User login
ADHD rates holding steady in U.S. children
TOPLINE:
While the prevalence of attention-deficit/hyperactivity disorder in U.S. children increased from the late 1990s to 2016,
METHODOLOGY:
- Based on prior data, the prevalence of ADHD in children rose from 6.1% in 1997-1998 to 10.2% in 2015-2016, with a 42.0% increase from 2003 to 2011. The new report provides updated prevalence data for 2017-2022.
- The cross-sectional analysis used data from the National Health Interview Survey (NHIS) from 2017 to 2022 for more than 37,609 U.S. children and adolescents 4-17 years old (52% male, 53% non-Hispanic White, 24% Hispanic, 11% non-Hispanic Black, and 12% non-Hispanic other race).
- Information on health care provider–diagnosed ADHD was reported by a parent or guardian.
TAKEAWAY:
- A total of 4,098 children and adolescents (10.9%) were reported to have an ADHD diagnosis during the study period.
- The weighted prevalence of ADHD ranged from 10.08% to 10.47% from 2017 to 2022, which is similar to the prevalence in 2015-2016 (10.20%).
- There was no significant change on an annual basis or in all subgroups evaluated. Notably, the estimated prevalence of ADHD among U.S. children and adolescents was higher than worldwide estimates (5.3%) in earlier years (1978-2005).
- The prevalence of ADHD in U.S. children differed significantly by age, sex, race/ethnicity, and family income, in line with previous findings, with higher rates in those 12-17 years (vs. 4-11 years), males, non-Hispanic populations, and those with higher family income.
IN PRACTICE:
The estimated ADHD prevalence remains “high” and “further investigation is warranted to assess potentially modifiable risk factors and provide adequate resources for treatment of individuals with ADHD in the future,” the authors write.
SOURCE:
The study, with first author Yanmei Li, Guangdong Pharmaceutical University, Guangzhou, China, was published online in JAMA Network Open.
LIMITATIONS:
Information on ADHD relied on parent-reported diagnosis, which may lead to misreporting and recall bias. The NHIS underwent a major redesign in 2019, which may affect comparability with prior years, and the COVID-19 pandemic affected collection in 2020.
DISCLOSURES:
The study had no specific funding. The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TOPLINE:
While the prevalence of attention-deficit/hyperactivity disorder in U.S. children increased from the late 1990s to 2016,
METHODOLOGY:
- Based on prior data, the prevalence of ADHD in children rose from 6.1% in 1997-1998 to 10.2% in 2015-2016, with a 42.0% increase from 2003 to 2011. The new report provides updated prevalence data for 2017-2022.
- The cross-sectional analysis used data from the National Health Interview Survey (NHIS) from 2017 to 2022 for more than 37,609 U.S. children and adolescents 4-17 years old (52% male, 53% non-Hispanic White, 24% Hispanic, 11% non-Hispanic Black, and 12% non-Hispanic other race).
- Information on health care provider–diagnosed ADHD was reported by a parent or guardian.
TAKEAWAY:
- A total of 4,098 children and adolescents (10.9%) were reported to have an ADHD diagnosis during the study period.
- The weighted prevalence of ADHD ranged from 10.08% to 10.47% from 2017 to 2022, which is similar to the prevalence in 2015-2016 (10.20%).
- There was no significant change on an annual basis or in all subgroups evaluated. Notably, the estimated prevalence of ADHD among U.S. children and adolescents was higher than worldwide estimates (5.3%) in earlier years (1978-2005).
- The prevalence of ADHD in U.S. children differed significantly by age, sex, race/ethnicity, and family income, in line with previous findings, with higher rates in those 12-17 years (vs. 4-11 years), males, non-Hispanic populations, and those with higher family income.
IN PRACTICE:
The estimated ADHD prevalence remains “high” and “further investigation is warranted to assess potentially modifiable risk factors and provide adequate resources for treatment of individuals with ADHD in the future,” the authors write.
SOURCE:
The study, with first author Yanmei Li, Guangdong Pharmaceutical University, Guangzhou, China, was published online in JAMA Network Open.
LIMITATIONS:
Information on ADHD relied on parent-reported diagnosis, which may lead to misreporting and recall bias. The NHIS underwent a major redesign in 2019, which may affect comparability with prior years, and the COVID-19 pandemic affected collection in 2020.
DISCLOSURES:
The study had no specific funding. The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TOPLINE:
While the prevalence of attention-deficit/hyperactivity disorder in U.S. children increased from the late 1990s to 2016,
METHODOLOGY:
- Based on prior data, the prevalence of ADHD in children rose from 6.1% in 1997-1998 to 10.2% in 2015-2016, with a 42.0% increase from 2003 to 2011. The new report provides updated prevalence data for 2017-2022.
- The cross-sectional analysis used data from the National Health Interview Survey (NHIS) from 2017 to 2022 for more than 37,609 U.S. children and adolescents 4-17 years old (52% male, 53% non-Hispanic White, 24% Hispanic, 11% non-Hispanic Black, and 12% non-Hispanic other race).
- Information on health care provider–diagnosed ADHD was reported by a parent or guardian.
TAKEAWAY:
- A total of 4,098 children and adolescents (10.9%) were reported to have an ADHD diagnosis during the study period.
- The weighted prevalence of ADHD ranged from 10.08% to 10.47% from 2017 to 2022, which is similar to the prevalence in 2015-2016 (10.20%).
- There was no significant change on an annual basis or in all subgroups evaluated. Notably, the estimated prevalence of ADHD among U.S. children and adolescents was higher than worldwide estimates (5.3%) in earlier years (1978-2005).
- The prevalence of ADHD in U.S. children differed significantly by age, sex, race/ethnicity, and family income, in line with previous findings, with higher rates in those 12-17 years (vs. 4-11 years), males, non-Hispanic populations, and those with higher family income.
IN PRACTICE:
The estimated ADHD prevalence remains “high” and “further investigation is warranted to assess potentially modifiable risk factors and provide adequate resources for treatment of individuals with ADHD in the future,” the authors write.
SOURCE:
The study, with first author Yanmei Li, Guangdong Pharmaceutical University, Guangzhou, China, was published online in JAMA Network Open.
LIMITATIONS:
Information on ADHD relied on parent-reported diagnosis, which may lead to misreporting and recall bias. The NHIS underwent a major redesign in 2019, which may affect comparability with prior years, and the COVID-19 pandemic affected collection in 2020.
DISCLOSURES:
The study had no specific funding. The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Intravenous formulation of secukinumab gets FDA approval
The Food and Drug Administration has approved an intravenous (IV) formulation of secukinumab (Cosentyx) for the treatment of adults with psoriatic arthritis (PsA), ankylosing spondylitis (AS), and nonradiographic axial spondyloarthritis (nr-axSpA).

Secukinumab is the only treatment approved in an IV formulation that specifically targets and blocks interleukin-17A and the only non–tumor necrosis factor alpha IV option available to treat the three indications of PsA, AS, and nr-axSpA, according to a press release from the drug’s manufacturer, Novartis.
The approval marks the first new IV treatment in 6 years for these three conditions. The drug was first approved in 2015 and up to now has been available only as a subcutaneous injection.
The new formulation is also approved for secukinumab’s other indications of plaque psoriasis in people aged 6 years or older, children aged 2 years or older with PsA, and enthesitis-related arthritis in patients aged 4 years or older.
“A significant portion of the millions of PsA, AS, and nr-axSpA patients in the United States require treatment through IV infusions for a variety of reasons, including not being comfortable with self-injections or simply preferring to have treatments administered in their health care provider’s office,” Philip J. Mease, MD, clinical professor at the University of Washington, Seattle, and director of rheumatology research at the Swedish Medical Center, Seattle, said in the press release. “The approval of Cosentyx as an IV formulation is an important milestone for patients because it expands the treatment options available to them with a different mechanism of action than existing biologic IV therapies, along with the comfort and familiarity of an established treatment.”
This IV formulation is administered monthly in a 30-minute, weight-based dosing regimen. This new option will become available before the end of the year, Novartis said.
“With this approval of Cosentyx as an IV formulation, along with the subcutaneous formulation, we can broaden the use of Cosentyx to help more patients manage their condition with a medicine backed by more than a decade of clinical research and 8 years of real-world experience,” said Christy Siegel, vice president and head of immunology, Novartis U.S.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has approved an intravenous (IV) formulation of secukinumab (Cosentyx) for the treatment of adults with psoriatic arthritis (PsA), ankylosing spondylitis (AS), and nonradiographic axial spondyloarthritis (nr-axSpA).
Secukinumab is the only treatment approved in an IV formulation that specifically targets and blocks interleukin-17A and the only non–tumor necrosis factor alpha IV option available to treat the three indications of PsA, AS, and nr-axSpA, according to a press release from the drug’s manufacturer, Novartis.
The approval marks the first new IV treatment in 6 years for these three conditions. The drug was first approved in 2015 and up to now has been available only as a subcutaneous injection.
The new formulation is also approved for secukinumab’s other indications of plaque psoriasis in people aged 6 years or older, children aged 2 years or older with PsA, and enthesitis-related arthritis in patients aged 4 years or older.
“A significant portion of the millions of PsA, AS, and nr-axSpA patients in the United States require treatment through IV infusions for a variety of reasons, including not being comfortable with self-injections or simply preferring to have treatments administered in their health care provider’s office,” Philip J. Mease, MD, clinical professor at the University of Washington, Seattle, and director of rheumatology research at the Swedish Medical Center, Seattle, said in the press release. “The approval of Cosentyx as an IV formulation is an important milestone for patients because it expands the treatment options available to them with a different mechanism of action than existing biologic IV therapies, along with the comfort and familiarity of an established treatment.”
This IV formulation is administered monthly in a 30-minute, weight-based dosing regimen. This new option will become available before the end of the year, Novartis said.
“With this approval of Cosentyx as an IV formulation, along with the subcutaneous formulation, we can broaden the use of Cosentyx to help more patients manage their condition with a medicine backed by more than a decade of clinical research and 8 years of real-world experience,” said Christy Siegel, vice president and head of immunology, Novartis U.S.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has approved an intravenous (IV) formulation of secukinumab (Cosentyx) for the treatment of adults with psoriatic arthritis (PsA), ankylosing spondylitis (AS), and nonradiographic axial spondyloarthritis (nr-axSpA).
Secukinumab is the only treatment approved in an IV formulation that specifically targets and blocks interleukin-17A and the only non–tumor necrosis factor alpha IV option available to treat the three indications of PsA, AS, and nr-axSpA, according to a press release from the drug’s manufacturer, Novartis.
The approval marks the first new IV treatment in 6 years for these three conditions. The drug was first approved in 2015 and up to now has been available only as a subcutaneous injection.
The new formulation is also approved for secukinumab’s other indications of plaque psoriasis in people aged 6 years or older, children aged 2 years or older with PsA, and enthesitis-related arthritis in patients aged 4 years or older.
“A significant portion of the millions of PsA, AS, and nr-axSpA patients in the United States require treatment through IV infusions for a variety of reasons, including not being comfortable with self-injections or simply preferring to have treatments administered in their health care provider’s office,” Philip J. Mease, MD, clinical professor at the University of Washington, Seattle, and director of rheumatology research at the Swedish Medical Center, Seattle, said in the press release. “The approval of Cosentyx as an IV formulation is an important milestone for patients because it expands the treatment options available to them with a different mechanism of action than existing biologic IV therapies, along with the comfort and familiarity of an established treatment.”
This IV formulation is administered monthly in a 30-minute, weight-based dosing regimen. This new option will become available before the end of the year, Novartis said.
“With this approval of Cosentyx as an IV formulation, along with the subcutaneous formulation, we can broaden the use of Cosentyx to help more patients manage their condition with a medicine backed by more than a decade of clinical research and 8 years of real-world experience,” said Christy Siegel, vice president and head of immunology, Novartis U.S.
A version of this article first appeared on Medscape.com.
Maternal pertussis vax effective for infants in most vulnerable months
Maternal pertussis vaccinations, given during pregnancy, prevent an estimated 65% of pertussis infections in infants, new research indicates.
The study, led by Annette K. Regan, PhD, MPH, a perinatal and pediatric infectious disease epidemiologist at Curtin University, Perth, Australia, was published online in Pediatrics.
Dr. Regan – who is also with the University of San Francisco and the University of California, Los Angeles – and colleagues reviewed data on 279,418 infants born to 252,444 mothers in Australia.
There, about 52% of the women in this study received the Tdap vaccine through a maternal pertussis vaccination program.
Duration of effectiveness in infants was one of the main questions the study sought to answer.
The authors wrote that they assessed vaccine effectiveness through 18 months of age. “We observed significant protection against disease until at least 8 months of age, 2 months longer than reported in previous studies.” From 70% to 90% of all pertussis-attributable hospitalizations and death occur in infancy.
Answering the ‘blunting’ question
This study also set out to clarify an important clinical question regarding a potential “blunting” effect in infants. Previous work had suggested that maternal antibodies from the vaccination could interfere with the effectiveness of infants’ DtaP (the version of Tdap for infants) and other vaccines.
Dr. Regan and colleagues found that, “although we observed slightly lower VE [vaccine effectiveness] point estimates for the third dose of infant pertussis vaccine among maternally vaccinated compared with unvaccinated infants (76.5% vs. 92.9%, P = .002), we did not observe higher rates of pertussis infection (hazard ratio, 0.70; 95% confidence interval, 0.61-3.39).
Best time to give mothers the vaccine
Another clinical debate has centered on when to give the mother the vaccine during pregnancy. The authors concluded: “Our findings support the infant health benefits of recommendations to administer a booster dose of pertussis vaccine near 28 weeks of gestational age.”
That 28-week mark was associated with lower risk of infection in infants through 8 months of age, they wrote.
Positive results in the United States
In an invited commentary, Kathryn M. Edwards, MD, with the division of infectious diseases, department of pediatrics, at Vanderbilt University Medical Center, Nashville, Tenn., highlighted similar positive findings for maternal pertussis vaccination in the United States.
The Centers for Disease Control and Prevention did an ecologic study of infant pertussis cases reported between Jan. 1, 2000, and Dec. 31, 2019. Rates were compared for the years before maternal Tdap vaccinations were recommended against the 7-year period after they were implemented.
That study found that in the period before maternal Tdap vaccination, annual pertussis incidence did not change among infants younger than 2 months and increased slightly in infants 6-12 months.
However, during the period after maternal Tdap vaccination had started (2012-2019), pertussis incidence significantly decreased in infants younger than 2 months and was unchanged in infants 6-12 months.
“As with the Australian data, the U.S. data support the overall benefit of the maternal Tdap program and, as with the Australian data, do not suggest that blunting has led to an increase in cases within the first year of life,” Dr. Edwards wrote.
The CDC notes that pertussis cases are rising and outbreaks are happening across the United States.
“On average, about 1,000 infants are hospitalized and typically between 5 and 15 infants die each year in the United States due to pertussis,” the CDC states.
Uptake low despite positive data
Dr. Edwards noted that, despite positive data supporting maternal vaccination to reduce pertussis, uptake rates are low – between 50% and 60% in Australia, the United Kingdom, and the United States. “Active engagement to increase these rates should be implemented.”
Maternal vaccination might also be implemented soon to protect against other diseases including respiratory syncytial virus and group B streptococcal disease after promising study data, she said.
As with pertussis, the potential “blunting” effect will need to be carefully monitored, she said, “as was done in the carefully conducted study of pertussis reported in this issue of Pediatrics.”
One coauthor has received institutional honoraria for participation in advisory groups for Merck Sharpe & Dohme and Pfizer unrelated to this work. Another coauthor was supported by scholarships provided by the Wesfarmers Centre of Vaccines and Infectious Disease at the Telethon Kids Institute. Dr. Edwards reported receiving grants from the CDC and consulting for Bionet, Dynavax, and IBM. She is a member of the data safety and monitoring board for Sanofi, X-4 Pharma, Seqirus, Moderna, Pfizer, Merck, Roche, Novavax, and Brighton Collaboration.
Maternal pertussis vaccinations, given during pregnancy, prevent an estimated 65% of pertussis infections in infants, new research indicates.
The study, led by Annette K. Regan, PhD, MPH, a perinatal and pediatric infectious disease epidemiologist at Curtin University, Perth, Australia, was published online in Pediatrics.
Dr. Regan – who is also with the University of San Francisco and the University of California, Los Angeles – and colleagues reviewed data on 279,418 infants born to 252,444 mothers in Australia.
There, about 52% of the women in this study received the Tdap vaccine through a maternal pertussis vaccination program.
Duration of effectiveness in infants was one of the main questions the study sought to answer.
The authors wrote that they assessed vaccine effectiveness through 18 months of age. “We observed significant protection against disease until at least 8 months of age, 2 months longer than reported in previous studies.” From 70% to 90% of all pertussis-attributable hospitalizations and death occur in infancy.
Answering the ‘blunting’ question
This study also set out to clarify an important clinical question regarding a potential “blunting” effect in infants. Previous work had suggested that maternal antibodies from the vaccination could interfere with the effectiveness of infants’ DtaP (the version of Tdap for infants) and other vaccines.
Dr. Regan and colleagues found that, “although we observed slightly lower VE [vaccine effectiveness] point estimates for the third dose of infant pertussis vaccine among maternally vaccinated compared with unvaccinated infants (76.5% vs. 92.9%, P = .002), we did not observe higher rates of pertussis infection (hazard ratio, 0.70; 95% confidence interval, 0.61-3.39).
Best time to give mothers the vaccine
Another clinical debate has centered on when to give the mother the vaccine during pregnancy. The authors concluded: “Our findings support the infant health benefits of recommendations to administer a booster dose of pertussis vaccine near 28 weeks of gestational age.”
That 28-week mark was associated with lower risk of infection in infants through 8 months of age, they wrote.
Positive results in the United States
In an invited commentary, Kathryn M. Edwards, MD, with the division of infectious diseases, department of pediatrics, at Vanderbilt University Medical Center, Nashville, Tenn., highlighted similar positive findings for maternal pertussis vaccination in the United States.
The Centers for Disease Control and Prevention did an ecologic study of infant pertussis cases reported between Jan. 1, 2000, and Dec. 31, 2019. Rates were compared for the years before maternal Tdap vaccinations were recommended against the 7-year period after they were implemented.
That study found that in the period before maternal Tdap vaccination, annual pertussis incidence did not change among infants younger than 2 months and increased slightly in infants 6-12 months.
However, during the period after maternal Tdap vaccination had started (2012-2019), pertussis incidence significantly decreased in infants younger than 2 months and was unchanged in infants 6-12 months.
“As with the Australian data, the U.S. data support the overall benefit of the maternal Tdap program and, as with the Australian data, do not suggest that blunting has led to an increase in cases within the first year of life,” Dr. Edwards wrote.
The CDC notes that pertussis cases are rising and outbreaks are happening across the United States.
“On average, about 1,000 infants are hospitalized and typically between 5 and 15 infants die each year in the United States due to pertussis,” the CDC states.
Uptake low despite positive data
Dr. Edwards noted that, despite positive data supporting maternal vaccination to reduce pertussis, uptake rates are low – between 50% and 60% in Australia, the United Kingdom, and the United States. “Active engagement to increase these rates should be implemented.”
Maternal vaccination might also be implemented soon to protect against other diseases including respiratory syncytial virus and group B streptococcal disease after promising study data, she said.
As with pertussis, the potential “blunting” effect will need to be carefully monitored, she said, “as was done in the carefully conducted study of pertussis reported in this issue of Pediatrics.”
One coauthor has received institutional honoraria for participation in advisory groups for Merck Sharpe & Dohme and Pfizer unrelated to this work. Another coauthor was supported by scholarships provided by the Wesfarmers Centre of Vaccines and Infectious Disease at the Telethon Kids Institute. Dr. Edwards reported receiving grants from the CDC and consulting for Bionet, Dynavax, and IBM. She is a member of the data safety and monitoring board for Sanofi, X-4 Pharma, Seqirus, Moderna, Pfizer, Merck, Roche, Novavax, and Brighton Collaboration.
Maternal pertussis vaccinations, given during pregnancy, prevent an estimated 65% of pertussis infections in infants, new research indicates.
The study, led by Annette K. Regan, PhD, MPH, a perinatal and pediatric infectious disease epidemiologist at Curtin University, Perth, Australia, was published online in Pediatrics.
Dr. Regan – who is also with the University of San Francisco and the University of California, Los Angeles – and colleagues reviewed data on 279,418 infants born to 252,444 mothers in Australia.
There, about 52% of the women in this study received the Tdap vaccine through a maternal pertussis vaccination program.
Duration of effectiveness in infants was one of the main questions the study sought to answer.
The authors wrote that they assessed vaccine effectiveness through 18 months of age. “We observed significant protection against disease until at least 8 months of age, 2 months longer than reported in previous studies.” From 70% to 90% of all pertussis-attributable hospitalizations and death occur in infancy.
Answering the ‘blunting’ question
This study also set out to clarify an important clinical question regarding a potential “blunting” effect in infants. Previous work had suggested that maternal antibodies from the vaccination could interfere with the effectiveness of infants’ DtaP (the version of Tdap for infants) and other vaccines.
Dr. Regan and colleagues found that, “although we observed slightly lower VE [vaccine effectiveness] point estimates for the third dose of infant pertussis vaccine among maternally vaccinated compared with unvaccinated infants (76.5% vs. 92.9%, P = .002), we did not observe higher rates of pertussis infection (hazard ratio, 0.70; 95% confidence interval, 0.61-3.39).
Best time to give mothers the vaccine
Another clinical debate has centered on when to give the mother the vaccine during pregnancy. The authors concluded: “Our findings support the infant health benefits of recommendations to administer a booster dose of pertussis vaccine near 28 weeks of gestational age.”
That 28-week mark was associated with lower risk of infection in infants through 8 months of age, they wrote.
Positive results in the United States
In an invited commentary, Kathryn M. Edwards, MD, with the division of infectious diseases, department of pediatrics, at Vanderbilt University Medical Center, Nashville, Tenn., highlighted similar positive findings for maternal pertussis vaccination in the United States.
The Centers for Disease Control and Prevention did an ecologic study of infant pertussis cases reported between Jan. 1, 2000, and Dec. 31, 2019. Rates were compared for the years before maternal Tdap vaccinations were recommended against the 7-year period after they were implemented.
That study found that in the period before maternal Tdap vaccination, annual pertussis incidence did not change among infants younger than 2 months and increased slightly in infants 6-12 months.
However, during the period after maternal Tdap vaccination had started (2012-2019), pertussis incidence significantly decreased in infants younger than 2 months and was unchanged in infants 6-12 months.
“As with the Australian data, the U.S. data support the overall benefit of the maternal Tdap program and, as with the Australian data, do not suggest that blunting has led to an increase in cases within the first year of life,” Dr. Edwards wrote.
The CDC notes that pertussis cases are rising and outbreaks are happening across the United States.
“On average, about 1,000 infants are hospitalized and typically between 5 and 15 infants die each year in the United States due to pertussis,” the CDC states.
Uptake low despite positive data
Dr. Edwards noted that, despite positive data supporting maternal vaccination to reduce pertussis, uptake rates are low – between 50% and 60% in Australia, the United Kingdom, and the United States. “Active engagement to increase these rates should be implemented.”
Maternal vaccination might also be implemented soon to protect against other diseases including respiratory syncytial virus and group B streptococcal disease after promising study data, she said.
As with pertussis, the potential “blunting” effect will need to be carefully monitored, she said, “as was done in the carefully conducted study of pertussis reported in this issue of Pediatrics.”
One coauthor has received institutional honoraria for participation in advisory groups for Merck Sharpe & Dohme and Pfizer unrelated to this work. Another coauthor was supported by scholarships provided by the Wesfarmers Centre of Vaccines and Infectious Disease at the Telethon Kids Institute. Dr. Edwards reported receiving grants from the CDC and consulting for Bionet, Dynavax, and IBM. She is a member of the data safety and monitoring board for Sanofi, X-4 Pharma, Seqirus, Moderna, Pfizer, Merck, Roche, Novavax, and Brighton Collaboration.
FROM PEDIATRICS
FDA approves topical roflumilast for psoriasis in children aged 6-11
On Oct. 6, the This marks an expanded indication for the drug, which was first approved for the same indication in July, 2022, for individuals aged 12 and older.
Roflumilast cream 0.3% is a phosphodiesterase-4 inhibitor approved for once-daily topical treatment of mild, moderate, and severe plaque psoriasis. According to a press release from the manufacturer, Arcutis Biotherapeutics, approval of the expanded indication is based on data from a 4-week Maximal Usage Systemic Exposure (MUSE) study in children ages 6-11 years with plaque psoriasis. It stated that pharmacokinetic, safety, tolerability, and efficacy data from this study were “generally consistent” with data from the DERMIS-1 and DERMIS-2 pivotal phase 3 trials in adults.
According to the press release, a future FDA review is planned for the results from a second MUSE study in children ages 2-5 years, as well as data from an ongoing open-label extension study evaluating the long-term safety of roflumilast cream in individuals with plaque psoriasis aged 2 years and older. The company markets topical roflumilast as Zoryve.
On Oct. 6, the This marks an expanded indication for the drug, which was first approved for the same indication in July, 2022, for individuals aged 12 and older.
Roflumilast cream 0.3% is a phosphodiesterase-4 inhibitor approved for once-daily topical treatment of mild, moderate, and severe plaque psoriasis. According to a press release from the manufacturer, Arcutis Biotherapeutics, approval of the expanded indication is based on data from a 4-week Maximal Usage Systemic Exposure (MUSE) study in children ages 6-11 years with plaque psoriasis. It stated that pharmacokinetic, safety, tolerability, and efficacy data from this study were “generally consistent” with data from the DERMIS-1 and DERMIS-2 pivotal phase 3 trials in adults.
According to the press release, a future FDA review is planned for the results from a second MUSE study in children ages 2-5 years, as well as data from an ongoing open-label extension study evaluating the long-term safety of roflumilast cream in individuals with plaque psoriasis aged 2 years and older. The company markets topical roflumilast as Zoryve.
On Oct. 6, the This marks an expanded indication for the drug, which was first approved for the same indication in July, 2022, for individuals aged 12 and older.
Roflumilast cream 0.3% is a phosphodiesterase-4 inhibitor approved for once-daily topical treatment of mild, moderate, and severe plaque psoriasis. According to a press release from the manufacturer, Arcutis Biotherapeutics, approval of the expanded indication is based on data from a 4-week Maximal Usage Systemic Exposure (MUSE) study in children ages 6-11 years with plaque psoriasis. It stated that pharmacokinetic, safety, tolerability, and efficacy data from this study were “generally consistent” with data from the DERMIS-1 and DERMIS-2 pivotal phase 3 trials in adults.
According to the press release, a future FDA review is planned for the results from a second MUSE study in children ages 2-5 years, as well as data from an ongoing open-label extension study evaluating the long-term safety of roflumilast cream in individuals with plaque psoriasis aged 2 years and older. The company markets topical roflumilast as Zoryve.
FDA approves ninth Humira biosimilar, with interchangeability
The Food and Drug Administration has granted an interchangeability designation to adalimumab-afzb (Abrilada), according to an announcement from Pfizer.
This is the second adalimumab biosimilar granted interchangeability. The first, adalimumab-adbm (Cyltezo), became available in July.
Biosimilars introduce market competition that can help lower drug prices. Adalimumab-afzb is one of nine approved biosimilars for Humira, and the last to launch in 2023.
Adalimumab-afzb is indicated for:
- Adults with rheumatoid arthritis.
- Polyarticular juvenile idiopathic arthritis in patients 2 years of age and older.
- Adults with psoriatic arthritis.
- Adults with ankylosing spondylitis.
- Crohn’s disease in adults and children 6 years of age and older.
- Adults with ulcerative colitis.
- Adults with plaque psoriasis.
- Adults with hidradenitis suppurativa.
- Adults with noninfectious intermediate and posterior uveitis and panuveitis.
“With this designation, Abrilada is now both biosimilar to and interchangeable with Humira, reinforcing confidence among physicians and pharmacists that there is no decrease in effectiveness or increase in safety risk associated with switching between Abrilada and the reference product,” Roy Fleischmann, MD, clinical professor of medicine, University of Texas Southwestern Medical Center, Dallas, said in Pfizer’s statement.
An interchangeability designation allows pharmacists to substitute the biosimilar for the reference product without involving the prescribing clinician (according to state law). To achieve this designation, Pfizer submitted data from a phase 3 study led by Dr. Fleischmann that evaluated adalimumab-afzb in patients with RA. Patients who were switched three times between the biosimilar and the reference product had outcomes similar to those of patients continuously treated with the reference product.
Adalimumab-afzb will be available later in October at a 5% discount from Humira’s price. Later this year, the drug will launch at a second price, a 60% discount from Humira.
Full prescribing information for adalimumab-afzb is available here.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has granted an interchangeability designation to adalimumab-afzb (Abrilada), according to an announcement from Pfizer.
This is the second adalimumab biosimilar granted interchangeability. The first, adalimumab-adbm (Cyltezo), became available in July.
Biosimilars introduce market competition that can help lower drug prices. Adalimumab-afzb is one of nine approved biosimilars for Humira, and the last to launch in 2023.
Adalimumab-afzb is indicated for:
- Adults with rheumatoid arthritis.
- Polyarticular juvenile idiopathic arthritis in patients 2 years of age and older.
- Adults with psoriatic arthritis.
- Adults with ankylosing spondylitis.
- Crohn’s disease in adults and children 6 years of age and older.
- Adults with ulcerative colitis.
- Adults with plaque psoriasis.
- Adults with hidradenitis suppurativa.
- Adults with noninfectious intermediate and posterior uveitis and panuveitis.
“With this designation, Abrilada is now both biosimilar to and interchangeable with Humira, reinforcing confidence among physicians and pharmacists that there is no decrease in effectiveness or increase in safety risk associated with switching between Abrilada and the reference product,” Roy Fleischmann, MD, clinical professor of medicine, University of Texas Southwestern Medical Center, Dallas, said in Pfizer’s statement.
An interchangeability designation allows pharmacists to substitute the biosimilar for the reference product without involving the prescribing clinician (according to state law). To achieve this designation, Pfizer submitted data from a phase 3 study led by Dr. Fleischmann that evaluated adalimumab-afzb in patients with RA. Patients who were switched three times between the biosimilar and the reference product had outcomes similar to those of patients continuously treated with the reference product.
Adalimumab-afzb will be available later in October at a 5% discount from Humira’s price. Later this year, the drug will launch at a second price, a 60% discount from Humira.
Full prescribing information for adalimumab-afzb is available here.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has granted an interchangeability designation to adalimumab-afzb (Abrilada), according to an announcement from Pfizer.
This is the second adalimumab biosimilar granted interchangeability. The first, adalimumab-adbm (Cyltezo), became available in July.
Biosimilars introduce market competition that can help lower drug prices. Adalimumab-afzb is one of nine approved biosimilars for Humira, and the last to launch in 2023.
Adalimumab-afzb is indicated for:
- Adults with rheumatoid arthritis.
- Polyarticular juvenile idiopathic arthritis in patients 2 years of age and older.
- Adults with psoriatic arthritis.
- Adults with ankylosing spondylitis.
- Crohn’s disease in adults and children 6 years of age and older.
- Adults with ulcerative colitis.
- Adults with plaque psoriasis.
- Adults with hidradenitis suppurativa.
- Adults with noninfectious intermediate and posterior uveitis and panuveitis.
“With this designation, Abrilada is now both biosimilar to and interchangeable with Humira, reinforcing confidence among physicians and pharmacists that there is no decrease in effectiveness or increase in safety risk associated with switching between Abrilada and the reference product,” Roy Fleischmann, MD, clinical professor of medicine, University of Texas Southwestern Medical Center, Dallas, said in Pfizer’s statement.
An interchangeability designation allows pharmacists to substitute the biosimilar for the reference product without involving the prescribing clinician (according to state law). To achieve this designation, Pfizer submitted data from a phase 3 study led by Dr. Fleischmann that evaluated adalimumab-afzb in patients with RA. Patients who were switched three times between the biosimilar and the reference product had outcomes similar to those of patients continuously treated with the reference product.
Adalimumab-afzb will be available later in October at a 5% discount from Humira’s price. Later this year, the drug will launch at a second price, a 60% discount from Humira.
Full prescribing information for adalimumab-afzb is available here.
A version of this article first appeared on Medscape.com.
Social media makes kids with type 1 diabetes feel less alone
After being diagnosed with type 1 diabetes in 2021, British teenager Johnny Bailey felt isolated. That’s when he turned to social media, where he found others living with type 1 diabetes. He began to share his experience and now has more than 329,000 followers on his TikTok account, where he regularly posts videos.
These include short clips of him demonstrating how he changes his FreeStyle Libre sensor for his flash glucose monitor. In the videos, Johnny appropriately places his sensor on the back of his arm with background music, makes facial expressions, and transforms a dreaded diabetes-related task into an experience that appears fun and entertaining. In the limited videos I was able to review, he follows all the appropriate steps for sensor placement.
Many youths living with type 1 diabetes struggle with living with a chronic medical condition. Because type 1 diabetes is a rare condition, affecting about 1 in 500 children in the United States, many youth may not meet anyone else their age with type 1 diabetes through school, social events, or extracurricular activities.
For adolescents with intensively managed conditions like type 1 diabetes, this can present numerous psychosocial challenges – specifically, many youth experience shame or stigma associated with managing type 1 diabetes.
Diabetes-specific tasks may include wearing an insulin pump, monitoring blood glucose with finger pricks or a continuous glucose monitor (CGM), giving injections of insulin before meals and snacks, adjusting times for meals and snacks based on metabolic needs, waking up in the middle of the night to treat high or low blood glucose – the list goes on and on.
One study estimated that the average time it takes a child with type 1 diabetes to perform diabetes-specific tasks is over 5 hours per day.
Although much of this diabetes management time is spent by parents, as children get older and become teenagers, they are gradually transitioning to taking on more of this responsibility themselves. Wearing diabetes technology (insulin pumps and CGMs) can draw unwanted attention, leading to diabetes-specific body image concerns. Kids may also have to excuse themselves from an activity to treat a low or high blood glucose, creating uncomfortable situations when others inquire about why the activity was interrupted. As a result, many youths will avoid managing their diabetes properly to avoid drawing unwanted attention, consequently put their health at risk.
Those who are afraid of placing their glucose sensor owing to fear of pain may be reassured by seeing Johnny placing his sensor with a smile on his face. Some of his content also highlights other stigmatizing situations that teens may face, for example someone with a judgmental look questioning why he needed to give an insulin injection here.
This highlights an important concept – that people with type 1 diabetes may face criticism when dosing insulin in public, but it doesn’t mean they should feel forced to manage diabetes in private unless they choose to. Johnny is an inspirational individual who has bravely taken his type 1 diabetes experiences and used his creative skills to make these seemingly boring health-related tasks fun, interesting, and accessible.
Social media has become an outlet for people with type 1 diabetes to connect with others who can relate to their experiences.
However, there’s another side to consider. Although social media may provide a great source of support for youth, it may also adversely affect mental health. Just as quickly as social media outlets have grown, so has concern over excessive social media use and its impact on adolescents’ mental health. There’s a growing body of literature that describes the negative mental health aspects related to social media use.
Some adolescents struggling to manage type 1 diabetes may feel worse when seeing others thrive on social media, which has the potential to worsen stigma and shame. Youth may wonder how someone else is able to manage their type 1 diabetes so well when they are facing so many challenges.
Short videos on social media provide an incomplete picture of living with type 1 diabetes – just a glimpse into others’ lives, and only the parts that they want others to see. Managing a chronic condition can’t be fully represented in 10-second videos. And if youths choose to post their type 1 diabetes experiences on social media, they also risk receiving backlash or criticism, which can negatively their impact mental health in return.
Furthermore, the content being posted may not always be accurate or educational, leading to the potential for some youth to misunderstand type 1 diabetes.
Although I wouldn’t discourage youth with type 1 diabetes from engaging on social media and viewing diabetes-related content, they need to know that social media is flooded with misinformation. Creating an open space for youth to ask their clinicians questions about type 1 diabetes–related topics they view on social media is vital to ensuring they are viewing accurate information, so they are able to continue to manage their diabetes safely.
As a pediatric endocrinologist, I sometimes share resources on social media with patients if I believe it will help them cope with their type 1 diabetes diagnosis and management. I have had numerous patients – many of whom have struggled to accept their diagnosis – mention with joy and excitement that they were following an organization addressing type 1 diabetes on social media.
When making suggestions, I may refer them to The Diabetes Link, an organization with resources for young adults with type 1 diabetes that creates a space to connect with other young adults with type 1 diabetes. diaTribe is another organization created and led by people with diabetes that has a plethora of resources and provides evidence-based education for patients. I have also shared Project 50-in-50, which highlights two individuals with type 1 diabetes hiking the highest peak in each state in less than 50 days. Being able to see type 1 diabetes in a positive light is a huge step toward a more positive outlook on diabetes management.
Dr. Nally is an assistant professor, department of pediatrics, and a pediatric endocrinologist, division of pediatric endocrinology, at Yale University, New Haven, Conn. She reported conflicts of interest with Medtronic and the National Institutes of Health.
A version of this article first appeared on Medscape.com.
After being diagnosed with type 1 diabetes in 2021, British teenager Johnny Bailey felt isolated. That’s when he turned to social media, where he found others living with type 1 diabetes. He began to share his experience and now has more than 329,000 followers on his TikTok account, where he regularly posts videos.
These include short clips of him demonstrating how he changes his FreeStyle Libre sensor for his flash glucose monitor. In the videos, Johnny appropriately places his sensor on the back of his arm with background music, makes facial expressions, and transforms a dreaded diabetes-related task into an experience that appears fun and entertaining. In the limited videos I was able to review, he follows all the appropriate steps for sensor placement.
Many youths living with type 1 diabetes struggle with living with a chronic medical condition. Because type 1 diabetes is a rare condition, affecting about 1 in 500 children in the United States, many youth may not meet anyone else their age with type 1 diabetes through school, social events, or extracurricular activities.
For adolescents with intensively managed conditions like type 1 diabetes, this can present numerous psychosocial challenges – specifically, many youth experience shame or stigma associated with managing type 1 diabetes.
Diabetes-specific tasks may include wearing an insulin pump, monitoring blood glucose with finger pricks or a continuous glucose monitor (CGM), giving injections of insulin before meals and snacks, adjusting times for meals and snacks based on metabolic needs, waking up in the middle of the night to treat high or low blood glucose – the list goes on and on.
One study estimated that the average time it takes a child with type 1 diabetes to perform diabetes-specific tasks is over 5 hours per day.
Although much of this diabetes management time is spent by parents, as children get older and become teenagers, they are gradually transitioning to taking on more of this responsibility themselves. Wearing diabetes technology (insulin pumps and CGMs) can draw unwanted attention, leading to diabetes-specific body image concerns. Kids may also have to excuse themselves from an activity to treat a low or high blood glucose, creating uncomfortable situations when others inquire about why the activity was interrupted. As a result, many youths will avoid managing their diabetes properly to avoid drawing unwanted attention, consequently put their health at risk.
Those who are afraid of placing their glucose sensor owing to fear of pain may be reassured by seeing Johnny placing his sensor with a smile on his face. Some of his content also highlights other stigmatizing situations that teens may face, for example someone with a judgmental look questioning why he needed to give an insulin injection here.
This highlights an important concept – that people with type 1 diabetes may face criticism when dosing insulin in public, but it doesn’t mean they should feel forced to manage diabetes in private unless they choose to. Johnny is an inspirational individual who has bravely taken his type 1 diabetes experiences and used his creative skills to make these seemingly boring health-related tasks fun, interesting, and accessible.
Social media has become an outlet for people with type 1 diabetes to connect with others who can relate to their experiences.
However, there’s another side to consider. Although social media may provide a great source of support for youth, it may also adversely affect mental health. Just as quickly as social media outlets have grown, so has concern over excessive social media use and its impact on adolescents’ mental health. There’s a growing body of literature that describes the negative mental health aspects related to social media use.
Some adolescents struggling to manage type 1 diabetes may feel worse when seeing others thrive on social media, which has the potential to worsen stigma and shame. Youth may wonder how someone else is able to manage their type 1 diabetes so well when they are facing so many challenges.
Short videos on social media provide an incomplete picture of living with type 1 diabetes – just a glimpse into others’ lives, and only the parts that they want others to see. Managing a chronic condition can’t be fully represented in 10-second videos. And if youths choose to post their type 1 diabetes experiences on social media, they also risk receiving backlash or criticism, which can negatively their impact mental health in return.
Furthermore, the content being posted may not always be accurate or educational, leading to the potential for some youth to misunderstand type 1 diabetes.
Although I wouldn’t discourage youth with type 1 diabetes from engaging on social media and viewing diabetes-related content, they need to know that social media is flooded with misinformation. Creating an open space for youth to ask their clinicians questions about type 1 diabetes–related topics they view on social media is vital to ensuring they are viewing accurate information, so they are able to continue to manage their diabetes safely.
As a pediatric endocrinologist, I sometimes share resources on social media with patients if I believe it will help them cope with their type 1 diabetes diagnosis and management. I have had numerous patients – many of whom have struggled to accept their diagnosis – mention with joy and excitement that they were following an organization addressing type 1 diabetes on social media.
When making suggestions, I may refer them to The Diabetes Link, an organization with resources for young adults with type 1 diabetes that creates a space to connect with other young adults with type 1 diabetes. diaTribe is another organization created and led by people with diabetes that has a plethora of resources and provides evidence-based education for patients. I have also shared Project 50-in-50, which highlights two individuals with type 1 diabetes hiking the highest peak in each state in less than 50 days. Being able to see type 1 diabetes in a positive light is a huge step toward a more positive outlook on diabetes management.
Dr. Nally is an assistant professor, department of pediatrics, and a pediatric endocrinologist, division of pediatric endocrinology, at Yale University, New Haven, Conn. She reported conflicts of interest with Medtronic and the National Institutes of Health.
A version of this article first appeared on Medscape.com.
After being diagnosed with type 1 diabetes in 2021, British teenager Johnny Bailey felt isolated. That’s when he turned to social media, where he found others living with type 1 diabetes. He began to share his experience and now has more than 329,000 followers on his TikTok account, where he regularly posts videos.
These include short clips of him demonstrating how he changes his FreeStyle Libre sensor for his flash glucose monitor. In the videos, Johnny appropriately places his sensor on the back of his arm with background music, makes facial expressions, and transforms a dreaded diabetes-related task into an experience that appears fun and entertaining. In the limited videos I was able to review, he follows all the appropriate steps for sensor placement.
Many youths living with type 1 diabetes struggle with living with a chronic medical condition. Because type 1 diabetes is a rare condition, affecting about 1 in 500 children in the United States, many youth may not meet anyone else their age with type 1 diabetes through school, social events, or extracurricular activities.
For adolescents with intensively managed conditions like type 1 diabetes, this can present numerous psychosocial challenges – specifically, many youth experience shame or stigma associated with managing type 1 diabetes.
Diabetes-specific tasks may include wearing an insulin pump, monitoring blood glucose with finger pricks or a continuous glucose monitor (CGM), giving injections of insulin before meals and snacks, adjusting times for meals and snacks based on metabolic needs, waking up in the middle of the night to treat high or low blood glucose – the list goes on and on.
One study estimated that the average time it takes a child with type 1 diabetes to perform diabetes-specific tasks is over 5 hours per day.
Although much of this diabetes management time is spent by parents, as children get older and become teenagers, they are gradually transitioning to taking on more of this responsibility themselves. Wearing diabetes technology (insulin pumps and CGMs) can draw unwanted attention, leading to diabetes-specific body image concerns. Kids may also have to excuse themselves from an activity to treat a low or high blood glucose, creating uncomfortable situations when others inquire about why the activity was interrupted. As a result, many youths will avoid managing their diabetes properly to avoid drawing unwanted attention, consequently put their health at risk.
Those who are afraid of placing their glucose sensor owing to fear of pain may be reassured by seeing Johnny placing his sensor with a smile on his face. Some of his content also highlights other stigmatizing situations that teens may face, for example someone with a judgmental look questioning why he needed to give an insulin injection here.
This highlights an important concept – that people with type 1 diabetes may face criticism when dosing insulin in public, but it doesn’t mean they should feel forced to manage diabetes in private unless they choose to. Johnny is an inspirational individual who has bravely taken his type 1 diabetes experiences and used his creative skills to make these seemingly boring health-related tasks fun, interesting, and accessible.
Social media has become an outlet for people with type 1 diabetes to connect with others who can relate to their experiences.
However, there’s another side to consider. Although social media may provide a great source of support for youth, it may also adversely affect mental health. Just as quickly as social media outlets have grown, so has concern over excessive social media use and its impact on adolescents’ mental health. There’s a growing body of literature that describes the negative mental health aspects related to social media use.
Some adolescents struggling to manage type 1 diabetes may feel worse when seeing others thrive on social media, which has the potential to worsen stigma and shame. Youth may wonder how someone else is able to manage their type 1 diabetes so well when they are facing so many challenges.
Short videos on social media provide an incomplete picture of living with type 1 diabetes – just a glimpse into others’ lives, and only the parts that they want others to see. Managing a chronic condition can’t be fully represented in 10-second videos. And if youths choose to post their type 1 diabetes experiences on social media, they also risk receiving backlash or criticism, which can negatively their impact mental health in return.
Furthermore, the content being posted may not always be accurate or educational, leading to the potential for some youth to misunderstand type 1 diabetes.
Although I wouldn’t discourage youth with type 1 diabetes from engaging on social media and viewing diabetes-related content, they need to know that social media is flooded with misinformation. Creating an open space for youth to ask their clinicians questions about type 1 diabetes–related topics they view on social media is vital to ensuring they are viewing accurate information, so they are able to continue to manage their diabetes safely.
As a pediatric endocrinologist, I sometimes share resources on social media with patients if I believe it will help them cope with their type 1 diabetes diagnosis and management. I have had numerous patients – many of whom have struggled to accept their diagnosis – mention with joy and excitement that they were following an organization addressing type 1 diabetes on social media.
When making suggestions, I may refer them to The Diabetes Link, an organization with resources for young adults with type 1 diabetes that creates a space to connect with other young adults with type 1 diabetes. diaTribe is another organization created and led by people with diabetes that has a plethora of resources and provides evidence-based education for patients. I have also shared Project 50-in-50, which highlights two individuals with type 1 diabetes hiking the highest peak in each state in less than 50 days. Being able to see type 1 diabetes in a positive light is a huge step toward a more positive outlook on diabetes management.
Dr. Nally is an assistant professor, department of pediatrics, and a pediatric endocrinologist, division of pediatric endocrinology, at Yale University, New Haven, Conn. She reported conflicts of interest with Medtronic and the National Institutes of Health.
A version of this article first appeared on Medscape.com.
Adolescents’ acute care use for eating disorders has risen
In a repeated cross-sectional study that examined population-based data from January 2017 through August 2022, ED visits increased by 121% above expected levels, and hospital admissions increased by 54% above expected among patients aged 10-17 years during the pandemic.
“We are hoping this study continues to heighten awareness of the importance of eating disorders, and also to bolster support for eating disorder programs so that we can adequately care for patients and address the increasing demand for treatment and services,” lead author Alene Toulany, MD, adolescent medicine specialist and researcher at the Hospital for Sick Children in Toronto, told this news organization.
The study was published in the Canadian Medical Association Journal.
‘A pressing concern’
The researchers used linked health administrative databases that included all patients in Ontario who were eligible for the Ontario Health Insurance Plan, which is publicly funded. They compared observed and expected rates of ED visits and hospitalizations for eating disorders between a prepandemic period (Jan. 1, 2017, to Feb. 29, 2020) and a pandemic period (Mar. 1, 2020, to Aug. 31, 2022). The researchers examined the following four age categories: adolescents (aged 10-17 years), young adults (aged 18-26 years), adults (aged 27-40 years), and older adults (aged 41-105 years).
Among adolescents, the observed rate of ED visits during the 30 pandemic months studied was 7.38 per 100,000 population, compared with 3.33 per 100,000 before the pandemic (incidence rate ratio [IRR], 2.21).
The rate of ED visits among young adults increased by 13% above the expected rate. It reached 2.79 per 100,000, compared with 2.46 per 100,000 in the prepandemic period (IRR, 1.13).
Among older adults, ED visits increased from 0.11 per 100,000 in the prepandemic period to 0.14 per 100,000 in the pandemic period (IRR, 1.15). The rate of ED visits among adults remained approximately the same.
The rate of hospital admissions among adolescents increased by 54% above the expected rate during the pandemic. The observed rate of hospital admissions before the pandemic was 5.74 per 100,000, vs. 8.82 per 100,000 during the pandemic (IRR, 1.54). Hospital admissions remained stable or decreased for the other age groups.
“Eating disorders have increased globally in children and adolescents during COVID,” said Dr. Toulany. “There are a number of risk factors contributing to this pandemic rise, including isolation, more time on social media, decreased access to care (as many in-person services were not available due to the pandemic), as well as fear of getting infected. All of these could contribute to an increased risk of developing an eating disorder or of making an existing one worse.”
Regardless of the cause, more investment in eating disorders research and eating disorder programs for adolescents and adults is needed, she said.
“The pandemic served as a catalyst, because it started to shed light on the prevalence of eating disorders, especially in young people. But it’s very important that we recognize that this has been a long-standing issue and a pressing concern that has been consistently overlooked and underfunded,” said Dr. Toulany.
Surging eating disorders
Commenting on the findings, Victor Fornari, MD, director of child and adolescent psychiatry at Zucker Hillside Hospital/Northwell Health in Glen Oaks, N.Y., said, “Our experience in the United States parallels what is described in this Canadian paper. This was a surge of eating disorders the likes of which I had not experienced in my career.” Dr. Fornari did not participate in the current study.
“I’ve been here for over 40 years, and the average number of our inpatients in our eating disorder program has been three to five and about a dozen patients in our day clinic at any one time. But in the spring of 2020, we surged to 20 inpatients and over 20 day patients,” Dr. Fornari said.
“We can speculate as to the reasons for this,” he continued. “Kids were isolated. School was closed. They spent more time on social media and the Internet. Their sports activities were curtailed. There was anxiety because the guidance that we were all offered to prevent contagion was increasing people’s anxiety about safety and danger. So, I think we saw dramatic rises in eating disorders in the same way we saw dramatic rises in anxiety and depression in adolescents, as well.”
Dr. Fornari cited social media as an important contributing factor to eating disorders, especially among vulnerable teenagers. “Many of these vulnerable kids are looking at pictures of people who are very thin and comparing themselves, feeling inadequate, feeling sad. Social media is one of the reasons why the rates of psychopathology amongst teens has skyrocketed in the last decade. The surgeon general recently said we should delay access to social media until age 16 because the younger kids are impressionable and vulnerable. I think there is wisdom there, but it is very hard to actually put into practice.”
Worsening mental health
“I thought this was very relevant research and an important contribution to our understanding of eating disorders during pandemic times,” said Simon Sherry, PhD, professor of psychology and neuroscience at Dalhousie University in Halifax, Nova Scotia. “It also dovetails with my own experience as a practitioner.” Dr. Sherry was not involved in the research.
The pandemic has been difficult for people with disordered eating for many reasons, Dr. Sherry said. “There was a massive disruption or ‘loss of normal’ around food. Restaurants closed, grocery shopping was disrupted, scarcity of food occurred, hoarding of food occurred. That meant that eating was difficult for all of us, but especially for individuals who were rigid and controlling around the consumption of food. In this COVID era, you would need flexibility and acceptance around eating, but if you had a narrow range of preferred foods and preferred shopping locations, no doubt the pandemic made this a lot worse.”
Certain forms of disordered eating would be much more likely during the pandemic, Dr. Sherry noted. “For example, binge eating is often triggered by psychological, social, and environmental events,” and those triggers were abundant at the beginning of the pandemic. Boredom, anxiety, depression, stress, loneliness, confinement, and isolation are among the triggers. “COVID-19-related stress was and is very fertile ground for the growth of emotional eating, binge eating, or turning to food to cope. Eating disorders tend to fester amid silence and isolation and inactivity, and that was very much our experience during the lockdown phase of the pandemic,” he said.
Dr. Sherry agrees with the need for more funding for eating disorders research. “We know in Canada that eating disorders are a very important and deadly issue that is chronically underfunded. We are not funding disordered eating in proportion to its prevalence or in proportion to the amount of harm and destruction it creates for individuals, their family members, and our society at large. The authors are absolutely correct to advocate for care in proportion to the prevalence and the damage associated with eating disorders,” he said.
The study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health, the Ministry of Long-Term Care, and the Canadian Institutes of Health Research (CIHR). Dr. Toulany, Dr. Fornari, and Dr. Sherry reported no relevant financial relationships. One study author reported receiving personal fees from the BMJ Group’s Archives of Diseases in Childhood and grants from CIHR, the Ontario Ministry of Health, the Centre for Addiction and Mental Health, and the Hospital for Sick Children. A second author reported funding from CIHR.
A version of this article first appeared on Medscape.com.
In a repeated cross-sectional study that examined population-based data from January 2017 through August 2022, ED visits increased by 121% above expected levels, and hospital admissions increased by 54% above expected among patients aged 10-17 years during the pandemic.
“We are hoping this study continues to heighten awareness of the importance of eating disorders, and also to bolster support for eating disorder programs so that we can adequately care for patients and address the increasing demand for treatment and services,” lead author Alene Toulany, MD, adolescent medicine specialist and researcher at the Hospital for Sick Children in Toronto, told this news organization.
The study was published in the Canadian Medical Association Journal.
‘A pressing concern’
The researchers used linked health administrative databases that included all patients in Ontario who were eligible for the Ontario Health Insurance Plan, which is publicly funded. They compared observed and expected rates of ED visits and hospitalizations for eating disorders between a prepandemic period (Jan. 1, 2017, to Feb. 29, 2020) and a pandemic period (Mar. 1, 2020, to Aug. 31, 2022). The researchers examined the following four age categories: adolescents (aged 10-17 years), young adults (aged 18-26 years), adults (aged 27-40 years), and older adults (aged 41-105 years).
Among adolescents, the observed rate of ED visits during the 30 pandemic months studied was 7.38 per 100,000 population, compared with 3.33 per 100,000 before the pandemic (incidence rate ratio [IRR], 2.21).
The rate of ED visits among young adults increased by 13% above the expected rate. It reached 2.79 per 100,000, compared with 2.46 per 100,000 in the prepandemic period (IRR, 1.13).
Among older adults, ED visits increased from 0.11 per 100,000 in the prepandemic period to 0.14 per 100,000 in the pandemic period (IRR, 1.15). The rate of ED visits among adults remained approximately the same.
The rate of hospital admissions among adolescents increased by 54% above the expected rate during the pandemic. The observed rate of hospital admissions before the pandemic was 5.74 per 100,000, vs. 8.82 per 100,000 during the pandemic (IRR, 1.54). Hospital admissions remained stable or decreased for the other age groups.
“Eating disorders have increased globally in children and adolescents during COVID,” said Dr. Toulany. “There are a number of risk factors contributing to this pandemic rise, including isolation, more time on social media, decreased access to care (as many in-person services were not available due to the pandemic), as well as fear of getting infected. All of these could contribute to an increased risk of developing an eating disorder or of making an existing one worse.”
Regardless of the cause, more investment in eating disorders research and eating disorder programs for adolescents and adults is needed, she said.
“The pandemic served as a catalyst, because it started to shed light on the prevalence of eating disorders, especially in young people. But it’s very important that we recognize that this has been a long-standing issue and a pressing concern that has been consistently overlooked and underfunded,” said Dr. Toulany.
Surging eating disorders
Commenting on the findings, Victor Fornari, MD, director of child and adolescent psychiatry at Zucker Hillside Hospital/Northwell Health in Glen Oaks, N.Y., said, “Our experience in the United States parallels what is described in this Canadian paper. This was a surge of eating disorders the likes of which I had not experienced in my career.” Dr. Fornari did not participate in the current study.
“I’ve been here for over 40 years, and the average number of our inpatients in our eating disorder program has been three to five and about a dozen patients in our day clinic at any one time. But in the spring of 2020, we surged to 20 inpatients and over 20 day patients,” Dr. Fornari said.
“We can speculate as to the reasons for this,” he continued. “Kids were isolated. School was closed. They spent more time on social media and the Internet. Their sports activities were curtailed. There was anxiety because the guidance that we were all offered to prevent contagion was increasing people’s anxiety about safety and danger. So, I think we saw dramatic rises in eating disorders in the same way we saw dramatic rises in anxiety and depression in adolescents, as well.”
Dr. Fornari cited social media as an important contributing factor to eating disorders, especially among vulnerable teenagers. “Many of these vulnerable kids are looking at pictures of people who are very thin and comparing themselves, feeling inadequate, feeling sad. Social media is one of the reasons why the rates of psychopathology amongst teens has skyrocketed in the last decade. The surgeon general recently said we should delay access to social media until age 16 because the younger kids are impressionable and vulnerable. I think there is wisdom there, but it is very hard to actually put into practice.”
Worsening mental health
“I thought this was very relevant research and an important contribution to our understanding of eating disorders during pandemic times,” said Simon Sherry, PhD, professor of psychology and neuroscience at Dalhousie University in Halifax, Nova Scotia. “It also dovetails with my own experience as a practitioner.” Dr. Sherry was not involved in the research.
The pandemic has been difficult for people with disordered eating for many reasons, Dr. Sherry said. “There was a massive disruption or ‘loss of normal’ around food. Restaurants closed, grocery shopping was disrupted, scarcity of food occurred, hoarding of food occurred. That meant that eating was difficult for all of us, but especially for individuals who were rigid and controlling around the consumption of food. In this COVID era, you would need flexibility and acceptance around eating, but if you had a narrow range of preferred foods and preferred shopping locations, no doubt the pandemic made this a lot worse.”
Certain forms of disordered eating would be much more likely during the pandemic, Dr. Sherry noted. “For example, binge eating is often triggered by psychological, social, and environmental events,” and those triggers were abundant at the beginning of the pandemic. Boredom, anxiety, depression, stress, loneliness, confinement, and isolation are among the triggers. “COVID-19-related stress was and is very fertile ground for the growth of emotional eating, binge eating, or turning to food to cope. Eating disorders tend to fester amid silence and isolation and inactivity, and that was very much our experience during the lockdown phase of the pandemic,” he said.
Dr. Sherry agrees with the need for more funding for eating disorders research. “We know in Canada that eating disorders are a very important and deadly issue that is chronically underfunded. We are not funding disordered eating in proportion to its prevalence or in proportion to the amount of harm and destruction it creates for individuals, their family members, and our society at large. The authors are absolutely correct to advocate for care in proportion to the prevalence and the damage associated with eating disorders,” he said.
The study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health, the Ministry of Long-Term Care, and the Canadian Institutes of Health Research (CIHR). Dr. Toulany, Dr. Fornari, and Dr. Sherry reported no relevant financial relationships. One study author reported receiving personal fees from the BMJ Group’s Archives of Diseases in Childhood and grants from CIHR, the Ontario Ministry of Health, the Centre for Addiction and Mental Health, and the Hospital for Sick Children. A second author reported funding from CIHR.
A version of this article first appeared on Medscape.com.
In a repeated cross-sectional study that examined population-based data from January 2017 through August 2022, ED visits increased by 121% above expected levels, and hospital admissions increased by 54% above expected among patients aged 10-17 years during the pandemic.
“We are hoping this study continues to heighten awareness of the importance of eating disorders, and also to bolster support for eating disorder programs so that we can adequately care for patients and address the increasing demand for treatment and services,” lead author Alene Toulany, MD, adolescent medicine specialist and researcher at the Hospital for Sick Children in Toronto, told this news organization.
The study was published in the Canadian Medical Association Journal.
‘A pressing concern’
The researchers used linked health administrative databases that included all patients in Ontario who were eligible for the Ontario Health Insurance Plan, which is publicly funded. They compared observed and expected rates of ED visits and hospitalizations for eating disorders between a prepandemic period (Jan. 1, 2017, to Feb. 29, 2020) and a pandemic period (Mar. 1, 2020, to Aug. 31, 2022). The researchers examined the following four age categories: adolescents (aged 10-17 years), young adults (aged 18-26 years), adults (aged 27-40 years), and older adults (aged 41-105 years).
Among adolescents, the observed rate of ED visits during the 30 pandemic months studied was 7.38 per 100,000 population, compared with 3.33 per 100,000 before the pandemic (incidence rate ratio [IRR], 2.21).
The rate of ED visits among young adults increased by 13% above the expected rate. It reached 2.79 per 100,000, compared with 2.46 per 100,000 in the prepandemic period (IRR, 1.13).
Among older adults, ED visits increased from 0.11 per 100,000 in the prepandemic period to 0.14 per 100,000 in the pandemic period (IRR, 1.15). The rate of ED visits among adults remained approximately the same.
The rate of hospital admissions among adolescents increased by 54% above the expected rate during the pandemic. The observed rate of hospital admissions before the pandemic was 5.74 per 100,000, vs. 8.82 per 100,000 during the pandemic (IRR, 1.54). Hospital admissions remained stable or decreased for the other age groups.
“Eating disorders have increased globally in children and adolescents during COVID,” said Dr. Toulany. “There are a number of risk factors contributing to this pandemic rise, including isolation, more time on social media, decreased access to care (as many in-person services were not available due to the pandemic), as well as fear of getting infected. All of these could contribute to an increased risk of developing an eating disorder or of making an existing one worse.”
Regardless of the cause, more investment in eating disorders research and eating disorder programs for adolescents and adults is needed, she said.
“The pandemic served as a catalyst, because it started to shed light on the prevalence of eating disorders, especially in young people. But it’s very important that we recognize that this has been a long-standing issue and a pressing concern that has been consistently overlooked and underfunded,” said Dr. Toulany.
Surging eating disorders
Commenting on the findings, Victor Fornari, MD, director of child and adolescent psychiatry at Zucker Hillside Hospital/Northwell Health in Glen Oaks, N.Y., said, “Our experience in the United States parallels what is described in this Canadian paper. This was a surge of eating disorders the likes of which I had not experienced in my career.” Dr. Fornari did not participate in the current study.
“I’ve been here for over 40 years, and the average number of our inpatients in our eating disorder program has been three to five and about a dozen patients in our day clinic at any one time. But in the spring of 2020, we surged to 20 inpatients and over 20 day patients,” Dr. Fornari said.
“We can speculate as to the reasons for this,” he continued. “Kids were isolated. School was closed. They spent more time on social media and the Internet. Their sports activities were curtailed. There was anxiety because the guidance that we were all offered to prevent contagion was increasing people’s anxiety about safety and danger. So, I think we saw dramatic rises in eating disorders in the same way we saw dramatic rises in anxiety and depression in adolescents, as well.”
Dr. Fornari cited social media as an important contributing factor to eating disorders, especially among vulnerable teenagers. “Many of these vulnerable kids are looking at pictures of people who are very thin and comparing themselves, feeling inadequate, feeling sad. Social media is one of the reasons why the rates of psychopathology amongst teens has skyrocketed in the last decade. The surgeon general recently said we should delay access to social media until age 16 because the younger kids are impressionable and vulnerable. I think there is wisdom there, but it is very hard to actually put into practice.”
Worsening mental health
“I thought this was very relevant research and an important contribution to our understanding of eating disorders during pandemic times,” said Simon Sherry, PhD, professor of psychology and neuroscience at Dalhousie University in Halifax, Nova Scotia. “It also dovetails with my own experience as a practitioner.” Dr. Sherry was not involved in the research.
The pandemic has been difficult for people with disordered eating for many reasons, Dr. Sherry said. “There was a massive disruption or ‘loss of normal’ around food. Restaurants closed, grocery shopping was disrupted, scarcity of food occurred, hoarding of food occurred. That meant that eating was difficult for all of us, but especially for individuals who were rigid and controlling around the consumption of food. In this COVID era, you would need flexibility and acceptance around eating, but if you had a narrow range of preferred foods and preferred shopping locations, no doubt the pandemic made this a lot worse.”
Certain forms of disordered eating would be much more likely during the pandemic, Dr. Sherry noted. “For example, binge eating is often triggered by psychological, social, and environmental events,” and those triggers were abundant at the beginning of the pandemic. Boredom, anxiety, depression, stress, loneliness, confinement, and isolation are among the triggers. “COVID-19-related stress was and is very fertile ground for the growth of emotional eating, binge eating, or turning to food to cope. Eating disorders tend to fester amid silence and isolation and inactivity, and that was very much our experience during the lockdown phase of the pandemic,” he said.
Dr. Sherry agrees with the need for more funding for eating disorders research. “We know in Canada that eating disorders are a very important and deadly issue that is chronically underfunded. We are not funding disordered eating in proportion to its prevalence or in proportion to the amount of harm and destruction it creates for individuals, their family members, and our society at large. The authors are absolutely correct to advocate for care in proportion to the prevalence and the damage associated with eating disorders,” he said.
The study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health, the Ministry of Long-Term Care, and the Canadian Institutes of Health Research (CIHR). Dr. Toulany, Dr. Fornari, and Dr. Sherry reported no relevant financial relationships. One study author reported receiving personal fees from the BMJ Group’s Archives of Diseases in Childhood and grants from CIHR, the Ontario Ministry of Health, the Centre for Addiction and Mental Health, and the Hospital for Sick Children. A second author reported funding from CIHR.
A version of this article first appeared on Medscape.com.
FROM THE CANADIAN MEDICAL ASSOCIATION JOURNAL
Long-Awaited RSV Vaccines Now Available for Older Adults and Pediatric Patients
- Jha A et al. Respiratory syncytial virus. In: Hui DS, Rossi GA, Johnston SL, eds. Respiratory Syncytial Virus. SARS, MERS and Other Viral Lung Infections. European Respiratory Society; 2016:chap 5. Accessed May 17, 2023.
- Ginsburg SA, Srikantiah P. Lancet Glob Health. 2021;9(12):e1644-e6145. doi:10.1016/S2214-109X(21)00455-1
- US Food and Drug Administration. FDA approves first respiratory syncytial virus (RSV) vaccine [press release]. Published May 3, 2023. Accessed May 17, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-first-respiratory-syncytial-virus-rsv-vaccine
- US Food and Drug Administration. FDA Approves New Drug to Prevent RSV in Babies and Toddlers [press release]. Published July 17, 2023. Accessed August 11, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-new-drug-prevent-rsv-babies-and-toddlers
- US Food and Drug Administration. FDA Approves First Vaccine for Pregnant Individuals to Prevent RSV in Infants. Published August 21, 2023. Accessed August 22, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-first-vaccine-pregnant-individuals-prevent-rsv-infants
- Madhi SA et al. N Engl J Med. 2020;383(5):426-439. doi:10.1056/ NEJMoa1908380
- Centers for Disease Control. Advisory Committee on Immunization Practices (ACIP) Meeting recommendations, August 2023. https://www.cdc.gov/vaccines/acip/recommendations.html
- Hammit LL et al. N Engl J Med. 2022;386(9):837-846. doi:10.1056/ NEJMoa2110275
- Centers for Disease Control and Prevention. RSV in infants and young children. Updated October 28, 2022. Accessed May 30, 2023. https://www.cdc.gov/rsv/ high-risk/infants-young-children.html
- Centers for Disease Control and Prevention. RSV in older adults and adults with chronic medical conditions. Updated October 28, 2022. Accessed May 30, 2023. https://www.cdc.gov/rsv/high-risk/older-adults.html
- Widmer K et al. J Infect Dis. 2012;206(1):56-62. doi:10.1093/infdis/jis309
- Hall CB et al. N Engl J Med. 2009;360(6):588-598. doi:10.1056/NEJMoa0804877
- McLaughlin JM et al. Open Forum Infect Dis. 2022;9(7):ofac300. doi:10.1093/ofid/ofac300
- Thompson et al. JAMA. 2003;289(2):179-186. doi:10.1001/jama.289.2.179
- Hansen CL et al. JAMA Netw Open. 2022;5(2):e220527. doi:10.1001/jamanetworkopen.2022.0527
- Walsh EE et al; RENOIR Clinical Trial Group. N Engl J Med. 2023;388(16):1465-1477. doi:10.1056/NEJMoa2213836
- Martin JA et al. Natl Vital Stat Rep. 2019;68(13):1-47. PMID:32501202
- Townsi N et al. Eur Clin Respir J. 2018;5(1):1487214. doi:10.1080/20018525.20 18.1487214
- Malek A et al. Am J Reprod Immunol. 1994;32(1):8-14. doi:10.1111/j.1600-0897.1994.tb00873.x
- Kampmann B et al; MATISSE Study Group. N Engl J Med. 2023;388(16):1451- 1464. doi:10.1056/NEJMoa2216480
- Synagis (palivizumab) injection prescribing information. Published June 2023. Accessed August 2023. https://www.synagis.com/synagis.pdf
- Jha A et al. Respiratory syncytial virus. In: Hui DS, Rossi GA, Johnston SL, eds. Respiratory Syncytial Virus. SARS, MERS and Other Viral Lung Infections. European Respiratory Society; 2016:chap 5. Accessed May 17, 2023.
- Ginsburg SA, Srikantiah P. Lancet Glob Health. 2021;9(12):e1644-e6145. doi:10.1016/S2214-109X(21)00455-1
- US Food and Drug Administration. FDA approves first respiratory syncytial virus (RSV) vaccine [press release]. Published May 3, 2023. Accessed May 17, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-first-respiratory-syncytial-virus-rsv-vaccine
- US Food and Drug Administration. FDA Approves New Drug to Prevent RSV in Babies and Toddlers [press release]. Published July 17, 2023. Accessed August 11, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-new-drug-prevent-rsv-babies-and-toddlers
- US Food and Drug Administration. FDA Approves First Vaccine for Pregnant Individuals to Prevent RSV in Infants. Published August 21, 2023. Accessed August 22, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-first-vaccine-pregnant-individuals-prevent-rsv-infants
- Madhi SA et al. N Engl J Med. 2020;383(5):426-439. doi:10.1056/ NEJMoa1908380
- Centers for Disease Control. Advisory Committee on Immunization Practices (ACIP) Meeting recommendations, August 2023. https://www.cdc.gov/vaccines/acip/recommendations.html
- Hammit LL et al. N Engl J Med. 2022;386(9):837-846. doi:10.1056/ NEJMoa2110275
- Centers for Disease Control and Prevention. RSV in infants and young children. Updated October 28, 2022. Accessed May 30, 2023. https://www.cdc.gov/rsv/ high-risk/infants-young-children.html
- Centers for Disease Control and Prevention. RSV in older adults and adults with chronic medical conditions. Updated October 28, 2022. Accessed May 30, 2023. https://www.cdc.gov/rsv/high-risk/older-adults.html
- Widmer K et al. J Infect Dis. 2012;206(1):56-62. doi:10.1093/infdis/jis309
- Hall CB et al. N Engl J Med. 2009;360(6):588-598. doi:10.1056/NEJMoa0804877
- McLaughlin JM et al. Open Forum Infect Dis. 2022;9(7):ofac300. doi:10.1093/ofid/ofac300
- Thompson et al. JAMA. 2003;289(2):179-186. doi:10.1001/jama.289.2.179
- Hansen CL et al. JAMA Netw Open. 2022;5(2):e220527. doi:10.1001/jamanetworkopen.2022.0527
- Walsh EE et al; RENOIR Clinical Trial Group. N Engl J Med. 2023;388(16):1465-1477. doi:10.1056/NEJMoa2213836
- Martin JA et al. Natl Vital Stat Rep. 2019;68(13):1-47. PMID:32501202
- Townsi N et al. Eur Clin Respir J. 2018;5(1):1487214. doi:10.1080/20018525.20 18.1487214
- Malek A et al. Am J Reprod Immunol. 1994;32(1):8-14. doi:10.1111/j.1600-0897.1994.tb00873.x
- Kampmann B et al; MATISSE Study Group. N Engl J Med. 2023;388(16):1451- 1464. doi:10.1056/NEJMoa2216480
- Synagis (palivizumab) injection prescribing information. Published June 2023. Accessed August 2023. https://www.synagis.com/synagis.pdf
- Jha A et al. Respiratory syncytial virus. In: Hui DS, Rossi GA, Johnston SL, eds. Respiratory Syncytial Virus. SARS, MERS and Other Viral Lung Infections. European Respiratory Society; 2016:chap 5. Accessed May 17, 2023.
- Ginsburg SA, Srikantiah P. Lancet Glob Health. 2021;9(12):e1644-e6145. doi:10.1016/S2214-109X(21)00455-1
- US Food and Drug Administration. FDA approves first respiratory syncytial virus (RSV) vaccine [press release]. Published May 3, 2023. Accessed May 17, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-first-respiratory-syncytial-virus-rsv-vaccine
- US Food and Drug Administration. FDA Approves New Drug to Prevent RSV in Babies and Toddlers [press release]. Published July 17, 2023. Accessed August 11, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-new-drug-prevent-rsv-babies-and-toddlers
- US Food and Drug Administration. FDA Approves First Vaccine for Pregnant Individuals to Prevent RSV in Infants. Published August 21, 2023. Accessed August 22, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-first-vaccine-pregnant-individuals-prevent-rsv-infants
- Madhi SA et al. N Engl J Med. 2020;383(5):426-439. doi:10.1056/ NEJMoa1908380
- Centers for Disease Control. Advisory Committee on Immunization Practices (ACIP) Meeting recommendations, August 2023. https://www.cdc.gov/vaccines/acip/recommendations.html
- Hammit LL et al. N Engl J Med. 2022;386(9):837-846. doi:10.1056/ NEJMoa2110275
- Centers for Disease Control and Prevention. RSV in infants and young children. Updated October 28, 2022. Accessed May 30, 2023. https://www.cdc.gov/rsv/ high-risk/infants-young-children.html
- Centers for Disease Control and Prevention. RSV in older adults and adults with chronic medical conditions. Updated October 28, 2022. Accessed May 30, 2023. https://www.cdc.gov/rsv/high-risk/older-adults.html
- Widmer K et al. J Infect Dis. 2012;206(1):56-62. doi:10.1093/infdis/jis309
- Hall CB et al. N Engl J Med. 2009;360(6):588-598. doi:10.1056/NEJMoa0804877
- McLaughlin JM et al. Open Forum Infect Dis. 2022;9(7):ofac300. doi:10.1093/ofid/ofac300
- Thompson et al. JAMA. 2003;289(2):179-186. doi:10.1001/jama.289.2.179
- Hansen CL et al. JAMA Netw Open. 2022;5(2):e220527. doi:10.1001/jamanetworkopen.2022.0527
- Walsh EE et al; RENOIR Clinical Trial Group. N Engl J Med. 2023;388(16):1465-1477. doi:10.1056/NEJMoa2213836
- Martin JA et al. Natl Vital Stat Rep. 2019;68(13):1-47. PMID:32501202
- Townsi N et al. Eur Clin Respir J. 2018;5(1):1487214. doi:10.1080/20018525.20 18.1487214
- Malek A et al. Am J Reprod Immunol. 1994;32(1):8-14. doi:10.1111/j.1600-0897.1994.tb00873.x
- Kampmann B et al; MATISSE Study Group. N Engl J Med. 2023;388(16):1451- 1464. doi:10.1056/NEJMoa2216480
- Synagis (palivizumab) injection prescribing information. Published June 2023. Accessed August 2023. https://www.synagis.com/synagis.pdf
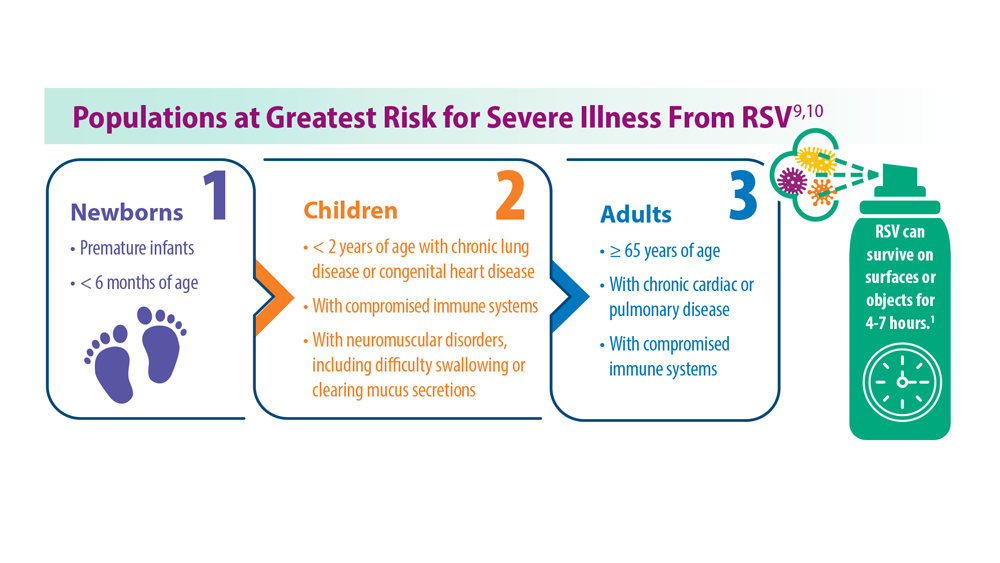
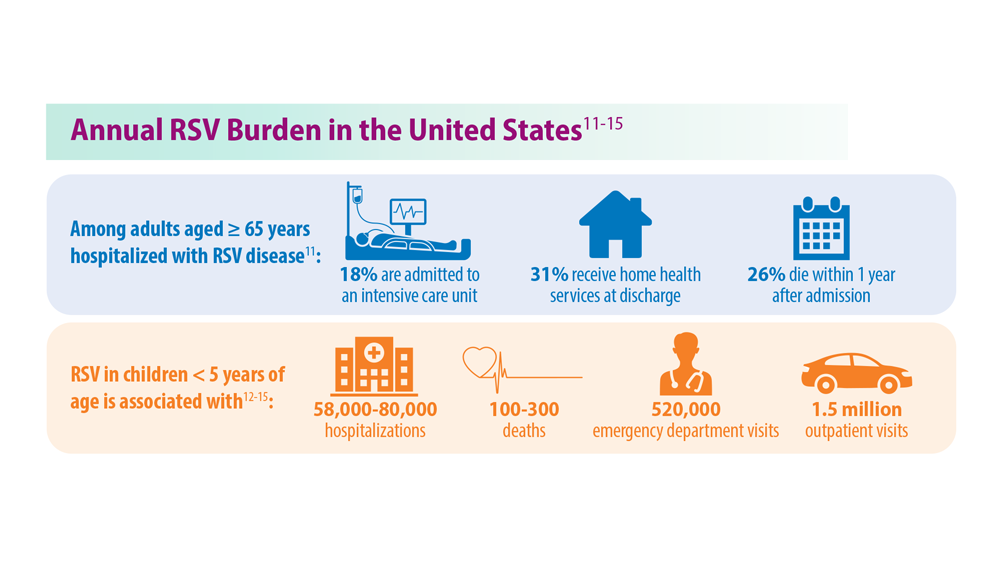
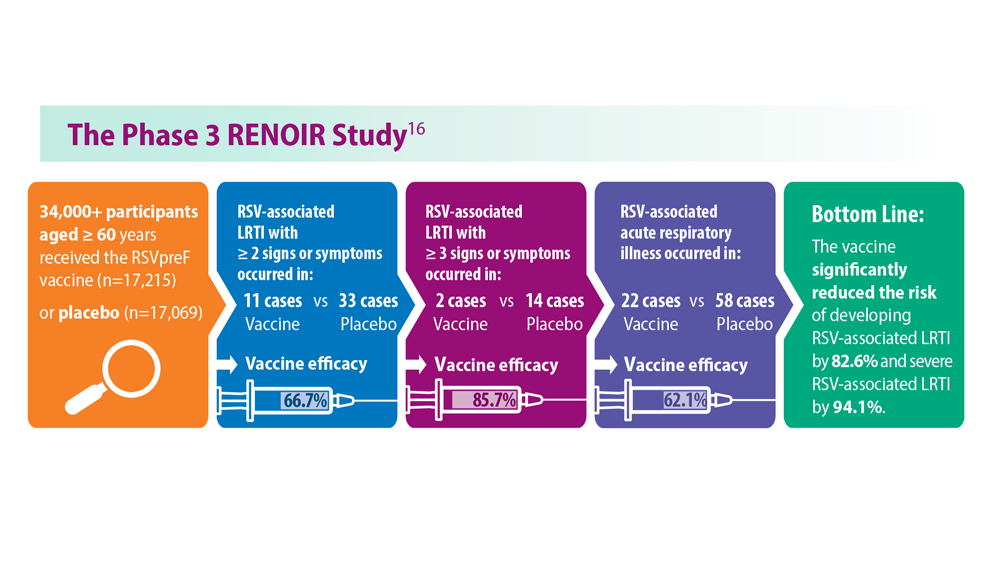
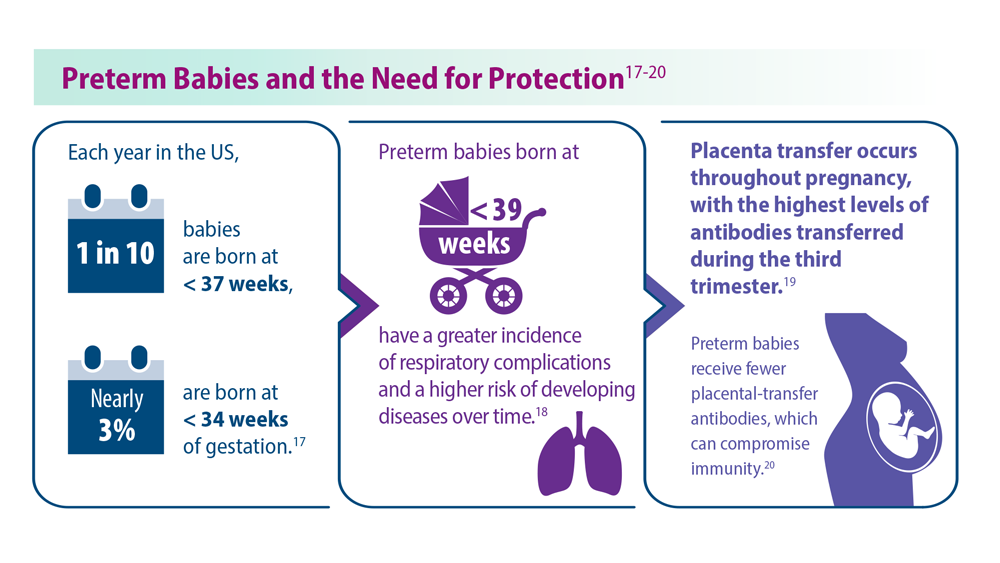
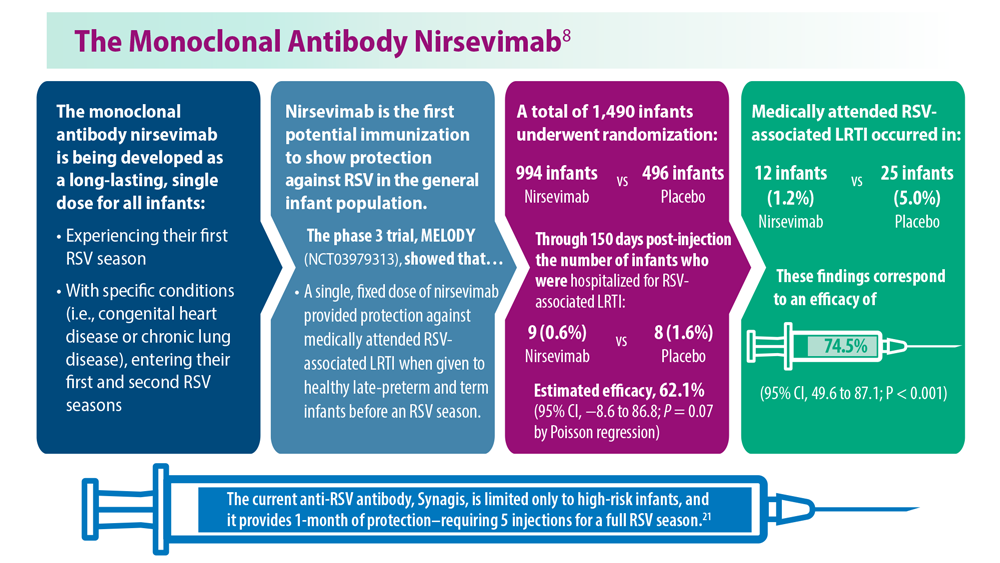
Salvage option to replace transplant in r/r Hodgkin lymphoma?
SAN DIEGO –
Patients who received second-line chemoimmunotherapy with nivolumab-brentuximab vedotin, with or without bendamustine, and proceeded to involved-site radiation appeared to have similar survival outcomes to those who received the chemoimmunotherapy combination plus the current second-line standard of care, which includes high-dose therapy and autologous stem cell transplant.
Among 28 patients with low-risk relapsed or refractory Hodgkin lymphoma followed for a median of 32 months, 3-year event-free survival without autologous stem cell transplant was 86.9% and 3-year progression-free survival was 95%, reported Brad Hoppe, MD, MPH, from the Mayo Clinic in Jacksonville, Fla. In contrast, 1-year progression-free survival was 91% among the 44 standard-risk patients who received high-dose therapy and autologous stem cell transplant, according to results of a trial the investigators published online in Blood in late 2022.
The latest results from the phase 2 CheckMate 744 trial were reported at the annual meeting of the American Society of Radiation Oncology.
“The findings suggest that children, adolescents, and young adults with low-risk relapsed classic Hodgkin lymphoma can be salvaged with low-toxicity chemoimmunotherapy and may not require high-dose therapy and transplant for a cure,” Dr. Hoppe said in an oral abstract session.
Andrea Ng, MD, MPH, a radiation oncologist who specializes in treating patients with Hodgkin lymphoma and other hematologic malignancies, said that, while the number of patients in the study was small and the follow-up too short, this option is “certainly something that’s very promising for the future.”
“The use of transplant in relapsed patients, which we have been doing for decades, is based on two very old, small, randomized studies,” said Dr. Ng, from the Dana-Farber Cancer Institute in Boston, who moderated the session.
“So, do we really need to transplant everybody? In the back of our minds, we think that we may be overtreating some patients,” she said.
Several small, retrospective studies exploring treatment with conventional chemotherapy with or without radiation therapy and without transplant in patients with relapsed or refractory Hodgkin lymphoma have demonstrated only modest results.
The CheckMate 744 trial, however, was designed to examine a risk-adapted and response-adapted approach to treating children, adolescents, and young adults with relapsed or refractory classic Hodgkin lymphoma within the setting of modern immunotherapy and targeted therapy. This approach was developed jointly by investigators with the Children’s Oncology Group and Euronet.
In the nonrandomized trial, patients were stratified into low-risk or standard-risk disease categories based on an algorithm that included factors at the time of initial diagnosis and relapse.
Patients were considered low-risk for relapse in three scenarios: (1) if they had initial stage IA or IIA disease that relapsed at least 1 year after the end of therapy; (2) if they had initial stage IA or IIA disease that relapsed between 3 and 12 months from the end of therapy but had received no more than three cycles of chemotherapy and no radiation therapy; or (3) if they had initial stage IB, IIB, or IIIA disease that relapsed more than 12 months after the end of first-line therapy.
To be included in the low-risk category, patients also had to be free of B symptoms or extranodal disease, free of relapse in prior radiation therapy fields, and have no more than four sites of lymphoma.
Low-risk patients were treated with a combination of nivolumab and brentuximab vedotin, which could be followed by additional brentuximab vedotin and bendamustine for those with a suboptimal response. Patients who achieved complete molecular remission after induction went on to consolidation therapy with involved-site radiation at a total dose of 30 Gy.
Patients considered standard-risk for relapse received the same nivolumab-brentuximab vedotin combination, with or without bendamustine, and then went on to high-dose therapy and autologous stem cell transplant.
In other results for the previously mentioned study published in Blood, the 44 standard-risk patients who received high-dose therapy and autologous stem cell transplant had an objective response rate of 95% – 86% of patients achieved complete molecular remission, and 9% achieved partial molecular remission.
At ASTRO, Dr. Hoppe reported results for the 28 patients with low-risk disease. One patient discontinued nivolumab/brentuximab vedotin after two cycles because of skin toxicity and was lost to follow-up. Of the remaining 27 patients, 21 had complete molecular remission after four cycles of the combination, and these patients went on to an additional two cycles of the combination, with 19 of 21 receiving involved-site radiation consolidation.
Six patients who had either a partial molecular remission or no response were given two additional cycles of brentuximab vedotin plus bendamustine. Of this group, three went on to complete molecular remission and received involved-site radiation consolidation on protocol. The remaining three patients who did not experience complete molecular remission received involved-site radiation off protocol.
The rate of complete molecular remission after four cycles of induction was 82.1%, and the rate of partial molecular remission was 14.3%, for an objective response rate of 96.4%. The respective response rates with the addition of two cycles of brentuximab vedotin and bendamustine were 92.9% and 7.1%, for an objective response rate of 100%, Dr. Hoppe reported.
Overall, at a median follow-up of 32 months, the 3-year event-free survival rate without transplant was 86.9%, and the 3-year progression-free survival rate was 95%.
Treatment-related adverse events of any grade occurred in 22 patients (78.6%) after induction, with 7 of those events (25%) being grade 3 or 4 in severity. Grade 3 or 4 events consisted of skin and subcutaneous tissue disorders in 3 patients, elevated liver function tests in 3 patients, and blood and lymphatic system disorders in 1 patient.
There were no new toxicities detected within 100 days of treatment.
“The results that Dr. Hoppe showed us are really, really good,” Dr. Ng said. And “the volume of treatment is pretty tiny, so I think we can safely say that long-term toxicities are very, very minimal.”
The study was supported by Bristol-Myers Squibb in collaboration with Seagen, Euronet-Paediatric Hodgkin Lymphoma, and the Children’s Oncology Group. Dr. Hoppe reported serving on a scientific advisory committee for Merck. Dr. Ng reported having no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
SAN DIEGO –
Patients who received second-line chemoimmunotherapy with nivolumab-brentuximab vedotin, with or without bendamustine, and proceeded to involved-site radiation appeared to have similar survival outcomes to those who received the chemoimmunotherapy combination plus the current second-line standard of care, which includes high-dose therapy and autologous stem cell transplant.
Among 28 patients with low-risk relapsed or refractory Hodgkin lymphoma followed for a median of 32 months, 3-year event-free survival without autologous stem cell transplant was 86.9% and 3-year progression-free survival was 95%, reported Brad Hoppe, MD, MPH, from the Mayo Clinic in Jacksonville, Fla. In contrast, 1-year progression-free survival was 91% among the 44 standard-risk patients who received high-dose therapy and autologous stem cell transplant, according to results of a trial the investigators published online in Blood in late 2022.
The latest results from the phase 2 CheckMate 744 trial were reported at the annual meeting of the American Society of Radiation Oncology.
“The findings suggest that children, adolescents, and young adults with low-risk relapsed classic Hodgkin lymphoma can be salvaged with low-toxicity chemoimmunotherapy and may not require high-dose therapy and transplant for a cure,” Dr. Hoppe said in an oral abstract session.
Andrea Ng, MD, MPH, a radiation oncologist who specializes in treating patients with Hodgkin lymphoma and other hematologic malignancies, said that, while the number of patients in the study was small and the follow-up too short, this option is “certainly something that’s very promising for the future.”
“The use of transplant in relapsed patients, which we have been doing for decades, is based on two very old, small, randomized studies,” said Dr. Ng, from the Dana-Farber Cancer Institute in Boston, who moderated the session.
“So, do we really need to transplant everybody? In the back of our minds, we think that we may be overtreating some patients,” she said.
Several small, retrospective studies exploring treatment with conventional chemotherapy with or without radiation therapy and without transplant in patients with relapsed or refractory Hodgkin lymphoma have demonstrated only modest results.
The CheckMate 744 trial, however, was designed to examine a risk-adapted and response-adapted approach to treating children, adolescents, and young adults with relapsed or refractory classic Hodgkin lymphoma within the setting of modern immunotherapy and targeted therapy. This approach was developed jointly by investigators with the Children’s Oncology Group and Euronet.
In the nonrandomized trial, patients were stratified into low-risk or standard-risk disease categories based on an algorithm that included factors at the time of initial diagnosis and relapse.
Patients were considered low-risk for relapse in three scenarios: (1) if they had initial stage IA or IIA disease that relapsed at least 1 year after the end of therapy; (2) if they had initial stage IA or IIA disease that relapsed between 3 and 12 months from the end of therapy but had received no more than three cycles of chemotherapy and no radiation therapy; or (3) if they had initial stage IB, IIB, or IIIA disease that relapsed more than 12 months after the end of first-line therapy.
To be included in the low-risk category, patients also had to be free of B symptoms or extranodal disease, free of relapse in prior radiation therapy fields, and have no more than four sites of lymphoma.
Low-risk patients were treated with a combination of nivolumab and brentuximab vedotin, which could be followed by additional brentuximab vedotin and bendamustine for those with a suboptimal response. Patients who achieved complete molecular remission after induction went on to consolidation therapy with involved-site radiation at a total dose of 30 Gy.
Patients considered standard-risk for relapse received the same nivolumab-brentuximab vedotin combination, with or without bendamustine, and then went on to high-dose therapy and autologous stem cell transplant.
In other results for the previously mentioned study published in Blood, the 44 standard-risk patients who received high-dose therapy and autologous stem cell transplant had an objective response rate of 95% – 86% of patients achieved complete molecular remission, and 9% achieved partial molecular remission.
At ASTRO, Dr. Hoppe reported results for the 28 patients with low-risk disease. One patient discontinued nivolumab/brentuximab vedotin after two cycles because of skin toxicity and was lost to follow-up. Of the remaining 27 patients, 21 had complete molecular remission after four cycles of the combination, and these patients went on to an additional two cycles of the combination, with 19 of 21 receiving involved-site radiation consolidation.
Six patients who had either a partial molecular remission or no response were given two additional cycles of brentuximab vedotin plus bendamustine. Of this group, three went on to complete molecular remission and received involved-site radiation consolidation on protocol. The remaining three patients who did not experience complete molecular remission received involved-site radiation off protocol.
The rate of complete molecular remission after four cycles of induction was 82.1%, and the rate of partial molecular remission was 14.3%, for an objective response rate of 96.4%. The respective response rates with the addition of two cycles of brentuximab vedotin and bendamustine were 92.9% and 7.1%, for an objective response rate of 100%, Dr. Hoppe reported.
Overall, at a median follow-up of 32 months, the 3-year event-free survival rate without transplant was 86.9%, and the 3-year progression-free survival rate was 95%.
Treatment-related adverse events of any grade occurred in 22 patients (78.6%) after induction, with 7 of those events (25%) being grade 3 or 4 in severity. Grade 3 or 4 events consisted of skin and subcutaneous tissue disorders in 3 patients, elevated liver function tests in 3 patients, and blood and lymphatic system disorders in 1 patient.
There were no new toxicities detected within 100 days of treatment.
“The results that Dr. Hoppe showed us are really, really good,” Dr. Ng said. And “the volume of treatment is pretty tiny, so I think we can safely say that long-term toxicities are very, very minimal.”
The study was supported by Bristol-Myers Squibb in collaboration with Seagen, Euronet-Paediatric Hodgkin Lymphoma, and the Children’s Oncology Group. Dr. Hoppe reported serving on a scientific advisory committee for Merck. Dr. Ng reported having no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
SAN DIEGO –
Patients who received second-line chemoimmunotherapy with nivolumab-brentuximab vedotin, with or without bendamustine, and proceeded to involved-site radiation appeared to have similar survival outcomes to those who received the chemoimmunotherapy combination plus the current second-line standard of care, which includes high-dose therapy and autologous stem cell transplant.
Among 28 patients with low-risk relapsed or refractory Hodgkin lymphoma followed for a median of 32 months, 3-year event-free survival without autologous stem cell transplant was 86.9% and 3-year progression-free survival was 95%, reported Brad Hoppe, MD, MPH, from the Mayo Clinic in Jacksonville, Fla. In contrast, 1-year progression-free survival was 91% among the 44 standard-risk patients who received high-dose therapy and autologous stem cell transplant, according to results of a trial the investigators published online in Blood in late 2022.
The latest results from the phase 2 CheckMate 744 trial were reported at the annual meeting of the American Society of Radiation Oncology.
“The findings suggest that children, adolescents, and young adults with low-risk relapsed classic Hodgkin lymphoma can be salvaged with low-toxicity chemoimmunotherapy and may not require high-dose therapy and transplant for a cure,” Dr. Hoppe said in an oral abstract session.
Andrea Ng, MD, MPH, a radiation oncologist who specializes in treating patients with Hodgkin lymphoma and other hematologic malignancies, said that, while the number of patients in the study was small and the follow-up too short, this option is “certainly something that’s very promising for the future.”
“The use of transplant in relapsed patients, which we have been doing for decades, is based on two very old, small, randomized studies,” said Dr. Ng, from the Dana-Farber Cancer Institute in Boston, who moderated the session.
“So, do we really need to transplant everybody? In the back of our minds, we think that we may be overtreating some patients,” she said.
Several small, retrospective studies exploring treatment with conventional chemotherapy with or without radiation therapy and without transplant in patients with relapsed or refractory Hodgkin lymphoma have demonstrated only modest results.
The CheckMate 744 trial, however, was designed to examine a risk-adapted and response-adapted approach to treating children, adolescents, and young adults with relapsed or refractory classic Hodgkin lymphoma within the setting of modern immunotherapy and targeted therapy. This approach was developed jointly by investigators with the Children’s Oncology Group and Euronet.
In the nonrandomized trial, patients were stratified into low-risk or standard-risk disease categories based on an algorithm that included factors at the time of initial diagnosis and relapse.
Patients were considered low-risk for relapse in three scenarios: (1) if they had initial stage IA or IIA disease that relapsed at least 1 year after the end of therapy; (2) if they had initial stage IA or IIA disease that relapsed between 3 and 12 months from the end of therapy but had received no more than three cycles of chemotherapy and no radiation therapy; or (3) if they had initial stage IB, IIB, or IIIA disease that relapsed more than 12 months after the end of first-line therapy.
To be included in the low-risk category, patients also had to be free of B symptoms or extranodal disease, free of relapse in prior radiation therapy fields, and have no more than four sites of lymphoma.
Low-risk patients were treated with a combination of nivolumab and brentuximab vedotin, which could be followed by additional brentuximab vedotin and bendamustine for those with a suboptimal response. Patients who achieved complete molecular remission after induction went on to consolidation therapy with involved-site radiation at a total dose of 30 Gy.
Patients considered standard-risk for relapse received the same nivolumab-brentuximab vedotin combination, with or without bendamustine, and then went on to high-dose therapy and autologous stem cell transplant.
In other results for the previously mentioned study published in Blood, the 44 standard-risk patients who received high-dose therapy and autologous stem cell transplant had an objective response rate of 95% – 86% of patients achieved complete molecular remission, and 9% achieved partial molecular remission.
At ASTRO, Dr. Hoppe reported results for the 28 patients with low-risk disease. One patient discontinued nivolumab/brentuximab vedotin after two cycles because of skin toxicity and was lost to follow-up. Of the remaining 27 patients, 21 had complete molecular remission after four cycles of the combination, and these patients went on to an additional two cycles of the combination, with 19 of 21 receiving involved-site radiation consolidation.
Six patients who had either a partial molecular remission or no response were given two additional cycles of brentuximab vedotin plus bendamustine. Of this group, three went on to complete molecular remission and received involved-site radiation consolidation on protocol. The remaining three patients who did not experience complete molecular remission received involved-site radiation off protocol.
The rate of complete molecular remission after four cycles of induction was 82.1%, and the rate of partial molecular remission was 14.3%, for an objective response rate of 96.4%. The respective response rates with the addition of two cycles of brentuximab vedotin and bendamustine were 92.9% and 7.1%, for an objective response rate of 100%, Dr. Hoppe reported.
Overall, at a median follow-up of 32 months, the 3-year event-free survival rate without transplant was 86.9%, and the 3-year progression-free survival rate was 95%.
Treatment-related adverse events of any grade occurred in 22 patients (78.6%) after induction, with 7 of those events (25%) being grade 3 or 4 in severity. Grade 3 or 4 events consisted of skin and subcutaneous tissue disorders in 3 patients, elevated liver function tests in 3 patients, and blood and lymphatic system disorders in 1 patient.
There were no new toxicities detected within 100 days of treatment.
“The results that Dr. Hoppe showed us are really, really good,” Dr. Ng said. And “the volume of treatment is pretty tiny, so I think we can safely say that long-term toxicities are very, very minimal.”
The study was supported by Bristol-Myers Squibb in collaboration with Seagen, Euronet-Paediatric Hodgkin Lymphoma, and the Children’s Oncology Group. Dr. Hoppe reported serving on a scientific advisory committee for Merck. Dr. Ng reported having no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
AT ASTRO 2023
Preparing for the viral trifecta: RSV, influenza, and COVID-19
New armamentaria available to fight an old disease.
In July 2023, nirsevimab (Beyfortus), a monoclonal antibody, was approved by the Food and Drug Administration for the prevention of respiratory syncytial virus (RSV) disease in infants and children younger than 2 years of age. On Aug. 3, 2023, the Advisory Committee on Immunization Practices (ACIP) of the Centers for Disease Control and Prevention recommended routine use of it for all infants younger than 8 months of age born during or entering their first RSV season. Its use is also recommended for certain children 8-19 months of age who are at increased risk for severe RSV disease at the start of their second RSV season. Hearing the approval, I immediately had a flashback to residency, recalling the multiple infants admitted each fall and winter exhibiting classic symptoms including cough, rhinorrhea, nasal flaring, retractions, and wheezing with many having oxygen requirements and others needing intubation. Only supportive care was available.
RSV is the leading cause of infant hospitalizations. Annually, the CDC estimates there are 50,000-80,000 RSV hospitalizations and 100-300 RSV-related deaths in the United States in persons younger than 5 years of age. While premature infants have the highest rates of hospitalization (three times a term infant) about 79% of hospitalized children younger than 2 years have no underlying medical risks.1 The majority of children will experience RSV as an upper respiratory infection within the first 2 years of life. However, severe disease requiring hospitalization is more likely to occur in premature infants and children younger than 6 months; children younger than 2 with congenital heart disease and/or chronic lung disease; children with severe cystic fibrosis; as well as the immunocompromised child and individuals with neuromuscular disorders that preclude clearing mucous secretions or have difficulty swallowing.

Palivizumab (Synagis), the first monoclonal antibody to prevent RSV in infants was licensed in 1998. Its use was limited to infants meeting specific criteria developed by the American Academy of Pediatrics. Only 5% of infants had access to it. It was a short-acting agent requiring monthly injections, which were very costly ($1,661-$2,584 per dose). Eligible infants could receive up to five injections per season. Several studies proved its use was not cost beneficial.
What are the advantages of nirsevimab? It’s a long-acting monoclonal antibody. Only one dose is required per season. Costs will significantly diminish. It is recommended for all infants younger than 8 months of age born during RSV season. Those children 8-19 months at risk for severe RSV disease can receive it prior to the start of their second RSV season. During RSV season (October 1 to March 31), the initial dose should be administered to newborns just prior to hospital discharge. Older infants and newborns who did not receive it prior to hospital discharge can receive it at their medical home. Newborns should receive it within the first week of life. It is covered by the Vaccine for Children Program. Simultaneous administration with routine childhood immunizations is recommended. Finally, RSV season may vary in tropical areas (Southern Florida, Puerto Rico. etc.) and Alaska. The timing of nirsevimab administration should be based on local RSV activity provided by state and local authorities.
In addition, the FDA approved an RSV vaccine (Abrysvo) for use in adults at least 60 years of age and in pregnant women at 32-36 weeks’ gestation. The latter is administered to prevent lower respiratory tract infection in infants from birth to 6 months. Recommendations have been published for administration in nonpregnant adults. Specific information is forthcoming in terms timing of administration of nirsevimab in infants whose mothers receive Abrysvo.
RSV season is quickly approaching. Detailed recommendations for administration and FAQ questions related to nirsevimab and palivizumab can be found at https://www.aap.org or https://www.cdc.gov/vaccines/hcp/acip-recs/index.html.
Influenza
So, what about influenza? Vaccine composition has been tweaked to match the circulating viruses but the recommended age for annual routine administration remains unchanged. All persons at least 6 months of age should be vaccinated. Children between 6 months and 8 years need two doses at least 4 weeks apart when receiving vaccine for the first time. Immunizing everyone in the household is encouraged especially if there are household contacts at risk for developing severe disease, including infants too young to be vaccinated. Keep in mind children may be coinfected with multiple viruses. Adams and colleagues reviewed the prevalence of coinfection of influenza and Sars-CoV-2 in persons younger than 18 years reported to three CDC surveillance platforms during the 2021-2022 season.2 Thirty-two of 575 hospitalized (6%) coinfections were analyzed and 7 of 44 (16%) deaths. Compared with patients without coinfections, the coinfected patients were more likely to require mechanical ventilation (13% vs. 4%) or CPAP (16% vs. 6%). Only 4 of 23 who were influenza vaccine eligible were vaccinated. Of seven coinfected children who died, none had received influenza vaccine and only one received an antiviral. Only 5 of 31 (16%) infected only with influenza were vaccinated.3
Influenza activity was lower than usual during the 2021-2022 season. However, this report revealed underuse of both influenza vaccine and antiviral therapy, both of which are routinely recommended.
COVID-19
What’s new with COVID-19? On Sept. 12, 2023, ACIP recommended that everyone at least 6 months of age receive the 2023-2024 (monovalent, XBB containing) COVID-19 vaccines. Children at least 5 years of age need one dose and those younger need one or two doses depending on the number of doses previously received. Why the change? Circulating variants continue to change. There is a current uptick in cases including hospitalizations (7.7%) and deaths (4.5%) and it’s just the beginning of the season.4 Symptoms, risk groups and complications have not changed. The primary goal is to prevent infection, hospitalization, long term complications, and death.
We are now armed with the most up-to-date interventions to help prevent the acquisition of these three viruses. Our next step is recommending and delivering them to our patients.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She reported no relevant financial disclosures.
References
1.Suh M et al. J Infect Dis. 2022;226(Suppl 2):S154-36. doi: 10.1093/infdis/jiac120.
2. Adams K et al. MMWR Morb Mortal Wkly Rep. 2022;71:1589-96. doi: http://dx.doi.org/10.15585/mmwr.mm7150a4.
3. Pingali C et al. MMWR Morb Mortal Wkly Rep. 2023 Aug 25;72:912-9. doi: http://dx.doi.org/10.15585/mmwr.mm7234a3.
4. CDC Covid Data Tracker.
New armamentaria available to fight an old disease.
New armamentaria available to fight an old disease.
In July 2023, nirsevimab (Beyfortus), a monoclonal antibody, was approved by the Food and Drug Administration for the prevention of respiratory syncytial virus (RSV) disease in infants and children younger than 2 years of age. On Aug. 3, 2023, the Advisory Committee on Immunization Practices (ACIP) of the Centers for Disease Control and Prevention recommended routine use of it for all infants younger than 8 months of age born during or entering their first RSV season. Its use is also recommended for certain children 8-19 months of age who are at increased risk for severe RSV disease at the start of their second RSV season. Hearing the approval, I immediately had a flashback to residency, recalling the multiple infants admitted each fall and winter exhibiting classic symptoms including cough, rhinorrhea, nasal flaring, retractions, and wheezing with many having oxygen requirements and others needing intubation. Only supportive care was available.
RSV is the leading cause of infant hospitalizations. Annually, the CDC estimates there are 50,000-80,000 RSV hospitalizations and 100-300 RSV-related deaths in the United States in persons younger than 5 years of age. While premature infants have the highest rates of hospitalization (three times a term infant) about 79% of hospitalized children younger than 2 years have no underlying medical risks.1 The majority of children will experience RSV as an upper respiratory infection within the first 2 years of life. However, severe disease requiring hospitalization is more likely to occur in premature infants and children younger than 6 months; children younger than 2 with congenital heart disease and/or chronic lung disease; children with severe cystic fibrosis; as well as the immunocompromised child and individuals with neuromuscular disorders that preclude clearing mucous secretions or have difficulty swallowing.
Palivizumab (Synagis), the first monoclonal antibody to prevent RSV in infants was licensed in 1998. Its use was limited to infants meeting specific criteria developed by the American Academy of Pediatrics. Only 5% of infants had access to it. It was a short-acting agent requiring monthly injections, which were very costly ($1,661-$2,584 per dose). Eligible infants could receive up to five injections per season. Several studies proved its use was not cost beneficial.
What are the advantages of nirsevimab? It’s a long-acting monoclonal antibody. Only one dose is required per season. Costs will significantly diminish. It is recommended for all infants younger than 8 months of age born during RSV season. Those children 8-19 months at risk for severe RSV disease can receive it prior to the start of their second RSV season. During RSV season (October 1 to March 31), the initial dose should be administered to newborns just prior to hospital discharge. Older infants and newborns who did not receive it prior to hospital discharge can receive it at their medical home. Newborns should receive it within the first week of life. It is covered by the Vaccine for Children Program. Simultaneous administration with routine childhood immunizations is recommended. Finally, RSV season may vary in tropical areas (Southern Florida, Puerto Rico. etc.) and Alaska. The timing of nirsevimab administration should be based on local RSV activity provided by state and local authorities.
In addition, the FDA approved an RSV vaccine (Abrysvo) for use in adults at least 60 years of age and in pregnant women at 32-36 weeks’ gestation. The latter is administered to prevent lower respiratory tract infection in infants from birth to 6 months. Recommendations have been published for administration in nonpregnant adults. Specific information is forthcoming in terms timing of administration of nirsevimab in infants whose mothers receive Abrysvo.
RSV season is quickly approaching. Detailed recommendations for administration and FAQ questions related to nirsevimab and palivizumab can be found at https://www.aap.org or https://www.cdc.gov/vaccines/hcp/acip-recs/index.html.
Influenza
So, what about influenza? Vaccine composition has been tweaked to match the circulating viruses but the recommended age for annual routine administration remains unchanged. All persons at least 6 months of age should be vaccinated. Children between 6 months and 8 years need two doses at least 4 weeks apart when receiving vaccine for the first time. Immunizing everyone in the household is encouraged especially if there are household contacts at risk for developing severe disease, including infants too young to be vaccinated. Keep in mind children may be coinfected with multiple viruses. Adams and colleagues reviewed the prevalence of coinfection of influenza and Sars-CoV-2 in persons younger than 18 years reported to three CDC surveillance platforms during the 2021-2022 season.2 Thirty-two of 575 hospitalized (6%) coinfections were analyzed and 7 of 44 (16%) deaths. Compared with patients without coinfections, the coinfected patients were more likely to require mechanical ventilation (13% vs. 4%) or CPAP (16% vs. 6%). Only 4 of 23 who were influenza vaccine eligible were vaccinated. Of seven coinfected children who died, none had received influenza vaccine and only one received an antiviral. Only 5 of 31 (16%) infected only with influenza were vaccinated.3
Influenza activity was lower than usual during the 2021-2022 season. However, this report revealed underuse of both influenza vaccine and antiviral therapy, both of which are routinely recommended.
COVID-19
What’s new with COVID-19? On Sept. 12, 2023, ACIP recommended that everyone at least 6 months of age receive the 2023-2024 (monovalent, XBB containing) COVID-19 vaccines. Children at least 5 years of age need one dose and those younger need one or two doses depending on the number of doses previously received. Why the change? Circulating variants continue to change. There is a current uptick in cases including hospitalizations (7.7%) and deaths (4.5%) and it’s just the beginning of the season.4 Symptoms, risk groups and complications have not changed. The primary goal is to prevent infection, hospitalization, long term complications, and death.
We are now armed with the most up-to-date interventions to help prevent the acquisition of these three viruses. Our next step is recommending and delivering them to our patients.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She reported no relevant financial disclosures.
References
1.Suh M et al. J Infect Dis. 2022;226(Suppl 2):S154-36. doi: 10.1093/infdis/jiac120.
2. Adams K et al. MMWR Morb Mortal Wkly Rep. 2022;71:1589-96. doi: http://dx.doi.org/10.15585/mmwr.mm7150a4.
3. Pingali C et al. MMWR Morb Mortal Wkly Rep. 2023 Aug 25;72:912-9. doi: http://dx.doi.org/10.15585/mmwr.mm7234a3.
4. CDC Covid Data Tracker.
In July 2023, nirsevimab (Beyfortus), a monoclonal antibody, was approved by the Food and Drug Administration for the prevention of respiratory syncytial virus (RSV) disease in infants and children younger than 2 years of age. On Aug. 3, 2023, the Advisory Committee on Immunization Practices (ACIP) of the Centers for Disease Control and Prevention recommended routine use of it for all infants younger than 8 months of age born during or entering their first RSV season. Its use is also recommended for certain children 8-19 months of age who are at increased risk for severe RSV disease at the start of their second RSV season. Hearing the approval, I immediately had a flashback to residency, recalling the multiple infants admitted each fall and winter exhibiting classic symptoms including cough, rhinorrhea, nasal flaring, retractions, and wheezing with many having oxygen requirements and others needing intubation. Only supportive care was available.
RSV is the leading cause of infant hospitalizations. Annually, the CDC estimates there are 50,000-80,000 RSV hospitalizations and 100-300 RSV-related deaths in the United States in persons younger than 5 years of age. While premature infants have the highest rates of hospitalization (three times a term infant) about 79% of hospitalized children younger than 2 years have no underlying medical risks.1 The majority of children will experience RSV as an upper respiratory infection within the first 2 years of life. However, severe disease requiring hospitalization is more likely to occur in premature infants and children younger than 6 months; children younger than 2 with congenital heart disease and/or chronic lung disease; children with severe cystic fibrosis; as well as the immunocompromised child and individuals with neuromuscular disorders that preclude clearing mucous secretions or have difficulty swallowing.
Palivizumab (Synagis), the first monoclonal antibody to prevent RSV in infants was licensed in 1998. Its use was limited to infants meeting specific criteria developed by the American Academy of Pediatrics. Only 5% of infants had access to it. It was a short-acting agent requiring monthly injections, which were very costly ($1,661-$2,584 per dose). Eligible infants could receive up to five injections per season. Several studies proved its use was not cost beneficial.
What are the advantages of nirsevimab? It’s a long-acting monoclonal antibody. Only one dose is required per season. Costs will significantly diminish. It is recommended for all infants younger than 8 months of age born during RSV season. Those children 8-19 months at risk for severe RSV disease can receive it prior to the start of their second RSV season. During RSV season (October 1 to March 31), the initial dose should be administered to newborns just prior to hospital discharge. Older infants and newborns who did not receive it prior to hospital discharge can receive it at their medical home. Newborns should receive it within the first week of life. It is covered by the Vaccine for Children Program. Simultaneous administration with routine childhood immunizations is recommended. Finally, RSV season may vary in tropical areas (Southern Florida, Puerto Rico. etc.) and Alaska. The timing of nirsevimab administration should be based on local RSV activity provided by state and local authorities.
In addition, the FDA approved an RSV vaccine (Abrysvo) for use in adults at least 60 years of age and in pregnant women at 32-36 weeks’ gestation. The latter is administered to prevent lower respiratory tract infection in infants from birth to 6 months. Recommendations have been published for administration in nonpregnant adults. Specific information is forthcoming in terms timing of administration of nirsevimab in infants whose mothers receive Abrysvo.
RSV season is quickly approaching. Detailed recommendations for administration and FAQ questions related to nirsevimab and palivizumab can be found at https://www.aap.org or https://www.cdc.gov/vaccines/hcp/acip-recs/index.html.
Influenza
So, what about influenza? Vaccine composition has been tweaked to match the circulating viruses but the recommended age for annual routine administration remains unchanged. All persons at least 6 months of age should be vaccinated. Children between 6 months and 8 years need two doses at least 4 weeks apart when receiving vaccine for the first time. Immunizing everyone in the household is encouraged especially if there are household contacts at risk for developing severe disease, including infants too young to be vaccinated. Keep in mind children may be coinfected with multiple viruses. Adams and colleagues reviewed the prevalence of coinfection of influenza and Sars-CoV-2 in persons younger than 18 years reported to three CDC surveillance platforms during the 2021-2022 season.2 Thirty-two of 575 hospitalized (6%) coinfections were analyzed and 7 of 44 (16%) deaths. Compared with patients without coinfections, the coinfected patients were more likely to require mechanical ventilation (13% vs. 4%) or CPAP (16% vs. 6%). Only 4 of 23 who were influenza vaccine eligible were vaccinated. Of seven coinfected children who died, none had received influenza vaccine and only one received an antiviral. Only 5 of 31 (16%) infected only with influenza were vaccinated.3
Influenza activity was lower than usual during the 2021-2022 season. However, this report revealed underuse of both influenza vaccine and antiviral therapy, both of which are routinely recommended.
COVID-19
What’s new with COVID-19? On Sept. 12, 2023, ACIP recommended that everyone at least 6 months of age receive the 2023-2024 (monovalent, XBB containing) COVID-19 vaccines. Children at least 5 years of age need one dose and those younger need one or two doses depending on the number of doses previously received. Why the change? Circulating variants continue to change. There is a current uptick in cases including hospitalizations (7.7%) and deaths (4.5%) and it’s just the beginning of the season.4 Symptoms, risk groups and complications have not changed. The primary goal is to prevent infection, hospitalization, long term complications, and death.
We are now armed with the most up-to-date interventions to help prevent the acquisition of these three viruses. Our next step is recommending and delivering them to our patients.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She reported no relevant financial disclosures.
References
1.Suh M et al. J Infect Dis. 2022;226(Suppl 2):S154-36. doi: 10.1093/infdis/jiac120.
2. Adams K et al. MMWR Morb Mortal Wkly Rep. 2022;71:1589-96. doi: http://dx.doi.org/10.15585/mmwr.mm7150a4.
3. Pingali C et al. MMWR Morb Mortal Wkly Rep. 2023 Aug 25;72:912-9. doi: http://dx.doi.org/10.15585/mmwr.mm7234a3.
4. CDC Covid Data Tracker.