User login
Changes to Healthcare that Hospitalists Should Expect in 2016
On the heels of last year’s repeal of the sustainable growth rate (SGR) formula, 2016 promises to be a year of significant changes for the healthcare system. These changes will require providers to focus not just on the immediate pressures and requirements coming from Medicare, of which there are many, but also to look down the road to how things will change in the coming years.
The final year of reporting on quality measures for the Physician Quality Reporting System (PQRS) is 2016, with performance impacting Medicare payments in 2018. Reporting on quality measures doesn’t end there, however. The Medicare Access and CHIP Reauthorization Act (MACRA) repealed the SGR and created two new pathways for pay-for-performance for physicians and most other providers: the Merit-based Incentive Payment System (MIPS) and alternative payment models. After this year, reporting quality measures becomes one component of the MIPS, a program similar to hospital value-based purchasing, but designed for providers.
Quality measures are here to stay. They form the backbone for evaluating whether healthcare is of value. Under the MIPS, quality measures are combined with cost measures, meaningful use, and clinical performance improvement activities to create an aggregate score for providers. That score will be used to determine payment adjustments for providers starting in 2019.
Also in 2016, the Centers for Medicare and Medicaid Services (CMS) will lay the foundation for the MIPS. It is a completely new program, and although it will build on elements of existing programs like PQRS, meaningful use, and the physician value-based payment modifier, its structure and ramifications are ultimately unknown. CMS has indicated its intention to issue the regulatory backbone of MIPS in just a few months. These regulations will be the new reality of Medicare’s fee-for-service for the foreseeable future.
The ramifications of MIPS cannot be understated. It will apply an adjustment based on performance on all Medicare Part B payments. That adjustment starts at +/- 4.0% in 2019 and rises to +/- 9.0% by 2022, a number that is not as far off as it seems based on how these programs operate.
SHM expects many of the current PQRS policies to be continued under MIPS, which means, unfortunately, that many of the challenges facing hospitalists will continue. Hospitalists do not have many measures to report on; most measures are developed for outpatient practices, are simply not reflective of the variability of hospitalist practice, and, even if specified for inpatient reporting, are not clinically relevant.
To meet the needs of hospitalists, SHM will advocate strongly for CMS to develop more flexible and relevant reporting options. We will work to ensure that hospitalists are not structurally disadvantaged by the policies set in place.
Given these upcoming changes, it is as important as ever for you to stay engaged and informed about the policy changes coming down the road. It might be just the start of the year, but already there’s a lot of critical work to do. To get involved and remain apprised of the changes, join SHM’s grassroots network at www.hospitalmedicine.org/grassroots. TH
Joshua Lapps is SHM’s government relations manager.
On the heels of last year’s repeal of the sustainable growth rate (SGR) formula, 2016 promises to be a year of significant changes for the healthcare system. These changes will require providers to focus not just on the immediate pressures and requirements coming from Medicare, of which there are many, but also to look down the road to how things will change in the coming years.
The final year of reporting on quality measures for the Physician Quality Reporting System (PQRS) is 2016, with performance impacting Medicare payments in 2018. Reporting on quality measures doesn’t end there, however. The Medicare Access and CHIP Reauthorization Act (MACRA) repealed the SGR and created two new pathways for pay-for-performance for physicians and most other providers: the Merit-based Incentive Payment System (MIPS) and alternative payment models. After this year, reporting quality measures becomes one component of the MIPS, a program similar to hospital value-based purchasing, but designed for providers.
Quality measures are here to stay. They form the backbone for evaluating whether healthcare is of value. Under the MIPS, quality measures are combined with cost measures, meaningful use, and clinical performance improvement activities to create an aggregate score for providers. That score will be used to determine payment adjustments for providers starting in 2019.
Also in 2016, the Centers for Medicare and Medicaid Services (CMS) will lay the foundation for the MIPS. It is a completely new program, and although it will build on elements of existing programs like PQRS, meaningful use, and the physician value-based payment modifier, its structure and ramifications are ultimately unknown. CMS has indicated its intention to issue the regulatory backbone of MIPS in just a few months. These regulations will be the new reality of Medicare’s fee-for-service for the foreseeable future.
The ramifications of MIPS cannot be understated. It will apply an adjustment based on performance on all Medicare Part B payments. That adjustment starts at +/- 4.0% in 2019 and rises to +/- 9.0% by 2022, a number that is not as far off as it seems based on how these programs operate.
SHM expects many of the current PQRS policies to be continued under MIPS, which means, unfortunately, that many of the challenges facing hospitalists will continue. Hospitalists do not have many measures to report on; most measures are developed for outpatient practices, are simply not reflective of the variability of hospitalist practice, and, even if specified for inpatient reporting, are not clinically relevant.
To meet the needs of hospitalists, SHM will advocate strongly for CMS to develop more flexible and relevant reporting options. We will work to ensure that hospitalists are not structurally disadvantaged by the policies set in place.
Given these upcoming changes, it is as important as ever for you to stay engaged and informed about the policy changes coming down the road. It might be just the start of the year, but already there’s a lot of critical work to do. To get involved and remain apprised of the changes, join SHM’s grassroots network at www.hospitalmedicine.org/grassroots. TH
Joshua Lapps is SHM’s government relations manager.
On the heels of last year’s repeal of the sustainable growth rate (SGR) formula, 2016 promises to be a year of significant changes for the healthcare system. These changes will require providers to focus not just on the immediate pressures and requirements coming from Medicare, of which there are many, but also to look down the road to how things will change in the coming years.
The final year of reporting on quality measures for the Physician Quality Reporting System (PQRS) is 2016, with performance impacting Medicare payments in 2018. Reporting on quality measures doesn’t end there, however. The Medicare Access and CHIP Reauthorization Act (MACRA) repealed the SGR and created two new pathways for pay-for-performance for physicians and most other providers: the Merit-based Incentive Payment System (MIPS) and alternative payment models. After this year, reporting quality measures becomes one component of the MIPS, a program similar to hospital value-based purchasing, but designed for providers.
Quality measures are here to stay. They form the backbone for evaluating whether healthcare is of value. Under the MIPS, quality measures are combined with cost measures, meaningful use, and clinical performance improvement activities to create an aggregate score for providers. That score will be used to determine payment adjustments for providers starting in 2019.
Also in 2016, the Centers for Medicare and Medicaid Services (CMS) will lay the foundation for the MIPS. It is a completely new program, and although it will build on elements of existing programs like PQRS, meaningful use, and the physician value-based payment modifier, its structure and ramifications are ultimately unknown. CMS has indicated its intention to issue the regulatory backbone of MIPS in just a few months. These regulations will be the new reality of Medicare’s fee-for-service for the foreseeable future.
The ramifications of MIPS cannot be understated. It will apply an adjustment based on performance on all Medicare Part B payments. That adjustment starts at +/- 4.0% in 2019 and rises to +/- 9.0% by 2022, a number that is not as far off as it seems based on how these programs operate.
SHM expects many of the current PQRS policies to be continued under MIPS, which means, unfortunately, that many of the challenges facing hospitalists will continue. Hospitalists do not have many measures to report on; most measures are developed for outpatient practices, are simply not reflective of the variability of hospitalist practice, and, even if specified for inpatient reporting, are not clinically relevant.
To meet the needs of hospitalists, SHM will advocate strongly for CMS to develop more flexible and relevant reporting options. We will work to ensure that hospitalists are not structurally disadvantaged by the policies set in place.
Given these upcoming changes, it is as important as ever for you to stay engaged and informed about the policy changes coming down the road. It might be just the start of the year, but already there’s a lot of critical work to do. To get involved and remain apprised of the changes, join SHM’s grassroots network at www.hospitalmedicine.org/grassroots. TH
Joshua Lapps is SHM’s government relations manager.
New SHM Members – January 2016
S. Godfrey, Alabama
W. Mohamed, MD, Alabama
S. Paladugu, MBBS, Alabama
E. Razzouk, Alabama
S. Bommena, MD, Arizona
L. Ledbetter, NP, Arizona
R. Nambusi, MD, Arkansas
S. Asarch, California
J. Barber, California
M. Bikhchandani, California
B. Boesch, DO, California
C. Brown, California
A. Bui, California
E. Collier, California
L. Demyan, California
S. Dowlatshahi, California
M. Edmunds, California
A. Eniasivam, MD, California
Z. Fernandez, California
S. George, MD, California
E. Granflor, ACNP, MSN, RN, California
V. Guitierrez, California
M. Incze, California
B. Jones-Linares, California
S. Judon, California
L. Khuu, MD, California
T. Kim, MD, California
A. Lakhanpal, California
B. Lee, California
E. Li, California
E. Liaw, California
V. Lieu, California
S. Lim, California
B. Lin, California
B. Lizarraga, California
J. Martinez-Cuellar, MD, California
M. Militante-Miller, DO, California
H. Montoya, California
D. Moon, California
L. Mukdad, California
N. Nardoni, California
K. Nguyen, California
B. Ramirez, California
R. Ramos, California
A. Reyes, California
W. Schlesinger, California
B. Scott, California
S. Singh, DO, California
C. Su, California
A. Tavakoli, California
O. Viramontes, California
J. Wassei, MD, California
R. Weiss, MD, California
J. Yuan, MD, California
W. Zellalem, DO, California
Y. Zheng, California
P. Filipowski, MD, Colorado
T. Guns, BHA, Colorado
A. Koch, DO, Colorado
N. Matthews, MD, Colorado
G. McGuire, MD, Colorado
M. Prakash, MBBS, Colorado
L. Stiff, MD, Colorado
J. Garcia, MD, Connecticut
L. Haut, Connecticut
O. Aly, MD, Washington, D.C.
C. Cole, MBA, Washington, D.C.
K. Allen, DO, Florida
S. Andrews, ANP, MS, Florida
G. Clayton, MD, Florida
P. Dubon, MD, Florida
S. Jadonath, MD, Florida
F. Keen, FACP, MD, Florida
A. Khanna, MD, Florida
J. Morrison, MD, PhD, Florida
K. Myint, MBBS, Florida
C. Riccard, MD, Florida
P. Russoniello, ARNP, RN, Florida
L. Staat, ARNP, Florida
K. Tamar, FACS, Florida
R. Torres, MD, Florida
M. Klimenko, MD, Georgia
S. Kommidi, MD, Georgia
H. Patel, MD, Georgia
T. Agni, Illinois
O. Al-Heeti, MD, Illinois
M. Allen, Illinois
C. Brines, Illinois
C. Campbell, Illinois
J. Cho, Illinois
A. Cordasco, Illinois
K. Cramer, Illinois
K. Crawford, Illinois
L. Crawford, Illinois
J. Dale, Illinois
R. Davidov, Illinois
O. Doolittle, Illinois
A. Fuller, Illinois
L. Garland, MD, Illinois
S. Godbois, Illinois
E. Gonzales, Illinois
S. Gupta, MD, Illinois
R. Hameeduddin, DO, Illinois
K. Hayes, Illinois
C. Hill, Illinois
M. Jackson, Illinois
S. Jackson, Illinois
H. Jang, Illinois
M. Keegan, Illinois
E. Kimmie, Illinois
T. Lombardo, Illinois
S. McGowan, Illinois
M. Megaly, Illinois
A. Morker, Illinois
L. Moyar, Illinois
V. Patel, Illinois
C. Pena, Illinois
C. Pinotti, Illinois
W. Poisson, Illinois
K. Puleo, Illinois
R. Schmidgall, Illinois
B. Segel, MD, Illinois
S. Teshale, MD, Illinois
N. Velasquez, Illinois
S. Yeom, Illinois
M. Deb Roy, MD, Indiana
N. Delecaris, MD, Indiana
J. Gilbert, MD, Indiana
M. Ali, Iowa
S. Patel, MD, Kentucky
H. Shah, DO, Kentucky
S. Abraham, MD, Louisiana
M. Bergstedt, MD, Louisiana
J. Burtch, Louisiana
S. Chaney, MD, Louisiana
P. Karam, Louisiana
D. Kim, Louisiana
J. Leong, Louisiana
A. Sheeder, MD, Louisiana
C. Yeh, Louisiana
M. Cunanan-Bush, Maryland
K. Gottlieb, MD, MBA, MS, Maryland
T. Halley, FAAP, Maryland
E. Sholder, PA-C, Maryland
S. Sumner, DO, Maryland
A. Diranian, PA-C, Massachusetts
M. Hunt, DO, Massachusetts
S. Sasidharan, Massachusetts
A. Abdulrazzak, MD, FACP, Michigan
M. Antonishen, Michigan
A. Dhaliwal, MD, Michigan
A. Drummond, MD, Michigan
K. Fitzgerald, MD, Michigan
J. Greenberg, MD, Michigan
C. Lang, MD, Michigan
S. McGinnis, DO, Michigan
L. McMann, Michigan
A. Uwaje, FACP, MD, Michigan
E. Wisniewski, MSN, RN, Michigan
J. Benson, DO, Minnesota
V. Chaudhary, MD, Minnesota
T. Wood, Minnesota
C. Yarke, MD, Minnesota
D. Phillippi, MD, Mississippi
D. Loa, Missouri
J. Loa, Missouri
N. Patel, MD, Missouri
E. Sauer, Missouri
K. Tompkins, MD, FAAP, Missouri
J. Price, FAAFP, Montana
J. Codjoe, MD, New Jersey
I. Khan, MD, New Jersey
E. Merrill, MD, New Jersey
S. Park, DO, New Jersey
T. Ronan, MD, New Mexico
N. Varvaresou, ACNP, New Mexico
E. Ahn, MD, New York
S. Anandan, New York
D. Buff, MD, New York
B. Kranitzky, MD, New York
E. Levine, MHS, MD, New York
J. Noworyta, PA-C, New York
M. Padial, New York
J. Tucker, PA-C, New York
A. Vien, New York
J. DeCoster, MD, MPH, North Carolina
P. Gambrell, NP-C, North Carolina
D. Shah, NP, North Carolina
L. Tlhabano, MD, North Carolina
O. Aduroja, MD, Ohio
A. Ahsan, MD, Ohio
A. Belagavi, Ohio
R. Carletti, Ohio
C. Cox, RN, BSN, Ohio
G. Farkas, Ohio
M. Lileas, MD, DO, FACP, Ohio
A. Lopez, MD, Ohio
S. Mall, Ohio
A. Moren, MD, Ohio
B. Sanaullah, MD, MBBS, Ohio
A. Singh, MBBS, MD, Ohio
A. Thakur, MBBS, Ohio
T. Klimenko, ACNP, Oklahoma
L. Van Dyke, ACNP, Oklahoma
K. Gandhi, Oregon
R. Petersen, Oregon
J. Pruett, MD, Oregon
C. Cobb, MSN, NP, CRNP, FNP-C, Pennsylvania
J. Hickland, Pennsylvania
O. Kufile, MD, Pennsylvania
E. McCullough, MPH, PA-C, Pennsylvania
M. McFall, Pennsylvania
S. Nazir, Pennsylvania
A. Puri, MD, Pennsylvania
W. Romeo, MS, Pennsylvania
J. Gelzhiser, MD, Rhode Island
S. Kim, BA, Rhode Island
K. Cooley, South Carolina
J. Katchman, South Carolina
T. Phillips, South Carolina
J. Oakley, PA, South Dakota
J. Douglass, DO, Tennessee
B. Herron, Tennessee
M. McCain, LPN, FNP, Tennessee
K. Zaman, MD, Tennessee
R. Desai, DO, Texas
P. LeGros, Texas
O. Nguyen, MS, Texas
S. Papineni, MD, Texas
B. Rhinehart, PA-C, Texas
C. Szych, MD, Texas
D. Allred, APRN, Utah
G. Price, Utah
K. Leonard, MD, FAAP, Vermont
D. Rand, DO, Vermont
G. Cabrera, MD, MBA, Virginia
M. Stanton, PA-C, Virginia
J. Voss, Virginia
J. Cameron, MD, Washington
K. Chaganur, MBBS, Washington
G. Dalmacion, MD, Washington
M. Lo, Washington
M. Mahal, BS, MD, Washington
D. Newton, MD, Washington
H. Bertelson, Wisconsin
E. Kitchin, MD, Wisconsin
S. Patel, MD, Wisconsin
E. Yanke, MD, Wisconsin
S. Negrete, BSC, CCFP, MD, Canada
C. Chu, MBBS, MRCP, China
J. Chan, China
N. Pillai, MBBS, MACP, Malaysia
J. Gonzalez Moreno, MD, Mexico
S. Godfrey, Alabama
W. Mohamed, MD, Alabama
S. Paladugu, MBBS, Alabama
E. Razzouk, Alabama
S. Bommena, MD, Arizona
L. Ledbetter, NP, Arizona
R. Nambusi, MD, Arkansas
S. Asarch, California
J. Barber, California
M. Bikhchandani, California
B. Boesch, DO, California
C. Brown, California
A. Bui, California
E. Collier, California
L. Demyan, California
S. Dowlatshahi, California
M. Edmunds, California
A. Eniasivam, MD, California
Z. Fernandez, California
S. George, MD, California
E. Granflor, ACNP, MSN, RN, California
V. Guitierrez, California
M. Incze, California
B. Jones-Linares, California
S. Judon, California
L. Khuu, MD, California
T. Kim, MD, California
A. Lakhanpal, California
B. Lee, California
E. Li, California
E. Liaw, California
V. Lieu, California
S. Lim, California
B. Lin, California
B. Lizarraga, California
J. Martinez-Cuellar, MD, California
M. Militante-Miller, DO, California
H. Montoya, California
D. Moon, California
L. Mukdad, California
N. Nardoni, California
K. Nguyen, California
B. Ramirez, California
R. Ramos, California
A. Reyes, California
W. Schlesinger, California
B. Scott, California
S. Singh, DO, California
C. Su, California
A. Tavakoli, California
O. Viramontes, California
J. Wassei, MD, California
R. Weiss, MD, California
J. Yuan, MD, California
W. Zellalem, DO, California
Y. Zheng, California
P. Filipowski, MD, Colorado
T. Guns, BHA, Colorado
A. Koch, DO, Colorado
N. Matthews, MD, Colorado
G. McGuire, MD, Colorado
M. Prakash, MBBS, Colorado
L. Stiff, MD, Colorado
J. Garcia, MD, Connecticut
L. Haut, Connecticut
O. Aly, MD, Washington, D.C.
C. Cole, MBA, Washington, D.C.
K. Allen, DO, Florida
S. Andrews, ANP, MS, Florida
G. Clayton, MD, Florida
P. Dubon, MD, Florida
S. Jadonath, MD, Florida
F. Keen, FACP, MD, Florida
A. Khanna, MD, Florida
J. Morrison, MD, PhD, Florida
K. Myint, MBBS, Florida
C. Riccard, MD, Florida
P. Russoniello, ARNP, RN, Florida
L. Staat, ARNP, Florida
K. Tamar, FACS, Florida
R. Torres, MD, Florida
M. Klimenko, MD, Georgia
S. Kommidi, MD, Georgia
H. Patel, MD, Georgia
T. Agni, Illinois
O. Al-Heeti, MD, Illinois
M. Allen, Illinois
C. Brines, Illinois
C. Campbell, Illinois
J. Cho, Illinois
A. Cordasco, Illinois
K. Cramer, Illinois
K. Crawford, Illinois
L. Crawford, Illinois
J. Dale, Illinois
R. Davidov, Illinois
O. Doolittle, Illinois
A. Fuller, Illinois
L. Garland, MD, Illinois
S. Godbois, Illinois
E. Gonzales, Illinois
S. Gupta, MD, Illinois
R. Hameeduddin, DO, Illinois
K. Hayes, Illinois
C. Hill, Illinois
M. Jackson, Illinois
S. Jackson, Illinois
H. Jang, Illinois
M. Keegan, Illinois
E. Kimmie, Illinois
T. Lombardo, Illinois
S. McGowan, Illinois
M. Megaly, Illinois
A. Morker, Illinois
L. Moyar, Illinois
V. Patel, Illinois
C. Pena, Illinois
C. Pinotti, Illinois
W. Poisson, Illinois
K. Puleo, Illinois
R. Schmidgall, Illinois
B. Segel, MD, Illinois
S. Teshale, MD, Illinois
N. Velasquez, Illinois
S. Yeom, Illinois
M. Deb Roy, MD, Indiana
N. Delecaris, MD, Indiana
J. Gilbert, MD, Indiana
M. Ali, Iowa
S. Patel, MD, Kentucky
H. Shah, DO, Kentucky
S. Abraham, MD, Louisiana
M. Bergstedt, MD, Louisiana
J. Burtch, Louisiana
S. Chaney, MD, Louisiana
P. Karam, Louisiana
D. Kim, Louisiana
J. Leong, Louisiana
A. Sheeder, MD, Louisiana
C. Yeh, Louisiana
M. Cunanan-Bush, Maryland
K. Gottlieb, MD, MBA, MS, Maryland
T. Halley, FAAP, Maryland
E. Sholder, PA-C, Maryland
S. Sumner, DO, Maryland
A. Diranian, PA-C, Massachusetts
M. Hunt, DO, Massachusetts
S. Sasidharan, Massachusetts
A. Abdulrazzak, MD, FACP, Michigan
M. Antonishen, Michigan
A. Dhaliwal, MD, Michigan
A. Drummond, MD, Michigan
K. Fitzgerald, MD, Michigan
J. Greenberg, MD, Michigan
C. Lang, MD, Michigan
S. McGinnis, DO, Michigan
L. McMann, Michigan
A. Uwaje, FACP, MD, Michigan
E. Wisniewski, MSN, RN, Michigan
J. Benson, DO, Minnesota
V. Chaudhary, MD, Minnesota
T. Wood, Minnesota
C. Yarke, MD, Minnesota
D. Phillippi, MD, Mississippi
D. Loa, Missouri
J. Loa, Missouri
N. Patel, MD, Missouri
E. Sauer, Missouri
K. Tompkins, MD, FAAP, Missouri
J. Price, FAAFP, Montana
J. Codjoe, MD, New Jersey
I. Khan, MD, New Jersey
E. Merrill, MD, New Jersey
S. Park, DO, New Jersey
T. Ronan, MD, New Mexico
N. Varvaresou, ACNP, New Mexico
E. Ahn, MD, New York
S. Anandan, New York
D. Buff, MD, New York
B. Kranitzky, MD, New York
E. Levine, MHS, MD, New York
J. Noworyta, PA-C, New York
M. Padial, New York
J. Tucker, PA-C, New York
A. Vien, New York
J. DeCoster, MD, MPH, North Carolina
P. Gambrell, NP-C, North Carolina
D. Shah, NP, North Carolina
L. Tlhabano, MD, North Carolina
O. Aduroja, MD, Ohio
A. Ahsan, MD, Ohio
A. Belagavi, Ohio
R. Carletti, Ohio
C. Cox, RN, BSN, Ohio
G. Farkas, Ohio
M. Lileas, MD, DO, FACP, Ohio
A. Lopez, MD, Ohio
S. Mall, Ohio
A. Moren, MD, Ohio
B. Sanaullah, MD, MBBS, Ohio
A. Singh, MBBS, MD, Ohio
A. Thakur, MBBS, Ohio
T. Klimenko, ACNP, Oklahoma
L. Van Dyke, ACNP, Oklahoma
K. Gandhi, Oregon
R. Petersen, Oregon
J. Pruett, MD, Oregon
C. Cobb, MSN, NP, CRNP, FNP-C, Pennsylvania
J. Hickland, Pennsylvania
O. Kufile, MD, Pennsylvania
E. McCullough, MPH, PA-C, Pennsylvania
M. McFall, Pennsylvania
S. Nazir, Pennsylvania
A. Puri, MD, Pennsylvania
W. Romeo, MS, Pennsylvania
J. Gelzhiser, MD, Rhode Island
S. Kim, BA, Rhode Island
K. Cooley, South Carolina
J. Katchman, South Carolina
T. Phillips, South Carolina
J. Oakley, PA, South Dakota
J. Douglass, DO, Tennessee
B. Herron, Tennessee
M. McCain, LPN, FNP, Tennessee
K. Zaman, MD, Tennessee
R. Desai, DO, Texas
P. LeGros, Texas
O. Nguyen, MS, Texas
S. Papineni, MD, Texas
B. Rhinehart, PA-C, Texas
C. Szych, MD, Texas
D. Allred, APRN, Utah
G. Price, Utah
K. Leonard, MD, FAAP, Vermont
D. Rand, DO, Vermont
G. Cabrera, MD, MBA, Virginia
M. Stanton, PA-C, Virginia
J. Voss, Virginia
J. Cameron, MD, Washington
K. Chaganur, MBBS, Washington
G. Dalmacion, MD, Washington
M. Lo, Washington
M. Mahal, BS, MD, Washington
D. Newton, MD, Washington
H. Bertelson, Wisconsin
E. Kitchin, MD, Wisconsin
S. Patel, MD, Wisconsin
E. Yanke, MD, Wisconsin
S. Negrete, BSC, CCFP, MD, Canada
C. Chu, MBBS, MRCP, China
J. Chan, China
N. Pillai, MBBS, MACP, Malaysia
J. Gonzalez Moreno, MD, Mexico
S. Godfrey, Alabama
W. Mohamed, MD, Alabama
S. Paladugu, MBBS, Alabama
E. Razzouk, Alabama
S. Bommena, MD, Arizona
L. Ledbetter, NP, Arizona
R. Nambusi, MD, Arkansas
S. Asarch, California
J. Barber, California
M. Bikhchandani, California
B. Boesch, DO, California
C. Brown, California
A. Bui, California
E. Collier, California
L. Demyan, California
S. Dowlatshahi, California
M. Edmunds, California
A. Eniasivam, MD, California
Z. Fernandez, California
S. George, MD, California
E. Granflor, ACNP, MSN, RN, California
V. Guitierrez, California
M. Incze, California
B. Jones-Linares, California
S. Judon, California
L. Khuu, MD, California
T. Kim, MD, California
A. Lakhanpal, California
B. Lee, California
E. Li, California
E. Liaw, California
V. Lieu, California
S. Lim, California
B. Lin, California
B. Lizarraga, California
J. Martinez-Cuellar, MD, California
M. Militante-Miller, DO, California
H. Montoya, California
D. Moon, California
L. Mukdad, California
N. Nardoni, California
K. Nguyen, California
B. Ramirez, California
R. Ramos, California
A. Reyes, California
W. Schlesinger, California
B. Scott, California
S. Singh, DO, California
C. Su, California
A. Tavakoli, California
O. Viramontes, California
J. Wassei, MD, California
R. Weiss, MD, California
J. Yuan, MD, California
W. Zellalem, DO, California
Y. Zheng, California
P. Filipowski, MD, Colorado
T. Guns, BHA, Colorado
A. Koch, DO, Colorado
N. Matthews, MD, Colorado
G. McGuire, MD, Colorado
M. Prakash, MBBS, Colorado
L. Stiff, MD, Colorado
J. Garcia, MD, Connecticut
L. Haut, Connecticut
O. Aly, MD, Washington, D.C.
C. Cole, MBA, Washington, D.C.
K. Allen, DO, Florida
S. Andrews, ANP, MS, Florida
G. Clayton, MD, Florida
P. Dubon, MD, Florida
S. Jadonath, MD, Florida
F. Keen, FACP, MD, Florida
A. Khanna, MD, Florida
J. Morrison, MD, PhD, Florida
K. Myint, MBBS, Florida
C. Riccard, MD, Florida
P. Russoniello, ARNP, RN, Florida
L. Staat, ARNP, Florida
K. Tamar, FACS, Florida
R. Torres, MD, Florida
M. Klimenko, MD, Georgia
S. Kommidi, MD, Georgia
H. Patel, MD, Georgia
T. Agni, Illinois
O. Al-Heeti, MD, Illinois
M. Allen, Illinois
C. Brines, Illinois
C. Campbell, Illinois
J. Cho, Illinois
A. Cordasco, Illinois
K. Cramer, Illinois
K. Crawford, Illinois
L. Crawford, Illinois
J. Dale, Illinois
R. Davidov, Illinois
O. Doolittle, Illinois
A. Fuller, Illinois
L. Garland, MD, Illinois
S. Godbois, Illinois
E. Gonzales, Illinois
S. Gupta, MD, Illinois
R. Hameeduddin, DO, Illinois
K. Hayes, Illinois
C. Hill, Illinois
M. Jackson, Illinois
S. Jackson, Illinois
H. Jang, Illinois
M. Keegan, Illinois
E. Kimmie, Illinois
T. Lombardo, Illinois
S. McGowan, Illinois
M. Megaly, Illinois
A. Morker, Illinois
L. Moyar, Illinois
V. Patel, Illinois
C. Pena, Illinois
C. Pinotti, Illinois
W. Poisson, Illinois
K. Puleo, Illinois
R. Schmidgall, Illinois
B. Segel, MD, Illinois
S. Teshale, MD, Illinois
N. Velasquez, Illinois
S. Yeom, Illinois
M. Deb Roy, MD, Indiana
N. Delecaris, MD, Indiana
J. Gilbert, MD, Indiana
M. Ali, Iowa
S. Patel, MD, Kentucky
H. Shah, DO, Kentucky
S. Abraham, MD, Louisiana
M. Bergstedt, MD, Louisiana
J. Burtch, Louisiana
S. Chaney, MD, Louisiana
P. Karam, Louisiana
D. Kim, Louisiana
J. Leong, Louisiana
A. Sheeder, MD, Louisiana
C. Yeh, Louisiana
M. Cunanan-Bush, Maryland
K. Gottlieb, MD, MBA, MS, Maryland
T. Halley, FAAP, Maryland
E. Sholder, PA-C, Maryland
S. Sumner, DO, Maryland
A. Diranian, PA-C, Massachusetts
M. Hunt, DO, Massachusetts
S. Sasidharan, Massachusetts
A. Abdulrazzak, MD, FACP, Michigan
M. Antonishen, Michigan
A. Dhaliwal, MD, Michigan
A. Drummond, MD, Michigan
K. Fitzgerald, MD, Michigan
J. Greenberg, MD, Michigan
C. Lang, MD, Michigan
S. McGinnis, DO, Michigan
L. McMann, Michigan
A. Uwaje, FACP, MD, Michigan
E. Wisniewski, MSN, RN, Michigan
J. Benson, DO, Minnesota
V. Chaudhary, MD, Minnesota
T. Wood, Minnesota
C. Yarke, MD, Minnesota
D. Phillippi, MD, Mississippi
D. Loa, Missouri
J. Loa, Missouri
N. Patel, MD, Missouri
E. Sauer, Missouri
K. Tompkins, MD, FAAP, Missouri
J. Price, FAAFP, Montana
J. Codjoe, MD, New Jersey
I. Khan, MD, New Jersey
E. Merrill, MD, New Jersey
S. Park, DO, New Jersey
T. Ronan, MD, New Mexico
N. Varvaresou, ACNP, New Mexico
E. Ahn, MD, New York
S. Anandan, New York
D. Buff, MD, New York
B. Kranitzky, MD, New York
E. Levine, MHS, MD, New York
J. Noworyta, PA-C, New York
M. Padial, New York
J. Tucker, PA-C, New York
A. Vien, New York
J. DeCoster, MD, MPH, North Carolina
P. Gambrell, NP-C, North Carolina
D. Shah, NP, North Carolina
L. Tlhabano, MD, North Carolina
O. Aduroja, MD, Ohio
A. Ahsan, MD, Ohio
A. Belagavi, Ohio
R. Carletti, Ohio
C. Cox, RN, BSN, Ohio
G. Farkas, Ohio
M. Lileas, MD, DO, FACP, Ohio
A. Lopez, MD, Ohio
S. Mall, Ohio
A. Moren, MD, Ohio
B. Sanaullah, MD, MBBS, Ohio
A. Singh, MBBS, MD, Ohio
A. Thakur, MBBS, Ohio
T. Klimenko, ACNP, Oklahoma
L. Van Dyke, ACNP, Oklahoma
K. Gandhi, Oregon
R. Petersen, Oregon
J. Pruett, MD, Oregon
C. Cobb, MSN, NP, CRNP, FNP-C, Pennsylvania
J. Hickland, Pennsylvania
O. Kufile, MD, Pennsylvania
E. McCullough, MPH, PA-C, Pennsylvania
M. McFall, Pennsylvania
S. Nazir, Pennsylvania
A. Puri, MD, Pennsylvania
W. Romeo, MS, Pennsylvania
J. Gelzhiser, MD, Rhode Island
S. Kim, BA, Rhode Island
K. Cooley, South Carolina
J. Katchman, South Carolina
T. Phillips, South Carolina
J. Oakley, PA, South Dakota
J. Douglass, DO, Tennessee
B. Herron, Tennessee
M. McCain, LPN, FNP, Tennessee
K. Zaman, MD, Tennessee
R. Desai, DO, Texas
P. LeGros, Texas
O. Nguyen, MS, Texas
S. Papineni, MD, Texas
B. Rhinehart, PA-C, Texas
C. Szych, MD, Texas
D. Allred, APRN, Utah
G. Price, Utah
K. Leonard, MD, FAAP, Vermont
D. Rand, DO, Vermont
G. Cabrera, MD, MBA, Virginia
M. Stanton, PA-C, Virginia
J. Voss, Virginia
J. Cameron, MD, Washington
K. Chaganur, MBBS, Washington
G. Dalmacion, MD, Washington
M. Lo, Washington
M. Mahal, BS, MD, Washington
D. Newton, MD, Washington
H. Bertelson, Wisconsin
E. Kitchin, MD, Wisconsin
S. Patel, MD, Wisconsin
E. Yanke, MD, Wisconsin
S. Negrete, BSC, CCFP, MD, Canada
C. Chu, MBBS, MRCP, China
J. Chan, China
N. Pillai, MBBS, MACP, Malaysia
J. Gonzalez Moreno, MD, Mexico
Combo prolongs PFS in phase 3 MM trial

Photo by Bill Branson
Results of the phase 3 ENDEAVOR trial suggest combination carfilzomib and dexamethasone prolongs progression-free survival (PFS) in patients with relapsed or refractory multiple myeloma (MM), when compared to bortezomib plus dexamethasone.
The median PFS was 18.7 months in the carfilzomib arm and 9.4 months in the bortezomib arm.
It is not clear whether this translates to an improvement in overall survival, as those data are not yet mature.
Treatment discontinuation due to adverse events (AEs) and on-study deaths were comparable between the treatment arms, although there were several AEs that occurred more frequently in the carfilzomib arm than the bortezomib arm.
These results were published in The Lancet Oncology. The trial was funded by Onyx Pharmaceuticals, Inc., a subsidiary of Amgen.
Patient treatment and characteristics
The ENDEAVOR trial included 929 patients with relapsed/refractory MM who had received 1 to 3 prior therapeutic regimens. They were randomized to receive carfilzomib in combination with low-dose dexamethasone (n=464) or bortezomib with low-dose dexamethasone (n=465) until progression.
Patients received carfilzomib as a 30-minute infusion on days 1, 2, 8, 9, 15, and 16 of 28-day treatment cycles, along with 20 mg of dexamethasone. For cycle 1 only, carfilzomib was administered at 20 mg/m2 on days 1 and 2, followed by escalation to 56 mg/m2 from day 8. Patients who tolerated 56 mg/m2 in cycle 1 were kept at this dose for subsequent cycles.
Patients who received bortezomib (1.3 mg/m2) with low-dose dexamethasone (20 mg) were given bortezomib subcutaneously or intravenously at the discretion of the investigator. More than 75% of the patients received bortezomib subcutaneously.
Baseline characteristics were generally balanced between the treatment arms. Both arms had a median age of 65 (overall range, 30-89), and about half were male. Three-quarters of patients in both arms were white, a little over 10% were Asian, 2% were black, and about 10% did not report race/ethnicity.
A majority of patients in both arms (more than 90%) had an ECOG score of 0 or 1. Most patients (more than 60%) had standard-risk cytogenetics.
The median number of prior treatment regimens was 2 in both arms. Patients in both arms had received prior lenalidomide (38% in both arms), thalidomide (45% in the carfilzomib arm and 53% in the bortezomib arm), bortezomib (54% in both arms), and carfilzomib (<1% in both arms).
Results
The median PFS in the carfilzomib arm was roughly double that of the bortezomib arm—18.7 months and 9.4 months, respectively. The hazard ratio was 0.53 (P<0.0001).
Overall survival data are not mature and are still being monitored.
The overall response rate was 77% in the carfilzomib arm and 63% in the bortezomib arm (P<0.0001). The duration of response was 21.3 months and 10.4 months, respectively.
The proportion of patients achieving a very good partial response or better was 54.3% in the carfilzomib arm and 29% in the bortezomib arm (P<0.0001). The complete response rates were 13% and 6%, respectively (P<0.001).
Treatment discontinuation due to AEs and on-study deaths were comparable between the arms. There were 75 deaths in the carfilzomib arm and 88 deaths in the bortezomib arm.
Of the 263 patients in the carfilzomib arm who discontinued treatment, 65 did so because of AEs. Of the 351 patients in the bortezomib arm who discontinued treatment, 73 did so because of AEs.
A number of known AEs were reported at a higher rate in the carfilzomib arm than the bortezomib arm, including any-grade dyspnea (28% vs 13%), hypertension (25% vs 3%), pyrexia (27% vs 14%), cough (25% vs 15%), cardiac failure (8% vs 3%), and acute renal failure (8% vs 5%).
Rates of grade 3 or higher AEs were 73% in the carfilzomib arm and 67% in the bortezomib arm. Grade 3 or higher AEs of interest in the carfilzomib and bortezomib arms, respectively, were hypertension (9% vs 3%), dyspnea (5% vs 2%), cardiac failure (5% vs 2%), acute renal failure (4% vs 3%), ischemic heart disease (2% vs 2%), and pulmonary hypertension (0.6% vs 0.2%). ![]()
Photo by Bill Branson
Results of the phase 3 ENDEAVOR trial suggest combination carfilzomib and dexamethasone prolongs progression-free survival (PFS) in patients with relapsed or refractory multiple myeloma (MM), when compared to bortezomib plus dexamethasone.
The median PFS was 18.7 months in the carfilzomib arm and 9.4 months in the bortezomib arm.
It is not clear whether this translates to an improvement in overall survival, as those data are not yet mature.
Treatment discontinuation due to adverse events (AEs) and on-study deaths were comparable between the treatment arms, although there were several AEs that occurred more frequently in the carfilzomib arm than the bortezomib arm.
These results were published in The Lancet Oncology. The trial was funded by Onyx Pharmaceuticals, Inc., a subsidiary of Amgen.
Patient treatment and characteristics
The ENDEAVOR trial included 929 patients with relapsed/refractory MM who had received 1 to 3 prior therapeutic regimens. They were randomized to receive carfilzomib in combination with low-dose dexamethasone (n=464) or bortezomib with low-dose dexamethasone (n=465) until progression.
Patients received carfilzomib as a 30-minute infusion on days 1, 2, 8, 9, 15, and 16 of 28-day treatment cycles, along with 20 mg of dexamethasone. For cycle 1 only, carfilzomib was administered at 20 mg/m2 on days 1 and 2, followed by escalation to 56 mg/m2 from day 8. Patients who tolerated 56 mg/m2 in cycle 1 were kept at this dose for subsequent cycles.
Patients who received bortezomib (1.3 mg/m2) with low-dose dexamethasone (20 mg) were given bortezomib subcutaneously or intravenously at the discretion of the investigator. More than 75% of the patients received bortezomib subcutaneously.
Baseline characteristics were generally balanced between the treatment arms. Both arms had a median age of 65 (overall range, 30-89), and about half were male. Three-quarters of patients in both arms were white, a little over 10% were Asian, 2% were black, and about 10% did not report race/ethnicity.
A majority of patients in both arms (more than 90%) had an ECOG score of 0 or 1. Most patients (more than 60%) had standard-risk cytogenetics.
The median number of prior treatment regimens was 2 in both arms. Patients in both arms had received prior lenalidomide (38% in both arms), thalidomide (45% in the carfilzomib arm and 53% in the bortezomib arm), bortezomib (54% in both arms), and carfilzomib (<1% in both arms).
Results
The median PFS in the carfilzomib arm was roughly double that of the bortezomib arm—18.7 months and 9.4 months, respectively. The hazard ratio was 0.53 (P<0.0001).
Overall survival data are not mature and are still being monitored.
The overall response rate was 77% in the carfilzomib arm and 63% in the bortezomib arm (P<0.0001). The duration of response was 21.3 months and 10.4 months, respectively.
The proportion of patients achieving a very good partial response or better was 54.3% in the carfilzomib arm and 29% in the bortezomib arm (P<0.0001). The complete response rates were 13% and 6%, respectively (P<0.001).
Treatment discontinuation due to AEs and on-study deaths were comparable between the arms. There were 75 deaths in the carfilzomib arm and 88 deaths in the bortezomib arm.
Of the 263 patients in the carfilzomib arm who discontinued treatment, 65 did so because of AEs. Of the 351 patients in the bortezomib arm who discontinued treatment, 73 did so because of AEs.
A number of known AEs were reported at a higher rate in the carfilzomib arm than the bortezomib arm, including any-grade dyspnea (28% vs 13%), hypertension (25% vs 3%), pyrexia (27% vs 14%), cough (25% vs 15%), cardiac failure (8% vs 3%), and acute renal failure (8% vs 5%).
Rates of grade 3 or higher AEs were 73% in the carfilzomib arm and 67% in the bortezomib arm. Grade 3 or higher AEs of interest in the carfilzomib and bortezomib arms, respectively, were hypertension (9% vs 3%), dyspnea (5% vs 2%), cardiac failure (5% vs 2%), acute renal failure (4% vs 3%), ischemic heart disease (2% vs 2%), and pulmonary hypertension (0.6% vs 0.2%). ![]()
Photo by Bill Branson
Results of the phase 3 ENDEAVOR trial suggest combination carfilzomib and dexamethasone prolongs progression-free survival (PFS) in patients with relapsed or refractory multiple myeloma (MM), when compared to bortezomib plus dexamethasone.
The median PFS was 18.7 months in the carfilzomib arm and 9.4 months in the bortezomib arm.
It is not clear whether this translates to an improvement in overall survival, as those data are not yet mature.
Treatment discontinuation due to adverse events (AEs) and on-study deaths were comparable between the treatment arms, although there were several AEs that occurred more frequently in the carfilzomib arm than the bortezomib arm.
These results were published in The Lancet Oncology. The trial was funded by Onyx Pharmaceuticals, Inc., a subsidiary of Amgen.
Patient treatment and characteristics
The ENDEAVOR trial included 929 patients with relapsed/refractory MM who had received 1 to 3 prior therapeutic regimens. They were randomized to receive carfilzomib in combination with low-dose dexamethasone (n=464) or bortezomib with low-dose dexamethasone (n=465) until progression.
Patients received carfilzomib as a 30-minute infusion on days 1, 2, 8, 9, 15, and 16 of 28-day treatment cycles, along with 20 mg of dexamethasone. For cycle 1 only, carfilzomib was administered at 20 mg/m2 on days 1 and 2, followed by escalation to 56 mg/m2 from day 8. Patients who tolerated 56 mg/m2 in cycle 1 were kept at this dose for subsequent cycles.
Patients who received bortezomib (1.3 mg/m2) with low-dose dexamethasone (20 mg) were given bortezomib subcutaneously or intravenously at the discretion of the investigator. More than 75% of the patients received bortezomib subcutaneously.
Baseline characteristics were generally balanced between the treatment arms. Both arms had a median age of 65 (overall range, 30-89), and about half were male. Three-quarters of patients in both arms were white, a little over 10% were Asian, 2% were black, and about 10% did not report race/ethnicity.
A majority of patients in both arms (more than 90%) had an ECOG score of 0 or 1. Most patients (more than 60%) had standard-risk cytogenetics.
The median number of prior treatment regimens was 2 in both arms. Patients in both arms had received prior lenalidomide (38% in both arms), thalidomide (45% in the carfilzomib arm and 53% in the bortezomib arm), bortezomib (54% in both arms), and carfilzomib (<1% in both arms).
Results
The median PFS in the carfilzomib arm was roughly double that of the bortezomib arm—18.7 months and 9.4 months, respectively. The hazard ratio was 0.53 (P<0.0001).
Overall survival data are not mature and are still being monitored.
The overall response rate was 77% in the carfilzomib arm and 63% in the bortezomib arm (P<0.0001). The duration of response was 21.3 months and 10.4 months, respectively.
The proportion of patients achieving a very good partial response or better was 54.3% in the carfilzomib arm and 29% in the bortezomib arm (P<0.0001). The complete response rates were 13% and 6%, respectively (P<0.001).
Treatment discontinuation due to AEs and on-study deaths were comparable between the arms. There were 75 deaths in the carfilzomib arm and 88 deaths in the bortezomib arm.
Of the 263 patients in the carfilzomib arm who discontinued treatment, 65 did so because of AEs. Of the 351 patients in the bortezomib arm who discontinued treatment, 73 did so because of AEs.
A number of known AEs were reported at a higher rate in the carfilzomib arm than the bortezomib arm, including any-grade dyspnea (28% vs 13%), hypertension (25% vs 3%), pyrexia (27% vs 14%), cough (25% vs 15%), cardiac failure (8% vs 3%), and acute renal failure (8% vs 5%).
Rates of grade 3 or higher AEs were 73% in the carfilzomib arm and 67% in the bortezomib arm. Grade 3 or higher AEs of interest in the carfilzomib and bortezomib arms, respectively, were hypertension (9% vs 3%), dyspnea (5% vs 2%), cardiac failure (5% vs 2%), acute renal failure (4% vs 3%), ischemic heart disease (2% vs 2%), and pulmonary hypertension (0.6% vs 0.2%). ![]()
Meta-analysis backs SPRINT findings, argues for lower BP targets
In high-risk patients, blood pressure lowering is associated with significant reductions in vascular events for a range of comorbidities and baseline blood pressures, said the authors of a meta-analysis of 123 randomized controlled trials published in the last 50 years.
Each 10–mm Hg reduction in systolic blood pressure was associated with a 20% reduction in major cardiovascular disease events (95% confidence interval, 0.77-0.83), a 17% reduction in coronary heart disease (95% CI, 0.78-0.88), a 27% reduction in stroke (95% CI, 0.68-0.77), and a 28% reduction in heart failure (95% CI, 0.67-0.78), based on the meta-analysis published Dec. 23 by the Lancet.

The exception was a lack of overall benefit of blood pressure lowering for renal failure events, a finding consistent with a previous meta-analysis of moderate versus intensive blood pressure reduction.
“Lowering of blood pressure into what has been regarded the normotensive range should therefore be routinely considered for the prevention of cardiovascular disease among those deemed to be of sufficient absolute risk,” wrote Dena Ettehad of the George Institute for Global Health, Oxford, and coauthors.
“Revision is urgently needed to recent blood pressure lowering guidelines that have relaxed the blood pressure lowering thresholds,” they added.
The researchers conducted a meta-analysis of blood pressure lowering treatment, involving a total of 613,815 participants and a minimum of 1,000 patient-years of follow-up in each study arm.
The analysis indicated that a 10–mm Hg reduction in systolic blood pressure achieved an overall 13% reduction in all-cause mortality (95% CI, 0.84-0.91) but had no significant impact on the risk of renal failure events.
These effects remained similar even when the effects were compared between strata of mean baseline systolic blood pressure, baseline coronary heart disease, or baseline cardiovascular disease (Lancet 2015 Dec 23. doi: 10.1016/S0140-6736(15)01225-8).
“In stratified analyses, we saw no strong evidence that proportional effects were diminished in trials that included people with lower baseline systolic blood pressure (less than 130 mm Hg), and major cardiovascular events were clearly reduced in high-risk patients with various baseline comorbidities,” the investigators wrote.
“Both of these major findings – the efficacy of blood pressure lowering below 130 mm Hg and the similar proportional effects in high-risk populations – are consistent with and extend the findings of the SPRINT trial,” they said.
The authors did note greater proportional reductions in the risk of stroke in populations without a history of cerebrovascular disease, compared with those with a history.
Populations without diabetes had significantly greater proportional reductions in risk, compared with those with diabetes, while populations without chronic kidney disease had greater proportional reductions in the risk of major cardiovascular disease events, compared with those with chronic kidney disease.
The five classes of antihypertensives were generally as effective as each other in reducing the risk of major outcomes.
The authors noted that, while there were small but significant differences between drug classes for outcomes, these effects may have been the result of differences in control regimens or the concurrent use of multiple drug classes in many trials.
Two authors were supported by the National Institute of Health Research, one by the Clarendon Fund, and one by the Rhodes Trust. The George Institute is supported by the Oxford Martin School. Two authors declared grants from Servier, and one also declared investments for the development of a polypill. No other conflicts of interest were declared.
The finding from this meta-analysis that there is no increased risk of any outcome with systolic blood pressure lowering shows that a J-shaped relationship could not be substantiated and that the treatment effects were unlikely to be attenuated in trials that included participants with low systolic blood pressures at baseline, particularly those with less than 130 mm Hg.
Since data are accumulating against the J-shaped relationship, and because energetic lowering of blood pressure seems safe and beneficial to patients, there is no reason not to apply this approach to high-risk patients.
Dr. Stéphane Laurent and Dr. Pierre Boutouyrie are with the department of pharmacology at European Georges Pompidou Hospital, Paris. These comments were taken from an accompanying editorial (Lancet 2015 Dec 23. doi: 10.1016/S0140-6736(15)01344-6). Dr. Boutouyrie declared grants and personal fees from Servier. Dr. Laurent had no conflicts of interest to declare.
The finding from this meta-analysis that there is no increased risk of any outcome with systolic blood pressure lowering shows that a J-shaped relationship could not be substantiated and that the treatment effects were unlikely to be attenuated in trials that included participants with low systolic blood pressures at baseline, particularly those with less than 130 mm Hg.
Since data are accumulating against the J-shaped relationship, and because energetic lowering of blood pressure seems safe and beneficial to patients, there is no reason not to apply this approach to high-risk patients.
Dr. Stéphane Laurent and Dr. Pierre Boutouyrie are with the department of pharmacology at European Georges Pompidou Hospital, Paris. These comments were taken from an accompanying editorial (Lancet 2015 Dec 23. doi: 10.1016/S0140-6736(15)01344-6). Dr. Boutouyrie declared grants and personal fees from Servier. Dr. Laurent had no conflicts of interest to declare.
The finding from this meta-analysis that there is no increased risk of any outcome with systolic blood pressure lowering shows that a J-shaped relationship could not be substantiated and that the treatment effects were unlikely to be attenuated in trials that included participants with low systolic blood pressures at baseline, particularly those with less than 130 mm Hg.
Since data are accumulating against the J-shaped relationship, and because energetic lowering of blood pressure seems safe and beneficial to patients, there is no reason not to apply this approach to high-risk patients.
Dr. Stéphane Laurent and Dr. Pierre Boutouyrie are with the department of pharmacology at European Georges Pompidou Hospital, Paris. These comments were taken from an accompanying editorial (Lancet 2015 Dec 23. doi: 10.1016/S0140-6736(15)01344-6). Dr. Boutouyrie declared grants and personal fees from Servier. Dr. Laurent had no conflicts of interest to declare.
In high-risk patients, blood pressure lowering is associated with significant reductions in vascular events for a range of comorbidities and baseline blood pressures, said the authors of a meta-analysis of 123 randomized controlled trials published in the last 50 years.
Each 10–mm Hg reduction in systolic blood pressure was associated with a 20% reduction in major cardiovascular disease events (95% confidence interval, 0.77-0.83), a 17% reduction in coronary heart disease (95% CI, 0.78-0.88), a 27% reduction in stroke (95% CI, 0.68-0.77), and a 28% reduction in heart failure (95% CI, 0.67-0.78), based on the meta-analysis published Dec. 23 by the Lancet.
The exception was a lack of overall benefit of blood pressure lowering for renal failure events, a finding consistent with a previous meta-analysis of moderate versus intensive blood pressure reduction.
“Lowering of blood pressure into what has been regarded the normotensive range should therefore be routinely considered for the prevention of cardiovascular disease among those deemed to be of sufficient absolute risk,” wrote Dena Ettehad of the George Institute for Global Health, Oxford, and coauthors.
“Revision is urgently needed to recent blood pressure lowering guidelines that have relaxed the blood pressure lowering thresholds,” they added.
The researchers conducted a meta-analysis of blood pressure lowering treatment, involving a total of 613,815 participants and a minimum of 1,000 patient-years of follow-up in each study arm.
The analysis indicated that a 10–mm Hg reduction in systolic blood pressure achieved an overall 13% reduction in all-cause mortality (95% CI, 0.84-0.91) but had no significant impact on the risk of renal failure events.
These effects remained similar even when the effects were compared between strata of mean baseline systolic blood pressure, baseline coronary heart disease, or baseline cardiovascular disease (Lancet 2015 Dec 23. doi: 10.1016/S0140-6736(15)01225-8).
“In stratified analyses, we saw no strong evidence that proportional effects were diminished in trials that included people with lower baseline systolic blood pressure (less than 130 mm Hg), and major cardiovascular events were clearly reduced in high-risk patients with various baseline comorbidities,” the investigators wrote.
“Both of these major findings – the efficacy of blood pressure lowering below 130 mm Hg and the similar proportional effects in high-risk populations – are consistent with and extend the findings of the SPRINT trial,” they said.
The authors did note greater proportional reductions in the risk of stroke in populations without a history of cerebrovascular disease, compared with those with a history.
Populations without diabetes had significantly greater proportional reductions in risk, compared with those with diabetes, while populations without chronic kidney disease had greater proportional reductions in the risk of major cardiovascular disease events, compared with those with chronic kidney disease.
The five classes of antihypertensives were generally as effective as each other in reducing the risk of major outcomes.
The authors noted that, while there were small but significant differences between drug classes for outcomes, these effects may have been the result of differences in control regimens or the concurrent use of multiple drug classes in many trials.
Two authors were supported by the National Institute of Health Research, one by the Clarendon Fund, and one by the Rhodes Trust. The George Institute is supported by the Oxford Martin School. Two authors declared grants from Servier, and one also declared investments for the development of a polypill. No other conflicts of interest were declared.
In high-risk patients, blood pressure lowering is associated with significant reductions in vascular events for a range of comorbidities and baseline blood pressures, said the authors of a meta-analysis of 123 randomized controlled trials published in the last 50 years.
Each 10–mm Hg reduction in systolic blood pressure was associated with a 20% reduction in major cardiovascular disease events (95% confidence interval, 0.77-0.83), a 17% reduction in coronary heart disease (95% CI, 0.78-0.88), a 27% reduction in stroke (95% CI, 0.68-0.77), and a 28% reduction in heart failure (95% CI, 0.67-0.78), based on the meta-analysis published Dec. 23 by the Lancet.
The exception was a lack of overall benefit of blood pressure lowering for renal failure events, a finding consistent with a previous meta-analysis of moderate versus intensive blood pressure reduction.
“Lowering of blood pressure into what has been regarded the normotensive range should therefore be routinely considered for the prevention of cardiovascular disease among those deemed to be of sufficient absolute risk,” wrote Dena Ettehad of the George Institute for Global Health, Oxford, and coauthors.
“Revision is urgently needed to recent blood pressure lowering guidelines that have relaxed the blood pressure lowering thresholds,” they added.
The researchers conducted a meta-analysis of blood pressure lowering treatment, involving a total of 613,815 participants and a minimum of 1,000 patient-years of follow-up in each study arm.
The analysis indicated that a 10–mm Hg reduction in systolic blood pressure achieved an overall 13% reduction in all-cause mortality (95% CI, 0.84-0.91) but had no significant impact on the risk of renal failure events.
These effects remained similar even when the effects were compared between strata of mean baseline systolic blood pressure, baseline coronary heart disease, or baseline cardiovascular disease (Lancet 2015 Dec 23. doi: 10.1016/S0140-6736(15)01225-8).
“In stratified analyses, we saw no strong evidence that proportional effects were diminished in trials that included people with lower baseline systolic blood pressure (less than 130 mm Hg), and major cardiovascular events were clearly reduced in high-risk patients with various baseline comorbidities,” the investigators wrote.
“Both of these major findings – the efficacy of blood pressure lowering below 130 mm Hg and the similar proportional effects in high-risk populations – are consistent with and extend the findings of the SPRINT trial,” they said.
The authors did note greater proportional reductions in the risk of stroke in populations without a history of cerebrovascular disease, compared with those with a history.
Populations without diabetes had significantly greater proportional reductions in risk, compared with those with diabetes, while populations without chronic kidney disease had greater proportional reductions in the risk of major cardiovascular disease events, compared with those with chronic kidney disease.
The five classes of antihypertensives were generally as effective as each other in reducing the risk of major outcomes.
The authors noted that, while there were small but significant differences between drug classes for outcomes, these effects may have been the result of differences in control regimens or the concurrent use of multiple drug classes in many trials.
Two authors were supported by the National Institute of Health Research, one by the Clarendon Fund, and one by the Rhodes Trust. The George Institute is supported by the Oxford Martin School. Two authors declared grants from Servier, and one also declared investments for the development of a polypill. No other conflicts of interest were declared.
FROM THE LANCET
Key clinical point: Blood pressure lowering is associated with significant reductions in vascular events in patients with a range of comorbidities and baseline blood pressures.
Major finding: Each 10–mm Hg reduction in systolic blood pressure is associated with a 20% reduction in major cardiovascular disease events.
Data source: A meta-analysis of 123 randomized controlled trials of blood pressure lowering treatment, involving a total of 613,815 participants.
Disclosures: Two authors were supported by the National Institute of Health Research, one by the Clarendon Fund, and one by the Rhodes Trust. The George Institute is supported by the Oxford Martin School. Two authors declared grants from Servier, and one also declared investments for the development of a polypill. No other conflicts of interest were declared.

Secukinumab cut ankylosing spondylitis symptoms in MEASURE trials
Secukinumab, an interleukin 17-A inhibitor approved for the treatment of moderate to severe psoriasis, significantly reduced the signs and symptoms of ankylosing spondylitis in two phase III trials, researchers reported Dec. 23 in the New England Journal of Medicine.
The results of the double-blind MEASURE 1 and MEASURE 2 trials extend the positive results of the phase II study, according to Dr. Dominique Baeten of the Academic Medical Center at the University of Amsterdam and his colleagues (N Engl J Med. 2015 Dec 23. doi: 10.1056/NEJMoa1505066).
“Although head-to-head trials would be required to fully assess the efficacy and safety of secukinumab versus TNF-inhibitors, the [20% improvement in Assessment of Spondyloarthritis International Society (ASAS20) response criteria] response rates achieved with secukinumab at week 16 in our studies were similar to those reported in phase III studies of anti-TNF agents in which most of the patients had not received previous anti-TNF therapy (response rates of 58% to 64% at weeks 12 to 24), even though 30% to 40% of the patients in our studies had had no response to previous anti-TNF treatment,” the authors wrote.
“Thus, secukinumab not only is effective in patients who have not received TNF agents previously but also may be effective in patients in whom previous anti-TNF treatment failed,” they added.
In MEASURE 1, 371 patients received intravenous secukinumab (10 mg/kg of body weight) or matched placebo at weeks 0, 2, and 4, followed by subcutaneous secukinumab (150 mg or 75 mg) or matched placebo every 4 weeks starting at week 8.
The study’s primary endpoint of ASAS20 response rates at week 16 were 61%, 60%, and 29% for subcutaneous secukinumab at doses of 150 mg and 75 mg and for placebo, respectively, (P less than .001 for both comparisons with placebo).
In MEASURE 2, 219 patients received subcutaneous secukinumab (150 mg or 75 mg) or matched placebo at baseline; at weeks 1, 2, and 3; and every 4 weeks starting at week 4.
At week 16, patients in the placebo group were randomly reassigned to subcutaneous secukinumab at a dose of 150 mg or 75 mg.
In this trial, ASAS20 rates were 61%, 41%, and 28% for subcutaneous secukinumab at doses of 150 mg and 75 mg and for placebo, respectively (P less than .001 for the 150-mg dose and P = .10 for the 75-mg dose).
The researchers noted that the ineffectiveness of the 75-mg dose in MEASURE 2 suggests that the efficacy of secukinumab at the 75-mg dose in MEASURE 1 may have been due to the greater exposure at week 16 as a result of the intravenous loading regimen, not to the 75-mg subcutaneous maintenance dose.
The safety profile of secukinumab in the present studies was consistent with previous studies of secukinumab for ankylosing spondylitis and moderate-to-severe plaque psoriasis, Dr. Baeten and his associates said.
During the entire treatment period, pooled exposure-adjusted incidence rates of grade 3 or 4 neutropenia, candida infections, and Crohn’s disease were 0.7, 0.9, and 0.7 cases per 100 patient-years, respectively, in secukinumab-treated patients.
Overall, the results suggest that interleukin-17A plays a role in the pathogenesis of ankylosing spondylitis, and they validate inhibition of this cytokine as a potential therapeutic approach, the study authors concluded.
The study was sponsored by Novartis Pharma. Dr. Baeten has received a grant from Novartis to study the impact of IL-17A blockade in experimental models of spondyloarthritis. He also has been a consultant for Novartis for the design and conduct of the secukinumab program in ankylosing spondylitis and psoriatic arthritis.
Secukinumab, an interleukin 17-A inhibitor approved for the treatment of moderate to severe psoriasis, significantly reduced the signs and symptoms of ankylosing spondylitis in two phase III trials, researchers reported Dec. 23 in the New England Journal of Medicine.
The results of the double-blind MEASURE 1 and MEASURE 2 trials extend the positive results of the phase II study, according to Dr. Dominique Baeten of the Academic Medical Center at the University of Amsterdam and his colleagues (N Engl J Med. 2015 Dec 23. doi: 10.1056/NEJMoa1505066).
“Although head-to-head trials would be required to fully assess the efficacy and safety of secukinumab versus TNF-inhibitors, the [20% improvement in Assessment of Spondyloarthritis International Society (ASAS20) response criteria] response rates achieved with secukinumab at week 16 in our studies were similar to those reported in phase III studies of anti-TNF agents in which most of the patients had not received previous anti-TNF therapy (response rates of 58% to 64% at weeks 12 to 24), even though 30% to 40% of the patients in our studies had had no response to previous anti-TNF treatment,” the authors wrote.
“Thus, secukinumab not only is effective in patients who have not received TNF agents previously but also may be effective in patients in whom previous anti-TNF treatment failed,” they added.
In MEASURE 1, 371 patients received intravenous secukinumab (10 mg/kg of body weight) or matched placebo at weeks 0, 2, and 4, followed by subcutaneous secukinumab (150 mg or 75 mg) or matched placebo every 4 weeks starting at week 8.
The study’s primary endpoint of ASAS20 response rates at week 16 were 61%, 60%, and 29% for subcutaneous secukinumab at doses of 150 mg and 75 mg and for placebo, respectively, (P less than .001 for both comparisons with placebo).
In MEASURE 2, 219 patients received subcutaneous secukinumab (150 mg or 75 mg) or matched placebo at baseline; at weeks 1, 2, and 3; and every 4 weeks starting at week 4.
At week 16, patients in the placebo group were randomly reassigned to subcutaneous secukinumab at a dose of 150 mg or 75 mg.
In this trial, ASAS20 rates were 61%, 41%, and 28% for subcutaneous secukinumab at doses of 150 mg and 75 mg and for placebo, respectively (P less than .001 for the 150-mg dose and P = .10 for the 75-mg dose).
The researchers noted that the ineffectiveness of the 75-mg dose in MEASURE 2 suggests that the efficacy of secukinumab at the 75-mg dose in MEASURE 1 may have been due to the greater exposure at week 16 as a result of the intravenous loading regimen, not to the 75-mg subcutaneous maintenance dose.
The safety profile of secukinumab in the present studies was consistent with previous studies of secukinumab for ankylosing spondylitis and moderate-to-severe plaque psoriasis, Dr. Baeten and his associates said.
During the entire treatment period, pooled exposure-adjusted incidence rates of grade 3 or 4 neutropenia, candida infections, and Crohn’s disease were 0.7, 0.9, and 0.7 cases per 100 patient-years, respectively, in secukinumab-treated patients.
Overall, the results suggest that interleukin-17A plays a role in the pathogenesis of ankylosing spondylitis, and they validate inhibition of this cytokine as a potential therapeutic approach, the study authors concluded.
The study was sponsored by Novartis Pharma. Dr. Baeten has received a grant from Novartis to study the impact of IL-17A blockade in experimental models of spondyloarthritis. He also has been a consultant for Novartis for the design and conduct of the secukinumab program in ankylosing spondylitis and psoriatic arthritis.
Secukinumab, an interleukin 17-A inhibitor approved for the treatment of moderate to severe psoriasis, significantly reduced the signs and symptoms of ankylosing spondylitis in two phase III trials, researchers reported Dec. 23 in the New England Journal of Medicine.
The results of the double-blind MEASURE 1 and MEASURE 2 trials extend the positive results of the phase II study, according to Dr. Dominique Baeten of the Academic Medical Center at the University of Amsterdam and his colleagues (N Engl J Med. 2015 Dec 23. doi: 10.1056/NEJMoa1505066).
“Although head-to-head trials would be required to fully assess the efficacy and safety of secukinumab versus TNF-inhibitors, the [20% improvement in Assessment of Spondyloarthritis International Society (ASAS20) response criteria] response rates achieved with secukinumab at week 16 in our studies were similar to those reported in phase III studies of anti-TNF agents in which most of the patients had not received previous anti-TNF therapy (response rates of 58% to 64% at weeks 12 to 24), even though 30% to 40% of the patients in our studies had had no response to previous anti-TNF treatment,” the authors wrote.
“Thus, secukinumab not only is effective in patients who have not received TNF agents previously but also may be effective in patients in whom previous anti-TNF treatment failed,” they added.
In MEASURE 1, 371 patients received intravenous secukinumab (10 mg/kg of body weight) or matched placebo at weeks 0, 2, and 4, followed by subcutaneous secukinumab (150 mg or 75 mg) or matched placebo every 4 weeks starting at week 8.
The study’s primary endpoint of ASAS20 response rates at week 16 were 61%, 60%, and 29% for subcutaneous secukinumab at doses of 150 mg and 75 mg and for placebo, respectively, (P less than .001 for both comparisons with placebo).
In MEASURE 2, 219 patients received subcutaneous secukinumab (150 mg or 75 mg) or matched placebo at baseline; at weeks 1, 2, and 3; and every 4 weeks starting at week 4.
At week 16, patients in the placebo group were randomly reassigned to subcutaneous secukinumab at a dose of 150 mg or 75 mg.
In this trial, ASAS20 rates were 61%, 41%, and 28% for subcutaneous secukinumab at doses of 150 mg and 75 mg and for placebo, respectively (P less than .001 for the 150-mg dose and P = .10 for the 75-mg dose).
The researchers noted that the ineffectiveness of the 75-mg dose in MEASURE 2 suggests that the efficacy of secukinumab at the 75-mg dose in MEASURE 1 may have been due to the greater exposure at week 16 as a result of the intravenous loading regimen, not to the 75-mg subcutaneous maintenance dose.
The safety profile of secukinumab in the present studies was consistent with previous studies of secukinumab for ankylosing spondylitis and moderate-to-severe plaque psoriasis, Dr. Baeten and his associates said.
During the entire treatment period, pooled exposure-adjusted incidence rates of grade 3 or 4 neutropenia, candida infections, and Crohn’s disease were 0.7, 0.9, and 0.7 cases per 100 patient-years, respectively, in secukinumab-treated patients.
Overall, the results suggest that interleukin-17A plays a role in the pathogenesis of ankylosing spondylitis, and they validate inhibition of this cytokine as a potential therapeutic approach, the study authors concluded.
The study was sponsored by Novartis Pharma. Dr. Baeten has received a grant from Novartis to study the impact of IL-17A blockade in experimental models of spondyloarthritis. He also has been a consultant for Novartis for the design and conduct of the secukinumab program in ankylosing spondylitis and psoriatic arthritis.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Interleukin-17A may play a role in ankylosing spondylitis, and secukinumab may prove to be an effective therapy for these patients.
Major finding: The primary endpoint of Assessment of Spondyloarthritis International Society (ASAS20) response rates at week 16 was met in both secukinumab groups in MEASURE 1 and in the group that received 150 mg of secukinumab subcutaneously in MEASURE 2.
Data source: Two double-blind, phase III studies: MEASURE 1 involving 371 patients with AS and MEASURE 2 involving 371 patients.
Disclosures: The studies were funded by Novartis Pharma. Dr. Baeten has received a grant from Novartis to study the impact of IL-17A blockade in experimental models of spondyloarthritis. He also has been a consultant for Novartis for the design and conduct of the secukinumab program in ankylosing spondylitis and psoriatic arthritis.

European societies issue aspergillosis diagnosis, management guidelines
European respiratory disease and infectious disease specialists have banded together to issue new clinical guidelines on the diagnosis and management of an uncommon but serious problem: chronic pulmonary aspergillosis (CPA).
Pulmonary infections with Aspergillus species, although uncommon, are a complicating factor in several lung diseases, especially tuberculosis, and aspergillosis is a serious, often fatal opportunistic infection in transplant recipients who are on chronic immunosuppression or patients who are immunocompromised from disease or cytotoxic chemotherapy.
Approximately 240,000 people in Europe and 3 million people worldwide have chronic pulmonary aspergillosis (CPA). The Centers for Disease Control and Prevention notes that because aspergillosis is not classified as a reportable disease, data on the actual incidence of infections in the United States are hard to come by.
“You don’t see this every day, whether you’re an infectious disease specialist or pulmonologist, so you really can’t rely on your experience to guide you in managing these cases, which is why guidelines such as this can be very helpful,” commented Dr. Norman Edelman, a pulmonologist and senior consultant for scientific affairs for the American Lung Association.
The guidelines, issued by the European Society for Clinical Microbiology and Infectious Diseases in cooperation with the European Confederation of Medical Mycology and the European Respiratory Society, are an attempt to provide clinicians with the best possible evidence-based guidance on managing patients with aspergillosis, primarily those with CPA (Eur Respir J. 2015. doi: 10.1183/13993003.00583-2015).
Dr. Edelman noted that the most frequent presentation he sees – and that very infrequently – is allergic bronchopulmonary aspergillosis in patients with asthma.
The most recent U.S. guidelines, issued under the aegis of the Infectious Diseases Society of America (IDSA) in 2000 and revised in 2008 (CID 2008;46:327-360), differ from the European recommendations in their level of detail, explained Prof. David W. Denning, professor of infectious diseases in global health at the University of Manchester (England) and lead author of the European guidelines.
“The IDSA guidelines assume that you know how to make the diagnosis, but actually for chronic pulmonary aspergillosis that’s not so easy with some patients,” he said in an interview.
“The European ones go into in great detail the diagnosis, the radiology, whether this test is better than that test, how they all add up, and all that sort of stuff,” he said,
The European guidelines also make recommendations for duration of therapy and comment on the use of steroids and immunotherapy with interferon-gamma, Dr. Denning noted.
Diagnostic criteria
The European guidelines categorize Aspergillus infections according to differences in clinical management:
• Simple aspergilloma. A single pulmonary cavity containing a fungal ball, supported by serologic or microbiologic evidence of infections with Aspergillus species in patients who are not immunocompromised and are asymptomatic or have only minor symptoms and no radiographic evidence of progression for at least 3 months.
• Chronic cavitary pulmonary aspergillosis (CCPA). The presence of one or more pulmonary cavities that may contain one or more aspergillomas or irregular intraluminal material, evidence of Aspergillus species, significant pulmonary/systemic symptoms, and overt progression on radiography over 3 or more months of observations.
• Chronic fibrosing pulmonary aspergillosis (CFPA). Severe, fibrotic destruction of at least two lung lobes as a complication of CCPA, causing a major loss of lung function. The guidelines note that destruction of a single lobe is designated as CCPA of that lobe.
• Aspergillus nodules. This unusual presentation is marked by the presence of one or more nodules that may or may not cavitate. The nodules may resemble tuberculoma, carcinoma of the lung, or coccidioidomycosis; histology is required to make an accurate diagnosis.
• Subacute invasive aspergillosis (SAIA). This can occur over the course of 1-3 months in patients who are mildly immunocompromised. Radiologic features can vary, and may include cavitation, the presence of nodules, and progressive consolidation with the appearance of abscess formation. Fungal hyphae (filaments) can be seen in biopsied lung tissues, and there may be evidence of Aspergillus galactomannan antigen in respiratory fluids or blood.
Treatment
The guidelines note that most of the evidence for managing CPA are based on cohort studies and case reports rather than randomized clinical trials, and that there have been no head-to-head trials comparing oral triazole agents.
For treatment of CPA, the European guidelines recommend:
• Itraconazole 200 mg twice daily, with therapeutic drug monitoring and dose adjustment as necessary (Grade A [strong] recommendation).
• Voriconazole 150-200 mg twice daily, with monitoring and dose adjustment. The guidelines recommend lower doses for patients older than 70 years, those with low body weight, significant liver disease, and/or those of Northeast Asian descent, who may be genetically inclined to slow drug metabolism (Grade A).
• Posaconazole liquid 400 mg twice daily, or tablets 300 mg once daily (Grade B [moderate] recommendation].
In general, the recommended duration of therapy for control of infection in patients with CPA or curative intent for patients with SAIA or chronic necrotizing pulmonary aspergillosis is 6 months or more, depending on patient status and drug tolerance.
For patients with CPA with progressive disease, those whom therapy has failed, or those who are intolerant of or have disease resistant to triazoles, intravenous therapy with micafungin, 150 mg day (Grade B); amphotericin B deoxycholate, 0.7-1.0 mg/kg per day (Grade C [marginal] recommendation); liposomal amphotericin B, 3 mg/kg per day (Grade B); or caspofungin, 50-70 mg/day (Grade C) are recommended.
The guidelines also recommend surgical excision of simple aspergilloma, preferably by a video-assisted thoracic surgery technique, if technically feasible.
“In my own experience, we resort to surgery very infrequently,” Dr. Edelman said.
He noted that it would be helpful if the guidelines had also allergic bronchopulmonary aspergillosis as a separate entity.
Ideal not always achievable
Prof. Denning points out that the optimum therapies and practices described in the guidelines can’t always be implemented. Worldwide, he said, antifungal therapy is not widely available, with the exception of fluconazole, which has no activity against Aspergillus, and is inferior to itraconazole and other extended azoles for other fungal diseases such as histoplasmosis, blastomycosis, and paracoccidioidomycosis.
The price of antifungal therapies can also be a barrier to effective treatment in many parts of the world.
“If you’re having to pay for your medicines and you’re living on $5 or $10 a day in Kenya, say, you can’t afford to buy them. So even if the drugs are physically there, it may not be really affordable for a course of therapy for these patients, and there’s some advocacy to be done around that for the whole world,” he said.
The guidelines were funded primarily by grants from ESCMID and ERS with additional support from ECMM. Authors’ travel expenses were funded jointly by ESCMID and ERS. Dr. Denning has received grant support and founder shares in F2G, and has received grants from the Fungal Research Trust, Wellcome Trust, Moulton Trust, Medical Research Council, Chronic Granulomatous Disease Research Trust, National Institute of Allergy and Infectious Diseases, National Institute of Health Research and the European Union, and AstraZeneca. Dr. Edelman reported no relevant disclosures.
European respiratory disease and infectious disease specialists have banded together to issue new clinical guidelines on the diagnosis and management of an uncommon but serious problem: chronic pulmonary aspergillosis (CPA).
Pulmonary infections with Aspergillus species, although uncommon, are a complicating factor in several lung diseases, especially tuberculosis, and aspergillosis is a serious, often fatal opportunistic infection in transplant recipients who are on chronic immunosuppression or patients who are immunocompromised from disease or cytotoxic chemotherapy.
Approximately 240,000 people in Europe and 3 million people worldwide have chronic pulmonary aspergillosis (CPA). The Centers for Disease Control and Prevention notes that because aspergillosis is not classified as a reportable disease, data on the actual incidence of infections in the United States are hard to come by.
“You don’t see this every day, whether you’re an infectious disease specialist or pulmonologist, so you really can’t rely on your experience to guide you in managing these cases, which is why guidelines such as this can be very helpful,” commented Dr. Norman Edelman, a pulmonologist and senior consultant for scientific affairs for the American Lung Association.
The guidelines, issued by the European Society for Clinical Microbiology and Infectious Diseases in cooperation with the European Confederation of Medical Mycology and the European Respiratory Society, are an attempt to provide clinicians with the best possible evidence-based guidance on managing patients with aspergillosis, primarily those with CPA (Eur Respir J. 2015. doi: 10.1183/13993003.00583-2015).
Dr. Edelman noted that the most frequent presentation he sees – and that very infrequently – is allergic bronchopulmonary aspergillosis in patients with asthma.
The most recent U.S. guidelines, issued under the aegis of the Infectious Diseases Society of America (IDSA) in 2000 and revised in 2008 (CID 2008;46:327-360), differ from the European recommendations in their level of detail, explained Prof. David W. Denning, professor of infectious diseases in global health at the University of Manchester (England) and lead author of the European guidelines.
“The IDSA guidelines assume that you know how to make the diagnosis, but actually for chronic pulmonary aspergillosis that’s not so easy with some patients,” he said in an interview.
“The European ones go into in great detail the diagnosis, the radiology, whether this test is better than that test, how they all add up, and all that sort of stuff,” he said,
The European guidelines also make recommendations for duration of therapy and comment on the use of steroids and immunotherapy with interferon-gamma, Dr. Denning noted.
Diagnostic criteria
The European guidelines categorize Aspergillus infections according to differences in clinical management:
• Simple aspergilloma. A single pulmonary cavity containing a fungal ball, supported by serologic or microbiologic evidence of infections with Aspergillus species in patients who are not immunocompromised and are asymptomatic or have only minor symptoms and no radiographic evidence of progression for at least 3 months.
• Chronic cavitary pulmonary aspergillosis (CCPA). The presence of one or more pulmonary cavities that may contain one or more aspergillomas or irregular intraluminal material, evidence of Aspergillus species, significant pulmonary/systemic symptoms, and overt progression on radiography over 3 or more months of observations.
• Chronic fibrosing pulmonary aspergillosis (CFPA). Severe, fibrotic destruction of at least two lung lobes as a complication of CCPA, causing a major loss of lung function. The guidelines note that destruction of a single lobe is designated as CCPA of that lobe.
• Aspergillus nodules. This unusual presentation is marked by the presence of one or more nodules that may or may not cavitate. The nodules may resemble tuberculoma, carcinoma of the lung, or coccidioidomycosis; histology is required to make an accurate diagnosis.
• Subacute invasive aspergillosis (SAIA). This can occur over the course of 1-3 months in patients who are mildly immunocompromised. Radiologic features can vary, and may include cavitation, the presence of nodules, and progressive consolidation with the appearance of abscess formation. Fungal hyphae (filaments) can be seen in biopsied lung tissues, and there may be evidence of Aspergillus galactomannan antigen in respiratory fluids or blood.
Treatment
The guidelines note that most of the evidence for managing CPA are based on cohort studies and case reports rather than randomized clinical trials, and that there have been no head-to-head trials comparing oral triazole agents.
For treatment of CPA, the European guidelines recommend:
• Itraconazole 200 mg twice daily, with therapeutic drug monitoring and dose adjustment as necessary (Grade A [strong] recommendation).
• Voriconazole 150-200 mg twice daily, with monitoring and dose adjustment. The guidelines recommend lower doses for patients older than 70 years, those with low body weight, significant liver disease, and/or those of Northeast Asian descent, who may be genetically inclined to slow drug metabolism (Grade A).
• Posaconazole liquid 400 mg twice daily, or tablets 300 mg once daily (Grade B [moderate] recommendation].
In general, the recommended duration of therapy for control of infection in patients with CPA or curative intent for patients with SAIA or chronic necrotizing pulmonary aspergillosis is 6 months or more, depending on patient status and drug tolerance.
For patients with CPA with progressive disease, those whom therapy has failed, or those who are intolerant of or have disease resistant to triazoles, intravenous therapy with micafungin, 150 mg day (Grade B); amphotericin B deoxycholate, 0.7-1.0 mg/kg per day (Grade C [marginal] recommendation); liposomal amphotericin B, 3 mg/kg per day (Grade B); or caspofungin, 50-70 mg/day (Grade C) are recommended.
The guidelines also recommend surgical excision of simple aspergilloma, preferably by a video-assisted thoracic surgery technique, if technically feasible.
“In my own experience, we resort to surgery very infrequently,” Dr. Edelman said.
He noted that it would be helpful if the guidelines had also allergic bronchopulmonary aspergillosis as a separate entity.
Ideal not always achievable
Prof. Denning points out that the optimum therapies and practices described in the guidelines can’t always be implemented. Worldwide, he said, antifungal therapy is not widely available, with the exception of fluconazole, which has no activity against Aspergillus, and is inferior to itraconazole and other extended azoles for other fungal diseases such as histoplasmosis, blastomycosis, and paracoccidioidomycosis.
The price of antifungal therapies can also be a barrier to effective treatment in many parts of the world.
“If you’re having to pay for your medicines and you’re living on $5 or $10 a day in Kenya, say, you can’t afford to buy them. So even if the drugs are physically there, it may not be really affordable for a course of therapy for these patients, and there’s some advocacy to be done around that for the whole world,” he said.
The guidelines were funded primarily by grants from ESCMID and ERS with additional support from ECMM. Authors’ travel expenses were funded jointly by ESCMID and ERS. Dr. Denning has received grant support and founder shares in F2G, and has received grants from the Fungal Research Trust, Wellcome Trust, Moulton Trust, Medical Research Council, Chronic Granulomatous Disease Research Trust, National Institute of Allergy and Infectious Diseases, National Institute of Health Research and the European Union, and AstraZeneca. Dr. Edelman reported no relevant disclosures.
European respiratory disease and infectious disease specialists have banded together to issue new clinical guidelines on the diagnosis and management of an uncommon but serious problem: chronic pulmonary aspergillosis (CPA).
Pulmonary infections with Aspergillus species, although uncommon, are a complicating factor in several lung diseases, especially tuberculosis, and aspergillosis is a serious, often fatal opportunistic infection in transplant recipients who are on chronic immunosuppression or patients who are immunocompromised from disease or cytotoxic chemotherapy.
Approximately 240,000 people in Europe and 3 million people worldwide have chronic pulmonary aspergillosis (CPA). The Centers for Disease Control and Prevention notes that because aspergillosis is not classified as a reportable disease, data on the actual incidence of infections in the United States are hard to come by.
“You don’t see this every day, whether you’re an infectious disease specialist or pulmonologist, so you really can’t rely on your experience to guide you in managing these cases, which is why guidelines such as this can be very helpful,” commented Dr. Norman Edelman, a pulmonologist and senior consultant for scientific affairs for the American Lung Association.
The guidelines, issued by the European Society for Clinical Microbiology and Infectious Diseases in cooperation with the European Confederation of Medical Mycology and the European Respiratory Society, are an attempt to provide clinicians with the best possible evidence-based guidance on managing patients with aspergillosis, primarily those with CPA (Eur Respir J. 2015. doi: 10.1183/13993003.00583-2015).
Dr. Edelman noted that the most frequent presentation he sees – and that very infrequently – is allergic bronchopulmonary aspergillosis in patients with asthma.
The most recent U.S. guidelines, issued under the aegis of the Infectious Diseases Society of America (IDSA) in 2000 and revised in 2008 (CID 2008;46:327-360), differ from the European recommendations in their level of detail, explained Prof. David W. Denning, professor of infectious diseases in global health at the University of Manchester (England) and lead author of the European guidelines.
“The IDSA guidelines assume that you know how to make the diagnosis, but actually for chronic pulmonary aspergillosis that’s not so easy with some patients,” he said in an interview.
“The European ones go into in great detail the diagnosis, the radiology, whether this test is better than that test, how they all add up, and all that sort of stuff,” he said,
The European guidelines also make recommendations for duration of therapy and comment on the use of steroids and immunotherapy with interferon-gamma, Dr. Denning noted.
Diagnostic criteria
The European guidelines categorize Aspergillus infections according to differences in clinical management:
• Simple aspergilloma. A single pulmonary cavity containing a fungal ball, supported by serologic or microbiologic evidence of infections with Aspergillus species in patients who are not immunocompromised and are asymptomatic or have only minor symptoms and no radiographic evidence of progression for at least 3 months.
• Chronic cavitary pulmonary aspergillosis (CCPA). The presence of one or more pulmonary cavities that may contain one or more aspergillomas or irregular intraluminal material, evidence of Aspergillus species, significant pulmonary/systemic symptoms, and overt progression on radiography over 3 or more months of observations.
• Chronic fibrosing pulmonary aspergillosis (CFPA). Severe, fibrotic destruction of at least two lung lobes as a complication of CCPA, causing a major loss of lung function. The guidelines note that destruction of a single lobe is designated as CCPA of that lobe.
• Aspergillus nodules. This unusual presentation is marked by the presence of one or more nodules that may or may not cavitate. The nodules may resemble tuberculoma, carcinoma of the lung, or coccidioidomycosis; histology is required to make an accurate diagnosis.
• Subacute invasive aspergillosis (SAIA). This can occur over the course of 1-3 months in patients who are mildly immunocompromised. Radiologic features can vary, and may include cavitation, the presence of nodules, and progressive consolidation with the appearance of abscess formation. Fungal hyphae (filaments) can be seen in biopsied lung tissues, and there may be evidence of Aspergillus galactomannan antigen in respiratory fluids or blood.
Treatment
The guidelines note that most of the evidence for managing CPA are based on cohort studies and case reports rather than randomized clinical trials, and that there have been no head-to-head trials comparing oral triazole agents.
For treatment of CPA, the European guidelines recommend:
• Itraconazole 200 mg twice daily, with therapeutic drug monitoring and dose adjustment as necessary (Grade A [strong] recommendation).
• Voriconazole 150-200 mg twice daily, with monitoring and dose adjustment. The guidelines recommend lower doses for patients older than 70 years, those with low body weight, significant liver disease, and/or those of Northeast Asian descent, who may be genetically inclined to slow drug metabolism (Grade A).
• Posaconazole liquid 400 mg twice daily, or tablets 300 mg once daily (Grade B [moderate] recommendation].
In general, the recommended duration of therapy for control of infection in patients with CPA or curative intent for patients with SAIA or chronic necrotizing pulmonary aspergillosis is 6 months or more, depending on patient status and drug tolerance.
For patients with CPA with progressive disease, those whom therapy has failed, or those who are intolerant of or have disease resistant to triazoles, intravenous therapy with micafungin, 150 mg day (Grade B); amphotericin B deoxycholate, 0.7-1.0 mg/kg per day (Grade C [marginal] recommendation); liposomal amphotericin B, 3 mg/kg per day (Grade B); or caspofungin, 50-70 mg/day (Grade C) are recommended.
The guidelines also recommend surgical excision of simple aspergilloma, preferably by a video-assisted thoracic surgery technique, if technically feasible.
“In my own experience, we resort to surgery very infrequently,” Dr. Edelman said.
He noted that it would be helpful if the guidelines had also allergic bronchopulmonary aspergillosis as a separate entity.
Ideal not always achievable
Prof. Denning points out that the optimum therapies and practices described in the guidelines can’t always be implemented. Worldwide, he said, antifungal therapy is not widely available, with the exception of fluconazole, which has no activity against Aspergillus, and is inferior to itraconazole and other extended azoles for other fungal diseases such as histoplasmosis, blastomycosis, and paracoccidioidomycosis.
The price of antifungal therapies can also be a barrier to effective treatment in many parts of the world.
“If you’re having to pay for your medicines and you’re living on $5 or $10 a day in Kenya, say, you can’t afford to buy them. So even if the drugs are physically there, it may not be really affordable for a course of therapy for these patients, and there’s some advocacy to be done around that for the whole world,” he said.
The guidelines were funded primarily by grants from ESCMID and ERS with additional support from ECMM. Authors’ travel expenses were funded jointly by ESCMID and ERS. Dr. Denning has received grant support and founder shares in F2G, and has received grants from the Fungal Research Trust, Wellcome Trust, Moulton Trust, Medical Research Council, Chronic Granulomatous Disease Research Trust, National Institute of Allergy and Infectious Diseases, National Institute of Health Research and the European Union, and AstraZeneca. Dr. Edelman reported no relevant disclosures.
FROM JOURNAL OF DRUGS IN DERMATOLOGY
Chutzpah
Chutzpah is a Yiddish word that entered American English, joining bagel and nosh. The usual translations of chutzpah – “nerve” or “effrontery” – are correct enough, but leave out the zest implied by chutzpah’s classic case: a man who kills his parents and throws himself on the mercy of the court because he is an orphan.
We all meet patients with chutzpah, which can be amusing, impressive – even breathtaking.

Take for instance the woman who paged me one evening last month. “I visit your nurse for cosmetic stuff,” she said when I called her back. “Your prices for laser hair removal were high, though, so I went to a spa where I could use a Groupon.”
How nice, I thought.
“Anyhow,” she continued, “I went for a treatment at the spa today, and now I have little red bumps all over my thighs. I thought it might be a reaction, and since you are my dermatologist I called to ask what to do.”
Good to be needed.
Then the next week I got another call, this time from a man I hadn’t seen in a long time. “I really like you as a dermatologist,” he began.
“Thank you,” I murmured.
“I saw this spot on my leg that worried me,” he said. “I was going to show it to you, but your office is in an old building, and old buildings don’t agree with me.”
As I scratched my head, he went on. “So I went to another dermatologist who works in a newer building. He did a biopsy and told me I have skin cancer. He said I should have surgery to take it off. I consider you my dermatologist, though, so I called to ask whether you think surgery is a good idea.”
I said I thought it was. I did not add that he should look for an old surgeon in a new building.
These patients are fresh in my mind, but it doesn’t take much effort to come up with others.
“Mr. Skillman wants a refill on his steroid cream,” says my secretary.
“Sure,” I tell her. “E-scribe it over.”
“No,” she says. “He wants a hard copy mailed to him.”
“Does he have one of those mail order pharmacies that requires a written script?”
“No.”
“But it’s so much simpler to call it in or do it by computer. Why does he have to have a hard copy?”
“I don’t know. But he insists on having one.”
I could go on and on. So could you, I’m sure.
When confronted with chutzpah, you have two options: challenge the person showing it and refuse to go along with his demands, or just sigh, comply, and move on. In general, I go with option #2.
First of all, anyone pushy enough to act this way will not react well to being pushed back. (“What’s your problem? Are you too busy to write a prescription? Too stingy to mail it?”)
Second, and perhaps more to the point, many people who display chutzpah don’t know that’s what they are doing. The woman who went for laser at the Groupon spa really has no idea I’d think it odd for her to call me about a complication instead of the spa personnel who lasered her legs. On some level, she figures that they probably don’t know (look how cheap they are), and thinks I should be flattered to be asked. After all, I’m her dermatologist.
Some people with chutzpah are aggressive and difficult and don’t care if they’re being offensive. A lot more are just clueless. The fellow who bores the daylights out of everyone at dinner parties with long, pointless stories doesn’t know he’s being tedious. He just doesn’t pick up social cues.
Most patients, like most people, are polite and deferential. The rest, though, are more memorable.
My building is indeed old. One hundred years ago it was the swankiest apartment house around. Every flat had rooms for a butler, a maid, and a chauffeur for their Packard motorcar. Then the builder went belly-up during the Depression, and the new owner converted it to medical offices. Downward mobility works for me.
Faced with chutzpah, I shrug, smile, and get on with it. Enough people can still tolerate old buildings, and old dermatologists.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. Write to him at [email protected].
Chutzpah is a Yiddish word that entered American English, joining bagel and nosh. The usual translations of chutzpah – “nerve” or “effrontery” – are correct enough, but leave out the zest implied by chutzpah’s classic case: a man who kills his parents and throws himself on the mercy of the court because he is an orphan.
We all meet patients with chutzpah, which can be amusing, impressive – even breathtaking.
Take for instance the woman who paged me one evening last month. “I visit your nurse for cosmetic stuff,” she said when I called her back. “Your prices for laser hair removal were high, though, so I went to a spa where I could use a Groupon.”
How nice, I thought.
“Anyhow,” she continued, “I went for a treatment at the spa today, and now I have little red bumps all over my thighs. I thought it might be a reaction, and since you are my dermatologist I called to ask what to do.”
Good to be needed.
Then the next week I got another call, this time from a man I hadn’t seen in a long time. “I really like you as a dermatologist,” he began.
“Thank you,” I murmured.
“I saw this spot on my leg that worried me,” he said. “I was going to show it to you, but your office is in an old building, and old buildings don’t agree with me.”
As I scratched my head, he went on. “So I went to another dermatologist who works in a newer building. He did a biopsy and told me I have skin cancer. He said I should have surgery to take it off. I consider you my dermatologist, though, so I called to ask whether you think surgery is a good idea.”
I said I thought it was. I did not add that he should look for an old surgeon in a new building.
These patients are fresh in my mind, but it doesn’t take much effort to come up with others.
“Mr. Skillman wants a refill on his steroid cream,” says my secretary.
“Sure,” I tell her. “E-scribe it over.”
“No,” she says. “He wants a hard copy mailed to him.”
“Does he have one of those mail order pharmacies that requires a written script?”
“No.”
“But it’s so much simpler to call it in or do it by computer. Why does he have to have a hard copy?”
“I don’t know. But he insists on having one.”
I could go on and on. So could you, I’m sure.
When confronted with chutzpah, you have two options: challenge the person showing it and refuse to go along with his demands, or just sigh, comply, and move on. In general, I go with option #2.
First of all, anyone pushy enough to act this way will not react well to being pushed back. (“What’s your problem? Are you too busy to write a prescription? Too stingy to mail it?”)
Second, and perhaps more to the point, many people who display chutzpah don’t know that’s what they are doing. The woman who went for laser at the Groupon spa really has no idea I’d think it odd for her to call me about a complication instead of the spa personnel who lasered her legs. On some level, she figures that they probably don’t know (look how cheap they are), and thinks I should be flattered to be asked. After all, I’m her dermatologist.
Some people with chutzpah are aggressive and difficult and don’t care if they’re being offensive. A lot more are just clueless. The fellow who bores the daylights out of everyone at dinner parties with long, pointless stories doesn’t know he’s being tedious. He just doesn’t pick up social cues.
Most patients, like most people, are polite and deferential. The rest, though, are more memorable.
My building is indeed old. One hundred years ago it was the swankiest apartment house around. Every flat had rooms for a butler, a maid, and a chauffeur for their Packard motorcar. Then the builder went belly-up during the Depression, and the new owner converted it to medical offices. Downward mobility works for me.
Faced with chutzpah, I shrug, smile, and get on with it. Enough people can still tolerate old buildings, and old dermatologists.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. Write to him at [email protected].
Chutzpah is a Yiddish word that entered American English, joining bagel and nosh. The usual translations of chutzpah – “nerve” or “effrontery” – are correct enough, but leave out the zest implied by chutzpah’s classic case: a man who kills his parents and throws himself on the mercy of the court because he is an orphan.
We all meet patients with chutzpah, which can be amusing, impressive – even breathtaking.
Take for instance the woman who paged me one evening last month. “I visit your nurse for cosmetic stuff,” she said when I called her back. “Your prices for laser hair removal were high, though, so I went to a spa where I could use a Groupon.”
How nice, I thought.
“Anyhow,” she continued, “I went for a treatment at the spa today, and now I have little red bumps all over my thighs. I thought it might be a reaction, and since you are my dermatologist I called to ask what to do.”
Good to be needed.
Then the next week I got another call, this time from a man I hadn’t seen in a long time. “I really like you as a dermatologist,” he began.
“Thank you,” I murmured.
“I saw this spot on my leg that worried me,” he said. “I was going to show it to you, but your office is in an old building, and old buildings don’t agree with me.”
As I scratched my head, he went on. “So I went to another dermatologist who works in a newer building. He did a biopsy and told me I have skin cancer. He said I should have surgery to take it off. I consider you my dermatologist, though, so I called to ask whether you think surgery is a good idea.”
I said I thought it was. I did not add that he should look for an old surgeon in a new building.
These patients are fresh in my mind, but it doesn’t take much effort to come up with others.
“Mr. Skillman wants a refill on his steroid cream,” says my secretary.
“Sure,” I tell her. “E-scribe it over.”
“No,” she says. “He wants a hard copy mailed to him.”
“Does he have one of those mail order pharmacies that requires a written script?”
“No.”
“But it’s so much simpler to call it in or do it by computer. Why does he have to have a hard copy?”
“I don’t know. But he insists on having one.”
I could go on and on. So could you, I’m sure.
When confronted with chutzpah, you have two options: challenge the person showing it and refuse to go along with his demands, or just sigh, comply, and move on. In general, I go with option #2.
First of all, anyone pushy enough to act this way will not react well to being pushed back. (“What’s your problem? Are you too busy to write a prescription? Too stingy to mail it?”)
Second, and perhaps more to the point, many people who display chutzpah don’t know that’s what they are doing. The woman who went for laser at the Groupon spa really has no idea I’d think it odd for her to call me about a complication instead of the spa personnel who lasered her legs. On some level, she figures that they probably don’t know (look how cheap they are), and thinks I should be flattered to be asked. After all, I’m her dermatologist.
Some people with chutzpah are aggressive and difficult and don’t care if they’re being offensive. A lot more are just clueless. The fellow who bores the daylights out of everyone at dinner parties with long, pointless stories doesn’t know he’s being tedious. He just doesn’t pick up social cues.
Most patients, like most people, are polite and deferential. The rest, though, are more memorable.
My building is indeed old. One hundred years ago it was the swankiest apartment house around. Every flat had rooms for a butler, a maid, and a chauffeur for their Packard motorcar. Then the builder went belly-up during the Depression, and the new owner converted it to medical offices. Downward mobility works for me.
Faced with chutzpah, I shrug, smile, and get on with it. Enough people can still tolerate old buildings, and old dermatologists.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. Write to him at [email protected].

Female Athletes: Unique Challenges Facing Women Warriors
Since Title IX passed in 1972, women have become exponentially more involved in competitive sports, from high school to professional levels. With more women engaging in serious athletics, the specific challenges they face have come to the forefront of sports medicine. These problems include the female athlete triad, concussions, exercise safety in pregnancy, anterior cruciate ligament (ACL) injuries, and continued sex discrimination and social injustice. Orthopedists treating female athletes should be aware of these problems, each of which is discussed in this review.
1. Female athlete triad
In 1992, the term female athlete triad was coined to describe 3 problems that often coexist in high-intensity female athletes.1 Since then, the definition has evolved, but the problem has remained essentially the same. The modern definition incorporates menstrual abnormalities, low energy availability with or without disordered eating, and decreased bone mineral density (BMD).2
With intense exercise and weight loss comes a variety of menstrual disturbances.3 In affected athletes, the hypothalamus is underactivated, and changes in gonadotropin-releasing hormone and luteinizing hormone lead to decreased estrogen production. Research suggests abnormal menses result from having inadequate energy and insufficient caloric intake to support extensive exercise.1 This phenomenon can occur in athletes in any sport but is most prevalent in lean-body sports, such as swimming, gymnastics, and ballet. The incidence of abnormal menses is as high as 79% in ballet dancers but only 5% in the general population.3 Menstrual abnormalities indicate hormonal abnormalities that can interfere with growth and maturation in young athletes.
Although full-blown eating disorders are uncommon among female athletes, disordered eating patterns are often found among women in competitive sports. Disordered eating can involve a spectrum of inadequate caloric intake and purging behavior, such as vomiting or laxative abuse, and has been reported in up to 25% of collegiate female athletes.4 Physicians must recognize these conditions and initiate counseling and treatment when appropriate. Women with disordered eating are at risk for developing electrolyte imbalances, malnutrition syndromes, and osteopenia.
Although careful evaluation and counseling are important, physicians must note that, in most cases, athletics participation may also protect against disordered eating and body image difficulties. A study of 146 college-age women found better body satisfaction among athletes than among nonathletes.5 Lean-sport athletes (eg, swimmers, gymnasts) were at higher risk for disordered eating and body image problems than other athletes were. Similarly, other studies have found that a majority of athletes have healthy eating habits.4
For poorly nourished and hormonally imbalanced female athletes, decreased BMD poses substantial risk. One study found a significant difference in BMD between athletes with amenorrhea and athletes with normal menses.6 In a cohort of female Navy recruits, those with amenorrhea were at 91% higher risk for stress fractures; calcium and vitamin D supplementation reduced risk by 20%.7 Osteopenia may be a special problem for prepubescent athletes. Girls who engage in intense exercise and have delayed menarche may have a low estrogen state, predisposing them to low BMD.3 Osteopenia and osteoporosis are difficult to reverse and can put these athletes at risk for stress fractures the rest of their lives. If unrecognized, stress fractures can end an athlete’s career.
Recommendations for dual-energy X-ray absorptiometry (DXA) include testing female athletes who have a diagnosed eating disorder, body mass index under 17.5, history of delayed menarche, oligomenorrhea, 2 prior stress fractures, or prior abnormal DXA scan. Complete testing recommendations appear in the 2014 consensus statement on the female athlete triad and return to sport.2,8
Orthopedists performing physical examinations for sports participation can screen for the female athlete triad through thoughtful questioning about menstrual history, nutrition habits, and stress fracture symptoms. Best treatment for a diagnosed case of the triad is multidisciplinary care with strong social support. When abnormal menses are an issue, referral to a gynecologist or endocrinologist and consideration of estrogen replacement should be discussed. Some cases require a psychiatrist’s assistance in treating disordered eating. Athletic trainers, coaches, and parents should be involved over the treatment course.1 Orthopedists must counsel women with osteopenia and osteoporosis about decreasing exercise to a safe level, improving nutritional intake, and supplementing with calcium (1200-1500 mg/d) and vitamin D (600-800 IU/d).3,7
2. Concussions
Increasing awareness of males’ sport-related concussions, particularly of concussions that occur during National Football League practice and games, has made physicians and researchers more aware of the rate of concussion in female athletes. That rate has increased, and, according to some reports, the risk for sport-related injury is higher for female athletes.9 A study of high school athletes found that the rate of concussion in girl’s soccer was second only to that in football.10
Concussions are categorized as mild traumatic brain injuries, and manifestations of the diagnosis are divided into physical, emotional, cognitive, and observed symptoms. The spectrum of symptoms is wide, ranging from difficulty concentrating and thinking clearly to headaches and dizziness.11 Compared with male athletes who sustain a concussion, female athletes report more of these concussive symptoms and have worse visual memory scores.12
Efforts to change sports at the player level have been resisted. Helmets have been proposed for field hockey and lacrosse but have not passed stringent concussion testing. In soccer, which has a high rate of concussion, a reform to eliminate heading the ball has been considered. Resistance to these suggestions stems from the thought that changes could alter the traditions of the games. Some individuals have indicated that helmets may give players a false sense of security and thereby cause them to play more aggressively.
Orthopedic surgeons must be aware of concussion symptoms. Multiple concussions may have a cumulative effect on functional ability and emotional well-being and may lead to chronic traumatic encephalopathy.13 Concern about the long-term effects of concussion has led to the implementation of universal “return to play” laws. These laws vary by state but have 3 steps in common: Educate coaches, players, and athletes; remove athletes from play; and obtain health care professionals’ permission to return to play.14 These guidelines set up an action plan for treating an athlete who has sustained a concussion.
Encouraging results of educating coaches have been noted. Coaches who were given Centers for Disease Control and Prevention–sponsored material on preventing, recognizing, and responding to concussions were able to effectively address concussions; 6 months later, 63% were better able to appreciate the severity of concussions.15 Continued education of athletic communities should help bring this injury to the attention of those treating female athletes.
3. Exercise safety in pregnancy
Women in sports can continue their athletic regimens during pregnancy. It is important to address challenges to the pregnant woman and to the fetus when assessing the risks of exercise.
The physiologic changes that occur during pregnancy may affect how a pregnant athlete responds to stress. Plasma volume, red blood cell volume, and cardiac function and output all increase during normal pregnancy.3,16 Abnormal heart rate during pregnancy can adversely affect the fetus. During and after exercise, fetal bradycardia can occur. Therefore, recommendations should include not exceeding pre-pregnancy activity levels.3 Careful monitoring of exercise intensity is recommended by the American College of Obstetrics and Gynecology; the guideline is to maintain less than 70% of maximal heart rate.17,18
The negative effects of exercise on the pregnant athlete are limited, but it is important to educate patients and to consider preventive strategies. One physiologic change that occurs during pregnancy is ligamentous laxity, which is caused by the hormone relaxin.16 Ligamentous laxity has the potential to put pregnant athletes at risk for soft-tissue and bony injury during impact sports. However, the positive effects of exercise during pregnancy include improved appetite, sleep, and emotional health.19 Aerobic exercise during pregnancy may reverse insulin resistance as demonstrated in animal studies; though this outcome has not been demonstrated in human studies,20 women should be reassured that moderate exercise has overall beneficial effects.
Some research suggests that exercise may expose the fetus to hyperthermia, blood sugar changes, physical injury, and premature labor.16 Typically, fetal heat is dissipated from the mother. After intense exercise, maternal body temperature rises and leads to some degree of fetal hyperthermia.16 Animal model studies have suggested that hyperthermia may result in a slightly higher rate of congenital abnormalities. Pregnant women should keep their exercise routines to less than 60 minutes, should exercise in a thermally regulated environment, and should keep themselves hydrated to avoid fetal hyperthermia.18
Reduced blood flow, accompanied by a deficit of oxygen to the uterus and the developing fetus, is another concern for pregnant athletes. During exercise, when more blood is flowing to the muscles, less is flowing to the uterus.16 Furthermore, during the third trimester, women should avoid supine exercise, as venous outflow is poor with the body in that position.21
Elite athletes who continue training during pregnancy should be carefully counseled about adjusting their training regimens. Because of increased cardiac output and blood volume, the heart rate will be lower than usual, demanding an adjustment in interpretation. Blood cell counts do not increase as much as plasma volume does—often leading to relative anemia. For elite athletes, this means iron supplementation is crucial.22 Thermal regulation may be more difficult, as training regimens may demand prolonged exercise. Physicians should recommend adequate hydration for these athletes.18
Although continued exercise is generally safe for a pregnant athlete and her fetus, caution is required when there is increased risk for premature delivery, or other special conditions exist. Multiple gestation, placenta previa, history of early labor or premature births, and incompetent cervix all contraindicate aerobic exercise during pregnancy.18 With these exceptions in mind, physicians can safely counsel pregnant women to do moderate exercise 30 minutes every day.17,18 Other recommendations are listed at the American College of Obstetricians and Gynecologists website.23
4. Anterior cruciate ligament injuries
ACL injuries affect a staggering number of athletes. In the United States, approximately 100,000 people sustain these injuries annually.24 As they occur up to 8 times more often in women than in men, ACL injuries are a top concern for physicians treating female athletes.
This disproportionate injury rate is influenced by differences between male and female anatomy. The width and shape of the femoral intercondylar notch have been studied as potential variables influencing the risk for ACL injury. Analysis of notch-view radiographs revealed a significant inverse relationship between notch width and ACL injury.25 A-shaped notches, notches with a significantly larger base and a narrowed roof, were more prevalent in women but did not correlate with increased risk for ACL injury. Studies have shown that female athletes with a noncontact ACL injury have a higher lateral tibial plateau posterior slope; this slope is associated with increased peak anteromedial ACL strain, which may contribute to injury.26 An analysis of magnetic resonance imaging scans in patients with and without ACL injury revealed that, for female patients, decreased femoral intercondylar notch width at the anterior outlet combined with increased lateral compartment posterior slope correlated best with risk for ACL injury.27
Although static anatomical factors contribute to ACL injuries in female athletes, dynamic neuromuscular influences are potential opportunities for intervention. Female athletes with high relative quadriceps strength and weak hamstring strength may be at increased risk for ACL injury.28 This “quadriceps dominance” becomes important in sports involving high-risk activities, such as running, cutting, pivoting, and jumping. In addition, compared with male athletes, female athletes demonstrate increased lateral trunk motion and knee valgus torque while landing during noncontact ACL tears, making core stability a factor in ACL injury.29
The collaborative efforts of physicians, physical therapists, athletic trainers, and coaches have yielded multifactorial neuromuscular training programs for the prevention of noncontact ACL injuries. Ideal ACL prevention protocols involve sessions that last for at least 10 minutes and take place 3 times a week. At these sessions, exercises are focused on strengthening, balance, and proprioceptive training.30 The programs last about 8 weeks, but sustained benefits require maintenance after the program has been completed and during the off-season. Program adherence must be encouraged and can be facilitated by varying workouts and raising risk awareness. The most effective programs have reduced the relative risk of noncontact ACL injuries by 75% to 100%.31 These promising results have led to increased focus on program implementation in an effort to prevent ACL injury.
5. Continued sex discrimination and social injustice
In 1972, Title IX was passed as part of the Education Amendments Act. Title IX states, “No person in the United States shall, on the basis of sex, be excluded from participation in, be denied the benefits of, or be subjected to discrimination under any educational program or activity receiving Federal financial assistance.” Passage of this law, which has implications outside of athletic participation, marked an important turning point in women’s ability to participate equally in college sports.32,33 The Civil Rights Restoration Act, passed in 1988, strengthened Title IX and made it applicable to all institutions receiving federal funding.34 Before the 1970s, women typically were restricted to club sports, and funding and participation opportunities were weighted heavily toward men. Over the past 40 years, women’s participation in high school, college, and professional sports has taken a huge leap forward.32 For example, the number of women participating in high school sports increased from 294,000 (7.4% of all athletes) in 1972 to 3.4 million (>41% of all athletes) in 2014.
Despite advances in women’s civil rights, examples of inequality in US schools remain, particularly in the distribution of funding, which still strongly favors men’s football.32 Men’s sports receive 90% of media coverage.33 In 2002, women represented 55% of college students but only 42% of varsity athletes.34 The schools that have complied the least with Title IX are schools in the Midwest and the South and those with football teams.34 Women are underrepresented as coaches, and funding continues to be disproportionately spent on men’s sports.
For women, the benefits of participating in sports are far-reaching and significant. These benefits include improvements in academic success, mental health, and responsible behavior.33 Women’s gaining acceptance and respect throughout the athletic world seems to have carried over elsewhere. Although many institutions remain noncompliant with Title IX, efforts continue to have a strongly positive effect on gender equality in the United States.
1. Nattiv A, Loucks AB, Manore MM, Sanborn CF, Sundgot-Borgen J, Warren MP; American College of Sports Medicine. American College of Sports Medicine position stand. The female athlete triad. Med Sci Sports Exerc. 2007;39(10):1867-1882.
2. De Souza MJ, Nattiv A, Joy E, et al; Expert Panel. 2014 Female Athlete Triad Coalition consensus statement on treatment and return to play of the female athlete triad: 1st international conference held in San Francisco, California, May 2012 and 2nd international conference held in Indianapolis, Indiana, May 2013. Br J Sports Med. 2014;48(4):289.
3. Warren MP, Shantha S. The female athlete. Baillieres Best Pract Res Clin Endocrinol Metab. 2000;14(1):37-53.
4. Greenleaf C, Petrie TA, Carter J, Reel JJ. Female collegiate athletes: prevalence of eating disorders and disordered eating behaviors. J Am Coll Health. 2009;57(5):489-495.
5. Reinking MF, Alexander LE. Prevalence of disordered-eating behaviors in undergraduate female collegiate athletes and nonathletes. J Athl Train. 2005;40(1):47-51.
6. Rencken ML, Chesnut CH 3rd, Drinkwater BL. Bone density at multiple skeletal sites in amenorrheic athletes. JAMA. 1996;276(3):238-240.
7. Lappe J, Cullen D, Haynatzki G, Recker R, Ahlf R, Thompson K. Calcium and vitamin D supplementation decreases incidence of stress fractures in female Navy recruits. J Bone Miner Res. 2008;23(5):741-749.
8. De Souza MJ. 2014 Female athlete triad consensus statement on guidelines for treatment and return to play. National Collegiate Athletic Association (NCAA) website. http://www.ncaa.org/health-and-safety/nutrition-and-performance/2014-female-athlete-triad-consensus-statement-guidelines. Accessed November 24, 2015.
9. Preiss-Farzanegan SJ, Chapman B, Wong TM, Wu J, Bazarian JJ. The relationship between gender and postconcussion symptoms after sport-related mild traumatic brain injury. PM R. 2009;1(3):245-253.
10. Marar M, McIlvain NM, Fields SK, Comstock RD. Epidemiology of concussions among United States high school athletes in 20 sports. Am J Sports Med. 2012;40(4):747-755.
11. Uhl RL, Rosenbaum AJ, Czajka C, Mulligan M, King C. Minor traumatic brain injury: a primer for the orthopaedic surgeon. J Am Acad Orthop Surg. 2013;21(10):624-631.
12. Covassin T, Elbin RJ, Harris W, Parker T, Kontos A. The role of age and sex in symptoms, neurocognitive performance, and postural stability in athletes after concussion. Am J Sports Med. 2012;40(6):1303-1312.
13. Covassin T, Moran R, Wilhelm K. Concussion symptoms and neurocognitive performance of high school and college athletes who incur multiple concussions. Am J Sports Med. 2013;41(12):2885-2889.
14. Sports concussion policies and laws: information for parents, coaches, and school & sports professionals. Centers for Disease Control and Prevention website. http://www.cdc.gov/headsup/policy/index.html. Updated February 16, 2015. Accessed November 24, 2015.
15. Covassin T, Elbin RJ, Sarmiento K. Educating coaches about concussion in sports: evaluation of the CDC’s “Heads Up: concussion in youth sports” initiative. J Sch Health. 2012;82(5):233-238.
16. Lumbers ER. Exercise in pregnancy: physiological basis of exercise prescription for the pregnant woman. J Sci Med Sport. 2002;5(1):20-31.
17. ACOG Committee Obstetric Practice. ACOG Committee opinion. Number 267, January 2002: exercise during pregnancy and the postpartum period. Obstet Gynecol. 2002;99(1):171-173.
18. Artal R, O’Toole M. Guidelines of the American College of Obstetricians and Gynecologists for exercise during pregnancy and the postpartum period. Br J Sports Med. 2003;37(1):6-12.
19. Kramer MS. Regular aerobic exercise during pregnancy. Cochrane Database Syst Rev. 2000;(2):CD000180. Update in: Cochrane Database Syst Rev. 2002;(2):CD000180.
20. Stafne SN, Salvesen KA, Romundstad PR, Stuge B, Morkved S. Does regular exercise during pregnancy influence lumbopelvic pain? A randomized controlled trial. Acta Obstet Gynecol Scand. 2012;91(5):552-559.
21. Nascimento SL, Surita FG, Cecatti JG. Physical exercise during pregnancy: a systematic review. Curr Opin Obstet Gynecol. 2012;24(6):387-394.
22. Hale RW, Milne L. The elite athlete and exercise in pregnancy. Semin Perinatol. 1996;20(4):277-284.
23. Exercise during pregnancy. American College of Obstetricians and Gynecologists website. http://www.acog.org/Patients/FAQs/Exercise-During-Pregnancy. Published August 2011. Accessed November 24, 2015.
24. Giugliano DN, Solomon JL. ACL tears in female athletes. Phys Med Rehabil Clin North Am. 2007;18(3):417-438, viii.
25. Ireland ML, Ballantyne BT, Little K, McClay IS. A radiographic analysis of the relationship between the size and shape of the intercondylar notch and anterior cruciate ligament injury. Knee Surg Sports Traumatol Arthrosc. 2001;9(4):200-205.
26. Lipps DB, Oh YK, Ashton-Miller JA, Wojtys EM. Morphologic characteristics help explain the gender difference in peak anterior cruciate ligament strain during a simulated pivot landing. Am J Sports Med. 2012;40(1):32-40.
27. Sturnick DR, Vacek PM, DeSarno MJ, et al. Combined anatomic factors predicting risk of anterior cruciate ligament injury for males and females. Am J Sports Med. 2015;43(4):839-847.
28. Myer GD, Ford KR, Barber Foss KD, Liu C, Nick TG, Hewett TE. The relationship of hamstrings and quadriceps strength to anterior cruciate ligament injury in female athletes. Clin J Sport Med. 2009;19(1):3-8.
29. Hewett TE, Torg JS, Boden BP. Video analysis of trunk and knee motion during non-contact anterior cruciate ligament injury in female athletes: lateral trunk and knee abduction motion are combined components of the injury mechanism. Br J Sports Med. 2009;43(6):417-422.
30. Sutton KM, Bullock JM. Anterior cruciate ligament rupture: differences between males and females. J Am Acad Orthop Surg. 2013;21(1):41-50.
31. Noyes FR, Barber-Westin SD. Neuromuscular retraining intervention programs: do they reduce noncontact anterior cruciate ligament injury rates in adolescent female athletes? Arthroscopy. 2014;30(2):245-255.
32. Ladd AL. The sports bra, the ACL, and Title IX—the game in play. Clin Orthop Relat Res. 2014;472(6):1681-1684.
33. Lopiano DA. Modern history of women in sports. Twenty-five years of Title IX. Clin Sports Med. 2000;19(2):163-173, vii.
34. Anderson DJ, Cheslock JJ, Ehrenberg RG. Gender equity in intercollegiate athletics: determinants of Title IX compliance. J High Educ. 2006;77(2):225-250.
Since Title IX passed in 1972, women have become exponentially more involved in competitive sports, from high school to professional levels. With more women engaging in serious athletics, the specific challenges they face have come to the forefront of sports medicine. These problems include the female athlete triad, concussions, exercise safety in pregnancy, anterior cruciate ligament (ACL) injuries, and continued sex discrimination and social injustice. Orthopedists treating female athletes should be aware of these problems, each of which is discussed in this review.
1. Female athlete triad
In 1992, the term female athlete triad was coined to describe 3 problems that often coexist in high-intensity female athletes.1 Since then, the definition has evolved, but the problem has remained essentially the same. The modern definition incorporates menstrual abnormalities, low energy availability with or without disordered eating, and decreased bone mineral density (BMD).2
With intense exercise and weight loss comes a variety of menstrual disturbances.3 In affected athletes, the hypothalamus is underactivated, and changes in gonadotropin-releasing hormone and luteinizing hormone lead to decreased estrogen production. Research suggests abnormal menses result from having inadequate energy and insufficient caloric intake to support extensive exercise.1 This phenomenon can occur in athletes in any sport but is most prevalent in lean-body sports, such as swimming, gymnastics, and ballet. The incidence of abnormal menses is as high as 79% in ballet dancers but only 5% in the general population.3 Menstrual abnormalities indicate hormonal abnormalities that can interfere with growth and maturation in young athletes.
Although full-blown eating disorders are uncommon among female athletes, disordered eating patterns are often found among women in competitive sports. Disordered eating can involve a spectrum of inadequate caloric intake and purging behavior, such as vomiting or laxative abuse, and has been reported in up to 25% of collegiate female athletes.4 Physicians must recognize these conditions and initiate counseling and treatment when appropriate. Women with disordered eating are at risk for developing electrolyte imbalances, malnutrition syndromes, and osteopenia.
Although careful evaluation and counseling are important, physicians must note that, in most cases, athletics participation may also protect against disordered eating and body image difficulties. A study of 146 college-age women found better body satisfaction among athletes than among nonathletes.5 Lean-sport athletes (eg, swimmers, gymnasts) were at higher risk for disordered eating and body image problems than other athletes were. Similarly, other studies have found that a majority of athletes have healthy eating habits.4
For poorly nourished and hormonally imbalanced female athletes, decreased BMD poses substantial risk. One study found a significant difference in BMD between athletes with amenorrhea and athletes with normal menses.6 In a cohort of female Navy recruits, those with amenorrhea were at 91% higher risk for stress fractures; calcium and vitamin D supplementation reduced risk by 20%.7 Osteopenia may be a special problem for prepubescent athletes. Girls who engage in intense exercise and have delayed menarche may have a low estrogen state, predisposing them to low BMD.3 Osteopenia and osteoporosis are difficult to reverse and can put these athletes at risk for stress fractures the rest of their lives. If unrecognized, stress fractures can end an athlete’s career.
Recommendations for dual-energy X-ray absorptiometry (DXA) include testing female athletes who have a diagnosed eating disorder, body mass index under 17.5, history of delayed menarche, oligomenorrhea, 2 prior stress fractures, or prior abnormal DXA scan. Complete testing recommendations appear in the 2014 consensus statement on the female athlete triad and return to sport.2,8
Orthopedists performing physical examinations for sports participation can screen for the female athlete triad through thoughtful questioning about menstrual history, nutrition habits, and stress fracture symptoms. Best treatment for a diagnosed case of the triad is multidisciplinary care with strong social support. When abnormal menses are an issue, referral to a gynecologist or endocrinologist and consideration of estrogen replacement should be discussed. Some cases require a psychiatrist’s assistance in treating disordered eating. Athletic trainers, coaches, and parents should be involved over the treatment course.1 Orthopedists must counsel women with osteopenia and osteoporosis about decreasing exercise to a safe level, improving nutritional intake, and supplementing with calcium (1200-1500 mg/d) and vitamin D (600-800 IU/d).3,7
2. Concussions
Increasing awareness of males’ sport-related concussions, particularly of concussions that occur during National Football League practice and games, has made physicians and researchers more aware of the rate of concussion in female athletes. That rate has increased, and, according to some reports, the risk for sport-related injury is higher for female athletes.9 A study of high school athletes found that the rate of concussion in girl’s soccer was second only to that in football.10
Concussions are categorized as mild traumatic brain injuries, and manifestations of the diagnosis are divided into physical, emotional, cognitive, and observed symptoms. The spectrum of symptoms is wide, ranging from difficulty concentrating and thinking clearly to headaches and dizziness.11 Compared with male athletes who sustain a concussion, female athletes report more of these concussive symptoms and have worse visual memory scores.12
Efforts to change sports at the player level have been resisted. Helmets have been proposed for field hockey and lacrosse but have not passed stringent concussion testing. In soccer, which has a high rate of concussion, a reform to eliminate heading the ball has been considered. Resistance to these suggestions stems from the thought that changes could alter the traditions of the games. Some individuals have indicated that helmets may give players a false sense of security and thereby cause them to play more aggressively.
Orthopedic surgeons must be aware of concussion symptoms. Multiple concussions may have a cumulative effect on functional ability and emotional well-being and may lead to chronic traumatic encephalopathy.13 Concern about the long-term effects of concussion has led to the implementation of universal “return to play” laws. These laws vary by state but have 3 steps in common: Educate coaches, players, and athletes; remove athletes from play; and obtain health care professionals’ permission to return to play.14 These guidelines set up an action plan for treating an athlete who has sustained a concussion.
Encouraging results of educating coaches have been noted. Coaches who were given Centers for Disease Control and Prevention–sponsored material on preventing, recognizing, and responding to concussions were able to effectively address concussions; 6 months later, 63% were better able to appreciate the severity of concussions.15 Continued education of athletic communities should help bring this injury to the attention of those treating female athletes.
3. Exercise safety in pregnancy
Women in sports can continue their athletic regimens during pregnancy. It is important to address challenges to the pregnant woman and to the fetus when assessing the risks of exercise.
The physiologic changes that occur during pregnancy may affect how a pregnant athlete responds to stress. Plasma volume, red blood cell volume, and cardiac function and output all increase during normal pregnancy.3,16 Abnormal heart rate during pregnancy can adversely affect the fetus. During and after exercise, fetal bradycardia can occur. Therefore, recommendations should include not exceeding pre-pregnancy activity levels.3 Careful monitoring of exercise intensity is recommended by the American College of Obstetrics and Gynecology; the guideline is to maintain less than 70% of maximal heart rate.17,18
The negative effects of exercise on the pregnant athlete are limited, but it is important to educate patients and to consider preventive strategies. One physiologic change that occurs during pregnancy is ligamentous laxity, which is caused by the hormone relaxin.16 Ligamentous laxity has the potential to put pregnant athletes at risk for soft-tissue and bony injury during impact sports. However, the positive effects of exercise during pregnancy include improved appetite, sleep, and emotional health.19 Aerobic exercise during pregnancy may reverse insulin resistance as demonstrated in animal studies; though this outcome has not been demonstrated in human studies,20 women should be reassured that moderate exercise has overall beneficial effects.
Some research suggests that exercise may expose the fetus to hyperthermia, blood sugar changes, physical injury, and premature labor.16 Typically, fetal heat is dissipated from the mother. After intense exercise, maternal body temperature rises and leads to some degree of fetal hyperthermia.16 Animal model studies have suggested that hyperthermia may result in a slightly higher rate of congenital abnormalities. Pregnant women should keep their exercise routines to less than 60 minutes, should exercise in a thermally regulated environment, and should keep themselves hydrated to avoid fetal hyperthermia.18
Reduced blood flow, accompanied by a deficit of oxygen to the uterus and the developing fetus, is another concern for pregnant athletes. During exercise, when more blood is flowing to the muscles, less is flowing to the uterus.16 Furthermore, during the third trimester, women should avoid supine exercise, as venous outflow is poor with the body in that position.21
Elite athletes who continue training during pregnancy should be carefully counseled about adjusting their training regimens. Because of increased cardiac output and blood volume, the heart rate will be lower than usual, demanding an adjustment in interpretation. Blood cell counts do not increase as much as plasma volume does—often leading to relative anemia. For elite athletes, this means iron supplementation is crucial.22 Thermal regulation may be more difficult, as training regimens may demand prolonged exercise. Physicians should recommend adequate hydration for these athletes.18
Although continued exercise is generally safe for a pregnant athlete and her fetus, caution is required when there is increased risk for premature delivery, or other special conditions exist. Multiple gestation, placenta previa, history of early labor or premature births, and incompetent cervix all contraindicate aerobic exercise during pregnancy.18 With these exceptions in mind, physicians can safely counsel pregnant women to do moderate exercise 30 minutes every day.17,18 Other recommendations are listed at the American College of Obstetricians and Gynecologists website.23
4. Anterior cruciate ligament injuries
ACL injuries affect a staggering number of athletes. In the United States, approximately 100,000 people sustain these injuries annually.24 As they occur up to 8 times more often in women than in men, ACL injuries are a top concern for physicians treating female athletes.
This disproportionate injury rate is influenced by differences between male and female anatomy. The width and shape of the femoral intercondylar notch have been studied as potential variables influencing the risk for ACL injury. Analysis of notch-view radiographs revealed a significant inverse relationship between notch width and ACL injury.25 A-shaped notches, notches with a significantly larger base and a narrowed roof, were more prevalent in women but did not correlate with increased risk for ACL injury. Studies have shown that female athletes with a noncontact ACL injury have a higher lateral tibial plateau posterior slope; this slope is associated with increased peak anteromedial ACL strain, which may contribute to injury.26 An analysis of magnetic resonance imaging scans in patients with and without ACL injury revealed that, for female patients, decreased femoral intercondylar notch width at the anterior outlet combined with increased lateral compartment posterior slope correlated best with risk for ACL injury.27
Although static anatomical factors contribute to ACL injuries in female athletes, dynamic neuromuscular influences are potential opportunities for intervention. Female athletes with high relative quadriceps strength and weak hamstring strength may be at increased risk for ACL injury.28 This “quadriceps dominance” becomes important in sports involving high-risk activities, such as running, cutting, pivoting, and jumping. In addition, compared with male athletes, female athletes demonstrate increased lateral trunk motion and knee valgus torque while landing during noncontact ACL tears, making core stability a factor in ACL injury.29
The collaborative efforts of physicians, physical therapists, athletic trainers, and coaches have yielded multifactorial neuromuscular training programs for the prevention of noncontact ACL injuries. Ideal ACL prevention protocols involve sessions that last for at least 10 minutes and take place 3 times a week. At these sessions, exercises are focused on strengthening, balance, and proprioceptive training.30 The programs last about 8 weeks, but sustained benefits require maintenance after the program has been completed and during the off-season. Program adherence must be encouraged and can be facilitated by varying workouts and raising risk awareness. The most effective programs have reduced the relative risk of noncontact ACL injuries by 75% to 100%.31 These promising results have led to increased focus on program implementation in an effort to prevent ACL injury.
5. Continued sex discrimination and social injustice
In 1972, Title IX was passed as part of the Education Amendments Act. Title IX states, “No person in the United States shall, on the basis of sex, be excluded from participation in, be denied the benefits of, or be subjected to discrimination under any educational program or activity receiving Federal financial assistance.” Passage of this law, which has implications outside of athletic participation, marked an important turning point in women’s ability to participate equally in college sports.32,33 The Civil Rights Restoration Act, passed in 1988, strengthened Title IX and made it applicable to all institutions receiving federal funding.34 Before the 1970s, women typically were restricted to club sports, and funding and participation opportunities were weighted heavily toward men. Over the past 40 years, women’s participation in high school, college, and professional sports has taken a huge leap forward.32 For example, the number of women participating in high school sports increased from 294,000 (7.4% of all athletes) in 1972 to 3.4 million (>41% of all athletes) in 2014.
Despite advances in women’s civil rights, examples of inequality in US schools remain, particularly in the distribution of funding, which still strongly favors men’s football.32 Men’s sports receive 90% of media coverage.33 In 2002, women represented 55% of college students but only 42% of varsity athletes.34 The schools that have complied the least with Title IX are schools in the Midwest and the South and those with football teams.34 Women are underrepresented as coaches, and funding continues to be disproportionately spent on men’s sports.
For women, the benefits of participating in sports are far-reaching and significant. These benefits include improvements in academic success, mental health, and responsible behavior.33 Women’s gaining acceptance and respect throughout the athletic world seems to have carried over elsewhere. Although many institutions remain noncompliant with Title IX, efforts continue to have a strongly positive effect on gender equality in the United States.
Since Title IX passed in 1972, women have become exponentially more involved in competitive sports, from high school to professional levels. With more women engaging in serious athletics, the specific challenges they face have come to the forefront of sports medicine. These problems include the female athlete triad, concussions, exercise safety in pregnancy, anterior cruciate ligament (ACL) injuries, and continued sex discrimination and social injustice. Orthopedists treating female athletes should be aware of these problems, each of which is discussed in this review.
1. Female athlete triad
In 1992, the term female athlete triad was coined to describe 3 problems that often coexist in high-intensity female athletes.1 Since then, the definition has evolved, but the problem has remained essentially the same. The modern definition incorporates menstrual abnormalities, low energy availability with or without disordered eating, and decreased bone mineral density (BMD).2
With intense exercise and weight loss comes a variety of menstrual disturbances.3 In affected athletes, the hypothalamus is underactivated, and changes in gonadotropin-releasing hormone and luteinizing hormone lead to decreased estrogen production. Research suggests abnormal menses result from having inadequate energy and insufficient caloric intake to support extensive exercise.1 This phenomenon can occur in athletes in any sport but is most prevalent in lean-body sports, such as swimming, gymnastics, and ballet. The incidence of abnormal menses is as high as 79% in ballet dancers but only 5% in the general population.3 Menstrual abnormalities indicate hormonal abnormalities that can interfere with growth and maturation in young athletes.
Although full-blown eating disorders are uncommon among female athletes, disordered eating patterns are often found among women in competitive sports. Disordered eating can involve a spectrum of inadequate caloric intake and purging behavior, such as vomiting or laxative abuse, and has been reported in up to 25% of collegiate female athletes.4 Physicians must recognize these conditions and initiate counseling and treatment when appropriate. Women with disordered eating are at risk for developing electrolyte imbalances, malnutrition syndromes, and osteopenia.
Although careful evaluation and counseling are important, physicians must note that, in most cases, athletics participation may also protect against disordered eating and body image difficulties. A study of 146 college-age women found better body satisfaction among athletes than among nonathletes.5 Lean-sport athletes (eg, swimmers, gymnasts) were at higher risk for disordered eating and body image problems than other athletes were. Similarly, other studies have found that a majority of athletes have healthy eating habits.4
For poorly nourished and hormonally imbalanced female athletes, decreased BMD poses substantial risk. One study found a significant difference in BMD between athletes with amenorrhea and athletes with normal menses.6 In a cohort of female Navy recruits, those with amenorrhea were at 91% higher risk for stress fractures; calcium and vitamin D supplementation reduced risk by 20%.7 Osteopenia may be a special problem for prepubescent athletes. Girls who engage in intense exercise and have delayed menarche may have a low estrogen state, predisposing them to low BMD.3 Osteopenia and osteoporosis are difficult to reverse and can put these athletes at risk for stress fractures the rest of their lives. If unrecognized, stress fractures can end an athlete’s career.
Recommendations for dual-energy X-ray absorptiometry (DXA) include testing female athletes who have a diagnosed eating disorder, body mass index under 17.5, history of delayed menarche, oligomenorrhea, 2 prior stress fractures, or prior abnormal DXA scan. Complete testing recommendations appear in the 2014 consensus statement on the female athlete triad and return to sport.2,8
Orthopedists performing physical examinations for sports participation can screen for the female athlete triad through thoughtful questioning about menstrual history, nutrition habits, and stress fracture symptoms. Best treatment for a diagnosed case of the triad is multidisciplinary care with strong social support. When abnormal menses are an issue, referral to a gynecologist or endocrinologist and consideration of estrogen replacement should be discussed. Some cases require a psychiatrist’s assistance in treating disordered eating. Athletic trainers, coaches, and parents should be involved over the treatment course.1 Orthopedists must counsel women with osteopenia and osteoporosis about decreasing exercise to a safe level, improving nutritional intake, and supplementing with calcium (1200-1500 mg/d) and vitamin D (600-800 IU/d).3,7
2. Concussions
Increasing awareness of males’ sport-related concussions, particularly of concussions that occur during National Football League practice and games, has made physicians and researchers more aware of the rate of concussion in female athletes. That rate has increased, and, according to some reports, the risk for sport-related injury is higher for female athletes.9 A study of high school athletes found that the rate of concussion in girl’s soccer was second only to that in football.10
Concussions are categorized as mild traumatic brain injuries, and manifestations of the diagnosis are divided into physical, emotional, cognitive, and observed symptoms. The spectrum of symptoms is wide, ranging from difficulty concentrating and thinking clearly to headaches and dizziness.11 Compared with male athletes who sustain a concussion, female athletes report more of these concussive symptoms and have worse visual memory scores.12
Efforts to change sports at the player level have been resisted. Helmets have been proposed for field hockey and lacrosse but have not passed stringent concussion testing. In soccer, which has a high rate of concussion, a reform to eliminate heading the ball has been considered. Resistance to these suggestions stems from the thought that changes could alter the traditions of the games. Some individuals have indicated that helmets may give players a false sense of security and thereby cause them to play more aggressively.
Orthopedic surgeons must be aware of concussion symptoms. Multiple concussions may have a cumulative effect on functional ability and emotional well-being and may lead to chronic traumatic encephalopathy.13 Concern about the long-term effects of concussion has led to the implementation of universal “return to play” laws. These laws vary by state but have 3 steps in common: Educate coaches, players, and athletes; remove athletes from play; and obtain health care professionals’ permission to return to play.14 These guidelines set up an action plan for treating an athlete who has sustained a concussion.
Encouraging results of educating coaches have been noted. Coaches who were given Centers for Disease Control and Prevention–sponsored material on preventing, recognizing, and responding to concussions were able to effectively address concussions; 6 months later, 63% were better able to appreciate the severity of concussions.15 Continued education of athletic communities should help bring this injury to the attention of those treating female athletes.
3. Exercise safety in pregnancy
Women in sports can continue their athletic regimens during pregnancy. It is important to address challenges to the pregnant woman and to the fetus when assessing the risks of exercise.
The physiologic changes that occur during pregnancy may affect how a pregnant athlete responds to stress. Plasma volume, red blood cell volume, and cardiac function and output all increase during normal pregnancy.3,16 Abnormal heart rate during pregnancy can adversely affect the fetus. During and after exercise, fetal bradycardia can occur. Therefore, recommendations should include not exceeding pre-pregnancy activity levels.3 Careful monitoring of exercise intensity is recommended by the American College of Obstetrics and Gynecology; the guideline is to maintain less than 70% of maximal heart rate.17,18
The negative effects of exercise on the pregnant athlete are limited, but it is important to educate patients and to consider preventive strategies. One physiologic change that occurs during pregnancy is ligamentous laxity, which is caused by the hormone relaxin.16 Ligamentous laxity has the potential to put pregnant athletes at risk for soft-tissue and bony injury during impact sports. However, the positive effects of exercise during pregnancy include improved appetite, sleep, and emotional health.19 Aerobic exercise during pregnancy may reverse insulin resistance as demonstrated in animal studies; though this outcome has not been demonstrated in human studies,20 women should be reassured that moderate exercise has overall beneficial effects.
Some research suggests that exercise may expose the fetus to hyperthermia, blood sugar changes, physical injury, and premature labor.16 Typically, fetal heat is dissipated from the mother. After intense exercise, maternal body temperature rises and leads to some degree of fetal hyperthermia.16 Animal model studies have suggested that hyperthermia may result in a slightly higher rate of congenital abnormalities. Pregnant women should keep their exercise routines to less than 60 minutes, should exercise in a thermally regulated environment, and should keep themselves hydrated to avoid fetal hyperthermia.18
Reduced blood flow, accompanied by a deficit of oxygen to the uterus and the developing fetus, is another concern for pregnant athletes. During exercise, when more blood is flowing to the muscles, less is flowing to the uterus.16 Furthermore, during the third trimester, women should avoid supine exercise, as venous outflow is poor with the body in that position.21
Elite athletes who continue training during pregnancy should be carefully counseled about adjusting their training regimens. Because of increased cardiac output and blood volume, the heart rate will be lower than usual, demanding an adjustment in interpretation. Blood cell counts do not increase as much as plasma volume does—often leading to relative anemia. For elite athletes, this means iron supplementation is crucial.22 Thermal regulation may be more difficult, as training regimens may demand prolonged exercise. Physicians should recommend adequate hydration for these athletes.18
Although continued exercise is generally safe for a pregnant athlete and her fetus, caution is required when there is increased risk for premature delivery, or other special conditions exist. Multiple gestation, placenta previa, history of early labor or premature births, and incompetent cervix all contraindicate aerobic exercise during pregnancy.18 With these exceptions in mind, physicians can safely counsel pregnant women to do moderate exercise 30 minutes every day.17,18 Other recommendations are listed at the American College of Obstetricians and Gynecologists website.23
4. Anterior cruciate ligament injuries
ACL injuries affect a staggering number of athletes. In the United States, approximately 100,000 people sustain these injuries annually.24 As they occur up to 8 times more often in women than in men, ACL injuries are a top concern for physicians treating female athletes.
This disproportionate injury rate is influenced by differences between male and female anatomy. The width and shape of the femoral intercondylar notch have been studied as potential variables influencing the risk for ACL injury. Analysis of notch-view radiographs revealed a significant inverse relationship between notch width and ACL injury.25 A-shaped notches, notches with a significantly larger base and a narrowed roof, were more prevalent in women but did not correlate with increased risk for ACL injury. Studies have shown that female athletes with a noncontact ACL injury have a higher lateral tibial plateau posterior slope; this slope is associated with increased peak anteromedial ACL strain, which may contribute to injury.26 An analysis of magnetic resonance imaging scans in patients with and without ACL injury revealed that, for female patients, decreased femoral intercondylar notch width at the anterior outlet combined with increased lateral compartment posterior slope correlated best with risk for ACL injury.27
Although static anatomical factors contribute to ACL injuries in female athletes, dynamic neuromuscular influences are potential opportunities for intervention. Female athletes with high relative quadriceps strength and weak hamstring strength may be at increased risk for ACL injury.28 This “quadriceps dominance” becomes important in sports involving high-risk activities, such as running, cutting, pivoting, and jumping. In addition, compared with male athletes, female athletes demonstrate increased lateral trunk motion and knee valgus torque while landing during noncontact ACL tears, making core stability a factor in ACL injury.29
The collaborative efforts of physicians, physical therapists, athletic trainers, and coaches have yielded multifactorial neuromuscular training programs for the prevention of noncontact ACL injuries. Ideal ACL prevention protocols involve sessions that last for at least 10 minutes and take place 3 times a week. At these sessions, exercises are focused on strengthening, balance, and proprioceptive training.30 The programs last about 8 weeks, but sustained benefits require maintenance after the program has been completed and during the off-season. Program adherence must be encouraged and can be facilitated by varying workouts and raising risk awareness. The most effective programs have reduced the relative risk of noncontact ACL injuries by 75% to 100%.31 These promising results have led to increased focus on program implementation in an effort to prevent ACL injury.
5. Continued sex discrimination and social injustice
In 1972, Title IX was passed as part of the Education Amendments Act. Title IX states, “No person in the United States shall, on the basis of sex, be excluded from participation in, be denied the benefits of, or be subjected to discrimination under any educational program or activity receiving Federal financial assistance.” Passage of this law, which has implications outside of athletic participation, marked an important turning point in women’s ability to participate equally in college sports.32,33 The Civil Rights Restoration Act, passed in 1988, strengthened Title IX and made it applicable to all institutions receiving federal funding.34 Before the 1970s, women typically were restricted to club sports, and funding and participation opportunities were weighted heavily toward men. Over the past 40 years, women’s participation in high school, college, and professional sports has taken a huge leap forward.32 For example, the number of women participating in high school sports increased from 294,000 (7.4% of all athletes) in 1972 to 3.4 million (>41% of all athletes) in 2014.
Despite advances in women’s civil rights, examples of inequality in US schools remain, particularly in the distribution of funding, which still strongly favors men’s football.32 Men’s sports receive 90% of media coverage.33 In 2002, women represented 55% of college students but only 42% of varsity athletes.34 The schools that have complied the least with Title IX are schools in the Midwest and the South and those with football teams.34 Women are underrepresented as coaches, and funding continues to be disproportionately spent on men’s sports.
For women, the benefits of participating in sports are far-reaching and significant. These benefits include improvements in academic success, mental health, and responsible behavior.33 Women’s gaining acceptance and respect throughout the athletic world seems to have carried over elsewhere. Although many institutions remain noncompliant with Title IX, efforts continue to have a strongly positive effect on gender equality in the United States.
1. Nattiv A, Loucks AB, Manore MM, Sanborn CF, Sundgot-Borgen J, Warren MP; American College of Sports Medicine. American College of Sports Medicine position stand. The female athlete triad. Med Sci Sports Exerc. 2007;39(10):1867-1882.
2. De Souza MJ, Nattiv A, Joy E, et al; Expert Panel. 2014 Female Athlete Triad Coalition consensus statement on treatment and return to play of the female athlete triad: 1st international conference held in San Francisco, California, May 2012 and 2nd international conference held in Indianapolis, Indiana, May 2013. Br J Sports Med. 2014;48(4):289.
3. Warren MP, Shantha S. The female athlete. Baillieres Best Pract Res Clin Endocrinol Metab. 2000;14(1):37-53.
4. Greenleaf C, Petrie TA, Carter J, Reel JJ. Female collegiate athletes: prevalence of eating disorders and disordered eating behaviors. J Am Coll Health. 2009;57(5):489-495.
5. Reinking MF, Alexander LE. Prevalence of disordered-eating behaviors in undergraduate female collegiate athletes and nonathletes. J Athl Train. 2005;40(1):47-51.
6. Rencken ML, Chesnut CH 3rd, Drinkwater BL. Bone density at multiple skeletal sites in amenorrheic athletes. JAMA. 1996;276(3):238-240.
7. Lappe J, Cullen D, Haynatzki G, Recker R, Ahlf R, Thompson K. Calcium and vitamin D supplementation decreases incidence of stress fractures in female Navy recruits. J Bone Miner Res. 2008;23(5):741-749.
8. De Souza MJ. 2014 Female athlete triad consensus statement on guidelines for treatment and return to play. National Collegiate Athletic Association (NCAA) website. http://www.ncaa.org/health-and-safety/nutrition-and-performance/2014-female-athlete-triad-consensus-statement-guidelines. Accessed November 24, 2015.
9. Preiss-Farzanegan SJ, Chapman B, Wong TM, Wu J, Bazarian JJ. The relationship between gender and postconcussion symptoms after sport-related mild traumatic brain injury. PM R. 2009;1(3):245-253.
10. Marar M, McIlvain NM, Fields SK, Comstock RD. Epidemiology of concussions among United States high school athletes in 20 sports. Am J Sports Med. 2012;40(4):747-755.
11. Uhl RL, Rosenbaum AJ, Czajka C, Mulligan M, King C. Minor traumatic brain injury: a primer for the orthopaedic surgeon. J Am Acad Orthop Surg. 2013;21(10):624-631.
12. Covassin T, Elbin RJ, Harris W, Parker T, Kontos A. The role of age and sex in symptoms, neurocognitive performance, and postural stability in athletes after concussion. Am J Sports Med. 2012;40(6):1303-1312.
13. Covassin T, Moran R, Wilhelm K. Concussion symptoms and neurocognitive performance of high school and college athletes who incur multiple concussions. Am J Sports Med. 2013;41(12):2885-2889.
14. Sports concussion policies and laws: information for parents, coaches, and school & sports professionals. Centers for Disease Control and Prevention website. http://www.cdc.gov/headsup/policy/index.html. Updated February 16, 2015. Accessed November 24, 2015.
15. Covassin T, Elbin RJ, Sarmiento K. Educating coaches about concussion in sports: evaluation of the CDC’s “Heads Up: concussion in youth sports” initiative. J Sch Health. 2012;82(5):233-238.
16. Lumbers ER. Exercise in pregnancy: physiological basis of exercise prescription for the pregnant woman. J Sci Med Sport. 2002;5(1):20-31.
17. ACOG Committee Obstetric Practice. ACOG Committee opinion. Number 267, January 2002: exercise during pregnancy and the postpartum period. Obstet Gynecol. 2002;99(1):171-173.
18. Artal R, O’Toole M. Guidelines of the American College of Obstetricians and Gynecologists for exercise during pregnancy and the postpartum period. Br J Sports Med. 2003;37(1):6-12.
19. Kramer MS. Regular aerobic exercise during pregnancy. Cochrane Database Syst Rev. 2000;(2):CD000180. Update in: Cochrane Database Syst Rev. 2002;(2):CD000180.
20. Stafne SN, Salvesen KA, Romundstad PR, Stuge B, Morkved S. Does regular exercise during pregnancy influence lumbopelvic pain? A randomized controlled trial. Acta Obstet Gynecol Scand. 2012;91(5):552-559.
21. Nascimento SL, Surita FG, Cecatti JG. Physical exercise during pregnancy: a systematic review. Curr Opin Obstet Gynecol. 2012;24(6):387-394.
22. Hale RW, Milne L. The elite athlete and exercise in pregnancy. Semin Perinatol. 1996;20(4):277-284.
23. Exercise during pregnancy. American College of Obstetricians and Gynecologists website. http://www.acog.org/Patients/FAQs/Exercise-During-Pregnancy. Published August 2011. Accessed November 24, 2015.
24. Giugliano DN, Solomon JL. ACL tears in female athletes. Phys Med Rehabil Clin North Am. 2007;18(3):417-438, viii.
25. Ireland ML, Ballantyne BT, Little K, McClay IS. A radiographic analysis of the relationship between the size and shape of the intercondylar notch and anterior cruciate ligament injury. Knee Surg Sports Traumatol Arthrosc. 2001;9(4):200-205.
26. Lipps DB, Oh YK, Ashton-Miller JA, Wojtys EM. Morphologic characteristics help explain the gender difference in peak anterior cruciate ligament strain during a simulated pivot landing. Am J Sports Med. 2012;40(1):32-40.
27. Sturnick DR, Vacek PM, DeSarno MJ, et al. Combined anatomic factors predicting risk of anterior cruciate ligament injury for males and females. Am J Sports Med. 2015;43(4):839-847.
28. Myer GD, Ford KR, Barber Foss KD, Liu C, Nick TG, Hewett TE. The relationship of hamstrings and quadriceps strength to anterior cruciate ligament injury in female athletes. Clin J Sport Med. 2009;19(1):3-8.
29. Hewett TE, Torg JS, Boden BP. Video analysis of trunk and knee motion during non-contact anterior cruciate ligament injury in female athletes: lateral trunk and knee abduction motion are combined components of the injury mechanism. Br J Sports Med. 2009;43(6):417-422.
30. Sutton KM, Bullock JM. Anterior cruciate ligament rupture: differences between males and females. J Am Acad Orthop Surg. 2013;21(1):41-50.
31. Noyes FR, Barber-Westin SD. Neuromuscular retraining intervention programs: do they reduce noncontact anterior cruciate ligament injury rates in adolescent female athletes? Arthroscopy. 2014;30(2):245-255.
32. Ladd AL. The sports bra, the ACL, and Title IX—the game in play. Clin Orthop Relat Res. 2014;472(6):1681-1684.
33. Lopiano DA. Modern history of women in sports. Twenty-five years of Title IX. Clin Sports Med. 2000;19(2):163-173, vii.
34. Anderson DJ, Cheslock JJ, Ehrenberg RG. Gender equity in intercollegiate athletics: determinants of Title IX compliance. J High Educ. 2006;77(2):225-250.
1. Nattiv A, Loucks AB, Manore MM, Sanborn CF, Sundgot-Borgen J, Warren MP; American College of Sports Medicine. American College of Sports Medicine position stand. The female athlete triad. Med Sci Sports Exerc. 2007;39(10):1867-1882.
2. De Souza MJ, Nattiv A, Joy E, et al; Expert Panel. 2014 Female Athlete Triad Coalition consensus statement on treatment and return to play of the female athlete triad: 1st international conference held in San Francisco, California, May 2012 and 2nd international conference held in Indianapolis, Indiana, May 2013. Br J Sports Med. 2014;48(4):289.
3. Warren MP, Shantha S. The female athlete. Baillieres Best Pract Res Clin Endocrinol Metab. 2000;14(1):37-53.
4. Greenleaf C, Petrie TA, Carter J, Reel JJ. Female collegiate athletes: prevalence of eating disorders and disordered eating behaviors. J Am Coll Health. 2009;57(5):489-495.
5. Reinking MF, Alexander LE. Prevalence of disordered-eating behaviors in undergraduate female collegiate athletes and nonathletes. J Athl Train. 2005;40(1):47-51.
6. Rencken ML, Chesnut CH 3rd, Drinkwater BL. Bone density at multiple skeletal sites in amenorrheic athletes. JAMA. 1996;276(3):238-240.
7. Lappe J, Cullen D, Haynatzki G, Recker R, Ahlf R, Thompson K. Calcium and vitamin D supplementation decreases incidence of stress fractures in female Navy recruits. J Bone Miner Res. 2008;23(5):741-749.
8. De Souza MJ. 2014 Female athlete triad consensus statement on guidelines for treatment and return to play. National Collegiate Athletic Association (NCAA) website. http://www.ncaa.org/health-and-safety/nutrition-and-performance/2014-female-athlete-triad-consensus-statement-guidelines. Accessed November 24, 2015.
9. Preiss-Farzanegan SJ, Chapman B, Wong TM, Wu J, Bazarian JJ. The relationship between gender and postconcussion symptoms after sport-related mild traumatic brain injury. PM R. 2009;1(3):245-253.
10. Marar M, McIlvain NM, Fields SK, Comstock RD. Epidemiology of concussions among United States high school athletes in 20 sports. Am J Sports Med. 2012;40(4):747-755.
11. Uhl RL, Rosenbaum AJ, Czajka C, Mulligan M, King C. Minor traumatic brain injury: a primer for the orthopaedic surgeon. J Am Acad Orthop Surg. 2013;21(10):624-631.
12. Covassin T, Elbin RJ, Harris W, Parker T, Kontos A. The role of age and sex in symptoms, neurocognitive performance, and postural stability in athletes after concussion. Am J Sports Med. 2012;40(6):1303-1312.
13. Covassin T, Moran R, Wilhelm K. Concussion symptoms and neurocognitive performance of high school and college athletes who incur multiple concussions. Am J Sports Med. 2013;41(12):2885-2889.
14. Sports concussion policies and laws: information for parents, coaches, and school & sports professionals. Centers for Disease Control and Prevention website. http://www.cdc.gov/headsup/policy/index.html. Updated February 16, 2015. Accessed November 24, 2015.
15. Covassin T, Elbin RJ, Sarmiento K. Educating coaches about concussion in sports: evaluation of the CDC’s “Heads Up: concussion in youth sports” initiative. J Sch Health. 2012;82(5):233-238.
16. Lumbers ER. Exercise in pregnancy: physiological basis of exercise prescription for the pregnant woman. J Sci Med Sport. 2002;5(1):20-31.
17. ACOG Committee Obstetric Practice. ACOG Committee opinion. Number 267, January 2002: exercise during pregnancy and the postpartum period. Obstet Gynecol. 2002;99(1):171-173.
18. Artal R, O’Toole M. Guidelines of the American College of Obstetricians and Gynecologists for exercise during pregnancy and the postpartum period. Br J Sports Med. 2003;37(1):6-12.
19. Kramer MS. Regular aerobic exercise during pregnancy. Cochrane Database Syst Rev. 2000;(2):CD000180. Update in: Cochrane Database Syst Rev. 2002;(2):CD000180.
20. Stafne SN, Salvesen KA, Romundstad PR, Stuge B, Morkved S. Does regular exercise during pregnancy influence lumbopelvic pain? A randomized controlled trial. Acta Obstet Gynecol Scand. 2012;91(5):552-559.
21. Nascimento SL, Surita FG, Cecatti JG. Physical exercise during pregnancy: a systematic review. Curr Opin Obstet Gynecol. 2012;24(6):387-394.
22. Hale RW, Milne L. The elite athlete and exercise in pregnancy. Semin Perinatol. 1996;20(4):277-284.
23. Exercise during pregnancy. American College of Obstetricians and Gynecologists website. http://www.acog.org/Patients/FAQs/Exercise-During-Pregnancy. Published August 2011. Accessed November 24, 2015.
24. Giugliano DN, Solomon JL. ACL tears in female athletes. Phys Med Rehabil Clin North Am. 2007;18(3):417-438, viii.
25. Ireland ML, Ballantyne BT, Little K, McClay IS. A radiographic analysis of the relationship between the size and shape of the intercondylar notch and anterior cruciate ligament injury. Knee Surg Sports Traumatol Arthrosc. 2001;9(4):200-205.
26. Lipps DB, Oh YK, Ashton-Miller JA, Wojtys EM. Morphologic characteristics help explain the gender difference in peak anterior cruciate ligament strain during a simulated pivot landing. Am J Sports Med. 2012;40(1):32-40.
27. Sturnick DR, Vacek PM, DeSarno MJ, et al. Combined anatomic factors predicting risk of anterior cruciate ligament injury for males and females. Am J Sports Med. 2015;43(4):839-847.
28. Myer GD, Ford KR, Barber Foss KD, Liu C, Nick TG, Hewett TE. The relationship of hamstrings and quadriceps strength to anterior cruciate ligament injury in female athletes. Clin J Sport Med. 2009;19(1):3-8.
29. Hewett TE, Torg JS, Boden BP. Video analysis of trunk and knee motion during non-contact anterior cruciate ligament injury in female athletes: lateral trunk and knee abduction motion are combined components of the injury mechanism. Br J Sports Med. 2009;43(6):417-422.
30. Sutton KM, Bullock JM. Anterior cruciate ligament rupture: differences between males and females. J Am Acad Orthop Surg. 2013;21(1):41-50.
31. Noyes FR, Barber-Westin SD. Neuromuscular retraining intervention programs: do they reduce noncontact anterior cruciate ligament injury rates in adolescent female athletes? Arthroscopy. 2014;30(2):245-255.
32. Ladd AL. The sports bra, the ACL, and Title IX—the game in play. Clin Orthop Relat Res. 2014;472(6):1681-1684.
33. Lopiano DA. Modern history of women in sports. Twenty-five years of Title IX. Clin Sports Med. 2000;19(2):163-173, vii.
34. Anderson DJ, Cheslock JJ, Ehrenberg RG. Gender equity in intercollegiate athletics: determinants of Title IX compliance. J High Educ. 2006;77(2):225-250.

Patient-Directed Valgus Stress Radiograph of the Knee: A New and Novel Technique
A new and novel technique for obtaining the patient-directed valgus stress radiograph of the knee.
To read the authors' full article click here.

A new and novel technique for obtaining the patient-directed valgus stress radiograph of the knee.
To read the authors' full article click here.
A new and novel technique for obtaining the patient-directed valgus stress radiograph of the knee.
To read the authors' full article click here.

Patient-Directed Valgus Stress Radiograph of the Knee: A New and Novel Technique
Medial-compartment partial knee arthroplasty (unicompartmental replacement) is an accepted surgical intervention for anteromedial osteoarthritis of the knee.1 The radiographic investigations required in the workup of these patients should include weight-bearing standing anteroposterior (AP), lateral, and sunrise (Merchant) views, as well as a valgus stress AP radiograph to assess the functionality of the lateral compartment. The method of properly obtaining the valgus stress film has been well described by the Oxford Group.2 Its recommended radiographic technique requires that a surgeon or a radiologic technologist perform the valgus stress maneuver, manually, while another technologist shoots the film. The 2 consequences of this technique are that it requires 2 individuals to obtain the film, and it subjects the individual who is applying the stress to some level of radiation exposure, which is undesirable. Because of this and the time inconvenience, many surgeons omit the valgus stress radiograph, which can lead to the adverse outcome of missing a lateral compartment that is functionally incompetent, resulting in the potential for early lateral compartment progression of osteoarthritis and the need for revision surgery, usually to a total knee arthroplasty.
In an attempt to mitigate these barriers to obtaining the necessary valgus stress radiograph, Dr. Mauerhan’s team developed a technique that could be done with the assistance of the patient and would require only 1 technologist to perform. Additionally, this project was a quality improvement initiative, because it lowered radiation exposure to all personnel involved in obtaining the correct films.
Materials and Methods
We initiated the project using weight-bearing strategies to impart the valgus stress view of the knee. After trying several different wedges and blocks, and varying patient instructions, we realized a different approach to this problem would be required to find an acceptable solution. We redirected our efforts to effectively performing the stress view with the patient in a supine position on the radiograph table. Ultimately, we decided that a much stiffer wedge and a denser object to squeeze would facilitate obtaining a proper film. Considering all available options, a youth size 4 soccer ball (diameter, 11 in) was introduced along with a slightly larger positioning wedge. The soccer ball was wrapped with 4-in Coban wrap (3M) to create a nonslip surface. This change in patient positioning, along with a standardized 7º to 10º cephalic radiographic tube angulation, helped to correct issues with tibial plateau visualization. Once these changes were enacted, we obtained fairly consistent positive results, and we instituted this patient-directed valgus stress view of the knee, along with a manual valgus stress view for comparison.
The protocol for obtaining the patient-directed valgus stress view of the knee is as follows: The patient lays supine with a dense 45º spine-positioning wedge (Burlington Medical Supplies) placed under both knees and the patient’s heels on the examining table. The radiographic tube is angled cephalad 7º to 10º centered on the inferior pole of the patella, using a 40-in source to image-receptor distance, collimated to part; the image receptor is placed under the affected knee, below the positioning wedge. The affected knee is rotated to the “true” AP position (the patella will be centered between the femoral condyles on the AP exposure), and the ball is placed between the patient’s legs just above the ankle joint. The technologist demonstrates to the patient how to squeeze the ball while maintaining contact of heels with the table. The technologist can exit the room and obtain the exposure, which is taken while the patient is squeezing the ball, as shown in Figures 1A and 1B. Examples of the standing AP, manual stress, and patient-directed valgus radiographs are shown in Figures 2A-2C. The entire technique is demonstrated in the Video.
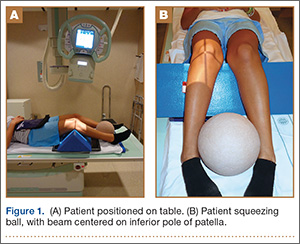
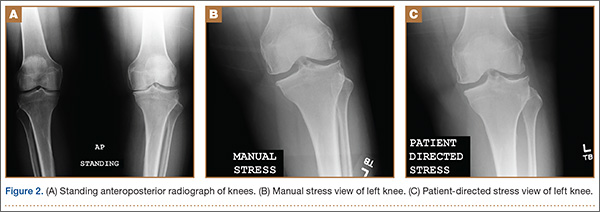
Results
During the 9 months of this quality improvement project, 78 examinations were performed. Five studies did not show complete correction of the varus deformity. Of these, 3 showed complete correction on a manual valgus stress radiograph, and 2 did not, contraindicating the use of partial knee replacement. Three patients displayed collapse of the lateral compartment, indicating a nonfunctional lateral compartment, and, therefore, were also a contraindication to partial knee arthroplasty. The remaining 70 patients had identical radiographic results with both the manual and patient-directed valgus stress tests. There was no instance of examination failure or need to repeat as a result of difficulty of the examination for the patient. Repeat films because of positioning errors were very rare, usually early in the learning curve, and no more prevalent than when using the manual stress method. The technique was reproducible and easy to teach and adopt.
Discussion
In total, 73 patients (93.5%) with the patient-directed stress film showed the desired result, either correction of the medial compartment narrowing in conjunction with an intact lateral compartment or narrowing of the lateral compartment. Of the 5 patients (6.5%) whose patient-directed stress films did not show correction of the varus deformity, 3 patients displayed correction with a manually applied stress radiograph and 2 did not. Based on this observation, our recommendation would be for those patients who do not show adequate correction on the patient-directed stress radiograph to have a manual examination to establish the presence or absence of the desired correction.
Performing a valgus stress radiograph is an integral part of the investigation to determine if the patient is an appropriate candidate for partial knee arthroplasty.3 The historical, manually performed valgus stress radiograph requires 2 individuals, 1 to apply the stress with the patient on the table and 1 to shoot the exposure. For the individual or individuals applying this stress, there is an increased radiation exposure that would be undesirable over a long career. The authors developed a new technique using a commercially available spinal positioning wedge and 11-in youth soccer ball wrapped with Coban wrap, as described, which is economical and easy to obtain and use in the clinical setting. We believe this cost-effective method will offer surgeons who perform partial knee arthroplasty a novel method to obtain the important information gleaned from the valgus stress radiograph and to improve surgical outcomes through the preoperative assessment of the lateral compartment. Additionally, as a quality and safety improvement initiative, we believe this technique will reduce radiographic exposure for those performing these studies, and, because the examination can be carried out by a single technologist, it will significantly improve efficiency in the radiology suite.
Conclusion
We have developed a new method of obtaining the important valgus stress radiograph as part of the workup of patients with medial-compartment osteoarthritis of the knee. The technique can be performed with easily obtainable, commercially available products and is reliable 93.5% of the time. It also adds to the efficiency of the radiology suite and reduces radiographic exposure for technologists.
1. White SH, Ludkowski PF, Goodfellow JW. Anteromedial osteoarthritis of the knee. J Bone Joint Surg Br. 1991;73(4):582-586.
2. Goodfellow JW, O’Conner JJ, Dodd CA, Murray DW. Unicompartmental Arthroplasty with the Oxford Knee. Woodeaton, Oxford, England: Goodfellow Publishers Limited; 2006:38-39.
3. Gibson PH, Goodfellow JW. Stress radiography in degenerative arthritis of the knee. J Bone Joint Surg Br. 1986;68(4):608-609.
Medial-compartment partial knee arthroplasty (unicompartmental replacement) is an accepted surgical intervention for anteromedial osteoarthritis of the knee.1 The radiographic investigations required in the workup of these patients should include weight-bearing standing anteroposterior (AP), lateral, and sunrise (Merchant) views, as well as a valgus stress AP radiograph to assess the functionality of the lateral compartment. The method of properly obtaining the valgus stress film has been well described by the Oxford Group.2 Its recommended radiographic technique requires that a surgeon or a radiologic technologist perform the valgus stress maneuver, manually, while another technologist shoots the film. The 2 consequences of this technique are that it requires 2 individuals to obtain the film, and it subjects the individual who is applying the stress to some level of radiation exposure, which is undesirable. Because of this and the time inconvenience, many surgeons omit the valgus stress radiograph, which can lead to the adverse outcome of missing a lateral compartment that is functionally incompetent, resulting in the potential for early lateral compartment progression of osteoarthritis and the need for revision surgery, usually to a total knee arthroplasty.
In an attempt to mitigate these barriers to obtaining the necessary valgus stress radiograph, Dr. Mauerhan’s team developed a technique that could be done with the assistance of the patient and would require only 1 technologist to perform. Additionally, this project was a quality improvement initiative, because it lowered radiation exposure to all personnel involved in obtaining the correct films.
Materials and Methods
We initiated the project using weight-bearing strategies to impart the valgus stress view of the knee. After trying several different wedges and blocks, and varying patient instructions, we realized a different approach to this problem would be required to find an acceptable solution. We redirected our efforts to effectively performing the stress view with the patient in a supine position on the radiograph table. Ultimately, we decided that a much stiffer wedge and a denser object to squeeze would facilitate obtaining a proper film. Considering all available options, a youth size 4 soccer ball (diameter, 11 in) was introduced along with a slightly larger positioning wedge. The soccer ball was wrapped with 4-in Coban wrap (3M) to create a nonslip surface. This change in patient positioning, along with a standardized 7º to 10º cephalic radiographic tube angulation, helped to correct issues with tibial plateau visualization. Once these changes were enacted, we obtained fairly consistent positive results, and we instituted this patient-directed valgus stress view of the knee, along with a manual valgus stress view for comparison.
The protocol for obtaining the patient-directed valgus stress view of the knee is as follows: The patient lays supine with a dense 45º spine-positioning wedge (Burlington Medical Supplies) placed under both knees and the patient’s heels on the examining table. The radiographic tube is angled cephalad 7º to 10º centered on the inferior pole of the patella, using a 40-in source to image-receptor distance, collimated to part; the image receptor is placed under the affected knee, below the positioning wedge. The affected knee is rotated to the “true” AP position (the patella will be centered between the femoral condyles on the AP exposure), and the ball is placed between the patient’s legs just above the ankle joint. The technologist demonstrates to the patient how to squeeze the ball while maintaining contact of heels with the table. The technologist can exit the room and obtain the exposure, which is taken while the patient is squeezing the ball, as shown in Figures 1A and 1B. Examples of the standing AP, manual stress, and patient-directed valgus radiographs are shown in Figures 2A-2C. The entire technique is demonstrated in the Video.
Results
During the 9 months of this quality improvement project, 78 examinations were performed. Five studies did not show complete correction of the varus deformity. Of these, 3 showed complete correction on a manual valgus stress radiograph, and 2 did not, contraindicating the use of partial knee replacement. Three patients displayed collapse of the lateral compartment, indicating a nonfunctional lateral compartment, and, therefore, were also a contraindication to partial knee arthroplasty. The remaining 70 patients had identical radiographic results with both the manual and patient-directed valgus stress tests. There was no instance of examination failure or need to repeat as a result of difficulty of the examination for the patient. Repeat films because of positioning errors were very rare, usually early in the learning curve, and no more prevalent than when using the manual stress method. The technique was reproducible and easy to teach and adopt.
Discussion
In total, 73 patients (93.5%) with the patient-directed stress film showed the desired result, either correction of the medial compartment narrowing in conjunction with an intact lateral compartment or narrowing of the lateral compartment. Of the 5 patients (6.5%) whose patient-directed stress films did not show correction of the varus deformity, 3 patients displayed correction with a manually applied stress radiograph and 2 did not. Based on this observation, our recommendation would be for those patients who do not show adequate correction on the patient-directed stress radiograph to have a manual examination to establish the presence or absence of the desired correction.
Performing a valgus stress radiograph is an integral part of the investigation to determine if the patient is an appropriate candidate for partial knee arthroplasty.3 The historical, manually performed valgus stress radiograph requires 2 individuals, 1 to apply the stress with the patient on the table and 1 to shoot the exposure. For the individual or individuals applying this stress, there is an increased radiation exposure that would be undesirable over a long career. The authors developed a new technique using a commercially available spinal positioning wedge and 11-in youth soccer ball wrapped with Coban wrap, as described, which is economical and easy to obtain and use in the clinical setting. We believe this cost-effective method will offer surgeons who perform partial knee arthroplasty a novel method to obtain the important information gleaned from the valgus stress radiograph and to improve surgical outcomes through the preoperative assessment of the lateral compartment. Additionally, as a quality and safety improvement initiative, we believe this technique will reduce radiographic exposure for those performing these studies, and, because the examination can be carried out by a single technologist, it will significantly improve efficiency in the radiology suite.
Conclusion
We have developed a new method of obtaining the important valgus stress radiograph as part of the workup of patients with medial-compartment osteoarthritis of the knee. The technique can be performed with easily obtainable, commercially available products and is reliable 93.5% of the time. It also adds to the efficiency of the radiology suite and reduces radiographic exposure for technologists.
Medial-compartment partial knee arthroplasty (unicompartmental replacement) is an accepted surgical intervention for anteromedial osteoarthritis of the knee.1 The radiographic investigations required in the workup of these patients should include weight-bearing standing anteroposterior (AP), lateral, and sunrise (Merchant) views, as well as a valgus stress AP radiograph to assess the functionality of the lateral compartment. The method of properly obtaining the valgus stress film has been well described by the Oxford Group.2 Its recommended radiographic technique requires that a surgeon or a radiologic technologist perform the valgus stress maneuver, manually, while another technologist shoots the film. The 2 consequences of this technique are that it requires 2 individuals to obtain the film, and it subjects the individual who is applying the stress to some level of radiation exposure, which is undesirable. Because of this and the time inconvenience, many surgeons omit the valgus stress radiograph, which can lead to the adverse outcome of missing a lateral compartment that is functionally incompetent, resulting in the potential for early lateral compartment progression of osteoarthritis and the need for revision surgery, usually to a total knee arthroplasty.
In an attempt to mitigate these barriers to obtaining the necessary valgus stress radiograph, Dr. Mauerhan’s team developed a technique that could be done with the assistance of the patient and would require only 1 technologist to perform. Additionally, this project was a quality improvement initiative, because it lowered radiation exposure to all personnel involved in obtaining the correct films.
Materials and Methods
We initiated the project using weight-bearing strategies to impart the valgus stress view of the knee. After trying several different wedges and blocks, and varying patient instructions, we realized a different approach to this problem would be required to find an acceptable solution. We redirected our efforts to effectively performing the stress view with the patient in a supine position on the radiograph table. Ultimately, we decided that a much stiffer wedge and a denser object to squeeze would facilitate obtaining a proper film. Considering all available options, a youth size 4 soccer ball (diameter, 11 in) was introduced along with a slightly larger positioning wedge. The soccer ball was wrapped with 4-in Coban wrap (3M) to create a nonslip surface. This change in patient positioning, along with a standardized 7º to 10º cephalic radiographic tube angulation, helped to correct issues with tibial plateau visualization. Once these changes were enacted, we obtained fairly consistent positive results, and we instituted this patient-directed valgus stress view of the knee, along with a manual valgus stress view for comparison.
The protocol for obtaining the patient-directed valgus stress view of the knee is as follows: The patient lays supine with a dense 45º spine-positioning wedge (Burlington Medical Supplies) placed under both knees and the patient’s heels on the examining table. The radiographic tube is angled cephalad 7º to 10º centered on the inferior pole of the patella, using a 40-in source to image-receptor distance, collimated to part; the image receptor is placed under the affected knee, below the positioning wedge. The affected knee is rotated to the “true” AP position (the patella will be centered between the femoral condyles on the AP exposure), and the ball is placed between the patient’s legs just above the ankle joint. The technologist demonstrates to the patient how to squeeze the ball while maintaining contact of heels with the table. The technologist can exit the room and obtain the exposure, which is taken while the patient is squeezing the ball, as shown in Figures 1A and 1B. Examples of the standing AP, manual stress, and patient-directed valgus radiographs are shown in Figures 2A-2C. The entire technique is demonstrated in the Video.
Results
During the 9 months of this quality improvement project, 78 examinations were performed. Five studies did not show complete correction of the varus deformity. Of these, 3 showed complete correction on a manual valgus stress radiograph, and 2 did not, contraindicating the use of partial knee replacement. Three patients displayed collapse of the lateral compartment, indicating a nonfunctional lateral compartment, and, therefore, were also a contraindication to partial knee arthroplasty. The remaining 70 patients had identical radiographic results with both the manual and patient-directed valgus stress tests. There was no instance of examination failure or need to repeat as a result of difficulty of the examination for the patient. Repeat films because of positioning errors were very rare, usually early in the learning curve, and no more prevalent than when using the manual stress method. The technique was reproducible and easy to teach and adopt.
Discussion
In total, 73 patients (93.5%) with the patient-directed stress film showed the desired result, either correction of the medial compartment narrowing in conjunction with an intact lateral compartment or narrowing of the lateral compartment. Of the 5 patients (6.5%) whose patient-directed stress films did not show correction of the varus deformity, 3 patients displayed correction with a manually applied stress radiograph and 2 did not. Based on this observation, our recommendation would be for those patients who do not show adequate correction on the patient-directed stress radiograph to have a manual examination to establish the presence or absence of the desired correction.
Performing a valgus stress radiograph is an integral part of the investigation to determine if the patient is an appropriate candidate for partial knee arthroplasty.3 The historical, manually performed valgus stress radiograph requires 2 individuals, 1 to apply the stress with the patient on the table and 1 to shoot the exposure. For the individual or individuals applying this stress, there is an increased radiation exposure that would be undesirable over a long career. The authors developed a new technique using a commercially available spinal positioning wedge and 11-in youth soccer ball wrapped with Coban wrap, as described, which is economical and easy to obtain and use in the clinical setting. We believe this cost-effective method will offer surgeons who perform partial knee arthroplasty a novel method to obtain the important information gleaned from the valgus stress radiograph and to improve surgical outcomes through the preoperative assessment of the lateral compartment. Additionally, as a quality and safety improvement initiative, we believe this technique will reduce radiographic exposure for those performing these studies, and, because the examination can be carried out by a single technologist, it will significantly improve efficiency in the radiology suite.
Conclusion
We have developed a new method of obtaining the important valgus stress radiograph as part of the workup of patients with medial-compartment osteoarthritis of the knee. The technique can be performed with easily obtainable, commercially available products and is reliable 93.5% of the time. It also adds to the efficiency of the radiology suite and reduces radiographic exposure for technologists.
1. White SH, Ludkowski PF, Goodfellow JW. Anteromedial osteoarthritis of the knee. J Bone Joint Surg Br. 1991;73(4):582-586.
2. Goodfellow JW, O’Conner JJ, Dodd CA, Murray DW. Unicompartmental Arthroplasty with the Oxford Knee. Woodeaton, Oxford, England: Goodfellow Publishers Limited; 2006:38-39.
3. Gibson PH, Goodfellow JW. Stress radiography in degenerative arthritis of the knee. J Bone Joint Surg Br. 1986;68(4):608-609.
1. White SH, Ludkowski PF, Goodfellow JW. Anteromedial osteoarthritis of the knee. J Bone Joint Surg Br. 1991;73(4):582-586.
2. Goodfellow JW, O’Conner JJ, Dodd CA, Murray DW. Unicompartmental Arthroplasty with the Oxford Knee. Woodeaton, Oxford, England: Goodfellow Publishers Limited; 2006:38-39.
3. Gibson PH, Goodfellow JW. Stress radiography in degenerative arthritis of the knee. J Bone Joint Surg Br. 1986;68(4):608-609.
