User login
Premature return to play after concussion has decreased
, according to a recent chart review. Rates of premature return to learn (RTL) are essentially unchanged, however.
“Delay in recovery is the major reason why it’s important not to RTL or RTP prematurely,” said James Carson, MD, associate professor of family and community medicine, University of Toronto.
“That delay in recovery only sets students further back in terms of the stress they get from being delayed with their schoolwork – they could lose their year in school, lose all their social contacts. So, there are a number of psychosocial issues that come into play if recovery is delayed, and that is what premature RTL and premature RTP will do – they delay the student’s recovery,” he emphasized.
The study was published in Canadian Family Physician.
Differences by sex
The study involved 241 students who had 258 distinct cases of SRC. The researchers defined premature RTP and RTL as chart records documenting the relapse, recurrence, or worsening of concussion symptoms that accompanied the patient’s RTP or RTL. Between 2011 and 2016, 26.7% of students had evidence of premature RTP, while 42.6% of them had evidence of premature RTL, the authors noted.
Compared with findings from an earlier survey of data from 2006 to 2011, the incidence of premature RTP dropped by 38.6% (P = .0003). In contrast, symptoms associated with premature RTL dropped by only 4.7% from the previous survey. This change was not statistically significant.
There was also a significant difference between males and females in the proportion of SRC cases with relapse of symptoms. Relapse occurred in 43.4% of female athletes with SRC versus 29.7% of male athletes with SRC (P = .023).
Female athletes also had significantly longer times before being cleared for RTP. The mean time was 74.5 days for females, compared with a mean of 42.3 days for male athletes (P < .001). “The median time to RTP clearance was nearly double [for female athletes] at 49 days versus 25 days [for male athletes],” wrote the authors.
The rate of premature RTL was also higher among secondary school students (48.8%), compared with 28% among elementary students and 42% among postsecondary students.
More concussions coming?
Before the first consensus conference, organized by the Concussion in Sport Group in 2001, management of concussion was based on rating and grading scales that had no medical evidence to support them, said Dr. Carson. After the consensus conference, it was recommended that physicians manage each concussion individually and, when it came to RTP, recommendations were based upon symptom resolution.
In contrast, there was nothing in the literature regarding how student athletes who sustain a concussion should RTL. Some schools made generous accommodations, and others none. This situation changed around 2011, when experts started publishing data about how better to accommodate student athletes who have a temporary disability for which schools need to introduce temporary accommodations to help them recover.
“Recommendations for RTP essentially had a 12-year head-start,” Dr. Carson emphasized, “and RTL had a much slower start.” Unfortunately, Dr. Carson foresees more athletes sustaining concussions as pandemic restrictions ease over the next few months. “As athletes RTP after the pandemic, they just will not be in game shape,” he said.
“In other words, athletes may not have the neuromuscular control to avoid these injuries as easily,” he added. Worse, athletes may not realize they are not quite ready to return to the expected level of participation so quickly. “I believe this scenario will lead to more concussions that will be difficult to manage in the context of an already strained health care system,” said Dr. Carson.
A limitation of the study was that it was difficult to assess whether all patients followed medical advice consistently.
“Very positive shifts”
Commenting on the findings, Nick Reed, PhD, Canada research chair in pediatric concussion and associate professor of occupational science and occupational therapy, University of Toronto, said that sports medicine physicians are seeing “very positive shifts” in concussion awareness and related behaviors such as providing education, support, and accommodations to students within the school environment. “More and more teachers are seeking education to learn what a concussion is and what to do to best support their students with concussion,” he said. Dr. Reed was not involved in the current study.
Indeed, this increasing awareness led to the development of a concussion education tool for teachers – SCHOOLFirst – although Dr. Reed did acknowledge that not all teachers have either the knowledge or the resources they need to optimally support their students with concussion. In the meantime, to reduce the risk of injury, Dr. Reed stressed that it is important for students to wear equipment appropriate for the game being played and to play by the rules.
“It is key to play sports in a way that is fair and respectful and not [engage] in behaviors with the intent of injuring an opponent,” he stressed. It is also important for athletes themselves to know the signs and symptoms of concussion and, if they think they have a concussion, to immediately stop playing, report how they are feeling to a coach, teacher, or parent, and to seek medical assessment to determine if they have a concussion or not.
“The key here is to focus on what the athlete can do after a concussion rather than what they can’t do,” Dr. Reed said. After even a few days of complete rest, students with a concussion can gradually introduce low levels of physical and cognitive activity that won’t make their symptoms worse. This activity can include going back to school with temporary accommodations in place, such as shorter school days and increased rest breaks. “When returning to school and to sport after a concussion, it is important to follow a stepwise and gradual return to activities so that you aren’t doing too much too fast,” Dr. Reed emphasized.
The study was conducted without external funding. Dr. Carson and Dr. Reed reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
, according to a recent chart review. Rates of premature return to learn (RTL) are essentially unchanged, however.
“Delay in recovery is the major reason why it’s important not to RTL or RTP prematurely,” said James Carson, MD, associate professor of family and community medicine, University of Toronto.
“That delay in recovery only sets students further back in terms of the stress they get from being delayed with their schoolwork – they could lose their year in school, lose all their social contacts. So, there are a number of psychosocial issues that come into play if recovery is delayed, and that is what premature RTL and premature RTP will do – they delay the student’s recovery,” he emphasized.
The study was published in Canadian Family Physician.
Differences by sex
The study involved 241 students who had 258 distinct cases of SRC. The researchers defined premature RTP and RTL as chart records documenting the relapse, recurrence, or worsening of concussion symptoms that accompanied the patient’s RTP or RTL. Between 2011 and 2016, 26.7% of students had evidence of premature RTP, while 42.6% of them had evidence of premature RTL, the authors noted.
Compared with findings from an earlier survey of data from 2006 to 2011, the incidence of premature RTP dropped by 38.6% (P = .0003). In contrast, symptoms associated with premature RTL dropped by only 4.7% from the previous survey. This change was not statistically significant.
There was also a significant difference between males and females in the proportion of SRC cases with relapse of symptoms. Relapse occurred in 43.4% of female athletes with SRC versus 29.7% of male athletes with SRC (P = .023).
Female athletes also had significantly longer times before being cleared for RTP. The mean time was 74.5 days for females, compared with a mean of 42.3 days for male athletes (P < .001). “The median time to RTP clearance was nearly double [for female athletes] at 49 days versus 25 days [for male athletes],” wrote the authors.
The rate of premature RTL was also higher among secondary school students (48.8%), compared with 28% among elementary students and 42% among postsecondary students.
More concussions coming?
Before the first consensus conference, organized by the Concussion in Sport Group in 2001, management of concussion was based on rating and grading scales that had no medical evidence to support them, said Dr. Carson. After the consensus conference, it was recommended that physicians manage each concussion individually and, when it came to RTP, recommendations were based upon symptom resolution.
In contrast, there was nothing in the literature regarding how student athletes who sustain a concussion should RTL. Some schools made generous accommodations, and others none. This situation changed around 2011, when experts started publishing data about how better to accommodate student athletes who have a temporary disability for which schools need to introduce temporary accommodations to help them recover.
“Recommendations for RTP essentially had a 12-year head-start,” Dr. Carson emphasized, “and RTL had a much slower start.” Unfortunately, Dr. Carson foresees more athletes sustaining concussions as pandemic restrictions ease over the next few months. “As athletes RTP after the pandemic, they just will not be in game shape,” he said.
“In other words, athletes may not have the neuromuscular control to avoid these injuries as easily,” he added. Worse, athletes may not realize they are not quite ready to return to the expected level of participation so quickly. “I believe this scenario will lead to more concussions that will be difficult to manage in the context of an already strained health care system,” said Dr. Carson.
A limitation of the study was that it was difficult to assess whether all patients followed medical advice consistently.
“Very positive shifts”
Commenting on the findings, Nick Reed, PhD, Canada research chair in pediatric concussion and associate professor of occupational science and occupational therapy, University of Toronto, said that sports medicine physicians are seeing “very positive shifts” in concussion awareness and related behaviors such as providing education, support, and accommodations to students within the school environment. “More and more teachers are seeking education to learn what a concussion is and what to do to best support their students with concussion,” he said. Dr. Reed was not involved in the current study.
Indeed, this increasing awareness led to the development of a concussion education tool for teachers – SCHOOLFirst – although Dr. Reed did acknowledge that not all teachers have either the knowledge or the resources they need to optimally support their students with concussion. In the meantime, to reduce the risk of injury, Dr. Reed stressed that it is important for students to wear equipment appropriate for the game being played and to play by the rules.
“It is key to play sports in a way that is fair and respectful and not [engage] in behaviors with the intent of injuring an opponent,” he stressed. It is also important for athletes themselves to know the signs and symptoms of concussion and, if they think they have a concussion, to immediately stop playing, report how they are feeling to a coach, teacher, or parent, and to seek medical assessment to determine if they have a concussion or not.
“The key here is to focus on what the athlete can do after a concussion rather than what they can’t do,” Dr. Reed said. After even a few days of complete rest, students with a concussion can gradually introduce low levels of physical and cognitive activity that won’t make their symptoms worse. This activity can include going back to school with temporary accommodations in place, such as shorter school days and increased rest breaks. “When returning to school and to sport after a concussion, it is important to follow a stepwise and gradual return to activities so that you aren’t doing too much too fast,” Dr. Reed emphasized.
The study was conducted without external funding. Dr. Carson and Dr. Reed reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
, according to a recent chart review. Rates of premature return to learn (RTL) are essentially unchanged, however.
“Delay in recovery is the major reason why it’s important not to RTL or RTP prematurely,” said James Carson, MD, associate professor of family and community medicine, University of Toronto.
“That delay in recovery only sets students further back in terms of the stress they get from being delayed with their schoolwork – they could lose their year in school, lose all their social contacts. So, there are a number of psychosocial issues that come into play if recovery is delayed, and that is what premature RTL and premature RTP will do – they delay the student’s recovery,” he emphasized.
The study was published in Canadian Family Physician.
Differences by sex
The study involved 241 students who had 258 distinct cases of SRC. The researchers defined premature RTP and RTL as chart records documenting the relapse, recurrence, or worsening of concussion symptoms that accompanied the patient’s RTP or RTL. Between 2011 and 2016, 26.7% of students had evidence of premature RTP, while 42.6% of them had evidence of premature RTL, the authors noted.
Compared with findings from an earlier survey of data from 2006 to 2011, the incidence of premature RTP dropped by 38.6% (P = .0003). In contrast, symptoms associated with premature RTL dropped by only 4.7% from the previous survey. This change was not statistically significant.
There was also a significant difference between males and females in the proportion of SRC cases with relapse of symptoms. Relapse occurred in 43.4% of female athletes with SRC versus 29.7% of male athletes with SRC (P = .023).
Female athletes also had significantly longer times before being cleared for RTP. The mean time was 74.5 days for females, compared with a mean of 42.3 days for male athletes (P < .001). “The median time to RTP clearance was nearly double [for female athletes] at 49 days versus 25 days [for male athletes],” wrote the authors.
The rate of premature RTL was also higher among secondary school students (48.8%), compared with 28% among elementary students and 42% among postsecondary students.
More concussions coming?
Before the first consensus conference, organized by the Concussion in Sport Group in 2001, management of concussion was based on rating and grading scales that had no medical evidence to support them, said Dr. Carson. After the consensus conference, it was recommended that physicians manage each concussion individually and, when it came to RTP, recommendations were based upon symptom resolution.
In contrast, there was nothing in the literature regarding how student athletes who sustain a concussion should RTL. Some schools made generous accommodations, and others none. This situation changed around 2011, when experts started publishing data about how better to accommodate student athletes who have a temporary disability for which schools need to introduce temporary accommodations to help them recover.
“Recommendations for RTP essentially had a 12-year head-start,” Dr. Carson emphasized, “and RTL had a much slower start.” Unfortunately, Dr. Carson foresees more athletes sustaining concussions as pandemic restrictions ease over the next few months. “As athletes RTP after the pandemic, they just will not be in game shape,” he said.
“In other words, athletes may not have the neuromuscular control to avoid these injuries as easily,” he added. Worse, athletes may not realize they are not quite ready to return to the expected level of participation so quickly. “I believe this scenario will lead to more concussions that will be difficult to manage in the context of an already strained health care system,” said Dr. Carson.
A limitation of the study was that it was difficult to assess whether all patients followed medical advice consistently.
“Very positive shifts”
Commenting on the findings, Nick Reed, PhD, Canada research chair in pediatric concussion and associate professor of occupational science and occupational therapy, University of Toronto, said that sports medicine physicians are seeing “very positive shifts” in concussion awareness and related behaviors such as providing education, support, and accommodations to students within the school environment. “More and more teachers are seeking education to learn what a concussion is and what to do to best support their students with concussion,” he said. Dr. Reed was not involved in the current study.
Indeed, this increasing awareness led to the development of a concussion education tool for teachers – SCHOOLFirst – although Dr. Reed did acknowledge that not all teachers have either the knowledge or the resources they need to optimally support their students with concussion. In the meantime, to reduce the risk of injury, Dr. Reed stressed that it is important for students to wear equipment appropriate for the game being played and to play by the rules.
“It is key to play sports in a way that is fair and respectful and not [engage] in behaviors with the intent of injuring an opponent,” he stressed. It is also important for athletes themselves to know the signs and symptoms of concussion and, if they think they have a concussion, to immediately stop playing, report how they are feeling to a coach, teacher, or parent, and to seek medical assessment to determine if they have a concussion or not.
“The key here is to focus on what the athlete can do after a concussion rather than what they can’t do,” Dr. Reed said. After even a few days of complete rest, students with a concussion can gradually introduce low levels of physical and cognitive activity that won’t make their symptoms worse. This activity can include going back to school with temporary accommodations in place, such as shorter school days and increased rest breaks. “When returning to school and to sport after a concussion, it is important to follow a stepwise and gradual return to activities so that you aren’t doing too much too fast,” Dr. Reed emphasized.
The study was conducted without external funding. Dr. Carson and Dr. Reed reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Cutting dementia risk in atrial fibrillation: Does rhythm control strategy matter?
The risk for dementia goes up in patients with atrial fibrillation (AFib), but some evidence suggests that risk can be blunted with therapies that restore sinus rhythm. But a new cohort study suggests that the treatment effect’s magnitude might depend on the rhythm control strategy. It hinted that AFib catheter ablation might be more effective than pharmacologic rhythm control alone at cutting the risk for dementia.
The case-matched study of more than 38,000 adults with AFib saw a 41% reduction (P < .0001) in risk for dementia among those who underwent catheter ablation after attempted rhythm control with antiarrhythmic drugs (AAD), compared with those managed with pharmacologic rhythm control therapy alone.
The observational study comprising 20 years of data comes with big limitations and can’t say for sure whether catheter ablation is better than AAD alone at cutting the dementia risk in AFib. But it and other evidence support the idea, which has yet to be explored in a randomized fashion.
In a secondary finding, the analysis showed a similar reduction in dementia risk from catheter ablation, compared with AAD, in women and in men by 40% and 45%, respectively (P < .0001 for both). The findings are particularly relevant “given the higher life-long risk of dementia among women and the lower likelihood that women will be offered ablation, which has been demonstrated repeatedly,” Emily P. Zeitler, MD, MHS, Dartmouth-Hitchcock Medical Center, Lebanon, N.H., said in an interview. “I think this is another reason to try to be more generous in offering ablation to women.”
Management of AFib certainly evolved in important ways from 2000 to 2021, the period covered by the study. But a sensitivity analysis based on data from 2010 to 2021 showed “no meaningful differences” in the results, said Dr. Zeitler, who is slated to present the findings at the annual scientific sessions of the Heart Rhythm Society.
Dr. Zeitler acknowledged that the observational study, even with its propensity-matched ablation and AAD cohorts, can only hint at a preference for ablation over AAD for lowering risk for AFib-associated dementia. “We know there’s unmeasured and unfixable confounding between those two groups, so we see this really as hypothesis-generating.”
It was “a well-done analysis,” and the conclusion that the dementia risk was lower with catheter ablation is “absolutely correct,” but only as far as the study and its limitations allow, agreed David Conen, MD, MPH, McMaster University, Hamilton, Ont., who is not a coauthor.
“Even with propensity matching, you can get rid of some sorts of confounding, but you can never get rid of all selection bias issues.” That, he said when interviewed, takes randomized trials.
Dr. Conen, who is studying cognitive decline in AFib as a SWISS-AF trial principal investigator, pointed to a secondary finding of the analysis as evidence for such confounding. He said the ablation group’s nearly 50% drop (P < .0001) in competing risk for death, compared with patients managed with AAD, isn’t plausible.
The finding “strongly suggests these people were healthier and that there’s some sort of selection bias. They were at lower risk of death, they were at lower risk of dementia, and they were probably also at lower risk of stroke, myocardial infarction, thrombosis, and cancer because they were just probably a little healthier than the others,” Dr. Conen said. The ablation and AAD groups “were two very different populations from the get-go.”
The analysis was based on U.S. insurance and Medicare claims data from AFib patients who either underwent catheter ablation after at least one AAD trial or filled prescriptions for at least two different antiarrhythmic agents in the year after AFib diagnosis. Patients with history of dementia, catheter or surgical AFib ablation, or a valve procedure were excluded.
The ablation and AAD-only groups each consisted of 19,066 patients after propensity matching, and the groups were balanced with respect to age, sex, type of insurance, CHA2DS2-VASc scores, and use of renin-angiotensin system inhibitors, oral anticoagulants, and antiplatelets.
The overall risk for dementia was 1.9% for the ablation group and 3.3% for AAD-only patients (hazard ratio, 0.59; 95% confidence interval, 0.52-0.67). Corresponding HRs by sex were 0.55 (95% CI, 0.46-0.66) for men and 0.60 (95% CI, 0.50-0.72) for women.
The competing risk for death was also significantly decreased in the ablation group (HR, 0.51; 95% CI, 0.46-0.55).
Dr. Zeitler pointed to a randomized trial now in the early stages called Neurocognition and Greater Maintenance of Sinus Rhythm in Atrial Fibrillation, or NOGGIN-AF, which will explore relationships between rhythm control therapy and dementia in patients with AFib, whether catheter ablation or AAD can mitigate that risk, and whether either strategy works better than the other, among other goals.
“I’m optimistic,” she said, “and I think it’s going to add to the growing motivations to get patients ablated more quickly and more broadly.”
The analysis was funded by Biosense-Webster. Dr. Zeitler disclosed consulting for Biosense-Webster and Arena Pharmaceuticals (now Pfizer); fees for speaking from Medtronic; and receiving research support from Boston Scientific, Sanofi, and Biosense-Webster. Dr. Conen has previously reported receiving speaker fees from Servier Canada.
A version of this article first appeared on Medscape.com.
The risk for dementia goes up in patients with atrial fibrillation (AFib), but some evidence suggests that risk can be blunted with therapies that restore sinus rhythm. But a new cohort study suggests that the treatment effect’s magnitude might depend on the rhythm control strategy. It hinted that AFib catheter ablation might be more effective than pharmacologic rhythm control alone at cutting the risk for dementia.
The case-matched study of more than 38,000 adults with AFib saw a 41% reduction (P < .0001) in risk for dementia among those who underwent catheter ablation after attempted rhythm control with antiarrhythmic drugs (AAD), compared with those managed with pharmacologic rhythm control therapy alone.
The observational study comprising 20 years of data comes with big limitations and can’t say for sure whether catheter ablation is better than AAD alone at cutting the dementia risk in AFib. But it and other evidence support the idea, which has yet to be explored in a randomized fashion.
In a secondary finding, the analysis showed a similar reduction in dementia risk from catheter ablation, compared with AAD, in women and in men by 40% and 45%, respectively (P < .0001 for both). The findings are particularly relevant “given the higher life-long risk of dementia among women and the lower likelihood that women will be offered ablation, which has been demonstrated repeatedly,” Emily P. Zeitler, MD, MHS, Dartmouth-Hitchcock Medical Center, Lebanon, N.H., said in an interview. “I think this is another reason to try to be more generous in offering ablation to women.”
Management of AFib certainly evolved in important ways from 2000 to 2021, the period covered by the study. But a sensitivity analysis based on data from 2010 to 2021 showed “no meaningful differences” in the results, said Dr. Zeitler, who is slated to present the findings at the annual scientific sessions of the Heart Rhythm Society.
Dr. Zeitler acknowledged that the observational study, even with its propensity-matched ablation and AAD cohorts, can only hint at a preference for ablation over AAD for lowering risk for AFib-associated dementia. “We know there’s unmeasured and unfixable confounding between those two groups, so we see this really as hypothesis-generating.”
It was “a well-done analysis,” and the conclusion that the dementia risk was lower with catheter ablation is “absolutely correct,” but only as far as the study and its limitations allow, agreed David Conen, MD, MPH, McMaster University, Hamilton, Ont., who is not a coauthor.
“Even with propensity matching, you can get rid of some sorts of confounding, but you can never get rid of all selection bias issues.” That, he said when interviewed, takes randomized trials.
Dr. Conen, who is studying cognitive decline in AFib as a SWISS-AF trial principal investigator, pointed to a secondary finding of the analysis as evidence for such confounding. He said the ablation group’s nearly 50% drop (P < .0001) in competing risk for death, compared with patients managed with AAD, isn’t plausible.
The finding “strongly suggests these people were healthier and that there’s some sort of selection bias. They were at lower risk of death, they were at lower risk of dementia, and they were probably also at lower risk of stroke, myocardial infarction, thrombosis, and cancer because they were just probably a little healthier than the others,” Dr. Conen said. The ablation and AAD groups “were two very different populations from the get-go.”
The analysis was based on U.S. insurance and Medicare claims data from AFib patients who either underwent catheter ablation after at least one AAD trial or filled prescriptions for at least two different antiarrhythmic agents in the year after AFib diagnosis. Patients with history of dementia, catheter or surgical AFib ablation, or a valve procedure were excluded.
The ablation and AAD-only groups each consisted of 19,066 patients after propensity matching, and the groups were balanced with respect to age, sex, type of insurance, CHA2DS2-VASc scores, and use of renin-angiotensin system inhibitors, oral anticoagulants, and antiplatelets.
The overall risk for dementia was 1.9% for the ablation group and 3.3% for AAD-only patients (hazard ratio, 0.59; 95% confidence interval, 0.52-0.67). Corresponding HRs by sex were 0.55 (95% CI, 0.46-0.66) for men and 0.60 (95% CI, 0.50-0.72) for women.
The competing risk for death was also significantly decreased in the ablation group (HR, 0.51; 95% CI, 0.46-0.55).
Dr. Zeitler pointed to a randomized trial now in the early stages called Neurocognition and Greater Maintenance of Sinus Rhythm in Atrial Fibrillation, or NOGGIN-AF, which will explore relationships between rhythm control therapy and dementia in patients with AFib, whether catheter ablation or AAD can mitigate that risk, and whether either strategy works better than the other, among other goals.
“I’m optimistic,” she said, “and I think it’s going to add to the growing motivations to get patients ablated more quickly and more broadly.”
The analysis was funded by Biosense-Webster. Dr. Zeitler disclosed consulting for Biosense-Webster and Arena Pharmaceuticals (now Pfizer); fees for speaking from Medtronic; and receiving research support from Boston Scientific, Sanofi, and Biosense-Webster. Dr. Conen has previously reported receiving speaker fees from Servier Canada.
A version of this article first appeared on Medscape.com.
The risk for dementia goes up in patients with atrial fibrillation (AFib), but some evidence suggests that risk can be blunted with therapies that restore sinus rhythm. But a new cohort study suggests that the treatment effect’s magnitude might depend on the rhythm control strategy. It hinted that AFib catheter ablation might be more effective than pharmacologic rhythm control alone at cutting the risk for dementia.
The case-matched study of more than 38,000 adults with AFib saw a 41% reduction (P < .0001) in risk for dementia among those who underwent catheter ablation after attempted rhythm control with antiarrhythmic drugs (AAD), compared with those managed with pharmacologic rhythm control therapy alone.
The observational study comprising 20 years of data comes with big limitations and can’t say for sure whether catheter ablation is better than AAD alone at cutting the dementia risk in AFib. But it and other evidence support the idea, which has yet to be explored in a randomized fashion.
In a secondary finding, the analysis showed a similar reduction in dementia risk from catheter ablation, compared with AAD, in women and in men by 40% and 45%, respectively (P < .0001 for both). The findings are particularly relevant “given the higher life-long risk of dementia among women and the lower likelihood that women will be offered ablation, which has been demonstrated repeatedly,” Emily P. Zeitler, MD, MHS, Dartmouth-Hitchcock Medical Center, Lebanon, N.H., said in an interview. “I think this is another reason to try to be more generous in offering ablation to women.”
Management of AFib certainly evolved in important ways from 2000 to 2021, the period covered by the study. But a sensitivity analysis based on data from 2010 to 2021 showed “no meaningful differences” in the results, said Dr. Zeitler, who is slated to present the findings at the annual scientific sessions of the Heart Rhythm Society.
Dr. Zeitler acknowledged that the observational study, even with its propensity-matched ablation and AAD cohorts, can only hint at a preference for ablation over AAD for lowering risk for AFib-associated dementia. “We know there’s unmeasured and unfixable confounding between those two groups, so we see this really as hypothesis-generating.”
It was “a well-done analysis,” and the conclusion that the dementia risk was lower with catheter ablation is “absolutely correct,” but only as far as the study and its limitations allow, agreed David Conen, MD, MPH, McMaster University, Hamilton, Ont., who is not a coauthor.
“Even with propensity matching, you can get rid of some sorts of confounding, but you can never get rid of all selection bias issues.” That, he said when interviewed, takes randomized trials.
Dr. Conen, who is studying cognitive decline in AFib as a SWISS-AF trial principal investigator, pointed to a secondary finding of the analysis as evidence for such confounding. He said the ablation group’s nearly 50% drop (P < .0001) in competing risk for death, compared with patients managed with AAD, isn’t plausible.
The finding “strongly suggests these people were healthier and that there’s some sort of selection bias. They were at lower risk of death, they were at lower risk of dementia, and they were probably also at lower risk of stroke, myocardial infarction, thrombosis, and cancer because they were just probably a little healthier than the others,” Dr. Conen said. The ablation and AAD groups “were two very different populations from the get-go.”
The analysis was based on U.S. insurance and Medicare claims data from AFib patients who either underwent catheter ablation after at least one AAD trial or filled prescriptions for at least two different antiarrhythmic agents in the year after AFib diagnosis. Patients with history of dementia, catheter or surgical AFib ablation, or a valve procedure were excluded.
The ablation and AAD-only groups each consisted of 19,066 patients after propensity matching, and the groups were balanced with respect to age, sex, type of insurance, CHA2DS2-VASc scores, and use of renin-angiotensin system inhibitors, oral anticoagulants, and antiplatelets.
The overall risk for dementia was 1.9% for the ablation group and 3.3% for AAD-only patients (hazard ratio, 0.59; 95% confidence interval, 0.52-0.67). Corresponding HRs by sex were 0.55 (95% CI, 0.46-0.66) for men and 0.60 (95% CI, 0.50-0.72) for women.
The competing risk for death was also significantly decreased in the ablation group (HR, 0.51; 95% CI, 0.46-0.55).
Dr. Zeitler pointed to a randomized trial now in the early stages called Neurocognition and Greater Maintenance of Sinus Rhythm in Atrial Fibrillation, or NOGGIN-AF, which will explore relationships between rhythm control therapy and dementia in patients with AFib, whether catheter ablation or AAD can mitigate that risk, and whether either strategy works better than the other, among other goals.
“I’m optimistic,” she said, “and I think it’s going to add to the growing motivations to get patients ablated more quickly and more broadly.”
The analysis was funded by Biosense-Webster. Dr. Zeitler disclosed consulting for Biosense-Webster and Arena Pharmaceuticals (now Pfizer); fees for speaking from Medtronic; and receiving research support from Boston Scientific, Sanofi, and Biosense-Webster. Dr. Conen has previously reported receiving speaker fees from Servier Canada.
A version of this article first appeared on Medscape.com.
HEART RHYTHM 2022
Traumatic brain injury linked to ‘striking’ risk for CVD, diabetes, brain disorders
Mild traumatic brain injury (TBI) is linked to a significantly increased risk for a host of subsequent cardiovascular, endocrine, neurologic, and psychiatric disorders, new research shows.
Incidence of hypertension, coronary heart disease, diabetes, stroke, depression, and dementia all began to increase soon after the brain injury and persisted over a decade in both mild and moderate to severe TBI.
Researchers found the multisystem comorbidities in all age groups, including in patients as young as 18. They also found that patients who developed multiple postinjury problems had higher mortality during the decade-long follow-up.
The findings suggest patients with TBI may require longer follow-up and proactive screening for multisystem disease, regardless of age or injury severity.
“The fact that both patients with mild and moderate to severe injuries both had long-term ongoing associations with comorbidities that continued over time and that they are cardiovascular, endocrine, neurologic, and behavioral health oriented was pretty striking,” study author Ross Zafonte, DO, PhD, president of Spaulding Rehab Hospital and professor and chair of physical medicine and rehab at Harvard Medical School, both in Boston, told this news organization.
The study was published online in JAMA Network Open.
Injury severity not a factor
An estimated 2.8 million individuals in the United States experience TBI every year. Worldwide, the figure may be as high as 74 million.
Studies have long suggested a link between brain injury and subsequent neurologic disorders, but research suggesting a possible link to cardiovascular and endocrine problems has recently gained attention.
Building on a 2021 study that showed increased incidence of cardiovascular issues following a concussion, the researchers examined medical records of previously healthy patients treated for TBI between 2000 and 2015 who also had at least 1 follow-up visit between 6 months and 10 years after the initial injury.
Researchers analyzed data from 13,053 individuals – 4,351 with mild injury (mTBI), 4351 with moderate to severe injury (msTBI), and 4351 with no TBI. The most common cause of injury was a fall. Patients with sports-related injuries were excluded.
Incidence of hypertension was significantly higher among patients with mTBI (hazard ratio, 2.5; 95% confidence interval, 2.1-2.9) and msTBI (HR, 2.4; 95% CI, 2.0-2.9), compared with the unaffected group. Risk for other cardiovascular problems, including hyperlipidemia, obesity, and coronary artery disease, were also higher in the affected groups.
TBI patients also reported higher incidence of endocrine diseases, including diabetes (mTBI: HR, 1.9; 95% CI, 1.4-2.7; msTBI: HR, 1.9; 95% CI, 1.4-2.6). Elevated risk for ischemic stroke or transient ischemic attack was also increased (mTBI: HR, 2.2; 95% CI, 1.4-3.3; msTBI: HR, 3.6; 95% CI, 2.4-5.3).
Regardless of injury severity, patients with TBI had a higher risk for neurologic and psychiatric diseases, particularly depression, dementia, and psychotic disorders. “This tells us that mild TBI is not clean of events,” Dr. Zafonte said.
Surprising rate of comorbidity in youth
Investigators found increased risk for posttrauma comorbidities in all age groups, but researchers were struck by the high rates in younger patients, aged 18-40. Compared with age-matched individuals with no TBI history, hypertension risk was nearly six times higher in those with mTBI (HR, 5.9; 95% CI, 3.9-9.1) and nearly four times higher in patients with msTBI (HR, 3.9; 95% CI, 2.5-6.1).
Rates of hyperlipidemia and diabetes were also higher in younger patients in the mTBI group and posttraumatic seizures and psychiatric disorders were elevated regardless of TBI severity.
Overall, patients with msTBI, but not those with mTBI, were at higher risk for mortality, compared with the unexposed group (432 deaths [9.9%] vs. 250 deaths [5.7%]; P < .001).
“It’s clear that what we may be dealing with is that it holds up even for the younger people,” Dr. Zafonte said. “We used to think brain injury risk is worse in the severe cases, which it is, and it’s worse later on among those who are older, which it is. But our younger folks don’t get away either.”
While the study offers associations between TBI and multisystem health problems, Dr. Zafonte said it’s impossible to say at this point whether the brain injury caused the increased risk for cardiovascular or endocrine problems. Other organ injuries sustained in the trauma may be a contributing factor.
“Further data is needed to elucidate the mechanism and the causative relationships, which we do not have here,” he said.
Many of the postinjury comorbidities emerged a median of 3.5 years after TBI, regardless of severity. But some of the cardiovascular and psychiatric conditions emerged far sooner than that.
That’s important because research suggests less than half of patients with TBI receive follow-up care.
“It does make sense for folks who are interacting with people who’ve had a TBI to be suspicious of medical comorbidities relatively early on, within the first couple of years,” Dr. Zafonte said.
In an invited commentary, Vijay Krishnamoorthy, MD, MPH, PhD, Duke University, Durham, N.C., and Monica S. Vavilala, MD, University of Washington, Seattle, highlight some of the study’s limitations, including a lack of information on comorbidity severity and the lack of a matched group of patients who experienced non-head trauma.
Despite those limitations, the study offers important information on how TBI may affect organs beyond the brain, they noted.
“These observations, if replicated in future studies, raise intriguing implications in the future care of patients with TBI, including heightened chronic disease-screening measures and possibly enhanced guidelines for chronic extracranial organ system care for patients who experience TBI,” Dr. Krishnamoorthy and Dr. Vavilala wrote.
The study received no specific funding. Dr. Zafonte reported having received personal fees from Springer/Demos, serving on scientific advisory boards for Myomo and OnCare and has received funding from the Football Players Health Study at Harvard, funded in part by the National Football League Players Association. Dr. Krishnamoorthy and Dr. Vavilala disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Mild traumatic brain injury (TBI) is linked to a significantly increased risk for a host of subsequent cardiovascular, endocrine, neurologic, and psychiatric disorders, new research shows.
Incidence of hypertension, coronary heart disease, diabetes, stroke, depression, and dementia all began to increase soon after the brain injury and persisted over a decade in both mild and moderate to severe TBI.
Researchers found the multisystem comorbidities in all age groups, including in patients as young as 18. They also found that patients who developed multiple postinjury problems had higher mortality during the decade-long follow-up.
The findings suggest patients with TBI may require longer follow-up and proactive screening for multisystem disease, regardless of age or injury severity.
“The fact that both patients with mild and moderate to severe injuries both had long-term ongoing associations with comorbidities that continued over time and that they are cardiovascular, endocrine, neurologic, and behavioral health oriented was pretty striking,” study author Ross Zafonte, DO, PhD, president of Spaulding Rehab Hospital and professor and chair of physical medicine and rehab at Harvard Medical School, both in Boston, told this news organization.
The study was published online in JAMA Network Open.
Injury severity not a factor
An estimated 2.8 million individuals in the United States experience TBI every year. Worldwide, the figure may be as high as 74 million.
Studies have long suggested a link between brain injury and subsequent neurologic disorders, but research suggesting a possible link to cardiovascular and endocrine problems has recently gained attention.
Building on a 2021 study that showed increased incidence of cardiovascular issues following a concussion, the researchers examined medical records of previously healthy patients treated for TBI between 2000 and 2015 who also had at least 1 follow-up visit between 6 months and 10 years after the initial injury.
Researchers analyzed data from 13,053 individuals – 4,351 with mild injury (mTBI), 4351 with moderate to severe injury (msTBI), and 4351 with no TBI. The most common cause of injury was a fall. Patients with sports-related injuries were excluded.
Incidence of hypertension was significantly higher among patients with mTBI (hazard ratio, 2.5; 95% confidence interval, 2.1-2.9) and msTBI (HR, 2.4; 95% CI, 2.0-2.9), compared with the unaffected group. Risk for other cardiovascular problems, including hyperlipidemia, obesity, and coronary artery disease, were also higher in the affected groups.
TBI patients also reported higher incidence of endocrine diseases, including diabetes (mTBI: HR, 1.9; 95% CI, 1.4-2.7; msTBI: HR, 1.9; 95% CI, 1.4-2.6). Elevated risk for ischemic stroke or transient ischemic attack was also increased (mTBI: HR, 2.2; 95% CI, 1.4-3.3; msTBI: HR, 3.6; 95% CI, 2.4-5.3).
Regardless of injury severity, patients with TBI had a higher risk for neurologic and psychiatric diseases, particularly depression, dementia, and psychotic disorders. “This tells us that mild TBI is not clean of events,” Dr. Zafonte said.
Surprising rate of comorbidity in youth
Investigators found increased risk for posttrauma comorbidities in all age groups, but researchers were struck by the high rates in younger patients, aged 18-40. Compared with age-matched individuals with no TBI history, hypertension risk was nearly six times higher in those with mTBI (HR, 5.9; 95% CI, 3.9-9.1) and nearly four times higher in patients with msTBI (HR, 3.9; 95% CI, 2.5-6.1).
Rates of hyperlipidemia and diabetes were also higher in younger patients in the mTBI group and posttraumatic seizures and psychiatric disorders were elevated regardless of TBI severity.
Overall, patients with msTBI, but not those with mTBI, were at higher risk for mortality, compared with the unexposed group (432 deaths [9.9%] vs. 250 deaths [5.7%]; P < .001).
“It’s clear that what we may be dealing with is that it holds up even for the younger people,” Dr. Zafonte said. “We used to think brain injury risk is worse in the severe cases, which it is, and it’s worse later on among those who are older, which it is. But our younger folks don’t get away either.”
While the study offers associations between TBI and multisystem health problems, Dr. Zafonte said it’s impossible to say at this point whether the brain injury caused the increased risk for cardiovascular or endocrine problems. Other organ injuries sustained in the trauma may be a contributing factor.
“Further data is needed to elucidate the mechanism and the causative relationships, which we do not have here,” he said.
Many of the postinjury comorbidities emerged a median of 3.5 years after TBI, regardless of severity. But some of the cardiovascular and psychiatric conditions emerged far sooner than that.
That’s important because research suggests less than half of patients with TBI receive follow-up care.
“It does make sense for folks who are interacting with people who’ve had a TBI to be suspicious of medical comorbidities relatively early on, within the first couple of years,” Dr. Zafonte said.
In an invited commentary, Vijay Krishnamoorthy, MD, MPH, PhD, Duke University, Durham, N.C., and Monica S. Vavilala, MD, University of Washington, Seattle, highlight some of the study’s limitations, including a lack of information on comorbidity severity and the lack of a matched group of patients who experienced non-head trauma.
Despite those limitations, the study offers important information on how TBI may affect organs beyond the brain, they noted.
“These observations, if replicated in future studies, raise intriguing implications in the future care of patients with TBI, including heightened chronic disease-screening measures and possibly enhanced guidelines for chronic extracranial organ system care for patients who experience TBI,” Dr. Krishnamoorthy and Dr. Vavilala wrote.
The study received no specific funding. Dr. Zafonte reported having received personal fees from Springer/Demos, serving on scientific advisory boards for Myomo and OnCare and has received funding from the Football Players Health Study at Harvard, funded in part by the National Football League Players Association. Dr. Krishnamoorthy and Dr. Vavilala disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Mild traumatic brain injury (TBI) is linked to a significantly increased risk for a host of subsequent cardiovascular, endocrine, neurologic, and psychiatric disorders, new research shows.
Incidence of hypertension, coronary heart disease, diabetes, stroke, depression, and dementia all began to increase soon after the brain injury and persisted over a decade in both mild and moderate to severe TBI.
Researchers found the multisystem comorbidities in all age groups, including in patients as young as 18. They also found that patients who developed multiple postinjury problems had higher mortality during the decade-long follow-up.
The findings suggest patients with TBI may require longer follow-up and proactive screening for multisystem disease, regardless of age or injury severity.
“The fact that both patients with mild and moderate to severe injuries both had long-term ongoing associations with comorbidities that continued over time and that they are cardiovascular, endocrine, neurologic, and behavioral health oriented was pretty striking,” study author Ross Zafonte, DO, PhD, president of Spaulding Rehab Hospital and professor and chair of physical medicine and rehab at Harvard Medical School, both in Boston, told this news organization.
The study was published online in JAMA Network Open.
Injury severity not a factor
An estimated 2.8 million individuals in the United States experience TBI every year. Worldwide, the figure may be as high as 74 million.
Studies have long suggested a link between brain injury and subsequent neurologic disorders, but research suggesting a possible link to cardiovascular and endocrine problems has recently gained attention.
Building on a 2021 study that showed increased incidence of cardiovascular issues following a concussion, the researchers examined medical records of previously healthy patients treated for TBI between 2000 and 2015 who also had at least 1 follow-up visit between 6 months and 10 years after the initial injury.
Researchers analyzed data from 13,053 individuals – 4,351 with mild injury (mTBI), 4351 with moderate to severe injury (msTBI), and 4351 with no TBI. The most common cause of injury was a fall. Patients with sports-related injuries were excluded.
Incidence of hypertension was significantly higher among patients with mTBI (hazard ratio, 2.5; 95% confidence interval, 2.1-2.9) and msTBI (HR, 2.4; 95% CI, 2.0-2.9), compared with the unaffected group. Risk for other cardiovascular problems, including hyperlipidemia, obesity, and coronary artery disease, were also higher in the affected groups.
TBI patients also reported higher incidence of endocrine diseases, including diabetes (mTBI: HR, 1.9; 95% CI, 1.4-2.7; msTBI: HR, 1.9; 95% CI, 1.4-2.6). Elevated risk for ischemic stroke or transient ischemic attack was also increased (mTBI: HR, 2.2; 95% CI, 1.4-3.3; msTBI: HR, 3.6; 95% CI, 2.4-5.3).
Regardless of injury severity, patients with TBI had a higher risk for neurologic and psychiatric diseases, particularly depression, dementia, and psychotic disorders. “This tells us that mild TBI is not clean of events,” Dr. Zafonte said.
Surprising rate of comorbidity in youth
Investigators found increased risk for posttrauma comorbidities in all age groups, but researchers were struck by the high rates in younger patients, aged 18-40. Compared with age-matched individuals with no TBI history, hypertension risk was nearly six times higher in those with mTBI (HR, 5.9; 95% CI, 3.9-9.1) and nearly four times higher in patients with msTBI (HR, 3.9; 95% CI, 2.5-6.1).
Rates of hyperlipidemia and diabetes were also higher in younger patients in the mTBI group and posttraumatic seizures and psychiatric disorders were elevated regardless of TBI severity.
Overall, patients with msTBI, but not those with mTBI, were at higher risk for mortality, compared with the unexposed group (432 deaths [9.9%] vs. 250 deaths [5.7%]; P < .001).
“It’s clear that what we may be dealing with is that it holds up even for the younger people,” Dr. Zafonte said. “We used to think brain injury risk is worse in the severe cases, which it is, and it’s worse later on among those who are older, which it is. But our younger folks don’t get away either.”
While the study offers associations between TBI and multisystem health problems, Dr. Zafonte said it’s impossible to say at this point whether the brain injury caused the increased risk for cardiovascular or endocrine problems. Other organ injuries sustained in the trauma may be a contributing factor.
“Further data is needed to elucidate the mechanism and the causative relationships, which we do not have here,” he said.
Many of the postinjury comorbidities emerged a median of 3.5 years after TBI, regardless of severity. But some of the cardiovascular and psychiatric conditions emerged far sooner than that.
That’s important because research suggests less than half of patients with TBI receive follow-up care.
“It does make sense for folks who are interacting with people who’ve had a TBI to be suspicious of medical comorbidities relatively early on, within the first couple of years,” Dr. Zafonte said.
In an invited commentary, Vijay Krishnamoorthy, MD, MPH, PhD, Duke University, Durham, N.C., and Monica S. Vavilala, MD, University of Washington, Seattle, highlight some of the study’s limitations, including a lack of information on comorbidity severity and the lack of a matched group of patients who experienced non-head trauma.
Despite those limitations, the study offers important information on how TBI may affect organs beyond the brain, they noted.
“These observations, if replicated in future studies, raise intriguing implications in the future care of patients with TBI, including heightened chronic disease-screening measures and possibly enhanced guidelines for chronic extracranial organ system care for patients who experience TBI,” Dr. Krishnamoorthy and Dr. Vavilala wrote.
The study received no specific funding. Dr. Zafonte reported having received personal fees from Springer/Demos, serving on scientific advisory boards for Myomo and OnCare and has received funding from the Football Players Health Study at Harvard, funded in part by the National Football League Players Association. Dr. Krishnamoorthy and Dr. Vavilala disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Two MS meds tied to higher COVID rates
Patients taking ocrelizumab (Ocrevus) or fingolimod (Gilenya) for treat multiple sclerosis (MS) have higher rates of COVID-19 infection and hospitalization before and after COVID vaccination, compared with those taking other treatments, a nationwide study in England found.
The study draws on a database that includes every patient with MS in England treated with a disease-modifying therapy (DMT) and national data on rates of COVID infection, hospitalization, mortality, and vaccination in those patients.
It’s the latest work to suggest varying levels of vaccine efficacy based on DMT use and is the first known study to offer this level of detail on the subject.
“What is obvious is that current vaccination protocols for these DMTs are not really working properly,” lead investigator Afagh Garjani, MD, clinical research fellow at the University of Nottingham (England), said in an interview.
Although the differences in infection rates and efficacy are significant in those two DMTs, the overall infection and hospitalization rates were low, Dr. Garjani noted, offering further evidence that vaccines are effective in most patients with MS.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Low mortality rate
The prospective, longitudinal study included National Health Service data on 44,170 people with MS. The data on hospitalization came from 29,353 patients with MS who had received at least two doses of a COVID-19 vaccine.
Patients taking dimethyl fumarate, the most commonly prescribed DMT in England, had similar rates of COVID infection in January 2021 – before they were fully vaccinated – and in December 2022, after they had received at least two vaccine doses.
However, among patients taking fingolimod and ocrelizumab there were significant increases in infection rates in that same time period. The incidence rate ratio in the fingolimod group was 0.50 (95% confidence interval, 0.37-0.66) in January 2021 and rose to 0.91 (95% CI, 0.80-1.03) in December 2022. In the ocrelizumab group, the IRR rose from 1.01 (95% CI, 0.79-1.26) to 1.57 (95% CI, 1.44-1.72) during that time frame.
Hospitalization rates were also higher in fully vaccinated patients with MS taking fingolimod and ocrelizumab. People taking dimethyl fumarate had a hospitalization rate of 32 (per 10,000 people), compared with a rate of 140 in patients on ocrelizumab and 94 in patients on fingolimod.
Mortality rates were low in all groups, but were slightly higher in the ocrelizumab group.
“However, the number of people who died due to COVID overall was small,” Dr. Garjani noted.
Following receipt of a third COVID-19 vaccine, the only hospitalizations were in patients taking ocrelizumab (4 out of 65 infections) and fingolimod (11 out of 78 infections), with no deaths.
Potential mechanism
Researchers suspect the reason for varying COVID-19 infection rates and vaccine efficacy among DMTs is related to their mode of action.
“With MS, the immune system attacks the central nervous system and the aim of these treatments is to modulate or suppress the immune system,” Dr. Garjani said. “Some of these medications are immune suppressants and therefore, in addition to preventing MS, might also put people at increased risk of infection from COVID or other diseases.”
Ocrelizumab and fingolimod have different modes of action, but both act as immunosuppressants.
Study data on beta-interferon offered an interesting twist. Patients taking that medication had far lower infection rates, compared with other DMTs and to the general population, and no COVID-related hospitalizations.
Interferons are known to have some antiviral effects, Dr. Garjani said. In fact, interferon is one of several existing drugs that scientists have considered as possible candidates to fight COVID infection.
Studies on COVID infection rates and vaccine efficacy have yielded conflicting results. Some suggest no differences based on DMT use, whereas others have shown immunological evidence pointing to lower or higher infections rates among the different therapies.
Based on some of those findings, up to 80% of specialists who treat MS in the United States said the pandemic may have changed their use of DMTs, one study found, which later studies suggested may not have been necessary.
While the findings shouldn’t necessarily prompt clinicians to consider changing their treatment approach, Dr. Garjani noted that her team tells patients who have not yet started treatment to get vaccinated before initiating MS treatment.
A balancing act
Commenting on the findings, Tyler Smith, MD, clinical assistant professor of neurology at New York University, said that, although the data suggest these MS therapies may affect COVID vaccine efficacy to varying degrees, there’s more to the story.
“This data builds upon a growing body of evidence that these treatments may attenuate vaccine responses to different degrees, and this should be balanced with their efficacy in controlling multiple sclerosis relapses, Dr. Smith said, adding that “real-life studies examining the effect of vaccines show benefit in limiting hospitalization and death.”
“Developing evidence continues to demonstrate the benefits of vaccination,” he said, “and I encourage all patients to follow the latest federal health guidelines regarding COVID-19 vaccinations.”
Dr. Garjani has received personal compensation for serving as a speaker with MS Academy and Biogen. Dr. Smith’s 2020-2021 fellowship was supported in part by Biogen and the National Multiple Sclerosis Society Clinical Care Physician Fellowship 2020-2021. Dr. Smith also received honoraria from the American Academy of Neurology in 2020.
A version of this article first appeared on Medscape.com.
Patients taking ocrelizumab (Ocrevus) or fingolimod (Gilenya) for treat multiple sclerosis (MS) have higher rates of COVID-19 infection and hospitalization before and after COVID vaccination, compared with those taking other treatments, a nationwide study in England found.
The study draws on a database that includes every patient with MS in England treated with a disease-modifying therapy (DMT) and national data on rates of COVID infection, hospitalization, mortality, and vaccination in those patients.
It’s the latest work to suggest varying levels of vaccine efficacy based on DMT use and is the first known study to offer this level of detail on the subject.
“What is obvious is that current vaccination protocols for these DMTs are not really working properly,” lead investigator Afagh Garjani, MD, clinical research fellow at the University of Nottingham (England), said in an interview.
Although the differences in infection rates and efficacy are significant in those two DMTs, the overall infection and hospitalization rates were low, Dr. Garjani noted, offering further evidence that vaccines are effective in most patients with MS.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Low mortality rate
The prospective, longitudinal study included National Health Service data on 44,170 people with MS. The data on hospitalization came from 29,353 patients with MS who had received at least two doses of a COVID-19 vaccine.
Patients taking dimethyl fumarate, the most commonly prescribed DMT in England, had similar rates of COVID infection in January 2021 – before they were fully vaccinated – and in December 2022, after they had received at least two vaccine doses.
However, among patients taking fingolimod and ocrelizumab there were significant increases in infection rates in that same time period. The incidence rate ratio in the fingolimod group was 0.50 (95% confidence interval, 0.37-0.66) in January 2021 and rose to 0.91 (95% CI, 0.80-1.03) in December 2022. In the ocrelizumab group, the IRR rose from 1.01 (95% CI, 0.79-1.26) to 1.57 (95% CI, 1.44-1.72) during that time frame.
Hospitalization rates were also higher in fully vaccinated patients with MS taking fingolimod and ocrelizumab. People taking dimethyl fumarate had a hospitalization rate of 32 (per 10,000 people), compared with a rate of 140 in patients on ocrelizumab and 94 in patients on fingolimod.
Mortality rates were low in all groups, but were slightly higher in the ocrelizumab group.
“However, the number of people who died due to COVID overall was small,” Dr. Garjani noted.
Following receipt of a third COVID-19 vaccine, the only hospitalizations were in patients taking ocrelizumab (4 out of 65 infections) and fingolimod (11 out of 78 infections), with no deaths.
Potential mechanism
Researchers suspect the reason for varying COVID-19 infection rates and vaccine efficacy among DMTs is related to their mode of action.
“With MS, the immune system attacks the central nervous system and the aim of these treatments is to modulate or suppress the immune system,” Dr. Garjani said. “Some of these medications are immune suppressants and therefore, in addition to preventing MS, might also put people at increased risk of infection from COVID or other diseases.”
Ocrelizumab and fingolimod have different modes of action, but both act as immunosuppressants.
Study data on beta-interferon offered an interesting twist. Patients taking that medication had far lower infection rates, compared with other DMTs and to the general population, and no COVID-related hospitalizations.
Interferons are known to have some antiviral effects, Dr. Garjani said. In fact, interferon is one of several existing drugs that scientists have considered as possible candidates to fight COVID infection.
Studies on COVID infection rates and vaccine efficacy have yielded conflicting results. Some suggest no differences based on DMT use, whereas others have shown immunological evidence pointing to lower or higher infections rates among the different therapies.
Based on some of those findings, up to 80% of specialists who treat MS in the United States said the pandemic may have changed their use of DMTs, one study found, which later studies suggested may not have been necessary.
While the findings shouldn’t necessarily prompt clinicians to consider changing their treatment approach, Dr. Garjani noted that her team tells patients who have not yet started treatment to get vaccinated before initiating MS treatment.
A balancing act
Commenting on the findings, Tyler Smith, MD, clinical assistant professor of neurology at New York University, said that, although the data suggest these MS therapies may affect COVID vaccine efficacy to varying degrees, there’s more to the story.
“This data builds upon a growing body of evidence that these treatments may attenuate vaccine responses to different degrees, and this should be balanced with their efficacy in controlling multiple sclerosis relapses, Dr. Smith said, adding that “real-life studies examining the effect of vaccines show benefit in limiting hospitalization and death.”
“Developing evidence continues to demonstrate the benefits of vaccination,” he said, “and I encourage all patients to follow the latest federal health guidelines regarding COVID-19 vaccinations.”
Dr. Garjani has received personal compensation for serving as a speaker with MS Academy and Biogen. Dr. Smith’s 2020-2021 fellowship was supported in part by Biogen and the National Multiple Sclerosis Society Clinical Care Physician Fellowship 2020-2021. Dr. Smith also received honoraria from the American Academy of Neurology in 2020.
A version of this article first appeared on Medscape.com.
Patients taking ocrelizumab (Ocrevus) or fingolimod (Gilenya) for treat multiple sclerosis (MS) have higher rates of COVID-19 infection and hospitalization before and after COVID vaccination, compared with those taking other treatments, a nationwide study in England found.
The study draws on a database that includes every patient with MS in England treated with a disease-modifying therapy (DMT) and national data on rates of COVID infection, hospitalization, mortality, and vaccination in those patients.
It’s the latest work to suggest varying levels of vaccine efficacy based on DMT use and is the first known study to offer this level of detail on the subject.
“What is obvious is that current vaccination protocols for these DMTs are not really working properly,” lead investigator Afagh Garjani, MD, clinical research fellow at the University of Nottingham (England), said in an interview.
Although the differences in infection rates and efficacy are significant in those two DMTs, the overall infection and hospitalization rates were low, Dr. Garjani noted, offering further evidence that vaccines are effective in most patients with MS.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Low mortality rate
The prospective, longitudinal study included National Health Service data on 44,170 people with MS. The data on hospitalization came from 29,353 patients with MS who had received at least two doses of a COVID-19 vaccine.
Patients taking dimethyl fumarate, the most commonly prescribed DMT in England, had similar rates of COVID infection in January 2021 – before they were fully vaccinated – and in December 2022, after they had received at least two vaccine doses.
However, among patients taking fingolimod and ocrelizumab there were significant increases in infection rates in that same time period. The incidence rate ratio in the fingolimod group was 0.50 (95% confidence interval, 0.37-0.66) in January 2021 and rose to 0.91 (95% CI, 0.80-1.03) in December 2022. In the ocrelizumab group, the IRR rose from 1.01 (95% CI, 0.79-1.26) to 1.57 (95% CI, 1.44-1.72) during that time frame.
Hospitalization rates were also higher in fully vaccinated patients with MS taking fingolimod and ocrelizumab. People taking dimethyl fumarate had a hospitalization rate of 32 (per 10,000 people), compared with a rate of 140 in patients on ocrelizumab and 94 in patients on fingolimod.
Mortality rates were low in all groups, but were slightly higher in the ocrelizumab group.
“However, the number of people who died due to COVID overall was small,” Dr. Garjani noted.
Following receipt of a third COVID-19 vaccine, the only hospitalizations were in patients taking ocrelizumab (4 out of 65 infections) and fingolimod (11 out of 78 infections), with no deaths.
Potential mechanism
Researchers suspect the reason for varying COVID-19 infection rates and vaccine efficacy among DMTs is related to their mode of action.
“With MS, the immune system attacks the central nervous system and the aim of these treatments is to modulate or suppress the immune system,” Dr. Garjani said. “Some of these medications are immune suppressants and therefore, in addition to preventing MS, might also put people at increased risk of infection from COVID or other diseases.”
Ocrelizumab and fingolimod have different modes of action, but both act as immunosuppressants.
Study data on beta-interferon offered an interesting twist. Patients taking that medication had far lower infection rates, compared with other DMTs and to the general population, and no COVID-related hospitalizations.
Interferons are known to have some antiviral effects, Dr. Garjani said. In fact, interferon is one of several existing drugs that scientists have considered as possible candidates to fight COVID infection.
Studies on COVID infection rates and vaccine efficacy have yielded conflicting results. Some suggest no differences based on DMT use, whereas others have shown immunological evidence pointing to lower or higher infections rates among the different therapies.
Based on some of those findings, up to 80% of specialists who treat MS in the United States said the pandemic may have changed their use of DMTs, one study found, which later studies suggested may not have been necessary.
While the findings shouldn’t necessarily prompt clinicians to consider changing their treatment approach, Dr. Garjani noted that her team tells patients who have not yet started treatment to get vaccinated before initiating MS treatment.
A balancing act
Commenting on the findings, Tyler Smith, MD, clinical assistant professor of neurology at New York University, said that, although the data suggest these MS therapies may affect COVID vaccine efficacy to varying degrees, there’s more to the story.
“This data builds upon a growing body of evidence that these treatments may attenuate vaccine responses to different degrees, and this should be balanced with their efficacy in controlling multiple sclerosis relapses, Dr. Smith said, adding that “real-life studies examining the effect of vaccines show benefit in limiting hospitalization and death.”
“Developing evidence continues to demonstrate the benefits of vaccination,” he said, “and I encourage all patients to follow the latest federal health guidelines regarding COVID-19 vaccinations.”
Dr. Garjani has received personal compensation for serving as a speaker with MS Academy and Biogen. Dr. Smith’s 2020-2021 fellowship was supported in part by Biogen and the National Multiple Sclerosis Society Clinical Care Physician Fellowship 2020-2021. Dr. Smith also received honoraria from the American Academy of Neurology in 2020.
A version of this article first appeared on Medscape.com.
FROM AAN 2022
The neurobiology of Jeopardy! champions
As a regular viewer of Jeopardy! I find it both interesting and educational. But the psychiatric neuroscientist in me marvels at the splendid cerebral attributes embedded in the brains of Jeopardy! champions.
Back in my college days, I participated in what were then called “general knowledge contests” and won a couple of trophies, the most gratifying of which was when our team of medical students beat the faculty team! Later, when my wife and I had children, Trivial Pursuit was a game frequently played in our household. So it is no wonder I have often thought of the remarkable, sometimes stunning intellectual performances of Jeopardy! champions.
What does it take to excel at Jeopardy!?
Watching contestants successfully answer a bewildering array of questions across an extensive spectrum of topics is simply dazzling and prompts me to ask: Which neurologic structures play a central role in the brains of Jeopardy! champions? So I channeled my inner neurobiologist and came up with the following prerequisites to excel at Jeopardy!:
- A hippocampus on steroids! Memory is obviously a core ingredient for responding to Jeopardy! questions. Unlike ordinary mortals, Jeopardy! champions appear to retain and instantaneously, accurately recall everything they have read, saw, or heard.
- A sublime network of dendritic spines, where learning is immediately transduced to biological memories, thanks to the wonders of experiential neuroplasticity in homo sapiens.
- A superlative frontal lobe, which provides the champion with an ultra-rapid abstraction ability in the dorsolateral prefrontal cortex, along with razor-sharp concentration and attention.
- An extremely well-myelinated network of the 137,000 miles of white matter fibers in the human brain. This is what leads to fabulous processing speed. Rapid neurotransmission is impossible without very well-myelinated axons and dendrites. It is not enough for a Jeopardy! champion to know the answer and retrieve it from the hippocampus—they also must transmit the answer at lightning speed to the speech area, and then activate the motor area to enunciate the answer. Processing speed is the foundation of overall cognitive functioning.
- A first-rate Broca’s area, referred to as “the brain’s scriptwriter,” which shapes human speech. It receives the flow of sensory information from the temporal cortex, devises a plan for speaking, and passes that plan seamlessly to the motor cortex, which controls the movements of the mouth.
- Blistering speed reflexes to click the handheld response buzzer within a fraction of a millisecond after the host finishes reading the clue (not before, or a penalty is incurred). Jeopardy! champions always click the buzzer faster than their competitors, who may know the answer but have ordinary motor reflexes (also related to the degree of myelination and a motoric component of processing speed).
- A thick corpus callosum, the largest interhemispheric commissure, a bundle of 200 million white matter fibers connecting analogous regions in the right and left hemispheres, is vital for the rapid bidirectional transfer of bits of information from the intuitive/nonverbal right hemisphere to the mathematical/verbal left hemisphere, when the answer requires right hemispheric input.
- A bright occipital cortex and exceptional optic nerve and retina, so that champions can recognize faces or locations and read the questions before the host finishes reading them, which gives them an awesome edge on other contestants.
Obviously, the brains of Jeopardy! champions are a breed of their own, with exceptional performances by multiple regions converging to produce a winning performance. But during their childhood and youthful years, such brains also generate motivation, curiosity, and interest in a wide range of topics, from cultures, regions, music genres, and word games to history, geography, sports, science, medicine, astronomy, and Greek mythology.
Jeopardy! champions may appear to have regular jobs and ordinary lives, but they have resplendent “renaissance” brains. I wonder how they spent their childhood, who mentored them, what type of family lives they had, and what they dream of accomplishing other than winning on Jeopardy!. Will their awe-inspiring performance in Jeopardy! translate to overall success in life? That’s a story that remains to be told.
As a regular viewer of Jeopardy! I find it both interesting and educational. But the psychiatric neuroscientist in me marvels at the splendid cerebral attributes embedded in the brains of Jeopardy! champions.
Back in my college days, I participated in what were then called “general knowledge contests” and won a couple of trophies, the most gratifying of which was when our team of medical students beat the faculty team! Later, when my wife and I had children, Trivial Pursuit was a game frequently played in our household. So it is no wonder I have often thought of the remarkable, sometimes stunning intellectual performances of Jeopardy! champions.
What does it take to excel at Jeopardy!?
Watching contestants successfully answer a bewildering array of questions across an extensive spectrum of topics is simply dazzling and prompts me to ask: Which neurologic structures play a central role in the brains of Jeopardy! champions? So I channeled my inner neurobiologist and came up with the following prerequisites to excel at Jeopardy!:
- A hippocampus on steroids! Memory is obviously a core ingredient for responding to Jeopardy! questions. Unlike ordinary mortals, Jeopardy! champions appear to retain and instantaneously, accurately recall everything they have read, saw, or heard.
- A sublime network of dendritic spines, where learning is immediately transduced to biological memories, thanks to the wonders of experiential neuroplasticity in homo sapiens.
- A superlative frontal lobe, which provides the champion with an ultra-rapid abstraction ability in the dorsolateral prefrontal cortex, along with razor-sharp concentration and attention.
- An extremely well-myelinated network of the 137,000 miles of white matter fibers in the human brain. This is what leads to fabulous processing speed. Rapid neurotransmission is impossible without very well-myelinated axons and dendrites. It is not enough for a Jeopardy! champion to know the answer and retrieve it from the hippocampus—they also must transmit the answer at lightning speed to the speech area, and then activate the motor area to enunciate the answer. Processing speed is the foundation of overall cognitive functioning.
- A first-rate Broca’s area, referred to as “the brain’s scriptwriter,” which shapes human speech. It receives the flow of sensory information from the temporal cortex, devises a plan for speaking, and passes that plan seamlessly to the motor cortex, which controls the movements of the mouth.
- Blistering speed reflexes to click the handheld response buzzer within a fraction of a millisecond after the host finishes reading the clue (not before, or a penalty is incurred). Jeopardy! champions always click the buzzer faster than their competitors, who may know the answer but have ordinary motor reflexes (also related to the degree of myelination and a motoric component of processing speed).
- A thick corpus callosum, the largest interhemispheric commissure, a bundle of 200 million white matter fibers connecting analogous regions in the right and left hemispheres, is vital for the rapid bidirectional transfer of bits of information from the intuitive/nonverbal right hemisphere to the mathematical/verbal left hemisphere, when the answer requires right hemispheric input.
- A bright occipital cortex and exceptional optic nerve and retina, so that champions can recognize faces or locations and read the questions before the host finishes reading them, which gives them an awesome edge on other contestants.
Obviously, the brains of Jeopardy! champions are a breed of their own, with exceptional performances by multiple regions converging to produce a winning performance. But during their childhood and youthful years, such brains also generate motivation, curiosity, and interest in a wide range of topics, from cultures, regions, music genres, and word games to history, geography, sports, science, medicine, astronomy, and Greek mythology.
Jeopardy! champions may appear to have regular jobs and ordinary lives, but they have resplendent “renaissance” brains. I wonder how they spent their childhood, who mentored them, what type of family lives they had, and what they dream of accomplishing other than winning on Jeopardy!. Will their awe-inspiring performance in Jeopardy! translate to overall success in life? That’s a story that remains to be told.
As a regular viewer of Jeopardy! I find it both interesting and educational. But the psychiatric neuroscientist in me marvels at the splendid cerebral attributes embedded in the brains of Jeopardy! champions.
Back in my college days, I participated in what were then called “general knowledge contests” and won a couple of trophies, the most gratifying of which was when our team of medical students beat the faculty team! Later, when my wife and I had children, Trivial Pursuit was a game frequently played in our household. So it is no wonder I have often thought of the remarkable, sometimes stunning intellectual performances of Jeopardy! champions.
What does it take to excel at Jeopardy!?
Watching contestants successfully answer a bewildering array of questions across an extensive spectrum of topics is simply dazzling and prompts me to ask: Which neurologic structures play a central role in the brains of Jeopardy! champions? So I channeled my inner neurobiologist and came up with the following prerequisites to excel at Jeopardy!:
- A hippocampus on steroids! Memory is obviously a core ingredient for responding to Jeopardy! questions. Unlike ordinary mortals, Jeopardy! champions appear to retain and instantaneously, accurately recall everything they have read, saw, or heard.
- A sublime network of dendritic spines, where learning is immediately transduced to biological memories, thanks to the wonders of experiential neuroplasticity in homo sapiens.
- A superlative frontal lobe, which provides the champion with an ultra-rapid abstraction ability in the dorsolateral prefrontal cortex, along with razor-sharp concentration and attention.
- An extremely well-myelinated network of the 137,000 miles of white matter fibers in the human brain. This is what leads to fabulous processing speed. Rapid neurotransmission is impossible without very well-myelinated axons and dendrites. It is not enough for a Jeopardy! champion to know the answer and retrieve it from the hippocampus—they also must transmit the answer at lightning speed to the speech area, and then activate the motor area to enunciate the answer. Processing speed is the foundation of overall cognitive functioning.
- A first-rate Broca’s area, referred to as “the brain’s scriptwriter,” which shapes human speech. It receives the flow of sensory information from the temporal cortex, devises a plan for speaking, and passes that plan seamlessly to the motor cortex, which controls the movements of the mouth.
- Blistering speed reflexes to click the handheld response buzzer within a fraction of a millisecond after the host finishes reading the clue (not before, or a penalty is incurred). Jeopardy! champions always click the buzzer faster than their competitors, who may know the answer but have ordinary motor reflexes (also related to the degree of myelination and a motoric component of processing speed).
- A thick corpus callosum, the largest interhemispheric commissure, a bundle of 200 million white matter fibers connecting analogous regions in the right and left hemispheres, is vital for the rapid bidirectional transfer of bits of information from the intuitive/nonverbal right hemisphere to the mathematical/verbal left hemisphere, when the answer requires right hemispheric input.
- A bright occipital cortex and exceptional optic nerve and retina, so that champions can recognize faces or locations and read the questions before the host finishes reading them, which gives them an awesome edge on other contestants.
Obviously, the brains of Jeopardy! champions are a breed of their own, with exceptional performances by multiple regions converging to produce a winning performance. But during their childhood and youthful years, such brains also generate motivation, curiosity, and interest in a wide range of topics, from cultures, regions, music genres, and word games to history, geography, sports, science, medicine, astronomy, and Greek mythology.
Jeopardy! champions may appear to have regular jobs and ordinary lives, but they have resplendent “renaissance” brains. I wonder how they spent their childhood, who mentored them, what type of family lives they had, and what they dream of accomplishing other than winning on Jeopardy!. Will their awe-inspiring performance in Jeopardy! translate to overall success in life? That’s a story that remains to be told.

Impaired vision an overlooked dementia risk factor
Investigators analyzed estimated population attributable fractions (PAFs) associated with dementia in more than 16,000 older adults. A PAF represents the number of dementia cases that could be prevented if a given risk factor were eliminated.
Results showed the PAF of vision impairment was 1.8%, suggesting that healthy vision had the potential to prevent more than 100,000 cases of dementia in the United States.
“Vision impairment and blindness disproportionately impact older adults, yet vision impairment is often preventable or even correctable,” study investigator Joshua Ehrlich MD, assistant professor of ophthalmology and visual sciences, University of Michigan, Ann Arbor, said in an interview.
Poor vision affects not only how individuals see the world, but also their systemic health and well-being, Dr. Ehrlich said.
“Accordingly, ensuring that older adults receive appropriate eye care is vital to promoting health, independence, and optimal aging,” he added.
The findings were published online in JAMA Neurology.
A surprising omission
There is an “urgent need to identify modifiable risk factors for dementia that can be targeted with interventions to slow cognitive decline and prevent dementia,” the investigators wrote.
In 2020, the Lancet Commission report on dementia prevention, intervention, and care proposed a life-course model of 12 potentially modifiable dementia risk factors. This included lower educational level, hearing loss, traumatic brain injury, hypertension, excessive alcohol consumption, obesity, smoking, depression, social isolation, physical inactivity, diabetes, and air pollution.
Together, these factors are associated with about 40% of dementia cases worldwide, the report notes.
Vision impairment was not included in this model, “despite considerable evidence that it is associated with an elevated risk of incident dementia and that it may operate through the same pathways as hearing loss,” the current researchers wrote.
“We have known for some time that vision impairment is a risk factor for dementia [and] we also know that a very large fraction of vision impairment, possibly in excess of 80%, is avoidable or has simply yet to be addressed,” Dr. Ehrlich said.
He and his colleagues found it “surprising that vision impairment had been ignored in key models of modifiable dementia risk factors that are used to shape health policy and resource allocation.” They set out to demonstrate that, “in fact, vision impairment is just as influential as a number of other long accepted modifiable dementia risk factors.”
The investigators assessed data from the Health and Retirement Study (HRS), a panel study that surveys more than 20,000 U.S. adults aged 50 years or older every 2 years.
The investigators applied the same methods used by the Lancet Commission to the HRS dataset and added vision impairment to the Lancet life-course model. Air pollution was excluded in their model “because those data were not readily available in the HRS,” the researchers wrote.
They noted the PAF is “based on the population prevalence and relative risk of dementia for each risk factor” and is “weighted, based on a principal components analysis, to account for communality (clustering of risk factors).”
A missed prevention opportunity
The sample included 16,690 participants (54% were women, 51.5% were at least age 65, 80.2% were White, 10.6% were Black, 9.2% were other).
In total, the 12 potentially modifiable risk factors used in the researchers’ model were associated with an estimated 62.4% of dementia cases in the United States, with hypertension as the most prevalent risk factor with the highest weighted PAF.
A new focus for prevention
Commenting for this article, Suzann Pershing, MD, associate professor of ophthalmology, Stanford (Calif.) University, called the study “particularly important because, despite growing recognition of its importance in relation to cognition, visual impairment is often an underrecognized risk factor.”
The current research “builds on increasingly robust medical literature linking visual impairment and dementia, applying analogous methods to those used for the life course model recently presented by the Lancet Commission to evaluate potentially modifiable dementia risk factors,” said Dr. Pershing, who was not involved with the study.
The investigators “make a compelling argument for inclusion of visual impairment as one of the potentially modifiable risk factors; practicing clinicians and health care systems may consider screening and targeted therapies to address visual impairment, with a goal of population health and contributing to a reduction in future dementia disease burden,” she added.
In an accompanying editorial), Jennifer Deal, PhD, department of epidemiology and Cochlear Center for Hearing and Public Health, Baltimore, and Julio Rojas, MD, PhD, Memory and Aging Center, department of neurology, Weill Institute for Neurosciences, University of California, San Francisco, call the findings “an important reminder that dementia is a social problem in which potentially treatable risk factors, including visual impairment, are highly prevalent in disadvantaged populations.”
The editorialists noted that 90% of cases of vision impairment are “preventable or have yet to be treated. The two “highly cost-effective interventions” of eyeglasses and/or cataract surgery “remain underused both in the U.S. and globally, especially in disadvantaged communities,” they wrote.
They added that more research is needed to “test the effectiveness of interventions to preserve cognitive health by promoting healthy vision.”
The study was supported by grants from the National Institute on Aging, the National Institutes of Health, and Research to Prevent Blindness. The investigators reported no relevant financial relationships. Dr. Deal reported having received grants from the National Institute on Aging. Dr. Rojas reported serving as site principal investigator on clinical trials for Eli Lilly and Eisai and receiving grants from the National Institute on Aging. Dr. Pershing is a consultant for Acumen, and Verana Health (as DigiSight Technologies).
A version of this article first appeared on Medscape.com.
Investigators analyzed estimated population attributable fractions (PAFs) associated with dementia in more than 16,000 older adults. A PAF represents the number of dementia cases that could be prevented if a given risk factor were eliminated.
Results showed the PAF of vision impairment was 1.8%, suggesting that healthy vision had the potential to prevent more than 100,000 cases of dementia in the United States.
“Vision impairment and blindness disproportionately impact older adults, yet vision impairment is often preventable or even correctable,” study investigator Joshua Ehrlich MD, assistant professor of ophthalmology and visual sciences, University of Michigan, Ann Arbor, said in an interview.
Poor vision affects not only how individuals see the world, but also their systemic health and well-being, Dr. Ehrlich said.
“Accordingly, ensuring that older adults receive appropriate eye care is vital to promoting health, independence, and optimal aging,” he added.
The findings were published online in JAMA Neurology.
A surprising omission
There is an “urgent need to identify modifiable risk factors for dementia that can be targeted with interventions to slow cognitive decline and prevent dementia,” the investigators wrote.
In 2020, the Lancet Commission report on dementia prevention, intervention, and care proposed a life-course model of 12 potentially modifiable dementia risk factors. This included lower educational level, hearing loss, traumatic brain injury, hypertension, excessive alcohol consumption, obesity, smoking, depression, social isolation, physical inactivity, diabetes, and air pollution.
Together, these factors are associated with about 40% of dementia cases worldwide, the report notes.
Vision impairment was not included in this model, “despite considerable evidence that it is associated with an elevated risk of incident dementia and that it may operate through the same pathways as hearing loss,” the current researchers wrote.
“We have known for some time that vision impairment is a risk factor for dementia [and] we also know that a very large fraction of vision impairment, possibly in excess of 80%, is avoidable or has simply yet to be addressed,” Dr. Ehrlich said.
He and his colleagues found it “surprising that vision impairment had been ignored in key models of modifiable dementia risk factors that are used to shape health policy and resource allocation.” They set out to demonstrate that, “in fact, vision impairment is just as influential as a number of other long accepted modifiable dementia risk factors.”
The investigators assessed data from the Health and Retirement Study (HRS), a panel study that surveys more than 20,000 U.S. adults aged 50 years or older every 2 years.
The investigators applied the same methods used by the Lancet Commission to the HRS dataset and added vision impairment to the Lancet life-course model. Air pollution was excluded in their model “because those data were not readily available in the HRS,” the researchers wrote.
They noted the PAF is “based on the population prevalence and relative risk of dementia for each risk factor” and is “weighted, based on a principal components analysis, to account for communality (clustering of risk factors).”
A missed prevention opportunity
The sample included 16,690 participants (54% were women, 51.5% were at least age 65, 80.2% were White, 10.6% were Black, 9.2% were other).
In total, the 12 potentially modifiable risk factors used in the researchers’ model were associated with an estimated 62.4% of dementia cases in the United States, with hypertension as the most prevalent risk factor with the highest weighted PAF.
A new focus for prevention
Commenting for this article, Suzann Pershing, MD, associate professor of ophthalmology, Stanford (Calif.) University, called the study “particularly important because, despite growing recognition of its importance in relation to cognition, visual impairment is often an underrecognized risk factor.”
The current research “builds on increasingly robust medical literature linking visual impairment and dementia, applying analogous methods to those used for the life course model recently presented by the Lancet Commission to evaluate potentially modifiable dementia risk factors,” said Dr. Pershing, who was not involved with the study.
The investigators “make a compelling argument for inclusion of visual impairment as one of the potentially modifiable risk factors; practicing clinicians and health care systems may consider screening and targeted therapies to address visual impairment, with a goal of population health and contributing to a reduction in future dementia disease burden,” she added.
In an accompanying editorial), Jennifer Deal, PhD, department of epidemiology and Cochlear Center for Hearing and Public Health, Baltimore, and Julio Rojas, MD, PhD, Memory and Aging Center, department of neurology, Weill Institute for Neurosciences, University of California, San Francisco, call the findings “an important reminder that dementia is a social problem in which potentially treatable risk factors, including visual impairment, are highly prevalent in disadvantaged populations.”
The editorialists noted that 90% of cases of vision impairment are “preventable or have yet to be treated. The two “highly cost-effective interventions” of eyeglasses and/or cataract surgery “remain underused both in the U.S. and globally, especially in disadvantaged communities,” they wrote.
They added that more research is needed to “test the effectiveness of interventions to preserve cognitive health by promoting healthy vision.”
The study was supported by grants from the National Institute on Aging, the National Institutes of Health, and Research to Prevent Blindness. The investigators reported no relevant financial relationships. Dr. Deal reported having received grants from the National Institute on Aging. Dr. Rojas reported serving as site principal investigator on clinical trials for Eli Lilly and Eisai and receiving grants from the National Institute on Aging. Dr. Pershing is a consultant for Acumen, and Verana Health (as DigiSight Technologies).
A version of this article first appeared on Medscape.com.
Investigators analyzed estimated population attributable fractions (PAFs) associated with dementia in more than 16,000 older adults. A PAF represents the number of dementia cases that could be prevented if a given risk factor were eliminated.
Results showed the PAF of vision impairment was 1.8%, suggesting that healthy vision had the potential to prevent more than 100,000 cases of dementia in the United States.
“Vision impairment and blindness disproportionately impact older adults, yet vision impairment is often preventable or even correctable,” study investigator Joshua Ehrlich MD, assistant professor of ophthalmology and visual sciences, University of Michigan, Ann Arbor, said in an interview.
Poor vision affects not only how individuals see the world, but also their systemic health and well-being, Dr. Ehrlich said.
“Accordingly, ensuring that older adults receive appropriate eye care is vital to promoting health, independence, and optimal aging,” he added.
The findings were published online in JAMA Neurology.
A surprising omission
There is an “urgent need to identify modifiable risk factors for dementia that can be targeted with interventions to slow cognitive decline and prevent dementia,” the investigators wrote.
In 2020, the Lancet Commission report on dementia prevention, intervention, and care proposed a life-course model of 12 potentially modifiable dementia risk factors. This included lower educational level, hearing loss, traumatic brain injury, hypertension, excessive alcohol consumption, obesity, smoking, depression, social isolation, physical inactivity, diabetes, and air pollution.
Together, these factors are associated with about 40% of dementia cases worldwide, the report notes.
Vision impairment was not included in this model, “despite considerable evidence that it is associated with an elevated risk of incident dementia and that it may operate through the same pathways as hearing loss,” the current researchers wrote.
“We have known for some time that vision impairment is a risk factor for dementia [and] we also know that a very large fraction of vision impairment, possibly in excess of 80%, is avoidable or has simply yet to be addressed,” Dr. Ehrlich said.
He and his colleagues found it “surprising that vision impairment had been ignored in key models of modifiable dementia risk factors that are used to shape health policy and resource allocation.” They set out to demonstrate that, “in fact, vision impairment is just as influential as a number of other long accepted modifiable dementia risk factors.”
The investigators assessed data from the Health and Retirement Study (HRS), a panel study that surveys more than 20,000 U.S. adults aged 50 years or older every 2 years.
The investigators applied the same methods used by the Lancet Commission to the HRS dataset and added vision impairment to the Lancet life-course model. Air pollution was excluded in their model “because those data were not readily available in the HRS,” the researchers wrote.
They noted the PAF is “based on the population prevalence and relative risk of dementia for each risk factor” and is “weighted, based on a principal components analysis, to account for communality (clustering of risk factors).”
A missed prevention opportunity
The sample included 16,690 participants (54% were women, 51.5% were at least age 65, 80.2% were White, 10.6% were Black, 9.2% were other).
In total, the 12 potentially modifiable risk factors used in the researchers’ model were associated with an estimated 62.4% of dementia cases in the United States, with hypertension as the most prevalent risk factor with the highest weighted PAF.
A new focus for prevention
Commenting for this article, Suzann Pershing, MD, associate professor of ophthalmology, Stanford (Calif.) University, called the study “particularly important because, despite growing recognition of its importance in relation to cognition, visual impairment is often an underrecognized risk factor.”
The current research “builds on increasingly robust medical literature linking visual impairment and dementia, applying analogous methods to those used for the life course model recently presented by the Lancet Commission to evaluate potentially modifiable dementia risk factors,” said Dr. Pershing, who was not involved with the study.
The investigators “make a compelling argument for inclusion of visual impairment as one of the potentially modifiable risk factors; practicing clinicians and health care systems may consider screening and targeted therapies to address visual impairment, with a goal of population health and contributing to a reduction in future dementia disease burden,” she added.
In an accompanying editorial), Jennifer Deal, PhD, department of epidemiology and Cochlear Center for Hearing and Public Health, Baltimore, and Julio Rojas, MD, PhD, Memory and Aging Center, department of neurology, Weill Institute for Neurosciences, University of California, San Francisco, call the findings “an important reminder that dementia is a social problem in which potentially treatable risk factors, including visual impairment, are highly prevalent in disadvantaged populations.”
The editorialists noted that 90% of cases of vision impairment are “preventable or have yet to be treated. The two “highly cost-effective interventions” of eyeglasses and/or cataract surgery “remain underused both in the U.S. and globally, especially in disadvantaged communities,” they wrote.
They added that more research is needed to “test the effectiveness of interventions to preserve cognitive health by promoting healthy vision.”
The study was supported by grants from the National Institute on Aging, the National Institutes of Health, and Research to Prevent Blindness. The investigators reported no relevant financial relationships. Dr. Deal reported having received grants from the National Institute on Aging. Dr. Rojas reported serving as site principal investigator on clinical trials for Eli Lilly and Eisai and receiving grants from the National Institute on Aging. Dr. Pershing is a consultant for Acumen, and Verana Health (as DigiSight Technologies).
A version of this article first appeared on Medscape.com.
Lupus may lead to worse stroke outcomes for women, but not men
Women with systemic lupus erythematosus (SLE) experience worse outcomes after an acute stroke than does the general population, but men with SLE do not, according to an analysis of the U.S. National Inpatient Sample presented at the annual meeting of the British Society for Rheumatology.
In a study of more than 1.5 million cases of acute stroke recorded in the United States between 2015 and 2018, women with SLE were more likely to be hospitalized for longer and less likely to be routinely discharged into their home environment than were those without SLE. No such association was found for men with SLE.
“The findings imply that primary stroke prevention is of utmost importance, especially in females with SLE,” said Sona Jesenakova, a fourth-year medical student at the University of Aberdeen (Scotland).
“There might be a need to explore more effective and targeted treatment strategies to try and minimize these excessive adverse acute stroke outcomes, especially in females with SLE suffering from stroke,” she suggested.
“Even though males form only a minority of the SLE patient population, some studies have shown that they are prone to suffer from worse disease outcomes,” Ms. Jesenakova said.
Importantly, “male sex has been identified as a risk factor for death early in the course of SLE,” she added, highlighting that sex differences do seem to exist in SLE.
Stroke is an important outcome to look at because people with SLE are known to be at higher risk for developing atherosclerosis, which is a widely known risk factor for ischemic stroke, and with antiphospholipid antibody positivity and uncontrolled disease activity, that risk can be increased. A meta-analysis of older studies has suggested that the risk for death after a stroke is 68% higher in people with SLE than in those without.
To examine the risk for death and other in-hospital outcomes in a more contemporary population, Ms. Jesenakova and associates used data from the National Inpatient Sample, a large, publicly available database that contains inpatient health care information from across the United States. Their sample population consisted of 1,581,430 individuals who had been hospitalized for stroke. Of these, there were 6,100 women and 940 men who had SLE; the remainder served as the ‘no-SLE’ control population.
As might be expected, patients with SLE were about 10 years younger than those without SLE; the median age of women and men with SLE and those without SLE were a respective 60, 61, and 71 years.
There was no difference in the type of stroke between the SLE and no-SLE groups; most had an ischemic stroke (around 89%) rather than a hemorrhagic stroke (around 11%).
The researchers analyzed three key outcomes: mortality at discharge, hospitalization prolonged to a stay of more than 4 days, and routine home discharge, meaning that the patient was able to be discharged home versus more specialist facilities such as a nursing home.
They conducted a multivariate analysis with adjustments made for potential confounding factors such as age, ethnicity, type of stroke, and revascularization treatment. Comorbidities, including major cardiovascular disease, were also accounted for.
Although women with SLE were 21% more likely to die than patients without SLE, men with SLE were 24% less likely to die than was the no-SLE population. However, these differences were not statistically significant.
Women with SLE were 20% more likely to have a prolonged hospital stay and 28% less likely to have a routine home discharge, compared with patients who did not have SLE. The 95% confidence intervals were statistically significant, which was not seen when comparing the same outcomes in men with SLE (odds ratios of 1.06 and 1.18, respectively).
“As for males, even though we didn’t find anything of statistical significance, we have to bear in mind that the sample we had was quite small, and thus these results need to be interpreted with caution,” Ms. Jesenakova said. “We also think that we identified a gap in the current knowledge, and as such, further research is needed to help us understand the influence of male sex on acute stroke outcomes in patients with comorbid SLE.”
The researchers performed a secondary analysis looking at the use of revascularization treatments for ischemic stroke and found that there were no differences between individuals with and without SLE. This analysis considered the use of intravenous thrombolysis and endovascular thrombectomy in just over 1.4 million cases but did not look at sex-specific differences.
Ms. Jesenakova had no conflicts of interest to disclose.
Women with systemic lupus erythematosus (SLE) experience worse outcomes after an acute stroke than does the general population, but men with SLE do not, according to an analysis of the U.S. National Inpatient Sample presented at the annual meeting of the British Society for Rheumatology.
In a study of more than 1.5 million cases of acute stroke recorded in the United States between 2015 and 2018, women with SLE were more likely to be hospitalized for longer and less likely to be routinely discharged into their home environment than were those without SLE. No such association was found for men with SLE.
“The findings imply that primary stroke prevention is of utmost importance, especially in females with SLE,” said Sona Jesenakova, a fourth-year medical student at the University of Aberdeen (Scotland).
“There might be a need to explore more effective and targeted treatment strategies to try and minimize these excessive adverse acute stroke outcomes, especially in females with SLE suffering from stroke,” she suggested.
“Even though males form only a minority of the SLE patient population, some studies have shown that they are prone to suffer from worse disease outcomes,” Ms. Jesenakova said.
Importantly, “male sex has been identified as a risk factor for death early in the course of SLE,” she added, highlighting that sex differences do seem to exist in SLE.
Stroke is an important outcome to look at because people with SLE are known to be at higher risk for developing atherosclerosis, which is a widely known risk factor for ischemic stroke, and with antiphospholipid antibody positivity and uncontrolled disease activity, that risk can be increased. A meta-analysis of older studies has suggested that the risk for death after a stroke is 68% higher in people with SLE than in those without.
To examine the risk for death and other in-hospital outcomes in a more contemporary population, Ms. Jesenakova and associates used data from the National Inpatient Sample, a large, publicly available database that contains inpatient health care information from across the United States. Their sample population consisted of 1,581,430 individuals who had been hospitalized for stroke. Of these, there were 6,100 women and 940 men who had SLE; the remainder served as the ‘no-SLE’ control population.
As might be expected, patients with SLE were about 10 years younger than those without SLE; the median age of women and men with SLE and those without SLE were a respective 60, 61, and 71 years.
There was no difference in the type of stroke between the SLE and no-SLE groups; most had an ischemic stroke (around 89%) rather than a hemorrhagic stroke (around 11%).
The researchers analyzed three key outcomes: mortality at discharge, hospitalization prolonged to a stay of more than 4 days, and routine home discharge, meaning that the patient was able to be discharged home versus more specialist facilities such as a nursing home.
They conducted a multivariate analysis with adjustments made for potential confounding factors such as age, ethnicity, type of stroke, and revascularization treatment. Comorbidities, including major cardiovascular disease, were also accounted for.
Although women with SLE were 21% more likely to die than patients without SLE, men with SLE were 24% less likely to die than was the no-SLE population. However, these differences were not statistically significant.
Women with SLE were 20% more likely to have a prolonged hospital stay and 28% less likely to have a routine home discharge, compared with patients who did not have SLE. The 95% confidence intervals were statistically significant, which was not seen when comparing the same outcomes in men with SLE (odds ratios of 1.06 and 1.18, respectively).
“As for males, even though we didn’t find anything of statistical significance, we have to bear in mind that the sample we had was quite small, and thus these results need to be interpreted with caution,” Ms. Jesenakova said. “We also think that we identified a gap in the current knowledge, and as such, further research is needed to help us understand the influence of male sex on acute stroke outcomes in patients with comorbid SLE.”
The researchers performed a secondary analysis looking at the use of revascularization treatments for ischemic stroke and found that there were no differences between individuals with and without SLE. This analysis considered the use of intravenous thrombolysis and endovascular thrombectomy in just over 1.4 million cases but did not look at sex-specific differences.
Ms. Jesenakova had no conflicts of interest to disclose.
Women with systemic lupus erythematosus (SLE) experience worse outcomes after an acute stroke than does the general population, but men with SLE do not, according to an analysis of the U.S. National Inpatient Sample presented at the annual meeting of the British Society for Rheumatology.
In a study of more than 1.5 million cases of acute stroke recorded in the United States between 2015 and 2018, women with SLE were more likely to be hospitalized for longer and less likely to be routinely discharged into their home environment than were those without SLE. No such association was found for men with SLE.
“The findings imply that primary stroke prevention is of utmost importance, especially in females with SLE,” said Sona Jesenakova, a fourth-year medical student at the University of Aberdeen (Scotland).
“There might be a need to explore more effective and targeted treatment strategies to try and minimize these excessive adverse acute stroke outcomes, especially in females with SLE suffering from stroke,” she suggested.
“Even though males form only a minority of the SLE patient population, some studies have shown that they are prone to suffer from worse disease outcomes,” Ms. Jesenakova said.
Importantly, “male sex has been identified as a risk factor for death early in the course of SLE,” she added, highlighting that sex differences do seem to exist in SLE.
Stroke is an important outcome to look at because people with SLE are known to be at higher risk for developing atherosclerosis, which is a widely known risk factor for ischemic stroke, and with antiphospholipid antibody positivity and uncontrolled disease activity, that risk can be increased. A meta-analysis of older studies has suggested that the risk for death after a stroke is 68% higher in people with SLE than in those without.
To examine the risk for death and other in-hospital outcomes in a more contemporary population, Ms. Jesenakova and associates used data from the National Inpatient Sample, a large, publicly available database that contains inpatient health care information from across the United States. Their sample population consisted of 1,581,430 individuals who had been hospitalized for stroke. Of these, there were 6,100 women and 940 men who had SLE; the remainder served as the ‘no-SLE’ control population.
As might be expected, patients with SLE were about 10 years younger than those without SLE; the median age of women and men with SLE and those without SLE were a respective 60, 61, and 71 years.
There was no difference in the type of stroke between the SLE and no-SLE groups; most had an ischemic stroke (around 89%) rather than a hemorrhagic stroke (around 11%).
The researchers analyzed three key outcomes: mortality at discharge, hospitalization prolonged to a stay of more than 4 days, and routine home discharge, meaning that the patient was able to be discharged home versus more specialist facilities such as a nursing home.
They conducted a multivariate analysis with adjustments made for potential confounding factors such as age, ethnicity, type of stroke, and revascularization treatment. Comorbidities, including major cardiovascular disease, were also accounted for.
Although women with SLE were 21% more likely to die than patients without SLE, men with SLE were 24% less likely to die than was the no-SLE population. However, these differences were not statistically significant.
Women with SLE were 20% more likely to have a prolonged hospital stay and 28% less likely to have a routine home discharge, compared with patients who did not have SLE. The 95% confidence intervals were statistically significant, which was not seen when comparing the same outcomes in men with SLE (odds ratios of 1.06 and 1.18, respectively).
“As for males, even though we didn’t find anything of statistical significance, we have to bear in mind that the sample we had was quite small, and thus these results need to be interpreted with caution,” Ms. Jesenakova said. “We also think that we identified a gap in the current knowledge, and as such, further research is needed to help us understand the influence of male sex on acute stroke outcomes in patients with comorbid SLE.”
The researchers performed a secondary analysis looking at the use of revascularization treatments for ischemic stroke and found that there were no differences between individuals with and without SLE. This analysis considered the use of intravenous thrombolysis and endovascular thrombectomy in just over 1.4 million cases but did not look at sex-specific differences.
Ms. Jesenakova had no conflicts of interest to disclose.
FROM BSR 2022
Smartphone diagnosis in infant seizures could be highly effective
This video transcript has been edited for clarity.
Andrew N. Wilner, MD: Welcome to Medscape. I’m Dr Andrew Wilner, reporting from the American Epilepsy Society meeting.
Today, I have the pleasure of speaking with Dr. Chethan Rao, a child and adolescent neurology resident from the Mayo Clinic in Jacksonville, Fla. Dr. Rao has a particular interest in pediatric epilepsy. Welcome, Dr. Rao.
Chethan Rao, DO: Thank you, Dr. Wilner. It’s a pleasure to be here, and thanks for taking the time to highlight our work.
Dr. Wilner: You had a very interesting paper at the meeting that I wanted to talk about, focused on infantile spasms and smartphone video. Before we dive into the paper, tell us: What are infantile spasms, and why is it important to diagnose them early?
Dr. Rao: Infantile spasms, also known as epileptic spasms, are 1- to 2-second seizures, and they typically consist of sudden stiffening of the body with brief bending forward or backward of the arms, legs, and head. They usually happen around age 3-8 months, and they typically occur in clusters, most often after awakening from sleep.
The incidence is about 1 in 2,000-3,000 children. Many kids with spasms go on to develop seizures that are very difficult to treat, like Lennox-Gastaut epilepsy, and many go on to have developmental delays as well.
Dr. Wilner: Are these subtle? In other words, could a parent have a child like that and not really recognize that this is something abnormal? Or are they so dramatic that parents say: “We’re going to the emergency room?”
Dr. Rao: One of the problems that we encounter often is that in this age group of infants, they have benign sleep myoclonus; they have Sandifer syndrome related to reflux. Those can be very difficult mimics of spasms. They’re not the most clear-cut, but they look usually different enough from normal baby movements that they get parents to seek medical attention.
Dr. Wilner: You mentioned that the infantile spasms really are a type of epilepsy and symptomatic, usually, of some underlying neurologic condition. Why is it so important to diagnose them early?
Dr. Rao: Great question. Many studies have looked at developmental outcomes based on when spasms were diagnosed and treated, and all of them have replicated time over time that the earlier you get to treatment for the spasms, the better the outcomes are for seizure control and for development.
For this reason, infantile spasm is considered a neurologic urgency in our world. Like I said, accurate diagnosis is often complicated by these potential mimics. Prompt EEG is one of the most important things for confirmation of diagnosis.
Dr. Wilner: But to get that EEG, it has to get all the way to the neurologist, right? It’s not something they’re going to do in the ER. I saw a statistic: There are millions, if not billions, of smartphones out there. Where does the smartphone come in?
Dr. Rao: Absolutely. One of the things that we have on our side these days is that almost everyone has a smartphone at their disposal. One of the recent polls in 2021 showed that more than 95% of adults of childbearing age have smartphones with video access. As some other studies have shown in the adult world, we all really have an epilepsy monitoring unit minus the EEG in our own pockets.
It’s definitely a useful tool, as that first screening video can be used in adjunct to history and physical. There have been many of studies on the adult epilepsy side showing the predictive value of smartphone video for differentiating things like epileptic seizures and nonepileptic spells. What we wanted to do is use smartphone video to pin the diagnosis early of infantile spasms and get it treated as quickly as possible.
Dr. Wilner: I’m a fan. Every now and then, I do have a patient who brings in a video of some spell. I’m an adult neurologist. The patient had a spell, and you ask them – of course they don’t remember – and you ask the witness, who usually is not a trained observer. There have been one or two occasions where I thought: “Well, I don’t know if that was really a seizure.” Then they show me the video and it’s like, “Wow, that is definitely a convulsion.” A picture definitely can be worth a thousand words.
You studied this systematically for your poster. Tell me about what you did.
Dr. Rao: Since the poster, we’ve actually expanded the study, so I’ll give you the updated version. We looked at 101 infants retrospectively at two large children’s health care centers: Nemours Children’s, associated with Mayo Clinic in Jacksonville, Fla., and Texas Children’s Hospital in Houston. We narrowed it down to 80 patients whom we included. Of these, 43 had smartphone video capture when they first presented and 37 had no video when they first presented.
We found a 17-day difference by median in the time to diagnosis and treatment. In other words, the video group was diagnosed and treated 17 days by median, compared with the no-video group. Although 17 days may not sound like a big number, in this context it can make a huge difference. That’s been shown by one of these key studies in our field called the UK Infantile Spasms Study. The 2-week difference made about a 10-point difference on the developmental scale that they use – so pretty significant.
Dr. Wilner: Let me think about this for a minute. Was that because the parents brought the child in with their video and the doctor said, “Hey, that’s infantile spasms. Here’s your shot of ACTH [or whatever they’re using these days].” Or was it because the parents who were attentive enough to use video brought their kids in sooner?
Or was this the time from when they brought the child in to treatment? Is that the time you looked at? So it wasn’t just that these were more attentive parents and more likely to use the video – you’re looking at the time from presentation with or without video until treatment, is that right?
Dr. Rao: We looked to the time from the start of the spasms, as reported by the parents, to the time of diagnosis and then the start of spasms to the time of treatment. What you asked was a fantastic question. We wanted to know who these parents are who are taking videos versus the ones that are not.
We looked at the race/ethnicity data and socioeconomic status data. There were no significant differences between the video and nonvideo group. That would not explain the difference in our results here.
Dr. Wilner: Do you have plans to follow these approximately 40 children 5 years from now and see who’s riding a bicycle and who’s still stuck in the stroller? Is there going to be a difference?
Dr. Rao: Because time to diagnosis and time to treatment were our primary outcomes, long-term follow-up may not really help as much in this study. We did have a couple of other ideas for future studies. One that we wanted to look at was kids who have risk factors for developing spasms, such as trisomy 21, tuberous sclerosis, and congenital cortical malformations; those kids are at a much higher risk for developing spasms around 3-8 months of life.
In giving targeted counseling to those families about how they can use smartphone video to minimize the time to diagnosis and treatment, we think we may be able to learn more and maybe do that prospectively.
The other interesting idea is using artificial intelligence technology for spasm detection in some of these smartphone videos. They’re already using it for different seizure types. It could be an efficient first pass when we get a whole bunch of smartphone videos to determine which ones we need to pursue further steps – to see whether we need to get long-term EEG monitoring or not.
Dr. Wilner: As an epileptologist, I was going to say that we have smartphone EKG. All we need now is smartphone EEG, and then you’ll have all the information you need on day one. It may be a ways away.
As a bottom line, would it be fair to say that parents should not hesitate to take a video of any suspiciously abnormal behavior and bring it to their family doctor or pediatric neurologist?
Dr. Rao: Yes. I was happy to see the Tuberous Sclerosis Alliance put out a promotional video that had some steps for when parents see things that are suspicious for spasms, and they do recommend using smartphone video and promptly showing it to their doctors. I think the difference that we hope to provide in this study is that we can now quantify the effect of having that smartphone video when they first present.
My takeaway from this study that I would like to show is encouraging the use of smartphone video as an adjunct tool and for providers to ask for the videos, but also for these pediatric centers to develop an infrastructure – either a secure, monitored email address like we have at our center or a patient portal – where parents can submit video concerning for spasms.
Dr. Wilner: Save the trip to the doctor. Get that video out there first.
Dr. Rao: Especially in the pandemic world, right?
Dr. Wilner: Yes. I understand that you are a neurology resident. To wrap up, what’s the next step for you?
Dr. Rao: I’m finishing up my child neurology residency this year, and I’m moving out to Stanford for pediatric epilepsy fellowship. We’re preparing this project we’re talking about for submission soon, and we’re working on another project, which is a systematic review of genetic testing and the presurgical workup for pediatric drug-resistant focal epilepsy.
Dr. Wilner: Excellent. That’s pretty exciting. Good luck to you. I want to thank you very much for telling us about your research.
Dr. Rao: It was a pleasure speaking with you, and I look forward to the next time.
Dr. Wilner: I’m Dr Andrew Wilner, reporting for Medscape. Thanks for watching.
A version of this article first appeared on Medscape.com.
This video transcript has been edited for clarity.
Andrew N. Wilner, MD: Welcome to Medscape. I’m Dr Andrew Wilner, reporting from the American Epilepsy Society meeting.
Today, I have the pleasure of speaking with Dr. Chethan Rao, a child and adolescent neurology resident from the Mayo Clinic in Jacksonville, Fla. Dr. Rao has a particular interest in pediatric epilepsy. Welcome, Dr. Rao.
Chethan Rao, DO: Thank you, Dr. Wilner. It’s a pleasure to be here, and thanks for taking the time to highlight our work.
Dr. Wilner: You had a very interesting paper at the meeting that I wanted to talk about, focused on infantile spasms and smartphone video. Before we dive into the paper, tell us: What are infantile spasms, and why is it important to diagnose them early?
Dr. Rao: Infantile spasms, also known as epileptic spasms, are 1- to 2-second seizures, and they typically consist of sudden stiffening of the body with brief bending forward or backward of the arms, legs, and head. They usually happen around age 3-8 months, and they typically occur in clusters, most often after awakening from sleep.
The incidence is about 1 in 2,000-3,000 children. Many kids with spasms go on to develop seizures that are very difficult to treat, like Lennox-Gastaut epilepsy, and many go on to have developmental delays as well.
Dr. Wilner: Are these subtle? In other words, could a parent have a child like that and not really recognize that this is something abnormal? Or are they so dramatic that parents say: “We’re going to the emergency room?”
Dr. Rao: One of the problems that we encounter often is that in this age group of infants, they have benign sleep myoclonus; they have Sandifer syndrome related to reflux. Those can be very difficult mimics of spasms. They’re not the most clear-cut, but they look usually different enough from normal baby movements that they get parents to seek medical attention.
Dr. Wilner: You mentioned that the infantile spasms really are a type of epilepsy and symptomatic, usually, of some underlying neurologic condition. Why is it so important to diagnose them early?
Dr. Rao: Great question. Many studies have looked at developmental outcomes based on when spasms were diagnosed and treated, and all of them have replicated time over time that the earlier you get to treatment for the spasms, the better the outcomes are for seizure control and for development.
For this reason, infantile spasm is considered a neurologic urgency in our world. Like I said, accurate diagnosis is often complicated by these potential mimics. Prompt EEG is one of the most important things for confirmation of diagnosis.
Dr. Wilner: But to get that EEG, it has to get all the way to the neurologist, right? It’s not something they’re going to do in the ER. I saw a statistic: There are millions, if not billions, of smartphones out there. Where does the smartphone come in?
Dr. Rao: Absolutely. One of the things that we have on our side these days is that almost everyone has a smartphone at their disposal. One of the recent polls in 2021 showed that more than 95% of adults of childbearing age have smartphones with video access. As some other studies have shown in the adult world, we all really have an epilepsy monitoring unit minus the EEG in our own pockets.
It’s definitely a useful tool, as that first screening video can be used in adjunct to history and physical. There have been many of studies on the adult epilepsy side showing the predictive value of smartphone video for differentiating things like epileptic seizures and nonepileptic spells. What we wanted to do is use smartphone video to pin the diagnosis early of infantile spasms and get it treated as quickly as possible.
Dr. Wilner: I’m a fan. Every now and then, I do have a patient who brings in a video of some spell. I’m an adult neurologist. The patient had a spell, and you ask them – of course they don’t remember – and you ask the witness, who usually is not a trained observer. There have been one or two occasions where I thought: “Well, I don’t know if that was really a seizure.” Then they show me the video and it’s like, “Wow, that is definitely a convulsion.” A picture definitely can be worth a thousand words.
You studied this systematically for your poster. Tell me about what you did.
Dr. Rao: Since the poster, we’ve actually expanded the study, so I’ll give you the updated version. We looked at 101 infants retrospectively at two large children’s health care centers: Nemours Children’s, associated with Mayo Clinic in Jacksonville, Fla., and Texas Children’s Hospital in Houston. We narrowed it down to 80 patients whom we included. Of these, 43 had smartphone video capture when they first presented and 37 had no video when they first presented.
We found a 17-day difference by median in the time to diagnosis and treatment. In other words, the video group was diagnosed and treated 17 days by median, compared with the no-video group. Although 17 days may not sound like a big number, in this context it can make a huge difference. That’s been shown by one of these key studies in our field called the UK Infantile Spasms Study. The 2-week difference made about a 10-point difference on the developmental scale that they use – so pretty significant.
Dr. Wilner: Let me think about this for a minute. Was that because the parents brought the child in with their video and the doctor said, “Hey, that’s infantile spasms. Here’s your shot of ACTH [or whatever they’re using these days].” Or was it because the parents who were attentive enough to use video brought their kids in sooner?
Or was this the time from when they brought the child in to treatment? Is that the time you looked at? So it wasn’t just that these were more attentive parents and more likely to use the video – you’re looking at the time from presentation with or without video until treatment, is that right?
Dr. Rao: We looked to the time from the start of the spasms, as reported by the parents, to the time of diagnosis and then the start of spasms to the time of treatment. What you asked was a fantastic question. We wanted to know who these parents are who are taking videos versus the ones that are not.
We looked at the race/ethnicity data and socioeconomic status data. There were no significant differences between the video and nonvideo group. That would not explain the difference in our results here.
Dr. Wilner: Do you have plans to follow these approximately 40 children 5 years from now and see who’s riding a bicycle and who’s still stuck in the stroller? Is there going to be a difference?
Dr. Rao: Because time to diagnosis and time to treatment were our primary outcomes, long-term follow-up may not really help as much in this study. We did have a couple of other ideas for future studies. One that we wanted to look at was kids who have risk factors for developing spasms, such as trisomy 21, tuberous sclerosis, and congenital cortical malformations; those kids are at a much higher risk for developing spasms around 3-8 months of life.
In giving targeted counseling to those families about how they can use smartphone video to minimize the time to diagnosis and treatment, we think we may be able to learn more and maybe do that prospectively.
The other interesting idea is using artificial intelligence technology for spasm detection in some of these smartphone videos. They’re already using it for different seizure types. It could be an efficient first pass when we get a whole bunch of smartphone videos to determine which ones we need to pursue further steps – to see whether we need to get long-term EEG monitoring or not.
Dr. Wilner: As an epileptologist, I was going to say that we have smartphone EKG. All we need now is smartphone EEG, and then you’ll have all the information you need on day one. It may be a ways away.
As a bottom line, would it be fair to say that parents should not hesitate to take a video of any suspiciously abnormal behavior and bring it to their family doctor or pediatric neurologist?
Dr. Rao: Yes. I was happy to see the Tuberous Sclerosis Alliance put out a promotional video that had some steps for when parents see things that are suspicious for spasms, and they do recommend using smartphone video and promptly showing it to their doctors. I think the difference that we hope to provide in this study is that we can now quantify the effect of having that smartphone video when they first present.
My takeaway from this study that I would like to show is encouraging the use of smartphone video as an adjunct tool and for providers to ask for the videos, but also for these pediatric centers to develop an infrastructure – either a secure, monitored email address like we have at our center or a patient portal – where parents can submit video concerning for spasms.
Dr. Wilner: Save the trip to the doctor. Get that video out there first.
Dr. Rao: Especially in the pandemic world, right?
Dr. Wilner: Yes. I understand that you are a neurology resident. To wrap up, what’s the next step for you?
Dr. Rao: I’m finishing up my child neurology residency this year, and I’m moving out to Stanford for pediatric epilepsy fellowship. We’re preparing this project we’re talking about for submission soon, and we’re working on another project, which is a systematic review of genetic testing and the presurgical workup for pediatric drug-resistant focal epilepsy.
Dr. Wilner: Excellent. That’s pretty exciting. Good luck to you. I want to thank you very much for telling us about your research.
Dr. Rao: It was a pleasure speaking with you, and I look forward to the next time.
Dr. Wilner: I’m Dr Andrew Wilner, reporting for Medscape. Thanks for watching.
A version of this article first appeared on Medscape.com.
This video transcript has been edited for clarity.
Andrew N. Wilner, MD: Welcome to Medscape. I’m Dr Andrew Wilner, reporting from the American Epilepsy Society meeting.
Today, I have the pleasure of speaking with Dr. Chethan Rao, a child and adolescent neurology resident from the Mayo Clinic in Jacksonville, Fla. Dr. Rao has a particular interest in pediatric epilepsy. Welcome, Dr. Rao.
Chethan Rao, DO: Thank you, Dr. Wilner. It’s a pleasure to be here, and thanks for taking the time to highlight our work.
Dr. Wilner: You had a very interesting paper at the meeting that I wanted to talk about, focused on infantile spasms and smartphone video. Before we dive into the paper, tell us: What are infantile spasms, and why is it important to diagnose them early?
Dr. Rao: Infantile spasms, also known as epileptic spasms, are 1- to 2-second seizures, and they typically consist of sudden stiffening of the body with brief bending forward or backward of the arms, legs, and head. They usually happen around age 3-8 months, and they typically occur in clusters, most often after awakening from sleep.
The incidence is about 1 in 2,000-3,000 children. Many kids with spasms go on to develop seizures that are very difficult to treat, like Lennox-Gastaut epilepsy, and many go on to have developmental delays as well.
Dr. Wilner: Are these subtle? In other words, could a parent have a child like that and not really recognize that this is something abnormal? Or are they so dramatic that parents say: “We’re going to the emergency room?”
Dr. Rao: One of the problems that we encounter often is that in this age group of infants, they have benign sleep myoclonus; they have Sandifer syndrome related to reflux. Those can be very difficult mimics of spasms. They’re not the most clear-cut, but they look usually different enough from normal baby movements that they get parents to seek medical attention.
Dr. Wilner: You mentioned that the infantile spasms really are a type of epilepsy and symptomatic, usually, of some underlying neurologic condition. Why is it so important to diagnose them early?
Dr. Rao: Great question. Many studies have looked at developmental outcomes based on when spasms were diagnosed and treated, and all of them have replicated time over time that the earlier you get to treatment for the spasms, the better the outcomes are for seizure control and for development.
For this reason, infantile spasm is considered a neurologic urgency in our world. Like I said, accurate diagnosis is often complicated by these potential mimics. Prompt EEG is one of the most important things for confirmation of diagnosis.
Dr. Wilner: But to get that EEG, it has to get all the way to the neurologist, right? It’s not something they’re going to do in the ER. I saw a statistic: There are millions, if not billions, of smartphones out there. Where does the smartphone come in?
Dr. Rao: Absolutely. One of the things that we have on our side these days is that almost everyone has a smartphone at their disposal. One of the recent polls in 2021 showed that more than 95% of adults of childbearing age have smartphones with video access. As some other studies have shown in the adult world, we all really have an epilepsy monitoring unit minus the EEG in our own pockets.
It’s definitely a useful tool, as that first screening video can be used in adjunct to history and physical. There have been many of studies on the adult epilepsy side showing the predictive value of smartphone video for differentiating things like epileptic seizures and nonepileptic spells. What we wanted to do is use smartphone video to pin the diagnosis early of infantile spasms and get it treated as quickly as possible.
Dr. Wilner: I’m a fan. Every now and then, I do have a patient who brings in a video of some spell. I’m an adult neurologist. The patient had a spell, and you ask them – of course they don’t remember – and you ask the witness, who usually is not a trained observer. There have been one or two occasions where I thought: “Well, I don’t know if that was really a seizure.” Then they show me the video and it’s like, “Wow, that is definitely a convulsion.” A picture definitely can be worth a thousand words.
You studied this systematically for your poster. Tell me about what you did.
Dr. Rao: Since the poster, we’ve actually expanded the study, so I’ll give you the updated version. We looked at 101 infants retrospectively at two large children’s health care centers: Nemours Children’s, associated with Mayo Clinic in Jacksonville, Fla., and Texas Children’s Hospital in Houston. We narrowed it down to 80 patients whom we included. Of these, 43 had smartphone video capture when they first presented and 37 had no video when they first presented.
We found a 17-day difference by median in the time to diagnosis and treatment. In other words, the video group was diagnosed and treated 17 days by median, compared with the no-video group. Although 17 days may not sound like a big number, in this context it can make a huge difference. That’s been shown by one of these key studies in our field called the UK Infantile Spasms Study. The 2-week difference made about a 10-point difference on the developmental scale that they use – so pretty significant.
Dr. Wilner: Let me think about this for a minute. Was that because the parents brought the child in with their video and the doctor said, “Hey, that’s infantile spasms. Here’s your shot of ACTH [or whatever they’re using these days].” Or was it because the parents who were attentive enough to use video brought their kids in sooner?
Or was this the time from when they brought the child in to treatment? Is that the time you looked at? So it wasn’t just that these were more attentive parents and more likely to use the video – you’re looking at the time from presentation with or without video until treatment, is that right?
Dr. Rao: We looked to the time from the start of the spasms, as reported by the parents, to the time of diagnosis and then the start of spasms to the time of treatment. What you asked was a fantastic question. We wanted to know who these parents are who are taking videos versus the ones that are not.
We looked at the race/ethnicity data and socioeconomic status data. There were no significant differences between the video and nonvideo group. That would not explain the difference in our results here.
Dr. Wilner: Do you have plans to follow these approximately 40 children 5 years from now and see who’s riding a bicycle and who’s still stuck in the stroller? Is there going to be a difference?
Dr. Rao: Because time to diagnosis and time to treatment were our primary outcomes, long-term follow-up may not really help as much in this study. We did have a couple of other ideas for future studies. One that we wanted to look at was kids who have risk factors for developing spasms, such as trisomy 21, tuberous sclerosis, and congenital cortical malformations; those kids are at a much higher risk for developing spasms around 3-8 months of life.
In giving targeted counseling to those families about how they can use smartphone video to minimize the time to diagnosis and treatment, we think we may be able to learn more and maybe do that prospectively.
The other interesting idea is using artificial intelligence technology for spasm detection in some of these smartphone videos. They’re already using it for different seizure types. It could be an efficient first pass when we get a whole bunch of smartphone videos to determine which ones we need to pursue further steps – to see whether we need to get long-term EEG monitoring or not.
Dr. Wilner: As an epileptologist, I was going to say that we have smartphone EKG. All we need now is smartphone EEG, and then you’ll have all the information you need on day one. It may be a ways away.
As a bottom line, would it be fair to say that parents should not hesitate to take a video of any suspiciously abnormal behavior and bring it to their family doctor or pediatric neurologist?
Dr. Rao: Yes. I was happy to see the Tuberous Sclerosis Alliance put out a promotional video that had some steps for when parents see things that are suspicious for spasms, and they do recommend using smartphone video and promptly showing it to their doctors. I think the difference that we hope to provide in this study is that we can now quantify the effect of having that smartphone video when they first present.
My takeaway from this study that I would like to show is encouraging the use of smartphone video as an adjunct tool and for providers to ask for the videos, but also for these pediatric centers to develop an infrastructure – either a secure, monitored email address like we have at our center or a patient portal – where parents can submit video concerning for spasms.
Dr. Wilner: Save the trip to the doctor. Get that video out there first.
Dr. Rao: Especially in the pandemic world, right?
Dr. Wilner: Yes. I understand that you are a neurology resident. To wrap up, what’s the next step for you?
Dr. Rao: I’m finishing up my child neurology residency this year, and I’m moving out to Stanford for pediatric epilepsy fellowship. We’re preparing this project we’re talking about for submission soon, and we’re working on another project, which is a systematic review of genetic testing and the presurgical workup for pediatric drug-resistant focal epilepsy.
Dr. Wilner: Excellent. That’s pretty exciting. Good luck to you. I want to thank you very much for telling us about your research.
Dr. Rao: It was a pleasure speaking with you, and I look forward to the next time.
Dr. Wilner: I’m Dr Andrew Wilner, reporting for Medscape. Thanks for watching.
A version of this article first appeared on Medscape.com.
Nap length linked to cognitive changes
No wonder we feel worse after naps
Some of us have hectic schedules that may make a nap feel more necessary. It’s common knowledge that naps shouldn’t be too long – maybe 20 minutes or so – but if you frequently take 3-hour naps and wake up thinking you’re late for school even though you’re 47 and have your PhD, this LOTME is for you.

Studies have shown that there is a link between napping during the day and Alzheimer’s/cognitive decline, but now we’ve got a double whammy for you: Longer and more frequent napping is linked to worse cognition after a year, and in turn, those with cognitive decline and Alzheimer’s are known to nap longer and more frequently during the day.
“We now know that the pathology related to cognitive decline can cause other changes in function,” he said. “It’s really a multisystem disorder, also including difficulty sleeping, changes in movement, changes in body composition, depression symptoms, behavioral changes, etc.,” coauthor Aron Buchman, MD, said in a statement from Rush University Medical Center.
The investigators monitored 1,400 patients over the course of 14 years with wrist bracelets that recorded when a person was not active during the day and considered that a nap.
At the beginning of the study, 75% of the study subjects had no cognitive impairment, 19.5% had some cognitive impairment, and approximately 4% had Alzheimer’s. Napping during the day only increased about 11 minutes a year for those with no signs of cognitive impairment, but those who showed significantly more signs of cognitive decline doubled their nap time and those actually diagnosed with Alzheimer’s tripled theirs.
The investigators did not imply that napping causes Alzheimer’s, but they noted that people who are older and nap more than an hour a day are 40% more likely to be at risk. It is something to consider and monitor.
Sometimes, after all, a nap seems like the best idea ever, but more often than not we wake up feeling 10 times worse. Our bodies may be giving us a heads up.
Pokemon Go away depression
The summer of 2016 was a great time if you happened to be a fan of Pokemon. Which is quite a lot of people. For almost 20 years millions have enjoyed the games and animated series, but Pokemon Go brought the thrill of catching Pokemon to life in a whole new way. For the first time, you could go out into the world and pretend you were a real Pokemon trainer, and everywhere you went, there would be others like you.

The ability to chase after Pikachu and Charizard in real life (well, augmented reality, but close enough) seemed to bring people a lot of joy, but seemed is never good enough for science. Can’t have anecdotes, we need data! So researchers at the London School of Economics and Political Science conducted a study into how Pokemon Go affected local Internet search rates of depression as the game was released slowly around the world.
Through analyzing Google Trend data of words like “depression,” “anxiety,” and “stress,” the researchers found that the release of Pokemon Go was significantly associated with a noticeable, though short-term, drop in depression-related Internet searches. Location-based augmented reality games may alleviate symptoms of mild depression, the researchers said, as they encourage physical activity, face-to-face socialization, and exposure to nature, though they added that simply going outside is likely not enough to combat clinical cases of severe depression.
Still, augmented reality games represent a viable target for public health investment, since they’re easy to use and inexpensive to make. That said, we’re not sure we want the FDA or CDC making a new Pokemon Go game. They’d probably end up filling the streets with Mr. Mime. And no one would leave their house for that.
And now a word from our sponsor
How many times has this happened to you? You need to repair a jet engine, inspect a nuclear reactor cooling system, AND perform bowel surgery, but you can’t carry around all the heavy, old-fashioned tools needed for those jobs.
Well, we’ve got one tool that can do it all! And that tool is a snake. No, it’s a robot.
It’s both! It’s the COntinuum roBot for Remote Applications. COBRA is the robot that looks like a snake! A snake that’s 5 meters long but only as thick as a pencil (about 9 mm in diameter). A robot with “extraordinary manoeuvrability and responsiveness due to … a compliant-joint structure and multiple continuous sections that enable it to bend at around 90 degrees,” according to the team at the University of Nottingham (England) that developed it.
COBRA comes equipped with a stereovision camera and a miniature cutting tool to perform complex industrial repair, but other devices can be interchanged for possible medical use.
COBRA and its joystick-like controller were designed to be easy to use. Dr. Oladejo Olaleye, the ear, nose, and throat and robotic surgeon at University Hospitals of Leicester who is directing its surgical development, was able to use COBRA on a dummy after just 5 minutes of training. He called it “the future of diagnostic endoscopy and therapeutic surgery.”
Don’t be the last aircraft engineer/nuclear technician/surgeon on your block to have this ultraslender, ultramaneuverable reptilian repair robot. Get your COBRA now! Operators are standing by.
Disclaimer: Robot is still under development and not yet on sale.
Rule, (worm) Britannia!
As long as there have been people, there have been parasitic worms living in their guts. Helminth infection is a continuing and largely ignored crisis in poor, tropical nations, though worm-based diseases have been basically eliminated from wealthier countries.

This wasn’t always the case, however, as a study published in PLOS Neglected Tropical Diseases (now there’s a specific topic) has found. The researchers detail the glorious history of helminth infestation in the United Kingdom from the Victorian era all the way back to prehistory, scouring hundreds of skeletons found in 17 sites across the country for eggs, which can remain intact for thousands of years.
The researchers found that two eras in particular had very high rates of infection. Unsurprisingly, the late medieval era was one of them, but the other is less obvious. The Romans were famous for their hygiene, their baths, and their plumbing, but maybe they also should be famous for the abundance of worms in their bellies. That doesn’t make sense at first: Shouldn’t good hygiene lower infection? The benefits of a good sewer system, however, are lessened when the waste containing said infectious organisms is used to fertilize crops. Recycling is generally a good thing, but less so when you’re recycling parasitic worms.
Curiously, of the three sites from the industrial age, only the one in London had high levels of worm infestation. Considering how dirty and cramped 19th-century British cities were, one might expect disease to run rampant (tuberculosis certainly did), but the sites in Oxford and Birmingham were almost devoid of worms. The researchers theorized that this was because of access to clean well water. Or maybe worms just have a thing for London. [Editor’s note: It’s probably not that.]
No wonder we feel worse after naps
Some of us have hectic schedules that may make a nap feel more necessary. It’s common knowledge that naps shouldn’t be too long – maybe 20 minutes or so – but if you frequently take 3-hour naps and wake up thinking you’re late for school even though you’re 47 and have your PhD, this LOTME is for you.
Studies have shown that there is a link between napping during the day and Alzheimer’s/cognitive decline, but now we’ve got a double whammy for you: Longer and more frequent napping is linked to worse cognition after a year, and in turn, those with cognitive decline and Alzheimer’s are known to nap longer and more frequently during the day.
“We now know that the pathology related to cognitive decline can cause other changes in function,” he said. “It’s really a multisystem disorder, also including difficulty sleeping, changes in movement, changes in body composition, depression symptoms, behavioral changes, etc.,” coauthor Aron Buchman, MD, said in a statement from Rush University Medical Center.
The investigators monitored 1,400 patients over the course of 14 years with wrist bracelets that recorded when a person was not active during the day and considered that a nap.
At the beginning of the study, 75% of the study subjects had no cognitive impairment, 19.5% had some cognitive impairment, and approximately 4% had Alzheimer’s. Napping during the day only increased about 11 minutes a year for those with no signs of cognitive impairment, but those who showed significantly more signs of cognitive decline doubled their nap time and those actually diagnosed with Alzheimer’s tripled theirs.
The investigators did not imply that napping causes Alzheimer’s, but they noted that people who are older and nap more than an hour a day are 40% more likely to be at risk. It is something to consider and monitor.
Sometimes, after all, a nap seems like the best idea ever, but more often than not we wake up feeling 10 times worse. Our bodies may be giving us a heads up.
Pokemon Go away depression
The summer of 2016 was a great time if you happened to be a fan of Pokemon. Which is quite a lot of people. For almost 20 years millions have enjoyed the games and animated series, but Pokemon Go brought the thrill of catching Pokemon to life in a whole new way. For the first time, you could go out into the world and pretend you were a real Pokemon trainer, and everywhere you went, there would be others like you.
The ability to chase after Pikachu and Charizard in real life (well, augmented reality, but close enough) seemed to bring people a lot of joy, but seemed is never good enough for science. Can’t have anecdotes, we need data! So researchers at the London School of Economics and Political Science conducted a study into how Pokemon Go affected local Internet search rates of depression as the game was released slowly around the world.
Through analyzing Google Trend data of words like “depression,” “anxiety,” and “stress,” the researchers found that the release of Pokemon Go was significantly associated with a noticeable, though short-term, drop in depression-related Internet searches. Location-based augmented reality games may alleviate symptoms of mild depression, the researchers said, as they encourage physical activity, face-to-face socialization, and exposure to nature, though they added that simply going outside is likely not enough to combat clinical cases of severe depression.
Still, augmented reality games represent a viable target for public health investment, since they’re easy to use and inexpensive to make. That said, we’re not sure we want the FDA or CDC making a new Pokemon Go game. They’d probably end up filling the streets with Mr. Mime. And no one would leave their house for that.
And now a word from our sponsor
How many times has this happened to you? You need to repair a jet engine, inspect a nuclear reactor cooling system, AND perform bowel surgery, but you can’t carry around all the heavy, old-fashioned tools needed for those jobs.
Well, we’ve got one tool that can do it all! And that tool is a snake. No, it’s a robot.
It’s both! It’s the COntinuum roBot for Remote Applications. COBRA is the robot that looks like a snake! A snake that’s 5 meters long but only as thick as a pencil (about 9 mm in diameter). A robot with “extraordinary manoeuvrability and responsiveness due to … a compliant-joint structure and multiple continuous sections that enable it to bend at around 90 degrees,” according to the team at the University of Nottingham (England) that developed it.
COBRA comes equipped with a stereovision camera and a miniature cutting tool to perform complex industrial repair, but other devices can be interchanged for possible medical use.
COBRA and its joystick-like controller were designed to be easy to use. Dr. Oladejo Olaleye, the ear, nose, and throat and robotic surgeon at University Hospitals of Leicester who is directing its surgical development, was able to use COBRA on a dummy after just 5 minutes of training. He called it “the future of diagnostic endoscopy and therapeutic surgery.”
Don’t be the last aircraft engineer/nuclear technician/surgeon on your block to have this ultraslender, ultramaneuverable reptilian repair robot. Get your COBRA now! Operators are standing by.
Disclaimer: Robot is still under development and not yet on sale.
Rule, (worm) Britannia!
As long as there have been people, there have been parasitic worms living in their guts. Helminth infection is a continuing and largely ignored crisis in poor, tropical nations, though worm-based diseases have been basically eliminated from wealthier countries.
This wasn’t always the case, however, as a study published in PLOS Neglected Tropical Diseases (now there’s a specific topic) has found. The researchers detail the glorious history of helminth infestation in the United Kingdom from the Victorian era all the way back to prehistory, scouring hundreds of skeletons found in 17 sites across the country for eggs, which can remain intact for thousands of years.
The researchers found that two eras in particular had very high rates of infection. Unsurprisingly, the late medieval era was one of them, but the other is less obvious. The Romans were famous for their hygiene, their baths, and their plumbing, but maybe they also should be famous for the abundance of worms in their bellies. That doesn’t make sense at first: Shouldn’t good hygiene lower infection? The benefits of a good sewer system, however, are lessened when the waste containing said infectious organisms is used to fertilize crops. Recycling is generally a good thing, but less so when you’re recycling parasitic worms.
Curiously, of the three sites from the industrial age, only the one in London had high levels of worm infestation. Considering how dirty and cramped 19th-century British cities were, one might expect disease to run rampant (tuberculosis certainly did), but the sites in Oxford and Birmingham were almost devoid of worms. The researchers theorized that this was because of access to clean well water. Or maybe worms just have a thing for London. [Editor’s note: It’s probably not that.]
No wonder we feel worse after naps
Some of us have hectic schedules that may make a nap feel more necessary. It’s common knowledge that naps shouldn’t be too long – maybe 20 minutes or so – but if you frequently take 3-hour naps and wake up thinking you’re late for school even though you’re 47 and have your PhD, this LOTME is for you.
Studies have shown that there is a link between napping during the day and Alzheimer’s/cognitive decline, but now we’ve got a double whammy for you: Longer and more frequent napping is linked to worse cognition after a year, and in turn, those with cognitive decline and Alzheimer’s are known to nap longer and more frequently during the day.
“We now know that the pathology related to cognitive decline can cause other changes in function,” he said. “It’s really a multisystem disorder, also including difficulty sleeping, changes in movement, changes in body composition, depression symptoms, behavioral changes, etc.,” coauthor Aron Buchman, MD, said in a statement from Rush University Medical Center.
The investigators monitored 1,400 patients over the course of 14 years with wrist bracelets that recorded when a person was not active during the day and considered that a nap.
At the beginning of the study, 75% of the study subjects had no cognitive impairment, 19.5% had some cognitive impairment, and approximately 4% had Alzheimer’s. Napping during the day only increased about 11 minutes a year for those with no signs of cognitive impairment, but those who showed significantly more signs of cognitive decline doubled their nap time and those actually diagnosed with Alzheimer’s tripled theirs.
The investigators did not imply that napping causes Alzheimer’s, but they noted that people who are older and nap more than an hour a day are 40% more likely to be at risk. It is something to consider and monitor.
Sometimes, after all, a nap seems like the best idea ever, but more often than not we wake up feeling 10 times worse. Our bodies may be giving us a heads up.
Pokemon Go away depression
The summer of 2016 was a great time if you happened to be a fan of Pokemon. Which is quite a lot of people. For almost 20 years millions have enjoyed the games and animated series, but Pokemon Go brought the thrill of catching Pokemon to life in a whole new way. For the first time, you could go out into the world and pretend you were a real Pokemon trainer, and everywhere you went, there would be others like you.
The ability to chase after Pikachu and Charizard in real life (well, augmented reality, but close enough) seemed to bring people a lot of joy, but seemed is never good enough for science. Can’t have anecdotes, we need data! So researchers at the London School of Economics and Political Science conducted a study into how Pokemon Go affected local Internet search rates of depression as the game was released slowly around the world.
Through analyzing Google Trend data of words like “depression,” “anxiety,” and “stress,” the researchers found that the release of Pokemon Go was significantly associated with a noticeable, though short-term, drop in depression-related Internet searches. Location-based augmented reality games may alleviate symptoms of mild depression, the researchers said, as they encourage physical activity, face-to-face socialization, and exposure to nature, though they added that simply going outside is likely not enough to combat clinical cases of severe depression.
Still, augmented reality games represent a viable target for public health investment, since they’re easy to use and inexpensive to make. That said, we’re not sure we want the FDA or CDC making a new Pokemon Go game. They’d probably end up filling the streets with Mr. Mime. And no one would leave their house for that.
And now a word from our sponsor
How many times has this happened to you? You need to repair a jet engine, inspect a nuclear reactor cooling system, AND perform bowel surgery, but you can’t carry around all the heavy, old-fashioned tools needed for those jobs.
Well, we’ve got one tool that can do it all! And that tool is a snake. No, it’s a robot.
It’s both! It’s the COntinuum roBot for Remote Applications. COBRA is the robot that looks like a snake! A snake that’s 5 meters long but only as thick as a pencil (about 9 mm in diameter). A robot with “extraordinary manoeuvrability and responsiveness due to … a compliant-joint structure and multiple continuous sections that enable it to bend at around 90 degrees,” according to the team at the University of Nottingham (England) that developed it.
COBRA comes equipped with a stereovision camera and a miniature cutting tool to perform complex industrial repair, but other devices can be interchanged for possible medical use.
COBRA and its joystick-like controller were designed to be easy to use. Dr. Oladejo Olaleye, the ear, nose, and throat and robotic surgeon at University Hospitals of Leicester who is directing its surgical development, was able to use COBRA on a dummy after just 5 minutes of training. He called it “the future of diagnostic endoscopy and therapeutic surgery.”
Don’t be the last aircraft engineer/nuclear technician/surgeon on your block to have this ultraslender, ultramaneuverable reptilian repair robot. Get your COBRA now! Operators are standing by.
Disclaimer: Robot is still under development and not yet on sale.
Rule, (worm) Britannia!
As long as there have been people, there have been parasitic worms living in their guts. Helminth infection is a continuing and largely ignored crisis in poor, tropical nations, though worm-based diseases have been basically eliminated from wealthier countries.
This wasn’t always the case, however, as a study published in PLOS Neglected Tropical Diseases (now there’s a specific topic) has found. The researchers detail the glorious history of helminth infestation in the United Kingdom from the Victorian era all the way back to prehistory, scouring hundreds of skeletons found in 17 sites across the country for eggs, which can remain intact for thousands of years.
The researchers found that two eras in particular had very high rates of infection. Unsurprisingly, the late medieval era was one of them, but the other is less obvious. The Romans were famous for their hygiene, their baths, and their plumbing, but maybe they also should be famous for the abundance of worms in their bellies. That doesn’t make sense at first: Shouldn’t good hygiene lower infection? The benefits of a good sewer system, however, are lessened when the waste containing said infectious organisms is used to fertilize crops. Recycling is generally a good thing, but less so when you’re recycling parasitic worms.
Curiously, of the three sites from the industrial age, only the one in London had high levels of worm infestation. Considering how dirty and cramped 19th-century British cities were, one might expect disease to run rampant (tuberculosis certainly did), but the sites in Oxford and Birmingham were almost devoid of worms. The researchers theorized that this was because of access to clean well water. Or maybe worms just have a thing for London. [Editor’s note: It’s probably not that.]
How do we distinguish between viral and bacterial meningitis?
Bacteria and viruses are the leading causes of community-acquired meningitis. Bacterial meningitis is associated with high morbidity and mortality, and prompt treatment with appropriate antibiotics is essential to optimize outcomes. Early diagnosis is therefore crucial for selecting patients who need antibiotics. On the other hand, the course of viral meningitis is generally benign, and there is usually no specific antimicrobial treatment required. Distinguishing between viral and bacterial causes of meningitis can be challenging; therefore, many patients receive empiric antibiotic treatment.
Etiology
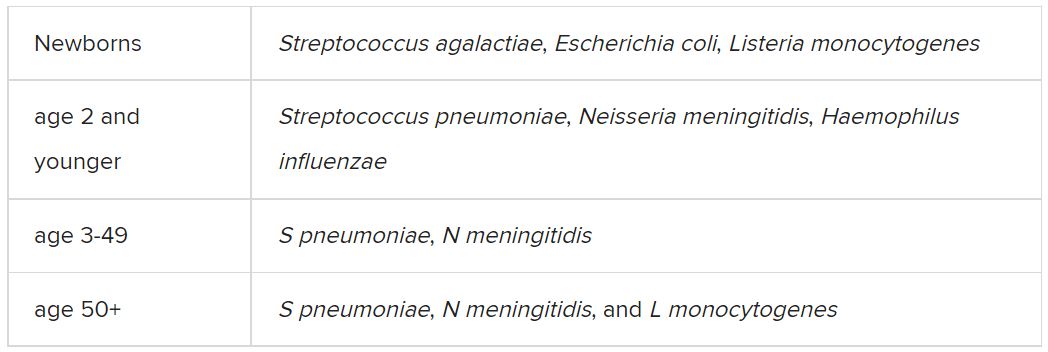
Among the etiologic agents of viral meningitis, the nonpolio enteroviruses (Echovirus 30, 11, 9, 6, 7, 18, 16, 71, 25; Coxsackie B2, A9, B1, B3, B4) are the most common, responsible for more than 85% of cases. Other viruses potentially responsible for meningitis include the herpes simplex virus (HSV), primarily type 2, and flavivirus (such as the Dengue virus).
Clinical presentation
The clinical presentation of bacterial meningitis is more severe than that of viral meningitis. The classic clinical triad of bacterial meningitis consists of fever, neck stiffness, and altered mental status. Only 41% of cases present with these three symptoms, however. Other clinical characteristics include severe headaches, decreased level of consciousness, nausea, vomiting, seizures, focal neurologic signs, and skin rash.
Viral meningitis is usually not associated with a decreased level of consciousness or significant decline in overall health status. The most frequently reported symptoms are unusual headaches, fever, nausea, vomiting, sensitivity to light, and neck stiffness. Patients may also present with skin changes and lymphadenopathy, and, depending on etiology, genital ulcers.
Diagnosis
The diagnosis of bacterial meningitis is based on clinical symptoms, blood panels (blood count, inflammation markers, cultures), and cerebrospinal fluid (CSF) cultures. Gram staining and latex agglutination may lead to false-negative results, and cultures may take a few days to provide a definitive result. Therefore, empiric antibiotic treatment is often started until the etiology can be determined.
A spinal tap must always be performed, preferably after a scan is taken, to rule out the risk of herniation. After CSF samples have been collected, they must undergo complete analysis, including cytological, biochemical, and microbiological evaluation, using conventional and molecular testing methods, when available.
Cytological and biochemical analyses of CSF may be helpful, as findings may indicate a higher probability of either bacterial or viral etiology.
CSF samples collected from patients with acute bacterial meningitis present characteristic neutrophilic pleocytosis (cell count usually ranging from hundreds to a few thousand, with >80% polymorphonuclear cells). In some cases of L. monocytogenes meningitis (from 25% to 30%), a lymphocytic predominance may occur. Normally, glucose is low (CSF glucose-to-blood-glucose ratio of ≤0.4 or <40 mg/dL), protein is very high (>200 mg/dL), and the CSF lactate level is high (≥31.53 mg/dL).
In viral meningitis, the white blood cell count is generally 10-300 cells/mm3. Although glucose levels are normal in most cases, they may be below normal limits in lymphocytic choriomeningitis virus (LCMV), HSV, mumps virus, and poliovirus meningitis. Protein levels tend to be slightly elevated, but they may still be within the reference range.
A recent study investigated which of the cytological or biochemical markers best correlate with the definite etiologic diagnosis. This study, in which CSF samples were collected and analyzed from 2013 to 2017, considered cases of bacterial or viral meningitis confirmed via microbiological evaluation or polymerase chain reaction (PCR). CSF lactate was the best single CSF parameter, and CSF lactate above 30 mg/dL virtually excludes the possibility of a viral etiology.
Etiologic determination
Despite the major contribution of globally analyzing CSF and secondary parameters, particularly CSF lactate, the precise etiologic definition is of great importance in cases of acute meningitis. Such precise definition is not simple, as identification of the causative microorganism is often difficult. Moreover, there are limits to conventional microbiological methods. Bacterioscopy is poorly sensitive, and although bacterial cultures are more sensitive, they can delay diagnosis because of the time it takes for the bacteria to grow in culture media.
Targeted molecular detection methods are usually more sensitive than conventional microbiological methods. Panel-based molecular tests identify multiple pathogens in a single test. In 2015, the U.S. Food and Drug Administration authorized the first commercial multiplex detection system for infectious causes of community-acquired meningitis and encephalitis. This test, the BioFire FilmArray system, detects 14 bacterial, viral, and fungal pathogens in a turnaround time of about 1 hour, including S. pneumoniae, N. meningitidis, H. influenzae, S. agalactiae (i.e., group B Streptococcus), E. coli (serotype K1), L. monocytogenes, HSV-1, HSV-2, varicella-zoster virus (VZV), cytomegalovirus (CMV), human herpesvirus 6 (HHV-6), human parechovirus (HPeV), and Cryptococcus neoformans/gattii.
A meta-analysis of eight precise diagnostic studies evaluating the BioFire FilmArray system showed a high sensitivity of 90% (95% confidence interval, 86%-93%) and specificity of 97% (95% CI, 94%-99%). The FilmArray ME panel can halve the time to microbiological result, allowing for earlier discontinuation of antimicrobial agents and hospital discharge in cases of viral meningitis.
Conclusion
Acute community-acquired meningitis is usually the result of viral or bacterial infections. Given the low specificity of clinical symptoms and, very often, of the general laboratory panel findings, many patients are empirically treated with antibiotics. High-sensitivity and -specificity molecular techniques allow for rapid identification of the bacterial etiology (which requires antibiotic therapy) or the viral etiology of meningitis. The latter can be managed only with symptom-specific medications and does not usually require extended hospitalization. Therefore, these new techniques can improve the quality of care for these patients with viral meningitis.
A version of this article first appeared on Medscape.com.
Bacteria and viruses are the leading causes of community-acquired meningitis. Bacterial meningitis is associated with high morbidity and mortality, and prompt treatment with appropriate antibiotics is essential to optimize outcomes. Early diagnosis is therefore crucial for selecting patients who need antibiotics. On the other hand, the course of viral meningitis is generally benign, and there is usually no specific antimicrobial treatment required. Distinguishing between viral and bacterial causes of meningitis can be challenging; therefore, many patients receive empiric antibiotic treatment.
Etiology
Among the etiologic agents of viral meningitis, the nonpolio enteroviruses (Echovirus 30, 11, 9, 6, 7, 18, 16, 71, 25; Coxsackie B2, A9, B1, B3, B4) are the most common, responsible for more than 85% of cases. Other viruses potentially responsible for meningitis include the herpes simplex virus (HSV), primarily type 2, and flavivirus (such as the Dengue virus).
Clinical presentation
The clinical presentation of bacterial meningitis is more severe than that of viral meningitis. The classic clinical triad of bacterial meningitis consists of fever, neck stiffness, and altered mental status. Only 41% of cases present with these three symptoms, however. Other clinical characteristics include severe headaches, decreased level of consciousness, nausea, vomiting, seizures, focal neurologic signs, and skin rash.
Viral meningitis is usually not associated with a decreased level of consciousness or significant decline in overall health status. The most frequently reported symptoms are unusual headaches, fever, nausea, vomiting, sensitivity to light, and neck stiffness. Patients may also present with skin changes and lymphadenopathy, and, depending on etiology, genital ulcers.
Diagnosis
The diagnosis of bacterial meningitis is based on clinical symptoms, blood panels (blood count, inflammation markers, cultures), and cerebrospinal fluid (CSF) cultures. Gram staining and latex agglutination may lead to false-negative results, and cultures may take a few days to provide a definitive result. Therefore, empiric antibiotic treatment is often started until the etiology can be determined.
A spinal tap must always be performed, preferably after a scan is taken, to rule out the risk of herniation. After CSF samples have been collected, they must undergo complete analysis, including cytological, biochemical, and microbiological evaluation, using conventional and molecular testing methods, when available.
Cytological and biochemical analyses of CSF may be helpful, as findings may indicate a higher probability of either bacterial or viral etiology.
CSF samples collected from patients with acute bacterial meningitis present characteristic neutrophilic pleocytosis (cell count usually ranging from hundreds to a few thousand, with >80% polymorphonuclear cells). In some cases of L. monocytogenes meningitis (from 25% to 30%), a lymphocytic predominance may occur. Normally, glucose is low (CSF glucose-to-blood-glucose ratio of ≤0.4 or <40 mg/dL), protein is very high (>200 mg/dL), and the CSF lactate level is high (≥31.53 mg/dL).
In viral meningitis, the white blood cell count is generally 10-300 cells/mm3. Although glucose levels are normal in most cases, they may be below normal limits in lymphocytic choriomeningitis virus (LCMV), HSV, mumps virus, and poliovirus meningitis. Protein levels tend to be slightly elevated, but they may still be within the reference range.
A recent study investigated which of the cytological or biochemical markers best correlate with the definite etiologic diagnosis. This study, in which CSF samples were collected and analyzed from 2013 to 2017, considered cases of bacterial or viral meningitis confirmed via microbiological evaluation or polymerase chain reaction (PCR). CSF lactate was the best single CSF parameter, and CSF lactate above 30 mg/dL virtually excludes the possibility of a viral etiology.
Etiologic determination
Despite the major contribution of globally analyzing CSF and secondary parameters, particularly CSF lactate, the precise etiologic definition is of great importance in cases of acute meningitis. Such precise definition is not simple, as identification of the causative microorganism is often difficult. Moreover, there are limits to conventional microbiological methods. Bacterioscopy is poorly sensitive, and although bacterial cultures are more sensitive, they can delay diagnosis because of the time it takes for the bacteria to grow in culture media.
Targeted molecular detection methods are usually more sensitive than conventional microbiological methods. Panel-based molecular tests identify multiple pathogens in a single test. In 2015, the U.S. Food and Drug Administration authorized the first commercial multiplex detection system for infectious causes of community-acquired meningitis and encephalitis. This test, the BioFire FilmArray system, detects 14 bacterial, viral, and fungal pathogens in a turnaround time of about 1 hour, including S. pneumoniae, N. meningitidis, H. influenzae, S. agalactiae (i.e., group B Streptococcus), E. coli (serotype K1), L. monocytogenes, HSV-1, HSV-2, varicella-zoster virus (VZV), cytomegalovirus (CMV), human herpesvirus 6 (HHV-6), human parechovirus (HPeV), and Cryptococcus neoformans/gattii.
A meta-analysis of eight precise diagnostic studies evaluating the BioFire FilmArray system showed a high sensitivity of 90% (95% confidence interval, 86%-93%) and specificity of 97% (95% CI, 94%-99%). The FilmArray ME panel can halve the time to microbiological result, allowing for earlier discontinuation of antimicrobial agents and hospital discharge in cases of viral meningitis.
Conclusion
Acute community-acquired meningitis is usually the result of viral or bacterial infections. Given the low specificity of clinical symptoms and, very often, of the general laboratory panel findings, many patients are empirically treated with antibiotics. High-sensitivity and -specificity molecular techniques allow for rapid identification of the bacterial etiology (which requires antibiotic therapy) or the viral etiology of meningitis. The latter can be managed only with symptom-specific medications and does not usually require extended hospitalization. Therefore, these new techniques can improve the quality of care for these patients with viral meningitis.
A version of this article first appeared on Medscape.com.
Bacteria and viruses are the leading causes of community-acquired meningitis. Bacterial meningitis is associated with high morbidity and mortality, and prompt treatment with appropriate antibiotics is essential to optimize outcomes. Early diagnosis is therefore crucial for selecting patients who need antibiotics. On the other hand, the course of viral meningitis is generally benign, and there is usually no specific antimicrobial treatment required. Distinguishing between viral and bacterial causes of meningitis can be challenging; therefore, many patients receive empiric antibiotic treatment.
Etiology
Among the etiologic agents of viral meningitis, the nonpolio enteroviruses (Echovirus 30, 11, 9, 6, 7, 18, 16, 71, 25; Coxsackie B2, A9, B1, B3, B4) are the most common, responsible for more than 85% of cases. Other viruses potentially responsible for meningitis include the herpes simplex virus (HSV), primarily type 2, and flavivirus (such as the Dengue virus).
Clinical presentation
The clinical presentation of bacterial meningitis is more severe than that of viral meningitis. The classic clinical triad of bacterial meningitis consists of fever, neck stiffness, and altered mental status. Only 41% of cases present with these three symptoms, however. Other clinical characteristics include severe headaches, decreased level of consciousness, nausea, vomiting, seizures, focal neurologic signs, and skin rash.
Viral meningitis is usually not associated with a decreased level of consciousness or significant decline in overall health status. The most frequently reported symptoms are unusual headaches, fever, nausea, vomiting, sensitivity to light, and neck stiffness. Patients may also present with skin changes and lymphadenopathy, and, depending on etiology, genital ulcers.
Diagnosis
The diagnosis of bacterial meningitis is based on clinical symptoms, blood panels (blood count, inflammation markers, cultures), and cerebrospinal fluid (CSF) cultures. Gram staining and latex agglutination may lead to false-negative results, and cultures may take a few days to provide a definitive result. Therefore, empiric antibiotic treatment is often started until the etiology can be determined.
A spinal tap must always be performed, preferably after a scan is taken, to rule out the risk of herniation. After CSF samples have been collected, they must undergo complete analysis, including cytological, biochemical, and microbiological evaluation, using conventional and molecular testing methods, when available.
Cytological and biochemical analyses of CSF may be helpful, as findings may indicate a higher probability of either bacterial or viral etiology.
CSF samples collected from patients with acute bacterial meningitis present characteristic neutrophilic pleocytosis (cell count usually ranging from hundreds to a few thousand, with >80% polymorphonuclear cells). In some cases of L. monocytogenes meningitis (from 25% to 30%), a lymphocytic predominance may occur. Normally, glucose is low (CSF glucose-to-blood-glucose ratio of ≤0.4 or <40 mg/dL), protein is very high (>200 mg/dL), and the CSF lactate level is high (≥31.53 mg/dL).
In viral meningitis, the white blood cell count is generally 10-300 cells/mm3. Although glucose levels are normal in most cases, they may be below normal limits in lymphocytic choriomeningitis virus (LCMV), HSV, mumps virus, and poliovirus meningitis. Protein levels tend to be slightly elevated, but they may still be within the reference range.
A recent study investigated which of the cytological or biochemical markers best correlate with the definite etiologic diagnosis. This study, in which CSF samples were collected and analyzed from 2013 to 2017, considered cases of bacterial or viral meningitis confirmed via microbiological evaluation or polymerase chain reaction (PCR). CSF lactate was the best single CSF parameter, and CSF lactate above 30 mg/dL virtually excludes the possibility of a viral etiology.
Etiologic determination
Despite the major contribution of globally analyzing CSF and secondary parameters, particularly CSF lactate, the precise etiologic definition is of great importance in cases of acute meningitis. Such precise definition is not simple, as identification of the causative microorganism is often difficult. Moreover, there are limits to conventional microbiological methods. Bacterioscopy is poorly sensitive, and although bacterial cultures are more sensitive, they can delay diagnosis because of the time it takes for the bacteria to grow in culture media.
Targeted molecular detection methods are usually more sensitive than conventional microbiological methods. Panel-based molecular tests identify multiple pathogens in a single test. In 2015, the U.S. Food and Drug Administration authorized the first commercial multiplex detection system for infectious causes of community-acquired meningitis and encephalitis. This test, the BioFire FilmArray system, detects 14 bacterial, viral, and fungal pathogens in a turnaround time of about 1 hour, including S. pneumoniae, N. meningitidis, H. influenzae, S. agalactiae (i.e., group B Streptococcus), E. coli (serotype K1), L. monocytogenes, HSV-1, HSV-2, varicella-zoster virus (VZV), cytomegalovirus (CMV), human herpesvirus 6 (HHV-6), human parechovirus (HPeV), and Cryptococcus neoformans/gattii.
A meta-analysis of eight precise diagnostic studies evaluating the BioFire FilmArray system showed a high sensitivity of 90% (95% confidence interval, 86%-93%) and specificity of 97% (95% CI, 94%-99%). The FilmArray ME panel can halve the time to microbiological result, allowing for earlier discontinuation of antimicrobial agents and hospital discharge in cases of viral meningitis.
Conclusion
Acute community-acquired meningitis is usually the result of viral or bacterial infections. Given the low specificity of clinical symptoms and, very often, of the general laboratory panel findings, many patients are empirically treated with antibiotics. High-sensitivity and -specificity molecular techniques allow for rapid identification of the bacterial etiology (which requires antibiotic therapy) or the viral etiology of meningitis. The latter can be managed only with symptom-specific medications and does not usually require extended hospitalization. Therefore, these new techniques can improve the quality of care for these patients with viral meningitis.
A version of this article first appeared on Medscape.com.