User login
The far-reaching implications of weight gain in pregnancy
It is not surprising that a pregnant woman’s actions heavily influence her developing baby. Ob.gyns. advise patients to stop smoking or to stop using illicit drugs, and limit their alcohol consumption during pregnancy because we know that these substances can cause serious, even fatal, consequences for the fetus. Although we routinely provide nutrition information and guidelines on healthy weight gain in pregnancy, we may not stress the importance of healthy eating to the same degree as we may emphasize the need to eliminate tobacco use. But should we?
In 2011, a study by researchers at Yale University, the University of Texas, and Arizona State University suggested that food can have effects on the brain similar to those of addictive substances (Arch Gen Psychiatry. 2011 Aug;68[8]:808-16). Using MRI, the investigators examined which areas of the brain became active in response to the consumption of a chocolate milkshake, and compared these results to brain scans of people addicted to opioids. The study enrolled 48 women who were lean to obese, based on body mass index. The researchers found that people who were obese had brain activity patterns in response to food that were similar to patterns that people with drug addiction had in response to opioids. Although the sample size was small, the investigators showed, in essence, that food is a “drug.”

Ob.gyns. working with patients who are overweight or obese typically encourage weight loss prior to pregnancy, or suggest limited weight gain during gestation, because obesity increases complications for both the pregnant mother and her unborn baby. If, as the 2011 study suggests, we were to think of food addiction as we do any other drug addiction – tobacco, opioids, alcohol – that should be curbed out of concern for the developing baby, ob.gyns. might tell our patients to reduce or completely eliminate their “trans-fat food habit” before and during pregnancy.
Importantly, a mother’s nutrition, or lack thereof, may exert harmful effects on her child’s long-term health. This idea was intimated decades ago when Dr. David Barker proposed that a person’s future risk for disease began during pregnancy. Exactly how this type of early programming may occur remains to be determined. Therefore, this month we examine the fetal origins of obesity, and have invited Dr. Michael G. Ross, professor of obstetrics and gynecology, and Mina Desai, Ph.D., assistant professor of obstetrics and gynecology, at the University of California, Los Angeles, to discuss this important topic.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column. Contact him at [email protected].
It is not surprising that a pregnant woman’s actions heavily influence her developing baby. Ob.gyns. advise patients to stop smoking or to stop using illicit drugs, and limit their alcohol consumption during pregnancy because we know that these substances can cause serious, even fatal, consequences for the fetus. Although we routinely provide nutrition information and guidelines on healthy weight gain in pregnancy, we may not stress the importance of healthy eating to the same degree as we may emphasize the need to eliminate tobacco use. But should we?
In 2011, a study by researchers at Yale University, the University of Texas, and Arizona State University suggested that food can have effects on the brain similar to those of addictive substances (Arch Gen Psychiatry. 2011 Aug;68[8]:808-16). Using MRI, the investigators examined which areas of the brain became active in response to the consumption of a chocolate milkshake, and compared these results to brain scans of people addicted to opioids. The study enrolled 48 women who were lean to obese, based on body mass index. The researchers found that people who were obese had brain activity patterns in response to food that were similar to patterns that people with drug addiction had in response to opioids. Although the sample size was small, the investigators showed, in essence, that food is a “drug.”
Ob.gyns. working with patients who are overweight or obese typically encourage weight loss prior to pregnancy, or suggest limited weight gain during gestation, because obesity increases complications for both the pregnant mother and her unborn baby. If, as the 2011 study suggests, we were to think of food addiction as we do any other drug addiction – tobacco, opioids, alcohol – that should be curbed out of concern for the developing baby, ob.gyns. might tell our patients to reduce or completely eliminate their “trans-fat food habit” before and during pregnancy.
Importantly, a mother’s nutrition, or lack thereof, may exert harmful effects on her child’s long-term health. This idea was intimated decades ago when Dr. David Barker proposed that a person’s future risk for disease began during pregnancy. Exactly how this type of early programming may occur remains to be determined. Therefore, this month we examine the fetal origins of obesity, and have invited Dr. Michael G. Ross, professor of obstetrics and gynecology, and Mina Desai, Ph.D., assistant professor of obstetrics and gynecology, at the University of California, Los Angeles, to discuss this important topic.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column. Contact him at [email protected].
It is not surprising that a pregnant woman’s actions heavily influence her developing baby. Ob.gyns. advise patients to stop smoking or to stop using illicit drugs, and limit their alcohol consumption during pregnancy because we know that these substances can cause serious, even fatal, consequences for the fetus. Although we routinely provide nutrition information and guidelines on healthy weight gain in pregnancy, we may not stress the importance of healthy eating to the same degree as we may emphasize the need to eliminate tobacco use. But should we?
In 2011, a study by researchers at Yale University, the University of Texas, and Arizona State University suggested that food can have effects on the brain similar to those of addictive substances (Arch Gen Psychiatry. 2011 Aug;68[8]:808-16). Using MRI, the investigators examined which areas of the brain became active in response to the consumption of a chocolate milkshake, and compared these results to brain scans of people addicted to opioids. The study enrolled 48 women who were lean to obese, based on body mass index. The researchers found that people who were obese had brain activity patterns in response to food that were similar to patterns that people with drug addiction had in response to opioids. Although the sample size was small, the investigators showed, in essence, that food is a “drug.”
Ob.gyns. working with patients who are overweight or obese typically encourage weight loss prior to pregnancy, or suggest limited weight gain during gestation, because obesity increases complications for both the pregnant mother and her unborn baby. If, as the 2011 study suggests, we were to think of food addiction as we do any other drug addiction – tobacco, opioids, alcohol – that should be curbed out of concern for the developing baby, ob.gyns. might tell our patients to reduce or completely eliminate their “trans-fat food habit” before and during pregnancy.
Importantly, a mother’s nutrition, or lack thereof, may exert harmful effects on her child’s long-term health. This idea was intimated decades ago when Dr. David Barker proposed that a person’s future risk for disease began during pregnancy. Exactly how this type of early programming may occur remains to be determined. Therefore, this month we examine the fetal origins of obesity, and have invited Dr. Michael G. Ross, professor of obstetrics and gynecology, and Mina Desai, Ph.D., assistant professor of obstetrics and gynecology, at the University of California, Los Angeles, to discuss this important topic.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column. Contact him at [email protected].

Understanding ovarian germ cell neoplasms
Germ cell neoplasms arise from primordial germ cells of the gonad that differentiate to embryonic and extraembryonic tissues. Approximately 20%-25% of ovarian neoplasms are germ cell in origin but they account for only 3%-5% of ovarian malignancies. Importantly, germ cell neoplasms encompass 70% of the ovarian neoplasms among girls and young women aged 10-30 years, of which approximately one-third are malignant.
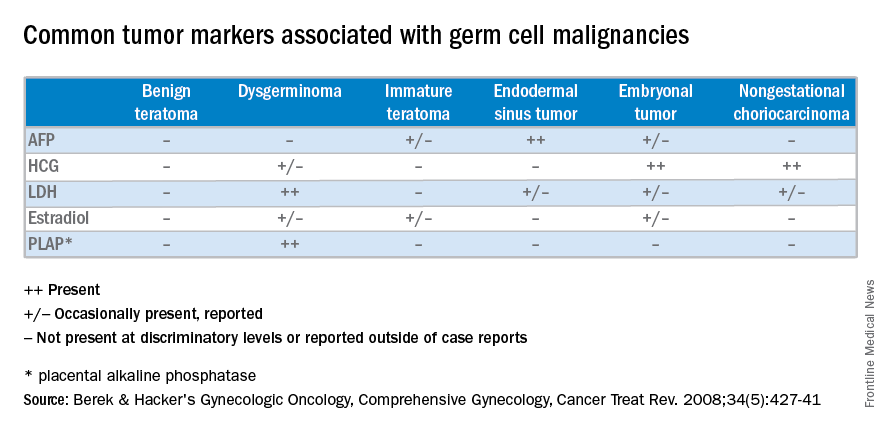
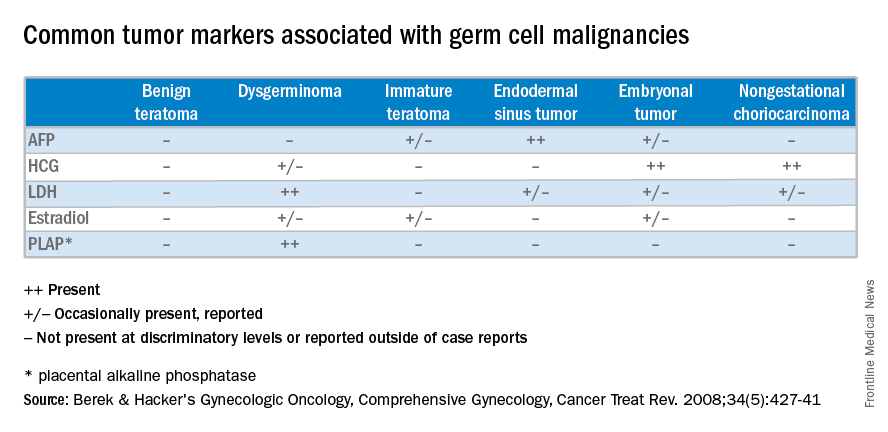
Unlike epithelial ovarian cancers, malignant germ cell neoplasms are typically diagnosed at early stages. They can present as a palpable mass or cause acute abdominal pain secondary to their rapid growth, penchant for necrosis, torsion, hemorrhage, infection, or rupture. Since malignant germ cell neoplasms can excrete hormonally-active tumor markers, such as human chorionic gonadotropin (HCG), many women present with menstrual irregularities.
Management of malignant germ cell neoplasms generally includes fertility-sparing surgery – with or without neoadjuvant combination bleomycin, etoposide, and cisplatin (BEP) – and is typically associated with a favorable prognosis (Cancer Treat Rev. 2008 Aug;34[5]:427-41).
Teratomas
Benign teratomas represent about a quarter of all ovarian neoplasms. Benign teratomas can be solid or cystic, and contain components representing all three cell layers: endoderm, mesoderm, and ectoderm. Due to the presence of differentiated adult tissues, benign teratomas have a characteristic radiographic appearance. They can appear as cystic echogenic masses with intense acoustic shadowing, homogenous nodules or bands, and rounded protuberances called “Rokitansky nodules.”
Treatment of benign teratomas in reproductive-age women includes ovarian cystectomy and careful inspection of the contralateral ovary as 10%-15% may be bilateral. In postmenopausal women, there is less than a 2% risk for malignant transformation of the associated cell lines, most commonly a squamous cell carcinoma. In these cases, spread beyond the ovarian capsule is associated with a poor prognosis and chemotherapy and/or radiation are indicated (Int J Gynecol Cancer. 2006 Jan-Feb;16[1]:140-4). Malignant monodermal teratomas are composed of single cell lines with malignant transformations of that tissue type; struma ovarii composed of thyroid tissue, for example, is exceedingly rare.

Dysgerminoma
Dysgerminomas are the most common malignant germ cell neoplasms, accounting for about one-third of cases. They typically present in girls and young women between 10 and 30 years of age, and rarely occur after 50 years of age. As a result, a quarter of cases are identified during pregnancy and another 5% are found in patients presenting with amenorrhea secondary to gonadal dysgenesis, such as is associated with Turner’s syndrome.
At diagnosis, lactate dehydrogenase (LDH) may be elevated and 10% may have an elevation of HCG. Ultrasound findings include a solid, mostly echoic, but heterogeneous mass with apparent lobulations. About two-thirds are stage I at the time of diagnosis, and 10%-15% are bilateral, making dysgerminomas the only malignant germ cell neoplasm with significant risk for bilaterality.
Treatment for early stage dysgerminoma is surgical; young women should have at least unilateral oophorectomy performed; if the contralateral ovary is spared there’s a 10% risk for recurrence over the next 2 years. Comprehensive fertility-sparing surgery is recommended with pelvic and para-aortic lymphadenectomy. Women with gonadal dysgenesis should have a bilateral salpingo-oophorectomy, and those beyond childbearing should undergo a total hysterectomy, with bilateral salpingo-oophorectomy and appropriate staging. BEP should be added for patients with advanced disease.

Other malignant germ cell neoplasms
Uncommon malignant germ cell neoplasms include immature teratomas and endodermal sinus tumors. Though uncommon, the majority of immature teratomas present between the ages of 10 and 20 years and account for nearly 30% of the ovarian cancer deaths in this age group. Immature teratomas usually have negative serum markers, though about one-third will excrete HCG. Immature teratomas are graded by the proportion of neuro-epithelium. Treatment includes unilateral oophorectomy, and surgical staging with adjuvant chemotherapy (BEP) for patients with greater than stage 1A grade 1 disease.
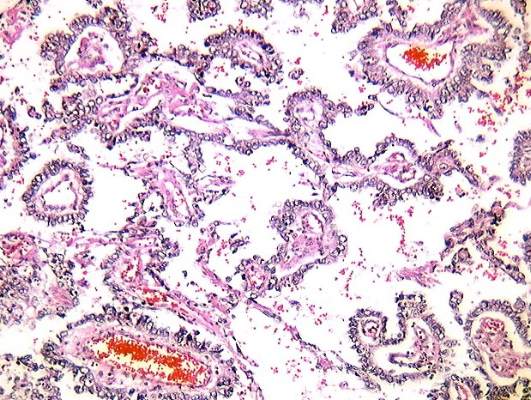
Endodermal sinus tumors are derived from the primitive yolk sac, are unilateral, and most will secrete alpha-fetoprotein (AFP). The median age of diagnosis of an endodermal sinus tumor is 18 years, thus treatment includes unilateral salpingo-oophorectomy and comprehensive fertility-sparing surgical staging followed by BEP.
Embryonal and nongestational choriocarcinomas are rare malignant germ cell neoplasms found in prepubertal girls to young women. Embryonal carcinomas can secrete estrogens, HCG and/or AFP, so patients may present with precocious puberty. Treatment is similar to that of endodermal sinus tumors. Nongestational choriocarcinomas, like the gestational forms, have a poor prognosis and are monitored and treated similarly.
Understanding presentation and treatments for malignant germ cell neoplasms is important in the evaluation of a young patient with a pelvic mass and should prompt the practicing gynecologist to test for AFP and HCG, with or without LDH and CA-125. If encountered inadvertently, every attempt should be made to preserve fertility in these young patients and expedient referral to a gynecologic oncologist, pediatric gynecologist, and/or a reproductive endocrinologist is warranted. Rarely, a second look laparotomy is indicated without obvious intraperitoneal spread and reproductive potential is preserved even in those requiring BEP. If managed appropriately, the overall prognosis remains good for these young women.
Dr. Gehrig is professor and director of gynecologic oncology at the University of North Carolina at Chapel Hill. Dr. Castellano is a resident physician in the obstetrics and gynecology program at the university. They reported having no relevant financial disclosures. To comment, email them at [email protected].
Germ cell neoplasms arise from primordial germ cells of the gonad that differentiate to embryonic and extraembryonic tissues. Approximately 20%-25% of ovarian neoplasms are germ cell in origin but they account for only 3%-5% of ovarian malignancies. Importantly, germ cell neoplasms encompass 70% of the ovarian neoplasms among girls and young women aged 10-30 years, of which approximately one-third are malignant.
Unlike epithelial ovarian cancers, malignant germ cell neoplasms are typically diagnosed at early stages. They can present as a palpable mass or cause acute abdominal pain secondary to their rapid growth, penchant for necrosis, torsion, hemorrhage, infection, or rupture. Since malignant germ cell neoplasms can excrete hormonally-active tumor markers, such as human chorionic gonadotropin (HCG), many women present with menstrual irregularities.
Management of malignant germ cell neoplasms generally includes fertility-sparing surgery – with or without neoadjuvant combination bleomycin, etoposide, and cisplatin (BEP) – and is typically associated with a favorable prognosis (Cancer Treat Rev. 2008 Aug;34[5]:427-41).
Teratomas
Benign teratomas represent about a quarter of all ovarian neoplasms. Benign teratomas can be solid or cystic, and contain components representing all three cell layers: endoderm, mesoderm, and ectoderm. Due to the presence of differentiated adult tissues, benign teratomas have a characteristic radiographic appearance. They can appear as cystic echogenic masses with intense acoustic shadowing, homogenous nodules or bands, and rounded protuberances called “Rokitansky nodules.”
Treatment of benign teratomas in reproductive-age women includes ovarian cystectomy and careful inspection of the contralateral ovary as 10%-15% may be bilateral. In postmenopausal women, there is less than a 2% risk for malignant transformation of the associated cell lines, most commonly a squamous cell carcinoma. In these cases, spread beyond the ovarian capsule is associated with a poor prognosis and chemotherapy and/or radiation are indicated (Int J Gynecol Cancer. 2006 Jan-Feb;16[1]:140-4). Malignant monodermal teratomas are composed of single cell lines with malignant transformations of that tissue type; struma ovarii composed of thyroid tissue, for example, is exceedingly rare.
Dysgerminoma
Dysgerminomas are the most common malignant germ cell neoplasms, accounting for about one-third of cases. They typically present in girls and young women between 10 and 30 years of age, and rarely occur after 50 years of age. As a result, a quarter of cases are identified during pregnancy and another 5% are found in patients presenting with amenorrhea secondary to gonadal dysgenesis, such as is associated with Turner’s syndrome.
At diagnosis, lactate dehydrogenase (LDH) may be elevated and 10% may have an elevation of HCG. Ultrasound findings include a solid, mostly echoic, but heterogeneous mass with apparent lobulations. About two-thirds are stage I at the time of diagnosis, and 10%-15% are bilateral, making dysgerminomas the only malignant germ cell neoplasm with significant risk for bilaterality.
Treatment for early stage dysgerminoma is surgical; young women should have at least unilateral oophorectomy performed; if the contralateral ovary is spared there’s a 10% risk for recurrence over the next 2 years. Comprehensive fertility-sparing surgery is recommended with pelvic and para-aortic lymphadenectomy. Women with gonadal dysgenesis should have a bilateral salpingo-oophorectomy, and those beyond childbearing should undergo a total hysterectomy, with bilateral salpingo-oophorectomy and appropriate staging. BEP should be added for patients with advanced disease.
Other malignant germ cell neoplasms
Uncommon malignant germ cell neoplasms include immature teratomas and endodermal sinus tumors. Though uncommon, the majority of immature teratomas present between the ages of 10 and 20 years and account for nearly 30% of the ovarian cancer deaths in this age group. Immature teratomas usually have negative serum markers, though about one-third will excrete HCG. Immature teratomas are graded by the proportion of neuro-epithelium. Treatment includes unilateral oophorectomy, and surgical staging with adjuvant chemotherapy (BEP) for patients with greater than stage 1A grade 1 disease.
Endodermal sinus tumors are derived from the primitive yolk sac, are unilateral, and most will secrete alpha-fetoprotein (AFP). The median age of diagnosis of an endodermal sinus tumor is 18 years, thus treatment includes unilateral salpingo-oophorectomy and comprehensive fertility-sparing surgical staging followed by BEP.
Embryonal and nongestational choriocarcinomas are rare malignant germ cell neoplasms found in prepubertal girls to young women. Embryonal carcinomas can secrete estrogens, HCG and/or AFP, so patients may present with precocious puberty. Treatment is similar to that of endodermal sinus tumors. Nongestational choriocarcinomas, like the gestational forms, have a poor prognosis and are monitored and treated similarly.
Understanding presentation and treatments for malignant germ cell neoplasms is important in the evaluation of a young patient with a pelvic mass and should prompt the practicing gynecologist to test for AFP and HCG, with or without LDH and CA-125. If encountered inadvertently, every attempt should be made to preserve fertility in these young patients and expedient referral to a gynecologic oncologist, pediatric gynecologist, and/or a reproductive endocrinologist is warranted. Rarely, a second look laparotomy is indicated without obvious intraperitoneal spread and reproductive potential is preserved even in those requiring BEP. If managed appropriately, the overall prognosis remains good for these young women.
Dr. Gehrig is professor and director of gynecologic oncology at the University of North Carolina at Chapel Hill. Dr. Castellano is a resident physician in the obstetrics and gynecology program at the university. They reported having no relevant financial disclosures. To comment, email them at [email protected].
Germ cell neoplasms arise from primordial germ cells of the gonad that differentiate to embryonic and extraembryonic tissues. Approximately 20%-25% of ovarian neoplasms are germ cell in origin but they account for only 3%-5% of ovarian malignancies. Importantly, germ cell neoplasms encompass 70% of the ovarian neoplasms among girls and young women aged 10-30 years, of which approximately one-third are malignant.
Unlike epithelial ovarian cancers, malignant germ cell neoplasms are typically diagnosed at early stages. They can present as a palpable mass or cause acute abdominal pain secondary to their rapid growth, penchant for necrosis, torsion, hemorrhage, infection, or rupture. Since malignant germ cell neoplasms can excrete hormonally-active tumor markers, such as human chorionic gonadotropin (HCG), many women present with menstrual irregularities.
Management of malignant germ cell neoplasms generally includes fertility-sparing surgery – with or without neoadjuvant combination bleomycin, etoposide, and cisplatin (BEP) – and is typically associated with a favorable prognosis (Cancer Treat Rev. 2008 Aug;34[5]:427-41).
Teratomas
Benign teratomas represent about a quarter of all ovarian neoplasms. Benign teratomas can be solid or cystic, and contain components representing all three cell layers: endoderm, mesoderm, and ectoderm. Due to the presence of differentiated adult tissues, benign teratomas have a characteristic radiographic appearance. They can appear as cystic echogenic masses with intense acoustic shadowing, homogenous nodules or bands, and rounded protuberances called “Rokitansky nodules.”
Treatment of benign teratomas in reproductive-age women includes ovarian cystectomy and careful inspection of the contralateral ovary as 10%-15% may be bilateral. In postmenopausal women, there is less than a 2% risk for malignant transformation of the associated cell lines, most commonly a squamous cell carcinoma. In these cases, spread beyond the ovarian capsule is associated with a poor prognosis and chemotherapy and/or radiation are indicated (Int J Gynecol Cancer. 2006 Jan-Feb;16[1]:140-4). Malignant monodermal teratomas are composed of single cell lines with malignant transformations of that tissue type; struma ovarii composed of thyroid tissue, for example, is exceedingly rare.
Dysgerminoma
Dysgerminomas are the most common malignant germ cell neoplasms, accounting for about one-third of cases. They typically present in girls and young women between 10 and 30 years of age, and rarely occur after 50 years of age. As a result, a quarter of cases are identified during pregnancy and another 5% are found in patients presenting with amenorrhea secondary to gonadal dysgenesis, such as is associated with Turner’s syndrome.
At diagnosis, lactate dehydrogenase (LDH) may be elevated and 10% may have an elevation of HCG. Ultrasound findings include a solid, mostly echoic, but heterogeneous mass with apparent lobulations. About two-thirds are stage I at the time of diagnosis, and 10%-15% are bilateral, making dysgerminomas the only malignant germ cell neoplasm with significant risk for bilaterality.
Treatment for early stage dysgerminoma is surgical; young women should have at least unilateral oophorectomy performed; if the contralateral ovary is spared there’s a 10% risk for recurrence over the next 2 years. Comprehensive fertility-sparing surgery is recommended with pelvic and para-aortic lymphadenectomy. Women with gonadal dysgenesis should have a bilateral salpingo-oophorectomy, and those beyond childbearing should undergo a total hysterectomy, with bilateral salpingo-oophorectomy and appropriate staging. BEP should be added for patients with advanced disease.
Other malignant germ cell neoplasms
Uncommon malignant germ cell neoplasms include immature teratomas and endodermal sinus tumors. Though uncommon, the majority of immature teratomas present between the ages of 10 and 20 years and account for nearly 30% of the ovarian cancer deaths in this age group. Immature teratomas usually have negative serum markers, though about one-third will excrete HCG. Immature teratomas are graded by the proportion of neuro-epithelium. Treatment includes unilateral oophorectomy, and surgical staging with adjuvant chemotherapy (BEP) for patients with greater than stage 1A grade 1 disease.
Endodermal sinus tumors are derived from the primitive yolk sac, are unilateral, and most will secrete alpha-fetoprotein (AFP). The median age of diagnosis of an endodermal sinus tumor is 18 years, thus treatment includes unilateral salpingo-oophorectomy and comprehensive fertility-sparing surgical staging followed by BEP.
Embryonal and nongestational choriocarcinomas are rare malignant germ cell neoplasms found in prepubertal girls to young women. Embryonal carcinomas can secrete estrogens, HCG and/or AFP, so patients may present with precocious puberty. Treatment is similar to that of endodermal sinus tumors. Nongestational choriocarcinomas, like the gestational forms, have a poor prognosis and are monitored and treated similarly.
Understanding presentation and treatments for malignant germ cell neoplasms is important in the evaluation of a young patient with a pelvic mass and should prompt the practicing gynecologist to test for AFP and HCG, with or without LDH and CA-125. If encountered inadvertently, every attempt should be made to preserve fertility in these young patients and expedient referral to a gynecologic oncologist, pediatric gynecologist, and/or a reproductive endocrinologist is warranted. Rarely, a second look laparotomy is indicated without obvious intraperitoneal spread and reproductive potential is preserved even in those requiring BEP. If managed appropriately, the overall prognosis remains good for these young women.
Dr. Gehrig is professor and director of gynecologic oncology at the University of North Carolina at Chapel Hill. Dr. Castellano is a resident physician in the obstetrics and gynecology program at the university. They reported having no relevant financial disclosures. To comment, email them at [email protected].
Establishing a Role for Polysomnography in Hospitalized Children
Clinical question: What is the role for inpatient polysomnograms for children with medical complexity?

Background: Sleep-disordered breathing is more common in certain pediatric populations. Children with neuromuscular disease, craniofacial or tracheobronchial malformations, or developmental delay have up to 10 times the rate of sleep-disordered breathing as compared to the general pediatric population, with a prevalence as high as 40%. It is recommended that patients with neuromuscular conditions get annual polysomnograms (PSGs). The medical complexity and requirement for nursing and respiratory care makes it challenging to obtain routine outpatient PSGs in this population. This study is the first of its kind to examine the characteristics of patients receiving inpatient PSGs and to determine the effects the findings of these studies had on the patients’ care.
Study design: Retrospective case series.
Setting: Single, large, academic medical center.
Synopsis: Eight-five PSGs were completed on 70 patients during the study period. These occurred primarily in the pediatric intensive care unit (50 patients) but also in the neonatal intensive care unit (five patients) and the general pediatric floor (15 patients). The mean age of patients was 6.5 years, and 60% were male.
The most common diagnoses in this group were airway obstruction due to craniofacial abnormalities or defects of the tracheobronchial tree (54%), chronic respiratory failure (34%), hypoxic ischemic encephalopathy (23%), and genetic syndromes (14%). All sleep studies were successfully completed using the center’s dedicated sleep technicians and PSG scoring staff. There were no complications associated with the PSGs.
The most common specific indications for obtaining the PSGs were chronic pulmonary failure with airway obstruction and ventilator requirement assessment. Eighty-nine percent of patients had some abnormality of their PSG. Obstructive sleep apnea, tachypnea and desaturation, and disorders of sleep architecture were the most commonly found abnormalities.
The most common interventions based upon the PSG results were adjustment of ventilator parameters (46%), ENT referral for upper airway assessment (31%), and initiation of positive pressure ventilation (CPAP or BiPAP, 25%). Follow-up PSGs after these interventions demonstrated statistically significant improvement in apnea-hypopnea index, arousal index, and lowest oxygen saturation.
Bottom line: Inpatient PSGs for children with medical complexity are safe and often have significant findings that alter care for the patient.
Citation: Tkachenko N, Singh K, Abreu N, et al. Establishing a role for polysomnography in hospitalized children. Pediatr Neurol. 2016;57:39-45.e1. doi:10.1016/j.pediatrneurol.2015.12.020.
Dr. Stubblefield is a pediatric hospitalist at Nemours/Alfred I. Dupont Hospital for Children in Wilmington, Del., and assistant professor of pediatrics at Thomas Jefferson Medical College in Philadelphia.
Clinical question: What is the role for inpatient polysomnograms for children with medical complexity?
Background: Sleep-disordered breathing is more common in certain pediatric populations. Children with neuromuscular disease, craniofacial or tracheobronchial malformations, or developmental delay have up to 10 times the rate of sleep-disordered breathing as compared to the general pediatric population, with a prevalence as high as 40%. It is recommended that patients with neuromuscular conditions get annual polysomnograms (PSGs). The medical complexity and requirement for nursing and respiratory care makes it challenging to obtain routine outpatient PSGs in this population. This study is the first of its kind to examine the characteristics of patients receiving inpatient PSGs and to determine the effects the findings of these studies had on the patients’ care.
Study design: Retrospective case series.
Setting: Single, large, academic medical center.
Synopsis: Eight-five PSGs were completed on 70 patients during the study period. These occurred primarily in the pediatric intensive care unit (50 patients) but also in the neonatal intensive care unit (five patients) and the general pediatric floor (15 patients). The mean age of patients was 6.5 years, and 60% were male.
The most common diagnoses in this group were airway obstruction due to craniofacial abnormalities or defects of the tracheobronchial tree (54%), chronic respiratory failure (34%), hypoxic ischemic encephalopathy (23%), and genetic syndromes (14%). All sleep studies were successfully completed using the center’s dedicated sleep technicians and PSG scoring staff. There were no complications associated with the PSGs.
The most common specific indications for obtaining the PSGs were chronic pulmonary failure with airway obstruction and ventilator requirement assessment. Eighty-nine percent of patients had some abnormality of their PSG. Obstructive sleep apnea, tachypnea and desaturation, and disorders of sleep architecture were the most commonly found abnormalities.
The most common interventions based upon the PSG results were adjustment of ventilator parameters (46%), ENT referral for upper airway assessment (31%), and initiation of positive pressure ventilation (CPAP or BiPAP, 25%). Follow-up PSGs after these interventions demonstrated statistically significant improvement in apnea-hypopnea index, arousal index, and lowest oxygen saturation.
Bottom line: Inpatient PSGs for children with medical complexity are safe and often have significant findings that alter care for the patient.
Citation: Tkachenko N, Singh K, Abreu N, et al. Establishing a role for polysomnography in hospitalized children. Pediatr Neurol. 2016;57:39-45.e1. doi:10.1016/j.pediatrneurol.2015.12.020.
Dr. Stubblefield is a pediatric hospitalist at Nemours/Alfred I. Dupont Hospital for Children in Wilmington, Del., and assistant professor of pediatrics at Thomas Jefferson Medical College in Philadelphia.
Clinical question: What is the role for inpatient polysomnograms for children with medical complexity?
Background: Sleep-disordered breathing is more common in certain pediatric populations. Children with neuromuscular disease, craniofacial or tracheobronchial malformations, or developmental delay have up to 10 times the rate of sleep-disordered breathing as compared to the general pediatric population, with a prevalence as high as 40%. It is recommended that patients with neuromuscular conditions get annual polysomnograms (PSGs). The medical complexity and requirement for nursing and respiratory care makes it challenging to obtain routine outpatient PSGs in this population. This study is the first of its kind to examine the characteristics of patients receiving inpatient PSGs and to determine the effects the findings of these studies had on the patients’ care.
Study design: Retrospective case series.
Setting: Single, large, academic medical center.
Synopsis: Eight-five PSGs were completed on 70 patients during the study period. These occurred primarily in the pediatric intensive care unit (50 patients) but also in the neonatal intensive care unit (five patients) and the general pediatric floor (15 patients). The mean age of patients was 6.5 years, and 60% were male.
The most common diagnoses in this group were airway obstruction due to craniofacial abnormalities or defects of the tracheobronchial tree (54%), chronic respiratory failure (34%), hypoxic ischemic encephalopathy (23%), and genetic syndromes (14%). All sleep studies were successfully completed using the center’s dedicated sleep technicians and PSG scoring staff. There were no complications associated with the PSGs.
The most common specific indications for obtaining the PSGs were chronic pulmonary failure with airway obstruction and ventilator requirement assessment. Eighty-nine percent of patients had some abnormality of their PSG. Obstructive sleep apnea, tachypnea and desaturation, and disorders of sleep architecture were the most commonly found abnormalities.
The most common interventions based upon the PSG results were adjustment of ventilator parameters (46%), ENT referral for upper airway assessment (31%), and initiation of positive pressure ventilation (CPAP or BiPAP, 25%). Follow-up PSGs after these interventions demonstrated statistically significant improvement in apnea-hypopnea index, arousal index, and lowest oxygen saturation.
Bottom line: Inpatient PSGs for children with medical complexity are safe and often have significant findings that alter care for the patient.
Citation: Tkachenko N, Singh K, Abreu N, et al. Establishing a role for polysomnography in hospitalized children. Pediatr Neurol. 2016;57:39-45.e1. doi:10.1016/j.pediatrneurol.2015.12.020.
Dr. Stubblefield is a pediatric hospitalist at Nemours/Alfred I. Dupont Hospital for Children in Wilmington, Del., and assistant professor of pediatrics at Thomas Jefferson Medical College in Philadelphia.
Study links radon and hematologic cancers in women

New research suggests there is a significant positive association between high levels of residential radon and the risk of hematologic malignancies in women.
The study is the first prospective, population-based study of residential radon exposure and hematologic malignancy risk.
Therefore, the researchers caution that it requires replication to better understand the association and whether it truly differs by sex.
Lauren Teras, PhD, of the American Cancer Society in Atlanta, Georgia, and her colleagues conducted this study and reported the results in Environmental Research.
Radon is a naturally occurring byproduct of the decay of radium and is a known human lung carcinogen. It is the second-leading cause of lung cancer in the US.
Modeling studies have shown that radon delivers a non-negligible dose of alpha radiation to the bone marrow and therefore could increase the risk of hematologic malignancies. However, studies investigating the link between radon and hematologic malignancies have produced inconsistent results.
For the current study, Dr Teras and her colleagues used data from the American Cancer Society Cancer Prevention Study-II Nutrition Cohort to examine the association between county-level residential radon exposure and the risk of hematologic cancer.
The analysis included 140,652 participants, including 3019 who had hematologic malignancies during 19 years of follow-up (1992 to 2011).
The researchers found that women living in counties with the highest mean radon concentration (> 148 Bq/m3) had a significantly higher risk of developing a hematologic malignancy than women living in counties with the lowest radon levels (< 74 Bq/m3).
The adjusted hazard ratio (adjusted for age, race, family history of hematologic malignancy, etc.) was 1.63 (P=0.0010).
The researchers also found evidence of a dose-response relationship, with an adjusted hazard ratio of 1.38 (P=0.001).
The team said there was evidence of a positive exposure-response relationship between radon concentration and the risk of all lymphoid malignancy subtypes in women. But the highest risk was observed for follicular lymphoma, with an adjusted hazard ratio of 2.74 (P=0.02).
On the other hand, there was a non-significant inverse association between radon and myeloid leukemias in women.
There was no association between hematologic malignancy and radon exposure among the men.
The researchers said a possible explanation for this finding is that men may have a higher baseline risk of hematologic malignancy, possibly because of more exposure to occupational or other risk factors, which would reduce the impact of any additional risk from residential radon.
In women, who have a smaller baseline risk, residential radon exposure might be a larger contributor to overall risk.
Another reason for the sex difference observed in this study may be that the women of this generation spent more time in their homes, so they had more residential exposure than men.
“The overall lifetime risk of hematological cancers in the United States is about 2%, so even a 60% relative increase would still mean a relatively small absolute risk,” Dr Teras noted.
“Nonetheless, radon is already associated with lung cancer, and if other studies confirm the link to blood cancers, we think it would warrant strengthened public health efforts to mitigate residential radon risks.” ![]()
New research suggests there is a significant positive association between high levels of residential radon and the risk of hematologic malignancies in women.
The study is the first prospective, population-based study of residential radon exposure and hematologic malignancy risk.
Therefore, the researchers caution that it requires replication to better understand the association and whether it truly differs by sex.
Lauren Teras, PhD, of the American Cancer Society in Atlanta, Georgia, and her colleagues conducted this study and reported the results in Environmental Research.
Radon is a naturally occurring byproduct of the decay of radium and is a known human lung carcinogen. It is the second-leading cause of lung cancer in the US.
Modeling studies have shown that radon delivers a non-negligible dose of alpha radiation to the bone marrow and therefore could increase the risk of hematologic malignancies. However, studies investigating the link between radon and hematologic malignancies have produced inconsistent results.
For the current study, Dr Teras and her colleagues used data from the American Cancer Society Cancer Prevention Study-II Nutrition Cohort to examine the association between county-level residential radon exposure and the risk of hematologic cancer.
The analysis included 140,652 participants, including 3019 who had hematologic malignancies during 19 years of follow-up (1992 to 2011).
The researchers found that women living in counties with the highest mean radon concentration (> 148 Bq/m3) had a significantly higher risk of developing a hematologic malignancy than women living in counties with the lowest radon levels (< 74 Bq/m3).
The adjusted hazard ratio (adjusted for age, race, family history of hematologic malignancy, etc.) was 1.63 (P=0.0010).
The researchers also found evidence of a dose-response relationship, with an adjusted hazard ratio of 1.38 (P=0.001).
The team said there was evidence of a positive exposure-response relationship between radon concentration and the risk of all lymphoid malignancy subtypes in women. But the highest risk was observed for follicular lymphoma, with an adjusted hazard ratio of 2.74 (P=0.02).
On the other hand, there was a non-significant inverse association between radon and myeloid leukemias in women.
There was no association between hematologic malignancy and radon exposure among the men.
The researchers said a possible explanation for this finding is that men may have a higher baseline risk of hematologic malignancy, possibly because of more exposure to occupational or other risk factors, which would reduce the impact of any additional risk from residential radon.
In women, who have a smaller baseline risk, residential radon exposure might be a larger contributor to overall risk.
Another reason for the sex difference observed in this study may be that the women of this generation spent more time in their homes, so they had more residential exposure than men.
“The overall lifetime risk of hematological cancers in the United States is about 2%, so even a 60% relative increase would still mean a relatively small absolute risk,” Dr Teras noted.
“Nonetheless, radon is already associated with lung cancer, and if other studies confirm the link to blood cancers, we think it would warrant strengthened public health efforts to mitigate residential radon risks.” ![]()
New research suggests there is a significant positive association between high levels of residential radon and the risk of hematologic malignancies in women.
The study is the first prospective, population-based study of residential radon exposure and hematologic malignancy risk.
Therefore, the researchers caution that it requires replication to better understand the association and whether it truly differs by sex.
Lauren Teras, PhD, of the American Cancer Society in Atlanta, Georgia, and her colleagues conducted this study and reported the results in Environmental Research.
Radon is a naturally occurring byproduct of the decay of radium and is a known human lung carcinogen. It is the second-leading cause of lung cancer in the US.
Modeling studies have shown that radon delivers a non-negligible dose of alpha radiation to the bone marrow and therefore could increase the risk of hematologic malignancies. However, studies investigating the link between radon and hematologic malignancies have produced inconsistent results.
For the current study, Dr Teras and her colleagues used data from the American Cancer Society Cancer Prevention Study-II Nutrition Cohort to examine the association between county-level residential radon exposure and the risk of hematologic cancer.
The analysis included 140,652 participants, including 3019 who had hematologic malignancies during 19 years of follow-up (1992 to 2011).
The researchers found that women living in counties with the highest mean radon concentration (> 148 Bq/m3) had a significantly higher risk of developing a hematologic malignancy than women living in counties with the lowest radon levels (< 74 Bq/m3).
The adjusted hazard ratio (adjusted for age, race, family history of hematologic malignancy, etc.) was 1.63 (P=0.0010).
The researchers also found evidence of a dose-response relationship, with an adjusted hazard ratio of 1.38 (P=0.001).
The team said there was evidence of a positive exposure-response relationship between radon concentration and the risk of all lymphoid malignancy subtypes in women. But the highest risk was observed for follicular lymphoma, with an adjusted hazard ratio of 2.74 (P=0.02).
On the other hand, there was a non-significant inverse association between radon and myeloid leukemias in women.
There was no association between hematologic malignancy and radon exposure among the men.
The researchers said a possible explanation for this finding is that men may have a higher baseline risk of hematologic malignancy, possibly because of more exposure to occupational or other risk factors, which would reduce the impact of any additional risk from residential radon.
In women, who have a smaller baseline risk, residential radon exposure might be a larger contributor to overall risk.
Another reason for the sex difference observed in this study may be that the women of this generation spent more time in their homes, so they had more residential exposure than men.
“The overall lifetime risk of hematological cancers in the United States is about 2%, so even a 60% relative increase would still mean a relatively small absolute risk,” Dr Teras noted.
“Nonetheless, radon is already associated with lung cancer, and if other studies confirm the link to blood cancers, we think it would warrant strengthened public health efforts to mitigate residential radon risks.” ![]()
CHMP recommends approving drug to treat FL

The European Medicine Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended that obinutuzumab (Gazyvaro), an anti-CD20 monoclonal antibody, be approved for use in patients with follicular lymphoma (FL).
The recommended indication is for obinutuzumab to be given first in combination with bendamustine and then as maintenance therapy in FL patients who did not respond to, progressed during, or progressed up to 6 months after treatment with rituximab or a rituximab-containing regimen.
Based on the CHMP’s recommendation, a final decision regarding the approval of obinutuzumab in FL is expected from the European Commission in the coming months.
Obinutuzumab is already approved in the European Union for use in combination with chlorambucil to treat patients with previously untreated chronic lymphocytic leukemia and comorbidities that make them unsuitable for full-dose fludarabine-based therapy.
Obinutuzumab is being developed by Roche.
GADOLIN trial
The CHMP’s recommendation to approve obinutuzumab in FL is based on results from the phase 3 GADOLIN trial. The study included 413 patients with rituximab-refractory non-Hodgkin lymphoma, including 321 patients with FL, 46 with marginal zone lymphoma, and 28 with small lymphocytic lymphoma.
The patients were randomized to receive bendamustine alone (control arm) or a combination of bendamustine and obinutuzumab followed by obinutuzumab maintenance (every 2 months for 2 years or until progression).
The primary endpoint of the study was progression-free survival (PFS), as assessed by an independent review committee (IRC). The secondary endpoints were PFS assessed by investigator review, best overall response, complete response (CR), partial response (PR), duration of response, overall survival, and safety profile.
Among patients with FL, the obinutuzumab regimen improved PFS compared to bendamustine alone, as assessed by IRC (hazard ratio [HR]=0.48, P<0.0001). The median PFS was not reached in patients receiving the obinutuzumab regimen but was 13.8 months in those receiving bendamustine alone.
Investigator-assessed PFS was consistent with IRC-assessed PFS. Investigators said the median PFS with the obinutuzumab regimen was more than double that with bendamustine alone—29.2 months vs 13.7 months (HR=0.48, P<0.0001).
The best overall response for patients receiving the obinutuzumab regimen was 78.7% (15.5% CR, 63.2% PR), compared to 74.7% for those receiving bendamustine alone (18.7% CR, 56% PR), as assessed by the IRC.
The median duration of response was not reached for patients receiving the obinutuzumab regimen and was 11.6 months for those receiving bendamustine alone.
The median overall survival has not yet been reached in either study arm.
The most common grade 3/4 adverse events observed in patients receiving the obinutuzumab regimen were neutropenia (33%), infusion reactions (11%), and thrombocytopenia (10%).
The most common adverse events of any grade were infusion reactions (69%), neutropenia (35%), nausea (54%), fatigue (39%), cough (26%), diarrhea (27%), constipation (19%), fever (18%), thrombocytopenia (15%), vomiting (22%), upper respiratory tract infection (13%), decreased appetite (18%), joint or muscle pain (12%), sinusitis (12%), anemia (12%), general weakness (11%), and urinary tract infection (10%). ![]()
The European Medicine Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended that obinutuzumab (Gazyvaro), an anti-CD20 monoclonal antibody, be approved for use in patients with follicular lymphoma (FL).
The recommended indication is for obinutuzumab to be given first in combination with bendamustine and then as maintenance therapy in FL patients who did not respond to, progressed during, or progressed up to 6 months after treatment with rituximab or a rituximab-containing regimen.
Based on the CHMP’s recommendation, a final decision regarding the approval of obinutuzumab in FL is expected from the European Commission in the coming months.
Obinutuzumab is already approved in the European Union for use in combination with chlorambucil to treat patients with previously untreated chronic lymphocytic leukemia and comorbidities that make them unsuitable for full-dose fludarabine-based therapy.
Obinutuzumab is being developed by Roche.
GADOLIN trial
The CHMP’s recommendation to approve obinutuzumab in FL is based on results from the phase 3 GADOLIN trial. The study included 413 patients with rituximab-refractory non-Hodgkin lymphoma, including 321 patients with FL, 46 with marginal zone lymphoma, and 28 with small lymphocytic lymphoma.
The patients were randomized to receive bendamustine alone (control arm) or a combination of bendamustine and obinutuzumab followed by obinutuzumab maintenance (every 2 months for 2 years or until progression).
The primary endpoint of the study was progression-free survival (PFS), as assessed by an independent review committee (IRC). The secondary endpoints were PFS assessed by investigator review, best overall response, complete response (CR), partial response (PR), duration of response, overall survival, and safety profile.
Among patients with FL, the obinutuzumab regimen improved PFS compared to bendamustine alone, as assessed by IRC (hazard ratio [HR]=0.48, P<0.0001). The median PFS was not reached in patients receiving the obinutuzumab regimen but was 13.8 months in those receiving bendamustine alone.
Investigator-assessed PFS was consistent with IRC-assessed PFS. Investigators said the median PFS with the obinutuzumab regimen was more than double that with bendamustine alone—29.2 months vs 13.7 months (HR=0.48, P<0.0001).
The best overall response for patients receiving the obinutuzumab regimen was 78.7% (15.5% CR, 63.2% PR), compared to 74.7% for those receiving bendamustine alone (18.7% CR, 56% PR), as assessed by the IRC.
The median duration of response was not reached for patients receiving the obinutuzumab regimen and was 11.6 months for those receiving bendamustine alone.
The median overall survival has not yet been reached in either study arm.
The most common grade 3/4 adverse events observed in patients receiving the obinutuzumab regimen were neutropenia (33%), infusion reactions (11%), and thrombocytopenia (10%).
The most common adverse events of any grade were infusion reactions (69%), neutropenia (35%), nausea (54%), fatigue (39%), cough (26%), diarrhea (27%), constipation (19%), fever (18%), thrombocytopenia (15%), vomiting (22%), upper respiratory tract infection (13%), decreased appetite (18%), joint or muscle pain (12%), sinusitis (12%), anemia (12%), general weakness (11%), and urinary tract infection (10%). ![]()
The European Medicine Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended that obinutuzumab (Gazyvaro), an anti-CD20 monoclonal antibody, be approved for use in patients with follicular lymphoma (FL).
The recommended indication is for obinutuzumab to be given first in combination with bendamustine and then as maintenance therapy in FL patients who did not respond to, progressed during, or progressed up to 6 months after treatment with rituximab or a rituximab-containing regimen.
Based on the CHMP’s recommendation, a final decision regarding the approval of obinutuzumab in FL is expected from the European Commission in the coming months.
Obinutuzumab is already approved in the European Union for use in combination with chlorambucil to treat patients with previously untreated chronic lymphocytic leukemia and comorbidities that make them unsuitable for full-dose fludarabine-based therapy.
Obinutuzumab is being developed by Roche.
GADOLIN trial
The CHMP’s recommendation to approve obinutuzumab in FL is based on results from the phase 3 GADOLIN trial. The study included 413 patients with rituximab-refractory non-Hodgkin lymphoma, including 321 patients with FL, 46 with marginal zone lymphoma, and 28 with small lymphocytic lymphoma.
The patients were randomized to receive bendamustine alone (control arm) or a combination of bendamustine and obinutuzumab followed by obinutuzumab maintenance (every 2 months for 2 years or until progression).
The primary endpoint of the study was progression-free survival (PFS), as assessed by an independent review committee (IRC). The secondary endpoints were PFS assessed by investigator review, best overall response, complete response (CR), partial response (PR), duration of response, overall survival, and safety profile.
Among patients with FL, the obinutuzumab regimen improved PFS compared to bendamustine alone, as assessed by IRC (hazard ratio [HR]=0.48, P<0.0001). The median PFS was not reached in patients receiving the obinutuzumab regimen but was 13.8 months in those receiving bendamustine alone.
Investigator-assessed PFS was consistent with IRC-assessed PFS. Investigators said the median PFS with the obinutuzumab regimen was more than double that with bendamustine alone—29.2 months vs 13.7 months (HR=0.48, P<0.0001).
The best overall response for patients receiving the obinutuzumab regimen was 78.7% (15.5% CR, 63.2% PR), compared to 74.7% for those receiving bendamustine alone (18.7% CR, 56% PR), as assessed by the IRC.
The median duration of response was not reached for patients receiving the obinutuzumab regimen and was 11.6 months for those receiving bendamustine alone.
The median overall survival has not yet been reached in either study arm.
The most common grade 3/4 adverse events observed in patients receiving the obinutuzumab regimen were neutropenia (33%), infusion reactions (11%), and thrombocytopenia (10%).
The most common adverse events of any grade were infusion reactions (69%), neutropenia (35%), nausea (54%), fatigue (39%), cough (26%), diarrhea (27%), constipation (19%), fever (18%), thrombocytopenia (15%), vomiting (22%), upper respiratory tract infection (13%), decreased appetite (18%), joint or muscle pain (12%), sinusitis (12%), anemia (12%), general weakness (11%), and urinary tract infection (10%). ![]()
FIRST reflections: Impact of ACGME duty hours on CT practitioners
Several months ago, Dr. Bilimoria and his colleagues published the long awaited study in NEJM essentially contradicting adverse effects of strict duty hours on patient outcomes (N Engl J Med. 2016 374:713-2). The study, known as the FIRST trial, was published in the March issue of Thoracic Surgery News. Although the study enrolled general surgery residents, its conclusion impacts no specialty more than cardiothoracic surgery, where frequent handoffs complicate tedious perioperative care of sick patients stall learning opportunities for young trainees.

As Dr. Shari Meyerson eloquently noted in her perspective piece for Thoracic Surgery News (March 2016, page 4), surgery training needs to adapt to meet the modern day needs of trainees to rest and spend time with family and friends, with those of exposure to complex clinical scenarios in a short residency period. Arguably, CT surgery trainees are some of the most motivated and driven; to limit their experience on a national level may be shortsighted. On the other hand, appropriate incorporation of advanced practice providers (APPs) may help allay some patient care challenges, free valuable family time, and allow thoracic residents to function well in a more flexible ACGME duty-hour paradigm. To add thoracic relevance to the findings of Dr. Bilimoria and his colleagues, the debate is brought to Thoracic Surgery News by our colleagues from different training pathways below:
Dr. Antonoff: “Due to the timing of my medical school matriculation, I completed my surgical clerkships in the preregulated duty-hour era. I had expectations of what my life would be like as a surgeon when I applied for the general surgery match, and frankly, my expectations prepared me for a life that would revolve around my education, my technical training, and my commitment to patient care. During my years as a junior resident, my surgical training program gradually adapted in recognition of the new guidelines, but it took time. I spent 3 years in the research lab, and, after I came out as a senior resident, I discovered that the rules of the game had totally changed. While duty hours for me, as a senior trainee, were still fairly open, I found that my interns and junior residents had to play by completely new rules. In some ways, on rare occasions, I felt frustrated and resentful of the fact that my duties as a chief resident and thoracic fellow included many of the tasks that I’d done as an intern, because my interns would ‘expire’ after 16 hours. However, much more often, I felt bad for those who came after me.

They seemed desperate to operate, eager to see their patients’ problems through to resolution, and embarrassed to have to end their days earlier than the more senior members of the team. I feel fortunate that I had years of frequent in-house call after long days in the operating room and followed by post-call days of more operating. I finished my junior years without fear of any sick patient in the hospital, I finished my general surgery training without fear of any emergent operation, and I finished my fellowship with confidence that I could get a patient through just about anything if I had access to a cannula.
My early experiences as an attending have certainly kept me humble, and I’ve spent many a night worried about my patients, rethinking choices that I’ve made and stitches that I’ve thrown. But I thank my lucky stars that I was exposed to phenomenal training, and that I had the privilege and opportunity to work the hours needed to reach a reasonable level of safety! I can only imagine that if I’d have spent fewer nights in the hospital, that I’d feel even more anxiety and nausea at this early stage of my surgical career.
As elaborated in the editorial by Dr. Birkmeyer (N Engl J Med. 2016;374:783-4), it is not surprising that patient outcomes did not immediately depend on whether the programs had adhered strictly to the ACGME duty-hour rules. Limited numbers of patients experience critical events during shift change, and hospitals are evolving to function with greater reliance on midlevel practitioners and attending physicians. I would not expect the short-term results of duty-hour flexibility to demonstrate any impact on patient care. However, I do fear that there will be a mid-term impact on trainee accountability and autonomy, which will ultimately impact the competence of the attending surgeons of the future, and downstream potential long-term impact on day-to-day patient outcomes.
As a wife and mother of 3, I recognize that we, as a specialty, need to find ways to support our trainees and their families and to help them live happy lives conducive to functioning outside the hospital. I believe that we can do this with support, mentorship, and advocacy; I do not believe that it requires cutting back on the training that we are all, in the end, so incredibly grateful to receive.”
Dr. Mara Antonoff is an assistant professor of thoracic and cardiovascular surgery at UT MD Anderson Cancer Center. She performed her General Surgery training at the University of Minnesota, 2004-2012, and her Thoracic Surgery Training at Washington University, as a traditional 2-year resident, 2012-2014.
Dr. Stephens: “There is nothing that replaces being bedside. Whether it be a postoperative patient struggling with low cardiac output syndrome overnight, or a patient with a high pressor requirement the etiology of which you are trying to uncover, or a patient you have been following who suddenly arrests, the value of seeing a patient’s trajectory longitudinally is critical to developing clinical acumen. When as an attending I will get called in the middle of the night about a postoperative patient not “doing well,” I will be drawing on my years of being on call and being bedside with my patients.

Patient care is the ultimate goal, and it is clear that overworked residents are at higher risk for making mistakes that jeopardize patient care, which nobody wants. However, the restrictions that duty hours place don’t allow the flexibility necessary for a specialty such as ours, and in fact strict adherence to such regulations inhibits opportunities for our learning. Also concerning is the “shift-work” mentality that seems to be increasingly pervasive with the implementation of duty hours. As has been well documented, and as I have seen personally, the constant patient handoffs that are requisite to implementation of duty hours pose their own perils in terms of patient safety.
Ultimately, these are our patients and we are responsible. Once we are attendings, those responsibilities will not be turned off after we have reached some prespecified hour limit.
The question then remains how best to implement a system across a wide variety of programs that ensures both patient safety and adequate clinical experience in the context of a culture of patient responsibility for the residents. As the NEJM study (N Engl J Med. 2016 374:713-2) shows, flexibility in implementation of duty hours did not result in increased complications, but resulted in improved resident satisfaction in continuity of care and handoffs. In my opinion, this study then encourages specialties such as ours to be more flexible in work hours, to encourage residents when there is a learning opportunity that previously they would be prohibited from taking part in to take hold of that opportunity, and to use this flexibility in implementation of duty hours to combat the invading “shift-work” mentality that will only jeopardize patient care.”
Dr. Elizabeth H. Stephens, MD, PhD is a Cardiothoracic Surgery, resident, PGY4, at Columbia University, New York, as an Integrated I-6 Resident.

Dr. Brown: “I took the traditional 5-year of General Surgery + 2 years of Cardiothoracic Surgery training route to becoming a General Thoracic Surgeon. My General Surgery experience was invaluable to my development as a surgeon. However, after all of those years of General Surgery cases and minimal exposure to Cardiothoracic Surgery cases, coupled with minimal overlap between the two specialties with regard to patient care, I found the learning curve in fellowship to be very steep. I was fortunate to train in a program with phenomenal physician extender support [APPs] in addition to top-notch colleagues in other specialties and excellent nursing, which allowed me to spend the majority of those 2 years in the operating room and completely focused on patient care. During that final phase of training, I welcomed flexibility with regard to the work-hour restrictions to ensure that I was acquiring the experience I needed prior to starting my own practice.”
Lisa M. Brown, MD, MAS, Assistant Professor of Thoracic Surgery, UC Davis Health System, Calif.; Training Institution: Washington University
Dr. Lee: “I started my surgical training in 2005, 2 years after the implementation of the 80-hour workweek restriction. Fortunately for my personal life, my training program took the restriction very seriously and strictly enforced it. As a result, I had scheduled periods off from work, and rarely worked more than 80 hours per week over the course of general surgery. On those occasions that I did, the next weeks, or preceding weeks would be shorter, to compensate. As a product of a 4+3 Thoracic Surgery residency in this environment, the 80-hour workweek extended to my subspecialty training. Our cardiac surgery time strictly enforced the go-home post-call policy. As a result, I believe my duty hours during Thoracic Surgery are likely shorter overall than many other programs.

Everyone hears the rumors of other programs lying about their duty hours. Fortunately, mine was not one of these. Despite this, or because of this, I received top-notch training. At the same time and more importantly, I started a family. I married my wife a week before my internship started, and am still married to the same person. We had two precious daughters during my Thoracic Surgery years. I don’t believe this would have been possible without duty-hours restrictions.
To create an environment where such a task was possible, my program hired an army of mid-level practitioners to deal with the day-to-day tasks of providing cardiothoracic surgical care to the patients, both in the intensive care unit and on the ward.
I rarely had to write a history and physical during Thoracic Surgery training. I consented fewer patients than I have fingers on my hands. I pulled even fewer chest tubes. I can now no longer remember having pulled a central line. I learned these tasks when I was a junior resident. What I did instead as a senior resident was perform over 900 cardiothoracic procedures as the primary surgeon. Now, as an attending surgeon, I still don’t write full histories and physicals by myself. I certainly don’t pull chest tubes and central lines. I consent patients by having a conversation with them, which I did as a resident, but I don’t bring a piece of paper with me in to the clinic room. I have a physician assistant who helps me fill in the gaps.

In 8 months of practice, I have performed over 15 thoracic organ transplants, repaired over 15 aortic dissections, half of whom required root replacements, performed more double-valve surgeries than straightforward single-valve replacements, started a minimally invasive atrial fibrillation surgical program, and applied almost every shred of knowledge and experience gained in 3 years of Thoracic Surgery Residency to a busy clinical practice. Most importantly, I continue to come home and watch my two daughters grow up.
With that perspective, I don’t believe the question should be whether or not programs should have the flexibility to enforce or not enforce duty-hours restrictions. It should be, how could every program find a way to effectively train residents to be good physicians and still allow them a personal life?”
Dr. Anson Lee is an Assistant Professor of Cardiac Surgery, Stanford University, Calif.; Training: 4+3 CT Residency, at Washington University, St. Louis.
Ms. Bohlman: “As a physician assistant in cardiac surgery, I represent the reality that physicians with a critical patient population appreciate consistency in their patient management. However, working in a university hospital setting also requires that surgical residents receive appropriate training. With the recently implemented duty restriction hours on resident training programs, advanced practice providers (APPs) have been utilized as an excellent solution for scheduling conflicts without compromising patient care. An example to this point is evident in my own place of work.

Approximately 1 year ago, our surgical intensive care unit transitioned from resident care to a combination of residents and APPs. At that time, the APPs were tasked with the complete care of all cardiac surgery patients. This change reduced the quantity and acuity of patients for which the residents were responsible and therefore allowed for more flexible hours along with a more manageable patient load. These changes, among others, have contributed to improved patient outcomes in the cardiac surgery patient population within our institution. With the increase in APPs that have training in various specialties, there comes an increasing ability to not only fill the gaps in scheduling but to do so with an extension of the providing physician. Although the NEJM article demonstrated no difference in patient outcomes between resident programs with restricted duty hours versus more flexible duty-hour policies, I foresee the future of medicine focusing on trained APPs as a complement to the care that the residents provide.”
Allison Bohlman is a Physician Assistant at Rush University Medical Center in the Integrated cardiovascular thoracic intensive care unit.
Several months ago, Dr. Bilimoria and his colleagues published the long awaited study in NEJM essentially contradicting adverse effects of strict duty hours on patient outcomes (N Engl J Med. 2016 374:713-2). The study, known as the FIRST trial, was published in the March issue of Thoracic Surgery News. Although the study enrolled general surgery residents, its conclusion impacts no specialty more than cardiothoracic surgery, where frequent handoffs complicate tedious perioperative care of sick patients stall learning opportunities for young trainees.
As Dr. Shari Meyerson eloquently noted in her perspective piece for Thoracic Surgery News (March 2016, page 4), surgery training needs to adapt to meet the modern day needs of trainees to rest and spend time with family and friends, with those of exposure to complex clinical scenarios in a short residency period. Arguably, CT surgery trainees are some of the most motivated and driven; to limit their experience on a national level may be shortsighted. On the other hand, appropriate incorporation of advanced practice providers (APPs) may help allay some patient care challenges, free valuable family time, and allow thoracic residents to function well in a more flexible ACGME duty-hour paradigm. To add thoracic relevance to the findings of Dr. Bilimoria and his colleagues, the debate is brought to Thoracic Surgery News by our colleagues from different training pathways below:
Dr. Antonoff: “Due to the timing of my medical school matriculation, I completed my surgical clerkships in the preregulated duty-hour era. I had expectations of what my life would be like as a surgeon when I applied for the general surgery match, and frankly, my expectations prepared me for a life that would revolve around my education, my technical training, and my commitment to patient care. During my years as a junior resident, my surgical training program gradually adapted in recognition of the new guidelines, but it took time. I spent 3 years in the research lab, and, after I came out as a senior resident, I discovered that the rules of the game had totally changed. While duty hours for me, as a senior trainee, were still fairly open, I found that my interns and junior residents had to play by completely new rules. In some ways, on rare occasions, I felt frustrated and resentful of the fact that my duties as a chief resident and thoracic fellow included many of the tasks that I’d done as an intern, because my interns would ‘expire’ after 16 hours. However, much more often, I felt bad for those who came after me.
They seemed desperate to operate, eager to see their patients’ problems through to resolution, and embarrassed to have to end their days earlier than the more senior members of the team. I feel fortunate that I had years of frequent in-house call after long days in the operating room and followed by post-call days of more operating. I finished my junior years without fear of any sick patient in the hospital, I finished my general surgery training without fear of any emergent operation, and I finished my fellowship with confidence that I could get a patient through just about anything if I had access to a cannula.
My early experiences as an attending have certainly kept me humble, and I’ve spent many a night worried about my patients, rethinking choices that I’ve made and stitches that I’ve thrown. But I thank my lucky stars that I was exposed to phenomenal training, and that I had the privilege and opportunity to work the hours needed to reach a reasonable level of safety! I can only imagine that if I’d have spent fewer nights in the hospital, that I’d feel even more anxiety and nausea at this early stage of my surgical career.
As elaborated in the editorial by Dr. Birkmeyer (N Engl J Med. 2016;374:783-4), it is not surprising that patient outcomes did not immediately depend on whether the programs had adhered strictly to the ACGME duty-hour rules. Limited numbers of patients experience critical events during shift change, and hospitals are evolving to function with greater reliance on midlevel practitioners and attending physicians. I would not expect the short-term results of duty-hour flexibility to demonstrate any impact on patient care. However, I do fear that there will be a mid-term impact on trainee accountability and autonomy, which will ultimately impact the competence of the attending surgeons of the future, and downstream potential long-term impact on day-to-day patient outcomes.
As a wife and mother of 3, I recognize that we, as a specialty, need to find ways to support our trainees and their families and to help them live happy lives conducive to functioning outside the hospital. I believe that we can do this with support, mentorship, and advocacy; I do not believe that it requires cutting back on the training that we are all, in the end, so incredibly grateful to receive.”
Dr. Mara Antonoff is an assistant professor of thoracic and cardiovascular surgery at UT MD Anderson Cancer Center. She performed her General Surgery training at the University of Minnesota, 2004-2012, and her Thoracic Surgery Training at Washington University, as a traditional 2-year resident, 2012-2014.
Dr. Stephens: “There is nothing that replaces being bedside. Whether it be a postoperative patient struggling with low cardiac output syndrome overnight, or a patient with a high pressor requirement the etiology of which you are trying to uncover, or a patient you have been following who suddenly arrests, the value of seeing a patient’s trajectory longitudinally is critical to developing clinical acumen. When as an attending I will get called in the middle of the night about a postoperative patient not “doing well,” I will be drawing on my years of being on call and being bedside with my patients.
Patient care is the ultimate goal, and it is clear that overworked residents are at higher risk for making mistakes that jeopardize patient care, which nobody wants. However, the restrictions that duty hours place don’t allow the flexibility necessary for a specialty such as ours, and in fact strict adherence to such regulations inhibits opportunities for our learning. Also concerning is the “shift-work” mentality that seems to be increasingly pervasive with the implementation of duty hours. As has been well documented, and as I have seen personally, the constant patient handoffs that are requisite to implementation of duty hours pose their own perils in terms of patient safety.
Ultimately, these are our patients and we are responsible. Once we are attendings, those responsibilities will not be turned off after we have reached some prespecified hour limit.
The question then remains how best to implement a system across a wide variety of programs that ensures both patient safety and adequate clinical experience in the context of a culture of patient responsibility for the residents. As the NEJM study (N Engl J Med. 2016 374:713-2) shows, flexibility in implementation of duty hours did not result in increased complications, but resulted in improved resident satisfaction in continuity of care and handoffs. In my opinion, this study then encourages specialties such as ours to be more flexible in work hours, to encourage residents when there is a learning opportunity that previously they would be prohibited from taking part in to take hold of that opportunity, and to use this flexibility in implementation of duty hours to combat the invading “shift-work” mentality that will only jeopardize patient care.”
Dr. Elizabeth H. Stephens, MD, PhD is a Cardiothoracic Surgery, resident, PGY4, at Columbia University, New York, as an Integrated I-6 Resident.
Dr. Brown: “I took the traditional 5-year of General Surgery + 2 years of Cardiothoracic Surgery training route to becoming a General Thoracic Surgeon. My General Surgery experience was invaluable to my development as a surgeon. However, after all of those years of General Surgery cases and minimal exposure to Cardiothoracic Surgery cases, coupled with minimal overlap between the two specialties with regard to patient care, I found the learning curve in fellowship to be very steep. I was fortunate to train in a program with phenomenal physician extender support [APPs] in addition to top-notch colleagues in other specialties and excellent nursing, which allowed me to spend the majority of those 2 years in the operating room and completely focused on patient care. During that final phase of training, I welcomed flexibility with regard to the work-hour restrictions to ensure that I was acquiring the experience I needed prior to starting my own practice.”
Lisa M. Brown, MD, MAS, Assistant Professor of Thoracic Surgery, UC Davis Health System, Calif.; Training Institution: Washington University
Dr. Lee: “I started my surgical training in 2005, 2 years after the implementation of the 80-hour workweek restriction. Fortunately for my personal life, my training program took the restriction very seriously and strictly enforced it. As a result, I had scheduled periods off from work, and rarely worked more than 80 hours per week over the course of general surgery. On those occasions that I did, the next weeks, or preceding weeks would be shorter, to compensate. As a product of a 4+3 Thoracic Surgery residency in this environment, the 80-hour workweek extended to my subspecialty training. Our cardiac surgery time strictly enforced the go-home post-call policy. As a result, I believe my duty hours during Thoracic Surgery are likely shorter overall than many other programs.
Everyone hears the rumors of other programs lying about their duty hours. Fortunately, mine was not one of these. Despite this, or because of this, I received top-notch training. At the same time and more importantly, I started a family. I married my wife a week before my internship started, and am still married to the same person. We had two precious daughters during my Thoracic Surgery years. I don’t believe this would have been possible without duty-hours restrictions.
To create an environment where such a task was possible, my program hired an army of mid-level practitioners to deal with the day-to-day tasks of providing cardiothoracic surgical care to the patients, both in the intensive care unit and on the ward.
I rarely had to write a history and physical during Thoracic Surgery training. I consented fewer patients than I have fingers on my hands. I pulled even fewer chest tubes. I can now no longer remember having pulled a central line. I learned these tasks when I was a junior resident. What I did instead as a senior resident was perform over 900 cardiothoracic procedures as the primary surgeon. Now, as an attending surgeon, I still don’t write full histories and physicals by myself. I certainly don’t pull chest tubes and central lines. I consent patients by having a conversation with them, which I did as a resident, but I don’t bring a piece of paper with me in to the clinic room. I have a physician assistant who helps me fill in the gaps.
In 8 months of practice, I have performed over 15 thoracic organ transplants, repaired over 15 aortic dissections, half of whom required root replacements, performed more double-valve surgeries than straightforward single-valve replacements, started a minimally invasive atrial fibrillation surgical program, and applied almost every shred of knowledge and experience gained in 3 years of Thoracic Surgery Residency to a busy clinical practice. Most importantly, I continue to come home and watch my two daughters grow up.
With that perspective, I don’t believe the question should be whether or not programs should have the flexibility to enforce or not enforce duty-hours restrictions. It should be, how could every program find a way to effectively train residents to be good physicians and still allow them a personal life?”
Dr. Anson Lee is an Assistant Professor of Cardiac Surgery, Stanford University, Calif.; Training: 4+3 CT Residency, at Washington University, St. Louis.
Ms. Bohlman: “As a physician assistant in cardiac surgery, I represent the reality that physicians with a critical patient population appreciate consistency in their patient management. However, working in a university hospital setting also requires that surgical residents receive appropriate training. With the recently implemented duty restriction hours on resident training programs, advanced practice providers (APPs) have been utilized as an excellent solution for scheduling conflicts without compromising patient care. An example to this point is evident in my own place of work.
Approximately 1 year ago, our surgical intensive care unit transitioned from resident care to a combination of residents and APPs. At that time, the APPs were tasked with the complete care of all cardiac surgery patients. This change reduced the quantity and acuity of patients for which the residents were responsible and therefore allowed for more flexible hours along with a more manageable patient load. These changes, among others, have contributed to improved patient outcomes in the cardiac surgery patient population within our institution. With the increase in APPs that have training in various specialties, there comes an increasing ability to not only fill the gaps in scheduling but to do so with an extension of the providing physician. Although the NEJM article demonstrated no difference in patient outcomes between resident programs with restricted duty hours versus more flexible duty-hour policies, I foresee the future of medicine focusing on trained APPs as a complement to the care that the residents provide.”
Allison Bohlman is a Physician Assistant at Rush University Medical Center in the Integrated cardiovascular thoracic intensive care unit.
Several months ago, Dr. Bilimoria and his colleagues published the long awaited study in NEJM essentially contradicting adverse effects of strict duty hours on patient outcomes (N Engl J Med. 2016 374:713-2). The study, known as the FIRST trial, was published in the March issue of Thoracic Surgery News. Although the study enrolled general surgery residents, its conclusion impacts no specialty more than cardiothoracic surgery, where frequent handoffs complicate tedious perioperative care of sick patients stall learning opportunities for young trainees.
As Dr. Shari Meyerson eloquently noted in her perspective piece for Thoracic Surgery News (March 2016, page 4), surgery training needs to adapt to meet the modern day needs of trainees to rest and spend time with family and friends, with those of exposure to complex clinical scenarios in a short residency period. Arguably, CT surgery trainees are some of the most motivated and driven; to limit their experience on a national level may be shortsighted. On the other hand, appropriate incorporation of advanced practice providers (APPs) may help allay some patient care challenges, free valuable family time, and allow thoracic residents to function well in a more flexible ACGME duty-hour paradigm. To add thoracic relevance to the findings of Dr. Bilimoria and his colleagues, the debate is brought to Thoracic Surgery News by our colleagues from different training pathways below:
Dr. Antonoff: “Due to the timing of my medical school matriculation, I completed my surgical clerkships in the preregulated duty-hour era. I had expectations of what my life would be like as a surgeon when I applied for the general surgery match, and frankly, my expectations prepared me for a life that would revolve around my education, my technical training, and my commitment to patient care. During my years as a junior resident, my surgical training program gradually adapted in recognition of the new guidelines, but it took time. I spent 3 years in the research lab, and, after I came out as a senior resident, I discovered that the rules of the game had totally changed. While duty hours for me, as a senior trainee, were still fairly open, I found that my interns and junior residents had to play by completely new rules. In some ways, on rare occasions, I felt frustrated and resentful of the fact that my duties as a chief resident and thoracic fellow included many of the tasks that I’d done as an intern, because my interns would ‘expire’ after 16 hours. However, much more often, I felt bad for those who came after me.
They seemed desperate to operate, eager to see their patients’ problems through to resolution, and embarrassed to have to end their days earlier than the more senior members of the team. I feel fortunate that I had years of frequent in-house call after long days in the operating room and followed by post-call days of more operating. I finished my junior years without fear of any sick patient in the hospital, I finished my general surgery training without fear of any emergent operation, and I finished my fellowship with confidence that I could get a patient through just about anything if I had access to a cannula.
My early experiences as an attending have certainly kept me humble, and I’ve spent many a night worried about my patients, rethinking choices that I’ve made and stitches that I’ve thrown. But I thank my lucky stars that I was exposed to phenomenal training, and that I had the privilege and opportunity to work the hours needed to reach a reasonable level of safety! I can only imagine that if I’d have spent fewer nights in the hospital, that I’d feel even more anxiety and nausea at this early stage of my surgical career.
As elaborated in the editorial by Dr. Birkmeyer (N Engl J Med. 2016;374:783-4), it is not surprising that patient outcomes did not immediately depend on whether the programs had adhered strictly to the ACGME duty-hour rules. Limited numbers of patients experience critical events during shift change, and hospitals are evolving to function with greater reliance on midlevel practitioners and attending physicians. I would not expect the short-term results of duty-hour flexibility to demonstrate any impact on patient care. However, I do fear that there will be a mid-term impact on trainee accountability and autonomy, which will ultimately impact the competence of the attending surgeons of the future, and downstream potential long-term impact on day-to-day patient outcomes.
As a wife and mother of 3, I recognize that we, as a specialty, need to find ways to support our trainees and their families and to help them live happy lives conducive to functioning outside the hospital. I believe that we can do this with support, mentorship, and advocacy; I do not believe that it requires cutting back on the training that we are all, in the end, so incredibly grateful to receive.”
Dr. Mara Antonoff is an assistant professor of thoracic and cardiovascular surgery at UT MD Anderson Cancer Center. She performed her General Surgery training at the University of Minnesota, 2004-2012, and her Thoracic Surgery Training at Washington University, as a traditional 2-year resident, 2012-2014.
Dr. Stephens: “There is nothing that replaces being bedside. Whether it be a postoperative patient struggling with low cardiac output syndrome overnight, or a patient with a high pressor requirement the etiology of which you are trying to uncover, or a patient you have been following who suddenly arrests, the value of seeing a patient’s trajectory longitudinally is critical to developing clinical acumen. When as an attending I will get called in the middle of the night about a postoperative patient not “doing well,” I will be drawing on my years of being on call and being bedside with my patients.
Patient care is the ultimate goal, and it is clear that overworked residents are at higher risk for making mistakes that jeopardize patient care, which nobody wants. However, the restrictions that duty hours place don’t allow the flexibility necessary for a specialty such as ours, and in fact strict adherence to such regulations inhibits opportunities for our learning. Also concerning is the “shift-work” mentality that seems to be increasingly pervasive with the implementation of duty hours. As has been well documented, and as I have seen personally, the constant patient handoffs that are requisite to implementation of duty hours pose their own perils in terms of patient safety.
Ultimately, these are our patients and we are responsible. Once we are attendings, those responsibilities will not be turned off after we have reached some prespecified hour limit.
The question then remains how best to implement a system across a wide variety of programs that ensures both patient safety and adequate clinical experience in the context of a culture of patient responsibility for the residents. As the NEJM study (N Engl J Med. 2016 374:713-2) shows, flexibility in implementation of duty hours did not result in increased complications, but resulted in improved resident satisfaction in continuity of care and handoffs. In my opinion, this study then encourages specialties such as ours to be more flexible in work hours, to encourage residents when there is a learning opportunity that previously they would be prohibited from taking part in to take hold of that opportunity, and to use this flexibility in implementation of duty hours to combat the invading “shift-work” mentality that will only jeopardize patient care.”
Dr. Elizabeth H. Stephens, MD, PhD is a Cardiothoracic Surgery, resident, PGY4, at Columbia University, New York, as an Integrated I-6 Resident.
Dr. Brown: “I took the traditional 5-year of General Surgery + 2 years of Cardiothoracic Surgery training route to becoming a General Thoracic Surgeon. My General Surgery experience was invaluable to my development as a surgeon. However, after all of those years of General Surgery cases and minimal exposure to Cardiothoracic Surgery cases, coupled with minimal overlap between the two specialties with regard to patient care, I found the learning curve in fellowship to be very steep. I was fortunate to train in a program with phenomenal physician extender support [APPs] in addition to top-notch colleagues in other specialties and excellent nursing, which allowed me to spend the majority of those 2 years in the operating room and completely focused on patient care. During that final phase of training, I welcomed flexibility with regard to the work-hour restrictions to ensure that I was acquiring the experience I needed prior to starting my own practice.”
Lisa M. Brown, MD, MAS, Assistant Professor of Thoracic Surgery, UC Davis Health System, Calif.; Training Institution: Washington University
Dr. Lee: “I started my surgical training in 2005, 2 years after the implementation of the 80-hour workweek restriction. Fortunately for my personal life, my training program took the restriction very seriously and strictly enforced it. As a result, I had scheduled periods off from work, and rarely worked more than 80 hours per week over the course of general surgery. On those occasions that I did, the next weeks, or preceding weeks would be shorter, to compensate. As a product of a 4+3 Thoracic Surgery residency in this environment, the 80-hour workweek extended to my subspecialty training. Our cardiac surgery time strictly enforced the go-home post-call policy. As a result, I believe my duty hours during Thoracic Surgery are likely shorter overall than many other programs.
Everyone hears the rumors of other programs lying about their duty hours. Fortunately, mine was not one of these. Despite this, or because of this, I received top-notch training. At the same time and more importantly, I started a family. I married my wife a week before my internship started, and am still married to the same person. We had two precious daughters during my Thoracic Surgery years. I don’t believe this would have been possible without duty-hours restrictions.
To create an environment where such a task was possible, my program hired an army of mid-level practitioners to deal with the day-to-day tasks of providing cardiothoracic surgical care to the patients, both in the intensive care unit and on the ward.
I rarely had to write a history and physical during Thoracic Surgery training. I consented fewer patients than I have fingers on my hands. I pulled even fewer chest tubes. I can now no longer remember having pulled a central line. I learned these tasks when I was a junior resident. What I did instead as a senior resident was perform over 900 cardiothoracic procedures as the primary surgeon. Now, as an attending surgeon, I still don’t write full histories and physicals by myself. I certainly don’t pull chest tubes and central lines. I consent patients by having a conversation with them, which I did as a resident, but I don’t bring a piece of paper with me in to the clinic room. I have a physician assistant who helps me fill in the gaps.
In 8 months of practice, I have performed over 15 thoracic organ transplants, repaired over 15 aortic dissections, half of whom required root replacements, performed more double-valve surgeries than straightforward single-valve replacements, started a minimally invasive atrial fibrillation surgical program, and applied almost every shred of knowledge and experience gained in 3 years of Thoracic Surgery Residency to a busy clinical practice. Most importantly, I continue to come home and watch my two daughters grow up.
With that perspective, I don’t believe the question should be whether or not programs should have the flexibility to enforce or not enforce duty-hours restrictions. It should be, how could every program find a way to effectively train residents to be good physicians and still allow them a personal life?”
Dr. Anson Lee is an Assistant Professor of Cardiac Surgery, Stanford University, Calif.; Training: 4+3 CT Residency, at Washington University, St. Louis.
Ms. Bohlman: “As a physician assistant in cardiac surgery, I represent the reality that physicians with a critical patient population appreciate consistency in their patient management. However, working in a university hospital setting also requires that surgical residents receive appropriate training. With the recently implemented duty restriction hours on resident training programs, advanced practice providers (APPs) have been utilized as an excellent solution for scheduling conflicts without compromising patient care. An example to this point is evident in my own place of work.
Approximately 1 year ago, our surgical intensive care unit transitioned from resident care to a combination of residents and APPs. At that time, the APPs were tasked with the complete care of all cardiac surgery patients. This change reduced the quantity and acuity of patients for which the residents were responsible and therefore allowed for more flexible hours along with a more manageable patient load. These changes, among others, have contributed to improved patient outcomes in the cardiac surgery patient population within our institution. With the increase in APPs that have training in various specialties, there comes an increasing ability to not only fill the gaps in scheduling but to do so with an extension of the providing physician. Although the NEJM article demonstrated no difference in patient outcomes between resident programs with restricted duty hours versus more flexible duty-hour policies, I foresee the future of medicine focusing on trained APPs as a complement to the care that the residents provide.”
Allison Bohlman is a Physician Assistant at Rush University Medical Center in the Integrated cardiovascular thoracic intensive care unit.

Vitamin C
Vitamin C (ascorbic acid) is one of the four most important ingredients in skin care products.
• It is proven to increase collagen production when applied topically to skin.
• It inhibits tyrosinase to even skin tone and has a strong antioxidant activity.
• It is absorbed well orally, but not enough gets to the skin.
• It is best absorbed at a pH of 2.0.
• It is unstable when exposed to light and air. Instruct patients to discard 6 months after opening.
In addition, the proper formulation is patented and expensive. Stick with brands you trust. Use vitamin C on skin prior to procedures to speed healing. It will sting when used on inflamed skin because of the low pH.

In my opinion, all patients need to be on the proper skin care regimen for their skin type. This includes a daily sun protection factor (SPF), a cleanser, a retinoid, and an antioxidant. Ascorbic acid is one of my favorite antioxidants because it is the only one shown to increase the production of collagen by fibroblasts and inhibit tyrosinase while scavenging free radicals. Sure it is expensive – but that is because formulating and packaging it properly is expensive. Unfortunately, many subpar brands have entered the market. Ask to see the company’s research data on its formulation before choosing to recommend or sell ascorbic acid/vitamin C in your practice.
An essential water-soluble nutrient for the development of bone and connective tissue, vitamin C is found in citrus fruits and green leafy vegetables. It is produced in most plants and animals, but a mutated gene in humans has resulted in a deficiency of L-gulono-gamma-lactone oxidase, the enzyme required for its production.1,2 Although ascorbic acid cannot be synthesized by the human body, dietary consumption renders it the most abundant antioxidant in human skin and blood, and vitamin C plays an important role in endogenous collagen production and the inhibition of collagen degradation.3-6 Ascorbic acid also is known to regenerate alpha-tocopherol (vitamin E) levels and, therefore, is thought to protect against diseases related to oxidative stress.7
Epidermal vitamin C can be depleted by sunlight and environmental pollution, such as ozone in urban pollution.8,9 Known to exhibit a wide range of biologic activities, ascorbic acid has been shown to deliver rejuvenating effects on skin wrinkles, texture, strength, and evenness of tone through its antioxidant, tyrosinase-inhibiting, and collagen production-promoting activities.10 Indeed, as a topical agent, vitamin C has been used to prevent photodamage, and to treat melasma, striae alba, and postoperative erythema in laser patients.11,12 It is regularly used to treat aging skin, and as a depigmenting agent.2,10,13 This column will discuss the antioxidant, antiaging, and depigmenting activity of vitamin C in the context of recent human studies.
Antioxidant and anti-aging activity
Vitamin C is unique among antioxidants because of its ability to increase collagen production in addition to its free radical scavenging antioxidant activity. Due to its capacity to interfere with the UV-induced generation of reactive oxygen species by reacting with the superoxide anion or the hydroxyl radical, vitamin C has become a popular addition to “after-sun” products,14,15 and been shown to be effective in mitigating the effects of UVB, such as erythema and signs of photoaging, on porcine and human skin.2,16-17
A 2001 study in 10 postmenopausal women by Nusgens et al. found that daily topical application of 5% L-ascorbic acid enhanced the levels of procollagen types I and III, their posttranslational maturation enzymes, and tissue inhibitor of matrix metalloproteinase.18 This led to increased levels of collagen in the skin.
In 2003, Humbert et al. conducted a 6-month, double-blind, vehicle-controlled trial with 20 healthy female volunteers showing that patients treated with 5% vitamin C cream experienced significant improvements in deep furrows on the neck and forearms.19
In a small study of nine adults with Fitzpatrick skin types II or III in 2008, Murray et al. studied whether a stable topical preparation of 15% L-ascorbic acid, 1% alpha-tocopherol, and 0.5% ferulic acid could protect human skin in vivo from UV-induced damage. They found that the antioxidant formulation supplemented the antioxidant pool of the skin and conferred significant photoprotection, guarding the skin against erythema and apoptosis as well as effectively suppressing p53 activation and reducing thymine dimer mutations known to be associated with skin cancer.13
In 2012, Xu et al. evaluated the efficacy and safety of topical 23.8% L-ascorbic acid on photoaged skin in a split-face study of 20 Chinese women. Significant improvements in fine lines, dyspigmentation, and surface roughness were observed, without adverse side effects.20
In a 2015 study of 60 healthy female subjects, Crisan et al. used high-frequency ultrasound to determine that the use of a topical vitamin C formulation yielded significant increases in collagen synthesis, revealing the solution to be an effective rejuvenation therapy.21
Skin lightening activity
Melasma
In 2004, Espinal-Perez et al. conducted a double-blind randomized trial of 5% ascorbic acid, compared with 4% hydroquinone (HQ) water–oil emulsion in 16 female patients with melasma, aged 23-43 years (mean 36 years). Of those treated with vitamin C, 62.5% exhibited good or excellent subjectively assessed skin lightening. There was no statistically significant difference in depigmenting activity in the HQ group, of which 68.7% experienced irritation whereas vitamin C was well tolerated.22

In a randomized, double-blind, placebo-controlled study, researchers used iontophoresis to enhance the penetration of vitamin C into the skin and significantly reduce pigmentation, compared with placebo.23
Although ascorbic acid is viewed by many as ineffective as a depigmenting agent alone, particularly in 5%-10% concentrations, when used in combination with other ingredients such as HQ, it is considered effective.24 In the magnesium-L-ascorbyl-2-phosphate esterified form, however, vitamin C is among the most popular prescribed depigmenting agents around the world, especially in countries where HQ and its derivatives are prohibited.25 In a 2009 16-week open-label study by Hwang et al. of 25% L-ascorbic acid and a chemical penetration enhancer for treating melasma in 40 patients, researchers observed significant reductions in pigmentation.26
In a small split-face study early in 2015, Lee et al. showed that the combination of 1,064-nm Q-switched neodymium-doped yttrium aluminum garnet (QS-Nd:YAG) laser and ultrasonic application of vitamin C was more effective than was the laser treatment alone in achieving a cosmetically acceptable treatment for melasma.27
PIPA
Vitamin C can be used to diminish or prevent post-inflammatory pigment alteration (PIPA) after procedures because it inhibits tyrosinase, lowers inflammation, and quenches free radicals. In a study of 10 patients, the application of topical vitamin C 2 or more weeks after surgery reduced the duration and degree of erythema after skin resurfacing with a carbon dioxide laser.28
Stretch marks
The depigmenting effects of vitamin C can lighten the pigmentation associated with stretch marks and its anti-inflammatory activity can contribute to blunting related redness.12
Conclusion
Although orally administered ascorbic acid is readily bioavailable, ascorbic acid in the skin is quickly depleted and oral supplementation alone does not yield optimal skin levels. Therefore, topical use of vitamin C is desirable. In fact, I tell my patients to use it topically in the morning and add a vitamin C supplement to their diet. Numerous formulation considerations (e.g., packaging, exposure to air or light during use, skin sensitivity, and user preference) are involved in the stabilization and effective penetration of ascorbic acid into the skin, and the process of developing, manufacturing, and packaging of effective, stable vitamin C products is expensive.
Vitamin C, particularly when combined with other ingredients, has been shown to be an integral constituent in topical antioxidant, antiaging, and depigmenting formulations that show promise in the dermatologic armamentarium. It is a great choice for use in a prep-procedure skin care regimen to speed healing. Use after a procedure is prohibited by the stinging associated with the low pH of properly formulated products.
References
1. J Biol Chem. 1994 May 6;269(18):13685-8.
2. Dermatol Surg. 2001 Feb;27(2):137-42.
3. J Invest Dermatol. 1994 Jan;102(1):122-4.
4. Dermatol Surg. 2005 Jul;31(7 Pt 2):814-7.
5. Annu Rev Nutr. 1994;14:371-91.
6. J Drugs Dermatol. 2008 Jul;7(7 Suppl):s2-6.
7. J Am Acad Dermatol. 2003 Jun;48(6):866-74.
8. J Invest Dermatol. 1994 Apr;102(4):470-5.
9. Free Radic Biol Med. 1997;23:85-91.
10. J Drugs Dermatol. 2014 Oct;13(10):1208-13.
11. J Am Acad Dermatol. 1996 Jan;34(1):29-33.
12. Dermatol Surg. 1998 Aug;24(8):849-56.
13. J Am Acad Dermatol. 2008 Sep;59(3):418-25.
14. J Biol Chem. 1983 Jun 10;258(11):6695-7.
15. J Phys Chem. 1983;87:1809-12.
16. Br J Dermatol. 1992 Sep;127(3):247-53.
17. J Invest Dermatol. 1991;96:587.
18. J Invest Dermatol. 2001 Jun;116(6):853-9.
19. Exp Dermatol. 2003 Jun;12(3):237-44.
20. J Drugs Dermatol. 2012 Jan;11(1):51-6.
21. Clin Cosmet Investig Dermatol. 2015 Sep 2;8:463-70
22. Int J Dermatol. 2004 Aug;43(8):604-7.
23. Dermatology. 2003;206(4):316-20.
24. Am J Clin Dermatol. 2011 Apr 1;12(2):87-99.
25. Phytother Res. 2006 Nov;20(11):921-34.
26. J Cutan Med Surg. 2009 Mar-Apr;13(2):74-81.
27. Lasers Med Sci. 2015 Jan;30(1):159-63.
28. Dermatol Surg. 1998 Mar;24(3):331-4.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera Biopharmaceuticals, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever.
Vitamin C (ascorbic acid) is one of the four most important ingredients in skin care products.
• It is proven to increase collagen production when applied topically to skin.
• It inhibits tyrosinase to even skin tone and has a strong antioxidant activity.
• It is absorbed well orally, but not enough gets to the skin.
• It is best absorbed at a pH of 2.0.
• It is unstable when exposed to light and air. Instruct patients to discard 6 months after opening.
In addition, the proper formulation is patented and expensive. Stick with brands you trust. Use vitamin C on skin prior to procedures to speed healing. It will sting when used on inflamed skin because of the low pH.
In my opinion, all patients need to be on the proper skin care regimen for their skin type. This includes a daily sun protection factor (SPF), a cleanser, a retinoid, and an antioxidant. Ascorbic acid is one of my favorite antioxidants because it is the only one shown to increase the production of collagen by fibroblasts and inhibit tyrosinase while scavenging free radicals. Sure it is expensive – but that is because formulating and packaging it properly is expensive. Unfortunately, many subpar brands have entered the market. Ask to see the company’s research data on its formulation before choosing to recommend or sell ascorbic acid/vitamin C in your practice.
An essential water-soluble nutrient for the development of bone and connective tissue, vitamin C is found in citrus fruits and green leafy vegetables. It is produced in most plants and animals, but a mutated gene in humans has resulted in a deficiency of L-gulono-gamma-lactone oxidase, the enzyme required for its production.1,2 Although ascorbic acid cannot be synthesized by the human body, dietary consumption renders it the most abundant antioxidant in human skin and blood, and vitamin C plays an important role in endogenous collagen production and the inhibition of collagen degradation.3-6 Ascorbic acid also is known to regenerate alpha-tocopherol (vitamin E) levels and, therefore, is thought to protect against diseases related to oxidative stress.7
Epidermal vitamin C can be depleted by sunlight and environmental pollution, such as ozone in urban pollution.8,9 Known to exhibit a wide range of biologic activities, ascorbic acid has been shown to deliver rejuvenating effects on skin wrinkles, texture, strength, and evenness of tone through its antioxidant, tyrosinase-inhibiting, and collagen production-promoting activities.10 Indeed, as a topical agent, vitamin C has been used to prevent photodamage, and to treat melasma, striae alba, and postoperative erythema in laser patients.11,12 It is regularly used to treat aging skin, and as a depigmenting agent.2,10,13 This column will discuss the antioxidant, antiaging, and depigmenting activity of vitamin C in the context of recent human studies.
Antioxidant and anti-aging activity
Vitamin C is unique among antioxidants because of its ability to increase collagen production in addition to its free radical scavenging antioxidant activity. Due to its capacity to interfere with the UV-induced generation of reactive oxygen species by reacting with the superoxide anion or the hydroxyl radical, vitamin C has become a popular addition to “after-sun” products,14,15 and been shown to be effective in mitigating the effects of UVB, such as erythema and signs of photoaging, on porcine and human skin.2,16-17
A 2001 study in 10 postmenopausal women by Nusgens et al. found that daily topical application of 5% L-ascorbic acid enhanced the levels of procollagen types I and III, their posttranslational maturation enzymes, and tissue inhibitor of matrix metalloproteinase.18 This led to increased levels of collagen in the skin.
In 2003, Humbert et al. conducted a 6-month, double-blind, vehicle-controlled trial with 20 healthy female volunteers showing that patients treated with 5% vitamin C cream experienced significant improvements in deep furrows on the neck and forearms.19
In a small study of nine adults with Fitzpatrick skin types II or III in 2008, Murray et al. studied whether a stable topical preparation of 15% L-ascorbic acid, 1% alpha-tocopherol, and 0.5% ferulic acid could protect human skin in vivo from UV-induced damage. They found that the antioxidant formulation supplemented the antioxidant pool of the skin and conferred significant photoprotection, guarding the skin against erythema and apoptosis as well as effectively suppressing p53 activation and reducing thymine dimer mutations known to be associated with skin cancer.13
In 2012, Xu et al. evaluated the efficacy and safety of topical 23.8% L-ascorbic acid on photoaged skin in a split-face study of 20 Chinese women. Significant improvements in fine lines, dyspigmentation, and surface roughness were observed, without adverse side effects.20
In a 2015 study of 60 healthy female subjects, Crisan et al. used high-frequency ultrasound to determine that the use of a topical vitamin C formulation yielded significant increases in collagen synthesis, revealing the solution to be an effective rejuvenation therapy.21
Skin lightening activity
Melasma
In 2004, Espinal-Perez et al. conducted a double-blind randomized trial of 5% ascorbic acid, compared with 4% hydroquinone (HQ) water–oil emulsion in 16 female patients with melasma, aged 23-43 years (mean 36 years). Of those treated with vitamin C, 62.5% exhibited good or excellent subjectively assessed skin lightening. There was no statistically significant difference in depigmenting activity in the HQ group, of which 68.7% experienced irritation whereas vitamin C was well tolerated.22
In a randomized, double-blind, placebo-controlled study, researchers used iontophoresis to enhance the penetration of vitamin C into the skin and significantly reduce pigmentation, compared with placebo.23
Although ascorbic acid is viewed by many as ineffective as a depigmenting agent alone, particularly in 5%-10% concentrations, when used in combination with other ingredients such as HQ, it is considered effective.24 In the magnesium-L-ascorbyl-2-phosphate esterified form, however, vitamin C is among the most popular prescribed depigmenting agents around the world, especially in countries where HQ and its derivatives are prohibited.25 In a 2009 16-week open-label study by Hwang et al. of 25% L-ascorbic acid and a chemical penetration enhancer for treating melasma in 40 patients, researchers observed significant reductions in pigmentation.26
In a small split-face study early in 2015, Lee et al. showed that the combination of 1,064-nm Q-switched neodymium-doped yttrium aluminum garnet (QS-Nd:YAG) laser and ultrasonic application of vitamin C was more effective than was the laser treatment alone in achieving a cosmetically acceptable treatment for melasma.27
PIPA
Vitamin C can be used to diminish or prevent post-inflammatory pigment alteration (PIPA) after procedures because it inhibits tyrosinase, lowers inflammation, and quenches free radicals. In a study of 10 patients, the application of topical vitamin C 2 or more weeks after surgery reduced the duration and degree of erythema after skin resurfacing with a carbon dioxide laser.28
Stretch marks
The depigmenting effects of vitamin C can lighten the pigmentation associated with stretch marks and its anti-inflammatory activity can contribute to blunting related redness.12
Conclusion
Although orally administered ascorbic acid is readily bioavailable, ascorbic acid in the skin is quickly depleted and oral supplementation alone does not yield optimal skin levels. Therefore, topical use of vitamin C is desirable. In fact, I tell my patients to use it topically in the morning and add a vitamin C supplement to their diet. Numerous formulation considerations (e.g., packaging, exposure to air or light during use, skin sensitivity, and user preference) are involved in the stabilization and effective penetration of ascorbic acid into the skin, and the process of developing, manufacturing, and packaging of effective, stable vitamin C products is expensive.
Vitamin C, particularly when combined with other ingredients, has been shown to be an integral constituent in topical antioxidant, antiaging, and depigmenting formulations that show promise in the dermatologic armamentarium. It is a great choice for use in a prep-procedure skin care regimen to speed healing. Use after a procedure is prohibited by the stinging associated with the low pH of properly formulated products.
References
1. J Biol Chem. 1994 May 6;269(18):13685-8.
2. Dermatol Surg. 2001 Feb;27(2):137-42.
3. J Invest Dermatol. 1994 Jan;102(1):122-4.
4. Dermatol Surg. 2005 Jul;31(7 Pt 2):814-7.
5. Annu Rev Nutr. 1994;14:371-91.
6. J Drugs Dermatol. 2008 Jul;7(7 Suppl):s2-6.
7. J Am Acad Dermatol. 2003 Jun;48(6):866-74.
8. J Invest Dermatol. 1994 Apr;102(4):470-5.
9. Free Radic Biol Med. 1997;23:85-91.
10. J Drugs Dermatol. 2014 Oct;13(10):1208-13.
11. J Am Acad Dermatol. 1996 Jan;34(1):29-33.
12. Dermatol Surg. 1998 Aug;24(8):849-56.
13. J Am Acad Dermatol. 2008 Sep;59(3):418-25.
14. J Biol Chem. 1983 Jun 10;258(11):6695-7.
15. J Phys Chem. 1983;87:1809-12.
16. Br J Dermatol. 1992 Sep;127(3):247-53.
17. J Invest Dermatol. 1991;96:587.
18. J Invest Dermatol. 2001 Jun;116(6):853-9.
19. Exp Dermatol. 2003 Jun;12(3):237-44.
20. J Drugs Dermatol. 2012 Jan;11(1):51-6.
21. Clin Cosmet Investig Dermatol. 2015 Sep 2;8:463-70
22. Int J Dermatol. 2004 Aug;43(8):604-7.
23. Dermatology. 2003;206(4):316-20.
24. Am J Clin Dermatol. 2011 Apr 1;12(2):87-99.
25. Phytother Res. 2006 Nov;20(11):921-34.
26. J Cutan Med Surg. 2009 Mar-Apr;13(2):74-81.
27. Lasers Med Sci. 2015 Jan;30(1):159-63.
28. Dermatol Surg. 1998 Mar;24(3):331-4.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera Biopharmaceuticals, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever.
Vitamin C (ascorbic acid) is one of the four most important ingredients in skin care products.
• It is proven to increase collagen production when applied topically to skin.
• It inhibits tyrosinase to even skin tone and has a strong antioxidant activity.
• It is absorbed well orally, but not enough gets to the skin.
• It is best absorbed at a pH of 2.0.
• It is unstable when exposed to light and air. Instruct patients to discard 6 months after opening.
In addition, the proper formulation is patented and expensive. Stick with brands you trust. Use vitamin C on skin prior to procedures to speed healing. It will sting when used on inflamed skin because of the low pH.
In my opinion, all patients need to be on the proper skin care regimen for their skin type. This includes a daily sun protection factor (SPF), a cleanser, a retinoid, and an antioxidant. Ascorbic acid is one of my favorite antioxidants because it is the only one shown to increase the production of collagen by fibroblasts and inhibit tyrosinase while scavenging free radicals. Sure it is expensive – but that is because formulating and packaging it properly is expensive. Unfortunately, many subpar brands have entered the market. Ask to see the company’s research data on its formulation before choosing to recommend or sell ascorbic acid/vitamin C in your practice.
An essential water-soluble nutrient for the development of bone and connective tissue, vitamin C is found in citrus fruits and green leafy vegetables. It is produced in most plants and animals, but a mutated gene in humans has resulted in a deficiency of L-gulono-gamma-lactone oxidase, the enzyme required for its production.1,2 Although ascorbic acid cannot be synthesized by the human body, dietary consumption renders it the most abundant antioxidant in human skin and blood, and vitamin C plays an important role in endogenous collagen production and the inhibition of collagen degradation.3-6 Ascorbic acid also is known to regenerate alpha-tocopherol (vitamin E) levels and, therefore, is thought to protect against diseases related to oxidative stress.7
Epidermal vitamin C can be depleted by sunlight and environmental pollution, such as ozone in urban pollution.8,9 Known to exhibit a wide range of biologic activities, ascorbic acid has been shown to deliver rejuvenating effects on skin wrinkles, texture, strength, and evenness of tone through its antioxidant, tyrosinase-inhibiting, and collagen production-promoting activities.10 Indeed, as a topical agent, vitamin C has been used to prevent photodamage, and to treat melasma, striae alba, and postoperative erythema in laser patients.11,12 It is regularly used to treat aging skin, and as a depigmenting agent.2,10,13 This column will discuss the antioxidant, antiaging, and depigmenting activity of vitamin C in the context of recent human studies.
Antioxidant and anti-aging activity
Vitamin C is unique among antioxidants because of its ability to increase collagen production in addition to its free radical scavenging antioxidant activity. Due to its capacity to interfere with the UV-induced generation of reactive oxygen species by reacting with the superoxide anion or the hydroxyl radical, vitamin C has become a popular addition to “after-sun” products,14,15 and been shown to be effective in mitigating the effects of UVB, such as erythema and signs of photoaging, on porcine and human skin.2,16-17
A 2001 study in 10 postmenopausal women by Nusgens et al. found that daily topical application of 5% L-ascorbic acid enhanced the levels of procollagen types I and III, their posttranslational maturation enzymes, and tissue inhibitor of matrix metalloproteinase.18 This led to increased levels of collagen in the skin.
In 2003, Humbert et al. conducted a 6-month, double-blind, vehicle-controlled trial with 20 healthy female volunteers showing that patients treated with 5% vitamin C cream experienced significant improvements in deep furrows on the neck and forearms.19
In a small study of nine adults with Fitzpatrick skin types II or III in 2008, Murray et al. studied whether a stable topical preparation of 15% L-ascorbic acid, 1% alpha-tocopherol, and 0.5% ferulic acid could protect human skin in vivo from UV-induced damage. They found that the antioxidant formulation supplemented the antioxidant pool of the skin and conferred significant photoprotection, guarding the skin against erythema and apoptosis as well as effectively suppressing p53 activation and reducing thymine dimer mutations known to be associated with skin cancer.13
In 2012, Xu et al. evaluated the efficacy and safety of topical 23.8% L-ascorbic acid on photoaged skin in a split-face study of 20 Chinese women. Significant improvements in fine lines, dyspigmentation, and surface roughness were observed, without adverse side effects.20
In a 2015 study of 60 healthy female subjects, Crisan et al. used high-frequency ultrasound to determine that the use of a topical vitamin C formulation yielded significant increases in collagen synthesis, revealing the solution to be an effective rejuvenation therapy.21
Skin lightening activity
Melasma
In 2004, Espinal-Perez et al. conducted a double-blind randomized trial of 5% ascorbic acid, compared with 4% hydroquinone (HQ) water–oil emulsion in 16 female patients with melasma, aged 23-43 years (mean 36 years). Of those treated with vitamin C, 62.5% exhibited good or excellent subjectively assessed skin lightening. There was no statistically significant difference in depigmenting activity in the HQ group, of which 68.7% experienced irritation whereas vitamin C was well tolerated.22
In a randomized, double-blind, placebo-controlled study, researchers used iontophoresis to enhance the penetration of vitamin C into the skin and significantly reduce pigmentation, compared with placebo.23
Although ascorbic acid is viewed by many as ineffective as a depigmenting agent alone, particularly in 5%-10% concentrations, when used in combination with other ingredients such as HQ, it is considered effective.24 In the magnesium-L-ascorbyl-2-phosphate esterified form, however, vitamin C is among the most popular prescribed depigmenting agents around the world, especially in countries where HQ and its derivatives are prohibited.25 In a 2009 16-week open-label study by Hwang et al. of 25% L-ascorbic acid and a chemical penetration enhancer for treating melasma in 40 patients, researchers observed significant reductions in pigmentation.26
In a small split-face study early in 2015, Lee et al. showed that the combination of 1,064-nm Q-switched neodymium-doped yttrium aluminum garnet (QS-Nd:YAG) laser and ultrasonic application of vitamin C was more effective than was the laser treatment alone in achieving a cosmetically acceptable treatment for melasma.27
PIPA
Vitamin C can be used to diminish or prevent post-inflammatory pigment alteration (PIPA) after procedures because it inhibits tyrosinase, lowers inflammation, and quenches free radicals. In a study of 10 patients, the application of topical vitamin C 2 or more weeks after surgery reduced the duration and degree of erythema after skin resurfacing with a carbon dioxide laser.28
Stretch marks
The depigmenting effects of vitamin C can lighten the pigmentation associated with stretch marks and its anti-inflammatory activity can contribute to blunting related redness.12
Conclusion
Although orally administered ascorbic acid is readily bioavailable, ascorbic acid in the skin is quickly depleted and oral supplementation alone does not yield optimal skin levels. Therefore, topical use of vitamin C is desirable. In fact, I tell my patients to use it topically in the morning and add a vitamin C supplement to their diet. Numerous formulation considerations (e.g., packaging, exposure to air or light during use, skin sensitivity, and user preference) are involved in the stabilization and effective penetration of ascorbic acid into the skin, and the process of developing, manufacturing, and packaging of effective, stable vitamin C products is expensive.
Vitamin C, particularly when combined with other ingredients, has been shown to be an integral constituent in topical antioxidant, antiaging, and depigmenting formulations that show promise in the dermatologic armamentarium. It is a great choice for use in a prep-procedure skin care regimen to speed healing. Use after a procedure is prohibited by the stinging associated with the low pH of properly formulated products.
References
1. J Biol Chem. 1994 May 6;269(18):13685-8.
2. Dermatol Surg. 2001 Feb;27(2):137-42.
3. J Invest Dermatol. 1994 Jan;102(1):122-4.
4. Dermatol Surg. 2005 Jul;31(7 Pt 2):814-7.
5. Annu Rev Nutr. 1994;14:371-91.
6. J Drugs Dermatol. 2008 Jul;7(7 Suppl):s2-6.
7. J Am Acad Dermatol. 2003 Jun;48(6):866-74.
8. J Invest Dermatol. 1994 Apr;102(4):470-5.
9. Free Radic Biol Med. 1997;23:85-91.
10. J Drugs Dermatol. 2014 Oct;13(10):1208-13.
11. J Am Acad Dermatol. 1996 Jan;34(1):29-33.
12. Dermatol Surg. 1998 Aug;24(8):849-56.
13. J Am Acad Dermatol. 2008 Sep;59(3):418-25.
14. J Biol Chem. 1983 Jun 10;258(11):6695-7.
15. J Phys Chem. 1983;87:1809-12.
16. Br J Dermatol. 1992 Sep;127(3):247-53.
17. J Invest Dermatol. 1991;96:587.
18. J Invest Dermatol. 2001 Jun;116(6):853-9.
19. Exp Dermatol. 2003 Jun;12(3):237-44.
20. J Drugs Dermatol. 2012 Jan;11(1):51-6.
21. Clin Cosmet Investig Dermatol. 2015 Sep 2;8:463-70
22. Int J Dermatol. 2004 Aug;43(8):604-7.
23. Dermatology. 2003;206(4):316-20.
24. Am J Clin Dermatol. 2011 Apr 1;12(2):87-99.
25. Phytother Res. 2006 Nov;20(11):921-34.
26. J Cutan Med Surg. 2009 Mar-Apr;13(2):74-81.
27. Lasers Med Sci. 2015 Jan;30(1):159-63.
28. Dermatol Surg. 1998 Mar;24(3):331-4.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera Biopharmaceuticals, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever.

TSH antibody levels predict Graves relapse after thionamides
BOSTON – Eighty-six percent of Graves disease patients with TSH receptor antibody levels of at least 2.0 mU/L at the end of thionamide therapy will relapse within 4 years, according to a British review.
TSH receptor antibody (TRAb) levels “are useful not only as a diagnostic tool but also as a prognostic tool. In patients where the risks of recurrent thyrotoxicosis are unacceptably high” – the elderly and those at risk for cardiovascular disease – “strong consideration should be given to primary radioiodine therapy” instead of thionamides, said investigator Nyo Nyo Tun of the Edinburgh Centre for Endocrinology and Diabetes.

Previous studies have suggested age and other risk factors for relapse after thionamides, but “have not [definitively] shown if elevation of TRAb levels” are predictive, she said at the annual meeting of the Endocrine Society.
Primary therapy with thionamides is more common in Europe than in the United States, where radioiodine tends to be the first choice. Part of the problem is that recurrence is known to be high after thionamides. The study suggests that using TRAb can help weed out patients who are likely to fail so that thionamides can be used with greater long-term success. Ms. Tun said the Edinburgh center routinely uses TRAb to guide Graves treatment; patients with high levels either stay on thionamide for prolonged periods or opt for radioiodine.
The investigators retrospectively studied 266 patients with a first presentation of Graves disease who completed a course of thionamide at two U.K. hospitals. In addition to TRAb levels at diagnosis and cessation of thionamide, they assessed age, sex, smoking status, free T4 levels, total T3, and time to normalization of thyroid function over 4 years of follow-up.
After thionamide cessation, thyrotoxicosis recurred in 31% of patients (82/266) at 1 year, 43% (111/261) at 2 years, 54% (125/232) at 3 years, and 66% (128/193) at 4 years.
Very high TRAb levels at diagnosis – those above 12 mU/L – were associated with a statistically significant 84% risk of recurrence over a 4-year period, compared with a 57% risk with diagnosis levels below 5mU/L (P = .002).
TRAb levels below 0.9 mU/L at cessation of an 18-month course of thionamide treatment were associated with a 22% risk of recurrence at 1 year and a 58% risk at 4 years. Those risks were significantly higher in patients whose TRAb levels were at least 2 mU/L at thionamide cessation, who had a 51% risk at 1 year and an 86% risk at 4 years (P less than 0.001). Relapse risk was highest in the first 18 months after cessation.
Younger age and time to TSH normalization also predicted relapse to some extent. Among patients who stayed in remission for 4 years, TSH normalized at a median of about 4 months after the start of drug treatment, but 6 months in those who relapsed. Similarly, patients who relapsed were a median of 39 years old at diagnosis; those who did not were a median of 47.
The investigators had no relevant financial disclosures.
The measurement of antibodies to the thyroid-stimulating hormone receptor is a useful clinical test that should be much more widely used in the United States. It’s a very accurate predictor of who’s going to get recurrent Grave’s disease after antithyroid drugs, but it’s misunderstood and not trusted.

|
Dr. Terry Davies |
When the test was first introduced, many major thyroid experts didn’t accept it and didn’t believe it was useful based on research at the time. The difference with the current study is that it was done carefully.
Dr. Terry Davies is the director of the division of endocrinology, diabetes, and bone diseases at the Mount Sinai Beth Israel Medical Center in New York. He moderated the presentation and was not involved in the work.
The measurement of antibodies to the thyroid-stimulating hormone receptor is a useful clinical test that should be much more widely used in the United States. It’s a very accurate predictor of who’s going to get recurrent Grave’s disease after antithyroid drugs, but it’s misunderstood and not trusted.
|
|
Dr. Terry Davies |
When the test was first introduced, many major thyroid experts didn’t accept it and didn’t believe it was useful based on research at the time. The difference with the current study is that it was done carefully.
Dr. Terry Davies is the director of the division of endocrinology, diabetes, and bone diseases at the Mount Sinai Beth Israel Medical Center in New York. He moderated the presentation and was not involved in the work.
The measurement of antibodies to the thyroid-stimulating hormone receptor is a useful clinical test that should be much more widely used in the United States. It’s a very accurate predictor of who’s going to get recurrent Grave’s disease after antithyroid drugs, but it’s misunderstood and not trusted.
|
|
Dr. Terry Davies |
When the test was first introduced, many major thyroid experts didn’t accept it and didn’t believe it was useful based on research at the time. The difference with the current study is that it was done carefully.
Dr. Terry Davies is the director of the division of endocrinology, diabetes, and bone diseases at the Mount Sinai Beth Israel Medical Center in New York. He moderated the presentation and was not involved in the work.
BOSTON – Eighty-six percent of Graves disease patients with TSH receptor antibody levels of at least 2.0 mU/L at the end of thionamide therapy will relapse within 4 years, according to a British review.
TSH receptor antibody (TRAb) levels “are useful not only as a diagnostic tool but also as a prognostic tool. In patients where the risks of recurrent thyrotoxicosis are unacceptably high” – the elderly and those at risk for cardiovascular disease – “strong consideration should be given to primary radioiodine therapy” instead of thionamides, said investigator Nyo Nyo Tun of the Edinburgh Centre for Endocrinology and Diabetes.
Previous studies have suggested age and other risk factors for relapse after thionamides, but “have not [definitively] shown if elevation of TRAb levels” are predictive, she said at the annual meeting of the Endocrine Society.
Primary therapy with thionamides is more common in Europe than in the United States, where radioiodine tends to be the first choice. Part of the problem is that recurrence is known to be high after thionamides. The study suggests that using TRAb can help weed out patients who are likely to fail so that thionamides can be used with greater long-term success. Ms. Tun said the Edinburgh center routinely uses TRAb to guide Graves treatment; patients with high levels either stay on thionamide for prolonged periods or opt for radioiodine.
The investigators retrospectively studied 266 patients with a first presentation of Graves disease who completed a course of thionamide at two U.K. hospitals. In addition to TRAb levels at diagnosis and cessation of thionamide, they assessed age, sex, smoking status, free T4 levels, total T3, and time to normalization of thyroid function over 4 years of follow-up.
After thionamide cessation, thyrotoxicosis recurred in 31% of patients (82/266) at 1 year, 43% (111/261) at 2 years, 54% (125/232) at 3 years, and 66% (128/193) at 4 years.
Very high TRAb levels at diagnosis – those above 12 mU/L – were associated with a statistically significant 84% risk of recurrence over a 4-year period, compared with a 57% risk with diagnosis levels below 5mU/L (P = .002).
TRAb levels below 0.9 mU/L at cessation of an 18-month course of thionamide treatment were associated with a 22% risk of recurrence at 1 year and a 58% risk at 4 years. Those risks were significantly higher in patients whose TRAb levels were at least 2 mU/L at thionamide cessation, who had a 51% risk at 1 year and an 86% risk at 4 years (P less than 0.001). Relapse risk was highest in the first 18 months after cessation.
Younger age and time to TSH normalization also predicted relapse to some extent. Among patients who stayed in remission for 4 years, TSH normalized at a median of about 4 months after the start of drug treatment, but 6 months in those who relapsed. Similarly, patients who relapsed were a median of 39 years old at diagnosis; those who did not were a median of 47.
The investigators had no relevant financial disclosures.
BOSTON – Eighty-six percent of Graves disease patients with TSH receptor antibody levels of at least 2.0 mU/L at the end of thionamide therapy will relapse within 4 years, according to a British review.
TSH receptor antibody (TRAb) levels “are useful not only as a diagnostic tool but also as a prognostic tool. In patients where the risks of recurrent thyrotoxicosis are unacceptably high” – the elderly and those at risk for cardiovascular disease – “strong consideration should be given to primary radioiodine therapy” instead of thionamides, said investigator Nyo Nyo Tun of the Edinburgh Centre for Endocrinology and Diabetes.
Previous studies have suggested age and other risk factors for relapse after thionamides, but “have not [definitively] shown if elevation of TRAb levels” are predictive, she said at the annual meeting of the Endocrine Society.
Primary therapy with thionamides is more common in Europe than in the United States, where radioiodine tends to be the first choice. Part of the problem is that recurrence is known to be high after thionamides. The study suggests that using TRAb can help weed out patients who are likely to fail so that thionamides can be used with greater long-term success. Ms. Tun said the Edinburgh center routinely uses TRAb to guide Graves treatment; patients with high levels either stay on thionamide for prolonged periods or opt for radioiodine.
The investigators retrospectively studied 266 patients with a first presentation of Graves disease who completed a course of thionamide at two U.K. hospitals. In addition to TRAb levels at diagnosis and cessation of thionamide, they assessed age, sex, smoking status, free T4 levels, total T3, and time to normalization of thyroid function over 4 years of follow-up.
After thionamide cessation, thyrotoxicosis recurred in 31% of patients (82/266) at 1 year, 43% (111/261) at 2 years, 54% (125/232) at 3 years, and 66% (128/193) at 4 years.
Very high TRAb levels at diagnosis – those above 12 mU/L – were associated with a statistically significant 84% risk of recurrence over a 4-year period, compared with a 57% risk with diagnosis levels below 5mU/L (P = .002).
TRAb levels below 0.9 mU/L at cessation of an 18-month course of thionamide treatment were associated with a 22% risk of recurrence at 1 year and a 58% risk at 4 years. Those risks were significantly higher in patients whose TRAb levels were at least 2 mU/L at thionamide cessation, who had a 51% risk at 1 year and an 86% risk at 4 years (P less than 0.001). Relapse risk was highest in the first 18 months after cessation.
Younger age and time to TSH normalization also predicted relapse to some extent. Among patients who stayed in remission for 4 years, TSH normalized at a median of about 4 months after the start of drug treatment, but 6 months in those who relapsed. Similarly, patients who relapsed were a median of 39 years old at diagnosis; those who did not were a median of 47.
The investigators had no relevant financial disclosures.
AT ENDO 2016
Key clinical point: Opt for radioiodine when Grave’s patients present with thyroid-stimulating hormone receptor antibody levels above 12 mU/L.
Major finding: Eighty-six percent of Grave’s disease patients with TSH receptor antibody levels of at least 2.0 mU/L at the end of thionamide therapy will relapse within 4 years.
Data source: A British review of 266 Grave’s patients treated with thionamides for 18 months.
Disclosures: The investigators had no relevant financial disclosures.

Tiotropium inhalation spray effective for asthma regardless of allergic status
LOS ANGELES – Once-daily tiotropium bromide inhalation spray as long-term, add-on maintenance therapy in patients with poorly controlled symptomatic asthma is similarly effective in both allergic and nonallergic asthma, according to Dr. Donald P. Tashkin.
In a series of analyses presented at the annual meeting of the American Academy of Allergy, Asthma, and Immunology, he and his coinvestigators showed that tiotropium bromide inhalation spray (Spiriva Respimat) given as add-on maintenance therapy resulted in significantly improved lung function, enhanced asthma symptom control, and fewer asthma exacerbations. The important new finding in these post hoc analyses was that the medication was similarly effective across the full range of baseline serum IgE and blood eosinophil levels, said Dr. Tashkin, director of the pulmonary function laboratories at the University of California, Los Angeles.

Last fall, the Food and Drug Administration approved an expanded indication for tiotropium bromide inhalation spray as long-term, add-on maintenance therapy of asthma in patients aged 12 and up who remain symptomatic despite taking other maintenance therapies. The once-daily medication had already been approved in the fall of 2014 for maintenance therapy of chronic obstructive pulmonary disease. Spiriva Respimat delivers a once-daily 2.5-mcg dose of tiotropium bromide via two 1.25-mcg puffs in a slow-moving, propellant-free mist designed to get the drug into the distal lungs independent of a patient’s skill in using a conventional metered-dose inhaler.
Dr. Tashkin and his coinvestigators presented a series of post hoc analyses combining data on 3,012 participants in the two prospective PrimoTinA-asthma and two MezzoTinA-asthma clinical trials. These phase III, double-blind, placebo-controlled trials defined participants’ allergic phenotype on the basis of the conventional cut points of a serum IgE level above or below 430 mcg/mL or a blood eosinophil count above or below 600 cells/mcL.
“The question is, are these appropriate cut points? Can we be sure that somebody below those cut points doesn’t have atopy? To answer that question, we looked at the whole spectrum of eosinophils in the blood from 5/mcL to 2,000/mcL and serum IgE levels from 2 mcg/mL to 2,000 mcg/mL. We found that the efficacy was similar across the entire spectrum of these measures of allergy,” he said in an interview.
Thus, these new findings support the use of this novel maintenance therapy without any need for lab tests to determine whether an individual patient’s asthma is T helper 2–cell dominant or not, Dr. Tashkin added.
The PrimoTinA-asthma trials were 48-week studies of add-on Spiriva Respimat or placebo conducted in patients with symptomatic asthma despite treatment with an inhaled corticosteroid plus a long-acting beta-agonist. The MezzoTinA-asthma studies were 24 weeks long and focused on patients who remained symptomatic despite at least moderate-dose inhaled corticosteroid therapy. Key endpoints included improvement in asthma symptom control as measured by the seven-question Asthma Control Questionnaire, improved peak and trough forced expiratory volume in 1 second, and time to a first severe asthma exacerbation.
Dr. Tashkin reported serving as a paid speaker on behalf of Boehringer Ingelheim, which markets Spiriva Respimat and sponsored the studies.
LOS ANGELES – Once-daily tiotropium bromide inhalation spray as long-term, add-on maintenance therapy in patients with poorly controlled symptomatic asthma is similarly effective in both allergic and nonallergic asthma, according to Dr. Donald P. Tashkin.
In a series of analyses presented at the annual meeting of the American Academy of Allergy, Asthma, and Immunology, he and his coinvestigators showed that tiotropium bromide inhalation spray (Spiriva Respimat) given as add-on maintenance therapy resulted in significantly improved lung function, enhanced asthma symptom control, and fewer asthma exacerbations. The important new finding in these post hoc analyses was that the medication was similarly effective across the full range of baseline serum IgE and blood eosinophil levels, said Dr. Tashkin, director of the pulmonary function laboratories at the University of California, Los Angeles.
Last fall, the Food and Drug Administration approved an expanded indication for tiotropium bromide inhalation spray as long-term, add-on maintenance therapy of asthma in patients aged 12 and up who remain symptomatic despite taking other maintenance therapies. The once-daily medication had already been approved in the fall of 2014 for maintenance therapy of chronic obstructive pulmonary disease. Spiriva Respimat delivers a once-daily 2.5-mcg dose of tiotropium bromide via two 1.25-mcg puffs in a slow-moving, propellant-free mist designed to get the drug into the distal lungs independent of a patient’s skill in using a conventional metered-dose inhaler.
Dr. Tashkin and his coinvestigators presented a series of post hoc analyses combining data on 3,012 participants in the two prospective PrimoTinA-asthma and two MezzoTinA-asthma clinical trials. These phase III, double-blind, placebo-controlled trials defined participants’ allergic phenotype on the basis of the conventional cut points of a serum IgE level above or below 430 mcg/mL or a blood eosinophil count above or below 600 cells/mcL.
“The question is, are these appropriate cut points? Can we be sure that somebody below those cut points doesn’t have atopy? To answer that question, we looked at the whole spectrum of eosinophils in the blood from 5/mcL to 2,000/mcL and serum IgE levels from 2 mcg/mL to 2,000 mcg/mL. We found that the efficacy was similar across the entire spectrum of these measures of allergy,” he said in an interview.
Thus, these new findings support the use of this novel maintenance therapy without any need for lab tests to determine whether an individual patient’s asthma is T helper 2–cell dominant or not, Dr. Tashkin added.
The PrimoTinA-asthma trials were 48-week studies of add-on Spiriva Respimat or placebo conducted in patients with symptomatic asthma despite treatment with an inhaled corticosteroid plus a long-acting beta-agonist. The MezzoTinA-asthma studies were 24 weeks long and focused on patients who remained symptomatic despite at least moderate-dose inhaled corticosteroid therapy. Key endpoints included improvement in asthma symptom control as measured by the seven-question Asthma Control Questionnaire, improved peak and trough forced expiratory volume in 1 second, and time to a first severe asthma exacerbation.
Dr. Tashkin reported serving as a paid speaker on behalf of Boehringer Ingelheim, which markets Spiriva Respimat and sponsored the studies.
LOS ANGELES – Once-daily tiotropium bromide inhalation spray as long-term, add-on maintenance therapy in patients with poorly controlled symptomatic asthma is similarly effective in both allergic and nonallergic asthma, according to Dr. Donald P. Tashkin.
In a series of analyses presented at the annual meeting of the American Academy of Allergy, Asthma, and Immunology, he and his coinvestigators showed that tiotropium bromide inhalation spray (Spiriva Respimat) given as add-on maintenance therapy resulted in significantly improved lung function, enhanced asthma symptom control, and fewer asthma exacerbations. The important new finding in these post hoc analyses was that the medication was similarly effective across the full range of baseline serum IgE and blood eosinophil levels, said Dr. Tashkin, director of the pulmonary function laboratories at the University of California, Los Angeles.
Last fall, the Food and Drug Administration approved an expanded indication for tiotropium bromide inhalation spray as long-term, add-on maintenance therapy of asthma in patients aged 12 and up who remain symptomatic despite taking other maintenance therapies. The once-daily medication had already been approved in the fall of 2014 for maintenance therapy of chronic obstructive pulmonary disease. Spiriva Respimat delivers a once-daily 2.5-mcg dose of tiotropium bromide via two 1.25-mcg puffs in a slow-moving, propellant-free mist designed to get the drug into the distal lungs independent of a patient’s skill in using a conventional metered-dose inhaler.
Dr. Tashkin and his coinvestigators presented a series of post hoc analyses combining data on 3,012 participants in the two prospective PrimoTinA-asthma and two MezzoTinA-asthma clinical trials. These phase III, double-blind, placebo-controlled trials defined participants’ allergic phenotype on the basis of the conventional cut points of a serum IgE level above or below 430 mcg/mL or a blood eosinophil count above or below 600 cells/mcL.
“The question is, are these appropriate cut points? Can we be sure that somebody below those cut points doesn’t have atopy? To answer that question, we looked at the whole spectrum of eosinophils in the blood from 5/mcL to 2,000/mcL and serum IgE levels from 2 mcg/mL to 2,000 mcg/mL. We found that the efficacy was similar across the entire spectrum of these measures of allergy,” he said in an interview.
Thus, these new findings support the use of this novel maintenance therapy without any need for lab tests to determine whether an individual patient’s asthma is T helper 2–cell dominant or not, Dr. Tashkin added.
The PrimoTinA-asthma trials were 48-week studies of add-on Spiriva Respimat or placebo conducted in patients with symptomatic asthma despite treatment with an inhaled corticosteroid plus a long-acting beta-agonist. The MezzoTinA-asthma studies were 24 weeks long and focused on patients who remained symptomatic despite at least moderate-dose inhaled corticosteroid therapy. Key endpoints included improvement in asthma symptom control as measured by the seven-question Asthma Control Questionnaire, improved peak and trough forced expiratory volume in 1 second, and time to a first severe asthma exacerbation.
Dr. Tashkin reported serving as a paid speaker on behalf of Boehringer Ingelheim, which markets Spiriva Respimat and sponsored the studies.
EXPERT ANALYSIS FROM THE 2016 AAAAI ANNUAL MEETING

Resistant Hypertension? Time to Consider This Fourth-line Drug
PRACTICE CHANGER
When a triple regimen (ACE inhibitor or ARB, calcium channel blocker, and thiazide diuretic) fails to achieve the target blood pressure, try adding spironolactone.
Strength of recommendation
C: Based on a high-quality disease-oriented randomized controlled trial.1
Willie S, a 56-year-old man with chronic essential hypertension, has been on an optimally dosed three-drug regimen of an ACE inhibitor, a calcium channel blocker, and a thiazide diuretic for more than three months, but his blood pressure is still not at goal. What is the best antihypertensive agent to add to his regimen?
About 5% to 30% of those being treated for hypertension have resistant hypertension, defined as inadequate blood pressure (BP) control despite a triple regimen of an ACE inhibitor or angiotensin receptor blocker (ARB), calcium channel blocker (CCB), and thiazide diuretic.1,2Guidelines from the Eighth Joint National Committee (JNC-8) on the management of high BP recommend ß-blockers, α-blockers, or aldosterone antagonists (AAs) as equivalent choices for a fourth-line agent. The recommendation is based on expert opinion.3
Earlier hypertension guidelines from the UK’s National Institute for Health and Care Excellence recommend an AA if BP targets have not been met with the triple regimen. But this recommendation is based on lower-quality evidence, without comparison to ß-blockers, α-blockers, or other drug classes.4
More evidence since guideline’s release
A 2015 meta-analysis of 15 studies and a total of more than 1,200 participants (three randomized controlled trials [RCTs], one non-randomized placebo-controlled comparative trial, and 11 single-arm observational studies) demonstrated the effectiveness of the AAs spironolactone and eplerenone on resistant hypertension.5In the four comparative studies, AAs decreased office systolic blood pressure (SBP) by 24.3 mm Hg and diastolic blood pressure (DBP) by 7.8 mm Hg more than placebo. In the 11 single-arm studies, AAs reduced SBP by 22.74 mm Hg and DBP by 10.49 mm Hg.
Another RCT examined the effect of low-dose (25-mg) spironolactone, compared with placebo, in 161 patients with resistant hypertension.6At eight weeks, 73% of those receiving spironolactone reached a goal SBP < 140 mm Hg versus 41% of patients on placebo. The same proportion (73%) achieved a goal DBP < 90 mm Hg in the spironolactone group, compared with 63% of those in the placebo group. Ambulatory BP was also found to be significantly improved among those receiving spironolactone versus placebo, with a decrease in SBP of 9.8 mm Hg and in DSP of 3.2 mm Hg.6
Continue for the study summary >>
STUDY SUMMARY
Spironolactone vs other drugs
The placebo-controlled crossover RCT conducted in the UK by Williams et al was the first to directly compare spironolactone with other medications for the treatment of resistant hypertension in adults already taking triple therapy.1The trial randomized 335 individuals with a mean age of 61.4 (range, 18 to 79), 69% of whom were male; 314 were included in the intention-to-treat analysis.1
Enrollment criteria for resistant hypertension specified a clinic-recorded SBP of ≥ 140 mm Hg (or ≥ 135 mm Hg in those with diabetes) and home SBP (in 18 readings over four days) of ≥ 130 mm Hg.1 To ensure fidelity to treatment protocols, the investigators directly observed therapy, took tablet counts, measured serum ACE activity, and assessed BP measurement technique, with all participants adhering to a minimum of three months on a maximally dosed triple regimen.
Among subjects, 14% had diabetes and 7.8% reported tobacco use. Average weight was 93.5 kg (205.7 lbs).1 Because of the expected inverse relationship between plasma renin and response to AAs, plasma renin was measured at baseline to test whether resistant hypertension was primarily due to sodium retention.1
Four 12-week rotations
All participants began the trial with four weeks of placebo, followed by randomization to 12-week rotations of once-daily oral treatment with (1) spironolactone 25 to 50 mg, (2) doxazosin modified release 4 to 8 mg, (3) bisoprolol 5 to 10 mg, and (4) placebo.1 Six weeks after initiation of each study medication, participants were titrated to the higher dose. There was no washout period between cycles.
The primary outcome was mean SBP measured at home on four consecutive days prior to the study visits in weeks 6 and 12. Participants were required to have at least six BP measurements per each six-week period in order to establish a valid average. Primary endpoints included the difference in home SBP between spironolactone and placebo, the difference in home SBP between spironolactone and the mean of the other two drugs, and the difference in home SBP between spironolactone and each of the other two drugs.
The results. Spironolactone lowered SBP more than placebo, doxazosin, and bisoprolol (see the Table).1 Clinic measurements were consistent with home BP readings.
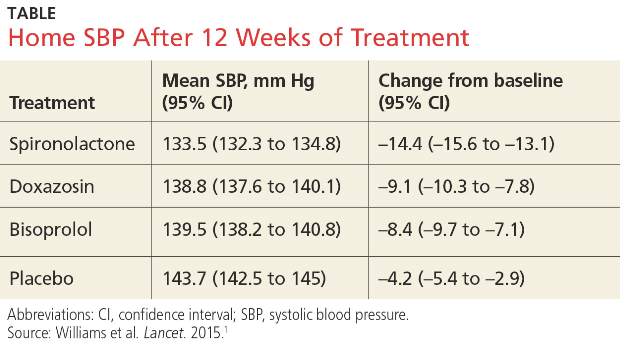
Overall, 58% of participants achieved goal SBP < 135 mm Hg on spironolactone, compared with 42% on doxazosin, 44% on bisoprolol, and 24% on placebo.1 The effectiveness of spironolactone on SBP reduction was shown to exhibit an inverse relationship to plasma renin levels, a finding that was not apparent with the other two study drugs. However, spironolactone had a superior BP-lowering effect throughout nearly the entire renin distribution of the cohort.
The mean difference between spironolactone and placebo was –10.2 mm Hg; compared with the other drugs, spironolactone lowered SBP, on average, by 5.64 mm Hg more than bisoprolol and doxazosin; 5.3 mm Hg more than doxazosin alone; and 5.98 mm Hg more than bisoprolol alone.
Only 1% of trial participants had to discontinue spironolactone due to adverse events—the same proportion of withdrawals as that for bisoprolol and placebo and three times less than for doxazosin.1
Continue for what's new >>
WHAT’S NEW
Evidence of superiority
This is the first RCT to compare spironolactone with two other commonly used fourth-line antihypertensives—bisoprolol and doxazosin—in patients with resistant hypertension. The study demonstrated clear superiority of spironolactone in achieving carefully measured ambulatory and clinic-recorded BP targets versus a ß-blocker or an α-blocker.
CAVEATS
Findings not universal
Spironolactone is contraindicated in patients with severe renal impairment. Although multiple drug trials have demonstrated the medication’s safety and effectiveness, especially in patients with resistant hypertension, we should factor in the need for monitoring electrolytes and renal function within weeks of treatment initiation and periodically thereafter.7,8 In this study, spironolactone increased potassium levels, on average, by 0.45 mmol/L. No gynecomastia (typically seen in about 6% of men) was found in those taking spironolactone for a 12-week cycle.1
This single trial enrolled mostly Caucasian men with a mean age of 61. Although smaller observational studies that included African-American patients have shown promising results for spironolactone, the question of external validity or applicability to a diverse population has yet to be decisively answered.9
CHALLENGES TO IMPLEMENTATION
Potential for adverse reactions
The evidence supporting this change in practice has been accumulating for the past few years. However, clinicians who treat patients with resistant hypertension may have concerns about hyperkalemia, gynecomastia, and effects on renal function. More patient-oriented evidence is likewise needed to assist with the revision of guidelines and wider adoption of AAs by primary care providers.
References
1. Williams B, MacDonald TM, Morant S, et al. Spironolactone versus placebo, bisoprolol, and doxazosin to determine the optimal treatment for drug-resistant hypertension (PATHWAY-2): a randomised, double-blind, crossover trial. Lancet. 2015;386:2059-2068.
2. Rosa J, Widimsky P, Tousek P, et al. Randomized comparison of renal denervation versus intensified pharmacotherapy including spironolactone in true-resistant hypertension: six-month results from the Prague-15 Study. Hypertension. 2015;65:407-413.
3. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults. JAMA. 2014;311:507-520.
4. National Institute for Health and Care Excellence. Hypertension in adults: diagnosis and management (Clinical Guideline CG127). August 2011. https://www.nice.org.uk/guidance/cg127. Accessed March 4, 2016.
5. Dahal K, Kunwar S, Rijal J, et al. The effects of aldosterone antagonists in patients with resistant hypertension: a meta-analysis of randomized and nonrandomized studies. Am J Hypertens. 2015;28:1376-1385.
6. Václavík J, Sedlák R, Jarkovský J, et al. Effect of spironolactone in resistant arterial hypertension: a randomized, double-blind, placebo-controlled trial (ASPIRANT-EXT). Medicine (Baltimore). 2014;93:e162.
7. Wei L, Struthers AD, Fahey T, et al. Spironolactone use and renal toxicity: population based longitudinal analysis. BMJ. 2010;340:c1768.
8. Oxlund CS, Henriksen JE, Tarnow L, et al. Low dose spironolactone reduces blood pressure in patients with resistant hypertension and type 2 diabetes mellitus. J Hypertens. 2013;31:2094-2102.
9. Nishizaka M, Zaman MA, Calhoun DA. Efficacy of low-dose spironolactone in subjects with resistant hypertension. Am J Hypertens. 2003;16:925-930.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2016. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2016;65(4):266-268.
PRACTICE CHANGER
When a triple regimen (ACE inhibitor or ARB, calcium channel blocker, and thiazide diuretic) fails to achieve the target blood pressure, try adding spironolactone.
Strength of recommendation
C: Based on a high-quality disease-oriented randomized controlled trial.1
Willie S, a 56-year-old man with chronic essential hypertension, has been on an optimally dosed three-drug regimen of an ACE inhibitor, a calcium channel blocker, and a thiazide diuretic for more than three months, but his blood pressure is still not at goal. What is the best antihypertensive agent to add to his regimen?
About 5% to 30% of those being treated for hypertension have resistant hypertension, defined as inadequate blood pressure (BP) control despite a triple regimen of an ACE inhibitor or angiotensin receptor blocker (ARB), calcium channel blocker (CCB), and thiazide diuretic.1,2Guidelines from the Eighth Joint National Committee (JNC-8) on the management of high BP recommend ß-blockers, α-blockers, or aldosterone antagonists (AAs) as equivalent choices for a fourth-line agent. The recommendation is based on expert opinion.3
Earlier hypertension guidelines from the UK’s National Institute for Health and Care Excellence recommend an AA if BP targets have not been met with the triple regimen. But this recommendation is based on lower-quality evidence, without comparison to ß-blockers, α-blockers, or other drug classes.4
More evidence since guideline’s release
A 2015 meta-analysis of 15 studies and a total of more than 1,200 participants (three randomized controlled trials [RCTs], one non-randomized placebo-controlled comparative trial, and 11 single-arm observational studies) demonstrated the effectiveness of the AAs spironolactone and eplerenone on resistant hypertension.5In the four comparative studies, AAs decreased office systolic blood pressure (SBP) by 24.3 mm Hg and diastolic blood pressure (DBP) by 7.8 mm Hg more than placebo. In the 11 single-arm studies, AAs reduced SBP by 22.74 mm Hg and DBP by 10.49 mm Hg.
Another RCT examined the effect of low-dose (25-mg) spironolactone, compared with placebo, in 161 patients with resistant hypertension.6At eight weeks, 73% of those receiving spironolactone reached a goal SBP < 140 mm Hg versus 41% of patients on placebo. The same proportion (73%) achieved a goal DBP < 90 mm Hg in the spironolactone group, compared with 63% of those in the placebo group. Ambulatory BP was also found to be significantly improved among those receiving spironolactone versus placebo, with a decrease in SBP of 9.8 mm Hg and in DSP of 3.2 mm Hg.6
Continue for the study summary >>
STUDY SUMMARY
Spironolactone vs other drugs
The placebo-controlled crossover RCT conducted in the UK by Williams et al was the first to directly compare spironolactone with other medications for the treatment of resistant hypertension in adults already taking triple therapy.1The trial randomized 335 individuals with a mean age of 61.4 (range, 18 to 79), 69% of whom were male; 314 were included in the intention-to-treat analysis.1
Enrollment criteria for resistant hypertension specified a clinic-recorded SBP of ≥ 140 mm Hg (or ≥ 135 mm Hg in those with diabetes) and home SBP (in 18 readings over four days) of ≥ 130 mm Hg.1 To ensure fidelity to treatment protocols, the investigators directly observed therapy, took tablet counts, measured serum ACE activity, and assessed BP measurement technique, with all participants adhering to a minimum of three months on a maximally dosed triple regimen.
Among subjects, 14% had diabetes and 7.8% reported tobacco use. Average weight was 93.5 kg (205.7 lbs).1 Because of the expected inverse relationship between plasma renin and response to AAs, plasma renin was measured at baseline to test whether resistant hypertension was primarily due to sodium retention.1
Four 12-week rotations
All participants began the trial with four weeks of placebo, followed by randomization to 12-week rotations of once-daily oral treatment with (1) spironolactone 25 to 50 mg, (2) doxazosin modified release 4 to 8 mg, (3) bisoprolol 5 to 10 mg, and (4) placebo.1 Six weeks after initiation of each study medication, participants were titrated to the higher dose. There was no washout period between cycles.
The primary outcome was mean SBP measured at home on four consecutive days prior to the study visits in weeks 6 and 12. Participants were required to have at least six BP measurements per each six-week period in order to establish a valid average. Primary endpoints included the difference in home SBP between spironolactone and placebo, the difference in home SBP between spironolactone and the mean of the other two drugs, and the difference in home SBP between spironolactone and each of the other two drugs.
The results. Spironolactone lowered SBP more than placebo, doxazosin, and bisoprolol (see the Table).1 Clinic measurements were consistent with home BP readings.
Overall, 58% of participants achieved goal SBP < 135 mm Hg on spironolactone, compared with 42% on doxazosin, 44% on bisoprolol, and 24% on placebo.1 The effectiveness of spironolactone on SBP reduction was shown to exhibit an inverse relationship to plasma renin levels, a finding that was not apparent with the other two study drugs. However, spironolactone had a superior BP-lowering effect throughout nearly the entire renin distribution of the cohort.
The mean difference between spironolactone and placebo was –10.2 mm Hg; compared with the other drugs, spironolactone lowered SBP, on average, by 5.64 mm Hg more than bisoprolol and doxazosin; 5.3 mm Hg more than doxazosin alone; and 5.98 mm Hg more than bisoprolol alone.
Only 1% of trial participants had to discontinue spironolactone due to adverse events—the same proportion of withdrawals as that for bisoprolol and placebo and three times less than for doxazosin.1
Continue for what's new >>
WHAT’S NEW
Evidence of superiority
This is the first RCT to compare spironolactone with two other commonly used fourth-line antihypertensives—bisoprolol and doxazosin—in patients with resistant hypertension. The study demonstrated clear superiority of spironolactone in achieving carefully measured ambulatory and clinic-recorded BP targets versus a ß-blocker or an α-blocker.
CAVEATS
Findings not universal
Spironolactone is contraindicated in patients with severe renal impairment. Although multiple drug trials have demonstrated the medication’s safety and effectiveness, especially in patients with resistant hypertension, we should factor in the need for monitoring electrolytes and renal function within weeks of treatment initiation and periodically thereafter.7,8 In this study, spironolactone increased potassium levels, on average, by 0.45 mmol/L. No gynecomastia (typically seen in about 6% of men) was found in those taking spironolactone for a 12-week cycle.1
This single trial enrolled mostly Caucasian men with a mean age of 61. Although smaller observational studies that included African-American patients have shown promising results for spironolactone, the question of external validity or applicability to a diverse population has yet to be decisively answered.9
CHALLENGES TO IMPLEMENTATION
Potential for adverse reactions
The evidence supporting this change in practice has been accumulating for the past few years. However, clinicians who treat patients with resistant hypertension may have concerns about hyperkalemia, gynecomastia, and effects on renal function. More patient-oriented evidence is likewise needed to assist with the revision of guidelines and wider adoption of AAs by primary care providers.
References
1. Williams B, MacDonald TM, Morant S, et al. Spironolactone versus placebo, bisoprolol, and doxazosin to determine the optimal treatment for drug-resistant hypertension (PATHWAY-2): a randomised, double-blind, crossover trial. Lancet. 2015;386:2059-2068.
2. Rosa J, Widimsky P, Tousek P, et al. Randomized comparison of renal denervation versus intensified pharmacotherapy including spironolactone in true-resistant hypertension: six-month results from the Prague-15 Study. Hypertension. 2015;65:407-413.
3. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults. JAMA. 2014;311:507-520.
4. National Institute for Health and Care Excellence. Hypertension in adults: diagnosis and management (Clinical Guideline CG127). August 2011. https://www.nice.org.uk/guidance/cg127. Accessed March 4, 2016.
5. Dahal K, Kunwar S, Rijal J, et al. The effects of aldosterone antagonists in patients with resistant hypertension: a meta-analysis of randomized and nonrandomized studies. Am J Hypertens. 2015;28:1376-1385.
6. Václavík J, Sedlák R, Jarkovský J, et al. Effect of spironolactone in resistant arterial hypertension: a randomized, double-blind, placebo-controlled trial (ASPIRANT-EXT). Medicine (Baltimore). 2014;93:e162.
7. Wei L, Struthers AD, Fahey T, et al. Spironolactone use and renal toxicity: population based longitudinal analysis. BMJ. 2010;340:c1768.
8. Oxlund CS, Henriksen JE, Tarnow L, et al. Low dose spironolactone reduces blood pressure in patients with resistant hypertension and type 2 diabetes mellitus. J Hypertens. 2013;31:2094-2102.
9. Nishizaka M, Zaman MA, Calhoun DA. Efficacy of low-dose spironolactone in subjects with resistant hypertension. Am J Hypertens. 2003;16:925-930.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2016. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2016;65(4):266-268.
PRACTICE CHANGER
When a triple regimen (ACE inhibitor or ARB, calcium channel blocker, and thiazide diuretic) fails to achieve the target blood pressure, try adding spironolactone.
Strength of recommendation
C: Based on a high-quality disease-oriented randomized controlled trial.1
Willie S, a 56-year-old man with chronic essential hypertension, has been on an optimally dosed three-drug regimen of an ACE inhibitor, a calcium channel blocker, and a thiazide diuretic for more than three months, but his blood pressure is still not at goal. What is the best antihypertensive agent to add to his regimen?
About 5% to 30% of those being treated for hypertension have resistant hypertension, defined as inadequate blood pressure (BP) control despite a triple regimen of an ACE inhibitor or angiotensin receptor blocker (ARB), calcium channel blocker (CCB), and thiazide diuretic.1,2Guidelines from the Eighth Joint National Committee (JNC-8) on the management of high BP recommend ß-blockers, α-blockers, or aldosterone antagonists (AAs) as equivalent choices for a fourth-line agent. The recommendation is based on expert opinion.3
Earlier hypertension guidelines from the UK’s National Institute for Health and Care Excellence recommend an AA if BP targets have not been met with the triple regimen. But this recommendation is based on lower-quality evidence, without comparison to ß-blockers, α-blockers, or other drug classes.4
More evidence since guideline’s release
A 2015 meta-analysis of 15 studies and a total of more than 1,200 participants (three randomized controlled trials [RCTs], one non-randomized placebo-controlled comparative trial, and 11 single-arm observational studies) demonstrated the effectiveness of the AAs spironolactone and eplerenone on resistant hypertension.5In the four comparative studies, AAs decreased office systolic blood pressure (SBP) by 24.3 mm Hg and diastolic blood pressure (DBP) by 7.8 mm Hg more than placebo. In the 11 single-arm studies, AAs reduced SBP by 22.74 mm Hg and DBP by 10.49 mm Hg.
Another RCT examined the effect of low-dose (25-mg) spironolactone, compared with placebo, in 161 patients with resistant hypertension.6At eight weeks, 73% of those receiving spironolactone reached a goal SBP < 140 mm Hg versus 41% of patients on placebo. The same proportion (73%) achieved a goal DBP < 90 mm Hg in the spironolactone group, compared with 63% of those in the placebo group. Ambulatory BP was also found to be significantly improved among those receiving spironolactone versus placebo, with a decrease in SBP of 9.8 mm Hg and in DSP of 3.2 mm Hg.6
Continue for the study summary >>
STUDY SUMMARY
Spironolactone vs other drugs
The placebo-controlled crossover RCT conducted in the UK by Williams et al was the first to directly compare spironolactone with other medications for the treatment of resistant hypertension in adults already taking triple therapy.1The trial randomized 335 individuals with a mean age of 61.4 (range, 18 to 79), 69% of whom were male; 314 were included in the intention-to-treat analysis.1
Enrollment criteria for resistant hypertension specified a clinic-recorded SBP of ≥ 140 mm Hg (or ≥ 135 mm Hg in those with diabetes) and home SBP (in 18 readings over four days) of ≥ 130 mm Hg.1 To ensure fidelity to treatment protocols, the investigators directly observed therapy, took tablet counts, measured serum ACE activity, and assessed BP measurement technique, with all participants adhering to a minimum of three months on a maximally dosed triple regimen.
Among subjects, 14% had diabetes and 7.8% reported tobacco use. Average weight was 93.5 kg (205.7 lbs).1 Because of the expected inverse relationship between plasma renin and response to AAs, plasma renin was measured at baseline to test whether resistant hypertension was primarily due to sodium retention.1
Four 12-week rotations
All participants began the trial with four weeks of placebo, followed by randomization to 12-week rotations of once-daily oral treatment with (1) spironolactone 25 to 50 mg, (2) doxazosin modified release 4 to 8 mg, (3) bisoprolol 5 to 10 mg, and (4) placebo.1 Six weeks after initiation of each study medication, participants were titrated to the higher dose. There was no washout period between cycles.
The primary outcome was mean SBP measured at home on four consecutive days prior to the study visits in weeks 6 and 12. Participants were required to have at least six BP measurements per each six-week period in order to establish a valid average. Primary endpoints included the difference in home SBP between spironolactone and placebo, the difference in home SBP between spironolactone and the mean of the other two drugs, and the difference in home SBP between spironolactone and each of the other two drugs.
The results. Spironolactone lowered SBP more than placebo, doxazosin, and bisoprolol (see the Table).1 Clinic measurements were consistent with home BP readings.
Overall, 58% of participants achieved goal SBP < 135 mm Hg on spironolactone, compared with 42% on doxazosin, 44% on bisoprolol, and 24% on placebo.1 The effectiveness of spironolactone on SBP reduction was shown to exhibit an inverse relationship to plasma renin levels, a finding that was not apparent with the other two study drugs. However, spironolactone had a superior BP-lowering effect throughout nearly the entire renin distribution of the cohort.
The mean difference between spironolactone and placebo was –10.2 mm Hg; compared with the other drugs, spironolactone lowered SBP, on average, by 5.64 mm Hg more than bisoprolol and doxazosin; 5.3 mm Hg more than doxazosin alone; and 5.98 mm Hg more than bisoprolol alone.
Only 1% of trial participants had to discontinue spironolactone due to adverse events—the same proportion of withdrawals as that for bisoprolol and placebo and three times less than for doxazosin.1
Continue for what's new >>
WHAT’S NEW
Evidence of superiority
This is the first RCT to compare spironolactone with two other commonly used fourth-line antihypertensives—bisoprolol and doxazosin—in patients with resistant hypertension. The study demonstrated clear superiority of spironolactone in achieving carefully measured ambulatory and clinic-recorded BP targets versus a ß-blocker or an α-blocker.
CAVEATS
Findings not universal
Spironolactone is contraindicated in patients with severe renal impairment. Although multiple drug trials have demonstrated the medication’s safety and effectiveness, especially in patients with resistant hypertension, we should factor in the need for monitoring electrolytes and renal function within weeks of treatment initiation and periodically thereafter.7,8 In this study, spironolactone increased potassium levels, on average, by 0.45 mmol/L. No gynecomastia (typically seen in about 6% of men) was found in those taking spironolactone for a 12-week cycle.1
This single trial enrolled mostly Caucasian men with a mean age of 61. Although smaller observational studies that included African-American patients have shown promising results for spironolactone, the question of external validity or applicability to a diverse population has yet to be decisively answered.9
CHALLENGES TO IMPLEMENTATION
Potential for adverse reactions
The evidence supporting this change in practice has been accumulating for the past few years. However, clinicians who treat patients with resistant hypertension may have concerns about hyperkalemia, gynecomastia, and effects on renal function. More patient-oriented evidence is likewise needed to assist with the revision of guidelines and wider adoption of AAs by primary care providers.
References
1. Williams B, MacDonald TM, Morant S, et al. Spironolactone versus placebo, bisoprolol, and doxazosin to determine the optimal treatment for drug-resistant hypertension (PATHWAY-2): a randomised, double-blind, crossover trial. Lancet. 2015;386:2059-2068.
2. Rosa J, Widimsky P, Tousek P, et al. Randomized comparison of renal denervation versus intensified pharmacotherapy including spironolactone in true-resistant hypertension: six-month results from the Prague-15 Study. Hypertension. 2015;65:407-413.
3. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults. JAMA. 2014;311:507-520.
4. National Institute for Health and Care Excellence. Hypertension in adults: diagnosis and management (Clinical Guideline CG127). August 2011. https://www.nice.org.uk/guidance/cg127. Accessed March 4, 2016.
5. Dahal K, Kunwar S, Rijal J, et al. The effects of aldosterone antagonists in patients with resistant hypertension: a meta-analysis of randomized and nonrandomized studies. Am J Hypertens. 2015;28:1376-1385.
6. Václavík J, Sedlák R, Jarkovský J, et al. Effect of spironolactone in resistant arterial hypertension: a randomized, double-blind, placebo-controlled trial (ASPIRANT-EXT). Medicine (Baltimore). 2014;93:e162.
7. Wei L, Struthers AD, Fahey T, et al. Spironolactone use and renal toxicity: population based longitudinal analysis. BMJ. 2010;340:c1768.
8. Oxlund CS, Henriksen JE, Tarnow L, et al. Low dose spironolactone reduces blood pressure in patients with resistant hypertension and type 2 diabetes mellitus. J Hypertens. 2013;31:2094-2102.
9. Nishizaka M, Zaman MA, Calhoun DA. Efficacy of low-dose spironolactone in subjects with resistant hypertension. Am J Hypertens. 2003;16:925-930.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2016. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2016;65(4):266-268.