User login
Botanical over-the-counter regimen reduces acne lesions
An over-the-counter botanical acne regimen outperformed a conventional acne regimen, with improved skin appearance and fewer lesions after 12 weeks of treatment, in a double-blind randomized controlled trial.
Eighty individuals aged 12 years and older with mild to moderate acne were randomized either to a three-step botanical-based acne treatment regimen (Receutics) consisting of a skin cleanser, breakout treatment, and tone and complexion corrector twice daily, or the currently marketed acne treatment kit, Proactiv (Guthy-Renker).

The botanical-based acne treatment contains a range of botanical ingredients, including algae and lentil seed extracts; cranberry seed, grape seed, and pumpkin seed oils; and allantoin; with 3.4% benzoyl peroxide as the active ingredient. The active ingredient in the cleanser is 2% salicylic acid, and niacinamide is the active ingredient in the tone and complexion corrector; both also contain botanical ingredients.
In the study, published in December, the investigator, Dr. Zoe Diana Draelos, reported that the botanical regimen achieved a significantly greater reduction in lesion count, in terms of closed comedones and inflammatory lesions, by week four, compared with the control treatment (J Drugs Dermatol. 2015 Dec; 14 [12]:1418-21).
This effect persisted at 12 weeks, with fewer closed comedones (P = .006). The botanical regimen also achieved greater reductions in pus, erythema, lesion height, and inflammation at weeks 2 and 4; although this difference disappeared by week 12. By week four and onwards, the botanical regimen also outperformed the conventional treatment on all blinded, investigator-assessed cosmetic appearance parameters, including skin tone, blemishes, erythema, and overall appearance.
While both treatments were effective at improving acne, Dr. Draelos, of Dermatology Consulting Services, High Point, N.C., said the botanical three-step regimen had the advantage of cosmetic ingredients such as emollients, anti-inflammatory/antioxidants, and “sensitive skin modulators.”
“This study demonstrates the value of combining monographed acne ingredients with advanced cosmeceutical technology,” she wrote.
The author received a grant from manufacturer Receutics to conduct the study.
An over-the-counter botanical acne regimen outperformed a conventional acne regimen, with improved skin appearance and fewer lesions after 12 weeks of treatment, in a double-blind randomized controlled trial.
Eighty individuals aged 12 years and older with mild to moderate acne were randomized either to a three-step botanical-based acne treatment regimen (Receutics) consisting of a skin cleanser, breakout treatment, and tone and complexion corrector twice daily, or the currently marketed acne treatment kit, Proactiv (Guthy-Renker).
The botanical-based acne treatment contains a range of botanical ingredients, including algae and lentil seed extracts; cranberry seed, grape seed, and pumpkin seed oils; and allantoin; with 3.4% benzoyl peroxide as the active ingredient. The active ingredient in the cleanser is 2% salicylic acid, and niacinamide is the active ingredient in the tone and complexion corrector; both also contain botanical ingredients.
In the study, published in December, the investigator, Dr. Zoe Diana Draelos, reported that the botanical regimen achieved a significantly greater reduction in lesion count, in terms of closed comedones and inflammatory lesions, by week four, compared with the control treatment (J Drugs Dermatol. 2015 Dec; 14 [12]:1418-21).
This effect persisted at 12 weeks, with fewer closed comedones (P = .006). The botanical regimen also achieved greater reductions in pus, erythema, lesion height, and inflammation at weeks 2 and 4; although this difference disappeared by week 12. By week four and onwards, the botanical regimen also outperformed the conventional treatment on all blinded, investigator-assessed cosmetic appearance parameters, including skin tone, blemishes, erythema, and overall appearance.
While both treatments were effective at improving acne, Dr. Draelos, of Dermatology Consulting Services, High Point, N.C., said the botanical three-step regimen had the advantage of cosmetic ingredients such as emollients, anti-inflammatory/antioxidants, and “sensitive skin modulators.”
“This study demonstrates the value of combining monographed acne ingredients with advanced cosmeceutical technology,” she wrote.
The author received a grant from manufacturer Receutics to conduct the study.
An over-the-counter botanical acne regimen outperformed a conventional acne regimen, with improved skin appearance and fewer lesions after 12 weeks of treatment, in a double-blind randomized controlled trial.
Eighty individuals aged 12 years and older with mild to moderate acne were randomized either to a three-step botanical-based acne treatment regimen (Receutics) consisting of a skin cleanser, breakout treatment, and tone and complexion corrector twice daily, or the currently marketed acne treatment kit, Proactiv (Guthy-Renker).
The botanical-based acne treatment contains a range of botanical ingredients, including algae and lentil seed extracts; cranberry seed, grape seed, and pumpkin seed oils; and allantoin; with 3.4% benzoyl peroxide as the active ingredient. The active ingredient in the cleanser is 2% salicylic acid, and niacinamide is the active ingredient in the tone and complexion corrector; both also contain botanical ingredients.
In the study, published in December, the investigator, Dr. Zoe Diana Draelos, reported that the botanical regimen achieved a significantly greater reduction in lesion count, in terms of closed comedones and inflammatory lesions, by week four, compared with the control treatment (J Drugs Dermatol. 2015 Dec; 14 [12]:1418-21).
This effect persisted at 12 weeks, with fewer closed comedones (P = .006). The botanical regimen also achieved greater reductions in pus, erythema, lesion height, and inflammation at weeks 2 and 4; although this difference disappeared by week 12. By week four and onwards, the botanical regimen also outperformed the conventional treatment on all blinded, investigator-assessed cosmetic appearance parameters, including skin tone, blemishes, erythema, and overall appearance.
While both treatments were effective at improving acne, Dr. Draelos, of Dermatology Consulting Services, High Point, N.C., said the botanical three-step regimen had the advantage of cosmetic ingredients such as emollients, anti-inflammatory/antioxidants, and “sensitive skin modulators.”
“This study demonstrates the value of combining monographed acne ingredients with advanced cosmeceutical technology,” she wrote.
The author received a grant from manufacturer Receutics to conduct the study.
FROM THE JOURNAL OF DRUGS IN DERMATOLOGY
Key clinical point: A botanical over-the-counter acne regimen achieved greater reductions in lesions than a currently marketed acne treatment.
Major finding: A three-step botanical-based acne regimen achieved significantly greater reduction in lesion counts and improvements in skin appearance than a conventional acne treatment.
Data source: A randomized, double-blind, controlled trial of 80 patients with mild to moderate acne.
Disclosures: The author received a grant from treatment manufacturer Receutics to conduct the study.

Breast cancer

Should You Bypass Anticoagulant “Bridging” Before and After Surgery?
PRACTICE CHANGER
Stop using low molecular weight heparin (LMWH) for surgical procedures to “bridge” low- to moderate-risk patients with atrial fibrillation (CHADS2 score ≤ 4) who are receiving warfarin. The risks outweigh the benefits.1
STRENGTH OF RECOMMENDATION
B: Based on a single good-quality randomized controlled trial.1
CASE A 75-year-old man comes to your office for surgical clearance before right knee replacement surgery. He has diabetes and high blood pressure and is taking warfarin for atrial fibrillation. He is scheduled for surgery in a week. What is the safest way to manage his warfarin in the perioperative period?
More than 2 million people are being treated with oral anticoagulation in North America to prevent stroke or to prevent or treat venous thromboembolism.2 Since 2010, several new oral anticoagulants have been approved, including dabigatran, apixaban, and rivaroxaban. These new medications have a shorter half-life than older anticoagulants, which enables them to be stopped one to two days before surgery.
On the other hand, warfarin—which remains a common choice for anticoagulation—has a three- to seven-day onset and elimination.3,4 This long clinical half-life presents a special challenge during the perioperative period. To reduce the risk for operative bleeding, the warfarin must be stopped days prior to the procedure, but clinicians often worry that this will increase the risk for arterial or venous thromboembolism, including stroke.
An estimated 250,000 patients need perioperative management of their anticoagulation each year.5 As the US population continues to age and the incidence of conditions requiring anticoagulation (particularly atrial fibrillation) increases, this number is only going to rise.6
Current guidelines on bridging. American College of Chest Physicians (ACCP) guidelines recommend transition to “a short-acting anticoagulant, consisting of subcutaneous low molecular weight heparin (LMWH) or intravenous unfractionated heparin, for a 10- to 12-day period during interruption of vitamin K antagonist (VKA) therapy.”5Furthermore, for an appropriate bridging regimen, the ACCP guidelines recommend stopping VKA therapy five days prior to the procedure and utilizing LMWH from within 24 to 48 hours of stopping VKA therapy until up to 24 hours before surgery.5 Postoperatively, VKA or LMWH therapy should be reinitiated within 24 hours and 24 to 72 hours, respectively, depending on the patient’s risk for bleeding during surgery.5
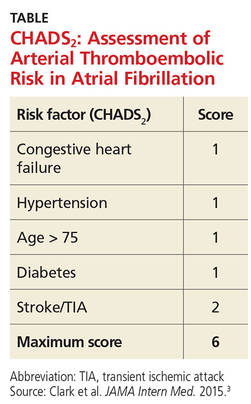
These guidelines recommend using CHADS2 scoring (see the table) to determine arterial thromboembolism (ATE) risk in atrial fibrillation.3,5 Patients at low risk for ATE (CHADS2 score, 0-2) should not be bridged, and patients at high risk (CHADS2 score, 5-6) should always be bridged.5 These guidelines are less clear about bridging recommendations for patients considered to be at moderate risk (CHADS2 score, 3-4).
Previous evidence on bridging. A 2012 meta-analysis of 34 studies evaluated the safety and efficacy of perioperative bridging with heparin in patients receiving VKA.7Researchers found no difference in ATE events in eight studies that compared groups that received bridging vs groups that simply stopped anticoagulation (odds ratio [OR], 0.80).7 The group that received bridging had an increased risk for overall bleeding in 13 studies and of major bleeding in five studies.7This meta-analysis was limited by poor study quality and variation in the indication for VKA therapy.
A 2015 subgroup analysis of a larger cohort study of patients receiving anticoagulants for atrial fibrillation found an increased risk for bleeding when their anticoagulation was interrupted for procedures (OR for major bleeding, 3.84).8
Douketis et al1 conducted a randomized trial to clarify the need for and safety of bridging anticoagulation for ATE in patients with atrial fibrillation who were receiving warfarin.
Continue for study summary >>
STUDY SUMMARY
When it comes to stroke/TIA, there’s no advantage to bridging
This double-blind, placebo-controlled trial compared bridging with dalteparin, a form of LMWH, to placebo among 1,884 patients with atrial fibrillation who were taking warfarin and whose anticoagulation therapy needed to be interrupted for an elective procedure. Patients were included if they were receiving warfarin to prevent stroke and had been taking it for at least 12 weeks, with a goal International Normalized Ratio (INR) of 2.0 to 3.0. Exclusion criteria included having a mechanical heart valve or having a stroke/transient ischemic attack (TIA; 12 weeks prior) or major bleeding (six weeks prior). Patients undergoing cardiac, intracranial, and intraspinal surgeries were also excluded from the study.
The mean CHADS2 score was 2.3; 38.3% of patients had a CHADS2 score ≥ 3, and 9.4% of patients had a history of stroke. Forty-four percent of patients underwent a gastrointestinal procedure, 17.2% underwent a cardiothoracic procedure, and 9.2% underwent an orthopedic procedure.
Patients stopped taking warfarin five days before their procedure and began subcutaneous dalteparin (100 IU/kg) or an identical placebo three days before the procedure. The dalteparin/placebo was stopped 24 hours before the procedure and restarted after the procedure, until the patient’s INR was in the therapeutic range. Warfarin was resumed on the evening of the procedure or the following day.
The primary efficacy outcome was ATE, including stroke, TIA, or systemic embolism. The primary safety endpoint was major bleeding (defined as bleeding at a critical anatomic site, symptomatic or clinically overt bleeding, or a decrease in hemoglobin > 2 g/dL). Secondary efficacy and safety outcomes included minor bleeding, acute myocardial infarction, deep vein thrombosis, pulmonary embolism, and death. Outcomes were assessed within 37 days of the procedure.
The incidence of ATE was 0.4% (four events) in the no-bridging group vs 0.3% (three events) in the bridging group. Major bleeding occurred in 1.3% of the no-bridging group (12 events) and in 3.2% of the bridging group (29 events), indicating that no bridging was superior in terms of the major bleeding outcome (number needed to harm [NNH], 53; relative risk [RR], 0.41).
The no-bridging group also had significantly fewer minor bleeds in comparison to the bridging group (NNH, 11; 12% vs 20.9%). There were no differences between groups in other secondary outcomes.
Continue for what's new >>
WHAT’S NEW
High-quality evidence suggests it’s OK to stop warfarin before surgery
This is the largest good-quality study to evaluate perioperative bridging in patients with atrial fibrillation who were at low or moderate risk for ATE (CHADS2 score, 0-4). Previous studies suggested bridging increased bleeding and offered limited benefit for reducing the risk for ATE. However, this is the first study to include a large group of moderate-risk patients (CHADS2 score, 3-4). This trial provides high-quality evidence to support the practice of simply stopping warfarin in the perioperative period, rather than bridging with LMWH.
CAVEATS
Findings might not apply to patients at highest risk
Most patients in this study had a CHADS2 score ≤ 3. About 3% had a CHADS2 score ≥ 5. It’s not clear whether these findings apply to patients with a CHADS2 score of 5 or 6.
This trial categorized ATE risk using the CHADS2 score, rather than the CHA2DS2-VASc, which includes additional risk factors and may more accurately predict stroke risk. Both patients who received bridging therapy and those who did not had a lower rate of stroke than predicted by CHADS2. This may reflect a limit of the predictive value of CHADS2 but should not have affected the rate of bleeding or ATE outcomes in this study.
Continue for challenges to implementation >>
CHALLENGES TO IMPLEMENTATION
Providers may hesitate to disregard current guidelines
Strokes are devastating events for patients, families, and clinicians, and they pose a greater risk for morbidity and mortality compared to bleeding. However, this study suggests patients who receive bridging have a higher risk for bleeding than stroke, which is in contrast to some providers’ experience and current recommendations.
A clinician caring for a patient who’s had a stroke may be inclined to recommend bridging despite the lack of efficacy and evidence of bleeding risk. Additionally, until guidelines reflect the most current research, clinicians may be reluctant to provide care in contrast to these recommendations.
REFERENCES
1. Douketis JD, Spyropoulos AC, Kaatz S, et al. Perioperative bridging anticoagulation in patients with atrial fibrillation. N Engl J Med. 2015;373:823-833.
2. Guyatt GH, Akl EA, Crowther M, et al; American College of Chest Physicians Antithrombotic Therapy and Prevention of Thrombosis Panel. Executive summary: Antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141:7S-47S.
3. Clark NP, Witt DM, Davies LE, et al. Bleeding, recurrent venous thromboembolism and mortality risks during warfarin interruption for invasive procedures. JAMA Intern Med. 2015; 175:1163-1168.
4. Lip GY, Lane DA. Stroke prevention in atrial fibrillation: a systematic review.JAMA. 2015;313:1950-1962.
5. Douketis JD, Spyropoulos AC, Spencer FA, et al; American College of Chest Physicians. Perioperative management of antithrombotic therapy: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141:e326S-e350S.
6. Miyasaka Y, Barnes ME, Gersh BJ, et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence.Circulation. 2006;114:119-125.
7. Siegal D, Yudin J, Kaatz S, et al. Periprocedural heparin bridging in patients receiving vitamin K antagonists: systematic review and meta-analysis of bleeding and thromboembolic rates.Circulation. 2012;126:1630-1639.
8. Steinberg B, Peterson E, Kim S, et al; Outcomes Registry for Better Informed Treatment of Atrial Fibrillation Investigators and Patients. Use and outcomes associated with bridging during anticoagulation interruptions in patients with atrial fibrillation: findings from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF).Circulation. 2015;131:488-494.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2015. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2015;64(12):794-795, 800.
PRACTICE CHANGER
Stop using low molecular weight heparin (LMWH) for surgical procedures to “bridge” low- to moderate-risk patients with atrial fibrillation (CHADS2 score ≤ 4) who are receiving warfarin. The risks outweigh the benefits.1
STRENGTH OF RECOMMENDATION
B: Based on a single good-quality randomized controlled trial.1
CASE A 75-year-old man comes to your office for surgical clearance before right knee replacement surgery. He has diabetes and high blood pressure and is taking warfarin for atrial fibrillation. He is scheduled for surgery in a week. What is the safest way to manage his warfarin in the perioperative period?
More than 2 million people are being treated with oral anticoagulation in North America to prevent stroke or to prevent or treat venous thromboembolism.2 Since 2010, several new oral anticoagulants have been approved, including dabigatran, apixaban, and rivaroxaban. These new medications have a shorter half-life than older anticoagulants, which enables them to be stopped one to two days before surgery.
On the other hand, warfarin—which remains a common choice for anticoagulation—has a three- to seven-day onset and elimination.3,4 This long clinical half-life presents a special challenge during the perioperative period. To reduce the risk for operative bleeding, the warfarin must be stopped days prior to the procedure, but clinicians often worry that this will increase the risk for arterial or venous thromboembolism, including stroke.
An estimated 250,000 patients need perioperative management of their anticoagulation each year.5 As the US population continues to age and the incidence of conditions requiring anticoagulation (particularly atrial fibrillation) increases, this number is only going to rise.6
Current guidelines on bridging. American College of Chest Physicians (ACCP) guidelines recommend transition to “a short-acting anticoagulant, consisting of subcutaneous low molecular weight heparin (LMWH) or intravenous unfractionated heparin, for a 10- to 12-day period during interruption of vitamin K antagonist (VKA) therapy.”5Furthermore, for an appropriate bridging regimen, the ACCP guidelines recommend stopping VKA therapy five days prior to the procedure and utilizing LMWH from within 24 to 48 hours of stopping VKA therapy until up to 24 hours before surgery.5 Postoperatively, VKA or LMWH therapy should be reinitiated within 24 hours and 24 to 72 hours, respectively, depending on the patient’s risk for bleeding during surgery.5
These guidelines recommend using CHADS2 scoring (see the table) to determine arterial thromboembolism (ATE) risk in atrial fibrillation.3,5 Patients at low risk for ATE (CHADS2 score, 0-2) should not be bridged, and patients at high risk (CHADS2 score, 5-6) should always be bridged.5 These guidelines are less clear about bridging recommendations for patients considered to be at moderate risk (CHADS2 score, 3-4).
Previous evidence on bridging. A 2012 meta-analysis of 34 studies evaluated the safety and efficacy of perioperative bridging with heparin in patients receiving VKA.7Researchers found no difference in ATE events in eight studies that compared groups that received bridging vs groups that simply stopped anticoagulation (odds ratio [OR], 0.80).7 The group that received bridging had an increased risk for overall bleeding in 13 studies and of major bleeding in five studies.7This meta-analysis was limited by poor study quality and variation in the indication for VKA therapy.
A 2015 subgroup analysis of a larger cohort study of patients receiving anticoagulants for atrial fibrillation found an increased risk for bleeding when their anticoagulation was interrupted for procedures (OR for major bleeding, 3.84).8
Douketis et al1 conducted a randomized trial to clarify the need for and safety of bridging anticoagulation for ATE in patients with atrial fibrillation who were receiving warfarin.
Continue for study summary >>
STUDY SUMMARY
When it comes to stroke/TIA, there’s no advantage to bridging
This double-blind, placebo-controlled trial compared bridging with dalteparin, a form of LMWH, to placebo among 1,884 patients with atrial fibrillation who were taking warfarin and whose anticoagulation therapy needed to be interrupted for an elective procedure. Patients were included if they were receiving warfarin to prevent stroke and had been taking it for at least 12 weeks, with a goal International Normalized Ratio (INR) of 2.0 to 3.0. Exclusion criteria included having a mechanical heart valve or having a stroke/transient ischemic attack (TIA; 12 weeks prior) or major bleeding (six weeks prior). Patients undergoing cardiac, intracranial, and intraspinal surgeries were also excluded from the study.
The mean CHADS2 score was 2.3; 38.3% of patients had a CHADS2 score ≥ 3, and 9.4% of patients had a history of stroke. Forty-four percent of patients underwent a gastrointestinal procedure, 17.2% underwent a cardiothoracic procedure, and 9.2% underwent an orthopedic procedure.
Patients stopped taking warfarin five days before their procedure and began subcutaneous dalteparin (100 IU/kg) or an identical placebo three days before the procedure. The dalteparin/placebo was stopped 24 hours before the procedure and restarted after the procedure, until the patient’s INR was in the therapeutic range. Warfarin was resumed on the evening of the procedure or the following day.
The primary efficacy outcome was ATE, including stroke, TIA, or systemic embolism. The primary safety endpoint was major bleeding (defined as bleeding at a critical anatomic site, symptomatic or clinically overt bleeding, or a decrease in hemoglobin > 2 g/dL). Secondary efficacy and safety outcomes included minor bleeding, acute myocardial infarction, deep vein thrombosis, pulmonary embolism, and death. Outcomes were assessed within 37 days of the procedure.
The incidence of ATE was 0.4% (four events) in the no-bridging group vs 0.3% (three events) in the bridging group. Major bleeding occurred in 1.3% of the no-bridging group (12 events) and in 3.2% of the bridging group (29 events), indicating that no bridging was superior in terms of the major bleeding outcome (number needed to harm [NNH], 53; relative risk [RR], 0.41).
The no-bridging group also had significantly fewer minor bleeds in comparison to the bridging group (NNH, 11; 12% vs 20.9%). There were no differences between groups in other secondary outcomes.
Continue for what's new >>
WHAT’S NEW
High-quality evidence suggests it’s OK to stop warfarin before surgery
This is the largest good-quality study to evaluate perioperative bridging in patients with atrial fibrillation who were at low or moderate risk for ATE (CHADS2 score, 0-4). Previous studies suggested bridging increased bleeding and offered limited benefit for reducing the risk for ATE. However, this is the first study to include a large group of moderate-risk patients (CHADS2 score, 3-4). This trial provides high-quality evidence to support the practice of simply stopping warfarin in the perioperative period, rather than bridging with LMWH.
CAVEATS
Findings might not apply to patients at highest risk
Most patients in this study had a CHADS2 score ≤ 3. About 3% had a CHADS2 score ≥ 5. It’s not clear whether these findings apply to patients with a CHADS2 score of 5 or 6.
This trial categorized ATE risk using the CHADS2 score, rather than the CHA2DS2-VASc, which includes additional risk factors and may more accurately predict stroke risk. Both patients who received bridging therapy and those who did not had a lower rate of stroke than predicted by CHADS2. This may reflect a limit of the predictive value of CHADS2 but should not have affected the rate of bleeding or ATE outcomes in this study.
Continue for challenges to implementation >>
CHALLENGES TO IMPLEMENTATION
Providers may hesitate to disregard current guidelines
Strokes are devastating events for patients, families, and clinicians, and they pose a greater risk for morbidity and mortality compared to bleeding. However, this study suggests patients who receive bridging have a higher risk for bleeding than stroke, which is in contrast to some providers’ experience and current recommendations.
A clinician caring for a patient who’s had a stroke may be inclined to recommend bridging despite the lack of efficacy and evidence of bleeding risk. Additionally, until guidelines reflect the most current research, clinicians may be reluctant to provide care in contrast to these recommendations.
REFERENCES
1. Douketis JD, Spyropoulos AC, Kaatz S, et al. Perioperative bridging anticoagulation in patients with atrial fibrillation. N Engl J Med. 2015;373:823-833.
2. Guyatt GH, Akl EA, Crowther M, et al; American College of Chest Physicians Antithrombotic Therapy and Prevention of Thrombosis Panel. Executive summary: Antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141:7S-47S.
3. Clark NP, Witt DM, Davies LE, et al. Bleeding, recurrent venous thromboembolism and mortality risks during warfarin interruption for invasive procedures. JAMA Intern Med. 2015; 175:1163-1168.
4. Lip GY, Lane DA. Stroke prevention in atrial fibrillation: a systematic review.JAMA. 2015;313:1950-1962.
5. Douketis JD, Spyropoulos AC, Spencer FA, et al; American College of Chest Physicians. Perioperative management of antithrombotic therapy: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141:e326S-e350S.
6. Miyasaka Y, Barnes ME, Gersh BJ, et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence.Circulation. 2006;114:119-125.
7. Siegal D, Yudin J, Kaatz S, et al. Periprocedural heparin bridging in patients receiving vitamin K antagonists: systematic review and meta-analysis of bleeding and thromboembolic rates.Circulation. 2012;126:1630-1639.
8. Steinberg B, Peterson E, Kim S, et al; Outcomes Registry for Better Informed Treatment of Atrial Fibrillation Investigators and Patients. Use and outcomes associated with bridging during anticoagulation interruptions in patients with atrial fibrillation: findings from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF).Circulation. 2015;131:488-494.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2015. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2015;64(12):794-795, 800.
PRACTICE CHANGER
Stop using low molecular weight heparin (LMWH) for surgical procedures to “bridge” low- to moderate-risk patients with atrial fibrillation (CHADS2 score ≤ 4) who are receiving warfarin. The risks outweigh the benefits.1
STRENGTH OF RECOMMENDATION
B: Based on a single good-quality randomized controlled trial.1
CASE A 75-year-old man comes to your office for surgical clearance before right knee replacement surgery. He has diabetes and high blood pressure and is taking warfarin for atrial fibrillation. He is scheduled for surgery in a week. What is the safest way to manage his warfarin in the perioperative period?
More than 2 million people are being treated with oral anticoagulation in North America to prevent stroke or to prevent or treat venous thromboembolism.2 Since 2010, several new oral anticoagulants have been approved, including dabigatran, apixaban, and rivaroxaban. These new medications have a shorter half-life than older anticoagulants, which enables them to be stopped one to two days before surgery.
On the other hand, warfarin—which remains a common choice for anticoagulation—has a three- to seven-day onset and elimination.3,4 This long clinical half-life presents a special challenge during the perioperative period. To reduce the risk for operative bleeding, the warfarin must be stopped days prior to the procedure, but clinicians often worry that this will increase the risk for arterial or venous thromboembolism, including stroke.
An estimated 250,000 patients need perioperative management of their anticoagulation each year.5 As the US population continues to age and the incidence of conditions requiring anticoagulation (particularly atrial fibrillation) increases, this number is only going to rise.6
Current guidelines on bridging. American College of Chest Physicians (ACCP) guidelines recommend transition to “a short-acting anticoagulant, consisting of subcutaneous low molecular weight heparin (LMWH) or intravenous unfractionated heparin, for a 10- to 12-day period during interruption of vitamin K antagonist (VKA) therapy.”5Furthermore, for an appropriate bridging regimen, the ACCP guidelines recommend stopping VKA therapy five days prior to the procedure and utilizing LMWH from within 24 to 48 hours of stopping VKA therapy until up to 24 hours before surgery.5 Postoperatively, VKA or LMWH therapy should be reinitiated within 24 hours and 24 to 72 hours, respectively, depending on the patient’s risk for bleeding during surgery.5
These guidelines recommend using CHADS2 scoring (see the table) to determine arterial thromboembolism (ATE) risk in atrial fibrillation.3,5 Patients at low risk for ATE (CHADS2 score, 0-2) should not be bridged, and patients at high risk (CHADS2 score, 5-6) should always be bridged.5 These guidelines are less clear about bridging recommendations for patients considered to be at moderate risk (CHADS2 score, 3-4).
Previous evidence on bridging. A 2012 meta-analysis of 34 studies evaluated the safety and efficacy of perioperative bridging with heparin in patients receiving VKA.7Researchers found no difference in ATE events in eight studies that compared groups that received bridging vs groups that simply stopped anticoagulation (odds ratio [OR], 0.80).7 The group that received bridging had an increased risk for overall bleeding in 13 studies and of major bleeding in five studies.7This meta-analysis was limited by poor study quality and variation in the indication for VKA therapy.
A 2015 subgroup analysis of a larger cohort study of patients receiving anticoagulants for atrial fibrillation found an increased risk for bleeding when their anticoagulation was interrupted for procedures (OR for major bleeding, 3.84).8
Douketis et al1 conducted a randomized trial to clarify the need for and safety of bridging anticoagulation for ATE in patients with atrial fibrillation who were receiving warfarin.
Continue for study summary >>
STUDY SUMMARY
When it comes to stroke/TIA, there’s no advantage to bridging
This double-blind, placebo-controlled trial compared bridging with dalteparin, a form of LMWH, to placebo among 1,884 patients with atrial fibrillation who were taking warfarin and whose anticoagulation therapy needed to be interrupted for an elective procedure. Patients were included if they were receiving warfarin to prevent stroke and had been taking it for at least 12 weeks, with a goal International Normalized Ratio (INR) of 2.0 to 3.0. Exclusion criteria included having a mechanical heart valve or having a stroke/transient ischemic attack (TIA; 12 weeks prior) or major bleeding (six weeks prior). Patients undergoing cardiac, intracranial, and intraspinal surgeries were also excluded from the study.
The mean CHADS2 score was 2.3; 38.3% of patients had a CHADS2 score ≥ 3, and 9.4% of patients had a history of stroke. Forty-four percent of patients underwent a gastrointestinal procedure, 17.2% underwent a cardiothoracic procedure, and 9.2% underwent an orthopedic procedure.
Patients stopped taking warfarin five days before their procedure and began subcutaneous dalteparin (100 IU/kg) or an identical placebo three days before the procedure. The dalteparin/placebo was stopped 24 hours before the procedure and restarted after the procedure, until the patient’s INR was in the therapeutic range. Warfarin was resumed on the evening of the procedure or the following day.
The primary efficacy outcome was ATE, including stroke, TIA, or systemic embolism. The primary safety endpoint was major bleeding (defined as bleeding at a critical anatomic site, symptomatic or clinically overt bleeding, or a decrease in hemoglobin > 2 g/dL). Secondary efficacy and safety outcomes included minor bleeding, acute myocardial infarction, deep vein thrombosis, pulmonary embolism, and death. Outcomes were assessed within 37 days of the procedure.
The incidence of ATE was 0.4% (four events) in the no-bridging group vs 0.3% (three events) in the bridging group. Major bleeding occurred in 1.3% of the no-bridging group (12 events) and in 3.2% of the bridging group (29 events), indicating that no bridging was superior in terms of the major bleeding outcome (number needed to harm [NNH], 53; relative risk [RR], 0.41).
The no-bridging group also had significantly fewer minor bleeds in comparison to the bridging group (NNH, 11; 12% vs 20.9%). There were no differences between groups in other secondary outcomes.
Continue for what's new >>
WHAT’S NEW
High-quality evidence suggests it’s OK to stop warfarin before surgery
This is the largest good-quality study to evaluate perioperative bridging in patients with atrial fibrillation who were at low or moderate risk for ATE (CHADS2 score, 0-4). Previous studies suggested bridging increased bleeding and offered limited benefit for reducing the risk for ATE. However, this is the first study to include a large group of moderate-risk patients (CHADS2 score, 3-4). This trial provides high-quality evidence to support the practice of simply stopping warfarin in the perioperative period, rather than bridging with LMWH.
CAVEATS
Findings might not apply to patients at highest risk
Most patients in this study had a CHADS2 score ≤ 3. About 3% had a CHADS2 score ≥ 5. It’s not clear whether these findings apply to patients with a CHADS2 score of 5 or 6.
This trial categorized ATE risk using the CHADS2 score, rather than the CHA2DS2-VASc, which includes additional risk factors and may more accurately predict stroke risk. Both patients who received bridging therapy and those who did not had a lower rate of stroke than predicted by CHADS2. This may reflect a limit of the predictive value of CHADS2 but should not have affected the rate of bleeding or ATE outcomes in this study.
Continue for challenges to implementation >>
CHALLENGES TO IMPLEMENTATION
Providers may hesitate to disregard current guidelines
Strokes are devastating events for patients, families, and clinicians, and they pose a greater risk for morbidity and mortality compared to bleeding. However, this study suggests patients who receive bridging have a higher risk for bleeding than stroke, which is in contrast to some providers’ experience and current recommendations.
A clinician caring for a patient who’s had a stroke may be inclined to recommend bridging despite the lack of efficacy and evidence of bleeding risk. Additionally, until guidelines reflect the most current research, clinicians may be reluctant to provide care in contrast to these recommendations.
REFERENCES
1. Douketis JD, Spyropoulos AC, Kaatz S, et al. Perioperative bridging anticoagulation in patients with atrial fibrillation. N Engl J Med. 2015;373:823-833.
2. Guyatt GH, Akl EA, Crowther M, et al; American College of Chest Physicians Antithrombotic Therapy and Prevention of Thrombosis Panel. Executive summary: Antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141:7S-47S.
3. Clark NP, Witt DM, Davies LE, et al. Bleeding, recurrent venous thromboembolism and mortality risks during warfarin interruption for invasive procedures. JAMA Intern Med. 2015; 175:1163-1168.
4. Lip GY, Lane DA. Stroke prevention in atrial fibrillation: a systematic review.JAMA. 2015;313:1950-1962.
5. Douketis JD, Spyropoulos AC, Spencer FA, et al; American College of Chest Physicians. Perioperative management of antithrombotic therapy: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141:e326S-e350S.
6. Miyasaka Y, Barnes ME, Gersh BJ, et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence.Circulation. 2006;114:119-125.
7. Siegal D, Yudin J, Kaatz S, et al. Periprocedural heparin bridging in patients receiving vitamin K antagonists: systematic review and meta-analysis of bleeding and thromboembolic rates.Circulation. 2012;126:1630-1639.
8. Steinberg B, Peterson E, Kim S, et al; Outcomes Registry for Better Informed Treatment of Atrial Fibrillation Investigators and Patients. Use and outcomes associated with bridging during anticoagulation interruptions in patients with atrial fibrillation: findings from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF).Circulation. 2015;131:488-494.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2015. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2015;64(12):794-795, 800.
Value of Ultra-Brief Cognitive Assessments in Predicting Negative Hospital Outcomes
Clinical question: What is the value of ultra-brief cognitive assessments in predicting hospital outcomes?

Background: Cognitive assessment tools can be used to predict patient outcomes in the hospital setting. Physician time constraints limit use of longer traditional cognitive testing, and little is known about the effectiveness of ultra-brief (less than one minute) assessments and their predictive value.
Study design: Secondary data analysis of a quality improvement project.
Setting: Tertiary, Veterans Administration hospital.
Synopsis: Using data from a prior inpatient database, 3,232 patients over the age of 60 were screened on admission using the modified Richmond Agitation and Sedation Scale (mRASS) for arousal and the months of the year backwards (MOTYB) for attention. Abnormal mRASS and incorrect MOTYB predicted negative hospital outcomes: increased length of stay (incident rate ratio 1.23, 95% CI 1.17-1.3); increased restraint use (risk ratio 5.05, 95% CI); increased hospital mortality (RR 3.46, 95% CI 1.24-9.63); and decreased rates of being discharged home (RR 2.97, 95% CI: 2.42-3.64).
This study highlights the value of two ultra-brief cognitive assessment tools in the prediction of potential poor outcomes during inpatient admission. Hospitalists need to identify high-risk patients, and these tools allow for rapid assessment at the time of admission, without a significant time constraint for the busy hospitalist.
Bottom Line: The use of ultra-brief cognitive assessment tools in patients over age 60 can predict negative inpatient outcomes.
Citation: Yevchak AM, Doherty K, Archambault EG, Kelly B, Fonda JR, Rudolph JL. The association between an ultra-brief cognitive screening in older adults and hospital outcomes. J Hosp Med. 2015;10(10):651-657.
Clinical question: What is the value of ultra-brief cognitive assessments in predicting hospital outcomes?
Background: Cognitive assessment tools can be used to predict patient outcomes in the hospital setting. Physician time constraints limit use of longer traditional cognitive testing, and little is known about the effectiveness of ultra-brief (less than one minute) assessments and their predictive value.
Study design: Secondary data analysis of a quality improvement project.
Setting: Tertiary, Veterans Administration hospital.
Synopsis: Using data from a prior inpatient database, 3,232 patients over the age of 60 were screened on admission using the modified Richmond Agitation and Sedation Scale (mRASS) for arousal and the months of the year backwards (MOTYB) for attention. Abnormal mRASS and incorrect MOTYB predicted negative hospital outcomes: increased length of stay (incident rate ratio 1.23, 95% CI 1.17-1.3); increased restraint use (risk ratio 5.05, 95% CI); increased hospital mortality (RR 3.46, 95% CI 1.24-9.63); and decreased rates of being discharged home (RR 2.97, 95% CI: 2.42-3.64).
This study highlights the value of two ultra-brief cognitive assessment tools in the prediction of potential poor outcomes during inpatient admission. Hospitalists need to identify high-risk patients, and these tools allow for rapid assessment at the time of admission, without a significant time constraint for the busy hospitalist.
Bottom Line: The use of ultra-brief cognitive assessment tools in patients over age 60 can predict negative inpatient outcomes.
Citation: Yevchak AM, Doherty K, Archambault EG, Kelly B, Fonda JR, Rudolph JL. The association between an ultra-brief cognitive screening in older adults and hospital outcomes. J Hosp Med. 2015;10(10):651-657.
Clinical question: What is the value of ultra-brief cognitive assessments in predicting hospital outcomes?
Background: Cognitive assessment tools can be used to predict patient outcomes in the hospital setting. Physician time constraints limit use of longer traditional cognitive testing, and little is known about the effectiveness of ultra-brief (less than one minute) assessments and their predictive value.
Study design: Secondary data analysis of a quality improvement project.
Setting: Tertiary, Veterans Administration hospital.
Synopsis: Using data from a prior inpatient database, 3,232 patients over the age of 60 were screened on admission using the modified Richmond Agitation and Sedation Scale (mRASS) for arousal and the months of the year backwards (MOTYB) for attention. Abnormal mRASS and incorrect MOTYB predicted negative hospital outcomes: increased length of stay (incident rate ratio 1.23, 95% CI 1.17-1.3); increased restraint use (risk ratio 5.05, 95% CI); increased hospital mortality (RR 3.46, 95% CI 1.24-9.63); and decreased rates of being discharged home (RR 2.97, 95% CI: 2.42-3.64).
This study highlights the value of two ultra-brief cognitive assessment tools in the prediction of potential poor outcomes during inpatient admission. Hospitalists need to identify high-risk patients, and these tools allow for rapid assessment at the time of admission, without a significant time constraint for the busy hospitalist.
Bottom Line: The use of ultra-brief cognitive assessment tools in patients over age 60 can predict negative inpatient outcomes.
Citation: Yevchak AM, Doherty K, Archambault EG, Kelly B, Fonda JR, Rudolph JL. The association between an ultra-brief cognitive screening in older adults and hospital outcomes. J Hosp Med. 2015;10(10):651-657.

Criteria for Appropriate Use of Peripherally Inserted Central Catheters
Clinical question: What are criteria for appropriate and inappropriate use of PICCs?
Background: PICCs are commonly used in medical care in a variety of clinical contexts; however, criteria defining the appropriate use of PICCs and practices related to PICC placement have not been previously established.
Study design: A multispecialty panel classified indications for PICC use as appropriate or inappropriate using the RAND/UCLA Appropriateness Method.
Synopsis: Selected appropriate PICC uses include:
- Infusion of peripherally compatible infusates, intermittent infusions, or infrequent phlebotomy in patients with poor or difficult venous access when the expected duration of use is at least six days;
- Phlebotomy at least every eight hours when the expected duration of use is at least six days; and
- Invasive hemodynamic monitoring in a critically ill patient only if the duration of use is expected to exceed 15 days.
Selected appropriate PICC-related practices:
- Verify PICC tip position using a chest radiograph only after non-ECG or non-fluoroscopically guided PICC insertion;
- Provide an interval without a PICC to allow resolution of bacteremia when managing PICC-related bloodstream infections; and
- For PICC-related DVT, provide at least three months of systemic anticoagulation if not otherwise contraindicated.
Selected inappropriate PICC-related practices:
- Adjustment of PICC tips that reside in the lower third of the superior vena cava, cavoatrial junction, or right atrium; and
- Removal or replacement of PICCs that are clinically necessary, well positioned, and functional in the setting of PICC-related DVT or without evidence of catheter-associated bloodstream infection.
Bottom line: A multispecialty expert panel provides guidance for appropriate use of PICCs and PICC-related practices.
Citation: Chopra V, Flanders SA, Saint S, et al. The Michigan appropriateness guide for intravenous catheters (MAGIC): results from a multispecialty panel using the RAND/UCLA appropriateness method. Ann Intern Med. 2015;163(6):S1-S40.
Clinical question: What are criteria for appropriate and inappropriate use of PICCs?
Background: PICCs are commonly used in medical care in a variety of clinical contexts; however, criteria defining the appropriate use of PICCs and practices related to PICC placement have not been previously established.
Study design: A multispecialty panel classified indications for PICC use as appropriate or inappropriate using the RAND/UCLA Appropriateness Method.
Synopsis: Selected appropriate PICC uses include:
- Infusion of peripherally compatible infusates, intermittent infusions, or infrequent phlebotomy in patients with poor or difficult venous access when the expected duration of use is at least six days;
- Phlebotomy at least every eight hours when the expected duration of use is at least six days; and
- Invasive hemodynamic monitoring in a critically ill patient only if the duration of use is expected to exceed 15 days.
Selected appropriate PICC-related practices:
- Verify PICC tip position using a chest radiograph only after non-ECG or non-fluoroscopically guided PICC insertion;
- Provide an interval without a PICC to allow resolution of bacteremia when managing PICC-related bloodstream infections; and
- For PICC-related DVT, provide at least three months of systemic anticoagulation if not otherwise contraindicated.
Selected inappropriate PICC-related practices:
- Adjustment of PICC tips that reside in the lower third of the superior vena cava, cavoatrial junction, or right atrium; and
- Removal or replacement of PICCs that are clinically necessary, well positioned, and functional in the setting of PICC-related DVT or without evidence of catheter-associated bloodstream infection.
Bottom line: A multispecialty expert panel provides guidance for appropriate use of PICCs and PICC-related practices.
Citation: Chopra V, Flanders SA, Saint S, et al. The Michigan appropriateness guide for intravenous catheters (MAGIC): results from a multispecialty panel using the RAND/UCLA appropriateness method. Ann Intern Med. 2015;163(6):S1-S40.
Clinical question: What are criteria for appropriate and inappropriate use of PICCs?
Background: PICCs are commonly used in medical care in a variety of clinical contexts; however, criteria defining the appropriate use of PICCs and practices related to PICC placement have not been previously established.
Study design: A multispecialty panel classified indications for PICC use as appropriate or inappropriate using the RAND/UCLA Appropriateness Method.
Synopsis: Selected appropriate PICC uses include:
- Infusion of peripherally compatible infusates, intermittent infusions, or infrequent phlebotomy in patients with poor or difficult venous access when the expected duration of use is at least six days;
- Phlebotomy at least every eight hours when the expected duration of use is at least six days; and
- Invasive hemodynamic monitoring in a critically ill patient only if the duration of use is expected to exceed 15 days.
Selected appropriate PICC-related practices:
- Verify PICC tip position using a chest radiograph only after non-ECG or non-fluoroscopically guided PICC insertion;
- Provide an interval without a PICC to allow resolution of bacteremia when managing PICC-related bloodstream infections; and
- For PICC-related DVT, provide at least three months of systemic anticoagulation if not otherwise contraindicated.
Selected inappropriate PICC-related practices:
- Adjustment of PICC tips that reside in the lower third of the superior vena cava, cavoatrial junction, or right atrium; and
- Removal or replacement of PICCs that are clinically necessary, well positioned, and functional in the setting of PICC-related DVT or without evidence of catheter-associated bloodstream infection.
Bottom line: A multispecialty expert panel provides guidance for appropriate use of PICCs and PICC-related practices.
Citation: Chopra V, Flanders SA, Saint S, et al. The Michigan appropriateness guide for intravenous catheters (MAGIC): results from a multispecialty panel using the RAND/UCLA appropriateness method. Ann Intern Med. 2015;163(6):S1-S40.
Kidney Transplants
Q) All I hear about is the shortage of kidneys for transplantation. A friend of mine is on the local transplant list, and it is eight years long! Are there any ideas out there to grow your own kidneys?
Eight years is a long time for people dealing with the physical and emotional effects of kidney disease coupled with hemodialysis or peritoneal dialysis. Your friend is one of 110,000 patients (as of January 2015) in the United States on the United Network for Organ Sharing (UNOS) kidney transplant waiting list.1 The UNOS/Organ Procurement and Transplant Network (OPTN) implemented new polices in 2014 to shorten the wait.
Among them: For pediatric patients (those younger than 18), the wait list time starts when the glomerular filtration rate (GFR) is ≤ 20 mL/min or the child starts dialysis. UNOS also has attempted to match posttransplant survival time of the graft with posttransplant survival time of the recipient through use of calculations that classify kidneys on the basis of how long they are likely to function once transplanted. Priority is now given to candidates with high immune system sensitivity or uncommon blood types, as they are less likely to obtain a kidney otherwise.2
The million-dollar question is how to obtain a kidney transplant in a timely fashion. Grave robbing, in case you are wondering, is not a viable option! Nor is transplant tourism (traveling outside the US to obtain an organ transplant), which confers a higher risk for severe infectious complications and acute rejection, possibly related to less extensive donor screening.3
There are other possibilities: Living donors can donate one kidney. Or, as is becoming increasingly common, paired organ transplants can be arranged. These occur when a patient in need of a kidney has a willing but incompatible donor; if a different match can be found, a “swap” is orchestrated, in which Donor A’s kidney is transplanted into Recipient B and Donor B’s kidney is given to Recipient A. This can be and has been done with multiple donors and recipients—in some cases, dozens—allowing the gift of donation to go on and on. (See “Trading Kidneys: Innovative Program Could Save Thousands of Lives” for an overview of how this concept started.)
Some exciting research is going on with regard to 3D printing of kidneys; they are miniature for now but showing survival of the printed cells. Another area of exploration is regenerative medicine; researchers in the field are investigating the bioengineering of organs by taking the “scaffolding” of an organ and implanting a patient’s own cells to “grow” a new organ (which, if successful, would also eliminate the need for immunosuppressants). Other signs of progress include recent news that scientists are getting lab-grown kidneys to work in animals.
It will be several years before any of these options will be viable. In the meantime, it never hurts to ask loved ones if they are willing to donate a kidney. Best wishes to your friend. —DC
Della Connor, PhD, RN, FNP-BC
East Texas Nephrology Associates, Lufkin, Texas
REFERENCES
1. Organ Procurement and Transplantation Network. http://optn.transplant.hrsa.gov. Accessed December 10, 2015.
2. Organ Procurement and Transplantation Network. New OPTN requirements and resources for the living donor kidney transplant programs. Prog Transplant. 2013;23(2):117.
3. Gill J, Madhira BR, Gjertson D, et al. Transplant tourism in the United States: a single-center experience. Clin J Am Soc Nephrol. 2008;3(6):1820-1828.
| Clinician Reviews in partnership with |
Renal Consult is edited by Jane S. Davis, CRNP, DNP, a member of the Clinician Reviews editorial board, who is a nurse practitioner in the Division of Nephrology at the University of Alabama at Birmingham and is the communications chairperson for the National Kidney Foundation’s Council of Advanced Practitioners (NKF-CAP); and Kim Zuber, PA-C, MSPS, DFAAPA, a retired physician assistant who works with the American Academy of Nephrology PAs and is also past chair of the NKF-CAP. This month’s responses were authored by Della Connor, PhD, RN, FNP-BC, who is an Assistant Professor at Stephen F. Austin State University in Nacogdoches, Texas, and practices at East Texas Nephrology Associates in Lufkin, and the department editors.
| Clinician Reviews in partnership with |
Renal Consult is edited by Jane S. Davis, CRNP, DNP, a member of the Clinician Reviews editorial board, who is a nurse practitioner in the Division of Nephrology at the University of Alabama at Birmingham and is the communications chairperson for the National Kidney Foundation’s Council of Advanced Practitioners (NKF-CAP); and Kim Zuber, PA-C, MSPS, DFAAPA, a retired physician assistant who works with the American Academy of Nephrology PAs and is also past chair of the NKF-CAP. This month’s responses were authored by Della Connor, PhD, RN, FNP-BC, who is an Assistant Professor at Stephen F. Austin State University in Nacogdoches, Texas, and practices at East Texas Nephrology Associates in Lufkin, and the department editors.
| Clinician Reviews in partnership with |
Renal Consult is edited by Jane S. Davis, CRNP, DNP, a member of the Clinician Reviews editorial board, who is a nurse practitioner in the Division of Nephrology at the University of Alabama at Birmingham and is the communications chairperson for the National Kidney Foundation’s Council of Advanced Practitioners (NKF-CAP); and Kim Zuber, PA-C, MSPS, DFAAPA, a retired physician assistant who works with the American Academy of Nephrology PAs and is also past chair of the NKF-CAP. This month’s responses were authored by Della Connor, PhD, RN, FNP-BC, who is an Assistant Professor at Stephen F. Austin State University in Nacogdoches, Texas, and practices at East Texas Nephrology Associates in Lufkin, and the department editors.
Q) All I hear about is the shortage of kidneys for transplantation. A friend of mine is on the local transplant list, and it is eight years long! Are there any ideas out there to grow your own kidneys?
Eight years is a long time for people dealing with the physical and emotional effects of kidney disease coupled with hemodialysis or peritoneal dialysis. Your friend is one of 110,000 patients (as of January 2015) in the United States on the United Network for Organ Sharing (UNOS) kidney transplant waiting list.1 The UNOS/Organ Procurement and Transplant Network (OPTN) implemented new polices in 2014 to shorten the wait.
Among them: For pediatric patients (those younger than 18), the wait list time starts when the glomerular filtration rate (GFR) is ≤ 20 mL/min or the child starts dialysis. UNOS also has attempted to match posttransplant survival time of the graft with posttransplant survival time of the recipient through use of calculations that classify kidneys on the basis of how long they are likely to function once transplanted. Priority is now given to candidates with high immune system sensitivity or uncommon blood types, as they are less likely to obtain a kidney otherwise.2
The million-dollar question is how to obtain a kidney transplant in a timely fashion. Grave robbing, in case you are wondering, is not a viable option! Nor is transplant tourism (traveling outside the US to obtain an organ transplant), which confers a higher risk for severe infectious complications and acute rejection, possibly related to less extensive donor screening.3
There are other possibilities: Living donors can donate one kidney. Or, as is becoming increasingly common, paired organ transplants can be arranged. These occur when a patient in need of a kidney has a willing but incompatible donor; if a different match can be found, a “swap” is orchestrated, in which Donor A’s kidney is transplanted into Recipient B and Donor B’s kidney is given to Recipient A. This can be and has been done with multiple donors and recipients—in some cases, dozens—allowing the gift of donation to go on and on. (See “Trading Kidneys: Innovative Program Could Save Thousands of Lives” for an overview of how this concept started.)
Some exciting research is going on with regard to 3D printing of kidneys; they are miniature for now but showing survival of the printed cells. Another area of exploration is regenerative medicine; researchers in the field are investigating the bioengineering of organs by taking the “scaffolding” of an organ and implanting a patient’s own cells to “grow” a new organ (which, if successful, would also eliminate the need for immunosuppressants). Other signs of progress include recent news that scientists are getting lab-grown kidneys to work in animals.
It will be several years before any of these options will be viable. In the meantime, it never hurts to ask loved ones if they are willing to donate a kidney. Best wishes to your friend. —DC
Della Connor, PhD, RN, FNP-BC
East Texas Nephrology Associates, Lufkin, Texas
REFERENCES
1. Organ Procurement and Transplantation Network. http://optn.transplant.hrsa.gov. Accessed December 10, 2015.
2. Organ Procurement and Transplantation Network. New OPTN requirements and resources for the living donor kidney transplant programs. Prog Transplant. 2013;23(2):117.
3. Gill J, Madhira BR, Gjertson D, et al. Transplant tourism in the United States: a single-center experience. Clin J Am Soc Nephrol. 2008;3(6):1820-1828.
Q) All I hear about is the shortage of kidneys for transplantation. A friend of mine is on the local transplant list, and it is eight years long! Are there any ideas out there to grow your own kidneys?
Eight years is a long time for people dealing with the physical and emotional effects of kidney disease coupled with hemodialysis or peritoneal dialysis. Your friend is one of 110,000 patients (as of January 2015) in the United States on the United Network for Organ Sharing (UNOS) kidney transplant waiting list.1 The UNOS/Organ Procurement and Transplant Network (OPTN) implemented new polices in 2014 to shorten the wait.
Among them: For pediatric patients (those younger than 18), the wait list time starts when the glomerular filtration rate (GFR) is ≤ 20 mL/min or the child starts dialysis. UNOS also has attempted to match posttransplant survival time of the graft with posttransplant survival time of the recipient through use of calculations that classify kidneys on the basis of how long they are likely to function once transplanted. Priority is now given to candidates with high immune system sensitivity or uncommon blood types, as they are less likely to obtain a kidney otherwise.2
The million-dollar question is how to obtain a kidney transplant in a timely fashion. Grave robbing, in case you are wondering, is not a viable option! Nor is transplant tourism (traveling outside the US to obtain an organ transplant), which confers a higher risk for severe infectious complications and acute rejection, possibly related to less extensive donor screening.3
There are other possibilities: Living donors can donate one kidney. Or, as is becoming increasingly common, paired organ transplants can be arranged. These occur when a patient in need of a kidney has a willing but incompatible donor; if a different match can be found, a “swap” is orchestrated, in which Donor A’s kidney is transplanted into Recipient B and Donor B’s kidney is given to Recipient A. This can be and has been done with multiple donors and recipients—in some cases, dozens—allowing the gift of donation to go on and on. (See “Trading Kidneys: Innovative Program Could Save Thousands of Lives” for an overview of how this concept started.)
Some exciting research is going on with regard to 3D printing of kidneys; they are miniature for now but showing survival of the printed cells. Another area of exploration is regenerative medicine; researchers in the field are investigating the bioengineering of organs by taking the “scaffolding” of an organ and implanting a patient’s own cells to “grow” a new organ (which, if successful, would also eliminate the need for immunosuppressants). Other signs of progress include recent news that scientists are getting lab-grown kidneys to work in animals.
It will be several years before any of these options will be viable. In the meantime, it never hurts to ask loved ones if they are willing to donate a kidney. Best wishes to your friend. —DC
Della Connor, PhD, RN, FNP-BC
East Texas Nephrology Associates, Lufkin, Texas
REFERENCES
1. Organ Procurement and Transplantation Network. http://optn.transplant.hrsa.gov. Accessed December 10, 2015.
2. Organ Procurement and Transplantation Network. New OPTN requirements and resources for the living donor kidney transplant programs. Prog Transplant. 2013;23(2):117.
3. Gill J, Madhira BR, Gjertson D, et al. Transplant tourism in the United States: a single-center experience. Clin J Am Soc Nephrol. 2008;3(6):1820-1828.
De novo mutation linked to FA subtype

with Fanconi anemia
Researchers say they have established the cause of a subtype of Fanconi anemia (FA)—a de novo mutation in 1 allele of RAD51, a gene responsible for repairing DNA damage.
The team made this discovery in a child with an FA-like syndrome who has healthy parents and a healthy sister.
“The particular mutation in this patient was a surprise to us,” said Patrick May, PhD, of the University of Luxembourg.
“It occurred only in 1 of the 2 RAD51 gene copies, which every person carries in the genome, but every RAD51 gene copy was normal in the child’s parents.”
Dr May and his colleagues described the mutation in Nature Communications.
Specifically, the researchers found a de novo g.41022153G>A; p.Ala293Thr (NM_002875) missense mutation in 1 allele of RAD51.
They said this heterozygous mutation causes a novel FA subtype, dubbed “FA-R,” which appears to be the first subtype of FA caused by a dominant-negative mutation.
The patient the researchers analyzed has microcephaly and mental retardation but has reached adulthood without the bone marrow failure and pediatric cancers typically observed in patients with FA.
Until this case, researchers believed that mutations leading to FA showed recessive inheritance and therefore had to be derived from both parents to lead to FA. Spontaneous mutations of the RAD51 gene like in this case had not been observed.
Dr May and his colleagues said their finding has implications for genetic counseling of families with a high risk for FA. Previously, people who wanted to have children but had relatives suffering from FA were screened for mutations in 1 of the 17 genes connected with the disease. Now, the risk of having a child with FA has to be recalculated.
“Furthermore, understanding this mutation teaches us more about how the RAD51 gene product protects the DNA and how disruptions of DNA repair may lead to leukemia and solid tumors,” Dr May said. “Of course, understanding the origins of human cancer will help us diagnose it with more confidence earlier and devise new therapies to prevent or mitigate it.” ![]()
with Fanconi anemia
Researchers say they have established the cause of a subtype of Fanconi anemia (FA)—a de novo mutation in 1 allele of RAD51, a gene responsible for repairing DNA damage.
The team made this discovery in a child with an FA-like syndrome who has healthy parents and a healthy sister.
“The particular mutation in this patient was a surprise to us,” said Patrick May, PhD, of the University of Luxembourg.
“It occurred only in 1 of the 2 RAD51 gene copies, which every person carries in the genome, but every RAD51 gene copy was normal in the child’s parents.”
Dr May and his colleagues described the mutation in Nature Communications.
Specifically, the researchers found a de novo g.41022153G>A; p.Ala293Thr (NM_002875) missense mutation in 1 allele of RAD51.
They said this heterozygous mutation causes a novel FA subtype, dubbed “FA-R,” which appears to be the first subtype of FA caused by a dominant-negative mutation.
The patient the researchers analyzed has microcephaly and mental retardation but has reached adulthood without the bone marrow failure and pediatric cancers typically observed in patients with FA.
Until this case, researchers believed that mutations leading to FA showed recessive inheritance and therefore had to be derived from both parents to lead to FA. Spontaneous mutations of the RAD51 gene like in this case had not been observed.
Dr May and his colleagues said their finding has implications for genetic counseling of families with a high risk for FA. Previously, people who wanted to have children but had relatives suffering from FA were screened for mutations in 1 of the 17 genes connected with the disease. Now, the risk of having a child with FA has to be recalculated.
“Furthermore, understanding this mutation teaches us more about how the RAD51 gene product protects the DNA and how disruptions of DNA repair may lead to leukemia and solid tumors,” Dr May said. “Of course, understanding the origins of human cancer will help us diagnose it with more confidence earlier and devise new therapies to prevent or mitigate it.” ![]()
with Fanconi anemia
Researchers say they have established the cause of a subtype of Fanconi anemia (FA)—a de novo mutation in 1 allele of RAD51, a gene responsible for repairing DNA damage.
The team made this discovery in a child with an FA-like syndrome who has healthy parents and a healthy sister.
“The particular mutation in this patient was a surprise to us,” said Patrick May, PhD, of the University of Luxembourg.
“It occurred only in 1 of the 2 RAD51 gene copies, which every person carries in the genome, but every RAD51 gene copy was normal in the child’s parents.”
Dr May and his colleagues described the mutation in Nature Communications.
Specifically, the researchers found a de novo g.41022153G>A; p.Ala293Thr (NM_002875) missense mutation in 1 allele of RAD51.
They said this heterozygous mutation causes a novel FA subtype, dubbed “FA-R,” which appears to be the first subtype of FA caused by a dominant-negative mutation.
The patient the researchers analyzed has microcephaly and mental retardation but has reached adulthood without the bone marrow failure and pediatric cancers typically observed in patients with FA.
Until this case, researchers believed that mutations leading to FA showed recessive inheritance and therefore had to be derived from both parents to lead to FA. Spontaneous mutations of the RAD51 gene like in this case had not been observed.
Dr May and his colleagues said their finding has implications for genetic counseling of families with a high risk for FA. Previously, people who wanted to have children but had relatives suffering from FA were screened for mutations in 1 of the 17 genes connected with the disease. Now, the risk of having a child with FA has to be recalculated.
“Furthermore, understanding this mutation teaches us more about how the RAD51 gene product protects the DNA and how disruptions of DNA repair may lead to leukemia and solid tumors,” Dr May said. “Of course, understanding the origins of human cancer will help us diagnose it with more confidence earlier and devise new therapies to prevent or mitigate it.” ![]()
Women can take anticoagulants and hormones safely, study suggests

A study published in Blood indicates that women on anticoagulants can take estrogen-containing contraception or hormone replacement therapy
without an increased risk of venous thromboembolism (VTE) or uterine bleeding.
If a woman is diagnosed with VTE, she is often advised to stop hormone therapy, even while receiving anticoagulant therapy, because she is thought to have an increased risk of VTE recurrence.
However, this practice is based on the known association between hormone therapy and increased clotting risk in the absence of anticoagulants. The safety of the concurrent use of these medications had not been previously explored.
“While it has been common practice among healthcare providers to avoid prescribing hormone therapy and anticoagulants at the same time, there has been no evidence to support this decision,” said study author Ida Martinelli, MD, of the A. Bianchi Bonomi Hemophilia and Thrombosis Center in Milan, Italy.
“We conducted this study to address the fear felt by both the physician and patient when making the decision to stop or continue hormone therapy in this setting.”
The researchers compared the incidences of recurrent VTE and abnormal uterine bleeding in 1888 women who received anticoagulants with or without concurrent hormone therapy.
The team analyzed data from the EINSTEIN DVT and PE study, which was performed to evaluate the safety and efficacy of 2 anticoagulants—the direct oral anticoagulant rivaroxaban and the current standard of care, a low-molecular-weight heparin (enoxaparin) followed by a vitamin K antagonist (VKA).
Women of child-bearing potential were advised to use adequate methods of contraception to avoid birth defects.
Of all the women in the study, 475 used hormone therapy during the analysis period. Medications used included estrogen-only pills, combined estrogen-progestogen contraceptives, and progestin-only contraceptives.
Participants were questioned about symptoms or signs of recurrent VTE and bleeding, including uterine bleeding, during each follow-up visit.
Seven recurrent VTEs occurred while patients were using hormone therapy, while 38 events occurred during a period when patients were not using hormone therapy.
Based on this analysis, the researchers concluded that women on anticoagulants and hormone therapy experienced recurrent VTE at a rate of 3.7% per year. In contrast, those not on hormone therapy had a recurrence rate of 4.7% per year.
The incidence of abnormal uterine bleeding in patients on hormonal therapy was 22.5%, compared to 21.4% for women not on hormone therapy.
According to the study authors, the similar incidence of VTE and abnormal uterine bleeding in women who did and did not receive hormone therapy suggest that combined use of these therapies is safe.
The study also showed that abnormal uterine bleeding occurred more frequently with rivaroxaban than with enoxaparin/VKA. The bleeding rate was estimated at 29.8% per year for patients on rivaroxaban and 15.5% per year in the enoxaparin/VKA group.
The researchers said this outcome suggests the need for further studies on rivaroxaban, which may be preferred for its convenience over enoxaparin/VKA.
“For the first time, we demonstrate that women suffering from blood clots can safely take hormone-containing contraceptives or hormone replacement therapy with anticoagulants, providing women the freedom to choose the method of birth control and other hormone-containing medications they prefer,” Dr Martinelli said.
“While further investigation is needed to evaluate the inconvenience of abnormal uterine bleeding with rivaroxaban and the other direct oral anticoagulants, these results dispel former misconceptions and should allow clinicians to confidently treat their patients who take blood thinners and hormones concurrently.” ![]()
A study published in Blood indicates that women on anticoagulants can take estrogen-containing contraception or hormone replacement therapy
without an increased risk of venous thromboembolism (VTE) or uterine bleeding.
If a woman is diagnosed with VTE, she is often advised to stop hormone therapy, even while receiving anticoagulant therapy, because she is thought to have an increased risk of VTE recurrence.
However, this practice is based on the known association between hormone therapy and increased clotting risk in the absence of anticoagulants. The safety of the concurrent use of these medications had not been previously explored.
“While it has been common practice among healthcare providers to avoid prescribing hormone therapy and anticoagulants at the same time, there has been no evidence to support this decision,” said study author Ida Martinelli, MD, of the A. Bianchi Bonomi Hemophilia and Thrombosis Center in Milan, Italy.
“We conducted this study to address the fear felt by both the physician and patient when making the decision to stop or continue hormone therapy in this setting.”
The researchers compared the incidences of recurrent VTE and abnormal uterine bleeding in 1888 women who received anticoagulants with or without concurrent hormone therapy.
The team analyzed data from the EINSTEIN DVT and PE study, which was performed to evaluate the safety and efficacy of 2 anticoagulants—the direct oral anticoagulant rivaroxaban and the current standard of care, a low-molecular-weight heparin (enoxaparin) followed by a vitamin K antagonist (VKA).
Women of child-bearing potential were advised to use adequate methods of contraception to avoid birth defects.
Of all the women in the study, 475 used hormone therapy during the analysis period. Medications used included estrogen-only pills, combined estrogen-progestogen contraceptives, and progestin-only contraceptives.
Participants were questioned about symptoms or signs of recurrent VTE and bleeding, including uterine bleeding, during each follow-up visit.
Seven recurrent VTEs occurred while patients were using hormone therapy, while 38 events occurred during a period when patients were not using hormone therapy.
Based on this analysis, the researchers concluded that women on anticoagulants and hormone therapy experienced recurrent VTE at a rate of 3.7% per year. In contrast, those not on hormone therapy had a recurrence rate of 4.7% per year.
The incidence of abnormal uterine bleeding in patients on hormonal therapy was 22.5%, compared to 21.4% for women not on hormone therapy.
According to the study authors, the similar incidence of VTE and abnormal uterine bleeding in women who did and did not receive hormone therapy suggest that combined use of these therapies is safe.
The study also showed that abnormal uterine bleeding occurred more frequently with rivaroxaban than with enoxaparin/VKA. The bleeding rate was estimated at 29.8% per year for patients on rivaroxaban and 15.5% per year in the enoxaparin/VKA group.
The researchers said this outcome suggests the need for further studies on rivaroxaban, which may be preferred for its convenience over enoxaparin/VKA.
“For the first time, we demonstrate that women suffering from blood clots can safely take hormone-containing contraceptives or hormone replacement therapy with anticoagulants, providing women the freedom to choose the method of birth control and other hormone-containing medications they prefer,” Dr Martinelli said.
“While further investigation is needed to evaluate the inconvenience of abnormal uterine bleeding with rivaroxaban and the other direct oral anticoagulants, these results dispel former misconceptions and should allow clinicians to confidently treat their patients who take blood thinners and hormones concurrently.” ![]()
A study published in Blood indicates that women on anticoagulants can take estrogen-containing contraception or hormone replacement therapy
without an increased risk of venous thromboembolism (VTE) or uterine bleeding.
If a woman is diagnosed with VTE, she is often advised to stop hormone therapy, even while receiving anticoagulant therapy, because she is thought to have an increased risk of VTE recurrence.
However, this practice is based on the known association between hormone therapy and increased clotting risk in the absence of anticoagulants. The safety of the concurrent use of these medications had not been previously explored.
“While it has been common practice among healthcare providers to avoid prescribing hormone therapy and anticoagulants at the same time, there has been no evidence to support this decision,” said study author Ida Martinelli, MD, of the A. Bianchi Bonomi Hemophilia and Thrombosis Center in Milan, Italy.
“We conducted this study to address the fear felt by both the physician and patient when making the decision to stop or continue hormone therapy in this setting.”
The researchers compared the incidences of recurrent VTE and abnormal uterine bleeding in 1888 women who received anticoagulants with or without concurrent hormone therapy.
The team analyzed data from the EINSTEIN DVT and PE study, which was performed to evaluate the safety and efficacy of 2 anticoagulants—the direct oral anticoagulant rivaroxaban and the current standard of care, a low-molecular-weight heparin (enoxaparin) followed by a vitamin K antagonist (VKA).
Women of child-bearing potential were advised to use adequate methods of contraception to avoid birth defects.
Of all the women in the study, 475 used hormone therapy during the analysis period. Medications used included estrogen-only pills, combined estrogen-progestogen contraceptives, and progestin-only contraceptives.
Participants were questioned about symptoms or signs of recurrent VTE and bleeding, including uterine bleeding, during each follow-up visit.
Seven recurrent VTEs occurred while patients were using hormone therapy, while 38 events occurred during a period when patients were not using hormone therapy.
Based on this analysis, the researchers concluded that women on anticoagulants and hormone therapy experienced recurrent VTE at a rate of 3.7% per year. In contrast, those not on hormone therapy had a recurrence rate of 4.7% per year.
The incidence of abnormal uterine bleeding in patients on hormonal therapy was 22.5%, compared to 21.4% for women not on hormone therapy.
According to the study authors, the similar incidence of VTE and abnormal uterine bleeding in women who did and did not receive hormone therapy suggest that combined use of these therapies is safe.
The study also showed that abnormal uterine bleeding occurred more frequently with rivaroxaban than with enoxaparin/VKA. The bleeding rate was estimated at 29.8% per year for patients on rivaroxaban and 15.5% per year in the enoxaparin/VKA group.
The researchers said this outcome suggests the need for further studies on rivaroxaban, which may be preferred for its convenience over enoxaparin/VKA.
“For the first time, we demonstrate that women suffering from blood clots can safely take hormone-containing contraceptives or hormone replacement therapy with anticoagulants, providing women the freedom to choose the method of birth control and other hormone-containing medications they prefer,” Dr Martinelli said.
“While further investigation is needed to evaluate the inconvenience of abnormal uterine bleeding with rivaroxaban and the other direct oral anticoagulants, these results dispel former misconceptions and should allow clinicians to confidently treat their patients who take blood thinners and hormones concurrently.” ![]()
ACP Guidelines for Evaluation of Suspected Pulmonary Embolism
Clinical question: What are best practices for evaluating patients with suspected acute pulmonary embolism (PE)?
Background: Use of CT in the evaluation of PE has increased across all clinical settings without improving mortality. Contrast CT carries the risks of radiation exposure, contrast-induced nephropathy, and incidental findings that require further investigation. The authors highlight evidence-based strategies for evaluation of PE, focusing on delivering high-value care.
Study design: Clinical guideline.
Setting: Literature review of studies across all adult clinical settings.
Synopsis: The clinical guidelines committee of the American College of Physicians conducted a literature search surrounding evaluation of suspected acute PE. From their review, they concluded:
- Pretest probability should initially be determined based on validated prediction tools (Wells score, Revised Geneva);
- In patients found to have low pretest probability and meeting the pulmonary embolism rule-out criteria (PERC), clinicians can forego d-dimer testing;
- In those with intermediate pretest probability or those with low pre-test probability who do not pass PERC, d-dimer measurement should be obtained;
- The d-dimer threshold should be age adjusted and imaging should not be pursued in patients whose d-dimer level falls below this cutoff, while those with positive d-dimers should receive CT pulmonary angiography (CTPA); and
- Patients with high pretest probability should undergo CTPA (or V/Q scan if CTPA is contraindicated) without d-dimer testing.
Bottom line: In suspected acute PE, first determine pretest probability using Wells and Revised Geneva, and then use this probability in conjunction with the PERC and d-dimer (as indicated) to guide decisions about imaging.
Citation: Raja AS, Greenberg JO, Qaseem A, Denberg TD, Fitterman N, Schuur JD. Evaluation of patients with suspected acute pulmonary embolism: best practice advice from the clinical guidelines committee of the American College of Physicians. Ann Intern Med. 2015;163(9):701-711.
Clinical question: What are best practices for evaluating patients with suspected acute pulmonary embolism (PE)?
Background: Use of CT in the evaluation of PE has increased across all clinical settings without improving mortality. Contrast CT carries the risks of radiation exposure, contrast-induced nephropathy, and incidental findings that require further investigation. The authors highlight evidence-based strategies for evaluation of PE, focusing on delivering high-value care.
Study design: Clinical guideline.
Setting: Literature review of studies across all adult clinical settings.
Synopsis: The clinical guidelines committee of the American College of Physicians conducted a literature search surrounding evaluation of suspected acute PE. From their review, they concluded:
- Pretest probability should initially be determined based on validated prediction tools (Wells score, Revised Geneva);
- In patients found to have low pretest probability and meeting the pulmonary embolism rule-out criteria (PERC), clinicians can forego d-dimer testing;
- In those with intermediate pretest probability or those with low pre-test probability who do not pass PERC, d-dimer measurement should be obtained;
- The d-dimer threshold should be age adjusted and imaging should not be pursued in patients whose d-dimer level falls below this cutoff, while those with positive d-dimers should receive CT pulmonary angiography (CTPA); and
- Patients with high pretest probability should undergo CTPA (or V/Q scan if CTPA is contraindicated) without d-dimer testing.
Bottom line: In suspected acute PE, first determine pretest probability using Wells and Revised Geneva, and then use this probability in conjunction with the PERC and d-dimer (as indicated) to guide decisions about imaging.
Citation: Raja AS, Greenberg JO, Qaseem A, Denberg TD, Fitterman N, Schuur JD. Evaluation of patients with suspected acute pulmonary embolism: best practice advice from the clinical guidelines committee of the American College of Physicians. Ann Intern Med. 2015;163(9):701-711.
Clinical question: What are best practices for evaluating patients with suspected acute pulmonary embolism (PE)?
Background: Use of CT in the evaluation of PE has increased across all clinical settings without improving mortality. Contrast CT carries the risks of radiation exposure, contrast-induced nephropathy, and incidental findings that require further investigation. The authors highlight evidence-based strategies for evaluation of PE, focusing on delivering high-value care.
Study design: Clinical guideline.
Setting: Literature review of studies across all adult clinical settings.
Synopsis: The clinical guidelines committee of the American College of Physicians conducted a literature search surrounding evaluation of suspected acute PE. From their review, they concluded:
- Pretest probability should initially be determined based on validated prediction tools (Wells score, Revised Geneva);
- In patients found to have low pretest probability and meeting the pulmonary embolism rule-out criteria (PERC), clinicians can forego d-dimer testing;
- In those with intermediate pretest probability or those with low pre-test probability who do not pass PERC, d-dimer measurement should be obtained;
- The d-dimer threshold should be age adjusted and imaging should not be pursued in patients whose d-dimer level falls below this cutoff, while those with positive d-dimers should receive CT pulmonary angiography (CTPA); and
- Patients with high pretest probability should undergo CTPA (or V/Q scan if CTPA is contraindicated) without d-dimer testing.
Bottom line: In suspected acute PE, first determine pretest probability using Wells and Revised Geneva, and then use this probability in conjunction with the PERC and d-dimer (as indicated) to guide decisions about imaging.
Citation: Raja AS, Greenberg JO, Qaseem A, Denberg TD, Fitterman N, Schuur JD. Evaluation of patients with suspected acute pulmonary embolism: best practice advice from the clinical guidelines committee of the American College of Physicians. Ann Intern Med. 2015;163(9):701-711.
Early Palliative Care Can Save Money
Clinical question: Does time to consult after admission change the effect palliative care consultation has on cost of care?
Background: Studies have shown that early palliative care involvement improves quality of life and survival among cancer patients while reducing the cost of care. Little is known about the optimal timing of palliative care consultation and its effect on cost.
Study design: Prospective, observational study.
Setting: Multi-site, high-volume, tertiary care hospitals with established palliative care teams.
Synopsis: Clinical and cost data were collected for 969 adult patients with advanced cancer admitted to the five participating hospitals. Among those, 256 patients received palliative care consultation and 713 received usual care. Subsamples were created based on time to consultation after admission.
The study found that earlier consultation yielded larger effects on cost savings. There was a 24% reduction in total cost if consultation occurred within two days (95% CI, -$3,438 to -$1,122; P<0.001), with estimated savings of $2,280. For consultation within six days of admission, there was a $1,312 savings (95% CI, -$2,568 to -$ 1,122; P<0.04), consistent with a 14% reduction in total cost.
There are notable limitations to this study. Half of eligible patients were excluded due to incomplete data collection, resulting in a small sample size. Further, these results can be generalized only to inpatients with advanced cancer.
Bottom line: Reducing the time to consultation with palliative care increases cost savings. In advanced cancer patients, a 24% reduction in total costs was realized for consultation within two days following admission.
Citation: May P, Garrido MM, Cassel JB, et al. Prospective cohort study of hospital palliative care teams for inpatients with advanced cancer: earlier consultation is associated with larger cost-saving effect. J Clin Oncol. 2015;33(25):2745-2752.
Clinical question: Does time to consult after admission change the effect palliative care consultation has on cost of care?
Background: Studies have shown that early palliative care involvement improves quality of life and survival among cancer patients while reducing the cost of care. Little is known about the optimal timing of palliative care consultation and its effect on cost.
Study design: Prospective, observational study.
Setting: Multi-site, high-volume, tertiary care hospitals with established palliative care teams.
Synopsis: Clinical and cost data were collected for 969 adult patients with advanced cancer admitted to the five participating hospitals. Among those, 256 patients received palliative care consultation and 713 received usual care. Subsamples were created based on time to consultation after admission.
The study found that earlier consultation yielded larger effects on cost savings. There was a 24% reduction in total cost if consultation occurred within two days (95% CI, -$3,438 to -$1,122; P<0.001), with estimated savings of $2,280. For consultation within six days of admission, there was a $1,312 savings (95% CI, -$2,568 to -$ 1,122; P<0.04), consistent with a 14% reduction in total cost.
There are notable limitations to this study. Half of eligible patients were excluded due to incomplete data collection, resulting in a small sample size. Further, these results can be generalized only to inpatients with advanced cancer.
Bottom line: Reducing the time to consultation with palliative care increases cost savings. In advanced cancer patients, a 24% reduction in total costs was realized for consultation within two days following admission.
Citation: May P, Garrido MM, Cassel JB, et al. Prospective cohort study of hospital palliative care teams for inpatients with advanced cancer: earlier consultation is associated with larger cost-saving effect. J Clin Oncol. 2015;33(25):2745-2752.
Clinical question: Does time to consult after admission change the effect palliative care consultation has on cost of care?
Background: Studies have shown that early palliative care involvement improves quality of life and survival among cancer patients while reducing the cost of care. Little is known about the optimal timing of palliative care consultation and its effect on cost.
Study design: Prospective, observational study.
Setting: Multi-site, high-volume, tertiary care hospitals with established palliative care teams.
Synopsis: Clinical and cost data were collected for 969 adult patients with advanced cancer admitted to the five participating hospitals. Among those, 256 patients received palliative care consultation and 713 received usual care. Subsamples were created based on time to consultation after admission.
The study found that earlier consultation yielded larger effects on cost savings. There was a 24% reduction in total cost if consultation occurred within two days (95% CI, -$3,438 to -$1,122; P<0.001), with estimated savings of $2,280. For consultation within six days of admission, there was a $1,312 savings (95% CI, -$2,568 to -$ 1,122; P<0.04), consistent with a 14% reduction in total cost.
There are notable limitations to this study. Half of eligible patients were excluded due to incomplete data collection, resulting in a small sample size. Further, these results can be generalized only to inpatients with advanced cancer.
Bottom line: Reducing the time to consultation with palliative care increases cost savings. In advanced cancer patients, a 24% reduction in total costs was realized for consultation within two days following admission.
Citation: May P, Garrido MM, Cassel JB, et al. Prospective cohort study of hospital palliative care teams for inpatients with advanced cancer: earlier consultation is associated with larger cost-saving effect. J Clin Oncol. 2015;33(25):2745-2752.