User login
Making HIV Transmission a Rare Event
About 80% of new HIV transmissions are from people who do not know they have HIV or are not receiving regular care, according to a CDC report. That makes improvements in early detection and “rapid entry into care” key to ending the HIV epidemic within 10 years—the current US Department of Health and Human Services goal.
Recent studies have shown that viral suppression prevents sexual transmission of HIV, the researchers say. The studies found no HIV transmissions attributable to sex between HIV-discordant couples when the HIV-infected partner was maintaining viral suppression through treatment—even when the HIV-negative partner was not using preexposure prophylaxis. Those findings mean HIV transmission can become a “rare event,” the researchers say.
Today’s treatments have gotten simpler than the hills of pills that patients used to take. Sometimes the patient needs only a single-tablet regimen. Most people, according to the CDC, can achieve viral suppression within 6 months of starting treatment.
But many of the 1.1 million people with HIV infection are not effectively treated. In 2015, the CDC researchers say, 14.5% of people with HIV infection did not have a diagnosis, and 37.2% were not in care (receiving ≥ 1 CD4 tests in a measurement year). Nearly half were not virally suppressed. Lack of effective treatment results in worse outcomes and higher rates of transmission: It was associated with 38,700 new HIV infections in 2016.
The researchers used a model to estimate transmission rates in 2016 along the HIV continuum of care. Overall, the rate was 3.5 per 100 person-years. Among 9,600 people who were acutely infected and unaware of their infection, the rate was 16.1 per 100 person-years. Among 154,400 people who were nonacutely infected and unaware, the rate was 8.4.
Of the nearly 250,000 people who were aware of HIV infection but not in care, 16,500 transmissions were generated (6.6/100 person-years). Among the 125,300 who were receiving HIV care but not virally suppressed, 7,700 transmissions were generated (6.1).
The transmission rate was 0 for patients who were virally suppressed. The researchers note that 100% efficacy was assumed based on trial results for sexual transmission; no data are available on the efficacy of viral suppression on reducing HIV transmission from IV drug use.
Better detection and linkage to treatment will address most of the problem, but what about the patients who do not maintain viral suppression? Among patients in clinical care, about 80% were virally suppressed at their most recent visit, but about one-third did not sustain viral suppression over 1 year. For those patients, the researchers say, a tailored approach aimed at the barriers that are most relevant for the patient is critical to improving adherence.
The CDC recommends routine screening of all Americans aged 13 to 64 years at least once in their life and at least annual testing for those at high risk. In addition, the researchers say, it is important to spread the word that maintaining viral suppression prevents sexual transmission. Sharing this knowledge more generally might reduce the stigma associated with HIV and help engage patients in consistent care.
About 80% of new HIV transmissions are from people who do not know they have HIV or are not receiving regular care, according to a CDC report. That makes improvements in early detection and “rapid entry into care” key to ending the HIV epidemic within 10 years—the current US Department of Health and Human Services goal.
Recent studies have shown that viral suppression prevents sexual transmission of HIV, the researchers say. The studies found no HIV transmissions attributable to sex between HIV-discordant couples when the HIV-infected partner was maintaining viral suppression through treatment—even when the HIV-negative partner was not using preexposure prophylaxis. Those findings mean HIV transmission can become a “rare event,” the researchers say.
Today’s treatments have gotten simpler than the hills of pills that patients used to take. Sometimes the patient needs only a single-tablet regimen. Most people, according to the CDC, can achieve viral suppression within 6 months of starting treatment.
But many of the 1.1 million people with HIV infection are not effectively treated. In 2015, the CDC researchers say, 14.5% of people with HIV infection did not have a diagnosis, and 37.2% were not in care (receiving ≥ 1 CD4 tests in a measurement year). Nearly half were not virally suppressed. Lack of effective treatment results in worse outcomes and higher rates of transmission: It was associated with 38,700 new HIV infections in 2016.
The researchers used a model to estimate transmission rates in 2016 along the HIV continuum of care. Overall, the rate was 3.5 per 100 person-years. Among 9,600 people who were acutely infected and unaware of their infection, the rate was 16.1 per 100 person-years. Among 154,400 people who were nonacutely infected and unaware, the rate was 8.4.
Of the nearly 250,000 people who were aware of HIV infection but not in care, 16,500 transmissions were generated (6.6/100 person-years). Among the 125,300 who were receiving HIV care but not virally suppressed, 7,700 transmissions were generated (6.1).
The transmission rate was 0 for patients who were virally suppressed. The researchers note that 100% efficacy was assumed based on trial results for sexual transmission; no data are available on the efficacy of viral suppression on reducing HIV transmission from IV drug use.
Better detection and linkage to treatment will address most of the problem, but what about the patients who do not maintain viral suppression? Among patients in clinical care, about 80% were virally suppressed at their most recent visit, but about one-third did not sustain viral suppression over 1 year. For those patients, the researchers say, a tailored approach aimed at the barriers that are most relevant for the patient is critical to improving adherence.
The CDC recommends routine screening of all Americans aged 13 to 64 years at least once in their life and at least annual testing for those at high risk. In addition, the researchers say, it is important to spread the word that maintaining viral suppression prevents sexual transmission. Sharing this knowledge more generally might reduce the stigma associated with HIV and help engage patients in consistent care.
About 80% of new HIV transmissions are from people who do not know they have HIV or are not receiving regular care, according to a CDC report. That makes improvements in early detection and “rapid entry into care” key to ending the HIV epidemic within 10 years—the current US Department of Health and Human Services goal.
Recent studies have shown that viral suppression prevents sexual transmission of HIV, the researchers say. The studies found no HIV transmissions attributable to sex between HIV-discordant couples when the HIV-infected partner was maintaining viral suppression through treatment—even when the HIV-negative partner was not using preexposure prophylaxis. Those findings mean HIV transmission can become a “rare event,” the researchers say.
Today’s treatments have gotten simpler than the hills of pills that patients used to take. Sometimes the patient needs only a single-tablet regimen. Most people, according to the CDC, can achieve viral suppression within 6 months of starting treatment.
But many of the 1.1 million people with HIV infection are not effectively treated. In 2015, the CDC researchers say, 14.5% of people with HIV infection did not have a diagnosis, and 37.2% were not in care (receiving ≥ 1 CD4 tests in a measurement year). Nearly half were not virally suppressed. Lack of effective treatment results in worse outcomes and higher rates of transmission: It was associated with 38,700 new HIV infections in 2016.
The researchers used a model to estimate transmission rates in 2016 along the HIV continuum of care. Overall, the rate was 3.5 per 100 person-years. Among 9,600 people who were acutely infected and unaware of their infection, the rate was 16.1 per 100 person-years. Among 154,400 people who were nonacutely infected and unaware, the rate was 8.4.
Of the nearly 250,000 people who were aware of HIV infection but not in care, 16,500 transmissions were generated (6.6/100 person-years). Among the 125,300 who were receiving HIV care but not virally suppressed, 7,700 transmissions were generated (6.1).
The transmission rate was 0 for patients who were virally suppressed. The researchers note that 100% efficacy was assumed based on trial results for sexual transmission; no data are available on the efficacy of viral suppression on reducing HIV transmission from IV drug use.
Better detection and linkage to treatment will address most of the problem, but what about the patients who do not maintain viral suppression? Among patients in clinical care, about 80% were virally suppressed at their most recent visit, but about one-third did not sustain viral suppression over 1 year. For those patients, the researchers say, a tailored approach aimed at the barriers that are most relevant for the patient is critical to improving adherence.
The CDC recommends routine screening of all Americans aged 13 to 64 years at least once in their life and at least annual testing for those at high risk. In addition, the researchers say, it is important to spread the word that maintaining viral suppression prevents sexual transmission. Sharing this knowledge more generally might reduce the stigma associated with HIV and help engage patients in consistent care.
Poor oral health predicts children’s school problems
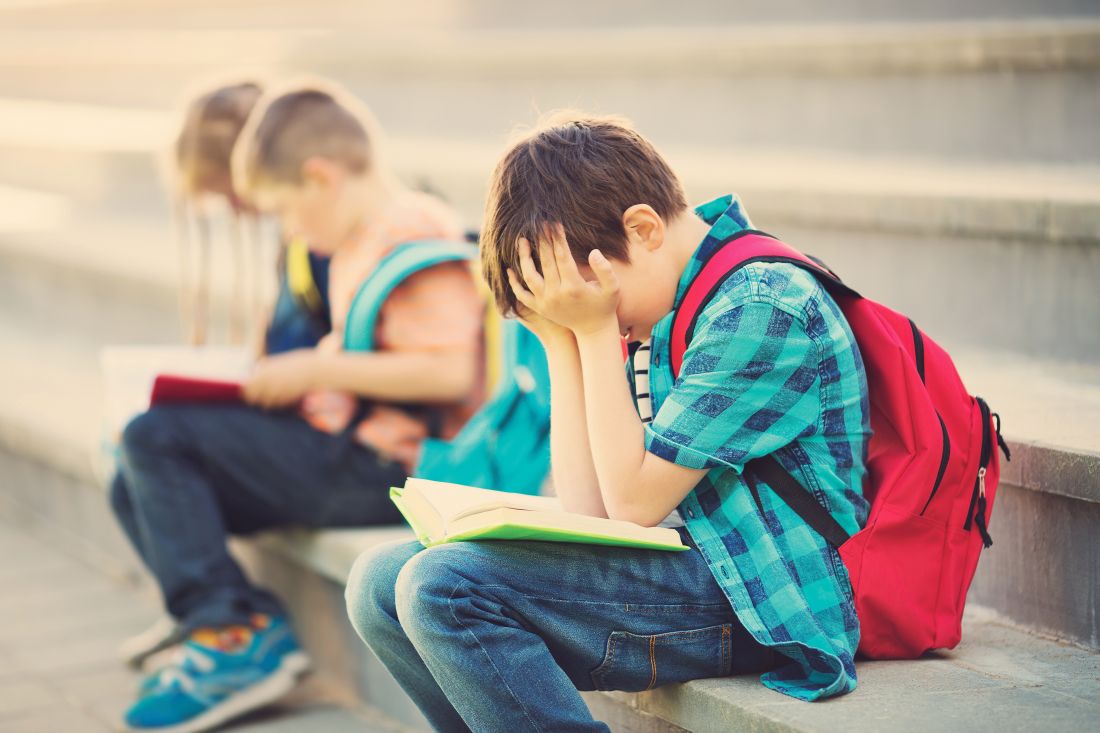
Poor oral health was significantly associated with poor academic performance in children aged 6-17 years, based on data from more than 45,000 children in the United States.
The study, published in the Journal of Pediatrics, updates an assessment from 2007 of a similarly representative sample of U.S. children.
“Providing an updated analysis is especially important to understand the dynamics between children’s oral health status and academic performance, given reported improvements in dental care use among children and dental treatment quality and the implementation or expansion of some state-level preventive strategies,” wrote Carol Cristina Guarnizo-Herreño, DDS, PhD, of Universidad Nacional de Colombia, Bogotá, and her colleagues.
The researchers analyzed data from the 2016 and 2017 versions of National Survey of Children’s Health that included 45,711 children aged 6-17 years. Survey data were collected from parents or other primary caregivers. In the study population, 16% of the children had a least one dental problem, defined as toothache, tooth decay or cavities, or bleeding gums, and 25% of the children had school problems: 67% missed any school, 23% missed more than 3 days of school, and 10% missed more than 6 days of school.
Overall, children with at least 1 dental problem were significantly more likely than those without dental problems to have problems at school (odds ratio, 1.56) or miss at least 1 school day (OR, 1.54) – more than 50% more likely. In addition, children with at least one dental problem were approximately 40% more likely to miss more than 3 days or more than 6 days of school (OR, 1.39 for both).
The association increased when the investigators used children’s oral health ratings; those with oral health rated as poor/fair were approximately 80% more likely to have school problems (OR, 1.77), almost 60% more likely to miss more than 3 days of school (OR, 1.56), and 90% more likely to miss more than 6 days of school, compared with children with oral health rankings of good, very good, or excellent.
Despite some variations in subgroups when the population was stratified by age, sex, race, household income, and health insurance, the associations between oral health problems and academic problems showed “remarkable stability,” across demographic and socioeconomic categories, the researchers said.
The study results were limited by several factors including the inability to identify the mechanisms behind the oral health and academic outcomes relationship, as well as the potential errors in parent or caregiver reports of children’s oral health and school performance, Dr. Guarnizo-Herreño and her associates said. However, the findings support those from an earlier study using 2007 data, and suggest that the link between poor oral health and poor academic performance has lasted for the past decade.
“The relationship between oral health and academic achievement is complex and likely involves multiple and intertwined pathways,” such as the impact of oral pain or discomfort on eating and sleeping that may affect academic performance, they said.
“These findings highlight the need for broad population-wide policies and integrated approaches to promote children’s development and reduce academic deficits that include among other components initiatives to improve oral health through prevention and treatment access strategies,” Dr. Guarnizo-Herreño and her associates concluded.
The study was supported by the National Institute of Dental and Craniofacial Research. The researchers had no financial conflicts to disclose.
SOURCE: Guarnizo-Herreño C et al. J Pediatr. 2019. doi: 10.1016/j.jpeds.2019.01.045.
“Dental caries remains the most common chronic disease of childhood in the United States and is known to affect multiple domains of health and well-being. Academic success is an important predictor of future employment and economic performance, as well as life and health outcomes. Therefore, it is important that we understand the impact oral disease has on academic performance,” Melinda Clark, MD, said in an interview. “This study demonstrated that middle schoolers are at greatest risk of dental disease impacting school performance, with poor dental health doubling the risk of having problems at school and missing school days in children 12-14 years of age.

“Pediatricians care a great deal about the overall health and academic success of children, and the science informs us that poor oral health adversely impacts both of those domains. Pediatric primary care providers can adopt the Department of Health and Human Services Oral Health Framework to combat dental caries by integrating oral health services into practice and advocating for community water fluoridation. Application of fluoride varnish in the primary care office for all children from tooth eruption to age 6 years is recommended by the U.S. Preventive Services Task Force, the American Academy of Pediatrics, and is on the Bright Futures Periodicity schedule.
“Now is the time for action. The majority of dental disease in children is preventable with timely risk assessment, healthy diet choices, oral hygiene, and relatively simple office interventions. Future research should examine the effects of oral health changes on children’s academic outcomes to capture the full impact on children’s well-being.”
Dr. Clark is an associate professor of pediatrics at the Albany Medical Center, New York, and a member of the Pediatric News editorial advisory board. She was asked to comment on the article by Dr. Guarnizo-Herreño and associates. She has no relevant financial disclosures.
“Dental caries remains the most common chronic disease of childhood in the United States and is known to affect multiple domains of health and well-being. Academic success is an important predictor of future employment and economic performance, as well as life and health outcomes. Therefore, it is important that we understand the impact oral disease has on academic performance,” Melinda Clark, MD, said in an interview. “This study demonstrated that middle schoolers are at greatest risk of dental disease impacting school performance, with poor dental health doubling the risk of having problems at school and missing school days in children 12-14 years of age.
“Pediatricians care a great deal about the overall health and academic success of children, and the science informs us that poor oral health adversely impacts both of those domains. Pediatric primary care providers can adopt the Department of Health and Human Services Oral Health Framework to combat dental caries by integrating oral health services into practice and advocating for community water fluoridation. Application of fluoride varnish in the primary care office for all children from tooth eruption to age 6 years is recommended by the U.S. Preventive Services Task Force, the American Academy of Pediatrics, and is on the Bright Futures Periodicity schedule.
“Now is the time for action. The majority of dental disease in children is preventable with timely risk assessment, healthy diet choices, oral hygiene, and relatively simple office interventions. Future research should examine the effects of oral health changes on children’s academic outcomes to capture the full impact on children’s well-being.”
Dr. Clark is an associate professor of pediatrics at the Albany Medical Center, New York, and a member of the Pediatric News editorial advisory board. She was asked to comment on the article by Dr. Guarnizo-Herreño and associates. She has no relevant financial disclosures.
“Dental caries remains the most common chronic disease of childhood in the United States and is known to affect multiple domains of health and well-being. Academic success is an important predictor of future employment and economic performance, as well as life and health outcomes. Therefore, it is important that we understand the impact oral disease has on academic performance,” Melinda Clark, MD, said in an interview. “This study demonstrated that middle schoolers are at greatest risk of dental disease impacting school performance, with poor dental health doubling the risk of having problems at school and missing school days in children 12-14 years of age.
“Pediatricians care a great deal about the overall health and academic success of children, and the science informs us that poor oral health adversely impacts both of those domains. Pediatric primary care providers can adopt the Department of Health and Human Services Oral Health Framework to combat dental caries by integrating oral health services into practice and advocating for community water fluoridation. Application of fluoride varnish in the primary care office for all children from tooth eruption to age 6 years is recommended by the U.S. Preventive Services Task Force, the American Academy of Pediatrics, and is on the Bright Futures Periodicity schedule.
“Now is the time for action. The majority of dental disease in children is preventable with timely risk assessment, healthy diet choices, oral hygiene, and relatively simple office interventions. Future research should examine the effects of oral health changes on children’s academic outcomes to capture the full impact on children’s well-being.”
Dr. Clark is an associate professor of pediatrics at the Albany Medical Center, New York, and a member of the Pediatric News editorial advisory board. She was asked to comment on the article by Dr. Guarnizo-Herreño and associates. She has no relevant financial disclosures.
Poor oral health was significantly associated with poor academic performance in children aged 6-17 years, based on data from more than 45,000 children in the United States.
The study, published in the Journal of Pediatrics, updates an assessment from 2007 of a similarly representative sample of U.S. children.
“Providing an updated analysis is especially important to understand the dynamics between children’s oral health status and academic performance, given reported improvements in dental care use among children and dental treatment quality and the implementation or expansion of some state-level preventive strategies,” wrote Carol Cristina Guarnizo-Herreño, DDS, PhD, of Universidad Nacional de Colombia, Bogotá, and her colleagues.
The researchers analyzed data from the 2016 and 2017 versions of National Survey of Children’s Health that included 45,711 children aged 6-17 years. Survey data were collected from parents or other primary caregivers. In the study population, 16% of the children had a least one dental problem, defined as toothache, tooth decay or cavities, or bleeding gums, and 25% of the children had school problems: 67% missed any school, 23% missed more than 3 days of school, and 10% missed more than 6 days of school.
Overall, children with at least 1 dental problem were significantly more likely than those without dental problems to have problems at school (odds ratio, 1.56) or miss at least 1 school day (OR, 1.54) – more than 50% more likely. In addition, children with at least one dental problem were approximately 40% more likely to miss more than 3 days or more than 6 days of school (OR, 1.39 for both).
The association increased when the investigators used children’s oral health ratings; those with oral health rated as poor/fair were approximately 80% more likely to have school problems (OR, 1.77), almost 60% more likely to miss more than 3 days of school (OR, 1.56), and 90% more likely to miss more than 6 days of school, compared with children with oral health rankings of good, very good, or excellent.
Despite some variations in subgroups when the population was stratified by age, sex, race, household income, and health insurance, the associations between oral health problems and academic problems showed “remarkable stability,” across demographic and socioeconomic categories, the researchers said.
The study results were limited by several factors including the inability to identify the mechanisms behind the oral health and academic outcomes relationship, as well as the potential errors in parent or caregiver reports of children’s oral health and school performance, Dr. Guarnizo-Herreño and her associates said. However, the findings support those from an earlier study using 2007 data, and suggest that the link between poor oral health and poor academic performance has lasted for the past decade.
“The relationship between oral health and academic achievement is complex and likely involves multiple and intertwined pathways,” such as the impact of oral pain or discomfort on eating and sleeping that may affect academic performance, they said.
“These findings highlight the need for broad population-wide policies and integrated approaches to promote children’s development and reduce academic deficits that include among other components initiatives to improve oral health through prevention and treatment access strategies,” Dr. Guarnizo-Herreño and her associates concluded.
The study was supported by the National Institute of Dental and Craniofacial Research. The researchers had no financial conflicts to disclose.
SOURCE: Guarnizo-Herreño C et al. J Pediatr. 2019. doi: 10.1016/j.jpeds.2019.01.045.
Poor oral health was significantly associated with poor academic performance in children aged 6-17 years, based on data from more than 45,000 children in the United States.
The study, published in the Journal of Pediatrics, updates an assessment from 2007 of a similarly representative sample of U.S. children.
“Providing an updated analysis is especially important to understand the dynamics between children’s oral health status and academic performance, given reported improvements in dental care use among children and dental treatment quality and the implementation or expansion of some state-level preventive strategies,” wrote Carol Cristina Guarnizo-Herreño, DDS, PhD, of Universidad Nacional de Colombia, Bogotá, and her colleagues.
The researchers analyzed data from the 2016 and 2017 versions of National Survey of Children’s Health that included 45,711 children aged 6-17 years. Survey data were collected from parents or other primary caregivers. In the study population, 16% of the children had a least one dental problem, defined as toothache, tooth decay or cavities, or bleeding gums, and 25% of the children had school problems: 67% missed any school, 23% missed more than 3 days of school, and 10% missed more than 6 days of school.
Overall, children with at least 1 dental problem were significantly more likely than those without dental problems to have problems at school (odds ratio, 1.56) or miss at least 1 school day (OR, 1.54) – more than 50% more likely. In addition, children with at least one dental problem were approximately 40% more likely to miss more than 3 days or more than 6 days of school (OR, 1.39 for both).
The association increased when the investigators used children’s oral health ratings; those with oral health rated as poor/fair were approximately 80% more likely to have school problems (OR, 1.77), almost 60% more likely to miss more than 3 days of school (OR, 1.56), and 90% more likely to miss more than 6 days of school, compared with children with oral health rankings of good, very good, or excellent.
Despite some variations in subgroups when the population was stratified by age, sex, race, household income, and health insurance, the associations between oral health problems and academic problems showed “remarkable stability,” across demographic and socioeconomic categories, the researchers said.
The study results were limited by several factors including the inability to identify the mechanisms behind the oral health and academic outcomes relationship, as well as the potential errors in parent or caregiver reports of children’s oral health and school performance, Dr. Guarnizo-Herreño and her associates said. However, the findings support those from an earlier study using 2007 data, and suggest that the link between poor oral health and poor academic performance has lasted for the past decade.
“The relationship between oral health and academic achievement is complex and likely involves multiple and intertwined pathways,” such as the impact of oral pain or discomfort on eating and sleeping that may affect academic performance, they said.
“These findings highlight the need for broad population-wide policies and integrated approaches to promote children’s development and reduce academic deficits that include among other components initiatives to improve oral health through prevention and treatment access strategies,” Dr. Guarnizo-Herreño and her associates concluded.
The study was supported by the National Institute of Dental and Craniofacial Research. The researchers had no financial conflicts to disclose.
SOURCE: Guarnizo-Herreño C et al. J Pediatr. 2019. doi: 10.1016/j.jpeds.2019.01.045.
FROM THE JOURNAL OF PEDIATRICS
Alternative regimen reduces narcotic use after pelvic reconstructive surgery
TUCSON, ARIZ. – compared with a standard regimen, with no difference in patient satisfaction scores.

The new study extends findings from other surgical procedures to pelvic reconstructive surgery.
“This can limit both inpatient and outpatient narcotic use. It uses oral Toradol on an outpatient basis. It’s totally underutilized. People are afraid of it, people think it causes more bleeding, and maybe there’s a cost issue,” Andrey Petrikovets, MD, a urogynecologist in Los Angeles, said in an interview.
The regimen, which he calls ICE-T, relies in part on 16 tablets of Toradol sent home with the patient – 4 days’ worth. “It’s just 16 tablets, so it’s cheap, and patients do great with it. If you really use Toradol appropriately, especially on an outpatient basis, you can pretty much eliminate outpatient narcotic use,” said Dr. Petrikovets, who presented the work at the annual scientific meeting of the Society of Gynecologic Surgeons.
He believes that ICE-T is a good option for vaginal surgery. It’s a possibility for benign laparoscopic and perhaps robotic surgery, although those applications need to be studied. ICE-T should be avoided in patients with chronic pain, as well as patients with contraindications to any of the regimen’s medications, Dr. Petrikovets said.
According to the protocol, until hospital discharge, patients receive 20 minutes of ice to the perineum every 2 hours, 30 mg IV Toradol every 6 hours, 1,000 mg oral Tylenol every 6 hours, and 0.2 mg IV Dilaudid every 3 hours as needed for breakthrough pain. The constant pain management is important, said Dr. Petrikovets. “Patients don’t have an opportunity for the pain to get really high,” he said. At-home management includes 1,000 mg oral Tylenol every 6 hours, as needed (pain level 1-5, 60 tablets), and 10 mg Toradol every 6 hours as needed (pain level 6-10, 16 tablets).
The trial was conducted at two centers, where 63 patients were randomized to ICE-T or a standard regimen, which at the hospital included 600 mg ibuprofen every 6 hours as needed for pain levels 1-3, one tablet of Percocet (5/325 mg) every 4-6 hours as needed for pain levels 4-6, two tablets of Percocet for pain levels 7-10, and 0.2 mg IV Dilaudid every 3 hours as needed for breakthrough pain. At-home management consisted of 600 mg ibuprofen every 6 hours for pain levels 1-5 (60 tablets), and Percocet 5/325 mg every 6 hours for pain levels 6-10 (16 tablets).
Using the visual analog scale, researchers found that the 30 patients in the ICE-T arm of the study had less morning pain (VAS score, 20 mm vs. 40 mm; P = .03), and lower numerical pain score at 96 hours (2 vs. 3; P = .04). During the mornings and at 96 hours, the two groups had similar quality of recovery and satisfaction scores.
Narcotic use, measured as oral morphine equivalents, was significantly lower in the ICE-T arm between exit from the postanesthesia care unit (PACU) and hospital discharge (3 vs. 20; P less than .001) and through PACU all the way to discharge (17 vs. 38; P less than .001); 70% of patients in the ICE-T arm required no narcotics after PACU discharge, compared with 12% in the standard care arm (P less than .001).
At 96 hours, there was no significant difference between the two groups in the number of emergency department visits, percentage who had a bowel movement since surgery, or the number of Percocet/Toradol tablets taken. The ICE-T group took more Tylenol tablets than did the standard group took ibuprofen (11 vs. 6; P = .012).
SOURCE: Petrikovets A et al. SGS 2019, Abstract 07.
TUCSON, ARIZ. – compared with a standard regimen, with no difference in patient satisfaction scores.
The new study extends findings from other surgical procedures to pelvic reconstructive surgery.
“This can limit both inpatient and outpatient narcotic use. It uses oral Toradol on an outpatient basis. It’s totally underutilized. People are afraid of it, people think it causes more bleeding, and maybe there’s a cost issue,” Andrey Petrikovets, MD, a urogynecologist in Los Angeles, said in an interview.
The regimen, which he calls ICE-T, relies in part on 16 tablets of Toradol sent home with the patient – 4 days’ worth. “It’s just 16 tablets, so it’s cheap, and patients do great with it. If you really use Toradol appropriately, especially on an outpatient basis, you can pretty much eliminate outpatient narcotic use,” said Dr. Petrikovets, who presented the work at the annual scientific meeting of the Society of Gynecologic Surgeons.
He believes that ICE-T is a good option for vaginal surgery. It’s a possibility for benign laparoscopic and perhaps robotic surgery, although those applications need to be studied. ICE-T should be avoided in patients with chronic pain, as well as patients with contraindications to any of the regimen’s medications, Dr. Petrikovets said.
According to the protocol, until hospital discharge, patients receive 20 minutes of ice to the perineum every 2 hours, 30 mg IV Toradol every 6 hours, 1,000 mg oral Tylenol every 6 hours, and 0.2 mg IV Dilaudid every 3 hours as needed for breakthrough pain. The constant pain management is important, said Dr. Petrikovets. “Patients don’t have an opportunity for the pain to get really high,” he said. At-home management includes 1,000 mg oral Tylenol every 6 hours, as needed (pain level 1-5, 60 tablets), and 10 mg Toradol every 6 hours as needed (pain level 6-10, 16 tablets).
The trial was conducted at two centers, where 63 patients were randomized to ICE-T or a standard regimen, which at the hospital included 600 mg ibuprofen every 6 hours as needed for pain levels 1-3, one tablet of Percocet (5/325 mg) every 4-6 hours as needed for pain levels 4-6, two tablets of Percocet for pain levels 7-10, and 0.2 mg IV Dilaudid every 3 hours as needed for breakthrough pain. At-home management consisted of 600 mg ibuprofen every 6 hours for pain levels 1-5 (60 tablets), and Percocet 5/325 mg every 6 hours for pain levels 6-10 (16 tablets).
Using the visual analog scale, researchers found that the 30 patients in the ICE-T arm of the study had less morning pain (VAS score, 20 mm vs. 40 mm; P = .03), and lower numerical pain score at 96 hours (2 vs. 3; P = .04). During the mornings and at 96 hours, the two groups had similar quality of recovery and satisfaction scores.
Narcotic use, measured as oral morphine equivalents, was significantly lower in the ICE-T arm between exit from the postanesthesia care unit (PACU) and hospital discharge (3 vs. 20; P less than .001) and through PACU all the way to discharge (17 vs. 38; P less than .001); 70% of patients in the ICE-T arm required no narcotics after PACU discharge, compared with 12% in the standard care arm (P less than .001).
At 96 hours, there was no significant difference between the two groups in the number of emergency department visits, percentage who had a bowel movement since surgery, or the number of Percocet/Toradol tablets taken. The ICE-T group took more Tylenol tablets than did the standard group took ibuprofen (11 vs. 6; P = .012).
SOURCE: Petrikovets A et al. SGS 2019, Abstract 07.
TUCSON, ARIZ. – compared with a standard regimen, with no difference in patient satisfaction scores.
The new study extends findings from other surgical procedures to pelvic reconstructive surgery.
“This can limit both inpatient and outpatient narcotic use. It uses oral Toradol on an outpatient basis. It’s totally underutilized. People are afraid of it, people think it causes more bleeding, and maybe there’s a cost issue,” Andrey Petrikovets, MD, a urogynecologist in Los Angeles, said in an interview.
The regimen, which he calls ICE-T, relies in part on 16 tablets of Toradol sent home with the patient – 4 days’ worth. “It’s just 16 tablets, so it’s cheap, and patients do great with it. If you really use Toradol appropriately, especially on an outpatient basis, you can pretty much eliminate outpatient narcotic use,” said Dr. Petrikovets, who presented the work at the annual scientific meeting of the Society of Gynecologic Surgeons.
He believes that ICE-T is a good option for vaginal surgery. It’s a possibility for benign laparoscopic and perhaps robotic surgery, although those applications need to be studied. ICE-T should be avoided in patients with chronic pain, as well as patients with contraindications to any of the regimen’s medications, Dr. Petrikovets said.
According to the protocol, until hospital discharge, patients receive 20 minutes of ice to the perineum every 2 hours, 30 mg IV Toradol every 6 hours, 1,000 mg oral Tylenol every 6 hours, and 0.2 mg IV Dilaudid every 3 hours as needed for breakthrough pain. The constant pain management is important, said Dr. Petrikovets. “Patients don’t have an opportunity for the pain to get really high,” he said. At-home management includes 1,000 mg oral Tylenol every 6 hours, as needed (pain level 1-5, 60 tablets), and 10 mg Toradol every 6 hours as needed (pain level 6-10, 16 tablets).
The trial was conducted at two centers, where 63 patients were randomized to ICE-T or a standard regimen, which at the hospital included 600 mg ibuprofen every 6 hours as needed for pain levels 1-3, one tablet of Percocet (5/325 mg) every 4-6 hours as needed for pain levels 4-6, two tablets of Percocet for pain levels 7-10, and 0.2 mg IV Dilaudid every 3 hours as needed for breakthrough pain. At-home management consisted of 600 mg ibuprofen every 6 hours for pain levels 1-5 (60 tablets), and Percocet 5/325 mg every 6 hours for pain levels 6-10 (16 tablets).
Using the visual analog scale, researchers found that the 30 patients in the ICE-T arm of the study had less morning pain (VAS score, 20 mm vs. 40 mm; P = .03), and lower numerical pain score at 96 hours (2 vs. 3; P = .04). During the mornings and at 96 hours, the two groups had similar quality of recovery and satisfaction scores.
Narcotic use, measured as oral morphine equivalents, was significantly lower in the ICE-T arm between exit from the postanesthesia care unit (PACU) and hospital discharge (3 vs. 20; P less than .001) and through PACU all the way to discharge (17 vs. 38; P less than .001); 70% of patients in the ICE-T arm required no narcotics after PACU discharge, compared with 12% in the standard care arm (P less than .001).
At 96 hours, there was no significant difference between the two groups in the number of emergency department visits, percentage who had a bowel movement since surgery, or the number of Percocet/Toradol tablets taken. The ICE-T group took more Tylenol tablets than did the standard group took ibuprofen (11 vs. 6; P = .012).
SOURCE: Petrikovets A et al. SGS 2019, Abstract 07.
REPORTING FROM SGS 2019

High levels of estradiol in older men may be associated with young biological age
NEW ORLEANS – In a large community-based study that evaluated sex hormone levels in older men, suggesting that sex hormones influence the aging process.
“There was a large effect size, comparable with being 2 or 3 years younger for those with relatively high levels of estradiol, compared with those with lower levels of the hormone,” said Bu Yeap, MBBS, PhD, professor of medicine, University of Western Australia Medical School, Perth, who reported the results at the annual meeting of the Endocrine Society.
In a video interview conducted at the meeting, Dr. Yeap explained the basis of the study, which is the variety of evidence showing that decline in sex hormones correlates with higher rates of age-related disease processes. For example, increasing rates of cardiovascular disease, dementia, and mortality in men all correlate with declining levels of testosterone.
In the study, 2,913 men between the ages of 70 and 89 years and living in the community were recruited. The average age of the men was 77 years. Serum levels of testosterone, dihydrotestosterone, and estradiol were measured. Telomere length was calculated with a polymerase chain reaction test.
Serum levels of testosterone and dihydrotestosterone did not correlate with telomere length, but incremental increases in serum estradiol levels were associated with incremental increases in telomere length.
“Telomeres are both a mediator and a biomarker for biological aging,” according to Dr. Yeap, who added that the telomeres protect chromosomes from degradation. As the telomeres shorten, cell senescence is increased along with an array of age-related diseases.
The next step for researchers is to evaluate whether administering exogenous sex hormones can favorably alter telomere length. If such an effect is demonstrated, then it could provide a step toward understanding how to slow the aging process, he said.
Dr Yeap and his colleagues reported no disclosures or financial conflicts of interest.

NEW ORLEANS – In a large community-based study that evaluated sex hormone levels in older men, suggesting that sex hormones influence the aging process.
“There was a large effect size, comparable with being 2 or 3 years younger for those with relatively high levels of estradiol, compared with those with lower levels of the hormone,” said Bu Yeap, MBBS, PhD, professor of medicine, University of Western Australia Medical School, Perth, who reported the results at the annual meeting of the Endocrine Society.
In a video interview conducted at the meeting, Dr. Yeap explained the basis of the study, which is the variety of evidence showing that decline in sex hormones correlates with higher rates of age-related disease processes. For example, increasing rates of cardiovascular disease, dementia, and mortality in men all correlate with declining levels of testosterone.
In the study, 2,913 men between the ages of 70 and 89 years and living in the community were recruited. The average age of the men was 77 years. Serum levels of testosterone, dihydrotestosterone, and estradiol were measured. Telomere length was calculated with a polymerase chain reaction test.
Serum levels of testosterone and dihydrotestosterone did not correlate with telomere length, but incremental increases in serum estradiol levels were associated with incremental increases in telomere length.
“Telomeres are both a mediator and a biomarker for biological aging,” according to Dr. Yeap, who added that the telomeres protect chromosomes from degradation. As the telomeres shorten, cell senescence is increased along with an array of age-related diseases.
The next step for researchers is to evaluate whether administering exogenous sex hormones can favorably alter telomere length. If such an effect is demonstrated, then it could provide a step toward understanding how to slow the aging process, he said.
Dr Yeap and his colleagues reported no disclosures or financial conflicts of interest.
NEW ORLEANS – In a large community-based study that evaluated sex hormone levels in older men, suggesting that sex hormones influence the aging process.
“There was a large effect size, comparable with being 2 or 3 years younger for those with relatively high levels of estradiol, compared with those with lower levels of the hormone,” said Bu Yeap, MBBS, PhD, professor of medicine, University of Western Australia Medical School, Perth, who reported the results at the annual meeting of the Endocrine Society.
In a video interview conducted at the meeting, Dr. Yeap explained the basis of the study, which is the variety of evidence showing that decline in sex hormones correlates with higher rates of age-related disease processes. For example, increasing rates of cardiovascular disease, dementia, and mortality in men all correlate with declining levels of testosterone.
In the study, 2,913 men between the ages of 70 and 89 years and living in the community were recruited. The average age of the men was 77 years. Serum levels of testosterone, dihydrotestosterone, and estradiol were measured. Telomere length was calculated with a polymerase chain reaction test.
Serum levels of testosterone and dihydrotestosterone did not correlate with telomere length, but incremental increases in serum estradiol levels were associated with incremental increases in telomere length.
“Telomeres are both a mediator and a biomarker for biological aging,” according to Dr. Yeap, who added that the telomeres protect chromosomes from degradation. As the telomeres shorten, cell senescence is increased along with an array of age-related diseases.
The next step for researchers is to evaluate whether administering exogenous sex hormones can favorably alter telomere length. If such an effect is demonstrated, then it could provide a step toward understanding how to slow the aging process, he said.
Dr Yeap and his colleagues reported no disclosures or financial conflicts of interest.
REPORTING FROM ENDO 2019
Cigna, Express Scripts to offer $25 cap on 30-day insulin supply
Cigna and Express Scripts have announced

The new program, open to Cigna members who are covered in commercial plans, would cap out-of-pocket costs for a 30-day supply of insulin at $25. For plan members, the only eligibility requirement is having an out-of-pocket cost higher than $25, according to a press release.
For a member to participate in the program, the plan administrator at the member’s place of employment has to opt in to it. There are no eligibility requirements imposed on the employer, other than a willingness to opt in.
A spokeswoman for Express Scripts said that there is no charge to sign up for the program, and most plans will not see an additional cost to get the copayment to $25 for the patient.
The announcement comes in the wake of the first of two hearings by the House Committee on Energy & Commerce aimed at understanding why insulin prices have spiked in recent years. The first hearing, held on April 2, examined the impact that the high list price of insulin is having on patients, and how out-of-pocket expenses are limiting access to this life-saving drug. The second hearing, expected to occur during the week of April 8 (the date had not been scheduled as of press time), will bring together various players in the supply chain, including the three major manufacturers of insulin.
“We are confident that our new program will remove cost as a barrier for people in participating plans who need insulin,” Steve Miller, MD, executive vice president and chief clinical officer at Cigna, said in a statement.
The Express Scripts spokeswoman noted that there were more than 700,000 people in a commercially insured plan across Cigna and Express Scripts who had a claim for insulin in 2018. The average out-of-pocket cost of a 30-day supply of insulin in 2018 across this population was $41.50.
Cigna and Express Scripts have announced
The new program, open to Cigna members who are covered in commercial plans, would cap out-of-pocket costs for a 30-day supply of insulin at $25. For plan members, the only eligibility requirement is having an out-of-pocket cost higher than $25, according to a press release.
For a member to participate in the program, the plan administrator at the member’s place of employment has to opt in to it. There are no eligibility requirements imposed on the employer, other than a willingness to opt in.
A spokeswoman for Express Scripts said that there is no charge to sign up for the program, and most plans will not see an additional cost to get the copayment to $25 for the patient.
The announcement comes in the wake of the first of two hearings by the House Committee on Energy & Commerce aimed at understanding why insulin prices have spiked in recent years. The first hearing, held on April 2, examined the impact that the high list price of insulin is having on patients, and how out-of-pocket expenses are limiting access to this life-saving drug. The second hearing, expected to occur during the week of April 8 (the date had not been scheduled as of press time), will bring together various players in the supply chain, including the three major manufacturers of insulin.
“We are confident that our new program will remove cost as a barrier for people in participating plans who need insulin,” Steve Miller, MD, executive vice president and chief clinical officer at Cigna, said in a statement.
The Express Scripts spokeswoman noted that there were more than 700,000 people in a commercially insured plan across Cigna and Express Scripts who had a claim for insulin in 2018. The average out-of-pocket cost of a 30-day supply of insulin in 2018 across this population was $41.50.
Cigna and Express Scripts have announced
The new program, open to Cigna members who are covered in commercial plans, would cap out-of-pocket costs for a 30-day supply of insulin at $25. For plan members, the only eligibility requirement is having an out-of-pocket cost higher than $25, according to a press release.
For a member to participate in the program, the plan administrator at the member’s place of employment has to opt in to it. There are no eligibility requirements imposed on the employer, other than a willingness to opt in.
A spokeswoman for Express Scripts said that there is no charge to sign up for the program, and most plans will not see an additional cost to get the copayment to $25 for the patient.
The announcement comes in the wake of the first of two hearings by the House Committee on Energy & Commerce aimed at understanding why insulin prices have spiked in recent years. The first hearing, held on April 2, examined the impact that the high list price of insulin is having on patients, and how out-of-pocket expenses are limiting access to this life-saving drug. The second hearing, expected to occur during the week of April 8 (the date had not been scheduled as of press time), will bring together various players in the supply chain, including the three major manufacturers of insulin.
“We are confident that our new program will remove cost as a barrier for people in participating plans who need insulin,” Steve Miller, MD, executive vice president and chief clinical officer at Cigna, said in a statement.
The Express Scripts spokeswoman noted that there were more than 700,000 people in a commercially insured plan across Cigna and Express Scripts who had a claim for insulin in 2018. The average out-of-pocket cost of a 30-day supply of insulin in 2018 across this population was $41.50.
ONC’s Dr. Rucker: Era of provider-controlled data is over
“The era of the provider controlling all of this, I think this is over,” Donald Rucker, MD, head of the Office of the National Coordinator (ONC) for Health Information Technology within the Department of Health and Human Services, said at an annual conference on health data and innovation. We need a “formal path to put patients back in control of their medical data.”
That path can be found in a pair of proposed rules issued earlier this year, one from the Centers for Medicare & Medicaid Services and the other from ONC, that are designed to give patients that control.
With smartphone apps under development that will allow patient access to health care data from a single point of entry, “technology now allows us to move from having to go portal to portal to portal to really having us in control,” Dr. Rucker said. “I think it is going to transform [health care] in the same way that the smartphone app has transformed other sectors. We are very excited about that.”
Access to data and information should further the transition to value-based care as patients become the center of the decision tree, Dr. Rucker said, making decisions based on benefits in a way that is not possible now.
“In particular, we think patients are going to start being able to shop for care,” he said, adding that if “they don’t like the price of the care they are getting, they are going to be able to move their business elsewhere.”
To that end, he said that much of the talk about interoperability “is really a conversation about affordability and the vast expenses in health care and how you get some control over that.”
“The era of the provider controlling all of this, I think this is over,” Donald Rucker, MD, head of the Office of the National Coordinator (ONC) for Health Information Technology within the Department of Health and Human Services, said at an annual conference on health data and innovation. We need a “formal path to put patients back in control of their medical data.”
That path can be found in a pair of proposed rules issued earlier this year, one from the Centers for Medicare & Medicaid Services and the other from ONC, that are designed to give patients that control.
With smartphone apps under development that will allow patient access to health care data from a single point of entry, “technology now allows us to move from having to go portal to portal to portal to really having us in control,” Dr. Rucker said. “I think it is going to transform [health care] in the same way that the smartphone app has transformed other sectors. We are very excited about that.”
Access to data and information should further the transition to value-based care as patients become the center of the decision tree, Dr. Rucker said, making decisions based on benefits in a way that is not possible now.
“In particular, we think patients are going to start being able to shop for care,” he said, adding that if “they don’t like the price of the care they are getting, they are going to be able to move their business elsewhere.”
To that end, he said that much of the talk about interoperability “is really a conversation about affordability and the vast expenses in health care and how you get some control over that.”
“The era of the provider controlling all of this, I think this is over,” Donald Rucker, MD, head of the Office of the National Coordinator (ONC) for Health Information Technology within the Department of Health and Human Services, said at an annual conference on health data and innovation. We need a “formal path to put patients back in control of their medical data.”
That path can be found in a pair of proposed rules issued earlier this year, one from the Centers for Medicare & Medicaid Services and the other from ONC, that are designed to give patients that control.
With smartphone apps under development that will allow patient access to health care data from a single point of entry, “technology now allows us to move from having to go portal to portal to portal to really having us in control,” Dr. Rucker said. “I think it is going to transform [health care] in the same way that the smartphone app has transformed other sectors. We are very excited about that.”
Access to data and information should further the transition to value-based care as patients become the center of the decision tree, Dr. Rucker said, making decisions based on benefits in a way that is not possible now.
“In particular, we think patients are going to start being able to shop for care,” he said, adding that if “they don’t like the price of the care they are getting, they are going to be able to move their business elsewhere.”
To that end, he said that much of the talk about interoperability “is really a conversation about affordability and the vast expenses in health care and how you get some control over that.”
REPORTING FROM HEALTH DATAPALOOZA 2019
Harness EHRs to identify PrEP candidates
SEATTLE – Kaiser Permanente Northern California has developed an EHR program that automatically flags patients at high risk for HIV.

The idea was to come up with a way to help clinicians focus their pre-exposure prophylaxis (PrEP) outreach on the people who need it most. PrEP prevents HIV, but often “it’s difficult for providers to identify patients who are at risk. Prediction models using EHR data can identify patients who are at high risk but not using PrEP,” said study lead Julia Marcus, PhD, an assistant professor in the department of population medicine at Harvard Medical School, Boston.
She proved that assertion in a presentation at the Conference on Retroviruses & Opportunistic Infections.
The Kaiser program uses 44 variables routinely collected in EHRs from five categories: demographics, social history, lab data, medication use, and diagnoses. Specific variables include living in a zip code with high HIV incidence; men who have sex with men (MSM); black race; urine tests positive for cocaine or methadone; use of erectile dysfunction medications; and diagnoses of depression, anal warts, and other conditions.
The development cohort included 3,143,963 Kaiser members from 2007 to 2014 with 2 or more years of enrollment; at least one outpatient visit; no prior PrEP use; and no HIV diagnosis.
There were 701 incident HIV cases; the model did a good job at predicting them, with a C-statistic of 0.86 (95% confidence interval, 0.85-0.87). A score of 1.0 would be perfect prediction, and 0.5 no predictive value. Previous efforts at HIV prediction – relying generally on just MSM status and STD history – have C-statistics of around 0.6; prediction models commonly used for cardiovascular and other diseases often have C-statistics of around 0.7, Dr. Marcus explained.
The model was validated in 606,701 Kaiser members during 2015-2017. The validation cohort was slightly younger than the development cohort, with a mean age of 37 versus 45 years, and slightly more diverse, with fewer white patients, 44% versus 52%. Both cohorts had slightly more women than men.
There were 83 new HIV diagnoses in the validation cohort. The C-statistic for HIV prediction was 0.84 (95% CI, 0.8-0.89). The model predicted 32 of 69 (46%) incident HIV cases among men tagged as high risk – at least a 0.2% chance of contracting HIV within 3 years – or very high risk, a 1% chance or higher, which is more than 50 times the risk among the general population. Relying on just MSM and STD history predicted 32% of cases.
Overall, “our model identified nearly half of new HIV cases among males by flagging only 2% of the general population. The results suggest our model would perform well if implemented today. You could replicate our approach in any health system with an EHR. Our specific variables may not translate to every setting, but any health care system can develop this model based on the EHR data they do have,” Dr. Marcus said.
“You could embed this in any EHR system and have it update in real time to flag providers to do a sexual history and talk with patients about PrEP,” she said.
The next step is a pilot project at Kaiser Permanente San Francisco to evaluate the impact on PrEP prescribing and HIV incidence. The model failed to predict 14 incident HIV cases among women in the validation cohort, a problem that also needs to be addressed.
The work was funded by the National Institutes of Health and Kaiser Permanente. Dr. Marcus didn’t have any relevant disclosures.
SOURCE: Marcus JL et al. CROI 2019, Abstract 105.
SEATTLE – Kaiser Permanente Northern California has developed an EHR program that automatically flags patients at high risk for HIV.
The idea was to come up with a way to help clinicians focus their pre-exposure prophylaxis (PrEP) outreach on the people who need it most. PrEP prevents HIV, but often “it’s difficult for providers to identify patients who are at risk. Prediction models using EHR data can identify patients who are at high risk but not using PrEP,” said study lead Julia Marcus, PhD, an assistant professor in the department of population medicine at Harvard Medical School, Boston.
She proved that assertion in a presentation at the Conference on Retroviruses & Opportunistic Infections.
The Kaiser program uses 44 variables routinely collected in EHRs from five categories: demographics, social history, lab data, medication use, and diagnoses. Specific variables include living in a zip code with high HIV incidence; men who have sex with men (MSM); black race; urine tests positive for cocaine or methadone; use of erectile dysfunction medications; and diagnoses of depression, anal warts, and other conditions.
The development cohort included 3,143,963 Kaiser members from 2007 to 2014 with 2 or more years of enrollment; at least one outpatient visit; no prior PrEP use; and no HIV diagnosis.
There were 701 incident HIV cases; the model did a good job at predicting them, with a C-statistic of 0.86 (95% confidence interval, 0.85-0.87). A score of 1.0 would be perfect prediction, and 0.5 no predictive value. Previous efforts at HIV prediction – relying generally on just MSM status and STD history – have C-statistics of around 0.6; prediction models commonly used for cardiovascular and other diseases often have C-statistics of around 0.7, Dr. Marcus explained.
The model was validated in 606,701 Kaiser members during 2015-2017. The validation cohort was slightly younger than the development cohort, with a mean age of 37 versus 45 years, and slightly more diverse, with fewer white patients, 44% versus 52%. Both cohorts had slightly more women than men.
There were 83 new HIV diagnoses in the validation cohort. The C-statistic for HIV prediction was 0.84 (95% CI, 0.8-0.89). The model predicted 32 of 69 (46%) incident HIV cases among men tagged as high risk – at least a 0.2% chance of contracting HIV within 3 years – or very high risk, a 1% chance or higher, which is more than 50 times the risk among the general population. Relying on just MSM and STD history predicted 32% of cases.
Overall, “our model identified nearly half of new HIV cases among males by flagging only 2% of the general population. The results suggest our model would perform well if implemented today. You could replicate our approach in any health system with an EHR. Our specific variables may not translate to every setting, but any health care system can develop this model based on the EHR data they do have,” Dr. Marcus said.
“You could embed this in any EHR system and have it update in real time to flag providers to do a sexual history and talk with patients about PrEP,” she said.
The next step is a pilot project at Kaiser Permanente San Francisco to evaluate the impact on PrEP prescribing and HIV incidence. The model failed to predict 14 incident HIV cases among women in the validation cohort, a problem that also needs to be addressed.
The work was funded by the National Institutes of Health and Kaiser Permanente. Dr. Marcus didn’t have any relevant disclosures.
SOURCE: Marcus JL et al. CROI 2019, Abstract 105.
SEATTLE – Kaiser Permanente Northern California has developed an EHR program that automatically flags patients at high risk for HIV.
The idea was to come up with a way to help clinicians focus their pre-exposure prophylaxis (PrEP) outreach on the people who need it most. PrEP prevents HIV, but often “it’s difficult for providers to identify patients who are at risk. Prediction models using EHR data can identify patients who are at high risk but not using PrEP,” said study lead Julia Marcus, PhD, an assistant professor in the department of population medicine at Harvard Medical School, Boston.
She proved that assertion in a presentation at the Conference on Retroviruses & Opportunistic Infections.
The Kaiser program uses 44 variables routinely collected in EHRs from five categories: demographics, social history, lab data, medication use, and diagnoses. Specific variables include living in a zip code with high HIV incidence; men who have sex with men (MSM); black race; urine tests positive for cocaine or methadone; use of erectile dysfunction medications; and diagnoses of depression, anal warts, and other conditions.
The development cohort included 3,143,963 Kaiser members from 2007 to 2014 with 2 or more years of enrollment; at least one outpatient visit; no prior PrEP use; and no HIV diagnosis.
There were 701 incident HIV cases; the model did a good job at predicting them, with a C-statistic of 0.86 (95% confidence interval, 0.85-0.87). A score of 1.0 would be perfect prediction, and 0.5 no predictive value. Previous efforts at HIV prediction – relying generally on just MSM status and STD history – have C-statistics of around 0.6; prediction models commonly used for cardiovascular and other diseases often have C-statistics of around 0.7, Dr. Marcus explained.
The model was validated in 606,701 Kaiser members during 2015-2017. The validation cohort was slightly younger than the development cohort, with a mean age of 37 versus 45 years, and slightly more diverse, with fewer white patients, 44% versus 52%. Both cohorts had slightly more women than men.
There were 83 new HIV diagnoses in the validation cohort. The C-statistic for HIV prediction was 0.84 (95% CI, 0.8-0.89). The model predicted 32 of 69 (46%) incident HIV cases among men tagged as high risk – at least a 0.2% chance of contracting HIV within 3 years – or very high risk, a 1% chance or higher, which is more than 50 times the risk among the general population. Relying on just MSM and STD history predicted 32% of cases.
Overall, “our model identified nearly half of new HIV cases among males by flagging only 2% of the general population. The results suggest our model would perform well if implemented today. You could replicate our approach in any health system with an EHR. Our specific variables may not translate to every setting, but any health care system can develop this model based on the EHR data they do have,” Dr. Marcus said.
“You could embed this in any EHR system and have it update in real time to flag providers to do a sexual history and talk with patients about PrEP,” she said.
The next step is a pilot project at Kaiser Permanente San Francisco to evaluate the impact on PrEP prescribing and HIV incidence. The model failed to predict 14 incident HIV cases among women in the validation cohort, a problem that also needs to be addressed.
The work was funded by the National Institutes of Health and Kaiser Permanente. Dr. Marcus didn’t have any relevant disclosures.
SOURCE: Marcus JL et al. CROI 2019, Abstract 105.
REPORTING FROM CROI 2019
‘Update in Hospital Medicine’ offered practice pearls at HM19
Studies that question common practices
On the big stage at HM19 in late March, Carrie Herzke, MD, FAAP, FACP, SFHM, and Christopher Moriates, MD, FACP, SFHM, undertook the daunting task of summarizing a year’s worth of research relevant to the practice of hospital medicine – all within the span of an hour.
As has been standard with the “Update in Hospital Medicine” session at previous SHM Annual Conferences, the presenters touched on lighter topics in the medical literature: a prospective cohort study that found drinking coffee was inversely associated with mortality, even for those who drink up to eight cups a day; a cross-sectional observational study in which patients noted that what a physician wears is an important consideration for them during care, with a white coat preferred over formal attire as the most highly rated preference in a clinical care setting; and a study from a pediatric journal in which researchers calculated the average transit time for a Lego figurine head ingested by an adult.
But Dr. Herzke and Dr. Moriates mainly covered more serious subjects. In an interview before the session, Dr. Herzke, associate vice chair for clinical affairs in the department of medicine at Johns Hopkins Medicine in Baltimore, said she and Dr. Moriates chose studies across the fields of infectious diseases, cardiology, and hematology that should make hospitalists question common practices and consider changing how they practice medicine at their home institution.
Dr. Moriates, assistant dean for health care value at the University of Texas at Austin, said in an interview that their topic choices reflected the breadth and diversity of patients taken care of by hospitalists.

For example, he noted during the HM19 session that results from several studies suggest hospitalists may soon choose oral antibiotics over IV antibiotics for care of certain patient populations: the recent POET trial suggests use of oral antibiotics for patients with left-sided infective endocarditis resulted in a lower length of stay in hospital (19 inpatient days) when compared with use of IV antibiotics (3 inpatient days and 17 additional treatment days post discharge), while the OVIVA trial found a lower but noninferior treatment failure rate among patients who received oral antibiotics for bone and joint infection, compared with IV antibiotics. Although these were both well-done studies, Dr. Moriates and Dr. Herzke emphasized that the results challenge widely accepted standards of care, and it may not yet be time for a paradigm shift.
Direct oral anticoagulants (DOACs) also are being studied in patients with end-stage renal disease (ESRD) and cancer, Dr. Herzke said, and apixaban (Eliquis) 5 mg appears to be the preferred dose for a lower risk of stroke and mortality in patients with ESRD and atrial fibrillation. The speakers said there are further studies being developed for management of AF in patients with heart failure and DOACs for patients with ESRD.
Another retrospective cohort study from research in the Massachusetts Public Health Dataset found that buprenorphine may have a number needed to treat of 50 for opioid use disorder, which Dr. Moriates said is close in proximity for the number needed to treat for aspirin. “It seems like it’s time for this to become standard of care,” he said.
The speakers also highlighted common practices hospitalists should stop performing based on the latest evidence.
In one example, they revealed that there is conflicting research on angiotensin-converting enzyme (ACE) inhibitors. One study found transient preoperative interruption of ACE inhibitors was associated with a reduction in intraoperative hypotension during a noncardiac, nonvascular surgery. A second study linked ACE inhibitor use with a reduction in all-cause mortality. However, long-term use of ACE inhibitors also appears to be associated with a 14% increase in lung cancers, with an increased incidence based on longer use duration.
Hospitalists should also be aware of recommendations from a study on oxygen therapy, Dr. Herzke noted, which found that extra oxygen therapy may harm patients with MI or stroke; as a result, hospitalists should “wean oxygen as tolerated” in these patients. In addition, hospitalists also may want to consider using oral vancomycin (Vancocin) or fidaxomicin (Dificid) for treatment of Clostridium difficile infections, based on new evidence that found there is a higher cure rate for those treatments, compared with metronidazole.
Dr. Moriates and Dr. Herzke had no relevant financial conflicts.
Studies that question common practices
Studies that question common practices
On the big stage at HM19 in late March, Carrie Herzke, MD, FAAP, FACP, SFHM, and Christopher Moriates, MD, FACP, SFHM, undertook the daunting task of summarizing a year’s worth of research relevant to the practice of hospital medicine – all within the span of an hour.
As has been standard with the “Update in Hospital Medicine” session at previous SHM Annual Conferences, the presenters touched on lighter topics in the medical literature: a prospective cohort study that found drinking coffee was inversely associated with mortality, even for those who drink up to eight cups a day; a cross-sectional observational study in which patients noted that what a physician wears is an important consideration for them during care, with a white coat preferred over formal attire as the most highly rated preference in a clinical care setting; and a study from a pediatric journal in which researchers calculated the average transit time for a Lego figurine head ingested by an adult.
But Dr. Herzke and Dr. Moriates mainly covered more serious subjects. In an interview before the session, Dr. Herzke, associate vice chair for clinical affairs in the department of medicine at Johns Hopkins Medicine in Baltimore, said she and Dr. Moriates chose studies across the fields of infectious diseases, cardiology, and hematology that should make hospitalists question common practices and consider changing how they practice medicine at their home institution.
Dr. Moriates, assistant dean for health care value at the University of Texas at Austin, said in an interview that their topic choices reflected the breadth and diversity of patients taken care of by hospitalists.
For example, he noted during the HM19 session that results from several studies suggest hospitalists may soon choose oral antibiotics over IV antibiotics for care of certain patient populations: the recent POET trial suggests use of oral antibiotics for patients with left-sided infective endocarditis resulted in a lower length of stay in hospital (19 inpatient days) when compared with use of IV antibiotics (3 inpatient days and 17 additional treatment days post discharge), while the OVIVA trial found a lower but noninferior treatment failure rate among patients who received oral antibiotics for bone and joint infection, compared with IV antibiotics. Although these were both well-done studies, Dr. Moriates and Dr. Herzke emphasized that the results challenge widely accepted standards of care, and it may not yet be time for a paradigm shift.
Direct oral anticoagulants (DOACs) also are being studied in patients with end-stage renal disease (ESRD) and cancer, Dr. Herzke said, and apixaban (Eliquis) 5 mg appears to be the preferred dose for a lower risk of stroke and mortality in patients with ESRD and atrial fibrillation. The speakers said there are further studies being developed for management of AF in patients with heart failure and DOACs for patients with ESRD.
Another retrospective cohort study from research in the Massachusetts Public Health Dataset found that buprenorphine may have a number needed to treat of 50 for opioid use disorder, which Dr. Moriates said is close in proximity for the number needed to treat for aspirin. “It seems like it’s time for this to become standard of care,” he said.
The speakers also highlighted common practices hospitalists should stop performing based on the latest evidence.
In one example, they revealed that there is conflicting research on angiotensin-converting enzyme (ACE) inhibitors. One study found transient preoperative interruption of ACE inhibitors was associated with a reduction in intraoperative hypotension during a noncardiac, nonvascular surgery. A second study linked ACE inhibitor use with a reduction in all-cause mortality. However, long-term use of ACE inhibitors also appears to be associated with a 14% increase in lung cancers, with an increased incidence based on longer use duration.
Hospitalists should also be aware of recommendations from a study on oxygen therapy, Dr. Herzke noted, which found that extra oxygen therapy may harm patients with MI or stroke; as a result, hospitalists should “wean oxygen as tolerated” in these patients. In addition, hospitalists also may want to consider using oral vancomycin (Vancocin) or fidaxomicin (Dificid) for treatment of Clostridium difficile infections, based on new evidence that found there is a higher cure rate for those treatments, compared with metronidazole.
Dr. Moriates and Dr. Herzke had no relevant financial conflicts.
On the big stage at HM19 in late March, Carrie Herzke, MD, FAAP, FACP, SFHM, and Christopher Moriates, MD, FACP, SFHM, undertook the daunting task of summarizing a year’s worth of research relevant to the practice of hospital medicine – all within the span of an hour.
As has been standard with the “Update in Hospital Medicine” session at previous SHM Annual Conferences, the presenters touched on lighter topics in the medical literature: a prospective cohort study that found drinking coffee was inversely associated with mortality, even for those who drink up to eight cups a day; a cross-sectional observational study in which patients noted that what a physician wears is an important consideration for them during care, with a white coat preferred over formal attire as the most highly rated preference in a clinical care setting; and a study from a pediatric journal in which researchers calculated the average transit time for a Lego figurine head ingested by an adult.
But Dr. Herzke and Dr. Moriates mainly covered more serious subjects. In an interview before the session, Dr. Herzke, associate vice chair for clinical affairs in the department of medicine at Johns Hopkins Medicine in Baltimore, said she and Dr. Moriates chose studies across the fields of infectious diseases, cardiology, and hematology that should make hospitalists question common practices and consider changing how they practice medicine at their home institution.
Dr. Moriates, assistant dean for health care value at the University of Texas at Austin, said in an interview that their topic choices reflected the breadth and diversity of patients taken care of by hospitalists.
For example, he noted during the HM19 session that results from several studies suggest hospitalists may soon choose oral antibiotics over IV antibiotics for care of certain patient populations: the recent POET trial suggests use of oral antibiotics for patients with left-sided infective endocarditis resulted in a lower length of stay in hospital (19 inpatient days) when compared with use of IV antibiotics (3 inpatient days and 17 additional treatment days post discharge), while the OVIVA trial found a lower but noninferior treatment failure rate among patients who received oral antibiotics for bone and joint infection, compared with IV antibiotics. Although these were both well-done studies, Dr. Moriates and Dr. Herzke emphasized that the results challenge widely accepted standards of care, and it may not yet be time for a paradigm shift.
Direct oral anticoagulants (DOACs) also are being studied in patients with end-stage renal disease (ESRD) and cancer, Dr. Herzke said, and apixaban (Eliquis) 5 mg appears to be the preferred dose for a lower risk of stroke and mortality in patients with ESRD and atrial fibrillation. The speakers said there are further studies being developed for management of AF in patients with heart failure and DOACs for patients with ESRD.
Another retrospective cohort study from research in the Massachusetts Public Health Dataset found that buprenorphine may have a number needed to treat of 50 for opioid use disorder, which Dr. Moriates said is close in proximity for the number needed to treat for aspirin. “It seems like it’s time for this to become standard of care,” he said.
The speakers also highlighted common practices hospitalists should stop performing based on the latest evidence.
In one example, they revealed that there is conflicting research on angiotensin-converting enzyme (ACE) inhibitors. One study found transient preoperative interruption of ACE inhibitors was associated with a reduction in intraoperative hypotension during a noncardiac, nonvascular surgery. A second study linked ACE inhibitor use with a reduction in all-cause mortality. However, long-term use of ACE inhibitors also appears to be associated with a 14% increase in lung cancers, with an increased incidence based on longer use duration.
Hospitalists should also be aware of recommendations from a study on oxygen therapy, Dr. Herzke noted, which found that extra oxygen therapy may harm patients with MI or stroke; as a result, hospitalists should “wean oxygen as tolerated” in these patients. In addition, hospitalists also may want to consider using oral vancomycin (Vancocin) or fidaxomicin (Dificid) for treatment of Clostridium difficile infections, based on new evidence that found there is a higher cure rate for those treatments, compared with metronidazole.
Dr. Moriates and Dr. Herzke had no relevant financial conflicts.
How to cope with patients who get under your skin
DENVER – If you get the impression you’re dealing with more angry and manipulative patients than usual in the past several years, you’re not alone.

In 1999, as many as 15% of patient encounters were rated as difficult by health care providers, according to Tina S. Alster, MD (Arch Intern Med. 1999;159:1069-75). Today, upward of 30% of patient encounters are deemed difficult (Int J Res Med Sci. 2016;4[8]:3554-62). “That means one in three patients that you see have a problem that goes beyond the scope of our official training,” said Dr. Alster, who is the founding director of the Washington Institute of Dermatologic Laser Surgery and clinical professor of dermatology at Georgetown University, Washington. “If it was limited to a medical problem, we could handle it; that’s what we’re trained to do. The interpersonal issues and psychosocial implications of treatment are much more difficult.”
At the annual conference of the American Society for Laser Medicine and Surgery, Dr. Alster said that difficult patients put a strain on your practice and your relationship with them. “These patients put you on your heels. They often point out a problem that may or may not be related to something that you’re responsible for. It’s not usually because you are running late on the day of their visit and you make them late for something else. That situation is one you can prepare for, because you know you’re running late. It’s the other stuff you don’t realize that’s going on, which can cause problems.”
Setting limits
Being proactive can help lessen the ripple effect from patients who rock the boat. “You want to set limits with those patients before you even see them,” Dr. Alster said. “There are written contracts and policies that you should have in place. Since I perform mostly cosmetic procedures in my office, it is important that patients are made aware that payment is expected at the time of service and that my office does not bill nor accept insurance payments in order to prevent misunderstandings at check out.” She also declines requests to provide expert testimony for legal cases. “I’ve been in this business a long time, and every day I get requests to be an expert or to review a case involving a provider who may or may not have made a mistake. I really hate going down that rabbit hole.”
Another solution to keeping difficult patients in check is to collaborate with your entire office staff on how to best deal with them. “You need to present a united front with these patients: They’re going to divide and conquer, with complaints like, ‘How dare the doctor be so late. I’ve been waiting here for 30 minutes. Doesn’t she know I’m busy?’ ” Dr. Alster said. “You’re going to have to give them the tools to set limits as well. During our staff meetings, we review the upcoming patient schedule and identify potentially difficult situations in order to make sure the team is on the same page. Because my office is located in the power corridor of Washington [three blocks away from the White House] and my patient base is populated by prevalent personalities, expectations are extraordinarily high. As such, it is important that we set limits and rules that everyone can play by.”
Getting a sense of whether a patient is angry or manipulative can also help. An angry patient often holds an expectation that has been unmet, or harbors fears related to the treatment itself, she said, while a manipulative patient may engage in bullying, excessive flattery, or veiled threats. “They often expect specific treatments that have only worked for them in the past, even though it may be opposed to the treatment you recommend. They know better than you, even though you’re the expert.”
Communicating effectively with these two types of patients requires a slightly different approach. “With an angry patient, you want to share decision making,” Dr. Alster said. “Have them voice their concerns and come up with a plan together going forward. You’re not going to make that person less angry by telling them what to do.” The manipulative patient, meanwhile, requires a team approach. For example, she may ask your medical assistant for opinions on the treatment option you recommended during your office consultation with her, or second-guess your recommendation with that person altogether. “Everybody needs to know who the manipulative patients are and approach them as a team.”
The art of nonconfrontation
Dr. Alster brings a nonconfrontational approach to interactions with difficult patients. “You can apologize if you’ve kept them waiting, but you can’t apologize for everything all the time,” she said. “I may say something like, ‘I appreciate that your visit is running late. I apologize for the delay and want you to know that we take as much time as necessary for each patient and that unforeseen circumstances beyond our control sometimes arise.’ ” Another phrase she may use is, “I understand that this has been a stressful visit, but I want to talk to you about your experience and identify how we can improve subsequent appointments.”
Showing empathy never hurts. “Repeat back to them what you heard, and establish the fact that you understand,” Dr. Alster said. “Lower your voice, talk slowly, don’t get caught up in emotion. Otherwise, you’re going down in a sinkhole with them. Be wrong to be right. This encourages negotiation. You also want to document all patient interactions. Put every correspondence in the patient’s EMR.”
Dr. Alster advises clinicians to provide an outline of office policies and procedures to all patients, as well as written and verbal instructions related to their care. She also phones or emails patients undergoing a treatment for the first time. “Even if they’ve been in the practice for several years, if they received filler injections for the first time [instead of Botox], we still check in with those patients when they receive a first-time treatment to make sure they’re doing okay,” she said. “We’ll call them that evening or at the very least early the next morning to make sure that they don’t have any questions or concerns.”
If problems persist despite your best efforts, sometimes your best option is to dismiss difficult patients from your practice. “That’s only when everything else fails,” Dr. Alster said. “A concise termination letter should state a ‘breakdown in physician-patient relationship.’ I call it my ‘Dear John’ letter, and since 1990, I’ve only written six of these. A detailed explanation is usually not needed, but may be advisable depending on your state, to protect yourself from a liability standpoint. I instruct patients to contact the state medical society for referral to another provider and inform them that upon their written request, their medical records will be forwarded to their new provider. I also set up a reasonable timeline during which I will continue to see them for emergency visits to ensure that there is continuity of care, even when it is a cosmetic situation.”
Dr. Alster reported having no financial disclosures related to her presentation.
DENVER – If you get the impression you’re dealing with more angry and manipulative patients than usual in the past several years, you’re not alone.
In 1999, as many as 15% of patient encounters were rated as difficult by health care providers, according to Tina S. Alster, MD (Arch Intern Med. 1999;159:1069-75). Today, upward of 30% of patient encounters are deemed difficult (Int J Res Med Sci. 2016;4[8]:3554-62). “That means one in three patients that you see have a problem that goes beyond the scope of our official training,” said Dr. Alster, who is the founding director of the Washington Institute of Dermatologic Laser Surgery and clinical professor of dermatology at Georgetown University, Washington. “If it was limited to a medical problem, we could handle it; that’s what we’re trained to do. The interpersonal issues and psychosocial implications of treatment are much more difficult.”
At the annual conference of the American Society for Laser Medicine and Surgery, Dr. Alster said that difficult patients put a strain on your practice and your relationship with them. “These patients put you on your heels. They often point out a problem that may or may not be related to something that you’re responsible for. It’s not usually because you are running late on the day of their visit and you make them late for something else. That situation is one you can prepare for, because you know you’re running late. It’s the other stuff you don’t realize that’s going on, which can cause problems.”
Setting limits
Being proactive can help lessen the ripple effect from patients who rock the boat. “You want to set limits with those patients before you even see them,” Dr. Alster said. “There are written contracts and policies that you should have in place. Since I perform mostly cosmetic procedures in my office, it is important that patients are made aware that payment is expected at the time of service and that my office does not bill nor accept insurance payments in order to prevent misunderstandings at check out.” She also declines requests to provide expert testimony for legal cases. “I’ve been in this business a long time, and every day I get requests to be an expert or to review a case involving a provider who may or may not have made a mistake. I really hate going down that rabbit hole.”
Another solution to keeping difficult patients in check is to collaborate with your entire office staff on how to best deal with them. “You need to present a united front with these patients: They’re going to divide and conquer, with complaints like, ‘How dare the doctor be so late. I’ve been waiting here for 30 minutes. Doesn’t she know I’m busy?’ ” Dr. Alster said. “You’re going to have to give them the tools to set limits as well. During our staff meetings, we review the upcoming patient schedule and identify potentially difficult situations in order to make sure the team is on the same page. Because my office is located in the power corridor of Washington [three blocks away from the White House] and my patient base is populated by prevalent personalities, expectations are extraordinarily high. As such, it is important that we set limits and rules that everyone can play by.”
Getting a sense of whether a patient is angry or manipulative can also help. An angry patient often holds an expectation that has been unmet, or harbors fears related to the treatment itself, she said, while a manipulative patient may engage in bullying, excessive flattery, or veiled threats. “They often expect specific treatments that have only worked for them in the past, even though it may be opposed to the treatment you recommend. They know better than you, even though you’re the expert.”
Communicating effectively with these two types of patients requires a slightly different approach. “With an angry patient, you want to share decision making,” Dr. Alster said. “Have them voice their concerns and come up with a plan together going forward. You’re not going to make that person less angry by telling them what to do.” The manipulative patient, meanwhile, requires a team approach. For example, she may ask your medical assistant for opinions on the treatment option you recommended during your office consultation with her, or second-guess your recommendation with that person altogether. “Everybody needs to know who the manipulative patients are and approach them as a team.”
The art of nonconfrontation
Dr. Alster brings a nonconfrontational approach to interactions with difficult patients. “You can apologize if you’ve kept them waiting, but you can’t apologize for everything all the time,” she said. “I may say something like, ‘I appreciate that your visit is running late. I apologize for the delay and want you to know that we take as much time as necessary for each patient and that unforeseen circumstances beyond our control sometimes arise.’ ” Another phrase she may use is, “I understand that this has been a stressful visit, but I want to talk to you about your experience and identify how we can improve subsequent appointments.”
Showing empathy never hurts. “Repeat back to them what you heard, and establish the fact that you understand,” Dr. Alster said. “Lower your voice, talk slowly, don’t get caught up in emotion. Otherwise, you’re going down in a sinkhole with them. Be wrong to be right. This encourages negotiation. You also want to document all patient interactions. Put every correspondence in the patient’s EMR.”
Dr. Alster advises clinicians to provide an outline of office policies and procedures to all patients, as well as written and verbal instructions related to their care. She also phones or emails patients undergoing a treatment for the first time. “Even if they’ve been in the practice for several years, if they received filler injections for the first time [instead of Botox], we still check in with those patients when they receive a first-time treatment to make sure they’re doing okay,” she said. “We’ll call them that evening or at the very least early the next morning to make sure that they don’t have any questions or concerns.”
If problems persist despite your best efforts, sometimes your best option is to dismiss difficult patients from your practice. “That’s only when everything else fails,” Dr. Alster said. “A concise termination letter should state a ‘breakdown in physician-patient relationship.’ I call it my ‘Dear John’ letter, and since 1990, I’ve only written six of these. A detailed explanation is usually not needed, but may be advisable depending on your state, to protect yourself from a liability standpoint. I instruct patients to contact the state medical society for referral to another provider and inform them that upon their written request, their medical records will be forwarded to their new provider. I also set up a reasonable timeline during which I will continue to see them for emergency visits to ensure that there is continuity of care, even when it is a cosmetic situation.”
Dr. Alster reported having no financial disclosures related to her presentation.
DENVER – If you get the impression you’re dealing with more angry and manipulative patients than usual in the past several years, you’re not alone.
In 1999, as many as 15% of patient encounters were rated as difficult by health care providers, according to Tina S. Alster, MD (Arch Intern Med. 1999;159:1069-75). Today, upward of 30% of patient encounters are deemed difficult (Int J Res Med Sci. 2016;4[8]:3554-62). “That means one in three patients that you see have a problem that goes beyond the scope of our official training,” said Dr. Alster, who is the founding director of the Washington Institute of Dermatologic Laser Surgery and clinical professor of dermatology at Georgetown University, Washington. “If it was limited to a medical problem, we could handle it; that’s what we’re trained to do. The interpersonal issues and psychosocial implications of treatment are much more difficult.”
At the annual conference of the American Society for Laser Medicine and Surgery, Dr. Alster said that difficult patients put a strain on your practice and your relationship with them. “These patients put you on your heels. They often point out a problem that may or may not be related to something that you’re responsible for. It’s not usually because you are running late on the day of their visit and you make them late for something else. That situation is one you can prepare for, because you know you’re running late. It’s the other stuff you don’t realize that’s going on, which can cause problems.”
Setting limits
Being proactive can help lessen the ripple effect from patients who rock the boat. “You want to set limits with those patients before you even see them,” Dr. Alster said. “There are written contracts and policies that you should have in place. Since I perform mostly cosmetic procedures in my office, it is important that patients are made aware that payment is expected at the time of service and that my office does not bill nor accept insurance payments in order to prevent misunderstandings at check out.” She also declines requests to provide expert testimony for legal cases. “I’ve been in this business a long time, and every day I get requests to be an expert or to review a case involving a provider who may or may not have made a mistake. I really hate going down that rabbit hole.”
Another solution to keeping difficult patients in check is to collaborate with your entire office staff on how to best deal with them. “You need to present a united front with these patients: They’re going to divide and conquer, with complaints like, ‘How dare the doctor be so late. I’ve been waiting here for 30 minutes. Doesn’t she know I’m busy?’ ” Dr. Alster said. “You’re going to have to give them the tools to set limits as well. During our staff meetings, we review the upcoming patient schedule and identify potentially difficult situations in order to make sure the team is on the same page. Because my office is located in the power corridor of Washington [three blocks away from the White House] and my patient base is populated by prevalent personalities, expectations are extraordinarily high. As such, it is important that we set limits and rules that everyone can play by.”
Getting a sense of whether a patient is angry or manipulative can also help. An angry patient often holds an expectation that has been unmet, or harbors fears related to the treatment itself, she said, while a manipulative patient may engage in bullying, excessive flattery, or veiled threats. “They often expect specific treatments that have only worked for them in the past, even though it may be opposed to the treatment you recommend. They know better than you, even though you’re the expert.”
Communicating effectively with these two types of patients requires a slightly different approach. “With an angry patient, you want to share decision making,” Dr. Alster said. “Have them voice their concerns and come up with a plan together going forward. You’re not going to make that person less angry by telling them what to do.” The manipulative patient, meanwhile, requires a team approach. For example, she may ask your medical assistant for opinions on the treatment option you recommended during your office consultation with her, or second-guess your recommendation with that person altogether. “Everybody needs to know who the manipulative patients are and approach them as a team.”
The art of nonconfrontation
Dr. Alster brings a nonconfrontational approach to interactions with difficult patients. “You can apologize if you’ve kept them waiting, but you can’t apologize for everything all the time,” she said. “I may say something like, ‘I appreciate that your visit is running late. I apologize for the delay and want you to know that we take as much time as necessary for each patient and that unforeseen circumstances beyond our control sometimes arise.’ ” Another phrase she may use is, “I understand that this has been a stressful visit, but I want to talk to you about your experience and identify how we can improve subsequent appointments.”
Showing empathy never hurts. “Repeat back to them what you heard, and establish the fact that you understand,” Dr. Alster said. “Lower your voice, talk slowly, don’t get caught up in emotion. Otherwise, you’re going down in a sinkhole with them. Be wrong to be right. This encourages negotiation. You also want to document all patient interactions. Put every correspondence in the patient’s EMR.”
Dr. Alster advises clinicians to provide an outline of office policies and procedures to all patients, as well as written and verbal instructions related to their care. She also phones or emails patients undergoing a treatment for the first time. “Even if they’ve been in the practice for several years, if they received filler injections for the first time [instead of Botox], we still check in with those patients when they receive a first-time treatment to make sure they’re doing okay,” she said. “We’ll call them that evening or at the very least early the next morning to make sure that they don’t have any questions or concerns.”
If problems persist despite your best efforts, sometimes your best option is to dismiss difficult patients from your practice. “That’s only when everything else fails,” Dr. Alster said. “A concise termination letter should state a ‘breakdown in physician-patient relationship.’ I call it my ‘Dear John’ letter, and since 1990, I’ve only written six of these. A detailed explanation is usually not needed, but may be advisable depending on your state, to protect yourself from a liability standpoint. I instruct patients to contact the state medical society for referral to another provider and inform them that upon their written request, their medical records will be forwarded to their new provider. I also set up a reasonable timeline during which I will continue to see them for emergency visits to ensure that there is continuity of care, even when it is a cosmetic situation.”
Dr. Alster reported having no financial disclosures related to her presentation.
EXPERT ANALYSIS FROM ASLMS 2019
Highlights from the 2019 Society of Gynecologic Surgeons Scientific Meeting

- Rising to the challenges in gynecologic surgical care
- Anterior, apical, posterior: Vaginal anatomy for the gynecologic surgeon
- Beyond enhanced recovery after surgery
B. Star Hampton, MD
Professor
Department of Obstetrics and Gynecology
Division of Urogynecology and Reconstructive
Pelvic Surgery
The Warren Albert Medical School
of Brown University
Women & Infants Hospital
Providence, Rhode Island
Peter C. Jeppson, MD
Assistant Professor
Division of Urogynecology
Department of Obstetrics and Gynecology
University of New Mexico School of Medicine
Albuquerque, New Mexico
Audra Jolyn Hill, MD
Assistant Professor
Division of Urogynecology
Department of Obstetrics and Gynecology
University of Utah School of Medicine
Salt Lake City, Utah
Sunil Balgobin, MD
Assistant Professor
Department of Obstetrics and Gynecology
Division of Female Pelvic Medicine
and Reconstructive Surgery
University of Texas Southwestern Medical Center
Dallas, Texas
Sean C. Dowdy, MD
Professor and Chair
Division of Gynecologic Oncology
Mayo Clinic
Rochester, Minnesota
- Rising to the challenges in gynecologic surgical care
- Anterior, apical, posterior: Vaginal anatomy for the gynecologic surgeon
- Beyond enhanced recovery after surgery
B. Star Hampton, MD
Professor
Department of Obstetrics and Gynecology
Division of Urogynecology and Reconstructive
Pelvic Surgery
The Warren Albert Medical School
of Brown University
Women & Infants Hospital
Providence, Rhode Island
Peter C. Jeppson, MD
Assistant Professor
Division of Urogynecology
Department of Obstetrics and Gynecology
University of New Mexico School of Medicine
Albuquerque, New Mexico
Audra Jolyn Hill, MD
Assistant Professor
Division of Urogynecology
Department of Obstetrics and Gynecology
University of Utah School of Medicine
Salt Lake City, Utah
Sunil Balgobin, MD
Assistant Professor
Department of Obstetrics and Gynecology
Division of Female Pelvic Medicine
and Reconstructive Surgery
University of Texas Southwestern Medical Center
Dallas, Texas
Sean C. Dowdy, MD
Professor and Chair
Division of Gynecologic Oncology
Mayo Clinic
Rochester, Minnesota
- Rising to the challenges in gynecologic surgical care
- Anterior, apical, posterior: Vaginal anatomy for the gynecologic surgeon
- Beyond enhanced recovery after surgery
B. Star Hampton, MD
Professor
Department of Obstetrics and Gynecology
Division of Urogynecology and Reconstructive
Pelvic Surgery
The Warren Albert Medical School
of Brown University
Women & Infants Hospital
Providence, Rhode Island
Peter C. Jeppson, MD
Assistant Professor
Division of Urogynecology
Department of Obstetrics and Gynecology
University of New Mexico School of Medicine
Albuquerque, New Mexico
Audra Jolyn Hill, MD
Assistant Professor
Division of Urogynecology
Department of Obstetrics and Gynecology
University of Utah School of Medicine
Salt Lake City, Utah
Sunil Balgobin, MD
Assistant Professor
Department of Obstetrics and Gynecology
Division of Female Pelvic Medicine
and Reconstructive Surgery
University of Texas Southwestern Medical Center
Dallas, Texas
Sean C. Dowdy, MD
Professor and Chair
Division of Gynecologic Oncology
Mayo Clinic
Rochester, Minnesota
