User login
Artemisinin: Its global impact on the treatment of malaria
Malaria remains a major international public health concern. In 2015, the World Health Organization estimated that 212 million individuals were infected and that there were 429,000 deaths. This represents a 21% decline in incidence globally and a 29% decline in global mortality between 2010 and 2015. In 2016, malaria was endemic in 91 countries and territories, down from 108 in 2000. Although malaria has been eliminated from the United States since the early 1950s, approximately 1,700 cases are reported annually, most of which occur in returned travelers, according to the Centers for Disease Control and Prevention.

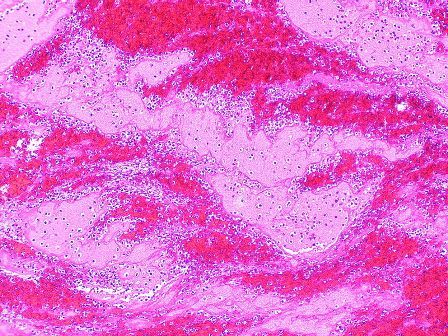
Five species of Plasmodium (P. falciparum, P. vivax, P. malariae, P. ovale, and, more recently, P. knowelsi) account for most of the infections in humans and are transmitted by the bite of an infected female Anopheles mosquito. The disease is rarely acquired by blood transfusion, by needle sharing, by organ transplantation, or congenitally. Once diagnosed, malaria can be treated; however, delay in initiating therapy can lead to both serious and fatal outcomes.
Treatment
Historically, drug development was driven by the need to protect the military. While quinine was isolated from the bark of the cinchona tree in 1820, chloroquine, proguanil, mefloquine, and atovaquone each were developed during or after a military conflict during 1945-1985. Tetracycline/doxycycline and clindamycin also have antimalarial activity. Use of any of these agents as monotherapy has led to drug resistance and treatment failure.
Artemisinin
Artemisinin (also known as qinghao su) and its derivatives are a new class of antimalarials derived from the sweet wormwood plant Artemisia annua. Initially developed in China in the 1970s, this class gained global attention in the 1990s. and have the fastest parasite clearance time, rapid resolution of symptoms, and an excellent safety profile. They have activity against all Plasmodium species.
Because of artemisinins’ rapid elimination, they are used in combination with an agent that also kills blood parasites but has a slower elimination rate and a different mechanism of action. The goal is to prevent and delay the development of resistance and reduce recrudescence. The superiority of artemisinin-based combination therapy (ACT) over monotherapies has been documented.

Resistance, always a concern, has remained limited to specific areas in Southeast Asia since reported in 2008. Monitoring drug efficacy, safety, quality of antimalarials is ongoing, as is discouraging monotherapy use of these agents. Globally, artemisinins are the mainstay of treatment. Spread of resistance would be a major setback for both malaria control and elimination.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures. Email her at [email protected].
Malaria remains a major international public health concern. In 2015, the World Health Organization estimated that 212 million individuals were infected and that there were 429,000 deaths. This represents a 21% decline in incidence globally and a 29% decline in global mortality between 2010 and 2015. In 2016, malaria was endemic in 91 countries and territories, down from 108 in 2000. Although malaria has been eliminated from the United States since the early 1950s, approximately 1,700 cases are reported annually, most of which occur in returned travelers, according to the Centers for Disease Control and Prevention.
Five species of Plasmodium (P. falciparum, P. vivax, P. malariae, P. ovale, and, more recently, P. knowelsi) account for most of the infections in humans and are transmitted by the bite of an infected female Anopheles mosquito. The disease is rarely acquired by blood transfusion, by needle sharing, by organ transplantation, or congenitally. Once diagnosed, malaria can be treated; however, delay in initiating therapy can lead to both serious and fatal outcomes.
Treatment
Historically, drug development was driven by the need to protect the military. While quinine was isolated from the bark of the cinchona tree in 1820, chloroquine, proguanil, mefloquine, and atovaquone each were developed during or after a military conflict during 1945-1985. Tetracycline/doxycycline and clindamycin also have antimalarial activity. Use of any of these agents as monotherapy has led to drug resistance and treatment failure.
Artemisinin
Artemisinin (also known as qinghao su) and its derivatives are a new class of antimalarials derived from the sweet wormwood plant Artemisia annua. Initially developed in China in the 1970s, this class gained global attention in the 1990s. and have the fastest parasite clearance time, rapid resolution of symptoms, and an excellent safety profile. They have activity against all Plasmodium species.
Because of artemisinins’ rapid elimination, they are used in combination with an agent that also kills blood parasites but has a slower elimination rate and a different mechanism of action. The goal is to prevent and delay the development of resistance and reduce recrudescence. The superiority of artemisinin-based combination therapy (ACT) over monotherapies has been documented.
Resistance, always a concern, has remained limited to specific areas in Southeast Asia since reported in 2008. Monitoring drug efficacy, safety, quality of antimalarials is ongoing, as is discouraging monotherapy use of these agents. Globally, artemisinins are the mainstay of treatment. Spread of resistance would be a major setback for both malaria control and elimination.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures. Email her at [email protected].
Malaria remains a major international public health concern. In 2015, the World Health Organization estimated that 212 million individuals were infected and that there were 429,000 deaths. This represents a 21% decline in incidence globally and a 29% decline in global mortality between 2010 and 2015. In 2016, malaria was endemic in 91 countries and territories, down from 108 in 2000. Although malaria has been eliminated from the United States since the early 1950s, approximately 1,700 cases are reported annually, most of which occur in returned travelers, according to the Centers for Disease Control and Prevention.
Five species of Plasmodium (P. falciparum, P. vivax, P. malariae, P. ovale, and, more recently, P. knowelsi) account for most of the infections in humans and are transmitted by the bite of an infected female Anopheles mosquito. The disease is rarely acquired by blood transfusion, by needle sharing, by organ transplantation, or congenitally. Once diagnosed, malaria can be treated; however, delay in initiating therapy can lead to both serious and fatal outcomes.
Treatment
Historically, drug development was driven by the need to protect the military. While quinine was isolated from the bark of the cinchona tree in 1820, chloroquine, proguanil, mefloquine, and atovaquone each were developed during or after a military conflict during 1945-1985. Tetracycline/doxycycline and clindamycin also have antimalarial activity. Use of any of these agents as monotherapy has led to drug resistance and treatment failure.
Artemisinin
Artemisinin (also known as qinghao su) and its derivatives are a new class of antimalarials derived from the sweet wormwood plant Artemisia annua. Initially developed in China in the 1970s, this class gained global attention in the 1990s. and have the fastest parasite clearance time, rapid resolution of symptoms, and an excellent safety profile. They have activity against all Plasmodium species.
Because of artemisinins’ rapid elimination, they are used in combination with an agent that also kills blood parasites but has a slower elimination rate and a different mechanism of action. The goal is to prevent and delay the development of resistance and reduce recrudescence. The superiority of artemisinin-based combination therapy (ACT) over monotherapies has been documented.
Resistance, always a concern, has remained limited to specific areas in Southeast Asia since reported in 2008. Monitoring drug efficacy, safety, quality of antimalarials is ongoing, as is discouraging monotherapy use of these agents. Globally, artemisinins are the mainstay of treatment. Spread of resistance would be a major setback for both malaria control and elimination.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures. Email her at [email protected].
Nurse practitioner/pediatrician collaboration: Try a pediatric health care/medical home model
The first nurse practitioner program owes much to Henry K. Silver, MD, a pediatrician, an endocrinologist, and a pioneer who was influential in the development of innovative educational programs for advanced pediatric health care providers. Dr. Silver, then a professor at the University of Colorado School of Medicine in Aurora, with Loretta Ford, EdD, a pediatric nurse and professor at the same university’s School of Nursing, developed that program in 1967 (Pediatrics. 1967;39[5]:756-60). They were responding to a serious shortage of pediatric providers, especially in rural and low socioeconomic areas. Pediatric nurses learned about primary care, office-based practice that included evaluating children with hearing and speech deficits, nutritional needs, vision impairment, and other congenital and acute problems. They made home visits and participated in follow-up of children with medical, surgical, and mental health concerns.

Now, more than 50 years later, an era when health care for children is at the forefront of policy and financial concerns, children are surviving longer with chronic and complex illness, and receive sophisticated therapies for medical and surgical problems. The definition of family is very different from that used in the 1960s, and challenges in health care provision begin with identification of basic needs such as food and shelter. In light of the risks for children today, there are many more opportunities for pediatricians and pediatric nurse practitioners (PNPs) to collaborate, especially in planning complex care strategies.
One example for collaboration is within the pediatric health care/medical home model (PHC/MHM). Practices, whether primary or subspecialty, can benefit patients and their families by providing a coordinated model of comprehensive care, especially for children who are at greatest identified risk. In addition, the PHC/MHM practice can receive insurance reimbursement benefits, and demonstrate a decrease in hospitalization rates, improved health care quality, and increased patient satisfaction (JAMA. 2014 Dec 24-31;312[24]:2640-8).
The American Academy of Pediatrics defines the medical home as “a model of delivering primary care that is accessible, continuous, family centered, coordinated, compassionate, and culturally effective to every child and adolescent” (Pediatrics. 2002. doi: 10.1542/peds.110.1.184). The National Association of Pediatric Nurse Practitioners (NAPNAP) describes the pediatric health care/medical home as a “model of care that promotes holistic care of children and their families where each patient/family has an ongoing relationship with a health care professional” (J Pediatr Health Care. 2015. doi: 10.1016/j.pedhc.2015.10.010). This is an approach to providing comprehensive pediatric care that facilitates partnerships between patients, providers, and families, which is not contained within the walls of the office or building.
By virtue of their designation and training, nurses provide care for the patient in a holistic fashion, including physical care, therapeutic treatments, education, and coordination of services. Primary care nurse practitioners are trained in health promotion and prevention. They receive advanced level education in pharmacology, pathophysiology, and physical assessment, diagnosis, and management. The combination of skills between the PNP and the pediatrician are complementary and, as history suggests, can result in improved patient care. In 1967, Dr. Silver and Ms. Ford reported: “It is becoming increasingly clear that competent professional nurses working cooperatively with physicians can make greater contributions to patient care.” The PHC/MHM is an excellent opportunity for collaboration between pediatricians and NPs.
Examples of collaboration in the PHC/MHM
Building the PHC/MHM requires an evidence base, with data obtained from EHRs and current research, but also founded on individual practice culture, type of practice, and patients served. Physician and NP collaboration in collecting, reviewing, and applying this evidence can result in the development of unique guidelines for that specific practice. Patients who are considered at risk for frequent illness and hospitalizations, or who have multisystem problems, including mental health or social issues, are primary candidates who can benefit from the medical home model. The NP, by virtue of leadership training, can assist in coordinating care teams, procedures, and office staff.
Cheryl Samuels, PNP, works at the University of Texas Health Science Center at Houston, McGovern Medical School in the UT Physicians High Risk Clinic, along with two other PNPs and two pediatricians. Their collaboration has resulted in the development of a certified health care home for children with complex illness. This practice has continued to collect data and publish research to document the effectiveness of their program. One recent study was a randomized controlled trial demonstrating cost efficiency and decreased serious illness when children with complex needs are cared for in a medical home (JAMA. 2014 Dec 24-31;312[24]:2640-8). Ms. Samuels and her colleagues published, “Case for the use of a nurse practitioner in the care of children with medical complexity,” in which they described the role of the NP and benefits in utilizing these skills in the multifaceted care of children with chronic and complex illness (Children [Basel]. 2017 Apr. doi: 10.3390/children4040024).

At the University of California, Los Angeles, Mattel Children’s Hospital, the pediatric medical home program provides primary care services and care coordination for more than 300 children, adolescents, and young adults with medical complexity. Nurse practitioner Siem Ia oversees the coordination of care for these patients, and collaborates with a team of four attending physicians, resident physicians, care coordinators, and an administrative assistant. These children have multisystem problems requiring multiple specialty services, and frequent hospitalizations. Ms. Ia works with her colleagues to ensure patients and families are provided with care that is aligned with the AAP and NAPNAP medical home principles. This team is now involved in a national collaborative project that aims to improve health outcomes for children with medical complexity, and enhance family partnerships to support the health of the child and promote family well being. She also has provided clinical expertise for the recently completed randomized, controlled trial aimed at reducing utilization for children with medical complexity through care coordination and health education.
These are just a few examples of the possibilities when pediatricians and NPs collaborate to influence and change models of primary patient care. The medical care of any child can be multifaceted, with increasing complexity, and require vigilance and thoughtful planning to be successful. Outcomes from these attempts documented in the literature include opportunities for certification and accreditation, insurance reimbursement at incentive levels, and, most importantly, patient and family satisfaction.
Dr. Haut is a PNP at Beacon Pediatrics, a large primary care practice in Rehoboth Beach, Del. She also works part time for Pediatrix Medical Group, serving the pediatric intensive care unit medical team at the Herman & Walter Samuelson Children’s Hospital at Sinai in Baltimore and as adjunct faculty at the University of Maryland School of Nursing, also in Baltimore.
The first nurse practitioner program owes much to Henry K. Silver, MD, a pediatrician, an endocrinologist, and a pioneer who was influential in the development of innovative educational programs for advanced pediatric health care providers. Dr. Silver, then a professor at the University of Colorado School of Medicine in Aurora, with Loretta Ford, EdD, a pediatric nurse and professor at the same university’s School of Nursing, developed that program in 1967 (Pediatrics. 1967;39[5]:756-60). They were responding to a serious shortage of pediatric providers, especially in rural and low socioeconomic areas. Pediatric nurses learned about primary care, office-based practice that included evaluating children with hearing and speech deficits, nutritional needs, vision impairment, and other congenital and acute problems. They made home visits and participated in follow-up of children with medical, surgical, and mental health concerns.
Now, more than 50 years later, an era when health care for children is at the forefront of policy and financial concerns, children are surviving longer with chronic and complex illness, and receive sophisticated therapies for medical and surgical problems. The definition of family is very different from that used in the 1960s, and challenges in health care provision begin with identification of basic needs such as food and shelter. In light of the risks for children today, there are many more opportunities for pediatricians and pediatric nurse practitioners (PNPs) to collaborate, especially in planning complex care strategies.
One example for collaboration is within the pediatric health care/medical home model (PHC/MHM). Practices, whether primary or subspecialty, can benefit patients and their families by providing a coordinated model of comprehensive care, especially for children who are at greatest identified risk. In addition, the PHC/MHM practice can receive insurance reimbursement benefits, and demonstrate a decrease in hospitalization rates, improved health care quality, and increased patient satisfaction (JAMA. 2014 Dec 24-31;312[24]:2640-8).
The American Academy of Pediatrics defines the medical home as “a model of delivering primary care that is accessible, continuous, family centered, coordinated, compassionate, and culturally effective to every child and adolescent” (Pediatrics. 2002. doi: 10.1542/peds.110.1.184). The National Association of Pediatric Nurse Practitioners (NAPNAP) describes the pediatric health care/medical home as a “model of care that promotes holistic care of children and their families where each patient/family has an ongoing relationship with a health care professional” (J Pediatr Health Care. 2015. doi: 10.1016/j.pedhc.2015.10.010). This is an approach to providing comprehensive pediatric care that facilitates partnerships between patients, providers, and families, which is not contained within the walls of the office or building.
By virtue of their designation and training, nurses provide care for the patient in a holistic fashion, including physical care, therapeutic treatments, education, and coordination of services. Primary care nurse practitioners are trained in health promotion and prevention. They receive advanced level education in pharmacology, pathophysiology, and physical assessment, diagnosis, and management. The combination of skills between the PNP and the pediatrician are complementary and, as history suggests, can result in improved patient care. In 1967, Dr. Silver and Ms. Ford reported: “It is becoming increasingly clear that competent professional nurses working cooperatively with physicians can make greater contributions to patient care.” The PHC/MHM is an excellent opportunity for collaboration between pediatricians and NPs.
Examples of collaboration in the PHC/MHM
Building the PHC/MHM requires an evidence base, with data obtained from EHRs and current research, but also founded on individual practice culture, type of practice, and patients served. Physician and NP collaboration in collecting, reviewing, and applying this evidence can result in the development of unique guidelines for that specific practice. Patients who are considered at risk for frequent illness and hospitalizations, or who have multisystem problems, including mental health or social issues, are primary candidates who can benefit from the medical home model. The NP, by virtue of leadership training, can assist in coordinating care teams, procedures, and office staff.
Cheryl Samuels, PNP, works at the University of Texas Health Science Center at Houston, McGovern Medical School in the UT Physicians High Risk Clinic, along with two other PNPs and two pediatricians. Their collaboration has resulted in the development of a certified health care home for children with complex illness. This practice has continued to collect data and publish research to document the effectiveness of their program. One recent study was a randomized controlled trial demonstrating cost efficiency and decreased serious illness when children with complex needs are cared for in a medical home (JAMA. 2014 Dec 24-31;312[24]:2640-8). Ms. Samuels and her colleagues published, “Case for the use of a nurse practitioner in the care of children with medical complexity,” in which they described the role of the NP and benefits in utilizing these skills in the multifaceted care of children with chronic and complex illness (Children [Basel]. 2017 Apr. doi: 10.3390/children4040024).
At the University of California, Los Angeles, Mattel Children’s Hospital, the pediatric medical home program provides primary care services and care coordination for more than 300 children, adolescents, and young adults with medical complexity. Nurse practitioner Siem Ia oversees the coordination of care for these patients, and collaborates with a team of four attending physicians, resident physicians, care coordinators, and an administrative assistant. These children have multisystem problems requiring multiple specialty services, and frequent hospitalizations. Ms. Ia works with her colleagues to ensure patients and families are provided with care that is aligned with the AAP and NAPNAP medical home principles. This team is now involved in a national collaborative project that aims to improve health outcomes for children with medical complexity, and enhance family partnerships to support the health of the child and promote family well being. She also has provided clinical expertise for the recently completed randomized, controlled trial aimed at reducing utilization for children with medical complexity through care coordination and health education.
These are just a few examples of the possibilities when pediatricians and NPs collaborate to influence and change models of primary patient care. The medical care of any child can be multifaceted, with increasing complexity, and require vigilance and thoughtful planning to be successful. Outcomes from these attempts documented in the literature include opportunities for certification and accreditation, insurance reimbursement at incentive levels, and, most importantly, patient and family satisfaction.
Dr. Haut is a PNP at Beacon Pediatrics, a large primary care practice in Rehoboth Beach, Del. She also works part time for Pediatrix Medical Group, serving the pediatric intensive care unit medical team at the Herman & Walter Samuelson Children’s Hospital at Sinai in Baltimore and as adjunct faculty at the University of Maryland School of Nursing, also in Baltimore.
The first nurse practitioner program owes much to Henry K. Silver, MD, a pediatrician, an endocrinologist, and a pioneer who was influential in the development of innovative educational programs for advanced pediatric health care providers. Dr. Silver, then a professor at the University of Colorado School of Medicine in Aurora, with Loretta Ford, EdD, a pediatric nurse and professor at the same university’s School of Nursing, developed that program in 1967 (Pediatrics. 1967;39[5]:756-60). They were responding to a serious shortage of pediatric providers, especially in rural and low socioeconomic areas. Pediatric nurses learned about primary care, office-based practice that included evaluating children with hearing and speech deficits, nutritional needs, vision impairment, and other congenital and acute problems. They made home visits and participated in follow-up of children with medical, surgical, and mental health concerns.
Now, more than 50 years later, an era when health care for children is at the forefront of policy and financial concerns, children are surviving longer with chronic and complex illness, and receive sophisticated therapies for medical and surgical problems. The definition of family is very different from that used in the 1960s, and challenges in health care provision begin with identification of basic needs such as food and shelter. In light of the risks for children today, there are many more opportunities for pediatricians and pediatric nurse practitioners (PNPs) to collaborate, especially in planning complex care strategies.
One example for collaboration is within the pediatric health care/medical home model (PHC/MHM). Practices, whether primary or subspecialty, can benefit patients and their families by providing a coordinated model of comprehensive care, especially for children who are at greatest identified risk. In addition, the PHC/MHM practice can receive insurance reimbursement benefits, and demonstrate a decrease in hospitalization rates, improved health care quality, and increased patient satisfaction (JAMA. 2014 Dec 24-31;312[24]:2640-8).
The American Academy of Pediatrics defines the medical home as “a model of delivering primary care that is accessible, continuous, family centered, coordinated, compassionate, and culturally effective to every child and adolescent” (Pediatrics. 2002. doi: 10.1542/peds.110.1.184). The National Association of Pediatric Nurse Practitioners (NAPNAP) describes the pediatric health care/medical home as a “model of care that promotes holistic care of children and their families where each patient/family has an ongoing relationship with a health care professional” (J Pediatr Health Care. 2015. doi: 10.1016/j.pedhc.2015.10.010). This is an approach to providing comprehensive pediatric care that facilitates partnerships between patients, providers, and families, which is not contained within the walls of the office or building.
By virtue of their designation and training, nurses provide care for the patient in a holistic fashion, including physical care, therapeutic treatments, education, and coordination of services. Primary care nurse practitioners are trained in health promotion and prevention. They receive advanced level education in pharmacology, pathophysiology, and physical assessment, diagnosis, and management. The combination of skills between the PNP and the pediatrician are complementary and, as history suggests, can result in improved patient care. In 1967, Dr. Silver and Ms. Ford reported: “It is becoming increasingly clear that competent professional nurses working cooperatively with physicians can make greater contributions to patient care.” The PHC/MHM is an excellent opportunity for collaboration between pediatricians and NPs.
Examples of collaboration in the PHC/MHM
Building the PHC/MHM requires an evidence base, with data obtained from EHRs and current research, but also founded on individual practice culture, type of practice, and patients served. Physician and NP collaboration in collecting, reviewing, and applying this evidence can result in the development of unique guidelines for that specific practice. Patients who are considered at risk for frequent illness and hospitalizations, or who have multisystem problems, including mental health or social issues, are primary candidates who can benefit from the medical home model. The NP, by virtue of leadership training, can assist in coordinating care teams, procedures, and office staff.
Cheryl Samuels, PNP, works at the University of Texas Health Science Center at Houston, McGovern Medical School in the UT Physicians High Risk Clinic, along with two other PNPs and two pediatricians. Their collaboration has resulted in the development of a certified health care home for children with complex illness. This practice has continued to collect data and publish research to document the effectiveness of their program. One recent study was a randomized controlled trial demonstrating cost efficiency and decreased serious illness when children with complex needs are cared for in a medical home (JAMA. 2014 Dec 24-31;312[24]:2640-8). Ms. Samuels and her colleagues published, “Case for the use of a nurse practitioner in the care of children with medical complexity,” in which they described the role of the NP and benefits in utilizing these skills in the multifaceted care of children with chronic and complex illness (Children [Basel]. 2017 Apr. doi: 10.3390/children4040024).
At the University of California, Los Angeles, Mattel Children’s Hospital, the pediatric medical home program provides primary care services and care coordination for more than 300 children, adolescents, and young adults with medical complexity. Nurse practitioner Siem Ia oversees the coordination of care for these patients, and collaborates with a team of four attending physicians, resident physicians, care coordinators, and an administrative assistant. These children have multisystem problems requiring multiple specialty services, and frequent hospitalizations. Ms. Ia works with her colleagues to ensure patients and families are provided with care that is aligned with the AAP and NAPNAP medical home principles. This team is now involved in a national collaborative project that aims to improve health outcomes for children with medical complexity, and enhance family partnerships to support the health of the child and promote family well being. She also has provided clinical expertise for the recently completed randomized, controlled trial aimed at reducing utilization for children with medical complexity through care coordination and health education.
These are just a few examples of the possibilities when pediatricians and NPs collaborate to influence and change models of primary patient care. The medical care of any child can be multifaceted, with increasing complexity, and require vigilance and thoughtful planning to be successful. Outcomes from these attempts documented in the literature include opportunities for certification and accreditation, insurance reimbursement at incentive levels, and, most importantly, patient and family satisfaction.
Dr. Haut is a PNP at Beacon Pediatrics, a large primary care practice in Rehoboth Beach, Del. She also works part time for Pediatrix Medical Group, serving the pediatric intensive care unit medical team at the Herman & Walter Samuelson Children’s Hospital at Sinai in Baltimore and as adjunct faculty at the University of Maryland School of Nursing, also in Baltimore.
DMTs Reduce the Risk of Conversion to Secondary Progressive MS
PARIS—Secondary progressive multiple sclerosis (MS) is at least partly a consequence of early inflammation, and the risk of conversion from relapsing-remitting MS to secondary progressive MS is modifiable over five years with existing disease-modifying therapies (DMTs), according to research described at the Seventh Joint ECTRIMS–ACTRIMS Meeting. High-efficacy therapies such as alemtuzumab and natalizumab reduce the risk to a greater extent than do other DMTs.
Current immunotherapies do not slow secondary progressive MS after disease onset. The extent to which secondary progressive MS reflects early inflammation is not certain. Also unclear is whether conversion to secondary progressive MS might be modified by immunomodulatory DMTs during the relapsing-remitting phase.
Using an objective definition of secondary progressive MS published by Lorscheider et al in 2016, J. William L. Brown, MD, of the Queen Square MS Center at University College of London Institute of Neurology, and colleagues examined whether DMTs delay or reduce conversion from relapsing-remitting MS to secondary progressive MS. They examined patients with relapsing-remitting MS who participated in the MSBase database and were treated with a single DMT with at least four years of on-treatment follow-up. In all, 240 patients received injectables (ie, interferons or glatiramer acetate), 109 took fingolimod, 93 received natalizumab, and 44 took alemtuzumab.
Participants were each propensity matched to untreated patients with relapsing-remitting MS from a historical cohort (n = 622; mean follow-up, 9.2 years) and then matched to different DMT groups. Patients were matched on gender, baseline age, annualized-relapse rate, Expanded Disability Status Scale (EDSS) score, and disease duration. The researchers used weighted conditional proportional hazards models adjusted for EDSS frequency with pairwise censoring to compare the proportions of patients in each group who were free from conversion to secondary progressive MS.
Because lower-efficacy drug groups may have been biased towards participants with milder disease through excluding patients with multiple DMTs (such as treatment escalators), the investigators limited the injectables group to patients followed up before higher-efficacy drugs became available in 2006.
All DMTs reduced the hazard of conversion to secondary progressive MS, compared with different groups of matched untreated patients, in a series of pairwise analyses. For injectables, the hazard ratio (HR) of conversion to secondary progressive MS was 0.31 (median censored on-treatment follow-up, 7.9 years). For fingolimod, the HR was 0.23 (follow-up, 4.6 years). Natalizumab was associated with an HR of 0.50 (follow-up, 4.9 years). Alemtuzumab had an HR of 0.60 (follow-up, 7.2 years).
When the investigators matched patients between the treated cohorts, they found no significant difference in rate of conversion to secondary progressive MS between alemtuzumab and natalizumab. Alemtuzumab and natalizumab were therefore combined in a category of high-efficacy therapies (n = 118) and matched and compared with the injectables group (n = 236). High-efficacy therapies conferred greater protection against conversion to secondary progressive MS than injectables did (HR, 0.65; follow-up, 5.7 years).
PARIS—Secondary progressive multiple sclerosis (MS) is at least partly a consequence of early inflammation, and the risk of conversion from relapsing-remitting MS to secondary progressive MS is modifiable over five years with existing disease-modifying therapies (DMTs), according to research described at the Seventh Joint ECTRIMS–ACTRIMS Meeting. High-efficacy therapies such as alemtuzumab and natalizumab reduce the risk to a greater extent than do other DMTs.
Current immunotherapies do not slow secondary progressive MS after disease onset. The extent to which secondary progressive MS reflects early inflammation is not certain. Also unclear is whether conversion to secondary progressive MS might be modified by immunomodulatory DMTs during the relapsing-remitting phase.
Using an objective definition of secondary progressive MS published by Lorscheider et al in 2016, J. William L. Brown, MD, of the Queen Square MS Center at University College of London Institute of Neurology, and colleagues examined whether DMTs delay or reduce conversion from relapsing-remitting MS to secondary progressive MS. They examined patients with relapsing-remitting MS who participated in the MSBase database and were treated with a single DMT with at least four years of on-treatment follow-up. In all, 240 patients received injectables (ie, interferons or glatiramer acetate), 109 took fingolimod, 93 received natalizumab, and 44 took alemtuzumab.
Participants were each propensity matched to untreated patients with relapsing-remitting MS from a historical cohort (n = 622; mean follow-up, 9.2 years) and then matched to different DMT groups. Patients were matched on gender, baseline age, annualized-relapse rate, Expanded Disability Status Scale (EDSS) score, and disease duration. The researchers used weighted conditional proportional hazards models adjusted for EDSS frequency with pairwise censoring to compare the proportions of patients in each group who were free from conversion to secondary progressive MS.
Because lower-efficacy drug groups may have been biased towards participants with milder disease through excluding patients with multiple DMTs (such as treatment escalators), the investigators limited the injectables group to patients followed up before higher-efficacy drugs became available in 2006.
All DMTs reduced the hazard of conversion to secondary progressive MS, compared with different groups of matched untreated patients, in a series of pairwise analyses. For injectables, the hazard ratio (HR) of conversion to secondary progressive MS was 0.31 (median censored on-treatment follow-up, 7.9 years). For fingolimod, the HR was 0.23 (follow-up, 4.6 years). Natalizumab was associated with an HR of 0.50 (follow-up, 4.9 years). Alemtuzumab had an HR of 0.60 (follow-up, 7.2 years).
When the investigators matched patients between the treated cohorts, they found no significant difference in rate of conversion to secondary progressive MS between alemtuzumab and natalizumab. Alemtuzumab and natalizumab were therefore combined in a category of high-efficacy therapies (n = 118) and matched and compared with the injectables group (n = 236). High-efficacy therapies conferred greater protection against conversion to secondary progressive MS than injectables did (HR, 0.65; follow-up, 5.7 years).
PARIS—Secondary progressive multiple sclerosis (MS) is at least partly a consequence of early inflammation, and the risk of conversion from relapsing-remitting MS to secondary progressive MS is modifiable over five years with existing disease-modifying therapies (DMTs), according to research described at the Seventh Joint ECTRIMS–ACTRIMS Meeting. High-efficacy therapies such as alemtuzumab and natalizumab reduce the risk to a greater extent than do other DMTs.
Current immunotherapies do not slow secondary progressive MS after disease onset. The extent to which secondary progressive MS reflects early inflammation is not certain. Also unclear is whether conversion to secondary progressive MS might be modified by immunomodulatory DMTs during the relapsing-remitting phase.
Using an objective definition of secondary progressive MS published by Lorscheider et al in 2016, J. William L. Brown, MD, of the Queen Square MS Center at University College of London Institute of Neurology, and colleagues examined whether DMTs delay or reduce conversion from relapsing-remitting MS to secondary progressive MS. They examined patients with relapsing-remitting MS who participated in the MSBase database and were treated with a single DMT with at least four years of on-treatment follow-up. In all, 240 patients received injectables (ie, interferons or glatiramer acetate), 109 took fingolimod, 93 received natalizumab, and 44 took alemtuzumab.
Participants were each propensity matched to untreated patients with relapsing-remitting MS from a historical cohort (n = 622; mean follow-up, 9.2 years) and then matched to different DMT groups. Patients were matched on gender, baseline age, annualized-relapse rate, Expanded Disability Status Scale (EDSS) score, and disease duration. The researchers used weighted conditional proportional hazards models adjusted for EDSS frequency with pairwise censoring to compare the proportions of patients in each group who were free from conversion to secondary progressive MS.
Because lower-efficacy drug groups may have been biased towards participants with milder disease through excluding patients with multiple DMTs (such as treatment escalators), the investigators limited the injectables group to patients followed up before higher-efficacy drugs became available in 2006.
All DMTs reduced the hazard of conversion to secondary progressive MS, compared with different groups of matched untreated patients, in a series of pairwise analyses. For injectables, the hazard ratio (HR) of conversion to secondary progressive MS was 0.31 (median censored on-treatment follow-up, 7.9 years). For fingolimod, the HR was 0.23 (follow-up, 4.6 years). Natalizumab was associated with an HR of 0.50 (follow-up, 4.9 years). Alemtuzumab had an HR of 0.60 (follow-up, 7.2 years).
When the investigators matched patients between the treated cohorts, they found no significant difference in rate of conversion to secondary progressive MS between alemtuzumab and natalizumab. Alemtuzumab and natalizumab were therefore combined in a category of high-efficacy therapies (n = 118) and matched and compared with the injectables group (n = 236). High-efficacy therapies conferred greater protection against conversion to secondary progressive MS than injectables did (HR, 0.65; follow-up, 5.7 years).
Measures needed to identify past pregnancy in transgender male blood donors
SAN DIEGO –
In study results presented at the annual meeting of the American Association of Blood Banks, 3% of transgender males who were identified as such reported a prior history of pregnancy. Importantly, this pregnancy history may not be divulged unless transgender males are asked “female” questions, said Kathleen M. Grima, MD, executive medical officer at the American Red Cross and medical director of the blood bank at the Brooklyn Hospital Center, New York.
Several studies have suggested that blood from ever-pregnant female donors can present increased risks to male recipients. Research also has suggested that antibodies or other immune system factors that women develop when pregnant could trigger transfusion-related acute lung injury (TRALI), a serious inflammatory reaction that can result in death, in male blood-transfusion recipients.
For this reason, it is important to have pregnancy histories from blood donors, and obtaining those histories from transgender males “presents a challenge for blood centers,” she said. “At our center, when a donor requests a gender change from female to male, an HLA test is requested for the next donation.” But as first-time donors are qualified based on their stated gender, transgender donors who have been pregnant will not be identified unless they volunteer the information or are asked about their pregnancy history.
The AABB recommends that a facility can perform HLA testing on all apheresis plasma donors and all whole blood donors whose units are intended for production into plasma components or, as an alternative, obtain a pregnancy history from all female donors and perform HLA typing only on women with a history of one or more full-term pregnancies.
Dr. Grima explained that, prior to the implementation of the Food and Drug Administration’s “final rule” on requirements for blood and blood components, blood centers asked donors to identify their birth gender to determine eligibility. If gender had changed, the donor was then asked to answer both the male and female questions. The FDA’s final rule now allows blood centers to accept the donor’s stated gender and eligibility can be determined based on that gender.
Dr. Grima and her colleagues conducted a review to determine the number of transgender males who were actively donating with a large blood center and to assess the risk of failing to ask a transgender male donor about pregnancy.
From 2013 to 2015, there were 121 female donors who had changed their gender to male and 60 male donors who had changed their gender to female. Of this group, seven (6%) transgender male donors (female at birth) stated at one of their donations that they had a pregnancy history; three were apheresis donors who had been tested for HLA antibodies (one was positive and two negative). The other four were whole blood donors and had not been tested.
After 2016, donors self-identified their gender, and 326 had requested a gender change from female to male. Of this group, 5 (1.5%) answered yes to pregnancy questions, 56 said no, and 265 did not respond.
“In our system, if a donor identifies as a male, then they only see male questions,” she pointed out. The center subsequently added in a test for HLA antibodies, and 101 donors were tested. Of this group, 13 (13%) tested positive; 2 had answered yes to pregnancy, 4 answered no, and 7 did not respond to the pregnancy question.
Combining the two cohorts, there were 447 transgender males who were identified; 12 (3%) responded yes to pregnancy, and 5 (1%) tested positive for HLA antibodies.
“We are continuing to add the HLA test,” said Dr. Grima. “I’m not sure this is the best [approach], but we will see over time.”
But if a donor comes in for the first time or identifies as a male or transgender male, they won’t be tested, and this is an opportunity that will be missed, she added. “Another option is to ask all donors if they have been pregnant or continue to ask donors their birth gender and then require that they answer both the male and female questions.”
Dr. Grima had no financial disclosures.
SAN DIEGO –
In study results presented at the annual meeting of the American Association of Blood Banks, 3% of transgender males who were identified as such reported a prior history of pregnancy. Importantly, this pregnancy history may not be divulged unless transgender males are asked “female” questions, said Kathleen M. Grima, MD, executive medical officer at the American Red Cross and medical director of the blood bank at the Brooklyn Hospital Center, New York.
Several studies have suggested that blood from ever-pregnant female donors can present increased risks to male recipients. Research also has suggested that antibodies or other immune system factors that women develop when pregnant could trigger transfusion-related acute lung injury (TRALI), a serious inflammatory reaction that can result in death, in male blood-transfusion recipients.
For this reason, it is important to have pregnancy histories from blood donors, and obtaining those histories from transgender males “presents a challenge for blood centers,” she said. “At our center, when a donor requests a gender change from female to male, an HLA test is requested for the next donation.” But as first-time donors are qualified based on their stated gender, transgender donors who have been pregnant will not be identified unless they volunteer the information or are asked about their pregnancy history.
The AABB recommends that a facility can perform HLA testing on all apheresis plasma donors and all whole blood donors whose units are intended for production into plasma components or, as an alternative, obtain a pregnancy history from all female donors and perform HLA typing only on women with a history of one or more full-term pregnancies.
Dr. Grima explained that, prior to the implementation of the Food and Drug Administration’s “final rule” on requirements for blood and blood components, blood centers asked donors to identify their birth gender to determine eligibility. If gender had changed, the donor was then asked to answer both the male and female questions. The FDA’s final rule now allows blood centers to accept the donor’s stated gender and eligibility can be determined based on that gender.
Dr. Grima and her colleagues conducted a review to determine the number of transgender males who were actively donating with a large blood center and to assess the risk of failing to ask a transgender male donor about pregnancy.
From 2013 to 2015, there were 121 female donors who had changed their gender to male and 60 male donors who had changed their gender to female. Of this group, seven (6%) transgender male donors (female at birth) stated at one of their donations that they had a pregnancy history; three were apheresis donors who had been tested for HLA antibodies (one was positive and two negative). The other four were whole blood donors and had not been tested.
After 2016, donors self-identified their gender, and 326 had requested a gender change from female to male. Of this group, 5 (1.5%) answered yes to pregnancy questions, 56 said no, and 265 did not respond.
“In our system, if a donor identifies as a male, then they only see male questions,” she pointed out. The center subsequently added in a test for HLA antibodies, and 101 donors were tested. Of this group, 13 (13%) tested positive; 2 had answered yes to pregnancy, 4 answered no, and 7 did not respond to the pregnancy question.
Combining the two cohorts, there were 447 transgender males who were identified; 12 (3%) responded yes to pregnancy, and 5 (1%) tested positive for HLA antibodies.
“We are continuing to add the HLA test,” said Dr. Grima. “I’m not sure this is the best [approach], but we will see over time.”
But if a donor comes in for the first time or identifies as a male or transgender male, they won’t be tested, and this is an opportunity that will be missed, she added. “Another option is to ask all donors if they have been pregnant or continue to ask donors their birth gender and then require that they answer both the male and female questions.”
Dr. Grima had no financial disclosures.
SAN DIEGO –
In study results presented at the annual meeting of the American Association of Blood Banks, 3% of transgender males who were identified as such reported a prior history of pregnancy. Importantly, this pregnancy history may not be divulged unless transgender males are asked “female” questions, said Kathleen M. Grima, MD, executive medical officer at the American Red Cross and medical director of the blood bank at the Brooklyn Hospital Center, New York.
Several studies have suggested that blood from ever-pregnant female donors can present increased risks to male recipients. Research also has suggested that antibodies or other immune system factors that women develop when pregnant could trigger transfusion-related acute lung injury (TRALI), a serious inflammatory reaction that can result in death, in male blood-transfusion recipients.
For this reason, it is important to have pregnancy histories from blood donors, and obtaining those histories from transgender males “presents a challenge for blood centers,” she said. “At our center, when a donor requests a gender change from female to male, an HLA test is requested for the next donation.” But as first-time donors are qualified based on their stated gender, transgender donors who have been pregnant will not be identified unless they volunteer the information or are asked about their pregnancy history.
The AABB recommends that a facility can perform HLA testing on all apheresis plasma donors and all whole blood donors whose units are intended for production into plasma components or, as an alternative, obtain a pregnancy history from all female donors and perform HLA typing only on women with a history of one or more full-term pregnancies.
Dr. Grima explained that, prior to the implementation of the Food and Drug Administration’s “final rule” on requirements for blood and blood components, blood centers asked donors to identify their birth gender to determine eligibility. If gender had changed, the donor was then asked to answer both the male and female questions. The FDA’s final rule now allows blood centers to accept the donor’s stated gender and eligibility can be determined based on that gender.
Dr. Grima and her colleagues conducted a review to determine the number of transgender males who were actively donating with a large blood center and to assess the risk of failing to ask a transgender male donor about pregnancy.
From 2013 to 2015, there were 121 female donors who had changed their gender to male and 60 male donors who had changed their gender to female. Of this group, seven (6%) transgender male donors (female at birth) stated at one of their donations that they had a pregnancy history; three were apheresis donors who had been tested for HLA antibodies (one was positive and two negative). The other four were whole blood donors and had not been tested.
After 2016, donors self-identified their gender, and 326 had requested a gender change from female to male. Of this group, 5 (1.5%) answered yes to pregnancy questions, 56 said no, and 265 did not respond.
“In our system, if a donor identifies as a male, then they only see male questions,” she pointed out. The center subsequently added in a test for HLA antibodies, and 101 donors were tested. Of this group, 13 (13%) tested positive; 2 had answered yes to pregnancy, 4 answered no, and 7 did not respond to the pregnancy question.
Combining the two cohorts, there were 447 transgender males who were identified; 12 (3%) responded yes to pregnancy, and 5 (1%) tested positive for HLA antibodies.
“We are continuing to add the HLA test,” said Dr. Grima. “I’m not sure this is the best [approach], but we will see over time.”
But if a donor comes in for the first time or identifies as a male or transgender male, they won’t be tested, and this is an opportunity that will be missed, she added. “Another option is to ask all donors if they have been pregnant or continue to ask donors their birth gender and then require that they answer both the male and female questions.”
Dr. Grima had no financial disclosures.
AT AABB17
Key clinical point: First-time transgender male donors with a history of pregnancy will not be identified, and HLA testing might not be performed unless these donors volunteer this information.
Major finding: Among 447 transgender males who were identified, 3% had been pregnant, and 1% tested positive for HLA antibodies.
Data source: A review of data from the blood bank at the Brooklyn Hospital Center, New York.
Disclosures: Dr. Grima had no financial disclosures.
Antibiotic exposure blunted metabolic improvement following vertical sleeve gastrectomy
SAN DIEGO – results from a mouse study demonstrated.
The finding raises the question of whether patients with suboptimal outcomes following vertical sleeve gastrectomy may benefit from microbial modulation.

According to Dr. Jahansouz of the University of Minnesota Microbiota Transplantation Program, mechanisms mediating metabolic improvement following bariatric surgery remain incompletely understood. “Outcomes are also somewhat variable: As many as 40%-75% of patients regain weight in the years following nadir of weight loss,” he said. “Human studies have shown an acute and sustained shift in the gut microbiota, and an altered bile acid profile. Bile acids increase following surgery.”
Meanwhile, mice deficient in Farnesoid X-receptor (FXR) and Takeda G protein–coupled Receptor 5 (TGR5) do not experience metabolic improvement following bariatric surgery; the composition of the microbiome can significantly impact the composition of bile acids.
“By altering the postsurgical composition of mice following bariatric surgery, we eliminate the metabolic benefits of surgery, possibly by altering bile acid profiles,” Dr. Jahansouz said.
For the trial, diet-induced obese mice were randomized to vertical sleeve gastrectomy (VSG) or sham surgery, with or without exposure to antibiotics that selectively suppress mainly gram-positive (fidaxomicin, streptomycin) or gram-negative (ceftriaxone) bacteria on postoperative days 1-4. The researchers characterized fecal microbiota before surgery and on postoperative days 7 and 28. Mice were metabolically characterized on postoperative days 30-32 and euthanized on postoperative day 35.
Mice in the VSG group experienced weight loss and shifts in the intestinal microbiota composition, compared with those in the sham surgery group.
“Antibiotic exposure resulted in sustained reductions in alpha (within sample) diversity of microbiota and shifts in its composition,” the researchers wrote in their abstract. “Different antimicrobial specificity of antibiotics led to functionally distinct physiologic effects. Specifically, fidaxomicin and streptomycin markedly altered hepatic bile acid signaling and lipid metabolism, while ceftriaxone resulted in greater reduction in the expression of key antimicrobial peptides.
“However, VSG mice exposed to antibiotics, regardless of their specificity, had significantly increased subcutaneous adiposity and impaired glucose homeostasis without changes in food intake, relative to control mice,” the investigators noted.
Dr. Jahansouz said that he was surprised by the fact that all three antibiotics tested, no matter their specificity in gut bacteria eliminated, resulted in significantly diminished weight loss and metabolic improvement following vertical sleeve gastrectomy in the mouse model. He acknowledged that translating the findings from mice to humans is a key limitation of the analysis.
“There are fundamental physiologic differences between mice and humans that need consideration in all murine models of metabolic disorders,” he said. “Therefore, it is critical that insights gained from these models are followed up in human studies.”
The study was funded by the American Diabetes Association and a Minnesota Discovery, Research and InnoVation Economy grant from the University of Minnesota. Dr. Jahansouz reported having no financial disclosures.
SAN DIEGO – results from a mouse study demonstrated.
The finding raises the question of whether patients with suboptimal outcomes following vertical sleeve gastrectomy may benefit from microbial modulation.
According to Dr. Jahansouz of the University of Minnesota Microbiota Transplantation Program, mechanisms mediating metabolic improvement following bariatric surgery remain incompletely understood. “Outcomes are also somewhat variable: As many as 40%-75% of patients regain weight in the years following nadir of weight loss,” he said. “Human studies have shown an acute and sustained shift in the gut microbiota, and an altered bile acid profile. Bile acids increase following surgery.”
Meanwhile, mice deficient in Farnesoid X-receptor (FXR) and Takeda G protein–coupled Receptor 5 (TGR5) do not experience metabolic improvement following bariatric surgery; the composition of the microbiome can significantly impact the composition of bile acids.
“By altering the postsurgical composition of mice following bariatric surgery, we eliminate the metabolic benefits of surgery, possibly by altering bile acid profiles,” Dr. Jahansouz said.
For the trial, diet-induced obese mice were randomized to vertical sleeve gastrectomy (VSG) or sham surgery, with or without exposure to antibiotics that selectively suppress mainly gram-positive (fidaxomicin, streptomycin) or gram-negative (ceftriaxone) bacteria on postoperative days 1-4. The researchers characterized fecal microbiota before surgery and on postoperative days 7 and 28. Mice were metabolically characterized on postoperative days 30-32 and euthanized on postoperative day 35.
Mice in the VSG group experienced weight loss and shifts in the intestinal microbiota composition, compared with those in the sham surgery group.
“Antibiotic exposure resulted in sustained reductions in alpha (within sample) diversity of microbiota and shifts in its composition,” the researchers wrote in their abstract. “Different antimicrobial specificity of antibiotics led to functionally distinct physiologic effects. Specifically, fidaxomicin and streptomycin markedly altered hepatic bile acid signaling and lipid metabolism, while ceftriaxone resulted in greater reduction in the expression of key antimicrobial peptides.
“However, VSG mice exposed to antibiotics, regardless of their specificity, had significantly increased subcutaneous adiposity and impaired glucose homeostasis without changes in food intake, relative to control mice,” the investigators noted.
Dr. Jahansouz said that he was surprised by the fact that all three antibiotics tested, no matter their specificity in gut bacteria eliminated, resulted in significantly diminished weight loss and metabolic improvement following vertical sleeve gastrectomy in the mouse model. He acknowledged that translating the findings from mice to humans is a key limitation of the analysis.
“There are fundamental physiologic differences between mice and humans that need consideration in all murine models of metabolic disorders,” he said. “Therefore, it is critical that insights gained from these models are followed up in human studies.”
The study was funded by the American Diabetes Association and a Minnesota Discovery, Research and InnoVation Economy grant from the University of Minnesota. Dr. Jahansouz reported having no financial disclosures.
SAN DIEGO – results from a mouse study demonstrated.
The finding raises the question of whether patients with suboptimal outcomes following vertical sleeve gastrectomy may benefit from microbial modulation.
According to Dr. Jahansouz of the University of Minnesota Microbiota Transplantation Program, mechanisms mediating metabolic improvement following bariatric surgery remain incompletely understood. “Outcomes are also somewhat variable: As many as 40%-75% of patients regain weight in the years following nadir of weight loss,” he said. “Human studies have shown an acute and sustained shift in the gut microbiota, and an altered bile acid profile. Bile acids increase following surgery.”
Meanwhile, mice deficient in Farnesoid X-receptor (FXR) and Takeda G protein–coupled Receptor 5 (TGR5) do not experience metabolic improvement following bariatric surgery; the composition of the microbiome can significantly impact the composition of bile acids.
“By altering the postsurgical composition of mice following bariatric surgery, we eliminate the metabolic benefits of surgery, possibly by altering bile acid profiles,” Dr. Jahansouz said.
For the trial, diet-induced obese mice were randomized to vertical sleeve gastrectomy (VSG) or sham surgery, with or without exposure to antibiotics that selectively suppress mainly gram-positive (fidaxomicin, streptomycin) or gram-negative (ceftriaxone) bacteria on postoperative days 1-4. The researchers characterized fecal microbiota before surgery and on postoperative days 7 and 28. Mice were metabolically characterized on postoperative days 30-32 and euthanized on postoperative day 35.
Mice in the VSG group experienced weight loss and shifts in the intestinal microbiota composition, compared with those in the sham surgery group.
“Antibiotic exposure resulted in sustained reductions in alpha (within sample) diversity of microbiota and shifts in its composition,” the researchers wrote in their abstract. “Different antimicrobial specificity of antibiotics led to functionally distinct physiologic effects. Specifically, fidaxomicin and streptomycin markedly altered hepatic bile acid signaling and lipid metabolism, while ceftriaxone resulted in greater reduction in the expression of key antimicrobial peptides.
“However, VSG mice exposed to antibiotics, regardless of their specificity, had significantly increased subcutaneous adiposity and impaired glucose homeostasis without changes in food intake, relative to control mice,” the investigators noted.
Dr. Jahansouz said that he was surprised by the fact that all three antibiotics tested, no matter their specificity in gut bacteria eliminated, resulted in significantly diminished weight loss and metabolic improvement following vertical sleeve gastrectomy in the mouse model. He acknowledged that translating the findings from mice to humans is a key limitation of the analysis.
“There are fundamental physiologic differences between mice and humans that need consideration in all murine models of metabolic disorders,” he said. “Therefore, it is critical that insights gained from these models are followed up in human studies.”
The study was funded by the American Diabetes Association and a Minnesota Discovery, Research and InnoVation Economy grant from the University of Minnesota. Dr. Jahansouz reported having no financial disclosures.
AT THE ACS CLINICAL CONGRESS
Key clinical point: Postsurgical disruption of intestinal microbiota composition attenuates the metabolic efficacy of vertical sleeve gastrectomy.
Major finding: VSG mice exposed to antibiotics had significantly increased subcutaneous adiposity and impaired glucose homeostasis without changes in food intake, compared with control mice.
Study details: A study of diet-induced obese mice that were randomized to VSG or sham surgery, with or without exposure to antibiotics.
Disclosures: The study was funded by the American Diabetes Association and a Minnesota Discovery, Research and InnoVation Economy grant from the University of Minnesota. Dr. Jahansouz reported having no financial disclosures.
Emphasizing an entrepreneurial spirit: Raman Palabindala, MD
Venkatraraman “Raman” Palabindala, MD, FACP, SFHM, was destined to be a doctor since his first breath. Born in India, his father decided Dr. Palabindala would take the mantle as the doctor of the family, while his siblings took to other professions like engineering.
Eager to be in the thick of things, Dr. Palabindala has voraciously pursued leadership positions, leading to his current role as chief of the Division of Hospital Medicine at the University of Mississippi Medical Center, Jackson.

Dr. Palabindala is enthusiastic about his role as one of the eight new members of The Hospitalist editorial advisory board, and took time to tell us more about himself in a recent interview.
Q: How did you get into medicine?
A: It’s all because of my dad’s motivation. My father believed in education, so when I was born, he said, “He’s going to be a doctor,” and as I grew up, I just worked towards being a physician and nothing else. I didn’t even have an option of choosing anything else. My dad said that I would be a doctor, and I am a doctor. I feel like that was the best thing that happened to me, though; it worked out well.
Q: How and when did you decide to go into hospital medicine?
A: After I came to the U.S., I joined residency in internal medicine at GBMC – that’s Greater Baltimore Medical Center – it’s affiliated with Johns Hopkins. I always wanted to be an internist, but my experiences in the clinic world were not so great. But I really enjoyed inpatient medicine, so in my 3rd year, when I was doing my chief residency year, I did get opportunities to join a fellowship, but I decided just to be a hospitalist at that time.
Q: What do you find to be rewarding about hospital medicine?

Q: What is one of the biggest challenges in hospital medicine?
A: I think talking about the business aspect of medicine, because it is like a taboo. We don’t really want to talk about whether the patient is covered or not covered by insurance, how much we are billing, and why we must discuss business issues while we are trying to focus on patient care, but these things are going to indirectly affect patient care, too. If you didn’t note the patient status accurately, they are going to get an inappropriate bill.
Q: What’s the best advice you have received that you try to pass on to your students?
A: Do the rounds at the bedside. We have the tendency of doing everything outside and then going in the room and just telling the patient what we are going to do. Instead, I encourage everyone to be at the bedside. Even without students, I go and sit at the bedside and then review the data in terms the patient can understand, and then explain the care plan, so they actually feel like we are at the bedside for a longer time. We are with the patient for at least 10 to 15 minutes, but at the same time, we are getting things done. I encourage my students and residents to do this.
Q: What is the worst advice you’ve received?
A: I don’t know if this is the “worst” advice, but in my second year, I was trying to take some leadership positions and was told I should wait, that leadership skills come with experience. I do think that’s a bad piece of advice. It’s all about learning how hard you work and then how fast you learn, and then how fast you implement. People who work, learn, and implement quickly can make a difference.
Q: Outside of patient care, what other career interests do you have?
A: I’m interested in smart clinics, and I actually have a patent for smart clinic chains. I’m a big fan of primary care, because, like hospitalists revolutionized inpatient care, I think we can revolutionize the outpatient care experience as well. I don’t think we are being very efficient with outpatient care.
But if I was not practicing medicine, I probably would be a chef. I like to cook, and I would open up my own restaurant if I was not doing this.
Q: Where do you see yourself in 10 years?
A: I want to be a consultant, evaluating hospitalist programs and guiding programs to grow and be more efficient. That, I think, would be the primary job that I would like to be doing, along with giving lectures and teaching about patient safety and quality, and educating younger physicians about the business of medicine.
Q: What experience with SHM has made the most lasting impact on you?
A: I would say the best impression was from the Academic Hospitalist Academy meeting I attended in Denver. I think that was helpful, because it was like a boot camp where you have only a limited number of attendees with a dedicated mentor. That was amazing, and I learned a lot. It helped me in redesigning my approach to where I would like to be both short- and long-term. I implemented at least 50 percent of what I learned at that meeting.
Q: What’s the best book that you’ve read recently and why was it the best?
A: Being Mortal by Atul Gawande. It’s a really beautiful book.
[email protected]
On Twitter @eaztweets
Venkatraraman “Raman” Palabindala, MD, FACP, SFHM, was destined to be a doctor since his first breath. Born in India, his father decided Dr. Palabindala would take the mantle as the doctor of the family, while his siblings took to other professions like engineering.
Eager to be in the thick of things, Dr. Palabindala has voraciously pursued leadership positions, leading to his current role as chief of the Division of Hospital Medicine at the University of Mississippi Medical Center, Jackson.
Dr. Palabindala is enthusiastic about his role as one of the eight new members of The Hospitalist editorial advisory board, and took time to tell us more about himself in a recent interview.
Q: How did you get into medicine?
A: It’s all because of my dad’s motivation. My father believed in education, so when I was born, he said, “He’s going to be a doctor,” and as I grew up, I just worked towards being a physician and nothing else. I didn’t even have an option of choosing anything else. My dad said that I would be a doctor, and I am a doctor. I feel like that was the best thing that happened to me, though; it worked out well.
Q: How and when did you decide to go into hospital medicine?
A: After I came to the U.S., I joined residency in internal medicine at GBMC – that’s Greater Baltimore Medical Center – it’s affiliated with Johns Hopkins. I always wanted to be an internist, but my experiences in the clinic world were not so great. But I really enjoyed inpatient medicine, so in my 3rd year, when I was doing my chief residency year, I did get opportunities to join a fellowship, but I decided just to be a hospitalist at that time.
Q: What do you find to be rewarding about hospital medicine?
Q: What is one of the biggest challenges in hospital medicine?
A: I think talking about the business aspect of medicine, because it is like a taboo. We don’t really want to talk about whether the patient is covered or not covered by insurance, how much we are billing, and why we must discuss business issues while we are trying to focus on patient care, but these things are going to indirectly affect patient care, too. If you didn’t note the patient status accurately, they are going to get an inappropriate bill.
Q: What’s the best advice you have received that you try to pass on to your students?
A: Do the rounds at the bedside. We have the tendency of doing everything outside and then going in the room and just telling the patient what we are going to do. Instead, I encourage everyone to be at the bedside. Even without students, I go and sit at the bedside and then review the data in terms the patient can understand, and then explain the care plan, so they actually feel like we are at the bedside for a longer time. We are with the patient for at least 10 to 15 minutes, but at the same time, we are getting things done. I encourage my students and residents to do this.
Q: What is the worst advice you’ve received?
A: I don’t know if this is the “worst” advice, but in my second year, I was trying to take some leadership positions and was told I should wait, that leadership skills come with experience. I do think that’s a bad piece of advice. It’s all about learning how hard you work and then how fast you learn, and then how fast you implement. People who work, learn, and implement quickly can make a difference.
Q: Outside of patient care, what other career interests do you have?
A: I’m interested in smart clinics, and I actually have a patent for smart clinic chains. I’m a big fan of primary care, because, like hospitalists revolutionized inpatient care, I think we can revolutionize the outpatient care experience as well. I don’t think we are being very efficient with outpatient care.
But if I was not practicing medicine, I probably would be a chef. I like to cook, and I would open up my own restaurant if I was not doing this.
Q: Where do you see yourself in 10 years?
A: I want to be a consultant, evaluating hospitalist programs and guiding programs to grow and be more efficient. That, I think, would be the primary job that I would like to be doing, along with giving lectures and teaching about patient safety and quality, and educating younger physicians about the business of medicine.
Q: What experience with SHM has made the most lasting impact on you?
A: I would say the best impression was from the Academic Hospitalist Academy meeting I attended in Denver. I think that was helpful, because it was like a boot camp where you have only a limited number of attendees with a dedicated mentor. That was amazing, and I learned a lot. It helped me in redesigning my approach to where I would like to be both short- and long-term. I implemented at least 50 percent of what I learned at that meeting.
Q: What’s the best book that you’ve read recently and why was it the best?
A: Being Mortal by Atul Gawande. It’s a really beautiful book.
[email protected]
On Twitter @eaztweets
Venkatraraman “Raman” Palabindala, MD, FACP, SFHM, was destined to be a doctor since his first breath. Born in India, his father decided Dr. Palabindala would take the mantle as the doctor of the family, while his siblings took to other professions like engineering.
Eager to be in the thick of things, Dr. Palabindala has voraciously pursued leadership positions, leading to his current role as chief of the Division of Hospital Medicine at the University of Mississippi Medical Center, Jackson.
Dr. Palabindala is enthusiastic about his role as one of the eight new members of The Hospitalist editorial advisory board, and took time to tell us more about himself in a recent interview.
Q: How did you get into medicine?
A: It’s all because of my dad’s motivation. My father believed in education, so when I was born, he said, “He’s going to be a doctor,” and as I grew up, I just worked towards being a physician and nothing else. I didn’t even have an option of choosing anything else. My dad said that I would be a doctor, and I am a doctor. I feel like that was the best thing that happened to me, though; it worked out well.
Q: How and when did you decide to go into hospital medicine?
A: After I came to the U.S., I joined residency in internal medicine at GBMC – that’s Greater Baltimore Medical Center – it’s affiliated with Johns Hopkins. I always wanted to be an internist, but my experiences in the clinic world were not so great. But I really enjoyed inpatient medicine, so in my 3rd year, when I was doing my chief residency year, I did get opportunities to join a fellowship, but I decided just to be a hospitalist at that time.
Q: What do you find to be rewarding about hospital medicine?
Q: What is one of the biggest challenges in hospital medicine?
A: I think talking about the business aspect of medicine, because it is like a taboo. We don’t really want to talk about whether the patient is covered or not covered by insurance, how much we are billing, and why we must discuss business issues while we are trying to focus on patient care, but these things are going to indirectly affect patient care, too. If you didn’t note the patient status accurately, they are going to get an inappropriate bill.
Q: What’s the best advice you have received that you try to pass on to your students?
A: Do the rounds at the bedside. We have the tendency of doing everything outside and then going in the room and just telling the patient what we are going to do. Instead, I encourage everyone to be at the bedside. Even without students, I go and sit at the bedside and then review the data in terms the patient can understand, and then explain the care plan, so they actually feel like we are at the bedside for a longer time. We are with the patient for at least 10 to 15 minutes, but at the same time, we are getting things done. I encourage my students and residents to do this.
Q: What is the worst advice you’ve received?
A: I don’t know if this is the “worst” advice, but in my second year, I was trying to take some leadership positions and was told I should wait, that leadership skills come with experience. I do think that’s a bad piece of advice. It’s all about learning how hard you work and then how fast you learn, and then how fast you implement. People who work, learn, and implement quickly can make a difference.
Q: Outside of patient care, what other career interests do you have?
A: I’m interested in smart clinics, and I actually have a patent for smart clinic chains. I’m a big fan of primary care, because, like hospitalists revolutionized inpatient care, I think we can revolutionize the outpatient care experience as well. I don’t think we are being very efficient with outpatient care.
But if I was not practicing medicine, I probably would be a chef. I like to cook, and I would open up my own restaurant if I was not doing this.
Q: Where do you see yourself in 10 years?
A: I want to be a consultant, evaluating hospitalist programs and guiding programs to grow and be more efficient. That, I think, would be the primary job that I would like to be doing, along with giving lectures and teaching about patient safety and quality, and educating younger physicians about the business of medicine.
Q: What experience with SHM has made the most lasting impact on you?
A: I would say the best impression was from the Academic Hospitalist Academy meeting I attended in Denver. I think that was helpful, because it was like a boot camp where you have only a limited number of attendees with a dedicated mentor. That was amazing, and I learned a lot. It helped me in redesigning my approach to where I would like to be both short- and long-term. I implemented at least 50 percent of what I learned at that meeting.
Q: What’s the best book that you’ve read recently and why was it the best?
A: Being Mortal by Atul Gawande. It’s a really beautiful book.
[email protected]
On Twitter @eaztweets
You can help with behavior of children with autism spectrum disorder
There are lots of reasons you may be eager to refer children with autism spectrum disorder (ASD) to specialty agencies. You want the fastest possible entry for the child into intervention and the families into a support system. , as well as the general health care, of their children.
“Wait!” you say, “I do not have the special knowledge to help with behavior of children with autism! There is much you can and should do, however, as the specialist(s) may not provide such guidance, entry into behavioral services may take months, and behavior issues may feel urgent to families.

So pick an example of a behavior that is concerning to the family. One problem might be lack of cooperation with activities of daily living such as eating. In this case, the A is being asked to stop playing and sit at the table; the B may be refusing to eat what is served or even to sit very long, ending in a tantrum that disrupts the family meal; and the C could be the child being sent from the table to play on their iPad. But what is the G?
Lack of social communication skills, restrictive interests, hypersensitivity, lack of coordination, and ADHD all may be playing a role. Lack of communication skills makes the social aspect of meals uninteresting. Giving verbal reasons for joining the family may not be effective. Hypersensitivity often is associated with extremes of food selectivity. Lack of fine motor coordination makes eating soup a challenge. And ADHD makes sitting for a long time difficult!

But what about that tantrum? Tantrums that are reinforced by allowing the child to leave and play on the iPad easily can turn into a chronic escape mechanism. Instead, parents need to watch for increasing restlessness, and allow the child to signal “all done” and be “excused” before any tantrum begins. Use of the iPad (a reward) should not be allowed until the family meal is over for everyone. Such accommodations are best decided on by all caregivers in advance, ideally also involving the higher-functioning child. A caregiver who persists in thinking that the child “should” be able to behave may be in denial or grief, and deserves counseling on ASD.
But he is so rigid, the parents say! The tendency of children with ASD to like sameness can be an asset to easing behavior. The key is to design and stick to routines as much as possible, 7 days per week. If the meal is at the same time each day, in the same seat, with the same plate, with no iPad, and the child is allowed to leave only after requesting to, the entire sequence is likely to be smoother. While flexibility does not come easily, it is acquired from the natural variability in family life, but only gradually and over time.
Creating and rehearsing “social stories” is an evidence-based way to help children with ASD have acceptable behaviors. Books, storyboards, and visual schedulers can be purchased to help. But even taking photos or a video of the components of a task and posting this online (private YouTube channel) or on the refrigerator, to review before, during, and/or after the activity, builds an internal image for the child. Children with ASD often watch the same YouTube videos over and over again, and even memorize and use chunks of the speech or songs at other times. Families can capitalize on this kind of repetition by using routines and songs to improve skills.
What to do when she only cares about her iPad? It is sometimes difficult to identify reinforcers to use to strengthen desired behaviors in a child with ASD. A smile or a hug or even candy may not be valued. Help parents think about an object, song, or touch the child tends to like. Media are a strong reinforcer, but need to be used sparingly, in specific situations, and kept under parental control, or else removing them can become a major source of upsets.
When a child with ASD gets upset or even violent, the behavior may be interpreted as defiance; it may scare or upset the whole family, and is not conducive to problem solving. Siblings may start screaming or begging for the parents to stop the behavior. While this creates a crisis, you can advise parents to first ensure that everyone is safe, take deep breaths, and then think about which gap is being stressed. A subtle change from what the child expected – new furniture, a guest at the table, a day off from school, or being interrupted mid video – can cause panic, especially for anxious children. Children with ASD also may act up when uncomfortable from a headache, tooth pain, constipation, hunger, or lack of sleep, but often are unable to vocalize the reason, even if they are verbal. Having parents make a few notes about the As, Bs, Cs, and Gs of each event (the essence of a functional behavioral assessment) to review with the child, each other, the teacher, or you is key to understanding the child with ASD and successfully shifting his behavior.
Dr. Howard is an assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News.
There are lots of reasons you may be eager to refer children with autism spectrum disorder (ASD) to specialty agencies. You want the fastest possible entry for the child into intervention and the families into a support system. , as well as the general health care, of their children.
“Wait!” you say, “I do not have the special knowledge to help with behavior of children with autism! There is much you can and should do, however, as the specialist(s) may not provide such guidance, entry into behavioral services may take months, and behavior issues may feel urgent to families.
So pick an example of a behavior that is concerning to the family. One problem might be lack of cooperation with activities of daily living such as eating. In this case, the A is being asked to stop playing and sit at the table; the B may be refusing to eat what is served or even to sit very long, ending in a tantrum that disrupts the family meal; and the C could be the child being sent from the table to play on their iPad. But what is the G?
Lack of social communication skills, restrictive interests, hypersensitivity, lack of coordination, and ADHD all may be playing a role. Lack of communication skills makes the social aspect of meals uninteresting. Giving verbal reasons for joining the family may not be effective. Hypersensitivity often is associated with extremes of food selectivity. Lack of fine motor coordination makes eating soup a challenge. And ADHD makes sitting for a long time difficult!
But what about that tantrum? Tantrums that are reinforced by allowing the child to leave and play on the iPad easily can turn into a chronic escape mechanism. Instead, parents need to watch for increasing restlessness, and allow the child to signal “all done” and be “excused” before any tantrum begins. Use of the iPad (a reward) should not be allowed until the family meal is over for everyone. Such accommodations are best decided on by all caregivers in advance, ideally also involving the higher-functioning child. A caregiver who persists in thinking that the child “should” be able to behave may be in denial or grief, and deserves counseling on ASD.
But he is so rigid, the parents say! The tendency of children with ASD to like sameness can be an asset to easing behavior. The key is to design and stick to routines as much as possible, 7 days per week. If the meal is at the same time each day, in the same seat, with the same plate, with no iPad, and the child is allowed to leave only after requesting to, the entire sequence is likely to be smoother. While flexibility does not come easily, it is acquired from the natural variability in family life, but only gradually and over time.
Creating and rehearsing “social stories” is an evidence-based way to help children with ASD have acceptable behaviors. Books, storyboards, and visual schedulers can be purchased to help. But even taking photos or a video of the components of a task and posting this online (private YouTube channel) or on the refrigerator, to review before, during, and/or after the activity, builds an internal image for the child. Children with ASD often watch the same YouTube videos over and over again, and even memorize and use chunks of the speech or songs at other times. Families can capitalize on this kind of repetition by using routines and songs to improve skills.
What to do when she only cares about her iPad? It is sometimes difficult to identify reinforcers to use to strengthen desired behaviors in a child with ASD. A smile or a hug or even candy may not be valued. Help parents think about an object, song, or touch the child tends to like. Media are a strong reinforcer, but need to be used sparingly, in specific situations, and kept under parental control, or else removing them can become a major source of upsets.
When a child with ASD gets upset or even violent, the behavior may be interpreted as defiance; it may scare or upset the whole family, and is not conducive to problem solving. Siblings may start screaming or begging for the parents to stop the behavior. While this creates a crisis, you can advise parents to first ensure that everyone is safe, take deep breaths, and then think about which gap is being stressed. A subtle change from what the child expected – new furniture, a guest at the table, a day off from school, or being interrupted mid video – can cause panic, especially for anxious children. Children with ASD also may act up when uncomfortable from a headache, tooth pain, constipation, hunger, or lack of sleep, but often are unable to vocalize the reason, even if they are verbal. Having parents make a few notes about the As, Bs, Cs, and Gs of each event (the essence of a functional behavioral assessment) to review with the child, each other, the teacher, or you is key to understanding the child with ASD and successfully shifting his behavior.
Dr. Howard is an assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News.
There are lots of reasons you may be eager to refer children with autism spectrum disorder (ASD) to specialty agencies. You want the fastest possible entry for the child into intervention and the families into a support system. , as well as the general health care, of their children.
“Wait!” you say, “I do not have the special knowledge to help with behavior of children with autism! There is much you can and should do, however, as the specialist(s) may not provide such guidance, entry into behavioral services may take months, and behavior issues may feel urgent to families.
So pick an example of a behavior that is concerning to the family. One problem might be lack of cooperation with activities of daily living such as eating. In this case, the A is being asked to stop playing and sit at the table; the B may be refusing to eat what is served or even to sit very long, ending in a tantrum that disrupts the family meal; and the C could be the child being sent from the table to play on their iPad. But what is the G?
Lack of social communication skills, restrictive interests, hypersensitivity, lack of coordination, and ADHD all may be playing a role. Lack of communication skills makes the social aspect of meals uninteresting. Giving verbal reasons for joining the family may not be effective. Hypersensitivity often is associated with extremes of food selectivity. Lack of fine motor coordination makes eating soup a challenge. And ADHD makes sitting for a long time difficult!
But what about that tantrum? Tantrums that are reinforced by allowing the child to leave and play on the iPad easily can turn into a chronic escape mechanism. Instead, parents need to watch for increasing restlessness, and allow the child to signal “all done” and be “excused” before any tantrum begins. Use of the iPad (a reward) should not be allowed until the family meal is over for everyone. Such accommodations are best decided on by all caregivers in advance, ideally also involving the higher-functioning child. A caregiver who persists in thinking that the child “should” be able to behave may be in denial or grief, and deserves counseling on ASD.
But he is so rigid, the parents say! The tendency of children with ASD to like sameness can be an asset to easing behavior. The key is to design and stick to routines as much as possible, 7 days per week. If the meal is at the same time each day, in the same seat, with the same plate, with no iPad, and the child is allowed to leave only after requesting to, the entire sequence is likely to be smoother. While flexibility does not come easily, it is acquired from the natural variability in family life, but only gradually and over time.
Creating and rehearsing “social stories” is an evidence-based way to help children with ASD have acceptable behaviors. Books, storyboards, and visual schedulers can be purchased to help. But even taking photos or a video of the components of a task and posting this online (private YouTube channel) or on the refrigerator, to review before, during, and/or after the activity, builds an internal image for the child. Children with ASD often watch the same YouTube videos over and over again, and even memorize and use chunks of the speech or songs at other times. Families can capitalize on this kind of repetition by using routines and songs to improve skills.
What to do when she only cares about her iPad? It is sometimes difficult to identify reinforcers to use to strengthen desired behaviors in a child with ASD. A smile or a hug or even candy may not be valued. Help parents think about an object, song, or touch the child tends to like. Media are a strong reinforcer, but need to be used sparingly, in specific situations, and kept under parental control, or else removing them can become a major source of upsets.
When a child with ASD gets upset or even violent, the behavior may be interpreted as defiance; it may scare or upset the whole family, and is not conducive to problem solving. Siblings may start screaming or begging for the parents to stop the behavior. While this creates a crisis, you can advise parents to first ensure that everyone is safe, take deep breaths, and then think about which gap is being stressed. A subtle change from what the child expected – new furniture, a guest at the table, a day off from school, or being interrupted mid video – can cause panic, especially for anxious children. Children with ASD also may act up when uncomfortable from a headache, tooth pain, constipation, hunger, or lack of sleep, but often are unable to vocalize the reason, even if they are verbal. Having parents make a few notes about the As, Bs, Cs, and Gs of each event (the essence of a functional behavioral assessment) to review with the child, each other, the teacher, or you is key to understanding the child with ASD and successfully shifting his behavior.
Dr. Howard is an assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News.
Caprini score is not a good predictor of PE in patients with DVT
The Caprini score, commonly used to risk stratify patients for the development of venous thromboembolism and to determine the optimal dose of prophylaxis, failed to predict the development of pulmonary embolism and hemodynamically significant PE in patients presenting with deep vein thrombosis (DVT), according to the results of a large, retrospective single-center study.
Recent surgery was not associated with the development of hemodynamically significant PE, but the presence of proximal DVT was, according to a report published online in the Journal of Vascular Surgery: Venous and Lymphatic Disorders (2017. doi: 10.1016/j.jvsv.2017.08.015).

Their results showed that patients who had undergone recent surgery were less likely to develop hemodynamically significant PE (13.3% vs. 27.2%; P = .01). In contrast, patients with proximal DVT were at higher risk for development of hemodynamically significant PE (80.7% vs. 64.2%; P = .007). They found no association between Caprini score and PE severity (P = .17) or the Caprini score and proximal DVT (P = .89).
“This study shows that the Caprini score does not correlate with the occurrence of PE or the severity of PE. On the other hand, a proximal location of DVT seems to have a high association with hemodynamically significant PE. Such patients may benefit from more aggressive anticoagulant therapy and work-up for PE,” the researchers concluded.
The authors reported that they had no conflicts of interest.
The Caprini score, commonly used to risk stratify patients for the development of venous thromboembolism and to determine the optimal dose of prophylaxis, failed to predict the development of pulmonary embolism and hemodynamically significant PE in patients presenting with deep vein thrombosis (DVT), according to the results of a large, retrospective single-center study.
Recent surgery was not associated with the development of hemodynamically significant PE, but the presence of proximal DVT was, according to a report published online in the Journal of Vascular Surgery: Venous and Lymphatic Disorders (2017. doi: 10.1016/j.jvsv.2017.08.015).
Their results showed that patients who had undergone recent surgery were less likely to develop hemodynamically significant PE (13.3% vs. 27.2%; P = .01). In contrast, patients with proximal DVT were at higher risk for development of hemodynamically significant PE (80.7% vs. 64.2%; P = .007). They found no association between Caprini score and PE severity (P = .17) or the Caprini score and proximal DVT (P = .89).
“This study shows that the Caprini score does not correlate with the occurrence of PE or the severity of PE. On the other hand, a proximal location of DVT seems to have a high association with hemodynamically significant PE. Such patients may benefit from more aggressive anticoagulant therapy and work-up for PE,” the researchers concluded.
The authors reported that they had no conflicts of interest.
The Caprini score, commonly used to risk stratify patients for the development of venous thromboembolism and to determine the optimal dose of prophylaxis, failed to predict the development of pulmonary embolism and hemodynamically significant PE in patients presenting with deep vein thrombosis (DVT), according to the results of a large, retrospective single-center study.
Recent surgery was not associated with the development of hemodynamically significant PE, but the presence of proximal DVT was, according to a report published online in the Journal of Vascular Surgery: Venous and Lymphatic Disorders (2017. doi: 10.1016/j.jvsv.2017.08.015).
Their results showed that patients who had undergone recent surgery were less likely to develop hemodynamically significant PE (13.3% vs. 27.2%; P = .01). In contrast, patients with proximal DVT were at higher risk for development of hemodynamically significant PE (80.7% vs. 64.2%; P = .007). They found no association between Caprini score and PE severity (P = .17) or the Caprini score and proximal DVT (P = .89).
“This study shows that the Caprini score does not correlate with the occurrence of PE or the severity of PE. On the other hand, a proximal location of DVT seems to have a high association with hemodynamically significant PE. Such patients may benefit from more aggressive anticoagulant therapy and work-up for PE,” the researchers concluded.
The authors reported that they had no conflicts of interest.
FROM THE JOURNAL OF VASCULAR SURGERY: VENOUS AND LYMPHATIC DISORDERS
Key clinical point:
Major finding: Among 838 patients presenting with DVT, nearly 26% had concomitant PE, more than half of which was hemodynamically significant.
Data source: A single-center, retrospective review of 838 patients diagnosed with DVT.
Disclosures: The authors reported that they had no conflicts of interest.
News from SVS: Post-thrombotic venous obstructions and stenting
Endovascular treatment of iliocaval and infrainguinal post-thrombotic venous obstruction results do not appear to be adversely affected by extension of the iliac vein stents into the femoral venous system, according to a report in the November edition of the Journal of Vascular Surgery: Venous and Lymphatic Diseases (J Vasc Surg: Venous and Lym Dis 2017;5:789-99).
Deep venous thrombosis remains a significant problem with well over 500,000 people affected in the United States. Over a quarter of these patients will experience post-thrombotic syndrome (PTS), despite appropriate anti-coagulation. Patients with iliocaval thrombosis face a three-fold risk of PTS. Treatment of the complications of PTS, including leg swelling, venous claudication, skin changes and ulceration, results in healthcare costs estimated at $7 to $10 billion per year.
Popularized by Drs. Seshadri Raju and Peter Neglen, venous stenting for symptomatic patients has increased significantly in this setting. Several large series since then have demonstrated safety, efficacy and good durability of this technique in iliocaval obstruction. Questions, however, remain as to the outcomes with regards to etiology (i.e., thrombotic versus non-thrombotic occlusion) and extent of stenting (i.e., extension below the inguinal ligament). Concern for the latter is raised as the mobility of the common femoral vein may result in stent fracture and thrombosis.
Researchers from UCLA, led by vascular surgeon Dr. Brian DeRubertis, retrospectively evaluated their single-center experience with percutaneous treatment of post-thrombotic iliocaval obstruction. In this series, 31 patients (42 limbs) presented with pain/swelling (100%) including venous claudication (81%) and active ulceration (10%). Percutaneous interventions, including iliocaval angioplasty/stent in 81% with extension into the femoral system (38%), resulted in 100% technical success. Of those with IVC filters, 46% were able to be removed.
At an average of 15 months follow-up (range 2-49 months), the following results were achieved:
- Improvement in pain/swelling 84%
- Resolved pain/swelling 42%
- Decreased CEAP classification 65%
- 1 year primary stent patency 66%
- 1 year secondary stent patency 75%
Those requiring infrainguinal extension of the stent realized no significant difference in primary stent patency at one year compared to those who did not (68% versus 65%). However, in those whose IVC filter could not be removed, resolution of symptoms was achieved in only 17%.
“Our aim was to better understand risk factors for poor clinical outcomes in patients undergoing percutaneous intervention for symptomatic chronic venous obstruction secondary to post-thrombotic lesions,” comments first author Dr. Johnathon Rollo. “Our results suggest that stenting below the inguinal ligament does not result in inferior outcomes, at least in the short-term, and may be necessary in a higher percentage of patients than previously reported. Additionally, the failure to remove an IVC filter in this setting appears to result in inferior outcome and an attempt to safely remove the filter should be made in this high-risk population.”
This data suggests a role for early filter removal after, or not even placing them at all, during ileocaval lytic therapy.
The authors emphasize stenting from normal vein above to normal vein below the occlusive disease, if technically possible. Based on these results, going below the inguinal ligament to achieve adequate inflow makes sense.
To download the complete article (link available free through 12/31/2017), click here.
Endovascular treatment of iliocaval and infrainguinal post-thrombotic venous obstruction results do not appear to be adversely affected by extension of the iliac vein stents into the femoral venous system, according to a report in the November edition of the Journal of Vascular Surgery: Venous and Lymphatic Diseases (J Vasc Surg: Venous and Lym Dis 2017;5:789-99).
Deep venous thrombosis remains a significant problem with well over 500,000 people affected in the United States. Over a quarter of these patients will experience post-thrombotic syndrome (PTS), despite appropriate anti-coagulation. Patients with iliocaval thrombosis face a three-fold risk of PTS. Treatment of the complications of PTS, including leg swelling, venous claudication, skin changes and ulceration, results in healthcare costs estimated at $7 to $10 billion per year.
Popularized by Drs. Seshadri Raju and Peter Neglen, venous stenting for symptomatic patients has increased significantly in this setting. Several large series since then have demonstrated safety, efficacy and good durability of this technique in iliocaval obstruction. Questions, however, remain as to the outcomes with regards to etiology (i.e., thrombotic versus non-thrombotic occlusion) and extent of stenting (i.e., extension below the inguinal ligament). Concern for the latter is raised as the mobility of the common femoral vein may result in stent fracture and thrombosis.
Researchers from UCLA, led by vascular surgeon Dr. Brian DeRubertis, retrospectively evaluated their single-center experience with percutaneous treatment of post-thrombotic iliocaval obstruction. In this series, 31 patients (42 limbs) presented with pain/swelling (100%) including venous claudication (81%) and active ulceration (10%). Percutaneous interventions, including iliocaval angioplasty/stent in 81% with extension into the femoral system (38%), resulted in 100% technical success. Of those with IVC filters, 46% were able to be removed.
At an average of 15 months follow-up (range 2-49 months), the following results were achieved:
- Improvement in pain/swelling 84%
- Resolved pain/swelling 42%
- Decreased CEAP classification 65%
- 1 year primary stent patency 66%
- 1 year secondary stent patency 75%
Those requiring infrainguinal extension of the stent realized no significant difference in primary stent patency at one year compared to those who did not (68% versus 65%). However, in those whose IVC filter could not be removed, resolution of symptoms was achieved in only 17%.
“Our aim was to better understand risk factors for poor clinical outcomes in patients undergoing percutaneous intervention for symptomatic chronic venous obstruction secondary to post-thrombotic lesions,” comments first author Dr. Johnathon Rollo. “Our results suggest that stenting below the inguinal ligament does not result in inferior outcomes, at least in the short-term, and may be necessary in a higher percentage of patients than previously reported. Additionally, the failure to remove an IVC filter in this setting appears to result in inferior outcome and an attempt to safely remove the filter should be made in this high-risk population.”
This data suggests a role for early filter removal after, or not even placing them at all, during ileocaval lytic therapy.
The authors emphasize stenting from normal vein above to normal vein below the occlusive disease, if technically possible. Based on these results, going below the inguinal ligament to achieve adequate inflow makes sense.
To download the complete article (link available free through 12/31/2017), click here.
Endovascular treatment of iliocaval and infrainguinal post-thrombotic venous obstruction results do not appear to be adversely affected by extension of the iliac vein stents into the femoral venous system, according to a report in the November edition of the Journal of Vascular Surgery: Venous and Lymphatic Diseases (J Vasc Surg: Venous and Lym Dis 2017;5:789-99).
Deep venous thrombosis remains a significant problem with well over 500,000 people affected in the United States. Over a quarter of these patients will experience post-thrombotic syndrome (PTS), despite appropriate anti-coagulation. Patients with iliocaval thrombosis face a three-fold risk of PTS. Treatment of the complications of PTS, including leg swelling, venous claudication, skin changes and ulceration, results in healthcare costs estimated at $7 to $10 billion per year.
Popularized by Drs. Seshadri Raju and Peter Neglen, venous stenting for symptomatic patients has increased significantly in this setting. Several large series since then have demonstrated safety, efficacy and good durability of this technique in iliocaval obstruction. Questions, however, remain as to the outcomes with regards to etiology (i.e., thrombotic versus non-thrombotic occlusion) and extent of stenting (i.e., extension below the inguinal ligament). Concern for the latter is raised as the mobility of the common femoral vein may result in stent fracture and thrombosis.
Researchers from UCLA, led by vascular surgeon Dr. Brian DeRubertis, retrospectively evaluated their single-center experience with percutaneous treatment of post-thrombotic iliocaval obstruction. In this series, 31 patients (42 limbs) presented with pain/swelling (100%) including venous claudication (81%) and active ulceration (10%). Percutaneous interventions, including iliocaval angioplasty/stent in 81% with extension into the femoral system (38%), resulted in 100% technical success. Of those with IVC filters, 46% were able to be removed.
At an average of 15 months follow-up (range 2-49 months), the following results were achieved:
- Improvement in pain/swelling 84%
- Resolved pain/swelling 42%
- Decreased CEAP classification 65%
- 1 year primary stent patency 66%
- 1 year secondary stent patency 75%
Those requiring infrainguinal extension of the stent realized no significant difference in primary stent patency at one year compared to those who did not (68% versus 65%). However, in those whose IVC filter could not be removed, resolution of symptoms was achieved in only 17%.
“Our aim was to better understand risk factors for poor clinical outcomes in patients undergoing percutaneous intervention for symptomatic chronic venous obstruction secondary to post-thrombotic lesions,” comments first author Dr. Johnathon Rollo. “Our results suggest that stenting below the inguinal ligament does not result in inferior outcomes, at least in the short-term, and may be necessary in a higher percentage of patients than previously reported. Additionally, the failure to remove an IVC filter in this setting appears to result in inferior outcome and an attempt to safely remove the filter should be made in this high-risk population.”
This data suggests a role for early filter removal after, or not even placing them at all, during ileocaval lytic therapy.
The authors emphasize stenting from normal vein above to normal vein below the occlusive disease, if technically possible. Based on these results, going below the inguinal ligament to achieve adequate inflow makes sense.
To download the complete article (link available free through 12/31/2017), click here.
Beware the risks associated with greater saphenous vein thrombosis
Isolated greater saphenous vein thrombosis is not as benign as generally thought, according to the results of a single institution retrospective study of 61 patients (67 limbs) with isolated GSVT.
Instead, patients had a significant risk of persistent symptoms, recurrence, deep vein thrombosis (DVT), and pulmonary embolism (PE), according to a report published in the Annals of Vascular Surgery by Elizabeth Kudlaty, MD, Ohio State University, Columbus, and her colleagues.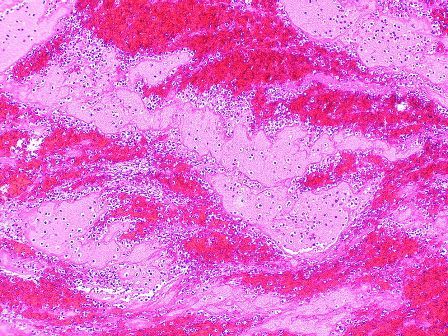
Location of the GSVT within 5 cm of the saphenous vein junction (SVJ; 32 patients) as compared with GSVT greater than 5 cm from the SVJ (29 patients) was significantly associated with malignancy (37.5% vs. 6.9%, respectively; P = .01), in-patient status (71.9% vs. 41.4%; P = .02), and diabetes (37.5% vs. 10.3%; P = .02). PE also was significantly greater in patients with GSVT within 5 cm of the SVJ (18.8% vs. 0.0%; P = .02). Patients with GSVT greater than 5 cm from the SVJ showed significantly more GSVT propagation/new saphenous vein thrombosis (0% vs. 31.3%, P = .048). There was a nonsignificant trend toward greater mortality for patients with GSVT within 5 cm of the SVJ (P = .052).
Dr. Kudlaty and her colleagues found that the different management options used, including anticoagulation, observation, and aspirin use, did not significantly affect outcomes (Ann Vasc Surg. 2017 Nov;45:154-9).
“Isolated GSVT can be viewed as a marker of more serious systemic diseases, notably diabetes and cancer, and leaves patients at high risk for thromboembolic events, recurrence, and persistent symptoms, despite a variety of managements,” the researchers concluded.
The authors reported that they had no conflicts of interest and that there were no outside funding sources.
Isolated greater saphenous vein thrombosis is not as benign as generally thought, according to the results of a single institution retrospective study of 61 patients (67 limbs) with isolated GSVT.
Instead, patients had a significant risk of persistent symptoms, recurrence, deep vein thrombosis (DVT), and pulmonary embolism (PE), according to a report published in the Annals of Vascular Surgery by Elizabeth Kudlaty, MD, Ohio State University, Columbus, and her colleagues.
Location of the GSVT within 5 cm of the saphenous vein junction (SVJ; 32 patients) as compared with GSVT greater than 5 cm from the SVJ (29 patients) was significantly associated with malignancy (37.5% vs. 6.9%, respectively; P = .01), in-patient status (71.9% vs. 41.4%; P = .02), and diabetes (37.5% vs. 10.3%; P = .02). PE also was significantly greater in patients with GSVT within 5 cm of the SVJ (18.8% vs. 0.0%; P = .02). Patients with GSVT greater than 5 cm from the SVJ showed significantly more GSVT propagation/new saphenous vein thrombosis (0% vs. 31.3%, P = .048). There was a nonsignificant trend toward greater mortality for patients with GSVT within 5 cm of the SVJ (P = .052).
Dr. Kudlaty and her colleagues found that the different management options used, including anticoagulation, observation, and aspirin use, did not significantly affect outcomes (Ann Vasc Surg. 2017 Nov;45:154-9).
“Isolated GSVT can be viewed as a marker of more serious systemic diseases, notably diabetes and cancer, and leaves patients at high risk for thromboembolic events, recurrence, and persistent symptoms, despite a variety of managements,” the researchers concluded.
The authors reported that they had no conflicts of interest and that there were no outside funding sources.
Isolated greater saphenous vein thrombosis is not as benign as generally thought, according to the results of a single institution retrospective study of 61 patients (67 limbs) with isolated GSVT.
Instead, patients had a significant risk of persistent symptoms, recurrence, deep vein thrombosis (DVT), and pulmonary embolism (PE), according to a report published in the Annals of Vascular Surgery by Elizabeth Kudlaty, MD, Ohio State University, Columbus, and her colleagues.
Location of the GSVT within 5 cm of the saphenous vein junction (SVJ; 32 patients) as compared with GSVT greater than 5 cm from the SVJ (29 patients) was significantly associated with malignancy (37.5% vs. 6.9%, respectively; P = .01), in-patient status (71.9% vs. 41.4%; P = .02), and diabetes (37.5% vs. 10.3%; P = .02). PE also was significantly greater in patients with GSVT within 5 cm of the SVJ (18.8% vs. 0.0%; P = .02). Patients with GSVT greater than 5 cm from the SVJ showed significantly more GSVT propagation/new saphenous vein thrombosis (0% vs. 31.3%, P = .048). There was a nonsignificant trend toward greater mortality for patients with GSVT within 5 cm of the SVJ (P = .052).
Dr. Kudlaty and her colleagues found that the different management options used, including anticoagulation, observation, and aspirin use, did not significantly affect outcomes (Ann Vasc Surg. 2017 Nov;45:154-9).
“Isolated GSVT can be viewed as a marker of more serious systemic diseases, notably diabetes and cancer, and leaves patients at high risk for thromboembolic events, recurrence, and persistent symptoms, despite a variety of managements,” the researchers concluded.
The authors reported that they had no conflicts of interest and that there were no outside funding sources.
FROM THE ANNALS OF VASCULAR SURGERY
Key clinical point:
Major finding: Patients with GSVT show a significant risk of persistent symptoms, recurrence, deep vein thrombosis, and pulmonary embolism.
Data source: A retrospective review of all 61 patients with isolated GSVT at a single institution between 2008 and 2014.
Disclosures: The authors reported that they had no conflicts of interest and that there were no outside funding sources.