User login
Granular Cell Tumor
Granular cell tumors (GCTs) tend to present as solitary nodules, not uncommonly affecting the dorsum of the tongue but also involving the skin, breasts, and internal organs.1 Cutaneous GCTs typically present as 0.5- to 3-cm firm nodules with a verrucous or eroded surface.2 They most commonly present in dark-skinned, middle-aged women but have been reported in all age groups and in both sexes.3 Multiple GCTs are reported in up to 25% of cases, rarely in association with LEOPARD syndrome (consisting of lentigines, electrocardiographic abnormalities, ocular hypertelorism, pulmonary stenosis, abnormalities of genitalia, retardation of growth, and deafness).4 Granular cell tumors generally are benign with a metastatic rate of approximately 3%.2
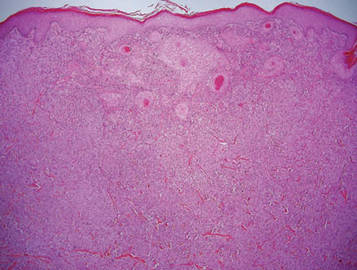
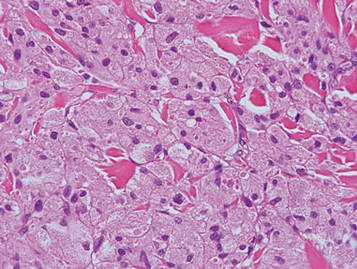
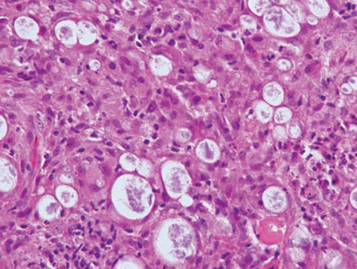
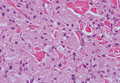
Granular cell tumors are histopathologically characterized by sheets of large polygonal cells with small, round, central nuclei; cytoplasm that is eosinophilic, coarse, and granular, as well as periodic acid–Schiff positive and diastase resistant; and distinct cytoplasmic membranes (Figure 1). Pustulo-ovoid bodies of Milian often generally appear as larger eosinophilic granules surrounded by a clear halo (Figure 2).5 Increased mitotic activity, a high nuclear-cytoplasmic ratio, pleomorphism, and necrosis suggest malignancy.6
|
|
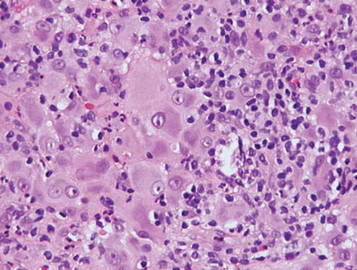
Lepromatous leprosy is characterized by sheets of histiocytes with vacuolated cytoplasm, some with clumped amphophilic bacilli known as globi (Figure 3). Mastocytoma can be distinguished from GCTs by the “fried egg” appearance of the mast cells (Figure 4). Although mast cells have a pale granular cytoplasm, they are smaller and lack pustulo-ovoid bodies and the polygonal shape of GCT cells. Reticulohistiocytoma, on the other hand, has two-toned dusty rose ground glass histiocytes (Figure 5), and xanthelasma can be distinguished histologically from GCT by the presence of a foamy rather than granular cytoplasm (Figure 6).
|
|
|
|


1. Elston DM, Ko C, Ferringer TC, et al, eds. Dermatopathology: Requisites in Dermatology. Philadelphia, PA: Saunders Elsevier; 2009.
2. Bolognia JL, Jorizzo JL, Schaffer JV. Dermatology. 3rd ed. Philadelphia, PA: Elsevier; 2012.
3. van de Loo S, Thunnissen E, Postmus P, et al. Granular cell tumor of the oral cavity; a case series including a case of metachronous occurrence in the tongue and the lung [published online ahead of print June 1, 2014]. Med Oral Patol Oral Cir Bucal. doi:10.4317/medoral.19867.
4. Schrader KA, Nelson TN, De Luca A, et al. Multiple granular cell tumors are an associated feature of LEOPARD syndrome caused by mutation in PTPN11. Clin Genet. 2009;75:185-189.
5. Epstein DS, Pashaei S, Hunt E Jr, et al. Pustulo-ovoid bodies of Milian in granular cell tumors. J Cutan Pathol. 2007;34:405-409.
6. Fanburg-Smith JC, Meis-Kindblom JM, Fante R, et al. Malignant granular cell tumor of soft tissue: diagnostic criteria and clinicopathologic correlation. Am J Surg Pathol. 1998;22:779-794.
Granular cell tumors (GCTs) tend to present as solitary nodules, not uncommonly affecting the dorsum of the tongue but also involving the skin, breasts, and internal organs.1 Cutaneous GCTs typically present as 0.5- to 3-cm firm nodules with a verrucous or eroded surface.2 They most commonly present in dark-skinned, middle-aged women but have been reported in all age groups and in both sexes.3 Multiple GCTs are reported in up to 25% of cases, rarely in association with LEOPARD syndrome (consisting of lentigines, electrocardiographic abnormalities, ocular hypertelorism, pulmonary stenosis, abnormalities of genitalia, retardation of growth, and deafness).4 Granular cell tumors generally are benign with a metastatic rate of approximately 3%.2
Granular cell tumors are histopathologically characterized by sheets of large polygonal cells with small, round, central nuclei; cytoplasm that is eosinophilic, coarse, and granular, as well as periodic acid–Schiff positive and diastase resistant; and distinct cytoplasmic membranes (Figure 1). Pustulo-ovoid bodies of Milian often generally appear as larger eosinophilic granules surrounded by a clear halo (Figure 2).5 Increased mitotic activity, a high nuclear-cytoplasmic ratio, pleomorphism, and necrosis suggest malignancy.6
|
|
Lepromatous leprosy is characterized by sheets of histiocytes with vacuolated cytoplasm, some with clumped amphophilic bacilli known as globi (Figure 3). Mastocytoma can be distinguished from GCTs by the “fried egg” appearance of the mast cells (Figure 4). Although mast cells have a pale granular cytoplasm, they are smaller and lack pustulo-ovoid bodies and the polygonal shape of GCT cells. Reticulohistiocytoma, on the other hand, has two-toned dusty rose ground glass histiocytes (Figure 5), and xanthelasma can be distinguished histologically from GCT by the presence of a foamy rather than granular cytoplasm (Figure 6).
|
|
|
|
Granular cell tumors (GCTs) tend to present as solitary nodules, not uncommonly affecting the dorsum of the tongue but also involving the skin, breasts, and internal organs.1 Cutaneous GCTs typically present as 0.5- to 3-cm firm nodules with a verrucous or eroded surface.2 They most commonly present in dark-skinned, middle-aged women but have been reported in all age groups and in both sexes.3 Multiple GCTs are reported in up to 25% of cases, rarely in association with LEOPARD syndrome (consisting of lentigines, electrocardiographic abnormalities, ocular hypertelorism, pulmonary stenosis, abnormalities of genitalia, retardation of growth, and deafness).4 Granular cell tumors generally are benign with a metastatic rate of approximately 3%.2
Granular cell tumors are histopathologically characterized by sheets of large polygonal cells with small, round, central nuclei; cytoplasm that is eosinophilic, coarse, and granular, as well as periodic acid–Schiff positive and diastase resistant; and distinct cytoplasmic membranes (Figure 1). Pustulo-ovoid bodies of Milian often generally appear as larger eosinophilic granules surrounded by a clear halo (Figure 2).5 Increased mitotic activity, a high nuclear-cytoplasmic ratio, pleomorphism, and necrosis suggest malignancy.6
|
|
Lepromatous leprosy is characterized by sheets of histiocytes with vacuolated cytoplasm, some with clumped amphophilic bacilli known as globi (Figure 3). Mastocytoma can be distinguished from GCTs by the “fried egg” appearance of the mast cells (Figure 4). Although mast cells have a pale granular cytoplasm, they are smaller and lack pustulo-ovoid bodies and the polygonal shape of GCT cells. Reticulohistiocytoma, on the other hand, has two-toned dusty rose ground glass histiocytes (Figure 5), and xanthelasma can be distinguished histologically from GCT by the presence of a foamy rather than granular cytoplasm (Figure 6).
|
|
|
|
1. Elston DM, Ko C, Ferringer TC, et al, eds. Dermatopathology: Requisites in Dermatology. Philadelphia, PA: Saunders Elsevier; 2009.
2. Bolognia JL, Jorizzo JL, Schaffer JV. Dermatology. 3rd ed. Philadelphia, PA: Elsevier; 2012.
3. van de Loo S, Thunnissen E, Postmus P, et al. Granular cell tumor of the oral cavity; a case series including a case of metachronous occurrence in the tongue and the lung [published online ahead of print June 1, 2014]. Med Oral Patol Oral Cir Bucal. doi:10.4317/medoral.19867.
4. Schrader KA, Nelson TN, De Luca A, et al. Multiple granular cell tumors are an associated feature of LEOPARD syndrome caused by mutation in PTPN11. Clin Genet. 2009;75:185-189.
5. Epstein DS, Pashaei S, Hunt E Jr, et al. Pustulo-ovoid bodies of Milian in granular cell tumors. J Cutan Pathol. 2007;34:405-409.
6. Fanburg-Smith JC, Meis-Kindblom JM, Fante R, et al. Malignant granular cell tumor of soft tissue: diagnostic criteria and clinicopathologic correlation. Am J Surg Pathol. 1998;22:779-794.
1. Elston DM, Ko C, Ferringer TC, et al, eds. Dermatopathology: Requisites in Dermatology. Philadelphia, PA: Saunders Elsevier; 2009.
2. Bolognia JL, Jorizzo JL, Schaffer JV. Dermatology. 3rd ed. Philadelphia, PA: Elsevier; 2012.
3. van de Loo S, Thunnissen E, Postmus P, et al. Granular cell tumor of the oral cavity; a case series including a case of metachronous occurrence in the tongue and the lung [published online ahead of print June 1, 2014]. Med Oral Patol Oral Cir Bucal. doi:10.4317/medoral.19867.
4. Schrader KA, Nelson TN, De Luca A, et al. Multiple granular cell tumors are an associated feature of LEOPARD syndrome caused by mutation in PTPN11. Clin Genet. 2009;75:185-189.
5. Epstein DS, Pashaei S, Hunt E Jr, et al. Pustulo-ovoid bodies of Milian in granular cell tumors. J Cutan Pathol. 2007;34:405-409.
6. Fanburg-Smith JC, Meis-Kindblom JM, Fante R, et al. Malignant granular cell tumor of soft tissue: diagnostic criteria and clinicopathologic correlation. Am J Surg Pathol. 1998;22:779-794.
Two activin receptor fusion proteins show promise in anemia

site of the ASH Annual Meeting
Photo courtesy of ASH
SAN FRANCISCO—Two activin receptor fusion proteins, luspatercept and sotatercept, increased hemoglobin levels and transfusion independence in patients with β-thalassemia and myelodysplastic syndromes (MDS)/chronic myelomonocytic leukemia (CMML), respectively, in phase 2 trials.
Luspatercept is a type IIB activin receptor, while sotatercept is type IIA. Both impact late-stage erythropoiesis and improve anemia.
Investigators reported the trial results at the 2014 ASH Annual Meeting.
Luspatercept in β-thalassemia
Antonio G. Piga, MD, of Turin University in Italy, explained that luspatercept binds to GDF11 and other ligands in the TGF-β superfamily and promotes late-stage erythroid maturation.
The study was designed in the US and conducted abroad, he said, because while β-thalassemia is rare in the US, it is not so in Europe.
Investigators evaluated whether luspatercept could increase hemoglobin levels 1.5 g/dL or more for at least 2 weeks in non-transfusion-dependent (NTD) patients.
And in transfusion-dependent (TD) patients, luspatercept was expected to decrease the transfusion burden by 20% or more over 12 weeks.
Thirty patients, 7 TD and 23 NTD, received an injection of luspatercept every 3 weeks for 3 months at doses ranging from 0.2 to 1.0 mg/kg.
The median age was 35, and 53% of patients were male. Eighty-three percent had had a splenectomy.
Luspatercept efficacy
Three-quarters of patients treated with 0.8 to 1.0 mg/kg increased their hemoglobin levels or reduced their transfusion burden.
Of the NTD patients, 8 of 12 with iron overload at baseline experienced a reduction in liver iron concentration of 1 mg or more at 16 weeks.
And in the TD group, “All patients had clinically improved reduction of transfusion dependence,” Dr Piga said.
They had a more than 60% reduction in transfusion burden over 12 weeks. This included 2 patients with β0 β0 genotype, who experienced a 79% and 75% reduction.
“There was a trend to lower liver iron concentration in TD patients,” Dr Piga noted, “except in 1 patient.”
And 5 of 5 TD patients experienced decreases in serum ferritin ranging from 12% to 60%.
Luspatercept safety
Luspatercept did not cause any treatment-related serious or severe adverse events. The most common adverse events were bone pain (20%), headache (17%), myalgia (13%), and asthenia (10%).
There was 1 grade 3 dose-limiting toxicity of worsening lumbar spine bone pain, and 3 patients discontinued early, 1 each with occipital headache, ankle pain, and back pain.
Luspatercept had beneficial effects on other complications of the disease, Dr Piga noted, such as the healing of leg ulcers in the 3 patients with this complication, 1 who is just ending the trial.
With these promising results, Dr Piga said the investigators are “anxious to start phase 3.”
Dr Piga reported the data as abstract 53. The study was supported by Acceleron Pharma and Celgene Corporation.
Sotatercept in MDS and CMML with anemia
Rami Komrokji, MD, of the Moffit Cancer Center in Tampa, Florida, explained that sotaterept increases the release of mature erythrocytes into circulation by a mechanism distinct from erythropoietin.
Sotatercept was shown to stimulate erythropoiesis and increase hemoglobin levels in healthy volunteers, so investigators undertook to study its potential to treat anemia.
They conducted a phase 2 dose-finding study to determine the best effective dose in patients with anemia and lower-risk MDS or nonproliferative CMML who were refractory to erythropoiesis-stimulating agents (ESAs).
Investigators evaluated 53 patients who had anemia of 9 g/dL or less requiring 2 or more units of red blood cells (RBCs) in the 12 weeks prior to enrollment.
Their white blood cell counts had to be under 13,000/μL, and they had to have no response, loss of response, or low chance of response to ESAs, reflected by serum erythropoietin of more than 500 mIU/mL.
Patients were a median age of 71, and 70% were male.
They received subcutaneous sotatercept at dose levels of 0.1, 0.3, 0.5, or 1.0 mg/kg once every 3 weeks for up to 24 months following the first treatment.
Sotatercept efficacy
The investigators evaluated efficacy for the entire cohort as well as in subgroups of patients with high transfusion burden (HTB) and low transfusion burden (LTB). Patients were defined as HTB if they required RBC transfusions of 4 or more units every 8 weeks and LTB as less than 4 units per 8 weeks.
Overall, 45% (24/53) of the evaluable patients achieved hematologic improvement as defined by IWG 2006 criteria.
Forty-two percent of HTB patients had a reduction in their transfusion burden of 4 or more RBC units per 8 weeks, with a median duration of longest response of 106 days (range, 62 to 345+). Eleven percent (5/44) achieved RBC transfusion independence of 56 days or more.
Sixty-three percent (5/8) of LTB patients achieved both RBC transfusion independence of 56 days or more and a mean hemoglobin increase of 1.5 mg/dL or more for at least 8 weeks.
Their maximum mean hemoglobin increase ranged from 1.9 to 4.4 g/dL, and the mean duration of RBC transfusion independence ranged from 76 to 233+ days. Of these 8 patients, 67% were in the 1.0 mg/kg cohort.
Sotatercept safety
“Most of the adverse events were not necessarily related to the treatment,” Dr Komrokji said, “and they were grade 1 or grade 2 toxicity.”
Twenty of 54* patients (37%) experienced 1 or more treatment-related adverse events, the most common of which were fatigue/asthenia (13%), headache (9%), decreased appetite (7%), nausea (7%), and dyspnea (6%).
Three patients discontinued the study due to treatment-emergent adverse events that were possibly related to sotatercept. One was for grade 2 hemolytic anemia, 1 for grade 3 hypertension, and 1 for grade 2 muscle weakness.
Dr Komrokji concluded saying the results showed “promising evidence of clinical activity” in these ESA-refractory, anemic, lower-risk MDS and CMML patients who have a “challenging and unmet need for treatment.”
He indicated that further exploration of sotatercept at higher dose levels and for longer treatment periods is planned and ongoing.
He presented the data as abstract 3251. The study was supported by Celgene Corporation. ![]()
*One patient was excluded from the efficacy analysis due to a protocol violation.
site of the ASH Annual Meeting
Photo courtesy of ASH
SAN FRANCISCO—Two activin receptor fusion proteins, luspatercept and sotatercept, increased hemoglobin levels and transfusion independence in patients with β-thalassemia and myelodysplastic syndromes (MDS)/chronic myelomonocytic leukemia (CMML), respectively, in phase 2 trials.
Luspatercept is a type IIB activin receptor, while sotatercept is type IIA. Both impact late-stage erythropoiesis and improve anemia.
Investigators reported the trial results at the 2014 ASH Annual Meeting.
Luspatercept in β-thalassemia
Antonio G. Piga, MD, of Turin University in Italy, explained that luspatercept binds to GDF11 and other ligands in the TGF-β superfamily and promotes late-stage erythroid maturation.
The study was designed in the US and conducted abroad, he said, because while β-thalassemia is rare in the US, it is not so in Europe.
Investigators evaluated whether luspatercept could increase hemoglobin levels 1.5 g/dL or more for at least 2 weeks in non-transfusion-dependent (NTD) patients.
And in transfusion-dependent (TD) patients, luspatercept was expected to decrease the transfusion burden by 20% or more over 12 weeks.
Thirty patients, 7 TD and 23 NTD, received an injection of luspatercept every 3 weeks for 3 months at doses ranging from 0.2 to 1.0 mg/kg.
The median age was 35, and 53% of patients were male. Eighty-three percent had had a splenectomy.
Luspatercept efficacy
Three-quarters of patients treated with 0.8 to 1.0 mg/kg increased their hemoglobin levels or reduced their transfusion burden.
Of the NTD patients, 8 of 12 with iron overload at baseline experienced a reduction in liver iron concentration of 1 mg or more at 16 weeks.
And in the TD group, “All patients had clinically improved reduction of transfusion dependence,” Dr Piga said.
They had a more than 60% reduction in transfusion burden over 12 weeks. This included 2 patients with β0 β0 genotype, who experienced a 79% and 75% reduction.
“There was a trend to lower liver iron concentration in TD patients,” Dr Piga noted, “except in 1 patient.”
And 5 of 5 TD patients experienced decreases in serum ferritin ranging from 12% to 60%.
Luspatercept safety
Luspatercept did not cause any treatment-related serious or severe adverse events. The most common adverse events were bone pain (20%), headache (17%), myalgia (13%), and asthenia (10%).
There was 1 grade 3 dose-limiting toxicity of worsening lumbar spine bone pain, and 3 patients discontinued early, 1 each with occipital headache, ankle pain, and back pain.
Luspatercept had beneficial effects on other complications of the disease, Dr Piga noted, such as the healing of leg ulcers in the 3 patients with this complication, 1 who is just ending the trial.
With these promising results, Dr Piga said the investigators are “anxious to start phase 3.”
Dr Piga reported the data as abstract 53. The study was supported by Acceleron Pharma and Celgene Corporation.
Sotatercept in MDS and CMML with anemia
Rami Komrokji, MD, of the Moffit Cancer Center in Tampa, Florida, explained that sotaterept increases the release of mature erythrocytes into circulation by a mechanism distinct from erythropoietin.
Sotatercept was shown to stimulate erythropoiesis and increase hemoglobin levels in healthy volunteers, so investigators undertook to study its potential to treat anemia.
They conducted a phase 2 dose-finding study to determine the best effective dose in patients with anemia and lower-risk MDS or nonproliferative CMML who were refractory to erythropoiesis-stimulating agents (ESAs).
Investigators evaluated 53 patients who had anemia of 9 g/dL or less requiring 2 or more units of red blood cells (RBCs) in the 12 weeks prior to enrollment.
Their white blood cell counts had to be under 13,000/μL, and they had to have no response, loss of response, or low chance of response to ESAs, reflected by serum erythropoietin of more than 500 mIU/mL.
Patients were a median age of 71, and 70% were male.
They received subcutaneous sotatercept at dose levels of 0.1, 0.3, 0.5, or 1.0 mg/kg once every 3 weeks for up to 24 months following the first treatment.
Sotatercept efficacy
The investigators evaluated efficacy for the entire cohort as well as in subgroups of patients with high transfusion burden (HTB) and low transfusion burden (LTB). Patients were defined as HTB if they required RBC transfusions of 4 or more units every 8 weeks and LTB as less than 4 units per 8 weeks.
Overall, 45% (24/53) of the evaluable patients achieved hematologic improvement as defined by IWG 2006 criteria.
Forty-two percent of HTB patients had a reduction in their transfusion burden of 4 or more RBC units per 8 weeks, with a median duration of longest response of 106 days (range, 62 to 345+). Eleven percent (5/44) achieved RBC transfusion independence of 56 days or more.
Sixty-three percent (5/8) of LTB patients achieved both RBC transfusion independence of 56 days or more and a mean hemoglobin increase of 1.5 mg/dL or more for at least 8 weeks.
Their maximum mean hemoglobin increase ranged from 1.9 to 4.4 g/dL, and the mean duration of RBC transfusion independence ranged from 76 to 233+ days. Of these 8 patients, 67% were in the 1.0 mg/kg cohort.
Sotatercept safety
“Most of the adverse events were not necessarily related to the treatment,” Dr Komrokji said, “and they were grade 1 or grade 2 toxicity.”
Twenty of 54* patients (37%) experienced 1 or more treatment-related adverse events, the most common of which were fatigue/asthenia (13%), headache (9%), decreased appetite (7%), nausea (7%), and dyspnea (6%).
Three patients discontinued the study due to treatment-emergent adverse events that were possibly related to sotatercept. One was for grade 2 hemolytic anemia, 1 for grade 3 hypertension, and 1 for grade 2 muscle weakness.
Dr Komrokji concluded saying the results showed “promising evidence of clinical activity” in these ESA-refractory, anemic, lower-risk MDS and CMML patients who have a “challenging and unmet need for treatment.”
He indicated that further exploration of sotatercept at higher dose levels and for longer treatment periods is planned and ongoing.
He presented the data as abstract 3251. The study was supported by Celgene Corporation. ![]()
*One patient was excluded from the efficacy analysis due to a protocol violation.
site of the ASH Annual Meeting
Photo courtesy of ASH
SAN FRANCISCO—Two activin receptor fusion proteins, luspatercept and sotatercept, increased hemoglobin levels and transfusion independence in patients with β-thalassemia and myelodysplastic syndromes (MDS)/chronic myelomonocytic leukemia (CMML), respectively, in phase 2 trials.
Luspatercept is a type IIB activin receptor, while sotatercept is type IIA. Both impact late-stage erythropoiesis and improve anemia.
Investigators reported the trial results at the 2014 ASH Annual Meeting.
Luspatercept in β-thalassemia
Antonio G. Piga, MD, of Turin University in Italy, explained that luspatercept binds to GDF11 and other ligands in the TGF-β superfamily and promotes late-stage erythroid maturation.
The study was designed in the US and conducted abroad, he said, because while β-thalassemia is rare in the US, it is not so in Europe.
Investigators evaluated whether luspatercept could increase hemoglobin levels 1.5 g/dL or more for at least 2 weeks in non-transfusion-dependent (NTD) patients.
And in transfusion-dependent (TD) patients, luspatercept was expected to decrease the transfusion burden by 20% or more over 12 weeks.
Thirty patients, 7 TD and 23 NTD, received an injection of luspatercept every 3 weeks for 3 months at doses ranging from 0.2 to 1.0 mg/kg.
The median age was 35, and 53% of patients were male. Eighty-three percent had had a splenectomy.
Luspatercept efficacy
Three-quarters of patients treated with 0.8 to 1.0 mg/kg increased their hemoglobin levels or reduced their transfusion burden.
Of the NTD patients, 8 of 12 with iron overload at baseline experienced a reduction in liver iron concentration of 1 mg or more at 16 weeks.
And in the TD group, “All patients had clinically improved reduction of transfusion dependence,” Dr Piga said.
They had a more than 60% reduction in transfusion burden over 12 weeks. This included 2 patients with β0 β0 genotype, who experienced a 79% and 75% reduction.
“There was a trend to lower liver iron concentration in TD patients,” Dr Piga noted, “except in 1 patient.”
And 5 of 5 TD patients experienced decreases in serum ferritin ranging from 12% to 60%.
Luspatercept safety
Luspatercept did not cause any treatment-related serious or severe adverse events. The most common adverse events were bone pain (20%), headache (17%), myalgia (13%), and asthenia (10%).
There was 1 grade 3 dose-limiting toxicity of worsening lumbar spine bone pain, and 3 patients discontinued early, 1 each with occipital headache, ankle pain, and back pain.
Luspatercept had beneficial effects on other complications of the disease, Dr Piga noted, such as the healing of leg ulcers in the 3 patients with this complication, 1 who is just ending the trial.
With these promising results, Dr Piga said the investigators are “anxious to start phase 3.”
Dr Piga reported the data as abstract 53. The study was supported by Acceleron Pharma and Celgene Corporation.
Sotatercept in MDS and CMML with anemia
Rami Komrokji, MD, of the Moffit Cancer Center in Tampa, Florida, explained that sotaterept increases the release of mature erythrocytes into circulation by a mechanism distinct from erythropoietin.
Sotatercept was shown to stimulate erythropoiesis and increase hemoglobin levels in healthy volunteers, so investigators undertook to study its potential to treat anemia.
They conducted a phase 2 dose-finding study to determine the best effective dose in patients with anemia and lower-risk MDS or nonproliferative CMML who were refractory to erythropoiesis-stimulating agents (ESAs).
Investigators evaluated 53 patients who had anemia of 9 g/dL or less requiring 2 or more units of red blood cells (RBCs) in the 12 weeks prior to enrollment.
Their white blood cell counts had to be under 13,000/μL, and they had to have no response, loss of response, or low chance of response to ESAs, reflected by serum erythropoietin of more than 500 mIU/mL.
Patients were a median age of 71, and 70% were male.
They received subcutaneous sotatercept at dose levels of 0.1, 0.3, 0.5, or 1.0 mg/kg once every 3 weeks for up to 24 months following the first treatment.
Sotatercept efficacy
The investigators evaluated efficacy for the entire cohort as well as in subgroups of patients with high transfusion burden (HTB) and low transfusion burden (LTB). Patients were defined as HTB if they required RBC transfusions of 4 or more units every 8 weeks and LTB as less than 4 units per 8 weeks.
Overall, 45% (24/53) of the evaluable patients achieved hematologic improvement as defined by IWG 2006 criteria.
Forty-two percent of HTB patients had a reduction in their transfusion burden of 4 or more RBC units per 8 weeks, with a median duration of longest response of 106 days (range, 62 to 345+). Eleven percent (5/44) achieved RBC transfusion independence of 56 days or more.
Sixty-three percent (5/8) of LTB patients achieved both RBC transfusion independence of 56 days or more and a mean hemoglobin increase of 1.5 mg/dL or more for at least 8 weeks.
Their maximum mean hemoglobin increase ranged from 1.9 to 4.4 g/dL, and the mean duration of RBC transfusion independence ranged from 76 to 233+ days. Of these 8 patients, 67% were in the 1.0 mg/kg cohort.
Sotatercept safety
“Most of the adverse events were not necessarily related to the treatment,” Dr Komrokji said, “and they were grade 1 or grade 2 toxicity.”
Twenty of 54* patients (37%) experienced 1 or more treatment-related adverse events, the most common of which were fatigue/asthenia (13%), headache (9%), decreased appetite (7%), nausea (7%), and dyspnea (6%).
Three patients discontinued the study due to treatment-emergent adverse events that were possibly related to sotatercept. One was for grade 2 hemolytic anemia, 1 for grade 3 hypertension, and 1 for grade 2 muscle weakness.
Dr Komrokji concluded saying the results showed “promising evidence of clinical activity” in these ESA-refractory, anemic, lower-risk MDS and CMML patients who have a “challenging and unmet need for treatment.”
He indicated that further exploration of sotatercept at higher dose levels and for longer treatment periods is planned and ongoing.
He presented the data as abstract 3251. The study was supported by Celgene Corporation. ![]()
*One patient was excluded from the efficacy analysis due to a protocol violation.
Civilian Stress Compounds Service-Related Stress
The stresses of civilian life—job problems, divorce, money—can add to the burden when a service member is already under strain from deployment-related traumatic events, such as being wounded or sexually harassed. Those extramilitary stressors may make it more likely for reserve soldiers to abuse alcohol, say researchers from Columbia University in New York City; University of Michigan in Ann Arbor; Case Western Reserve University in Cleveland, and University of Toledo, both in Ohio.
The researchers surveyed 1,095 members of the Ohio Army National Guard who served mostly in Afghanistan and Iraq from June 2008 to February 2009. They wanted to find out the relative influence of both deployment-related trauma and civilian stress, including the influence of both or either on alcohol abuse.
Almost 60% of soldiers surveyed reported experiencing combat-related traumatic events; 13% of that group was abusing alcohol. Of the 17% who reported being sexually harassed, about 5% were abusing alcohol. Of the nearly 36% of respondents who also experienced civilian stressors, 7.1% were abusing alcohol. In a final model, only civilian stressors were associated with subsequent alcohol use disorder (AUD), independent of deployment-related traumatic events.
Of the respondents, 106 had experienced mental illness personally or in someone close to them, 156 had been through a divorce or breakup, and 105 had been unemployed for ≥ 3 months. While serving, 364 had encountered land mines, water mines, or booby traps; 573 had received hostile incoming fire; and 471 had been attacked by terrorists, insurgents, or civilians.
The civilian stressors found to be most closely associated with AUD were having a family member with a serious drug or alcohol problem (adjusted odds ratio [OR] 1.36; 95% CI, 0.96-1.94), being robbed or having the house broken into (adjusted OR, 1.48; 95% CI, 1.02-2.21), and having problems in getting access to adequate health care (adjusted OR, 1.97; 95% CI, 1.07-3.63). Having experienced sexual harassment was the most closely associated combat trauma.
It was clear to the researchers that the combination of deployment-related trauma and civilian stressors were associated with new onset of AUD. That could mean that adult-onset AUD constitutes a different phenotype from recurrent AUDs, the researchers say. They cite previous research that identified 2 “types” of people who abuse alcohol. One type has a later onset, has “greater malleability to the social environment,” uses alcohol to soothe anxiety, and has less severe alcohol dependence symptoms. The other type turns to alcohol earlier, may be genetically predisposed to alcohol abuse, uses alcohol for its euphoric effect, and has a chronic treatment history.
A consideration when evaluating the findings, the researchers say, is that the soldiers who were interviewed shortly after their deployment may have been misclassified because psychiatric symptoms tend to appear 3 to 4 months after deployment.
Source
Cerdá M, Richards C, Cohen GH, et al. Am J Prev Med. 2014;47(4):461-466.
doi: 10.1016/j.amepre.2014.06.015.
The stresses of civilian life—job problems, divorce, money—can add to the burden when a service member is already under strain from deployment-related traumatic events, such as being wounded or sexually harassed. Those extramilitary stressors may make it more likely for reserve soldiers to abuse alcohol, say researchers from Columbia University in New York City; University of Michigan in Ann Arbor; Case Western Reserve University in Cleveland, and University of Toledo, both in Ohio.
The researchers surveyed 1,095 members of the Ohio Army National Guard who served mostly in Afghanistan and Iraq from June 2008 to February 2009. They wanted to find out the relative influence of both deployment-related trauma and civilian stress, including the influence of both or either on alcohol abuse.
Almost 60% of soldiers surveyed reported experiencing combat-related traumatic events; 13% of that group was abusing alcohol. Of the 17% who reported being sexually harassed, about 5% were abusing alcohol. Of the nearly 36% of respondents who also experienced civilian stressors, 7.1% were abusing alcohol. In a final model, only civilian stressors were associated with subsequent alcohol use disorder (AUD), independent of deployment-related traumatic events.
Of the respondents, 106 had experienced mental illness personally or in someone close to them, 156 had been through a divorce or breakup, and 105 had been unemployed for ≥ 3 months. While serving, 364 had encountered land mines, water mines, or booby traps; 573 had received hostile incoming fire; and 471 had been attacked by terrorists, insurgents, or civilians.
The civilian stressors found to be most closely associated with AUD were having a family member with a serious drug or alcohol problem (adjusted odds ratio [OR] 1.36; 95% CI, 0.96-1.94), being robbed or having the house broken into (adjusted OR, 1.48; 95% CI, 1.02-2.21), and having problems in getting access to adequate health care (adjusted OR, 1.97; 95% CI, 1.07-3.63). Having experienced sexual harassment was the most closely associated combat trauma.
It was clear to the researchers that the combination of deployment-related trauma and civilian stressors were associated with new onset of AUD. That could mean that adult-onset AUD constitutes a different phenotype from recurrent AUDs, the researchers say. They cite previous research that identified 2 “types” of people who abuse alcohol. One type has a later onset, has “greater malleability to the social environment,” uses alcohol to soothe anxiety, and has less severe alcohol dependence symptoms. The other type turns to alcohol earlier, may be genetically predisposed to alcohol abuse, uses alcohol for its euphoric effect, and has a chronic treatment history.
A consideration when evaluating the findings, the researchers say, is that the soldiers who were interviewed shortly after their deployment may have been misclassified because psychiatric symptoms tend to appear 3 to 4 months after deployment.
Source
Cerdá M, Richards C, Cohen GH, et al. Am J Prev Med. 2014;47(4):461-466.
doi: 10.1016/j.amepre.2014.06.015.
The stresses of civilian life—job problems, divorce, money—can add to the burden when a service member is already under strain from deployment-related traumatic events, such as being wounded or sexually harassed. Those extramilitary stressors may make it more likely for reserve soldiers to abuse alcohol, say researchers from Columbia University in New York City; University of Michigan in Ann Arbor; Case Western Reserve University in Cleveland, and University of Toledo, both in Ohio.
The researchers surveyed 1,095 members of the Ohio Army National Guard who served mostly in Afghanistan and Iraq from June 2008 to February 2009. They wanted to find out the relative influence of both deployment-related trauma and civilian stress, including the influence of both or either on alcohol abuse.
Almost 60% of soldiers surveyed reported experiencing combat-related traumatic events; 13% of that group was abusing alcohol. Of the 17% who reported being sexually harassed, about 5% were abusing alcohol. Of the nearly 36% of respondents who also experienced civilian stressors, 7.1% were abusing alcohol. In a final model, only civilian stressors were associated with subsequent alcohol use disorder (AUD), independent of deployment-related traumatic events.
Of the respondents, 106 had experienced mental illness personally or in someone close to them, 156 had been through a divorce or breakup, and 105 had been unemployed for ≥ 3 months. While serving, 364 had encountered land mines, water mines, or booby traps; 573 had received hostile incoming fire; and 471 had been attacked by terrorists, insurgents, or civilians.
The civilian stressors found to be most closely associated with AUD were having a family member with a serious drug or alcohol problem (adjusted odds ratio [OR] 1.36; 95% CI, 0.96-1.94), being robbed or having the house broken into (adjusted OR, 1.48; 95% CI, 1.02-2.21), and having problems in getting access to adequate health care (adjusted OR, 1.97; 95% CI, 1.07-3.63). Having experienced sexual harassment was the most closely associated combat trauma.
It was clear to the researchers that the combination of deployment-related trauma and civilian stressors were associated with new onset of AUD. That could mean that adult-onset AUD constitutes a different phenotype from recurrent AUDs, the researchers say. They cite previous research that identified 2 “types” of people who abuse alcohol. One type has a later onset, has “greater malleability to the social environment,” uses alcohol to soothe anxiety, and has less severe alcohol dependence symptoms. The other type turns to alcohol earlier, may be genetically predisposed to alcohol abuse, uses alcohol for its euphoric effect, and has a chronic treatment history.
A consideration when evaluating the findings, the researchers say, is that the soldiers who were interviewed shortly after their deployment may have been misclassified because psychiatric symptoms tend to appear 3 to 4 months after deployment.
Source
Cerdá M, Richards C, Cohen GH, et al. Am J Prev Med. 2014;47(4):461-466.
doi: 10.1016/j.amepre.2014.06.015.
Discovery could help predict, prevent therapy-related AML

Credit: Rhoda Baer
A new study challenges the view that cancer treatment is a direct cause of therapy-related acute myeloid leukemia (AML).
The research suggests that mutations in p53 can accumulate in hematopoietic stem cells (HSCs) as a person ages, years before a cancer diagnosis.
If and when cancer develops, these mutated cells are more resistant to treatment and multiply at an accelerated pace after exposure to chemotherapy or radiation therapy, which can then lead to AML.
The findings, reported in Nature, open up new avenues for research to predict which patients are at risk of developing therapy-related AML and to find ways to prevent it.
“Until now, we’ve really understood very little about therapy-related AML and why it is so difficult to treat,” said study author Daniel Link, MD, of Washington University in St Louis, Missouri.
“This gives us some important clues for further studies aimed at treatment and prevention.”
Dr Link and his colleagues began this research by sequencing the genomes of 22 patients with therapy-related AML. The patients had similar numbers and types of mutations in their leukemia cells as other patients who developed AML without prior exposure to chemotherapy or radiation, an indication that cancer treatment does not cause widespread DNA damage.
“This is contrary to what physicians and scientists have long accepted as fact,” said study author Richard K. Wilson, PhD, of The Genome Institute at Washington University.
“It led us to consider a novel hypothesis: p53 mutations accumulate randomly as part of the aging process and are present in blood stem cells long before a patient is diagnosed with therapy-related AML.”
When therapy-related AML occurs, it typically develops 1 to 5 years after treatment with chemotherapy or radiation. Its incidence varies by cancer type. For example, 10% of lymphoma patients who relapse after chemotherapy go on to develop therapy-related AML, compared to 0.1% of breast cancer patients.
The researchers knew that patients with therapy-related AML are more likely than other AML patients to have a high rate of p53 mutations in their blood cells.
But the team was surprised to find that nearly 50% of 19 healthy subjects (aged 68 to 89 with no history of cancer or chemotherapy) had mutations in one copy of p53, an indicator that many people acquire mutations in this gene as they age.
The finding encouraged the researchers to dig further. They scoured the US to find bone marrow samples from patients with therapy-related AML that had been stored before the patients developed leukemia.
“We wanted to know whether we could go back in time—before a patient is diagnosed with therapy-related AML—to find the exact p53 mutation that caused them to develop leukemia years later,” Dr Link said.
The researchers found 7 bone marrow samples that fit the criteria. In 4 samples, they detected specific mutations in p53 that were present at very low rates in blood cells or bone marrow 3 to 6 years before the patients developed AML.
In the 3 cases in which p53 mutations could not be found, the researchers said it’s possible the mutations were present but at rates too low to be detected, or it may be that other age-related mutations contributed to the onset of therapy-related AML.
In related work in mice, the team showed that chemotherapy causes HSCs with mutations in p53 to divide rapidly, which gives them a competitive advantage. But that was not the case in HSCs with both copies of the gene intact.
The researchers suspect the early accumulation of p53 mutations in HSCs likely contributes to the frequent chromosomal and genetic abnormalities seen in patients with therapy-related AML and their poor responses to chemotherapy. The team believes other age-related mutations may be involved in the disease as well.
“We’re already conducting follow-up studies to look for other age-related mutations that may be at play in therapy-related AML,” Dr Link said. “As individuals, we’re not genetically homogeneous throughout our lives. Our DNA is constantly changing as we age, and we know this plays an important role in the development of cancer.”
“With advanced genomics, we can investigate the interplay between aging and the random accumulation of mutations, as a means to improve the diagnosis, treatment, and prevention of cancer.” ![]()
Credit: Rhoda Baer
A new study challenges the view that cancer treatment is a direct cause of therapy-related acute myeloid leukemia (AML).
The research suggests that mutations in p53 can accumulate in hematopoietic stem cells (HSCs) as a person ages, years before a cancer diagnosis.
If and when cancer develops, these mutated cells are more resistant to treatment and multiply at an accelerated pace after exposure to chemotherapy or radiation therapy, which can then lead to AML.
The findings, reported in Nature, open up new avenues for research to predict which patients are at risk of developing therapy-related AML and to find ways to prevent it.
“Until now, we’ve really understood very little about therapy-related AML and why it is so difficult to treat,” said study author Daniel Link, MD, of Washington University in St Louis, Missouri.
“This gives us some important clues for further studies aimed at treatment and prevention.”
Dr Link and his colleagues began this research by sequencing the genomes of 22 patients with therapy-related AML. The patients had similar numbers and types of mutations in their leukemia cells as other patients who developed AML without prior exposure to chemotherapy or radiation, an indication that cancer treatment does not cause widespread DNA damage.
“This is contrary to what physicians and scientists have long accepted as fact,” said study author Richard K. Wilson, PhD, of The Genome Institute at Washington University.
“It led us to consider a novel hypothesis: p53 mutations accumulate randomly as part of the aging process and are present in blood stem cells long before a patient is diagnosed with therapy-related AML.”
When therapy-related AML occurs, it typically develops 1 to 5 years after treatment with chemotherapy or radiation. Its incidence varies by cancer type. For example, 10% of lymphoma patients who relapse after chemotherapy go on to develop therapy-related AML, compared to 0.1% of breast cancer patients.
The researchers knew that patients with therapy-related AML are more likely than other AML patients to have a high rate of p53 mutations in their blood cells.
But the team was surprised to find that nearly 50% of 19 healthy subjects (aged 68 to 89 with no history of cancer or chemotherapy) had mutations in one copy of p53, an indicator that many people acquire mutations in this gene as they age.
The finding encouraged the researchers to dig further. They scoured the US to find bone marrow samples from patients with therapy-related AML that had been stored before the patients developed leukemia.
“We wanted to know whether we could go back in time—before a patient is diagnosed with therapy-related AML—to find the exact p53 mutation that caused them to develop leukemia years later,” Dr Link said.
The researchers found 7 bone marrow samples that fit the criteria. In 4 samples, they detected specific mutations in p53 that were present at very low rates in blood cells or bone marrow 3 to 6 years before the patients developed AML.
In the 3 cases in which p53 mutations could not be found, the researchers said it’s possible the mutations were present but at rates too low to be detected, or it may be that other age-related mutations contributed to the onset of therapy-related AML.
In related work in mice, the team showed that chemotherapy causes HSCs with mutations in p53 to divide rapidly, which gives them a competitive advantage. But that was not the case in HSCs with both copies of the gene intact.
The researchers suspect the early accumulation of p53 mutations in HSCs likely contributes to the frequent chromosomal and genetic abnormalities seen in patients with therapy-related AML and their poor responses to chemotherapy. The team believes other age-related mutations may be involved in the disease as well.
“We’re already conducting follow-up studies to look for other age-related mutations that may be at play in therapy-related AML,” Dr Link said. “As individuals, we’re not genetically homogeneous throughout our lives. Our DNA is constantly changing as we age, and we know this plays an important role in the development of cancer.”
“With advanced genomics, we can investigate the interplay between aging and the random accumulation of mutations, as a means to improve the diagnosis, treatment, and prevention of cancer.” ![]()
Credit: Rhoda Baer
A new study challenges the view that cancer treatment is a direct cause of therapy-related acute myeloid leukemia (AML).
The research suggests that mutations in p53 can accumulate in hematopoietic stem cells (HSCs) as a person ages, years before a cancer diagnosis.
If and when cancer develops, these mutated cells are more resistant to treatment and multiply at an accelerated pace after exposure to chemotherapy or radiation therapy, which can then lead to AML.
The findings, reported in Nature, open up new avenues for research to predict which patients are at risk of developing therapy-related AML and to find ways to prevent it.
“Until now, we’ve really understood very little about therapy-related AML and why it is so difficult to treat,” said study author Daniel Link, MD, of Washington University in St Louis, Missouri.
“This gives us some important clues for further studies aimed at treatment and prevention.”
Dr Link and his colleagues began this research by sequencing the genomes of 22 patients with therapy-related AML. The patients had similar numbers and types of mutations in their leukemia cells as other patients who developed AML without prior exposure to chemotherapy or radiation, an indication that cancer treatment does not cause widespread DNA damage.
“This is contrary to what physicians and scientists have long accepted as fact,” said study author Richard K. Wilson, PhD, of The Genome Institute at Washington University.
“It led us to consider a novel hypothesis: p53 mutations accumulate randomly as part of the aging process and are present in blood stem cells long before a patient is diagnosed with therapy-related AML.”
When therapy-related AML occurs, it typically develops 1 to 5 years after treatment with chemotherapy or radiation. Its incidence varies by cancer type. For example, 10% of lymphoma patients who relapse after chemotherapy go on to develop therapy-related AML, compared to 0.1% of breast cancer patients.
The researchers knew that patients with therapy-related AML are more likely than other AML patients to have a high rate of p53 mutations in their blood cells.
But the team was surprised to find that nearly 50% of 19 healthy subjects (aged 68 to 89 with no history of cancer or chemotherapy) had mutations in one copy of p53, an indicator that many people acquire mutations in this gene as they age.
The finding encouraged the researchers to dig further. They scoured the US to find bone marrow samples from patients with therapy-related AML that had been stored before the patients developed leukemia.
“We wanted to know whether we could go back in time—before a patient is diagnosed with therapy-related AML—to find the exact p53 mutation that caused them to develop leukemia years later,” Dr Link said.
The researchers found 7 bone marrow samples that fit the criteria. In 4 samples, they detected specific mutations in p53 that were present at very low rates in blood cells or bone marrow 3 to 6 years before the patients developed AML.
In the 3 cases in which p53 mutations could not be found, the researchers said it’s possible the mutations were present but at rates too low to be detected, or it may be that other age-related mutations contributed to the onset of therapy-related AML.
In related work in mice, the team showed that chemotherapy causes HSCs with mutations in p53 to divide rapidly, which gives them a competitive advantage. But that was not the case in HSCs with both copies of the gene intact.
The researchers suspect the early accumulation of p53 mutations in HSCs likely contributes to the frequent chromosomal and genetic abnormalities seen in patients with therapy-related AML and their poor responses to chemotherapy. The team believes other age-related mutations may be involved in the disease as well.
“We’re already conducting follow-up studies to look for other age-related mutations that may be at play in therapy-related AML,” Dr Link said. “As individuals, we’re not genetically homogeneous throughout our lives. Our DNA is constantly changing as we age, and we know this plays an important role in the development of cancer.”
“With advanced genomics, we can investigate the interplay between aging and the random accumulation of mutations, as a means to improve the diagnosis, treatment, and prevention of cancer.” ![]()
Ixazomib induces durable responses in hard-to-treat amyloidosis

Photo courtesy of ASH
SAN FRANCISCO—The oral proteasome inhibitor ixazomib induces high-quality hematologic responses in patients with relapsed/refractory systemic light-chain (AL) amyloidosis, with generally manageable side effects, a phase 1 study suggests.
Preliminary results from this study indicated that ixazomib had promise for treating AL amyloidosis.
Now, researchers have reported updated safety data and figures for hematologic and organ responses, progression-free survival, and overall survival.
The study was presented at the 2014 ASH Annual Meeting (abstract 3450) 5 days after the US Food and Drug Administration granted ixazomib breakthrough status for the treatment of relapsed/refractory AL amyloidosis.
“To have an oral drug that is well-tolerated and extremely effective in patients exposed to all lines of other therapy is remarkable in this disease,” said study investigator Giampaolo Merlini, MD, of the Amyloidosis Research and Treatment Center, Fondazione IRCCS Policlinico San Matteo, at the University of Pavia in Italy.
He and his colleagues evaluated ixazomib in 22 patients with a median age of 65 years. They were heavily pretreated, with 95% exposed to melphalan and 73% to bortezomib.
The patients received 4 mg of ixazomib on days 1, 8, and 15 of 28-day cycles for up to 12 cycles. Those who did not achieve a hematologic partial response after 3 cycles received added dexamethasone.
In 21 evaluable patients, the overall response rate was 52%, including a complete response and very good partial response in 43% of patients.
Dr Merlini noted that responses were deep and durable. And the high response rates translated into high organ response rates.
“End-organ damage is what kills patients,” he said. “In 18 evaluable patients, both the heart and kidney response rate was 45%.”
At 1 year, progression-free survival was 60%. At 2 years, overall survival was 63%.
The drug was well-tolerated as well. The 3 most common side effects—nausea, diarrhea, and fatigue—were mild and seen in about 30% of patients.
Severe grade 3 or higher side effects included thrombocytopenia, diarrhea, and rash, occurring in about 10% of patients.
The development program for ixazomib in AL amyloidosis progressed directly from this phase 1 trial to a phase 3 study, TOURMALINE-AL1. The trial is already underway, with 80 patients enrolled thus far.
TOURMALINE-AL1 investigators are comparing ixazomib plus dexamethasone to physician’s choice of treatment in patients with relapsed/refractory AL amyloidosis. Data from this trial are expected by the end of 2015.
“For the first time, we have evidence of an oral drug that is extremely effective,” Dr Merlini said. “We need to see the phase 3 data, but it could be a breakthrough.” ![]()
Photo courtesy of ASH
SAN FRANCISCO—The oral proteasome inhibitor ixazomib induces high-quality hematologic responses in patients with relapsed/refractory systemic light-chain (AL) amyloidosis, with generally manageable side effects, a phase 1 study suggests.
Preliminary results from this study indicated that ixazomib had promise for treating AL amyloidosis.
Now, researchers have reported updated safety data and figures for hematologic and organ responses, progression-free survival, and overall survival.
The study was presented at the 2014 ASH Annual Meeting (abstract 3450) 5 days after the US Food and Drug Administration granted ixazomib breakthrough status for the treatment of relapsed/refractory AL amyloidosis.
“To have an oral drug that is well-tolerated and extremely effective in patients exposed to all lines of other therapy is remarkable in this disease,” said study investigator Giampaolo Merlini, MD, of the Amyloidosis Research and Treatment Center, Fondazione IRCCS Policlinico San Matteo, at the University of Pavia in Italy.
He and his colleagues evaluated ixazomib in 22 patients with a median age of 65 years. They were heavily pretreated, with 95% exposed to melphalan and 73% to bortezomib.
The patients received 4 mg of ixazomib on days 1, 8, and 15 of 28-day cycles for up to 12 cycles. Those who did not achieve a hematologic partial response after 3 cycles received added dexamethasone.
In 21 evaluable patients, the overall response rate was 52%, including a complete response and very good partial response in 43% of patients.
Dr Merlini noted that responses were deep and durable. And the high response rates translated into high organ response rates.
“End-organ damage is what kills patients,” he said. “In 18 evaluable patients, both the heart and kidney response rate was 45%.”
At 1 year, progression-free survival was 60%. At 2 years, overall survival was 63%.
The drug was well-tolerated as well. The 3 most common side effects—nausea, diarrhea, and fatigue—were mild and seen in about 30% of patients.
Severe grade 3 or higher side effects included thrombocytopenia, diarrhea, and rash, occurring in about 10% of patients.
The development program for ixazomib in AL amyloidosis progressed directly from this phase 1 trial to a phase 3 study, TOURMALINE-AL1. The trial is already underway, with 80 patients enrolled thus far.
TOURMALINE-AL1 investigators are comparing ixazomib plus dexamethasone to physician’s choice of treatment in patients with relapsed/refractory AL amyloidosis. Data from this trial are expected by the end of 2015.
“For the first time, we have evidence of an oral drug that is extremely effective,” Dr Merlini said. “We need to see the phase 3 data, but it could be a breakthrough.” ![]()
Photo courtesy of ASH
SAN FRANCISCO—The oral proteasome inhibitor ixazomib induces high-quality hematologic responses in patients with relapsed/refractory systemic light-chain (AL) amyloidosis, with generally manageable side effects, a phase 1 study suggests.
Preliminary results from this study indicated that ixazomib had promise for treating AL amyloidosis.
Now, researchers have reported updated safety data and figures for hematologic and organ responses, progression-free survival, and overall survival.
The study was presented at the 2014 ASH Annual Meeting (abstract 3450) 5 days after the US Food and Drug Administration granted ixazomib breakthrough status for the treatment of relapsed/refractory AL amyloidosis.
“To have an oral drug that is well-tolerated and extremely effective in patients exposed to all lines of other therapy is remarkable in this disease,” said study investigator Giampaolo Merlini, MD, of the Amyloidosis Research and Treatment Center, Fondazione IRCCS Policlinico San Matteo, at the University of Pavia in Italy.
He and his colleagues evaluated ixazomib in 22 patients with a median age of 65 years. They were heavily pretreated, with 95% exposed to melphalan and 73% to bortezomib.
The patients received 4 mg of ixazomib on days 1, 8, and 15 of 28-day cycles for up to 12 cycles. Those who did not achieve a hematologic partial response after 3 cycles received added dexamethasone.
In 21 evaluable patients, the overall response rate was 52%, including a complete response and very good partial response in 43% of patients.
Dr Merlini noted that responses were deep and durable. And the high response rates translated into high organ response rates.
“End-organ damage is what kills patients,” he said. “In 18 evaluable patients, both the heart and kidney response rate was 45%.”
At 1 year, progression-free survival was 60%. At 2 years, overall survival was 63%.
The drug was well-tolerated as well. The 3 most common side effects—nausea, diarrhea, and fatigue—were mild and seen in about 30% of patients.
Severe grade 3 or higher side effects included thrombocytopenia, diarrhea, and rash, occurring in about 10% of patients.
The development program for ixazomib in AL amyloidosis progressed directly from this phase 1 trial to a phase 3 study, TOURMALINE-AL1. The trial is already underway, with 80 patients enrolled thus far.
TOURMALINE-AL1 investigators are comparing ixazomib plus dexamethasone to physician’s choice of treatment in patients with relapsed/refractory AL amyloidosis. Data from this trial are expected by the end of 2015.
“For the first time, we have evidence of an oral drug that is extremely effective,” Dr Merlini said. “We need to see the phase 3 data, but it could be a breakthrough.” ![]()
FDA approves first supplemental test for HTLV-I/II

Credit: Daniel Gay
The US Food and Drug Administration (FDA) has approved the first supplemental test for human T-cell lymphotropic virus-I/II (HTLV-I/II).
The test, MP Diagnostics HTLV Blot 2.4, is a qualitative enzyme immunoassay intended for use as an additional, more specific test for human serum or plasma specimens that have previously tested positive for HTLV-I/II.
MP Diagnostics HTLV Blot 2.4 can confirm infection with HTLV and differentiate between HTLV-I and HTLV-II.
The HTLVs are a group of human retroviruses known to cause diseases such as adult T-cell leukemia/lymphoma and myelopathy. HTLV can be transmitted from person to person through breastfeeding, unprotected sexual contact, or transfusion of blood from an infected donor.
Therefore, the FDA requires that donated blood be tested for HTLV-I/II antibodies. Currently, there are 2 FDA-licensed screening tests for HTLV-I/II. If a test is positive, the donation is discarded, and the donor is notified of his or her deferral.
The MP Diagnostics HTLV Blot 2.4 can provide blood establishments with additional information to convey to the donor. Specifically, the test can confirm HTLV infection and determine which virus type is causing the infection, HTLV-I or HTLV-II.
“The approval of MP Diagnostics HTLV Blot 2.4 will help blood establishments better counsel donors who have had positive results on an FDA-licensed HTLV-I/II screening test,” said Karen Midthun, MD, director of the FDA’s Center for Biologics Evaluation and Research.
MP Diagnostics HTLV Blot 2.4 is manufactured by MP Biomedicals Asia Pacific Pte. Ltd. in Singapore, a company of MP Biomedicals LLC in Santa Ana, California. For more information on the test, visit the MP Biomedicals website. ![]()
Credit: Daniel Gay
The US Food and Drug Administration (FDA) has approved the first supplemental test for human T-cell lymphotropic virus-I/II (HTLV-I/II).
The test, MP Diagnostics HTLV Blot 2.4, is a qualitative enzyme immunoassay intended for use as an additional, more specific test for human serum or plasma specimens that have previously tested positive for HTLV-I/II.
MP Diagnostics HTLV Blot 2.4 can confirm infection with HTLV and differentiate between HTLV-I and HTLV-II.
The HTLVs are a group of human retroviruses known to cause diseases such as adult T-cell leukemia/lymphoma and myelopathy. HTLV can be transmitted from person to person through breastfeeding, unprotected sexual contact, or transfusion of blood from an infected donor.
Therefore, the FDA requires that donated blood be tested for HTLV-I/II antibodies. Currently, there are 2 FDA-licensed screening tests for HTLV-I/II. If a test is positive, the donation is discarded, and the donor is notified of his or her deferral.
The MP Diagnostics HTLV Blot 2.4 can provide blood establishments with additional information to convey to the donor. Specifically, the test can confirm HTLV infection and determine which virus type is causing the infection, HTLV-I or HTLV-II.
“The approval of MP Diagnostics HTLV Blot 2.4 will help blood establishments better counsel donors who have had positive results on an FDA-licensed HTLV-I/II screening test,” said Karen Midthun, MD, director of the FDA’s Center for Biologics Evaluation and Research.
MP Diagnostics HTLV Blot 2.4 is manufactured by MP Biomedicals Asia Pacific Pte. Ltd. in Singapore, a company of MP Biomedicals LLC in Santa Ana, California. For more information on the test, visit the MP Biomedicals website. ![]()
Credit: Daniel Gay
The US Food and Drug Administration (FDA) has approved the first supplemental test for human T-cell lymphotropic virus-I/II (HTLV-I/II).
The test, MP Diagnostics HTLV Blot 2.4, is a qualitative enzyme immunoassay intended for use as an additional, more specific test for human serum or plasma specimens that have previously tested positive for HTLV-I/II.
MP Diagnostics HTLV Blot 2.4 can confirm infection with HTLV and differentiate between HTLV-I and HTLV-II.
The HTLVs are a group of human retroviruses known to cause diseases such as adult T-cell leukemia/lymphoma and myelopathy. HTLV can be transmitted from person to person through breastfeeding, unprotected sexual contact, or transfusion of blood from an infected donor.
Therefore, the FDA requires that donated blood be tested for HTLV-I/II antibodies. Currently, there are 2 FDA-licensed screening tests for HTLV-I/II. If a test is positive, the donation is discarded, and the donor is notified of his or her deferral.
The MP Diagnostics HTLV Blot 2.4 can provide blood establishments with additional information to convey to the donor. Specifically, the test can confirm HTLV infection and determine which virus type is causing the infection, HTLV-I or HTLV-II.
“The approval of MP Diagnostics HTLV Blot 2.4 will help blood establishments better counsel donors who have had positive results on an FDA-licensed HTLV-I/II screening test,” said Karen Midthun, MD, director of the FDA’s Center for Biologics Evaluation and Research.
MP Diagnostics HTLV Blot 2.4 is manufactured by MP Biomedicals Asia Pacific Pte. Ltd. in Singapore, a company of MP Biomedicals LLC in Santa Ana, California. For more information on the test, visit the MP Biomedicals website. ![]()
Experts debate venous sinus stenting for intracranial hypertension
SCOTTSDALE, ARIZ. – Venous sinus stenting remains a controversial treatment for headache associated with benign intracranial hypertension. Opponents highlight potentially serious adverse effects and a lack of rigorous studies on the procedure, while supporters describe it as safe and effective. Experts recently debated the procedure at a symposium sponsored by the American Headache Society.
Which came first?
Stenting is based on the rationale that lowering venous sinus pressure might lower intracranial pressure, said Dr. Deborah Friedman, a neuro-ophthalmologist at the University of Texas Southwestern Medical Center in Dallas.

“Other surgical techniques create a fistula the body wants to close,” she said. “Stenting may provide a permanent solution.”
The crux of the debate on stenting is whether venous sinus stenosis is a cause or outcome of benign intracranial hypertension (BIH), said Dr. Felipe Albuquerque, an endovascular neurosurgeon at the Barrow Neurological Institute in Phoenix. The fact that 90% of affected patients have venous sinus stenosis on MRI suggests stenosis is a valid etiology the condition, he said.
But Dr. Friedman disagreed. In a retrospective study of 51 patients with BIH and transverse sinus stenosis, 71% had more than 50% stenosis, but the degree and location of stenosis did not predict clinical outcome. The analysis also found no link between cerebrospinal fluid pressure and the location, degree, or residual area of stenosis. Nonetheless, the procedure may be useful in patients who have persistent transverse sinus stenosis after undergoing a shunt procedure, she said.
The cons of stenting
“Stenting carries a high risk of morbidity and mortality, compared with currently used treatments, and should only be used as a last resort in patients who are losing vision,” Dr. Friedman asserted. Most patients do well, but others suffer serious complications, including life-threatening anaphylaxis, subdural hematomas, subarachnoid hemorrhage, and brain herniation, she said.
In contrast, optic nerve sheath fenestration for BIH has no associated fatalities, according to Dr. Friedman. And in a National Inpatient Sample database analysis of 1,224 shunts, mortality was only 0.9% for ventriculoperitoneal shunt and 0.3% for lumbar-peritoneal shunt. No deaths were recorded for shunts performed for BIH or pseudotumor cerebri, she added.
The literature on venous sinus stenting “is a mess,” Dr. Friedman continued. “All data are from retrospective case series, and the diagnosis of idiopathic intracranial hypertension is questionable in some cases,” she said. “The indication for stenting is not well defined.”
Studies on the safety and efficacy of stenting have lacked a common primary outcome variable and may reflect reporting bias, Dr. Friedman said. Studies have been heterogeneous with regard to disease duration and the presence or absence of papilledema, visual status, previous treatments, and definitions of treatment failure, she added. No randomized, controlled trials have been carried out with sham stenting to assess the possibility of placebo effect, she noted.
“I think stenting may have utility in patients who have failed conventional therapy and have had another procedure that did not work. I think it very likely that there is a strong placebo effect in this group,” Dr. Friedman said.
“It’s not like our existing procedures are wonderful,” she added. “I wish we had something better to offer our patients.”
The pros
Venous sinus stenting “is usually effective in ameliorating both subjective headache and objective papilledema symptoms,” Dr. Albuquerque said. “One could argue that both ventriculoperitoneal shunt and lumbar-peritoneal shunt, the most commonly performed surgical interventions for benign intracranial hypertension, are substantially more invasive than stenting is and associated with far more severe complications.”
Dr. Albuquerque described a prospective study he conducted with his associates on 15 patients with BIH who underwent venous sinus stenting. In all, 80% of patients said their headaches improved, and 60% reported at least a 50% decrease in headache pain. Rates of patency and technical success were 100%, and no patients had permanent complications from the procedure, although one patient developed acute retroperitoneal hematoma, he said.
Dr. Albuquerque also reported his long-term follow-up of 27 patients who underwent venous sinus stenting to treat pseudotumors. All patients had more than 50% stenosis confirmed by retrograde venogram and a transstenotic pressure gradient that was greater than 12 mm Hg. Fully 70% of patients improved symptomatically, but five underwent a shunt procedure after they failed to improve. Patients experienced no permanent complications, although one required a stent for femoral artery pseudoaneurysm. Angiographies performed an average of 23 months later showed that all stents remained patent, although four patients had mild (less than 25%) stenosis. Five patients had narrowing of the sinus proximal to the stent.
Patients need dual antiplatelet therapy after venous sinus stenting, and the rate of chronic patency after the procedure is unknown, Dr. Albuquerque noted. Patients can develop scalp pain over the stented segment, he added.
“I think if you limit this procedure to a very select group of patients, I think its efficacy is tremendous,” Dr. Albuquerque concluded.
Dr. Albuquerque declared no conflicts of interest. Dr. Friedman reported serving on the speakers bureau of Allergan, receiving research grants from the National Eye Institute, Merck & Co., and ElectroCore, and having served as an expert witness (for the plaintiff and defense) on idiopathic intracranial hypertension.
SCOTTSDALE, ARIZ. – Venous sinus stenting remains a controversial treatment for headache associated with benign intracranial hypertension. Opponents highlight potentially serious adverse effects and a lack of rigorous studies on the procedure, while supporters describe it as safe and effective. Experts recently debated the procedure at a symposium sponsored by the American Headache Society.
Which came first?
Stenting is based on the rationale that lowering venous sinus pressure might lower intracranial pressure, said Dr. Deborah Friedman, a neuro-ophthalmologist at the University of Texas Southwestern Medical Center in Dallas.
“Other surgical techniques create a fistula the body wants to close,” she said. “Stenting may provide a permanent solution.”
The crux of the debate on stenting is whether venous sinus stenosis is a cause or outcome of benign intracranial hypertension (BIH), said Dr. Felipe Albuquerque, an endovascular neurosurgeon at the Barrow Neurological Institute in Phoenix. The fact that 90% of affected patients have venous sinus stenosis on MRI suggests stenosis is a valid etiology the condition, he said.
But Dr. Friedman disagreed. In a retrospective study of 51 patients with BIH and transverse sinus stenosis, 71% had more than 50% stenosis, but the degree and location of stenosis did not predict clinical outcome. The analysis also found no link between cerebrospinal fluid pressure and the location, degree, or residual area of stenosis. Nonetheless, the procedure may be useful in patients who have persistent transverse sinus stenosis after undergoing a shunt procedure, she said.
The cons of stenting
“Stenting carries a high risk of morbidity and mortality, compared with currently used treatments, and should only be used as a last resort in patients who are losing vision,” Dr. Friedman asserted. Most patients do well, but others suffer serious complications, including life-threatening anaphylaxis, subdural hematomas, subarachnoid hemorrhage, and brain herniation, she said.
In contrast, optic nerve sheath fenestration for BIH has no associated fatalities, according to Dr. Friedman. And in a National Inpatient Sample database analysis of 1,224 shunts, mortality was only 0.9% for ventriculoperitoneal shunt and 0.3% for lumbar-peritoneal shunt. No deaths were recorded for shunts performed for BIH or pseudotumor cerebri, she added.
The literature on venous sinus stenting “is a mess,” Dr. Friedman continued. “All data are from retrospective case series, and the diagnosis of idiopathic intracranial hypertension is questionable in some cases,” she said. “The indication for stenting is not well defined.”
Studies on the safety and efficacy of stenting have lacked a common primary outcome variable and may reflect reporting bias, Dr. Friedman said. Studies have been heterogeneous with regard to disease duration and the presence or absence of papilledema, visual status, previous treatments, and definitions of treatment failure, she added. No randomized, controlled trials have been carried out with sham stenting to assess the possibility of placebo effect, she noted.
“I think stenting may have utility in patients who have failed conventional therapy and have had another procedure that did not work. I think it very likely that there is a strong placebo effect in this group,” Dr. Friedman said.
“It’s not like our existing procedures are wonderful,” she added. “I wish we had something better to offer our patients.”
The pros
Venous sinus stenting “is usually effective in ameliorating both subjective headache and objective papilledema symptoms,” Dr. Albuquerque said. “One could argue that both ventriculoperitoneal shunt and lumbar-peritoneal shunt, the most commonly performed surgical interventions for benign intracranial hypertension, are substantially more invasive than stenting is and associated with far more severe complications.”
Dr. Albuquerque described a prospective study he conducted with his associates on 15 patients with BIH who underwent venous sinus stenting. In all, 80% of patients said their headaches improved, and 60% reported at least a 50% decrease in headache pain. Rates of patency and technical success were 100%, and no patients had permanent complications from the procedure, although one patient developed acute retroperitoneal hematoma, he said.
Dr. Albuquerque also reported his long-term follow-up of 27 patients who underwent venous sinus stenting to treat pseudotumors. All patients had more than 50% stenosis confirmed by retrograde venogram and a transstenotic pressure gradient that was greater than 12 mm Hg. Fully 70% of patients improved symptomatically, but five underwent a shunt procedure after they failed to improve. Patients experienced no permanent complications, although one required a stent for femoral artery pseudoaneurysm. Angiographies performed an average of 23 months later showed that all stents remained patent, although four patients had mild (less than 25%) stenosis. Five patients had narrowing of the sinus proximal to the stent.
Patients need dual antiplatelet therapy after venous sinus stenting, and the rate of chronic patency after the procedure is unknown, Dr. Albuquerque noted. Patients can develop scalp pain over the stented segment, he added.
“I think if you limit this procedure to a very select group of patients, I think its efficacy is tremendous,” Dr. Albuquerque concluded.
Dr. Albuquerque declared no conflicts of interest. Dr. Friedman reported serving on the speakers bureau of Allergan, receiving research grants from the National Eye Institute, Merck & Co., and ElectroCore, and having served as an expert witness (for the plaintiff and defense) on idiopathic intracranial hypertension.
SCOTTSDALE, ARIZ. – Venous sinus stenting remains a controversial treatment for headache associated with benign intracranial hypertension. Opponents highlight potentially serious adverse effects and a lack of rigorous studies on the procedure, while supporters describe it as safe and effective. Experts recently debated the procedure at a symposium sponsored by the American Headache Society.
Which came first?
Stenting is based on the rationale that lowering venous sinus pressure might lower intracranial pressure, said Dr. Deborah Friedman, a neuro-ophthalmologist at the University of Texas Southwestern Medical Center in Dallas.
“Other surgical techniques create a fistula the body wants to close,” she said. “Stenting may provide a permanent solution.”
The crux of the debate on stenting is whether venous sinus stenosis is a cause or outcome of benign intracranial hypertension (BIH), said Dr. Felipe Albuquerque, an endovascular neurosurgeon at the Barrow Neurological Institute in Phoenix. The fact that 90% of affected patients have venous sinus stenosis on MRI suggests stenosis is a valid etiology the condition, he said.
But Dr. Friedman disagreed. In a retrospective study of 51 patients with BIH and transverse sinus stenosis, 71% had more than 50% stenosis, but the degree and location of stenosis did not predict clinical outcome. The analysis also found no link between cerebrospinal fluid pressure and the location, degree, or residual area of stenosis. Nonetheless, the procedure may be useful in patients who have persistent transverse sinus stenosis after undergoing a shunt procedure, she said.
The cons of stenting
“Stenting carries a high risk of morbidity and mortality, compared with currently used treatments, and should only be used as a last resort in patients who are losing vision,” Dr. Friedman asserted. Most patients do well, but others suffer serious complications, including life-threatening anaphylaxis, subdural hematomas, subarachnoid hemorrhage, and brain herniation, she said.
In contrast, optic nerve sheath fenestration for BIH has no associated fatalities, according to Dr. Friedman. And in a National Inpatient Sample database analysis of 1,224 shunts, mortality was only 0.9% for ventriculoperitoneal shunt and 0.3% for lumbar-peritoneal shunt. No deaths were recorded for shunts performed for BIH or pseudotumor cerebri, she added.
The literature on venous sinus stenting “is a mess,” Dr. Friedman continued. “All data are from retrospective case series, and the diagnosis of idiopathic intracranial hypertension is questionable in some cases,” she said. “The indication for stenting is not well defined.”
Studies on the safety and efficacy of stenting have lacked a common primary outcome variable and may reflect reporting bias, Dr. Friedman said. Studies have been heterogeneous with regard to disease duration and the presence or absence of papilledema, visual status, previous treatments, and definitions of treatment failure, she added. No randomized, controlled trials have been carried out with sham stenting to assess the possibility of placebo effect, she noted.
“I think stenting may have utility in patients who have failed conventional therapy and have had another procedure that did not work. I think it very likely that there is a strong placebo effect in this group,” Dr. Friedman said.
“It’s not like our existing procedures are wonderful,” she added. “I wish we had something better to offer our patients.”
The pros
Venous sinus stenting “is usually effective in ameliorating both subjective headache and objective papilledema symptoms,” Dr. Albuquerque said. “One could argue that both ventriculoperitoneal shunt and lumbar-peritoneal shunt, the most commonly performed surgical interventions for benign intracranial hypertension, are substantially more invasive than stenting is and associated with far more severe complications.”
Dr. Albuquerque described a prospective study he conducted with his associates on 15 patients with BIH who underwent venous sinus stenting. In all, 80% of patients said their headaches improved, and 60% reported at least a 50% decrease in headache pain. Rates of patency and technical success were 100%, and no patients had permanent complications from the procedure, although one patient developed acute retroperitoneal hematoma, he said.
Dr. Albuquerque also reported his long-term follow-up of 27 patients who underwent venous sinus stenting to treat pseudotumors. All patients had more than 50% stenosis confirmed by retrograde venogram and a transstenotic pressure gradient that was greater than 12 mm Hg. Fully 70% of patients improved symptomatically, but five underwent a shunt procedure after they failed to improve. Patients experienced no permanent complications, although one required a stent for femoral artery pseudoaneurysm. Angiographies performed an average of 23 months later showed that all stents remained patent, although four patients had mild (less than 25%) stenosis. Five patients had narrowing of the sinus proximal to the stent.
Patients need dual antiplatelet therapy after venous sinus stenting, and the rate of chronic patency after the procedure is unknown, Dr. Albuquerque noted. Patients can develop scalp pain over the stented segment, he added.
“I think if you limit this procedure to a very select group of patients, I think its efficacy is tremendous,” Dr. Albuquerque concluded.
Dr. Albuquerque declared no conflicts of interest. Dr. Friedman reported serving on the speakers bureau of Allergan, receiving research grants from the National Eye Institute, Merck & Co., and ElectroCore, and having served as an expert witness (for the plaintiff and defense) on idiopathic intracranial hypertension.
EXPERT ANALYSIS AT THE SCOTTSDALE HEADACHE SYMPOSIUM

At-home radiofrequency devices
The field of body contouring and tissue tightening has expanded over the years, with many new devices appearing on the market that utilize radiofrequency (RF) energy to tighten and rejuvenate the skin. What originally began with a single monopolar RF device has progressed to a world in which there are skin-tightening devices that use bipolar energy and tripolar energy, as well as monopolar, and newer machines that boast five and eight poles of RF energy.
In addition to in-office radiofrequency devices, at-home devices are now available.
Radiofrequency energy uses the tissue’s resistance within the various layers of the skin to transform the RF energy given to the skin into thermal energy. This process induces collagen remodeling and neocollagenesis, resulting in skin tightening. Since RF energy produces an electrical current instead of a light source like lasers, tissue damage can be minimized, and epidermal melanin is not targeted or typically damaged. Therefore, RF energies can be used for patients of all skin types and colors. Adverse events to RF therapy in general may include pain, erythema, swelling, and rare reports of burns or fat atrophy with first-generation devices.
Many at-home devices delivering RF energy have been developed and are now on the market for skin tightening and rejuvenation. These devices range in cost from about $30 to more than $1,000, and are marketed for skin tightening as well as body contouring. Most machines require multiple uses, daily or weekly, to achieve desired results, compared with in-office devices that are typically used once, or not more than once every 6 months. A recent study published in the Journal of Drugs in Dermatology of a newer at-home device that uses phase-controlled multisource radiofrequency technology found statistically significant improvement using a Fitzpatrick wrinkle and elastosis scale of 62 patients when pre- and post-photographs of 62 patients were evaluated by three independent board-certified dermatologists.
At-home devices do not deliver energies as high as in-office devices, and no head-to-head studies comparing in-office versus at-home RF devices are currently available. As even in-office radiofrequency device results can be subtle, or occur over 6 months, patient expectations should be managed, and clinicians should be realistic when counseling patients about the use of these devices. Patient selection is key for successful therapy. If skin laxity is severe enough that the patient warrants a face lift or surgical correction to achieve the desired results, then they may not be the best candidate for RF therapy alone.
Dr. Talakoub and Dr. Wesley are co-contributors to a monthly Aesthetic Dermatology column in Skin & Allergy News. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Wesley.
The field of body contouring and tissue tightening has expanded over the years, with many new devices appearing on the market that utilize radiofrequency (RF) energy to tighten and rejuvenate the skin. What originally began with a single monopolar RF device has progressed to a world in which there are skin-tightening devices that use bipolar energy and tripolar energy, as well as monopolar, and newer machines that boast five and eight poles of RF energy.
In addition to in-office radiofrequency devices, at-home devices are now available.
Radiofrequency energy uses the tissue’s resistance within the various layers of the skin to transform the RF energy given to the skin into thermal energy. This process induces collagen remodeling and neocollagenesis, resulting in skin tightening. Since RF energy produces an electrical current instead of a light source like lasers, tissue damage can be minimized, and epidermal melanin is not targeted or typically damaged. Therefore, RF energies can be used for patients of all skin types and colors. Adverse events to RF therapy in general may include pain, erythema, swelling, and rare reports of burns or fat atrophy with first-generation devices.
Many at-home devices delivering RF energy have been developed and are now on the market for skin tightening and rejuvenation. These devices range in cost from about $30 to more than $1,000, and are marketed for skin tightening as well as body contouring. Most machines require multiple uses, daily or weekly, to achieve desired results, compared with in-office devices that are typically used once, or not more than once every 6 months. A recent study published in the Journal of Drugs in Dermatology of a newer at-home device that uses phase-controlled multisource radiofrequency technology found statistically significant improvement using a Fitzpatrick wrinkle and elastosis scale of 62 patients when pre- and post-photographs of 62 patients were evaluated by three independent board-certified dermatologists.
At-home devices do not deliver energies as high as in-office devices, and no head-to-head studies comparing in-office versus at-home RF devices are currently available. As even in-office radiofrequency device results can be subtle, or occur over 6 months, patient expectations should be managed, and clinicians should be realistic when counseling patients about the use of these devices. Patient selection is key for successful therapy. If skin laxity is severe enough that the patient warrants a face lift or surgical correction to achieve the desired results, then they may not be the best candidate for RF therapy alone.
Dr. Talakoub and Dr. Wesley are co-contributors to a monthly Aesthetic Dermatology column in Skin & Allergy News. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Wesley.
The field of body contouring and tissue tightening has expanded over the years, with many new devices appearing on the market that utilize radiofrequency (RF) energy to tighten and rejuvenate the skin. What originally began with a single monopolar RF device has progressed to a world in which there are skin-tightening devices that use bipolar energy and tripolar energy, as well as monopolar, and newer machines that boast five and eight poles of RF energy.
In addition to in-office radiofrequency devices, at-home devices are now available.
Radiofrequency energy uses the tissue’s resistance within the various layers of the skin to transform the RF energy given to the skin into thermal energy. This process induces collagen remodeling and neocollagenesis, resulting in skin tightening. Since RF energy produces an electrical current instead of a light source like lasers, tissue damage can be minimized, and epidermal melanin is not targeted or typically damaged. Therefore, RF energies can be used for patients of all skin types and colors. Adverse events to RF therapy in general may include pain, erythema, swelling, and rare reports of burns or fat atrophy with first-generation devices.
Many at-home devices delivering RF energy have been developed and are now on the market for skin tightening and rejuvenation. These devices range in cost from about $30 to more than $1,000, and are marketed for skin tightening as well as body contouring. Most machines require multiple uses, daily or weekly, to achieve desired results, compared with in-office devices that are typically used once, or not more than once every 6 months. A recent study published in the Journal of Drugs in Dermatology of a newer at-home device that uses phase-controlled multisource radiofrequency technology found statistically significant improvement using a Fitzpatrick wrinkle and elastosis scale of 62 patients when pre- and post-photographs of 62 patients were evaluated by three independent board-certified dermatologists.
At-home devices do not deliver energies as high as in-office devices, and no head-to-head studies comparing in-office versus at-home RF devices are currently available. As even in-office radiofrequency device results can be subtle, or occur over 6 months, patient expectations should be managed, and clinicians should be realistic when counseling patients about the use of these devices. Patient selection is key for successful therapy. If skin laxity is severe enough that the patient warrants a face lift or surgical correction to achieve the desired results, then they may not be the best candidate for RF therapy alone.
Dr. Talakoub and Dr. Wesley are co-contributors to a monthly Aesthetic Dermatology column in Skin & Allergy News. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Wesley.

Maintaining Adequate Third-Party Compensation
In a previous column I discussed the challenges inherent to incorporating the Patient Protection and Affordable Care Act’s health insurance exchanges into private practices.1 While it is important to pay close attention to newer third-party vehicles, do not ignore established payers or assume their compensation schedules are up-to-date.
Because traditional insurers and managed care organizations typically do not take it upon themselves to update their payment schedules for private practices on a regular basis, you should take a close look at your third-party plans; you may be surprised to find that you have unknowingly remained associated with an outdated plan with an inappropriate fee schedule or with few patients generating negligible remuneration for your practice when you could have replaced it with a young, aggressive, well-paying organization long ago.
As is usually the case, you will never know unless you look. The process is the sort of disagreeable task that smaller practices often postpone or ignore completely, but the effort is well worth it. First, ask your employees to assemble some data. Start with lists of the last 50 patients affiliated with each third-party contract; your electronic records should allow you to assemble these data easily. For each patient, note the diagnoses; the procedure codes billed; the amounts billed and paid for each code; and any problems encountered, especially payment delays and records requests. Also ask for any correspondence you have on file with claims departments and medical directors over the last year.
Next, send out a questionnaire to the provider relations department for each third-party payer. Tell them you are updating your managed care data. Include a list of your 25 most commonly used Current Procedural Terminology (CPT) codes and ask for their maximum allowable reimbursement on each code. Then ask some basic questions. There are 5 questions we routinely ask in my practice:
- Does your organization recognize the use of CPT modifier 25?
- If a diagnostic or surgical procedure and an evaluation and management encounter are performed during the same patient visit, does your organization reimburse them as separate (unbundled) services?
- If multiple diagnostic or surgical procedures are performed on the same day, how does your organization reimburse such procedures?
- What are your official criteria for coding consultations versus office visits?
- What is your average and maximum time for processing a clean claim?
Have a staffer follow-up with a telephone call 10 days later on each letter to make sure it was received and will be answered promptly.
Once these questions have been answered, schedule a meeting with your office manager and your insurance specialist. Put the telephones on service, ask someone else to cover emergencies, and otherwise make sure you will not be disturbed during this time. Armed with the answers received from each payer and the data you have collected, analyze each plan in detail during this meeting. How many of the payer’s patients are currently active in your practice? Is that number increasing or decreasing? How well does each one compensate you compared to other payers, Medicare, and your regular fees, and how promptly are you paid? What problems have you had with referral and claim forms? Are you permitted to bill patients for uncovered charges?
More specific issues also should be addressed. For instance, what services, precisely, are not covered? Which procedures are paid particularly well and which are paid poorly (or not at all) despite being ostensibly “covered”? Are there any unusual or unorthodox rules for certain surgical or diagnostic procedures? Do you get an inordinate number of requests for further information from the payer? Are you asked for the same information repeatedly? Are there problems with CPT modifiers 25 and 78, or other modifiers?
Then take a hard look at the numbers. What fraction of your accounts receivable is attributed to each plan at any particular moment? Is that number increasing? If so, is it because the number of patients in that plan is increasing, or is it because the plan is losing momentum in paying its bills? The latter is a red flag; either growth is outstripping efficiency or financial problems are looming.
It also is important to look at mechanics of each plan. How easy is it for patients to get a referral to your office? Do primary care practitioners dole out referrals as if they were diamonds? Be sure to review the referral requirements in each of your contracts. On those all-too-common occasions when patients show up for an appointment without a valid referral, how easy does the plan make it to get them one quickly?
Finally, talk to your insurance representatives, the staffers who deal with these plans on a daily basis. Their subjective impressions are just as important as any hard data. They will immediately separate the good plans from the bad, but it also is important to ask them some specific questions. Is your staff constantly cutting through red tape to get patients seen? Are claim forms confusing or hard to file? How hard is it to get a hold of provider relations representatives, and once contacted, are they helpful and courteous? Are provider relations representatives constantly calling your office with unnecessary or inappropriate questions?
After you collect all of this information, you will have your own up-to-the-minute managed care database, which you can consult immediately to determine which plans you will keep and which you should disengage. Repeat this exercise regularly—we now do it yearly in my practice—because the private insurance environment is evolving ever more rapidly due to the advent of the Patient Protection and Affordable Care Act and other factors.
Another important use for your managed care database is to renegotiate your fee schedule. Any payer with fees that are below your average remuneration should receive a letter informing them that the payments are below the level that is recognized as usual and customary in your area. Inform them that your office will be pleased to give them the opportunity to remain associated with your practice if their reimbursements are immediately increased. Although insurers are not always receptive to requests for increased compensation, they are usually willing to open a dialogue; if not, you will need to reconsider your practice’s continued association with that plan.
This exercise requires a lot of work, but your time and effort will be well spent. In addition to ensuring that your services are properly compensated, you will be putting your third-party payers on notice that you are paying attention and that your office will not tolerate unfair remuneration or inordinate delays in payment.
- Eastern J. Should you accept insurance exchange coverage? Cutis. 2014;94:75-77.
In a previous column I discussed the challenges inherent to incorporating the Patient Protection and Affordable Care Act’s health insurance exchanges into private practices.1 While it is important to pay close attention to newer third-party vehicles, do not ignore established payers or assume their compensation schedules are up-to-date.
Because traditional insurers and managed care organizations typically do not take it upon themselves to update their payment schedules for private practices on a regular basis, you should take a close look at your third-party plans; you may be surprised to find that you have unknowingly remained associated with an outdated plan with an inappropriate fee schedule or with few patients generating negligible remuneration for your practice when you could have replaced it with a young, aggressive, well-paying organization long ago.
As is usually the case, you will never know unless you look. The process is the sort of disagreeable task that smaller practices often postpone or ignore completely, but the effort is well worth it. First, ask your employees to assemble some data. Start with lists of the last 50 patients affiliated with each third-party contract; your electronic records should allow you to assemble these data easily. For each patient, note the diagnoses; the procedure codes billed; the amounts billed and paid for each code; and any problems encountered, especially payment delays and records requests. Also ask for any correspondence you have on file with claims departments and medical directors over the last year.
Next, send out a questionnaire to the provider relations department for each third-party payer. Tell them you are updating your managed care data. Include a list of your 25 most commonly used Current Procedural Terminology (CPT) codes and ask for their maximum allowable reimbursement on each code. Then ask some basic questions. There are 5 questions we routinely ask in my practice:
- Does your organization recognize the use of CPT modifier 25?
- If a diagnostic or surgical procedure and an evaluation and management encounter are performed during the same patient visit, does your organization reimburse them as separate (unbundled) services?
- If multiple diagnostic or surgical procedures are performed on the same day, how does your organization reimburse such procedures?
- What are your official criteria for coding consultations versus office visits?
- What is your average and maximum time for processing a clean claim?
Have a staffer follow-up with a telephone call 10 days later on each letter to make sure it was received and will be answered promptly.
Once these questions have been answered, schedule a meeting with your office manager and your insurance specialist. Put the telephones on service, ask someone else to cover emergencies, and otherwise make sure you will not be disturbed during this time. Armed with the answers received from each payer and the data you have collected, analyze each plan in detail during this meeting. How many of the payer’s patients are currently active in your practice? Is that number increasing or decreasing? How well does each one compensate you compared to other payers, Medicare, and your regular fees, and how promptly are you paid? What problems have you had with referral and claim forms? Are you permitted to bill patients for uncovered charges?
More specific issues also should be addressed. For instance, what services, precisely, are not covered? Which procedures are paid particularly well and which are paid poorly (or not at all) despite being ostensibly “covered”? Are there any unusual or unorthodox rules for certain surgical or diagnostic procedures? Do you get an inordinate number of requests for further information from the payer? Are you asked for the same information repeatedly? Are there problems with CPT modifiers 25 and 78, or other modifiers?
Then take a hard look at the numbers. What fraction of your accounts receivable is attributed to each plan at any particular moment? Is that number increasing? If so, is it because the number of patients in that plan is increasing, or is it because the plan is losing momentum in paying its bills? The latter is a red flag; either growth is outstripping efficiency or financial problems are looming.
It also is important to look at mechanics of each plan. How easy is it for patients to get a referral to your office? Do primary care practitioners dole out referrals as if they were diamonds? Be sure to review the referral requirements in each of your contracts. On those all-too-common occasions when patients show up for an appointment without a valid referral, how easy does the plan make it to get them one quickly?
Finally, talk to your insurance representatives, the staffers who deal with these plans on a daily basis. Their subjective impressions are just as important as any hard data. They will immediately separate the good plans from the bad, but it also is important to ask them some specific questions. Is your staff constantly cutting through red tape to get patients seen? Are claim forms confusing or hard to file? How hard is it to get a hold of provider relations representatives, and once contacted, are they helpful and courteous? Are provider relations representatives constantly calling your office with unnecessary or inappropriate questions?
After you collect all of this information, you will have your own up-to-the-minute managed care database, which you can consult immediately to determine which plans you will keep and which you should disengage. Repeat this exercise regularly—we now do it yearly in my practice—because the private insurance environment is evolving ever more rapidly due to the advent of the Patient Protection and Affordable Care Act and other factors.
Another important use for your managed care database is to renegotiate your fee schedule. Any payer with fees that are below your average remuneration should receive a letter informing them that the payments are below the level that is recognized as usual and customary in your area. Inform them that your office will be pleased to give them the opportunity to remain associated with your practice if their reimbursements are immediately increased. Although insurers are not always receptive to requests for increased compensation, they are usually willing to open a dialogue; if not, you will need to reconsider your practice’s continued association with that plan.
This exercise requires a lot of work, but your time and effort will be well spent. In addition to ensuring that your services are properly compensated, you will be putting your third-party payers on notice that you are paying attention and that your office will not tolerate unfair remuneration or inordinate delays in payment.
In a previous column I discussed the challenges inherent to incorporating the Patient Protection and Affordable Care Act’s health insurance exchanges into private practices.1 While it is important to pay close attention to newer third-party vehicles, do not ignore established payers or assume their compensation schedules are up-to-date.
Because traditional insurers and managed care organizations typically do not take it upon themselves to update their payment schedules for private practices on a regular basis, you should take a close look at your third-party plans; you may be surprised to find that you have unknowingly remained associated with an outdated plan with an inappropriate fee schedule or with few patients generating negligible remuneration for your practice when you could have replaced it with a young, aggressive, well-paying organization long ago.
As is usually the case, you will never know unless you look. The process is the sort of disagreeable task that smaller practices often postpone or ignore completely, but the effort is well worth it. First, ask your employees to assemble some data. Start with lists of the last 50 patients affiliated with each third-party contract; your electronic records should allow you to assemble these data easily. For each patient, note the diagnoses; the procedure codes billed; the amounts billed and paid for each code; and any problems encountered, especially payment delays and records requests. Also ask for any correspondence you have on file with claims departments and medical directors over the last year.
Next, send out a questionnaire to the provider relations department for each third-party payer. Tell them you are updating your managed care data. Include a list of your 25 most commonly used Current Procedural Terminology (CPT) codes and ask for their maximum allowable reimbursement on each code. Then ask some basic questions. There are 5 questions we routinely ask in my practice:
- Does your organization recognize the use of CPT modifier 25?
- If a diagnostic or surgical procedure and an evaluation and management encounter are performed during the same patient visit, does your organization reimburse them as separate (unbundled) services?
- If multiple diagnostic or surgical procedures are performed on the same day, how does your organization reimburse such procedures?
- What are your official criteria for coding consultations versus office visits?
- What is your average and maximum time for processing a clean claim?
Have a staffer follow-up with a telephone call 10 days later on each letter to make sure it was received and will be answered promptly.
Once these questions have been answered, schedule a meeting with your office manager and your insurance specialist. Put the telephones on service, ask someone else to cover emergencies, and otherwise make sure you will not be disturbed during this time. Armed with the answers received from each payer and the data you have collected, analyze each plan in detail during this meeting. How many of the payer’s patients are currently active in your practice? Is that number increasing or decreasing? How well does each one compensate you compared to other payers, Medicare, and your regular fees, and how promptly are you paid? What problems have you had with referral and claim forms? Are you permitted to bill patients for uncovered charges?
More specific issues also should be addressed. For instance, what services, precisely, are not covered? Which procedures are paid particularly well and which are paid poorly (or not at all) despite being ostensibly “covered”? Are there any unusual or unorthodox rules for certain surgical or diagnostic procedures? Do you get an inordinate number of requests for further information from the payer? Are you asked for the same information repeatedly? Are there problems with CPT modifiers 25 and 78, or other modifiers?
Then take a hard look at the numbers. What fraction of your accounts receivable is attributed to each plan at any particular moment? Is that number increasing? If so, is it because the number of patients in that plan is increasing, or is it because the plan is losing momentum in paying its bills? The latter is a red flag; either growth is outstripping efficiency or financial problems are looming.
It also is important to look at mechanics of each plan. How easy is it for patients to get a referral to your office? Do primary care practitioners dole out referrals as if they were diamonds? Be sure to review the referral requirements in each of your contracts. On those all-too-common occasions when patients show up for an appointment without a valid referral, how easy does the plan make it to get them one quickly?
Finally, talk to your insurance representatives, the staffers who deal with these plans on a daily basis. Their subjective impressions are just as important as any hard data. They will immediately separate the good plans from the bad, but it also is important to ask them some specific questions. Is your staff constantly cutting through red tape to get patients seen? Are claim forms confusing or hard to file? How hard is it to get a hold of provider relations representatives, and once contacted, are they helpful and courteous? Are provider relations representatives constantly calling your office with unnecessary or inappropriate questions?
After you collect all of this information, you will have your own up-to-the-minute managed care database, which you can consult immediately to determine which plans you will keep and which you should disengage. Repeat this exercise regularly—we now do it yearly in my practice—because the private insurance environment is evolving ever more rapidly due to the advent of the Patient Protection and Affordable Care Act and other factors.
Another important use for your managed care database is to renegotiate your fee schedule. Any payer with fees that are below your average remuneration should receive a letter informing them that the payments are below the level that is recognized as usual and customary in your area. Inform them that your office will be pleased to give them the opportunity to remain associated with your practice if their reimbursements are immediately increased. Although insurers are not always receptive to requests for increased compensation, they are usually willing to open a dialogue; if not, you will need to reconsider your practice’s continued association with that plan.
This exercise requires a lot of work, but your time and effort will be well spent. In addition to ensuring that your services are properly compensated, you will be putting your third-party payers on notice that you are paying attention and that your office will not tolerate unfair remuneration or inordinate delays in payment.
- Eastern J. Should you accept insurance exchange coverage? Cutis. 2014;94:75-77.
- Eastern J. Should you accept insurance exchange coverage? Cutis. 2014;94:75-77.
Practice Points
- Third-party payers do not typically update their compensation schedules on a regular basis; therefore, a regular review of all your third-party contracts is mandatory.
- Discarding outdated plans and regularly renegotiating fee schedules with payers who are retained is essential to the financial solvency of any private practice.

Autologous stem-cell transplant boosts survival in sequential transformed indolent lymphoma
Autologous stem-cell transplantation can be highly effective in securing better long-term results for patients undergoing rituximab-based chemotherapy for transformed indolent lymphoma with high-grade histologies, according to a retrospective study published online in Annals of Oncology.
ASCT improved outcomes in patients with sequential TIL (S-TIL), but not in those with composite/discordant TIL (CD-TIL). The benefits of ASCT were greater in patients who were rituximab-naive at transformation, wrote Dr. Carsten Madsen of Denmark’s Aarhus University Hospital, and his coauthors (Ann. Oncol. 2014 Nov. 18 [doi: 10.1093/annonc/mdu537]).
Patients with “CD-TIL had a better outcome than [did those with] S-TIL regardless of treatment strategy at transformation. With regard to ASCT in particular, we found that it had a beneficial influence on outcome limited to S-TIL,” the investigators concluded.
In a multicenter cohort study, Dr. Madsen and his associates used the National Danish Pathology Registry to identify patients aged 18-68 years with histologically verified TIL diagnosed between 1999 and 2012 at the Aarhus, Odense, and Aalborg university hospitals in Denmark. Researchers looked for TIL, defined as “a biopsy proven IL in addition to a DLBCL [diffuse large B-cell lymphoma] lesion that was either coexisting at primary diagnosis or histologically ascertained over time through a subsequent biopsy.” In total, 85 patients were selected for the study – 72 subjects with follicular lymphoma at histological grades between 1 and 3A, and 13 subjects with otherwise unspecified forms of indolent lymphoma (IL).
Data for all patients were used to calculate 5-year overall survival (OS) and progression-free survival (PFS) rates. Calculations were done in three cohorts: an “all TIL” whole cohort, a CD-TIL cohort of subjects with “coexisting evidence of both indolent and aggressive histology at diagnosis,” and an S-TIL cohort of subjects who transformed after having indolent lymphoma for a prolonged period of time.
Of the 85 subjects, 54 (64%) received ASCT consolidation and 31 (36%) did not.
In the “all TIL” cohort, the OS and PFS rates were higher in subjects who received rituximab-containing regimens and ASCT compared with those who received only the chemotherapy. The OS rates were 67% vs. 48% (P = .11); the PFS rates were 60% versus 30% (P = .02).
There was no evidence of an advantage in the CD-TIL cohort, the OS rates were 76% for the combined therapy versus 67% for those given rituximab-based chemo only (P = .66), and the PFS rates were 71% versus 36% (P = .54).
The sequential TIL cohort, however, saw improvements in both OS and PFS – 62% versus 36% (P = .07) and 53% versus 6% (P = .002), respectively – regardless of whether or not patients had previously received rituximab-based chemo.
Prospective clinical trials, specifically designed for TIL patients, should be encouraged to investigate the optimal treatment strategy for this still largely unmet clinical need, the researchers concluded.
The authors disclosed no conflicts of interest.
Autologous stem-cell transplantation can be highly effective in securing better long-term results for patients undergoing rituximab-based chemotherapy for transformed indolent lymphoma with high-grade histologies, according to a retrospective study published online in Annals of Oncology.
ASCT improved outcomes in patients with sequential TIL (S-TIL), but not in those with composite/discordant TIL (CD-TIL). The benefits of ASCT were greater in patients who were rituximab-naive at transformation, wrote Dr. Carsten Madsen of Denmark’s Aarhus University Hospital, and his coauthors (Ann. Oncol. 2014 Nov. 18 [doi: 10.1093/annonc/mdu537]).
Patients with “CD-TIL had a better outcome than [did those with] S-TIL regardless of treatment strategy at transformation. With regard to ASCT in particular, we found that it had a beneficial influence on outcome limited to S-TIL,” the investigators concluded.
In a multicenter cohort study, Dr. Madsen and his associates used the National Danish Pathology Registry to identify patients aged 18-68 years with histologically verified TIL diagnosed between 1999 and 2012 at the Aarhus, Odense, and Aalborg university hospitals in Denmark. Researchers looked for TIL, defined as “a biopsy proven IL in addition to a DLBCL [diffuse large B-cell lymphoma] lesion that was either coexisting at primary diagnosis or histologically ascertained over time through a subsequent biopsy.” In total, 85 patients were selected for the study – 72 subjects with follicular lymphoma at histological grades between 1 and 3A, and 13 subjects with otherwise unspecified forms of indolent lymphoma (IL).
Data for all patients were used to calculate 5-year overall survival (OS) and progression-free survival (PFS) rates. Calculations were done in three cohorts: an “all TIL” whole cohort, a CD-TIL cohort of subjects with “coexisting evidence of both indolent and aggressive histology at diagnosis,” and an S-TIL cohort of subjects who transformed after having indolent lymphoma for a prolonged period of time.
Of the 85 subjects, 54 (64%) received ASCT consolidation and 31 (36%) did not.
In the “all TIL” cohort, the OS and PFS rates were higher in subjects who received rituximab-containing regimens and ASCT compared with those who received only the chemotherapy. The OS rates were 67% vs. 48% (P = .11); the PFS rates were 60% versus 30% (P = .02).
There was no evidence of an advantage in the CD-TIL cohort, the OS rates were 76% for the combined therapy versus 67% for those given rituximab-based chemo only (P = .66), and the PFS rates were 71% versus 36% (P = .54).
The sequential TIL cohort, however, saw improvements in both OS and PFS – 62% versus 36% (P = .07) and 53% versus 6% (P = .002), respectively – regardless of whether or not patients had previously received rituximab-based chemo.
Prospective clinical trials, specifically designed for TIL patients, should be encouraged to investigate the optimal treatment strategy for this still largely unmet clinical need, the researchers concluded.
The authors disclosed no conflicts of interest.
Autologous stem-cell transplantation can be highly effective in securing better long-term results for patients undergoing rituximab-based chemotherapy for transformed indolent lymphoma with high-grade histologies, according to a retrospective study published online in Annals of Oncology.
ASCT improved outcomes in patients with sequential TIL (S-TIL), but not in those with composite/discordant TIL (CD-TIL). The benefits of ASCT were greater in patients who were rituximab-naive at transformation, wrote Dr. Carsten Madsen of Denmark’s Aarhus University Hospital, and his coauthors (Ann. Oncol. 2014 Nov. 18 [doi: 10.1093/annonc/mdu537]).
Patients with “CD-TIL had a better outcome than [did those with] S-TIL regardless of treatment strategy at transformation. With regard to ASCT in particular, we found that it had a beneficial influence on outcome limited to S-TIL,” the investigators concluded.
In a multicenter cohort study, Dr. Madsen and his associates used the National Danish Pathology Registry to identify patients aged 18-68 years with histologically verified TIL diagnosed between 1999 and 2012 at the Aarhus, Odense, and Aalborg university hospitals in Denmark. Researchers looked for TIL, defined as “a biopsy proven IL in addition to a DLBCL [diffuse large B-cell lymphoma] lesion that was either coexisting at primary diagnosis or histologically ascertained over time through a subsequent biopsy.” In total, 85 patients were selected for the study – 72 subjects with follicular lymphoma at histological grades between 1 and 3A, and 13 subjects with otherwise unspecified forms of indolent lymphoma (IL).
Data for all patients were used to calculate 5-year overall survival (OS) and progression-free survival (PFS) rates. Calculations were done in three cohorts: an “all TIL” whole cohort, a CD-TIL cohort of subjects with “coexisting evidence of both indolent and aggressive histology at diagnosis,” and an S-TIL cohort of subjects who transformed after having indolent lymphoma for a prolonged period of time.
Of the 85 subjects, 54 (64%) received ASCT consolidation and 31 (36%) did not.
In the “all TIL” cohort, the OS and PFS rates were higher in subjects who received rituximab-containing regimens and ASCT compared with those who received only the chemotherapy. The OS rates were 67% vs. 48% (P = .11); the PFS rates were 60% versus 30% (P = .02).
There was no evidence of an advantage in the CD-TIL cohort, the OS rates were 76% for the combined therapy versus 67% for those given rituximab-based chemo only (P = .66), and the PFS rates were 71% versus 36% (P = .54).
The sequential TIL cohort, however, saw improvements in both OS and PFS – 62% versus 36% (P = .07) and 53% versus 6% (P = .002), respectively – regardless of whether or not patients had previously received rituximab-based chemo.
Prospective clinical trials, specifically designed for TIL patients, should be encouraged to investigate the optimal treatment strategy for this still largely unmet clinical need, the researchers concluded.
The authors disclosed no conflicts of interest.
FROM ANNALS OF ONCOLOGY
Key clinical point: Autologous stem-cell transplantation (ASCT) plus chemo improved responses for patients with sequential indolent lymphoma transformed to high-grade histology (TIL), and was most effective in patients who were rituximab-naive at transformation.
Major finding: The sequential TIL cohort had better outcomes with ASCT plus chemo than did those with chemo alone: OS was 62% versus 36% (P = .07) and PFS was 53% versus 6% (P = .002), respectively.
Data source: A total of 85 patients selected from a registry of those with histologically verified TIL at the Aarhus, Odense, and Aalborg university hospitals in Denmark.
Disclosures: The authors disclosed no conflicts of interest.