User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Topical Ruxolitinib Effective for AD in Study of Children Ages 2-11 years
) affecting ≥ 35% or more of their body surface area (BSA), results from a small open-label maximum-use trial showed.
When approved for this age group, ruxolitinib cream will provide a topical nonsteroidal option for patients aged 2-11, which will “simplify the treatment regimen,” one of the study investigators, Linda Stein Gold, MD, director of clinical research and division head of dermatology at the Henry Ford Health System, Detroit, said in an interview after the Revolutionizing Atopic Dermatitis conference, where the study was presented during a late-breaking abstract session.

A topical formulation of the selective Janus kinase (JAK) 1/JAK2 inhibitor, ruxolitinib cream 1.5% is currently approved by the Food and Drug Administration for the short-term and noncontinuous chronic treatment of mild to moderate AD in non-immunocompromised adult and pediatric patients aged 12 years and older, whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable.
In previous reports of this trial in children aged 2-11 years with ≥ 35% affected BSA, ruxolitinib cream 1.5% was generally well tolerated, with rapid anti-inflammatory and antipruritic effects and improvements in patient-reported outcomes observed with ≤ 4 weeks of continuous treatment and maintained with as-needed treatment from 4 to 8 weeks.
For the current trial, investigators evaluated data on tolerability, safety, systemic exposure, and clinical and patient-reported outcomes through 52 weeks to determine whether clinical benefits and tolerability observed through 8 weeks were sustained.
Dr. Stein Gold and colleagues reported results from 29 children who received ruxolitinib cream 1.5% from baseline through week 8. Of these, 22 continued into the long-term safety period from week 8 through 52. From baseline through week 8, patients applied a mean of 6.5 g per day of ruxolitinib cream; this dropped to a mean of 3.2 g per day from weeks 8 through 52. The mean steady-state plasma concentration of ruxolitinib throughout the study was 98.2 nM, which is “well below half-maximal concentration of JAK-mediated myelosuppression in adults (281 nM),” the researchers stated in their abstract.
No treatment-related interruptions, discontinuations, or serious adverse events were observed between baseline and week 52. One patient (3.4%) had two treatment-related application site reactions (paresthesia and folliculitis). At weeks 4 and 52, 53.8% of patients achieved treatment success, which was defined as an Investigator Global Assessment of 0/1 with a ≥ 2-grade improvement from baseline. The mean affected BSA decreased from 58.0% at baseline to 11.4% at week 4 and continued to decrease to 2.2% through week 52. “I was surprised that patients could maintain control over the long-term using the medication as needed,” Dr. Stein Gold told this news organization. “I was also pleased to see that there was low systemic exposure even when used on large body surface areas.”
In other findings, the mean total Patient Oriented Eczema Measure score dropped from a baseline of 19.4 to a mean of 4.5 at week 8 and 3.6 at week 52 and the mean total Children’s Dermatology Life Quality Index score fell from a baseline of 15.4 to a mean of 5.3 at week 8 and a mean of 2.1 at week 52. Meanwhile, the mean total Infants’ Dermatology Quality of Life Index score fell from a mean of 12.3 at baseline to a mean of 2.8 at week 8 and a mean of 0.7 at week 52.
Dr. Stein Gold noted certain limitations of the study, including the fact that it did not study children aged younger than 2 years.
The study was funded by Incyte, which markets ruxolitinib cream 1.5% as Opzelura. Dr. Stein Gold disclosed that she has served as an investigator, advisor, and/or speaker for several pharmaceutical companies, including Incyte.
A version of this article appeared on Medscape.com.
) affecting ≥ 35% or more of their body surface area (BSA), results from a small open-label maximum-use trial showed.
When approved for this age group, ruxolitinib cream will provide a topical nonsteroidal option for patients aged 2-11, which will “simplify the treatment regimen,” one of the study investigators, Linda Stein Gold, MD, director of clinical research and division head of dermatology at the Henry Ford Health System, Detroit, said in an interview after the Revolutionizing Atopic Dermatitis conference, where the study was presented during a late-breaking abstract session.
A topical formulation of the selective Janus kinase (JAK) 1/JAK2 inhibitor, ruxolitinib cream 1.5% is currently approved by the Food and Drug Administration for the short-term and noncontinuous chronic treatment of mild to moderate AD in non-immunocompromised adult and pediatric patients aged 12 years and older, whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable.
In previous reports of this trial in children aged 2-11 years with ≥ 35% affected BSA, ruxolitinib cream 1.5% was generally well tolerated, with rapid anti-inflammatory and antipruritic effects and improvements in patient-reported outcomes observed with ≤ 4 weeks of continuous treatment and maintained with as-needed treatment from 4 to 8 weeks.
For the current trial, investigators evaluated data on tolerability, safety, systemic exposure, and clinical and patient-reported outcomes through 52 weeks to determine whether clinical benefits and tolerability observed through 8 weeks were sustained.
Dr. Stein Gold and colleagues reported results from 29 children who received ruxolitinib cream 1.5% from baseline through week 8. Of these, 22 continued into the long-term safety period from week 8 through 52. From baseline through week 8, patients applied a mean of 6.5 g per day of ruxolitinib cream; this dropped to a mean of 3.2 g per day from weeks 8 through 52. The mean steady-state plasma concentration of ruxolitinib throughout the study was 98.2 nM, which is “well below half-maximal concentration of JAK-mediated myelosuppression in adults (281 nM),” the researchers stated in their abstract.
No treatment-related interruptions, discontinuations, or serious adverse events were observed between baseline and week 52. One patient (3.4%) had two treatment-related application site reactions (paresthesia and folliculitis). At weeks 4 and 52, 53.8% of patients achieved treatment success, which was defined as an Investigator Global Assessment of 0/1 with a ≥ 2-grade improvement from baseline. The mean affected BSA decreased from 58.0% at baseline to 11.4% at week 4 and continued to decrease to 2.2% through week 52. “I was surprised that patients could maintain control over the long-term using the medication as needed,” Dr. Stein Gold told this news organization. “I was also pleased to see that there was low systemic exposure even when used on large body surface areas.”
In other findings, the mean total Patient Oriented Eczema Measure score dropped from a baseline of 19.4 to a mean of 4.5 at week 8 and 3.6 at week 52 and the mean total Children’s Dermatology Life Quality Index score fell from a baseline of 15.4 to a mean of 5.3 at week 8 and a mean of 2.1 at week 52. Meanwhile, the mean total Infants’ Dermatology Quality of Life Index score fell from a mean of 12.3 at baseline to a mean of 2.8 at week 8 and a mean of 0.7 at week 52.
Dr. Stein Gold noted certain limitations of the study, including the fact that it did not study children aged younger than 2 years.
The study was funded by Incyte, which markets ruxolitinib cream 1.5% as Opzelura. Dr. Stein Gold disclosed that she has served as an investigator, advisor, and/or speaker for several pharmaceutical companies, including Incyte.
A version of this article appeared on Medscape.com.
) affecting ≥ 35% or more of their body surface area (BSA), results from a small open-label maximum-use trial showed.
When approved for this age group, ruxolitinib cream will provide a topical nonsteroidal option for patients aged 2-11, which will “simplify the treatment regimen,” one of the study investigators, Linda Stein Gold, MD, director of clinical research and division head of dermatology at the Henry Ford Health System, Detroit, said in an interview after the Revolutionizing Atopic Dermatitis conference, where the study was presented during a late-breaking abstract session.
A topical formulation of the selective Janus kinase (JAK) 1/JAK2 inhibitor, ruxolitinib cream 1.5% is currently approved by the Food and Drug Administration for the short-term and noncontinuous chronic treatment of mild to moderate AD in non-immunocompromised adult and pediatric patients aged 12 years and older, whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable.
In previous reports of this trial in children aged 2-11 years with ≥ 35% affected BSA, ruxolitinib cream 1.5% was generally well tolerated, with rapid anti-inflammatory and antipruritic effects and improvements in patient-reported outcomes observed with ≤ 4 weeks of continuous treatment and maintained with as-needed treatment from 4 to 8 weeks.
For the current trial, investigators evaluated data on tolerability, safety, systemic exposure, and clinical and patient-reported outcomes through 52 weeks to determine whether clinical benefits and tolerability observed through 8 weeks were sustained.
Dr. Stein Gold and colleagues reported results from 29 children who received ruxolitinib cream 1.5% from baseline through week 8. Of these, 22 continued into the long-term safety period from week 8 through 52. From baseline through week 8, patients applied a mean of 6.5 g per day of ruxolitinib cream; this dropped to a mean of 3.2 g per day from weeks 8 through 52. The mean steady-state plasma concentration of ruxolitinib throughout the study was 98.2 nM, which is “well below half-maximal concentration of JAK-mediated myelosuppression in adults (281 nM),” the researchers stated in their abstract.
No treatment-related interruptions, discontinuations, or serious adverse events were observed between baseline and week 52. One patient (3.4%) had two treatment-related application site reactions (paresthesia and folliculitis). At weeks 4 and 52, 53.8% of patients achieved treatment success, which was defined as an Investigator Global Assessment of 0/1 with a ≥ 2-grade improvement from baseline. The mean affected BSA decreased from 58.0% at baseline to 11.4% at week 4 and continued to decrease to 2.2% through week 52. “I was surprised that patients could maintain control over the long-term using the medication as needed,” Dr. Stein Gold told this news organization. “I was also pleased to see that there was low systemic exposure even when used on large body surface areas.”
In other findings, the mean total Patient Oriented Eczema Measure score dropped from a baseline of 19.4 to a mean of 4.5 at week 8 and 3.6 at week 52 and the mean total Children’s Dermatology Life Quality Index score fell from a baseline of 15.4 to a mean of 5.3 at week 8 and a mean of 2.1 at week 52. Meanwhile, the mean total Infants’ Dermatology Quality of Life Index score fell from a mean of 12.3 at baseline to a mean of 2.8 at week 8 and a mean of 0.7 at week 52.
Dr. Stein Gold noted certain limitations of the study, including the fact that it did not study children aged younger than 2 years.
The study was funded by Incyte, which markets ruxolitinib cream 1.5% as Opzelura. Dr. Stein Gold disclosed that she has served as an investigator, advisor, and/or speaker for several pharmaceutical companies, including Incyte.
A version of this article appeared on Medscape.com.
Pediatric Atopic Dermatitis: Study Suggests Treatment May Impact Atopic March
TOPLINE:
METHODOLOGY:
- Researchers conducted a retrospective cohort study using data from the US Collaborative Network, focusing on pediatric patients aged 18 years and younger with two AD diagnoses at least 30 days apart.
- Patients were divided into two cohorts: Those treated with dupilumab (n = 2192) and those who received conventional therapies (n = 2192), including systemic corticosteroids or conventional immunomodulators. They were stratified into three age groups: Preschoolers (< 6 years), school-aged children (6 to < 12 years), and adolescents (12-18 years).
- Both cohorts underwent 1:1 propensity score matching based on current age, age at index (first prescription of dupilumab or conventional therapy), sex, race, comorbidities, laboratory measurements, and prior medications. The primary outcome was atopic march progression, defined by incident asthma or allergic rhinitis.
TAKEAWAY:
- Over 3 years, the dupilumab-treated cohort had a significantly lower cumulative incidence of atopic march progression (20.09% vs 27.22%; P < .001), asthma (9.43% vs 14.64%; P = .001), and allergic rhinitis (13.57% vs 20.52%; P = .003) than the conventional therapy cohort.
- The risk for atopic march progression, asthma, and allergic rhinitis was also significantly reduced by 32%, 40%, and 31%, respectively, in the dupilumab vs conventional therapy cohort.
- Age-specific analyses found that the protective effect of dupilumab against allergic rhinitis was the most pronounced in adolescents (hazard ratio [HR], 0.503; 95% CI, 0.322-0.784), followed by school-aged children (HR, 0.577; 95% CI, 0.399-0.834), and preschoolers (HR, 0.623; 95% CI, 0.412-0.942).
- However, dupilumab was associated with reduced risk for asthma only in preschoolers (HR, 0.427; 95% CI, 0.247-0.738) and not in school-aged children or adolescents.
IN PRACTICE:
“Dupilumab in AD not only treats the disease but may influence atopic march mechanisms, suggesting its role as a disease-modifying atopic march drug,” the authors wrote, adding that more research “with extended follow-up and proof-of-concept is warranted.”
SOURCE:
The study was led by Teng-Li Lin, MD, Department of Dermatology, Dalin Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Chiayi, Taiwan, and was published online on June 13, 2024, in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The observational nature of the study limited the ability to infer direct causality between dupilumab use and reduced atopic march risk. Lack of detailed information on AD severity, total dosage, and duration of medication treatment may affect the interpretation of the study’s findings. The demographic data suggest that the dupilumab cohort had more severe AD, so the observed risk reduction may be greater than that reported in this study.
DISCLOSURES:
The study was supported in part by the National Science and Technology Council, Taiwan, and Taichung Veterans General Hospital. The authors had no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article appeared on Medscape.com .
TOPLINE:
METHODOLOGY:
- Researchers conducted a retrospective cohort study using data from the US Collaborative Network, focusing on pediatric patients aged 18 years and younger with two AD diagnoses at least 30 days apart.
- Patients were divided into two cohorts: Those treated with dupilumab (n = 2192) and those who received conventional therapies (n = 2192), including systemic corticosteroids or conventional immunomodulators. They were stratified into three age groups: Preschoolers (< 6 years), school-aged children (6 to < 12 years), and adolescents (12-18 years).
- Both cohorts underwent 1:1 propensity score matching based on current age, age at index (first prescription of dupilumab or conventional therapy), sex, race, comorbidities, laboratory measurements, and prior medications. The primary outcome was atopic march progression, defined by incident asthma or allergic rhinitis.
TAKEAWAY:
- Over 3 years, the dupilumab-treated cohort had a significantly lower cumulative incidence of atopic march progression (20.09% vs 27.22%; P < .001), asthma (9.43% vs 14.64%; P = .001), and allergic rhinitis (13.57% vs 20.52%; P = .003) than the conventional therapy cohort.
- The risk for atopic march progression, asthma, and allergic rhinitis was also significantly reduced by 32%, 40%, and 31%, respectively, in the dupilumab vs conventional therapy cohort.
- Age-specific analyses found that the protective effect of dupilumab against allergic rhinitis was the most pronounced in adolescents (hazard ratio [HR], 0.503; 95% CI, 0.322-0.784), followed by school-aged children (HR, 0.577; 95% CI, 0.399-0.834), and preschoolers (HR, 0.623; 95% CI, 0.412-0.942).
- However, dupilumab was associated with reduced risk for asthma only in preschoolers (HR, 0.427; 95% CI, 0.247-0.738) and not in school-aged children or adolescents.
IN PRACTICE:
“Dupilumab in AD not only treats the disease but may influence atopic march mechanisms, suggesting its role as a disease-modifying atopic march drug,” the authors wrote, adding that more research “with extended follow-up and proof-of-concept is warranted.”
SOURCE:
The study was led by Teng-Li Lin, MD, Department of Dermatology, Dalin Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Chiayi, Taiwan, and was published online on June 13, 2024, in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The observational nature of the study limited the ability to infer direct causality between dupilumab use and reduced atopic march risk. Lack of detailed information on AD severity, total dosage, and duration of medication treatment may affect the interpretation of the study’s findings. The demographic data suggest that the dupilumab cohort had more severe AD, so the observed risk reduction may be greater than that reported in this study.
DISCLOSURES:
The study was supported in part by the National Science and Technology Council, Taiwan, and Taichung Veterans General Hospital. The authors had no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article appeared on Medscape.com .
TOPLINE:
METHODOLOGY:
- Researchers conducted a retrospective cohort study using data from the US Collaborative Network, focusing on pediatric patients aged 18 years and younger with two AD diagnoses at least 30 days apart.
- Patients were divided into two cohorts: Those treated with dupilumab (n = 2192) and those who received conventional therapies (n = 2192), including systemic corticosteroids or conventional immunomodulators. They were stratified into three age groups: Preschoolers (< 6 years), school-aged children (6 to < 12 years), and adolescents (12-18 years).
- Both cohorts underwent 1:1 propensity score matching based on current age, age at index (first prescription of dupilumab or conventional therapy), sex, race, comorbidities, laboratory measurements, and prior medications. The primary outcome was atopic march progression, defined by incident asthma or allergic rhinitis.
TAKEAWAY:
- Over 3 years, the dupilumab-treated cohort had a significantly lower cumulative incidence of atopic march progression (20.09% vs 27.22%; P < .001), asthma (9.43% vs 14.64%; P = .001), and allergic rhinitis (13.57% vs 20.52%; P = .003) than the conventional therapy cohort.
- The risk for atopic march progression, asthma, and allergic rhinitis was also significantly reduced by 32%, 40%, and 31%, respectively, in the dupilumab vs conventional therapy cohort.
- Age-specific analyses found that the protective effect of dupilumab against allergic rhinitis was the most pronounced in adolescents (hazard ratio [HR], 0.503; 95% CI, 0.322-0.784), followed by school-aged children (HR, 0.577; 95% CI, 0.399-0.834), and preschoolers (HR, 0.623; 95% CI, 0.412-0.942).
- However, dupilumab was associated with reduced risk for asthma only in preschoolers (HR, 0.427; 95% CI, 0.247-0.738) and not in school-aged children or adolescents.
IN PRACTICE:
“Dupilumab in AD not only treats the disease but may influence atopic march mechanisms, suggesting its role as a disease-modifying atopic march drug,” the authors wrote, adding that more research “with extended follow-up and proof-of-concept is warranted.”
SOURCE:
The study was led by Teng-Li Lin, MD, Department of Dermatology, Dalin Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Chiayi, Taiwan, and was published online on June 13, 2024, in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The observational nature of the study limited the ability to infer direct causality between dupilumab use and reduced atopic march risk. Lack of detailed information on AD severity, total dosage, and duration of medication treatment may affect the interpretation of the study’s findings. The demographic data suggest that the dupilumab cohort had more severe AD, so the observed risk reduction may be greater than that reported in this study.
DISCLOSURES:
The study was supported in part by the National Science and Technology Council, Taiwan, and Taichung Veterans General Hospital. The authors had no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article appeared on Medscape.com .
Meta-Analysis Finds Combination Cream Plus Tranexamic Acid Effective for Melasma
TOPLINE:
A meta-analysis showed that .
METHODOLOGY:
- Current treatments for melasma focus on inducing remission and preventing relapse. Tranexamic acid, an antifibrinolytic drug, has shown promise in recent studies, but its optimal use, either alone or as an adjunct to TCC, remains unclear.
- Researchers conducted a meta-analysis of four randomized controlled trials patients that compared oral tranexamic acid plus TCC (hydroquinone, retinoic acid, and hydrocortisone) and TCC alone in 480 patients with melasma, divided almost evenly into the two treatment groups.
- The main outcome was the change in the Melasma Severity Area Index (MASI) score and recurrence rate from baseline.
TAKEAWAY:
- Patients treated with oral tranexamic acid plus TCC showed a greater reduction in MASI scores compared with those who received TCC alone (mean difference, −3.10; P = .03).
- The recurrence rate of melasma was significantly lower in the tranexamic acid plus TCC group (risk ratio [RR], 0.28; P < .001).
- There was no significant difference in the incidences of erythema (RR, 0.63; P = .147) and burning (RR, 0.59; P = .131).
IN PRACTICE:
“Evidence indicates that oral tranexamic acid confers clinical benefits, contributing to the enhancement of treatment outcomes in melasma when used in conjunction with TCC therapy,” and results are promising with regards to minimizing recurrence, the authors concluded.
SOURCE:
The study was led by Ocílio Ribeiro Gonçalves, MS, of the Federal University of Piauí, Teresina, Brazil, and was published online on June 8, 2024, in Clinical and Experimental Dermatology.
LIMITATIONS:
There was heterogeneity across studies, including different methods of administration, treatment protocols (including dosage), and timing of treatment.
DISCLOSURES:
The study reported receiving no funding. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
A meta-analysis showed that .
METHODOLOGY:
- Current treatments for melasma focus on inducing remission and preventing relapse. Tranexamic acid, an antifibrinolytic drug, has shown promise in recent studies, but its optimal use, either alone or as an adjunct to TCC, remains unclear.
- Researchers conducted a meta-analysis of four randomized controlled trials patients that compared oral tranexamic acid plus TCC (hydroquinone, retinoic acid, and hydrocortisone) and TCC alone in 480 patients with melasma, divided almost evenly into the two treatment groups.
- The main outcome was the change in the Melasma Severity Area Index (MASI) score and recurrence rate from baseline.
TAKEAWAY:
- Patients treated with oral tranexamic acid plus TCC showed a greater reduction in MASI scores compared with those who received TCC alone (mean difference, −3.10; P = .03).
- The recurrence rate of melasma was significantly lower in the tranexamic acid plus TCC group (risk ratio [RR], 0.28; P < .001).
- There was no significant difference in the incidences of erythema (RR, 0.63; P = .147) and burning (RR, 0.59; P = .131).
IN PRACTICE:
“Evidence indicates that oral tranexamic acid confers clinical benefits, contributing to the enhancement of treatment outcomes in melasma when used in conjunction with TCC therapy,” and results are promising with regards to minimizing recurrence, the authors concluded.
SOURCE:
The study was led by Ocílio Ribeiro Gonçalves, MS, of the Federal University of Piauí, Teresina, Brazil, and was published online on June 8, 2024, in Clinical and Experimental Dermatology.
LIMITATIONS:
There was heterogeneity across studies, including different methods of administration, treatment protocols (including dosage), and timing of treatment.
DISCLOSURES:
The study reported receiving no funding. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
A meta-analysis showed that .
METHODOLOGY:
- Current treatments for melasma focus on inducing remission and preventing relapse. Tranexamic acid, an antifibrinolytic drug, has shown promise in recent studies, but its optimal use, either alone or as an adjunct to TCC, remains unclear.
- Researchers conducted a meta-analysis of four randomized controlled trials patients that compared oral tranexamic acid plus TCC (hydroquinone, retinoic acid, and hydrocortisone) and TCC alone in 480 patients with melasma, divided almost evenly into the two treatment groups.
- The main outcome was the change in the Melasma Severity Area Index (MASI) score and recurrence rate from baseline.
TAKEAWAY:
- Patients treated with oral tranexamic acid plus TCC showed a greater reduction in MASI scores compared with those who received TCC alone (mean difference, −3.10; P = .03).
- The recurrence rate of melasma was significantly lower in the tranexamic acid plus TCC group (risk ratio [RR], 0.28; P < .001).
- There was no significant difference in the incidences of erythema (RR, 0.63; P = .147) and burning (RR, 0.59; P = .131).
IN PRACTICE:
“Evidence indicates that oral tranexamic acid confers clinical benefits, contributing to the enhancement of treatment outcomes in melasma when used in conjunction with TCC therapy,” and results are promising with regards to minimizing recurrence, the authors concluded.
SOURCE:
The study was led by Ocílio Ribeiro Gonçalves, MS, of the Federal University of Piauí, Teresina, Brazil, and was published online on June 8, 2024, in Clinical and Experimental Dermatology.
LIMITATIONS:
There was heterogeneity across studies, including different methods of administration, treatment protocols (including dosage), and timing of treatment.
DISCLOSURES:
The study reported receiving no funding. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
OTC Supplement Linked to Hyperpigmentation
CHICAGO —The .
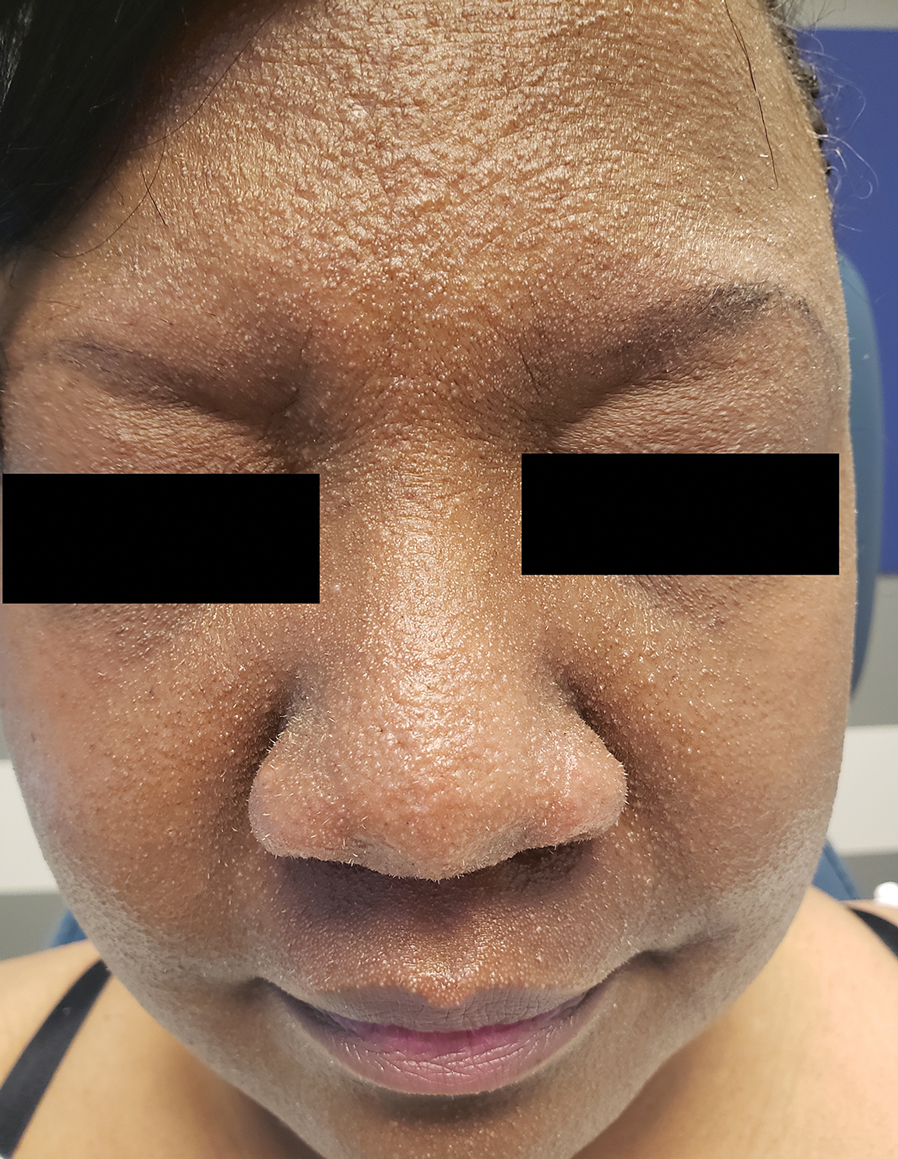
“This is something we will see more and more,” Heather Woolery-Lloyd, MD, director of the Skin of Color Division at the University of Miami Department of Dermatology, said at the Pigmentary Disorders Exchange Symposium. The key marker of this hyperpigmentation, she said, is that “it’s strongly photoaccentuated,” affecting areas exposed to the sun — but it also tends to spare the knuckles on patients’ hands.
Used Like an Opioid, But It’s Not Regulated
Kratom is a plant common in southeast Asia and is used as an analgesic. It’s marketed as a “legal opioid” or “legal high” and is sold in 2- or 3-ounce containers of extract or sold as a powder, Dr. Woolery-Lloyd said. The leaves may be boiled into a tea, smoked, chewed, or put into capsules, according to a case report published in February in the Journal of Integrative Dermatology. It is used worldwide and is not regulated in the United States.
“Many of our patients think kratom is a safe, herbal supplement” but often don’t know it can have several side effects and can be addictive, Dr. Woolery-Lloyd said. Its popularity is increasing as reflected by the number of posts related to kratom on social media platforms.
In the February case report, Shaina Patel, BA, and Nathaniel Phelan, MD, from Kansas City University, Kansas City, Missouri, wrote that side effects of kratom include drowsiness, tachycardia, vomiting, respiratory depression, and cardiac arrest, in addition to confusion and hallucinations.
Kratom also has many different effects on the psyche, Dr. Woolery-Lloyd said at the meeting. At low doses, it blocks the reuptake of norepinephrine, serotonin, and dopamine, producing a motivational effect, and at high doses, it creates an analgesic, calming effect. And people who chronically consume high doses of kratom may be susceptible to hyperpigmentation.
Kratom-associated hyperpigmentation should be considered as a diagnosis when evaluating patients for other drug-associated pigmentary disorders, “especially if pigment is photodistributed,” she said. “If you see new-onset hyperpigmentation or onset over several months and it’s very photoaccentuated, definitely ask about use of kratom.”
Case Reports Show Patterns of Presentation
A 2022 report from Landon R. Powell, BS, with the department of biology, Whitworth University in Spokane, Washington, and coauthors, published in JAAD Case Reports, noted that kratom use in the United States has increased dramatically. “As measured by call reports to the United States National Poison Data System, in 2011, there were 11 reported kratom exposures, and in the first 7 months of 2018, there were 357 reported exposures,” they wrote.
An estimated 1.7 million Americans aged ≥ 12 years said they had used kratom in the previous year, according to the Substance Abuse and Mental Health Services Administration 2021 National Survey on Drug Use and Health.
In the case report, Mr. Powell and coauthors described a 54-year-old White male patient who had been using kratom for the previous four to five years to reduce opioid use. During this period, he consumed kratom powder mixed with orange juice three to four times a day. He presented with “diffuse hyperpigmented patches on his arms and face in a photodistributed manner, with notable sparing of the knuckles on both hands.”
Dark Gray-Blue Skin
In the more recent case report, Ms. Patel and Dr. Phelan described a 30-year-old White male patient who presented with dark gray-blue skin coloring on his cheeks, back of his neck, and the backs of his hands and forearms. He had no other medical conditions and did not take any medications or supplements that cause hyperpigmentation while using kratom.
The patient had been taking kratom for years in the wake of an opioid addiction following medications for a high school injury. He developed an opioid use disorder and tried to replace his pain medications with kratom.
“The patient stopped using kratom in May 2022, but the discoloration remains. It has not regressed in the following 16 months after discontinuing kratom use,” the authors wrote, noting that “whether or not the hyperpigmentation is able to regress is unknown.”
Dr. Woolery-Lloyd is a consultant for AbbVie, Incyte, Johnson & Johnson Consumer, LivDerm, and L’Oreal; a speaker for Eli Lilly, Incyte, L’Oreal, and Ortho Dermatologics; and a researcher/investigator for AbbVie, Allergan, Eirion Therapeutics, Galderma, Pfizer, Sanofi, and Vyne Therapeutics.
According to an information page on kratom on the Food and Drug Administration website, health care professionals and consumers can report adverse reactions associated with kratom to the FDA’s MedWatch program.
A version of this article appeared on Medscape.com.
CHICAGO —The .
“This is something we will see more and more,” Heather Woolery-Lloyd, MD, director of the Skin of Color Division at the University of Miami Department of Dermatology, said at the Pigmentary Disorders Exchange Symposium. The key marker of this hyperpigmentation, she said, is that “it’s strongly photoaccentuated,” affecting areas exposed to the sun — but it also tends to spare the knuckles on patients’ hands.
Used Like an Opioid, But It’s Not Regulated
Kratom is a plant common in southeast Asia and is used as an analgesic. It’s marketed as a “legal opioid” or “legal high” and is sold in 2- or 3-ounce containers of extract or sold as a powder, Dr. Woolery-Lloyd said. The leaves may be boiled into a tea, smoked, chewed, or put into capsules, according to a case report published in February in the Journal of Integrative Dermatology. It is used worldwide and is not regulated in the United States.
“Many of our patients think kratom is a safe, herbal supplement” but often don’t know it can have several side effects and can be addictive, Dr. Woolery-Lloyd said. Its popularity is increasing as reflected by the number of posts related to kratom on social media platforms.
In the February case report, Shaina Patel, BA, and Nathaniel Phelan, MD, from Kansas City University, Kansas City, Missouri, wrote that side effects of kratom include drowsiness, tachycardia, vomiting, respiratory depression, and cardiac arrest, in addition to confusion and hallucinations.
Kratom also has many different effects on the psyche, Dr. Woolery-Lloyd said at the meeting. At low doses, it blocks the reuptake of norepinephrine, serotonin, and dopamine, producing a motivational effect, and at high doses, it creates an analgesic, calming effect. And people who chronically consume high doses of kratom may be susceptible to hyperpigmentation.
Kratom-associated hyperpigmentation should be considered as a diagnosis when evaluating patients for other drug-associated pigmentary disorders, “especially if pigment is photodistributed,” she said. “If you see new-onset hyperpigmentation or onset over several months and it’s very photoaccentuated, definitely ask about use of kratom.”
Case Reports Show Patterns of Presentation
A 2022 report from Landon R. Powell, BS, with the department of biology, Whitworth University in Spokane, Washington, and coauthors, published in JAAD Case Reports, noted that kratom use in the United States has increased dramatically. “As measured by call reports to the United States National Poison Data System, in 2011, there were 11 reported kratom exposures, and in the first 7 months of 2018, there were 357 reported exposures,” they wrote.
An estimated 1.7 million Americans aged ≥ 12 years said they had used kratom in the previous year, according to the Substance Abuse and Mental Health Services Administration 2021 National Survey on Drug Use and Health.
In the case report, Mr. Powell and coauthors described a 54-year-old White male patient who had been using kratom for the previous four to five years to reduce opioid use. During this period, he consumed kratom powder mixed with orange juice three to four times a day. He presented with “diffuse hyperpigmented patches on his arms and face in a photodistributed manner, with notable sparing of the knuckles on both hands.”
Dark Gray-Blue Skin
In the more recent case report, Ms. Patel and Dr. Phelan described a 30-year-old White male patient who presented with dark gray-blue skin coloring on his cheeks, back of his neck, and the backs of his hands and forearms. He had no other medical conditions and did not take any medications or supplements that cause hyperpigmentation while using kratom.
The patient had been taking kratom for years in the wake of an opioid addiction following medications for a high school injury. He developed an opioid use disorder and tried to replace his pain medications with kratom.
“The patient stopped using kratom in May 2022, but the discoloration remains. It has not regressed in the following 16 months after discontinuing kratom use,” the authors wrote, noting that “whether or not the hyperpigmentation is able to regress is unknown.”
Dr. Woolery-Lloyd is a consultant for AbbVie, Incyte, Johnson & Johnson Consumer, LivDerm, and L’Oreal; a speaker for Eli Lilly, Incyte, L’Oreal, and Ortho Dermatologics; and a researcher/investigator for AbbVie, Allergan, Eirion Therapeutics, Galderma, Pfizer, Sanofi, and Vyne Therapeutics.
According to an information page on kratom on the Food and Drug Administration website, health care professionals and consumers can report adverse reactions associated with kratom to the FDA’s MedWatch program.
A version of this article appeared on Medscape.com.
CHICAGO —The .
“This is something we will see more and more,” Heather Woolery-Lloyd, MD, director of the Skin of Color Division at the University of Miami Department of Dermatology, said at the Pigmentary Disorders Exchange Symposium. The key marker of this hyperpigmentation, she said, is that “it’s strongly photoaccentuated,” affecting areas exposed to the sun — but it also tends to spare the knuckles on patients’ hands.
Used Like an Opioid, But It’s Not Regulated
Kratom is a plant common in southeast Asia and is used as an analgesic. It’s marketed as a “legal opioid” or “legal high” and is sold in 2- or 3-ounce containers of extract or sold as a powder, Dr. Woolery-Lloyd said. The leaves may be boiled into a tea, smoked, chewed, or put into capsules, according to a case report published in February in the Journal of Integrative Dermatology. It is used worldwide and is not regulated in the United States.
“Many of our patients think kratom is a safe, herbal supplement” but often don’t know it can have several side effects and can be addictive, Dr. Woolery-Lloyd said. Its popularity is increasing as reflected by the number of posts related to kratom on social media platforms.
In the February case report, Shaina Patel, BA, and Nathaniel Phelan, MD, from Kansas City University, Kansas City, Missouri, wrote that side effects of kratom include drowsiness, tachycardia, vomiting, respiratory depression, and cardiac arrest, in addition to confusion and hallucinations.
Kratom also has many different effects on the psyche, Dr. Woolery-Lloyd said at the meeting. At low doses, it blocks the reuptake of norepinephrine, serotonin, and dopamine, producing a motivational effect, and at high doses, it creates an analgesic, calming effect. And people who chronically consume high doses of kratom may be susceptible to hyperpigmentation.
Kratom-associated hyperpigmentation should be considered as a diagnosis when evaluating patients for other drug-associated pigmentary disorders, “especially if pigment is photodistributed,” she said. “If you see new-onset hyperpigmentation or onset over several months and it’s very photoaccentuated, definitely ask about use of kratom.”
Case Reports Show Patterns of Presentation
A 2022 report from Landon R. Powell, BS, with the department of biology, Whitworth University in Spokane, Washington, and coauthors, published in JAAD Case Reports, noted that kratom use in the United States has increased dramatically. “As measured by call reports to the United States National Poison Data System, in 2011, there were 11 reported kratom exposures, and in the first 7 months of 2018, there were 357 reported exposures,” they wrote.
An estimated 1.7 million Americans aged ≥ 12 years said they had used kratom in the previous year, according to the Substance Abuse and Mental Health Services Administration 2021 National Survey on Drug Use and Health.
In the case report, Mr. Powell and coauthors described a 54-year-old White male patient who had been using kratom for the previous four to five years to reduce opioid use. During this period, he consumed kratom powder mixed with orange juice three to four times a day. He presented with “diffuse hyperpigmented patches on his arms and face in a photodistributed manner, with notable sparing of the knuckles on both hands.”
Dark Gray-Blue Skin
In the more recent case report, Ms. Patel and Dr. Phelan described a 30-year-old White male patient who presented with dark gray-blue skin coloring on his cheeks, back of his neck, and the backs of his hands and forearms. He had no other medical conditions and did not take any medications or supplements that cause hyperpigmentation while using kratom.
The patient had been taking kratom for years in the wake of an opioid addiction following medications for a high school injury. He developed an opioid use disorder and tried to replace his pain medications with kratom.
“The patient stopped using kratom in May 2022, but the discoloration remains. It has not regressed in the following 16 months after discontinuing kratom use,” the authors wrote, noting that “whether or not the hyperpigmentation is able to regress is unknown.”
Dr. Woolery-Lloyd is a consultant for AbbVie, Incyte, Johnson & Johnson Consumer, LivDerm, and L’Oreal; a speaker for Eli Lilly, Incyte, L’Oreal, and Ortho Dermatologics; and a researcher/investigator for AbbVie, Allergan, Eirion Therapeutics, Galderma, Pfizer, Sanofi, and Vyne Therapeutics.
According to an information page on kratom on the Food and Drug Administration website, health care professionals and consumers can report adverse reactions associated with kratom to the FDA’s MedWatch program.
A version of this article appeared on Medscape.com.
US Hospitals Prone to Cyberattacks Like One That Impacted Patient Care at Ascension, Experts Say
In the wake of a debilitating cyberattack against one of the nation’s largest health care systems, Marvin Ruckle, a nurse at an Ascension hospital in Wichita, Kansas, said he had a frightening experience: He nearly gave a baby “the wrong dose of narcotic” because of confusing paperwork.
A May 8 ransomware attack against Ascension, a Catholic health system with 140 hospitals in at least 10 states, locked providers out of systems that track and coordinate nearly every aspect of patient care. They include its systems for electronic health records, some phones, and ones “utilized to order certain tests, procedures and medications,” the company said in a May 9 statement.
More than a dozen doctors and nurses who work for the sprawling health system told Michigan Public and KFF Health News that patient care at its hospitals across the nation was compromised in the fallout of the cyberattack over the past several weeks. Clinicians working for hospitals in three states described harrowing lapses, including delayed or lost lab results, medication errors, and an absence of routine safety checks via technology to prevent potentially fatal mistakes.
Despite a precipitous rise in cyberattacks against the health sector in recent years, a weeks-long disruption of this magnitude is beyond what most health systems are prepared for, said John S. Clark, an associate chief pharmacy officer at the University of Michigan health system.
“I don’t believe that anyone is fully prepared,” he said. Most emergency management plans “are designed around long-term downtimes that are into one, two, or three days.”
Ascension in a public statement May 9 said its care teams were “trained for these kinds of disruptions,” but did not respond to questions in early June about whether it had prepared for longer periods of downtime. Ascension said June 14 it had restored access to electronic health records across its network, but that patient “medical records and other information collected between May 8” and when the service was restored “may be temporarily inaccessible as we work to update the portal with information collected during the system downtime.”
Ruckle said he “had no training” for the cyberattack.
Back to Paper
Lisa Watson, an intensive care unit nurse at Ascension Via Christi St. Francis hospital in Wichita, described her own close call. She said she nearly administered the wrong medication to a critically ill patient because she couldn’t scan it as she normally would. “My patient probably would have passed away had I not caught it,” she said.
Watson is no stranger to using paper for patients’ medical charts, saying she did so “for probably half of my career,” before electronic health records became ubiquitous in hospitals. What happened after the cyberattack was “by no means the same.”
“When we paper-charted, we had systems in place to get those orders to other departments in a timely manner,” she said, “and those have all gone away.”
Melissa LaRue, an ICU nurse at Ascension Saint Agnes Hospital in Baltimore, described a close call with “administering the wrong dosage” of a patient’s blood pressure medication. “Luckily,” she said, it was “triple-checked and remedied before that could happen. But I think the potential for harm is there when you have so much information and paperwork that you have to go through.”
Clinicians say their hospitals have relied on slapdash workarounds, using handwritten notes, faxes, sticky notes, and basic computer spreadsheets — many devised on the fly by doctors and nurses — to care for patients.
More than a dozen other nurses and doctors, some of them without union protections, at Ascension hospitals in Michigan recounted situations in which they say patient care was compromised. Those clinicians spoke on the condition that they not be named for fear of retaliation by their employer.
An Ascension hospital emergency room doctor in Detroit said a man on the city’s east side was given a dangerous narcotic intended for another patient because of a paperwork mix-up. As a result, the patient’s breathing slowed to the point that he had to be put on a ventilator. “We intubated him and we sent him to the ICU because he got the wrong medication.”
A nurse in a Michigan Ascension hospital ER said a woman with low blood sugar and “altered mental status” went into cardiac arrest and died after staff said they waited four hours for lab results they needed to determine how to treat her, but never received. “If I started having crushing chest pain in the middle of work and thought I was having a big one, I would grab someone to drive me down the street to another hospital,” the same ER nurse said.
Similar concerns reportedly led a travel nurse at an Ascension hospital in Indiana to quit. “I just want to warn those patients that are coming to any of the Ascension facilities that there will be delays in care. There is potential for error and for harm,” Justin Neisser told CBS4 in Indianapolis in May.
Several nurses and doctors at Ascension hospitals said they feared the errors they’ve witnessed since the cyberattack began could threaten their professional licenses. “This is how a RaDonda Vaught happens,” one nurse said, referring to the Tennessee nurse who was convicted of criminally negligent homicide in 2022 for a fatal drug error.
Reporters were not able to review records to verify clinicians’ claims because of privacy laws surrounding patients’ medical information that apply to health care professionals.
Ascension declined to answer questions about claims that care has been affected by the ransomware attack. “As we have made clear throughout this cyber attack which has impacted our system and our dedicated clinical providers, caring for our patients is our highest priority,” Sean Fitzpatrick, Ascension’s vice president of external communications, said via email on June 3. “We are confident that our care providers in our hospitals and facilities continue to provide quality medical care.”
The federal government requires hospitals to protect patients’ sensitive health data, according to cybersecurity experts. However, there are no federal requirements for hospitals to prevent or prepare for cyberattacks that could compromise their electronic systems.
Hospitals: ‘The No.1 Target of Ransomware’
“We’ve started to think about these as public health issues and disasters on the scale of earthquakes or hurricanes,” said Jeff Tully, a co-director of the Center for Healthcare Cybersecurity at the University of California-San Diego. “These types of cybersecurity incidents should be thought of as a matter of when, and not if.”
Josh Corman, a cybersecurity expert and advocate, said ransom crews regard hospitals as the perfect prey: “They have terrible security and they’ll pay. So almost immediately, hospitals went to the No. 1 target of ransomware.”
In 2023, the health sector experienced the largest share of ransomware attacks of 16 infrastructure sectors considered vital to national security or safety, according to an FBI report on internet crimes. In March, the federal Department of Health and Human Services said reported large breaches involving ransomware had jumped by 264% over the past five years.
A cyberattack this year on Change Healthcare, a unit of UnitedHealth Group’s Optum division that processes billions of health care transactions every year, crippled the business of providers, pharmacies, and hospitals.
In May, UnitedHealth Group CEO Andrew Witty told lawmakers the company paid a $22 million ransom as a result of the Change Healthcare attack — which occurred after hackers accessed a company portal that didn’t have multifactor authentication, a basic cybersecurity tool.
The Biden administration in recent months has pushed to bolster health care cybersecurity standards, but it’s not clear which new measures will be required.
In January, HHS nudged companies to improve email security, add multifactor authentication, and institute cybersecurity training and testing, among other voluntary measures. The Centers for Medicare & Medicaid Services is expected to release new requirements for hospitals, but the scope and timing are unclear. The same is true of an update HHS is expected to make to patient privacy regulations.
HHS said the voluntary measures “will inform the creation of new enforceable cybersecurity standards,” department spokesperson Jeff Nesbit said in a statement.
“The recent cyberattack at Ascension only underscores the need for everyone in the health care ecosystem to do their part to secure their systems and protect patients,” Nesbit said.
Meanwhile, lobbyists for the hospital industry contend cybersecurity mandates or penalties are misplaced and would curtail hospitals’ resources to fend off attacks.
“Hospitals and health systems are not the primary source of cyber risk exposure facing the health care sector,” the American Hospital Association, the largest lobbying group for U.S. hospitals, said in an April statement prepared for U.S. House lawmakers. Most large data breaches that hit hospitals in 2023 originated with third-party “business associates” or other health entities, including CMS itself, the AHA statement said.
Hospitals consolidating into large multistate health systems face increased risk of data breaches and ransomware attacks, according to one study. Ascension in 2022 was the third-largest hospital chain in the U.S. by number of beds, according to the most recent data from the federal Agency for Healthcare Research and Quality.
And while cybersecurity regulations can quickly become outdated, they can at least make it clear that if health systems fail to implement basic protections there “should be consequences for that,” Jim Bagian, a former director of the National Center for Patient Safety at the Veterans Health Administration, told Michigan Public’s Stateside.
Patients can pay the price when lapses occur. Those in hospital care face a greater likelihood of death during a cyberattack, according to researchers at the University of Minnesota School of Public Health.
Workers concerned about patient safety at Ascension hospitals in Michigan have called for the company to make changes.
“We implore Ascension to recognize the internal problems that continue to plague its hospitals, both publicly and transparently,” said Dina Carlisle, a nurse and the president of the OPEIU Local 40 union, which represents nurses at Ascension Providence Rochester. At least 125 staff members at that Ascension hospital have signed a petition asking administrators to temporarily reduce elective surgeries and nonemergency patient admissions, like under the protocols many hospitals adopted early in the covid-19 pandemic.
Watson, the Kansas ICU nurse, said in late May that nurses had urged management to bring in more nurses to help manage the workflow. “Everything that we say has fallen on deaf ears,” she said.
“It is very hard to be a nurse at Ascension right now,” Watson said in late May. “It is very hard to be a patient at Ascension right now.”
If you’re a patient or worker at an Ascension hospital and would like to tell KFF Health News about your experiences, click here to share your story with us.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
In the wake of a debilitating cyberattack against one of the nation’s largest health care systems, Marvin Ruckle, a nurse at an Ascension hospital in Wichita, Kansas, said he had a frightening experience: He nearly gave a baby “the wrong dose of narcotic” because of confusing paperwork.
A May 8 ransomware attack against Ascension, a Catholic health system with 140 hospitals in at least 10 states, locked providers out of systems that track and coordinate nearly every aspect of patient care. They include its systems for electronic health records, some phones, and ones “utilized to order certain tests, procedures and medications,” the company said in a May 9 statement.
More than a dozen doctors and nurses who work for the sprawling health system told Michigan Public and KFF Health News that patient care at its hospitals across the nation was compromised in the fallout of the cyberattack over the past several weeks. Clinicians working for hospitals in three states described harrowing lapses, including delayed or lost lab results, medication errors, and an absence of routine safety checks via technology to prevent potentially fatal mistakes.
Despite a precipitous rise in cyberattacks against the health sector in recent years, a weeks-long disruption of this magnitude is beyond what most health systems are prepared for, said John S. Clark, an associate chief pharmacy officer at the University of Michigan health system.
“I don’t believe that anyone is fully prepared,” he said. Most emergency management plans “are designed around long-term downtimes that are into one, two, or three days.”
Ascension in a public statement May 9 said its care teams were “trained for these kinds of disruptions,” but did not respond to questions in early June about whether it had prepared for longer periods of downtime. Ascension said June 14 it had restored access to electronic health records across its network, but that patient “medical records and other information collected between May 8” and when the service was restored “may be temporarily inaccessible as we work to update the portal with information collected during the system downtime.”
Ruckle said he “had no training” for the cyberattack.
Back to Paper
Lisa Watson, an intensive care unit nurse at Ascension Via Christi St. Francis hospital in Wichita, described her own close call. She said she nearly administered the wrong medication to a critically ill patient because she couldn’t scan it as she normally would. “My patient probably would have passed away had I not caught it,” she said.
Watson is no stranger to using paper for patients’ medical charts, saying she did so “for probably half of my career,” before electronic health records became ubiquitous in hospitals. What happened after the cyberattack was “by no means the same.”
“When we paper-charted, we had systems in place to get those orders to other departments in a timely manner,” she said, “and those have all gone away.”
Melissa LaRue, an ICU nurse at Ascension Saint Agnes Hospital in Baltimore, described a close call with “administering the wrong dosage” of a patient’s blood pressure medication. “Luckily,” she said, it was “triple-checked and remedied before that could happen. But I think the potential for harm is there when you have so much information and paperwork that you have to go through.”
Clinicians say their hospitals have relied on slapdash workarounds, using handwritten notes, faxes, sticky notes, and basic computer spreadsheets — many devised on the fly by doctors and nurses — to care for patients.
More than a dozen other nurses and doctors, some of them without union protections, at Ascension hospitals in Michigan recounted situations in which they say patient care was compromised. Those clinicians spoke on the condition that they not be named for fear of retaliation by their employer.
An Ascension hospital emergency room doctor in Detroit said a man on the city’s east side was given a dangerous narcotic intended for another patient because of a paperwork mix-up. As a result, the patient’s breathing slowed to the point that he had to be put on a ventilator. “We intubated him and we sent him to the ICU because he got the wrong medication.”
A nurse in a Michigan Ascension hospital ER said a woman with low blood sugar and “altered mental status” went into cardiac arrest and died after staff said they waited four hours for lab results they needed to determine how to treat her, but never received. “If I started having crushing chest pain in the middle of work and thought I was having a big one, I would grab someone to drive me down the street to another hospital,” the same ER nurse said.
Similar concerns reportedly led a travel nurse at an Ascension hospital in Indiana to quit. “I just want to warn those patients that are coming to any of the Ascension facilities that there will be delays in care. There is potential for error and for harm,” Justin Neisser told CBS4 in Indianapolis in May.
Several nurses and doctors at Ascension hospitals said they feared the errors they’ve witnessed since the cyberattack began could threaten their professional licenses. “This is how a RaDonda Vaught happens,” one nurse said, referring to the Tennessee nurse who was convicted of criminally negligent homicide in 2022 for a fatal drug error.
Reporters were not able to review records to verify clinicians’ claims because of privacy laws surrounding patients’ medical information that apply to health care professionals.
Ascension declined to answer questions about claims that care has been affected by the ransomware attack. “As we have made clear throughout this cyber attack which has impacted our system and our dedicated clinical providers, caring for our patients is our highest priority,” Sean Fitzpatrick, Ascension’s vice president of external communications, said via email on June 3. “We are confident that our care providers in our hospitals and facilities continue to provide quality medical care.”
The federal government requires hospitals to protect patients’ sensitive health data, according to cybersecurity experts. However, there are no federal requirements for hospitals to prevent or prepare for cyberattacks that could compromise their electronic systems.
Hospitals: ‘The No.1 Target of Ransomware’
“We’ve started to think about these as public health issues and disasters on the scale of earthquakes or hurricanes,” said Jeff Tully, a co-director of the Center for Healthcare Cybersecurity at the University of California-San Diego. “These types of cybersecurity incidents should be thought of as a matter of when, and not if.”
Josh Corman, a cybersecurity expert and advocate, said ransom crews regard hospitals as the perfect prey: “They have terrible security and they’ll pay. So almost immediately, hospitals went to the No. 1 target of ransomware.”
In 2023, the health sector experienced the largest share of ransomware attacks of 16 infrastructure sectors considered vital to national security or safety, according to an FBI report on internet crimes. In March, the federal Department of Health and Human Services said reported large breaches involving ransomware had jumped by 264% over the past five years.
A cyberattack this year on Change Healthcare, a unit of UnitedHealth Group’s Optum division that processes billions of health care transactions every year, crippled the business of providers, pharmacies, and hospitals.
In May, UnitedHealth Group CEO Andrew Witty told lawmakers the company paid a $22 million ransom as a result of the Change Healthcare attack — which occurred after hackers accessed a company portal that didn’t have multifactor authentication, a basic cybersecurity tool.
The Biden administration in recent months has pushed to bolster health care cybersecurity standards, but it’s not clear which new measures will be required.
In January, HHS nudged companies to improve email security, add multifactor authentication, and institute cybersecurity training and testing, among other voluntary measures. The Centers for Medicare & Medicaid Services is expected to release new requirements for hospitals, but the scope and timing are unclear. The same is true of an update HHS is expected to make to patient privacy regulations.
HHS said the voluntary measures “will inform the creation of new enforceable cybersecurity standards,” department spokesperson Jeff Nesbit said in a statement.
“The recent cyberattack at Ascension only underscores the need for everyone in the health care ecosystem to do their part to secure their systems and protect patients,” Nesbit said.
Meanwhile, lobbyists for the hospital industry contend cybersecurity mandates or penalties are misplaced and would curtail hospitals’ resources to fend off attacks.
“Hospitals and health systems are not the primary source of cyber risk exposure facing the health care sector,” the American Hospital Association, the largest lobbying group for U.S. hospitals, said in an April statement prepared for U.S. House lawmakers. Most large data breaches that hit hospitals in 2023 originated with third-party “business associates” or other health entities, including CMS itself, the AHA statement said.
Hospitals consolidating into large multistate health systems face increased risk of data breaches and ransomware attacks, according to one study. Ascension in 2022 was the third-largest hospital chain in the U.S. by number of beds, according to the most recent data from the federal Agency for Healthcare Research and Quality.
And while cybersecurity regulations can quickly become outdated, they can at least make it clear that if health systems fail to implement basic protections there “should be consequences for that,” Jim Bagian, a former director of the National Center for Patient Safety at the Veterans Health Administration, told Michigan Public’s Stateside.
Patients can pay the price when lapses occur. Those in hospital care face a greater likelihood of death during a cyberattack, according to researchers at the University of Minnesota School of Public Health.
Workers concerned about patient safety at Ascension hospitals in Michigan have called for the company to make changes.
“We implore Ascension to recognize the internal problems that continue to plague its hospitals, both publicly and transparently,” said Dina Carlisle, a nurse and the president of the OPEIU Local 40 union, which represents nurses at Ascension Providence Rochester. At least 125 staff members at that Ascension hospital have signed a petition asking administrators to temporarily reduce elective surgeries and nonemergency patient admissions, like under the protocols many hospitals adopted early in the covid-19 pandemic.
Watson, the Kansas ICU nurse, said in late May that nurses had urged management to bring in more nurses to help manage the workflow. “Everything that we say has fallen on deaf ears,” she said.
“It is very hard to be a nurse at Ascension right now,” Watson said in late May. “It is very hard to be a patient at Ascension right now.”
If you’re a patient or worker at an Ascension hospital and would like to tell KFF Health News about your experiences, click here to share your story with us.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
In the wake of a debilitating cyberattack against one of the nation’s largest health care systems, Marvin Ruckle, a nurse at an Ascension hospital in Wichita, Kansas, said he had a frightening experience: He nearly gave a baby “the wrong dose of narcotic” because of confusing paperwork.
A May 8 ransomware attack against Ascension, a Catholic health system with 140 hospitals in at least 10 states, locked providers out of systems that track and coordinate nearly every aspect of patient care. They include its systems for electronic health records, some phones, and ones “utilized to order certain tests, procedures and medications,” the company said in a May 9 statement.
More than a dozen doctors and nurses who work for the sprawling health system told Michigan Public and KFF Health News that patient care at its hospitals across the nation was compromised in the fallout of the cyberattack over the past several weeks. Clinicians working for hospitals in three states described harrowing lapses, including delayed or lost lab results, medication errors, and an absence of routine safety checks via technology to prevent potentially fatal mistakes.
Despite a precipitous rise in cyberattacks against the health sector in recent years, a weeks-long disruption of this magnitude is beyond what most health systems are prepared for, said John S. Clark, an associate chief pharmacy officer at the University of Michigan health system.
“I don’t believe that anyone is fully prepared,” he said. Most emergency management plans “are designed around long-term downtimes that are into one, two, or three days.”
Ascension in a public statement May 9 said its care teams were “trained for these kinds of disruptions,” but did not respond to questions in early June about whether it had prepared for longer periods of downtime. Ascension said June 14 it had restored access to electronic health records across its network, but that patient “medical records and other information collected between May 8” and when the service was restored “may be temporarily inaccessible as we work to update the portal with information collected during the system downtime.”
Ruckle said he “had no training” for the cyberattack.
Back to Paper
Lisa Watson, an intensive care unit nurse at Ascension Via Christi St. Francis hospital in Wichita, described her own close call. She said she nearly administered the wrong medication to a critically ill patient because she couldn’t scan it as she normally would. “My patient probably would have passed away had I not caught it,” she said.
Watson is no stranger to using paper for patients’ medical charts, saying she did so “for probably half of my career,” before electronic health records became ubiquitous in hospitals. What happened after the cyberattack was “by no means the same.”
“When we paper-charted, we had systems in place to get those orders to other departments in a timely manner,” she said, “and those have all gone away.”
Melissa LaRue, an ICU nurse at Ascension Saint Agnes Hospital in Baltimore, described a close call with “administering the wrong dosage” of a patient’s blood pressure medication. “Luckily,” she said, it was “triple-checked and remedied before that could happen. But I think the potential for harm is there when you have so much information and paperwork that you have to go through.”
Clinicians say their hospitals have relied on slapdash workarounds, using handwritten notes, faxes, sticky notes, and basic computer spreadsheets — many devised on the fly by doctors and nurses — to care for patients.
More than a dozen other nurses and doctors, some of them without union protections, at Ascension hospitals in Michigan recounted situations in which they say patient care was compromised. Those clinicians spoke on the condition that they not be named for fear of retaliation by their employer.
An Ascension hospital emergency room doctor in Detroit said a man on the city’s east side was given a dangerous narcotic intended for another patient because of a paperwork mix-up. As a result, the patient’s breathing slowed to the point that he had to be put on a ventilator. “We intubated him and we sent him to the ICU because he got the wrong medication.”
A nurse in a Michigan Ascension hospital ER said a woman with low blood sugar and “altered mental status” went into cardiac arrest and died after staff said they waited four hours for lab results they needed to determine how to treat her, but never received. “If I started having crushing chest pain in the middle of work and thought I was having a big one, I would grab someone to drive me down the street to another hospital,” the same ER nurse said.
Similar concerns reportedly led a travel nurse at an Ascension hospital in Indiana to quit. “I just want to warn those patients that are coming to any of the Ascension facilities that there will be delays in care. There is potential for error and for harm,” Justin Neisser told CBS4 in Indianapolis in May.
Several nurses and doctors at Ascension hospitals said they feared the errors they’ve witnessed since the cyberattack began could threaten their professional licenses. “This is how a RaDonda Vaught happens,” one nurse said, referring to the Tennessee nurse who was convicted of criminally negligent homicide in 2022 for a fatal drug error.
Reporters were not able to review records to verify clinicians’ claims because of privacy laws surrounding patients’ medical information that apply to health care professionals.
Ascension declined to answer questions about claims that care has been affected by the ransomware attack. “As we have made clear throughout this cyber attack which has impacted our system and our dedicated clinical providers, caring for our patients is our highest priority,” Sean Fitzpatrick, Ascension’s vice president of external communications, said via email on June 3. “We are confident that our care providers in our hospitals and facilities continue to provide quality medical care.”
The federal government requires hospitals to protect patients’ sensitive health data, according to cybersecurity experts. However, there are no federal requirements for hospitals to prevent or prepare for cyberattacks that could compromise their electronic systems.
Hospitals: ‘The No.1 Target of Ransomware’
“We’ve started to think about these as public health issues and disasters on the scale of earthquakes or hurricanes,” said Jeff Tully, a co-director of the Center for Healthcare Cybersecurity at the University of California-San Diego. “These types of cybersecurity incidents should be thought of as a matter of when, and not if.”
Josh Corman, a cybersecurity expert and advocate, said ransom crews regard hospitals as the perfect prey: “They have terrible security and they’ll pay. So almost immediately, hospitals went to the No. 1 target of ransomware.”
In 2023, the health sector experienced the largest share of ransomware attacks of 16 infrastructure sectors considered vital to national security or safety, according to an FBI report on internet crimes. In March, the federal Department of Health and Human Services said reported large breaches involving ransomware had jumped by 264% over the past five years.
A cyberattack this year on Change Healthcare, a unit of UnitedHealth Group’s Optum division that processes billions of health care transactions every year, crippled the business of providers, pharmacies, and hospitals.
In May, UnitedHealth Group CEO Andrew Witty told lawmakers the company paid a $22 million ransom as a result of the Change Healthcare attack — which occurred after hackers accessed a company portal that didn’t have multifactor authentication, a basic cybersecurity tool.
The Biden administration in recent months has pushed to bolster health care cybersecurity standards, but it’s not clear which new measures will be required.
In January, HHS nudged companies to improve email security, add multifactor authentication, and institute cybersecurity training and testing, among other voluntary measures. The Centers for Medicare & Medicaid Services is expected to release new requirements for hospitals, but the scope and timing are unclear. The same is true of an update HHS is expected to make to patient privacy regulations.
HHS said the voluntary measures “will inform the creation of new enforceable cybersecurity standards,” department spokesperson Jeff Nesbit said in a statement.
“The recent cyberattack at Ascension only underscores the need for everyone in the health care ecosystem to do their part to secure their systems and protect patients,” Nesbit said.
Meanwhile, lobbyists for the hospital industry contend cybersecurity mandates or penalties are misplaced and would curtail hospitals’ resources to fend off attacks.
“Hospitals and health systems are not the primary source of cyber risk exposure facing the health care sector,” the American Hospital Association, the largest lobbying group for U.S. hospitals, said in an April statement prepared for U.S. House lawmakers. Most large data breaches that hit hospitals in 2023 originated with third-party “business associates” or other health entities, including CMS itself, the AHA statement said.
Hospitals consolidating into large multistate health systems face increased risk of data breaches and ransomware attacks, according to one study. Ascension in 2022 was the third-largest hospital chain in the U.S. by number of beds, according to the most recent data from the federal Agency for Healthcare Research and Quality.
And while cybersecurity regulations can quickly become outdated, they can at least make it clear that if health systems fail to implement basic protections there “should be consequences for that,” Jim Bagian, a former director of the National Center for Patient Safety at the Veterans Health Administration, told Michigan Public’s Stateside.
Patients can pay the price when lapses occur. Those in hospital care face a greater likelihood of death during a cyberattack, according to researchers at the University of Minnesota School of Public Health.
Workers concerned about patient safety at Ascension hospitals in Michigan have called for the company to make changes.
“We implore Ascension to recognize the internal problems that continue to plague its hospitals, both publicly and transparently,” said Dina Carlisle, a nurse and the president of the OPEIU Local 40 union, which represents nurses at Ascension Providence Rochester. At least 125 staff members at that Ascension hospital have signed a petition asking administrators to temporarily reduce elective surgeries and nonemergency patient admissions, like under the protocols many hospitals adopted early in the covid-19 pandemic.
Watson, the Kansas ICU nurse, said in late May that nurses had urged management to bring in more nurses to help manage the workflow. “Everything that we say has fallen on deaf ears,” she said.
“It is very hard to be a nurse at Ascension right now,” Watson said in late May. “It is very hard to be a patient at Ascension right now.”
If you’re a patient or worker at an Ascension hospital and would like to tell KFF Health News about your experiences, click here to share your story with us.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Should You Offer Medical Credit Cards?
Editor’s note: This is Dr. Eastern’s last “Managing Your Practice” column for Dermatology News. After his first column was published in 1986, Dr. Eastern continued writing his column monthly until the mid-1990s, resuming in 2005. In total, he has written over 300 columns on topics relevant to medical practice, ranging from hiring employees, selling and merging practices, complying with OSHA, and avoiding embezzlement, to electronic health records, burnout, medical assistants, negative online reviews, artificial intelligence in the office, and more. In the future, he will continue to provide commentary on practice issues with an occasional guest editorial.
Medicare reimbursement cuts, increasing overhead and staff salaries, and inflation have made running a profitable private practice increasingly challenging, particularly for rural and smaller offices. Medical credit cards are an increasingly popular choice to fill this gap.

Traditionally, these cards were used to help cover procedures insurance didn’t cover — such as cosmetic procedures — but over the years, they have been expanded to cover other healthcare charges, mostly for patients who are paying out of pocket due to inadequate insurance or other reasons.
Advantages for physicians include immediate payment from the credit card company and reduced billing and collection costs. Patients are also less likely to delay or defer treatment if they can charge the payment and pay it back in installments.
The first step in offering medical credit cards is signing up with one or more third-party card companies. CareCredit is the most common provider in the medical credit card market. Other vendors include Wells Fargo, AccessOne, Alphaeon Credit, and iCare Financial. (As always, I have no financial interest in any product or service mentioned in this column.) A member of your staff signs patients up, and the credit card company checks their credit. If approved, the card company pays you your fee and assumes responsibility for collecting from the patient.
The interest charge on medical credit cards is often deferred for a period of time, typically between 6 and 24 months. If patients pay off the debt within this time, they can avoid paying interest. But, like other credit cards, if they make late payments or have an unpaid balance once the promotional period ends, they may end up with interest and fees totaling 25%-30% or more. It is important to make it very clear to your patients that payments are interest-free only if they are all made on time and within the promotional period.

According to a Consumer Financial Protection Bureau report released earlier this year, deferred interest medical credit cards or loans were used to pay nearly $23 billion in healthcare expenses from 2018 to 2020. Individuals unable to complete payment during the promotional period paid $1 billion in deferred interest payments during that period.
Despite the growing popularity of medical credit cards among physicians, it is worth noting that some consumer groups view them as predatory financial products, marketed toward people in tough financial situations. A coalition of 60 health advocacy groups has urged the Biden Administration to ban deferred interest medical credit cards. So there is that much more reason to choose candidates for medical credit cards carefully, and to make them fully aware of what obligations they are assuming.
Patients who do not think they can pay off the balance within the interest-free time frame should probably be advised to pursue an alternative payment method, such as using a conventional credit card, taking out a personal or home-equity loan, or borrowing from a retirement savings account. Some physicians are willing to negotiate a reduced fee for patients who agree to pay cash at the time of service.
Those who do choose to apply for a medical credit card should be informed of their options, which can vary considerably depending on the product and the third-party vendor. Some medical credit products can be used only for elective procedures, but some can be used more broadly for various medical expenses. Check to make sure that each patient’s financing option can be used for his or her desired medical service.
Some payment products can only be used at specific practices or groups, while others can be used at a variety of medical offices and hospitals. If a patient arrives with a medical credit card already in hand, confirm that it is one that your office accepts.
Interest rates generally vary with each card and vendor. Make patients aware of when interest rates start accruing and if the plan offers a fixed or variable APR, or if it charges compounding interest. Confirm if there is a deferred interest option, and if so, for how long.
Different medical credit products also have varying fees and payment schedules. See that each patient reads the terms of the agreement to understand when interest may start to accrue or change, as well as when certain fees may apply. Understanding when the payments are due will help them avoid additional fees, including late fees. Some medical payment plans may also have administrative or processing fees. If so, patients should be made aware of them.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, New Jersey. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Editor’s note: This is Dr. Eastern’s last “Managing Your Practice” column for Dermatology News. After his first column was published in 1986, Dr. Eastern continued writing his column monthly until the mid-1990s, resuming in 2005. In total, he has written over 300 columns on topics relevant to medical practice, ranging from hiring employees, selling and merging practices, complying with OSHA, and avoiding embezzlement, to electronic health records, burnout, medical assistants, negative online reviews, artificial intelligence in the office, and more. In the future, he will continue to provide commentary on practice issues with an occasional guest editorial.
Medicare reimbursement cuts, increasing overhead and staff salaries, and inflation have made running a profitable private practice increasingly challenging, particularly for rural and smaller offices. Medical credit cards are an increasingly popular choice to fill this gap.
Traditionally, these cards were used to help cover procedures insurance didn’t cover — such as cosmetic procedures — but over the years, they have been expanded to cover other healthcare charges, mostly for patients who are paying out of pocket due to inadequate insurance or other reasons.
Advantages for physicians include immediate payment from the credit card company and reduced billing and collection costs. Patients are also less likely to delay or defer treatment if they can charge the payment and pay it back in installments.
The first step in offering medical credit cards is signing up with one or more third-party card companies. CareCredit is the most common provider in the medical credit card market. Other vendors include Wells Fargo, AccessOne, Alphaeon Credit, and iCare Financial. (As always, I have no financial interest in any product or service mentioned in this column.) A member of your staff signs patients up, and the credit card company checks their credit. If approved, the card company pays you your fee and assumes responsibility for collecting from the patient.
The interest charge on medical credit cards is often deferred for a period of time, typically between 6 and 24 months. If patients pay off the debt within this time, they can avoid paying interest. But, like other credit cards, if they make late payments or have an unpaid balance once the promotional period ends, they may end up with interest and fees totaling 25%-30% or more. It is important to make it very clear to your patients that payments are interest-free only if they are all made on time and within the promotional period.
According to a Consumer Financial Protection Bureau report released earlier this year, deferred interest medical credit cards or loans were used to pay nearly $23 billion in healthcare expenses from 2018 to 2020. Individuals unable to complete payment during the promotional period paid $1 billion in deferred interest payments during that period.
Despite the growing popularity of medical credit cards among physicians, it is worth noting that some consumer groups view them as predatory financial products, marketed toward people in tough financial situations. A coalition of 60 health advocacy groups has urged the Biden Administration to ban deferred interest medical credit cards. So there is that much more reason to choose candidates for medical credit cards carefully, and to make them fully aware of what obligations they are assuming.
Patients who do not think they can pay off the balance within the interest-free time frame should probably be advised to pursue an alternative payment method, such as using a conventional credit card, taking out a personal or home-equity loan, or borrowing from a retirement savings account. Some physicians are willing to negotiate a reduced fee for patients who agree to pay cash at the time of service.
Those who do choose to apply for a medical credit card should be informed of their options, which can vary considerably depending on the product and the third-party vendor. Some medical credit products can be used only for elective procedures, but some can be used more broadly for various medical expenses. Check to make sure that each patient’s financing option can be used for his or her desired medical service.
Some payment products can only be used at specific practices or groups, while others can be used at a variety of medical offices and hospitals. If a patient arrives with a medical credit card already in hand, confirm that it is one that your office accepts.
Interest rates generally vary with each card and vendor. Make patients aware of when interest rates start accruing and if the plan offers a fixed or variable APR, or if it charges compounding interest. Confirm if there is a deferred interest option, and if so, for how long.
Different medical credit products also have varying fees and payment schedules. See that each patient reads the terms of the agreement to understand when interest may start to accrue or change, as well as when certain fees may apply. Understanding when the payments are due will help them avoid additional fees, including late fees. Some medical payment plans may also have administrative or processing fees. If so, patients should be made aware of them.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, New Jersey. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Editor’s note: This is Dr. Eastern’s last “Managing Your Practice” column for Dermatology News. After his first column was published in 1986, Dr. Eastern continued writing his column monthly until the mid-1990s, resuming in 2005. In total, he has written over 300 columns on topics relevant to medical practice, ranging from hiring employees, selling and merging practices, complying with OSHA, and avoiding embezzlement, to electronic health records, burnout, medical assistants, negative online reviews, artificial intelligence in the office, and more. In the future, he will continue to provide commentary on practice issues with an occasional guest editorial.
Medicare reimbursement cuts, increasing overhead and staff salaries, and inflation have made running a profitable private practice increasingly challenging, particularly for rural and smaller offices. Medical credit cards are an increasingly popular choice to fill this gap.
Traditionally, these cards were used to help cover procedures insurance didn’t cover — such as cosmetic procedures — but over the years, they have been expanded to cover other healthcare charges, mostly for patients who are paying out of pocket due to inadequate insurance or other reasons.
Advantages for physicians include immediate payment from the credit card company and reduced billing and collection costs. Patients are also less likely to delay or defer treatment if they can charge the payment and pay it back in installments.
The first step in offering medical credit cards is signing up with one or more third-party card companies. CareCredit is the most common provider in the medical credit card market. Other vendors include Wells Fargo, AccessOne, Alphaeon Credit, and iCare Financial. (As always, I have no financial interest in any product or service mentioned in this column.) A member of your staff signs patients up, and the credit card company checks their credit. If approved, the card company pays you your fee and assumes responsibility for collecting from the patient.
The interest charge on medical credit cards is often deferred for a period of time, typically between 6 and 24 months. If patients pay off the debt within this time, they can avoid paying interest. But, like other credit cards, if they make late payments or have an unpaid balance once the promotional period ends, they may end up with interest and fees totaling 25%-30% or more. It is important to make it very clear to your patients that payments are interest-free only if they are all made on time and within the promotional period.
According to a Consumer Financial Protection Bureau report released earlier this year, deferred interest medical credit cards or loans were used to pay nearly $23 billion in healthcare expenses from 2018 to 2020. Individuals unable to complete payment during the promotional period paid $1 billion in deferred interest payments during that period.
Despite the growing popularity of medical credit cards among physicians, it is worth noting that some consumer groups view them as predatory financial products, marketed toward people in tough financial situations. A coalition of 60 health advocacy groups has urged the Biden Administration to ban deferred interest medical credit cards. So there is that much more reason to choose candidates for medical credit cards carefully, and to make them fully aware of what obligations they are assuming.
Patients who do not think they can pay off the balance within the interest-free time frame should probably be advised to pursue an alternative payment method, such as using a conventional credit card, taking out a personal or home-equity loan, or borrowing from a retirement savings account. Some physicians are willing to negotiate a reduced fee for patients who agree to pay cash at the time of service.
Those who do choose to apply for a medical credit card should be informed of their options, which can vary considerably depending on the product and the third-party vendor. Some medical credit products can be used only for elective procedures, but some can be used more broadly for various medical expenses. Check to make sure that each patient’s financing option can be used for his or her desired medical service.
Some payment products can only be used at specific practices or groups, while others can be used at a variety of medical offices and hospitals. If a patient arrives with a medical credit card already in hand, confirm that it is one that your office accepts.
Interest rates generally vary with each card and vendor. Make patients aware of when interest rates start accruing and if the plan offers a fixed or variable APR, or if it charges compounding interest. Confirm if there is a deferred interest option, and if so, for how long.
Different medical credit products also have varying fees and payment schedules. See that each patient reads the terms of the agreement to understand when interest may start to accrue or change, as well as when certain fees may apply. Understanding when the payments are due will help them avoid additional fees, including late fees. Some medical payment plans may also have administrative or processing fees. If so, patients should be made aware of them.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, New Jersey. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Latest Izokibep Trial for PsA Shows Promise But Misses on Enthesitis
VIENNA — The investigational interleukin (IL)-17 inhibitor izokibep hit its mark when it came to improving overall disease activity in people with active psoriatic arthritis (PsA) in a phase 2b/3 trial, but it was no better than placebo at reducing inflammation of the entheses.
This apparent and unexpected lack of effect in the entheses was a key talking point after Philip J. Mease, MD, presented the late-breaking trial findings at the annual European Congress of Rheumatology.

At just 18.6 kilodaltons in size, izokibep is just “one tenth the size of a standard monoclonal antibody” and is classed as a small protein therapeutic, Dr. Mease said. It has a “very tight” binding affinity for IL-17A, and because it also binds to albumin, it has a prolonged half-life compared with other IL-17 inhibitors. Potentially, it should be able to “penetrate into difficult areas,” such as the entheses, he said.
Prespecified Enthesitis Analysis
However, results of a prespecified secondary analysis conducted in 209 of the 343 trial participants who had received treatment showed no significant difference in the proportions with enthesis resolution at 16 weeks, defined as a Leeds Enthesitis Index (LEI) of 0.
Comparing two dosing regimens of izokibep 160 mg once weekly (QW) vs every other week (Q2W) with placebo, enthesitis resolution was seen in 45%, 56%, and 47%, respectively, of patients.
The LEI is “sometimes subject to problems with evaluation because of placebo response, which is what we see here,” noted Dr. Mease, director of rheumatology research at the Providence Swedish Medical Center and a rheumatology professor at the University of Washington School of Medicine in Seattle.
An exploratory analysis showed that there was a better response for izokibep vs placebo if the analysis included only patients with higher LEI scores at baseline, at 8.0% (n = 12) for placebo, 22.0% (n = 9) for izokibep 160 mg QW, and 50.0% (n = 12) for izokibep 160 mg Q2W.
Main Efficacy Data
The primary endpoint for the trial was the proportion of patients who had 50% improvement in American College of Rheumatology response criteria (ACR50) at 16 weeks. This showed a clear advantage for treatment with izokibep 160 QW and Q2W compared with placebo, with a respective 40%, 43%, and 15% of patients meeting this endpoint.
Corresponding ACR20 response rates were 59%, 64%, and 35%, respectively; ACR70 response rates were a respective 25%, 23%, and 5%.
In addition to ACR70, izokibep 160 QW and Q2W met a number of other “high hurdle” efficacy endpoints better than did placebo, Dr. Mease reported. A 90% reduction from baseline in the Psoriasis Area and Severity Index (PASI90) was achieved by a respective 64%, 58%, and 12% of patients, and a 100% reduction in this index (PASI100) was achieved by a respective 51%, 47%, and 12%. And 41%, 42%, and 14% of patients, respectively, met the criteria for minimal disease activity.
Patient Population
Mease pointed out during his presentation that the trial included patients with adult-onset PsA that had been ongoing for ≥ 6 months. Patients had to have at least three tender or swollen joints and an inadequate response, intolerance, or contraindication to commonly used front-line therapies such as nonsteroidal anti-inflammatory drugs, conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), and tumor necrosis factor inhibitors (TNFi).
In fact, around half of the participants across the three treatment arms had received prior csDMARDs, and almost a quarter had received a TNFi.
The mean duration of disease was around 7 years, the average age was about 50 years, and the majority of the participants were White individuals. There were more women than men in the placebo vs the izokibep arms (43.4% vs about 60.0%).
Adverse Events
Injection site reactions were the most common adverse events, most of which were mild to moderate. Very few (< 1% to 4%) led to any need to discontinue the drug.
Serious adverse events occurred at low rates in all study arms: 0.8% for placebo, 2.7% for izokibep QW, and 1.8% for izokibep Q2W.
One patient each (0.9%) in the izokibep arms developed ulcerative colitis, whereas none in the placebo group did. Only two patients developed candidiasis. One was in the placebo group and had a skin infection, and the other was an oral infection in the QW izokibep arm.
There were no cases of uveitis, suicidal ideation, or deaths reported.
Comments on the Study
During the discussion that followed the presentation, Walter P. Maksymowych, MBChB, of the University of Alberta in Edmonton, Alberta, Canada, addressed the dosing regimens used.

“Looking at the side effect profile and then looking at the response rate, comparing the weekly dosing and every 2 weeks, do you think, in hindsight, you might be remiss that there wasn’t an additional dosing on a monthly basis, especially since this is a construct that is meant to prolong the half-life of the molecule?” he asked, adding that perhaps this should be something to consider in future studies.
Mease responded that there had been a fourth dosing arm in the trial — izokibep 80 mg once a month — but because there were only eight patients, the data were not sufficiently robust to analyze.
Commenting on the study, Laura C. Coates, MBChB, PhD, said: “It’s a pretty standard phase 2b/3 study,” and the outcomes were not wildly different from what has been seen with other IL-17A inhibitors.
“In phase 2, the enthesitis data looked really good; in phase 3, the enthesitis data looks the same as for any other IL-17 inhibitor,” Dr. Coates said.

More and longer-term data are needed to see if “the theoretical biological difference in the drug design translates to a different clinical outcome or whether it’s another IL-17,” added Dr. Coates, a clinician scientist and senior clinical research fellow at the University of Oxford in England.
Dennis McGonagle, MB MCH BAO, PhD, of the University of Leeds, England, also picked up on the enthesitis data, echoing the conclusion that the phase 2 enthesitis data were “spectacular” and noting that “it’s a real inversion of what was expected, given the small molecule.”
The study was funded by Acelyrin. Dr. Mease disclosed ties with Acelyrin and other pharmaceutical companies. Dr. Maksymowych, Dr. Coates, and Dr. McGonagle reported having a variety of financial relationships with pharmaceutical companies outside of this study.
A version of this article appeared on Medscape.com.
VIENNA — The investigational interleukin (IL)-17 inhibitor izokibep hit its mark when it came to improving overall disease activity in people with active psoriatic arthritis (PsA) in a phase 2b/3 trial, but it was no better than placebo at reducing inflammation of the entheses.
This apparent and unexpected lack of effect in the entheses was a key talking point after Philip J. Mease, MD, presented the late-breaking trial findings at the annual European Congress of Rheumatology.
At just 18.6 kilodaltons in size, izokibep is just “one tenth the size of a standard monoclonal antibody” and is classed as a small protein therapeutic, Dr. Mease said. It has a “very tight” binding affinity for IL-17A, and because it also binds to albumin, it has a prolonged half-life compared with other IL-17 inhibitors. Potentially, it should be able to “penetrate into difficult areas,” such as the entheses, he said.
Prespecified Enthesitis Analysis
However, results of a prespecified secondary analysis conducted in 209 of the 343 trial participants who had received treatment showed no significant difference in the proportions with enthesis resolution at 16 weeks, defined as a Leeds Enthesitis Index (LEI) of 0.
Comparing two dosing regimens of izokibep 160 mg once weekly (QW) vs every other week (Q2W) with placebo, enthesitis resolution was seen in 45%, 56%, and 47%, respectively, of patients.
The LEI is “sometimes subject to problems with evaluation because of placebo response, which is what we see here,” noted Dr. Mease, director of rheumatology research at the Providence Swedish Medical Center and a rheumatology professor at the University of Washington School of Medicine in Seattle.
An exploratory analysis showed that there was a better response for izokibep vs placebo if the analysis included only patients with higher LEI scores at baseline, at 8.0% (n = 12) for placebo, 22.0% (n = 9) for izokibep 160 mg QW, and 50.0% (n = 12) for izokibep 160 mg Q2W.
Main Efficacy Data
The primary endpoint for the trial was the proportion of patients who had 50% improvement in American College of Rheumatology response criteria (ACR50) at 16 weeks. This showed a clear advantage for treatment with izokibep 160 QW and Q2W compared with placebo, with a respective 40%, 43%, and 15% of patients meeting this endpoint.
Corresponding ACR20 response rates were 59%, 64%, and 35%, respectively; ACR70 response rates were a respective 25%, 23%, and 5%.
In addition to ACR70, izokibep 160 QW and Q2W met a number of other “high hurdle” efficacy endpoints better than did placebo, Dr. Mease reported. A 90% reduction from baseline in the Psoriasis Area and Severity Index (PASI90) was achieved by a respective 64%, 58%, and 12% of patients, and a 100% reduction in this index (PASI100) was achieved by a respective 51%, 47%, and 12%. And 41%, 42%, and 14% of patients, respectively, met the criteria for minimal disease activity.
Patient Population
Mease pointed out during his presentation that the trial included patients with adult-onset PsA that had been ongoing for ≥ 6 months. Patients had to have at least three tender or swollen joints and an inadequate response, intolerance, or contraindication to commonly used front-line therapies such as nonsteroidal anti-inflammatory drugs, conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), and tumor necrosis factor inhibitors (TNFi).
In fact, around half of the participants across the three treatment arms had received prior csDMARDs, and almost a quarter had received a TNFi.
The mean duration of disease was around 7 years, the average age was about 50 years, and the majority of the participants were White individuals. There were more women than men in the placebo vs the izokibep arms (43.4% vs about 60.0%).
Adverse Events
Injection site reactions were the most common adverse events, most of which were mild to moderate. Very few (< 1% to 4%) led to any need to discontinue the drug.
Serious adverse events occurred at low rates in all study arms: 0.8% for placebo, 2.7% for izokibep QW, and 1.8% for izokibep Q2W.
One patient each (0.9%) in the izokibep arms developed ulcerative colitis, whereas none in the placebo group did. Only two patients developed candidiasis. One was in the placebo group and had a skin infection, and the other was an oral infection in the QW izokibep arm.
There were no cases of uveitis, suicidal ideation, or deaths reported.
Comments on the Study
During the discussion that followed the presentation, Walter P. Maksymowych, MBChB, of the University of Alberta in Edmonton, Alberta, Canada, addressed the dosing regimens used.
“Looking at the side effect profile and then looking at the response rate, comparing the weekly dosing and every 2 weeks, do you think, in hindsight, you might be remiss that there wasn’t an additional dosing on a monthly basis, especially since this is a construct that is meant to prolong the half-life of the molecule?” he asked, adding that perhaps this should be something to consider in future studies.
Mease responded that there had been a fourth dosing arm in the trial — izokibep 80 mg once a month — but because there were only eight patients, the data were not sufficiently robust to analyze.
Commenting on the study, Laura C. Coates, MBChB, PhD, said: “It’s a pretty standard phase 2b/3 study,” and the outcomes were not wildly different from what has been seen with other IL-17A inhibitors.
“In phase 2, the enthesitis data looked really good; in phase 3, the enthesitis data looks the same as for any other IL-17 inhibitor,” Dr. Coates said.
More and longer-term data are needed to see if “the theoretical biological difference in the drug design translates to a different clinical outcome or whether it’s another IL-17,” added Dr. Coates, a clinician scientist and senior clinical research fellow at the University of Oxford in England.
Dennis McGonagle, MB MCH BAO, PhD, of the University of Leeds, England, also picked up on the enthesitis data, echoing the conclusion that the phase 2 enthesitis data were “spectacular” and noting that “it’s a real inversion of what was expected, given the small molecule.”
The study was funded by Acelyrin. Dr. Mease disclosed ties with Acelyrin and other pharmaceutical companies. Dr. Maksymowych, Dr. Coates, and Dr. McGonagle reported having a variety of financial relationships with pharmaceutical companies outside of this study.
A version of this article appeared on Medscape.com.
VIENNA — The investigational interleukin (IL)-17 inhibitor izokibep hit its mark when it came to improving overall disease activity in people with active psoriatic arthritis (PsA) in a phase 2b/3 trial, but it was no better than placebo at reducing inflammation of the entheses.
This apparent and unexpected lack of effect in the entheses was a key talking point after Philip J. Mease, MD, presented the late-breaking trial findings at the annual European Congress of Rheumatology.
At just 18.6 kilodaltons in size, izokibep is just “one tenth the size of a standard monoclonal antibody” and is classed as a small protein therapeutic, Dr. Mease said. It has a “very tight” binding affinity for IL-17A, and because it also binds to albumin, it has a prolonged half-life compared with other IL-17 inhibitors. Potentially, it should be able to “penetrate into difficult areas,” such as the entheses, he said.
Prespecified Enthesitis Analysis
However, results of a prespecified secondary analysis conducted in 209 of the 343 trial participants who had received treatment showed no significant difference in the proportions with enthesis resolution at 16 weeks, defined as a Leeds Enthesitis Index (LEI) of 0.
Comparing two dosing regimens of izokibep 160 mg once weekly (QW) vs every other week (Q2W) with placebo, enthesitis resolution was seen in 45%, 56%, and 47%, respectively, of patients.
The LEI is “sometimes subject to problems with evaluation because of placebo response, which is what we see here,” noted Dr. Mease, director of rheumatology research at the Providence Swedish Medical Center and a rheumatology professor at the University of Washington School of Medicine in Seattle.
An exploratory analysis showed that there was a better response for izokibep vs placebo if the analysis included only patients with higher LEI scores at baseline, at 8.0% (n = 12) for placebo, 22.0% (n = 9) for izokibep 160 mg QW, and 50.0% (n = 12) for izokibep 160 mg Q2W.
Main Efficacy Data
The primary endpoint for the trial was the proportion of patients who had 50% improvement in American College of Rheumatology response criteria (ACR50) at 16 weeks. This showed a clear advantage for treatment with izokibep 160 QW and Q2W compared with placebo, with a respective 40%, 43%, and 15% of patients meeting this endpoint.
Corresponding ACR20 response rates were 59%, 64%, and 35%, respectively; ACR70 response rates were a respective 25%, 23%, and 5%.
In addition to ACR70, izokibep 160 QW and Q2W met a number of other “high hurdle” efficacy endpoints better than did placebo, Dr. Mease reported. A 90% reduction from baseline in the Psoriasis Area and Severity Index (PASI90) was achieved by a respective 64%, 58%, and 12% of patients, and a 100% reduction in this index (PASI100) was achieved by a respective 51%, 47%, and 12%. And 41%, 42%, and 14% of patients, respectively, met the criteria for minimal disease activity.
Patient Population
Mease pointed out during his presentation that the trial included patients with adult-onset PsA that had been ongoing for ≥ 6 months. Patients had to have at least three tender or swollen joints and an inadequate response, intolerance, or contraindication to commonly used front-line therapies such as nonsteroidal anti-inflammatory drugs, conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), and tumor necrosis factor inhibitors (TNFi).
In fact, around half of the participants across the three treatment arms had received prior csDMARDs, and almost a quarter had received a TNFi.
The mean duration of disease was around 7 years, the average age was about 50 years, and the majority of the participants were White individuals. There were more women than men in the placebo vs the izokibep arms (43.4% vs about 60.0%).
Adverse Events
Injection site reactions were the most common adverse events, most of which were mild to moderate. Very few (< 1% to 4%) led to any need to discontinue the drug.
Serious adverse events occurred at low rates in all study arms: 0.8% for placebo, 2.7% for izokibep QW, and 1.8% for izokibep Q2W.
One patient each (0.9%) in the izokibep arms developed ulcerative colitis, whereas none in the placebo group did. Only two patients developed candidiasis. One was in the placebo group and had a skin infection, and the other was an oral infection in the QW izokibep arm.
There were no cases of uveitis, suicidal ideation, or deaths reported.
Comments on the Study
During the discussion that followed the presentation, Walter P. Maksymowych, MBChB, of the University of Alberta in Edmonton, Alberta, Canada, addressed the dosing regimens used.
“Looking at the side effect profile and then looking at the response rate, comparing the weekly dosing and every 2 weeks, do you think, in hindsight, you might be remiss that there wasn’t an additional dosing on a monthly basis, especially since this is a construct that is meant to prolong the half-life of the molecule?” he asked, adding that perhaps this should be something to consider in future studies.
Mease responded that there had been a fourth dosing arm in the trial — izokibep 80 mg once a month — but because there were only eight patients, the data were not sufficiently robust to analyze.
Commenting on the study, Laura C. Coates, MBChB, PhD, said: “It’s a pretty standard phase 2b/3 study,” and the outcomes were not wildly different from what has been seen with other IL-17A inhibitors.
“In phase 2, the enthesitis data looked really good; in phase 3, the enthesitis data looks the same as for any other IL-17 inhibitor,” Dr. Coates said.
More and longer-term data are needed to see if “the theoretical biological difference in the drug design translates to a different clinical outcome or whether it’s another IL-17,” added Dr. Coates, a clinician scientist and senior clinical research fellow at the University of Oxford in England.
Dennis McGonagle, MB MCH BAO, PhD, of the University of Leeds, England, also picked up on the enthesitis data, echoing the conclusion that the phase 2 enthesitis data were “spectacular” and noting that “it’s a real inversion of what was expected, given the small molecule.”
The study was funded by Acelyrin. Dr. Mease disclosed ties with Acelyrin and other pharmaceutical companies. Dr. Maksymowych, Dr. Coates, and Dr. McGonagle reported having a variety of financial relationships with pharmaceutical companies outside of this study.
A version of this article appeared on Medscape.com.
FROM EULAR 2024
VEXAS Syndrome: Study Highlights Cutaneous Symptoms
Additionally, the most common histologic findings include leukocytoclastic vasculitis, neutrophilic dermatosis, and perivascular dermatitis; different variants in the UBA1 gene are associated with specific skin manifestations.
Those are key findings from a cohort study of 112 patients with VEXAS published online in JAMA Dermatology. The study, conducted by researchers at the National Institutes of Health (NIH) and several other institutions, aimed to define the spectrum of cutaneous manifestations in VEXAS in association with genetic, histologic, and other clinical findings.
First described in 2020, VEXAS syndrome is an adult-onset multisystem disease that can pose a diagnostic challenge to clinicians, the study’s corresponding author, Edward W. Cowen, MD, MHSc, of the dermatology branch at the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), said in an interview. The disease is caused by pathogenic variants in the UBA1 gene, located on the X chromosome. Affected individuals exhibit a wide range of manifestations, including cytopenia/myelodysplasia, multiorgan systemic inflammation, and cutaneous involvement.
“Patients may present to a variety of disease specialists depending on their symptoms and providers may not immediately consider a genetic etiology in an older individual,” Dr. Cowen said in an interview. “Although skin involvement occurs in more than 80% of patients, it is pleomorphic and may resemble a variety of other conditions such as vasculitis and Sweet syndrome.”
To better understand the cutaneous manifestations of VEXAS syndrome, the researchers evaluated data from 112 patients with VEXAS-defining genetic variants in the UBA1 gene between 2019 and 2023. Of the 112 patients, 73 underwent medical record review only, and 39 were prospectively evaluated at NIH. All but one of the patients were men, 94% were White individuals, and their mean age was 64 years. Skin involvement occurred in 83% of cases and was the most common presenting feature of VEXAS in 61% of cases.
Of the 64 histopathologic reports available from 60 patients, the main skin histopathologic findings were leukocytoclastic vasculitis in 23 patients (36%), neutrophilic dermatosis in 22 patients (34%), and perivascular dermatitis in 19 patients (30%). According to Dr. Cowen, one key histologic finding was a distinct pattern of “histiocytoid” dermal neutrophilic inflammation, which was present in 13 of 15 specimens (86%) that underwent central re-review. “This pattern can occasionally also be seen in patients with Sweet syndrome, unrelated to VEXAS, but was a hallmark feature found in the majority of skin biopsies of patients with VEXAS,” he said.
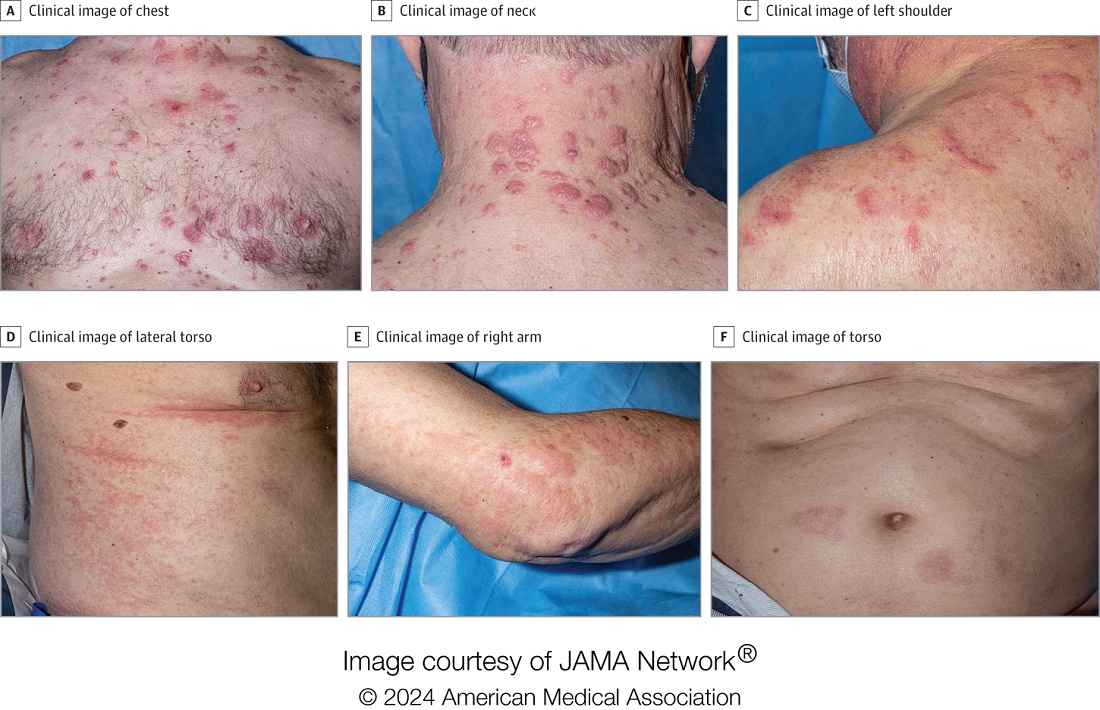
“Together with another pathologic finding, leukocytoclasia, these features can be useful clues to alert the pathologist to a potential diagnosis of VEXAS. This myeloid predominant pattern of skin inflammation was also most strongly associated with the leucine pathogenic variant of the UBA1 gene.” In contrast, cutaneous vasculitis was most strongly associated with the valine pathogenic variant of UBA1. “This is important because the valine variant has been previously independently linked to decreased survival,” he said.
In findings related to pathogenic genetic variants, the researchers observed that the p.Met41Leu variant was most frequently associated with neutrophilic dermal infiltrates in 14 of 17 patients (82%) with this variant and often resembled histiocytoid Sweet syndrome. In addition, the p.Met41Val variant was associated with vasculitic lesions in 11 of 20 patients (55%) with this variant and with a mixed leukocytic infiltrate in 17 of these 20 patients (85%).
Treatment Outcomes
In the realm of therapies, skin manifestations improved in 67 of 73 patients (92%) treated with oral prednisone, while treatment with the interleukin-1 receptor antagonist anakinra improved cutaneous disease in 9 of the 16 (56%) who received it. However, 12 (75%) of those who received anakinra developed severe injection-site reactions, including ulceration in two patients and abscess formation in one patient.
Dr. Cowen noted that VEXAS is associated with high mortality (22% in this cohort), and a high degree of suspicion is required to diagnose patients with VEXAS before significant end organ damage has occurred. “This diagnosis should be considered in all older male patients who present with neutrophilic dermatosis — particularly histiocytoid Sweet syndrome, vasculitis, or leukocytoclasia without vasculitis. Patients who appear to have isolated skin involvement may have cytopenias and acute phase reactants. Therefore, complete blood count with differential and ESR and CRP should be considered to investigate for macrocytosis, cytopenias, and systemic inflammation.”
He acknowledged certain limitations of the study, including the fact that many patients were first evaluated at the NIH after having disease symptoms for many months or years. “It is possible that patients with VEXAS referred to the NIH, either for genetic testing or in person evaluation, represent a population with more aggressive disease.”
Christine Ko, MD, professor of dermatology and pathology at Yale University, New Haven, Connecticut, who was asked to comment on the study, emphasized the importance of the UBA1 mutation in the diagnosis of this complex syndrome. “Dermatologists should be aware of VEXAS syndrome as the majority of patients present with skin lesions, which can range from urticarial to Sweet syndrome–like to palpable purpura,” Dr. Ko said.
“Chondritis and periorbital edema, sometimes unilateral, are also associated. Histopathologic clues include a predominantly histiocytoid infiltrate,” she noted. In addition, “the prominent myxoid stroma around blood vessels and adnexal structures as a clue to VEXAS syndrome surprised me; I had not read that before.”
The study was supported by the Intramural Research Program of NIAMS. One of the study authors reported personal fees from Alexion, Novartis, and Sobi outside of the submitted work. No other disclosures were reported. Dr. Ko reported having no disclosures.
A version of this article appeared on Medscape.com .
Additionally, the most common histologic findings include leukocytoclastic vasculitis, neutrophilic dermatosis, and perivascular dermatitis; different variants in the UBA1 gene are associated with specific skin manifestations.
Those are key findings from a cohort study of 112 patients with VEXAS published online in JAMA Dermatology. The study, conducted by researchers at the National Institutes of Health (NIH) and several other institutions, aimed to define the spectrum of cutaneous manifestations in VEXAS in association with genetic, histologic, and other clinical findings.
First described in 2020, VEXAS syndrome is an adult-onset multisystem disease that can pose a diagnostic challenge to clinicians, the study’s corresponding author, Edward W. Cowen, MD, MHSc, of the dermatology branch at the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), said in an interview. The disease is caused by pathogenic variants in the UBA1 gene, located on the X chromosome. Affected individuals exhibit a wide range of manifestations, including cytopenia/myelodysplasia, multiorgan systemic inflammation, and cutaneous involvement.
“Patients may present to a variety of disease specialists depending on their symptoms and providers may not immediately consider a genetic etiology in an older individual,” Dr. Cowen said in an interview. “Although skin involvement occurs in more than 80% of patients, it is pleomorphic and may resemble a variety of other conditions such as vasculitis and Sweet syndrome.”
To better understand the cutaneous manifestations of VEXAS syndrome, the researchers evaluated data from 112 patients with VEXAS-defining genetic variants in the UBA1 gene between 2019 and 2023. Of the 112 patients, 73 underwent medical record review only, and 39 were prospectively evaluated at NIH. All but one of the patients were men, 94% were White individuals, and their mean age was 64 years. Skin involvement occurred in 83% of cases and was the most common presenting feature of VEXAS in 61% of cases.
Of the 64 histopathologic reports available from 60 patients, the main skin histopathologic findings were leukocytoclastic vasculitis in 23 patients (36%), neutrophilic dermatosis in 22 patients (34%), and perivascular dermatitis in 19 patients (30%). According to Dr. Cowen, one key histologic finding was a distinct pattern of “histiocytoid” dermal neutrophilic inflammation, which was present in 13 of 15 specimens (86%) that underwent central re-review. “This pattern can occasionally also be seen in patients with Sweet syndrome, unrelated to VEXAS, but was a hallmark feature found in the majority of skin biopsies of patients with VEXAS,” he said.
“Together with another pathologic finding, leukocytoclasia, these features can be useful clues to alert the pathologist to a potential diagnosis of VEXAS. This myeloid predominant pattern of skin inflammation was also most strongly associated with the leucine pathogenic variant of the UBA1 gene.” In contrast, cutaneous vasculitis was most strongly associated with the valine pathogenic variant of UBA1. “This is important because the valine variant has been previously independently linked to decreased survival,” he said.
In findings related to pathogenic genetic variants, the researchers observed that the p.Met41Leu variant was most frequently associated with neutrophilic dermal infiltrates in 14 of 17 patients (82%) with this variant and often resembled histiocytoid Sweet syndrome. In addition, the p.Met41Val variant was associated with vasculitic lesions in 11 of 20 patients (55%) with this variant and with a mixed leukocytic infiltrate in 17 of these 20 patients (85%).
Treatment Outcomes
In the realm of therapies, skin manifestations improved in 67 of 73 patients (92%) treated with oral prednisone, while treatment with the interleukin-1 receptor antagonist anakinra improved cutaneous disease in 9 of the 16 (56%) who received it. However, 12 (75%) of those who received anakinra developed severe injection-site reactions, including ulceration in two patients and abscess formation in one patient.
Dr. Cowen noted that VEXAS is associated with high mortality (22% in this cohort), and a high degree of suspicion is required to diagnose patients with VEXAS before significant end organ damage has occurred. “This diagnosis should be considered in all older male patients who present with neutrophilic dermatosis — particularly histiocytoid Sweet syndrome, vasculitis, or leukocytoclasia without vasculitis. Patients who appear to have isolated skin involvement may have cytopenias and acute phase reactants. Therefore, complete blood count with differential and ESR and CRP should be considered to investigate for macrocytosis, cytopenias, and systemic inflammation.”
He acknowledged certain limitations of the study, including the fact that many patients were first evaluated at the NIH after having disease symptoms for many months or years. “It is possible that patients with VEXAS referred to the NIH, either for genetic testing or in person evaluation, represent a population with more aggressive disease.”
Christine Ko, MD, professor of dermatology and pathology at Yale University, New Haven, Connecticut, who was asked to comment on the study, emphasized the importance of the UBA1 mutation in the diagnosis of this complex syndrome. “Dermatologists should be aware of VEXAS syndrome as the majority of patients present with skin lesions, which can range from urticarial to Sweet syndrome–like to palpable purpura,” Dr. Ko said.
“Chondritis and periorbital edema, sometimes unilateral, are also associated. Histopathologic clues include a predominantly histiocytoid infiltrate,” she noted. In addition, “the prominent myxoid stroma around blood vessels and adnexal structures as a clue to VEXAS syndrome surprised me; I had not read that before.”
The study was supported by the Intramural Research Program of NIAMS. One of the study authors reported personal fees from Alexion, Novartis, and Sobi outside of the submitted work. No other disclosures were reported. Dr. Ko reported having no disclosures.
A version of this article appeared on Medscape.com .
Additionally, the most common histologic findings include leukocytoclastic vasculitis, neutrophilic dermatosis, and perivascular dermatitis; different variants in the UBA1 gene are associated with specific skin manifestations.
Those are key findings from a cohort study of 112 patients with VEXAS published online in JAMA Dermatology. The study, conducted by researchers at the National Institutes of Health (NIH) and several other institutions, aimed to define the spectrum of cutaneous manifestations in VEXAS in association with genetic, histologic, and other clinical findings.
First described in 2020, VEXAS syndrome is an adult-onset multisystem disease that can pose a diagnostic challenge to clinicians, the study’s corresponding author, Edward W. Cowen, MD, MHSc, of the dermatology branch at the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), said in an interview. The disease is caused by pathogenic variants in the UBA1 gene, located on the X chromosome. Affected individuals exhibit a wide range of manifestations, including cytopenia/myelodysplasia, multiorgan systemic inflammation, and cutaneous involvement.
“Patients may present to a variety of disease specialists depending on their symptoms and providers may not immediately consider a genetic etiology in an older individual,” Dr. Cowen said in an interview. “Although skin involvement occurs in more than 80% of patients, it is pleomorphic and may resemble a variety of other conditions such as vasculitis and Sweet syndrome.”
To better understand the cutaneous manifestations of VEXAS syndrome, the researchers evaluated data from 112 patients with VEXAS-defining genetic variants in the UBA1 gene between 2019 and 2023. Of the 112 patients, 73 underwent medical record review only, and 39 were prospectively evaluated at NIH. All but one of the patients were men, 94% were White individuals, and their mean age was 64 years. Skin involvement occurred in 83% of cases and was the most common presenting feature of VEXAS in 61% of cases.
Of the 64 histopathologic reports available from 60 patients, the main skin histopathologic findings were leukocytoclastic vasculitis in 23 patients (36%), neutrophilic dermatosis in 22 patients (34%), and perivascular dermatitis in 19 patients (30%). According to Dr. Cowen, one key histologic finding was a distinct pattern of “histiocytoid” dermal neutrophilic inflammation, which was present in 13 of 15 specimens (86%) that underwent central re-review. “This pattern can occasionally also be seen in patients with Sweet syndrome, unrelated to VEXAS, but was a hallmark feature found in the majority of skin biopsies of patients with VEXAS,” he said.
“Together with another pathologic finding, leukocytoclasia, these features can be useful clues to alert the pathologist to a potential diagnosis of VEXAS. This myeloid predominant pattern of skin inflammation was also most strongly associated with the leucine pathogenic variant of the UBA1 gene.” In contrast, cutaneous vasculitis was most strongly associated with the valine pathogenic variant of UBA1. “This is important because the valine variant has been previously independently linked to decreased survival,” he said.
In findings related to pathogenic genetic variants, the researchers observed that the p.Met41Leu variant was most frequently associated with neutrophilic dermal infiltrates in 14 of 17 patients (82%) with this variant and often resembled histiocytoid Sweet syndrome. In addition, the p.Met41Val variant was associated with vasculitic lesions in 11 of 20 patients (55%) with this variant and with a mixed leukocytic infiltrate in 17 of these 20 patients (85%).
Treatment Outcomes
In the realm of therapies, skin manifestations improved in 67 of 73 patients (92%) treated with oral prednisone, while treatment with the interleukin-1 receptor antagonist anakinra improved cutaneous disease in 9 of the 16 (56%) who received it. However, 12 (75%) of those who received anakinra developed severe injection-site reactions, including ulceration in two patients and abscess formation in one patient.
Dr. Cowen noted that VEXAS is associated with high mortality (22% in this cohort), and a high degree of suspicion is required to diagnose patients with VEXAS before significant end organ damage has occurred. “This diagnosis should be considered in all older male patients who present with neutrophilic dermatosis — particularly histiocytoid Sweet syndrome, vasculitis, or leukocytoclasia without vasculitis. Patients who appear to have isolated skin involvement may have cytopenias and acute phase reactants. Therefore, complete blood count with differential and ESR and CRP should be considered to investigate for macrocytosis, cytopenias, and systemic inflammation.”
He acknowledged certain limitations of the study, including the fact that many patients were first evaluated at the NIH after having disease symptoms for many months or years. “It is possible that patients with VEXAS referred to the NIH, either for genetic testing or in person evaluation, represent a population with more aggressive disease.”
Christine Ko, MD, professor of dermatology and pathology at Yale University, New Haven, Connecticut, who was asked to comment on the study, emphasized the importance of the UBA1 mutation in the diagnosis of this complex syndrome. “Dermatologists should be aware of VEXAS syndrome as the majority of patients present with skin lesions, which can range from urticarial to Sweet syndrome–like to palpable purpura,” Dr. Ko said.
“Chondritis and periorbital edema, sometimes unilateral, are also associated. Histopathologic clues include a predominantly histiocytoid infiltrate,” she noted. In addition, “the prominent myxoid stroma around blood vessels and adnexal structures as a clue to VEXAS syndrome surprised me; I had not read that before.”
The study was supported by the Intramural Research Program of NIAMS. One of the study authors reported personal fees from Alexion, Novartis, and Sobi outside of the submitted work. No other disclosures were reported. Dr. Ko reported having no disclosures.
A version of this article appeared on Medscape.com .
FROM JAMA DERMATOLOGY
Pruritic, violaceous papules in a patient with renal cell carcinoma
Pembrolizumab (Keytruda) is a programmed cell death protein 1 (PD-1) blocking antibody used to treat different malignancies including melanoma, non–small cell lung cancer, and other advanced solid tumors and hematologic malignancies. and drug rash with eosinophilia and systemic symptoms (DRESS).
Lichen planus-like adverse drug reactions, as seen in this patient, are also referred to as lichenoid drug eruption or drug-induced lichen planus. This cutaneous reaction is one of the more rare side effects of pembrolizumab. It should be noted that in lichenoid reactions, keratinocytes expressing PD-L1 are particularly affected, leading to a dense CD4/CD8 positive lymphocytic infiltration in the basal layer, necrosis of keratinocytes, acanthosis, and hypergranulosis. Subsequently, the cutaneous adverse reaction is a target effect of the PD-1/PD-L1 pathway and not a general hypersensitivity reaction. Clinically, both lichen planus and lichenoid drug eruptions exhibit erythematous papules and plaques. Lichenoid drug eruptions, however, can be scaly, pruritic, and heal with more hyperpigmentation.
A skin biopsy revealed irregular epidermal hyperplasia with jagged rete ridges. Within the dermis, there was a lichenoid inflammatory cell infiltrate obscuring the dermal-epidermal junction. The inflammatory cell infiltrate contained lymphocytes, histiocytes, and eosinophils. A diagnosis of a lichen planus-like adverse drug reaction to pembrolizumab was favored.
If the reaction is mild, topical corticosteroids and oral antihistamines can help with the drug-induced lichen planus. For more severe cases, systemic steroids can be given to help ease the reaction. Physicians should be aware of potential adverse drug effects that can mimic other medical conditions.

The case and photo were submitted by Ms. Towe, Nova Southeastern University College of Osteopathic Medicine, Davie, Florida, and Dr. Berke, Three Rivers Dermatology, Coraopolis, Pennsylvania. The column was edited by Donna Bilu Martin, MD.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
Bansal A et al. Indian Dermatol Online J. 2023 Apr 4;14(3):391-4. doi: 10.4103/idoj.idoj_377_22.
Sethi A, Raj M. Cureus. 2021 Mar 8;13(3):e13768. doi: 10.7759/cureus.13768.
Pembrolizumab (Keytruda) is a programmed cell death protein 1 (PD-1) blocking antibody used to treat different malignancies including melanoma, non–small cell lung cancer, and other advanced solid tumors and hematologic malignancies. and drug rash with eosinophilia and systemic symptoms (DRESS).
Lichen planus-like adverse drug reactions, as seen in this patient, are also referred to as lichenoid drug eruption or drug-induced lichen planus. This cutaneous reaction is one of the more rare side effects of pembrolizumab. It should be noted that in lichenoid reactions, keratinocytes expressing PD-L1 are particularly affected, leading to a dense CD4/CD8 positive lymphocytic infiltration in the basal layer, necrosis of keratinocytes, acanthosis, and hypergranulosis. Subsequently, the cutaneous adverse reaction is a target effect of the PD-1/PD-L1 pathway and not a general hypersensitivity reaction. Clinically, both lichen planus and lichenoid drug eruptions exhibit erythematous papules and plaques. Lichenoid drug eruptions, however, can be scaly, pruritic, and heal with more hyperpigmentation.
A skin biopsy revealed irregular epidermal hyperplasia with jagged rete ridges. Within the dermis, there was a lichenoid inflammatory cell infiltrate obscuring the dermal-epidermal junction. The inflammatory cell infiltrate contained lymphocytes, histiocytes, and eosinophils. A diagnosis of a lichen planus-like adverse drug reaction to pembrolizumab was favored.
If the reaction is mild, topical corticosteroids and oral antihistamines can help with the drug-induced lichen planus. For more severe cases, systemic steroids can be given to help ease the reaction. Physicians should be aware of potential adverse drug effects that can mimic other medical conditions.
The case and photo were submitted by Ms. Towe, Nova Southeastern University College of Osteopathic Medicine, Davie, Florida, and Dr. Berke, Three Rivers Dermatology, Coraopolis, Pennsylvania. The column was edited by Donna Bilu Martin, MD.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
Bansal A et al. Indian Dermatol Online J. 2023 Apr 4;14(3):391-4. doi: 10.4103/idoj.idoj_377_22.
Sethi A, Raj M. Cureus. 2021 Mar 8;13(3):e13768. doi: 10.7759/cureus.13768.
Pembrolizumab (Keytruda) is a programmed cell death protein 1 (PD-1) blocking antibody used to treat different malignancies including melanoma, non–small cell lung cancer, and other advanced solid tumors and hematologic malignancies. and drug rash with eosinophilia and systemic symptoms (DRESS).
Lichen planus-like adverse drug reactions, as seen in this patient, are also referred to as lichenoid drug eruption or drug-induced lichen planus. This cutaneous reaction is one of the more rare side effects of pembrolizumab. It should be noted that in lichenoid reactions, keratinocytes expressing PD-L1 are particularly affected, leading to a dense CD4/CD8 positive lymphocytic infiltration in the basal layer, necrosis of keratinocytes, acanthosis, and hypergranulosis. Subsequently, the cutaneous adverse reaction is a target effect of the PD-1/PD-L1 pathway and not a general hypersensitivity reaction. Clinically, both lichen planus and lichenoid drug eruptions exhibit erythematous papules and plaques. Lichenoid drug eruptions, however, can be scaly, pruritic, and heal with more hyperpigmentation.
A skin biopsy revealed irregular epidermal hyperplasia with jagged rete ridges. Within the dermis, there was a lichenoid inflammatory cell infiltrate obscuring the dermal-epidermal junction. The inflammatory cell infiltrate contained lymphocytes, histiocytes, and eosinophils. A diagnosis of a lichen planus-like adverse drug reaction to pembrolizumab was favored.
If the reaction is mild, topical corticosteroids and oral antihistamines can help with the drug-induced lichen planus. For more severe cases, systemic steroids can be given to help ease the reaction. Physicians should be aware of potential adverse drug effects that can mimic other medical conditions.
The case and photo were submitted by Ms. Towe, Nova Southeastern University College of Osteopathic Medicine, Davie, Florida, and Dr. Berke, Three Rivers Dermatology, Coraopolis, Pennsylvania. The column was edited by Donna Bilu Martin, MD.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
Bansal A et al. Indian Dermatol Online J. 2023 Apr 4;14(3):391-4. doi: 10.4103/idoj.idoj_377_22.
Sethi A, Raj M. Cureus. 2021 Mar 8;13(3):e13768. doi: 10.7759/cureus.13768.

Flesh-Colored Pinpoint Papules With Fine White Spicules on the Upper Body
The Diagnosis: Trichodysplasia Spinulosa
A diagnosis of trichodysplasia spinulosa (TS) was rendered based on the clinical presentation— diffuse folliculocentric keratotic papules with spicules and leonine facies—coinciding with cyclosporine initiation. Biopsy was deferred given the classic presentation. The patient applied cidofovir cream 1% daily to lesions on the face. She was prescribed leflunomide 10 mg daily, which was later increased to 20 mg daily, for polyarthritis associated with systemic lupus erythematosus (SLE). Her transplant physician increased her cyclosporine dosage from 50 mg twice daily to 75 mg each morning and 50 mg each evening due to rising creatinine and donor-specific antibodies from the renal transplant. The patient’s TS eruption mildly improved 3 months after the cyclosporine dose was increased. To treat persistent lesions, oral valganciclovir was started at 450 mg once daily and later reduced to every other day due to leukopenia. After 3 months of taking valganciclovir 450 mg every other day, the patient’s TS rash resolved.
Trichodysplasia spinulosa is a rare condition caused by TS-associated polyomavirus1 that may arise in immunosuppressed patients, especially in solid organ transplant recipients.2 It is characterized by spiculated and folliculocentric papules, mainly on the face,1 and often is diagnosed clinically, but if the presentation is not classic, a skin biopsy can help to confirm the diagnosis. Because of its rarity, treatment options do not have well-established efficacy1 but include reducing immunosuppression and using the antivirals cidofovir1 or valganciclovir3 to treat the polyomavirus. Topical retinoids,3 photodynamic therapy, 4 and leflunomide5 also may be effective.
Although the typical approach to treating TS is to reduce immunosuppression, this was not an option for our patient, as she required increased immunosuppression for the treatment of active SLE. Leflunomide can be used for SLE, and in some reports it can be effective for BK viremia in kidney transplant recipients5 as well as for TS in solid organ transplant recipients.6 Our patient showed improvement of the TS, BK viremia, renal function, and SLE while taking leflunomide and valganciclovir.
The differential diagnosis includes keratosis pilaris, lichen nitidus, scleromyxedema, and trichostasis spinulosa. Keratosis pilaris is a benign skin disorder consisting of patches of keratotic papules with varying degrees of erythema and inflammation that are formed by dead keratinocytes plugging the hair follicles and often are seen on the extremities, face, and trunk.7 Our patient’s papules were flesh colored with no notable background erythema. Additionally, the presence of leonine facies was atypical for keratosis pilaris. Acids, steroids, and kinase inhibitors are the most frequently used treatments for keratosis pilaris.8
Lichen nitidus is a skin condition characterized by multiple shiny, dome-shaped, flesh-colored papules usually found on the flexor surfaces of the arms, anterior trunk, and genitalia. It is mostly asymptomatic, but patients may experience pruritus. Most cases occur in children and young adults, with no obvious racial or gender predilection. The diagnosis often is clinical, but biopsy shows downward enlargement of the epidermal rete ridges surrounding a focal inflammatory infiltrate, known as a ball-in-claw configuration.9-11 Lichen nitidus spontaneously resolves within a few years without treatment. Our patient did have flesh-colored papules on the arms and chest; however, major involvement of the face is not typical in lichen nitidus. Additionally, fine white spicules would not be seen in lichen nitidus. For severe generalized lichen nitidus, treatment options include topical corticosteroids, topical calcineurin inhibitors, oral antihistamines, or UV light to decrease inflammation.9-11
Scleromyxedema is a rare condition involving the deposition of mucinous material in the papillary dermis to cause the formation of infiltrative skin lesions.12 It is thought that immunoglobulins and cytokines secreted by inflammatory cells lead to the synthesis of glycosaminoglycans, which then causes deposition of mucin in the dermis.13 The classic cutaneous features of scleromyxedema include waxy indurated papules and plaques with skin thickening throughout the entire body.12 Our patient’s papules were not notably indurated and involved less than 50% of the total body surface area. An important diagnostic feature of scleromyxedema is monoclonal gammopathy, which our patient did not have. Intravenous immunoglobulin is the first-line treatment of scleromyxedema, and second-line treatments include systemic corticosteroids and thalidomide.14 Our patient also did not require treatment with intravenous immunoglobulin, as her rash improved with antiviral medication, which would not address the underlying inflammatory processes associated with scleromyxedema.
Trichostasis spinulosa is a rare hair follicle disorder consisting of dark, spiny, hyperkeratotic follicular papules that can be found on the extremities and face, especially the nose. The etiology is unknown, but risk factors include congenital dysplasia of hair follicles; exposure to UV light, dust, oil, or heat; chronic renal failure; Malassezia yeast; and Propionibacterium acnes. Adult women with darker skin types are most commonly affected by trichostasis spinulosa.15,16 Our patient fit the epidemiologic demographic of trichostasis spinulosa, including a history of chronic renal failure. Her rash covered the face, nose, and arms; however, the papules were flesh colored, whereas trichostasis spinulosa would appear as black papules. Furthermore, yeast and bacterial infections have been identified as potential agents associated with trichostasis spinulosa; therefore, antiviral agents would be ineffective. Viable treatments for trichostasis spinulosa include emollients, topical keratolytic agents, retinoic acids, and lasers to remove abnormal hair follicles.15,16
- Curman P, Näsman A, Brauner H. Trichodysplasia spinulosa: a comprehensive disease and its treatment. J Eur Acad Dermatol Venereol. 2021;35:1067-1076.
- Fischer MK, Kao GF, Nguyen HP, et al. Specific detection of trichodysplasia spinulosa-associated polyomavirus DNA in skin and renal allograft tissues in a patient with trichodysplasia spinulosa. Arch Dermatol. 2021;148:726-733.
- Shah PR, Esaa FS, Gupta P, et al. Trichodysplasia spinulosa successfully treated with adapalene 0.1% gel and oral valganciclovir in a renal transplant recipient. JAAD Case Rep. 2020;6:23-25.
- Liew YCC, Kee TYS, Kwek JL, et al. Photodynamic therapy for the treatment of trichodysplasia spinulosa in an Asian renal transplant recipient: a case report and review of the literature. JAAD Case Rep. 2021;7:74-83.
- Pierrotti LC, Urbano PRP, da Silva Nali LH, et al. Viremia and viuria of trichodysplasia spinulosa-associated polyomavirus before the development of clinical disease in a kidney transplant recipient. Transpl Infect Dis. 2019;21:E13133.
- Kassar R, Chang J, Chan AW, et al. Leflunomide for the treatment of trichodysplasia spinulosa in a liver transplant recipient. Transpl Infect Dis. 2017;19:E12702.
- Eckburg A, Kazemi T, Maguiness S. Keratosis pilaris rubra successfully treated with topical sirolimus: report of a case and review of the literature. Pediatr Dermatol. 2022;39:429-431.
- Reddy S, Brahmbhatt H. A narrative review on the role of acids, steroids, and kinase inhibitors in the treatment of keratosis pilaris. Cureus. 2021;13:E18917.
- Jordan AS, Green MC, Sulit DJ. Lichen nitidus. J Am Osteopath Assoc. 2019;119:704.
- Arizaga AT, Gaughan MD, Bang RH. Generalized lichen nitidus. Clin Exp Dermatol. 2002;27:115-117.
- Chu J, Lam JM. Lichen nitidus. CMAJ. 2014;186:E688.
- Haber R, Bachour J, El Gemayel M. Scleromyxedema treatment: a systematic review and update. Int J Dermatol. 2020;59:1191-1201.
- Christman MP, Sukhdeo K, Kim RH, et al. Papular mucinosis, or localized lichen myxedematosis (LM) (discrete papular type). Dermatol Online J. 2017;23:8.
- Hoffman JHO, Enk AH. Scleromyxedema. J Dtsch Dermatol Ges. 2020;18:1449-1467.
- Kositkuljorn C, Suchonwanit P. Trichostasis spinulosa: a case report with an unusual presentation. Case Rep Dermatol. 2020;12:178-185.
- Ramteke MN, Bhide AA. Trichostasis spinulosa at an unusual site. Int J Trichology. 2016;8:78-80.
The Diagnosis: Trichodysplasia Spinulosa
A diagnosis of trichodysplasia spinulosa (TS) was rendered based on the clinical presentation— diffuse folliculocentric keratotic papules with spicules and leonine facies—coinciding with cyclosporine initiation. Biopsy was deferred given the classic presentation. The patient applied cidofovir cream 1% daily to lesions on the face. She was prescribed leflunomide 10 mg daily, which was later increased to 20 mg daily, for polyarthritis associated with systemic lupus erythematosus (SLE). Her transplant physician increased her cyclosporine dosage from 50 mg twice daily to 75 mg each morning and 50 mg each evening due to rising creatinine and donor-specific antibodies from the renal transplant. The patient’s TS eruption mildly improved 3 months after the cyclosporine dose was increased. To treat persistent lesions, oral valganciclovir was started at 450 mg once daily and later reduced to every other day due to leukopenia. After 3 months of taking valganciclovir 450 mg every other day, the patient’s TS rash resolved.
Trichodysplasia spinulosa is a rare condition caused by TS-associated polyomavirus1 that may arise in immunosuppressed patients, especially in solid organ transplant recipients.2 It is characterized by spiculated and folliculocentric papules, mainly on the face,1 and often is diagnosed clinically, but if the presentation is not classic, a skin biopsy can help to confirm the diagnosis. Because of its rarity, treatment options do not have well-established efficacy1 but include reducing immunosuppression and using the antivirals cidofovir1 or valganciclovir3 to treat the polyomavirus. Topical retinoids,3 photodynamic therapy, 4 and leflunomide5 also may be effective.
Although the typical approach to treating TS is to reduce immunosuppression, this was not an option for our patient, as she required increased immunosuppression for the treatment of active SLE. Leflunomide can be used for SLE, and in some reports it can be effective for BK viremia in kidney transplant recipients5 as well as for TS in solid organ transplant recipients.6 Our patient showed improvement of the TS, BK viremia, renal function, and SLE while taking leflunomide and valganciclovir.
The differential diagnosis includes keratosis pilaris, lichen nitidus, scleromyxedema, and trichostasis spinulosa. Keratosis pilaris is a benign skin disorder consisting of patches of keratotic papules with varying degrees of erythema and inflammation that are formed by dead keratinocytes plugging the hair follicles and often are seen on the extremities, face, and trunk.7 Our patient’s papules were flesh colored with no notable background erythema. Additionally, the presence of leonine facies was atypical for keratosis pilaris. Acids, steroids, and kinase inhibitors are the most frequently used treatments for keratosis pilaris.8
Lichen nitidus is a skin condition characterized by multiple shiny, dome-shaped, flesh-colored papules usually found on the flexor surfaces of the arms, anterior trunk, and genitalia. It is mostly asymptomatic, but patients may experience pruritus. Most cases occur in children and young adults, with no obvious racial or gender predilection. The diagnosis often is clinical, but biopsy shows downward enlargement of the epidermal rete ridges surrounding a focal inflammatory infiltrate, known as a ball-in-claw configuration.9-11 Lichen nitidus spontaneously resolves within a few years without treatment. Our patient did have flesh-colored papules on the arms and chest; however, major involvement of the face is not typical in lichen nitidus. Additionally, fine white spicules would not be seen in lichen nitidus. For severe generalized lichen nitidus, treatment options include topical corticosteroids, topical calcineurin inhibitors, oral antihistamines, or UV light to decrease inflammation.9-11
Scleromyxedema is a rare condition involving the deposition of mucinous material in the papillary dermis to cause the formation of infiltrative skin lesions.12 It is thought that immunoglobulins and cytokines secreted by inflammatory cells lead to the synthesis of glycosaminoglycans, which then causes deposition of mucin in the dermis.13 The classic cutaneous features of scleromyxedema include waxy indurated papules and plaques with skin thickening throughout the entire body.12 Our patient’s papules were not notably indurated and involved less than 50% of the total body surface area. An important diagnostic feature of scleromyxedema is monoclonal gammopathy, which our patient did not have. Intravenous immunoglobulin is the first-line treatment of scleromyxedema, and second-line treatments include systemic corticosteroids and thalidomide.14 Our patient also did not require treatment with intravenous immunoglobulin, as her rash improved with antiviral medication, which would not address the underlying inflammatory processes associated with scleromyxedema.
Trichostasis spinulosa is a rare hair follicle disorder consisting of dark, spiny, hyperkeratotic follicular papules that can be found on the extremities and face, especially the nose. The etiology is unknown, but risk factors include congenital dysplasia of hair follicles; exposure to UV light, dust, oil, or heat; chronic renal failure; Malassezia yeast; and Propionibacterium acnes. Adult women with darker skin types are most commonly affected by trichostasis spinulosa.15,16 Our patient fit the epidemiologic demographic of trichostasis spinulosa, including a history of chronic renal failure. Her rash covered the face, nose, and arms; however, the papules were flesh colored, whereas trichostasis spinulosa would appear as black papules. Furthermore, yeast and bacterial infections have been identified as potential agents associated with trichostasis spinulosa; therefore, antiviral agents would be ineffective. Viable treatments for trichostasis spinulosa include emollients, topical keratolytic agents, retinoic acids, and lasers to remove abnormal hair follicles.15,16
The Diagnosis: Trichodysplasia Spinulosa
A diagnosis of trichodysplasia spinulosa (TS) was rendered based on the clinical presentation— diffuse folliculocentric keratotic papules with spicules and leonine facies—coinciding with cyclosporine initiation. Biopsy was deferred given the classic presentation. The patient applied cidofovir cream 1% daily to lesions on the face. She was prescribed leflunomide 10 mg daily, which was later increased to 20 mg daily, for polyarthritis associated with systemic lupus erythematosus (SLE). Her transplant physician increased her cyclosporine dosage from 50 mg twice daily to 75 mg each morning and 50 mg each evening due to rising creatinine and donor-specific antibodies from the renal transplant. The patient’s TS eruption mildly improved 3 months after the cyclosporine dose was increased. To treat persistent lesions, oral valganciclovir was started at 450 mg once daily and later reduced to every other day due to leukopenia. After 3 months of taking valganciclovir 450 mg every other day, the patient’s TS rash resolved.
Trichodysplasia spinulosa is a rare condition caused by TS-associated polyomavirus1 that may arise in immunosuppressed patients, especially in solid organ transplant recipients.2 It is characterized by spiculated and folliculocentric papules, mainly on the face,1 and often is diagnosed clinically, but if the presentation is not classic, a skin biopsy can help to confirm the diagnosis. Because of its rarity, treatment options do not have well-established efficacy1 but include reducing immunosuppression and using the antivirals cidofovir1 or valganciclovir3 to treat the polyomavirus. Topical retinoids,3 photodynamic therapy, 4 and leflunomide5 also may be effective.
Although the typical approach to treating TS is to reduce immunosuppression, this was not an option for our patient, as she required increased immunosuppression for the treatment of active SLE. Leflunomide can be used for SLE, and in some reports it can be effective for BK viremia in kidney transplant recipients5 as well as for TS in solid organ transplant recipients.6 Our patient showed improvement of the TS, BK viremia, renal function, and SLE while taking leflunomide and valganciclovir.
The differential diagnosis includes keratosis pilaris, lichen nitidus, scleromyxedema, and trichostasis spinulosa. Keratosis pilaris is a benign skin disorder consisting of patches of keratotic papules with varying degrees of erythema and inflammation that are formed by dead keratinocytes plugging the hair follicles and often are seen on the extremities, face, and trunk.7 Our patient’s papules were flesh colored with no notable background erythema. Additionally, the presence of leonine facies was atypical for keratosis pilaris. Acids, steroids, and kinase inhibitors are the most frequently used treatments for keratosis pilaris.8
Lichen nitidus is a skin condition characterized by multiple shiny, dome-shaped, flesh-colored papules usually found on the flexor surfaces of the arms, anterior trunk, and genitalia. It is mostly asymptomatic, but patients may experience pruritus. Most cases occur in children and young adults, with no obvious racial or gender predilection. The diagnosis often is clinical, but biopsy shows downward enlargement of the epidermal rete ridges surrounding a focal inflammatory infiltrate, known as a ball-in-claw configuration.9-11 Lichen nitidus spontaneously resolves within a few years without treatment. Our patient did have flesh-colored papules on the arms and chest; however, major involvement of the face is not typical in lichen nitidus. Additionally, fine white spicules would not be seen in lichen nitidus. For severe generalized lichen nitidus, treatment options include topical corticosteroids, topical calcineurin inhibitors, oral antihistamines, or UV light to decrease inflammation.9-11
Scleromyxedema is a rare condition involving the deposition of mucinous material in the papillary dermis to cause the formation of infiltrative skin lesions.12 It is thought that immunoglobulins and cytokines secreted by inflammatory cells lead to the synthesis of glycosaminoglycans, which then causes deposition of mucin in the dermis.13 The classic cutaneous features of scleromyxedema include waxy indurated papules and plaques with skin thickening throughout the entire body.12 Our patient’s papules were not notably indurated and involved less than 50% of the total body surface area. An important diagnostic feature of scleromyxedema is monoclonal gammopathy, which our patient did not have. Intravenous immunoglobulin is the first-line treatment of scleromyxedema, and second-line treatments include systemic corticosteroids and thalidomide.14 Our patient also did not require treatment with intravenous immunoglobulin, as her rash improved with antiviral medication, which would not address the underlying inflammatory processes associated with scleromyxedema.
Trichostasis spinulosa is a rare hair follicle disorder consisting of dark, spiny, hyperkeratotic follicular papules that can be found on the extremities and face, especially the nose. The etiology is unknown, but risk factors include congenital dysplasia of hair follicles; exposure to UV light, dust, oil, or heat; chronic renal failure; Malassezia yeast; and Propionibacterium acnes. Adult women with darker skin types are most commonly affected by trichostasis spinulosa.15,16 Our patient fit the epidemiologic demographic of trichostasis spinulosa, including a history of chronic renal failure. Her rash covered the face, nose, and arms; however, the papules were flesh colored, whereas trichostasis spinulosa would appear as black papules. Furthermore, yeast and bacterial infections have been identified as potential agents associated with trichostasis spinulosa; therefore, antiviral agents would be ineffective. Viable treatments for trichostasis spinulosa include emollients, topical keratolytic agents, retinoic acids, and lasers to remove abnormal hair follicles.15,16
- Curman P, Näsman A, Brauner H. Trichodysplasia spinulosa: a comprehensive disease and its treatment. J Eur Acad Dermatol Venereol. 2021;35:1067-1076.
- Fischer MK, Kao GF, Nguyen HP, et al. Specific detection of trichodysplasia spinulosa-associated polyomavirus DNA in skin and renal allograft tissues in a patient with trichodysplasia spinulosa. Arch Dermatol. 2021;148:726-733.
- Shah PR, Esaa FS, Gupta P, et al. Trichodysplasia spinulosa successfully treated with adapalene 0.1% gel and oral valganciclovir in a renal transplant recipient. JAAD Case Rep. 2020;6:23-25.
- Liew YCC, Kee TYS, Kwek JL, et al. Photodynamic therapy for the treatment of trichodysplasia spinulosa in an Asian renal transplant recipient: a case report and review of the literature. JAAD Case Rep. 2021;7:74-83.
- Pierrotti LC, Urbano PRP, da Silva Nali LH, et al. Viremia and viuria of trichodysplasia spinulosa-associated polyomavirus before the development of clinical disease in a kidney transplant recipient. Transpl Infect Dis. 2019;21:E13133.
- Kassar R, Chang J, Chan AW, et al. Leflunomide for the treatment of trichodysplasia spinulosa in a liver transplant recipient. Transpl Infect Dis. 2017;19:E12702.
- Eckburg A, Kazemi T, Maguiness S. Keratosis pilaris rubra successfully treated with topical sirolimus: report of a case and review of the literature. Pediatr Dermatol. 2022;39:429-431.
- Reddy S, Brahmbhatt H. A narrative review on the role of acids, steroids, and kinase inhibitors in the treatment of keratosis pilaris. Cureus. 2021;13:E18917.
- Jordan AS, Green MC, Sulit DJ. Lichen nitidus. J Am Osteopath Assoc. 2019;119:704.
- Arizaga AT, Gaughan MD, Bang RH. Generalized lichen nitidus. Clin Exp Dermatol. 2002;27:115-117.
- Chu J, Lam JM. Lichen nitidus. CMAJ. 2014;186:E688.
- Haber R, Bachour J, El Gemayel M. Scleromyxedema treatment: a systematic review and update. Int J Dermatol. 2020;59:1191-1201.
- Christman MP, Sukhdeo K, Kim RH, et al. Papular mucinosis, or localized lichen myxedematosis (LM) (discrete papular type). Dermatol Online J. 2017;23:8.
- Hoffman JHO, Enk AH. Scleromyxedema. J Dtsch Dermatol Ges. 2020;18:1449-1467.
- Kositkuljorn C, Suchonwanit P. Trichostasis spinulosa: a case report with an unusual presentation. Case Rep Dermatol. 2020;12:178-185.
- Ramteke MN, Bhide AA. Trichostasis spinulosa at an unusual site. Int J Trichology. 2016;8:78-80.
- Curman P, Näsman A, Brauner H. Trichodysplasia spinulosa: a comprehensive disease and its treatment. J Eur Acad Dermatol Venereol. 2021;35:1067-1076.
- Fischer MK, Kao GF, Nguyen HP, et al. Specific detection of trichodysplasia spinulosa-associated polyomavirus DNA in skin and renal allograft tissues in a patient with trichodysplasia spinulosa. Arch Dermatol. 2021;148:726-733.
- Shah PR, Esaa FS, Gupta P, et al. Trichodysplasia spinulosa successfully treated with adapalene 0.1% gel and oral valganciclovir in a renal transplant recipient. JAAD Case Rep. 2020;6:23-25.
- Liew YCC, Kee TYS, Kwek JL, et al. Photodynamic therapy for the treatment of trichodysplasia spinulosa in an Asian renal transplant recipient: a case report and review of the literature. JAAD Case Rep. 2021;7:74-83.
- Pierrotti LC, Urbano PRP, da Silva Nali LH, et al. Viremia and viuria of trichodysplasia spinulosa-associated polyomavirus before the development of clinical disease in a kidney transplant recipient. Transpl Infect Dis. 2019;21:E13133.
- Kassar R, Chang J, Chan AW, et al. Leflunomide for the treatment of trichodysplasia spinulosa in a liver transplant recipient. Transpl Infect Dis. 2017;19:E12702.
- Eckburg A, Kazemi T, Maguiness S. Keratosis pilaris rubra successfully treated with topical sirolimus: report of a case and review of the literature. Pediatr Dermatol. 2022;39:429-431.
- Reddy S, Brahmbhatt H. A narrative review on the role of acids, steroids, and kinase inhibitors in the treatment of keratosis pilaris. Cureus. 2021;13:E18917.
- Jordan AS, Green MC, Sulit DJ. Lichen nitidus. J Am Osteopath Assoc. 2019;119:704.
- Arizaga AT, Gaughan MD, Bang RH. Generalized lichen nitidus. Clin Exp Dermatol. 2002;27:115-117.
- Chu J, Lam JM. Lichen nitidus. CMAJ. 2014;186:E688.
- Haber R, Bachour J, El Gemayel M. Scleromyxedema treatment: a systematic review and update. Int J Dermatol. 2020;59:1191-1201.
- Christman MP, Sukhdeo K, Kim RH, et al. Papular mucinosis, or localized lichen myxedematosis (LM) (discrete papular type). Dermatol Online J. 2017;23:8.
- Hoffman JHO, Enk AH. Scleromyxedema. J Dtsch Dermatol Ges. 2020;18:1449-1467.
- Kositkuljorn C, Suchonwanit P. Trichostasis spinulosa: a case report with an unusual presentation. Case Rep Dermatol. 2020;12:178-185.
- Ramteke MN, Bhide AA. Trichostasis spinulosa at an unusual site. Int J Trichology. 2016;8:78-80.
A 54-year-old Black woman presented with a rash that developed 6 months after a renal transplant due to a history of systemic lupus erythematosus with lupus nephritis. She was started on mycophenolate mofetil and tacrolimus after the transplant but was switched to cyclosporine because of BK viremia. The rash developed 1 week after cyclosporine was initiated and consisted of pruritic papules that started on the face and spread to the trunk and arms. Physical examination revealed innumerable follicular-based, keratotic, flesh-colored, pinpoint papules with fine white spicules on the face (top), neck, chest, arms, and back. Leonine facies was seen along the glabella with madarosis of the lateral eyebrows (top) and ears (bottom).