User login
Even ‘Just a Few’ Cigarettes Have Long-Term Consequences
“There is no safe level of smoking”—that’s the conclusion of National Cancer Institute researchers, based on data from 290,215 adults in the 2004-2005 NIH-AARP Diet and Health Study. “[S]moking even a small number of cigarettes per day has substantial negative health effects,” said Maki Inoue-Choi, PhD, lead author.
The participants responded to a questionnaire that assessed lifetime smoking intensity. Those who smoked between 1 and 10 cigarettes a day had an 87% higher risk of earlier death. But even people who smoked an average of < 1 cigarette per day over their lifetime still had a 64% higher risk of earlier death, compared with never-smokers.
The researchers also looked at specific causes of death. Not surprisingly, they found a “particularly strong” association for lung cancer mortality. But again, even people who consistently averaged < 1 cigarette per day over their lifetime had 9 times the risk of dying from lung cancer than never-smokers. Among those who smoked between 1 and 10 cigarettes a day, the risk of dying from lung cancer was nearly 12 times higher.
People who smoked between 1 and 10 cigarettes a day also had > 6 times the risk of dying from respiratory disease and about 1 and a half times the risk of dying of cardiovascular disease, compared with never-smokers.
The younger people were when they quit smoking, the lower their risk of early death.
“There is no safe level of smoking”—that’s the conclusion of National Cancer Institute researchers, based on data from 290,215 adults in the 2004-2005 NIH-AARP Diet and Health Study. “[S]moking even a small number of cigarettes per day has substantial negative health effects,” said Maki Inoue-Choi, PhD, lead author.
The participants responded to a questionnaire that assessed lifetime smoking intensity. Those who smoked between 1 and 10 cigarettes a day had an 87% higher risk of earlier death. But even people who smoked an average of < 1 cigarette per day over their lifetime still had a 64% higher risk of earlier death, compared with never-smokers.
The researchers also looked at specific causes of death. Not surprisingly, they found a “particularly strong” association for lung cancer mortality. But again, even people who consistently averaged < 1 cigarette per day over their lifetime had 9 times the risk of dying from lung cancer than never-smokers. Among those who smoked between 1 and 10 cigarettes a day, the risk of dying from lung cancer was nearly 12 times higher.
People who smoked between 1 and 10 cigarettes a day also had > 6 times the risk of dying from respiratory disease and about 1 and a half times the risk of dying of cardiovascular disease, compared with never-smokers.
The younger people were when they quit smoking, the lower their risk of early death.
“There is no safe level of smoking”—that’s the conclusion of National Cancer Institute researchers, based on data from 290,215 adults in the 2004-2005 NIH-AARP Diet and Health Study. “[S]moking even a small number of cigarettes per day has substantial negative health effects,” said Maki Inoue-Choi, PhD, lead author.
The participants responded to a questionnaire that assessed lifetime smoking intensity. Those who smoked between 1 and 10 cigarettes a day had an 87% higher risk of earlier death. But even people who smoked an average of < 1 cigarette per day over their lifetime still had a 64% higher risk of earlier death, compared with never-smokers.
The researchers also looked at specific causes of death. Not surprisingly, they found a “particularly strong” association for lung cancer mortality. But again, even people who consistently averaged < 1 cigarette per day over their lifetime had 9 times the risk of dying from lung cancer than never-smokers. Among those who smoked between 1 and 10 cigarettes a day, the risk of dying from lung cancer was nearly 12 times higher.
People who smoked between 1 and 10 cigarettes a day also had > 6 times the risk of dying from respiratory disease and about 1 and a half times the risk of dying of cardiovascular disease, compared with never-smokers.
The younger people were when they quit smoking, the lower their risk of early death.
Targeting disease stem cells in AML, MDS

Image by Robert Paulson
The cell surface molecule CD99 occurs more frequently than normal on stem cells responsible for acute myeloid leukemia (AML) and myelodysplastic syndromes (MDS), according to research published in Science Translational Medicine.
Building on this discovery, researchers designed anti-CD99 monoclonal antibodies (mAbs).
In vitro and in vivo experiments
showed that these mAbs can recognize
and destroy AML and MDS stem/progenitor cells.
“Our findings not only identify a new molecule expressed on stem cells that drive these human malignancies, but we show that antibodies against this target can directly kill human AML stem cells,” said study author Christopher Y. Park, MD, PhD, of NYU Langone Medical Center in New York, New York.
“While we still have important details to work out, CD99 is likely to be an exploitable therapeutic target for most AML and MDS patients, and we are working urgently to finalize a therapy for human testing.”
Dr Park and his colleagues first examined stem cell populations from 79 patients with AML and 24 with MDS. More than 80% of stem cells in both groups expressed high levels of CD99.
The levels were so high that leukemia stem cells could be cleanly separated from normal hematopoietic stem cells in AML samples.
Upon confirming that CD99 was abundant on AML and MDS stem cells, the researchers made several anti-CD99 mAbs and tested them in vitro and in mouse models.
The mAbs destroyed AML and MDS stem cells by causing a sudden spike in the activity of SRC family kinases—a group of proteins that are implicated in invasion, tumor progression, and metastasis in a variety of cancers.
However, the mAbs had minimal effects on normal hematopoietic stem cells.
“With the appropriate support, we believe we can rapidly determine the best antibodies for use in patients, produce them at the quality needed to verify our results, and apply for permission to begin clinical trials,” Dr Park said. ![]()
Image by Robert Paulson
The cell surface molecule CD99 occurs more frequently than normal on stem cells responsible for acute myeloid leukemia (AML) and myelodysplastic syndromes (MDS), according to research published in Science Translational Medicine.
Building on this discovery, researchers designed anti-CD99 monoclonal antibodies (mAbs).
In vitro and in vivo experiments
showed that these mAbs can recognize
and destroy AML and MDS stem/progenitor cells.
“Our findings not only identify a new molecule expressed on stem cells that drive these human malignancies, but we show that antibodies against this target can directly kill human AML stem cells,” said study author Christopher Y. Park, MD, PhD, of NYU Langone Medical Center in New York, New York.
“While we still have important details to work out, CD99 is likely to be an exploitable therapeutic target for most AML and MDS patients, and we are working urgently to finalize a therapy for human testing.”
Dr Park and his colleagues first examined stem cell populations from 79 patients with AML and 24 with MDS. More than 80% of stem cells in both groups expressed high levels of CD99.
The levels were so high that leukemia stem cells could be cleanly separated from normal hematopoietic stem cells in AML samples.
Upon confirming that CD99 was abundant on AML and MDS stem cells, the researchers made several anti-CD99 mAbs and tested them in vitro and in mouse models.
The mAbs destroyed AML and MDS stem cells by causing a sudden spike in the activity of SRC family kinases—a group of proteins that are implicated in invasion, tumor progression, and metastasis in a variety of cancers.
However, the mAbs had minimal effects on normal hematopoietic stem cells.
“With the appropriate support, we believe we can rapidly determine the best antibodies for use in patients, produce them at the quality needed to verify our results, and apply for permission to begin clinical trials,” Dr Park said. ![]()
Image by Robert Paulson
The cell surface molecule CD99 occurs more frequently than normal on stem cells responsible for acute myeloid leukemia (AML) and myelodysplastic syndromes (MDS), according to research published in Science Translational Medicine.
Building on this discovery, researchers designed anti-CD99 monoclonal antibodies (mAbs).
In vitro and in vivo experiments
showed that these mAbs can recognize
and destroy AML and MDS stem/progenitor cells.
“Our findings not only identify a new molecule expressed on stem cells that drive these human malignancies, but we show that antibodies against this target can directly kill human AML stem cells,” said study author Christopher Y. Park, MD, PhD, of NYU Langone Medical Center in New York, New York.
“While we still have important details to work out, CD99 is likely to be an exploitable therapeutic target for most AML and MDS patients, and we are working urgently to finalize a therapy for human testing.”
Dr Park and his colleagues first examined stem cell populations from 79 patients with AML and 24 with MDS. More than 80% of stem cells in both groups expressed high levels of CD99.
The levels were so high that leukemia stem cells could be cleanly separated from normal hematopoietic stem cells in AML samples.
Upon confirming that CD99 was abundant on AML and MDS stem cells, the researchers made several anti-CD99 mAbs and tested them in vitro and in mouse models.
The mAbs destroyed AML and MDS stem cells by causing a sudden spike in the activity of SRC family kinases—a group of proteins that are implicated in invasion, tumor progression, and metastasis in a variety of cancers.
However, the mAbs had minimal effects on normal hematopoietic stem cells.
“With the appropriate support, we believe we can rapidly determine the best antibodies for use in patients, produce them at the quality needed to verify our results, and apply for permission to begin clinical trials,” Dr Park said. ![]()
Gene therapy granted breakthrough designation to treat hemophilia B

Image by Spencer Phillips
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation for the investigational gene therapy AMT-060 as a treatment for patients with severe hemophilia B.
AMT-060 consists of a codon-optimized wild-type factor IX (FIX) gene cassette, the LP1 liver promoter, and an AAV5 viral vector manufactured by uniQure using its proprietary insect cell-based technology platform. uniQure is the company developing AMT-060.
The FDA’s breakthrough therapy designation is intended to expedite the development and review of new treatments for serious or life-threatening conditions.
Breakthrough designation entitles the company developing a therapy to more intensive FDA guidance on an efficient and accelerated development program, as well as eligibility for other actions to expedite FDA review, such as a rolling submission and priority review.
To earn breakthrough designation, a treatment must show encouraging early clinical results demonstrating substantial improvement over available therapies with regard to a clinically significant endpoint, or it must fulfill an unmet need.
Phase 1/2 trial
The breakthrough designation for AMT-060 is based on results from an ongoing phase 1/2 study. Updated data from this study were recently presented at the 2016 ASH Annual Meeting (abstract 2314).
In this trial, researchers are testing AMT-060 in 10 patients. All patients had severe or moderately severe hemophilia at baseline, including documented FIX levels less than 1% to 2% of normal, and required chronic infusions of prophylactic or on-demand FIX therapy at the time of enrollment.
Each patient received a 1-time, 30-minute, intravenous dose of AMT-060, without the use of corticosteroids. Five patients received AMT-060 at 5 x 1012 gc/kg, and 5 received AMT-060 at 2 x 1013 gc/kg.
The data presented at ASH included up to 52 weeks of follow-up from the low-dose cohort and up to 31 weeks of follow-up from the higher-dose cohort.
Data from the higher-dose cohort show a dose response with improvement in disease state in all 5 patients. Four patients who previously required prophylactic FIX replacement therapy were able to stop this therapy.
As of the data cutoff date for the ASH presentation, 1 unconfirmed spontaneous bleed had been reported during an aggregate of 94 weeks of follow-up after the discontinuation of prophylaxis.
Researchers previously reported that 4 patients in the low-dose cohort were able to discontinue prophylactic therapy. The 1 patient who
remained on prophylaxis sustained an improved disease
phenotype and also required materially less FIX concentrate after
treatment with AMT-060.
According to uniQure, all 5 patients in the low-dose cohort continue to maintain “constant and clinically meaningful” levels of FIX activity for up to 52 weeks post-treatment. In fact, there were no spontaneous bleeds in these patients in the last 14 weeks of observation.
uniQure also said AMT-060 continues to be well-tolerated, and there have been no severe adverse events.
Three patients (2 in the higher-dose cohort and 1 previously reported from the low-dose cohort) experienced mild, asymptomatic elevations of alanine aminotransferase and received a tapering course of corticosteroids per protocol.
These temporary alanine aminotransferase elevations were not associated with any loss of endogenous FIX activity or T-cell response to the AAV5 capsid.
None of the patients in either cohort have developed inhibitory antibodies against FIX, and none of the patients screened tested positive for anti-AAV5 antibodies. ![]()
Image by Spencer Phillips
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation for the investigational gene therapy AMT-060 as a treatment for patients with severe hemophilia B.
AMT-060 consists of a codon-optimized wild-type factor IX (FIX) gene cassette, the LP1 liver promoter, and an AAV5 viral vector manufactured by uniQure using its proprietary insect cell-based technology platform. uniQure is the company developing AMT-060.
The FDA’s breakthrough therapy designation is intended to expedite the development and review of new treatments for serious or life-threatening conditions.
Breakthrough designation entitles the company developing a therapy to more intensive FDA guidance on an efficient and accelerated development program, as well as eligibility for other actions to expedite FDA review, such as a rolling submission and priority review.
To earn breakthrough designation, a treatment must show encouraging early clinical results demonstrating substantial improvement over available therapies with regard to a clinically significant endpoint, or it must fulfill an unmet need.
Phase 1/2 trial
The breakthrough designation for AMT-060 is based on results from an ongoing phase 1/2 study. Updated data from this study were recently presented at the 2016 ASH Annual Meeting (abstract 2314).
In this trial, researchers are testing AMT-060 in 10 patients. All patients had severe or moderately severe hemophilia at baseline, including documented FIX levels less than 1% to 2% of normal, and required chronic infusions of prophylactic or on-demand FIX therapy at the time of enrollment.
Each patient received a 1-time, 30-minute, intravenous dose of AMT-060, without the use of corticosteroids. Five patients received AMT-060 at 5 x 1012 gc/kg, and 5 received AMT-060 at 2 x 1013 gc/kg.
The data presented at ASH included up to 52 weeks of follow-up from the low-dose cohort and up to 31 weeks of follow-up from the higher-dose cohort.
Data from the higher-dose cohort show a dose response with improvement in disease state in all 5 patients. Four patients who previously required prophylactic FIX replacement therapy were able to stop this therapy.
As of the data cutoff date for the ASH presentation, 1 unconfirmed spontaneous bleed had been reported during an aggregate of 94 weeks of follow-up after the discontinuation of prophylaxis.
Researchers previously reported that 4 patients in the low-dose cohort were able to discontinue prophylactic therapy. The 1 patient who
remained on prophylaxis sustained an improved disease
phenotype and also required materially less FIX concentrate after
treatment with AMT-060.
According to uniQure, all 5 patients in the low-dose cohort continue to maintain “constant and clinically meaningful” levels of FIX activity for up to 52 weeks post-treatment. In fact, there were no spontaneous bleeds in these patients in the last 14 weeks of observation.
uniQure also said AMT-060 continues to be well-tolerated, and there have been no severe adverse events.
Three patients (2 in the higher-dose cohort and 1 previously reported from the low-dose cohort) experienced mild, asymptomatic elevations of alanine aminotransferase and received a tapering course of corticosteroids per protocol.
These temporary alanine aminotransferase elevations were not associated with any loss of endogenous FIX activity or T-cell response to the AAV5 capsid.
None of the patients in either cohort have developed inhibitory antibodies against FIX, and none of the patients screened tested positive for anti-AAV5 antibodies. ![]()
Image by Spencer Phillips
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation for the investigational gene therapy AMT-060 as a treatment for patients with severe hemophilia B.
AMT-060 consists of a codon-optimized wild-type factor IX (FIX) gene cassette, the LP1 liver promoter, and an AAV5 viral vector manufactured by uniQure using its proprietary insect cell-based technology platform. uniQure is the company developing AMT-060.
The FDA’s breakthrough therapy designation is intended to expedite the development and review of new treatments for serious or life-threatening conditions.
Breakthrough designation entitles the company developing a therapy to more intensive FDA guidance on an efficient and accelerated development program, as well as eligibility for other actions to expedite FDA review, such as a rolling submission and priority review.
To earn breakthrough designation, a treatment must show encouraging early clinical results demonstrating substantial improvement over available therapies with regard to a clinically significant endpoint, or it must fulfill an unmet need.
Phase 1/2 trial
The breakthrough designation for AMT-060 is based on results from an ongoing phase 1/2 study. Updated data from this study were recently presented at the 2016 ASH Annual Meeting (abstract 2314).
In this trial, researchers are testing AMT-060 in 10 patients. All patients had severe or moderately severe hemophilia at baseline, including documented FIX levels less than 1% to 2% of normal, and required chronic infusions of prophylactic or on-demand FIX therapy at the time of enrollment.
Each patient received a 1-time, 30-minute, intravenous dose of AMT-060, without the use of corticosteroids. Five patients received AMT-060 at 5 x 1012 gc/kg, and 5 received AMT-060 at 2 x 1013 gc/kg.
The data presented at ASH included up to 52 weeks of follow-up from the low-dose cohort and up to 31 weeks of follow-up from the higher-dose cohort.
Data from the higher-dose cohort show a dose response with improvement in disease state in all 5 patients. Four patients who previously required prophylactic FIX replacement therapy were able to stop this therapy.
As of the data cutoff date for the ASH presentation, 1 unconfirmed spontaneous bleed had been reported during an aggregate of 94 weeks of follow-up after the discontinuation of prophylaxis.
Researchers previously reported that 4 patients in the low-dose cohort were able to discontinue prophylactic therapy. The 1 patient who
remained on prophylaxis sustained an improved disease
phenotype and also required materially less FIX concentrate after
treatment with AMT-060.
According to uniQure, all 5 patients in the low-dose cohort continue to maintain “constant and clinically meaningful” levels of FIX activity for up to 52 weeks post-treatment. In fact, there were no spontaneous bleeds in these patients in the last 14 weeks of observation.
uniQure also said AMT-060 continues to be well-tolerated, and there have been no severe adverse events.
Three patients (2 in the higher-dose cohort and 1 previously reported from the low-dose cohort) experienced mild, asymptomatic elevations of alanine aminotransferase and received a tapering course of corticosteroids per protocol.
These temporary alanine aminotransferase elevations were not associated with any loss of endogenous FIX activity or T-cell response to the AAV5 capsid.
None of the patients in either cohort have developed inhibitory antibodies against FIX, and none of the patients screened tested positive for anti-AAV5 antibodies. ![]()
Long-term oxygen for COPD with moderate desaturation
Clinical question: Does using supplemental oxygen in patients with stable chronic obstructive pulmonary disease (COPD) result in a longer time to death or first hospitalization?
Background: Previous trials have shown that use of long-term, supplemental oxygen in COPD and severe resting hypoxia reduced mortality, however, data is inconclusive if its use in mild-moderate COPD has the same effect.
Study design: Parallel-group, randomized, unblinded clinical trial.

Synopsis: Researchers randomized 738 patients from 42 outpatient centers with stable COPD and moderate resting desaturation (SpO2, 89%-93%) or moderate exercise induced desaturation (6-minute walk test, SpO2 greater than 80% for five minutes, and greater than 90% for 10 seconds) to long-term supplemental oxygen or no supplemental oxygen. Time-to-event analysis found no differences in the composite primary outcome of death or first hospitalization (HR, 0.94; 95% confidence interval, 0.79-1.12), or in any other secondary outcomes of COPD exacerbations, or COPD-related or all-cause hospitalizations.
Limitations included lack of blinding, possible exclusion of patients with higher COPD severity, and lack of assessment of immediate effects of oxygen on symptoms or exercise performance.
Bottom line: Long-term, supplemental oxygen provided no benefit in mortality or time to first hospitalization among other outcomes in patients with stable COPD and resting or exercise-induced moderate desaturations.
Citation: The Long-Term Oxygen Treatment Trial Research Group. A randomized trial of long-term oxygen for COPD with moderate desaturation. N Engl J Med. 2016;375:1617-27.
Dr. Ciarkowski is a clinical instructor at the University of Utah School of Medicine and an academic hospitalist at the University of Utah Hospital.
Clinical question: Does using supplemental oxygen in patients with stable chronic obstructive pulmonary disease (COPD) result in a longer time to death or first hospitalization?
Background: Previous trials have shown that use of long-term, supplemental oxygen in COPD and severe resting hypoxia reduced mortality, however, data is inconclusive if its use in mild-moderate COPD has the same effect.
Study design: Parallel-group, randomized, unblinded clinical trial.
Synopsis: Researchers randomized 738 patients from 42 outpatient centers with stable COPD and moderate resting desaturation (SpO2, 89%-93%) or moderate exercise induced desaturation (6-minute walk test, SpO2 greater than 80% for five minutes, and greater than 90% for 10 seconds) to long-term supplemental oxygen or no supplemental oxygen. Time-to-event analysis found no differences in the composite primary outcome of death or first hospitalization (HR, 0.94; 95% confidence interval, 0.79-1.12), or in any other secondary outcomes of COPD exacerbations, or COPD-related or all-cause hospitalizations.
Limitations included lack of blinding, possible exclusion of patients with higher COPD severity, and lack of assessment of immediate effects of oxygen on symptoms or exercise performance.
Bottom line: Long-term, supplemental oxygen provided no benefit in mortality or time to first hospitalization among other outcomes in patients with stable COPD and resting or exercise-induced moderate desaturations.
Citation: The Long-Term Oxygen Treatment Trial Research Group. A randomized trial of long-term oxygen for COPD with moderate desaturation. N Engl J Med. 2016;375:1617-27.
Dr. Ciarkowski is a clinical instructor at the University of Utah School of Medicine and an academic hospitalist at the University of Utah Hospital.
Clinical question: Does using supplemental oxygen in patients with stable chronic obstructive pulmonary disease (COPD) result in a longer time to death or first hospitalization?
Background: Previous trials have shown that use of long-term, supplemental oxygen in COPD and severe resting hypoxia reduced mortality, however, data is inconclusive if its use in mild-moderate COPD has the same effect.
Study design: Parallel-group, randomized, unblinded clinical trial.
Synopsis: Researchers randomized 738 patients from 42 outpatient centers with stable COPD and moderate resting desaturation (SpO2, 89%-93%) or moderate exercise induced desaturation (6-minute walk test, SpO2 greater than 80% for five minutes, and greater than 90% for 10 seconds) to long-term supplemental oxygen or no supplemental oxygen. Time-to-event analysis found no differences in the composite primary outcome of death or first hospitalization (HR, 0.94; 95% confidence interval, 0.79-1.12), or in any other secondary outcomes of COPD exacerbations, or COPD-related or all-cause hospitalizations.
Limitations included lack of blinding, possible exclusion of patients with higher COPD severity, and lack of assessment of immediate effects of oxygen on symptoms or exercise performance.
Bottom line: Long-term, supplemental oxygen provided no benefit in mortality or time to first hospitalization among other outcomes in patients with stable COPD and resting or exercise-induced moderate desaturations.
Citation: The Long-Term Oxygen Treatment Trial Research Group. A randomized trial of long-term oxygen for COPD with moderate desaturation. N Engl J Med. 2016;375:1617-27.
Dr. Ciarkowski is a clinical instructor at the University of Utah School of Medicine and an academic hospitalist at the University of Utah Hospital.
Breath test aims to sniff out GEJ cancers
AMSTERDAM – A test that samples exhaled breath and looks for the presence of just five volatile organic compounds shows promise as an inexpensive method for screening patients with suspected cancers of the gastroesophageal junction (GEJ), investigators from the United Kingdom reported.
In a multicenter clinical trial testing breath samples from patients with adenocarcinoma of the GEJ and matched controls, the test had an overall sensitivity of 80% and specificity of 81% for adenocarcinoma of the GEJ, said Sheraz R. Markar, MD, PhD, from Imperial College London.

If the test can be validated in larger studies, it could increase the number of patients screened and has the potential to save medical costs by reducing the number of unnecessary endoscopies and by catching GEJ cancers at earlier, potentially curable stages, he said.
The test uses selected ion flow tube mass spectrometry, or SIFT-MS to identify the olfactory signatures of specific chemical components among the millions of possible odors in a sample of air.
The investigators previously identified 13 volatile organic compounds (VOCs) associated with GEJ cancers and through additional analysis pared the number down to five: butyric acid, pentanoic acid, hexanoic acid, butanal, and decanal.
In tests of the five-VOC breath model, they found it had an area under the curve (AUC) of the receiver operating characteristic of 0.90, sensitivity of 84%, and a specificity of 88%.
They then sought to validate the model in a multicenter blinded study. They enrolled 163 treatment-naive patients diagnosed with nonmetastatic GEJ cancer (stages I-III), and 172 controls matched on a 1:1 basis.
Breath samples from all participants were collected in steel breath bags and sent to a central lab for SIFT-MS analysis. A statistician blinded to patient diagnosis then determined cancer risk based on previously determined odds ratios for each VOC.
The investigators used quality assurance measures to minimize the risk of errors, including sampling of the ambient air where the samples were collected, training of all researchers in uniform breath collection technique, and calibration to water.
They found that in this validation study, four of the five VOCs were significantly dysregulated in cases, compared with controls; pentanoic acid was the exception. The AUC was 0.85, with a sensitivity of 80% and specificity of 81%.
Looking at the association between VOCs and demographics of the patients as possible confounders, they saw that hexanoic acid levels could be affected by smoking history, and that butanal could be affected by smoking, white race, or history of using an ACE inhibitor.
Dr. Markar said that among the strengths of the study are that is was adequately powered, performed in multiple centers, and had quality assurance measures in place. In addition, the results compared well with results from the use of a cytosponge.
He acknowledged, however, that there were more late- than early-stage cancers among patients in the study, and that the 80% sensitivity level meant that one in five cancers would be missed.
Nonetheless, if the test is refined and can be further validated in an unenriched population, it could serve as an endoscopy triage test, he said.

He noted that we are just beginning to understand the importance of smell, the “most primitive” of the five senses, in relation to human health and joked that, just as many airports have drug-sniffing dogs, clinical practices could have patient-sniffing dogs that could be used to direct patients to the right specialist.
He was not involved in the study, but commented on it as part of a media briefing.
The study was supported by the UK National Institute for Health Research. The authors reported no competing interests.
AMSTERDAM – A test that samples exhaled breath and looks for the presence of just five volatile organic compounds shows promise as an inexpensive method for screening patients with suspected cancers of the gastroesophageal junction (GEJ), investigators from the United Kingdom reported.
In a multicenter clinical trial testing breath samples from patients with adenocarcinoma of the GEJ and matched controls, the test had an overall sensitivity of 80% and specificity of 81% for adenocarcinoma of the GEJ, said Sheraz R. Markar, MD, PhD, from Imperial College London.
If the test can be validated in larger studies, it could increase the number of patients screened and has the potential to save medical costs by reducing the number of unnecessary endoscopies and by catching GEJ cancers at earlier, potentially curable stages, he said.
The test uses selected ion flow tube mass spectrometry, or SIFT-MS to identify the olfactory signatures of specific chemical components among the millions of possible odors in a sample of air.
The investigators previously identified 13 volatile organic compounds (VOCs) associated with GEJ cancers and through additional analysis pared the number down to five: butyric acid, pentanoic acid, hexanoic acid, butanal, and decanal.
In tests of the five-VOC breath model, they found it had an area under the curve (AUC) of the receiver operating characteristic of 0.90, sensitivity of 84%, and a specificity of 88%.
They then sought to validate the model in a multicenter blinded study. They enrolled 163 treatment-naive patients diagnosed with nonmetastatic GEJ cancer (stages I-III), and 172 controls matched on a 1:1 basis.
Breath samples from all participants were collected in steel breath bags and sent to a central lab for SIFT-MS analysis. A statistician blinded to patient diagnosis then determined cancer risk based on previously determined odds ratios for each VOC.
The investigators used quality assurance measures to minimize the risk of errors, including sampling of the ambient air where the samples were collected, training of all researchers in uniform breath collection technique, and calibration to water.
They found that in this validation study, four of the five VOCs were significantly dysregulated in cases, compared with controls; pentanoic acid was the exception. The AUC was 0.85, with a sensitivity of 80% and specificity of 81%.
Looking at the association between VOCs and demographics of the patients as possible confounders, they saw that hexanoic acid levels could be affected by smoking history, and that butanal could be affected by smoking, white race, or history of using an ACE inhibitor.
Dr. Markar said that among the strengths of the study are that is was adequately powered, performed in multiple centers, and had quality assurance measures in place. In addition, the results compared well with results from the use of a cytosponge.
He acknowledged, however, that there were more late- than early-stage cancers among patients in the study, and that the 80% sensitivity level meant that one in five cancers would be missed.
Nonetheless, if the test is refined and can be further validated in an unenriched population, it could serve as an endoscopy triage test, he said.
He noted that we are just beginning to understand the importance of smell, the “most primitive” of the five senses, in relation to human health and joked that, just as many airports have drug-sniffing dogs, clinical practices could have patient-sniffing dogs that could be used to direct patients to the right specialist.
He was not involved in the study, but commented on it as part of a media briefing.
The study was supported by the UK National Institute for Health Research. The authors reported no competing interests.
AMSTERDAM – A test that samples exhaled breath and looks for the presence of just five volatile organic compounds shows promise as an inexpensive method for screening patients with suspected cancers of the gastroesophageal junction (GEJ), investigators from the United Kingdom reported.
In a multicenter clinical trial testing breath samples from patients with adenocarcinoma of the GEJ and matched controls, the test had an overall sensitivity of 80% and specificity of 81% for adenocarcinoma of the GEJ, said Sheraz R. Markar, MD, PhD, from Imperial College London.
If the test can be validated in larger studies, it could increase the number of patients screened and has the potential to save medical costs by reducing the number of unnecessary endoscopies and by catching GEJ cancers at earlier, potentially curable stages, he said.
The test uses selected ion flow tube mass spectrometry, or SIFT-MS to identify the olfactory signatures of specific chemical components among the millions of possible odors in a sample of air.
The investigators previously identified 13 volatile organic compounds (VOCs) associated with GEJ cancers and through additional analysis pared the number down to five: butyric acid, pentanoic acid, hexanoic acid, butanal, and decanal.
In tests of the five-VOC breath model, they found it had an area under the curve (AUC) of the receiver operating characteristic of 0.90, sensitivity of 84%, and a specificity of 88%.
They then sought to validate the model in a multicenter blinded study. They enrolled 163 treatment-naive patients diagnosed with nonmetastatic GEJ cancer (stages I-III), and 172 controls matched on a 1:1 basis.
Breath samples from all participants were collected in steel breath bags and sent to a central lab for SIFT-MS analysis. A statistician blinded to patient diagnosis then determined cancer risk based on previously determined odds ratios for each VOC.
The investigators used quality assurance measures to minimize the risk of errors, including sampling of the ambient air where the samples were collected, training of all researchers in uniform breath collection technique, and calibration to water.
They found that in this validation study, four of the five VOCs were significantly dysregulated in cases, compared with controls; pentanoic acid was the exception. The AUC was 0.85, with a sensitivity of 80% and specificity of 81%.
Looking at the association between VOCs and demographics of the patients as possible confounders, they saw that hexanoic acid levels could be affected by smoking history, and that butanal could be affected by smoking, white race, or history of using an ACE inhibitor.
Dr. Markar said that among the strengths of the study are that is was adequately powered, performed in multiple centers, and had quality assurance measures in place. In addition, the results compared well with results from the use of a cytosponge.
He acknowledged, however, that there were more late- than early-stage cancers among patients in the study, and that the 80% sensitivity level meant that one in five cancers would be missed.
Nonetheless, if the test is refined and can be further validated in an unenriched population, it could serve as an endoscopy triage test, he said.
He noted that we are just beginning to understand the importance of smell, the “most primitive” of the five senses, in relation to human health and joked that, just as many airports have drug-sniffing dogs, clinical practices could have patient-sniffing dogs that could be used to direct patients to the right specialist.
He was not involved in the study, but commented on it as part of a media briefing.
The study was supported by the UK National Institute for Health Research. The authors reported no competing interests.
Key clinical point: Breath analysis may be able detect early cancers of the gastroesophagel junction.
Major finding: A breath test had 80% sensitivity and 81% specificity for GEJ cancer.
Data source: Multicenter case-control study with 335 participants.
Disclosures: The study was supported by the UK National Institute for Health Research. The authors reported no competing interests.
Even small weight loss can improve long-term atrial fib ablation success
ORLANDO – Excess body weight exerts a major negative impact on the likelihood of remaining free of atrial fibrillation long term after an ablation procedure, according to a new set of data and a review of published studies.
“Just losing 3 pounds can dramatically improve the long-term success of an ablation when compared to a weight gain,” reported John D. Day, MD, medical director, Intermountain Heart Rhythm Specialists, Salt Lake City, at the annual International AF Symposium.

“As BMI goes up, long-term success in controlling AF goes down. The difference at 1 year may not be a big deal, but if you follow patients for a long time, weight control is a very big deal,” Dr. Day advised. He emphasized repeatedly, “We are just talking about a few pounds” for a favorable effect.
New data presented at the meeting supported the message. In the study, ablation outcomes in relationship to body mass index (BMI) were evaluated in 2,715 AF patients undergoing 3,742 ablations. Patients were stratified into five groups by BMI: less than 25 kg/m2, 25 to less than 30; 30 to less than 35; 35 to less than 40, and at least 40.
As BMI increased from less than 25 to at least 40, there were significant increases in left atrial size (P less than .005), CHADS2 scores (P = .002), persistent AF (P less than .0001), and longstanding AF (P less than .0001). Unlike persistent and long-term AF, rates of paroxysmal AF fell (48% to 16.3%; P less than .0001).

Not surprisingly and consistent with other published reports, increasing BMI was associated with increases in many of the key risk factors for AF in the study.
Specifically, as BMI increased from less than 25 to at least 40, the proportion of patients with cardiomyopathy climbed from 7.6% to 12.4% (P less than .001), hypertension climbed from 41% to 72.9% (P less than .0001), diabetes climbed from 4.3% to 23.3% (P less than .0001), and sleep apnea climbed from 7.0% to 46.9% (P less than .0001).
Dr. Day cited the LEGACY trial as one of the most influential studies associating weight loss with a reduction in AF burden (J Am Coll Cardiol. 2015 May 26;65[20]:2159-69). In that study, weight loss of at least 10% resulted in a sixfold increased likelihood of AF-free survival. Independent of AF, Dr. Day also pointed out that the sense of well-being among patients who achieved weight loss improved 200%.
Recognizing that major weight loss is difficult to achieve, Dr. Day repeatedly returned to the theme of weight control.
He cited one study in which AF patients were randomized to a weight loss program or usual care. In the usual care group, which included physician advice to lose weight, there was a small but significant weight loss. Even though the effect of that weight loss on AF burden was a fraction of that achieved in the group that achieved greater reductions in weight on active management, it, too, was significant, according to Dr. Day.
“Even brief physician advice can have a meaningful influence on waist circumference,” said Dr. Day, who urged physicians to inform their AF patients about the benefits of weight loss. Failing to do so might deprive patients of achieving the very modest reductions in weight loss required to improve their likelihood of freedom from AF, he added.
Dr. Winkle had no relevant financial relationships. Dr. Day reported a financial relationship with St. Jude Medical.
ORLANDO – Excess body weight exerts a major negative impact on the likelihood of remaining free of atrial fibrillation long term after an ablation procedure, according to a new set of data and a review of published studies.
“Just losing 3 pounds can dramatically improve the long-term success of an ablation when compared to a weight gain,” reported John D. Day, MD, medical director, Intermountain Heart Rhythm Specialists, Salt Lake City, at the annual International AF Symposium.
“As BMI goes up, long-term success in controlling AF goes down. The difference at 1 year may not be a big deal, but if you follow patients for a long time, weight control is a very big deal,” Dr. Day advised. He emphasized repeatedly, “We are just talking about a few pounds” for a favorable effect.
New data presented at the meeting supported the message. In the study, ablation outcomes in relationship to body mass index (BMI) were evaluated in 2,715 AF patients undergoing 3,742 ablations. Patients were stratified into five groups by BMI: less than 25 kg/m2, 25 to less than 30; 30 to less than 35; 35 to less than 40, and at least 40.
As BMI increased from less than 25 to at least 40, there were significant increases in left atrial size (P less than .005), CHADS2 scores (P = .002), persistent AF (P less than .0001), and longstanding AF (P less than .0001). Unlike persistent and long-term AF, rates of paroxysmal AF fell (48% to 16.3%; P less than .0001).
Not surprisingly and consistent with other published reports, increasing BMI was associated with increases in many of the key risk factors for AF in the study.
Specifically, as BMI increased from less than 25 to at least 40, the proportion of patients with cardiomyopathy climbed from 7.6% to 12.4% (P less than .001), hypertension climbed from 41% to 72.9% (P less than .0001), diabetes climbed from 4.3% to 23.3% (P less than .0001), and sleep apnea climbed from 7.0% to 46.9% (P less than .0001).
Dr. Day cited the LEGACY trial as one of the most influential studies associating weight loss with a reduction in AF burden (J Am Coll Cardiol. 2015 May 26;65[20]:2159-69). In that study, weight loss of at least 10% resulted in a sixfold increased likelihood of AF-free survival. Independent of AF, Dr. Day also pointed out that the sense of well-being among patients who achieved weight loss improved 200%.
Recognizing that major weight loss is difficult to achieve, Dr. Day repeatedly returned to the theme of weight control.
He cited one study in which AF patients were randomized to a weight loss program or usual care. In the usual care group, which included physician advice to lose weight, there was a small but significant weight loss. Even though the effect of that weight loss on AF burden was a fraction of that achieved in the group that achieved greater reductions in weight on active management, it, too, was significant, according to Dr. Day.
“Even brief physician advice can have a meaningful influence on waist circumference,” said Dr. Day, who urged physicians to inform their AF patients about the benefits of weight loss. Failing to do so might deprive patients of achieving the very modest reductions in weight loss required to improve their likelihood of freedom from AF, he added.
Dr. Winkle had no relevant financial relationships. Dr. Day reported a financial relationship with St. Jude Medical.
ORLANDO – Excess body weight exerts a major negative impact on the likelihood of remaining free of atrial fibrillation long term after an ablation procedure, according to a new set of data and a review of published studies.
“Just losing 3 pounds can dramatically improve the long-term success of an ablation when compared to a weight gain,” reported John D. Day, MD, medical director, Intermountain Heart Rhythm Specialists, Salt Lake City, at the annual International AF Symposium.
“As BMI goes up, long-term success in controlling AF goes down. The difference at 1 year may not be a big deal, but if you follow patients for a long time, weight control is a very big deal,” Dr. Day advised. He emphasized repeatedly, “We are just talking about a few pounds” for a favorable effect.
New data presented at the meeting supported the message. In the study, ablation outcomes in relationship to body mass index (BMI) were evaluated in 2,715 AF patients undergoing 3,742 ablations. Patients were stratified into five groups by BMI: less than 25 kg/m2, 25 to less than 30; 30 to less than 35; 35 to less than 40, and at least 40.
As BMI increased from less than 25 to at least 40, there were significant increases in left atrial size (P less than .005), CHADS2 scores (P = .002), persistent AF (P less than .0001), and longstanding AF (P less than .0001). Unlike persistent and long-term AF, rates of paroxysmal AF fell (48% to 16.3%; P less than .0001).
Not surprisingly and consistent with other published reports, increasing BMI was associated with increases in many of the key risk factors for AF in the study.
Specifically, as BMI increased from less than 25 to at least 40, the proportion of patients with cardiomyopathy climbed from 7.6% to 12.4% (P less than .001), hypertension climbed from 41% to 72.9% (P less than .0001), diabetes climbed from 4.3% to 23.3% (P less than .0001), and sleep apnea climbed from 7.0% to 46.9% (P less than .0001).
Dr. Day cited the LEGACY trial as one of the most influential studies associating weight loss with a reduction in AF burden (J Am Coll Cardiol. 2015 May 26;65[20]:2159-69). In that study, weight loss of at least 10% resulted in a sixfold increased likelihood of AF-free survival. Independent of AF, Dr. Day also pointed out that the sense of well-being among patients who achieved weight loss improved 200%.
Recognizing that major weight loss is difficult to achieve, Dr. Day repeatedly returned to the theme of weight control.
He cited one study in which AF patients were randomized to a weight loss program or usual care. In the usual care group, which included physician advice to lose weight, there was a small but significant weight loss. Even though the effect of that weight loss on AF burden was a fraction of that achieved in the group that achieved greater reductions in weight on active management, it, too, was significant, according to Dr. Day.
“Even brief physician advice can have a meaningful influence on waist circumference,” said Dr. Day, who urged physicians to inform their AF patients about the benefits of weight loss. Failing to do so might deprive patients of achieving the very modest reductions in weight loss required to improve their likelihood of freedom from AF, he added.
Dr. Winkle had no relevant financial relationships. Dr. Day reported a financial relationship with St. Jude Medical.
Key clinical point: New data expand evidence that obesity reduces long-term success of ablation for atrial fibrillation.
Major finding: Freedom from AF 5 years after ablation fell from 70% in patients with a BMI of less than 35 kg/m2 to 57% in those with BMIs of at least 35.
Data source: A retrospective observational study.
Disclosures: Dr. Winkle had no relevant financial relationships; Dr. Day reported a financial relationship with St. Jude Medical.
Residual disease burden is prognostic across breast cancer phenotypes
The Residual Cancer Burden (RCB), a standardized measure of residual disease in pathologic resection specimens following neoadjuvant chemotherapy, was found to be prognostic of long-term survival across all three phenotypic subtypes when it was applied to five breast cancer cohorts totaling 1,158 patients from a single institution, investigators report in the Journal of Clinical Oncology.
If the findings of this retrospective cohort analysis are validated in other cohorts, it would indicate that assessing patients’ RCB index could add “meaningful information to pretreatement clinical and pathologic information and posttreatment yp stage [American Joint Commission on Cancer stage],” said W. Fraser Symmans, MD, of the University of Texas M.D. Anderson Cancer Center, Houston, and his associates.
Residual disease is categorized into four groups: an index of zero (RCB-0) reflects a complete pathologic response to neoadjuvant treatment, RCB-I indicates minimal residual disease, RCB-II indicates moderate residual disease, and RCB-III indicates extensive residual disease. The investigators reviewed pathology specimens to determine the RCB index in a cohort of 219 patients followed for 13 years, a cohort of 262 patients followed for 9 years, a cohort of 342 patients followed for 7 years, a cohort of 132 patients followed for more than 16 years, and a cohort of 203 patients followed for 7 years.
They found that the RCB index predicted the risk of relapse or death across all five cohorts, regardless of other clinical and pathologic variables such as tumor stage or grade, patient age, and type of surgery (J Clin Oncol. 2017 Jan 30. doi: 10.1200/JCO.2015.63.1010).
RCB also was predictive regardless of whether patients had triple-negative disease, HR-positive/HER2-negative disease, HER2-positive disease treated with paclitaxel plus combined fluorouracil, doxorubicin, and cyclophosphamide alone, or HER2-positive disease treated with paclitaxel plus combined fluorouracil, doxorubicin, and cyclophosphamide plus trastuzumab.
In two especially high-risk groups of patients – those with triple-negative breast cancer and those with HER2-positive breast cancer – RCB was the only or the most important predictor of survival. Approximately half of the patients with triple-negative disease had an index of RCB-0 or RCB-I and a good prognosis, while those with an RCB-II or RCB-III index had poor survival, Dr. Symmans and his associates said.
The authors use their main finding – that RCB index provides additional and independent prognostic information to yp stage and other clinical factors – to support their opinion that clinicians should be provided this information.

Sibylle Loibl, MD, is with the German Breast Group in Neu-Isenburg, Germany. Carsten Denkert, MD, is with the German Breast Group and with Charite University Hospital, Berlin. They reported having no relevant financial disclosures. Dr. Loibl and Dr. Denkert made these remarks in an editorial accompanying Dr. Symmans’ report (J Clin Oncol. 2017 Jan 30. doi: 10.1200/JCO.2016.71.3503).
The authors use their main finding – that RCB index provides additional and independent prognostic information to yp stage and other clinical factors – to support their opinion that clinicians should be provided this information.
Sibylle Loibl, MD, is with the German Breast Group in Neu-Isenburg, Germany. Carsten Denkert, MD, is with the German Breast Group and with Charite University Hospital, Berlin. They reported having no relevant financial disclosures. Dr. Loibl and Dr. Denkert made these remarks in an editorial accompanying Dr. Symmans’ report (J Clin Oncol. 2017 Jan 30. doi: 10.1200/JCO.2016.71.3503).
The authors use their main finding – that RCB index provides additional and independent prognostic information to yp stage and other clinical factors – to support their opinion that clinicians should be provided this information.
Sibylle Loibl, MD, is with the German Breast Group in Neu-Isenburg, Germany. Carsten Denkert, MD, is with the German Breast Group and with Charite University Hospital, Berlin. They reported having no relevant financial disclosures. Dr. Loibl and Dr. Denkert made these remarks in an editorial accompanying Dr. Symmans’ report (J Clin Oncol. 2017 Jan 30. doi: 10.1200/JCO.2016.71.3503).
The Residual Cancer Burden (RCB), a standardized measure of residual disease in pathologic resection specimens following neoadjuvant chemotherapy, was found to be prognostic of long-term survival across all three phenotypic subtypes when it was applied to five breast cancer cohorts totaling 1,158 patients from a single institution, investigators report in the Journal of Clinical Oncology.
If the findings of this retrospective cohort analysis are validated in other cohorts, it would indicate that assessing patients’ RCB index could add “meaningful information to pretreatement clinical and pathologic information and posttreatment yp stage [American Joint Commission on Cancer stage],” said W. Fraser Symmans, MD, of the University of Texas M.D. Anderson Cancer Center, Houston, and his associates.
Residual disease is categorized into four groups: an index of zero (RCB-0) reflects a complete pathologic response to neoadjuvant treatment, RCB-I indicates minimal residual disease, RCB-II indicates moderate residual disease, and RCB-III indicates extensive residual disease. The investigators reviewed pathology specimens to determine the RCB index in a cohort of 219 patients followed for 13 years, a cohort of 262 patients followed for 9 years, a cohort of 342 patients followed for 7 years, a cohort of 132 patients followed for more than 16 years, and a cohort of 203 patients followed for 7 years.
They found that the RCB index predicted the risk of relapse or death across all five cohorts, regardless of other clinical and pathologic variables such as tumor stage or grade, patient age, and type of surgery (J Clin Oncol. 2017 Jan 30. doi: 10.1200/JCO.2015.63.1010).
RCB also was predictive regardless of whether patients had triple-negative disease, HR-positive/HER2-negative disease, HER2-positive disease treated with paclitaxel plus combined fluorouracil, doxorubicin, and cyclophosphamide alone, or HER2-positive disease treated with paclitaxel plus combined fluorouracil, doxorubicin, and cyclophosphamide plus trastuzumab.
In two especially high-risk groups of patients – those with triple-negative breast cancer and those with HER2-positive breast cancer – RCB was the only or the most important predictor of survival. Approximately half of the patients with triple-negative disease had an index of RCB-0 or RCB-I and a good prognosis, while those with an RCB-II or RCB-III index had poor survival, Dr. Symmans and his associates said.
The Residual Cancer Burden (RCB), a standardized measure of residual disease in pathologic resection specimens following neoadjuvant chemotherapy, was found to be prognostic of long-term survival across all three phenotypic subtypes when it was applied to five breast cancer cohorts totaling 1,158 patients from a single institution, investigators report in the Journal of Clinical Oncology.
If the findings of this retrospective cohort analysis are validated in other cohorts, it would indicate that assessing patients’ RCB index could add “meaningful information to pretreatement clinical and pathologic information and posttreatment yp stage [American Joint Commission on Cancer stage],” said W. Fraser Symmans, MD, of the University of Texas M.D. Anderson Cancer Center, Houston, and his associates.
Residual disease is categorized into four groups: an index of zero (RCB-0) reflects a complete pathologic response to neoadjuvant treatment, RCB-I indicates minimal residual disease, RCB-II indicates moderate residual disease, and RCB-III indicates extensive residual disease. The investigators reviewed pathology specimens to determine the RCB index in a cohort of 219 patients followed for 13 years, a cohort of 262 patients followed for 9 years, a cohort of 342 patients followed for 7 years, a cohort of 132 patients followed for more than 16 years, and a cohort of 203 patients followed for 7 years.
They found that the RCB index predicted the risk of relapse or death across all five cohorts, regardless of other clinical and pathologic variables such as tumor stage or grade, patient age, and type of surgery (J Clin Oncol. 2017 Jan 30. doi: 10.1200/JCO.2015.63.1010).
RCB also was predictive regardless of whether patients had triple-negative disease, HR-positive/HER2-negative disease, HER2-positive disease treated with paclitaxel plus combined fluorouracil, doxorubicin, and cyclophosphamide alone, or HER2-positive disease treated with paclitaxel plus combined fluorouracil, doxorubicin, and cyclophosphamide plus trastuzumab.
In two especially high-risk groups of patients – those with triple-negative breast cancer and those with HER2-positive breast cancer – RCB was the only or the most important predictor of survival. Approximately half of the patients with triple-negative disease had an index of RCB-0 or RCB-I and a good prognosis, while those with an RCB-II or RCB-III index had poor survival, Dr. Symmans and his associates said.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: The RCB measure is prognostic of long-term survival across all three phenotypic subtypes of breast cancer.
Major finding: The RCB index predicted the risk of relapse or death across five cohorts at a single institution, regardless of other clinical and pathologic variables such as tumor stage or grade, patient age, and type of surgery.
Data source: A retrospective cohort study assessing the RCB’s ability to predict long-term survival using data from five breast cancer cohorts (1,158 patients) with 6-17 years of follow-up.
Disclosures: This study was supported by the Department of Defense Congressionally Directed Funds for Breast Cancer Research, the Breast Cancer Research Foundation, Susan G. Komen for the Cure, and the Nellie B. Connally Breast Center at M.D. Anderson Cancer Center. Dr. Symmans reported ties to ISIS Pharmaceuticals, Nuvera Biosciences, Affymetrix, Celgene, Genentech, and AbbVie, and his associates reported ties to numerous industry sources.
Adding bevacizumab improves PFS in extensive SCLC
Adding the antiangiogenic agent bevacizumab to standard first-line chemotherapy improves progression-free survival in extensive small-cell lung cancer, according to a report published online Jan. 30.
In what they described as the first prospective randomized, controlled phase III trial comparing these two approaches, researchers studied 204 adults who had extensive SCLC, including brain and bone metastases, at 29 medical centers in Italy. These participants (mean age, 64 years) were randomly assigned to receive a combination of standard cisplatin, etoposide, and bevacizumab every 3 weeks or cisplatin and etoposide chemotherapy every 3 weeks. Patients who developed cisplatin contraindications or toxicity related to the drug could substitute carboplatin. In the experimental arm of the study, patients could opt to continue bevacizumab alone as maintenance therapy for a maximum of 18 cycles. Forty-one patients (42%) did so, said Marcello Tiseo, MD, PhD, of Azienda Ospedaliero Universitaria, Parma, Italy, and his associates.
After a median follow-up of 35 months, the median progression-free survival was 5.7 months with standard therapy and 6.7 months with add-on bevacizumab (hazard ratio, 0.72; 95% confidence interval, 0.54 to 0.97; P = .030). However, adding bevacizumab did not significantly improve overall survival, which was the primary endpoint of the trial. A subgroup analysis showed that bevacizumab significantly extended overall survival among men (HR, 0.55) but not among women (HR, 1.55), an association that has been reported in previous studies, Dr. Tiseo and his associates said (J Clin Oncol. 2017 Jan 30. doi:10.1200/JCO.2016.69.4844).
These findings, together with those of other investigators assessing the same class of agents, justify “further studies with novel and better antiangiogenic agents in extensive SCLC, particularly in the maintenance setting,” they added.
This trial was supported by the Agenzia Italiana del Farmaco. Dr. Tiseo reported serving as a consultant for AstraZeneca, Eli Lilly, Boehringer Ingelheim, Novartis, Bristol-Myers Squibb, Pierre Fabre, and Otsuka; his associates reported ties to numerous industry sources.
Adding the antiangiogenic agent bevacizumab to standard first-line chemotherapy improves progression-free survival in extensive small-cell lung cancer, according to a report published online Jan. 30.
In what they described as the first prospective randomized, controlled phase III trial comparing these two approaches, researchers studied 204 adults who had extensive SCLC, including brain and bone metastases, at 29 medical centers in Italy. These participants (mean age, 64 years) were randomly assigned to receive a combination of standard cisplatin, etoposide, and bevacizumab every 3 weeks or cisplatin and etoposide chemotherapy every 3 weeks. Patients who developed cisplatin contraindications or toxicity related to the drug could substitute carboplatin. In the experimental arm of the study, patients could opt to continue bevacizumab alone as maintenance therapy for a maximum of 18 cycles. Forty-one patients (42%) did so, said Marcello Tiseo, MD, PhD, of Azienda Ospedaliero Universitaria, Parma, Italy, and his associates.
After a median follow-up of 35 months, the median progression-free survival was 5.7 months with standard therapy and 6.7 months with add-on bevacizumab (hazard ratio, 0.72; 95% confidence interval, 0.54 to 0.97; P = .030). However, adding bevacizumab did not significantly improve overall survival, which was the primary endpoint of the trial. A subgroup analysis showed that bevacizumab significantly extended overall survival among men (HR, 0.55) but not among women (HR, 1.55), an association that has been reported in previous studies, Dr. Tiseo and his associates said (J Clin Oncol. 2017 Jan 30. doi:10.1200/JCO.2016.69.4844).
These findings, together with those of other investigators assessing the same class of agents, justify “further studies with novel and better antiangiogenic agents in extensive SCLC, particularly in the maintenance setting,” they added.
This trial was supported by the Agenzia Italiana del Farmaco. Dr. Tiseo reported serving as a consultant for AstraZeneca, Eli Lilly, Boehringer Ingelheim, Novartis, Bristol-Myers Squibb, Pierre Fabre, and Otsuka; his associates reported ties to numerous industry sources.
Adding the antiangiogenic agent bevacizumab to standard first-line chemotherapy improves progression-free survival in extensive small-cell lung cancer, according to a report published online Jan. 30.
In what they described as the first prospective randomized, controlled phase III trial comparing these two approaches, researchers studied 204 adults who had extensive SCLC, including brain and bone metastases, at 29 medical centers in Italy. These participants (mean age, 64 years) were randomly assigned to receive a combination of standard cisplatin, etoposide, and bevacizumab every 3 weeks or cisplatin and etoposide chemotherapy every 3 weeks. Patients who developed cisplatin contraindications or toxicity related to the drug could substitute carboplatin. In the experimental arm of the study, patients could opt to continue bevacizumab alone as maintenance therapy for a maximum of 18 cycles. Forty-one patients (42%) did so, said Marcello Tiseo, MD, PhD, of Azienda Ospedaliero Universitaria, Parma, Italy, and his associates.
After a median follow-up of 35 months, the median progression-free survival was 5.7 months with standard therapy and 6.7 months with add-on bevacizumab (hazard ratio, 0.72; 95% confidence interval, 0.54 to 0.97; P = .030). However, adding bevacizumab did not significantly improve overall survival, which was the primary endpoint of the trial. A subgroup analysis showed that bevacizumab significantly extended overall survival among men (HR, 0.55) but not among women (HR, 1.55), an association that has been reported in previous studies, Dr. Tiseo and his associates said (J Clin Oncol. 2017 Jan 30. doi:10.1200/JCO.2016.69.4844).
These findings, together with those of other investigators assessing the same class of agents, justify “further studies with novel and better antiangiogenic agents in extensive SCLC, particularly in the maintenance setting,” they added.
This trial was supported by the Agenzia Italiana del Farmaco. Dr. Tiseo reported serving as a consultant for AstraZeneca, Eli Lilly, Boehringer Ingelheim, Novartis, Bristol-Myers Squibb, Pierre Fabre, and Otsuka; his associates reported ties to numerous industry sources.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Adding bevacizumab to standard first-line chemotherapy improves progression-free survival in extensive small-cell lung cancer.
Major finding: After a median follow-up of 35 months, the median progression-free survival was 5.7 months with standard therapy and 6.7 months with add-on bevacizumab (hazard ratio, 0.72; 95% confidence interval, 0.54 to 0.97; P = .030).
Data source: A multicenter open-label randomized, controlled phase III trial involving 204 adults in Italy.
Disclosures: This trial was supported by the Agenzia Italiana del Farmaco. Dr. Tiseo reported serving as a consultant for AstraZeneca, Eli Lilly, Boehringer Ingelheim, Novartis, Bristol-Myers Squibb, Pierre Fabre, and Otsuka; his associates reported ties to numerous industry sources.
February Hot Threads in ACS Communities
Your colleagues already have a lot to say in 2017. Here are the top discussion threads in ACS Communities just prior to press time (communities in which the threads appear are listed in parentheses):
1. Care for the Vulnerable vs Cash for the Powerful... (General Surgery)
2. Car lease or buy (General Surgery)
3. Interval cholecystectomy (General Surgery)
4. Enemy of good is better (General Surgery)
5. Crushed meds and elixirs (Bariatric Surgery)
6. Unsuspected cancer on reduction mammoplasty (Breast Surgery)
7. UC with sigmoid tumor (Colon and Rectal Surgery)
8. Transverse colostomy problems (Colon and Rectal Surgery)
9. Complex anal fistula (Colon and Rectal Surgery)
10. Ethical dilemma (Trauma Surgery)
To join communities, log in to ACS Communities at http://acscommunities.facs.org/home, go to “Browse All Communities” near the top of any page, and click the blue “Join” button next to the community you’d like to join. If you have any questions, please send them to [email protected].
Your colleagues already have a lot to say in 2017. Here are the top discussion threads in ACS Communities just prior to press time (communities in which the threads appear are listed in parentheses):
1. Care for the Vulnerable vs Cash for the Powerful... (General Surgery)
2. Car lease or buy (General Surgery)
3. Interval cholecystectomy (General Surgery)
4. Enemy of good is better (General Surgery)
5. Crushed meds and elixirs (Bariatric Surgery)
6. Unsuspected cancer on reduction mammoplasty (Breast Surgery)
7. UC with sigmoid tumor (Colon and Rectal Surgery)
8. Transverse colostomy problems (Colon and Rectal Surgery)
9. Complex anal fistula (Colon and Rectal Surgery)
10. Ethical dilemma (Trauma Surgery)
To join communities, log in to ACS Communities at http://acscommunities.facs.org/home, go to “Browse All Communities” near the top of any page, and click the blue “Join” button next to the community you’d like to join. If you have any questions, please send them to [email protected].
Your colleagues already have a lot to say in 2017. Here are the top discussion threads in ACS Communities just prior to press time (communities in which the threads appear are listed in parentheses):
1. Care for the Vulnerable vs Cash for the Powerful... (General Surgery)
2. Car lease or buy (General Surgery)
3. Interval cholecystectomy (General Surgery)
4. Enemy of good is better (General Surgery)
5. Crushed meds and elixirs (Bariatric Surgery)
6. Unsuspected cancer on reduction mammoplasty (Breast Surgery)
7. UC with sigmoid tumor (Colon and Rectal Surgery)
8. Transverse colostomy problems (Colon and Rectal Surgery)
9. Complex anal fistula (Colon and Rectal Surgery)
10. Ethical dilemma (Trauma Surgery)
To join communities, log in to ACS Communities at http://acscommunities.facs.org/home, go to “Browse All Communities” near the top of any page, and click the blue “Join” button next to the community you’d like to join. If you have any questions, please send them to [email protected].
Increase brings flu activity back to seasonal high
for the week ending Jan. 21, compared with three states the week before, according to the Centers for Disease Control and Prevention.
Alabama, Kansas, New Jersey, Oklahoma, and South Carolina were at level 10 on the CDC’s 1-10 scale of ILI activity, with Oklahoma reaching that level for the third consecutive week. Georgia (level 9) and Louisiana, Minnesota, Missouri, and Tennessee (level 8) were also in the “high” range, the CDC reported.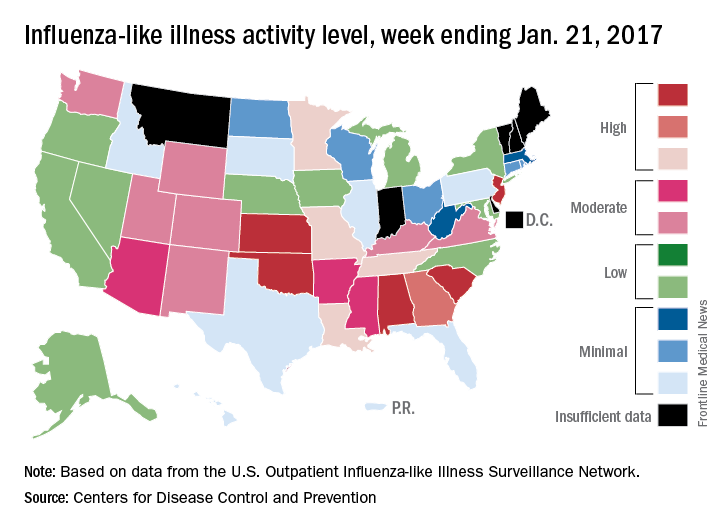
Three flu-related pediatric deaths were reported for the week, although two occurred during the week ending Jan. 14. The two earlier deaths were associated with an influenza A (H3) virus, and the more recent death was associated with an influenza B virus. For the 2016-2017 season so far, there have been a total of eight pediatric deaths, the CDC said.
for the week ending Jan. 21, compared with three states the week before, according to the Centers for Disease Control and Prevention.
Alabama, Kansas, New Jersey, Oklahoma, and South Carolina were at level 10 on the CDC’s 1-10 scale of ILI activity, with Oklahoma reaching that level for the third consecutive week. Georgia (level 9) and Louisiana, Minnesota, Missouri, and Tennessee (level 8) were also in the “high” range, the CDC reported.
Three flu-related pediatric deaths were reported for the week, although two occurred during the week ending Jan. 14. The two earlier deaths were associated with an influenza A (H3) virus, and the more recent death was associated with an influenza B virus. For the 2016-2017 season so far, there have been a total of eight pediatric deaths, the CDC said.
for the week ending Jan. 21, compared with three states the week before, according to the Centers for Disease Control and Prevention.
Alabama, Kansas, New Jersey, Oklahoma, and South Carolina were at level 10 on the CDC’s 1-10 scale of ILI activity, with Oklahoma reaching that level for the third consecutive week. Georgia (level 9) and Louisiana, Minnesota, Missouri, and Tennessee (level 8) were also in the “high” range, the CDC reported.
Three flu-related pediatric deaths were reported for the week, although two occurred during the week ending Jan. 14. The two earlier deaths were associated with an influenza A (H3) virus, and the more recent death was associated with an influenza B virus. For the 2016-2017 season so far, there have been a total of eight pediatric deaths, the CDC said.