User login
Measles: 26 new cases reported last week
according to the Centers for Disease Control and Prevention.
On Jan. 31, total measles cases stood at 79, which means that the number of individuals with measles has risen by 61% in just the last 2 weeks. Of the five outbreaks (defined as three or more cases) so far in 2019, three have occurred in New York (57 cases in three counties), one in Texas (8 cases in five counties), and one in Washington (62 cases in two counties), the CDC reported Feb. 18.
The majority of the Washington cases (61 of the 62) have occurred in Clark County, which is located just across the Columbia River from Portland, Ore. Oregon, in turn, has a higher percentage of kindergartners with nonmedical exemptions from vaccination (7.5%) than any other state, the CDC reported in October 2018. Washington’s rate of 3.9% was nearly double the national median of 2.0% for the 2017-2018 school year, while Texas (1.8%) and New York (1.0%) were below it, the CDC said.
In the Pacific Northwest, however, some parents may be changing their minds about vaccinations, according to the New York Times, which reported that “about triple the number of children have been vaccinated this year, compared with the same period in 2018,” in Oregon and southwest Washington.
Individual cases of measles have been reported to the CDC by seven other states: California, Colorado, Connecticut, Georgia, Illinois, Kentucky, and Oregon.
according to the Centers for Disease Control and Prevention.
On Jan. 31, total measles cases stood at 79, which means that the number of individuals with measles has risen by 61% in just the last 2 weeks. Of the five outbreaks (defined as three or more cases) so far in 2019, three have occurred in New York (57 cases in three counties), one in Texas (8 cases in five counties), and one in Washington (62 cases in two counties), the CDC reported Feb. 18.
The majority of the Washington cases (61 of the 62) have occurred in Clark County, which is located just across the Columbia River from Portland, Ore. Oregon, in turn, has a higher percentage of kindergartners with nonmedical exemptions from vaccination (7.5%) than any other state, the CDC reported in October 2018. Washington’s rate of 3.9% was nearly double the national median of 2.0% for the 2017-2018 school year, while Texas (1.8%) and New York (1.0%) were below it, the CDC said.
In the Pacific Northwest, however, some parents may be changing their minds about vaccinations, according to the New York Times, which reported that “about triple the number of children have been vaccinated this year, compared with the same period in 2018,” in Oregon and southwest Washington.
Individual cases of measles have been reported to the CDC by seven other states: California, Colorado, Connecticut, Georgia, Illinois, Kentucky, and Oregon.
according to the Centers for Disease Control and Prevention.
On Jan. 31, total measles cases stood at 79, which means that the number of individuals with measles has risen by 61% in just the last 2 weeks. Of the five outbreaks (defined as three or more cases) so far in 2019, three have occurred in New York (57 cases in three counties), one in Texas (8 cases in five counties), and one in Washington (62 cases in two counties), the CDC reported Feb. 18.
The majority of the Washington cases (61 of the 62) have occurred in Clark County, which is located just across the Columbia River from Portland, Ore. Oregon, in turn, has a higher percentage of kindergartners with nonmedical exemptions from vaccination (7.5%) than any other state, the CDC reported in October 2018. Washington’s rate of 3.9% was nearly double the national median of 2.0% for the 2017-2018 school year, while Texas (1.8%) and New York (1.0%) were below it, the CDC said.
In the Pacific Northwest, however, some parents may be changing their minds about vaccinations, according to the New York Times, which reported that “about triple the number of children have been vaccinated this year, compared with the same period in 2018,” in Oregon and southwest Washington.
Individual cases of measles have been reported to the CDC by seven other states: California, Colorado, Connecticut, Georgia, Illinois, Kentucky, and Oregon.
Conservatism spreads in prostate cancer
, the United States now has more than 100 measles cases for the year, e-cigarette use reverses progress in reducing teens’ tobacco use, and consider adopting the MESA 10-year coronary heart disease risk calculator.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
, the United States now has more than 100 measles cases for the year, e-cigarette use reverses progress in reducing teens’ tobacco use, and consider adopting the MESA 10-year coronary heart disease risk calculator.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
, the United States now has more than 100 measles cases for the year, e-cigarette use reverses progress in reducing teens’ tobacco use, and consider adopting the MESA 10-year coronary heart disease risk calculator.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify

Vaccination and antiviral treatment do not affect stroke risk following shingles
HONOLULU – according to findings from a retrospective study of Medicare beneficiaries with shingles and ischemic stroke.

The findings suggest that primary prevention of shingles through vaccination might be the most effective approach to prevent shingles-associated acute ischemic stroke, said the researchers, who presented the study at the International Stroke Conference sponsored by the American Heart Association.
Almost one in three people in the United States will develop shingles, also known as herpes zoster, in their lifetime, according to the Centers for Disease Control and Prevention. Previous research has not simultaneously examined the effect of shingles vaccination and antiviral treatment following shingles onset on the risk of acute ischemic stroke.
Quanhe Yang, PhD, a senior scientist at the CDC, and his colleagues examined data for 35,186 Medicare fee-for-service beneficiaries who were 66 years or older, diagnosed with shingles during 2008-2014, and diagnosed with acute ischemic stroke within a year of shingles diagnosis. Using a self-controlled case series design, the investigators analyzed the association between shingles and stroke. Dr. Yang and his colleagues estimated the incident rate ratio (IRR) by comparing the incidence of stroke during risk periods (i.e., periods following shingles), compared with control periods. To minimize confounding by age, they restricted their analyses to approximately 365 days from the shingles index date.
To investigate how vaccination against shingles with Zostavax and antiviral treatment following shingles affected stroke risk, the researchers classified beneficiaries into the following four groups: Group 1 had no vaccination and no antiviral treatment (49% of beneficiaries), Group 2 had vaccination only (9%), Group 3 had antiviral treatment only (34%), and Group 4 had vaccination and antiviral treatment (8%). The researchers tested for interaction to examine the changes in IRRs across the four groups.
IRRs for stroke progressively declined as time passed from the index shingles date, from 1.61 at 0-14 days following shingles to 1.35 at 15-30 days, 1.16 at 31-90 days, and 1.05 at 91-180 days. The researchers found no evidence that shingles vaccination and antiviral treatment modified the risk of acute ischemic stroke. The association between shingles and risk for acute ischemic stroke was consistent across age groups (i.e., 66-74 years, 75-84 years, and 85 years or older), sex, and race (i.e., non-Hispanic white, non-Hispanic black, and Hispanic, other).
One of the study’s strengths was that its sample was a large national cohort of Medicare fee-for-service beneficiaries, Dr. Yang said. In addition, the study design eliminated all fixed confounding effects. Potential weaknesses, however, included the fact that herpes zoster diagnosis was based on administrative data and that the vaccine’s efficacy declines over time.
The findings suggest that the importance of following the recommended shingles vaccination protocol in the prevention of shingles, Dr. Yang said. Shingrix, a vaccine that the Food and Drug Administration approved in 2017, prevents shingles with an efficacy greater than 90%, he added.
The investigators reported no funding source or disclosures for this study.
SOURCE: Yang Q et al. Circulation. 2019;50(Suppl_1): Abstract 39
HONOLULU – according to findings from a retrospective study of Medicare beneficiaries with shingles and ischemic stroke.
The findings suggest that primary prevention of shingles through vaccination might be the most effective approach to prevent shingles-associated acute ischemic stroke, said the researchers, who presented the study at the International Stroke Conference sponsored by the American Heart Association.
Almost one in three people in the United States will develop shingles, also known as herpes zoster, in their lifetime, according to the Centers for Disease Control and Prevention. Previous research has not simultaneously examined the effect of shingles vaccination and antiviral treatment following shingles onset on the risk of acute ischemic stroke.
Quanhe Yang, PhD, a senior scientist at the CDC, and his colleagues examined data for 35,186 Medicare fee-for-service beneficiaries who were 66 years or older, diagnosed with shingles during 2008-2014, and diagnosed with acute ischemic stroke within a year of shingles diagnosis. Using a self-controlled case series design, the investigators analyzed the association between shingles and stroke. Dr. Yang and his colleagues estimated the incident rate ratio (IRR) by comparing the incidence of stroke during risk periods (i.e., periods following shingles), compared with control periods. To minimize confounding by age, they restricted their analyses to approximately 365 days from the shingles index date.
To investigate how vaccination against shingles with Zostavax and antiviral treatment following shingles affected stroke risk, the researchers classified beneficiaries into the following four groups: Group 1 had no vaccination and no antiviral treatment (49% of beneficiaries), Group 2 had vaccination only (9%), Group 3 had antiviral treatment only (34%), and Group 4 had vaccination and antiviral treatment (8%). The researchers tested for interaction to examine the changes in IRRs across the four groups.
IRRs for stroke progressively declined as time passed from the index shingles date, from 1.61 at 0-14 days following shingles to 1.35 at 15-30 days, 1.16 at 31-90 days, and 1.05 at 91-180 days. The researchers found no evidence that shingles vaccination and antiviral treatment modified the risk of acute ischemic stroke. The association between shingles and risk for acute ischemic stroke was consistent across age groups (i.e., 66-74 years, 75-84 years, and 85 years or older), sex, and race (i.e., non-Hispanic white, non-Hispanic black, and Hispanic, other).
One of the study’s strengths was that its sample was a large national cohort of Medicare fee-for-service beneficiaries, Dr. Yang said. In addition, the study design eliminated all fixed confounding effects. Potential weaknesses, however, included the fact that herpes zoster diagnosis was based on administrative data and that the vaccine’s efficacy declines over time.
The findings suggest that the importance of following the recommended shingles vaccination protocol in the prevention of shingles, Dr. Yang said. Shingrix, a vaccine that the Food and Drug Administration approved in 2017, prevents shingles with an efficacy greater than 90%, he added.
The investigators reported no funding source or disclosures for this study.
SOURCE: Yang Q et al. Circulation. 2019;50(Suppl_1): Abstract 39
HONOLULU – according to findings from a retrospective study of Medicare beneficiaries with shingles and ischemic stroke.
The findings suggest that primary prevention of shingles through vaccination might be the most effective approach to prevent shingles-associated acute ischemic stroke, said the researchers, who presented the study at the International Stroke Conference sponsored by the American Heart Association.
Almost one in three people in the United States will develop shingles, also known as herpes zoster, in their lifetime, according to the Centers for Disease Control and Prevention. Previous research has not simultaneously examined the effect of shingles vaccination and antiviral treatment following shingles onset on the risk of acute ischemic stroke.
Quanhe Yang, PhD, a senior scientist at the CDC, and his colleagues examined data for 35,186 Medicare fee-for-service beneficiaries who were 66 years or older, diagnosed with shingles during 2008-2014, and diagnosed with acute ischemic stroke within a year of shingles diagnosis. Using a self-controlled case series design, the investigators analyzed the association between shingles and stroke. Dr. Yang and his colleagues estimated the incident rate ratio (IRR) by comparing the incidence of stroke during risk periods (i.e., periods following shingles), compared with control periods. To minimize confounding by age, they restricted their analyses to approximately 365 days from the shingles index date.
To investigate how vaccination against shingles with Zostavax and antiviral treatment following shingles affected stroke risk, the researchers classified beneficiaries into the following four groups: Group 1 had no vaccination and no antiviral treatment (49% of beneficiaries), Group 2 had vaccination only (9%), Group 3 had antiviral treatment only (34%), and Group 4 had vaccination and antiviral treatment (8%). The researchers tested for interaction to examine the changes in IRRs across the four groups.
IRRs for stroke progressively declined as time passed from the index shingles date, from 1.61 at 0-14 days following shingles to 1.35 at 15-30 days, 1.16 at 31-90 days, and 1.05 at 91-180 days. The researchers found no evidence that shingles vaccination and antiviral treatment modified the risk of acute ischemic stroke. The association between shingles and risk for acute ischemic stroke was consistent across age groups (i.e., 66-74 years, 75-84 years, and 85 years or older), sex, and race (i.e., non-Hispanic white, non-Hispanic black, and Hispanic, other).
One of the study’s strengths was that its sample was a large national cohort of Medicare fee-for-service beneficiaries, Dr. Yang said. In addition, the study design eliminated all fixed confounding effects. Potential weaknesses, however, included the fact that herpes zoster diagnosis was based on administrative data and that the vaccine’s efficacy declines over time.
The findings suggest that the importance of following the recommended shingles vaccination protocol in the prevention of shingles, Dr. Yang said. Shingrix, a vaccine that the Food and Drug Administration approved in 2017, prevents shingles with an efficacy greater than 90%, he added.
The investigators reported no funding source or disclosures for this study.
SOURCE: Yang Q et al. Circulation. 2019;50(Suppl_1): Abstract 39
REPORTING FROM ISC 2019
Key clinical point: After a patient develops shingles, prior vaccination or treatment with antiviral medication does not change the risk of acute ischemic stroke.
Major finding: Stroke incidence increased by 61% within 14 days after shingles onset.
Study details: A self-controlled case series of 35,186 Medicare beneficiaries with shingles and acute ischemic stroke.
Disclosures: The authors reported no funding source or disclosures for this study.
Source: Yang Q et al. Circulation. 2019;50(Suppl_1), Abstract 39
Adult HIV patients should receive standard vaccinations, with caveats
Patients infected with HIV have an increased risk of mortality and morbidity from diseases that are preventable with vaccines. Undervaccination of these patients poses a major concern, according to a literature review of the vaccine response in the adult patient with HIV published in The American Journal of Medicine.

Despite the fact that data are limited, patients infected with HIV are advised to receive their age-specific and risk group−based vaccines, according to Firas El Chaer, MD, of the University of Maryland, Baltimore, and his colleague.
HIV patients are of particular concern regarding vaccination, because, despite the use of retroviral therapy, CD4+ T-lymphocytes in individuals infected with HIV remain lower than in those without HIV. In addition, HIV causes an inappropriate response to B-cell stimulation, which results in suboptimal primary and secondary response to vaccination, according to Dr. El Chaer and his colleague. Despite this and initial concerns about vaccine safety in this population, it is now recommended that adult patients infected with HIV receive their age-specific and risk group−based vaccines, they stated.
Inactivated or subunit vaccines
Haemophilus influenzae type b vaccine is not recommended under current guidelines for individuals older than age 18 with HIV infection, unless they have a clinical indication.
Vaccination against hepatitis A virus is recommended for HIV-infected patients who are hepatitis A virus seronegative and have chronic liver disease, men who have sex with men, intravenous drug users, and travelers to endemic regions. However, research has shown that the immunogenicity of the vaccine is lower in patients with HIV than in uninfected individuals. It was found that the CD4 count at the time of vaccination, not the CD4 low point, was the major predictor of the immune response.
Patients coinfected with HIV and hepatitis B virus have an 8-fold and 19-fold increase in mortality, respectively, compared with either virus monoinfection. Although vaccination is recommended, the optimal hepatitis B virus vaccination schedule in patients with HIV remains controversial, according to the authors. They indicated that new strategies to improve hepatitis B virus vaccine immunogenicity for those infected with HIV are needed.
Individuals infected with HIV have been found to have a higher risk of human papillomavirus (HPV) infection. The safety and immunogenicity results and prospect of benefits has led to a consensus on the benefit of vaccinating HIV-infected patients who meet the HPV vaccine age criteria, the authors indicated.
With regard to standard flu vaccinations: “An annual inactivated influenza vaccine is recommended during the influenza season for all adult individuals with HIV; however, a live attenuated influenza vaccine is contraindicated in this population,” according to the review.
Patients with HIV have a more than 10-fold increased risk of invasive meningococcal disease, compared with the general population, with the risk being particularly higher in those individuals with CD4 counts less than 200 cells/mm3 and in men who have sex with men in cities with meningococcal outbreaks. For these reasons, the “quadrivalent meningococcal vaccine is recommended for all patients with HIV regardless of their CD4 count, with 2-dose primary series at least 2 months apart and with a booster every 5 years.”
Pneumonia is known to be especially dangerous in the HIV-infected population. With regard to pneumonia vaccination, the 13-valent pneumococcal conjugate vaccine is recommended for all patients with HIV, regardless of their CD4 cell counts. According to Dr. El Chaer and his colleague, it should be followed by the 23-valent pneumococcal polysaccharide vaccine at least 8 weeks later as a prime-boost regimen, preferably when CD4 counts are greater than 200 cells/mm3 and in patients receiving ART.
“Tetanus toxoid, diphtheria toxoid, and acellular pertussis vaccines are recommended once for all individuals infected with HIV, regardless of the CD4 count, with a tetanus toxoid and diphtheria toxoid booster every 10 years,” according to the review.
Live vaccines
Live vaccines are a concerning issue for HIV-infected adults and recommendations for use are generally tied to the CD4 T-cell count. The measles, mumps, and rubella vaccine seems to be safe in patients infected with HIV with a CD4 count greater than 200 cells/mm3, according to Dr. El Chaer and his colleague. Similarly, patients with HIV with CD4 counts greater than 200 cells/mm3 and no evidence of documented immunity to varicella should receive the varicella vaccine.
In contrast, the live, attenuated varicella zoster virus vaccine is not recommended for patients infected with HIV, and it is contraindicated if CD4 count is less than 200 cells/mm3. Recently, a herpes zoster subunit vaccine (HZ/su) was tested in a phase 1/2a randomized, placebo-controlled study and was found to be safe and immunogenic regardless of CD4 count, although it has not yet been given a specific recommendation for immunocompromised patients.
“With the widespread use of ART resulting in better HIV control, ,” the authors concluded.
The study was not sponsored. Dr. El Chaer and his colleague reported that they had no conflicts.
SOURCE: El Chaer F et al. Am J Med. 2019. doi: 10.1016/j.amjmed.2018.12.011.
Patients infected with HIV have an increased risk of mortality and morbidity from diseases that are preventable with vaccines. Undervaccination of these patients poses a major concern, according to a literature review of the vaccine response in the adult patient with HIV published in The American Journal of Medicine.
Despite the fact that data are limited, patients infected with HIV are advised to receive their age-specific and risk group−based vaccines, according to Firas El Chaer, MD, of the University of Maryland, Baltimore, and his colleague.
HIV patients are of particular concern regarding vaccination, because, despite the use of retroviral therapy, CD4+ T-lymphocytes in individuals infected with HIV remain lower than in those without HIV. In addition, HIV causes an inappropriate response to B-cell stimulation, which results in suboptimal primary and secondary response to vaccination, according to Dr. El Chaer and his colleague. Despite this and initial concerns about vaccine safety in this population, it is now recommended that adult patients infected with HIV receive their age-specific and risk group−based vaccines, they stated.
Inactivated or subunit vaccines
Haemophilus influenzae type b vaccine is not recommended under current guidelines for individuals older than age 18 with HIV infection, unless they have a clinical indication.
Vaccination against hepatitis A virus is recommended for HIV-infected patients who are hepatitis A virus seronegative and have chronic liver disease, men who have sex with men, intravenous drug users, and travelers to endemic regions. However, research has shown that the immunogenicity of the vaccine is lower in patients with HIV than in uninfected individuals. It was found that the CD4 count at the time of vaccination, not the CD4 low point, was the major predictor of the immune response.
Patients coinfected with HIV and hepatitis B virus have an 8-fold and 19-fold increase in mortality, respectively, compared with either virus monoinfection. Although vaccination is recommended, the optimal hepatitis B virus vaccination schedule in patients with HIV remains controversial, according to the authors. They indicated that new strategies to improve hepatitis B virus vaccine immunogenicity for those infected with HIV are needed.
Individuals infected with HIV have been found to have a higher risk of human papillomavirus (HPV) infection. The safety and immunogenicity results and prospect of benefits has led to a consensus on the benefit of vaccinating HIV-infected patients who meet the HPV vaccine age criteria, the authors indicated.
With regard to standard flu vaccinations: “An annual inactivated influenza vaccine is recommended during the influenza season for all adult individuals with HIV; however, a live attenuated influenza vaccine is contraindicated in this population,” according to the review.
Patients with HIV have a more than 10-fold increased risk of invasive meningococcal disease, compared with the general population, with the risk being particularly higher in those individuals with CD4 counts less than 200 cells/mm3 and in men who have sex with men in cities with meningococcal outbreaks. For these reasons, the “quadrivalent meningococcal vaccine is recommended for all patients with HIV regardless of their CD4 count, with 2-dose primary series at least 2 months apart and with a booster every 5 years.”
Pneumonia is known to be especially dangerous in the HIV-infected population. With regard to pneumonia vaccination, the 13-valent pneumococcal conjugate vaccine is recommended for all patients with HIV, regardless of their CD4 cell counts. According to Dr. El Chaer and his colleague, it should be followed by the 23-valent pneumococcal polysaccharide vaccine at least 8 weeks later as a prime-boost regimen, preferably when CD4 counts are greater than 200 cells/mm3 and in patients receiving ART.
“Tetanus toxoid, diphtheria toxoid, and acellular pertussis vaccines are recommended once for all individuals infected with HIV, regardless of the CD4 count, with a tetanus toxoid and diphtheria toxoid booster every 10 years,” according to the review.
Live vaccines
Live vaccines are a concerning issue for HIV-infected adults and recommendations for use are generally tied to the CD4 T-cell count. The measles, mumps, and rubella vaccine seems to be safe in patients infected with HIV with a CD4 count greater than 200 cells/mm3, according to Dr. El Chaer and his colleague. Similarly, patients with HIV with CD4 counts greater than 200 cells/mm3 and no evidence of documented immunity to varicella should receive the varicella vaccine.
In contrast, the live, attenuated varicella zoster virus vaccine is not recommended for patients infected with HIV, and it is contraindicated if CD4 count is less than 200 cells/mm3. Recently, a herpes zoster subunit vaccine (HZ/su) was tested in a phase 1/2a randomized, placebo-controlled study and was found to be safe and immunogenic regardless of CD4 count, although it has not yet been given a specific recommendation for immunocompromised patients.
“With the widespread use of ART resulting in better HIV control, ,” the authors concluded.
The study was not sponsored. Dr. El Chaer and his colleague reported that they had no conflicts.
SOURCE: El Chaer F et al. Am J Med. 2019. doi: 10.1016/j.amjmed.2018.12.011.
Patients infected with HIV have an increased risk of mortality and morbidity from diseases that are preventable with vaccines. Undervaccination of these patients poses a major concern, according to a literature review of the vaccine response in the adult patient with HIV published in The American Journal of Medicine.
Despite the fact that data are limited, patients infected with HIV are advised to receive their age-specific and risk group−based vaccines, according to Firas El Chaer, MD, of the University of Maryland, Baltimore, and his colleague.
HIV patients are of particular concern regarding vaccination, because, despite the use of retroviral therapy, CD4+ T-lymphocytes in individuals infected with HIV remain lower than in those without HIV. In addition, HIV causes an inappropriate response to B-cell stimulation, which results in suboptimal primary and secondary response to vaccination, according to Dr. El Chaer and his colleague. Despite this and initial concerns about vaccine safety in this population, it is now recommended that adult patients infected with HIV receive their age-specific and risk group−based vaccines, they stated.
Inactivated or subunit vaccines
Haemophilus influenzae type b vaccine is not recommended under current guidelines for individuals older than age 18 with HIV infection, unless they have a clinical indication.
Vaccination against hepatitis A virus is recommended for HIV-infected patients who are hepatitis A virus seronegative and have chronic liver disease, men who have sex with men, intravenous drug users, and travelers to endemic regions. However, research has shown that the immunogenicity of the vaccine is lower in patients with HIV than in uninfected individuals. It was found that the CD4 count at the time of vaccination, not the CD4 low point, was the major predictor of the immune response.
Patients coinfected with HIV and hepatitis B virus have an 8-fold and 19-fold increase in mortality, respectively, compared with either virus monoinfection. Although vaccination is recommended, the optimal hepatitis B virus vaccination schedule in patients with HIV remains controversial, according to the authors. They indicated that new strategies to improve hepatitis B virus vaccine immunogenicity for those infected with HIV are needed.
Individuals infected with HIV have been found to have a higher risk of human papillomavirus (HPV) infection. The safety and immunogenicity results and prospect of benefits has led to a consensus on the benefit of vaccinating HIV-infected patients who meet the HPV vaccine age criteria, the authors indicated.
With regard to standard flu vaccinations: “An annual inactivated influenza vaccine is recommended during the influenza season for all adult individuals with HIV; however, a live attenuated influenza vaccine is contraindicated in this population,” according to the review.
Patients with HIV have a more than 10-fold increased risk of invasive meningococcal disease, compared with the general population, with the risk being particularly higher in those individuals with CD4 counts less than 200 cells/mm3 and in men who have sex with men in cities with meningococcal outbreaks. For these reasons, the “quadrivalent meningococcal vaccine is recommended for all patients with HIV regardless of their CD4 count, with 2-dose primary series at least 2 months apart and with a booster every 5 years.”
Pneumonia is known to be especially dangerous in the HIV-infected population. With regard to pneumonia vaccination, the 13-valent pneumococcal conjugate vaccine is recommended for all patients with HIV, regardless of their CD4 cell counts. According to Dr. El Chaer and his colleague, it should be followed by the 23-valent pneumococcal polysaccharide vaccine at least 8 weeks later as a prime-boost regimen, preferably when CD4 counts are greater than 200 cells/mm3 and in patients receiving ART.
“Tetanus toxoid, diphtheria toxoid, and acellular pertussis vaccines are recommended once for all individuals infected with HIV, regardless of the CD4 count, with a tetanus toxoid and diphtheria toxoid booster every 10 years,” according to the review.
Live vaccines
Live vaccines are a concerning issue for HIV-infected adults and recommendations for use are generally tied to the CD4 T-cell count. The measles, mumps, and rubella vaccine seems to be safe in patients infected with HIV with a CD4 count greater than 200 cells/mm3, according to Dr. El Chaer and his colleague. Similarly, patients with HIV with CD4 counts greater than 200 cells/mm3 and no evidence of documented immunity to varicella should receive the varicella vaccine.
In contrast, the live, attenuated varicella zoster virus vaccine is not recommended for patients infected with HIV, and it is contraindicated if CD4 count is less than 200 cells/mm3. Recently, a herpes zoster subunit vaccine (HZ/su) was tested in a phase 1/2a randomized, placebo-controlled study and was found to be safe and immunogenic regardless of CD4 count, although it has not yet been given a specific recommendation for immunocompromised patients.
“With the widespread use of ART resulting in better HIV control, ,” the authors concluded.
The study was not sponsored. Dr. El Chaer and his colleague reported that they had no conflicts.
SOURCE: El Chaer F et al. Am J Med. 2019. doi: 10.1016/j.amjmed.2018.12.011.
FROM THE AMERICAN JOURNAL OF MEDICINE
Key clinical point: Undervaccination is too common among HIV-infected patients.
Major finding: Data on vaccine effectiveness in HIV patients are limited, but do not contraindicate the need for vaccination.
Study details: Literature review of immunogenicity and vaccine efficacy in HIV-infected adults.
Disclosures: The study was unsponsored and the authors reported they had no conflicts.
Source: El Chaer F et al. Am J Med. 2019. doi: 10.1016/j.amjmed.2018.12.011.
Measles outbreak sends vaccine demand soaring, even among the hesitant
Demand for measles vaccine has surged in the Washington county in which the highly contagious virus is linked to more than 50 confirmed illnesses this year – including among people who had previously shunned the shots.
Orders for two types of measles vaccines in Clark County were up nearly 500% in January, compared with the same month last year, jumping from 530 doses to 3,150, according to state health department figures.
Area health clinics are scrambling to keep up with sudden demand, mostly among parents of children who had not been inoculated.
“During an outbreak is when you see an influx of patients who would otherwise be vaccine hesitant,” said Virginia Ramos, infection control nurse with Sea Mar Community Health Center, which runs six sites that offer vaccines in Clark County.
“We’re just happy that we’re prepared and that there is vaccine available.”
The Vancouver Clinic, which operates medical offices and urgent care centers in the area, reported that shots administered jumped from 263 in January 2018 to 1,444 last month, a nearly 450% increase.
That’s a huge rise in a county in which vaccination rates lag – only 76.5% of kindergartners had all the required immunizations for the 2017-2018 school year. Health officials have long worried about the potential for an outbreak in the region.
Statewide in Washington, orders for measles vaccine jumped about 30% in January, compared with the same month last year, climbing from 12,140 doses to 15,780 doses, figures showed. The vaccines include MMR, which protects against measles, mumps and rubella, and MMR-V, which also protects against the varicella-zoster virus, which causes chickenpox. The vaccine takes effect within 72 hours, health officials said.
The orders represent only state-supplied vaccines requested through the federal Vaccines for Children program, which provides free immunizations to children who otherwise couldn’t afford them.
But it’s a snapshot of the scare an outbreak can cause, said Alan Melnick, MD, the health officer and public health director for Clark County overseeing the response.

“I would rather it not take an outbreak for this to happen,” he said.
Since Jan. 1, 2019, 50 cases of measles have been confirmed in Clark County, with 11 more cases suspected, officials said. The Pacific Northwest outbreak includes one confirmed case in King County, where Seattle is located, and four in Multnomah County, which includes Portland, Ore.
On Feb. 6, officials sent letters to families of 5,000 children in Multnomah County telling them they’ll be excluded from school if they don’t have up-to-date immunizations or valid exemptions by Feb. 20.
Most of the infections have occurred in children, under age 18 years, who were unvaccinated. The outbreak includes 43 cases among those who were not immunized, 6 cases in which immunization has not been verified, and 1 case in which the person had received only a single dose of vaccine.
The Centers for Disease Control and Prevention recommends two doses of measles vaccine, one given at between 12 and 15 months of age and one between ages 4 and 6. Health officials say the shots are safe and effective, providing about 93% protection with one dose and 97% with two doses.
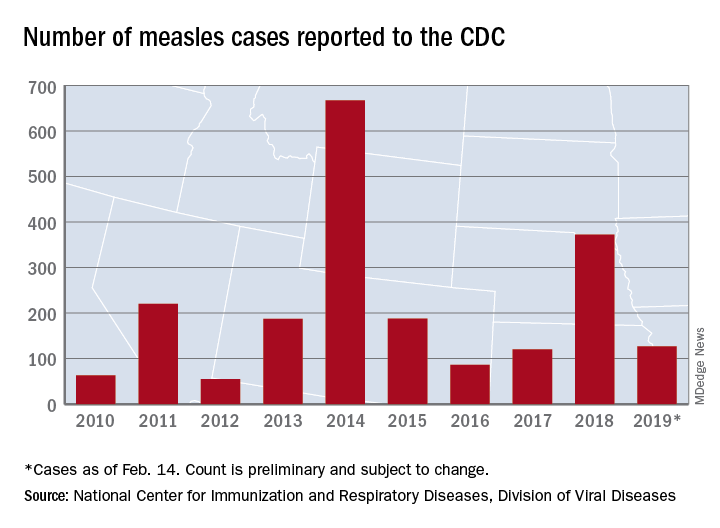
The Northwest cases are among three ongoing measles outbreaks in the United States that sickened 79 people in January, according to the CDC. Last year, 372 measles cases were confirmed nationwide, the most since an outbreak in 2014 sickened 667 people.
Washington and Oregon are among 17 states that allow nonmedical exemptions from vaccination requirements for school entry, according to the National Conference of State Legislatures.
Washington state Rep. Paul Harris (R-Vancouver) has introduced a measure that would remove personal belief exemptions for the MMR vaccine.
Research has confirmed that vaccines don’t cause autism, a common reason cited by parents who reject vaccinations. Others object to the timing and combinations of the vaccines and to being forced to inoculate their children.
Kaiser Health News is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Demand for measles vaccine has surged in the Washington county in which the highly contagious virus is linked to more than 50 confirmed illnesses this year – including among people who had previously shunned the shots.
Orders for two types of measles vaccines in Clark County were up nearly 500% in January, compared with the same month last year, jumping from 530 doses to 3,150, according to state health department figures.
Area health clinics are scrambling to keep up with sudden demand, mostly among parents of children who had not been inoculated.
“During an outbreak is when you see an influx of patients who would otherwise be vaccine hesitant,” said Virginia Ramos, infection control nurse with Sea Mar Community Health Center, which runs six sites that offer vaccines in Clark County.
“We’re just happy that we’re prepared and that there is vaccine available.”
The Vancouver Clinic, which operates medical offices and urgent care centers in the area, reported that shots administered jumped from 263 in January 2018 to 1,444 last month, a nearly 450% increase.
That’s a huge rise in a county in which vaccination rates lag – only 76.5% of kindergartners had all the required immunizations for the 2017-2018 school year. Health officials have long worried about the potential for an outbreak in the region.
Statewide in Washington, orders for measles vaccine jumped about 30% in January, compared with the same month last year, climbing from 12,140 doses to 15,780 doses, figures showed. The vaccines include MMR, which protects against measles, mumps and rubella, and MMR-V, which also protects against the varicella-zoster virus, which causes chickenpox. The vaccine takes effect within 72 hours, health officials said.
The orders represent only state-supplied vaccines requested through the federal Vaccines for Children program, which provides free immunizations to children who otherwise couldn’t afford them.
But it’s a snapshot of the scare an outbreak can cause, said Alan Melnick, MD, the health officer and public health director for Clark County overseeing the response.
“I would rather it not take an outbreak for this to happen,” he said.
Since Jan. 1, 2019, 50 cases of measles have been confirmed in Clark County, with 11 more cases suspected, officials said. The Pacific Northwest outbreak includes one confirmed case in King County, where Seattle is located, and four in Multnomah County, which includes Portland, Ore.
On Feb. 6, officials sent letters to families of 5,000 children in Multnomah County telling them they’ll be excluded from school if they don’t have up-to-date immunizations or valid exemptions by Feb. 20.
Most of the infections have occurred in children, under age 18 years, who were unvaccinated. The outbreak includes 43 cases among those who were not immunized, 6 cases in which immunization has not been verified, and 1 case in which the person had received only a single dose of vaccine.
The Centers for Disease Control and Prevention recommends two doses of measles vaccine, one given at between 12 and 15 months of age and one between ages 4 and 6. Health officials say the shots are safe and effective, providing about 93% protection with one dose and 97% with two doses.
The Northwest cases are among three ongoing measles outbreaks in the United States that sickened 79 people in January, according to the CDC. Last year, 372 measles cases were confirmed nationwide, the most since an outbreak in 2014 sickened 667 people.
Washington and Oregon are among 17 states that allow nonmedical exemptions from vaccination requirements for school entry, according to the National Conference of State Legislatures.
Washington state Rep. Paul Harris (R-Vancouver) has introduced a measure that would remove personal belief exemptions for the MMR vaccine.
Research has confirmed that vaccines don’t cause autism, a common reason cited by parents who reject vaccinations. Others object to the timing and combinations of the vaccines and to being forced to inoculate their children.
Kaiser Health News is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Demand for measles vaccine has surged in the Washington county in which the highly contagious virus is linked to more than 50 confirmed illnesses this year – including among people who had previously shunned the shots.
Orders for two types of measles vaccines in Clark County were up nearly 500% in January, compared with the same month last year, jumping from 530 doses to 3,150, according to state health department figures.
Area health clinics are scrambling to keep up with sudden demand, mostly among parents of children who had not been inoculated.
“During an outbreak is when you see an influx of patients who would otherwise be vaccine hesitant,” said Virginia Ramos, infection control nurse with Sea Mar Community Health Center, which runs six sites that offer vaccines in Clark County.
“We’re just happy that we’re prepared and that there is vaccine available.”
The Vancouver Clinic, which operates medical offices and urgent care centers in the area, reported that shots administered jumped from 263 in January 2018 to 1,444 last month, a nearly 450% increase.
That’s a huge rise in a county in which vaccination rates lag – only 76.5% of kindergartners had all the required immunizations for the 2017-2018 school year. Health officials have long worried about the potential for an outbreak in the region.
Statewide in Washington, orders for measles vaccine jumped about 30% in January, compared with the same month last year, climbing from 12,140 doses to 15,780 doses, figures showed. The vaccines include MMR, which protects against measles, mumps and rubella, and MMR-V, which also protects against the varicella-zoster virus, which causes chickenpox. The vaccine takes effect within 72 hours, health officials said.
The orders represent only state-supplied vaccines requested through the federal Vaccines for Children program, which provides free immunizations to children who otherwise couldn’t afford them.
But it’s a snapshot of the scare an outbreak can cause, said Alan Melnick, MD, the health officer and public health director for Clark County overseeing the response.
“I would rather it not take an outbreak for this to happen,” he said.
Since Jan. 1, 2019, 50 cases of measles have been confirmed in Clark County, with 11 more cases suspected, officials said. The Pacific Northwest outbreak includes one confirmed case in King County, where Seattle is located, and four in Multnomah County, which includes Portland, Ore.
On Feb. 6, officials sent letters to families of 5,000 children in Multnomah County telling them they’ll be excluded from school if they don’t have up-to-date immunizations or valid exemptions by Feb. 20.
Most of the infections have occurred in children, under age 18 years, who were unvaccinated. The outbreak includes 43 cases among those who were not immunized, 6 cases in which immunization has not been verified, and 1 case in which the person had received only a single dose of vaccine.
The Centers for Disease Control and Prevention recommends two doses of measles vaccine, one given at between 12 and 15 months of age and one between ages 4 and 6. Health officials say the shots are safe and effective, providing about 93% protection with one dose and 97% with two doses.
The Northwest cases are among three ongoing measles outbreaks in the United States that sickened 79 people in January, according to the CDC. Last year, 372 measles cases were confirmed nationwide, the most since an outbreak in 2014 sickened 667 people.
Washington and Oregon are among 17 states that allow nonmedical exemptions from vaccination requirements for school entry, according to the National Conference of State Legislatures.
Washington state Rep. Paul Harris (R-Vancouver) has introduced a measure that would remove personal belief exemptions for the MMR vaccine.
Research has confirmed that vaccines don’t cause autism, a common reason cited by parents who reject vaccinations. Others object to the timing and combinations of the vaccines and to being forced to inoculate their children.
Kaiser Health News is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
No increase in severe community-acquired pneumonia after PCV13
Despite concern about the rise of nonvaccine serotypes following widespread PCV13 immunization, cases of community-acquired pneumonia (CAP) remain nearly as low as after initial implementation of the vaccine and severe cases have not risen at all.

This was the finding of a prospective time-series analysis study from eight French pediatric emergency departments between June 2009 and May 2017.
The 12,587 children with CAP enrolled in the study between June 2009 and May 2017 were all aged 15 years or younger and came from one of eight French pediatric EDs.
Pediatric pneumonia cases per 1,000 ED visits dropped 44% after PCV13 was implemented, a decrease from 6.3 to 3.5 cases of CAP per 1,000 pediatric visits from June 2011 to May 2014, with a slight but statistically significant increase to 3.8 cases of CAP per 1,000 pediatric visits from June 2014 to May 2017. However, there was no statistically significant increase in cases with pleural effusion, hospitalization, or high inflammatory biomarkers.
“These results contrast with the recent increase in frequency of invasive pneumococcal disease observed in several countries during the same period linked to serotype replacement beyond 5 years after PCV13 implementation,” reported Naïm Ouldali, MD, of the Association Clinique et Thérapeutique Infantile du Val-de-Marne in France, and associates. The report is in JAMA Pediatrics.
“This difference in the trends suggests different consequences of serotype replacement on pneumococcal CAP vs invasive pneumococcal disease,” they wrote. “The recent slight increase in the number of all CAP cases and virus involvement may reflect changes in the epidemiology of other pathogens and/or serotype replacement with less pathogenic serotypes.”
This latter point arose from discovering no dominant serotype during the study period. Of the 11 serotypes not covered by PCV13, none appeared in more than four cases.
“The implementation of PCV13 has led to the quasi-disappearance of the more invasive serotypes and increase in others in nasopharyngeal flora, which greatly reduces the frequency of the more severe forms of CAP, but could also play a role in the slight increase in frequency of the more benign forms,” the authors reported.
Among the study’s limitations was lack of a control group, precluding the ability to attribute findings to any changes in case reporting. And “participating physicians were encouraged to not change their practice, including test use, and no other potential interfering intervention.”
Funding sources for this study included the Pediatric Infectious Diseases Group of the French Pediatrics Society, Association Clinique et Thérapeutique Infantile du Val-de-Marne, the Foundation for Medical Research and a Pfizer Investigator Initiated Research grant.
Dr Ouldali has received grants from GlaxoSmithKline, and many of the authors have financial ties and/or have received non-financial support from AstraZeneca, Biocodex, GlaxoSmithKline, Merck, Novartis, Pfizer and/or Sanofi Pasteur.
SOURCE: Ouldali N et al. JAMA Pediatrics. 2019 Feb 4. doi: 10.1001/jamapediatrics.2018.5273.
Despite concern about the rise of nonvaccine serotypes following widespread PCV13 immunization, cases of community-acquired pneumonia (CAP) remain nearly as low as after initial implementation of the vaccine and severe cases have not risen at all.
This was the finding of a prospective time-series analysis study from eight French pediatric emergency departments between June 2009 and May 2017.
The 12,587 children with CAP enrolled in the study between June 2009 and May 2017 were all aged 15 years or younger and came from one of eight French pediatric EDs.
Pediatric pneumonia cases per 1,000 ED visits dropped 44% after PCV13 was implemented, a decrease from 6.3 to 3.5 cases of CAP per 1,000 pediatric visits from June 2011 to May 2014, with a slight but statistically significant increase to 3.8 cases of CAP per 1,000 pediatric visits from June 2014 to May 2017. However, there was no statistically significant increase in cases with pleural effusion, hospitalization, or high inflammatory biomarkers.
“These results contrast with the recent increase in frequency of invasive pneumococcal disease observed in several countries during the same period linked to serotype replacement beyond 5 years after PCV13 implementation,” reported Naïm Ouldali, MD, of the Association Clinique et Thérapeutique Infantile du Val-de-Marne in France, and associates. The report is in JAMA Pediatrics.
“This difference in the trends suggests different consequences of serotype replacement on pneumococcal CAP vs invasive pneumococcal disease,” they wrote. “The recent slight increase in the number of all CAP cases and virus involvement may reflect changes in the epidemiology of other pathogens and/or serotype replacement with less pathogenic serotypes.”
This latter point arose from discovering no dominant serotype during the study period. Of the 11 serotypes not covered by PCV13, none appeared in more than four cases.
“The implementation of PCV13 has led to the quasi-disappearance of the more invasive serotypes and increase in others in nasopharyngeal flora, which greatly reduces the frequency of the more severe forms of CAP, but could also play a role in the slight increase in frequency of the more benign forms,” the authors reported.
Among the study’s limitations was lack of a control group, precluding the ability to attribute findings to any changes in case reporting. And “participating physicians were encouraged to not change their practice, including test use, and no other potential interfering intervention.”
Funding sources for this study included the Pediatric Infectious Diseases Group of the French Pediatrics Society, Association Clinique et Thérapeutique Infantile du Val-de-Marne, the Foundation for Medical Research and a Pfizer Investigator Initiated Research grant.
Dr Ouldali has received grants from GlaxoSmithKline, and many of the authors have financial ties and/or have received non-financial support from AstraZeneca, Biocodex, GlaxoSmithKline, Merck, Novartis, Pfizer and/or Sanofi Pasteur.
SOURCE: Ouldali N et al. JAMA Pediatrics. 2019 Feb 4. doi: 10.1001/jamapediatrics.2018.5273.
Despite concern about the rise of nonvaccine serotypes following widespread PCV13 immunization, cases of community-acquired pneumonia (CAP) remain nearly as low as after initial implementation of the vaccine and severe cases have not risen at all.
This was the finding of a prospective time-series analysis study from eight French pediatric emergency departments between June 2009 and May 2017.
The 12,587 children with CAP enrolled in the study between June 2009 and May 2017 were all aged 15 years or younger and came from one of eight French pediatric EDs.
Pediatric pneumonia cases per 1,000 ED visits dropped 44% after PCV13 was implemented, a decrease from 6.3 to 3.5 cases of CAP per 1,000 pediatric visits from June 2011 to May 2014, with a slight but statistically significant increase to 3.8 cases of CAP per 1,000 pediatric visits from June 2014 to May 2017. However, there was no statistically significant increase in cases with pleural effusion, hospitalization, or high inflammatory biomarkers.
“These results contrast with the recent increase in frequency of invasive pneumococcal disease observed in several countries during the same period linked to serotype replacement beyond 5 years after PCV13 implementation,” reported Naïm Ouldali, MD, of the Association Clinique et Thérapeutique Infantile du Val-de-Marne in France, and associates. The report is in JAMA Pediatrics.
“This difference in the trends suggests different consequences of serotype replacement on pneumococcal CAP vs invasive pneumococcal disease,” they wrote. “The recent slight increase in the number of all CAP cases and virus involvement may reflect changes in the epidemiology of other pathogens and/or serotype replacement with less pathogenic serotypes.”
This latter point arose from discovering no dominant serotype during the study period. Of the 11 serotypes not covered by PCV13, none appeared in more than four cases.
“The implementation of PCV13 has led to the quasi-disappearance of the more invasive serotypes and increase in others in nasopharyngeal flora, which greatly reduces the frequency of the more severe forms of CAP, but could also play a role in the slight increase in frequency of the more benign forms,” the authors reported.
Among the study’s limitations was lack of a control group, precluding the ability to attribute findings to any changes in case reporting. And “participating physicians were encouraged to not change their practice, including test use, and no other potential interfering intervention.”
Funding sources for this study included the Pediatric Infectious Diseases Group of the French Pediatrics Society, Association Clinique et Thérapeutique Infantile du Val-de-Marne, the Foundation for Medical Research and a Pfizer Investigator Initiated Research grant.
Dr Ouldali has received grants from GlaxoSmithKline, and many of the authors have financial ties and/or have received non-financial support from AstraZeneca, Biocodex, GlaxoSmithKline, Merck, Novartis, Pfizer and/or Sanofi Pasteur.
SOURCE: Ouldali N et al. JAMA Pediatrics. 2019 Feb 4. doi: 10.1001/jamapediatrics.2018.5273.
FROM JAMA PEDIATRICS
Key clinical point:
Major finding: Pediatric community-acquired pneumonia cases dropped from 6.3 to 3.5 cases per 1,000 visits from 2010 to 2014 and increased to 3.8 cases per 1,000 visits in May 2017.
Study details: The findings are based on a prospective time series analysis of 12,587 pediatric pneumonia cases (under 15 years old) in eight French emergency departments from June 2009 to May 2017.
Disclosures: Funding sources for this study included the Pediatric Infectious Diseases Group of the French Pediatrics Society, Association Clinique et Thérapeutique Infantile du Val-de-Marne, the Foundation for Medical Research, and a Pfizer Investigator Initiated Research grant. Dr. Ouldali has received grants from GlaxoSmithKline, and many of the authors have financial ties and/or have received nonfinancial support from AstraZeneca, Biocodex, GlaxoSmithKline, Merck, Novartis, Pfizer, and/or Sanofi Pasteur.
Source: Ouldali N et al. JAMA Pediatrics. 2019 Feb 4. doi: 10.1001/jamapediatrics.2018.5273.
FDA approves 0.5-mL Fluzone Quadrivalent vaccine in young children
according to Sanofi Pasteur, the vaccine’s manufacturer.

FDA approval was based on results of a phase 4 safety and immunogenicity study of nearly 2,000 children. Children aged 6-35 months who received one or two doses of Fluzone at 0.50 mL had a safety profile similar to that of children who received one or two doses of Fluzone at 0.25 mL. Results from the study were presented at the Pediatric Academic Societies annual meeting in April 2018.
This flu vaccine should not be given to anyone with a severe allergic reaction (anaphylaxis) to egg or egg products, according to the press release.
In children, the most common adverse events are injection site reactions, muscle aches, fatigue, and headache; in young children, irritability, abnormal crying, drowsiness, appetite loss, vomiting, and fever are common.
“Offering pediatricians the convenience of the same 0.5-mL dose option for children may help streamline immunization efforts. The potentially life-threatening effects of influenza in children reported during the 2017-18 season, especially among those who were not vaccinated, is sobering,” David P. Greenberg, MD, regional medical head of Sanofi Pasteur of North America, said in the press release.
Find the full press release on the Sanofi website.
according to Sanofi Pasteur, the vaccine’s manufacturer.
FDA approval was based on results of a phase 4 safety and immunogenicity study of nearly 2,000 children. Children aged 6-35 months who received one or two doses of Fluzone at 0.50 mL had a safety profile similar to that of children who received one or two doses of Fluzone at 0.25 mL. Results from the study were presented at the Pediatric Academic Societies annual meeting in April 2018.
This flu vaccine should not be given to anyone with a severe allergic reaction (anaphylaxis) to egg or egg products, according to the press release.
In children, the most common adverse events are injection site reactions, muscle aches, fatigue, and headache; in young children, irritability, abnormal crying, drowsiness, appetite loss, vomiting, and fever are common.
“Offering pediatricians the convenience of the same 0.5-mL dose option for children may help streamline immunization efforts. The potentially life-threatening effects of influenza in children reported during the 2017-18 season, especially among those who were not vaccinated, is sobering,” David P. Greenberg, MD, regional medical head of Sanofi Pasteur of North America, said in the press release.
Find the full press release on the Sanofi website.
according to Sanofi Pasteur, the vaccine’s manufacturer.
FDA approval was based on results of a phase 4 safety and immunogenicity study of nearly 2,000 children. Children aged 6-35 months who received one or two doses of Fluzone at 0.50 mL had a safety profile similar to that of children who received one or two doses of Fluzone at 0.25 mL. Results from the study were presented at the Pediatric Academic Societies annual meeting in April 2018.
This flu vaccine should not be given to anyone with a severe allergic reaction (anaphylaxis) to egg or egg products, according to the press release.
In children, the most common adverse events are injection site reactions, muscle aches, fatigue, and headache; in young children, irritability, abnormal crying, drowsiness, appetite loss, vomiting, and fever are common.
“Offering pediatricians the convenience of the same 0.5-mL dose option for children may help streamline immunization efforts. The potentially life-threatening effects of influenza in children reported during the 2017-18 season, especially among those who were not vaccinated, is sobering,” David P. Greenberg, MD, regional medical head of Sanofi Pasteur of North America, said in the press release.
Find the full press release on the Sanofi website.
Study shows evidence of herd immunity with HPV vaccine
Introduction of the quadrivalent human papillomavirus (HPV) vaccine was associated with significant declines in the incidence of vaccine-type virus both in vaccinated and unvaccinated young women, according to a study published in Pediatrics.
Four surveillance studies, conducted between 2006 and 2017, examined the rate of positive tests for vaccine-type HPV among 1,580 vaccinated and unvaccinated women aged 13-26 years. The majority of participants identified as African American or multiracial.
Overall, 97% of study participants received the quadrivalent vaccine, with vaccination rates increasing from 0% to 84% over the four waves of vaccination. Vaccine effectiveness – representing the relative risk of infection in vaccinated individuals, compared with unvaccinated risk before introduction of the vaccine – increased by 72% from wave 1 to wave 2, 91% from wave 1 to wave 3, and 80% from wave 1 to wave 4.
Among women who were vaccinated, rates of the quadrivalent vaccine–type HPV decreased by 81%, from 35% to 7%. But even among women who were unvaccinated, detection of the vaccine-targeted strains of HPV decreased by 40%, from 32% to 19%.
Chelse Spinner of the University of Cincinnati and her coauthors wrote that the decline in the quadrivalent vaccine–type HPV provided evidence of direct protection and high vaccine effectiveness in this real-world setting.
“This degree of effectiveness is remarkable given the fact that vaccination was defined as having received one or more doses (i.e., was not defined as having completed the vaccination series) and that women in this study were likely at a substantially higher risk for preexisting HPV infection than [were] those in the HPV vaccine clinical trials because of their reported sexual behaviors,” they wrote. “As noted in a recent review, evidence about herd protection will be a key component of cost-effectiveness analysis evaluating cervical cancer screening strategies.”
Twelve percent of women in the studies received the nine-valent HPV vaccine, and among these women, the rate of infection with the nine-valent vaccine-type HPV decreased from 47% in the first wave of vaccination to 14% in the last wave, representing a 71% decline.
The proportion of vaccinated women in the study who were infected with one or more of the five viral subtypes included in the nine-valent but not in the quadrivalent vaccine decreased significantly by 69%, from 23% to 7%.
However, these data also suggested a nonsignificant 58% increase among unvaccinated women in infections with one of the five subtypes covered by the nine-valent vaccine but not the quadrivalent vaccine.
Ms. Spinner and her associates noted this increase was unexpected and suggested the increase may be caused by the differences between vaccinated and unvaccinated women.
“For example, if women who are unvaccinated versus women who are vaccinated are more likely to practice riskier behaviors that would increase their risk of acquiring HPV, they would be more likely to acquire non–vaccine-type HPV,” they wrote.
Ms. Spinner graduated from the University of Cincinnati and now is a graduate student at the University of South Florida, Tampa. The study was funded by the National Institutes of Health. Darron R. Brown declared shares of Merck, but the other coauthors declared no other relevant financial disclosures.
SOURCE: Spinner C et al. Pediatrics. 2019, Jan 22. doi: 10.1542/peds.2018-1902.
This study of the real-world effectiveness of the HPV vaccine adds to the growing body of literature, and has produced three important results.
The first is that women who had received at least one dose of the vaccine were considered vaccinated, and because of their level of sexual activity, many likely would have already been infected with some HPV subtypes. The high vaccine effectiveness seen in this study despite these factors adds weight to evidence that this HPV vaccine is highly protective.
The study also showed evidence of cross-protection, in that even women who had received only the quadrivalent vaccine still had significantly reduced rates of infection with the HPV subtypes included in the nine-valent vaccine.
It also provides significant evidence of the herd immunity effect against the subtypes included in the quadrivalent vaccine.
Amanda F. Dempsey, MD, PhD, is from the adult and child consortium for health outcomes research and delivery science at the University of Colorado, Denver. These comments are taken from an accompanying editorial (Pediatrics. 2019 Jan 22. doi: 10.1542/peds.2018-3427). Dr. Dempsey declared advisory board roles for Merck, Sanofi, and Pfizer and a consultancy for Pfizer. She received no external funding.
This study of the real-world effectiveness of the HPV vaccine adds to the growing body of literature, and has produced three important results.
The first is that women who had received at least one dose of the vaccine were considered vaccinated, and because of their level of sexual activity, many likely would have already been infected with some HPV subtypes. The high vaccine effectiveness seen in this study despite these factors adds weight to evidence that this HPV vaccine is highly protective.
The study also showed evidence of cross-protection, in that even women who had received only the quadrivalent vaccine still had significantly reduced rates of infection with the HPV subtypes included in the nine-valent vaccine.
It also provides significant evidence of the herd immunity effect against the subtypes included in the quadrivalent vaccine.
Amanda F. Dempsey, MD, PhD, is from the adult and child consortium for health outcomes research and delivery science at the University of Colorado, Denver. These comments are taken from an accompanying editorial (Pediatrics. 2019 Jan 22. doi: 10.1542/peds.2018-3427). Dr. Dempsey declared advisory board roles for Merck, Sanofi, and Pfizer and a consultancy for Pfizer. She received no external funding.
This study of the real-world effectiveness of the HPV vaccine adds to the growing body of literature, and has produced three important results.
The first is that women who had received at least one dose of the vaccine were considered vaccinated, and because of their level of sexual activity, many likely would have already been infected with some HPV subtypes. The high vaccine effectiveness seen in this study despite these factors adds weight to evidence that this HPV vaccine is highly protective.
The study also showed evidence of cross-protection, in that even women who had received only the quadrivalent vaccine still had significantly reduced rates of infection with the HPV subtypes included in the nine-valent vaccine.
It also provides significant evidence of the herd immunity effect against the subtypes included in the quadrivalent vaccine.
Amanda F. Dempsey, MD, PhD, is from the adult and child consortium for health outcomes research and delivery science at the University of Colorado, Denver. These comments are taken from an accompanying editorial (Pediatrics. 2019 Jan 22. doi: 10.1542/peds.2018-3427). Dr. Dempsey declared advisory board roles for Merck, Sanofi, and Pfizer and a consultancy for Pfizer. She received no external funding.
Introduction of the quadrivalent human papillomavirus (HPV) vaccine was associated with significant declines in the incidence of vaccine-type virus both in vaccinated and unvaccinated young women, according to a study published in Pediatrics.
Four surveillance studies, conducted between 2006 and 2017, examined the rate of positive tests for vaccine-type HPV among 1,580 vaccinated and unvaccinated women aged 13-26 years. The majority of participants identified as African American or multiracial.
Overall, 97% of study participants received the quadrivalent vaccine, with vaccination rates increasing from 0% to 84% over the four waves of vaccination. Vaccine effectiveness – representing the relative risk of infection in vaccinated individuals, compared with unvaccinated risk before introduction of the vaccine – increased by 72% from wave 1 to wave 2, 91% from wave 1 to wave 3, and 80% from wave 1 to wave 4.
Among women who were vaccinated, rates of the quadrivalent vaccine–type HPV decreased by 81%, from 35% to 7%. But even among women who were unvaccinated, detection of the vaccine-targeted strains of HPV decreased by 40%, from 32% to 19%.
Chelse Spinner of the University of Cincinnati and her coauthors wrote that the decline in the quadrivalent vaccine–type HPV provided evidence of direct protection and high vaccine effectiveness in this real-world setting.
“This degree of effectiveness is remarkable given the fact that vaccination was defined as having received one or more doses (i.e., was not defined as having completed the vaccination series) and that women in this study were likely at a substantially higher risk for preexisting HPV infection than [were] those in the HPV vaccine clinical trials because of their reported sexual behaviors,” they wrote. “As noted in a recent review, evidence about herd protection will be a key component of cost-effectiveness analysis evaluating cervical cancer screening strategies.”
Twelve percent of women in the studies received the nine-valent HPV vaccine, and among these women, the rate of infection with the nine-valent vaccine-type HPV decreased from 47% in the first wave of vaccination to 14% in the last wave, representing a 71% decline.
The proportion of vaccinated women in the study who were infected with one or more of the five viral subtypes included in the nine-valent but not in the quadrivalent vaccine decreased significantly by 69%, from 23% to 7%.
However, these data also suggested a nonsignificant 58% increase among unvaccinated women in infections with one of the five subtypes covered by the nine-valent vaccine but not the quadrivalent vaccine.
Ms. Spinner and her associates noted this increase was unexpected and suggested the increase may be caused by the differences between vaccinated and unvaccinated women.
“For example, if women who are unvaccinated versus women who are vaccinated are more likely to practice riskier behaviors that would increase their risk of acquiring HPV, they would be more likely to acquire non–vaccine-type HPV,” they wrote.
Ms. Spinner graduated from the University of Cincinnati and now is a graduate student at the University of South Florida, Tampa. The study was funded by the National Institutes of Health. Darron R. Brown declared shares of Merck, but the other coauthors declared no other relevant financial disclosures.
SOURCE: Spinner C et al. Pediatrics. 2019, Jan 22. doi: 10.1542/peds.2018-1902.
Introduction of the quadrivalent human papillomavirus (HPV) vaccine was associated with significant declines in the incidence of vaccine-type virus both in vaccinated and unvaccinated young women, according to a study published in Pediatrics.
Four surveillance studies, conducted between 2006 and 2017, examined the rate of positive tests for vaccine-type HPV among 1,580 vaccinated and unvaccinated women aged 13-26 years. The majority of participants identified as African American or multiracial.
Overall, 97% of study participants received the quadrivalent vaccine, with vaccination rates increasing from 0% to 84% over the four waves of vaccination. Vaccine effectiveness – representing the relative risk of infection in vaccinated individuals, compared with unvaccinated risk before introduction of the vaccine – increased by 72% from wave 1 to wave 2, 91% from wave 1 to wave 3, and 80% from wave 1 to wave 4.
Among women who were vaccinated, rates of the quadrivalent vaccine–type HPV decreased by 81%, from 35% to 7%. But even among women who were unvaccinated, detection of the vaccine-targeted strains of HPV decreased by 40%, from 32% to 19%.
Chelse Spinner of the University of Cincinnati and her coauthors wrote that the decline in the quadrivalent vaccine–type HPV provided evidence of direct protection and high vaccine effectiveness in this real-world setting.
“This degree of effectiveness is remarkable given the fact that vaccination was defined as having received one or more doses (i.e., was not defined as having completed the vaccination series) and that women in this study were likely at a substantially higher risk for preexisting HPV infection than [were] those in the HPV vaccine clinical trials because of their reported sexual behaviors,” they wrote. “As noted in a recent review, evidence about herd protection will be a key component of cost-effectiveness analysis evaluating cervical cancer screening strategies.”
Twelve percent of women in the studies received the nine-valent HPV vaccine, and among these women, the rate of infection with the nine-valent vaccine-type HPV decreased from 47% in the first wave of vaccination to 14% in the last wave, representing a 71% decline.
The proportion of vaccinated women in the study who were infected with one or more of the five viral subtypes included in the nine-valent but not in the quadrivalent vaccine decreased significantly by 69%, from 23% to 7%.
However, these data also suggested a nonsignificant 58% increase among unvaccinated women in infections with one of the five subtypes covered by the nine-valent vaccine but not the quadrivalent vaccine.
Ms. Spinner and her associates noted this increase was unexpected and suggested the increase may be caused by the differences between vaccinated and unvaccinated women.
“For example, if women who are unvaccinated versus women who are vaccinated are more likely to practice riskier behaviors that would increase their risk of acquiring HPV, they would be more likely to acquire non–vaccine-type HPV,” they wrote.
Ms. Spinner graduated from the University of Cincinnati and now is a graduate student at the University of South Florida, Tampa. The study was funded by the National Institutes of Health. Darron R. Brown declared shares of Merck, but the other coauthors declared no other relevant financial disclosures.
SOURCE: Spinner C et al. Pediatrics. 2019, Jan 22. doi: 10.1542/peds.2018-1902.
FROM PEDIATRICS
Key clinical point:
Major finding: Infection rates for quadrivalent vaccine-covered HPV strains declined by 81% among vaccinated women.
Study details: Surveillance studies in 1,580 vaccinated and unvaccinated young women.
Disclosures: The study was funded by the National Institutes of Health. One author declared shares of Merck, but no other conflicts of interest were declared.
Source: Spinner C et al. Pediatrics. 2019, Jan 22. doi: 10.1542/peds.2018-1902.
Emphasize disease prevention in communications about HPV vaccine
Parents were much more confident about vaccinating their children against the human papillomavirus (HPV) when they were told about the diseases that the vaccine prevents rather than about safety, new research found.

In Pediatrics, researchers reported the outcomes of an online video-messaging study that attempted to address the most common parental questions and concerns about the HPV vaccine. They surveyed a national sample of 1,196 parents of children (aged 9-17 years) who watched four brief videos of a pediatrician talking about one of seven common concerns regarding HPV vaccination. The parents then were asked how each video affected them.
Parents who were exposed to messages about the diseases that the HPV vaccine prevented had the highest confidence in the HPV vaccine (46%). These messages included “HPV is a common virus that millions of people get every year. The HPV vaccine will protect your child from some cancers and genital warts” and “HPV infection can cause cancer in both men and women. The HPV vaccine will protect your child from many of these cancers.”
Similarly, parents exposed to messages about the need for HPV vaccination for both boys and girls also had the highest levels of confidence about HPV vaccination (44%).
Confidence was lower in parents exposed to messages about safety and side effects (30%)
“As such, reiterating vaccination benefits (including cancer prevention) when addressing concerns may also improve the impact of messages,” wrote Parth D. Shah, PhD, from the Fred Hutchinson Cancer Research Center, Seattle, and his coauthors.
Parents who received messages that expressed urgency about vaccination had lower confidence in the HPV vaccine.
“One reason may be that parents who are hesitant feel inappropriately rushed or that their concerns are not being treated with appropriate care,” the authors wrote.
However, messages that required a higher reading grade level and messages that were longer also seemed to inspire more confidence among parents. Parents who were exposed to messages about cancer prevention additionally were even more confident in HPV vaccine, Dr. Shah and his associates reported.
The study also found that 84% of parents wanted to talk to their children’s doctor about the diseases that the HPV vaccine prevented, while 68% wanted to talk about safety and side effects.
The study was funded by the Centers for Disease Control and Prevention and the National Cancer Institute. Dr. Shah was partially supported by an Agency for Healthcare Research and Quality grant. Another author declared being on paid advisory boards of research grants from Merck, Pfizer, and GlaxoSmithKline. No other conflicts of interest were declared.
SOURCE: Shah PD et al. Pediatrics. 2019 Feb. doi: 10.1542/peds.2018-1872.
Parents were much more confident about vaccinating their children against the human papillomavirus (HPV) when they were told about the diseases that the vaccine prevents rather than about safety, new research found.
In Pediatrics, researchers reported the outcomes of an online video-messaging study that attempted to address the most common parental questions and concerns about the HPV vaccine. They surveyed a national sample of 1,196 parents of children (aged 9-17 years) who watched four brief videos of a pediatrician talking about one of seven common concerns regarding HPV vaccination. The parents then were asked how each video affected them.
Parents who were exposed to messages about the diseases that the HPV vaccine prevented had the highest confidence in the HPV vaccine (46%). These messages included “HPV is a common virus that millions of people get every year. The HPV vaccine will protect your child from some cancers and genital warts” and “HPV infection can cause cancer in both men and women. The HPV vaccine will protect your child from many of these cancers.”
Similarly, parents exposed to messages about the need for HPV vaccination for both boys and girls also had the highest levels of confidence about HPV vaccination (44%).
Confidence was lower in parents exposed to messages about safety and side effects (30%)
“As such, reiterating vaccination benefits (including cancer prevention) when addressing concerns may also improve the impact of messages,” wrote Parth D. Shah, PhD, from the Fred Hutchinson Cancer Research Center, Seattle, and his coauthors.
Parents who received messages that expressed urgency about vaccination had lower confidence in the HPV vaccine.
“One reason may be that parents who are hesitant feel inappropriately rushed or that their concerns are not being treated with appropriate care,” the authors wrote.
However, messages that required a higher reading grade level and messages that were longer also seemed to inspire more confidence among parents. Parents who were exposed to messages about cancer prevention additionally were even more confident in HPV vaccine, Dr. Shah and his associates reported.
The study also found that 84% of parents wanted to talk to their children’s doctor about the diseases that the HPV vaccine prevented, while 68% wanted to talk about safety and side effects.
The study was funded by the Centers for Disease Control and Prevention and the National Cancer Institute. Dr. Shah was partially supported by an Agency for Healthcare Research and Quality grant. Another author declared being on paid advisory boards of research grants from Merck, Pfizer, and GlaxoSmithKline. No other conflicts of interest were declared.
SOURCE: Shah PD et al. Pediatrics. 2019 Feb. doi: 10.1542/peds.2018-1872.
Parents were much more confident about vaccinating their children against the human papillomavirus (HPV) when they were told about the diseases that the vaccine prevents rather than about safety, new research found.
In Pediatrics, researchers reported the outcomes of an online video-messaging study that attempted to address the most common parental questions and concerns about the HPV vaccine. They surveyed a national sample of 1,196 parents of children (aged 9-17 years) who watched four brief videos of a pediatrician talking about one of seven common concerns regarding HPV vaccination. The parents then were asked how each video affected them.
Parents who were exposed to messages about the diseases that the HPV vaccine prevented had the highest confidence in the HPV vaccine (46%). These messages included “HPV is a common virus that millions of people get every year. The HPV vaccine will protect your child from some cancers and genital warts” and “HPV infection can cause cancer in both men and women. The HPV vaccine will protect your child from many of these cancers.”
Similarly, parents exposed to messages about the need for HPV vaccination for both boys and girls also had the highest levels of confidence about HPV vaccination (44%).
Confidence was lower in parents exposed to messages about safety and side effects (30%)
“As such, reiterating vaccination benefits (including cancer prevention) when addressing concerns may also improve the impact of messages,” wrote Parth D. Shah, PhD, from the Fred Hutchinson Cancer Research Center, Seattle, and his coauthors.
Parents who received messages that expressed urgency about vaccination had lower confidence in the HPV vaccine.
“One reason may be that parents who are hesitant feel inappropriately rushed or that their concerns are not being treated with appropriate care,” the authors wrote.
However, messages that required a higher reading grade level and messages that were longer also seemed to inspire more confidence among parents. Parents who were exposed to messages about cancer prevention additionally were even more confident in HPV vaccine, Dr. Shah and his associates reported.
The study also found that 84% of parents wanted to talk to their children’s doctor about the diseases that the HPV vaccine prevented, while 68% wanted to talk about safety and side effects.
The study was funded by the Centers for Disease Control and Prevention and the National Cancer Institute. Dr. Shah was partially supported by an Agency for Healthcare Research and Quality grant. Another author declared being on paid advisory boards of research grants from Merck, Pfizer, and GlaxoSmithKline. No other conflicts of interest were declared.
SOURCE: Shah PD et al. Pediatrics. 2019 Feb. doi: 10.1542/peds.2018-1872.
FROM PEDIATRICS
Key clinical point: Information on the benefits of HPV vaccination can improve parent confidence.
Major finding: Messages about the disease and cancer prevention benefits of HPV vaccination inspired greater parent confidence.
Study details: Study in 1,196 parents of children aged 9-17 years.
Disclosures: The study was funded by the Centers for Disease Control and Prevention and the National Cancer Institute. Dr. Shah was partially supported by an Agency for Healthcare Research and Quality grant. Another author declared being on paid advisory boards of research grants from Merck, Pfizer, and GlaxoSmithKline. No other conflicts of interest were declared.
Source: Shah P et al. Pediatrics. 2019 Feb. doi. 10.1542/peds.2018-1872.
Confidential, parent-free discussion should occur by age 13
Discussing confidentiality is essential to the appropriate health care of adolescents, especially prior to discussing sensitive subjects, reported John S. Santelli, MD, MPH, of Mailman School of Public Health, Columbia University, New York, N.Y., and his associates.

“Previous research has shown that when adolescents and young adults (AYAs) are not assured of confidentiality, they are less willing to discuss sensitive topics with their providers,” they wrote. The report is in Pediatrics.
According to national guidelines, although discussions concerning confidentiality can begin with parents in early adolescence, over time, the goal should be to allow fully for alone time for the AYA with you without parents present in the room.
You have a unique opportunity to help parents understand confidentiality and aid them in transitioning over time, with full respect and support for the developing adolescent-provider relationship, so that it can be fully realized by the time the adolescent reaches 13 years of age.
Using a nationally representative age-, race/ethnicity-, and income-matched sample of AYAs, the authors surveyed youth aged 13-26 years concerning preventive services received and discussions held with health care providers. Of the 1,918 individuals who completed the survey, the authors’ analysis was limited to the 1,509 (79%) youth who had seen their providers in the past 2 years.
The study focused on 11 youth-provider discussion topics. For 10 of the 11 topics, less than half of the young people said they had a discussion on the topic with a health care provider on their last visit. The most commonly discussed topics overall included mental health/emotional issues (55%), drug or alcohol use (46%), tobacco use (44%), and school performance (43%); the least common were gun safety (14%), sexual orientation (20%), and sexual or physical abuse (21%). There were more discussions concerning birth control among young women (from 26% at ages 13-14 to 54% by ages 23-26) compared with young men (13% at ages 13-14 to 12% by ages 23-26).
On average, young women reported discussing just 3.7 of the 11 topics during their last preventive care visit; young men similarly reported an average of 3.6 topics. Overall, the mean number of youth-provider discussions declined over time from 4.1 at ages 13-14 and 4.4 at ages 15-18 to 2.6 by ages 23-26.
Compared with white youth, who reported 3.3 topics at their last visit, Hispanic and African American youth reported discussing 4.2 topics. Similar differences were seen when comparing rural (2.7 topics) and urban or suburban youth (3.8 topics) or incomes greater than $75,000 (3.6 topics) compared with incomes of $25,000 or less (4.2 topics).
Youth who previously discussed confidentiality also reported discussing more topics (4.4), compared with those who had not talked about confidentiality (2.9).
Before the implementation of the Patient Protection and Affordable Care Act (ACA), which requires the provision of prevention services without cost sharing, less than half of adolescents visited a medical provider for annual preventive care visits, other studies have shown.
Although professional guidelines for adolescent preventive care recommend youth access to confidential services, “young people report that health care encounters often do not include an explanation of confidentiality by their health care provider.” Without the assurance of confidentiality, adolescents are more likely to not seek care or to opt not to disclose risky behaviors.
Current systems tend to rely on parent reporting regarding uses of services, and there is no mechanism in place for collection of data on discussion of sensitive health topics. The authors also noted a lack of time available for dialogue during visits as well as an absence of screening questionnaires prior to visits that might invite opportunities to disclose information on sensitive topics.
“Young people who reported ever having talked about confidentiality with their regular provider were more likely to engage in health discussions with providers,” emphasized Dr. Santelli and his associates. “The use of a health checklist and/or questionnaire and having spent more time with their provider during the visit were consistently associated with more of these discussions.”
You can build rapport with AYAs during preventive care visits that include screening and counseling. Immunizations, screening, and treatment of sexually transmitted infections, and dispensing of reproductive and sexual health services, including contraception, offer good opportunities for these discussions. Other sensitive topics are tobacco, alcohol, and drug use; depression and mental health; and obesity and physical activity.
Dr. Santelli and his associates consider the results of their research to serve as a “valuable addition to the literature.” They did, however, note several limitations. Because the data are cross-sectional, they cannot demonstrate causality. The use of self-report data may have contributed to underreporting of risk behaviors because adolescents were interviewed directly following parents on the same computer. Survey questions did account for the existence of youth-provider discussions, but the researchers were not able to measure the impact or quality of the resulting conversations.
It is important to note that because providers were not interviewed, the time pressures and other expected barriers were not fully accounted for in this research, Dr. Santelli and his colleagues cautioned. “Future research should ask specifically about provider-level barriers to providing preventive care to better understand their impact,” they advised.
Ultimately, the clinicians who are providing care to youth and their families will need support in implementing such changes, especially where education in the importance of discussion confidentiality and private time are concerned, they added.
The authors had no relevant financial disclosures. The study was funded by an unrestricted research grant from the Merck Foundation.
SOURCE: Santelli J et. al. Pediatrics. 2019. doi: 10.1542/peds.2018-1403.
Passage of the Affordable Care Act “provides a rich opportunity to improve the delivery of adolescent preventive services,” by lowering the financial barriers that had impeded preventive care, Jeanne Van Cleave, MD, wrote in an editorial published with the study. The findings in Santelli et al. “provide important direction for efforts to improve the delivery of adolescent preventive care.”
Specifically, changing office culture to ensure consistent screening, private time with providers, and policies that ensure discussion of confidentiality, can be accomplished by incorporating new roles for office staff, establishing team-based care, and requiring performance measurement. “By involving the whole practice, the burden of ensuring the elements of adolescent preventive care that facilitate discussion of potentially sensitive topics is lifted from individual providers,” advised Dr. Van Cleave.
Essential to the success of such a revised model of care is the practice-wide implementation and understanding of confidentiality. Dr. Van Cleave envisions a partnership between front-desk staff, medical assistants, and providers for administering screening tools and explaining to families the role of private time as well as confidentiality policies. Also essential is routine measurement of performance; the success of such a system would depend upon identifying where the gaps in care exist and what the options are for improving those gaps, she explained.
The use of alternative providers, such as nurses, social workers, or even properly trained parents, is a concept that has been tested previously. They afford greater flexibility, both during and outside of regular office hours, and they have been shown to raise the level of comfort among some youth who might otherwise be reluctant to discuss sensitive topics with their regular providers. These providers can be contacted by families outside of office visits when there are questions, giving advice and counseling by phone and electronic communication.
Dr. Van Cleave points out that while adolescents have many resources at their disposal for researching sensitive topics, including parents, social media, and even school health programs, such sources have been known to provide less accurate or incomplete information, compared with the specific, individually-tailored advice that only the primary care provider can give.
The important take-away message from the Santelli et al. report is that regular discussion of potentially sensitive topics in pediatric primary care leads to “positive patterns for seeking help later in adulthood,” Dr. Van Cleave observed. Their research offers important evidence concerning what needs to change in the practice care environment to facilitate these improvements.
What comes next, namely development and testing of appropriate interventions, will determine whether we can effectively change the role health care has to play in mitigating health risks for this population, she concluded.
Dr. Van Cleave is affiliated with Children’s Hospital Colorado and adult and child consortium for health outcomes research and delivery science, University of Colorado, Aurora. These comments are excerpted from an editorial by Dr. Van Cleave on the study by Santelli et al. (Pediatrics. 2019. doi: 10.1542/peds.2018-3618). She had no relevant financial disclosures and received no external funding.
Passage of the Affordable Care Act “provides a rich opportunity to improve the delivery of adolescent preventive services,” by lowering the financial barriers that had impeded preventive care, Jeanne Van Cleave, MD, wrote in an editorial published with the study. The findings in Santelli et al. “provide important direction for efforts to improve the delivery of adolescent preventive care.”
Specifically, changing office culture to ensure consistent screening, private time with providers, and policies that ensure discussion of confidentiality, can be accomplished by incorporating new roles for office staff, establishing team-based care, and requiring performance measurement. “By involving the whole practice, the burden of ensuring the elements of adolescent preventive care that facilitate discussion of potentially sensitive topics is lifted from individual providers,” advised Dr. Van Cleave.
Essential to the success of such a revised model of care is the practice-wide implementation and understanding of confidentiality. Dr. Van Cleave envisions a partnership between front-desk staff, medical assistants, and providers for administering screening tools and explaining to families the role of private time as well as confidentiality policies. Also essential is routine measurement of performance; the success of such a system would depend upon identifying where the gaps in care exist and what the options are for improving those gaps, she explained.
The use of alternative providers, such as nurses, social workers, or even properly trained parents, is a concept that has been tested previously. They afford greater flexibility, both during and outside of regular office hours, and they have been shown to raise the level of comfort among some youth who might otherwise be reluctant to discuss sensitive topics with their regular providers. These providers can be contacted by families outside of office visits when there are questions, giving advice and counseling by phone and electronic communication.
Dr. Van Cleave points out that while adolescents have many resources at their disposal for researching sensitive topics, including parents, social media, and even school health programs, such sources have been known to provide less accurate or incomplete information, compared with the specific, individually-tailored advice that only the primary care provider can give.
The important take-away message from the Santelli et al. report is that regular discussion of potentially sensitive topics in pediatric primary care leads to “positive patterns for seeking help later in adulthood,” Dr. Van Cleave observed. Their research offers important evidence concerning what needs to change in the practice care environment to facilitate these improvements.
What comes next, namely development and testing of appropriate interventions, will determine whether we can effectively change the role health care has to play in mitigating health risks for this population, she concluded.
Dr. Van Cleave is affiliated with Children’s Hospital Colorado and adult and child consortium for health outcomes research and delivery science, University of Colorado, Aurora. These comments are excerpted from an editorial by Dr. Van Cleave on the study by Santelli et al. (Pediatrics. 2019. doi: 10.1542/peds.2018-3618). She had no relevant financial disclosures and received no external funding.
Passage of the Affordable Care Act “provides a rich opportunity to improve the delivery of adolescent preventive services,” by lowering the financial barriers that had impeded preventive care, Jeanne Van Cleave, MD, wrote in an editorial published with the study. The findings in Santelli et al. “provide important direction for efforts to improve the delivery of adolescent preventive care.”
Specifically, changing office culture to ensure consistent screening, private time with providers, and policies that ensure discussion of confidentiality, can be accomplished by incorporating new roles for office staff, establishing team-based care, and requiring performance measurement. “By involving the whole practice, the burden of ensuring the elements of adolescent preventive care that facilitate discussion of potentially sensitive topics is lifted from individual providers,” advised Dr. Van Cleave.
Essential to the success of such a revised model of care is the practice-wide implementation and understanding of confidentiality. Dr. Van Cleave envisions a partnership between front-desk staff, medical assistants, and providers for administering screening tools and explaining to families the role of private time as well as confidentiality policies. Also essential is routine measurement of performance; the success of such a system would depend upon identifying where the gaps in care exist and what the options are for improving those gaps, she explained.
The use of alternative providers, such as nurses, social workers, or even properly trained parents, is a concept that has been tested previously. They afford greater flexibility, both during and outside of regular office hours, and they have been shown to raise the level of comfort among some youth who might otherwise be reluctant to discuss sensitive topics with their regular providers. These providers can be contacted by families outside of office visits when there are questions, giving advice and counseling by phone and electronic communication.
Dr. Van Cleave points out that while adolescents have many resources at their disposal for researching sensitive topics, including parents, social media, and even school health programs, such sources have been known to provide less accurate or incomplete information, compared with the specific, individually-tailored advice that only the primary care provider can give.
The important take-away message from the Santelli et al. report is that regular discussion of potentially sensitive topics in pediatric primary care leads to “positive patterns for seeking help later in adulthood,” Dr. Van Cleave observed. Their research offers important evidence concerning what needs to change in the practice care environment to facilitate these improvements.
What comes next, namely development and testing of appropriate interventions, will determine whether we can effectively change the role health care has to play in mitigating health risks for this population, she concluded.
Dr. Van Cleave is affiliated with Children’s Hospital Colorado and adult and child consortium for health outcomes research and delivery science, University of Colorado, Aurora. These comments are excerpted from an editorial by Dr. Van Cleave on the study by Santelli et al. (Pediatrics. 2019. doi: 10.1542/peds.2018-3618). She had no relevant financial disclosures and received no external funding.
Discussing confidentiality is essential to the appropriate health care of adolescents, especially prior to discussing sensitive subjects, reported John S. Santelli, MD, MPH, of Mailman School of Public Health, Columbia University, New York, N.Y., and his associates.
“Previous research has shown that when adolescents and young adults (AYAs) are not assured of confidentiality, they are less willing to discuss sensitive topics with their providers,” they wrote. The report is in Pediatrics.
According to national guidelines, although discussions concerning confidentiality can begin with parents in early adolescence, over time, the goal should be to allow fully for alone time for the AYA with you without parents present in the room.
You have a unique opportunity to help parents understand confidentiality and aid them in transitioning over time, with full respect and support for the developing adolescent-provider relationship, so that it can be fully realized by the time the adolescent reaches 13 years of age.
Using a nationally representative age-, race/ethnicity-, and income-matched sample of AYAs, the authors surveyed youth aged 13-26 years concerning preventive services received and discussions held with health care providers. Of the 1,918 individuals who completed the survey, the authors’ analysis was limited to the 1,509 (79%) youth who had seen their providers in the past 2 years.
The study focused on 11 youth-provider discussion topics. For 10 of the 11 topics, less than half of the young people said they had a discussion on the topic with a health care provider on their last visit. The most commonly discussed topics overall included mental health/emotional issues (55%), drug or alcohol use (46%), tobacco use (44%), and school performance (43%); the least common were gun safety (14%), sexual orientation (20%), and sexual or physical abuse (21%). There were more discussions concerning birth control among young women (from 26% at ages 13-14 to 54% by ages 23-26) compared with young men (13% at ages 13-14 to 12% by ages 23-26).
On average, young women reported discussing just 3.7 of the 11 topics during their last preventive care visit; young men similarly reported an average of 3.6 topics. Overall, the mean number of youth-provider discussions declined over time from 4.1 at ages 13-14 and 4.4 at ages 15-18 to 2.6 by ages 23-26.
Compared with white youth, who reported 3.3 topics at their last visit, Hispanic and African American youth reported discussing 4.2 topics. Similar differences were seen when comparing rural (2.7 topics) and urban or suburban youth (3.8 topics) or incomes greater than $75,000 (3.6 topics) compared with incomes of $25,000 or less (4.2 topics).
Youth who previously discussed confidentiality also reported discussing more topics (4.4), compared with those who had not talked about confidentiality (2.9).
Before the implementation of the Patient Protection and Affordable Care Act (ACA), which requires the provision of prevention services without cost sharing, less than half of adolescents visited a medical provider for annual preventive care visits, other studies have shown.
Although professional guidelines for adolescent preventive care recommend youth access to confidential services, “young people report that health care encounters often do not include an explanation of confidentiality by their health care provider.” Without the assurance of confidentiality, adolescents are more likely to not seek care or to opt not to disclose risky behaviors.
Current systems tend to rely on parent reporting regarding uses of services, and there is no mechanism in place for collection of data on discussion of sensitive health topics. The authors also noted a lack of time available for dialogue during visits as well as an absence of screening questionnaires prior to visits that might invite opportunities to disclose information on sensitive topics.
“Young people who reported ever having talked about confidentiality with their regular provider were more likely to engage in health discussions with providers,” emphasized Dr. Santelli and his associates. “The use of a health checklist and/or questionnaire and having spent more time with their provider during the visit were consistently associated with more of these discussions.”
You can build rapport with AYAs during preventive care visits that include screening and counseling. Immunizations, screening, and treatment of sexually transmitted infections, and dispensing of reproductive and sexual health services, including contraception, offer good opportunities for these discussions. Other sensitive topics are tobacco, alcohol, and drug use; depression and mental health; and obesity and physical activity.
Dr. Santelli and his associates consider the results of their research to serve as a “valuable addition to the literature.” They did, however, note several limitations. Because the data are cross-sectional, they cannot demonstrate causality. The use of self-report data may have contributed to underreporting of risk behaviors because adolescents were interviewed directly following parents on the same computer. Survey questions did account for the existence of youth-provider discussions, but the researchers were not able to measure the impact or quality of the resulting conversations.
It is important to note that because providers were not interviewed, the time pressures and other expected barriers were not fully accounted for in this research, Dr. Santelli and his colleagues cautioned. “Future research should ask specifically about provider-level barriers to providing preventive care to better understand their impact,” they advised.
Ultimately, the clinicians who are providing care to youth and their families will need support in implementing such changes, especially where education in the importance of discussion confidentiality and private time are concerned, they added.
The authors had no relevant financial disclosures. The study was funded by an unrestricted research grant from the Merck Foundation.
SOURCE: Santelli J et. al. Pediatrics. 2019. doi: 10.1542/peds.2018-1403.
Discussing confidentiality is essential to the appropriate health care of adolescents, especially prior to discussing sensitive subjects, reported John S. Santelli, MD, MPH, of Mailman School of Public Health, Columbia University, New York, N.Y., and his associates.
“Previous research has shown that when adolescents and young adults (AYAs) are not assured of confidentiality, they are less willing to discuss sensitive topics with their providers,” they wrote. The report is in Pediatrics.
According to national guidelines, although discussions concerning confidentiality can begin with parents in early adolescence, over time, the goal should be to allow fully for alone time for the AYA with you without parents present in the room.
You have a unique opportunity to help parents understand confidentiality and aid them in transitioning over time, with full respect and support for the developing adolescent-provider relationship, so that it can be fully realized by the time the adolescent reaches 13 years of age.
Using a nationally representative age-, race/ethnicity-, and income-matched sample of AYAs, the authors surveyed youth aged 13-26 years concerning preventive services received and discussions held with health care providers. Of the 1,918 individuals who completed the survey, the authors’ analysis was limited to the 1,509 (79%) youth who had seen their providers in the past 2 years.
The study focused on 11 youth-provider discussion topics. For 10 of the 11 topics, less than half of the young people said they had a discussion on the topic with a health care provider on their last visit. The most commonly discussed topics overall included mental health/emotional issues (55%), drug or alcohol use (46%), tobacco use (44%), and school performance (43%); the least common were gun safety (14%), sexual orientation (20%), and sexual or physical abuse (21%). There were more discussions concerning birth control among young women (from 26% at ages 13-14 to 54% by ages 23-26) compared with young men (13% at ages 13-14 to 12% by ages 23-26).
On average, young women reported discussing just 3.7 of the 11 topics during their last preventive care visit; young men similarly reported an average of 3.6 topics. Overall, the mean number of youth-provider discussions declined over time from 4.1 at ages 13-14 and 4.4 at ages 15-18 to 2.6 by ages 23-26.
Compared with white youth, who reported 3.3 topics at their last visit, Hispanic and African American youth reported discussing 4.2 topics. Similar differences were seen when comparing rural (2.7 topics) and urban or suburban youth (3.8 topics) or incomes greater than $75,000 (3.6 topics) compared with incomes of $25,000 or less (4.2 topics).
Youth who previously discussed confidentiality also reported discussing more topics (4.4), compared with those who had not talked about confidentiality (2.9).
Before the implementation of the Patient Protection and Affordable Care Act (ACA), which requires the provision of prevention services without cost sharing, less than half of adolescents visited a medical provider for annual preventive care visits, other studies have shown.
Although professional guidelines for adolescent preventive care recommend youth access to confidential services, “young people report that health care encounters often do not include an explanation of confidentiality by their health care provider.” Without the assurance of confidentiality, adolescents are more likely to not seek care or to opt not to disclose risky behaviors.
Current systems tend to rely on parent reporting regarding uses of services, and there is no mechanism in place for collection of data on discussion of sensitive health topics. The authors also noted a lack of time available for dialogue during visits as well as an absence of screening questionnaires prior to visits that might invite opportunities to disclose information on sensitive topics.
“Young people who reported ever having talked about confidentiality with their regular provider were more likely to engage in health discussions with providers,” emphasized Dr. Santelli and his associates. “The use of a health checklist and/or questionnaire and having spent more time with their provider during the visit were consistently associated with more of these discussions.”
You can build rapport with AYAs during preventive care visits that include screening and counseling. Immunizations, screening, and treatment of sexually transmitted infections, and dispensing of reproductive and sexual health services, including contraception, offer good opportunities for these discussions. Other sensitive topics are tobacco, alcohol, and drug use; depression and mental health; and obesity and physical activity.
Dr. Santelli and his associates consider the results of their research to serve as a “valuable addition to the literature.” They did, however, note several limitations. Because the data are cross-sectional, they cannot demonstrate causality. The use of self-report data may have contributed to underreporting of risk behaviors because adolescents were interviewed directly following parents on the same computer. Survey questions did account for the existence of youth-provider discussions, but the researchers were not able to measure the impact or quality of the resulting conversations.
It is important to note that because providers were not interviewed, the time pressures and other expected barriers were not fully accounted for in this research, Dr. Santelli and his colleagues cautioned. “Future research should ask specifically about provider-level barriers to providing preventive care to better understand their impact,” they advised.
Ultimately, the clinicians who are providing care to youth and their families will need support in implementing such changes, especially where education in the importance of discussion confidentiality and private time are concerned, they added.
The authors had no relevant financial disclosures. The study was funded by an unrestricted research grant from the Merck Foundation.
SOURCE: Santelli J et. al. Pediatrics. 2019. doi: 10.1542/peds.2018-1403.
FROM PEDIATRICS
Key clinical point:
Major finding: The most commonly discussed topics overall included mental health/emotional issues (55%), drug or alcohol use (46%), tobacco use (44%), and school performance (43%); the least common were gun safety (14%), sexual orientation (20%), and sexual or physical abuse (21%).
Study details: Self-report survey.
Disclosures: The authors had no financial relationships relevant to this article to disclose. The study was funded by an unrestricted research grant from the Merck Foundation.
Source: Santelli J. et. al. Pediatrics. 2019;143(2):e20181403.
