User login
Exenatide Aids Motor Function in Parkinson’s Disease
Exenatide improves motor function in patients with Parkinson’s disease, according to research published online ahead of print August 3 in Lancet. The improvements may persist for months after treatment exposure.
Exenatide, an analogue of glucagon-like peptide-1, is used to treat type 2 diabetes. In rodent models of Parkinson’s disease, exenatide had neuroprotective effects and improved motor performance, behavior, learning, and memory. The drug also provided motor and cognitive benefits in a proof-of-concept study including patients with Parkinson’s disease.
Active Group Was Slightly Older
Dilan Athauda, MBBS, Senior Clinical Research Associate at University College London, and colleagues conducted a double-blind study to assess exenatide’s potential disease-modifying effects. At screening for study entry, patients with idiopathic Parkinson’s disease underwent physical and neurologic examinations, assessments of mood and cognition, and blood sampling. The investigators randomized eligible participants to subcutaneous injections of exenatide (2 mg) or placebo once weekly for 48 weeks. Participants continued to take their regular medications. Investigators examined patients in an off-medication state and collected blood and urine at baseline and weeks 12, 24, 36, and 48. Study drugs were withdrawn after 48 weeks, and the final follow-up visit was at week 60.
The primary outcome was change in Movement Disorders Society Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) part 3 score at 60 weeks. Secondary outcomes included differences between exenatide and placebo in each subsection of the MDS-UPDRS in the on-medication state, and the Mattis Dementia Rating Scale at weeks 48 and 60.
In all, 62 participants were randomized. Patients assigned to exenatide were slightly older, had higher baseline MDS-UPDRS part 3 scores, and had lower levodopa equivalent dose than did controls. Average age was about 62 in the exenatide group and about 58 among controls. About 26% of the population was female, and the mean disease duration at baseline was 6.4 years. Approximately 97% of the population were between Hoehn and Yahr stage 1 and 2 at baseline.
Exenatide Yielded Motor Improvement
At week 60, off-medication MDS-UPDRS part 3 scores had worsened by 2.1 points in the placebo group and improved by 1.0 point in the exenatide group, yielding a significant adjusted difference of –3.5 points. At week 48, scores among controls had deteriorated by 1.7 points, and those in the exenatide group had improved by 2.3 points, resulting in a significant adjusted between-group difference of –4.3 points.
On-medication scores on MDS-UPDRS parts 1 through 4 did not differ significantly between groups at weeks 48 or 60. The researchers also did not observe a significant difference between groups in Mattis Dementia Rating Scale score at those time points. The frequency of adverse events was similar between groups.
“Exenatide could have a longer-lasting effect on disease severity beyond conventional drug effects on dopaminergic receptors,” said the researchers. “Whether exenatide affects the underlying disease pathophysiology or simply induces long-lasting symptomatic effects is uncertain. Exenatide represents a major new avenue for investigation in Parkinson’s disease, and effects on everyday symptoms should be examined in longer-term trials.”
—Erik Greb
Suggested Reading
Athauda D, Maclagan K, Skene SS, et al. Exenatide once weekly versus placebo in Parkinson’s disease: a randomised, double-blind, placebo-controlled trial. Lancet. 2017 Aug 3 [Epub ahead of print].
Exenatide improves motor function in patients with Parkinson’s disease, according to research published online ahead of print August 3 in Lancet. The improvements may persist for months after treatment exposure.
Exenatide, an analogue of glucagon-like peptide-1, is used to treat type 2 diabetes. In rodent models of Parkinson’s disease, exenatide had neuroprotective effects and improved motor performance, behavior, learning, and memory. The drug also provided motor and cognitive benefits in a proof-of-concept study including patients with Parkinson’s disease.
Active Group Was Slightly Older
Dilan Athauda, MBBS, Senior Clinical Research Associate at University College London, and colleagues conducted a double-blind study to assess exenatide’s potential disease-modifying effects. At screening for study entry, patients with idiopathic Parkinson’s disease underwent physical and neurologic examinations, assessments of mood and cognition, and blood sampling. The investigators randomized eligible participants to subcutaneous injections of exenatide (2 mg) or placebo once weekly for 48 weeks. Participants continued to take their regular medications. Investigators examined patients in an off-medication state and collected blood and urine at baseline and weeks 12, 24, 36, and 48. Study drugs were withdrawn after 48 weeks, and the final follow-up visit was at week 60.
The primary outcome was change in Movement Disorders Society Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) part 3 score at 60 weeks. Secondary outcomes included differences between exenatide and placebo in each subsection of the MDS-UPDRS in the on-medication state, and the Mattis Dementia Rating Scale at weeks 48 and 60.
In all, 62 participants were randomized. Patients assigned to exenatide were slightly older, had higher baseline MDS-UPDRS part 3 scores, and had lower levodopa equivalent dose than did controls. Average age was about 62 in the exenatide group and about 58 among controls. About 26% of the population was female, and the mean disease duration at baseline was 6.4 years. Approximately 97% of the population were between Hoehn and Yahr stage 1 and 2 at baseline.
Exenatide Yielded Motor Improvement
At week 60, off-medication MDS-UPDRS part 3 scores had worsened by 2.1 points in the placebo group and improved by 1.0 point in the exenatide group, yielding a significant adjusted difference of –3.5 points. At week 48, scores among controls had deteriorated by 1.7 points, and those in the exenatide group had improved by 2.3 points, resulting in a significant adjusted between-group difference of –4.3 points.
On-medication scores on MDS-UPDRS parts 1 through 4 did not differ significantly between groups at weeks 48 or 60. The researchers also did not observe a significant difference between groups in Mattis Dementia Rating Scale score at those time points. The frequency of adverse events was similar between groups.
“Exenatide could have a longer-lasting effect on disease severity beyond conventional drug effects on dopaminergic receptors,” said the researchers. “Whether exenatide affects the underlying disease pathophysiology or simply induces long-lasting symptomatic effects is uncertain. Exenatide represents a major new avenue for investigation in Parkinson’s disease, and effects on everyday symptoms should be examined in longer-term trials.”
—Erik Greb
Suggested Reading
Athauda D, Maclagan K, Skene SS, et al. Exenatide once weekly versus placebo in Parkinson’s disease: a randomised, double-blind, placebo-controlled trial. Lancet. 2017 Aug 3 [Epub ahead of print].
Exenatide improves motor function in patients with Parkinson’s disease, according to research published online ahead of print August 3 in Lancet. The improvements may persist for months after treatment exposure.
Exenatide, an analogue of glucagon-like peptide-1, is used to treat type 2 diabetes. In rodent models of Parkinson’s disease, exenatide had neuroprotective effects and improved motor performance, behavior, learning, and memory. The drug also provided motor and cognitive benefits in a proof-of-concept study including patients with Parkinson’s disease.
Active Group Was Slightly Older
Dilan Athauda, MBBS, Senior Clinical Research Associate at University College London, and colleagues conducted a double-blind study to assess exenatide’s potential disease-modifying effects. At screening for study entry, patients with idiopathic Parkinson’s disease underwent physical and neurologic examinations, assessments of mood and cognition, and blood sampling. The investigators randomized eligible participants to subcutaneous injections of exenatide (2 mg) or placebo once weekly for 48 weeks. Participants continued to take their regular medications. Investigators examined patients in an off-medication state and collected blood and urine at baseline and weeks 12, 24, 36, and 48. Study drugs were withdrawn after 48 weeks, and the final follow-up visit was at week 60.
The primary outcome was change in Movement Disorders Society Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) part 3 score at 60 weeks. Secondary outcomes included differences between exenatide and placebo in each subsection of the MDS-UPDRS in the on-medication state, and the Mattis Dementia Rating Scale at weeks 48 and 60.
In all, 62 participants were randomized. Patients assigned to exenatide were slightly older, had higher baseline MDS-UPDRS part 3 scores, and had lower levodopa equivalent dose than did controls. Average age was about 62 in the exenatide group and about 58 among controls. About 26% of the population was female, and the mean disease duration at baseline was 6.4 years. Approximately 97% of the population were between Hoehn and Yahr stage 1 and 2 at baseline.
Exenatide Yielded Motor Improvement
At week 60, off-medication MDS-UPDRS part 3 scores had worsened by 2.1 points in the placebo group and improved by 1.0 point in the exenatide group, yielding a significant adjusted difference of –3.5 points. At week 48, scores among controls had deteriorated by 1.7 points, and those in the exenatide group had improved by 2.3 points, resulting in a significant adjusted between-group difference of –4.3 points.
On-medication scores on MDS-UPDRS parts 1 through 4 did not differ significantly between groups at weeks 48 or 60. The researchers also did not observe a significant difference between groups in Mattis Dementia Rating Scale score at those time points. The frequency of adverse events was similar between groups.
“Exenatide could have a longer-lasting effect on disease severity beyond conventional drug effects on dopaminergic receptors,” said the researchers. “Whether exenatide affects the underlying disease pathophysiology or simply induces long-lasting symptomatic effects is uncertain. Exenatide represents a major new avenue for investigation in Parkinson’s disease, and effects on everyday symptoms should be examined in longer-term trials.”
—Erik Greb
Suggested Reading
Athauda D, Maclagan K, Skene SS, et al. Exenatide once weekly versus placebo in Parkinson’s disease: a randomised, double-blind, placebo-controlled trial. Lancet. 2017 Aug 3 [Epub ahead of print].
Peer-to-peer learning about robotic surgery is happening on social media
Social media is now being used by surgeons for interaction among peers, informal learning, exchange of technical information, and diffusion of ideas.
A study has examined posting and membership data from a closed Facebook page, the “Robotic Surgery Collaboration,” created by surgeons who practice robotic-assisted procedures. Overall, the findings show exponential growth in membership in January 2015 through August 2016, some signs of stagnating engagement, and use of the platform for peer-to-peer learning and discussion.
“The growth in this group over time suggests that surgeons found it useful for engaging in informal interactions and learning vicariously from one another, but also reveals that not all users were actively engaged in these interactions each month and that growth in active membership differed from growth in overall group membership (as evident in the stagnating growth of active members, despite continued growth in total members),” the investigators concluded. Read the full study at Ann Surg. 2017 Aug 29. doi: 10.1097/SLA.0000000000002479. (Epub ahead of print).
Social media is now being used by surgeons for interaction among peers, informal learning, exchange of technical information, and diffusion of ideas.
A study has examined posting and membership data from a closed Facebook page, the “Robotic Surgery Collaboration,” created by surgeons who practice robotic-assisted procedures. Overall, the findings show exponential growth in membership in January 2015 through August 2016, some signs of stagnating engagement, and use of the platform for peer-to-peer learning and discussion.
“The growth in this group over time suggests that surgeons found it useful for engaging in informal interactions and learning vicariously from one another, but also reveals that not all users were actively engaged in these interactions each month and that growth in active membership differed from growth in overall group membership (as evident in the stagnating growth of active members, despite continued growth in total members),” the investigators concluded. Read the full study at Ann Surg. 2017 Aug 29. doi: 10.1097/SLA.0000000000002479. (Epub ahead of print).
Social media is now being used by surgeons for interaction among peers, informal learning, exchange of technical information, and diffusion of ideas.
A study has examined posting and membership data from a closed Facebook page, the “Robotic Surgery Collaboration,” created by surgeons who practice robotic-assisted procedures. Overall, the findings show exponential growth in membership in January 2015 through August 2016, some signs of stagnating engagement, and use of the platform for peer-to-peer learning and discussion.
“The growth in this group over time suggests that surgeons found it useful for engaging in informal interactions and learning vicariously from one another, but also reveals that not all users were actively engaged in these interactions each month and that growth in active membership differed from growth in overall group membership (as evident in the stagnating growth of active members, despite continued growth in total members),” the investigators concluded. Read the full study at Ann Surg. 2017 Aug 29. doi: 10.1097/SLA.0000000000002479. (Epub ahead of print).
Immunogenicity concerns for biosimilars so far don’t go beyond originator biologics
A key factor that impacts the efficacy and the toxicity of biologics used for rheumatic diseases is their immunogenicity, and this factor doesn’t appear to be any different for biosimilars in studies conducted so far.
In a meta-analysis of 63 studies of tumor necrosis factor (TNF) inhibitors, investigators including Daniel E. Furst, MD, professor of rheumatology at the University of Washington, Seattle, who also is affiliated with the University of California, Los Angeles, and the University of Florence, Italy, found that antidrug antibodies developed in 17% of patients (BioDrugs 2015;29:241-58).
“That doesn’t sound too bad, but does it differ by medication?” asked Dr. Furst, who spoke at the annual Perspectives in Rheumatic Diseases held by Global Academy for Medical Education. “For infliximab, 30% of the time, there are antidrug antibodies. So if that has a clinical effect, that’s a big deal. For certolizumab ... it’s only 6%, so there is a huge difference within the TNF inhibitors.” At the same time, antidrug antibodies developed in patients on adalimumab 23% of the time, followed by certolizumab (6%), golimumab (4%), and etanercept (2%).

One approach to circumventing the impact of antidrug antibodies on clinical response is by using immunosuppression, which in the meta-analysis had a 70% probability for decreasing antidrug antibodies. But this approach comes with a hitch, Dr. Furst said. The effect of immunosuppression on antidrug antibody positivity differs by disease. Immunosuppression had a 78% probability for decreasing antidrug antibody positivity in RA, 63% probability in inflammatory bowel disease, and 32% probability in ankylosing spondylitis. “That’s a wild mix of immunogenicity and the possibility that it’s going to affect the underlying response,” he said. The best studies in this area are of infliximab and adalimumab, which showed that antidrug antibodies in patients on infliximab reduced the probability of a clinical response by 54% and for adalimumab by 65%.
The same meta-analysis found that there were more antibodies to adalimumab than to certolizumab, golimumab, or etanercept, and also more antibodies to infliximab than to certolizumab, golimumab, or etanercept, but no difference between adalimumab and infliximab. “You’d think that maybe there is a difference between adalimumab and infliximab, but that’s not true,” Dr. Furst said. The apparent effect on the percentage of antidrug antibodies depends on what type of assay is used. For example, radioimmunoassay measures about 11% more antidrug antibodies, compared with enzyme-linked immunosorbent assay. Disease duration also matters. Each year of disease duration increases the antidrug antibodies by 1%.
What about the non-TNF inhibitors? A meta-analysis of five core trials of tocilizumab for RA found that the antidrug antibodies ranged from 1.7% at baseline to 2.3% during the respective trials (Clin Ther. 2010;32:1597-1609). “Anywhere along the way, the percentage of antidrug antibodies was about 1.5%,” said Dr. Furst, who was not involved with the study. “So as opposed to the TNF inhibitors, when you look at tocilizumab, this whole immunity question is probably a non-issue. The same is true for abatacept. With rituximab, the question is a little bit different. In one randomized, controlled trial, immunogenicity was 2.9%, while in the next it was 7.9%. In an open-label trial, it was 11.5%. So I think for rituximab we have to assume that you have some potentially important antidrug antibodies that might affect response.”
Studies have shown that antidrug antibodies do affect the pharmacokinetics of a biologic (and thereby clinical response) by producing lower trough levels of the biologic through an increase in its clearance. However, studies of infliximab and its biosimilars have not yielded any significant differences in clinical responses rates despite small differences in rates of antidrug antibodies or in rates of treatment-emergent adverse events, he said.
There has also been no difference in disease worsening in the only reported double-blind, randomized, switching study for infliximab and an infliximab biosimilar, the NOR-SWITCH study. However, the small numbers of patients in the study with certain diseases for which infliximab is indicated do not allow for conclusions to be drawn for specific diseases, Dr. Furst said.
Dr. Furst disclosed that he has received grant/research support from AbbVie, Actelion, Amgen, Bristol-Myers Squibb, Corbus, the National Institutes of Health, Novartis, and Roche/Genentech. He is also a consultant for AbbVie, Actelion, Amgen, Bristol-Myers Squibb, Cytori, Novartis, Pfizer, and Roche/Genentech. Global Academy for Medical Education and this news organization are owned by the same parent company.
A key factor that impacts the efficacy and the toxicity of biologics used for rheumatic diseases is their immunogenicity, and this factor doesn’t appear to be any different for biosimilars in studies conducted so far.
In a meta-analysis of 63 studies of tumor necrosis factor (TNF) inhibitors, investigators including Daniel E. Furst, MD, professor of rheumatology at the University of Washington, Seattle, who also is affiliated with the University of California, Los Angeles, and the University of Florence, Italy, found that antidrug antibodies developed in 17% of patients (BioDrugs 2015;29:241-58).
“That doesn’t sound too bad, but does it differ by medication?” asked Dr. Furst, who spoke at the annual Perspectives in Rheumatic Diseases held by Global Academy for Medical Education. “For infliximab, 30% of the time, there are antidrug antibodies. So if that has a clinical effect, that’s a big deal. For certolizumab ... it’s only 6%, so there is a huge difference within the TNF inhibitors.” At the same time, antidrug antibodies developed in patients on adalimumab 23% of the time, followed by certolizumab (6%), golimumab (4%), and etanercept (2%).
One approach to circumventing the impact of antidrug antibodies on clinical response is by using immunosuppression, which in the meta-analysis had a 70% probability for decreasing antidrug antibodies. But this approach comes with a hitch, Dr. Furst said. The effect of immunosuppression on antidrug antibody positivity differs by disease. Immunosuppression had a 78% probability for decreasing antidrug antibody positivity in RA, 63% probability in inflammatory bowel disease, and 32% probability in ankylosing spondylitis. “That’s a wild mix of immunogenicity and the possibility that it’s going to affect the underlying response,” he said. The best studies in this area are of infliximab and adalimumab, which showed that antidrug antibodies in patients on infliximab reduced the probability of a clinical response by 54% and for adalimumab by 65%.
The same meta-analysis found that there were more antibodies to adalimumab than to certolizumab, golimumab, or etanercept, and also more antibodies to infliximab than to certolizumab, golimumab, or etanercept, but no difference between adalimumab and infliximab. “You’d think that maybe there is a difference between adalimumab and infliximab, but that’s not true,” Dr. Furst said. The apparent effect on the percentage of antidrug antibodies depends on what type of assay is used. For example, radioimmunoassay measures about 11% more antidrug antibodies, compared with enzyme-linked immunosorbent assay. Disease duration also matters. Each year of disease duration increases the antidrug antibodies by 1%.
What about the non-TNF inhibitors? A meta-analysis of five core trials of tocilizumab for RA found that the antidrug antibodies ranged from 1.7% at baseline to 2.3% during the respective trials (Clin Ther. 2010;32:1597-1609). “Anywhere along the way, the percentage of antidrug antibodies was about 1.5%,” said Dr. Furst, who was not involved with the study. “So as opposed to the TNF inhibitors, when you look at tocilizumab, this whole immunity question is probably a non-issue. The same is true for abatacept. With rituximab, the question is a little bit different. In one randomized, controlled trial, immunogenicity was 2.9%, while in the next it was 7.9%. In an open-label trial, it was 11.5%. So I think for rituximab we have to assume that you have some potentially important antidrug antibodies that might affect response.”
Studies have shown that antidrug antibodies do affect the pharmacokinetics of a biologic (and thereby clinical response) by producing lower trough levels of the biologic through an increase in its clearance. However, studies of infliximab and its biosimilars have not yielded any significant differences in clinical responses rates despite small differences in rates of antidrug antibodies or in rates of treatment-emergent adverse events, he said.
There has also been no difference in disease worsening in the only reported double-blind, randomized, switching study for infliximab and an infliximab biosimilar, the NOR-SWITCH study. However, the small numbers of patients in the study with certain diseases for which infliximab is indicated do not allow for conclusions to be drawn for specific diseases, Dr. Furst said.
Dr. Furst disclosed that he has received grant/research support from AbbVie, Actelion, Amgen, Bristol-Myers Squibb, Corbus, the National Institutes of Health, Novartis, and Roche/Genentech. He is also a consultant for AbbVie, Actelion, Amgen, Bristol-Myers Squibb, Cytori, Novartis, Pfizer, and Roche/Genentech. Global Academy for Medical Education and this news organization are owned by the same parent company.
A key factor that impacts the efficacy and the toxicity of biologics used for rheumatic diseases is their immunogenicity, and this factor doesn’t appear to be any different for biosimilars in studies conducted so far.
In a meta-analysis of 63 studies of tumor necrosis factor (TNF) inhibitors, investigators including Daniel E. Furst, MD, professor of rheumatology at the University of Washington, Seattle, who also is affiliated with the University of California, Los Angeles, and the University of Florence, Italy, found that antidrug antibodies developed in 17% of patients (BioDrugs 2015;29:241-58).
“That doesn’t sound too bad, but does it differ by medication?” asked Dr. Furst, who spoke at the annual Perspectives in Rheumatic Diseases held by Global Academy for Medical Education. “For infliximab, 30% of the time, there are antidrug antibodies. So if that has a clinical effect, that’s a big deal. For certolizumab ... it’s only 6%, so there is a huge difference within the TNF inhibitors.” At the same time, antidrug antibodies developed in patients on adalimumab 23% of the time, followed by certolizumab (6%), golimumab (4%), and etanercept (2%).
One approach to circumventing the impact of antidrug antibodies on clinical response is by using immunosuppression, which in the meta-analysis had a 70% probability for decreasing antidrug antibodies. But this approach comes with a hitch, Dr. Furst said. The effect of immunosuppression on antidrug antibody positivity differs by disease. Immunosuppression had a 78% probability for decreasing antidrug antibody positivity in RA, 63% probability in inflammatory bowel disease, and 32% probability in ankylosing spondylitis. “That’s a wild mix of immunogenicity and the possibility that it’s going to affect the underlying response,” he said. The best studies in this area are of infliximab and adalimumab, which showed that antidrug antibodies in patients on infliximab reduced the probability of a clinical response by 54% and for adalimumab by 65%.
The same meta-analysis found that there were more antibodies to adalimumab than to certolizumab, golimumab, or etanercept, and also more antibodies to infliximab than to certolizumab, golimumab, or etanercept, but no difference between adalimumab and infliximab. “You’d think that maybe there is a difference between adalimumab and infliximab, but that’s not true,” Dr. Furst said. The apparent effect on the percentage of antidrug antibodies depends on what type of assay is used. For example, radioimmunoassay measures about 11% more antidrug antibodies, compared with enzyme-linked immunosorbent assay. Disease duration also matters. Each year of disease duration increases the antidrug antibodies by 1%.
What about the non-TNF inhibitors? A meta-analysis of five core trials of tocilizumab for RA found that the antidrug antibodies ranged from 1.7% at baseline to 2.3% during the respective trials (Clin Ther. 2010;32:1597-1609). “Anywhere along the way, the percentage of antidrug antibodies was about 1.5%,” said Dr. Furst, who was not involved with the study. “So as opposed to the TNF inhibitors, when you look at tocilizumab, this whole immunity question is probably a non-issue. The same is true for abatacept. With rituximab, the question is a little bit different. In one randomized, controlled trial, immunogenicity was 2.9%, while in the next it was 7.9%. In an open-label trial, it was 11.5%. So I think for rituximab we have to assume that you have some potentially important antidrug antibodies that might affect response.”
Studies have shown that antidrug antibodies do affect the pharmacokinetics of a biologic (and thereby clinical response) by producing lower trough levels of the biologic through an increase in its clearance. However, studies of infliximab and its biosimilars have not yielded any significant differences in clinical responses rates despite small differences in rates of antidrug antibodies or in rates of treatment-emergent adverse events, he said.
There has also been no difference in disease worsening in the only reported double-blind, randomized, switching study for infliximab and an infliximab biosimilar, the NOR-SWITCH study. However, the small numbers of patients in the study with certain diseases for which infliximab is indicated do not allow for conclusions to be drawn for specific diseases, Dr. Furst said.
Dr. Furst disclosed that he has received grant/research support from AbbVie, Actelion, Amgen, Bristol-Myers Squibb, Corbus, the National Institutes of Health, Novartis, and Roche/Genentech. He is also a consultant for AbbVie, Actelion, Amgen, Bristol-Myers Squibb, Cytori, Novartis, Pfizer, and Roche/Genentech. Global Academy for Medical Education and this news organization are owned by the same parent company.
EXPERT ANALYSIS FROM THE ANNUAL PERSPECTIVES IN RHEUMATIC DISEASES
In hypoparathyroidism, phosphate, calcium levels may matter
DENVER – Most patients maintained time-weighted serum levels in the normal range in a case-control study of hypoparathyroidism, but serum levels of phosphate and calcium phosphate above median values were associated with a higher mortality and risk of complications.
Patients with calcium levels in the lowest tertile also had an increased risk of cardiovascular disease, while those who experienced episodes of hypercalcemia had a higher risk of mortality and infections.
Denmark has a well-established cohort of patients with hypoparathyroidism, and previous epidemiologic studies have shown that those patients have increased risks of cardiovascular disease, renal diseases, and infections.
“From our epidemiologic study, we did not see increased mortality when we compared patients with hypoparathyroidism to [the] Danish population. So, we were actually a bit surprised that the phosphate and the calcium phosphate product had an influence on mortality,” said Dr. Underbjerg.
To find out if there were any associations between the biochemical findings and complications, the researchers collected biochemical data on 431 patients with hypoparathyroidism (81% of whom were women, with an average age of 41 years and a median disease duration of 12 years); 88% of the patients had the condition as a result of surgery, and 95% of patients received daily calcium and/or activated vitamin D supplements.
The researchers looked at four complications: mortality, cardiovascular disease, renal disease, and any infection. For each complication, they compared patients who had experienced the complication to hypoparathyroidism patients who did not experience the complication.
The subjects had a median time-weighted serum level of ionized calcium of 1.17 mmol/L (interquartile range [IQR], 1.14-1.21), a median of value of 1.21 mmol/L of phosphate (IQR, 1.11-1.32), and a median value of 2.80 mmol2/L2 of the calcium-phosphate product (IQR, 2.51-3.03).
Patients in the lowest tertile of ionized calcium (less than or equal to 1.16) had a greater risk of developing cardiovascular diseases than patients in the midtertile (1.16-1.19; odds ratio [OR], 2.96; 95% confidence interval [CI], 1.02-8.59).
Compared with patients in the midquartile, patients with serum phosphate levels above the median value of 1.21 were at a higher risk of mortality (OR, 2.76; 95% CI, 1.32-5.80) and infections (OR, 1.77; 95% CI, 1.04-3.01).
Calcium-phosphate product levels above the median value of 2.80 were associated with heightened mortality (OR, 2.67; 95% CI, 1.27-5.63) and renal diseases (OR, 1.71; 95% CI, 1.03-2.86).
Hypercalcemia occurred in 41% of patients and was also tied to increased mortality (OR, 1.76; 95% CI, 1.02-3.05) and risk of infections (OR, 1.86; 95% CI, 1.18-2.93).
The results suggest that those values have the potential to be clinically important. “I think you have to be aware that phosphate and calcium phosphate levels have an influence on a patient’s well-being,” said Dr. Underbjerg.
Shire funded the study. Dr. Underbjerg reported having no relevant financial disclosures.
DENVER – Most patients maintained time-weighted serum levels in the normal range in a case-control study of hypoparathyroidism, but serum levels of phosphate and calcium phosphate above median values were associated with a higher mortality and risk of complications.
Patients with calcium levels in the lowest tertile also had an increased risk of cardiovascular disease, while those who experienced episodes of hypercalcemia had a higher risk of mortality and infections.
Denmark has a well-established cohort of patients with hypoparathyroidism, and previous epidemiologic studies have shown that those patients have increased risks of cardiovascular disease, renal diseases, and infections.
“From our epidemiologic study, we did not see increased mortality when we compared patients with hypoparathyroidism to [the] Danish population. So, we were actually a bit surprised that the phosphate and the calcium phosphate product had an influence on mortality,” said Dr. Underbjerg.
To find out if there were any associations between the biochemical findings and complications, the researchers collected biochemical data on 431 patients with hypoparathyroidism (81% of whom were women, with an average age of 41 years and a median disease duration of 12 years); 88% of the patients had the condition as a result of surgery, and 95% of patients received daily calcium and/or activated vitamin D supplements.
The researchers looked at four complications: mortality, cardiovascular disease, renal disease, and any infection. For each complication, they compared patients who had experienced the complication to hypoparathyroidism patients who did not experience the complication.
The subjects had a median time-weighted serum level of ionized calcium of 1.17 mmol/L (interquartile range [IQR], 1.14-1.21), a median of value of 1.21 mmol/L of phosphate (IQR, 1.11-1.32), and a median value of 2.80 mmol2/L2 of the calcium-phosphate product (IQR, 2.51-3.03).
Patients in the lowest tertile of ionized calcium (less than or equal to 1.16) had a greater risk of developing cardiovascular diseases than patients in the midtertile (1.16-1.19; odds ratio [OR], 2.96; 95% confidence interval [CI], 1.02-8.59).
Compared with patients in the midquartile, patients with serum phosphate levels above the median value of 1.21 were at a higher risk of mortality (OR, 2.76; 95% CI, 1.32-5.80) and infections (OR, 1.77; 95% CI, 1.04-3.01).
Calcium-phosphate product levels above the median value of 2.80 were associated with heightened mortality (OR, 2.67; 95% CI, 1.27-5.63) and renal diseases (OR, 1.71; 95% CI, 1.03-2.86).
Hypercalcemia occurred in 41% of patients and was also tied to increased mortality (OR, 1.76; 95% CI, 1.02-3.05) and risk of infections (OR, 1.86; 95% CI, 1.18-2.93).
The results suggest that those values have the potential to be clinically important. “I think you have to be aware that phosphate and calcium phosphate levels have an influence on a patient’s well-being,” said Dr. Underbjerg.
Shire funded the study. Dr. Underbjerg reported having no relevant financial disclosures.
DENVER – Most patients maintained time-weighted serum levels in the normal range in a case-control study of hypoparathyroidism, but serum levels of phosphate and calcium phosphate above median values were associated with a higher mortality and risk of complications.
Patients with calcium levels in the lowest tertile also had an increased risk of cardiovascular disease, while those who experienced episodes of hypercalcemia had a higher risk of mortality and infections.
Denmark has a well-established cohort of patients with hypoparathyroidism, and previous epidemiologic studies have shown that those patients have increased risks of cardiovascular disease, renal diseases, and infections.
“From our epidemiologic study, we did not see increased mortality when we compared patients with hypoparathyroidism to [the] Danish population. So, we were actually a bit surprised that the phosphate and the calcium phosphate product had an influence on mortality,” said Dr. Underbjerg.
To find out if there were any associations between the biochemical findings and complications, the researchers collected biochemical data on 431 patients with hypoparathyroidism (81% of whom were women, with an average age of 41 years and a median disease duration of 12 years); 88% of the patients had the condition as a result of surgery, and 95% of patients received daily calcium and/or activated vitamin D supplements.
The researchers looked at four complications: mortality, cardiovascular disease, renal disease, and any infection. For each complication, they compared patients who had experienced the complication to hypoparathyroidism patients who did not experience the complication.
The subjects had a median time-weighted serum level of ionized calcium of 1.17 mmol/L (interquartile range [IQR], 1.14-1.21), a median of value of 1.21 mmol/L of phosphate (IQR, 1.11-1.32), and a median value of 2.80 mmol2/L2 of the calcium-phosphate product (IQR, 2.51-3.03).
Patients in the lowest tertile of ionized calcium (less than or equal to 1.16) had a greater risk of developing cardiovascular diseases than patients in the midtertile (1.16-1.19; odds ratio [OR], 2.96; 95% confidence interval [CI], 1.02-8.59).
Compared with patients in the midquartile, patients with serum phosphate levels above the median value of 1.21 were at a higher risk of mortality (OR, 2.76; 95% CI, 1.32-5.80) and infections (OR, 1.77; 95% CI, 1.04-3.01).
Calcium-phosphate product levels above the median value of 2.80 were associated with heightened mortality (OR, 2.67; 95% CI, 1.27-5.63) and renal diseases (OR, 1.71; 95% CI, 1.03-2.86).
Hypercalcemia occurred in 41% of patients and was also tied to increased mortality (OR, 1.76; 95% CI, 1.02-3.05) and risk of infections (OR, 1.86; 95% CI, 1.18-2.93).
The results suggest that those values have the potential to be clinically important. “I think you have to be aware that phosphate and calcium phosphate levels have an influence on a patient’s well-being,” said Dr. Underbjerg.
Shire funded the study. Dr. Underbjerg reported having no relevant financial disclosures.
AT ASBMR
Key clinical point: Serum phosphate and calcium-phosphate levels may influence patient outcomes in hypoparathyroidism.
Major finding: Higher phosphate levels are tied to an increased risk of mortality (OR, 2.76) and infections (OR, 1.77).
Data source: A case-control study of 431 patients with hypoparathyroidism.
Disclosures: Shire funded the study. Dr. Underbjerg reported having no relevant financial disclosures.
Laser Interstitial Thermal Ablation: A Promising Approach to TLE
Laser interstitial thermal ablation (LiTT) appears to benefit patients with temporal lobe epilepsy (TLE) according to a recent article published in Epilepsy Research.
- According to the author, LiTT has been found to eliminate seizures in about half of patients with mesial temporal lobe epilepsy who undergo the procedure.
- Neuropsychological side effects of the procedure seem to be less severe, when compared to surgeries that require large resections.
- LiTT involves inserting a probe into the area of the brain responsible for the seizures, including the mesial temporal lobe and hypothalamic hamartoma, and heating the tip of the probe by means of laser energy.
- Advantages include the fact that LiTT is less invasive than open surgery and allows patients to leave the hospital sooner and experience less pain.
- The minimally invasive surgery typically requires a single day of hospitalization and allows patients to return to work in 3 days.
- It remains uncertain whether LiTT is as efficacious as more invasive procedures but appears to be about as efficacious as anterior temporal lobectomy.
Kang JY, Sperling MR. Epileptologist’s view: Laser interstitial thermal ablation for treatment of temporal lobe epilepsy. [Published online ahead of print July 25, 2017] Epilepsy Res. https://doi.org/10.1016/j.eplepsyres.2017.07.007
Laser interstitial thermal ablation (LiTT) appears to benefit patients with temporal lobe epilepsy (TLE) according to a recent article published in Epilepsy Research.
- According to the author, LiTT has been found to eliminate seizures in about half of patients with mesial temporal lobe epilepsy who undergo the procedure.
- Neuropsychological side effects of the procedure seem to be less severe, when compared to surgeries that require large resections.
- LiTT involves inserting a probe into the area of the brain responsible for the seizures, including the mesial temporal lobe and hypothalamic hamartoma, and heating the tip of the probe by means of laser energy.
- Advantages include the fact that LiTT is less invasive than open surgery and allows patients to leave the hospital sooner and experience less pain.
- The minimally invasive surgery typically requires a single day of hospitalization and allows patients to return to work in 3 days.
- It remains uncertain whether LiTT is as efficacious as more invasive procedures but appears to be about as efficacious as anterior temporal lobectomy.
Kang JY, Sperling MR. Epileptologist’s view: Laser interstitial thermal ablation for treatment of temporal lobe epilepsy. [Published online ahead of print July 25, 2017] Epilepsy Res. https://doi.org/10.1016/j.eplepsyres.2017.07.007
Laser interstitial thermal ablation (LiTT) appears to benefit patients with temporal lobe epilepsy (TLE) according to a recent article published in Epilepsy Research.
- According to the author, LiTT has been found to eliminate seizures in about half of patients with mesial temporal lobe epilepsy who undergo the procedure.
- Neuropsychological side effects of the procedure seem to be less severe, when compared to surgeries that require large resections.
- LiTT involves inserting a probe into the area of the brain responsible for the seizures, including the mesial temporal lobe and hypothalamic hamartoma, and heating the tip of the probe by means of laser energy.
- Advantages include the fact that LiTT is less invasive than open surgery and allows patients to leave the hospital sooner and experience less pain.
- The minimally invasive surgery typically requires a single day of hospitalization and allows patients to return to work in 3 days.
- It remains uncertain whether LiTT is as efficacious as more invasive procedures but appears to be about as efficacious as anterior temporal lobectomy.
Kang JY, Sperling MR. Epileptologist’s view: Laser interstitial thermal ablation for treatment of temporal lobe epilepsy. [Published online ahead of print July 25, 2017] Epilepsy Res. https://doi.org/10.1016/j.eplepsyres.2017.07.007
The Link Between Ischemic Stroke and Seizures
The threat of seizures and epilepsy is a significant concern for patients who have had a stroke, according to a review of 41 studies published in Neurology.
- Investigators found 35 studies that reported stroke-related seizures and 6 studies that found details on the effects of antiepileptic drugs.
- Seizures occurred early on in 3.3% of patients who had experienced a stroke.
- Late-onset seizures or epilepsy was reported in 18/1000 person-years.
- Researchers were unable to find any evidence to suggest that a specific drug was more effective among patients who had seizures after a stroke.
- Newer drugs caused fewer side effects than older medications.
- The systematic review and meta-analysis included measurement of I2 statistic to evaluate heterogeneity and sensitivity analyses were also performed.
- Early onset and late onset seizures generated I2 statistics of 92.8% and 94.1%, respectively.
- Sensitivity analyses was unable to explain the high degree of heterogeneity.
Wang JZ, Vyas MV, Saposnik G, Burneo JG. Incidence and management of seizures after ischemic stroke. Neurology. 2017;89:1220-1228.
The threat of seizures and epilepsy is a significant concern for patients who have had a stroke, according to a review of 41 studies published in Neurology.
- Investigators found 35 studies that reported stroke-related seizures and 6 studies that found details on the effects of antiepileptic drugs.
- Seizures occurred early on in 3.3% of patients who had experienced a stroke.
- Late-onset seizures or epilepsy was reported in 18/1000 person-years.
- Researchers were unable to find any evidence to suggest that a specific drug was more effective among patients who had seizures after a stroke.
- Newer drugs caused fewer side effects than older medications.
- The systematic review and meta-analysis included measurement of I2 statistic to evaluate heterogeneity and sensitivity analyses were also performed.
- Early onset and late onset seizures generated I2 statistics of 92.8% and 94.1%, respectively.
- Sensitivity analyses was unable to explain the high degree of heterogeneity.
Wang JZ, Vyas MV, Saposnik G, Burneo JG. Incidence and management of seizures after ischemic stroke. Neurology. 2017;89:1220-1228.
The threat of seizures and epilepsy is a significant concern for patients who have had a stroke, according to a review of 41 studies published in Neurology.
- Investigators found 35 studies that reported stroke-related seizures and 6 studies that found details on the effects of antiepileptic drugs.
- Seizures occurred early on in 3.3% of patients who had experienced a stroke.
- Late-onset seizures or epilepsy was reported in 18/1000 person-years.
- Researchers were unable to find any evidence to suggest that a specific drug was more effective among patients who had seizures after a stroke.
- Newer drugs caused fewer side effects than older medications.
- The systematic review and meta-analysis included measurement of I2 statistic to evaluate heterogeneity and sensitivity analyses were also performed.
- Early onset and late onset seizures generated I2 statistics of 92.8% and 94.1%, respectively.
- Sensitivity analyses was unable to explain the high degree of heterogeneity.
Wang JZ, Vyas MV, Saposnik G, Burneo JG. Incidence and management of seizures after ischemic stroke. Neurology. 2017;89:1220-1228.
Sleep, Age, and Prone Position Linked to SUDEP
Patients are more likely to die of sudden unexpected death in epilepsy (SUDEP) while they are asleep, according to a review of over 1000 SUDEP cases gleaned from 67 studies.
- Among 1025 patients with SUDEP, 880 cases had a circadian pattern.
- Of the 880 cases with a circadian pattern, 69.3% of the deaths occurred during sleep and 30.7% while patients were awake (P<0.001).
- Subgroup analysis found 272 patients in which both circadian pattern and age could be established.
- In this subgroup, patients aged 40 years and younger were more likely to die while asleep, when compared with older patients (odds ratio, 2.0).
- Among patients whose body position could also be verified, prone position was more often associated with death, when compared with those in prone position who were awake (87.6% vs 52.9%).
Ali A, Wu S, Issa NP, et al. Association of sleep with sudden unexpected death in epilepsy. [Published online ahead of print September 13, 2017] Epilepsy Behav. https://doi.org/10.1016/j.yebeh.2017.08.021
Patients are more likely to die of sudden unexpected death in epilepsy (SUDEP) while they are asleep, according to a review of over 1000 SUDEP cases gleaned from 67 studies.
- Among 1025 patients with SUDEP, 880 cases had a circadian pattern.
- Of the 880 cases with a circadian pattern, 69.3% of the deaths occurred during sleep and 30.7% while patients were awake (P<0.001).
- Subgroup analysis found 272 patients in which both circadian pattern and age could be established.
- In this subgroup, patients aged 40 years and younger were more likely to die while asleep, when compared with older patients (odds ratio, 2.0).
- Among patients whose body position could also be verified, prone position was more often associated with death, when compared with those in prone position who were awake (87.6% vs 52.9%).
Ali A, Wu S, Issa NP, et al. Association of sleep with sudden unexpected death in epilepsy. [Published online ahead of print September 13, 2017] Epilepsy Behav. https://doi.org/10.1016/j.yebeh.2017.08.021
Patients are more likely to die of sudden unexpected death in epilepsy (SUDEP) while they are asleep, according to a review of over 1000 SUDEP cases gleaned from 67 studies.
- Among 1025 patients with SUDEP, 880 cases had a circadian pattern.
- Of the 880 cases with a circadian pattern, 69.3% of the deaths occurred during sleep and 30.7% while patients were awake (P<0.001).
- Subgroup analysis found 272 patients in which both circadian pattern and age could be established.
- In this subgroup, patients aged 40 years and younger were more likely to die while asleep, when compared with older patients (odds ratio, 2.0).
- Among patients whose body position could also be verified, prone position was more often associated with death, when compared with those in prone position who were awake (87.6% vs 52.9%).
Ali A, Wu S, Issa NP, et al. Association of sleep with sudden unexpected death in epilepsy. [Published online ahead of print September 13, 2017] Epilepsy Behav. https://doi.org/10.1016/j.yebeh.2017.08.021
Leukocyte activation test–based elimination diet improves IBS symptoms
Elimination diets guided by leukocyte activation tests reduced symptoms in patients with irritable bowel syndrome (IBS) in a parallel-group, double-blind, randomized controlled trial.
Study participants were randomized to a 4-week diet with individualized guidance to either eliminate foods with positive assay results and to allow foods with negative assay results (intervention group), or to eliminate foods with negative assay results and allow foods with positive assay results (comparison group). The 29 patients in the intervention group had significantly greater increases in mean IBS Global Improvement Scale scores at 4 weeks and 8 weeks vs. the 29 patients in the comparison group (mean between-group differences, 0.86 and 1.22 points, respectively), reported Ather Ali, ND, of Yale University, New Haven, Conn., and colleagues (BMJ Open Gastro. 2017;0:e000164. doi: 10.1136/bmjgast-2017-000164).
Improvements were seen in IBS Adequate Relief and Quality of Life scores in the intervention group, but the differences between the groups were not statistically significant. No adverse effects related to the intervention were reported, they said.
Of note, strong responders in the intervention group experienced significant reductions in neutrophil elastase.
IBS is a prevalent, costly, and often disabling condition, but assessing food intolerance in clinical practice is challenging, the investigators said, adding that while a number of commercially available blood tests claim to diagnose food intolerance – including leukocyte activation tests, which are among the most widely used for this purpose – no rigorous studies of the tests have been published.
For the current study, adults aged 18-75 years who met Rome III criteria for any subtype of IBS and had active symptoms were enrolled from an academic health center in Connecticut. The leukocyte activation test was used to culture peripheral blood leukocytes with standardized individual food extracts, producing either a positive or negative result, which then guided the food elimination.
The findings demonstrate that “a diet guided by leukocyte activation testing results in demonstrable clinical improvement in IBS,” they wrote, noting that dietary changes based on a leukocyte activation test may be less restrictive than those associated with a low–fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (low FODMAPs) diet (which has also shown promise as “an efficacious, although burdensome, dietary intervention for IBS”), and may result in better long-term adherence.
“These clinical results, associated with a reduction in plasma neutrophil elastase, have implication for better understanding the role of food intolerance and the pathophysiology of IBS,” they said, adding that “future studies, ideally multisite and in larger samples, can assess comparative effects of other dietary interventions in IBS, the effects of restricting specific foods, and whether dietary changes guided by leukocyte activation testing affect other conditions.”
Cell Science Systems funded the study. The authors reported having no disclosures.
Elimination diets guided by leukocyte activation tests reduced symptoms in patients with irritable bowel syndrome (IBS) in a parallel-group, double-blind, randomized controlled trial.
Study participants were randomized to a 4-week diet with individualized guidance to either eliminate foods with positive assay results and to allow foods with negative assay results (intervention group), or to eliminate foods with negative assay results and allow foods with positive assay results (comparison group). The 29 patients in the intervention group had significantly greater increases in mean IBS Global Improvement Scale scores at 4 weeks and 8 weeks vs. the 29 patients in the comparison group (mean between-group differences, 0.86 and 1.22 points, respectively), reported Ather Ali, ND, of Yale University, New Haven, Conn., and colleagues (BMJ Open Gastro. 2017;0:e000164. doi: 10.1136/bmjgast-2017-000164).
Improvements were seen in IBS Adequate Relief and Quality of Life scores in the intervention group, but the differences between the groups were not statistically significant. No adverse effects related to the intervention were reported, they said.
Of note, strong responders in the intervention group experienced significant reductions in neutrophil elastase.
IBS is a prevalent, costly, and often disabling condition, but assessing food intolerance in clinical practice is challenging, the investigators said, adding that while a number of commercially available blood tests claim to diagnose food intolerance – including leukocyte activation tests, which are among the most widely used for this purpose – no rigorous studies of the tests have been published.
For the current study, adults aged 18-75 years who met Rome III criteria for any subtype of IBS and had active symptoms were enrolled from an academic health center in Connecticut. The leukocyte activation test was used to culture peripheral blood leukocytes with standardized individual food extracts, producing either a positive or negative result, which then guided the food elimination.
The findings demonstrate that “a diet guided by leukocyte activation testing results in demonstrable clinical improvement in IBS,” they wrote, noting that dietary changes based on a leukocyte activation test may be less restrictive than those associated with a low–fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (low FODMAPs) diet (which has also shown promise as “an efficacious, although burdensome, dietary intervention for IBS”), and may result in better long-term adherence.
“These clinical results, associated with a reduction in plasma neutrophil elastase, have implication for better understanding the role of food intolerance and the pathophysiology of IBS,” they said, adding that “future studies, ideally multisite and in larger samples, can assess comparative effects of other dietary interventions in IBS, the effects of restricting specific foods, and whether dietary changes guided by leukocyte activation testing affect other conditions.”
Cell Science Systems funded the study. The authors reported having no disclosures.
Elimination diets guided by leukocyte activation tests reduced symptoms in patients with irritable bowel syndrome (IBS) in a parallel-group, double-blind, randomized controlled trial.
Study participants were randomized to a 4-week diet with individualized guidance to either eliminate foods with positive assay results and to allow foods with negative assay results (intervention group), or to eliminate foods with negative assay results and allow foods with positive assay results (comparison group). The 29 patients in the intervention group had significantly greater increases in mean IBS Global Improvement Scale scores at 4 weeks and 8 weeks vs. the 29 patients in the comparison group (mean between-group differences, 0.86 and 1.22 points, respectively), reported Ather Ali, ND, of Yale University, New Haven, Conn., and colleagues (BMJ Open Gastro. 2017;0:e000164. doi: 10.1136/bmjgast-2017-000164).
Improvements were seen in IBS Adequate Relief and Quality of Life scores in the intervention group, but the differences between the groups were not statistically significant. No adverse effects related to the intervention were reported, they said.
Of note, strong responders in the intervention group experienced significant reductions in neutrophil elastase.
IBS is a prevalent, costly, and often disabling condition, but assessing food intolerance in clinical practice is challenging, the investigators said, adding that while a number of commercially available blood tests claim to diagnose food intolerance – including leukocyte activation tests, which are among the most widely used for this purpose – no rigorous studies of the tests have been published.
For the current study, adults aged 18-75 years who met Rome III criteria for any subtype of IBS and had active symptoms were enrolled from an academic health center in Connecticut. The leukocyte activation test was used to culture peripheral blood leukocytes with standardized individual food extracts, producing either a positive or negative result, which then guided the food elimination.
The findings demonstrate that “a diet guided by leukocyte activation testing results in demonstrable clinical improvement in IBS,” they wrote, noting that dietary changes based on a leukocyte activation test may be less restrictive than those associated with a low–fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (low FODMAPs) diet (which has also shown promise as “an efficacious, although burdensome, dietary intervention for IBS”), and may result in better long-term adherence.
“These clinical results, associated with a reduction in plasma neutrophil elastase, have implication for better understanding the role of food intolerance and the pathophysiology of IBS,” they said, adding that “future studies, ideally multisite and in larger samples, can assess comparative effects of other dietary interventions in IBS, the effects of restricting specific foods, and whether dietary changes guided by leukocyte activation testing affect other conditions.”
Cell Science Systems funded the study. The authors reported having no disclosures.
FROM BMJ OPEN GASTROENTEROLOGY
Key clinical point:
Major finding: Mean IBS Global Improvement Scale scores improved significantly more in the intervention vs. comparison group at 4 weeks and 8 weeks (mean between-group differences of 0.86 and 1.22 points, respectively).
Data source: A parallel-group, double-blind, randomized controlled trial of 58 IBS patients.
Disclosures: Cell Science Systems funded the study. The authors reported having no disclosures.
Benzodiazepines and antidepressants do not impair cognition in midlife schizophrenia
PARIS – Cumulative lifetime exposure to benzodiazepines and antidepressants in the relatively modest amounts typically prescribed in schizophrenia did not appear to adversely affect patients’ cognition in midlife, according to a first-of-its-kind study from Finland.
“These findings are reassuring,” said Anja P. Hulkko, MD, a psychiatric resident at the University of Oulu (Finland).

“Similarly, you don’t need to worry about using benzodiazepines in schizophrenia if you are using small doses or for short periods to treat a specific condition like anxiety or sleeplessness,” Dr. Hulkko said at the annual congress of the European College of Neuropsychopharmacology.
These observations were among the key findings of her analysis from the Northern Finnish Birth Cohort 1966. This ongoing unique and naturalistic observational study – or actually, more than 20 different studies conducted in the same population – was designed to study risk factors involved in preterm birth and intrauterine growth retardation, as well as the consequences of these early adverse events on later morbidity and mortality. Data including maternal health during pregnancy have been prospectively collected from first prenatal contact at weeks 10-16 well into adulthood.
The 1966 cohort included 12,058 live births in the two northernmost provinces of Finland, which was 96% of all births there in that year. DNA samples were obtained from nearly 6,000 subjects in the cohort. After birth and again every 7-15 years, the offspring were examined and underwent clinical evaluation in which a wide range of phenotypic, behavioral, and demographic data were collected. Linkage to Finland’s comprehensive national registries provides investigators with up-to-date information about participants’ education, medication, hospitalizations, significant medical diagnoses, pensions, and death. These prospective data allow investigations of the importance of genetic, biologic, social, and behavioral risk factors in the emergence of various target diseases, one of which is schizophrenia.
Dr. Hulkko’s presentation focused on 60 patients with various schizophrenia spectrum disorders who underwent an extensive battery of neuropsychological tests at age 43, when they averaged 16.5 years of illness.
Lifetime cumulative exposure to benzodiazepines or antidepressants was not significantly associated with a global composite cognition score in a multivariate analysis adjusted for potential confounders including sex, age at schizophrenia onset, and lifetime psychiatric hospital treatment days.
The comprehensive test battery included the California Verbal Learning Test, the Abstraction Inhibition and Working Memory Task, Digit Span and Matrix Reasoning, verbal fluency and vocabulary testing, and the Visual Object Learning Test.
This, she said, is the first report to look at the cognitive impact of these drug classes in midlife schizophrenia. Long-term, high-dose use of benzodiazepines has in recent years been linked to increased risk for cognitive impairment in other populations, but that’s not ordinarily how those drugs are employed in schizophrenia.
In contrast to the new Finnish antidepressant and benzodiazepine findings, higher lifetime antipsychotic dose-years in the study population were recently reported by Dr. Hulkko’s senior coinvestigators to be significantly associated with a worse adjusted cognition score, with no difference between typical and atypical antipsychotics. “It is possible that large antipsychotic doses harm cognition in schizophrenia in the long term,” the researchers concluded (Psychiatry Res. 2017 Jan;247:130-8).
At the meeting, Dr. Hulkko presented new data on the cognitive impact of cumulative exposure to antipsychotics in the midlife schizophrenia cohort. The new finding is that having an antipsychotic-free period of at least 1 year at any point since treatment started an average of more than 16 years earlier was associated with a better adjusted cognitive performance.
The same was true for having an antipsychotic-free interval of at least 11 months directly before administration of the neuropsychological test battery. This is an encouraging finding because it suggests that an antipsychotic drug holiday might promote a measurable degree of cognitive recovery. But this observation must be viewed as hypothesis generating rather than conclusive, given the relatively small size of the study population, the observational nature of the study, and the possibility that the patients on a pretest antipsychotic break had less severe illness.
“Although we have tried to control for many factors, still, it’s possible that we cannot control for everything,” she noted. “It seems likely that both the illness itself and treatment are associated with the course of cognition.”
Kamilla W. Miskowiak, PhD, a neuropsychologist at the University of Copenhagen deemed the Finnish results “highly interesting.”
“This is reassuring, since many patients are worried about taking these medications [antidepressants and benzodiazepines] because of their potential negative effects on cognition. In contrast, long-term high-dose antipsychotic medication was associated with poorer cognitive outcome. This underscores the importance of close dose monitoring of antipsychotic medication for these patients to improve their cognitive outcome,” said Dr. Miskowiak, who was not involved in the study.
The study was supported by the Academy of Finland, the Finnish Cultural Foundation Lapland Regional Fund, and grants from various nonprofit foundations. Dr. Hulkko reported having no financial conflicts of interest.
PARIS – Cumulative lifetime exposure to benzodiazepines and antidepressants in the relatively modest amounts typically prescribed in schizophrenia did not appear to adversely affect patients’ cognition in midlife, according to a first-of-its-kind study from Finland.
“These findings are reassuring,” said Anja P. Hulkko, MD, a psychiatric resident at the University of Oulu (Finland).
“Similarly, you don’t need to worry about using benzodiazepines in schizophrenia if you are using small doses or for short periods to treat a specific condition like anxiety or sleeplessness,” Dr. Hulkko said at the annual congress of the European College of Neuropsychopharmacology.
These observations were among the key findings of her analysis from the Northern Finnish Birth Cohort 1966. This ongoing unique and naturalistic observational study – or actually, more than 20 different studies conducted in the same population – was designed to study risk factors involved in preterm birth and intrauterine growth retardation, as well as the consequences of these early adverse events on later morbidity and mortality. Data including maternal health during pregnancy have been prospectively collected from first prenatal contact at weeks 10-16 well into adulthood.
The 1966 cohort included 12,058 live births in the two northernmost provinces of Finland, which was 96% of all births there in that year. DNA samples were obtained from nearly 6,000 subjects in the cohort. After birth and again every 7-15 years, the offspring were examined and underwent clinical evaluation in which a wide range of phenotypic, behavioral, and demographic data were collected. Linkage to Finland’s comprehensive national registries provides investigators with up-to-date information about participants’ education, medication, hospitalizations, significant medical diagnoses, pensions, and death. These prospective data allow investigations of the importance of genetic, biologic, social, and behavioral risk factors in the emergence of various target diseases, one of which is schizophrenia.
Dr. Hulkko’s presentation focused on 60 patients with various schizophrenia spectrum disorders who underwent an extensive battery of neuropsychological tests at age 43, when they averaged 16.5 years of illness.
Lifetime cumulative exposure to benzodiazepines or antidepressants was not significantly associated with a global composite cognition score in a multivariate analysis adjusted for potential confounders including sex, age at schizophrenia onset, and lifetime psychiatric hospital treatment days.
The comprehensive test battery included the California Verbal Learning Test, the Abstraction Inhibition and Working Memory Task, Digit Span and Matrix Reasoning, verbal fluency and vocabulary testing, and the Visual Object Learning Test.
This, she said, is the first report to look at the cognitive impact of these drug classes in midlife schizophrenia. Long-term, high-dose use of benzodiazepines has in recent years been linked to increased risk for cognitive impairment in other populations, but that’s not ordinarily how those drugs are employed in schizophrenia.
In contrast to the new Finnish antidepressant and benzodiazepine findings, higher lifetime antipsychotic dose-years in the study population were recently reported by Dr. Hulkko’s senior coinvestigators to be significantly associated with a worse adjusted cognition score, with no difference between typical and atypical antipsychotics. “It is possible that large antipsychotic doses harm cognition in schizophrenia in the long term,” the researchers concluded (Psychiatry Res. 2017 Jan;247:130-8).
At the meeting, Dr. Hulkko presented new data on the cognitive impact of cumulative exposure to antipsychotics in the midlife schizophrenia cohort. The new finding is that having an antipsychotic-free period of at least 1 year at any point since treatment started an average of more than 16 years earlier was associated with a better adjusted cognitive performance.
The same was true for having an antipsychotic-free interval of at least 11 months directly before administration of the neuropsychological test battery. This is an encouraging finding because it suggests that an antipsychotic drug holiday might promote a measurable degree of cognitive recovery. But this observation must be viewed as hypothesis generating rather than conclusive, given the relatively small size of the study population, the observational nature of the study, and the possibility that the patients on a pretest antipsychotic break had less severe illness.
“Although we have tried to control for many factors, still, it’s possible that we cannot control for everything,” she noted. “It seems likely that both the illness itself and treatment are associated with the course of cognition.”
Kamilla W. Miskowiak, PhD, a neuropsychologist at the University of Copenhagen deemed the Finnish results “highly interesting.”
“This is reassuring, since many patients are worried about taking these medications [antidepressants and benzodiazepines] because of their potential negative effects on cognition. In contrast, long-term high-dose antipsychotic medication was associated with poorer cognitive outcome. This underscores the importance of close dose monitoring of antipsychotic medication for these patients to improve their cognitive outcome,” said Dr. Miskowiak, who was not involved in the study.
The study was supported by the Academy of Finland, the Finnish Cultural Foundation Lapland Regional Fund, and grants from various nonprofit foundations. Dr. Hulkko reported having no financial conflicts of interest.
PARIS – Cumulative lifetime exposure to benzodiazepines and antidepressants in the relatively modest amounts typically prescribed in schizophrenia did not appear to adversely affect patients’ cognition in midlife, according to a first-of-its-kind study from Finland.
“These findings are reassuring,” said Anja P. Hulkko, MD, a psychiatric resident at the University of Oulu (Finland).
“Similarly, you don’t need to worry about using benzodiazepines in schizophrenia if you are using small doses or for short periods to treat a specific condition like anxiety or sleeplessness,” Dr. Hulkko said at the annual congress of the European College of Neuropsychopharmacology.
These observations were among the key findings of her analysis from the Northern Finnish Birth Cohort 1966. This ongoing unique and naturalistic observational study – or actually, more than 20 different studies conducted in the same population – was designed to study risk factors involved in preterm birth and intrauterine growth retardation, as well as the consequences of these early adverse events on later morbidity and mortality. Data including maternal health during pregnancy have been prospectively collected from first prenatal contact at weeks 10-16 well into adulthood.
The 1966 cohort included 12,058 live births in the two northernmost provinces of Finland, which was 96% of all births there in that year. DNA samples were obtained from nearly 6,000 subjects in the cohort. After birth and again every 7-15 years, the offspring were examined and underwent clinical evaluation in which a wide range of phenotypic, behavioral, and demographic data were collected. Linkage to Finland’s comprehensive national registries provides investigators with up-to-date information about participants’ education, medication, hospitalizations, significant medical diagnoses, pensions, and death. These prospective data allow investigations of the importance of genetic, biologic, social, and behavioral risk factors in the emergence of various target diseases, one of which is schizophrenia.
Dr. Hulkko’s presentation focused on 60 patients with various schizophrenia spectrum disorders who underwent an extensive battery of neuropsychological tests at age 43, when they averaged 16.5 years of illness.
Lifetime cumulative exposure to benzodiazepines or antidepressants was not significantly associated with a global composite cognition score in a multivariate analysis adjusted for potential confounders including sex, age at schizophrenia onset, and lifetime psychiatric hospital treatment days.
The comprehensive test battery included the California Verbal Learning Test, the Abstraction Inhibition and Working Memory Task, Digit Span and Matrix Reasoning, verbal fluency and vocabulary testing, and the Visual Object Learning Test.
This, she said, is the first report to look at the cognitive impact of these drug classes in midlife schizophrenia. Long-term, high-dose use of benzodiazepines has in recent years been linked to increased risk for cognitive impairment in other populations, but that’s not ordinarily how those drugs are employed in schizophrenia.
In contrast to the new Finnish antidepressant and benzodiazepine findings, higher lifetime antipsychotic dose-years in the study population were recently reported by Dr. Hulkko’s senior coinvestigators to be significantly associated with a worse adjusted cognition score, with no difference between typical and atypical antipsychotics. “It is possible that large antipsychotic doses harm cognition in schizophrenia in the long term,” the researchers concluded (Psychiatry Res. 2017 Jan;247:130-8).
At the meeting, Dr. Hulkko presented new data on the cognitive impact of cumulative exposure to antipsychotics in the midlife schizophrenia cohort. The new finding is that having an antipsychotic-free period of at least 1 year at any point since treatment started an average of more than 16 years earlier was associated with a better adjusted cognitive performance.
The same was true for having an antipsychotic-free interval of at least 11 months directly before administration of the neuropsychological test battery. This is an encouraging finding because it suggests that an antipsychotic drug holiday might promote a measurable degree of cognitive recovery. But this observation must be viewed as hypothesis generating rather than conclusive, given the relatively small size of the study population, the observational nature of the study, and the possibility that the patients on a pretest antipsychotic break had less severe illness.
“Although we have tried to control for many factors, still, it’s possible that we cannot control for everything,” she noted. “It seems likely that both the illness itself and treatment are associated with the course of cognition.”
Kamilla W. Miskowiak, PhD, a neuropsychologist at the University of Copenhagen deemed the Finnish results “highly interesting.”
“This is reassuring, since many patients are worried about taking these medications [antidepressants and benzodiazepines] because of their potential negative effects on cognition. In contrast, long-term high-dose antipsychotic medication was associated with poorer cognitive outcome. This underscores the importance of close dose monitoring of antipsychotic medication for these patients to improve their cognitive outcome,” said Dr. Miskowiak, who was not involved in the study.
The study was supported by the Academy of Finland, the Finnish Cultural Foundation Lapland Regional Fund, and grants from various nonprofit foundations. Dr. Hulkko reported having no financial conflicts of interest.
AT THE ECNP CONGRESS
Key clinical point:
Major finding: As-needed prescription of antidepressants and benzodiazepines in the dose typically used in schizophrenia does not impair midlife cognition.
Data source: An ongoing naturalistic, observational, general population-based study of more than 12,000 babies born in Northern Finland in 1966 from fetal life through middle age.
Disclosures: The study was supported by the Academy of Finland, the Finnish Cultural Foundation Lapland Regional Fund, and grants from various nonprofit charitable foundations. The presenter reported having no financial conflicts of interest.
DETOUR system shows early promise for long SFA lesions
A new, percutaneous bypass system appeared safe and effective for treating long-segment blockages in the femoropopliteal artery, a subset of the DETOUR I trial showed. Data at 30 days showed low levels of major adverse events and the results showed that there was promising graft patency at 6 months.
Sean Lyden, MD, chairman of the department of vascular surgery at the Cleveland Clinic, presented the results in a late-breaking clinical trial session at the 2017 Vascular Interventional Advances meeting. The study evaluated the safety and effectiveness of the DETOUR System for treating long-segment (greater than 25 cm) blockages in the femoropopliteal artery.
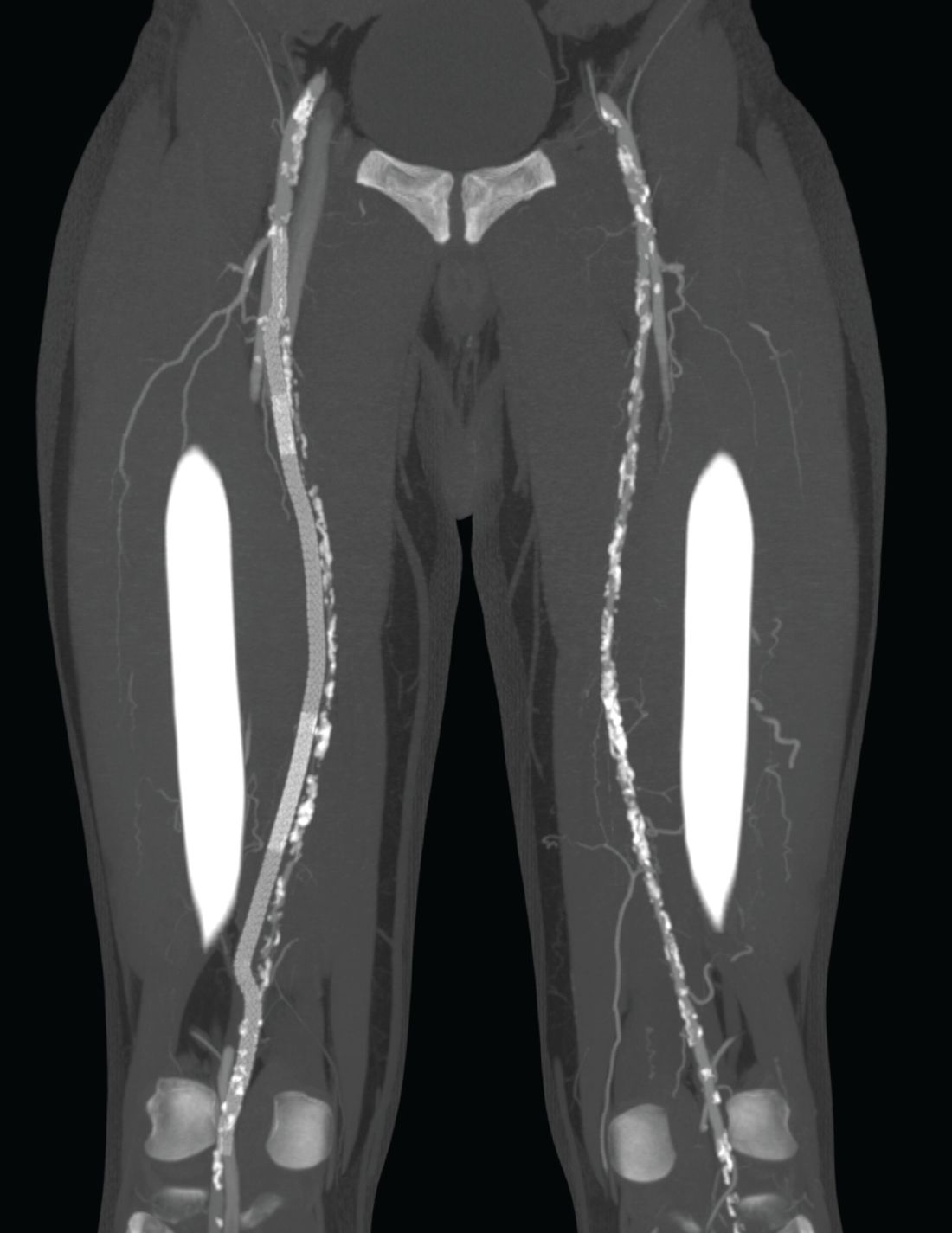
To address this problem, the PQ Bypass DETOUR System was developed as a fully percutaneous bypass approach designed to achieve comparable end results as open bypass surgery, by using the femoral vein as a pathway for created a modular stent graft bypass.
“The DETOUR procedure creates a pathway around a lesion by placing stent grafts that cross from the superficial femoral artery (SFA) into the femoral vein and back into the artery. The new path through the stent grafts redirects oxygen-rich blood around the blockage and restores blood flow to the lower leg and foot of the patient,” according to a company press release.
The DETOUR 1 trial was a prospective, single-arm study of 77 patients (81 limbs) treated at eight global sites. Dr. Lyden reported on a subset analysis of 50 patients with long lesions (greater than 25 cm). The mean age of the patients was 65 years; 84% were men.
Comorbidities included diabetes (30%), history of renal insufficiency (26%), smoking (90%), and previous peripheral intervention (30%). There were 53 lesions treated in all, with a mean length of 33.5 cm. The percentage of total occlusions was 96% and the percentage of lesions with zero, one, two, or three runoff vessels was 0%, 4%, 26%, and 70%, respectively, according to Dr. Lyden.
The primary safety endpoint of 2% major adverse events defined as death, target vessel revascularization or amputation at 30 days was met, with no deaths or amputations and only one target vessel revascularization.
The primary patency was 89% at 6 months with optimal placement, with an overall primary patency of 77%.
Both the delivery and removal of the device was successful in all the lesions treated.
The Rutherford Class improved at least 2 grades in 92% of the patients, and there was a statistically significant improvement in ankle brachial index from 0.64 to 0.92 (P less than .0001).

“Percutaneous bypass using the femoral vein as a pathway may end up being an important step forward in the treatment of long-segment SFA disease,” Dr. Lyden concluded.
In March 2017, the DETOUR System received CE (Conformité Européenne) Mark approval, but the system is not yet approved by the Food and Drug Administration for sale in the United States.
The DETOUR trial was sponsored by PQ Bypass Inc. Dr. Lyden reported receiving fees Spectranetics Corp and VIVA Physicians. He has no financial conflicts with regard to PQ Bypass.
A new, percutaneous bypass system appeared safe and effective for treating long-segment blockages in the femoropopliteal artery, a subset of the DETOUR I trial showed. Data at 30 days showed low levels of major adverse events and the results showed that there was promising graft patency at 6 months.
Sean Lyden, MD, chairman of the department of vascular surgery at the Cleveland Clinic, presented the results in a late-breaking clinical trial session at the 2017 Vascular Interventional Advances meeting. The study evaluated the safety and effectiveness of the DETOUR System for treating long-segment (greater than 25 cm) blockages in the femoropopliteal artery.
To address this problem, the PQ Bypass DETOUR System was developed as a fully percutaneous bypass approach designed to achieve comparable end results as open bypass surgery, by using the femoral vein as a pathway for created a modular stent graft bypass.
“The DETOUR procedure creates a pathway around a lesion by placing stent grafts that cross from the superficial femoral artery (SFA) into the femoral vein and back into the artery. The new path through the stent grafts redirects oxygen-rich blood around the blockage and restores blood flow to the lower leg and foot of the patient,” according to a company press release.
The DETOUR 1 trial was a prospective, single-arm study of 77 patients (81 limbs) treated at eight global sites. Dr. Lyden reported on a subset analysis of 50 patients with long lesions (greater than 25 cm). The mean age of the patients was 65 years; 84% were men.
Comorbidities included diabetes (30%), history of renal insufficiency (26%), smoking (90%), and previous peripheral intervention (30%). There were 53 lesions treated in all, with a mean length of 33.5 cm. The percentage of total occlusions was 96% and the percentage of lesions with zero, one, two, or three runoff vessels was 0%, 4%, 26%, and 70%, respectively, according to Dr. Lyden.
The primary safety endpoint of 2% major adverse events defined as death, target vessel revascularization or amputation at 30 days was met, with no deaths or amputations and only one target vessel revascularization.
The primary patency was 89% at 6 months with optimal placement, with an overall primary patency of 77%.
Both the delivery and removal of the device was successful in all the lesions treated.
The Rutherford Class improved at least 2 grades in 92% of the patients, and there was a statistically significant improvement in ankle brachial index from 0.64 to 0.92 (P less than .0001).
“Percutaneous bypass using the femoral vein as a pathway may end up being an important step forward in the treatment of long-segment SFA disease,” Dr. Lyden concluded.
In March 2017, the DETOUR System received CE (Conformité Européenne) Mark approval, but the system is not yet approved by the Food and Drug Administration for sale in the United States.
The DETOUR trial was sponsored by PQ Bypass Inc. Dr. Lyden reported receiving fees Spectranetics Corp and VIVA Physicians. He has no financial conflicts with regard to PQ Bypass.
A new, percutaneous bypass system appeared safe and effective for treating long-segment blockages in the femoropopliteal artery, a subset of the DETOUR I trial showed. Data at 30 days showed low levels of major adverse events and the results showed that there was promising graft patency at 6 months.
Sean Lyden, MD, chairman of the department of vascular surgery at the Cleveland Clinic, presented the results in a late-breaking clinical trial session at the 2017 Vascular Interventional Advances meeting. The study evaluated the safety and effectiveness of the DETOUR System for treating long-segment (greater than 25 cm) blockages in the femoropopliteal artery.
To address this problem, the PQ Bypass DETOUR System was developed as a fully percutaneous bypass approach designed to achieve comparable end results as open bypass surgery, by using the femoral vein as a pathway for created a modular stent graft bypass.
“The DETOUR procedure creates a pathway around a lesion by placing stent grafts that cross from the superficial femoral artery (SFA) into the femoral vein and back into the artery. The new path through the stent grafts redirects oxygen-rich blood around the blockage and restores blood flow to the lower leg and foot of the patient,” according to a company press release.
The DETOUR 1 trial was a prospective, single-arm study of 77 patients (81 limbs) treated at eight global sites. Dr. Lyden reported on a subset analysis of 50 patients with long lesions (greater than 25 cm). The mean age of the patients was 65 years; 84% were men.
Comorbidities included diabetes (30%), history of renal insufficiency (26%), smoking (90%), and previous peripheral intervention (30%). There were 53 lesions treated in all, with a mean length of 33.5 cm. The percentage of total occlusions was 96% and the percentage of lesions with zero, one, two, or three runoff vessels was 0%, 4%, 26%, and 70%, respectively, according to Dr. Lyden.
The primary safety endpoint of 2% major adverse events defined as death, target vessel revascularization or amputation at 30 days was met, with no deaths or amputations and only one target vessel revascularization.
The primary patency was 89% at 6 months with optimal placement, with an overall primary patency of 77%.
Both the delivery and removal of the device was successful in all the lesions treated.
The Rutherford Class improved at least 2 grades in 92% of the patients, and there was a statistically significant improvement in ankle brachial index from 0.64 to 0.92 (P less than .0001).
“Percutaneous bypass using the femoral vein as a pathway may end up being an important step forward in the treatment of long-segment SFA disease,” Dr. Lyden concluded.
In March 2017, the DETOUR System received CE (Conformité Européenne) Mark approval, but the system is not yet approved by the Food and Drug Administration for sale in the United States.
The DETOUR trial was sponsored by PQ Bypass Inc. Dr. Lyden reported receiving fees Spectranetics Corp and VIVA Physicians. He has no financial conflicts with regard to PQ Bypass.
FROM VIVA 17
Key clinical point:
Major finding: Primary patency was 89% at 6 months, with low MAE at 30 days.
Data source: Subset analysis of 50 patients with long lesions in the multicenter, prospective, single-arm DETOUR 1 trial.
Disclosures: The DETOUR trial was sponsored by PQ Bypass. Dr. Lyden reported receiving fees from Spectranetics Corp and VIVA Physicians. He has no financial conflicts with regard to PQ Bypass.