User login
When adolescents visit the ED, 10% leave with an opioid
although there was a small but significant decrease in prescriptions over that time, according to an analysis of two nationwide ambulatory care surveys.
For adolescents aged 13-17 years, 10.4% of ED visits were associated with a prescription for an opioid versus 1.6% among outpatient visits. There was a slight but significant decrease in the rate of opioid prescriptions in the ED setting over the study period, with an odds ratio of 0.95 (95% confidence interval, 0.92-0.97), but there was no significant change in the trend over time in the outpatient setting (OR, 1.02; 95% CI, 0.99-1.09), Joel D. Hudgins, MD, and associates reported in Pediatrics.
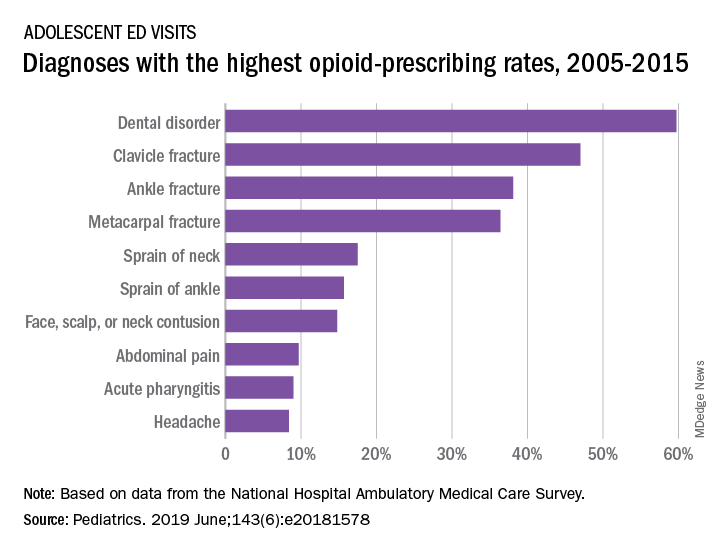
“Opioid prescribing in ambulatory care visits is particularly high in the ED setting and … certain diagnoses appear to be routinely treated with an opioid,” said Dr. Hudgins and associates from Boston Children’s Hospital.
The highest rates of opioid prescribing among adolescents visiting the ED involved dental disorders (60%) and acute injuries such as fractures of the clavicle (47%), ankle (38%), and metacarpals (36%). “However, when considering the total volume of opioid prescriptions dispensed [over 7.8 million during 2005-2015], certain common conditions, including abdominal pain, acute pharyngitis, urinary tract infection, and headache, contributed large numbers of prescriptions as well,” they added.
The study involved data from the National Hospital Ambulatory Medical Care Survey (hospital-based EDs) and the National Ambulatory Medical Care Survey (office-based practices), which both are conducted annually by the National Center for Health Statistics.
The senior investigator is supported by an award from the Burroughs Wellcome Fund by the Harvard-MIT Center for Regulatory Science. The authors said that they have no relevant financial relationships.
SOURCE: Hudgins JD et al. Pediatrics. 2019 June. doi: 10.1542/peds.2018-1578.
although there was a small but significant decrease in prescriptions over that time, according to an analysis of two nationwide ambulatory care surveys.
For adolescents aged 13-17 years, 10.4% of ED visits were associated with a prescription for an opioid versus 1.6% among outpatient visits. There was a slight but significant decrease in the rate of opioid prescriptions in the ED setting over the study period, with an odds ratio of 0.95 (95% confidence interval, 0.92-0.97), but there was no significant change in the trend over time in the outpatient setting (OR, 1.02; 95% CI, 0.99-1.09), Joel D. Hudgins, MD, and associates reported in Pediatrics.
“Opioid prescribing in ambulatory care visits is particularly high in the ED setting and … certain diagnoses appear to be routinely treated with an opioid,” said Dr. Hudgins and associates from Boston Children’s Hospital.
The highest rates of opioid prescribing among adolescents visiting the ED involved dental disorders (60%) and acute injuries such as fractures of the clavicle (47%), ankle (38%), and metacarpals (36%). “However, when considering the total volume of opioid prescriptions dispensed [over 7.8 million during 2005-2015], certain common conditions, including abdominal pain, acute pharyngitis, urinary tract infection, and headache, contributed large numbers of prescriptions as well,” they added.
The study involved data from the National Hospital Ambulatory Medical Care Survey (hospital-based EDs) and the National Ambulatory Medical Care Survey (office-based practices), which both are conducted annually by the National Center for Health Statistics.
The senior investigator is supported by an award from the Burroughs Wellcome Fund by the Harvard-MIT Center for Regulatory Science. The authors said that they have no relevant financial relationships.
SOURCE: Hudgins JD et al. Pediatrics. 2019 June. doi: 10.1542/peds.2018-1578.
although there was a small but significant decrease in prescriptions over that time, according to an analysis of two nationwide ambulatory care surveys.
For adolescents aged 13-17 years, 10.4% of ED visits were associated with a prescription for an opioid versus 1.6% among outpatient visits. There was a slight but significant decrease in the rate of opioid prescriptions in the ED setting over the study period, with an odds ratio of 0.95 (95% confidence interval, 0.92-0.97), but there was no significant change in the trend over time in the outpatient setting (OR, 1.02; 95% CI, 0.99-1.09), Joel D. Hudgins, MD, and associates reported in Pediatrics.
“Opioid prescribing in ambulatory care visits is particularly high in the ED setting and … certain diagnoses appear to be routinely treated with an opioid,” said Dr. Hudgins and associates from Boston Children’s Hospital.
The highest rates of opioid prescribing among adolescents visiting the ED involved dental disorders (60%) and acute injuries such as fractures of the clavicle (47%), ankle (38%), and metacarpals (36%). “However, when considering the total volume of opioid prescriptions dispensed [over 7.8 million during 2005-2015], certain common conditions, including abdominal pain, acute pharyngitis, urinary tract infection, and headache, contributed large numbers of prescriptions as well,” they added.
The study involved data from the National Hospital Ambulatory Medical Care Survey (hospital-based EDs) and the National Ambulatory Medical Care Survey (office-based practices), which both are conducted annually by the National Center for Health Statistics.
The senior investigator is supported by an award from the Burroughs Wellcome Fund by the Harvard-MIT Center for Regulatory Science. The authors said that they have no relevant financial relationships.
SOURCE: Hudgins JD et al. Pediatrics. 2019 June. doi: 10.1542/peds.2018-1578.
FROM PEDIATRICS
FDA approves Zolgensma for infantile-onset SMA treatment
The Food and Drug Administration has approved Zolgensma (onasemnogene abeparvovec-xioi), the first gene therapy for the treatment of infantile-onset spinal muscular atrophy in children aged less than 2 years.

The FDA granted the approval of Zolgensma to AveXis Inc.
Spinal muscular atrophy (SMA) is a genetic disorder caused by a mutation in the SMN1 gene, which encodes the survival motor neuron protein. This protein is necessary for motor function throughout the body; without it, motor neurons die, causing severe, often fatal muscle weakness. Infantile-onset SMA is the most severe and most common form of the disease; children will have difficulty holding their head up, swallowing, or breathing. Symptoms can be present at birth or appear by 6 months.
FDA approval of Zolgensma is based on results of a pair of clinical trials – one ongoing, one completed – comprising 36 patients with infantile-onset SMA aged between 2 weeks and 8 months at study entry. Of the 21 patients initially enrolled in the ongoing trial, 19 remain, aged between 9.4 and 18.5 months; most of these patients are at least 14 months. Compared with natural disease course, patients treated with Zolgensma are more likely to reach developmental motor milestones such as head control and the ability to sit without support.
The most common adverse events associated with Zolgensma include elevated liver enzymes and vomiting. The labeling includes a warning that acute serious liver injury can occur, and patients with preexisting liver conditions are at a higher risk for serious liver injury. Liver function should be monitored for at least 3 months following initiation of Zolgensma treatment.
“Children with SMA experience difficulty performing essential functions of life. Most children with this disease do not survive past early childhood due to respiratory failure. Patients with SMA now have another treatment option to minimize the progression of SMA and improve survival,” Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research, said in the press release.
Find the full press release on the FDA website.
The Food and Drug Administration has approved Zolgensma (onasemnogene abeparvovec-xioi), the first gene therapy for the treatment of infantile-onset spinal muscular atrophy in children aged less than 2 years.
The FDA granted the approval of Zolgensma to AveXis Inc.
Spinal muscular atrophy (SMA) is a genetic disorder caused by a mutation in the SMN1 gene, which encodes the survival motor neuron protein. This protein is necessary for motor function throughout the body; without it, motor neurons die, causing severe, often fatal muscle weakness. Infantile-onset SMA is the most severe and most common form of the disease; children will have difficulty holding their head up, swallowing, or breathing. Symptoms can be present at birth or appear by 6 months.
FDA approval of Zolgensma is based on results of a pair of clinical trials – one ongoing, one completed – comprising 36 patients with infantile-onset SMA aged between 2 weeks and 8 months at study entry. Of the 21 patients initially enrolled in the ongoing trial, 19 remain, aged between 9.4 and 18.5 months; most of these patients are at least 14 months. Compared with natural disease course, patients treated with Zolgensma are more likely to reach developmental motor milestones such as head control and the ability to sit without support.
The most common adverse events associated with Zolgensma include elevated liver enzymes and vomiting. The labeling includes a warning that acute serious liver injury can occur, and patients with preexisting liver conditions are at a higher risk for serious liver injury. Liver function should be monitored for at least 3 months following initiation of Zolgensma treatment.
“Children with SMA experience difficulty performing essential functions of life. Most children with this disease do not survive past early childhood due to respiratory failure. Patients with SMA now have another treatment option to minimize the progression of SMA and improve survival,” Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research, said in the press release.
Find the full press release on the FDA website.
The Food and Drug Administration has approved Zolgensma (onasemnogene abeparvovec-xioi), the first gene therapy for the treatment of infantile-onset spinal muscular atrophy in children aged less than 2 years.
The FDA granted the approval of Zolgensma to AveXis Inc.
Spinal muscular atrophy (SMA) is a genetic disorder caused by a mutation in the SMN1 gene, which encodes the survival motor neuron protein. This protein is necessary for motor function throughout the body; without it, motor neurons die, causing severe, often fatal muscle weakness. Infantile-onset SMA is the most severe and most common form of the disease; children will have difficulty holding their head up, swallowing, or breathing. Symptoms can be present at birth or appear by 6 months.
FDA approval of Zolgensma is based on results of a pair of clinical trials – one ongoing, one completed – comprising 36 patients with infantile-onset SMA aged between 2 weeks and 8 months at study entry. Of the 21 patients initially enrolled in the ongoing trial, 19 remain, aged between 9.4 and 18.5 months; most of these patients are at least 14 months. Compared with natural disease course, patients treated with Zolgensma are more likely to reach developmental motor milestones such as head control and the ability to sit without support.
The most common adverse events associated with Zolgensma include elevated liver enzymes and vomiting. The labeling includes a warning that acute serious liver injury can occur, and patients with preexisting liver conditions are at a higher risk for serious liver injury. Liver function should be monitored for at least 3 months following initiation of Zolgensma treatment.
“Children with SMA experience difficulty performing essential functions of life. Most children with this disease do not survive past early childhood due to respiratory failure. Patients with SMA now have another treatment option to minimize the progression of SMA and improve survival,” Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research, said in the press release.
Find the full press release on the FDA website.
Entrectinib exhibits activity in children with solid tumors
Entrectinib demonstrated “very promising” antitumor activity in children and adolescents with recurrent or refractory solid tumors, according to an investigator involved in a phase 1/1b trial.
Twelve of 29 patients enrolled in the trial have responded to entrectinib. All responders had fusions in genes targeted by the drug – NTRK1/2/3 (TRKA/B/C), ROS1, or ALK – or an ALK mutation.
Details of this study are scheduled to be presented at the annual meeting of the American Society of Clinical Oncology.
Giles W. Robinson, MD, of St. Jude Children’s Research Hospital in Memphis, Tenn., discussed the study during a press briefing in advance of the meeting.
“Entrectinib is an oral and potent inhibitor of the TRKA/B/C, ROS1, and ALK proteins, but it also penetrates into the brain to reach tumors in the brain and spine, which can be a hard area to get drugs to,” Dr. Robinson explained.
“Promising clinical activity was initially seen in the adult solid tumor patients with target rearrangements, and it was encouraging to see these patients also had responses when the tumors were located in their brains. And what got us really excited as pediatric oncologists was that a variety of pediatric cancers harbor these fusions and mutations within certain tumors.”
With this in mind, Dr. Robinson and colleagues conducted a phase 1/1b study (NCT02650401) of entrectinib in 29 patients with recurrent or refractory solid tumors, including central nervous system (CNS) tumors.
The patients’ median age was 7 years (range, 0-20 years), and roughly half of them were male (n = 15). Patients were diagnosed with neuroblastoma (n = 16), high-grade glioma (n = 5), inflammatory myofibroblastic tumors (n = 3), infantile fibrosarcoma (n = 2), CNS embryonal tumor (n = 1), melanoma (n = 1), and synovial sarcoma (n = 1).
In the dose-finding portion of the trial, patients received entrectinib at 250 mg/m2 (n = 3), 400 mg/m2 (n = 3), 550 mg/m2 (n = 7), or 750 mg/m2 (n = 3).
In the phase 1b portion, patients received entrectinib at 550 mg/m2 (n = 7) – the recommended dose – or 400 mg/m2 (n = 6) if they were unable to swallow intact capsules.
Dr. Robinson said entrectinib was “quite well tolerated” overall, but he did not present any data on adverse events. He did say dose-limiting toxicities included fatigue, elevated creatinine levels, dysgeusia resulting in loss of taste, weight gain, and, in one patient, pulmonary edema.
“Entrectinib produced striking, rapid, and durable responses in all children with refractory CNS and solid tumors that actually harbored these fusions in NTRK1/2/3, ROS1, or ALK,” Dr. Robinson said. “It also produced a significant response in one ALK-mutated neuroblastoma patient. [N]o responses were seen in tumors lacking aberrations in the target kinases.”
In all, 12 patients responded. The three complete responders had an ALK F1174L mutation, an ALK fusion, and an NTRK fusion, respectively. Five partial responders had NTRK fusions, three had ROS1 fusions, and one had an ALK fusion.
Three responders discontinued treatment. Ten patients were still receiving entrectinib at last follow-up, and 11 patients had died.
Progression-free survival was significantly longer among patients who had fusions than among those who did not (P less than .0001).
“To sum up, entrectinib really is very promising,” Dr. Robinson said. “It has very promising antitumor activity and progression-free survival but [only] in patients with target gene fusions.”
Dr. Robinson said this trial is ongoing, but it is now limited to patients with fusions targeted by entrectinib.
The trial is sponsored by Hoffman-La Roche Ltd. and supported by Alex’s Lemonade Stand Center of Excellence. Dr. Robinson has relationships with Lilly, Genentech/Roche, and Novartis.
SOURCE: Robinson GW et al. ASCO 2019. Abstract 10009.
Entrectinib demonstrated “very promising” antitumor activity in children and adolescents with recurrent or refractory solid tumors, according to an investigator involved in a phase 1/1b trial.
Twelve of 29 patients enrolled in the trial have responded to entrectinib. All responders had fusions in genes targeted by the drug – NTRK1/2/3 (TRKA/B/C), ROS1, or ALK – or an ALK mutation.
Details of this study are scheduled to be presented at the annual meeting of the American Society of Clinical Oncology.
Giles W. Robinson, MD, of St. Jude Children’s Research Hospital in Memphis, Tenn., discussed the study during a press briefing in advance of the meeting.
“Entrectinib is an oral and potent inhibitor of the TRKA/B/C, ROS1, and ALK proteins, but it also penetrates into the brain to reach tumors in the brain and spine, which can be a hard area to get drugs to,” Dr. Robinson explained.
“Promising clinical activity was initially seen in the adult solid tumor patients with target rearrangements, and it was encouraging to see these patients also had responses when the tumors were located in their brains. And what got us really excited as pediatric oncologists was that a variety of pediatric cancers harbor these fusions and mutations within certain tumors.”
With this in mind, Dr. Robinson and colleagues conducted a phase 1/1b study (NCT02650401) of entrectinib in 29 patients with recurrent or refractory solid tumors, including central nervous system (CNS) tumors.
The patients’ median age was 7 years (range, 0-20 years), and roughly half of them were male (n = 15). Patients were diagnosed with neuroblastoma (n = 16), high-grade glioma (n = 5), inflammatory myofibroblastic tumors (n = 3), infantile fibrosarcoma (n = 2), CNS embryonal tumor (n = 1), melanoma (n = 1), and synovial sarcoma (n = 1).
In the dose-finding portion of the trial, patients received entrectinib at 250 mg/m2 (n = 3), 400 mg/m2 (n = 3), 550 mg/m2 (n = 7), or 750 mg/m2 (n = 3).
In the phase 1b portion, patients received entrectinib at 550 mg/m2 (n = 7) – the recommended dose – or 400 mg/m2 (n = 6) if they were unable to swallow intact capsules.
Dr. Robinson said entrectinib was “quite well tolerated” overall, but he did not present any data on adverse events. He did say dose-limiting toxicities included fatigue, elevated creatinine levels, dysgeusia resulting in loss of taste, weight gain, and, in one patient, pulmonary edema.
“Entrectinib produced striking, rapid, and durable responses in all children with refractory CNS and solid tumors that actually harbored these fusions in NTRK1/2/3, ROS1, or ALK,” Dr. Robinson said. “It also produced a significant response in one ALK-mutated neuroblastoma patient. [N]o responses were seen in tumors lacking aberrations in the target kinases.”
In all, 12 patients responded. The three complete responders had an ALK F1174L mutation, an ALK fusion, and an NTRK fusion, respectively. Five partial responders had NTRK fusions, three had ROS1 fusions, and one had an ALK fusion.
Three responders discontinued treatment. Ten patients were still receiving entrectinib at last follow-up, and 11 patients had died.
Progression-free survival was significantly longer among patients who had fusions than among those who did not (P less than .0001).
“To sum up, entrectinib really is very promising,” Dr. Robinson said. “It has very promising antitumor activity and progression-free survival but [only] in patients with target gene fusions.”
Dr. Robinson said this trial is ongoing, but it is now limited to patients with fusions targeted by entrectinib.
The trial is sponsored by Hoffman-La Roche Ltd. and supported by Alex’s Lemonade Stand Center of Excellence. Dr. Robinson has relationships with Lilly, Genentech/Roche, and Novartis.
SOURCE: Robinson GW et al. ASCO 2019. Abstract 10009.
Entrectinib demonstrated “very promising” antitumor activity in children and adolescents with recurrent or refractory solid tumors, according to an investigator involved in a phase 1/1b trial.
Twelve of 29 patients enrolled in the trial have responded to entrectinib. All responders had fusions in genes targeted by the drug – NTRK1/2/3 (TRKA/B/C), ROS1, or ALK – or an ALK mutation.
Details of this study are scheduled to be presented at the annual meeting of the American Society of Clinical Oncology.
Giles W. Robinson, MD, of St. Jude Children’s Research Hospital in Memphis, Tenn., discussed the study during a press briefing in advance of the meeting.
“Entrectinib is an oral and potent inhibitor of the TRKA/B/C, ROS1, and ALK proteins, but it also penetrates into the brain to reach tumors in the brain and spine, which can be a hard area to get drugs to,” Dr. Robinson explained.
“Promising clinical activity was initially seen in the adult solid tumor patients with target rearrangements, and it was encouraging to see these patients also had responses when the tumors were located in their brains. And what got us really excited as pediatric oncologists was that a variety of pediatric cancers harbor these fusions and mutations within certain tumors.”
With this in mind, Dr. Robinson and colleagues conducted a phase 1/1b study (NCT02650401) of entrectinib in 29 patients with recurrent or refractory solid tumors, including central nervous system (CNS) tumors.
The patients’ median age was 7 years (range, 0-20 years), and roughly half of them were male (n = 15). Patients were diagnosed with neuroblastoma (n = 16), high-grade glioma (n = 5), inflammatory myofibroblastic tumors (n = 3), infantile fibrosarcoma (n = 2), CNS embryonal tumor (n = 1), melanoma (n = 1), and synovial sarcoma (n = 1).
In the dose-finding portion of the trial, patients received entrectinib at 250 mg/m2 (n = 3), 400 mg/m2 (n = 3), 550 mg/m2 (n = 7), or 750 mg/m2 (n = 3).
In the phase 1b portion, patients received entrectinib at 550 mg/m2 (n = 7) – the recommended dose – or 400 mg/m2 (n = 6) if they were unable to swallow intact capsules.
Dr. Robinson said entrectinib was “quite well tolerated” overall, but he did not present any data on adverse events. He did say dose-limiting toxicities included fatigue, elevated creatinine levels, dysgeusia resulting in loss of taste, weight gain, and, in one patient, pulmonary edema.
“Entrectinib produced striking, rapid, and durable responses in all children with refractory CNS and solid tumors that actually harbored these fusions in NTRK1/2/3, ROS1, or ALK,” Dr. Robinson said. “It also produced a significant response in one ALK-mutated neuroblastoma patient. [N]o responses were seen in tumors lacking aberrations in the target kinases.”
In all, 12 patients responded. The three complete responders had an ALK F1174L mutation, an ALK fusion, and an NTRK fusion, respectively. Five partial responders had NTRK fusions, three had ROS1 fusions, and one had an ALK fusion.
Three responders discontinued treatment. Ten patients were still receiving entrectinib at last follow-up, and 11 patients had died.
Progression-free survival was significantly longer among patients who had fusions than among those who did not (P less than .0001).
“To sum up, entrectinib really is very promising,” Dr. Robinson said. “It has very promising antitumor activity and progression-free survival but [only] in patients with target gene fusions.”
Dr. Robinson said this trial is ongoing, but it is now limited to patients with fusions targeted by entrectinib.
The trial is sponsored by Hoffman-La Roche Ltd. and supported by Alex’s Lemonade Stand Center of Excellence. Dr. Robinson has relationships with Lilly, Genentech/Roche, and Novartis.
SOURCE: Robinson GW et al. ASCO 2019. Abstract 10009.
REPORTING FROM ASCO 2019
Connected care
I previously shared my concerns about the compromises some physicians are making when they consent to practicing in a telemedicine arrangement in which the system’s technical limitations prevents them from obtaining information critical to making an accurate diagnosis. In the scenarios that I described, a physician would have great difficulty being a good steward of antibiotic usage if he were willing to make a diagnosis of otitis media or strep throat without access to tympanic membrane visualization or the results of a rapid strep test.

In response to my observation, I received an email from Dr. Kenneth McConnochie, a name out of my deep past from when we were teammates in college. Now a professor of pediatrics at University of Rochester (N.Y.) Medical Center, Dr. McConnochie has studied telemedicine in primary care extensively. He has thought a lot about telemedicine and more specifically about how it relates to quality. As he pointed out to me,
I suspect that like me, whenever you look at an article or study that has “telemedicine” in its title or headline, you are never sure what you’re going to be reading about. Is it going to be a discussion of telephone triaging in a suburban primary practice or will the article describe how a pediatric cardiologist in Anchorage can follow his little patients in the Aleutians via an audio/video hookup that provides him with the ability to auscultate and review electrocardiograms and radiographic images? Dr. McConnochie suggests that by using the broader term “connected care” for care that is delivered at a distance, and by clearly specifying different types or levels, we will be one big step closer to a more meaningful way to understand the usefulness of that care.
In the conceptual framework he proposes, level 1 is text-only care because it offers the physician the least capacity for the acquisition of (1) diagnostically relevant information and (2) interpersonal connection. Phone care can provide more and videoconferencing still more. Level 4 would be what Dr. McConnochie labels “information rich” care providing the most abundant capacity. Here, think of an arrangement in which someone at the patient’s end of the connection has been trained to use an electronic otoscope that can capture an image of the child’s tympanic membrane, an electronic stethoscope that can record heart and breath sounds, and a high resolution camera to capture images of the patient’s skin, throat, and eyes, then transmit them to the child’s electronic health record (EHR) in real time. Someone in the school or day care center where the child spends his day has been taught how to obtain and process a rapid strep test. The physician who has instant access to the child’s EHR can communicate “face to face” via teleconferencing with the day care providers and with the parent who is at work to discuss the diagnosis, treatment plan, and follow-up. If any of the parties feels the exchange of information is insufficiently robust, a traditional office visit can be arranged.
The challenge of assigning value to each level care still remains. Is the level 4 scenario I just described as valuable as a face to face traditional office visit? In some situations, it is likely to be more valuable than a visit with a physician in an urgent care clinic or emergency department who has never seen the patient and/or lacks access to the EHR because her computer doesn’t interface with the primary care physician’s EHR. It certainly may be more convenient for the family.

But who is going to assign value? A connected visit may be more efficient for the patient and the parent, but will it be more costly? And who is going to pay? Dr. McConnochie’s observations should be taken seriously by those folks who assign value and pay.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
I previously shared my concerns about the compromises some physicians are making when they consent to practicing in a telemedicine arrangement in which the system’s technical limitations prevents them from obtaining information critical to making an accurate diagnosis. In the scenarios that I described, a physician would have great difficulty being a good steward of antibiotic usage if he were willing to make a diagnosis of otitis media or strep throat without access to tympanic membrane visualization or the results of a rapid strep test.
In response to my observation, I received an email from Dr. Kenneth McConnochie, a name out of my deep past from when we were teammates in college. Now a professor of pediatrics at University of Rochester (N.Y.) Medical Center, Dr. McConnochie has studied telemedicine in primary care extensively. He has thought a lot about telemedicine and more specifically about how it relates to quality. As he pointed out to me,
I suspect that like me, whenever you look at an article or study that has “telemedicine” in its title or headline, you are never sure what you’re going to be reading about. Is it going to be a discussion of telephone triaging in a suburban primary practice or will the article describe how a pediatric cardiologist in Anchorage can follow his little patients in the Aleutians via an audio/video hookup that provides him with the ability to auscultate and review electrocardiograms and radiographic images? Dr. McConnochie suggests that by using the broader term “connected care” for care that is delivered at a distance, and by clearly specifying different types or levels, we will be one big step closer to a more meaningful way to understand the usefulness of that care.
In the conceptual framework he proposes, level 1 is text-only care because it offers the physician the least capacity for the acquisition of (1) diagnostically relevant information and (2) interpersonal connection. Phone care can provide more and videoconferencing still more. Level 4 would be what Dr. McConnochie labels “information rich” care providing the most abundant capacity. Here, think of an arrangement in which someone at the patient’s end of the connection has been trained to use an electronic otoscope that can capture an image of the child’s tympanic membrane, an electronic stethoscope that can record heart and breath sounds, and a high resolution camera to capture images of the patient’s skin, throat, and eyes, then transmit them to the child’s electronic health record (EHR) in real time. Someone in the school or day care center where the child spends his day has been taught how to obtain and process a rapid strep test. The physician who has instant access to the child’s EHR can communicate “face to face” via teleconferencing with the day care providers and with the parent who is at work to discuss the diagnosis, treatment plan, and follow-up. If any of the parties feels the exchange of information is insufficiently robust, a traditional office visit can be arranged.
The challenge of assigning value to each level care still remains. Is the level 4 scenario I just described as valuable as a face to face traditional office visit? In some situations, it is likely to be more valuable than a visit with a physician in an urgent care clinic or emergency department who has never seen the patient and/or lacks access to the EHR because her computer doesn’t interface with the primary care physician’s EHR. It certainly may be more convenient for the family.
But who is going to assign value? A connected visit may be more efficient for the patient and the parent, but will it be more costly? And who is going to pay? Dr. McConnochie’s observations should be taken seriously by those folks who assign value and pay.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
I previously shared my concerns about the compromises some physicians are making when they consent to practicing in a telemedicine arrangement in which the system’s technical limitations prevents them from obtaining information critical to making an accurate diagnosis. In the scenarios that I described, a physician would have great difficulty being a good steward of antibiotic usage if he were willing to make a diagnosis of otitis media or strep throat without access to tympanic membrane visualization or the results of a rapid strep test.
In response to my observation, I received an email from Dr. Kenneth McConnochie, a name out of my deep past from when we were teammates in college. Now a professor of pediatrics at University of Rochester (N.Y.) Medical Center, Dr. McConnochie has studied telemedicine in primary care extensively. He has thought a lot about telemedicine and more specifically about how it relates to quality. As he pointed out to me,
I suspect that like me, whenever you look at an article or study that has “telemedicine” in its title or headline, you are never sure what you’re going to be reading about. Is it going to be a discussion of telephone triaging in a suburban primary practice or will the article describe how a pediatric cardiologist in Anchorage can follow his little patients in the Aleutians via an audio/video hookup that provides him with the ability to auscultate and review electrocardiograms and radiographic images? Dr. McConnochie suggests that by using the broader term “connected care” for care that is delivered at a distance, and by clearly specifying different types or levels, we will be one big step closer to a more meaningful way to understand the usefulness of that care.
In the conceptual framework he proposes, level 1 is text-only care because it offers the physician the least capacity for the acquisition of (1) diagnostically relevant information and (2) interpersonal connection. Phone care can provide more and videoconferencing still more. Level 4 would be what Dr. McConnochie labels “information rich” care providing the most abundant capacity. Here, think of an arrangement in which someone at the patient’s end of the connection has been trained to use an electronic otoscope that can capture an image of the child’s tympanic membrane, an electronic stethoscope that can record heart and breath sounds, and a high resolution camera to capture images of the patient’s skin, throat, and eyes, then transmit them to the child’s electronic health record (EHR) in real time. Someone in the school or day care center where the child spends his day has been taught how to obtain and process a rapid strep test. The physician who has instant access to the child’s EHR can communicate “face to face” via teleconferencing with the day care providers and with the parent who is at work to discuss the diagnosis, treatment plan, and follow-up. If any of the parties feels the exchange of information is insufficiently robust, a traditional office visit can be arranged.
The challenge of assigning value to each level care still remains. Is the level 4 scenario I just described as valuable as a face to face traditional office visit? In some situations, it is likely to be more valuable than a visit with a physician in an urgent care clinic or emergency department who has never seen the patient and/or lacks access to the EHR because her computer doesn’t interface with the primary care physician’s EHR. It certainly may be more convenient for the family.
But who is going to assign value? A connected visit may be more efficient for the patient and the parent, but will it be more costly? And who is going to pay? Dr. McConnochie’s observations should be taken seriously by those folks who assign value and pay.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
Beyond symptom improvement: Practicing happiness
Kailah is a 13-year-old cisgender female with two working parents, two younger siblings, and a history of mild asthma and overweight who recently presented for a problem-focused visit related to increasing anxiety. An interview of Kailah and her parents led to a diagnosis of generalized anxiety disorder, and she was referred for cognitive-behavioral therapy (CBT) and started on a low-dose SSRI. She now presents 3 months later with decreased anxiety and is compliant with the SSRI and CBT. What next?
Positive psychology and psychiatry have emerged as scientific disciplines since Seligman et al.1 charged the field of psychology with reclaiming its stake in helping everyday people to thrive, as well as cultivating strengths and talents at each level of society – individual, family, institutional, and beyond. This call to action revealed the shift over time from mental health care toward a focus only on mental illness. And study after study confirmed that being “not depressed,” “not anxious” and so on was not the same as flourishing.2
Returning to Kailah, from a mental-health-as-usual approach, your job may be done. Her symptoms have responded to first-line treatments. Perhaps you even tracked her symptoms with a freely available standardized assessment tool like the Screen for Child Anxiety Related Disorders (SCARED)3 and noted a significant drop in her generalized anxiety score.
After a couple decades of research, the science of well-being has led to some consistent findings that can be translated into office practice with children and families. As with any new science, the first steps to building well-being are defining and measuring what we are talking about. I recommend the Flourishing Scale4 for its brevity, availability, and ease of use. It covers the domains included in Seligman’s formula for thriving: PERMA. This acronym represents a consolidation of the first decades of research on well-being, and stands for Positive Emotions, Engagement, (Positive) Relationships, Meaning, and Accomplishments. For a readable but deeper look at the science behind this, check out Seligman’s “Flourish.”5
With the Flourishing Scale total score as a starting point, the acronym PERMA itself can be a good rubric to guide assessment and treatment planning in the office. You can query each of the elements to understand a youth’s current status and areas for building strengths. What brings positive emotions? What activities bring a sense of harmonious engagement without self-consciousness or awareness of time (such as a flow state)? What supportive relationships exist? Where does the youth find meaning or purpose – connection to something larger than themselves (family, work, community, teams, religion, and so on)? And where does the youth derive a sense of competence or self-esteem – something they are good at (accomplishment)?
Your clinical recommendations can flow from this assessment discussion, melding the patient’s and family’s strengths and priorities with evidence-based interventions. “The Resilience Drive,” by Alexia Michiels,6 is a good source for the latter – each chapter has segments relating research to straightforward happiness practices. The Growing Happy card deck (available online) also has brief and usable recommendations suitable for many young people. You can use these during office visits, loan out cards, gift them to families, or recommend families purchase a deck.

To build relationships, I recommend the StoryCorps and 36 Questions To Fall In Love apps. They are free and can be used with parents, peers, or others to build relationship supports and positive intimacy. Try them out yourself first; they essentially provide a platform to generate vulnerable conversations.
Mindfulness is a great antidote to lack of engagement, and it can be practiced in a variety of forms. Card decks make good office props or giveaways, including Growing Mindful (mindfulness practices for all ages) and the YogaKids Toolbox. Plus, there’s an app for that – in fact, many. Two that are free and include materials accessible for younger age groups are Smiling Mind (a nonprofit) and Insight Timer (searchable). This can build engagement and counter negative emotions.
For increasing engagement and flow, I recommend patients and family members assess their character strengths at Strengths-Based Resilience by the University of Toronto SSQ72. Research shows that using your strengths in novel ways lowers depression risk, increases happiness,7 and may be a key to increasing engagement in everyday activities.
When Kailah came in for her next visit, a discussion of PERMA led to identifying time with her family and time with her dog as significant relationship supports that bring positive emotions. However, she struggled to identify a realm where she felt some sense of mastery or competence. Taking the strengths survey (SSQ72) brought out her strengths of love of learning and curiosity. This led to her volunteering at her local library – assisting with programs and eventually creating and leading a teens’ book group. Her CBT therapist supported her through these challenges, and she was able to taper the frequency of therapy sessions so that Kailah only returns for a booster session now every 6 months or so. While she still identifies as an anxious person, Kailah has broadened her self-image to include her resilience and love of learning as core strengths.
Dr. Andrew J. Rosenfeld is an assistant professor in the departments of psychiatry and pediatrics at the University of Vermont Medical Center, Burlington. He said he has no relevant disclosures. Email him at [email protected].
References
1. Am Psychol. 2000;55(1):5-14.
2. Am Psychol. 2007 Feb-Mar;62(2):95-108.
3. J Am Acad Child Adolesc Psychiatry. 1999 Oct;38(10):1230-6.
4. Soc Indic Res. 2009; 39:247-66.
5. “Flourish: A visionary new understanding of happiness and well-being” (New York: Free Press, 2011).
6. “The Resilience Drive” (Switzerland: Favre, 2017).
7. Am Psychol. 2005 Jul-Aug;60(5):410-21.
Kailah is a 13-year-old cisgender female with two working parents, two younger siblings, and a history of mild asthma and overweight who recently presented for a problem-focused visit related to increasing anxiety. An interview of Kailah and her parents led to a diagnosis of generalized anxiety disorder, and she was referred for cognitive-behavioral therapy (CBT) and started on a low-dose SSRI. She now presents 3 months later with decreased anxiety and is compliant with the SSRI and CBT. What next?
Positive psychology and psychiatry have emerged as scientific disciplines since Seligman et al.1 charged the field of psychology with reclaiming its stake in helping everyday people to thrive, as well as cultivating strengths and talents at each level of society – individual, family, institutional, and beyond. This call to action revealed the shift over time from mental health care toward a focus only on mental illness. And study after study confirmed that being “not depressed,” “not anxious” and so on was not the same as flourishing.2
Returning to Kailah, from a mental-health-as-usual approach, your job may be done. Her symptoms have responded to first-line treatments. Perhaps you even tracked her symptoms with a freely available standardized assessment tool like the Screen for Child Anxiety Related Disorders (SCARED)3 and noted a significant drop in her generalized anxiety score.
After a couple decades of research, the science of well-being has led to some consistent findings that can be translated into office practice with children and families. As with any new science, the first steps to building well-being are defining and measuring what we are talking about. I recommend the Flourishing Scale4 for its brevity, availability, and ease of use. It covers the domains included in Seligman’s formula for thriving: PERMA. This acronym represents a consolidation of the first decades of research on well-being, and stands for Positive Emotions, Engagement, (Positive) Relationships, Meaning, and Accomplishments. For a readable but deeper look at the science behind this, check out Seligman’s “Flourish.”5
With the Flourishing Scale total score as a starting point, the acronym PERMA itself can be a good rubric to guide assessment and treatment planning in the office. You can query each of the elements to understand a youth’s current status and areas for building strengths. What brings positive emotions? What activities bring a sense of harmonious engagement without self-consciousness or awareness of time (such as a flow state)? What supportive relationships exist? Where does the youth find meaning or purpose – connection to something larger than themselves (family, work, community, teams, religion, and so on)? And where does the youth derive a sense of competence or self-esteem – something they are good at (accomplishment)?
Your clinical recommendations can flow from this assessment discussion, melding the patient’s and family’s strengths and priorities with evidence-based interventions. “The Resilience Drive,” by Alexia Michiels,6 is a good source for the latter – each chapter has segments relating research to straightforward happiness practices. The Growing Happy card deck (available online) also has brief and usable recommendations suitable for many young people. You can use these during office visits, loan out cards, gift them to families, or recommend families purchase a deck.
To build relationships, I recommend the StoryCorps and 36 Questions To Fall In Love apps. They are free and can be used with parents, peers, or others to build relationship supports and positive intimacy. Try them out yourself first; they essentially provide a platform to generate vulnerable conversations.
Mindfulness is a great antidote to lack of engagement, and it can be practiced in a variety of forms. Card decks make good office props or giveaways, including Growing Mindful (mindfulness practices for all ages) and the YogaKids Toolbox. Plus, there’s an app for that – in fact, many. Two that are free and include materials accessible for younger age groups are Smiling Mind (a nonprofit) and Insight Timer (searchable). This can build engagement and counter negative emotions.
For increasing engagement and flow, I recommend patients and family members assess their character strengths at Strengths-Based Resilience by the University of Toronto SSQ72. Research shows that using your strengths in novel ways lowers depression risk, increases happiness,7 and may be a key to increasing engagement in everyday activities.
When Kailah came in for her next visit, a discussion of PERMA led to identifying time with her family and time with her dog as significant relationship supports that bring positive emotions. However, she struggled to identify a realm where she felt some sense of mastery or competence. Taking the strengths survey (SSQ72) brought out her strengths of love of learning and curiosity. This led to her volunteering at her local library – assisting with programs and eventually creating and leading a teens’ book group. Her CBT therapist supported her through these challenges, and she was able to taper the frequency of therapy sessions so that Kailah only returns for a booster session now every 6 months or so. While she still identifies as an anxious person, Kailah has broadened her self-image to include her resilience and love of learning as core strengths.
Dr. Andrew J. Rosenfeld is an assistant professor in the departments of psychiatry and pediatrics at the University of Vermont Medical Center, Burlington. He said he has no relevant disclosures. Email him at [email protected].
References
1. Am Psychol. 2000;55(1):5-14.
2. Am Psychol. 2007 Feb-Mar;62(2):95-108.
3. J Am Acad Child Adolesc Psychiatry. 1999 Oct;38(10):1230-6.
4. Soc Indic Res. 2009; 39:247-66.
5. “Flourish: A visionary new understanding of happiness and well-being” (New York: Free Press, 2011).
6. “The Resilience Drive” (Switzerland: Favre, 2017).
7. Am Psychol. 2005 Jul-Aug;60(5):410-21.
Kailah is a 13-year-old cisgender female with two working parents, two younger siblings, and a history of mild asthma and overweight who recently presented for a problem-focused visit related to increasing anxiety. An interview of Kailah and her parents led to a diagnosis of generalized anxiety disorder, and she was referred for cognitive-behavioral therapy (CBT) and started on a low-dose SSRI. She now presents 3 months later with decreased anxiety and is compliant with the SSRI and CBT. What next?
Positive psychology and psychiatry have emerged as scientific disciplines since Seligman et al.1 charged the field of psychology with reclaiming its stake in helping everyday people to thrive, as well as cultivating strengths and talents at each level of society – individual, family, institutional, and beyond. This call to action revealed the shift over time from mental health care toward a focus only on mental illness. And study after study confirmed that being “not depressed,” “not anxious” and so on was not the same as flourishing.2
Returning to Kailah, from a mental-health-as-usual approach, your job may be done. Her symptoms have responded to first-line treatments. Perhaps you even tracked her symptoms with a freely available standardized assessment tool like the Screen for Child Anxiety Related Disorders (SCARED)3 and noted a significant drop in her generalized anxiety score.
After a couple decades of research, the science of well-being has led to some consistent findings that can be translated into office practice with children and families. As with any new science, the first steps to building well-being are defining and measuring what we are talking about. I recommend the Flourishing Scale4 for its brevity, availability, and ease of use. It covers the domains included in Seligman’s formula for thriving: PERMA. This acronym represents a consolidation of the first decades of research on well-being, and stands for Positive Emotions, Engagement, (Positive) Relationships, Meaning, and Accomplishments. For a readable but deeper look at the science behind this, check out Seligman’s “Flourish.”5
With the Flourishing Scale total score as a starting point, the acronym PERMA itself can be a good rubric to guide assessment and treatment planning in the office. You can query each of the elements to understand a youth’s current status and areas for building strengths. What brings positive emotions? What activities bring a sense of harmonious engagement without self-consciousness or awareness of time (such as a flow state)? What supportive relationships exist? Where does the youth find meaning or purpose – connection to something larger than themselves (family, work, community, teams, religion, and so on)? And where does the youth derive a sense of competence or self-esteem – something they are good at (accomplishment)?
Your clinical recommendations can flow from this assessment discussion, melding the patient’s and family’s strengths and priorities with evidence-based interventions. “The Resilience Drive,” by Alexia Michiels,6 is a good source for the latter – each chapter has segments relating research to straightforward happiness practices. The Growing Happy card deck (available online) also has brief and usable recommendations suitable for many young people. You can use these during office visits, loan out cards, gift them to families, or recommend families purchase a deck.
To build relationships, I recommend the StoryCorps and 36 Questions To Fall In Love apps. They are free and can be used with parents, peers, or others to build relationship supports and positive intimacy. Try them out yourself first; they essentially provide a platform to generate vulnerable conversations.
Mindfulness is a great antidote to lack of engagement, and it can be practiced in a variety of forms. Card decks make good office props or giveaways, including Growing Mindful (mindfulness practices for all ages) and the YogaKids Toolbox. Plus, there’s an app for that – in fact, many. Two that are free and include materials accessible for younger age groups are Smiling Mind (a nonprofit) and Insight Timer (searchable). This can build engagement and counter negative emotions.
For increasing engagement and flow, I recommend patients and family members assess their character strengths at Strengths-Based Resilience by the University of Toronto SSQ72. Research shows that using your strengths in novel ways lowers depression risk, increases happiness,7 and may be a key to increasing engagement in everyday activities.
When Kailah came in for her next visit, a discussion of PERMA led to identifying time with her family and time with her dog as significant relationship supports that bring positive emotions. However, she struggled to identify a realm where she felt some sense of mastery or competence. Taking the strengths survey (SSQ72) brought out her strengths of love of learning and curiosity. This led to her volunteering at her local library – assisting with programs and eventually creating and leading a teens’ book group. Her CBT therapist supported her through these challenges, and she was able to taper the frequency of therapy sessions so that Kailah only returns for a booster session now every 6 months or so. While she still identifies as an anxious person, Kailah has broadened her self-image to include her resilience and love of learning as core strengths.
Dr. Andrew J. Rosenfeld is an assistant professor in the departments of psychiatry and pediatrics at the University of Vermont Medical Center, Burlington. He said he has no relevant disclosures. Email him at [email protected].
References
1. Am Psychol. 2000;55(1):5-14.
2. Am Psychol. 2007 Feb-Mar;62(2):95-108.
3. J Am Acad Child Adolesc Psychiatry. 1999 Oct;38(10):1230-6.
4. Soc Indic Res. 2009; 39:247-66.
5. “Flourish: A visionary new understanding of happiness and well-being” (New York: Free Press, 2011).
6. “The Resilience Drive” (Switzerland: Favre, 2017).
7. Am Psychol. 2005 Jul-Aug;60(5):410-21.

Risk of suicide attempt is higher in children of opioid users
according to an evaluation of a medical claims database from which a sample of more than 200,00 privately insured parents was evaluated.

Based on data collected between the years 2010 and 2016, the study raises the possibility that rising rates of opioid prescriptions and rising rates of suicide in adolescents and children are linked, said David A. Brent, of the University of Pittsburgh, and associates.
The relationship was considered sufficiently strong that the authors recommended clinicians consider mental health screening of children whose parents are known to have had extensive opioid exposure.
Addressing both opioid use in parents and the mental health in their children “may help, at least in part, to reverse the current upward trend in mortality due to the twin epidemics of suicide and opioid overdose,” said Dr. Brent and associates, whose findings were published in JAMA Psychiatry.
From a pool of more than 1 million parents aged 30-50 years in the claims database, 121,306 parents with extensive opioid use – defined as receiving opioid prescriptions for more than 365 days between 2010 and 2016 – were matched with 121,306 controls in the same age range. Children aged 10-19 years in both groups were compared for suicide attempts.
Overall, the rate of prescription opioid use as defined for inclusion in this study was 5% in the target parent population evaluated in this claims database.
Of the 184,142 children with parents exposed to opioids, 678 (0.37%) attempted suicide versus 212 (0.14%) of the 148,395 children from the nonopioid group. Expressed as a rate per 10,000 person years, the figures were 11.7 and 5.9 for the opioid and nonopioid groups, respectively.
When translated into an odds ratio (OR), the increased risk of suicide was found to be almost twice as high (OR 1.99) among children with parents meeting the study criteria for prescription opioid use. The OR was only slightly reduced (OR 1.85) after adjustment for sex and age.
Suicide attempts overall were higher in daughters than sons and in older children (15 years of age or older) than younger (ages 10 to less than 15 years) whether or not parents were taking opioids, but the relative risk remained consistently higher across all these subgroups when comparing those whose parents were taking prescription opioids with those whose parents were not.
As in past studies, children were more likely to make a suicide attempt if they had a parent who had a history of attempting suicide. However, the authors reported a significantly elevated risk of a suicide attempt for children of prescription opioid users after adjustment for this factor as well as for child depression, parental depression, and parental substance use disorder (OR, 1.45).
The OR of a suicide attempt was not significantly higher for a suicide attempt among those children with both parents taking prescription opioids relative to opioid use in only one parent (OR 1.05).
Dr. Brent and associates acknowledged that these data do not confirm that the rising rate of prescription opioid use is linked to the recent parallel rise in suicide attempts among children. However, they did conclude that children of parents using opioid prescriptions are at risk and might be an appropriate target for suicide prevention.
“Recognition and treatment of patients with opioid use disorder, attendance to comorbid conditions in affected parents, and screening and appropriate referral of their children may help” address both major public health issues, they maintained.
The study was supported by a National Institutes of Health grant. Dr Brent reported receiving royalties from Guilford Press, eRT, and UpToDate. Dr. Gibbons has served as an expert witness in cases related to suicide involving pharmaceutical companies, such as Pfizer and GlaxoSmithKline.
SOURCE: Brent DA et al. JAMA Psychiatry. 2019 May 22 doi: 10.1001/jamapsychiatry.2019.0940.
according to an evaluation of a medical claims database from which a sample of more than 200,00 privately insured parents was evaluated.
Based on data collected between the years 2010 and 2016, the study raises the possibility that rising rates of opioid prescriptions and rising rates of suicide in adolescents and children are linked, said David A. Brent, of the University of Pittsburgh, and associates.
The relationship was considered sufficiently strong that the authors recommended clinicians consider mental health screening of children whose parents are known to have had extensive opioid exposure.
Addressing both opioid use in parents and the mental health in their children “may help, at least in part, to reverse the current upward trend in mortality due to the twin epidemics of suicide and opioid overdose,” said Dr. Brent and associates, whose findings were published in JAMA Psychiatry.
From a pool of more than 1 million parents aged 30-50 years in the claims database, 121,306 parents with extensive opioid use – defined as receiving opioid prescriptions for more than 365 days between 2010 and 2016 – were matched with 121,306 controls in the same age range. Children aged 10-19 years in both groups were compared for suicide attempts.
Overall, the rate of prescription opioid use as defined for inclusion in this study was 5% in the target parent population evaluated in this claims database.
Of the 184,142 children with parents exposed to opioids, 678 (0.37%) attempted suicide versus 212 (0.14%) of the 148,395 children from the nonopioid group. Expressed as a rate per 10,000 person years, the figures were 11.7 and 5.9 for the opioid and nonopioid groups, respectively.
When translated into an odds ratio (OR), the increased risk of suicide was found to be almost twice as high (OR 1.99) among children with parents meeting the study criteria for prescription opioid use. The OR was only slightly reduced (OR 1.85) after adjustment for sex and age.
Suicide attempts overall were higher in daughters than sons and in older children (15 years of age or older) than younger (ages 10 to less than 15 years) whether or not parents were taking opioids, but the relative risk remained consistently higher across all these subgroups when comparing those whose parents were taking prescription opioids with those whose parents were not.
As in past studies, children were more likely to make a suicide attempt if they had a parent who had a history of attempting suicide. However, the authors reported a significantly elevated risk of a suicide attempt for children of prescription opioid users after adjustment for this factor as well as for child depression, parental depression, and parental substance use disorder (OR, 1.45).
The OR of a suicide attempt was not significantly higher for a suicide attempt among those children with both parents taking prescription opioids relative to opioid use in only one parent (OR 1.05).
Dr. Brent and associates acknowledged that these data do not confirm that the rising rate of prescription opioid use is linked to the recent parallel rise in suicide attempts among children. However, they did conclude that children of parents using opioid prescriptions are at risk and might be an appropriate target for suicide prevention.
“Recognition and treatment of patients with opioid use disorder, attendance to comorbid conditions in affected parents, and screening and appropriate referral of their children may help” address both major public health issues, they maintained.
The study was supported by a National Institutes of Health grant. Dr Brent reported receiving royalties from Guilford Press, eRT, and UpToDate. Dr. Gibbons has served as an expert witness in cases related to suicide involving pharmaceutical companies, such as Pfizer and GlaxoSmithKline.
SOURCE: Brent DA et al. JAMA Psychiatry. 2019 May 22 doi: 10.1001/jamapsychiatry.2019.0940.
according to an evaluation of a medical claims database from which a sample of more than 200,00 privately insured parents was evaluated.
Based on data collected between the years 2010 and 2016, the study raises the possibility that rising rates of opioid prescriptions and rising rates of suicide in adolescents and children are linked, said David A. Brent, of the University of Pittsburgh, and associates.
The relationship was considered sufficiently strong that the authors recommended clinicians consider mental health screening of children whose parents are known to have had extensive opioid exposure.
Addressing both opioid use in parents and the mental health in their children “may help, at least in part, to reverse the current upward trend in mortality due to the twin epidemics of suicide and opioid overdose,” said Dr. Brent and associates, whose findings were published in JAMA Psychiatry.
From a pool of more than 1 million parents aged 30-50 years in the claims database, 121,306 parents with extensive opioid use – defined as receiving opioid prescriptions for more than 365 days between 2010 and 2016 – were matched with 121,306 controls in the same age range. Children aged 10-19 years in both groups were compared for suicide attempts.
Overall, the rate of prescription opioid use as defined for inclusion in this study was 5% in the target parent population evaluated in this claims database.
Of the 184,142 children with parents exposed to opioids, 678 (0.37%) attempted suicide versus 212 (0.14%) of the 148,395 children from the nonopioid group. Expressed as a rate per 10,000 person years, the figures were 11.7 and 5.9 for the opioid and nonopioid groups, respectively.
When translated into an odds ratio (OR), the increased risk of suicide was found to be almost twice as high (OR 1.99) among children with parents meeting the study criteria for prescription opioid use. The OR was only slightly reduced (OR 1.85) after adjustment for sex and age.
Suicide attempts overall were higher in daughters than sons and in older children (15 years of age or older) than younger (ages 10 to less than 15 years) whether or not parents were taking opioids, but the relative risk remained consistently higher across all these subgroups when comparing those whose parents were taking prescription opioids with those whose parents were not.
As in past studies, children were more likely to make a suicide attempt if they had a parent who had a history of attempting suicide. However, the authors reported a significantly elevated risk of a suicide attempt for children of prescription opioid users after adjustment for this factor as well as for child depression, parental depression, and parental substance use disorder (OR, 1.45).
The OR of a suicide attempt was not significantly higher for a suicide attempt among those children with both parents taking prescription opioids relative to opioid use in only one parent (OR 1.05).
Dr. Brent and associates acknowledged that these data do not confirm that the rising rate of prescription opioid use is linked to the recent parallel rise in suicide attempts among children. However, they did conclude that children of parents using opioid prescriptions are at risk and might be an appropriate target for suicide prevention.
“Recognition and treatment of patients with opioid use disorder, attendance to comorbid conditions in affected parents, and screening and appropriate referral of their children may help” address both major public health issues, they maintained.
The study was supported by a National Institutes of Health grant. Dr Brent reported receiving royalties from Guilford Press, eRT, and UpToDate. Dr. Gibbons has served as an expert witness in cases related to suicide involving pharmaceutical companies, such as Pfizer and GlaxoSmithKline.
SOURCE: Brent DA et al. JAMA Psychiatry. 2019 May 22 doi: 10.1001/jamapsychiatry.2019.0940.
FROM JAMA PSYCHIATRY
Addressing the sexual and reproductive health needs of trans and gender nonconforming patients
Separating gender identity from sexual identity to allow for more comprehensive history-taking
Grouping the term “transgender” in the abbreviation LGBT (lesbian, gay, bisexual, transgender) has historically been empowering for trans and gender nonconforming (GNC) persons. However, it also has contributed to the misunderstanding that gender identity is interchangeable with sexual identity. This common misconception can be a barrier to trans and GNC patients seeking care from ob.gyns. for their reproductive health needs.

By definition, gender identity refers to an internal experience of one’s gender, of one’s self.1 While gender identity has social implications, it ultimately is something that a person experiences independently of interactions with others. By contrast, sexual orientation has an explicitly relational underpinning because sexual orientation involves attraction to others. The distinction between gender identity and sexual orientation is similar to an internal-versus-external, or a self-versus-other dichotomy. A further nuance to add is that sexual behavior does not always reflect sexual orientation, and sexual behavior can vary along a wide spectrum when gender identity is added to the equation.
Overall, When approaching a sexual history with any patient, but especially a transgender or GNC patient, providers should think deeply about what information is medically relevant.2 The purpose of a sexual history is to identify behaviors that contribute to health risk, including pregnancy, sexually transmitted infection, and social problems such as sex-trafficking or intimate partner violence. The health care provider’s job is to ask questions that will uncover these risk factors.
With the advent of a more inclusive attitude toward gay and lesbian partnership, many providers already have learned to collect the sexual history without assuming the gender of a person’s sexual contacts. Still, when a provider is taking the sexual history, gender often is inappropriately used as proxy for the type of sex that a patient may be having. For example, a provider asking a cisgender woman about her sexual activity may ask, “how many sexual partners have you had in the last year?” But then, the provider may follow-up her response of “three sexual partners in the last year” by asking “men, women, or both?” By asking a patient if the patient’s sexual partners are “men, women, or both,” providers fail to accurately elucidate the risk factors that they are actually seeking when taking a sexual history. The cisgender woman from the above scenario may reply that she has been sleeping only with women for the last year, but if the sexual partners are transgender women, aka a woman who was assigned male at birth and therefore still may use her penis/testes for sexual purposes, then the patient actually may be at risk for pregnancy and may also have a different risk factor profile for sexually transmitted infections than if the patient were sexually active with cisgender women.

A different approach to using gender in taking the sexual history is to speak plainly about which sex organs come into contact during sexual activity. When patients identify as transgender or GNC, a provider first should start by asking them what language they would like providers to use when discussing sex organs.3 One example is that many trans men, both those who have undergone mastectomy as well as those who have not, may not use the word “breasts” to describe their “chests.” This distinction may make the difference between gaining and losing the trust of a trans/GNC patient in your clinic. After identifying how a patient would like to refer to sex organs, a provider can continue by asking which of the patient’s sex partners’ organs come into contact with the patient’s organs during sexual activity. Alternatively, starting with an even more broad line of questioning may be best for some patients, such as “how do you like to have sex?”

Carefully identifying the type of sex and what sex organs are involved has concrete medical implications. Patients assigned female at birth who are on hormone therapy with testosterone may need supportive care if they continue to use their vaginas in sexual encounters because testosterone can lead to a relatively hypoestrogenic state. Patients assigned male at birth who have undergone vaginoplasty procedures may need counseling about how to use and support their neovaginas as well as adjusted testing for dysplasia. Patients assigned female at birth who want to avoid pregnancy may need a nuanced consultation regarding contraception. These are just a few examples of how obstetrician-gynecologists can better support the sexual health of their trans/GNC patients by having an accurate understanding of how a trans/GNC person has sex.
Dr. Joyner is an assistant professor at Emory University, Atlanta, and is the director of gynecologic services in the Gender Center at Grady Memorial Hospital in Atlanta. Dr. Joyner identifies as a cisgender female and uses she/hers/her as her personal pronouns. Dr. Joey Bahng is a PGY-1 resident physician in Emory University’s gynecology & obstetrics residency program. Dr. Bahng identifies as nonbinary and uses they/them/their as their personal pronouns. Dr. Bahng and Dr. Joyner reported no relevant financial disclosures
References
1. Sexual orientation and gender identity definitions. Human Rights Campaign.
2. Taking a sexual history from transgender people. Transforming Health at the Centers for Disease Control and Prevention.
3. Sexual health history: Talking sex with gender non-conforming and trans patients. National LGBT Health Education Center at The Fenway Institute.
Separating gender identity from sexual identity to allow for more comprehensive history-taking
Separating gender identity from sexual identity to allow for more comprehensive history-taking
Grouping the term “transgender” in the abbreviation LGBT (lesbian, gay, bisexual, transgender) has historically been empowering for trans and gender nonconforming (GNC) persons. However, it also has contributed to the misunderstanding that gender identity is interchangeable with sexual identity. This common misconception can be a barrier to trans and GNC patients seeking care from ob.gyns. for their reproductive health needs.
By definition, gender identity refers to an internal experience of one’s gender, of one’s self.1 While gender identity has social implications, it ultimately is something that a person experiences independently of interactions with others. By contrast, sexual orientation has an explicitly relational underpinning because sexual orientation involves attraction to others. The distinction between gender identity and sexual orientation is similar to an internal-versus-external, or a self-versus-other dichotomy. A further nuance to add is that sexual behavior does not always reflect sexual orientation, and sexual behavior can vary along a wide spectrum when gender identity is added to the equation.
Overall, When approaching a sexual history with any patient, but especially a transgender or GNC patient, providers should think deeply about what information is medically relevant.2 The purpose of a sexual history is to identify behaviors that contribute to health risk, including pregnancy, sexually transmitted infection, and social problems such as sex-trafficking or intimate partner violence. The health care provider’s job is to ask questions that will uncover these risk factors.
With the advent of a more inclusive attitude toward gay and lesbian partnership, many providers already have learned to collect the sexual history without assuming the gender of a person’s sexual contacts. Still, when a provider is taking the sexual history, gender often is inappropriately used as proxy for the type of sex that a patient may be having. For example, a provider asking a cisgender woman about her sexual activity may ask, “how many sexual partners have you had in the last year?” But then, the provider may follow-up her response of “three sexual partners in the last year” by asking “men, women, or both?” By asking a patient if the patient’s sexual partners are “men, women, or both,” providers fail to accurately elucidate the risk factors that they are actually seeking when taking a sexual history. The cisgender woman from the above scenario may reply that she has been sleeping only with women for the last year, but if the sexual partners are transgender women, aka a woman who was assigned male at birth and therefore still may use her penis/testes for sexual purposes, then the patient actually may be at risk for pregnancy and may also have a different risk factor profile for sexually transmitted infections than if the patient were sexually active with cisgender women.
A different approach to using gender in taking the sexual history is to speak plainly about which sex organs come into contact during sexual activity. When patients identify as transgender or GNC, a provider first should start by asking them what language they would like providers to use when discussing sex organs.3 One example is that many trans men, both those who have undergone mastectomy as well as those who have not, may not use the word “breasts” to describe their “chests.” This distinction may make the difference between gaining and losing the trust of a trans/GNC patient in your clinic. After identifying how a patient would like to refer to sex organs, a provider can continue by asking which of the patient’s sex partners’ organs come into contact with the patient’s organs during sexual activity. Alternatively, starting with an even more broad line of questioning may be best for some patients, such as “how do you like to have sex?”
Carefully identifying the type of sex and what sex organs are involved has concrete medical implications. Patients assigned female at birth who are on hormone therapy with testosterone may need supportive care if they continue to use their vaginas in sexual encounters because testosterone can lead to a relatively hypoestrogenic state. Patients assigned male at birth who have undergone vaginoplasty procedures may need counseling about how to use and support their neovaginas as well as adjusted testing for dysplasia. Patients assigned female at birth who want to avoid pregnancy may need a nuanced consultation regarding contraception. These are just a few examples of how obstetrician-gynecologists can better support the sexual health of their trans/GNC patients by having an accurate understanding of how a trans/GNC person has sex.
Dr. Joyner is an assistant professor at Emory University, Atlanta, and is the director of gynecologic services in the Gender Center at Grady Memorial Hospital in Atlanta. Dr. Joyner identifies as a cisgender female and uses she/hers/her as her personal pronouns. Dr. Joey Bahng is a PGY-1 resident physician in Emory University’s gynecology & obstetrics residency program. Dr. Bahng identifies as nonbinary and uses they/them/their as their personal pronouns. Dr. Bahng and Dr. Joyner reported no relevant financial disclosures
References
1. Sexual orientation and gender identity definitions. Human Rights Campaign.
2. Taking a sexual history from transgender people. Transforming Health at the Centers for Disease Control and Prevention.
3. Sexual health history: Talking sex with gender non-conforming and trans patients. National LGBT Health Education Center at The Fenway Institute.
Grouping the term “transgender” in the abbreviation LGBT (lesbian, gay, bisexual, transgender) has historically been empowering for trans and gender nonconforming (GNC) persons. However, it also has contributed to the misunderstanding that gender identity is interchangeable with sexual identity. This common misconception can be a barrier to trans and GNC patients seeking care from ob.gyns. for their reproductive health needs.
By definition, gender identity refers to an internal experience of one’s gender, of one’s self.1 While gender identity has social implications, it ultimately is something that a person experiences independently of interactions with others. By contrast, sexual orientation has an explicitly relational underpinning because sexual orientation involves attraction to others. The distinction between gender identity and sexual orientation is similar to an internal-versus-external, or a self-versus-other dichotomy. A further nuance to add is that sexual behavior does not always reflect sexual orientation, and sexual behavior can vary along a wide spectrum when gender identity is added to the equation.
Overall, When approaching a sexual history with any patient, but especially a transgender or GNC patient, providers should think deeply about what information is medically relevant.2 The purpose of a sexual history is to identify behaviors that contribute to health risk, including pregnancy, sexually transmitted infection, and social problems such as sex-trafficking or intimate partner violence. The health care provider’s job is to ask questions that will uncover these risk factors.
With the advent of a more inclusive attitude toward gay and lesbian partnership, many providers already have learned to collect the sexual history without assuming the gender of a person’s sexual contacts. Still, when a provider is taking the sexual history, gender often is inappropriately used as proxy for the type of sex that a patient may be having. For example, a provider asking a cisgender woman about her sexual activity may ask, “how many sexual partners have you had in the last year?” But then, the provider may follow-up her response of “three sexual partners in the last year” by asking “men, women, or both?” By asking a patient if the patient’s sexual partners are “men, women, or both,” providers fail to accurately elucidate the risk factors that they are actually seeking when taking a sexual history. The cisgender woman from the above scenario may reply that she has been sleeping only with women for the last year, but if the sexual partners are transgender women, aka a woman who was assigned male at birth and therefore still may use her penis/testes for sexual purposes, then the patient actually may be at risk for pregnancy and may also have a different risk factor profile for sexually transmitted infections than if the patient were sexually active with cisgender women.
A different approach to using gender in taking the sexual history is to speak plainly about which sex organs come into contact during sexual activity. When patients identify as transgender or GNC, a provider first should start by asking them what language they would like providers to use when discussing sex organs.3 One example is that many trans men, both those who have undergone mastectomy as well as those who have not, may not use the word “breasts” to describe their “chests.” This distinction may make the difference between gaining and losing the trust of a trans/GNC patient in your clinic. After identifying how a patient would like to refer to sex organs, a provider can continue by asking which of the patient’s sex partners’ organs come into contact with the patient’s organs during sexual activity. Alternatively, starting with an even more broad line of questioning may be best for some patients, such as “how do you like to have sex?”
Carefully identifying the type of sex and what sex organs are involved has concrete medical implications. Patients assigned female at birth who are on hormone therapy with testosterone may need supportive care if they continue to use their vaginas in sexual encounters because testosterone can lead to a relatively hypoestrogenic state. Patients assigned male at birth who have undergone vaginoplasty procedures may need counseling about how to use and support their neovaginas as well as adjusted testing for dysplasia. Patients assigned female at birth who want to avoid pregnancy may need a nuanced consultation regarding contraception. These are just a few examples of how obstetrician-gynecologists can better support the sexual health of their trans/GNC patients by having an accurate understanding of how a trans/GNC person has sex.
Dr. Joyner is an assistant professor at Emory University, Atlanta, and is the director of gynecologic services in the Gender Center at Grady Memorial Hospital in Atlanta. Dr. Joyner identifies as a cisgender female and uses she/hers/her as her personal pronouns. Dr. Joey Bahng is a PGY-1 resident physician in Emory University’s gynecology & obstetrics residency program. Dr. Bahng identifies as nonbinary and uses they/them/their as their personal pronouns. Dr. Bahng and Dr. Joyner reported no relevant financial disclosures
References
1. Sexual orientation and gender identity definitions. Human Rights Campaign.
2. Taking a sexual history from transgender people. Transforming Health at the Centers for Disease Control and Prevention.
3. Sexual health history: Talking sex with gender non-conforming and trans patients. National LGBT Health Education Center at The Fenway Institute.

Low-dose FVIII prophylaxis reduced bleeding in hemophilia A
The findings have implications for low resource countries, the researchers reported.
Novie A. Chozie, MD, of Universitas Indonesia in Jakarta, along with colleagues, conducted a parallel-group, randomized controlled study of 50 children with severe hemophilia A. Study participants were randomized to receive either low‐dose FVIII prophylaxis (n = 25) or on‐demand treatment (n = 25) for a total of 12 months. The findings were published in Haemophilia.
Participants in the prophylaxis arm received FVIII at a dose of 10 IU/kg, infused twice weekly. If patients experienced an episode of acute bleeding, prophylaxis was delayed until the episode resolved.
The primary outcome was the number of total and joint bleeding events from the start of therapy to 12 months. Secondary outcomes included evidence of FVIII inhibitor, Hemophilia Joint Health Score (HJHS), and Hemophilia Early Arthropathy Detection Ultrasound (HEAD‐US) score.
After analysis, the team found that the number of joint and total bleeding events was significantly lower in the prophylaxis group. For total bleeding events, there was a median of 8 events with the prophylaxis group, compared with 25 in the on-demand treatment group (P less than .001). There was a median of three joint bleeding events in the prophylaxis group versus nine in the on-demand group (P less than .001).
Patients in the prophylaxis arm also showed improved joint function (P = .004), while those in the on‐demand arm showed evidence of deterioration (P = .001).
Two key limitations of the study were short duration of follow-up and single‐center design, which could have limited the generalizability of the results.
“In countries with limited resources, low‐dose prophylaxis is strongly recommended as a therapeutic option for severe haemophilia A [in] children,” the researchers wrote.
The study was funded by Grifols. The authors reported having no conflicts of interest.
SOURCE: Chozie NA et al. Haemophilia. 2019 May 2. doi: 10.1111/hae.13770.
The findings have implications for low resource countries, the researchers reported.
Novie A. Chozie, MD, of Universitas Indonesia in Jakarta, along with colleagues, conducted a parallel-group, randomized controlled study of 50 children with severe hemophilia A. Study participants were randomized to receive either low‐dose FVIII prophylaxis (n = 25) or on‐demand treatment (n = 25) for a total of 12 months. The findings were published in Haemophilia.
Participants in the prophylaxis arm received FVIII at a dose of 10 IU/kg, infused twice weekly. If patients experienced an episode of acute bleeding, prophylaxis was delayed until the episode resolved.
The primary outcome was the number of total and joint bleeding events from the start of therapy to 12 months. Secondary outcomes included evidence of FVIII inhibitor, Hemophilia Joint Health Score (HJHS), and Hemophilia Early Arthropathy Detection Ultrasound (HEAD‐US) score.
After analysis, the team found that the number of joint and total bleeding events was significantly lower in the prophylaxis group. For total bleeding events, there was a median of 8 events with the prophylaxis group, compared with 25 in the on-demand treatment group (P less than .001). There was a median of three joint bleeding events in the prophylaxis group versus nine in the on-demand group (P less than .001).
Patients in the prophylaxis arm also showed improved joint function (P = .004), while those in the on‐demand arm showed evidence of deterioration (P = .001).
Two key limitations of the study were short duration of follow-up and single‐center design, which could have limited the generalizability of the results.
“In countries with limited resources, low‐dose prophylaxis is strongly recommended as a therapeutic option for severe haemophilia A [in] children,” the researchers wrote.
The study was funded by Grifols. The authors reported having no conflicts of interest.
SOURCE: Chozie NA et al. Haemophilia. 2019 May 2. doi: 10.1111/hae.13770.
The findings have implications for low resource countries, the researchers reported.
Novie A. Chozie, MD, of Universitas Indonesia in Jakarta, along with colleagues, conducted a parallel-group, randomized controlled study of 50 children with severe hemophilia A. Study participants were randomized to receive either low‐dose FVIII prophylaxis (n = 25) or on‐demand treatment (n = 25) for a total of 12 months. The findings were published in Haemophilia.
Participants in the prophylaxis arm received FVIII at a dose of 10 IU/kg, infused twice weekly. If patients experienced an episode of acute bleeding, prophylaxis was delayed until the episode resolved.
The primary outcome was the number of total and joint bleeding events from the start of therapy to 12 months. Secondary outcomes included evidence of FVIII inhibitor, Hemophilia Joint Health Score (HJHS), and Hemophilia Early Arthropathy Detection Ultrasound (HEAD‐US) score.
After analysis, the team found that the number of joint and total bleeding events was significantly lower in the prophylaxis group. For total bleeding events, there was a median of 8 events with the prophylaxis group, compared with 25 in the on-demand treatment group (P less than .001). There was a median of three joint bleeding events in the prophylaxis group versus nine in the on-demand group (P less than .001).
Patients in the prophylaxis arm also showed improved joint function (P = .004), while those in the on‐demand arm showed evidence of deterioration (P = .001).
Two key limitations of the study were short duration of follow-up and single‐center design, which could have limited the generalizability of the results.
“In countries with limited resources, low‐dose prophylaxis is strongly recommended as a therapeutic option for severe haemophilia A [in] children,” the researchers wrote.
The study was funded by Grifols. The authors reported having no conflicts of interest.
SOURCE: Chozie NA et al. Haemophilia. 2019 May 2. doi: 10.1111/hae.13770.
FROM HAEMOPHILIA
HM19: Pediatric sepsis
Improving recognition and treatment
Presenters
Elise van der Jagt, MD, MPH
Workshop title
What you need to know about pediatric sepsis
Session summary
Dr. Elise van der Jagt of the University of Rochester (N.Y.) Medical Center, introduced the topic of pediatric sepsis and its epidemiology with the story of 12-year-old Rory Staunton, who died in 2012 of sepsis. In pediatrics, sepsis is the 10th leading cause of death, with severe sepsis having a mortality rate of 4%-10%. As a response to Rory Staunton’s death from sepsis, New York Governor Andrew Cuomo mandated all hospitals to implement ways to improve recognition and treatment of septic shock, especially in children.
The definition and management of sepsis in pediatrics is complex, and forms a spectrum of disease from sepsis to severe sepsis, and septic shock. Dr. van der Jagt advised not to use the adult sepsis definition in children. Sepsis, stated Dr. van der Jagt, is systemic inflammatory response syndrome in association with suspected or proven infection. Severe sepsis is sepsis with cardiovascular dysfunction, respiratory dysfunction, or dysfunction of two other systems. Septic shock is sepsis with cardiovascular dysfunction that persists despite 40 mL/kg of fluid bolus in 1 hour.
Early recognition and management of sepsis decreases mortality. Early recognition can be improved by initiating a recognition bundle. Multiple trigger tools are available such as pSOFA (Pediatric Sequential Organ Failure Assessment). Any trigger tool, however, must be combined with physician evaluation. This clinician assessment should be initiated within 15 minutes for any patient who screens positive with a trigger tool.
Resuscitation bundles also decrease mortality. A good goal is establishing intravenous or intraosseous access within 5 minutes, fluid administration within 30 minutes, and antibiotics and inotrope administration (if needed) in 60 minutes. Resuscitation bundles could include a sepsis clock, rapid response team, check list, protocol, and order set. Additional studies are needed to determine which of the components of a sepsis bundle is most important. Studies show that mortality increases with delays in initiating fluids and less fluids given. However, giving too much fluid also increases morbidity. It is imperative, stated Dr. van der Jagt, to reassess after fluid boluses. Use of lactate measurement can be problematic in pediatrics, as normal lactate can be seen with florid sepsis.
Stabilization bundles are more common in the ICU setting. They include an arterial line, central venous pressure, cardiopulmonary monitor, urinary catheter, and pulse oximeter. A performance bundle is important to assess adherence to the other bundles. This could include providing debriefing, data review, feedback, and formal quality improvement projects. Assigning a sepsis champion in each area helps to overcome barriers and continue performance bundles.
Key takeaways for HM
- Patients with severe sepsis/septic shock should be rapidly identified with the 2014/2017 American College of Critical Care Medicine consensus criteria.
- Efficient, time-based care should be provided during the first hour after recognizing pediatric severe sepsis/septic shock.
- Overcoming systems barriers to rapid sepsis recognition and treatment requires sepsis champions in each area, continuous data collection and feedback, persistence, and patience.
Dr. Eboh is a pediatric hospitalist at Covenant Children’s Hospital in Lubbock, Texas, and assistant professor of pediatrics at Texas Tech University Health Sciences Center. Dr. Wright is a pediatric hospitalist at Texas Tech University Health Sciences Center.
Improving recognition and treatment
Improving recognition and treatment
Presenters
Elise van der Jagt, MD, MPH
Workshop title
What you need to know about pediatric sepsis
Session summary
Dr. Elise van der Jagt of the University of Rochester (N.Y.) Medical Center, introduced the topic of pediatric sepsis and its epidemiology with the story of 12-year-old Rory Staunton, who died in 2012 of sepsis. In pediatrics, sepsis is the 10th leading cause of death, with severe sepsis having a mortality rate of 4%-10%. As a response to Rory Staunton’s death from sepsis, New York Governor Andrew Cuomo mandated all hospitals to implement ways to improve recognition and treatment of septic shock, especially in children.
The definition and management of sepsis in pediatrics is complex, and forms a spectrum of disease from sepsis to severe sepsis, and septic shock. Dr. van der Jagt advised not to use the adult sepsis definition in children. Sepsis, stated Dr. van der Jagt, is systemic inflammatory response syndrome in association with suspected or proven infection. Severe sepsis is sepsis with cardiovascular dysfunction, respiratory dysfunction, or dysfunction of two other systems. Septic shock is sepsis with cardiovascular dysfunction that persists despite 40 mL/kg of fluid bolus in 1 hour.
Early recognition and management of sepsis decreases mortality. Early recognition can be improved by initiating a recognition bundle. Multiple trigger tools are available such as pSOFA (Pediatric Sequential Organ Failure Assessment). Any trigger tool, however, must be combined with physician evaluation. This clinician assessment should be initiated within 15 minutes for any patient who screens positive with a trigger tool.
Resuscitation bundles also decrease mortality. A good goal is establishing intravenous or intraosseous access within 5 minutes, fluid administration within 30 minutes, and antibiotics and inotrope administration (if needed) in 60 minutes. Resuscitation bundles could include a sepsis clock, rapid response team, check list, protocol, and order set. Additional studies are needed to determine which of the components of a sepsis bundle is most important. Studies show that mortality increases with delays in initiating fluids and less fluids given. However, giving too much fluid also increases morbidity. It is imperative, stated Dr. van der Jagt, to reassess after fluid boluses. Use of lactate measurement can be problematic in pediatrics, as normal lactate can be seen with florid sepsis.
Stabilization bundles are more common in the ICU setting. They include an arterial line, central venous pressure, cardiopulmonary monitor, urinary catheter, and pulse oximeter. A performance bundle is important to assess adherence to the other bundles. This could include providing debriefing, data review, feedback, and formal quality improvement projects. Assigning a sepsis champion in each area helps to overcome barriers and continue performance bundles.
Key takeaways for HM
- Patients with severe sepsis/septic shock should be rapidly identified with the 2014/2017 American College of Critical Care Medicine consensus criteria.
- Efficient, time-based care should be provided during the first hour after recognizing pediatric severe sepsis/septic shock.
- Overcoming systems barriers to rapid sepsis recognition and treatment requires sepsis champions in each area, continuous data collection and feedback, persistence, and patience.
Dr. Eboh is a pediatric hospitalist at Covenant Children’s Hospital in Lubbock, Texas, and assistant professor of pediatrics at Texas Tech University Health Sciences Center. Dr. Wright is a pediatric hospitalist at Texas Tech University Health Sciences Center.
Presenters
Elise van der Jagt, MD, MPH
Workshop title
What you need to know about pediatric sepsis
Session summary
Dr. Elise van der Jagt of the University of Rochester (N.Y.) Medical Center, introduced the topic of pediatric sepsis and its epidemiology with the story of 12-year-old Rory Staunton, who died in 2012 of sepsis. In pediatrics, sepsis is the 10th leading cause of death, with severe sepsis having a mortality rate of 4%-10%. As a response to Rory Staunton’s death from sepsis, New York Governor Andrew Cuomo mandated all hospitals to implement ways to improve recognition and treatment of septic shock, especially in children.
The definition and management of sepsis in pediatrics is complex, and forms a spectrum of disease from sepsis to severe sepsis, and septic shock. Dr. van der Jagt advised not to use the adult sepsis definition in children. Sepsis, stated Dr. van der Jagt, is systemic inflammatory response syndrome in association with suspected or proven infection. Severe sepsis is sepsis with cardiovascular dysfunction, respiratory dysfunction, or dysfunction of two other systems. Septic shock is sepsis with cardiovascular dysfunction that persists despite 40 mL/kg of fluid bolus in 1 hour.
Early recognition and management of sepsis decreases mortality. Early recognition can be improved by initiating a recognition bundle. Multiple trigger tools are available such as pSOFA (Pediatric Sequential Organ Failure Assessment). Any trigger tool, however, must be combined with physician evaluation. This clinician assessment should be initiated within 15 minutes for any patient who screens positive with a trigger tool.
Resuscitation bundles also decrease mortality. A good goal is establishing intravenous or intraosseous access within 5 minutes, fluid administration within 30 minutes, and antibiotics and inotrope administration (if needed) in 60 minutes. Resuscitation bundles could include a sepsis clock, rapid response team, check list, protocol, and order set. Additional studies are needed to determine which of the components of a sepsis bundle is most important. Studies show that mortality increases with delays in initiating fluids and less fluids given. However, giving too much fluid also increases morbidity. It is imperative, stated Dr. van der Jagt, to reassess after fluid boluses. Use of lactate measurement can be problematic in pediatrics, as normal lactate can be seen with florid sepsis.
Stabilization bundles are more common in the ICU setting. They include an arterial line, central venous pressure, cardiopulmonary monitor, urinary catheter, and pulse oximeter. A performance bundle is important to assess adherence to the other bundles. This could include providing debriefing, data review, feedback, and formal quality improvement projects. Assigning a sepsis champion in each area helps to overcome barriers and continue performance bundles.
Key takeaways for HM
- Patients with severe sepsis/septic shock should be rapidly identified with the 2014/2017 American College of Critical Care Medicine consensus criteria.
- Efficient, time-based care should be provided during the first hour after recognizing pediatric severe sepsis/septic shock.
- Overcoming systems barriers to rapid sepsis recognition and treatment requires sepsis champions in each area, continuous data collection and feedback, persistence, and patience.
Dr. Eboh is a pediatric hospitalist at Covenant Children’s Hospital in Lubbock, Texas, and assistant professor of pediatrics at Texas Tech University Health Sciences Center. Dr. Wright is a pediatric hospitalist at Texas Tech University Health Sciences Center.

Keep sports fun, keep kids playing
according to a clinical report from the American Academy of Pediatrics’ Council on Sports Medicine and Fitness.

In the report, “Organized Sports for Children, Preadolescents, and Adolescents,” published online in Pediatrics, the authors addressed the risks and benefits of organized sports for children and teens and offered guidance for how clinicians, schools, and communities can involve more children in sports programs.
The authors emphasized the role of free play and the development of skills for children younger than 6 years. However, they wrote that you and parents should encourage organized sports – with emphasis on physical activity enjoyment – for children older than 6 years at a range of skill levels.
“Aspects of readiness to consider are motor skill acquisition, ability to combine those skills, and attention span,” according to the authors, who noted that most children younger than 6 years may not yet have the skills and attention for organized sports.
You also can remind parents to step back from pushing children into particular sports. Allowing children to choose which activities to try helps keep the focus on fun, even if the child’s idea of fun may differ from parental ideas. “Forcing children to participate in organized sports (or any physical activity) is likely to decrease fun in the activity and discourage future participation,” according to the authors.
They recognize barriers to organized sports for children from low socioeconomic backgrounds and advise communities to try to reduce them; other recommendations include having more options for organized sports at a range of skill levels to encourage participation and long-term involvement, and promoting physical activity.
“If we offer children a variety of sports for all skill levels, they are more likely to try new activities and stick with the ones they enjoy,” Kelsey Logan, MD, a coauthor of the report, said in a statement. “The interest should start with the child, not the parent.”
“Families can help by encouraging children to ‘sample’ sports, so they can figure out what they find enjoyable,” he said. “Ideally, there is an activity for everyone, with the focus on having fun.”
“Given the epidemic of obesity and all of its accompanying medical conditions, it is important to find ways to keep kids physically active. Organized sports participation is one tactic to accomplish this,” the authors said.
They acknowledge the potential risks involved in organized sports such as sports injuries, bullying, and burnout, but also advise empowering parents to support a positive coaching environment with playing time for all participants so they can enjoy the physical and mental benefits of being on a team.
“Young athletes typically learn skills and values that they can use in everyday life,” Steven Cuff, MD, coauthor of the report, said in a statement. “The camaraderie and teamwork needed on a playing field offers lasting lessons on personal responsibility, sportsmanship, goal-setting, and emotional control.”
Children with developmental and neurologic disabilities also can benefit from organized sports participation in programs such as Special Olympics, the authors said.
The report authors had no financial conflicts to disclose.
SOURCE: Logan K et al. Pediatrics. 2019 May 20. doi: 10.1542/peds.2019-0997.
“I think it is quite timely with the obesity epidemic and lack of PE in schools to highlight how important physical activity is for children, and organized sports is one of the ways to accomplish that,” Andrew Gregory, MD, said in an interview.
“I think the summary of both benefits and risks is well informed and complete,” he said.
However, “I think most pediatricians and parents are aware of the physical benefits of exercise, but many may be unaware of the psychological and social benefits,” Dr. Gregory noted. “It is also important that parents and coaches understand that bullying and hazing have no place in organized sports and should not be tolerated.”
“I think the most important thing for clinicians to pass on is that the benefits of organized sports far outweigh the risks,” he said. The challenge is, “How do we better incorporate organized sports into schools and community organizations so that more children have access?”
Dr. Gregory is an associate professor of orthopaedics, neurosurgery & pediatrics at Vanderbilt University in Nashville, Tenn., and serves as codirector of the Vanderbilt Sports Concussion Center. He had no financial conflicts to disclose.
“I think it is quite timely with the obesity epidemic and lack of PE in schools to highlight how important physical activity is for children, and organized sports is one of the ways to accomplish that,” Andrew Gregory, MD, said in an interview.
“I think the summary of both benefits and risks is well informed and complete,” he said.
However, “I think most pediatricians and parents are aware of the physical benefits of exercise, but many may be unaware of the psychological and social benefits,” Dr. Gregory noted. “It is also important that parents and coaches understand that bullying and hazing have no place in organized sports and should not be tolerated.”
“I think the most important thing for clinicians to pass on is that the benefits of organized sports far outweigh the risks,” he said. The challenge is, “How do we better incorporate organized sports into schools and community organizations so that more children have access?”
Dr. Gregory is an associate professor of orthopaedics, neurosurgery & pediatrics at Vanderbilt University in Nashville, Tenn., and serves as codirector of the Vanderbilt Sports Concussion Center. He had no financial conflicts to disclose.
“I think it is quite timely with the obesity epidemic and lack of PE in schools to highlight how important physical activity is for children, and organized sports is one of the ways to accomplish that,” Andrew Gregory, MD, said in an interview.
“I think the summary of both benefits and risks is well informed and complete,” he said.
However, “I think most pediatricians and parents are aware of the physical benefits of exercise, but many may be unaware of the psychological and social benefits,” Dr. Gregory noted. “It is also important that parents and coaches understand that bullying and hazing have no place in organized sports and should not be tolerated.”
“I think the most important thing for clinicians to pass on is that the benefits of organized sports far outweigh the risks,” he said. The challenge is, “How do we better incorporate organized sports into schools and community organizations so that more children have access?”
Dr. Gregory is an associate professor of orthopaedics, neurosurgery & pediatrics at Vanderbilt University in Nashville, Tenn., and serves as codirector of the Vanderbilt Sports Concussion Center. He had no financial conflicts to disclose.
according to a clinical report from the American Academy of Pediatrics’ Council on Sports Medicine and Fitness.
In the report, “Organized Sports for Children, Preadolescents, and Adolescents,” published online in Pediatrics, the authors addressed the risks and benefits of organized sports for children and teens and offered guidance for how clinicians, schools, and communities can involve more children in sports programs.
The authors emphasized the role of free play and the development of skills for children younger than 6 years. However, they wrote that you and parents should encourage organized sports – with emphasis on physical activity enjoyment – for children older than 6 years at a range of skill levels.
“Aspects of readiness to consider are motor skill acquisition, ability to combine those skills, and attention span,” according to the authors, who noted that most children younger than 6 years may not yet have the skills and attention for organized sports.
You also can remind parents to step back from pushing children into particular sports. Allowing children to choose which activities to try helps keep the focus on fun, even if the child’s idea of fun may differ from parental ideas. “Forcing children to participate in organized sports (or any physical activity) is likely to decrease fun in the activity and discourage future participation,” according to the authors.
They recognize barriers to organized sports for children from low socioeconomic backgrounds and advise communities to try to reduce them; other recommendations include having more options for organized sports at a range of skill levels to encourage participation and long-term involvement, and promoting physical activity.
“If we offer children a variety of sports for all skill levels, they are more likely to try new activities and stick with the ones they enjoy,” Kelsey Logan, MD, a coauthor of the report, said in a statement. “The interest should start with the child, not the parent.”
“Families can help by encouraging children to ‘sample’ sports, so they can figure out what they find enjoyable,” he said. “Ideally, there is an activity for everyone, with the focus on having fun.”
“Given the epidemic of obesity and all of its accompanying medical conditions, it is important to find ways to keep kids physically active. Organized sports participation is one tactic to accomplish this,” the authors said.
They acknowledge the potential risks involved in organized sports such as sports injuries, bullying, and burnout, but also advise empowering parents to support a positive coaching environment with playing time for all participants so they can enjoy the physical and mental benefits of being on a team.
“Young athletes typically learn skills and values that they can use in everyday life,” Steven Cuff, MD, coauthor of the report, said in a statement. “The camaraderie and teamwork needed on a playing field offers lasting lessons on personal responsibility, sportsmanship, goal-setting, and emotional control.”
Children with developmental and neurologic disabilities also can benefit from organized sports participation in programs such as Special Olympics, the authors said.
The report authors had no financial conflicts to disclose.
SOURCE: Logan K et al. Pediatrics. 2019 May 20. doi: 10.1542/peds.2019-0997.
according to a clinical report from the American Academy of Pediatrics’ Council on Sports Medicine and Fitness.
In the report, “Organized Sports for Children, Preadolescents, and Adolescents,” published online in Pediatrics, the authors addressed the risks and benefits of organized sports for children and teens and offered guidance for how clinicians, schools, and communities can involve more children in sports programs.
The authors emphasized the role of free play and the development of skills for children younger than 6 years. However, they wrote that you and parents should encourage organized sports – with emphasis on physical activity enjoyment – for children older than 6 years at a range of skill levels.
“Aspects of readiness to consider are motor skill acquisition, ability to combine those skills, and attention span,” according to the authors, who noted that most children younger than 6 years may not yet have the skills and attention for organized sports.
You also can remind parents to step back from pushing children into particular sports. Allowing children to choose which activities to try helps keep the focus on fun, even if the child’s idea of fun may differ from parental ideas. “Forcing children to participate in organized sports (or any physical activity) is likely to decrease fun in the activity and discourage future participation,” according to the authors.
They recognize barriers to organized sports for children from low socioeconomic backgrounds and advise communities to try to reduce them; other recommendations include having more options for organized sports at a range of skill levels to encourage participation and long-term involvement, and promoting physical activity.
“If we offer children a variety of sports for all skill levels, they are more likely to try new activities and stick with the ones they enjoy,” Kelsey Logan, MD, a coauthor of the report, said in a statement. “The interest should start with the child, not the parent.”
“Families can help by encouraging children to ‘sample’ sports, so they can figure out what they find enjoyable,” he said. “Ideally, there is an activity for everyone, with the focus on having fun.”
“Given the epidemic of obesity and all of its accompanying medical conditions, it is important to find ways to keep kids physically active. Organized sports participation is one tactic to accomplish this,” the authors said.
They acknowledge the potential risks involved in organized sports such as sports injuries, bullying, and burnout, but also advise empowering parents to support a positive coaching environment with playing time for all participants so they can enjoy the physical and mental benefits of being on a team.
“Young athletes typically learn skills and values that they can use in everyday life,” Steven Cuff, MD, coauthor of the report, said in a statement. “The camaraderie and teamwork needed on a playing field offers lasting lessons on personal responsibility, sportsmanship, goal-setting, and emotional control.”
Children with developmental and neurologic disabilities also can benefit from organized sports participation in programs such as Special Olympics, the authors said.
The report authors had no financial conflicts to disclose.
SOURCE: Logan K et al. Pediatrics. 2019 May 20. doi: 10.1542/peds.2019-0997.
FROM PEDIATRICS