out of pocket are a pretty limited group.”
Dr. Scharre agreed that the costs of treatment were concerning, and that “at least you should be able to narrow it down and hopefully just use health care dollars for people who might stand to benefit,” he said – namely patients in an earlier stage of disease.
The Alzheimer’s Association’s Dr. Carrillo declined to address the high price of aducanumab or its implications, saying only that the association is “very invested in all aspects of access including covering costs associated with the drug and the rest of treatment.”
Access also means “infrastructure, access to physicians to diagnose, access to diagnostics,” Dr. Carrillo said.
Dr. Cummings said aducanumab’s price would likely come down through negotiations with the Centers for Medicare & Medicaid Services, copayments, and bulk purchases.
The FDA has offered no guidance on how long treatment with aducanumab should last, or what should prompt withdrawal of treatment, meaning that patients could, in theory, stay on it to the end of their lives – raising costs further.
Critics have also noted that a built-in financial incentive under Medicare Part B, which covers infusion drugs, could result in overprescription of aducanumab. Under Medicare Part B, prescribing physicians are reimbursed 6% of a drug’s average sales price.
Geriatricians wary
On social media and in the lay press, geriatricians have been among the most outspoken opponents of the FDA decision and the Alzheimer’s Association’s advocacy of aducanumab.
Eric Widera, MD, a geriatrician at the University of California, San Francisco, said that the specialty might be less likely than others to embrace aducanumab. “I think part of the reasons geriatricians don’t make a lot of money is they have strong commitment to their values,” Dr. Widera said.
The American Geriatrics Society opposed the drug’s approval, citing concerns about evidence, side effects, and cost. “Additional considerations are the unintended consequences of overstressing Medicare’s limited financial reserves, and of challenging health care systems … to divert precious resources to an expensive treatment of uncertain value,” the society’s president, Peter Hollmann, MD, and chief executive officer, Nancy E. Lundebjerg, wrote in a June 2 letter to the FDA.
Dr. Widera said the approval was likely to undermine confidence in the FDA and in the Alzheimer’s Association, which receives significant funding from drug manufacturers, including Biogen and Eisai. “There’s a lot of reasons that the Geriatrics Society could have done what the Alzheimer’s Association did, and yet they came out against it, which I applaud.”
Dr. Widera pointed to a study showing that dementia patients were less likely to be on an antidementia drug if they were treated by a geriatrician, compared with a psychiatrist or a neurologist. But whether the specialty will prove as cautious with aducanumab remains to be seen. Some geriatricians will be tempted to open lucrative infusion centers, he predicted.
What is especially worrisome, Dr. Widera said, is that aducanumab’s label offers no guidance as to when to withdraw treatment. “We’ll probably see something similar to what happened with the cholinesterase inhibitors” – the class of marginally effective antidementia drugs that includes donepezil (Aricept, Pfizer) and rivastigmine (Exelon, Novartis). “No one thinks about deprescribing them. People are prescribed them even in their last months of life. There is no reason to think these infusions won’t be continued for a very long time, well beyond how long people were dosed in the trials.”
“Taking care of someone with dementia is hard enough,” Dr. Widera added. “We can’t even get normal support in the home for someone with dementia. But we are more than happy to throw money to Biogen for a drug they have not yet showed benefit for. Hopefully in 5 years we’ll have a drug that actually works,” Dr. Widera said. “After 5 years of giving this to people at $50,000 a year.”
A fractured research community
Ever since October 2019, when Biogen and Eisai announced that despite two trials halted for futility, they would go ahead and seek FDA approval for aducanumab, the Alzheimer’s research community has been bitterly divided over the drug and the FDA’s accelerated approval process.
Top researchers published critical editorials in journals, with some eventually taking their case to major newspapers as well. The Alzheimer’s Association’s position on the drug has clashed with that of many researchers whose work it supports.
“The Alzheimer’s community has been wonderfully collegial – we all have a common purpose,” Dr. Cummings said. “Now we have people taking extreme positions and I’m hoping this will not result in a permanent fracturing of the community.”
Chief among the critics’ concerns is that the FDA decision ratified the use of antiamyloid therapies based on biomarker evidence, opening the door for makers of similar drugs – those still under development or even those whose development has been halted – to seek approval on weak evidence of clinical benefit.
Whether the approval will chill research into drugs targeting pathways other than amyloid is uncertain.
Dr. Cummings said he felt that while the aducanumab decision would spur other manufacturers of antiamyloid drugs to seek accelerated approval, other classes of Alzheimer’s therapies in development also stand to get a boost. Many Alzheimer’s experts believe that a combination of drugs targeting different elements of the disease pathway – not just amyloid – will be needed in the long run.
Dr. Scharre said that the buzz over aducanumab’s approval will have at least one concrete benefit: people getting into doctors’ offices sooner.
“The people who come into our memory centers represent only a fraction of people walking around with MCI – there are people out there who may have heard that it’s normal aging; they have decreased insight; there’s denial, there’s embarrassment – there’s hundreds of reasons people avoid getting seen,” he said.
“Perhaps they come in and learn that they don’t have any degenerative process but their thyroid is out of whack, or there’s something else causing cognitive impairment. And if they do have a degenerative process, they’ll have time to start [aducanumab], and hopefully get to see a reduction in the decline.”
Dr. Knopman was a site investigator for the Biogen aducanumab trials and has consulted for Samus Therapeutics, Third Rock, Roche, and Alzeca Biosciences. A former member of the FDA’s Peripheral and Central Nervous System Drugs Advisory Committee, he was recused from the Nov. 6, 2020, meeting that voted against aducanumab. Dr. Cummings has consulted for Biogen, Eisai, and other manufacturers. Dr. Scharre reports financial relationships with Biogen, Brain Test, Acadia, and Vascular Scientific. Dr. Widera has no disclosures. Dr. Delio is a speaker for Gore Medical, Allergan, and Biohaven Pharmaceuticals.
Moving more, sitting less vital for migraine patients
according to a presentation at the American Headache Society’s 2021 annual meeting.
Though reliable research is sparse overall on how much physical activity people with migraine get, enough exists to reveal the need for clinicians to help patients identify ways to increase their levels of physical activity and make it a habit, said Dale S. Bond, PhD, a professor of psychiatry and human behavior at the Miriam Hospital and Brown University, both in Providence, R.I.
He emphasized the need not only to replace sedentary time with physical activity but also to reduce sedentary time overall.
“It’s important to note that because active and sedentary represent different behavioral domains, people can still be active – that is, achieving recommended levels of moderate to vigorous physical activity [MVPA] – but still be highly sedentary because they sit for long hours throughout the day,” Dr. Bond said. “This is important because MVPA will not necessarily eliminate the health risks of long hours of sitting.”
Dr. Bond reviewed the existing literature on physical activity and sedentary behavior among patients with migraine. His presentation, “Move More, Sit Less,” aimed at finding ways to incorporate more physical activity into the daily lives of those with migraine. Dr. Bond began by briefly reviewing the well-established benefits of physical activity, including healthy sleep; cardiovascular, respiratory, musculoskeletal, mental, and cognitive health; and metabolic functioning.
“Physical activity and exercise in particular enhances the functioning of bodily systems, including those that have direct relevance to migraine in its comorbidities,” Dr. Bond said. “The positive systemic effects of exercise on bodily systems carries potential to reduce migraine severity and related disability and morbidity.”
He also explained the ways in which excessive sedentary time can exacerbate migraine triggers. “Long periods of interrupted sitting elevated levels of glucose and fat in the bloodstream, which in turn triggers the immune system to attack the body via inflammation,” Dr. Bond said. “Low grade chronic inflammation has long been hypothesized to play a role in migraine pathogenesis.”
Recommended levels of exercise
The World Health Organization and the U.S. Department of Health & Human Services recommends at least 150-300 minutes of moderate-intensity aerobic physical activity or 75-150 minutes of vigorous activity each week. An additional recommendation is at least 2 days per week of muscle strengthening activities that involve all major muscle groups.
While neither of those organizations has specific guidelines on how much reduction of sedentary time is recommended, the Canadian Society for Exercise Physiology recommends limiting sedentary time to 8 or fewer hours per day.
Exercise and migraine
“Unfortunately, at present, we have very few studies from which to draw conclusions about the extent to which individuals with migraine adhere to physical activity and sedentary guidelines,” Dr. Bond said. Existing studies vary widely in sample types, study design, physical activity measure and MVPA outcome, including the type or definition of MVPA. “This wide variability in measures and outcomes makes it challenging to draw any conclusions about adherence to guidelines among individuals with migraine,” he said.
Existing evidence suggests anywhere from 32% to 66% of migraine patients are at least moderately active, though it’s not clear what constitutes “moderately active” behavior. It appears that activity levels of patients with migraine are low overall, but it’s less clear the extent to which these levels are lower than in controls given the paucity of evidence.
In one of the few studies using objective measures to assess physical activity in migraine patients, the daily level of MVPA was significantly lower in 25 women with migraine than in 25 age- and body mass index–matched women without migraine (P <. 003). Both groups had obesity. The same study found that virtually no women with migraine adhered to the guidelines recommending less than 8 hours a day of sedentary time, compared with 30% of women without migraine.
“Also, low physical activity and high sedentary levels appear to be consistent across headache and nonheadache days,” Dr. Bond said. “This finding in particular raises an interesting question: If migraine severity is not related to physical activity and sedentary time, what is it about migraine that contributes to an inactive and sedentary lifestyle?”
Dr. Bond noted that future research needs to include reports of frequency, duration, and intensity of activities performed as well as the percentage of participants who meet guidelines for physical activity and sedentary time. Ideally, these studies should include not only self-report but also objective measures of activity as well as assess sleep and identify barriers and facilitators to physical activity in patients.
Exercise avoidance
Dr. Bond described findings from survey of 100 women he conducted to better understand potential barriers and reported that 78% of patients report intentionally avoiding physical activity. These patients typically avoided it an average of 4 days per week, regardless of intensity, and additional survey findings found “that participants who reported any avoidance had stronger beliefs that physical activity would both trigger and worsen a migraine attack, compared with participants who reported no avoidance,” he said.
That finding matches the clinical experience of Jennifer Robblee, MD, MSc, assistant professor of neurology at Barrow Neurological Institute in Phoenix, who viewed the presentation but was not involved with it.
“They often feel that it is a trigger for worsening an attack or, for some people, can actually trigger an attack, and that they feel worse in the midst of an attack when they’re exercising,” Dr. Robblee said in an interview regarding her patients who exercise less frequently. “Since so many of the patients I see have a daily and constant headache, it’s about how they can get themselves to start to exercise when something makes them feel worse, even if it makes them feel better in the long run.”
Yet, experimental research suggests that physical activity is not necessarily a reliable trigger of migraine attacks and only worsens migraine in a minority of attacks, Dr. Bond said, revealing an interesting paradox: “While engaging in regular physical activity is an important migraine management strategy, most individuals in the study reported doing the exact opposite – that is, avoiding physical activity as a management strategy – and this strategy was associated with higher frequency and duration of attacks. Research from our group and others also suggested individuals with migraine could be overestimating the role that physical activity hasn’t triggering or worsening of attacks.”
Encouraging patients to exercise
Since the benefits of physical activity and limiting sedentary time outweigh the potential harms, “some physical activity is better than none,” Dr. Bond said. To help patients begin increasing their physical activity, he recommended advising them to start with small amounts and then gradually increase frequency, intensity, and duration over time.
Dr. Robblee follows a similar approach, taking into account each patient’s particular circumstances and any medications they’re taking, including the side effects of those medications.
“It’s about starting where they are,” Dr. Robblee said. “Some patients, despite having severe migraine, have built themselves up so they’re doing exercise three or four times per week, or every day, and I have other people who never exercise,” she said. “For those patients who are very sedentary, if I can get them to start with 5 minutes per week so they have that sense of accomplishment, then that’s where I start. Then slowly build it up over time. Like most things in the migraine world, I individualize it for the person.”
Dr. Bond offered the following specific tips to clinicians in educating and encouraging patients to increase physical activity:
- Educate patients regarding the short-and long-term benefits of moving more and sitting less, both for their migraines and for overall health.
- Correct misconceptions about the negative effects of physical activity as it relates to migraines.
- Personalize the rationale for physical activity to that patient’s specific values and personal goals.
- Encourage patients to use an activity tracker, both for tracking physical activity and sedentary time, and to monitor migraine attacks, stress, energy levels, and fatigue on days they do and do not exercise.
- Help patients set goals for eventually meeting MVPA recommendations and interrupting prolonged periods of sitting with brief movement breaks.
- Help patients identify rewards for meeting goals that are tied to the activity, such as new exercise clothing.
- Encourage patients to identify a consistent time for physical activity each day to establish a habit, “ideally in the morning before barriers and life get in the way,” he said.
Eventually, physical activity itself should become intrinsically rewarding, Dr. Bond said.
“To limit sitting and encourage more movement throughout the day, we want to make the choice to engage in physical activity easier by adding environmental cues that encourage physical activity,” he said. “Conversely, we want to make the choice to engage in sedentary behavior more difficult by increasing the amount of effort that is required to engage in these behaviors.”
Dr. Robblee found Dr. Bond’s emphasis on sitting less – distinct from moving more – a helpful frame to consider with her patients. “I really like the approach of looking at it from that approach: in addition to how do we get you up and moving, how much time are you sitting, and how often can you break that up into smaller increments so that you’re up more often?” Dr. Robblee said. “That sometimes sounds less scary than ‘let’s get you exercising.’ So ‘let’s get you sitting a little bit less.’ I think that is something I might start to adopt.”
No external funding was noted. Dr. Robblee is a principal investigator for a study sponsored by Eli Lilly and receives stipends for MedLink Neurology and Neurodiem. Dr. Bond reported no disclosures.
according to a presentation at the American Headache Society’s 2021 annual meeting.
Though reliable research is sparse overall on how much physical activity people with migraine get, enough exists to reveal the need for clinicians to help patients identify ways to increase their levels of physical activity and make it a habit, said Dale S. Bond, PhD, a professor of psychiatry and human behavior at the Miriam Hospital and Brown University, both in Providence, R.I.
He emphasized the need not only to replace sedentary time with physical activity but also to reduce sedentary time overall.
“It’s important to note that because active and sedentary represent different behavioral domains, people can still be active – that is, achieving recommended levels of moderate to vigorous physical activity [MVPA] – but still be highly sedentary because they sit for long hours throughout the day,” Dr. Bond said. “This is important because MVPA will not necessarily eliminate the health risks of long hours of sitting.”
Dr. Bond reviewed the existing literature on physical activity and sedentary behavior among patients with migraine. His presentation, “Move More, Sit Less,” aimed at finding ways to incorporate more physical activity into the daily lives of those with migraine. Dr. Bond began by briefly reviewing the well-established benefits of physical activity, including healthy sleep; cardiovascular, respiratory, musculoskeletal, mental, and cognitive health; and metabolic functioning.
“Physical activity and exercise in particular enhances the functioning of bodily systems, including those that have direct relevance to migraine in its comorbidities,” Dr. Bond said. “The positive systemic effects of exercise on bodily systems carries potential to reduce migraine severity and related disability and morbidity.”
He also explained the ways in which excessive sedentary time can exacerbate migraine triggers. “Long periods of interrupted sitting elevated levels of glucose and fat in the bloodstream, which in turn triggers the immune system to attack the body via inflammation,” Dr. Bond said. “Low grade chronic inflammation has long been hypothesized to play a role in migraine pathogenesis.”
Recommended levels of exercise
The World Health Organization and the U.S. Department of Health & Human Services recommends at least 150-300 minutes of moderate-intensity aerobic physical activity or 75-150 minutes of vigorous activity each week. An additional recommendation is at least 2 days per week of muscle strengthening activities that involve all major muscle groups.
While neither of those organizations has specific guidelines on how much reduction of sedentary time is recommended, the Canadian Society for Exercise Physiology recommends limiting sedentary time to 8 or fewer hours per day.
Exercise and migraine
“Unfortunately, at present, we have very few studies from which to draw conclusions about the extent to which individuals with migraine adhere to physical activity and sedentary guidelines,” Dr. Bond said. Existing studies vary widely in sample types, study design, physical activity measure and MVPA outcome, including the type or definition of MVPA. “This wide variability in measures and outcomes makes it challenging to draw any conclusions about adherence to guidelines among individuals with migraine,” he said.
Existing evidence suggests anywhere from 32% to 66% of migraine patients are at least moderately active, though it’s not clear what constitutes “moderately active” behavior. It appears that activity levels of patients with migraine are low overall, but it’s less clear the extent to which these levels are lower than in controls given the paucity of evidence.
In one of the few studies using objective measures to assess physical activity in migraine patients, the daily level of MVPA was significantly lower in 25 women with migraine than in 25 age- and body mass index–matched women without migraine (P <. 003). Both groups had obesity. The same study found that virtually no women with migraine adhered to the guidelines recommending less than 8 hours a day of sedentary time, compared with 30% of women without migraine.
“Also, low physical activity and high sedentary levels appear to be consistent across headache and nonheadache days,” Dr. Bond said. “This finding in particular raises an interesting question: If migraine severity is not related to physical activity and sedentary time, what is it about migraine that contributes to an inactive and sedentary lifestyle?”
Dr. Bond noted that future research needs to include reports of frequency, duration, and intensity of activities performed as well as the percentage of participants who meet guidelines for physical activity and sedentary time. Ideally, these studies should include not only self-report but also objective measures of activity as well as assess sleep and identify barriers and facilitators to physical activity in patients.
Exercise avoidance
Dr. Bond described findings from survey of 100 women he conducted to better understand potential barriers and reported that 78% of patients report intentionally avoiding physical activity. These patients typically avoided it an average of 4 days per week, regardless of intensity, and additional survey findings found “that participants who reported any avoidance had stronger beliefs that physical activity would both trigger and worsen a migraine attack, compared with participants who reported no avoidance,” he said.
That finding matches the clinical experience of Jennifer Robblee, MD, MSc, assistant professor of neurology at Barrow Neurological Institute in Phoenix, who viewed the presentation but was not involved with it.
“They often feel that it is a trigger for worsening an attack or, for some people, can actually trigger an attack, and that they feel worse in the midst of an attack when they’re exercising,” Dr. Robblee said in an interview regarding her patients who exercise less frequently. “Since so many of the patients I see have a daily and constant headache, it’s about how they can get themselves to start to exercise when something makes them feel worse, even if it makes them feel better in the long run.”
Yet, experimental research suggests that physical activity is not necessarily a reliable trigger of migraine attacks and only worsens migraine in a minority of attacks, Dr. Bond said, revealing an interesting paradox: “While engaging in regular physical activity is an important migraine management strategy, most individuals in the study reported doing the exact opposite – that is, avoiding physical activity as a management strategy – and this strategy was associated with higher frequency and duration of attacks. Research from our group and others also suggested individuals with migraine could be overestimating the role that physical activity hasn’t triggering or worsening of attacks.”
Encouraging patients to exercise
Since the benefits of physical activity and limiting sedentary time outweigh the potential harms, “some physical activity is better than none,” Dr. Bond said. To help patients begin increasing their physical activity, he recommended advising them to start with small amounts and then gradually increase frequency, intensity, and duration over time.
Dr. Robblee follows a similar approach, taking into account each patient’s particular circumstances and any medications they’re taking, including the side effects of those medications.
“It’s about starting where they are,” Dr. Robblee said. “Some patients, despite having severe migraine, have built themselves up so they’re doing exercise three or four times per week, or every day, and I have other people who never exercise,” she said. “For those patients who are very sedentary, if I can get them to start with 5 minutes per week so they have that sense of accomplishment, then that’s where I start. Then slowly build it up over time. Like most things in the migraine world, I individualize it for the person.”
Dr. Bond offered the following specific tips to clinicians in educating and encouraging patients to increase physical activity:
- Educate patients regarding the short-and long-term benefits of moving more and sitting less, both for their migraines and for overall health.
- Correct misconceptions about the negative effects of physical activity as it relates to migraines.
- Personalize the rationale for physical activity to that patient’s specific values and personal goals.
- Encourage patients to use an activity tracker, both for tracking physical activity and sedentary time, and to monitor migraine attacks, stress, energy levels, and fatigue on days they do and do not exercise.
- Help patients set goals for eventually meeting MVPA recommendations and interrupting prolonged periods of sitting with brief movement breaks.
- Help patients identify rewards for meeting goals that are tied to the activity, such as new exercise clothing.
- Encourage patients to identify a consistent time for physical activity each day to establish a habit, “ideally in the morning before barriers and life get in the way,” he said.
Eventually, physical activity itself should become intrinsically rewarding, Dr. Bond said.
“To limit sitting and encourage more movement throughout the day, we want to make the choice to engage in physical activity easier by adding environmental cues that encourage physical activity,” he said. “Conversely, we want to make the choice to engage in sedentary behavior more difficult by increasing the amount of effort that is required to engage in these behaviors.”
Dr. Robblee found Dr. Bond’s emphasis on sitting less – distinct from moving more – a helpful frame to consider with her patients. “I really like the approach of looking at it from that approach: in addition to how do we get you up and moving, how much time are you sitting, and how often can you break that up into smaller increments so that you’re up more often?” Dr. Robblee said. “That sometimes sounds less scary than ‘let’s get you exercising.’ So ‘let’s get you sitting a little bit less.’ I think that is something I might start to adopt.”
No external funding was noted. Dr. Robblee is a principal investigator for a study sponsored by Eli Lilly and receives stipends for MedLink Neurology and Neurodiem. Dr. Bond reported no disclosures.
according to a presentation at the American Headache Society’s 2021 annual meeting.
Though reliable research is sparse overall on how much physical activity people with migraine get, enough exists to reveal the need for clinicians to help patients identify ways to increase their levels of physical activity and make it a habit, said Dale S. Bond, PhD, a professor of psychiatry and human behavior at the Miriam Hospital and Brown University, both in Providence, R.I.
He emphasized the need not only to replace sedentary time with physical activity but also to reduce sedentary time overall.
“It’s important to note that because active and sedentary represent different behavioral domains, people can still be active – that is, achieving recommended levels of moderate to vigorous physical activity [MVPA] – but still be highly sedentary because they sit for long hours throughout the day,” Dr. Bond said. “This is important because MVPA will not necessarily eliminate the health risks of long hours of sitting.”
Dr. Bond reviewed the existing literature on physical activity and sedentary behavior among patients with migraine. His presentation, “Move More, Sit Less,” aimed at finding ways to incorporate more physical activity into the daily lives of those with migraine. Dr. Bond began by briefly reviewing the well-established benefits of physical activity, including healthy sleep; cardiovascular, respiratory, musculoskeletal, mental, and cognitive health; and metabolic functioning.
“Physical activity and exercise in particular enhances the functioning of bodily systems, including those that have direct relevance to migraine in its comorbidities,” Dr. Bond said. “The positive systemic effects of exercise on bodily systems carries potential to reduce migraine severity and related disability and morbidity.”
He also explained the ways in which excessive sedentary time can exacerbate migraine triggers. “Long periods of interrupted sitting elevated levels of glucose and fat in the bloodstream, which in turn triggers the immune system to attack the body via inflammation,” Dr. Bond said. “Low grade chronic inflammation has long been hypothesized to play a role in migraine pathogenesis.”
Recommended levels of exercise
The World Health Organization and the U.S. Department of Health & Human Services recommends at least 150-300 minutes of moderate-intensity aerobic physical activity or 75-150 minutes of vigorous activity each week. An additional recommendation is at least 2 days per week of muscle strengthening activities that involve all major muscle groups.
While neither of those organizations has specific guidelines on how much reduction of sedentary time is recommended, the Canadian Society for Exercise Physiology recommends limiting sedentary time to 8 or fewer hours per day.
Exercise and migraine
“Unfortunately, at present, we have very few studies from which to draw conclusions about the extent to which individuals with migraine adhere to physical activity and sedentary guidelines,” Dr. Bond said. Existing studies vary widely in sample types, study design, physical activity measure and MVPA outcome, including the type or definition of MVPA. “This wide variability in measures and outcomes makes it challenging to draw any conclusions about adherence to guidelines among individuals with migraine,” he said.
Existing evidence suggests anywhere from 32% to 66% of migraine patients are at least moderately active, though it’s not clear what constitutes “moderately active” behavior. It appears that activity levels of patients with migraine are low overall, but it’s less clear the extent to which these levels are lower than in controls given the paucity of evidence.
In one of the few studies using objective measures to assess physical activity in migraine patients, the daily level of MVPA was significantly lower in 25 women with migraine than in 25 age- and body mass index–matched women without migraine (P <. 003). Both groups had obesity. The same study found that virtually no women with migraine adhered to the guidelines recommending less than 8 hours a day of sedentary time, compared with 30% of women without migraine.
“Also, low physical activity and high sedentary levels appear to be consistent across headache and nonheadache days,” Dr. Bond said. “This finding in particular raises an interesting question: If migraine severity is not related to physical activity and sedentary time, what is it about migraine that contributes to an inactive and sedentary lifestyle?”
Dr. Bond noted that future research needs to include reports of frequency, duration, and intensity of activities performed as well as the percentage of participants who meet guidelines for physical activity and sedentary time. Ideally, these studies should include not only self-report but also objective measures of activity as well as assess sleep and identify barriers and facilitators to physical activity in patients.
Exercise avoidance
Dr. Bond described findings from survey of 100 women he conducted to better understand potential barriers and reported that 78% of patients report intentionally avoiding physical activity. These patients typically avoided it an average of 4 days per week, regardless of intensity, and additional survey findings found “that participants who reported any avoidance had stronger beliefs that physical activity would both trigger and worsen a migraine attack, compared with participants who reported no avoidance,” he said.
That finding matches the clinical experience of Jennifer Robblee, MD, MSc, assistant professor of neurology at Barrow Neurological Institute in Phoenix, who viewed the presentation but was not involved with it.
“They often feel that it is a trigger for worsening an attack or, for some people, can actually trigger an attack, and that they feel worse in the midst of an attack when they’re exercising,” Dr. Robblee said in an interview regarding her patients who exercise less frequently. “Since so many of the patients I see have a daily and constant headache, it’s about how they can get themselves to start to exercise when something makes them feel worse, even if it makes them feel better in the long run.”
Yet, experimental research suggests that physical activity is not necessarily a reliable trigger of migraine attacks and only worsens migraine in a minority of attacks, Dr. Bond said, revealing an interesting paradox: “While engaging in regular physical activity is an important migraine management strategy, most individuals in the study reported doing the exact opposite – that is, avoiding physical activity as a management strategy – and this strategy was associated with higher frequency and duration of attacks. Research from our group and others also suggested individuals with migraine could be overestimating the role that physical activity hasn’t triggering or worsening of attacks.”
Encouraging patients to exercise
Since the benefits of physical activity and limiting sedentary time outweigh the potential harms, “some physical activity is better than none,” Dr. Bond said. To help patients begin increasing their physical activity, he recommended advising them to start with small amounts and then gradually increase frequency, intensity, and duration over time.
Dr. Robblee follows a similar approach, taking into account each patient’s particular circumstances and any medications they’re taking, including the side effects of those medications.
“It’s about starting where they are,” Dr. Robblee said. “Some patients, despite having severe migraine, have built themselves up so they’re doing exercise three or four times per week, or every day, and I have other people who never exercise,” she said. “For those patients who are very sedentary, if I can get them to start with 5 minutes per week so they have that sense of accomplishment, then that’s where I start. Then slowly build it up over time. Like most things in the migraine world, I individualize it for the person.”
Dr. Bond offered the following specific tips to clinicians in educating and encouraging patients to increase physical activity:
- Educate patients regarding the short-and long-term benefits of moving more and sitting less, both for their migraines and for overall health.
- Correct misconceptions about the negative effects of physical activity as it relates to migraines.
- Personalize the rationale for physical activity to that patient’s specific values and personal goals.
- Encourage patients to use an activity tracker, both for tracking physical activity and sedentary time, and to monitor migraine attacks, stress, energy levels, and fatigue on days they do and do not exercise.
- Help patients set goals for eventually meeting MVPA recommendations and interrupting prolonged periods of sitting with brief movement breaks.
- Help patients identify rewards for meeting goals that are tied to the activity, such as new exercise clothing.
- Encourage patients to identify a consistent time for physical activity each day to establish a habit, “ideally in the morning before barriers and life get in the way,” he said.
Eventually, physical activity itself should become intrinsically rewarding, Dr. Bond said.
“To limit sitting and encourage more movement throughout the day, we want to make the choice to engage in physical activity easier by adding environmental cues that encourage physical activity,” he said. “Conversely, we want to make the choice to engage in sedentary behavior more difficult by increasing the amount of effort that is required to engage in these behaviors.”
Dr. Robblee found Dr. Bond’s emphasis on sitting less – distinct from moving more – a helpful frame to consider with her patients. “I really like the approach of looking at it from that approach: in addition to how do we get you up and moving, how much time are you sitting, and how often can you break that up into smaller increments so that you’re up more often?” Dr. Robblee said. “That sometimes sounds less scary than ‘let’s get you exercising.’ So ‘let’s get you sitting a little bit less.’ I think that is something I might start to adopt.”
No external funding was noted. Dr. Robblee is a principal investigator for a study sponsored by Eli Lilly and receives stipends for MedLink Neurology and Neurodiem. Dr. Bond reported no disclosures.
FROM AHS 2021
Ubrogepant effective for acute migraine even with preventive monoclonal antibody therapy
according to preliminary findings presented at the American Headache Society’s 2021 annual meeting.

“Because prevention [with mAbs] is rarely 100% effective, virtually everyone on preventive treatment needs to also take acute treatment,” presenter Richard B. Lipton, MD, a professor of neurology and director of the Montefiore Headache Center at Albert Einstein College of Medicine, New York, said in an interview after his presentation. He explained that ubrogepant, a small-molecule CGRP receptor blocker, is approved for acute treatment of migraine, while mAbs, which block the CGRP receptor or CGRP itself, are approved for prevention. “Many people predicted that gepants would not work in people on CGRP-targeted mAbs because of overlapping mechanisms.”
Dr. Lipton himself was not surprised by the findings, however. “For me, the surprise was that ubrogepant worked so well,” he said.
Novel data collection
Uniquely, his study used an entirely remote design with mobile applications to safely evaluate the drug’s real-world effectiveness in the midst of the COVID-19 pandemic. The prospective, observational study used the mobile app Migraine Buddy to collect data and assess outcomes from the use of 50 mg or 100 mg of ubrogepant along with a mAb, onabotA, or both.
In most migraine trials, researchers ask patients to track their symptoms in electronic diaries they learn how to use in the clinic.
“One disadvantage of this approach is that people usually need to carry two devices, the study device and their smartphone,” Dr. Lipton said in an interview. “In this study, people download an app at home to their smartphone and only need to carry one device. Though remote studies are particularly valuable in the time of pandemic, I believe that apps like Migraine Buddy are and will remain a valuable tool for addressing many research questions.”
Jennifer Robblee, MD, MSc, an assistant professor of neurology at Barrow Neurological Institute in Phoenix, viewed the presentation and was also impressed with the novel use of a smartphone app to conduct the study. “I think that was a unique and cool demonstration of what can be done with the apps out there now,” Dr. Robblee said in an interview. “If you want to have really good tracking and more through tracking, apps like this are fabulous and are very patient forward and patient friendly.”
Combination therapy
The researchers invited 4,541 adults to participate in the study if they had previously reported at least three migraine attacks in the past 30 days and if they had treated at least three prior attacks with ubrogepant. The 483 participants who enrolled after consent and screening included 272 taking ubrogepant with mAb, 132 participants taking ubrogepant with onabotA, and 79 taking ubrogepant with both onabotA and mAb.
For 30 days, participants reported in the app’s diary their pain relief and the time elapsed since taking ubrogepant until they returned to normal functioning. Endpoints included meaningful pain relief – defined as “a level of pain relief that is meaningful to you” – and return to normal function at 2 and 4 hours.
During the study, 352 participants reported treating a migraine attack with a single dose of ubrogepant, and 78 participants treated migraine with two doses. The former group included 193 patients in the ubrogepant plus mAb group, 102 patients in the ubrogepant plus onabotA group, and 57 patients in the ubrogepant plus both group. Because of the limited enrollment in the second two arms, the data Dr. Lipton presented data only on the ubrogepant with mAb arm.
Most of this group (89.1%) was female, with an average age of 40 years and an average Migraine Disability Assessment score of 72.2. Most of the patients were taking erenumab (44.6%) or galcanezumab (34.2%) with the remaining patients taking fremanezumab (17.6%), eptinezumab (3.1%) or multiple mAbs (0.5%). Most participants (59.6%) were prescribed 100-mg ubrogepant dose while the remaining participants took 50 mg.
The analysis of the ubrogepant plus mAb group revealed that 64.2% of patients reported meaningful pain relief at 2 hours, and 84.5% had meaningful pain relief 4 hours after taking ubrogepant. The odds of achieving meaningful pain relief were statistically significant at both time points and remained significant after adjustment for participants’ age, Migraine Disability Assessment score and self-reported prescribed ubrogepant dose (P < .001).
“This study shows that in patients with migraine on CGRP-targeted monoclonal antibodies, ubrogepant is an acute treatment to consider for breakthrough headaches,” Dr. Lipton said. He added that they have now completed the study with more participants and begun analyzing all three groups.
“Full analyses will include data from multiple attacks, attacks treated with a second dose of ubrogepant, additional daily and 30-day effectiveness measures for use of ubrogepant with onabotA and use of ubrogepant with both onabotA and CGRP mAbs,” Dr. Lipton said.
While the findings did not surprise Dr. Robblee, she was happy to see a study that explicitly testing the combination of these treatments, especially given access challenges. “Right now, because treatments are new, we get a lot of insurance denials,” Dr. Robblee said in an interview. “It’s great to have a study out there that we can turn to and say, ‘hey, look, they had all these patients safely using these together.’ It’s going to help us improve access for patients.”
Though Dr. Robblee typically uses old-school pen-and-calendar diaries with her patients, she also sees potential for the use of apps going forward, just as she sees for virtual health care.
“I’ve found telemedicine in general to be a really great addition to the migraine world, and this plays into our ability to use telemedicine paired with tracking,” Dr. Robblee said. “In so many studies, we’re doing a diary anyway, so if there are standard diaries and programs we’re all using, that would be a nice way to do these.”
She notes that most symptom tracking for pain is subjective already, and these apps often include the options to print out the data or to export or transfer it electronically to physicians. “It’s giving us meaningful data,” she said.
The research was funded by AbbVie. Dr. Lipton has received honoraria or research support from AbbVie, Amgen, Biohaven, Dr. Reddy’s Laboratories, electroCore, Eli Lilly, eNeura Therapeutics, GlaxoSmithKline, Merck, Novartis, Teva, Vector and Vedanta Research. He holds stock options in Biohaven and Ctrl M. Dr. Robblee is a principal investigator for a study sponsored by Eli Lilly and receives stipends for MedLink Neurology and Neurodiem.
according to preliminary findings presented at the American Headache Society’s 2021 annual meeting.
“Because prevention [with mAbs] is rarely 100% effective, virtually everyone on preventive treatment needs to also take acute treatment,” presenter Richard B. Lipton, MD, a professor of neurology and director of the Montefiore Headache Center at Albert Einstein College of Medicine, New York, said in an interview after his presentation. He explained that ubrogepant, a small-molecule CGRP receptor blocker, is approved for acute treatment of migraine, while mAbs, which block the CGRP receptor or CGRP itself, are approved for prevention. “Many people predicted that gepants would not work in people on CGRP-targeted mAbs because of overlapping mechanisms.”
Dr. Lipton himself was not surprised by the findings, however. “For me, the surprise was that ubrogepant worked so well,” he said.
Novel data collection
Uniquely, his study used an entirely remote design with mobile applications to safely evaluate the drug’s real-world effectiveness in the midst of the COVID-19 pandemic. The prospective, observational study used the mobile app Migraine Buddy to collect data and assess outcomes from the use of 50 mg or 100 mg of ubrogepant along with a mAb, onabotA, or both.
In most migraine trials, researchers ask patients to track their symptoms in electronic diaries they learn how to use in the clinic.
“One disadvantage of this approach is that people usually need to carry two devices, the study device and their smartphone,” Dr. Lipton said in an interview. “In this study, people download an app at home to their smartphone and only need to carry one device. Though remote studies are particularly valuable in the time of pandemic, I believe that apps like Migraine Buddy are and will remain a valuable tool for addressing many research questions.”
Jennifer Robblee, MD, MSc, an assistant professor of neurology at Barrow Neurological Institute in Phoenix, viewed the presentation and was also impressed with the novel use of a smartphone app to conduct the study. “I think that was a unique and cool demonstration of what can be done with the apps out there now,” Dr. Robblee said in an interview. “If you want to have really good tracking and more through tracking, apps like this are fabulous and are very patient forward and patient friendly.”
Combination therapy
The researchers invited 4,541 adults to participate in the study if they had previously reported at least three migraine attacks in the past 30 days and if they had treated at least three prior attacks with ubrogepant. The 483 participants who enrolled after consent and screening included 272 taking ubrogepant with mAb, 132 participants taking ubrogepant with onabotA, and 79 taking ubrogepant with both onabotA and mAb.
For 30 days, participants reported in the app’s diary their pain relief and the time elapsed since taking ubrogepant until they returned to normal functioning. Endpoints included meaningful pain relief – defined as “a level of pain relief that is meaningful to you” – and return to normal function at 2 and 4 hours.
During the study, 352 participants reported treating a migraine attack with a single dose of ubrogepant, and 78 participants treated migraine with two doses. The former group included 193 patients in the ubrogepant plus mAb group, 102 patients in the ubrogepant plus onabotA group, and 57 patients in the ubrogepant plus both group. Because of the limited enrollment in the second two arms, the data Dr. Lipton presented data only on the ubrogepant with mAb arm.
Most of this group (89.1%) was female, with an average age of 40 years and an average Migraine Disability Assessment score of 72.2. Most of the patients were taking erenumab (44.6%) or galcanezumab (34.2%) with the remaining patients taking fremanezumab (17.6%), eptinezumab (3.1%) or multiple mAbs (0.5%). Most participants (59.6%) were prescribed 100-mg ubrogepant dose while the remaining participants took 50 mg.
The analysis of the ubrogepant plus mAb group revealed that 64.2% of patients reported meaningful pain relief at 2 hours, and 84.5% had meaningful pain relief 4 hours after taking ubrogepant. The odds of achieving meaningful pain relief were statistically significant at both time points and remained significant after adjustment for participants’ age, Migraine Disability Assessment score and self-reported prescribed ubrogepant dose (P < .001).
“This study shows that in patients with migraine on CGRP-targeted monoclonal antibodies, ubrogepant is an acute treatment to consider for breakthrough headaches,” Dr. Lipton said. He added that they have now completed the study with more participants and begun analyzing all three groups.
“Full analyses will include data from multiple attacks, attacks treated with a second dose of ubrogepant, additional daily and 30-day effectiveness measures for use of ubrogepant with onabotA and use of ubrogepant with both onabotA and CGRP mAbs,” Dr. Lipton said.
While the findings did not surprise Dr. Robblee, she was happy to see a study that explicitly testing the combination of these treatments, especially given access challenges. “Right now, because treatments are new, we get a lot of insurance denials,” Dr. Robblee said in an interview. “It’s great to have a study out there that we can turn to and say, ‘hey, look, they had all these patients safely using these together.’ It’s going to help us improve access for patients.”
Though Dr. Robblee typically uses old-school pen-and-calendar diaries with her patients, she also sees potential for the use of apps going forward, just as she sees for virtual health care.
“I’ve found telemedicine in general to be a really great addition to the migraine world, and this plays into our ability to use telemedicine paired with tracking,” Dr. Robblee said. “In so many studies, we’re doing a diary anyway, so if there are standard diaries and programs we’re all using, that would be a nice way to do these.”
She notes that most symptom tracking for pain is subjective already, and these apps often include the options to print out the data or to export or transfer it electronically to physicians. “It’s giving us meaningful data,” she said.
The research was funded by AbbVie. Dr. Lipton has received honoraria or research support from AbbVie, Amgen, Biohaven, Dr. Reddy’s Laboratories, electroCore, Eli Lilly, eNeura Therapeutics, GlaxoSmithKline, Merck, Novartis, Teva, Vector and Vedanta Research. He holds stock options in Biohaven and Ctrl M. Dr. Robblee is a principal investigator for a study sponsored by Eli Lilly and receives stipends for MedLink Neurology and Neurodiem.
according to preliminary findings presented at the American Headache Society’s 2021 annual meeting.
“Because prevention [with mAbs] is rarely 100% effective, virtually everyone on preventive treatment needs to also take acute treatment,” presenter Richard B. Lipton, MD, a professor of neurology and director of the Montefiore Headache Center at Albert Einstein College of Medicine, New York, said in an interview after his presentation. He explained that ubrogepant, a small-molecule CGRP receptor blocker, is approved for acute treatment of migraine, while mAbs, which block the CGRP receptor or CGRP itself, are approved for prevention. “Many people predicted that gepants would not work in people on CGRP-targeted mAbs because of overlapping mechanisms.”
Dr. Lipton himself was not surprised by the findings, however. “For me, the surprise was that ubrogepant worked so well,” he said.
Novel data collection
Uniquely, his study used an entirely remote design with mobile applications to safely evaluate the drug’s real-world effectiveness in the midst of the COVID-19 pandemic. The prospective, observational study used the mobile app Migraine Buddy to collect data and assess outcomes from the use of 50 mg or 100 mg of ubrogepant along with a mAb, onabotA, or both.
In most migraine trials, researchers ask patients to track their symptoms in electronic diaries they learn how to use in the clinic.
“One disadvantage of this approach is that people usually need to carry two devices, the study device and their smartphone,” Dr. Lipton said in an interview. “In this study, people download an app at home to their smartphone and only need to carry one device. Though remote studies are particularly valuable in the time of pandemic, I believe that apps like Migraine Buddy are and will remain a valuable tool for addressing many research questions.”
Jennifer Robblee, MD, MSc, an assistant professor of neurology at Barrow Neurological Institute in Phoenix, viewed the presentation and was also impressed with the novel use of a smartphone app to conduct the study. “I think that was a unique and cool demonstration of what can be done with the apps out there now,” Dr. Robblee said in an interview. “If you want to have really good tracking and more through tracking, apps like this are fabulous and are very patient forward and patient friendly.”
Combination therapy
The researchers invited 4,541 adults to participate in the study if they had previously reported at least three migraine attacks in the past 30 days and if they had treated at least three prior attacks with ubrogepant. The 483 participants who enrolled after consent and screening included 272 taking ubrogepant with mAb, 132 participants taking ubrogepant with onabotA, and 79 taking ubrogepant with both onabotA and mAb.
For 30 days, participants reported in the app’s diary their pain relief and the time elapsed since taking ubrogepant until they returned to normal functioning. Endpoints included meaningful pain relief – defined as “a level of pain relief that is meaningful to you” – and return to normal function at 2 and 4 hours.
During the study, 352 participants reported treating a migraine attack with a single dose of ubrogepant, and 78 participants treated migraine with two doses. The former group included 193 patients in the ubrogepant plus mAb group, 102 patients in the ubrogepant plus onabotA group, and 57 patients in the ubrogepant plus both group. Because of the limited enrollment in the second two arms, the data Dr. Lipton presented data only on the ubrogepant with mAb arm.
Most of this group (89.1%) was female, with an average age of 40 years and an average Migraine Disability Assessment score of 72.2. Most of the patients were taking erenumab (44.6%) or galcanezumab (34.2%) with the remaining patients taking fremanezumab (17.6%), eptinezumab (3.1%) or multiple mAbs (0.5%). Most participants (59.6%) were prescribed 100-mg ubrogepant dose while the remaining participants took 50 mg.
The analysis of the ubrogepant plus mAb group revealed that 64.2% of patients reported meaningful pain relief at 2 hours, and 84.5% had meaningful pain relief 4 hours after taking ubrogepant. The odds of achieving meaningful pain relief were statistically significant at both time points and remained significant after adjustment for participants’ age, Migraine Disability Assessment score and self-reported prescribed ubrogepant dose (P < .001).
“This study shows that in patients with migraine on CGRP-targeted monoclonal antibodies, ubrogepant is an acute treatment to consider for breakthrough headaches,” Dr. Lipton said. He added that they have now completed the study with more participants and begun analyzing all three groups.
“Full analyses will include data from multiple attacks, attacks treated with a second dose of ubrogepant, additional daily and 30-day effectiveness measures for use of ubrogepant with onabotA and use of ubrogepant with both onabotA and CGRP mAbs,” Dr. Lipton said.
While the findings did not surprise Dr. Robblee, she was happy to see a study that explicitly testing the combination of these treatments, especially given access challenges. “Right now, because treatments are new, we get a lot of insurance denials,” Dr. Robblee said in an interview. “It’s great to have a study out there that we can turn to and say, ‘hey, look, they had all these patients safely using these together.’ It’s going to help us improve access for patients.”
Though Dr. Robblee typically uses old-school pen-and-calendar diaries with her patients, she also sees potential for the use of apps going forward, just as she sees for virtual health care.
“I’ve found telemedicine in general to be a really great addition to the migraine world, and this plays into our ability to use telemedicine paired with tracking,” Dr. Robblee said. “In so many studies, we’re doing a diary anyway, so if there are standard diaries and programs we’re all using, that would be a nice way to do these.”
She notes that most symptom tracking for pain is subjective already, and these apps often include the options to print out the data or to export or transfer it electronically to physicians. “It’s giving us meaningful data,” she said.
The research was funded by AbbVie. Dr. Lipton has received honoraria or research support from AbbVie, Amgen, Biohaven, Dr. Reddy’s Laboratories, electroCore, Eli Lilly, eNeura Therapeutics, GlaxoSmithKline, Merck, Novartis, Teva, Vector and Vedanta Research. He holds stock options in Biohaven and Ctrl M. Dr. Robblee is a principal investigator for a study sponsored by Eli Lilly and receives stipends for MedLink Neurology and Neurodiem.
FROM AHS 2021
Migraine linked to more COVID-19 infections, symptoms but less health care utilization
, according to a study presented at the American Headache Society’s 2021 annual meeting.

“These data suggest that people with migraine are either more susceptible to contracting COVID-19, or that they may be more sensitive to the development of symptoms once COVID-19 has been contracted, or both,” Robert Shapiro, MD, PhD, professor of neurological science at the University of Vermont, Burlington. “Further, once COVID-19 has been contracted, people with migraine may be less likely to develop serious COVID-19 outcomes, or they may be less likely to seek health care for COVID-19, or both.”
In providing background information, Dr. Shapiro noted previous research showing that headache is associated with a positive prognosis in COVID-19 inpatients, including lower IL-6 levels throughout the disease course, a 1-week shorter disease course, and a 2.2 times greater relative risk of survival.
Yet in a study across 171 countries, a higher population prevalence of migraine is associated with higher COVID-19 mortality rates. It’s unclear what conclusions can be drawn from that association, however, said Deborah I. Friedman, MD, MPH, professor of neurology and ophthalmology at University of Texas, Dallas, who was not involved in the research.
Dr. Shapiro suggested a theoretical possibility, noting that two genes linked to migraine susceptibility – SCN1A and IFNAR2 – are among 15 host loci also associated with COVID-19 outcomes. Further, Dr. Shapiro noted in his background information, COVID-19 is linked to lower serum calcitonin gene-related peptide levels.
For the study, Dr. Shapiro and colleagues analyzed data from U.S. adults who responded to the National Health and Wellness Survey from April to July 2020. The researchers limited their analysis to the 41,155 participants who had not received the flu vaccine in 2020 since previous research has suggested reduced morbidity among those with COVID-19 who had been vaccinated against the flu. In this group, 4,550 participants had ever been diagnosed by a doctor with migraine (11%) and 36,605 participants had not (89%).
The majority of those with a history of migraine were female (78%), compared with the overall sample (50% female), and tended to be younger, with an average age of 39 compared with 45 for those without migraine (P < .001).
Among those with a previous migraine diagnosis, 3.8% self-reported having had a COVID-19 infection, compared with infection in 2.4% of those without a history of migraine (P < .001). That translated to a 58% increased risk of COVID-19 infection in those with migraine history, with a similar rate of test positivity in both groups (33.7% with migraine history vs. 34.5% without). Test negativity was also similar in both groups (15.9% vs. 17.8%).
Of 360 respondents who had tested positive for COVID-19, the 60 with a history of migraine reported more frequent symptoms than those without migraine. The increased frequency was statistically significant (P < .001 unless otherwise indicated) for the following symptoms:
- Difficulty breathing or shortness of breath (P = .005).
- Fever.
- Headache, sore throat, and/or congestion.
- Fatigue.
- Loss of smell and taste.
- Chills and body aches.
- Persistent pain or pressure in the chest.
- Confusion or inability to arouse.
- Digestive issues (P = .005).
- Bluish lips or face.
For several of these symptoms – such as headache/sore throat/congestion, persistent pain or pressure in the chest, confusion/inability to arouse, and digestive issues – more than twice as many respondents with migraine reported the symptom, vs. those without migraine.
Changes in health care utilization
“I think that people with migraine are aware of their bodies and aware of their symptoms more than the average person,” Dr. Friedman said. Yet those with migraine were less likely to use health care while diagnosed with COVID-19 than were those without migraine. Migraine sufferers with a COVID-19 infection were 1.2 times more likely to visit a health care provider than were those without an infection, but the similar relative risk was 1.35 greater for those with COVID-19 infections and no migraines.
Similarly, those with a migraine history were more than twice as likely to visit the emergency department when they had a COVID-19 vaccine infection than were those without an infection (RR = 2.6), but among those without a history of migraine, respondents were nearly five times more likely to visit the emergency department when they had a COVID-19 infection than when they didn’t (RR = 4.9).
Dr. Friedman suggested that the lower utilization rate may have to do with the nature of migraine itself. “There are people with migraine who go to the emergency room all the time, but then there’s most of the people with migraine, who would rather die than go to the emergency room because with the light and the noise, it’s just a horrible place to be if you have migraine,” Dr. Friedman said. “I think the majority of people would prefer not to go to the emergency room if given the choice.”
Increased likelihood of hospitalization among those with migraine and a COVID-19 infection was 4.6 compared with those with a migraine and no infection; the corresponding hospitalization risk for COVID-19 among those without migraine was 7.6 times greater than for those with no infection. All these risk ratios were statistically significant.
Dr. Shapiro then speculated on what it might mean that headache is a positive prognostic indicator for COVID-19 inpatients and that migraine population prevalence is linked to higher COVID-19 mortality.
“A hypothesis emerges that headache as a symptom, and migraine as a disease, may reflect adaptive processes associated with host defenses against viruses,” Dr. Shapiro said. “For example, migraine-driven behaviors, such as social distancing due to photophobia, in the setting of viral illness may play adaptive roles in reducing viral spread.”
The researchers did not receive external funding. Dr. Shapiro has consulted for Eli Lilly and Lundbeck. Dr. Friedman reports grant support and/or advisory board participation for Allergan, Biohaven Pharmaceuticals, Eli Lilly, Impel NeuroPharma, Invex, Lundbeck, Merck, Revance Therapeutics, Satsuma Pharmaceuticals, Teva Pharmaceuticals, Theranica, and Zosano Pharma.
, according to a study presented at the American Headache Society’s 2021 annual meeting.
“These data suggest that people with migraine are either more susceptible to contracting COVID-19, or that they may be more sensitive to the development of symptoms once COVID-19 has been contracted, or both,” Robert Shapiro, MD, PhD, professor of neurological science at the University of Vermont, Burlington. “Further, once COVID-19 has been contracted, people with migraine may be less likely to develop serious COVID-19 outcomes, or they may be less likely to seek health care for COVID-19, or both.”
In providing background information, Dr. Shapiro noted previous research showing that headache is associated with a positive prognosis in COVID-19 inpatients, including lower IL-6 levels throughout the disease course, a 1-week shorter disease course, and a 2.2 times greater relative risk of survival.
Yet in a study across 171 countries, a higher population prevalence of migraine is associated with higher COVID-19 mortality rates. It’s unclear what conclusions can be drawn from that association, however, said Deborah I. Friedman, MD, MPH, professor of neurology and ophthalmology at University of Texas, Dallas, who was not involved in the research.
Dr. Shapiro suggested a theoretical possibility, noting that two genes linked to migraine susceptibility – SCN1A and IFNAR2 – are among 15 host loci also associated with COVID-19 outcomes. Further, Dr. Shapiro noted in his background information, COVID-19 is linked to lower serum calcitonin gene-related peptide levels.
For the study, Dr. Shapiro and colleagues analyzed data from U.S. adults who responded to the National Health and Wellness Survey from April to July 2020. The researchers limited their analysis to the 41,155 participants who had not received the flu vaccine in 2020 since previous research has suggested reduced morbidity among those with COVID-19 who had been vaccinated against the flu. In this group, 4,550 participants had ever been diagnosed by a doctor with migraine (11%) and 36,605 participants had not (89%).
The majority of those with a history of migraine were female (78%), compared with the overall sample (50% female), and tended to be younger, with an average age of 39 compared with 45 for those without migraine (P < .001).
Among those with a previous migraine diagnosis, 3.8% self-reported having had a COVID-19 infection, compared with infection in 2.4% of those without a history of migraine (P < .001). That translated to a 58% increased risk of COVID-19 infection in those with migraine history, with a similar rate of test positivity in both groups (33.7% with migraine history vs. 34.5% without). Test negativity was also similar in both groups (15.9% vs. 17.8%).
Of 360 respondents who had tested positive for COVID-19, the 60 with a history of migraine reported more frequent symptoms than those without migraine. The increased frequency was statistically significant (P < .001 unless otherwise indicated) for the following symptoms:
- Difficulty breathing or shortness of breath (P = .005).
- Fever.
- Headache, sore throat, and/or congestion.
- Fatigue.
- Loss of smell and taste.
- Chills and body aches.
- Persistent pain or pressure in the chest.
- Confusion or inability to arouse.
- Digestive issues (P = .005).
- Bluish lips or face.
For several of these symptoms – such as headache/sore throat/congestion, persistent pain or pressure in the chest, confusion/inability to arouse, and digestive issues – more than twice as many respondents with migraine reported the symptom, vs. those without migraine.
Changes in health care utilization
“I think that people with migraine are aware of their bodies and aware of their symptoms more than the average person,” Dr. Friedman said. Yet those with migraine were less likely to use health care while diagnosed with COVID-19 than were those without migraine. Migraine sufferers with a COVID-19 infection were 1.2 times more likely to visit a health care provider than were those without an infection, but the similar relative risk was 1.35 greater for those with COVID-19 infections and no migraines.
Similarly, those with a migraine history were more than twice as likely to visit the emergency department when they had a COVID-19 vaccine infection than were those without an infection (RR = 2.6), but among those without a history of migraine, respondents were nearly five times more likely to visit the emergency department when they had a COVID-19 infection than when they didn’t (RR = 4.9).
Dr. Friedman suggested that the lower utilization rate may have to do with the nature of migraine itself. “There are people with migraine who go to the emergency room all the time, but then there’s most of the people with migraine, who would rather die than go to the emergency room because with the light and the noise, it’s just a horrible place to be if you have migraine,” Dr. Friedman said. “I think the majority of people would prefer not to go to the emergency room if given the choice.”
Increased likelihood of hospitalization among those with migraine and a COVID-19 infection was 4.6 compared with those with a migraine and no infection; the corresponding hospitalization risk for COVID-19 among those without migraine was 7.6 times greater than for those with no infection. All these risk ratios were statistically significant.
Dr. Shapiro then speculated on what it might mean that headache is a positive prognostic indicator for COVID-19 inpatients and that migraine population prevalence is linked to higher COVID-19 mortality.
“A hypothesis emerges that headache as a symptom, and migraine as a disease, may reflect adaptive processes associated with host defenses against viruses,” Dr. Shapiro said. “For example, migraine-driven behaviors, such as social distancing due to photophobia, in the setting of viral illness may play adaptive roles in reducing viral spread.”
The researchers did not receive external funding. Dr. Shapiro has consulted for Eli Lilly and Lundbeck. Dr. Friedman reports grant support and/or advisory board participation for Allergan, Biohaven Pharmaceuticals, Eli Lilly, Impel NeuroPharma, Invex, Lundbeck, Merck, Revance Therapeutics, Satsuma Pharmaceuticals, Teva Pharmaceuticals, Theranica, and Zosano Pharma.
, according to a study presented at the American Headache Society’s 2021 annual meeting.
“These data suggest that people with migraine are either more susceptible to contracting COVID-19, or that they may be more sensitive to the development of symptoms once COVID-19 has been contracted, or both,” Robert Shapiro, MD, PhD, professor of neurological science at the University of Vermont, Burlington. “Further, once COVID-19 has been contracted, people with migraine may be less likely to develop serious COVID-19 outcomes, or they may be less likely to seek health care for COVID-19, or both.”
In providing background information, Dr. Shapiro noted previous research showing that headache is associated with a positive prognosis in COVID-19 inpatients, including lower IL-6 levels throughout the disease course, a 1-week shorter disease course, and a 2.2 times greater relative risk of survival.
Yet in a study across 171 countries, a higher population prevalence of migraine is associated with higher COVID-19 mortality rates. It’s unclear what conclusions can be drawn from that association, however, said Deborah I. Friedman, MD, MPH, professor of neurology and ophthalmology at University of Texas, Dallas, who was not involved in the research.
Dr. Shapiro suggested a theoretical possibility, noting that two genes linked to migraine susceptibility – SCN1A and IFNAR2 – are among 15 host loci also associated with COVID-19 outcomes. Further, Dr. Shapiro noted in his background information, COVID-19 is linked to lower serum calcitonin gene-related peptide levels.
For the study, Dr. Shapiro and colleagues analyzed data from U.S. adults who responded to the National Health and Wellness Survey from April to July 2020. The researchers limited their analysis to the 41,155 participants who had not received the flu vaccine in 2020 since previous research has suggested reduced morbidity among those with COVID-19 who had been vaccinated against the flu. In this group, 4,550 participants had ever been diagnosed by a doctor with migraine (11%) and 36,605 participants had not (89%).
The majority of those with a history of migraine were female (78%), compared with the overall sample (50% female), and tended to be younger, with an average age of 39 compared with 45 for those without migraine (P < .001).
Among those with a previous migraine diagnosis, 3.8% self-reported having had a COVID-19 infection, compared with infection in 2.4% of those without a history of migraine (P < .001). That translated to a 58% increased risk of COVID-19 infection in those with migraine history, with a similar rate of test positivity in both groups (33.7% with migraine history vs. 34.5% without). Test negativity was also similar in both groups (15.9% vs. 17.8%).
Of 360 respondents who had tested positive for COVID-19, the 60 with a history of migraine reported more frequent symptoms than those without migraine. The increased frequency was statistically significant (P < .001 unless otherwise indicated) for the following symptoms:
- Difficulty breathing or shortness of breath (P = .005).
- Fever.
- Headache, sore throat, and/or congestion.
- Fatigue.
- Loss of smell and taste.
- Chills and body aches.
- Persistent pain or pressure in the chest.
- Confusion or inability to arouse.
- Digestive issues (P = .005).
- Bluish lips or face.
For several of these symptoms – such as headache/sore throat/congestion, persistent pain or pressure in the chest, confusion/inability to arouse, and digestive issues – more than twice as many respondents with migraine reported the symptom, vs. those without migraine.
Changes in health care utilization
“I think that people with migraine are aware of their bodies and aware of their symptoms more than the average person,” Dr. Friedman said. Yet those with migraine were less likely to use health care while diagnosed with COVID-19 than were those without migraine. Migraine sufferers with a COVID-19 infection were 1.2 times more likely to visit a health care provider than were those without an infection, but the similar relative risk was 1.35 greater for those with COVID-19 infections and no migraines.
Similarly, those with a migraine history were more than twice as likely to visit the emergency department when they had a COVID-19 vaccine infection than were those without an infection (RR = 2.6), but among those without a history of migraine, respondents were nearly five times more likely to visit the emergency department when they had a COVID-19 infection than when they didn’t (RR = 4.9).
Dr. Friedman suggested that the lower utilization rate may have to do with the nature of migraine itself. “There are people with migraine who go to the emergency room all the time, but then there’s most of the people with migraine, who would rather die than go to the emergency room because with the light and the noise, it’s just a horrible place to be if you have migraine,” Dr. Friedman said. “I think the majority of people would prefer not to go to the emergency room if given the choice.”
Increased likelihood of hospitalization among those with migraine and a COVID-19 infection was 4.6 compared with those with a migraine and no infection; the corresponding hospitalization risk for COVID-19 among those without migraine was 7.6 times greater than for those with no infection. All these risk ratios were statistically significant.
Dr. Shapiro then speculated on what it might mean that headache is a positive prognostic indicator for COVID-19 inpatients and that migraine population prevalence is linked to higher COVID-19 mortality.
“A hypothesis emerges that headache as a symptom, and migraine as a disease, may reflect adaptive processes associated with host defenses against viruses,” Dr. Shapiro said. “For example, migraine-driven behaviors, such as social distancing due to photophobia, in the setting of viral illness may play adaptive roles in reducing viral spread.”
The researchers did not receive external funding. Dr. Shapiro has consulted for Eli Lilly and Lundbeck. Dr. Friedman reports grant support and/or advisory board participation for Allergan, Biohaven Pharmaceuticals, Eli Lilly, Impel NeuroPharma, Invex, Lundbeck, Merck, Revance Therapeutics, Satsuma Pharmaceuticals, Teva Pharmaceuticals, Theranica, and Zosano Pharma.
FROM AHS 2021

Chronic headache pain in veterans linked to suicide attempts
, according to findings presented at the American Headache Society’s 2021 annual meeting. Risk rose even more in those with chronic headache pain and a comorbid traumatic brain injury (TBI).
“In addition, as expected, veterans with psychiatric conditions have increased risk of suicide attempt with the exception of anxiety in men and dependent personality in women,” said X. Michelle Androulakis, MD, associate professor of neurology at the University of South Carolina, Columbia.
‘Surprising’ findings
“These findings are eye-opening but not surprising since we know that veterans in general and people with chronic pain are at higher risk for suicidal behaviors compared with their civilian counterparts,” said Amy. S Grinberg, PhD, a clinical health psychologist who practices in New Rochelle, N.Y. Dr. Grinberg, who also works at VA Connecticut Healthcare System, was not involved in the study.
“It is, however, very interesting that suicidal attempts are higher in veterans with chronic headache compared with other chronic pain disorders, such as chronic neck and back pain,” Dr Grinberg said. “This really highlights the impact of living with a chronic headache disorder, and emphasizes the continued efforts that should be put into place to support veterans with chronic headache, including improved access to a range of treatment options and continued funding for future research.”
Veterans with chronic pain
The researchers retrospectively analyzed Veterans Health Administration electronic health records of 3,252,704 veterans, predominantly male and White, who had been diagnosed with any type of chronic pain from 2000 to 2010.
The researchers looked at overall headache diagnoses instead of specific diagnoses, such as migraine, cluster headache, or posttraumatic headache, since specific headache disorders are frequently underdiagnosed.
The population included 14.7% of patients with chronic headache, 14.9% with chronic neck pain, 59.2% with chronic back pain, and 60.2% with other types of chronic pain, including arthritis, fibromyalgia, joint pain, and reflex sympathetic dystrophy.
Traumatic brain injury occurred in 11.2% of those with chronic headaches, compared with 6.8% of those with chronic back pain, 8.5% of those with chronic neck pain, and 5.9% of those with other chronic pain.
More than half (56.4%) of those with chronic headache had depression, the most common comorbidity in the group, followed by 31.5% who had posttraumatic stress disorder (PTSD), and 21.8% who had adjustment disorder. Other rates of psychiatric disorders were all below 10%. Prevalence of depression occurred in 44.5% of those with back pain, 52.4% of those with neck pain, and 39% of those with other chronic pain. PTSD rates were also lower in those with back (22%), neck (27.2%), or other chronic pain (18.6%).
“Interestingly, this study found that those veterans with a history of traumatic brain injury and psychiatric comorbidities, such as depression, are at greater risk for suicide attempts,” said Dr. Grinberg. “The good news is that these are modifiable risk factors, and evidence-based treatments for depression, PTSD, and headache, for example, are widely disseminated within the VA.”
The majority of headache diagnoses were not otherwise specified (80.1%). Half (50.2%) were migraine headaches while rates were much lower for tension-type headache (8.8%), trigeminal neuralgia (5%), cluster headache (0.8%), and posttraumatic headache (0.7%).
The highest incidence of suicide attempts occurred among those with chronic headaches, ranging from 329 to 396 per 100,000, aside from a peak of 482 per 100,000 in 2005. Suicide attempts peaked among all patients with chronic pain in 2005, “likely related to the deployment and policy changes in the Veterans Health Administration,” Dr. Androulakis said.
Those with neck pain had the next highest rate of suicide attempts, ranging from 263 to 314 per 100,000, excluding the peak of 398 per 100,000 in 2005.
Male veterans with chronic headaches had a 1.5 times greater likelihood of a suicide attempt than did those with back or neck pain (relative risk [RR] = 1.5), which increased to a relative risk of 2.8 greater for those with concurrent TBI. Among female veterans, chronic headache was associated with a 1.6 times greater risk of a suicide attempt, which rose to 2.15 times greater with concurrent TBI.
“Knowing that veterans with chronic headache disorders have an elevated rate of suicide, it is imperative that doctors and other clinical providers continue to conduct in-depth risk assessments and implement strategies to support those veterans who are at risk,” said Dr. Grinberg. “Clinical providers should continue in their efforts to reduce stigma associated with headache disorders and mental health treatment in order to effectively engage veterans in evidence-based treatments that are likely a step towards reducing symptoms and suicidal attempts.”
No external funding was noted. Dr. Androulakis and Dr. Grinberg had no disclosures.
, according to findings presented at the American Headache Society’s 2021 annual meeting. Risk rose even more in those with chronic headache pain and a comorbid traumatic brain injury (TBI).
“In addition, as expected, veterans with psychiatric conditions have increased risk of suicide attempt with the exception of anxiety in men and dependent personality in women,” said X. Michelle Androulakis, MD, associate professor of neurology at the University of South Carolina, Columbia.
‘Surprising’ findings
“These findings are eye-opening but not surprising since we know that veterans in general and people with chronic pain are at higher risk for suicidal behaviors compared with their civilian counterparts,” said Amy. S Grinberg, PhD, a clinical health psychologist who practices in New Rochelle, N.Y. Dr. Grinberg, who also works at VA Connecticut Healthcare System, was not involved in the study.
“It is, however, very interesting that suicidal attempts are higher in veterans with chronic headache compared with other chronic pain disorders, such as chronic neck and back pain,” Dr Grinberg said. “This really highlights the impact of living with a chronic headache disorder, and emphasizes the continued efforts that should be put into place to support veterans with chronic headache, including improved access to a range of treatment options and continued funding for future research.”
Veterans with chronic pain
The researchers retrospectively analyzed Veterans Health Administration electronic health records of 3,252,704 veterans, predominantly male and White, who had been diagnosed with any type of chronic pain from 2000 to 2010.
The researchers looked at overall headache diagnoses instead of specific diagnoses, such as migraine, cluster headache, or posttraumatic headache, since specific headache disorders are frequently underdiagnosed.
The population included 14.7% of patients with chronic headache, 14.9% with chronic neck pain, 59.2% with chronic back pain, and 60.2% with other types of chronic pain, including arthritis, fibromyalgia, joint pain, and reflex sympathetic dystrophy.
Traumatic brain injury occurred in 11.2% of those with chronic headaches, compared with 6.8% of those with chronic back pain, 8.5% of those with chronic neck pain, and 5.9% of those with other chronic pain.
More than half (56.4%) of those with chronic headache had depression, the most common comorbidity in the group, followed by 31.5% who had posttraumatic stress disorder (PTSD), and 21.8% who had adjustment disorder. Other rates of psychiatric disorders were all below 10%. Prevalence of depression occurred in 44.5% of those with back pain, 52.4% of those with neck pain, and 39% of those with other chronic pain. PTSD rates were also lower in those with back (22%), neck (27.2%), or other chronic pain (18.6%).
“Interestingly, this study found that those veterans with a history of traumatic brain injury and psychiatric comorbidities, such as depression, are at greater risk for suicide attempts,” said Dr. Grinberg. “The good news is that these are modifiable risk factors, and evidence-based treatments for depression, PTSD, and headache, for example, are widely disseminated within the VA.”
The majority of headache diagnoses were not otherwise specified (80.1%). Half (50.2%) were migraine headaches while rates were much lower for tension-type headache (8.8%), trigeminal neuralgia (5%), cluster headache (0.8%), and posttraumatic headache (0.7%).
The highest incidence of suicide attempts occurred among those with chronic headaches, ranging from 329 to 396 per 100,000, aside from a peak of 482 per 100,000 in 2005. Suicide attempts peaked among all patients with chronic pain in 2005, “likely related to the deployment and policy changes in the Veterans Health Administration,” Dr. Androulakis said.
Those with neck pain had the next highest rate of suicide attempts, ranging from 263 to 314 per 100,000, excluding the peak of 398 per 100,000 in 2005.
Male veterans with chronic headaches had a 1.5 times greater likelihood of a suicide attempt than did those with back or neck pain (relative risk [RR] = 1.5), which increased to a relative risk of 2.8 greater for those with concurrent TBI. Among female veterans, chronic headache was associated with a 1.6 times greater risk of a suicide attempt, which rose to 2.15 times greater with concurrent TBI.
“Knowing that veterans with chronic headache disorders have an elevated rate of suicide, it is imperative that doctors and other clinical providers continue to conduct in-depth risk assessments and implement strategies to support those veterans who are at risk,” said Dr. Grinberg. “Clinical providers should continue in their efforts to reduce stigma associated with headache disorders and mental health treatment in order to effectively engage veterans in evidence-based treatments that are likely a step towards reducing symptoms and suicidal attempts.”
No external funding was noted. Dr. Androulakis and Dr. Grinberg had no disclosures.
, according to findings presented at the American Headache Society’s 2021 annual meeting. Risk rose even more in those with chronic headache pain and a comorbid traumatic brain injury (TBI).
“In addition, as expected, veterans with psychiatric conditions have increased risk of suicide attempt with the exception of anxiety in men and dependent personality in women,” said X. Michelle Androulakis, MD, associate professor of neurology at the University of South Carolina, Columbia.
‘Surprising’ findings
“These findings are eye-opening but not surprising since we know that veterans in general and people with chronic pain are at higher risk for suicidal behaviors compared with their civilian counterparts,” said Amy. S Grinberg, PhD, a clinical health psychologist who practices in New Rochelle, N.Y. Dr. Grinberg, who also works at VA Connecticut Healthcare System, was not involved in the study.
“It is, however, very interesting that suicidal attempts are higher in veterans with chronic headache compared with other chronic pain disorders, such as chronic neck and back pain,” Dr Grinberg said. “This really highlights the impact of living with a chronic headache disorder, and emphasizes the continued efforts that should be put into place to support veterans with chronic headache, including improved access to a range of treatment options and continued funding for future research.”
Veterans with chronic pain
The researchers retrospectively analyzed Veterans Health Administration electronic health records of 3,252,704 veterans, predominantly male and White, who had been diagnosed with any type of chronic pain from 2000 to 2010.
The researchers looked at overall headache diagnoses instead of specific diagnoses, such as migraine, cluster headache, or posttraumatic headache, since specific headache disorders are frequently underdiagnosed.
The population included 14.7% of patients with chronic headache, 14.9% with chronic neck pain, 59.2% with chronic back pain, and 60.2% with other types of chronic pain, including arthritis, fibromyalgia, joint pain, and reflex sympathetic dystrophy.
Traumatic brain injury occurred in 11.2% of those with chronic headaches, compared with 6.8% of those with chronic back pain, 8.5% of those with chronic neck pain, and 5.9% of those with other chronic pain.
More than half (56.4%) of those with chronic headache had depression, the most common comorbidity in the group, followed by 31.5% who had posttraumatic stress disorder (PTSD), and 21.8% who had adjustment disorder. Other rates of psychiatric disorders were all below 10%. Prevalence of depression occurred in 44.5% of those with back pain, 52.4% of those with neck pain, and 39% of those with other chronic pain. PTSD rates were also lower in those with back (22%), neck (27.2%), or other chronic pain (18.6%).
“Interestingly, this study found that those veterans with a history of traumatic brain injury and psychiatric comorbidities, such as depression, are at greater risk for suicide attempts,” said Dr. Grinberg. “The good news is that these are modifiable risk factors, and evidence-based treatments for depression, PTSD, and headache, for example, are widely disseminated within the VA.”
The majority of headache diagnoses were not otherwise specified (80.1%). Half (50.2%) were migraine headaches while rates were much lower for tension-type headache (8.8%), trigeminal neuralgia (5%), cluster headache (0.8%), and posttraumatic headache (0.7%).
The highest incidence of suicide attempts occurred among those with chronic headaches, ranging from 329 to 396 per 100,000, aside from a peak of 482 per 100,000 in 2005. Suicide attempts peaked among all patients with chronic pain in 2005, “likely related to the deployment and policy changes in the Veterans Health Administration,” Dr. Androulakis said.
Those with neck pain had the next highest rate of suicide attempts, ranging from 263 to 314 per 100,000, excluding the peak of 398 per 100,000 in 2005.
Male veterans with chronic headaches had a 1.5 times greater likelihood of a suicide attempt than did those with back or neck pain (relative risk [RR] = 1.5), which increased to a relative risk of 2.8 greater for those with concurrent TBI. Among female veterans, chronic headache was associated with a 1.6 times greater risk of a suicide attempt, which rose to 2.15 times greater with concurrent TBI.
“Knowing that veterans with chronic headache disorders have an elevated rate of suicide, it is imperative that doctors and other clinical providers continue to conduct in-depth risk assessments and implement strategies to support those veterans who are at risk,” said Dr. Grinberg. “Clinical providers should continue in their efforts to reduce stigma associated with headache disorders and mental health treatment in order to effectively engage veterans in evidence-based treatments that are likely a step towards reducing symptoms and suicidal attempts.”
No external funding was noted. Dr. Androulakis and Dr. Grinberg had no disclosures.
FROM AHS 2021
e-TNS device passes at-home test
The study also demonstrated that the device, manufactured by Cefaly and cleared in 2020 by the Food and Drug Administration for over-the-counter use, can be safely and effectively used at home.

The study also explored the benefits of 2 hours of use, rather than the 1 hour of use tested in a previous study. “The programming on the device is currently [set to] turn off at 1 hour. As a result of this study, I tell patients if they don’t have adequate relief, and they’re tolerating it, that they can activate it again for a second hour,” Stewart Tepper, MD, said in an interview. Dr. Tepper is a professor of neurology at Geisel School of Medicine at Dartmouth, Hanover, N.H., and a coauthor of the study that was presented by Deena Kuruvilla, MD, at the American Headache Society’s 2021 annual meeting. Dr. Kuruvilla is a neurologist and director of the Westport (Conn.) Headache Institute.
The improvements seen over the sham were significant but not overwhelming, according to Deborah Friedman, MD, MPH, professor of neurology and ophthalmology at the University of Texas, Dallas.

“The numbers are not super impressive when you compare them with other devices. I thought it was interesting that the most bothersome symptom went away in a much higher percentage of people than the headache. That was actually pretty impressive,” said Dr. Friedman, who was asked to comment on the study. She also wondered if the sham device may have inadvertently provided a small amount of stimulation, which could explain the smaller than expected efficacy difference. “It just kind of makes me wonder because I would expect to see a larger separation, even though it was statistically significant.”
The study was an overall success according to Dr. Tepper, who noted that the efficacy of pain freedom was comparable with what has been seen with calcitonin gene-related peptide receptor antagonists (gepants), as well as relieving the most bothersome symptom at 2 hours. The device failed to reduce the usage of rescue medication, suggesting that it might be a candidate to combine with rescue medications. “I think the main thing is it works. It works in a sham-controlled trial, it works at home, and it works comparably to acute medication. And it is further evidence that the lack of access is something that needs to be addressed,” said Dr. Tepper.
Access will depend on insurance companies, who have so far been reluctant to pay for the device. Dr. Tepper is not optimistic they will come around on their own. “My feeling about it is that the only way that payers will finally start to cover this is with a concerted, organized advocacy campaign by patients. The analogy is that when the disease-modifying therapies became available for multiple sclerosis, the National MS Society organized the MS patients and they demanded that the payers cover the disease modifying therapies. That’s the kind of intense focus of advocacy that needs to be done for these noninvasive neuromodulation devices,” said Dr. Tepper.
The TEAM study was a double blind, randomized, sham-controlled trial of 538 patients who were asked to use neurostimulation for a 2-hour, continuous session within 4 hours of a moderate to severe migraine accompanied by at least one migraine-associated symptom. At 2 hours, 25.5% of those using the device achieved pain freedom, compared with 18.3% of those using the sham (P < .05). Among those using the device, 56.4% had freedom from most bothersome symptom, compared with 42.3% of those using the sham (P < .01).
Pain relief at 2 hours was more common in the device group (69.5% vs. 55.2%; P < .01), as was absence of all migraine-associated symptoms at 2 hours (42.5% vs. 34.1%; P < .05), sustained pain freedom at 24 hours (22.8% vs. 15.8%; P < .05), and sustained pain relief at 24 hours (45.9% vs. 34.4%; P < .01). There was no statistically significant between-group difference in use of rescue medications.
In the device group, 8.5% of patients experienced an adverse event, versus 2.9% in the sham group (P = .004). The only adverse reaction that occurred more frequently in the device group was forehead paresthesia, discomfort, and burning (3.5% vs. 0.4%; P = .009).
The study was funded by Cefaly. Dr. Tepper and Dr. Friedman have no relevant financial disclosures.
The study also demonstrated that the device, manufactured by Cefaly and cleared in 2020 by the Food and Drug Administration for over-the-counter use, can be safely and effectively used at home.
The study also explored the benefits of 2 hours of use, rather than the 1 hour of use tested in a previous study. “The programming on the device is currently [set to] turn off at 1 hour. As a result of this study, I tell patients if they don’t have adequate relief, and they’re tolerating it, that they can activate it again for a second hour,” Stewart Tepper, MD, said in an interview. Dr. Tepper is a professor of neurology at Geisel School of Medicine at Dartmouth, Hanover, N.H., and a coauthor of the study that was presented by Deena Kuruvilla, MD, at the American Headache Society’s 2021 annual meeting. Dr. Kuruvilla is a neurologist and director of the Westport (Conn.) Headache Institute.
The improvements seen over the sham were significant but not overwhelming, according to Deborah Friedman, MD, MPH, professor of neurology and ophthalmology at the University of Texas, Dallas.
“The numbers are not super impressive when you compare them with other devices. I thought it was interesting that the most bothersome symptom went away in a much higher percentage of people than the headache. That was actually pretty impressive,” said Dr. Friedman, who was asked to comment on the study. She also wondered if the sham device may have inadvertently provided a small amount of stimulation, which could explain the smaller than expected efficacy difference. “It just kind of makes me wonder because I would expect to see a larger separation, even though it was statistically significant.”
The study was an overall success according to Dr. Tepper, who noted that the efficacy of pain freedom was comparable with what has been seen with calcitonin gene-related peptide receptor antagonists (gepants), as well as relieving the most bothersome symptom at 2 hours. The device failed to reduce the usage of rescue medication, suggesting that it might be a candidate to combine with rescue medications. “I think the main thing is it works. It works in a sham-controlled trial, it works at home, and it works comparably to acute medication. And it is further evidence that the lack of access is something that needs to be addressed,” said Dr. Tepper.
Access will depend on insurance companies, who have so far been reluctant to pay for the device. Dr. Tepper is not optimistic they will come around on their own. “My feeling about it is that the only way that payers will finally start to cover this is with a concerted, organized advocacy campaign by patients. The analogy is that when the disease-modifying therapies became available for multiple sclerosis, the National MS Society organized the MS patients and they demanded that the payers cover the disease modifying therapies. That’s the kind of intense focus of advocacy that needs to be done for these noninvasive neuromodulation devices,” said Dr. Tepper.
The TEAM study was a double blind, randomized, sham-controlled trial of 538 patients who were asked to use neurostimulation for a 2-hour, continuous session within 4 hours of a moderate to severe migraine accompanied by at least one migraine-associated symptom. At 2 hours, 25.5% of those using the device achieved pain freedom, compared with 18.3% of those using the sham (P < .05). Among those using the device, 56.4% had freedom from most bothersome symptom, compared with 42.3% of those using the sham (P < .01).
Pain relief at 2 hours was more common in the device group (69.5% vs. 55.2%; P < .01), as was absence of all migraine-associated symptoms at 2 hours (42.5% vs. 34.1%; P < .05), sustained pain freedom at 24 hours (22.8% vs. 15.8%; P < .05), and sustained pain relief at 24 hours (45.9% vs. 34.4%; P < .01). There was no statistically significant between-group difference in use of rescue medications.
In the device group, 8.5% of patients experienced an adverse event, versus 2.9% in the sham group (P = .004). The only adverse reaction that occurred more frequently in the device group was forehead paresthesia, discomfort, and burning (3.5% vs. 0.4%; P = .009).
The study was funded by Cefaly. Dr. Tepper and Dr. Friedman have no relevant financial disclosures.
The study also demonstrated that the device, manufactured by Cefaly and cleared in 2020 by the Food and Drug Administration for over-the-counter use, can be safely and effectively used at home.
The study also explored the benefits of 2 hours of use, rather than the 1 hour of use tested in a previous study. “The programming on the device is currently [set to] turn off at 1 hour. As a result of this study, I tell patients if they don’t have adequate relief, and they’re tolerating it, that they can activate it again for a second hour,” Stewart Tepper, MD, said in an interview. Dr. Tepper is a professor of neurology at Geisel School of Medicine at Dartmouth, Hanover, N.H., and a coauthor of the study that was presented by Deena Kuruvilla, MD, at the American Headache Society’s 2021 annual meeting. Dr. Kuruvilla is a neurologist and director of the Westport (Conn.) Headache Institute.
The improvements seen over the sham were significant but not overwhelming, according to Deborah Friedman, MD, MPH, professor of neurology and ophthalmology at the University of Texas, Dallas.
“The numbers are not super impressive when you compare them with other devices. I thought it was interesting that the most bothersome symptom went away in a much higher percentage of people than the headache. That was actually pretty impressive,” said Dr. Friedman, who was asked to comment on the study. She also wondered if the sham device may have inadvertently provided a small amount of stimulation, which could explain the smaller than expected efficacy difference. “It just kind of makes me wonder because I would expect to see a larger separation, even though it was statistically significant.”
The study was an overall success according to Dr. Tepper, who noted that the efficacy of pain freedom was comparable with what has been seen with calcitonin gene-related peptide receptor antagonists (gepants), as well as relieving the most bothersome symptom at 2 hours. The device failed to reduce the usage of rescue medication, suggesting that it might be a candidate to combine with rescue medications. “I think the main thing is it works. It works in a sham-controlled trial, it works at home, and it works comparably to acute medication. And it is further evidence that the lack of access is something that needs to be addressed,” said Dr. Tepper.
Access will depend on insurance companies, who have so far been reluctant to pay for the device. Dr. Tepper is not optimistic they will come around on their own. “My feeling about it is that the only way that payers will finally start to cover this is with a concerted, organized advocacy campaign by patients. The analogy is that when the disease-modifying therapies became available for multiple sclerosis, the National MS Society organized the MS patients and they demanded that the payers cover the disease modifying therapies. That’s the kind of intense focus of advocacy that needs to be done for these noninvasive neuromodulation devices,” said Dr. Tepper.
The TEAM study was a double blind, randomized, sham-controlled trial of 538 patients who were asked to use neurostimulation for a 2-hour, continuous session within 4 hours of a moderate to severe migraine accompanied by at least one migraine-associated symptom. At 2 hours, 25.5% of those using the device achieved pain freedom, compared with 18.3% of those using the sham (P < .05). Among those using the device, 56.4% had freedom from most bothersome symptom, compared with 42.3% of those using the sham (P < .01).
Pain relief at 2 hours was more common in the device group (69.5% vs. 55.2%; P < .01), as was absence of all migraine-associated symptoms at 2 hours (42.5% vs. 34.1%; P < .05), sustained pain freedom at 24 hours (22.8% vs. 15.8%; P < .05), and sustained pain relief at 24 hours (45.9% vs. 34.4%; P < .01). There was no statistically significant between-group difference in use of rescue medications.
In the device group, 8.5% of patients experienced an adverse event, versus 2.9% in the sham group (P = .004). The only adverse reaction that occurred more frequently in the device group was forehead paresthesia, discomfort, and burning (3.5% vs. 0.4%; P = .009).
The study was funded by Cefaly. Dr. Tepper and Dr. Friedman have no relevant financial disclosures.
FROM AHS 2021

Role of 3D Printing and Modeling to Aid in Neuroradiology Education for Medical Trainees
Applications of 3-dimensional (3D) printing in medical imaging and health care are expanding. 3D printing may serve a variety of roles and is used increasingly in the context of presurgical planning, as specific medical models may be created using individual patient imaging data.1 These patient-specific models may assist in medical trainee education, decrease operating room time, improve patient education for potential planned surgery, and guide clinicians for optimizing therapy.1,2 This article discusses the utility of 3D printing at a single institution to serve in enhancing specifically neuroradiology education.
Background
As digital imaging and 3D printing have increased in popularity, the potential application of using imaging data to guide patient therapy has shown significant promise. Computed tomography (CT) is a commonly used modality that can be used to create 3D anatomical models, as it is frequently used in the medical setting, demonstrates excellent resolution to the millimeter scale, and can readily pinpoint pathology on imaging.
Image Acquisition
CT scans can be rapidly obtained, which adds significant value, particularly in the context of point-of-care 3D printing. Another modality commonly used for 3D printing is magnetic resonance imaging (MRI), which unlike CT, does not expose the patient to ionizing radiation. The 3D printing process is initiated with patient-specific CT or MRI data stored in the digital imaging and communications in medicine (DICOM) format, which is the international standard for communication and management of medical imaging information and related data. DICOM allows for faster and robust collaboration among imaging professionals.3
Image Processing
To print 3D anatomical models, patient-specific data must be converted from DICOM into standard tessellation language (STL) format, which can be created and edited with a variety of softwares.3 At James A. Haley Veterans’ Hospital in Tampa, Florida, we use an image processing package that includes the Materialise 3-matic and interactive medical image control system. Image quality is essential; therefore, careful attention to details such as pixel dimensions, slice thickness, and slice increments must be considered.3,4
An STL file creates a 3D image from triangle approximations. The entire 3D shape will be made of numerous large or small triangles, depending on the slice thickness, therefore, quality of the original radiologic image. The size and position of the triangles used to make the model can be varied to approximate the object’s shape. The smaller the triangles, the better the image quality and vice versa. This concept is analogous to approximating a circle using straight lines of equal length—more, smaller lines will result in better approximation of a circle (Figure 1).5,6 Similarly, using smaller triangles allows for better approximation of the image. As the human body is a complex structure, mimicking the body requires a system able to create nongeometrical shapes, which is made possible via these triangle approximations in a 3D STL file.
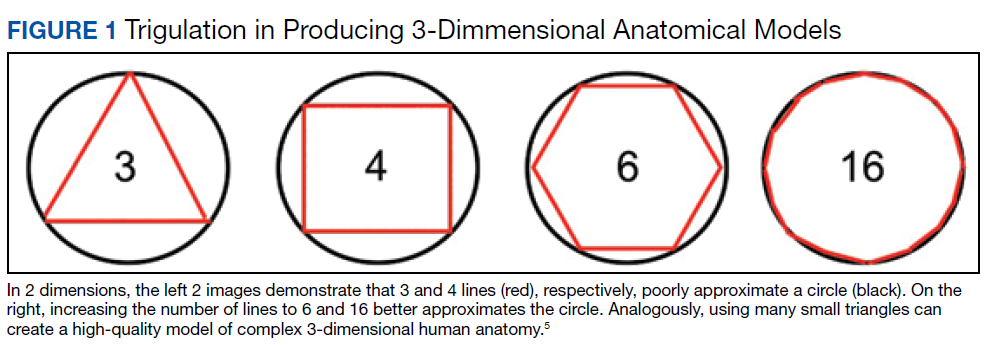
The creation of an STL file from DICOM data starts with a threshold-based segmentation process followed by additional fine-tuning and edits, and ends in the creation of a 3D part. The initial segmentation can be created with the threshold tool, using a Hounsfield unit range based on the area of interest desired (eg, bone, blood, fat). This is used to create an initial mask, which can be further optimized. The region grow tool allows the user to focus the segmentation by discarding areas that are not directly connected to the region of interest. In contrast, the split mask tool divides areas that are connected. Next, fine-tuning the segmentation using tools such as multiple slice edit helps to optimize the model. After all edits are made, the calculate part tool converts the mask into a 3D component that can be used in downstream applications. For the purposes of demonstration and proof of concept, the models provided in this article were created via open-source hardware designs under free or open licenses.7-9
3D Printing in Neuroradiology Education
Neuroradiologists focus on diagnosing pathology related to the brain, head and neck, and spine. CT and MRI scans are the primary modalities used to diagnose these conditions. 3D printing is a useful tool for the trainee who wishes to fully understand neuroanatomy and obtain further appreciation of imaging pathology as it relates to 3D anatomy. Head and neck imaging are a complex subdiscipline of neuroradiology that often require further training beyond radiology residency. A neuroradiology fellowship that focuses on head and neck imaging extends the training.
3D printing has the potential to improve the understanding of various imaging pathologies by providing the trainee with a more in-depth appreciation of the anterior, middle, and posterior cranial fossa, the skull base foramina (ie, foramen ovale, spinosum, rotundum), and complex 3D areas, such as the pterygopalatine fossa, which are all critical areas to investigate on imaging. Figure 2 highlights how a complex anatomical structure, such as the sphenoid bone when printed in 3D, can be correlated with CT cross-sectional images to supplement the educational experience.
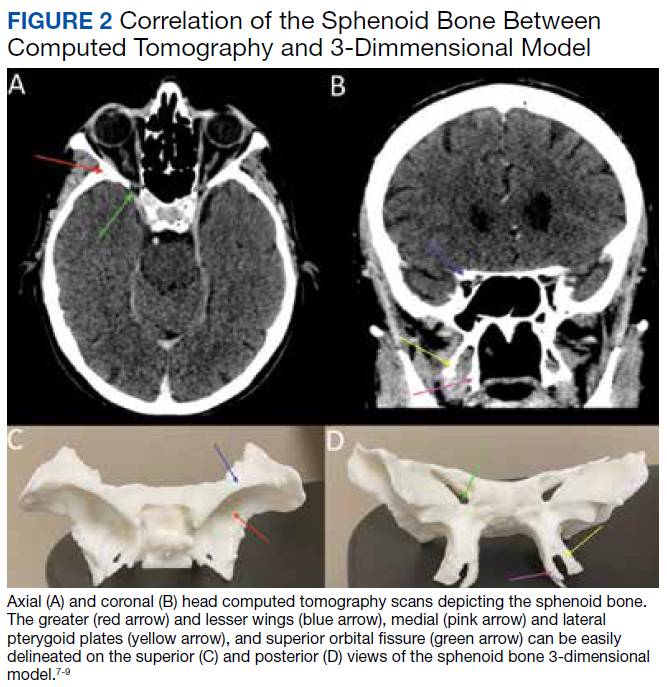
Furthermore, the various lobes, sulci, and gyri of the brain and cerebellum and how they interrelate to nearby vasculature and bony structures can be difficult to conceptualize for early trainees. A 3D-printed cerebellum and its relation to the brainstem is illustrated in Figure 3A. Additional complex head and neck structures of the middle ear membranous and bony labyrinth and ossicles and multiple views of the mandible are shown in Figures 3B through 3E.
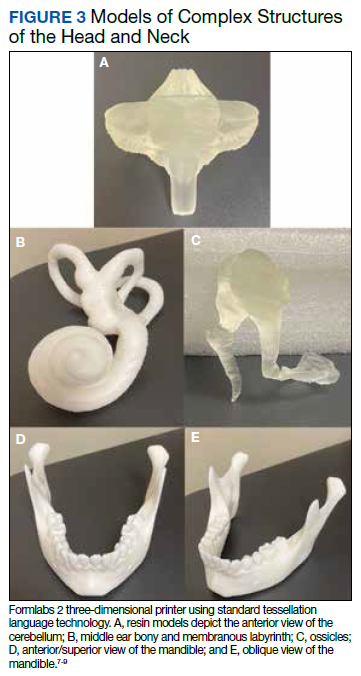
3D printing in the context of neurovascular pathology holds great promise, particularly as these models may provide the trainee, patient, and proceduralist essential details such as appearance and morphology of an intracranial aneurysm, relationship and size of the neck of aneurysm, incorporation of vessels emanating from the aneurysmal sac, and details of the dome of the aneurysm. For example, the normal circle of Willis in Figure 4A is juxtaposed with an example of a saccular internal carotid artery aneurysm (Figure 4B).
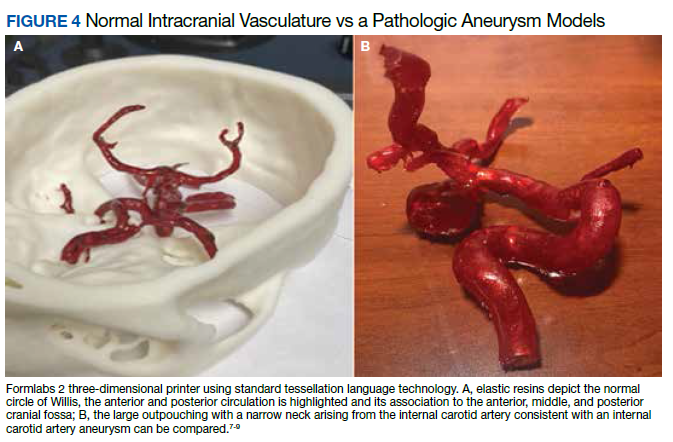
A variety of conditions can affect the bony spine from degenerative, trauma, neoplastic, and inflammatory etiologies. A CT scan of the spine is readily used to detect these different conditions and often is used in the initial evaluation of trauma as indicated in the American College of Radiology appropriateness criteria.10 In addition, MRI is used to evaluate the spinal cord and to further define spinal stenosis as well as evaluate radiculopathy. An appreciation of the bony and soft tissue structures within the spine can be garnered with the use of 3D models (Figure 5).
Trainees can further their understanding of approaches in spinal procedures, including lumbar puncture, myelography, and facet injections. A variety of approaches to access the spinal canal have been documented, such as interspinous, paraspinous, and interlaminar oblique; 3D-printed models can aid in practicing these procedures.11 For example, a water-filled tube can be inserted into the vertebral canal to provide realistic tactile feedback for simulation of a lumbar puncture. An appreciation of the 3D anatomy can guide the clinician on the optimal approach, which can help limit time and potentially improve outcomes.
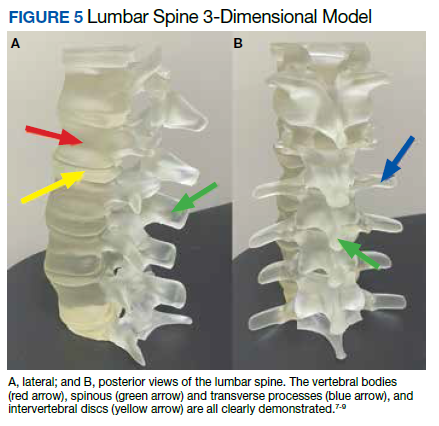
Future Directions
Artificial Intelligence (AI) offers the ability to teach computers to perform tasks that ordinarily require human intelligence. In the context of 3D printing, the ability to use AI to readily convert and process DICOM data into printable STL models holds significant promise. Currently, the manual conversion of a DICOM file into a segmented 3D model may take several days, necessitating a number of productive hours even from the imaging and engineering champion. If machines could aid in this process, the ability to readily scale clinical 3D printing and promote widespread adoption would be feasible. Several studies already are looking into this concept to determine how deep learning networks may automatically recognize lesions on medical imaging to assist a human operator, potentially cutting hours from the clinical 3D printing workflow.12,13
Furthermore, there are several applications for AI in the context of 3D printing upstream or before the creation of a 3D model. A number of AI tools are already in use at the CT and MRI scanner. Current strategies leverage deep learning and advances in neural networks to improve image quality and create thin section DICOM data, which can be converted into printable 3D files. Additionally, the ability to automate tasks using AI can improve production capacity by assessing material costs and ensuring cost efficiency, which will be critical as point-of-care 3D printing develops widespread adoption. AI also can reduce printing errors by using automated adaptive feedback, using machine learning to search for possible print errors, and sending feedback to the computer to ensure appropriate settings (eg, temperature settings/environmental conditions).
Conclusions
Based on this single-institution experience, 3D-printed complex neuroanatomical structures seems feasible and may enhance resident education and patient safety. Interested trainees may have the opportunity to learn and be involved in the printing process of new and innovative ideas. Further studies may involve printing various pathologic processes and applying these same steps and principles to other subspecialties of radiology. Finally, AI has the potential to advance the 3D printing process in the future.
1. Rengier F, Mehndiratta A, von Tengg-Kobligk H, et al. 3D printing based on imaging data: review of medical applications. Int J Comput Assist Radiol Surg. 2010;5(4):335-341. doi:10.1007/s11548-010-0476-x
2. Perica E, Sun Z. Patient-specific three-dimensional printing for pre-surgical planning in hepatocellular carcinoma treatment. Quant Imaging Med Surg. 2017;7(6):668-677. doi:10.21037/qims.2017.11.02
3. Hwang JJ, Jung Y-H, Cho B-H. The need for DICOM encapsulation of 3D scanning STL data. Imaging Sci Dent. 2018;48(4):301-302. doi:10.5624/isd.2018.48.4.301
4. Whyms BJ, Vorperian HK, Gentry LR, Schimek EM, Bersu ET, Chung MK. The effect of computed tomographic scanner parameters and 3-dimensional volume rendering techniques on the accuracy of linear, angular, and volumetric measurements of the mandible. Oral Surg Oral Med, Oral Pathol Oral Radiol. 2013;115(5):682-691. doi:10.1016/j.oooo.2013.02.008
5. Materialise Cloud. Triangle reduction. Accessed May 20, 2021. https://cloud.materialise.com/tools/triangle-reduction
6. Comaneanu RM, Tarcolea M, Vlasceanu D, Cotrut MC. Virtual 3D reconstruction, diagnosis and surgical planning with Mimics software. Int J Nano Biomaterials. 2012;4(1);69-77.
7. Thingiverse: Digital designs for physical objects. Accessed May 20, 2021. https://www.thingiverse.com
8. Cults. Download for free 3D models for 3D printers. Accessed May 20, 2021. https://cults3d.com/en
9. yeggi. Search engine for 3D printer models. Accessed May 20, 2021. https://www.yeggi.com
10. Expert Panel on Neurological Imaging and Musculoskeletal Imaging; Beckmann NM, West OC, Nunez D, et al. ACR appropriateness criteria suspected spine trauma. J Am Coll Radiol. 2919;16(5):S264-285. doi:10.1016/j.jacr.2019.02.002
11. McKinney AM. Normal variants of the lumbar and sacral spine. In: Atlas of Head/Neck and Spine Normal Imaging Variants. Springer; 2018:263-321.
12. Sollini M, Bartoli F, Marciano A, et al. Artificial intelligence and hybrid imaging: the best match for personalized medicine in oncology. Eur J Hybrid Imaging. 2020;4(1):24. doi:10.1186/s41824-020-00094-8
13. Küstner T, Hepp T, Fischer M, et al. Fully automated and standardized segmentation of adipose tissue compartments via deep learning in 3D whole-body MRI of epidemiologic cohort studies. Radiol Artif Intell.2020;2(6):e200010. doi:10.1148/ryai.2020200010
Applications of 3-dimensional (3D) printing in medical imaging and health care are expanding. 3D printing may serve a variety of roles and is used increasingly in the context of presurgical planning, as specific medical models may be created using individual patient imaging data.1 These patient-specific models may assist in medical trainee education, decrease operating room time, improve patient education for potential planned surgery, and guide clinicians for optimizing therapy.1,2 This article discusses the utility of 3D printing at a single institution to serve in enhancing specifically neuroradiology education.
Background
As digital imaging and 3D printing have increased in popularity, the potential application of using imaging data to guide patient therapy has shown significant promise. Computed tomography (CT) is a commonly used modality that can be used to create 3D anatomical models, as it is frequently used in the medical setting, demonstrates excellent resolution to the millimeter scale, and can readily pinpoint pathology on imaging.
Image Acquisition
CT scans can be rapidly obtained, which adds significant value, particularly in the context of point-of-care 3D printing. Another modality commonly used for 3D printing is magnetic resonance imaging (MRI), which unlike CT, does not expose the patient to ionizing radiation. The 3D printing process is initiated with patient-specific CT or MRI data stored in the digital imaging and communications in medicine (DICOM) format, which is the international standard for communication and management of medical imaging information and related data. DICOM allows for faster and robust collaboration among imaging professionals.3
Image Processing
To print 3D anatomical models, patient-specific data must be converted from DICOM into standard tessellation language (STL) format, which can be created and edited with a variety of softwares.3 At James A. Haley Veterans’ Hospital in Tampa, Florida, we use an image processing package that includes the Materialise 3-matic and interactive medical image control system. Image quality is essential; therefore, careful attention to details such as pixel dimensions, slice thickness, and slice increments must be considered.3,4
An STL file creates a 3D image from triangle approximations. The entire 3D shape will be made of numerous large or small triangles, depending on the slice thickness, therefore, quality of the original radiologic image. The size and position of the triangles used to make the model can be varied to approximate the object’s shape. The smaller the triangles, the better the image quality and vice versa. This concept is analogous to approximating a circle using straight lines of equal length—more, smaller lines will result in better approximation of a circle (Figure 1).5,6 Similarly, using smaller triangles allows for better approximation of the image. As the human body is a complex structure, mimicking the body requires a system able to create nongeometrical shapes, which is made possible via these triangle approximations in a 3D STL file.
The creation of an STL file from DICOM data starts with a threshold-based segmentation process followed by additional fine-tuning and edits, and ends in the creation of a 3D part. The initial segmentation can be created with the threshold tool, using a Hounsfield unit range based on the area of interest desired (eg, bone, blood, fat). This is used to create an initial mask, which can be further optimized. The region grow tool allows the user to focus the segmentation by discarding areas that are not directly connected to the region of interest. In contrast, the split mask tool divides areas that are connected. Next, fine-tuning the segmentation using tools such as multiple slice edit helps to optimize the model. After all edits are made, the calculate part tool converts the mask into a 3D component that can be used in downstream applications. For the purposes of demonstration and proof of concept, the models provided in this article were created via open-source hardware designs under free or open licenses.7-9
3D Printing in Neuroradiology Education
Neuroradiologists focus on diagnosing pathology related to the brain, head and neck, and spine. CT and MRI scans are the primary modalities used to diagnose these conditions. 3D printing is a useful tool for the trainee who wishes to fully understand neuroanatomy and obtain further appreciation of imaging pathology as it relates to 3D anatomy. Head and neck imaging are a complex subdiscipline of neuroradiology that often require further training beyond radiology residency. A neuroradiology fellowship that focuses on head and neck imaging extends the training.
3D printing has the potential to improve the understanding of various imaging pathologies by providing the trainee with a more in-depth appreciation of the anterior, middle, and posterior cranial fossa, the skull base foramina (ie, foramen ovale, spinosum, rotundum), and complex 3D areas, such as the pterygopalatine fossa, which are all critical areas to investigate on imaging. Figure 2 highlights how a complex anatomical structure, such as the sphenoid bone when printed in 3D, can be correlated with CT cross-sectional images to supplement the educational experience.
Furthermore, the various lobes, sulci, and gyri of the brain and cerebellum and how they interrelate to nearby vasculature and bony structures can be difficult to conceptualize for early trainees. A 3D-printed cerebellum and its relation to the brainstem is illustrated in Figure 3A. Additional complex head and neck structures of the middle ear membranous and bony labyrinth and ossicles and multiple views of the mandible are shown in Figures 3B through 3E.
3D printing in the context of neurovascular pathology holds great promise, particularly as these models may provide the trainee, patient, and proceduralist essential details such as appearance and morphology of an intracranial aneurysm, relationship and size of the neck of aneurysm, incorporation of vessels emanating from the aneurysmal sac, and details of the dome of the aneurysm. For example, the normal circle of Willis in Figure 4A is juxtaposed with an example of a saccular internal carotid artery aneurysm (Figure 4B).
A variety of conditions can affect the bony spine from degenerative, trauma, neoplastic, and inflammatory etiologies. A CT scan of the spine is readily used to detect these different conditions and often is used in the initial evaluation of trauma as indicated in the American College of Radiology appropriateness criteria.10 In addition, MRI is used to evaluate the spinal cord and to further define spinal stenosis as well as evaluate radiculopathy. An appreciation of the bony and soft tissue structures within the spine can be garnered with the use of 3D models (Figure 5).
Trainees can further their understanding of approaches in spinal procedures, including lumbar puncture, myelography, and facet injections. A variety of approaches to access the spinal canal have been documented, such as interspinous, paraspinous, and interlaminar oblique; 3D-printed models can aid in practicing these procedures.11 For example, a water-filled tube can be inserted into the vertebral canal to provide realistic tactile feedback for simulation of a lumbar puncture. An appreciation of the 3D anatomy can guide the clinician on the optimal approach, which can help limit time and potentially improve outcomes.
Future Directions
Artificial Intelligence (AI) offers the ability to teach computers to perform tasks that ordinarily require human intelligence. In the context of 3D printing, the ability to use AI to readily convert and process DICOM data into printable STL models holds significant promise. Currently, the manual conversion of a DICOM file into a segmented 3D model may take several days, necessitating a number of productive hours even from the imaging and engineering champion. If machines could aid in this process, the ability to readily scale clinical 3D printing and promote widespread adoption would be feasible. Several studies already are looking into this concept to determine how deep learning networks may automatically recognize lesions on medical imaging to assist a human operator, potentially cutting hours from the clinical 3D printing workflow.12,13
Furthermore, there are several applications for AI in the context of 3D printing upstream or before the creation of a 3D model. A number of AI tools are already in use at the CT and MRI scanner. Current strategies leverage deep learning and advances in neural networks to improve image quality and create thin section DICOM data, which can be converted into printable 3D files. Additionally, the ability to automate tasks using AI can improve production capacity by assessing material costs and ensuring cost efficiency, which will be critical as point-of-care 3D printing develops widespread adoption. AI also can reduce printing errors by using automated adaptive feedback, using machine learning to search for possible print errors, and sending feedback to the computer to ensure appropriate settings (eg, temperature settings/environmental conditions).
Conclusions
Based on this single-institution experience, 3D-printed complex neuroanatomical structures seems feasible and may enhance resident education and patient safety. Interested trainees may have the opportunity to learn and be involved in the printing process of new and innovative ideas. Further studies may involve printing various pathologic processes and applying these same steps and principles to other subspecialties of radiology. Finally, AI has the potential to advance the 3D printing process in the future.
Applications of 3-dimensional (3D) printing in medical imaging and health care are expanding. 3D printing may serve a variety of roles and is used increasingly in the context of presurgical planning, as specific medical models may be created using individual patient imaging data.1 These patient-specific models may assist in medical trainee education, decrease operating room time, improve patient education for potential planned surgery, and guide clinicians for optimizing therapy.1,2 This article discusses the utility of 3D printing at a single institution to serve in enhancing specifically neuroradiology education.
Background
As digital imaging and 3D printing have increased in popularity, the potential application of using imaging data to guide patient therapy has shown significant promise. Computed tomography (CT) is a commonly used modality that can be used to create 3D anatomical models, as it is frequently used in the medical setting, demonstrates excellent resolution to the millimeter scale, and can readily pinpoint pathology on imaging.
Image Acquisition
CT scans can be rapidly obtained, which adds significant value, particularly in the context of point-of-care 3D printing. Another modality commonly used for 3D printing is magnetic resonance imaging (MRI), which unlike CT, does not expose the patient to ionizing radiation. The 3D printing process is initiated with patient-specific CT or MRI data stored in the digital imaging and communications in medicine (DICOM) format, which is the international standard for communication and management of medical imaging information and related data. DICOM allows for faster and robust collaboration among imaging professionals.3
Image Processing
To print 3D anatomical models, patient-specific data must be converted from DICOM into standard tessellation language (STL) format, which can be created and edited with a variety of softwares.3 At James A. Haley Veterans’ Hospital in Tampa, Florida, we use an image processing package that includes the Materialise 3-matic and interactive medical image control system. Image quality is essential; therefore, careful attention to details such as pixel dimensions, slice thickness, and slice increments must be considered.3,4
An STL file creates a 3D image from triangle approximations. The entire 3D shape will be made of numerous large or small triangles, depending on the slice thickness, therefore, quality of the original radiologic image. The size and position of the triangles used to make the model can be varied to approximate the object’s shape. The smaller the triangles, the better the image quality and vice versa. This concept is analogous to approximating a circle using straight lines of equal length—more, smaller lines will result in better approximation of a circle (Figure 1).5,6 Similarly, using smaller triangles allows for better approximation of the image. As the human body is a complex structure, mimicking the body requires a system able to create nongeometrical shapes, which is made possible via these triangle approximations in a 3D STL file.
The creation of an STL file from DICOM data starts with a threshold-based segmentation process followed by additional fine-tuning and edits, and ends in the creation of a 3D part. The initial segmentation can be created with the threshold tool, using a Hounsfield unit range based on the area of interest desired (eg, bone, blood, fat). This is used to create an initial mask, which can be further optimized. The region grow tool allows the user to focus the segmentation by discarding areas that are not directly connected to the region of interest. In contrast, the split mask tool divides areas that are connected. Next, fine-tuning the segmentation using tools such as multiple slice edit helps to optimize the model. After all edits are made, the calculate part tool converts the mask into a 3D component that can be used in downstream applications. For the purposes of demonstration and proof of concept, the models provided in this article were created via open-source hardware designs under free or open licenses.7-9
3D Printing in Neuroradiology Education
Neuroradiologists focus on diagnosing pathology related to the brain, head and neck, and spine. CT and MRI scans are the primary modalities used to diagnose these conditions. 3D printing is a useful tool for the trainee who wishes to fully understand neuroanatomy and obtain further appreciation of imaging pathology as it relates to 3D anatomy. Head and neck imaging are a complex subdiscipline of neuroradiology that often require further training beyond radiology residency. A neuroradiology fellowship that focuses on head and neck imaging extends the training.
3D printing has the potential to improve the understanding of various imaging pathologies by providing the trainee with a more in-depth appreciation of the anterior, middle, and posterior cranial fossa, the skull base foramina (ie, foramen ovale, spinosum, rotundum), and complex 3D areas, such as the pterygopalatine fossa, which are all critical areas to investigate on imaging. Figure 2 highlights how a complex anatomical structure, such as the sphenoid bone when printed in 3D, can be correlated with CT cross-sectional images to supplement the educational experience.
Furthermore, the various lobes, sulci, and gyri of the brain and cerebellum and how they interrelate to nearby vasculature and bony structures can be difficult to conceptualize for early trainees. A 3D-printed cerebellum and its relation to the brainstem is illustrated in Figure 3A. Additional complex head and neck structures of the middle ear membranous and bony labyrinth and ossicles and multiple views of the mandible are shown in Figures 3B through 3E.
3D printing in the context of neurovascular pathology holds great promise, particularly as these models may provide the trainee, patient, and proceduralist essential details such as appearance and morphology of an intracranial aneurysm, relationship and size of the neck of aneurysm, incorporation of vessels emanating from the aneurysmal sac, and details of the dome of the aneurysm. For example, the normal circle of Willis in Figure 4A is juxtaposed with an example of a saccular internal carotid artery aneurysm (Figure 4B).
A variety of conditions can affect the bony spine from degenerative, trauma, neoplastic, and inflammatory etiologies. A CT scan of the spine is readily used to detect these different conditions and often is used in the initial evaluation of trauma as indicated in the American College of Radiology appropriateness criteria.10 In addition, MRI is used to evaluate the spinal cord and to further define spinal stenosis as well as evaluate radiculopathy. An appreciation of the bony and soft tissue structures within the spine can be garnered with the use of 3D models (Figure 5).
Trainees can further their understanding of approaches in spinal procedures, including lumbar puncture, myelography, and facet injections. A variety of approaches to access the spinal canal have been documented, such as interspinous, paraspinous, and interlaminar oblique; 3D-printed models can aid in practicing these procedures.11 For example, a water-filled tube can be inserted into the vertebral canal to provide realistic tactile feedback for simulation of a lumbar puncture. An appreciation of the 3D anatomy can guide the clinician on the optimal approach, which can help limit time and potentially improve outcomes.
Future Directions
Artificial Intelligence (AI) offers the ability to teach computers to perform tasks that ordinarily require human intelligence. In the context of 3D printing, the ability to use AI to readily convert and process DICOM data into printable STL models holds significant promise. Currently, the manual conversion of a DICOM file into a segmented 3D model may take several days, necessitating a number of productive hours even from the imaging and engineering champion. If machines could aid in this process, the ability to readily scale clinical 3D printing and promote widespread adoption would be feasible. Several studies already are looking into this concept to determine how deep learning networks may automatically recognize lesions on medical imaging to assist a human operator, potentially cutting hours from the clinical 3D printing workflow.12,13
Furthermore, there are several applications for AI in the context of 3D printing upstream or before the creation of a 3D model. A number of AI tools are already in use at the CT and MRI scanner. Current strategies leverage deep learning and advances in neural networks to improve image quality and create thin section DICOM data, which can be converted into printable 3D files. Additionally, the ability to automate tasks using AI can improve production capacity by assessing material costs and ensuring cost efficiency, which will be critical as point-of-care 3D printing develops widespread adoption. AI also can reduce printing errors by using automated adaptive feedback, using machine learning to search for possible print errors, and sending feedback to the computer to ensure appropriate settings (eg, temperature settings/environmental conditions).
Conclusions
Based on this single-institution experience, 3D-printed complex neuroanatomical structures seems feasible and may enhance resident education and patient safety. Interested trainees may have the opportunity to learn and be involved in the printing process of new and innovative ideas. Further studies may involve printing various pathologic processes and applying these same steps and principles to other subspecialties of radiology. Finally, AI has the potential to advance the 3D printing process in the future.
1. Rengier F, Mehndiratta A, von Tengg-Kobligk H, et al. 3D printing based on imaging data: review of medical applications. Int J Comput Assist Radiol Surg. 2010;5(4):335-341. doi:10.1007/s11548-010-0476-x
2. Perica E, Sun Z. Patient-specific three-dimensional printing for pre-surgical planning in hepatocellular carcinoma treatment. Quant Imaging Med Surg. 2017;7(6):668-677. doi:10.21037/qims.2017.11.02
3. Hwang JJ, Jung Y-H, Cho B-H. The need for DICOM encapsulation of 3D scanning STL data. Imaging Sci Dent. 2018;48(4):301-302. doi:10.5624/isd.2018.48.4.301
4. Whyms BJ, Vorperian HK, Gentry LR, Schimek EM, Bersu ET, Chung MK. The effect of computed tomographic scanner parameters and 3-dimensional volume rendering techniques on the accuracy of linear, angular, and volumetric measurements of the mandible. Oral Surg Oral Med, Oral Pathol Oral Radiol. 2013;115(5):682-691. doi:10.1016/j.oooo.2013.02.008
5. Materialise Cloud. Triangle reduction. Accessed May 20, 2021. https://cloud.materialise.com/tools/triangle-reduction
6. Comaneanu RM, Tarcolea M, Vlasceanu D, Cotrut MC. Virtual 3D reconstruction, diagnosis and surgical planning with Mimics software. Int J Nano Biomaterials. 2012;4(1);69-77.
7. Thingiverse: Digital designs for physical objects. Accessed May 20, 2021. https://www.thingiverse.com
8. Cults. Download for free 3D models for 3D printers. Accessed May 20, 2021. https://cults3d.com/en
9. yeggi. Search engine for 3D printer models. Accessed May 20, 2021. https://www.yeggi.com
10. Expert Panel on Neurological Imaging and Musculoskeletal Imaging; Beckmann NM, West OC, Nunez D, et al. ACR appropriateness criteria suspected spine trauma. J Am Coll Radiol. 2919;16(5):S264-285. doi:10.1016/j.jacr.2019.02.002
11. McKinney AM. Normal variants of the lumbar and sacral spine. In: Atlas of Head/Neck and Spine Normal Imaging Variants. Springer; 2018:263-321.
12. Sollini M, Bartoli F, Marciano A, et al. Artificial intelligence and hybrid imaging: the best match for personalized medicine in oncology. Eur J Hybrid Imaging. 2020;4(1):24. doi:10.1186/s41824-020-00094-8
13. Küstner T, Hepp T, Fischer M, et al. Fully automated and standardized segmentation of adipose tissue compartments via deep learning in 3D whole-body MRI of epidemiologic cohort studies. Radiol Artif Intell.2020;2(6):e200010. doi:10.1148/ryai.2020200010
1. Rengier F, Mehndiratta A, von Tengg-Kobligk H, et al. 3D printing based on imaging data: review of medical applications. Int J Comput Assist Radiol Surg. 2010;5(4):335-341. doi:10.1007/s11548-010-0476-x
2. Perica E, Sun Z. Patient-specific three-dimensional printing for pre-surgical planning in hepatocellular carcinoma treatment. Quant Imaging Med Surg. 2017;7(6):668-677. doi:10.21037/qims.2017.11.02
3. Hwang JJ, Jung Y-H, Cho B-H. The need for DICOM encapsulation of 3D scanning STL data. Imaging Sci Dent. 2018;48(4):301-302. doi:10.5624/isd.2018.48.4.301
4. Whyms BJ, Vorperian HK, Gentry LR, Schimek EM, Bersu ET, Chung MK. The effect of computed tomographic scanner parameters and 3-dimensional volume rendering techniques on the accuracy of linear, angular, and volumetric measurements of the mandible. Oral Surg Oral Med, Oral Pathol Oral Radiol. 2013;115(5):682-691. doi:10.1016/j.oooo.2013.02.008
5. Materialise Cloud. Triangle reduction. Accessed May 20, 2021. https://cloud.materialise.com/tools/triangle-reduction
6. Comaneanu RM, Tarcolea M, Vlasceanu D, Cotrut MC. Virtual 3D reconstruction, diagnosis and surgical planning with Mimics software. Int J Nano Biomaterials. 2012;4(1);69-77.
7. Thingiverse: Digital designs for physical objects. Accessed May 20, 2021. https://www.thingiverse.com
8. Cults. Download for free 3D models for 3D printers. Accessed May 20, 2021. https://cults3d.com/en
9. yeggi. Search engine for 3D printer models. Accessed May 20, 2021. https://www.yeggi.com
10. Expert Panel on Neurological Imaging and Musculoskeletal Imaging; Beckmann NM, West OC, Nunez D, et al. ACR appropriateness criteria suspected spine trauma. J Am Coll Radiol. 2919;16(5):S264-285. doi:10.1016/j.jacr.2019.02.002
11. McKinney AM. Normal variants of the lumbar and sacral spine. In: Atlas of Head/Neck and Spine Normal Imaging Variants. Springer; 2018:263-321.
12. Sollini M, Bartoli F, Marciano A, et al. Artificial intelligence and hybrid imaging: the best match for personalized medicine in oncology. Eur J Hybrid Imaging. 2020;4(1):24. doi:10.1186/s41824-020-00094-8
13. Küstner T, Hepp T, Fischer M, et al. Fully automated and standardized segmentation of adipose tissue compartments via deep learning in 3D whole-body MRI of epidemiologic cohort studies. Radiol Artif Intell.2020;2(6):e200010. doi:10.1148/ryai.2020200010
A large proportion of migraine patients are not offered preventive treatment
, new research suggests. Investigators found that among patients with migraine who are eligible for preventive therapy, more than a third were not offered this option. In addition, fewer than 10% were currently taking preventive medication, and an additional 10% had discontinued preventive therapy.

“We confirmed that as of 2012 to 2013 – the years these data were collected from a large, comprehensive survey – gaps in care remained,” said study investigator Stephanie J. Nahas, MD, director of the headache medicine fellowship program, Thomas Jefferson University, Philadelphia. “In this preventive-eligible population, 35% reported never even being offered preventive medication.”
Furthermore, only 28% of patients taking preventive medication experienced a reduction in headache frequency to less than 4 days per month, which is a primary goal of treatment, said Dr. Nahas. Disease burden, as measured with scales of disability and affective comorbidities, remained substantial.
The findings were presented at the American Headache Society’s 2021 annual meeting.
Lack of efficacy?
In 2019, the American Headache Society published a position statement recommending that preventive treatment be considered for patients who have migraine and four or more monthly headache days (MHDs), regardless of their level of associated disability. However, previous data suggest few patients who are eligible for preventive treatment receive it. In addition, many who have used preventive medications do not adhere to their regimens because of problems with tolerability, efficacy, or both.
To identify treatment gaps and characterize self-reported use of preventive medications for migraine, the investigators examined data from the Chronic Migraine Epidemiology and Outcomes (CaMEO) study, a web-based survey conducted in a representative U.S. sample from September 2012 through November 2013.
The survey identified and characterized patients who met modified criteria for migraine consistent with those in ICHD-3. The researchers classified respondents who had migraine and four or more MHDs as potentially eligible for migraine preventive treatment.
The investigators assessed the study population’s use of oral preventive medications, migraine-related disability and burden, willingness to take preventive treatment, and reasons for discontinuation.
Assessments included the Migraine Disability Assessment Questionnaire, the Patient Health Questionnaire–9 for depression, the Generalized Anxiety Disorder 7-Item Scale, the Migraine Specific Quality of Life questionnaire, and the Migraine Symptom Severity Scale.
In all, 16,789 respondents met criteria for migraine, and 6,579 (39.2%) reported having at least four MHDs. The median age of this subgroup that was eligible for preventive treatment was 40.3 years, and approximately 79% were women.
Only 9.8% of respondents who were eligible for preventive medications were currently using an oral preventive medication. Among those who had ever tried an oral preventive medication, 53.6% discontinued it. Efficacy for patients who used medications appeared to be inadequate. Among all current users of preventive treatment, 68.4% continued to have at least four MHDs.
The researchers assessed treatment eligibility among patients not taking preventive medication. Among respondents who had never used a preventive treatment, 35.7% were eligible to receive it. Among all users who had discontinued preventive medication, 61.0% were still eligible to receive it.
Attitudes toward injectables
Among respondents who had never used a preventive treatment, 64.3% had zero to three MHDs. The remaining 35.7% had 4-7, 8-14, or 15 or more MHDs. Among current users of preventive treatments, 68.4% had four or more MHDs. Among those who had discontinued preventive treatment, 61.0% had four or more MHDs.
Patients who have never used preventive medication “have substantial management gaps,” said Dr. Nahas. High proportions of these patients have moderate or severe disability (64.7%), depression (43%), and anxiety (39%). The rates of these outcomes are higher in users who discontinued treatment, likely because of confounding by indication, she added.
The prevalence of anxiety was similar between those who currently used, formerly used, or never used preventive medications. However, there were differences between never-users and current or former users with respect to moderate to severe depression (never-users, 43%; current users, 49.4%; discontinued users, 46.5%) and moderate to severe disability (never-users, 64.7%; current users, 80.4%; discontinued users, 78.9%).
In all, 44.6% of those who discontinued preventive therapy reported safety and tolerability problems as reasons for stopping treatment. In addition, 39.7% reported that these medications did not prevent enough headaches. Some patients reported partial or temporary efficacy as a reason for discontinuation. Other reasons were related to health care costs and access and personal preferences. Only 9.2% of patients who discontinued treatment said that their headaches improved enough to stop medication.
The investigators also analyzed respondents’ interest in preventive therapies. Among respondents who had never used preventive therapies, 61.8% of those who were eligible to use them were somewhat or very interested in trying an oral prescription medication for migraine prevention. However, 59.1% of never-users who were eligible for preventive medications were not at all interested, not sure, or needed more information about trying an injectable preventive medication. About 40% were not at all interested in injectables. In general, current users and those who had discontinued medication were more interested in preventive medication, including injectables.
‘Disheartening’ discontinuation rates
There are likely multiple reasons for the low rate of migraine prevention treatment, said Dr. Nahas. Many people with migraine never consult a clinician, owing to factors such as stigma, cost, lack of access, and lack of awareness. In addition, patients with migraine are frequently misdiagnosed, she added.
“Other data suggest that only about a quarter of people with episodic migraine and under 5% of people with chronic migraine consult a clinician, receive an accurate diagnosis, and are prescribed appropriate therapy,” said Dr. Nahas.
When the data in this analysis were gathered, public awareness of migraine was much lower than it is today, and injectable migraine therapies had not gained broad acceptance, she noted. Dr. Nahas added it is possible that attitudes toward injectable preventive medications have changed.
“Would people still prefer daily oral medications? We can’t know for sure until we start asking,” she said. In addition, scientific advances and educational outreach have increased clinicians’ awareness, interest, and skill regarding injectable medications, she said.
“I would certainly hope to see that a much greater proportion of preventive-eligible persons with migraine were at least offered, if not currently taking, preventive medication,” said Dr. Nahas. “But there’s no pleasing everyone, so I think we would still see somewhat disheartening discontinuation rates. The reasons for discontinuation, however, might be less typified by concerns about safety and tolerability.”
Still relevant
Commenting on the study, Mia Tova Minen, MD, chief of headache research and associate professor of neurology and population health at NYU Langone Health, New York, noted that although CaMEO is an older study, its results are still highly relevant.

“Unfortunately, primary care providers are still uncomfortable prescribing migraine preventive medications, and this accounts for the large percentage [of patients] with migraine who, while eligible for migraine preventive therapy, are not offered it,” she said.
Although the public and primary care physicians are now more aware of preventive treatments for migraine, “the number of people offered migraine preventive medication still needs to increase dramatically,” said Dr. Minen.
The American Academy of Neurology’s guidelines for migraine prevention were published in 2012 and are currently being updated. The updated guidelines may include new evidence for candesartan and emerging treatments, such as melatonin and aerobic exercise.
“It is my hope that primary care providers will become more comfortable prescribing migraine preventive medications sooner,” said Dr. Minen.
The current findings suggest a need for additional ways of educating patients with migraine who are eligible for preventive therapies so that they can advocate for themselves, she added. They also suggest the idea of demanding more insurance coverage of behavioral therapies for migraine, because data indicate that these treatments have long-term efficacy and good safety profiles, said Dr. Minen.
An ‘invisible’ disorder
Also commenting on the study, Barbara L. Nye, MD, director of the headache fellowship and codirector of the headache clinic at Dartmouth-Hitchcock Medical Center, Lebanon, N.H., said the CaMEO cohort likely is representative of the general population of patients with migraine.
She noted that a significant weakness of the current study is that it examined data collected before the Food and Drug Administration approved monoclonal antibodies and therefore does not reflect patients’ current experience with medications.
“I believe that the attitudes and fears surrounding the use of injectable medication are now likely far less than previously reported, given the positive track record the new generation of once-a-month injectable medications has,” said Dr. Nye.
The findings reinforce the idea that either patients are not talking to their primary care physicians about their headaches and disability or that clinicians are not asking about them, she added. “Both issues are likely linked to the stigma that this disease state has surrounding it. This is an invisible neurological disorder to most,” Dr. Nye said.
The study was sponsored by Allergan before it was acquired by AbbVie. Dr. Nahas has served as a consultant, advisory board member, or speaker for AbbVie/Allergan, Alder/Lundbeck, Amgen/Novartis, Biohaven, Eli Lilly, Impel, Nesos Corp, Supernus, Teva, Theranica, and Zosano. She has not received and will not receive monetary compensation for this research. Dr. Minen has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests. Investigators found that among patients with migraine who are eligible for preventive therapy, more than a third were not offered this option. In addition, fewer than 10% were currently taking preventive medication, and an additional 10% had discontinued preventive therapy.
“We confirmed that as of 2012 to 2013 – the years these data were collected from a large, comprehensive survey – gaps in care remained,” said study investigator Stephanie J. Nahas, MD, director of the headache medicine fellowship program, Thomas Jefferson University, Philadelphia. “In this preventive-eligible population, 35% reported never even being offered preventive medication.”
Furthermore, only 28% of patients taking preventive medication experienced a reduction in headache frequency to less than 4 days per month, which is a primary goal of treatment, said Dr. Nahas. Disease burden, as measured with scales of disability and affective comorbidities, remained substantial.
The findings were presented at the American Headache Society’s 2021 annual meeting.
Lack of efficacy?
In 2019, the American Headache Society published a position statement recommending that preventive treatment be considered for patients who have migraine and four or more monthly headache days (MHDs), regardless of their level of associated disability. However, previous data suggest few patients who are eligible for preventive treatment receive it. In addition, many who have used preventive medications do not adhere to their regimens because of problems with tolerability, efficacy, or both.
To identify treatment gaps and characterize self-reported use of preventive medications for migraine, the investigators examined data from the Chronic Migraine Epidemiology and Outcomes (CaMEO) study, a web-based survey conducted in a representative U.S. sample from September 2012 through November 2013.
The survey identified and characterized patients who met modified criteria for migraine consistent with those in ICHD-3. The researchers classified respondents who had migraine and four or more MHDs as potentially eligible for migraine preventive treatment.
The investigators assessed the study population’s use of oral preventive medications, migraine-related disability and burden, willingness to take preventive treatment, and reasons for discontinuation.
Assessments included the Migraine Disability Assessment Questionnaire, the Patient Health Questionnaire–9 for depression, the Generalized Anxiety Disorder 7-Item Scale, the Migraine Specific Quality of Life questionnaire, and the Migraine Symptom Severity Scale.
In all, 16,789 respondents met criteria for migraine, and 6,579 (39.2%) reported having at least four MHDs. The median age of this subgroup that was eligible for preventive treatment was 40.3 years, and approximately 79% were women.
Only 9.8% of respondents who were eligible for preventive medications were currently using an oral preventive medication. Among those who had ever tried an oral preventive medication, 53.6% discontinued it. Efficacy for patients who used medications appeared to be inadequate. Among all current users of preventive treatment, 68.4% continued to have at least four MHDs.
The researchers assessed treatment eligibility among patients not taking preventive medication. Among respondents who had never used a preventive treatment, 35.7% were eligible to receive it. Among all users who had discontinued preventive medication, 61.0% were still eligible to receive it.
Attitudes toward injectables
Among respondents who had never used a preventive treatment, 64.3% had zero to three MHDs. The remaining 35.7% had 4-7, 8-14, or 15 or more MHDs. Among current users of preventive treatments, 68.4% had four or more MHDs. Among those who had discontinued preventive treatment, 61.0% had four or more MHDs.
Patients who have never used preventive medication “have substantial management gaps,” said Dr. Nahas. High proportions of these patients have moderate or severe disability (64.7%), depression (43%), and anxiety (39%). The rates of these outcomes are higher in users who discontinued treatment, likely because of confounding by indication, she added.
The prevalence of anxiety was similar between those who currently used, formerly used, or never used preventive medications. However, there were differences between never-users and current or former users with respect to moderate to severe depression (never-users, 43%; current users, 49.4%; discontinued users, 46.5%) and moderate to severe disability (never-users, 64.7%; current users, 80.4%; discontinued users, 78.9%).
In all, 44.6% of those who discontinued preventive therapy reported safety and tolerability problems as reasons for stopping treatment. In addition, 39.7% reported that these medications did not prevent enough headaches. Some patients reported partial or temporary efficacy as a reason for discontinuation. Other reasons were related to health care costs and access and personal preferences. Only 9.2% of patients who discontinued treatment said that their headaches improved enough to stop medication.
The investigators also analyzed respondents’ interest in preventive therapies. Among respondents who had never used preventive therapies, 61.8% of those who were eligible to use them were somewhat or very interested in trying an oral prescription medication for migraine prevention. However, 59.1% of never-users who were eligible for preventive medications were not at all interested, not sure, or needed more information about trying an injectable preventive medication. About 40% were not at all interested in injectables. In general, current users and those who had discontinued medication were more interested in preventive medication, including injectables.
‘Disheartening’ discontinuation rates
There are likely multiple reasons for the low rate of migraine prevention treatment, said Dr. Nahas. Many people with migraine never consult a clinician, owing to factors such as stigma, cost, lack of access, and lack of awareness. In addition, patients with migraine are frequently misdiagnosed, she added.
“Other data suggest that only about a quarter of people with episodic migraine and under 5% of people with chronic migraine consult a clinician, receive an accurate diagnosis, and are prescribed appropriate therapy,” said Dr. Nahas.
When the data in this analysis were gathered, public awareness of migraine was much lower than it is today, and injectable migraine therapies had not gained broad acceptance, she noted. Dr. Nahas added it is possible that attitudes toward injectable preventive medications have changed.
“Would people still prefer daily oral medications? We can’t know for sure until we start asking,” she said. In addition, scientific advances and educational outreach have increased clinicians’ awareness, interest, and skill regarding injectable medications, she said.
“I would certainly hope to see that a much greater proportion of preventive-eligible persons with migraine were at least offered, if not currently taking, preventive medication,” said Dr. Nahas. “But there’s no pleasing everyone, so I think we would still see somewhat disheartening discontinuation rates. The reasons for discontinuation, however, might be less typified by concerns about safety and tolerability.”
Still relevant
Commenting on the study, Mia Tova Minen, MD, chief of headache research and associate professor of neurology and population health at NYU Langone Health, New York, noted that although CaMEO is an older study, its results are still highly relevant.
“Unfortunately, primary care providers are still uncomfortable prescribing migraine preventive medications, and this accounts for the large percentage [of patients] with migraine who, while eligible for migraine preventive therapy, are not offered it,” she said.
Although the public and primary care physicians are now more aware of preventive treatments for migraine, “the number of people offered migraine preventive medication still needs to increase dramatically,” said Dr. Minen.
The American Academy of Neurology’s guidelines for migraine prevention were published in 2012 and are currently being updated. The updated guidelines may include new evidence for candesartan and emerging treatments, such as melatonin and aerobic exercise.
“It is my hope that primary care providers will become more comfortable prescribing migraine preventive medications sooner,” said Dr. Minen.
The current findings suggest a need for additional ways of educating patients with migraine who are eligible for preventive therapies so that they can advocate for themselves, she added. They also suggest the idea of demanding more insurance coverage of behavioral therapies for migraine, because data indicate that these treatments have long-term efficacy and good safety profiles, said Dr. Minen.
An ‘invisible’ disorder
Also commenting on the study, Barbara L. Nye, MD, director of the headache fellowship and codirector of the headache clinic at Dartmouth-Hitchcock Medical Center, Lebanon, N.H., said the CaMEO cohort likely is representative of the general population of patients with migraine.
She noted that a significant weakness of the current study is that it examined data collected before the Food and Drug Administration approved monoclonal antibodies and therefore does not reflect patients’ current experience with medications.
“I believe that the attitudes and fears surrounding the use of injectable medication are now likely far less than previously reported, given the positive track record the new generation of once-a-month injectable medications has,” said Dr. Nye.
The findings reinforce the idea that either patients are not talking to their primary care physicians about their headaches and disability or that clinicians are not asking about them, she added. “Both issues are likely linked to the stigma that this disease state has surrounding it. This is an invisible neurological disorder to most,” Dr. Nye said.
The study was sponsored by Allergan before it was acquired by AbbVie. Dr. Nahas has served as a consultant, advisory board member, or speaker for AbbVie/Allergan, Alder/Lundbeck, Amgen/Novartis, Biohaven, Eli Lilly, Impel, Nesos Corp, Supernus, Teva, Theranica, and Zosano. She has not received and will not receive monetary compensation for this research. Dr. Minen has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests. Investigators found that among patients with migraine who are eligible for preventive therapy, more than a third were not offered this option. In addition, fewer than 10% were currently taking preventive medication, and an additional 10% had discontinued preventive therapy.
“We confirmed that as of 2012 to 2013 – the years these data were collected from a large, comprehensive survey – gaps in care remained,” said study investigator Stephanie J. Nahas, MD, director of the headache medicine fellowship program, Thomas Jefferson University, Philadelphia. “In this preventive-eligible population, 35% reported never even being offered preventive medication.”
Furthermore, only 28% of patients taking preventive medication experienced a reduction in headache frequency to less than 4 days per month, which is a primary goal of treatment, said Dr. Nahas. Disease burden, as measured with scales of disability and affective comorbidities, remained substantial.
The findings were presented at the American Headache Society’s 2021 annual meeting.
Lack of efficacy?
In 2019, the American Headache Society published a position statement recommending that preventive treatment be considered for patients who have migraine and four or more monthly headache days (MHDs), regardless of their level of associated disability. However, previous data suggest few patients who are eligible for preventive treatment receive it. In addition, many who have used preventive medications do not adhere to their regimens because of problems with tolerability, efficacy, or both.
To identify treatment gaps and characterize self-reported use of preventive medications for migraine, the investigators examined data from the Chronic Migraine Epidemiology and Outcomes (CaMEO) study, a web-based survey conducted in a representative U.S. sample from September 2012 through November 2013.
The survey identified and characterized patients who met modified criteria for migraine consistent with those in ICHD-3. The researchers classified respondents who had migraine and four or more MHDs as potentially eligible for migraine preventive treatment.
The investigators assessed the study population’s use of oral preventive medications, migraine-related disability and burden, willingness to take preventive treatment, and reasons for discontinuation.
Assessments included the Migraine Disability Assessment Questionnaire, the Patient Health Questionnaire–9 for depression, the Generalized Anxiety Disorder 7-Item Scale, the Migraine Specific Quality of Life questionnaire, and the Migraine Symptom Severity Scale.
In all, 16,789 respondents met criteria for migraine, and 6,579 (39.2%) reported having at least four MHDs. The median age of this subgroup that was eligible for preventive treatment was 40.3 years, and approximately 79% were women.
Only 9.8% of respondents who were eligible for preventive medications were currently using an oral preventive medication. Among those who had ever tried an oral preventive medication, 53.6% discontinued it. Efficacy for patients who used medications appeared to be inadequate. Among all current users of preventive treatment, 68.4% continued to have at least four MHDs.
The researchers assessed treatment eligibility among patients not taking preventive medication. Among respondents who had never used a preventive treatment, 35.7% were eligible to receive it. Among all users who had discontinued preventive medication, 61.0% were still eligible to receive it.
Attitudes toward injectables
Among respondents who had never used a preventive treatment, 64.3% had zero to three MHDs. The remaining 35.7% had 4-7, 8-14, or 15 or more MHDs. Among current users of preventive treatments, 68.4% had four or more MHDs. Among those who had discontinued preventive treatment, 61.0% had four or more MHDs.
Patients who have never used preventive medication “have substantial management gaps,” said Dr. Nahas. High proportions of these patients have moderate or severe disability (64.7%), depression (43%), and anxiety (39%). The rates of these outcomes are higher in users who discontinued treatment, likely because of confounding by indication, she added.
The prevalence of anxiety was similar between those who currently used, formerly used, or never used preventive medications. However, there were differences between never-users and current or former users with respect to moderate to severe depression (never-users, 43%; current users, 49.4%; discontinued users, 46.5%) and moderate to severe disability (never-users, 64.7%; current users, 80.4%; discontinued users, 78.9%).
In all, 44.6% of those who discontinued preventive therapy reported safety and tolerability problems as reasons for stopping treatment. In addition, 39.7% reported that these medications did not prevent enough headaches. Some patients reported partial or temporary efficacy as a reason for discontinuation. Other reasons were related to health care costs and access and personal preferences. Only 9.2% of patients who discontinued treatment said that their headaches improved enough to stop medication.
The investigators also analyzed respondents’ interest in preventive therapies. Among respondents who had never used preventive therapies, 61.8% of those who were eligible to use them were somewhat or very interested in trying an oral prescription medication for migraine prevention. However, 59.1% of never-users who were eligible for preventive medications were not at all interested, not sure, or needed more information about trying an injectable preventive medication. About 40% were not at all interested in injectables. In general, current users and those who had discontinued medication were more interested in preventive medication, including injectables.
‘Disheartening’ discontinuation rates
There are likely multiple reasons for the low rate of migraine prevention treatment, said Dr. Nahas. Many people with migraine never consult a clinician, owing to factors such as stigma, cost, lack of access, and lack of awareness. In addition, patients with migraine are frequently misdiagnosed, she added.
“Other data suggest that only about a quarter of people with episodic migraine and under 5% of people with chronic migraine consult a clinician, receive an accurate diagnosis, and are prescribed appropriate therapy,” said Dr. Nahas.
When the data in this analysis were gathered, public awareness of migraine was much lower than it is today, and injectable migraine therapies had not gained broad acceptance, she noted. Dr. Nahas added it is possible that attitudes toward injectable preventive medications have changed.
“Would people still prefer daily oral medications? We can’t know for sure until we start asking,” she said. In addition, scientific advances and educational outreach have increased clinicians’ awareness, interest, and skill regarding injectable medications, she said.
“I would certainly hope to see that a much greater proportion of preventive-eligible persons with migraine were at least offered, if not currently taking, preventive medication,” said Dr. Nahas. “But there’s no pleasing everyone, so I think we would still see somewhat disheartening discontinuation rates. The reasons for discontinuation, however, might be less typified by concerns about safety and tolerability.”
Still relevant
Commenting on the study, Mia Tova Minen, MD, chief of headache research and associate professor of neurology and population health at NYU Langone Health, New York, noted that although CaMEO is an older study, its results are still highly relevant.
“Unfortunately, primary care providers are still uncomfortable prescribing migraine preventive medications, and this accounts for the large percentage [of patients] with migraine who, while eligible for migraine preventive therapy, are not offered it,” she said.
Although the public and primary care physicians are now more aware of preventive treatments for migraine, “the number of people offered migraine preventive medication still needs to increase dramatically,” said Dr. Minen.
The American Academy of Neurology’s guidelines for migraine prevention were published in 2012 and are currently being updated. The updated guidelines may include new evidence for candesartan and emerging treatments, such as melatonin and aerobic exercise.
“It is my hope that primary care providers will become more comfortable prescribing migraine preventive medications sooner,” said Dr. Minen.
The current findings suggest a need for additional ways of educating patients with migraine who are eligible for preventive therapies so that they can advocate for themselves, she added. They also suggest the idea of demanding more insurance coverage of behavioral therapies for migraine, because data indicate that these treatments have long-term efficacy and good safety profiles, said Dr. Minen.
An ‘invisible’ disorder
Also commenting on the study, Barbara L. Nye, MD, director of the headache fellowship and codirector of the headache clinic at Dartmouth-Hitchcock Medical Center, Lebanon, N.H., said the CaMEO cohort likely is representative of the general population of patients with migraine.
She noted that a significant weakness of the current study is that it examined data collected before the Food and Drug Administration approved monoclonal antibodies and therefore does not reflect patients’ current experience with medications.
“I believe that the attitudes and fears surrounding the use of injectable medication are now likely far less than previously reported, given the positive track record the new generation of once-a-month injectable medications has,” said Dr. Nye.
The findings reinforce the idea that either patients are not talking to their primary care physicians about their headaches and disability or that clinicians are not asking about them, she added. “Both issues are likely linked to the stigma that this disease state has surrounding it. This is an invisible neurological disorder to most,” Dr. Nye said.
The study was sponsored by Allergan before it was acquired by AbbVie. Dr. Nahas has served as a consultant, advisory board member, or speaker for AbbVie/Allergan, Alder/Lundbeck, Amgen/Novartis, Biohaven, Eli Lilly, Impel, Nesos Corp, Supernus, Teva, Theranica, and Zosano. She has not received and will not receive monetary compensation for this research. Dr. Minen has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AHS 2021
FDA clears next-generation DBS system for movement disorders
The SenSight Directional Lead System for DBS therapy combines two recent advancements: sensing capability that allows real-time monitoring of brain signals to optimize settings for stimulation, and a “directional lead” that enables steering of electric current for more precise targeting of stimulation through the electrode.
“Until now, sensing capability and directional leads have not been available in the same DBS system, so we have had to choose one technology or the other, based on the predicted needs of each patient,” neurosurgeon Kelly Foote, MD, who performed the first implant of the SenSight System at University of Florida (UF) Health, said in a news release.
“Now, by coupling this new directional lead with a pulse generator capable of brain sensing, we are excited to be able to offer our patients the synergistic benefits of both technologies,” added Dr. Foote, codirector of the Norman Fixel Institute for Neurological Diseases at UF Health.
Dr. Foote said DBS systems capable of adjusting therapeutic stimulation in response to continuously recorded brain signals may lead to better DBS outcomes with fewer adverse effects.
“Adding a directional lead to such a system will improve our ability to localize abnormal signals and enable us to steer current more effectively to areas in the brain where it is most beneficial,” Dr. Foote said.
“We are excited to see the clinical benefits that the new SenSight directional lead system will provide to patients and physicians in the U.S.,” added Mike Daly, vice president and general manager of brain modulation at Medtronic.
Medtronic’s SenSight directional lead DBS system received CE Mark approval in Europe in March.
A version of this article first appeared on Medscape.com.
The SenSight Directional Lead System for DBS therapy combines two recent advancements: sensing capability that allows real-time monitoring of brain signals to optimize settings for stimulation, and a “directional lead” that enables steering of electric current for more precise targeting of stimulation through the electrode.
“Until now, sensing capability and directional leads have not been available in the same DBS system, so we have had to choose one technology or the other, based on the predicted needs of each patient,” neurosurgeon Kelly Foote, MD, who performed the first implant of the SenSight System at University of Florida (UF) Health, said in a news release.
“Now, by coupling this new directional lead with a pulse generator capable of brain sensing, we are excited to be able to offer our patients the synergistic benefits of both technologies,” added Dr. Foote, codirector of the Norman Fixel Institute for Neurological Diseases at UF Health.
Dr. Foote said DBS systems capable of adjusting therapeutic stimulation in response to continuously recorded brain signals may lead to better DBS outcomes with fewer adverse effects.
“Adding a directional lead to such a system will improve our ability to localize abnormal signals and enable us to steer current more effectively to areas in the brain where it is most beneficial,” Dr. Foote said.
“We are excited to see the clinical benefits that the new SenSight directional lead system will provide to patients and physicians in the U.S.,” added Mike Daly, vice president and general manager of brain modulation at Medtronic.
Medtronic’s SenSight directional lead DBS system received CE Mark approval in Europe in March.
A version of this article first appeared on Medscape.com.
The SenSight Directional Lead System for DBS therapy combines two recent advancements: sensing capability that allows real-time monitoring of brain signals to optimize settings for stimulation, and a “directional lead” that enables steering of electric current for more precise targeting of stimulation through the electrode.
“Until now, sensing capability and directional leads have not been available in the same DBS system, so we have had to choose one technology or the other, based on the predicted needs of each patient,” neurosurgeon Kelly Foote, MD, who performed the first implant of the SenSight System at University of Florida (UF) Health, said in a news release.
“Now, by coupling this new directional lead with a pulse generator capable of brain sensing, we are excited to be able to offer our patients the synergistic benefits of both technologies,” added Dr. Foote, codirector of the Norman Fixel Institute for Neurological Diseases at UF Health.
Dr. Foote said DBS systems capable of adjusting therapeutic stimulation in response to continuously recorded brain signals may lead to better DBS outcomes with fewer adverse effects.
“Adding a directional lead to such a system will improve our ability to localize abnormal signals and enable us to steer current more effectively to areas in the brain where it is most beneficial,” Dr. Foote said.
“We are excited to see the clinical benefits that the new SenSight directional lead system will provide to patients and physicians in the U.S.,” added Mike Daly, vice president and general manager of brain modulation at Medtronic.
Medtronic’s SenSight directional lead DBS system received CE Mark approval in Europe in March.
A version of this article first appeared on Medscape.com.