User login
Epidermolysis bullosa classification criteria refined and ready
LONDON – have come in understanding this debilitating group of genetic skin diseases, but also how far there is still to go towards improving the management of those affected.

Previous criteria issued in 2014 represented “important progress” and “built on the achievements of several generations of physicians and researchers who described the phenotypes, the level of skin cleavage, developed and characterized antibodies, and discovered EB-associated genes,” Cristina Has, MD, said at the EB World Congress, organized by the Dystrophic Epidermolysis Bullosa Association (DEBRA).
Dr. Has, a senior dermatologist and professor of experimental dermatology at the University of Freiburg (Germany), observed that prior criteria had “introduced genetic and molecular data in a so-called onion-skin classification of EB, and removed most of the eponyms,” which had been maintained in the latest update.
“What is new, and probably the most important change, is making the distinction between classical EB and other disorders with skin fragility,” she said, noting that the revised classification criteria for EB included minor changes to the nomenclature of EB. Six new EB subtypes and genes have also been added, and there are new sections on genotype/phenotype correlations, disease modifying factors, and the natural history of EB. Furthermore, supporting information included a concise description of clinical and genetic features of all EB types and subtypes.
The updated criteria are the result of an expert meeting held in April 2019 and have been accepted for publication. The expert panel that developed the criteria think that the revised classification criteria will be “useful and, we hope, inspiring and motivating for the young generation of dermatologists, pediatricians, and for the researchers who work in this field,” Dr. Has said.
“The term EB has been used in the last years for many new disorders, and this is the reason why we thought we have to somehow control this, and to make the distinction between classical epidermolysis bullosa due to defects at the dermal junction and other disorders with skin fragility where the anomalies occur within other layers of the epidermis or in the dermis,” Dr. Has explained.
There are still 4 main types of classical EB: EB simplex (EBS), dystrophic EB (DEB), junctional EB, and Kindler EB, but there are now 34 subtypes, slightly fewer than before. The updated criteria distinguish between the types and subtypes according to the level of skin cleavage, the inheritance pattern, the mutated gene, and the targeted protein, Dr. Has said.
As for peeling disorders, these have been classified as being erosive or hyperkeratotic, or as affecting the connective tissue with skin blistering. Similar to classical EB, these disorders are associated with fragility of the skin and mucosa and share some pathogenetic mechanisms. Moreover, as “the suffering of the patient is similar,” Dr. Has said, “we’d like to consider them under the umbrella of EB.” Most of the disorders she listed were inherited via an autosomal recessive mechanism, with intraepidermal disorders inherited via an autosomal dominant mechanism. New genes are being identified the time, she added, so these groupings will no doubt be subject to future revisions.
Minor changes to nomenclature were made to avoid confusion among clinicians and those living with the condition. As such, Kindler EB replaces Kindler syndrome, names of some subtypes were simplified, and a new “self-improving” type of DEB was introduced to replace the term “transient dermolysis of the newborn.” Altogether, there are now 11 subtypes of DEB. A distinction was also made between syndromic and nonsyndromic EB. “We all know that EB can be a systemic disorder with secondary manifestations within different organs,” Dr. Has told conference attendees. Anemia and failure to thrive can be associated, but it still remains a nonsyndromic disorder, she said. By contrast, “syndromic EB is due to genetic defects, which are also expressed in other organs than the skin or mucosal membranes, and lead to primary extracutaneous manifestations, such as cardiomyopathy, nephropathy, and so on.”
There are fewer subtypes of EBS and “we think they are better defined,” Dr. Has stated. “EB simplex is the most heterogenous EB type, clinically and genetically, and includes several syndromic disorders,” and the new classification criteria should be useful in helping categorize individuals with EBS and thus help target their management.
One of the six new subtypes of EB included in the revised classification criteria is “syndromic EBS with cardiomyopathy” caused by the KLH24 mutation. This gene was discovered in 2016 and more than 40 cases have so far been identified, 50% of which have been sporadic de novo mutations.
Other new EB subtypes are:
- “EBS with localized nephropathy” caused by a mutation in the CD151 gene.
- An autosomal recessive EBS linked to the KRT5 gene.
- A new phenotype that manifests with oral mucosal blisters linked to the DSG3 gene. (Although only a single case has been reported to date, it was felt worthy of inclusion.)
- Another linked to DSG3 that leads to skin fragility and hypertrichosis.
- A new dystrophic EB subtype linked to mutations in the PLOD3 gene.
In an interview, Dr. Has reiterated the importance of keeping classification criteria updated in line with current research findings. She emphasized that there were many types of EB and how important it was to refine how these were classified based on the underlying genetics.
“We brought much more genetic data into the paper, because we are in the era of personalized medicine,” she said. “There are specific therapies for mutations and for different subtypes and that’s why we think that, step by step, we have to bring in more and more data into the classification.”
There are many people with EBS, she observed, and while these individuals may not have such a dramatic clinical presentation as those with recessive DEB, for example, the effect of the condition on their daily lives is no less. “These people are active, they have jobs, they have to work, and they have pain, they have blister,” Dr. Has said.
While the criteria are intended only for classification of EB, they might help in practice. Dr. Has gave an anecdotal example of a woman that has been misdiagnosed as having a type of DEB with a high risk of squamous cell carcinoma but in fact had a different form of EB with no risk of developing SCC. “That’s why criteria are important,” she said.
Dr. Has had no conflicts of interest to disclose.
LONDON – have come in understanding this debilitating group of genetic skin diseases, but also how far there is still to go towards improving the management of those affected.
Previous criteria issued in 2014 represented “important progress” and “built on the achievements of several generations of physicians and researchers who described the phenotypes, the level of skin cleavage, developed and characterized antibodies, and discovered EB-associated genes,” Cristina Has, MD, said at the EB World Congress, organized by the Dystrophic Epidermolysis Bullosa Association (DEBRA).
Dr. Has, a senior dermatologist and professor of experimental dermatology at the University of Freiburg (Germany), observed that prior criteria had “introduced genetic and molecular data in a so-called onion-skin classification of EB, and removed most of the eponyms,” which had been maintained in the latest update.
“What is new, and probably the most important change, is making the distinction between classical EB and other disorders with skin fragility,” she said, noting that the revised classification criteria for EB included minor changes to the nomenclature of EB. Six new EB subtypes and genes have also been added, and there are new sections on genotype/phenotype correlations, disease modifying factors, and the natural history of EB. Furthermore, supporting information included a concise description of clinical and genetic features of all EB types and subtypes.
The updated criteria are the result of an expert meeting held in April 2019 and have been accepted for publication. The expert panel that developed the criteria think that the revised classification criteria will be “useful and, we hope, inspiring and motivating for the young generation of dermatologists, pediatricians, and for the researchers who work in this field,” Dr. Has said.
“The term EB has been used in the last years for many new disorders, and this is the reason why we thought we have to somehow control this, and to make the distinction between classical epidermolysis bullosa due to defects at the dermal junction and other disorders with skin fragility where the anomalies occur within other layers of the epidermis or in the dermis,” Dr. Has explained.
There are still 4 main types of classical EB: EB simplex (EBS), dystrophic EB (DEB), junctional EB, and Kindler EB, but there are now 34 subtypes, slightly fewer than before. The updated criteria distinguish between the types and subtypes according to the level of skin cleavage, the inheritance pattern, the mutated gene, and the targeted protein, Dr. Has said.
As for peeling disorders, these have been classified as being erosive or hyperkeratotic, or as affecting the connective tissue with skin blistering. Similar to classical EB, these disorders are associated with fragility of the skin and mucosa and share some pathogenetic mechanisms. Moreover, as “the suffering of the patient is similar,” Dr. Has said, “we’d like to consider them under the umbrella of EB.” Most of the disorders she listed were inherited via an autosomal recessive mechanism, with intraepidermal disorders inherited via an autosomal dominant mechanism. New genes are being identified the time, she added, so these groupings will no doubt be subject to future revisions.
Minor changes to nomenclature were made to avoid confusion among clinicians and those living with the condition. As such, Kindler EB replaces Kindler syndrome, names of some subtypes were simplified, and a new “self-improving” type of DEB was introduced to replace the term “transient dermolysis of the newborn.” Altogether, there are now 11 subtypes of DEB. A distinction was also made between syndromic and nonsyndromic EB. “We all know that EB can be a systemic disorder with secondary manifestations within different organs,” Dr. Has told conference attendees. Anemia and failure to thrive can be associated, but it still remains a nonsyndromic disorder, she said. By contrast, “syndromic EB is due to genetic defects, which are also expressed in other organs than the skin or mucosal membranes, and lead to primary extracutaneous manifestations, such as cardiomyopathy, nephropathy, and so on.”
There are fewer subtypes of EBS and “we think they are better defined,” Dr. Has stated. “EB simplex is the most heterogenous EB type, clinically and genetically, and includes several syndromic disorders,” and the new classification criteria should be useful in helping categorize individuals with EBS and thus help target their management.
One of the six new subtypes of EB included in the revised classification criteria is “syndromic EBS with cardiomyopathy” caused by the KLH24 mutation. This gene was discovered in 2016 and more than 40 cases have so far been identified, 50% of which have been sporadic de novo mutations.
Other new EB subtypes are:
- “EBS with localized nephropathy” caused by a mutation in the CD151 gene.
- An autosomal recessive EBS linked to the KRT5 gene.
- A new phenotype that manifests with oral mucosal blisters linked to the DSG3 gene. (Although only a single case has been reported to date, it was felt worthy of inclusion.)
- Another linked to DSG3 that leads to skin fragility and hypertrichosis.
- A new dystrophic EB subtype linked to mutations in the PLOD3 gene.
In an interview, Dr. Has reiterated the importance of keeping classification criteria updated in line with current research findings. She emphasized that there were many types of EB and how important it was to refine how these were classified based on the underlying genetics.
“We brought much more genetic data into the paper, because we are in the era of personalized medicine,” she said. “There are specific therapies for mutations and for different subtypes and that’s why we think that, step by step, we have to bring in more and more data into the classification.”
There are many people with EBS, she observed, and while these individuals may not have such a dramatic clinical presentation as those with recessive DEB, for example, the effect of the condition on their daily lives is no less. “These people are active, they have jobs, they have to work, and they have pain, they have blister,” Dr. Has said.
While the criteria are intended only for classification of EB, they might help in practice. Dr. Has gave an anecdotal example of a woman that has been misdiagnosed as having a type of DEB with a high risk of squamous cell carcinoma but in fact had a different form of EB with no risk of developing SCC. “That’s why criteria are important,” she said.
Dr. Has had no conflicts of interest to disclose.
LONDON – have come in understanding this debilitating group of genetic skin diseases, but also how far there is still to go towards improving the management of those affected.
Previous criteria issued in 2014 represented “important progress” and “built on the achievements of several generations of physicians and researchers who described the phenotypes, the level of skin cleavage, developed and characterized antibodies, and discovered EB-associated genes,” Cristina Has, MD, said at the EB World Congress, organized by the Dystrophic Epidermolysis Bullosa Association (DEBRA).
Dr. Has, a senior dermatologist and professor of experimental dermatology at the University of Freiburg (Germany), observed that prior criteria had “introduced genetic and molecular data in a so-called onion-skin classification of EB, and removed most of the eponyms,” which had been maintained in the latest update.
“What is new, and probably the most important change, is making the distinction between classical EB and other disorders with skin fragility,” she said, noting that the revised classification criteria for EB included minor changes to the nomenclature of EB. Six new EB subtypes and genes have also been added, and there are new sections on genotype/phenotype correlations, disease modifying factors, and the natural history of EB. Furthermore, supporting information included a concise description of clinical and genetic features of all EB types and subtypes.
The updated criteria are the result of an expert meeting held in April 2019 and have been accepted for publication. The expert panel that developed the criteria think that the revised classification criteria will be “useful and, we hope, inspiring and motivating for the young generation of dermatologists, pediatricians, and for the researchers who work in this field,” Dr. Has said.
“The term EB has been used in the last years for many new disorders, and this is the reason why we thought we have to somehow control this, and to make the distinction between classical epidermolysis bullosa due to defects at the dermal junction and other disorders with skin fragility where the anomalies occur within other layers of the epidermis or in the dermis,” Dr. Has explained.
There are still 4 main types of classical EB: EB simplex (EBS), dystrophic EB (DEB), junctional EB, and Kindler EB, but there are now 34 subtypes, slightly fewer than before. The updated criteria distinguish between the types and subtypes according to the level of skin cleavage, the inheritance pattern, the mutated gene, and the targeted protein, Dr. Has said.
As for peeling disorders, these have been classified as being erosive or hyperkeratotic, or as affecting the connective tissue with skin blistering. Similar to classical EB, these disorders are associated with fragility of the skin and mucosa and share some pathogenetic mechanisms. Moreover, as “the suffering of the patient is similar,” Dr. Has said, “we’d like to consider them under the umbrella of EB.” Most of the disorders she listed were inherited via an autosomal recessive mechanism, with intraepidermal disorders inherited via an autosomal dominant mechanism. New genes are being identified the time, she added, so these groupings will no doubt be subject to future revisions.
Minor changes to nomenclature were made to avoid confusion among clinicians and those living with the condition. As such, Kindler EB replaces Kindler syndrome, names of some subtypes were simplified, and a new “self-improving” type of DEB was introduced to replace the term “transient dermolysis of the newborn.” Altogether, there are now 11 subtypes of DEB. A distinction was also made between syndromic and nonsyndromic EB. “We all know that EB can be a systemic disorder with secondary manifestations within different organs,” Dr. Has told conference attendees. Anemia and failure to thrive can be associated, but it still remains a nonsyndromic disorder, she said. By contrast, “syndromic EB is due to genetic defects, which are also expressed in other organs than the skin or mucosal membranes, and lead to primary extracutaneous manifestations, such as cardiomyopathy, nephropathy, and so on.”
There are fewer subtypes of EBS and “we think they are better defined,” Dr. Has stated. “EB simplex is the most heterogenous EB type, clinically and genetically, and includes several syndromic disorders,” and the new classification criteria should be useful in helping categorize individuals with EBS and thus help target their management.
One of the six new subtypes of EB included in the revised classification criteria is “syndromic EBS with cardiomyopathy” caused by the KLH24 mutation. This gene was discovered in 2016 and more than 40 cases have so far been identified, 50% of which have been sporadic de novo mutations.
Other new EB subtypes are:
- “EBS with localized nephropathy” caused by a mutation in the CD151 gene.
- An autosomal recessive EBS linked to the KRT5 gene.
- A new phenotype that manifests with oral mucosal blisters linked to the DSG3 gene. (Although only a single case has been reported to date, it was felt worthy of inclusion.)
- Another linked to DSG3 that leads to skin fragility and hypertrichosis.
- A new dystrophic EB subtype linked to mutations in the PLOD3 gene.
In an interview, Dr. Has reiterated the importance of keeping classification criteria updated in line with current research findings. She emphasized that there were many types of EB and how important it was to refine how these were classified based on the underlying genetics.
“We brought much more genetic data into the paper, because we are in the era of personalized medicine,” she said. “There are specific therapies for mutations and for different subtypes and that’s why we think that, step by step, we have to bring in more and more data into the classification.”
There are many people with EBS, she observed, and while these individuals may not have such a dramatic clinical presentation as those with recessive DEB, for example, the effect of the condition on their daily lives is no less. “These people are active, they have jobs, they have to work, and they have pain, they have blister,” Dr. Has said.
While the criteria are intended only for classification of EB, they might help in practice. Dr. Has gave an anecdotal example of a woman that has been misdiagnosed as having a type of DEB with a high risk of squamous cell carcinoma but in fact had a different form of EB with no risk of developing SCC. “That’s why criteria are important,” she said.
Dr. Has had no conflicts of interest to disclose.
REPORTING FROM EB 2020
Weight bias against teens: Understand it and combat it
NEW ORLEANS – and support your patients regardless of weight.
Rebecca Puhl, PhD, a deputy director of the Rudd Center for Food Policy and Obesity at the University of Connecticut, Hartford, said that weight-based discrimination can occur whatever a person’s size or body shape, but it’s most often targeted at youth who are overweight or obese.
These children and teens commonly face teasing, harassment, cyberbullying, physical aggression, and social bullying from peers, coaches, teachers, and even parents, Dr. Puhl told attendees at the annual meeting of the American Academy of Pediatrics.
Common beliefs about overweight people – that they have little self discipline or poor eating and activity habits – only perpetuate stereotypes, she said. Common stereotypes are that people with obesity are noncompliant, lazy, sloppy, unsuccessful, unintelligent, dishonest, and awkward.
And health professionals of every type have been found to harbor these biases. In one study of more than 4,000 first-year medical students, well over half the respondents revealed explicit (74%) and implicit (67%) weight bias (Obesity. 2014 Apr;22[4]:1201-8). The study also found that explicit weight bias was stronger than explicit bias against blacks, Hispanics, LGBTQ people, and poor people.
Know the effects of weight stigma
Far from a minor issue, the discrimination that begins in childhood against those who are overweight can have a long-lasting impact on their future prospects and mental health. Being overweight is overwhelmingly cited as the most common reason for bullying (Pediatr Obes. 2016 Aug;11[4]:241-50). Dr. Puhl described to attendees how weight bias shifts throughout a lifetime, beginning as early as preschool. In childhood, the stereotypes about being overweight worsen, and the teasing and bullying increase. By adolescence, this treatment affects teens’ psychological, social, and physical well-being. It then translates in adulthood into reduced opportunities in employment and education, and poorer access and treatment in health care.
The mental distress caused by weight bullying often takes the form of depression, anxiety, and substance use, Dr. Puhl said, and children’s academic success can be hampered by bullying about their weight. One study found a higher risk of poor grades and school avoidance with each additional teasing incident (J Youth Adolesc. 2012 Jan;41[1]:27-40).
Weight stigma also can contribute to more weight gain, obesity, and lower physical activity levels. Maladaptive eating behaviors can result from weight stigmatization as well: binge eating, emotional eating, increased consumption in general, and other eating disorders. Severe binge eating is 80% more likely among teens who are bullied about their weight, Dr. Puhl said, and the risk increases with increased frequency and types of bullying.
Children who are teased about their weight often become less willing to engage in physical activity, she noted. They may skip gym class, feel less competent about physical activity, and end up enjoying sports participation less.
Further, sexual- and gender-minority youth report high rates of weight-related teasing from friends and family regardless of their body mass index (BMI) percentile, Dr. Puhl emphasized. Researchers have found bullying about weight in this population linked to dieting, difficulty sleeping, high stress levels, binge drinking, smoking, and marijuana use.
Know how to combat weight bias
Dr. Puhl described strategies for reducing weight bias based on clinical practice recommendations in the American Academy of Pediatrics’ policy statement entitled “Stigma Experienced by Children and Adolescents With Obesity” (Pediatrics. 2017 Dec;140[6]:e20173034).
Be aware. Consider how personal assumptions and attitudes about weight can affect your body language, tone of voice, facial expression, gestures, eye contact (or lack thereof), and spatial distance from the patient.
Recognizing the biological, genetic, and environmental causes of obesity can reduce stigma and improve understanding of the complexity of obesity etiology. It’s also important that you help parents understand this complexity and the negative impact of weight stigma.
Consider language and word choice. “Carefully consider language that might unintentionally communicate bias, blame, or negative judgment,” Dr. Puhl told attendees. “Use language that is supportive and empowering.”
Terms such as “unhealthy weight” and “high BMI” are less stigmatizing than “fat” and “morbidly obese” to parents, she said, and research has found nearly a quarter of parents would avoid future doctor appointments if their child’s doctor used stigmatizing terms to discuss weight (Pediatrics. 2011 Oct;128[4]:e786-93).
Teens themselves may have diverse preferences for the language used. Start by asking: “Could we talk about your weight today?” and then follow up by directly asking, “what words would you feel most comfortable with as we talk about your weight?”
Person-first language – such as “person with obesity” instead of “obese person” also is important to reducing stigma, she said.
It’s normal for you to feel uneasy about bringing up weight with patients, so Dr. Puhl recommended you practice dialogue out loud.
“Acknowledge your strengths,” she said. “You already have the skills and experience of engaging in difficult conversations with patients and families on a range of other health issues,” so apply that in this context as well.
Screen for negative experiences that could indicate weight-based bullying. These could include teasing and bullying, low self-esteem, poor school performance, depression, and anxiety.
“Remember that weight-based victimization can occur at diverse body sizes, not just in youth with obesity,” Dr. Puhl said. If you discover your patient is experiencing weight-related bullying, determine whether they have a support system in place and whether a mental health referral is appropriate. Provide or refer for behavior change counseling with motivational interviewing and patient-centered, empathic approaches. Parents should be aware of the issue and should contact the child’s teachers and school administration to help address it.
But before you do that, keep in mind that it’s not just peers doing the bullying. According to a study of teens with obesity enrolled in a national weight-loss camp, 37% of teen participants in 2012 said that their parents bully them (Pediatrics. 2013 Jan;131[1]:e1-9).
You should assess whether family interactions or the parents’ own history with weight is involved. If parents make disparaging comments about their child’s weight, “use this as an opportunity to model appropriate language and educate parents about weight bias,” Dr. Puhl said.
It’s also important to realize that parents themselves often are frustrated, so critical comments about their language or approach can backfire, she warned. Instead, help parents understand how to create a home setting that encourages healthy food choices, praises children for healthy decision making, and models positive health behaviors. It is key for them to focus on improving their children’s health behaviors rather than focusing on weight.
And before you contact the school, remember teachers also are common perpetrators of weight stigma, Dr. Puhl noted. She gave as an example a study in which investigators assessed 133 teachers’ perceptions of middle or high school students’ abilities based on photos that had been digitally altered to show each girl both as average weight or as overweight. Each photo was associated with an essay specifically chosen because it was neither particularly good nor bad (Brit J Educ Psychol. 2019 Oct 26. doi: 10.1111/bjep.12322). The teachers judged the essays believed to be submitted by overweight girls to be “similar in structural quality,” but they gave the overweight girls lower grades than the average-weight girls. They also indicated that they considered the overweight girls “put forth more effort, needed more remedial assistance, and had lower overall grades in school.” The teachers also rated other teachers’ weight bias to be at a low level, and their own weight bias to be “significantly lower” than the others.
Assess your clinical environment. Be aware of your clinical environment and whether it meets the needs of youth with diverse body sizes. That includes having a range of sturdy armless seating options and adequately sized doorways, hallways, and restrooms. You also should have beds, wheelchairs, and exam tables with adequate weight capacity. Also check that you have supplies, such as robes or blood pressure cuffs, on hand for a variety of body sizes.
NEW ORLEANS – and support your patients regardless of weight.
Rebecca Puhl, PhD, a deputy director of the Rudd Center for Food Policy and Obesity at the University of Connecticut, Hartford, said that weight-based discrimination can occur whatever a person’s size or body shape, but it’s most often targeted at youth who are overweight or obese.
These children and teens commonly face teasing, harassment, cyberbullying, physical aggression, and social bullying from peers, coaches, teachers, and even parents, Dr. Puhl told attendees at the annual meeting of the American Academy of Pediatrics.
Common beliefs about overweight people – that they have little self discipline or poor eating and activity habits – only perpetuate stereotypes, she said. Common stereotypes are that people with obesity are noncompliant, lazy, sloppy, unsuccessful, unintelligent, dishonest, and awkward.
And health professionals of every type have been found to harbor these biases. In one study of more than 4,000 first-year medical students, well over half the respondents revealed explicit (74%) and implicit (67%) weight bias (Obesity. 2014 Apr;22[4]:1201-8). The study also found that explicit weight bias was stronger than explicit bias against blacks, Hispanics, LGBTQ people, and poor people.
Know the effects of weight stigma
Far from a minor issue, the discrimination that begins in childhood against those who are overweight can have a long-lasting impact on their future prospects and mental health. Being overweight is overwhelmingly cited as the most common reason for bullying (Pediatr Obes. 2016 Aug;11[4]:241-50). Dr. Puhl described to attendees how weight bias shifts throughout a lifetime, beginning as early as preschool. In childhood, the stereotypes about being overweight worsen, and the teasing and bullying increase. By adolescence, this treatment affects teens’ psychological, social, and physical well-being. It then translates in adulthood into reduced opportunities in employment and education, and poorer access and treatment in health care.
The mental distress caused by weight bullying often takes the form of depression, anxiety, and substance use, Dr. Puhl said, and children’s academic success can be hampered by bullying about their weight. One study found a higher risk of poor grades and school avoidance with each additional teasing incident (J Youth Adolesc. 2012 Jan;41[1]:27-40).
Weight stigma also can contribute to more weight gain, obesity, and lower physical activity levels. Maladaptive eating behaviors can result from weight stigmatization as well: binge eating, emotional eating, increased consumption in general, and other eating disorders. Severe binge eating is 80% more likely among teens who are bullied about their weight, Dr. Puhl said, and the risk increases with increased frequency and types of bullying.
Children who are teased about their weight often become less willing to engage in physical activity, she noted. They may skip gym class, feel less competent about physical activity, and end up enjoying sports participation less.
Further, sexual- and gender-minority youth report high rates of weight-related teasing from friends and family regardless of their body mass index (BMI) percentile, Dr. Puhl emphasized. Researchers have found bullying about weight in this population linked to dieting, difficulty sleeping, high stress levels, binge drinking, smoking, and marijuana use.
Know how to combat weight bias
Dr. Puhl described strategies for reducing weight bias based on clinical practice recommendations in the American Academy of Pediatrics’ policy statement entitled “Stigma Experienced by Children and Adolescents With Obesity” (Pediatrics. 2017 Dec;140[6]:e20173034).
Be aware. Consider how personal assumptions and attitudes about weight can affect your body language, tone of voice, facial expression, gestures, eye contact (or lack thereof), and spatial distance from the patient.
Recognizing the biological, genetic, and environmental causes of obesity can reduce stigma and improve understanding of the complexity of obesity etiology. It’s also important that you help parents understand this complexity and the negative impact of weight stigma.
Consider language and word choice. “Carefully consider language that might unintentionally communicate bias, blame, or negative judgment,” Dr. Puhl told attendees. “Use language that is supportive and empowering.”
Terms such as “unhealthy weight” and “high BMI” are less stigmatizing than “fat” and “morbidly obese” to parents, she said, and research has found nearly a quarter of parents would avoid future doctor appointments if their child’s doctor used stigmatizing terms to discuss weight (Pediatrics. 2011 Oct;128[4]:e786-93).
Teens themselves may have diverse preferences for the language used. Start by asking: “Could we talk about your weight today?” and then follow up by directly asking, “what words would you feel most comfortable with as we talk about your weight?”
Person-first language – such as “person with obesity” instead of “obese person” also is important to reducing stigma, she said.
It’s normal for you to feel uneasy about bringing up weight with patients, so Dr. Puhl recommended you practice dialogue out loud.
“Acknowledge your strengths,” she said. “You already have the skills and experience of engaging in difficult conversations with patients and families on a range of other health issues,” so apply that in this context as well.
Screen for negative experiences that could indicate weight-based bullying. These could include teasing and bullying, low self-esteem, poor school performance, depression, and anxiety.
“Remember that weight-based victimization can occur at diverse body sizes, not just in youth with obesity,” Dr. Puhl said. If you discover your patient is experiencing weight-related bullying, determine whether they have a support system in place and whether a mental health referral is appropriate. Provide or refer for behavior change counseling with motivational interviewing and patient-centered, empathic approaches. Parents should be aware of the issue and should contact the child’s teachers and school administration to help address it.
But before you do that, keep in mind that it’s not just peers doing the bullying. According to a study of teens with obesity enrolled in a national weight-loss camp, 37% of teen participants in 2012 said that their parents bully them (Pediatrics. 2013 Jan;131[1]:e1-9).
You should assess whether family interactions or the parents’ own history with weight is involved. If parents make disparaging comments about their child’s weight, “use this as an opportunity to model appropriate language and educate parents about weight bias,” Dr. Puhl said.
It’s also important to realize that parents themselves often are frustrated, so critical comments about their language or approach can backfire, she warned. Instead, help parents understand how to create a home setting that encourages healthy food choices, praises children for healthy decision making, and models positive health behaviors. It is key for them to focus on improving their children’s health behaviors rather than focusing on weight.
And before you contact the school, remember teachers also are common perpetrators of weight stigma, Dr. Puhl noted. She gave as an example a study in which investigators assessed 133 teachers’ perceptions of middle or high school students’ abilities based on photos that had been digitally altered to show each girl both as average weight or as overweight. Each photo was associated with an essay specifically chosen because it was neither particularly good nor bad (Brit J Educ Psychol. 2019 Oct 26. doi: 10.1111/bjep.12322). The teachers judged the essays believed to be submitted by overweight girls to be “similar in structural quality,” but they gave the overweight girls lower grades than the average-weight girls. They also indicated that they considered the overweight girls “put forth more effort, needed more remedial assistance, and had lower overall grades in school.” The teachers also rated other teachers’ weight bias to be at a low level, and their own weight bias to be “significantly lower” than the others.
Assess your clinical environment. Be aware of your clinical environment and whether it meets the needs of youth with diverse body sizes. That includes having a range of sturdy armless seating options and adequately sized doorways, hallways, and restrooms. You also should have beds, wheelchairs, and exam tables with adequate weight capacity. Also check that you have supplies, such as robes or blood pressure cuffs, on hand for a variety of body sizes.
NEW ORLEANS – and support your patients regardless of weight.
Rebecca Puhl, PhD, a deputy director of the Rudd Center for Food Policy and Obesity at the University of Connecticut, Hartford, said that weight-based discrimination can occur whatever a person’s size or body shape, but it’s most often targeted at youth who are overweight or obese.
These children and teens commonly face teasing, harassment, cyberbullying, physical aggression, and social bullying from peers, coaches, teachers, and even parents, Dr. Puhl told attendees at the annual meeting of the American Academy of Pediatrics.
Common beliefs about overweight people – that they have little self discipline or poor eating and activity habits – only perpetuate stereotypes, she said. Common stereotypes are that people with obesity are noncompliant, lazy, sloppy, unsuccessful, unintelligent, dishonest, and awkward.
And health professionals of every type have been found to harbor these biases. In one study of more than 4,000 first-year medical students, well over half the respondents revealed explicit (74%) and implicit (67%) weight bias (Obesity. 2014 Apr;22[4]:1201-8). The study also found that explicit weight bias was stronger than explicit bias against blacks, Hispanics, LGBTQ people, and poor people.
Know the effects of weight stigma
Far from a minor issue, the discrimination that begins in childhood against those who are overweight can have a long-lasting impact on their future prospects and mental health. Being overweight is overwhelmingly cited as the most common reason for bullying (Pediatr Obes. 2016 Aug;11[4]:241-50). Dr. Puhl described to attendees how weight bias shifts throughout a lifetime, beginning as early as preschool. In childhood, the stereotypes about being overweight worsen, and the teasing and bullying increase. By adolescence, this treatment affects teens’ psychological, social, and physical well-being. It then translates in adulthood into reduced opportunities in employment and education, and poorer access and treatment in health care.
The mental distress caused by weight bullying often takes the form of depression, anxiety, and substance use, Dr. Puhl said, and children’s academic success can be hampered by bullying about their weight. One study found a higher risk of poor grades and school avoidance with each additional teasing incident (J Youth Adolesc. 2012 Jan;41[1]:27-40).
Weight stigma also can contribute to more weight gain, obesity, and lower physical activity levels. Maladaptive eating behaviors can result from weight stigmatization as well: binge eating, emotional eating, increased consumption in general, and other eating disorders. Severe binge eating is 80% more likely among teens who are bullied about their weight, Dr. Puhl said, and the risk increases with increased frequency and types of bullying.
Children who are teased about their weight often become less willing to engage in physical activity, she noted. They may skip gym class, feel less competent about physical activity, and end up enjoying sports participation less.
Further, sexual- and gender-minority youth report high rates of weight-related teasing from friends and family regardless of their body mass index (BMI) percentile, Dr. Puhl emphasized. Researchers have found bullying about weight in this population linked to dieting, difficulty sleeping, high stress levels, binge drinking, smoking, and marijuana use.
Know how to combat weight bias
Dr. Puhl described strategies for reducing weight bias based on clinical practice recommendations in the American Academy of Pediatrics’ policy statement entitled “Stigma Experienced by Children and Adolescents With Obesity” (Pediatrics. 2017 Dec;140[6]:e20173034).
Be aware. Consider how personal assumptions and attitudes about weight can affect your body language, tone of voice, facial expression, gestures, eye contact (or lack thereof), and spatial distance from the patient.
Recognizing the biological, genetic, and environmental causes of obesity can reduce stigma and improve understanding of the complexity of obesity etiology. It’s also important that you help parents understand this complexity and the negative impact of weight stigma.
Consider language and word choice. “Carefully consider language that might unintentionally communicate bias, blame, or negative judgment,” Dr. Puhl told attendees. “Use language that is supportive and empowering.”
Terms such as “unhealthy weight” and “high BMI” are less stigmatizing than “fat” and “morbidly obese” to parents, she said, and research has found nearly a quarter of parents would avoid future doctor appointments if their child’s doctor used stigmatizing terms to discuss weight (Pediatrics. 2011 Oct;128[4]:e786-93).
Teens themselves may have diverse preferences for the language used. Start by asking: “Could we talk about your weight today?” and then follow up by directly asking, “what words would you feel most comfortable with as we talk about your weight?”
Person-first language – such as “person with obesity” instead of “obese person” also is important to reducing stigma, she said.
It’s normal for you to feel uneasy about bringing up weight with patients, so Dr. Puhl recommended you practice dialogue out loud.
“Acknowledge your strengths,” she said. “You already have the skills and experience of engaging in difficult conversations with patients and families on a range of other health issues,” so apply that in this context as well.
Screen for negative experiences that could indicate weight-based bullying. These could include teasing and bullying, low self-esteem, poor school performance, depression, and anxiety.
“Remember that weight-based victimization can occur at diverse body sizes, not just in youth with obesity,” Dr. Puhl said. If you discover your patient is experiencing weight-related bullying, determine whether they have a support system in place and whether a mental health referral is appropriate. Provide or refer for behavior change counseling with motivational interviewing and patient-centered, empathic approaches. Parents should be aware of the issue and should contact the child’s teachers and school administration to help address it.
But before you do that, keep in mind that it’s not just peers doing the bullying. According to a study of teens with obesity enrolled in a national weight-loss camp, 37% of teen participants in 2012 said that their parents bully them (Pediatrics. 2013 Jan;131[1]:e1-9).
You should assess whether family interactions or the parents’ own history with weight is involved. If parents make disparaging comments about their child’s weight, “use this as an opportunity to model appropriate language and educate parents about weight bias,” Dr. Puhl said.
It’s also important to realize that parents themselves often are frustrated, so critical comments about their language or approach can backfire, she warned. Instead, help parents understand how to create a home setting that encourages healthy food choices, praises children for healthy decision making, and models positive health behaviors. It is key for them to focus on improving their children’s health behaviors rather than focusing on weight.
And before you contact the school, remember teachers also are common perpetrators of weight stigma, Dr. Puhl noted. She gave as an example a study in which investigators assessed 133 teachers’ perceptions of middle or high school students’ abilities based on photos that had been digitally altered to show each girl both as average weight or as overweight. Each photo was associated with an essay specifically chosen because it was neither particularly good nor bad (Brit J Educ Psychol. 2019 Oct 26. doi: 10.1111/bjep.12322). The teachers judged the essays believed to be submitted by overweight girls to be “similar in structural quality,” but they gave the overweight girls lower grades than the average-weight girls. They also indicated that they considered the overweight girls “put forth more effort, needed more remedial assistance, and had lower overall grades in school.” The teachers also rated other teachers’ weight bias to be at a low level, and their own weight bias to be “significantly lower” than the others.
Assess your clinical environment. Be aware of your clinical environment and whether it meets the needs of youth with diverse body sizes. That includes having a range of sturdy armless seating options and adequately sized doorways, hallways, and restrooms. You also should have beds, wheelchairs, and exam tables with adequate weight capacity. Also check that you have supplies, such as robes or blood pressure cuffs, on hand for a variety of body sizes.
EXPERT ANALYSIS FROM AAP 19
Genetic testing helps avoid false hemoglobinopathy diagnoses in newborns
Confirmatory genetic testing may be useful in the diagnosis of hemoglobinopathies for newborns with an abnormal hemoglobin (Hb) pattern, according to a recent study.
The findings suggest further research is needed to evaluate whether genetic testing programs for newborns could have diagnostic value in the clinical setting.
“We studied a consecutive cohort of newborns with an ‘FSA’ pattern (a suspected diagnosis of HbSbeta+) on the initial newborn screening test,” explained Lisa M. Shook of the University of Cincinnati and colleagues. The results were published in the International Journal of Neonatal Screening.
The retrospective study included a total of 1,151 newborns with an abnormal Hb pattern, 31 of which had an FSA pattern. The newborns were screened for hemoglobinopathies from 2015 to 2018. The findings of the initial newborn screening test (a suspected diagnosis of HbSbeta+) were compared with the diagnosis established using both protein-based and genetic confirmatory testing. Protein-based testing cannot accurately detect several hemoglobinopathies in newborns, especially when beta-thalassemia mutations are involved, according to the authors.
“During this study period, genetic testing was not universally applied in advance; it was used based on clinical suspicion,” the researchers wrote.
Among newborns with an FSA pattern, the mean gestational age was 38.7 weeks. In total, 17 newborns received genetic testing, and 30 had protein-based confirmatory testing.
“In this consecutive cohort of 31 newborns with a suspected diagnosis of HbSbeta+ based on initial newborn screening (an FSA pattern), none actually had HbSbeta+. All had the sickle cell trait (HbAS), instead; that is, we found that an initial FSA pattern was much more likely to indicate a final diagnosis of HbAS than HbSbeta+,” the authors wrote.
This meant that two-thirds of these newborns had a correct diagnosis of HbAS established at 2-4 weeks of age by protein-based confirmatory testing (and confirmed by genetic testing in a subset), but that the remaining one-third still had an incorrect, suspected diagnosis of HbSbeta+. This could lead to unnecessary treatment and testing of infants and incorrect, disease-focused counseling of parents and family members, according to the authors.
Two key limitations of the study were the small sample size and retrospective design.
“Based on this experience in which genetic testing was not universally applied, we now perform simultaneous protein-based and genetic testing as our standard clinical practice,” they concluded.
The study was funded by the National Institutes of Health and the Ohio Department of Health. The authors reported having no conflicts of interest.
SOURCE: Shook LM et al. Int J Neonatal Screen. 2020 Jan 31. doi: 10.3390/ijns6010007
Confirmatory genetic testing may be useful in the diagnosis of hemoglobinopathies for newborns with an abnormal hemoglobin (Hb) pattern, according to a recent study.
The findings suggest further research is needed to evaluate whether genetic testing programs for newborns could have diagnostic value in the clinical setting.
“We studied a consecutive cohort of newborns with an ‘FSA’ pattern (a suspected diagnosis of HbSbeta+) on the initial newborn screening test,” explained Lisa M. Shook of the University of Cincinnati and colleagues. The results were published in the International Journal of Neonatal Screening.
The retrospective study included a total of 1,151 newborns with an abnormal Hb pattern, 31 of which had an FSA pattern. The newborns were screened for hemoglobinopathies from 2015 to 2018. The findings of the initial newborn screening test (a suspected diagnosis of HbSbeta+) were compared with the diagnosis established using both protein-based and genetic confirmatory testing. Protein-based testing cannot accurately detect several hemoglobinopathies in newborns, especially when beta-thalassemia mutations are involved, according to the authors.
“During this study period, genetic testing was not universally applied in advance; it was used based on clinical suspicion,” the researchers wrote.
Among newborns with an FSA pattern, the mean gestational age was 38.7 weeks. In total, 17 newborns received genetic testing, and 30 had protein-based confirmatory testing.
“In this consecutive cohort of 31 newborns with a suspected diagnosis of HbSbeta+ based on initial newborn screening (an FSA pattern), none actually had HbSbeta+. All had the sickle cell trait (HbAS), instead; that is, we found that an initial FSA pattern was much more likely to indicate a final diagnosis of HbAS than HbSbeta+,” the authors wrote.
This meant that two-thirds of these newborns had a correct diagnosis of HbAS established at 2-4 weeks of age by protein-based confirmatory testing (and confirmed by genetic testing in a subset), but that the remaining one-third still had an incorrect, suspected diagnosis of HbSbeta+. This could lead to unnecessary treatment and testing of infants and incorrect, disease-focused counseling of parents and family members, according to the authors.
Two key limitations of the study were the small sample size and retrospective design.
“Based on this experience in which genetic testing was not universally applied, we now perform simultaneous protein-based and genetic testing as our standard clinical practice,” they concluded.
The study was funded by the National Institutes of Health and the Ohio Department of Health. The authors reported having no conflicts of interest.
SOURCE: Shook LM et al. Int J Neonatal Screen. 2020 Jan 31. doi: 10.3390/ijns6010007
Confirmatory genetic testing may be useful in the diagnosis of hemoglobinopathies for newborns with an abnormal hemoglobin (Hb) pattern, according to a recent study.
The findings suggest further research is needed to evaluate whether genetic testing programs for newborns could have diagnostic value in the clinical setting.
“We studied a consecutive cohort of newborns with an ‘FSA’ pattern (a suspected diagnosis of HbSbeta+) on the initial newborn screening test,” explained Lisa M. Shook of the University of Cincinnati and colleagues. The results were published in the International Journal of Neonatal Screening.
The retrospective study included a total of 1,151 newborns with an abnormal Hb pattern, 31 of which had an FSA pattern. The newborns were screened for hemoglobinopathies from 2015 to 2018. The findings of the initial newborn screening test (a suspected diagnosis of HbSbeta+) were compared with the diagnosis established using both protein-based and genetic confirmatory testing. Protein-based testing cannot accurately detect several hemoglobinopathies in newborns, especially when beta-thalassemia mutations are involved, according to the authors.
“During this study period, genetic testing was not universally applied in advance; it was used based on clinical suspicion,” the researchers wrote.
Among newborns with an FSA pattern, the mean gestational age was 38.7 weeks. In total, 17 newborns received genetic testing, and 30 had protein-based confirmatory testing.
“In this consecutive cohort of 31 newborns with a suspected diagnosis of HbSbeta+ based on initial newborn screening (an FSA pattern), none actually had HbSbeta+. All had the sickle cell trait (HbAS), instead; that is, we found that an initial FSA pattern was much more likely to indicate a final diagnosis of HbAS than HbSbeta+,” the authors wrote.
This meant that two-thirds of these newborns had a correct diagnosis of HbAS established at 2-4 weeks of age by protein-based confirmatory testing (and confirmed by genetic testing in a subset), but that the remaining one-third still had an incorrect, suspected diagnosis of HbSbeta+. This could lead to unnecessary treatment and testing of infants and incorrect, disease-focused counseling of parents and family members, according to the authors.
Two key limitations of the study were the small sample size and retrospective design.
“Based on this experience in which genetic testing was not universally applied, we now perform simultaneous protein-based and genetic testing as our standard clinical practice,” they concluded.
The study was funded by the National Institutes of Health and the Ohio Department of Health. The authors reported having no conflicts of interest.
SOURCE: Shook LM et al. Int J Neonatal Screen. 2020 Jan 31. doi: 10.3390/ijns6010007
FROM THE INTERNATIONAL JOURNAL OF NEONATAL SCREENING
Psoriasis ointment helped with itch, healing in phase 2 EB study
LONDON – , in a small, placebo-controlled, phase 2 study.

More importantly, use of the ointment promoted wound healing in those with the severe skin-blistering condition. Indeed, compared with placebo, a greater reduction in wound size was observed after 2 weeks when the ointment was applied (a mean reduction of 65.5% vs. 88.4%; P less than .006). However, at 1 month, no significant differences were seen in the size of the wounds between the two treatment arms.
“Calcipotriol is a vitamin D analog and it is well known that vitamin D is a very critical factor for skin homeostasis and proper wound healing,” Christina Guttmann-Gruber, PhD, said at the EB World Congress, organized by the Dystrophic Epidermolysis Bullosa Association (DEBRA). Dr. Guttmann-Gruber, a group lead researcher for EB House Austria, which is based at the Salzburg (Austria) University Clinic for Dermatology, noted that vitamin D also helps with tissue repair and immune modulation, and enhances local antimicrobial activity.
During an oral poster presentation at the meeting, Dr. Guttmann-Gruber explained that in previous in vitro studies, it was found that low concentrations (100 nmol) of calcipotriol inhibited proliferation of RDEB tumor cells (Sci Rep. 2018 Sep 7;8:13430). Calcipotriol (also known as calcipotriene) also was found to improve the expression of antimicrobial peptides and promote wound closure. “Therefore, we thought that applying calcipotriol at the site of injury, on chronic wounds prone to superinfection where it is needed, might be beneficial for our patients.”
She and her associates designed a two-arm, randomized, double-blind crossover study to assess the effects of an existing calcipotriol-containing ointment on wound healing in patients with RDEB. The ointment used in the study is approved for treating psoriasis but was adapted by the in-house pharmacy team to reduce the concentration of calcipotriol to about 0.05 mcg/g, or around 121 nmol. The reason for the reduction was that, at higher doses, keratinocyte proliferation was reduced, which would be detrimental in RDEB patients.
Nine patients were included in the study and were randomized to either apply 1 g of the active or placebo ointment to each of two designated wounds, of at least 6 cm2 in size, every day for 4 weeks. A 2-month washout period then followed before the groups switched to use the other ointment for 1 month. Six out of the nine patients completed both treatment phases. The reasons for the patients not completing both intervention phases were not related to the drug.
Calcipotriol treatment resulted in a significant and steady reduction in itch over the entire course of treatment, which was not seen among those on placebo, Dr. Guttmann-Gruber observed. The reduction in itch was “striking,” but only while the treatment was being used, she said. Results for pain were less clear, with a significant reduction in pain after 2 weeks seen only in the placebo group, while both treatments reduced pain to the same degree by 1 month.
No serious adverse events were observed at any time point and topical use of the low-dose calcipotriol did not significantly change serum levels of calcium or vitamin D in the two patients in which this was studied, Dr. Guttmann-Gruber said.
“This is an approved drug; it’s used in psoriasis, but at a very high concentration. We were able to use it off label and make a diluted version,” she observed. “Any pharmacy can do it.” Although it was applied topically, it could be done by applying it to the dressing rather directly onto the wounded skin, she said.
Data on the skin microbiome response to treatment were also collected but were not available to analyze in time for presentation, but it appeared that there was improvement with the low-dose calcipotriol treatment, Dr. Guttmann-Gruber said. “When the wounds are healing, the microbial flora is improving.”
The next step will probably be to plan a multicenter trial of this treatment, Dr. Guttmann-Gruber said in an interview. The questions is whether such a trial would get the financial backing it needed, but if an orphan drug designation could be obtained for calcipotriol for EB, then it would be possible to conduct such a trial.
The study was funded by DEBRA Austria. The presenting author, Dr. Guttmann-Gruber, had no conflicts of interest to disclose.
SOURCE: Guttmann-Gruber C et al. EB World Congress 2020. Poster 34.
LONDON – , in a small, placebo-controlled, phase 2 study.
More importantly, use of the ointment promoted wound healing in those with the severe skin-blistering condition. Indeed, compared with placebo, a greater reduction in wound size was observed after 2 weeks when the ointment was applied (a mean reduction of 65.5% vs. 88.4%; P less than .006). However, at 1 month, no significant differences were seen in the size of the wounds between the two treatment arms.
“Calcipotriol is a vitamin D analog and it is well known that vitamin D is a very critical factor for skin homeostasis and proper wound healing,” Christina Guttmann-Gruber, PhD, said at the EB World Congress, organized by the Dystrophic Epidermolysis Bullosa Association (DEBRA). Dr. Guttmann-Gruber, a group lead researcher for EB House Austria, which is based at the Salzburg (Austria) University Clinic for Dermatology, noted that vitamin D also helps with tissue repair and immune modulation, and enhances local antimicrobial activity.
During an oral poster presentation at the meeting, Dr. Guttmann-Gruber explained that in previous in vitro studies, it was found that low concentrations (100 nmol) of calcipotriol inhibited proliferation of RDEB tumor cells (Sci Rep. 2018 Sep 7;8:13430). Calcipotriol (also known as calcipotriene) also was found to improve the expression of antimicrobial peptides and promote wound closure. “Therefore, we thought that applying calcipotriol at the site of injury, on chronic wounds prone to superinfection where it is needed, might be beneficial for our patients.”
She and her associates designed a two-arm, randomized, double-blind crossover study to assess the effects of an existing calcipotriol-containing ointment on wound healing in patients with RDEB. The ointment used in the study is approved for treating psoriasis but was adapted by the in-house pharmacy team to reduce the concentration of calcipotriol to about 0.05 mcg/g, or around 121 nmol. The reason for the reduction was that, at higher doses, keratinocyte proliferation was reduced, which would be detrimental in RDEB patients.
Nine patients were included in the study and were randomized to either apply 1 g of the active or placebo ointment to each of two designated wounds, of at least 6 cm2 in size, every day for 4 weeks. A 2-month washout period then followed before the groups switched to use the other ointment for 1 month. Six out of the nine patients completed both treatment phases. The reasons for the patients not completing both intervention phases were not related to the drug.
Calcipotriol treatment resulted in a significant and steady reduction in itch over the entire course of treatment, which was not seen among those on placebo, Dr. Guttmann-Gruber observed. The reduction in itch was “striking,” but only while the treatment was being used, she said. Results for pain were less clear, with a significant reduction in pain after 2 weeks seen only in the placebo group, while both treatments reduced pain to the same degree by 1 month.
No serious adverse events were observed at any time point and topical use of the low-dose calcipotriol did not significantly change serum levels of calcium or vitamin D in the two patients in which this was studied, Dr. Guttmann-Gruber said.
“This is an approved drug; it’s used in psoriasis, but at a very high concentration. We were able to use it off label and make a diluted version,” she observed. “Any pharmacy can do it.” Although it was applied topically, it could be done by applying it to the dressing rather directly onto the wounded skin, she said.
Data on the skin microbiome response to treatment were also collected but were not available to analyze in time for presentation, but it appeared that there was improvement with the low-dose calcipotriol treatment, Dr. Guttmann-Gruber said. “When the wounds are healing, the microbial flora is improving.”
The next step will probably be to plan a multicenter trial of this treatment, Dr. Guttmann-Gruber said in an interview. The questions is whether such a trial would get the financial backing it needed, but if an orphan drug designation could be obtained for calcipotriol for EB, then it would be possible to conduct such a trial.
The study was funded by DEBRA Austria. The presenting author, Dr. Guttmann-Gruber, had no conflicts of interest to disclose.
SOURCE: Guttmann-Gruber C et al. EB World Congress 2020. Poster 34.
LONDON – , in a small, placebo-controlled, phase 2 study.
More importantly, use of the ointment promoted wound healing in those with the severe skin-blistering condition. Indeed, compared with placebo, a greater reduction in wound size was observed after 2 weeks when the ointment was applied (a mean reduction of 65.5% vs. 88.4%; P less than .006). However, at 1 month, no significant differences were seen in the size of the wounds between the two treatment arms.
“Calcipotriol is a vitamin D analog and it is well known that vitamin D is a very critical factor for skin homeostasis and proper wound healing,” Christina Guttmann-Gruber, PhD, said at the EB World Congress, organized by the Dystrophic Epidermolysis Bullosa Association (DEBRA). Dr. Guttmann-Gruber, a group lead researcher for EB House Austria, which is based at the Salzburg (Austria) University Clinic for Dermatology, noted that vitamin D also helps with tissue repair and immune modulation, and enhances local antimicrobial activity.
During an oral poster presentation at the meeting, Dr. Guttmann-Gruber explained that in previous in vitro studies, it was found that low concentrations (100 nmol) of calcipotriol inhibited proliferation of RDEB tumor cells (Sci Rep. 2018 Sep 7;8:13430). Calcipotriol (also known as calcipotriene) also was found to improve the expression of antimicrobial peptides and promote wound closure. “Therefore, we thought that applying calcipotriol at the site of injury, on chronic wounds prone to superinfection where it is needed, might be beneficial for our patients.”
She and her associates designed a two-arm, randomized, double-blind crossover study to assess the effects of an existing calcipotriol-containing ointment on wound healing in patients with RDEB. The ointment used in the study is approved for treating psoriasis but was adapted by the in-house pharmacy team to reduce the concentration of calcipotriol to about 0.05 mcg/g, or around 121 nmol. The reason for the reduction was that, at higher doses, keratinocyte proliferation was reduced, which would be detrimental in RDEB patients.
Nine patients were included in the study and were randomized to either apply 1 g of the active or placebo ointment to each of two designated wounds, of at least 6 cm2 in size, every day for 4 weeks. A 2-month washout period then followed before the groups switched to use the other ointment for 1 month. Six out of the nine patients completed both treatment phases. The reasons for the patients not completing both intervention phases were not related to the drug.
Calcipotriol treatment resulted in a significant and steady reduction in itch over the entire course of treatment, which was not seen among those on placebo, Dr. Guttmann-Gruber observed. The reduction in itch was “striking,” but only while the treatment was being used, she said. Results for pain were less clear, with a significant reduction in pain after 2 weeks seen only in the placebo group, while both treatments reduced pain to the same degree by 1 month.
No serious adverse events were observed at any time point and topical use of the low-dose calcipotriol did not significantly change serum levels of calcium or vitamin D in the two patients in which this was studied, Dr. Guttmann-Gruber said.
“This is an approved drug; it’s used in psoriasis, but at a very high concentration. We were able to use it off label and make a diluted version,” she observed. “Any pharmacy can do it.” Although it was applied topically, it could be done by applying it to the dressing rather directly onto the wounded skin, she said.
Data on the skin microbiome response to treatment were also collected but were not available to analyze in time for presentation, but it appeared that there was improvement with the low-dose calcipotriol treatment, Dr. Guttmann-Gruber said. “When the wounds are healing, the microbial flora is improving.”
The next step will probably be to plan a multicenter trial of this treatment, Dr. Guttmann-Gruber said in an interview. The questions is whether such a trial would get the financial backing it needed, but if an orphan drug designation could be obtained for calcipotriol for EB, then it would be possible to conduct such a trial.
The study was funded by DEBRA Austria. The presenting author, Dr. Guttmann-Gruber, had no conflicts of interest to disclose.
SOURCE: Guttmann-Gruber C et al. EB World Congress 2020. Poster 34.
REPORTING FROM EB 2020
Pharmacologic prophylaxis fails in pediatric migraine

Clinicians hoped that medications used in adults – such as antidepressants, antiepileptics, antihypertensive agents, calcium channel blockers, and food supplements – would find similar success in children. Unfortunately, researchers found only short-term signs of efficacy over placebo, with no benefit lasting more than 6 months.
The study, conducted by a team led by Cosima Locher, PhD, of Boston Children’s Hospital, included 23 double-blind, randomized, controlled trials with a total of 2,217 patients; the mean age was 11 years. They compared 12 pharmacologic agents with each other or with placebo in the study, published online in JAMA Pediatrics.
In a main efficacy analysis that included 19 studies, only two treatments outperformed placebo: propranolol (standardized mean difference, 0.60; 95% confidence interval, 0.03-1.17) and topiramate (SMD, 0.59; 95% CI, 0.03-1.15). There were no statistically significant between-treatment differences.
The results had an overall low to moderate certainty.
When propranolol was compared to placebo, the 95% prediction interval (–0.62 to 1.82) was wider than the significant confidence interval (0.03-1.17), and comprised both beneficial and detrimental effects. A similar result was found with topiramate, with a prediction interval of –0.62 to 1.80 extending into nonsignificant effects (95% CI, 0.03-1.15). In both cases, significant effects were found only when the prediction interval was 70%.
In a long-term analysis (greater than 6 months), no treatment outperformed placebo.
The treatments generally were acceptable. The researchers found no significant difference in tolerability between any of the treatments and each other or placebo. Safety data analyzed from 13 trials revealed no significant differences between treatments and placebo.
“Because specific effects of drugs are associated with the size of the placebo effect, the lack of drug efficacy in our NMA [network meta-analysis] could be owing to a comparatively high placebo effect in children. In fact, there is indirect evidence [from other studies] that the placebo effect is more pronounced in children and adolescents than in adults,” Dr. Locher and associates said. They suggested that studies were needed to quantify the placebo effect in pediatric migraine, and if it was large, to develop innovative therapies making use of this.
The findings should lead to some changes in practice, Boris Zernikow, MD, PhD, of Children’s and Adolescents’ Hospital Datteln (Germany) wrote in an accompanying editorial.
Pharmacological prophylactic treatment of childhood migraine should be an exception rather than the rule, and nonpharmacologic approaches should be emphasized, particularly because the placebo effect is magnified in children, he said.
Many who suffer migraines in childhood will continue to be affected in adulthood, so pediatric intervention is a good opportunity to instill effective strategies. These include: using abortive medication early in an attack and using antimigraine medications for only that specific type of headache; engaging in physical activity to reduce migraine attacks; getting sufficient sleep; and learning relaxation and other psychological approaches to counter migraines.
Dr. Zernikow had no relevant financial disclosures. One study author received grants from Amgen and other support from Grunenthal and Akelos. The study received funding from the Sara Page Mayo Endowment for Pediatric Pain Research, Education, and Treatment; the Swiss National Science Foundation; the Schweizer-Arau-Foundation; and the Theophrastus Foundation.
SOURCES: Locher C et al. JAMA Pediatrics. 2020 Feb 10. doi: 10.1001/jamapediatrics.2019.5856; Zernikow B. JAMA Pediatrics. 2020 Feb 10. doi: 10.1001/jamapediatrics.2019.5907.
Clinicians hoped that medications used in adults – such as antidepressants, antiepileptics, antihypertensive agents, calcium channel blockers, and food supplements – would find similar success in children. Unfortunately, researchers found only short-term signs of efficacy over placebo, with no benefit lasting more than 6 months.
The study, conducted by a team led by Cosima Locher, PhD, of Boston Children’s Hospital, included 23 double-blind, randomized, controlled trials with a total of 2,217 patients; the mean age was 11 years. They compared 12 pharmacologic agents with each other or with placebo in the study, published online in JAMA Pediatrics.
In a main efficacy analysis that included 19 studies, only two treatments outperformed placebo: propranolol (standardized mean difference, 0.60; 95% confidence interval, 0.03-1.17) and topiramate (SMD, 0.59; 95% CI, 0.03-1.15). There were no statistically significant between-treatment differences.
The results had an overall low to moderate certainty.
When propranolol was compared to placebo, the 95% prediction interval (–0.62 to 1.82) was wider than the significant confidence interval (0.03-1.17), and comprised both beneficial and detrimental effects. A similar result was found with topiramate, with a prediction interval of –0.62 to 1.80 extending into nonsignificant effects (95% CI, 0.03-1.15). In both cases, significant effects were found only when the prediction interval was 70%.
In a long-term analysis (greater than 6 months), no treatment outperformed placebo.
The treatments generally were acceptable. The researchers found no significant difference in tolerability between any of the treatments and each other or placebo. Safety data analyzed from 13 trials revealed no significant differences between treatments and placebo.
“Because specific effects of drugs are associated with the size of the placebo effect, the lack of drug efficacy in our NMA [network meta-analysis] could be owing to a comparatively high placebo effect in children. In fact, there is indirect evidence [from other studies] that the placebo effect is more pronounced in children and adolescents than in adults,” Dr. Locher and associates said. They suggested that studies were needed to quantify the placebo effect in pediatric migraine, and if it was large, to develop innovative therapies making use of this.
The findings should lead to some changes in practice, Boris Zernikow, MD, PhD, of Children’s and Adolescents’ Hospital Datteln (Germany) wrote in an accompanying editorial.
Pharmacological prophylactic treatment of childhood migraine should be an exception rather than the rule, and nonpharmacologic approaches should be emphasized, particularly because the placebo effect is magnified in children, he said.
Many who suffer migraines in childhood will continue to be affected in adulthood, so pediatric intervention is a good opportunity to instill effective strategies. These include: using abortive medication early in an attack and using antimigraine medications for only that specific type of headache; engaging in physical activity to reduce migraine attacks; getting sufficient sleep; and learning relaxation and other psychological approaches to counter migraines.
Dr. Zernikow had no relevant financial disclosures. One study author received grants from Amgen and other support from Grunenthal and Akelos. The study received funding from the Sara Page Mayo Endowment for Pediatric Pain Research, Education, and Treatment; the Swiss National Science Foundation; the Schweizer-Arau-Foundation; and the Theophrastus Foundation.
SOURCES: Locher C et al. JAMA Pediatrics. 2020 Feb 10. doi: 10.1001/jamapediatrics.2019.5856; Zernikow B. JAMA Pediatrics. 2020 Feb 10. doi: 10.1001/jamapediatrics.2019.5907.
Clinicians hoped that medications used in adults – such as antidepressants, antiepileptics, antihypertensive agents, calcium channel blockers, and food supplements – would find similar success in children. Unfortunately, researchers found only short-term signs of efficacy over placebo, with no benefit lasting more than 6 months.
The study, conducted by a team led by Cosima Locher, PhD, of Boston Children’s Hospital, included 23 double-blind, randomized, controlled trials with a total of 2,217 patients; the mean age was 11 years. They compared 12 pharmacologic agents with each other or with placebo in the study, published online in JAMA Pediatrics.
In a main efficacy analysis that included 19 studies, only two treatments outperformed placebo: propranolol (standardized mean difference, 0.60; 95% confidence interval, 0.03-1.17) and topiramate (SMD, 0.59; 95% CI, 0.03-1.15). There were no statistically significant between-treatment differences.
The results had an overall low to moderate certainty.
When propranolol was compared to placebo, the 95% prediction interval (–0.62 to 1.82) was wider than the significant confidence interval (0.03-1.17), and comprised both beneficial and detrimental effects. A similar result was found with topiramate, with a prediction interval of –0.62 to 1.80 extending into nonsignificant effects (95% CI, 0.03-1.15). In both cases, significant effects were found only when the prediction interval was 70%.
In a long-term analysis (greater than 6 months), no treatment outperformed placebo.
The treatments generally were acceptable. The researchers found no significant difference in tolerability between any of the treatments and each other or placebo. Safety data analyzed from 13 trials revealed no significant differences between treatments and placebo.
“Because specific effects of drugs are associated with the size of the placebo effect, the lack of drug efficacy in our NMA [network meta-analysis] could be owing to a comparatively high placebo effect in children. In fact, there is indirect evidence [from other studies] that the placebo effect is more pronounced in children and adolescents than in adults,” Dr. Locher and associates said. They suggested that studies were needed to quantify the placebo effect in pediatric migraine, and if it was large, to develop innovative therapies making use of this.
The findings should lead to some changes in practice, Boris Zernikow, MD, PhD, of Children’s and Adolescents’ Hospital Datteln (Germany) wrote in an accompanying editorial.
Pharmacological prophylactic treatment of childhood migraine should be an exception rather than the rule, and nonpharmacologic approaches should be emphasized, particularly because the placebo effect is magnified in children, he said.
Many who suffer migraines in childhood will continue to be affected in adulthood, so pediatric intervention is a good opportunity to instill effective strategies. These include: using abortive medication early in an attack and using antimigraine medications for only that specific type of headache; engaging in physical activity to reduce migraine attacks; getting sufficient sleep; and learning relaxation and other psychological approaches to counter migraines.
Dr. Zernikow had no relevant financial disclosures. One study author received grants from Amgen and other support from Grunenthal and Akelos. The study received funding from the Sara Page Mayo Endowment for Pediatric Pain Research, Education, and Treatment; the Swiss National Science Foundation; the Schweizer-Arau-Foundation; and the Theophrastus Foundation.
SOURCES: Locher C et al. JAMA Pediatrics. 2020 Feb 10. doi: 10.1001/jamapediatrics.2019.5856; Zernikow B. JAMA Pediatrics. 2020 Feb 10. doi: 10.1001/jamapediatrics.2019.5907.
FROM JAMA PEDIATRICS
Flu activity increases for third straight week
For the second time during the 2019-2020 flu season, activity measures have climbed into noteworthy territory.
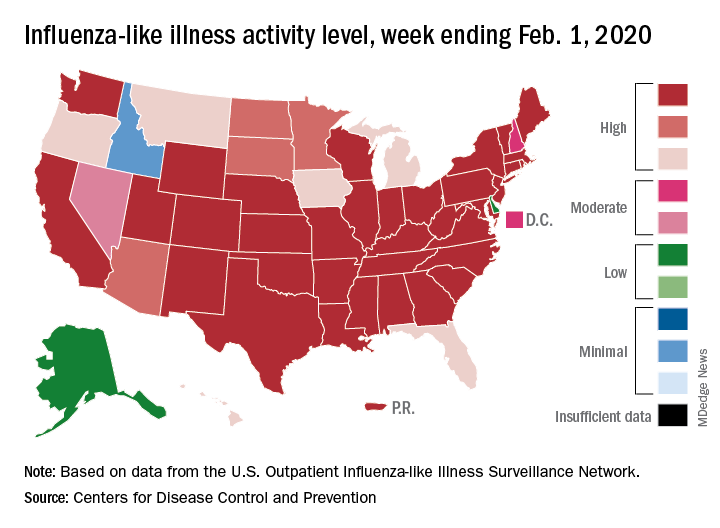
The proportion of outpatient visits for influenza-like illness (ILI) reached its highest December level, 7.1%, since 2003 and then dropped for 2 weeks. Three weeks of increases since then, however, have the outpatient-visit rate at 6.7% for the week ending Feb. 1, 2020, the Centers for Disease Control and Prevention reported. The baseline rate for the United States is 2.4%.
That rate of 6.7% is already above the highest rates recorded in eight of the last nine flu seasons, and another increase could mean a second, separate trip above 7.0% in the 2019-2020 season – something that has not occurred since national tracking began in 1997, CDC data show.
Those same data also show that,
Another important measure on the rise, the proportion of respiratory specimens testing positive for influenza, reached a new high for the season, 29.8%, during the week of Feb. 1, the CDC’s influenza division said.
Tests at clinical laboratories also show that predominance is continuing to switch from type B (45.6%) to type A (54.4%), the influenza division noted. Overall predominance for the season, however, continues to favor type B, 59.3% to 40.7%.
The percentage of deaths caused by pneumonia and influenza, which passed the threshold for epidemic of 7.2% back in early January, has been trending downward for the last 3 weeks and was 7.1% as of Feb. 1, according to the influenza division.
ILI-related deaths among children continue to remain high, with a total count of 78 for the season after another 10 deaths were reported during the week ending Feb. 1, the CDC reported. Comparable numbers for the last three seasons are 44 (2018-2019), 97 (2017-2018), and 35 (2016-2017).
The CDC estimates put the total number of ILIs at around 22 million for the season so far, leading to 210,000 hospitalizations. The agency said that it expects to release estimates of vaccine effectiveness later this month.
For the second time during the 2019-2020 flu season, activity measures have climbed into noteworthy territory.
The proportion of outpatient visits for influenza-like illness (ILI) reached its highest December level, 7.1%, since 2003 and then dropped for 2 weeks. Three weeks of increases since then, however, have the outpatient-visit rate at 6.7% for the week ending Feb. 1, 2020, the Centers for Disease Control and Prevention reported. The baseline rate for the United States is 2.4%.
That rate of 6.7% is already above the highest rates recorded in eight of the last nine flu seasons, and another increase could mean a second, separate trip above 7.0% in the 2019-2020 season – something that has not occurred since national tracking began in 1997, CDC data show.
Those same data also show that,
Another important measure on the rise, the proportion of respiratory specimens testing positive for influenza, reached a new high for the season, 29.8%, during the week of Feb. 1, the CDC’s influenza division said.
Tests at clinical laboratories also show that predominance is continuing to switch from type B (45.6%) to type A (54.4%), the influenza division noted. Overall predominance for the season, however, continues to favor type B, 59.3% to 40.7%.
The percentage of deaths caused by pneumonia and influenza, which passed the threshold for epidemic of 7.2% back in early January, has been trending downward for the last 3 weeks and was 7.1% as of Feb. 1, according to the influenza division.
ILI-related deaths among children continue to remain high, with a total count of 78 for the season after another 10 deaths were reported during the week ending Feb. 1, the CDC reported. Comparable numbers for the last three seasons are 44 (2018-2019), 97 (2017-2018), and 35 (2016-2017).
The CDC estimates put the total number of ILIs at around 22 million for the season so far, leading to 210,000 hospitalizations. The agency said that it expects to release estimates of vaccine effectiveness later this month.
For the second time during the 2019-2020 flu season, activity measures have climbed into noteworthy territory.
The proportion of outpatient visits for influenza-like illness (ILI) reached its highest December level, 7.1%, since 2003 and then dropped for 2 weeks. Three weeks of increases since then, however, have the outpatient-visit rate at 6.7% for the week ending Feb. 1, 2020, the Centers for Disease Control and Prevention reported. The baseline rate for the United States is 2.4%.
That rate of 6.7% is already above the highest rates recorded in eight of the last nine flu seasons, and another increase could mean a second, separate trip above 7.0% in the 2019-2020 season – something that has not occurred since national tracking began in 1997, CDC data show.
Those same data also show that,
Another important measure on the rise, the proportion of respiratory specimens testing positive for influenza, reached a new high for the season, 29.8%, during the week of Feb. 1, the CDC’s influenza division said.
Tests at clinical laboratories also show that predominance is continuing to switch from type B (45.6%) to type A (54.4%), the influenza division noted. Overall predominance for the season, however, continues to favor type B, 59.3% to 40.7%.
The percentage of deaths caused by pneumonia and influenza, which passed the threshold for epidemic of 7.2% back in early January, has been trending downward for the last 3 weeks and was 7.1% as of Feb. 1, according to the influenza division.
ILI-related deaths among children continue to remain high, with a total count of 78 for the season after another 10 deaths were reported during the week ending Feb. 1, the CDC reported. Comparable numbers for the last three seasons are 44 (2018-2019), 97 (2017-2018), and 35 (2016-2017).
The CDC estimates put the total number of ILIs at around 22 million for the season so far, leading to 210,000 hospitalizations. The agency said that it expects to release estimates of vaccine effectiveness later this month.
EEG abnormalities may indicate increased risk for epilepsy in patients with autism
BALTIMORE – , according to research presented at the annual meeting of the American Epilepsy Society. In addition, a positive family history of febrile seizures also is associated with an increased risk of epilepsy in this population.
The literature suggests that the prevalence of epilepsy in patients with ASD ranges from 5% to 40%. This broad range may result from the heterogeneity of epilepsy risk factors among patients with ASD. These risk factors include intellectual disability, age, and syndromic forms of ASD such as tuberous sclerosis complex. Regardless of whether they have epilepsy, approximately 60% of patients with ASD have EEG abnormalities. The prognostic implications of these abnormalities are uncertain.
Investigators reviewed patients’ charts retrospectively
Divya Nadkarni, MD, a neurologist at Ronald Reagan UCLA Medical Center in Los Angeles, and colleagues sought to clarify the relationship between risk factors such as EEG abnormalities and subsequent epilepsy in patients with ASD. They retrospectively identified patients who were followed jointly at UCLA and at Pediatric Minds, a neurodevelopmental clinic in Torrance, Calif. Eligible patients had a diagnosis of ASD, based on criteria from DSM-IV, DSM-5, or the Autism Diagnostic Observation Schedule. In addition, patients had overnight, continuous video EEG evaluation and a minimum follow-up of 1 week after EEG. Patients with a history of epilepsy before the initial EEG evaluation were excluded. Dr. Nadkarni and colleagues collected clinical and electrographic data by chart review.
The study’s primary outcome was time to onset of epilepsy. Among the variables that the investigators analyzed were EEG abnormalities, which they defined as focal slowing or generalized or focal epileptiform discharges. The other variables were history of febrile seizures, family history of epilepsy, family history of febrile seizures, and family history of ASD. Dr. Nadkarni and colleagues analyzed the data using the Kaplan–Meier method and Cox proportional hazards models.
In all, 164 patients met the study’s inclusion criteria. The population’s median age at the initial EEG evaluation was 4.5 years. The median follow-up after this evaluation was 2.4 years. The investigators found 63 patients (38.4%) with abnormal EEGs, and 18 patients (11%) subsequently developed epilepsy after a median of 1.9 years.
Family history of febrile seizures was associated with time to epilepsy onset
The time to epilepsy onset was associated with abnormalities on the initial overnight continuous EEG. The hazard ratio of epilepsy among patients with EEG abnormalities was 8.0. Approximately one-third of patients with EEG abnormalities developed subsequent epilepsy, compared with approximately 5% of patients without EEG abnormalities, said Dr. Nadkarni.
In addition, time to epilepsy onset was independently associated with a positive family history of febrile seizures. This finding was unexpected, said Dr. Nadkarni. The hazard ratio of epilepsy among patients with a positive family history of febrile seizures was 12.6.
The patient’s own history of febrile seizures was not associated with time to epilepsy onset. One potential explanation for this result is that it is difficult to distinguish between febrile seizure and seizure with fever in the general pediatric population. Making this distinction in children with ASD, who may have atypical febrile seizures, might be still more difficult, said Dr. Nadkarni.
Time for guideline updates?
“Statements from the Centers for Disease Control and Prevention, the American Academy of Pediatrics, the American Academy of Neurology, and the Child Neurology Society do not currently recommend routine EEG screening for all children with ASD,” said Dr. Nadkarni. Investigators are suggesting that the guidelines should be reevaluated, however. “Research shows that EEG abnormalities, particularly epileptiform abnormalities, are associated with worse outcome, in terms of developmental and adaptive functioning. EEG endophenotypes in ASD are starting to be elucidated ... That’s one reason to consider EEG screening.” Furthermore, preliminary connectivity research suggests that EEG screening of high-risk siblings of children with ASD may predict the development of ASD.
The small cohort and retrospective design were among the study’s limitations, said Dr. Nadkarni. Some patients were lost to follow-up, and some data were missing from patients’ charts.
“In our opinion, further study – ideally, a prospective, observational cohort study – might be warranted to determine whether overnight continuous EEG monitoring might be useful as a screening tool for epilepsy in patients with ASD,” Dr. Nadkarni concluded.
The study was conducted without external funding, and the investigators had no disclosures.
SOURCE: Nadkarni D et al. AES 2019. Abstract 1.29.
BALTIMORE – , according to research presented at the annual meeting of the American Epilepsy Society. In addition, a positive family history of febrile seizures also is associated with an increased risk of epilepsy in this population.
The literature suggests that the prevalence of epilepsy in patients with ASD ranges from 5% to 40%. This broad range may result from the heterogeneity of epilepsy risk factors among patients with ASD. These risk factors include intellectual disability, age, and syndromic forms of ASD such as tuberous sclerosis complex. Regardless of whether they have epilepsy, approximately 60% of patients with ASD have EEG abnormalities. The prognostic implications of these abnormalities are uncertain.
Investigators reviewed patients’ charts retrospectively
Divya Nadkarni, MD, a neurologist at Ronald Reagan UCLA Medical Center in Los Angeles, and colleagues sought to clarify the relationship between risk factors such as EEG abnormalities and subsequent epilepsy in patients with ASD. They retrospectively identified patients who were followed jointly at UCLA and at Pediatric Minds, a neurodevelopmental clinic in Torrance, Calif. Eligible patients had a diagnosis of ASD, based on criteria from DSM-IV, DSM-5, or the Autism Diagnostic Observation Schedule. In addition, patients had overnight, continuous video EEG evaluation and a minimum follow-up of 1 week after EEG. Patients with a history of epilepsy before the initial EEG evaluation were excluded. Dr. Nadkarni and colleagues collected clinical and electrographic data by chart review.
The study’s primary outcome was time to onset of epilepsy. Among the variables that the investigators analyzed were EEG abnormalities, which they defined as focal slowing or generalized or focal epileptiform discharges. The other variables were history of febrile seizures, family history of epilepsy, family history of febrile seizures, and family history of ASD. Dr. Nadkarni and colleagues analyzed the data using the Kaplan–Meier method and Cox proportional hazards models.
In all, 164 patients met the study’s inclusion criteria. The population’s median age at the initial EEG evaluation was 4.5 years. The median follow-up after this evaluation was 2.4 years. The investigators found 63 patients (38.4%) with abnormal EEGs, and 18 patients (11%) subsequently developed epilepsy after a median of 1.9 years.
Family history of febrile seizures was associated with time to epilepsy onset
The time to epilepsy onset was associated with abnormalities on the initial overnight continuous EEG. The hazard ratio of epilepsy among patients with EEG abnormalities was 8.0. Approximately one-third of patients with EEG abnormalities developed subsequent epilepsy, compared with approximately 5% of patients without EEG abnormalities, said Dr. Nadkarni.
In addition, time to epilepsy onset was independently associated with a positive family history of febrile seizures. This finding was unexpected, said Dr. Nadkarni. The hazard ratio of epilepsy among patients with a positive family history of febrile seizures was 12.6.
The patient’s own history of febrile seizures was not associated with time to epilepsy onset. One potential explanation for this result is that it is difficult to distinguish between febrile seizure and seizure with fever in the general pediatric population. Making this distinction in children with ASD, who may have atypical febrile seizures, might be still more difficult, said Dr. Nadkarni.
Time for guideline updates?
“Statements from the Centers for Disease Control and Prevention, the American Academy of Pediatrics, the American Academy of Neurology, and the Child Neurology Society do not currently recommend routine EEG screening for all children with ASD,” said Dr. Nadkarni. Investigators are suggesting that the guidelines should be reevaluated, however. “Research shows that EEG abnormalities, particularly epileptiform abnormalities, are associated with worse outcome, in terms of developmental and adaptive functioning. EEG endophenotypes in ASD are starting to be elucidated ... That’s one reason to consider EEG screening.” Furthermore, preliminary connectivity research suggests that EEG screening of high-risk siblings of children with ASD may predict the development of ASD.
The small cohort and retrospective design were among the study’s limitations, said Dr. Nadkarni. Some patients were lost to follow-up, and some data were missing from patients’ charts.
“In our opinion, further study – ideally, a prospective, observational cohort study – might be warranted to determine whether overnight continuous EEG monitoring might be useful as a screening tool for epilepsy in patients with ASD,” Dr. Nadkarni concluded.
The study was conducted without external funding, and the investigators had no disclosures.
SOURCE: Nadkarni D et al. AES 2019. Abstract 1.29.
BALTIMORE – , according to research presented at the annual meeting of the American Epilepsy Society. In addition, a positive family history of febrile seizures also is associated with an increased risk of epilepsy in this population.
The literature suggests that the prevalence of epilepsy in patients with ASD ranges from 5% to 40%. This broad range may result from the heterogeneity of epilepsy risk factors among patients with ASD. These risk factors include intellectual disability, age, and syndromic forms of ASD such as tuberous sclerosis complex. Regardless of whether they have epilepsy, approximately 60% of patients with ASD have EEG abnormalities. The prognostic implications of these abnormalities are uncertain.
Investigators reviewed patients’ charts retrospectively
Divya Nadkarni, MD, a neurologist at Ronald Reagan UCLA Medical Center in Los Angeles, and colleagues sought to clarify the relationship between risk factors such as EEG abnormalities and subsequent epilepsy in patients with ASD. They retrospectively identified patients who were followed jointly at UCLA and at Pediatric Minds, a neurodevelopmental clinic in Torrance, Calif. Eligible patients had a diagnosis of ASD, based on criteria from DSM-IV, DSM-5, or the Autism Diagnostic Observation Schedule. In addition, patients had overnight, continuous video EEG evaluation and a minimum follow-up of 1 week after EEG. Patients with a history of epilepsy before the initial EEG evaluation were excluded. Dr. Nadkarni and colleagues collected clinical and electrographic data by chart review.
The study’s primary outcome was time to onset of epilepsy. Among the variables that the investigators analyzed were EEG abnormalities, which they defined as focal slowing or generalized or focal epileptiform discharges. The other variables were history of febrile seizures, family history of epilepsy, family history of febrile seizures, and family history of ASD. Dr. Nadkarni and colleagues analyzed the data using the Kaplan–Meier method and Cox proportional hazards models.
In all, 164 patients met the study’s inclusion criteria. The population’s median age at the initial EEG evaluation was 4.5 years. The median follow-up after this evaluation was 2.4 years. The investigators found 63 patients (38.4%) with abnormal EEGs, and 18 patients (11%) subsequently developed epilepsy after a median of 1.9 years.
Family history of febrile seizures was associated with time to epilepsy onset
The time to epilepsy onset was associated with abnormalities on the initial overnight continuous EEG. The hazard ratio of epilepsy among patients with EEG abnormalities was 8.0. Approximately one-third of patients with EEG abnormalities developed subsequent epilepsy, compared with approximately 5% of patients without EEG abnormalities, said Dr. Nadkarni.
In addition, time to epilepsy onset was independently associated with a positive family history of febrile seizures. This finding was unexpected, said Dr. Nadkarni. The hazard ratio of epilepsy among patients with a positive family history of febrile seizures was 12.6.
The patient’s own history of febrile seizures was not associated with time to epilepsy onset. One potential explanation for this result is that it is difficult to distinguish between febrile seizure and seizure with fever in the general pediatric population. Making this distinction in children with ASD, who may have atypical febrile seizures, might be still more difficult, said Dr. Nadkarni.
Time for guideline updates?
“Statements from the Centers for Disease Control and Prevention, the American Academy of Pediatrics, the American Academy of Neurology, and the Child Neurology Society do not currently recommend routine EEG screening for all children with ASD,” said Dr. Nadkarni. Investigators are suggesting that the guidelines should be reevaluated, however. “Research shows that EEG abnormalities, particularly epileptiform abnormalities, are associated with worse outcome, in terms of developmental and adaptive functioning. EEG endophenotypes in ASD are starting to be elucidated ... That’s one reason to consider EEG screening.” Furthermore, preliminary connectivity research suggests that EEG screening of high-risk siblings of children with ASD may predict the development of ASD.
The small cohort and retrospective design were among the study’s limitations, said Dr. Nadkarni. Some patients were lost to follow-up, and some data were missing from patients’ charts.
“In our opinion, further study – ideally, a prospective, observational cohort study – might be warranted to determine whether overnight continuous EEG monitoring might be useful as a screening tool for epilepsy in patients with ASD,” Dr. Nadkarni concluded.
The study was conducted without external funding, and the investigators had no disclosures.
SOURCE: Nadkarni D et al. AES 2019. Abstract 1.29.
REPORTING FROM AES 2019
Consider allergic contact dermatitis in children with AD with disease flares, new rash
ORLANDO – Do you have ? Consider patch testing to assess whether they have allergic contact dermatitis.

“Of the patients who are sent to me by local pediatric dermatologists, 50% of them are positive” for allergens, said Jonathan H. Zippin, MD, PhD, director of the contact, occupational, and photodermatitis service at Cornell University, New York.
Speaking at the ODAC Dermatology, Aesthetic, and Surgical Conference, Dr. Zippin noted the prevalence of allergen sensitization is between 13% and 25% among children who are asymptomatic, while the prevalence of sensitization to at least one allergen among children with suspected allergic contact dermatitis (ACD) is between 25% and 96%. In 2014, a study from the National American Contact Dermatitis Group (NACDG) showed that of 883 children who were patch tested, 56.7% had at least one relevant positive patch test (RPPT) result.
“The take-home message here is that pediatric contact dermatitis is common, much more common than a lot of people realize,” Dr. Zippin said.
He described three common scenarios to keep in mind: a worsening rash, a new rash, and failure of a rash to improve after the patient avoids all of his or her positive allergens.
When a rash worsens, patch testing is likely to offer answers. In an analysis of 1,142 patients with suspected ACD aged 18 years or younger (mean age, 10.5 years; 64% female) in the Pediatric Contact Dermatitis Registry study database, 65% had at least one positive patch test, and 48% had at least 1 RPPT (Dermatitis 2016; 27[5] 293-302).
But not all patch testing is the same: The study also found that 24% of the RPPT cases would have been missed if assessed with the T.R.U.E. TEST compared with extended patch testing. If a T.R.U.E. TEST fails to explain generalized atopic dermatitis, the patient should be sent for more comprehensive testing where available, Dr. Zippin advised.
Pediatric patients also have unique allergens clinicians should consider. In the same study, children had a number of allergens similar to those of adults as reported in previous studies, such as nickel, cobalt, and neomycin. However, propylene glycol and cocamidopropyl betaine were allergens identified as unique to the pediatric population.
Another study looking at the same group of patients found that compared with children who did not have AD, children with AD had 7.4 times higher odds of having an RPPT to cocamidopropyl betaine, 7.6 times higher odds of having an RPPT to parthenolide, 5.3 times higher odds of having an RPPT to tixocortol pivalate, 4.2 times higher odds of having an RPPT to wool alcohols, and 4 times higher odds of having an RPPT to lanolin (JAMA Dermatology 2017;153[8]:765-70).
All of these are components of topical medicaments used to treat AD, “either components of emollients that we recommend, or components of steroids that we recommend,” Dr. Zippin pointed out.
One of these allergens could be the culprit when a child develops a new rash but there are no new apparent changes in products, exposures, and activities. Lanolin, also called wool grease, is used in many skin care products, for example. Dr. Zippin described the case of a 6-year-old girl with a history of AD, who presented with a new rash on her scalp and behind her ears, not explained by any obvious changes to products, exposures, or activities. Subsequent patch testing determined that the rash was caused by baby shampoo, which contained cocamidopropyl betaine, which is used in hypoallergenic products. The rash resolved after a different shampoo was used.
“Sometimes, we really have to be thinking when the rash is getting worse, is there something they’re being exposed to that might be an allergen?” Dr. Zippin said.
In patients who have avoided all their positive allergens but a rash has not improved, clinicians should consider systemic contact dermatitis (SCD). Patients can develop SCD through different types of exposures, including transepidermal, transmucosal, oral, intravenous, subcutaneous, intramuscular, inhalation, and implantation routes.
SCD also has a variety of presentations, including pompholyx/dyshidrosis/vesicular dermatitis, maculopapular eruption, chronic pruritus, exfoliative erythroderma/toxiderma, chronic urticaria, erythema multiforme and vasculitis, hyperkeratotic papules of the elbows, acute generalized exanthematous pustulosis, and pruritus ani, according to Dr. Zippin.
SCD should be considered when a patient has a positive patch test to an allergen that is known to cause SCD, and does not clear after avoiding cutaneous exposure to the allergen, Dr. Zippin advised.
Patients will most often develop SCD from plants and herbs, Dr. Zippin noted. Chrysanthemums and chamomile tea are common culprits for compositae allergy and can trigger SCD; other causes are Anacardiaceae, Balsam of Peru, and propolis. Metals (nickel, cobalt, gold, and chromium), medications (aminoglycosides, corticosteroids, and ethylenediamine), and other sources (formaldehyde, propylene glycol in frozen foods, gallates, and methylisothiazolinone) can cause SCD as well.
Methylisothiazolinone in particular is a very common sensitizer, Dr. Zippin said. “If you have a patient who is positive to this, it’s almost always the cause of their problem.”
Balsam of Peru is in a number of different foods, and patients who need to follow a diet free of Balsam of Peru should avoid a long list of foods including citrus; bakery goods; Danish pastry; candy; gum; spices such as cinnamon, cloves, vanilla, curry, allspice, anise, and ginger; spicy condiments such as ketchup, chili sauce, barbecue sauce; chili, pizza, and foods with red sauces; tomatoes; pickles; alcohol (wine, beer, gin, vermouth); tea (perfumed or flavored); tobacco; chocolate and ice cream; and soft drinks (cola or spiced soft drinks).
Patients starting a nickel-free diet should avoid soy, peanuts and other nuts, legumes, chocolate, cocoa, oats, fish, and whole wheat flours. Any elimination diet should last for 3 months but should at least be tried for 3-4 weeks, with gradual reintroduction of foods suspected as triggers once per week. Any type I allergies that are discovered or suspected can be referred to an allergist for allergen challenge and desensitization therapy.
For more information, Dr. Zippin recommended the American Contact Dermatitis Society website for more information.
Dr. Zippin reported that he is the founder and holds stock options at CEP Biotech; is on the medical advisory board and receives stock options from YouV Labs., is a paid consultant and performs industry-sponsored research for Pfizer, receives stock options from Regeneron, and is on the medical advisory board for Hoth Therapeutics Inc. He is on the board of directors for the American Contact Dermatitis Society.
ORLANDO – Do you have ? Consider patch testing to assess whether they have allergic contact dermatitis.
“Of the patients who are sent to me by local pediatric dermatologists, 50% of them are positive” for allergens, said Jonathan H. Zippin, MD, PhD, director of the contact, occupational, and photodermatitis service at Cornell University, New York.
Speaking at the ODAC Dermatology, Aesthetic, and Surgical Conference, Dr. Zippin noted the prevalence of allergen sensitization is between 13% and 25% among children who are asymptomatic, while the prevalence of sensitization to at least one allergen among children with suspected allergic contact dermatitis (ACD) is between 25% and 96%. In 2014, a study from the National American Contact Dermatitis Group (NACDG) showed that of 883 children who were patch tested, 56.7% had at least one relevant positive patch test (RPPT) result.
“The take-home message here is that pediatric contact dermatitis is common, much more common than a lot of people realize,” Dr. Zippin said.
He described three common scenarios to keep in mind: a worsening rash, a new rash, and failure of a rash to improve after the patient avoids all of his or her positive allergens.
When a rash worsens, patch testing is likely to offer answers. In an analysis of 1,142 patients with suspected ACD aged 18 years or younger (mean age, 10.5 years; 64% female) in the Pediatric Contact Dermatitis Registry study database, 65% had at least one positive patch test, and 48% had at least 1 RPPT (Dermatitis 2016; 27[5] 293-302).
But not all patch testing is the same: The study also found that 24% of the RPPT cases would have been missed if assessed with the T.R.U.E. TEST compared with extended patch testing. If a T.R.U.E. TEST fails to explain generalized atopic dermatitis, the patient should be sent for more comprehensive testing where available, Dr. Zippin advised.
Pediatric patients also have unique allergens clinicians should consider. In the same study, children had a number of allergens similar to those of adults as reported in previous studies, such as nickel, cobalt, and neomycin. However, propylene glycol and cocamidopropyl betaine were allergens identified as unique to the pediatric population.
Another study looking at the same group of patients found that compared with children who did not have AD, children with AD had 7.4 times higher odds of having an RPPT to cocamidopropyl betaine, 7.6 times higher odds of having an RPPT to parthenolide, 5.3 times higher odds of having an RPPT to tixocortol pivalate, 4.2 times higher odds of having an RPPT to wool alcohols, and 4 times higher odds of having an RPPT to lanolin (JAMA Dermatology 2017;153[8]:765-70).
All of these are components of topical medicaments used to treat AD, “either components of emollients that we recommend, or components of steroids that we recommend,” Dr. Zippin pointed out.
One of these allergens could be the culprit when a child develops a new rash but there are no new apparent changes in products, exposures, and activities. Lanolin, also called wool grease, is used in many skin care products, for example. Dr. Zippin described the case of a 6-year-old girl with a history of AD, who presented with a new rash on her scalp and behind her ears, not explained by any obvious changes to products, exposures, or activities. Subsequent patch testing determined that the rash was caused by baby shampoo, which contained cocamidopropyl betaine, which is used in hypoallergenic products. The rash resolved after a different shampoo was used.
“Sometimes, we really have to be thinking when the rash is getting worse, is there something they’re being exposed to that might be an allergen?” Dr. Zippin said.
In patients who have avoided all their positive allergens but a rash has not improved, clinicians should consider systemic contact dermatitis (SCD). Patients can develop SCD through different types of exposures, including transepidermal, transmucosal, oral, intravenous, subcutaneous, intramuscular, inhalation, and implantation routes.
SCD also has a variety of presentations, including pompholyx/dyshidrosis/vesicular dermatitis, maculopapular eruption, chronic pruritus, exfoliative erythroderma/toxiderma, chronic urticaria, erythema multiforme and vasculitis, hyperkeratotic papules of the elbows, acute generalized exanthematous pustulosis, and pruritus ani, according to Dr. Zippin.
SCD should be considered when a patient has a positive patch test to an allergen that is known to cause SCD, and does not clear after avoiding cutaneous exposure to the allergen, Dr. Zippin advised.
Patients will most often develop SCD from plants and herbs, Dr. Zippin noted. Chrysanthemums and chamomile tea are common culprits for compositae allergy and can trigger SCD; other causes are Anacardiaceae, Balsam of Peru, and propolis. Metals (nickel, cobalt, gold, and chromium), medications (aminoglycosides, corticosteroids, and ethylenediamine), and other sources (formaldehyde, propylene glycol in frozen foods, gallates, and methylisothiazolinone) can cause SCD as well.
Methylisothiazolinone in particular is a very common sensitizer, Dr. Zippin said. “If you have a patient who is positive to this, it’s almost always the cause of their problem.”
Balsam of Peru is in a number of different foods, and patients who need to follow a diet free of Balsam of Peru should avoid a long list of foods including citrus; bakery goods; Danish pastry; candy; gum; spices such as cinnamon, cloves, vanilla, curry, allspice, anise, and ginger; spicy condiments such as ketchup, chili sauce, barbecue sauce; chili, pizza, and foods with red sauces; tomatoes; pickles; alcohol (wine, beer, gin, vermouth); tea (perfumed or flavored); tobacco; chocolate and ice cream; and soft drinks (cola or spiced soft drinks).
Patients starting a nickel-free diet should avoid soy, peanuts and other nuts, legumes, chocolate, cocoa, oats, fish, and whole wheat flours. Any elimination diet should last for 3 months but should at least be tried for 3-4 weeks, with gradual reintroduction of foods suspected as triggers once per week. Any type I allergies that are discovered or suspected can be referred to an allergist for allergen challenge and desensitization therapy.
For more information, Dr. Zippin recommended the American Contact Dermatitis Society website for more information.
Dr. Zippin reported that he is the founder and holds stock options at CEP Biotech; is on the medical advisory board and receives stock options from YouV Labs., is a paid consultant and performs industry-sponsored research for Pfizer, receives stock options from Regeneron, and is on the medical advisory board for Hoth Therapeutics Inc. He is on the board of directors for the American Contact Dermatitis Society.
ORLANDO – Do you have ? Consider patch testing to assess whether they have allergic contact dermatitis.
“Of the patients who are sent to me by local pediatric dermatologists, 50% of them are positive” for allergens, said Jonathan H. Zippin, MD, PhD, director of the contact, occupational, and photodermatitis service at Cornell University, New York.
Speaking at the ODAC Dermatology, Aesthetic, and Surgical Conference, Dr. Zippin noted the prevalence of allergen sensitization is between 13% and 25% among children who are asymptomatic, while the prevalence of sensitization to at least one allergen among children with suspected allergic contact dermatitis (ACD) is between 25% and 96%. In 2014, a study from the National American Contact Dermatitis Group (NACDG) showed that of 883 children who were patch tested, 56.7% had at least one relevant positive patch test (RPPT) result.
“The take-home message here is that pediatric contact dermatitis is common, much more common than a lot of people realize,” Dr. Zippin said.
He described three common scenarios to keep in mind: a worsening rash, a new rash, and failure of a rash to improve after the patient avoids all of his or her positive allergens.
When a rash worsens, patch testing is likely to offer answers. In an analysis of 1,142 patients with suspected ACD aged 18 years or younger (mean age, 10.5 years; 64% female) in the Pediatric Contact Dermatitis Registry study database, 65% had at least one positive patch test, and 48% had at least 1 RPPT (Dermatitis 2016; 27[5] 293-302).
But not all patch testing is the same: The study also found that 24% of the RPPT cases would have been missed if assessed with the T.R.U.E. TEST compared with extended patch testing. If a T.R.U.E. TEST fails to explain generalized atopic dermatitis, the patient should be sent for more comprehensive testing where available, Dr. Zippin advised.
Pediatric patients also have unique allergens clinicians should consider. In the same study, children had a number of allergens similar to those of adults as reported in previous studies, such as nickel, cobalt, and neomycin. However, propylene glycol and cocamidopropyl betaine were allergens identified as unique to the pediatric population.
Another study looking at the same group of patients found that compared with children who did not have AD, children with AD had 7.4 times higher odds of having an RPPT to cocamidopropyl betaine, 7.6 times higher odds of having an RPPT to parthenolide, 5.3 times higher odds of having an RPPT to tixocortol pivalate, 4.2 times higher odds of having an RPPT to wool alcohols, and 4 times higher odds of having an RPPT to lanolin (JAMA Dermatology 2017;153[8]:765-70).
All of these are components of topical medicaments used to treat AD, “either components of emollients that we recommend, or components of steroids that we recommend,” Dr. Zippin pointed out.
One of these allergens could be the culprit when a child develops a new rash but there are no new apparent changes in products, exposures, and activities. Lanolin, also called wool grease, is used in many skin care products, for example. Dr. Zippin described the case of a 6-year-old girl with a history of AD, who presented with a new rash on her scalp and behind her ears, not explained by any obvious changes to products, exposures, or activities. Subsequent patch testing determined that the rash was caused by baby shampoo, which contained cocamidopropyl betaine, which is used in hypoallergenic products. The rash resolved after a different shampoo was used.
“Sometimes, we really have to be thinking when the rash is getting worse, is there something they’re being exposed to that might be an allergen?” Dr. Zippin said.
In patients who have avoided all their positive allergens but a rash has not improved, clinicians should consider systemic contact dermatitis (SCD). Patients can develop SCD through different types of exposures, including transepidermal, transmucosal, oral, intravenous, subcutaneous, intramuscular, inhalation, and implantation routes.
SCD also has a variety of presentations, including pompholyx/dyshidrosis/vesicular dermatitis, maculopapular eruption, chronic pruritus, exfoliative erythroderma/toxiderma, chronic urticaria, erythema multiforme and vasculitis, hyperkeratotic papules of the elbows, acute generalized exanthematous pustulosis, and pruritus ani, according to Dr. Zippin.
SCD should be considered when a patient has a positive patch test to an allergen that is known to cause SCD, and does not clear after avoiding cutaneous exposure to the allergen, Dr. Zippin advised.
Patients will most often develop SCD from plants and herbs, Dr. Zippin noted. Chrysanthemums and chamomile tea are common culprits for compositae allergy and can trigger SCD; other causes are Anacardiaceae, Balsam of Peru, and propolis. Metals (nickel, cobalt, gold, and chromium), medications (aminoglycosides, corticosteroids, and ethylenediamine), and other sources (formaldehyde, propylene glycol in frozen foods, gallates, and methylisothiazolinone) can cause SCD as well.
Methylisothiazolinone in particular is a very common sensitizer, Dr. Zippin said. “If you have a patient who is positive to this, it’s almost always the cause of their problem.”
Balsam of Peru is in a number of different foods, and patients who need to follow a diet free of Balsam of Peru should avoid a long list of foods including citrus; bakery goods; Danish pastry; candy; gum; spices such as cinnamon, cloves, vanilla, curry, allspice, anise, and ginger; spicy condiments such as ketchup, chili sauce, barbecue sauce; chili, pizza, and foods with red sauces; tomatoes; pickles; alcohol (wine, beer, gin, vermouth); tea (perfumed or flavored); tobacco; chocolate and ice cream; and soft drinks (cola or spiced soft drinks).
Patients starting a nickel-free diet should avoid soy, peanuts and other nuts, legumes, chocolate, cocoa, oats, fish, and whole wheat flours. Any elimination diet should last for 3 months but should at least be tried for 3-4 weeks, with gradual reintroduction of foods suspected as triggers once per week. Any type I allergies that are discovered or suspected can be referred to an allergist for allergen challenge and desensitization therapy.
For more information, Dr. Zippin recommended the American Contact Dermatitis Society website for more information.
Dr. Zippin reported that he is the founder and holds stock options at CEP Biotech; is on the medical advisory board and receives stock options from YouV Labs., is a paid consultant and performs industry-sponsored research for Pfizer, receives stock options from Regeneron, and is on the medical advisory board for Hoth Therapeutics Inc. He is on the board of directors for the American Contact Dermatitis Society.
EXPERT ANALYSIS FROM ODAC 2020
Choice of infant sleep location is multifactorial
according to a recent nationally representative study.

Of 3,260 mothers surveyed, 59% of mothers said that they intended to room-share without bed-sharing, but only 45% practiced – and also had the intent to practice – room-sharing without bed-sharing. Of the 41% who said that they did not intend to bed-share, 24% actually did intend to practice at least some bed-sharing with their infants, who were all aged 2-6 months at the time of survey administration.
Mothers who were African American and those who were breastfeeding exclusively were most likely to report that they intended to bed-share, reported Ann Kellams, MD, of the department of pediatrics at the University of Virginia,Charlottesville, and coauthors. Mothers who were exclusively breastfeeding had a nearly threefold higher rate of intending to bed-share than mothers whose infants were fed formula.
How mothers perceived social norms about bed- and room-sharing practices also plays a role. Women who considered that social norms supported bed-sharing and discouraged room-sharing had almost 200 times the odds of intending to bed-share, compared with those who perceived that social norms supported room-sharing without bed-sharing.
Conversely, being advised by a doctor to follow the American Academy of Pediatrics–recommended practice of room-sharing without bed-sharing made it less likely that mothers would plan to share a bed with their infant (adjusted odds ratio, 0.56). Yet women who intended to room-share without bed-sharing but who actually did bed-share some of the time, their doctor’s advice to room-share only had no impact (aOR, 1.01).
The investigators noted that, “although other studies have investigated factors influencing maternal decisions, no studies to date have examined maternal intention regarding sleep location and what factors influence intention.”
The Study of Attitudes and Factors Effecting Infant Care drew from 32 U.S. hospitals, and asked mothers about feeding and care practices, including the infant’s usual sleep locations and all sleep locations over the 2 weeks preceding the survey. Additionally, the survey asked about future intent for sleeping practices, looking ahead to the next 2 weeks.
The survey design and the analysis performed in the study were based on the theory of planned behavior (TPB), “which hypothesizes that attitudes, subjective social norms, and perceptions about control over behavior impact one’s intention, which leads to actual behavior,” explained Dr. Kellams and coinvestigators. They reported that they had previously used TPB to analyze mothers’ intentions and actions regarding supine sleep position for infants, finding that a variety of behavioral and social facets accounted for by TPB affected maternal intention and decision making.
Additionally, the study’s design captured partial-night bed-sharing, where an infant may start the night in a separate bed but be brought to bed for feeding or comforting, then share a bed with the mother for the remainder of the night. “Unintended bed-sharing may explain our finding that there is frequent inconsistency between those whose near-future intention is to room-share without bed-sharing but whose actual practice includes bed-sharing,” the authors wrote.
“Attitudes, social norms, and doctor advice are associated with infant sleep location and may be potential targets for educational interventions,” concluded Dr. Kellams and coinvestigators.
Dr. Kellams and associates reported no relevant financial disclosures. The study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Institutes of Health.
SOURCE: Kellams A et al. Pediatrics. 2020 Feb 7;145(3):e20191523.
according to a recent nationally representative study.
Of 3,260 mothers surveyed, 59% of mothers said that they intended to room-share without bed-sharing, but only 45% practiced – and also had the intent to practice – room-sharing without bed-sharing. Of the 41% who said that they did not intend to bed-share, 24% actually did intend to practice at least some bed-sharing with their infants, who were all aged 2-6 months at the time of survey administration.
Mothers who were African American and those who were breastfeeding exclusively were most likely to report that they intended to bed-share, reported Ann Kellams, MD, of the department of pediatrics at the University of Virginia,Charlottesville, and coauthors. Mothers who were exclusively breastfeeding had a nearly threefold higher rate of intending to bed-share than mothers whose infants were fed formula.
How mothers perceived social norms about bed- and room-sharing practices also plays a role. Women who considered that social norms supported bed-sharing and discouraged room-sharing had almost 200 times the odds of intending to bed-share, compared with those who perceived that social norms supported room-sharing without bed-sharing.
Conversely, being advised by a doctor to follow the American Academy of Pediatrics–recommended practice of room-sharing without bed-sharing made it less likely that mothers would plan to share a bed with their infant (adjusted odds ratio, 0.56). Yet women who intended to room-share without bed-sharing but who actually did bed-share some of the time, their doctor’s advice to room-share only had no impact (aOR, 1.01).
The investigators noted that, “although other studies have investigated factors influencing maternal decisions, no studies to date have examined maternal intention regarding sleep location and what factors influence intention.”
The Study of Attitudes and Factors Effecting Infant Care drew from 32 U.S. hospitals, and asked mothers about feeding and care practices, including the infant’s usual sleep locations and all sleep locations over the 2 weeks preceding the survey. Additionally, the survey asked about future intent for sleeping practices, looking ahead to the next 2 weeks.
The survey design and the analysis performed in the study were based on the theory of planned behavior (TPB), “which hypothesizes that attitudes, subjective social norms, and perceptions about control over behavior impact one’s intention, which leads to actual behavior,” explained Dr. Kellams and coinvestigators. They reported that they had previously used TPB to analyze mothers’ intentions and actions regarding supine sleep position for infants, finding that a variety of behavioral and social facets accounted for by TPB affected maternal intention and decision making.
Additionally, the study’s design captured partial-night bed-sharing, where an infant may start the night in a separate bed but be brought to bed for feeding or comforting, then share a bed with the mother for the remainder of the night. “Unintended bed-sharing may explain our finding that there is frequent inconsistency between those whose near-future intention is to room-share without bed-sharing but whose actual practice includes bed-sharing,” the authors wrote.
“Attitudes, social norms, and doctor advice are associated with infant sleep location and may be potential targets for educational interventions,” concluded Dr. Kellams and coinvestigators.
Dr. Kellams and associates reported no relevant financial disclosures. The study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Institutes of Health.
SOURCE: Kellams A et al. Pediatrics. 2020 Feb 7;145(3):e20191523.
according to a recent nationally representative study.
Of 3,260 mothers surveyed, 59% of mothers said that they intended to room-share without bed-sharing, but only 45% practiced – and also had the intent to practice – room-sharing without bed-sharing. Of the 41% who said that they did not intend to bed-share, 24% actually did intend to practice at least some bed-sharing with their infants, who were all aged 2-6 months at the time of survey administration.
Mothers who were African American and those who were breastfeeding exclusively were most likely to report that they intended to bed-share, reported Ann Kellams, MD, of the department of pediatrics at the University of Virginia,Charlottesville, and coauthors. Mothers who were exclusively breastfeeding had a nearly threefold higher rate of intending to bed-share than mothers whose infants were fed formula.
How mothers perceived social norms about bed- and room-sharing practices also plays a role. Women who considered that social norms supported bed-sharing and discouraged room-sharing had almost 200 times the odds of intending to bed-share, compared with those who perceived that social norms supported room-sharing without bed-sharing.
Conversely, being advised by a doctor to follow the American Academy of Pediatrics–recommended practice of room-sharing without bed-sharing made it less likely that mothers would plan to share a bed with their infant (adjusted odds ratio, 0.56). Yet women who intended to room-share without bed-sharing but who actually did bed-share some of the time, their doctor’s advice to room-share only had no impact (aOR, 1.01).
The investigators noted that, “although other studies have investigated factors influencing maternal decisions, no studies to date have examined maternal intention regarding sleep location and what factors influence intention.”
The Study of Attitudes and Factors Effecting Infant Care drew from 32 U.S. hospitals, and asked mothers about feeding and care practices, including the infant’s usual sleep locations and all sleep locations over the 2 weeks preceding the survey. Additionally, the survey asked about future intent for sleeping practices, looking ahead to the next 2 weeks.
The survey design and the analysis performed in the study were based on the theory of planned behavior (TPB), “which hypothesizes that attitudes, subjective social norms, and perceptions about control over behavior impact one’s intention, which leads to actual behavior,” explained Dr. Kellams and coinvestigators. They reported that they had previously used TPB to analyze mothers’ intentions and actions regarding supine sleep position for infants, finding that a variety of behavioral and social facets accounted for by TPB affected maternal intention and decision making.
Additionally, the study’s design captured partial-night bed-sharing, where an infant may start the night in a separate bed but be brought to bed for feeding or comforting, then share a bed with the mother for the remainder of the night. “Unintended bed-sharing may explain our finding that there is frequent inconsistency between those whose near-future intention is to room-share without bed-sharing but whose actual practice includes bed-sharing,” the authors wrote.
“Attitudes, social norms, and doctor advice are associated with infant sleep location and may be potential targets for educational interventions,” concluded Dr. Kellams and coinvestigators.
Dr. Kellams and associates reported no relevant financial disclosures. The study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Institutes of Health.
SOURCE: Kellams A et al. Pediatrics. 2020 Feb 7;145(3):e20191523.
FROM PEDIATRICS
Like a hot potato
Most of us did our postgraduate training in tertiary medical centers, ivory towers of medicine often attached to or closely affiliated with medical schools. These are the places where the buck stops. Occasionally, a very complex patient might be sent to another tertiary center that claims to have a supersubspecialist, a one-of-a-kind physician with nationally recognized expertise. But for most patients, the tertiary medical center is the end of the line, and his or her physicians must manage with the resources at hand. They may confer with one another but there is no place for them to pass the buck.

But most of us who chose primary care left the comforting cocoon of the teaching hospital complex when we finished our training. Those first few months and years in the hinterland can be angst producing. Until we have established our own personal networks of consultants and mentors, patients with more than run-of-the-mill complaints may prompt us to reach for the phone or fire off an email call for help to our recently departed mother ship.
It can take awhile to establish the self-confidence – or at least the appearance of self-confidence – that physicians are expected to exude. But even after years of experience, none of us wants to watch a patient die or suffer preventable complications under our care when we know there is another facility that can provide a higher lever of care just an ambulance ride or short helicopter trip away.
Our primary concern is of course assuring that our patient is receiving the best care. How quickly we reach for the phone to refer out the most fragile patients depends on several factors. Do we practice in a community that has a historic reputation of having a low threshold for malpractice suits? How well do we know the patient and her family? Have we had time to establish bidirectional trust?
Is the patient’s diagnosis one that we feel comfortable with or is the diagnosis one that we believe could quickly deteriorate without warning? For example, a recently published study revealed that 20% of pediatric trauma patients were overtriaged and that the mechanism of injury – firearms or motor vehicle accidents – appeared to have an outsized influence in the triage decision (Trauma Surg Acute Care Open. 2019 Dec 29. doi: 10.1136/tsaco-2019-000300).

Because I have no experience with firearm injuries and minimal experience with motor vehicle injuries I can understand why the emergency medical technicians might be quick to ship these patients to the trauma center. However, I hope that, were I offered better training and more opportunities to gain experience with these types of injuries, I would have a lower overtriage percentage.
Which begs the question of what is an acceptable rate of overtriage or overreferral? It’s the same old question of how many normal appendixes should one remove to avoid a fatal outcome. Each of us arrives at a given clinical crossroads with our own level of experience and comfort level.
But in the final analysis it boils down to a personal decision and our own basic level of anxiety. Let’s face it, some of us worry more than others. Physicians come in all shades of anxiety. A hot potato in your hands may feel only room temperature to me.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
Most of us did our postgraduate training in tertiary medical centers, ivory towers of medicine often attached to or closely affiliated with medical schools. These are the places where the buck stops. Occasionally, a very complex patient might be sent to another tertiary center that claims to have a supersubspecialist, a one-of-a-kind physician with nationally recognized expertise. But for most patients, the tertiary medical center is the end of the line, and his or her physicians must manage with the resources at hand. They may confer with one another but there is no place for them to pass the buck.
But most of us who chose primary care left the comforting cocoon of the teaching hospital complex when we finished our training. Those first few months and years in the hinterland can be angst producing. Until we have established our own personal networks of consultants and mentors, patients with more than run-of-the-mill complaints may prompt us to reach for the phone or fire off an email call for help to our recently departed mother ship.
It can take awhile to establish the self-confidence – or at least the appearance of self-confidence – that physicians are expected to exude. But even after years of experience, none of us wants to watch a patient die or suffer preventable complications under our care when we know there is another facility that can provide a higher lever of care just an ambulance ride or short helicopter trip away.
Our primary concern is of course assuring that our patient is receiving the best care. How quickly we reach for the phone to refer out the most fragile patients depends on several factors. Do we practice in a community that has a historic reputation of having a low threshold for malpractice suits? How well do we know the patient and her family? Have we had time to establish bidirectional trust?
Is the patient’s diagnosis one that we feel comfortable with or is the diagnosis one that we believe could quickly deteriorate without warning? For example, a recently published study revealed that 20% of pediatric trauma patients were overtriaged and that the mechanism of injury – firearms or motor vehicle accidents – appeared to have an outsized influence in the triage decision (Trauma Surg Acute Care Open. 2019 Dec 29. doi: 10.1136/tsaco-2019-000300).
Because I have no experience with firearm injuries and minimal experience with motor vehicle injuries I can understand why the emergency medical technicians might be quick to ship these patients to the trauma center. However, I hope that, were I offered better training and more opportunities to gain experience with these types of injuries, I would have a lower overtriage percentage.
Which begs the question of what is an acceptable rate of overtriage or overreferral? It’s the same old question of how many normal appendixes should one remove to avoid a fatal outcome. Each of us arrives at a given clinical crossroads with our own level of experience and comfort level.
But in the final analysis it boils down to a personal decision and our own basic level of anxiety. Let’s face it, some of us worry more than others. Physicians come in all shades of anxiety. A hot potato in your hands may feel only room temperature to me.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
Most of us did our postgraduate training in tertiary medical centers, ivory towers of medicine often attached to or closely affiliated with medical schools. These are the places where the buck stops. Occasionally, a very complex patient might be sent to another tertiary center that claims to have a supersubspecialist, a one-of-a-kind physician with nationally recognized expertise. But for most patients, the tertiary medical center is the end of the line, and his or her physicians must manage with the resources at hand. They may confer with one another but there is no place for them to pass the buck.
But most of us who chose primary care left the comforting cocoon of the teaching hospital complex when we finished our training. Those first few months and years in the hinterland can be angst producing. Until we have established our own personal networks of consultants and mentors, patients with more than run-of-the-mill complaints may prompt us to reach for the phone or fire off an email call for help to our recently departed mother ship.
It can take awhile to establish the self-confidence – or at least the appearance of self-confidence – that physicians are expected to exude. But even after years of experience, none of us wants to watch a patient die or suffer preventable complications under our care when we know there is another facility that can provide a higher lever of care just an ambulance ride or short helicopter trip away.
Our primary concern is of course assuring that our patient is receiving the best care. How quickly we reach for the phone to refer out the most fragile patients depends on several factors. Do we practice in a community that has a historic reputation of having a low threshold for malpractice suits? How well do we know the patient and her family? Have we had time to establish bidirectional trust?
Is the patient’s diagnosis one that we feel comfortable with or is the diagnosis one that we believe could quickly deteriorate without warning? For example, a recently published study revealed that 20% of pediatric trauma patients were overtriaged and that the mechanism of injury – firearms or motor vehicle accidents – appeared to have an outsized influence in the triage decision (Trauma Surg Acute Care Open. 2019 Dec 29. doi: 10.1136/tsaco-2019-000300).
Because I have no experience with firearm injuries and minimal experience with motor vehicle injuries I can understand why the emergency medical technicians might be quick to ship these patients to the trauma center. However, I hope that, were I offered better training and more opportunities to gain experience with these types of injuries, I would have a lower overtriage percentage.
Which begs the question of what is an acceptable rate of overtriage or overreferral? It’s the same old question of how many normal appendixes should one remove to avoid a fatal outcome. Each of us arrives at a given clinical crossroads with our own level of experience and comfort level.
But in the final analysis it boils down to a personal decision and our own basic level of anxiety. Let’s face it, some of us worry more than others. Physicians come in all shades of anxiety. A hot potato in your hands may feel only room temperature to me.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].