User login
Cardiac Cases: How Not to Lose Your License

Hospitalists can meet the demand for physician executives
HM provides “foundational leadership skills”
Hospitals and health systems are increasingly looking to physicians to provide leadership at the most senior executive level. While the chief medical officer (CMO) or similar role has given physicians a seat at the executive table at many organizations, physicians are also being sought for the CEO role at the head of that table.

A commonly referenced study from 2011 by Amanda Goodall, MD, in Social Science & Medicine concluded that, among a cohort of highly ranked hospitals, overall quality metrics were approximately 25% higher in hospitals where a physician was CEO, in comparison to hospitals with non-physician CEOs (2011 Aug;73[4]:535-9). In addition, new positions at both the hospital and health system level are coming into existence: Examples include chief (or VP) of population health, chief innovation officer, chief quality officer, chief patient experience officer, and others.
There is every reason to think that these senior executive physician roles can – and in many cases perhaps should – be filled by hospitalists. Hospital medicine is an ideal “proving ground” for future physician executives and leaders. I believe that the best practitioners of hospital medicine are also the best candidates for hospital, health care, and health system physician executive leadership, because many of the characteristics essential for success as an executive are the same characteristics that are essential for success as a hospitalist. Strong candidates should have the following characteristics:
- A patient-centered perspective. Perhaps the most important characteristic of a leader is empathy. To appreciate the complex, and often (if not usual) challenging emotional states of our patients keeps us connected at the most fundamental, human level to the work we do and to our patients and families. Empathy can – and should – extend to fellow caregivers as well, and allows us to practice and lead teams in the most human of professions. No leader – in health care, anyway – can last long without being able to demonstrate empathy, through words and behavior.
- A systems-based practice: A hospitalist must be able to have a foot in each of two canoes – to be able to see each patient and their family individually and develop preference-based plans of care, and also to be able to focus on process, structure, and outcomes for the hospital system as a whole. The former trait is imbued in us during training and is the critical foundation for the patient-physician relationship. The latter, however, is something different entirely and reflects an ability to have perspective on the entire ecosystem of care – and apply principles of process and quality improvement to achieve forward looking results. That’s leadership.
- Team leadership: Another fundamental attribute of leaders is to assemble a talented and diverse team around an objective, and then to delegate both tasks and their ownership, deferring to expertise. Hospitalists – the best ones, anyway – similarly recognize that for the vast majority of a patient’s hospital stay, the most important caregiver in a patient’s care is someone other than themselves. At any given time, it might be the nurse, aide, pharmacist, care manager, transporter, radiology tech, urologist, housekeeper, surgical resident, or anyone involved in that patient’s care. The hospitalist’s greatest value is in developing the plan of care with the patient and their family, and then communicating – and therefore delegating – that plan to individuals with the expertise to execute that plan. I believe the biggest difficulty hospitalists have in assuming leadership roles is getting out of the comfortable weeds of daily clinical operations and instead focusing on goals, strategies, and teams to accomplish them. The best hospitalists are doing this already as part of their daily care.
- The ability to manage relationships: Hospitalists manage and work among a team of diverse talents. They also often have accountability relationships to a myriad of clinical and administrative leaders in the hospital, each of whom may be in a position of authority to place demands on the hospitalists: A partial list might include the CEO, the chief medical officer, chief nurse, chief of staff, other medical staff departments, academic leaders, and of course, patients and their families. Functioning in a “matrixed” organization – in which lines of authority can go in many directions, depending on the situation – is standard fare, even at the executive level, and the key competency is open and frequent communication.
- Experience: Already, hospitalists assume leadership roles in their hospitals – leaders in quality, medical informatics, patient experience, and continuous improvement. In these roles, physicians work with senior executives and other hospital leaders to both set goals and implement strategies, providing visibility and working relationships that can be helpful to aspiring leaders.
Perhaps more so than most other specialties, then, hospitalists demonstrate foundational leadership skills in their day-to-day practice – an ideal start to a leadership path. This is not to say or suggest that a career devoted purely to clinical practice is somehow inferior – far from it. However, as health care organizations turn to the medical community to provider leadership, hospitalists are well positioned to develop and be developed as executive leaders.
How can the Society of Hospital Medicine help? While management degrees become a common pathway for many, some health systems and professional organizations support their membership with a leadership development curriculum which may be a better place to start. In my opinion, SHM provides one of the most thorough and relevant experiences available. The SHM Leadership Academy focuses on developing a broad set of additional leadership competencies across a spectrum of experience. The format varies depending on the course, but all rely heavily upon experienced hospitalist leaders – in fact, many current and former Board members and officers volunteer their time to facilitate and teach at the Academy, including at the entry level. It’s a powerful way to learn from others who have started walking the leadership path.
Dr. Harte is a past president of SHM and president of Cleveland Clinic Akron General and Southern Region.
HM provides “foundational leadership skills”
HM provides “foundational leadership skills”
Hospitals and health systems are increasingly looking to physicians to provide leadership at the most senior executive level. While the chief medical officer (CMO) or similar role has given physicians a seat at the executive table at many organizations, physicians are also being sought for the CEO role at the head of that table.
A commonly referenced study from 2011 by Amanda Goodall, MD, in Social Science & Medicine concluded that, among a cohort of highly ranked hospitals, overall quality metrics were approximately 25% higher in hospitals where a physician was CEO, in comparison to hospitals with non-physician CEOs (2011 Aug;73[4]:535-9). In addition, new positions at both the hospital and health system level are coming into existence: Examples include chief (or VP) of population health, chief innovation officer, chief quality officer, chief patient experience officer, and others.
There is every reason to think that these senior executive physician roles can – and in many cases perhaps should – be filled by hospitalists. Hospital medicine is an ideal “proving ground” for future physician executives and leaders. I believe that the best practitioners of hospital medicine are also the best candidates for hospital, health care, and health system physician executive leadership, because many of the characteristics essential for success as an executive are the same characteristics that are essential for success as a hospitalist. Strong candidates should have the following characteristics:
- A patient-centered perspective. Perhaps the most important characteristic of a leader is empathy. To appreciate the complex, and often (if not usual) challenging emotional states of our patients keeps us connected at the most fundamental, human level to the work we do and to our patients and families. Empathy can – and should – extend to fellow caregivers as well, and allows us to practice and lead teams in the most human of professions. No leader – in health care, anyway – can last long without being able to demonstrate empathy, through words and behavior.
- A systems-based practice: A hospitalist must be able to have a foot in each of two canoes – to be able to see each patient and their family individually and develop preference-based plans of care, and also to be able to focus on process, structure, and outcomes for the hospital system as a whole. The former trait is imbued in us during training and is the critical foundation for the patient-physician relationship. The latter, however, is something different entirely and reflects an ability to have perspective on the entire ecosystem of care – and apply principles of process and quality improvement to achieve forward looking results. That’s leadership.
- Team leadership: Another fundamental attribute of leaders is to assemble a talented and diverse team around an objective, and then to delegate both tasks and their ownership, deferring to expertise. Hospitalists – the best ones, anyway – similarly recognize that for the vast majority of a patient’s hospital stay, the most important caregiver in a patient’s care is someone other than themselves. At any given time, it might be the nurse, aide, pharmacist, care manager, transporter, radiology tech, urologist, housekeeper, surgical resident, or anyone involved in that patient’s care. The hospitalist’s greatest value is in developing the plan of care with the patient and their family, and then communicating – and therefore delegating – that plan to individuals with the expertise to execute that plan. I believe the biggest difficulty hospitalists have in assuming leadership roles is getting out of the comfortable weeds of daily clinical operations and instead focusing on goals, strategies, and teams to accomplish them. The best hospitalists are doing this already as part of their daily care.
- The ability to manage relationships: Hospitalists manage and work among a team of diverse talents. They also often have accountability relationships to a myriad of clinical and administrative leaders in the hospital, each of whom may be in a position of authority to place demands on the hospitalists: A partial list might include the CEO, the chief medical officer, chief nurse, chief of staff, other medical staff departments, academic leaders, and of course, patients and their families. Functioning in a “matrixed” organization – in which lines of authority can go in many directions, depending on the situation – is standard fare, even at the executive level, and the key competency is open and frequent communication.
- Experience: Already, hospitalists assume leadership roles in their hospitals – leaders in quality, medical informatics, patient experience, and continuous improvement. In these roles, physicians work with senior executives and other hospital leaders to both set goals and implement strategies, providing visibility and working relationships that can be helpful to aspiring leaders.
Perhaps more so than most other specialties, then, hospitalists demonstrate foundational leadership skills in their day-to-day practice – an ideal start to a leadership path. This is not to say or suggest that a career devoted purely to clinical practice is somehow inferior – far from it. However, as health care organizations turn to the medical community to provider leadership, hospitalists are well positioned to develop and be developed as executive leaders.
How can the Society of Hospital Medicine help? While management degrees become a common pathway for many, some health systems and professional organizations support their membership with a leadership development curriculum which may be a better place to start. In my opinion, SHM provides one of the most thorough and relevant experiences available. The SHM Leadership Academy focuses on developing a broad set of additional leadership competencies across a spectrum of experience. The format varies depending on the course, but all rely heavily upon experienced hospitalist leaders – in fact, many current and former Board members and officers volunteer their time to facilitate and teach at the Academy, including at the entry level. It’s a powerful way to learn from others who have started walking the leadership path.
Dr. Harte is a past president of SHM and president of Cleveland Clinic Akron General and Southern Region.
Hospitals and health systems are increasingly looking to physicians to provide leadership at the most senior executive level. While the chief medical officer (CMO) or similar role has given physicians a seat at the executive table at many organizations, physicians are also being sought for the CEO role at the head of that table.
A commonly referenced study from 2011 by Amanda Goodall, MD, in Social Science & Medicine concluded that, among a cohort of highly ranked hospitals, overall quality metrics were approximately 25% higher in hospitals where a physician was CEO, in comparison to hospitals with non-physician CEOs (2011 Aug;73[4]:535-9). In addition, new positions at both the hospital and health system level are coming into existence: Examples include chief (or VP) of population health, chief innovation officer, chief quality officer, chief patient experience officer, and others.
There is every reason to think that these senior executive physician roles can – and in many cases perhaps should – be filled by hospitalists. Hospital medicine is an ideal “proving ground” for future physician executives and leaders. I believe that the best practitioners of hospital medicine are also the best candidates for hospital, health care, and health system physician executive leadership, because many of the characteristics essential for success as an executive are the same characteristics that are essential for success as a hospitalist. Strong candidates should have the following characteristics:
- A patient-centered perspective. Perhaps the most important characteristic of a leader is empathy. To appreciate the complex, and often (if not usual) challenging emotional states of our patients keeps us connected at the most fundamental, human level to the work we do and to our patients and families. Empathy can – and should – extend to fellow caregivers as well, and allows us to practice and lead teams in the most human of professions. No leader – in health care, anyway – can last long without being able to demonstrate empathy, through words and behavior.
- A systems-based practice: A hospitalist must be able to have a foot in each of two canoes – to be able to see each patient and their family individually and develop preference-based plans of care, and also to be able to focus on process, structure, and outcomes for the hospital system as a whole. The former trait is imbued in us during training and is the critical foundation for the patient-physician relationship. The latter, however, is something different entirely and reflects an ability to have perspective on the entire ecosystem of care – and apply principles of process and quality improvement to achieve forward looking results. That’s leadership.
- Team leadership: Another fundamental attribute of leaders is to assemble a talented and diverse team around an objective, and then to delegate both tasks and their ownership, deferring to expertise. Hospitalists – the best ones, anyway – similarly recognize that for the vast majority of a patient’s hospital stay, the most important caregiver in a patient’s care is someone other than themselves. At any given time, it might be the nurse, aide, pharmacist, care manager, transporter, radiology tech, urologist, housekeeper, surgical resident, or anyone involved in that patient’s care. The hospitalist’s greatest value is in developing the plan of care with the patient and their family, and then communicating – and therefore delegating – that plan to individuals with the expertise to execute that plan. I believe the biggest difficulty hospitalists have in assuming leadership roles is getting out of the comfortable weeds of daily clinical operations and instead focusing on goals, strategies, and teams to accomplish them. The best hospitalists are doing this already as part of their daily care.
- The ability to manage relationships: Hospitalists manage and work among a team of diverse talents. They also often have accountability relationships to a myriad of clinical and administrative leaders in the hospital, each of whom may be in a position of authority to place demands on the hospitalists: A partial list might include the CEO, the chief medical officer, chief nurse, chief of staff, other medical staff departments, academic leaders, and of course, patients and their families. Functioning in a “matrixed” organization – in which lines of authority can go in many directions, depending on the situation – is standard fare, even at the executive level, and the key competency is open and frequent communication.
- Experience: Already, hospitalists assume leadership roles in their hospitals – leaders in quality, medical informatics, patient experience, and continuous improvement. In these roles, physicians work with senior executives and other hospital leaders to both set goals and implement strategies, providing visibility and working relationships that can be helpful to aspiring leaders.
Perhaps more so than most other specialties, then, hospitalists demonstrate foundational leadership skills in their day-to-day practice – an ideal start to a leadership path. This is not to say or suggest that a career devoted purely to clinical practice is somehow inferior – far from it. However, as health care organizations turn to the medical community to provider leadership, hospitalists are well positioned to develop and be developed as executive leaders.
How can the Society of Hospital Medicine help? While management degrees become a common pathway for many, some health systems and professional organizations support their membership with a leadership development curriculum which may be a better place to start. In my opinion, SHM provides one of the most thorough and relevant experiences available. The SHM Leadership Academy focuses on developing a broad set of additional leadership competencies across a spectrum of experience. The format varies depending on the course, but all rely heavily upon experienced hospitalist leaders – in fact, many current and former Board members and officers volunteer their time to facilitate and teach at the Academy, including at the entry level. It’s a powerful way to learn from others who have started walking the leadership path.
Dr. Harte is a past president of SHM and president of Cleveland Clinic Akron General and Southern Region.
Peripheral Arterial Disease: Putting Guidelines into Practice

Myths debunked around guns, mental illness, and video games
For some Americans, fears surrounding random gun violence are all too common.

In fact, a poll of people aged 13-24 years released earlier this year showed that, for young Americans, fear of gun violence ranks higher than the fear of climate change, terrorism, and rising college costs.
After nearly every mass shooting, the specter of mental illness comes up as a possible explanation. America’s rate of gun-related deaths is eight times that found in the European Union, according to Fareed Zakaria of CNN. “Does America have eight times the rate of mental illness?” he asked in a recent special episode of his public affairs show, “Fareed Zakaria GPS.” “Where is the disconnect?”
Mr. Zakaria went on to examine the 1996 Port Arthur massacre, in which a 28-year-old gunman with no history of mental illness killed 35 people and injured 18. After that incident, Australia sponsored a buyback program and eliminated more than 600,000 weapons. Afterward, the rate of gun-related homicides and suicides in Australia reportedly fell.
He also explored possible ties between video games and gun violence by examining the video game phenomenon in Japan. He reported that in Japan, a country of about 127 million people, about 13 people died in gun-related murders in 2016. Meanwhile, that year in the United States, the per-capita gun homicide rate was 300 times higher.
Finally, he examined the gun culture in Switzerland, where there are about 28 guns per 100 people. The country has citizen militias, and soldiers take home their weapons – but not their ammunition.
“We in America have been remarkably passive when it comes to gun violence,” Mr. Zakaria said. “One of the most important tasks for a government is to keep its citizens – especially its children – safe. Every other developed country in the world is able to fulfill this mandate. America is not. And the greatest tragedy is we know how to do it.”
Veterans’ friendship “like family”
John Nordeen and Kay Lee are on the far side of 70. During their youth, some of which was spent serving together in the Vietnam War, the two men forged a friendship. But back stateside, they lost touch.
In 2015, after years of searching by Mr. Nordeen, they reconnected. In a recent interview with NPR, they described their experiences in Vietnam and its aftermath.
“Our platoon went from like 29 guys to 10 guys in 2 days. So, the guys that were left, we had even stronger bonds because we had survived this together,” Mr. Nordeen said. The intense feeling of togetherness was tempered by equally intense feeling of the loss of their platoon mates.
The loss lingered for Mr. Nordeen once he returned home. “When you lose friends, you develop a hard exterior, and you don’t want to make friends with anyone else. So I don’t have a big circle of friends. I think that’s just one of many hang-ups I brought home with me.”
Mr. Lee concurred. “When I got home, most of the time I tried to forget the whole experience and not think about it too much. And I didn’t try to contact anyone because I’m not sure if you guys wanted to be contacted.”
It took years, but the two reunited. The reconnection has been welcomed by both men.
“It’s hard to describe, but the friendship and the bond that you form during battle is different than most friendship,” Mr. Lee said. “It’s like family now, so I’m very grateful for your effort to find me.”
Mr. Nordeen agreed. “Well, I feel like I’m a treasure hunter, and I found the treasure when I found you.”
Changing “embedded attitudes”
Kyle Fraser, a former student at St. Michael’s College School in Toronto, said he left because of its “toxic environment.”
The elite private Catholic school for boys in grades 7-12 is in the midst of a controversy involving allegations of several incidents involving brutal hazing perpetrated by returning members of the school’s junior football team on rookie players. In an official statement, the school administrators profess they are “heartbroken,” and the school’s president and principal have both resigned. Yet, Mr. Fraser said, he is not surprised by what has occurred.
“That’s the culture at that school,” he said in an interview with CBC News. During his years at St. Michael’s, Mr. Fraser said, he was verbally harassed every day.
Margery Holman, PhD, said she is not surprised about the environment at St. Michael’s. “It’s those male-dominated environments,” said Dr. Holman, an associate professor emeritus at the University of Windsor (Ont.) and coeditor of the book “Making the Team: Inside the World of Sport Hazing and Initiations”. “This is part of a history and tradition that is tolerated and accepted, and people turn a blind eye to it. It’s happening everywhere, not just at St. Mike’s. These are embedded attitudes that are going to take a long time to change. It took a long time to build on them, and it escalates every year.”
Susan Lipkins, PhD, a New York–based psychologist, agreed that the turmoil at St. Michael’s is not unique. “It’s being accepted as a norm, as a rite of passage. It’s becoming normalized for the kids, and they are not really attending to how awful and usually how illegal these events are.”
“Drive-by activism” turns sour
Even in an era in which photos can be altered digitally and disagreeable news can be dubbed fictitious, many people are moved to act when they become aware of others’ misfortune. But altruism turns into something else entirely when con artists become involved.
An example reported by NBC News involved a scheme that played out on a crowdfunding site.
On the site, Mark D’Amico and Kate McClure described an encounter Ms. McClure had with Johnny Bobbit, in which she ran out of gas by a roadside in New Jersey. The homeless veteran trudged to a gas station and used his last $20 to pay for gas. Later, the couple launched a GoFundMe campaign to solicit money to allow Mr. Bobbit a place to live and some transportation.
The response was overwhelming; more than 14,000 people contributed more than $400,000 in a single month. But the fairy tale turned sour after Mr. Bobbit complained about receiving only a small portion of the money. The remainder, contended lawyers prosecuting the couple, was spent on a new car and trips.
The case is “a perfect example of the inherent risks and weaknesses of giving over a crowdfunding site,” said Stephanie Kalivas, an analyst for Charity Watch in Chicago. Donating anonymously is a way for many people to feel they are doing something good and then moving on with their day – “drive-by activism,” according to Adrienne Gonzalez, founder of the watchdog website GoFraudMe. “We give five dollars, move on, and forget about it.”
GoFundMe agreed to reimburse everyone who contributed, the report said.
Layoff leads to $500 million
Change can be scary, especially when it hits the wallet. But being able to recognize opportunities that have opened up and seizing the moment can turn out far better than the old job ever was.
As described in a recent article in the Atlantic, Tim Chen is the poster person for adversity as opportunity. Mr. Chen is founder and CEO of the NerdWallet personal finance website, which compares products available from banks and insurance companies. Each month, 10 million people use the site to help make financial decisions. Begun in 2009, the site is valued at more than $500 million.
And it started when Mr. Chen was laid off as a financial analyst in the bust times of 2008. “[I was] totally blindsided. Never in a million years would I have thought that the institutions that I worked for, or the banks themselves, would be worried about going out of business. In hindsight, I feel very fortunate that there was a recession, from a personal perspective, because I never would have gotten into entrepreneurship, even though it was an ambition of mine. It’s just too hard to take that risk when you have a stable job and you’re living in a really expensive city like New York,” Mr. Chen explained in the article.
The bust-to-boom journey has taught Mr. Chen “that you can’t just put your head down and work hard and do things. You have to communicate well what it is you’re trying to do – the vision behind what you’re trying to do – to get other people inspired to understand what you’re doing and help you out.”
In contrast to the “job-for-life” world of the mid-20th century, the present reality for millennials is a series of jobs, and Mr. Chen said he relishes this shift. “I really want to learn from the person I’m working for, and 3 or 4 years from now, I’m going to come out with a different set of skills. I think the best opportunities in 30 years, while we can’t anticipate them now, are going to go to the people who have picked up a lot of skills along the way.”
For some Americans, fears surrounding random gun violence are all too common.
In fact, a poll of people aged 13-24 years released earlier this year showed that, for young Americans, fear of gun violence ranks higher than the fear of climate change, terrorism, and rising college costs.
After nearly every mass shooting, the specter of mental illness comes up as a possible explanation. America’s rate of gun-related deaths is eight times that found in the European Union, according to Fareed Zakaria of CNN. “Does America have eight times the rate of mental illness?” he asked in a recent special episode of his public affairs show, “Fareed Zakaria GPS.” “Where is the disconnect?”
Mr. Zakaria went on to examine the 1996 Port Arthur massacre, in which a 28-year-old gunman with no history of mental illness killed 35 people and injured 18. After that incident, Australia sponsored a buyback program and eliminated more than 600,000 weapons. Afterward, the rate of gun-related homicides and suicides in Australia reportedly fell.
He also explored possible ties between video games and gun violence by examining the video game phenomenon in Japan. He reported that in Japan, a country of about 127 million people, about 13 people died in gun-related murders in 2016. Meanwhile, that year in the United States, the per-capita gun homicide rate was 300 times higher.
Finally, he examined the gun culture in Switzerland, where there are about 28 guns per 100 people. The country has citizen militias, and soldiers take home their weapons – but not their ammunition.
“We in America have been remarkably passive when it comes to gun violence,” Mr. Zakaria said. “One of the most important tasks for a government is to keep its citizens – especially its children – safe. Every other developed country in the world is able to fulfill this mandate. America is not. And the greatest tragedy is we know how to do it.”
Veterans’ friendship “like family”
John Nordeen and Kay Lee are on the far side of 70. During their youth, some of which was spent serving together in the Vietnam War, the two men forged a friendship. But back stateside, they lost touch.
In 2015, after years of searching by Mr. Nordeen, they reconnected. In a recent interview with NPR, they described their experiences in Vietnam and its aftermath.
“Our platoon went from like 29 guys to 10 guys in 2 days. So, the guys that were left, we had even stronger bonds because we had survived this together,” Mr. Nordeen said. The intense feeling of togetherness was tempered by equally intense feeling of the loss of their platoon mates.
The loss lingered for Mr. Nordeen once he returned home. “When you lose friends, you develop a hard exterior, and you don’t want to make friends with anyone else. So I don’t have a big circle of friends. I think that’s just one of many hang-ups I brought home with me.”
Mr. Lee concurred. “When I got home, most of the time I tried to forget the whole experience and not think about it too much. And I didn’t try to contact anyone because I’m not sure if you guys wanted to be contacted.”
It took years, but the two reunited. The reconnection has been welcomed by both men.
“It’s hard to describe, but the friendship and the bond that you form during battle is different than most friendship,” Mr. Lee said. “It’s like family now, so I’m very grateful for your effort to find me.”
Mr. Nordeen agreed. “Well, I feel like I’m a treasure hunter, and I found the treasure when I found you.”
Changing “embedded attitudes”
Kyle Fraser, a former student at St. Michael’s College School in Toronto, said he left because of its “toxic environment.”
The elite private Catholic school for boys in grades 7-12 is in the midst of a controversy involving allegations of several incidents involving brutal hazing perpetrated by returning members of the school’s junior football team on rookie players. In an official statement, the school administrators profess they are “heartbroken,” and the school’s president and principal have both resigned. Yet, Mr. Fraser said, he is not surprised by what has occurred.
“That’s the culture at that school,” he said in an interview with CBC News. During his years at St. Michael’s, Mr. Fraser said, he was verbally harassed every day.
Margery Holman, PhD, said she is not surprised about the environment at St. Michael’s. “It’s those male-dominated environments,” said Dr. Holman, an associate professor emeritus at the University of Windsor (Ont.) and coeditor of the book “Making the Team: Inside the World of Sport Hazing and Initiations”. “This is part of a history and tradition that is tolerated and accepted, and people turn a blind eye to it. It’s happening everywhere, not just at St. Mike’s. These are embedded attitudes that are going to take a long time to change. It took a long time to build on them, and it escalates every year.”
Susan Lipkins, PhD, a New York–based psychologist, agreed that the turmoil at St. Michael’s is not unique. “It’s being accepted as a norm, as a rite of passage. It’s becoming normalized for the kids, and they are not really attending to how awful and usually how illegal these events are.”
“Drive-by activism” turns sour
Even in an era in which photos can be altered digitally and disagreeable news can be dubbed fictitious, many people are moved to act when they become aware of others’ misfortune. But altruism turns into something else entirely when con artists become involved.
An example reported by NBC News involved a scheme that played out on a crowdfunding site.
On the site, Mark D’Amico and Kate McClure described an encounter Ms. McClure had with Johnny Bobbit, in which she ran out of gas by a roadside in New Jersey. The homeless veteran trudged to a gas station and used his last $20 to pay for gas. Later, the couple launched a GoFundMe campaign to solicit money to allow Mr. Bobbit a place to live and some transportation.
The response was overwhelming; more than 14,000 people contributed more than $400,000 in a single month. But the fairy tale turned sour after Mr. Bobbit complained about receiving only a small portion of the money. The remainder, contended lawyers prosecuting the couple, was spent on a new car and trips.
The case is “a perfect example of the inherent risks and weaknesses of giving over a crowdfunding site,” said Stephanie Kalivas, an analyst for Charity Watch in Chicago. Donating anonymously is a way for many people to feel they are doing something good and then moving on with their day – “drive-by activism,” according to Adrienne Gonzalez, founder of the watchdog website GoFraudMe. “We give five dollars, move on, and forget about it.”
GoFundMe agreed to reimburse everyone who contributed, the report said.
Layoff leads to $500 million
Change can be scary, especially when it hits the wallet. But being able to recognize opportunities that have opened up and seizing the moment can turn out far better than the old job ever was.
As described in a recent article in the Atlantic, Tim Chen is the poster person for adversity as opportunity. Mr. Chen is founder and CEO of the NerdWallet personal finance website, which compares products available from banks and insurance companies. Each month, 10 million people use the site to help make financial decisions. Begun in 2009, the site is valued at more than $500 million.
And it started when Mr. Chen was laid off as a financial analyst in the bust times of 2008. “[I was] totally blindsided. Never in a million years would I have thought that the institutions that I worked for, or the banks themselves, would be worried about going out of business. In hindsight, I feel very fortunate that there was a recession, from a personal perspective, because I never would have gotten into entrepreneurship, even though it was an ambition of mine. It’s just too hard to take that risk when you have a stable job and you’re living in a really expensive city like New York,” Mr. Chen explained in the article.
The bust-to-boom journey has taught Mr. Chen “that you can’t just put your head down and work hard and do things. You have to communicate well what it is you’re trying to do – the vision behind what you’re trying to do – to get other people inspired to understand what you’re doing and help you out.”
In contrast to the “job-for-life” world of the mid-20th century, the present reality for millennials is a series of jobs, and Mr. Chen said he relishes this shift. “I really want to learn from the person I’m working for, and 3 or 4 years from now, I’m going to come out with a different set of skills. I think the best opportunities in 30 years, while we can’t anticipate them now, are going to go to the people who have picked up a lot of skills along the way.”
For some Americans, fears surrounding random gun violence are all too common.
In fact, a poll of people aged 13-24 years released earlier this year showed that, for young Americans, fear of gun violence ranks higher than the fear of climate change, terrorism, and rising college costs.
After nearly every mass shooting, the specter of mental illness comes up as a possible explanation. America’s rate of gun-related deaths is eight times that found in the European Union, according to Fareed Zakaria of CNN. “Does America have eight times the rate of mental illness?” he asked in a recent special episode of his public affairs show, “Fareed Zakaria GPS.” “Where is the disconnect?”
Mr. Zakaria went on to examine the 1996 Port Arthur massacre, in which a 28-year-old gunman with no history of mental illness killed 35 people and injured 18. After that incident, Australia sponsored a buyback program and eliminated more than 600,000 weapons. Afterward, the rate of gun-related homicides and suicides in Australia reportedly fell.
He also explored possible ties between video games and gun violence by examining the video game phenomenon in Japan. He reported that in Japan, a country of about 127 million people, about 13 people died in gun-related murders in 2016. Meanwhile, that year in the United States, the per-capita gun homicide rate was 300 times higher.
Finally, he examined the gun culture in Switzerland, where there are about 28 guns per 100 people. The country has citizen militias, and soldiers take home their weapons – but not their ammunition.
“We in America have been remarkably passive when it comes to gun violence,” Mr. Zakaria said. “One of the most important tasks for a government is to keep its citizens – especially its children – safe. Every other developed country in the world is able to fulfill this mandate. America is not. And the greatest tragedy is we know how to do it.”
Veterans’ friendship “like family”
John Nordeen and Kay Lee are on the far side of 70. During their youth, some of which was spent serving together in the Vietnam War, the two men forged a friendship. But back stateside, they lost touch.
In 2015, after years of searching by Mr. Nordeen, they reconnected. In a recent interview with NPR, they described their experiences in Vietnam and its aftermath.
“Our platoon went from like 29 guys to 10 guys in 2 days. So, the guys that were left, we had even stronger bonds because we had survived this together,” Mr. Nordeen said. The intense feeling of togetherness was tempered by equally intense feeling of the loss of their platoon mates.
The loss lingered for Mr. Nordeen once he returned home. “When you lose friends, you develop a hard exterior, and you don’t want to make friends with anyone else. So I don’t have a big circle of friends. I think that’s just one of many hang-ups I brought home with me.”
Mr. Lee concurred. “When I got home, most of the time I tried to forget the whole experience and not think about it too much. And I didn’t try to contact anyone because I’m not sure if you guys wanted to be contacted.”
It took years, but the two reunited. The reconnection has been welcomed by both men.
“It’s hard to describe, but the friendship and the bond that you form during battle is different than most friendship,” Mr. Lee said. “It’s like family now, so I’m very grateful for your effort to find me.”
Mr. Nordeen agreed. “Well, I feel like I’m a treasure hunter, and I found the treasure when I found you.”
Changing “embedded attitudes”
Kyle Fraser, a former student at St. Michael’s College School in Toronto, said he left because of its “toxic environment.”
The elite private Catholic school for boys in grades 7-12 is in the midst of a controversy involving allegations of several incidents involving brutal hazing perpetrated by returning members of the school’s junior football team on rookie players. In an official statement, the school administrators profess they are “heartbroken,” and the school’s president and principal have both resigned. Yet, Mr. Fraser said, he is not surprised by what has occurred.
“That’s the culture at that school,” he said in an interview with CBC News. During his years at St. Michael’s, Mr. Fraser said, he was verbally harassed every day.
Margery Holman, PhD, said she is not surprised about the environment at St. Michael’s. “It’s those male-dominated environments,” said Dr. Holman, an associate professor emeritus at the University of Windsor (Ont.) and coeditor of the book “Making the Team: Inside the World of Sport Hazing and Initiations”. “This is part of a history and tradition that is tolerated and accepted, and people turn a blind eye to it. It’s happening everywhere, not just at St. Mike’s. These are embedded attitudes that are going to take a long time to change. It took a long time to build on them, and it escalates every year.”
Susan Lipkins, PhD, a New York–based psychologist, agreed that the turmoil at St. Michael’s is not unique. “It’s being accepted as a norm, as a rite of passage. It’s becoming normalized for the kids, and they are not really attending to how awful and usually how illegal these events are.”
“Drive-by activism” turns sour
Even in an era in which photos can be altered digitally and disagreeable news can be dubbed fictitious, many people are moved to act when they become aware of others’ misfortune. But altruism turns into something else entirely when con artists become involved.
An example reported by NBC News involved a scheme that played out on a crowdfunding site.
On the site, Mark D’Amico and Kate McClure described an encounter Ms. McClure had with Johnny Bobbit, in which she ran out of gas by a roadside in New Jersey. The homeless veteran trudged to a gas station and used his last $20 to pay for gas. Later, the couple launched a GoFundMe campaign to solicit money to allow Mr. Bobbit a place to live and some transportation.
The response was overwhelming; more than 14,000 people contributed more than $400,000 in a single month. But the fairy tale turned sour after Mr. Bobbit complained about receiving only a small portion of the money. The remainder, contended lawyers prosecuting the couple, was spent on a new car and trips.
The case is “a perfect example of the inherent risks and weaknesses of giving over a crowdfunding site,” said Stephanie Kalivas, an analyst for Charity Watch in Chicago. Donating anonymously is a way for many people to feel they are doing something good and then moving on with their day – “drive-by activism,” according to Adrienne Gonzalez, founder of the watchdog website GoFraudMe. “We give five dollars, move on, and forget about it.”
GoFundMe agreed to reimburse everyone who contributed, the report said.
Layoff leads to $500 million
Change can be scary, especially when it hits the wallet. But being able to recognize opportunities that have opened up and seizing the moment can turn out far better than the old job ever was.
As described in a recent article in the Atlantic, Tim Chen is the poster person for adversity as opportunity. Mr. Chen is founder and CEO of the NerdWallet personal finance website, which compares products available from banks and insurance companies. Each month, 10 million people use the site to help make financial decisions. Begun in 2009, the site is valued at more than $500 million.
And it started when Mr. Chen was laid off as a financial analyst in the bust times of 2008. “[I was] totally blindsided. Never in a million years would I have thought that the institutions that I worked for, or the banks themselves, would be worried about going out of business. In hindsight, I feel very fortunate that there was a recession, from a personal perspective, because I never would have gotten into entrepreneurship, even though it was an ambition of mine. It’s just too hard to take that risk when you have a stable job and you’re living in a really expensive city like New York,” Mr. Chen explained in the article.
The bust-to-boom journey has taught Mr. Chen “that you can’t just put your head down and work hard and do things. You have to communicate well what it is you’re trying to do – the vision behind what you’re trying to do – to get other people inspired to understand what you’re doing and help you out.”
In contrast to the “job-for-life” world of the mid-20th century, the present reality for millennials is a series of jobs, and Mr. Chen said he relishes this shift. “I really want to learn from the person I’m working for, and 3 or 4 years from now, I’m going to come out with a different set of skills. I think the best opportunities in 30 years, while we can’t anticipate them now, are going to go to the people who have picked up a lot of skills along the way.”
U.S. life expectancy down; drug overdose, suicide up sharply
Average life expectancy fell in the United States fell from 78.7 years to 78.6 years from 2016 to 2017, according to a new report on the nation’s health. The decrease is primarily attributable to increases in suicide and drug overdose rates, according to new data from the Centers for Disease Control (CDC).

“The latest CDC data show that the U.S. life expectancy has declined over the past few years. Tragically, this troubling trend is largely driven by deaths from drug overdose and suicide,” said CDC Director Robert Redfield, MD, in a statement.
Two subreports that looked specifically at suicide mortality and drug overdose deaths mapped out where, when, and for whom the sharpest increases in mortality are being seen.
For suicide, though rates have increased by 33% overall for both men and women since 1999, the greatest annual increases in suicide rates have happened since 2006, according to a new report from the CDC’s National Center for Health Statistics (NCHS).
Overall, suicide rates have climbed from 10.5 to 14.0 per 100,000 individuals, with statistically significant increases in suicide rates among all age groups except those aged 75 years and older.
Suicide rates rose more steeply in the most rural counties. The age-adjusted increase in the most rural counties was 53%, compared with an increase of 16% in suicide rates for the nation’s most urban counties over the 1999-2017 time period.
Over the entire period studied, men were more likely than women to experience suicide, as rates rose among most age groups. For example, the rates of suicide for men aged 15-24 years rose from 16.8 to 22.7 per 100,000; for women in that age group, suicide rates went from 3.0 to 5.8 per 100,000.
Though suicide has remained the 10th leading cause of death overall in the United States, suicide was the second leading cause of death for adolescents and young adults (aged 10-34) in 2016, and the fourth leading cause of death for those aged 35-54 in that year.
These increases come despite a goal set by the CDC and a national coalition of health partners to reduce suicide rates to 10.2 per 100,000 by 2020, as part of the Healthy People 2020 initiative, noted Molly Hedegaard, MD, of NCHS, and her coauthors, in the suicide mortality data briefing.
Drug overdoses increased by nearly 10% in one year, with the highest rates seen in adults aged 25-54 years, according to a second CDC data briefing.
The number of people who died of drug overdoses in the United States in 2017 was 70,237. This represents a year-over-year age-adjusted increase of 9.6%, from 19.8 to 21.7 per 100,000 individuals, said Dr. Hedegaard and the coauthors of the drug overdose mortality report.
Reflecting known national trends in opioid use disorder, age-adjusted drug overdose deaths were highest in the states of West Virginia, Ohio, and Pennsylvania, where rates were 57.8, 46.3, and 44.3 per 100,000 residents, respectively. The District of Columbia had the fourth-highest age adjusted drug overdose death rate, at 44 per 100,000.
Twenty states, clustered primarily in the Eastern half of the United States, “had age-adjusted drug overdose death rate that were statistically higher than the national rate,” wrote Dr. Hedegaard and her coauthors.
Compared with 1999, more than six times as many adults in older midlife (aged 55-64 years) died from drug overdoses in 2017 (4.2 versus 28 per 100,000).
Adults aged 25-34 years, 35-44 years, and 45-54 years also had significant increases in drug overdose rates; in 2017, rates were 38.4, 29, and 37.7 per 100,000, respectively. Adolescent and young adults died from drug overdoses at a rate of 12.6 per 100,000, and those over 65 years old had a death rate of 6.9 per 100,000.
Deaths attributable to synthetic opioid use, excluding methadone, rose by 45% in just one year, going from 6.2 to 9.0 per 100,000 nationally. In 1999, synthetic opioids other than methadone were implicated in just 0.3 per 100,000 deaths. Synthetic opioids include fentanyl and fentanyl analogs, such as carfentanyl.
Deaths involving heroin remained stable from 2016 to 2017, at 4.9 per 100,000. Deaths attributable to natural and semisynthetic prescription opioids, such as oxycodone and hydrocodone, also were the same in 2017 as 2016, at 4.4 per 100,000.
Looking at trends over time since 1999, the rate of increase in drug overdose deaths had risen slowly since 1999 and stabilized in the mid-2000s. However, beginning in 2012, rates have increased steeply, particularly for males.
“Male rates were significantly higher than female rates for all years,” reported Dr. Hedegaard and her coauthors (P less than .05). Though female drug overdose death rates have climbed from 3.9 to 14.4 per 100,000 since 1999, the male death rate has gone from 8.2 to 29.1 per 100,000 during the study period.
“Life expectancy gives us a snapshot of the nation’s overall health and these sobering statistics are a wakeup call that we are losing too many Americans, too early and too often, to conditions that are preventable. CDC is committed to putting science into action to protect U.S. health, but we must all work together to reverse this trend and help ensure that all Americans live longer and healthier lives,” said Dr. Redfield.
Average life expectancy fell in the United States fell from 78.7 years to 78.6 years from 2016 to 2017, according to a new report on the nation’s health. The decrease is primarily attributable to increases in suicide and drug overdose rates, according to new data from the Centers for Disease Control (CDC).
“The latest CDC data show that the U.S. life expectancy has declined over the past few years. Tragically, this troubling trend is largely driven by deaths from drug overdose and suicide,” said CDC Director Robert Redfield, MD, in a statement.
Two subreports that looked specifically at suicide mortality and drug overdose deaths mapped out where, when, and for whom the sharpest increases in mortality are being seen.
For suicide, though rates have increased by 33% overall for both men and women since 1999, the greatest annual increases in suicide rates have happened since 2006, according to a new report from the CDC’s National Center for Health Statistics (NCHS).
Overall, suicide rates have climbed from 10.5 to 14.0 per 100,000 individuals, with statistically significant increases in suicide rates among all age groups except those aged 75 years and older.
Suicide rates rose more steeply in the most rural counties. The age-adjusted increase in the most rural counties was 53%, compared with an increase of 16% in suicide rates for the nation’s most urban counties over the 1999-2017 time period.
Over the entire period studied, men were more likely than women to experience suicide, as rates rose among most age groups. For example, the rates of suicide for men aged 15-24 years rose from 16.8 to 22.7 per 100,000; for women in that age group, suicide rates went from 3.0 to 5.8 per 100,000.
Though suicide has remained the 10th leading cause of death overall in the United States, suicide was the second leading cause of death for adolescents and young adults (aged 10-34) in 2016, and the fourth leading cause of death for those aged 35-54 in that year.
These increases come despite a goal set by the CDC and a national coalition of health partners to reduce suicide rates to 10.2 per 100,000 by 2020, as part of the Healthy People 2020 initiative, noted Molly Hedegaard, MD, of NCHS, and her coauthors, in the suicide mortality data briefing.
Drug overdoses increased by nearly 10% in one year, with the highest rates seen in adults aged 25-54 years, according to a second CDC data briefing.
The number of people who died of drug overdoses in the United States in 2017 was 70,237. This represents a year-over-year age-adjusted increase of 9.6%, from 19.8 to 21.7 per 100,000 individuals, said Dr. Hedegaard and the coauthors of the drug overdose mortality report.
Reflecting known national trends in opioid use disorder, age-adjusted drug overdose deaths were highest in the states of West Virginia, Ohio, and Pennsylvania, where rates were 57.8, 46.3, and 44.3 per 100,000 residents, respectively. The District of Columbia had the fourth-highest age adjusted drug overdose death rate, at 44 per 100,000.
Twenty states, clustered primarily in the Eastern half of the United States, “had age-adjusted drug overdose death rate that were statistically higher than the national rate,” wrote Dr. Hedegaard and her coauthors.
Compared with 1999, more than six times as many adults in older midlife (aged 55-64 years) died from drug overdoses in 2017 (4.2 versus 28 per 100,000).
Adults aged 25-34 years, 35-44 years, and 45-54 years also had significant increases in drug overdose rates; in 2017, rates were 38.4, 29, and 37.7 per 100,000, respectively. Adolescent and young adults died from drug overdoses at a rate of 12.6 per 100,000, and those over 65 years old had a death rate of 6.9 per 100,000.
Deaths attributable to synthetic opioid use, excluding methadone, rose by 45% in just one year, going from 6.2 to 9.0 per 100,000 nationally. In 1999, synthetic opioids other than methadone were implicated in just 0.3 per 100,000 deaths. Synthetic opioids include fentanyl and fentanyl analogs, such as carfentanyl.
Deaths involving heroin remained stable from 2016 to 2017, at 4.9 per 100,000. Deaths attributable to natural and semisynthetic prescription opioids, such as oxycodone and hydrocodone, also were the same in 2017 as 2016, at 4.4 per 100,000.
Looking at trends over time since 1999, the rate of increase in drug overdose deaths had risen slowly since 1999 and stabilized in the mid-2000s. However, beginning in 2012, rates have increased steeply, particularly for males.
“Male rates were significantly higher than female rates for all years,” reported Dr. Hedegaard and her coauthors (P less than .05). Though female drug overdose death rates have climbed from 3.9 to 14.4 per 100,000 since 1999, the male death rate has gone from 8.2 to 29.1 per 100,000 during the study period.
“Life expectancy gives us a snapshot of the nation’s overall health and these sobering statistics are a wakeup call that we are losing too many Americans, too early and too often, to conditions that are preventable. CDC is committed to putting science into action to protect U.S. health, but we must all work together to reverse this trend and help ensure that all Americans live longer and healthier lives,” said Dr. Redfield.
Average life expectancy fell in the United States fell from 78.7 years to 78.6 years from 2016 to 2017, according to a new report on the nation’s health. The decrease is primarily attributable to increases in suicide and drug overdose rates, according to new data from the Centers for Disease Control (CDC).
“The latest CDC data show that the U.S. life expectancy has declined over the past few years. Tragically, this troubling trend is largely driven by deaths from drug overdose and suicide,” said CDC Director Robert Redfield, MD, in a statement.
Two subreports that looked specifically at suicide mortality and drug overdose deaths mapped out where, when, and for whom the sharpest increases in mortality are being seen.
For suicide, though rates have increased by 33% overall for both men and women since 1999, the greatest annual increases in suicide rates have happened since 2006, according to a new report from the CDC’s National Center for Health Statistics (NCHS).
Overall, suicide rates have climbed from 10.5 to 14.0 per 100,000 individuals, with statistically significant increases in suicide rates among all age groups except those aged 75 years and older.
Suicide rates rose more steeply in the most rural counties. The age-adjusted increase in the most rural counties was 53%, compared with an increase of 16% in suicide rates for the nation’s most urban counties over the 1999-2017 time period.
Over the entire period studied, men were more likely than women to experience suicide, as rates rose among most age groups. For example, the rates of suicide for men aged 15-24 years rose from 16.8 to 22.7 per 100,000; for women in that age group, suicide rates went from 3.0 to 5.8 per 100,000.
Though suicide has remained the 10th leading cause of death overall in the United States, suicide was the second leading cause of death for adolescents and young adults (aged 10-34) in 2016, and the fourth leading cause of death for those aged 35-54 in that year.
These increases come despite a goal set by the CDC and a national coalition of health partners to reduce suicide rates to 10.2 per 100,000 by 2020, as part of the Healthy People 2020 initiative, noted Molly Hedegaard, MD, of NCHS, and her coauthors, in the suicide mortality data briefing.
Drug overdoses increased by nearly 10% in one year, with the highest rates seen in adults aged 25-54 years, according to a second CDC data briefing.
The number of people who died of drug overdoses in the United States in 2017 was 70,237. This represents a year-over-year age-adjusted increase of 9.6%, from 19.8 to 21.7 per 100,000 individuals, said Dr. Hedegaard and the coauthors of the drug overdose mortality report.
Reflecting known national trends in opioid use disorder, age-adjusted drug overdose deaths were highest in the states of West Virginia, Ohio, and Pennsylvania, where rates were 57.8, 46.3, and 44.3 per 100,000 residents, respectively. The District of Columbia had the fourth-highest age adjusted drug overdose death rate, at 44 per 100,000.
Twenty states, clustered primarily in the Eastern half of the United States, “had age-adjusted drug overdose death rate that were statistically higher than the national rate,” wrote Dr. Hedegaard and her coauthors.
Compared with 1999, more than six times as many adults in older midlife (aged 55-64 years) died from drug overdoses in 2017 (4.2 versus 28 per 100,000).
Adults aged 25-34 years, 35-44 years, and 45-54 years also had significant increases in drug overdose rates; in 2017, rates were 38.4, 29, and 37.7 per 100,000, respectively. Adolescent and young adults died from drug overdoses at a rate of 12.6 per 100,000, and those over 65 years old had a death rate of 6.9 per 100,000.
Deaths attributable to synthetic opioid use, excluding methadone, rose by 45% in just one year, going from 6.2 to 9.0 per 100,000 nationally. In 1999, synthetic opioids other than methadone were implicated in just 0.3 per 100,000 deaths. Synthetic opioids include fentanyl and fentanyl analogs, such as carfentanyl.
Deaths involving heroin remained stable from 2016 to 2017, at 4.9 per 100,000. Deaths attributable to natural and semisynthetic prescription opioids, such as oxycodone and hydrocodone, also were the same in 2017 as 2016, at 4.4 per 100,000.
Looking at trends over time since 1999, the rate of increase in drug overdose deaths had risen slowly since 1999 and stabilized in the mid-2000s. However, beginning in 2012, rates have increased steeply, particularly for males.
“Male rates were significantly higher than female rates for all years,” reported Dr. Hedegaard and her coauthors (P less than .05). Though female drug overdose death rates have climbed from 3.9 to 14.4 per 100,000 since 1999, the male death rate has gone from 8.2 to 29.1 per 100,000 during the study period.
“Life expectancy gives us a snapshot of the nation’s overall health and these sobering statistics are a wakeup call that we are losing too many Americans, too early and too often, to conditions that are preventable. CDC is committed to putting science into action to protect U.S. health, but we must all work together to reverse this trend and help ensure that all Americans live longer and healthier lives,” said Dr. Redfield.
Democrats taking key leadership jobs have pocketed millions from Pharma
Three of the lawmakers who will lead the House next year as Congress focuses on skyrocketing drug costs are among the biggest recipients of campaign contributions from the pharmaceutical industry, a new KHN analysis shows.
On Nov. 28, House Democrats selected Rep. Steny Hoyer of Maryland to serve as the next majority leader and Rep. James Clyburn of South Carolina as majority whip, making them the No. 2 and No. 3 most powerful Democrats as their party regains control of the House in January.
Both lawmakers have received more than $1 million from pharmaceutical company political action committees (PACs) in the past decade. Just four members of Congress hold that distinction, including Rep. Kevin McCarthy of California, whom Republicans chose as the next House minority leader earlier this month.
Adding Rep. Nancy Pelosi, the California Democrat expected to be the next speaker, the three-person House Democratic leadership team has collected more than $2.3 million total in campaign contributions from drugmakers since the 2007-2008 election cycle, according to KHN’s database.
High drug prices surfaced as a major campaign issue in 2018. With almost half of Americans saying they were worried about prescription drug costs last summer, many Democrats told voters they’d tackle the issue in the next Congress. But the large amount of money going to key Democrats, and Republicans, raises questions about whether Congress will take on the pharmaceutical industry.
In the past decade, members of Congress from both parties have received about $81 million from 68 pharma PACs run by employees of companies that make drugs and industry trade groups.
Brendan Fischer, who directs federal reform programs at the nonpartisan Campaign Legal Center, said drugmakers, like other wealthy industries, “shower money” on congressional leaders who are mulling legislation that could affect the pharmaceutical industry.
“Both Democrats and Republicans have discussed taking action on prescription drug prices, and drug companies likely expect that big contributions will help them maintain access to, and influence over, powerful lawmakers,” he said.
Mr. McCarthy, who has close ties to President Donald Trump, has received more than $1.08 million from drugmaker PACs since 2007. According to the latest data, which runs through September, he received about $250,000 this election cycle.
The fourth lawmaker to top $1 million is Sen. Richard Burr, a North Carolina Republican who serves on both the Senate Committee on Health, Education, Labor and Pensions and the Senate Committee on Finance. North Carolina is also home to a number of research universities and drugmakers’ headquarters.
While campaign contributions may seem tantalizing as a metric for influence, industries are not necessarily buying votes with their cash. More likely, they are buying access – a sizable donation from a drugmaker’s PAC may increase the chances its lobbyists get a meeting with an influential lawmaker, for example.
Mr. Clyburn, who like Mr. Hoyer has served as a top Democratic leader since 2007, has received more from drugmaker PACs over the past decade than any other member of Congress – more than $1.09 million. During the 2018 election cycle, he received at least $170,000, despite trouncing his Republican opponent in his safely Democratic district.
A party leader and the highest-ranking African-American in Congress, Mr. Clyburn has had ties to the pharmaceutical industry over the years. In 2013, he was a featured speaker at a conference hosted by PhRMA, the industry’s leading trade group. The conference was held at the James E. Clyburn Research Center at the Medical University of South Carolina, a hub for biopharmaceutical research.
This fall, Mr. Hoyer topped the million-dollar mark in drugmaker PAC contributions over the past decade, collecting more than $1.02 million since 2007 and more than $128,000 this election cycle.
“Mr. Hoyer’s positions on legislation are based on what is in the best interest of his constituents and the American people, and he has made it clear the new Congress will tackle rising health care and prescription drug costs,” said Mariel Saez, a Hoyer spokeswoman.
The offices of Mr. Clyburn, Mr. McCarthy, and Ms. Pelosi did not respond to requests for comment.
Ms. Pelosi, in contrast to her deputies, has received nearly $193,000 total from drugmaker PACs the past decade. In the month before the midterm elections, she intensified her calls for action to control drug prices, saying on Election Day that she believed Democrats could find “common ground” with Trump on addressing the problem.
Senior committee members also tend to draw huge sums from the industries they oversee. Rep. Frank Pallone of New Jersey, the Democrat who is expected to chair the House Committee on Energy and Commerce, received nearly $169,000 this election cycle from drugmaker PACs, according to KHN’s database. Since 2007, he has collected more than $840,000.
Similarly, Rep. Greg Walden, the Oregon Republican who is finishing his term as chair of the committee, received $302,300, the most of any member this election cycle in contributions from drugmaker PACs.
By contrast, Rep. Elijah Cummings – the Maryland Democrat who is expected to head the House Committee on Oversight and Government Reform – has attracted minimal drugmaker cash, receiving just $18,500 since the 2007-2008 election cycle. He has made it clear that he intends to target pharmaceutical companies next year as he investigates climbing drug costs.
Kaiser Health News is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Three of the lawmakers who will lead the House next year as Congress focuses on skyrocketing drug costs are among the biggest recipients of campaign contributions from the pharmaceutical industry, a new KHN analysis shows.
On Nov. 28, House Democrats selected Rep. Steny Hoyer of Maryland to serve as the next majority leader and Rep. James Clyburn of South Carolina as majority whip, making them the No. 2 and No. 3 most powerful Democrats as their party regains control of the House in January.
Both lawmakers have received more than $1 million from pharmaceutical company political action committees (PACs) in the past decade. Just four members of Congress hold that distinction, including Rep. Kevin McCarthy of California, whom Republicans chose as the next House minority leader earlier this month.
Adding Rep. Nancy Pelosi, the California Democrat expected to be the next speaker, the three-person House Democratic leadership team has collected more than $2.3 million total in campaign contributions from drugmakers since the 2007-2008 election cycle, according to KHN’s database.
High drug prices surfaced as a major campaign issue in 2018. With almost half of Americans saying they were worried about prescription drug costs last summer, many Democrats told voters they’d tackle the issue in the next Congress. But the large amount of money going to key Democrats, and Republicans, raises questions about whether Congress will take on the pharmaceutical industry.
In the past decade, members of Congress from both parties have received about $81 million from 68 pharma PACs run by employees of companies that make drugs and industry trade groups.
Brendan Fischer, who directs federal reform programs at the nonpartisan Campaign Legal Center, said drugmakers, like other wealthy industries, “shower money” on congressional leaders who are mulling legislation that could affect the pharmaceutical industry.
“Both Democrats and Republicans have discussed taking action on prescription drug prices, and drug companies likely expect that big contributions will help them maintain access to, and influence over, powerful lawmakers,” he said.
Mr. McCarthy, who has close ties to President Donald Trump, has received more than $1.08 million from drugmaker PACs since 2007. According to the latest data, which runs through September, he received about $250,000 this election cycle.
The fourth lawmaker to top $1 million is Sen. Richard Burr, a North Carolina Republican who serves on both the Senate Committee on Health, Education, Labor and Pensions and the Senate Committee on Finance. North Carolina is also home to a number of research universities and drugmakers’ headquarters.
While campaign contributions may seem tantalizing as a metric for influence, industries are not necessarily buying votes with their cash. More likely, they are buying access – a sizable donation from a drugmaker’s PAC may increase the chances its lobbyists get a meeting with an influential lawmaker, for example.
Mr. Clyburn, who like Mr. Hoyer has served as a top Democratic leader since 2007, has received more from drugmaker PACs over the past decade than any other member of Congress – more than $1.09 million. During the 2018 election cycle, he received at least $170,000, despite trouncing his Republican opponent in his safely Democratic district.
A party leader and the highest-ranking African-American in Congress, Mr. Clyburn has had ties to the pharmaceutical industry over the years. In 2013, he was a featured speaker at a conference hosted by PhRMA, the industry’s leading trade group. The conference was held at the James E. Clyburn Research Center at the Medical University of South Carolina, a hub for biopharmaceutical research.
This fall, Mr. Hoyer topped the million-dollar mark in drugmaker PAC contributions over the past decade, collecting more than $1.02 million since 2007 and more than $128,000 this election cycle.
“Mr. Hoyer’s positions on legislation are based on what is in the best interest of his constituents and the American people, and he has made it clear the new Congress will tackle rising health care and prescription drug costs,” said Mariel Saez, a Hoyer spokeswoman.
The offices of Mr. Clyburn, Mr. McCarthy, and Ms. Pelosi did not respond to requests for comment.
Ms. Pelosi, in contrast to her deputies, has received nearly $193,000 total from drugmaker PACs the past decade. In the month before the midterm elections, she intensified her calls for action to control drug prices, saying on Election Day that she believed Democrats could find “common ground” with Trump on addressing the problem.
Senior committee members also tend to draw huge sums from the industries they oversee. Rep. Frank Pallone of New Jersey, the Democrat who is expected to chair the House Committee on Energy and Commerce, received nearly $169,000 this election cycle from drugmaker PACs, according to KHN’s database. Since 2007, he has collected more than $840,000.
Similarly, Rep. Greg Walden, the Oregon Republican who is finishing his term as chair of the committee, received $302,300, the most of any member this election cycle in contributions from drugmaker PACs.
By contrast, Rep. Elijah Cummings – the Maryland Democrat who is expected to head the House Committee on Oversight and Government Reform – has attracted minimal drugmaker cash, receiving just $18,500 since the 2007-2008 election cycle. He has made it clear that he intends to target pharmaceutical companies next year as he investigates climbing drug costs.
Kaiser Health News is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Three of the lawmakers who will lead the House next year as Congress focuses on skyrocketing drug costs are among the biggest recipients of campaign contributions from the pharmaceutical industry, a new KHN analysis shows.
On Nov. 28, House Democrats selected Rep. Steny Hoyer of Maryland to serve as the next majority leader and Rep. James Clyburn of South Carolina as majority whip, making them the No. 2 and No. 3 most powerful Democrats as their party regains control of the House in January.
Both lawmakers have received more than $1 million from pharmaceutical company political action committees (PACs) in the past decade. Just four members of Congress hold that distinction, including Rep. Kevin McCarthy of California, whom Republicans chose as the next House minority leader earlier this month.
Adding Rep. Nancy Pelosi, the California Democrat expected to be the next speaker, the three-person House Democratic leadership team has collected more than $2.3 million total in campaign contributions from drugmakers since the 2007-2008 election cycle, according to KHN’s database.
High drug prices surfaced as a major campaign issue in 2018. With almost half of Americans saying they were worried about prescription drug costs last summer, many Democrats told voters they’d tackle the issue in the next Congress. But the large amount of money going to key Democrats, and Republicans, raises questions about whether Congress will take on the pharmaceutical industry.
In the past decade, members of Congress from both parties have received about $81 million from 68 pharma PACs run by employees of companies that make drugs and industry trade groups.
Brendan Fischer, who directs federal reform programs at the nonpartisan Campaign Legal Center, said drugmakers, like other wealthy industries, “shower money” on congressional leaders who are mulling legislation that could affect the pharmaceutical industry.
“Both Democrats and Republicans have discussed taking action on prescription drug prices, and drug companies likely expect that big contributions will help them maintain access to, and influence over, powerful lawmakers,” he said.
Mr. McCarthy, who has close ties to President Donald Trump, has received more than $1.08 million from drugmaker PACs since 2007. According to the latest data, which runs through September, he received about $250,000 this election cycle.
The fourth lawmaker to top $1 million is Sen. Richard Burr, a North Carolina Republican who serves on both the Senate Committee on Health, Education, Labor and Pensions and the Senate Committee on Finance. North Carolina is also home to a number of research universities and drugmakers’ headquarters.
While campaign contributions may seem tantalizing as a metric for influence, industries are not necessarily buying votes with their cash. More likely, they are buying access – a sizable donation from a drugmaker’s PAC may increase the chances its lobbyists get a meeting with an influential lawmaker, for example.
Mr. Clyburn, who like Mr. Hoyer has served as a top Democratic leader since 2007, has received more from drugmaker PACs over the past decade than any other member of Congress – more than $1.09 million. During the 2018 election cycle, he received at least $170,000, despite trouncing his Republican opponent in his safely Democratic district.
A party leader and the highest-ranking African-American in Congress, Mr. Clyburn has had ties to the pharmaceutical industry over the years. In 2013, he was a featured speaker at a conference hosted by PhRMA, the industry’s leading trade group. The conference was held at the James E. Clyburn Research Center at the Medical University of South Carolina, a hub for biopharmaceutical research.
This fall, Mr. Hoyer topped the million-dollar mark in drugmaker PAC contributions over the past decade, collecting more than $1.02 million since 2007 and more than $128,000 this election cycle.
“Mr. Hoyer’s positions on legislation are based on what is in the best interest of his constituents and the American people, and he has made it clear the new Congress will tackle rising health care and prescription drug costs,” said Mariel Saez, a Hoyer spokeswoman.
The offices of Mr. Clyburn, Mr. McCarthy, and Ms. Pelosi did not respond to requests for comment.
Ms. Pelosi, in contrast to her deputies, has received nearly $193,000 total from drugmaker PACs the past decade. In the month before the midterm elections, she intensified her calls for action to control drug prices, saying on Election Day that she believed Democrats could find “common ground” with Trump on addressing the problem.
Senior committee members also tend to draw huge sums from the industries they oversee. Rep. Frank Pallone of New Jersey, the Democrat who is expected to chair the House Committee on Energy and Commerce, received nearly $169,000 this election cycle from drugmaker PACs, according to KHN’s database. Since 2007, he has collected more than $840,000.
Similarly, Rep. Greg Walden, the Oregon Republican who is finishing his term as chair of the committee, received $302,300, the most of any member this election cycle in contributions from drugmaker PACs.
By contrast, Rep. Elijah Cummings – the Maryland Democrat who is expected to head the House Committee on Oversight and Government Reform – has attracted minimal drugmaker cash, receiving just $18,500 since the 2007-2008 election cycle. He has made it clear that he intends to target pharmaceutical companies next year as he investigates climbing drug costs.
Kaiser Health News is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Intra-articular Wnt inhibitor for knee OA sails through phase 2
CHICAGO – A single intra-articular injection of a novel drug known for now as SMO4690 resulted in statistically significant and clinically meaningful improvements in pain and physical function through 6 months of follow-up in a phase 2b study including 695 patients with moderately to severely symptomatic knee OA, Yusuf Yazici, MD, reported at the annual meeting of the American College of Rheumatology.
Based on the encouraging results of this and another large phase 2 study, two pivotal phase 3, randomized clinical trials are due to start in the spring of 2019. If the results are positive, SMO4690 could become the first approved disease-modifying OA drug (DMOAD), something that’s been a long-sought, high-priority goal in rheumatology, noted Dr. Yazici, chief medical officer at San Diego–based Samumed, which is developing the drug, and a rheumatologist at New York University.
SMO4690 is a small molecule inhibitor of the Wnt signaling pathway. The drug has two distinct mechanisms of action for treatment of knee OA: It has an anti-inflammatory effect and it protects cartilage from degeneration, as demonstrated by a clinically significant improvement in joint space width by x-ray, compared with placebo at 12 months of follow-up after a single baseline injection in the earlier 455-patient, phase 2 study. Also, animal studies suggest SMO4690 generates cartilage, an exciting possibility now being evaluated in two ongoing serial MRI studies in knee OA patients.
Dr. Yazici presented patient-reported outcomes from the 695-patient, 24-week, multicenter, randomized, placebo-controlled, double-blind, phase 2b study, which evaluated four different concentrations of SMO4690. The 0.07- and 0.23-mg per 2-mL injection doses proved significantly better than placebo at 12 weeks – the primary endpoint – for all patient-reported outcomes.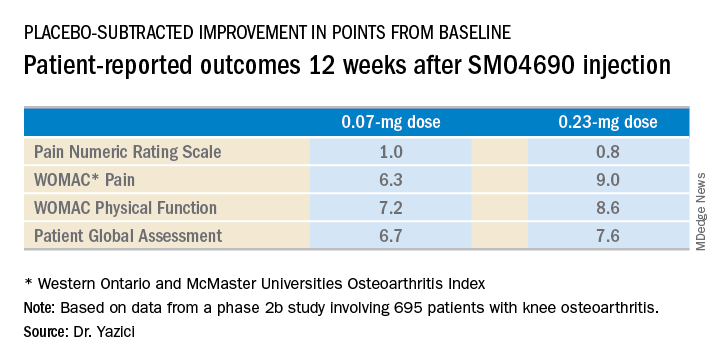
The 0.23-mg dose of SMO4690 remained superior to placebo for all four patient-reported outcomes at subsequent assessments at weeks 16, 20, and 24. The 0.07-mg dose remained significantly better than placebo through week 20.
As in the earlier phase 2 study, SMO4690 raised no significant safety concerns. Adverse events were similar in type and frequency in the active-treatment and placebo groups.
The study was sponsored by Samumed, where Dr. Yazici is employed as chief medical officer.
SOURCE: Yazici Y et al. Arthritis Rheumatol. 2018;70(Suppl 10), Abstract L03.
CHICAGO – A single intra-articular injection of a novel drug known for now as SMO4690 resulted in statistically significant and clinically meaningful improvements in pain and physical function through 6 months of follow-up in a phase 2b study including 695 patients with moderately to severely symptomatic knee OA, Yusuf Yazici, MD, reported at the annual meeting of the American College of Rheumatology.
Based on the encouraging results of this and another large phase 2 study, two pivotal phase 3, randomized clinical trials are due to start in the spring of 2019. If the results are positive, SMO4690 could become the first approved disease-modifying OA drug (DMOAD), something that’s been a long-sought, high-priority goal in rheumatology, noted Dr. Yazici, chief medical officer at San Diego–based Samumed, which is developing the drug, and a rheumatologist at New York University.
SMO4690 is a small molecule inhibitor of the Wnt signaling pathway. The drug has two distinct mechanisms of action for treatment of knee OA: It has an anti-inflammatory effect and it protects cartilage from degeneration, as demonstrated by a clinically significant improvement in joint space width by x-ray, compared with placebo at 12 months of follow-up after a single baseline injection in the earlier 455-patient, phase 2 study. Also, animal studies suggest SMO4690 generates cartilage, an exciting possibility now being evaluated in two ongoing serial MRI studies in knee OA patients.
Dr. Yazici presented patient-reported outcomes from the 695-patient, 24-week, multicenter, randomized, placebo-controlled, double-blind, phase 2b study, which evaluated four different concentrations of SMO4690. The 0.07- and 0.23-mg per 2-mL injection doses proved significantly better than placebo at 12 weeks – the primary endpoint – for all patient-reported outcomes.
The 0.23-mg dose of SMO4690 remained superior to placebo for all four patient-reported outcomes at subsequent assessments at weeks 16, 20, and 24. The 0.07-mg dose remained significantly better than placebo through week 20.
As in the earlier phase 2 study, SMO4690 raised no significant safety concerns. Adverse events were similar in type and frequency in the active-treatment and placebo groups.
The study was sponsored by Samumed, where Dr. Yazici is employed as chief medical officer.
SOURCE: Yazici Y et al. Arthritis Rheumatol. 2018;70(Suppl 10), Abstract L03.
CHICAGO – A single intra-articular injection of a novel drug known for now as SMO4690 resulted in statistically significant and clinically meaningful improvements in pain and physical function through 6 months of follow-up in a phase 2b study including 695 patients with moderately to severely symptomatic knee OA, Yusuf Yazici, MD, reported at the annual meeting of the American College of Rheumatology.
Based on the encouraging results of this and another large phase 2 study, two pivotal phase 3, randomized clinical trials are due to start in the spring of 2019. If the results are positive, SMO4690 could become the first approved disease-modifying OA drug (DMOAD), something that’s been a long-sought, high-priority goal in rheumatology, noted Dr. Yazici, chief medical officer at San Diego–based Samumed, which is developing the drug, and a rheumatologist at New York University.
SMO4690 is a small molecule inhibitor of the Wnt signaling pathway. The drug has two distinct mechanisms of action for treatment of knee OA: It has an anti-inflammatory effect and it protects cartilage from degeneration, as demonstrated by a clinically significant improvement in joint space width by x-ray, compared with placebo at 12 months of follow-up after a single baseline injection in the earlier 455-patient, phase 2 study. Also, animal studies suggest SMO4690 generates cartilage, an exciting possibility now being evaluated in two ongoing serial MRI studies in knee OA patients.
Dr. Yazici presented patient-reported outcomes from the 695-patient, 24-week, multicenter, randomized, placebo-controlled, double-blind, phase 2b study, which evaluated four different concentrations of SMO4690. The 0.07- and 0.23-mg per 2-mL injection doses proved significantly better than placebo at 12 weeks – the primary endpoint – for all patient-reported outcomes.
The 0.23-mg dose of SMO4690 remained superior to placebo for all four patient-reported outcomes at subsequent assessments at weeks 16, 20, and 24. The 0.07-mg dose remained significantly better than placebo through week 20.
As in the earlier phase 2 study, SMO4690 raised no significant safety concerns. Adverse events were similar in type and frequency in the active-treatment and placebo groups.
The study was sponsored by Samumed, where Dr. Yazici is employed as chief medical officer.
SOURCE: Yazici Y et al. Arthritis Rheumatol. 2018;70(Suppl 10), Abstract L03.
REPORTING FROM THE ACR ANNUAL MEETING
Key clinical point:
Major finding: The 0.23-mg dose of SMO4690 proved superior to placebo for four key patient-reported outcomes.
Study details: This was a 24-week, randomized, multicenter, placebo-controlled, double-blind, phase 2b study in 695 patients with moderately to severely symptomatic knee OA.
Disclosures: The presenter is chief medical officer at Samumed, the study sponsor.
Source: Yazici Y et al. Arthritis Rheumatol. 2018;70(Suppl 10), Abstract L03.
Anthralin shows promise as second-line agent for pediatric alopecia areata
Given its limited systemic toxicity, , according to Sean Z. Wu, MD, of the department of dermatology, University of Cincinnati, and his associates.
In a retrospective study of 37 pediatric patients with AA, published in Pediatric Dermatology, Dr. Wu and his colleagues found that almost two-thirds experienced at least 50% regrowth of hair with topical anthralin treatment, but they described severe dermatitis and relapses as “potential drawbacks” of treatment.
The 37 patients were in the Cleveland Clinic AA areata database and began treatment with anthralin between 2004 and 2015, at aged 2-17 years (mean age 9). Over half (22) were females and most (31) were white. About 65% had patchy AA; the remainder had either alopecia totalis or alopecia universalis. Prior treatments included topical corticosteroids, minoxidil, and intralesional corticosteroids; four patients had not been treated previously. Patients were followed up from 51 days to more than 10 years, with a mean duration of 2.5 years. Treatment regimens, titrated up to achieve a mild to moderate dermatitis, included application of 0.5% cream for 5 minutes twice a week up to 1.0% cream for 30 minutes a day.
With topical anthralin, 12 (32%) of patients had complete scalp regrowth, 25 (68%) experienced at least 50% regrowth, and 5 (14%) had no response; in five patients, no follow-up information was available. Among those with at least 50% regrowth, the initial response was first noted at a mean of 3.4 months, and the mean time to maximal response was 15 months. This timeline suggests that treatment with anthralin should be continued beyond 1 year to ensure maximum beneficial results with hair regrowth, the authors wrote.
Factors associated with a positive response to treatment included less than 50% of scalp involvement. The two patients who used anthralin as monotherapy did not achieve a 50% scalp response, but the four treatment-naive patients were among those with at least 50% scalp regrowth, versus three of the five patients (60%) who had been treated previously with systemic steroids.
Two potential clinical limitations were noted during the study. Four patients had to stop treatment because of dermatitis, which suggests that patients and parents should be counseled about the potential for severe skin irritation with this treatment, the authors said. And among those who achieved at least 50% scalp regrowth, 16 of the 25 (64%) relapsed. The authors speculated that the effects of the drug could be temporary “or that the disease process may be able to overcome the anthralin effect over time.”
Dr. Wu and his coauthors cited the retrospective design and the small population size as major limitations of the study. Because some patients continued other treatments, it is “difficult to attribute scalp regrowth entirely to anthralin,” and variations in formulation and in treatment regimens are also factors to be considered, they cautioned. That AA has been found to spontaneously resolve, depending upon the severity of the disease, presents additional challenges for clinicians attempting to determine the extent to which anthralin offers therapeutic benefit, they pointed out.
In spite of the drug’s limitations, the authors concluded that the treatment was a safe and useful option as an “adjunct for those who fail first-line therapy with topical or intralesional corticosteroids.” They added that more work is needed to tailor treatment formulation, frequency, and duration to the specific needs of pediatric patients.
The authors had no relevant financial disclosures to report.
SOURCE: Wu SZ et al. Pediatr Dermatol. 2018;35:817-20.
Given its limited systemic toxicity, , according to Sean Z. Wu, MD, of the department of dermatology, University of Cincinnati, and his associates.
In a retrospective study of 37 pediatric patients with AA, published in Pediatric Dermatology, Dr. Wu and his colleagues found that almost two-thirds experienced at least 50% regrowth of hair with topical anthralin treatment, but they described severe dermatitis and relapses as “potential drawbacks” of treatment.
The 37 patients were in the Cleveland Clinic AA areata database and began treatment with anthralin between 2004 and 2015, at aged 2-17 years (mean age 9). Over half (22) were females and most (31) were white. About 65% had patchy AA; the remainder had either alopecia totalis or alopecia universalis. Prior treatments included topical corticosteroids, minoxidil, and intralesional corticosteroids; four patients had not been treated previously. Patients were followed up from 51 days to more than 10 years, with a mean duration of 2.5 years. Treatment regimens, titrated up to achieve a mild to moderate dermatitis, included application of 0.5% cream for 5 minutes twice a week up to 1.0% cream for 30 minutes a day.
With topical anthralin, 12 (32%) of patients had complete scalp regrowth, 25 (68%) experienced at least 50% regrowth, and 5 (14%) had no response; in five patients, no follow-up information was available. Among those with at least 50% regrowth, the initial response was first noted at a mean of 3.4 months, and the mean time to maximal response was 15 months. This timeline suggests that treatment with anthralin should be continued beyond 1 year to ensure maximum beneficial results with hair regrowth, the authors wrote.
Factors associated with a positive response to treatment included less than 50% of scalp involvement. The two patients who used anthralin as monotherapy did not achieve a 50% scalp response, but the four treatment-naive patients were among those with at least 50% scalp regrowth, versus three of the five patients (60%) who had been treated previously with systemic steroids.
Two potential clinical limitations were noted during the study. Four patients had to stop treatment because of dermatitis, which suggests that patients and parents should be counseled about the potential for severe skin irritation with this treatment, the authors said. And among those who achieved at least 50% scalp regrowth, 16 of the 25 (64%) relapsed. The authors speculated that the effects of the drug could be temporary “or that the disease process may be able to overcome the anthralin effect over time.”
Dr. Wu and his coauthors cited the retrospective design and the small population size as major limitations of the study. Because some patients continued other treatments, it is “difficult to attribute scalp regrowth entirely to anthralin,” and variations in formulation and in treatment regimens are also factors to be considered, they cautioned. That AA has been found to spontaneously resolve, depending upon the severity of the disease, presents additional challenges for clinicians attempting to determine the extent to which anthralin offers therapeutic benefit, they pointed out.
In spite of the drug’s limitations, the authors concluded that the treatment was a safe and useful option as an “adjunct for those who fail first-line therapy with topical or intralesional corticosteroids.” They added that more work is needed to tailor treatment formulation, frequency, and duration to the specific needs of pediatric patients.
The authors had no relevant financial disclosures to report.
SOURCE: Wu SZ et al. Pediatr Dermatol. 2018;35:817-20.
Given its limited systemic toxicity, , according to Sean Z. Wu, MD, of the department of dermatology, University of Cincinnati, and his associates.
In a retrospective study of 37 pediatric patients with AA, published in Pediatric Dermatology, Dr. Wu and his colleagues found that almost two-thirds experienced at least 50% regrowth of hair with topical anthralin treatment, but they described severe dermatitis and relapses as “potential drawbacks” of treatment.
The 37 patients were in the Cleveland Clinic AA areata database and began treatment with anthralin between 2004 and 2015, at aged 2-17 years (mean age 9). Over half (22) were females and most (31) were white. About 65% had patchy AA; the remainder had either alopecia totalis or alopecia universalis. Prior treatments included topical corticosteroids, minoxidil, and intralesional corticosteroids; four patients had not been treated previously. Patients were followed up from 51 days to more than 10 years, with a mean duration of 2.5 years. Treatment regimens, titrated up to achieve a mild to moderate dermatitis, included application of 0.5% cream for 5 minutes twice a week up to 1.0% cream for 30 minutes a day.
With topical anthralin, 12 (32%) of patients had complete scalp regrowth, 25 (68%) experienced at least 50% regrowth, and 5 (14%) had no response; in five patients, no follow-up information was available. Among those with at least 50% regrowth, the initial response was first noted at a mean of 3.4 months, and the mean time to maximal response was 15 months. This timeline suggests that treatment with anthralin should be continued beyond 1 year to ensure maximum beneficial results with hair regrowth, the authors wrote.
Factors associated with a positive response to treatment included less than 50% of scalp involvement. The two patients who used anthralin as monotherapy did not achieve a 50% scalp response, but the four treatment-naive patients were among those with at least 50% scalp regrowth, versus three of the five patients (60%) who had been treated previously with systemic steroids.
Two potential clinical limitations were noted during the study. Four patients had to stop treatment because of dermatitis, which suggests that patients and parents should be counseled about the potential for severe skin irritation with this treatment, the authors said. And among those who achieved at least 50% scalp regrowth, 16 of the 25 (64%) relapsed. The authors speculated that the effects of the drug could be temporary “or that the disease process may be able to overcome the anthralin effect over time.”
Dr. Wu and his coauthors cited the retrospective design and the small population size as major limitations of the study. Because some patients continued other treatments, it is “difficult to attribute scalp regrowth entirely to anthralin,” and variations in formulation and in treatment regimens are also factors to be considered, they cautioned. That AA has been found to spontaneously resolve, depending upon the severity of the disease, presents additional challenges for clinicians attempting to determine the extent to which anthralin offers therapeutic benefit, they pointed out.
In spite of the drug’s limitations, the authors concluded that the treatment was a safe and useful option as an “adjunct for those who fail first-line therapy with topical or intralesional corticosteroids.” They added that more work is needed to tailor treatment formulation, frequency, and duration to the specific needs of pediatric patients.
The authors had no relevant financial disclosures to report.
SOURCE: Wu SZ et al. Pediatr Dermatol. 2018;35:817-20.
FROM PEDIATRIC DERMATOLOGY
Key clinical point: Additional research is needed to pinpoint protocols for optimal formulation, dosage, and duration of anthralin in pediatric patients.
Major finding: At least 50% regrowth of scalp hair was achieved in 68% of patients treated with topical anthralin.
Study details: A retrospective chart review of 37 patients with alopecia areata who started treatment at a mean age of 9 years.
Disclosures: The authors reported no relevant financial disclosures.
Source: Wu SZ et al. Pediatr Dermatol. 2018;35:817-20.
Infant mortality generally unchanged in 2016
Infant mortality in the United Sates dropped very slightly from 2015 to 2016 and has not changed significantly since 2011, according to the National Center for Health Statistics.
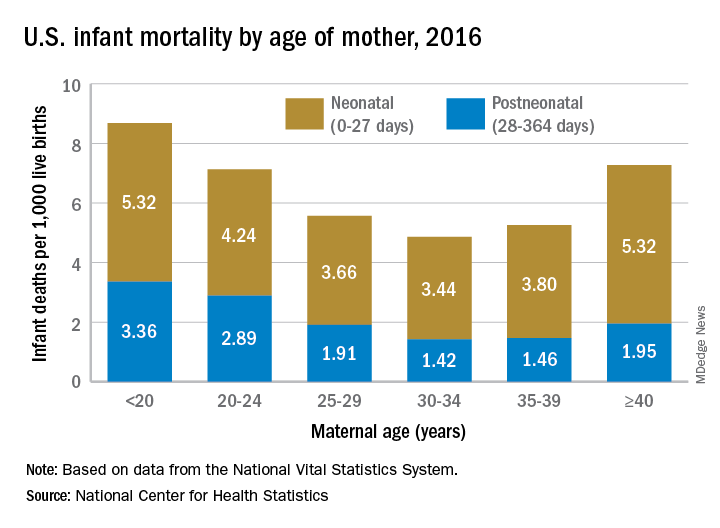
Overall infant mortality was 5.87 per 1,000 live births in 2016, which was not significantly less than the 2015 rate of 5.90 per 1,000 or the rate of 6.07 per 1,000 recorded in 2011, the NCHS said in a recent Data Brief. The rate for 2016 works out to 3.88 per 1,000 for the neonatal period (0-27 days) and 1.99 per 1,000 during the postneonatal period (28-364 days).
The rate was lowest for mothers aged 30-34 years (4.86 per 1,000) and highest for those under 20 years (8.69). All overall rates by maternal age were significantly different from each other, except for those of mothers aged 20-24 years (7.13) and those aged 40 years and over (7.27). Neonatal mortality was highest for the under-20 group and the 40-and-over group at 5.32 per 1,000, with the difference between them coming during the postneonatal period: 3.36 for those under 20 and 1.95 for the 40-and-overs, the NCHS investigators reported based on data from the National Vital Statistics System.
The leading cause of death during the neonatal period in 2016 was low birth weight at 98 per 1,000 live births, with congenital malformations second at 86 per 1,000. The leading cause of death in the postneonatal period was congenital malformations at 36 per 1,000, followed by sudden infant death syndrome (35 per 1,000), unintentional injuries (27 per 1,000), diseases of the circulatory system (9 per 1,000), and homicide (6 per 1,000), they added.
Infant mortality in the United Sates dropped very slightly from 2015 to 2016 and has not changed significantly since 2011, according to the National Center for Health Statistics.
Overall infant mortality was 5.87 per 1,000 live births in 2016, which was not significantly less than the 2015 rate of 5.90 per 1,000 or the rate of 6.07 per 1,000 recorded in 2011, the NCHS said in a recent Data Brief. The rate for 2016 works out to 3.88 per 1,000 for the neonatal period (0-27 days) and 1.99 per 1,000 during the postneonatal period (28-364 days).
The rate was lowest for mothers aged 30-34 years (4.86 per 1,000) and highest for those under 20 years (8.69). All overall rates by maternal age were significantly different from each other, except for those of mothers aged 20-24 years (7.13) and those aged 40 years and over (7.27). Neonatal mortality was highest for the under-20 group and the 40-and-over group at 5.32 per 1,000, with the difference between them coming during the postneonatal period: 3.36 for those under 20 and 1.95 for the 40-and-overs, the NCHS investigators reported based on data from the National Vital Statistics System.
The leading cause of death during the neonatal period in 2016 was low birth weight at 98 per 1,000 live births, with congenital malformations second at 86 per 1,000. The leading cause of death in the postneonatal period was congenital malformations at 36 per 1,000, followed by sudden infant death syndrome (35 per 1,000), unintentional injuries (27 per 1,000), diseases of the circulatory system (9 per 1,000), and homicide (6 per 1,000), they added.
Infant mortality in the United Sates dropped very slightly from 2015 to 2016 and has not changed significantly since 2011, according to the National Center for Health Statistics.
Overall infant mortality was 5.87 per 1,000 live births in 2016, which was not significantly less than the 2015 rate of 5.90 per 1,000 or the rate of 6.07 per 1,000 recorded in 2011, the NCHS said in a recent Data Brief. The rate for 2016 works out to 3.88 per 1,000 for the neonatal period (0-27 days) and 1.99 per 1,000 during the postneonatal period (28-364 days).
The rate was lowest for mothers aged 30-34 years (4.86 per 1,000) and highest for those under 20 years (8.69). All overall rates by maternal age were significantly different from each other, except for those of mothers aged 20-24 years (7.13) and those aged 40 years and over (7.27). Neonatal mortality was highest for the under-20 group and the 40-and-over group at 5.32 per 1,000, with the difference between them coming during the postneonatal period: 3.36 for those under 20 and 1.95 for the 40-and-overs, the NCHS investigators reported based on data from the National Vital Statistics System.
The leading cause of death during the neonatal period in 2016 was low birth weight at 98 per 1,000 live births, with congenital malformations second at 86 per 1,000. The leading cause of death in the postneonatal period was congenital malformations at 36 per 1,000, followed by sudden infant death syndrome (35 per 1,000), unintentional injuries (27 per 1,000), diseases of the circulatory system (9 per 1,000), and homicide (6 per 1,000), they added.
MVP Data Reveals Gene Mutations Ruling Cholesterol
Using data from the Million Veteran Program (MVP), researchers found people with mutations for PDE3B, PCSK9, and ANGPTL4 had better cholesterol and triglyceride levels than did those without the mutations.
The PDE3B mutation seems to protect against heart disease. A PCSK9 mutation may reduce the risk not only of heart disease, but also abdominal aortic aneurysm. The ANGPTL4 mutation was linked to lower risk of type 2 DM.
MVP, 1 of the world’s largest databases of health and genomic information, partners with veterans receiving care in the VHA to study how genes affect health. It has enrolled > 700,000 veterans to date.
Using data from the Million Veteran Program (MVP), researchers found people with mutations for PDE3B, PCSK9, and ANGPTL4 had better cholesterol and triglyceride levels than did those without the mutations.
The PDE3B mutation seems to protect against heart disease. A PCSK9 mutation may reduce the risk not only of heart disease, but also abdominal aortic aneurysm. The ANGPTL4 mutation was linked to lower risk of type 2 DM.
MVP, 1 of the world’s largest databases of health and genomic information, partners with veterans receiving care in the VHA to study how genes affect health. It has enrolled > 700,000 veterans to date.
Using data from the Million Veteran Program (MVP), researchers found people with mutations for PDE3B, PCSK9, and ANGPTL4 had better cholesterol and triglyceride levels than did those without the mutations.
The PDE3B mutation seems to protect against heart disease. A PCSK9 mutation may reduce the risk not only of heart disease, but also abdominal aortic aneurysm. The ANGPTL4 mutation was linked to lower risk of type 2 DM.
MVP, 1 of the world’s largest databases of health and genomic information, partners with veterans receiving care in the VHA to study how genes affect health. It has enrolled > 700,000 veterans to date.