User login
Unhealthy Alcohol Use May Increase in the Years After Bariatric Surgery
After bariatric surgery, patients have a “much higher” risk of unhealthy alcohol use—even if they had no documented unhealthy drinking at baseline, according to researchers from the Durham Veteran Affairs (VA) Medical Center in North Carolina.
Based on their findings, the researchers estimate that for every 21 patients who undergo laparoscopic sleeve gastrectomy (LSG) or Roux-en-Y gastric bypass (RYGB), on average one from each group will develop unhealthy alcohol use.
The researchers collected electronic health record (EHR) data from 2,608 veterans who underwent LSG or RYGB at any bariatric center in the VA health system between 2008 and 2016, and compared that group with a nonsurgical control group.
Nearly all the patients screened negative for unhealthy alcohol use in the 2-year baseline period; however, their mean AUDIT-C scores and the probability of unhealthy alcohol use both increased significantly 3 to 8 years after surgery when compared with the control group. Eight years after an LSG, the probability was 3.4% higher (7.9% vs 4.5%). Eight years after an RYGB, the probability was 9.2% vs 4.4%, a difference of 4.8%.
The estimated prevalence of unhealthy alcohol use 8 years after bariatric surgery was higher for patients with unhealthy drinking at baseline (30 40%) than it was for those without baseline unhealthy drinking (5 - 10%). However, the probability was significantly higher for patients who had an RYGB than it was for nonsurgical control patients after 8 years, which might reflect alcohol pharmacokinetics changes, the researchers say.
Not drinking alcohol is the safest option after bariatric surgery, the researchers say, given that blood alcohol concentration peaks at higher levels after the operation. They advise monitoring patients long-term, using the three-item AUDIT-C scale. And, importantly, they advise cautioning patients undergoing bariatric surgery that drinking alcohol can escalate, even if they have had no history of drinking above recommended limits.
After bariatric surgery, patients have a “much higher” risk of unhealthy alcohol use—even if they had no documented unhealthy drinking at baseline, according to researchers from the Durham Veteran Affairs (VA) Medical Center in North Carolina.
Based on their findings, the researchers estimate that for every 21 patients who undergo laparoscopic sleeve gastrectomy (LSG) or Roux-en-Y gastric bypass (RYGB), on average one from each group will develop unhealthy alcohol use.
The researchers collected electronic health record (EHR) data from 2,608 veterans who underwent LSG or RYGB at any bariatric center in the VA health system between 2008 and 2016, and compared that group with a nonsurgical control group.
Nearly all the patients screened negative for unhealthy alcohol use in the 2-year baseline period; however, their mean AUDIT-C scores and the probability of unhealthy alcohol use both increased significantly 3 to 8 years after surgery when compared with the control group. Eight years after an LSG, the probability was 3.4% higher (7.9% vs 4.5%). Eight years after an RYGB, the probability was 9.2% vs 4.4%, a difference of 4.8%.
The estimated prevalence of unhealthy alcohol use 8 years after bariatric surgery was higher for patients with unhealthy drinking at baseline (30 40%) than it was for those without baseline unhealthy drinking (5 - 10%). However, the probability was significantly higher for patients who had an RYGB than it was for nonsurgical control patients after 8 years, which might reflect alcohol pharmacokinetics changes, the researchers say.
Not drinking alcohol is the safest option after bariatric surgery, the researchers say, given that blood alcohol concentration peaks at higher levels after the operation. They advise monitoring patients long-term, using the three-item AUDIT-C scale. And, importantly, they advise cautioning patients undergoing bariatric surgery that drinking alcohol can escalate, even if they have had no history of drinking above recommended limits.
After bariatric surgery, patients have a “much higher” risk of unhealthy alcohol use—even if they had no documented unhealthy drinking at baseline, according to researchers from the Durham Veteran Affairs (VA) Medical Center in North Carolina.
Based on their findings, the researchers estimate that for every 21 patients who undergo laparoscopic sleeve gastrectomy (LSG) or Roux-en-Y gastric bypass (RYGB), on average one from each group will develop unhealthy alcohol use.
The researchers collected electronic health record (EHR) data from 2,608 veterans who underwent LSG or RYGB at any bariatric center in the VA health system between 2008 and 2016, and compared that group with a nonsurgical control group.
Nearly all the patients screened negative for unhealthy alcohol use in the 2-year baseline period; however, their mean AUDIT-C scores and the probability of unhealthy alcohol use both increased significantly 3 to 8 years after surgery when compared with the control group. Eight years after an LSG, the probability was 3.4% higher (7.9% vs 4.5%). Eight years after an RYGB, the probability was 9.2% vs 4.4%, a difference of 4.8%.
The estimated prevalence of unhealthy alcohol use 8 years after bariatric surgery was higher for patients with unhealthy drinking at baseline (30 40%) than it was for those without baseline unhealthy drinking (5 - 10%). However, the probability was significantly higher for patients who had an RYGB than it was for nonsurgical control patients after 8 years, which might reflect alcohol pharmacokinetics changes, the researchers say.
Not drinking alcohol is the safest option after bariatric surgery, the researchers say, given that blood alcohol concentration peaks at higher levels after the operation. They advise monitoring patients long-term, using the three-item AUDIT-C scale. And, importantly, they advise cautioning patients undergoing bariatric surgery that drinking alcohol can escalate, even if they have had no history of drinking above recommended limits.
COVID-19 in children: Latest weekly increase is largest yet
according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
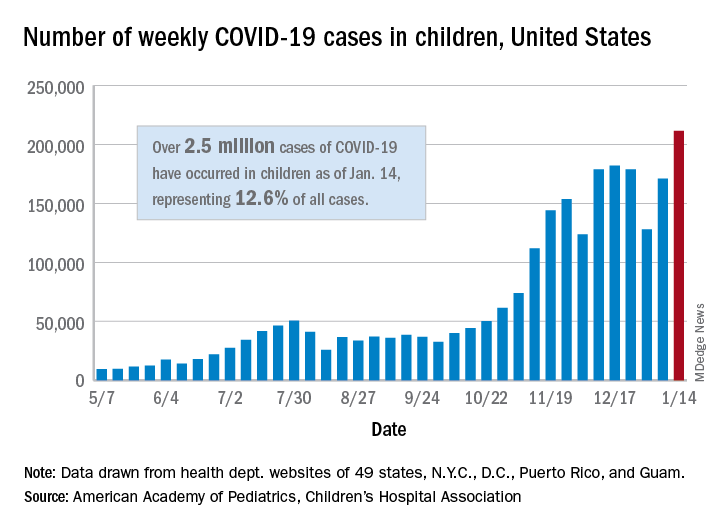
There were 211,466 new cases reported in children during the week of Jan. 8-14, topping the previous high (Dec. 11-17) by almost 30,000. Those new cases bring the total for the pandemic to over 2.5 million children infected with the coronavirus, which represents 12.6% of all reported cases, the AAP and the CHA said Jan. 19 in their weekly COVID-19 report.
The rise in cases also brought an increase in the proportion reported among children. The week before (Jan. 1-7), cases in children were 12.9% of all cases reported, but the most recent week saw that number rise to 14.5% of all cases, the highest it’s been since early October, based on data collected from the health department websites of 49 states (excluding New York), the District of Columbia, New York City, Puerto Rio, and Guam.
The corresponding figures for severe illness continue to be low: Children represent 1.8% of all hospitalizations from COVID-19 in 24 states and New York City and 0.06% of all deaths in 43 states and New York City. Three deaths were reported for the week of Jan. 8-14, making for a total of 191 since the pandemic started, the AAP and CHA said in their report.
Among the states, California has the most overall cases at just over 350,000, Wyoming has the highest proportion of cases in children (20.3%), and North Dakota has the highest rate of infection (over 8,100 per 100,000 children). The infection rate for the nation is now above 3,300 per 100,000 children, and 11 states reported rates over 5,000, according to the AAP and the CHA.
according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
There were 211,466 new cases reported in children during the week of Jan. 8-14, topping the previous high (Dec. 11-17) by almost 30,000. Those new cases bring the total for the pandemic to over 2.5 million children infected with the coronavirus, which represents 12.6% of all reported cases, the AAP and the CHA said Jan. 19 in their weekly COVID-19 report.
The rise in cases also brought an increase in the proportion reported among children. The week before (Jan. 1-7), cases in children were 12.9% of all cases reported, but the most recent week saw that number rise to 14.5% of all cases, the highest it’s been since early October, based on data collected from the health department websites of 49 states (excluding New York), the District of Columbia, New York City, Puerto Rio, and Guam.
The corresponding figures for severe illness continue to be low: Children represent 1.8% of all hospitalizations from COVID-19 in 24 states and New York City and 0.06% of all deaths in 43 states and New York City. Three deaths were reported for the week of Jan. 8-14, making for a total of 191 since the pandemic started, the AAP and CHA said in their report.
Among the states, California has the most overall cases at just over 350,000, Wyoming has the highest proportion of cases in children (20.3%), and North Dakota has the highest rate of infection (over 8,100 per 100,000 children). The infection rate for the nation is now above 3,300 per 100,000 children, and 11 states reported rates over 5,000, according to the AAP and the CHA.
according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
There were 211,466 new cases reported in children during the week of Jan. 8-14, topping the previous high (Dec. 11-17) by almost 30,000. Those new cases bring the total for the pandemic to over 2.5 million children infected with the coronavirus, which represents 12.6% of all reported cases, the AAP and the CHA said Jan. 19 in their weekly COVID-19 report.
The rise in cases also brought an increase in the proportion reported among children. The week before (Jan. 1-7), cases in children were 12.9% of all cases reported, but the most recent week saw that number rise to 14.5% of all cases, the highest it’s been since early October, based on data collected from the health department websites of 49 states (excluding New York), the District of Columbia, New York City, Puerto Rio, and Guam.
The corresponding figures for severe illness continue to be low: Children represent 1.8% of all hospitalizations from COVID-19 in 24 states and New York City and 0.06% of all deaths in 43 states and New York City. Three deaths were reported for the week of Jan. 8-14, making for a total of 191 since the pandemic started, the AAP and CHA said in their report.
Among the states, California has the most overall cases at just over 350,000, Wyoming has the highest proportion of cases in children (20.3%), and North Dakota has the highest rate of infection (over 8,100 per 100,000 children). The infection rate for the nation is now above 3,300 per 100,000 children, and 11 states reported rates over 5,000, according to the AAP and the CHA.
Gut microbiome may predict nivolumab efficacy in gastric cancer
Researchers have demonstrated bacterial invasion of the epithelial cell pathway in the gut microbiome and suggest that this could potentially become a novel biomarker.
“In addition, we found gastric cancer–specific gut microbiome predictive of responses to immune checkpoint inhibitors,” said study author Yu Sunakawa, MD, PhD, an associate professor in the department of clinical oncology at St. Marianna University, Kawasaki, Japan.
Dr. Sunakawa presented the study’s results at the 2021 Gastrointestinal Cancers Symposium.
The gut microbiome holds great interest as a potential biomarker for response. Previous studies suggested that it may hold the key to immunotherapy responses. The concept has been demonstrated in several studies involving patients with melanoma, but this is the first study in patients with gastric cancer.
Nivolumab monotherapy has been shown to provide a survival benefit with a manageable safety profile in previously treated patients with gastric cancer or gastroesophageal junction (GEJ) cancer, Dr. Sunakawa noted. However, fewer than half of patients responded to therapy.
“The disease control rate was about 40%, and many patients did not experience any tumor degradation,” he said. “About 60% of the patients did not respond to nivolumab as a late-line therapy.”
In the observational/translational DELIVER trial, investigators enrolled 501 patients with recurrent or metastatic adenocarcinoma of the stomach or GEJ. The patients were recruited from 50 sites in Japan.
The primary endpoint was the relationship between the genomic pathway in the gut microbiome and efficacy of nivolumab and whether there was progressive disease or not at the first evaluation, as determined in accordance with Response Evaluation Criteria in Solid Tumors criteria.
Genomic data were measured by genome shotgun sequence at a central laboratory. Biomarkers were analyzed by Wilcoxon rank sum test in the first 200 patients, who constituted the training cohort. The top 30 biomarker candidates were validated in the last 300 patients (the validation cohort) using the Bonferroni method.
Clinical and genomic data were available for 437 patients (87%). Of this group, 180 constituted the training cohort, and 257, the validation cohort.
The phylogenetic composition of common bacterial taxa was similar for both cohorts.
In the training cohort, 62.2% of patients had progressive disease, as did 53.2% in the validation cohort. The microbiome was more diverse among the patients who did not have progressive disease than among those who did have progressive disease.
The authors noted that, although there was no statistically significant pathway to be validated for a primary endpoint using the Bonferroni method, bacterial invasion of epithelial cells in the KEGG pathway was associated with clinical outcomes in both the training cohort (P = .057) and the validation cohort (P = .014). However, these pathways were not significantly associated with progressive disease after Bonferroni correction, a conservative test that adjusts for multiple comparisons.
An exploratory analysis of genus showed that Odoribacter and Veillonella species were associated with tumor response to nivolumab in both cohorts.
Dr. Sunakawa noted that biomarker analyses are ongoing. The researchers are investigating the relationships between microbiome and survival times, as well as other endpoints.
Still some gaps
In a discussion of the study, Jonathan Yeung, MD, PhD, of Princess Margaret Cancer Center, Toronto, congratulated the investigators on their study, noting that “the logistical hurdles must have been tremendous to obtain these data.”
However, Dr. Yeung pointed out some limitations and gaps in the data that were presented. For example, he found that the ratio of the training set to the validation set was unusual. “The training set is usually larger and usually an 80/20 ratio,” he said. “In their design, the validation set is larger, and I’m quite curious about their rationale.
“The conclusion of the study is that a more diverse microbiome was observed in patients with a tumor response than in those without a response,” he continued, “but they don’t actually show the statistical test used to make this conclusion. There is considerable overlap between the groups, and more compelling data are needed to make that conclusion.”
Another limitation was the marked imbalance in the number of patients whose condition responded to nivolumab in comparison with those whose condition did not (20 vs. 417 patients). This could have affected the statistical power of the study.
But overall, Dr. Yeung congratulated the authors for presenting a very impressive dataset. “The preliminary data are very interesting, and I look forward to the final results,” he said.
The study was funded by Ono Pharmaceutical and Bristol-Myers Squibb, which markets nivolumab. Dr. Sunakawa has received honoraria from Bayer Yakuhin, Bristol-Myers Squibb Japan, Chugai, Kyowa Hakko Kirin, Lilly Japan, Nippon Kayaku, Sanofi, Taiho, Takeda, and Yakult Honsha. He has held a consulting or advisory role for Bristol-Myers Squibb Japan, Daiichi Sankyo, and Takeda and has received research funding from Chugai Pharma, Daiichi Sankyo, Lilly Japan, Sanofi, Taiho Pharmaceutical, and Takeda. The Gastrointestinal Cancers Symposium is sponsored by the American Gastroenterological Association, the American Society for Clinical Oncology, the American Society for Radiation Oncology, and the Society of Surgical Oncology.
A version of this article first appeared on Medscape.com.
Researchers have demonstrated bacterial invasion of the epithelial cell pathway in the gut microbiome and suggest that this could potentially become a novel biomarker.
“In addition, we found gastric cancer–specific gut microbiome predictive of responses to immune checkpoint inhibitors,” said study author Yu Sunakawa, MD, PhD, an associate professor in the department of clinical oncology at St. Marianna University, Kawasaki, Japan.
Dr. Sunakawa presented the study’s results at the 2021 Gastrointestinal Cancers Symposium.
The gut microbiome holds great interest as a potential biomarker for response. Previous studies suggested that it may hold the key to immunotherapy responses. The concept has been demonstrated in several studies involving patients with melanoma, but this is the first study in patients with gastric cancer.
Nivolumab monotherapy has been shown to provide a survival benefit with a manageable safety profile in previously treated patients with gastric cancer or gastroesophageal junction (GEJ) cancer, Dr. Sunakawa noted. However, fewer than half of patients responded to therapy.
“The disease control rate was about 40%, and many patients did not experience any tumor degradation,” he said. “About 60% of the patients did not respond to nivolumab as a late-line therapy.”
In the observational/translational DELIVER trial, investigators enrolled 501 patients with recurrent or metastatic adenocarcinoma of the stomach or GEJ. The patients were recruited from 50 sites in Japan.
The primary endpoint was the relationship between the genomic pathway in the gut microbiome and efficacy of nivolumab and whether there was progressive disease or not at the first evaluation, as determined in accordance with Response Evaluation Criteria in Solid Tumors criteria.
Genomic data were measured by genome shotgun sequence at a central laboratory. Biomarkers were analyzed by Wilcoxon rank sum test in the first 200 patients, who constituted the training cohort. The top 30 biomarker candidates were validated in the last 300 patients (the validation cohort) using the Bonferroni method.
Clinical and genomic data were available for 437 patients (87%). Of this group, 180 constituted the training cohort, and 257, the validation cohort.
The phylogenetic composition of common bacterial taxa was similar for both cohorts.
In the training cohort, 62.2% of patients had progressive disease, as did 53.2% in the validation cohort. The microbiome was more diverse among the patients who did not have progressive disease than among those who did have progressive disease.
The authors noted that, although there was no statistically significant pathway to be validated for a primary endpoint using the Bonferroni method, bacterial invasion of epithelial cells in the KEGG pathway was associated with clinical outcomes in both the training cohort (P = .057) and the validation cohort (P = .014). However, these pathways were not significantly associated with progressive disease after Bonferroni correction, a conservative test that adjusts for multiple comparisons.
An exploratory analysis of genus showed that Odoribacter and Veillonella species were associated with tumor response to nivolumab in both cohorts.
Dr. Sunakawa noted that biomarker analyses are ongoing. The researchers are investigating the relationships between microbiome and survival times, as well as other endpoints.
Still some gaps
In a discussion of the study, Jonathan Yeung, MD, PhD, of Princess Margaret Cancer Center, Toronto, congratulated the investigators on their study, noting that “the logistical hurdles must have been tremendous to obtain these data.”
However, Dr. Yeung pointed out some limitations and gaps in the data that were presented. For example, he found that the ratio of the training set to the validation set was unusual. “The training set is usually larger and usually an 80/20 ratio,” he said. “In their design, the validation set is larger, and I’m quite curious about their rationale.
“The conclusion of the study is that a more diverse microbiome was observed in patients with a tumor response than in those without a response,” he continued, “but they don’t actually show the statistical test used to make this conclusion. There is considerable overlap between the groups, and more compelling data are needed to make that conclusion.”
Another limitation was the marked imbalance in the number of patients whose condition responded to nivolumab in comparison with those whose condition did not (20 vs. 417 patients). This could have affected the statistical power of the study.
But overall, Dr. Yeung congratulated the authors for presenting a very impressive dataset. “The preliminary data are very interesting, and I look forward to the final results,” he said.
The study was funded by Ono Pharmaceutical and Bristol-Myers Squibb, which markets nivolumab. Dr. Sunakawa has received honoraria from Bayer Yakuhin, Bristol-Myers Squibb Japan, Chugai, Kyowa Hakko Kirin, Lilly Japan, Nippon Kayaku, Sanofi, Taiho, Takeda, and Yakult Honsha. He has held a consulting or advisory role for Bristol-Myers Squibb Japan, Daiichi Sankyo, and Takeda and has received research funding from Chugai Pharma, Daiichi Sankyo, Lilly Japan, Sanofi, Taiho Pharmaceutical, and Takeda. The Gastrointestinal Cancers Symposium is sponsored by the American Gastroenterological Association, the American Society for Clinical Oncology, the American Society for Radiation Oncology, and the Society of Surgical Oncology.
A version of this article first appeared on Medscape.com.
Researchers have demonstrated bacterial invasion of the epithelial cell pathway in the gut microbiome and suggest that this could potentially become a novel biomarker.
“In addition, we found gastric cancer–specific gut microbiome predictive of responses to immune checkpoint inhibitors,” said study author Yu Sunakawa, MD, PhD, an associate professor in the department of clinical oncology at St. Marianna University, Kawasaki, Japan.
Dr. Sunakawa presented the study’s results at the 2021 Gastrointestinal Cancers Symposium.
The gut microbiome holds great interest as a potential biomarker for response. Previous studies suggested that it may hold the key to immunotherapy responses. The concept has been demonstrated in several studies involving patients with melanoma, but this is the first study in patients with gastric cancer.
Nivolumab monotherapy has been shown to provide a survival benefit with a manageable safety profile in previously treated patients with gastric cancer or gastroesophageal junction (GEJ) cancer, Dr. Sunakawa noted. However, fewer than half of patients responded to therapy.
“The disease control rate was about 40%, and many patients did not experience any tumor degradation,” he said. “About 60% of the patients did not respond to nivolumab as a late-line therapy.”
In the observational/translational DELIVER trial, investigators enrolled 501 patients with recurrent or metastatic adenocarcinoma of the stomach or GEJ. The patients were recruited from 50 sites in Japan.
The primary endpoint was the relationship between the genomic pathway in the gut microbiome and efficacy of nivolumab and whether there was progressive disease or not at the first evaluation, as determined in accordance with Response Evaluation Criteria in Solid Tumors criteria.
Genomic data were measured by genome shotgun sequence at a central laboratory. Biomarkers were analyzed by Wilcoxon rank sum test in the first 200 patients, who constituted the training cohort. The top 30 biomarker candidates were validated in the last 300 patients (the validation cohort) using the Bonferroni method.
Clinical and genomic data were available for 437 patients (87%). Of this group, 180 constituted the training cohort, and 257, the validation cohort.
The phylogenetic composition of common bacterial taxa was similar for both cohorts.
In the training cohort, 62.2% of patients had progressive disease, as did 53.2% in the validation cohort. The microbiome was more diverse among the patients who did not have progressive disease than among those who did have progressive disease.
The authors noted that, although there was no statistically significant pathway to be validated for a primary endpoint using the Bonferroni method, bacterial invasion of epithelial cells in the KEGG pathway was associated with clinical outcomes in both the training cohort (P = .057) and the validation cohort (P = .014). However, these pathways were not significantly associated with progressive disease after Bonferroni correction, a conservative test that adjusts for multiple comparisons.
An exploratory analysis of genus showed that Odoribacter and Veillonella species were associated with tumor response to nivolumab in both cohorts.
Dr. Sunakawa noted that biomarker analyses are ongoing. The researchers are investigating the relationships between microbiome and survival times, as well as other endpoints.
Still some gaps
In a discussion of the study, Jonathan Yeung, MD, PhD, of Princess Margaret Cancer Center, Toronto, congratulated the investigators on their study, noting that “the logistical hurdles must have been tremendous to obtain these data.”
However, Dr. Yeung pointed out some limitations and gaps in the data that were presented. For example, he found that the ratio of the training set to the validation set was unusual. “The training set is usually larger and usually an 80/20 ratio,” he said. “In their design, the validation set is larger, and I’m quite curious about their rationale.
“The conclusion of the study is that a more diverse microbiome was observed in patients with a tumor response than in those without a response,” he continued, “but they don’t actually show the statistical test used to make this conclusion. There is considerable overlap between the groups, and more compelling data are needed to make that conclusion.”
Another limitation was the marked imbalance in the number of patients whose condition responded to nivolumab in comparison with those whose condition did not (20 vs. 417 patients). This could have affected the statistical power of the study.
But overall, Dr. Yeung congratulated the authors for presenting a very impressive dataset. “The preliminary data are very interesting, and I look forward to the final results,” he said.
The study was funded by Ono Pharmaceutical and Bristol-Myers Squibb, which markets nivolumab. Dr. Sunakawa has received honoraria from Bayer Yakuhin, Bristol-Myers Squibb Japan, Chugai, Kyowa Hakko Kirin, Lilly Japan, Nippon Kayaku, Sanofi, Taiho, Takeda, and Yakult Honsha. He has held a consulting or advisory role for Bristol-Myers Squibb Japan, Daiichi Sankyo, and Takeda and has received research funding from Chugai Pharma, Daiichi Sankyo, Lilly Japan, Sanofi, Taiho Pharmaceutical, and Takeda. The Gastrointestinal Cancers Symposium is sponsored by the American Gastroenterological Association, the American Society for Clinical Oncology, the American Society for Radiation Oncology, and the Society of Surgical Oncology.
A version of this article first appeared on Medscape.com.
Von Willebrand disease guidelines address women’s bleeding concerns
New guidelines issued jointly by four major international hematology groups focus on the management of patients with von Willebrand disease (VWD), the most common bleeding disorder in the world.
The evidence-based guidelines, published in Blood Advances, were developed in collaboration by the American Society of Hematology (ASH), the International Society on Thrombosis and Haemostasis, the National Hemophilia Foundation, and the World Federation of Hemophilia. They outline key recommendations spanning the care of patients with a broad range of therapeutic needs.
“We addressed some of the questions that were most important to the community, but certainly there are a lot of areas that we couldn’t cover” said coauthor Veronica H. Flood, MD, of the Medical College of Wisconsin in Milwaukee.
The guidelines process began with a survey sent to the von Willebrand disease community, including patients, caregivers, nurses, physicians, and scientists. The respondents were asked to prioritize issues that they felt should be addressed in the guidelines.
“Interestingly, some of the issues were the same between patients and caregivers and physicians, and some were different, but there were obviously some areas that we just couldn’t cover,” she said in an interview.
One of the areas of greatest concern for respondents was bleeding in women, and many of the recommendations include specific considerations for management of gynecologic and obstetric patients, Dr. Flood said.
“We also tried to make the questions applicable to as many patients with von Willebrand disease as possible,” she added.
Some of the questions, such as recommendation 1, regarding prophylaxis, are geared toward management of patients with severe disease, while others, such as recommendations for treatment of menstrual bleeding, are more suited for patients with milder VWD.
All of the recommendations in the guidelines are “conditional” (suggested), due to very low certainty in the evidence of effects, the authors noted.
Prophylaxis
The guidelines suggest long-term prophylaxis for patients with a history of severe and frequent bleeds, with periodic assessment of the need for prophylaxis.
Desmopressin
For those patients who may benefit from the use of desmopressin, primarily those with type 1 VWD, and who have a baseline von Willebrand factor (VWF) level below 0.30 IU/mL, the panel issued a conditional recommendation for a desmopressin trial with treatment based on the patient’s results compared with not performing a trial and treating with tranexamic acid or factor concentrate. The guidelines also advise against treating with desmopressin in the absence of a trial. In a section of “good practice statements,” the guidelines indicate that using desmopressin in patients with type 2B VWD is generally contraindicated, because of the risk of thrombocytopenia as a result of increased platelet binding. In addition, desmopressin is generally contraindicated in patients with active cardiovascular disease, patients with seizure disorders, patients less than 2 years old, and patients with type 1C VWD in the setting of surgery.
Antithrombotic therapy
The guideline panelists conditionally recommend antithrombotic therapy with either antiplatelet agents or anticoagulants, with an emphasis on reassessing bleeding risk throughout the course of treatment.
An accompanying good practice statement calls for individualized assessments of risks and benefits of specific antithrombotic therapies by a multidisciplinary team including hematologists, cardiovascular specialists, and the patient.
Major surgery
This section includes a recommendation for targeting both factor VIII and VWF activity levels to a minimum of 50 IU/mL for at least 3 days after surgery, and a suggestion against using factor VIII target levels alone.
Minor surgery/invasive procedures
The panelists suggest increasing VWF activity levels to a minimum of 0.50 IU/mL with desmopressin or factor concentrate with the addition of tranexamic acid over raising VWF levels to at least 0.50 IU/mL with desmopressin or factor concentrate alone.
In addition, the panelists suggest “giving tranexamic acid alone over increasing VWF activity levels to a minimum threshold of 0.50 IU/mL with any intervention in patients with type 1 VWD with baseline VWF activity levels of 0.30 IU/mL and a mild bleeding phenotype undergoing minor mucosal procedures.”
Heavy menstrual bleeding
In women with heavy menstrual bleeding who do not plan to conceive, the panel suggests either combined hormonal therapy or levonorgestrel-releasing intrauterine system, or tranexamic acid over desmopressin.
In women who wish to conceive, the panel suggests using tranexamic acid over desmopressin.
Neuraxial anesthesia during labor
For women in labor for whom neuraxial anesthesia is considered, the guidelines suggest targeting a VWF activity level from 0.50 to 1.50 IU/mL over targeting a level above 1.50 IU/mL.
Postpartum management
“The guideline panel suggests the use of tranexamic acid over not using it in women with type 1 VWD or low VWF levels (and this may also apply to types 2 and 3 VWD) during the postpartum period,” the guidelines say.
An accompanying good practice statement says that tranexamic acid can be provided orally or intravenously. The oral dose is 25 mg/kg three times daily for 10-14 days, or longer if blood loss remains heavy.
Dr. Flood said that the guidelines were developed under the assumption that they would apply to care of patients in regions with a high or moderately high degree of clinical resources.
“We recognize that this eliminates a great deal of the globe, and our hope is that ASH and the other sponsoring organizations are going to let us revise this and do a version for lower-resourced settings,” she said.
New guidelines issued jointly by four major international hematology groups focus on the management of patients with von Willebrand disease (VWD), the most common bleeding disorder in the world.
The evidence-based guidelines, published in Blood Advances, were developed in collaboration by the American Society of Hematology (ASH), the International Society on Thrombosis and Haemostasis, the National Hemophilia Foundation, and the World Federation of Hemophilia. They outline key recommendations spanning the care of patients with a broad range of therapeutic needs.
“We addressed some of the questions that were most important to the community, but certainly there are a lot of areas that we couldn’t cover” said coauthor Veronica H. Flood, MD, of the Medical College of Wisconsin in Milwaukee.
The guidelines process began with a survey sent to the von Willebrand disease community, including patients, caregivers, nurses, physicians, and scientists. The respondents were asked to prioritize issues that they felt should be addressed in the guidelines.
“Interestingly, some of the issues were the same between patients and caregivers and physicians, and some were different, but there were obviously some areas that we just couldn’t cover,” she said in an interview.
One of the areas of greatest concern for respondents was bleeding in women, and many of the recommendations include specific considerations for management of gynecologic and obstetric patients, Dr. Flood said.
“We also tried to make the questions applicable to as many patients with von Willebrand disease as possible,” she added.
Some of the questions, such as recommendation 1, regarding prophylaxis, are geared toward management of patients with severe disease, while others, such as recommendations for treatment of menstrual bleeding, are more suited for patients with milder VWD.
All of the recommendations in the guidelines are “conditional” (suggested), due to very low certainty in the evidence of effects, the authors noted.
Prophylaxis
The guidelines suggest long-term prophylaxis for patients with a history of severe and frequent bleeds, with periodic assessment of the need for prophylaxis.
Desmopressin
For those patients who may benefit from the use of desmopressin, primarily those with type 1 VWD, and who have a baseline von Willebrand factor (VWF) level below 0.30 IU/mL, the panel issued a conditional recommendation for a desmopressin trial with treatment based on the patient’s results compared with not performing a trial and treating with tranexamic acid or factor concentrate. The guidelines also advise against treating with desmopressin in the absence of a trial. In a section of “good practice statements,” the guidelines indicate that using desmopressin in patients with type 2B VWD is generally contraindicated, because of the risk of thrombocytopenia as a result of increased platelet binding. In addition, desmopressin is generally contraindicated in patients with active cardiovascular disease, patients with seizure disorders, patients less than 2 years old, and patients with type 1C VWD in the setting of surgery.
Antithrombotic therapy
The guideline panelists conditionally recommend antithrombotic therapy with either antiplatelet agents or anticoagulants, with an emphasis on reassessing bleeding risk throughout the course of treatment.
An accompanying good practice statement calls for individualized assessments of risks and benefits of specific antithrombotic therapies by a multidisciplinary team including hematologists, cardiovascular specialists, and the patient.
Major surgery
This section includes a recommendation for targeting both factor VIII and VWF activity levels to a minimum of 50 IU/mL for at least 3 days after surgery, and a suggestion against using factor VIII target levels alone.
Minor surgery/invasive procedures
The panelists suggest increasing VWF activity levels to a minimum of 0.50 IU/mL with desmopressin or factor concentrate with the addition of tranexamic acid over raising VWF levels to at least 0.50 IU/mL with desmopressin or factor concentrate alone.
In addition, the panelists suggest “giving tranexamic acid alone over increasing VWF activity levels to a minimum threshold of 0.50 IU/mL with any intervention in patients with type 1 VWD with baseline VWF activity levels of 0.30 IU/mL and a mild bleeding phenotype undergoing minor mucosal procedures.”
Heavy menstrual bleeding
In women with heavy menstrual bleeding who do not plan to conceive, the panel suggests either combined hormonal therapy or levonorgestrel-releasing intrauterine system, or tranexamic acid over desmopressin.
In women who wish to conceive, the panel suggests using tranexamic acid over desmopressin.
Neuraxial anesthesia during labor
For women in labor for whom neuraxial anesthesia is considered, the guidelines suggest targeting a VWF activity level from 0.50 to 1.50 IU/mL over targeting a level above 1.50 IU/mL.
Postpartum management
“The guideline panel suggests the use of tranexamic acid over not using it in women with type 1 VWD or low VWF levels (and this may also apply to types 2 and 3 VWD) during the postpartum period,” the guidelines say.
An accompanying good practice statement says that tranexamic acid can be provided orally or intravenously. The oral dose is 25 mg/kg three times daily for 10-14 days, or longer if blood loss remains heavy.
Dr. Flood said that the guidelines were developed under the assumption that they would apply to care of patients in regions with a high or moderately high degree of clinical resources.
“We recognize that this eliminates a great deal of the globe, and our hope is that ASH and the other sponsoring organizations are going to let us revise this and do a version for lower-resourced settings,” she said.
New guidelines issued jointly by four major international hematology groups focus on the management of patients with von Willebrand disease (VWD), the most common bleeding disorder in the world.
The evidence-based guidelines, published in Blood Advances, were developed in collaboration by the American Society of Hematology (ASH), the International Society on Thrombosis and Haemostasis, the National Hemophilia Foundation, and the World Federation of Hemophilia. They outline key recommendations spanning the care of patients with a broad range of therapeutic needs.
“We addressed some of the questions that were most important to the community, but certainly there are a lot of areas that we couldn’t cover” said coauthor Veronica H. Flood, MD, of the Medical College of Wisconsin in Milwaukee.
The guidelines process began with a survey sent to the von Willebrand disease community, including patients, caregivers, nurses, physicians, and scientists. The respondents were asked to prioritize issues that they felt should be addressed in the guidelines.
“Interestingly, some of the issues were the same between patients and caregivers and physicians, and some were different, but there were obviously some areas that we just couldn’t cover,” she said in an interview.
One of the areas of greatest concern for respondents was bleeding in women, and many of the recommendations include specific considerations for management of gynecologic and obstetric patients, Dr. Flood said.
“We also tried to make the questions applicable to as many patients with von Willebrand disease as possible,” she added.
Some of the questions, such as recommendation 1, regarding prophylaxis, are geared toward management of patients with severe disease, while others, such as recommendations for treatment of menstrual bleeding, are more suited for patients with milder VWD.
All of the recommendations in the guidelines are “conditional” (suggested), due to very low certainty in the evidence of effects, the authors noted.
Prophylaxis
The guidelines suggest long-term prophylaxis for patients with a history of severe and frequent bleeds, with periodic assessment of the need for prophylaxis.
Desmopressin
For those patients who may benefit from the use of desmopressin, primarily those with type 1 VWD, and who have a baseline von Willebrand factor (VWF) level below 0.30 IU/mL, the panel issued a conditional recommendation for a desmopressin trial with treatment based on the patient’s results compared with not performing a trial and treating with tranexamic acid or factor concentrate. The guidelines also advise against treating with desmopressin in the absence of a trial. In a section of “good practice statements,” the guidelines indicate that using desmopressin in patients with type 2B VWD is generally contraindicated, because of the risk of thrombocytopenia as a result of increased platelet binding. In addition, desmopressin is generally contraindicated in patients with active cardiovascular disease, patients with seizure disorders, patients less than 2 years old, and patients with type 1C VWD in the setting of surgery.
Antithrombotic therapy
The guideline panelists conditionally recommend antithrombotic therapy with either antiplatelet agents or anticoagulants, with an emphasis on reassessing bleeding risk throughout the course of treatment.
An accompanying good practice statement calls for individualized assessments of risks and benefits of specific antithrombotic therapies by a multidisciplinary team including hematologists, cardiovascular specialists, and the patient.
Major surgery
This section includes a recommendation for targeting both factor VIII and VWF activity levels to a minimum of 50 IU/mL for at least 3 days after surgery, and a suggestion against using factor VIII target levels alone.
Minor surgery/invasive procedures
The panelists suggest increasing VWF activity levels to a minimum of 0.50 IU/mL with desmopressin or factor concentrate with the addition of tranexamic acid over raising VWF levels to at least 0.50 IU/mL with desmopressin or factor concentrate alone.
In addition, the panelists suggest “giving tranexamic acid alone over increasing VWF activity levels to a minimum threshold of 0.50 IU/mL with any intervention in patients with type 1 VWD with baseline VWF activity levels of 0.30 IU/mL and a mild bleeding phenotype undergoing minor mucosal procedures.”
Heavy menstrual bleeding
In women with heavy menstrual bleeding who do not plan to conceive, the panel suggests either combined hormonal therapy or levonorgestrel-releasing intrauterine system, or tranexamic acid over desmopressin.
In women who wish to conceive, the panel suggests using tranexamic acid over desmopressin.
Neuraxial anesthesia during labor
For women in labor for whom neuraxial anesthesia is considered, the guidelines suggest targeting a VWF activity level from 0.50 to 1.50 IU/mL over targeting a level above 1.50 IU/mL.
Postpartum management
“The guideline panel suggests the use of tranexamic acid over not using it in women with type 1 VWD or low VWF levels (and this may also apply to types 2 and 3 VWD) during the postpartum period,” the guidelines say.
An accompanying good practice statement says that tranexamic acid can be provided orally or intravenously. The oral dose is 25 mg/kg three times daily for 10-14 days, or longer if blood loss remains heavy.
Dr. Flood said that the guidelines were developed under the assumption that they would apply to care of patients in regions with a high or moderately high degree of clinical resources.
“We recognize that this eliminates a great deal of the globe, and our hope is that ASH and the other sponsoring organizations are going to let us revise this and do a version for lower-resourced settings,” she said.
FROM BLOOD ADVANCES
Topical tranexamic acid for melasma
By addressing the vascular component of melasma, off-label use of oral tranexamic acid has been a beneficial adjunct for this difficult-to-treat condition. For on-label use treating menorrhagia (the oral form) and short-term prophylaxis of bleeding in hemophilia patients undergoing dental procedures – (the injectable form), tranexamic acid acts as an antifibrinolytic.

By inhibiting plasminogen activation, according to a 2018 review article “tranexamic acid mitigates UV radiation–induced melanogenesis and neovascularization,” both exhibited in the clinical manifestations of melasma.1 In addition to inhibiting fibrinolysis, tranexamic acid has direct effects on UV-induced pigmentation, “via its inhibitory effects on UV light–induced plasminogen activator on keratinocytes and [subsequent] plasmin activity,” the article states. “Plasminogen activator induces tyrosinase activity, resulting in increased melanin synthesis. The presence of plasmin [which dissolves clots by degrading fibrin] results in increased production of both arachidonic acid and fibroblast growth factor, which stimulate melanogenesis and neovascularization, respectively.”
With oral use, the risk of clot formation, especially in those who have a history of blood clots, clotting disorders (such as factor V Leiden), smoking, or other hypercoagulability risks should be weighed.
Topical tranexamic acid used locally mitigates systemic risk, and according to published studies, has been found to be efficacious for hemostasis in knee and hip arthroplasty surgery and for epistaxis. However, clinical outcomes with the topical treatment have largely not been on par with regards to efficacy for melasma when compared with oral tranexamic acid.
. Topical tranexamic acid, in my experience, when applied immediately after fractional 1927-nm diode laser treatment, not only has been noted by patients to feel soothing, but anecdotally has been found to improve pigmentation.
Moreover, there are now several peer-reviewed studies showing some benefit for treating pigmentation from photodamage or melasma with laser-assisted delivery of topical tranexamic acid. Treatment of these conditions may also benefit from nonablative 1927-nm laser alone.
In one recently published study, 10 female melasma patients, Fitzpatrick skin types II-IV, underwent five full-face low-energy, low-density (power 4-5 W, fluence 2-8 mJ, 2-8 passes) 1927-nm fractional thulium fiber laser treatment.2 Topical tranexamic acid was applied immediately after laser treatment and continued twice daily for 7 days. Seven patients completed the study. Based on the Global Aesthetics Improvement Scale (GAIS) ratings, all seven patients noted improvement at day 180, at which time six of the patients were considered to have improved from baseline, according to the investigator GAIS ratings. Using the Melasma Area Severity Index (MASI) score, the greatest degree of improvement was seen at day 90; there were three recurrences of melasma with worsening of the MASI score between day 90 and day 180.
In a split-face, double-blind, randomized controlled study, 46 patients with Fitzpatrick skin types III-V, with recalcitrant melasma received four weekly treatments of full-face fractional 1927-nm thulium laser; topical tranexamic acid was applied to one side of the face and normal saline applied to the other side under occlusion, immediately after treatment.3 At 3 months, significant improvements from baseline were seen with Melanin Index (MI) and modified MASI (mMASI) scores for the sides treated with tranexamic acid and the control side, with no statistically significant differences between the two. However, at month 6, among the 29 patients available for follow-up, significant differences in MI and mMASI scores from baseline were still evident, with the exception of MI scores on the control sides.
No adverse events from using topical tranexamic acid with laser were noted in either study. Split-face randomized control studies with use of topical tranexamic acid after fractional 1927-nm diode laser in comparison to fractional 1927-nm thulium laser would be notable in this vascular and heat-sensitive condition as well.
Dr. Wesley and Dr. Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Wesley. Write to them at [email protected]. They had no relevant disclosures.
References
1. Sheu SL. Cutis. 2018 Feb;101(2):E7-E8.
2. Wang, JV et al. J Cosmet Dermatol. 2021 Jan;20(1):105-9.
3. Wanitphakdeedecha R. et al. Lasers Med Sci. 2020 Dec;35(9):2015-21.
By addressing the vascular component of melasma, off-label use of oral tranexamic acid has been a beneficial adjunct for this difficult-to-treat condition. For on-label use treating menorrhagia (the oral form) and short-term prophylaxis of bleeding in hemophilia patients undergoing dental procedures – (the injectable form), tranexamic acid acts as an antifibrinolytic.
By inhibiting plasminogen activation, according to a 2018 review article “tranexamic acid mitigates UV radiation–induced melanogenesis and neovascularization,” both exhibited in the clinical manifestations of melasma.1 In addition to inhibiting fibrinolysis, tranexamic acid has direct effects on UV-induced pigmentation, “via its inhibitory effects on UV light–induced plasminogen activator on keratinocytes and [subsequent] plasmin activity,” the article states. “Plasminogen activator induces tyrosinase activity, resulting in increased melanin synthesis. The presence of plasmin [which dissolves clots by degrading fibrin] results in increased production of both arachidonic acid and fibroblast growth factor, which stimulate melanogenesis and neovascularization, respectively.”
With oral use, the risk of clot formation, especially in those who have a history of blood clots, clotting disorders (such as factor V Leiden), smoking, or other hypercoagulability risks should be weighed.
Topical tranexamic acid used locally mitigates systemic risk, and according to published studies, has been found to be efficacious for hemostasis in knee and hip arthroplasty surgery and for epistaxis. However, clinical outcomes with the topical treatment have largely not been on par with regards to efficacy for melasma when compared with oral tranexamic acid.
. Topical tranexamic acid, in my experience, when applied immediately after fractional 1927-nm diode laser treatment, not only has been noted by patients to feel soothing, but anecdotally has been found to improve pigmentation.
Moreover, there are now several peer-reviewed studies showing some benefit for treating pigmentation from photodamage or melasma with laser-assisted delivery of topical tranexamic acid. Treatment of these conditions may also benefit from nonablative 1927-nm laser alone.
In one recently published study, 10 female melasma patients, Fitzpatrick skin types II-IV, underwent five full-face low-energy, low-density (power 4-5 W, fluence 2-8 mJ, 2-8 passes) 1927-nm fractional thulium fiber laser treatment.2 Topical tranexamic acid was applied immediately after laser treatment and continued twice daily for 7 days. Seven patients completed the study. Based on the Global Aesthetics Improvement Scale (GAIS) ratings, all seven patients noted improvement at day 180, at which time six of the patients were considered to have improved from baseline, according to the investigator GAIS ratings. Using the Melasma Area Severity Index (MASI) score, the greatest degree of improvement was seen at day 90; there were three recurrences of melasma with worsening of the MASI score between day 90 and day 180.
In a split-face, double-blind, randomized controlled study, 46 patients with Fitzpatrick skin types III-V, with recalcitrant melasma received four weekly treatments of full-face fractional 1927-nm thulium laser; topical tranexamic acid was applied to one side of the face and normal saline applied to the other side under occlusion, immediately after treatment.3 At 3 months, significant improvements from baseline were seen with Melanin Index (MI) and modified MASI (mMASI) scores for the sides treated with tranexamic acid and the control side, with no statistically significant differences between the two. However, at month 6, among the 29 patients available for follow-up, significant differences in MI and mMASI scores from baseline were still evident, with the exception of MI scores on the control sides.
No adverse events from using topical tranexamic acid with laser were noted in either study. Split-face randomized control studies with use of topical tranexamic acid after fractional 1927-nm diode laser in comparison to fractional 1927-nm thulium laser would be notable in this vascular and heat-sensitive condition as well.
Dr. Wesley and Dr. Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Wesley. Write to them at [email protected]. They had no relevant disclosures.
References
1. Sheu SL. Cutis. 2018 Feb;101(2):E7-E8.
2. Wang, JV et al. J Cosmet Dermatol. 2021 Jan;20(1):105-9.
3. Wanitphakdeedecha R. et al. Lasers Med Sci. 2020 Dec;35(9):2015-21.
By addressing the vascular component of melasma, off-label use of oral tranexamic acid has been a beneficial adjunct for this difficult-to-treat condition. For on-label use treating menorrhagia (the oral form) and short-term prophylaxis of bleeding in hemophilia patients undergoing dental procedures – (the injectable form), tranexamic acid acts as an antifibrinolytic.
By inhibiting plasminogen activation, according to a 2018 review article “tranexamic acid mitigates UV radiation–induced melanogenesis and neovascularization,” both exhibited in the clinical manifestations of melasma.1 In addition to inhibiting fibrinolysis, tranexamic acid has direct effects on UV-induced pigmentation, “via its inhibitory effects on UV light–induced plasminogen activator on keratinocytes and [subsequent] plasmin activity,” the article states. “Plasminogen activator induces tyrosinase activity, resulting in increased melanin synthesis. The presence of plasmin [which dissolves clots by degrading fibrin] results in increased production of both arachidonic acid and fibroblast growth factor, which stimulate melanogenesis and neovascularization, respectively.”
With oral use, the risk of clot formation, especially in those who have a history of blood clots, clotting disorders (such as factor V Leiden), smoking, or other hypercoagulability risks should be weighed.
Topical tranexamic acid used locally mitigates systemic risk, and according to published studies, has been found to be efficacious for hemostasis in knee and hip arthroplasty surgery and for epistaxis. However, clinical outcomes with the topical treatment have largely not been on par with regards to efficacy for melasma when compared with oral tranexamic acid.
. Topical tranexamic acid, in my experience, when applied immediately after fractional 1927-nm diode laser treatment, not only has been noted by patients to feel soothing, but anecdotally has been found to improve pigmentation.
Moreover, there are now several peer-reviewed studies showing some benefit for treating pigmentation from photodamage or melasma with laser-assisted delivery of topical tranexamic acid. Treatment of these conditions may also benefit from nonablative 1927-nm laser alone.
In one recently published study, 10 female melasma patients, Fitzpatrick skin types II-IV, underwent five full-face low-energy, low-density (power 4-5 W, fluence 2-8 mJ, 2-8 passes) 1927-nm fractional thulium fiber laser treatment.2 Topical tranexamic acid was applied immediately after laser treatment and continued twice daily for 7 days. Seven patients completed the study. Based on the Global Aesthetics Improvement Scale (GAIS) ratings, all seven patients noted improvement at day 180, at which time six of the patients were considered to have improved from baseline, according to the investigator GAIS ratings. Using the Melasma Area Severity Index (MASI) score, the greatest degree of improvement was seen at day 90; there were three recurrences of melasma with worsening of the MASI score between day 90 and day 180.
In a split-face, double-blind, randomized controlled study, 46 patients with Fitzpatrick skin types III-V, with recalcitrant melasma received four weekly treatments of full-face fractional 1927-nm thulium laser; topical tranexamic acid was applied to one side of the face and normal saline applied to the other side under occlusion, immediately after treatment.3 At 3 months, significant improvements from baseline were seen with Melanin Index (MI) and modified MASI (mMASI) scores for the sides treated with tranexamic acid and the control side, with no statistically significant differences between the two. However, at month 6, among the 29 patients available for follow-up, significant differences in MI and mMASI scores from baseline were still evident, with the exception of MI scores on the control sides.
No adverse events from using topical tranexamic acid with laser were noted in either study. Split-face randomized control studies with use of topical tranexamic acid after fractional 1927-nm diode laser in comparison to fractional 1927-nm thulium laser would be notable in this vascular and heat-sensitive condition as well.
Dr. Wesley and Dr. Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Wesley. Write to them at [email protected]. They had no relevant disclosures.
References
1. Sheu SL. Cutis. 2018 Feb;101(2):E7-E8.
2. Wang, JV et al. J Cosmet Dermatol. 2021 Jan;20(1):105-9.
3. Wanitphakdeedecha R. et al. Lasers Med Sci. 2020 Dec;35(9):2015-21.
Schools, COVID-19, and Jan. 6, 2021
The first weeks of 2021 have us considering how best to face compound challenges and we expect parents will be looking to their pediatricians for guidance. There are daily stories of the COVID-19 death toll, an abstraction made real by tragic stories of shattered families. Most families are approaching the first anniversary of their children being in virtual school, with growing concerns about the quality of virtual education, loss of socialization and group activities, and additional risks facing poor and vulnerable children. There are real concerns about the future impact of children spending so much time every day on their screens for school, extracurricular activities, social time, and relaxation. While the COVID-19 vaccines promise a return to “normal” sometime in 2021, in-person school may not return until late in the spring or next fall.

After the events of Jan. 6, families face an additional challenge: Discussing the violent invasion of the U.S. Capitol by the president’s supporters. This event was shocking, frightening, and confusing for most, and continues to be heavily covered in the news and online. There is a light in all this darkness. We have the opportunity to talk with our children – and to share explanations, perspectives, values, and even the discomfort of the unknowns – about COVID-19, use of the Internet, and the violence of Jan 6. We will consider how parents can approach this challenge for three age groups. With each group, parents will need to be calm and curious and will need time to give their children their full attention. We are all living through history. When parents can be fully present with their children, even for short periods at meals or at bedtime, it will help all to get their balance back and start to make sense of the extraordinary events we have been facing.
The youngest children (aged 3-6 years), those who were in preschool or kindergarten before the pandemic, need the most from their parents during this time. If they are attending school virtually, their online school days are likely short and challenging. Children at this age are mastering behavior rather than cognitive tasks. They are learning how to manage their bodies in space (stay in their seats!), how to be patient and kind (take turns!), and how to manage frustration (math is hard, try again!). Without the physical presence of their teacher and classmates, these lessons are tougher to internalize. Given their age-appropriate short attention spans, they often walk away from a screen, even if it’s class time. They are more likely to be paying attention to their parents, responding to the emotional climate at home. Even if they are not watching news websites themselves, they are likely to have overheard or noticed the news about recent events. Parents of young children should take care to turn off the television or their own computer, as repeated frightening videos of the insurrection can cause their children to worry that these events continue to unfold. These children need their parents’ undivided attention, even just for a little while. Play a board game with them (good chance to stay in their seats, take turns, and manage losing). Or get them outside for some physical play. While playing, parents can ask what they have seen, heard, or understand about what happened in the Capitol. Then they can correct misperceptions that might be frightening and offer reasonable reassurances in language these young children can understand. They might tell their children that sometimes people get angry when they have lost, and even adults can behave badly and make mistakes. They can focus on who the helpers are, and what they could do to help also. They could write letters of appreciation to their elected officials or to the Capitol police who were so brave in protecting others. If their children are curious, parents can find books or videos that are age appropriate about the Constitution and how elections work in a democracy. Parents don’t need to be able to answer every question, watching “Schoolhouse Rock” videos on YouTube together is a wonderful way to complement their online school and support their healthy development.

School-aged children (7-12 years) are developmentally focused on mastery experiences, whether they are social, academic, or athletic. They may be better equipped to pay attention and do homework than their younger siblings, but they will miss building friendships and having a real audience for their efforts as they build emotional maturity. They are prone to worry and distress about the big events that they can understand, at least in concrete terms, but have never faced before. These children usually have been able to use social media and online games to stay connected to friends, but they are less likely than their older siblings to independently exercise or explore new interests without a parent or teacher to guide and support them. These children are likely to be spending a lot of their time online on websites their parents don’t know about, and most likely to be curious about the events of Jan. 6. Parents should close their own device and invite their school-age children to show them what they are working on in school. Be curious about all of it, even how they are doing gym or music class. Then ask about what they have seen or heard about the election and its aftermath at school, from friends, or on their own. Let them be the teachers about what happened and how they learned about it. Parents can correct misinformation or offer reliable sources of information they can investigate together. What they will need is validation of the difficult feelings that events like these can cause; that is, acknowledgment, acceptance, and understanding of big feelings, without trying to just make those feelings go away. Parents might help them to be curious about what can make people get angry, break laws, and even hurt others, and how we protest injustices in a democracy. These children may be ready to take a deeper dive into history, via a good film or documentary, with their parents’ company for discussion afterward. Be their audience and model curiosity and patience, all the while validating the feelings that might arise.
Teenagers are developmentally focused on building their own identities, cultivating independence, and deeper relationships beyond their family. While they may be well equipped to manage online learning and to stay connected to their friends and teachers through electronic means, they are also facing considerable challenge, as their ability to explore new interests, build new relationships, and be meaningfully independent has been profoundly restrained over the past year. And they are facing other losses, as milestones like proms, performances, and competitions have been altered or missed. Parents still know when their teenager is most likely to talk, and they should check in with them during those times. They can ask them about what classes are working online and which ones aren’t, and what extracurriculars are still possible. They should not be discouraged if their teenager only offers cursory responses, it matters that they are showing up and showing interest. The election and its aftermath provide a meaningful matter to discuss; parents can find out if it is being discussed by any teachers or friends. What do they think triggered the events of Jan. 6? Who should be held responsible? How to reasonably protest injustice? What does a society do when citizens can’t agree on facts? More than offering reassurance, parents should be curious about their adolescent’s developing identity and their values, how they are thinking about complex issues around free speech and justice. It is a wonderful opportunity for parents to learn about their adolescent’s emerging identity, to be tolerant of their autonomy, and an opportunity to offer their perspective and values.
At every age, parents need to be present by listening and drawing their children out without distraction. Now is a time to build relationships and to use the difficult events of the day to shed light on deeper issues and values. This is hard, but far better than having children deal with these issues in darkness or alone.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics at Harvard Medical School, Boston. Email them at [email protected].
The first weeks of 2021 have us considering how best to face compound challenges and we expect parents will be looking to their pediatricians for guidance. There are daily stories of the COVID-19 death toll, an abstraction made real by tragic stories of shattered families. Most families are approaching the first anniversary of their children being in virtual school, with growing concerns about the quality of virtual education, loss of socialization and group activities, and additional risks facing poor and vulnerable children. There are real concerns about the future impact of children spending so much time every day on their screens for school, extracurricular activities, social time, and relaxation. While the COVID-19 vaccines promise a return to “normal” sometime in 2021, in-person school may not return until late in the spring or next fall.
After the events of Jan. 6, families face an additional challenge: Discussing the violent invasion of the U.S. Capitol by the president’s supporters. This event was shocking, frightening, and confusing for most, and continues to be heavily covered in the news and online. There is a light in all this darkness. We have the opportunity to talk with our children – and to share explanations, perspectives, values, and even the discomfort of the unknowns – about COVID-19, use of the Internet, and the violence of Jan 6. We will consider how parents can approach this challenge for three age groups. With each group, parents will need to be calm and curious and will need time to give their children their full attention. We are all living through history. When parents can be fully present with their children, even for short periods at meals or at bedtime, it will help all to get their balance back and start to make sense of the extraordinary events we have been facing.
The youngest children (aged 3-6 years), those who were in preschool or kindergarten before the pandemic, need the most from their parents during this time. If they are attending school virtually, their online school days are likely short and challenging. Children at this age are mastering behavior rather than cognitive tasks. They are learning how to manage their bodies in space (stay in their seats!), how to be patient and kind (take turns!), and how to manage frustration (math is hard, try again!). Without the physical presence of their teacher and classmates, these lessons are tougher to internalize. Given their age-appropriate short attention spans, they often walk away from a screen, even if it’s class time. They are more likely to be paying attention to their parents, responding to the emotional climate at home. Even if they are not watching news websites themselves, they are likely to have overheard or noticed the news about recent events. Parents of young children should take care to turn off the television or their own computer, as repeated frightening videos of the insurrection can cause their children to worry that these events continue to unfold. These children need their parents’ undivided attention, even just for a little while. Play a board game with them (good chance to stay in their seats, take turns, and manage losing). Or get them outside for some physical play. While playing, parents can ask what they have seen, heard, or understand about what happened in the Capitol. Then they can correct misperceptions that might be frightening and offer reasonable reassurances in language these young children can understand. They might tell their children that sometimes people get angry when they have lost, and even adults can behave badly and make mistakes. They can focus on who the helpers are, and what they could do to help also. They could write letters of appreciation to their elected officials or to the Capitol police who were so brave in protecting others. If their children are curious, parents can find books or videos that are age appropriate about the Constitution and how elections work in a democracy. Parents don’t need to be able to answer every question, watching “Schoolhouse Rock” videos on YouTube together is a wonderful way to complement their online school and support their healthy development.
School-aged children (7-12 years) are developmentally focused on mastery experiences, whether they are social, academic, or athletic. They may be better equipped to pay attention and do homework than their younger siblings, but they will miss building friendships and having a real audience for their efforts as they build emotional maturity. They are prone to worry and distress about the big events that they can understand, at least in concrete terms, but have never faced before. These children usually have been able to use social media and online games to stay connected to friends, but they are less likely than their older siblings to independently exercise or explore new interests without a parent or teacher to guide and support them. These children are likely to be spending a lot of their time online on websites their parents don’t know about, and most likely to be curious about the events of Jan. 6. Parents should close their own device and invite their school-age children to show them what they are working on in school. Be curious about all of it, even how they are doing gym or music class. Then ask about what they have seen or heard about the election and its aftermath at school, from friends, or on their own. Let them be the teachers about what happened and how they learned about it. Parents can correct misinformation or offer reliable sources of information they can investigate together. What they will need is validation of the difficult feelings that events like these can cause; that is, acknowledgment, acceptance, and understanding of big feelings, without trying to just make those feelings go away. Parents might help them to be curious about what can make people get angry, break laws, and even hurt others, and how we protest injustices in a democracy. These children may be ready to take a deeper dive into history, via a good film or documentary, with their parents’ company for discussion afterward. Be their audience and model curiosity and patience, all the while validating the feelings that might arise.
Teenagers are developmentally focused on building their own identities, cultivating independence, and deeper relationships beyond their family. While they may be well equipped to manage online learning and to stay connected to their friends and teachers through electronic means, they are also facing considerable challenge, as their ability to explore new interests, build new relationships, and be meaningfully independent has been profoundly restrained over the past year. And they are facing other losses, as milestones like proms, performances, and competitions have been altered or missed. Parents still know when their teenager is most likely to talk, and they should check in with them during those times. They can ask them about what classes are working online and which ones aren’t, and what extracurriculars are still possible. They should not be discouraged if their teenager only offers cursory responses, it matters that they are showing up and showing interest. The election and its aftermath provide a meaningful matter to discuss; parents can find out if it is being discussed by any teachers or friends. What do they think triggered the events of Jan. 6? Who should be held responsible? How to reasonably protest injustice? What does a society do when citizens can’t agree on facts? More than offering reassurance, parents should be curious about their adolescent’s developing identity and their values, how they are thinking about complex issues around free speech and justice. It is a wonderful opportunity for parents to learn about their adolescent’s emerging identity, to be tolerant of their autonomy, and an opportunity to offer their perspective and values.
At every age, parents need to be present by listening and drawing their children out without distraction. Now is a time to build relationships and to use the difficult events of the day to shed light on deeper issues and values. This is hard, but far better than having children deal with these issues in darkness or alone.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics at Harvard Medical School, Boston. Email them at [email protected].
The first weeks of 2021 have us considering how best to face compound challenges and we expect parents will be looking to their pediatricians for guidance. There are daily stories of the COVID-19 death toll, an abstraction made real by tragic stories of shattered families. Most families are approaching the first anniversary of their children being in virtual school, with growing concerns about the quality of virtual education, loss of socialization and group activities, and additional risks facing poor and vulnerable children. There are real concerns about the future impact of children spending so much time every day on their screens for school, extracurricular activities, social time, and relaxation. While the COVID-19 vaccines promise a return to “normal” sometime in 2021, in-person school may not return until late in the spring or next fall.
After the events of Jan. 6, families face an additional challenge: Discussing the violent invasion of the U.S. Capitol by the president’s supporters. This event was shocking, frightening, and confusing for most, and continues to be heavily covered in the news and online. There is a light in all this darkness. We have the opportunity to talk with our children – and to share explanations, perspectives, values, and even the discomfort of the unknowns – about COVID-19, use of the Internet, and the violence of Jan 6. We will consider how parents can approach this challenge for three age groups. With each group, parents will need to be calm and curious and will need time to give their children their full attention. We are all living through history. When parents can be fully present with their children, even for short periods at meals or at bedtime, it will help all to get their balance back and start to make sense of the extraordinary events we have been facing.
The youngest children (aged 3-6 years), those who were in preschool or kindergarten before the pandemic, need the most from their parents during this time. If they are attending school virtually, their online school days are likely short and challenging. Children at this age are mastering behavior rather than cognitive tasks. They are learning how to manage their bodies in space (stay in their seats!), how to be patient and kind (take turns!), and how to manage frustration (math is hard, try again!). Without the physical presence of their teacher and classmates, these lessons are tougher to internalize. Given their age-appropriate short attention spans, they often walk away from a screen, even if it’s class time. They are more likely to be paying attention to their parents, responding to the emotional climate at home. Even if they are not watching news websites themselves, they are likely to have overheard or noticed the news about recent events. Parents of young children should take care to turn off the television or their own computer, as repeated frightening videos of the insurrection can cause their children to worry that these events continue to unfold. These children need their parents’ undivided attention, even just for a little while. Play a board game with them (good chance to stay in their seats, take turns, and manage losing). Or get them outside for some physical play. While playing, parents can ask what they have seen, heard, or understand about what happened in the Capitol. Then they can correct misperceptions that might be frightening and offer reasonable reassurances in language these young children can understand. They might tell their children that sometimes people get angry when they have lost, and even adults can behave badly and make mistakes. They can focus on who the helpers are, and what they could do to help also. They could write letters of appreciation to their elected officials or to the Capitol police who were so brave in protecting others. If their children are curious, parents can find books or videos that are age appropriate about the Constitution and how elections work in a democracy. Parents don’t need to be able to answer every question, watching “Schoolhouse Rock” videos on YouTube together is a wonderful way to complement their online school and support their healthy development.
School-aged children (7-12 years) are developmentally focused on mastery experiences, whether they are social, academic, or athletic. They may be better equipped to pay attention and do homework than their younger siblings, but they will miss building friendships and having a real audience for their efforts as they build emotional maturity. They are prone to worry and distress about the big events that they can understand, at least in concrete terms, but have never faced before. These children usually have been able to use social media and online games to stay connected to friends, but they are less likely than their older siblings to independently exercise or explore new interests without a parent or teacher to guide and support them. These children are likely to be spending a lot of their time online on websites their parents don’t know about, and most likely to be curious about the events of Jan. 6. Parents should close their own device and invite their school-age children to show them what they are working on in school. Be curious about all of it, even how they are doing gym or music class. Then ask about what they have seen or heard about the election and its aftermath at school, from friends, or on their own. Let them be the teachers about what happened and how they learned about it. Parents can correct misinformation or offer reliable sources of information they can investigate together. What they will need is validation of the difficult feelings that events like these can cause; that is, acknowledgment, acceptance, and understanding of big feelings, without trying to just make those feelings go away. Parents might help them to be curious about what can make people get angry, break laws, and even hurt others, and how we protest injustices in a democracy. These children may be ready to take a deeper dive into history, via a good film or documentary, with their parents’ company for discussion afterward. Be their audience and model curiosity and patience, all the while validating the feelings that might arise.
Teenagers are developmentally focused on building their own identities, cultivating independence, and deeper relationships beyond their family. While they may be well equipped to manage online learning and to stay connected to their friends and teachers through electronic means, they are also facing considerable challenge, as their ability to explore new interests, build new relationships, and be meaningfully independent has been profoundly restrained over the past year. And they are facing other losses, as milestones like proms, performances, and competitions have been altered or missed. Parents still know when their teenager is most likely to talk, and they should check in with them during those times. They can ask them about what classes are working online and which ones aren’t, and what extracurriculars are still possible. They should not be discouraged if their teenager only offers cursory responses, it matters that they are showing up and showing interest. The election and its aftermath provide a meaningful matter to discuss; parents can find out if it is being discussed by any teachers or friends. What do they think triggered the events of Jan. 6? Who should be held responsible? How to reasonably protest injustice? What does a society do when citizens can’t agree on facts? More than offering reassurance, parents should be curious about their adolescent’s developing identity and their values, how they are thinking about complex issues around free speech and justice. It is a wonderful opportunity for parents to learn about their adolescent’s emerging identity, to be tolerant of their autonomy, and an opportunity to offer their perspective and values.
At every age, parents need to be present by listening and drawing their children out without distraction. Now is a time to build relationships and to use the difficult events of the day to shed light on deeper issues and values. This is hard, but far better than having children deal with these issues in darkness or alone.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics at Harvard Medical School, Boston. Email them at [email protected].
Age at menarche signals potential cardiovascular health risk
“Increases in age at menarche are significantly associated with increases in cardiovascular health among women,” reported Yi Zheng, MPH, and colleagues at the University of Florida, Gainesville.
Mr. Zheng and colleagues conducted a cross-sectional analysis of 20,447 women aged 18 or older using data from a nationally representative sample of the 1999-2016 National Health and Nutrition Examinations Survey (NHANES). In all, 2,292 (11.2%) were determined to have ideal cardiovascular health (CVH).
Early menarche was confirmed to be related to increases in body mass index and greater incidence of type 2 diabetes, consistent with earlier studies, the authors confirmed. Those with nonideal CVH were more likely to have reported early menarche; those with ideal CVH were not only younger, but they also had college or graduate level education or above and higher poverty income ratio. Those with ideal CVH were also less likely to be to be of non-Hispanic Black heritage or to have been previously married.
BMI may be the missing link between early menarche and CVH
Unlike previous studies, the researchers found no significant link between early menarche and blood pressure, total cholesterol, smoking, physical activity, or diet using fully adjusted model data, leading them to conclude that “the associations between early menarche and CVH might be mainly driven by its associations with BMI.”
Mr. Zheng and colleagues suggested that future studies should evaluate the causal relationships between age at menarche and BMI and whether genetic factors and childhood lifestyle predispose women to early menarche and obesity.
“Our findings further highlighted that age at menarche may be used to identify high-risk population[s] and to guide targeted preventions to maintain and improve CVH,” the authors noted. Although they cited several strengths and limitations of the study, they emphasized that the wide use of Life’s Simple 7 factors (blood pressure, total cholesterol, glucose levels, smoking, BMI, physical activity, and diet) to measure CVH should “only be regarded as a surrogate construct, and future efforts are needed to better characterize CVH,” they cautioned.
The findings offer an opportunity to more closely track CVH in racial and ethnic groups
In a separate editorial, Ewa M. Gross-Sawicka, MD, PhD, and Eiran Z. Gorodeski, MD, MPH, both of the Harrington Heart and Vascular Institute, Cleveland, observed: “That the authors found African American women had the lowest overall CVH scores, even after adjusting for differences, highlights the importance of beginning cardiovascular health education earlier, especially for those in certain racial and ethnic groups.”
Dr. Gross-Sawicka and Dr. Gorodeski also raised several key questions that warrant further research: “1) Why do women who experience late menarche have improved cardiovascular health while those who experience early menarche have reduced cardiovascular health? 2) Why do the ‘beneficial’ effects of late menarche on CVH last 10 years longer than the ‘detrimental’ effects of early menarche? 3) Since both early and late menarche are associated with increased risk of cardiovascular disease, are women who experience menarche at an older age more cognizant of the cardiovascular risks compared with younger women and adjust their CVH accordingly?”
A key point also worth further consideration: “It is unclear whether age at menarche is directly associated with CVH, or if this relationship is mediated by the association of age at menarche and BMI and/or hyperglycemia,” said Dr. Gross-Sawicka and Dr. Gorodeski.
In an interview, Jan Shifren, MD, director, Midlife Women’s Health Center, Massachusetts General Hospital, Boston, noted, “The principal finding is that early menarche is associated with worse cardiovascular health, which may reflect the adverse impact of obesity and glucose intolerance on CVH, as obesity also is a risk factor for early menarche. The association between early menarche and worse CVH was significant only in women aged 25-34 years, but not in older women, possibly as other risk factors become more important as women age. One of the most concerning findings in this study ... is that only 11% had ideal CVH based on a combination of behavioral and health factors. As cardiovascular disease is the leading cause of death for women, we must do a better job of optimizing [their] cardiovascular health. Clinicians need to focus on optimizing cardiovascular health for all of their midlife patients, whether or not they experienced early menarche!”
Mr. Zheng and colleagues, as well as Dr. Shifren and Dr. Grodeski, had no conflicts of interest to report. Dr. Gross-Sawicka has received funding from Abbott and Novartis.
“Increases in age at menarche are significantly associated with increases in cardiovascular health among women,” reported Yi Zheng, MPH, and colleagues at the University of Florida, Gainesville.
Mr. Zheng and colleagues conducted a cross-sectional analysis of 20,447 women aged 18 or older using data from a nationally representative sample of the 1999-2016 National Health and Nutrition Examinations Survey (NHANES). In all, 2,292 (11.2%) were determined to have ideal cardiovascular health (CVH).
Early menarche was confirmed to be related to increases in body mass index and greater incidence of type 2 diabetes, consistent with earlier studies, the authors confirmed. Those with nonideal CVH were more likely to have reported early menarche; those with ideal CVH were not only younger, but they also had college or graduate level education or above and higher poverty income ratio. Those with ideal CVH were also less likely to be to be of non-Hispanic Black heritage or to have been previously married.
BMI may be the missing link between early menarche and CVH
Unlike previous studies, the researchers found no significant link between early menarche and blood pressure, total cholesterol, smoking, physical activity, or diet using fully adjusted model data, leading them to conclude that “the associations between early menarche and CVH might be mainly driven by its associations with BMI.”
Mr. Zheng and colleagues suggested that future studies should evaluate the causal relationships between age at menarche and BMI and whether genetic factors and childhood lifestyle predispose women to early menarche and obesity.
“Our findings further highlighted that age at menarche may be used to identify high-risk population[s] and to guide targeted preventions to maintain and improve CVH,” the authors noted. Although they cited several strengths and limitations of the study, they emphasized that the wide use of Life’s Simple 7 factors (blood pressure, total cholesterol, glucose levels, smoking, BMI, physical activity, and diet) to measure CVH should “only be regarded as a surrogate construct, and future efforts are needed to better characterize CVH,” they cautioned.
The findings offer an opportunity to more closely track CVH in racial and ethnic groups
In a separate editorial, Ewa M. Gross-Sawicka, MD, PhD, and Eiran Z. Gorodeski, MD, MPH, both of the Harrington Heart and Vascular Institute, Cleveland, observed: “That the authors found African American women had the lowest overall CVH scores, even after adjusting for differences, highlights the importance of beginning cardiovascular health education earlier, especially for those in certain racial and ethnic groups.”
Dr. Gross-Sawicka and Dr. Gorodeski also raised several key questions that warrant further research: “1) Why do women who experience late menarche have improved cardiovascular health while those who experience early menarche have reduced cardiovascular health? 2) Why do the ‘beneficial’ effects of late menarche on CVH last 10 years longer than the ‘detrimental’ effects of early menarche? 3) Since both early and late menarche are associated with increased risk of cardiovascular disease, are women who experience menarche at an older age more cognizant of the cardiovascular risks compared with younger women and adjust their CVH accordingly?”
A key point also worth further consideration: “It is unclear whether age at menarche is directly associated with CVH, or if this relationship is mediated by the association of age at menarche and BMI and/or hyperglycemia,” said Dr. Gross-Sawicka and Dr. Gorodeski.
In an interview, Jan Shifren, MD, director, Midlife Women’s Health Center, Massachusetts General Hospital, Boston, noted, “The principal finding is that early menarche is associated with worse cardiovascular health, which may reflect the adverse impact of obesity and glucose intolerance on CVH, as obesity also is a risk factor for early menarche. The association between early menarche and worse CVH was significant only in women aged 25-34 years, but not in older women, possibly as other risk factors become more important as women age. One of the most concerning findings in this study ... is that only 11% had ideal CVH based on a combination of behavioral and health factors. As cardiovascular disease is the leading cause of death for women, we must do a better job of optimizing [their] cardiovascular health. Clinicians need to focus on optimizing cardiovascular health for all of their midlife patients, whether or not they experienced early menarche!”
Mr. Zheng and colleagues, as well as Dr. Shifren and Dr. Grodeski, had no conflicts of interest to report. Dr. Gross-Sawicka has received funding from Abbott and Novartis.
“Increases in age at menarche are significantly associated with increases in cardiovascular health among women,” reported Yi Zheng, MPH, and colleagues at the University of Florida, Gainesville.
Mr. Zheng and colleagues conducted a cross-sectional analysis of 20,447 women aged 18 or older using data from a nationally representative sample of the 1999-2016 National Health and Nutrition Examinations Survey (NHANES). In all, 2,292 (11.2%) were determined to have ideal cardiovascular health (CVH).
Early menarche was confirmed to be related to increases in body mass index and greater incidence of type 2 diabetes, consistent with earlier studies, the authors confirmed. Those with nonideal CVH were more likely to have reported early menarche; those with ideal CVH were not only younger, but they also had college or graduate level education or above and higher poverty income ratio. Those with ideal CVH were also less likely to be to be of non-Hispanic Black heritage or to have been previously married.
BMI may be the missing link between early menarche and CVH
Unlike previous studies, the researchers found no significant link between early menarche and blood pressure, total cholesterol, smoking, physical activity, or diet using fully adjusted model data, leading them to conclude that “the associations between early menarche and CVH might be mainly driven by its associations with BMI.”
Mr. Zheng and colleagues suggested that future studies should evaluate the causal relationships between age at menarche and BMI and whether genetic factors and childhood lifestyle predispose women to early menarche and obesity.
“Our findings further highlighted that age at menarche may be used to identify high-risk population[s] and to guide targeted preventions to maintain and improve CVH,” the authors noted. Although they cited several strengths and limitations of the study, they emphasized that the wide use of Life’s Simple 7 factors (blood pressure, total cholesterol, glucose levels, smoking, BMI, physical activity, and diet) to measure CVH should “only be regarded as a surrogate construct, and future efforts are needed to better characterize CVH,” they cautioned.
The findings offer an opportunity to more closely track CVH in racial and ethnic groups
In a separate editorial, Ewa M. Gross-Sawicka, MD, PhD, and Eiran Z. Gorodeski, MD, MPH, both of the Harrington Heart and Vascular Institute, Cleveland, observed: “That the authors found African American women had the lowest overall CVH scores, even after adjusting for differences, highlights the importance of beginning cardiovascular health education earlier, especially for those in certain racial and ethnic groups.”
Dr. Gross-Sawicka and Dr. Gorodeski also raised several key questions that warrant further research: “1) Why do women who experience late menarche have improved cardiovascular health while those who experience early menarche have reduced cardiovascular health? 2) Why do the ‘beneficial’ effects of late menarche on CVH last 10 years longer than the ‘detrimental’ effects of early menarche? 3) Since both early and late menarche are associated with increased risk of cardiovascular disease, are women who experience menarche at an older age more cognizant of the cardiovascular risks compared with younger women and adjust their CVH accordingly?”
A key point also worth further consideration: “It is unclear whether age at menarche is directly associated with CVH, or if this relationship is mediated by the association of age at menarche and BMI and/or hyperglycemia,” said Dr. Gross-Sawicka and Dr. Gorodeski.
In an interview, Jan Shifren, MD, director, Midlife Women’s Health Center, Massachusetts General Hospital, Boston, noted, “The principal finding is that early menarche is associated with worse cardiovascular health, which may reflect the adverse impact of obesity and glucose intolerance on CVH, as obesity also is a risk factor for early menarche. The association between early menarche and worse CVH was significant only in women aged 25-34 years, but not in older women, possibly as other risk factors become more important as women age. One of the most concerning findings in this study ... is that only 11% had ideal CVH based on a combination of behavioral and health factors. As cardiovascular disease is the leading cause of death for women, we must do a better job of optimizing [their] cardiovascular health. Clinicians need to focus on optimizing cardiovascular health for all of their midlife patients, whether or not they experienced early menarche!”
Mr. Zheng and colleagues, as well as Dr. Shifren and Dr. Grodeski, had no conflicts of interest to report. Dr. Gross-Sawicka has received funding from Abbott and Novartis.
FROM THE JOURNAL OF THE NORTH AMERICAN MENOPAUSE SOCIETY
Tiger parenting, Earl Woods, and the ABPD template
The Tiger Woods saga, which has been broadcast on HBO, is a “child” of the ESPN Michael Jordan series – which riveted early pandemic America. It is likely to exert a similar vicelike hold on the imagination of Biden transition/Trump impeachment II United States, despite not having the express participation of Woods himself.
The differences in parenting styles of these young African American men, at least superficially, appears in amazingly stark contrast.
Whereas Michael Jordan’s parents appear to have shown good old, red-blooded North Carolina ambitious and hard-driven tough parenting, Earl and Kultida Woods seem to have exerted a textbook example of what we call “achievement by proxy distortion” (ABPD) parenting style.1-5
By deciding, even prior to birth, what their son’s future career would be, Earl, aided by Kultida Woods, created a master plan that came to fruition when Eldrick Tont “Tiger” Woods won his first Masters Tournament at the ripe old age of 21.
His parents’ fine-tuning of the ABPD template for professional sports parenting is often emulated. It had been earlier developed, in an industrial model – especially in women’s gymnastics – where Bela Karolyi and others in the Romanian Eastern Bloc system had developed Nadia Comaneci and others to be prepubescent superstars of the 1970s. When it was transferred to the more financially supportive, fertile base of the U.S., physical and sexual abuse were the acceptable price paid for Olympic gold medals.
When Tiger first appeared on the U.S. radar at the age of 2 on the Mike Douglas show in 1977, he was already definitively on the way to “prodigy” territory. Earl, a retired Vietnam veteran and product of the U.S. Marines, was able to model his own extraordinarily rigorous training where breaking down soldiers psychologically helps them survive special ops behind enemy lines. He trained his son essentially from birth, imprinting through somatic and postural echo these golf skills and habits for playing under pressure, handling annoying distraction, and self-hypnosis. These all clearly accelerated his son’s ability to enter the “zone,” a level of high attunement required, even demanded, at the highest levels of professional golf.
His parents’ ruthless approach, clearly accompanied by undoubted love and enthusiasm, to ending what appears to have been an age-appropriate high school relationship with his then “sweetheart,” appears on the surface a little cruel. But their approach achieved its purpose of sacrificing a distraction on the glorious golden path toward inevitable success and superstardom. This likely also produced a degree of self-objectification and further compartmentalization.
The typical outcome of ABPD is a fairly unidimensional identity defined by the activity, or in this case, the sport. In this case, where Earl was building or imagining a Messianic role for Tiger, multidimensionality was important as the self-described “Cablinasian” moniker suggests, whereby all of Tiger’s background of Caucasian, Black, Indian, and Asian ancestry was acknowledged as they all became lifelong fans.
What most likely saved Tiger Woods from the most debilitating aspects of his father’s master plan was that golfers cannot compete and achieve mega endorsements at the professional level until they have established credentials and grow into their adult bodies, when their stroke making becomes fully competitive and their product image ideal.
Therefore, a 6-year-old JonBenet Ramsey competing in beauty contests, or a 7-year-old Jessica Dubroff flying across country could have been Tiger, but they were not.
While awaiting his preordained career and endorsement deals, Tiger still needed to at least spend some time at college, in his case on a Stanford (Calif.) University golfing scholarship, while he accumulated U.S. amateur titles and fully established his credentials during this crucial time of normal development and “adolescent moratorium.”
According to the documentary,* being exposed to the “secret” extracurricular fringe benefits and sexual proclivities of golf pros with his father is likely to have been part of a traumatic “adultification” and compartmentalizing process. Whereby, one of Tiger’s roles became keeping his parents’ marriage together. That alleged exposure may also have planted the seeds for the “groupie” and sexual acting out challenges he so publicly experienced later in his career.
While Michael Jordan’s career has almost receded into the ancient and “hoary” past, Tiger Woods’s career at age 45, after overcoming significant back injuries and multiple failed surgeries, continues to astonish the golf and sporting world in general.
Most of his now deceased father Earl’s ambitions have indeed been realized despite some hiccups, setbacks, and loss of endorsements.
As parents in these challenging times, we all make sacrifices for our children, and in turn, expect them to step up to the plate and within reason, sacrifice and defer short-term excitement and fun for long-term educational, social, and life goals. How we as parents, and that includes Tiger Woods now, rise to this challenge is often a daily and humbling struggle.
While you watch this series, please keep your psychiatrist and family dynamics eyes wide open.
Dr. Tofler is a child and adolescent, sport psychiatrist, and is affiliated with Kaiser Permanente Psychiatry in West Los Angeles. He also is a visiting faculty member in the department of psychiatry and biobehavioral sciences at the University of California, Los Angeles. Dr. Tofler has no conflicts of interest.
References
1. Tofler IR et al. N Engl J Med. 1996 Jul 25;335(4):281-3.
2. Jellinek MS et al. J Am Acad Child Adolesc Psychiatry. 1999 Feb;38(2):213-6.
3. Tofler IR and DiGeronimo TF. “Keeping Your Kids Out Front Without Kicking Them From Behind: How to Nurture High-Achieving Athletes, Scholars, and Performing Artists.” (Hoboken, N.J,: Jossey-Bass, 2000).
4. Tofler IR et al. Clin Sports Med. 2005 Oct;24(4):805-28.
5. Clark TP et al. Clin Sports Med. 2005 Oct;24(4):959-71.
*Updated 1/25/2021
The Tiger Woods saga, which has been broadcast on HBO, is a “child” of the ESPN Michael Jordan series – which riveted early pandemic America. It is likely to exert a similar vicelike hold on the imagination of Biden transition/Trump impeachment II United States, despite not having the express participation of Woods himself.
The differences in parenting styles of these young African American men, at least superficially, appears in amazingly stark contrast.
Whereas Michael Jordan’s parents appear to have shown good old, red-blooded North Carolina ambitious and hard-driven tough parenting, Earl and Kultida Woods seem to have exerted a textbook example of what we call “achievement by proxy distortion” (ABPD) parenting style.1-5
By deciding, even prior to birth, what their son’s future career would be, Earl, aided by Kultida Woods, created a master plan that came to fruition when Eldrick Tont “Tiger” Woods won his first Masters Tournament at the ripe old age of 21.
His parents’ fine-tuning of the ABPD template for professional sports parenting is often emulated. It had been earlier developed, in an industrial model – especially in women’s gymnastics – where Bela Karolyi and others in the Romanian Eastern Bloc system had developed Nadia Comaneci and others to be prepubescent superstars of the 1970s. When it was transferred to the more financially supportive, fertile base of the U.S., physical and sexual abuse were the acceptable price paid for Olympic gold medals.
When Tiger first appeared on the U.S. radar at the age of 2 on the Mike Douglas show in 1977, he was already definitively on the way to “prodigy” territory. Earl, a retired Vietnam veteran and product of the U.S. Marines, was able to model his own extraordinarily rigorous training where breaking down soldiers psychologically helps them survive special ops behind enemy lines. He trained his son essentially from birth, imprinting through somatic and postural echo these golf skills and habits for playing under pressure, handling annoying distraction, and self-hypnosis. These all clearly accelerated his son’s ability to enter the “zone,” a level of high attunement required, even demanded, at the highest levels of professional golf.
His parents’ ruthless approach, clearly accompanied by undoubted love and enthusiasm, to ending what appears to have been an age-appropriate high school relationship with his then “sweetheart,” appears on the surface a little cruel. But their approach achieved its purpose of sacrificing a distraction on the glorious golden path toward inevitable success and superstardom. This likely also produced a degree of self-objectification and further compartmentalization.
The typical outcome of ABPD is a fairly unidimensional identity defined by the activity, or in this case, the sport. In this case, where Earl was building or imagining a Messianic role for Tiger, multidimensionality was important as the self-described “Cablinasian” moniker suggests, whereby all of Tiger’s background of Caucasian, Black, Indian, and Asian ancestry was acknowledged as they all became lifelong fans.
What most likely saved Tiger Woods from the most debilitating aspects of his father’s master plan was that golfers cannot compete and achieve mega endorsements at the professional level until they have established credentials and grow into their adult bodies, when their stroke making becomes fully competitive and their product image ideal.
Therefore, a 6-year-old JonBenet Ramsey competing in beauty contests, or a 7-year-old Jessica Dubroff flying across country could have been Tiger, but they were not.
While awaiting his preordained career and endorsement deals, Tiger still needed to at least spend some time at college, in his case on a Stanford (Calif.) University golfing scholarship, while he accumulated U.S. amateur titles and fully established his credentials during this crucial time of normal development and “adolescent moratorium.”
According to the documentary,* being exposed to the “secret” extracurricular fringe benefits and sexual proclivities of golf pros with his father is likely to have been part of a traumatic “adultification” and compartmentalizing process. Whereby, one of Tiger’s roles became keeping his parents’ marriage together. That alleged exposure may also have planted the seeds for the “groupie” and sexual acting out challenges he so publicly experienced later in his career.
While Michael Jordan’s career has almost receded into the ancient and “hoary” past, Tiger Woods’s career at age 45, after overcoming significant back injuries and multiple failed surgeries, continues to astonish the golf and sporting world in general.
Most of his now deceased father Earl’s ambitions have indeed been realized despite some hiccups, setbacks, and loss of endorsements.
As parents in these challenging times, we all make sacrifices for our children, and in turn, expect them to step up to the plate and within reason, sacrifice and defer short-term excitement and fun for long-term educational, social, and life goals. How we as parents, and that includes Tiger Woods now, rise to this challenge is often a daily and humbling struggle.
While you watch this series, please keep your psychiatrist and family dynamics eyes wide open.
Dr. Tofler is a child and adolescent, sport psychiatrist, and is affiliated with Kaiser Permanente Psychiatry in West Los Angeles. He also is a visiting faculty member in the department of psychiatry and biobehavioral sciences at the University of California, Los Angeles. Dr. Tofler has no conflicts of interest.
References
1. Tofler IR et al. N Engl J Med. 1996 Jul 25;335(4):281-3.
2. Jellinek MS et al. J Am Acad Child Adolesc Psychiatry. 1999 Feb;38(2):213-6.
3. Tofler IR and DiGeronimo TF. “Keeping Your Kids Out Front Without Kicking Them From Behind: How to Nurture High-Achieving Athletes, Scholars, and Performing Artists.” (Hoboken, N.J,: Jossey-Bass, 2000).
4. Tofler IR et al. Clin Sports Med. 2005 Oct;24(4):805-28.
5. Clark TP et al. Clin Sports Med. 2005 Oct;24(4):959-71.
*Updated 1/25/2021
The Tiger Woods saga, which has been broadcast on HBO, is a “child” of the ESPN Michael Jordan series – which riveted early pandemic America. It is likely to exert a similar vicelike hold on the imagination of Biden transition/Trump impeachment II United States, despite not having the express participation of Woods himself.
The differences in parenting styles of these young African American men, at least superficially, appears in amazingly stark contrast.
Whereas Michael Jordan’s parents appear to have shown good old, red-blooded North Carolina ambitious and hard-driven tough parenting, Earl and Kultida Woods seem to have exerted a textbook example of what we call “achievement by proxy distortion” (ABPD) parenting style.1-5
By deciding, even prior to birth, what their son’s future career would be, Earl, aided by Kultida Woods, created a master plan that came to fruition when Eldrick Tont “Tiger” Woods won his first Masters Tournament at the ripe old age of 21.
His parents’ fine-tuning of the ABPD template for professional sports parenting is often emulated. It had been earlier developed, in an industrial model – especially in women’s gymnastics – where Bela Karolyi and others in the Romanian Eastern Bloc system had developed Nadia Comaneci and others to be prepubescent superstars of the 1970s. When it was transferred to the more financially supportive, fertile base of the U.S., physical and sexual abuse were the acceptable price paid for Olympic gold medals.
When Tiger first appeared on the U.S. radar at the age of 2 on the Mike Douglas show in 1977, he was already definitively on the way to “prodigy” territory. Earl, a retired Vietnam veteran and product of the U.S. Marines, was able to model his own extraordinarily rigorous training where breaking down soldiers psychologically helps them survive special ops behind enemy lines. He trained his son essentially from birth, imprinting through somatic and postural echo these golf skills and habits for playing under pressure, handling annoying distraction, and self-hypnosis. These all clearly accelerated his son’s ability to enter the “zone,” a level of high attunement required, even demanded, at the highest levels of professional golf.
His parents’ ruthless approach, clearly accompanied by undoubted love and enthusiasm, to ending what appears to have been an age-appropriate high school relationship with his then “sweetheart,” appears on the surface a little cruel. But their approach achieved its purpose of sacrificing a distraction on the glorious golden path toward inevitable success and superstardom. This likely also produced a degree of self-objectification and further compartmentalization.
The typical outcome of ABPD is a fairly unidimensional identity defined by the activity, or in this case, the sport. In this case, where Earl was building or imagining a Messianic role for Tiger, multidimensionality was important as the self-described “Cablinasian” moniker suggests, whereby all of Tiger’s background of Caucasian, Black, Indian, and Asian ancestry was acknowledged as they all became lifelong fans.
What most likely saved Tiger Woods from the most debilitating aspects of his father’s master plan was that golfers cannot compete and achieve mega endorsements at the professional level until they have established credentials and grow into their adult bodies, when their stroke making becomes fully competitive and their product image ideal.
Therefore, a 6-year-old JonBenet Ramsey competing in beauty contests, or a 7-year-old Jessica Dubroff flying across country could have been Tiger, but they were not.
While awaiting his preordained career and endorsement deals, Tiger still needed to at least spend some time at college, in his case on a Stanford (Calif.) University golfing scholarship, while he accumulated U.S. amateur titles and fully established his credentials during this crucial time of normal development and “adolescent moratorium.”
According to the documentary,* being exposed to the “secret” extracurricular fringe benefits and sexual proclivities of golf pros with his father is likely to have been part of a traumatic “adultification” and compartmentalizing process. Whereby, one of Tiger’s roles became keeping his parents’ marriage together. That alleged exposure may also have planted the seeds for the “groupie” and sexual acting out challenges he so publicly experienced later in his career.
While Michael Jordan’s career has almost receded into the ancient and “hoary” past, Tiger Woods’s career at age 45, after overcoming significant back injuries and multiple failed surgeries, continues to astonish the golf and sporting world in general.
Most of his now deceased father Earl’s ambitions have indeed been realized despite some hiccups, setbacks, and loss of endorsements.
As parents in these challenging times, we all make sacrifices for our children, and in turn, expect them to step up to the plate and within reason, sacrifice and defer short-term excitement and fun for long-term educational, social, and life goals. How we as parents, and that includes Tiger Woods now, rise to this challenge is often a daily and humbling struggle.
While you watch this series, please keep your psychiatrist and family dynamics eyes wide open.
Dr. Tofler is a child and adolescent, sport psychiatrist, and is affiliated with Kaiser Permanente Psychiatry in West Los Angeles. He also is a visiting faculty member in the department of psychiatry and biobehavioral sciences at the University of California, Los Angeles. Dr. Tofler has no conflicts of interest.
References
1. Tofler IR et al. N Engl J Med. 1996 Jul 25;335(4):281-3.
2. Jellinek MS et al. J Am Acad Child Adolesc Psychiatry. 1999 Feb;38(2):213-6.
3. Tofler IR and DiGeronimo TF. “Keeping Your Kids Out Front Without Kicking Them From Behind: How to Nurture High-Achieving Athletes, Scholars, and Performing Artists.” (Hoboken, N.J,: Jossey-Bass, 2000).
4. Tofler IR et al. Clin Sports Med. 2005 Oct;24(4):805-28.
5. Clark TP et al. Clin Sports Med. 2005 Oct;24(4):959-71.
*Updated 1/25/2021
Childhood growth hormones raise risk for adult cardiovascular events
Childhood treatment with recombinant human growth hormone was associated with a significantly increased risk of cardiovascular events, based on data from more than 3,000 individuals.
“Both excess levels of growth hormone and [growth hormone deficiency] have been associated with increased cardiovascular morbidity and mortality,” but data on long-term cardiovascular morbidity in individuals treated with growth hormone in childhood are lacking, wrote Anders Tinblad, MD, of Karolinska Institutet, Stockholm, and colleagues.
In a population-based cohort study published in JAMA Pediatrics, the researchers identified 3,408 Swedish patients treated as children with recombinant human growth hormone (rhGH) between Jan. 1, 1985, and Dec. 31, 2010, and compared each with 15 matched controls (a total of 50,036 controls). The patients were treated for one of three conditions: isolated growth hormone deficiency (GHD), small for gestational age (SGA), and idiopathic short stature (ISS).
Data on cardiovascular outcomes were collected from health care and population-based registers and analyzed between Jan. 1, 1985, and Dec. 31, 2014. The average age of the participants at the study’s end was 25.1 years.
In all, 1,809 cardiovascular disease events were recorded over a median follow-up period of 14.9 years, for an incidence rate of 25.6 events per 10,000 person-years in patients and 22.6 events per 10,000 person-years in controls.
When separated by sex, the incidence was higher in female patients compared with controls (31.2 vs. 23.4 events per 10,000 person-years, respectively, but similar in male patients vs. controls (23.3 vs. 22.3 events per 10,000 person-years). “Differences in estrogen levels or responsiveness to rhGH treatment have previously been hypothesized as possible explanations, but the underlying mechanism for this sex difference still remains unclear and merits further investigation,” the researchers wrote.
Overall, the highest adjusted hazard ratios occurred in subgroups of patients with the longest treatment duration (HR 2.08) and highest cumulative dose of growth hormone (HR 2.05), but no association was noted between highest daily hormone dose and cardiovascular event risk. Hazard ratios were higher across all three treatment subgroups of SGA, GHD, and ISS compared with controls (HR 1.97, 1.66, and 1.55, respectively).
“The association between childhood rhGH treatment and CVD events was also seen when assessing only severe CVD outcomes, but with even lower absolute risks,” the researchers noted.
The study findings were limited by several factors including the potential for confounding by treatment indication and the lack of long-term follow-up data given the relatively young age of the study population, the researchers said. The results were strengthened by the large sample size and showed that the absolute risk for overall and severe cardiovascular disease in children treated with growth hormones was low, “which could be reassuring to individual patients,” they added. However, “At the group level, and perhaps especially for female patients and those treated for SGA indication, further close monitoring and future studies of CVD safety are warranted,” they concluded.
Safety and ethical concerns persist
Although the study authors cite limited conclusions on causality and low absolute risk, several issues persist that prompt ongoing analysis of pediatric growth hormone use, namely “worrisome indirect evidence, challenges and limitations in the direct evidence, and the changing world of growth hormone treatment,” Adda Grimberg, MD, of the University of Pennsylvania, Philadelphia, wrote in an accompanying editorial.
“Although evidence asserts that neither growth hormone nor insulinlike growth factor I is carcinogenic, the basic science and oncology literatures are rife with reports showing that they can make aberrant cells more aggressive,” and such indirect evidence supports the need for more direct evidence of possible harm from growth hormone treatment, Dr. Grimberg wrote. Most current safety data on growth hormone come from postmarketing surveillance studies, but these studies do not include controls or data on outcomes after discontinuation of treatment, she noted.
The current study, while able to follow patients across the lifespan, cannot indicate “whether the small but increased risk of cardiovascular disease found in this study was caused by the pediatric growth hormone treatment that identified the participants, by the conditions being treated, by other potential confounder(s) not captured by the study’s methods, or by a combination of the above,” said Dr. Grimberg.
In addition, “the move from replacement of GHD to pharmacologic height augmentation in children who already make sufficient growth hormone had the potential to change the safety profile of treatment,” she said.
“Parents of patients in pediatric primary care practices and of patients seeking growth-related care in a subspecialty endocrine clinic rated treatment characteristics (i.e., proven efficacy and safety) as the factor most having a big or extreme effect on their growth-related medical decision-making,” Dr. Grimberg said. “The centrality of treatment safety to patient-family decision-making underscores the importance of continued scrutiny of growth hormone safety as the treatment and its recipients continue to evolve,” she concluded.
The study was supported by the Swedish Research Council, the Stockholm City Council, the Karolinska Institute, the Society for Child Care, Sahlgrenska University Hospital, and the Stockholm County Council’s combined clinical residency and PhD training program. Lead author Dr. Tidblad disclosed funding from the Society for Child Care and Stockholm County Council during the conduct of the study and personal fees from Pfizer. Dr. Grimberg disclosed serving as a member of the steering committee for the Pfizer International Growth Study Database, and as a consultant for the Pediatric Endocrine Society GH Deficiency Knowledge Center, sponsored by Sandoz AG.
Childhood treatment with recombinant human growth hormone was associated with a significantly increased risk of cardiovascular events, based on data from more than 3,000 individuals.
“Both excess levels of growth hormone and [growth hormone deficiency] have been associated with increased cardiovascular morbidity and mortality,” but data on long-term cardiovascular morbidity in individuals treated with growth hormone in childhood are lacking, wrote Anders Tinblad, MD, of Karolinska Institutet, Stockholm, and colleagues.
In a population-based cohort study published in JAMA Pediatrics, the researchers identified 3,408 Swedish patients treated as children with recombinant human growth hormone (rhGH) between Jan. 1, 1985, and Dec. 31, 2010, and compared each with 15 matched controls (a total of 50,036 controls). The patients were treated for one of three conditions: isolated growth hormone deficiency (GHD), small for gestational age (SGA), and idiopathic short stature (ISS).
Data on cardiovascular outcomes were collected from health care and population-based registers and analyzed between Jan. 1, 1985, and Dec. 31, 2014. The average age of the participants at the study’s end was 25.1 years.
In all, 1,809 cardiovascular disease events were recorded over a median follow-up period of 14.9 years, for an incidence rate of 25.6 events per 10,000 person-years in patients and 22.6 events per 10,000 person-years in controls.
When separated by sex, the incidence was higher in female patients compared with controls (31.2 vs. 23.4 events per 10,000 person-years, respectively, but similar in male patients vs. controls (23.3 vs. 22.3 events per 10,000 person-years). “Differences in estrogen levels or responsiveness to rhGH treatment have previously been hypothesized as possible explanations, but the underlying mechanism for this sex difference still remains unclear and merits further investigation,” the researchers wrote.
Overall, the highest adjusted hazard ratios occurred in subgroups of patients with the longest treatment duration (HR 2.08) and highest cumulative dose of growth hormone (HR 2.05), but no association was noted between highest daily hormone dose and cardiovascular event risk. Hazard ratios were higher across all three treatment subgroups of SGA, GHD, and ISS compared with controls (HR 1.97, 1.66, and 1.55, respectively).
“The association between childhood rhGH treatment and CVD events was also seen when assessing only severe CVD outcomes, but with even lower absolute risks,” the researchers noted.
The study findings were limited by several factors including the potential for confounding by treatment indication and the lack of long-term follow-up data given the relatively young age of the study population, the researchers said. The results were strengthened by the large sample size and showed that the absolute risk for overall and severe cardiovascular disease in children treated with growth hormones was low, “which could be reassuring to individual patients,” they added. However, “At the group level, and perhaps especially for female patients and those treated for SGA indication, further close monitoring and future studies of CVD safety are warranted,” they concluded.
Safety and ethical concerns persist
Although the study authors cite limited conclusions on causality and low absolute risk, several issues persist that prompt ongoing analysis of pediatric growth hormone use, namely “worrisome indirect evidence, challenges and limitations in the direct evidence, and the changing world of growth hormone treatment,” Adda Grimberg, MD, of the University of Pennsylvania, Philadelphia, wrote in an accompanying editorial.
“Although evidence asserts that neither growth hormone nor insulinlike growth factor I is carcinogenic, the basic science and oncology literatures are rife with reports showing that they can make aberrant cells more aggressive,” and such indirect evidence supports the need for more direct evidence of possible harm from growth hormone treatment, Dr. Grimberg wrote. Most current safety data on growth hormone come from postmarketing surveillance studies, but these studies do not include controls or data on outcomes after discontinuation of treatment, she noted.
The current study, while able to follow patients across the lifespan, cannot indicate “whether the small but increased risk of cardiovascular disease found in this study was caused by the pediatric growth hormone treatment that identified the participants, by the conditions being treated, by other potential confounder(s) not captured by the study’s methods, or by a combination of the above,” said Dr. Grimberg.
In addition, “the move from replacement of GHD to pharmacologic height augmentation in children who already make sufficient growth hormone had the potential to change the safety profile of treatment,” she said.
“Parents of patients in pediatric primary care practices and of patients seeking growth-related care in a subspecialty endocrine clinic rated treatment characteristics (i.e., proven efficacy and safety) as the factor most having a big or extreme effect on their growth-related medical decision-making,” Dr. Grimberg said. “The centrality of treatment safety to patient-family decision-making underscores the importance of continued scrutiny of growth hormone safety as the treatment and its recipients continue to evolve,” she concluded.
The study was supported by the Swedish Research Council, the Stockholm City Council, the Karolinska Institute, the Society for Child Care, Sahlgrenska University Hospital, and the Stockholm County Council’s combined clinical residency and PhD training program. Lead author Dr. Tidblad disclosed funding from the Society for Child Care and Stockholm County Council during the conduct of the study and personal fees from Pfizer. Dr. Grimberg disclosed serving as a member of the steering committee for the Pfizer International Growth Study Database, and as a consultant for the Pediatric Endocrine Society GH Deficiency Knowledge Center, sponsored by Sandoz AG.
Childhood treatment with recombinant human growth hormone was associated with a significantly increased risk of cardiovascular events, based on data from more than 3,000 individuals.
“Both excess levels of growth hormone and [growth hormone deficiency] have been associated with increased cardiovascular morbidity and mortality,” but data on long-term cardiovascular morbidity in individuals treated with growth hormone in childhood are lacking, wrote Anders Tinblad, MD, of Karolinska Institutet, Stockholm, and colleagues.
In a population-based cohort study published in JAMA Pediatrics, the researchers identified 3,408 Swedish patients treated as children with recombinant human growth hormone (rhGH) between Jan. 1, 1985, and Dec. 31, 2010, and compared each with 15 matched controls (a total of 50,036 controls). The patients were treated for one of three conditions: isolated growth hormone deficiency (GHD), small for gestational age (SGA), and idiopathic short stature (ISS).
Data on cardiovascular outcomes were collected from health care and population-based registers and analyzed between Jan. 1, 1985, and Dec. 31, 2014. The average age of the participants at the study’s end was 25.1 years.
In all, 1,809 cardiovascular disease events were recorded over a median follow-up period of 14.9 years, for an incidence rate of 25.6 events per 10,000 person-years in patients and 22.6 events per 10,000 person-years in controls.
When separated by sex, the incidence was higher in female patients compared with controls (31.2 vs. 23.4 events per 10,000 person-years, respectively, but similar in male patients vs. controls (23.3 vs. 22.3 events per 10,000 person-years). “Differences in estrogen levels or responsiveness to rhGH treatment have previously been hypothesized as possible explanations, but the underlying mechanism for this sex difference still remains unclear and merits further investigation,” the researchers wrote.
Overall, the highest adjusted hazard ratios occurred in subgroups of patients with the longest treatment duration (HR 2.08) and highest cumulative dose of growth hormone (HR 2.05), but no association was noted between highest daily hormone dose and cardiovascular event risk. Hazard ratios were higher across all three treatment subgroups of SGA, GHD, and ISS compared with controls (HR 1.97, 1.66, and 1.55, respectively).
“The association between childhood rhGH treatment and CVD events was also seen when assessing only severe CVD outcomes, but with even lower absolute risks,” the researchers noted.
The study findings were limited by several factors including the potential for confounding by treatment indication and the lack of long-term follow-up data given the relatively young age of the study population, the researchers said. The results were strengthened by the large sample size and showed that the absolute risk for overall and severe cardiovascular disease in children treated with growth hormones was low, “which could be reassuring to individual patients,” they added. However, “At the group level, and perhaps especially for female patients and those treated for SGA indication, further close monitoring and future studies of CVD safety are warranted,” they concluded.
Safety and ethical concerns persist
Although the study authors cite limited conclusions on causality and low absolute risk, several issues persist that prompt ongoing analysis of pediatric growth hormone use, namely “worrisome indirect evidence, challenges and limitations in the direct evidence, and the changing world of growth hormone treatment,” Adda Grimberg, MD, of the University of Pennsylvania, Philadelphia, wrote in an accompanying editorial.
“Although evidence asserts that neither growth hormone nor insulinlike growth factor I is carcinogenic, the basic science and oncology literatures are rife with reports showing that they can make aberrant cells more aggressive,” and such indirect evidence supports the need for more direct evidence of possible harm from growth hormone treatment, Dr. Grimberg wrote. Most current safety data on growth hormone come from postmarketing surveillance studies, but these studies do not include controls or data on outcomes after discontinuation of treatment, she noted.
The current study, while able to follow patients across the lifespan, cannot indicate “whether the small but increased risk of cardiovascular disease found in this study was caused by the pediatric growth hormone treatment that identified the participants, by the conditions being treated, by other potential confounder(s) not captured by the study’s methods, or by a combination of the above,” said Dr. Grimberg.
In addition, “the move from replacement of GHD to pharmacologic height augmentation in children who already make sufficient growth hormone had the potential to change the safety profile of treatment,” she said.
“Parents of patients in pediatric primary care practices and of patients seeking growth-related care in a subspecialty endocrine clinic rated treatment characteristics (i.e., proven efficacy and safety) as the factor most having a big or extreme effect on their growth-related medical decision-making,” Dr. Grimberg said. “The centrality of treatment safety to patient-family decision-making underscores the importance of continued scrutiny of growth hormone safety as the treatment and its recipients continue to evolve,” she concluded.
The study was supported by the Swedish Research Council, the Stockholm City Council, the Karolinska Institute, the Society for Child Care, Sahlgrenska University Hospital, and the Stockholm County Council’s combined clinical residency and PhD training program. Lead author Dr. Tidblad disclosed funding from the Society for Child Care and Stockholm County Council during the conduct of the study and personal fees from Pfizer. Dr. Grimberg disclosed serving as a member of the steering committee for the Pfizer International Growth Study Database, and as a consultant for the Pediatric Endocrine Society GH Deficiency Knowledge Center, sponsored by Sandoz AG.
FROM JAMA PEDIATRICS
How do you answer patients’ emails?
The pandemic has isolated our patients to an unprecedented degree, forcing them to find other ways to communicate with us, including email.

Responses varied all over the map. Some refuse the medium entirely. “I politely say that I don’t practice dermatology via email,” said one. “Please schedule a teledermatology appointment and I’d be happy to help.”
Others are ambivalent: “I do email with some patients who have complex situations or quick questions, but if it gets out of hand then I let them know someone will call to make an appointment.” Another office treats them as a one-way street: “We set up one account to receive patients’ emails, but we tell them clearly that we don’t respond ... my staff or I call them back.”
Still others have assimilated it completely. “Patients email through the portal and my MA routes [them] to me. I answer questions and the MA responds ... staff loves it because it’s so much faster than the phone.”
A 1998 study in JAMA was more scientifically designed, but basically reached the same conclusion. The authors found “a striking lack of consensus” on how to deal with patient emails: 50% responded to them, but 31% of responders refused to give advice without seeing the patient, while 59% offered a diagnosis, and a third of that group went on to provide specific advice about therapy. In response to a follow-up questionnaire, 28% said that they tended not to answer any patient emails, 24% said they usually replied with a standard message, and 24% said they answer each request individually. The authors concluded that “standards for physician response to unsolicited patient emails are needed.”
Indeed, my own unscientific survey suggests that, more than 20 years later, there is still nothing resembling a consensus on this issue. In the interim, several groups, including the American Medical Informatics Association and the American Medical Association have proposed standards, but none have been generally accepted. Until that happens, it seems prudent for each individual practice to adopt its own guidelines. For ideas, take a look at the proposals from the groups I mentioned, plus any others you can find. When you’re done, consider running your list past your attorney to make sure you haven’t forgotten anything, and that there are no unique requirements in your state.
Your guidelines may be very simple (if you decide never to answer any queries) or very complex, depending on your situation and personal philosophy. But all guidelines should cover such issues as authentication of correspondents, informed consent, licensing jurisdiction (if you receive emails from states in which you are not licensed), and of course, confidentiality.
Contrary to popular belief, HIPAA does not prohibit email communication with patients, nor require that it be encrypted. The HIPAA website specifically says: “Patients may initiate communications with a provider using email. If this situation occurs, the health care provider can assume (unless the patient has explicitly stated otherwise) that e-mail communications are acceptable to the individual.”
Still, if you are not comfortable with unencrypted communication, encryption software can be added to your practice’s email system. Proofpoint, Tumbleweed, Zix, and many other vendors sell encryption packages. (As always, I have no financial interest in any product or enterprise mentioned in this column.)
Another option is web-based messaging: Patients enter your website and send a message using an electronic template that you design. A designated staffer will be notified by regular email when messages are received, and can post a reply on a page that can only be accessed by the patient. Besides enhancing privacy and security, you can state your guidelines in plain English to preclude any misunderstanding of what you will and will not address online.
Web-based messaging services can be freestanding or incorporated into existing secure websites. Medfusion and klara are among the leading vendors of secure messaging services.
The important thing is to make a firm decision on how you want to deal with emails, and stick with that method. And follow your guidelines.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
The pandemic has isolated our patients to an unprecedented degree, forcing them to find other ways to communicate with us, including email.
Responses varied all over the map. Some refuse the medium entirely. “I politely say that I don’t practice dermatology via email,” said one. “Please schedule a teledermatology appointment and I’d be happy to help.”
Others are ambivalent: “I do email with some patients who have complex situations or quick questions, but if it gets out of hand then I let them know someone will call to make an appointment.” Another office treats them as a one-way street: “We set up one account to receive patients’ emails, but we tell them clearly that we don’t respond ... my staff or I call them back.”
Still others have assimilated it completely. “Patients email through the portal and my MA routes [them] to me. I answer questions and the MA responds ... staff loves it because it’s so much faster than the phone.”
A 1998 study in JAMA was more scientifically designed, but basically reached the same conclusion. The authors found “a striking lack of consensus” on how to deal with patient emails: 50% responded to them, but 31% of responders refused to give advice without seeing the patient, while 59% offered a diagnosis, and a third of that group went on to provide specific advice about therapy. In response to a follow-up questionnaire, 28% said that they tended not to answer any patient emails, 24% said they usually replied with a standard message, and 24% said they answer each request individually. The authors concluded that “standards for physician response to unsolicited patient emails are needed.”
Indeed, my own unscientific survey suggests that, more than 20 years later, there is still nothing resembling a consensus on this issue. In the interim, several groups, including the American Medical Informatics Association and the American Medical Association have proposed standards, but none have been generally accepted. Until that happens, it seems prudent for each individual practice to adopt its own guidelines. For ideas, take a look at the proposals from the groups I mentioned, plus any others you can find. When you’re done, consider running your list past your attorney to make sure you haven’t forgotten anything, and that there are no unique requirements in your state.
Your guidelines may be very simple (if you decide never to answer any queries) or very complex, depending on your situation and personal philosophy. But all guidelines should cover such issues as authentication of correspondents, informed consent, licensing jurisdiction (if you receive emails from states in which you are not licensed), and of course, confidentiality.
Contrary to popular belief, HIPAA does not prohibit email communication with patients, nor require that it be encrypted. The HIPAA website specifically says: “Patients may initiate communications with a provider using email. If this situation occurs, the health care provider can assume (unless the patient has explicitly stated otherwise) that e-mail communications are acceptable to the individual.”
Still, if you are not comfortable with unencrypted communication, encryption software can be added to your practice’s email system. Proofpoint, Tumbleweed, Zix, and many other vendors sell encryption packages. (As always, I have no financial interest in any product or enterprise mentioned in this column.)
Another option is web-based messaging: Patients enter your website and send a message using an electronic template that you design. A designated staffer will be notified by regular email when messages are received, and can post a reply on a page that can only be accessed by the patient. Besides enhancing privacy and security, you can state your guidelines in plain English to preclude any misunderstanding of what you will and will not address online.
Web-based messaging services can be freestanding or incorporated into existing secure websites. Medfusion and klara are among the leading vendors of secure messaging services.
The important thing is to make a firm decision on how you want to deal with emails, and stick with that method. And follow your guidelines.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
The pandemic has isolated our patients to an unprecedented degree, forcing them to find other ways to communicate with us, including email.
Responses varied all over the map. Some refuse the medium entirely. “I politely say that I don’t practice dermatology via email,” said one. “Please schedule a teledermatology appointment and I’d be happy to help.”
Others are ambivalent: “I do email with some patients who have complex situations or quick questions, but if it gets out of hand then I let them know someone will call to make an appointment.” Another office treats them as a one-way street: “We set up one account to receive patients’ emails, but we tell them clearly that we don’t respond ... my staff or I call them back.”
Still others have assimilated it completely. “Patients email through the portal and my MA routes [them] to me. I answer questions and the MA responds ... staff loves it because it’s so much faster than the phone.”
A 1998 study in JAMA was more scientifically designed, but basically reached the same conclusion. The authors found “a striking lack of consensus” on how to deal with patient emails: 50% responded to them, but 31% of responders refused to give advice without seeing the patient, while 59% offered a diagnosis, and a third of that group went on to provide specific advice about therapy. In response to a follow-up questionnaire, 28% said that they tended not to answer any patient emails, 24% said they usually replied with a standard message, and 24% said they answer each request individually. The authors concluded that “standards for physician response to unsolicited patient emails are needed.”
Indeed, my own unscientific survey suggests that, more than 20 years later, there is still nothing resembling a consensus on this issue. In the interim, several groups, including the American Medical Informatics Association and the American Medical Association have proposed standards, but none have been generally accepted. Until that happens, it seems prudent for each individual practice to adopt its own guidelines. For ideas, take a look at the proposals from the groups I mentioned, plus any others you can find. When you’re done, consider running your list past your attorney to make sure you haven’t forgotten anything, and that there are no unique requirements in your state.
Your guidelines may be very simple (if you decide never to answer any queries) or very complex, depending on your situation and personal philosophy. But all guidelines should cover such issues as authentication of correspondents, informed consent, licensing jurisdiction (if you receive emails from states in which you are not licensed), and of course, confidentiality.
Contrary to popular belief, HIPAA does not prohibit email communication with patients, nor require that it be encrypted. The HIPAA website specifically says: “Patients may initiate communications with a provider using email. If this situation occurs, the health care provider can assume (unless the patient has explicitly stated otherwise) that e-mail communications are acceptable to the individual.”
Still, if you are not comfortable with unencrypted communication, encryption software can be added to your practice’s email system. Proofpoint, Tumbleweed, Zix, and many other vendors sell encryption packages. (As always, I have no financial interest in any product or enterprise mentioned in this column.)
Another option is web-based messaging: Patients enter your website and send a message using an electronic template that you design. A designated staffer will be notified by regular email when messages are received, and can post a reply on a page that can only be accessed by the patient. Besides enhancing privacy and security, you can state your guidelines in plain English to preclude any misunderstanding of what you will and will not address online.
Web-based messaging services can be freestanding or incorporated into existing secure websites. Medfusion and klara are among the leading vendors of secure messaging services.
The important thing is to make a firm decision on how you want to deal with emails, and stick with that method. And follow your guidelines.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
