User login
VIDEO: Dermatologists often miss adult onset atopic dermatitis
WAILEA, HAWAII – Evidence from several recent studies suggests that the prevalence of adult onset atopic dermatitis in the United States may be as high as 7%-10%, said Jonathan I. Silverberg, MD, of the department of dermatology, preventive medicine, and medical social sciences, Northwestern University, Chicago.
Many features are similar to atopic dermatitis (AD) seen in childhood, but in adults the eczema is more likely to affect the hands and the eyelids. “We often have a hard time telling that apart from contact dermatitis,” Dr. Silverberg said in a video interview at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
Some adults may have forgotten they had AD as children and don’t recognize it if it reappears in adulthood, but sometimes AD appears with no childhood history, he noted. “There’s a skepticism that if it is adult onset, it must not be atopic dermatitis,” but he has found that is not always the case.
A take-home message for clinicians: “Don’t be surprised when a patient walks in the door as an adult meeting all criteria for atopic dermatitis. It can be, and you can diagnose them comfortably,” said Dr. Silverberg, who is also director of the Northwestern Medicine Multidisciplinary Eczema Center, Northwestern Memorial Hospital, Chicago.
Most of the treatments for adult AD “cover many different arms of the immune system,” and include topical steroids and immunosuppressants, he added.
Dr. Silverberg disclosed relationships with companies including AbbVie, Anacor, Celgene, Chugai, GlaxoSmithKline, Lilly, MedImmune-AstraZeneca, Pfizer, Procter & Gamble, Puricore, and Regeneron-Sanofi. SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAILEA, HAWAII – Evidence from several recent studies suggests that the prevalence of adult onset atopic dermatitis in the United States may be as high as 7%-10%, said Jonathan I. Silverberg, MD, of the department of dermatology, preventive medicine, and medical social sciences, Northwestern University, Chicago.
Many features are similar to atopic dermatitis (AD) seen in childhood, but in adults the eczema is more likely to affect the hands and the eyelids. “We often have a hard time telling that apart from contact dermatitis,” Dr. Silverberg said in a video interview at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
Some adults may have forgotten they had AD as children and don’t recognize it if it reappears in adulthood, but sometimes AD appears with no childhood history, he noted. “There’s a skepticism that if it is adult onset, it must not be atopic dermatitis,” but he has found that is not always the case.
A take-home message for clinicians: “Don’t be surprised when a patient walks in the door as an adult meeting all criteria for atopic dermatitis. It can be, and you can diagnose them comfortably,” said Dr. Silverberg, who is also director of the Northwestern Medicine Multidisciplinary Eczema Center, Northwestern Memorial Hospital, Chicago.
Most of the treatments for adult AD “cover many different arms of the immune system,” and include topical steroids and immunosuppressants, he added.
Dr. Silverberg disclosed relationships with companies including AbbVie, Anacor, Celgene, Chugai, GlaxoSmithKline, Lilly, MedImmune-AstraZeneca, Pfizer, Procter & Gamble, Puricore, and Regeneron-Sanofi. SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAILEA, HAWAII – Evidence from several recent studies suggests that the prevalence of adult onset atopic dermatitis in the United States may be as high as 7%-10%, said Jonathan I. Silverberg, MD, of the department of dermatology, preventive medicine, and medical social sciences, Northwestern University, Chicago.
Many features are similar to atopic dermatitis (AD) seen in childhood, but in adults the eczema is more likely to affect the hands and the eyelids. “We often have a hard time telling that apart from contact dermatitis,” Dr. Silverberg said in a video interview at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
Some adults may have forgotten they had AD as children and don’t recognize it if it reappears in adulthood, but sometimes AD appears with no childhood history, he noted. “There’s a skepticism that if it is adult onset, it must not be atopic dermatitis,” but he has found that is not always the case.
A take-home message for clinicians: “Don’t be surprised when a patient walks in the door as an adult meeting all criteria for atopic dermatitis. It can be, and you can diagnose them comfortably,” said Dr. Silverberg, who is also director of the Northwestern Medicine Multidisciplinary Eczema Center, Northwestern Memorial Hospital, Chicago.
Most of the treatments for adult AD “cover many different arms of the immune system,” and include topical steroids and immunosuppressants, he added.
Dr. Silverberg disclosed relationships with companies including AbbVie, Anacor, Celgene, Chugai, GlaxoSmithKline, Lilly, MedImmune-AstraZeneca, Pfizer, Procter & Gamble, Puricore, and Regeneron-Sanofi. SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT SDEF HAWAII DERMATOLOGY SEMINAR

AAN Guideline Assesses fMRI for Presurgical Evaluation of Patients With Epilepsy
When preparing for epilepsy surgery, neurologists may consider using functional MRI (fMRI) instead of the intracarotid amobarbital procedure (IAP) to map language and memory functions in the brain, according to a practice guideline developed by the American Academy of Neurology (AAN). The current evidence is weak, however, and clinicians should advise patients carefully about the benefits and risks of IAP (also known as the Wada test) and fMRI, according to the guideline, which was published online ahead of print January 11 in Neurology.
IAP, an invasive technique, is the current standard for presurgical evaluation in epilepsy. fMRI is noninvasive and also considered safe. Neither of the two methods has been standardized. “Because fMRI is becoming more widely available, we wanted to see how it compares to the Wada test,” said lead author Jerzy Szaflarski, MD, PhD, Professor of Neurology at the University of Alabama at Birmingham. “While the risks associated with the Wada test are rare, they can be serious, including stroke and injury to the carotid artery.”

The AAN formed an 11-member panel to draft the guidelines. Two panelists independently selected 37 possibly relevant articles. Studies with fewer than 15 cases, case reports, meta-analyses, and editorials were excluded. Two panelists rated each article according to the AAN’s diagnostic and prognostic classification of evidence, and the panel ultimately developed consensus recommendations.
Data Support fMRI for Certain Situations
Class II data indicated that fMRI possibly provides language lateralization information concordant with that of IAP in 87% of people with medial temporal lobe epilepsy and in 81% of patients with extratemporal epilepsy. Current comparative data for temporal tumors or lateral temporal cases are insufficient to draw conclusions. Thus, fMRI may be considered as an option for lateralizing language functions in place of IAP in patients with medial temporal lobe epilepsy (Level C), temporal epilepsy in general (Level C), or extratemporal epilepsy (Level C), said the authors. The evidence is unclear for patients with temporal neocortical epilepsy or temporal tumors (Level U).
One Class II study and one Class III study suggested that fMRI is possibly effective in aiding the prediction of postsurgical language deficits in patients undergoing presurgical evaluation for possible temporal lobectomy. The authors recommended that fMRI may be considered for predicting postsurgical language outcomes after anterior temporal lobe resection for the control of temporal lobe epilepsy (Level C).
Class II evidence suggests that in patients with medial temporal lobe epilepsy, fMRI is comparable with IAP in its ability to lateralize memory functions and may be used for this purpose. The authors recommended that fMRI may be considered as an option to lateralize memory functions in place of IAP in patients with medial temporal lobe epilepsy (Level C).
Nine Class II studies with different methods together suggested that fMRI leftward activation asymmetry during encoding of verbal material, regardless of whether measured in the medial temporal lobe or in the language network, probably predicts verbal memory decline after left medial temporal lobe surgery. The authors therefore recommended that presurgical fMRI of verbal memory or of language encoding should be considered as an option to predict verbal memory outcome in patients with epilepsy who are undergoing evaluation for left medial temporal lobe surgery (Level B).
A Class II study indicated that fMRI activation asymmetry during nonverbal (ie, scene and face recognition) memory tasks possibly predicts nonverbal memory decline after medial temporal lobe surgery. The authors recommended that presurgical fMRI using nonverbal memory encoding may be considered as a means to predict visuospatial memory outcomes in patients with epilepsy who are undergoing evaluation for temporal lobe surgery (Level C).
Based on data from one Class II study and one Class III study, the authors recommended that presurgical fMRI may be used instead of the IAP for language lateralization in patients with epilepsy who are undergoing evaluation for brain surgery (Level C). “However, when fMRI is used for this purpose, task design, data analysis methods, and epilepsy type should be considered,” they added.
In addition, based on nine Class II studies, the authors recommended that fMRI of language and verbal memory lateralization may be an alternative to IAP memory testing for prediction of verbal memory outcome in medial temporal lobe epilepsy (Level C). The authors note that fMRI is not yet established as an alternative to the IAP for prediction of global amnesia in patients who have undergone anterior temporal lobe surgery.
More and Larger Studies Are Needed
“The imperfect concordance between fMRI and IAP language lateralization leaves open the question of which test is more accurate in discordant cases,” said the authors. Although the IAP is the reference standard, it is subject to limitations resulting from individual variation in arterial anatomy, variable effects of anesthesia, the rate of amobarbital injection, variability in patient cooperation, and variation in testing methods.
Like the IAP, cognitive fMRI “is a complex diagnostic procedure that requires both advanced technical expertise in imaging and expert interaction with patients to elicit adequate levels of task performance, select a set of activation tasks appropriate to the patient’s ability and the clinical aims of the study, instruct the patient on the tasks, administer the tasks during scanning, and evaluate and provide corrective feedback on task performance during the scanning session,” said the authors.
Global amnesia may result from bilateral medial temporal lobe damage, and some neurologists depend on the IAP to evaluate a patient’s risk for this outcome. “Global amnesia is rare after unilateral temporal lobe surgery, however, and occurs mainly when there is preexisting contralateral medial temporal lobe dysfunction,” said the authors. “One possible approach, therefore, is to reserve use of the IAP memory test for those patients at greatest risk for global amnesia, that is, patients undergoing unilateral anterior temporal lobe resection who have structural or functional evidence of damage to the contralateral medial temporal lobe.”
“Larger studies need to be conducted to increase the quality of available evidence,” Dr. Szaflarski concluded.
—Erik Greb
Suggested Reading
Szaflarski JP, Gloss D, Binder JR, et al. Practice guideline summary: Use of fMRI in the presurgical evaluation of patients with epilepsy—Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology. 2017 Jan 11 [Epub ahead of print].
When preparing for epilepsy surgery, neurologists may consider using functional MRI (fMRI) instead of the intracarotid amobarbital procedure (IAP) to map language and memory functions in the brain, according to a practice guideline developed by the American Academy of Neurology (AAN). The current evidence is weak, however, and clinicians should advise patients carefully about the benefits and risks of IAP (also known as the Wada test) and fMRI, according to the guideline, which was published online ahead of print January 11 in Neurology.
IAP, an invasive technique, is the current standard for presurgical evaluation in epilepsy. fMRI is noninvasive and also considered safe. Neither of the two methods has been standardized. “Because fMRI is becoming more widely available, we wanted to see how it compares to the Wada test,” said lead author Jerzy Szaflarski, MD, PhD, Professor of Neurology at the University of Alabama at Birmingham. “While the risks associated with the Wada test are rare, they can be serious, including stroke and injury to the carotid artery.”
The AAN formed an 11-member panel to draft the guidelines. Two panelists independently selected 37 possibly relevant articles. Studies with fewer than 15 cases, case reports, meta-analyses, and editorials were excluded. Two panelists rated each article according to the AAN’s diagnostic and prognostic classification of evidence, and the panel ultimately developed consensus recommendations.
Data Support fMRI for Certain Situations
Class II data indicated that fMRI possibly provides language lateralization information concordant with that of IAP in 87% of people with medial temporal lobe epilepsy and in 81% of patients with extratemporal epilepsy. Current comparative data for temporal tumors or lateral temporal cases are insufficient to draw conclusions. Thus, fMRI may be considered as an option for lateralizing language functions in place of IAP in patients with medial temporal lobe epilepsy (Level C), temporal epilepsy in general (Level C), or extratemporal epilepsy (Level C), said the authors. The evidence is unclear for patients with temporal neocortical epilepsy or temporal tumors (Level U).
One Class II study and one Class III study suggested that fMRI is possibly effective in aiding the prediction of postsurgical language deficits in patients undergoing presurgical evaluation for possible temporal lobectomy. The authors recommended that fMRI may be considered for predicting postsurgical language outcomes after anterior temporal lobe resection for the control of temporal lobe epilepsy (Level C).
Class II evidence suggests that in patients with medial temporal lobe epilepsy, fMRI is comparable with IAP in its ability to lateralize memory functions and may be used for this purpose. The authors recommended that fMRI may be considered as an option to lateralize memory functions in place of IAP in patients with medial temporal lobe epilepsy (Level C).
Nine Class II studies with different methods together suggested that fMRI leftward activation asymmetry during encoding of verbal material, regardless of whether measured in the medial temporal lobe or in the language network, probably predicts verbal memory decline after left medial temporal lobe surgery. The authors therefore recommended that presurgical fMRI of verbal memory or of language encoding should be considered as an option to predict verbal memory outcome in patients with epilepsy who are undergoing evaluation for left medial temporal lobe surgery (Level B).
A Class II study indicated that fMRI activation asymmetry during nonverbal (ie, scene and face recognition) memory tasks possibly predicts nonverbal memory decline after medial temporal lobe surgery. The authors recommended that presurgical fMRI using nonverbal memory encoding may be considered as a means to predict visuospatial memory outcomes in patients with epilepsy who are undergoing evaluation for temporal lobe surgery (Level C).
Based on data from one Class II study and one Class III study, the authors recommended that presurgical fMRI may be used instead of the IAP for language lateralization in patients with epilepsy who are undergoing evaluation for brain surgery (Level C). “However, when fMRI is used for this purpose, task design, data analysis methods, and epilepsy type should be considered,” they added.
In addition, based on nine Class II studies, the authors recommended that fMRI of language and verbal memory lateralization may be an alternative to IAP memory testing for prediction of verbal memory outcome in medial temporal lobe epilepsy (Level C). The authors note that fMRI is not yet established as an alternative to the IAP for prediction of global amnesia in patients who have undergone anterior temporal lobe surgery.
More and Larger Studies Are Needed
“The imperfect concordance between fMRI and IAP language lateralization leaves open the question of which test is more accurate in discordant cases,” said the authors. Although the IAP is the reference standard, it is subject to limitations resulting from individual variation in arterial anatomy, variable effects of anesthesia, the rate of amobarbital injection, variability in patient cooperation, and variation in testing methods.
Like the IAP, cognitive fMRI “is a complex diagnostic procedure that requires both advanced technical expertise in imaging and expert interaction with patients to elicit adequate levels of task performance, select a set of activation tasks appropriate to the patient’s ability and the clinical aims of the study, instruct the patient on the tasks, administer the tasks during scanning, and evaluate and provide corrective feedback on task performance during the scanning session,” said the authors.
Global amnesia may result from bilateral medial temporal lobe damage, and some neurologists depend on the IAP to evaluate a patient’s risk for this outcome. “Global amnesia is rare after unilateral temporal lobe surgery, however, and occurs mainly when there is preexisting contralateral medial temporal lobe dysfunction,” said the authors. “One possible approach, therefore, is to reserve use of the IAP memory test for those patients at greatest risk for global amnesia, that is, patients undergoing unilateral anterior temporal lobe resection who have structural or functional evidence of damage to the contralateral medial temporal lobe.”
“Larger studies need to be conducted to increase the quality of available evidence,” Dr. Szaflarski concluded.
—Erik Greb
Suggested Reading
Szaflarski JP, Gloss D, Binder JR, et al. Practice guideline summary: Use of fMRI in the presurgical evaluation of patients with epilepsy—Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology. 2017 Jan 11 [Epub ahead of print].
When preparing for epilepsy surgery, neurologists may consider using functional MRI (fMRI) instead of the intracarotid amobarbital procedure (IAP) to map language and memory functions in the brain, according to a practice guideline developed by the American Academy of Neurology (AAN). The current evidence is weak, however, and clinicians should advise patients carefully about the benefits and risks of IAP (also known as the Wada test) and fMRI, according to the guideline, which was published online ahead of print January 11 in Neurology.
IAP, an invasive technique, is the current standard for presurgical evaluation in epilepsy. fMRI is noninvasive and also considered safe. Neither of the two methods has been standardized. “Because fMRI is becoming more widely available, we wanted to see how it compares to the Wada test,” said lead author Jerzy Szaflarski, MD, PhD, Professor of Neurology at the University of Alabama at Birmingham. “While the risks associated with the Wada test are rare, they can be serious, including stroke and injury to the carotid artery.”
The AAN formed an 11-member panel to draft the guidelines. Two panelists independently selected 37 possibly relevant articles. Studies with fewer than 15 cases, case reports, meta-analyses, and editorials were excluded. Two panelists rated each article according to the AAN’s diagnostic and prognostic classification of evidence, and the panel ultimately developed consensus recommendations.
Data Support fMRI for Certain Situations
Class II data indicated that fMRI possibly provides language lateralization information concordant with that of IAP in 87% of people with medial temporal lobe epilepsy and in 81% of patients with extratemporal epilepsy. Current comparative data for temporal tumors or lateral temporal cases are insufficient to draw conclusions. Thus, fMRI may be considered as an option for lateralizing language functions in place of IAP in patients with medial temporal lobe epilepsy (Level C), temporal epilepsy in general (Level C), or extratemporal epilepsy (Level C), said the authors. The evidence is unclear for patients with temporal neocortical epilepsy or temporal tumors (Level U).
One Class II study and one Class III study suggested that fMRI is possibly effective in aiding the prediction of postsurgical language deficits in patients undergoing presurgical evaluation for possible temporal lobectomy. The authors recommended that fMRI may be considered for predicting postsurgical language outcomes after anterior temporal lobe resection for the control of temporal lobe epilepsy (Level C).
Class II evidence suggests that in patients with medial temporal lobe epilepsy, fMRI is comparable with IAP in its ability to lateralize memory functions and may be used for this purpose. The authors recommended that fMRI may be considered as an option to lateralize memory functions in place of IAP in patients with medial temporal lobe epilepsy (Level C).
Nine Class II studies with different methods together suggested that fMRI leftward activation asymmetry during encoding of verbal material, regardless of whether measured in the medial temporal lobe or in the language network, probably predicts verbal memory decline after left medial temporal lobe surgery. The authors therefore recommended that presurgical fMRI of verbal memory or of language encoding should be considered as an option to predict verbal memory outcome in patients with epilepsy who are undergoing evaluation for left medial temporal lobe surgery (Level B).
A Class II study indicated that fMRI activation asymmetry during nonverbal (ie, scene and face recognition) memory tasks possibly predicts nonverbal memory decline after medial temporal lobe surgery. The authors recommended that presurgical fMRI using nonverbal memory encoding may be considered as a means to predict visuospatial memory outcomes in patients with epilepsy who are undergoing evaluation for temporal lobe surgery (Level C).
Based on data from one Class II study and one Class III study, the authors recommended that presurgical fMRI may be used instead of the IAP for language lateralization in patients with epilepsy who are undergoing evaluation for brain surgery (Level C). “However, when fMRI is used for this purpose, task design, data analysis methods, and epilepsy type should be considered,” they added.
In addition, based on nine Class II studies, the authors recommended that fMRI of language and verbal memory lateralization may be an alternative to IAP memory testing for prediction of verbal memory outcome in medial temporal lobe epilepsy (Level C). The authors note that fMRI is not yet established as an alternative to the IAP for prediction of global amnesia in patients who have undergone anterior temporal lobe surgery.
More and Larger Studies Are Needed
“The imperfect concordance between fMRI and IAP language lateralization leaves open the question of which test is more accurate in discordant cases,” said the authors. Although the IAP is the reference standard, it is subject to limitations resulting from individual variation in arterial anatomy, variable effects of anesthesia, the rate of amobarbital injection, variability in patient cooperation, and variation in testing methods.
Like the IAP, cognitive fMRI “is a complex diagnostic procedure that requires both advanced technical expertise in imaging and expert interaction with patients to elicit adequate levels of task performance, select a set of activation tasks appropriate to the patient’s ability and the clinical aims of the study, instruct the patient on the tasks, administer the tasks during scanning, and evaluate and provide corrective feedback on task performance during the scanning session,” said the authors.
Global amnesia may result from bilateral medial temporal lobe damage, and some neurologists depend on the IAP to evaluate a patient’s risk for this outcome. “Global amnesia is rare after unilateral temporal lobe surgery, however, and occurs mainly when there is preexisting contralateral medial temporal lobe dysfunction,” said the authors. “One possible approach, therefore, is to reserve use of the IAP memory test for those patients at greatest risk for global amnesia, that is, patients undergoing unilateral anterior temporal lobe resection who have structural or functional evidence of damage to the contralateral medial temporal lobe.”
“Larger studies need to be conducted to increase the quality of available evidence,” Dr. Szaflarski concluded.
—Erik Greb
Suggested Reading
Szaflarski JP, Gloss D, Binder JR, et al. Practice guideline summary: Use of fMRI in the presurgical evaluation of patients with epilepsy—Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology. 2017 Jan 11 [Epub ahead of print].

What Are the Best Treatments for Nonmotor Symptoms in Parkinson’s Disease?
PORTLAND, OR—Nonmotor symptoms are common in patients with Parkinson’s disease and they can substantially impact quality of life, according to an overview presented at the Fourth World Parkinson Congress.
“Nonmotor symptoms in Parkinson’s disease have become increasingly recognized, and the number of clinical trials that are now out there is also on the increase,” said Susan H. Fox, MD, PhD, Associate Professor of Neurology at the University of Toronto.

Over the course of the illness, nonmotor symptoms become increasingly prevalent and are major determinants of the progression of overall disability. Conflicting evidence can make it difficult to choose appropriate treatments for some nonmotor symptoms such as depression and psychosis. Additionally, neurologists lack validated scales that accurately measure nonmotor symptoms, which further complicates treatment. Nevertheless, the literature does provide guidance for neurologists.
Managing Depression
Depression can affect as much as 60% of patients with Parkinson’s disease, according to the Parkinson’s Disease Foundation. Most interventions for depression have not been assessed extensively in patients with Parkinson’s disease, said Dr. Fox. Tricyclic antidepressants such as amitriptyline were evaluated in Parkinson’s disease, but study populations have been small, and the evidence has been conflicting. Other interventions for depression include selective serotonin reuptake inhibitors (SSRIs) such as citalopram, sertraline, paroxetine, and fluoxetine. Evidence for these drugs is considered insufficient.
A study of nortriptyline and paroxetine versus placebo found that nortriptyline significantly reduced depression, but that paroxetine did not. A follow-up study, however, comparing paroxetine to venlafaxine showed that paroxetine was effective in patients with Parkinson’s disease and depression.
Pramipexole, a dopamine agonist, may be an effective intervention for depression in Parkinson’s disease, according to Barone et al. Additionally, rasagiline, a monoamine oxidase-B inhibitor, has been tested in patients with Parkinson’s disease. Evidence suggests that rasagiline has a nonsignificant clinical effect on depression in these patients. Richard et al concluded that venlafaxine may be effective in this population. Their study did not identify any safety concerns. According to Dobkin et al, cognitive behavioral therapy may be an effective nonpharmacologic treatment for depression in Parkinson’s disease.
Cognitive Problems
Clinical trials so far have provided insufficient evidence about the efficacy of the acetylcholinesterase inhibitors donepezil and galantamine for treating cognitive impairment such as dementia in Parkinson’s disease. Studies do suggest, however, that rivastigmine promotes positive outcomes among patients with cognitive problems, but adverse events are common. Researchers compared oral and patch preparations of rivastigmine in a long-term open-label study that included a large number of patients. Fewer patients experienced tremor with the patch, compared with the oral formulation.
The data for memantine as an intervention for cognitive impairment in Parkinson’s disease are mixed. The drug is considered to have insufficient evidence. Exercise and cognitive behavioral therapy have also been studied for cognitive impairment, but experts have not developed evidence-based recommendations about these interventions.
Measuring Psychosis
Psychosis can cause significant morbidity in patients with Parkinson’s disease. Treating psychosis can be complicated because symptoms such as hallucinations, delusions, and paranoia may not persist. It may be difficult to determine whether the intervention reduced these psychotic symptoms or whether they resolved themselves, said Dr. Fox.
In addition, a lack of widely used validated scales makes measuring psychosis in Parkinson’s disease more difficult. Trials often have used rating scales borrowed from Alzheimer’s disease research. The difference between Alzheimer’s disease and Parkinson’s disease may bias the study results or cause researchers to overlook a drug that may provide benefit, said Dr. Fox.
Still, the literature does provide guidance. Overall, clozapine is considered effective in controlling psychosis in Parkinson’s disease. The associated risk of agranulocytosis makes this treatment less popular, however. As a result, some physicians avoid prescribing clozapine because it requires patients to undergo specialized blood monitoring.
Quetiapine may help to manage psychosis in Parkinson’s disease; most physicians would consider it a first-line agent for treating psychosis because of its ease of use, said Dr. Fox. However, insufficient evidence supports the drug’s use. Pimavanserin, a 5-HT2A inverse agonist, was recently approved for treatment of psychosis in Parkinson’s disease.
Other Nonmotor Symptoms
Autonomic dysfunctions such as overactive bladder syndrome, sialorrhoea, and constipation are also common nonmotor symptoms of Parkinson’s disease. Studies show that botulinum toxins are efficacious for treating sialorrhoea in Parkinson’s disease. Side effects such as dry mouth, transient swallowing difficulties, and severe dysphagia have been reported, although the latter is rare.
Lubiprostrone is considered likely efficacious for treating constipation in Parkinson’s disease. Researchers concluded that there is insufficient evidence for the drug’s safety in patients with Parkinson’s disease, however. Typical adverse events include nausea, diarrhea, and dyspnea.
When it comes to treating sleep disorders associated with Parkinson’s disease (eg, insomnia, excessive daytime somnolence, and sudden onset of sleep), there is insufficient evidence. Drugs such as melatonin and eszopiclone are not well studied in this population.
“I don’t think we fully understand the pathology or the cause of many nonmotor symptoms. Certainly we have a better understanding than we did a few years ago, but we still have a long way to go,” said Dr. Fox.
—Erica Tricarico
Suggested Reading
Seppi K, Weintraub D, Coelho M, et al. The Movement Disorder Society evidence-based medicine review update: treatments for the non-motor symptoms of Parkinson’s disease. Mov Disord. 2011;26 Suppl 3:S42-S80.
PORTLAND, OR—Nonmotor symptoms are common in patients with Parkinson’s disease and they can substantially impact quality of life, according to an overview presented at the Fourth World Parkinson Congress.
“Nonmotor symptoms in Parkinson’s disease have become increasingly recognized, and the number of clinical trials that are now out there is also on the increase,” said Susan H. Fox, MD, PhD, Associate Professor of Neurology at the University of Toronto.
Over the course of the illness, nonmotor symptoms become increasingly prevalent and are major determinants of the progression of overall disability. Conflicting evidence can make it difficult to choose appropriate treatments for some nonmotor symptoms such as depression and psychosis. Additionally, neurologists lack validated scales that accurately measure nonmotor symptoms, which further complicates treatment. Nevertheless, the literature does provide guidance for neurologists.
Managing Depression
Depression can affect as much as 60% of patients with Parkinson’s disease, according to the Parkinson’s Disease Foundation. Most interventions for depression have not been assessed extensively in patients with Parkinson’s disease, said Dr. Fox. Tricyclic antidepressants such as amitriptyline were evaluated in Parkinson’s disease, but study populations have been small, and the evidence has been conflicting. Other interventions for depression include selective serotonin reuptake inhibitors (SSRIs) such as citalopram, sertraline, paroxetine, and fluoxetine. Evidence for these drugs is considered insufficient.
A study of nortriptyline and paroxetine versus placebo found that nortriptyline significantly reduced depression, but that paroxetine did not. A follow-up study, however, comparing paroxetine to venlafaxine showed that paroxetine was effective in patients with Parkinson’s disease and depression.
Pramipexole, a dopamine agonist, may be an effective intervention for depression in Parkinson’s disease, according to Barone et al. Additionally, rasagiline, a monoamine oxidase-B inhibitor, has been tested in patients with Parkinson’s disease. Evidence suggests that rasagiline has a nonsignificant clinical effect on depression in these patients. Richard et al concluded that venlafaxine may be effective in this population. Their study did not identify any safety concerns. According to Dobkin et al, cognitive behavioral therapy may be an effective nonpharmacologic treatment for depression in Parkinson’s disease.
Cognitive Problems
Clinical trials so far have provided insufficient evidence about the efficacy of the acetylcholinesterase inhibitors donepezil and galantamine for treating cognitive impairment such as dementia in Parkinson’s disease. Studies do suggest, however, that rivastigmine promotes positive outcomes among patients with cognitive problems, but adverse events are common. Researchers compared oral and patch preparations of rivastigmine in a long-term open-label study that included a large number of patients. Fewer patients experienced tremor with the patch, compared with the oral formulation.
The data for memantine as an intervention for cognitive impairment in Parkinson’s disease are mixed. The drug is considered to have insufficient evidence. Exercise and cognitive behavioral therapy have also been studied for cognitive impairment, but experts have not developed evidence-based recommendations about these interventions.
Measuring Psychosis
Psychosis can cause significant morbidity in patients with Parkinson’s disease. Treating psychosis can be complicated because symptoms such as hallucinations, delusions, and paranoia may not persist. It may be difficult to determine whether the intervention reduced these psychotic symptoms or whether they resolved themselves, said Dr. Fox.
In addition, a lack of widely used validated scales makes measuring psychosis in Parkinson’s disease more difficult. Trials often have used rating scales borrowed from Alzheimer’s disease research. The difference between Alzheimer’s disease and Parkinson’s disease may bias the study results or cause researchers to overlook a drug that may provide benefit, said Dr. Fox.
Still, the literature does provide guidance. Overall, clozapine is considered effective in controlling psychosis in Parkinson’s disease. The associated risk of agranulocytosis makes this treatment less popular, however. As a result, some physicians avoid prescribing clozapine because it requires patients to undergo specialized blood monitoring.
Quetiapine may help to manage psychosis in Parkinson’s disease; most physicians would consider it a first-line agent for treating psychosis because of its ease of use, said Dr. Fox. However, insufficient evidence supports the drug’s use. Pimavanserin, a 5-HT2A inverse agonist, was recently approved for treatment of psychosis in Parkinson’s disease.
Other Nonmotor Symptoms
Autonomic dysfunctions such as overactive bladder syndrome, sialorrhoea, and constipation are also common nonmotor symptoms of Parkinson’s disease. Studies show that botulinum toxins are efficacious for treating sialorrhoea in Parkinson’s disease. Side effects such as dry mouth, transient swallowing difficulties, and severe dysphagia have been reported, although the latter is rare.
Lubiprostrone is considered likely efficacious for treating constipation in Parkinson’s disease. Researchers concluded that there is insufficient evidence for the drug’s safety in patients with Parkinson’s disease, however. Typical adverse events include nausea, diarrhea, and dyspnea.
When it comes to treating sleep disorders associated with Parkinson’s disease (eg, insomnia, excessive daytime somnolence, and sudden onset of sleep), there is insufficient evidence. Drugs such as melatonin and eszopiclone are not well studied in this population.
“I don’t think we fully understand the pathology or the cause of many nonmotor symptoms. Certainly we have a better understanding than we did a few years ago, but we still have a long way to go,” said Dr. Fox.
—Erica Tricarico
Suggested Reading
Seppi K, Weintraub D, Coelho M, et al. The Movement Disorder Society evidence-based medicine review update: treatments for the non-motor symptoms of Parkinson’s disease. Mov Disord. 2011;26 Suppl 3:S42-S80.
PORTLAND, OR—Nonmotor symptoms are common in patients with Parkinson’s disease and they can substantially impact quality of life, according to an overview presented at the Fourth World Parkinson Congress.
“Nonmotor symptoms in Parkinson’s disease have become increasingly recognized, and the number of clinical trials that are now out there is also on the increase,” said Susan H. Fox, MD, PhD, Associate Professor of Neurology at the University of Toronto.
Over the course of the illness, nonmotor symptoms become increasingly prevalent and are major determinants of the progression of overall disability. Conflicting evidence can make it difficult to choose appropriate treatments for some nonmotor symptoms such as depression and psychosis. Additionally, neurologists lack validated scales that accurately measure nonmotor symptoms, which further complicates treatment. Nevertheless, the literature does provide guidance for neurologists.
Managing Depression
Depression can affect as much as 60% of patients with Parkinson’s disease, according to the Parkinson’s Disease Foundation. Most interventions for depression have not been assessed extensively in patients with Parkinson’s disease, said Dr. Fox. Tricyclic antidepressants such as amitriptyline were evaluated in Parkinson’s disease, but study populations have been small, and the evidence has been conflicting. Other interventions for depression include selective serotonin reuptake inhibitors (SSRIs) such as citalopram, sertraline, paroxetine, and fluoxetine. Evidence for these drugs is considered insufficient.
A study of nortriptyline and paroxetine versus placebo found that nortriptyline significantly reduced depression, but that paroxetine did not. A follow-up study, however, comparing paroxetine to venlafaxine showed that paroxetine was effective in patients with Parkinson’s disease and depression.
Pramipexole, a dopamine agonist, may be an effective intervention for depression in Parkinson’s disease, according to Barone et al. Additionally, rasagiline, a monoamine oxidase-B inhibitor, has been tested in patients with Parkinson’s disease. Evidence suggests that rasagiline has a nonsignificant clinical effect on depression in these patients. Richard et al concluded that venlafaxine may be effective in this population. Their study did not identify any safety concerns. According to Dobkin et al, cognitive behavioral therapy may be an effective nonpharmacologic treatment for depression in Parkinson’s disease.
Cognitive Problems
Clinical trials so far have provided insufficient evidence about the efficacy of the acetylcholinesterase inhibitors donepezil and galantamine for treating cognitive impairment such as dementia in Parkinson’s disease. Studies do suggest, however, that rivastigmine promotes positive outcomes among patients with cognitive problems, but adverse events are common. Researchers compared oral and patch preparations of rivastigmine in a long-term open-label study that included a large number of patients. Fewer patients experienced tremor with the patch, compared with the oral formulation.
The data for memantine as an intervention for cognitive impairment in Parkinson’s disease are mixed. The drug is considered to have insufficient evidence. Exercise and cognitive behavioral therapy have also been studied for cognitive impairment, but experts have not developed evidence-based recommendations about these interventions.
Measuring Psychosis
Psychosis can cause significant morbidity in patients with Parkinson’s disease. Treating psychosis can be complicated because symptoms such as hallucinations, delusions, and paranoia may not persist. It may be difficult to determine whether the intervention reduced these psychotic symptoms or whether they resolved themselves, said Dr. Fox.
In addition, a lack of widely used validated scales makes measuring psychosis in Parkinson’s disease more difficult. Trials often have used rating scales borrowed from Alzheimer’s disease research. The difference between Alzheimer’s disease and Parkinson’s disease may bias the study results or cause researchers to overlook a drug that may provide benefit, said Dr. Fox.
Still, the literature does provide guidance. Overall, clozapine is considered effective in controlling psychosis in Parkinson’s disease. The associated risk of agranulocytosis makes this treatment less popular, however. As a result, some physicians avoid prescribing clozapine because it requires patients to undergo specialized blood monitoring.
Quetiapine may help to manage psychosis in Parkinson’s disease; most physicians would consider it a first-line agent for treating psychosis because of its ease of use, said Dr. Fox. However, insufficient evidence supports the drug’s use. Pimavanserin, a 5-HT2A inverse agonist, was recently approved for treatment of psychosis in Parkinson’s disease.
Other Nonmotor Symptoms
Autonomic dysfunctions such as overactive bladder syndrome, sialorrhoea, and constipation are also common nonmotor symptoms of Parkinson’s disease. Studies show that botulinum toxins are efficacious for treating sialorrhoea in Parkinson’s disease. Side effects such as dry mouth, transient swallowing difficulties, and severe dysphagia have been reported, although the latter is rare.
Lubiprostrone is considered likely efficacious for treating constipation in Parkinson’s disease. Researchers concluded that there is insufficient evidence for the drug’s safety in patients with Parkinson’s disease, however. Typical adverse events include nausea, diarrhea, and dyspnea.
When it comes to treating sleep disorders associated with Parkinson’s disease (eg, insomnia, excessive daytime somnolence, and sudden onset of sleep), there is insufficient evidence. Drugs such as melatonin and eszopiclone are not well studied in this population.
“I don’t think we fully understand the pathology or the cause of many nonmotor symptoms. Certainly we have a better understanding than we did a few years ago, but we still have a long way to go,” said Dr. Fox.
—Erica Tricarico
Suggested Reading
Seppi K, Weintraub D, Coelho M, et al. The Movement Disorder Society evidence-based medicine review update: treatments for the non-motor symptoms of Parkinson’s disease. Mov Disord. 2011;26 Suppl 3:S42-S80.

Trials Will Address Unanswered Questions About Endovascular Therapy
BALTIMORE—Data from five large trials, including the MR CLEAN trial, published in the New England Journal of Medicine have greatly improved understanding of endovascular therapy for acute stroke. They have indicated that the therapy is effective if initiated within six hours of onset and suggested that baseline collateral flow predicts successful reperfusion and response to therapy. Research currently under way could address several questions that remain unanswered, according to an overview presented at the 141st Annual Meeting of the American Neurological Association.
Defining the Treatment Window
The most important of these questions is whether thrombectomy is effective in appropriately selected patients if administered at more than six hours from onset, said Joseph P. Broderick, MD, Professor of Neurology and Rehabilitation Medicine at the University of Cincinnati College of Medicine. “We are going away from chronological measures of infarction to physiological measures of brain ischemia. That is how we are going to try to appropriately select patients.”

The DEFUSE 3 trial is based on the premise that after six hours from onset, many patients with stroke still have salvageable tissue. The investigators are examining whether imaging can identify these patients and whether devices cleared by the FDA can benefit them. Eligible patients have an occlusion of the internal carotid artery or an M1 occlusion and a target mismatch profile. The inclusion criteria are similar to those of other endovascular trials, except that baseline NIH Stroke Scale (NIHSS) score must be 6 or higher. Patients with a contraindication to MRI or CT perfusion are excluded from the trial, as are patients with an Alberta Stroke Program Early CT Score (ASPECTS) of less than 6 on a noncontrast CT.
Patients are randomized to thrombectomy plus standard medical therapy or standard medical therapy alone. Treatment is delivered within 16 hours of stroke onset using any device that has been cleared for thrombectomy by the FDA (eg, the Solitaire device or the Penumbra aspiration system). Intra-arterial t-PA is not allowed in the trial, and the investigators strongly recommend conscious sedation rather than general anesthesia. The trial’s adaptive design will identify, at interim analyses, the group with the best prospect for showing benefit from endovascular treatment, based on baseline core lesion volumes and the times since stroke onset. The investigators plan to enroll a maximum sample size of 476 and to perform interim analyses when enrollment reaches 200 patients and 340 patients.
The DAWN trial will test endovascular therapy when administered at six to 24 hours after onset. Its primary objective is to evaluate the hypothesis that Trevo thrombectomy plus medical management provides superior clinical outcome at 90 days, compared with medical management alone, in appropriately selected patients. The primary end point is modified Rankin scale (mRS) score at 90 days. Participants will be randomized in a 1:1 ratio at as many as 50 sites. Unlike in DEFUSE 3, the DAWN investigators will be examining patients with a clinical–imaging mismatch. “It will end up having a different but overlapping population of patients, as compared to DEFUSE 3,” said Dr. Broderick. “My prediction is that patients, no matter which arm they are randomized to, will have better outcomes in this particular trial because their core volumes will be smaller than in DEFUSE III.”
In addition, the POSITIVE trial will examine whether patients with acute ischemic stroke who are refractory to or ineligible for t-PA have less stroke-related disability and better functional outcomes if they receive thrombectomy, compared with best medical therapy, at six to 12 hours after onset. Patients without an associated large penumbra, as defined by physiologic imaging, will be excluded from the trial. Disability will be assessed by mRS.
Finally, the MR CLEAN LATE trial will compare endovascular therapy and best medical therapy with endovascular therapy alone in patients with acute stroke and moderate to good collateral flow. Treatment will be administered at six to 12 hours after stroke onset. The trial has not begun, but will enroll 500 patients, including some with wake-up stoke. The investigators will examine whether the two groups’ outcomes differ by 10%.
Triaging Patients With Suspected Large Artery Occlusions
Another unanswered question is how emergency physicians can best triage patients with acute stroke who are most likely to have large artery occlusions. Mobile stroke units, for example, can identify large right occlusion on a baseline thin-slice CT or on CT angiography. Or emergency medical responders can use brief prehospital scales (eg, the Cincinnati Stroke Triage Assessment Tool), which take less time to administer than CT. Identifying the best method of triage could greatly reduce time to reperfusion, said Dr. Broderick.
The RACECAT trial, which has not yet been initiated, may provide evidence to address this question. Emergency responders in Catalonia, Spain, will use the Rapid Arterial Occlusion Evaluation (RACE) scale, which has more items than some of the other triage scales, to identify patients with acute stroke and suspected large vessel occlusion. After the responders contact the stroke neurologists on call using a telestroke system, eligible participants will be randomized according to a predetermined sequence to either transfer to the closest local stroke center or direct transfer to an endovascular stroke center. The study allocations will allow for three additional comparisons: between two groups of 12 hours, between metropolitan and provincial areas, and between workdays and weekends. The primary end point is the mRS at 90 days.
Identifying the Best Level of Anesthesia
Other trials will seek to determine whether general anesthesia or planned conscious sedation is more cost-effective in patients who are eligible for either procedure. Researchers previously examined this question in the IMS III trial. Setting aside patients who underwent medically indicated general anesthesia (who had large strokes and many comorbidities and tended to have poor outcomes), the researchers found a trend toward better outcomes among patients who underwent conscious sedation, compared with patients who received general anesthesia. In addition, general anesthesia cost approximately $16,000 more than conscious sedation did.
In the prospective SIESTA trial, patients with acute ischemic stroke were randomized in a 1:1 ratio to a nonintubated state or to an intubated state for endovascular stroke treatment. The primary outcome measure was NIHSS at 24 hours after the intervention. Secondary outcome measures included mRS at three months and inpatient mortality. Conscious sedation was not associated with any advantage over general anesthesia in this small randomized trial, according to the researchers.
In addition, investigators are recruiting patients for the GOLIATH trial, in which patients will be randomized to general anesthesia or local anesthesia. The primary outcome measure will be growth of the ischemic lesion on diffusion-weighted imaging (DWI). Secondary outcome measures will include time from arrival to groin puncture and recanalization, blood pressure during intervention, and mRS.
Thrombectomy With or Without Thrombolysis
Another unanswered question is whether thrombectomy alone provides greater benefit than IV t-PA followed by thrombectomy for patients with acute ischemic stroke. Investigators in the Netherlands are conducting the MR CLEAN NO IV trial to answer this question. They plan to include 500 patients who are taken directly to a comprehensive stroke center. One group will receive IV t-PA plus endovascular treatment, and the other group will receive endovascular treatment alone.
—Erik Greb
Suggested Reading
Goyal M, Menon BK, van Zwam WH, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. 2016;387(10029):1723-1731.
Lansberg MG, Cereda CW, Mlynash M, et al. Response to endovascular reperfusion is not time-dependent in patients with salvageable tissue. Neurology. 2015;85(8):708-714.
Schönenberger S, Uhlmann L, Hacke W, et al. Effect of conscious sedation vs general anesthesia on early neurological improvement among patients with ischemic stroke undergoing endovascular thrombectomy: a randomized clinical trial. JAMA. 2016;316(19):1986-1996.
BALTIMORE—Data from five large trials, including the MR CLEAN trial, published in the New England Journal of Medicine have greatly improved understanding of endovascular therapy for acute stroke. They have indicated that the therapy is effective if initiated within six hours of onset and suggested that baseline collateral flow predicts successful reperfusion and response to therapy. Research currently under way could address several questions that remain unanswered, according to an overview presented at the 141st Annual Meeting of the American Neurological Association.
Defining the Treatment Window
The most important of these questions is whether thrombectomy is effective in appropriately selected patients if administered at more than six hours from onset, said Joseph P. Broderick, MD, Professor of Neurology and Rehabilitation Medicine at the University of Cincinnati College of Medicine. “We are going away from chronological measures of infarction to physiological measures of brain ischemia. That is how we are going to try to appropriately select patients.”
The DEFUSE 3 trial is based on the premise that after six hours from onset, many patients with stroke still have salvageable tissue. The investigators are examining whether imaging can identify these patients and whether devices cleared by the FDA can benefit them. Eligible patients have an occlusion of the internal carotid artery or an M1 occlusion and a target mismatch profile. The inclusion criteria are similar to those of other endovascular trials, except that baseline NIH Stroke Scale (NIHSS) score must be 6 or higher. Patients with a contraindication to MRI or CT perfusion are excluded from the trial, as are patients with an Alberta Stroke Program Early CT Score (ASPECTS) of less than 6 on a noncontrast CT.
Patients are randomized to thrombectomy plus standard medical therapy or standard medical therapy alone. Treatment is delivered within 16 hours of stroke onset using any device that has been cleared for thrombectomy by the FDA (eg, the Solitaire device or the Penumbra aspiration system). Intra-arterial t-PA is not allowed in the trial, and the investigators strongly recommend conscious sedation rather than general anesthesia. The trial’s adaptive design will identify, at interim analyses, the group with the best prospect for showing benefit from endovascular treatment, based on baseline core lesion volumes and the times since stroke onset. The investigators plan to enroll a maximum sample size of 476 and to perform interim analyses when enrollment reaches 200 patients and 340 patients.
The DAWN trial will test endovascular therapy when administered at six to 24 hours after onset. Its primary objective is to evaluate the hypothesis that Trevo thrombectomy plus medical management provides superior clinical outcome at 90 days, compared with medical management alone, in appropriately selected patients. The primary end point is modified Rankin scale (mRS) score at 90 days. Participants will be randomized in a 1:1 ratio at as many as 50 sites. Unlike in DEFUSE 3, the DAWN investigators will be examining patients with a clinical–imaging mismatch. “It will end up having a different but overlapping population of patients, as compared to DEFUSE 3,” said Dr. Broderick. “My prediction is that patients, no matter which arm they are randomized to, will have better outcomes in this particular trial because their core volumes will be smaller than in DEFUSE III.”
In addition, the POSITIVE trial will examine whether patients with acute ischemic stroke who are refractory to or ineligible for t-PA have less stroke-related disability and better functional outcomes if they receive thrombectomy, compared with best medical therapy, at six to 12 hours after onset. Patients without an associated large penumbra, as defined by physiologic imaging, will be excluded from the trial. Disability will be assessed by mRS.
Finally, the MR CLEAN LATE trial will compare endovascular therapy and best medical therapy with endovascular therapy alone in patients with acute stroke and moderate to good collateral flow. Treatment will be administered at six to 12 hours after stroke onset. The trial has not begun, but will enroll 500 patients, including some with wake-up stoke. The investigators will examine whether the two groups’ outcomes differ by 10%.
Triaging Patients With Suspected Large Artery Occlusions
Another unanswered question is how emergency physicians can best triage patients with acute stroke who are most likely to have large artery occlusions. Mobile stroke units, for example, can identify large right occlusion on a baseline thin-slice CT or on CT angiography. Or emergency medical responders can use brief prehospital scales (eg, the Cincinnati Stroke Triage Assessment Tool), which take less time to administer than CT. Identifying the best method of triage could greatly reduce time to reperfusion, said Dr. Broderick.
The RACECAT trial, which has not yet been initiated, may provide evidence to address this question. Emergency responders in Catalonia, Spain, will use the Rapid Arterial Occlusion Evaluation (RACE) scale, which has more items than some of the other triage scales, to identify patients with acute stroke and suspected large vessel occlusion. After the responders contact the stroke neurologists on call using a telestroke system, eligible participants will be randomized according to a predetermined sequence to either transfer to the closest local stroke center or direct transfer to an endovascular stroke center. The study allocations will allow for three additional comparisons: between two groups of 12 hours, between metropolitan and provincial areas, and between workdays and weekends. The primary end point is the mRS at 90 days.
Identifying the Best Level of Anesthesia
Other trials will seek to determine whether general anesthesia or planned conscious sedation is more cost-effective in patients who are eligible for either procedure. Researchers previously examined this question in the IMS III trial. Setting aside patients who underwent medically indicated general anesthesia (who had large strokes and many comorbidities and tended to have poor outcomes), the researchers found a trend toward better outcomes among patients who underwent conscious sedation, compared with patients who received general anesthesia. In addition, general anesthesia cost approximately $16,000 more than conscious sedation did.
In the prospective SIESTA trial, patients with acute ischemic stroke were randomized in a 1:1 ratio to a nonintubated state or to an intubated state for endovascular stroke treatment. The primary outcome measure was NIHSS at 24 hours after the intervention. Secondary outcome measures included mRS at three months and inpatient mortality. Conscious sedation was not associated with any advantage over general anesthesia in this small randomized trial, according to the researchers.
In addition, investigators are recruiting patients for the GOLIATH trial, in which patients will be randomized to general anesthesia or local anesthesia. The primary outcome measure will be growth of the ischemic lesion on diffusion-weighted imaging (DWI). Secondary outcome measures will include time from arrival to groin puncture and recanalization, blood pressure during intervention, and mRS.
Thrombectomy With or Without Thrombolysis
Another unanswered question is whether thrombectomy alone provides greater benefit than IV t-PA followed by thrombectomy for patients with acute ischemic stroke. Investigators in the Netherlands are conducting the MR CLEAN NO IV trial to answer this question. They plan to include 500 patients who are taken directly to a comprehensive stroke center. One group will receive IV t-PA plus endovascular treatment, and the other group will receive endovascular treatment alone.
—Erik Greb
Suggested Reading
Goyal M, Menon BK, van Zwam WH, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. 2016;387(10029):1723-1731.
Lansberg MG, Cereda CW, Mlynash M, et al. Response to endovascular reperfusion is not time-dependent in patients with salvageable tissue. Neurology. 2015;85(8):708-714.
Schönenberger S, Uhlmann L, Hacke W, et al. Effect of conscious sedation vs general anesthesia on early neurological improvement among patients with ischemic stroke undergoing endovascular thrombectomy: a randomized clinical trial. JAMA. 2016;316(19):1986-1996.
BALTIMORE—Data from five large trials, including the MR CLEAN trial, published in the New England Journal of Medicine have greatly improved understanding of endovascular therapy for acute stroke. They have indicated that the therapy is effective if initiated within six hours of onset and suggested that baseline collateral flow predicts successful reperfusion and response to therapy. Research currently under way could address several questions that remain unanswered, according to an overview presented at the 141st Annual Meeting of the American Neurological Association.
Defining the Treatment Window
The most important of these questions is whether thrombectomy is effective in appropriately selected patients if administered at more than six hours from onset, said Joseph P. Broderick, MD, Professor of Neurology and Rehabilitation Medicine at the University of Cincinnati College of Medicine. “We are going away from chronological measures of infarction to physiological measures of brain ischemia. That is how we are going to try to appropriately select patients.”
The DEFUSE 3 trial is based on the premise that after six hours from onset, many patients with stroke still have salvageable tissue. The investigators are examining whether imaging can identify these patients and whether devices cleared by the FDA can benefit them. Eligible patients have an occlusion of the internal carotid artery or an M1 occlusion and a target mismatch profile. The inclusion criteria are similar to those of other endovascular trials, except that baseline NIH Stroke Scale (NIHSS) score must be 6 or higher. Patients with a contraindication to MRI or CT perfusion are excluded from the trial, as are patients with an Alberta Stroke Program Early CT Score (ASPECTS) of less than 6 on a noncontrast CT.
Patients are randomized to thrombectomy plus standard medical therapy or standard medical therapy alone. Treatment is delivered within 16 hours of stroke onset using any device that has been cleared for thrombectomy by the FDA (eg, the Solitaire device or the Penumbra aspiration system). Intra-arterial t-PA is not allowed in the trial, and the investigators strongly recommend conscious sedation rather than general anesthesia. The trial’s adaptive design will identify, at interim analyses, the group with the best prospect for showing benefit from endovascular treatment, based on baseline core lesion volumes and the times since stroke onset. The investigators plan to enroll a maximum sample size of 476 and to perform interim analyses when enrollment reaches 200 patients and 340 patients.
The DAWN trial will test endovascular therapy when administered at six to 24 hours after onset. Its primary objective is to evaluate the hypothesis that Trevo thrombectomy plus medical management provides superior clinical outcome at 90 days, compared with medical management alone, in appropriately selected patients. The primary end point is modified Rankin scale (mRS) score at 90 days. Participants will be randomized in a 1:1 ratio at as many as 50 sites. Unlike in DEFUSE 3, the DAWN investigators will be examining patients with a clinical–imaging mismatch. “It will end up having a different but overlapping population of patients, as compared to DEFUSE 3,” said Dr. Broderick. “My prediction is that patients, no matter which arm they are randomized to, will have better outcomes in this particular trial because their core volumes will be smaller than in DEFUSE III.”
In addition, the POSITIVE trial will examine whether patients with acute ischemic stroke who are refractory to or ineligible for t-PA have less stroke-related disability and better functional outcomes if they receive thrombectomy, compared with best medical therapy, at six to 12 hours after onset. Patients without an associated large penumbra, as defined by physiologic imaging, will be excluded from the trial. Disability will be assessed by mRS.
Finally, the MR CLEAN LATE trial will compare endovascular therapy and best medical therapy with endovascular therapy alone in patients with acute stroke and moderate to good collateral flow. Treatment will be administered at six to 12 hours after stroke onset. The trial has not begun, but will enroll 500 patients, including some with wake-up stoke. The investigators will examine whether the two groups’ outcomes differ by 10%.
Triaging Patients With Suspected Large Artery Occlusions
Another unanswered question is how emergency physicians can best triage patients with acute stroke who are most likely to have large artery occlusions. Mobile stroke units, for example, can identify large right occlusion on a baseline thin-slice CT or on CT angiography. Or emergency medical responders can use brief prehospital scales (eg, the Cincinnati Stroke Triage Assessment Tool), which take less time to administer than CT. Identifying the best method of triage could greatly reduce time to reperfusion, said Dr. Broderick.
The RACECAT trial, which has not yet been initiated, may provide evidence to address this question. Emergency responders in Catalonia, Spain, will use the Rapid Arterial Occlusion Evaluation (RACE) scale, which has more items than some of the other triage scales, to identify patients with acute stroke and suspected large vessel occlusion. After the responders contact the stroke neurologists on call using a telestroke system, eligible participants will be randomized according to a predetermined sequence to either transfer to the closest local stroke center or direct transfer to an endovascular stroke center. The study allocations will allow for three additional comparisons: between two groups of 12 hours, between metropolitan and provincial areas, and between workdays and weekends. The primary end point is the mRS at 90 days.
Identifying the Best Level of Anesthesia
Other trials will seek to determine whether general anesthesia or planned conscious sedation is more cost-effective in patients who are eligible for either procedure. Researchers previously examined this question in the IMS III trial. Setting aside patients who underwent medically indicated general anesthesia (who had large strokes and many comorbidities and tended to have poor outcomes), the researchers found a trend toward better outcomes among patients who underwent conscious sedation, compared with patients who received general anesthesia. In addition, general anesthesia cost approximately $16,000 more than conscious sedation did.
In the prospective SIESTA trial, patients with acute ischemic stroke were randomized in a 1:1 ratio to a nonintubated state or to an intubated state for endovascular stroke treatment. The primary outcome measure was NIHSS at 24 hours after the intervention. Secondary outcome measures included mRS at three months and inpatient mortality. Conscious sedation was not associated with any advantage over general anesthesia in this small randomized trial, according to the researchers.
In addition, investigators are recruiting patients for the GOLIATH trial, in which patients will be randomized to general anesthesia or local anesthesia. The primary outcome measure will be growth of the ischemic lesion on diffusion-weighted imaging (DWI). Secondary outcome measures will include time from arrival to groin puncture and recanalization, blood pressure during intervention, and mRS.
Thrombectomy With or Without Thrombolysis
Another unanswered question is whether thrombectomy alone provides greater benefit than IV t-PA followed by thrombectomy for patients with acute ischemic stroke. Investigators in the Netherlands are conducting the MR CLEAN NO IV trial to answer this question. They plan to include 500 patients who are taken directly to a comprehensive stroke center. One group will receive IV t-PA plus endovascular treatment, and the other group will receive endovascular treatment alone.
—Erik Greb
Suggested Reading
Goyal M, Menon BK, van Zwam WH, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. 2016;387(10029):1723-1731.
Lansberg MG, Cereda CW, Mlynash M, et al. Response to endovascular reperfusion is not time-dependent in patients with salvageable tissue. Neurology. 2015;85(8):708-714.
Schönenberger S, Uhlmann L, Hacke W, et al. Effect of conscious sedation vs general anesthesia on early neurological improvement among patients with ischemic stroke undergoing endovascular thrombectomy: a randomized clinical trial. JAMA. 2016;316(19):1986-1996.
‘I can handle it’– The state of hospitalist group backup systems
It took my hospital medicine group (HMG) 20 years to implement a formal backup system. Of all the reasons we resisted creating a backup system, foremost was that we did not want to mandate additional work. Because our compensation model did not have a mechanism to financially reward hospitalists for unexpectedly having to come in on unscheduled work days (other than the work relative value units generated by seeing patients), there was not enough motivational energy to get a system started.
It turns out our group is not unlike many other HMGs across the nation. According to the 2016 State of Hospital Medicine report (SoHM), 58.3% of adult-only HMGs, 72.2% of pediatric-only HMGs, and 52.6% of HMGs serving both adults and children did not have staffing backup systems. Interestingly, the report also showed that for groups serving adults only, academic HMGs were more likely to have formal backup systems in place (62.6%, compared with 37.3% in nonacademic HMGs).
The reason most HMGs create backup systems is to have a consistent and fair approach for dealing with unanticipated absences and/or high-volume census. In addition to creating a safety net, implementing a backup system addresses the common problem of the same hospitalists disproportionately filling in during times of crisis.
Although our group created a formal backup system starting January 2015, it is not comprehensive and deals only with high patient volumes occurring during the late evening and night hours. Hospitalists rotate through a schedule, taking a week of backup call for which no additional compensation is offered. Then, if they are actually called to come in, an hourly stipend is paid in addition to work RVUs generated. Implementing a backup system was not necessarily a popular idea. Nevertheless, the system has successfully remained in place. Triggering the system infrequently, having a clear set of criteria for when to activate backup, and providing additional compensation for the additional work are key factors in our system’s success.

When data from the 2016 SoHM report are compared with the 2014 SoHM report, the proportion of groups with formal backup systems actually decreases for both adults-only HMGs and HMGs serving both adults and children. For adult-only HMGs, there was a decline to 41.8% from 57.6%. For adult/pediatric HMGs, there was a decline to 47.4% from 58.8%. It also is notable that pediatric HMGs in particular are much less likely to have formal backup systems, only 27.8%, which has changed little since the last survey (28.8 % in 2014).
All in all, the reasons for the decline in backup systems are unclear. Possibly, the decrease is because of issues surrounding compensation, as approximately one-third of survey respondents with backup systems received no additional compensation. But in my view, it’s more likely that the reason for the decreased percentage of groups with backup systems has to do with differences in the particular set of HMGs that responded to the survey this year.
Dr. Stephan is a hospitalist at Abbott Northwestern Hospital in Minneapolis and a member of SHM’s Practice Analysis Committee.
It took my hospital medicine group (HMG) 20 years to implement a formal backup system. Of all the reasons we resisted creating a backup system, foremost was that we did not want to mandate additional work. Because our compensation model did not have a mechanism to financially reward hospitalists for unexpectedly having to come in on unscheduled work days (other than the work relative value units generated by seeing patients), there was not enough motivational energy to get a system started.
It turns out our group is not unlike many other HMGs across the nation. According to the 2016 State of Hospital Medicine report (SoHM), 58.3% of adult-only HMGs, 72.2% of pediatric-only HMGs, and 52.6% of HMGs serving both adults and children did not have staffing backup systems. Interestingly, the report also showed that for groups serving adults only, academic HMGs were more likely to have formal backup systems in place (62.6%, compared with 37.3% in nonacademic HMGs).
The reason most HMGs create backup systems is to have a consistent and fair approach for dealing with unanticipated absences and/or high-volume census. In addition to creating a safety net, implementing a backup system addresses the common problem of the same hospitalists disproportionately filling in during times of crisis.
Although our group created a formal backup system starting January 2015, it is not comprehensive and deals only with high patient volumes occurring during the late evening and night hours. Hospitalists rotate through a schedule, taking a week of backup call for which no additional compensation is offered. Then, if they are actually called to come in, an hourly stipend is paid in addition to work RVUs generated. Implementing a backup system was not necessarily a popular idea. Nevertheless, the system has successfully remained in place. Triggering the system infrequently, having a clear set of criteria for when to activate backup, and providing additional compensation for the additional work are key factors in our system’s success.
When data from the 2016 SoHM report are compared with the 2014 SoHM report, the proportion of groups with formal backup systems actually decreases for both adults-only HMGs and HMGs serving both adults and children. For adult-only HMGs, there was a decline to 41.8% from 57.6%. For adult/pediatric HMGs, there was a decline to 47.4% from 58.8%. It also is notable that pediatric HMGs in particular are much less likely to have formal backup systems, only 27.8%, which has changed little since the last survey (28.8 % in 2014).
All in all, the reasons for the decline in backup systems are unclear. Possibly, the decrease is because of issues surrounding compensation, as approximately one-third of survey respondents with backup systems received no additional compensation. But in my view, it’s more likely that the reason for the decreased percentage of groups with backup systems has to do with differences in the particular set of HMGs that responded to the survey this year.
Dr. Stephan is a hospitalist at Abbott Northwestern Hospital in Minneapolis and a member of SHM’s Practice Analysis Committee.
It took my hospital medicine group (HMG) 20 years to implement a formal backup system. Of all the reasons we resisted creating a backup system, foremost was that we did not want to mandate additional work. Because our compensation model did not have a mechanism to financially reward hospitalists for unexpectedly having to come in on unscheduled work days (other than the work relative value units generated by seeing patients), there was not enough motivational energy to get a system started.
It turns out our group is not unlike many other HMGs across the nation. According to the 2016 State of Hospital Medicine report (SoHM), 58.3% of adult-only HMGs, 72.2% of pediatric-only HMGs, and 52.6% of HMGs serving both adults and children did not have staffing backup systems. Interestingly, the report also showed that for groups serving adults only, academic HMGs were more likely to have formal backup systems in place (62.6%, compared with 37.3% in nonacademic HMGs).
The reason most HMGs create backup systems is to have a consistent and fair approach for dealing with unanticipated absences and/or high-volume census. In addition to creating a safety net, implementing a backup system addresses the common problem of the same hospitalists disproportionately filling in during times of crisis.
Although our group created a formal backup system starting January 2015, it is not comprehensive and deals only with high patient volumes occurring during the late evening and night hours. Hospitalists rotate through a schedule, taking a week of backup call for which no additional compensation is offered. Then, if they are actually called to come in, an hourly stipend is paid in addition to work RVUs generated. Implementing a backup system was not necessarily a popular idea. Nevertheless, the system has successfully remained in place. Triggering the system infrequently, having a clear set of criteria for when to activate backup, and providing additional compensation for the additional work are key factors in our system’s success.
When data from the 2016 SoHM report are compared with the 2014 SoHM report, the proportion of groups with formal backup systems actually decreases for both adults-only HMGs and HMGs serving both adults and children. For adult-only HMGs, there was a decline to 41.8% from 57.6%. For adult/pediatric HMGs, there was a decline to 47.4% from 58.8%. It also is notable that pediatric HMGs in particular are much less likely to have formal backup systems, only 27.8%, which has changed little since the last survey (28.8 % in 2014).
All in all, the reasons for the decline in backup systems are unclear. Possibly, the decrease is because of issues surrounding compensation, as approximately one-third of survey respondents with backup systems received no additional compensation. But in my view, it’s more likely that the reason for the decreased percentage of groups with backup systems has to do with differences in the particular set of HMGs that responded to the survey this year.
Dr. Stephan is a hospitalist at Abbott Northwestern Hospital in Minneapolis and a member of SHM’s Practice Analysis Committee.
Don’t miss these drug reactions
WAILEA, HAWAII – New drugs can mean new drug reactions affecting the skin, notably those associated with hepatitis C therapies and new cancer drugs, according to J. Mark Jackson, MD, of the University of Louisville (Ky.).
When dermatologists recognize the side effects from hepatitis C and cancer drugs, they can monitor patients appropriately and initiate the correct treatments, Dr. Jackson said at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/ Skin Disease Education Foundation.

Finally, “telaprevir-related dermatitis, which accounts for 95% of skin events in telaprevir-treated patients, is clinically and histologically eczematous and different from the classic ‘maculopapular’ drug-induced eruptions,” he explained. Some patients develop DRESS syndrome or drug rash with eosinophilia and systemic symptoms, he added.
In addition, four approved hepatitis C antivirals – simeprevir, telaprevir, boceprevir, and sofosbuvir – may cause photosensitivity, Dr. Jackson said. He cited a case of a patient who took simeprevir and developed photodistributed lichenoid eruptions (J Cutan Pathol. 2015 Oct;42[10]:769-73).
New cancer treatments have brought new side effects as well, Dr. Jackson said. Epidermal growth factor receptor inhibitors cause papulopustular and follicular eruptions in many cancer patients, and some of these patients also experience conditions including xerosis cutis, changes to the hair and nails, skin hyperpigmentation, and enhanced radiation dermatitis, he said. Multikinase inhibitors, a common cause of hand-foot syndrome (HFS), are also associated with facial erythema, subungual splinter hemorrhages, and other skin changes, he added.
Capecitabine-induced HFS, while not life-threatening, can affect a patient’s quality of life, Dr. Jackson pointed out. “Dose modification of the inciting agent serves as the most effective management of HFS, although a variety of anecdotal reports suggest that other agents may also be efficacious,” he explained.
Dr. Jackson noted one extreme case of a 61-year-old woman with metastatic breast cancer who was treated with capecitabine and developed HFS that led to a pseudomonal superinfection, followed by bacterial sepsis and rapid death. The case suggests that “early adjustment of therapy may prevent adverse outcomes from secondary cutaneous infections while maintaining tumor response,” he noted.
Dr. Jackson disclosed relationships with companies including AbbVie, Amgen, Celgene, Dermira, Galderma, Genentech, Janssen, Lilly, Medimetriks, Merck, Novartis, Pfizer, Promius, and Top MD.
SDEF and this news organization are owned by the same parent company.
WAILEA, HAWAII – New drugs can mean new drug reactions affecting the skin, notably those associated with hepatitis C therapies and new cancer drugs, according to J. Mark Jackson, MD, of the University of Louisville (Ky.).
When dermatologists recognize the side effects from hepatitis C and cancer drugs, they can monitor patients appropriately and initiate the correct treatments, Dr. Jackson said at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/ Skin Disease Education Foundation.
Finally, “telaprevir-related dermatitis, which accounts for 95% of skin events in telaprevir-treated patients, is clinically and histologically eczematous and different from the classic ‘maculopapular’ drug-induced eruptions,” he explained. Some patients develop DRESS syndrome or drug rash with eosinophilia and systemic symptoms, he added.
In addition, four approved hepatitis C antivirals – simeprevir, telaprevir, boceprevir, and sofosbuvir – may cause photosensitivity, Dr. Jackson said. He cited a case of a patient who took simeprevir and developed photodistributed lichenoid eruptions (J Cutan Pathol. 2015 Oct;42[10]:769-73).
New cancer treatments have brought new side effects as well, Dr. Jackson said. Epidermal growth factor receptor inhibitors cause papulopustular and follicular eruptions in many cancer patients, and some of these patients also experience conditions including xerosis cutis, changes to the hair and nails, skin hyperpigmentation, and enhanced radiation dermatitis, he said. Multikinase inhibitors, a common cause of hand-foot syndrome (HFS), are also associated with facial erythema, subungual splinter hemorrhages, and other skin changes, he added.
Capecitabine-induced HFS, while not life-threatening, can affect a patient’s quality of life, Dr. Jackson pointed out. “Dose modification of the inciting agent serves as the most effective management of HFS, although a variety of anecdotal reports suggest that other agents may also be efficacious,” he explained.
Dr. Jackson noted one extreme case of a 61-year-old woman with metastatic breast cancer who was treated with capecitabine and developed HFS that led to a pseudomonal superinfection, followed by bacterial sepsis and rapid death. The case suggests that “early adjustment of therapy may prevent adverse outcomes from secondary cutaneous infections while maintaining tumor response,” he noted.
Dr. Jackson disclosed relationships with companies including AbbVie, Amgen, Celgene, Dermira, Galderma, Genentech, Janssen, Lilly, Medimetriks, Merck, Novartis, Pfizer, Promius, and Top MD.
SDEF and this news organization are owned by the same parent company.
WAILEA, HAWAII – New drugs can mean new drug reactions affecting the skin, notably those associated with hepatitis C therapies and new cancer drugs, according to J. Mark Jackson, MD, of the University of Louisville (Ky.).
When dermatologists recognize the side effects from hepatitis C and cancer drugs, they can monitor patients appropriately and initiate the correct treatments, Dr. Jackson said at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/ Skin Disease Education Foundation.
Finally, “telaprevir-related dermatitis, which accounts for 95% of skin events in telaprevir-treated patients, is clinically and histologically eczematous and different from the classic ‘maculopapular’ drug-induced eruptions,” he explained. Some patients develop DRESS syndrome or drug rash with eosinophilia and systemic symptoms, he added.
In addition, four approved hepatitis C antivirals – simeprevir, telaprevir, boceprevir, and sofosbuvir – may cause photosensitivity, Dr. Jackson said. He cited a case of a patient who took simeprevir and developed photodistributed lichenoid eruptions (J Cutan Pathol. 2015 Oct;42[10]:769-73).
New cancer treatments have brought new side effects as well, Dr. Jackson said. Epidermal growth factor receptor inhibitors cause papulopustular and follicular eruptions in many cancer patients, and some of these patients also experience conditions including xerosis cutis, changes to the hair and nails, skin hyperpigmentation, and enhanced radiation dermatitis, he said. Multikinase inhibitors, a common cause of hand-foot syndrome (HFS), are also associated with facial erythema, subungual splinter hemorrhages, and other skin changes, he added.
Capecitabine-induced HFS, while not life-threatening, can affect a patient’s quality of life, Dr. Jackson pointed out. “Dose modification of the inciting agent serves as the most effective management of HFS, although a variety of anecdotal reports suggest that other agents may also be efficacious,” he explained.
Dr. Jackson noted one extreme case of a 61-year-old woman with metastatic breast cancer who was treated with capecitabine and developed HFS that led to a pseudomonal superinfection, followed by bacterial sepsis and rapid death. The case suggests that “early adjustment of therapy may prevent adverse outcomes from secondary cutaneous infections while maintaining tumor response,” he noted.
Dr. Jackson disclosed relationships with companies including AbbVie, Amgen, Celgene, Dermira, Galderma, Genentech, Janssen, Lilly, Medimetriks, Merck, Novartis, Pfizer, Promius, and Top MD.
SDEF and this news organization are owned by the same parent company.
AT SDEF HAWAII DERMATOLOGY SEMINAR
Poorer Arthroscopic Outcomes of Mild Dysplasia With Cam Femoroacetabular Impingement Versus Mixed Femoroacetabular Impingement in Absence of Capsular Repair
Take-Home Points
- Cam deformity often occurs with dysplasia.
- Borderline or mild dysplasia has been treated with isolated hip arthroscopy.
- Avoid rim trimming that can make mild dysplasia more severe.
- Labral preservation, cam decompression, and capsular repair or plication are currently suggested.
- Poorer outcomes occurred in borderline or mild dysplasia with cam impingement relative to controls following hip arthroscopy without capsular repair.
- Initial clinical improvement may be followed by clinical deterioration suggesting close long-term follow-up with prompt addition of reorientation acetabular osteotomy if indicated.
- It is unknown whether small capsulotomies may yield comparable outcomes with larger capsulotomies plus repair.
It is unknown whether small capsulotomies may yield comparable outcomes with larger capsulotomies plus repair. There is growing interest in hip preservation surgery in general and arthroscopic hip preservation in particular. Chondrolabral pathology leading to symptoms and degenerative progression typically is caused by structural abnormalities, mainly femoroacetabular impingement (FAI) and developmental dysplasia of the hip. Unlike the bony overcoverage of pincer FAI, developmental dysplasia of the hip typically exhibits insufficient anterolateral coverage of the femoral head.
The role of hip arthroscopy in the treatment of dysplasia remains undefined. Emerging evidence shows a high incidence of dysplasia with associated cam deformity,1,2 but there is a paucity of evidence-based information for this specific patient population. Clinical outcomes of hip arthroscopy in the setting of dysplasia are conflicting: some poor3-5 and others successful.1,6-9 Although reorientation periacetabular osteotomy (PAO) is considered a mainstay in the treatment of dysplasia—providing improvement in symptoms, deficient anterolateral acetabular coverage, and hip biomechanics—midterm failure rates approaching 24% have been reported.10-12 Many young patients with symptomatic dysplasia want a surgical option that is less invasive than open PAO.4 Intra-articular central compartment pathology and cam FAI commonly occur with dysplasia and are amenable to arthroscopic treatment.1,13,14 Moreover, staged PAO may be successful in cases in which arthroscopic intervention fails to provide clinical improvement.5,15
Emerging evidence suggests beneficial effects of arthroscopic capsular repair or plication in the setting of borderline or mild dysplasia.7,9 However, the literature provides little information on arthroscopic outcomes without capsular repair. One study found poor outcomes of arthroscopic surgery for dysplasia, but its patients underwent labral débridement, not repair.3 Two patients in a case report demonstrated rapidly progressive osteoarthritis after arthroscopic labral repairs and concurrent femoroplasties for cam FAI, but each had marked dysplasia with a lateral center-edge angle (LCEA) of <15°.4
Arthroscopy with capsular repair has been assumed to provide better outcomes than arthroscopy without repair, but to our knowledge there are no studies that have compared outcomes of mild dysplasia with cam FAI and outcomes of mixed FAI treated without capsular repair. Clinical equipoise makes it ethically challenging to perform a prospective study comparing dysplasia treated with and without capsular repair. We conducted a study to compare outcomes of mild dysplasia with cam FAI and outcomes of mixed FAI treated with arthroscopic surgery and to fill the knowledge gap regarding outcomes of mild dysplasia treated without capsular repair.
Methods
In this study, which received Institutional Review Board approval, we retrospectively reviewed radiographs and data from a prospective 3-center study of arthroscopic outcomes of FAI in 150 patients (159 hips) who underwent arthroscopic surgery by 1 of 3 surgeons between March 2009 and June 2010. In all cases, digital images of anteroposterior pelvic radiographs were used for radiographic measurements. On these images, the LCEA is formed by the intersection of the vertical line (corrected for obliquity using a horizontal reference line connecting the inferior extents of both radiographic teardrops) through the center of the femoral head (determined with a digital centering tool) with the line extending to the lateral edge of the sourcil (radiographic eyebrow of the weight-bearing region or roof of the acetabulum). Measurements were made in blinded fashion (by a nonsurgeon coauthor, Dr. Nikhil Gupta, who completed training modules) and were confirmed without alteration by the principal investigator Dr. Dean K. Matsuda. Inclusion criteria were mild acetabular dysplasia (LCEA, 15°-24°) and mixed FAI including focal pincer component (LCEA, 25°-39°), radiographic crossover sign, and successful completion of patient-reported outcome (PRO) measures at minimum 2-year follow-up. Exclusion criteria were severe dysplasia (LCEA, <15°), hip subluxation, broken Shenton line, global pincer FAI (LCEA, ≥40°), Tönnis grade 3 osteoarthritis, Legg-Calvé-Perthes disease, osteonecrosis, prior hip surgery, and unsuccessful completion of PRO measures. Outcome measures included investigator-blinded preoperative and postoperative Nonarthritic Hip Score (NAHS) and 5-point Likert satisfaction score. Complications, revision surgeries, and conversion arthroplasties were recorded.
Statistical Analysis
We examined outcomes with descriptive statistics for each of the candidate covariates in the model classified by femoroacetabular subtype: focal pincer and cam (mixed FAI) and dysplasia with cam. We examined the variables of sex, age, weight, height, body mass index, preoperative NAHS, presence of dysplasia (yes/no), presence of osteoarthritis (yes/no), Tönnis osteoarthritis grade, Outerbridge class, American Society of Anesthesiologists (ASA) score, months of pain, bilateral procedure (yes/no), and pincer involvement with cam FAI (yes/no). Before beginning linear regression modeling, we screened the candidate variables for strong correlations with other variables and looked for those variables with minimal missing data. For all these covariates, we then performed linear regression with a selection process—both a stepwise selection method and a backward elimination method—to verify we determined the same model for 24-month NAHS, or to understand why we could not. Finally, we ran the model we found from the linear regression as a linear mixed model of 24-month NAHS with the dichotomous variables taken as fixed effects and the other variables taken as random effects, using variance-components representation for the random effects. We then examined 3-month and 12-month NAHS with the same variables selected for the 24-month model.
To further examine and verify the effects of dysplasia on outcomes found in our linear mixed model, we performed a nested case–control analysis matching each member of cohort D (cases) with 2 members of cohort M (controls). We used an optimal-matching algorithm to match focal patients in the linear regression dataset with dysplasia patients in the linear regression dataset in such a way as to minimize the overall differences between the datasets. We matched cases and controls on preoperative NAHS, age, sex, presence of osteoarthritis, months of pain, ASA score, and body mass index. The differences between the matched cases and controls (control value minus case value) were compared using Wilcoxon rank sum tests for statistical significance of differences from 0 (with differences generated for each control group member, 2 differences per case) to examine the quality of the match. Finally, we examined the statistical significance of the difference of the outcome variables (3-, 12-, and 24-month NAHS) from 0, again using Wilcoxon rank sum tests. Statistical significance was set at P < .05 using SAS Version 9.3 (SAS Institute).
Surgical Procedure
In all cases, supine outpatient hip arthroscopy was performed under general anesthesia. Anterolateral and modified midanterior portals16 were used. T-capsulotomies were performed in both cohorts. Cohort M underwent anterosuperior acetabuloplasty with a motorized burr. Labral refixation or selective débridement was performed in cohort M, whereas labral repair (with limited freshening of acetabular rim attachment site) or selective débridement (but no segmental resection) was performed in cohort D. Arthroscopic femoroplasty was performed with similar endpoints of 120° minimum hip flexion and 30° minimum flexed hip internal rotation with retention of the labral fluid seal. Capsular repair or plication was not performed for either cohort during the study period.
The cohorts underwent similar postoperative protocols: 2 weeks of protected ambulation using 2 crutches, exercise cycling without resistance beginning postoperative day 1, swimming at 2 weeks, elliptical machine workouts at 6 weeks, jogging at 12 weeks, and return to unrestricted athletics at 5 months.
Results
In cohort D, which consisted of 8 patients (5 female), mean age was 49.6 years, and mean LCEA was 19° (range, 16°-24°). 
In cohort D, mean (SD) change in NAHS was +20.00 (6.24) (P = .25) at 3 months (n = 3), +14.33 (9.77) (P = .03) at 12 months (n = 6), and –0.75 (19.86) (P = .74) at 24 months (n = 8). 

In cohort M, mean (SD) change in NAHS was +12.09 (18.98) (P < .0001) at 3 months (n = 45), +20.39 (16.49) (P < .0001) at 12 months (n = 57), and +21.99 (17.32) (P < .0001) at 24 months (n = 69). 
In a pairwise case–control comparison, the mean (SD) change-from-baseline difference between cohorts D and M was +8.2 (12.85) (P = .31) at 3 months (n = 5), –8.7 (11.52) (P = .03) at 12 months (n = 10), and –31.06 (23.55) (P = .0002) at 24 months (n = 16). Dysplasia had an impact of –23.4 points on 24-month NAHS (standard error = 5.35 points; P < .0001), which corresponds to a 95% confidence interval of –12.9 to –33.9 points on NAHS.

Compared with cohort M, cohort D had significantly less NAHS improvement (P = .002), less satisfaction (P = .15) and more hip arthroplasty conversions (P = .22, not statistically significant).
There were no statistically significant differences between cohorts in demographics, preoperative variables, intraoperative findings, or surgical procedures in the regression analysis. Of the investigated variables, only group membership (cohort D) was a statistically significant predictor of poorer outcomes in the model of change from preoperative to 24 months. However, older age was associated with cohort D (older patients with dysplasia, P = .07), and therefore in the nested case–control analysis we were able to match on all variables except age (8.74 years older in cohort D, P = .0013) to a level of statistical nonsignificance.
Discussion
The principal finding of this study is the significantly poorer outcomes of mild dysplasia and cam FAI relative to mixed FAI after hip arthroscopy without capsular repair. Study group (cohort D) and control group (cohort M) had associated cam deformities treated with femoroplasty with similar decompression endpoints and labral preservation in the form of selective débridement or labral repair (no labral resections in either cohort) with similar rehabilitation protocols.
Our study findings suggest short-term improvement may be followed by midterm worsening in patients with mild dysplasia and sustained improvement in patients with mixed FAI. These findings have practical clinical applications. Jackson and colleagues5 reported on a patient who, after undergoing “successful” arthroscopic surgery for mild dysplasia, clinically deteriorated after 13 months and eventually required PAO. Patients undergoing isolated hip arthroscopy for mild dysplasia with cam FAI should be informed of the possible need for secondary PAO or even hip arthroplasty, be followed up more often and longer than comparable patients with FAI, and have follow-up supplemented with interval radiographs.4 If even subtle subluxation or joint narrowing occurs, we suggest resumption of protected weight-bearing and prompt progression to PAO in younger patients with joint congruency or eventual conversion arthroplasty in older ones.
Although mean preoperative NAHS (52.88) and mean 24-month postoperative NAHS (52.13) suggest essentially no change in PROs for cohort D, all patients with dysplasia either worsened or improved, though those who improved did so at a lesser relative magnitude than those with mixed FAI (cohort M). This finding may help explain the divergent outcomes reported in the literature on dysplasia treated with hip arthroscopy.
Cohort D was older than cohort M, but the difference was not statistically significant. Age may still be a confounding variable, and it may have contributed in part to the poorer outcomes for the patients with dysplasia. However, emerging studies demonstrate select older patients with FAI and/or labral tears may have successful outcomes with arthroscopic intervention.17,18 Our findings support mild dysplasia as the main contributor to the poor outcomes observed in this study.
With identical postoperative rehabilitation protocols, patients in both cohorts typically were ambulating without crutches by the end of postoperative week 2. Delayed weight-bearing has been suggested as contributing to successful outcomes in the setting of dysplasia7,19,20 but has not been shown to adversely affect nondysplastic hips.21 Whether delayed weight-bearing contributed to the poor outcomes in our dysplasia cohort is unknown, but the early successful outcomes may discount its influence.
Our findings support successful outcomes of arthroscopic treatment of mixed FAI (specifically focal pincer plus cam FAI) without capsular repair. Perhaps more important, we found inferior outcomes of arthroscopic treatment of mild dysplasia plus cam FAI without capsular repair—filling the knowledge gap regarding the need for arthroscopic capsular repair for mild dysplasia. Although a recent study demonstrated no significant difference in outcomes between hip arthroscopy with and without capsular repair,22 2 studies specific to mild dysplasia demonstrated successful outcomes of capsular repair.7,9 One found that mild dysplasia treated with arthroscopy, including capsular plication, resulted in 77% good/excellent outcomes and LCEA as low as 18° at minimum 2-year follow-up.7 The other found clinical improvement in mild dysplasia (LCEA, 15°-19°) when capsular repair was performed as part of arthroscopic treatment.9 In the present study, we retrospectively reviewed outcomes from a prospective study performed in 2009 to 2010, before the era of common capsular repair. It appears that capsular repair9 or plication7 in the setting of mild dysplasia may yield improved outcomes approaching those of arthroscopic FAI surgery. Our study results showed that, despite labral preservation and cam decompression, mild dysplasia without the closure of T-capsulotomy had inferior outcomes at 2 years. However, we do not know if outcomes would have been better with capsular repair or plication and/or smaller capsulotomies, perhaps with minimal violation of the iliofemoral ligament in this specific subset of patients. Furthermore, we do not know if optimal outcomes can best be achieved with arthroscopic and/or open surgery, with or without acetabular reorientation, in patients with mild dysplasia and cam FAI.
Dysplasia with cam FAI is an emerging common condition for which patients may seek less invasive treatment in the form of hip arthroscopy. The findings of this study suggest caution in using hip arthroscopy without capsular repair in the treatment of mild dysplasia with cam FAI, even in the presence of cam decompression and labral and acetabular rim preservation.
Study Strengths and Limitations
One strength was the relative lack of surgeon bias. When the surgeries were performed (2009-2010), we recognized cam and pincer FAI but did not discriminate for mild dysplasia, because at that time it was not known to be a potential predictor of poorer outcomes. Another strength was the strict methodology, with blinding of all investigator surgeons to PROs and stringent retention of all PROs, including “failures” (eg, total hip arthroplasty conversions and complications), in both cohorts. Moreover, the crucial case-control analysis matched on multiple variables verified statistically significant results demonstrating poorer outcomes at minimum 2-year follow-up, despite more improvement in the dysplasia cohort at 3 months. The latter, we think, is also valuable new information; it emphasizes the need for close and prolonged follow-up of patients with mild dysplasia despite early improvement.
Limitations include the small number of study patients, the retrospective study design (using prospectively collected data), and the isolated use of LCEA to define dysplasia. Pereira and colleagues23 recommended using LCEA with Tönnis angle to define minor dysplasia. Although dysplasia cannot be precisely defined with only this radiographic measurement, LCEA has been shown to be a reliable, clinically relevant measure.24 In addition, LCEA has been used in most reports on arthroscopic management of dysplastic hips and thus allows for comparison. Furthermore, other studies have used LCEA of <15° as a threshold between mild and severe dysplasia, and we did as well. This broad inclusion criterion allowed for heterogeneity in our mild dysplasia cohort and was a study limitation. Interobserver reliability of measured LCEA was not assessed and is another limitation.
The initial prospective study (2009) did not record α angles to quantify cam FAI. This is a study limitation. However, the surgical range-of-motion endpoints considered sufficient for cam decompression were the same in both cohorts. In addition, femoral version was not assessed in the original database (2009-2010), as this aspect of hip anatomy was not thought significant during initial data collection. These areas of interest merit further investigation.
Use of a focal pincer cohort may be challenged as a suboptimal control group. However, there were very few completely normal acetabulae with pure cam FAI in the original prospective study, and the focal pincer cohort was used as a control cohort in previous studies.25
Conclusion
The common combination of mild dysplasia and cam FAI has poorer outcomes than mixed FAI after arthroscopic surgery without capsular repair.
Am J Orthop. 2017;46(1):E47-E53. Copyright Frontline Medical Communications Inc. 2017. All rights reserved.
1. Paliobeis CP, Villar RN. The prevalence of dysplasia in femoroacetabular impingement. Hip Int. 2011;21(2):141-145.
2. Clohisy JC, Nunley RM, Carlisle JC, Schoenecker PL. Incidence and characteristics of femoral deformities in the dysplastic hip. Clin Orthop Relat Res. 2009;467(1):128-134.
3. Parvizi J, Bican O, Bender B, et al. Arthroscopy for labral tears in patients with developmental dysplasia of the hip: a cautionary note. J Arthroplasty. 2009;24(6 suppl):110-113.
4. Matsuda DK, Khatod M. Rapidly progressive osteoarthritis after arthroscopic labral repair in patients with hip dysplasia. Arthroscopy. 2012;28(11):1738-1743.
5. Jackson TJ, Watson J, LaReau JM, Domb BG. Periacetabular osteotomy and arthroscopic labral repair after failed hip arthroscopy due to iatrogenic aggravation of hip dysplasia. Knee Surg Sports Traumatol Arthrosc. 2014;22(4):911-914.
6. Byrd JW, Jones KS. Hip arthroscopy in the presence of dysplasia. Arthroscopy. 2003;19(10):1055-1060.
7. Domb BG, Stake CE, Lindner D, El-Bitar Y, Jackson TJ. Arthroscopic capsular plication and labral preservation in borderline hip dysplasia: two-year clinical outcomes of a surgical approach to a challenging problem. Am J Sports Med. 2013;41(11):2591-2598.
8. Jayasekera N, Aprato A, Villar RN. Hip arthroscopy in the presence of acetabular dysplasia. Open Orthop J. 2015;9:185-187.
9. Fukui K, Briggs KK, Trindade CA, Philippon MJ. Outcomes after labral repair in patients with femoroacetabular impingement and borderline dysplasia. Arthroscopy. 2015;31(12):2371-2379.
10. Siebenrock KA, Leunig M, Ganz R. Periacetabular osteotomy: the Bernese experience. Instr Course Lect. 2001;50:239-245.
11. Garras DN, Crowder TT, Olson SA. Medium-term results of the Bernese periacetabular osteotomy in the treatment of symptomatic developmental dysplasia of the hip. J Bone Joint Surg Br. 2007;89(6):721-724.
12. Biedermann R, Donnan L, Gabriel A, Wachter R, Krismer M, Behensky H. Complications and patient satisfaction after periacetabular pelvic osteotomy. Int Orthop. 2008;32(5):611-617.
13. Ross JR, Zaltz I, Nepple JJ, Schoenecker PL, Clohisy JC. Arthroscopic disease classification and interventions as an adjunct in the treatment of acetabular dysplasia. Am J Sports Med. 2011;39(suppl):72S-78S.
14. Domb BG, LaReau JM, Baydoun H, Botser I, Millis MB, Yen YM. Is intraarticular pathology common in patients with hip dysplasia undergoing periacetabular osteotomy? Clin Orthop Relat Res. 2014;472(2):674-680.
15. Kain MS, Novais EN, Vallim C, Millis MB, Kim YJ. Periacetabular osteotomy after failed hip arthroscopy for labral tears in patients with acetabular dysplasia. J Bone Joint Surg Am. 2011;93(suppl 2):57-61.
16. Matsuda DK, Villamor A. The modified mid-anterior portal for hip arthroscopy. Arthrosc Tech. 2014;3(4):e469-e474.
17. Javed A, O’Donnell JM. Arthroscopic femoral osteochondroplasty for cam femoroacetabular impingement in patients over 60 years of age. J Bone Joint Surg Br. 2011;93(3):326-331.
18. Redmond JM, Gupta A, Cregar WM, Hammarstedt JE, Gui C, Domb BG. Arthroscopic treatment of labral tears in patients aged 60 years or older. Arthroscopy. 2015;31(10):1921-1927.
19. Mei-Dan O, McConkey MO, Brick M. Catastrophic failure of hip arthroscopy due to iatrogenic instability: can partial division of the ligamentum teres and iliofemoral ligament cause subluxation? Arthroscopy. 2012;28(3):440-445.
20. Benali Y, Katthagen BD. Hip subluxation as a complication of arthroscopic debridement. Arthroscopy. 2009;25(4):405-407.
21. Jayasekera N, Aprato A, Villar RN. Are crutches required after hip arthroscopy? A case–control study. Hip Int. 2013;23(3):269-273.
22. Domb BG, Stake CE, Finley ZJ, Chen T, Giordano BD. Influence of capsular repair versus unrepaired capsulotomy on 2-year clinical outcomes after arthroscopic hip preservation surgery. Arthroscopy. 2015;31(4):643-650.
23. Pereira F, Giles A, Wood G, Board TN. Recognition of minor adult hip dysplasia: which anatomical indices are important? Hip Int. 2014;24(2):175-179.
24. Murphy SB, Ganz R, Müller ME. The prognosis in untreated dysplasia of the hip. A study of radiographic factors that predict the outcome. J Bone Joint Surg Am. 1995;77(7):985-989.
25. Matsuda DK, Gupta N, Burchette R, Sehgal B. Arthroscopic surgery for global versus focal pincer femoroacetabular impingement: are the outcomes different? J Hip Preserv Surg. 2015;2(1):42-50.
Take-Home Points
- Cam deformity often occurs with dysplasia.
- Borderline or mild dysplasia has been treated with isolated hip arthroscopy.
- Avoid rim trimming that can make mild dysplasia more severe.
- Labral preservation, cam decompression, and capsular repair or plication are currently suggested.
- Poorer outcomes occurred in borderline or mild dysplasia with cam impingement relative to controls following hip arthroscopy without capsular repair.
- Initial clinical improvement may be followed by clinical deterioration suggesting close long-term follow-up with prompt addition of reorientation acetabular osteotomy if indicated.
- It is unknown whether small capsulotomies may yield comparable outcomes with larger capsulotomies plus repair.
It is unknown whether small capsulotomies may yield comparable outcomes with larger capsulotomies plus repair. There is growing interest in hip preservation surgery in general and arthroscopic hip preservation in particular. Chondrolabral pathology leading to symptoms and degenerative progression typically is caused by structural abnormalities, mainly femoroacetabular impingement (FAI) and developmental dysplasia of the hip. Unlike the bony overcoverage of pincer FAI, developmental dysplasia of the hip typically exhibits insufficient anterolateral coverage of the femoral head.
The role of hip arthroscopy in the treatment of dysplasia remains undefined. Emerging evidence shows a high incidence of dysplasia with associated cam deformity,1,2 but there is a paucity of evidence-based information for this specific patient population. Clinical outcomes of hip arthroscopy in the setting of dysplasia are conflicting: some poor3-5 and others successful.1,6-9 Although reorientation periacetabular osteotomy (PAO) is considered a mainstay in the treatment of dysplasia—providing improvement in symptoms, deficient anterolateral acetabular coverage, and hip biomechanics—midterm failure rates approaching 24% have been reported.10-12 Many young patients with symptomatic dysplasia want a surgical option that is less invasive than open PAO.4 Intra-articular central compartment pathology and cam FAI commonly occur with dysplasia and are amenable to arthroscopic treatment.1,13,14 Moreover, staged PAO may be successful in cases in which arthroscopic intervention fails to provide clinical improvement.5,15
Emerging evidence suggests beneficial effects of arthroscopic capsular repair or plication in the setting of borderline or mild dysplasia.7,9 However, the literature provides little information on arthroscopic outcomes without capsular repair. One study found poor outcomes of arthroscopic surgery for dysplasia, but its patients underwent labral débridement, not repair.3 Two patients in a case report demonstrated rapidly progressive osteoarthritis after arthroscopic labral repairs and concurrent femoroplasties for cam FAI, but each had marked dysplasia with a lateral center-edge angle (LCEA) of <15°.4
Arthroscopy with capsular repair has been assumed to provide better outcomes than arthroscopy without repair, but to our knowledge there are no studies that have compared outcomes of mild dysplasia with cam FAI and outcomes of mixed FAI treated without capsular repair. Clinical equipoise makes it ethically challenging to perform a prospective study comparing dysplasia treated with and without capsular repair. We conducted a study to compare outcomes of mild dysplasia with cam FAI and outcomes of mixed FAI treated with arthroscopic surgery and to fill the knowledge gap regarding outcomes of mild dysplasia treated without capsular repair.
Methods
In this study, which received Institutional Review Board approval, we retrospectively reviewed radiographs and data from a prospective 3-center study of arthroscopic outcomes of FAI in 150 patients (159 hips) who underwent arthroscopic surgery by 1 of 3 surgeons between March 2009 and June 2010. In all cases, digital images of anteroposterior pelvic radiographs were used for radiographic measurements. On these images, the LCEA is formed by the intersection of the vertical line (corrected for obliquity using a horizontal reference line connecting the inferior extents of both radiographic teardrops) through the center of the femoral head (determined with a digital centering tool) with the line extending to the lateral edge of the sourcil (radiographic eyebrow of the weight-bearing region or roof of the acetabulum). Measurements were made in blinded fashion (by a nonsurgeon coauthor, Dr. Nikhil Gupta, who completed training modules) and were confirmed without alteration by the principal investigator Dr. Dean K. Matsuda. Inclusion criteria were mild acetabular dysplasia (LCEA, 15°-24°) and mixed FAI including focal pincer component (LCEA, 25°-39°), radiographic crossover sign, and successful completion of patient-reported outcome (PRO) measures at minimum 2-year follow-up. Exclusion criteria were severe dysplasia (LCEA, <15°), hip subluxation, broken Shenton line, global pincer FAI (LCEA, ≥40°), Tönnis grade 3 osteoarthritis, Legg-Calvé-Perthes disease, osteonecrosis, prior hip surgery, and unsuccessful completion of PRO measures. Outcome measures included investigator-blinded preoperative and postoperative Nonarthritic Hip Score (NAHS) and 5-point Likert satisfaction score. Complications, revision surgeries, and conversion arthroplasties were recorded.
Statistical Analysis
We examined outcomes with descriptive statistics for each of the candidate covariates in the model classified by femoroacetabular subtype: focal pincer and cam (mixed FAI) and dysplasia with cam. We examined the variables of sex, age, weight, height, body mass index, preoperative NAHS, presence of dysplasia (yes/no), presence of osteoarthritis (yes/no), Tönnis osteoarthritis grade, Outerbridge class, American Society of Anesthesiologists (ASA) score, months of pain, bilateral procedure (yes/no), and pincer involvement with cam FAI (yes/no). Before beginning linear regression modeling, we screened the candidate variables for strong correlations with other variables and looked for those variables with minimal missing data. For all these covariates, we then performed linear regression with a selection process—both a stepwise selection method and a backward elimination method—to verify we determined the same model for 24-month NAHS, or to understand why we could not. Finally, we ran the model we found from the linear regression as a linear mixed model of 24-month NAHS with the dichotomous variables taken as fixed effects and the other variables taken as random effects, using variance-components representation for the random effects. We then examined 3-month and 12-month NAHS with the same variables selected for the 24-month model.
To further examine and verify the effects of dysplasia on outcomes found in our linear mixed model, we performed a nested case–control analysis matching each member of cohort D (cases) with 2 members of cohort M (controls). We used an optimal-matching algorithm to match focal patients in the linear regression dataset with dysplasia patients in the linear regression dataset in such a way as to minimize the overall differences between the datasets. We matched cases and controls on preoperative NAHS, age, sex, presence of osteoarthritis, months of pain, ASA score, and body mass index. The differences between the matched cases and controls (control value minus case value) were compared using Wilcoxon rank sum tests for statistical significance of differences from 0 (with differences generated for each control group member, 2 differences per case) to examine the quality of the match. Finally, we examined the statistical significance of the difference of the outcome variables (3-, 12-, and 24-month NAHS) from 0, again using Wilcoxon rank sum tests. Statistical significance was set at P < .05 using SAS Version 9.3 (SAS Institute).
Surgical Procedure
In all cases, supine outpatient hip arthroscopy was performed under general anesthesia. Anterolateral and modified midanterior portals16 were used. T-capsulotomies were performed in both cohorts. Cohort M underwent anterosuperior acetabuloplasty with a motorized burr. Labral refixation or selective débridement was performed in cohort M, whereas labral repair (with limited freshening of acetabular rim attachment site) or selective débridement (but no segmental resection) was performed in cohort D. Arthroscopic femoroplasty was performed with similar endpoints of 120° minimum hip flexion and 30° minimum flexed hip internal rotation with retention of the labral fluid seal. Capsular repair or plication was not performed for either cohort during the study period.
The cohorts underwent similar postoperative protocols: 2 weeks of protected ambulation using 2 crutches, exercise cycling without resistance beginning postoperative day 1, swimming at 2 weeks, elliptical machine workouts at 6 weeks, jogging at 12 weeks, and return to unrestricted athletics at 5 months.
Results
In cohort D, which consisted of 8 patients (5 female), mean age was 49.6 years, and mean LCEA was 19° (range, 16°-24°).
In cohort D, mean (SD) change in NAHS was +20.00 (6.24) (P = .25) at 3 months (n = 3), +14.33 (9.77) (P = .03) at 12 months (n = 6), and –0.75 (19.86) (P = .74) at 24 months (n = 8).
In cohort M, mean (SD) change in NAHS was +12.09 (18.98) (P < .0001) at 3 months (n = 45), +20.39 (16.49) (P < .0001) at 12 months (n = 57), and +21.99 (17.32) (P < .0001) at 24 months (n = 69).
In a pairwise case–control comparison, the mean (SD) change-from-baseline difference between cohorts D and M was +8.2 (12.85) (P = .31) at 3 months (n = 5), –8.7 (11.52) (P = .03) at 12 months (n = 10), and –31.06 (23.55) (P = .0002) at 24 months (n = 16). Dysplasia had an impact of –23.4 points on 24-month NAHS (standard error = 5.35 points; P < .0001), which corresponds to a 95% confidence interval of –12.9 to –33.9 points on NAHS.
Compared with cohort M, cohort D had significantly less NAHS improvement (P = .002), less satisfaction (P = .15) and more hip arthroplasty conversions (P = .22, not statistically significant).
There were no statistically significant differences between cohorts in demographics, preoperative variables, intraoperative findings, or surgical procedures in the regression analysis. Of the investigated variables, only group membership (cohort D) was a statistically significant predictor of poorer outcomes in the model of change from preoperative to 24 months. However, older age was associated with cohort D (older patients with dysplasia, P = .07), and therefore in the nested case–control analysis we were able to match on all variables except age (8.74 years older in cohort D, P = .0013) to a level of statistical nonsignificance.
Discussion
The principal finding of this study is the significantly poorer outcomes of mild dysplasia and cam FAI relative to mixed FAI after hip arthroscopy without capsular repair. Study group (cohort D) and control group (cohort M) had associated cam deformities treated with femoroplasty with similar decompression endpoints and labral preservation in the form of selective débridement or labral repair (no labral resections in either cohort) with similar rehabilitation protocols.
Our study findings suggest short-term improvement may be followed by midterm worsening in patients with mild dysplasia and sustained improvement in patients with mixed FAI. These findings have practical clinical applications. Jackson and colleagues5 reported on a patient who, after undergoing “successful” arthroscopic surgery for mild dysplasia, clinically deteriorated after 13 months and eventually required PAO. Patients undergoing isolated hip arthroscopy for mild dysplasia with cam FAI should be informed of the possible need for secondary PAO or even hip arthroplasty, be followed up more often and longer than comparable patients with FAI, and have follow-up supplemented with interval radiographs.4 If even subtle subluxation or joint narrowing occurs, we suggest resumption of protected weight-bearing and prompt progression to PAO in younger patients with joint congruency or eventual conversion arthroplasty in older ones.
Although mean preoperative NAHS (52.88) and mean 24-month postoperative NAHS (52.13) suggest essentially no change in PROs for cohort D, all patients with dysplasia either worsened or improved, though those who improved did so at a lesser relative magnitude than those with mixed FAI (cohort M). This finding may help explain the divergent outcomes reported in the literature on dysplasia treated with hip arthroscopy.
Cohort D was older than cohort M, but the difference was not statistically significant. Age may still be a confounding variable, and it may have contributed in part to the poorer outcomes for the patients with dysplasia. However, emerging studies demonstrate select older patients with FAI and/or labral tears may have successful outcomes with arthroscopic intervention.17,18 Our findings support mild dysplasia as the main contributor to the poor outcomes observed in this study.
With identical postoperative rehabilitation protocols, patients in both cohorts typically were ambulating without crutches by the end of postoperative week 2. Delayed weight-bearing has been suggested as contributing to successful outcomes in the setting of dysplasia7,19,20 but has not been shown to adversely affect nondysplastic hips.21 Whether delayed weight-bearing contributed to the poor outcomes in our dysplasia cohort is unknown, but the early successful outcomes may discount its influence.
Our findings support successful outcomes of arthroscopic treatment of mixed FAI (specifically focal pincer plus cam FAI) without capsular repair. Perhaps more important, we found inferior outcomes of arthroscopic treatment of mild dysplasia plus cam FAI without capsular repair—filling the knowledge gap regarding the need for arthroscopic capsular repair for mild dysplasia. Although a recent study demonstrated no significant difference in outcomes between hip arthroscopy with and without capsular repair,22 2 studies specific to mild dysplasia demonstrated successful outcomes of capsular repair.7,9 One found that mild dysplasia treated with arthroscopy, including capsular plication, resulted in 77% good/excellent outcomes and LCEA as low as 18° at minimum 2-year follow-up.7 The other found clinical improvement in mild dysplasia (LCEA, 15°-19°) when capsular repair was performed as part of arthroscopic treatment.9 In the present study, we retrospectively reviewed outcomes from a prospective study performed in 2009 to 2010, before the era of common capsular repair. It appears that capsular repair9 or plication7 in the setting of mild dysplasia may yield improved outcomes approaching those of arthroscopic FAI surgery. Our study results showed that, despite labral preservation and cam decompression, mild dysplasia without the closure of T-capsulotomy had inferior outcomes at 2 years. However, we do not know if outcomes would have been better with capsular repair or plication and/or smaller capsulotomies, perhaps with minimal violation of the iliofemoral ligament in this specific subset of patients. Furthermore, we do not know if optimal outcomes can best be achieved with arthroscopic and/or open surgery, with or without acetabular reorientation, in patients with mild dysplasia and cam FAI.
Dysplasia with cam FAI is an emerging common condition for which patients may seek less invasive treatment in the form of hip arthroscopy. The findings of this study suggest caution in using hip arthroscopy without capsular repair in the treatment of mild dysplasia with cam FAI, even in the presence of cam decompression and labral and acetabular rim preservation.
Study Strengths and Limitations
One strength was the relative lack of surgeon bias. When the surgeries were performed (2009-2010), we recognized cam and pincer FAI but did not discriminate for mild dysplasia, because at that time it was not known to be a potential predictor of poorer outcomes. Another strength was the strict methodology, with blinding of all investigator surgeons to PROs and stringent retention of all PROs, including “failures” (eg, total hip arthroplasty conversions and complications), in both cohorts. Moreover, the crucial case-control analysis matched on multiple variables verified statistically significant results demonstrating poorer outcomes at minimum 2-year follow-up, despite more improvement in the dysplasia cohort at 3 months. The latter, we think, is also valuable new information; it emphasizes the need for close and prolonged follow-up of patients with mild dysplasia despite early improvement.
Limitations include the small number of study patients, the retrospective study design (using prospectively collected data), and the isolated use of LCEA to define dysplasia. Pereira and colleagues23 recommended using LCEA with Tönnis angle to define minor dysplasia. Although dysplasia cannot be precisely defined with only this radiographic measurement, LCEA has been shown to be a reliable, clinically relevant measure.24 In addition, LCEA has been used in most reports on arthroscopic management of dysplastic hips and thus allows for comparison. Furthermore, other studies have used LCEA of <15° as a threshold between mild and severe dysplasia, and we did as well. This broad inclusion criterion allowed for heterogeneity in our mild dysplasia cohort and was a study limitation. Interobserver reliability of measured LCEA was not assessed and is another limitation.
The initial prospective study (2009) did not record α angles to quantify cam FAI. This is a study limitation. However, the surgical range-of-motion endpoints considered sufficient for cam decompression were the same in both cohorts. In addition, femoral version was not assessed in the original database (2009-2010), as this aspect of hip anatomy was not thought significant during initial data collection. These areas of interest merit further investigation.
Use of a focal pincer cohort may be challenged as a suboptimal control group. However, there were very few completely normal acetabulae with pure cam FAI in the original prospective study, and the focal pincer cohort was used as a control cohort in previous studies.25
Conclusion
The common combination of mild dysplasia and cam FAI has poorer outcomes than mixed FAI after arthroscopic surgery without capsular repair.
Am J Orthop. 2017;46(1):E47-E53. Copyright Frontline Medical Communications Inc. 2017. All rights reserved.
Take-Home Points
- Cam deformity often occurs with dysplasia.
- Borderline or mild dysplasia has been treated with isolated hip arthroscopy.
- Avoid rim trimming that can make mild dysplasia more severe.
- Labral preservation, cam decompression, and capsular repair or plication are currently suggested.
- Poorer outcomes occurred in borderline or mild dysplasia with cam impingement relative to controls following hip arthroscopy without capsular repair.
- Initial clinical improvement may be followed by clinical deterioration suggesting close long-term follow-up with prompt addition of reorientation acetabular osteotomy if indicated.
- It is unknown whether small capsulotomies may yield comparable outcomes with larger capsulotomies plus repair.
It is unknown whether small capsulotomies may yield comparable outcomes with larger capsulotomies plus repair. There is growing interest in hip preservation surgery in general and arthroscopic hip preservation in particular. Chondrolabral pathology leading to symptoms and degenerative progression typically is caused by structural abnormalities, mainly femoroacetabular impingement (FAI) and developmental dysplasia of the hip. Unlike the bony overcoverage of pincer FAI, developmental dysplasia of the hip typically exhibits insufficient anterolateral coverage of the femoral head.
The role of hip arthroscopy in the treatment of dysplasia remains undefined. Emerging evidence shows a high incidence of dysplasia with associated cam deformity,1,2 but there is a paucity of evidence-based information for this specific patient population. Clinical outcomes of hip arthroscopy in the setting of dysplasia are conflicting: some poor3-5 and others successful.1,6-9 Although reorientation periacetabular osteotomy (PAO) is considered a mainstay in the treatment of dysplasia—providing improvement in symptoms, deficient anterolateral acetabular coverage, and hip biomechanics—midterm failure rates approaching 24% have been reported.10-12 Many young patients with symptomatic dysplasia want a surgical option that is less invasive than open PAO.4 Intra-articular central compartment pathology and cam FAI commonly occur with dysplasia and are amenable to arthroscopic treatment.1,13,14 Moreover, staged PAO may be successful in cases in which arthroscopic intervention fails to provide clinical improvement.5,15
Emerging evidence suggests beneficial effects of arthroscopic capsular repair or plication in the setting of borderline or mild dysplasia.7,9 However, the literature provides little information on arthroscopic outcomes without capsular repair. One study found poor outcomes of arthroscopic surgery for dysplasia, but its patients underwent labral débridement, not repair.3 Two patients in a case report demonstrated rapidly progressive osteoarthritis after arthroscopic labral repairs and concurrent femoroplasties for cam FAI, but each had marked dysplasia with a lateral center-edge angle (LCEA) of <15°.4
Arthroscopy with capsular repair has been assumed to provide better outcomes than arthroscopy without repair, but to our knowledge there are no studies that have compared outcomes of mild dysplasia with cam FAI and outcomes of mixed FAI treated without capsular repair. Clinical equipoise makes it ethically challenging to perform a prospective study comparing dysplasia treated with and without capsular repair. We conducted a study to compare outcomes of mild dysplasia with cam FAI and outcomes of mixed FAI treated with arthroscopic surgery and to fill the knowledge gap regarding outcomes of mild dysplasia treated without capsular repair.
Methods
In this study, which received Institutional Review Board approval, we retrospectively reviewed radiographs and data from a prospective 3-center study of arthroscopic outcomes of FAI in 150 patients (159 hips) who underwent arthroscopic surgery by 1 of 3 surgeons between March 2009 and June 2010. In all cases, digital images of anteroposterior pelvic radiographs were used for radiographic measurements. On these images, the LCEA is formed by the intersection of the vertical line (corrected for obliquity using a horizontal reference line connecting the inferior extents of both radiographic teardrops) through the center of the femoral head (determined with a digital centering tool) with the line extending to the lateral edge of the sourcil (radiographic eyebrow of the weight-bearing region or roof of the acetabulum). Measurements were made in blinded fashion (by a nonsurgeon coauthor, Dr. Nikhil Gupta, who completed training modules) and were confirmed without alteration by the principal investigator Dr. Dean K. Matsuda. Inclusion criteria were mild acetabular dysplasia (LCEA, 15°-24°) and mixed FAI including focal pincer component (LCEA, 25°-39°), radiographic crossover sign, and successful completion of patient-reported outcome (PRO) measures at minimum 2-year follow-up. Exclusion criteria were severe dysplasia (LCEA, <15°), hip subluxation, broken Shenton line, global pincer FAI (LCEA, ≥40°), Tönnis grade 3 osteoarthritis, Legg-Calvé-Perthes disease, osteonecrosis, prior hip surgery, and unsuccessful completion of PRO measures. Outcome measures included investigator-blinded preoperative and postoperative Nonarthritic Hip Score (NAHS) and 5-point Likert satisfaction score. Complications, revision surgeries, and conversion arthroplasties were recorded.
Statistical Analysis
We examined outcomes with descriptive statistics for each of the candidate covariates in the model classified by femoroacetabular subtype: focal pincer and cam (mixed FAI) and dysplasia with cam. We examined the variables of sex, age, weight, height, body mass index, preoperative NAHS, presence of dysplasia (yes/no), presence of osteoarthritis (yes/no), Tönnis osteoarthritis grade, Outerbridge class, American Society of Anesthesiologists (ASA) score, months of pain, bilateral procedure (yes/no), and pincer involvement with cam FAI (yes/no). Before beginning linear regression modeling, we screened the candidate variables for strong correlations with other variables and looked for those variables with minimal missing data. For all these covariates, we then performed linear regression with a selection process—both a stepwise selection method and a backward elimination method—to verify we determined the same model for 24-month NAHS, or to understand why we could not. Finally, we ran the model we found from the linear regression as a linear mixed model of 24-month NAHS with the dichotomous variables taken as fixed effects and the other variables taken as random effects, using variance-components representation for the random effects. We then examined 3-month and 12-month NAHS with the same variables selected for the 24-month model.
To further examine and verify the effects of dysplasia on outcomes found in our linear mixed model, we performed a nested case–control analysis matching each member of cohort D (cases) with 2 members of cohort M (controls). We used an optimal-matching algorithm to match focal patients in the linear regression dataset with dysplasia patients in the linear regression dataset in such a way as to minimize the overall differences between the datasets. We matched cases and controls on preoperative NAHS, age, sex, presence of osteoarthritis, months of pain, ASA score, and body mass index. The differences between the matched cases and controls (control value minus case value) were compared using Wilcoxon rank sum tests for statistical significance of differences from 0 (with differences generated for each control group member, 2 differences per case) to examine the quality of the match. Finally, we examined the statistical significance of the difference of the outcome variables (3-, 12-, and 24-month NAHS) from 0, again using Wilcoxon rank sum tests. Statistical significance was set at P < .05 using SAS Version 9.3 (SAS Institute).
Surgical Procedure
In all cases, supine outpatient hip arthroscopy was performed under general anesthesia. Anterolateral and modified midanterior portals16 were used. T-capsulotomies were performed in both cohorts. Cohort M underwent anterosuperior acetabuloplasty with a motorized burr. Labral refixation or selective débridement was performed in cohort M, whereas labral repair (with limited freshening of acetabular rim attachment site) or selective débridement (but no segmental resection) was performed in cohort D. Arthroscopic femoroplasty was performed with similar endpoints of 120° minimum hip flexion and 30° minimum flexed hip internal rotation with retention of the labral fluid seal. Capsular repair or plication was not performed for either cohort during the study period.
The cohorts underwent similar postoperative protocols: 2 weeks of protected ambulation using 2 crutches, exercise cycling without resistance beginning postoperative day 1, swimming at 2 weeks, elliptical machine workouts at 6 weeks, jogging at 12 weeks, and return to unrestricted athletics at 5 months.
Results
In cohort D, which consisted of 8 patients (5 female), mean age was 49.6 years, and mean LCEA was 19° (range, 16°-24°).
In cohort D, mean (SD) change in NAHS was +20.00 (6.24) (P = .25) at 3 months (n = 3), +14.33 (9.77) (P = .03) at 12 months (n = 6), and –0.75 (19.86) (P = .74) at 24 months (n = 8).
In cohort M, mean (SD) change in NAHS was +12.09 (18.98) (P < .0001) at 3 months (n = 45), +20.39 (16.49) (P < .0001) at 12 months (n = 57), and +21.99 (17.32) (P < .0001) at 24 months (n = 69).
In a pairwise case–control comparison, the mean (SD) change-from-baseline difference between cohorts D and M was +8.2 (12.85) (P = .31) at 3 months (n = 5), –8.7 (11.52) (P = .03) at 12 months (n = 10), and –31.06 (23.55) (P = .0002) at 24 months (n = 16). Dysplasia had an impact of –23.4 points on 24-month NAHS (standard error = 5.35 points; P < .0001), which corresponds to a 95% confidence interval of –12.9 to –33.9 points on NAHS.
Compared with cohort M, cohort D had significantly less NAHS improvement (P = .002), less satisfaction (P = .15) and more hip arthroplasty conversions (P = .22, not statistically significant).
There were no statistically significant differences between cohorts in demographics, preoperative variables, intraoperative findings, or surgical procedures in the regression analysis. Of the investigated variables, only group membership (cohort D) was a statistically significant predictor of poorer outcomes in the model of change from preoperative to 24 months. However, older age was associated with cohort D (older patients with dysplasia, P = .07), and therefore in the nested case–control analysis we were able to match on all variables except age (8.74 years older in cohort D, P = .0013) to a level of statistical nonsignificance.
Discussion
The principal finding of this study is the significantly poorer outcomes of mild dysplasia and cam FAI relative to mixed FAI after hip arthroscopy without capsular repair. Study group (cohort D) and control group (cohort M) had associated cam deformities treated with femoroplasty with similar decompression endpoints and labral preservation in the form of selective débridement or labral repair (no labral resections in either cohort) with similar rehabilitation protocols.
Our study findings suggest short-term improvement may be followed by midterm worsening in patients with mild dysplasia and sustained improvement in patients with mixed FAI. These findings have practical clinical applications. Jackson and colleagues5 reported on a patient who, after undergoing “successful” arthroscopic surgery for mild dysplasia, clinically deteriorated after 13 months and eventually required PAO. Patients undergoing isolated hip arthroscopy for mild dysplasia with cam FAI should be informed of the possible need for secondary PAO or even hip arthroplasty, be followed up more often and longer than comparable patients with FAI, and have follow-up supplemented with interval radiographs.4 If even subtle subluxation or joint narrowing occurs, we suggest resumption of protected weight-bearing and prompt progression to PAO in younger patients with joint congruency or eventual conversion arthroplasty in older ones.
Although mean preoperative NAHS (52.88) and mean 24-month postoperative NAHS (52.13) suggest essentially no change in PROs for cohort D, all patients with dysplasia either worsened or improved, though those who improved did so at a lesser relative magnitude than those with mixed FAI (cohort M). This finding may help explain the divergent outcomes reported in the literature on dysplasia treated with hip arthroscopy.
Cohort D was older than cohort M, but the difference was not statistically significant. Age may still be a confounding variable, and it may have contributed in part to the poorer outcomes for the patients with dysplasia. However, emerging studies demonstrate select older patients with FAI and/or labral tears may have successful outcomes with arthroscopic intervention.17,18 Our findings support mild dysplasia as the main contributor to the poor outcomes observed in this study.
With identical postoperative rehabilitation protocols, patients in both cohorts typically were ambulating without crutches by the end of postoperative week 2. Delayed weight-bearing has been suggested as contributing to successful outcomes in the setting of dysplasia7,19,20 but has not been shown to adversely affect nondysplastic hips.21 Whether delayed weight-bearing contributed to the poor outcomes in our dysplasia cohort is unknown, but the early successful outcomes may discount its influence.
Our findings support successful outcomes of arthroscopic treatment of mixed FAI (specifically focal pincer plus cam FAI) without capsular repair. Perhaps more important, we found inferior outcomes of arthroscopic treatment of mild dysplasia plus cam FAI without capsular repair—filling the knowledge gap regarding the need for arthroscopic capsular repair for mild dysplasia. Although a recent study demonstrated no significant difference in outcomes between hip arthroscopy with and without capsular repair,22 2 studies specific to mild dysplasia demonstrated successful outcomes of capsular repair.7,9 One found that mild dysplasia treated with arthroscopy, including capsular plication, resulted in 77% good/excellent outcomes and LCEA as low as 18° at minimum 2-year follow-up.7 The other found clinical improvement in mild dysplasia (LCEA, 15°-19°) when capsular repair was performed as part of arthroscopic treatment.9 In the present study, we retrospectively reviewed outcomes from a prospective study performed in 2009 to 2010, before the era of common capsular repair. It appears that capsular repair9 or plication7 in the setting of mild dysplasia may yield improved outcomes approaching those of arthroscopic FAI surgery. Our study results showed that, despite labral preservation and cam decompression, mild dysplasia without the closure of T-capsulotomy had inferior outcomes at 2 years. However, we do not know if outcomes would have been better with capsular repair or plication and/or smaller capsulotomies, perhaps with minimal violation of the iliofemoral ligament in this specific subset of patients. Furthermore, we do not know if optimal outcomes can best be achieved with arthroscopic and/or open surgery, with or without acetabular reorientation, in patients with mild dysplasia and cam FAI.
Dysplasia with cam FAI is an emerging common condition for which patients may seek less invasive treatment in the form of hip arthroscopy. The findings of this study suggest caution in using hip arthroscopy without capsular repair in the treatment of mild dysplasia with cam FAI, even in the presence of cam decompression and labral and acetabular rim preservation.
Study Strengths and Limitations
One strength was the relative lack of surgeon bias. When the surgeries were performed (2009-2010), we recognized cam and pincer FAI but did not discriminate for mild dysplasia, because at that time it was not known to be a potential predictor of poorer outcomes. Another strength was the strict methodology, with blinding of all investigator surgeons to PROs and stringent retention of all PROs, including “failures” (eg, total hip arthroplasty conversions and complications), in both cohorts. Moreover, the crucial case-control analysis matched on multiple variables verified statistically significant results demonstrating poorer outcomes at minimum 2-year follow-up, despite more improvement in the dysplasia cohort at 3 months. The latter, we think, is also valuable new information; it emphasizes the need for close and prolonged follow-up of patients with mild dysplasia despite early improvement.
Limitations include the small number of study patients, the retrospective study design (using prospectively collected data), and the isolated use of LCEA to define dysplasia. Pereira and colleagues23 recommended using LCEA with Tönnis angle to define minor dysplasia. Although dysplasia cannot be precisely defined with only this radiographic measurement, LCEA has been shown to be a reliable, clinically relevant measure.24 In addition, LCEA has been used in most reports on arthroscopic management of dysplastic hips and thus allows for comparison. Furthermore, other studies have used LCEA of <15° as a threshold between mild and severe dysplasia, and we did as well. This broad inclusion criterion allowed for heterogeneity in our mild dysplasia cohort and was a study limitation. Interobserver reliability of measured LCEA was not assessed and is another limitation.
The initial prospective study (2009) did not record α angles to quantify cam FAI. This is a study limitation. However, the surgical range-of-motion endpoints considered sufficient for cam decompression were the same in both cohorts. In addition, femoral version was not assessed in the original database (2009-2010), as this aspect of hip anatomy was not thought significant during initial data collection. These areas of interest merit further investigation.
Use of a focal pincer cohort may be challenged as a suboptimal control group. However, there were very few completely normal acetabulae with pure cam FAI in the original prospective study, and the focal pincer cohort was used as a control cohort in previous studies.25
Conclusion
The common combination of mild dysplasia and cam FAI has poorer outcomes than mixed FAI after arthroscopic surgery without capsular repair.
Am J Orthop. 2017;46(1):E47-E53. Copyright Frontline Medical Communications Inc. 2017. All rights reserved.
1. Paliobeis CP, Villar RN. The prevalence of dysplasia in femoroacetabular impingement. Hip Int. 2011;21(2):141-145.
2. Clohisy JC, Nunley RM, Carlisle JC, Schoenecker PL. Incidence and characteristics of femoral deformities in the dysplastic hip. Clin Orthop Relat Res. 2009;467(1):128-134.
3. Parvizi J, Bican O, Bender B, et al. Arthroscopy for labral tears in patients with developmental dysplasia of the hip: a cautionary note. J Arthroplasty. 2009;24(6 suppl):110-113.
4. Matsuda DK, Khatod M. Rapidly progressive osteoarthritis after arthroscopic labral repair in patients with hip dysplasia. Arthroscopy. 2012;28(11):1738-1743.
5. Jackson TJ, Watson J, LaReau JM, Domb BG. Periacetabular osteotomy and arthroscopic labral repair after failed hip arthroscopy due to iatrogenic aggravation of hip dysplasia. Knee Surg Sports Traumatol Arthrosc. 2014;22(4):911-914.
6. Byrd JW, Jones KS. Hip arthroscopy in the presence of dysplasia. Arthroscopy. 2003;19(10):1055-1060.
7. Domb BG, Stake CE, Lindner D, El-Bitar Y, Jackson TJ. Arthroscopic capsular plication and labral preservation in borderline hip dysplasia: two-year clinical outcomes of a surgical approach to a challenging problem. Am J Sports Med. 2013;41(11):2591-2598.
8. Jayasekera N, Aprato A, Villar RN. Hip arthroscopy in the presence of acetabular dysplasia. Open Orthop J. 2015;9:185-187.
9. Fukui K, Briggs KK, Trindade CA, Philippon MJ. Outcomes after labral repair in patients with femoroacetabular impingement and borderline dysplasia. Arthroscopy. 2015;31(12):2371-2379.
10. Siebenrock KA, Leunig M, Ganz R. Periacetabular osteotomy: the Bernese experience. Instr Course Lect. 2001;50:239-245.
11. Garras DN, Crowder TT, Olson SA. Medium-term results of the Bernese periacetabular osteotomy in the treatment of symptomatic developmental dysplasia of the hip. J Bone Joint Surg Br. 2007;89(6):721-724.
12. Biedermann R, Donnan L, Gabriel A, Wachter R, Krismer M, Behensky H. Complications and patient satisfaction after periacetabular pelvic osteotomy. Int Orthop. 2008;32(5):611-617.
13. Ross JR, Zaltz I, Nepple JJ, Schoenecker PL, Clohisy JC. Arthroscopic disease classification and interventions as an adjunct in the treatment of acetabular dysplasia. Am J Sports Med. 2011;39(suppl):72S-78S.
14. Domb BG, LaReau JM, Baydoun H, Botser I, Millis MB, Yen YM. Is intraarticular pathology common in patients with hip dysplasia undergoing periacetabular osteotomy? Clin Orthop Relat Res. 2014;472(2):674-680.
15. Kain MS, Novais EN, Vallim C, Millis MB, Kim YJ. Periacetabular osteotomy after failed hip arthroscopy for labral tears in patients with acetabular dysplasia. J Bone Joint Surg Am. 2011;93(suppl 2):57-61.
16. Matsuda DK, Villamor A. The modified mid-anterior portal for hip arthroscopy. Arthrosc Tech. 2014;3(4):e469-e474.
17. Javed A, O’Donnell JM. Arthroscopic femoral osteochondroplasty for cam femoroacetabular impingement in patients over 60 years of age. J Bone Joint Surg Br. 2011;93(3):326-331.
18. Redmond JM, Gupta A, Cregar WM, Hammarstedt JE, Gui C, Domb BG. Arthroscopic treatment of labral tears in patients aged 60 years or older. Arthroscopy. 2015;31(10):1921-1927.
19. Mei-Dan O, McConkey MO, Brick M. Catastrophic failure of hip arthroscopy due to iatrogenic instability: can partial division of the ligamentum teres and iliofemoral ligament cause subluxation? Arthroscopy. 2012;28(3):440-445.
20. Benali Y, Katthagen BD. Hip subluxation as a complication of arthroscopic debridement. Arthroscopy. 2009;25(4):405-407.
21. Jayasekera N, Aprato A, Villar RN. Are crutches required after hip arthroscopy? A case–control study. Hip Int. 2013;23(3):269-273.
22. Domb BG, Stake CE, Finley ZJ, Chen T, Giordano BD. Influence of capsular repair versus unrepaired capsulotomy on 2-year clinical outcomes after arthroscopic hip preservation surgery. Arthroscopy. 2015;31(4):643-650.
23. Pereira F, Giles A, Wood G, Board TN. Recognition of minor adult hip dysplasia: which anatomical indices are important? Hip Int. 2014;24(2):175-179.
24. Murphy SB, Ganz R, Müller ME. The prognosis in untreated dysplasia of the hip. A study of radiographic factors that predict the outcome. J Bone Joint Surg Am. 1995;77(7):985-989.
25. Matsuda DK, Gupta N, Burchette R, Sehgal B. Arthroscopic surgery for global versus focal pincer femoroacetabular impingement: are the outcomes different? J Hip Preserv Surg. 2015;2(1):42-50.
1. Paliobeis CP, Villar RN. The prevalence of dysplasia in femoroacetabular impingement. Hip Int. 2011;21(2):141-145.
2. Clohisy JC, Nunley RM, Carlisle JC, Schoenecker PL. Incidence and characteristics of femoral deformities in the dysplastic hip. Clin Orthop Relat Res. 2009;467(1):128-134.
3. Parvizi J, Bican O, Bender B, et al. Arthroscopy for labral tears in patients with developmental dysplasia of the hip: a cautionary note. J Arthroplasty. 2009;24(6 suppl):110-113.
4. Matsuda DK, Khatod M. Rapidly progressive osteoarthritis after arthroscopic labral repair in patients with hip dysplasia. Arthroscopy. 2012;28(11):1738-1743.
5. Jackson TJ, Watson J, LaReau JM, Domb BG. Periacetabular osteotomy and arthroscopic labral repair after failed hip arthroscopy due to iatrogenic aggravation of hip dysplasia. Knee Surg Sports Traumatol Arthrosc. 2014;22(4):911-914.
6. Byrd JW, Jones KS. Hip arthroscopy in the presence of dysplasia. Arthroscopy. 2003;19(10):1055-1060.
7. Domb BG, Stake CE, Lindner D, El-Bitar Y, Jackson TJ. Arthroscopic capsular plication and labral preservation in borderline hip dysplasia: two-year clinical outcomes of a surgical approach to a challenging problem. Am J Sports Med. 2013;41(11):2591-2598.
8. Jayasekera N, Aprato A, Villar RN. Hip arthroscopy in the presence of acetabular dysplasia. Open Orthop J. 2015;9:185-187.
9. Fukui K, Briggs KK, Trindade CA, Philippon MJ. Outcomes after labral repair in patients with femoroacetabular impingement and borderline dysplasia. Arthroscopy. 2015;31(12):2371-2379.
10. Siebenrock KA, Leunig M, Ganz R. Periacetabular osteotomy: the Bernese experience. Instr Course Lect. 2001;50:239-245.
11. Garras DN, Crowder TT, Olson SA. Medium-term results of the Bernese periacetabular osteotomy in the treatment of symptomatic developmental dysplasia of the hip. J Bone Joint Surg Br. 2007;89(6):721-724.
12. Biedermann R, Donnan L, Gabriel A, Wachter R, Krismer M, Behensky H. Complications and patient satisfaction after periacetabular pelvic osteotomy. Int Orthop. 2008;32(5):611-617.
13. Ross JR, Zaltz I, Nepple JJ, Schoenecker PL, Clohisy JC. Arthroscopic disease classification and interventions as an adjunct in the treatment of acetabular dysplasia. Am J Sports Med. 2011;39(suppl):72S-78S.
14. Domb BG, LaReau JM, Baydoun H, Botser I, Millis MB, Yen YM. Is intraarticular pathology common in patients with hip dysplasia undergoing periacetabular osteotomy? Clin Orthop Relat Res. 2014;472(2):674-680.
15. Kain MS, Novais EN, Vallim C, Millis MB, Kim YJ. Periacetabular osteotomy after failed hip arthroscopy for labral tears in patients with acetabular dysplasia. J Bone Joint Surg Am. 2011;93(suppl 2):57-61.
16. Matsuda DK, Villamor A. The modified mid-anterior portal for hip arthroscopy. Arthrosc Tech. 2014;3(4):e469-e474.
17. Javed A, O’Donnell JM. Arthroscopic femoral osteochondroplasty for cam femoroacetabular impingement in patients over 60 years of age. J Bone Joint Surg Br. 2011;93(3):326-331.
18. Redmond JM, Gupta A, Cregar WM, Hammarstedt JE, Gui C, Domb BG. Arthroscopic treatment of labral tears in patients aged 60 years or older. Arthroscopy. 2015;31(10):1921-1927.
19. Mei-Dan O, McConkey MO, Brick M. Catastrophic failure of hip arthroscopy due to iatrogenic instability: can partial division of the ligamentum teres and iliofemoral ligament cause subluxation? Arthroscopy. 2012;28(3):440-445.
20. Benali Y, Katthagen BD. Hip subluxation as a complication of arthroscopic debridement. Arthroscopy. 2009;25(4):405-407.
21. Jayasekera N, Aprato A, Villar RN. Are crutches required after hip arthroscopy? A case–control study. Hip Int. 2013;23(3):269-273.
22. Domb BG, Stake CE, Finley ZJ, Chen T, Giordano BD. Influence of capsular repair versus unrepaired capsulotomy on 2-year clinical outcomes after arthroscopic hip preservation surgery. Arthroscopy. 2015;31(4):643-650.
23. Pereira F, Giles A, Wood G, Board TN. Recognition of minor adult hip dysplasia: which anatomical indices are important? Hip Int. 2014;24(2):175-179.
24. Murphy SB, Ganz R, Müller ME. The prognosis in untreated dysplasia of the hip. A study of radiographic factors that predict the outcome. J Bone Joint Surg Am. 1995;77(7):985-989.
25. Matsuda DK, Gupta N, Burchette R, Sehgal B. Arthroscopic surgery for global versus focal pincer femoroacetabular impingement: are the outcomes different? J Hip Preserv Surg. 2015;2(1):42-50.
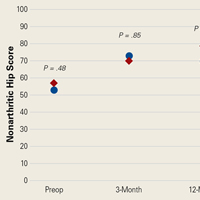
Metformin for acne
Acne is the most common skin condition, affecting up to 50 million individuals annually. Self-esteem is affected, and scarring can result if left untreated or inadequately treated. Although still somewhat controversial in some circles, available data have linked acne to dairy products, refined sugar ingestion, and high glycemic loads.
Acne has been linked to insulin levels and insulin-like growth factor (IGF-1). Glycemic loads are associated with both insulin and IGF-1. Metformin reduces glucose release from the liver while increasing glucose uptake in muscles and adipocytes.

So, can interventions that reduce glycemic load, such as diet and metformin, decrease the incidence of acne in patients among whom other standard interventions have been tried?
Gabriella Fabbrocini, MD, of the University of Naples, Italy, and her colleagues tested this hypothesis by conducting a randomized, clinical trial evaluating the impact of a low glycemic diet and metformin on acne (Clin Exp Dermatol. 2016 Jan;41[1]:38-42). Twenty males aged 17-24 years with acne for at least 1 year were randomized to either metformin 500 mg twice daily with a 1,500- to 2,000-kcal diet rich in fruits, vegetables, fish, and low carbohydrates with standard therapy; or standard therapy alone. Standard therapy consisted of a bland skin detergent and a sebostatic cream. Acne severity was rated by four observers.
Patients in the metformin group demonstrated a statistically significant improvement in acne severity, compared with patients in the standard care only group. No side effects were reported with metformin.
In this study, only patients with an “altered metabolic profile” were enrolled and randomized. An “altered metabolic profile” was defined as impaired fasting glucose, high total cholesterol or LDL, reduced HDL, and elevated waist circumference and body mass index. Results should be generalizable only to patients with these characteristics. The sample size in this study was small, but the included picture of acne resolution on one subject was indeed impressive.
For patients among whom traditional acne treatment approaches have not been effective, and knowing the tolerability and affordability of metformin, this may be a reasonable intervention.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author and do not necessarily represent the views and opinions of the Mayo Clinic. The opinions expressed in this article should not be used to diagnose or treat any medical condition, nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician. Dr. Ebbert has no relevant financial disclosures about this article.
Acne is the most common skin condition, affecting up to 50 million individuals annually. Self-esteem is affected, and scarring can result if left untreated or inadequately treated. Although still somewhat controversial in some circles, available data have linked acne to dairy products, refined sugar ingestion, and high glycemic loads.
Acne has been linked to insulin levels and insulin-like growth factor (IGF-1). Glycemic loads are associated with both insulin and IGF-1. Metformin reduces glucose release from the liver while increasing glucose uptake in muscles and adipocytes.
So, can interventions that reduce glycemic load, such as diet and metformin, decrease the incidence of acne in patients among whom other standard interventions have been tried?
Gabriella Fabbrocini, MD, of the University of Naples, Italy, and her colleagues tested this hypothesis by conducting a randomized, clinical trial evaluating the impact of a low glycemic diet and metformin on acne (Clin Exp Dermatol. 2016 Jan;41[1]:38-42). Twenty males aged 17-24 years with acne for at least 1 year were randomized to either metformin 500 mg twice daily with a 1,500- to 2,000-kcal diet rich in fruits, vegetables, fish, and low carbohydrates with standard therapy; or standard therapy alone. Standard therapy consisted of a bland skin detergent and a sebostatic cream. Acne severity was rated by four observers.
Patients in the metformin group demonstrated a statistically significant improvement in acne severity, compared with patients in the standard care only group. No side effects were reported with metformin.
In this study, only patients with an “altered metabolic profile” were enrolled and randomized. An “altered metabolic profile” was defined as impaired fasting glucose, high total cholesterol or LDL, reduced HDL, and elevated waist circumference and body mass index. Results should be generalizable only to patients with these characteristics. The sample size in this study was small, but the included picture of acne resolution on one subject was indeed impressive.
For patients among whom traditional acne treatment approaches have not been effective, and knowing the tolerability and affordability of metformin, this may be a reasonable intervention.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author and do not necessarily represent the views and opinions of the Mayo Clinic. The opinions expressed in this article should not be used to diagnose or treat any medical condition, nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician. Dr. Ebbert has no relevant financial disclosures about this article.
Acne is the most common skin condition, affecting up to 50 million individuals annually. Self-esteem is affected, and scarring can result if left untreated or inadequately treated. Although still somewhat controversial in some circles, available data have linked acne to dairy products, refined sugar ingestion, and high glycemic loads.
Acne has been linked to insulin levels and insulin-like growth factor (IGF-1). Glycemic loads are associated with both insulin and IGF-1. Metformin reduces glucose release from the liver while increasing glucose uptake in muscles and adipocytes.
So, can interventions that reduce glycemic load, such as diet and metformin, decrease the incidence of acne in patients among whom other standard interventions have been tried?
Gabriella Fabbrocini, MD, of the University of Naples, Italy, and her colleagues tested this hypothesis by conducting a randomized, clinical trial evaluating the impact of a low glycemic diet and metformin on acne (Clin Exp Dermatol. 2016 Jan;41[1]:38-42). Twenty males aged 17-24 years with acne for at least 1 year were randomized to either metformin 500 mg twice daily with a 1,500- to 2,000-kcal diet rich in fruits, vegetables, fish, and low carbohydrates with standard therapy; or standard therapy alone. Standard therapy consisted of a bland skin detergent and a sebostatic cream. Acne severity was rated by four observers.
Patients in the metformin group demonstrated a statistically significant improvement in acne severity, compared with patients in the standard care only group. No side effects were reported with metformin.
In this study, only patients with an “altered metabolic profile” were enrolled and randomized. An “altered metabolic profile” was defined as impaired fasting glucose, high total cholesterol or LDL, reduced HDL, and elevated waist circumference and body mass index. Results should be generalizable only to patients with these characteristics. The sample size in this study was small, but the included picture of acne resolution on one subject was indeed impressive.
For patients among whom traditional acne treatment approaches have not been effective, and knowing the tolerability and affordability of metformin, this may be a reasonable intervention.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author and do not necessarily represent the views and opinions of the Mayo Clinic. The opinions expressed in this article should not be used to diagnose or treat any medical condition, nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician. Dr. Ebbert has no relevant financial disclosures about this article.
Stroke rates high when catheter ablation of AF fails
ORLANDO – In patients with atrial fibrillation (AF) who fail to achieve rhythm control after catheter ablation, the risk of ischemic stroke may approach 30% over 5 or more years of follow-up, despite optimized anticoagulation therapy, according to data from 1,002 consecutive patients presented at the annual International AF Symposium.
“The risk of stroke is high among patients after unsuccessful catheter ablation,” confirmed Mihran Martirosyan, MD, Erasmus Medical Center, Rotterdam, the Netherlands. He asserted that this is the first study to investigate long-term clinical outcomes of AF patients with unsuccessful rhythm control following repeated catheter ablation.
The retrospective analysis was conducted in 1,002 patients who underwent catheter ablation after failing pharmacologic treatment of AF. Of these, 169 (17%) failed the ablation, but the focus of this study was on the subgroup of 67 catheter ablation treatment failures that have been followed for at least 5 years. All had been maintained on anticoagulation therapy.
Within this group, 18 (27%) had an ischemic stroke over the course of follow-up. The average time to stroke after the first ablation procedure was 3.9 years.
Prior to being declared catheter ablation failures, the average number of ablation procedures in this long-term follow-up group was 1.7. In 55.2% of patients, the first ablation was performed with a cryoballoon. The remaining first ablations were delivered with radiofrequency. For a second or third ablation, the same techniques were commonly repeated, but 25% received a cavotricuspid isthmus ablation, and 12% underwent a VATS-Maze procedure.
There were no deaths in this series, in which the average patient age was 66 years. The average duration of AF was 12 years, the mean left atrial size was 45 mm, and the average left ventricular ejection fraction was 55%.
In this study, catheter ablation failure was defined as inability to regain rhythm control despite repeated ablation procedures. However, many patients who initially achieve rhythm control after catheter ablation have recurrence of AF over time. It is unclear whether patients who initially achieve but then lose rhythm control face the same high risk for stroke as seen in the Dutch series if followed long-term.
One study suggests that they may not. In 631 consecutive patients who underwent a mean 1.5 catheter ablations before achieving rhythm control, 34% had an AF recurrence at 1 year (Europace 2014 Oct 21;17[3]:403-8). When followed for a mean 4.1 years of additional follow-up (5.1 years from the initial ablation), only 10% had a serious adverse event, such as heart failure or hemorrhage, and only 2% had a cerebrovascular event.
Numerous clinical studies have shown that catheter ablation is more effective than pharmacologic therapy for both regaining rhythm control in AF patients and reducing symptoms, according to Dr. Martirosyan, but these long-term follow-up data confirm that the risk of thromboembolic complications remains high in those who fail the initial catheter ablation. Of the 18 strokes, only 4 occurred in the first year of follow-up. The remaining strokes accrued slowly over time. Strokes were recorded up until 10 years after the ablation, the longest period that any patient was followed.
Dr. Martirosyan reports no relevant financial relationships.
ORLANDO – In patients with atrial fibrillation (AF) who fail to achieve rhythm control after catheter ablation, the risk of ischemic stroke may approach 30% over 5 or more years of follow-up, despite optimized anticoagulation therapy, according to data from 1,002 consecutive patients presented at the annual International AF Symposium.
“The risk of stroke is high among patients after unsuccessful catheter ablation,” confirmed Mihran Martirosyan, MD, Erasmus Medical Center, Rotterdam, the Netherlands. He asserted that this is the first study to investigate long-term clinical outcomes of AF patients with unsuccessful rhythm control following repeated catheter ablation.
The retrospective analysis was conducted in 1,002 patients who underwent catheter ablation after failing pharmacologic treatment of AF. Of these, 169 (17%) failed the ablation, but the focus of this study was on the subgroup of 67 catheter ablation treatment failures that have been followed for at least 5 years. All had been maintained on anticoagulation therapy.
Within this group, 18 (27%) had an ischemic stroke over the course of follow-up. The average time to stroke after the first ablation procedure was 3.9 years.
Prior to being declared catheter ablation failures, the average number of ablation procedures in this long-term follow-up group was 1.7. In 55.2% of patients, the first ablation was performed with a cryoballoon. The remaining first ablations were delivered with radiofrequency. For a second or third ablation, the same techniques were commonly repeated, but 25% received a cavotricuspid isthmus ablation, and 12% underwent a VATS-Maze procedure.
There were no deaths in this series, in which the average patient age was 66 years. The average duration of AF was 12 years, the mean left atrial size was 45 mm, and the average left ventricular ejection fraction was 55%.
In this study, catheter ablation failure was defined as inability to regain rhythm control despite repeated ablation procedures. However, many patients who initially achieve rhythm control after catheter ablation have recurrence of AF over time. It is unclear whether patients who initially achieve but then lose rhythm control face the same high risk for stroke as seen in the Dutch series if followed long-term.
One study suggests that they may not. In 631 consecutive patients who underwent a mean 1.5 catheter ablations before achieving rhythm control, 34% had an AF recurrence at 1 year (Europace 2014 Oct 21;17[3]:403-8). When followed for a mean 4.1 years of additional follow-up (5.1 years from the initial ablation), only 10% had a serious adverse event, such as heart failure or hemorrhage, and only 2% had a cerebrovascular event.
Numerous clinical studies have shown that catheter ablation is more effective than pharmacologic therapy for both regaining rhythm control in AF patients and reducing symptoms, according to Dr. Martirosyan, but these long-term follow-up data confirm that the risk of thromboembolic complications remains high in those who fail the initial catheter ablation. Of the 18 strokes, only 4 occurred in the first year of follow-up. The remaining strokes accrued slowly over time. Strokes were recorded up until 10 years after the ablation, the longest period that any patient was followed.
Dr. Martirosyan reports no relevant financial relationships.
ORLANDO – In patients with atrial fibrillation (AF) who fail to achieve rhythm control after catheter ablation, the risk of ischemic stroke may approach 30% over 5 or more years of follow-up, despite optimized anticoagulation therapy, according to data from 1,002 consecutive patients presented at the annual International AF Symposium.
“The risk of stroke is high among patients after unsuccessful catheter ablation,” confirmed Mihran Martirosyan, MD, Erasmus Medical Center, Rotterdam, the Netherlands. He asserted that this is the first study to investigate long-term clinical outcomes of AF patients with unsuccessful rhythm control following repeated catheter ablation.
The retrospective analysis was conducted in 1,002 patients who underwent catheter ablation after failing pharmacologic treatment of AF. Of these, 169 (17%) failed the ablation, but the focus of this study was on the subgroup of 67 catheter ablation treatment failures that have been followed for at least 5 years. All had been maintained on anticoagulation therapy.
Within this group, 18 (27%) had an ischemic stroke over the course of follow-up. The average time to stroke after the first ablation procedure was 3.9 years.
Prior to being declared catheter ablation failures, the average number of ablation procedures in this long-term follow-up group was 1.7. In 55.2% of patients, the first ablation was performed with a cryoballoon. The remaining first ablations were delivered with radiofrequency. For a second or third ablation, the same techniques were commonly repeated, but 25% received a cavotricuspid isthmus ablation, and 12% underwent a VATS-Maze procedure.
There were no deaths in this series, in which the average patient age was 66 years. The average duration of AF was 12 years, the mean left atrial size was 45 mm, and the average left ventricular ejection fraction was 55%.
In this study, catheter ablation failure was defined as inability to regain rhythm control despite repeated ablation procedures. However, many patients who initially achieve rhythm control after catheter ablation have recurrence of AF over time. It is unclear whether patients who initially achieve but then lose rhythm control face the same high risk for stroke as seen in the Dutch series if followed long-term.
One study suggests that they may not. In 631 consecutive patients who underwent a mean 1.5 catheter ablations before achieving rhythm control, 34% had an AF recurrence at 1 year (Europace 2014 Oct 21;17[3]:403-8). When followed for a mean 4.1 years of additional follow-up (5.1 years from the initial ablation), only 10% had a serious adverse event, such as heart failure or hemorrhage, and only 2% had a cerebrovascular event.
Numerous clinical studies have shown that catheter ablation is more effective than pharmacologic therapy for both regaining rhythm control in AF patients and reducing symptoms, according to Dr. Martirosyan, but these long-term follow-up data confirm that the risk of thromboembolic complications remains high in those who fail the initial catheter ablation. Of the 18 strokes, only 4 occurred in the first year of follow-up. The remaining strokes accrued slowly over time. Strokes were recorded up until 10 years after the ablation, the longest period that any patient was followed.
Dr. Martirosyan reports no relevant financial relationships.
AT THE AF SYMPOSIUM 2017
Key clinical point: If catheter ablation of atrial fibrillation fails, stroke rates are high despite optimized anticoagulation therapy.
Major finding: In a median follow-up of up to 5 years after ablation, 27% of patients had an ischemic stroke.
Data source: Retrospective analysis.
Disclosures: Dr. Martirosyan reports no relevant financial relationships.
Strokes cut by extended NOAC prophylaxis in hospitalized, medically ill patients
NEW ORLEANS – Thromboprophylaxis for 35-42 days with the new oral anticoagulant betrixaban led to a significant reduction in all-cause and ischemic strokes in medically ill patients who required hospitalization as compared with conventional prophylaxis for 10 days, based on a post-hoc analysis of data from a randomized trial with more than 7,500 patients.
But the trial’s unusual design left it unclear whether the incremental benefit seen from prolonged prophylaxis with a NOAC resulted primarily from a longer period of treatment, the drug used, or both.

The safety analysis showed that prolonged treatment with betrixaban roughly doubled the rate of major or clinically relevant nonmajor bleeding events during the period of treatment and for the first 7 days after treatment stopped. The incidence of these bleeds was 1.6% among control patients on 10 days of enoxaparin treatment and 3.1% among patients who received extended treatment with betrixaban, a statistically significant difference. The rates of fatal bleeds and intracranial hemorrhages in the two study groups did not significantly differ.
The data Dr. Gibson reported came from the Multicenter, Randomized, Active-Controlled Efficacy And Safety Study Comparing Extended Duration Betrixaban With Standard Of Care Enoxaparin For The Prevention Of Venous Thromboembolism In Acute Medically Ill Patients (APEX). The study’s primary aim was testing in 7,513 hospitalized medically ill patients the safety and efficacy of prolonged prophylaxis with the oral, factor Xa inhibitor betrixaban, compared with 10 days of prophylaxis with the low molecular weight heparin enoxaparin. The primary endpoint was the rate of venous thromboembolic events and deaths from venous thromboembolism (VTE) out to 47 days after the start of treatment.
APEX enrolled patients hospitalized for acute decompensated heart failure, chronic respiratory failure, acute infection without septic shock, acute rheumatic disorders or acute ischemic stroke. All enrolled patients had to be expected to be immobilized for at least 24 hours following randomization and to be hospitalized for at least 3 days. Patients also had to have an additional risk marker for high thrombotic risk: They had to be at least 75 years old, or 60-74 years old with a D-dimer level at least twice the upper limit of normal, or 40-59 years old with a D-dimer level at least twice the upper limit of normal and a history of either VTE or cancer.
Results for the primary endpoint, reported in 2016, showed that prolonged betrixaban prophylaxis linked with an absolute 1.6% reduction in the combined endpoint, which resulted in a 19% relative risk reduction that fell just short of the trial’s prespecified definition of statistical significance. The study’s primary safety endpoint was the occurrence of major bleeding events through 7 days after the stop of treatment, which occurred in 0.7% of the betrixaban patients and in 0.6% of those on enoxaparin (N Engl J Med. 2016 Aug 11;375[6]:534-44).
Even thought the primary results from this pivotal trial failed to meet the prespecified threshold for statistical significance, the company developing betrixaban, Portola, submitted an application to the Food and Drug Administration to approve marketing of extended-duration betrixaban for VTE prophylaxis in acute medically-ill patients with VTE risk factors. In December 2016, Portola announced that the FDA had given the application priority status for a decision.
The post-hoc analysis that Dr. Gibson presented at the meeting looked at the impact of betrixaban compared with enoxaparin on the incidence of all-cause and ischemic stroke during 77 days of follow-up after the start of treatment in the 7,432 patients who received at least one dose of their assigned drug, two endpoints that weren’t even secondary outcomes in APEX’s original design.
Among the 3,716 treated with betrixaban, the all-cause stroke incidence was 0.54%; among the 3,716 patients treated with enoxaparin, the all-cause stroke incidence was 0.97%. The 56% relative risk reduction was statistically significant. The incidence of ischemic strokes was 0.48% with betrixaban and 0.91% with enoxaparin, a 53% relative risk reduction that was also statistically significant.
The post-hoc analysis also looked specifically at the comparison between betrixaban and enoxaparin for stroke prevention in a subgroup of patients who had the highest stroke rate, the patients who were hospitalized because of an index stroke or an index heart failure episode. In this high-risk subgroup, prophylaxis with betrixaban cut the all-cause stroke rate compared with enoxaparin by 49% and the ischemic stroke rate by 45%, both statistically significant effects. When the high-risk subgroup also included patients hospitalized for an index episode of atrial fibrillation, betrixaban cut the rate of all-cause strokes by a relative 48% and ischemic strokes by a relative 44%.
Concurrently with Dr. Gibson’s report at the meeting, the results also appeared online (Circulation. 2016 Nov 14. doi: 10.1161/CIRCULATIONAHA.116.025427).
APEX was sponsored by Portola, the company developing betrixaban. Dr. Gibson has been a consultant to Eli Lilly, Gilead, The Medicines Company, Novo Nordisk, Pfizer, and St. Jude. He has received research support from Portola and several other companies.
[email protected]
On Twitter @mitchelzoler
The APEX study identified a group of patients hospitalized for medical reasons who were at high risk for both venous thromboembolism and for stroke. We are comfortable with the concept of thromboprophylaxis for hospitalized patients who are at high risk for venous thromboembolism, but we have generally not paid attention to prophylaxis against stroke during and immediately after hospitalization.
The results suggest that extending thromboprophylaxis beyond the standard period of 10 days may be a good idea. Because patients in the two treatment arms of the study differed in both the drugs they received and in the duration of prophylaxis, the results cannot distinguish which of these two variables was more important. Treating patients with enoxaparin for 35-42 days may provide a similar benefit to what was seen with extended-duration betrixaban.

The findings are a wake-up call to the high thromboembolic risk faced by the types of patients enrolled in APEX, and they point to a new way to manage these patients. Guidelines already call for putting high-risk patients, such as those with heart failure, on anticoagulant prophylaxis if they have no contraindications. These new data suggest that thromboprophylaxis in appropriate patients should extend beyond 10 days and beyond acute hospitalization.
Steven R. Lentz, MD, is a professor of medicine and a hematologist oncologist at the University of Iowa in Iowa City. He has been a consultant to Novo Nordisk and Opko, has an ownership interest in Celgene, and has received research grants from Novo Nordisk. He made these comments in an interview.
The APEX study identified a group of patients hospitalized for medical reasons who were at high risk for both venous thromboembolism and for stroke. We are comfortable with the concept of thromboprophylaxis for hospitalized patients who are at high risk for venous thromboembolism, but we have generally not paid attention to prophylaxis against stroke during and immediately after hospitalization.
The results suggest that extending thromboprophylaxis beyond the standard period of 10 days may be a good idea. Because patients in the two treatment arms of the study differed in both the drugs they received and in the duration of prophylaxis, the results cannot distinguish which of these two variables was more important. Treating patients with enoxaparin for 35-42 days may provide a similar benefit to what was seen with extended-duration betrixaban.
The findings are a wake-up call to the high thromboembolic risk faced by the types of patients enrolled in APEX, and they point to a new way to manage these patients. Guidelines already call for putting high-risk patients, such as those with heart failure, on anticoagulant prophylaxis if they have no contraindications. These new data suggest that thromboprophylaxis in appropriate patients should extend beyond 10 days and beyond acute hospitalization.
Steven R. Lentz, MD, is a professor of medicine and a hematologist oncologist at the University of Iowa in Iowa City. He has been a consultant to Novo Nordisk and Opko, has an ownership interest in Celgene, and has received research grants from Novo Nordisk. He made these comments in an interview.
The APEX study identified a group of patients hospitalized for medical reasons who were at high risk for both venous thromboembolism and for stroke. We are comfortable with the concept of thromboprophylaxis for hospitalized patients who are at high risk for venous thromboembolism, but we have generally not paid attention to prophylaxis against stroke during and immediately after hospitalization.
The results suggest that extending thromboprophylaxis beyond the standard period of 10 days may be a good idea. Because patients in the two treatment arms of the study differed in both the drugs they received and in the duration of prophylaxis, the results cannot distinguish which of these two variables was more important. Treating patients with enoxaparin for 35-42 days may provide a similar benefit to what was seen with extended-duration betrixaban.
The findings are a wake-up call to the high thromboembolic risk faced by the types of patients enrolled in APEX, and they point to a new way to manage these patients. Guidelines already call for putting high-risk patients, such as those with heart failure, on anticoagulant prophylaxis if they have no contraindications. These new data suggest that thromboprophylaxis in appropriate patients should extend beyond 10 days and beyond acute hospitalization.
Steven R. Lentz, MD, is a professor of medicine and a hematologist oncologist at the University of Iowa in Iowa City. He has been a consultant to Novo Nordisk and Opko, has an ownership interest in Celgene, and has received research grants from Novo Nordisk. He made these comments in an interview.
NEW ORLEANS – Thromboprophylaxis for 35-42 days with the new oral anticoagulant betrixaban led to a significant reduction in all-cause and ischemic strokes in medically ill patients who required hospitalization as compared with conventional prophylaxis for 10 days, based on a post-hoc analysis of data from a randomized trial with more than 7,500 patients.
But the trial’s unusual design left it unclear whether the incremental benefit seen from prolonged prophylaxis with a NOAC resulted primarily from a longer period of treatment, the drug used, or both.
The safety analysis showed that prolonged treatment with betrixaban roughly doubled the rate of major or clinically relevant nonmajor bleeding events during the period of treatment and for the first 7 days after treatment stopped. The incidence of these bleeds was 1.6% among control patients on 10 days of enoxaparin treatment and 3.1% among patients who received extended treatment with betrixaban, a statistically significant difference. The rates of fatal bleeds and intracranial hemorrhages in the two study groups did not significantly differ.
The data Dr. Gibson reported came from the Multicenter, Randomized, Active-Controlled Efficacy And Safety Study Comparing Extended Duration Betrixaban With Standard Of Care Enoxaparin For The Prevention Of Venous Thromboembolism In Acute Medically Ill Patients (APEX). The study’s primary aim was testing in 7,513 hospitalized medically ill patients the safety and efficacy of prolonged prophylaxis with the oral, factor Xa inhibitor betrixaban, compared with 10 days of prophylaxis with the low molecular weight heparin enoxaparin. The primary endpoint was the rate of venous thromboembolic events and deaths from venous thromboembolism (VTE) out to 47 days after the start of treatment.
APEX enrolled patients hospitalized for acute decompensated heart failure, chronic respiratory failure, acute infection without septic shock, acute rheumatic disorders or acute ischemic stroke. All enrolled patients had to be expected to be immobilized for at least 24 hours following randomization and to be hospitalized for at least 3 days. Patients also had to have an additional risk marker for high thrombotic risk: They had to be at least 75 years old, or 60-74 years old with a D-dimer level at least twice the upper limit of normal, or 40-59 years old with a D-dimer level at least twice the upper limit of normal and a history of either VTE or cancer.
Results for the primary endpoint, reported in 2016, showed that prolonged betrixaban prophylaxis linked with an absolute 1.6% reduction in the combined endpoint, which resulted in a 19% relative risk reduction that fell just short of the trial’s prespecified definition of statistical significance. The study’s primary safety endpoint was the occurrence of major bleeding events through 7 days after the stop of treatment, which occurred in 0.7% of the betrixaban patients and in 0.6% of those on enoxaparin (N Engl J Med. 2016 Aug 11;375[6]:534-44).
Even thought the primary results from this pivotal trial failed to meet the prespecified threshold for statistical significance, the company developing betrixaban, Portola, submitted an application to the Food and Drug Administration to approve marketing of extended-duration betrixaban for VTE prophylaxis in acute medically-ill patients with VTE risk factors. In December 2016, Portola announced that the FDA had given the application priority status for a decision.
The post-hoc analysis that Dr. Gibson presented at the meeting looked at the impact of betrixaban compared with enoxaparin on the incidence of all-cause and ischemic stroke during 77 days of follow-up after the start of treatment in the 7,432 patients who received at least one dose of their assigned drug, two endpoints that weren’t even secondary outcomes in APEX’s original design.
Among the 3,716 treated with betrixaban, the all-cause stroke incidence was 0.54%; among the 3,716 patients treated with enoxaparin, the all-cause stroke incidence was 0.97%. The 56% relative risk reduction was statistically significant. The incidence of ischemic strokes was 0.48% with betrixaban and 0.91% with enoxaparin, a 53% relative risk reduction that was also statistically significant.
The post-hoc analysis also looked specifically at the comparison between betrixaban and enoxaparin for stroke prevention in a subgroup of patients who had the highest stroke rate, the patients who were hospitalized because of an index stroke or an index heart failure episode. In this high-risk subgroup, prophylaxis with betrixaban cut the all-cause stroke rate compared with enoxaparin by 49% and the ischemic stroke rate by 45%, both statistically significant effects. When the high-risk subgroup also included patients hospitalized for an index episode of atrial fibrillation, betrixaban cut the rate of all-cause strokes by a relative 48% and ischemic strokes by a relative 44%.
Concurrently with Dr. Gibson’s report at the meeting, the results also appeared online (Circulation. 2016 Nov 14. doi: 10.1161/CIRCULATIONAHA.116.025427).
APEX was sponsored by Portola, the company developing betrixaban. Dr. Gibson has been a consultant to Eli Lilly, Gilead, The Medicines Company, Novo Nordisk, Pfizer, and St. Jude. He has received research support from Portola and several other companies.
[email protected]
On Twitter @mitchelzoler
NEW ORLEANS – Thromboprophylaxis for 35-42 days with the new oral anticoagulant betrixaban led to a significant reduction in all-cause and ischemic strokes in medically ill patients who required hospitalization as compared with conventional prophylaxis for 10 days, based on a post-hoc analysis of data from a randomized trial with more than 7,500 patients.
But the trial’s unusual design left it unclear whether the incremental benefit seen from prolonged prophylaxis with a NOAC resulted primarily from a longer period of treatment, the drug used, or both.
The safety analysis showed that prolonged treatment with betrixaban roughly doubled the rate of major or clinically relevant nonmajor bleeding events during the period of treatment and for the first 7 days after treatment stopped. The incidence of these bleeds was 1.6% among control patients on 10 days of enoxaparin treatment and 3.1% among patients who received extended treatment with betrixaban, a statistically significant difference. The rates of fatal bleeds and intracranial hemorrhages in the two study groups did not significantly differ.
The data Dr. Gibson reported came from the Multicenter, Randomized, Active-Controlled Efficacy And Safety Study Comparing Extended Duration Betrixaban With Standard Of Care Enoxaparin For The Prevention Of Venous Thromboembolism In Acute Medically Ill Patients (APEX). The study’s primary aim was testing in 7,513 hospitalized medically ill patients the safety and efficacy of prolonged prophylaxis with the oral, factor Xa inhibitor betrixaban, compared with 10 days of prophylaxis with the low molecular weight heparin enoxaparin. The primary endpoint was the rate of venous thromboembolic events and deaths from venous thromboembolism (VTE) out to 47 days after the start of treatment.
APEX enrolled patients hospitalized for acute decompensated heart failure, chronic respiratory failure, acute infection without septic shock, acute rheumatic disorders or acute ischemic stroke. All enrolled patients had to be expected to be immobilized for at least 24 hours following randomization and to be hospitalized for at least 3 days. Patients also had to have an additional risk marker for high thrombotic risk: They had to be at least 75 years old, or 60-74 years old with a D-dimer level at least twice the upper limit of normal, or 40-59 years old with a D-dimer level at least twice the upper limit of normal and a history of either VTE or cancer.
Results for the primary endpoint, reported in 2016, showed that prolonged betrixaban prophylaxis linked with an absolute 1.6% reduction in the combined endpoint, which resulted in a 19% relative risk reduction that fell just short of the trial’s prespecified definition of statistical significance. The study’s primary safety endpoint was the occurrence of major bleeding events through 7 days after the stop of treatment, which occurred in 0.7% of the betrixaban patients and in 0.6% of those on enoxaparin (N Engl J Med. 2016 Aug 11;375[6]:534-44).
Even thought the primary results from this pivotal trial failed to meet the prespecified threshold for statistical significance, the company developing betrixaban, Portola, submitted an application to the Food and Drug Administration to approve marketing of extended-duration betrixaban for VTE prophylaxis in acute medically-ill patients with VTE risk factors. In December 2016, Portola announced that the FDA had given the application priority status for a decision.
The post-hoc analysis that Dr. Gibson presented at the meeting looked at the impact of betrixaban compared with enoxaparin on the incidence of all-cause and ischemic stroke during 77 days of follow-up after the start of treatment in the 7,432 patients who received at least one dose of their assigned drug, two endpoints that weren’t even secondary outcomes in APEX’s original design.
Among the 3,716 treated with betrixaban, the all-cause stroke incidence was 0.54%; among the 3,716 patients treated with enoxaparin, the all-cause stroke incidence was 0.97%. The 56% relative risk reduction was statistically significant. The incidence of ischemic strokes was 0.48% with betrixaban and 0.91% with enoxaparin, a 53% relative risk reduction that was also statistically significant.
The post-hoc analysis also looked specifically at the comparison between betrixaban and enoxaparin for stroke prevention in a subgroup of patients who had the highest stroke rate, the patients who were hospitalized because of an index stroke or an index heart failure episode. In this high-risk subgroup, prophylaxis with betrixaban cut the all-cause stroke rate compared with enoxaparin by 49% and the ischemic stroke rate by 45%, both statistically significant effects. When the high-risk subgroup also included patients hospitalized for an index episode of atrial fibrillation, betrixaban cut the rate of all-cause strokes by a relative 48% and ischemic strokes by a relative 44%.
Concurrently with Dr. Gibson’s report at the meeting, the results also appeared online (Circulation. 2016 Nov 14. doi: 10.1161/CIRCULATIONAHA.116.025427).
APEX was sponsored by Portola, the company developing betrixaban. Dr. Gibson has been a consultant to Eli Lilly, Gilead, The Medicines Company, Novo Nordisk, Pfizer, and St. Jude. He has received research support from Portola and several other companies.
[email protected]
On Twitter @mitchelzoler
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: Strokes occurred in 0.54% of patients on extended-duration betrixaban prophylaxis and in 0.97% of patients on standard-duration enoxaparin.
Data source: APEX, a multicenter randomized trial with 7,513 patients.
Disclosures: APEX was sponsored by Portola, the company developing betrixaban. Dr. Gibson has been a consultant to Eli Lilly, Gilead, The Medicines Company, Novo Nordisk, Pfizer and St. Jude. He has received research support from Portola and several other companies.