User login
USPSTF should reconsider recommendation to lower mammogram age: Experts
The updated draft recommendation from the U.S. Preventive Services Task Force that would lower the recommended start age for routine screening mammograms by a decade for all average-risk women is not justified, experts argue in a “dissenting view” published in the New England Journal of Medicine.
The proposed change would affect more than 20 million U.S. women, and it’s “hard to see any potential benefits associated with lowering the starting age,” coauthor Steven Woloshin, MD, with Dartmouth Cancer Center, Lebanon, N.H., said in an NEJM podcast.
Back in May, when USPSTF released the draft recommendation, task force member John Wong, MD, with Tufts Medical Center, Boston, said in an interview, “It is now clear that screening every other year starting at age 40 has the potential to save about 20% more lives among all women.”
But, according to Dr. Woloshin, there is no recent evidence that mortality from breast cancer is increasing in young women.
In fact, the United States has seen a steady decrease in breast cancer mortality, especially among younger women. Breast cancer mortality among women under 50 “has been cut in half over the past 30 years,” Dr. Woloshin and coauthors explained.
Another wrinkle: The task force did not base its recent recommendation on randomized trial data. In fact, there have been no new randomized trials of screening mammography for women in their 40s since 2016. Instead, the task force relied on statistical models to “estimate what might happen if the starting age were lowered,” Dr. Woloshin and colleagues said.
Relying on a statistical model, however, “is problematic because it has some very optimistic assumptions about the benefit of mammography,” Dr. Woloshin said in the podcast. For instance, the models assume that screening mammography reduces breast cancer mortality by about 25%.
That 25% reduction is “far greater than what’s reported in the meta-analyses of the available randomized trials,” Dr. Woloshin explained. The meta-analyses report about a 16% reduction for all the trials combined and an estimated 13% for trials at low risk of bias. But “even these meta-analyses are likely to overstate the effect of screening since the trials were done before the major advances in treatment.”
In their own calculations, Dr. Woloshin and colleagues found that lowering the screening age to 40 came with a small potential benefit and a substantial risk for harm.
Combing data from the National Cancer Institute, the team reported that the risk for death for women in their 40s from any cause over the next 10 years was about 3% whether or not they received their biennial mammogram.
The risk for death from breast cancer in that time was 0.23% with mammograms – about 2 in every 1,000 women – and 0.31% without. “That’s 1 less breast cancer death per 1,000 women screened for 10 years,” Dr. Woloshin said.
Put another way, with mammography screening, “the chance of not dying from breast cancer over the next 10 years increases from 99.7% to 99.8%,” Dr. Woloshin said.
The benefit is arguably small, while the harms appear quite significant, Dr. Woloshin said. About 36% of women who begin screening at age 40 would have at least one false alarm over 10 years, and almost 7% would have a false alarm requiring a biopsy in that time frame.
Ease or exacerbate racial disparity?
Another argument that the USPSTF highlighted for lowering the screening age: Research indicates that Black women get breast cancer at younger ages and are more likely to die of the disease, compared with White women.
Dr. Woloshin and coauthors, however, also took issue with the view that lowering the screening age could reduce disparities between Black and White women.
“There’s no question that there are substantial differences between Black and White women in terms of breast cancer mortality, but there’s actually very little disparity in breast cancer screening – about 60% of Black and White women in their 40s are screened regularly in the United States,” Dr. Woloshin explained in the podcast.
Therefore, it’s “really hard to imagine” how recommending the same intervention to both groups could possibly reduce the disparity, he said.
“The disparity is not a reflection of screening. It reflects differences in cancer biology,” he added. “Black women are at higher risk for more aggressive, fast-growing cancers that are less likely to be caught by screening and unfortunately are less likely to benefit from treatment.”
Earlier screening would also not address the problems facing poor women, who tend to be disproportionately Black, such as lower quality of available medical services, follow-up delays after abnormal scans, treatment delays, and less use of adjuvant therapy, Dr. Woloshin cautioned.
In Dr. Woloshin’s view, lowering the screening age, which broadens the eligible population, may actually “exacerbate problems contributing to disparity by diverting resources toward expanded screening rather than doing what we know works by ensuring that high-quality treatments are more readily accessible to poor women with breast cancer.”
Reconsider the change?
Because task force recommendations are so influential, Dr. Woloshin and colleagues worry that mammography screening for women in their 40s will probably become a performance measure.
“Our concern is that, rather than fostering informed decisions, clinicians and practices are going to be judged and rewarded and punished based on compliance with this quality metric,” Dr. Woloshin said.
That’s a problem, he noted, “because women should be able to make the decision for themselves rather than having this be a public health imperative, which is imposed by physicians and practices who are incentivized to meet a quality metric.”
The hope, said Dr. Woloshin, is that this prospective piece will help influence the task force to “reconsider the recommendation, because we think that the bottom line is that their models are insufficient to support a new imperative. The benefits are really limited, and there are really common and important harms for healthy women.”
The comment period for the draft recommendation is now closed, and a final decision from the task force is forthcoming.
The research had no funding. Dr. Woloshin has no relevant disclosures.
A version of this article first appeared on Medscape.com.
The updated draft recommendation from the U.S. Preventive Services Task Force that would lower the recommended start age for routine screening mammograms by a decade for all average-risk women is not justified, experts argue in a “dissenting view” published in the New England Journal of Medicine.
The proposed change would affect more than 20 million U.S. women, and it’s “hard to see any potential benefits associated with lowering the starting age,” coauthor Steven Woloshin, MD, with Dartmouth Cancer Center, Lebanon, N.H., said in an NEJM podcast.
Back in May, when USPSTF released the draft recommendation, task force member John Wong, MD, with Tufts Medical Center, Boston, said in an interview, “It is now clear that screening every other year starting at age 40 has the potential to save about 20% more lives among all women.”
But, according to Dr. Woloshin, there is no recent evidence that mortality from breast cancer is increasing in young women.
In fact, the United States has seen a steady decrease in breast cancer mortality, especially among younger women. Breast cancer mortality among women under 50 “has been cut in half over the past 30 years,” Dr. Woloshin and coauthors explained.
Another wrinkle: The task force did not base its recent recommendation on randomized trial data. In fact, there have been no new randomized trials of screening mammography for women in their 40s since 2016. Instead, the task force relied on statistical models to “estimate what might happen if the starting age were lowered,” Dr. Woloshin and colleagues said.
Relying on a statistical model, however, “is problematic because it has some very optimistic assumptions about the benefit of mammography,” Dr. Woloshin said in the podcast. For instance, the models assume that screening mammography reduces breast cancer mortality by about 25%.
That 25% reduction is “far greater than what’s reported in the meta-analyses of the available randomized trials,” Dr. Woloshin explained. The meta-analyses report about a 16% reduction for all the trials combined and an estimated 13% for trials at low risk of bias. But “even these meta-analyses are likely to overstate the effect of screening since the trials were done before the major advances in treatment.”
In their own calculations, Dr. Woloshin and colleagues found that lowering the screening age to 40 came with a small potential benefit and a substantial risk for harm.
Combing data from the National Cancer Institute, the team reported that the risk for death for women in their 40s from any cause over the next 10 years was about 3% whether or not they received their biennial mammogram.
The risk for death from breast cancer in that time was 0.23% with mammograms – about 2 in every 1,000 women – and 0.31% without. “That’s 1 less breast cancer death per 1,000 women screened for 10 years,” Dr. Woloshin said.
Put another way, with mammography screening, “the chance of not dying from breast cancer over the next 10 years increases from 99.7% to 99.8%,” Dr. Woloshin said.
The benefit is arguably small, while the harms appear quite significant, Dr. Woloshin said. About 36% of women who begin screening at age 40 would have at least one false alarm over 10 years, and almost 7% would have a false alarm requiring a biopsy in that time frame.
Ease or exacerbate racial disparity?
Another argument that the USPSTF highlighted for lowering the screening age: Research indicates that Black women get breast cancer at younger ages and are more likely to die of the disease, compared with White women.
Dr. Woloshin and coauthors, however, also took issue with the view that lowering the screening age could reduce disparities between Black and White women.
“There’s no question that there are substantial differences between Black and White women in terms of breast cancer mortality, but there’s actually very little disparity in breast cancer screening – about 60% of Black and White women in their 40s are screened regularly in the United States,” Dr. Woloshin explained in the podcast.
Therefore, it’s “really hard to imagine” how recommending the same intervention to both groups could possibly reduce the disparity, he said.
“The disparity is not a reflection of screening. It reflects differences in cancer biology,” he added. “Black women are at higher risk for more aggressive, fast-growing cancers that are less likely to be caught by screening and unfortunately are less likely to benefit from treatment.”
Earlier screening would also not address the problems facing poor women, who tend to be disproportionately Black, such as lower quality of available medical services, follow-up delays after abnormal scans, treatment delays, and less use of adjuvant therapy, Dr. Woloshin cautioned.
In Dr. Woloshin’s view, lowering the screening age, which broadens the eligible population, may actually “exacerbate problems contributing to disparity by diverting resources toward expanded screening rather than doing what we know works by ensuring that high-quality treatments are more readily accessible to poor women with breast cancer.”
Reconsider the change?
Because task force recommendations are so influential, Dr. Woloshin and colleagues worry that mammography screening for women in their 40s will probably become a performance measure.
“Our concern is that, rather than fostering informed decisions, clinicians and practices are going to be judged and rewarded and punished based on compliance with this quality metric,” Dr. Woloshin said.
That’s a problem, he noted, “because women should be able to make the decision for themselves rather than having this be a public health imperative, which is imposed by physicians and practices who are incentivized to meet a quality metric.”
The hope, said Dr. Woloshin, is that this prospective piece will help influence the task force to “reconsider the recommendation, because we think that the bottom line is that their models are insufficient to support a new imperative. The benefits are really limited, and there are really common and important harms for healthy women.”
The comment period for the draft recommendation is now closed, and a final decision from the task force is forthcoming.
The research had no funding. Dr. Woloshin has no relevant disclosures.
A version of this article first appeared on Medscape.com.
The updated draft recommendation from the U.S. Preventive Services Task Force that would lower the recommended start age for routine screening mammograms by a decade for all average-risk women is not justified, experts argue in a “dissenting view” published in the New England Journal of Medicine.
The proposed change would affect more than 20 million U.S. women, and it’s “hard to see any potential benefits associated with lowering the starting age,” coauthor Steven Woloshin, MD, with Dartmouth Cancer Center, Lebanon, N.H., said in an NEJM podcast.
Back in May, when USPSTF released the draft recommendation, task force member John Wong, MD, with Tufts Medical Center, Boston, said in an interview, “It is now clear that screening every other year starting at age 40 has the potential to save about 20% more lives among all women.”
But, according to Dr. Woloshin, there is no recent evidence that mortality from breast cancer is increasing in young women.
In fact, the United States has seen a steady decrease in breast cancer mortality, especially among younger women. Breast cancer mortality among women under 50 “has been cut in half over the past 30 years,” Dr. Woloshin and coauthors explained.
Another wrinkle: The task force did not base its recent recommendation on randomized trial data. In fact, there have been no new randomized trials of screening mammography for women in their 40s since 2016. Instead, the task force relied on statistical models to “estimate what might happen if the starting age were lowered,” Dr. Woloshin and colleagues said.
Relying on a statistical model, however, “is problematic because it has some very optimistic assumptions about the benefit of mammography,” Dr. Woloshin said in the podcast. For instance, the models assume that screening mammography reduces breast cancer mortality by about 25%.
That 25% reduction is “far greater than what’s reported in the meta-analyses of the available randomized trials,” Dr. Woloshin explained. The meta-analyses report about a 16% reduction for all the trials combined and an estimated 13% for trials at low risk of bias. But “even these meta-analyses are likely to overstate the effect of screening since the trials were done before the major advances in treatment.”
In their own calculations, Dr. Woloshin and colleagues found that lowering the screening age to 40 came with a small potential benefit and a substantial risk for harm.
Combing data from the National Cancer Institute, the team reported that the risk for death for women in their 40s from any cause over the next 10 years was about 3% whether or not they received their biennial mammogram.
The risk for death from breast cancer in that time was 0.23% with mammograms – about 2 in every 1,000 women – and 0.31% without. “That’s 1 less breast cancer death per 1,000 women screened for 10 years,” Dr. Woloshin said.
Put another way, with mammography screening, “the chance of not dying from breast cancer over the next 10 years increases from 99.7% to 99.8%,” Dr. Woloshin said.
The benefit is arguably small, while the harms appear quite significant, Dr. Woloshin said. About 36% of women who begin screening at age 40 would have at least one false alarm over 10 years, and almost 7% would have a false alarm requiring a biopsy in that time frame.
Ease or exacerbate racial disparity?
Another argument that the USPSTF highlighted for lowering the screening age: Research indicates that Black women get breast cancer at younger ages and are more likely to die of the disease, compared with White women.
Dr. Woloshin and coauthors, however, also took issue with the view that lowering the screening age could reduce disparities between Black and White women.
“There’s no question that there are substantial differences between Black and White women in terms of breast cancer mortality, but there’s actually very little disparity in breast cancer screening – about 60% of Black and White women in their 40s are screened regularly in the United States,” Dr. Woloshin explained in the podcast.
Therefore, it’s “really hard to imagine” how recommending the same intervention to both groups could possibly reduce the disparity, he said.
“The disparity is not a reflection of screening. It reflects differences in cancer biology,” he added. “Black women are at higher risk for more aggressive, fast-growing cancers that are less likely to be caught by screening and unfortunately are less likely to benefit from treatment.”
Earlier screening would also not address the problems facing poor women, who tend to be disproportionately Black, such as lower quality of available medical services, follow-up delays after abnormal scans, treatment delays, and less use of adjuvant therapy, Dr. Woloshin cautioned.
In Dr. Woloshin’s view, lowering the screening age, which broadens the eligible population, may actually “exacerbate problems contributing to disparity by diverting resources toward expanded screening rather than doing what we know works by ensuring that high-quality treatments are more readily accessible to poor women with breast cancer.”
Reconsider the change?
Because task force recommendations are so influential, Dr. Woloshin and colleagues worry that mammography screening for women in their 40s will probably become a performance measure.
“Our concern is that, rather than fostering informed decisions, clinicians and practices are going to be judged and rewarded and punished based on compliance with this quality metric,” Dr. Woloshin said.
That’s a problem, he noted, “because women should be able to make the decision for themselves rather than having this be a public health imperative, which is imposed by physicians and practices who are incentivized to meet a quality metric.”
The hope, said Dr. Woloshin, is that this prospective piece will help influence the task force to “reconsider the recommendation, because we think that the bottom line is that their models are insufficient to support a new imperative. The benefits are really limited, and there are really common and important harms for healthy women.”
The comment period for the draft recommendation is now closed, and a final decision from the task force is forthcoming.
The research had no funding. Dr. Woloshin has no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Severity score predicts mortality in pulmonary tuberculosis
, based on data from approximately 400 individuals.
Although a mortality risk-prediction score could improve treatment for pulmonary tuberculosis patients, such a score has not been previously reported, wrote Takeshi Osawa, MD, of Fukujuji Hospital, Tokyo, and colleagues.
In a study published in the journal CHEST, the researchers used 252 patients from a previous perspective study of newly diagnosed pulmonary tuberculosis as the development cohort, and recruited 165 additional patients between March 2021 and September 2022.
The primary endpoint was all-cause in-hospital mortality. Based on data from the development group, the researchers found that age 65 years and older and age 80 years and older, hypoxemia, activities of daily living, bilateral pulmonary lesions, lymphocyte count of less than 720 microliters, serum albumin less than 2.86 mg/dL, C-reactive protein (CRP) 3.97 mg/dL or higher, and procalcitonin (PCT) 0.130 ng/mL or higher were predictors of all-cause in hospital mortality.
The researchers used this information to create the disease severity score, known as the AHL score. The AHL included three clinical parameters: activity in daily living (semi-dependent, 1 point; totally dependent, 2 points); hypoxemia (1 point) and lymphocytes (< 720 /mcL, 1 point).
The scoring systems for the three parameters were, respectively, 1 point for semi-dependent and 2 points totally dependent (for activity in daily living), 1 point for presence of hypoxemia, and 1 point for lymphocytes less than 720 per microliter. The researchers stratified the scores into levels of low, intermediate, and high risk, with scores of 0, 1-2, and 3-4, respectively.
All-cause in hospital mortality occurred in 39 (15.5%) and 17 (10.3%) of patients in the developmental and validation cohorts, respectively.
The AHL score effectively predicted mortality, dividing patients into three groups of 1.3% low-risk, 8.9% intermediate risk, and 39.3% high-risk in the validation cohort, with a Harrell’s c-statistic of 0.842.
The corresponding numbers for the development cohort were 0, 13.5%, and 55.8%, with a c-statistic of 0.902.
The findings were limited by several factors, including the lack of data from “smear-negative” patients who were treated as outpatients, and more research is needed to determine the applicability of the AHL score in an outpatient population, the researchers noted. Other limitations included the lack of data on long-term mortality in surviving patients who were discharged, and the reliance on assessments that can be performed only in clinical settings in developed countries, they said.
However, the results support the feasibility of the AHL score in clinical settings to accurately predict mortality in patients with pulmonary TB, and may help optimize treatments for this population, they concluded.
The study received no outside funding. All authors disclosed nonfinancial support in the form of measuring reagents from Fujifilm Wako Pure Chemical Corporation during the study but had no relevant financial conflicts to disclose.
, based on data from approximately 400 individuals.
Although a mortality risk-prediction score could improve treatment for pulmonary tuberculosis patients, such a score has not been previously reported, wrote Takeshi Osawa, MD, of Fukujuji Hospital, Tokyo, and colleagues.
In a study published in the journal CHEST, the researchers used 252 patients from a previous perspective study of newly diagnosed pulmonary tuberculosis as the development cohort, and recruited 165 additional patients between March 2021 and September 2022.
The primary endpoint was all-cause in-hospital mortality. Based on data from the development group, the researchers found that age 65 years and older and age 80 years and older, hypoxemia, activities of daily living, bilateral pulmonary lesions, lymphocyte count of less than 720 microliters, serum albumin less than 2.86 mg/dL, C-reactive protein (CRP) 3.97 mg/dL or higher, and procalcitonin (PCT) 0.130 ng/mL or higher were predictors of all-cause in hospital mortality.
The researchers used this information to create the disease severity score, known as the AHL score. The AHL included three clinical parameters: activity in daily living (semi-dependent, 1 point; totally dependent, 2 points); hypoxemia (1 point) and lymphocytes (< 720 /mcL, 1 point).
The scoring systems for the three parameters were, respectively, 1 point for semi-dependent and 2 points totally dependent (for activity in daily living), 1 point for presence of hypoxemia, and 1 point for lymphocytes less than 720 per microliter. The researchers stratified the scores into levels of low, intermediate, and high risk, with scores of 0, 1-2, and 3-4, respectively.
All-cause in hospital mortality occurred in 39 (15.5%) and 17 (10.3%) of patients in the developmental and validation cohorts, respectively.
The AHL score effectively predicted mortality, dividing patients into three groups of 1.3% low-risk, 8.9% intermediate risk, and 39.3% high-risk in the validation cohort, with a Harrell’s c-statistic of 0.842.
The corresponding numbers for the development cohort were 0, 13.5%, and 55.8%, with a c-statistic of 0.902.
The findings were limited by several factors, including the lack of data from “smear-negative” patients who were treated as outpatients, and more research is needed to determine the applicability of the AHL score in an outpatient population, the researchers noted. Other limitations included the lack of data on long-term mortality in surviving patients who were discharged, and the reliance on assessments that can be performed only in clinical settings in developed countries, they said.
However, the results support the feasibility of the AHL score in clinical settings to accurately predict mortality in patients with pulmonary TB, and may help optimize treatments for this population, they concluded.
The study received no outside funding. All authors disclosed nonfinancial support in the form of measuring reagents from Fujifilm Wako Pure Chemical Corporation during the study but had no relevant financial conflicts to disclose.
, based on data from approximately 400 individuals.
Although a mortality risk-prediction score could improve treatment for pulmonary tuberculosis patients, such a score has not been previously reported, wrote Takeshi Osawa, MD, of Fukujuji Hospital, Tokyo, and colleagues.
In a study published in the journal CHEST, the researchers used 252 patients from a previous perspective study of newly diagnosed pulmonary tuberculosis as the development cohort, and recruited 165 additional patients between March 2021 and September 2022.
The primary endpoint was all-cause in-hospital mortality. Based on data from the development group, the researchers found that age 65 years and older and age 80 years and older, hypoxemia, activities of daily living, bilateral pulmonary lesions, lymphocyte count of less than 720 microliters, serum albumin less than 2.86 mg/dL, C-reactive protein (CRP) 3.97 mg/dL or higher, and procalcitonin (PCT) 0.130 ng/mL or higher were predictors of all-cause in hospital mortality.
The researchers used this information to create the disease severity score, known as the AHL score. The AHL included three clinical parameters: activity in daily living (semi-dependent, 1 point; totally dependent, 2 points); hypoxemia (1 point) and lymphocytes (< 720 /mcL, 1 point).
The scoring systems for the three parameters were, respectively, 1 point for semi-dependent and 2 points totally dependent (for activity in daily living), 1 point for presence of hypoxemia, and 1 point for lymphocytes less than 720 per microliter. The researchers stratified the scores into levels of low, intermediate, and high risk, with scores of 0, 1-2, and 3-4, respectively.
All-cause in hospital mortality occurred in 39 (15.5%) and 17 (10.3%) of patients in the developmental and validation cohorts, respectively.
The AHL score effectively predicted mortality, dividing patients into three groups of 1.3% low-risk, 8.9% intermediate risk, and 39.3% high-risk in the validation cohort, with a Harrell’s c-statistic of 0.842.
The corresponding numbers for the development cohort were 0, 13.5%, and 55.8%, with a c-statistic of 0.902.
The findings were limited by several factors, including the lack of data from “smear-negative” patients who were treated as outpatients, and more research is needed to determine the applicability of the AHL score in an outpatient population, the researchers noted. Other limitations included the lack of data on long-term mortality in surviving patients who were discharged, and the reliance on assessments that can be performed only in clinical settings in developed countries, they said.
However, the results support the feasibility of the AHL score in clinical settings to accurately predict mortality in patients with pulmonary TB, and may help optimize treatments for this population, they concluded.
The study received no outside funding. All authors disclosed nonfinancial support in the form of measuring reagents from Fujifilm Wako Pure Chemical Corporation during the study but had no relevant financial conflicts to disclose.
FROM THE JOURNAL CHEST
Hold blood thinners during thyroid nodule biopsy?
WASHINGTON – The routine practice of holding use of blood-thinning medications at the time of an ultrasound-guided thyroid nodule fine needle aspiration (FNA) biopsy shows no significant safety benefit in preventing the risk of complications such as hematomas or nondiagnostic results; however, experts suggest using individualized decision-making with the practice.
first author Michelle Lundholm, MD, of the Cleveland Clinic said in an interview.
“[The practice] impacts neither the safety of the FNA procedure nor the adequacy of the sample,” she said.
The late-breaking research was presented at the annual meeting of the American Thyroid Association.
Key concerns in the use of anticoagulants and/or antiplatelet medications during thyroid nodule FNA biopsy include the increased risk of postprocedural hematoma or nondiagnostic results, with, for instance, one study showing higher rates of nondiagnostic results among patients remaining on aspirin therapy during the FNA biopsy.
However, holding the medically indicated therapies can have risks of its own, including concerns of thrombotic events such as deep vein thrombosis or stroke. However, evidence comparing the risks with each strategy in thyroid nodule FNA is lacking.
To investigate, Dr. Lundholm and colleagues conducted a review of data on 2,945 patients who had undergone a total of 4,741 thyroid nodule FNAs in the Cleveland Clinic’s diverse network of centers between 2010 and 2023. The patients had a mean age of 66.2; 69.6% were female and 75.7% were White.
All patients had an active prescription for an anticoagulant or antiplatelet medication up to 10 days prior to their thyroid nodule FNA biopsy. Specifically, 73.7% were on 81 mg aspirin, 8.5% were on 325 mg aspirin, 7.4% were taking other antiplatelet medication such as clopidogrel or ticagrelor; 7.0% were on warfarin, 8.2% were on a direct oral anticoagulant (DOAC); 6.3% were on heparin products; and 10.3% of patients were on two or more blood-thinning medications.
The results show that, overall, 13.0% (n = 614) of the thyroid nodule FNA biopsies had nondiagnostic results, which is within the average rates in the literature ranging from 6% to 36%, Dr. Lundholm noted.
Blood-thinning medications were held in 20.8% of the FNA biopsies, however, there were no differences in nondiagnostic results between those who had drugs held (12.2%) or who continued on the medications (13.2%; P = .41).
After multivariate adjustment for age and sex, the lack of significant differences in receiving nondiagnostic results among those who did or did not continue blood thinners was consistent overall (odds ratio, 1.10; P = .38), and in the specific groups of 81 mg aspirin (OR, 1.00; P = .99); 325 mg aspirin or clopidogrel/ticagrelor (OR, 1.50; P = .15); or warfarin, DOAC, or heparin/enoxaparin (OR, 1.27; P = .27).
In terms of hematoma risk, ED records within 48 hours of the FNA showed that such events were rare, with only one hematoma occurring overall, involving a patient who was on 81 mg of aspirin for secondary stroke prevention that was not interrupted for FNA biopsy. The patient was discharged and did not require medical intervention.
Four other hematomas occurred among patients who were not being treated with blood thinners, with none requiring intervention.
The findings indicate that “hematoma can happen in any patient, but rarely requires intervention,” Dr. Lundholm said.
However, while thrombotic events were also rare, serious events occurred in three patients within 48 hours of the thyroid nodule FNA biopsy when a blood thinner was withheld, including ischemic strokes among two patients who were on a DOAC and 81 mg of aspirin that were withheld, and one MI occurring in a patient on a DOAC that was held for the FNA.
Unlike hematomas, the thrombotic events each had significant long‐term sequelae, Dr. Lundholm noted.
“Having these ischemic strokes and heart attack really led to a change in these patients’ lives,” she said. “While we can never assume that [the events occurred] because the blood-thinner therapy was held, the timing within 48 hours is certainly very suspicious.”
There were no deep vein thrombosis or pulmonary embolism events.
Withholding practices vary
In a previous survey of 60 clinicians conducted by Dr. Lundholm and colleagues, wide variation was reported in the rates of withholding antiplatelet or anticoagulant medications prior to thyroid nodule FNA biopsy.
The survey of endocrinologists, interventional radiologists, and ear, nose, and throat providers showed rates of withholding 81 mg of aspirin prior to FNA biopsy of just 13.3%, withholding 325 mg of aspirin, 15%, other antiplatelets, 41.7%, warfarin, 73.3%, DOACs, 43.3%, and heparin, 43.3%.
“We found heterogeneity in withholding patterns even within the same department,” she said. “This is reflective of the fact that evidence is mixed.”
Guidelines on the issue from the Society of Interventional Radiology and the International Society on Thrombosis and Hemostasis recommend that providers consider the balance of the procedure and patient bleeding risk versus the clotting risk, Dr. Lundholm noted.
However, a caveat is that those recommendations are based on pooled data from similar minimal risk procedures, she explained.
“There is a lack of data on bleeding risks for individual interventions like thyroid biopsy, and, as such, there is no specific procedure-related risk determination.”
Meanwhile, Dr. Lundholm said that notable limitations regarding the current research include that the study may not have caught all patient cases that presented with complications to an outside ED.
Furthermore, the study results pertain to the safety of blood thinners in routine use, with key aspects that can influence complication rates, such as provider experience, needle size, and nodule features unavailable for analysis.
At MD Anderson, case-by-case
Commenting on the research, Anastasios Maniakas, MD, PhD, of the department of head and neck surgery, division of surgery, University of Texas MD Anderson Cancer Center, Houston, said the study is important, noting that, at his institution, the approach regarding holding blood-thinning medications is generally determined on an individual basis.
“I think this was a good study, but I don’t think it’s practice changing because these decisions may differ on a case-by-case basis,” Dr. Maniakas, who comoderated the session, said in an interview.
“At MD Anderson, we probably have one of the highest volumes in the country for thyroid nodule FNAs, and we do hold blood thinners because we often have to do more significant biopsies, with multiple passages and larger needles to be used,” Dr. Maniakas said.
“If you’re going to use perhaps the smallest possible gauge needle, then I think it is reasonable to not hold blood thinners, but if you’re going to be doing multiple passages and you need to do a core biopsy and use a large needle, then it is wiser to try to hold the medications for a day or 2.
“We haven’t had any complications, but I think there’s still a lot of apprehension to not hold blood thinners,” Dr. Maniakas said. “So, overall, I think the message is that it has to be on a case-by-case basis.”
Dr. Lundholm and Dr. Maniakas reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
WASHINGTON – The routine practice of holding use of blood-thinning medications at the time of an ultrasound-guided thyroid nodule fine needle aspiration (FNA) biopsy shows no significant safety benefit in preventing the risk of complications such as hematomas or nondiagnostic results; however, experts suggest using individualized decision-making with the practice.
first author Michelle Lundholm, MD, of the Cleveland Clinic said in an interview.
“[The practice] impacts neither the safety of the FNA procedure nor the adequacy of the sample,” she said.
The late-breaking research was presented at the annual meeting of the American Thyroid Association.
Key concerns in the use of anticoagulants and/or antiplatelet medications during thyroid nodule FNA biopsy include the increased risk of postprocedural hematoma or nondiagnostic results, with, for instance, one study showing higher rates of nondiagnostic results among patients remaining on aspirin therapy during the FNA biopsy.
However, holding the medically indicated therapies can have risks of its own, including concerns of thrombotic events such as deep vein thrombosis or stroke. However, evidence comparing the risks with each strategy in thyroid nodule FNA is lacking.
To investigate, Dr. Lundholm and colleagues conducted a review of data on 2,945 patients who had undergone a total of 4,741 thyroid nodule FNAs in the Cleveland Clinic’s diverse network of centers between 2010 and 2023. The patients had a mean age of 66.2; 69.6% were female and 75.7% were White.
All patients had an active prescription for an anticoagulant or antiplatelet medication up to 10 days prior to their thyroid nodule FNA biopsy. Specifically, 73.7% were on 81 mg aspirin, 8.5% were on 325 mg aspirin, 7.4% were taking other antiplatelet medication such as clopidogrel or ticagrelor; 7.0% were on warfarin, 8.2% were on a direct oral anticoagulant (DOAC); 6.3% were on heparin products; and 10.3% of patients were on two or more blood-thinning medications.
The results show that, overall, 13.0% (n = 614) of the thyroid nodule FNA biopsies had nondiagnostic results, which is within the average rates in the literature ranging from 6% to 36%, Dr. Lundholm noted.
Blood-thinning medications were held in 20.8% of the FNA biopsies, however, there were no differences in nondiagnostic results between those who had drugs held (12.2%) or who continued on the medications (13.2%; P = .41).
After multivariate adjustment for age and sex, the lack of significant differences in receiving nondiagnostic results among those who did or did not continue blood thinners was consistent overall (odds ratio, 1.10; P = .38), and in the specific groups of 81 mg aspirin (OR, 1.00; P = .99); 325 mg aspirin or clopidogrel/ticagrelor (OR, 1.50; P = .15); or warfarin, DOAC, or heparin/enoxaparin (OR, 1.27; P = .27).
In terms of hematoma risk, ED records within 48 hours of the FNA showed that such events were rare, with only one hematoma occurring overall, involving a patient who was on 81 mg of aspirin for secondary stroke prevention that was not interrupted for FNA biopsy. The patient was discharged and did not require medical intervention.
Four other hematomas occurred among patients who were not being treated with blood thinners, with none requiring intervention.
The findings indicate that “hematoma can happen in any patient, but rarely requires intervention,” Dr. Lundholm said.
However, while thrombotic events were also rare, serious events occurred in three patients within 48 hours of the thyroid nodule FNA biopsy when a blood thinner was withheld, including ischemic strokes among two patients who were on a DOAC and 81 mg of aspirin that were withheld, and one MI occurring in a patient on a DOAC that was held for the FNA.
Unlike hematomas, the thrombotic events each had significant long‐term sequelae, Dr. Lundholm noted.
“Having these ischemic strokes and heart attack really led to a change in these patients’ lives,” she said. “While we can never assume that [the events occurred] because the blood-thinner therapy was held, the timing within 48 hours is certainly very suspicious.”
There were no deep vein thrombosis or pulmonary embolism events.
Withholding practices vary
In a previous survey of 60 clinicians conducted by Dr. Lundholm and colleagues, wide variation was reported in the rates of withholding antiplatelet or anticoagulant medications prior to thyroid nodule FNA biopsy.
The survey of endocrinologists, interventional radiologists, and ear, nose, and throat providers showed rates of withholding 81 mg of aspirin prior to FNA biopsy of just 13.3%, withholding 325 mg of aspirin, 15%, other antiplatelets, 41.7%, warfarin, 73.3%, DOACs, 43.3%, and heparin, 43.3%.
“We found heterogeneity in withholding patterns even within the same department,” she said. “This is reflective of the fact that evidence is mixed.”
Guidelines on the issue from the Society of Interventional Radiology and the International Society on Thrombosis and Hemostasis recommend that providers consider the balance of the procedure and patient bleeding risk versus the clotting risk, Dr. Lundholm noted.
However, a caveat is that those recommendations are based on pooled data from similar minimal risk procedures, she explained.
“There is a lack of data on bleeding risks for individual interventions like thyroid biopsy, and, as such, there is no specific procedure-related risk determination.”
Meanwhile, Dr. Lundholm said that notable limitations regarding the current research include that the study may not have caught all patient cases that presented with complications to an outside ED.
Furthermore, the study results pertain to the safety of blood thinners in routine use, with key aspects that can influence complication rates, such as provider experience, needle size, and nodule features unavailable for analysis.
At MD Anderson, case-by-case
Commenting on the research, Anastasios Maniakas, MD, PhD, of the department of head and neck surgery, division of surgery, University of Texas MD Anderson Cancer Center, Houston, said the study is important, noting that, at his institution, the approach regarding holding blood-thinning medications is generally determined on an individual basis.
“I think this was a good study, but I don’t think it’s practice changing because these decisions may differ on a case-by-case basis,” Dr. Maniakas, who comoderated the session, said in an interview.
“At MD Anderson, we probably have one of the highest volumes in the country for thyroid nodule FNAs, and we do hold blood thinners because we often have to do more significant biopsies, with multiple passages and larger needles to be used,” Dr. Maniakas said.
“If you’re going to use perhaps the smallest possible gauge needle, then I think it is reasonable to not hold blood thinners, but if you’re going to be doing multiple passages and you need to do a core biopsy and use a large needle, then it is wiser to try to hold the medications for a day or 2.
“We haven’t had any complications, but I think there’s still a lot of apprehension to not hold blood thinners,” Dr. Maniakas said. “So, overall, I think the message is that it has to be on a case-by-case basis.”
Dr. Lundholm and Dr. Maniakas reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
WASHINGTON – The routine practice of holding use of blood-thinning medications at the time of an ultrasound-guided thyroid nodule fine needle aspiration (FNA) biopsy shows no significant safety benefit in preventing the risk of complications such as hematomas or nondiagnostic results; however, experts suggest using individualized decision-making with the practice.
first author Michelle Lundholm, MD, of the Cleveland Clinic said in an interview.
“[The practice] impacts neither the safety of the FNA procedure nor the adequacy of the sample,” she said.
The late-breaking research was presented at the annual meeting of the American Thyroid Association.
Key concerns in the use of anticoagulants and/or antiplatelet medications during thyroid nodule FNA biopsy include the increased risk of postprocedural hematoma or nondiagnostic results, with, for instance, one study showing higher rates of nondiagnostic results among patients remaining on aspirin therapy during the FNA biopsy.
However, holding the medically indicated therapies can have risks of its own, including concerns of thrombotic events such as deep vein thrombosis or stroke. However, evidence comparing the risks with each strategy in thyroid nodule FNA is lacking.
To investigate, Dr. Lundholm and colleagues conducted a review of data on 2,945 patients who had undergone a total of 4,741 thyroid nodule FNAs in the Cleveland Clinic’s diverse network of centers between 2010 and 2023. The patients had a mean age of 66.2; 69.6% were female and 75.7% were White.
All patients had an active prescription for an anticoagulant or antiplatelet medication up to 10 days prior to their thyroid nodule FNA biopsy. Specifically, 73.7% were on 81 mg aspirin, 8.5% were on 325 mg aspirin, 7.4% were taking other antiplatelet medication such as clopidogrel or ticagrelor; 7.0% were on warfarin, 8.2% were on a direct oral anticoagulant (DOAC); 6.3% were on heparin products; and 10.3% of patients were on two or more blood-thinning medications.
The results show that, overall, 13.0% (n = 614) of the thyroid nodule FNA biopsies had nondiagnostic results, which is within the average rates in the literature ranging from 6% to 36%, Dr. Lundholm noted.
Blood-thinning medications were held in 20.8% of the FNA biopsies, however, there were no differences in nondiagnostic results between those who had drugs held (12.2%) or who continued on the medications (13.2%; P = .41).
After multivariate adjustment for age and sex, the lack of significant differences in receiving nondiagnostic results among those who did or did not continue blood thinners was consistent overall (odds ratio, 1.10; P = .38), and in the specific groups of 81 mg aspirin (OR, 1.00; P = .99); 325 mg aspirin or clopidogrel/ticagrelor (OR, 1.50; P = .15); or warfarin, DOAC, or heparin/enoxaparin (OR, 1.27; P = .27).
In terms of hematoma risk, ED records within 48 hours of the FNA showed that such events were rare, with only one hematoma occurring overall, involving a patient who was on 81 mg of aspirin for secondary stroke prevention that was not interrupted for FNA biopsy. The patient was discharged and did not require medical intervention.
Four other hematomas occurred among patients who were not being treated with blood thinners, with none requiring intervention.
The findings indicate that “hematoma can happen in any patient, but rarely requires intervention,” Dr. Lundholm said.
However, while thrombotic events were also rare, serious events occurred in three patients within 48 hours of the thyroid nodule FNA biopsy when a blood thinner was withheld, including ischemic strokes among two patients who were on a DOAC and 81 mg of aspirin that were withheld, and one MI occurring in a patient on a DOAC that was held for the FNA.
Unlike hematomas, the thrombotic events each had significant long‐term sequelae, Dr. Lundholm noted.
“Having these ischemic strokes and heart attack really led to a change in these patients’ lives,” she said. “While we can never assume that [the events occurred] because the blood-thinner therapy was held, the timing within 48 hours is certainly very suspicious.”
There were no deep vein thrombosis or pulmonary embolism events.
Withholding practices vary
In a previous survey of 60 clinicians conducted by Dr. Lundholm and colleagues, wide variation was reported in the rates of withholding antiplatelet or anticoagulant medications prior to thyroid nodule FNA biopsy.
The survey of endocrinologists, interventional radiologists, and ear, nose, and throat providers showed rates of withholding 81 mg of aspirin prior to FNA biopsy of just 13.3%, withholding 325 mg of aspirin, 15%, other antiplatelets, 41.7%, warfarin, 73.3%, DOACs, 43.3%, and heparin, 43.3%.
“We found heterogeneity in withholding patterns even within the same department,” she said. “This is reflective of the fact that evidence is mixed.”
Guidelines on the issue from the Society of Interventional Radiology and the International Society on Thrombosis and Hemostasis recommend that providers consider the balance of the procedure and patient bleeding risk versus the clotting risk, Dr. Lundholm noted.
However, a caveat is that those recommendations are based on pooled data from similar minimal risk procedures, she explained.
“There is a lack of data on bleeding risks for individual interventions like thyroid biopsy, and, as such, there is no specific procedure-related risk determination.”
Meanwhile, Dr. Lundholm said that notable limitations regarding the current research include that the study may not have caught all patient cases that presented with complications to an outside ED.
Furthermore, the study results pertain to the safety of blood thinners in routine use, with key aspects that can influence complication rates, such as provider experience, needle size, and nodule features unavailable for analysis.
At MD Anderson, case-by-case
Commenting on the research, Anastasios Maniakas, MD, PhD, of the department of head and neck surgery, division of surgery, University of Texas MD Anderson Cancer Center, Houston, said the study is important, noting that, at his institution, the approach regarding holding blood-thinning medications is generally determined on an individual basis.
“I think this was a good study, but I don’t think it’s practice changing because these decisions may differ on a case-by-case basis,” Dr. Maniakas, who comoderated the session, said in an interview.
“At MD Anderson, we probably have one of the highest volumes in the country for thyroid nodule FNAs, and we do hold blood thinners because we often have to do more significant biopsies, with multiple passages and larger needles to be used,” Dr. Maniakas said.
“If you’re going to use perhaps the smallest possible gauge needle, then I think it is reasonable to not hold blood thinners, but if you’re going to be doing multiple passages and you need to do a core biopsy and use a large needle, then it is wiser to try to hold the medications for a day or 2.
“We haven’t had any complications, but I think there’s still a lot of apprehension to not hold blood thinners,” Dr. Maniakas said. “So, overall, I think the message is that it has to be on a case-by-case basis.”
Dr. Lundholm and Dr. Maniakas reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT ATA 2023
Tirzepatide with insulin glargine improves type 2 diabetes
HAMBURG, GERMANY – Once-weekly tirzepatide (Mounjaro, Lilly) added to insulin glargine resulted in greater reductions in hemoglobin A1c along with more weight loss and less hypoglycemia, compared with prandial insulin lispro (Humalog, Sanofi), for patients with inadequately controlled type 2 diabetes, show data from the SURPASS-6 randomized clinical trial.
It also resulted in a higher percentage of participants meeting an A1c target of less than 7.0%, wrote the researchers, whose study was presented at the annual meeting of the European Association for the Study of Diabetes and was published simultaneously in JAMA.
Also, daily insulin glargine use was substantially lower among participants who received tirzepatide, compared with insulin lispro. Insulin glargine was administered at a dosage 13 IU/day; insulin lispro was administered at a dosage of 62 IU/day. “At the highest dose, some patients stopped their insulin [glargine] in the tirzepatide arm,” said Juan Pablo Frias, MD, medical director and principal investigator of Velocity Clinical Research, Los Angeles, who presented the findings. “We demonstrated clinically meaningful and superior glycemic and body weight control with tirzepatide compared with insulin lispro, while tirzepatide was also associated with less clinically significant hypoglycemia.”
Weight improved for participants who received tirzepatide compared with those who received insulin lispro, at –10 kg and +4 kg respectively. The rate of clinically significant hypoglycemia (blood glucose < 54 mg/dL) or severe hypoglycemia was tenfold lower with tirzepatide, compared with insulin lispro.
The session dedicated to tirzepatide was comoderated by Apostolos Tsapas, MD, professor of medicine and diabetes, Aristotle University, Thessaloniki, Greece, and Konstantinos Toulis, MD, consultant in endocrinology and diabetes, General Military Hospital, Thessaloniki, Greece. Dr. Toulis remarked that, in the chronic disease setting, management and treatment intensification are challenging to integrate, and there are barriers to adoption in routine practice. “This is particularly true when it adds complexity, as in the case of multiple prandial insulin injections on top of basal insulin in suboptimally treated individuals with type 2 diabetes.
“Demonstrating superiority over insulin lispro in terms of the so-called trio of A1c, weight loss, and hypoglycemic events, tirzepatide offers both a simpler to adhere to and a more efficacious treatment intensification option.” He noted that, while long-term safety data are awaited, “this seems to be a definite step forward from any viewpoint, with the possible exception of the taxpayer’s perspective.”
Dr. Tsapas added: “These data further support the very high dual glucose and weight efficacy of tirzepatide and the primary role of incretin-related therapies amongst the injectables for the treatment of type 2 diabetes.”
Tirzepatide 5, 10, 15 mg vs. insulin lispro in addition to insulin glargine
The researchers aimed to assess the efficacy and safety of adding once-weekly tirzepatide, compared with thrice-daily prandial insulin lispro, as an adjunctive therapy to insulin glargine for patients with type 2 diabetes that was inadequately controlled with basal insulin.
Tirzepatide activates the body’s receptors for glucose-dependent insulinotropic polypeptide and glucagonlike peptide–1 (GLP-1). The study authors noted that “recent guidelines support adding an injectable incretin-related therapy such as GLP-1 receptor agonist for glycemic control, rather than basal insulin, when oral medications are inadequate.”
The open-label, phase 3b clinical trial drew data from 135 sites across 15 countries and included 1,428 adults with type 2 diabetes who were taking basal insulin. Participants were randomly assigned in a 1:1:1:3 ratio to receive once-weekly subcutaneous injections of tirzepatide (5 mg [n = 243], 10 mg [n = 238], or 15 mg [n = 236]) or prandial thrice-daily insulin lispro (n = 708).
Both arms were well matched. The average age was 60 years, and 60% of participants were women. The average amount of time patients had type 2 diabetes was 14 years; 85% of participants continued taking metformin. The average A1c level was 8.8% at baseline. Patients were categorized as having obesity (average body mass index, 33 kg/m2). The average insulin glargine dose was 46 units, or 0.5 units/kg.
Outcomes included noninferiority of tirzepatide (pooled cohort) compared with insulin lispro, both in addition to insulin glargine; and A1c change from baseline to week 52 (noninferiority margin, 0.3%). Key secondary endpoints included change in body weight and percentage of participants who achieved an A1c target of less than 7.0%.
About 90% of participants who received the study drug completed the study, said Dr. Frias. “Only 0.5% of tirzepatide patients needed rescue therapy, while only 2% of the insulin lispro did.”
Prior to optimization, the average insulin glargine dose was 42 IU/kg; during optimization, it rose to an average of 46 IU/kg. “At 52 weeks, those on basal-bolus insulin found their insulin glargine dose stayed flat while insulin lispro was 62 units,” reported Dr. Frias. “The three tirzepatide doses show a reduction in insulin glargine, such that the pooled dose reached an average of 11 units, while 20% actually came off their basal insulin altogether [pooled tirzepatide].”
Tirzepatide (pooled) led to the recommended A1c target of less than 7.0% for 68% of patients versus 36% of patients in the insulin lispro group.
About 68% of the patients who received tirzepatide (pooled) achieved the recommended A1c target of less than 7.0% versus 36% of patients in the insulin lispro group.
“Individual tirzepatide doses and pooled doses showed significant reduction in A1c and up to a 2.5% reduction,” Dr. Frias added. “Normoglycemia was obtained by a greater proportion of patients on tirzepatide doses versus basal-bolus insulin – one-third in the 15-mg tirzepatide dose.”
Body weight reduction of 10% or more with tirzepatide
Further, at week 52, weight loss of 5% or more was achieved by 75.4% of participants in the pooled tirzepatide group, compared with 6.3% in the prandial lispro group. The weight loss was accompanied by clinically relevant improvements in cardiometabolic parameters.
In an exploratory analysis, weight loss of 10% or more was achieved by a mean of 48.9% of pooled tirzepatide-treated participants at week 52, compared with 2% of those taking insulin lispro, said Dr. Frias.
“It is possible that the body weight loss induced by tirzepatide therapy and its reported effect in reducing liver fat content may have led to an improvement in insulin sensitivity and decreased insulin requirements,” wrote the researchers in their article.
Hypoglycemia risk and the weight gain observed with complex insulin regimens that include prandial insulin have been main limitations to optimally up-titrate insulin therapy in clinical practice, wrote the authors.
Dr. Frias noted that, in this study, 48% of patients who received insulin lispro experienced clinically significant hypoglycemia, while only 10% of patients in the tirzepatide arms did. “This was 0.4 episodes per patient-year versus 4.4 in tirzepatide and insulin lispro respectively.”
There were more reports of adverse events among the tirzepatide groups than the insulin lispro group. “Typically, with tirzepatide, the commonest adverse events were GI in origin and were mild to moderate.” Rates were 14%-26% for nausea, 11%-15% for diarrhea, and 5%-13% for vomiting.
The study was sponsored by Eli Lilly. Dr. Frias has received grants from Eli Lilly paid to his institution during the conduct of the study and grants, personal fees, or nonfinancial support from Boehringer Ingelheim, Pfizer, Merck, Altimmune, 89BIO, Akero, Carmot Therapeutics, Intercept, Janssen, Madrigal, Novartis, Eli Lilly, Sanofi, and Novo Nordisk outside the submitted work. Dr. Toulis and Dr. Tsapas declared no relevant disclosures.
A version of this article first appeared on Medscape.com.
HAMBURG, GERMANY – Once-weekly tirzepatide (Mounjaro, Lilly) added to insulin glargine resulted in greater reductions in hemoglobin A1c along with more weight loss and less hypoglycemia, compared with prandial insulin lispro (Humalog, Sanofi), for patients with inadequately controlled type 2 diabetes, show data from the SURPASS-6 randomized clinical trial.
It also resulted in a higher percentage of participants meeting an A1c target of less than 7.0%, wrote the researchers, whose study was presented at the annual meeting of the European Association for the Study of Diabetes and was published simultaneously in JAMA.
Also, daily insulin glargine use was substantially lower among participants who received tirzepatide, compared with insulin lispro. Insulin glargine was administered at a dosage 13 IU/day; insulin lispro was administered at a dosage of 62 IU/day. “At the highest dose, some patients stopped their insulin [glargine] in the tirzepatide arm,” said Juan Pablo Frias, MD, medical director and principal investigator of Velocity Clinical Research, Los Angeles, who presented the findings. “We demonstrated clinically meaningful and superior glycemic and body weight control with tirzepatide compared with insulin lispro, while tirzepatide was also associated with less clinically significant hypoglycemia.”
Weight improved for participants who received tirzepatide compared with those who received insulin lispro, at –10 kg and +4 kg respectively. The rate of clinically significant hypoglycemia (blood glucose < 54 mg/dL) or severe hypoglycemia was tenfold lower with tirzepatide, compared with insulin lispro.
The session dedicated to tirzepatide was comoderated by Apostolos Tsapas, MD, professor of medicine and diabetes, Aristotle University, Thessaloniki, Greece, and Konstantinos Toulis, MD, consultant in endocrinology and diabetes, General Military Hospital, Thessaloniki, Greece. Dr. Toulis remarked that, in the chronic disease setting, management and treatment intensification are challenging to integrate, and there are barriers to adoption in routine practice. “This is particularly true when it adds complexity, as in the case of multiple prandial insulin injections on top of basal insulin in suboptimally treated individuals with type 2 diabetes.
“Demonstrating superiority over insulin lispro in terms of the so-called trio of A1c, weight loss, and hypoglycemic events, tirzepatide offers both a simpler to adhere to and a more efficacious treatment intensification option.” He noted that, while long-term safety data are awaited, “this seems to be a definite step forward from any viewpoint, with the possible exception of the taxpayer’s perspective.”
Dr. Tsapas added: “These data further support the very high dual glucose and weight efficacy of tirzepatide and the primary role of incretin-related therapies amongst the injectables for the treatment of type 2 diabetes.”
Tirzepatide 5, 10, 15 mg vs. insulin lispro in addition to insulin glargine
The researchers aimed to assess the efficacy and safety of adding once-weekly tirzepatide, compared with thrice-daily prandial insulin lispro, as an adjunctive therapy to insulin glargine for patients with type 2 diabetes that was inadequately controlled with basal insulin.
Tirzepatide activates the body’s receptors for glucose-dependent insulinotropic polypeptide and glucagonlike peptide–1 (GLP-1). The study authors noted that “recent guidelines support adding an injectable incretin-related therapy such as GLP-1 receptor agonist for glycemic control, rather than basal insulin, when oral medications are inadequate.”
The open-label, phase 3b clinical trial drew data from 135 sites across 15 countries and included 1,428 adults with type 2 diabetes who were taking basal insulin. Participants were randomly assigned in a 1:1:1:3 ratio to receive once-weekly subcutaneous injections of tirzepatide (5 mg [n = 243], 10 mg [n = 238], or 15 mg [n = 236]) or prandial thrice-daily insulin lispro (n = 708).
Both arms were well matched. The average age was 60 years, and 60% of participants were women. The average amount of time patients had type 2 diabetes was 14 years; 85% of participants continued taking metformin. The average A1c level was 8.8% at baseline. Patients were categorized as having obesity (average body mass index, 33 kg/m2). The average insulin glargine dose was 46 units, or 0.5 units/kg.
Outcomes included noninferiority of tirzepatide (pooled cohort) compared with insulin lispro, both in addition to insulin glargine; and A1c change from baseline to week 52 (noninferiority margin, 0.3%). Key secondary endpoints included change in body weight and percentage of participants who achieved an A1c target of less than 7.0%.
About 90% of participants who received the study drug completed the study, said Dr. Frias. “Only 0.5% of tirzepatide patients needed rescue therapy, while only 2% of the insulin lispro did.”
Prior to optimization, the average insulin glargine dose was 42 IU/kg; during optimization, it rose to an average of 46 IU/kg. “At 52 weeks, those on basal-bolus insulin found their insulin glargine dose stayed flat while insulin lispro was 62 units,” reported Dr. Frias. “The three tirzepatide doses show a reduction in insulin glargine, such that the pooled dose reached an average of 11 units, while 20% actually came off their basal insulin altogether [pooled tirzepatide].”
Tirzepatide (pooled) led to the recommended A1c target of less than 7.0% for 68% of patients versus 36% of patients in the insulin lispro group.
About 68% of the patients who received tirzepatide (pooled) achieved the recommended A1c target of less than 7.0% versus 36% of patients in the insulin lispro group.
“Individual tirzepatide doses and pooled doses showed significant reduction in A1c and up to a 2.5% reduction,” Dr. Frias added. “Normoglycemia was obtained by a greater proportion of patients on tirzepatide doses versus basal-bolus insulin – one-third in the 15-mg tirzepatide dose.”
Body weight reduction of 10% or more with tirzepatide
Further, at week 52, weight loss of 5% or more was achieved by 75.4% of participants in the pooled tirzepatide group, compared with 6.3% in the prandial lispro group. The weight loss was accompanied by clinically relevant improvements in cardiometabolic parameters.
In an exploratory analysis, weight loss of 10% or more was achieved by a mean of 48.9% of pooled tirzepatide-treated participants at week 52, compared with 2% of those taking insulin lispro, said Dr. Frias.
“It is possible that the body weight loss induced by tirzepatide therapy and its reported effect in reducing liver fat content may have led to an improvement in insulin sensitivity and decreased insulin requirements,” wrote the researchers in their article.
Hypoglycemia risk and the weight gain observed with complex insulin regimens that include prandial insulin have been main limitations to optimally up-titrate insulin therapy in clinical practice, wrote the authors.
Dr. Frias noted that, in this study, 48% of patients who received insulin lispro experienced clinically significant hypoglycemia, while only 10% of patients in the tirzepatide arms did. “This was 0.4 episodes per patient-year versus 4.4 in tirzepatide and insulin lispro respectively.”
There were more reports of adverse events among the tirzepatide groups than the insulin lispro group. “Typically, with tirzepatide, the commonest adverse events were GI in origin and were mild to moderate.” Rates were 14%-26% for nausea, 11%-15% for diarrhea, and 5%-13% for vomiting.
The study was sponsored by Eli Lilly. Dr. Frias has received grants from Eli Lilly paid to his institution during the conduct of the study and grants, personal fees, or nonfinancial support from Boehringer Ingelheim, Pfizer, Merck, Altimmune, 89BIO, Akero, Carmot Therapeutics, Intercept, Janssen, Madrigal, Novartis, Eli Lilly, Sanofi, and Novo Nordisk outside the submitted work. Dr. Toulis and Dr. Tsapas declared no relevant disclosures.
A version of this article first appeared on Medscape.com.
HAMBURG, GERMANY – Once-weekly tirzepatide (Mounjaro, Lilly) added to insulin glargine resulted in greater reductions in hemoglobin A1c along with more weight loss and less hypoglycemia, compared with prandial insulin lispro (Humalog, Sanofi), for patients with inadequately controlled type 2 diabetes, show data from the SURPASS-6 randomized clinical trial.
It also resulted in a higher percentage of participants meeting an A1c target of less than 7.0%, wrote the researchers, whose study was presented at the annual meeting of the European Association for the Study of Diabetes and was published simultaneously in JAMA.
Also, daily insulin glargine use was substantially lower among participants who received tirzepatide, compared with insulin lispro. Insulin glargine was administered at a dosage 13 IU/day; insulin lispro was administered at a dosage of 62 IU/day. “At the highest dose, some patients stopped their insulin [glargine] in the tirzepatide arm,” said Juan Pablo Frias, MD, medical director and principal investigator of Velocity Clinical Research, Los Angeles, who presented the findings. “We demonstrated clinically meaningful and superior glycemic and body weight control with tirzepatide compared with insulin lispro, while tirzepatide was also associated with less clinically significant hypoglycemia.”
Weight improved for participants who received tirzepatide compared with those who received insulin lispro, at –10 kg and +4 kg respectively. The rate of clinically significant hypoglycemia (blood glucose < 54 mg/dL) or severe hypoglycemia was tenfold lower with tirzepatide, compared with insulin lispro.
The session dedicated to tirzepatide was comoderated by Apostolos Tsapas, MD, professor of medicine and diabetes, Aristotle University, Thessaloniki, Greece, and Konstantinos Toulis, MD, consultant in endocrinology and diabetes, General Military Hospital, Thessaloniki, Greece. Dr. Toulis remarked that, in the chronic disease setting, management and treatment intensification are challenging to integrate, and there are barriers to adoption in routine practice. “This is particularly true when it adds complexity, as in the case of multiple prandial insulin injections on top of basal insulin in suboptimally treated individuals with type 2 diabetes.
“Demonstrating superiority over insulin lispro in terms of the so-called trio of A1c, weight loss, and hypoglycemic events, tirzepatide offers both a simpler to adhere to and a more efficacious treatment intensification option.” He noted that, while long-term safety data are awaited, “this seems to be a definite step forward from any viewpoint, with the possible exception of the taxpayer’s perspective.”
Dr. Tsapas added: “These data further support the very high dual glucose and weight efficacy of tirzepatide and the primary role of incretin-related therapies amongst the injectables for the treatment of type 2 diabetes.”
Tirzepatide 5, 10, 15 mg vs. insulin lispro in addition to insulin glargine
The researchers aimed to assess the efficacy and safety of adding once-weekly tirzepatide, compared with thrice-daily prandial insulin lispro, as an adjunctive therapy to insulin glargine for patients with type 2 diabetes that was inadequately controlled with basal insulin.
Tirzepatide activates the body’s receptors for glucose-dependent insulinotropic polypeptide and glucagonlike peptide–1 (GLP-1). The study authors noted that “recent guidelines support adding an injectable incretin-related therapy such as GLP-1 receptor agonist for glycemic control, rather than basal insulin, when oral medications are inadequate.”
The open-label, phase 3b clinical trial drew data from 135 sites across 15 countries and included 1,428 adults with type 2 diabetes who were taking basal insulin. Participants were randomly assigned in a 1:1:1:3 ratio to receive once-weekly subcutaneous injections of tirzepatide (5 mg [n = 243], 10 mg [n = 238], or 15 mg [n = 236]) or prandial thrice-daily insulin lispro (n = 708).
Both arms were well matched. The average age was 60 years, and 60% of participants were women. The average amount of time patients had type 2 diabetes was 14 years; 85% of participants continued taking metformin. The average A1c level was 8.8% at baseline. Patients were categorized as having obesity (average body mass index, 33 kg/m2). The average insulin glargine dose was 46 units, or 0.5 units/kg.
Outcomes included noninferiority of tirzepatide (pooled cohort) compared with insulin lispro, both in addition to insulin glargine; and A1c change from baseline to week 52 (noninferiority margin, 0.3%). Key secondary endpoints included change in body weight and percentage of participants who achieved an A1c target of less than 7.0%.
About 90% of participants who received the study drug completed the study, said Dr. Frias. “Only 0.5% of tirzepatide patients needed rescue therapy, while only 2% of the insulin lispro did.”
Prior to optimization, the average insulin glargine dose was 42 IU/kg; during optimization, it rose to an average of 46 IU/kg. “At 52 weeks, those on basal-bolus insulin found their insulin glargine dose stayed flat while insulin lispro was 62 units,” reported Dr. Frias. “The three tirzepatide doses show a reduction in insulin glargine, such that the pooled dose reached an average of 11 units, while 20% actually came off their basal insulin altogether [pooled tirzepatide].”
Tirzepatide (pooled) led to the recommended A1c target of less than 7.0% for 68% of patients versus 36% of patients in the insulin lispro group.
About 68% of the patients who received tirzepatide (pooled) achieved the recommended A1c target of less than 7.0% versus 36% of patients in the insulin lispro group.
“Individual tirzepatide doses and pooled doses showed significant reduction in A1c and up to a 2.5% reduction,” Dr. Frias added. “Normoglycemia was obtained by a greater proportion of patients on tirzepatide doses versus basal-bolus insulin – one-third in the 15-mg tirzepatide dose.”
Body weight reduction of 10% or more with tirzepatide
Further, at week 52, weight loss of 5% or more was achieved by 75.4% of participants in the pooled tirzepatide group, compared with 6.3% in the prandial lispro group. The weight loss was accompanied by clinically relevant improvements in cardiometabolic parameters.
In an exploratory analysis, weight loss of 10% or more was achieved by a mean of 48.9% of pooled tirzepatide-treated participants at week 52, compared with 2% of those taking insulin lispro, said Dr. Frias.
“It is possible that the body weight loss induced by tirzepatide therapy and its reported effect in reducing liver fat content may have led to an improvement in insulin sensitivity and decreased insulin requirements,” wrote the researchers in their article.
Hypoglycemia risk and the weight gain observed with complex insulin regimens that include prandial insulin have been main limitations to optimally up-titrate insulin therapy in clinical practice, wrote the authors.
Dr. Frias noted that, in this study, 48% of patients who received insulin lispro experienced clinically significant hypoglycemia, while only 10% of patients in the tirzepatide arms did. “This was 0.4 episodes per patient-year versus 4.4 in tirzepatide and insulin lispro respectively.”
There were more reports of adverse events among the tirzepatide groups than the insulin lispro group. “Typically, with tirzepatide, the commonest adverse events were GI in origin and were mild to moderate.” Rates were 14%-26% for nausea, 11%-15% for diarrhea, and 5%-13% for vomiting.
The study was sponsored by Eli Lilly. Dr. Frias has received grants from Eli Lilly paid to his institution during the conduct of the study and grants, personal fees, or nonfinancial support from Boehringer Ingelheim, Pfizer, Merck, Altimmune, 89BIO, Akero, Carmot Therapeutics, Intercept, Janssen, Madrigal, Novartis, Eli Lilly, Sanofi, and Novo Nordisk outside the submitted work. Dr. Toulis and Dr. Tsapas declared no relevant disclosures.
A version of this article first appeared on Medscape.com.
AT EASD 2023
Salvage option to replace transplant in r/r Hodgkin lymphoma?
SAN DIEGO –
Patients who received second-line chemoimmunotherapy with nivolumab-brentuximab vedotin, with or without bendamustine, and proceeded to involved-site radiation appeared to have similar survival outcomes to those who received the chemoimmunotherapy combination plus the current second-line standard of care, which includes high-dose therapy and autologous stem cell transplant.
Among 28 patients with low-risk relapsed or refractory Hodgkin lymphoma followed for a median of 32 months, 3-year event-free survival without autologous stem cell transplant was 86.9% and 3-year progression-free survival was 95%, reported Brad Hoppe, MD, MPH, from the Mayo Clinic in Jacksonville, Fla. In contrast, 1-year progression-free survival was 91% among the 44 standard-risk patients who received high-dose therapy and autologous stem cell transplant, according to results of a trial the investigators published online in Blood in late 2022.
The latest results from the phase 2 CheckMate 744 trial were reported at the annual meeting of the American Society of Radiation Oncology.
“The findings suggest that children, adolescents, and young adults with low-risk relapsed classic Hodgkin lymphoma can be salvaged with low-toxicity chemoimmunotherapy and may not require high-dose therapy and transplant for a cure,” Dr. Hoppe said in an oral abstract session.
Andrea Ng, MD, MPH, a radiation oncologist who specializes in treating patients with Hodgkin lymphoma and other hematologic malignancies, said that, while the number of patients in the study was small and the follow-up too short, this option is “certainly something that’s very promising for the future.”
“The use of transplant in relapsed patients, which we have been doing for decades, is based on two very old, small, randomized studies,” said Dr. Ng, from the Dana-Farber Cancer Institute in Boston, who moderated the session.
“So, do we really need to transplant everybody? In the back of our minds, we think that we may be overtreating some patients,” she said.
Several small, retrospective studies exploring treatment with conventional chemotherapy with or without radiation therapy and without transplant in patients with relapsed or refractory Hodgkin lymphoma have demonstrated only modest results.
The CheckMate 744 trial, however, was designed to examine a risk-adapted and response-adapted approach to treating children, adolescents, and young adults with relapsed or refractory classic Hodgkin lymphoma within the setting of modern immunotherapy and targeted therapy. This approach was developed jointly by investigators with the Children’s Oncology Group and Euronet.
In the nonrandomized trial, patients were stratified into low-risk or standard-risk disease categories based on an algorithm that included factors at the time of initial diagnosis and relapse.
Patients were considered low-risk for relapse in three scenarios: (1) if they had initial stage IA or IIA disease that relapsed at least 1 year after the end of therapy; (2) if they had initial stage IA or IIA disease that relapsed between 3 and 12 months from the end of therapy but had received no more than three cycles of chemotherapy and no radiation therapy; or (3) if they had initial stage IB, IIB, or IIIA disease that relapsed more than 12 months after the end of first-line therapy.
To be included in the low-risk category, patients also had to be free of B symptoms or extranodal disease, free of relapse in prior radiation therapy fields, and have no more than four sites of lymphoma.
Low-risk patients were treated with a combination of nivolumab and brentuximab vedotin, which could be followed by additional brentuximab vedotin and bendamustine for those with a suboptimal response. Patients who achieved complete molecular remission after induction went on to consolidation therapy with involved-site radiation at a total dose of 30 Gy.
Patients considered standard-risk for relapse received the same nivolumab-brentuximab vedotin combination, with or without bendamustine, and then went on to high-dose therapy and autologous stem cell transplant.
In other results for the previously mentioned study published in Blood, the 44 standard-risk patients who received high-dose therapy and autologous stem cell transplant had an objective response rate of 95% – 86% of patients achieved complete molecular remission, and 9% achieved partial molecular remission.
At ASTRO, Dr. Hoppe reported results for the 28 patients with low-risk disease. One patient discontinued nivolumab/brentuximab vedotin after two cycles because of skin toxicity and was lost to follow-up. Of the remaining 27 patients, 21 had complete molecular remission after four cycles of the combination, and these patients went on to an additional two cycles of the combination, with 19 of 21 receiving involved-site radiation consolidation.
Six patients who had either a partial molecular remission or no response were given two additional cycles of brentuximab vedotin plus bendamustine. Of this group, three went on to complete molecular remission and received involved-site radiation consolidation on protocol. The remaining three patients who did not experience complete molecular remission received involved-site radiation off protocol.
The rate of complete molecular remission after four cycles of induction was 82.1%, and the rate of partial molecular remission was 14.3%, for an objective response rate of 96.4%. The respective response rates with the addition of two cycles of brentuximab vedotin and bendamustine were 92.9% and 7.1%, for an objective response rate of 100%, Dr. Hoppe reported.
Overall, at a median follow-up of 32 months, the 3-year event-free survival rate without transplant was 86.9%, and the 3-year progression-free survival rate was 95%.
Treatment-related adverse events of any grade occurred in 22 patients (78.6%) after induction, with 7 of those events (25%) being grade 3 or 4 in severity. Grade 3 or 4 events consisted of skin and subcutaneous tissue disorders in 3 patients, elevated liver function tests in 3 patients, and blood and lymphatic system disorders in 1 patient.
There were no new toxicities detected within 100 days of treatment.
“The results that Dr. Hoppe showed us are really, really good,” Dr. Ng said. And “the volume of treatment is pretty tiny, so I think we can safely say that long-term toxicities are very, very minimal.”
The study was supported by Bristol-Myers Squibb in collaboration with Seagen, Euronet-Paediatric Hodgkin Lymphoma, and the Children’s Oncology Group. Dr. Hoppe reported serving on a scientific advisory committee for Merck. Dr. Ng reported having no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
SAN DIEGO –
Patients who received second-line chemoimmunotherapy with nivolumab-brentuximab vedotin, with or without bendamustine, and proceeded to involved-site radiation appeared to have similar survival outcomes to those who received the chemoimmunotherapy combination plus the current second-line standard of care, which includes high-dose therapy and autologous stem cell transplant.
Among 28 patients with low-risk relapsed or refractory Hodgkin lymphoma followed for a median of 32 months, 3-year event-free survival without autologous stem cell transplant was 86.9% and 3-year progression-free survival was 95%, reported Brad Hoppe, MD, MPH, from the Mayo Clinic in Jacksonville, Fla. In contrast, 1-year progression-free survival was 91% among the 44 standard-risk patients who received high-dose therapy and autologous stem cell transplant, according to results of a trial the investigators published online in Blood in late 2022.
The latest results from the phase 2 CheckMate 744 trial were reported at the annual meeting of the American Society of Radiation Oncology.
“The findings suggest that children, adolescents, and young adults with low-risk relapsed classic Hodgkin lymphoma can be salvaged with low-toxicity chemoimmunotherapy and may not require high-dose therapy and transplant for a cure,” Dr. Hoppe said in an oral abstract session.
Andrea Ng, MD, MPH, a radiation oncologist who specializes in treating patients with Hodgkin lymphoma and other hematologic malignancies, said that, while the number of patients in the study was small and the follow-up too short, this option is “certainly something that’s very promising for the future.”
“The use of transplant in relapsed patients, which we have been doing for decades, is based on two very old, small, randomized studies,” said Dr. Ng, from the Dana-Farber Cancer Institute in Boston, who moderated the session.
“So, do we really need to transplant everybody? In the back of our minds, we think that we may be overtreating some patients,” she said.
Several small, retrospective studies exploring treatment with conventional chemotherapy with or without radiation therapy and without transplant in patients with relapsed or refractory Hodgkin lymphoma have demonstrated only modest results.
The CheckMate 744 trial, however, was designed to examine a risk-adapted and response-adapted approach to treating children, adolescents, and young adults with relapsed or refractory classic Hodgkin lymphoma within the setting of modern immunotherapy and targeted therapy. This approach was developed jointly by investigators with the Children’s Oncology Group and Euronet.
In the nonrandomized trial, patients were stratified into low-risk or standard-risk disease categories based on an algorithm that included factors at the time of initial diagnosis and relapse.
Patients were considered low-risk for relapse in three scenarios: (1) if they had initial stage IA or IIA disease that relapsed at least 1 year after the end of therapy; (2) if they had initial stage IA or IIA disease that relapsed between 3 and 12 months from the end of therapy but had received no more than three cycles of chemotherapy and no radiation therapy; or (3) if they had initial stage IB, IIB, or IIIA disease that relapsed more than 12 months after the end of first-line therapy.
To be included in the low-risk category, patients also had to be free of B symptoms or extranodal disease, free of relapse in prior radiation therapy fields, and have no more than four sites of lymphoma.
Low-risk patients were treated with a combination of nivolumab and brentuximab vedotin, which could be followed by additional brentuximab vedotin and bendamustine for those with a suboptimal response. Patients who achieved complete molecular remission after induction went on to consolidation therapy with involved-site radiation at a total dose of 30 Gy.
Patients considered standard-risk for relapse received the same nivolumab-brentuximab vedotin combination, with or without bendamustine, and then went on to high-dose therapy and autologous stem cell transplant.
In other results for the previously mentioned study published in Blood, the 44 standard-risk patients who received high-dose therapy and autologous stem cell transplant had an objective response rate of 95% – 86% of patients achieved complete molecular remission, and 9% achieved partial molecular remission.
At ASTRO, Dr. Hoppe reported results for the 28 patients with low-risk disease. One patient discontinued nivolumab/brentuximab vedotin after two cycles because of skin toxicity and was lost to follow-up. Of the remaining 27 patients, 21 had complete molecular remission after four cycles of the combination, and these patients went on to an additional two cycles of the combination, with 19 of 21 receiving involved-site radiation consolidation.
Six patients who had either a partial molecular remission or no response were given two additional cycles of brentuximab vedotin plus bendamustine. Of this group, three went on to complete molecular remission and received involved-site radiation consolidation on protocol. The remaining three patients who did not experience complete molecular remission received involved-site radiation off protocol.
The rate of complete molecular remission after four cycles of induction was 82.1%, and the rate of partial molecular remission was 14.3%, for an objective response rate of 96.4%. The respective response rates with the addition of two cycles of brentuximab vedotin and bendamustine were 92.9% and 7.1%, for an objective response rate of 100%, Dr. Hoppe reported.
Overall, at a median follow-up of 32 months, the 3-year event-free survival rate without transplant was 86.9%, and the 3-year progression-free survival rate was 95%.
Treatment-related adverse events of any grade occurred in 22 patients (78.6%) after induction, with 7 of those events (25%) being grade 3 or 4 in severity. Grade 3 or 4 events consisted of skin and subcutaneous tissue disorders in 3 patients, elevated liver function tests in 3 patients, and blood and lymphatic system disorders in 1 patient.
There were no new toxicities detected within 100 days of treatment.
“The results that Dr. Hoppe showed us are really, really good,” Dr. Ng said. And “the volume of treatment is pretty tiny, so I think we can safely say that long-term toxicities are very, very minimal.”
The study was supported by Bristol-Myers Squibb in collaboration with Seagen, Euronet-Paediatric Hodgkin Lymphoma, and the Children’s Oncology Group. Dr. Hoppe reported serving on a scientific advisory committee for Merck. Dr. Ng reported having no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
SAN DIEGO –
Patients who received second-line chemoimmunotherapy with nivolumab-brentuximab vedotin, with or without bendamustine, and proceeded to involved-site radiation appeared to have similar survival outcomes to those who received the chemoimmunotherapy combination plus the current second-line standard of care, which includes high-dose therapy and autologous stem cell transplant.
Among 28 patients with low-risk relapsed or refractory Hodgkin lymphoma followed for a median of 32 months, 3-year event-free survival without autologous stem cell transplant was 86.9% and 3-year progression-free survival was 95%, reported Brad Hoppe, MD, MPH, from the Mayo Clinic in Jacksonville, Fla. In contrast, 1-year progression-free survival was 91% among the 44 standard-risk patients who received high-dose therapy and autologous stem cell transplant, according to results of a trial the investigators published online in Blood in late 2022.
The latest results from the phase 2 CheckMate 744 trial were reported at the annual meeting of the American Society of Radiation Oncology.
“The findings suggest that children, adolescents, and young adults with low-risk relapsed classic Hodgkin lymphoma can be salvaged with low-toxicity chemoimmunotherapy and may not require high-dose therapy and transplant for a cure,” Dr. Hoppe said in an oral abstract session.
Andrea Ng, MD, MPH, a radiation oncologist who specializes in treating patients with Hodgkin lymphoma and other hematologic malignancies, said that, while the number of patients in the study was small and the follow-up too short, this option is “certainly something that’s very promising for the future.”
“The use of transplant in relapsed patients, which we have been doing for decades, is based on two very old, small, randomized studies,” said Dr. Ng, from the Dana-Farber Cancer Institute in Boston, who moderated the session.
“So, do we really need to transplant everybody? In the back of our minds, we think that we may be overtreating some patients,” she said.
Several small, retrospective studies exploring treatment with conventional chemotherapy with or without radiation therapy and without transplant in patients with relapsed or refractory Hodgkin lymphoma have demonstrated only modest results.
The CheckMate 744 trial, however, was designed to examine a risk-adapted and response-adapted approach to treating children, adolescents, and young adults with relapsed or refractory classic Hodgkin lymphoma within the setting of modern immunotherapy and targeted therapy. This approach was developed jointly by investigators with the Children’s Oncology Group and Euronet.
In the nonrandomized trial, patients were stratified into low-risk or standard-risk disease categories based on an algorithm that included factors at the time of initial diagnosis and relapse.
Patients were considered low-risk for relapse in three scenarios: (1) if they had initial stage IA or IIA disease that relapsed at least 1 year after the end of therapy; (2) if they had initial stage IA or IIA disease that relapsed between 3 and 12 months from the end of therapy but had received no more than three cycles of chemotherapy and no radiation therapy; or (3) if they had initial stage IB, IIB, or IIIA disease that relapsed more than 12 months after the end of first-line therapy.
To be included in the low-risk category, patients also had to be free of B symptoms or extranodal disease, free of relapse in prior radiation therapy fields, and have no more than four sites of lymphoma.
Low-risk patients were treated with a combination of nivolumab and brentuximab vedotin, which could be followed by additional brentuximab vedotin and bendamustine for those with a suboptimal response. Patients who achieved complete molecular remission after induction went on to consolidation therapy with involved-site radiation at a total dose of 30 Gy.
Patients considered standard-risk for relapse received the same nivolumab-brentuximab vedotin combination, with or without bendamustine, and then went on to high-dose therapy and autologous stem cell transplant.
In other results for the previously mentioned study published in Blood, the 44 standard-risk patients who received high-dose therapy and autologous stem cell transplant had an objective response rate of 95% – 86% of patients achieved complete molecular remission, and 9% achieved partial molecular remission.
At ASTRO, Dr. Hoppe reported results for the 28 patients with low-risk disease. One patient discontinued nivolumab/brentuximab vedotin after two cycles because of skin toxicity and was lost to follow-up. Of the remaining 27 patients, 21 had complete molecular remission after four cycles of the combination, and these patients went on to an additional two cycles of the combination, with 19 of 21 receiving involved-site radiation consolidation.
Six patients who had either a partial molecular remission or no response were given two additional cycles of brentuximab vedotin plus bendamustine. Of this group, three went on to complete molecular remission and received involved-site radiation consolidation on protocol. The remaining three patients who did not experience complete molecular remission received involved-site radiation off protocol.
The rate of complete molecular remission after four cycles of induction was 82.1%, and the rate of partial molecular remission was 14.3%, for an objective response rate of 96.4%. The respective response rates with the addition of two cycles of brentuximab vedotin and bendamustine were 92.9% and 7.1%, for an objective response rate of 100%, Dr. Hoppe reported.
Overall, at a median follow-up of 32 months, the 3-year event-free survival rate without transplant was 86.9%, and the 3-year progression-free survival rate was 95%.
Treatment-related adverse events of any grade occurred in 22 patients (78.6%) after induction, with 7 of those events (25%) being grade 3 or 4 in severity. Grade 3 or 4 events consisted of skin and subcutaneous tissue disorders in 3 patients, elevated liver function tests in 3 patients, and blood and lymphatic system disorders in 1 patient.
There were no new toxicities detected within 100 days of treatment.
“The results that Dr. Hoppe showed us are really, really good,” Dr. Ng said. And “the volume of treatment is pretty tiny, so I think we can safely say that long-term toxicities are very, very minimal.”
The study was supported by Bristol-Myers Squibb in collaboration with Seagen, Euronet-Paediatric Hodgkin Lymphoma, and the Children’s Oncology Group. Dr. Hoppe reported serving on a scientific advisory committee for Merck. Dr. Ng reported having no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
AT ASTRO 2023
Cervical cancer: Vaginal dilation linked to less stenosis after treatment
SAN DIEGO – , a new 5-year prospective study reports.
Findings from the EMBRACE study were presented at the annual American Society for Radiation Oncology (ASTRO) meeting and included 882 women with locally advanced cervical cancer. Of those, 565 women reported regular vaginal dilation and/or sexual intercourse during at least three of their follow-up assessments. Patients who reported both dilation and intercourse had the lowest risk of developing vaginal stenosis of grade ≥ 2 (18%) at 5 years.
The other 317 women were described in the study as having no penetration (13%) or infrequent penetration (23%) and were more likely to experience stenosis of grade ≥ 2 (36% and 37% respectively (P ≤ 0.001)), reported psycho-oncologist, clinical psychologist Kathrin Kirchheiner, PhD, MSc, of the Medical University of Vienna, and colleagues at ASTRO 2023.
While noting that the observational study cannot determine cause and effect, “these long-term data support clinical recommendations worldwide,” said Dr. Kirchheiner at an ASTRO news briefing.
According to Dr. Kirchheiner, external beam radiotherapy, chemotherapy, and internal brachytherapy are the standard of care for locally advanced cervical cancer that cannot be removed by surgery.
Studies have shown that the treatment can cause vaginal shortening and narrowing due to the formation of scar tissue, she said. As a result, there can be “permanent changes in the vaginal tissue that lead to a loss of elasticity. This can often cause problems during the gynecological follow-up examination and pain during sexual intercourse.”
In an earlier reported 2-year analysis of the EMBRACE study (median follow-up of 15 months), the study authors reported that 89% of 588 patients developed grade ≥ 1 vaginal stenosis following their treatment, with 29% at grade ≥ 2 and 3.6% at grade ≥ 3.
The use of medical dilators is commonly recommended after cervical cancer treatment to stretch the vaginal canal. Women are instructed to increase the dilator size over time. But research suggests that adherence may be low.
For the observational, multi-institution study, researchers tracked 1,416 cervical cancer patients from 2008 to 2015 for a median follow-up of 5 years. The new analysis focuses on 882 patients with at least three follow-up assessments, with a median age of 49. Researchers reported that patients who didn’t engage in intercourse or use dilators were most likely to experience vaginal stenosis (37%) vs. those who did both (18%), those who just had intercourse (23%), and those who only used dilators (28%) (P ≤ 0.001).
The findings were confirmed in a multivariable analysis with adjustments for tumor infiltration, age, treatment parameters, and hormonal replacement therapy, the researchers reported.
Regular sexual activity, vaginal dilation, or both were linked to higher risk of mild vaginal dryness at grade ≥ 1 (72% vs. 67% in the no/infrequent penetration group, P = 0.028) and vaginal bleeding at grade ≥ 1 (61% vs. 34% in the no/infrequent penetration group, P ≤ 0.001). There was no link to higher rates of vaginal mucositis.
Dr. Kirchheiner noted that these symptoms can be treated with lubricants, moisturizer, and hormonal replacement therapy.
As for limitations, Dr. Kirchheiner, in a press release provided by ASTRO, noted that “we cannot and should not randomize patients in a clinical trial into groups with and without regular dilation.” She also noted that future research should explore why sexual intercourse had slightly better results than use of dilators, a finding that could be related to blood flow during sexual arousal.
In comments at the news briefing, Akila Viswanathan, MD, MPH, MSc, director of Radiation Oncology and Molecular Radiation Sciences at Johns Hopkins Medicine, Baltimore, praised the new study and noted that quality of life after cervical cancer treatment is “very understudied.”
Vaginal side effects in particular are underreported because physicians often fail to ask about them and patients “are hesitant to accurately describe what they’re feeling,” she said.
The interventions of providing medical dilators and encouraging sexual activity are “very low cost,” Dr. Viswanathan said. But she noted that women – especially older women – may “find the concepts of using a dilator very difficult to understand.”
The study offers the “best evidence to date” supporting vaginal dilation, said Yale University, New Haven, Conn., radiation oncologist Shari Damast, MD, in an interview. It has “a large dataset, longitudinal design, lengthy follow-up, and uses validated tools of measurement. It gives us strong confidence in the efficacy of vaginal dilators.”
In an interview, Deborah Watkins Bruner, RN, PhD, senior vice president for research at Emory University, Atlanta, also praised the research. But she noted that it’s not clear how often vaginal dilation/sexual intercourse should be performed in order to reduce stenosis. “In addition, it is clear that vaginal dilation only is not enough to treat the myriad of symptoms that survivors must deal with,” she said.
Dr. Bruner urged colleagues “to routinely assess symptoms at each visit and offer treatments which should include hormone replacement therapy, vaginal dilation, and appropriate referral for anxiety, depression, or marital problems.”
The study was funded by Elekta and Varian Medical System via the Medical University of Vienna. The study authors, Dr. Bruner, and Dr. Damast have no disclosures. Disclosure information for Dr. Viswanathan was not available.
SAN DIEGO – , a new 5-year prospective study reports.
Findings from the EMBRACE study were presented at the annual American Society for Radiation Oncology (ASTRO) meeting and included 882 women with locally advanced cervical cancer. Of those, 565 women reported regular vaginal dilation and/or sexual intercourse during at least three of their follow-up assessments. Patients who reported both dilation and intercourse had the lowest risk of developing vaginal stenosis of grade ≥ 2 (18%) at 5 years.
The other 317 women were described in the study as having no penetration (13%) or infrequent penetration (23%) and were more likely to experience stenosis of grade ≥ 2 (36% and 37% respectively (P ≤ 0.001)), reported psycho-oncologist, clinical psychologist Kathrin Kirchheiner, PhD, MSc, of the Medical University of Vienna, and colleagues at ASTRO 2023.
While noting that the observational study cannot determine cause and effect, “these long-term data support clinical recommendations worldwide,” said Dr. Kirchheiner at an ASTRO news briefing.
According to Dr. Kirchheiner, external beam radiotherapy, chemotherapy, and internal brachytherapy are the standard of care for locally advanced cervical cancer that cannot be removed by surgery.
Studies have shown that the treatment can cause vaginal shortening and narrowing due to the formation of scar tissue, she said. As a result, there can be “permanent changes in the vaginal tissue that lead to a loss of elasticity. This can often cause problems during the gynecological follow-up examination and pain during sexual intercourse.”
In an earlier reported 2-year analysis of the EMBRACE study (median follow-up of 15 months), the study authors reported that 89% of 588 patients developed grade ≥ 1 vaginal stenosis following their treatment, with 29% at grade ≥ 2 and 3.6% at grade ≥ 3.
The use of medical dilators is commonly recommended after cervical cancer treatment to stretch the vaginal canal. Women are instructed to increase the dilator size over time. But research suggests that adherence may be low.
For the observational, multi-institution study, researchers tracked 1,416 cervical cancer patients from 2008 to 2015 for a median follow-up of 5 years. The new analysis focuses on 882 patients with at least three follow-up assessments, with a median age of 49. Researchers reported that patients who didn’t engage in intercourse or use dilators were most likely to experience vaginal stenosis (37%) vs. those who did both (18%), those who just had intercourse (23%), and those who only used dilators (28%) (P ≤ 0.001).
The findings were confirmed in a multivariable analysis with adjustments for tumor infiltration, age, treatment parameters, and hormonal replacement therapy, the researchers reported.
Regular sexual activity, vaginal dilation, or both were linked to higher risk of mild vaginal dryness at grade ≥ 1 (72% vs. 67% in the no/infrequent penetration group, P = 0.028) and vaginal bleeding at grade ≥ 1 (61% vs. 34% in the no/infrequent penetration group, P ≤ 0.001). There was no link to higher rates of vaginal mucositis.
Dr. Kirchheiner noted that these symptoms can be treated with lubricants, moisturizer, and hormonal replacement therapy.
As for limitations, Dr. Kirchheiner, in a press release provided by ASTRO, noted that “we cannot and should not randomize patients in a clinical trial into groups with and without regular dilation.” She also noted that future research should explore why sexual intercourse had slightly better results than use of dilators, a finding that could be related to blood flow during sexual arousal.
In comments at the news briefing, Akila Viswanathan, MD, MPH, MSc, director of Radiation Oncology and Molecular Radiation Sciences at Johns Hopkins Medicine, Baltimore, praised the new study and noted that quality of life after cervical cancer treatment is “very understudied.”
Vaginal side effects in particular are underreported because physicians often fail to ask about them and patients “are hesitant to accurately describe what they’re feeling,” she said.
The interventions of providing medical dilators and encouraging sexual activity are “very low cost,” Dr. Viswanathan said. But she noted that women – especially older women – may “find the concepts of using a dilator very difficult to understand.”
The study offers the “best evidence to date” supporting vaginal dilation, said Yale University, New Haven, Conn., radiation oncologist Shari Damast, MD, in an interview. It has “a large dataset, longitudinal design, lengthy follow-up, and uses validated tools of measurement. It gives us strong confidence in the efficacy of vaginal dilators.”
In an interview, Deborah Watkins Bruner, RN, PhD, senior vice president for research at Emory University, Atlanta, also praised the research. But she noted that it’s not clear how often vaginal dilation/sexual intercourse should be performed in order to reduce stenosis. “In addition, it is clear that vaginal dilation only is not enough to treat the myriad of symptoms that survivors must deal with,” she said.
Dr. Bruner urged colleagues “to routinely assess symptoms at each visit and offer treatments which should include hormone replacement therapy, vaginal dilation, and appropriate referral for anxiety, depression, or marital problems.”
The study was funded by Elekta and Varian Medical System via the Medical University of Vienna. The study authors, Dr. Bruner, and Dr. Damast have no disclosures. Disclosure information for Dr. Viswanathan was not available.
SAN DIEGO – , a new 5-year prospective study reports.
Findings from the EMBRACE study were presented at the annual American Society for Radiation Oncology (ASTRO) meeting and included 882 women with locally advanced cervical cancer. Of those, 565 women reported regular vaginal dilation and/or sexual intercourse during at least three of their follow-up assessments. Patients who reported both dilation and intercourse had the lowest risk of developing vaginal stenosis of grade ≥ 2 (18%) at 5 years.
The other 317 women were described in the study as having no penetration (13%) or infrequent penetration (23%) and were more likely to experience stenosis of grade ≥ 2 (36% and 37% respectively (P ≤ 0.001)), reported psycho-oncologist, clinical psychologist Kathrin Kirchheiner, PhD, MSc, of the Medical University of Vienna, and colleagues at ASTRO 2023.
While noting that the observational study cannot determine cause and effect, “these long-term data support clinical recommendations worldwide,” said Dr. Kirchheiner at an ASTRO news briefing.
According to Dr. Kirchheiner, external beam radiotherapy, chemotherapy, and internal brachytherapy are the standard of care for locally advanced cervical cancer that cannot be removed by surgery.
Studies have shown that the treatment can cause vaginal shortening and narrowing due to the formation of scar tissue, she said. As a result, there can be “permanent changes in the vaginal tissue that lead to a loss of elasticity. This can often cause problems during the gynecological follow-up examination and pain during sexual intercourse.”
In an earlier reported 2-year analysis of the EMBRACE study (median follow-up of 15 months), the study authors reported that 89% of 588 patients developed grade ≥ 1 vaginal stenosis following their treatment, with 29% at grade ≥ 2 and 3.6% at grade ≥ 3.
The use of medical dilators is commonly recommended after cervical cancer treatment to stretch the vaginal canal. Women are instructed to increase the dilator size over time. But research suggests that adherence may be low.
For the observational, multi-institution study, researchers tracked 1,416 cervical cancer patients from 2008 to 2015 for a median follow-up of 5 years. The new analysis focuses on 882 patients with at least three follow-up assessments, with a median age of 49. Researchers reported that patients who didn’t engage in intercourse or use dilators were most likely to experience vaginal stenosis (37%) vs. those who did both (18%), those who just had intercourse (23%), and those who only used dilators (28%) (P ≤ 0.001).
The findings were confirmed in a multivariable analysis with adjustments for tumor infiltration, age, treatment parameters, and hormonal replacement therapy, the researchers reported.
Regular sexual activity, vaginal dilation, or both were linked to higher risk of mild vaginal dryness at grade ≥ 1 (72% vs. 67% in the no/infrequent penetration group, P = 0.028) and vaginal bleeding at grade ≥ 1 (61% vs. 34% in the no/infrequent penetration group, P ≤ 0.001). There was no link to higher rates of vaginal mucositis.
Dr. Kirchheiner noted that these symptoms can be treated with lubricants, moisturizer, and hormonal replacement therapy.
As for limitations, Dr. Kirchheiner, in a press release provided by ASTRO, noted that “we cannot and should not randomize patients in a clinical trial into groups with and without regular dilation.” She also noted that future research should explore why sexual intercourse had slightly better results than use of dilators, a finding that could be related to blood flow during sexual arousal.
In comments at the news briefing, Akila Viswanathan, MD, MPH, MSc, director of Radiation Oncology and Molecular Radiation Sciences at Johns Hopkins Medicine, Baltimore, praised the new study and noted that quality of life after cervical cancer treatment is “very understudied.”
Vaginal side effects in particular are underreported because physicians often fail to ask about them and patients “are hesitant to accurately describe what they’re feeling,” she said.
The interventions of providing medical dilators and encouraging sexual activity are “very low cost,” Dr. Viswanathan said. But she noted that women – especially older women – may “find the concepts of using a dilator very difficult to understand.”
The study offers the “best evidence to date” supporting vaginal dilation, said Yale University, New Haven, Conn., radiation oncologist Shari Damast, MD, in an interview. It has “a large dataset, longitudinal design, lengthy follow-up, and uses validated tools of measurement. It gives us strong confidence in the efficacy of vaginal dilators.”
In an interview, Deborah Watkins Bruner, RN, PhD, senior vice president for research at Emory University, Atlanta, also praised the research. But she noted that it’s not clear how often vaginal dilation/sexual intercourse should be performed in order to reduce stenosis. “In addition, it is clear that vaginal dilation only is not enough to treat the myriad of symptoms that survivors must deal with,” she said.
Dr. Bruner urged colleagues “to routinely assess symptoms at each visit and offer treatments which should include hormone replacement therapy, vaginal dilation, and appropriate referral for anxiety, depression, or marital problems.”
The study was funded by Elekta and Varian Medical System via the Medical University of Vienna. The study authors, Dr. Bruner, and Dr. Damast have no disclosures. Disclosure information for Dr. Viswanathan was not available.
AT ASTRO 2023
Data Trends 2023: Access to Women's Health Care
- US Department of Veteran Affairs. Facts and statistics: women veterans in focus. Updated January 31, 2023. Accessed May 5, 2023. https://www.womenshealth.va.gov/materials-and-resources/facts-and-statistics.asp
- US Department of Defense. Department of Defense Releases Annual Demographics Report — Upward Trend in Number of Women Serving Continues. Published December 14, 2022. Accessed June 12, 2023. https://www.defense.gov/News/Releases/Release/Article/3246268/department-of-defense-releases-annual-demographics-report-upwardtrend-in-numbe/
- Meadows SO, Collins RL, Schuler MS, Beckman RL, Cefalu M. The Women’s Reproductive Health Survey (WRHS) of active-duty service members. RAND Corporation. Published 2022. Accessed May 5, 2023. https://www.rand.org/content/dam/rand/pubs/research_reports/RRA1000/RRA1031-1/RAND_RRA1031-1.pdf
- US Department of Veteran Affairs. Facts and statistics: women veterans in focus. Updated January 31, 2023. Accessed May 5, 2023. https://www.womenshealth.va.gov/materials-and-resources/facts-and-statistics.asp
- US Department of Defense. Department of Defense Releases Annual Demographics Report — Upward Trend in Number of Women Serving Continues. Published December 14, 2022. Accessed June 12, 2023. https://www.defense.gov/News/Releases/Release/Article/3246268/department-of-defense-releases-annual-demographics-report-upwardtrend-in-numbe/
- Meadows SO, Collins RL, Schuler MS, Beckman RL, Cefalu M. The Women’s Reproductive Health Survey (WRHS) of active-duty service members. RAND Corporation. Published 2022. Accessed May 5, 2023. https://www.rand.org/content/dam/rand/pubs/research_reports/RRA1000/RRA1031-1/RAND_RRA1031-1.pdf
- US Department of Veteran Affairs. Facts and statistics: women veterans in focus. Updated January 31, 2023. Accessed May 5, 2023. https://www.womenshealth.va.gov/materials-and-resources/facts-and-statistics.asp
- US Department of Defense. Department of Defense Releases Annual Demographics Report — Upward Trend in Number of Women Serving Continues. Published December 14, 2022. Accessed June 12, 2023. https://www.defense.gov/News/Releases/Release/Article/3246268/department-of-defense-releases-annual-demographics-report-upwardtrend-in-numbe/
- Meadows SO, Collins RL, Schuler MS, Beckman RL, Cefalu M. The Women’s Reproductive Health Survey (WRHS) of active-duty service members. RAND Corporation. Published 2022. Accessed May 5, 2023. https://www.rand.org/content/dam/rand/pubs/research_reports/RRA1000/RRA1031-1/RAND_RRA1031-1.pdf
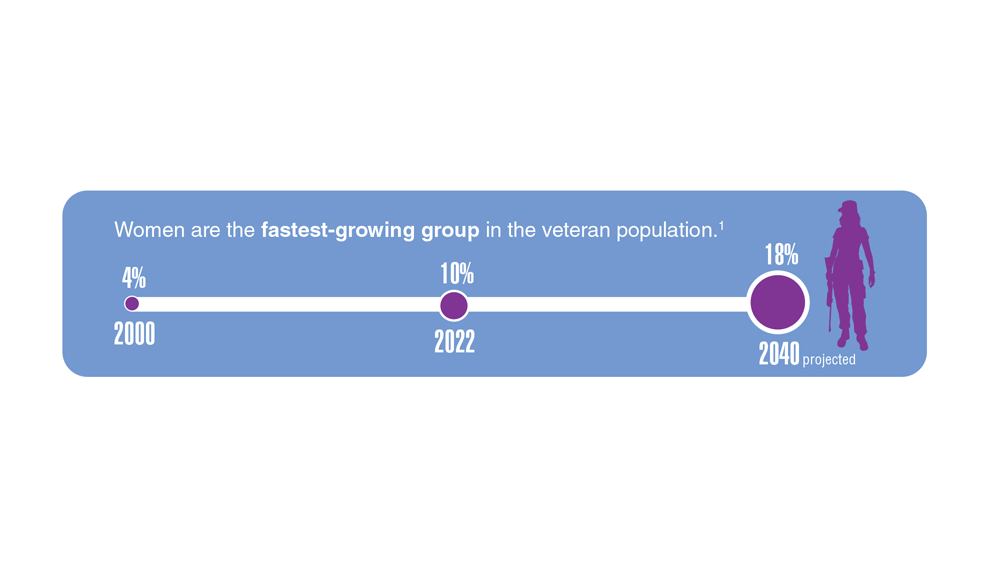
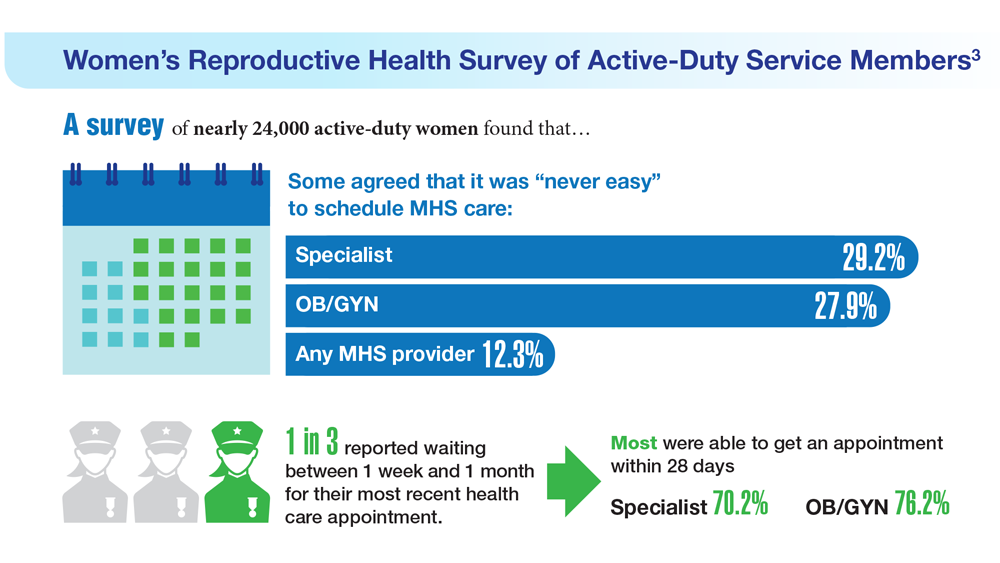
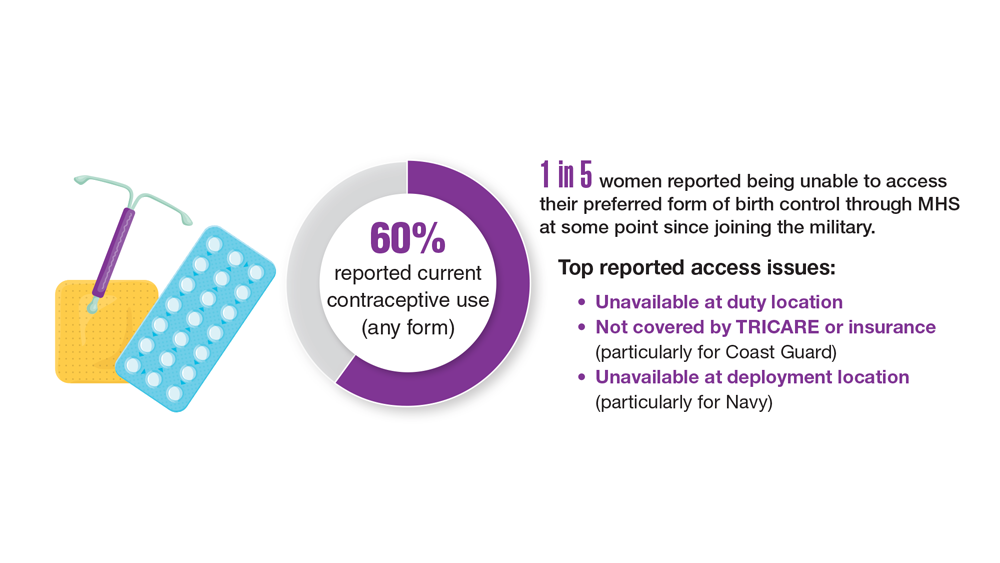
Data Trends 2023: Rheumatoid Arthritis
- Morse JL et al. J Psychiatr Res. 2023;159:224-229. doi:10.1016/j.jpsychires.2023.01.039
- van Vollenhoven RF. BMC Med. 2009;7:12. doi:10.1186/1741-7015-7-12
- US Department of Veteran Affairs, National Center for Veteran Analysis and Statistics. Profile of veterans: 2017. Published March 2019. Accessed April 27, 2023. https://www.va.gov/vetdata/docs/SpecialReports/Profile_of_Veterans_2017.pdf
- Johnson TM et al. Arthritis Care Res (Hoboken). 2022 Nov 4. doi:10.1002/acr.25053
- Ebel AV et al. Arthritis Rheumatol. 2021;73(3):392-400. doi:10.1002/art.41559
- Sokolove J et al. Rheumatology (Oxford). 2016;55(11):1969-1977. doi:10.1093/rheumatology/kew285
- Alpizar-Rodriguez D et al. Rheumatology (Oxford). 2019;58(3):432-440. doi:10.1093/rheumatology/key311
- Chancay MG et al. Womens Midlife Health. 2019;5:3. doi:10.1186/s40695-019-0047-4
- Bongartz T et al. Arthritis Rheum. 2010;62(6):1583-1591. doi:10.1002/art.27405
- Kelly CA et al. Rheumatology (Oxford). 2014;53(9):1676-1682. doi:10.1093/rheumatology/keu165
- Koduri G et al. Rheumatology (Oxford). 2010;49(8):1483-1489. doi:10.1093/rheumatology/keq035
- Olson AL et al. Am J Respir Crit Care Med. 2011;183(3):372-378. doi:10.1164/rccm.201004-0622OC
- Mikuls TR et al. Rheumatology (Oxford). 2011;50(1):101-109. doi:10.1093/rheumatology/keq232
- England BR et al. Arthritis Care Res. 2016;68(1):36-45. doi:10.1002/acr.22642
- Morse JL et al. J Psychiatr Res. 2023;159:224-229. doi:10.1016/j.jpsychires.2023.01.039
- van Vollenhoven RF. BMC Med. 2009;7:12. doi:10.1186/1741-7015-7-12
- US Department of Veteran Affairs, National Center for Veteran Analysis and Statistics. Profile of veterans: 2017. Published March 2019. Accessed April 27, 2023. https://www.va.gov/vetdata/docs/SpecialReports/Profile_of_Veterans_2017.pdf
- Johnson TM et al. Arthritis Care Res (Hoboken). 2022 Nov 4. doi:10.1002/acr.25053
- Ebel AV et al. Arthritis Rheumatol. 2021;73(3):392-400. doi:10.1002/art.41559
- Sokolove J et al. Rheumatology (Oxford). 2016;55(11):1969-1977. doi:10.1093/rheumatology/kew285
- Alpizar-Rodriguez D et al. Rheumatology (Oxford). 2019;58(3):432-440. doi:10.1093/rheumatology/key311
- Chancay MG et al. Womens Midlife Health. 2019;5:3. doi:10.1186/s40695-019-0047-4
- Bongartz T et al. Arthritis Rheum. 2010;62(6):1583-1591. doi:10.1002/art.27405
- Kelly CA et al. Rheumatology (Oxford). 2014;53(9):1676-1682. doi:10.1093/rheumatology/keu165
- Koduri G et al. Rheumatology (Oxford). 2010;49(8):1483-1489. doi:10.1093/rheumatology/keq035
- Olson AL et al. Am J Respir Crit Care Med. 2011;183(3):372-378. doi:10.1164/rccm.201004-0622OC
- Mikuls TR et al. Rheumatology (Oxford). 2011;50(1):101-109. doi:10.1093/rheumatology/keq232
- England BR et al. Arthritis Care Res. 2016;68(1):36-45. doi:10.1002/acr.22642
- Morse JL et al. J Psychiatr Res. 2023;159:224-229. doi:10.1016/j.jpsychires.2023.01.039
- van Vollenhoven RF. BMC Med. 2009;7:12. doi:10.1186/1741-7015-7-12
- US Department of Veteran Affairs, National Center for Veteran Analysis and Statistics. Profile of veterans: 2017. Published March 2019. Accessed April 27, 2023. https://www.va.gov/vetdata/docs/SpecialReports/Profile_of_Veterans_2017.pdf
- Johnson TM et al. Arthritis Care Res (Hoboken). 2022 Nov 4. doi:10.1002/acr.25053
- Ebel AV et al. Arthritis Rheumatol. 2021;73(3):392-400. doi:10.1002/art.41559
- Sokolove J et al. Rheumatology (Oxford). 2016;55(11):1969-1977. doi:10.1093/rheumatology/kew285
- Alpizar-Rodriguez D et al. Rheumatology (Oxford). 2019;58(3):432-440. doi:10.1093/rheumatology/key311
- Chancay MG et al. Womens Midlife Health. 2019;5:3. doi:10.1186/s40695-019-0047-4
- Bongartz T et al. Arthritis Rheum. 2010;62(6):1583-1591. doi:10.1002/art.27405
- Kelly CA et al. Rheumatology (Oxford). 2014;53(9):1676-1682. doi:10.1093/rheumatology/keu165
- Koduri G et al. Rheumatology (Oxford). 2010;49(8):1483-1489. doi:10.1093/rheumatology/keq035
- Olson AL et al. Am J Respir Crit Care Med. 2011;183(3):372-378. doi:10.1164/rccm.201004-0622OC
- Mikuls TR et al. Rheumatology (Oxford). 2011;50(1):101-109. doi:10.1093/rheumatology/keq232
- England BR et al. Arthritis Care Res. 2016;68(1):36-45. doi:10.1002/acr.22642
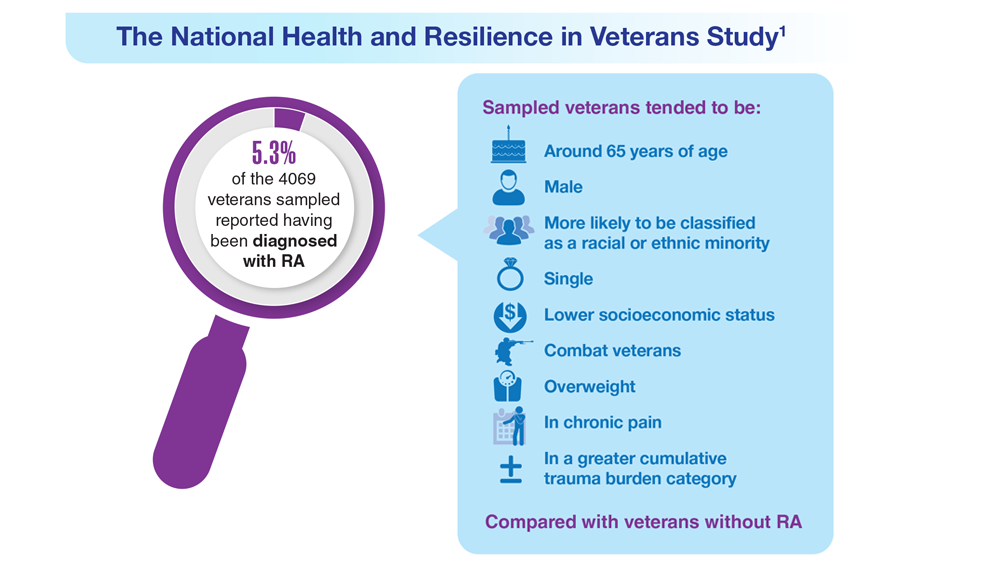
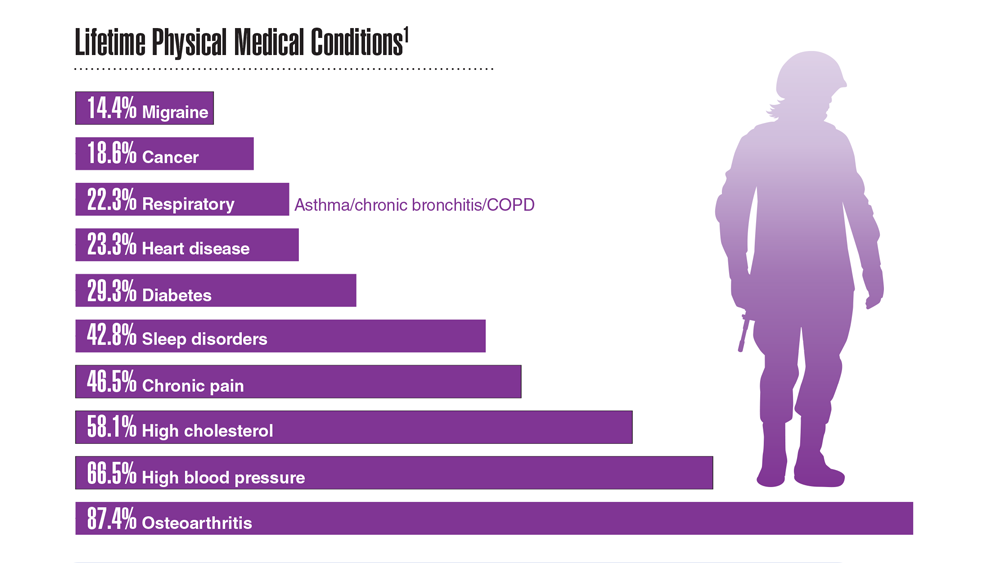
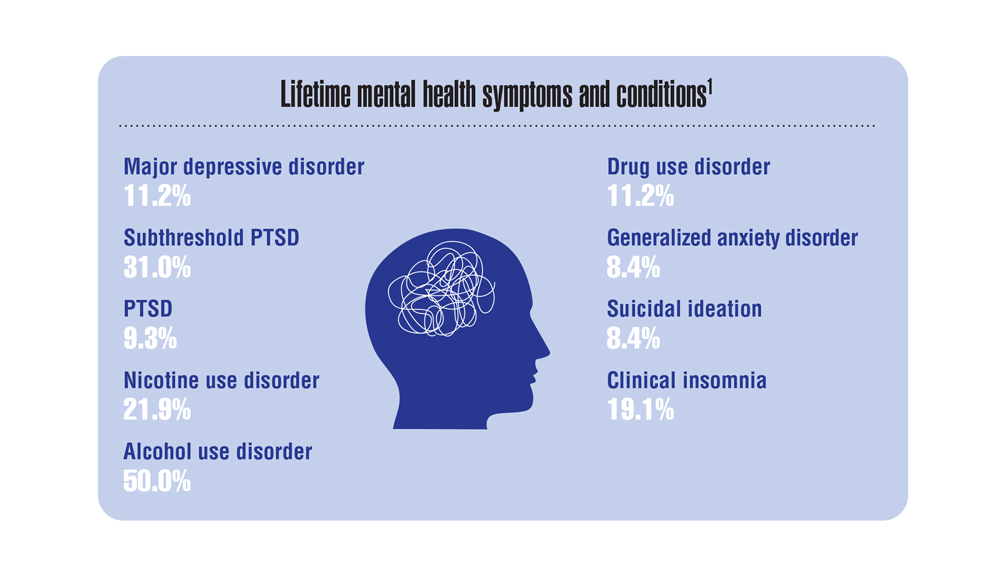
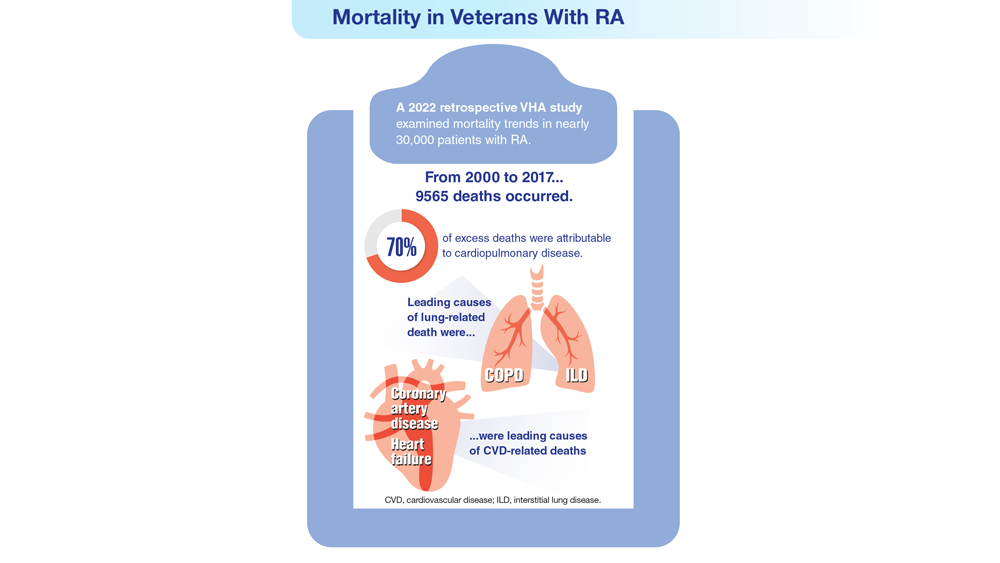


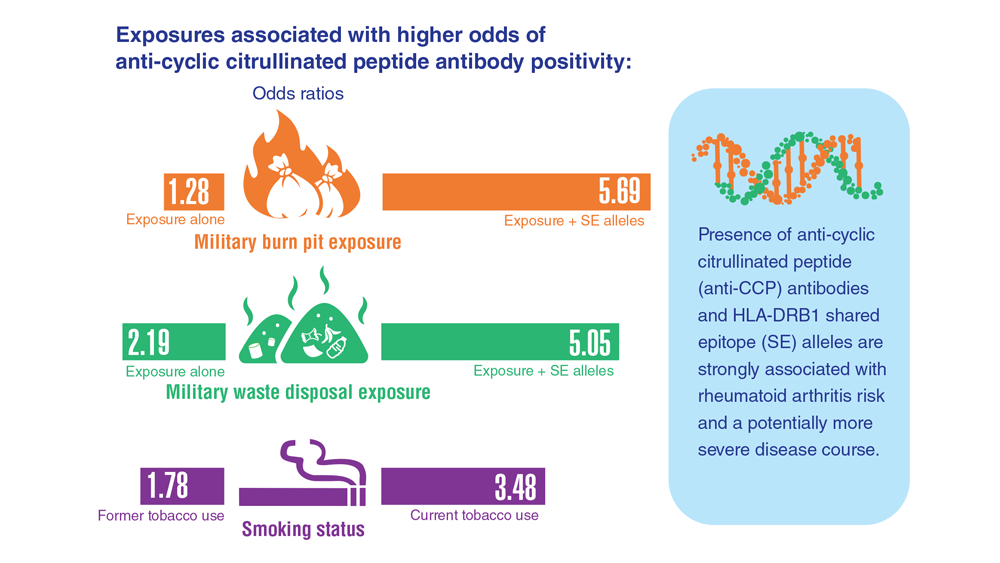
Data Trends 2023: Migraine and Headache
22. Seng EK et al. Neurology. 2022;99(18):e1979-e1992. doi:10.1212/WNL.0000000000200888
23. Coffman C et al. Neurology. 2022;99(2):e187-e198. doi:10.1212/WNL.0000000000200518
24. Hesselbrock RR et al. Aerosp Med Hum Perform. 2022;93(1):26-31. doi:10.3357/amhp.5980.2022
25. Kuruvilla DE et al. BMC Complement Med Ther. 2022;22(1):22. doi:10.1186/s12906-022-03511-6
22. Seng EK et al. Neurology. 2022;99(18):e1979-e1992. doi:10.1212/WNL.0000000000200888
23. Coffman C et al. Neurology. 2022;99(2):e187-e198. doi:10.1212/WNL.0000000000200518
24. Hesselbrock RR et al. Aerosp Med Hum Perform. 2022;93(1):26-31. doi:10.3357/amhp.5980.2022
25. Kuruvilla DE et al. BMC Complement Med Ther. 2022;22(1):22. doi:10.1186/s12906-022-03511-6
22. Seng EK et al. Neurology. 2022;99(18):e1979-e1992. doi:10.1212/WNL.0000000000200888
23. Coffman C et al. Neurology. 2022;99(2):e187-e198. doi:10.1212/WNL.0000000000200518
24. Hesselbrock RR et al. Aerosp Med Hum Perform. 2022;93(1):26-31. doi:10.3357/amhp.5980.2022
25. Kuruvilla DE et al. BMC Complement Med Ther. 2022;22(1):22. doi:10.1186/s12906-022-03511-6
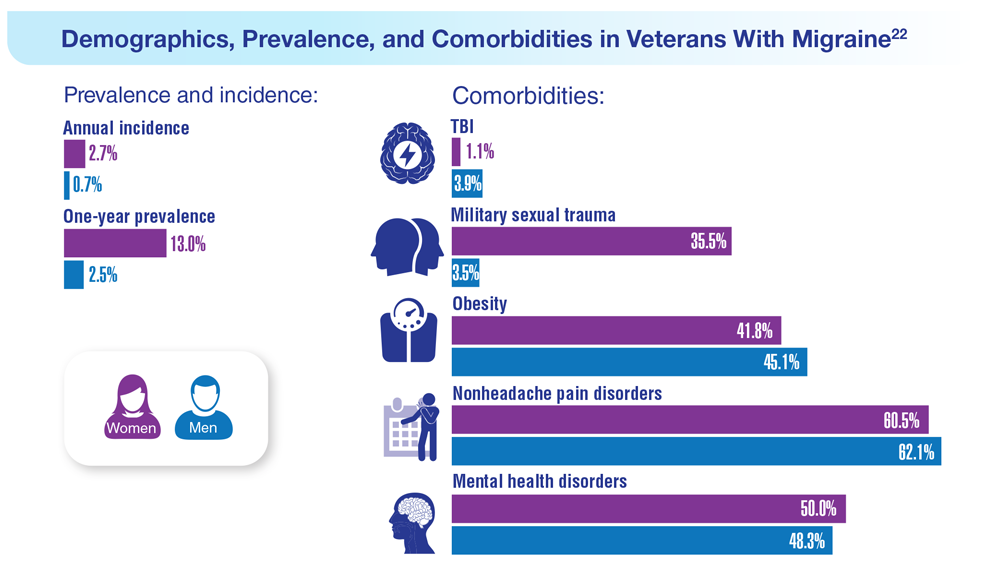
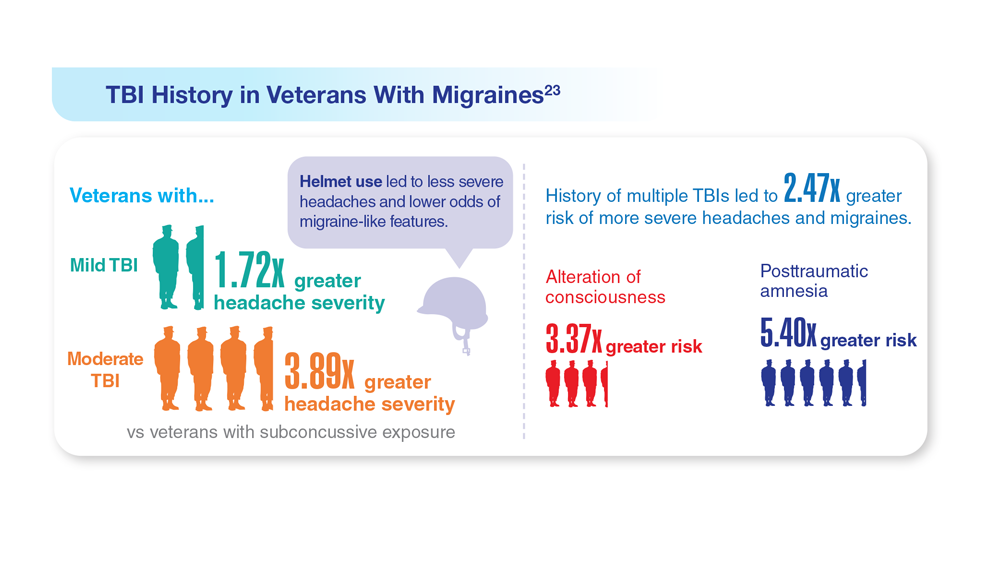
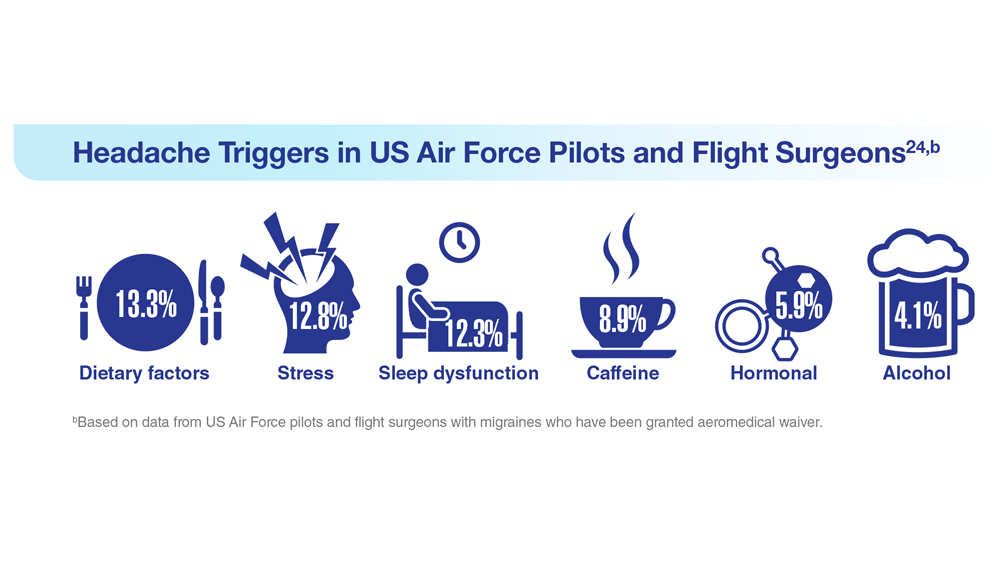
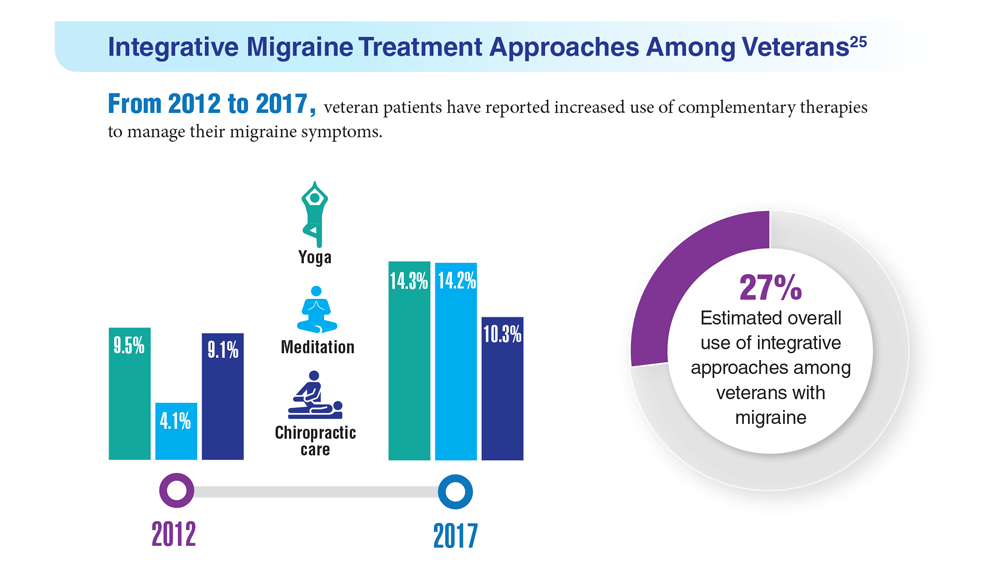
Data Trends 2023: Parkinson’s Disease
17. US Department of Veterans Affairs, Office of Research and Development.
Parkinson’s disease. Updated October 28, 2021. Accessed May 5, 2023.
https://www.research.va.gov/topics/parkinsons.cfm
18. Feeney M et al. Front Neurol. 2022;13:924999. doi:10.3389/fneur.2022.924999
19. Heronemus M et al. Parkinsonism Relat Disord. 2022;105:58-61. doi:10.1016/j.parkreldis.2022.11.003
20. Nejtek VA et al. PLoS One. 2021;16(11):e0258851. doi:10.1371/journal.pone.0258851
21. Yang Y et al. Dement Neurocogn Disord. 2016;15(3):75-81. doi:10.12779/dnd.2016.15.3.75
17. US Department of Veterans Affairs, Office of Research and Development.
Parkinson’s disease. Updated October 28, 2021. Accessed May 5, 2023.
https://www.research.va.gov/topics/parkinsons.cfm
18. Feeney M et al. Front Neurol. 2022;13:924999. doi:10.3389/fneur.2022.924999
19. Heronemus M et al. Parkinsonism Relat Disord. 2022;105:58-61. doi:10.1016/j.parkreldis.2022.11.003
20. Nejtek VA et al. PLoS One. 2021;16(11):e0258851. doi:10.1371/journal.pone.0258851
21. Yang Y et al. Dement Neurocogn Disord. 2016;15(3):75-81. doi:10.12779/dnd.2016.15.3.75
17. US Department of Veterans Affairs, Office of Research and Development.
Parkinson’s disease. Updated October 28, 2021. Accessed May 5, 2023.
https://www.research.va.gov/topics/parkinsons.cfm
18. Feeney M et al. Front Neurol. 2022;13:924999. doi:10.3389/fneur.2022.924999
19. Heronemus M et al. Parkinsonism Relat Disord. 2022;105:58-61. doi:10.1016/j.parkreldis.2022.11.003
20. Nejtek VA et al. PLoS One. 2021;16(11):e0258851. doi:10.1371/journal.pone.0258851
21. Yang Y et al. Dement Neurocogn Disord. 2016;15(3):75-81. doi:10.12779/dnd.2016.15.3.75