User login
Most dermatologic drugs safe for breastfeeding mothers
CHICAGO – A common reason why a women stops breastfeeding is the use of medication her doctor has claimed is unsafe during lactation. But most drugs have little or no effect on an infant’s well-being or milk supply, explained Jenny Eileen Murase, MD, of Palo Alto (Calif.) Foundation Medical Group.

“The bottom line I want you to take away from this [session] is that ,” Dr. Murase told attendees at the American Academy of Dermatology summer meeting. “I really want everyone in this room to understand that most of the time, you should not be recommending that a woman is pumping and dumping her milk or stopping breastfeeding because she’s on an agent.”
Dr. Murase, also affiliated with the University of California, San Francisco, provided an overview of drug safety during lactation for major categories of medications that dermatologists prescribe. She recommended that physicians get a copy of Medications and Mother’s Milk by Thomas Hale, PhD, which she considers the best reference for looking up specific drugs. It categorizes drugs as L1 (safest) to L5 (contraindicated), and L2 as “safer,” L3 as “moderately safe,” and L4 as “possibly hazardous.”
Steroids
Contrary to what many believe, prednisone is not contraindicated in breastfeeding, Dr. Murase said. Instead of advising patients to “pump and dump their milk,” she said, “the only recommendation you need to make is that they wait 4 hours after taking the medicine to breastfeed.” For example, a mother can take prednisone before bed and then wake 4 hours later to nurse. Higher doses, such as more than 40 mg daily over long periods, may have the potential to affect growth and development, but more typical doses don’t pose the same risk.
Topical steroids (except for those that are class 1) also are safe to apply directly to the nipple in breastfeeding women, she noted.
Biologics and immunosuppressants
One of the few medications that are contraindicated are topical pimecrolimus and tacrolimus if applied directly to the nipple, since “oral consumption in the infant could be significant,” Dr. Murase said.
Biologics, on the other hand, are not a concern during lactation. “They have low oral bioavailability because of their large molecular size,” and are broken down in the stomach “in a proteolytic environment,” Dr. Murase explained. The CRADLE study, for example, examined the concentration of certolizumab (Cimzia) in mothers’ mature breast milk and found the highest concentration to be just 0.077 mcg/mL, resulting in an average daily infant dose of less than 0.01 mg/kg per day.
Antihistamines and cosmetic topicals
The major antihistamines – brompheniramine, chlorpheniramine, diphenhydramine, hydroxyzine, cetirizine, fexofenadine and loratadine – are likewise safe as L1-L3 drugs. It is preferable to prescribe nonsedating antihistamines, opting for loratadine as the first-line choice. But dermatologists should be reassured that no data support concerns about milk supply reduction from antihistamines, Dr. Murase said.
It’s best to avoid cosmetic topical products, but hydroquinone (L3), topical minoxidil (L2), and botulinum toxin A (L3) do not pose significant risk to the infant. Neither do the anesthetics lidocaine (L2) and epinephrine (L1) for breastfeeding women who need surgery.
Antibiotics
The vast majority of antibiotics are safe for women to use while breastfeeding, but a few notable exceptions exist, including erythromycin.
“People associate erythromycin as safe in lactation because it’s safe in pregnancy, but that’s not the case,” Dr. Murase pointed out. Erythromycin has been linked to pyloric stenosis in newborns and therefore should be avoided in the early months of breastfeeding. In older infants, however, erythromycin becomes an L1 medication.”
Tetracyclines fall into a borderline category. “Tetracyclines would be fine for a complicated infection,” but should not be used for more than 3 weeks, at which point they are regarded as L4, Dr. Murase said. “So long-term use of the tetracyclines should be avoided.”
Aside from these, topical antibiotics are considered safe. Women taking other oral antibiotics should be monitored for gastrointestinal symptoms or allergic responses.
Antifungals
As for antifungals, topicals are safe, and nystatin and clotrimazole are the best first-line options (both L1). Oral antifungals are similarly fine, with griseofulvin, fluconazole, ketoconazole, itraconazole, and terbinafine all classified as L2 and amphotericin B as L3.
If antifungals or antibiotics are being prescribed for a breast fungal infection or for mastitis, Dr. Murase underscored the importance of not stopping breastfeeding.
“The most important thing is that they continue to actually breastfeed on the affected breast that has the staph infection,” she said. She then reiterated that physicians should “reassure new mothers that the majority of oral and topical medications are safe.”
Dr. Murase disclosed serving on the advisory boards of Dermira, UCB, and Genzyme/Sanofi, and she has consulted for Ferndale and UpToDate.
CHICAGO – A common reason why a women stops breastfeeding is the use of medication her doctor has claimed is unsafe during lactation. But most drugs have little or no effect on an infant’s well-being or milk supply, explained Jenny Eileen Murase, MD, of Palo Alto (Calif.) Foundation Medical Group.
“The bottom line I want you to take away from this [session] is that ,” Dr. Murase told attendees at the American Academy of Dermatology summer meeting. “I really want everyone in this room to understand that most of the time, you should not be recommending that a woman is pumping and dumping her milk or stopping breastfeeding because she’s on an agent.”
Dr. Murase, also affiliated with the University of California, San Francisco, provided an overview of drug safety during lactation for major categories of medications that dermatologists prescribe. She recommended that physicians get a copy of Medications and Mother’s Milk by Thomas Hale, PhD, which she considers the best reference for looking up specific drugs. It categorizes drugs as L1 (safest) to L5 (contraindicated), and L2 as “safer,” L3 as “moderately safe,” and L4 as “possibly hazardous.”
Steroids
Contrary to what many believe, prednisone is not contraindicated in breastfeeding, Dr. Murase said. Instead of advising patients to “pump and dump their milk,” she said, “the only recommendation you need to make is that they wait 4 hours after taking the medicine to breastfeed.” For example, a mother can take prednisone before bed and then wake 4 hours later to nurse. Higher doses, such as more than 40 mg daily over long periods, may have the potential to affect growth and development, but more typical doses don’t pose the same risk.
Topical steroids (except for those that are class 1) also are safe to apply directly to the nipple in breastfeeding women, she noted.
Biologics and immunosuppressants
One of the few medications that are contraindicated are topical pimecrolimus and tacrolimus if applied directly to the nipple, since “oral consumption in the infant could be significant,” Dr. Murase said.
Biologics, on the other hand, are not a concern during lactation. “They have low oral bioavailability because of their large molecular size,” and are broken down in the stomach “in a proteolytic environment,” Dr. Murase explained. The CRADLE study, for example, examined the concentration of certolizumab (Cimzia) in mothers’ mature breast milk and found the highest concentration to be just 0.077 mcg/mL, resulting in an average daily infant dose of less than 0.01 mg/kg per day.
Antihistamines and cosmetic topicals
The major antihistamines – brompheniramine, chlorpheniramine, diphenhydramine, hydroxyzine, cetirizine, fexofenadine and loratadine – are likewise safe as L1-L3 drugs. It is preferable to prescribe nonsedating antihistamines, opting for loratadine as the first-line choice. But dermatologists should be reassured that no data support concerns about milk supply reduction from antihistamines, Dr. Murase said.
It’s best to avoid cosmetic topical products, but hydroquinone (L3), topical minoxidil (L2), and botulinum toxin A (L3) do not pose significant risk to the infant. Neither do the anesthetics lidocaine (L2) and epinephrine (L1) for breastfeeding women who need surgery.
Antibiotics
The vast majority of antibiotics are safe for women to use while breastfeeding, but a few notable exceptions exist, including erythromycin.
“People associate erythromycin as safe in lactation because it’s safe in pregnancy, but that’s not the case,” Dr. Murase pointed out. Erythromycin has been linked to pyloric stenosis in newborns and therefore should be avoided in the early months of breastfeeding. In older infants, however, erythromycin becomes an L1 medication.”
Tetracyclines fall into a borderline category. “Tetracyclines would be fine for a complicated infection,” but should not be used for more than 3 weeks, at which point they are regarded as L4, Dr. Murase said. “So long-term use of the tetracyclines should be avoided.”
Aside from these, topical antibiotics are considered safe. Women taking other oral antibiotics should be monitored for gastrointestinal symptoms or allergic responses.
Antifungals
As for antifungals, topicals are safe, and nystatin and clotrimazole are the best first-line options (both L1). Oral antifungals are similarly fine, with griseofulvin, fluconazole, ketoconazole, itraconazole, and terbinafine all classified as L2 and amphotericin B as L3.
If antifungals or antibiotics are being prescribed for a breast fungal infection or for mastitis, Dr. Murase underscored the importance of not stopping breastfeeding.
“The most important thing is that they continue to actually breastfeed on the affected breast that has the staph infection,” she said. She then reiterated that physicians should “reassure new mothers that the majority of oral and topical medications are safe.”
Dr. Murase disclosed serving on the advisory boards of Dermira, UCB, and Genzyme/Sanofi, and she has consulted for Ferndale and UpToDate.
CHICAGO – A common reason why a women stops breastfeeding is the use of medication her doctor has claimed is unsafe during lactation. But most drugs have little or no effect on an infant’s well-being or milk supply, explained Jenny Eileen Murase, MD, of Palo Alto (Calif.) Foundation Medical Group.
“The bottom line I want you to take away from this [session] is that ,” Dr. Murase told attendees at the American Academy of Dermatology summer meeting. “I really want everyone in this room to understand that most of the time, you should not be recommending that a woman is pumping and dumping her milk or stopping breastfeeding because she’s on an agent.”
Dr. Murase, also affiliated with the University of California, San Francisco, provided an overview of drug safety during lactation for major categories of medications that dermatologists prescribe. She recommended that physicians get a copy of Medications and Mother’s Milk by Thomas Hale, PhD, which she considers the best reference for looking up specific drugs. It categorizes drugs as L1 (safest) to L5 (contraindicated), and L2 as “safer,” L3 as “moderately safe,” and L4 as “possibly hazardous.”
Steroids
Contrary to what many believe, prednisone is not contraindicated in breastfeeding, Dr. Murase said. Instead of advising patients to “pump and dump their milk,” she said, “the only recommendation you need to make is that they wait 4 hours after taking the medicine to breastfeed.” For example, a mother can take prednisone before bed and then wake 4 hours later to nurse. Higher doses, such as more than 40 mg daily over long periods, may have the potential to affect growth and development, but more typical doses don’t pose the same risk.
Topical steroids (except for those that are class 1) also are safe to apply directly to the nipple in breastfeeding women, she noted.
Biologics and immunosuppressants
One of the few medications that are contraindicated are topical pimecrolimus and tacrolimus if applied directly to the nipple, since “oral consumption in the infant could be significant,” Dr. Murase said.
Biologics, on the other hand, are not a concern during lactation. “They have low oral bioavailability because of their large molecular size,” and are broken down in the stomach “in a proteolytic environment,” Dr. Murase explained. The CRADLE study, for example, examined the concentration of certolizumab (Cimzia) in mothers’ mature breast milk and found the highest concentration to be just 0.077 mcg/mL, resulting in an average daily infant dose of less than 0.01 mg/kg per day.
Antihistamines and cosmetic topicals
The major antihistamines – brompheniramine, chlorpheniramine, diphenhydramine, hydroxyzine, cetirizine, fexofenadine and loratadine – are likewise safe as L1-L3 drugs. It is preferable to prescribe nonsedating antihistamines, opting for loratadine as the first-line choice. But dermatologists should be reassured that no data support concerns about milk supply reduction from antihistamines, Dr. Murase said.
It’s best to avoid cosmetic topical products, but hydroquinone (L3), topical minoxidil (L2), and botulinum toxin A (L3) do not pose significant risk to the infant. Neither do the anesthetics lidocaine (L2) and epinephrine (L1) for breastfeeding women who need surgery.
Antibiotics
The vast majority of antibiotics are safe for women to use while breastfeeding, but a few notable exceptions exist, including erythromycin.
“People associate erythromycin as safe in lactation because it’s safe in pregnancy, but that’s not the case,” Dr. Murase pointed out. Erythromycin has been linked to pyloric stenosis in newborns and therefore should be avoided in the early months of breastfeeding. In older infants, however, erythromycin becomes an L1 medication.”
Tetracyclines fall into a borderline category. “Tetracyclines would be fine for a complicated infection,” but should not be used for more than 3 weeks, at which point they are regarded as L4, Dr. Murase said. “So long-term use of the tetracyclines should be avoided.”
Aside from these, topical antibiotics are considered safe. Women taking other oral antibiotics should be monitored for gastrointestinal symptoms or allergic responses.
Antifungals
As for antifungals, topicals are safe, and nystatin and clotrimazole are the best first-line options (both L1). Oral antifungals are similarly fine, with griseofulvin, fluconazole, ketoconazole, itraconazole, and terbinafine all classified as L2 and amphotericin B as L3.
If antifungals or antibiotics are being prescribed for a breast fungal infection or for mastitis, Dr. Murase underscored the importance of not stopping breastfeeding.
“The most important thing is that they continue to actually breastfeed on the affected breast that has the staph infection,” she said. She then reiterated that physicians should “reassure new mothers that the majority of oral and topical medications are safe.”
Dr. Murase disclosed serving on the advisory boards of Dermira, UCB, and Genzyme/Sanofi, and she has consulted for Ferndale and UpToDate.
EXPERT ANALYSIS FROM SUMMER AAD 2018
ESMO 2018 to highlight research on advanced breast cancer
Oncology Practice will have on-site reporters in Munich covering the European Society for Medical Oncology 2018 Congress, held October 19-23.
A total of 2,051 abstracts will be presented, covering the latest in immunotherapy, technologies of the future, biomarkers, basic and translational research, and prevention, according to an ESMO press release.
Results from four studies on advanced breast cancer will be featured in the first presidential symposium:
- LBA1 – Results of IMpassion130: Results from a global, randomized, double-blind, phase 3 study of atezolizumab + nab-paclitaxel vs. placebo + nab-paclitaxel in treatment-naive locally advanced or metastatic triple-negative breast cancer.
- LBA2 – Analyses from PALOMA-3: Overall survival with palbociclib plus fulvestrant in women with hormone receptor–positive, human epidermal growth factor receptor 2–negative advanced breast cancer.
- LBA3 – Results of the phase 3 SOLAR-1 trial: Alpelisib + fulvestrant for advanced breast cancer.
- 283O PR – Results of the phase 3 trial: Chidamide, a subtype-selective histone deacetylase inhibitor, in combination with exemestane in patients with hormone receptor–positive advanced breast cancer.
Additional late-breaking plenary sessions will cover research on alectinib vs. crizotinib for treatment-naive anaplastic lymphoma kinase positive advanced non–small cell lung cancer, avelumab + axitinib vs. sunitinib as first-line treatment of advanced renal cell carcinoma, and a poly ADP-ribose polymerase inhibitor for maintenance therapy in advanced ovarian cancer
.
Oncology Practice will have on-site reporters in Munich covering the European Society for Medical Oncology 2018 Congress, held October 19-23.
A total of 2,051 abstracts will be presented, covering the latest in immunotherapy, technologies of the future, biomarkers, basic and translational research, and prevention, according to an ESMO press release.
Results from four studies on advanced breast cancer will be featured in the first presidential symposium:
- LBA1 – Results of IMpassion130: Results from a global, randomized, double-blind, phase 3 study of atezolizumab + nab-paclitaxel vs. placebo + nab-paclitaxel in treatment-naive locally advanced or metastatic triple-negative breast cancer.
- LBA2 – Analyses from PALOMA-3: Overall survival with palbociclib plus fulvestrant in women with hormone receptor–positive, human epidermal growth factor receptor 2–negative advanced breast cancer.
- LBA3 – Results of the phase 3 SOLAR-1 trial: Alpelisib + fulvestrant for advanced breast cancer.
- 283O PR – Results of the phase 3 trial: Chidamide, a subtype-selective histone deacetylase inhibitor, in combination with exemestane in patients with hormone receptor–positive advanced breast cancer.
Additional late-breaking plenary sessions will cover research on alectinib vs. crizotinib for treatment-naive anaplastic lymphoma kinase positive advanced non–small cell lung cancer, avelumab + axitinib vs. sunitinib as first-line treatment of advanced renal cell carcinoma, and a poly ADP-ribose polymerase inhibitor for maintenance therapy in advanced ovarian cancer
.
Oncology Practice will have on-site reporters in Munich covering the European Society for Medical Oncology 2018 Congress, held October 19-23.
A total of 2,051 abstracts will be presented, covering the latest in immunotherapy, technologies of the future, biomarkers, basic and translational research, and prevention, according to an ESMO press release.
Results from four studies on advanced breast cancer will be featured in the first presidential symposium:
- LBA1 – Results of IMpassion130: Results from a global, randomized, double-blind, phase 3 study of atezolizumab + nab-paclitaxel vs. placebo + nab-paclitaxel in treatment-naive locally advanced or metastatic triple-negative breast cancer.
- LBA2 – Analyses from PALOMA-3: Overall survival with palbociclib plus fulvestrant in women with hormone receptor–positive, human epidermal growth factor receptor 2–negative advanced breast cancer.
- LBA3 – Results of the phase 3 SOLAR-1 trial: Alpelisib + fulvestrant for advanced breast cancer.
- 283O PR – Results of the phase 3 trial: Chidamide, a subtype-selective histone deacetylase inhibitor, in combination with exemestane in patients with hormone receptor–positive advanced breast cancer.
Additional late-breaking plenary sessions will cover research on alectinib vs. crizotinib for treatment-naive anaplastic lymphoma kinase positive advanced non–small cell lung cancer, avelumab + axitinib vs. sunitinib as first-line treatment of advanced renal cell carcinoma, and a poly ADP-ribose polymerase inhibitor for maintenance therapy in advanced ovarian cancer
.
New secondary fracture–prevention recommendations carry simple messages
Ensuring that older adults who have experienced a hip or vertebral fracture understand they likely have osteoporosis, and offering prompt drug treatment for the condition, are among five fundamental
The recommendations were announced at the annual meeting of the American Society for Bone and Mineral Research (ASBMR) in Montreal. The 40-member group that developed the recommendations, called the ASBMR Secondary Fracture Prevention Initiative Coalition, includes the American Association of Clinical Endocrinologists/American College of Endocrinology, the Endocrine Society, the American College of Rheumatology, the American College of Physicians, the American Geriatrics Society, the American Academy of Physical Medicine and Rehabilitation, and the American Academy of Orthopaedic Surgeons.
Additional fundamental recommendations from the Coalition advised ensuring that patients’ primary health care providers are aware of the fracture, regularly assessing the risk of falls, and routinely reevaluating patients who are being treated for osteoporosis. These suggestions were developed in response to growing evidence of a rising trend in osteoporosis patients not being prescribed appropriate medications or not taking them, the ASBMR said.
“The very simple message is if you’ve got somebody who has had a hip fracture or a vertebral fracture, that needs secondary prevention just like somebody who’s had an MI needs to be on a statin and a beta blocker,” said coalition cochair Sundeep Khosla, MD, a past president of the ASBMR and director of the Center for Clinical and Translational Science at the Mayo Clinic, Rochester, Minn. “You can’t ignore the fracture because it’s not immediately life-threatening. Down the road they’re going to have another hip fracture if nothing is done.”
Only 23% of elderly patients who have a hip fracture receive osteoporosis medication to reduce future fracture risk, according to the ASBMR. A 30-year downward trend in the number of hip fractures in the United States has recently plateaued, raising concerns this may have been caused by doctors and patients not following diagnostic and treatment guidelines, the organization noted.
The reasons for the plateau are uncertain, Dr. Khosla said, but could include a reluctance by patients to take bisphosphonates following some reports of relatively rare side effects, such as atypical femoral fractures and osteonecrosis of the jaw. In addition, he said, reimbursement for dual-energy x-ray absorptiometry (DEXA) scans to measure bone mineral density has gone down, which has led to fewer osteoporosis diagnoses. But fracture prevention is important, he said. Of the 300,000 hip fractures in the United States each year, one of every two patients never regains their previous functioning. In addition, one of every four hip fracture patients ends up in a nursing home or dies within a year, according to the ASBMR.
The recommendations and more data about osteoporosis treatment are available on the coalition’s website, www.secondaryfractures.org. An action plan for clinicians should be added to the site sometime this fall, Dr. Khosla said.
There are five fundamental recommendations:
First, communicate three simple messages to patients and their family/caregivers throughout the fracture care and healing process. These include: Their broken bone likely means they have osteoporosis and are at high risk for breaking more bones; breaking bones means they may have to use a walker, cane, or wheelchair or move from their home to a residential facility and will be at higher risk for premature death; and there are actions they can take to reduce their risk.

This is key, said coalition cochair Douglas P. Kiel, MD, a past president of ASBMR, the director of the Musculoskeletal Research Center at the Institute for Aging Research at Hebrew SeniorLife in Boston, and a professor of medicine at Harvard Medical School, also in Boston.
“If you talk to people who have had a broken bone, they view this as an accident and not that they have anything wrong with them,” he said. “The communication should be that if you broke something, it is not a random, chance event. You have osteoporosis, and if you don’t do anything about it, you’re going to be at great risk of a life-threatening, independence-threatening fracture in the future.”
Second, ensure the patient’s primary health care provider is made aware of the occurrence of the fracture. Take action to be sure the communication is made.
Third, regularly assess the risk of falling in women and men age 65 years or older who have had a hip or vertebral fracture. At minimum, take a history of falls within the last year, minimize the use of medications associated with increased risk for falls, evaluate patients for conditions associated with an increased risk for falls, and strongly consider referring patients to physical and/or occupational therapy or a physiatrist for evaluation and interventions to improve impairments in mobility, gait, and balance to reduce the risk for falls.
Fourth, reduce the risk of additional fractures by offering pharmacologic therapy for osteoporosis to women and men age 65 years or older who have had a hip or vertebral fracture. This can begin in the hospital and be included in discharge orders. Do not delay initiation of therapy for bone mineral density (BMD) testing. Consider patients’ oral health before starting therapy with bisphosphonates or denosumab (Prolia).
Most hip fracture patients leave the hospital without osteoporosis medications, Dr. Kiel said. It could be that hospital-based physicians are concerned patients are still unsteady such that they may not want to start patients on a new medication when they’re discharging them. Physicians in rehabilitation units may not prescribe these medications because they feel they have the patients for a short time, so by the time the patient returns to their primary care provider, the patient may have the same mistaken impression the fracture was an accident.
“We’re advocating not to delay treatment for any of these care transitions or because you think they need a BMD test,” Dr. Kiel said. “Just get them treated like they do with heart attacks.”
Finally, follow and reevaluate women and men age 65 years or older who have had a hip or vertebral fracture and are being treated for osteoporosis because it is a life-long chronic condition. This can help reinforce key messages about osteoporosis and associated fractures, identify any barriers to treatment adherence, assess the risk of falls, evaluate the effectiveness of a treatment plan, monitor for adverse effects, and determine whether any changes in treatment should be made, including whether any osteoporosis pharmacotherapy should be changed or discontinued.
Ideally, patients should be managed in the context of a multidisciplinary clinical system that includes case management, such as a fracture liaison service, according to the recommendations.
Besides the fundamental five recommendations, the documents lists another seven that deal with referring patients, prescribing vitamin D, counseling on lifestyle and diet, discussing pharmacotherapy benefits and risks, weighing first-line therapy options, and determining the duration of pharmacotherapy.
Ensuring that older adults who have experienced a hip or vertebral fracture understand they likely have osteoporosis, and offering prompt drug treatment for the condition, are among five fundamental
The recommendations were announced at the annual meeting of the American Society for Bone and Mineral Research (ASBMR) in Montreal. The 40-member group that developed the recommendations, called the ASBMR Secondary Fracture Prevention Initiative Coalition, includes the American Association of Clinical Endocrinologists/American College of Endocrinology, the Endocrine Society, the American College of Rheumatology, the American College of Physicians, the American Geriatrics Society, the American Academy of Physical Medicine and Rehabilitation, and the American Academy of Orthopaedic Surgeons.
Additional fundamental recommendations from the Coalition advised ensuring that patients’ primary health care providers are aware of the fracture, regularly assessing the risk of falls, and routinely reevaluating patients who are being treated for osteoporosis. These suggestions were developed in response to growing evidence of a rising trend in osteoporosis patients not being prescribed appropriate medications or not taking them, the ASBMR said.
“The very simple message is if you’ve got somebody who has had a hip fracture or a vertebral fracture, that needs secondary prevention just like somebody who’s had an MI needs to be on a statin and a beta blocker,” said coalition cochair Sundeep Khosla, MD, a past president of the ASBMR and director of the Center for Clinical and Translational Science at the Mayo Clinic, Rochester, Minn. “You can’t ignore the fracture because it’s not immediately life-threatening. Down the road they’re going to have another hip fracture if nothing is done.”
Only 23% of elderly patients who have a hip fracture receive osteoporosis medication to reduce future fracture risk, according to the ASBMR. A 30-year downward trend in the number of hip fractures in the United States has recently plateaued, raising concerns this may have been caused by doctors and patients not following diagnostic and treatment guidelines, the organization noted.
The reasons for the plateau are uncertain, Dr. Khosla said, but could include a reluctance by patients to take bisphosphonates following some reports of relatively rare side effects, such as atypical femoral fractures and osteonecrosis of the jaw. In addition, he said, reimbursement for dual-energy x-ray absorptiometry (DEXA) scans to measure bone mineral density has gone down, which has led to fewer osteoporosis diagnoses. But fracture prevention is important, he said. Of the 300,000 hip fractures in the United States each year, one of every two patients never regains their previous functioning. In addition, one of every four hip fracture patients ends up in a nursing home or dies within a year, according to the ASBMR.
The recommendations and more data about osteoporosis treatment are available on the coalition’s website, www.secondaryfractures.org. An action plan for clinicians should be added to the site sometime this fall, Dr. Khosla said.
There are five fundamental recommendations:
First, communicate three simple messages to patients and their family/caregivers throughout the fracture care and healing process. These include: Their broken bone likely means they have osteoporosis and are at high risk for breaking more bones; breaking bones means they may have to use a walker, cane, or wheelchair or move from their home to a residential facility and will be at higher risk for premature death; and there are actions they can take to reduce their risk.
This is key, said coalition cochair Douglas P. Kiel, MD, a past president of ASBMR, the director of the Musculoskeletal Research Center at the Institute for Aging Research at Hebrew SeniorLife in Boston, and a professor of medicine at Harvard Medical School, also in Boston.
“If you talk to people who have had a broken bone, they view this as an accident and not that they have anything wrong with them,” he said. “The communication should be that if you broke something, it is not a random, chance event. You have osteoporosis, and if you don’t do anything about it, you’re going to be at great risk of a life-threatening, independence-threatening fracture in the future.”
Second, ensure the patient’s primary health care provider is made aware of the occurrence of the fracture. Take action to be sure the communication is made.
Third, regularly assess the risk of falling in women and men age 65 years or older who have had a hip or vertebral fracture. At minimum, take a history of falls within the last year, minimize the use of medications associated with increased risk for falls, evaluate patients for conditions associated with an increased risk for falls, and strongly consider referring patients to physical and/or occupational therapy or a physiatrist for evaluation and interventions to improve impairments in mobility, gait, and balance to reduce the risk for falls.
Fourth, reduce the risk of additional fractures by offering pharmacologic therapy for osteoporosis to women and men age 65 years or older who have had a hip or vertebral fracture. This can begin in the hospital and be included in discharge orders. Do not delay initiation of therapy for bone mineral density (BMD) testing. Consider patients’ oral health before starting therapy with bisphosphonates or denosumab (Prolia).
Most hip fracture patients leave the hospital without osteoporosis medications, Dr. Kiel said. It could be that hospital-based physicians are concerned patients are still unsteady such that they may not want to start patients on a new medication when they’re discharging them. Physicians in rehabilitation units may not prescribe these medications because they feel they have the patients for a short time, so by the time the patient returns to their primary care provider, the patient may have the same mistaken impression the fracture was an accident.
“We’re advocating not to delay treatment for any of these care transitions or because you think they need a BMD test,” Dr. Kiel said. “Just get them treated like they do with heart attacks.”
Finally, follow and reevaluate women and men age 65 years or older who have had a hip or vertebral fracture and are being treated for osteoporosis because it is a life-long chronic condition. This can help reinforce key messages about osteoporosis and associated fractures, identify any barriers to treatment adherence, assess the risk of falls, evaluate the effectiveness of a treatment plan, monitor for adverse effects, and determine whether any changes in treatment should be made, including whether any osteoporosis pharmacotherapy should be changed or discontinued.
Ideally, patients should be managed in the context of a multidisciplinary clinical system that includes case management, such as a fracture liaison service, according to the recommendations.
Besides the fundamental five recommendations, the documents lists another seven that deal with referring patients, prescribing vitamin D, counseling on lifestyle and diet, discussing pharmacotherapy benefits and risks, weighing first-line therapy options, and determining the duration of pharmacotherapy.
Ensuring that older adults who have experienced a hip or vertebral fracture understand they likely have osteoporosis, and offering prompt drug treatment for the condition, are among five fundamental
The recommendations were announced at the annual meeting of the American Society for Bone and Mineral Research (ASBMR) in Montreal. The 40-member group that developed the recommendations, called the ASBMR Secondary Fracture Prevention Initiative Coalition, includes the American Association of Clinical Endocrinologists/American College of Endocrinology, the Endocrine Society, the American College of Rheumatology, the American College of Physicians, the American Geriatrics Society, the American Academy of Physical Medicine and Rehabilitation, and the American Academy of Orthopaedic Surgeons.
Additional fundamental recommendations from the Coalition advised ensuring that patients’ primary health care providers are aware of the fracture, regularly assessing the risk of falls, and routinely reevaluating patients who are being treated for osteoporosis. These suggestions were developed in response to growing evidence of a rising trend in osteoporosis patients not being prescribed appropriate medications or not taking them, the ASBMR said.
“The very simple message is if you’ve got somebody who has had a hip fracture or a vertebral fracture, that needs secondary prevention just like somebody who’s had an MI needs to be on a statin and a beta blocker,” said coalition cochair Sundeep Khosla, MD, a past president of the ASBMR and director of the Center for Clinical and Translational Science at the Mayo Clinic, Rochester, Minn. “You can’t ignore the fracture because it’s not immediately life-threatening. Down the road they’re going to have another hip fracture if nothing is done.”
Only 23% of elderly patients who have a hip fracture receive osteoporosis medication to reduce future fracture risk, according to the ASBMR. A 30-year downward trend in the number of hip fractures in the United States has recently plateaued, raising concerns this may have been caused by doctors and patients not following diagnostic and treatment guidelines, the organization noted.
The reasons for the plateau are uncertain, Dr. Khosla said, but could include a reluctance by patients to take bisphosphonates following some reports of relatively rare side effects, such as atypical femoral fractures and osteonecrosis of the jaw. In addition, he said, reimbursement for dual-energy x-ray absorptiometry (DEXA) scans to measure bone mineral density has gone down, which has led to fewer osteoporosis diagnoses. But fracture prevention is important, he said. Of the 300,000 hip fractures in the United States each year, one of every two patients never regains their previous functioning. In addition, one of every four hip fracture patients ends up in a nursing home or dies within a year, according to the ASBMR.
The recommendations and more data about osteoporosis treatment are available on the coalition’s website, www.secondaryfractures.org. An action plan for clinicians should be added to the site sometime this fall, Dr. Khosla said.
There are five fundamental recommendations:
First, communicate three simple messages to patients and their family/caregivers throughout the fracture care and healing process. These include: Their broken bone likely means they have osteoporosis and are at high risk for breaking more bones; breaking bones means they may have to use a walker, cane, or wheelchair or move from their home to a residential facility and will be at higher risk for premature death; and there are actions they can take to reduce their risk.
This is key, said coalition cochair Douglas P. Kiel, MD, a past president of ASBMR, the director of the Musculoskeletal Research Center at the Institute for Aging Research at Hebrew SeniorLife in Boston, and a professor of medicine at Harvard Medical School, also in Boston.
“If you talk to people who have had a broken bone, they view this as an accident and not that they have anything wrong with them,” he said. “The communication should be that if you broke something, it is not a random, chance event. You have osteoporosis, and if you don’t do anything about it, you’re going to be at great risk of a life-threatening, independence-threatening fracture in the future.”
Second, ensure the patient’s primary health care provider is made aware of the occurrence of the fracture. Take action to be sure the communication is made.
Third, regularly assess the risk of falling in women and men age 65 years or older who have had a hip or vertebral fracture. At minimum, take a history of falls within the last year, minimize the use of medications associated with increased risk for falls, evaluate patients for conditions associated with an increased risk for falls, and strongly consider referring patients to physical and/or occupational therapy or a physiatrist for evaluation and interventions to improve impairments in mobility, gait, and balance to reduce the risk for falls.
Fourth, reduce the risk of additional fractures by offering pharmacologic therapy for osteoporosis to women and men age 65 years or older who have had a hip or vertebral fracture. This can begin in the hospital and be included in discharge orders. Do not delay initiation of therapy for bone mineral density (BMD) testing. Consider patients’ oral health before starting therapy with bisphosphonates or denosumab (Prolia).
Most hip fracture patients leave the hospital without osteoporosis medications, Dr. Kiel said. It could be that hospital-based physicians are concerned patients are still unsteady such that they may not want to start patients on a new medication when they’re discharging them. Physicians in rehabilitation units may not prescribe these medications because they feel they have the patients for a short time, so by the time the patient returns to their primary care provider, the patient may have the same mistaken impression the fracture was an accident.
“We’re advocating not to delay treatment for any of these care transitions or because you think they need a BMD test,” Dr. Kiel said. “Just get them treated like they do with heart attacks.”
Finally, follow and reevaluate women and men age 65 years or older who have had a hip or vertebral fracture and are being treated for osteoporosis because it is a life-long chronic condition. This can help reinforce key messages about osteoporosis and associated fractures, identify any barriers to treatment adherence, assess the risk of falls, evaluate the effectiveness of a treatment plan, monitor for adverse effects, and determine whether any changes in treatment should be made, including whether any osteoporosis pharmacotherapy should be changed or discontinued.
Ideally, patients should be managed in the context of a multidisciplinary clinical system that includes case management, such as a fracture liaison service, according to the recommendations.
Besides the fundamental five recommendations, the documents lists another seven that deal with referring patients, prescribing vitamin D, counseling on lifestyle and diet, discussing pharmacotherapy benefits and risks, weighing first-line therapy options, and determining the duration of pharmacotherapy.
EXPERT ANALYSIS FROM ASBMR 2018
Modeling favors immediate AED after unprovoked first seizure
including those who are at low risk of recurrent seizures, results of a decision analysis suggest.
Taking into account quality of life, seizure risk, and antiepileptic drug (AED) side effects, the model favored treatment of a patient with a single unprovoked seizure who did not meet the International League Against Epilepsy (ILAE) definition of epilepsy, investigators reported.
The model also favored treatment of patients who did meet ILAE criteria, namely, a 10-year recurrence risk greater than 60% in a patients with a single unprovoked seizure, according to their report in Neurology.
Together, these findings suggest that the current ILAE epilepsy definition is “too simplistic” for deciding whether to start or withhold AED treatment after a first unprovoked seizure, said M. Brandon Westover, MD, PhD, of the department of neurology, Massachusetts General Hospital, Boston, and his coauthors in their report.
“A more precise and patient-personalized definition of epilepsy should encompass not only seizure recurrence probability but also a multitude of other risks and benefits associated with AED treatment,” they said in a discussion of their study results.
To determine which patients with a first unprovoked seizure might benefit from immediate AED treatment, Dr. Westover and his colleagues used a decision model with measures constructed from retrospective clinical trial data.
The goal of the simulation was to determine which treatment strategy – immediate or delayed AED – would maximize the patient’s expected quality-adjusted life years (QALYs). Toward that end, Dr. Westover and his coinvestigators considered three base cases, which represented various degrees of seizure-recurrence risk.
The first base case was a 30-year-old man with no other risk factors for recurrent seizure, other than having had a first seizure. In that case, immediate and deferred AED treatment resulted in 19.04 and 18.65 QALYs, respectively.
“In dollar values, using the conservative approximation of $50,000/QALY gained, this difference in treatment outcomes would amount to $19,500 gained per individual,” Dr. Westover and his coauthors wrote in their report.
The second case was a 30-year-old woman who presented with a first unprovoked seizure and had positive MRI results that establish a high risk of recurrence. As expected, because of the high recurrence risk, this scenario also favored immediate treatment, with 15.23 and 14.75 QALYs, respectively, for the immediate and deferred strategies.
The final case was a wheelchair-bound 60-year-old woman with a first unprovoked seizure and high risk of recurrence, but also a high risk of AED adverse effects and a smaller expected quality of life reduction from further seizures. In this scenario, in which treatment might be “intuitively discouraged” because of the AED side-effect risk, the cohort simulation indeed favored deferred AED treatment by a small margin, the investigators said.
“A high baseline risk for recurrent seizures does not by itself always favor immediate AED treatment,” they wrote.
The study was supported by the National Institutes of Health-National Institute of Neurological Disorders and Stroke. Dr. Westover and his coauthors had no relevant disclosures to report.
SOURCE: Bao EL et al. Neurology. 2018 Sep 12. pii: 10.1212/WNL.0000000000006319.
The conclusion of this decision analysis by Bao and colleagues is “likely correct” that early treatment of a first unprovoked seizure could be favorable in a wide range of clinical scenarios, according to authors of an accompanying editorial.
The decision analysis is based on a reasonable though not comprehensive set of parameters to simulate base cases representative of common first-ever seizure clinical scenarios, Claire S. Jacobs, MD, PhD, and Jong Woo Lee, MD, PhD, said in the editorial.
Potentially the most controversial scenario addressed in the decision model, they noted, is the patient with low seizure recurrence risk but substantial quality of life decline upon recurrence. While that patient would not meet the commonly accepted 60% recurrence risk threshold that would indicate treatment is warranted, this model favors immediate treatment because of the potentially disruptive effect of recurrence.
This study does not address important issues such as the cost of medication and patient preferences, they pointed out, and furthermore, quality-adjusted life years (QALYs) can be difficult to integrate into clinical decision making.
Nonetheless, the findings are worth considering in clinical practice, authors suggested. “At the very least, this study should, however subtly, shift the starting point of discussion with the patient toward a default of immediate, rather than deferred, treatment after a first unprovoked seizure and apparent absence of disease,” they wrote.
Claire S. Jacobs, MD, PhD, and Jong Woo Lee, MD, PhD , are with department of neurology, Brigham and Women’s Hospital, Boston. Their editorial appeared in Neurology . Dr. Jacobs reported being partially supported by NIH/National Institute of Neurological Disorders and Stroke and is an inventor on patents related to synthesis and use of DNA-binding small molecules targeted to transcription factor–binding sites. Dr. Lee reported that he has received prior NIH funding, has served on the scientific advisory board of Lundbeck, has done contract work for SleepMed/DigiTrace and Advance Medical.
The conclusion of this decision analysis by Bao and colleagues is “likely correct” that early treatment of a first unprovoked seizure could be favorable in a wide range of clinical scenarios, according to authors of an accompanying editorial.
The decision analysis is based on a reasonable though not comprehensive set of parameters to simulate base cases representative of common first-ever seizure clinical scenarios, Claire S. Jacobs, MD, PhD, and Jong Woo Lee, MD, PhD, said in the editorial.
Potentially the most controversial scenario addressed in the decision model, they noted, is the patient with low seizure recurrence risk but substantial quality of life decline upon recurrence. While that patient would not meet the commonly accepted 60% recurrence risk threshold that would indicate treatment is warranted, this model favors immediate treatment because of the potentially disruptive effect of recurrence.
This study does not address important issues such as the cost of medication and patient preferences, they pointed out, and furthermore, quality-adjusted life years (QALYs) can be difficult to integrate into clinical decision making.
Nonetheless, the findings are worth considering in clinical practice, authors suggested. “At the very least, this study should, however subtly, shift the starting point of discussion with the patient toward a default of immediate, rather than deferred, treatment after a first unprovoked seizure and apparent absence of disease,” they wrote.
Claire S. Jacobs, MD, PhD, and Jong Woo Lee, MD, PhD , are with department of neurology, Brigham and Women’s Hospital, Boston. Their editorial appeared in Neurology . Dr. Jacobs reported being partially supported by NIH/National Institute of Neurological Disorders and Stroke and is an inventor on patents related to synthesis and use of DNA-binding small molecules targeted to transcription factor–binding sites. Dr. Lee reported that he has received prior NIH funding, has served on the scientific advisory board of Lundbeck, has done contract work for SleepMed/DigiTrace and Advance Medical.
The conclusion of this decision analysis by Bao and colleagues is “likely correct” that early treatment of a first unprovoked seizure could be favorable in a wide range of clinical scenarios, according to authors of an accompanying editorial.
The decision analysis is based on a reasonable though not comprehensive set of parameters to simulate base cases representative of common first-ever seizure clinical scenarios, Claire S. Jacobs, MD, PhD, and Jong Woo Lee, MD, PhD, said in the editorial.
Potentially the most controversial scenario addressed in the decision model, they noted, is the patient with low seizure recurrence risk but substantial quality of life decline upon recurrence. While that patient would not meet the commonly accepted 60% recurrence risk threshold that would indicate treatment is warranted, this model favors immediate treatment because of the potentially disruptive effect of recurrence.
This study does not address important issues such as the cost of medication and patient preferences, they pointed out, and furthermore, quality-adjusted life years (QALYs) can be difficult to integrate into clinical decision making.
Nonetheless, the findings are worth considering in clinical practice, authors suggested. “At the very least, this study should, however subtly, shift the starting point of discussion with the patient toward a default of immediate, rather than deferred, treatment after a first unprovoked seizure and apparent absence of disease,” they wrote.
Claire S. Jacobs, MD, PhD, and Jong Woo Lee, MD, PhD , are with department of neurology, Brigham and Women’s Hospital, Boston. Their editorial appeared in Neurology . Dr. Jacobs reported being partially supported by NIH/National Institute of Neurological Disorders and Stroke and is an inventor on patents related to synthesis and use of DNA-binding small molecules targeted to transcription factor–binding sites. Dr. Lee reported that he has received prior NIH funding, has served on the scientific advisory board of Lundbeck, has done contract work for SleepMed/DigiTrace and Advance Medical.
including those who are at low risk of recurrent seizures, results of a decision analysis suggest.
Taking into account quality of life, seizure risk, and antiepileptic drug (AED) side effects, the model favored treatment of a patient with a single unprovoked seizure who did not meet the International League Against Epilepsy (ILAE) definition of epilepsy, investigators reported.
The model also favored treatment of patients who did meet ILAE criteria, namely, a 10-year recurrence risk greater than 60% in a patients with a single unprovoked seizure, according to their report in Neurology.
Together, these findings suggest that the current ILAE epilepsy definition is “too simplistic” for deciding whether to start or withhold AED treatment after a first unprovoked seizure, said M. Brandon Westover, MD, PhD, of the department of neurology, Massachusetts General Hospital, Boston, and his coauthors in their report.
“A more precise and patient-personalized definition of epilepsy should encompass not only seizure recurrence probability but also a multitude of other risks and benefits associated with AED treatment,” they said in a discussion of their study results.
To determine which patients with a first unprovoked seizure might benefit from immediate AED treatment, Dr. Westover and his colleagues used a decision model with measures constructed from retrospective clinical trial data.
The goal of the simulation was to determine which treatment strategy – immediate or delayed AED – would maximize the patient’s expected quality-adjusted life years (QALYs). Toward that end, Dr. Westover and his coinvestigators considered three base cases, which represented various degrees of seizure-recurrence risk.
The first base case was a 30-year-old man with no other risk factors for recurrent seizure, other than having had a first seizure. In that case, immediate and deferred AED treatment resulted in 19.04 and 18.65 QALYs, respectively.
“In dollar values, using the conservative approximation of $50,000/QALY gained, this difference in treatment outcomes would amount to $19,500 gained per individual,” Dr. Westover and his coauthors wrote in their report.
The second case was a 30-year-old woman who presented with a first unprovoked seizure and had positive MRI results that establish a high risk of recurrence. As expected, because of the high recurrence risk, this scenario also favored immediate treatment, with 15.23 and 14.75 QALYs, respectively, for the immediate and deferred strategies.
The final case was a wheelchair-bound 60-year-old woman with a first unprovoked seizure and high risk of recurrence, but also a high risk of AED adverse effects and a smaller expected quality of life reduction from further seizures. In this scenario, in which treatment might be “intuitively discouraged” because of the AED side-effect risk, the cohort simulation indeed favored deferred AED treatment by a small margin, the investigators said.
“A high baseline risk for recurrent seizures does not by itself always favor immediate AED treatment,” they wrote.
The study was supported by the National Institutes of Health-National Institute of Neurological Disorders and Stroke. Dr. Westover and his coauthors had no relevant disclosures to report.
SOURCE: Bao EL et al. Neurology. 2018 Sep 12. pii: 10.1212/WNL.0000000000006319.
including those who are at low risk of recurrent seizures, results of a decision analysis suggest.
Taking into account quality of life, seizure risk, and antiepileptic drug (AED) side effects, the model favored treatment of a patient with a single unprovoked seizure who did not meet the International League Against Epilepsy (ILAE) definition of epilepsy, investigators reported.
The model also favored treatment of patients who did meet ILAE criteria, namely, a 10-year recurrence risk greater than 60% in a patients with a single unprovoked seizure, according to their report in Neurology.
Together, these findings suggest that the current ILAE epilepsy definition is “too simplistic” for deciding whether to start or withhold AED treatment after a first unprovoked seizure, said M. Brandon Westover, MD, PhD, of the department of neurology, Massachusetts General Hospital, Boston, and his coauthors in their report.
“A more precise and patient-personalized definition of epilepsy should encompass not only seizure recurrence probability but also a multitude of other risks and benefits associated with AED treatment,” they said in a discussion of their study results.
To determine which patients with a first unprovoked seizure might benefit from immediate AED treatment, Dr. Westover and his colleagues used a decision model with measures constructed from retrospective clinical trial data.
The goal of the simulation was to determine which treatment strategy – immediate or delayed AED – would maximize the patient’s expected quality-adjusted life years (QALYs). Toward that end, Dr. Westover and his coinvestigators considered three base cases, which represented various degrees of seizure-recurrence risk.
The first base case was a 30-year-old man with no other risk factors for recurrent seizure, other than having had a first seizure. In that case, immediate and deferred AED treatment resulted in 19.04 and 18.65 QALYs, respectively.
“In dollar values, using the conservative approximation of $50,000/QALY gained, this difference in treatment outcomes would amount to $19,500 gained per individual,” Dr. Westover and his coauthors wrote in their report.
The second case was a 30-year-old woman who presented with a first unprovoked seizure and had positive MRI results that establish a high risk of recurrence. As expected, because of the high recurrence risk, this scenario also favored immediate treatment, with 15.23 and 14.75 QALYs, respectively, for the immediate and deferred strategies.
The final case was a wheelchair-bound 60-year-old woman with a first unprovoked seizure and high risk of recurrence, but also a high risk of AED adverse effects and a smaller expected quality of life reduction from further seizures. In this scenario, in which treatment might be “intuitively discouraged” because of the AED side-effect risk, the cohort simulation indeed favored deferred AED treatment by a small margin, the investigators said.
“A high baseline risk for recurrent seizures does not by itself always favor immediate AED treatment,” they wrote.
The study was supported by the National Institutes of Health-National Institute of Neurological Disorders and Stroke. Dr. Westover and his coauthors had no relevant disclosures to report.
SOURCE: Bao EL et al. Neurology. 2018 Sep 12. pii: 10.1212/WNL.0000000000006319.
FROM NEUROLOGY
Key clinical point: Based on quality-adjusted life years (QALYs), immediate treatment of a first unprovoked seizure may be preferable to delayed treatment over a wide range of patients, including those who are at low risk of recurrent seizures.
Major finding: In a base case of a first unprovoked seizure and no other risk factors for recurrent seizure, immediate, and deferred antiepileptic drug treatment resulted in 19.04 and 18.65 QALYs, respectively.
Study details: A simulated clinical trial using decision analysis modeling, which included three base cases representing various degrees of seizure recurrence risk.
Disclosures: The study was supported by the National Institute of Neurological Disorders and Stroke. Study authors had no relevant disclosures to report.
Source: Bao EL et al. Neurology. 2018 Sep 12. pii: 10.1212/WNL.0000000000006319.
SSRIs linked to reduced height in risperidone-treated boys
according to results of an analysis reported in The Journal of Pediatrics.
The inverse association between SSRI use and height was particularly notable in boys undergoing puberty, according to the authors of the retrospective study. Follow-up into adulthood will be needed to see if the effects are reversible or have a negative impact on adult height.
“In the meantime, clinicians should continue to closely monitor children and adolescents starting antidepressant treatment to minimize side effects,” said Chadi A. Calarge, MD, of Baylor College of Medicine, Houston, and his coauthors.
These observations by Dr. Calarge and his colleagues were based on an analysis of 267 boys, of whom 190 had been treated with SSRIs. The boys had been in one of four previous studies, three of which included risperidone treatment for at least 6 or 12 months, and one small longitudinal observational study including children who had initiated risperidone in the month prior to enrollment. All four studies excluded subjects with chronic medical or neurologic conditions and those taking more than one antipsychotic medication.
Use of an SSRI was associated with reduced growth in height, particularly among boys in Tanner stages 3 and 4. “This effect is of a moderate magnitude of about 1 cm for every 1 year of treatment with SSRIs during adolescence,” Dr. Calarge and his coauthors said.
Among boys who took SSRIs continuously, the strongest inverse association with height z scores was in boys in Tanner stages 3 and 4 (r = –0.69; P less than .009). By contrast, this correlation was “negligible” in boys in Tanner stage 1 and stage 5, and there were only 5 boys of Tanner stage 2 in this analysis, the investigators said.
The mechanism by which SSRIs may have an effect on longitudinal growth has not been well investigated, according to Dr. Calarge and his coauthors. “Impaired growth hormone secretion or activity has been implicated, given that SSRIs alter serotonin signaling, which is known to control GH secretion.”
Funding for the study came from the National Institutes of Health, and other grants. One study coauthor reported funding support from Pfizer and Aeterna Zentaris.
SOURCE: Calarge CA et al. J Pediatr. 2018 Oct;201:245-51.
Although results of this secondary analysis require confirmation, they do underscore the need to consider how “complex combinations” of psychotropic agents may affect growth and development, according to Philip S. Zeitler, MD, PhD.
Such combinations are increasingly seen in the management of behavioral disorders in children and adolescents, Dr. Zeitler noted in a commentary on the findings by Calarge et al.
While side effects are well described for individual drugs used to treat youths with complex mental and behavioral disorders, the potential for side effects particular to combinations of these drugs are less well understood, he said.
The present study shows that in risperidone-treated youth, SSRI use was associated with decreased longitudinal growth. The estimated decrease of 1 cm per year of exposure to SSRIs suggests “a potentially significant decrease in adult height for peripubertal youth who are treated for many years,” according to the author.
“Unlike with stimulants, the decreased longitudinal growth was not associated with suppression of weight gain, suggesting an independent effect of SSRIs on growth during puberty,” he added.
Dr. Zeitler, of Aurora, Colo., is on the editorial board of The Journal of Pediatrics. His commentary on this study appeared in the October 2018 issue (J Pediatr. 2018;201:3). Dr. Zeitler also serves on the editorial board of the Journal of Clinical Endocrinology & Metabolism and Current Diabetes Reports, and is the editor-in-chief of Pediatric Diabetes. He reported serving on the data and safety monitoring board for Tolmar Pharmaceuticals, and serving as a consultant for Daiichi Sankyo, Merck, Boehringer-Ingelheim, and Janssen Pharmaceuticals.
Although results of this secondary analysis require confirmation, they do underscore the need to consider how “complex combinations” of psychotropic agents may affect growth and development, according to Philip S. Zeitler, MD, PhD.
Such combinations are increasingly seen in the management of behavioral disorders in children and adolescents, Dr. Zeitler noted in a commentary on the findings by Calarge et al.
While side effects are well described for individual drugs used to treat youths with complex mental and behavioral disorders, the potential for side effects particular to combinations of these drugs are less well understood, he said.
The present study shows that in risperidone-treated youth, SSRI use was associated with decreased longitudinal growth. The estimated decrease of 1 cm per year of exposure to SSRIs suggests “a potentially significant decrease in adult height for peripubertal youth who are treated for many years,” according to the author.
“Unlike with stimulants, the decreased longitudinal growth was not associated with suppression of weight gain, suggesting an independent effect of SSRIs on growth during puberty,” he added.
Dr. Zeitler, of Aurora, Colo., is on the editorial board of The Journal of Pediatrics. His commentary on this study appeared in the October 2018 issue (J Pediatr. 2018;201:3). Dr. Zeitler also serves on the editorial board of the Journal of Clinical Endocrinology & Metabolism and Current Diabetes Reports, and is the editor-in-chief of Pediatric Diabetes. He reported serving on the data and safety monitoring board for Tolmar Pharmaceuticals, and serving as a consultant for Daiichi Sankyo, Merck, Boehringer-Ingelheim, and Janssen Pharmaceuticals.
Although results of this secondary analysis require confirmation, they do underscore the need to consider how “complex combinations” of psychotropic agents may affect growth and development, according to Philip S. Zeitler, MD, PhD.
Such combinations are increasingly seen in the management of behavioral disorders in children and adolescents, Dr. Zeitler noted in a commentary on the findings by Calarge et al.
While side effects are well described for individual drugs used to treat youths with complex mental and behavioral disorders, the potential for side effects particular to combinations of these drugs are less well understood, he said.
The present study shows that in risperidone-treated youth, SSRI use was associated with decreased longitudinal growth. The estimated decrease of 1 cm per year of exposure to SSRIs suggests “a potentially significant decrease in adult height for peripubertal youth who are treated for many years,” according to the author.
“Unlike with stimulants, the decreased longitudinal growth was not associated with suppression of weight gain, suggesting an independent effect of SSRIs on growth during puberty,” he added.
Dr. Zeitler, of Aurora, Colo., is on the editorial board of The Journal of Pediatrics. His commentary on this study appeared in the October 2018 issue (J Pediatr. 2018;201:3). Dr. Zeitler also serves on the editorial board of the Journal of Clinical Endocrinology & Metabolism and Current Diabetes Reports, and is the editor-in-chief of Pediatric Diabetes. He reported serving on the data and safety monitoring board for Tolmar Pharmaceuticals, and serving as a consultant for Daiichi Sankyo, Merck, Boehringer-Ingelheim, and Janssen Pharmaceuticals.
according to results of an analysis reported in The Journal of Pediatrics.
The inverse association between SSRI use and height was particularly notable in boys undergoing puberty, according to the authors of the retrospective study. Follow-up into adulthood will be needed to see if the effects are reversible or have a negative impact on adult height.
“In the meantime, clinicians should continue to closely monitor children and adolescents starting antidepressant treatment to minimize side effects,” said Chadi A. Calarge, MD, of Baylor College of Medicine, Houston, and his coauthors.
These observations by Dr. Calarge and his colleagues were based on an analysis of 267 boys, of whom 190 had been treated with SSRIs. The boys had been in one of four previous studies, three of which included risperidone treatment for at least 6 or 12 months, and one small longitudinal observational study including children who had initiated risperidone in the month prior to enrollment. All four studies excluded subjects with chronic medical or neurologic conditions and those taking more than one antipsychotic medication.
Use of an SSRI was associated with reduced growth in height, particularly among boys in Tanner stages 3 and 4. “This effect is of a moderate magnitude of about 1 cm for every 1 year of treatment with SSRIs during adolescence,” Dr. Calarge and his coauthors said.
Among boys who took SSRIs continuously, the strongest inverse association with height z scores was in boys in Tanner stages 3 and 4 (r = –0.69; P less than .009). By contrast, this correlation was “negligible” in boys in Tanner stage 1 and stage 5, and there were only 5 boys of Tanner stage 2 in this analysis, the investigators said.
The mechanism by which SSRIs may have an effect on longitudinal growth has not been well investigated, according to Dr. Calarge and his coauthors. “Impaired growth hormone secretion or activity has been implicated, given that SSRIs alter serotonin signaling, which is known to control GH secretion.”
Funding for the study came from the National Institutes of Health, and other grants. One study coauthor reported funding support from Pfizer and Aeterna Zentaris.
SOURCE: Calarge CA et al. J Pediatr. 2018 Oct;201:245-51.
according to results of an analysis reported in The Journal of Pediatrics.
The inverse association between SSRI use and height was particularly notable in boys undergoing puberty, according to the authors of the retrospective study. Follow-up into adulthood will be needed to see if the effects are reversible or have a negative impact on adult height.
“In the meantime, clinicians should continue to closely monitor children and adolescents starting antidepressant treatment to minimize side effects,” said Chadi A. Calarge, MD, of Baylor College of Medicine, Houston, and his coauthors.
These observations by Dr. Calarge and his colleagues were based on an analysis of 267 boys, of whom 190 had been treated with SSRIs. The boys had been in one of four previous studies, three of which included risperidone treatment for at least 6 or 12 months, and one small longitudinal observational study including children who had initiated risperidone in the month prior to enrollment. All four studies excluded subjects with chronic medical or neurologic conditions and those taking more than one antipsychotic medication.
Use of an SSRI was associated with reduced growth in height, particularly among boys in Tanner stages 3 and 4. “This effect is of a moderate magnitude of about 1 cm for every 1 year of treatment with SSRIs during adolescence,” Dr. Calarge and his coauthors said.
Among boys who took SSRIs continuously, the strongest inverse association with height z scores was in boys in Tanner stages 3 and 4 (r = –0.69; P less than .009). By contrast, this correlation was “negligible” in boys in Tanner stage 1 and stage 5, and there were only 5 boys of Tanner stage 2 in this analysis, the investigators said.
The mechanism by which SSRIs may have an effect on longitudinal growth has not been well investigated, according to Dr. Calarge and his coauthors. “Impaired growth hormone secretion or activity has been implicated, given that SSRIs alter serotonin signaling, which is known to control GH secretion.”
Funding for the study came from the National Institutes of Health, and other grants. One study coauthor reported funding support from Pfizer and Aeterna Zentaris.
SOURCE: Calarge CA et al. J Pediatr. 2018 Oct;201:245-51.
FROM THE JOURNAL OF PEDIATRICS
Key clinical point: Among risperidone-treated boys, use of SSRIs was linked to reduced longitudinal growth, according to results of an analysis.
Major finding: The strongest inverse association between continuous SSRI use and height z scores was in boys in Tanner stages 3 and 4 (r = −0.69; P less than .009).
Study details: Retrospective analysis of 267 boys enrolled in four previous studies evaluating risperidone use.
Disclosures: Funding for the study came from the National Institutes of Health and other grants. One study coauthor reported funding support from Pfizer and Aeterna Zentaris.
Source: Calarge CA et al. J Pediatr. 2018;201:245-51.
Rosacea likely underdiagnosed, suboptimally treated in skin of color
in this population, according to the authors of a clinical review article on the topic.

“Current reports of rosacea in patients with skin of color may point to a large pool of undiagnosed patients,” said Andrew F. Alexis, MD, chairman of the department of dermatology, Mount Sinai St. Luke’s and Mount Sinai West, New York, and his coauthors.
Increased awareness of rosacea in these patients may reduce disparities in disease management, they wrote in the review, published in the Journal of the American Academy of Dermatology, which outlines strategies for timely diagnosis and effective treatment of rosacea in skin of color.
The erroneous perception that rosacea does not occur in skin of color may arise from epidemiologic reports, which frequently position it as a disease that occurs in fair-skinned individuals of Northern European or Celtic background, they said.
The reported prevalence of rosacea in skin of color varies worldwide and is as high as 10%, according to the authors. Moreover, a recent U.S. medical care survey found that 3.9% of rosacea patients were Hispanic or Latino, 2.3% were Asian or Pacific Islander, and 2% were black.

A low index of suspicion for rosacea in skin of color may lead to delayed diagnosis, and consequently, advanced disease that could include disfigurement with disease progression (such as rhinophyma and otophyma) and, in the case of ocular disease, loss of sight, Dr. Alexis and his coauthors pointed out.
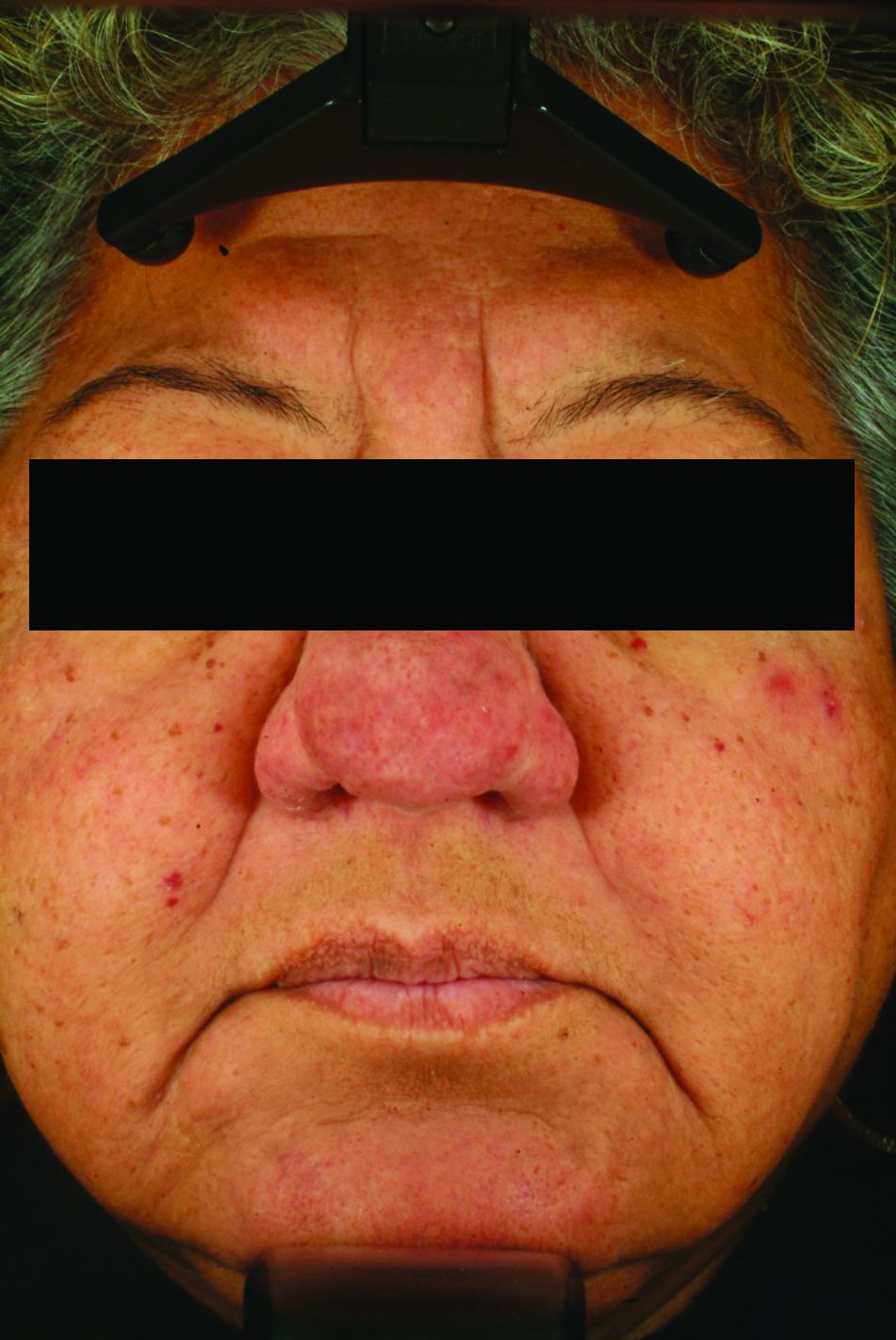
One clinical aspect of rosacea in skin of color is that persistent facial erythema is less frequently reported than are papules and pustules. That may be due to the difficulty of visualizing erythema in darker skin, they suggested, noting that the postinflammatory hyperpigmentation that is more common in skin of color could also mask erythema.
A rosacea variant seen more often in these patients is the granulomatous subtype, which may not present with flushing, persistent erythema, or other typical rosacea signs, they pointed out.
One key to accurately diagnosing rosacea in skin of color is the patient’s own observations, such as whether they experience flushing or a warm sensation in the face, according to the authors, who said patients may report stinging or burning with certain skin care products.
Dr. Alexis and his coauthors said they have tried various strategies to assess dark skin for erythema and telangiectasia. Photographing subjects on a dark-blue background may better highlight any redness, they said, while using a dermatoscope may help differentiate skin pigment from blood vessels.
A magnifying glass or microscope slide can be used to test skin for blanching: “If the skin pales when pressed under the glass or slide, erythema is present,” they wrote.

Although data on treatment of rosacea in skin of color is limited, the general treatment approach is similar to that of lighter skin and may include topical and oral therapies, laser or light-based treatment, or surgery. “Patients with skin of color may have unique clinical features that need to be addressed during the treatment of rosacea, such as postinflammatory pigment alteration or risk of developing this complication with laser/light-based therapies,” they noted.
In the review, they referred to a few studies of oral or topical treatments that suggest similar benefits in Fitzpatrick skin phototypes I-III (lighter) and IV-VI (darker) that the authors describe in their review.
Allergan sponsored development of the paper, which was developed with editorial assistance from Peloton Advantage. Dr. Alexis and his coauthors provided disclosures related to Allergan, BioPharmx, Galderma, Bayer, Beiersdorf, Croma-Pharma, Aclaris, and Unilever.
SOURCE: Alexis AF et al. J Am Acad Dermatol. 2018 Sep 18. pii: S0190-9622(18)32576-3. doi: 10.1016/j.jaad.2018.08.049.
in this population, according to the authors of a clinical review article on the topic.
“Current reports of rosacea in patients with skin of color may point to a large pool of undiagnosed patients,” said Andrew F. Alexis, MD, chairman of the department of dermatology, Mount Sinai St. Luke’s and Mount Sinai West, New York, and his coauthors.
Increased awareness of rosacea in these patients may reduce disparities in disease management, they wrote in the review, published in the Journal of the American Academy of Dermatology, which outlines strategies for timely diagnosis and effective treatment of rosacea in skin of color.
The erroneous perception that rosacea does not occur in skin of color may arise from epidemiologic reports, which frequently position it as a disease that occurs in fair-skinned individuals of Northern European or Celtic background, they said.
The reported prevalence of rosacea in skin of color varies worldwide and is as high as 10%, according to the authors. Moreover, a recent U.S. medical care survey found that 3.9% of rosacea patients were Hispanic or Latino, 2.3% were Asian or Pacific Islander, and 2% were black.
A low index of suspicion for rosacea in skin of color may lead to delayed diagnosis, and consequently, advanced disease that could include disfigurement with disease progression (such as rhinophyma and otophyma) and, in the case of ocular disease, loss of sight, Dr. Alexis and his coauthors pointed out.
One clinical aspect of rosacea in skin of color is that persistent facial erythema is less frequently reported than are papules and pustules. That may be due to the difficulty of visualizing erythema in darker skin, they suggested, noting that the postinflammatory hyperpigmentation that is more common in skin of color could also mask erythema.
A rosacea variant seen more often in these patients is the granulomatous subtype, which may not present with flushing, persistent erythema, or other typical rosacea signs, they pointed out.
One key to accurately diagnosing rosacea in skin of color is the patient’s own observations, such as whether they experience flushing or a warm sensation in the face, according to the authors, who said patients may report stinging or burning with certain skin care products.
Dr. Alexis and his coauthors said they have tried various strategies to assess dark skin for erythema and telangiectasia. Photographing subjects on a dark-blue background may better highlight any redness, they said, while using a dermatoscope may help differentiate skin pigment from blood vessels.
A magnifying glass or microscope slide can be used to test skin for blanching: “If the skin pales when pressed under the glass or slide, erythema is present,” they wrote.
Although data on treatment of rosacea in skin of color is limited, the general treatment approach is similar to that of lighter skin and may include topical and oral therapies, laser or light-based treatment, or surgery. “Patients with skin of color may have unique clinical features that need to be addressed during the treatment of rosacea, such as postinflammatory pigment alteration or risk of developing this complication with laser/light-based therapies,” they noted.
In the review, they referred to a few studies of oral or topical treatments that suggest similar benefits in Fitzpatrick skin phototypes I-III (lighter) and IV-VI (darker) that the authors describe in their review.
Allergan sponsored development of the paper, which was developed with editorial assistance from Peloton Advantage. Dr. Alexis and his coauthors provided disclosures related to Allergan, BioPharmx, Galderma, Bayer, Beiersdorf, Croma-Pharma, Aclaris, and Unilever.
SOURCE: Alexis AF et al. J Am Acad Dermatol. 2018 Sep 18. pii: S0190-9622(18)32576-3. doi: 10.1016/j.jaad.2018.08.049.
in this population, according to the authors of a clinical review article on the topic.
“Current reports of rosacea in patients with skin of color may point to a large pool of undiagnosed patients,” said Andrew F. Alexis, MD, chairman of the department of dermatology, Mount Sinai St. Luke’s and Mount Sinai West, New York, and his coauthors.
Increased awareness of rosacea in these patients may reduce disparities in disease management, they wrote in the review, published in the Journal of the American Academy of Dermatology, which outlines strategies for timely diagnosis and effective treatment of rosacea in skin of color.
The erroneous perception that rosacea does not occur in skin of color may arise from epidemiologic reports, which frequently position it as a disease that occurs in fair-skinned individuals of Northern European or Celtic background, they said.
The reported prevalence of rosacea in skin of color varies worldwide and is as high as 10%, according to the authors. Moreover, a recent U.S. medical care survey found that 3.9% of rosacea patients were Hispanic or Latino, 2.3% were Asian or Pacific Islander, and 2% were black.
A low index of suspicion for rosacea in skin of color may lead to delayed diagnosis, and consequently, advanced disease that could include disfigurement with disease progression (such as rhinophyma and otophyma) and, in the case of ocular disease, loss of sight, Dr. Alexis and his coauthors pointed out.
One clinical aspect of rosacea in skin of color is that persistent facial erythema is less frequently reported than are papules and pustules. That may be due to the difficulty of visualizing erythema in darker skin, they suggested, noting that the postinflammatory hyperpigmentation that is more common in skin of color could also mask erythema.
A rosacea variant seen more often in these patients is the granulomatous subtype, which may not present with flushing, persistent erythema, or other typical rosacea signs, they pointed out.
One key to accurately diagnosing rosacea in skin of color is the patient’s own observations, such as whether they experience flushing or a warm sensation in the face, according to the authors, who said patients may report stinging or burning with certain skin care products.
Dr. Alexis and his coauthors said they have tried various strategies to assess dark skin for erythema and telangiectasia. Photographing subjects on a dark-blue background may better highlight any redness, they said, while using a dermatoscope may help differentiate skin pigment from blood vessels.
A magnifying glass or microscope slide can be used to test skin for blanching: “If the skin pales when pressed under the glass or slide, erythema is present,” they wrote.
Although data on treatment of rosacea in skin of color is limited, the general treatment approach is similar to that of lighter skin and may include topical and oral therapies, laser or light-based treatment, or surgery. “Patients with skin of color may have unique clinical features that need to be addressed during the treatment of rosacea, such as postinflammatory pigment alteration or risk of developing this complication with laser/light-based therapies,” they noted.
In the review, they referred to a few studies of oral or topical treatments that suggest similar benefits in Fitzpatrick skin phototypes I-III (lighter) and IV-VI (darker) that the authors describe in their review.
Allergan sponsored development of the paper, which was developed with editorial assistance from Peloton Advantage. Dr. Alexis and his coauthors provided disclosures related to Allergan, BioPharmx, Galderma, Bayer, Beiersdorf, Croma-Pharma, Aclaris, and Unilever.
SOURCE: Alexis AF et al. J Am Acad Dermatol. 2018 Sep 18. pii: S0190-9622(18)32576-3. doi: 10.1016/j.jaad.2018.08.049.
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
‘Twincreatin’ produces ‘impressive’ HbA1c, weight control in T2DM
BERLIN – Patients with type 2 diabetes mellitus (T2DM) achieved “impressive” drops in glycated hemoglobin, or HbA1c, of up to 2.4% and in body weight of up to 11.3 kg with the investigational drug LY3298176 in a phase 2b trial.

The primary endpoint was the change in HbA1c at 26 weeks, which showed significant reductions from baseline of 1.6%, 2%, and 2.4% for the 5-mg, 10-mg, and 15-mg doses, respectively, of the drug tested. By comparison, a drop of just 1.1% was seen for dulaglutide, and 0.1% for placebo.
The higher doses of LY3298176, which is a dual agonist of glucose-dependent insulinotropic polypeptide (GIP) and the glucagonlike peptide–1 (GLP-1) receptor, used in the trial helped up to 90% of patients achieve an HbA1c of 7% or less, 82% of patients to achieve an HbA1c of 6.5% or less, and up to 30% of patients to achieve an HbA1c of less than 5.7%, a range which is considered normal for people without diabetes.
As for weight loss, the 5-mg, 10-mg, and 15-mg doses of LY3298176 helped patients achieve significant –4.8-kg, –8.7-kg, and –11.3-kg changes from baseline, respectively. These were greater than those seen with dulaglutide (–2.7 kg) and placebo (–0.4 kg).
More than one third of patients treated with the novel drug achieved at least a 10% or more change in their starting body weight, with a quarter of patients on the 15-mg dose achieving a 15% or more change in bodyweight.
“These are very, very impressive data both from an A1c-lowering perspective and also from a weight reduction perspective,” said the study’s principal investigator Juan Frias, MD, at a press briefing held at the annual meeting of the European Association for the Study of Diabetes (EASD).
GLP-1 receptor agonist therapy is a recommended treatment for T2DM because it addresses many of the important pathophysiologic problems, from blood glucose control and weight loss to reducing cardiovascular risk, Dr. Frias observed.
He added that the first GLP-1 receptor agonists became available in the United States in 2005. Their use in T2DM has recently been further endorsed in a consensus report (Diabetes Care. 2018 Sep. doi: rg/10.2337/dci18-0033; Diabetologia. 2018. doi: 10.1007/s00125-018-4729-5) issued jointly by the American Diabetes Association and the EASD.
“Despite the potency of these agents, many of our patients are not achieving adequate glycemic or weight control, so we could always use new agents that are more potent as long as they’re safe for the patient,” said Dr. Frias, who is a clinical endocrinologist and the chief executive officer at the National Research Institute in Los Angeles
LY3298176 is a novel unimolecular, multifunctional peptide that is being developed by Eli Lilly as a dual GIP/GLP-1 receptor agonist for the treatment of T2DM. It consists of 39 amino acids linked to a C20 fatty–diacid moiety and has a mean half-life of around 5 days, which means it can be dosed weekly, Dr. Frias observed.
The effect of targeting both GIP and the GLP-1 receptor simultaneously is possibly both additive and complementary, Dr. Frias suggested. Additive effects may include a decrease in food intake and an increase in insulin secretion, with opposing effects on glucagon secretion, with the additional effects of increased glucose uptake with GIP and delayed gastric emptying with GLP-1 receptor agonism.

“When you think back on what the history, biology, and discovery of these compounds was, it isn’t at all obvious you’d pair these two [to make] a so-called ‘twincreatin’ – there is so much overlap,” said Matthias Tschöp, MD, who was invited to discuss the findings after the presentation at the EASD meeting.
Dr. Tschöp, who is the head of the division of neuroendocrinology at the Institute for Diabetes and Obesity at Helmholtz Zentrum München in Neuherberg , Germany, noted that it’s an interesting combination, but it’s not the only approach being tested – there are other twincretin combinations. GIP on its own doesn’t seem to do much, but it must be the combination that is important, it was suggested during discussion.
A total of 318 patients with T2DM and a starting HbA1c of 7%-10.5% were studied and randomized equally to one of six weekly treatment groups: LY3298176 at doses of either 1 mg, 5 mg, 10 mg, or 15 mg, given subcutaneously; 1.5 mg of dulaglutide; or a placebo injection.
The two highest doses of LY3298176 were titrated rather quickly, Dr. Frias said, and this is important when it comes to the side effect profile. In a subsequent study, the dose titration schedule was amended to prolong the titration period to try to avoid some of the side effects seen, according to Dr. Frias.
Adverse events predominantly affected the gastrointestinal system, with any grade nausea, vomiting, and diarrhea seen in a respective 20%-40%, 7%-26%, and 24%-32% of patients taking the 5-mg, 10-mg, and 15-mg doses. Corresponding rates in dulaglutide-treated patients were, approximately, 30%, 9%, and 17%.
“The safety profile of the dual agonist is really similar to that which you see with selective GLP-1 receptor agonists,” Dr. Frias observed. “The most common adverse events were seen at the higher doses and pertained to GI tolerability, but the majority of these events were mild to moderate and dissipated with time and [could] be reduced significantly by appropriate titration.”
Dr. Frias said: “This novel dual GIP/GLP-1 receptor agonist certainly has the potential to be become a very promising treatment option for patients with type 2 diabetes.”
He added: “In my experience as an investigator, as a clinician, I’ve never really seen this magnitude of A1c reduction in this percentage of patients and also with this level of weight loss as well, certainly greater than with a selective GLP-1 receptor agonist.”
Further long-term studies are needed, and the phase 3 program in T2DM will be called SURPASS, according to a press statement issued by Eli Lilly. The phase 3 studies are expected to begin “no later than early 2019,” the statement said, and be completed in late 2021. The drug company also noted that it is “evaluating next steps in the study of GIP/GLP-1 RA for obesity and other conditions.”
SOURCE: Frias JP et al. EASD 2018, Session S31; Frias JP et al. Lancet. 2018 Oct 4. doi: 10.1016/S0140-6736(18)32260-8.
BERLIN – Patients with type 2 diabetes mellitus (T2DM) achieved “impressive” drops in glycated hemoglobin, or HbA1c, of up to 2.4% and in body weight of up to 11.3 kg with the investigational drug LY3298176 in a phase 2b trial.
The primary endpoint was the change in HbA1c at 26 weeks, which showed significant reductions from baseline of 1.6%, 2%, and 2.4% for the 5-mg, 10-mg, and 15-mg doses, respectively, of the drug tested. By comparison, a drop of just 1.1% was seen for dulaglutide, and 0.1% for placebo.
The higher doses of LY3298176, which is a dual agonist of glucose-dependent insulinotropic polypeptide (GIP) and the glucagonlike peptide–1 (GLP-1) receptor, used in the trial helped up to 90% of patients achieve an HbA1c of 7% or less, 82% of patients to achieve an HbA1c of 6.5% or less, and up to 30% of patients to achieve an HbA1c of less than 5.7%, a range which is considered normal for people without diabetes.
As for weight loss, the 5-mg, 10-mg, and 15-mg doses of LY3298176 helped patients achieve significant –4.8-kg, –8.7-kg, and –11.3-kg changes from baseline, respectively. These were greater than those seen with dulaglutide (–2.7 kg) and placebo (–0.4 kg).
More than one third of patients treated with the novel drug achieved at least a 10% or more change in their starting body weight, with a quarter of patients on the 15-mg dose achieving a 15% or more change in bodyweight.
“These are very, very impressive data both from an A1c-lowering perspective and also from a weight reduction perspective,” said the study’s principal investigator Juan Frias, MD, at a press briefing held at the annual meeting of the European Association for the Study of Diabetes (EASD).
GLP-1 receptor agonist therapy is a recommended treatment for T2DM because it addresses many of the important pathophysiologic problems, from blood glucose control and weight loss to reducing cardiovascular risk, Dr. Frias observed.
He added that the first GLP-1 receptor agonists became available in the United States in 2005. Their use in T2DM has recently been further endorsed in a consensus report (Diabetes Care. 2018 Sep. doi: rg/10.2337/dci18-0033; Diabetologia. 2018. doi: 10.1007/s00125-018-4729-5) issued jointly by the American Diabetes Association and the EASD.
“Despite the potency of these agents, many of our patients are not achieving adequate glycemic or weight control, so we could always use new agents that are more potent as long as they’re safe for the patient,” said Dr. Frias, who is a clinical endocrinologist and the chief executive officer at the National Research Institute in Los Angeles
LY3298176 is a novel unimolecular, multifunctional peptide that is being developed by Eli Lilly as a dual GIP/GLP-1 receptor agonist for the treatment of T2DM. It consists of 39 amino acids linked to a C20 fatty–diacid moiety and has a mean half-life of around 5 days, which means it can be dosed weekly, Dr. Frias observed.
The effect of targeting both GIP and the GLP-1 receptor simultaneously is possibly both additive and complementary, Dr. Frias suggested. Additive effects may include a decrease in food intake and an increase in insulin secretion, with opposing effects on glucagon secretion, with the additional effects of increased glucose uptake with GIP and delayed gastric emptying with GLP-1 receptor agonism.
“When you think back on what the history, biology, and discovery of these compounds was, it isn’t at all obvious you’d pair these two [to make] a so-called ‘twincreatin’ – there is so much overlap,” said Matthias Tschöp, MD, who was invited to discuss the findings after the presentation at the EASD meeting.
Dr. Tschöp, who is the head of the division of neuroendocrinology at the Institute for Diabetes and Obesity at Helmholtz Zentrum München in Neuherberg , Germany, noted that it’s an interesting combination, but it’s not the only approach being tested – there are other twincretin combinations. GIP on its own doesn’t seem to do much, but it must be the combination that is important, it was suggested during discussion.
A total of 318 patients with T2DM and a starting HbA1c of 7%-10.5% were studied and randomized equally to one of six weekly treatment groups: LY3298176 at doses of either 1 mg, 5 mg, 10 mg, or 15 mg, given subcutaneously; 1.5 mg of dulaglutide; or a placebo injection.
The two highest doses of LY3298176 were titrated rather quickly, Dr. Frias said, and this is important when it comes to the side effect profile. In a subsequent study, the dose titration schedule was amended to prolong the titration period to try to avoid some of the side effects seen, according to Dr. Frias.
Adverse events predominantly affected the gastrointestinal system, with any grade nausea, vomiting, and diarrhea seen in a respective 20%-40%, 7%-26%, and 24%-32% of patients taking the 5-mg, 10-mg, and 15-mg doses. Corresponding rates in dulaglutide-treated patients were, approximately, 30%, 9%, and 17%.
“The safety profile of the dual agonist is really similar to that which you see with selective GLP-1 receptor agonists,” Dr. Frias observed. “The most common adverse events were seen at the higher doses and pertained to GI tolerability, but the majority of these events were mild to moderate and dissipated with time and [could] be reduced significantly by appropriate titration.”
Dr. Frias said: “This novel dual GIP/GLP-1 receptor agonist certainly has the potential to be become a very promising treatment option for patients with type 2 diabetes.”
He added: “In my experience as an investigator, as a clinician, I’ve never really seen this magnitude of A1c reduction in this percentage of patients and also with this level of weight loss as well, certainly greater than with a selective GLP-1 receptor agonist.”
Further long-term studies are needed, and the phase 3 program in T2DM will be called SURPASS, according to a press statement issued by Eli Lilly. The phase 3 studies are expected to begin “no later than early 2019,” the statement said, and be completed in late 2021. The drug company also noted that it is “evaluating next steps in the study of GIP/GLP-1 RA for obesity and other conditions.”
SOURCE: Frias JP et al. EASD 2018, Session S31; Frias JP et al. Lancet. 2018 Oct 4. doi: 10.1016/S0140-6736(18)32260-8.
BERLIN – Patients with type 2 diabetes mellitus (T2DM) achieved “impressive” drops in glycated hemoglobin, or HbA1c, of up to 2.4% and in body weight of up to 11.3 kg with the investigational drug LY3298176 in a phase 2b trial.
The primary endpoint was the change in HbA1c at 26 weeks, which showed significant reductions from baseline of 1.6%, 2%, and 2.4% for the 5-mg, 10-mg, and 15-mg doses, respectively, of the drug tested. By comparison, a drop of just 1.1% was seen for dulaglutide, and 0.1% for placebo.
The higher doses of LY3298176, which is a dual agonist of glucose-dependent insulinotropic polypeptide (GIP) and the glucagonlike peptide–1 (GLP-1) receptor, used in the trial helped up to 90% of patients achieve an HbA1c of 7% or less, 82% of patients to achieve an HbA1c of 6.5% or less, and up to 30% of patients to achieve an HbA1c of less than 5.7%, a range which is considered normal for people without diabetes.
As for weight loss, the 5-mg, 10-mg, and 15-mg doses of LY3298176 helped patients achieve significant –4.8-kg, –8.7-kg, and –11.3-kg changes from baseline, respectively. These were greater than those seen with dulaglutide (–2.7 kg) and placebo (–0.4 kg).
More than one third of patients treated with the novel drug achieved at least a 10% or more change in their starting body weight, with a quarter of patients on the 15-mg dose achieving a 15% or more change in bodyweight.
“These are very, very impressive data both from an A1c-lowering perspective and also from a weight reduction perspective,” said the study’s principal investigator Juan Frias, MD, at a press briefing held at the annual meeting of the European Association for the Study of Diabetes (EASD).
GLP-1 receptor agonist therapy is a recommended treatment for T2DM because it addresses many of the important pathophysiologic problems, from blood glucose control and weight loss to reducing cardiovascular risk, Dr. Frias observed.
He added that the first GLP-1 receptor agonists became available in the United States in 2005. Their use in T2DM has recently been further endorsed in a consensus report (Diabetes Care. 2018 Sep. doi: rg/10.2337/dci18-0033; Diabetologia. 2018. doi: 10.1007/s00125-018-4729-5) issued jointly by the American Diabetes Association and the EASD.
“Despite the potency of these agents, many of our patients are not achieving adequate glycemic or weight control, so we could always use new agents that are more potent as long as they’re safe for the patient,” said Dr. Frias, who is a clinical endocrinologist and the chief executive officer at the National Research Institute in Los Angeles
LY3298176 is a novel unimolecular, multifunctional peptide that is being developed by Eli Lilly as a dual GIP/GLP-1 receptor agonist for the treatment of T2DM. It consists of 39 amino acids linked to a C20 fatty–diacid moiety and has a mean half-life of around 5 days, which means it can be dosed weekly, Dr. Frias observed.
The effect of targeting both GIP and the GLP-1 receptor simultaneously is possibly both additive and complementary, Dr. Frias suggested. Additive effects may include a decrease in food intake and an increase in insulin secretion, with opposing effects on glucagon secretion, with the additional effects of increased glucose uptake with GIP and delayed gastric emptying with GLP-1 receptor agonism.
“When you think back on what the history, biology, and discovery of these compounds was, it isn’t at all obvious you’d pair these two [to make] a so-called ‘twincreatin’ – there is so much overlap,” said Matthias Tschöp, MD, who was invited to discuss the findings after the presentation at the EASD meeting.
Dr. Tschöp, who is the head of the division of neuroendocrinology at the Institute for Diabetes and Obesity at Helmholtz Zentrum München in Neuherberg , Germany, noted that it’s an interesting combination, but it’s not the only approach being tested – there are other twincretin combinations. GIP on its own doesn’t seem to do much, but it must be the combination that is important, it was suggested during discussion.
A total of 318 patients with T2DM and a starting HbA1c of 7%-10.5% were studied and randomized equally to one of six weekly treatment groups: LY3298176 at doses of either 1 mg, 5 mg, 10 mg, or 15 mg, given subcutaneously; 1.5 mg of dulaglutide; or a placebo injection.
The two highest doses of LY3298176 were titrated rather quickly, Dr. Frias said, and this is important when it comes to the side effect profile. In a subsequent study, the dose titration schedule was amended to prolong the titration period to try to avoid some of the side effects seen, according to Dr. Frias.
Adverse events predominantly affected the gastrointestinal system, with any grade nausea, vomiting, and diarrhea seen in a respective 20%-40%, 7%-26%, and 24%-32% of patients taking the 5-mg, 10-mg, and 15-mg doses. Corresponding rates in dulaglutide-treated patients were, approximately, 30%, 9%, and 17%.
“The safety profile of the dual agonist is really similar to that which you see with selective GLP-1 receptor agonists,” Dr. Frias observed. “The most common adverse events were seen at the higher doses and pertained to GI tolerability, but the majority of these events were mild to moderate and dissipated with time and [could] be reduced significantly by appropriate titration.”
Dr. Frias said: “This novel dual GIP/GLP-1 receptor agonist certainly has the potential to be become a very promising treatment option for patients with type 2 diabetes.”
He added: “In my experience as an investigator, as a clinician, I’ve never really seen this magnitude of A1c reduction in this percentage of patients and also with this level of weight loss as well, certainly greater than with a selective GLP-1 receptor agonist.”
Further long-term studies are needed, and the phase 3 program in T2DM will be called SURPASS, according to a press statement issued by Eli Lilly. The phase 3 studies are expected to begin “no later than early 2019,” the statement said, and be completed in late 2021. The drug company also noted that it is “evaluating next steps in the study of GIP/GLP-1 RA for obesity and other conditions.”
SOURCE: Frias JP et al. EASD 2018, Session S31; Frias JP et al. Lancet. 2018 Oct 4. doi: 10.1016/S0140-6736(18)32260-8.
REPORTING FROM EASD 2018
Key clinical point: The investigational dual GIP/GLP-1 receptor agonist LY3298176 could prove to be a promising treatment for T2DM.
Major finding: HbA1c fell by up to 2.4%, and body weight reduced by up to 11.3 kg depending on the dose tested.
Study details: A 26-week, phase 2b, double-blind, placebo-controlled study of 318 subjects with T2DM and a starting HbA1c of 7%-10.5%.
Disclosures: The study was funded by Eli Lilly. The presenting author Dr. Frias declared receiving research support and consulting honorarium from the company, as well as from multiple other pharmaceutical companies. The commentator Dr. Tschöp disclosed being a scientific advisory board member of ERX Pharmaceuticals.
Sources: Frias JP et al. EASD 2018, Session S31; Frias JP et al. Lancet. 2018 Oct 4. doi: 10.1016/S0140-6736(18)32260-8.
For surgeons, 1 on-call night equals 3 sleep-disrupted nights
SAN DIEGO – Almost 70% of surgeons who pull in-house call duty may be sleep deprived, Jamie Jones Coleman, MD, said at the annual meeting of the American Association for the Surgery of Trauma.

Even extra sleep the night after call doesn’t even things out, said Dr. Coleman of the University of Colorado, Denver. Her prospective study found that it takes 3 nights for sleep patterns to return to normal – a potential problem for surgeons who have frequent on-call nights.
“Sleep deprivation slows reaction time, decreases fine motor coordination, and increases the risk of chronic disease,” said Dr. Coleman. “A single period of 24 hours without sleep results in a neurocognitive performance that’s similar to having a blood alcohol content of 0.1%. It’s also associated with decreased empathy and increased depression. We need to take this issue seriously.”
Dr. Coleman measured sleep hours and architecture on 17 surgeons over 3 months, collecting data on 1,421 nights. Each surgeon wore a biometric measuring device called “Whoop” for the entire study. Worn on the wrist, the device measures heart rate, heart rate variability, and movement 100 times per second. It also records sleep onset and termination and can determine stages of sleep (light, slow wave, and REM).
In addition to wearing the device, the subjects also recorded all of their call schedules. The study compared sleep patterns on pre-call day 1 to those on post-call days 1, 2, and 3. Acute sleep deprivation was defined as two or more cycles of slow-wave sleep before REM; chronic sleep deprivation was one or more cycles of REM before slow-wave sleep onset.
Most of the subjects (65%) were men; the mean age was 45 years. Of the 1,421 nights recorded, 227 were on-call. Surgeons were already getting fewer hours of sleep than generally recommended, averaging 6.5 hours excluding call nights.
Subjects tried to “catch up” on sleep the day after call, Dr. Coleman said. On the day before call, they recorded an average of 6.4 hours of sleep; that increased to about 7 hours on post-call day 1. On post-call day 2, the average sleep time was about 6.3 hours, and increased to 6.5 hours by the third day.
Most of these recovery nights (70%) had abnormal amounts of REM sleep; 56% had abnormal amounts of slow-wave sleep. The majority of subjects (65%) showed patterns that qualified as either acute or chronic sleep deprivation.
“A recent study of football players found that correcting sleep issues was associated with both decreased alcohol consumption and decreased injuries,” Dr. Coleman said. “Well, we are being injured too. Shouldn’t surgeons take this as seriously as people who throw a ball for a living?”
She had no financial disclosures.
[email protected]
SOURCE: Coleman JJ et al. AAST 2018, Abstract 29.
SAN DIEGO – Almost 70% of surgeons who pull in-house call duty may be sleep deprived, Jamie Jones Coleman, MD, said at the annual meeting of the American Association for the Surgery of Trauma.
Even extra sleep the night after call doesn’t even things out, said Dr. Coleman of the University of Colorado, Denver. Her prospective study found that it takes 3 nights for sleep patterns to return to normal – a potential problem for surgeons who have frequent on-call nights.
“Sleep deprivation slows reaction time, decreases fine motor coordination, and increases the risk of chronic disease,” said Dr. Coleman. “A single period of 24 hours without sleep results in a neurocognitive performance that’s similar to having a blood alcohol content of 0.1%. It’s also associated with decreased empathy and increased depression. We need to take this issue seriously.”
Dr. Coleman measured sleep hours and architecture on 17 surgeons over 3 months, collecting data on 1,421 nights. Each surgeon wore a biometric measuring device called “Whoop” for the entire study. Worn on the wrist, the device measures heart rate, heart rate variability, and movement 100 times per second. It also records sleep onset and termination and can determine stages of sleep (light, slow wave, and REM).
In addition to wearing the device, the subjects also recorded all of their call schedules. The study compared sleep patterns on pre-call day 1 to those on post-call days 1, 2, and 3. Acute sleep deprivation was defined as two or more cycles of slow-wave sleep before REM; chronic sleep deprivation was one or more cycles of REM before slow-wave sleep onset.
Most of the subjects (65%) were men; the mean age was 45 years. Of the 1,421 nights recorded, 227 were on-call. Surgeons were already getting fewer hours of sleep than generally recommended, averaging 6.5 hours excluding call nights.
Subjects tried to “catch up” on sleep the day after call, Dr. Coleman said. On the day before call, they recorded an average of 6.4 hours of sleep; that increased to about 7 hours on post-call day 1. On post-call day 2, the average sleep time was about 6.3 hours, and increased to 6.5 hours by the third day.
Most of these recovery nights (70%) had abnormal amounts of REM sleep; 56% had abnormal amounts of slow-wave sleep. The majority of subjects (65%) showed patterns that qualified as either acute or chronic sleep deprivation.
“A recent study of football players found that correcting sleep issues was associated with both decreased alcohol consumption and decreased injuries,” Dr. Coleman said. “Well, we are being injured too. Shouldn’t surgeons take this as seriously as people who throw a ball for a living?”
She had no financial disclosures.
[email protected]
SOURCE: Coleman JJ et al. AAST 2018, Abstract 29.
SAN DIEGO – Almost 70% of surgeons who pull in-house call duty may be sleep deprived, Jamie Jones Coleman, MD, said at the annual meeting of the American Association for the Surgery of Trauma.
Even extra sleep the night after call doesn’t even things out, said Dr. Coleman of the University of Colorado, Denver. Her prospective study found that it takes 3 nights for sleep patterns to return to normal – a potential problem for surgeons who have frequent on-call nights.
“Sleep deprivation slows reaction time, decreases fine motor coordination, and increases the risk of chronic disease,” said Dr. Coleman. “A single period of 24 hours without sleep results in a neurocognitive performance that’s similar to having a blood alcohol content of 0.1%. It’s also associated with decreased empathy and increased depression. We need to take this issue seriously.”
Dr. Coleman measured sleep hours and architecture on 17 surgeons over 3 months, collecting data on 1,421 nights. Each surgeon wore a biometric measuring device called “Whoop” for the entire study. Worn on the wrist, the device measures heart rate, heart rate variability, and movement 100 times per second. It also records sleep onset and termination and can determine stages of sleep (light, slow wave, and REM).
In addition to wearing the device, the subjects also recorded all of their call schedules. The study compared sleep patterns on pre-call day 1 to those on post-call days 1, 2, and 3. Acute sleep deprivation was defined as two or more cycles of slow-wave sleep before REM; chronic sleep deprivation was one or more cycles of REM before slow-wave sleep onset.
Most of the subjects (65%) were men; the mean age was 45 years. Of the 1,421 nights recorded, 227 were on-call. Surgeons were already getting fewer hours of sleep than generally recommended, averaging 6.5 hours excluding call nights.
Subjects tried to “catch up” on sleep the day after call, Dr. Coleman said. On the day before call, they recorded an average of 6.4 hours of sleep; that increased to about 7 hours on post-call day 1. On post-call day 2, the average sleep time was about 6.3 hours, and increased to 6.5 hours by the third day.
Most of these recovery nights (70%) had abnormal amounts of REM sleep; 56% had abnormal amounts of slow-wave sleep. The majority of subjects (65%) showed patterns that qualified as either acute or chronic sleep deprivation.
“A recent study of football players found that correcting sleep issues was associated with both decreased alcohol consumption and decreased injuries,” Dr. Coleman said. “Well, we are being injured too. Shouldn’t surgeons take this as seriously as people who throw a ball for a living?”
She had no financial disclosures.
[email protected]
SOURCE: Coleman JJ et al. AAST 2018, Abstract 29.
REPORTING FROM THE AAST ANNUAL MEETING
Key clinical point: On-call duty disrupts sleep for many surgeons.
Major finding: About 65% qualify as having acute or chronic sleep deprivation.
Study details: The prospective study involved 17 surgeons.
Disclosures: Dr. Coleman had no relevant financial disclosures.
Source: Coleman JJ et al. AAST 2018, Abstract 29.
Anxiety and depression widespread among arthritis patients
Adults with arthritis are almost twice as likely to have symptoms of anxiety than depression, but the depressed patients are more likely to receive treatment, according to the Centers for Disease Control and Prevention.
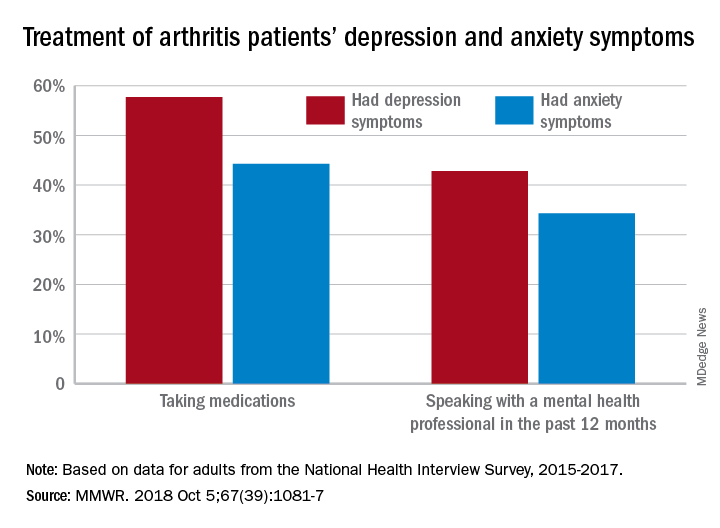
During 2015-2017, the prevalence of anxiety symptoms was 22.5% in adults with arthritis, compared with 12.1% for depression symptoms. Treatment of those symptoms, however, was another story: 57.7% of arthritis patients with depression symptoms were taking medications, versus 44.3% of those with anxiety symptoms, and 42.8% of those with symptoms of depression reported seeing a mental health professional the past 12 months, compared with 34.3% of adults with anxiety, Dana Guglielmo, MPH, of the CDC’s National Center for Chronic Disease Prevention and Health Promotion, Atlanta, and her associates reported in the Morbidity and Mortality Weekly Report.
Prevalences of anxiety and depression symptoms varied considerably by sociodemographic characteristic during 2015-2017. Anxiety and depression were both more common in those aged 18-44 years (28.3% and 13.7%, respectively) than in those aged over 65 (9.7% and 6.2%), and women with arthritis were more likely than were men to experience symptoms of anxiety (26.9% vs. 16%) and depression (14% vs. 9.2%), the investigators said, based on data from the National Health Interview Survey.
Among racial/ethnic groups, the prevalence of anxiety was highest for whites (23.9%) and lowest for Asians (10.6%), who also had lowest depression symptom prevalence at 3.3%, with American Indians/Alaska Natives highest at 15.4%. Adults categorized as other/multiple race, however, were highest in both cases at 32.3% for anxiety and 17.4% for depression, Ms. Guglielmo and her associates said.
The overall prevalence of anxiety and depression symptoms in patients with arthritis was much higher than in those without arthritis – 10.7% for anxiety and 4.7% for depression – which “suggests that all adults with arthritis would benefit from mental health screening,” they noted.
, and encouraging physical activity, which is an effective nonpharmacologic strategy that can help reduce the symptoms of anxiety and depression, improve arthritis symptoms, and promote better quality of life,” the investigators wrote.
SOURCE: Guglielmo D et al. MMWR. 2018 Oct 5;67(39):1081-7.
Adults with arthritis are almost twice as likely to have symptoms of anxiety than depression, but the depressed patients are more likely to receive treatment, according to the Centers for Disease Control and Prevention.
During 2015-2017, the prevalence of anxiety symptoms was 22.5% in adults with arthritis, compared with 12.1% for depression symptoms. Treatment of those symptoms, however, was another story: 57.7% of arthritis patients with depression symptoms were taking medications, versus 44.3% of those with anxiety symptoms, and 42.8% of those with symptoms of depression reported seeing a mental health professional the past 12 months, compared with 34.3% of adults with anxiety, Dana Guglielmo, MPH, of the CDC’s National Center for Chronic Disease Prevention and Health Promotion, Atlanta, and her associates reported in the Morbidity and Mortality Weekly Report.
Prevalences of anxiety and depression symptoms varied considerably by sociodemographic characteristic during 2015-2017. Anxiety and depression were both more common in those aged 18-44 years (28.3% and 13.7%, respectively) than in those aged over 65 (9.7% and 6.2%), and women with arthritis were more likely than were men to experience symptoms of anxiety (26.9% vs. 16%) and depression (14% vs. 9.2%), the investigators said, based on data from the National Health Interview Survey.
Among racial/ethnic groups, the prevalence of anxiety was highest for whites (23.9%) and lowest for Asians (10.6%), who also had lowest depression symptom prevalence at 3.3%, with American Indians/Alaska Natives highest at 15.4%. Adults categorized as other/multiple race, however, were highest in both cases at 32.3% for anxiety and 17.4% for depression, Ms. Guglielmo and her associates said.
The overall prevalence of anxiety and depression symptoms in patients with arthritis was much higher than in those without arthritis – 10.7% for anxiety and 4.7% for depression – which “suggests that all adults with arthritis would benefit from mental health screening,” they noted.
, and encouraging physical activity, which is an effective nonpharmacologic strategy that can help reduce the symptoms of anxiety and depression, improve arthritis symptoms, and promote better quality of life,” the investigators wrote.
SOURCE: Guglielmo D et al. MMWR. 2018 Oct 5;67(39):1081-7.
Adults with arthritis are almost twice as likely to have symptoms of anxiety than depression, but the depressed patients are more likely to receive treatment, according to the Centers for Disease Control and Prevention.
During 2015-2017, the prevalence of anxiety symptoms was 22.5% in adults with arthritis, compared with 12.1% for depression symptoms. Treatment of those symptoms, however, was another story: 57.7% of arthritis patients with depression symptoms were taking medications, versus 44.3% of those with anxiety symptoms, and 42.8% of those with symptoms of depression reported seeing a mental health professional the past 12 months, compared with 34.3% of adults with anxiety, Dana Guglielmo, MPH, of the CDC’s National Center for Chronic Disease Prevention and Health Promotion, Atlanta, and her associates reported in the Morbidity and Mortality Weekly Report.
Prevalences of anxiety and depression symptoms varied considerably by sociodemographic characteristic during 2015-2017. Anxiety and depression were both more common in those aged 18-44 years (28.3% and 13.7%, respectively) than in those aged over 65 (9.7% and 6.2%), and women with arthritis were more likely than were men to experience symptoms of anxiety (26.9% vs. 16%) and depression (14% vs. 9.2%), the investigators said, based on data from the National Health Interview Survey.
Among racial/ethnic groups, the prevalence of anxiety was highest for whites (23.9%) and lowest for Asians (10.6%), who also had lowest depression symptom prevalence at 3.3%, with American Indians/Alaska Natives highest at 15.4%. Adults categorized as other/multiple race, however, were highest in both cases at 32.3% for anxiety and 17.4% for depression, Ms. Guglielmo and her associates said.
The overall prevalence of anxiety and depression symptoms in patients with arthritis was much higher than in those without arthritis – 10.7% for anxiety and 4.7% for depression – which “suggests that all adults with arthritis would benefit from mental health screening,” they noted.
, and encouraging physical activity, which is an effective nonpharmacologic strategy that can help reduce the symptoms of anxiety and depression, improve arthritis symptoms, and promote better quality of life,” the investigators wrote.
SOURCE: Guglielmo D et al. MMWR. 2018 Oct 5;67(39):1081-7.
FROM MMWR
Short-term NSAIDs appear safe for high-risk patients
in a retrospective, observational study.
The findings of the study challenge the Choosing Wisely campaign of the American Society of Nephrology, which recommends against NSAIDs for high-risk patients, according to lead author Zachary Bouck, MPH, of the department of medicine at Sunnybrook Health Sciences Centre in Toronto, and his coauthors.
“While these recommendations offer basic analgesics and nonpharmacological treatments as preferable alternatives, it is both possible and disconcerting that some physicians might instead prescribe opioids, which typically pose elevated risk of adverse events and dependence vs. NSAIDs,” the investigators wrote. The report is in JAMA Internal Medicine.
They sought to estimate the frequency and characteristics of NSAID prescriptions while also looking for associations with acute renal and cardiovascular complications. The retrospective, observational study involved 814,049 adults with musculoskeletal disease and 7,365 primary care physicians in Ontario, Canada. All patients were aged 65 years and older, and had been diagnosed with hypertension, chronic kidney disease, or heart failure in the past year. Instances in which a patient was prescribed an NSAID within 7 days of presentation were included.
To assess for associations between prescription NSAIDs and negative outcomes, the investigators searched for renal or cardiovascular complications within 37 days of presentation. Over-the-counter NSAID usage was not evaluated.
There were 224,825 visits. An NSAID was prescribed after 9.3% of these visits.
Renal and cardiovascular outcomes were similar between high-risk patients who received a prescription NSAID and those who did not (absolute risk reduction, .0003; P = .74).
“The similarity in risk between users and nonusers, each group primarily consisting of patients with hypertension, suggests that the short-term association of NSAIDs in high-risk patients with musculoskeletal pain may not be as dangerous as initially thought,” the authors concluded.
The investigators found that prescribing rates varied widely, ranging from 6.7% to 14.4% of different health regions, and from 0.9% to 60.3% among 688 primary care practices, with “substantial variation in use” among primary care physicians.
The authors acknowledged limitations, including the use of administrative data, but noted that their study, showing substantial variations in NSAID prescribing, “along with the identification of patient and physician characteristics associated with NSAID use, presents an opportunity for quality improvement, with some potential targets for any resulting interventions,” they wrote.
The Institute for Clinical Evaluative Sciences funded the study. The authors reported compensation from the Canadian Institute of Health Research, the department of family and community medicine at the University of Toronto, the Heart and Stroke Foundation of Canada, and Women’s College Hospital.
SOURCE: Bouck et al. JAMA Intern Med. 2018 Oct 8. doi: 10.1001/jamainternmed.2018.4273.
The study by Bouck and colleagues found that short-term prescription NSAIDs were safe for high-risk patients; however, physicians should consider the inherent limitations of observational studies before altering clinical decisions, according to Jonathan Zipursky, MD, and David N. Juurlink, MD, PhD. This is particularly important since the findings challenge the American Society of Nephrology, which recommends against NSAIDs in patients with chronic kidney disease (CKD), heart failure, or hypertension.
Among the advantages of observational studies over randomized trials is that they often include patients not eligible for randomized controlled trials, “and extended follow-up enables examination of outcomes that might not have arisen earlier in treatment,” they wrote in an editorial. “Moreover, sample sizes often greatly exceed those of RCTs, facilitating detection of less common adverse events. Consequently, population-based observational studies are critical to postmarketing surveillance and, increasingly, evidence-based prescribing recommendations.”
On the other hand, observational studies are less tightly controlled than randomized trials, with nonrandomized allocation, which “raises the possibilities of selection bias and confounding by indication,” they wrote. Furthermore, “readers are left questioning whether patients who were not prescribed NSAIDs were simply taking over-the-counter medications (including NSAIDs),” they wrote.
“Although we rely on observational studies to answer questions poorly suited to clinical trials, we have to interpret these findings with caution,” they added.
Jonathan Zipursky, MD, and Dr. Juurlink are affiliated with the department of medicine at Sunnybrook Health Sciences Centre in Toronto. These comments are adapted from their accompanying editorial (JAMA Intern Med 2018 Oct 8. doi: 10.1136/ebmed-2016-110401).
The study by Bouck and colleagues found that short-term prescription NSAIDs were safe for high-risk patients; however, physicians should consider the inherent limitations of observational studies before altering clinical decisions, according to Jonathan Zipursky, MD, and David N. Juurlink, MD, PhD. This is particularly important since the findings challenge the American Society of Nephrology, which recommends against NSAIDs in patients with chronic kidney disease (CKD), heart failure, or hypertension.
Among the advantages of observational studies over randomized trials is that they often include patients not eligible for randomized controlled trials, “and extended follow-up enables examination of outcomes that might not have arisen earlier in treatment,” they wrote in an editorial. “Moreover, sample sizes often greatly exceed those of RCTs, facilitating detection of less common adverse events. Consequently, population-based observational studies are critical to postmarketing surveillance and, increasingly, evidence-based prescribing recommendations.”
On the other hand, observational studies are less tightly controlled than randomized trials, with nonrandomized allocation, which “raises the possibilities of selection bias and confounding by indication,” they wrote. Furthermore, “readers are left questioning whether patients who were not prescribed NSAIDs were simply taking over-the-counter medications (including NSAIDs),” they wrote.
“Although we rely on observational studies to answer questions poorly suited to clinical trials, we have to interpret these findings with caution,” they added.
Jonathan Zipursky, MD, and Dr. Juurlink are affiliated with the department of medicine at Sunnybrook Health Sciences Centre in Toronto. These comments are adapted from their accompanying editorial (JAMA Intern Med 2018 Oct 8. doi: 10.1136/ebmed-2016-110401).
The study by Bouck and colleagues found that short-term prescription NSAIDs were safe for high-risk patients; however, physicians should consider the inherent limitations of observational studies before altering clinical decisions, according to Jonathan Zipursky, MD, and David N. Juurlink, MD, PhD. This is particularly important since the findings challenge the American Society of Nephrology, which recommends against NSAIDs in patients with chronic kidney disease (CKD), heart failure, or hypertension.
Among the advantages of observational studies over randomized trials is that they often include patients not eligible for randomized controlled trials, “and extended follow-up enables examination of outcomes that might not have arisen earlier in treatment,” they wrote in an editorial. “Moreover, sample sizes often greatly exceed those of RCTs, facilitating detection of less common adverse events. Consequently, population-based observational studies are critical to postmarketing surveillance and, increasingly, evidence-based prescribing recommendations.”
On the other hand, observational studies are less tightly controlled than randomized trials, with nonrandomized allocation, which “raises the possibilities of selection bias and confounding by indication,” they wrote. Furthermore, “readers are left questioning whether patients who were not prescribed NSAIDs were simply taking over-the-counter medications (including NSAIDs),” they wrote.
“Although we rely on observational studies to answer questions poorly suited to clinical trials, we have to interpret these findings with caution,” they added.
Jonathan Zipursky, MD, and Dr. Juurlink are affiliated with the department of medicine at Sunnybrook Health Sciences Centre in Toronto. These comments are adapted from their accompanying editorial (JAMA Intern Med 2018 Oct 8. doi: 10.1136/ebmed-2016-110401).
in a retrospective, observational study.
The findings of the study challenge the Choosing Wisely campaign of the American Society of Nephrology, which recommends against NSAIDs for high-risk patients, according to lead author Zachary Bouck, MPH, of the department of medicine at Sunnybrook Health Sciences Centre in Toronto, and his coauthors.
“While these recommendations offer basic analgesics and nonpharmacological treatments as preferable alternatives, it is both possible and disconcerting that some physicians might instead prescribe opioids, which typically pose elevated risk of adverse events and dependence vs. NSAIDs,” the investigators wrote. The report is in JAMA Internal Medicine.
They sought to estimate the frequency and characteristics of NSAID prescriptions while also looking for associations with acute renal and cardiovascular complications. The retrospective, observational study involved 814,049 adults with musculoskeletal disease and 7,365 primary care physicians in Ontario, Canada. All patients were aged 65 years and older, and had been diagnosed with hypertension, chronic kidney disease, or heart failure in the past year. Instances in which a patient was prescribed an NSAID within 7 days of presentation were included.
To assess for associations between prescription NSAIDs and negative outcomes, the investigators searched for renal or cardiovascular complications within 37 days of presentation. Over-the-counter NSAID usage was not evaluated.
There were 224,825 visits. An NSAID was prescribed after 9.3% of these visits.
Renal and cardiovascular outcomes were similar between high-risk patients who received a prescription NSAID and those who did not (absolute risk reduction, .0003; P = .74).
“The similarity in risk between users and nonusers, each group primarily consisting of patients with hypertension, suggests that the short-term association of NSAIDs in high-risk patients with musculoskeletal pain may not be as dangerous as initially thought,” the authors concluded.
The investigators found that prescribing rates varied widely, ranging from 6.7% to 14.4% of different health regions, and from 0.9% to 60.3% among 688 primary care practices, with “substantial variation in use” among primary care physicians.
The authors acknowledged limitations, including the use of administrative data, but noted that their study, showing substantial variations in NSAID prescribing, “along with the identification of patient and physician characteristics associated with NSAID use, presents an opportunity for quality improvement, with some potential targets for any resulting interventions,” they wrote.
The Institute for Clinical Evaluative Sciences funded the study. The authors reported compensation from the Canadian Institute of Health Research, the department of family and community medicine at the University of Toronto, the Heart and Stroke Foundation of Canada, and Women’s College Hospital.
SOURCE: Bouck et al. JAMA Intern Med. 2018 Oct 8. doi: 10.1001/jamainternmed.2018.4273.
in a retrospective, observational study.
The findings of the study challenge the Choosing Wisely campaign of the American Society of Nephrology, which recommends against NSAIDs for high-risk patients, according to lead author Zachary Bouck, MPH, of the department of medicine at Sunnybrook Health Sciences Centre in Toronto, and his coauthors.
“While these recommendations offer basic analgesics and nonpharmacological treatments as preferable alternatives, it is both possible and disconcerting that some physicians might instead prescribe opioids, which typically pose elevated risk of adverse events and dependence vs. NSAIDs,” the investigators wrote. The report is in JAMA Internal Medicine.
They sought to estimate the frequency and characteristics of NSAID prescriptions while also looking for associations with acute renal and cardiovascular complications. The retrospective, observational study involved 814,049 adults with musculoskeletal disease and 7,365 primary care physicians in Ontario, Canada. All patients were aged 65 years and older, and had been diagnosed with hypertension, chronic kidney disease, or heart failure in the past year. Instances in which a patient was prescribed an NSAID within 7 days of presentation were included.
To assess for associations between prescription NSAIDs and negative outcomes, the investigators searched for renal or cardiovascular complications within 37 days of presentation. Over-the-counter NSAID usage was not evaluated.
There were 224,825 visits. An NSAID was prescribed after 9.3% of these visits.
Renal and cardiovascular outcomes were similar between high-risk patients who received a prescription NSAID and those who did not (absolute risk reduction, .0003; P = .74).
“The similarity in risk between users and nonusers, each group primarily consisting of patients with hypertension, suggests that the short-term association of NSAIDs in high-risk patients with musculoskeletal pain may not be as dangerous as initially thought,” the authors concluded.
The investigators found that prescribing rates varied widely, ranging from 6.7% to 14.4% of different health regions, and from 0.9% to 60.3% among 688 primary care practices, with “substantial variation in use” among primary care physicians.
The authors acknowledged limitations, including the use of administrative data, but noted that their study, showing substantial variations in NSAID prescribing, “along with the identification of patient and physician characteristics associated with NSAID use, presents an opportunity for quality improvement, with some potential targets for any resulting interventions,” they wrote.
The Institute for Clinical Evaluative Sciences funded the study. The authors reported compensation from the Canadian Institute of Health Research, the department of family and community medicine at the University of Toronto, the Heart and Stroke Foundation of Canada, and Women’s College Hospital.
SOURCE: Bouck et al. JAMA Intern Med. 2018 Oct 8. doi: 10.1001/jamainternmed.2018.4273.
FROM JAMA INTERNAL MEDICINE
Key clinical point: In patients with musculoskeletal disease and hypertension, chronic kidney disease, or heart failure, short-term prescription NSAIDs may be safer than once thought.
Major finding: Renal and cardiovascular outcomes were similar between high-risk patients who received a prescription NSAID and those who did not (absolute risk reduction, .0003; P = .74).
Study details: A retrospective, observational study involving 814,049 adults with musculoskeletal disease and 7,365 primary care physicians in Ontario, Canada.
Disclosures: The Institute for Clinical Evaluative Sciences funded the study. The authors reported compensation from the Canadian Institute of Health Research, the Heart and Stroke Foundation of Canada, and Women’s College Hospital.
Source: Bouck et al. JAMA Intern Med. 2018 Oct 8. doi: 10.1001/jamainternmed.2018.4273.