User login
Treating Acne During Pregnancy and Lactation
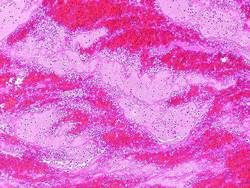
Acne during pregnancy and lactation is common and poses a considerable treatment challenge for dermatologists. It is a disease that often is trivialized, viewed by the ill informed as cosmetic in nature. Combined with fetal and neonatal health concerns plus a healthy dose of medicolegal overlay, treatment of acne in this patient population may be complicated.
Pregnant and lactating women have been summarily orphaned from advances in drug therapy. Due to, in no small part, the pervasive litigious atmosphere surrounding birth defects in pregnancy, many health care providers have defaulted to avoiding all medications in this patient population to be “on the safe side,” and many have convinced pregnant women that taking medication to relieve pain and discomfort while pregnant is selfish and vain, especially where acne is concerned. However, erring on the safe side is not always safe. Drug avoidance can lead to increased physical and psychiatric morbidity.
Numerous studies have shown that acne is not trivial or inconsequential and may even be associated with suicidal ideations.1,2 In one study, female gender and acne were both jointly and independently associated with the risk for major depression and suicide.3 The traditional notion that pregnancy is a time of joy and emotional well-being is not supported by data. There is a marked increase of mood instability during pregnancy. According to the American Psychological Association, the incidence of true clinical postpartum depression in the United States is 1 in 7 pregnancies but is likely much higher, as it often remains undiagnosed.4 These women may consider suicide and may even harm their children. Therefore, “first, do no harm” might indeed involve aggressive therapy in this patient population; at the very least, it warrants a thorough consideration of the risks and benefits rather than a knee-jerk “wait until you stop breastfeeding” default. Without adequate knowledge of true drug risks and with the stakes so high, we find ourselves in medicolegal quicksand. As clinicians, we understand the concept of weighing risks and benefits, but the balance of the scale cannot be determined when no evidence exists regarding the relative weight of the risk side.
Most drug risks in pregnancy are noted after market approval and are obtained from published case reports and retrospective birth defect registries. Reported problems likely represent a small fraction of actual cases. The absence of direct information regarding drug use during pregnancy is exacerbated by the knowledge that there are large gender differences in drug pharmacokinetics. This dichotomy would be expected to be especially pronounced between men and pregnant women in whom drug absorption, distribution, and elimination are all notably altered. A poorly publicized aberration in the drug approval process is that gender information is not required from generic medication bioequivalence studies. Although studies for drugs indicated for both sexes need to include male and female participants, resulting data showing gender differences are not required to be disclosed, which means that it is theoretically possible for a generic drug to be approved based on results in men only.
The pregnancy categories for drugs (A, B, C, D, and X), which were initially defined in 1979, have been our only aid in risk assessment but have little clinical relevance beyond defining the level of medicolegal risk. Furthermore, these drug categories are poised to disappear before the publication of this editorial, as new guidelines for labeling human prescription drugs are mandated to begin on June 30, 2015.5 Although guaranteed to be confusing at first, it seems the new labeling guidelines will be much more helpful for clinicians. One of the most important changes is the inclusion of the following statement in pregnancy and lactation subsections on drug labels: “All pregnancies have a background risk of birth defect, loss, or other adverse outcome regardless of drug exposure. The fetal risk summary below describes (name of drug)’s potential to increase the risk of developmental abnormalities above the background risk.”5 In the absence of concerning human data, efforts will be made to put positive animal data into perspective. In the absence of systemic exposure the label will state: “(Name of drug) is not absorbed systemically from (part of body) and cannot be detected in the blood. Maternal use is not expected to result in fetal exposure to the drug.”5 This final rule includes virtually all topical acne products, including topical retinoids.
As weak as the evidence-based risk information is for drugs in pregnancy, it is worse for lactation. It is a commonly mistaken belief among practitioners that the safety, or lack thereof, of medications during pregnancy indicates safety during lactation. In actuality, decisions should instead be based on safety data on the drug during the neonatal period. Levels of neonatal drug exposure through breast milk is 5- to 10-fold less than fetal exposure in utero.6 Therefore, it generally is safer for women to take drugs during lactation than during pregnancy. For the most part, medications enter the breast milk by passive diffusion from the maternal bloodstream. Several hours after a medication is taken, maternal blood levels fall and drug from the breast milk flows back along the concentration gradient into the maternal circulation. Therefore, safety is maximized by administering maternal medications immediately after the last feed and just prior to the longest sleep period of the child, usually at night.
In the lactation section of the new labeling guidelines ruling, the verbiage is completely different and highly clinically relevant. If the data demonstrate that a drug does not affect the quantity and/or quality of human breast milk, the product label must state: “The use of (name of drug) is compatible with breastfeeding.”5 If the drug is not systemically absorbed, the label will state simply and clearly, “Breastfeeding is not expected to result in fetal exposure to the drug.” Therefore, if these labeling guidelines are followed, it appears that all topical acne medications will be interpreted as safe during lactation under the new guidelines.
Dermatologists have taken an oath to “first, do no harm,” but in the case of acne in pregnancy and especially in lactation, we may need to treat aggressively and push the envelope beyond our current category B medications. Erring on the side of caution may be the wrong approach, especially in lactation where psychological consequences are high and neonatal exposure is minimal. The new US Food and Drug Administration guidelines should be helpful in the process of risk assessment and aid us in discussing rational, thoughtful, practical approaches with our patients.
1. Halvorsen J, Stern R, Dalgard F, et al. Suicidal ideation, mental health problems and social impairment are increased in adolescents with acne: a population-based study. J Invest Dermatol. 2001;13:363-370.
2. Ramrakha S, Fergusson D, Horwood L, et al. Cumulative health consequences of acne: 23-year follow-up in a general population birth cohort study [published online ahead of print March 27, 2015]. Br J Dermatol. doi:10.1111/bjd.13786.
3. Yang YC, Tu HP, Hong CH, et al. Female gender and acne disease are jointly and independently associated with the risk of major depression and suicide: a national population-based study [published online ahead of print February 11, 2014]. Biomed Res Int. 2014;2014:504279.
4. Postpartum depression. American Psychological Association Web site. http://www.apa.org/pi/women/programs/depression/postpartum.aspx. Accessed June 20, 2015.
5. Content and format of labeling for human prescription drugs and biologics; requirements for pregnancy and lactation labeling. Fed Regist. 2004;79(233):72064-72103. To be codified at 21 CFR §201.
6. Wright-Hale T, Rowe HE, eds. Medications and Mother’s Milk. 3rd ed. Plano, TX: Hale Publishing; 2008.
Acne during pregnancy and lactation is common and poses a considerable treatment challenge for dermatologists. It is a disease that often is trivialized, viewed by the ill informed as cosmetic in nature. Combined with fetal and neonatal health concerns plus a healthy dose of medicolegal overlay, treatment of acne in this patient population may be complicated.
Pregnant and lactating women have been summarily orphaned from advances in drug therapy. Due to, in no small part, the pervasive litigious atmosphere surrounding birth defects in pregnancy, many health care providers have defaulted to avoiding all medications in this patient population to be “on the safe side,” and many have convinced pregnant women that taking medication to relieve pain and discomfort while pregnant is selfish and vain, especially where acne is concerned. However, erring on the safe side is not always safe. Drug avoidance can lead to increased physical and psychiatric morbidity.
Numerous studies have shown that acne is not trivial or inconsequential and may even be associated with suicidal ideations.1,2 In one study, female gender and acne were both jointly and independently associated with the risk for major depression and suicide.3 The traditional notion that pregnancy is a time of joy and emotional well-being is not supported by data. There is a marked increase of mood instability during pregnancy. According to the American Psychological Association, the incidence of true clinical postpartum depression in the United States is 1 in 7 pregnancies but is likely much higher, as it often remains undiagnosed.4 These women may consider suicide and may even harm their children. Therefore, “first, do no harm” might indeed involve aggressive therapy in this patient population; at the very least, it warrants a thorough consideration of the risks and benefits rather than a knee-jerk “wait until you stop breastfeeding” default. Without adequate knowledge of true drug risks and with the stakes so high, we find ourselves in medicolegal quicksand. As clinicians, we understand the concept of weighing risks and benefits, but the balance of the scale cannot be determined when no evidence exists regarding the relative weight of the risk side.
Most drug risks in pregnancy are noted after market approval and are obtained from published case reports and retrospective birth defect registries. Reported problems likely represent a small fraction of actual cases. The absence of direct information regarding drug use during pregnancy is exacerbated by the knowledge that there are large gender differences in drug pharmacokinetics. This dichotomy would be expected to be especially pronounced between men and pregnant women in whom drug absorption, distribution, and elimination are all notably altered. A poorly publicized aberration in the drug approval process is that gender information is not required from generic medication bioequivalence studies. Although studies for drugs indicated for both sexes need to include male and female participants, resulting data showing gender differences are not required to be disclosed, which means that it is theoretically possible for a generic drug to be approved based on results in men only.
The pregnancy categories for drugs (A, B, C, D, and X), which were initially defined in 1979, have been our only aid in risk assessment but have little clinical relevance beyond defining the level of medicolegal risk. Furthermore, these drug categories are poised to disappear before the publication of this editorial, as new guidelines for labeling human prescription drugs are mandated to begin on June 30, 2015.5 Although guaranteed to be confusing at first, it seems the new labeling guidelines will be much more helpful for clinicians. One of the most important changes is the inclusion of the following statement in pregnancy and lactation subsections on drug labels: “All pregnancies have a background risk of birth defect, loss, or other adverse outcome regardless of drug exposure. The fetal risk summary below describes (name of drug)’s potential to increase the risk of developmental abnormalities above the background risk.”5 In the absence of concerning human data, efforts will be made to put positive animal data into perspective. In the absence of systemic exposure the label will state: “(Name of drug) is not absorbed systemically from (part of body) and cannot be detected in the blood. Maternal use is not expected to result in fetal exposure to the drug.”5 This final rule includes virtually all topical acne products, including topical retinoids.
As weak as the evidence-based risk information is for drugs in pregnancy, it is worse for lactation. It is a commonly mistaken belief among practitioners that the safety, or lack thereof, of medications during pregnancy indicates safety during lactation. In actuality, decisions should instead be based on safety data on the drug during the neonatal period. Levels of neonatal drug exposure through breast milk is 5- to 10-fold less than fetal exposure in utero.6 Therefore, it generally is safer for women to take drugs during lactation than during pregnancy. For the most part, medications enter the breast milk by passive diffusion from the maternal bloodstream. Several hours after a medication is taken, maternal blood levels fall and drug from the breast milk flows back along the concentration gradient into the maternal circulation. Therefore, safety is maximized by administering maternal medications immediately after the last feed and just prior to the longest sleep period of the child, usually at night.
In the lactation section of the new labeling guidelines ruling, the verbiage is completely different and highly clinically relevant. If the data demonstrate that a drug does not affect the quantity and/or quality of human breast milk, the product label must state: “The use of (name of drug) is compatible with breastfeeding.”5 If the drug is not systemically absorbed, the label will state simply and clearly, “Breastfeeding is not expected to result in fetal exposure to the drug.” Therefore, if these labeling guidelines are followed, it appears that all topical acne medications will be interpreted as safe during lactation under the new guidelines.
Dermatologists have taken an oath to “first, do no harm,” but in the case of acne in pregnancy and especially in lactation, we may need to treat aggressively and push the envelope beyond our current category B medications. Erring on the side of caution may be the wrong approach, especially in lactation where psychological consequences are high and neonatal exposure is minimal. The new US Food and Drug Administration guidelines should be helpful in the process of risk assessment and aid us in discussing rational, thoughtful, practical approaches with our patients.
Acne during pregnancy and lactation is common and poses a considerable treatment challenge for dermatologists. It is a disease that often is trivialized, viewed by the ill informed as cosmetic in nature. Combined with fetal and neonatal health concerns plus a healthy dose of medicolegal overlay, treatment of acne in this patient population may be complicated.
Pregnant and lactating women have been summarily orphaned from advances in drug therapy. Due to, in no small part, the pervasive litigious atmosphere surrounding birth defects in pregnancy, many health care providers have defaulted to avoiding all medications in this patient population to be “on the safe side,” and many have convinced pregnant women that taking medication to relieve pain and discomfort while pregnant is selfish and vain, especially where acne is concerned. However, erring on the safe side is not always safe. Drug avoidance can lead to increased physical and psychiatric morbidity.
Numerous studies have shown that acne is not trivial or inconsequential and may even be associated with suicidal ideations.1,2 In one study, female gender and acne were both jointly and independently associated with the risk for major depression and suicide.3 The traditional notion that pregnancy is a time of joy and emotional well-being is not supported by data. There is a marked increase of mood instability during pregnancy. According to the American Psychological Association, the incidence of true clinical postpartum depression in the United States is 1 in 7 pregnancies but is likely much higher, as it often remains undiagnosed.4 These women may consider suicide and may even harm their children. Therefore, “first, do no harm” might indeed involve aggressive therapy in this patient population; at the very least, it warrants a thorough consideration of the risks and benefits rather than a knee-jerk “wait until you stop breastfeeding” default. Without adequate knowledge of true drug risks and with the stakes so high, we find ourselves in medicolegal quicksand. As clinicians, we understand the concept of weighing risks and benefits, but the balance of the scale cannot be determined when no evidence exists regarding the relative weight of the risk side.
Most drug risks in pregnancy are noted after market approval and are obtained from published case reports and retrospective birth defect registries. Reported problems likely represent a small fraction of actual cases. The absence of direct information regarding drug use during pregnancy is exacerbated by the knowledge that there are large gender differences in drug pharmacokinetics. This dichotomy would be expected to be especially pronounced between men and pregnant women in whom drug absorption, distribution, and elimination are all notably altered. A poorly publicized aberration in the drug approval process is that gender information is not required from generic medication bioequivalence studies. Although studies for drugs indicated for both sexes need to include male and female participants, resulting data showing gender differences are not required to be disclosed, which means that it is theoretically possible for a generic drug to be approved based on results in men only.
The pregnancy categories for drugs (A, B, C, D, and X), which were initially defined in 1979, have been our only aid in risk assessment but have little clinical relevance beyond defining the level of medicolegal risk. Furthermore, these drug categories are poised to disappear before the publication of this editorial, as new guidelines for labeling human prescription drugs are mandated to begin on June 30, 2015.5 Although guaranteed to be confusing at first, it seems the new labeling guidelines will be much more helpful for clinicians. One of the most important changes is the inclusion of the following statement in pregnancy and lactation subsections on drug labels: “All pregnancies have a background risk of birth defect, loss, or other adverse outcome regardless of drug exposure. The fetal risk summary below describes (name of drug)’s potential to increase the risk of developmental abnormalities above the background risk.”5 In the absence of concerning human data, efforts will be made to put positive animal data into perspective. In the absence of systemic exposure the label will state: “(Name of drug) is not absorbed systemically from (part of body) and cannot be detected in the blood. Maternal use is not expected to result in fetal exposure to the drug.”5 This final rule includes virtually all topical acne products, including topical retinoids.
As weak as the evidence-based risk information is for drugs in pregnancy, it is worse for lactation. It is a commonly mistaken belief among practitioners that the safety, or lack thereof, of medications during pregnancy indicates safety during lactation. In actuality, decisions should instead be based on safety data on the drug during the neonatal period. Levels of neonatal drug exposure through breast milk is 5- to 10-fold less than fetal exposure in utero.6 Therefore, it generally is safer for women to take drugs during lactation than during pregnancy. For the most part, medications enter the breast milk by passive diffusion from the maternal bloodstream. Several hours after a medication is taken, maternal blood levels fall and drug from the breast milk flows back along the concentration gradient into the maternal circulation. Therefore, safety is maximized by administering maternal medications immediately after the last feed and just prior to the longest sleep period of the child, usually at night.
In the lactation section of the new labeling guidelines ruling, the verbiage is completely different and highly clinically relevant. If the data demonstrate that a drug does not affect the quantity and/or quality of human breast milk, the product label must state: “The use of (name of drug) is compatible with breastfeeding.”5 If the drug is not systemically absorbed, the label will state simply and clearly, “Breastfeeding is not expected to result in fetal exposure to the drug.” Therefore, if these labeling guidelines are followed, it appears that all topical acne medications will be interpreted as safe during lactation under the new guidelines.
Dermatologists have taken an oath to “first, do no harm,” but in the case of acne in pregnancy and especially in lactation, we may need to treat aggressively and push the envelope beyond our current category B medications. Erring on the side of caution may be the wrong approach, especially in lactation where psychological consequences are high and neonatal exposure is minimal. The new US Food and Drug Administration guidelines should be helpful in the process of risk assessment and aid us in discussing rational, thoughtful, practical approaches with our patients.
1. Halvorsen J, Stern R, Dalgard F, et al. Suicidal ideation, mental health problems and social impairment are increased in adolescents with acne: a population-based study. J Invest Dermatol. 2001;13:363-370.
2. Ramrakha S, Fergusson D, Horwood L, et al. Cumulative health consequences of acne: 23-year follow-up in a general population birth cohort study [published online ahead of print March 27, 2015]. Br J Dermatol. doi:10.1111/bjd.13786.
3. Yang YC, Tu HP, Hong CH, et al. Female gender and acne disease are jointly and independently associated with the risk of major depression and suicide: a national population-based study [published online ahead of print February 11, 2014]. Biomed Res Int. 2014;2014:504279.
4. Postpartum depression. American Psychological Association Web site. http://www.apa.org/pi/women/programs/depression/postpartum.aspx. Accessed June 20, 2015.
5. Content and format of labeling for human prescription drugs and biologics; requirements for pregnancy and lactation labeling. Fed Regist. 2004;79(233):72064-72103. To be codified at 21 CFR §201.
6. Wright-Hale T, Rowe HE, eds. Medications and Mother’s Milk. 3rd ed. Plano, TX: Hale Publishing; 2008.
1. Halvorsen J, Stern R, Dalgard F, et al. Suicidal ideation, mental health problems and social impairment are increased in adolescents with acne: a population-based study. J Invest Dermatol. 2001;13:363-370.
2. Ramrakha S, Fergusson D, Horwood L, et al. Cumulative health consequences of acne: 23-year follow-up in a general population birth cohort study [published online ahead of print March 27, 2015]. Br J Dermatol. doi:10.1111/bjd.13786.
3. Yang YC, Tu HP, Hong CH, et al. Female gender and acne disease are jointly and independently associated with the risk of major depression and suicide: a national population-based study [published online ahead of print February 11, 2014]. Biomed Res Int. 2014;2014:504279.
4. Postpartum depression. American Psychological Association Web site. http://www.apa.org/pi/women/programs/depression/postpartum.aspx. Accessed June 20, 2015.
5. Content and format of labeling for human prescription drugs and biologics; requirements for pregnancy and lactation labeling. Fed Regist. 2004;79(233):72064-72103. To be codified at 21 CFR §201.
6. Wright-Hale T, Rowe HE, eds. Medications and Mother’s Milk. 3rd ed. Plano, TX: Hale Publishing; 2008.

Myth of the Month: Why can’t I give my patient hydrochlorothiazide?
A 56-year-old woman presents with hypertension. Her blood pressures have been about 160/100 mm Hg. Past medical history includes depression, GERD, and hypothyroidism, and the patient has an allergy to sulfamethoxazole (rash).
She receives a prescription for hydrochlorothiazide. The pharmacist calls later to report that the pharmacy did not fill the prescription because the patient has a sulfa allergy.
What would you recommend?
A. Call in a prescription for a calcium channel blocker.
B. Call in a prescription for an ACE inhibitor.
C. Call in a prescription for a beta-blocker.
D. Call and ask the pharmacist to fill the hydrochlorothiazide prescription.
I have received this call from pharmacies many times. The patients are usually very frustrated because they could not pick up their medications. Is this the right call from the pharmacist? Does the fact that the patient has a sulfa allergy make prescribing hydrochlorothiazide wrong?
Allergies to sulfonamide antibiotics occur in about 3% of patients who are prescribed the drugs. Sulfa-containing antibiotics contain a five- or six-member nitrogen-containing ring attached to the N1 nitrogen of the sulfonamide group and an arylamine group (H2N) at the N4 position of the sulfonamide group (Pharmacotherapy 2004;24:856-70). Sulfa-containing nonantibiotics – including thiazides and loop diuretics, as well as COX-2 inhibitors – do not contain these same features.
There has always been concern that there is a possibility of increased risk of drug reactions in patients who receive a sulfa nonantibiotic, and frequently prescriptions for these medicines are not filled by pharmacies without directly confirming the intent by speaking with the prescriber.
Brian Hemstreet, Pharm.D., and Robert Page II, Pharm.D., did a prospective, observational study of patients admitted to a hospital with a history of sulfa allergy (Pharmacotherapy 2006;26:551-7). A total of 94 patients were studied who had a reported sulfa allergy. Forty of these patients were taking a sulfonamide nonantibiotic at the time of admission (most commonly furosemide). Nine of the patients received a sulfonamide nonantibiotic during their hospitalization. None of the patients had a drug reaction, either while receiving a sulfonamide nonantibiotic in the hospital, or previously while receiving one as an outpatient.
Dr. Pilar Tornero and colleagues used patch testing and control oral challenge in patients with previous fixed drug eruptions to trimethoprim-sulfamethoxazole or an unknown sulfonamide (Contact Dermatitis 2004;51:57-62). All patients received low doses of oral sulfonamide antibiotics (trimethoprim-sulfamethoxazole, sulfadiazine, or sulfamethizole). All patients also received furosemide.
Every patient with previous known sulfa reaction had a positive oral challenge test when given sulfamethoxazole. There was cross reactivity with other sulfa antibiotics: Seven of 18 patients with prior sulfamethoxazole allergy reacted to oral challenge with sulfadiazine, and 4 of 9 patients with prior allergy with sulfamethoxazole reacted to challenge with sulfamethazine. All 28 patients in the study were challenged with furosemide (a sulfa nonantibiotic) with no allergic reactions.
Dr. Brian Strom and colleagues conducted a retrospective cohort study using general practice research database, looking at risk of allergic reactions within 30 days of receipt of a sulfonamide nonantibiotic (N. Engl. J. Med. 2003;349:1628-35).
Patients who had a history of prior hypersensitivity to a sulfonamide antibiotic were compared with those with no previous history of allergy. Analyses were also performed in patients with a prior penicillin allergy. A total of 969 patients who had an allergic reaction after a sulfonamide antibiotic were evaluated.
Of those patients, 9.1% had an allergic reaction after receiving a sulfonamide nonantibiotic. In those patients without a sulfa antibiotic allergy, only 1.6% had a reaction to a sulfa nonantibiotic. Interestingly, in patients with a prior history of penicillin reaction, 14.6% had an allergic reaction when receiving a sulfa nonantibiotic.
Patients with a history of sulfa allergy to a sulfa antibiotic are more likely to have a reaction to a sulfa nonantibiotic than are those without a previous allergy history. But this appears to be due to overall increased reactiveness and not a cross reactivity, because those with history of penicillin allergy had an even higher allergy rate to sulfa nonantibiotics than did patients with a prior sulfa allergy.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at [email protected].
A 56-year-old woman presents with hypertension. Her blood pressures have been about 160/100 mm Hg. Past medical history includes depression, GERD, and hypothyroidism, and the patient has an allergy to sulfamethoxazole (rash).
She receives a prescription for hydrochlorothiazide. The pharmacist calls later to report that the pharmacy did not fill the prescription because the patient has a sulfa allergy.
What would you recommend?
A. Call in a prescription for a calcium channel blocker.
B. Call in a prescription for an ACE inhibitor.
C. Call in a prescription for a beta-blocker.
D. Call and ask the pharmacist to fill the hydrochlorothiazide prescription.
I have received this call from pharmacies many times. The patients are usually very frustrated because they could not pick up their medications. Is this the right call from the pharmacist? Does the fact that the patient has a sulfa allergy make prescribing hydrochlorothiazide wrong?
Allergies to sulfonamide antibiotics occur in about 3% of patients who are prescribed the drugs. Sulfa-containing antibiotics contain a five- or six-member nitrogen-containing ring attached to the N1 nitrogen of the sulfonamide group and an arylamine group (H2N) at the N4 position of the sulfonamide group (Pharmacotherapy 2004;24:856-70). Sulfa-containing nonantibiotics – including thiazides and loop diuretics, as well as COX-2 inhibitors – do not contain these same features.
There has always been concern that there is a possibility of increased risk of drug reactions in patients who receive a sulfa nonantibiotic, and frequently prescriptions for these medicines are not filled by pharmacies without directly confirming the intent by speaking with the prescriber.
Brian Hemstreet, Pharm.D., and Robert Page II, Pharm.D., did a prospective, observational study of patients admitted to a hospital with a history of sulfa allergy (Pharmacotherapy 2006;26:551-7). A total of 94 patients were studied who had a reported sulfa allergy. Forty of these patients were taking a sulfonamide nonantibiotic at the time of admission (most commonly furosemide). Nine of the patients received a sulfonamide nonantibiotic during their hospitalization. None of the patients had a drug reaction, either while receiving a sulfonamide nonantibiotic in the hospital, or previously while receiving one as an outpatient.
Dr. Pilar Tornero and colleagues used patch testing and control oral challenge in patients with previous fixed drug eruptions to trimethoprim-sulfamethoxazole or an unknown sulfonamide (Contact Dermatitis 2004;51:57-62). All patients received low doses of oral sulfonamide antibiotics (trimethoprim-sulfamethoxazole, sulfadiazine, or sulfamethizole). All patients also received furosemide.
Every patient with previous known sulfa reaction had a positive oral challenge test when given sulfamethoxazole. There was cross reactivity with other sulfa antibiotics: Seven of 18 patients with prior sulfamethoxazole allergy reacted to oral challenge with sulfadiazine, and 4 of 9 patients with prior allergy with sulfamethoxazole reacted to challenge with sulfamethazine. All 28 patients in the study were challenged with furosemide (a sulfa nonantibiotic) with no allergic reactions.
Dr. Brian Strom and colleagues conducted a retrospective cohort study using general practice research database, looking at risk of allergic reactions within 30 days of receipt of a sulfonamide nonantibiotic (N. Engl. J. Med. 2003;349:1628-35).
Patients who had a history of prior hypersensitivity to a sulfonamide antibiotic were compared with those with no previous history of allergy. Analyses were also performed in patients with a prior penicillin allergy. A total of 969 patients who had an allergic reaction after a sulfonamide antibiotic were evaluated.
Of those patients, 9.1% had an allergic reaction after receiving a sulfonamide nonantibiotic. In those patients without a sulfa antibiotic allergy, only 1.6% had a reaction to a sulfa nonantibiotic. Interestingly, in patients with a prior history of penicillin reaction, 14.6% had an allergic reaction when receiving a sulfa nonantibiotic.
Patients with a history of sulfa allergy to a sulfa antibiotic are more likely to have a reaction to a sulfa nonantibiotic than are those without a previous allergy history. But this appears to be due to overall increased reactiveness and not a cross reactivity, because those with history of penicillin allergy had an even higher allergy rate to sulfa nonantibiotics than did patients with a prior sulfa allergy.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at [email protected].
A 56-year-old woman presents with hypertension. Her blood pressures have been about 160/100 mm Hg. Past medical history includes depression, GERD, and hypothyroidism, and the patient has an allergy to sulfamethoxazole (rash).
She receives a prescription for hydrochlorothiazide. The pharmacist calls later to report that the pharmacy did not fill the prescription because the patient has a sulfa allergy.
What would you recommend?
A. Call in a prescription for a calcium channel blocker.
B. Call in a prescription for an ACE inhibitor.
C. Call in a prescription for a beta-blocker.
D. Call and ask the pharmacist to fill the hydrochlorothiazide prescription.
I have received this call from pharmacies many times. The patients are usually very frustrated because they could not pick up their medications. Is this the right call from the pharmacist? Does the fact that the patient has a sulfa allergy make prescribing hydrochlorothiazide wrong?
Allergies to sulfonamide antibiotics occur in about 3% of patients who are prescribed the drugs. Sulfa-containing antibiotics contain a five- or six-member nitrogen-containing ring attached to the N1 nitrogen of the sulfonamide group and an arylamine group (H2N) at the N4 position of the sulfonamide group (Pharmacotherapy 2004;24:856-70). Sulfa-containing nonantibiotics – including thiazides and loop diuretics, as well as COX-2 inhibitors – do not contain these same features.
There has always been concern that there is a possibility of increased risk of drug reactions in patients who receive a sulfa nonantibiotic, and frequently prescriptions for these medicines are not filled by pharmacies without directly confirming the intent by speaking with the prescriber.
Brian Hemstreet, Pharm.D., and Robert Page II, Pharm.D., did a prospective, observational study of patients admitted to a hospital with a history of sulfa allergy (Pharmacotherapy 2006;26:551-7). A total of 94 patients were studied who had a reported sulfa allergy. Forty of these patients were taking a sulfonamide nonantibiotic at the time of admission (most commonly furosemide). Nine of the patients received a sulfonamide nonantibiotic during their hospitalization. None of the patients had a drug reaction, either while receiving a sulfonamide nonantibiotic in the hospital, or previously while receiving one as an outpatient.
Dr. Pilar Tornero and colleagues used patch testing and control oral challenge in patients with previous fixed drug eruptions to trimethoprim-sulfamethoxazole or an unknown sulfonamide (Contact Dermatitis 2004;51:57-62). All patients received low doses of oral sulfonamide antibiotics (trimethoprim-sulfamethoxazole, sulfadiazine, or sulfamethizole). All patients also received furosemide.
Every patient with previous known sulfa reaction had a positive oral challenge test when given sulfamethoxazole. There was cross reactivity with other sulfa antibiotics: Seven of 18 patients with prior sulfamethoxazole allergy reacted to oral challenge with sulfadiazine, and 4 of 9 patients with prior allergy with sulfamethoxazole reacted to challenge with sulfamethazine. All 28 patients in the study were challenged with furosemide (a sulfa nonantibiotic) with no allergic reactions.
Dr. Brian Strom and colleagues conducted a retrospective cohort study using general practice research database, looking at risk of allergic reactions within 30 days of receipt of a sulfonamide nonantibiotic (N. Engl. J. Med. 2003;349:1628-35).
Patients who had a history of prior hypersensitivity to a sulfonamide antibiotic were compared with those with no previous history of allergy. Analyses were also performed in patients with a prior penicillin allergy. A total of 969 patients who had an allergic reaction after a sulfonamide antibiotic were evaluated.
Of those patients, 9.1% had an allergic reaction after receiving a sulfonamide nonantibiotic. In those patients without a sulfa antibiotic allergy, only 1.6% had a reaction to a sulfa nonantibiotic. Interestingly, in patients with a prior history of penicillin reaction, 14.6% had an allergic reaction when receiving a sulfa nonantibiotic.
Patients with a history of sulfa allergy to a sulfa antibiotic are more likely to have a reaction to a sulfa nonantibiotic than are those without a previous allergy history. But this appears to be due to overall increased reactiveness and not a cross reactivity, because those with history of penicillin allergy had an even higher allergy rate to sulfa nonantibiotics than did patients with a prior sulfa allergy.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at [email protected].

Index discriminates prognostic groups in CLL
An international prognostic index for patients with chronic lymphocytic leukemia (CLL) may help to inform treatment decisions, based on a meta-analysis presented at the International Congress on Malignant Lymphoma in Lugano, Switzerland.
The International Prognostic Index for patients with CLL (CLL-IPI) combines the most important genetic risk factors and traditional clinical stage, age, and serum beta-2-microglobulin measures. By discriminating between prognostic groups, the index may aid in informing treatment of CLL patients, Dr. Jasmin Bahlo of the University Hospital Cologne, Köln, Germany, said.
The CLL-IPI consists of five risk factors – age, clinical stage, IgHV (immunoglobulin heavy-chain variable-region) gene mutation status, serum beta-2-microglobulin measure, and the presence of del(17p) and/or TP53 mutation, Dr. Bahlo said.
To develop the index, Dr. Bahlo and colleagues performed an analysis of 26 possible prognostic factors by using data from eight phase III trials from France, Germany, the United Kingdom, the United States, and Poland. The data included a full analysis set of 3,742 previously untreated patients at early and advanced stages of disease. The median age of the patients was 61 years, the median observation time was 80 months, and the main endpoint was overall survival.
From the 26 variables, the researchers identified five independent predictors for overall survival: age (65 years or more), clinical stage (Binet A/Rai 0 vs. Binet B-C/Rai I-IV), del(17p) and/or TP53 mutation status, IgHV mutation status, and serum beta-2-microglobulin measure (3.5 mg/L or more).
The index was used to identify four risk groups – low risk (score 0-1), intermediate (score 2-3), high (score 4-6), and very high (score 7-10)) – with significantly different overall survival rates at 5 years of 93%, 79%, 64%, and 23%, respectively.
The value of the index was then confirmed in 575 patients, with a 5-year overall survival rate of 91%, 80%, 52%, and 19%, respectively.
Similar findings were seen in an external data set of patients from the Mayo Clinic data set, with 5-year overall survivals of 97%, 91%, 68%, and 21%, respectively. The CLL-IPI also provided accurate estimation regarding time to first treatment; 81%, 47%, 30%, and 19% of patients in the respective risk groups were free from treatment at 5 years.
In the era of more effective treatments for CLL, the established clinical staging systems (Rai and Binet) do not accurately discriminate between prognostic groups because they do not integrate the major clinical, biologic, and genetic variables into one widely accepted prognostic system, Dr. Bahlo noted. The CLL-IPI is, therefore, an important contribution to management of this condition.
The researchers had no relevant financial disclosures.
Until very recently, most treatment decisions in CLL have been based on age, overall fitness of the patient and presence of cytopenias. Biologic prognostic markers have been delineated, but not acted upon, with the recent exception of del17p given the advent of effective novel agents in this setting. This is an admirable attempt to establish a better prognostic index, building upon prior German CLL group data (Pflug et al Blood 2014), but it has limitations. It is a weighted score, heavily dependent on p53 mutation/del17p, which is uncommon at initial diagnosis, and today such patients should be receiving a targeted agent. It would be useful to have a CLL-IPI for patients without del17p. Further, while its ability to predict time to require therapy will remain useful, its survival predictions are likely already outdated given the array of new agents already, or soon to be, available.
Until very recently, most treatment decisions in CLL have been based on age, overall fitness of the patient and presence of cytopenias. Biologic prognostic markers have been delineated, but not acted upon, with the recent exception of del17p given the advent of effective novel agents in this setting. This is an admirable attempt to establish a better prognostic index, building upon prior German CLL group data (Pflug et al Blood 2014), but it has limitations. It is a weighted score, heavily dependent on p53 mutation/del17p, which is uncommon at initial diagnosis, and today such patients should be receiving a targeted agent. It would be useful to have a CLL-IPI for patients without del17p. Further, while its ability to predict time to require therapy will remain useful, its survival predictions are likely already outdated given the array of new agents already, or soon to be, available.
Until very recently, most treatment decisions in CLL have been based on age, overall fitness of the patient and presence of cytopenias. Biologic prognostic markers have been delineated, but not acted upon, with the recent exception of del17p given the advent of effective novel agents in this setting. This is an admirable attempt to establish a better prognostic index, building upon prior German CLL group data (Pflug et al Blood 2014), but it has limitations. It is a weighted score, heavily dependent on p53 mutation/del17p, which is uncommon at initial diagnosis, and today such patients should be receiving a targeted agent. It would be useful to have a CLL-IPI for patients without del17p. Further, while its ability to predict time to require therapy will remain useful, its survival predictions are likely already outdated given the array of new agents already, or soon to be, available.
An international prognostic index for patients with chronic lymphocytic leukemia (CLL) may help to inform treatment decisions, based on a meta-analysis presented at the International Congress on Malignant Lymphoma in Lugano, Switzerland.
The International Prognostic Index for patients with CLL (CLL-IPI) combines the most important genetic risk factors and traditional clinical stage, age, and serum beta-2-microglobulin measures. By discriminating between prognostic groups, the index may aid in informing treatment of CLL patients, Dr. Jasmin Bahlo of the University Hospital Cologne, Köln, Germany, said.
The CLL-IPI consists of five risk factors – age, clinical stage, IgHV (immunoglobulin heavy-chain variable-region) gene mutation status, serum beta-2-microglobulin measure, and the presence of del(17p) and/or TP53 mutation, Dr. Bahlo said.
To develop the index, Dr. Bahlo and colleagues performed an analysis of 26 possible prognostic factors by using data from eight phase III trials from France, Germany, the United Kingdom, the United States, and Poland. The data included a full analysis set of 3,742 previously untreated patients at early and advanced stages of disease. The median age of the patients was 61 years, the median observation time was 80 months, and the main endpoint was overall survival.
From the 26 variables, the researchers identified five independent predictors for overall survival: age (65 years or more), clinical stage (Binet A/Rai 0 vs. Binet B-C/Rai I-IV), del(17p) and/or TP53 mutation status, IgHV mutation status, and serum beta-2-microglobulin measure (3.5 mg/L or more).
The index was used to identify four risk groups – low risk (score 0-1), intermediate (score 2-3), high (score 4-6), and very high (score 7-10)) – with significantly different overall survival rates at 5 years of 93%, 79%, 64%, and 23%, respectively.
The value of the index was then confirmed in 575 patients, with a 5-year overall survival rate of 91%, 80%, 52%, and 19%, respectively.
Similar findings were seen in an external data set of patients from the Mayo Clinic data set, with 5-year overall survivals of 97%, 91%, 68%, and 21%, respectively. The CLL-IPI also provided accurate estimation regarding time to first treatment; 81%, 47%, 30%, and 19% of patients in the respective risk groups were free from treatment at 5 years.
In the era of more effective treatments for CLL, the established clinical staging systems (Rai and Binet) do not accurately discriminate between prognostic groups because they do not integrate the major clinical, biologic, and genetic variables into one widely accepted prognostic system, Dr. Bahlo noted. The CLL-IPI is, therefore, an important contribution to management of this condition.
The researchers had no relevant financial disclosures.
An international prognostic index for patients with chronic lymphocytic leukemia (CLL) may help to inform treatment decisions, based on a meta-analysis presented at the International Congress on Malignant Lymphoma in Lugano, Switzerland.
The International Prognostic Index for patients with CLL (CLL-IPI) combines the most important genetic risk factors and traditional clinical stage, age, and serum beta-2-microglobulin measures. By discriminating between prognostic groups, the index may aid in informing treatment of CLL patients, Dr. Jasmin Bahlo of the University Hospital Cologne, Köln, Germany, said.
The CLL-IPI consists of five risk factors – age, clinical stage, IgHV (immunoglobulin heavy-chain variable-region) gene mutation status, serum beta-2-microglobulin measure, and the presence of del(17p) and/or TP53 mutation, Dr. Bahlo said.
To develop the index, Dr. Bahlo and colleagues performed an analysis of 26 possible prognostic factors by using data from eight phase III trials from France, Germany, the United Kingdom, the United States, and Poland. The data included a full analysis set of 3,742 previously untreated patients at early and advanced stages of disease. The median age of the patients was 61 years, the median observation time was 80 months, and the main endpoint was overall survival.
From the 26 variables, the researchers identified five independent predictors for overall survival: age (65 years or more), clinical stage (Binet A/Rai 0 vs. Binet B-C/Rai I-IV), del(17p) and/or TP53 mutation status, IgHV mutation status, and serum beta-2-microglobulin measure (3.5 mg/L or more).
The index was used to identify four risk groups – low risk (score 0-1), intermediate (score 2-3), high (score 4-6), and very high (score 7-10)) – with significantly different overall survival rates at 5 years of 93%, 79%, 64%, and 23%, respectively.
The value of the index was then confirmed in 575 patients, with a 5-year overall survival rate of 91%, 80%, 52%, and 19%, respectively.
Similar findings were seen in an external data set of patients from the Mayo Clinic data set, with 5-year overall survivals of 97%, 91%, 68%, and 21%, respectively. The CLL-IPI also provided accurate estimation regarding time to first treatment; 81%, 47%, 30%, and 19% of patients in the respective risk groups were free from treatment at 5 years.
In the era of more effective treatments for CLL, the established clinical staging systems (Rai and Binet) do not accurately discriminate between prognostic groups because they do not integrate the major clinical, biologic, and genetic variables into one widely accepted prognostic system, Dr. Bahlo noted. The CLL-IPI is, therefore, an important contribution to management of this condition.
The researchers had no relevant financial disclosures.
FROM 13-ICML
Key clinical point: An international prognostic index for patients with chronic lymphocytic leukemia may help to inform treatment decisions.
Major finding: The index was used to identify four risk groups – low risk (score 0-1), intermediate (score 2-3), high (score 4-6), and very high (score 7-10)) – with significantly different overall survival rates at 5 years of 93%, 79%, 64%, and 23%, respectively.
Data source: A multivariate analysis of 3,742 previously untreated patients at early and advanced CLL stages.
Disclosures: The researchers had no relevant financial disclosures.
High VTE recurrence risk persists for at least 3 years
TORONTO – The risk of recurrence following an initial episode of venous thromboembolism is highest in the first 3 months, but remains high for up to 3 years, according to findings from a population-based study involving 2,989 adults.
Over a mean of 23 months (median, 30 months), there were 329 VTE recurrences in the study subjects. Cumulative incidence rates were 5.1% at 3 months, and 14.5% at 3 years. The corresponding rates were 8.7% and 24.8% among those with active cancer, 5.2% and 13.0% among those with provoked VTE, and 3.8% and 13.1% among those with unprovoked VTE, Dr. Wei Huang reported at the International Society on Thrombosis and Haemostasis congress.
Independent predictors of recurrence within 3 years after the index event were active cancer with chemotherapy (hazard ratio, 2.59), active cancer without chemotherapy (HR, 1.59), hypercoagulable state (HR, 2.53) superficial thrombophlebitis (HR, 1.62), varicose vein stripping (HR, 1.75), and inferior vena cava (IVC) filter placement (HR, 2.04), said Dr. Huang of the University of Massachusetts, Worcester.
Individuals included in the study were all residents of the Worcester Metropolitan Statistical Area (WMSA) who had a validated diagnosis of acute first-time deep vein thrombosis and/or pulmonary embolism in a hospital or ambulatory care center that provided short-term care for WMSA residents between 1999 and 2009. Medical records and national and local death registry data were reviewed to examine outcomes up to 3 years after the index event.
Subjects were adults with a mean age of 64 years; 44% were men, and 94% where white. Pulmonary embolism with or without deep vein thrombosis occurred in 42%, and 17% of cases were associated with cancer, 43% involved provoked VTE, and 40% involved unprovoked VTE.
Provoked VTE was defined as VTE occurring within 3 months of a prior surgery, pregnancy, trauma, fracture, or hospitalization in patients without presence of active cancer.
Though limited by the lack of information about variations in physician practices across regions, and by the high proportion of white resident in the WMSA, which both raise questions about whether the findings are generalizable to the U.S. population, the identification of these predictors could allow for improved estimation of risk for individual patients, and may aid in the design of new interventional studies, Dr. Huang concluded.
This study was supported by the National Institutes of Health.
TORONTO – The risk of recurrence following an initial episode of venous thromboembolism is highest in the first 3 months, but remains high for up to 3 years, according to findings from a population-based study involving 2,989 adults.
Over a mean of 23 months (median, 30 months), there were 329 VTE recurrences in the study subjects. Cumulative incidence rates were 5.1% at 3 months, and 14.5% at 3 years. The corresponding rates were 8.7% and 24.8% among those with active cancer, 5.2% and 13.0% among those with provoked VTE, and 3.8% and 13.1% among those with unprovoked VTE, Dr. Wei Huang reported at the International Society on Thrombosis and Haemostasis congress.
Independent predictors of recurrence within 3 years after the index event were active cancer with chemotherapy (hazard ratio, 2.59), active cancer without chemotherapy (HR, 1.59), hypercoagulable state (HR, 2.53) superficial thrombophlebitis (HR, 1.62), varicose vein stripping (HR, 1.75), and inferior vena cava (IVC) filter placement (HR, 2.04), said Dr. Huang of the University of Massachusetts, Worcester.
Individuals included in the study were all residents of the Worcester Metropolitan Statistical Area (WMSA) who had a validated diagnosis of acute first-time deep vein thrombosis and/or pulmonary embolism in a hospital or ambulatory care center that provided short-term care for WMSA residents between 1999 and 2009. Medical records and national and local death registry data were reviewed to examine outcomes up to 3 years after the index event.
Subjects were adults with a mean age of 64 years; 44% were men, and 94% where white. Pulmonary embolism with or without deep vein thrombosis occurred in 42%, and 17% of cases were associated with cancer, 43% involved provoked VTE, and 40% involved unprovoked VTE.
Provoked VTE was defined as VTE occurring within 3 months of a prior surgery, pregnancy, trauma, fracture, or hospitalization in patients without presence of active cancer.
Though limited by the lack of information about variations in physician practices across regions, and by the high proportion of white resident in the WMSA, which both raise questions about whether the findings are generalizable to the U.S. population, the identification of these predictors could allow for improved estimation of risk for individual patients, and may aid in the design of new interventional studies, Dr. Huang concluded.
This study was supported by the National Institutes of Health.
TORONTO – The risk of recurrence following an initial episode of venous thromboembolism is highest in the first 3 months, but remains high for up to 3 years, according to findings from a population-based study involving 2,989 adults.
Over a mean of 23 months (median, 30 months), there were 329 VTE recurrences in the study subjects. Cumulative incidence rates were 5.1% at 3 months, and 14.5% at 3 years. The corresponding rates were 8.7% and 24.8% among those with active cancer, 5.2% and 13.0% among those with provoked VTE, and 3.8% and 13.1% among those with unprovoked VTE, Dr. Wei Huang reported at the International Society on Thrombosis and Haemostasis congress.
Independent predictors of recurrence within 3 years after the index event were active cancer with chemotherapy (hazard ratio, 2.59), active cancer without chemotherapy (HR, 1.59), hypercoagulable state (HR, 2.53) superficial thrombophlebitis (HR, 1.62), varicose vein stripping (HR, 1.75), and inferior vena cava (IVC) filter placement (HR, 2.04), said Dr. Huang of the University of Massachusetts, Worcester.
Individuals included in the study were all residents of the Worcester Metropolitan Statistical Area (WMSA) who had a validated diagnosis of acute first-time deep vein thrombosis and/or pulmonary embolism in a hospital or ambulatory care center that provided short-term care for WMSA residents between 1999 and 2009. Medical records and national and local death registry data were reviewed to examine outcomes up to 3 years after the index event.
Subjects were adults with a mean age of 64 years; 44% were men, and 94% where white. Pulmonary embolism with or without deep vein thrombosis occurred in 42%, and 17% of cases were associated with cancer, 43% involved provoked VTE, and 40% involved unprovoked VTE.
Provoked VTE was defined as VTE occurring within 3 months of a prior surgery, pregnancy, trauma, fracture, or hospitalization in patients without presence of active cancer.
Though limited by the lack of information about variations in physician practices across regions, and by the high proportion of white resident in the WMSA, which both raise questions about whether the findings are generalizable to the U.S. population, the identification of these predictors could allow for improved estimation of risk for individual patients, and may aid in the design of new interventional studies, Dr. Huang concluded.
This study was supported by the National Institutes of Health.
AT THE 2015 ISTH CONGRESS
Key clinical point: The risk of recurrence following an initial episode of venous thromboembolism is highest in the first 3 months, but remains high for up to 3 years, according to findings from a population-based study involving 2,989 adults.
Major finding: Active cancer with chemotherapy was the strongest predictor of VTE recurrence (hazard ratio, 2.59).
Data source: Population-based surveillance of 2,989 adults patients.
Disclosures: The National Institutes of Health supported the study.
Statins showed no benefit in reducing risk of recurrent VTE
TORONTO – The use of statins showed no benefit in reducing the risk of recurrent venous thromboembolism in patients enrolled in phase III trials comparing direct oral anticoagulants with vitamin K antagonists, a large meta-analysis demonstrated.
Recurrence after an unprovoked VTE is 10%-15% in the first 6-12 months, and recurrence risk in the first 6 months is reduced by 80%-90% with anticoagulants, Dr. Mandy N. Lauw said at the International Society on Thrombosis and Haemostasis congress.

“However, the use of anticoagulants has the risk of bleeding, and therefore the long-term risk-benefit ratio is unclear,” said Dr. Lauw of the department of vascular medicine at Academic Medical Center, Amsterdam. “Therefore it’s interesting to look at modalities outside the coagulation cascade to treat patients for longer term and to prevent recurrent thrombosis. One of these modalities has been the use of statins, which are known to reduce arterial vascular events by lowering cholesterol levels. However, recent studies have also indicated that they may have an effect on VTE events.”
In an effort to evaluate the effects of statins on recurrent VTE, Dr. Lauw and her associates conducted a meta-analysis of statins in three randomized, phase III trials comparing non–vitamin K oral anticoagulant (NOAC) with vitamin K antagonist (VKA) therapy in patients with acute symptomatic VTE.
The trials included 5,153 patients enrolled in RE-COVER I and II (an analysis of dabigatran vs. standard therapy for acute VTE), 8,281 enrolled in the EINSTEIN clinical trials for DVT and pulmonary embolism (an analysis of rivaroxaban vs. standard therapy for symptomatic VTE), and 8,292 enrolled in a trial conducted by the Hokusai-DVT investigators (an analysis of edoxaban vs. standard therapy for symptomatic VTE). The researchers examined the effect of statin use on recurrent VTE or VTE-related death, recurrent DVT or PE, and major bleeding. To do this they conducted a pooled meta-analysis and an analysis per study, adjusted for age, gender, diabetes mellitus, creatinine clearance of less than 50 mL/min, hypertension, prior VTE, and use of aspirin.
Dr. Lauw reported results from 21,587 patients included in the analysis. Among all three studies, 2,754 patients (12.8%) used statins and 18,833 (87.2%) did not. In an unadjusted pooled analysis, the use of statins at baseline did not have an influence on the risk of recurrent VTE or VTE-related death, with an odds ratio of 0.91. There was also no effect of statins on the risk of recurrent PE or DVT (ORs of 0.84 and 1.05, respectively), while major bleeding seemed to be increased with the use of statins (OR, 1.65). A subanalysis in patients getting NOAC or VKA separately showed a non–statistically significant benefit of statins with NOACs, compared with VKAs on the risk of recurrent VTE or VTE-related death (ORs of 0.60 vs. OR 1.24, respectively). The results were similar for NOACs, compared with VKA, on the risk of recurrent DVT (ORs of 0.47 vs. OR 1.67) and the risk of recurrent PE (ORs of 0.73 vs. 1.02).
On adjusted analysis, the risk of recurrent VTE or VTE-related death between all three studies was similar and nonsignificant (hazard ratio of 0.99 in RE-COVER I and II, HR of 0.78 in the EINSTEIN clinical trials for DVT & PE, and HR of 0.99 in the trial conducted by the Hokusai-DVT Investigators). There also were no significant differences between the study groups in recurrent PE, recurrent DVT, or major bleeding. “So statins have no beneficial effect, but also no harmful effect,” Dr. Lauw said.
She acknowledged certain limitations of the study, including the fact that it was an on-treatment analysis, “so it could be that we had inadequate follow-up duration,” she said. “Also, we don’t have any assessment of statin effects without anticoagulation in these patients. Perhaps it would be interesting to use the extension trials to explore these results as well.”
For now, “there is no evidence that statins reduce the recurrence of VTE,” she concluded. “The only way to explore this is to do a randomized controlled trial properly designed and powered to estimate this effect prospectively.”
Dr. Lauw reported having no financial disclosures.
TORONTO – The use of statins showed no benefit in reducing the risk of recurrent venous thromboembolism in patients enrolled in phase III trials comparing direct oral anticoagulants with vitamin K antagonists, a large meta-analysis demonstrated.
Recurrence after an unprovoked VTE is 10%-15% in the first 6-12 months, and recurrence risk in the first 6 months is reduced by 80%-90% with anticoagulants, Dr. Mandy N. Lauw said at the International Society on Thrombosis and Haemostasis congress.
“However, the use of anticoagulants has the risk of bleeding, and therefore the long-term risk-benefit ratio is unclear,” said Dr. Lauw of the department of vascular medicine at Academic Medical Center, Amsterdam. “Therefore it’s interesting to look at modalities outside the coagulation cascade to treat patients for longer term and to prevent recurrent thrombosis. One of these modalities has been the use of statins, which are known to reduce arterial vascular events by lowering cholesterol levels. However, recent studies have also indicated that they may have an effect on VTE events.”
In an effort to evaluate the effects of statins on recurrent VTE, Dr. Lauw and her associates conducted a meta-analysis of statins in three randomized, phase III trials comparing non–vitamin K oral anticoagulant (NOAC) with vitamin K antagonist (VKA) therapy in patients with acute symptomatic VTE.
The trials included 5,153 patients enrolled in RE-COVER I and II (an analysis of dabigatran vs. standard therapy for acute VTE), 8,281 enrolled in the EINSTEIN clinical trials for DVT and pulmonary embolism (an analysis of rivaroxaban vs. standard therapy for symptomatic VTE), and 8,292 enrolled in a trial conducted by the Hokusai-DVT investigators (an analysis of edoxaban vs. standard therapy for symptomatic VTE). The researchers examined the effect of statin use on recurrent VTE or VTE-related death, recurrent DVT or PE, and major bleeding. To do this they conducted a pooled meta-analysis and an analysis per study, adjusted for age, gender, diabetes mellitus, creatinine clearance of less than 50 mL/min, hypertension, prior VTE, and use of aspirin.
Dr. Lauw reported results from 21,587 patients included in the analysis. Among all three studies, 2,754 patients (12.8%) used statins and 18,833 (87.2%) did not. In an unadjusted pooled analysis, the use of statins at baseline did not have an influence on the risk of recurrent VTE or VTE-related death, with an odds ratio of 0.91. There was also no effect of statins on the risk of recurrent PE or DVT (ORs of 0.84 and 1.05, respectively), while major bleeding seemed to be increased with the use of statins (OR, 1.65). A subanalysis in patients getting NOAC or VKA separately showed a non–statistically significant benefit of statins with NOACs, compared with VKAs on the risk of recurrent VTE or VTE-related death (ORs of 0.60 vs. OR 1.24, respectively). The results were similar for NOACs, compared with VKA, on the risk of recurrent DVT (ORs of 0.47 vs. OR 1.67) and the risk of recurrent PE (ORs of 0.73 vs. 1.02).
On adjusted analysis, the risk of recurrent VTE or VTE-related death between all three studies was similar and nonsignificant (hazard ratio of 0.99 in RE-COVER I and II, HR of 0.78 in the EINSTEIN clinical trials for DVT & PE, and HR of 0.99 in the trial conducted by the Hokusai-DVT Investigators). There also were no significant differences between the study groups in recurrent PE, recurrent DVT, or major bleeding. “So statins have no beneficial effect, but also no harmful effect,” Dr. Lauw said.
She acknowledged certain limitations of the study, including the fact that it was an on-treatment analysis, “so it could be that we had inadequate follow-up duration,” she said. “Also, we don’t have any assessment of statin effects without anticoagulation in these patients. Perhaps it would be interesting to use the extension trials to explore these results as well.”
For now, “there is no evidence that statins reduce the recurrence of VTE,” she concluded. “The only way to explore this is to do a randomized controlled trial properly designed and powered to estimate this effect prospectively.”
Dr. Lauw reported having no financial disclosures.
TORONTO – The use of statins showed no benefit in reducing the risk of recurrent venous thromboembolism in patients enrolled in phase III trials comparing direct oral anticoagulants with vitamin K antagonists, a large meta-analysis demonstrated.
Recurrence after an unprovoked VTE is 10%-15% in the first 6-12 months, and recurrence risk in the first 6 months is reduced by 80%-90% with anticoagulants, Dr. Mandy N. Lauw said at the International Society on Thrombosis and Haemostasis congress.
“However, the use of anticoagulants has the risk of bleeding, and therefore the long-term risk-benefit ratio is unclear,” said Dr. Lauw of the department of vascular medicine at Academic Medical Center, Amsterdam. “Therefore it’s interesting to look at modalities outside the coagulation cascade to treat patients for longer term and to prevent recurrent thrombosis. One of these modalities has been the use of statins, which are known to reduce arterial vascular events by lowering cholesterol levels. However, recent studies have also indicated that they may have an effect on VTE events.”
In an effort to evaluate the effects of statins on recurrent VTE, Dr. Lauw and her associates conducted a meta-analysis of statins in three randomized, phase III trials comparing non–vitamin K oral anticoagulant (NOAC) with vitamin K antagonist (VKA) therapy in patients with acute symptomatic VTE.
The trials included 5,153 patients enrolled in RE-COVER I and II (an analysis of dabigatran vs. standard therapy for acute VTE), 8,281 enrolled in the EINSTEIN clinical trials for DVT and pulmonary embolism (an analysis of rivaroxaban vs. standard therapy for symptomatic VTE), and 8,292 enrolled in a trial conducted by the Hokusai-DVT investigators (an analysis of edoxaban vs. standard therapy for symptomatic VTE). The researchers examined the effect of statin use on recurrent VTE or VTE-related death, recurrent DVT or PE, and major bleeding. To do this they conducted a pooled meta-analysis and an analysis per study, adjusted for age, gender, diabetes mellitus, creatinine clearance of less than 50 mL/min, hypertension, prior VTE, and use of aspirin.
Dr. Lauw reported results from 21,587 patients included in the analysis. Among all three studies, 2,754 patients (12.8%) used statins and 18,833 (87.2%) did not. In an unadjusted pooled analysis, the use of statins at baseline did not have an influence on the risk of recurrent VTE or VTE-related death, with an odds ratio of 0.91. There was also no effect of statins on the risk of recurrent PE or DVT (ORs of 0.84 and 1.05, respectively), while major bleeding seemed to be increased with the use of statins (OR, 1.65). A subanalysis in patients getting NOAC or VKA separately showed a non–statistically significant benefit of statins with NOACs, compared with VKAs on the risk of recurrent VTE or VTE-related death (ORs of 0.60 vs. OR 1.24, respectively). The results were similar for NOACs, compared with VKA, on the risk of recurrent DVT (ORs of 0.47 vs. OR 1.67) and the risk of recurrent PE (ORs of 0.73 vs. 1.02).
On adjusted analysis, the risk of recurrent VTE or VTE-related death between all three studies was similar and nonsignificant (hazard ratio of 0.99 in RE-COVER I and II, HR of 0.78 in the EINSTEIN clinical trials for DVT & PE, and HR of 0.99 in the trial conducted by the Hokusai-DVT Investigators). There also were no significant differences between the study groups in recurrent PE, recurrent DVT, or major bleeding. “So statins have no beneficial effect, but also no harmful effect,” Dr. Lauw said.
She acknowledged certain limitations of the study, including the fact that it was an on-treatment analysis, “so it could be that we had inadequate follow-up duration,” she said. “Also, we don’t have any assessment of statin effects without anticoagulation in these patients. Perhaps it would be interesting to use the extension trials to explore these results as well.”
For now, “there is no evidence that statins reduce the recurrence of VTE,” she concluded. “The only way to explore this is to do a randomized controlled trial properly designed and powered to estimate this effect prospectively.”
Dr. Lauw reported having no financial disclosures.
AT THE 2015 ISTH CONGRESS
Key clinical point: No beneficial effect of statins in reducing recurrent VTE was observed in patients threated in phase III acute VTE trials.
Major finding: On adjusted analysis, the risk of recurrent VTE or VTE-related death between all three studies was similar and nonsignificant (HR of 0.99 in RE-COVER I and II, HR of 0.78 in the EINSTEIN clinical trials for DVT and PE, and HR of 0.99 in the trial conducted by the Hokusai-DVT investigators).
Data source: A meta-analysis of 21,587 patients enrolled in three phase III trials comparing non–vitamin K oral anticoagulant (NOAC) with vitamin K antagonist (VKA) therapy in patients with acute symptomatic VTE.
Disclosures: Dr. Lauw reported having no financial disclosures.

Combo shows potential for treating PEL
reviewing an image
Photo from the University
of Southern California
Immunomodulatory drugs (IMiDs) and BRD4 inhibitors hold promise for treating primary effusion lymphoma (PEL), according to preclinical research.
The IMiDs lenalidomide and pomalidomide had antiproliferative effects in PEL cell lines, and lenalidomide exhibited synergistic cytotoxicity with the BRD4 inhibitors JQ-1, IBET151, and PFI-1.
In mouse models of PEL, treatment with lenalidomide and JQ-1 significantly prolonged survival.
Preet Chaudhary, MD, PhD, of the University of Southern California, Los Angeles, and his colleagues reported these results in Oncogene.
The researchers first tested lenalidomide and pomalidomide in 9 PEL cell lines. Both drugs exhibited antiproliferative effects, at clinically achievable doses, in 6 of the cell lines (BC-3, BCBL-1, JSC-1, VG-1, UMPEL-1, and UMPEL-3).
The IMiDs displayed activity in the remaining 3 cells lines (BC-1, BCP-1, and APK-1) as well, but only at high doses (ranging from 2.6 μM to 10 μM for lenalidomide and from 226 nM to 744 nM for pomalidomide).
Looking into the mechanism of IMiDs in PEL, the researchers found these drugs induce G1 cell-cycle arrest without inducing Kaposi’s sarcoma-associated herpes virus lytic cycle reactivation.
Further investigation revealed that interferon α, β, and γ are cytotoxic to PEL, but they are not essential for the antiproliferative effects of IMiDs. On the other hand, cereblon-dependent suppression of IRF4 and rapid degradation of IKZF1 are essential.
The researchers also found that knocking down MYC enhanced IMiD activity. This led them to BRD4 inhibitors, which are known to target MYC transcription.
The team tested lenalidomide in combination with JQ-1, IBET151, and PFI-1. The IMiD was “highly synergistic” with all 3 BRD4 inhibitors in BC-3 and BCBL-1 cell lines.
In both cell lines, treatment with lenalidomide and JQ-1 significantly decreased the expression of MYC and IRF4 at protein and mRNA levels. The treatment also resulted in G1 cell cycle arrest, cleavage of poly (ADP-ribose) polymerase, and apoptosis.
So the researchers tested this combination in a mouse model of PEL (NOD-SCID mice injected with BC-3 cells). And they observed a significant improvement in median survival for mice that received combination treatment, compared to lenalidomide or JQ-1 alone—51 days, 35 days, and 42 days, respectively (P≤0.01).![]()
reviewing an image
Photo from the University
of Southern California
Immunomodulatory drugs (IMiDs) and BRD4 inhibitors hold promise for treating primary effusion lymphoma (PEL), according to preclinical research.
The IMiDs lenalidomide and pomalidomide had antiproliferative effects in PEL cell lines, and lenalidomide exhibited synergistic cytotoxicity with the BRD4 inhibitors JQ-1, IBET151, and PFI-1.
In mouse models of PEL, treatment with lenalidomide and JQ-1 significantly prolonged survival.
Preet Chaudhary, MD, PhD, of the University of Southern California, Los Angeles, and his colleagues reported these results in Oncogene.
The researchers first tested lenalidomide and pomalidomide in 9 PEL cell lines. Both drugs exhibited antiproliferative effects, at clinically achievable doses, in 6 of the cell lines (BC-3, BCBL-1, JSC-1, VG-1, UMPEL-1, and UMPEL-3).
The IMiDs displayed activity in the remaining 3 cells lines (BC-1, BCP-1, and APK-1) as well, but only at high doses (ranging from 2.6 μM to 10 μM for lenalidomide and from 226 nM to 744 nM for pomalidomide).
Looking into the mechanism of IMiDs in PEL, the researchers found these drugs induce G1 cell-cycle arrest without inducing Kaposi’s sarcoma-associated herpes virus lytic cycle reactivation.
Further investigation revealed that interferon α, β, and γ are cytotoxic to PEL, but they are not essential for the antiproliferative effects of IMiDs. On the other hand, cereblon-dependent suppression of IRF4 and rapid degradation of IKZF1 are essential.
The researchers also found that knocking down MYC enhanced IMiD activity. This led them to BRD4 inhibitors, which are known to target MYC transcription.
The team tested lenalidomide in combination with JQ-1, IBET151, and PFI-1. The IMiD was “highly synergistic” with all 3 BRD4 inhibitors in BC-3 and BCBL-1 cell lines.
In both cell lines, treatment with lenalidomide and JQ-1 significantly decreased the expression of MYC and IRF4 at protein and mRNA levels. The treatment also resulted in G1 cell cycle arrest, cleavage of poly (ADP-ribose) polymerase, and apoptosis.
So the researchers tested this combination in a mouse model of PEL (NOD-SCID mice injected with BC-3 cells). And they observed a significant improvement in median survival for mice that received combination treatment, compared to lenalidomide or JQ-1 alone—51 days, 35 days, and 42 days, respectively (P≤0.01).![]()
reviewing an image
Photo from the University
of Southern California
Immunomodulatory drugs (IMiDs) and BRD4 inhibitors hold promise for treating primary effusion lymphoma (PEL), according to preclinical research.
The IMiDs lenalidomide and pomalidomide had antiproliferative effects in PEL cell lines, and lenalidomide exhibited synergistic cytotoxicity with the BRD4 inhibitors JQ-1, IBET151, and PFI-1.
In mouse models of PEL, treatment with lenalidomide and JQ-1 significantly prolonged survival.
Preet Chaudhary, MD, PhD, of the University of Southern California, Los Angeles, and his colleagues reported these results in Oncogene.
The researchers first tested lenalidomide and pomalidomide in 9 PEL cell lines. Both drugs exhibited antiproliferative effects, at clinically achievable doses, in 6 of the cell lines (BC-3, BCBL-1, JSC-1, VG-1, UMPEL-1, and UMPEL-3).
The IMiDs displayed activity in the remaining 3 cells lines (BC-1, BCP-1, and APK-1) as well, but only at high doses (ranging from 2.6 μM to 10 μM for lenalidomide and from 226 nM to 744 nM for pomalidomide).
Looking into the mechanism of IMiDs in PEL, the researchers found these drugs induce G1 cell-cycle arrest without inducing Kaposi’s sarcoma-associated herpes virus lytic cycle reactivation.
Further investigation revealed that interferon α, β, and γ are cytotoxic to PEL, but they are not essential for the antiproliferative effects of IMiDs. On the other hand, cereblon-dependent suppression of IRF4 and rapid degradation of IKZF1 are essential.
The researchers also found that knocking down MYC enhanced IMiD activity. This led them to BRD4 inhibitors, which are known to target MYC transcription.
The team tested lenalidomide in combination with JQ-1, IBET151, and PFI-1. The IMiD was “highly synergistic” with all 3 BRD4 inhibitors in BC-3 and BCBL-1 cell lines.
In both cell lines, treatment with lenalidomide and JQ-1 significantly decreased the expression of MYC and IRF4 at protein and mRNA levels. The treatment also resulted in G1 cell cycle arrest, cleavage of poly (ADP-ribose) polymerase, and apoptosis.
So the researchers tested this combination in a mouse model of PEL (NOD-SCID mice injected with BC-3 cells). And they observed a significant improvement in median survival for mice that received combination treatment, compared to lenalidomide or JQ-1 alone—51 days, 35 days, and 42 days, respectively (P≤0.01).![]()
Model helps explain chaotic angiogenesis

Image by Louis Heiser
and Robert Ackland
Scientists say they have developed a model that provides new insight into chaotic angiogenesis, a hallmark of cancer.
The model shows how proteins involved in angiogenesis communicate with each other and how tumors take charge of the protein signaling chain that controls blood vessel growth.
The work, published in PNAS, suggests that Jagged ligands play a major role in the chaotic vessel growth observed around tumors.
In normal growth, an endothelial cell sprouts from an existing blood vessel as a tip. Others that follow the tip cell become the stalk cells that ultimately form vessel walls. The Notch signaling pathway directs the endothelial cell’s decision to become a tip or stalk.
Notch receptors bind with Delta ligand or Jagged ligand molecules produced by cells. How they interact determines the cell’s fate.
When Notch and Delta bind, they prompt a few cells to be tips and adjacent ones to be stalks. The Notch-Delta pathway has been studied extensively and is the target of many angiogenesis inhibitors now in use, according to the scientists.
“We wondered exactly what Notch-Jagged signaling does that is not done in Notch-Delta signaling,” said study author Marcelo Boareto, PhD, of the Swiss Federal Institute of Technology in Zurich.
“We find that when the cells communicate mostly via Jagged, we see a new kind of cell that is not exactly tip and not exactly stalk, but somewhere in between. This compromised cell is the major difference between normal and tumor angiogenesis and suggests that if Notch-Jagged signaling can be somehow suppressed without affecting Notch-Delta, we can probably disrupt tumor angiogenesis.”
The scientists found the tip/stalk hybrid cells do form new blood vessels, but these vessels rarely mature.
“High levels of Jagged in the environment can trigger the formation of blood vessels that are useful to the tumor: fast-developing, leaky, and spread chaotically all over the tumor mass,” Dr Boareto said.
“Tumors don’t have to wait for the vessels to develop,” added study author José Onuchic, PhD, of Rice University in Houston, Texas. “They take advantage of the leakiness of the structure.”
The scientists’ model also takes into account the effect of vascular endothelial growth factor, which triggers angiogenesis and is overexpressed by tumor cells.
“It is very interesting how the tumor hijacks this important mechanism, which is needed for the development of a functional vessel, and amplifies it to generate pathological angiogenesis that leads to uncontrolled growth,” Dr Onuchic said. ![]()
Image by Louis Heiser
and Robert Ackland
Scientists say they have developed a model that provides new insight into chaotic angiogenesis, a hallmark of cancer.
The model shows how proteins involved in angiogenesis communicate with each other and how tumors take charge of the protein signaling chain that controls blood vessel growth.
The work, published in PNAS, suggests that Jagged ligands play a major role in the chaotic vessel growth observed around tumors.
In normal growth, an endothelial cell sprouts from an existing blood vessel as a tip. Others that follow the tip cell become the stalk cells that ultimately form vessel walls. The Notch signaling pathway directs the endothelial cell’s decision to become a tip or stalk.
Notch receptors bind with Delta ligand or Jagged ligand molecules produced by cells. How they interact determines the cell’s fate.
When Notch and Delta bind, they prompt a few cells to be tips and adjacent ones to be stalks. The Notch-Delta pathway has been studied extensively and is the target of many angiogenesis inhibitors now in use, according to the scientists.
“We wondered exactly what Notch-Jagged signaling does that is not done in Notch-Delta signaling,” said study author Marcelo Boareto, PhD, of the Swiss Federal Institute of Technology in Zurich.
“We find that when the cells communicate mostly via Jagged, we see a new kind of cell that is not exactly tip and not exactly stalk, but somewhere in between. This compromised cell is the major difference between normal and tumor angiogenesis and suggests that if Notch-Jagged signaling can be somehow suppressed without affecting Notch-Delta, we can probably disrupt tumor angiogenesis.”
The scientists found the tip/stalk hybrid cells do form new blood vessels, but these vessels rarely mature.
“High levels of Jagged in the environment can trigger the formation of blood vessels that are useful to the tumor: fast-developing, leaky, and spread chaotically all over the tumor mass,” Dr Boareto said.
“Tumors don’t have to wait for the vessels to develop,” added study author José Onuchic, PhD, of Rice University in Houston, Texas. “They take advantage of the leakiness of the structure.”
The scientists’ model also takes into account the effect of vascular endothelial growth factor, which triggers angiogenesis and is overexpressed by tumor cells.
“It is very interesting how the tumor hijacks this important mechanism, which is needed for the development of a functional vessel, and amplifies it to generate pathological angiogenesis that leads to uncontrolled growth,” Dr Onuchic said. ![]()
Image by Louis Heiser
and Robert Ackland
Scientists say they have developed a model that provides new insight into chaotic angiogenesis, a hallmark of cancer.
The model shows how proteins involved in angiogenesis communicate with each other and how tumors take charge of the protein signaling chain that controls blood vessel growth.
The work, published in PNAS, suggests that Jagged ligands play a major role in the chaotic vessel growth observed around tumors.
In normal growth, an endothelial cell sprouts from an existing blood vessel as a tip. Others that follow the tip cell become the stalk cells that ultimately form vessel walls. The Notch signaling pathway directs the endothelial cell’s decision to become a tip or stalk.
Notch receptors bind with Delta ligand or Jagged ligand molecules produced by cells. How they interact determines the cell’s fate.
When Notch and Delta bind, they prompt a few cells to be tips and adjacent ones to be stalks. The Notch-Delta pathway has been studied extensively and is the target of many angiogenesis inhibitors now in use, according to the scientists.
“We wondered exactly what Notch-Jagged signaling does that is not done in Notch-Delta signaling,” said study author Marcelo Boareto, PhD, of the Swiss Federal Institute of Technology in Zurich.
“We find that when the cells communicate mostly via Jagged, we see a new kind of cell that is not exactly tip and not exactly stalk, but somewhere in between. This compromised cell is the major difference between normal and tumor angiogenesis and suggests that if Notch-Jagged signaling can be somehow suppressed without affecting Notch-Delta, we can probably disrupt tumor angiogenesis.”
The scientists found the tip/stalk hybrid cells do form new blood vessels, but these vessels rarely mature.
“High levels of Jagged in the environment can trigger the formation of blood vessels that are useful to the tumor: fast-developing, leaky, and spread chaotically all over the tumor mass,” Dr Boareto said.
“Tumors don’t have to wait for the vessels to develop,” added study author José Onuchic, PhD, of Rice University in Houston, Texas. “They take advantage of the leakiness of the structure.”
The scientists’ model also takes into account the effect of vascular endothelial growth factor, which triggers angiogenesis and is overexpressed by tumor cells.
“It is very interesting how the tumor hijacks this important mechanism, which is needed for the development of a functional vessel, and amplifies it to generate pathological angiogenesis that leads to uncontrolled growth,” Dr Onuchic said. ![]()
Sepsis readmissions common and costly, group says

Photo courtesy of the CDC
Hospital readmissions for sepsis are under-recognized, and additional measures are needed to prevent these readmissions, researchers say.
The group conducted a study of California hospitals that showed sepsis accounts for roughly the same percentage of readmissions as heart attacks and congestive heart failure.
However, sepsis readmissions cost the healthcare system more than heart attack and congestive heart failure readmissions combined.
The research was published in Critical Care Medicine.
“Our study shows how common sepsis readmissions are and [elucidates] some of the factors that are associated with higher risk of readmission after these severe infections,” said study author Dong Chang, MD, of Harbor-UCLA Medical Center in Los Angeles, California.
“In addition, we show that sepsis readmissions have a significant impact on healthcare expenditures relative to other high-risk conditions that are receiving active attention and interventions. Based on these results, we believe that sepsis readmissions are under-recognized and should be among the conditions that are targeted for intervention by policymakers.”
The researchers analyzed data on sepsis admissions for adults 18 years of age and older at all California hospitals from 2009 through 2011. The team also analyzed data for congestive heart failure and heart attack admissions during the same period.
There were 240,198 admissions for sepsis, 193,153 for congestive heart failure, and 105,684 for heart attacks. The all-cause, 30-day readmission rate was 20.4% for sepsis, 23.6% for congestive heart failure, and 17.7% for heart attacks.
Patients with sepsis were readmitted because of respiratory failure; pneumonia; urinary tract infections; renal infections; renal failure; intestinal infections; complications with devices, implants, or grafts; and other causes.
Sepsis readmission rates were higher among young adults than older adults, among men than women, among black and Native American patients than other racial groups, and among lower-income patients than those with higher incomes. In addition, patients with other concurrent health problems were more likely to be readmitted than those with sepsis alone.
The estimated annual cost of sepsis-related readmissions in California during the study period was $500 million, compared with $229 million for congestive heart failure and $142 million for heart attacks.
“These findings suggest that efforts to reduce hospital readmissions need to include sepsis prominently, at least on par with heart failure and myocardial infarction,” said study author Martin Shapiro, MD, PhD, of the David Geffen School of Medicine at UCLA.
Next, the researchers plan to examine why patients are readmitted after sepsis and the percentage of those readmissions that are due to processes that can be improved upon, such as discharge practices, follow-up care, and teaching patients how to take their medications. ![]()
Photo courtesy of the CDC
Hospital readmissions for sepsis are under-recognized, and additional measures are needed to prevent these readmissions, researchers say.
The group conducted a study of California hospitals that showed sepsis accounts for roughly the same percentage of readmissions as heart attacks and congestive heart failure.
However, sepsis readmissions cost the healthcare system more than heart attack and congestive heart failure readmissions combined.
The research was published in Critical Care Medicine.
“Our study shows how common sepsis readmissions are and [elucidates] some of the factors that are associated with higher risk of readmission after these severe infections,” said study author Dong Chang, MD, of Harbor-UCLA Medical Center in Los Angeles, California.
“In addition, we show that sepsis readmissions have a significant impact on healthcare expenditures relative to other high-risk conditions that are receiving active attention and interventions. Based on these results, we believe that sepsis readmissions are under-recognized and should be among the conditions that are targeted for intervention by policymakers.”
The researchers analyzed data on sepsis admissions for adults 18 years of age and older at all California hospitals from 2009 through 2011. The team also analyzed data for congestive heart failure and heart attack admissions during the same period.
There were 240,198 admissions for sepsis, 193,153 for congestive heart failure, and 105,684 for heart attacks. The all-cause, 30-day readmission rate was 20.4% for sepsis, 23.6% for congestive heart failure, and 17.7% for heart attacks.
Patients with sepsis were readmitted because of respiratory failure; pneumonia; urinary tract infections; renal infections; renal failure; intestinal infections; complications with devices, implants, or grafts; and other causes.
Sepsis readmission rates were higher among young adults than older adults, among men than women, among black and Native American patients than other racial groups, and among lower-income patients than those with higher incomes. In addition, patients with other concurrent health problems were more likely to be readmitted than those with sepsis alone.
The estimated annual cost of sepsis-related readmissions in California during the study period was $500 million, compared with $229 million for congestive heart failure and $142 million for heart attacks.
“These findings suggest that efforts to reduce hospital readmissions need to include sepsis prominently, at least on par with heart failure and myocardial infarction,” said study author Martin Shapiro, MD, PhD, of the David Geffen School of Medicine at UCLA.
Next, the researchers plan to examine why patients are readmitted after sepsis and the percentage of those readmissions that are due to processes that can be improved upon, such as discharge practices, follow-up care, and teaching patients how to take their medications. ![]()
Photo courtesy of the CDC
Hospital readmissions for sepsis are under-recognized, and additional measures are needed to prevent these readmissions, researchers say.
The group conducted a study of California hospitals that showed sepsis accounts for roughly the same percentage of readmissions as heart attacks and congestive heart failure.
However, sepsis readmissions cost the healthcare system more than heart attack and congestive heart failure readmissions combined.
The research was published in Critical Care Medicine.
“Our study shows how common sepsis readmissions are and [elucidates] some of the factors that are associated with higher risk of readmission after these severe infections,” said study author Dong Chang, MD, of Harbor-UCLA Medical Center in Los Angeles, California.
“In addition, we show that sepsis readmissions have a significant impact on healthcare expenditures relative to other high-risk conditions that are receiving active attention and interventions. Based on these results, we believe that sepsis readmissions are under-recognized and should be among the conditions that are targeted for intervention by policymakers.”
The researchers analyzed data on sepsis admissions for adults 18 years of age and older at all California hospitals from 2009 through 2011. The team also analyzed data for congestive heart failure and heart attack admissions during the same period.
There were 240,198 admissions for sepsis, 193,153 for congestive heart failure, and 105,684 for heart attacks. The all-cause, 30-day readmission rate was 20.4% for sepsis, 23.6% for congestive heart failure, and 17.7% for heart attacks.
Patients with sepsis were readmitted because of respiratory failure; pneumonia; urinary tract infections; renal infections; renal failure; intestinal infections; complications with devices, implants, or grafts; and other causes.
Sepsis readmission rates were higher among young adults than older adults, among men than women, among black and Native American patients than other racial groups, and among lower-income patients than those with higher incomes. In addition, patients with other concurrent health problems were more likely to be readmitted than those with sepsis alone.
The estimated annual cost of sepsis-related readmissions in California during the study period was $500 million, compared with $229 million for congestive heart failure and $142 million for heart attacks.
“These findings suggest that efforts to reduce hospital readmissions need to include sepsis prominently, at least on par with heart failure and myocardial infarction,” said study author Martin Shapiro, MD, PhD, of the David Geffen School of Medicine at UCLA.
Next, the researchers plan to examine why patients are readmitted after sepsis and the percentage of those readmissions that are due to processes that can be improved upon, such as discharge practices, follow-up care, and teaching patients how to take their medications. ![]()
Early progression predicts overall survival in FL

Photo by Rhoda Baer
The goal for many cancer patients is to reach the 5-year mark without progression, but a new study suggests 2 years might be a more appropriate goal for patients with follicular lymphoma (FL).
Previous research indicated that about 20% of FL patients relapse within 2 years of treatment.
Now, researchers have found these patients have a significantly worse 5-year survival rate than patients who make it past the 2-year mark without progressing.
Carla Casulo, MD, of the University of Rochester in New York, and her colleagues recounted these findings in the Journal of Clinical Oncology.
The team analyzed data from 588 patients with stage 2-4 FL who received first-line therapy with rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP).
These patients could be separated into 2 groups: those with disease progression within 2 years of diagnosis (19%, n=110) and those who did not progress within the 2-year period (71%, n=420).
Eight percent of patients (n=46) were lost to follow-up, and 2% (n=12) died of causes other than progression within the 2-year period.
At 2 years, the overall survival (OS) rate was 68% in the early progression group and 97% in the group that did not progress. At 5 years, OS rates were 50% and 90%, respectively.
In unadjusted Cox regression analysis, early progression was associated with lower OS (hazard ratio[HR]=7.17). The same was true after the researchers adjusted for FLIPI score (HR=6.44).
The team observed similar results in a validation cohort of 147 FL patients who received first-line R-CHOP. At 2 years, the OS rate was 64% in the early progression group and 98% in the group that did not progress. At 5 years, OS rates were 34% and 94%, respectively.
Again, in an unadjusted analysis, early progression was associated with lower OS (HR=20.0). And this trend was maintained after the researchers adjusted for FLIPI score (HR=19.8).
The researchers also found that, for patients in the early progression group, clinical factors that were predictive of inferior OS were age, ECOG performance score, nodal sites, and disease stage. For the group that did not progress within 2 years, clinical factors that were predictive of OS were age and extranodal sites.
In a Cox regression analysis that encompassed these factors and early progression, only early progression, age, and ECOG performance scores remained significantly predictive of OS.
“[W]e have confirmed that all relapsed patients are not equal and therefore should not be approached the same at diagnosis, nor at the time of relapse, in terms of therapies,” Dr Casulo said.
“It will be critical to predict who is most likely to relapse early. We believe that targeted sequencing or gene-expression profiling will be important to understanding how to improve the outcomes of this group.” ![]()
Photo by Rhoda Baer
The goal for many cancer patients is to reach the 5-year mark without progression, but a new study suggests 2 years might be a more appropriate goal for patients with follicular lymphoma (FL).
Previous research indicated that about 20% of FL patients relapse within 2 years of treatment.
Now, researchers have found these patients have a significantly worse 5-year survival rate than patients who make it past the 2-year mark without progressing.
Carla Casulo, MD, of the University of Rochester in New York, and her colleagues recounted these findings in the Journal of Clinical Oncology.
The team analyzed data from 588 patients with stage 2-4 FL who received first-line therapy with rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP).
These patients could be separated into 2 groups: those with disease progression within 2 years of diagnosis (19%, n=110) and those who did not progress within the 2-year period (71%, n=420).
Eight percent of patients (n=46) were lost to follow-up, and 2% (n=12) died of causes other than progression within the 2-year period.
At 2 years, the overall survival (OS) rate was 68% in the early progression group and 97% in the group that did not progress. At 5 years, OS rates were 50% and 90%, respectively.
In unadjusted Cox regression analysis, early progression was associated with lower OS (hazard ratio[HR]=7.17). The same was true after the researchers adjusted for FLIPI score (HR=6.44).
The team observed similar results in a validation cohort of 147 FL patients who received first-line R-CHOP. At 2 years, the OS rate was 64% in the early progression group and 98% in the group that did not progress. At 5 years, OS rates were 34% and 94%, respectively.
Again, in an unadjusted analysis, early progression was associated with lower OS (HR=20.0). And this trend was maintained after the researchers adjusted for FLIPI score (HR=19.8).
The researchers also found that, for patients in the early progression group, clinical factors that were predictive of inferior OS were age, ECOG performance score, nodal sites, and disease stage. For the group that did not progress within 2 years, clinical factors that were predictive of OS were age and extranodal sites.
In a Cox regression analysis that encompassed these factors and early progression, only early progression, age, and ECOG performance scores remained significantly predictive of OS.
“[W]e have confirmed that all relapsed patients are not equal and therefore should not be approached the same at diagnosis, nor at the time of relapse, in terms of therapies,” Dr Casulo said.
“It will be critical to predict who is most likely to relapse early. We believe that targeted sequencing or gene-expression profiling will be important to understanding how to improve the outcomes of this group.” ![]()
Photo by Rhoda Baer
The goal for many cancer patients is to reach the 5-year mark without progression, but a new study suggests 2 years might be a more appropriate goal for patients with follicular lymphoma (FL).
Previous research indicated that about 20% of FL patients relapse within 2 years of treatment.
Now, researchers have found these patients have a significantly worse 5-year survival rate than patients who make it past the 2-year mark without progressing.
Carla Casulo, MD, of the University of Rochester in New York, and her colleagues recounted these findings in the Journal of Clinical Oncology.
The team analyzed data from 588 patients with stage 2-4 FL who received first-line therapy with rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP).
These patients could be separated into 2 groups: those with disease progression within 2 years of diagnosis (19%, n=110) and those who did not progress within the 2-year period (71%, n=420).
Eight percent of patients (n=46) were lost to follow-up, and 2% (n=12) died of causes other than progression within the 2-year period.
At 2 years, the overall survival (OS) rate was 68% in the early progression group and 97% in the group that did not progress. At 5 years, OS rates were 50% and 90%, respectively.
In unadjusted Cox regression analysis, early progression was associated with lower OS (hazard ratio[HR]=7.17). The same was true after the researchers adjusted for FLIPI score (HR=6.44).
The team observed similar results in a validation cohort of 147 FL patients who received first-line R-CHOP. At 2 years, the OS rate was 64% in the early progression group and 98% in the group that did not progress. At 5 years, OS rates were 34% and 94%, respectively.
Again, in an unadjusted analysis, early progression was associated with lower OS (HR=20.0). And this trend was maintained after the researchers adjusted for FLIPI score (HR=19.8).
The researchers also found that, for patients in the early progression group, clinical factors that were predictive of inferior OS were age, ECOG performance score, nodal sites, and disease stage. For the group that did not progress within 2 years, clinical factors that were predictive of OS were age and extranodal sites.
In a Cox regression analysis that encompassed these factors and early progression, only early progression, age, and ECOG performance scores remained significantly predictive of OS.
“[W]e have confirmed that all relapsed patients are not equal and therefore should not be approached the same at diagnosis, nor at the time of relapse, in terms of therapies,” Dr Casulo said.
“It will be critical to predict who is most likely to relapse early. We believe that targeted sequencing or gene-expression profiling will be important to understanding how to improve the outcomes of this group.” ![]()
Interim PET results guide ongoing therapy in Hodgkin lymphoma
Bleomycin can be eliminated after two cycles of the ABVD chemotherapeutic regimen based on a negative interim PET scan finding in patients with Hodgkin lymphoma, according to the 3-year findings of the RATHL study.
Being able to omit bleomycin after a negative interim PET scan was associated with a lower rate of pulmonary toxicity, but no loss in efficacy. For patients with positive interim PET scans, a more aggressive therapy was associated with good outcomes, suggesting that response-adapted therapy can yield good results, Dr. Peter Johnson said at the International Congress on Malignant Lymphoma in Lugano, Switzerland.
In the large international RATHL study (Response-Adapted Therapy in Hodgkin Lymphoma study) 1,137 adults with newly diagnosed disease (41% stage II, 31% stage III, 28% stage IV) underwent PET-CT scans at baseline and after completing two cycles of ABVD (adriamycin, bleomycin, vinblastine, dacarbazine). The patients’ PET images were centrally reviewed using a 5-point scale as either negative (1-3) or positive (4-5),
The majority of patients (84%) had negative scans after two cycles of the ABVD regimen and were randomized to receive four additional cycles either with or without bleomycin (ABVD or AVD). Consolidation radiotherapy was not advised for patients whose interim PET scans were negative, regardless of baseline bulk or residual masses, Dr. Johnson, of the Cancer Research UK Centre at University of Southampton, England, reported.
Patients with positive interim PET scans received escalated therapy with a BEACOPP (bleomycin, etoposide, doxorubicin [Adriamycin], cyclophosphamide, vincristine [Oncovin], procarbazine, prednisolone) regimen. They received either eBEACOPP and BEASCOPP-14.
At the 3-year follow-up, progression-free survival in the PET-negative group was 85% for both the ABVD- and AVD-treated patients. Similarly, overall survival was 97% for both groups.
Factors that predicted treatment failure after a negative interim PET scan were initial tumor stage and international prognostic score, but not bulk, B symptoms, or score of the interim PET scan.
ABVD was associated with more pulmonary toxicity than was AVD.
Of 174 patients who had a positive interim PET scan and received escalated therapy, 74% had a subsequent negative PET scan after treatment. Their 3-year, progression-free survival rate was 68%, and their overall survival was 86% with no difference in outcome between two variations of BEACOPP (eBEACOPP and BEASCOPP-14).
Of the 53 deaths in the study, 19 were caused by Hodgkin lymphoma. The overall 3-year progression-free survival is 83%, and overall survival is 95%.
The results of the RATHL study have important implications for therapy of Hodgkin lymphoma, Dr. Johnson stated. First, interim PET scans are highly predictive for response to ABVD, providing valuable prognostic information to support decisions related to escalation of therapy. Secondly, after two cycles of ABVD, “it is safe to omit bleomycin from subsequent cycles, without consolidation radiotherapy,” he reported.
Omitting bleomycin has the potential to reduce pulmonary toxicity from chemotherapy, especially dyspnea, thromboembolism, and neutropenic fever, Dr. Johnson added. In the RATHL study, rates of pulmonary toxicity were significantly higher in the group receiving bleomycin.
This large randomized phase 3 RATHL trial has practice changing implications for advanced stage Hodgkin lymphoma. This trial had a simple straightforward design uniting two themes in Hodgkin research: (1) desire to minimizeor omit bleomycin due to its somewhat unpredictable pulmonary toxicity; and (2) utilizing early PET response- adapted strategies, though most such studies have focused on early stage patients. This trial demonstrates that patients with advanced stage Hodgkin lymphoma who achieve PET negativity after 2 cycles of ABVD, representing 84% of patients, do not need to be exposed to bleomycin during the last 4 cycles, reducing pulmonary toxicity. This has immediate clinical utility. Whether this can be extrapolated to early stage patients remains an interesting research question.
This large randomized phase 3 RATHL trial has practice changing implications for advanced stage Hodgkin lymphoma. This trial had a simple straightforward design uniting two themes in Hodgkin research: (1) desire to minimizeor omit bleomycin due to its somewhat unpredictable pulmonary toxicity; and (2) utilizing early PET response- adapted strategies, though most such studies have focused on early stage patients. This trial demonstrates that patients with advanced stage Hodgkin lymphoma who achieve PET negativity after 2 cycles of ABVD, representing 84% of patients, do not need to be exposed to bleomycin during the last 4 cycles, reducing pulmonary toxicity. This has immediate clinical utility. Whether this can be extrapolated to early stage patients remains an interesting research question.
This large randomized phase 3 RATHL trial has practice changing implications for advanced stage Hodgkin lymphoma. This trial had a simple straightforward design uniting two themes in Hodgkin research: (1) desire to minimizeor omit bleomycin due to its somewhat unpredictable pulmonary toxicity; and (2) utilizing early PET response- adapted strategies, though most such studies have focused on early stage patients. This trial demonstrates that patients with advanced stage Hodgkin lymphoma who achieve PET negativity after 2 cycles of ABVD, representing 84% of patients, do not need to be exposed to bleomycin during the last 4 cycles, reducing pulmonary toxicity. This has immediate clinical utility. Whether this can be extrapolated to early stage patients remains an interesting research question.
Bleomycin can be eliminated after two cycles of the ABVD chemotherapeutic regimen based on a negative interim PET scan finding in patients with Hodgkin lymphoma, according to the 3-year findings of the RATHL study.
Being able to omit bleomycin after a negative interim PET scan was associated with a lower rate of pulmonary toxicity, but no loss in efficacy. For patients with positive interim PET scans, a more aggressive therapy was associated with good outcomes, suggesting that response-adapted therapy can yield good results, Dr. Peter Johnson said at the International Congress on Malignant Lymphoma in Lugano, Switzerland.
In the large international RATHL study (Response-Adapted Therapy in Hodgkin Lymphoma study) 1,137 adults with newly diagnosed disease (41% stage II, 31% stage III, 28% stage IV) underwent PET-CT scans at baseline and after completing two cycles of ABVD (adriamycin, bleomycin, vinblastine, dacarbazine). The patients’ PET images were centrally reviewed using a 5-point scale as either negative (1-3) or positive (4-5),
The majority of patients (84%) had negative scans after two cycles of the ABVD regimen and were randomized to receive four additional cycles either with or without bleomycin (ABVD or AVD). Consolidation radiotherapy was not advised for patients whose interim PET scans were negative, regardless of baseline bulk or residual masses, Dr. Johnson, of the Cancer Research UK Centre at University of Southampton, England, reported.
Patients with positive interim PET scans received escalated therapy with a BEACOPP (bleomycin, etoposide, doxorubicin [Adriamycin], cyclophosphamide, vincristine [Oncovin], procarbazine, prednisolone) regimen. They received either eBEACOPP and BEASCOPP-14.
At the 3-year follow-up, progression-free survival in the PET-negative group was 85% for both the ABVD- and AVD-treated patients. Similarly, overall survival was 97% for both groups.
Factors that predicted treatment failure after a negative interim PET scan were initial tumor stage and international prognostic score, but not bulk, B symptoms, or score of the interim PET scan.
ABVD was associated with more pulmonary toxicity than was AVD.
Of 174 patients who had a positive interim PET scan and received escalated therapy, 74% had a subsequent negative PET scan after treatment. Their 3-year, progression-free survival rate was 68%, and their overall survival was 86% with no difference in outcome between two variations of BEACOPP (eBEACOPP and BEASCOPP-14).
Of the 53 deaths in the study, 19 were caused by Hodgkin lymphoma. The overall 3-year progression-free survival is 83%, and overall survival is 95%.
The results of the RATHL study have important implications for therapy of Hodgkin lymphoma, Dr. Johnson stated. First, interim PET scans are highly predictive for response to ABVD, providing valuable prognostic information to support decisions related to escalation of therapy. Secondly, after two cycles of ABVD, “it is safe to omit bleomycin from subsequent cycles, without consolidation radiotherapy,” he reported.
Omitting bleomycin has the potential to reduce pulmonary toxicity from chemotherapy, especially dyspnea, thromboembolism, and neutropenic fever, Dr. Johnson added. In the RATHL study, rates of pulmonary toxicity were significantly higher in the group receiving bleomycin.
Bleomycin can be eliminated after two cycles of the ABVD chemotherapeutic regimen based on a negative interim PET scan finding in patients with Hodgkin lymphoma, according to the 3-year findings of the RATHL study.
Being able to omit bleomycin after a negative interim PET scan was associated with a lower rate of pulmonary toxicity, but no loss in efficacy. For patients with positive interim PET scans, a more aggressive therapy was associated with good outcomes, suggesting that response-adapted therapy can yield good results, Dr. Peter Johnson said at the International Congress on Malignant Lymphoma in Lugano, Switzerland.
In the large international RATHL study (Response-Adapted Therapy in Hodgkin Lymphoma study) 1,137 adults with newly diagnosed disease (41% stage II, 31% stage III, 28% stage IV) underwent PET-CT scans at baseline and after completing two cycles of ABVD (adriamycin, bleomycin, vinblastine, dacarbazine). The patients’ PET images were centrally reviewed using a 5-point scale as either negative (1-3) or positive (4-5),
The majority of patients (84%) had negative scans after two cycles of the ABVD regimen and were randomized to receive four additional cycles either with or without bleomycin (ABVD or AVD). Consolidation radiotherapy was not advised for patients whose interim PET scans were negative, regardless of baseline bulk or residual masses, Dr. Johnson, of the Cancer Research UK Centre at University of Southampton, England, reported.
Patients with positive interim PET scans received escalated therapy with a BEACOPP (bleomycin, etoposide, doxorubicin [Adriamycin], cyclophosphamide, vincristine [Oncovin], procarbazine, prednisolone) regimen. They received either eBEACOPP and BEASCOPP-14.
At the 3-year follow-up, progression-free survival in the PET-negative group was 85% for both the ABVD- and AVD-treated patients. Similarly, overall survival was 97% for both groups.
Factors that predicted treatment failure after a negative interim PET scan were initial tumor stage and international prognostic score, but not bulk, B symptoms, or score of the interim PET scan.
ABVD was associated with more pulmonary toxicity than was AVD.
Of 174 patients who had a positive interim PET scan and received escalated therapy, 74% had a subsequent negative PET scan after treatment. Their 3-year, progression-free survival rate was 68%, and their overall survival was 86% with no difference in outcome between two variations of BEACOPP (eBEACOPP and BEASCOPP-14).
Of the 53 deaths in the study, 19 were caused by Hodgkin lymphoma. The overall 3-year progression-free survival is 83%, and overall survival is 95%.
The results of the RATHL study have important implications for therapy of Hodgkin lymphoma, Dr. Johnson stated. First, interim PET scans are highly predictive for response to ABVD, providing valuable prognostic information to support decisions related to escalation of therapy. Secondly, after two cycles of ABVD, “it is safe to omit bleomycin from subsequent cycles, without consolidation radiotherapy,” he reported.
Omitting bleomycin has the potential to reduce pulmonary toxicity from chemotherapy, especially dyspnea, thromboembolism, and neutropenic fever, Dr. Johnson added. In the RATHL study, rates of pulmonary toxicity were significantly higher in the group receiving bleomycin.
AT 13-ICML
Key clinical point: Bleomycin can be eliminated after two cycles of the ABVD chemotherapeutic regimen based on a negative interim PET scan finding in patients with Hodgkin lymphoma.
Major finding: At the 3-year follow-up, progression-free survival in the PET-negative group was 85% for both the ABVD- and AVD-treated patients. Similarly, overall survival was 97% for both groups.
Data source: The international RATHL study (Response-Adapted Therapy in Hodgkin Lymphoma study).
Disclosures: The study was supported by Cancer Research UK, Experimental Cancer Medicine Centre (ECMC), and the National Institute for Health Research Cancer Research Network (NCRN). The researchers had no relevant financial disclosures.