User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Oncology Mergers Are on the Rise. How Can Independent Practices Survive?
When he completed his fellowship at Fox Chase Cancer Center in Philadelphia, Moshe Chasky, MD, joined a small five-person practice that rented space from the city’s Jefferson Hospital in Philadelphia. The arrangement seemed to work well for the hospital and the small practice, which remained independent.
Within 10 years, the hospital sought to buy the practice, Alliance Cancer Specialists.
But the oncologists at Alliance did not want to join Jefferson.
The hospital eventually entered into an exclusive agreement with its own medical group to provide inpatient oncology/hematology services at three Jefferson Health–Northeast hospitals and stripped Dr. Chasky and his colleagues of their privileges at those facilities, Medscape Medical News reported last year.
said Jeff Patton, MD, CEO of OneOncology, a management services organization.
A 2020 report from the Community Oncology Alliance (COA), for instance, tracked mergers, acquisitions, and closures in the community oncology setting and found the number of practices acquired by hospitals, known as vertical integration, nearly tripled from 2010 to 2020.
“Some hospitals are pretty predatory in their approach,” Dr. Patton said. If hospitals have their own oncology program, “they’ll employ the referring doctors and then discourage them or prevent them from referring patients to our independent practices that are not owned by the hospital.”
Still, in the face of growing pressure to join hospitals, some community oncology practices are finding ways to survive and maintain their independence.
A Growing Trend
The latest data continue to show a clear trend: Consolidation in oncology is on the rise.
A 2024 study revealed that the pace of consolidation seems to be increasing.
The analysis found that, between 2015 and 2022, the number of medical oncologists increased by 14% and the number of medical oncologists per practice increased by 40%, while the number of practices decreased by 18%.
While about 44% of practices remain independent, the percentage of medical oncologists working in practices with more than 25 clinicians has increased from 34% in 2015 to 44% in 2022. By 2022, the largest 102 practices in the United States employed more than 40% of all medical oncologists.
“The rate of consolidation seems to be rapid,” study coauthor Parsa Erfani, MD, an internal medicine resident at Brigham & Women’s Hospital, Boston, explained.
Consolidation appears to breed more consolidation. The researchers found, for instance, that markets with greater hospital consolidation and more hospital beds per capita were more likely to undergo consolidation in oncology.
Consolidation may be higher in these markets “because hospitals or health systems are buying up oncology practices or conversely because oncology practices are merging to compete more effectively with larger hospitals in the area,” Dr. Erfani told this news organization.
Mergers among independent practices, known as horizontal integration, have also been on the rise, according to the 2020 COA report. These mergers can help counter pressures from hospitals seeking to acquire community practices as well as prevent practices and their clinics from closing.
Although Dr. Erfani’s research wasn’t designed to determine the factors behind consolidation, he and his colleagues point to the Affordable Care Act (ACA) and the federal 340B Drug Pricing Program as potential drivers of this trend.
The ACA encouraged consolidation as a way to improve efficiency and created the need for ever-larger information systems to collect and report quality data. But these data collection and reporting requirements have become increasingly difficult for smaller practices to take on.
The 340B Program, however, may be a bigger contributing factor to consolidation. Created in 1992, the 340B Program allows qualifying hospitals and clinics that treat low-income and uninsured patients to buy outpatient prescription drugs at a 25%-50% discount.
Hospitals seeking to capitalize on the margins possible under the 340B Program will “buy all the referring physicians in a market so that the medical oncology group is left with little choice but to sell to the hospital,” said Dr. Patton.
“Those 340B dollars are worth a lot to hospitals,” said David A. Eagle, MD, a hematologist/oncologist with New York Cancer & Blood Specialists and past president of COA. The program “creates an appetite for nonprofit hospitals to want to grow their medical oncology programs,” he told this news organization.
Declining Medicare reimbursement has also hit independent practices hard.
Over the past 15 years, compared with inflation, physicians have gotten “a pay rate decrease from Medicare,” said Dr. Patton. Payers have followed that lead and tried to cut pay for clinicians, especially those who do not have market share, he said. Paying them less is “disingenuous knowing that our costs of providing care are going up,” he said.
Less Access, Higher Costs, Worse Care?
Many studies have demonstrated that, when hospitals become behemoths in a given market, healthcare costs go up.
“There are robust data showing that consolidation increases healthcare costs by reducing competition, including in oncology,” wrote Dr. Erfani and colleagues.
Oncology practices that are owned by hospitals bill facility fees for outpatient chemotherapy treatment, adding another layer of cost, the researchers explained, citing a 2019 Health Economics study.
Another analysis, published in 2020, found that hospital prices for the top 37 infused cancer drugs averaged 86% more per unit than the price charged by physician offices. Hospital outpatient departments charged even more, on average, for drugs — 128% more for nivolumab and 428% more for fluorouracil, for instance.
In their 2024 analysis, Dr. Erfani and colleagues also found that increased hospital market concentration was associated with worse quality of care, across all assessed patient satisfaction measures, and may result in worse access to care as well.
Overall, these consolidation “trends have important implications for cancer care cost, quality, and access,” the authors concluded.
Navigating the Consolidation Trend
In the face of mounting pressure to join hospitals, community oncology practices have typically relied on horizontal mergers to maintain their independence. An increasing number of practices, however, are now turning to another strategy: Management services organizations.
According to some oncologists, a core benefit of joining a management services organization is their community practices can maintain autonomy, hold on to referrals, and benefit from access to a wider network of peers and recently approved treatments such as chimeric antigen receptor T-cell therapies.
In these arrangements, the management company also provides business assistance to practices, including help with billing and collection, payer negotiations, supply chain issues, and credentialing, as well as recruiting, hiring, and marketing.
These management organizations, which include American Oncology Network, Integrated Oncology Network, OneOncology, and Verdi Oncology, are, however, backed by private equity. According to a 2022 report, private equity–backed management organizations have ramped up arrangements with community oncology practices over the past few years — a trend that has concerned some experts.
The authors of a recent analysis in JAMA Internal Medicine explained that, although private equity involvement in physician practices may enable operational efficiencies, “critics point to potential conflicts of interest” and highlight concerns that patients “may face additional barriers to both accessibility and affordability of care.”
The difference, according to some oncologists, is their practices are not owned by the management services organization; instead, the practices enter contracts that outline the boundaries of the relationship and stipulate fees to the management organizations.
In 2020, Dr. Chasky’s practice, Alliance Cancer Specialists, joined The US Oncology Network, a management services organization wholly owned by McKesson. The organization provides the practice with capital and other resources, as well as access to the Sarah Cannon Research Institute, so patients can participate in clinical trials.
“We totally function as an independent practice,” said Dr. Chasky. “We make our own management decisions,” he said. For instance, if Alliance wants to hire a new clinician, US Oncology helps with the recruitment. “But at the end of the day, it’s our practice,” he said.
Davey Daniel, MD — whose community practice joined the management services organization OneOncology — has seen the benefits of being part of a larger network. For instance, bispecific therapies for leukemias, lymphomas, and multiple myeloma are typically administered at academic centers because of the risk for cytokine release syndrome.
However, physician leaders in the OneOncology network “came up with a playbook on how to do it safely” in the community setting, said Dr. Daniel. “It meant that we were adopting FDA newly approved therapies in a very short course.”
Being able to draw from a wider pool of expertise has had other advantages. Dr. Daniel can lean on pathologists and research scientists in the network for advice on targeted therapy use. “We’re actually bringing precision medicine expertise to the community,” Dr. Daniel said.
Dr. Chasky and Dr. Eagle, whose practice is also part of OneOncology, said that continuing to work in the community setting has allowed them greater flexibility.
Dr. Eagle explained that New York Cancer & Blood Specialists tries to offer patients an appointment within 2 days of a referral, and it allows walk-in visits.
Dr. Chasky leans into the flexibility by having staff stay late, when needed, to ensure that all patients are seen. “We’re there for our patients at all hours,” Dr. Chasky said, adding that often “you don’t have that flexibility when you work for a big hospital system.”
The bottom line is community oncology can still thrive, said Nick Ferreyros, managing director of COA, “as long as we have a healthy competitive ecosystem where [we] are valued and seen as an important part of our cancer care system.”
A version of this article first appeared on Medscape.com.
When he completed his fellowship at Fox Chase Cancer Center in Philadelphia, Moshe Chasky, MD, joined a small five-person practice that rented space from the city’s Jefferson Hospital in Philadelphia. The arrangement seemed to work well for the hospital and the small practice, which remained independent.
Within 10 years, the hospital sought to buy the practice, Alliance Cancer Specialists.
But the oncologists at Alliance did not want to join Jefferson.
The hospital eventually entered into an exclusive agreement with its own medical group to provide inpatient oncology/hematology services at three Jefferson Health–Northeast hospitals and stripped Dr. Chasky and his colleagues of their privileges at those facilities, Medscape Medical News reported last year.
said Jeff Patton, MD, CEO of OneOncology, a management services organization.
A 2020 report from the Community Oncology Alliance (COA), for instance, tracked mergers, acquisitions, and closures in the community oncology setting and found the number of practices acquired by hospitals, known as vertical integration, nearly tripled from 2010 to 2020.
“Some hospitals are pretty predatory in their approach,” Dr. Patton said. If hospitals have their own oncology program, “they’ll employ the referring doctors and then discourage them or prevent them from referring patients to our independent practices that are not owned by the hospital.”
Still, in the face of growing pressure to join hospitals, some community oncology practices are finding ways to survive and maintain their independence.
A Growing Trend
The latest data continue to show a clear trend: Consolidation in oncology is on the rise.
A 2024 study revealed that the pace of consolidation seems to be increasing.
The analysis found that, between 2015 and 2022, the number of medical oncologists increased by 14% and the number of medical oncologists per practice increased by 40%, while the number of practices decreased by 18%.
While about 44% of practices remain independent, the percentage of medical oncologists working in practices with more than 25 clinicians has increased from 34% in 2015 to 44% in 2022. By 2022, the largest 102 practices in the United States employed more than 40% of all medical oncologists.
“The rate of consolidation seems to be rapid,” study coauthor Parsa Erfani, MD, an internal medicine resident at Brigham & Women’s Hospital, Boston, explained.
Consolidation appears to breed more consolidation. The researchers found, for instance, that markets with greater hospital consolidation and more hospital beds per capita were more likely to undergo consolidation in oncology.
Consolidation may be higher in these markets “because hospitals or health systems are buying up oncology practices or conversely because oncology practices are merging to compete more effectively with larger hospitals in the area,” Dr. Erfani told this news organization.
Mergers among independent practices, known as horizontal integration, have also been on the rise, according to the 2020 COA report. These mergers can help counter pressures from hospitals seeking to acquire community practices as well as prevent practices and their clinics from closing.
Although Dr. Erfani’s research wasn’t designed to determine the factors behind consolidation, he and his colleagues point to the Affordable Care Act (ACA) and the federal 340B Drug Pricing Program as potential drivers of this trend.
The ACA encouraged consolidation as a way to improve efficiency and created the need for ever-larger information systems to collect and report quality data. But these data collection and reporting requirements have become increasingly difficult for smaller practices to take on.
The 340B Program, however, may be a bigger contributing factor to consolidation. Created in 1992, the 340B Program allows qualifying hospitals and clinics that treat low-income and uninsured patients to buy outpatient prescription drugs at a 25%-50% discount.
Hospitals seeking to capitalize on the margins possible under the 340B Program will “buy all the referring physicians in a market so that the medical oncology group is left with little choice but to sell to the hospital,” said Dr. Patton.
“Those 340B dollars are worth a lot to hospitals,” said David A. Eagle, MD, a hematologist/oncologist with New York Cancer & Blood Specialists and past president of COA. The program “creates an appetite for nonprofit hospitals to want to grow their medical oncology programs,” he told this news organization.
Declining Medicare reimbursement has also hit independent practices hard.
Over the past 15 years, compared with inflation, physicians have gotten “a pay rate decrease from Medicare,” said Dr. Patton. Payers have followed that lead and tried to cut pay for clinicians, especially those who do not have market share, he said. Paying them less is “disingenuous knowing that our costs of providing care are going up,” he said.
Less Access, Higher Costs, Worse Care?
Many studies have demonstrated that, when hospitals become behemoths in a given market, healthcare costs go up.
“There are robust data showing that consolidation increases healthcare costs by reducing competition, including in oncology,” wrote Dr. Erfani and colleagues.
Oncology practices that are owned by hospitals bill facility fees for outpatient chemotherapy treatment, adding another layer of cost, the researchers explained, citing a 2019 Health Economics study.
Another analysis, published in 2020, found that hospital prices for the top 37 infused cancer drugs averaged 86% more per unit than the price charged by physician offices. Hospital outpatient departments charged even more, on average, for drugs — 128% more for nivolumab and 428% more for fluorouracil, for instance.
In their 2024 analysis, Dr. Erfani and colleagues also found that increased hospital market concentration was associated with worse quality of care, across all assessed patient satisfaction measures, and may result in worse access to care as well.
Overall, these consolidation “trends have important implications for cancer care cost, quality, and access,” the authors concluded.
Navigating the Consolidation Trend
In the face of mounting pressure to join hospitals, community oncology practices have typically relied on horizontal mergers to maintain their independence. An increasing number of practices, however, are now turning to another strategy: Management services organizations.
According to some oncologists, a core benefit of joining a management services organization is their community practices can maintain autonomy, hold on to referrals, and benefit from access to a wider network of peers and recently approved treatments such as chimeric antigen receptor T-cell therapies.
In these arrangements, the management company also provides business assistance to practices, including help with billing and collection, payer negotiations, supply chain issues, and credentialing, as well as recruiting, hiring, and marketing.
These management organizations, which include American Oncology Network, Integrated Oncology Network, OneOncology, and Verdi Oncology, are, however, backed by private equity. According to a 2022 report, private equity–backed management organizations have ramped up arrangements with community oncology practices over the past few years — a trend that has concerned some experts.
The authors of a recent analysis in JAMA Internal Medicine explained that, although private equity involvement in physician practices may enable operational efficiencies, “critics point to potential conflicts of interest” and highlight concerns that patients “may face additional barriers to both accessibility and affordability of care.”
The difference, according to some oncologists, is their practices are not owned by the management services organization; instead, the practices enter contracts that outline the boundaries of the relationship and stipulate fees to the management organizations.
In 2020, Dr. Chasky’s practice, Alliance Cancer Specialists, joined The US Oncology Network, a management services organization wholly owned by McKesson. The organization provides the practice with capital and other resources, as well as access to the Sarah Cannon Research Institute, so patients can participate in clinical trials.
“We totally function as an independent practice,” said Dr. Chasky. “We make our own management decisions,” he said. For instance, if Alliance wants to hire a new clinician, US Oncology helps with the recruitment. “But at the end of the day, it’s our practice,” he said.
Davey Daniel, MD — whose community practice joined the management services organization OneOncology — has seen the benefits of being part of a larger network. For instance, bispecific therapies for leukemias, lymphomas, and multiple myeloma are typically administered at academic centers because of the risk for cytokine release syndrome.
However, physician leaders in the OneOncology network “came up with a playbook on how to do it safely” in the community setting, said Dr. Daniel. “It meant that we were adopting FDA newly approved therapies in a very short course.”
Being able to draw from a wider pool of expertise has had other advantages. Dr. Daniel can lean on pathologists and research scientists in the network for advice on targeted therapy use. “We’re actually bringing precision medicine expertise to the community,” Dr. Daniel said.
Dr. Chasky and Dr. Eagle, whose practice is also part of OneOncology, said that continuing to work in the community setting has allowed them greater flexibility.
Dr. Eagle explained that New York Cancer & Blood Specialists tries to offer patients an appointment within 2 days of a referral, and it allows walk-in visits.
Dr. Chasky leans into the flexibility by having staff stay late, when needed, to ensure that all patients are seen. “We’re there for our patients at all hours,” Dr. Chasky said, adding that often “you don’t have that flexibility when you work for a big hospital system.”
The bottom line is community oncology can still thrive, said Nick Ferreyros, managing director of COA, “as long as we have a healthy competitive ecosystem where [we] are valued and seen as an important part of our cancer care system.”
A version of this article first appeared on Medscape.com.
When he completed his fellowship at Fox Chase Cancer Center in Philadelphia, Moshe Chasky, MD, joined a small five-person practice that rented space from the city’s Jefferson Hospital in Philadelphia. The arrangement seemed to work well for the hospital and the small practice, which remained independent.
Within 10 years, the hospital sought to buy the practice, Alliance Cancer Specialists.
But the oncologists at Alliance did not want to join Jefferson.
The hospital eventually entered into an exclusive agreement with its own medical group to provide inpatient oncology/hematology services at three Jefferson Health–Northeast hospitals and stripped Dr. Chasky and his colleagues of their privileges at those facilities, Medscape Medical News reported last year.
said Jeff Patton, MD, CEO of OneOncology, a management services organization.
A 2020 report from the Community Oncology Alliance (COA), for instance, tracked mergers, acquisitions, and closures in the community oncology setting and found the number of practices acquired by hospitals, known as vertical integration, nearly tripled from 2010 to 2020.
“Some hospitals are pretty predatory in their approach,” Dr. Patton said. If hospitals have their own oncology program, “they’ll employ the referring doctors and then discourage them or prevent them from referring patients to our independent practices that are not owned by the hospital.”
Still, in the face of growing pressure to join hospitals, some community oncology practices are finding ways to survive and maintain their independence.
A Growing Trend
The latest data continue to show a clear trend: Consolidation in oncology is on the rise.
A 2024 study revealed that the pace of consolidation seems to be increasing.
The analysis found that, between 2015 and 2022, the number of medical oncologists increased by 14% and the number of medical oncologists per practice increased by 40%, while the number of practices decreased by 18%.
While about 44% of practices remain independent, the percentage of medical oncologists working in practices with more than 25 clinicians has increased from 34% in 2015 to 44% in 2022. By 2022, the largest 102 practices in the United States employed more than 40% of all medical oncologists.
“The rate of consolidation seems to be rapid,” study coauthor Parsa Erfani, MD, an internal medicine resident at Brigham & Women’s Hospital, Boston, explained.
Consolidation appears to breed more consolidation. The researchers found, for instance, that markets with greater hospital consolidation and more hospital beds per capita were more likely to undergo consolidation in oncology.
Consolidation may be higher in these markets “because hospitals or health systems are buying up oncology practices or conversely because oncology practices are merging to compete more effectively with larger hospitals in the area,” Dr. Erfani told this news organization.
Mergers among independent practices, known as horizontal integration, have also been on the rise, according to the 2020 COA report. These mergers can help counter pressures from hospitals seeking to acquire community practices as well as prevent practices and their clinics from closing.
Although Dr. Erfani’s research wasn’t designed to determine the factors behind consolidation, he and his colleagues point to the Affordable Care Act (ACA) and the federal 340B Drug Pricing Program as potential drivers of this trend.
The ACA encouraged consolidation as a way to improve efficiency and created the need for ever-larger information systems to collect and report quality data. But these data collection and reporting requirements have become increasingly difficult for smaller practices to take on.
The 340B Program, however, may be a bigger contributing factor to consolidation. Created in 1992, the 340B Program allows qualifying hospitals and clinics that treat low-income and uninsured patients to buy outpatient prescription drugs at a 25%-50% discount.
Hospitals seeking to capitalize on the margins possible under the 340B Program will “buy all the referring physicians in a market so that the medical oncology group is left with little choice but to sell to the hospital,” said Dr. Patton.
“Those 340B dollars are worth a lot to hospitals,” said David A. Eagle, MD, a hematologist/oncologist with New York Cancer & Blood Specialists and past president of COA. The program “creates an appetite for nonprofit hospitals to want to grow their medical oncology programs,” he told this news organization.
Declining Medicare reimbursement has also hit independent practices hard.
Over the past 15 years, compared with inflation, physicians have gotten “a pay rate decrease from Medicare,” said Dr. Patton. Payers have followed that lead and tried to cut pay for clinicians, especially those who do not have market share, he said. Paying them less is “disingenuous knowing that our costs of providing care are going up,” he said.
Less Access, Higher Costs, Worse Care?
Many studies have demonstrated that, when hospitals become behemoths in a given market, healthcare costs go up.
“There are robust data showing that consolidation increases healthcare costs by reducing competition, including in oncology,” wrote Dr. Erfani and colleagues.
Oncology practices that are owned by hospitals bill facility fees for outpatient chemotherapy treatment, adding another layer of cost, the researchers explained, citing a 2019 Health Economics study.
Another analysis, published in 2020, found that hospital prices for the top 37 infused cancer drugs averaged 86% more per unit than the price charged by physician offices. Hospital outpatient departments charged even more, on average, for drugs — 128% more for nivolumab and 428% more for fluorouracil, for instance.
In their 2024 analysis, Dr. Erfani and colleagues also found that increased hospital market concentration was associated with worse quality of care, across all assessed patient satisfaction measures, and may result in worse access to care as well.
Overall, these consolidation “trends have important implications for cancer care cost, quality, and access,” the authors concluded.
Navigating the Consolidation Trend
In the face of mounting pressure to join hospitals, community oncology practices have typically relied on horizontal mergers to maintain their independence. An increasing number of practices, however, are now turning to another strategy: Management services organizations.
According to some oncologists, a core benefit of joining a management services organization is their community practices can maintain autonomy, hold on to referrals, and benefit from access to a wider network of peers and recently approved treatments such as chimeric antigen receptor T-cell therapies.
In these arrangements, the management company also provides business assistance to practices, including help with billing and collection, payer negotiations, supply chain issues, and credentialing, as well as recruiting, hiring, and marketing.
These management organizations, which include American Oncology Network, Integrated Oncology Network, OneOncology, and Verdi Oncology, are, however, backed by private equity. According to a 2022 report, private equity–backed management organizations have ramped up arrangements with community oncology practices over the past few years — a trend that has concerned some experts.
The authors of a recent analysis in JAMA Internal Medicine explained that, although private equity involvement in physician practices may enable operational efficiencies, “critics point to potential conflicts of interest” and highlight concerns that patients “may face additional barriers to both accessibility and affordability of care.”
The difference, according to some oncologists, is their practices are not owned by the management services organization; instead, the practices enter contracts that outline the boundaries of the relationship and stipulate fees to the management organizations.
In 2020, Dr. Chasky’s practice, Alliance Cancer Specialists, joined The US Oncology Network, a management services organization wholly owned by McKesson. The organization provides the practice with capital and other resources, as well as access to the Sarah Cannon Research Institute, so patients can participate in clinical trials.
“We totally function as an independent practice,” said Dr. Chasky. “We make our own management decisions,” he said. For instance, if Alliance wants to hire a new clinician, US Oncology helps with the recruitment. “But at the end of the day, it’s our practice,” he said.
Davey Daniel, MD — whose community practice joined the management services organization OneOncology — has seen the benefits of being part of a larger network. For instance, bispecific therapies for leukemias, lymphomas, and multiple myeloma are typically administered at academic centers because of the risk for cytokine release syndrome.
However, physician leaders in the OneOncology network “came up with a playbook on how to do it safely” in the community setting, said Dr. Daniel. “It meant that we were adopting FDA newly approved therapies in a very short course.”
Being able to draw from a wider pool of expertise has had other advantages. Dr. Daniel can lean on pathologists and research scientists in the network for advice on targeted therapy use. “We’re actually bringing precision medicine expertise to the community,” Dr. Daniel said.
Dr. Chasky and Dr. Eagle, whose practice is also part of OneOncology, said that continuing to work in the community setting has allowed them greater flexibility.
Dr. Eagle explained that New York Cancer & Blood Specialists tries to offer patients an appointment within 2 days of a referral, and it allows walk-in visits.
Dr. Chasky leans into the flexibility by having staff stay late, when needed, to ensure that all patients are seen. “We’re there for our patients at all hours,” Dr. Chasky said, adding that often “you don’t have that flexibility when you work for a big hospital system.”
The bottom line is community oncology can still thrive, said Nick Ferreyros, managing director of COA, “as long as we have a healthy competitive ecosystem where [we] are valued and seen as an important part of our cancer care system.”
A version of this article first appeared on Medscape.com.
Treatment of Infantile Hemangiomas in Concomitant Tuberous Sclerosis Complex Should Prompt Evaluation for Cardiac Rhabdomyomas Prior to Initiation of Propranolol
To the Editor:
Cardiac rhabdomyomas are benign hamartomas that are common in patients with tuberous sclerosis complex (TSC).1 We describe a patient who presented with large infantile hemangiomas (IHs) and hypopigmented macules, which prompted further testing that eventually showed concomitant multiple cardiac rhabdomyomas in the context of TSC.
A 5-week-old girl—who was born at 38 weeks and 3 days’ gestation via uncomplicated vaginal delivery—was referred to our pediatric dermatology clinic for evaluation of multiple erythematous lesions on the scalp and left buttock that were first noticed 2 weeks prior to presentation. There was a family history of seizures in the patient’s mother. The patient’s older brother did not have similar symptoms.
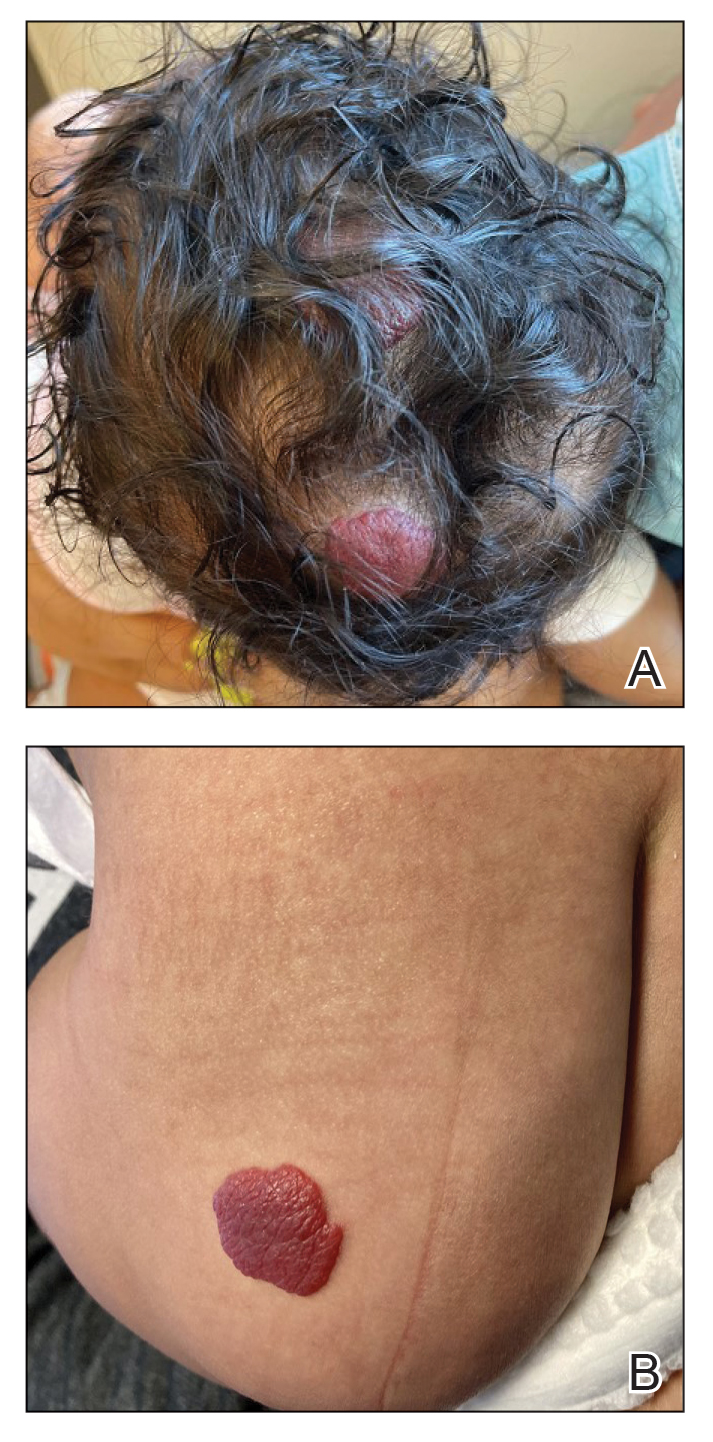
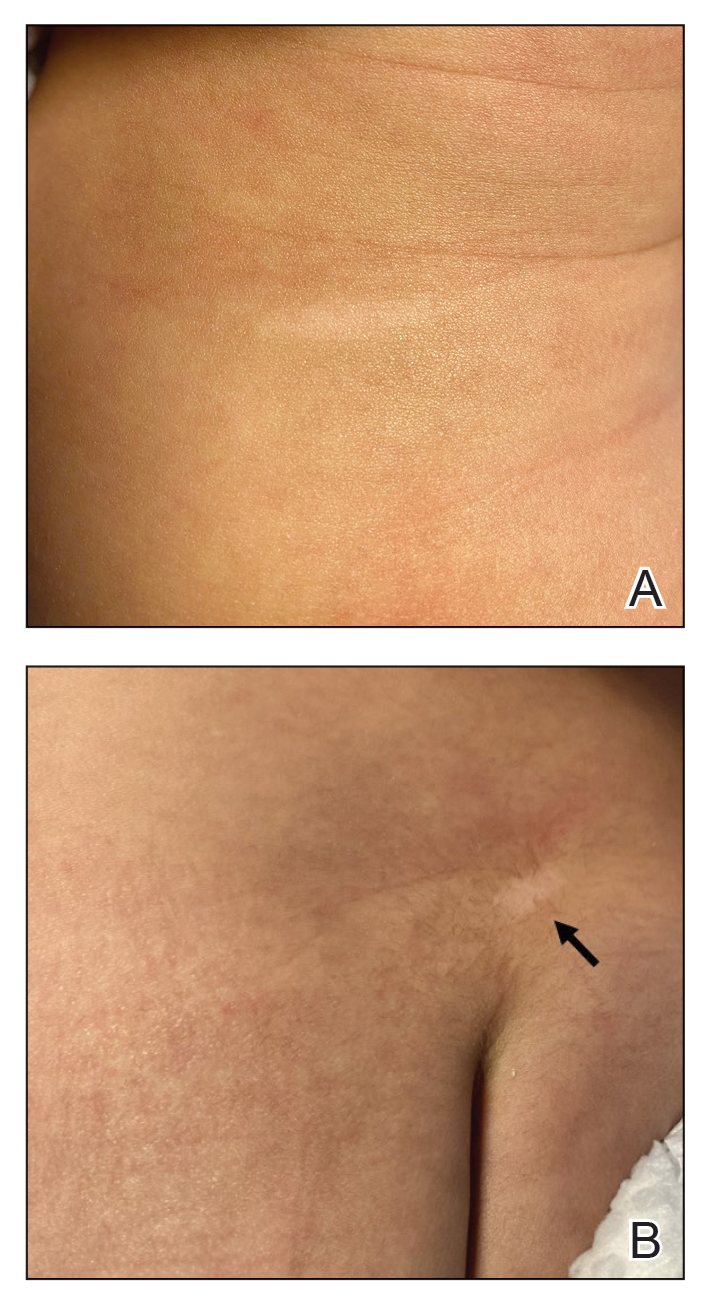
Physical examination revealed 2 nonulcerating erythematous nodules on the middle and posterior left vertex scalp that measured 2.5×2 cm (Figure 1A) as well as 1 bright red plaque on the left buttock (Figure 1B). Five hypopigmented macules, ranging from 5 mm to 1.5 cm in diameter, also were detected on the left thorax (Figure 2A) as well as the middle and lower back (Figure 2B). These findings, along with the history of seizures in the patient’s mother, prompted further evaluation of the family history, which uncovered TSC in the patient’s mother, maternal aunt, and maternal grandmother.
The large IHs on the scalp did not pose concerns for potential functional impairment but were still considered high risk for permanent alopecia based on clinical practice guidelines for the management of IH.2 Treatment with oral propranolol was recommended; however, because of a strong suspicion of TSC due to the presence of 5 hypopigmented macules measuring more than 5 mm in diameter (≥3 hypopigmented macules of ≥5 mm is one of the major criterion for TSC), the patient was referred to cardiology prior to initiation of propranolol.
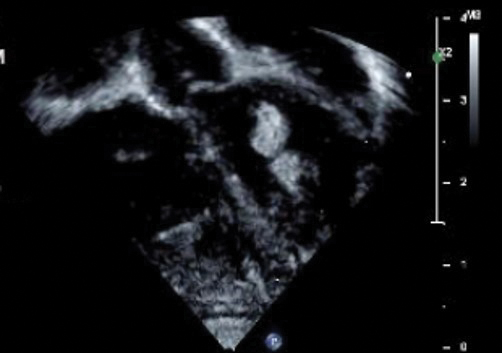
Echocardiography revealed 3 intracardiac masses measuring 4 to 5 mm in diameter in the left ventricle (LV), along the interventricular septum and the LV posterior wall. These masses were consistent with rhabdomyomas (Figure 3)—a major criterion for TSC—which had not been detected by prenatal ultrasonography. No obstruction to LV inflow or outflow was observed. Additionally, no arrhythmias were detected on electrocardiography.
The patient was cleared for propranolol, which was slowly uptitrated to 2 mg/kg/d. She completed the course without adverse effects. The treatment of IH was successful with substantial reduction in size over the following months until clearance. She also was referred to neurology for magnetic resonance imaging of the brain, which showed a 3-mm subependymal nodule in the lateral right ventricle, another major feature of TSC.
Cardiac rhabdomyomas are benign hamartomas that affect as many as 80% of patients with TSC1 and are primarily localized in the ventricles. Although cardiac rhabdomyomas usually regress over time, they can compromise ventricular function or valvular function, or both, and result in outflow obstruction, arrhythmias, and Wolff- Parkinson-White syndrome.3 Surgical resection may be needed in patients whose condition is refractory to medical management for heart failure.
The pathophysiologic mechanism behind the natural involution of cardiac rhabdomyomas has not been fully elucidated. It has been hypothesized that these masses stem from the inability of rhabdomyoma cells to divide after birth due to their embryonic myocyte derivation.4
According to the TSC diagnostic criteria from the Tuberous Sclerosis Complex International Consensus Group, at least 2 major features or 1 major and 2 minor features are required to make a definitive diagnosis of TSC. Cutaneous signs represent more than one-third of major features of TSC; almost all patients with TSC have skin findings.5
Identification of pathogenic mutations in either TSC1 (on chromosome 9q34.3, encoding for hamartin) or TSC2 (on chromosome 16p13.3, encoding for tuberin), resulting in constitutive activation of mammalian target of rapamycin and subsequent increased cell growth, is sufficient for a definitive diagnosis of TSC. However, mutations cannot be identified by conventional genetic testing in as many as one-quarter of patients with TSC; therefore, a negative result does not exclude TSC if the patient meets clinical diagnostic criteria.
Although a cardiology workup is indicated prior to initiating propranolol in the presence of possible cardiac rhabdomyomas, most of those lesions are hemodynamically stable and do not require treatment. There also is no contraindication for β-blocker therapy. In fact, propranolol has been reported as a successful treatment in rhabdomyoma-associated arrhythmias in children.6 Notably, obstructive cardiac rhabdomyomas have been successfully treated with mammalian target of rapamycin inhibitors, such as sirolimus7 and everolimus.8
Baseline cardiology screening with echocardiography prior to initiating propranolol for treatment of IH is not routinely indicated in babies with uncomplicated IH. However, in a patient with TSC, cardiology screening is necessary to rule out rhabdomyomas with associated arrhythmias or obstructed blood flow, or both, prior to initiating treatment.
We presented a case of concomitant IH and TSC in a patient with cardiac rhabdomyomas. The manifestation of large IHs in our patient prompted further testing that revealed multiple cardiac rhabdomyomas in the context of TSC. It is imperative for cardiologists, cardiac surgeons, and dermatologists to be familiar with the TSC diagnostic criteria so that they can reach a prompt diagnosis and make appropriate referrals for further evaluation of cardiac, neurologic, and ophthalmologic signs.
- Frudit P, Vitturi BK, Navarro FC, et al. Multiple cardiac rhabdomyomas in tuberous sclerosis complex: case report and review of the literature. Autops Case Rep. 2019;9:e2019125. doi:10.4322/acr.2019.125
- Krowchuk DP, Frieden IJ, Mancini AJ, et al; Subcommittee on the Management of Infantile Hemangiomas. Clinical practice guideline for the management of infantile hemangiomas. Pediatrics. 2019;143:e20183475. doi:10.1542/peds.2018-3475
- Venugopalan P, Babu JS, Al-Bulushi A. Right atrial rhabdomyoma acting as the substrate for Wolff-Parkinson-White syndrome in a 3-month-old infant. Acta Cardiol. 2005;60:543-545. doi:10.2143/AC.60.5.2004977
- DiMario FJ Jr, Diana D, Leopold H, et al. Evolution of cardiac rhabdomyoma in tuberous sclerosis complex. Clin Pediatr (Phila). 1996;35:615-619. doi:10.1177/000992289603501202
- Northrup H, Krueger DA; International Tuberous Sclerosis Complex Consensus Group. Tuberous sclerosis complex diagnostic criteria update: recommendations of the 2012 International Tuberous Sclerosis Complex Consensus Conference. Pediatr Neurol. 2013;49:243-254. doi:10.1016/j.pediatrneurol.2013.08.001
- Kathare PA, Muthuswamy KS, Sadasivan J, et al. Incessant ventricular tachycardia due to multiple cardiac rhabdomyomas in an infant with tuberous sclerosis. Indian Heart J. 2013;65:111-113. doi:10.1016/j.ihj.2012.12.003
- Breathnach C, Pears J, Franklin O, et al. Rapid regression of left ventricular outflow tract rhabdomyoma after sirolimus therapy. Pediatrics. 2014;134:e1199-e1202. doi:10.1542/peds.2013-3293
- Chang J-S, Chiou P-Y, Yao S-H, et al. Regression of neonatal cardiac rhabdomyoma in two months through low-dose everolimus therapy: a report of three cases. Pediatr Cardiol. 2017;38:1478-1484. doi:10.1007/s00246-017-1688-4
To the Editor:
Cardiac rhabdomyomas are benign hamartomas that are common in patients with tuberous sclerosis complex (TSC).1 We describe a patient who presented with large infantile hemangiomas (IHs) and hypopigmented macules, which prompted further testing that eventually showed concomitant multiple cardiac rhabdomyomas in the context of TSC.
A 5-week-old girl—who was born at 38 weeks and 3 days’ gestation via uncomplicated vaginal delivery—was referred to our pediatric dermatology clinic for evaluation of multiple erythematous lesions on the scalp and left buttock that were first noticed 2 weeks prior to presentation. There was a family history of seizures in the patient’s mother. The patient’s older brother did not have similar symptoms.
Physical examination revealed 2 nonulcerating erythematous nodules on the middle and posterior left vertex scalp that measured 2.5×2 cm (Figure 1A) as well as 1 bright red plaque on the left buttock (Figure 1B). Five hypopigmented macules, ranging from 5 mm to 1.5 cm in diameter, also were detected on the left thorax (Figure 2A) as well as the middle and lower back (Figure 2B). These findings, along with the history of seizures in the patient’s mother, prompted further evaluation of the family history, which uncovered TSC in the patient’s mother, maternal aunt, and maternal grandmother.
The large IHs on the scalp did not pose concerns for potential functional impairment but were still considered high risk for permanent alopecia based on clinical practice guidelines for the management of IH.2 Treatment with oral propranolol was recommended; however, because of a strong suspicion of TSC due to the presence of 5 hypopigmented macules measuring more than 5 mm in diameter (≥3 hypopigmented macules of ≥5 mm is one of the major criterion for TSC), the patient was referred to cardiology prior to initiation of propranolol.
Echocardiography revealed 3 intracardiac masses measuring 4 to 5 mm in diameter in the left ventricle (LV), along the interventricular septum and the LV posterior wall. These masses were consistent with rhabdomyomas (Figure 3)—a major criterion for TSC—which had not been detected by prenatal ultrasonography. No obstruction to LV inflow or outflow was observed. Additionally, no arrhythmias were detected on electrocardiography.
The patient was cleared for propranolol, which was slowly uptitrated to 2 mg/kg/d. She completed the course without adverse effects. The treatment of IH was successful with substantial reduction in size over the following months until clearance. She also was referred to neurology for magnetic resonance imaging of the brain, which showed a 3-mm subependymal nodule in the lateral right ventricle, another major feature of TSC.
Cardiac rhabdomyomas are benign hamartomas that affect as many as 80% of patients with TSC1 and are primarily localized in the ventricles. Although cardiac rhabdomyomas usually regress over time, they can compromise ventricular function or valvular function, or both, and result in outflow obstruction, arrhythmias, and Wolff- Parkinson-White syndrome.3 Surgical resection may be needed in patients whose condition is refractory to medical management for heart failure.
The pathophysiologic mechanism behind the natural involution of cardiac rhabdomyomas has not been fully elucidated. It has been hypothesized that these masses stem from the inability of rhabdomyoma cells to divide after birth due to their embryonic myocyte derivation.4
According to the TSC diagnostic criteria from the Tuberous Sclerosis Complex International Consensus Group, at least 2 major features or 1 major and 2 minor features are required to make a definitive diagnosis of TSC. Cutaneous signs represent more than one-third of major features of TSC; almost all patients with TSC have skin findings.5
Identification of pathogenic mutations in either TSC1 (on chromosome 9q34.3, encoding for hamartin) or TSC2 (on chromosome 16p13.3, encoding for tuberin), resulting in constitutive activation of mammalian target of rapamycin and subsequent increased cell growth, is sufficient for a definitive diagnosis of TSC. However, mutations cannot be identified by conventional genetic testing in as many as one-quarter of patients with TSC; therefore, a negative result does not exclude TSC if the patient meets clinical diagnostic criteria.
Although a cardiology workup is indicated prior to initiating propranolol in the presence of possible cardiac rhabdomyomas, most of those lesions are hemodynamically stable and do not require treatment. There also is no contraindication for β-blocker therapy. In fact, propranolol has been reported as a successful treatment in rhabdomyoma-associated arrhythmias in children.6 Notably, obstructive cardiac rhabdomyomas have been successfully treated with mammalian target of rapamycin inhibitors, such as sirolimus7 and everolimus.8
Baseline cardiology screening with echocardiography prior to initiating propranolol for treatment of IH is not routinely indicated in babies with uncomplicated IH. However, in a patient with TSC, cardiology screening is necessary to rule out rhabdomyomas with associated arrhythmias or obstructed blood flow, or both, prior to initiating treatment.
We presented a case of concomitant IH and TSC in a patient with cardiac rhabdomyomas. The manifestation of large IHs in our patient prompted further testing that revealed multiple cardiac rhabdomyomas in the context of TSC. It is imperative for cardiologists, cardiac surgeons, and dermatologists to be familiar with the TSC diagnostic criteria so that they can reach a prompt diagnosis and make appropriate referrals for further evaluation of cardiac, neurologic, and ophthalmologic signs.
To the Editor:
Cardiac rhabdomyomas are benign hamartomas that are common in patients with tuberous sclerosis complex (TSC).1 We describe a patient who presented with large infantile hemangiomas (IHs) and hypopigmented macules, which prompted further testing that eventually showed concomitant multiple cardiac rhabdomyomas in the context of TSC.
A 5-week-old girl—who was born at 38 weeks and 3 days’ gestation via uncomplicated vaginal delivery—was referred to our pediatric dermatology clinic for evaluation of multiple erythematous lesions on the scalp and left buttock that were first noticed 2 weeks prior to presentation. There was a family history of seizures in the patient’s mother. The patient’s older brother did not have similar symptoms.
Physical examination revealed 2 nonulcerating erythematous nodules on the middle and posterior left vertex scalp that measured 2.5×2 cm (Figure 1A) as well as 1 bright red plaque on the left buttock (Figure 1B). Five hypopigmented macules, ranging from 5 mm to 1.5 cm in diameter, also were detected on the left thorax (Figure 2A) as well as the middle and lower back (Figure 2B). These findings, along with the history of seizures in the patient’s mother, prompted further evaluation of the family history, which uncovered TSC in the patient’s mother, maternal aunt, and maternal grandmother.
The large IHs on the scalp did not pose concerns for potential functional impairment but were still considered high risk for permanent alopecia based on clinical practice guidelines for the management of IH.2 Treatment with oral propranolol was recommended; however, because of a strong suspicion of TSC due to the presence of 5 hypopigmented macules measuring more than 5 mm in diameter (≥3 hypopigmented macules of ≥5 mm is one of the major criterion for TSC), the patient was referred to cardiology prior to initiation of propranolol.
Echocardiography revealed 3 intracardiac masses measuring 4 to 5 mm in diameter in the left ventricle (LV), along the interventricular septum and the LV posterior wall. These masses were consistent with rhabdomyomas (Figure 3)—a major criterion for TSC—which had not been detected by prenatal ultrasonography. No obstruction to LV inflow or outflow was observed. Additionally, no arrhythmias were detected on electrocardiography.
The patient was cleared for propranolol, which was slowly uptitrated to 2 mg/kg/d. She completed the course without adverse effects. The treatment of IH was successful with substantial reduction in size over the following months until clearance. She also was referred to neurology for magnetic resonance imaging of the brain, which showed a 3-mm subependymal nodule in the lateral right ventricle, another major feature of TSC.
Cardiac rhabdomyomas are benign hamartomas that affect as many as 80% of patients with TSC1 and are primarily localized in the ventricles. Although cardiac rhabdomyomas usually regress over time, they can compromise ventricular function or valvular function, or both, and result in outflow obstruction, arrhythmias, and Wolff- Parkinson-White syndrome.3 Surgical resection may be needed in patients whose condition is refractory to medical management for heart failure.
The pathophysiologic mechanism behind the natural involution of cardiac rhabdomyomas has not been fully elucidated. It has been hypothesized that these masses stem from the inability of rhabdomyoma cells to divide after birth due to their embryonic myocyte derivation.4
According to the TSC diagnostic criteria from the Tuberous Sclerosis Complex International Consensus Group, at least 2 major features or 1 major and 2 minor features are required to make a definitive diagnosis of TSC. Cutaneous signs represent more than one-third of major features of TSC; almost all patients with TSC have skin findings.5
Identification of pathogenic mutations in either TSC1 (on chromosome 9q34.3, encoding for hamartin) or TSC2 (on chromosome 16p13.3, encoding for tuberin), resulting in constitutive activation of mammalian target of rapamycin and subsequent increased cell growth, is sufficient for a definitive diagnosis of TSC. However, mutations cannot be identified by conventional genetic testing in as many as one-quarter of patients with TSC; therefore, a negative result does not exclude TSC if the patient meets clinical diagnostic criteria.
Although a cardiology workup is indicated prior to initiating propranolol in the presence of possible cardiac rhabdomyomas, most of those lesions are hemodynamically stable and do not require treatment. There also is no contraindication for β-blocker therapy. In fact, propranolol has been reported as a successful treatment in rhabdomyoma-associated arrhythmias in children.6 Notably, obstructive cardiac rhabdomyomas have been successfully treated with mammalian target of rapamycin inhibitors, such as sirolimus7 and everolimus.8
Baseline cardiology screening with echocardiography prior to initiating propranolol for treatment of IH is not routinely indicated in babies with uncomplicated IH. However, in a patient with TSC, cardiology screening is necessary to rule out rhabdomyomas with associated arrhythmias or obstructed blood flow, or both, prior to initiating treatment.
We presented a case of concomitant IH and TSC in a patient with cardiac rhabdomyomas. The manifestation of large IHs in our patient prompted further testing that revealed multiple cardiac rhabdomyomas in the context of TSC. It is imperative for cardiologists, cardiac surgeons, and dermatologists to be familiar with the TSC diagnostic criteria so that they can reach a prompt diagnosis and make appropriate referrals for further evaluation of cardiac, neurologic, and ophthalmologic signs.
- Frudit P, Vitturi BK, Navarro FC, et al. Multiple cardiac rhabdomyomas in tuberous sclerosis complex: case report and review of the literature. Autops Case Rep. 2019;9:e2019125. doi:10.4322/acr.2019.125
- Krowchuk DP, Frieden IJ, Mancini AJ, et al; Subcommittee on the Management of Infantile Hemangiomas. Clinical practice guideline for the management of infantile hemangiomas. Pediatrics. 2019;143:e20183475. doi:10.1542/peds.2018-3475
- Venugopalan P, Babu JS, Al-Bulushi A. Right atrial rhabdomyoma acting as the substrate for Wolff-Parkinson-White syndrome in a 3-month-old infant. Acta Cardiol. 2005;60:543-545. doi:10.2143/AC.60.5.2004977
- DiMario FJ Jr, Diana D, Leopold H, et al. Evolution of cardiac rhabdomyoma in tuberous sclerosis complex. Clin Pediatr (Phila). 1996;35:615-619. doi:10.1177/000992289603501202
- Northrup H, Krueger DA; International Tuberous Sclerosis Complex Consensus Group. Tuberous sclerosis complex diagnostic criteria update: recommendations of the 2012 International Tuberous Sclerosis Complex Consensus Conference. Pediatr Neurol. 2013;49:243-254. doi:10.1016/j.pediatrneurol.2013.08.001
- Kathare PA, Muthuswamy KS, Sadasivan J, et al. Incessant ventricular tachycardia due to multiple cardiac rhabdomyomas in an infant with tuberous sclerosis. Indian Heart J. 2013;65:111-113. doi:10.1016/j.ihj.2012.12.003
- Breathnach C, Pears J, Franklin O, et al. Rapid regression of left ventricular outflow tract rhabdomyoma after sirolimus therapy. Pediatrics. 2014;134:e1199-e1202. doi:10.1542/peds.2013-3293
- Chang J-S, Chiou P-Y, Yao S-H, et al. Regression of neonatal cardiac rhabdomyoma in two months through low-dose everolimus therapy: a report of three cases. Pediatr Cardiol. 2017;38:1478-1484. doi:10.1007/s00246-017-1688-4
- Frudit P, Vitturi BK, Navarro FC, et al. Multiple cardiac rhabdomyomas in tuberous sclerosis complex: case report and review of the literature. Autops Case Rep. 2019;9:e2019125. doi:10.4322/acr.2019.125
- Krowchuk DP, Frieden IJ, Mancini AJ, et al; Subcommittee on the Management of Infantile Hemangiomas. Clinical practice guideline for the management of infantile hemangiomas. Pediatrics. 2019;143:e20183475. doi:10.1542/peds.2018-3475
- Venugopalan P, Babu JS, Al-Bulushi A. Right atrial rhabdomyoma acting as the substrate for Wolff-Parkinson-White syndrome in a 3-month-old infant. Acta Cardiol. 2005;60:543-545. doi:10.2143/AC.60.5.2004977
- DiMario FJ Jr, Diana D, Leopold H, et al. Evolution of cardiac rhabdomyoma in tuberous sclerosis complex. Clin Pediatr (Phila). 1996;35:615-619. doi:10.1177/000992289603501202
- Northrup H, Krueger DA; International Tuberous Sclerosis Complex Consensus Group. Tuberous sclerosis complex diagnostic criteria update: recommendations of the 2012 International Tuberous Sclerosis Complex Consensus Conference. Pediatr Neurol. 2013;49:243-254. doi:10.1016/j.pediatrneurol.2013.08.001
- Kathare PA, Muthuswamy KS, Sadasivan J, et al. Incessant ventricular tachycardia due to multiple cardiac rhabdomyomas in an infant with tuberous sclerosis. Indian Heart J. 2013;65:111-113. doi:10.1016/j.ihj.2012.12.003
- Breathnach C, Pears J, Franklin O, et al. Rapid regression of left ventricular outflow tract rhabdomyoma after sirolimus therapy. Pediatrics. 2014;134:e1199-e1202. doi:10.1542/peds.2013-3293
- Chang J-S, Chiou P-Y, Yao S-H, et al. Regression of neonatal cardiac rhabdomyoma in two months through low-dose everolimus therapy: a report of three cases. Pediatr Cardiol. 2017;38:1478-1484. doi:10.1007/s00246-017-1688-4
Practice Points
- Dermatologists may see patients with infantile hemangiomas (IHs) and tuberous sclerosis complex (TSC); therefore, they should be familiar with TSC diagnostic criteria to reach a prompt diagnosis and make appropriate referrals.
- Cardiologic evaluation is not routinely required prior to systemic treatment of IH, but knowledge of cardiac findings in TSC should prompt cardiologic clearance prior to β-blocker initiation.

Online Diagnosis of Sexually Transmitted Infections? Ethicist Says We Are Nowhere Close
This transcript has been edited for clarity.
There has been a large amount of news lately about dating online and dating apps. Probably the most common way younger people find potential partners is to go online and see who’s there that they might want to meet.
Online dating is also notorious for being full of scammers. There are all kinds of people out there that you have to be careful of, who are trying to rip you off by saying, “Send me money, I’m in trouble,” or “Now that we have a relationship, will you support my particular entrepreneurial idea?” Certainly, dangers are there.
Another danger we don’t talk much about is meeting people who have sexually transmitted diseases. That’s been a problem before websites and before dating apps. I think the opportunity of meeting more people — strangers, people you don’t really know — who may not tell you the truth about their health, and particularly their sexual health, is really out there.
It’s always good medical advice to tell people to practice safe sex, and that often involves a man wearing a condom. It certainly is the case that we want to attend not just to the prevention of unwanted pregnancy but also to the transmission of diseases. I think it’s very important to tell women of reproductive age to get their HPV shot to try to reduce cancers in their reproductive systems, or sometimes in men — anal cancers, or even being a transmitter of disease.
Even then, certainly one wants to recommend that, in an age where some people are going to meet many partners that they don’t know well or don’t have much background with, it’s wise to try to prevent diseases using the vaccines we’ve got, using the contraceptive methods that will prevent disease transmission, and reminding people to ask about sex life.
I did come across a website that just startled me. It’s called HeHealth, and basically it says to men, if you are conscientious about your sex life, take a picture of your penis, send it to us, and we have doctors — I presume they’re US doctors but I don’t know — who will diagnose venereal diseases based on that picture. I presume women could also say, “Before we have sex, or now that we’re approaching that possibility, I want you to send a picture to this company on this website.”
Now, a couple of reminders. I think we all know this, but just because you’re not manifesting symptoms on your reproductive organs doesn’t mean you don’t have a sexual disease. It’s not a reliable measure. Yes, maybe you could have somebody say: “Oh, that looks nasty. I’m not sure you ought to have sex right now, and maybe you should go get some treatment.” This is going to miss many cases and is not a reliable indicator that your partner is safe in terms of not transmitting diseases to you.
It also isn’t clear what they do with these images. Do they keep them? Who can see them? Could they resell them? What sort of privacy protection have you got if you decide to use this?
There’s another issue here, which is, if they misdiagnose someone and you do catch a sexual disease, who’s liable? Can you go after them for using doctors who weren’t competent or transmitting images that weren’t really adequate because you didn’t know how to take that picture properly when you sent that off to them? There are many unknowns.
The bottom line is that we’re in a different world, I think, of romance. We’re in a world where some people are going to meet more partners. Some people are going to meet more strangers. One approach is to have us take pictures of ourselves, send them off to who knows where, and ask for a green light to go ahead and have sexual relations. I don’t think we’re anywhere close to being able to rely on that as a way to avoid the risks of unprotected sexual behavior.
We do know what to do in dealing with patients who are sexually active. First, we have to ask them. Then we’ve got to recommend available vaccinations to prevent the transmission of some cancers, the HPV vaccine. Then they need that reminder about safe sexual practices not only to protect against unwanted pregnancy, but still, in this day and age, to protect against syphilis, which is on the rise, plus HIV, gonorrhea, chlamydia, and other sexually transmissible diseases.
I’m not going to rely on the penis picture to make the world safe for sex. I think we have to still use the old-fashioned techniques of education and prevention to do the best we can.
Dr. Caplan is director of the Division of Medical Ethics at New York University Langone Medical Center, New York City. He reported conflicts of interest with Johnson & Johnson’s Panel for Compassionate Drug Use and Medscape.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
There has been a large amount of news lately about dating online and dating apps. Probably the most common way younger people find potential partners is to go online and see who’s there that they might want to meet.
Online dating is also notorious for being full of scammers. There are all kinds of people out there that you have to be careful of, who are trying to rip you off by saying, “Send me money, I’m in trouble,” or “Now that we have a relationship, will you support my particular entrepreneurial idea?” Certainly, dangers are there.
Another danger we don’t talk much about is meeting people who have sexually transmitted diseases. That’s been a problem before websites and before dating apps. I think the opportunity of meeting more people — strangers, people you don’t really know — who may not tell you the truth about their health, and particularly their sexual health, is really out there.
It’s always good medical advice to tell people to practice safe sex, and that often involves a man wearing a condom. It certainly is the case that we want to attend not just to the prevention of unwanted pregnancy but also to the transmission of diseases. I think it’s very important to tell women of reproductive age to get their HPV shot to try to reduce cancers in their reproductive systems, or sometimes in men — anal cancers, or even being a transmitter of disease.
Even then, certainly one wants to recommend that, in an age where some people are going to meet many partners that they don’t know well or don’t have much background with, it’s wise to try to prevent diseases using the vaccines we’ve got, using the contraceptive methods that will prevent disease transmission, and reminding people to ask about sex life.
I did come across a website that just startled me. It’s called HeHealth, and basically it says to men, if you are conscientious about your sex life, take a picture of your penis, send it to us, and we have doctors — I presume they’re US doctors but I don’t know — who will diagnose venereal diseases based on that picture. I presume women could also say, “Before we have sex, or now that we’re approaching that possibility, I want you to send a picture to this company on this website.”
Now, a couple of reminders. I think we all know this, but just because you’re not manifesting symptoms on your reproductive organs doesn’t mean you don’t have a sexual disease. It’s not a reliable measure. Yes, maybe you could have somebody say: “Oh, that looks nasty. I’m not sure you ought to have sex right now, and maybe you should go get some treatment.” This is going to miss many cases and is not a reliable indicator that your partner is safe in terms of not transmitting diseases to you.
It also isn’t clear what they do with these images. Do they keep them? Who can see them? Could they resell them? What sort of privacy protection have you got if you decide to use this?
There’s another issue here, which is, if they misdiagnose someone and you do catch a sexual disease, who’s liable? Can you go after them for using doctors who weren’t competent or transmitting images that weren’t really adequate because you didn’t know how to take that picture properly when you sent that off to them? There are many unknowns.
The bottom line is that we’re in a different world, I think, of romance. We’re in a world where some people are going to meet more partners. Some people are going to meet more strangers. One approach is to have us take pictures of ourselves, send them off to who knows where, and ask for a green light to go ahead and have sexual relations. I don’t think we’re anywhere close to being able to rely on that as a way to avoid the risks of unprotected sexual behavior.
We do know what to do in dealing with patients who are sexually active. First, we have to ask them. Then we’ve got to recommend available vaccinations to prevent the transmission of some cancers, the HPV vaccine. Then they need that reminder about safe sexual practices not only to protect against unwanted pregnancy, but still, in this day and age, to protect against syphilis, which is on the rise, plus HIV, gonorrhea, chlamydia, and other sexually transmissible diseases.
I’m not going to rely on the penis picture to make the world safe for sex. I think we have to still use the old-fashioned techniques of education and prevention to do the best we can.
Dr. Caplan is director of the Division of Medical Ethics at New York University Langone Medical Center, New York City. He reported conflicts of interest with Johnson & Johnson’s Panel for Compassionate Drug Use and Medscape.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
There has been a large amount of news lately about dating online and dating apps. Probably the most common way younger people find potential partners is to go online and see who’s there that they might want to meet.
Online dating is also notorious for being full of scammers. There are all kinds of people out there that you have to be careful of, who are trying to rip you off by saying, “Send me money, I’m in trouble,” or “Now that we have a relationship, will you support my particular entrepreneurial idea?” Certainly, dangers are there.
Another danger we don’t talk much about is meeting people who have sexually transmitted diseases. That’s been a problem before websites and before dating apps. I think the opportunity of meeting more people — strangers, people you don’t really know — who may not tell you the truth about their health, and particularly their sexual health, is really out there.
It’s always good medical advice to tell people to practice safe sex, and that often involves a man wearing a condom. It certainly is the case that we want to attend not just to the prevention of unwanted pregnancy but also to the transmission of diseases. I think it’s very important to tell women of reproductive age to get their HPV shot to try to reduce cancers in their reproductive systems, or sometimes in men — anal cancers, or even being a transmitter of disease.
Even then, certainly one wants to recommend that, in an age where some people are going to meet many partners that they don’t know well or don’t have much background with, it’s wise to try to prevent diseases using the vaccines we’ve got, using the contraceptive methods that will prevent disease transmission, and reminding people to ask about sex life.
I did come across a website that just startled me. It’s called HeHealth, and basically it says to men, if you are conscientious about your sex life, take a picture of your penis, send it to us, and we have doctors — I presume they’re US doctors but I don’t know — who will diagnose venereal diseases based on that picture. I presume women could also say, “Before we have sex, or now that we’re approaching that possibility, I want you to send a picture to this company on this website.”
Now, a couple of reminders. I think we all know this, but just because you’re not manifesting symptoms on your reproductive organs doesn’t mean you don’t have a sexual disease. It’s not a reliable measure. Yes, maybe you could have somebody say: “Oh, that looks nasty. I’m not sure you ought to have sex right now, and maybe you should go get some treatment.” This is going to miss many cases and is not a reliable indicator that your partner is safe in terms of not transmitting diseases to you.
It also isn’t clear what they do with these images. Do they keep them? Who can see them? Could they resell them? What sort of privacy protection have you got if you decide to use this?
There’s another issue here, which is, if they misdiagnose someone and you do catch a sexual disease, who’s liable? Can you go after them for using doctors who weren’t competent or transmitting images that weren’t really adequate because you didn’t know how to take that picture properly when you sent that off to them? There are many unknowns.
The bottom line is that we’re in a different world, I think, of romance. We’re in a world where some people are going to meet more partners. Some people are going to meet more strangers. One approach is to have us take pictures of ourselves, send them off to who knows where, and ask for a green light to go ahead and have sexual relations. I don’t think we’re anywhere close to being able to rely on that as a way to avoid the risks of unprotected sexual behavior.
We do know what to do in dealing with patients who are sexually active. First, we have to ask them. Then we’ve got to recommend available vaccinations to prevent the transmission of some cancers, the HPV vaccine. Then they need that reminder about safe sexual practices not only to protect against unwanted pregnancy, but still, in this day and age, to protect against syphilis, which is on the rise, plus HIV, gonorrhea, chlamydia, and other sexually transmissible diseases.
I’m not going to rely on the penis picture to make the world safe for sex. I think we have to still use the old-fashioned techniques of education and prevention to do the best we can.
Dr. Caplan is director of the Division of Medical Ethics at New York University Langone Medical Center, New York City. He reported conflicts of interest with Johnson & Johnson’s Panel for Compassionate Drug Use and Medscape.
A version of this article first appeared on Medscape.com.
FDA Approves Topical Anticholinergic for Axillary Hyperhidrosis
The .
According to a press release from Botanix Pharmaceuticals, which developed the product and will market it under the brand name Sofdra, approval was based on results from two phase 3 studies that enrolled 710 patients with primary axillary hyperhidrosis. In the trials, patients treated with sofpironium topical gel, 12.45%, experienced “clinically and statistically meaningful changes” from baseline in the Gravimetric Sweat Production and the Hyperhidrosis Disease Severity Measure–Axillary seven-item score, according to the company.
Botanix plans to enable qualified patients to gain early access to the product in the third quarter of 2024, with commercial sales expected in the fourth quarter of 2024.
A version of this article first appeared on Medscape.com.
The .
According to a press release from Botanix Pharmaceuticals, which developed the product and will market it under the brand name Sofdra, approval was based on results from two phase 3 studies that enrolled 710 patients with primary axillary hyperhidrosis. In the trials, patients treated with sofpironium topical gel, 12.45%, experienced “clinically and statistically meaningful changes” from baseline in the Gravimetric Sweat Production and the Hyperhidrosis Disease Severity Measure–Axillary seven-item score, according to the company.
Botanix plans to enable qualified patients to gain early access to the product in the third quarter of 2024, with commercial sales expected in the fourth quarter of 2024.
A version of this article first appeared on Medscape.com.
The .
According to a press release from Botanix Pharmaceuticals, which developed the product and will market it under the brand name Sofdra, approval was based on results from two phase 3 studies that enrolled 710 patients with primary axillary hyperhidrosis. In the trials, patients treated with sofpironium topical gel, 12.45%, experienced “clinically and statistically meaningful changes” from baseline in the Gravimetric Sweat Production and the Hyperhidrosis Disease Severity Measure–Axillary seven-item score, according to the company.
Botanix plans to enable qualified patients to gain early access to the product in the third quarter of 2024, with commercial sales expected in the fourth quarter of 2024.
A version of this article first appeared on Medscape.com.
Rethinking Management of Skin Cancer in Older Patients
WASHINGTON — In 2013, Vishal A. Patel, MD, was completing a fellowship in Mohs surgery and cutaneous oncology at Columbia University Irving Medical Center, New York City, when a study was published showing that most nonmelanoma skin cancers (NMSCs) were treated with surgery, regardless of the patient’s life expectancy. Life expectancy “should enter into treatment decisions,” the authors concluded.
“ Dr. Patel recalled at the ElderDerm conference hosted by the Department of Dermatology at George Washington University, Washington, DC, and described as a first-of-its-kind meeting dedicated to improving dermatologic care for older adults.

Today, however, more than a decade later, guidelines still promote surgical therapy as the gold standard across the board, and questions raised by the study are still unaddressed, Dr. Patel, associate professor of dermatology and medicine/oncology at George Washington University, said at the meeting. These questions are becoming increasingly urgent as the incidence of skin cancer, especially NMSC, rises in the older adult population, especially in patients older than 85 years. “It’s a function of our training and our treatment guidelines that we reach for the most definitive treatment, which happens to be the most aggressive, in these patients,” added Dr. Patel, who is also director of the cutaneous oncology program at the GW Cancer Center.
“Sometimes we lose track of what ... we need to do” to provide care that reflects the best interests of the older patient, he continued. “Surgery may be the gold standard for treating the majority of NMSCs ... but is it the [best option] for what our older patients and patients with limited life expectancy need?”
Learning about what truly matters to the patient is a key element of the “age-friendly, whole-person care” that dermatologists must embrace as older adults become an increasingly large subset of their patient population, Christina Prather, MD, director and associate professor of geriatrics and palliative medicine at George Washington University, said at the meeting.
By 2040, projections are that the number of adults aged 85 years and older in the United States will be nearly quadruple the number in 2000, according to one estimate.
“We know that there are less than 6000 practicing geriatricians in the country ... [so the healthcare system] needs more of you who know how to bring an age-friendly approach to care,” Dr. Prather said. Dermatology is among the specialties that need to be “geriatricized.”
NMSC Increasing in the Older Population
The incidence of skin cancer is rising faster than that of any other cancer, Dr. Patel said. One window into the epidemiology, he said, comes from recently published data showing that an average of 6.1 million adults were treated each year for skin cancer during 2016-2018 (5.2 million of them for NMSC) — an increase from an average of 5.8 million annually in the 2012-2015 period. The data come from the Medical Expenditure Panel Survey (MEPS), which is conducted by the US Public Health Service through the Agency for Healthcare Research and Quality and the Centers for Disease Control and Prevention.
As a frame of reference, the average number of adults treated each year for nonskin cancers during these periods rose from 10.8 to 11.9 million, according to the 2023 MEPS data. “Skin cancer is about one-third of all cancers combined,” Dr. Patel said.
Not only is the incidence of NMSC significantly higher than that of melanoma but it also shows a more prominent aging trend. This was documented recently in a long-term observational study from Japan, in which researchers looked at the change in the median age of patients with NMSC and melanoma, compared with cancers of other organs, from 1991 to 2020 and found that NMSC had by far the greatest rise in median age, to a median age of 80 years in 2021.
Even more notable, Dr. Patel said, was a particularly marked increase in the number of patients with skin cancer aged 90 years and older. In 2021, this group of older adults accounted for 17% of patients receiving treatment for skin cancer at the Japanese hospital where the data were collected.
The 2013 study that stirred Dr. Patel as a fellow was of 1536 consecutive patients diagnosed with NMSC at two dermatology clinics (a University of California San Francisco–based private clinic and a Veterans Affairs Medical Center clinic) and followed for 6 years. “What’s interesting and worth thinking about is that, regardless of patients’ life expectancy, NMSCs were treated aggressively and surgically, and the choice of surgery was not influenced by the patient’s poor prognosis in a multivariate model” adjusted for tumor and patient characteristics, he said at the meeting.
The researchers defined limited life expectancy as either 85 years or older or having a Charleston Comorbidity Index ≥ 3. Approximately half of the patients with limited life expectancy died within 5 years, none of NMSC. Most patients with limited life expectancy were not often bothered by their tumors, and approximately one in five reported a treatment complication within 2 years. The 5-year tumor recurrence rate was 3.7%.
A more recent study looked at 1181 patients older than 85 years with NMSC referred for Mohs surgery. Almost all patients in the multicenter, prospective cohort study (91.3%) were treated with Mohs.
Treated patients were more likely to have facial tumors and higher functional status than those not treated with Mohs surgery, and the most common reasons provided by surgeons for proceeding with the surgery were a patient desire for a high cure rate (66%), higher functional status for age (57%), and high-risk tumor type (40%). Almost 42% of the referred patients were 89 years or older.
“Granted, [the reasons] are justified indications for surgery,” Dr. Patel said. Yet the study brings up the question of “whether we need to do Mohs surgery this frequently in elderly patients?” In an email after the meeting, he added, “it’s a question we may need to reconsider as the elderly population continues to increase and median age of NMSC rises.”
Underutilized Management Options for NMSC
In his practice, discussions of treatment options are preceded by a thorough discussion of the disease itself. Many lesions are low risk, and helping patients understand risks, as well as understanding what is important to the patient — especially those with limited life expectancy — will guide shared decision-making to choose the best treatment, Dr. Patel said at the meeting.
The dermatologist’s risk assessment — both staging and stratifying risk as it relates to specific outcomes such as recurrence, metastases, or death — takes on added importance in the older patient, he emphasized. “I think we underutilize the risk assessment.”
Also underutilized is the option of shave removal for low-risk squamous cell carcinomas and basal cell carcinomas, Dr. Patel said, noting that, in the National Comprehensive Cancer Network guidelines, “there’s an option for shave removal and nothing more if you have clear margins.”
Alternatively, disc excision with the initial biopsy can often be considered. “Having that intent to treat at the time of biopsy may be all that needs to be done” in older patients with obvious or highly suspicious lesions, he said.
Systemic immunotherapy has joined the treatment armamentarium for advanced basal cell carcinoma and advanced cutaneous squamous cell carcinoma, and if early, ongoing research of intralesional programmed cell death protein 1 inhibitor treatment advances, this could be another option for older adults in the future, Dr. Patel said. Targeting drug delivery directly to the tumor would lower the total dose, decrease systemic exposure, and could be used to avoid surgery for some groups of patients, such as those with limited life expectancy.
A Personal Story, a Word on Melanoma
Dr. Prather recalled when her 97-year-old grandfather had a skin lesion on his forehead removed, and a conversation he had with her mother about whether he really needed to have the procedure because he had cognitive impairment and was on oral anticoagulants.
The clinician “said it absolutely had to go. ... I can’t tell you how much his doctors’ visits and wound care consumed my family’s life for the next few years — for this thing that never quite healed,” she said.
“Was it necessary? The more I’ve learned over time is that it wasn’t,” Dr. Prather added. “We have to take time [with our older patients] and think critically. What is feasible? What makes the most sense? What is the most important thing I need to know about the patient?”
Also important, Dr. Patel noted, is the big-picture consideration of skin cancer treatment costs. The MEPS survey data showing the rising prevalence of skin cancer treatment also documented the economic burden: A nearly 30% increase in the average annual cost of treating NMSC from $5 billion in 2012-2015 to $6.5 billion in 2016-2018. (The average annual costs of treating melanoma decreased slightly.) “Skin cancer is a big drain on our limited resources,” he said.
With melanoma as well, dermatologists must think critically and holistically about the individual patient — and not have “a single view lens of the disease and how we treat the disease,” said Dr. Patel, urging the audience to read a “Sounding Board” article published in The New England Journal of Medicine in 2021. The article argued that there is overdiagnosis of cutaneous melanoma stemming from increased screening, falling clinical thresholds for biopsy, and falling pathological thresholds for labeling morphologic changes as cancer.
“There’s a diagnostic disconnect and a problem of overdiagnosis ... because we’re afraid to miss or make a mistake,” he said. “It leads to the question, do all lesions denoted as skin cancers need aggressive treatment? What does it mean for the patient in front of you?”
Dr. Patel reported receiving honoraria from Regeneron, Almirall, Biofrontera, Sun Pharma, and SkylineDx and serving on the speaker bureau of Regeneron and Almirall. He is chief medical officer for Lazarus AI and is cofounder of the Skin Cancer Outcomes consortium. Dr. Prather disclosed relationships with the National Institutes of Health, AHRQ, The Washington Home Foundation, and the Alzheimer’s Association.
A version of this article appeared on Medscape.com.
WASHINGTON — In 2013, Vishal A. Patel, MD, was completing a fellowship in Mohs surgery and cutaneous oncology at Columbia University Irving Medical Center, New York City, when a study was published showing that most nonmelanoma skin cancers (NMSCs) were treated with surgery, regardless of the patient’s life expectancy. Life expectancy “should enter into treatment decisions,” the authors concluded.
“ Dr. Patel recalled at the ElderDerm conference hosted by the Department of Dermatology at George Washington University, Washington, DC, and described as a first-of-its-kind meeting dedicated to improving dermatologic care for older adults.
Today, however, more than a decade later, guidelines still promote surgical therapy as the gold standard across the board, and questions raised by the study are still unaddressed, Dr. Patel, associate professor of dermatology and medicine/oncology at George Washington University, said at the meeting. These questions are becoming increasingly urgent as the incidence of skin cancer, especially NMSC, rises in the older adult population, especially in patients older than 85 years. “It’s a function of our training and our treatment guidelines that we reach for the most definitive treatment, which happens to be the most aggressive, in these patients,” added Dr. Patel, who is also director of the cutaneous oncology program at the GW Cancer Center.
“Sometimes we lose track of what ... we need to do” to provide care that reflects the best interests of the older patient, he continued. “Surgery may be the gold standard for treating the majority of NMSCs ... but is it the [best option] for what our older patients and patients with limited life expectancy need?”
Learning about what truly matters to the patient is a key element of the “age-friendly, whole-person care” that dermatologists must embrace as older adults become an increasingly large subset of their patient population, Christina Prather, MD, director and associate professor of geriatrics and palliative medicine at George Washington University, said at the meeting.
By 2040, projections are that the number of adults aged 85 years and older in the United States will be nearly quadruple the number in 2000, according to one estimate.
“We know that there are less than 6000 practicing geriatricians in the country ... [so the healthcare system] needs more of you who know how to bring an age-friendly approach to care,” Dr. Prather said. Dermatology is among the specialties that need to be “geriatricized.”
NMSC Increasing in the Older Population
The incidence of skin cancer is rising faster than that of any other cancer, Dr. Patel said. One window into the epidemiology, he said, comes from recently published data showing that an average of 6.1 million adults were treated each year for skin cancer during 2016-2018 (5.2 million of them for NMSC) — an increase from an average of 5.8 million annually in the 2012-2015 period. The data come from the Medical Expenditure Panel Survey (MEPS), which is conducted by the US Public Health Service through the Agency for Healthcare Research and Quality and the Centers for Disease Control and Prevention.
As a frame of reference, the average number of adults treated each year for nonskin cancers during these periods rose from 10.8 to 11.9 million, according to the 2023 MEPS data. “Skin cancer is about one-third of all cancers combined,” Dr. Patel said.
Not only is the incidence of NMSC significantly higher than that of melanoma but it also shows a more prominent aging trend. This was documented recently in a long-term observational study from Japan, in which researchers looked at the change in the median age of patients with NMSC and melanoma, compared with cancers of other organs, from 1991 to 2020 and found that NMSC had by far the greatest rise in median age, to a median age of 80 years in 2021.
Even more notable, Dr. Patel said, was a particularly marked increase in the number of patients with skin cancer aged 90 years and older. In 2021, this group of older adults accounted for 17% of patients receiving treatment for skin cancer at the Japanese hospital where the data were collected.
The 2013 study that stirred Dr. Patel as a fellow was of 1536 consecutive patients diagnosed with NMSC at two dermatology clinics (a University of California San Francisco–based private clinic and a Veterans Affairs Medical Center clinic) and followed for 6 years. “What’s interesting and worth thinking about is that, regardless of patients’ life expectancy, NMSCs were treated aggressively and surgically, and the choice of surgery was not influenced by the patient’s poor prognosis in a multivariate model” adjusted for tumor and patient characteristics, he said at the meeting.
The researchers defined limited life expectancy as either 85 years or older or having a Charleston Comorbidity Index ≥ 3. Approximately half of the patients with limited life expectancy died within 5 years, none of NMSC. Most patients with limited life expectancy were not often bothered by their tumors, and approximately one in five reported a treatment complication within 2 years. The 5-year tumor recurrence rate was 3.7%.
A more recent study looked at 1181 patients older than 85 years with NMSC referred for Mohs surgery. Almost all patients in the multicenter, prospective cohort study (91.3%) were treated with Mohs.
Treated patients were more likely to have facial tumors and higher functional status than those not treated with Mohs surgery, and the most common reasons provided by surgeons for proceeding with the surgery were a patient desire for a high cure rate (66%), higher functional status for age (57%), and high-risk tumor type (40%). Almost 42% of the referred patients were 89 years or older.
“Granted, [the reasons] are justified indications for surgery,” Dr. Patel said. Yet the study brings up the question of “whether we need to do Mohs surgery this frequently in elderly patients?” In an email after the meeting, he added, “it’s a question we may need to reconsider as the elderly population continues to increase and median age of NMSC rises.”
Underutilized Management Options for NMSC
In his practice, discussions of treatment options are preceded by a thorough discussion of the disease itself. Many lesions are low risk, and helping patients understand risks, as well as understanding what is important to the patient — especially those with limited life expectancy — will guide shared decision-making to choose the best treatment, Dr. Patel said at the meeting.
The dermatologist’s risk assessment — both staging and stratifying risk as it relates to specific outcomes such as recurrence, metastases, or death — takes on added importance in the older patient, he emphasized. “I think we underutilize the risk assessment.”
Also underutilized is the option of shave removal for low-risk squamous cell carcinomas and basal cell carcinomas, Dr. Patel said, noting that, in the National Comprehensive Cancer Network guidelines, “there’s an option for shave removal and nothing more if you have clear margins.”
Alternatively, disc excision with the initial biopsy can often be considered. “Having that intent to treat at the time of biopsy may be all that needs to be done” in older patients with obvious or highly suspicious lesions, he said.
Systemic immunotherapy has joined the treatment armamentarium for advanced basal cell carcinoma and advanced cutaneous squamous cell carcinoma, and if early, ongoing research of intralesional programmed cell death protein 1 inhibitor treatment advances, this could be another option for older adults in the future, Dr. Patel said. Targeting drug delivery directly to the tumor would lower the total dose, decrease systemic exposure, and could be used to avoid surgery for some groups of patients, such as those with limited life expectancy.
A Personal Story, a Word on Melanoma
Dr. Prather recalled when her 97-year-old grandfather had a skin lesion on his forehead removed, and a conversation he had with her mother about whether he really needed to have the procedure because he had cognitive impairment and was on oral anticoagulants.
The clinician “said it absolutely had to go. ... I can’t tell you how much his doctors’ visits and wound care consumed my family’s life for the next few years — for this thing that never quite healed,” she said.
“Was it necessary? The more I’ve learned over time is that it wasn’t,” Dr. Prather added. “We have to take time [with our older patients] and think critically. What is feasible? What makes the most sense? What is the most important thing I need to know about the patient?”
Also important, Dr. Patel noted, is the big-picture consideration of skin cancer treatment costs. The MEPS survey data showing the rising prevalence of skin cancer treatment also documented the economic burden: A nearly 30% increase in the average annual cost of treating NMSC from $5 billion in 2012-2015 to $6.5 billion in 2016-2018. (The average annual costs of treating melanoma decreased slightly.) “Skin cancer is a big drain on our limited resources,” he said.
With melanoma as well, dermatologists must think critically and holistically about the individual patient — and not have “a single view lens of the disease and how we treat the disease,” said Dr. Patel, urging the audience to read a “Sounding Board” article published in The New England Journal of Medicine in 2021. The article argued that there is overdiagnosis of cutaneous melanoma stemming from increased screening, falling clinical thresholds for biopsy, and falling pathological thresholds for labeling morphologic changes as cancer.
“There’s a diagnostic disconnect and a problem of overdiagnosis ... because we’re afraid to miss or make a mistake,” he said. “It leads to the question, do all lesions denoted as skin cancers need aggressive treatment? What does it mean for the patient in front of you?”
Dr. Patel reported receiving honoraria from Regeneron, Almirall, Biofrontera, Sun Pharma, and SkylineDx and serving on the speaker bureau of Regeneron and Almirall. He is chief medical officer for Lazarus AI and is cofounder of the Skin Cancer Outcomes consortium. Dr. Prather disclosed relationships with the National Institutes of Health, AHRQ, The Washington Home Foundation, and the Alzheimer’s Association.
A version of this article appeared on Medscape.com.
WASHINGTON — In 2013, Vishal A. Patel, MD, was completing a fellowship in Mohs surgery and cutaneous oncology at Columbia University Irving Medical Center, New York City, when a study was published showing that most nonmelanoma skin cancers (NMSCs) were treated with surgery, regardless of the patient’s life expectancy. Life expectancy “should enter into treatment decisions,” the authors concluded.
“ Dr. Patel recalled at the ElderDerm conference hosted by the Department of Dermatology at George Washington University, Washington, DC, and described as a first-of-its-kind meeting dedicated to improving dermatologic care for older adults.
Today, however, more than a decade later, guidelines still promote surgical therapy as the gold standard across the board, and questions raised by the study are still unaddressed, Dr. Patel, associate professor of dermatology and medicine/oncology at George Washington University, said at the meeting. These questions are becoming increasingly urgent as the incidence of skin cancer, especially NMSC, rises in the older adult population, especially in patients older than 85 years. “It’s a function of our training and our treatment guidelines that we reach for the most definitive treatment, which happens to be the most aggressive, in these patients,” added Dr. Patel, who is also director of the cutaneous oncology program at the GW Cancer Center.
“Sometimes we lose track of what ... we need to do” to provide care that reflects the best interests of the older patient, he continued. “Surgery may be the gold standard for treating the majority of NMSCs ... but is it the [best option] for what our older patients and patients with limited life expectancy need?”
Learning about what truly matters to the patient is a key element of the “age-friendly, whole-person care” that dermatologists must embrace as older adults become an increasingly large subset of their patient population, Christina Prather, MD, director and associate professor of geriatrics and palliative medicine at George Washington University, said at the meeting.
By 2040, projections are that the number of adults aged 85 years and older in the United States will be nearly quadruple the number in 2000, according to one estimate.
“We know that there are less than 6000 practicing geriatricians in the country ... [so the healthcare system] needs more of you who know how to bring an age-friendly approach to care,” Dr. Prather said. Dermatology is among the specialties that need to be “geriatricized.”
NMSC Increasing in the Older Population
The incidence of skin cancer is rising faster than that of any other cancer, Dr. Patel said. One window into the epidemiology, he said, comes from recently published data showing that an average of 6.1 million adults were treated each year for skin cancer during 2016-2018 (5.2 million of them for NMSC) — an increase from an average of 5.8 million annually in the 2012-2015 period. The data come from the Medical Expenditure Panel Survey (MEPS), which is conducted by the US Public Health Service through the Agency for Healthcare Research and Quality and the Centers for Disease Control and Prevention.
As a frame of reference, the average number of adults treated each year for nonskin cancers during these periods rose from 10.8 to 11.9 million, according to the 2023 MEPS data. “Skin cancer is about one-third of all cancers combined,” Dr. Patel said.
Not only is the incidence of NMSC significantly higher than that of melanoma but it also shows a more prominent aging trend. This was documented recently in a long-term observational study from Japan, in which researchers looked at the change in the median age of patients with NMSC and melanoma, compared with cancers of other organs, from 1991 to 2020 and found that NMSC had by far the greatest rise in median age, to a median age of 80 years in 2021.
Even more notable, Dr. Patel said, was a particularly marked increase in the number of patients with skin cancer aged 90 years and older. In 2021, this group of older adults accounted for 17% of patients receiving treatment for skin cancer at the Japanese hospital where the data were collected.
The 2013 study that stirred Dr. Patel as a fellow was of 1536 consecutive patients diagnosed with NMSC at two dermatology clinics (a University of California San Francisco–based private clinic and a Veterans Affairs Medical Center clinic) and followed for 6 years. “What’s interesting and worth thinking about is that, regardless of patients’ life expectancy, NMSCs were treated aggressively and surgically, and the choice of surgery was not influenced by the patient’s poor prognosis in a multivariate model” adjusted for tumor and patient characteristics, he said at the meeting.
The researchers defined limited life expectancy as either 85 years or older or having a Charleston Comorbidity Index ≥ 3. Approximately half of the patients with limited life expectancy died within 5 years, none of NMSC. Most patients with limited life expectancy were not often bothered by their tumors, and approximately one in five reported a treatment complication within 2 years. The 5-year tumor recurrence rate was 3.7%.
A more recent study looked at 1181 patients older than 85 years with NMSC referred for Mohs surgery. Almost all patients in the multicenter, prospective cohort study (91.3%) were treated with Mohs.
Treated patients were more likely to have facial tumors and higher functional status than those not treated with Mohs surgery, and the most common reasons provided by surgeons for proceeding with the surgery were a patient desire for a high cure rate (66%), higher functional status for age (57%), and high-risk tumor type (40%). Almost 42% of the referred patients were 89 years or older.
“Granted, [the reasons] are justified indications for surgery,” Dr. Patel said. Yet the study brings up the question of “whether we need to do Mohs surgery this frequently in elderly patients?” In an email after the meeting, he added, “it’s a question we may need to reconsider as the elderly population continues to increase and median age of NMSC rises.”
Underutilized Management Options for NMSC
In his practice, discussions of treatment options are preceded by a thorough discussion of the disease itself. Many lesions are low risk, and helping patients understand risks, as well as understanding what is important to the patient — especially those with limited life expectancy — will guide shared decision-making to choose the best treatment, Dr. Patel said at the meeting.
The dermatologist’s risk assessment — both staging and stratifying risk as it relates to specific outcomes such as recurrence, metastases, or death — takes on added importance in the older patient, he emphasized. “I think we underutilize the risk assessment.”
Also underutilized is the option of shave removal for low-risk squamous cell carcinomas and basal cell carcinomas, Dr. Patel said, noting that, in the National Comprehensive Cancer Network guidelines, “there’s an option for shave removal and nothing more if you have clear margins.”
Alternatively, disc excision with the initial biopsy can often be considered. “Having that intent to treat at the time of biopsy may be all that needs to be done” in older patients with obvious or highly suspicious lesions, he said.
Systemic immunotherapy has joined the treatment armamentarium for advanced basal cell carcinoma and advanced cutaneous squamous cell carcinoma, and if early, ongoing research of intralesional programmed cell death protein 1 inhibitor treatment advances, this could be another option for older adults in the future, Dr. Patel said. Targeting drug delivery directly to the tumor would lower the total dose, decrease systemic exposure, and could be used to avoid surgery for some groups of patients, such as those with limited life expectancy.
A Personal Story, a Word on Melanoma
Dr. Prather recalled when her 97-year-old grandfather had a skin lesion on his forehead removed, and a conversation he had with her mother about whether he really needed to have the procedure because he had cognitive impairment and was on oral anticoagulants.
The clinician “said it absolutely had to go. ... I can’t tell you how much his doctors’ visits and wound care consumed my family’s life for the next few years — for this thing that never quite healed,” she said.
“Was it necessary? The more I’ve learned over time is that it wasn’t,” Dr. Prather added. “We have to take time [with our older patients] and think critically. What is feasible? What makes the most sense? What is the most important thing I need to know about the patient?”
Also important, Dr. Patel noted, is the big-picture consideration of skin cancer treatment costs. The MEPS survey data showing the rising prevalence of skin cancer treatment also documented the economic burden: A nearly 30% increase in the average annual cost of treating NMSC from $5 billion in 2012-2015 to $6.5 billion in 2016-2018. (The average annual costs of treating melanoma decreased slightly.) “Skin cancer is a big drain on our limited resources,” he said.
With melanoma as well, dermatologists must think critically and holistically about the individual patient — and not have “a single view lens of the disease and how we treat the disease,” said Dr. Patel, urging the audience to read a “Sounding Board” article published in The New England Journal of Medicine in 2021. The article argued that there is overdiagnosis of cutaneous melanoma stemming from increased screening, falling clinical thresholds for biopsy, and falling pathological thresholds for labeling morphologic changes as cancer.
“There’s a diagnostic disconnect and a problem of overdiagnosis ... because we’re afraid to miss or make a mistake,” he said. “It leads to the question, do all lesions denoted as skin cancers need aggressive treatment? What does it mean for the patient in front of you?”
Dr. Patel reported receiving honoraria from Regeneron, Almirall, Biofrontera, Sun Pharma, and SkylineDx and serving on the speaker bureau of Regeneron and Almirall. He is chief medical officer for Lazarus AI and is cofounder of the Skin Cancer Outcomes consortium. Dr. Prather disclosed relationships with the National Institutes of Health, AHRQ, The Washington Home Foundation, and the Alzheimer’s Association.
A version of this article appeared on Medscape.com.
Ixekizumab Met Phase 3 Trial Endpoint in Juvenile PsA, Enthesitis-Related Arthritis
VIENNA — Ixekizumab (Taltz), an interleukin-17A inhibitor that’s already approved for the treatment of psoriatic arthritis and axial spondyloarthritis in adults appears likely to be granted the same corresponding indications for children, based on initial results from an open-label, phase 3 trial that employed adalimumab as a reference.
With a safety profile comparable with that seen in adult patients, ixekizumab “met the prespecified criterion for success at 16 weeks,” reported Athimalaipet V. Ramanan, MD, PhD, of Bristol Royal Hospital for Children and Translational Health Sciences, Bristol, England.
In this multicenter, randomized, open-label trial called COSPIRIT-JIA, which is still ongoing, investigators enrolled 101 children with active juvenile PsA (JPsA) or enthesitis-related arthritis (ERA), which is akin to spondyloarthritis in adults.
The efficacy and safety data at 16 weeks were presented as a late-breaking abstract at the annual European Congress of Rheumatology. Dr. Ramanan said that the open-label extension to 104 weeks is underway and further follow-up out to 264 weeks is planned.
Nearly 90% Achieve ACR30
The trial had an adaptive design in which the first 40 patients without biologics experience were randomized to ixekizumab or adalimumab, stratified by JPsA or ERA diagnosis, and the following 61 patients with either no biologic experience or an inadequate response or intolerance to biologics all received ixekizumab. The drugs were dosed according to weight. Dr. Ramanan explained that a placebo-controlled trial was considered unethical because of the strong evidence of benefit from biologics for JPsA and ERA.
The trial easily met its predefined threshold for success, which required ≥ 80% probability, based on Bayesian analysis, that ≥ 50% of patients would have 30% improvement in American College of Rheumatology response criteria (ACR30) at week 16. ACR30 was achieved in 88.9% of those treated with ixekizumab overall vs 95.0% of those treated with adalimumab, but the trial was not designed as a head-to-head comparison. Rather, adalimumab served as a reference.
When compared for the distinct diseases, the ACR30 rates were also numerically lower for ixekizumab relative to adalimumab for both ERA (88.9% vs 93.8%) and JPsA (88.9% vs 100%), but all of the adalimumab patients were naive to biologics. In comparison, about 75% of patients receiving ixekizumab were biologic-therapy naive.
Response rates to ixekizumab overall were numerically higher for patients without previous biologic experience than for those with experience (90.0% vs 85.7%), and this was also the case for patients with ERA (92.5% vs 78.6%). However, in the JPsA group, biologic-experienced patients had higher numerical response rates to ixekizumab (100% vs 85.0%).
An ACR30 is not a clinical goal that satisfies most patients and clinicians, Dr. Ramanan conceded, but he noted that ACR50 was reached with ixekizumab by 81.5% with ERA and 74.1% with JPsA, and ACR70 was reached by 68.5% and 55.6%, respectively. The highest responses of ACR90 (27.8% and 33.3%) and ACR100 (14.8% and 25.9%) were lower but still substantial in the ERA and JPsA groups, respectively.
Through week 16, 58.0% of those treated with ixekizumab had an adverse event considered treatment-related. Nearly half were of mild severity, and the remainder were moderate. Only 3.7% were considered serious. No patient discontinued study treatment because of an adverse event.
In this study, the presence of at least three active peripheral joints was an inclusion criterion. The median age was about 13 years in the biologic-naive adalimumab and ixekizumab groups and 14 years in the ixekizumab biologic-experienced group. The youngest patient in the study was aged 5 years, and the oldest was aged 18 years. Although about 40% of patients were women in the two biologic-naive subgroups, it was 60% in the biologic-experienced group.
On average, patients in the biologic-naive group were entered about 1 year after diagnosis. In the experienced patients, the average duration of disease at entry was nearly 4 years. About 45% of patients remained on conventional synthetic disease-modifying antirheumatic drugs while receiving ixekizumab. The proportion was 35% in the adalimumab reference arm.
Ixekizumab Might Fulfill Need for More Options
There are several biologics that have received regulatory approval or are already widely used for the treatment of JPsA or ERA, but more options are needed, according to Dr. Ramanan and the chair of the abstract session in which these data were reported. According to Caroline Ospelt, MD, PhD, a researcher at the Center for Experimental Rheumatology, University Hospital Zurich, Switzerland, regulatory approval of ixekizumab will depend on sustained efficacy and safety in longer follow-up from the COSPIRIT-JIA trial, but this trial supports continued development.
Despite a novel mechanism of action, “the data so far suggest a level of efficacy similar to that of anti-TNF [anti-tumor necrosis factor] biologics,” said Dr. Ospelt, who, in addition to moderating the late-breaking session, served as Scientific Program Chair of EULAR 2024.
While Dr. Ospelt emphasized that she is a researcher involved in translational rheumatology studies and not a clinician, she said there was consensus within the program committee to select this abstract from other high-quality latebreaker submissions on the basis of its potential clinical significance.
Dr. Ramanan reported financial relationships with AbbVie, AstraZeneca, Novartis, Pfizer, Roche, SOBI, UCB, and Eli Lilly, which provided funding for this study. Dr. Ospelt reported no potential conflicts of interest.
A version of this article first appeared on Medscape.com.
VIENNA — Ixekizumab (Taltz), an interleukin-17A inhibitor that’s already approved for the treatment of psoriatic arthritis and axial spondyloarthritis in adults appears likely to be granted the same corresponding indications for children, based on initial results from an open-label, phase 3 trial that employed adalimumab as a reference.
With a safety profile comparable with that seen in adult patients, ixekizumab “met the prespecified criterion for success at 16 weeks,” reported Athimalaipet V. Ramanan, MD, PhD, of Bristol Royal Hospital for Children and Translational Health Sciences, Bristol, England.
In this multicenter, randomized, open-label trial called COSPIRIT-JIA, which is still ongoing, investigators enrolled 101 children with active juvenile PsA (JPsA) or enthesitis-related arthritis (ERA), which is akin to spondyloarthritis in adults.
The efficacy and safety data at 16 weeks were presented as a late-breaking abstract at the annual European Congress of Rheumatology. Dr. Ramanan said that the open-label extension to 104 weeks is underway and further follow-up out to 264 weeks is planned.
Nearly 90% Achieve ACR30
The trial had an adaptive design in which the first 40 patients without biologics experience were randomized to ixekizumab or adalimumab, stratified by JPsA or ERA diagnosis, and the following 61 patients with either no biologic experience or an inadequate response or intolerance to biologics all received ixekizumab. The drugs were dosed according to weight. Dr. Ramanan explained that a placebo-controlled trial was considered unethical because of the strong evidence of benefit from biologics for JPsA and ERA.
The trial easily met its predefined threshold for success, which required ≥ 80% probability, based on Bayesian analysis, that ≥ 50% of patients would have 30% improvement in American College of Rheumatology response criteria (ACR30) at week 16. ACR30 was achieved in 88.9% of those treated with ixekizumab overall vs 95.0% of those treated with adalimumab, but the trial was not designed as a head-to-head comparison. Rather, adalimumab served as a reference.
When compared for the distinct diseases, the ACR30 rates were also numerically lower for ixekizumab relative to adalimumab for both ERA (88.9% vs 93.8%) and JPsA (88.9% vs 100%), but all of the adalimumab patients were naive to biologics. In comparison, about 75% of patients receiving ixekizumab were biologic-therapy naive.
Response rates to ixekizumab overall were numerically higher for patients without previous biologic experience than for those with experience (90.0% vs 85.7%), and this was also the case for patients with ERA (92.5% vs 78.6%). However, in the JPsA group, biologic-experienced patients had higher numerical response rates to ixekizumab (100% vs 85.0%).
An ACR30 is not a clinical goal that satisfies most patients and clinicians, Dr. Ramanan conceded, but he noted that ACR50 was reached with ixekizumab by 81.5% with ERA and 74.1% with JPsA, and ACR70 was reached by 68.5% and 55.6%, respectively. The highest responses of ACR90 (27.8% and 33.3%) and ACR100 (14.8% and 25.9%) were lower but still substantial in the ERA and JPsA groups, respectively.
Through week 16, 58.0% of those treated with ixekizumab had an adverse event considered treatment-related. Nearly half were of mild severity, and the remainder were moderate. Only 3.7% were considered serious. No patient discontinued study treatment because of an adverse event.
In this study, the presence of at least three active peripheral joints was an inclusion criterion. The median age was about 13 years in the biologic-naive adalimumab and ixekizumab groups and 14 years in the ixekizumab biologic-experienced group. The youngest patient in the study was aged 5 years, and the oldest was aged 18 years. Although about 40% of patients were women in the two biologic-naive subgroups, it was 60% in the biologic-experienced group.
On average, patients in the biologic-naive group were entered about 1 year after diagnosis. In the experienced patients, the average duration of disease at entry was nearly 4 years. About 45% of patients remained on conventional synthetic disease-modifying antirheumatic drugs while receiving ixekizumab. The proportion was 35% in the adalimumab reference arm.
Ixekizumab Might Fulfill Need for More Options
There are several biologics that have received regulatory approval or are already widely used for the treatment of JPsA or ERA, but more options are needed, according to Dr. Ramanan and the chair of the abstract session in which these data were reported. According to Caroline Ospelt, MD, PhD, a researcher at the Center for Experimental Rheumatology, University Hospital Zurich, Switzerland, regulatory approval of ixekizumab will depend on sustained efficacy and safety in longer follow-up from the COSPIRIT-JIA trial, but this trial supports continued development.
Despite a novel mechanism of action, “the data so far suggest a level of efficacy similar to that of anti-TNF [anti-tumor necrosis factor] biologics,” said Dr. Ospelt, who, in addition to moderating the late-breaking session, served as Scientific Program Chair of EULAR 2024.
While Dr. Ospelt emphasized that she is a researcher involved in translational rheumatology studies and not a clinician, she said there was consensus within the program committee to select this abstract from other high-quality latebreaker submissions on the basis of its potential clinical significance.
Dr. Ramanan reported financial relationships with AbbVie, AstraZeneca, Novartis, Pfizer, Roche, SOBI, UCB, and Eli Lilly, which provided funding for this study. Dr. Ospelt reported no potential conflicts of interest.
A version of this article first appeared on Medscape.com.
VIENNA — Ixekizumab (Taltz), an interleukin-17A inhibitor that’s already approved for the treatment of psoriatic arthritis and axial spondyloarthritis in adults appears likely to be granted the same corresponding indications for children, based on initial results from an open-label, phase 3 trial that employed adalimumab as a reference.
With a safety profile comparable with that seen in adult patients, ixekizumab “met the prespecified criterion for success at 16 weeks,” reported Athimalaipet V. Ramanan, MD, PhD, of Bristol Royal Hospital for Children and Translational Health Sciences, Bristol, England.
In this multicenter, randomized, open-label trial called COSPIRIT-JIA, which is still ongoing, investigators enrolled 101 children with active juvenile PsA (JPsA) or enthesitis-related arthritis (ERA), which is akin to spondyloarthritis in adults.
The efficacy and safety data at 16 weeks were presented as a late-breaking abstract at the annual European Congress of Rheumatology. Dr. Ramanan said that the open-label extension to 104 weeks is underway and further follow-up out to 264 weeks is planned.
Nearly 90% Achieve ACR30
The trial had an adaptive design in which the first 40 patients without biologics experience were randomized to ixekizumab or adalimumab, stratified by JPsA or ERA diagnosis, and the following 61 patients with either no biologic experience or an inadequate response or intolerance to biologics all received ixekizumab. The drugs were dosed according to weight. Dr. Ramanan explained that a placebo-controlled trial was considered unethical because of the strong evidence of benefit from biologics for JPsA and ERA.
The trial easily met its predefined threshold for success, which required ≥ 80% probability, based on Bayesian analysis, that ≥ 50% of patients would have 30% improvement in American College of Rheumatology response criteria (ACR30) at week 16. ACR30 was achieved in 88.9% of those treated with ixekizumab overall vs 95.0% of those treated with adalimumab, but the trial was not designed as a head-to-head comparison. Rather, adalimumab served as a reference.
When compared for the distinct diseases, the ACR30 rates were also numerically lower for ixekizumab relative to adalimumab for both ERA (88.9% vs 93.8%) and JPsA (88.9% vs 100%), but all of the adalimumab patients were naive to biologics. In comparison, about 75% of patients receiving ixekizumab were biologic-therapy naive.
Response rates to ixekizumab overall were numerically higher for patients without previous biologic experience than for those with experience (90.0% vs 85.7%), and this was also the case for patients with ERA (92.5% vs 78.6%). However, in the JPsA group, biologic-experienced patients had higher numerical response rates to ixekizumab (100% vs 85.0%).
An ACR30 is not a clinical goal that satisfies most patients and clinicians, Dr. Ramanan conceded, but he noted that ACR50 was reached with ixekizumab by 81.5% with ERA and 74.1% with JPsA, and ACR70 was reached by 68.5% and 55.6%, respectively. The highest responses of ACR90 (27.8% and 33.3%) and ACR100 (14.8% and 25.9%) were lower but still substantial in the ERA and JPsA groups, respectively.
Through week 16, 58.0% of those treated with ixekizumab had an adverse event considered treatment-related. Nearly half were of mild severity, and the remainder were moderate. Only 3.7% were considered serious. No patient discontinued study treatment because of an adverse event.
In this study, the presence of at least three active peripheral joints was an inclusion criterion. The median age was about 13 years in the biologic-naive adalimumab and ixekizumab groups and 14 years in the ixekizumab biologic-experienced group. The youngest patient in the study was aged 5 years, and the oldest was aged 18 years. Although about 40% of patients were women in the two biologic-naive subgroups, it was 60% in the biologic-experienced group.
On average, patients in the biologic-naive group were entered about 1 year after diagnosis. In the experienced patients, the average duration of disease at entry was nearly 4 years. About 45% of patients remained on conventional synthetic disease-modifying antirheumatic drugs while receiving ixekizumab. The proportion was 35% in the adalimumab reference arm.
Ixekizumab Might Fulfill Need for More Options
There are several biologics that have received regulatory approval or are already widely used for the treatment of JPsA or ERA, but more options are needed, according to Dr. Ramanan and the chair of the abstract session in which these data were reported. According to Caroline Ospelt, MD, PhD, a researcher at the Center for Experimental Rheumatology, University Hospital Zurich, Switzerland, regulatory approval of ixekizumab will depend on sustained efficacy and safety in longer follow-up from the COSPIRIT-JIA trial, but this trial supports continued development.
Despite a novel mechanism of action, “the data so far suggest a level of efficacy similar to that of anti-TNF [anti-tumor necrosis factor] biologics,” said Dr. Ospelt, who, in addition to moderating the late-breaking session, served as Scientific Program Chair of EULAR 2024.
While Dr. Ospelt emphasized that she is a researcher involved in translational rheumatology studies and not a clinician, she said there was consensus within the program committee to select this abstract from other high-quality latebreaker submissions on the basis of its potential clinical significance.
Dr. Ramanan reported financial relationships with AbbVie, AstraZeneca, Novartis, Pfizer, Roche, SOBI, UCB, and Eli Lilly, which provided funding for this study. Dr. Ospelt reported no potential conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM EULAR 2024
Medicare Advantage Plans Not Always Advantageous
While Medicare Advantage (MA) plans are marketed as providing more generous benefits than traditional Medicare (TM), differences in the financial burden between beneficiaries switching to MA and staying with TM, are minimal, a longitudinal cohort analysis found.
In fact, according to a study by Sungchul Park, PhD, a health economist at Korea University in Seoul, and colleagues, the estimated annual out-of-pocket spending when switching to MA was $168 higher than staying in TM. That amounted to a 10.5% relative increase based on baseline out-of-pocket spending of $1597 annually among switchers, ranging widely, however, from a $133 decrease to a $469 increase. And for some, MA enrollment was associated with a higher likelihood of catastrophic financial burden.
“Our findings contrast with the notion that MA’s apparently more generous health insurance benefits lead to financial savings for enrollees,” Dr. Park and associates wrote in Annals of Internal Medicine.
The study
The analysis looked at costs for 7054 TM stayers and 1544 TM-to-MA switchers from the 2014-2020 Medical Expenditure Panel Survey, focusing on a cohort in which 18% of TM-covered individuals in year 1 switched to MA in year 2.
Comparative financial outcome measures included individual healthcare costs (out-of-pocket spending/cost sharing), financial burden (high/catastrophic), and subjective financial hardship (difficulty paying medical bills).
Although the overall out-of-pocket differences for MA were minimal and amounted to less than 1% of total healthcare expenses, MA was associated with a greater financial burden in vulnerable, especially in low-income populations. For every 100 beneficiaries with family incomes below 200% of the federal poverty level, one to six more switchers faced a catastrophic financial burden, with their out-of-pocket costs consuming more than 40% of household income in the year after switching.
The gap between the perception of lower costs and reality may be caused by a substantially heavier cost-sharing burden for certain services in MA plans, Dr. Park and associates pointed out. While MA enrollees generally paid less in some studies than the Part A hospital deductible for TM for inpatient stays of 3 days, they were more likely to face higher cost sharing for stays exceeding 7 days
Furthermore, whereas TM covers home health services without cost sharing, some MA plans have copayments. In addition, out-of-network health services can cost more. MA enrollees paid an average of $9 more for mental health services than for other in-network services and often encountered limited access to in-network providers. According to a 2021 study, only 18.2% of mental health professionals, 34.4% of cardiologists, 50.0% of psychiatrists, and 57.9% of primary care providers were included in MA networks,
An accompanying editorial noted that private MA plans will reap $83 billion in overpayments from U.S. taxpayers this year, according to Congress’s Medicare Payment Advisory Commission.
And as the data from Dr. Park and colleagues reveal, switchers don’t get much financial protection, according to primary care physician and healthcare researcher Steffi J. Woolhandler, MD, MPH, and internist David U. Himmelstein, MD, both of City University of New York at Hunter College in New York City.
“Medicare Advantage looks good when you’re healthy and don’t need much care. But when you need coverage, it often fails, leaving you with big bills and narrow choices for care,” Dr. Woolhandler said in an interview.
So how do these findings square with insurers’ hard-sell claims and enrollees’ perceptions that MA cuts out-of-pocket costs? “The likeliest explanation is that MA insurers have structured their benefits to advantage low-cost (that is, profitable) enrollees and disadvantage those requiring expensive care,” the editorial commentators wrote. For beneficiaries on inexpensive medications, MA plans would be a financial win. “But for patients requiring expensive chemotherapies, the 20% coinsurance that most MA plans charge could be financially ruinous.”
Commenting on the study but not involved in it, David A. Lipschutz, JD, LLB, associate director of the Center for Medicare Advocacy in Washington, DC, called the study an important one that provides more evidence that significant overpayments to MA plans don’t translate to better financial protections for plan enrollees, particularly lower-income individuals. “While there has been some recent movement to hold plans more accountable for providing necessary care, much more impactful action by policymakers is required to mitigate the harms of the growing privatization of the Medicare program,” he said. “MA overpayments could be redistributed to traditional Medicare in order to enrich all Medicare beneficiaries instead of just insurance companies.”
This study was supported by the National Research Foundation of Korea. Dr. Park disclosed no competing interests. One study coauthor reported support from government and not-for-profit research-funding bodies. Editorialists Dr. Woolhandler and Dr. Himmelstein had no competing interests to declare. Dr. Lipschutz disclosed Medicare advocacy work.
While Medicare Advantage (MA) plans are marketed as providing more generous benefits than traditional Medicare (TM), differences in the financial burden between beneficiaries switching to MA and staying with TM, are minimal, a longitudinal cohort analysis found.
In fact, according to a study by Sungchul Park, PhD, a health economist at Korea University in Seoul, and colleagues, the estimated annual out-of-pocket spending when switching to MA was $168 higher than staying in TM. That amounted to a 10.5% relative increase based on baseline out-of-pocket spending of $1597 annually among switchers, ranging widely, however, from a $133 decrease to a $469 increase. And for some, MA enrollment was associated with a higher likelihood of catastrophic financial burden.
“Our findings contrast with the notion that MA’s apparently more generous health insurance benefits lead to financial savings for enrollees,” Dr. Park and associates wrote in Annals of Internal Medicine.
The study
The analysis looked at costs for 7054 TM stayers and 1544 TM-to-MA switchers from the 2014-2020 Medical Expenditure Panel Survey, focusing on a cohort in which 18% of TM-covered individuals in year 1 switched to MA in year 2.
Comparative financial outcome measures included individual healthcare costs (out-of-pocket spending/cost sharing), financial burden (high/catastrophic), and subjective financial hardship (difficulty paying medical bills).
Although the overall out-of-pocket differences for MA were minimal and amounted to less than 1% of total healthcare expenses, MA was associated with a greater financial burden in vulnerable, especially in low-income populations. For every 100 beneficiaries with family incomes below 200% of the federal poverty level, one to six more switchers faced a catastrophic financial burden, with their out-of-pocket costs consuming more than 40% of household income in the year after switching.
The gap between the perception of lower costs and reality may be caused by a substantially heavier cost-sharing burden for certain services in MA plans, Dr. Park and associates pointed out. While MA enrollees generally paid less in some studies than the Part A hospital deductible for TM for inpatient stays of 3 days, they were more likely to face higher cost sharing for stays exceeding 7 days
Furthermore, whereas TM covers home health services without cost sharing, some MA plans have copayments. In addition, out-of-network health services can cost more. MA enrollees paid an average of $9 more for mental health services than for other in-network services and often encountered limited access to in-network providers. According to a 2021 study, only 18.2% of mental health professionals, 34.4% of cardiologists, 50.0% of psychiatrists, and 57.9% of primary care providers were included in MA networks,
An accompanying editorial noted that private MA plans will reap $83 billion in overpayments from U.S. taxpayers this year, according to Congress’s Medicare Payment Advisory Commission.
And as the data from Dr. Park and colleagues reveal, switchers don’t get much financial protection, according to primary care physician and healthcare researcher Steffi J. Woolhandler, MD, MPH, and internist David U. Himmelstein, MD, both of City University of New York at Hunter College in New York City.
“Medicare Advantage looks good when you’re healthy and don’t need much care. But when you need coverage, it often fails, leaving you with big bills and narrow choices for care,” Dr. Woolhandler said in an interview.
So how do these findings square with insurers’ hard-sell claims and enrollees’ perceptions that MA cuts out-of-pocket costs? “The likeliest explanation is that MA insurers have structured their benefits to advantage low-cost (that is, profitable) enrollees and disadvantage those requiring expensive care,” the editorial commentators wrote. For beneficiaries on inexpensive medications, MA plans would be a financial win. “But for patients requiring expensive chemotherapies, the 20% coinsurance that most MA plans charge could be financially ruinous.”
Commenting on the study but not involved in it, David A. Lipschutz, JD, LLB, associate director of the Center for Medicare Advocacy in Washington, DC, called the study an important one that provides more evidence that significant overpayments to MA plans don’t translate to better financial protections for plan enrollees, particularly lower-income individuals. “While there has been some recent movement to hold plans more accountable for providing necessary care, much more impactful action by policymakers is required to mitigate the harms of the growing privatization of the Medicare program,” he said. “MA overpayments could be redistributed to traditional Medicare in order to enrich all Medicare beneficiaries instead of just insurance companies.”
This study was supported by the National Research Foundation of Korea. Dr. Park disclosed no competing interests. One study coauthor reported support from government and not-for-profit research-funding bodies. Editorialists Dr. Woolhandler and Dr. Himmelstein had no competing interests to declare. Dr. Lipschutz disclosed Medicare advocacy work.
While Medicare Advantage (MA) plans are marketed as providing more generous benefits than traditional Medicare (TM), differences in the financial burden between beneficiaries switching to MA and staying with TM, are minimal, a longitudinal cohort analysis found.
In fact, according to a study by Sungchul Park, PhD, a health economist at Korea University in Seoul, and colleagues, the estimated annual out-of-pocket spending when switching to MA was $168 higher than staying in TM. That amounted to a 10.5% relative increase based on baseline out-of-pocket spending of $1597 annually among switchers, ranging widely, however, from a $133 decrease to a $469 increase. And for some, MA enrollment was associated with a higher likelihood of catastrophic financial burden.
“Our findings contrast with the notion that MA’s apparently more generous health insurance benefits lead to financial savings for enrollees,” Dr. Park and associates wrote in Annals of Internal Medicine.
The study
The analysis looked at costs for 7054 TM stayers and 1544 TM-to-MA switchers from the 2014-2020 Medical Expenditure Panel Survey, focusing on a cohort in which 18% of TM-covered individuals in year 1 switched to MA in year 2.
Comparative financial outcome measures included individual healthcare costs (out-of-pocket spending/cost sharing), financial burden (high/catastrophic), and subjective financial hardship (difficulty paying medical bills).
Although the overall out-of-pocket differences for MA were minimal and amounted to less than 1% of total healthcare expenses, MA was associated with a greater financial burden in vulnerable, especially in low-income populations. For every 100 beneficiaries with family incomes below 200% of the federal poverty level, one to six more switchers faced a catastrophic financial burden, with their out-of-pocket costs consuming more than 40% of household income in the year after switching.
The gap between the perception of lower costs and reality may be caused by a substantially heavier cost-sharing burden for certain services in MA plans, Dr. Park and associates pointed out. While MA enrollees generally paid less in some studies than the Part A hospital deductible for TM for inpatient stays of 3 days, they were more likely to face higher cost sharing for stays exceeding 7 days
Furthermore, whereas TM covers home health services without cost sharing, some MA plans have copayments. In addition, out-of-network health services can cost more. MA enrollees paid an average of $9 more for mental health services than for other in-network services and often encountered limited access to in-network providers. According to a 2021 study, only 18.2% of mental health professionals, 34.4% of cardiologists, 50.0% of psychiatrists, and 57.9% of primary care providers were included in MA networks,
An accompanying editorial noted that private MA plans will reap $83 billion in overpayments from U.S. taxpayers this year, according to Congress’s Medicare Payment Advisory Commission.
And as the data from Dr. Park and colleagues reveal, switchers don’t get much financial protection, according to primary care physician and healthcare researcher Steffi J. Woolhandler, MD, MPH, and internist David U. Himmelstein, MD, both of City University of New York at Hunter College in New York City.
“Medicare Advantage looks good when you’re healthy and don’t need much care. But when you need coverage, it often fails, leaving you with big bills and narrow choices for care,” Dr. Woolhandler said in an interview.
So how do these findings square with insurers’ hard-sell claims and enrollees’ perceptions that MA cuts out-of-pocket costs? “The likeliest explanation is that MA insurers have structured their benefits to advantage low-cost (that is, profitable) enrollees and disadvantage those requiring expensive care,” the editorial commentators wrote. For beneficiaries on inexpensive medications, MA plans would be a financial win. “But for patients requiring expensive chemotherapies, the 20% coinsurance that most MA plans charge could be financially ruinous.”
Commenting on the study but not involved in it, David A. Lipschutz, JD, LLB, associate director of the Center for Medicare Advocacy in Washington, DC, called the study an important one that provides more evidence that significant overpayments to MA plans don’t translate to better financial protections for plan enrollees, particularly lower-income individuals. “While there has been some recent movement to hold plans more accountable for providing necessary care, much more impactful action by policymakers is required to mitigate the harms of the growing privatization of the Medicare program,” he said. “MA overpayments could be redistributed to traditional Medicare in order to enrich all Medicare beneficiaries instead of just insurance companies.”
This study was supported by the National Research Foundation of Korea. Dr. Park disclosed no competing interests. One study coauthor reported support from government and not-for-profit research-funding bodies. Editorialists Dr. Woolhandler and Dr. Himmelstein had no competing interests to declare. Dr. Lipschutz disclosed Medicare advocacy work.
FROM ANNALS OF INTERNAL MEDICINE
See the Medical World Through Neurodivergent Doctors’ Eyes
Some 15%-20% of the world’s population are neurodivergent, with conditions such as autism, dyslexia, Tourette syndrome, attention-deficit/hyperactivity disorder (ADHD), and others. With different strengths and challenges around learning, engaging socially, or completing certain tasks, neurodivergent people can face barriers in the workforce.
Meanwhile, studies suggest that neurodivergent people may be overrepresented in STEM fields such as medicine. The medical field may self-select for traits associated with neurodivergent conditions, researchers say, including a hyperfocus on intense interests, pattern recognition, increased curiosity and empathy, and thinking quickly under pressure.
But . They struggle with stigma, a culture of nondisclosure, and lack of accommodations, which can lead to burnout and poor mental health.
“The medical system and the mental health system are some of the spaces that are holding on tightly to some of the outdated understandings of things like autism and ADHD,” says Megan Anna Neff, PsyD, a psychologist with autism and ADHD based in Portland, Oregon.
Situations can get dire: A 2023 survey of more than 200 autistic doctors from several countries found that 77% had considered suicide and 24% had attempted it.
But here’s the crux of it: Many neurodivergent doctors believe their unique ways of thinking and outside-the-box creativity are skills and strengths that can benefit the field. And they say making medicine more inclusive — and better understanding how a neurodivergent physician’s brain works — would allow them to thrive.
Blending In and Breaking Down
The exact number of neurodivergent physicians in the workforce remains unknown. Existing studies are small and focus mainly on autism. But researchers believe the percentage could be higher than we think, because neurodiversity can be underidentified.
Although autism can sometimes be diagnosed as early as 18 months, it’s not uncommon to receive a diagnosis well into adulthood. “Like many late-identified autistic adults, I got my autism diagnosis in the context of autistic burnout,” says Melissa Houser, MD, a primary care physician who received a diagnosis in 2021. Dr. Houser, who uses the pronouns she/they, explains that her experience is common, “a consequence of chronically having your life’s demands exceed your capacity.”
Dr. Houser, who also has ADHD and dyslexia, among other neurodivergent conditions, says that before her diagnosis, she worked in a traditional practice setting. Eventually, she began to notice intense dysregulation and fatigue. “I began to have a lot more difficulties with communication and my motor planning and sequencing,” Dr. Houser says. “I was sleep-deprived, and my needs were not being met. I was in a situation where I had a complete lack of autonomy over my practice.”
Deep in burnout, Dr. Houser says she lost her ability to “mask,” a term used to describe how some neurodivergent people work to “blend in” with societal expectations. This led to further communication breakdowns with her supervisor. Finally, Dr. Houser saw a psychiatrist.
Shortly after her diagnosis, Dr. Houser quit her job and founded All Brains Belong, a nonprofit that provides neurodiversity-affirming medical care, education, and advocacy. Research has found that people with autism are at increased risk for physical health conditions, including immune conditions, gastrointestinal disorders, metabolic conditions, and increased mortality in hospital settings. Understanding these connections can “mean the difference between life and death” for neurodivergent patients, Dr. Houser says.
Yet, in a 2015 study that assessed providers’ ability to recognize autism, a high proportion were not aware that they had patients with autism spectrum disorder, and most reported lacking both the skills and the tools to care for them.
Different as a Doctor and a Patient
Bernadette Grosjean, MD, a retired associate professor of psychiatry at David Geffen School of Medicine at UCLA and a distinguished Fellow of the American Psychiatric Association, also found insight into lifelong experiences as both a doctor and a patient with her autism diagnosis, which came when she was 61.
“Looking back, I was a smart kid but kind of clumsy and different in other ways,” Dr. Grosjean says. According to a 2021 survey by Cambridge University, autistic individuals are significantly more likely to identify as LGBTQ+, and Dr. Grosjean, who is gay, says that not being fully accepted by family or friends played a role in her struggles with mental health issues.
Throughout her mental health treatment, Dr. Grosjean felt as though her providers “were expecting from me things that I didn’t know how to do or fix. I didn’t know how to be a ‘good’ patient,” she recalls.
As a psychiatrist, Dr. Grosjean started to notice that many of the women she treated for borderline personality disorder, which is categorized by unstable relationships and emotions, were autistic. “I then started asking lots of questions about myself — the fact that I’ve always been very sensitive or that I’ve been accused of being both hypersensitive and not having emotions, and I understood a lot.”
When Dr. Grosjean came across Autistic Doctors International, a group of over 800 autistic doctors worldwide, she says, “I found my tribe.” She now serves as the US lead for psychiatry for the group, which is focused on support, advocacy, research, and education around neurodiversity.
Psychiatric comorbidities can accompany neurodivergent conditions. But a growing body of research, including a 2022 study published in the European Archives of Psychiatry and Clinical Neuroscience, indicates that autism and ADHD are frequently misdiagnosed as depression or anxiety.
Dr. Neff was unaware of her conditions until one of her children was diagnosed with autism in 2021. She started to research it. “As I was learning about autism and girls, I was like, ‘Oh, my gosh, this is me,’ ” Dr. Neff recalls. Within a few weeks, she had her own diagnosis.
In hindsight, Dr. Neff has more clarity regarding her struggles in the traditional medical space. She had found it difficult to fit patients into short appointment windows and keep their notes concise. Although she loved hospital work, the environment had been overwhelming and led to burnout.
‘A Deficit-Based Lens’
Dr. Houser believes that too often, autism is viewed through a “deficit-based lens.” Stressors like sensory overload, changes in routine, or unexpected events can exacerbate behavioral challenges for neurodivergent people in the workplace. The DSM-5 criteria for autism, she points out, are largely based on autistic “stress behaviors.”
The result, Dr. Houser says, is that neurodivergent doctors are judged by their response to stressors that put them at a disadvantage rather than their capabilities under more positive circumstances. “The more dysregulated someone is,” she says, “the more likely they are to manifest those observable behaviors.”
Dr. Neff notes that medicine is a very “sensory overwhelming work environment.” Working in ob.gyn. and primary care clinics, she remembers often coming home with a headache and a low-grade fever. “I had no idea why, but I now realize it’s because I was so sensory sick.”
Fearing for her job, Dr. Neff intentionally waited until she was in private practice to disclose her neurodiversity. “I don’t think it would have been received well if I was in a hospital system,” she says. “There’s a lot of invalidation that can come when someone chooses to self-disclose, and their colleagues don’t have a framework in mind to understand.” In one instance, after revealing her diagnosis, she remembers a well-known researcher telling her she wasn’t autistic.
Dr. Grosjean has also had former colleagues invalidate her diagnosis, something she says “keeps people quiet.”
Understanding the Neurodivergent Brain
The general lack of education on how neurodivergent brains work, physicians with these conditions say, means they are not often recognized for how they can function with certain accommodations and how they could contribute in unique ways if their workplace challenges were reduced.
“What we know about autistic brains is that we are systems-thinking pattern matchers,” says Dr. Houser, who formed an interdisciplinary task force to explore medical conditions that are more common in autistic people. Through that comprehensive approach, she has worked to find best practices to treat the constellation of conditions that can arise among these patients. “My autistic brain allowed me to do that,” Dr. Houser says.
Catriona McVey, a medical student in the United Kingdom and creator of the blog Attention Deficit Doctor, points out that “ADHD brains are interest-driven; they can be very focused when you’re doing something enjoyable or new due to increased dopaminergic stimulation.” Ms. McVey speaks from personal experience. “I’ve hyperfocused before on an essay that interested me for over 10 hours,” she recalls, “so I imagine if I was interested in surgery, I could easily hyperfocus on a long operation.”
Empathy is another key part of medical practice. Contrary to stereotypes of neurodivergent people lacking empathy, current research suggests this isn’t true. A concept known as the “double empathy problem,” a term coined by British researcher Damian Milton in 2012, challenges the misconception that autistic people do not have empathy, explains Dr. Grosjean.
Mr. Milton theorized that there are two types of empathy: emotional, when you feel someone else’s pain, and cognitive, which involves critical thinking to understand someone’s emotions or thoughts. “Autistic people have, in general, a lot of emotional empathy,” Dr. Grosjean says, “but the cognitive empathy they don’t have as well.”
Dr. Neff has experienced this in her practice. “I will often feel what my clients are feeling as they’re feeling it,” she says, adding that she has always had an innate ability to analyze and connect with clients. She’s good at observing the interplay of health conditions, incorporating biology, psychology, and social conceptualizations of issues, with nuance. She feels that recognizing behavioral patterns or psychological triggers in her patients helps her see them holistically and provide better care. “That was a skill even before I realized I was autistic, but I always thought it was just intuitive to everyone,” she says.
Support Can Lead to Success
The Americans with Disabilities Act requires employers to provide reasonable accommodations to neurodivergent employees. However, getting those accommodations involves disclosure, which many physicians have reasons to avoid.
It also means more work. Requesting and putting adjustments in place can take a lot of time and energy to organize. Ms. McVey says they can be “long-winded, multistep tasks” that are not very compatible with ADHD. “Some doctors report that service pressures and funding are used as excuses to refuse adjustments,” she adds.
Ms. McVey lists several workplace accommodations that could be helpful, including flexible working hours, a quiet space to complete paperwork, dictation software, and extra time for medical students to complete written exams.
Neurodivergent physicians have also called for increased diversity of senior leadership and utilizing “cognitive apprenticeship models,” where employees explain their thought processes and receive timely feedback.
But far too often, there is little intervention until a doctor reaches a crisis point. “I look forward to the day when we don’t have to wait until people are profoundly depleted to discover how their brains work,” says Dr. Houser.
Beyond logistical and structural changes in the medical field, Dr. Grosjean speaks of the simple need to listen to colleagues with an open mind and believe them when they express their feelings and experiences. “Everyone has a role to play in challenging stigma, misconceptions, and stereotypes,” Ms. McVey agrees. Ask yourself the old question, she suggests: “If not me, then who? If not now, then when?”
A version of this article first appeared on Medscape.com.
Some 15%-20% of the world’s population are neurodivergent, with conditions such as autism, dyslexia, Tourette syndrome, attention-deficit/hyperactivity disorder (ADHD), and others. With different strengths and challenges around learning, engaging socially, or completing certain tasks, neurodivergent people can face barriers in the workforce.
Meanwhile, studies suggest that neurodivergent people may be overrepresented in STEM fields such as medicine. The medical field may self-select for traits associated with neurodivergent conditions, researchers say, including a hyperfocus on intense interests, pattern recognition, increased curiosity and empathy, and thinking quickly under pressure.
But . They struggle with stigma, a culture of nondisclosure, and lack of accommodations, which can lead to burnout and poor mental health.
“The medical system and the mental health system are some of the spaces that are holding on tightly to some of the outdated understandings of things like autism and ADHD,” says Megan Anna Neff, PsyD, a psychologist with autism and ADHD based in Portland, Oregon.
Situations can get dire: A 2023 survey of more than 200 autistic doctors from several countries found that 77% had considered suicide and 24% had attempted it.
But here’s the crux of it: Many neurodivergent doctors believe their unique ways of thinking and outside-the-box creativity are skills and strengths that can benefit the field. And they say making medicine more inclusive — and better understanding how a neurodivergent physician’s brain works — would allow them to thrive.
Blending In and Breaking Down
The exact number of neurodivergent physicians in the workforce remains unknown. Existing studies are small and focus mainly on autism. But researchers believe the percentage could be higher than we think, because neurodiversity can be underidentified.
Although autism can sometimes be diagnosed as early as 18 months, it’s not uncommon to receive a diagnosis well into adulthood. “Like many late-identified autistic adults, I got my autism diagnosis in the context of autistic burnout,” says Melissa Houser, MD, a primary care physician who received a diagnosis in 2021. Dr. Houser, who uses the pronouns she/they, explains that her experience is common, “a consequence of chronically having your life’s demands exceed your capacity.”
Dr. Houser, who also has ADHD and dyslexia, among other neurodivergent conditions, says that before her diagnosis, she worked in a traditional practice setting. Eventually, she began to notice intense dysregulation and fatigue. “I began to have a lot more difficulties with communication and my motor planning and sequencing,” Dr. Houser says. “I was sleep-deprived, and my needs were not being met. I was in a situation where I had a complete lack of autonomy over my practice.”
Deep in burnout, Dr. Houser says she lost her ability to “mask,” a term used to describe how some neurodivergent people work to “blend in” with societal expectations. This led to further communication breakdowns with her supervisor. Finally, Dr. Houser saw a psychiatrist.
Shortly after her diagnosis, Dr. Houser quit her job and founded All Brains Belong, a nonprofit that provides neurodiversity-affirming medical care, education, and advocacy. Research has found that people with autism are at increased risk for physical health conditions, including immune conditions, gastrointestinal disorders, metabolic conditions, and increased mortality in hospital settings. Understanding these connections can “mean the difference between life and death” for neurodivergent patients, Dr. Houser says.
Yet, in a 2015 study that assessed providers’ ability to recognize autism, a high proportion were not aware that they had patients with autism spectrum disorder, and most reported lacking both the skills and the tools to care for them.
Different as a Doctor and a Patient
Bernadette Grosjean, MD, a retired associate professor of psychiatry at David Geffen School of Medicine at UCLA and a distinguished Fellow of the American Psychiatric Association, also found insight into lifelong experiences as both a doctor and a patient with her autism diagnosis, which came when she was 61.
“Looking back, I was a smart kid but kind of clumsy and different in other ways,” Dr. Grosjean says. According to a 2021 survey by Cambridge University, autistic individuals are significantly more likely to identify as LGBTQ+, and Dr. Grosjean, who is gay, says that not being fully accepted by family or friends played a role in her struggles with mental health issues.
Throughout her mental health treatment, Dr. Grosjean felt as though her providers “were expecting from me things that I didn’t know how to do or fix. I didn’t know how to be a ‘good’ patient,” she recalls.
As a psychiatrist, Dr. Grosjean started to notice that many of the women she treated for borderline personality disorder, which is categorized by unstable relationships and emotions, were autistic. “I then started asking lots of questions about myself — the fact that I’ve always been very sensitive or that I’ve been accused of being both hypersensitive and not having emotions, and I understood a lot.”
When Dr. Grosjean came across Autistic Doctors International, a group of over 800 autistic doctors worldwide, she says, “I found my tribe.” She now serves as the US lead for psychiatry for the group, which is focused on support, advocacy, research, and education around neurodiversity.
Psychiatric comorbidities can accompany neurodivergent conditions. But a growing body of research, including a 2022 study published in the European Archives of Psychiatry and Clinical Neuroscience, indicates that autism and ADHD are frequently misdiagnosed as depression or anxiety.
Dr. Neff was unaware of her conditions until one of her children was diagnosed with autism in 2021. She started to research it. “As I was learning about autism and girls, I was like, ‘Oh, my gosh, this is me,’ ” Dr. Neff recalls. Within a few weeks, she had her own diagnosis.
In hindsight, Dr. Neff has more clarity regarding her struggles in the traditional medical space. She had found it difficult to fit patients into short appointment windows and keep their notes concise. Although she loved hospital work, the environment had been overwhelming and led to burnout.
‘A Deficit-Based Lens’
Dr. Houser believes that too often, autism is viewed through a “deficit-based lens.” Stressors like sensory overload, changes in routine, or unexpected events can exacerbate behavioral challenges for neurodivergent people in the workplace. The DSM-5 criteria for autism, she points out, are largely based on autistic “stress behaviors.”
The result, Dr. Houser says, is that neurodivergent doctors are judged by their response to stressors that put them at a disadvantage rather than their capabilities under more positive circumstances. “The more dysregulated someone is,” she says, “the more likely they are to manifest those observable behaviors.”
Dr. Neff notes that medicine is a very “sensory overwhelming work environment.” Working in ob.gyn. and primary care clinics, she remembers often coming home with a headache and a low-grade fever. “I had no idea why, but I now realize it’s because I was so sensory sick.”
Fearing for her job, Dr. Neff intentionally waited until she was in private practice to disclose her neurodiversity. “I don’t think it would have been received well if I was in a hospital system,” she says. “There’s a lot of invalidation that can come when someone chooses to self-disclose, and their colleagues don’t have a framework in mind to understand.” In one instance, after revealing her diagnosis, she remembers a well-known researcher telling her she wasn’t autistic.
Dr. Grosjean has also had former colleagues invalidate her diagnosis, something she says “keeps people quiet.”
Understanding the Neurodivergent Brain
The general lack of education on how neurodivergent brains work, physicians with these conditions say, means they are not often recognized for how they can function with certain accommodations and how they could contribute in unique ways if their workplace challenges were reduced.
“What we know about autistic brains is that we are systems-thinking pattern matchers,” says Dr. Houser, who formed an interdisciplinary task force to explore medical conditions that are more common in autistic people. Through that comprehensive approach, she has worked to find best practices to treat the constellation of conditions that can arise among these patients. “My autistic brain allowed me to do that,” Dr. Houser says.
Catriona McVey, a medical student in the United Kingdom and creator of the blog Attention Deficit Doctor, points out that “ADHD brains are interest-driven; they can be very focused when you’re doing something enjoyable or new due to increased dopaminergic stimulation.” Ms. McVey speaks from personal experience. “I’ve hyperfocused before on an essay that interested me for over 10 hours,” she recalls, “so I imagine if I was interested in surgery, I could easily hyperfocus on a long operation.”
Empathy is another key part of medical practice. Contrary to stereotypes of neurodivergent people lacking empathy, current research suggests this isn’t true. A concept known as the “double empathy problem,” a term coined by British researcher Damian Milton in 2012, challenges the misconception that autistic people do not have empathy, explains Dr. Grosjean.
Mr. Milton theorized that there are two types of empathy: emotional, when you feel someone else’s pain, and cognitive, which involves critical thinking to understand someone’s emotions or thoughts. “Autistic people have, in general, a lot of emotional empathy,” Dr. Grosjean says, “but the cognitive empathy they don’t have as well.”
Dr. Neff has experienced this in her practice. “I will often feel what my clients are feeling as they’re feeling it,” she says, adding that she has always had an innate ability to analyze and connect with clients. She’s good at observing the interplay of health conditions, incorporating biology, psychology, and social conceptualizations of issues, with nuance. She feels that recognizing behavioral patterns or psychological triggers in her patients helps her see them holistically and provide better care. “That was a skill even before I realized I was autistic, but I always thought it was just intuitive to everyone,” she says.
Support Can Lead to Success
The Americans with Disabilities Act requires employers to provide reasonable accommodations to neurodivergent employees. However, getting those accommodations involves disclosure, which many physicians have reasons to avoid.
It also means more work. Requesting and putting adjustments in place can take a lot of time and energy to organize. Ms. McVey says they can be “long-winded, multistep tasks” that are not very compatible with ADHD. “Some doctors report that service pressures and funding are used as excuses to refuse adjustments,” she adds.
Ms. McVey lists several workplace accommodations that could be helpful, including flexible working hours, a quiet space to complete paperwork, dictation software, and extra time for medical students to complete written exams.
Neurodivergent physicians have also called for increased diversity of senior leadership and utilizing “cognitive apprenticeship models,” where employees explain their thought processes and receive timely feedback.
But far too often, there is little intervention until a doctor reaches a crisis point. “I look forward to the day when we don’t have to wait until people are profoundly depleted to discover how their brains work,” says Dr. Houser.
Beyond logistical and structural changes in the medical field, Dr. Grosjean speaks of the simple need to listen to colleagues with an open mind and believe them when they express their feelings and experiences. “Everyone has a role to play in challenging stigma, misconceptions, and stereotypes,” Ms. McVey agrees. Ask yourself the old question, she suggests: “If not me, then who? If not now, then when?”
A version of this article first appeared on Medscape.com.
Some 15%-20% of the world’s population are neurodivergent, with conditions such as autism, dyslexia, Tourette syndrome, attention-deficit/hyperactivity disorder (ADHD), and others. With different strengths and challenges around learning, engaging socially, or completing certain tasks, neurodivergent people can face barriers in the workforce.
Meanwhile, studies suggest that neurodivergent people may be overrepresented in STEM fields such as medicine. The medical field may self-select for traits associated with neurodivergent conditions, researchers say, including a hyperfocus on intense interests, pattern recognition, increased curiosity and empathy, and thinking quickly under pressure.
But . They struggle with stigma, a culture of nondisclosure, and lack of accommodations, which can lead to burnout and poor mental health.
“The medical system and the mental health system are some of the spaces that are holding on tightly to some of the outdated understandings of things like autism and ADHD,” says Megan Anna Neff, PsyD, a psychologist with autism and ADHD based in Portland, Oregon.
Situations can get dire: A 2023 survey of more than 200 autistic doctors from several countries found that 77% had considered suicide and 24% had attempted it.
But here’s the crux of it: Many neurodivergent doctors believe their unique ways of thinking and outside-the-box creativity are skills and strengths that can benefit the field. And they say making medicine more inclusive — and better understanding how a neurodivergent physician’s brain works — would allow them to thrive.
Blending In and Breaking Down
The exact number of neurodivergent physicians in the workforce remains unknown. Existing studies are small and focus mainly on autism. But researchers believe the percentage could be higher than we think, because neurodiversity can be underidentified.
Although autism can sometimes be diagnosed as early as 18 months, it’s not uncommon to receive a diagnosis well into adulthood. “Like many late-identified autistic adults, I got my autism diagnosis in the context of autistic burnout,” says Melissa Houser, MD, a primary care physician who received a diagnosis in 2021. Dr. Houser, who uses the pronouns she/they, explains that her experience is common, “a consequence of chronically having your life’s demands exceed your capacity.”
Dr. Houser, who also has ADHD and dyslexia, among other neurodivergent conditions, says that before her diagnosis, she worked in a traditional practice setting. Eventually, she began to notice intense dysregulation and fatigue. “I began to have a lot more difficulties with communication and my motor planning and sequencing,” Dr. Houser says. “I was sleep-deprived, and my needs were not being met. I was in a situation where I had a complete lack of autonomy over my practice.”
Deep in burnout, Dr. Houser says she lost her ability to “mask,” a term used to describe how some neurodivergent people work to “blend in” with societal expectations. This led to further communication breakdowns with her supervisor. Finally, Dr. Houser saw a psychiatrist.
Shortly after her diagnosis, Dr. Houser quit her job and founded All Brains Belong, a nonprofit that provides neurodiversity-affirming medical care, education, and advocacy. Research has found that people with autism are at increased risk for physical health conditions, including immune conditions, gastrointestinal disorders, metabolic conditions, and increased mortality in hospital settings. Understanding these connections can “mean the difference between life and death” for neurodivergent patients, Dr. Houser says.
Yet, in a 2015 study that assessed providers’ ability to recognize autism, a high proportion were not aware that they had patients with autism spectrum disorder, and most reported lacking both the skills and the tools to care for them.
Different as a Doctor and a Patient
Bernadette Grosjean, MD, a retired associate professor of psychiatry at David Geffen School of Medicine at UCLA and a distinguished Fellow of the American Psychiatric Association, also found insight into lifelong experiences as both a doctor and a patient with her autism diagnosis, which came when she was 61.
“Looking back, I was a smart kid but kind of clumsy and different in other ways,” Dr. Grosjean says. According to a 2021 survey by Cambridge University, autistic individuals are significantly more likely to identify as LGBTQ+, and Dr. Grosjean, who is gay, says that not being fully accepted by family or friends played a role in her struggles with mental health issues.
Throughout her mental health treatment, Dr. Grosjean felt as though her providers “were expecting from me things that I didn’t know how to do or fix. I didn’t know how to be a ‘good’ patient,” she recalls.
As a psychiatrist, Dr. Grosjean started to notice that many of the women she treated for borderline personality disorder, which is categorized by unstable relationships and emotions, were autistic. “I then started asking lots of questions about myself — the fact that I’ve always been very sensitive or that I’ve been accused of being both hypersensitive and not having emotions, and I understood a lot.”
When Dr. Grosjean came across Autistic Doctors International, a group of over 800 autistic doctors worldwide, she says, “I found my tribe.” She now serves as the US lead for psychiatry for the group, which is focused on support, advocacy, research, and education around neurodiversity.
Psychiatric comorbidities can accompany neurodivergent conditions. But a growing body of research, including a 2022 study published in the European Archives of Psychiatry and Clinical Neuroscience, indicates that autism and ADHD are frequently misdiagnosed as depression or anxiety.
Dr. Neff was unaware of her conditions until one of her children was diagnosed with autism in 2021. She started to research it. “As I was learning about autism and girls, I was like, ‘Oh, my gosh, this is me,’ ” Dr. Neff recalls. Within a few weeks, she had her own diagnosis.
In hindsight, Dr. Neff has more clarity regarding her struggles in the traditional medical space. She had found it difficult to fit patients into short appointment windows and keep their notes concise. Although she loved hospital work, the environment had been overwhelming and led to burnout.
‘A Deficit-Based Lens’
Dr. Houser believes that too often, autism is viewed through a “deficit-based lens.” Stressors like sensory overload, changes in routine, or unexpected events can exacerbate behavioral challenges for neurodivergent people in the workplace. The DSM-5 criteria for autism, she points out, are largely based on autistic “stress behaviors.”
The result, Dr. Houser says, is that neurodivergent doctors are judged by their response to stressors that put them at a disadvantage rather than their capabilities under more positive circumstances. “The more dysregulated someone is,” she says, “the more likely they are to manifest those observable behaviors.”
Dr. Neff notes that medicine is a very “sensory overwhelming work environment.” Working in ob.gyn. and primary care clinics, she remembers often coming home with a headache and a low-grade fever. “I had no idea why, but I now realize it’s because I was so sensory sick.”
Fearing for her job, Dr. Neff intentionally waited until she was in private practice to disclose her neurodiversity. “I don’t think it would have been received well if I was in a hospital system,” she says. “There’s a lot of invalidation that can come when someone chooses to self-disclose, and their colleagues don’t have a framework in mind to understand.” In one instance, after revealing her diagnosis, she remembers a well-known researcher telling her she wasn’t autistic.
Dr. Grosjean has also had former colleagues invalidate her diagnosis, something she says “keeps people quiet.”
Understanding the Neurodivergent Brain
The general lack of education on how neurodivergent brains work, physicians with these conditions say, means they are not often recognized for how they can function with certain accommodations and how they could contribute in unique ways if their workplace challenges were reduced.
“What we know about autistic brains is that we are systems-thinking pattern matchers,” says Dr. Houser, who formed an interdisciplinary task force to explore medical conditions that are more common in autistic people. Through that comprehensive approach, she has worked to find best practices to treat the constellation of conditions that can arise among these patients. “My autistic brain allowed me to do that,” Dr. Houser says.
Catriona McVey, a medical student in the United Kingdom and creator of the blog Attention Deficit Doctor, points out that “ADHD brains are interest-driven; they can be very focused when you’re doing something enjoyable or new due to increased dopaminergic stimulation.” Ms. McVey speaks from personal experience. “I’ve hyperfocused before on an essay that interested me for over 10 hours,” she recalls, “so I imagine if I was interested in surgery, I could easily hyperfocus on a long operation.”
Empathy is another key part of medical practice. Contrary to stereotypes of neurodivergent people lacking empathy, current research suggests this isn’t true. A concept known as the “double empathy problem,” a term coined by British researcher Damian Milton in 2012, challenges the misconception that autistic people do not have empathy, explains Dr. Grosjean.
Mr. Milton theorized that there are two types of empathy: emotional, when you feel someone else’s pain, and cognitive, which involves critical thinking to understand someone’s emotions or thoughts. “Autistic people have, in general, a lot of emotional empathy,” Dr. Grosjean says, “but the cognitive empathy they don’t have as well.”
Dr. Neff has experienced this in her practice. “I will often feel what my clients are feeling as they’re feeling it,” she says, adding that she has always had an innate ability to analyze and connect with clients. She’s good at observing the interplay of health conditions, incorporating biology, psychology, and social conceptualizations of issues, with nuance. She feels that recognizing behavioral patterns or psychological triggers in her patients helps her see them holistically and provide better care. “That was a skill even before I realized I was autistic, but I always thought it was just intuitive to everyone,” she says.
Support Can Lead to Success
The Americans with Disabilities Act requires employers to provide reasonable accommodations to neurodivergent employees. However, getting those accommodations involves disclosure, which many physicians have reasons to avoid.
It also means more work. Requesting and putting adjustments in place can take a lot of time and energy to organize. Ms. McVey says they can be “long-winded, multistep tasks” that are not very compatible with ADHD. “Some doctors report that service pressures and funding are used as excuses to refuse adjustments,” she adds.
Ms. McVey lists several workplace accommodations that could be helpful, including flexible working hours, a quiet space to complete paperwork, dictation software, and extra time for medical students to complete written exams.
Neurodivergent physicians have also called for increased diversity of senior leadership and utilizing “cognitive apprenticeship models,” where employees explain their thought processes and receive timely feedback.
But far too often, there is little intervention until a doctor reaches a crisis point. “I look forward to the day when we don’t have to wait until people are profoundly depleted to discover how their brains work,” says Dr. Houser.
Beyond logistical and structural changes in the medical field, Dr. Grosjean speaks of the simple need to listen to colleagues with an open mind and believe them when they express their feelings and experiences. “Everyone has a role to play in challenging stigma, misconceptions, and stereotypes,” Ms. McVey agrees. Ask yourself the old question, she suggests: “If not me, then who? If not now, then when?”
A version of this article first appeared on Medscape.com.
Study Finds Major CV Event Risk in Patients With AD Similar to Controls
(RA), according to an analysis of national claims data.
The results of the analysis were presented during a poster session at the Revolutionizing Atopic Dermatitis conference in Chicago. “While it is known that atopic dermatitis is associated with some comorbidities, the specific risk of major adverse cardiovascular events in patients with AD, especially those with moderate to severe AD within the US population, is unclear,” the study’s first author Christopher G. Bunick, MD, PhD, said in an interview following the conference.

To characterize the risk for MACE in patients with AD vs matched controls without AD (non-AD) and patients with RA, Dr. Bunick, associate professor of dermatology at Yale University, New Haven, Connecticut, and colleagues retrospectively evaluated US claims data from Optum’s Clinformatics Data Mart. The study population consisted of 381,221 patients aged 18 years and older who were diagnosed with AD from March 2017 to March 2023. Comparator groups included 381,221 non-AD controls matched by age, sex, and cohort entry, and 97,445 patients diagnosed with RA based on at least two claims for RA ≥ 7 days apart.
Patients were classified as having moderate to severe disease if they received dupilumab for AD or advanced systemic therapy for RA at any time during the follow-up period. The matched moderate to severe AD and non-AD cohorts were composed of 7134 patients each. The incidence of MACE was defined as inpatient hospitalization with myocardial infarction or stroke. The researchers used multivariable Cox proportional hazard models adjusted for baseline demographics, comorbidities, and medications to calculate the relative risk for MACE.
MACE Incidence, Relative Risk
The mean age of the AD cohort and non-AD matched controls was 58 years, and the mean age of the RA cohort was 67 years. The incidence of MACE per 100 patient-years was 1.78 among patients with AD, 1.83 among non-AD matched controls, and 2.12 among patients with RA. Patients with moderate to severe AD had a MACE incidence of 1.18 per 100 patient-years, which was lower than that of non-AD matched controls (1.52) and patients with moderate to severe RA (1.67).
In other findings, the relative risk for MACE in patients with AD was lower vs non-AD controls (adjusted hazard ratio [aHR], 0.91; 95% CI, 0.89-0.93; P < .001) and patients with RA (aHR, 0.83; 95% CI, 0.80-0.85; P < .001). Among patients with moderate to severe AD, MACE risk was similar to that of non-AD matched controls (aHR, 0.92; 95% CI, 0.73-1.14) and lower vs those with moderate to severe RA (aHR, 0.83; 95% CI, 0.73-0.94; P < .01).
MACE risk associated with AD was greater in patients who were older (per year, aHR, 1.05; 95% CI, 1.05-1.05), male (aHR, 0.81; 95% CI, 0.79-0.84), and Black vs White (aHR, 1.16; 95% CI, 1.11-1.21), and among those who received systemic corticosteroids in the 3 months before diagnosis (aHR, 1.10; 95% CI, 1.06-1.14), were hospitalized in the year before diagnosis (aHR, 1.35; 95% CI, 1.30-1.41), and had a history of smoking (aHR, 1.20; 95% CI, 1.16-1.24) and drug abuse (aHR, 1.34; 95% CI, 1.25-1.43).
Unexpected Results
“One surprising finding was that the incidence of MACE in patients with moderate to severe AD was actually lower than that in non-AD matched controls and significantly lower compared to patients with moderate to severe RA,” Dr. Bunick said. “This contrasts with the expectation that increased systemic inflammation in moderate to severe AD would correspond with a higher incidence of MACE.”
Another unexpected result, he said, was that, among patients with moderate to severe AD, the risk for MACE was not significantly different from that of non-AD matched controls, suggesting that the inflammatory burden in AD might not translate to as high a cardiovascular risk as previously assumed.
Dr. Bunick noted that advanced treatments for AD such as Janus kinase (JAK) inhibitors (upadacitinib and abrocitinib) have a class boxed warning for MACE based on a study of another JAK inhibitor (tofacitinib) in patients with RA, but “this may not apply to AD because patients with AD have a lower risk for MACE.”
In his opinion, he said, the study “underscores the importance of understanding the specific risks associated with different inflammatory conditions.” Moreover, “it emphasizes the potential benefits of newer systemic therapies in potentially mitigating cardiovascular risks in patients with moderate to severe AD.”
Dr. Bunick acknowledged certain limitations of the study, including its retrospective design and reliance on administrative claims data, which “may introduce coding errors and misclassification,” and the generalizability of the results, which may be limited to the US population.
AbbVie funded the study, and three of the coauthors are employees of the company. Dr. Bunick disclosed that he has served as an investigator and/or a consultant for AbbVie, Almirall, Apogee, Arcutis Biotherapeutics, Connect Biopharma, Daiichi Sankyo, EPI Health/Novan, LEO, Lilly, Novartis, Ortho Dermatologics, Palvella Therapeutics, Pfizer, Sanofi Regeneron, Sun, Takeda, Timber, and UCB.
A version of this article appeared on Medscape.com.
(RA), according to an analysis of national claims data.
The results of the analysis were presented during a poster session at the Revolutionizing Atopic Dermatitis conference in Chicago. “While it is known that atopic dermatitis is associated with some comorbidities, the specific risk of major adverse cardiovascular events in patients with AD, especially those with moderate to severe AD within the US population, is unclear,” the study’s first author Christopher G. Bunick, MD, PhD, said in an interview following the conference.
To characterize the risk for MACE in patients with AD vs matched controls without AD (non-AD) and patients with RA, Dr. Bunick, associate professor of dermatology at Yale University, New Haven, Connecticut, and colleagues retrospectively evaluated US claims data from Optum’s Clinformatics Data Mart. The study population consisted of 381,221 patients aged 18 years and older who were diagnosed with AD from March 2017 to March 2023. Comparator groups included 381,221 non-AD controls matched by age, sex, and cohort entry, and 97,445 patients diagnosed with RA based on at least two claims for RA ≥ 7 days apart.
Patients were classified as having moderate to severe disease if they received dupilumab for AD or advanced systemic therapy for RA at any time during the follow-up period. The matched moderate to severe AD and non-AD cohorts were composed of 7134 patients each. The incidence of MACE was defined as inpatient hospitalization with myocardial infarction or stroke. The researchers used multivariable Cox proportional hazard models adjusted for baseline demographics, comorbidities, and medications to calculate the relative risk for MACE.
MACE Incidence, Relative Risk
The mean age of the AD cohort and non-AD matched controls was 58 years, and the mean age of the RA cohort was 67 years. The incidence of MACE per 100 patient-years was 1.78 among patients with AD, 1.83 among non-AD matched controls, and 2.12 among patients with RA. Patients with moderate to severe AD had a MACE incidence of 1.18 per 100 patient-years, which was lower than that of non-AD matched controls (1.52) and patients with moderate to severe RA (1.67).
In other findings, the relative risk for MACE in patients with AD was lower vs non-AD controls (adjusted hazard ratio [aHR], 0.91; 95% CI, 0.89-0.93; P < .001) and patients with RA (aHR, 0.83; 95% CI, 0.80-0.85; P < .001). Among patients with moderate to severe AD, MACE risk was similar to that of non-AD matched controls (aHR, 0.92; 95% CI, 0.73-1.14) and lower vs those with moderate to severe RA (aHR, 0.83; 95% CI, 0.73-0.94; P < .01).
MACE risk associated with AD was greater in patients who were older (per year, aHR, 1.05; 95% CI, 1.05-1.05), male (aHR, 0.81; 95% CI, 0.79-0.84), and Black vs White (aHR, 1.16; 95% CI, 1.11-1.21), and among those who received systemic corticosteroids in the 3 months before diagnosis (aHR, 1.10; 95% CI, 1.06-1.14), were hospitalized in the year before diagnosis (aHR, 1.35; 95% CI, 1.30-1.41), and had a history of smoking (aHR, 1.20; 95% CI, 1.16-1.24) and drug abuse (aHR, 1.34; 95% CI, 1.25-1.43).
Unexpected Results
“One surprising finding was that the incidence of MACE in patients with moderate to severe AD was actually lower than that in non-AD matched controls and significantly lower compared to patients with moderate to severe RA,” Dr. Bunick said. “This contrasts with the expectation that increased systemic inflammation in moderate to severe AD would correspond with a higher incidence of MACE.”
Another unexpected result, he said, was that, among patients with moderate to severe AD, the risk for MACE was not significantly different from that of non-AD matched controls, suggesting that the inflammatory burden in AD might not translate to as high a cardiovascular risk as previously assumed.
Dr. Bunick noted that advanced treatments for AD such as Janus kinase (JAK) inhibitors (upadacitinib and abrocitinib) have a class boxed warning for MACE based on a study of another JAK inhibitor (tofacitinib) in patients with RA, but “this may not apply to AD because patients with AD have a lower risk for MACE.”
In his opinion, he said, the study “underscores the importance of understanding the specific risks associated with different inflammatory conditions.” Moreover, “it emphasizes the potential benefits of newer systemic therapies in potentially mitigating cardiovascular risks in patients with moderate to severe AD.”
Dr. Bunick acknowledged certain limitations of the study, including its retrospective design and reliance on administrative claims data, which “may introduce coding errors and misclassification,” and the generalizability of the results, which may be limited to the US population.
AbbVie funded the study, and three of the coauthors are employees of the company. Dr. Bunick disclosed that he has served as an investigator and/or a consultant for AbbVie, Almirall, Apogee, Arcutis Biotherapeutics, Connect Biopharma, Daiichi Sankyo, EPI Health/Novan, LEO, Lilly, Novartis, Ortho Dermatologics, Palvella Therapeutics, Pfizer, Sanofi Regeneron, Sun, Takeda, Timber, and UCB.
A version of this article appeared on Medscape.com.
(RA), according to an analysis of national claims data.
The results of the analysis were presented during a poster session at the Revolutionizing Atopic Dermatitis conference in Chicago. “While it is known that atopic dermatitis is associated with some comorbidities, the specific risk of major adverse cardiovascular events in patients with AD, especially those with moderate to severe AD within the US population, is unclear,” the study’s first author Christopher G. Bunick, MD, PhD, said in an interview following the conference.
To characterize the risk for MACE in patients with AD vs matched controls without AD (non-AD) and patients with RA, Dr. Bunick, associate professor of dermatology at Yale University, New Haven, Connecticut, and colleagues retrospectively evaluated US claims data from Optum’s Clinformatics Data Mart. The study population consisted of 381,221 patients aged 18 years and older who were diagnosed with AD from March 2017 to March 2023. Comparator groups included 381,221 non-AD controls matched by age, sex, and cohort entry, and 97,445 patients diagnosed with RA based on at least two claims for RA ≥ 7 days apart.
Patients were classified as having moderate to severe disease if they received dupilumab for AD or advanced systemic therapy for RA at any time during the follow-up period. The matched moderate to severe AD and non-AD cohorts were composed of 7134 patients each. The incidence of MACE was defined as inpatient hospitalization with myocardial infarction or stroke. The researchers used multivariable Cox proportional hazard models adjusted for baseline demographics, comorbidities, and medications to calculate the relative risk for MACE.
MACE Incidence, Relative Risk
The mean age of the AD cohort and non-AD matched controls was 58 years, and the mean age of the RA cohort was 67 years. The incidence of MACE per 100 patient-years was 1.78 among patients with AD, 1.83 among non-AD matched controls, and 2.12 among patients with RA. Patients with moderate to severe AD had a MACE incidence of 1.18 per 100 patient-years, which was lower than that of non-AD matched controls (1.52) and patients with moderate to severe RA (1.67).
In other findings, the relative risk for MACE in patients with AD was lower vs non-AD controls (adjusted hazard ratio [aHR], 0.91; 95% CI, 0.89-0.93; P < .001) and patients with RA (aHR, 0.83; 95% CI, 0.80-0.85; P < .001). Among patients with moderate to severe AD, MACE risk was similar to that of non-AD matched controls (aHR, 0.92; 95% CI, 0.73-1.14) and lower vs those with moderate to severe RA (aHR, 0.83; 95% CI, 0.73-0.94; P < .01).
MACE risk associated with AD was greater in patients who were older (per year, aHR, 1.05; 95% CI, 1.05-1.05), male (aHR, 0.81; 95% CI, 0.79-0.84), and Black vs White (aHR, 1.16; 95% CI, 1.11-1.21), and among those who received systemic corticosteroids in the 3 months before diagnosis (aHR, 1.10; 95% CI, 1.06-1.14), were hospitalized in the year before diagnosis (aHR, 1.35; 95% CI, 1.30-1.41), and had a history of smoking (aHR, 1.20; 95% CI, 1.16-1.24) and drug abuse (aHR, 1.34; 95% CI, 1.25-1.43).
Unexpected Results
“One surprising finding was that the incidence of MACE in patients with moderate to severe AD was actually lower than that in non-AD matched controls and significantly lower compared to patients with moderate to severe RA,” Dr. Bunick said. “This contrasts with the expectation that increased systemic inflammation in moderate to severe AD would correspond with a higher incidence of MACE.”
Another unexpected result, he said, was that, among patients with moderate to severe AD, the risk for MACE was not significantly different from that of non-AD matched controls, suggesting that the inflammatory burden in AD might not translate to as high a cardiovascular risk as previously assumed.
Dr. Bunick noted that advanced treatments for AD such as Janus kinase (JAK) inhibitors (upadacitinib and abrocitinib) have a class boxed warning for MACE based on a study of another JAK inhibitor (tofacitinib) in patients with RA, but “this may not apply to AD because patients with AD have a lower risk for MACE.”
In his opinion, he said, the study “underscores the importance of understanding the specific risks associated with different inflammatory conditions.” Moreover, “it emphasizes the potential benefits of newer systemic therapies in potentially mitigating cardiovascular risks in patients with moderate to severe AD.”
Dr. Bunick acknowledged certain limitations of the study, including its retrospective design and reliance on administrative claims data, which “may introduce coding errors and misclassification,” and the generalizability of the results, which may be limited to the US population.
AbbVie funded the study, and three of the coauthors are employees of the company. Dr. Bunick disclosed that he has served as an investigator and/or a consultant for AbbVie, Almirall, Apogee, Arcutis Biotherapeutics, Connect Biopharma, Daiichi Sankyo, EPI Health/Novan, LEO, Lilly, Novartis, Ortho Dermatologics, Palvella Therapeutics, Pfizer, Sanofi Regeneron, Sun, Takeda, Timber, and UCB.
A version of this article appeared on Medscape.com.
Atopic Dermatitis: Study Compares Prevalence by Gender, Age, and Ethnic Background
than adults from other ethnic backgrounds.
Those are among the key findings from an analysis of nationally representative cross-sectional data that were presented during a late-breaking abstract session at the Revolutionizing Atopic Dermatitis conference in Chicago.
“In the past few years, there has been a much-needed focus on better understanding disparities in atopic dermatitis,” one of the study authors, Raj Chovatiya, MD, PhD, clinical associate professor at Chicago Medical School, Rosalind Franklin University, North Chicago, told this news organization after the conference.

“Epidemiology is one of the key ways in which we can query differences in AD at a population level.”
Drawing from the 2021 National Health Interview Survey, the researchers identified 3103 respondents who reported being diagnosed with AD or eczema. They estimated the prevalence rates of AD for the overall population and each subgroup by dividing US frequency estimates by their corresponding US population totals and used multivariable logistic regression to assess the odds of having AD.
More than half of the respondents (1643) were aged between 18 and 64 years, 522 were aged 65 years and older, and 922 were children younger than 18 years. Overall, the prevalence of AD was 7.6% in adults aged 18-64 years and 6.1% in adults aged 65 years and older, for a weighted US estimate of 15.3 and 3.2 million, respectively. The prevalence of AD varied by race/ethnicity and was highest for those from “other single and multiple races” group (12.4%), followed by Black/African American (8.5%), White (7.7%), Asian (6.5%), American Indian/Alaskan Native (4.9%), and Hispanic (4.8%) populations.
In children, race/ethnicity prevalence were highest for those from other single and multiple races (15.2.%), followed by Black/African American (14.2%), American Indian/Alaskan Native (12%), White (10.2%), Hispanic (9.5%), and Asian (9%) populations.
When the researchers combined all age groups, they observed higher prevalence rates of AD among females than among males. However, in an analysis limited to children, the prevalence rates were similar between girls and boys (10.8% vs 10.7%, respectively), for a weighted US estimate of 7.8 million children with AD.
On multiple regression, the odds of having AD were greater among women than among men (odds ratio [OR], 1.4), among adults aged 18-64 years than among those aged 65 years and older (OR, 1.4), among those younger than 18 years than among those aged 65 years and older (OR, 2.0), and among Black/African American individuals than among White individuals (OR, 1.2). Hispanic adults had a lower risk for AD than non-Hispanic White adults (OR, 0.69) as did Asian adults than White adults (OR, 0.82).
“We found AD prevalence rates were higher in children and adult females, Hispanic adults had a lower prevalence of AD than all other adult groups, and there were numerical differences in AD prevalence across racial groups,” Dr. Chovatiya said in the interview. “While there are of course limitations to the use of any nationally representative cross-sectional dataset that requires weighting to project results from a smaller sample to reflect a larger more heterogeneous group, these results are important for us to consider targeted strategies to address AD burden.”
Jonathan I. Silverberg, MD, PhD, professor of dermatology at The George Washington University, Washington, who was asked to comment on the study, said that while the prevalence of AD in children has been well documented in prior research, “this study fills an important gap by showing us that the prevalence does remain high in adults.”
In addition, “it has not shown any evidence of AD decreasing over time; if anything, it might be slightly increasing,” he said. “We’re also seeing differences [in AD] by race and ethnicity. We have seen that demonstrated in children but [has been] less clearly demonstrated in adults.”
Eli Lilly and Company funded the analysis. Dr. Chovatiya and Dr. Silverberg disclosed ties to several pharmaceutical companies, including Eli Lilly.
A version of this article appeared on Medscape.com .
than adults from other ethnic backgrounds.
Those are among the key findings from an analysis of nationally representative cross-sectional data that were presented during a late-breaking abstract session at the Revolutionizing Atopic Dermatitis conference in Chicago.
“In the past few years, there has been a much-needed focus on better understanding disparities in atopic dermatitis,” one of the study authors, Raj Chovatiya, MD, PhD, clinical associate professor at Chicago Medical School, Rosalind Franklin University, North Chicago, told this news organization after the conference.
“Epidemiology is one of the key ways in which we can query differences in AD at a population level.”
Drawing from the 2021 National Health Interview Survey, the researchers identified 3103 respondents who reported being diagnosed with AD or eczema. They estimated the prevalence rates of AD for the overall population and each subgroup by dividing US frequency estimates by their corresponding US population totals and used multivariable logistic regression to assess the odds of having AD.
More than half of the respondents (1643) were aged between 18 and 64 years, 522 were aged 65 years and older, and 922 were children younger than 18 years. Overall, the prevalence of AD was 7.6% in adults aged 18-64 years and 6.1% in adults aged 65 years and older, for a weighted US estimate of 15.3 and 3.2 million, respectively. The prevalence of AD varied by race/ethnicity and was highest for those from “other single and multiple races” group (12.4%), followed by Black/African American (8.5%), White (7.7%), Asian (6.5%), American Indian/Alaskan Native (4.9%), and Hispanic (4.8%) populations.
In children, race/ethnicity prevalence were highest for those from other single and multiple races (15.2.%), followed by Black/African American (14.2%), American Indian/Alaskan Native (12%), White (10.2%), Hispanic (9.5%), and Asian (9%) populations.
When the researchers combined all age groups, they observed higher prevalence rates of AD among females than among males. However, in an analysis limited to children, the prevalence rates were similar between girls and boys (10.8% vs 10.7%, respectively), for a weighted US estimate of 7.8 million children with AD.
On multiple regression, the odds of having AD were greater among women than among men (odds ratio [OR], 1.4), among adults aged 18-64 years than among those aged 65 years and older (OR, 1.4), among those younger than 18 years than among those aged 65 years and older (OR, 2.0), and among Black/African American individuals than among White individuals (OR, 1.2). Hispanic adults had a lower risk for AD than non-Hispanic White adults (OR, 0.69) as did Asian adults than White adults (OR, 0.82).
“We found AD prevalence rates were higher in children and adult females, Hispanic adults had a lower prevalence of AD than all other adult groups, and there were numerical differences in AD prevalence across racial groups,” Dr. Chovatiya said in the interview. “While there are of course limitations to the use of any nationally representative cross-sectional dataset that requires weighting to project results from a smaller sample to reflect a larger more heterogeneous group, these results are important for us to consider targeted strategies to address AD burden.”
Jonathan I. Silverberg, MD, PhD, professor of dermatology at The George Washington University, Washington, who was asked to comment on the study, said that while the prevalence of AD in children has been well documented in prior research, “this study fills an important gap by showing us that the prevalence does remain high in adults.”
In addition, “it has not shown any evidence of AD decreasing over time; if anything, it might be slightly increasing,” he said. “We’re also seeing differences [in AD] by race and ethnicity. We have seen that demonstrated in children but [has been] less clearly demonstrated in adults.”
Eli Lilly and Company funded the analysis. Dr. Chovatiya and Dr. Silverberg disclosed ties to several pharmaceutical companies, including Eli Lilly.
A version of this article appeared on Medscape.com .
than adults from other ethnic backgrounds.
Those are among the key findings from an analysis of nationally representative cross-sectional data that were presented during a late-breaking abstract session at the Revolutionizing Atopic Dermatitis conference in Chicago.
“In the past few years, there has been a much-needed focus on better understanding disparities in atopic dermatitis,” one of the study authors, Raj Chovatiya, MD, PhD, clinical associate professor at Chicago Medical School, Rosalind Franklin University, North Chicago, told this news organization after the conference.
“Epidemiology is one of the key ways in which we can query differences in AD at a population level.”
Drawing from the 2021 National Health Interview Survey, the researchers identified 3103 respondents who reported being diagnosed with AD or eczema. They estimated the prevalence rates of AD for the overall population and each subgroup by dividing US frequency estimates by their corresponding US population totals and used multivariable logistic regression to assess the odds of having AD.
More than half of the respondents (1643) were aged between 18 and 64 years, 522 were aged 65 years and older, and 922 were children younger than 18 years. Overall, the prevalence of AD was 7.6% in adults aged 18-64 years and 6.1% in adults aged 65 years and older, for a weighted US estimate of 15.3 and 3.2 million, respectively. The prevalence of AD varied by race/ethnicity and was highest for those from “other single and multiple races” group (12.4%), followed by Black/African American (8.5%), White (7.7%), Asian (6.5%), American Indian/Alaskan Native (4.9%), and Hispanic (4.8%) populations.
In children, race/ethnicity prevalence were highest for those from other single and multiple races (15.2.%), followed by Black/African American (14.2%), American Indian/Alaskan Native (12%), White (10.2%), Hispanic (9.5%), and Asian (9%) populations.
When the researchers combined all age groups, they observed higher prevalence rates of AD among females than among males. However, in an analysis limited to children, the prevalence rates were similar between girls and boys (10.8% vs 10.7%, respectively), for a weighted US estimate of 7.8 million children with AD.
On multiple regression, the odds of having AD were greater among women than among men (odds ratio [OR], 1.4), among adults aged 18-64 years than among those aged 65 years and older (OR, 1.4), among those younger than 18 years than among those aged 65 years and older (OR, 2.0), and among Black/African American individuals than among White individuals (OR, 1.2). Hispanic adults had a lower risk for AD than non-Hispanic White adults (OR, 0.69) as did Asian adults than White adults (OR, 0.82).
“We found AD prevalence rates were higher in children and adult females, Hispanic adults had a lower prevalence of AD than all other adult groups, and there were numerical differences in AD prevalence across racial groups,” Dr. Chovatiya said in the interview. “While there are of course limitations to the use of any nationally representative cross-sectional dataset that requires weighting to project results from a smaller sample to reflect a larger more heterogeneous group, these results are important for us to consider targeted strategies to address AD burden.”
Jonathan I. Silverberg, MD, PhD, professor of dermatology at The George Washington University, Washington, who was asked to comment on the study, said that while the prevalence of AD in children has been well documented in prior research, “this study fills an important gap by showing us that the prevalence does remain high in adults.”
In addition, “it has not shown any evidence of AD decreasing over time; if anything, it might be slightly increasing,” he said. “We’re also seeing differences [in AD] by race and ethnicity. We have seen that demonstrated in children but [has been] less clearly demonstrated in adults.”
Eli Lilly and Company funded the analysis. Dr. Chovatiya and Dr. Silverberg disclosed ties to several pharmaceutical companies, including Eli Lilly.
A version of this article appeared on Medscape.com .