User login
Light therapy for nonseasonal major depressive disorder?
Consider treatment with bright light therapy, alone or in combination with fluoxetine, for patients with nonseasonal major depressive disorder (MDD).1
Strength of recommendation
B: Based on a single moderate-quality randomized control trial.
Lam RW, Levitt AJ, Levitan RD, et al. Efficacy of bright light treatment, fluoxetine, and the combination in patients with nonseasonal major depressive disorder: a randomized clinical trial. JAMA Psychiatry. 2016;73:56-63.
Illustrative Case
A 38-year-old woman recently diagnosed with MDD without a seasonal pattern comes to see you for her treatment options. Her Hamilton Depression Rating Scale (HAM-D) is 22, and she is not suicidal. Should you consider bright light therapy in addition to pharmacotherapy?
MDD is one of the most common psychiatric illnesses in the United States, affecting approximately one in 5 adults at some point in their lives.2 Selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors are considered effective first-line pharmacotherapy options for MDD.2,3 Despite their effectiveness, however, studies have shown that only about 40% of patients with MDD achieve remission with first- or second-line drugs.2 In addition, pharmacologic agents have a higher frequency of treatment-associated adverse effects than fluorescent light therapy.4
A Cochrane systematic review of 20 studies (N=620) showed the effectiveness of combined light therapy and pharmacotherapy in treating nonseasonal MDD, but found no benefit to light used as a monotherapy.5 However, the majority of the studies were of poor quality, occurred in the inpatient setting, and lasted fewer than 4 weeks.
In a 5-week, controlled, double-blind trial not included in the Cochrane review, 102 patients with nonseasonal MDD were randomized to receive either active treatment (bright light therapy) plus sertraline 50 mg daily or sham light treatment (using a dim red light) plus sertraline 50 mg daily. The investigators found a statistically significant larger reduction in depression score in the active treatment group than in the sham light group, based on the HAM-D, the Hamilton 6-Item Subscale, the Melancholia Scale, and the 7 atypical items from the Structured Interview Guide for the Seasonal Affective Disorder version of the HAM-D.6,7
Study Summary
Light therapy improves depression without a seasonal component
This latest study was an 8-week randomized, double-blind, placebo- and sham-controlled clinical trial evaluating the benefit of light therapy with and without pharmacotherapy for nonseasonal MDD.1 The investigators enrolled 122 adult patients (ages 19-60 years) from outpatient psychiatry clinics with a diagnosis of MDD (as diagnosed by a psychiatrist) and a HAM-D8 score of at least 20. Subjects had to be off psychotropic medication for at least 2 weeks prior to the first visit and were subsequently monitored for one week to identify spontaneous responders and to give patients time to better regulate their sleep-wake cycle (with the goal of sleeping only between 10:00 pm and 8:00 am daily).
The investigators randomly assigned patients to one of 4 treatment groups: active light monotherapy (10,000-lux fluorescent white light for 30 min/d early in the morning) plus a placebo pill; fluoxetine 20 mg/d plus sham light therapy; placebo pills with sham light therapy; and combined active light therapy with fluoxetine 20 mg daily. Sham light therapy consisted of the use of an inactivated negative ion generator, used in the same fashion as a light box. All patients were analyzed based on modified intention to treat.
The investigators monitored patients for adherence to active and sham treatment by review of their daily logs of device treatment times. Pill counts were used to assess medication adherence. The primary outcome at 8 weeks was the change from baseline in the Montgomery-Asberg Depression Rating Scale (MADRS), a 10-item questionnaire with a worst score of 60.9 Secondary outcomes were treatment response (≥50% MADRS score reduction) and remission (≤10 MADRS score) at the final 8th-week visit. MADRS scoring was used because of its higher sensitivity to treatment-induced changes and its high correlation with the HAM-D scale.
At the end of 8 weeks, the mean (standard deviation [SD]) changes in MADRS scores from baseline were: light monotherapy 13.4 (7.5), fluoxetine monotherapy 8.8 (9.9), combination therapy 16.9 (9.2), and placebo 6.5 (9.6). The improvement was significant in the light monotherapy treatment group vs the placebo group (P=.006), in the combination treatment group vs the vs placebo group (P<.001), and in the combination group vs the fluoxetine treatment group (P=.02), but not for the fluoxetine treatment group vs the placebo group (P=.32). The effect sizes vs placebo were: fluoxetine, d=0.24 (95% confidence interval [CI], −0.27 to 0.74); light monotherapy, 0.80 (95% CI, 0.28 to 1.31); and combination therapy, 1.11 (95% CI, 0.54 to 1.64). Effect sizes of more than 0.8 are often considered large.10
The treatment response (≥50% MADRS improvement) rate was highest in the combination treatment group (75.9%) with response rates to light monotherapy, placebo, and fluoxetine monotherapy of 50%, 33.3%, and 29%, respectively. There was a significant response effect for the combination vs placebo treatment group (P=.005). Similarly, there was a higher remission rate in the combination treatment group (58.6%) than in the placebo, light monotherapy, or fluoxetine treatment groups (30%, 43.8%, and 19.4%, respectively) with a significant effect for the combination vs placebo treatment group (P=.02).
Combination therapy was superior to placebo in treatment response (≥50% reduction in the MADRS score) and remission (MADRS ≤10) with numbers needed to treat of 2.4 (95% CI, 1.6-5.8) and 3.5 (95% CI, 2.0-29.9), respectively.
By the end of the 8-week study period, 16 of 122 patients had dropped out; 2 reported lack of efficacy, 5 reported adverse effects, and the remainder cited administrative reasons, were lost to follow-up, or withdrew consent.
What’s New?
New evidence on a not-so-new treatment
We now have evidence that bright light therapy, either alone or in combination with fluoxetine, is efficacious in increasing the remission rate of nonseasonal MDD.
Caveats
Choice of SSRI, geography, and trial duration may have affected results
A single SSRI (fluoxetine) was used in this study; other more potent SSRIs might work better. This study was conducted in southern Canada, and light therapy may not demonstrate as large a benefit in regions located farther south. The study excluded pregnant and breastfeeding women.
The trial duration was relatively short, and the investigators did not attain their pre-planned sample size for the study, which limited the power to detect clinically significant seasonal treatment effects and differences between the fluoxetine and placebo groups, regardless of whether they received active phototherapy.
Also, it’s worth noting that there were trends for some adverse events (nausea, heartburn, weight gain, agitation, sexual dysfunction, and skin rash) to occur less frequently in the combination group than in the fluoxetine monotherapy group. Possible explanations are that the study had inadequate power, that the sham treatment did not adequately blind patients, or that light therapy can ameliorate some of the adverse effects of fluoxetine.
Challenges to Implementation
Commercial insurance doesn’t usually cover light therapy
Bright light therapy is fairly safe, and some evidence exists supporting its use in the treatment of nonseasonal MDD; however, the data for its use in this area are limited.11 Since only a few studies have tested light therapy for nonseasonal MDD, significant uncertainty remains about patient selection, as well as optimal dose, timing, and duration of light therapy in the management of nonseasonal MDD.12 Although the risks associated with bright light therapy are minimal, the therapy can lead to mania or hypomania,3 so clinicians need to monitor for such effects when initiating therapy.
Lastly, commercial insurance does not usually cover light therapy. The average price of the bright light devices, which can be found in medical supply stores and online outlets, ranges between $118 and $237.4,12 However, such devices are reusable, making the amortized cost almost negligible.13
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Lam RW, Levitt AJ, Levitan RD, et al. Efficacy of bright light treatment, fluoxetine, and the combination in patients with nonseasonal major depressive disorder: a randomized clinical trial. JAMA Psychiatry. 2016;73:56-63.
2. Weihs K, Wert JM. A primary care focus on the treatment of patients with major depressive disorder. Am J Med Sci. 2011;342:324-330.
3. Gelenberg AJ, Freeman CMP, Markowitz JC, et al. Practice guideline for the treatment of patients with major depressive disorder. 3rd edition. 2010. Available at: http://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/mdd.pdf. Accessed April 20, 2016.
4. Lam RW, Tam EM. A Clinician’s Guide to Using Light Therapy. New York, NY: Cambridge University Press; 2009. Available at: http://www.ubcmood.ca/sad/SAD%20resources%20package%202009.pdf. Accessed April 20, 2016.
5. Tuunainen A, Kripke DF, Endo T. Light therapy for non-seasonal depression. Cochrane Database Syst Rev. 2004;2:CD004050.
6. Martiny K. Adjunctive bright light in non-seasonal major depression. Acta Psychiatr Scand Suppl. 2004;425:7-28.
7. Martiny K, Lunde M, Unden M, et al. Adjunctive bright light in non-seasonal major depression: results from clinician-rated depression scales. Acta Psychiatr Scand. 2005;112:117-125.
8. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23:56-62.
9. Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry. 1979;134:382-389.
10. Sullivan GM, Feinn R. Using effect size—or why the P value is not enough. J Grad Med Educ. 2012;4:279-282.
11. Oldham MA, Ciraulo DA. Use of bright light therapy among psychiatrists in Massachusetts: an e-mail survey. The Primary Care Companion for CNS Disorders. 2014;16.
12. Sloane PD, Figueiro M, Cohen L. Light as therapy for sleep disorders and depression in older adults. Clin Geriatr. 2008;16:25-31.
13. Kripke DF. A breakthrough treatment for major depression. J Clin Psychiatry. 2015;76:e660-e661.
Consider treatment with bright light therapy, alone or in combination with fluoxetine, for patients with nonseasonal major depressive disorder (MDD).1
Strength of recommendation
B: Based on a single moderate-quality randomized control trial.
Lam RW, Levitt AJ, Levitan RD, et al. Efficacy of bright light treatment, fluoxetine, and the combination in patients with nonseasonal major depressive disorder: a randomized clinical trial. JAMA Psychiatry. 2016;73:56-63.
Illustrative Case
A 38-year-old woman recently diagnosed with MDD without a seasonal pattern comes to see you for her treatment options. Her Hamilton Depression Rating Scale (HAM-D) is 22, and she is not suicidal. Should you consider bright light therapy in addition to pharmacotherapy?
MDD is one of the most common psychiatric illnesses in the United States, affecting approximately one in 5 adults at some point in their lives.2 Selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors are considered effective first-line pharmacotherapy options for MDD.2,3 Despite their effectiveness, however, studies have shown that only about 40% of patients with MDD achieve remission with first- or second-line drugs.2 In addition, pharmacologic agents have a higher frequency of treatment-associated adverse effects than fluorescent light therapy.4
A Cochrane systematic review of 20 studies (N=620) showed the effectiveness of combined light therapy and pharmacotherapy in treating nonseasonal MDD, but found no benefit to light used as a monotherapy.5 However, the majority of the studies were of poor quality, occurred in the inpatient setting, and lasted fewer than 4 weeks.
In a 5-week, controlled, double-blind trial not included in the Cochrane review, 102 patients with nonseasonal MDD were randomized to receive either active treatment (bright light therapy) plus sertraline 50 mg daily or sham light treatment (using a dim red light) plus sertraline 50 mg daily. The investigators found a statistically significant larger reduction in depression score in the active treatment group than in the sham light group, based on the HAM-D, the Hamilton 6-Item Subscale, the Melancholia Scale, and the 7 atypical items from the Structured Interview Guide for the Seasonal Affective Disorder version of the HAM-D.6,7
Study Summary
Light therapy improves depression without a seasonal component
This latest study was an 8-week randomized, double-blind, placebo- and sham-controlled clinical trial evaluating the benefit of light therapy with and without pharmacotherapy for nonseasonal MDD.1 The investigators enrolled 122 adult patients (ages 19-60 years) from outpatient psychiatry clinics with a diagnosis of MDD (as diagnosed by a psychiatrist) and a HAM-D8 score of at least 20. Subjects had to be off psychotropic medication for at least 2 weeks prior to the first visit and were subsequently monitored for one week to identify spontaneous responders and to give patients time to better regulate their sleep-wake cycle (with the goal of sleeping only between 10:00 pm and 8:00 am daily).
The investigators randomly assigned patients to one of 4 treatment groups: active light monotherapy (10,000-lux fluorescent white light for 30 min/d early in the morning) plus a placebo pill; fluoxetine 20 mg/d plus sham light therapy; placebo pills with sham light therapy; and combined active light therapy with fluoxetine 20 mg daily. Sham light therapy consisted of the use of an inactivated negative ion generator, used in the same fashion as a light box. All patients were analyzed based on modified intention to treat.
The investigators monitored patients for adherence to active and sham treatment by review of their daily logs of device treatment times. Pill counts were used to assess medication adherence. The primary outcome at 8 weeks was the change from baseline in the Montgomery-Asberg Depression Rating Scale (MADRS), a 10-item questionnaire with a worst score of 60.9 Secondary outcomes were treatment response (≥50% MADRS score reduction) and remission (≤10 MADRS score) at the final 8th-week visit. MADRS scoring was used because of its higher sensitivity to treatment-induced changes and its high correlation with the HAM-D scale.
At the end of 8 weeks, the mean (standard deviation [SD]) changes in MADRS scores from baseline were: light monotherapy 13.4 (7.5), fluoxetine monotherapy 8.8 (9.9), combination therapy 16.9 (9.2), and placebo 6.5 (9.6). The improvement was significant in the light monotherapy treatment group vs the placebo group (P=.006), in the combination treatment group vs the vs placebo group (P<.001), and in the combination group vs the fluoxetine treatment group (P=.02), but not for the fluoxetine treatment group vs the placebo group (P=.32). The effect sizes vs placebo were: fluoxetine, d=0.24 (95% confidence interval [CI], −0.27 to 0.74); light monotherapy, 0.80 (95% CI, 0.28 to 1.31); and combination therapy, 1.11 (95% CI, 0.54 to 1.64). Effect sizes of more than 0.8 are often considered large.10
The treatment response (≥50% MADRS improvement) rate was highest in the combination treatment group (75.9%) with response rates to light monotherapy, placebo, and fluoxetine monotherapy of 50%, 33.3%, and 29%, respectively. There was a significant response effect for the combination vs placebo treatment group (P=.005). Similarly, there was a higher remission rate in the combination treatment group (58.6%) than in the placebo, light monotherapy, or fluoxetine treatment groups (30%, 43.8%, and 19.4%, respectively) with a significant effect for the combination vs placebo treatment group (P=.02).
Combination therapy was superior to placebo in treatment response (≥50% reduction in the MADRS score) and remission (MADRS ≤10) with numbers needed to treat of 2.4 (95% CI, 1.6-5.8) and 3.5 (95% CI, 2.0-29.9), respectively.
By the end of the 8-week study period, 16 of 122 patients had dropped out; 2 reported lack of efficacy, 5 reported adverse effects, and the remainder cited administrative reasons, were lost to follow-up, or withdrew consent.
What’s New?
New evidence on a not-so-new treatment
We now have evidence that bright light therapy, either alone or in combination with fluoxetine, is efficacious in increasing the remission rate of nonseasonal MDD.
Caveats
Choice of SSRI, geography, and trial duration may have affected results
A single SSRI (fluoxetine) was used in this study; other more potent SSRIs might work better. This study was conducted in southern Canada, and light therapy may not demonstrate as large a benefit in regions located farther south. The study excluded pregnant and breastfeeding women.
The trial duration was relatively short, and the investigators did not attain their pre-planned sample size for the study, which limited the power to detect clinically significant seasonal treatment effects and differences between the fluoxetine and placebo groups, regardless of whether they received active phototherapy.
Also, it’s worth noting that there were trends for some adverse events (nausea, heartburn, weight gain, agitation, sexual dysfunction, and skin rash) to occur less frequently in the combination group than in the fluoxetine monotherapy group. Possible explanations are that the study had inadequate power, that the sham treatment did not adequately blind patients, or that light therapy can ameliorate some of the adverse effects of fluoxetine.
Challenges to Implementation
Commercial insurance doesn’t usually cover light therapy
Bright light therapy is fairly safe, and some evidence exists supporting its use in the treatment of nonseasonal MDD; however, the data for its use in this area are limited.11 Since only a few studies have tested light therapy for nonseasonal MDD, significant uncertainty remains about patient selection, as well as optimal dose, timing, and duration of light therapy in the management of nonseasonal MDD.12 Although the risks associated with bright light therapy are minimal, the therapy can lead to mania or hypomania,3 so clinicians need to monitor for such effects when initiating therapy.
Lastly, commercial insurance does not usually cover light therapy. The average price of the bright light devices, which can be found in medical supply stores and online outlets, ranges between $118 and $237.4,12 However, such devices are reusable, making the amortized cost almost negligible.13
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Consider treatment with bright light therapy, alone or in combination with fluoxetine, for patients with nonseasonal major depressive disorder (MDD).1
Strength of recommendation
B: Based on a single moderate-quality randomized control trial.
Lam RW, Levitt AJ, Levitan RD, et al. Efficacy of bright light treatment, fluoxetine, and the combination in patients with nonseasonal major depressive disorder: a randomized clinical trial. JAMA Psychiatry. 2016;73:56-63.
Illustrative Case
A 38-year-old woman recently diagnosed with MDD without a seasonal pattern comes to see you for her treatment options. Her Hamilton Depression Rating Scale (HAM-D) is 22, and she is not suicidal. Should you consider bright light therapy in addition to pharmacotherapy?
MDD is one of the most common psychiatric illnesses in the United States, affecting approximately one in 5 adults at some point in their lives.2 Selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors are considered effective first-line pharmacotherapy options for MDD.2,3 Despite their effectiveness, however, studies have shown that only about 40% of patients with MDD achieve remission with first- or second-line drugs.2 In addition, pharmacologic agents have a higher frequency of treatment-associated adverse effects than fluorescent light therapy.4
A Cochrane systematic review of 20 studies (N=620) showed the effectiveness of combined light therapy and pharmacotherapy in treating nonseasonal MDD, but found no benefit to light used as a monotherapy.5 However, the majority of the studies were of poor quality, occurred in the inpatient setting, and lasted fewer than 4 weeks.
In a 5-week, controlled, double-blind trial not included in the Cochrane review, 102 patients with nonseasonal MDD were randomized to receive either active treatment (bright light therapy) plus sertraline 50 mg daily or sham light treatment (using a dim red light) plus sertraline 50 mg daily. The investigators found a statistically significant larger reduction in depression score in the active treatment group than in the sham light group, based on the HAM-D, the Hamilton 6-Item Subscale, the Melancholia Scale, and the 7 atypical items from the Structured Interview Guide for the Seasonal Affective Disorder version of the HAM-D.6,7
Study Summary
Light therapy improves depression without a seasonal component
This latest study was an 8-week randomized, double-blind, placebo- and sham-controlled clinical trial evaluating the benefit of light therapy with and without pharmacotherapy for nonseasonal MDD.1 The investigators enrolled 122 adult patients (ages 19-60 years) from outpatient psychiatry clinics with a diagnosis of MDD (as diagnosed by a psychiatrist) and a HAM-D8 score of at least 20. Subjects had to be off psychotropic medication for at least 2 weeks prior to the first visit and were subsequently monitored for one week to identify spontaneous responders and to give patients time to better regulate their sleep-wake cycle (with the goal of sleeping only between 10:00 pm and 8:00 am daily).
The investigators randomly assigned patients to one of 4 treatment groups: active light monotherapy (10,000-lux fluorescent white light for 30 min/d early in the morning) plus a placebo pill; fluoxetine 20 mg/d plus sham light therapy; placebo pills with sham light therapy; and combined active light therapy with fluoxetine 20 mg daily. Sham light therapy consisted of the use of an inactivated negative ion generator, used in the same fashion as a light box. All patients were analyzed based on modified intention to treat.
The investigators monitored patients for adherence to active and sham treatment by review of their daily logs of device treatment times. Pill counts were used to assess medication adherence. The primary outcome at 8 weeks was the change from baseline in the Montgomery-Asberg Depression Rating Scale (MADRS), a 10-item questionnaire with a worst score of 60.9 Secondary outcomes were treatment response (≥50% MADRS score reduction) and remission (≤10 MADRS score) at the final 8th-week visit. MADRS scoring was used because of its higher sensitivity to treatment-induced changes and its high correlation with the HAM-D scale.
At the end of 8 weeks, the mean (standard deviation [SD]) changes in MADRS scores from baseline were: light monotherapy 13.4 (7.5), fluoxetine monotherapy 8.8 (9.9), combination therapy 16.9 (9.2), and placebo 6.5 (9.6). The improvement was significant in the light monotherapy treatment group vs the placebo group (P=.006), in the combination treatment group vs the vs placebo group (P<.001), and in the combination group vs the fluoxetine treatment group (P=.02), but not for the fluoxetine treatment group vs the placebo group (P=.32). The effect sizes vs placebo were: fluoxetine, d=0.24 (95% confidence interval [CI], −0.27 to 0.74); light monotherapy, 0.80 (95% CI, 0.28 to 1.31); and combination therapy, 1.11 (95% CI, 0.54 to 1.64). Effect sizes of more than 0.8 are often considered large.10
The treatment response (≥50% MADRS improvement) rate was highest in the combination treatment group (75.9%) with response rates to light monotherapy, placebo, and fluoxetine monotherapy of 50%, 33.3%, and 29%, respectively. There was a significant response effect for the combination vs placebo treatment group (P=.005). Similarly, there was a higher remission rate in the combination treatment group (58.6%) than in the placebo, light monotherapy, or fluoxetine treatment groups (30%, 43.8%, and 19.4%, respectively) with a significant effect for the combination vs placebo treatment group (P=.02).
Combination therapy was superior to placebo in treatment response (≥50% reduction in the MADRS score) and remission (MADRS ≤10) with numbers needed to treat of 2.4 (95% CI, 1.6-5.8) and 3.5 (95% CI, 2.0-29.9), respectively.
By the end of the 8-week study period, 16 of 122 patients had dropped out; 2 reported lack of efficacy, 5 reported adverse effects, and the remainder cited administrative reasons, were lost to follow-up, or withdrew consent.
What’s New?
New evidence on a not-so-new treatment
We now have evidence that bright light therapy, either alone or in combination with fluoxetine, is efficacious in increasing the remission rate of nonseasonal MDD.
Caveats
Choice of SSRI, geography, and trial duration may have affected results
A single SSRI (fluoxetine) was used in this study; other more potent SSRIs might work better. This study was conducted in southern Canada, and light therapy may not demonstrate as large a benefit in regions located farther south. The study excluded pregnant and breastfeeding women.
The trial duration was relatively short, and the investigators did not attain their pre-planned sample size for the study, which limited the power to detect clinically significant seasonal treatment effects and differences between the fluoxetine and placebo groups, regardless of whether they received active phototherapy.
Also, it’s worth noting that there were trends for some adverse events (nausea, heartburn, weight gain, agitation, sexual dysfunction, and skin rash) to occur less frequently in the combination group than in the fluoxetine monotherapy group. Possible explanations are that the study had inadequate power, that the sham treatment did not adequately blind patients, or that light therapy can ameliorate some of the adverse effects of fluoxetine.
Challenges to Implementation
Commercial insurance doesn’t usually cover light therapy
Bright light therapy is fairly safe, and some evidence exists supporting its use in the treatment of nonseasonal MDD; however, the data for its use in this area are limited.11 Since only a few studies have tested light therapy for nonseasonal MDD, significant uncertainty remains about patient selection, as well as optimal dose, timing, and duration of light therapy in the management of nonseasonal MDD.12 Although the risks associated with bright light therapy are minimal, the therapy can lead to mania or hypomania,3 so clinicians need to monitor for such effects when initiating therapy.
Lastly, commercial insurance does not usually cover light therapy. The average price of the bright light devices, which can be found in medical supply stores and online outlets, ranges between $118 and $237.4,12 However, such devices are reusable, making the amortized cost almost negligible.13
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Lam RW, Levitt AJ, Levitan RD, et al. Efficacy of bright light treatment, fluoxetine, and the combination in patients with nonseasonal major depressive disorder: a randomized clinical trial. JAMA Psychiatry. 2016;73:56-63.
2. Weihs K, Wert JM. A primary care focus on the treatment of patients with major depressive disorder. Am J Med Sci. 2011;342:324-330.
3. Gelenberg AJ, Freeman CMP, Markowitz JC, et al. Practice guideline for the treatment of patients with major depressive disorder. 3rd edition. 2010. Available at: http://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/mdd.pdf. Accessed April 20, 2016.
4. Lam RW, Tam EM. A Clinician’s Guide to Using Light Therapy. New York, NY: Cambridge University Press; 2009. Available at: http://www.ubcmood.ca/sad/SAD%20resources%20package%202009.pdf. Accessed April 20, 2016.
5. Tuunainen A, Kripke DF, Endo T. Light therapy for non-seasonal depression. Cochrane Database Syst Rev. 2004;2:CD004050.
6. Martiny K. Adjunctive bright light in non-seasonal major depression. Acta Psychiatr Scand Suppl. 2004;425:7-28.
7. Martiny K, Lunde M, Unden M, et al. Adjunctive bright light in non-seasonal major depression: results from clinician-rated depression scales. Acta Psychiatr Scand. 2005;112:117-125.
8. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23:56-62.
9. Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry. 1979;134:382-389.
10. Sullivan GM, Feinn R. Using effect size—or why the P value is not enough. J Grad Med Educ. 2012;4:279-282.
11. Oldham MA, Ciraulo DA. Use of bright light therapy among psychiatrists in Massachusetts: an e-mail survey. The Primary Care Companion for CNS Disorders. 2014;16.
12. Sloane PD, Figueiro M, Cohen L. Light as therapy for sleep disorders and depression in older adults. Clin Geriatr. 2008;16:25-31.
13. Kripke DF. A breakthrough treatment for major depression. J Clin Psychiatry. 2015;76:e660-e661.
1. Lam RW, Levitt AJ, Levitan RD, et al. Efficacy of bright light treatment, fluoxetine, and the combination in patients with nonseasonal major depressive disorder: a randomized clinical trial. JAMA Psychiatry. 2016;73:56-63.
2. Weihs K, Wert JM. A primary care focus on the treatment of patients with major depressive disorder. Am J Med Sci. 2011;342:324-330.
3. Gelenberg AJ, Freeman CMP, Markowitz JC, et al. Practice guideline for the treatment of patients with major depressive disorder. 3rd edition. 2010. Available at: http://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/mdd.pdf. Accessed April 20, 2016.
4. Lam RW, Tam EM. A Clinician’s Guide to Using Light Therapy. New York, NY: Cambridge University Press; 2009. Available at: http://www.ubcmood.ca/sad/SAD%20resources%20package%202009.pdf. Accessed April 20, 2016.
5. Tuunainen A, Kripke DF, Endo T. Light therapy for non-seasonal depression. Cochrane Database Syst Rev. 2004;2:CD004050.
6. Martiny K. Adjunctive bright light in non-seasonal major depression. Acta Psychiatr Scand Suppl. 2004;425:7-28.
7. Martiny K, Lunde M, Unden M, et al. Adjunctive bright light in non-seasonal major depression: results from clinician-rated depression scales. Acta Psychiatr Scand. 2005;112:117-125.
8. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23:56-62.
9. Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry. 1979;134:382-389.
10. Sullivan GM, Feinn R. Using effect size—or why the P value is not enough. J Grad Med Educ. 2012;4:279-282.
11. Oldham MA, Ciraulo DA. Use of bright light therapy among psychiatrists in Massachusetts: an e-mail survey. The Primary Care Companion for CNS Disorders. 2014;16.
12. Sloane PD, Figueiro M, Cohen L. Light as therapy for sleep disorders and depression in older adults. Clin Geriatr. 2008;16:25-31.
13. Kripke DF. A breakthrough treatment for major depression. J Clin Psychiatry. 2015;76:e660-e661.
Copyright © 2016. The Family Physicians Inquiries Network. All rights reserved.

Evolving therapeutic strategies maintain clinical momentum in melanoma
The past 5 years have witnessed a watershed moment in the management of metastatic melanoma. The successes of molecularly targeted and immune-based therapies have transformed it from an aggressively lethal malignancy into one that is readily treatable. Here, we discuss continued efforts to find new therapies and broaden the clinical impact of existing options to maintain the unprecedented momentum of improving patient outcomes.
Click on the PDF icon at the top of this introduction to read the full article.
The past 5 years have witnessed a watershed moment in the management of metastatic melanoma. The successes of molecularly targeted and immune-based therapies have transformed it from an aggressively lethal malignancy into one that is readily treatable. Here, we discuss continued efforts to find new therapies and broaden the clinical impact of existing options to maintain the unprecedented momentum of improving patient outcomes.
Click on the PDF icon at the top of this introduction to read the full article.
The past 5 years have witnessed a watershed moment in the management of metastatic melanoma. The successes of molecularly targeted and immune-based therapies have transformed it from an aggressively lethal malignancy into one that is readily treatable. Here, we discuss continued efforts to find new therapies and broaden the clinical impact of existing options to maintain the unprecedented momentum of improving patient outcomes.
Click on the PDF icon at the top of this introduction to read the full article.
Group-based psychosocial services: assessing outpatient oncology needs
Background Group-based services can improve quality-of-life outcomes for oncology patients.
Objective To assess patient preferences for supportive and wellness programming to better meet patient needs and allocate resources.
Methods Patients from 3 cancer centers in New York City completed a 15-item questionnaire about their interest in educational topics (wellness, nutrition, legal issues, etc) and services (support groups, lectures, and exercise programs).
Results 311 patients participated in the survey. Mean age was 59 years, and 74% were women. The most common cancer was breast (40%), followed by genitourinary (15%). Women preferred wellness workshops most, followed by informative sessions; men most preferred informative sessions, followed equally by posttreatment support and wellness workshops. Older age was related to an increased likelihood of group attendance. Overall, 68% of participants reported that they would be likely to attend groups. For lectures, nutrition was of greatest interest for men (43%) and women (34%), followed by anxiety management (17% and 18%, respectively). Overall, 64% of participants reported that they would be likely to attend a lecture. A majority of respondents (54%) expressed a desire for exercise programs.
Limitations Generalizability to all cancer centers is limited, because data was not tracked on those who refused to complete the questionnaire.
Conclusions Obtaining patient feedback on psychosocial programs is imperative for understanding patient preferences and developing effective support programming.
Click on the PDF icon at the top of this introduction to read the full article.
Background Group-based services can improve quality-of-life outcomes for oncology patients.
Objective To assess patient preferences for supportive and wellness programming to better meet patient needs and allocate resources.
Methods Patients from 3 cancer centers in New York City completed a 15-item questionnaire about their interest in educational topics (wellness, nutrition, legal issues, etc) and services (support groups, lectures, and exercise programs).
Results 311 patients participated in the survey. Mean age was 59 years, and 74% were women. The most common cancer was breast (40%), followed by genitourinary (15%). Women preferred wellness workshops most, followed by informative sessions; men most preferred informative sessions, followed equally by posttreatment support and wellness workshops. Older age was related to an increased likelihood of group attendance. Overall, 68% of participants reported that they would be likely to attend groups. For lectures, nutrition was of greatest interest for men (43%) and women (34%), followed by anxiety management (17% and 18%, respectively). Overall, 64% of participants reported that they would be likely to attend a lecture. A majority of respondents (54%) expressed a desire for exercise programs.
Limitations Generalizability to all cancer centers is limited, because data was not tracked on those who refused to complete the questionnaire.
Conclusions Obtaining patient feedback on psychosocial programs is imperative for understanding patient preferences and developing effective support programming.
Click on the PDF icon at the top of this introduction to read the full article.
Background Group-based services can improve quality-of-life outcomes for oncology patients.
Objective To assess patient preferences for supportive and wellness programming to better meet patient needs and allocate resources.
Methods Patients from 3 cancer centers in New York City completed a 15-item questionnaire about their interest in educational topics (wellness, nutrition, legal issues, etc) and services (support groups, lectures, and exercise programs).
Results 311 patients participated in the survey. Mean age was 59 years, and 74% were women. The most common cancer was breast (40%), followed by genitourinary (15%). Women preferred wellness workshops most, followed by informative sessions; men most preferred informative sessions, followed equally by posttreatment support and wellness workshops. Older age was related to an increased likelihood of group attendance. Overall, 68% of participants reported that they would be likely to attend groups. For lectures, nutrition was of greatest interest for men (43%) and women (34%), followed by anxiety management (17% and 18%, respectively). Overall, 64% of participants reported that they would be likely to attend a lecture. A majority of respondents (54%) expressed a desire for exercise programs.
Limitations Generalizability to all cancer centers is limited, because data was not tracked on those who refused to complete the questionnaire.
Conclusions Obtaining patient feedback on psychosocial programs is imperative for understanding patient preferences and developing effective support programming.
Click on the PDF icon at the top of this introduction to read the full article.
Tips for Living With Dystonia

Early results positive for nivolumab as first-line therapy in advanced NSCLC
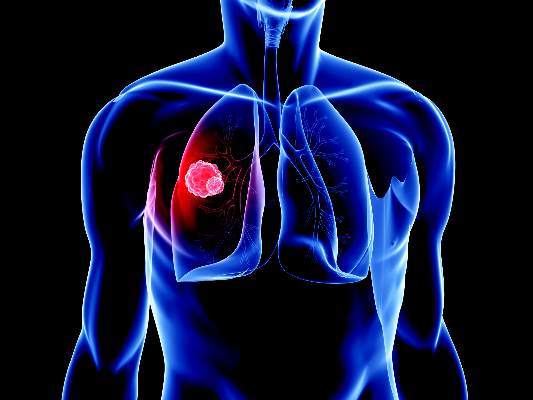
The PD-1 immune checkpoint inhibitor nivolumab may be safe and effective as a first-line therapy in adult patients with non–small cell lung cancer (NSCLC), according to the results of the phase I CheckMate 012 trial.
Of 52 adult patients with advanced NSCLC who received nivolumab, 19% experienced grade three or four adverse events, and the overall response rate was 23% with four ongoing complete responses, reported Scott Gettinger, MD, of the Yale Cancer Center, New Haven, Conn., and his associates (J Clin Oncol. 2016 June. doi: 10.1200/JCO.2016.66.9929).
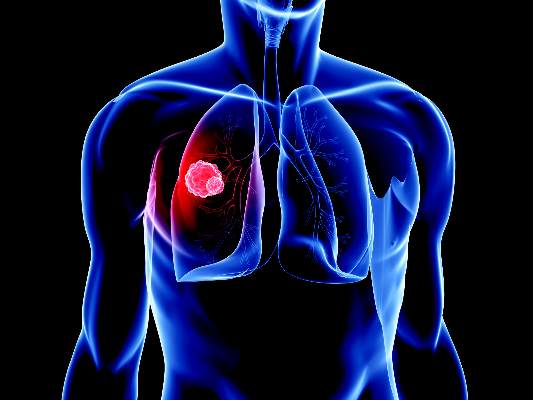
In the study cohort, 94% had stage IV NSCLC, 79% were former or current smokers, and 65% had received either radiotherapy, adjuvant or neoadjuvant chemotherapy.
Treatment-related adverse events were reported in 71% of patients, the most common being fatigue (29%), rash (19%), and nausea (14%). Grade 3 or 4 adverse events including rash, cardiac failure, and lung infection occurred in 10 patients (19%). There were no treatment-related deaths, but adverse events led to the discontinuation of the drug treatment in six patients.
Responses to nivolumab (overall response rate, 23%) were durable with duration of responses ranging from 4.2 to 25.8 months. In addition, the median overall survival was 19.4 months, median progression-free survival was 3.5 months, and the 24-week progression-free survival rate was 31% (95% confidence interval, 28%-60%).
Forty-six patients had tumor specimens evaluable for PD-L1 expression. Clinical activity was observed regardless of PD-L1 expression, the investigators reported. However, the overall response rate was higher in patients with tumors that expressed PD-L1, compared with non-PD-L1-expressing tumors.
All investigators reported serving in advisory roles for, receiving financial compensation or honoraria from, or having ownership or stock in multiple companies including Bristol-Myers Squibb, which funded the study.
On Twitter @jessnicolecraig
The PD-1 immune checkpoint inhibitor nivolumab may be safe and effective as a first-line therapy in adult patients with non–small cell lung cancer (NSCLC), according to the results of the phase I CheckMate 012 trial.
Of 52 adult patients with advanced NSCLC who received nivolumab, 19% experienced grade three or four adverse events, and the overall response rate was 23% with four ongoing complete responses, reported Scott Gettinger, MD, of the Yale Cancer Center, New Haven, Conn., and his associates (J Clin Oncol. 2016 June. doi: 10.1200/JCO.2016.66.9929).
In the study cohort, 94% had stage IV NSCLC, 79% were former or current smokers, and 65% had received either radiotherapy, adjuvant or neoadjuvant chemotherapy.
Treatment-related adverse events were reported in 71% of patients, the most common being fatigue (29%), rash (19%), and nausea (14%). Grade 3 or 4 adverse events including rash, cardiac failure, and lung infection occurred in 10 patients (19%). There were no treatment-related deaths, but adverse events led to the discontinuation of the drug treatment in six patients.
Responses to nivolumab (overall response rate, 23%) were durable with duration of responses ranging from 4.2 to 25.8 months. In addition, the median overall survival was 19.4 months, median progression-free survival was 3.5 months, and the 24-week progression-free survival rate was 31% (95% confidence interval, 28%-60%).
Forty-six patients had tumor specimens evaluable for PD-L1 expression. Clinical activity was observed regardless of PD-L1 expression, the investigators reported. However, the overall response rate was higher in patients with tumors that expressed PD-L1, compared with non-PD-L1-expressing tumors.
All investigators reported serving in advisory roles for, receiving financial compensation or honoraria from, or having ownership or stock in multiple companies including Bristol-Myers Squibb, which funded the study.
On Twitter @jessnicolecraig
The PD-1 immune checkpoint inhibitor nivolumab may be safe and effective as a first-line therapy in adult patients with non–small cell lung cancer (NSCLC), according to the results of the phase I CheckMate 012 trial.
Of 52 adult patients with advanced NSCLC who received nivolumab, 19% experienced grade three or four adverse events, and the overall response rate was 23% with four ongoing complete responses, reported Scott Gettinger, MD, of the Yale Cancer Center, New Haven, Conn., and his associates (J Clin Oncol. 2016 June. doi: 10.1200/JCO.2016.66.9929).
In the study cohort, 94% had stage IV NSCLC, 79% were former or current smokers, and 65% had received either radiotherapy, adjuvant or neoadjuvant chemotherapy.
Treatment-related adverse events were reported in 71% of patients, the most common being fatigue (29%), rash (19%), and nausea (14%). Grade 3 or 4 adverse events including rash, cardiac failure, and lung infection occurred in 10 patients (19%). There were no treatment-related deaths, but adverse events led to the discontinuation of the drug treatment in six patients.
Responses to nivolumab (overall response rate, 23%) were durable with duration of responses ranging from 4.2 to 25.8 months. In addition, the median overall survival was 19.4 months, median progression-free survival was 3.5 months, and the 24-week progression-free survival rate was 31% (95% confidence interval, 28%-60%).
Forty-six patients had tumor specimens evaluable for PD-L1 expression. Clinical activity was observed regardless of PD-L1 expression, the investigators reported. However, the overall response rate was higher in patients with tumors that expressed PD-L1, compared with non-PD-L1-expressing tumors.
All investigators reported serving in advisory roles for, receiving financial compensation or honoraria from, or having ownership or stock in multiple companies including Bristol-Myers Squibb, which funded the study.
On Twitter @jessnicolecraig
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: A phase I trial indicates that nivolumab is safe and shows durable activity as a first-line therapy in treating patients with advanced NSCLC.
Major finding: Grade 3 or 4 adverse events were reported in 19% of patients. The overall response rate was 23% with four ongoing complete responses.
Data source: A phase I trial of 52 patients with stage 3 or 4 non–small-cell lung cancer.
Disclosures: All investigators reported serving in advisory roles for, receiving financial compensation or honoraria from, or having ownership or stock interest in multiple companies including Bristol-Myers Squibb, which funded the study.
The impact of a nurse practitioner-led symptom clinic on emergency department use in cancer patients
Background Emergency department (ED) use and hospitalization is distressing to cancer patients and drives up the cost of health care. A growing body of evidence demonstrates that more than half of those visits may be avoidable.
Objective To examine the impact of a nurse practitioner (NP)-led, physician-supervised, outpatient symptom management clinic on ED use.
Methods We conducted a retrospective review of ED encounters to quantify the frequency of ED use by oncology patients at a community cancer institute 6 months before (October 2012-March 2013) and after (April-September 2013) the initiation of an NP-staffed symptom management clinic.
Results The highest use of the ED and supportive clinic was among patients with advanced cancer, most commonly with lung or breast cancer, who were receiving cytotoxic chemotherapy. Uncontrolled symptoms of shortness of breath, pain, weakness, fever, nausea, vomiting, and diarrhea commonly led to ED visits. Despite instituting the NP-staffed symptom management clinic to manage those symptoms, there was a 17.9% increase in ED use. However, of the patients seen by the NP, 95% may have avoided hospitalization.
Limitations Retrospective study
Conclusions Our study identifies a high-risk population of patients who use the ED frequently. NP-led clinics could aggressively manage the symptom burden of these patients and potentially reduce ED visits as other studies have demonstrated. Although our study did not directly demonstrate this, we have identified weaknesses of care delivery in our clinic that could be optimized. In addition, we have demonstrated that the majority of patients seen for acute symptoms by an NP avoided an ED visit.
Click on the PDF icon at the top of this introduction to read the full article.
Background Emergency department (ED) use and hospitalization is distressing to cancer patients and drives up the cost of health care. A growing body of evidence demonstrates that more than half of those visits may be avoidable.
Objective To examine the impact of a nurse practitioner (NP)-led, physician-supervised, outpatient symptom management clinic on ED use.
Methods We conducted a retrospective review of ED encounters to quantify the frequency of ED use by oncology patients at a community cancer institute 6 months before (October 2012-March 2013) and after (April-September 2013) the initiation of an NP-staffed symptom management clinic.
Results The highest use of the ED and supportive clinic was among patients with advanced cancer, most commonly with lung or breast cancer, who were receiving cytotoxic chemotherapy. Uncontrolled symptoms of shortness of breath, pain, weakness, fever, nausea, vomiting, and diarrhea commonly led to ED visits. Despite instituting the NP-staffed symptom management clinic to manage those symptoms, there was a 17.9% increase in ED use. However, of the patients seen by the NP, 95% may have avoided hospitalization.
Limitations Retrospective study
Conclusions Our study identifies a high-risk population of patients who use the ED frequently. NP-led clinics could aggressively manage the symptom burden of these patients and potentially reduce ED visits as other studies have demonstrated. Although our study did not directly demonstrate this, we have identified weaknesses of care delivery in our clinic that could be optimized. In addition, we have demonstrated that the majority of patients seen for acute symptoms by an NP avoided an ED visit.
Click on the PDF icon at the top of this introduction to read the full article.
Background Emergency department (ED) use and hospitalization is distressing to cancer patients and drives up the cost of health care. A growing body of evidence demonstrates that more than half of those visits may be avoidable.
Objective To examine the impact of a nurse practitioner (NP)-led, physician-supervised, outpatient symptom management clinic on ED use.
Methods We conducted a retrospective review of ED encounters to quantify the frequency of ED use by oncology patients at a community cancer institute 6 months before (October 2012-March 2013) and after (April-September 2013) the initiation of an NP-staffed symptom management clinic.
Results The highest use of the ED and supportive clinic was among patients with advanced cancer, most commonly with lung or breast cancer, who were receiving cytotoxic chemotherapy. Uncontrolled symptoms of shortness of breath, pain, weakness, fever, nausea, vomiting, and diarrhea commonly led to ED visits. Despite instituting the NP-staffed symptom management clinic to manage those symptoms, there was a 17.9% increase in ED use. However, of the patients seen by the NP, 95% may have avoided hospitalization.
Limitations Retrospective study
Conclusions Our study identifies a high-risk population of patients who use the ED frequently. NP-led clinics could aggressively manage the symptom burden of these patients and potentially reduce ED visits as other studies have demonstrated. Although our study did not directly demonstrate this, we have identified weaknesses of care delivery in our clinic that could be optimized. In addition, we have demonstrated that the majority of patients seen for acute symptoms by an NP avoided an ED visit.
Click on the PDF icon at the top of this introduction to read the full article.
Hereditary breast and ovarian cancer: risk assessment in minority women and provider knowledge gaps
Methods The Georgia Department of Public Health established this project through a cooperative agreement with the Centers for Disease Control and Prevention. HBOC screening and genetic services were provided in 13 public health centers and federally qualified health centers. Staff received training on genetics and risk assessment using the Breast Cancer Genetics Referral Screening Tool (B-RST). Providers and medical residents were surveyed on their knowledge of HBOC. Young women with breast cancer were surveyed on receipt of genetic services.
Conclusions The genomics project demonstrated the efficacy of population-based screening to identify high-risk women before they receive a diagnosis of cancer. A high percentage of women who screened positive also completed genetic counseling and testing. Access to the benefits of HBOC management to prevent cancer and decrease mortality among minority and underserved women depends on improvements in knowledge of genetics and evidence-based practice by providers.
Funding/sponsorship This project was funded through a cooperative agreement from the Centers for Disease Control and Prevention to the Georgia Department of Public Health from 2011-2014.
Click on the PDF icon at the top of this introduction to read the full article.
Methods The Georgia Department of Public Health established this project through a cooperative agreement with the Centers for Disease Control and Prevention. HBOC screening and genetic services were provided in 13 public health centers and federally qualified health centers. Staff received training on genetics and risk assessment using the Breast Cancer Genetics Referral Screening Tool (B-RST). Providers and medical residents were surveyed on their knowledge of HBOC. Young women with breast cancer were surveyed on receipt of genetic services.
Conclusions The genomics project demonstrated the efficacy of population-based screening to identify high-risk women before they receive a diagnosis of cancer. A high percentage of women who screened positive also completed genetic counseling and testing. Access to the benefits of HBOC management to prevent cancer and decrease mortality among minority and underserved women depends on improvements in knowledge of genetics and evidence-based practice by providers.
Funding/sponsorship This project was funded through a cooperative agreement from the Centers for Disease Control and Prevention to the Georgia Department of Public Health from 2011-2014.
Click on the PDF icon at the top of this introduction to read the full article.
Methods The Georgia Department of Public Health established this project through a cooperative agreement with the Centers for Disease Control and Prevention. HBOC screening and genetic services were provided in 13 public health centers and federally qualified health centers. Staff received training on genetics and risk assessment using the Breast Cancer Genetics Referral Screening Tool (B-RST). Providers and medical residents were surveyed on their knowledge of HBOC. Young women with breast cancer were surveyed on receipt of genetic services.
Conclusions The genomics project demonstrated the efficacy of population-based screening to identify high-risk women before they receive a diagnosis of cancer. A high percentage of women who screened positive also completed genetic counseling and testing. Access to the benefits of HBOC management to prevent cancer and decrease mortality among minority and underserved women depends on improvements in knowledge of genetics and evidence-based practice by providers.
Funding/sponsorship This project was funded through a cooperative agreement from the Centers for Disease Control and Prevention to the Georgia Department of Public Health from 2011-2014.
Click on the PDF icon at the top of this introduction to read the full article.
HBV/HIV coinfection a significant risk factor for inpatient mortality
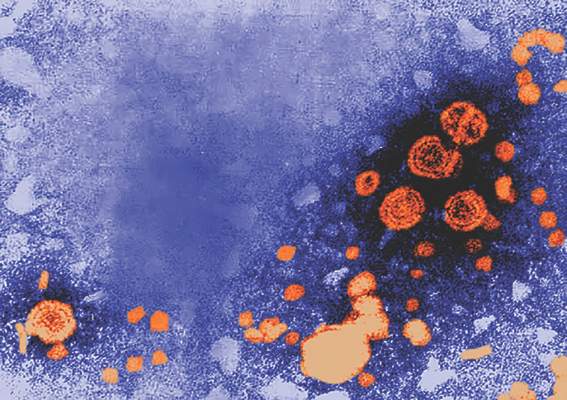
Patients coinfected with hepatitis B virus and HIV are at greater risk for in-hospital mortality, particularly in liver-related admissions, compared with HBV monoinfection, according to a study in the Journal of Viral Hepatitis.
Researchers at Massachusetts General Hospital, Boston, identified patients in the 2011 U.S. Nationwide Inpatient Sample who had been hospitalized with HBV or HIV monoinfection or HBV/HIV coinfection using ICD-9-CM codes. A total of 72,584 discharges with HBV monoinfection, 133,880 discharges with HIV monoinfection and 8,156 discharges with HBV/HIV coinfection were included. The researchers then compared liver-related hospital admissions among the three groups and performed multivariable logistic regression to identify independent predictors of in-hospital mortality, length of stay, and total charges.
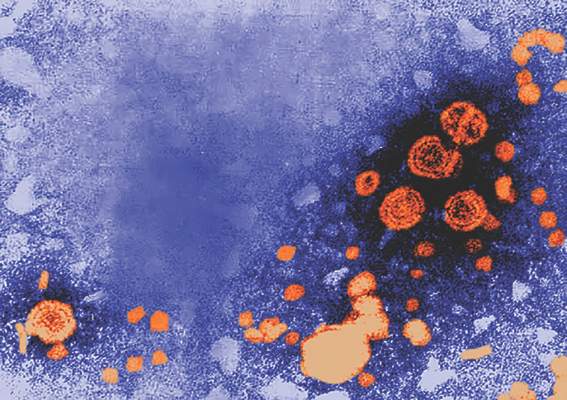
According to Raymond T. Chung, MD, director of hepatology at Massachusetts General Hospital, and his coauthors, this study is the first to examine outcomes of HBV/HIV coinfection among hospitalized patients, a “group that represents those with advanced disease and vulnerable to poor outcomes and high health care utilization.” (J Viral Hepat. 2016 Jun 13. doi: 10.1111/jvh.12555)
Patients in the study with HBV monoinfection tended to be older than those with HIV monoinfection or HBV/HIV coinfection. Of those aged 51-65 years, 42% had HBV monoinfection, 34% had HIV monoinfection, and 31% had HBV/HIV coinfection (P less than .001). Males were overrepresented in the HBV/HIV coinfection group (77%), compared with those with HBV monoinfection (57%), and HIV monoinfection (67%). Additionally, the investigators found that patients with HBV monoinfection were more likely to be white (42%) than were those with HIV monoinfection (26%) or HBV/HIV coinfection (27%).
Dr. Chung and his colleagues found that HBV/HIV coinfection was associated with significantly higher adjusted in-hospital mortality, compared with patients with HBV monoinfection (adjusted odds ratio, 1.67; 95% confidence interval, 1.30-2.15), but not compared with HIV monoinfection (aOR, 1.22; 95% CI, 0.96-1.54).
“Interestingly, [the] increase in risk of mortality was primarily observed in liver-related admissions … and not infectious-related hospitalizations,” Dr. Chung and his coauthors said.
The overall adjusted hospital length of stay (LOS;1.53 days; 95% CI, 0.93-2.13; less than .001) and total hospitalization charges ($17,595; 95% CI 11,120-24,069; P less than .0001) were higher in the coinfected group, compared with the HBV monoinfection group – even after adjustment for comorbidity- and disease-related complications, the authors wrote. LOS and total charges also were higher in the coinfected group, compared with the HIV monoinfection group (+0.62 days; P = .034; $8,840; P = .005).
While HBV/HIV coinfection by itself was not associated with higher in-hospital mortality, the presence of HBV along with cirrhosis or complications of portal hypertension was associated with three times greater in-hospital mortality in patients with HIV, compared with those without such complications (odds ratio, 3.00; 95% CI, 1.80-5.02). Researchers also found that LOS (0.62 days; 95% CI, 0.05-1.20; P = .034) and hospitalization cost ($8,840; 95% CI, 2,604-15,077; P = .005) were increased in patients with HBV/HIV coinfection, compared with HIV monoinfection.
“Overall health care utilization from HBV/HIV coinfection is … higher than for either infection alone and higher than the national average for all hospitalizations, emphasizing the health care burden from these illnesses,” the authors concluded.
Three study coauthors were supported in part by grants from the National Institutes of Health, while one coauthor was supported by a career development award from the American Gastroenterological Association and by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Chung reported no financial conflict of interests. One coauthor reported participation on scientific advisory boards of AbbVie and Cubist pharmaceuticals.
On Twitter @richpizzi
Patients coinfected with hepatitis B virus and HIV are at greater risk for in-hospital mortality, particularly in liver-related admissions, compared with HBV monoinfection, according to a study in the Journal of Viral Hepatitis.
Researchers at Massachusetts General Hospital, Boston, identified patients in the 2011 U.S. Nationwide Inpatient Sample who had been hospitalized with HBV or HIV monoinfection or HBV/HIV coinfection using ICD-9-CM codes. A total of 72,584 discharges with HBV monoinfection, 133,880 discharges with HIV monoinfection and 8,156 discharges with HBV/HIV coinfection were included. The researchers then compared liver-related hospital admissions among the three groups and performed multivariable logistic regression to identify independent predictors of in-hospital mortality, length of stay, and total charges.
According to Raymond T. Chung, MD, director of hepatology at Massachusetts General Hospital, and his coauthors, this study is the first to examine outcomes of HBV/HIV coinfection among hospitalized patients, a “group that represents those with advanced disease and vulnerable to poor outcomes and high health care utilization.” (J Viral Hepat. 2016 Jun 13. doi: 10.1111/jvh.12555)
Patients in the study with HBV monoinfection tended to be older than those with HIV monoinfection or HBV/HIV coinfection. Of those aged 51-65 years, 42% had HBV monoinfection, 34% had HIV monoinfection, and 31% had HBV/HIV coinfection (P less than .001). Males were overrepresented in the HBV/HIV coinfection group (77%), compared with those with HBV monoinfection (57%), and HIV monoinfection (67%). Additionally, the investigators found that patients with HBV monoinfection were more likely to be white (42%) than were those with HIV monoinfection (26%) or HBV/HIV coinfection (27%).
Dr. Chung and his colleagues found that HBV/HIV coinfection was associated with significantly higher adjusted in-hospital mortality, compared with patients with HBV monoinfection (adjusted odds ratio, 1.67; 95% confidence interval, 1.30-2.15), but not compared with HIV monoinfection (aOR, 1.22; 95% CI, 0.96-1.54).
“Interestingly, [the] increase in risk of mortality was primarily observed in liver-related admissions … and not infectious-related hospitalizations,” Dr. Chung and his coauthors said.
The overall adjusted hospital length of stay (LOS;1.53 days; 95% CI, 0.93-2.13; less than .001) and total hospitalization charges ($17,595; 95% CI 11,120-24,069; P less than .0001) were higher in the coinfected group, compared with the HBV monoinfection group – even after adjustment for comorbidity- and disease-related complications, the authors wrote. LOS and total charges also were higher in the coinfected group, compared with the HIV monoinfection group (+0.62 days; P = .034; $8,840; P = .005).
While HBV/HIV coinfection by itself was not associated with higher in-hospital mortality, the presence of HBV along with cirrhosis or complications of portal hypertension was associated with three times greater in-hospital mortality in patients with HIV, compared with those without such complications (odds ratio, 3.00; 95% CI, 1.80-5.02). Researchers also found that LOS (0.62 days; 95% CI, 0.05-1.20; P = .034) and hospitalization cost ($8,840; 95% CI, 2,604-15,077; P = .005) were increased in patients with HBV/HIV coinfection, compared with HIV monoinfection.
“Overall health care utilization from HBV/HIV coinfection is … higher than for either infection alone and higher than the national average for all hospitalizations, emphasizing the health care burden from these illnesses,” the authors concluded.
Three study coauthors were supported in part by grants from the National Institutes of Health, while one coauthor was supported by a career development award from the American Gastroenterological Association and by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Chung reported no financial conflict of interests. One coauthor reported participation on scientific advisory boards of AbbVie and Cubist pharmaceuticals.
On Twitter @richpizzi
Patients coinfected with hepatitis B virus and HIV are at greater risk for in-hospital mortality, particularly in liver-related admissions, compared with HBV monoinfection, according to a study in the Journal of Viral Hepatitis.
Researchers at Massachusetts General Hospital, Boston, identified patients in the 2011 U.S. Nationwide Inpatient Sample who had been hospitalized with HBV or HIV monoinfection or HBV/HIV coinfection using ICD-9-CM codes. A total of 72,584 discharges with HBV monoinfection, 133,880 discharges with HIV monoinfection and 8,156 discharges with HBV/HIV coinfection were included. The researchers then compared liver-related hospital admissions among the three groups and performed multivariable logistic regression to identify independent predictors of in-hospital mortality, length of stay, and total charges.
According to Raymond T. Chung, MD, director of hepatology at Massachusetts General Hospital, and his coauthors, this study is the first to examine outcomes of HBV/HIV coinfection among hospitalized patients, a “group that represents those with advanced disease and vulnerable to poor outcomes and high health care utilization.” (J Viral Hepat. 2016 Jun 13. doi: 10.1111/jvh.12555)
Patients in the study with HBV monoinfection tended to be older than those with HIV monoinfection or HBV/HIV coinfection. Of those aged 51-65 years, 42% had HBV monoinfection, 34% had HIV monoinfection, and 31% had HBV/HIV coinfection (P less than .001). Males were overrepresented in the HBV/HIV coinfection group (77%), compared with those with HBV monoinfection (57%), and HIV monoinfection (67%). Additionally, the investigators found that patients with HBV monoinfection were more likely to be white (42%) than were those with HIV monoinfection (26%) or HBV/HIV coinfection (27%).
Dr. Chung and his colleagues found that HBV/HIV coinfection was associated with significantly higher adjusted in-hospital mortality, compared with patients with HBV monoinfection (adjusted odds ratio, 1.67; 95% confidence interval, 1.30-2.15), but not compared with HIV monoinfection (aOR, 1.22; 95% CI, 0.96-1.54).
“Interestingly, [the] increase in risk of mortality was primarily observed in liver-related admissions … and not infectious-related hospitalizations,” Dr. Chung and his coauthors said.
The overall adjusted hospital length of stay (LOS;1.53 days; 95% CI, 0.93-2.13; less than .001) and total hospitalization charges ($17,595; 95% CI 11,120-24,069; P less than .0001) were higher in the coinfected group, compared with the HBV monoinfection group – even after adjustment for comorbidity- and disease-related complications, the authors wrote. LOS and total charges also were higher in the coinfected group, compared with the HIV monoinfection group (+0.62 days; P = .034; $8,840; P = .005).
While HBV/HIV coinfection by itself was not associated with higher in-hospital mortality, the presence of HBV along with cirrhosis or complications of portal hypertension was associated with three times greater in-hospital mortality in patients with HIV, compared with those without such complications (odds ratio, 3.00; 95% CI, 1.80-5.02). Researchers also found that LOS (0.62 days; 95% CI, 0.05-1.20; P = .034) and hospitalization cost ($8,840; 95% CI, 2,604-15,077; P = .005) were increased in patients with HBV/HIV coinfection, compared with HIV monoinfection.
“Overall health care utilization from HBV/HIV coinfection is … higher than for either infection alone and higher than the national average for all hospitalizations, emphasizing the health care burden from these illnesses,” the authors concluded.
Three study coauthors were supported in part by grants from the National Institutes of Health, while one coauthor was supported by a career development award from the American Gastroenterological Association and by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Chung reported no financial conflict of interests. One coauthor reported participation on scientific advisory boards of AbbVie and Cubist pharmaceuticals.
On Twitter @richpizzi
FROM THE JOURNAL OF VIRAL HEPATITIS
Key clinical point: Patients coinfected with HBV and HIV are at greater risk for in-hospital mortality, particularly in liver-related admissions, compared with HBV monoinfection.
Major finding: HBV/HIV coinfection was associated with significantly higher adjusted in-hospital mortality, compared with patients with HBV monoinfection, but not when compared with HIV monoinfection.
Data source: Comparison study of patient discharges from the 2011 U.S. Nationwide Inpatient Sample: 72,584 discharges with HBV monoinfection, 133,880 discharges with HIV monoinfection and 8,156 discharges with HBV/HIV coinfection.
Disclosures: Three study coauthors were supported in part by grants from the National Institutes of Health, while one coauthor was supported by a career development award from the American Gastroenterological Association and by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Chung reported no financial conflict of interests. One coauthor reported participation on scientific advisory boards of AbbVie and Cubist pharmaceuticals.
New Guideline for Stroke Rehabilitation
The American Heart Association/American Stroke Association has issued its first guideline on adult stroke rehabilitation. Published in the June issue of Stroke, the guideline calls for intensive, multidisciplinary treatment in an inpatient rehabilitation facility.
“Previous guidelines have focused on the medical issues involved in the initial management of stroke, but many people survive a stroke with some level of disability. There is increasing evidence that rehabilitation can have a big impact on the survivors’ quality of life, so the time is right to review the evidence in this complex field and highlight effective and important aspects of rehabilitation,” said Carolee J. Winstein, PhD, PT, lead author of the guideline and Professor of Biokinesiology and Physical Therapy at the University of Southern California in Los Angeles.

Carolee J. Winstein, PhD, PT
The American Stroke Association strongly recommends that stroke patients be treated at an inpatient rehabilitation facility whenever possible, rather than at a skilled nursing facility. While in an inpatient rehabilitation facility, a patient participates in at least three hours of rehabilitation per day with physical therapists, occupational therapists, and speech therapists. Nurses are continuously available, and doctors typically visit daily.
“There is considerable evidence that patients benefit from the team approach in a facility that understands the importance of rehabilitation during the early period after a stroke,” said Dr. Winstein.
According to Dr. Winstein and her coauthors, caregivers should advocate for discharge to an inpatient rehabilitation facility and insist that a stroke survivor not be discharged from the hospital until he or she has participated in a structured program on preventing falls. This program should include education about changes to make the home safer (eg, removing throw rugs and improving lighting), minimizing the fall risk resulting from the side effects of medication, and safely using assistive devices such as wheelchairs, walkers, and canes.
“This recommendation will probably change medical practice. Even the top stroke centers may not have a formal falls-prevention program, but it is very important because a high percentage of patients end up falling after a stroke,” Dr. Winstein said.
The guideline also recommends the following measures:
• Intense mobility-task training after stroke for all survivors with walking limitations to relearn activities such as climbing stairs
• An individually tailored exercise program that allows survivors to safely continue to improve their cardiovascular fitness through proper exercise and physical activity after formal rehabilitation is complete
• An enriched environment (which might include a computer, books, music, and games) to increase engagement and cognitive activities during rehabilitation
• Speech therapy for those with difficulty speaking following a stroke
• Eye exercises for survivors with difficulty focusing on near objects
• A balance training program for survivors with poor balance, or who are at risk for falls.
“For a person to fulfill his or her full potential after stroke, there needs to be a coordinated effort and ongoing communication between a team of professionals, as well as the patient, family, and caregivers,” Dr. Winstein said.
Suggested Reading
Winstein CJ, Stein J, Arena R, et al. Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2016;47(6):e98-e169.
The American Heart Association/American Stroke Association has issued its first guideline on adult stroke rehabilitation. Published in the June issue of Stroke, the guideline calls for intensive, multidisciplinary treatment in an inpatient rehabilitation facility.
“Previous guidelines have focused on the medical issues involved in the initial management of stroke, but many people survive a stroke with some level of disability. There is increasing evidence that rehabilitation can have a big impact on the survivors’ quality of life, so the time is right to review the evidence in this complex field and highlight effective and important aspects of rehabilitation,” said Carolee J. Winstein, PhD, PT, lead author of the guideline and Professor of Biokinesiology and Physical Therapy at the University of Southern California in Los Angeles.
Carolee J. Winstein, PhD, PT
The American Stroke Association strongly recommends that stroke patients be treated at an inpatient rehabilitation facility whenever possible, rather than at a skilled nursing facility. While in an inpatient rehabilitation facility, a patient participates in at least three hours of rehabilitation per day with physical therapists, occupational therapists, and speech therapists. Nurses are continuously available, and doctors typically visit daily.
“There is considerable evidence that patients benefit from the team approach in a facility that understands the importance of rehabilitation during the early period after a stroke,” said Dr. Winstein.
According to Dr. Winstein and her coauthors, caregivers should advocate for discharge to an inpatient rehabilitation facility and insist that a stroke survivor not be discharged from the hospital until he or she has participated in a structured program on preventing falls. This program should include education about changes to make the home safer (eg, removing throw rugs and improving lighting), minimizing the fall risk resulting from the side effects of medication, and safely using assistive devices such as wheelchairs, walkers, and canes.
“This recommendation will probably change medical practice. Even the top stroke centers may not have a formal falls-prevention program, but it is very important because a high percentage of patients end up falling after a stroke,” Dr. Winstein said.
The guideline also recommends the following measures:
• Intense mobility-task training after stroke for all survivors with walking limitations to relearn activities such as climbing stairs
• An individually tailored exercise program that allows survivors to safely continue to improve their cardiovascular fitness through proper exercise and physical activity after formal rehabilitation is complete
• An enriched environment (which might include a computer, books, music, and games) to increase engagement and cognitive activities during rehabilitation
• Speech therapy for those with difficulty speaking following a stroke
• Eye exercises for survivors with difficulty focusing on near objects
• A balance training program for survivors with poor balance, or who are at risk for falls.
“For a person to fulfill his or her full potential after stroke, there needs to be a coordinated effort and ongoing communication between a team of professionals, as well as the patient, family, and caregivers,” Dr. Winstein said.
The American Heart Association/American Stroke Association has issued its first guideline on adult stroke rehabilitation. Published in the June issue of Stroke, the guideline calls for intensive, multidisciplinary treatment in an inpatient rehabilitation facility.
“Previous guidelines have focused on the medical issues involved in the initial management of stroke, but many people survive a stroke with some level of disability. There is increasing evidence that rehabilitation can have a big impact on the survivors’ quality of life, so the time is right to review the evidence in this complex field and highlight effective and important aspects of rehabilitation,” said Carolee J. Winstein, PhD, PT, lead author of the guideline and Professor of Biokinesiology and Physical Therapy at the University of Southern California in Los Angeles.
Carolee J. Winstein, PhD, PT
The American Stroke Association strongly recommends that stroke patients be treated at an inpatient rehabilitation facility whenever possible, rather than at a skilled nursing facility. While in an inpatient rehabilitation facility, a patient participates in at least three hours of rehabilitation per day with physical therapists, occupational therapists, and speech therapists. Nurses are continuously available, and doctors typically visit daily.
“There is considerable evidence that patients benefit from the team approach in a facility that understands the importance of rehabilitation during the early period after a stroke,” said Dr. Winstein.
According to Dr. Winstein and her coauthors, caregivers should advocate for discharge to an inpatient rehabilitation facility and insist that a stroke survivor not be discharged from the hospital until he or she has participated in a structured program on preventing falls. This program should include education about changes to make the home safer (eg, removing throw rugs and improving lighting), minimizing the fall risk resulting from the side effects of medication, and safely using assistive devices such as wheelchairs, walkers, and canes.
“This recommendation will probably change medical practice. Even the top stroke centers may not have a formal falls-prevention program, but it is very important because a high percentage of patients end up falling after a stroke,” Dr. Winstein said.
The guideline also recommends the following measures:
• Intense mobility-task training after stroke for all survivors with walking limitations to relearn activities such as climbing stairs
• An individually tailored exercise program that allows survivors to safely continue to improve their cardiovascular fitness through proper exercise and physical activity after formal rehabilitation is complete
• An enriched environment (which might include a computer, books, music, and games) to increase engagement and cognitive activities during rehabilitation
• Speech therapy for those with difficulty speaking following a stroke
• Eye exercises for survivors with difficulty focusing on near objects
• A balance training program for survivors with poor balance, or who are at risk for falls.
“For a person to fulfill his or her full potential after stroke, there needs to be a coordinated effort and ongoing communication between a team of professionals, as well as the patient, family, and caregivers,” Dr. Winstein said.
Suggested Reading
Winstein CJ, Stein J, Arena R, et al. Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2016;47(6):e98-e169.
Suggested Reading
Winstein CJ, Stein J, Arena R, et al. Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2016;47(6):e98-e169.

Quality versus queasy: neurokinin 1 receptor antagonist use in moderately emetogenic chemotherapy
Background The American Society of Clinical Oncology (ASCO) launched the Quality Oncology Practice Initiative (QOPI) program in 2010 to promote quality cancer care. The association has subsequently influenced the use of neurokinin 1 (NK-1) receptor antagonists through articles published in peer-reviewed publications and its Choosing Wisely campaign.
Objective To explore the rationale behind the use of NK-1 receptor antagonists in clinical practice.
Methods We distributed an anonymous 12-question online survey to 650 medical oncologists in 5 states, inquiring about their use of these agents. A total of 155 responses were analyzed.
Results QOPI-certified physicians were significantly more likely than noncertified physicians to use NK-1 receptor antagonists with moderately emetogenic regimens, including weekly cisplatin for head and neck cancer (82.6% vs 27.0%, respectively; P < .001), cervical and bladder cancer (81.4% vs 32.7%, P < .001), and with CHOP (cyclophosphamide, hydroxydaunorubicin, oncovin, prednisone) with or without rituximab in lymphoma (81.4 vs 17.3%, P < .001). The majority of QOPI-certified physicians reported using these agents for the sole purpose of maintaining QOPI certification (80.0%-86.0%). Certified physicians were also significantly more likely to appropriately prescribe NK-1 antagonists with highly emetogenic chemotherapy.
Limitations Responder bias; short survey that precludes detailed analysis; small sample size may limit generalizability to the field of medical oncology.
Conclusion Our data demonstrate that providers in QOPI-certified practices are significantly more likely than those in noncertified practices to prescribe NK-1 receptor antagonists. Certified physicians report that satisfying ASCO-QOPI requirements is their primary motivation for offering these agents.
Click on the PDF icon at the top of this introduction to read the full article.
Background The American Society of Clinical Oncology (ASCO) launched the Quality Oncology Practice Initiative (QOPI) program in 2010 to promote quality cancer care. The association has subsequently influenced the use of neurokinin 1 (NK-1) receptor antagonists through articles published in peer-reviewed publications and its Choosing Wisely campaign.
Objective To explore the rationale behind the use of NK-1 receptor antagonists in clinical practice.
Methods We distributed an anonymous 12-question online survey to 650 medical oncologists in 5 states, inquiring about their use of these agents. A total of 155 responses were analyzed.
Results QOPI-certified physicians were significantly more likely than noncertified physicians to use NK-1 receptor antagonists with moderately emetogenic regimens, including weekly cisplatin for head and neck cancer (82.6% vs 27.0%, respectively; P < .001), cervical and bladder cancer (81.4% vs 32.7%, P < .001), and with CHOP (cyclophosphamide, hydroxydaunorubicin, oncovin, prednisone) with or without rituximab in lymphoma (81.4 vs 17.3%, P < .001). The majority of QOPI-certified physicians reported using these agents for the sole purpose of maintaining QOPI certification (80.0%-86.0%). Certified physicians were also significantly more likely to appropriately prescribe NK-1 antagonists with highly emetogenic chemotherapy.
Limitations Responder bias; short survey that precludes detailed analysis; small sample size may limit generalizability to the field of medical oncology.
Conclusion Our data demonstrate that providers in QOPI-certified practices are significantly more likely than those in noncertified practices to prescribe NK-1 receptor antagonists. Certified physicians report that satisfying ASCO-QOPI requirements is their primary motivation for offering these agents.
Click on the PDF icon at the top of this introduction to read the full article.
Background The American Society of Clinical Oncology (ASCO) launched the Quality Oncology Practice Initiative (QOPI) program in 2010 to promote quality cancer care. The association has subsequently influenced the use of neurokinin 1 (NK-1) receptor antagonists through articles published in peer-reviewed publications and its Choosing Wisely campaign.
Objective To explore the rationale behind the use of NK-1 receptor antagonists in clinical practice.
Methods We distributed an anonymous 12-question online survey to 650 medical oncologists in 5 states, inquiring about their use of these agents. A total of 155 responses were analyzed.
Results QOPI-certified physicians were significantly more likely than noncertified physicians to use NK-1 receptor antagonists with moderately emetogenic regimens, including weekly cisplatin for head and neck cancer (82.6% vs 27.0%, respectively; P < .001), cervical and bladder cancer (81.4% vs 32.7%, P < .001), and with CHOP (cyclophosphamide, hydroxydaunorubicin, oncovin, prednisone) with or without rituximab in lymphoma (81.4 vs 17.3%, P < .001). The majority of QOPI-certified physicians reported using these agents for the sole purpose of maintaining QOPI certification (80.0%-86.0%). Certified physicians were also significantly more likely to appropriately prescribe NK-1 antagonists with highly emetogenic chemotherapy.
Limitations Responder bias; short survey that precludes detailed analysis; small sample size may limit generalizability to the field of medical oncology.
Conclusion Our data demonstrate that providers in QOPI-certified practices are significantly more likely than those in noncertified practices to prescribe NK-1 receptor antagonists. Certified physicians report that satisfying ASCO-QOPI requirements is their primary motivation for offering these agents.
Click on the PDF icon at the top of this introduction to read the full article.