User login
Menopause and cardiovascular risk examined in type 1 diabetes
NEW ORLEANS – Premenopausal women with type 1 diabetes mellitus have a higher cardiovascular risk, compared with their diabetes-free counterparts. Among postmenopausal women, however, those with type 1 diabetes do not have a higher cardiovascular risk, compared with their peers who do not have diabetes, with the exception of those aged 54 and older.
Those are key findings from an analysis of women enrolled in the Coronary Artery Calcification in Type 1 Diabetes (CACTI) study.
“In general [premenopausal] women have a better cardiovascular profile than do men, but we don’t see that same effect in diabetic women,” lead author Amena Keshawarz said in an interview in advance of the annual scientific sessions of the American Diabetes Association. “They lose some of that protection. We’re wondering if that has some sort of relationship with menopause, because once women undergo menopause they tend to lose that protective factor.”
Ms. Keshawarz, a doctoral student and research assistant at the University of Colorado Barbara Davis Center for Childhood Diabetes, Aurora, and her associates used carotid intima-media thickness (cIMT) and the presence of coronary artery calcification to measure the cardiovascular risk by menopausal status in 106 women with type 1 diabetes and 140 nondiabetic women who were enrolled in CACTI. The patients ranged in age from 33-74 years and the data were collected between January 2014 and May 2016. Multivariable linear and logistic regressions were used to examine the differences in cIMT and to estimate the odds ratio for coronary artery calcification (CAC). The models were run for the following ages separately: 42, 42, 48, 51, 54, and 57 years.
As a group, women with type 1 diabetes were younger than their counterparts without diabetes (a mean age of 51 vs. 55 years, respectively; P = .002), but menopause age did not differ by diabetes status. Ms. Keshawarz reported that women with type 1 diabetes had significantly higher age-adjusted odds of significant CAC and higher cIMT, compared with those in the nondiabetic group, but these relationships differed by age and menopause status. For example, among premenopausal women, type 1 diabetes increased the odds of CAC at all ages, and cIMT was higher in women with type 1 diabetes, compared with those in the nondiabetic group at age 45 years and older. Among postmenopausal women, type 1 diabetes was associated with only higher CAC at age 54 years and older and with higher cIMT at age 57 years.
“Type 1 diabetic women face unique problems in their health that are not just endocrinology-related,” Ms. Keshawarz said. “If they haven’t undergone menopause yet, that needs to be taken into account when you’re proposing interventions and lifestyle and behavioral changes, because there is an increased possibility that they’re going to be at higher risk of coronary artery calcification and thicker [coronary] artery walls.”
The study was supported by grants from the American Diabetes Association and the National Institutes of Health. Ms. Keshawarz reported having no financial disclosures.
NEW ORLEANS – Premenopausal women with type 1 diabetes mellitus have a higher cardiovascular risk, compared with their diabetes-free counterparts. Among postmenopausal women, however, those with type 1 diabetes do not have a higher cardiovascular risk, compared with their peers who do not have diabetes, with the exception of those aged 54 and older.
Those are key findings from an analysis of women enrolled in the Coronary Artery Calcification in Type 1 Diabetes (CACTI) study.
“In general [premenopausal] women have a better cardiovascular profile than do men, but we don’t see that same effect in diabetic women,” lead author Amena Keshawarz said in an interview in advance of the annual scientific sessions of the American Diabetes Association. “They lose some of that protection. We’re wondering if that has some sort of relationship with menopause, because once women undergo menopause they tend to lose that protective factor.”
Ms. Keshawarz, a doctoral student and research assistant at the University of Colorado Barbara Davis Center for Childhood Diabetes, Aurora, and her associates used carotid intima-media thickness (cIMT) and the presence of coronary artery calcification to measure the cardiovascular risk by menopausal status in 106 women with type 1 diabetes and 140 nondiabetic women who were enrolled in CACTI. The patients ranged in age from 33-74 years and the data were collected between January 2014 and May 2016. Multivariable linear and logistic regressions were used to examine the differences in cIMT and to estimate the odds ratio for coronary artery calcification (CAC). The models were run for the following ages separately: 42, 42, 48, 51, 54, and 57 years.
As a group, women with type 1 diabetes were younger than their counterparts without diabetes (a mean age of 51 vs. 55 years, respectively; P = .002), but menopause age did not differ by diabetes status. Ms. Keshawarz reported that women with type 1 diabetes had significantly higher age-adjusted odds of significant CAC and higher cIMT, compared with those in the nondiabetic group, but these relationships differed by age and menopause status. For example, among premenopausal women, type 1 diabetes increased the odds of CAC at all ages, and cIMT was higher in women with type 1 diabetes, compared with those in the nondiabetic group at age 45 years and older. Among postmenopausal women, type 1 diabetes was associated with only higher CAC at age 54 years and older and with higher cIMT at age 57 years.
“Type 1 diabetic women face unique problems in their health that are not just endocrinology-related,” Ms. Keshawarz said. “If they haven’t undergone menopause yet, that needs to be taken into account when you’re proposing interventions and lifestyle and behavioral changes, because there is an increased possibility that they’re going to be at higher risk of coronary artery calcification and thicker [coronary] artery walls.”
The study was supported by grants from the American Diabetes Association and the National Institutes of Health. Ms. Keshawarz reported having no financial disclosures.
NEW ORLEANS – Premenopausal women with type 1 diabetes mellitus have a higher cardiovascular risk, compared with their diabetes-free counterparts. Among postmenopausal women, however, those with type 1 diabetes do not have a higher cardiovascular risk, compared with their peers who do not have diabetes, with the exception of those aged 54 and older.
Those are key findings from an analysis of women enrolled in the Coronary Artery Calcification in Type 1 Diabetes (CACTI) study.
“In general [premenopausal] women have a better cardiovascular profile than do men, but we don’t see that same effect in diabetic women,” lead author Amena Keshawarz said in an interview in advance of the annual scientific sessions of the American Diabetes Association. “They lose some of that protection. We’re wondering if that has some sort of relationship with menopause, because once women undergo menopause they tend to lose that protective factor.”
Ms. Keshawarz, a doctoral student and research assistant at the University of Colorado Barbara Davis Center for Childhood Diabetes, Aurora, and her associates used carotid intima-media thickness (cIMT) and the presence of coronary artery calcification to measure the cardiovascular risk by menopausal status in 106 women with type 1 diabetes and 140 nondiabetic women who were enrolled in CACTI. The patients ranged in age from 33-74 years and the data were collected between January 2014 and May 2016. Multivariable linear and logistic regressions were used to examine the differences in cIMT and to estimate the odds ratio for coronary artery calcification (CAC). The models were run for the following ages separately: 42, 42, 48, 51, 54, and 57 years.
As a group, women with type 1 diabetes were younger than their counterparts without diabetes (a mean age of 51 vs. 55 years, respectively; P = .002), but menopause age did not differ by diabetes status. Ms. Keshawarz reported that women with type 1 diabetes had significantly higher age-adjusted odds of significant CAC and higher cIMT, compared with those in the nondiabetic group, but these relationships differed by age and menopause status. For example, among premenopausal women, type 1 diabetes increased the odds of CAC at all ages, and cIMT was higher in women with type 1 diabetes, compared with those in the nondiabetic group at age 45 years and older. Among postmenopausal women, type 1 diabetes was associated with only higher CAC at age 54 years and older and with higher cIMT at age 57 years.
“Type 1 diabetic women face unique problems in their health that are not just endocrinology-related,” Ms. Keshawarz said. “If they haven’t undergone menopause yet, that needs to be taken into account when you’re proposing interventions and lifestyle and behavioral changes, because there is an increased possibility that they’re going to be at higher risk of coronary artery calcification and thicker [coronary] artery walls.”
The study was supported by grants from the American Diabetes Association and the National Institutes of Health. Ms. Keshawarz reported having no financial disclosures.
AT THE ADA ANNUAL SCIENTIFIC SESSIONS
Key clinical point: Premenopausal women with type 1 diabetes have a higher cardiovascular risk, compared with their peers who do not have diabetes.
Major finding: Women with type 1 diabetes had significantly higher age-adjusted odds of higher coronary artery calcification and higher carotid intima-media thickness, compared with those in the nondiabetic group, but these relationships differed by age and menopause status.
Data source: An analysis of 106 women with type 1 diabetes and 140 nondiabetic women who were enrolled in the Coronary Artery Calcification in Type 1 Diabetes (CACTI) study.
Disclosures: The study was supported by grants from the American Diabetes Association and the National Institutes of Health. Ms. Keshawarz reported having no financial disclosures.
Women’s Health Initiative May Account for Insomnia’s Upward Trend
DENVER – Much of the rising prevalence of insomnia among U.S. and Canadian adults may be driven by the sharp reduction in the use of hormone replacement therapy following the 2002 report from the Women’s Health Initiative, Sheila N. Garland, PhD, said at the annual meeting of the Associated Professional Sleep Societies.
“In 2002 the Women’s Health Initiative came out with findings that hormone replacement therapy increased the risk of coronary heart disease, breast cancer, stroke, and pulmonary embolism [JAMA. 2002 Jul 17;288(3):321-33]. A lot of women on hormone replacement therapy up until 2002 stopped using it then. The increase in difficulty sleeping we found between 2002 and 2012 could perhaps represent an untreated menopausal symptom,” according to Dr. Garland, a psychologist at Memorial University of Newfoundland in St. John’s.

She presented an analysis of data from the Canadian Community Health Survey, a national once-per-decade survey, which included 34,118 adults aged 20-80 years and older in the 2002 version and 23,089 in 2012.
The key finding from the standpoint of sleep medicine, the prevalence of self-reported trouble sleeping, increased from 15.6% in 2002 to 17.1% in 2012. And this increase was concentrated in 40- to 59-year-old women, where the prevalence of insomnia or poor sleep rose from 19% to 24.3%, the highest of any age group. Rates remained flat over time in men and women aged 20-39 years and 60-80 years and older as well as in 40- to 59-year-old men.
The sleep-related question put to survey participants in face-to-face or telephone interviews was this: “How often do you have trouble going to sleep or staying asleep?” If they answered “most of the time” or “all of the time” they were classified as having poor sleep.
When Dr. Garland saw the survey results she immediately asked herself, “What is happening with Canadian women?” She came up with two theories. They are not mutually exclusive. One hinges on the dramatic drop off in the use of hormone replacement therapy in response to the Women’s Health Initiative report. The other theory is that the increasing prevalence of insomnia in middle-aged women is a manifestation of stress among the growing population of what has been called “the sandwich generation,” people who care for their aging parents while also supporting their own children. Those responsibilities most often fall upon the mother.
She noted that a similar rise in the prevalence of insomnia or trouble sleeping is occurring south of the border – in the United States – as documented in a Centers for Disease Control and Prevention analysis. The CDC investigators examined data on 30,970 adult participants in the 2002 National Health Interview Survey, 23,344 in the 2007 survey, and 34,509 in the 2012 survey. The prevalence of insomnia or trouble sleeping increased from 17.5% in 2002 to 19.2% in 2012. That absolute 1.7% increase pairs well with the 1.5% rise over the same time frame in the Canadian survey. The prevalence was higher in U.S. women than men in all three survey years (Sleep Med. 2015 Mar;16[3]:372-8).
Dr. Garland said the Canadian national survey contains data on self-perceived stress levels. She plans to analyze those results to learn if being a member of the sandwich generation is a significant contributor to poor sleep.
Regardless of the underlying mechanism, she continued, it’s clear from these large national surveys that middle-aged women are particularly vulnerable to poor sleep.
“Increased recognition is necessary. Prevention and intervention programs may be warranted, given the individual and societal consequences of poor sleep, including increased psychiatric and medical disorders, work absenteeism, and health care costs,” she said.
One audience member rose to congratulate Dr. Garland on her detective work. He commented that her notion that the rise in insomnia can be traced to fallout from the 2002 Women’s Health Initiative is consistent with his own clinical experience.
“The most common way women over age 40 present to our sleep center with insomnia is because they’re menopausal and not on hormone replacement therapy,” he said.
The Canadian Community Health Survey is sponsored by Statistics Canada. Dr. Garland reported having no financial conflicts of interest.
DENVER – Much of the rising prevalence of insomnia among U.S. and Canadian adults may be driven by the sharp reduction in the use of hormone replacement therapy following the 2002 report from the Women’s Health Initiative, Sheila N. Garland, PhD, said at the annual meeting of the Associated Professional Sleep Societies.
“In 2002 the Women’s Health Initiative came out with findings that hormone replacement therapy increased the risk of coronary heart disease, breast cancer, stroke, and pulmonary embolism [JAMA. 2002 Jul 17;288(3):321-33]. A lot of women on hormone replacement therapy up until 2002 stopped using it then. The increase in difficulty sleeping we found between 2002 and 2012 could perhaps represent an untreated menopausal symptom,” according to Dr. Garland, a psychologist at Memorial University of Newfoundland in St. John’s.
She presented an analysis of data from the Canadian Community Health Survey, a national once-per-decade survey, which included 34,118 adults aged 20-80 years and older in the 2002 version and 23,089 in 2012.
The key finding from the standpoint of sleep medicine, the prevalence of self-reported trouble sleeping, increased from 15.6% in 2002 to 17.1% in 2012. And this increase was concentrated in 40- to 59-year-old women, where the prevalence of insomnia or poor sleep rose from 19% to 24.3%, the highest of any age group. Rates remained flat over time in men and women aged 20-39 years and 60-80 years and older as well as in 40- to 59-year-old men.
The sleep-related question put to survey participants in face-to-face or telephone interviews was this: “How often do you have trouble going to sleep or staying asleep?” If they answered “most of the time” or “all of the time” they were classified as having poor sleep.
When Dr. Garland saw the survey results she immediately asked herself, “What is happening with Canadian women?” She came up with two theories. They are not mutually exclusive. One hinges on the dramatic drop off in the use of hormone replacement therapy in response to the Women’s Health Initiative report. The other theory is that the increasing prevalence of insomnia in middle-aged women is a manifestation of stress among the growing population of what has been called “the sandwich generation,” people who care for their aging parents while also supporting their own children. Those responsibilities most often fall upon the mother.
She noted that a similar rise in the prevalence of insomnia or trouble sleeping is occurring south of the border – in the United States – as documented in a Centers for Disease Control and Prevention analysis. The CDC investigators examined data on 30,970 adult participants in the 2002 National Health Interview Survey, 23,344 in the 2007 survey, and 34,509 in the 2012 survey. The prevalence of insomnia or trouble sleeping increased from 17.5% in 2002 to 19.2% in 2012. That absolute 1.7% increase pairs well with the 1.5% rise over the same time frame in the Canadian survey. The prevalence was higher in U.S. women than men in all three survey years (Sleep Med. 2015 Mar;16[3]:372-8).
Dr. Garland said the Canadian national survey contains data on self-perceived stress levels. She plans to analyze those results to learn if being a member of the sandwich generation is a significant contributor to poor sleep.
Regardless of the underlying mechanism, she continued, it’s clear from these large national surveys that middle-aged women are particularly vulnerable to poor sleep.
“Increased recognition is necessary. Prevention and intervention programs may be warranted, given the individual and societal consequences of poor sleep, including increased psychiatric and medical disorders, work absenteeism, and health care costs,” she said.
One audience member rose to congratulate Dr. Garland on her detective work. He commented that her notion that the rise in insomnia can be traced to fallout from the 2002 Women’s Health Initiative is consistent with his own clinical experience.
“The most common way women over age 40 present to our sleep center with insomnia is because they’re menopausal and not on hormone replacement therapy,” he said.
The Canadian Community Health Survey is sponsored by Statistics Canada. Dr. Garland reported having no financial conflicts of interest.
DENVER – Much of the rising prevalence of insomnia among U.S. and Canadian adults may be driven by the sharp reduction in the use of hormone replacement therapy following the 2002 report from the Women’s Health Initiative, Sheila N. Garland, PhD, said at the annual meeting of the Associated Professional Sleep Societies.
“In 2002 the Women’s Health Initiative came out with findings that hormone replacement therapy increased the risk of coronary heart disease, breast cancer, stroke, and pulmonary embolism [JAMA. 2002 Jul 17;288(3):321-33]. A lot of women on hormone replacement therapy up until 2002 stopped using it then. The increase in difficulty sleeping we found between 2002 and 2012 could perhaps represent an untreated menopausal symptom,” according to Dr. Garland, a psychologist at Memorial University of Newfoundland in St. John’s.
She presented an analysis of data from the Canadian Community Health Survey, a national once-per-decade survey, which included 34,118 adults aged 20-80 years and older in the 2002 version and 23,089 in 2012.
The key finding from the standpoint of sleep medicine, the prevalence of self-reported trouble sleeping, increased from 15.6% in 2002 to 17.1% in 2012. And this increase was concentrated in 40- to 59-year-old women, where the prevalence of insomnia or poor sleep rose from 19% to 24.3%, the highest of any age group. Rates remained flat over time in men and women aged 20-39 years and 60-80 years and older as well as in 40- to 59-year-old men.
The sleep-related question put to survey participants in face-to-face or telephone interviews was this: “How often do you have trouble going to sleep or staying asleep?” If they answered “most of the time” or “all of the time” they were classified as having poor sleep.
When Dr. Garland saw the survey results she immediately asked herself, “What is happening with Canadian women?” She came up with two theories. They are not mutually exclusive. One hinges on the dramatic drop off in the use of hormone replacement therapy in response to the Women’s Health Initiative report. The other theory is that the increasing prevalence of insomnia in middle-aged women is a manifestation of stress among the growing population of what has been called “the sandwich generation,” people who care for their aging parents while also supporting their own children. Those responsibilities most often fall upon the mother.
She noted that a similar rise in the prevalence of insomnia or trouble sleeping is occurring south of the border – in the United States – as documented in a Centers for Disease Control and Prevention analysis. The CDC investigators examined data on 30,970 adult participants in the 2002 National Health Interview Survey, 23,344 in the 2007 survey, and 34,509 in the 2012 survey. The prevalence of insomnia or trouble sleeping increased from 17.5% in 2002 to 19.2% in 2012. That absolute 1.7% increase pairs well with the 1.5% rise over the same time frame in the Canadian survey. The prevalence was higher in U.S. women than men in all three survey years (Sleep Med. 2015 Mar;16[3]:372-8).
Dr. Garland said the Canadian national survey contains data on self-perceived stress levels. She plans to analyze those results to learn if being a member of the sandwich generation is a significant contributor to poor sleep.
Regardless of the underlying mechanism, she continued, it’s clear from these large national surveys that middle-aged women are particularly vulnerable to poor sleep.
“Increased recognition is necessary. Prevention and intervention programs may be warranted, given the individual and societal consequences of poor sleep, including increased psychiatric and medical disorders, work absenteeism, and health care costs,” she said.
One audience member rose to congratulate Dr. Garland on her detective work. He commented that her notion that the rise in insomnia can be traced to fallout from the 2002 Women’s Health Initiative is consistent with his own clinical experience.
“The most common way women over age 40 present to our sleep center with insomnia is because they’re menopausal and not on hormone replacement therapy,” he said.
The Canadian Community Health Survey is sponsored by Statistics Canada. Dr. Garland reported having no financial conflicts of interest.
AT SLEEP 2016

Women’s Health Initiative may account for insomnia’s upward trend
DENVER – Much of the rising prevalence of insomnia among U.S. and Canadian adults may be driven by the sharp reduction in the use of hormone replacement therapy following the 2002 report from the Women’s Health Initiative, Sheila N. Garland, PhD, said at the annual meeting of the Associated Professional Sleep Societies.
“In 2002 the Women’s Health Initiative came out with findings that hormone replacement therapy increased the risk of coronary heart disease, breast cancer, stroke, and pulmonary embolism [JAMA. 2002 Jul 17;288(3):321-33]. A lot of women on hormone replacement therapy up until 2002 stopped using it then. The increase in difficulty sleeping we found between 2002 and 2012 could perhaps represent an untreated menopausal symptom,” according to Dr. Garland, a psychologist at Memorial University of Newfoundland in St. John’s.

She presented an analysis of data from the Canadian Community Health Survey, a national once-per-decade survey, which included 34,118 adults aged 20-80 years and older in the 2002 version and 23,089 in 2012.
The key finding from the standpoint of sleep medicine, the prevalence of self-reported trouble sleeping, increased from 15.6% in 2002 to 17.1% in 2012. And this increase was concentrated in 40- to 59-year-old women, where the prevalence of insomnia or poor sleep rose from 19% to 24.3%, the highest of any age group. Rates remained flat over time in men and women aged 20-39 years and 60-80 years and older as well as in 40- to 59-year-old men.
The sleep-related question put to survey participants in face-to-face or telephone interviews was this: “How often do you have trouble going to sleep or staying asleep?” If they answered “most of the time” or “all of the time” they were classified as having poor sleep.
When Dr. Garland saw the survey results she immediately asked herself, “What is happening with Canadian women?” She came up with two theories. They are not mutually exclusive. One hinges on the dramatic drop off in the use of hormone replacement therapy in response to the Women’s Health Initiative report. The other theory is that the increasing prevalence of insomnia in middle-aged women is a manifestation of stress among the growing population of what has been called “the sandwich generation,” people who care for their aging parents while also supporting their own children. Those responsibilities most often fall upon the mother.
She noted that a similar rise in the prevalence of insomnia or trouble sleeping is occurring south of the border – in the United States – as documented in a Centers for Disease Control and Prevention analysis. The CDC investigators examined data on 30,970 adult participants in the 2002 National Health Interview Survey, 23,344 in the 2007 survey, and 34,509 in the 2012 survey. The prevalence of insomnia or trouble sleeping increased from 17.5% in 2002 to 19.2% in 2012. That absolute 1.7% increase pairs well with the 1.5% rise over the same time frame in the Canadian survey. The prevalence was higher in U.S. women than men in all three survey years (Sleep Med. 2015 Mar;16[3]:372-8).
Dr. Garland said the Canadian national survey contains data on self-perceived stress levels. She plans to analyze those results to learn if being a member of the sandwich generation is a significant contributor to poor sleep.
Regardless of the underlying mechanism, she continued, it’s clear from these large national surveys that middle-aged women are particularly vulnerable to poor sleep.
“Increased recognition is necessary. Prevention and intervention programs may be warranted, given the individual and societal consequences of poor sleep, including increased psychiatric and medical disorders, work absenteeism, and health care costs,” she said.
One audience member rose to congratulate Dr. Garland on her detective work. He commented that her notion that the rise in insomnia can be traced to fallout from the 2002 Women’s Health Initiative is consistent with his own clinical experience.
“The most common way women over age 40 present to our sleep center with insomnia is because they’re menopausal and not on hormone replacement therapy,” he said.
The Canadian Community Health Survey is sponsored by Statistics Canada. Dr. Garland reported having no financial conflicts of interest.
DENVER – Much of the rising prevalence of insomnia among U.S. and Canadian adults may be driven by the sharp reduction in the use of hormone replacement therapy following the 2002 report from the Women’s Health Initiative, Sheila N. Garland, PhD, said at the annual meeting of the Associated Professional Sleep Societies.
“In 2002 the Women’s Health Initiative came out with findings that hormone replacement therapy increased the risk of coronary heart disease, breast cancer, stroke, and pulmonary embolism [JAMA. 2002 Jul 17;288(3):321-33]. A lot of women on hormone replacement therapy up until 2002 stopped using it then. The increase in difficulty sleeping we found between 2002 and 2012 could perhaps represent an untreated menopausal symptom,” according to Dr. Garland, a psychologist at Memorial University of Newfoundland in St. John’s.
She presented an analysis of data from the Canadian Community Health Survey, a national once-per-decade survey, which included 34,118 adults aged 20-80 years and older in the 2002 version and 23,089 in 2012.
The key finding from the standpoint of sleep medicine, the prevalence of self-reported trouble sleeping, increased from 15.6% in 2002 to 17.1% in 2012. And this increase was concentrated in 40- to 59-year-old women, where the prevalence of insomnia or poor sleep rose from 19% to 24.3%, the highest of any age group. Rates remained flat over time in men and women aged 20-39 years and 60-80 years and older as well as in 40- to 59-year-old men.
The sleep-related question put to survey participants in face-to-face or telephone interviews was this: “How often do you have trouble going to sleep or staying asleep?” If they answered “most of the time” or “all of the time” they were classified as having poor sleep.
When Dr. Garland saw the survey results she immediately asked herself, “What is happening with Canadian women?” She came up with two theories. They are not mutually exclusive. One hinges on the dramatic drop off in the use of hormone replacement therapy in response to the Women’s Health Initiative report. The other theory is that the increasing prevalence of insomnia in middle-aged women is a manifestation of stress among the growing population of what has been called “the sandwich generation,” people who care for their aging parents while also supporting their own children. Those responsibilities most often fall upon the mother.
She noted that a similar rise in the prevalence of insomnia or trouble sleeping is occurring south of the border – in the United States – as documented in a Centers for Disease Control and Prevention analysis. The CDC investigators examined data on 30,970 adult participants in the 2002 National Health Interview Survey, 23,344 in the 2007 survey, and 34,509 in the 2012 survey. The prevalence of insomnia or trouble sleeping increased from 17.5% in 2002 to 19.2% in 2012. That absolute 1.7% increase pairs well with the 1.5% rise over the same time frame in the Canadian survey. The prevalence was higher in U.S. women than men in all three survey years (Sleep Med. 2015 Mar;16[3]:372-8).
Dr. Garland said the Canadian national survey contains data on self-perceived stress levels. She plans to analyze those results to learn if being a member of the sandwich generation is a significant contributor to poor sleep.
Regardless of the underlying mechanism, she continued, it’s clear from these large national surveys that middle-aged women are particularly vulnerable to poor sleep.
“Increased recognition is necessary. Prevention and intervention programs may be warranted, given the individual and societal consequences of poor sleep, including increased psychiatric and medical disorders, work absenteeism, and health care costs,” she said.
One audience member rose to congratulate Dr. Garland on her detective work. He commented that her notion that the rise in insomnia can be traced to fallout from the 2002 Women’s Health Initiative is consistent with his own clinical experience.
“The most common way women over age 40 present to our sleep center with insomnia is because they’re menopausal and not on hormone replacement therapy,” he said.
The Canadian Community Health Survey is sponsored by Statistics Canada. Dr. Garland reported having no financial conflicts of interest.
DENVER – Much of the rising prevalence of insomnia among U.S. and Canadian adults may be driven by the sharp reduction in the use of hormone replacement therapy following the 2002 report from the Women’s Health Initiative, Sheila N. Garland, PhD, said at the annual meeting of the Associated Professional Sleep Societies.
“In 2002 the Women’s Health Initiative came out with findings that hormone replacement therapy increased the risk of coronary heart disease, breast cancer, stroke, and pulmonary embolism [JAMA. 2002 Jul 17;288(3):321-33]. A lot of women on hormone replacement therapy up until 2002 stopped using it then. The increase in difficulty sleeping we found between 2002 and 2012 could perhaps represent an untreated menopausal symptom,” according to Dr. Garland, a psychologist at Memorial University of Newfoundland in St. John’s.
She presented an analysis of data from the Canadian Community Health Survey, a national once-per-decade survey, which included 34,118 adults aged 20-80 years and older in the 2002 version and 23,089 in 2012.
The key finding from the standpoint of sleep medicine, the prevalence of self-reported trouble sleeping, increased from 15.6% in 2002 to 17.1% in 2012. And this increase was concentrated in 40- to 59-year-old women, where the prevalence of insomnia or poor sleep rose from 19% to 24.3%, the highest of any age group. Rates remained flat over time in men and women aged 20-39 years and 60-80 years and older as well as in 40- to 59-year-old men.
The sleep-related question put to survey participants in face-to-face or telephone interviews was this: “How often do you have trouble going to sleep or staying asleep?” If they answered “most of the time” or “all of the time” they were classified as having poor sleep.
When Dr. Garland saw the survey results she immediately asked herself, “What is happening with Canadian women?” She came up with two theories. They are not mutually exclusive. One hinges on the dramatic drop off in the use of hormone replacement therapy in response to the Women’s Health Initiative report. The other theory is that the increasing prevalence of insomnia in middle-aged women is a manifestation of stress among the growing population of what has been called “the sandwich generation,” people who care for their aging parents while also supporting their own children. Those responsibilities most often fall upon the mother.
She noted that a similar rise in the prevalence of insomnia or trouble sleeping is occurring south of the border – in the United States – as documented in a Centers for Disease Control and Prevention analysis. The CDC investigators examined data on 30,970 adult participants in the 2002 National Health Interview Survey, 23,344 in the 2007 survey, and 34,509 in the 2012 survey. The prevalence of insomnia or trouble sleeping increased from 17.5% in 2002 to 19.2% in 2012. That absolute 1.7% increase pairs well with the 1.5% rise over the same time frame in the Canadian survey. The prevalence was higher in U.S. women than men in all three survey years (Sleep Med. 2015 Mar;16[3]:372-8).
Dr. Garland said the Canadian national survey contains data on self-perceived stress levels. She plans to analyze those results to learn if being a member of the sandwich generation is a significant contributor to poor sleep.
Regardless of the underlying mechanism, she continued, it’s clear from these large national surveys that middle-aged women are particularly vulnerable to poor sleep.
“Increased recognition is necessary. Prevention and intervention programs may be warranted, given the individual and societal consequences of poor sleep, including increased psychiatric and medical disorders, work absenteeism, and health care costs,” she said.
One audience member rose to congratulate Dr. Garland on her detective work. He commented that her notion that the rise in insomnia can be traced to fallout from the 2002 Women’s Health Initiative is consistent with his own clinical experience.
“The most common way women over age 40 present to our sleep center with insomnia is because they’re menopausal and not on hormone replacement therapy,” he said.
The Canadian Community Health Survey is sponsored by Statistics Canada. Dr. Garland reported having no financial conflicts of interest.
AT SLEEP 2016
Key clinical point: Middle-aged women are increasingly vulnerable to insomnia.
Major finding: The prevalence of insomnia or poor sleep among 40- to 59-year-old Canadian women climbed from 19% in 2002 to 24.3% in 2012.
Data source: The Canadian Community Health Survey included 34,118 adults aged 20-80 years and older in 2002 and 23,089 in 2012.
Disclosures: The survey is sponsored by Statistics Canada. The presenter reported having no financial conflicts of interest.

Editorial Board Biographies
Struan H. Coleman, MD, PhD
Associate Editor for Practice Management/Economics

Dr. Coleman is a board-certified orthopedic surgeon specializing in hip preservation and sports medicine at the Hospital for Special Surgery in New York and the Vincera Institute in Philadelphia, and currently is the Head Team Physician for the New York Mets. He earned a medical degree from Columbia College of Physicians and Surgeons and holds a D.Phil in Microbiology from Oxford University in England. He completed his residency in Orthopedic Surgery and a fellowship in Sports Medicine at the Hospital for Special Surgery. Dr. Coleman focuses on the treatment of sports-related injuries of the hip, knee, and shoulder with a particular interest in hip arthroscopy and hip preservation. He has published multiple articles and book chapters, and holds numerous patents for technologies that are utilized by sports medicine physicians and surgeons.
Jack Farr II, MD
Associate Editor for Patellofemoral

Dr. Farr is a board-certified orthopedic surgeon and has a subspecialty practice in knee and cartilage restoration. He is affiliated with the OrthoIndy Hospital and Community Hospital South. He is also the Vice President of the Patellofemoral Foundation, is on the board for the International Cartilage Repair Society, holds a board position with the Cartilage Research Foundation, and holds a voluntary clinical full professorship in Orthopedic Surgery at the Indiana University Medical Center. Dr. Farr earned his medical degree from Indiana University, and completed his Orthopedic Surgery residency at Indiana University Medical Center. He was a design surgeon for a meniscal allograft transplant system and 2 knee patellofemoral osteotomy systems. He is also a member of the American Academy of Orthopaedic Surgeons (AAOS), the Arthroscopy Association of North America (AANA), and the European Society of Sports Traumatology, Knee Surgery and Arthroscopy (ESSKA).
Kenneth Montgomery, MD
Associate Editor for Professional Sports

Dr. Montgomery is an orthopedic surgeon who is fellowship-trained in sports medicine and hand and upper extremity surgery. He is currently practicing at Tri-County Orthopedics and Sports Medicine in Morristown, New Jersey. He is also the Head Team Physician and Medical Director for the New York Jets. He served as a team orthopedist with the New York Islanders from 1997-2009, and was formerly the section chief of Sports Medicine at ProHEALTH Care Associates in Lake Success, New York. Dr. Montgomery completed his residency in Orthopedic Surgery at the Hospital for Special Surgery, and completed a Sports Medicine fellowship at Lenox Hill Hospital. He also completed a Hand and Upper Extremity fellowship at Harvard. He is one of the founders for OrthoNations, a nonprofit organization that helps educate orthopedic surgeons in developing countries. He is also one of the founding surgeons for Cayenne Medical, a medical device company specializing in sports medicine implants.
Struan H. Coleman, MD, PhD
Associate Editor for Practice Management/Economics
Dr. Coleman is a board-certified orthopedic surgeon specializing in hip preservation and sports medicine at the Hospital for Special Surgery in New York and the Vincera Institute in Philadelphia, and currently is the Head Team Physician for the New York Mets. He earned a medical degree from Columbia College of Physicians and Surgeons and holds a D.Phil in Microbiology from Oxford University in England. He completed his residency in Orthopedic Surgery and a fellowship in Sports Medicine at the Hospital for Special Surgery. Dr. Coleman focuses on the treatment of sports-related injuries of the hip, knee, and shoulder with a particular interest in hip arthroscopy and hip preservation. He has published multiple articles and book chapters, and holds numerous patents for technologies that are utilized by sports medicine physicians and surgeons.
Jack Farr II, MD
Associate Editor for Patellofemoral
Dr. Farr is a board-certified orthopedic surgeon and has a subspecialty practice in knee and cartilage restoration. He is affiliated with the OrthoIndy Hospital and Community Hospital South. He is also the Vice President of the Patellofemoral Foundation, is on the board for the International Cartilage Repair Society, holds a board position with the Cartilage Research Foundation, and holds a voluntary clinical full professorship in Orthopedic Surgery at the Indiana University Medical Center. Dr. Farr earned his medical degree from Indiana University, and completed his Orthopedic Surgery residency at Indiana University Medical Center. He was a design surgeon for a meniscal allograft transplant system and 2 knee patellofemoral osteotomy systems. He is also a member of the American Academy of Orthopaedic Surgeons (AAOS), the Arthroscopy Association of North America (AANA), and the European Society of Sports Traumatology, Knee Surgery and Arthroscopy (ESSKA).
Kenneth Montgomery, MD
Associate Editor for Professional Sports
Dr. Montgomery is an orthopedic surgeon who is fellowship-trained in sports medicine and hand and upper extremity surgery. He is currently practicing at Tri-County Orthopedics and Sports Medicine in Morristown, New Jersey. He is also the Head Team Physician and Medical Director for the New York Jets. He served as a team orthopedist with the New York Islanders from 1997-2009, and was formerly the section chief of Sports Medicine at ProHEALTH Care Associates in Lake Success, New York. Dr. Montgomery completed his residency in Orthopedic Surgery at the Hospital for Special Surgery, and completed a Sports Medicine fellowship at Lenox Hill Hospital. He also completed a Hand and Upper Extremity fellowship at Harvard. He is one of the founders for OrthoNations, a nonprofit organization that helps educate orthopedic surgeons in developing countries. He is also one of the founding surgeons for Cayenne Medical, a medical device company specializing in sports medicine implants.
Struan H. Coleman, MD, PhD
Associate Editor for Practice Management/Economics
Dr. Coleman is a board-certified orthopedic surgeon specializing in hip preservation and sports medicine at the Hospital for Special Surgery in New York and the Vincera Institute in Philadelphia, and currently is the Head Team Physician for the New York Mets. He earned a medical degree from Columbia College of Physicians and Surgeons and holds a D.Phil in Microbiology from Oxford University in England. He completed his residency in Orthopedic Surgery and a fellowship in Sports Medicine at the Hospital for Special Surgery. Dr. Coleman focuses on the treatment of sports-related injuries of the hip, knee, and shoulder with a particular interest in hip arthroscopy and hip preservation. He has published multiple articles and book chapters, and holds numerous patents for technologies that are utilized by sports medicine physicians and surgeons.
Jack Farr II, MD
Associate Editor for Patellofemoral
Dr. Farr is a board-certified orthopedic surgeon and has a subspecialty practice in knee and cartilage restoration. He is affiliated with the OrthoIndy Hospital and Community Hospital South. He is also the Vice President of the Patellofemoral Foundation, is on the board for the International Cartilage Repair Society, holds a board position with the Cartilage Research Foundation, and holds a voluntary clinical full professorship in Orthopedic Surgery at the Indiana University Medical Center. Dr. Farr earned his medical degree from Indiana University, and completed his Orthopedic Surgery residency at Indiana University Medical Center. He was a design surgeon for a meniscal allograft transplant system and 2 knee patellofemoral osteotomy systems. He is also a member of the American Academy of Orthopaedic Surgeons (AAOS), the Arthroscopy Association of North America (AANA), and the European Society of Sports Traumatology, Knee Surgery and Arthroscopy (ESSKA).
Kenneth Montgomery, MD
Associate Editor for Professional Sports
Dr. Montgomery is an orthopedic surgeon who is fellowship-trained in sports medicine and hand and upper extremity surgery. He is currently practicing at Tri-County Orthopedics and Sports Medicine in Morristown, New Jersey. He is also the Head Team Physician and Medical Director for the New York Jets. He served as a team orthopedist with the New York Islanders from 1997-2009, and was formerly the section chief of Sports Medicine at ProHEALTH Care Associates in Lake Success, New York. Dr. Montgomery completed his residency in Orthopedic Surgery at the Hospital for Special Surgery, and completed a Sports Medicine fellowship at Lenox Hill Hospital. He also completed a Hand and Upper Extremity fellowship at Harvard. He is one of the founders for OrthoNations, a nonprofit organization that helps educate orthopedic surgeons in developing countries. He is also one of the founding surgeons for Cayenne Medical, a medical device company specializing in sports medicine implants.
Who are the ‘no-shows’ to diabetes education classes?
NEW ORLEANS – Patients with diabetes who failed to show up for diabetes education classes were slightly younger and less likely to be insured, compared with those who attended the classes. Forty-one percent of those who failed to show were covered by private insurance, and 63% were women.
Those are key findings from an analysis by researchers to investigate the patterns of population characteristics related nonadherence to diabetes education classes that patients are referred to.
“What it shows us is that when we’re trying to get people to come to diabetes education classes, we have to be in tune with the sociodemographic characteristics that present different barriers or obstacles,” Ashby Walker, PhD, said in an interview at the annual scientific sessions of the American Diabetes Association.

Dr. Walker, of the department of health outcomes and policy at the University of Florida, Gainesville, and her associates, including Kathryn Parker, RD, program manager for diabetes education at the UF Health Shands Hospital, Gainesville, conducted a manual chart review to examine the demographics of 257 “no-shows” who were referred to a diabetes education class at the university’s hospital between January 2015 and March 2015. Data of interest included age, gender, diagnosis, reasons for referral, referring department, socioeconomic status, and race/ethnicity. For comparison purposes, the researchers also examined a cohort of 339 patients who showed up for their diabetes education classes between August 2014 and January 2015.
More than two-thirds of the no-shows (69%) had type 2 diabetes, 63% were women, and the mean age was 50 years. More than half (57%) were publicly insured or uninsured, while 41% had private insurance and 3% were self-pay or had missing data for insurance type.
The fact that a higher proportion of the insured no-shows were women surprised the researchers. “If you think about women who are working full time, they often shoulder the tremendous responsibility of household labor, too,” Dr. Walker said. “So for them to take time out of very busy lives to take care of themselves might create a different obstacle than someone who’s very low income or low health literacy who has transportation as a barrier. The findings show us that we have to tailor those interventions appropriately for different audiences.”
Another surprise finding, she said, was the fact that males were underrepresented in both the “no show” cohort (37%) and among those who honored their referrals (32%). “While there are some studies that indicate women fare worse with diabetes than men, the underrepresentation of men warrants further attention,” Dr. Walker said. “It begs the question: Are providers referring men less?”
Shannon Taylor, a fellow researcher at the University of Florida, said that the study’s findings underscore the need for clinicians “to be attuned to the different things about social life that can impact how people self-care, whether it’s gender differences or differences in socioeconomic status.”
The researchers reported having no financial disclosures.
NEW ORLEANS – Patients with diabetes who failed to show up for diabetes education classes were slightly younger and less likely to be insured, compared with those who attended the classes. Forty-one percent of those who failed to show were covered by private insurance, and 63% were women.
Those are key findings from an analysis by researchers to investigate the patterns of population characteristics related nonadherence to diabetes education classes that patients are referred to.
“What it shows us is that when we’re trying to get people to come to diabetes education classes, we have to be in tune with the sociodemographic characteristics that present different barriers or obstacles,” Ashby Walker, PhD, said in an interview at the annual scientific sessions of the American Diabetes Association.
Dr. Walker, of the department of health outcomes and policy at the University of Florida, Gainesville, and her associates, including Kathryn Parker, RD, program manager for diabetes education at the UF Health Shands Hospital, Gainesville, conducted a manual chart review to examine the demographics of 257 “no-shows” who were referred to a diabetes education class at the university’s hospital between January 2015 and March 2015. Data of interest included age, gender, diagnosis, reasons for referral, referring department, socioeconomic status, and race/ethnicity. For comparison purposes, the researchers also examined a cohort of 339 patients who showed up for their diabetes education classes between August 2014 and January 2015.
More than two-thirds of the no-shows (69%) had type 2 diabetes, 63% were women, and the mean age was 50 years. More than half (57%) were publicly insured or uninsured, while 41% had private insurance and 3% were self-pay or had missing data for insurance type.
The fact that a higher proportion of the insured no-shows were women surprised the researchers. “If you think about women who are working full time, they often shoulder the tremendous responsibility of household labor, too,” Dr. Walker said. “So for them to take time out of very busy lives to take care of themselves might create a different obstacle than someone who’s very low income or low health literacy who has transportation as a barrier. The findings show us that we have to tailor those interventions appropriately for different audiences.”
Another surprise finding, she said, was the fact that males were underrepresented in both the “no show” cohort (37%) and among those who honored their referrals (32%). “While there are some studies that indicate women fare worse with diabetes than men, the underrepresentation of men warrants further attention,” Dr. Walker said. “It begs the question: Are providers referring men less?”
Shannon Taylor, a fellow researcher at the University of Florida, said that the study’s findings underscore the need for clinicians “to be attuned to the different things about social life that can impact how people self-care, whether it’s gender differences or differences in socioeconomic status.”
The researchers reported having no financial disclosures.
NEW ORLEANS – Patients with diabetes who failed to show up for diabetes education classes were slightly younger and less likely to be insured, compared with those who attended the classes. Forty-one percent of those who failed to show were covered by private insurance, and 63% were women.
Those are key findings from an analysis by researchers to investigate the patterns of population characteristics related nonadherence to diabetes education classes that patients are referred to.
“What it shows us is that when we’re trying to get people to come to diabetes education classes, we have to be in tune with the sociodemographic characteristics that present different barriers or obstacles,” Ashby Walker, PhD, said in an interview at the annual scientific sessions of the American Diabetes Association.
Dr. Walker, of the department of health outcomes and policy at the University of Florida, Gainesville, and her associates, including Kathryn Parker, RD, program manager for diabetes education at the UF Health Shands Hospital, Gainesville, conducted a manual chart review to examine the demographics of 257 “no-shows” who were referred to a diabetes education class at the university’s hospital between January 2015 and March 2015. Data of interest included age, gender, diagnosis, reasons for referral, referring department, socioeconomic status, and race/ethnicity. For comparison purposes, the researchers also examined a cohort of 339 patients who showed up for their diabetes education classes between August 2014 and January 2015.
More than two-thirds of the no-shows (69%) had type 2 diabetes, 63% were women, and the mean age was 50 years. More than half (57%) were publicly insured or uninsured, while 41% had private insurance and 3% were self-pay or had missing data for insurance type.
The fact that a higher proportion of the insured no-shows were women surprised the researchers. “If you think about women who are working full time, they often shoulder the tremendous responsibility of household labor, too,” Dr. Walker said. “So for them to take time out of very busy lives to take care of themselves might create a different obstacle than someone who’s very low income or low health literacy who has transportation as a barrier. The findings show us that we have to tailor those interventions appropriately for different audiences.”
Another surprise finding, she said, was the fact that males were underrepresented in both the “no show” cohort (37%) and among those who honored their referrals (32%). “While there are some studies that indicate women fare worse with diabetes than men, the underrepresentation of men warrants further attention,” Dr. Walker said. “It begs the question: Are providers referring men less?”
Shannon Taylor, a fellow researcher at the University of Florida, said that the study’s findings underscore the need for clinicians “to be attuned to the different things about social life that can impact how people self-care, whether it’s gender differences or differences in socioeconomic status.”
The researchers reported having no financial disclosures.
AT THE ADA SCIENTIFIC SESSIONS

Engineered Bone Graft
Exactech
Optecure+ccc
(http://www.exac.com/products/biologics/optecure-optecure-ccc)
Autogenous bone graft remains the standard for augmenting the surgical care of severe fractures, promoting spinal fusion, filling bone voids, and treating nonunions. However, lingering problems with donor site morbidity, volume limitation, increased operative time, and increased case complexity have led to the growing use of bone graft substitutes.1 These alternatives include allograft bone, demineralized bone matrix, calcium sulfate and calcium phosphate, bioglass, growth factors (rhBMP-2, rhBMP-7, rhPDGF, and PRP [platelet-rich plasma]), collagen matrix, and new cellular-based compounds using mesenchymal stem cells. Since each individual class of bone substitute falls short of the optimal blend of osteoconduction, osteoinduction, and osteogenesis, novel composite grafts have been developed to combine the convenience, durability, and flexibility of synthetic grafts with the biologic activity of native bone.
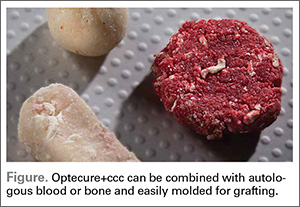
Optecure+ccc (Exactech) is an engineered composite bone graft that contains demineralized bone mixed with gamma irradiated cortical cancellous chips in an absorbable synthetic hydrogel matrix (Figure). When mixed with saline, blood, autogenous bone, bone marrow aspirate, or PRP, it becomes a surprisingly robust and malleable 3-dimensional matrix that allows easy bone void filling with excellent osteoconductive and osteoinductive characteristics. Each individual lot is tested for sterility and endotoxin levels to confirm safety as well as in vivo testing in athymic mice to confirm osteoinductive potential. Optecure+ccc has been successfully used to augment healing when combined with bone marrow aspirate in minimally invasive spine fusion surgery.2
Surgical pearl: I treat a large number of bicycle injuries on Nantucket; many are quite serious. I have found Optecure+ccc to be particularly useful during locked volar plating of severe distal radius wrist fractures as a way to restore and support radial length when autogenous bone access is limited. In this application, Optecure’s ability to expand and mold into a functional bone scaffold is critical to create a stable, stress-resistant fracture construct.
After exposure of the comminuted fracture line of the distal radius, gentle axial traction is applied and a small osteotome or freer is used to carefully wedge open the cortex to allow metaphyseal window access. The Optecure+ccc is mixed with either blood or bone marrow aspirate to reach a “grape nuts cereal”-like consistency and then carefully packed into the metaphyseal window to backfill the void. Multiplanar fluoroscopy is used to monitor graft placement and gradual joint line restoration. Traction is then released after the void is filled sufficiently to support the provisional reduction. Additional grafting with standard Optecure without bone chips can be used to fill more difficult-to-access areas. Both forms of Optecure are resistant to diluent migration, giving them good intraoperative behavior. Excess graft can be easily wiped away from the fracture site prior to plate application.
After elevation and restoration of the joint line, the locking volar plate is then affixed, wrist alignment confirmed fluoroscopically, and the procedure completed. The result is a well-filled void and an improved fracture construct. While Optecure+ccc has proven its battle readiness in wrist fracture surgery, I have also found it very helpful in reconstructing complex proximal humerus and clavicle fractures. Its unique combination of intraoperative versatility and durability provides a welcome edge in challenging cases.
1. Rodgers WB, Gerber EJ, Patterson JR. Fusion after minimally disruptive anterior lumbar interbody fusion: analysis of extreme lateral interbody fusion by computed tomography. SAS J. 2010;4(2):63-66.
2. Sasso RC, LeHuec JC, Shaffrey C; Spine Interbody Research Group. Iliac crest bone graft donor site pain after anterior lumbar interbody fusion: a prospective patient satisfaction outcome assessment. J Spinal Disord Tech. 2005;18 Suppl:S77-S81.
Exactech
Optecure+ccc
(http://www.exac.com/products/biologics/optecure-optecure-ccc)
Autogenous bone graft remains the standard for augmenting the surgical care of severe fractures, promoting spinal fusion, filling bone voids, and treating nonunions. However, lingering problems with donor site morbidity, volume limitation, increased operative time, and increased case complexity have led to the growing use of bone graft substitutes.1 These alternatives include allograft bone, demineralized bone matrix, calcium sulfate and calcium phosphate, bioglass, growth factors (rhBMP-2, rhBMP-7, rhPDGF, and PRP [platelet-rich plasma]), collagen matrix, and new cellular-based compounds using mesenchymal stem cells. Since each individual class of bone substitute falls short of the optimal blend of osteoconduction, osteoinduction, and osteogenesis, novel composite grafts have been developed to combine the convenience, durability, and flexibility of synthetic grafts with the biologic activity of native bone.
Optecure+ccc (Exactech) is an engineered composite bone graft that contains demineralized bone mixed with gamma irradiated cortical cancellous chips in an absorbable synthetic hydrogel matrix (Figure). When mixed with saline, blood, autogenous bone, bone marrow aspirate, or PRP, it becomes a surprisingly robust and malleable 3-dimensional matrix that allows easy bone void filling with excellent osteoconductive and osteoinductive characteristics. Each individual lot is tested for sterility and endotoxin levels to confirm safety as well as in vivo testing in athymic mice to confirm osteoinductive potential. Optecure+ccc has been successfully used to augment healing when combined with bone marrow aspirate in minimally invasive spine fusion surgery.2
Surgical pearl: I treat a large number of bicycle injuries on Nantucket; many are quite serious. I have found Optecure+ccc to be particularly useful during locked volar plating of severe distal radius wrist fractures as a way to restore and support radial length when autogenous bone access is limited. In this application, Optecure’s ability to expand and mold into a functional bone scaffold is critical to create a stable, stress-resistant fracture construct.
After exposure of the comminuted fracture line of the distal radius, gentle axial traction is applied and a small osteotome or freer is used to carefully wedge open the cortex to allow metaphyseal window access. The Optecure+ccc is mixed with either blood or bone marrow aspirate to reach a “grape nuts cereal”-like consistency and then carefully packed into the metaphyseal window to backfill the void. Multiplanar fluoroscopy is used to monitor graft placement and gradual joint line restoration. Traction is then released after the void is filled sufficiently to support the provisional reduction. Additional grafting with standard Optecure without bone chips can be used to fill more difficult-to-access areas. Both forms of Optecure are resistant to diluent migration, giving them good intraoperative behavior. Excess graft can be easily wiped away from the fracture site prior to plate application.
After elevation and restoration of the joint line, the locking volar plate is then affixed, wrist alignment confirmed fluoroscopically, and the procedure completed. The result is a well-filled void and an improved fracture construct. While Optecure+ccc has proven its battle readiness in wrist fracture surgery, I have also found it very helpful in reconstructing complex proximal humerus and clavicle fractures. Its unique combination of intraoperative versatility and durability provides a welcome edge in challenging cases.
Exactech
Optecure+ccc
(http://www.exac.com/products/biologics/optecure-optecure-ccc)
Autogenous bone graft remains the standard for augmenting the surgical care of severe fractures, promoting spinal fusion, filling bone voids, and treating nonunions. However, lingering problems with donor site morbidity, volume limitation, increased operative time, and increased case complexity have led to the growing use of bone graft substitutes.1 These alternatives include allograft bone, demineralized bone matrix, calcium sulfate and calcium phosphate, bioglass, growth factors (rhBMP-2, rhBMP-7, rhPDGF, and PRP [platelet-rich plasma]), collagen matrix, and new cellular-based compounds using mesenchymal stem cells. Since each individual class of bone substitute falls short of the optimal blend of osteoconduction, osteoinduction, and osteogenesis, novel composite grafts have been developed to combine the convenience, durability, and flexibility of synthetic grafts with the biologic activity of native bone.
Optecure+ccc (Exactech) is an engineered composite bone graft that contains demineralized bone mixed with gamma irradiated cortical cancellous chips in an absorbable synthetic hydrogel matrix (Figure). When mixed with saline, blood, autogenous bone, bone marrow aspirate, or PRP, it becomes a surprisingly robust and malleable 3-dimensional matrix that allows easy bone void filling with excellent osteoconductive and osteoinductive characteristics. Each individual lot is tested for sterility and endotoxin levels to confirm safety as well as in vivo testing in athymic mice to confirm osteoinductive potential. Optecure+ccc has been successfully used to augment healing when combined with bone marrow aspirate in minimally invasive spine fusion surgery.2
Surgical pearl: I treat a large number of bicycle injuries on Nantucket; many are quite serious. I have found Optecure+ccc to be particularly useful during locked volar plating of severe distal radius wrist fractures as a way to restore and support radial length when autogenous bone access is limited. In this application, Optecure’s ability to expand and mold into a functional bone scaffold is critical to create a stable, stress-resistant fracture construct.
After exposure of the comminuted fracture line of the distal radius, gentle axial traction is applied and a small osteotome or freer is used to carefully wedge open the cortex to allow metaphyseal window access. The Optecure+ccc is mixed with either blood or bone marrow aspirate to reach a “grape nuts cereal”-like consistency and then carefully packed into the metaphyseal window to backfill the void. Multiplanar fluoroscopy is used to monitor graft placement and gradual joint line restoration. Traction is then released after the void is filled sufficiently to support the provisional reduction. Additional grafting with standard Optecure without bone chips can be used to fill more difficult-to-access areas. Both forms of Optecure are resistant to diluent migration, giving them good intraoperative behavior. Excess graft can be easily wiped away from the fracture site prior to plate application.
After elevation and restoration of the joint line, the locking volar plate is then affixed, wrist alignment confirmed fluoroscopically, and the procedure completed. The result is a well-filled void and an improved fracture construct. While Optecure+ccc has proven its battle readiness in wrist fracture surgery, I have also found it very helpful in reconstructing complex proximal humerus and clavicle fractures. Its unique combination of intraoperative versatility and durability provides a welcome edge in challenging cases.
1. Rodgers WB, Gerber EJ, Patterson JR. Fusion after minimally disruptive anterior lumbar interbody fusion: analysis of extreme lateral interbody fusion by computed tomography. SAS J. 2010;4(2):63-66.
2. Sasso RC, LeHuec JC, Shaffrey C; Spine Interbody Research Group. Iliac crest bone graft donor site pain after anterior lumbar interbody fusion: a prospective patient satisfaction outcome assessment. J Spinal Disord Tech. 2005;18 Suppl:S77-S81.
1. Rodgers WB, Gerber EJ, Patterson JR. Fusion after minimally disruptive anterior lumbar interbody fusion: analysis of extreme lateral interbody fusion by computed tomography. SAS J. 2010;4(2):63-66.
2. Sasso RC, LeHuec JC, Shaffrey C; Spine Interbody Research Group. Iliac crest bone graft donor site pain after anterior lumbar interbody fusion: a prospective patient satisfaction outcome assessment. J Spinal Disord Tech. 2005;18 Suppl:S77-S81.

Innervation Is Maintained for 24 Years After Transplantation in Parkinson’s Disease
Transplanted nerve cells may survive for nearly a quarter of a century in a patient’s brain despite ongoing Parkinson’s disease, according to data published online ahead of print May 2 in the Proceedings of the National Academy of Sciences of the United States of America. A transplant of cells into the putamen yields dense reinnervation similar to that of healthy brains. The case study also suggests that the initial clinical benefits of the transplant gradually deteriorate when pathology spreads from the patient’s brain to the transplanted cells.
“This is the first time a patient has shown such a well-functioning transplant so many years after transplantation of nerve cells to the brain,” said Olle Lindvall, MD, PhD, Professor of Clinical Neurology and Chairman of Neurology at the University Hospital in Lund, Sweden. “At the same time, we have observed that the transplant’s positive effects on this patient gradually disappeared as the disease spread to more structures in the brain.”

Olle Lindvall, MD, PhD
Dr. Lindvall and colleagues followed a patient with Parkinson’s disease for 24 years after he received a transplant of embryonic dopaminergic neurons. The patient had developed Parkinson’s disease in 1980 and had started L-dopa treatment in 1982. The therapy appeared to be efficacious, but in 1986, the patient developed “on–off” symptoms. During “off” periods, he experienced resting tremor, hypokinetic movements, and rigidity, especially on the left side of his body. During “on” periods, he displayed mild parkinsonian symptoms.
In 1989, the patient, who was then age 59, underwent transplantation with ventral mesencephalic tissue from four human embryos into the right putamen. He was monitored for 10 years post transplantation. In the first three years, researchers noted significant improvement, and L-dopa was withdrawn at 32 months. At 64 months post transplantation, immunosuppressive treatment was stopped. When symptoms progressed at 74 months, a low dose of L-dopa was reintroduced. The patient had a marked clinical benefit, including a near-absence of rigidity, at 10 years. At 12 years, however, he had worsening hypokinesia; as a result, a low-dose dopamine agonist was added for two years, and the L-dopa dose was increased.
The patient responded well to his treatment change at first, but at 14 years, his condition worsened. He began to experience increasing rigidity, hypokinesia, and a gradual loss of beneficial L-dopa response. During this time, cognitive impairment and onset of progressive dementia were first noted. At 18 years, no graft-related motor improvement remained, and the patient was unable to walk, swallow, or speak. At 24 years, the patient died of cardiac insufficiency. Autopsy revealed no evidence of an ongoing immune or inflammatory response. The patient had a dense, near-normal dopaminergic reinnervation derived from the grafts at 24 years post transplantation.
This case study provides the first evidence that rich dopaminergic innervation that develops in the first three years after transplantation and causes dramatic motor improvement can be preserved for 24 years in Parkinson’s disease, according to the authors. The clinical results, however, showed that even a viable graft could eventually lose its efficacy if widespread alpha-synucleinopathy progresses and degeneration occurs in the host brain.
“This study is completely unique,” said Anders Bjorklund, Professor at the Wallenberg Neuroscience Center at Lund University. “No transplanted Parkinson’s patient has ever been followed so closely and over such a long period...What we have learnt from the study of this patient will be of great value for future attempts to transplant dopamine-producing nerve cells obtained from stem cells, a new development led by researchers in Lund.”
—Erica Robinson
Suggested Reading
Li W, Englund E, Wildner H, et al. Extensive graft-derived dopaminergic innervation is maintained 24 years after transplantation in the degenerating parkinsonian brain. Proc Natl Acad Sci U S A. 2016 May 2 [Epub ahead of print].
Transplanted nerve cells may survive for nearly a quarter of a century in a patient’s brain despite ongoing Parkinson’s disease, according to data published online ahead of print May 2 in the Proceedings of the National Academy of Sciences of the United States of America. A transplant of cells into the putamen yields dense reinnervation similar to that of healthy brains. The case study also suggests that the initial clinical benefits of the transplant gradually deteriorate when pathology spreads from the patient’s brain to the transplanted cells.
“This is the first time a patient has shown such a well-functioning transplant so many years after transplantation of nerve cells to the brain,” said Olle Lindvall, MD, PhD, Professor of Clinical Neurology and Chairman of Neurology at the University Hospital in Lund, Sweden. “At the same time, we have observed that the transplant’s positive effects on this patient gradually disappeared as the disease spread to more structures in the brain.”
Olle Lindvall, MD, PhD
Dr. Lindvall and colleagues followed a patient with Parkinson’s disease for 24 years after he received a transplant of embryonic dopaminergic neurons. The patient had developed Parkinson’s disease in 1980 and had started L-dopa treatment in 1982. The therapy appeared to be efficacious, but in 1986, the patient developed “on–off” symptoms. During “off” periods, he experienced resting tremor, hypokinetic movements, and rigidity, especially on the left side of his body. During “on” periods, he displayed mild parkinsonian symptoms.
In 1989, the patient, who was then age 59, underwent transplantation with ventral mesencephalic tissue from four human embryos into the right putamen. He was monitored for 10 years post transplantation. In the first three years, researchers noted significant improvement, and L-dopa was withdrawn at 32 months. At 64 months post transplantation, immunosuppressive treatment was stopped. When symptoms progressed at 74 months, a low dose of L-dopa was reintroduced. The patient had a marked clinical benefit, including a near-absence of rigidity, at 10 years. At 12 years, however, he had worsening hypokinesia; as a result, a low-dose dopamine agonist was added for two years, and the L-dopa dose was increased.
The patient responded well to his treatment change at first, but at 14 years, his condition worsened. He began to experience increasing rigidity, hypokinesia, and a gradual loss of beneficial L-dopa response. During this time, cognitive impairment and onset of progressive dementia were first noted. At 18 years, no graft-related motor improvement remained, and the patient was unable to walk, swallow, or speak. At 24 years, the patient died of cardiac insufficiency. Autopsy revealed no evidence of an ongoing immune or inflammatory response. The patient had a dense, near-normal dopaminergic reinnervation derived from the grafts at 24 years post transplantation.
This case study provides the first evidence that rich dopaminergic innervation that develops in the first three years after transplantation and causes dramatic motor improvement can be preserved for 24 years in Parkinson’s disease, according to the authors. The clinical results, however, showed that even a viable graft could eventually lose its efficacy if widespread alpha-synucleinopathy progresses and degeneration occurs in the host brain.
“This study is completely unique,” said Anders Bjorklund, Professor at the Wallenberg Neuroscience Center at Lund University. “No transplanted Parkinson’s patient has ever been followed so closely and over such a long period...What we have learnt from the study of this patient will be of great value for future attempts to transplant dopamine-producing nerve cells obtained from stem cells, a new development led by researchers in Lund.”
—Erica Robinson
Transplanted nerve cells may survive for nearly a quarter of a century in a patient’s brain despite ongoing Parkinson’s disease, according to data published online ahead of print May 2 in the Proceedings of the National Academy of Sciences of the United States of America. A transplant of cells into the putamen yields dense reinnervation similar to that of healthy brains. The case study also suggests that the initial clinical benefits of the transplant gradually deteriorate when pathology spreads from the patient’s brain to the transplanted cells.
“This is the first time a patient has shown such a well-functioning transplant so many years after transplantation of nerve cells to the brain,” said Olle Lindvall, MD, PhD, Professor of Clinical Neurology and Chairman of Neurology at the University Hospital in Lund, Sweden. “At the same time, we have observed that the transplant’s positive effects on this patient gradually disappeared as the disease spread to more structures in the brain.”
Olle Lindvall, MD, PhD
Dr. Lindvall and colleagues followed a patient with Parkinson’s disease for 24 years after he received a transplant of embryonic dopaminergic neurons. The patient had developed Parkinson’s disease in 1980 and had started L-dopa treatment in 1982. The therapy appeared to be efficacious, but in 1986, the patient developed “on–off” symptoms. During “off” periods, he experienced resting tremor, hypokinetic movements, and rigidity, especially on the left side of his body. During “on” periods, he displayed mild parkinsonian symptoms.
In 1989, the patient, who was then age 59, underwent transplantation with ventral mesencephalic tissue from four human embryos into the right putamen. He was monitored for 10 years post transplantation. In the first three years, researchers noted significant improvement, and L-dopa was withdrawn at 32 months. At 64 months post transplantation, immunosuppressive treatment was stopped. When symptoms progressed at 74 months, a low dose of L-dopa was reintroduced. The patient had a marked clinical benefit, including a near-absence of rigidity, at 10 years. At 12 years, however, he had worsening hypokinesia; as a result, a low-dose dopamine agonist was added for two years, and the L-dopa dose was increased.
The patient responded well to his treatment change at first, but at 14 years, his condition worsened. He began to experience increasing rigidity, hypokinesia, and a gradual loss of beneficial L-dopa response. During this time, cognitive impairment and onset of progressive dementia were first noted. At 18 years, no graft-related motor improvement remained, and the patient was unable to walk, swallow, or speak. At 24 years, the patient died of cardiac insufficiency. Autopsy revealed no evidence of an ongoing immune or inflammatory response. The patient had a dense, near-normal dopaminergic reinnervation derived from the grafts at 24 years post transplantation.
This case study provides the first evidence that rich dopaminergic innervation that develops in the first three years after transplantation and causes dramatic motor improvement can be preserved for 24 years in Parkinson’s disease, according to the authors. The clinical results, however, showed that even a viable graft could eventually lose its efficacy if widespread alpha-synucleinopathy progresses and degeneration occurs in the host brain.
“This study is completely unique,” said Anders Bjorklund, Professor at the Wallenberg Neuroscience Center at Lund University. “No transplanted Parkinson’s patient has ever been followed so closely and over such a long period...What we have learnt from the study of this patient will be of great value for future attempts to transplant dopamine-producing nerve cells obtained from stem cells, a new development led by researchers in Lund.”
—Erica Robinson
Suggested Reading
Li W, Englund E, Wildner H, et al. Extensive graft-derived dopaminergic innervation is maintained 24 years after transplantation in the degenerating parkinsonian brain. Proc Natl Acad Sci U S A. 2016 May 2 [Epub ahead of print].
Suggested Reading
Li W, Englund E, Wildner H, et al. Extensive graft-derived dopaminergic innervation is maintained 24 years after transplantation in the degenerating parkinsonian brain. Proc Natl Acad Sci U S A. 2016 May 2 [Epub ahead of print].

Choosing MS Treatments From the Therapeutic Armamentarium
VANCOUVER—When selecting a therapy for a patient with multiple sclerosis (MS), drug adherence, side effects, and the patient’s risk of aggressive disease are among the considerations that may influence treatment choice, said Scott Newsome, DO, Director of Neurology Outpatient Services and the Neurology Infusion Center at Johns Hopkins University School of Medicine in Baltimore. Patients’ risk tolerance, desire to pursue pregnancy, and John Cunningham virus (JCV) antibody status also can affect the treatment decision.

Scott Newsome, DO
“I wish we had a cookbook recipe. I wish we were able to say, … ‘This is what you’re going to go on, this is what we’re going to expect,’ but that’s not the case. Maybe one day it will be the case, but until then we have to look at many different factors in choosing therapies,” Dr. Newsome said at the 68th Annual Meeting of the American Academy of Neurology.
Two Decades of Advances
The FDA first approved an MS therapy, interferon beta-1b, in 1993. Now, more than 10 treatments with various routes of administration and mechanisms of action have FDA approval, including a new injectable agent approved in May. Additional promising therapies are on the horizon.
“The world of MS therapeutics is evolving and becoming more complicated,” and neurologists have an “ongoing need to balance efficacy, safety, and tolerability of therapeutic interventions for each patient,” Dr. Newsome said.
Dr. Newsome hopes that in the future, biomarkers will help clinicians identify which specific treatments are the best options for each patient. In addition, more research is needed to determine the best time to start a new drug after a patient develops lymphopenia on another MS therapy, and to better understand how prior treatment with other agents affects the risk of progressive multifocal leukoencephalopathy (PML) and other adverse outcomes, he said.
With current therapies, “treating early and having a low threshold to escalate therapy is very important,” Dr. Newsome said. Monitoring relapses and MRI activity may be helpful when evaluating the efficacy of a newly initiated therapy. If a patient has subclinical disease activity six to 12 months after starting a therapy, many clinicians switch therapies and consider treatments that have different mechanisms of action. If a patient develops one small T2 lesion a year out from starting a therapy, he or she does not necessarily need to switch therapies, however. “These drugs are not cures, so you have to look at various factors when you’re thinking about switching or escalating,” Dr. Newsome said. If a patient has a definite relapse, poor recovery from a relapse, disability progression, or robust MRI activity, even when the patient is asymptomatic, clinicians should consider switching therapies.
Risk of Aggressive Disease
Recommendations published in 2013 by the Canadian MS Working Group along with other groups have noted that patients who are male or African American, have an older age at MS onset, or have motor, cerebellar, sphincter, or brainstem involvement are more likely to have aggressive MS. Frequent relapses, poor recovery from relapses, high MRI lesion burden at presentation, brain atrophy, and a low level of vitamin D also are associated with more aggressive disease. Thus, if a patient is African American, does not recover well from a transverse myelitis attack, and has 15 lesions on MRI, including many that are gadolinium-enhancing, with a high spinal cord lesion load, the patient is at high risk of aggressive disease. “When I see this demographic, this phenotype, I’m thinking maybe we need to start with a stronger immune therapy,” said Dr. Newsome.
Based on a cross-comparison of results from the drugs’ pivotal trials, newer medications seem more effective. Head-to-head trials are the only way to establish drug equivalence or superiority, however. With newly diagnosed MS, especially aggressive MS, many clinicians first prescribe an oral agent or an IV therapy instead of an earlier injectable therapy, with the aim of preventing future disability, Dr. Newsome said.
Injectable, Oral, and IV Therapies
Injectable agents include interferon agents (IFN beta-1a, PEG IFN beta-1a, and IFN beta-1b) and glatiramer acetate. In phase III trials, the interferon agents and glatiramer acetate reduced relapses by about 30%, compared with placebo. They also affected MRI activity and had a modest effect on 12-week disability progression, as measured by the Expanded Disability Status Scale (EDSS), with reductions in the range of about 30% to 40%, compared with placebo.
More recently approved oral and infusion agents may be good options for patients who develop injection fatigue, which can affect adherence, or who have breakthrough disease activity on injectable therapies, Dr. Newsome said. Fingolimod, the first approved oral therapy, is given once daily. Teriflunomide is administered once daily, and two doses are available. Dimethyl fumarate, the newest oral medication, has a mechanism of action similar to that of glatiramer acetate, but also has a unique mechanism of action in that it activates a transcriptional pathway that may help with oxidative and metabolic stress in MS. It is given twice daily.
In clinical trials, fingolimod and dimethyl fumarate reduced patients’ annualized relapse rate by more than 50%, compared with placebo. The 14-mg dose of teriflunomide reduced relapses by 32%. The oral medications had a robust effect on MRI activity. They also reduced 12-week disability progression, compared with placebo (32% reduction with fingolimod, 30% with teriflunomide, and 38% with dimethyl fumarate).
Natalizumab, an IV therapy that targets VLA-4 antigen on immune cells, reduced patients’ annualized relapse rate by 68% and had a robust effect on MRI activity, compared with placebo, in a phase III trial. Treatment reduced 12-week disability progression by 42%. Alemtuzumab, another IV treatment, depletes mature B and T cells, and infusions are needed only once per year. Initial treatment is 12 mg/day for five consecutive days. The following year, patients receive the same dosing for three days. Afterwards, many clinicians monitor patients and do not treat patients further unless they observe relapses or MRI activity, Dr. Newsome said. In two phase III trials, treatment with alemtuzumab reduced relapses by about 50% and had a robust effect on MRI activity, compared with treatment with interferon beta-1a given three times per week. In addition, alemtuzumab significantly reduced disability progression in one of the phase III trials, Dr. Newsome said.
Daclizumab is a fully humanized monoclonal antibody that targets CD25 on T cells. The FDA approved the therapy, an injection administered by the patient monthly, on May 27. In a phase III trial, daclizumab reduced patients’ annualized relapse rate by 45%, compared with interferon beta-1a given once per week. It also reduced disability progression at six months by 27% and had a robust effect on MRI activity (65% reduction in new gadolinium-enhancing lesions), compared with interferon beta-1a.
The Importance of Laboratory Monitoring
“The higher the potency and efficacy of the drugs, the greater the risk” of adverse events, Dr. Newsome said. Laboratory monitoring is critical. “With all of the therapies that we have available today, with the exception maybe of glatiramer acetate, you need to check labs routinely,” he said. Complete blood counts with differential to monitor patients’ absolute lymphocyte counts and liver function tests “are the bare minimum” needed to monitor patients on most of these drugs, he said.
Certain therapies require additional safety monitoring. For example, patients treated with alemtuzumab require monthly blood work and urine tests. Patients must undergo cardiac monitoring when initiating treatment with fingolimod. With natalizumab, the serum JCV antibody test reliably stratifies patients’ risk of PML over time. Individual MS drugs are associated with a range of minor and major adverse events. Certain therapies may unmask or reactivate infections, cause secondary autoimmunity, or increase the risk of rare opportunistic infections.
The Future
Ocrelizumab, a fully humanized monoclonal antibody that targets CD20+ B cells, is a potential future therapy that is delivered as an infusion every six months. In two relapsing-remitting MS phase III trials, ocrelizumab reduced patients’ annualized relapse rate by close to 50%, compared with interferon beta-1a given three times per week. It also reduced disability progression by around 40% and had a robust effect on MRI activity (> 90% reduction in new gadolinium-enhancing lesions), compared with interferon beta-1a. Ocrelizumab was also found to reduce disability progression at three and six months (24% and 25%, respectively) and reduce worsening in walking speed in patients by 29% in primary progressive MS, compared with placebo.
Investigators also are evaluating strategies for remyelination. Despite the increasing number of available agents, more therapies are needed. “We need more medications and more interventions that impact neurodegeneration and have the potential to repair damage,” Dr. Newsome said.
—Jake Remaly
Suggested Reading
Butzkueven H, Calabresi PA. Is my MS patient failing treatment? Neurology. 2016 Jun 15 [Epub ahead of print].
Freedman MS, Selchen D, Arnold DL, et al. Treatment optimization in MS: Canadian MS Working Group updated recommendations. Can J Neurol Sci. 2013;40(3):307-323.
Lublin FD, Baier M, Cutter G. Effect of relapses on development of residual deficit in multiple sclerosis. Neurology. 2003;61(11):1528-1532.
VANCOUVER—When selecting a therapy for a patient with multiple sclerosis (MS), drug adherence, side effects, and the patient’s risk of aggressive disease are among the considerations that may influence treatment choice, said Scott Newsome, DO, Director of Neurology Outpatient Services and the Neurology Infusion Center at Johns Hopkins University School of Medicine in Baltimore. Patients’ risk tolerance, desire to pursue pregnancy, and John Cunningham virus (JCV) antibody status also can affect the treatment decision.
Scott Newsome, DO
“I wish we had a cookbook recipe. I wish we were able to say, … ‘This is what you’re going to go on, this is what we’re going to expect,’ but that’s not the case. Maybe one day it will be the case, but until then we have to look at many different factors in choosing therapies,” Dr. Newsome said at the 68th Annual Meeting of the American Academy of Neurology.
Two Decades of Advances
The FDA first approved an MS therapy, interferon beta-1b, in 1993. Now, more than 10 treatments with various routes of administration and mechanisms of action have FDA approval, including a new injectable agent approved in May. Additional promising therapies are on the horizon.
“The world of MS therapeutics is evolving and becoming more complicated,” and neurologists have an “ongoing need to balance efficacy, safety, and tolerability of therapeutic interventions for each patient,” Dr. Newsome said.
Dr. Newsome hopes that in the future, biomarkers will help clinicians identify which specific treatments are the best options for each patient. In addition, more research is needed to determine the best time to start a new drug after a patient develops lymphopenia on another MS therapy, and to better understand how prior treatment with other agents affects the risk of progressive multifocal leukoencephalopathy (PML) and other adverse outcomes, he said.
With current therapies, “treating early and having a low threshold to escalate therapy is very important,” Dr. Newsome said. Monitoring relapses and MRI activity may be helpful when evaluating the efficacy of a newly initiated therapy. If a patient has subclinical disease activity six to 12 months after starting a therapy, many clinicians switch therapies and consider treatments that have different mechanisms of action. If a patient develops one small T2 lesion a year out from starting a therapy, he or she does not necessarily need to switch therapies, however. “These drugs are not cures, so you have to look at various factors when you’re thinking about switching or escalating,” Dr. Newsome said. If a patient has a definite relapse, poor recovery from a relapse, disability progression, or robust MRI activity, even when the patient is asymptomatic, clinicians should consider switching therapies.
Risk of Aggressive Disease
Recommendations published in 2013 by the Canadian MS Working Group along with other groups have noted that patients who are male or African American, have an older age at MS onset, or have motor, cerebellar, sphincter, or brainstem involvement are more likely to have aggressive MS. Frequent relapses, poor recovery from relapses, high MRI lesion burden at presentation, brain atrophy, and a low level of vitamin D also are associated with more aggressive disease. Thus, if a patient is African American, does not recover well from a transverse myelitis attack, and has 15 lesions on MRI, including many that are gadolinium-enhancing, with a high spinal cord lesion load, the patient is at high risk of aggressive disease. “When I see this demographic, this phenotype, I’m thinking maybe we need to start with a stronger immune therapy,” said Dr. Newsome.
Based on a cross-comparison of results from the drugs’ pivotal trials, newer medications seem more effective. Head-to-head trials are the only way to establish drug equivalence or superiority, however. With newly diagnosed MS, especially aggressive MS, many clinicians first prescribe an oral agent or an IV therapy instead of an earlier injectable therapy, with the aim of preventing future disability, Dr. Newsome said.
Injectable, Oral, and IV Therapies
Injectable agents include interferon agents (IFN beta-1a, PEG IFN beta-1a, and IFN beta-1b) and glatiramer acetate. In phase III trials, the interferon agents and glatiramer acetate reduced relapses by about 30%, compared with placebo. They also affected MRI activity and had a modest effect on 12-week disability progression, as measured by the Expanded Disability Status Scale (EDSS), with reductions in the range of about 30% to 40%, compared with placebo.
More recently approved oral and infusion agents may be good options for patients who develop injection fatigue, which can affect adherence, or who have breakthrough disease activity on injectable therapies, Dr. Newsome said. Fingolimod, the first approved oral therapy, is given once daily. Teriflunomide is administered once daily, and two doses are available. Dimethyl fumarate, the newest oral medication, has a mechanism of action similar to that of glatiramer acetate, but also has a unique mechanism of action in that it activates a transcriptional pathway that may help with oxidative and metabolic stress in MS. It is given twice daily.
In clinical trials, fingolimod and dimethyl fumarate reduced patients’ annualized relapse rate by more than 50%, compared with placebo. The 14-mg dose of teriflunomide reduced relapses by 32%. The oral medications had a robust effect on MRI activity. They also reduced 12-week disability progression, compared with placebo (32% reduction with fingolimod, 30% with teriflunomide, and 38% with dimethyl fumarate).
Natalizumab, an IV therapy that targets VLA-4 antigen on immune cells, reduced patients’ annualized relapse rate by 68% and had a robust effect on MRI activity, compared with placebo, in a phase III trial. Treatment reduced 12-week disability progression by 42%. Alemtuzumab, another IV treatment, depletes mature B and T cells, and infusions are needed only once per year. Initial treatment is 12 mg/day for five consecutive days. The following year, patients receive the same dosing for three days. Afterwards, many clinicians monitor patients and do not treat patients further unless they observe relapses or MRI activity, Dr. Newsome said. In two phase III trials, treatment with alemtuzumab reduced relapses by about 50% and had a robust effect on MRI activity, compared with treatment with interferon beta-1a given three times per week. In addition, alemtuzumab significantly reduced disability progression in one of the phase III trials, Dr. Newsome said.
Daclizumab is a fully humanized monoclonal antibody that targets CD25 on T cells. The FDA approved the therapy, an injection administered by the patient monthly, on May 27. In a phase III trial, daclizumab reduced patients’ annualized relapse rate by 45%, compared with interferon beta-1a given once per week. It also reduced disability progression at six months by 27% and had a robust effect on MRI activity (65% reduction in new gadolinium-enhancing lesions), compared with interferon beta-1a.
The Importance of Laboratory Monitoring
“The higher the potency and efficacy of the drugs, the greater the risk” of adverse events, Dr. Newsome said. Laboratory monitoring is critical. “With all of the therapies that we have available today, with the exception maybe of glatiramer acetate, you need to check labs routinely,” he said. Complete blood counts with differential to monitor patients’ absolute lymphocyte counts and liver function tests “are the bare minimum” needed to monitor patients on most of these drugs, he said.
Certain therapies require additional safety monitoring. For example, patients treated with alemtuzumab require monthly blood work and urine tests. Patients must undergo cardiac monitoring when initiating treatment with fingolimod. With natalizumab, the serum JCV antibody test reliably stratifies patients’ risk of PML over time. Individual MS drugs are associated with a range of minor and major adverse events. Certain therapies may unmask or reactivate infections, cause secondary autoimmunity, or increase the risk of rare opportunistic infections.
The Future
Ocrelizumab, a fully humanized monoclonal antibody that targets CD20+ B cells, is a potential future therapy that is delivered as an infusion every six months. In two relapsing-remitting MS phase III trials, ocrelizumab reduced patients’ annualized relapse rate by close to 50%, compared with interferon beta-1a given three times per week. It also reduced disability progression by around 40% and had a robust effect on MRI activity (> 90% reduction in new gadolinium-enhancing lesions), compared with interferon beta-1a. Ocrelizumab was also found to reduce disability progression at three and six months (24% and 25%, respectively) and reduce worsening in walking speed in patients by 29% in primary progressive MS, compared with placebo.
Investigators also are evaluating strategies for remyelination. Despite the increasing number of available agents, more therapies are needed. “We need more medications and more interventions that impact neurodegeneration and have the potential to repair damage,” Dr. Newsome said.
—Jake Remaly
VANCOUVER—When selecting a therapy for a patient with multiple sclerosis (MS), drug adherence, side effects, and the patient’s risk of aggressive disease are among the considerations that may influence treatment choice, said Scott Newsome, DO, Director of Neurology Outpatient Services and the Neurology Infusion Center at Johns Hopkins University School of Medicine in Baltimore. Patients’ risk tolerance, desire to pursue pregnancy, and John Cunningham virus (JCV) antibody status also can affect the treatment decision.
Scott Newsome, DO
“I wish we had a cookbook recipe. I wish we were able to say, … ‘This is what you’re going to go on, this is what we’re going to expect,’ but that’s not the case. Maybe one day it will be the case, but until then we have to look at many different factors in choosing therapies,” Dr. Newsome said at the 68th Annual Meeting of the American Academy of Neurology.
Two Decades of Advances
The FDA first approved an MS therapy, interferon beta-1b, in 1993. Now, more than 10 treatments with various routes of administration and mechanisms of action have FDA approval, including a new injectable agent approved in May. Additional promising therapies are on the horizon.
“The world of MS therapeutics is evolving and becoming more complicated,” and neurologists have an “ongoing need to balance efficacy, safety, and tolerability of therapeutic interventions for each patient,” Dr. Newsome said.
Dr. Newsome hopes that in the future, biomarkers will help clinicians identify which specific treatments are the best options for each patient. In addition, more research is needed to determine the best time to start a new drug after a patient develops lymphopenia on another MS therapy, and to better understand how prior treatment with other agents affects the risk of progressive multifocal leukoencephalopathy (PML) and other adverse outcomes, he said.
With current therapies, “treating early and having a low threshold to escalate therapy is very important,” Dr. Newsome said. Monitoring relapses and MRI activity may be helpful when evaluating the efficacy of a newly initiated therapy. If a patient has subclinical disease activity six to 12 months after starting a therapy, many clinicians switch therapies and consider treatments that have different mechanisms of action. If a patient develops one small T2 lesion a year out from starting a therapy, he or she does not necessarily need to switch therapies, however. “These drugs are not cures, so you have to look at various factors when you’re thinking about switching or escalating,” Dr. Newsome said. If a patient has a definite relapse, poor recovery from a relapse, disability progression, or robust MRI activity, even when the patient is asymptomatic, clinicians should consider switching therapies.
Risk of Aggressive Disease
Recommendations published in 2013 by the Canadian MS Working Group along with other groups have noted that patients who are male or African American, have an older age at MS onset, or have motor, cerebellar, sphincter, or brainstem involvement are more likely to have aggressive MS. Frequent relapses, poor recovery from relapses, high MRI lesion burden at presentation, brain atrophy, and a low level of vitamin D also are associated with more aggressive disease. Thus, if a patient is African American, does not recover well from a transverse myelitis attack, and has 15 lesions on MRI, including many that are gadolinium-enhancing, with a high spinal cord lesion load, the patient is at high risk of aggressive disease. “When I see this demographic, this phenotype, I’m thinking maybe we need to start with a stronger immune therapy,” said Dr. Newsome.
Based on a cross-comparison of results from the drugs’ pivotal trials, newer medications seem more effective. Head-to-head trials are the only way to establish drug equivalence or superiority, however. With newly diagnosed MS, especially aggressive MS, many clinicians first prescribe an oral agent or an IV therapy instead of an earlier injectable therapy, with the aim of preventing future disability, Dr. Newsome said.
Injectable, Oral, and IV Therapies
Injectable agents include interferon agents (IFN beta-1a, PEG IFN beta-1a, and IFN beta-1b) and glatiramer acetate. In phase III trials, the interferon agents and glatiramer acetate reduced relapses by about 30%, compared with placebo. They also affected MRI activity and had a modest effect on 12-week disability progression, as measured by the Expanded Disability Status Scale (EDSS), with reductions in the range of about 30% to 40%, compared with placebo.
More recently approved oral and infusion agents may be good options for patients who develop injection fatigue, which can affect adherence, or who have breakthrough disease activity on injectable therapies, Dr. Newsome said. Fingolimod, the first approved oral therapy, is given once daily. Teriflunomide is administered once daily, and two doses are available. Dimethyl fumarate, the newest oral medication, has a mechanism of action similar to that of glatiramer acetate, but also has a unique mechanism of action in that it activates a transcriptional pathway that may help with oxidative and metabolic stress in MS. It is given twice daily.
In clinical trials, fingolimod and dimethyl fumarate reduced patients’ annualized relapse rate by more than 50%, compared with placebo. The 14-mg dose of teriflunomide reduced relapses by 32%. The oral medications had a robust effect on MRI activity. They also reduced 12-week disability progression, compared with placebo (32% reduction with fingolimod, 30% with teriflunomide, and 38% with dimethyl fumarate).
Natalizumab, an IV therapy that targets VLA-4 antigen on immune cells, reduced patients’ annualized relapse rate by 68% and had a robust effect on MRI activity, compared with placebo, in a phase III trial. Treatment reduced 12-week disability progression by 42%. Alemtuzumab, another IV treatment, depletes mature B and T cells, and infusions are needed only once per year. Initial treatment is 12 mg/day for five consecutive days. The following year, patients receive the same dosing for three days. Afterwards, many clinicians monitor patients and do not treat patients further unless they observe relapses or MRI activity, Dr. Newsome said. In two phase III trials, treatment with alemtuzumab reduced relapses by about 50% and had a robust effect on MRI activity, compared with treatment with interferon beta-1a given three times per week. In addition, alemtuzumab significantly reduced disability progression in one of the phase III trials, Dr. Newsome said.
Daclizumab is a fully humanized monoclonal antibody that targets CD25 on T cells. The FDA approved the therapy, an injection administered by the patient monthly, on May 27. In a phase III trial, daclizumab reduced patients’ annualized relapse rate by 45%, compared with interferon beta-1a given once per week. It also reduced disability progression at six months by 27% and had a robust effect on MRI activity (65% reduction in new gadolinium-enhancing lesions), compared with interferon beta-1a.
The Importance of Laboratory Monitoring
“The higher the potency and efficacy of the drugs, the greater the risk” of adverse events, Dr. Newsome said. Laboratory monitoring is critical. “With all of the therapies that we have available today, with the exception maybe of glatiramer acetate, you need to check labs routinely,” he said. Complete blood counts with differential to monitor patients’ absolute lymphocyte counts and liver function tests “are the bare minimum” needed to monitor patients on most of these drugs, he said.
Certain therapies require additional safety monitoring. For example, patients treated with alemtuzumab require monthly blood work and urine tests. Patients must undergo cardiac monitoring when initiating treatment with fingolimod. With natalizumab, the serum JCV antibody test reliably stratifies patients’ risk of PML over time. Individual MS drugs are associated with a range of minor and major adverse events. Certain therapies may unmask or reactivate infections, cause secondary autoimmunity, or increase the risk of rare opportunistic infections.
The Future
Ocrelizumab, a fully humanized monoclonal antibody that targets CD20+ B cells, is a potential future therapy that is delivered as an infusion every six months. In two relapsing-remitting MS phase III trials, ocrelizumab reduced patients’ annualized relapse rate by close to 50%, compared with interferon beta-1a given three times per week. It also reduced disability progression by around 40% and had a robust effect on MRI activity (> 90% reduction in new gadolinium-enhancing lesions), compared with interferon beta-1a. Ocrelizumab was also found to reduce disability progression at three and six months (24% and 25%, respectively) and reduce worsening in walking speed in patients by 29% in primary progressive MS, compared with placebo.
Investigators also are evaluating strategies for remyelination. Despite the increasing number of available agents, more therapies are needed. “We need more medications and more interventions that impact neurodegeneration and have the potential to repair damage,” Dr. Newsome said.
—Jake Remaly
Suggested Reading
Butzkueven H, Calabresi PA. Is my MS patient failing treatment? Neurology. 2016 Jun 15 [Epub ahead of print].
Freedman MS, Selchen D, Arnold DL, et al. Treatment optimization in MS: Canadian MS Working Group updated recommendations. Can J Neurol Sci. 2013;40(3):307-323.
Lublin FD, Baier M, Cutter G. Effect of relapses on development of residual deficit in multiple sclerosis. Neurology. 2003;61(11):1528-1532.
Suggested Reading
Butzkueven H, Calabresi PA. Is my MS patient failing treatment? Neurology. 2016 Jun 15 [Epub ahead of print].
Freedman MS, Selchen D, Arnold DL, et al. Treatment optimization in MS: Canadian MS Working Group updated recommendations. Can J Neurol Sci. 2013;40(3):307-323.
Lublin FD, Baier M, Cutter G. Effect of relapses on development of residual deficit in multiple sclerosis. Neurology. 2003;61(11):1528-1532.

CABG tops PCI for nondiabetic patients with multivessel CAD
Coronary artery bypass graft surgery was associated with a 35% lower rate of all-cause mortality rate and a 59% lower rate of cardiac death than was percutaneous coronary intervention in a pooled analysis of nondiabetic patients with multivessel coronary artery disease in two international randomized trials.
“The superiority of CABG over PCI was consistent across all major clinical subgroups. Likewise, the rate of myocardial infarction was remarkably lower after CABG than after PCI,” Mineok Chang, MD, of the University of Ulsan in Seoul, South Korea, and her associates reported online June 27 in the Journal of the American College of Cardiology.
The advent of drug-eluting stents has led to widespread use of PCI, but controversy persists regarding the best revascularization strategy for nondiabetic patients with multivessel CAD, the researchers said. All-cause mortality “is undoubtedly the most unbiased endpoint to determine treatment strategy,” but individual trials have lacked the power to evaluate this endpoint, they added. Accordingly, they pooled data from the SYNTAX (Synergy Between PCI with Taxus and Cardiac Surgery) trial – which included 1,800 patients with three-vessel or left main CAD from Europe and the United States – and from the BEST (Randomized Comparison of Coronary Artery Bypass Surgery and Everolimus-Eluting Stent Implantation in the Treatment of Patients With Multivessel Coronary Artery Disease) trial, which included 880 patients from Asia with two- or three-vessel CAD. Excluding patients with left main CAD or diabetes left 1,275 patients for analysis (J Am Coll Cardiol. 2016 Jun 27. 68:29-36).
After a median follow-up of 61 months, 38 (6%) CABG patients had died, compared with 59 (9.3%) PCI patients, for a statistically significant hazard ratio of 0.65 (95% confidence interval, 0.25-0.78; P = .039). Likewise, cardiac death was significantly less likely after CABG than PCI (HR, 0.41; 95% CI, 0.25-0.78; P = .005). “The statistical difference between the two groups was pronounced after 2 years of randomization for both all-cause and cardiac mortality,” the researchers reported. Although the latest drug-eluting stents “are reported to improve clinical outcomes,” they did not find a significant interaction between older and more recently developed stents when considering all-cause mortality, they noted.
The study was supported by a research grant from the CardioVascular Research Foundation in Seoul, South Korea. Dr. Chang had no disclosures. Senior author, Dr. Seung-Jung Park, disclosed research support from Abbott Vascular, Cordis, Boston Scientific, and Medtronic.
It is important to consider some limitations of the current study. First, the majority of patients were derived from the SYNTAX trial, which used first-generation paclitaxel drug-eluting stents (DES) that exhibit higher stent complication rates compared with current second- and third-generation everolimus-eluting stents. Second, although complete revascularization was more frequently obtained with CABG in the SYNTAX and BEST trials, current PCI approaches are narrowing this gap with chronic total occlusion PCI techniques and temporary hemodynamic support when needed. Third, selection bias may limit the applicability of these results to patients with more complex disease who are often excluded from clinical trials and may not be eligible for CABG.
Therefore, an adequately powered study of contemporary DES PCI versus CABG is warranted for real-world, nondiabetic patients with multivessel CAD. Guidelines and meta-analyses provide valuable recommendations for populations at large, but decision making for nondiabetic patients with multivessel CAD should be individualized. If equipoise between CABG and PCI exists, decision-making can be improved by engaging a local multidisciplinary CAD heart team. Well-informed cardiologists, interventionalists, and cardiac surgeons who engage in multidisciplinary heart team evaluations and patient-centered shared decision making will provide optimal guidance for patients with multivessel CAD.
Farouc A. Jaffer, MD, is at Massachusetts General Hospital; Patrick T. O’Gara, MD, is at Brigham and Women’s Hospital, both in Boston. Dr. Jaffer disclosed research grants from Siemens and Kowa and consulting relationships with Boston Scientific and Abbott Vascular. Dr. O’Gara had no disclosures. These comments are from their editorial (J Am Coll Cardiol. 2016 Jun 27. doi: 10.1016/j.jacc.2016.05.008).
It is important to consider some limitations of the current study. First, the majority of patients were derived from the SYNTAX trial, which used first-generation paclitaxel drug-eluting stents (DES) that exhibit higher stent complication rates compared with current second- and third-generation everolimus-eluting stents. Second, although complete revascularization was more frequently obtained with CABG in the SYNTAX and BEST trials, current PCI approaches are narrowing this gap with chronic total occlusion PCI techniques and temporary hemodynamic support when needed. Third, selection bias may limit the applicability of these results to patients with more complex disease who are often excluded from clinical trials and may not be eligible for CABG.
Therefore, an adequately powered study of contemporary DES PCI versus CABG is warranted for real-world, nondiabetic patients with multivessel CAD. Guidelines and meta-analyses provide valuable recommendations for populations at large, but decision making for nondiabetic patients with multivessel CAD should be individualized. If equipoise between CABG and PCI exists, decision-making can be improved by engaging a local multidisciplinary CAD heart team. Well-informed cardiologists, interventionalists, and cardiac surgeons who engage in multidisciplinary heart team evaluations and patient-centered shared decision making will provide optimal guidance for patients with multivessel CAD.
Farouc A. Jaffer, MD, is at Massachusetts General Hospital; Patrick T. O’Gara, MD, is at Brigham and Women’s Hospital, both in Boston. Dr. Jaffer disclosed research grants from Siemens and Kowa and consulting relationships with Boston Scientific and Abbott Vascular. Dr. O’Gara had no disclosures. These comments are from their editorial (J Am Coll Cardiol. 2016 Jun 27. doi: 10.1016/j.jacc.2016.05.008).
It is important to consider some limitations of the current study. First, the majority of patients were derived from the SYNTAX trial, which used first-generation paclitaxel drug-eluting stents (DES) that exhibit higher stent complication rates compared with current second- and third-generation everolimus-eluting stents. Second, although complete revascularization was more frequently obtained with CABG in the SYNTAX and BEST trials, current PCI approaches are narrowing this gap with chronic total occlusion PCI techniques and temporary hemodynamic support when needed. Third, selection bias may limit the applicability of these results to patients with more complex disease who are often excluded from clinical trials and may not be eligible for CABG.
Therefore, an adequately powered study of contemporary DES PCI versus CABG is warranted for real-world, nondiabetic patients with multivessel CAD. Guidelines and meta-analyses provide valuable recommendations for populations at large, but decision making for nondiabetic patients with multivessel CAD should be individualized. If equipoise between CABG and PCI exists, decision-making can be improved by engaging a local multidisciplinary CAD heart team. Well-informed cardiologists, interventionalists, and cardiac surgeons who engage in multidisciplinary heart team evaluations and patient-centered shared decision making will provide optimal guidance for patients with multivessel CAD.
Farouc A. Jaffer, MD, is at Massachusetts General Hospital; Patrick T. O’Gara, MD, is at Brigham and Women’s Hospital, both in Boston. Dr. Jaffer disclosed research grants from Siemens and Kowa and consulting relationships with Boston Scientific and Abbott Vascular. Dr. O’Gara had no disclosures. These comments are from their editorial (J Am Coll Cardiol. 2016 Jun 27. doi: 10.1016/j.jacc.2016.05.008).
Coronary artery bypass graft surgery was associated with a 35% lower rate of all-cause mortality rate and a 59% lower rate of cardiac death than was percutaneous coronary intervention in a pooled analysis of nondiabetic patients with multivessel coronary artery disease in two international randomized trials.
“The superiority of CABG over PCI was consistent across all major clinical subgroups. Likewise, the rate of myocardial infarction was remarkably lower after CABG than after PCI,” Mineok Chang, MD, of the University of Ulsan in Seoul, South Korea, and her associates reported online June 27 in the Journal of the American College of Cardiology.
The advent of drug-eluting stents has led to widespread use of PCI, but controversy persists regarding the best revascularization strategy for nondiabetic patients with multivessel CAD, the researchers said. All-cause mortality “is undoubtedly the most unbiased endpoint to determine treatment strategy,” but individual trials have lacked the power to evaluate this endpoint, they added. Accordingly, they pooled data from the SYNTAX (Synergy Between PCI with Taxus and Cardiac Surgery) trial – which included 1,800 patients with three-vessel or left main CAD from Europe and the United States – and from the BEST (Randomized Comparison of Coronary Artery Bypass Surgery and Everolimus-Eluting Stent Implantation in the Treatment of Patients With Multivessel Coronary Artery Disease) trial, which included 880 patients from Asia with two- or three-vessel CAD. Excluding patients with left main CAD or diabetes left 1,275 patients for analysis (J Am Coll Cardiol. 2016 Jun 27. 68:29-36).
After a median follow-up of 61 months, 38 (6%) CABG patients had died, compared with 59 (9.3%) PCI patients, for a statistically significant hazard ratio of 0.65 (95% confidence interval, 0.25-0.78; P = .039). Likewise, cardiac death was significantly less likely after CABG than PCI (HR, 0.41; 95% CI, 0.25-0.78; P = .005). “The statistical difference between the two groups was pronounced after 2 years of randomization for both all-cause and cardiac mortality,” the researchers reported. Although the latest drug-eluting stents “are reported to improve clinical outcomes,” they did not find a significant interaction between older and more recently developed stents when considering all-cause mortality, they noted.
The study was supported by a research grant from the CardioVascular Research Foundation in Seoul, South Korea. Dr. Chang had no disclosures. Senior author, Dr. Seung-Jung Park, disclosed research support from Abbott Vascular, Cordis, Boston Scientific, and Medtronic.
Coronary artery bypass graft surgery was associated with a 35% lower rate of all-cause mortality rate and a 59% lower rate of cardiac death than was percutaneous coronary intervention in a pooled analysis of nondiabetic patients with multivessel coronary artery disease in two international randomized trials.
“The superiority of CABG over PCI was consistent across all major clinical subgroups. Likewise, the rate of myocardial infarction was remarkably lower after CABG than after PCI,” Mineok Chang, MD, of the University of Ulsan in Seoul, South Korea, and her associates reported online June 27 in the Journal of the American College of Cardiology.
The advent of drug-eluting stents has led to widespread use of PCI, but controversy persists regarding the best revascularization strategy for nondiabetic patients with multivessel CAD, the researchers said. All-cause mortality “is undoubtedly the most unbiased endpoint to determine treatment strategy,” but individual trials have lacked the power to evaluate this endpoint, they added. Accordingly, they pooled data from the SYNTAX (Synergy Between PCI with Taxus and Cardiac Surgery) trial – which included 1,800 patients with three-vessel or left main CAD from Europe and the United States – and from the BEST (Randomized Comparison of Coronary Artery Bypass Surgery and Everolimus-Eluting Stent Implantation in the Treatment of Patients With Multivessel Coronary Artery Disease) trial, which included 880 patients from Asia with two- or three-vessel CAD. Excluding patients with left main CAD or diabetes left 1,275 patients for analysis (J Am Coll Cardiol. 2016 Jun 27. 68:29-36).
After a median follow-up of 61 months, 38 (6%) CABG patients had died, compared with 59 (9.3%) PCI patients, for a statistically significant hazard ratio of 0.65 (95% confidence interval, 0.25-0.78; P = .039). Likewise, cardiac death was significantly less likely after CABG than PCI (HR, 0.41; 95% CI, 0.25-0.78; P = .005). “The statistical difference between the two groups was pronounced after 2 years of randomization for both all-cause and cardiac mortality,” the researchers reported. Although the latest drug-eluting stents “are reported to improve clinical outcomes,” they did not find a significant interaction between older and more recently developed stents when considering all-cause mortality, they noted.
The study was supported by a research grant from the CardioVascular Research Foundation in Seoul, South Korea. Dr. Chang had no disclosures. Senior author, Dr. Seung-Jung Park, disclosed research support from Abbott Vascular, Cordis, Boston Scientific, and Medtronic.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Key clinical point: Coronary artery bypass graft is superior to percutaneous coronary intervention for nondiabetic patients with multivessel coronary artery disease.
Major finding: All-cause mortality rates were 6% for CABG and 9.3% for PCI (HR, 0.65; P = .039).
Data source: A pooled analysis of 1,275 nondiabetic patients with two- or three-vessel CAD from the SYNTAX and BEST trials.
Disclosures: The study was supported by a research grant from the CardioVascular Research Foundation in Seoul, South Korea. Dr. Chang had no disclosures. Senior author, Dr. Seung-Jung Park, disclosed research support from Abbott Vascular, Cordis, Boston Scientific, and Medtronic.
Hyperkeratotic Lesions in a Patient With Hepatitis C Virus
The Diagnosis: Necrolytic Acral Erythema
Histopathologic analysis of a biopsy specimen from the right leg revealed an erosion with parakeratosis containing neutrophils and marked spongiosis favoring the upper layer of the epidermis with focal individual necrotic keratinocytes. In addition, there was a lymphocytic and neutrophilic exocytosis with edema of the papillary dermal papillae, mild papillary dermal fibrosis, and a mild perivascular lymphocytic infiltrate with neutrophils and occasional eosinophils. Clinicopathologic correlation led to a diagnosis of necrolytic acral erythema (NAE).
The patient was prescribed clobetasol propionate ointment 0.05% and oral zinc sulfate 220 mg twice daily but was initially noncompliant with the topical corticosteroid regimen. He did, however, initiate zinc supplementation, which was later increased to 220 mg 3 times daily. At 3-month follow-up, the lesions had nearly completely cleared (Figure) and the serum zinc level was within reference range at 81 μg/dL.

Necrolytic acral erythema is a rare dermatosis that was first described in 1996 by el Darouti and Abu el Ela1 in a series of 7 Egyptian patients. Since then, most of the cases have reported concomitant hepatitis C virus (HCV) infection.2 Necrolytic acral erythema classically presents with symmetric, well-defined, hyperkeratotic plaques in an acral distribution, typically on the dorsal aspect of the feet.2,3 Lesions may involve the dorsal aspect of the toes and the lower legs, with less common involvement of the elbows, hands, and buttocks. Patients often report pruritus and/or burning.3
Abdallah et al4 proposed several stages of NAE development with erythematous papules with dusky eroded centers progressing to marginated, erythematous to violaceous, lichenified plaques. Over time, these lesions tend to thin with progressive hyperpigmentation.
Histologically, early findings of NAE include acanthosis with epidermal spongiosis and upper dermal perivascular dermatitis. Over time, lesions may exhibit psoriasiform hyperplasia with papillomatosis and parakeratosis, epidermal pallor, subcorneal pustules, vascular ectasia, papillary dermal inflammation, and necrotic keratinocytes. Minimal to moderate acanthosis with an inflammatory infiltrate may be observed later in disease progression.5
The differential diagnosis of NAE includes many benign inflammatory skin diseases. Given the acral/extensor distribution of hyperkeratotic lesions and psoriasiform pattern on histopathology, NAE initially may be misdiagnosed as psoriasis. Unlike psoriasis, however, NAE rarely involves palmoplantar skin or nails4 and may respond dramatically to treatment with zinc supplementation.6,7 Necrolytic acral erythema also may be confused with other necrolytic erythemas, including necrolytic migratory erythema, acrodermatitis enteropathica, and pellagra. A deficiency of biotin or essential fatty acids also may mimic NAE. Necrolytic acral erythema can be distinguished from these entities based on its characteristic appearance and distribution, along with comorbid HCV infection.2-4
Several reports of NAE have revealed an associated zinc deficiency.2,8 The underlying pathophysiology of zinc deficiency in NAE has not been elucidated but is thought to be related to HCV infection.2 Clinical improvement has been reported with zinc supplementation in patients with NAE at dosages of 220 mg twice daily, even in those with initial serum zinc levels within reference range.6,7 Our patient was observed to have a low serum zinc level that dramatically improved with oral supplementation.
The recognition of this uncommon entity is critical for dermatologists and dermatopathologists, as NAE has been proposed as an early cutaneous marker of HCV and may prompt the initial diagnosis of HCV.1-10 The severity of NAE has even been linked to HCV severity.1,8 Treatment of HCV has cleared NAE in several cases,4,10 implicating the virus in its pathogenesis. A proper workup for liver dysfunction and follow-up with an appropriate health care provider for HCV treatment is crucial. Our patient was encouraged to follow up with the hepatology department, as he had not been evaluated in several years.
- el Darouti M, Abu el Ela M. Necrolytic acral erythema: a cutaneous marker of viral hepatitis C. Int J Dermatol. 1996;35:252-256.
- Patel U, Loyd A, Patel R, et al. Necrolytic acral erythema. Dermatol Online J. 2010;16:15.
- Geria AN, Holcomb KZ, Scheinfeld NS. Necrolytic acral erythema: a review of the literature. Cutis. 2009;83:309-314.
- Abdallah MA, Ghozzi MY, Monib HA, et al. Necrolytic acral erythema: a cutaneous sign of hepatitis C virus infection. J Am Acad Dermatol. 2005;53:247-251.
- Abdallah MA, Ghozzi MY, Monib HA, et al. Histological study of necrolytic acral erythema. J Ark Med Soc. 2004;100:354-355.
- Khanna VJ, Shieh S, Benjamin J, et al. Necrolytic acral erythema associated with hepatitis C: effective treatment with interferon alfa and zinc. Arch Dermatol. 2000;136:755-757.
- Abdallah MA, Hull C, Horn TD. Necrolytic acral erythema: a patient from the United States successfully treated with oral zinc. Arch Dermatol. 2005;141:85-87.
- Najarian DJ, Lefkowitz I, Balfour E, et al. Zinc deficiency associated with necrolytic acral erythema. J Am Acad Dermatol. 2006;55(5 suppl):S108-S110.
- Nofal AA, Nofal E, Attwa E, et al. Necrolytic acral erythema: a variant of necrolytic migratory erythema or a distinct entity? Int J Dermatol. 2005;44:916-921.
- Hivnor CM, Yan AC, Junkins-Hopkins JM, et al. Necrolytic acral erythema: response to combination therapy with interferon and ribavirin. J Am Acad Dermatol. 2004;50(5 suppl):S121-S124.
The Diagnosis: Necrolytic Acral Erythema
Histopathologic analysis of a biopsy specimen from the right leg revealed an erosion with parakeratosis containing neutrophils and marked spongiosis favoring the upper layer of the epidermis with focal individual necrotic keratinocytes. In addition, there was a lymphocytic and neutrophilic exocytosis with edema of the papillary dermal papillae, mild papillary dermal fibrosis, and a mild perivascular lymphocytic infiltrate with neutrophils and occasional eosinophils. Clinicopathologic correlation led to a diagnosis of necrolytic acral erythema (NAE).
The patient was prescribed clobetasol propionate ointment 0.05% and oral zinc sulfate 220 mg twice daily but was initially noncompliant with the topical corticosteroid regimen. He did, however, initiate zinc supplementation, which was later increased to 220 mg 3 times daily. At 3-month follow-up, the lesions had nearly completely cleared (Figure) and the serum zinc level was within reference range at 81 μg/dL.
Necrolytic acral erythema is a rare dermatosis that was first described in 1996 by el Darouti and Abu el Ela1 in a series of 7 Egyptian patients. Since then, most of the cases have reported concomitant hepatitis C virus (HCV) infection.2 Necrolytic acral erythema classically presents with symmetric, well-defined, hyperkeratotic plaques in an acral distribution, typically on the dorsal aspect of the feet.2,3 Lesions may involve the dorsal aspect of the toes and the lower legs, with less common involvement of the elbows, hands, and buttocks. Patients often report pruritus and/or burning.3
Abdallah et al4 proposed several stages of NAE development with erythematous papules with dusky eroded centers progressing to marginated, erythematous to violaceous, lichenified plaques. Over time, these lesions tend to thin with progressive hyperpigmentation.
Histologically, early findings of NAE include acanthosis with epidermal spongiosis and upper dermal perivascular dermatitis. Over time, lesions may exhibit psoriasiform hyperplasia with papillomatosis and parakeratosis, epidermal pallor, subcorneal pustules, vascular ectasia, papillary dermal inflammation, and necrotic keratinocytes. Minimal to moderate acanthosis with an inflammatory infiltrate may be observed later in disease progression.5
The differential diagnosis of NAE includes many benign inflammatory skin diseases. Given the acral/extensor distribution of hyperkeratotic lesions and psoriasiform pattern on histopathology, NAE initially may be misdiagnosed as psoriasis. Unlike psoriasis, however, NAE rarely involves palmoplantar skin or nails4 and may respond dramatically to treatment with zinc supplementation.6,7 Necrolytic acral erythema also may be confused with other necrolytic erythemas, including necrolytic migratory erythema, acrodermatitis enteropathica, and pellagra. A deficiency of biotin or essential fatty acids also may mimic NAE. Necrolytic acral erythema can be distinguished from these entities based on its characteristic appearance and distribution, along with comorbid HCV infection.2-4
Several reports of NAE have revealed an associated zinc deficiency.2,8 The underlying pathophysiology of zinc deficiency in NAE has not been elucidated but is thought to be related to HCV infection.2 Clinical improvement has been reported with zinc supplementation in patients with NAE at dosages of 220 mg twice daily, even in those with initial serum zinc levels within reference range.6,7 Our patient was observed to have a low serum zinc level that dramatically improved with oral supplementation.
The recognition of this uncommon entity is critical for dermatologists and dermatopathologists, as NAE has been proposed as an early cutaneous marker of HCV and may prompt the initial diagnosis of HCV.1-10 The severity of NAE has even been linked to HCV severity.1,8 Treatment of HCV has cleared NAE in several cases,4,10 implicating the virus in its pathogenesis. A proper workup for liver dysfunction and follow-up with an appropriate health care provider for HCV treatment is crucial. Our patient was encouraged to follow up with the hepatology department, as he had not been evaluated in several years.
The Diagnosis: Necrolytic Acral Erythema
Histopathologic analysis of a biopsy specimen from the right leg revealed an erosion with parakeratosis containing neutrophils and marked spongiosis favoring the upper layer of the epidermis with focal individual necrotic keratinocytes. In addition, there was a lymphocytic and neutrophilic exocytosis with edema of the papillary dermal papillae, mild papillary dermal fibrosis, and a mild perivascular lymphocytic infiltrate with neutrophils and occasional eosinophils. Clinicopathologic correlation led to a diagnosis of necrolytic acral erythema (NAE).
The patient was prescribed clobetasol propionate ointment 0.05% and oral zinc sulfate 220 mg twice daily but was initially noncompliant with the topical corticosteroid regimen. He did, however, initiate zinc supplementation, which was later increased to 220 mg 3 times daily. At 3-month follow-up, the lesions had nearly completely cleared (Figure) and the serum zinc level was within reference range at 81 μg/dL.
Necrolytic acral erythema is a rare dermatosis that was first described in 1996 by el Darouti and Abu el Ela1 in a series of 7 Egyptian patients. Since then, most of the cases have reported concomitant hepatitis C virus (HCV) infection.2 Necrolytic acral erythema classically presents with symmetric, well-defined, hyperkeratotic plaques in an acral distribution, typically on the dorsal aspect of the feet.2,3 Lesions may involve the dorsal aspect of the toes and the lower legs, with less common involvement of the elbows, hands, and buttocks. Patients often report pruritus and/or burning.3
Abdallah et al4 proposed several stages of NAE development with erythematous papules with dusky eroded centers progressing to marginated, erythematous to violaceous, lichenified plaques. Over time, these lesions tend to thin with progressive hyperpigmentation.
Histologically, early findings of NAE include acanthosis with epidermal spongiosis and upper dermal perivascular dermatitis. Over time, lesions may exhibit psoriasiform hyperplasia with papillomatosis and parakeratosis, epidermal pallor, subcorneal pustules, vascular ectasia, papillary dermal inflammation, and necrotic keratinocytes. Minimal to moderate acanthosis with an inflammatory infiltrate may be observed later in disease progression.5
The differential diagnosis of NAE includes many benign inflammatory skin diseases. Given the acral/extensor distribution of hyperkeratotic lesions and psoriasiform pattern on histopathology, NAE initially may be misdiagnosed as psoriasis. Unlike psoriasis, however, NAE rarely involves palmoplantar skin or nails4 and may respond dramatically to treatment with zinc supplementation.6,7 Necrolytic acral erythema also may be confused with other necrolytic erythemas, including necrolytic migratory erythema, acrodermatitis enteropathica, and pellagra. A deficiency of biotin or essential fatty acids also may mimic NAE. Necrolytic acral erythema can be distinguished from these entities based on its characteristic appearance and distribution, along with comorbid HCV infection.2-4
Several reports of NAE have revealed an associated zinc deficiency.2,8 The underlying pathophysiology of zinc deficiency in NAE has not been elucidated but is thought to be related to HCV infection.2 Clinical improvement has been reported with zinc supplementation in patients with NAE at dosages of 220 mg twice daily, even in those with initial serum zinc levels within reference range.6,7 Our patient was observed to have a low serum zinc level that dramatically improved with oral supplementation.
The recognition of this uncommon entity is critical for dermatologists and dermatopathologists, as NAE has been proposed as an early cutaneous marker of HCV and may prompt the initial diagnosis of HCV.1-10 The severity of NAE has even been linked to HCV severity.1,8 Treatment of HCV has cleared NAE in several cases,4,10 implicating the virus in its pathogenesis. A proper workup for liver dysfunction and follow-up with an appropriate health care provider for HCV treatment is crucial. Our patient was encouraged to follow up with the hepatology department, as he had not been evaluated in several years.
- el Darouti M, Abu el Ela M. Necrolytic acral erythema: a cutaneous marker of viral hepatitis C. Int J Dermatol. 1996;35:252-256.
- Patel U, Loyd A, Patel R, et al. Necrolytic acral erythema. Dermatol Online J. 2010;16:15.
- Geria AN, Holcomb KZ, Scheinfeld NS. Necrolytic acral erythema: a review of the literature. Cutis. 2009;83:309-314.
- Abdallah MA, Ghozzi MY, Monib HA, et al. Necrolytic acral erythema: a cutaneous sign of hepatitis C virus infection. J Am Acad Dermatol. 2005;53:247-251.
- Abdallah MA, Ghozzi MY, Monib HA, et al. Histological study of necrolytic acral erythema. J Ark Med Soc. 2004;100:354-355.
- Khanna VJ, Shieh S, Benjamin J, et al. Necrolytic acral erythema associated with hepatitis C: effective treatment with interferon alfa and zinc. Arch Dermatol. 2000;136:755-757.
- Abdallah MA, Hull C, Horn TD. Necrolytic acral erythema: a patient from the United States successfully treated with oral zinc. Arch Dermatol. 2005;141:85-87.
- Najarian DJ, Lefkowitz I, Balfour E, et al. Zinc deficiency associated with necrolytic acral erythema. J Am Acad Dermatol. 2006;55(5 suppl):S108-S110.
- Nofal AA, Nofal E, Attwa E, et al. Necrolytic acral erythema: a variant of necrolytic migratory erythema or a distinct entity? Int J Dermatol. 2005;44:916-921.
- Hivnor CM, Yan AC, Junkins-Hopkins JM, et al. Necrolytic acral erythema: response to combination therapy with interferon and ribavirin. J Am Acad Dermatol. 2004;50(5 suppl):S121-S124.
- el Darouti M, Abu el Ela M. Necrolytic acral erythema: a cutaneous marker of viral hepatitis C. Int J Dermatol. 1996;35:252-256.
- Patel U, Loyd A, Patel R, et al. Necrolytic acral erythema. Dermatol Online J. 2010;16:15.
- Geria AN, Holcomb KZ, Scheinfeld NS. Necrolytic acral erythema: a review of the literature. Cutis. 2009;83:309-314.
- Abdallah MA, Ghozzi MY, Monib HA, et al. Necrolytic acral erythema: a cutaneous sign of hepatitis C virus infection. J Am Acad Dermatol. 2005;53:247-251.
- Abdallah MA, Ghozzi MY, Monib HA, et al. Histological study of necrolytic acral erythema. J Ark Med Soc. 2004;100:354-355.
- Khanna VJ, Shieh S, Benjamin J, et al. Necrolytic acral erythema associated with hepatitis C: effective treatment with interferon alfa and zinc. Arch Dermatol. 2000;136:755-757.
- Abdallah MA, Hull C, Horn TD. Necrolytic acral erythema: a patient from the United States successfully treated with oral zinc. Arch Dermatol. 2005;141:85-87.
- Najarian DJ, Lefkowitz I, Balfour E, et al. Zinc deficiency associated with necrolytic acral erythema. J Am Acad Dermatol. 2006;55(5 suppl):S108-S110.
- Nofal AA, Nofal E, Attwa E, et al. Necrolytic acral erythema: a variant of necrolytic migratory erythema or a distinct entity? Int J Dermatol. 2005;44:916-921.
- Hivnor CM, Yan AC, Junkins-Hopkins JM, et al. Necrolytic acral erythema: response to combination therapy with interferon and ribavirin. J Am Acad Dermatol. 2004;50(5 suppl):S121-S124.

