User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
COVID in pregnancy may affect boys’ neurodevelopment: Study
Boys born to mothers infected with SARS‐CoV‐2 during pregnancy may be more likely to receive a diagnosis of a neurodevelopmental disorder by age 12 months, according to new research.
Andrea G. Edlow, MD, MSc, with Massachusetts General Hospital and Harvard Medical School in Boston, and colleagues examined data from 18,355 births between March 1, 2020, and May 31, 2021, at eight hospitals across two health systems in Massachusetts.
Of these births, 883 (4.8%) were to individuals who tested positive for SARS‐CoV‐2 during pregnancy. Among the children exposed to SARS‐CoV‐2 in the womb, 26 (3%) received a neurodevelopmental diagnosis, including disorders of motor function, speech and language, and psychological development, by age 1 year. In the group unexposed to the virus, 1.8% received such a diagnosis.
After adjusting for factors such as race, insurance, maternal age, and preterm birth, Dr. Edlow’s group found that a positive test for SARS-CoV-2 during pregnancy was associated with an increased risk for neurodevelopmental diagnoses at 12 months among boys (adjusted odds ratio, 1.94; 95% confidence interval, 1.12-3.17; P = .01), but not among girls.
In a subset of children with data available at 18 months, the correlation among boys at that age was less pronounced and not statistically significant (aOR, 1.42; 95% CI, 0.92-2.11; P = .10).
The findings were published online in JAMA Network Open
Prior epidemiological research has suggested that maternal infection during pregnancy is associated with heightened risk for a range of neurodevelopmental disorders, including autism and schizophrenia, in offspring, the authors wrote.
“The neurodevelopmental risk associated with maternal SARS-CoV-2 infection was disproportionately high in male infants, consistent with the known increased vulnerability of males in the face of prenatal adverse exposures,” Dr. Edlow said in a news release about the findings.
Larger studies and longer follow‐up are needed to confirm and reliably estimate the risk, the researchers said.
“It is not clear that the changes we can detect at 12 and 18 months will be indicative of persistent risks for disorders such as autism spectrum disorder, intellectual disability, or schizophrenia,” they write.
New data published online by the Centers for Disease Control and Prevention show that in 11 communities in 2020, 1 in 36 (2.8%) 8-year-old children had been identified with autism spectrum disorder, an increase from 2.3% in 2018. The data also show that the early months of the pandemic may have disrupted autism detection efforts among 4-year-olds.
The investigators were supported by grants from the National Institutes of Health and the Simons Foundation Autism Research Initiative. Coauthors disclosed consulting for or receiving personal fees from biotechnology and pharmaceutical companies.
A version of this article first appeared on Medscape.com.
Boys born to mothers infected with SARS‐CoV‐2 during pregnancy may be more likely to receive a diagnosis of a neurodevelopmental disorder by age 12 months, according to new research.
Andrea G. Edlow, MD, MSc, with Massachusetts General Hospital and Harvard Medical School in Boston, and colleagues examined data from 18,355 births between March 1, 2020, and May 31, 2021, at eight hospitals across two health systems in Massachusetts.
Of these births, 883 (4.8%) were to individuals who tested positive for SARS‐CoV‐2 during pregnancy. Among the children exposed to SARS‐CoV‐2 in the womb, 26 (3%) received a neurodevelopmental diagnosis, including disorders of motor function, speech and language, and psychological development, by age 1 year. In the group unexposed to the virus, 1.8% received such a diagnosis.
After adjusting for factors such as race, insurance, maternal age, and preterm birth, Dr. Edlow’s group found that a positive test for SARS-CoV-2 during pregnancy was associated with an increased risk for neurodevelopmental diagnoses at 12 months among boys (adjusted odds ratio, 1.94; 95% confidence interval, 1.12-3.17; P = .01), but not among girls.
In a subset of children with data available at 18 months, the correlation among boys at that age was less pronounced and not statistically significant (aOR, 1.42; 95% CI, 0.92-2.11; P = .10).
The findings were published online in JAMA Network Open
Prior epidemiological research has suggested that maternal infection during pregnancy is associated with heightened risk for a range of neurodevelopmental disorders, including autism and schizophrenia, in offspring, the authors wrote.
“The neurodevelopmental risk associated with maternal SARS-CoV-2 infection was disproportionately high in male infants, consistent with the known increased vulnerability of males in the face of prenatal adverse exposures,” Dr. Edlow said in a news release about the findings.
Larger studies and longer follow‐up are needed to confirm and reliably estimate the risk, the researchers said.
“It is not clear that the changes we can detect at 12 and 18 months will be indicative of persistent risks for disorders such as autism spectrum disorder, intellectual disability, or schizophrenia,” they write.
New data published online by the Centers for Disease Control and Prevention show that in 11 communities in 2020, 1 in 36 (2.8%) 8-year-old children had been identified with autism spectrum disorder, an increase from 2.3% in 2018. The data also show that the early months of the pandemic may have disrupted autism detection efforts among 4-year-olds.
The investigators were supported by grants from the National Institutes of Health and the Simons Foundation Autism Research Initiative. Coauthors disclosed consulting for or receiving personal fees from biotechnology and pharmaceutical companies.
A version of this article first appeared on Medscape.com.
Boys born to mothers infected with SARS‐CoV‐2 during pregnancy may be more likely to receive a diagnosis of a neurodevelopmental disorder by age 12 months, according to new research.
Andrea G. Edlow, MD, MSc, with Massachusetts General Hospital and Harvard Medical School in Boston, and colleagues examined data from 18,355 births between March 1, 2020, and May 31, 2021, at eight hospitals across two health systems in Massachusetts.
Of these births, 883 (4.8%) were to individuals who tested positive for SARS‐CoV‐2 during pregnancy. Among the children exposed to SARS‐CoV‐2 in the womb, 26 (3%) received a neurodevelopmental diagnosis, including disorders of motor function, speech and language, and psychological development, by age 1 year. In the group unexposed to the virus, 1.8% received such a diagnosis.
After adjusting for factors such as race, insurance, maternal age, and preterm birth, Dr. Edlow’s group found that a positive test for SARS-CoV-2 during pregnancy was associated with an increased risk for neurodevelopmental diagnoses at 12 months among boys (adjusted odds ratio, 1.94; 95% confidence interval, 1.12-3.17; P = .01), but not among girls.
In a subset of children with data available at 18 months, the correlation among boys at that age was less pronounced and not statistically significant (aOR, 1.42; 95% CI, 0.92-2.11; P = .10).
The findings were published online in JAMA Network Open
Prior epidemiological research has suggested that maternal infection during pregnancy is associated with heightened risk for a range of neurodevelopmental disorders, including autism and schizophrenia, in offspring, the authors wrote.
“The neurodevelopmental risk associated with maternal SARS-CoV-2 infection was disproportionately high in male infants, consistent with the known increased vulnerability of males in the face of prenatal adverse exposures,” Dr. Edlow said in a news release about the findings.
Larger studies and longer follow‐up are needed to confirm and reliably estimate the risk, the researchers said.
“It is not clear that the changes we can detect at 12 and 18 months will be indicative of persistent risks for disorders such as autism spectrum disorder, intellectual disability, or schizophrenia,” they write.
New data published online by the Centers for Disease Control and Prevention show that in 11 communities in 2020, 1 in 36 (2.8%) 8-year-old children had been identified with autism spectrum disorder, an increase from 2.3% in 2018. The data also show that the early months of the pandemic may have disrupted autism detection efforts among 4-year-olds.
The investigators were supported by grants from the National Institutes of Health and the Simons Foundation Autism Research Initiative. Coauthors disclosed consulting for or receiving personal fees from biotechnology and pharmaceutical companies.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Headache before the revolution: A clinician looks back
Headache treatment before the early 1990s was marked by decades of improvisation with mostly unapproved agents, followed by an explosion of scientific interest and new treatments developed specifically for migraine.
But this is largely thanks to the sea change that occurred 30 years ago.
In an interview, Alan M. Rapoport, MD, editor-in-chief of Neurology Reviews, past president of the International Headache Society and clinical professor of neurology at UCLA’s David Geffen School of Medicine in Los Angeles, recalled what it was like to treat patients before and after triptan medications came onto the market.

After the first of these anti-migraine agents, sumatriptan, was approved by the Food and Drug Administration in late December 1992, headache specialists found themselves with a powerful, approved treatment that validated their commitment to solving the disorder, and helped put to rest a persistent but mistaken notion that migraine was a psychiatric condition affecting young women.
But in the 1970s and 1980s, “there wasn’t great science explaining the pathophysiology of common primary headaches like tension-type headache, cluster headache, and migraine,” Dr. Rapoport recalled. “There is often comorbid depression and anxiety with migraine, and sometimes more serious psychiatric disease, but it doesn’t mean migraine is caused by psychological issues. Now we see it clearly as a disease of the brain, but it took years of investigation to prove that.”
The early years
Dr. Rapoport’s journey with headache began in 1972, when he joined a private neurology practice in Stamford and Greenwich, Conn. Neurologists were frowned upon then for having too much interest in headache, he said. There was poor remuneration for doctors treating headache patients, who were hard to properly diagnose and effectively care for. Few medications could effectively stop a migraine attack or reliably reduce the frequency of headaches or the disability they caused.
On weekends Dr. Rapoport covered emergency departments and ICUs at three hospitals, where standard treatment for a migraine attack was injectable opiates. Not only did this treatment aggravate nausea, a common migraine symptom, “but it did not stop the migraine process.” Once the pain relief wore off, patients woke up with the same headache, Dr. Rapoport recalled. “The other drug that was available was ergotamine tartrate” – a fungal alkaloid used since medieval times to treat headache – “given sublingually. It helped the headache slightly but increased the nausea. DHE, or dihydroergotamine, was available only by injection and not used very much.”
DHE, a semi-synthetic molecule based on ergotamine, had FDA approval for migraine, but was complicated to administer. Like the opioids, it provoked vomiting when given intravenously, in patients already suffering migraine-induced nausea. But Dr. Rapoport, along with some of his colleagues, felt that there was a role for DHE for the most severe subtypes of patients, those with long histories of frequent migraines.
“We put people in the hospital and we gave them intravenous DHE. Eventually I got the idea to give it intramuscularly or subcutaneously in the emergency room or my office. When you give it that way, it doesn’t work as quickly but has fewer side effects.” Dr. Rapoport designed a cocktail by coadministering promethazine for nausea, and eventually added a steroid, dexamethasone. The triple shots worked on most patients experiencing severe daily or near-daily migraine attacks, Dr. Rapoport saw, and he began administering the drug combination at The New England Center for Headache in Stamford and Greenwich, Conn., which he opened with Dr. Fred D. Sheftell in 1979.
“The triple shots really worked,” Dr. Rapoport recalled. “There was no need to keep patients in the office or emergency room for intravenous therapy. The patients never called to complain or came back the next day,” he said, as often occurred with opioid treatment.
Dr. Rapoport had learned early in his residency, in the late 1960s, from Dr. David R. Coddon, a neurologist at Mount Sinai hospital in New York, that a tricyclic antidepressant, imipramine, could be helpful in some patients with frequent migraine attacks. As evidence trickled in that other antidepressants, beta-blockers, and antiepileptic drugs might have preventive properties, Dr. Rapoport and others prescribed them for certain patients. But of all the drugs in the headache specialists’ repertoire, few were approved for either treatment or prevention. “And this continued until the triptans,” Dr. Rapoport said.
The triptan era
Sumatriptan was developed by Glaxo for the acute treatment of migraine. The medication, first available only as self-administered subcutaneous injections, was originally designed to bind to vascular serotonin receptors to allow selective constriction of cranial vessels that dilate, causing pain, during a migraine attack. (Years later it was discovered that triptans also worked as anti-inflammatory agents that decreased the release of the neurotransmitter calcitonin gene-related peptide, or CGRP.)
Triptans “changed the world for migraine patients and for me,” Dr. Rapoport said. “I could now prescribe a medication that people could take at home to decrease or stop the migraine process in an hour or two.” The success of the triptans prompted pharmaceutical companies to search for new, more effective ways to treat migraine attacks, with better tolerability.
Seven different triptans were developed, some as injections or tablets and others as nasal sprays. “If one triptan didn’t work, we’d give a second and rarely a third,” Dr. Rapoport said. “We learned that if oral triptans did not work, the most likely issue was that it was not rapidly absorbed from the small intestine, as migraine patients have nausea, poor GI absorption, and slow transit times. This prompted the greater use of injections and nasal sprays.” Headache specialists began combining triptan treatment with nonsteroidal anti-inflammatory drugs, offering further relief for the acute care of migraine.
Medication overuse headache
The years between 1993 and 2000, which saw all the current triptan drugs come onto the market, was an exhilarating one for headache specialists. But even those who were thrilled by the possibilities of the triptans, like Dr. Rapoport, soon came to recognize their limitations, in terms of side effects and poor tolerability for some patients.
Specialists also noticed something unsettling about the triptans: that patients’ headaches seemed to recur within a day, or occur more frequently over time, with higher medication use.
Medication overuse headache (MOH) was known to occur when patients treated migraine too often with acute care medications, especially over-the-counter analgesics and prescription opioids and barbiturates. Dr. Rapoport began warning at conferences and in seminars that MOH seemed to occur with the triptans as well. “In the beginning other doctors didn’t think the triptans could cause MOH, but I observed that patients who were taking triptans daily or almost daily were having increased headache frequency and the triptans stopped being effective. If they didn’t take the drug they were overusing, they were going to get much worse, almost like a withdrawal.”
Today, all seven triptans are now generic, and they remain a mainstay of migraine treatment: “Almost all of my patients are using, or have used a triptan,” Dr. Rapoport said. Yet researchers came to recognize the need for treatments targeting different pathways, both for prevention and acute care.
The next revolution: CGRP and gepants
Studies in the early 2000s began to show a link between the release of one ubiquitous nervous system neurotransmitter, calcitonin gene-related peptide, or CGRP, and migraine. They also noticed that blocking meningeal inflammation could lead to improvement in headache. Two new drug classes emerged from this science: monoclonal antibodies against CGRP or its receptor that had to be given by injection, and oral CGRP receptor blockers that could be used both as a preventive or as an acute care medication.
In 2018 the first monoclonal antibody against the CGRP receptor, erenumab (Aimovig, marketed by Amgen), delivered by injection, was approved for migraine prevention. Three others followed, most given by autoinjector, and one by IV infusion in office or hospital settings. “Those drugs are great,” Dr. Rapoport said. “You take one shot a month or every 3 months, and your headaches drop by 50% or more with very few side effects. Some patients actually see their migraines disappear.”
The following year ubrogepant (Ubrelvy, marketed by AbbVie), the first of a novel class of oral CGRP receptor blockers known as “gepants,” was approved to treat acute migraine. The FDA soon approved another gepant, rimegepant (Nurtec, marketed by Pfizer), which received indications both for prevention and for stopping a migraine attack acutely.
Both classes of therapies – the antibodies and the gepants – are far costlier than the triptans, which are all generic, and may not be needed for every migraine patient. With the gepants, for example, insurers may restrict use to people who have not responded to triptans or for whom triptans are contraindicated or cause too many adverse events. But the CGRP-targeted therapies as a whole “have been every bit as revolutionary” as the triptans, Dr. Rapoport said. The treatments work quickly to resolve headache and disability and get the patient functioning within an hour or two, and there are fewer side effects.
In a review article published in CNS Drugs in 2021, Dr. Rapoport and his colleagues reported that the anti-CGRP treatment with gepants did not appear linked to medication overuse headache, as virtually all previous acute care medication classes did, and could be used in patients who had previously reported MOH. “I am confident that over the next few years, more people will be using them as insurance coverage will improve for patients living with migraine,” he said.
Headache treatment today
Migraine specialists and patients now have a staggering range of therapeutic options. Approved treatments now include prevention of migraine with onabotulinumtoxinA (Botox, marketed by the Allergan division of AbbVie) injections, which work alone and with other medicines; acute care treatment with ditans like lasmiditan (Reyvow, marketed by Lilly*), a category of acute care medicines that work like triptans but target different serotonin receptors. Five devices have been cleared for migraine and other types of headache by the FDA. These work alone or along with medication and can be used acutely or preventively. The devices “should be used more,” Dr. Rapoport said, but are not yet well covered by insurance.
Thirty years after the triptans, scientists and researchers continue to explore the pathophysiology of headache disorders, finding new pathways and identifying new potential targets.
“There are many parts of the brain and brain stem that are involved, as well as the thalamus and hypothalamus,” Dr. Rapoport said. “It’s interesting that the newer medications, and some of the older ones, work in the peripheral nervous system, outside the brain stem in the trigeminovascular system, to modulate the central nervous system. We also know that the CGRP system is involved with cellular second-order messengers. Stimulating and blocking this chain of reactions with newer drugs may become treatments in the future.”
Recent research has focused on a blood vessel dilating neurotransmitter, pituitary adenylate-cyclase-activating polypeptide, or PACAP-38, as a potential therapeutic target. Psychedelic medications such as psilocybin, strong pain medications such as ketamine, and even cannabinoids such as marijuana have all been investigated in migraine. Biofeedback therapies, mindfulness, and other behavioral interventions also have proved effective.
“I expect the next 2-5 years to bring us many important clinical trials on new types of pharmacological treatments,” Dr. Rapoport said. “This is a wonderful time to be a doctor or nurse treating patients living with migraine. When I started out treating headache, 51 years ago, we had only ergotamine tartrate. Today we have so many therapies and combinations of therapies that I hardly know where to start.”
Dr. Rapoport has served as a consultant to or speaker for AbbVie, Amgen, Biohaven, Cala Health, Lundbeck, Satsuma, and Teva, among others.
*Correction, 3/30/23: An earlier version of this article misstated the name of the company that markets Reyvow.
Headache treatment before the early 1990s was marked by decades of improvisation with mostly unapproved agents, followed by an explosion of scientific interest and new treatments developed specifically for migraine.
But this is largely thanks to the sea change that occurred 30 years ago.
In an interview, Alan M. Rapoport, MD, editor-in-chief of Neurology Reviews, past president of the International Headache Society and clinical professor of neurology at UCLA’s David Geffen School of Medicine in Los Angeles, recalled what it was like to treat patients before and after triptan medications came onto the market.
After the first of these anti-migraine agents, sumatriptan, was approved by the Food and Drug Administration in late December 1992, headache specialists found themselves with a powerful, approved treatment that validated their commitment to solving the disorder, and helped put to rest a persistent but mistaken notion that migraine was a psychiatric condition affecting young women.
But in the 1970s and 1980s, “there wasn’t great science explaining the pathophysiology of common primary headaches like tension-type headache, cluster headache, and migraine,” Dr. Rapoport recalled. “There is often comorbid depression and anxiety with migraine, and sometimes more serious psychiatric disease, but it doesn’t mean migraine is caused by psychological issues. Now we see it clearly as a disease of the brain, but it took years of investigation to prove that.”
The early years
Dr. Rapoport’s journey with headache began in 1972, when he joined a private neurology practice in Stamford and Greenwich, Conn. Neurologists were frowned upon then for having too much interest in headache, he said. There was poor remuneration for doctors treating headache patients, who were hard to properly diagnose and effectively care for. Few medications could effectively stop a migraine attack or reliably reduce the frequency of headaches or the disability they caused.
On weekends Dr. Rapoport covered emergency departments and ICUs at three hospitals, where standard treatment for a migraine attack was injectable opiates. Not only did this treatment aggravate nausea, a common migraine symptom, “but it did not stop the migraine process.” Once the pain relief wore off, patients woke up with the same headache, Dr. Rapoport recalled. “The other drug that was available was ergotamine tartrate” – a fungal alkaloid used since medieval times to treat headache – “given sublingually. It helped the headache slightly but increased the nausea. DHE, or dihydroergotamine, was available only by injection and not used very much.”
DHE, a semi-synthetic molecule based on ergotamine, had FDA approval for migraine, but was complicated to administer. Like the opioids, it provoked vomiting when given intravenously, in patients already suffering migraine-induced nausea. But Dr. Rapoport, along with some of his colleagues, felt that there was a role for DHE for the most severe subtypes of patients, those with long histories of frequent migraines.
“We put people in the hospital and we gave them intravenous DHE. Eventually I got the idea to give it intramuscularly or subcutaneously in the emergency room or my office. When you give it that way, it doesn’t work as quickly but has fewer side effects.” Dr. Rapoport designed a cocktail by coadministering promethazine for nausea, and eventually added a steroid, dexamethasone. The triple shots worked on most patients experiencing severe daily or near-daily migraine attacks, Dr. Rapoport saw, and he began administering the drug combination at The New England Center for Headache in Stamford and Greenwich, Conn., which he opened with Dr. Fred D. Sheftell in 1979.
“The triple shots really worked,” Dr. Rapoport recalled. “There was no need to keep patients in the office or emergency room for intravenous therapy. The patients never called to complain or came back the next day,” he said, as often occurred with opioid treatment.
Dr. Rapoport had learned early in his residency, in the late 1960s, from Dr. David R. Coddon, a neurologist at Mount Sinai hospital in New York, that a tricyclic antidepressant, imipramine, could be helpful in some patients with frequent migraine attacks. As evidence trickled in that other antidepressants, beta-blockers, and antiepileptic drugs might have preventive properties, Dr. Rapoport and others prescribed them for certain patients. But of all the drugs in the headache specialists’ repertoire, few were approved for either treatment or prevention. “And this continued until the triptans,” Dr. Rapoport said.
The triptan era
Sumatriptan was developed by Glaxo for the acute treatment of migraine. The medication, first available only as self-administered subcutaneous injections, was originally designed to bind to vascular serotonin receptors to allow selective constriction of cranial vessels that dilate, causing pain, during a migraine attack. (Years later it was discovered that triptans also worked as anti-inflammatory agents that decreased the release of the neurotransmitter calcitonin gene-related peptide, or CGRP.)
Triptans “changed the world for migraine patients and for me,” Dr. Rapoport said. “I could now prescribe a medication that people could take at home to decrease or stop the migraine process in an hour or two.” The success of the triptans prompted pharmaceutical companies to search for new, more effective ways to treat migraine attacks, with better tolerability.
Seven different triptans were developed, some as injections or tablets and others as nasal sprays. “If one triptan didn’t work, we’d give a second and rarely a third,” Dr. Rapoport said. “We learned that if oral triptans did not work, the most likely issue was that it was not rapidly absorbed from the small intestine, as migraine patients have nausea, poor GI absorption, and slow transit times. This prompted the greater use of injections and nasal sprays.” Headache specialists began combining triptan treatment with nonsteroidal anti-inflammatory drugs, offering further relief for the acute care of migraine.
Medication overuse headache
The years between 1993 and 2000, which saw all the current triptan drugs come onto the market, was an exhilarating one for headache specialists. But even those who were thrilled by the possibilities of the triptans, like Dr. Rapoport, soon came to recognize their limitations, in terms of side effects and poor tolerability for some patients.
Specialists also noticed something unsettling about the triptans: that patients’ headaches seemed to recur within a day, or occur more frequently over time, with higher medication use.
Medication overuse headache (MOH) was known to occur when patients treated migraine too often with acute care medications, especially over-the-counter analgesics and prescription opioids and barbiturates. Dr. Rapoport began warning at conferences and in seminars that MOH seemed to occur with the triptans as well. “In the beginning other doctors didn’t think the triptans could cause MOH, but I observed that patients who were taking triptans daily or almost daily were having increased headache frequency and the triptans stopped being effective. If they didn’t take the drug they were overusing, they were going to get much worse, almost like a withdrawal.”
Today, all seven triptans are now generic, and they remain a mainstay of migraine treatment: “Almost all of my patients are using, or have used a triptan,” Dr. Rapoport said. Yet researchers came to recognize the need for treatments targeting different pathways, both for prevention and acute care.
The next revolution: CGRP and gepants
Studies in the early 2000s began to show a link between the release of one ubiquitous nervous system neurotransmitter, calcitonin gene-related peptide, or CGRP, and migraine. They also noticed that blocking meningeal inflammation could lead to improvement in headache. Two new drug classes emerged from this science: monoclonal antibodies against CGRP or its receptor that had to be given by injection, and oral CGRP receptor blockers that could be used both as a preventive or as an acute care medication.
In 2018 the first monoclonal antibody against the CGRP receptor, erenumab (Aimovig, marketed by Amgen), delivered by injection, was approved for migraine prevention. Three others followed, most given by autoinjector, and one by IV infusion in office or hospital settings. “Those drugs are great,” Dr. Rapoport said. “You take one shot a month or every 3 months, and your headaches drop by 50% or more with very few side effects. Some patients actually see their migraines disappear.”
The following year ubrogepant (Ubrelvy, marketed by AbbVie), the first of a novel class of oral CGRP receptor blockers known as “gepants,” was approved to treat acute migraine. The FDA soon approved another gepant, rimegepant (Nurtec, marketed by Pfizer), which received indications both for prevention and for stopping a migraine attack acutely.
Both classes of therapies – the antibodies and the gepants – are far costlier than the triptans, which are all generic, and may not be needed for every migraine patient. With the gepants, for example, insurers may restrict use to people who have not responded to triptans or for whom triptans are contraindicated or cause too many adverse events. But the CGRP-targeted therapies as a whole “have been every bit as revolutionary” as the triptans, Dr. Rapoport said. The treatments work quickly to resolve headache and disability and get the patient functioning within an hour or two, and there are fewer side effects.
In a review article published in CNS Drugs in 2021, Dr. Rapoport and his colleagues reported that the anti-CGRP treatment with gepants did not appear linked to medication overuse headache, as virtually all previous acute care medication classes did, and could be used in patients who had previously reported MOH. “I am confident that over the next few years, more people will be using them as insurance coverage will improve for patients living with migraine,” he said.
Headache treatment today
Migraine specialists and patients now have a staggering range of therapeutic options. Approved treatments now include prevention of migraine with onabotulinumtoxinA (Botox, marketed by the Allergan division of AbbVie) injections, which work alone and with other medicines; acute care treatment with ditans like lasmiditan (Reyvow, marketed by Lilly*), a category of acute care medicines that work like triptans but target different serotonin receptors. Five devices have been cleared for migraine and other types of headache by the FDA. These work alone or along with medication and can be used acutely or preventively. The devices “should be used more,” Dr. Rapoport said, but are not yet well covered by insurance.
Thirty years after the triptans, scientists and researchers continue to explore the pathophysiology of headache disorders, finding new pathways and identifying new potential targets.
“There are many parts of the brain and brain stem that are involved, as well as the thalamus and hypothalamus,” Dr. Rapoport said. “It’s interesting that the newer medications, and some of the older ones, work in the peripheral nervous system, outside the brain stem in the trigeminovascular system, to modulate the central nervous system. We also know that the CGRP system is involved with cellular second-order messengers. Stimulating and blocking this chain of reactions with newer drugs may become treatments in the future.”
Recent research has focused on a blood vessel dilating neurotransmitter, pituitary adenylate-cyclase-activating polypeptide, or PACAP-38, as a potential therapeutic target. Psychedelic medications such as psilocybin, strong pain medications such as ketamine, and even cannabinoids such as marijuana have all been investigated in migraine. Biofeedback therapies, mindfulness, and other behavioral interventions also have proved effective.
“I expect the next 2-5 years to bring us many important clinical trials on new types of pharmacological treatments,” Dr. Rapoport said. “This is a wonderful time to be a doctor or nurse treating patients living with migraine. When I started out treating headache, 51 years ago, we had only ergotamine tartrate. Today we have so many therapies and combinations of therapies that I hardly know where to start.”
Dr. Rapoport has served as a consultant to or speaker for AbbVie, Amgen, Biohaven, Cala Health, Lundbeck, Satsuma, and Teva, among others.
*Correction, 3/30/23: An earlier version of this article misstated the name of the company that markets Reyvow.
Headache treatment before the early 1990s was marked by decades of improvisation with mostly unapproved agents, followed by an explosion of scientific interest and new treatments developed specifically for migraine.
But this is largely thanks to the sea change that occurred 30 years ago.
In an interview, Alan M. Rapoport, MD, editor-in-chief of Neurology Reviews, past president of the International Headache Society and clinical professor of neurology at UCLA’s David Geffen School of Medicine in Los Angeles, recalled what it was like to treat patients before and after triptan medications came onto the market.
After the first of these anti-migraine agents, sumatriptan, was approved by the Food and Drug Administration in late December 1992, headache specialists found themselves with a powerful, approved treatment that validated their commitment to solving the disorder, and helped put to rest a persistent but mistaken notion that migraine was a psychiatric condition affecting young women.
But in the 1970s and 1980s, “there wasn’t great science explaining the pathophysiology of common primary headaches like tension-type headache, cluster headache, and migraine,” Dr. Rapoport recalled. “There is often comorbid depression and anxiety with migraine, and sometimes more serious psychiatric disease, but it doesn’t mean migraine is caused by psychological issues. Now we see it clearly as a disease of the brain, but it took years of investigation to prove that.”
The early years
Dr. Rapoport’s journey with headache began in 1972, when he joined a private neurology practice in Stamford and Greenwich, Conn. Neurologists were frowned upon then for having too much interest in headache, he said. There was poor remuneration for doctors treating headache patients, who were hard to properly diagnose and effectively care for. Few medications could effectively stop a migraine attack or reliably reduce the frequency of headaches or the disability they caused.
On weekends Dr. Rapoport covered emergency departments and ICUs at three hospitals, where standard treatment for a migraine attack was injectable opiates. Not only did this treatment aggravate nausea, a common migraine symptom, “but it did not stop the migraine process.” Once the pain relief wore off, patients woke up with the same headache, Dr. Rapoport recalled. “The other drug that was available was ergotamine tartrate” – a fungal alkaloid used since medieval times to treat headache – “given sublingually. It helped the headache slightly but increased the nausea. DHE, or dihydroergotamine, was available only by injection and not used very much.”
DHE, a semi-synthetic molecule based on ergotamine, had FDA approval for migraine, but was complicated to administer. Like the opioids, it provoked vomiting when given intravenously, in patients already suffering migraine-induced nausea. But Dr. Rapoport, along with some of his colleagues, felt that there was a role for DHE for the most severe subtypes of patients, those with long histories of frequent migraines.
“We put people in the hospital and we gave them intravenous DHE. Eventually I got the idea to give it intramuscularly or subcutaneously in the emergency room or my office. When you give it that way, it doesn’t work as quickly but has fewer side effects.” Dr. Rapoport designed a cocktail by coadministering promethazine for nausea, and eventually added a steroid, dexamethasone. The triple shots worked on most patients experiencing severe daily or near-daily migraine attacks, Dr. Rapoport saw, and he began administering the drug combination at The New England Center for Headache in Stamford and Greenwich, Conn., which he opened with Dr. Fred D. Sheftell in 1979.
“The triple shots really worked,” Dr. Rapoport recalled. “There was no need to keep patients in the office or emergency room for intravenous therapy. The patients never called to complain or came back the next day,” he said, as often occurred with opioid treatment.
Dr. Rapoport had learned early in his residency, in the late 1960s, from Dr. David R. Coddon, a neurologist at Mount Sinai hospital in New York, that a tricyclic antidepressant, imipramine, could be helpful in some patients with frequent migraine attacks. As evidence trickled in that other antidepressants, beta-blockers, and antiepileptic drugs might have preventive properties, Dr. Rapoport and others prescribed them for certain patients. But of all the drugs in the headache specialists’ repertoire, few were approved for either treatment or prevention. “And this continued until the triptans,” Dr. Rapoport said.
The triptan era
Sumatriptan was developed by Glaxo for the acute treatment of migraine. The medication, first available only as self-administered subcutaneous injections, was originally designed to bind to vascular serotonin receptors to allow selective constriction of cranial vessels that dilate, causing pain, during a migraine attack. (Years later it was discovered that triptans also worked as anti-inflammatory agents that decreased the release of the neurotransmitter calcitonin gene-related peptide, or CGRP.)
Triptans “changed the world for migraine patients and for me,” Dr. Rapoport said. “I could now prescribe a medication that people could take at home to decrease or stop the migraine process in an hour or two.” The success of the triptans prompted pharmaceutical companies to search for new, more effective ways to treat migraine attacks, with better tolerability.
Seven different triptans were developed, some as injections or tablets and others as nasal sprays. “If one triptan didn’t work, we’d give a second and rarely a third,” Dr. Rapoport said. “We learned that if oral triptans did not work, the most likely issue was that it was not rapidly absorbed from the small intestine, as migraine patients have nausea, poor GI absorption, and slow transit times. This prompted the greater use of injections and nasal sprays.” Headache specialists began combining triptan treatment with nonsteroidal anti-inflammatory drugs, offering further relief for the acute care of migraine.
Medication overuse headache
The years between 1993 and 2000, which saw all the current triptan drugs come onto the market, was an exhilarating one for headache specialists. But even those who were thrilled by the possibilities of the triptans, like Dr. Rapoport, soon came to recognize their limitations, in terms of side effects and poor tolerability for some patients.
Specialists also noticed something unsettling about the triptans: that patients’ headaches seemed to recur within a day, or occur more frequently over time, with higher medication use.
Medication overuse headache (MOH) was known to occur when patients treated migraine too often with acute care medications, especially over-the-counter analgesics and prescription opioids and barbiturates. Dr. Rapoport began warning at conferences and in seminars that MOH seemed to occur with the triptans as well. “In the beginning other doctors didn’t think the triptans could cause MOH, but I observed that patients who were taking triptans daily or almost daily were having increased headache frequency and the triptans stopped being effective. If they didn’t take the drug they were overusing, they were going to get much worse, almost like a withdrawal.”
Today, all seven triptans are now generic, and they remain a mainstay of migraine treatment: “Almost all of my patients are using, or have used a triptan,” Dr. Rapoport said. Yet researchers came to recognize the need for treatments targeting different pathways, both for prevention and acute care.
The next revolution: CGRP and gepants
Studies in the early 2000s began to show a link between the release of one ubiquitous nervous system neurotransmitter, calcitonin gene-related peptide, or CGRP, and migraine. They also noticed that blocking meningeal inflammation could lead to improvement in headache. Two new drug classes emerged from this science: monoclonal antibodies against CGRP or its receptor that had to be given by injection, and oral CGRP receptor blockers that could be used both as a preventive or as an acute care medication.
In 2018 the first monoclonal antibody against the CGRP receptor, erenumab (Aimovig, marketed by Amgen), delivered by injection, was approved for migraine prevention. Three others followed, most given by autoinjector, and one by IV infusion in office or hospital settings. “Those drugs are great,” Dr. Rapoport said. “You take one shot a month or every 3 months, and your headaches drop by 50% or more with very few side effects. Some patients actually see their migraines disappear.”
The following year ubrogepant (Ubrelvy, marketed by AbbVie), the first of a novel class of oral CGRP receptor blockers known as “gepants,” was approved to treat acute migraine. The FDA soon approved another gepant, rimegepant (Nurtec, marketed by Pfizer), which received indications both for prevention and for stopping a migraine attack acutely.
Both classes of therapies – the antibodies and the gepants – are far costlier than the triptans, which are all generic, and may not be needed for every migraine patient. With the gepants, for example, insurers may restrict use to people who have not responded to triptans or for whom triptans are contraindicated or cause too many adverse events. But the CGRP-targeted therapies as a whole “have been every bit as revolutionary” as the triptans, Dr. Rapoport said. The treatments work quickly to resolve headache and disability and get the patient functioning within an hour or two, and there are fewer side effects.
In a review article published in CNS Drugs in 2021, Dr. Rapoport and his colleagues reported that the anti-CGRP treatment with gepants did not appear linked to medication overuse headache, as virtually all previous acute care medication classes did, and could be used in patients who had previously reported MOH. “I am confident that over the next few years, more people will be using them as insurance coverage will improve for patients living with migraine,” he said.
Headache treatment today
Migraine specialists and patients now have a staggering range of therapeutic options. Approved treatments now include prevention of migraine with onabotulinumtoxinA (Botox, marketed by the Allergan division of AbbVie) injections, which work alone and with other medicines; acute care treatment with ditans like lasmiditan (Reyvow, marketed by Lilly*), a category of acute care medicines that work like triptans but target different serotonin receptors. Five devices have been cleared for migraine and other types of headache by the FDA. These work alone or along with medication and can be used acutely or preventively. The devices “should be used more,” Dr. Rapoport said, but are not yet well covered by insurance.
Thirty years after the triptans, scientists and researchers continue to explore the pathophysiology of headache disorders, finding new pathways and identifying new potential targets.
“There are many parts of the brain and brain stem that are involved, as well as the thalamus and hypothalamus,” Dr. Rapoport said. “It’s interesting that the newer medications, and some of the older ones, work in the peripheral nervous system, outside the brain stem in the trigeminovascular system, to modulate the central nervous system. We also know that the CGRP system is involved with cellular second-order messengers. Stimulating and blocking this chain of reactions with newer drugs may become treatments in the future.”
Recent research has focused on a blood vessel dilating neurotransmitter, pituitary adenylate-cyclase-activating polypeptide, or PACAP-38, as a potential therapeutic target. Psychedelic medications such as psilocybin, strong pain medications such as ketamine, and even cannabinoids such as marijuana have all been investigated in migraine. Biofeedback therapies, mindfulness, and other behavioral interventions also have proved effective.
“I expect the next 2-5 years to bring us many important clinical trials on new types of pharmacological treatments,” Dr. Rapoport said. “This is a wonderful time to be a doctor or nurse treating patients living with migraine. When I started out treating headache, 51 years ago, we had only ergotamine tartrate. Today we have so many therapies and combinations of therapies that I hardly know where to start.”
Dr. Rapoport has served as a consultant to or speaker for AbbVie, Amgen, Biohaven, Cala Health, Lundbeck, Satsuma, and Teva, among others.
*Correction, 3/30/23: An earlier version of this article misstated the name of the company that markets Reyvow.
Tooth loss and diabetes together hasten mental decline
most specifically in those 65-74 years of age, new findings suggest.
The data come from a 12-year follow-up of older adults in a nationally representative U.S. survey.
“From a clinical perspective, our study demonstrates the importance of improving access to dental health care and integrating primary dental and medical care. Health care professionals and family caregivers should pay close attention to the cognitive status of diabetic older adults with poor oral health status,” lead author Bei Wu, PhD, of New York University, said in an interview. Dr. Wu is the Dean’s Professor in Global Health and codirector of the NYU Aging Incubator.
Moreover, said Dr. Wu: “For individuals with both poor oral health and diabetes, regular dental visits should be encouraged in addition to adherence to the diabetes self-care protocol.”
Diabetes has long been recognized as a risk factor for cognitive decline, but the findings have been inconsistent for different age groups. Tooth loss has also been linked to cognitive decline and dementia, as well as diabetes.
The mechanisms aren’t entirely clear, but “co-occurring diabetes and poor oral health may increase the risk for dementia, possibly via the potentially interrelated pathways of chronic inflammation and cardiovascular risk factors,” Dr. Wu said.
The new study, published in the Journal of Dental Research, is the first to examine the relationships between all three conditions by age group.
Diabetes, edentulism, and cognitive decline
The data came from a total of 9,948 participants in the Health and Retirement Study (HRS) from 2006 to 2018. At baseline, 5,440 participants were aged 65-74 years, 3,300 were aged 75-84, and 1,208 were aged 85 years or older.
They were assessed every 2 years using the 35-point Telephone Survey for Cognitive Status, which included tests of immediate and delayed word recall, repeated subtracting by 7, counting backward from 20, naming objects, and naming the president and vice president of the U.S. As might be expected, the youngest group scored the highest, averaging 23 points, while the oldest group scored lowest, at 18.5 points.
Participants were also asked if they had ever been told by a doctor that they have diabetes. Another question was: “Have you lost all of your upper and lower natural permanent teeth?”
The condition of having no teeth is known as edentulism.
The percentages of participants who reported having both diabetes and edentulism were 6.0%, 6.7%, and 5.0% for those aged 65-74 years, 75-84 years, and 85 years or older, respectively. The proportions with neither of those conditions were 63.5%, 60.4%, and 58.3% in those three age groups, respectively (P < .001).
Compared with their counterparts with neither diabetes nor edentulism at baseline, older adults with both conditions aged 65-74 years (P < .001) and aged 75-84 years had worse cognitive function (P < .001).
In terms of the rate of cognitive decline, compared with those with neither condition from the same age cohort, older adults aged 65-74 years with both conditions declined at a higher rate (P < .001).
Having diabetes alone led to accelerated cognitive decline in older adults aged 65-74 years (P < .001). Having edentulism alone led to accelerated decline in older adults aged 65-74 years (P < .001) and older adults aged 75-84 years (P < 0.01).
“Our study finds the co-occurrence of diabetes and edentulism led to a worse cognitive function and a faster cognitive decline in older adults aged 65-74 years,” say Wu and colleagues.
Study limitations: Better data needed
The study has several limitations, most of them due to the data source. For example, while the HRS collects detailed information on cognitive status, edentulism is its only measure of oral health. There were no data on whether individuals had replacements such as dentures or implants that would affect their ability to eat, which could influence other health factors.
“I have made repeated appeals for federal funding to collect more oral health-related information in large national surveys,” Dr. Wu told this news organization.
Similarly, assessments of diabetes status such as hemoglobin A1c were only available for small subsets and not sufficient to demonstrate statistical significance, she explained.
Dr. Wu suggested that both oral health and cognitive screening might be included in the “Welcome to Medicare” preventive visit. In addition, “Oral hygiene practice should also be highlighted to improve cognitive health. Developing dental care interventions and programs are needed for reducing the societal cost of dementia.”
The study was partially supported by the National Institutes of Health. The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
most specifically in those 65-74 years of age, new findings suggest.
The data come from a 12-year follow-up of older adults in a nationally representative U.S. survey.
“From a clinical perspective, our study demonstrates the importance of improving access to dental health care and integrating primary dental and medical care. Health care professionals and family caregivers should pay close attention to the cognitive status of diabetic older adults with poor oral health status,” lead author Bei Wu, PhD, of New York University, said in an interview. Dr. Wu is the Dean’s Professor in Global Health and codirector of the NYU Aging Incubator.
Moreover, said Dr. Wu: “For individuals with both poor oral health and diabetes, regular dental visits should be encouraged in addition to adherence to the diabetes self-care protocol.”
Diabetes has long been recognized as a risk factor for cognitive decline, but the findings have been inconsistent for different age groups. Tooth loss has also been linked to cognitive decline and dementia, as well as diabetes.
The mechanisms aren’t entirely clear, but “co-occurring diabetes and poor oral health may increase the risk for dementia, possibly via the potentially interrelated pathways of chronic inflammation and cardiovascular risk factors,” Dr. Wu said.
The new study, published in the Journal of Dental Research, is the first to examine the relationships between all three conditions by age group.
Diabetes, edentulism, and cognitive decline
The data came from a total of 9,948 participants in the Health and Retirement Study (HRS) from 2006 to 2018. At baseline, 5,440 participants were aged 65-74 years, 3,300 were aged 75-84, and 1,208 were aged 85 years or older.
They were assessed every 2 years using the 35-point Telephone Survey for Cognitive Status, which included tests of immediate and delayed word recall, repeated subtracting by 7, counting backward from 20, naming objects, and naming the president and vice president of the U.S. As might be expected, the youngest group scored the highest, averaging 23 points, while the oldest group scored lowest, at 18.5 points.
Participants were also asked if they had ever been told by a doctor that they have diabetes. Another question was: “Have you lost all of your upper and lower natural permanent teeth?”
The condition of having no teeth is known as edentulism.
The percentages of participants who reported having both diabetes and edentulism were 6.0%, 6.7%, and 5.0% for those aged 65-74 years, 75-84 years, and 85 years or older, respectively. The proportions with neither of those conditions were 63.5%, 60.4%, and 58.3% in those three age groups, respectively (P < .001).
Compared with their counterparts with neither diabetes nor edentulism at baseline, older adults with both conditions aged 65-74 years (P < .001) and aged 75-84 years had worse cognitive function (P < .001).
In terms of the rate of cognitive decline, compared with those with neither condition from the same age cohort, older adults aged 65-74 years with both conditions declined at a higher rate (P < .001).
Having diabetes alone led to accelerated cognitive decline in older adults aged 65-74 years (P < .001). Having edentulism alone led to accelerated decline in older adults aged 65-74 years (P < .001) and older adults aged 75-84 years (P < 0.01).
“Our study finds the co-occurrence of diabetes and edentulism led to a worse cognitive function and a faster cognitive decline in older adults aged 65-74 years,” say Wu and colleagues.
Study limitations: Better data needed
The study has several limitations, most of them due to the data source. For example, while the HRS collects detailed information on cognitive status, edentulism is its only measure of oral health. There were no data on whether individuals had replacements such as dentures or implants that would affect their ability to eat, which could influence other health factors.
“I have made repeated appeals for federal funding to collect more oral health-related information in large national surveys,” Dr. Wu told this news organization.
Similarly, assessments of diabetes status such as hemoglobin A1c were only available for small subsets and not sufficient to demonstrate statistical significance, she explained.
Dr. Wu suggested that both oral health and cognitive screening might be included in the “Welcome to Medicare” preventive visit. In addition, “Oral hygiene practice should also be highlighted to improve cognitive health. Developing dental care interventions and programs are needed for reducing the societal cost of dementia.”
The study was partially supported by the National Institutes of Health. The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
most specifically in those 65-74 years of age, new findings suggest.
The data come from a 12-year follow-up of older adults in a nationally representative U.S. survey.
“From a clinical perspective, our study demonstrates the importance of improving access to dental health care and integrating primary dental and medical care. Health care professionals and family caregivers should pay close attention to the cognitive status of diabetic older adults with poor oral health status,” lead author Bei Wu, PhD, of New York University, said in an interview. Dr. Wu is the Dean’s Professor in Global Health and codirector of the NYU Aging Incubator.
Moreover, said Dr. Wu: “For individuals with both poor oral health and diabetes, regular dental visits should be encouraged in addition to adherence to the diabetes self-care protocol.”
Diabetes has long been recognized as a risk factor for cognitive decline, but the findings have been inconsistent for different age groups. Tooth loss has also been linked to cognitive decline and dementia, as well as diabetes.
The mechanisms aren’t entirely clear, but “co-occurring diabetes and poor oral health may increase the risk for dementia, possibly via the potentially interrelated pathways of chronic inflammation and cardiovascular risk factors,” Dr. Wu said.
The new study, published in the Journal of Dental Research, is the first to examine the relationships between all three conditions by age group.
Diabetes, edentulism, and cognitive decline
The data came from a total of 9,948 participants in the Health and Retirement Study (HRS) from 2006 to 2018. At baseline, 5,440 participants were aged 65-74 years, 3,300 were aged 75-84, and 1,208 were aged 85 years or older.
They were assessed every 2 years using the 35-point Telephone Survey for Cognitive Status, which included tests of immediate and delayed word recall, repeated subtracting by 7, counting backward from 20, naming objects, and naming the president and vice president of the U.S. As might be expected, the youngest group scored the highest, averaging 23 points, while the oldest group scored lowest, at 18.5 points.
Participants were also asked if they had ever been told by a doctor that they have diabetes. Another question was: “Have you lost all of your upper and lower natural permanent teeth?”
The condition of having no teeth is known as edentulism.
The percentages of participants who reported having both diabetes and edentulism were 6.0%, 6.7%, and 5.0% for those aged 65-74 years, 75-84 years, and 85 years or older, respectively. The proportions with neither of those conditions were 63.5%, 60.4%, and 58.3% in those three age groups, respectively (P < .001).
Compared with their counterparts with neither diabetes nor edentulism at baseline, older adults with both conditions aged 65-74 years (P < .001) and aged 75-84 years had worse cognitive function (P < .001).
In terms of the rate of cognitive decline, compared with those with neither condition from the same age cohort, older adults aged 65-74 years with both conditions declined at a higher rate (P < .001).
Having diabetes alone led to accelerated cognitive decline in older adults aged 65-74 years (P < .001). Having edentulism alone led to accelerated decline in older adults aged 65-74 years (P < .001) and older adults aged 75-84 years (P < 0.01).
“Our study finds the co-occurrence of diabetes and edentulism led to a worse cognitive function and a faster cognitive decline in older adults aged 65-74 years,” say Wu and colleagues.
Study limitations: Better data needed
The study has several limitations, most of them due to the data source. For example, while the HRS collects detailed information on cognitive status, edentulism is its only measure of oral health. There were no data on whether individuals had replacements such as dentures or implants that would affect their ability to eat, which could influence other health factors.
“I have made repeated appeals for federal funding to collect more oral health-related information in large national surveys,” Dr. Wu told this news organization.
Similarly, assessments of diabetes status such as hemoglobin A1c were only available for small subsets and not sufficient to demonstrate statistical significance, she explained.
Dr. Wu suggested that both oral health and cognitive screening might be included in the “Welcome to Medicare” preventive visit. In addition, “Oral hygiene practice should also be highlighted to improve cognitive health. Developing dental care interventions and programs are needed for reducing the societal cost of dementia.”
The study was partially supported by the National Institutes of Health. The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF DENTAL RESEARCH
Mortality risk in epilepsy: New data
new research shows.
“To our knowledge, this is the only study that has assessed the cause-specific mortality risk among people with epilepsy according to age and disease course,” investigators led by Seo-Young Lee, MD, PhD, of Kangwon National University, Chuncheon, South Korea, write. “Understanding cause-specific mortality risk, particularly the risk of external causes, is important because they are mostly preventable.”
The findings were published online in Neurology.
Higher mortality risk
For the study, researchers analyzed data from the National Health Insurance Service database in Korea from 2006 to 2017 and vital statistics from Statistics Korea from 2008 to 2017.
The study population included 138,998 patients with newly treated epilepsy, with an average at diagnosis of 48.6 years.
Over 665,928 person years of follow-up (mean follow-up, 4.79 years), 20.095 patients died.
People with epilepsy had more than twice the risk for death, compared with the overall population (standardized mortality ratio, 2.25; 95% confidence interval, 2.22-2.28). Mortality was highest in children aged 4 years or younger and was higher in the first year after diagnosis and in women at all age points.
People with epilepsy had a higher mortality risk, compared with the general public, regardless of how many anti-seizure medications they were taking. Those taking only one medication had a 156% higher risk for death (SMR, 1.56; 95% CI, 1.53-1.60), compared with 493% higher risk in those taking four or more medications (SMR, 4.93; 95% CI, 4.76-5.10).
Where patients lived also played a role in mortality risk. Living in a rural area was associated with a 247% higher risk for death, compared with people without epilepsy who lived in the same area (SMR, 2.47; 95% CI, 2.41-2.53), and the risk was 203% higher risk among those living in urban centers (SMR, 2.03; 95% CI, 1.98-2.09).
Although people with comorbidities had higher mortality rates, even those without any other health conditions had a 161% higher risk for death, compared with people without epilepsy (SMR, 1.61; 95% CI, 1.50-1.72).
Causes of death
The most frequent causes of death were malignant neoplasm and cerebrovascular disease, which researchers noted are thought to be underlying causes of epilepsy.
Among external causes of death, suicide was the most common cause (2.6%). The suicide rate was highest among younger patients and gradually decreased with age.
Deaths tied directly to epilepsy, transport accidents, or falls were lower in this study than had been previously reported, which may be due to adequate seizure control or because the number of older people with epilepsy and comorbidities is higher in Korea than that reported in other countries.
“To reduce mortality in people with epilepsy, comprehensive efforts [are needed], including a national policy against stigma of epilepsy and clinicians’ total management such as risk stratification, education about injury prevention, and monitoring for suicidal ideation with psychological intervention, as well as active control of seizures,” the authors write.
Generalizable findings
Joseph Sirven, MD, professor of neurology at Mayo Clinic Florida, Jacksonville, said that although the study included only Korean patients, the findings are applicable to other counties.
That researchers found patients with epilepsy were more than twice as likely to die prematurely, compared with the general population wasn’t particularly surprising, Dr. Sirven said.
“What struck me the most was the fact that even patients who were on a single drug and seemingly well controlled also had excess mortality reported,” Dr. Sirven said. “That these risks occur should be part of what we tell all patients with epilepsy so that they can better arm themselves with information and help to address some of the risks that this study showed.”
Another important finding is the risk for suicide in patients with epilepsy, especially those who are newly diagnosed, he said.
“When we treat a patient with epilepsy, it should not just be about seizures, but we need to inquire about the psychiatric comorbidities and more importantly manage them in a comprehensive manner,” Dr. Sirven said.
The study was funded by Soonchunhyang University Research Fund and the Korea Health Technology R&D Project. The study authors and Dr. Sirven report no relevant financial conflicts.
A version of this article first appeared on Medscape.com.
new research shows.
“To our knowledge, this is the only study that has assessed the cause-specific mortality risk among people with epilepsy according to age and disease course,” investigators led by Seo-Young Lee, MD, PhD, of Kangwon National University, Chuncheon, South Korea, write. “Understanding cause-specific mortality risk, particularly the risk of external causes, is important because they are mostly preventable.”
The findings were published online in Neurology.
Higher mortality risk
For the study, researchers analyzed data from the National Health Insurance Service database in Korea from 2006 to 2017 and vital statistics from Statistics Korea from 2008 to 2017.
The study population included 138,998 patients with newly treated epilepsy, with an average at diagnosis of 48.6 years.
Over 665,928 person years of follow-up (mean follow-up, 4.79 years), 20.095 patients died.
People with epilepsy had more than twice the risk for death, compared with the overall population (standardized mortality ratio, 2.25; 95% confidence interval, 2.22-2.28). Mortality was highest in children aged 4 years or younger and was higher in the first year after diagnosis and in women at all age points.
People with epilepsy had a higher mortality risk, compared with the general public, regardless of how many anti-seizure medications they were taking. Those taking only one medication had a 156% higher risk for death (SMR, 1.56; 95% CI, 1.53-1.60), compared with 493% higher risk in those taking four or more medications (SMR, 4.93; 95% CI, 4.76-5.10).
Where patients lived also played a role in mortality risk. Living in a rural area was associated with a 247% higher risk for death, compared with people without epilepsy who lived in the same area (SMR, 2.47; 95% CI, 2.41-2.53), and the risk was 203% higher risk among those living in urban centers (SMR, 2.03; 95% CI, 1.98-2.09).
Although people with comorbidities had higher mortality rates, even those without any other health conditions had a 161% higher risk for death, compared with people without epilepsy (SMR, 1.61; 95% CI, 1.50-1.72).
Causes of death
The most frequent causes of death were malignant neoplasm and cerebrovascular disease, which researchers noted are thought to be underlying causes of epilepsy.
Among external causes of death, suicide was the most common cause (2.6%). The suicide rate was highest among younger patients and gradually decreased with age.
Deaths tied directly to epilepsy, transport accidents, or falls were lower in this study than had been previously reported, which may be due to adequate seizure control or because the number of older people with epilepsy and comorbidities is higher in Korea than that reported in other countries.
“To reduce mortality in people with epilepsy, comprehensive efforts [are needed], including a national policy against stigma of epilepsy and clinicians’ total management such as risk stratification, education about injury prevention, and monitoring for suicidal ideation with psychological intervention, as well as active control of seizures,” the authors write.
Generalizable findings
Joseph Sirven, MD, professor of neurology at Mayo Clinic Florida, Jacksonville, said that although the study included only Korean patients, the findings are applicable to other counties.
That researchers found patients with epilepsy were more than twice as likely to die prematurely, compared with the general population wasn’t particularly surprising, Dr. Sirven said.
“What struck me the most was the fact that even patients who were on a single drug and seemingly well controlled also had excess mortality reported,” Dr. Sirven said. “That these risks occur should be part of what we tell all patients with epilepsy so that they can better arm themselves with information and help to address some of the risks that this study showed.”
Another important finding is the risk for suicide in patients with epilepsy, especially those who are newly diagnosed, he said.
“When we treat a patient with epilepsy, it should not just be about seizures, but we need to inquire about the psychiatric comorbidities and more importantly manage them in a comprehensive manner,” Dr. Sirven said.
The study was funded by Soonchunhyang University Research Fund and the Korea Health Technology R&D Project. The study authors and Dr. Sirven report no relevant financial conflicts.
A version of this article first appeared on Medscape.com.
new research shows.
“To our knowledge, this is the only study that has assessed the cause-specific mortality risk among people with epilepsy according to age and disease course,” investigators led by Seo-Young Lee, MD, PhD, of Kangwon National University, Chuncheon, South Korea, write. “Understanding cause-specific mortality risk, particularly the risk of external causes, is important because they are mostly preventable.”
The findings were published online in Neurology.
Higher mortality risk
For the study, researchers analyzed data from the National Health Insurance Service database in Korea from 2006 to 2017 and vital statistics from Statistics Korea from 2008 to 2017.
The study population included 138,998 patients with newly treated epilepsy, with an average at diagnosis of 48.6 years.
Over 665,928 person years of follow-up (mean follow-up, 4.79 years), 20.095 patients died.
People with epilepsy had more than twice the risk for death, compared with the overall population (standardized mortality ratio, 2.25; 95% confidence interval, 2.22-2.28). Mortality was highest in children aged 4 years or younger and was higher in the first year after diagnosis and in women at all age points.
People with epilepsy had a higher mortality risk, compared with the general public, regardless of how many anti-seizure medications they were taking. Those taking only one medication had a 156% higher risk for death (SMR, 1.56; 95% CI, 1.53-1.60), compared with 493% higher risk in those taking four or more medications (SMR, 4.93; 95% CI, 4.76-5.10).
Where patients lived also played a role in mortality risk. Living in a rural area was associated with a 247% higher risk for death, compared with people without epilepsy who lived in the same area (SMR, 2.47; 95% CI, 2.41-2.53), and the risk was 203% higher risk among those living in urban centers (SMR, 2.03; 95% CI, 1.98-2.09).
Although people with comorbidities had higher mortality rates, even those without any other health conditions had a 161% higher risk for death, compared with people without epilepsy (SMR, 1.61; 95% CI, 1.50-1.72).
Causes of death
The most frequent causes of death were malignant neoplasm and cerebrovascular disease, which researchers noted are thought to be underlying causes of epilepsy.
Among external causes of death, suicide was the most common cause (2.6%). The suicide rate was highest among younger patients and gradually decreased with age.
Deaths tied directly to epilepsy, transport accidents, or falls were lower in this study than had been previously reported, which may be due to adequate seizure control or because the number of older people with epilepsy and comorbidities is higher in Korea than that reported in other countries.
“To reduce mortality in people with epilepsy, comprehensive efforts [are needed], including a national policy against stigma of epilepsy and clinicians’ total management such as risk stratification, education about injury prevention, and monitoring for suicidal ideation with psychological intervention, as well as active control of seizures,” the authors write.
Generalizable findings
Joseph Sirven, MD, professor of neurology at Mayo Clinic Florida, Jacksonville, said that although the study included only Korean patients, the findings are applicable to other counties.
That researchers found patients with epilepsy were more than twice as likely to die prematurely, compared with the general population wasn’t particularly surprising, Dr. Sirven said.
“What struck me the most was the fact that even patients who were on a single drug and seemingly well controlled also had excess mortality reported,” Dr. Sirven said. “That these risks occur should be part of what we tell all patients with epilepsy so that they can better arm themselves with information and help to address some of the risks that this study showed.”
Another important finding is the risk for suicide in patients with epilepsy, especially those who are newly diagnosed, he said.
“When we treat a patient with epilepsy, it should not just be about seizures, but we need to inquire about the psychiatric comorbidities and more importantly manage them in a comprehensive manner,” Dr. Sirven said.
The study was funded by Soonchunhyang University Research Fund and the Korea Health Technology R&D Project. The study authors and Dr. Sirven report no relevant financial conflicts.
A version of this article first appeared on Medscape.com.
FROM NEUROLOGY
Celebrity death finally solved – with locks of hair
This transcript has been edited for clarity.
I’m going to open this week with a case.
A 56-year-old musician presents with diffuse abdominal pain, cramping, and jaundice. His medical history is notable for years of diffuse abdominal complaints, characterized by disabling bouts of diarrhea.
In addition to the jaundice, this acute illness was accompanied by fever as well as diffuse edema and ascites. The patient underwent several abdominal paracenteses to drain excess fluid. One consulting physician administered alcohol to relieve pain, to little avail.
The patient succumbed to his illness. An autopsy showed diffuse liver injury, as well as papillary necrosis of the kidneys. Notably, the nerves of his auditory canal were noted to be thickened, along with the bony part of the skull, consistent with Paget disease of the bone and explaining, potentially, why the talented musician had gone deaf at such a young age.
An interesting note on social history: The patient had apparently developed some feelings for the niece of that doctor who prescribed alcohol. Her name was Therese, perhaps mistranscribed as Elise, and it seems that he may have written this song for her.

We’re talking about this paper in Current Biology, by Tristan Begg and colleagues, which gives us a look into the very genome of what some would argue is the world’s greatest composer.
The ability to extract DNA from older specimens has transformed the fields of anthropology, archaeology, and history, and now, perhaps, musicology as well.
The researchers identified eight locks of hair in private and public collections, all attributed to the maestro.
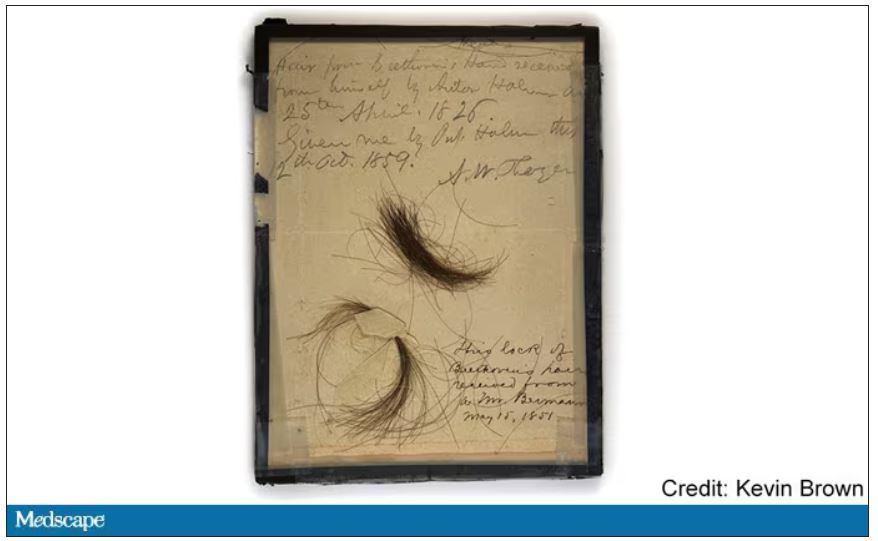
Four of the samples had an intact chain of custody from the time the hair was cut. DNA sequencing on these four and an additional one of the eight locks came from the same individual, a male of European heritage.
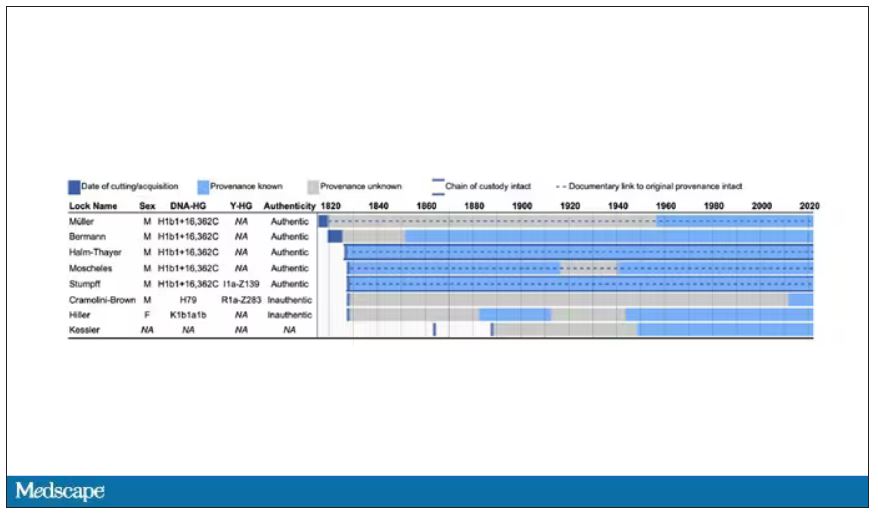
The three locks with less documentation came from three other unrelated individuals. Interestingly, analysis of one of those hair samples – the so-called Hiller Lock – had shown high levels of lead, leading historians to speculate that lead poisoning could account for some of Beethoven’s symptoms.
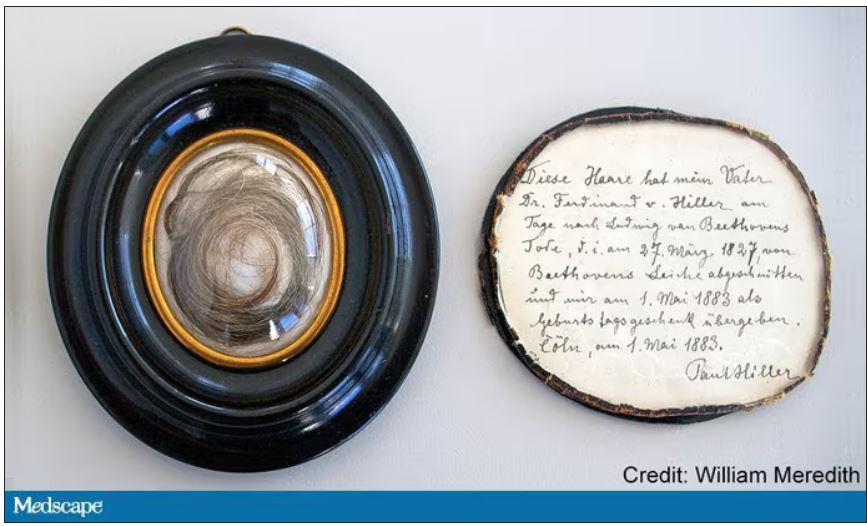
DNA analysis of that hair reveals it to have come from a woman likely of North African, Middle Eastern, or Jewish ancestry. We can no longer presume that plumbism was involved in Beethoven’s death. Beethoven’s ancestry turns out to be less exotic and maps quite well to ethnic German populations today.
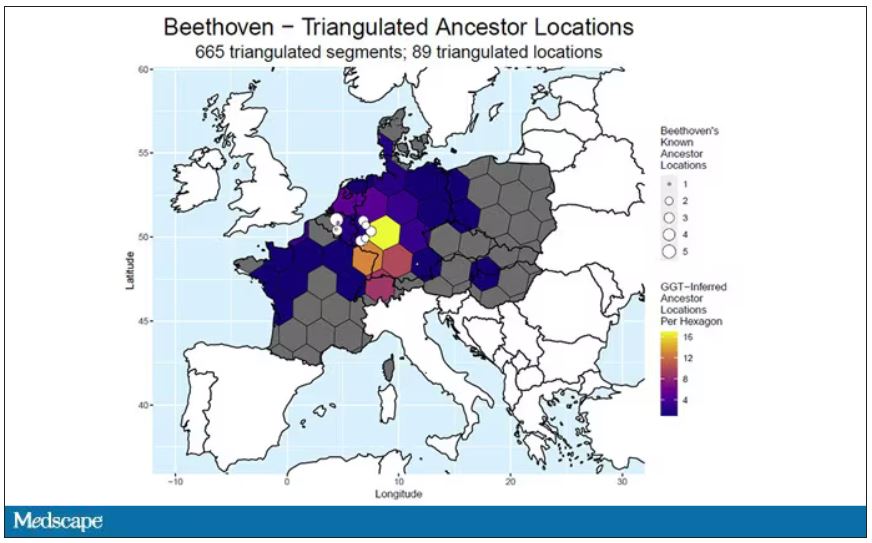
In fact, there are van Beethovens alive as we speak, primarily in Belgium. Genealogic records suggest that these van Beethovens share a common ancestor with the virtuoso composer, a man by the name of Aert van Beethoven.
But the DNA reveals a scandal.
The Y-chromosome that Beethoven inherited was not Aert van Beethoven’s. Questions of Beethoven’s paternity have been raised before, but this evidence strongly suggests an extramarital paternity event, at least in the generations preceding his birth. That’s right – Beethoven may not have been a Beethoven.
With five locks now essentially certain to have come from Beethoven himself, the authors could use DNA analysis to try to explain three significant health problems he experienced throughout his life and death: his hearing loss, his terrible gastrointestinal issues, and his liver failure.
Let’s start with the most disappointing results, explanations for his hearing loss. No genetic cause was forthcoming, though the authors note that they have little to go on in regard to the genetic risk for otosclerosis, to which his hearing loss has often been attributed. Lead poisoning is, of course, possible here, though this report focuses only on genetics – there was no testing for lead – and as I mentioned, the lock that was strongly lead-positive in prior studies is almost certainly inauthentic.
What about his lifelong GI complaints? Some have suggested celiac disease or lactose intolerance as explanations. These can essentially be ruled out by the genetic analysis, which shows no risk alleles for celiac disease and the presence of the lactase-persistence gene which confers the ability to metabolize lactose throughout one’s life. IBS is harder to assess genetically, but for what it’s worth, he scored quite low on a polygenic risk score for the condition, in just the 9th percentile of risk. We should probably be looking elsewhere to explain the GI distress.
The genetic information bore much more fruit in regard to his liver disease. Remember that Beethoven’s autopsy showed cirrhosis. His polygenic risk score for liver cirrhosis puts him in the 96th percentile of risk. He was also heterozygous for two variants that can cause hereditary hemochromatosis. The risk for cirrhosis among those with these variants is increased by the use of alcohol. And historical accounts are quite clear that Beethoven consumed more than his share.
But it wasn’t just Beethoven’s DNA in these hair follicles. Analysis of a follicle from later in his life revealed the unmistakable presence of hepatitis B virus. Endemic in Europe at the time, this was a common cause of liver failure and is likely to have contributed to, if not directly caused, Beethoven’s demise.
It’s hard to read these results and not marvel at the fact that, two centuries after his death, our fascination with Beethoven has led us to probe every corner of his life – his letters, his writings, his medical records, and now his very DNA. What are we actually looking for? Is it relevant to us today what caused his hearing loss? His stomach troubles? Even his death? Will it help any patients in the future? I propose that what we are actually trying to understand is something ineffable: Genius of magnitude that is rarely seen in one or many lifetimes. And our scientific tools, as sharp as they may have become, are still far too blunt to probe the depths of that transcendence.
In any case, friends, no more of these sounds. Let us sing more cheerful songs, more full of joy.
For Medscape, I’m Perry Wilson.
Dr. Wilson is associate professor, department of medicine, and director, Clinical and Translational Research Accelerator, at Yale University, New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I’m going to open this week with a case.
A 56-year-old musician presents with diffuse abdominal pain, cramping, and jaundice. His medical history is notable for years of diffuse abdominal complaints, characterized by disabling bouts of diarrhea.
In addition to the jaundice, this acute illness was accompanied by fever as well as diffuse edema and ascites. The patient underwent several abdominal paracenteses to drain excess fluid. One consulting physician administered alcohol to relieve pain, to little avail.
The patient succumbed to his illness. An autopsy showed diffuse liver injury, as well as papillary necrosis of the kidneys. Notably, the nerves of his auditory canal were noted to be thickened, along with the bony part of the skull, consistent with Paget disease of the bone and explaining, potentially, why the talented musician had gone deaf at such a young age.
An interesting note on social history: The patient had apparently developed some feelings for the niece of that doctor who prescribed alcohol. Her name was Therese, perhaps mistranscribed as Elise, and it seems that he may have written this song for her.
We’re talking about this paper in Current Biology, by Tristan Begg and colleagues, which gives us a look into the very genome of what some would argue is the world’s greatest composer.
The ability to extract DNA from older specimens has transformed the fields of anthropology, archaeology, and history, and now, perhaps, musicology as well.
The researchers identified eight locks of hair in private and public collections, all attributed to the maestro.
Four of the samples had an intact chain of custody from the time the hair was cut. DNA sequencing on these four and an additional one of the eight locks came from the same individual, a male of European heritage.
The three locks with less documentation came from three other unrelated individuals. Interestingly, analysis of one of those hair samples – the so-called Hiller Lock – had shown high levels of lead, leading historians to speculate that lead poisoning could account for some of Beethoven’s symptoms.
DNA analysis of that hair reveals it to have come from a woman likely of North African, Middle Eastern, or Jewish ancestry. We can no longer presume that plumbism was involved in Beethoven’s death. Beethoven’s ancestry turns out to be less exotic and maps quite well to ethnic German populations today.
In fact, there are van Beethovens alive as we speak, primarily in Belgium. Genealogic records suggest that these van Beethovens share a common ancestor with the virtuoso composer, a man by the name of Aert van Beethoven.
But the DNA reveals a scandal.
The Y-chromosome that Beethoven inherited was not Aert van Beethoven’s. Questions of Beethoven’s paternity have been raised before, but this evidence strongly suggests an extramarital paternity event, at least in the generations preceding his birth. That’s right – Beethoven may not have been a Beethoven.
With five locks now essentially certain to have come from Beethoven himself, the authors could use DNA analysis to try to explain three significant health problems he experienced throughout his life and death: his hearing loss, his terrible gastrointestinal issues, and his liver failure.
Let’s start with the most disappointing results, explanations for his hearing loss. No genetic cause was forthcoming, though the authors note that they have little to go on in regard to the genetic risk for otosclerosis, to which his hearing loss has often been attributed. Lead poisoning is, of course, possible here, though this report focuses only on genetics – there was no testing for lead – and as I mentioned, the lock that was strongly lead-positive in prior studies is almost certainly inauthentic.
What about his lifelong GI complaints? Some have suggested celiac disease or lactose intolerance as explanations. These can essentially be ruled out by the genetic analysis, which shows no risk alleles for celiac disease and the presence of the lactase-persistence gene which confers the ability to metabolize lactose throughout one’s life. IBS is harder to assess genetically, but for what it’s worth, he scored quite low on a polygenic risk score for the condition, in just the 9th percentile of risk. We should probably be looking elsewhere to explain the GI distress.
The genetic information bore much more fruit in regard to his liver disease. Remember that Beethoven’s autopsy showed cirrhosis. His polygenic risk score for liver cirrhosis puts him in the 96th percentile of risk. He was also heterozygous for two variants that can cause hereditary hemochromatosis. The risk for cirrhosis among those with these variants is increased by the use of alcohol. And historical accounts are quite clear that Beethoven consumed more than his share.
But it wasn’t just Beethoven’s DNA in these hair follicles. Analysis of a follicle from later in his life revealed the unmistakable presence of hepatitis B virus. Endemic in Europe at the time, this was a common cause of liver failure and is likely to have contributed to, if not directly caused, Beethoven’s demise.
It’s hard to read these results and not marvel at the fact that, two centuries after his death, our fascination with Beethoven has led us to probe every corner of his life – his letters, his writings, his medical records, and now his very DNA. What are we actually looking for? Is it relevant to us today what caused his hearing loss? His stomach troubles? Even his death? Will it help any patients in the future? I propose that what we are actually trying to understand is something ineffable: Genius of magnitude that is rarely seen in one or many lifetimes. And our scientific tools, as sharp as they may have become, are still far too blunt to probe the depths of that transcendence.
In any case, friends, no more of these sounds. Let us sing more cheerful songs, more full of joy.
For Medscape, I’m Perry Wilson.
Dr. Wilson is associate professor, department of medicine, and director, Clinical and Translational Research Accelerator, at Yale University, New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I’m going to open this week with a case.
A 56-year-old musician presents with diffuse abdominal pain, cramping, and jaundice. His medical history is notable for years of diffuse abdominal complaints, characterized by disabling bouts of diarrhea.
In addition to the jaundice, this acute illness was accompanied by fever as well as diffuse edema and ascites. The patient underwent several abdominal paracenteses to drain excess fluid. One consulting physician administered alcohol to relieve pain, to little avail.
The patient succumbed to his illness. An autopsy showed diffuse liver injury, as well as papillary necrosis of the kidneys. Notably, the nerves of his auditory canal were noted to be thickened, along with the bony part of the skull, consistent with Paget disease of the bone and explaining, potentially, why the talented musician had gone deaf at such a young age.
An interesting note on social history: The patient had apparently developed some feelings for the niece of that doctor who prescribed alcohol. Her name was Therese, perhaps mistranscribed as Elise, and it seems that he may have written this song for her.
We’re talking about this paper in Current Biology, by Tristan Begg and colleagues, which gives us a look into the very genome of what some would argue is the world’s greatest composer.
The ability to extract DNA from older specimens has transformed the fields of anthropology, archaeology, and history, and now, perhaps, musicology as well.
The researchers identified eight locks of hair in private and public collections, all attributed to the maestro.
Four of the samples had an intact chain of custody from the time the hair was cut. DNA sequencing on these four and an additional one of the eight locks came from the same individual, a male of European heritage.
The three locks with less documentation came from three other unrelated individuals. Interestingly, analysis of one of those hair samples – the so-called Hiller Lock – had shown high levels of lead, leading historians to speculate that lead poisoning could account for some of Beethoven’s symptoms.
DNA analysis of that hair reveals it to have come from a woman likely of North African, Middle Eastern, or Jewish ancestry. We can no longer presume that plumbism was involved in Beethoven’s death. Beethoven’s ancestry turns out to be less exotic and maps quite well to ethnic German populations today.
In fact, there are van Beethovens alive as we speak, primarily in Belgium. Genealogic records suggest that these van Beethovens share a common ancestor with the virtuoso composer, a man by the name of Aert van Beethoven.
But the DNA reveals a scandal.
The Y-chromosome that Beethoven inherited was not Aert van Beethoven’s. Questions of Beethoven’s paternity have been raised before, but this evidence strongly suggests an extramarital paternity event, at least in the generations preceding his birth. That’s right – Beethoven may not have been a Beethoven.
With five locks now essentially certain to have come from Beethoven himself, the authors could use DNA analysis to try to explain three significant health problems he experienced throughout his life and death: his hearing loss, his terrible gastrointestinal issues, and his liver failure.
Let’s start with the most disappointing results, explanations for his hearing loss. No genetic cause was forthcoming, though the authors note that they have little to go on in regard to the genetic risk for otosclerosis, to which his hearing loss has often been attributed. Lead poisoning is, of course, possible here, though this report focuses only on genetics – there was no testing for lead – and as I mentioned, the lock that was strongly lead-positive in prior studies is almost certainly inauthentic.
What about his lifelong GI complaints? Some have suggested celiac disease or lactose intolerance as explanations. These can essentially be ruled out by the genetic analysis, which shows no risk alleles for celiac disease and the presence of the lactase-persistence gene which confers the ability to metabolize lactose throughout one’s life. IBS is harder to assess genetically, but for what it’s worth, he scored quite low on a polygenic risk score for the condition, in just the 9th percentile of risk. We should probably be looking elsewhere to explain the GI distress.
The genetic information bore much more fruit in regard to his liver disease. Remember that Beethoven’s autopsy showed cirrhosis. His polygenic risk score for liver cirrhosis puts him in the 96th percentile of risk. He was also heterozygous for two variants that can cause hereditary hemochromatosis. The risk for cirrhosis among those with these variants is increased by the use of alcohol. And historical accounts are quite clear that Beethoven consumed more than his share.
But it wasn’t just Beethoven’s DNA in these hair follicles. Analysis of a follicle from later in his life revealed the unmistakable presence of hepatitis B virus. Endemic in Europe at the time, this was a common cause of liver failure and is likely to have contributed to, if not directly caused, Beethoven’s demise.
It’s hard to read these results and not marvel at the fact that, two centuries after his death, our fascination with Beethoven has led us to probe every corner of his life – his letters, his writings, his medical records, and now his very DNA. What are we actually looking for? Is it relevant to us today what caused his hearing loss? His stomach troubles? Even his death? Will it help any patients in the future? I propose that what we are actually trying to understand is something ineffable: Genius of magnitude that is rarely seen in one or many lifetimes. And our scientific tools, as sharp as they may have become, are still far too blunt to probe the depths of that transcendence.
In any case, friends, no more of these sounds. Let us sing more cheerful songs, more full of joy.
For Medscape, I’m Perry Wilson.
Dr. Wilson is associate professor, department of medicine, and director, Clinical and Translational Research Accelerator, at Yale University, New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Nurse makes millions selling her licensing exam study sheets
Ms. Beggs, 28, sells one-page study sheets or bundles of sheets, sometimes with colorful drawings, conversation bubbles and underlining, that boil down concepts for particular conditions into easy-to-understand language.
The biggest seller on Ms. Beggs’ online marketplace Etsy site, RNExplained, is a bundle of study guides covering eight core nursing classes. The notes range in price from $2 to $150. More than 70,000 customers have bought the $60 bundle, according to the website.
Ms. Beggs’ business developed in a “very unintentional” way when COVID hit with just months left in her nursing program at Mount Saint Mary’s University, Los Angeles, she told this news organization.
Classes had switched to Zoom, and she had no one to study with as she prepared to take her board exams.
“The best way I know how to study is to teach things out loud. But because I had nobody to teach out loud to, I would literally teach them to the wall,” Ms. Beggs said. “I would record myself so I could play it back and teach myself these topics that were hard for me to understand.”
Just for fun, she says, she posted them on TikTok and the responses started flowing in, with followers asking where she was selling the sheets. She now has more than 660,000 TikTok followers and 9 million likes.
Ms. Beggs said that every sheet highlights a condition, and she has made 308 of them.
Traditional classroom lessons typically teach one medical condition in 5-6 pages, Ms. Beggs said. “I go straight to the point.”
One reviewer on Ms. Beggs’ Etsy site appreciated the handwritten notes, calling them “simplified and concise.” Another commented: “Definitely helped me pass my last exam.”
Ms. Beggs says that her notes may seem simple, but each page represents comprehensive research.
“I have to go through not just one source of information to make sure my information is factual,” Ms. Beggs says. “What you teach in California might be a little different than what you teach in Florida. It’s very meticulous. The lab values will be a little different everywhere you go.”
She acknowledges her competition, noting that there are many other study guides for the NCLEX and nursing courses.
Nursing groups weigh in
Dawn Kappel, spokesperson for the National Council of State Boards of Nursing, which oversees NCLEX, said in an interview that “NCSBN has no issue with the current content of Stephanee Beggs’ business venture.”
For many students, the study guides will be helpful, especially for visual learners, said Carole Kenner, PhD, RN, dean and professor in the School of Nursing and Health Sciences at The College of New Jersey.
But for students “who are less confident in their knowledge, I would want to see a lot more in-depth explanation and rationale,” Dr. Kenner said.
“Since the NCLEX is moving to more cased-based scenarios, the next-gen unfolding cases, you really have to understand a lot of the rationale.”
The notes remind Dr. Kenner of traditional flash cards. “I don’t think it will work for all students, but even the fanciest of onsite review courses are useful to everyone,” she said.
‘Not cutting corners’
As an emergency nurse, Ms. Beggs said, “I have the experience as a nurse to show people that what you are learning will be seen in real life.”
“The way I teach my brand is not to take shortcuts. I love to teach to understand rather than teaching to memorize for an exam.”
She said she sees her guides as a supplement to learning, not a replacement.
“It’s not cutting corners,” she says. “I condense a medical condition that could take a very long time to understand and break it into layman’s terms.”
Ms. Beggs said when people hear about the $2 million, they often ask her whether she plans to give up her shifts in the emergency department for the more lucrative venture.
The answer is no, at least not yet.
“Aside from teaching, I genuinely love being at the bedside,” Ms. Beggs said. “I don’t foresee myself leaving that for good for as long as I can handle both.” She acknowledged, though, that her business now takes up most of her time.
“I love everything about both aspects, so it’s hard for me to choose.”
A version of this article first appeared on Medscape.com.
Ms. Beggs, 28, sells one-page study sheets or bundles of sheets, sometimes with colorful drawings, conversation bubbles and underlining, that boil down concepts for particular conditions into easy-to-understand language.
The biggest seller on Ms. Beggs’ online marketplace Etsy site, RNExplained, is a bundle of study guides covering eight core nursing classes. The notes range in price from $2 to $150. More than 70,000 customers have bought the $60 bundle, according to the website.
Ms. Beggs’ business developed in a “very unintentional” way when COVID hit with just months left in her nursing program at Mount Saint Mary’s University, Los Angeles, she told this news organization.
Classes had switched to Zoom, and she had no one to study with as she prepared to take her board exams.
“The best way I know how to study is to teach things out loud. But because I had nobody to teach out loud to, I would literally teach them to the wall,” Ms. Beggs said. “I would record myself so I could play it back and teach myself these topics that were hard for me to understand.”
Just for fun, she says, she posted them on TikTok and the responses started flowing in, with followers asking where she was selling the sheets. She now has more than 660,000 TikTok followers and 9 million likes.
Ms. Beggs said that every sheet highlights a condition, and she has made 308 of them.
Traditional classroom lessons typically teach one medical condition in 5-6 pages, Ms. Beggs said. “I go straight to the point.”
One reviewer on Ms. Beggs’ Etsy site appreciated the handwritten notes, calling them “simplified and concise.” Another commented: “Definitely helped me pass my last exam.”
Ms. Beggs says that her notes may seem simple, but each page represents comprehensive research.
“I have to go through not just one source of information to make sure my information is factual,” Ms. Beggs says. “What you teach in California might be a little different than what you teach in Florida. It’s very meticulous. The lab values will be a little different everywhere you go.”
She acknowledges her competition, noting that there are many other study guides for the NCLEX and nursing courses.
Nursing groups weigh in
Dawn Kappel, spokesperson for the National Council of State Boards of Nursing, which oversees NCLEX, said in an interview that “NCSBN has no issue with the current content of Stephanee Beggs’ business venture.”
For many students, the study guides will be helpful, especially for visual learners, said Carole Kenner, PhD, RN, dean and professor in the School of Nursing and Health Sciences at The College of New Jersey.
But for students “who are less confident in their knowledge, I would want to see a lot more in-depth explanation and rationale,” Dr. Kenner said.
“Since the NCLEX is moving to more cased-based scenarios, the next-gen unfolding cases, you really have to understand a lot of the rationale.”
The notes remind Dr. Kenner of traditional flash cards. “I don’t think it will work for all students, but even the fanciest of onsite review courses are useful to everyone,” she said.
‘Not cutting corners’
As an emergency nurse, Ms. Beggs said, “I have the experience as a nurse to show people that what you are learning will be seen in real life.”
“The way I teach my brand is not to take shortcuts. I love to teach to understand rather than teaching to memorize for an exam.”
She said she sees her guides as a supplement to learning, not a replacement.
“It’s not cutting corners,” she says. “I condense a medical condition that could take a very long time to understand and break it into layman’s terms.”
Ms. Beggs said when people hear about the $2 million, they often ask her whether she plans to give up her shifts in the emergency department for the more lucrative venture.
The answer is no, at least not yet.
“Aside from teaching, I genuinely love being at the bedside,” Ms. Beggs said. “I don’t foresee myself leaving that for good for as long as I can handle both.” She acknowledged, though, that her business now takes up most of her time.
“I love everything about both aspects, so it’s hard for me to choose.”
A version of this article first appeared on Medscape.com.
Ms. Beggs, 28, sells one-page study sheets or bundles of sheets, sometimes with colorful drawings, conversation bubbles and underlining, that boil down concepts for particular conditions into easy-to-understand language.
The biggest seller on Ms. Beggs’ online marketplace Etsy site, RNExplained, is a bundle of study guides covering eight core nursing classes. The notes range in price from $2 to $150. More than 70,000 customers have bought the $60 bundle, according to the website.
Ms. Beggs’ business developed in a “very unintentional” way when COVID hit with just months left in her nursing program at Mount Saint Mary’s University, Los Angeles, she told this news organization.
Classes had switched to Zoom, and she had no one to study with as she prepared to take her board exams.
“The best way I know how to study is to teach things out loud. But because I had nobody to teach out loud to, I would literally teach them to the wall,” Ms. Beggs said. “I would record myself so I could play it back and teach myself these topics that were hard for me to understand.”
Just for fun, she says, she posted them on TikTok and the responses started flowing in, with followers asking where she was selling the sheets. She now has more than 660,000 TikTok followers and 9 million likes.
Ms. Beggs said that every sheet highlights a condition, and she has made 308 of them.
Traditional classroom lessons typically teach one medical condition in 5-6 pages, Ms. Beggs said. “I go straight to the point.”
One reviewer on Ms. Beggs’ Etsy site appreciated the handwritten notes, calling them “simplified and concise.” Another commented: “Definitely helped me pass my last exam.”
Ms. Beggs says that her notes may seem simple, but each page represents comprehensive research.
“I have to go through not just one source of information to make sure my information is factual,” Ms. Beggs says. “What you teach in California might be a little different than what you teach in Florida. It’s very meticulous. The lab values will be a little different everywhere you go.”
She acknowledges her competition, noting that there are many other study guides for the NCLEX and nursing courses.
Nursing groups weigh in
Dawn Kappel, spokesperson for the National Council of State Boards of Nursing, which oversees NCLEX, said in an interview that “NCSBN has no issue with the current content of Stephanee Beggs’ business venture.”
For many students, the study guides will be helpful, especially for visual learners, said Carole Kenner, PhD, RN, dean and professor in the School of Nursing and Health Sciences at The College of New Jersey.
But for students “who are less confident in their knowledge, I would want to see a lot more in-depth explanation and rationale,” Dr. Kenner said.
“Since the NCLEX is moving to more cased-based scenarios, the next-gen unfolding cases, you really have to understand a lot of the rationale.”
The notes remind Dr. Kenner of traditional flash cards. “I don’t think it will work for all students, but even the fanciest of onsite review courses are useful to everyone,” she said.
‘Not cutting corners’
As an emergency nurse, Ms. Beggs said, “I have the experience as a nurse to show people that what you are learning will be seen in real life.”
“The way I teach my brand is not to take shortcuts. I love to teach to understand rather than teaching to memorize for an exam.”
She said she sees her guides as a supplement to learning, not a replacement.
“It’s not cutting corners,” she says. “I condense a medical condition that could take a very long time to understand and break it into layman’s terms.”
Ms. Beggs said when people hear about the $2 million, they often ask her whether she plans to give up her shifts in the emergency department for the more lucrative venture.
The answer is no, at least not yet.
“Aside from teaching, I genuinely love being at the bedside,” Ms. Beggs said. “I don’t foresee myself leaving that for good for as long as I can handle both.” She acknowledged, though, that her business now takes up most of her time.
“I love everything about both aspects, so it’s hard for me to choose.”
A version of this article first appeared on Medscape.com.
LAA closure device shown safe in groups omitted in trials
WASHINGTON – Left atrial appendage closure can be performed safely and effectively in older patients, those with end-stage renal disease, and likely others not included in the pivotal clinical trials, according to a series of new studies, including a late-breaker, presented on the both older and newer Watchman devices at the Cardiovascular Research Technologies conference.
In the case of the late-breaking clinical trial report, which included more than 60,000 patients, the goal was to look at the safety of the Watchman FLX, which is the newest of the devices in real-world practice, according to Samir R. Kapadia, MD, chairman of the department of cardiovascular medicine at the Cleveland Clinic.

In the SURPASS registry, the number of patients discharged on the Watchman FLX climbed from zero in August 2020, when data accrual began, to 66,894 by March 2022. For the current analysis, 45-day follow-up was available for 61,963 patients and 1-year follow-up was available for 18,233.
Based on this number of patients treated by more than 2,300 clinicians at more than 740 sites, the SURPASS registry establishes that Watchman FLX “can be accomplished safely with clinical outcomes similar to pivotal trials at 45 days and 1 year,” Dr. Kapadia reported.
No surprises found in real-world outcome
At 7 days or hospital discharge (whichever came last), the rate of all-cause death was 0.18%, the rate of ischemic stroke was 0.13%, and there were no systemic emboli. By 45 days, the rate of all-cause death (0.84%) and stroke of any kind (0.32%) remained less than 1% and there were still no systemic emboli. Major bleeding events, of which about one-third occurred during hospitalization, had reached 3.34% by day 45.
By 1 year, all-cause mortality had risen to 8.3%, the stroke rate was 1.6%, and major bleeding reached 6.7%. The rate of systemic emboli remained very low (0.1%). The rates of death and stroke rose at a slow but steady rate throughout the 1-year follow-up. In contrast, major bleeding events rose steeply in the first 90 days and were followed by a much slower accrual subsequently.
At 1 year, 84.4% of patients had a complete seal. Leaks ≤ 3 mm were observed in 12.1%. The remaining leaks were larger, but just 0.7% had a leak > 5 mm.
Relative to the first-generation Watchman, the Watchman FLX has numerous design changes, including a shorter profile, more struts, and a reduced metal exposure. Most of these changes were performed to make the device easier to deploy.
When the SURPASS data are compared to the pivotal trials with Watchman FLX or to the Ewolution and National Cardiovascular Data (NCD) registries, which were created to monitor efficacy and safety with the earlier generation Watchman, the outcomes are similar or, in many cases, numerically favorable for such outcomes as bleeding and rates of stroke.
In addition to providing reassurance for the real-world safety of Watchman FLX, Dr. Kapadia said that these data establish reasonable benchmarks for centers tracking in-hospital and 1-year outcomes.
Dr. Kapadia also reported that outcomes overall in SURPASS were similar in women and men with the exception of major bleeding, a finding common to other interventional studies.
The late-breaker panelists generally agreed that SURPASS provides a robust set of data by which to be reassured, but David J. Cohen, MD, director of Clinical and Outcomes Research at the Cardiovascular Research Foundation in New York, said that he thinks the rate of bleeding is unnecessarily high.
“You really need to figure out a way to get the rate of bleeding at 45 days down,” Dr. Cohen said. He called for studies of anticoagulation in the post-procedural period that offer a better benefit-to-risk ratio.
Elderly patients benefit equally from Watchman
Yet, Watchman devices are generally regarded as a success story, and this has led investigators to evaluate safety in patients not well represented or explicitly excluded from clinical trials, such as the elderly and those with end-stage renal disease (ESRD). New data derived from experience in both of these groups were presented at the conference, which was sponsored by MedStar Heart & Vascular Institute.
To tease out the relative safety of Watchman in octogenarians, Samian Sulaiman, MD, a cardiology fellow at West Virginia University Heart and Vascular Institute, Morgantown, performed a competing risk analysis to study the relative benefit of Watchman devices after controlling for the greater overall risk of complications in the elderly.
In raw data comparisons of those 80 years of age or older to those younger in published trials, the not-surprising result is that overall rates of death and ischemic events are far higher in the elderly, according to Dr. Sulaiman, but it’s an “unfair comparison,” he said.
“It is easy to mistakenly conclude that left atrial appendage closure is associated with worse outcomes, but older patients have far higher rates of these events independent of other factors,” Dr. Sulaiman noted.
In fact, in his comparison of 472 older patients to 1,404 younger patients, the seal rates at 45 days, 6 months, and 12 months are almost identical. Moreover, after the extensive adjustments performed for competing risk analysis, the rates of death, stroke, and bleeding were also almost identical for those 80 years or older whether or not they received a Watchman.
Although he acknowledged the risk for residual confounding, Dr. Sulaiman concluded that elderly patients derive about the same benefits as younger patients from the Watchman. He concluded age alone should not be a factor in selecting candidates for this device.
ESRD is not Watchman contraindication
A similar point was made about ESRD based on analysis of 237 patients who received either an earlier generation Watchman or the Watchman FLX. Initiated in Spain, the study was amended to collect data from centers elsewhere in Europe, the United States, and Australia.
Successful implantation was achieved in 99.2% of the patients, reported Armando Perez de Prado, MD, PhD, head of interventional cardiology at the University of Leon, Spain.

After a median follow-up of 480 days, stroke or transient ischemic attacks were observed in 3.1%, leaks > 5 mm were observed in 1.4%, and systemic emboli were observed in 0.9%. Major bleeding (BARC > 2) occurred in 13.3%.
Although the all-cause mortality over the period of follow-up was high (37.4%), most of the deaths (61.2%) were of noncardiovascular origin, according to Dr. Sulaiman. He said mortality and adverse events linked to the Watchman appeared to be roughly comparable to those seen in patients with ESRD.
“The Watchman device for patients on hemodialysis with nonvalvular atrial fibrillation is an effective and safe intervention to prevent embolic events,” he said. However, he also cautioned these the ESRD and the accompanying comorbidities place these patients at high risk of a limited life expectancy.
“Given the high mortality rate of this population, proper selection of candidates is paramount to ensure the optimal clinical benefit,” he cautioned.
Dr. Samir reported no potential conflicts of interest but stated that this study was funded by Boston Scientific. Dr. Cohen reported financial ties with Abbott Vascular, Boston Scientific, Corvia Medical, Edwards Lifesciences, Impulse Dynamics, MyoKardia, Phillips, Svelte, V-Wave, and Zoll. Dr. Sulaiman reported no potential conflicts of interest. Dr. Perez de Prado reported no potential conflicts of interest but stated that this study was funded by Boston Scientific.
WASHINGTON – Left atrial appendage closure can be performed safely and effectively in older patients, those with end-stage renal disease, and likely others not included in the pivotal clinical trials, according to a series of new studies, including a late-breaker, presented on the both older and newer Watchman devices at the Cardiovascular Research Technologies conference.
In the case of the late-breaking clinical trial report, which included more than 60,000 patients, the goal was to look at the safety of the Watchman FLX, which is the newest of the devices in real-world practice, according to Samir R. Kapadia, MD, chairman of the department of cardiovascular medicine at the Cleveland Clinic.
In the SURPASS registry, the number of patients discharged on the Watchman FLX climbed from zero in August 2020, when data accrual began, to 66,894 by March 2022. For the current analysis, 45-day follow-up was available for 61,963 patients and 1-year follow-up was available for 18,233.
Based on this number of patients treated by more than 2,300 clinicians at more than 740 sites, the SURPASS registry establishes that Watchman FLX “can be accomplished safely with clinical outcomes similar to pivotal trials at 45 days and 1 year,” Dr. Kapadia reported.
No surprises found in real-world outcome
At 7 days or hospital discharge (whichever came last), the rate of all-cause death was 0.18%, the rate of ischemic stroke was 0.13%, and there were no systemic emboli. By 45 days, the rate of all-cause death (0.84%) and stroke of any kind (0.32%) remained less than 1% and there were still no systemic emboli. Major bleeding events, of which about one-third occurred during hospitalization, had reached 3.34% by day 45.
By 1 year, all-cause mortality had risen to 8.3%, the stroke rate was 1.6%, and major bleeding reached 6.7%. The rate of systemic emboli remained very low (0.1%). The rates of death and stroke rose at a slow but steady rate throughout the 1-year follow-up. In contrast, major bleeding events rose steeply in the first 90 days and were followed by a much slower accrual subsequently.
At 1 year, 84.4% of patients had a complete seal. Leaks ≤ 3 mm were observed in 12.1%. The remaining leaks were larger, but just 0.7% had a leak > 5 mm.
Relative to the first-generation Watchman, the Watchman FLX has numerous design changes, including a shorter profile, more struts, and a reduced metal exposure. Most of these changes were performed to make the device easier to deploy.
When the SURPASS data are compared to the pivotal trials with Watchman FLX or to the Ewolution and National Cardiovascular Data (NCD) registries, which were created to monitor efficacy and safety with the earlier generation Watchman, the outcomes are similar or, in many cases, numerically favorable for such outcomes as bleeding and rates of stroke.
In addition to providing reassurance for the real-world safety of Watchman FLX, Dr. Kapadia said that these data establish reasonable benchmarks for centers tracking in-hospital and 1-year outcomes.
Dr. Kapadia also reported that outcomes overall in SURPASS were similar in women and men with the exception of major bleeding, a finding common to other interventional studies.
The late-breaker panelists generally agreed that SURPASS provides a robust set of data by which to be reassured, but David J. Cohen, MD, director of Clinical and Outcomes Research at the Cardiovascular Research Foundation in New York, said that he thinks the rate of bleeding is unnecessarily high.
“You really need to figure out a way to get the rate of bleeding at 45 days down,” Dr. Cohen said. He called for studies of anticoagulation in the post-procedural period that offer a better benefit-to-risk ratio.
Elderly patients benefit equally from Watchman
Yet, Watchman devices are generally regarded as a success story, and this has led investigators to evaluate safety in patients not well represented or explicitly excluded from clinical trials, such as the elderly and those with end-stage renal disease (ESRD). New data derived from experience in both of these groups were presented at the conference, which was sponsored by MedStar Heart & Vascular Institute.
To tease out the relative safety of Watchman in octogenarians, Samian Sulaiman, MD, a cardiology fellow at West Virginia University Heart and Vascular Institute, Morgantown, performed a competing risk analysis to study the relative benefit of Watchman devices after controlling for the greater overall risk of complications in the elderly.
In raw data comparisons of those 80 years of age or older to those younger in published trials, the not-surprising result is that overall rates of death and ischemic events are far higher in the elderly, according to Dr. Sulaiman, but it’s an “unfair comparison,” he said.
“It is easy to mistakenly conclude that left atrial appendage closure is associated with worse outcomes, but older patients have far higher rates of these events independent of other factors,” Dr. Sulaiman noted.
In fact, in his comparison of 472 older patients to 1,404 younger patients, the seal rates at 45 days, 6 months, and 12 months are almost identical. Moreover, after the extensive adjustments performed for competing risk analysis, the rates of death, stroke, and bleeding were also almost identical for those 80 years or older whether or not they received a Watchman.
Although he acknowledged the risk for residual confounding, Dr. Sulaiman concluded that elderly patients derive about the same benefits as younger patients from the Watchman. He concluded age alone should not be a factor in selecting candidates for this device.
ESRD is not Watchman contraindication
A similar point was made about ESRD based on analysis of 237 patients who received either an earlier generation Watchman or the Watchman FLX. Initiated in Spain, the study was amended to collect data from centers elsewhere in Europe, the United States, and Australia.
Successful implantation was achieved in 99.2% of the patients, reported Armando Perez de Prado, MD, PhD, head of interventional cardiology at the University of Leon, Spain.
After a median follow-up of 480 days, stroke or transient ischemic attacks were observed in 3.1%, leaks > 5 mm were observed in 1.4%, and systemic emboli were observed in 0.9%. Major bleeding (BARC > 2) occurred in 13.3%.
Although the all-cause mortality over the period of follow-up was high (37.4%), most of the deaths (61.2%) were of noncardiovascular origin, according to Dr. Sulaiman. He said mortality and adverse events linked to the Watchman appeared to be roughly comparable to those seen in patients with ESRD.
“The Watchman device for patients on hemodialysis with nonvalvular atrial fibrillation is an effective and safe intervention to prevent embolic events,” he said. However, he also cautioned these the ESRD and the accompanying comorbidities place these patients at high risk of a limited life expectancy.
“Given the high mortality rate of this population, proper selection of candidates is paramount to ensure the optimal clinical benefit,” he cautioned.
Dr. Samir reported no potential conflicts of interest but stated that this study was funded by Boston Scientific. Dr. Cohen reported financial ties with Abbott Vascular, Boston Scientific, Corvia Medical, Edwards Lifesciences, Impulse Dynamics, MyoKardia, Phillips, Svelte, V-Wave, and Zoll. Dr. Sulaiman reported no potential conflicts of interest. Dr. Perez de Prado reported no potential conflicts of interest but stated that this study was funded by Boston Scientific.
WASHINGTON – Left atrial appendage closure can be performed safely and effectively in older patients, those with end-stage renal disease, and likely others not included in the pivotal clinical trials, according to a series of new studies, including a late-breaker, presented on the both older and newer Watchman devices at the Cardiovascular Research Technologies conference.
In the case of the late-breaking clinical trial report, which included more than 60,000 patients, the goal was to look at the safety of the Watchman FLX, which is the newest of the devices in real-world practice, according to Samir R. Kapadia, MD, chairman of the department of cardiovascular medicine at the Cleveland Clinic.
In the SURPASS registry, the number of patients discharged on the Watchman FLX climbed from zero in August 2020, when data accrual began, to 66,894 by March 2022. For the current analysis, 45-day follow-up was available for 61,963 patients and 1-year follow-up was available for 18,233.
Based on this number of patients treated by more than 2,300 clinicians at more than 740 sites, the SURPASS registry establishes that Watchman FLX “can be accomplished safely with clinical outcomes similar to pivotal trials at 45 days and 1 year,” Dr. Kapadia reported.
No surprises found in real-world outcome
At 7 days or hospital discharge (whichever came last), the rate of all-cause death was 0.18%, the rate of ischemic stroke was 0.13%, and there were no systemic emboli. By 45 days, the rate of all-cause death (0.84%) and stroke of any kind (0.32%) remained less than 1% and there were still no systemic emboli. Major bleeding events, of which about one-third occurred during hospitalization, had reached 3.34% by day 45.
By 1 year, all-cause mortality had risen to 8.3%, the stroke rate was 1.6%, and major bleeding reached 6.7%. The rate of systemic emboli remained very low (0.1%). The rates of death and stroke rose at a slow but steady rate throughout the 1-year follow-up. In contrast, major bleeding events rose steeply in the first 90 days and were followed by a much slower accrual subsequently.
At 1 year, 84.4% of patients had a complete seal. Leaks ≤ 3 mm were observed in 12.1%. The remaining leaks were larger, but just 0.7% had a leak > 5 mm.
Relative to the first-generation Watchman, the Watchman FLX has numerous design changes, including a shorter profile, more struts, and a reduced metal exposure. Most of these changes were performed to make the device easier to deploy.
When the SURPASS data are compared to the pivotal trials with Watchman FLX or to the Ewolution and National Cardiovascular Data (NCD) registries, which were created to monitor efficacy and safety with the earlier generation Watchman, the outcomes are similar or, in many cases, numerically favorable for such outcomes as bleeding and rates of stroke.
In addition to providing reassurance for the real-world safety of Watchman FLX, Dr. Kapadia said that these data establish reasonable benchmarks for centers tracking in-hospital and 1-year outcomes.
Dr. Kapadia also reported that outcomes overall in SURPASS were similar in women and men with the exception of major bleeding, a finding common to other interventional studies.
The late-breaker panelists generally agreed that SURPASS provides a robust set of data by which to be reassured, but David J. Cohen, MD, director of Clinical and Outcomes Research at the Cardiovascular Research Foundation in New York, said that he thinks the rate of bleeding is unnecessarily high.
“You really need to figure out a way to get the rate of bleeding at 45 days down,” Dr. Cohen said. He called for studies of anticoagulation in the post-procedural period that offer a better benefit-to-risk ratio.
Elderly patients benefit equally from Watchman
Yet, Watchman devices are generally regarded as a success story, and this has led investigators to evaluate safety in patients not well represented or explicitly excluded from clinical trials, such as the elderly and those with end-stage renal disease (ESRD). New data derived from experience in both of these groups were presented at the conference, which was sponsored by MedStar Heart & Vascular Institute.
To tease out the relative safety of Watchman in octogenarians, Samian Sulaiman, MD, a cardiology fellow at West Virginia University Heart and Vascular Institute, Morgantown, performed a competing risk analysis to study the relative benefit of Watchman devices after controlling for the greater overall risk of complications in the elderly.
In raw data comparisons of those 80 years of age or older to those younger in published trials, the not-surprising result is that overall rates of death and ischemic events are far higher in the elderly, according to Dr. Sulaiman, but it’s an “unfair comparison,” he said.
“It is easy to mistakenly conclude that left atrial appendage closure is associated with worse outcomes, but older patients have far higher rates of these events independent of other factors,” Dr. Sulaiman noted.
In fact, in his comparison of 472 older patients to 1,404 younger patients, the seal rates at 45 days, 6 months, and 12 months are almost identical. Moreover, after the extensive adjustments performed for competing risk analysis, the rates of death, stroke, and bleeding were also almost identical for those 80 years or older whether or not they received a Watchman.
Although he acknowledged the risk for residual confounding, Dr. Sulaiman concluded that elderly patients derive about the same benefits as younger patients from the Watchman. He concluded age alone should not be a factor in selecting candidates for this device.
ESRD is not Watchman contraindication
A similar point was made about ESRD based on analysis of 237 patients who received either an earlier generation Watchman or the Watchman FLX. Initiated in Spain, the study was amended to collect data from centers elsewhere in Europe, the United States, and Australia.
Successful implantation was achieved in 99.2% of the patients, reported Armando Perez de Prado, MD, PhD, head of interventional cardiology at the University of Leon, Spain.
After a median follow-up of 480 days, stroke or transient ischemic attacks were observed in 3.1%, leaks > 5 mm were observed in 1.4%, and systemic emboli were observed in 0.9%. Major bleeding (BARC > 2) occurred in 13.3%.
Although the all-cause mortality over the period of follow-up was high (37.4%), most of the deaths (61.2%) were of noncardiovascular origin, according to Dr. Sulaiman. He said mortality and adverse events linked to the Watchman appeared to be roughly comparable to those seen in patients with ESRD.
“The Watchman device for patients on hemodialysis with nonvalvular atrial fibrillation is an effective and safe intervention to prevent embolic events,” he said. However, he also cautioned these the ESRD and the accompanying comorbidities place these patients at high risk of a limited life expectancy.
“Given the high mortality rate of this population, proper selection of candidates is paramount to ensure the optimal clinical benefit,” he cautioned.
Dr. Samir reported no potential conflicts of interest but stated that this study was funded by Boston Scientific. Dr. Cohen reported financial ties with Abbott Vascular, Boston Scientific, Corvia Medical, Edwards Lifesciences, Impulse Dynamics, MyoKardia, Phillips, Svelte, V-Wave, and Zoll. Dr. Sulaiman reported no potential conflicts of interest. Dr. Perez de Prado reported no potential conflicts of interest but stated that this study was funded by Boston Scientific.
AT CRT 2023
Fast, cheap ... or accurate?
A recent study on the JAMA Network found that, .
Does this surprise anyone?

One of my friends, a pharmacist, has a sign in his home office: “Fast. Accurate. Cheap. You can’t have all 3.” A true statement. I’ve also seen it at car repair places, but they’re doctors in their own way.
The problem here is that physicians are increasingly squeezed for time. If your only revenue stream is seeing patients, and your expenses are going up (and whose aren’t?) then your options are to either raise your prices or see more patients.
Of course, raising prices in medicine can’t happen for most of us. We’re all tied into insurance contracts, which themselves are pegged to Medicare, as to how much we get paid. I mean, yes, you can raise your prices, but that doesn’t matter. The insurance company will still pay a predetermined amount set years ago, in better economic times, no matter what you charge.
So the only real option for most is to see more patients. Which means less time with each one. Which, inevitably, leads to more snap judgments, inappropriate prescriptions, and mistakes.
Patients may get Fast and Cheap, but Accurate gets sidelined. This is the nature of things. If you don’t have enough time to gather and process data, then you’re less likely to reach the right answer.
There’s also the fact that sometimes it’s easier for anyone to just take the path of least resistance. The patient wants an antibiotic, and you realize it’s going to take less time to hand them a script for one than to explain why they don’t need it for what’s probably a viral infection. Not only that, but then you run the risk of their giving you a bad Yelp review (“incompetent, refused to give me antibiotics when I obviously needed them, 1 star”) and who needs that? If you’re employed by a large health care system a bad online review will get you a talking-to by some nonmedical admin from marketing, saying you’re hurting the practice’s “brand.”
Years ago the satire site The Onion had an article about a doctor who specialized in “giving a shit” - assumedly where Accurate dominates. While none of us may intentionally rush through patients or do half-assed jobs, we also have to deal with pressures of time. There never seems to be enough in a workday.
Nowhere is this more true than in primary care, where the pressures of time, overhead, and a large patient volume intersect. There are patients to see, labs to review, phone calls to return, forms to complete, meetings to attend, samples to sign for ... and probably many other things I’ve left out.
The fact that this situation exists shouldn’t surprise anyone. People talk about “burnout” and “making health care better” but that just seems to be lip service. They give you a free subscription to a meditation app, phone access to a counselor, and a mandatory early morning meeting to discuss stress reduction. Of course, these things take time away from seeing patients, which sort of defeats the whole purpose. Unless you want to do them at home – taking time away from your family, or doing the taxes, or other things you have to do besides your day job.
This is not sustainable for patients, doctors, or the health care system as a whole. But right now the situation is only getting worse, and there aren’t any easy answers.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
A recent study on the JAMA Network found that, .
Does this surprise anyone?
One of my friends, a pharmacist, has a sign in his home office: “Fast. Accurate. Cheap. You can’t have all 3.” A true statement. I’ve also seen it at car repair places, but they’re doctors in their own way.
The problem here is that physicians are increasingly squeezed for time. If your only revenue stream is seeing patients, and your expenses are going up (and whose aren’t?) then your options are to either raise your prices or see more patients.
Of course, raising prices in medicine can’t happen for most of us. We’re all tied into insurance contracts, which themselves are pegged to Medicare, as to how much we get paid. I mean, yes, you can raise your prices, but that doesn’t matter. The insurance company will still pay a predetermined amount set years ago, in better economic times, no matter what you charge.
So the only real option for most is to see more patients. Which means less time with each one. Which, inevitably, leads to more snap judgments, inappropriate prescriptions, and mistakes.
Patients may get Fast and Cheap, but Accurate gets sidelined. This is the nature of things. If you don’t have enough time to gather and process data, then you’re less likely to reach the right answer.
There’s also the fact that sometimes it’s easier for anyone to just take the path of least resistance. The patient wants an antibiotic, and you realize it’s going to take less time to hand them a script for one than to explain why they don’t need it for what’s probably a viral infection. Not only that, but then you run the risk of their giving you a bad Yelp review (“incompetent, refused to give me antibiotics when I obviously needed them, 1 star”) and who needs that? If you’re employed by a large health care system a bad online review will get you a talking-to by some nonmedical admin from marketing, saying you’re hurting the practice’s “brand.”
Years ago the satire site The Onion had an article about a doctor who specialized in “giving a shit” - assumedly where Accurate dominates. While none of us may intentionally rush through patients or do half-assed jobs, we also have to deal with pressures of time. There never seems to be enough in a workday.
Nowhere is this more true than in primary care, where the pressures of time, overhead, and a large patient volume intersect. There are patients to see, labs to review, phone calls to return, forms to complete, meetings to attend, samples to sign for ... and probably many other things I’ve left out.
The fact that this situation exists shouldn’t surprise anyone. People talk about “burnout” and “making health care better” but that just seems to be lip service. They give you a free subscription to a meditation app, phone access to a counselor, and a mandatory early morning meeting to discuss stress reduction. Of course, these things take time away from seeing patients, which sort of defeats the whole purpose. Unless you want to do them at home – taking time away from your family, or doing the taxes, or other things you have to do besides your day job.
This is not sustainable for patients, doctors, or the health care system as a whole. But right now the situation is only getting worse, and there aren’t any easy answers.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
A recent study on the JAMA Network found that, .
Does this surprise anyone?
One of my friends, a pharmacist, has a sign in his home office: “Fast. Accurate. Cheap. You can’t have all 3.” A true statement. I’ve also seen it at car repair places, but they’re doctors in their own way.
The problem here is that physicians are increasingly squeezed for time. If your only revenue stream is seeing patients, and your expenses are going up (and whose aren’t?) then your options are to either raise your prices or see more patients.
Of course, raising prices in medicine can’t happen for most of us. We’re all tied into insurance contracts, which themselves are pegged to Medicare, as to how much we get paid. I mean, yes, you can raise your prices, but that doesn’t matter. The insurance company will still pay a predetermined amount set years ago, in better economic times, no matter what you charge.
So the only real option for most is to see more patients. Which means less time with each one. Which, inevitably, leads to more snap judgments, inappropriate prescriptions, and mistakes.
Patients may get Fast and Cheap, but Accurate gets sidelined. This is the nature of things. If you don’t have enough time to gather and process data, then you’re less likely to reach the right answer.
There’s also the fact that sometimes it’s easier for anyone to just take the path of least resistance. The patient wants an antibiotic, and you realize it’s going to take less time to hand them a script for one than to explain why they don’t need it for what’s probably a viral infection. Not only that, but then you run the risk of their giving you a bad Yelp review (“incompetent, refused to give me antibiotics when I obviously needed them, 1 star”) and who needs that? If you’re employed by a large health care system a bad online review will get you a talking-to by some nonmedical admin from marketing, saying you’re hurting the practice’s “brand.”
Years ago the satire site The Onion had an article about a doctor who specialized in “giving a shit” - assumedly where Accurate dominates. While none of us may intentionally rush through patients or do half-assed jobs, we also have to deal with pressures of time. There never seems to be enough in a workday.
Nowhere is this more true than in primary care, where the pressures of time, overhead, and a large patient volume intersect. There are patients to see, labs to review, phone calls to return, forms to complete, meetings to attend, samples to sign for ... and probably many other things I’ve left out.
The fact that this situation exists shouldn’t surprise anyone. People talk about “burnout” and “making health care better” but that just seems to be lip service. They give you a free subscription to a meditation app, phone access to a counselor, and a mandatory early morning meeting to discuss stress reduction. Of course, these things take time away from seeing patients, which sort of defeats the whole purpose. Unless you want to do them at home – taking time away from your family, or doing the taxes, or other things you have to do besides your day job.
This is not sustainable for patients, doctors, or the health care system as a whole. But right now the situation is only getting worse, and there aren’t any easy answers.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Restless legs a new modifiable risk factor for dementia?
suggesting the disorder may be a risk factor for dementia or a very early noncognitive sign of dementia, researchers say.
In a large population-based cohort study, adults with RLS were significantly more likely to develop dementia over more than a decade than were their peers without RLS.
If confirmed in future studies, “regular check-ups for cognitive decline in older patients with RLS may facilitate earlier detection and intervention for those with dementia risk,” wrote investigators led by Eosu Kim, MD, PhD, with Yonsei University, Seoul, Republic of Korea.
The study was published online in Alzheimer’s Research and Therapy.
Sleep disorders and dementia
RLS is associated with poor sleep, depression/anxiety, poor diet, microvasculopathy, and hypoxia – all of which are known risk factors for dementia. However, the relationship between RLS and incident dementia has been unclear.
The researchers compared risk for all-cause dementia, Alzheimer’s disease (AD), and vascular dementia (VaD) among 2,501 adults with newly diagnosed RLS and 9,977 matched control persons participating in the Korean National Health Insurance Service–Elderly Cohort, a nationwide population-based cohort of adults aged 60 and older.
The mean age of the cohort was 73 years; most of the participants were women (65%). Among all 12,478 participants, 874 (7%) developed all-cause dementia during follow-up – 475 (54%) developed AD, and 194 (22%) developed VaD.
The incidence of all-cause dementia was significantly higher among the RLS group than among the control group (10.4% vs. 6.2%). Incidence rates of AD and VaD (5.6% and 2.6%, respectively) were also higher in the RLS group than in the control group (3.4% and 1.3%, respectively).
In Cox regression analysis, RLS was significantly associated with an increased risk of all-cause dementia (adjusted hazard ratio [aHR], 1.46; 95% confidence interval [CI], 1.24-1.72), AD (aHR 1.38; 95% CI, 1.11-1.72) and VaD (aHR, 1.81; 95% CI, 1.30-2.53).
The researchers noted that RLS may precede deterioration of cognitive function, leading to dementia, and they suggest that RLS could be regarded as a “newly identified” risk factor or prodromal sign of dementia.
Modifiable risk factor
Reached for comment, Thanh Dang-Vu, MD, PhD, professor and research chair in sleep, neuroimaging, and cognitive health at Concordia University in Montreal, said there is now “increasing literature that shows sleep as a modifiable risk factor for cognitive decline.
“Previous evidence indicates that both sleep apnea and insomnia disorder increase the risk for cognitive decline and possibly dementia. Here the study adds to this body of evidence linking sleep disorders to dementia, suggesting that RLS should also be considered as a sleep-related risk factor,” Dr. Dang-Vu told this news organization.
“More evidence is needed, though, as here, all diagnoses were based on national health insurance diagnostic codes, and it is likely there were missed diagnoses for RLS but also for other sleep disorders, as there was no systematic screening for them,” Dr. Dang-Vu cautioned.
Support for the study was provided by the Ministry of Health and Welfare, the Korean government, and Yonsei University. Dr. Kim and Dr. Dang-Vu reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
suggesting the disorder may be a risk factor for dementia or a very early noncognitive sign of dementia, researchers say.
In a large population-based cohort study, adults with RLS were significantly more likely to develop dementia over more than a decade than were their peers without RLS.
If confirmed in future studies, “regular check-ups for cognitive decline in older patients with RLS may facilitate earlier detection and intervention for those with dementia risk,” wrote investigators led by Eosu Kim, MD, PhD, with Yonsei University, Seoul, Republic of Korea.
The study was published online in Alzheimer’s Research and Therapy.
Sleep disorders and dementia
RLS is associated with poor sleep, depression/anxiety, poor diet, microvasculopathy, and hypoxia – all of which are known risk factors for dementia. However, the relationship between RLS and incident dementia has been unclear.
The researchers compared risk for all-cause dementia, Alzheimer’s disease (AD), and vascular dementia (VaD) among 2,501 adults with newly diagnosed RLS and 9,977 matched control persons participating in the Korean National Health Insurance Service–Elderly Cohort, a nationwide population-based cohort of adults aged 60 and older.
The mean age of the cohort was 73 years; most of the participants were women (65%). Among all 12,478 participants, 874 (7%) developed all-cause dementia during follow-up – 475 (54%) developed AD, and 194 (22%) developed VaD.
The incidence of all-cause dementia was significantly higher among the RLS group than among the control group (10.4% vs. 6.2%). Incidence rates of AD and VaD (5.6% and 2.6%, respectively) were also higher in the RLS group than in the control group (3.4% and 1.3%, respectively).
In Cox regression analysis, RLS was significantly associated with an increased risk of all-cause dementia (adjusted hazard ratio [aHR], 1.46; 95% confidence interval [CI], 1.24-1.72), AD (aHR 1.38; 95% CI, 1.11-1.72) and VaD (aHR, 1.81; 95% CI, 1.30-2.53).
The researchers noted that RLS may precede deterioration of cognitive function, leading to dementia, and they suggest that RLS could be regarded as a “newly identified” risk factor or prodromal sign of dementia.
Modifiable risk factor
Reached for comment, Thanh Dang-Vu, MD, PhD, professor and research chair in sleep, neuroimaging, and cognitive health at Concordia University in Montreal, said there is now “increasing literature that shows sleep as a modifiable risk factor for cognitive decline.
“Previous evidence indicates that both sleep apnea and insomnia disorder increase the risk for cognitive decline and possibly dementia. Here the study adds to this body of evidence linking sleep disorders to dementia, suggesting that RLS should also be considered as a sleep-related risk factor,” Dr. Dang-Vu told this news organization.
“More evidence is needed, though, as here, all diagnoses were based on national health insurance diagnostic codes, and it is likely there were missed diagnoses for RLS but also for other sleep disorders, as there was no systematic screening for them,” Dr. Dang-Vu cautioned.
Support for the study was provided by the Ministry of Health and Welfare, the Korean government, and Yonsei University. Dr. Kim and Dr. Dang-Vu reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
suggesting the disorder may be a risk factor for dementia or a very early noncognitive sign of dementia, researchers say.
In a large population-based cohort study, adults with RLS were significantly more likely to develop dementia over more than a decade than were their peers without RLS.
If confirmed in future studies, “regular check-ups for cognitive decline in older patients with RLS may facilitate earlier detection and intervention for those with dementia risk,” wrote investigators led by Eosu Kim, MD, PhD, with Yonsei University, Seoul, Republic of Korea.
The study was published online in Alzheimer’s Research and Therapy.
Sleep disorders and dementia
RLS is associated with poor sleep, depression/anxiety, poor diet, microvasculopathy, and hypoxia – all of which are known risk factors for dementia. However, the relationship between RLS and incident dementia has been unclear.
The researchers compared risk for all-cause dementia, Alzheimer’s disease (AD), and vascular dementia (VaD) among 2,501 adults with newly diagnosed RLS and 9,977 matched control persons participating in the Korean National Health Insurance Service–Elderly Cohort, a nationwide population-based cohort of adults aged 60 and older.
The mean age of the cohort was 73 years; most of the participants were women (65%). Among all 12,478 participants, 874 (7%) developed all-cause dementia during follow-up – 475 (54%) developed AD, and 194 (22%) developed VaD.
The incidence of all-cause dementia was significantly higher among the RLS group than among the control group (10.4% vs. 6.2%). Incidence rates of AD and VaD (5.6% and 2.6%, respectively) were also higher in the RLS group than in the control group (3.4% and 1.3%, respectively).
In Cox regression analysis, RLS was significantly associated with an increased risk of all-cause dementia (adjusted hazard ratio [aHR], 1.46; 95% confidence interval [CI], 1.24-1.72), AD (aHR 1.38; 95% CI, 1.11-1.72) and VaD (aHR, 1.81; 95% CI, 1.30-2.53).
The researchers noted that RLS may precede deterioration of cognitive function, leading to dementia, and they suggest that RLS could be regarded as a “newly identified” risk factor or prodromal sign of dementia.
Modifiable risk factor
Reached for comment, Thanh Dang-Vu, MD, PhD, professor and research chair in sleep, neuroimaging, and cognitive health at Concordia University in Montreal, said there is now “increasing literature that shows sleep as a modifiable risk factor for cognitive decline.
“Previous evidence indicates that both sleep apnea and insomnia disorder increase the risk for cognitive decline and possibly dementia. Here the study adds to this body of evidence linking sleep disorders to dementia, suggesting that RLS should also be considered as a sleep-related risk factor,” Dr. Dang-Vu told this news organization.
“More evidence is needed, though, as here, all diagnoses were based on national health insurance diagnostic codes, and it is likely there were missed diagnoses for RLS but also for other sleep disorders, as there was no systematic screening for them,” Dr. Dang-Vu cautioned.
Support for the study was provided by the Ministry of Health and Welfare, the Korean government, and Yonsei University. Dr. Kim and Dr. Dang-Vu reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ALZHEIMER’S RESEARCH AND THERAPY
After the Match: Next steps for new residents, unmatched
Medical school graduates around the US took to social media after last week's Match Day to share their joy ― or explore their options if they did not match.
Take this post March 19 on Twitter: “I went unmatched this year; looking for research position at any institute for internal medicine.”
including an international medical graduate who matched into his chosen specialty after multiple disappointments.
“I’ve waited for this email for 8 years,” Sahil Bawa, MD, posted on Twitter on March 13. A few days later, when he learned about his residency position, he posted: “I’m beyond grateful. Will be moving to Alabama soon #familymedicine.”
Dr. Bawa, who matched into UAB Medicine Selma (Ala.), graduated from medical school in India in 2014. He said in an interview that he has visited the United States periodically since then to pass medical tests, obtain letters of recommendation, and participate in research.
Over the years he watched his Indian colleagues give up on becoming American doctors, find alternative careers, or resolve to practice in their native country. But he held onto the few success stories he saw on social media. “There were always one to two every year. It kept me going. If they can do it, I can do it.”
International medical graduates (IMGs) like Dr. Bawa applied in record numbers to Match2023, according to the National Resident Matching Program (NRMP), which announced the results on March 13 of its main residency match and the Supplemental Offer and Acceptance Program (SOAP) for unfilled positions or unmatched applicants.
Overall, 48,156 total applicants registered for the match, which was driven by the increase of non-U.S. IMG applicants and U.S. DO seniors over the past year, NRMP stated in its release. U.S. MD seniors had a match rate of nearly 94%, and U.S. DO seniors, nearly 92%. U.S. IMGs had a match rate of nearly 68%, an “all-time high,” and non-U.S. IMGs, nearly 60%, NRMP stated.
Three specialties that filled all of their 30 or more available positions were orthopedic surgery, plastic surgery (integrated), radiology – diagnostic, and thoracic surgery. Specialties with 30 or more positions that filled with the highest percentage of U.S. MD and DO seniors were plastic surgery (integrated), internal medicine-pediatrics, ob.gyn., and orthopedic surgery.
The number of available primary care positions increased slightly, NRMP reported. Considering “a serious and growing shortage of primary care physicians across the U.S.,” there were 571 more primary care positions than 2022. That’s an increase of about 3% over last year and 17% over the past 5 years. Primary care positions filled at a rate of 94%, which remained steady from 2022.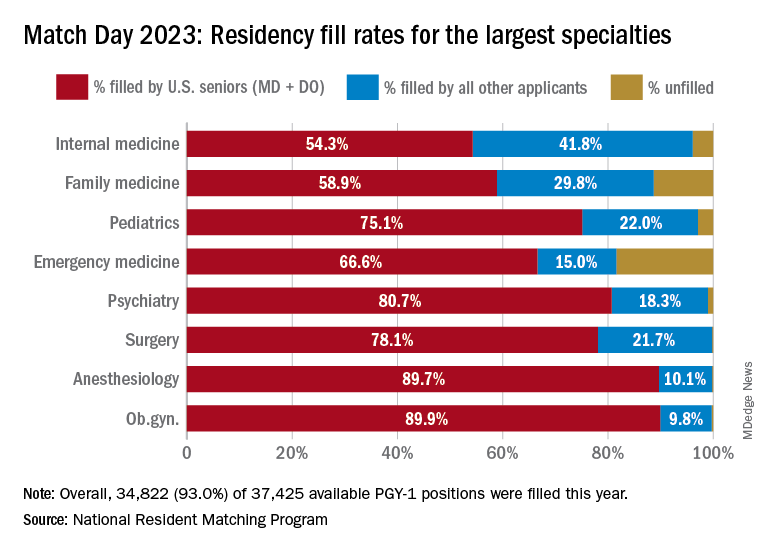
NRMP also pointed out specialties with increases in the number of positions filled by U.S. MD seniors of more than 10% and 10 positions in the past 5 years: anesthesiology, child neurology, interventional radiology, neurology, pathology, physical medicine and rehabilitation, plastic surgery (integrated), psychiatry, radiology-diagnostic, transitional year, and vascular surgery.
Bryan Carmody, MD, MPH, a pediatric nephrologist known for his medical school commentaries, said in an interview that the most competitive specialties he noted in 2023 were radiology, pathology, and neurology.
“The surgical specialties are always competitive, so it wasn’t a surprise that orthopedics, plastic surgery, and thoracic surgery filled all of their positions. But I was surprised to see diagnostic radiology fill every single one of their positions in the match. And although pathology and neurology aren’t typically considered extremely competitive specialties, they filled over 99% of their positions in the Match this year.”
On Dr. Carmody’s blog about the winners and losers of Match Day, he said that despite the record number of primary care positions offered, family medicine programs suffered. “Only 89% of family medicine programs filled in the Match, and graduating U.S. MD and DO students only filled a little more than half of all the available positions,” he wrote.
For a record number of applicants that match each year, and “the most favorable ratio in the past 2 decades” of applicants-to-positions in 2023, there are still a lot unmatched, Dr. Carmody said. “It’s a tough thing to talk about. The reality is the number of residency positions should be determined by the number of physicians needed.”
One student, Asim Ansari, didn’t match into a traditional residency or through SOAP. It was his fifth attempt. He was serving a transitional-year residency at Merit Health Wesley in Hattiesburg, Miss., and when he didn’t match, he accepted a child and adolescent psychiatry fellowship at the University of Kansas Medical Center, Kansas City.
He said he was “relieved and excited” to have found a program in his chosen specialty. Still, in 2 years, Mr. Ansari must again try to match into a traditional psychiatry residency.
Meanwhile, Dr. Bawa will prepare for his 3-year residency in Alabama after completing his interim research year in the surgery department at Wayne State University, Detroit, in May.
Despite his years in limbo, Dr. Bawa said, “I have no regrets, no complaints. I am still very happy.”
A version of this article originally appeared on Medscape.com.
Medical school graduates around the US took to social media after last week's Match Day to share their joy ― or explore their options if they did not match.
Take this post March 19 on Twitter: “I went unmatched this year; looking for research position at any institute for internal medicine.”
including an international medical graduate who matched into his chosen specialty after multiple disappointments.
“I’ve waited for this email for 8 years,” Sahil Bawa, MD, posted on Twitter on March 13. A few days later, when he learned about his residency position, he posted: “I’m beyond grateful. Will be moving to Alabama soon #familymedicine.”
Dr. Bawa, who matched into UAB Medicine Selma (Ala.), graduated from medical school in India in 2014. He said in an interview that he has visited the United States periodically since then to pass medical tests, obtain letters of recommendation, and participate in research.
Over the years he watched his Indian colleagues give up on becoming American doctors, find alternative careers, or resolve to practice in their native country. But he held onto the few success stories he saw on social media. “There were always one to two every year. It kept me going. If they can do it, I can do it.”
International medical graduates (IMGs) like Dr. Bawa applied in record numbers to Match2023, according to the National Resident Matching Program (NRMP), which announced the results on March 13 of its main residency match and the Supplemental Offer and Acceptance Program (SOAP) for unfilled positions or unmatched applicants.
Overall, 48,156 total applicants registered for the match, which was driven by the increase of non-U.S. IMG applicants and U.S. DO seniors over the past year, NRMP stated in its release. U.S. MD seniors had a match rate of nearly 94%, and U.S. DO seniors, nearly 92%. U.S. IMGs had a match rate of nearly 68%, an “all-time high,” and non-U.S. IMGs, nearly 60%, NRMP stated.
Three specialties that filled all of their 30 or more available positions were orthopedic surgery, plastic surgery (integrated), radiology – diagnostic, and thoracic surgery. Specialties with 30 or more positions that filled with the highest percentage of U.S. MD and DO seniors were plastic surgery (integrated), internal medicine-pediatrics, ob.gyn., and orthopedic surgery.
The number of available primary care positions increased slightly, NRMP reported. Considering “a serious and growing shortage of primary care physicians across the U.S.,” there were 571 more primary care positions than 2022. That’s an increase of about 3% over last year and 17% over the past 5 years. Primary care positions filled at a rate of 94%, which remained steady from 2022.
NRMP also pointed out specialties with increases in the number of positions filled by U.S. MD seniors of more than 10% and 10 positions in the past 5 years: anesthesiology, child neurology, interventional radiology, neurology, pathology, physical medicine and rehabilitation, plastic surgery (integrated), psychiatry, radiology-diagnostic, transitional year, and vascular surgery.
Bryan Carmody, MD, MPH, a pediatric nephrologist known for his medical school commentaries, said in an interview that the most competitive specialties he noted in 2023 were radiology, pathology, and neurology.
“The surgical specialties are always competitive, so it wasn’t a surprise that orthopedics, plastic surgery, and thoracic surgery filled all of their positions. But I was surprised to see diagnostic radiology fill every single one of their positions in the match. And although pathology and neurology aren’t typically considered extremely competitive specialties, they filled over 99% of their positions in the Match this year.”
On Dr. Carmody’s blog about the winners and losers of Match Day, he said that despite the record number of primary care positions offered, family medicine programs suffered. “Only 89% of family medicine programs filled in the Match, and graduating U.S. MD and DO students only filled a little more than half of all the available positions,” he wrote.
For a record number of applicants that match each year, and “the most favorable ratio in the past 2 decades” of applicants-to-positions in 2023, there are still a lot unmatched, Dr. Carmody said. “It’s a tough thing to talk about. The reality is the number of residency positions should be determined by the number of physicians needed.”
One student, Asim Ansari, didn’t match into a traditional residency or through SOAP. It was his fifth attempt. He was serving a transitional-year residency at Merit Health Wesley in Hattiesburg, Miss., and when he didn’t match, he accepted a child and adolescent psychiatry fellowship at the University of Kansas Medical Center, Kansas City.
He said he was “relieved and excited” to have found a program in his chosen specialty. Still, in 2 years, Mr. Ansari must again try to match into a traditional psychiatry residency.
Meanwhile, Dr. Bawa will prepare for his 3-year residency in Alabama after completing his interim research year in the surgery department at Wayne State University, Detroit, in May.
Despite his years in limbo, Dr. Bawa said, “I have no regrets, no complaints. I am still very happy.”
A version of this article originally appeared on Medscape.com.
Medical school graduates around the US took to social media after last week's Match Day to share their joy ― or explore their options if they did not match.
Take this post March 19 on Twitter: “I went unmatched this year; looking for research position at any institute for internal medicine.”
including an international medical graduate who matched into his chosen specialty after multiple disappointments.
“I’ve waited for this email for 8 years,” Sahil Bawa, MD, posted on Twitter on March 13. A few days later, when he learned about his residency position, he posted: “I’m beyond grateful. Will be moving to Alabama soon #familymedicine.”
Dr. Bawa, who matched into UAB Medicine Selma (Ala.), graduated from medical school in India in 2014. He said in an interview that he has visited the United States periodically since then to pass medical tests, obtain letters of recommendation, and participate in research.
Over the years he watched his Indian colleagues give up on becoming American doctors, find alternative careers, or resolve to practice in their native country. But he held onto the few success stories he saw on social media. “There were always one to two every year. It kept me going. If they can do it, I can do it.”
International medical graduates (IMGs) like Dr. Bawa applied in record numbers to Match2023, according to the National Resident Matching Program (NRMP), which announced the results on March 13 of its main residency match and the Supplemental Offer and Acceptance Program (SOAP) for unfilled positions or unmatched applicants.
Overall, 48,156 total applicants registered for the match, which was driven by the increase of non-U.S. IMG applicants and U.S. DO seniors over the past year, NRMP stated in its release. U.S. MD seniors had a match rate of nearly 94%, and U.S. DO seniors, nearly 92%. U.S. IMGs had a match rate of nearly 68%, an “all-time high,” and non-U.S. IMGs, nearly 60%, NRMP stated.
Three specialties that filled all of their 30 or more available positions were orthopedic surgery, plastic surgery (integrated), radiology – diagnostic, and thoracic surgery. Specialties with 30 or more positions that filled with the highest percentage of U.S. MD and DO seniors were plastic surgery (integrated), internal medicine-pediatrics, ob.gyn., and orthopedic surgery.
The number of available primary care positions increased slightly, NRMP reported. Considering “a serious and growing shortage of primary care physicians across the U.S.,” there were 571 more primary care positions than 2022. That’s an increase of about 3% over last year and 17% over the past 5 years. Primary care positions filled at a rate of 94%, which remained steady from 2022.
NRMP also pointed out specialties with increases in the number of positions filled by U.S. MD seniors of more than 10% and 10 positions in the past 5 years: anesthesiology, child neurology, interventional radiology, neurology, pathology, physical medicine and rehabilitation, plastic surgery (integrated), psychiatry, radiology-diagnostic, transitional year, and vascular surgery.
Bryan Carmody, MD, MPH, a pediatric nephrologist known for his medical school commentaries, said in an interview that the most competitive specialties he noted in 2023 were radiology, pathology, and neurology.
“The surgical specialties are always competitive, so it wasn’t a surprise that orthopedics, plastic surgery, and thoracic surgery filled all of their positions. But I was surprised to see diagnostic radiology fill every single one of their positions in the match. And although pathology and neurology aren’t typically considered extremely competitive specialties, they filled over 99% of their positions in the Match this year.”
On Dr. Carmody’s blog about the winners and losers of Match Day, he said that despite the record number of primary care positions offered, family medicine programs suffered. “Only 89% of family medicine programs filled in the Match, and graduating U.S. MD and DO students only filled a little more than half of all the available positions,” he wrote.
For a record number of applicants that match each year, and “the most favorable ratio in the past 2 decades” of applicants-to-positions in 2023, there are still a lot unmatched, Dr. Carmody said. “It’s a tough thing to talk about. The reality is the number of residency positions should be determined by the number of physicians needed.”
One student, Asim Ansari, didn’t match into a traditional residency or through SOAP. It was his fifth attempt. He was serving a transitional-year residency at Merit Health Wesley in Hattiesburg, Miss., and when he didn’t match, he accepted a child and adolescent psychiatry fellowship at the University of Kansas Medical Center, Kansas City.
He said he was “relieved and excited” to have found a program in his chosen specialty. Still, in 2 years, Mr. Ansari must again try to match into a traditional psychiatry residency.
Meanwhile, Dr. Bawa will prepare for his 3-year residency in Alabama after completing his interim research year in the surgery department at Wayne State University, Detroit, in May.
Despite his years in limbo, Dr. Bawa said, “I have no regrets, no complaints. I am still very happy.”
A version of this article originally appeared on Medscape.com.