User login
PODCAST: Highlights of the June 2014 issue of The Hospitalist
This month in our issue, 10 medical specialty groups offer Choosing Wisely guidelines for hospitalists. Among them, Dr. Linda Cox notes why comprehensive pulmonary assessment, including spirometry, is important to diagnosing or ruling out asthma; and otolaryngologist Dr. Rahul Shah tells why hospitalists should stop routine radiographic imaging for patients who meet the diagnostic criteria for uncomplicated acute rhinosinusitis. Meanwhile, ABIM Foundation executive vice president and CEO Daniel Wolfson talks about why the Choosing Wisely campaign is not just another attempt at cost-containment.
Also in this issue, legal advice for hospitalists on the intersection of social media and HIPAA rules, clinical practice guidelines on red blood cell transfusions, and our Key Clinical Question explores which patients should be screened for hepatitis C infection.
This month in our issue, 10 medical specialty groups offer Choosing Wisely guidelines for hospitalists. Among them, Dr. Linda Cox notes why comprehensive pulmonary assessment, including spirometry, is important to diagnosing or ruling out asthma; and otolaryngologist Dr. Rahul Shah tells why hospitalists should stop routine radiographic imaging for patients who meet the diagnostic criteria for uncomplicated acute rhinosinusitis. Meanwhile, ABIM Foundation executive vice president and CEO Daniel Wolfson talks about why the Choosing Wisely campaign is not just another attempt at cost-containment.
Also in this issue, legal advice for hospitalists on the intersection of social media and HIPAA rules, clinical practice guidelines on red blood cell transfusions, and our Key Clinical Question explores which patients should be screened for hepatitis C infection.
This month in our issue, 10 medical specialty groups offer Choosing Wisely guidelines for hospitalists. Among them, Dr. Linda Cox notes why comprehensive pulmonary assessment, including spirometry, is important to diagnosing or ruling out asthma; and otolaryngologist Dr. Rahul Shah tells why hospitalists should stop routine radiographic imaging for patients who meet the diagnostic criteria for uncomplicated acute rhinosinusitis. Meanwhile, ABIM Foundation executive vice president and CEO Daniel Wolfson talks about why the Choosing Wisely campaign is not just another attempt at cost-containment.
Also in this issue, legal advice for hospitalists on the intersection of social media and HIPAA rules, clinical practice guidelines on red blood cell transfusions, and our Key Clinical Question explores which patients should be screened for hepatitis C infection.
Fatigue, arthalgia, amenorrhea—Dx?
THE CASE
A 46-year-old Caucasian female with a history of epilepsy came into our family medicine center complaining of weakness, fatigue, and arthralgia that made it difficult for her to walk. She’d had these symptoms for 6 months and reported having amenorrhea and hot flashes for the past 2 years.
The patient’s blood pressure was 133/72 mm Hg, heart rate was 82 beats per min, and respiratory rate was 20 breaths per min. Her skin was dry without hyperpigmentation, and her sclerae were anicteric. A musculoskeletal examination revealed tenderness of the metacarpophalangeal and metatarsophalangeal joints without edema, deformity, or evidence of synovitis.
She had no history of skin bronzing, jaundice, transfusions, hepatitis, abdominal pain, or diabetes and denied using tobacco, alcohol, or illicit drugs. Her medications included lamotrigine (250 mg BID) and over-the-counter iron supplementation. She had no family history of rheumatoid arthritis, lupus, cirrhosis, hemochromatosis, or other liver disease. Her mother died from colorectal cancer and her father’s cause of death was unknown; her sisters did not have any medical issues. The patient’s lab tests were normal, except for the following: aspartate aminotransferase, 89 U/L (normal, 13-45 U/L); alanine aminotransferase, 80 U/L (normal, 5-57 U/L); and alkaline phosphatase, 132 U/L (normal, 39-117 U/L). Her coagulation panel revealed a prothrombin time of 13.1 seconds, and an international normalized ratio of 1.3. Serology was negative for hepatitis A, B, and C. Additional testing revealed the following: ferritin, 4014.1 ng/dL (normal, 7-282 ng/dL); iron, 210 mg/dL (normal, 40-170 mg/dL); total iron binding capacity, 258 mg/dL (normal, 260-445 mg/dL); and transferrin saturation, 81% (normal, 20%-55%).
Abdominal ultrasonography revealed gallstones, an enlarged spleen, a dilated portal vein, and a fatty liver consistent with cirrhosis. X-rays showed soft-tissue swelling and demineralization in her hands consistent with osteopenia and degenerative arthritis in both feet.
THE DIAGNOSIS
Based on our patient’s complaints of fatigue, weakness, arthralgia, and amenorrhea, as well as her abnormal iron levels, we suspected hereditary hemochromatosis (HH). We ordered HFE genotyping, and the results indicated that the patient was homozygous for the C282Y mutation, confirming our diagnosis.
DISCUSSION
HH is an autosomal recessive disorder of iron homeostasis characterized by increased gastrointestinal iron absorption and tissue deposition of iron. It is caused by mutations in the HFE gene (C282Y or H63D) located on chromosome 6 (locus 6p21) and commonly seen in Northern European Caucasians.1 Approximately 85% of patients with HH are homozygous for C282Y; the H63D mutation can cause HH when in the presence of a single C282Y mutation.1 Men manifest HH symptoms usually between the ages of 40 and 60 years,2 although women may be affected at a later age than men because physiologic blood loss from menstruation and parturition limit the rate at which excess iron is accumulated.2
|
Signs and symptoms of HH include depression, fatigue, restless legs syndrome, weakness, and weight loss.3 In advanced HH, patients may develop progressive skin pigmentation or bronzing, and hypogonadism. Advanced HH can affect the patient’s organs, including the pancreas (diabetes), liver (hepatomegaly, abnormal liver function tests), pituitary gland (amenorrhea, decreased libido, erectile dysfunction), and heart (arrhythmias, congestive heart failure), as well as the musculoskeletal system (joint pain).3,4 The spleen can also be affected after cirrhosis develops. Cirrhosis, hepatocellular carcinoma, and cardiomyopathy can reduce life expectancy.4
Testing for HH
Because symptoms of HH are common and nonspecific, a high degree of clinical suspicion is required for early diagnosis. The differential diagnosis includes conditions related to chronic liver disease or iron overload (TABLE).5 If the diagnosis goes undetected until complications arise, the risk of morbidity and mortality are greatly increased.5
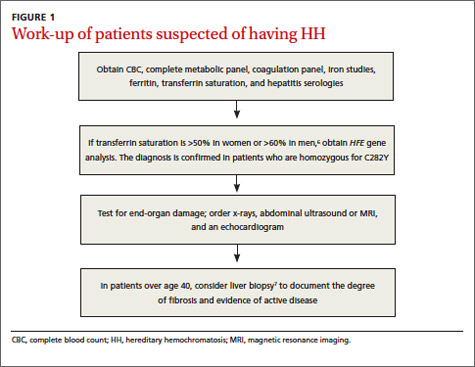
If HH is suspected, serum ferritin concentration and fasting serum transferrin saturation (the ratio of serum iron level to total iron-binding capacity × 100) are recommended as initial tests.5 The normal range of transferrin saturation for males is 15% to 50% and the normal range for females is 12% to 45%. If the transferrin saturation exceeds 50% in women or 60% in men, further evaluation is warranted (FIGURE 1).6,7 The sensitivity and specificity of elevated transferrin saturation for HH are 92% and 93%, respectively.5 These transferrin saturation cutoffs don’t apply to patients with a history of frequent blood transfusion (ie, patients with sickle cell disease or thalassemia).
Additional testing for patients in whom you suspect HH includes:
• a complete blood count, metabolic panel, and coagulation panel
• hepatitis serologies
• imaging (abdominal ultrasound, skeletal radiographs, echocardiogram, abdominal magnetic resonance imaging [MRI])
• a liver biopsy with iron staining and quantitative iron measurements.
The gold standard. Performing a liver biopsy to measure hepatic iron concentration by staining is considered the gold standard test for HH.8 But since genetic testing has become more readily available, liver biopsies aren’t widely used to confirm the diagnosis.8 The diagnosis of HH usually is confirmed by molecular testing for the C282Y and H63D mutations. Liver biopsy may be recommended to document the degree of fibrosis in all homozygotes over age 40 with elevated serum transaminase levels, clinical evidence of liver disease, or a serum ferritin level >1000 mcg/L.7
Phlebotomy helps lower iron levels
Treatment should not be delayed until symptoms develop.3 The mainstay of therapy is phlebotomy.9 If phlebotomy is started before the onset of organ damage, patients can anticipate a normal lifespan.9 Without treatment death may occur from cirrhosis, hepatocellular carcinoma, or cardiomyopathy.
Removal of 1 unit of red blood cells (450-500 mL) results in the loss of approximately 200 mg of iron. Serum ferritin level testing is the most reliable and least expensive method to monitor therapy.9 Iron depletion is complete when the serum ferritin level is 10 to 20 g/L, when the hemoglobin concentration is <11 g/dL, or the hematocrit is <33% for >3 weeks. HH patients need to undergo lifelong phlebotomy to maintain a serum ferritin level <50 g/L. Encourage patients to take in an adequate amount of dietary protein, vitamin B12, and folate to support the accelerated level of erythropoiesis that occurs during therapy.9
Chelation therapy is reserved for patients with advanced disease (eg, those with organ damage) or those who do not respond to phlebotomy.10 Deferoxamine given intravenously (IV) or subcutaneously has been the standard chelation agent. It’s usually administered by continuous subcutaneous infusion using a battery-operated pump at a dose of 40 mg/kg/d for 8 to 12 hours nightly for 5 to 7 nights weekly. A dose of approximately 2 g per 24 hours usually achieves maximal urinary iron excretion.
The use of deferoxamine therapy is limited by cost as well as the need for parenteral therapy, discomfort, inconvenience, and neurotoxicity.5 The US Food and Drug Administration recently approved an oral ironchelating agent, deferasirox, for the treatment of secondary iron overload due to ineffective erythropoiesis. Studies are ongoing to evaluate its potential use in HH.5,9
Our patient’s outcome
Our patient declined liver biopsy and her sisters declined HFE genotyping. Our patient did, however, complete 7 phlebotomies over 4 months. Two months later, she reported shortness of breath during exertion, leg swelling, and palpitations. A chest x-ray revealed a right-sided pleural effusion and an electrocardiogram showed atrial fibrillation with rapid ventricular response. Our patient was admitted for telemetry monitoring and started on diltiazem IV. Echocardiogram showed a restrictive cardiomyopathy, with an ejection fraction of 15% (normal range >55%).
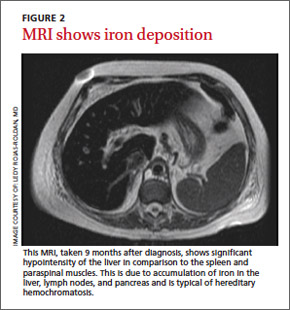
Six weeks later, her ejection fraction decreased to 10%. An MRI of her abdomen showed iron deposition in her liver, pancreas, and lymph nodes (FIGURE 2). She was started on deferoxamine IV and transferred to the coronary care unit for 3 weeks. She was discharged with a diagnosis of class IV heart failure and admitted 2 weeks later for exacerbation of heart failure symptoms. She did not want to pursue a heart transplant. Her condition deteriorated and she expired after a fatal cardiac arrhythmia.
THE TAKEAWAY
Patients with abnormal iron studies and those with evidence of liver disease should be evaluated for HH5 (strength of recommendation [SOR]: A). Fasting serum transferrin saturation and serum ferritin concentration are recommended as initial tests for HH11 (SOR C). Liver biopsy is the gold standard for diagnosis of HH, but the diagnosis usually is confirmed by genetic testing8 (SOR C). Phlebotomy is the mainstay of therapy9 (SOR B). Chelation therapy is reserved for patients with advanced disease or for those who do not respond to phlebotomy10 (SOR C).
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
1. Matthews AL, Grimes SJ, Wiesner GL, et al. Clinical consult: iron overload--hereditary hemochromatosis. Prim Care. 2004;31:767-770,xii-xiii.
2. Gochee PA, Powell LW. What’s new in hemochromatosis. Curr Opin Hematol. 2001;8:98-104.
3. Niederau C, Fischer R, Sonnenberg A, et al. Survival and causes of death in cirrhotic patients with primary hemochromatosis. N Engl J Med. 1985;313:1256-1262.
4. Adams PC. Hemochromatosis. Clin Liver Dis. 2004;8:735-753,vii.
5. Bacon BR, Adams PC, Kowdley KV, et al; American Association for the Study of Liver Diseases. Diagnosis and management of hemochromatosis: 2011 practice guideline by the American Association for the Study of Liver Diseases. Hepatology. 2011;54:328-343.
6. Brandhagen DJ, Fairbanks VF, Baldus W. Recognition and management of hereditary hemochromatosis. Am Fam Physician. 2002;65:853-860.
7. Hash RB. Hereditary hemochromatosis. J Am Board Fam Pract. 2001;14:266-273.
8. Qaseem A, Aronson M, Fitterman N, et al; Clinical Efficacy Assessment Subcommittee of the American College of Physicians. Screening for hereditary hemochromatosis: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2005;143:517-521.
9. Brissot P, de Bels F. Current approaches to the management of hemochromatosis. Hematology Am Soc Hematol Educ Program. 2006:36-41.
10. US Preventive Services Task Force. Screening for hemochromatosis: recommendation statement. Ann Intern Med. 2006;145:204-208.
11. Borwein S, Ghent CN, Valberg LS. Diagnostic efficacy of screening tests for hereditary hemochromatosis. Can Med Assoc J. 1984;131:895-901.
THE CASE
A 46-year-old Caucasian female with a history of epilepsy came into our family medicine center complaining of weakness, fatigue, and arthralgia that made it difficult for her to walk. She’d had these symptoms for 6 months and reported having amenorrhea and hot flashes for the past 2 years.
The patient’s blood pressure was 133/72 mm Hg, heart rate was 82 beats per min, and respiratory rate was 20 breaths per min. Her skin was dry without hyperpigmentation, and her sclerae were anicteric. A musculoskeletal examination revealed tenderness of the metacarpophalangeal and metatarsophalangeal joints without edema, deformity, or evidence of synovitis.
She had no history of skin bronzing, jaundice, transfusions, hepatitis, abdominal pain, or diabetes and denied using tobacco, alcohol, or illicit drugs. Her medications included lamotrigine (250 mg BID) and over-the-counter iron supplementation. She had no family history of rheumatoid arthritis, lupus, cirrhosis, hemochromatosis, or other liver disease. Her mother died from colorectal cancer and her father’s cause of death was unknown; her sisters did not have any medical issues. The patient’s lab tests were normal, except for the following: aspartate aminotransferase, 89 U/L (normal, 13-45 U/L); alanine aminotransferase, 80 U/L (normal, 5-57 U/L); and alkaline phosphatase, 132 U/L (normal, 39-117 U/L). Her coagulation panel revealed a prothrombin time of 13.1 seconds, and an international normalized ratio of 1.3. Serology was negative for hepatitis A, B, and C. Additional testing revealed the following: ferritin, 4014.1 ng/dL (normal, 7-282 ng/dL); iron, 210 mg/dL (normal, 40-170 mg/dL); total iron binding capacity, 258 mg/dL (normal, 260-445 mg/dL); and transferrin saturation, 81% (normal, 20%-55%).
Abdominal ultrasonography revealed gallstones, an enlarged spleen, a dilated portal vein, and a fatty liver consistent with cirrhosis. X-rays showed soft-tissue swelling and demineralization in her hands consistent with osteopenia and degenerative arthritis in both feet.
THE DIAGNOSIS
Based on our patient’s complaints of fatigue, weakness, arthralgia, and amenorrhea, as well as her abnormal iron levels, we suspected hereditary hemochromatosis (HH). We ordered HFE genotyping, and the results indicated that the patient was homozygous for the C282Y mutation, confirming our diagnosis.
DISCUSSION
HH is an autosomal recessive disorder of iron homeostasis characterized by increased gastrointestinal iron absorption and tissue deposition of iron. It is caused by mutations in the HFE gene (C282Y or H63D) located on chromosome 6 (locus 6p21) and commonly seen in Northern European Caucasians.1 Approximately 85% of patients with HH are homozygous for C282Y; the H63D mutation can cause HH when in the presence of a single C282Y mutation.1 Men manifest HH symptoms usually between the ages of 40 and 60 years,2 although women may be affected at a later age than men because physiologic blood loss from menstruation and parturition limit the rate at which excess iron is accumulated.2
|
Signs and symptoms of HH include depression, fatigue, restless legs syndrome, weakness, and weight loss.3 In advanced HH, patients may develop progressive skin pigmentation or bronzing, and hypogonadism. Advanced HH can affect the patient’s organs, including the pancreas (diabetes), liver (hepatomegaly, abnormal liver function tests), pituitary gland (amenorrhea, decreased libido, erectile dysfunction), and heart (arrhythmias, congestive heart failure), as well as the musculoskeletal system (joint pain).3,4 The spleen can also be affected after cirrhosis develops. Cirrhosis, hepatocellular carcinoma, and cardiomyopathy can reduce life expectancy.4
Testing for HH
Because symptoms of HH are common and nonspecific, a high degree of clinical suspicion is required for early diagnosis. The differential diagnosis includes conditions related to chronic liver disease or iron overload (TABLE).5 If the diagnosis goes undetected until complications arise, the risk of morbidity and mortality are greatly increased.5
If HH is suspected, serum ferritin concentration and fasting serum transferrin saturation (the ratio of serum iron level to total iron-binding capacity × 100) are recommended as initial tests.5 The normal range of transferrin saturation for males is 15% to 50% and the normal range for females is 12% to 45%. If the transferrin saturation exceeds 50% in women or 60% in men, further evaluation is warranted (FIGURE 1).6,7 The sensitivity and specificity of elevated transferrin saturation for HH are 92% and 93%, respectively.5 These transferrin saturation cutoffs don’t apply to patients with a history of frequent blood transfusion (ie, patients with sickle cell disease or thalassemia).
Additional testing for patients in whom you suspect HH includes:
• a complete blood count, metabolic panel, and coagulation panel
• hepatitis serologies
• imaging (abdominal ultrasound, skeletal radiographs, echocardiogram, abdominal magnetic resonance imaging [MRI])
• a liver biopsy with iron staining and quantitative iron measurements.
The gold standard. Performing a liver biopsy to measure hepatic iron concentration by staining is considered the gold standard test for HH.8 But since genetic testing has become more readily available, liver biopsies aren’t widely used to confirm the diagnosis.8 The diagnosis of HH usually is confirmed by molecular testing for the C282Y and H63D mutations. Liver biopsy may be recommended to document the degree of fibrosis in all homozygotes over age 40 with elevated serum transaminase levels, clinical evidence of liver disease, or a serum ferritin level >1000 mcg/L.7
Phlebotomy helps lower iron levels
Treatment should not be delayed until symptoms develop.3 The mainstay of therapy is phlebotomy.9 If phlebotomy is started before the onset of organ damage, patients can anticipate a normal lifespan.9 Without treatment death may occur from cirrhosis, hepatocellular carcinoma, or cardiomyopathy.
Removal of 1 unit of red blood cells (450-500 mL) results in the loss of approximately 200 mg of iron. Serum ferritin level testing is the most reliable and least expensive method to monitor therapy.9 Iron depletion is complete when the serum ferritin level is 10 to 20 g/L, when the hemoglobin concentration is <11 g/dL, or the hematocrit is <33% for >3 weeks. HH patients need to undergo lifelong phlebotomy to maintain a serum ferritin level <50 g/L. Encourage patients to take in an adequate amount of dietary protein, vitamin B12, and folate to support the accelerated level of erythropoiesis that occurs during therapy.9
Chelation therapy is reserved for patients with advanced disease (eg, those with organ damage) or those who do not respond to phlebotomy.10 Deferoxamine given intravenously (IV) or subcutaneously has been the standard chelation agent. It’s usually administered by continuous subcutaneous infusion using a battery-operated pump at a dose of 40 mg/kg/d for 8 to 12 hours nightly for 5 to 7 nights weekly. A dose of approximately 2 g per 24 hours usually achieves maximal urinary iron excretion.
The use of deferoxamine therapy is limited by cost as well as the need for parenteral therapy, discomfort, inconvenience, and neurotoxicity.5 The US Food and Drug Administration recently approved an oral ironchelating agent, deferasirox, for the treatment of secondary iron overload due to ineffective erythropoiesis. Studies are ongoing to evaluate its potential use in HH.5,9
Our patient’s outcome
Our patient declined liver biopsy and her sisters declined HFE genotyping. Our patient did, however, complete 7 phlebotomies over 4 months. Two months later, she reported shortness of breath during exertion, leg swelling, and palpitations. A chest x-ray revealed a right-sided pleural effusion and an electrocardiogram showed atrial fibrillation with rapid ventricular response. Our patient was admitted for telemetry monitoring and started on diltiazem IV. Echocardiogram showed a restrictive cardiomyopathy, with an ejection fraction of 15% (normal range >55%).
Six weeks later, her ejection fraction decreased to 10%. An MRI of her abdomen showed iron deposition in her liver, pancreas, and lymph nodes (FIGURE 2). She was started on deferoxamine IV and transferred to the coronary care unit for 3 weeks. She was discharged with a diagnosis of class IV heart failure and admitted 2 weeks later for exacerbation of heart failure symptoms. She did not want to pursue a heart transplant. Her condition deteriorated and she expired after a fatal cardiac arrhythmia.
THE TAKEAWAY
Patients with abnormal iron studies and those with evidence of liver disease should be evaluated for HH5 (strength of recommendation [SOR]: A). Fasting serum transferrin saturation and serum ferritin concentration are recommended as initial tests for HH11 (SOR C). Liver biopsy is the gold standard for diagnosis of HH, but the diagnosis usually is confirmed by genetic testing8 (SOR C). Phlebotomy is the mainstay of therapy9 (SOR B). Chelation therapy is reserved for patients with advanced disease or for those who do not respond to phlebotomy10 (SOR C).
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
THE CASE
A 46-year-old Caucasian female with a history of epilepsy came into our family medicine center complaining of weakness, fatigue, and arthralgia that made it difficult for her to walk. She’d had these symptoms for 6 months and reported having amenorrhea and hot flashes for the past 2 years.
The patient’s blood pressure was 133/72 mm Hg, heart rate was 82 beats per min, and respiratory rate was 20 breaths per min. Her skin was dry without hyperpigmentation, and her sclerae were anicteric. A musculoskeletal examination revealed tenderness of the metacarpophalangeal and metatarsophalangeal joints without edema, deformity, or evidence of synovitis.
She had no history of skin bronzing, jaundice, transfusions, hepatitis, abdominal pain, or diabetes and denied using tobacco, alcohol, or illicit drugs. Her medications included lamotrigine (250 mg BID) and over-the-counter iron supplementation. She had no family history of rheumatoid arthritis, lupus, cirrhosis, hemochromatosis, or other liver disease. Her mother died from colorectal cancer and her father’s cause of death was unknown; her sisters did not have any medical issues. The patient’s lab tests were normal, except for the following: aspartate aminotransferase, 89 U/L (normal, 13-45 U/L); alanine aminotransferase, 80 U/L (normal, 5-57 U/L); and alkaline phosphatase, 132 U/L (normal, 39-117 U/L). Her coagulation panel revealed a prothrombin time of 13.1 seconds, and an international normalized ratio of 1.3. Serology was negative for hepatitis A, B, and C. Additional testing revealed the following: ferritin, 4014.1 ng/dL (normal, 7-282 ng/dL); iron, 210 mg/dL (normal, 40-170 mg/dL); total iron binding capacity, 258 mg/dL (normal, 260-445 mg/dL); and transferrin saturation, 81% (normal, 20%-55%).
Abdominal ultrasonography revealed gallstones, an enlarged spleen, a dilated portal vein, and a fatty liver consistent with cirrhosis. X-rays showed soft-tissue swelling and demineralization in her hands consistent with osteopenia and degenerative arthritis in both feet.
THE DIAGNOSIS
Based on our patient’s complaints of fatigue, weakness, arthralgia, and amenorrhea, as well as her abnormal iron levels, we suspected hereditary hemochromatosis (HH). We ordered HFE genotyping, and the results indicated that the patient was homozygous for the C282Y mutation, confirming our diagnosis.
DISCUSSION
HH is an autosomal recessive disorder of iron homeostasis characterized by increased gastrointestinal iron absorption and tissue deposition of iron. It is caused by mutations in the HFE gene (C282Y or H63D) located on chromosome 6 (locus 6p21) and commonly seen in Northern European Caucasians.1 Approximately 85% of patients with HH are homozygous for C282Y; the H63D mutation can cause HH when in the presence of a single C282Y mutation.1 Men manifest HH symptoms usually between the ages of 40 and 60 years,2 although women may be affected at a later age than men because physiologic blood loss from menstruation and parturition limit the rate at which excess iron is accumulated.2
|
Signs and symptoms of HH include depression, fatigue, restless legs syndrome, weakness, and weight loss.3 In advanced HH, patients may develop progressive skin pigmentation or bronzing, and hypogonadism. Advanced HH can affect the patient’s organs, including the pancreas (diabetes), liver (hepatomegaly, abnormal liver function tests), pituitary gland (amenorrhea, decreased libido, erectile dysfunction), and heart (arrhythmias, congestive heart failure), as well as the musculoskeletal system (joint pain).3,4 The spleen can also be affected after cirrhosis develops. Cirrhosis, hepatocellular carcinoma, and cardiomyopathy can reduce life expectancy.4
Testing for HH
Because symptoms of HH are common and nonspecific, a high degree of clinical suspicion is required for early diagnosis. The differential diagnosis includes conditions related to chronic liver disease or iron overload (TABLE).5 If the diagnosis goes undetected until complications arise, the risk of morbidity and mortality are greatly increased.5
If HH is suspected, serum ferritin concentration and fasting serum transferrin saturation (the ratio of serum iron level to total iron-binding capacity × 100) are recommended as initial tests.5 The normal range of transferrin saturation for males is 15% to 50% and the normal range for females is 12% to 45%. If the transferrin saturation exceeds 50% in women or 60% in men, further evaluation is warranted (FIGURE 1).6,7 The sensitivity and specificity of elevated transferrin saturation for HH are 92% and 93%, respectively.5 These transferrin saturation cutoffs don’t apply to patients with a history of frequent blood transfusion (ie, patients with sickle cell disease or thalassemia).
Additional testing for patients in whom you suspect HH includes:
• a complete blood count, metabolic panel, and coagulation panel
• hepatitis serologies
• imaging (abdominal ultrasound, skeletal radiographs, echocardiogram, abdominal magnetic resonance imaging [MRI])
• a liver biopsy with iron staining and quantitative iron measurements.
The gold standard. Performing a liver biopsy to measure hepatic iron concentration by staining is considered the gold standard test for HH.8 But since genetic testing has become more readily available, liver biopsies aren’t widely used to confirm the diagnosis.8 The diagnosis of HH usually is confirmed by molecular testing for the C282Y and H63D mutations. Liver biopsy may be recommended to document the degree of fibrosis in all homozygotes over age 40 with elevated serum transaminase levels, clinical evidence of liver disease, or a serum ferritin level >1000 mcg/L.7
Phlebotomy helps lower iron levels
Treatment should not be delayed until symptoms develop.3 The mainstay of therapy is phlebotomy.9 If phlebotomy is started before the onset of organ damage, patients can anticipate a normal lifespan.9 Without treatment death may occur from cirrhosis, hepatocellular carcinoma, or cardiomyopathy.
Removal of 1 unit of red blood cells (450-500 mL) results in the loss of approximately 200 mg of iron. Serum ferritin level testing is the most reliable and least expensive method to monitor therapy.9 Iron depletion is complete when the serum ferritin level is 10 to 20 g/L, when the hemoglobin concentration is <11 g/dL, or the hematocrit is <33% for >3 weeks. HH patients need to undergo lifelong phlebotomy to maintain a serum ferritin level <50 g/L. Encourage patients to take in an adequate amount of dietary protein, vitamin B12, and folate to support the accelerated level of erythropoiesis that occurs during therapy.9
Chelation therapy is reserved for patients with advanced disease (eg, those with organ damage) or those who do not respond to phlebotomy.10 Deferoxamine given intravenously (IV) or subcutaneously has been the standard chelation agent. It’s usually administered by continuous subcutaneous infusion using a battery-operated pump at a dose of 40 mg/kg/d for 8 to 12 hours nightly for 5 to 7 nights weekly. A dose of approximately 2 g per 24 hours usually achieves maximal urinary iron excretion.
The use of deferoxamine therapy is limited by cost as well as the need for parenteral therapy, discomfort, inconvenience, and neurotoxicity.5 The US Food and Drug Administration recently approved an oral ironchelating agent, deferasirox, for the treatment of secondary iron overload due to ineffective erythropoiesis. Studies are ongoing to evaluate its potential use in HH.5,9
Our patient’s outcome
Our patient declined liver biopsy and her sisters declined HFE genotyping. Our patient did, however, complete 7 phlebotomies over 4 months. Two months later, she reported shortness of breath during exertion, leg swelling, and palpitations. A chest x-ray revealed a right-sided pleural effusion and an electrocardiogram showed atrial fibrillation with rapid ventricular response. Our patient was admitted for telemetry monitoring and started on diltiazem IV. Echocardiogram showed a restrictive cardiomyopathy, with an ejection fraction of 15% (normal range >55%).
Six weeks later, her ejection fraction decreased to 10%. An MRI of her abdomen showed iron deposition in her liver, pancreas, and lymph nodes (FIGURE 2). She was started on deferoxamine IV and transferred to the coronary care unit for 3 weeks. She was discharged with a diagnosis of class IV heart failure and admitted 2 weeks later for exacerbation of heart failure symptoms. She did not want to pursue a heart transplant. Her condition deteriorated and she expired after a fatal cardiac arrhythmia.
THE TAKEAWAY
Patients with abnormal iron studies and those with evidence of liver disease should be evaluated for HH5 (strength of recommendation [SOR]: A). Fasting serum transferrin saturation and serum ferritin concentration are recommended as initial tests for HH11 (SOR C). Liver biopsy is the gold standard for diagnosis of HH, but the diagnosis usually is confirmed by genetic testing8 (SOR C). Phlebotomy is the mainstay of therapy9 (SOR B). Chelation therapy is reserved for patients with advanced disease or for those who do not respond to phlebotomy10 (SOR C).
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
1. Matthews AL, Grimes SJ, Wiesner GL, et al. Clinical consult: iron overload--hereditary hemochromatosis. Prim Care. 2004;31:767-770,xii-xiii.
2. Gochee PA, Powell LW. What’s new in hemochromatosis. Curr Opin Hematol. 2001;8:98-104.
3. Niederau C, Fischer R, Sonnenberg A, et al. Survival and causes of death in cirrhotic patients with primary hemochromatosis. N Engl J Med. 1985;313:1256-1262.
4. Adams PC. Hemochromatosis. Clin Liver Dis. 2004;8:735-753,vii.
5. Bacon BR, Adams PC, Kowdley KV, et al; American Association for the Study of Liver Diseases. Diagnosis and management of hemochromatosis: 2011 practice guideline by the American Association for the Study of Liver Diseases. Hepatology. 2011;54:328-343.
6. Brandhagen DJ, Fairbanks VF, Baldus W. Recognition and management of hereditary hemochromatosis. Am Fam Physician. 2002;65:853-860.
7. Hash RB. Hereditary hemochromatosis. J Am Board Fam Pract. 2001;14:266-273.
8. Qaseem A, Aronson M, Fitterman N, et al; Clinical Efficacy Assessment Subcommittee of the American College of Physicians. Screening for hereditary hemochromatosis: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2005;143:517-521.
9. Brissot P, de Bels F. Current approaches to the management of hemochromatosis. Hematology Am Soc Hematol Educ Program. 2006:36-41.
10. US Preventive Services Task Force. Screening for hemochromatosis: recommendation statement. Ann Intern Med. 2006;145:204-208.
11. Borwein S, Ghent CN, Valberg LS. Diagnostic efficacy of screening tests for hereditary hemochromatosis. Can Med Assoc J. 1984;131:895-901.
1. Matthews AL, Grimes SJ, Wiesner GL, et al. Clinical consult: iron overload--hereditary hemochromatosis. Prim Care. 2004;31:767-770,xii-xiii.
2. Gochee PA, Powell LW. What’s new in hemochromatosis. Curr Opin Hematol. 2001;8:98-104.
3. Niederau C, Fischer R, Sonnenberg A, et al. Survival and causes of death in cirrhotic patients with primary hemochromatosis. N Engl J Med. 1985;313:1256-1262.
4. Adams PC. Hemochromatosis. Clin Liver Dis. 2004;8:735-753,vii.
5. Bacon BR, Adams PC, Kowdley KV, et al; American Association for the Study of Liver Diseases. Diagnosis and management of hemochromatosis: 2011 practice guideline by the American Association for the Study of Liver Diseases. Hepatology. 2011;54:328-343.
6. Brandhagen DJ, Fairbanks VF, Baldus W. Recognition and management of hereditary hemochromatosis. Am Fam Physician. 2002;65:853-860.
7. Hash RB. Hereditary hemochromatosis. J Am Board Fam Pract. 2001;14:266-273.
8. Qaseem A, Aronson M, Fitterman N, et al; Clinical Efficacy Assessment Subcommittee of the American College of Physicians. Screening for hereditary hemochromatosis: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2005;143:517-521.
9. Brissot P, de Bels F. Current approaches to the management of hemochromatosis. Hematology Am Soc Hematol Educ Program. 2006:36-41.
10. US Preventive Services Task Force. Screening for hemochromatosis: recommendation statement. Ann Intern Med. 2006;145:204-208.
11. Borwein S, Ghent CN, Valberg LS. Diagnostic efficacy of screening tests for hereditary hemochromatosis. Can Med Assoc J. 1984;131:895-901.

LISTEN NOW! ABIM Foundation EVP/COO Explains How the Choosing Wisely Campaign Got Started, and Its Impact on the U.S. Healthcare System
Listen to Daniel Wolfson explain how the Choosing Wisely campaign got started and its significance in U.S. healthcare
Listen to Daniel Wolfson explain how the Choosing Wisely campaign got started and its significance in U.S. healthcare
Listen to Daniel Wolfson explain how the Choosing Wisely campaign got started and its significance in U.S. healthcare
LISTEN NOW! Two Additional Choosing Wisely Recommendations from Specialty Societies
Listen to Dr. Cox, owner of Allergy and Asthma Center in Ft. Lauderdale, Fla., discuss why it's important for hospitalists to avoid diagnosing or managing asthma without spirometry.
Click here to listen to Dr. Shah, associate professor of otolaryngology and pediatrics at Children's National Medical Center in Washington, D.C, tell hospitalists why they should avoid routine radiographic imaging for patients who meet diagnostic criteria for uncomplicated acute rhinosinusitis.
Listen to Dr. Cox, owner of Allergy and Asthma Center in Ft. Lauderdale, Fla., discuss why it's important for hospitalists to avoid diagnosing or managing asthma without spirometry.
Click here to listen to Dr. Shah, associate professor of otolaryngology and pediatrics at Children's National Medical Center in Washington, D.C, tell hospitalists why they should avoid routine radiographic imaging for patients who meet diagnostic criteria for uncomplicated acute rhinosinusitis.
Listen to Dr. Cox, owner of Allergy and Asthma Center in Ft. Lauderdale, Fla., discuss why it's important for hospitalists to avoid diagnosing or managing asthma without spirometry.
Click here to listen to Dr. Shah, associate professor of otolaryngology and pediatrics at Children's National Medical Center in Washington, D.C, tell hospitalists why they should avoid routine radiographic imaging for patients who meet diagnostic criteria for uncomplicated acute rhinosinusitis.
What is the best treatment for impetigo?
Although evidence is lacking to support a single best treatment for impetigo, topical mupirocin, fusidic acid, gentamicin, and retapamulin are all at least 20% more likely than placebo to produce cure or improvement (strength of recommendation [SOR]: A, meta-analysis of randomized controlled trials [RCTs] and a single RCT of retapamulin).
Topical bacitracin and fusidic acid are 15% more likely than disinfectant solutions to cure or improve impetigo (SOR: A, systematic review of RCTs).
Oral antibiotics may be as effective as topical antibiotics (SOR: B, RCTs with different results).
EVIDENCE SUMMARY
Most data on the effectiveness of topical antibiotics focus on bacitracin, fusidic acid (not available in the United States), and mupirocin. Retapamulin 1% ointment, a topical antibiotic in the pleuromutilin class, is approved by the US Food and Drug Administration (FDA) for use in adults and children older than 9 months to treat impetigo caused by methicillin-susceptible Staphylococcus aureus and Streptococcus pyogenes.1
Topical antibiotics outperform placebo
A 2003 meta-analysis of 16 studies (1944 patients) evaluated treatments for impetigo in both adults and children.2 Investigators conducted most of the studies in outpatient settings in the United States, United Kingdom, Northern Europe, and Canada. They expressed outcomes in terms of cure or clinical improvement within 7 to 14 days of starting treatment.
Topical agents, including mupirocin, fusidic acid, and gentamicin, resulted in cure or improvement in more patients at 7 to 14 days than placebo (absolute benefit increase=20%; number needed to treat [NNT]=5; 95% confidence interval [CI], 1.49-4.86). Definitions of cure or improvement varied among the included studies, however.
A 2012 Cochrane review of various interventions included 68 RCTs with a total of 5708 participants, primarily from pediatric or dermatology hospital outpatient clinics in North America and Europe.3 Clinical cure (defined as clearance of crusts, blisters, and redness as determined by investigators) or improvement at one week were the primary outcomes (TABLE).3,4 Mupirocin (relative risk [RR]=2.21; 95% CI, 1.16-3.13), fusidic acid (RR=4.42; 95% CI, 2.39-8.17), and retapamulin (RR=1.64; 95% CI, 1.30-2.07) all demonstrated higher rates of cure or improvement than placebo.
Retapamulin produces greater clinical response than placebo in an RCT
A 2008 randomized, double-blind, multicenter, industry-funded, placebo-controlled trial of 213 patients evaluated the effectiveness of retapamulin to treat uncomplicated impetigo with an outcome of clinical response at 7 days.4 Clinical response was defined as total absence of lesions, drying of treated lesions without crusts or erythema, decrease in the size of the affected area or decrease in the number of lesions. Retapamulin ointment produced a higher rate of clinical response than placebo (absolute risk reduction=33.5%; 95% CI, 20.5-46.5; NNT=3, P<.001).
TABLE
How well do impetigo treatments work?3,4
Comparison | Number of patients | ARR for cure or improvement | NNT | Cost of treatment* |
Topical antibiotics vs placebo | 575 | 41.2% | 2 |
|
Retapamulin vs placebo | 213 | 33.5% | 3 | Retapamulin 1% ointment (15 g): $130.12 |
Topical antibiotics vs disinfectant solution | 292 | 11.4% | 9 |
|
Mupirocin vs fusidic acid | 440 | NS | NS | Mupirocin ointment 2% (22 g): $42.75 Fusidic acid is not available in the United States |
Mupirocin vs oral erythromycin | 581 | 5.1% | 20 | Erythromycin 100 tabs: $295.01 (250 mg), $314.23 (333 mg), $338.93 (500 mg) Erythromycin ethylsuccinate solution (100 mL): $170.50 (200 mg/5 mL), $218.14 (400 mg/5 mL) |
Mupirocin vs dicloxacillin | 53 | NS | NS | Dicloxacillin 100 tabs (250 mg):$66 |
Mupirocin vs ampicillin | 13 | NS | NS | Ampicillin 100 tabs (500 mg): $39.88 Ampicillin suspension 100 mL: $9.54 (125 mg/5 mL), $14.08 (250 mg/5 mL) |
Bacitracin vs oral erythromycin | 30 | NS | NS | Bacitracin ointment 500 units/g (28.4 g): $3.47 |
Bacitracin vs penicillin | 34 | NS | NS | Penicillin V oral 100 tabs (500 mg): $77.77 Penicillin V suspension 100 mL: $3.84 (125 mg/5 mL), $4.31 (250 mg/5 mL) |
Cephalexin vs bacitracin | 19 | 56.7% | 2 | Cephalexin 100 tabs (500 mg): $526.13 Cephalexin oral suspension 100 mL: $8.93 (125 mg/5 mL), $18.90 |
Erythromycin vs penicillin | 79 | 22.4% | 4 | See above |
Cloxacillin vs penicillin | 166 | 35.9% | 3 | Cloxacillin is not available in the United States |
ARR, absolute risk reduction; NNT, number needed to treat; NS, not significant.
*Cost data obtained from Medi-Span at www.uptodate.com. Accessed December 5, 2013.
Topical antibiotics work slightly better than disinfectant solutions
In a pooled analysis from the 2012 Cochrane review, topical bacitracin and fusidic acid demonstrated slightly higher rates of cure or improvement than disinfectant solutions (RR=1.15; 95% CI, 1.01-1.32).3 Oral antibiotics may work as well as, or better than, topicals The 2012 Cochrane review found better rates of cure or improvement for topical mupirocin than oral erythromycin (RR=1.07; 95% CI, 1.01-1.13).3 Investigators noted no significant differences between topical mupirocin and bacitracin and oral antibiotics other than erythromycin, although in one small study (10 patients), oral cephalexin resulted in a higher rate of cure or improvement than topical bacitracin (absolute risk reduction [ARR]=56.7%; NNT=2).
Studies comparing oral antibiotics found that both erythromycin and cloxacillin (not available in the United States) produced higher rates of cure or improvement than penicillin (erythromycin, RR=1.29; 95% CI, 1.07-1.56; cloxacillin, RR=1.14; 95% CI, 0.80-1.62).
RECOMMENDATIONS
The Infectious Diseases Society of America recommends topical mupirocin as first-line therapy for impetigo, although resistance to the drug exists. Patients with numerous lesions or who fail to respond to topical treatment should be treated with oral antibiotics active against S pyogenes and S aureus. Recommended oral antibiotics include dicloxacillin, amoxicillin/clavulanate, cephalexin, erythromycin, and clindamycin.5
1. Altabax. Med Library Web site. Available at: http://medlibrary.org/lib/rx/meds/altabax-3/. Accessed May 12, 2014.
2. George A, Rubin G. A systematic review and meta-analysis of treatments for impetigo. Br J Gen Practice. 2003;53:480-487.
3. Koning S, van der Sande R, Verhagen AP, et al. Interventions for impetigo. Cochrane Database Syst Rev. 2012;1:CD003261.
4. Koning S, van der Wouden JC, Chosidow O, et al. Efficacy and safety of retapamulin ointment as treatment of impetigo: randomized double-blind multicentre placebo-controlled trial. Br J Dermatol. 2008;158:1077-1082.
5. Stevens DL, Bisno AL, Chambers HF, et al; Infectious Diseases Society of America. Practice guidelines for diagnosis and management of skin and soft-tissue infections. Clin Infect Dis. 2005;41:1373–1406.
Although evidence is lacking to support a single best treatment for impetigo, topical mupirocin, fusidic acid, gentamicin, and retapamulin are all at least 20% more likely than placebo to produce cure or improvement (strength of recommendation [SOR]: A, meta-analysis of randomized controlled trials [RCTs] and a single RCT of retapamulin).
Topical bacitracin and fusidic acid are 15% more likely than disinfectant solutions to cure or improve impetigo (SOR: A, systematic review of RCTs).
Oral antibiotics may be as effective as topical antibiotics (SOR: B, RCTs with different results).
EVIDENCE SUMMARY
Most data on the effectiveness of topical antibiotics focus on bacitracin, fusidic acid (not available in the United States), and mupirocin. Retapamulin 1% ointment, a topical antibiotic in the pleuromutilin class, is approved by the US Food and Drug Administration (FDA) for use in adults and children older than 9 months to treat impetigo caused by methicillin-susceptible Staphylococcus aureus and Streptococcus pyogenes.1
Topical antibiotics outperform placebo
A 2003 meta-analysis of 16 studies (1944 patients) evaluated treatments for impetigo in both adults and children.2 Investigators conducted most of the studies in outpatient settings in the United States, United Kingdom, Northern Europe, and Canada. They expressed outcomes in terms of cure or clinical improvement within 7 to 14 days of starting treatment.
Topical agents, including mupirocin, fusidic acid, and gentamicin, resulted in cure or improvement in more patients at 7 to 14 days than placebo (absolute benefit increase=20%; number needed to treat [NNT]=5; 95% confidence interval [CI], 1.49-4.86). Definitions of cure or improvement varied among the included studies, however.
A 2012 Cochrane review of various interventions included 68 RCTs with a total of 5708 participants, primarily from pediatric or dermatology hospital outpatient clinics in North America and Europe.3 Clinical cure (defined as clearance of crusts, blisters, and redness as determined by investigators) or improvement at one week were the primary outcomes (TABLE).3,4 Mupirocin (relative risk [RR]=2.21; 95% CI, 1.16-3.13), fusidic acid (RR=4.42; 95% CI, 2.39-8.17), and retapamulin (RR=1.64; 95% CI, 1.30-2.07) all demonstrated higher rates of cure or improvement than placebo.
Retapamulin produces greater clinical response than placebo in an RCT
A 2008 randomized, double-blind, multicenter, industry-funded, placebo-controlled trial of 213 patients evaluated the effectiveness of retapamulin to treat uncomplicated impetigo with an outcome of clinical response at 7 days.4 Clinical response was defined as total absence of lesions, drying of treated lesions without crusts or erythema, decrease in the size of the affected area or decrease in the number of lesions. Retapamulin ointment produced a higher rate of clinical response than placebo (absolute risk reduction=33.5%; 95% CI, 20.5-46.5; NNT=3, P<.001).
TABLE
How well do impetigo treatments work?3,4
Comparison | Number of patients | ARR for cure or improvement | NNT | Cost of treatment* |
Topical antibiotics vs placebo | 575 | 41.2% | 2 |
|
Retapamulin vs placebo | 213 | 33.5% | 3 | Retapamulin 1% ointment (15 g): $130.12 |
Topical antibiotics vs disinfectant solution | 292 | 11.4% | 9 |
|
Mupirocin vs fusidic acid | 440 | NS | NS | Mupirocin ointment 2% (22 g): $42.75 Fusidic acid is not available in the United States |
Mupirocin vs oral erythromycin | 581 | 5.1% | 20 | Erythromycin 100 tabs: $295.01 (250 mg), $314.23 (333 mg), $338.93 (500 mg) Erythromycin ethylsuccinate solution (100 mL): $170.50 (200 mg/5 mL), $218.14 (400 mg/5 mL) |
Mupirocin vs dicloxacillin | 53 | NS | NS | Dicloxacillin 100 tabs (250 mg):$66 |
Mupirocin vs ampicillin | 13 | NS | NS | Ampicillin 100 tabs (500 mg): $39.88 Ampicillin suspension 100 mL: $9.54 (125 mg/5 mL), $14.08 (250 mg/5 mL) |
Bacitracin vs oral erythromycin | 30 | NS | NS | Bacitracin ointment 500 units/g (28.4 g): $3.47 |
Bacitracin vs penicillin | 34 | NS | NS | Penicillin V oral 100 tabs (500 mg): $77.77 Penicillin V suspension 100 mL: $3.84 (125 mg/5 mL), $4.31 (250 mg/5 mL) |
Cephalexin vs bacitracin | 19 | 56.7% | 2 | Cephalexin 100 tabs (500 mg): $526.13 Cephalexin oral suspension 100 mL: $8.93 (125 mg/5 mL), $18.90 |
Erythromycin vs penicillin | 79 | 22.4% | 4 | See above |
Cloxacillin vs penicillin | 166 | 35.9% | 3 | Cloxacillin is not available in the United States |
ARR, absolute risk reduction; NNT, number needed to treat; NS, not significant.
*Cost data obtained from Medi-Span at www.uptodate.com. Accessed December 5, 2013.
Topical antibiotics work slightly better than disinfectant solutions
In a pooled analysis from the 2012 Cochrane review, topical bacitracin and fusidic acid demonstrated slightly higher rates of cure or improvement than disinfectant solutions (RR=1.15; 95% CI, 1.01-1.32).3 Oral antibiotics may work as well as, or better than, topicals The 2012 Cochrane review found better rates of cure or improvement for topical mupirocin than oral erythromycin (RR=1.07; 95% CI, 1.01-1.13).3 Investigators noted no significant differences between topical mupirocin and bacitracin and oral antibiotics other than erythromycin, although in one small study (10 patients), oral cephalexin resulted in a higher rate of cure or improvement than topical bacitracin (absolute risk reduction [ARR]=56.7%; NNT=2).
Studies comparing oral antibiotics found that both erythromycin and cloxacillin (not available in the United States) produced higher rates of cure or improvement than penicillin (erythromycin, RR=1.29; 95% CI, 1.07-1.56; cloxacillin, RR=1.14; 95% CI, 0.80-1.62).
RECOMMENDATIONS
The Infectious Diseases Society of America recommends topical mupirocin as first-line therapy for impetigo, although resistance to the drug exists. Patients with numerous lesions or who fail to respond to topical treatment should be treated with oral antibiotics active against S pyogenes and S aureus. Recommended oral antibiotics include dicloxacillin, amoxicillin/clavulanate, cephalexin, erythromycin, and clindamycin.5
Although evidence is lacking to support a single best treatment for impetigo, topical mupirocin, fusidic acid, gentamicin, and retapamulin are all at least 20% more likely than placebo to produce cure or improvement (strength of recommendation [SOR]: A, meta-analysis of randomized controlled trials [RCTs] and a single RCT of retapamulin).
Topical bacitracin and fusidic acid are 15% more likely than disinfectant solutions to cure or improve impetigo (SOR: A, systematic review of RCTs).
Oral antibiotics may be as effective as topical antibiotics (SOR: B, RCTs with different results).
EVIDENCE SUMMARY
Most data on the effectiveness of topical antibiotics focus on bacitracin, fusidic acid (not available in the United States), and mupirocin. Retapamulin 1% ointment, a topical antibiotic in the pleuromutilin class, is approved by the US Food and Drug Administration (FDA) for use in adults and children older than 9 months to treat impetigo caused by methicillin-susceptible Staphylococcus aureus and Streptococcus pyogenes.1
Topical antibiotics outperform placebo
A 2003 meta-analysis of 16 studies (1944 patients) evaluated treatments for impetigo in both adults and children.2 Investigators conducted most of the studies in outpatient settings in the United States, United Kingdom, Northern Europe, and Canada. They expressed outcomes in terms of cure or clinical improvement within 7 to 14 days of starting treatment.
Topical agents, including mupirocin, fusidic acid, and gentamicin, resulted in cure or improvement in more patients at 7 to 14 days than placebo (absolute benefit increase=20%; number needed to treat [NNT]=5; 95% confidence interval [CI], 1.49-4.86). Definitions of cure or improvement varied among the included studies, however.
A 2012 Cochrane review of various interventions included 68 RCTs with a total of 5708 participants, primarily from pediatric or dermatology hospital outpatient clinics in North America and Europe.3 Clinical cure (defined as clearance of crusts, blisters, and redness as determined by investigators) or improvement at one week were the primary outcomes (TABLE).3,4 Mupirocin (relative risk [RR]=2.21; 95% CI, 1.16-3.13), fusidic acid (RR=4.42; 95% CI, 2.39-8.17), and retapamulin (RR=1.64; 95% CI, 1.30-2.07) all demonstrated higher rates of cure or improvement than placebo.
Retapamulin produces greater clinical response than placebo in an RCT
A 2008 randomized, double-blind, multicenter, industry-funded, placebo-controlled trial of 213 patients evaluated the effectiveness of retapamulin to treat uncomplicated impetigo with an outcome of clinical response at 7 days.4 Clinical response was defined as total absence of lesions, drying of treated lesions without crusts or erythema, decrease in the size of the affected area or decrease in the number of lesions. Retapamulin ointment produced a higher rate of clinical response than placebo (absolute risk reduction=33.5%; 95% CI, 20.5-46.5; NNT=3, P<.001).
TABLE
How well do impetigo treatments work?3,4
Comparison | Number of patients | ARR for cure or improvement | NNT | Cost of treatment* |
Topical antibiotics vs placebo | 575 | 41.2% | 2 |
|
Retapamulin vs placebo | 213 | 33.5% | 3 | Retapamulin 1% ointment (15 g): $130.12 |
Topical antibiotics vs disinfectant solution | 292 | 11.4% | 9 |
|
Mupirocin vs fusidic acid | 440 | NS | NS | Mupirocin ointment 2% (22 g): $42.75 Fusidic acid is not available in the United States |
Mupirocin vs oral erythromycin | 581 | 5.1% | 20 | Erythromycin 100 tabs: $295.01 (250 mg), $314.23 (333 mg), $338.93 (500 mg) Erythromycin ethylsuccinate solution (100 mL): $170.50 (200 mg/5 mL), $218.14 (400 mg/5 mL) |
Mupirocin vs dicloxacillin | 53 | NS | NS | Dicloxacillin 100 tabs (250 mg):$66 |
Mupirocin vs ampicillin | 13 | NS | NS | Ampicillin 100 tabs (500 mg): $39.88 Ampicillin suspension 100 mL: $9.54 (125 mg/5 mL), $14.08 (250 mg/5 mL) |
Bacitracin vs oral erythromycin | 30 | NS | NS | Bacitracin ointment 500 units/g (28.4 g): $3.47 |
Bacitracin vs penicillin | 34 | NS | NS | Penicillin V oral 100 tabs (500 mg): $77.77 Penicillin V suspension 100 mL: $3.84 (125 mg/5 mL), $4.31 (250 mg/5 mL) |
Cephalexin vs bacitracin | 19 | 56.7% | 2 | Cephalexin 100 tabs (500 mg): $526.13 Cephalexin oral suspension 100 mL: $8.93 (125 mg/5 mL), $18.90 |
Erythromycin vs penicillin | 79 | 22.4% | 4 | See above |
Cloxacillin vs penicillin | 166 | 35.9% | 3 | Cloxacillin is not available in the United States |
ARR, absolute risk reduction; NNT, number needed to treat; NS, not significant.
*Cost data obtained from Medi-Span at www.uptodate.com. Accessed December 5, 2013.
Topical antibiotics work slightly better than disinfectant solutions
In a pooled analysis from the 2012 Cochrane review, topical bacitracin and fusidic acid demonstrated slightly higher rates of cure or improvement than disinfectant solutions (RR=1.15; 95% CI, 1.01-1.32).3 Oral antibiotics may work as well as, or better than, topicals The 2012 Cochrane review found better rates of cure or improvement for topical mupirocin than oral erythromycin (RR=1.07; 95% CI, 1.01-1.13).3 Investigators noted no significant differences between topical mupirocin and bacitracin and oral antibiotics other than erythromycin, although in one small study (10 patients), oral cephalexin resulted in a higher rate of cure or improvement than topical bacitracin (absolute risk reduction [ARR]=56.7%; NNT=2).
Studies comparing oral antibiotics found that both erythromycin and cloxacillin (not available in the United States) produced higher rates of cure or improvement than penicillin (erythromycin, RR=1.29; 95% CI, 1.07-1.56; cloxacillin, RR=1.14; 95% CI, 0.80-1.62).
RECOMMENDATIONS
The Infectious Diseases Society of America recommends topical mupirocin as first-line therapy for impetigo, although resistance to the drug exists. Patients with numerous lesions or who fail to respond to topical treatment should be treated with oral antibiotics active against S pyogenes and S aureus. Recommended oral antibiotics include dicloxacillin, amoxicillin/clavulanate, cephalexin, erythromycin, and clindamycin.5
1. Altabax. Med Library Web site. Available at: http://medlibrary.org/lib/rx/meds/altabax-3/. Accessed May 12, 2014.
2. George A, Rubin G. A systematic review and meta-analysis of treatments for impetigo. Br J Gen Practice. 2003;53:480-487.
3. Koning S, van der Sande R, Verhagen AP, et al. Interventions for impetigo. Cochrane Database Syst Rev. 2012;1:CD003261.
4. Koning S, van der Wouden JC, Chosidow O, et al. Efficacy and safety of retapamulin ointment as treatment of impetigo: randomized double-blind multicentre placebo-controlled trial. Br J Dermatol. 2008;158:1077-1082.
5. Stevens DL, Bisno AL, Chambers HF, et al; Infectious Diseases Society of America. Practice guidelines for diagnosis and management of skin and soft-tissue infections. Clin Infect Dis. 2005;41:1373–1406.
1. Altabax. Med Library Web site. Available at: http://medlibrary.org/lib/rx/meds/altabax-3/. Accessed May 12, 2014.
2. George A, Rubin G. A systematic review and meta-analysis of treatments for impetigo. Br J Gen Practice. 2003;53:480-487.
3. Koning S, van der Sande R, Verhagen AP, et al. Interventions for impetigo. Cochrane Database Syst Rev. 2012;1:CD003261.
4. Koning S, van der Wouden JC, Chosidow O, et al. Efficacy and safety of retapamulin ointment as treatment of impetigo: randomized double-blind multicentre placebo-controlled trial. Br J Dermatol. 2008;158:1077-1082.
5. Stevens DL, Bisno AL, Chambers HF, et al; Infectious Diseases Society of America. Practice guidelines for diagnosis and management of skin and soft-tissue infections. Clin Infect Dis. 2005;41:1373–1406.
Evidence-based answers from the Family Physicians Inquiries Network
Do complementary agents lower HbA1c when used with standard type 2 diabetes therapy?
No, there is no high-quality evidence that supports using complementary or alternative agents to lower hemoglobin A1c (HbA1c) in patients with noninsulin-dependent type 2 diabetes. Oral chromium in widely varying doses reduces HbA1c a small amount (strength of recommendation [SOR]: C, meta-analysis of low-quality randomized, controlled trials [RCTs] of disease-oriented outcomes, with inconsistent results).
Oral cinnamon 1 to 3 g/d causes a small (<0.1%) drop in HbA1c (SOR: C, meta-analysis of low-quality RCTs of disease-oriented outcomes).
Fenugreek, milk thistle, safflower oil, and sweet potato extract may also reduce HbA1c (SOR: C, small, low-quality RCTs of disease-oriented outcomes).
EVIDENCE SUMMARY
Almost all complementary and alternative agents reviewed here were tested against placebo, and most were used in combination with standard therapy, usually identified as diet with or without oral hypoglycemic agents (TABLE).1-8
Meta-analyses evaluate effects of chromium and cinnamon
A meta-analysis of 13 RCTs evaluating the effect of oral chromium in patients with type 2 diabetes (age range not given) found a small improvement in HbA1c.1 Limitations of the meta-analysis included a wide range of chromium dosages and preparations. Ten studies showed no benefit, and of the 3 showing improvement, the researchers rated 2 as poor-quality.
A meta-analysis of 5 RCTs assessing the effect of oral cinnamon in patients with type 2 diabetes, 42 to 71 years of age, found that cinnamon produced a clinically irrelevant but statistically significant decrease in mean HbA1c.2 After analyzing the 2 RCTs with the largest effects, the researchers concluded that cinnamon might have a greater effect in patients with poorly controlled diabetes (baseline HbA1c>8.2%).
When they evaluated these RCTs for study homogeneity, they found significant differences among the studies in subject age, gender, ethnicity, body mass index, disease duration, concurrent medications, and baseline HbA1c levels, as well as variations in cinnamon dose, preparation, and therapy duration. Furthermore, only one of the studies reported randomization methods and whether allocation was concealed.
What about caiapo, fenugreek, milk thistle, and safflower oil?
Two small, moderate-quality RCTs of caiapo (sweet potato skin extract) in diet-controlled patients with diabetes demonstrated small but possibly clinically significant reductions in HbA1c between the intervention and control groups.3,4
TABLE
Effect of complementary or alternative agents on HbA1c in type 2 diabetes
CAA* | Dose/day | Concurrent diabetes therapy | Study type | Study size | Study duration | Difference in HbA1c (in HbA1c units) | 95% CI or P value |
Chromium1 | 1.28-1000 mcg | Not given | Meta-analysis of 13 RCTs | 381 | 3 wk-8 mo | -0.6† | -0.9 to -0.2 |
Cinnamon2 | 1-3 g | Various oral hypoglycemic agents‡ | Meta-analysis of 5 RCTs | 315 | 1.5-4 mo | -0.09 (WMD)† | -0.14 to -0.04 |
Caiapo3 | 4 g | Diet only | RCT | 61 | 5 mo | -0.21 (caiapo)§ +0.25 (placebo)§ | P=.08
P=.0001 |
Caiapo4 | 4 g | Diet only | RCT | 61 | 3 mo | -0.53 (caiapo)§ +0.06 (placebo)§ | P<.001
P=.23 |
Trigonella foenum-graecum (fenugreek)5 | 6.84 g | Sulfonylurea | RCT | 69 | 3 mo | -1.46 (fenugreek)§ -0.41 (placebo)§ | P<.05
P<.05 |
Silybum marianum (milk thistle)6 | 200 mg | Metformin and sulfonylurea | RCT | 51 | 4 mo | -1.0 (milk thistle)§ +1.2 (placebo)§ | P<.001
P<.0001 |
Silybum marianum (milk thistle)7 | 200 mg | Sulfonylurea | RCT | 38 | 4 mo | -1.5 (milk thistle)§ -0.5 (placebo)§ | P<.05
P=NS |
Safflower oil vs conjugated linoleic acid8 | 8 g | Various oral hypoglycemic agents‡ | DBRCD | 35 | 4 mo | -0.6 (safflower oil)§ +0.1 (conjugated linoleic acid)§ | P=.0007
P=NS |
CAA, complementary or alternative agents; CI, confidence interval; DBRCD, double-blind, randomized, crossover design; HbA1c, glycosylated hemoglobin A1c; NS, not significant; RCT, randomized controlled trial; WMD, weighted mean difference.
*All CAAs were compared against placebo, with the exception of safflower oil, which was compared against conjugated linoleic acid supplementation.
† Change in HbA1c means at study endpoint; the difference in HbA1c in intervention vs placebo groups.
‡ Oral hypoglycemic agents included a-glucosidase inhibitors, biguanides, glinides, glitazones, sulfonylureas, and thiazolidinediones.
§ Change in HbA1c means at study endpoint; the change in HbA1c from baseline.
Four small, placebo-controlled RCTs of fenugreek, milk thistle, and safflower oil found statistically and clinically significant reductions in HbA1c, but all these studies were of poor quality with unclear methods of randomization, threats to blinding, and a lack of baseline demographics.5-8
RECOMMENDATIONS
Both the American Diabetes Association (ADA) and the Diabetes UK Nutrition Working Group state that, “there is no clear evidence of benefit from vitamin or mineral supplementation in people with diabetes (compared with the general population), who do not have underlying deficiencies.”9,10 The ADA specifically states that chromium cannot be recommended because it lacks any clear benefit.9
1. Balk ME, Tatsioni A, Lichtenstein AH, et al. Effect of chromium supplementation on glucose metabolism and lipids: a systematic review of randomized controlled trials. Diabetes Care. 2007;30:2154-2163.
2. Akilen R, Tsiami A, Devendra D, et al. Cinnamon in glycaemic control: Systematic review and meta analysis. Clin Nutr. 2012;31:609-615.
3. Ludvik B, Hanefeld M, Pacini G. Improved metabolic control by Ipomoea batatas (Caiapo) is associated with increased adiponectin and decreased fibrinogen levels in type 2 diabetic subjects. Diabetes Obes Metab. 2008;10:586-592.
4. Ludvik, B, Neuffer, B, Pacini G. Efficacy of Ipomoea batatas (Caiapo) on diabetes control in type 2 diabetic subjects treated with diet. Diabetes Care. 2004;27:436-440.
5. Lu FR, Shen L, Qin Y, et al. Clinical observation on trigonella foenum-graecum L. total saponins in combination with sulfonylureas in the treatment of type 2 diabetes mellitus. Chin J Integr Med. 2008;14:56-60.
6. Huseini HF, Larijani B, Heshmat R, et al. The efficacy of Silybummarianum (L.) Gaertn. (silymarin) in the treatment of type II diabetes: a randomized, double-blind, placebo-controlled clinical trial. Phytother Res. 2006;20:1036-1039.
7. Hussain SA. Silymarin as an adjunct to glibenclamide therapy improves long-term and postprandial glycemic control and body mass index in type 2 diabetes. J Med Food. 2007;10:543-547.
8. Asp ML, Collene AL, Norris LE, et al. Time-dependent effects of safflower oil to improve glycemia, inflammation and blood lipids in obese, post-menopausal women with type 2 diabetes: a randomized,double-masked, crossover study. Clin Nutr. 2011;30:443-449.
9. American Diabetes Association; Bantle JP, Wylie-Rosett J, Albright AL, et al. Nutrition recommendations and interventions for diabetes: a position statement of the American Diabetes Association. Diabetes Care. 2008;31 suppl 1:S61-S78.
10. Diabetes UK Nutrition Working Group, Dyson PA, Kelly T, Deakin T, et al. Evidence-Based Nutrition Guidelines for the Prevention and Management of Diabetes. Diabetes UK Web site. Available at: www.diabetes.org.uk/Documents/Reports/nutritional-guidelines-2013-amendment-0413.pdf. Accessed October 2, 2013.
No, there is no high-quality evidence that supports using complementary or alternative agents to lower hemoglobin A1c (HbA1c) in patients with noninsulin-dependent type 2 diabetes. Oral chromium in widely varying doses reduces HbA1c a small amount (strength of recommendation [SOR]: C, meta-analysis of low-quality randomized, controlled trials [RCTs] of disease-oriented outcomes, with inconsistent results).
Oral cinnamon 1 to 3 g/d causes a small (<0.1%) drop in HbA1c (SOR: C, meta-analysis of low-quality RCTs of disease-oriented outcomes).
Fenugreek, milk thistle, safflower oil, and sweet potato extract may also reduce HbA1c (SOR: C, small, low-quality RCTs of disease-oriented outcomes).
EVIDENCE SUMMARY
Almost all complementary and alternative agents reviewed here were tested against placebo, and most were used in combination with standard therapy, usually identified as diet with or without oral hypoglycemic agents (TABLE).1-8
Meta-analyses evaluate effects of chromium and cinnamon
A meta-analysis of 13 RCTs evaluating the effect of oral chromium in patients with type 2 diabetes (age range not given) found a small improvement in HbA1c.1 Limitations of the meta-analysis included a wide range of chromium dosages and preparations. Ten studies showed no benefit, and of the 3 showing improvement, the researchers rated 2 as poor-quality.
A meta-analysis of 5 RCTs assessing the effect of oral cinnamon in patients with type 2 diabetes, 42 to 71 years of age, found that cinnamon produced a clinically irrelevant but statistically significant decrease in mean HbA1c.2 After analyzing the 2 RCTs with the largest effects, the researchers concluded that cinnamon might have a greater effect in patients with poorly controlled diabetes (baseline HbA1c>8.2%).
When they evaluated these RCTs for study homogeneity, they found significant differences among the studies in subject age, gender, ethnicity, body mass index, disease duration, concurrent medications, and baseline HbA1c levels, as well as variations in cinnamon dose, preparation, and therapy duration. Furthermore, only one of the studies reported randomization methods and whether allocation was concealed.
What about caiapo, fenugreek, milk thistle, and safflower oil?
Two small, moderate-quality RCTs of caiapo (sweet potato skin extract) in diet-controlled patients with diabetes demonstrated small but possibly clinically significant reductions in HbA1c between the intervention and control groups.3,4
TABLE
Effect of complementary or alternative agents on HbA1c in type 2 diabetes
CAA* | Dose/day | Concurrent diabetes therapy | Study type | Study size | Study duration | Difference in HbA1c (in HbA1c units) | 95% CI or P value |
Chromium1 | 1.28-1000 mcg | Not given | Meta-analysis of 13 RCTs | 381 | 3 wk-8 mo | -0.6† | -0.9 to -0.2 |
Cinnamon2 | 1-3 g | Various oral hypoglycemic agents‡ | Meta-analysis of 5 RCTs | 315 | 1.5-4 mo | -0.09 (WMD)† | -0.14 to -0.04 |
Caiapo3 | 4 g | Diet only | RCT | 61 | 5 mo | -0.21 (caiapo)§ +0.25 (placebo)§ | P=.08
P=.0001 |
Caiapo4 | 4 g | Diet only | RCT | 61 | 3 mo | -0.53 (caiapo)§ +0.06 (placebo)§ | P<.001
P=.23 |
Trigonella foenum-graecum (fenugreek)5 | 6.84 g | Sulfonylurea | RCT | 69 | 3 mo | -1.46 (fenugreek)§ -0.41 (placebo)§ | P<.05
P<.05 |
Silybum marianum (milk thistle)6 | 200 mg | Metformin and sulfonylurea | RCT | 51 | 4 mo | -1.0 (milk thistle)§ +1.2 (placebo)§ | P<.001
P<.0001 |
Silybum marianum (milk thistle)7 | 200 mg | Sulfonylurea | RCT | 38 | 4 mo | -1.5 (milk thistle)§ -0.5 (placebo)§ | P<.05
P=NS |
Safflower oil vs conjugated linoleic acid8 | 8 g | Various oral hypoglycemic agents‡ | DBRCD | 35 | 4 mo | -0.6 (safflower oil)§ +0.1 (conjugated linoleic acid)§ | P=.0007
P=NS |
CAA, complementary or alternative agents; CI, confidence interval; DBRCD, double-blind, randomized, crossover design; HbA1c, glycosylated hemoglobin A1c; NS, not significant; RCT, randomized controlled trial; WMD, weighted mean difference.
*All CAAs were compared against placebo, with the exception of safflower oil, which was compared against conjugated linoleic acid supplementation.
† Change in HbA1c means at study endpoint; the difference in HbA1c in intervention vs placebo groups.
‡ Oral hypoglycemic agents included a-glucosidase inhibitors, biguanides, glinides, glitazones, sulfonylureas, and thiazolidinediones.
§ Change in HbA1c means at study endpoint; the change in HbA1c from baseline.
Four small, placebo-controlled RCTs of fenugreek, milk thistle, and safflower oil found statistically and clinically significant reductions in HbA1c, but all these studies were of poor quality with unclear methods of randomization, threats to blinding, and a lack of baseline demographics.5-8
RECOMMENDATIONS
Both the American Diabetes Association (ADA) and the Diabetes UK Nutrition Working Group state that, “there is no clear evidence of benefit from vitamin or mineral supplementation in people with diabetes (compared with the general population), who do not have underlying deficiencies.”9,10 The ADA specifically states that chromium cannot be recommended because it lacks any clear benefit.9
No, there is no high-quality evidence that supports using complementary or alternative agents to lower hemoglobin A1c (HbA1c) in patients with noninsulin-dependent type 2 diabetes. Oral chromium in widely varying doses reduces HbA1c a small amount (strength of recommendation [SOR]: C, meta-analysis of low-quality randomized, controlled trials [RCTs] of disease-oriented outcomes, with inconsistent results).
Oral cinnamon 1 to 3 g/d causes a small (<0.1%) drop in HbA1c (SOR: C, meta-analysis of low-quality RCTs of disease-oriented outcomes).
Fenugreek, milk thistle, safflower oil, and sweet potato extract may also reduce HbA1c (SOR: C, small, low-quality RCTs of disease-oriented outcomes).
EVIDENCE SUMMARY
Almost all complementary and alternative agents reviewed here were tested against placebo, and most were used in combination with standard therapy, usually identified as diet with or without oral hypoglycemic agents (TABLE).1-8
Meta-analyses evaluate effects of chromium and cinnamon
A meta-analysis of 13 RCTs evaluating the effect of oral chromium in patients with type 2 diabetes (age range not given) found a small improvement in HbA1c.1 Limitations of the meta-analysis included a wide range of chromium dosages and preparations. Ten studies showed no benefit, and of the 3 showing improvement, the researchers rated 2 as poor-quality.
A meta-analysis of 5 RCTs assessing the effect of oral cinnamon in patients with type 2 diabetes, 42 to 71 years of age, found that cinnamon produced a clinically irrelevant but statistically significant decrease in mean HbA1c.2 After analyzing the 2 RCTs with the largest effects, the researchers concluded that cinnamon might have a greater effect in patients with poorly controlled diabetes (baseline HbA1c>8.2%).
When they evaluated these RCTs for study homogeneity, they found significant differences among the studies in subject age, gender, ethnicity, body mass index, disease duration, concurrent medications, and baseline HbA1c levels, as well as variations in cinnamon dose, preparation, and therapy duration. Furthermore, only one of the studies reported randomization methods and whether allocation was concealed.
What about caiapo, fenugreek, milk thistle, and safflower oil?
Two small, moderate-quality RCTs of caiapo (sweet potato skin extract) in diet-controlled patients with diabetes demonstrated small but possibly clinically significant reductions in HbA1c between the intervention and control groups.3,4
TABLE
Effect of complementary or alternative agents on HbA1c in type 2 diabetes
CAA* | Dose/day | Concurrent diabetes therapy | Study type | Study size | Study duration | Difference in HbA1c (in HbA1c units) | 95% CI or P value |
Chromium1 | 1.28-1000 mcg | Not given | Meta-analysis of 13 RCTs | 381 | 3 wk-8 mo | -0.6† | -0.9 to -0.2 |
Cinnamon2 | 1-3 g | Various oral hypoglycemic agents‡ | Meta-analysis of 5 RCTs | 315 | 1.5-4 mo | -0.09 (WMD)† | -0.14 to -0.04 |
Caiapo3 | 4 g | Diet only | RCT | 61 | 5 mo | -0.21 (caiapo)§ +0.25 (placebo)§ | P=.08
P=.0001 |
Caiapo4 | 4 g | Diet only | RCT | 61 | 3 mo | -0.53 (caiapo)§ +0.06 (placebo)§ | P<.001
P=.23 |
Trigonella foenum-graecum (fenugreek)5 | 6.84 g | Sulfonylurea | RCT | 69 | 3 mo | -1.46 (fenugreek)§ -0.41 (placebo)§ | P<.05
P<.05 |
Silybum marianum (milk thistle)6 | 200 mg | Metformin and sulfonylurea | RCT | 51 | 4 mo | -1.0 (milk thistle)§ +1.2 (placebo)§ | P<.001
P<.0001 |
Silybum marianum (milk thistle)7 | 200 mg | Sulfonylurea | RCT | 38 | 4 mo | -1.5 (milk thistle)§ -0.5 (placebo)§ | P<.05
P=NS |
Safflower oil vs conjugated linoleic acid8 | 8 g | Various oral hypoglycemic agents‡ | DBRCD | 35 | 4 mo | -0.6 (safflower oil)§ +0.1 (conjugated linoleic acid)§ | P=.0007
P=NS |
CAA, complementary or alternative agents; CI, confidence interval; DBRCD, double-blind, randomized, crossover design; HbA1c, glycosylated hemoglobin A1c; NS, not significant; RCT, randomized controlled trial; WMD, weighted mean difference.
*All CAAs were compared against placebo, with the exception of safflower oil, which was compared against conjugated linoleic acid supplementation.
† Change in HbA1c means at study endpoint; the difference in HbA1c in intervention vs placebo groups.
‡ Oral hypoglycemic agents included a-glucosidase inhibitors, biguanides, glinides, glitazones, sulfonylureas, and thiazolidinediones.
§ Change in HbA1c means at study endpoint; the change in HbA1c from baseline.
Four small, placebo-controlled RCTs of fenugreek, milk thistle, and safflower oil found statistically and clinically significant reductions in HbA1c, but all these studies were of poor quality with unclear methods of randomization, threats to blinding, and a lack of baseline demographics.5-8
RECOMMENDATIONS
Both the American Diabetes Association (ADA) and the Diabetes UK Nutrition Working Group state that, “there is no clear evidence of benefit from vitamin or mineral supplementation in people with diabetes (compared with the general population), who do not have underlying deficiencies.”9,10 The ADA specifically states that chromium cannot be recommended because it lacks any clear benefit.9
1. Balk ME, Tatsioni A, Lichtenstein AH, et al. Effect of chromium supplementation on glucose metabolism and lipids: a systematic review of randomized controlled trials. Diabetes Care. 2007;30:2154-2163.
2. Akilen R, Tsiami A, Devendra D, et al. Cinnamon in glycaemic control: Systematic review and meta analysis. Clin Nutr. 2012;31:609-615.
3. Ludvik B, Hanefeld M, Pacini G. Improved metabolic control by Ipomoea batatas (Caiapo) is associated with increased adiponectin and decreased fibrinogen levels in type 2 diabetic subjects. Diabetes Obes Metab. 2008;10:586-592.
4. Ludvik, B, Neuffer, B, Pacini G. Efficacy of Ipomoea batatas (Caiapo) on diabetes control in type 2 diabetic subjects treated with diet. Diabetes Care. 2004;27:436-440.
5. Lu FR, Shen L, Qin Y, et al. Clinical observation on trigonella foenum-graecum L. total saponins in combination with sulfonylureas in the treatment of type 2 diabetes mellitus. Chin J Integr Med. 2008;14:56-60.
6. Huseini HF, Larijani B, Heshmat R, et al. The efficacy of Silybummarianum (L.) Gaertn. (silymarin) in the treatment of type II diabetes: a randomized, double-blind, placebo-controlled clinical trial. Phytother Res. 2006;20:1036-1039.
7. Hussain SA. Silymarin as an adjunct to glibenclamide therapy improves long-term and postprandial glycemic control and body mass index in type 2 diabetes. J Med Food. 2007;10:543-547.
8. Asp ML, Collene AL, Norris LE, et al. Time-dependent effects of safflower oil to improve glycemia, inflammation and blood lipids in obese, post-menopausal women with type 2 diabetes: a randomized,double-masked, crossover study. Clin Nutr. 2011;30:443-449.
9. American Diabetes Association; Bantle JP, Wylie-Rosett J, Albright AL, et al. Nutrition recommendations and interventions for diabetes: a position statement of the American Diabetes Association. Diabetes Care. 2008;31 suppl 1:S61-S78.
10. Diabetes UK Nutrition Working Group, Dyson PA, Kelly T, Deakin T, et al. Evidence-Based Nutrition Guidelines for the Prevention and Management of Diabetes. Diabetes UK Web site. Available at: www.diabetes.org.uk/Documents/Reports/nutritional-guidelines-2013-amendment-0413.pdf. Accessed October 2, 2013.
1. Balk ME, Tatsioni A, Lichtenstein AH, et al. Effect of chromium supplementation on glucose metabolism and lipids: a systematic review of randomized controlled trials. Diabetes Care. 2007;30:2154-2163.
2. Akilen R, Tsiami A, Devendra D, et al. Cinnamon in glycaemic control: Systematic review and meta analysis. Clin Nutr. 2012;31:609-615.
3. Ludvik B, Hanefeld M, Pacini G. Improved metabolic control by Ipomoea batatas (Caiapo) is associated with increased adiponectin and decreased fibrinogen levels in type 2 diabetic subjects. Diabetes Obes Metab. 2008;10:586-592.
4. Ludvik, B, Neuffer, B, Pacini G. Efficacy of Ipomoea batatas (Caiapo) on diabetes control in type 2 diabetic subjects treated with diet. Diabetes Care. 2004;27:436-440.
5. Lu FR, Shen L, Qin Y, et al. Clinical observation on trigonella foenum-graecum L. total saponins in combination with sulfonylureas in the treatment of type 2 diabetes mellitus. Chin J Integr Med. 2008;14:56-60.
6. Huseini HF, Larijani B, Heshmat R, et al. The efficacy of Silybummarianum (L.) Gaertn. (silymarin) in the treatment of type II diabetes: a randomized, double-blind, placebo-controlled clinical trial. Phytother Res. 2006;20:1036-1039.
7. Hussain SA. Silymarin as an adjunct to glibenclamide therapy improves long-term and postprandial glycemic control and body mass index in type 2 diabetes. J Med Food. 2007;10:543-547.
8. Asp ML, Collene AL, Norris LE, et al. Time-dependent effects of safflower oil to improve glycemia, inflammation and blood lipids in obese, post-menopausal women with type 2 diabetes: a randomized,double-masked, crossover study. Clin Nutr. 2011;30:443-449.
9. American Diabetes Association; Bantle JP, Wylie-Rosett J, Albright AL, et al. Nutrition recommendations and interventions for diabetes: a position statement of the American Diabetes Association. Diabetes Care. 2008;31 suppl 1:S61-S78.
10. Diabetes UK Nutrition Working Group, Dyson PA, Kelly T, Deakin T, et al. Evidence-Based Nutrition Guidelines for the Prevention and Management of Diabetes. Diabetes UK Web site. Available at: www.diabetes.org.uk/Documents/Reports/nutritional-guidelines-2013-amendment-0413.pdf. Accessed October 2, 2013.
Evidence-based answers from the Family Physicians Inquiries Network
A better approach to opioid prescribing in primary care
ABSTRACT
Purpose Primary care physicians are at the center of a national prescription opioid epidemic, with little training or knowledge about the management of patients on opioids for chronic noncancer pain (CNCP). We developed an electronic medical record (EMR)-based protocol and educational intervention to standardize documentation and management of patients prescribed opioids by primary care providers. Our objective was to evaluate provider adherence to this protocol, attitudes toward the management of these patients, and knowledge of opioid prescribing.
Methods We trained providers and select staff from 3 primary care practices at the Division of General Internal Medicine at the University of Pennsylvania in the use of a protocol for managing patients taking opioids for CNCP. The following served as measures of protocol adherence: 1) the provider used a standard diagnosis (chronic pain, ICD-9 code 338.29A) in the problem list, 2) the provider ordered at least one urine drug screen (UDS) for the patient in the past year, and 3) the patient came in for at least one office visit every 6 months. We assessed physician and staff attitudes and knowledge with pre- and post-intervention surveys. Adherence to the protocol was linked to a monetary incentive.
Results Provider adherence to the protocol significantly improved measured outcomes. The number of UDSs ordered increased by 145%, and the diagnosis of chronic pain on the problem list increased by 424%. There was a statistically significant improvement in providers’ role adequacy, role support, and job satisfaction/role-related self-esteem when working with patients taking opioids. In addition, provider knowledge of proper management of these patients improved significantly. Eighty-nine percent of our physicians attained the monetary incentive.
Conclusions We developed a quality improvement intervention that addressed the need for better regulation of opioid prescribing, resulted in increased adherence to best-practice guidelines, and improved provider knowledge and attitudes.
Primary care physicians often express dissatisfaction with their competency in treating patients with opioids,1 and at our institution, this includes residents and faculty, as well. Their concern, combined with apprehension about patient safety and the potential for addiction, can hinder appropriate opioid management.1 We asked: Could a protocol that structures the intervention improve physician competence and performance in prescribing opioids and reduce patient risk?
Physician concerns are well-founded. Nonmedical use of prescription opioids is second only to smoking marijuana in the illicit use of drugs in the United States.2 Since 2003, more overdose deaths have involved opioid analgesics than heroin and cocaine combined, leading the Centers for Disease Control and Prevention to declare in 2012 that the problem was a “national epidemic.”3 The Washington State Medical Quality Assurance Commission now mandates extensive patient evaluation and documentation, the use of a Controlled Medication Agreement (CMA), and specific education requirements for physicians prescribing long-acting or high-dose opioids.4
Necessary adjustments going forward. As the nation moves toward more regulated prescribing of opioids, physicians will need to develop a consistent approach to this complicated task. Primary care doctors must be at the center of this effort, as they generate most opioid prescriptions for the treatment of CNCP. Currently, providers vary widely in their management of this condition,5-7 and recommended corrective steps include increased education8 and improved adherence to national guidelines. Our contention—and the basis of our study—was that a clinical protocol for opioid prescribing could improve the care that physicians and staff were providing to CNCP patients, as well as improve the satisfaction that clinicians felt in providing this care.
Our protocol intervention. Prior to our protocol intervention, no guidelines existed for managing patients on long-term opioid therapy in the clinical practices of the University of Pennsylvania Division of General Internal Medicine. Our providers, too, varied widely in their prescribing and management. Though regular urine drug screening is known to improve detection of opioid misuse and decrease the problem in patients treated for CNCP,9,10 a study reviewing opioid prescribing practices in our clinics from 2004 to 2007 showed that physicians ordered UDSs for only 8% of patients.11 Furthermore, only half of patients (49.8%) had regular office visits—even those at high risk for opioid misuse.11
|
Based on expert opinion and national best-practice guidelines, we created a division-wide quality improvement intervention for opioid prescribing. The protocol required standardized evaluation and documentation of a patient’s pain history and treatment plan, and the use of a UDS and a CMA, which is known to decrease emergency room visits and improve physician satisfaction, respectively.9,10 We trained attending physicians and staff on the protocol, and they in turn taught residents at their practice sites. The goal of this study was to determine whether this initiative would result in adherence to the protocol and improve provider and staff knowledge and satisfaction with management of patients prescribed opioids for CNCP.
METHODS
The intervention consisted of (1) the development of an EMR-based protocol to standardize documentation and management of patients with CNCP taking opioids; (2) instruction on using the protocol and on key components of opioid management; (3) collection of data; and (4) a monetary incentive for attending physicians to adhere to the protocol. We measured the impact of this intervention by assessing physician compliance with the protocol, provider satisfaction, and knowledge.
Protocol and process
We developed a division-wide protocol for managing primary-care patients with CNCP taking opioids, based on national guidelines, expert input, best practice data, and EMR capabilities (EpicCare Ambulatory Medical Record, version Summer 2009).
Health system experts from anesthesia, pain management, and psychiatry met regularly with our monthly workgroup to review the latest literature on UDSs and CMAs, and to assess best practices researched by the Center for Evidence Based Practice at our institution. We trained providers on the following steps:
• select patients who are taking opioids for CNCP (ie, receiving >2 opioid prescriptions in the 6 months prior to the intervention for a nonlimited pain condition)
• risk stratify these patients using the Opioid Risk Tool12
• follow high-risk patients monthly; low-to-moderate-risk patients every 3 to 6 months
• use a standard diagnosis (chronic pain, ICD-9 code 338.29A) in the EMR problem list
• complete a standardized EMR “smart set” documenting evaluation and management in the overview section of the EMR’s chronic pain diagnosis module (TABLE 1)
• complete a CMA
• order a UDS at regular intervals (at least one per year; every 1-3 months in high-risk patients)
• designate one provider (in the EMR) to be responsible for opioid prescribing. Medical residents were encouraged to specify a “Continuity Attending” to maintain continuity of care when they were not in clinic.
Educational intervention
The principal investigator conducted 4 training sessions that were available to all attending physicians and staff, to review the protocol as well as information on best practices in opioid prescribing. One session was a Quality Improvement Grand Rounds for the division, and 3 sessions were open presentations within each participating practice. During all sessions, we taught the protocol, provided instruction on riskstratifying patients, reviewed the definition and prevalence of chronic pain, described the national opioid problem, detailed the components of proper documentation, and explained how to interpret and manage UDS results.
We trained categorical internal medicine interns for 1 hour during their mandatory clinical lecture series. Primary care track residents received 4 hours of training as part of their regular educational program.
Ongoing education for attending physicians occurred at 4 bimonthly opioid management case conferences, where difficult cases were presented to a rotating panel of experts from pain medicine, addiction psychiatry, and primary care. We held regular noon conferences on opioid management for residents.
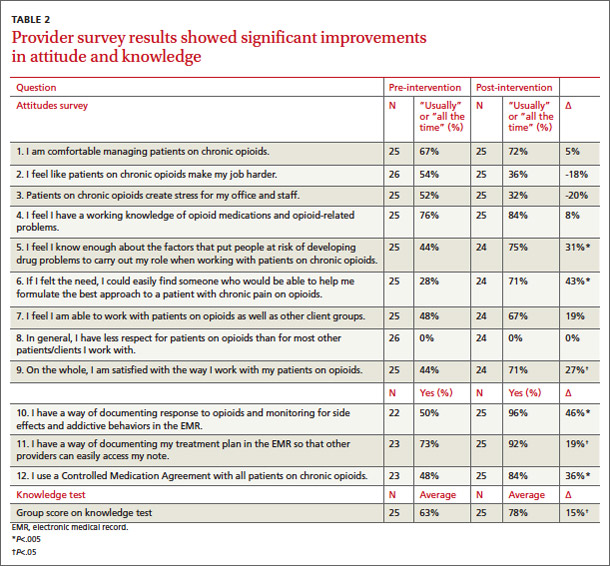
Monetary incentive for physicians
Our division further aided our efforts by offering a monetary incentive ($1500) to attending physicians who achieved all 3 of the following measures of adherence with at least 80% of their chronic pain patients: at least one UDS in the past year, an office visit at least every 6 months, and a chronic pain diagnosis on the problem list in the EMR.
Data feedback
We gave providers a list of their patients receiving >2 opioid prescriptions over 6 months, and were able to exclude those patients treated for a limited pain condition. For the remainder of patients, physicians received quarterly individual reports on their adherence to the protocol.
Study population
Three internal medicine clinical practices of the University of Pennsylvania in Philadelphia took part in this initiative. We included all attending providers at these practices in the analysis assessing adherence to the protocol. Those who consented and completed a survey were included in the survey analysis. Providers were attending physicians and nurse practitioners. In Practice 1, primary care track residents are fully integrated into the practice and were included in the survey as their extended training was timed with our intervention. We did not survey residents at the other practices due to their variable schedules and inability to train as a group.
Staff included registered nurses, licensed practical nurses, medical assistants, and patient service representatives. Because nurses and medical assistants are responsible for medication refills, they received education specifically about this intervention. The remaining staff also received instruction, as they have personal interactions with patients at the provider visit, and thus their attitudes were important to measure. Participants completed surveys at the time of the educational sessions and again 9 months following implementation of the intervention. This was a one-year intervention, with 3 initial months of teaching; the study period therefore lasted 9 months. Since surveys were anonymous, we could not link results to specific individuals. However, we provided post-intervention surveys only to those who reported completing the initial survey.
Survey design and administration
The provider survey contained an attitude component and a knowledge component (TABLE 2). The attitude component consisted of 6 items taken from the Drug Problems Perceptions Questionnaire,13 to address role adequacy, support, and self-esteem, as well as job satisfaction (the words “drug users” were replaced with “patients on [chronic] opioids”). We created an additional 3 items to further explore these domains (items 1-3). Three additional items addressed provider access to EMR specific tools (items 10-12).
The knowledge survey consisted of multiple choice questions created by the study team, and it reflected best practice guidelines for opioid management for CNCP and knowledge of protocol elements. Items included the definition of chronic pain, opioid medications not included on the UDS, interpretation of UDS results, addiction risk, intervals for office visits for patients on chronic opioid therapy, and pain medication dose escalation.
The staff survey included similar attitude components and a modified knowledge portion regarding which patients should have a CMA, where to document a CMA in the EMR, addiction risk, intervals for office visits, and how to handle early prescription refill requests.
Evaluation and statistical analysis
To assess the impact of the intervention, we chose 2 measures of physician adherence with the protocol (UDS and chronic pain diagnosis) because of our ability to access these measures within our approved protocol.
Individual attitude survey questions were compared using paired t-tests. We averaged knowledge test scores, and also used the paired t-test to compare pre- and posttest averages. We used Stata 11.2 (StataCorp LP, 2009) to analyze survey data.
This study was sponsored by the Matthew Slap Research Award and approved by the University of Pennsylvania Institutional Review Board.
RESULTS
Practice demographics
The 3 practices are located within the same zip code, a few city blocks from one another. Despite geographic proximity of the practices, their populations differ racially and ethnically as well as in neighborhood income distributions (TABLE 3). In all 3 practices, the total number of patients prescribed >2 opioid medications declined during the year-long study period. Practice 3 had the sharpest decline in the number of patients prescribed chronic opioids, likely due to provider turnover during the study period. Practices 1 and 2 had the highest adherence to guidelines. The marked variability in adoption of guidelines likely reflects a number of factors: the difference in baseline opioid prescribing (highest in Practice 3), the presence of physician champions in Practices 1 and 2, and more intensive training of the primary care residents in Practice 1.
Protocol adherence
We measured provider adherence to the protocol by comparing data from the year before the intervention to the year following the start of the intervention for the number of UDSs ordered, the number of chronic pain diagnoses on patients’ EMR problem lists, and the number of office visits with CNCP patients. UDSs ordered increased by 145% across all 3 practices, with the largest improvement seen in Practice 1 (430%; P<.05). Documentation of a chronic pain diagnosis in the EMR problem list increased by 424% across practices, with the largest improvement seen again in Practice 1 (918%, P<.05) (TABLE 4). Based on this performance, 24 of 27 (89%) full time physicians qualified for the financial incentive. We chose not to include the third measure (number of office visits) for analysis, as we discovered that >90% of patients were seen at least every 6 months before the intervention.
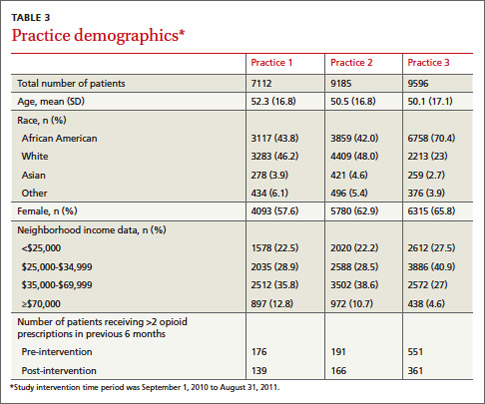
Survey results
Before the protocol training, we surveyed 26 providers and 33 staff members. Nine months after the initiation of the protocol, 25 providers and 26 staff were again surveyed. Surveys were anonymous so we were unable to link knowledge gains to individuals.
Providers exhibited statistically significant improvement of attitude for role adequacy (item 5), role support (item 6), job satisfaction/role-related self-esteem (item 9), and access to EMR-specific tools (items 10-12) (TABLE 2). In addition, the knowledge test score increased by 15% (P<.05) in the postintervention survey.
Staff surveys showed statistically significant improvement of attitude for job satisfaction/role-related self-esteem. There was no improvement in knowledge for staff, which is likely due to variability in training.
DISCUSSION
More than 40% of opioid prescriptions in the United States are written by primary care physicians.14 Therefore, interventions that enhance provider knowledge, institute best practices, and support role-related self-esteem in opioid management are vital to our profession.
Through a straightforward protocol, we greatly increased the number of UDSs ordered (145%) and documentation of chronic pain on the problem list (424%). By increasing adherence to best practice standards, we believe this protocol will lead to improved management of patients with CNCP by providing objective urine data to guide a treatment plan, patient education with the CMA, and a documented evaluation and care plan.
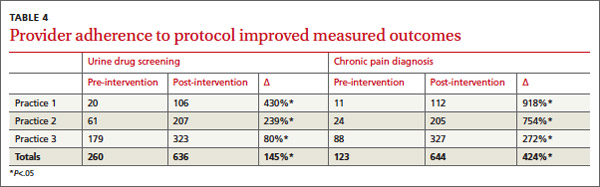
In addition to fostering adherence to the protocol, our multicomponent intervention resulted in marked improvement of provider and staff attitudes toward patients taking opioids for CNCP (TABLE 2). Participants’ satisfaction in working with these patients improved significantly (27%), as did their confidence in knowing whom to ask for help with management (43%). After this intervention, physicians reported a nonstatistically significant but large reductions in the perception that patients on opioids create stress for the office (-20%), and that patients on opioids make their job harder (-18%). Knowledge about chronic opioid prescribing also improved significantly for providers (15%).
At all practices, the number of patients receiving opioids decreased, likely due to the protocol intervention.
Previous studies have shown low adoption of best practices in opioid management without a structured intervention.10 Our findings suggest that a multicomponent quality improvement intervention that combines education, financial incentive, and a structured protocol can positively impact provider and staff attitudes and adherence to best practices in caring for patients with CNCP taking opioid medications. We believe that similar interventions could be adapted by other primary care clinics with a comparable favorable impact on physician behavior, attitudes, and knowledge.
Limitations
Our findings may not apply to nonacademic practices, as we required training and the use of an EMR. Additionally, our urban patient populations may not be generalizable to rural, suburban, or other populations in the management of patients taking prescription opioids. Further, the monetary incentive, which was included in a yearly incentive package at our institution, may not be feasible at other sites.
We did not design this study to allow for practice-level comparisons or to assess patient level variables. Analysis of patient data on safety, aberrant behavior, abnormal UDS results, and the impact of the intervention on these outcomes was outside of the scope of this study. We were unable to determine whether physician turnover, particularly high in one practice, could be linked to the results.
Providers often neglected to indicate their level of training on surveys, and we were therefore unable to compare adherence and knowledge between residents and attending physicians. Additionally, we lacked approval to search individual charts to completely investigate the components of our protocol (for example, completion of a CMA or UDS). Lastly, we did not design the study to control for confounders on a provider level (such as age, gender, and years of experience). A more comprehensive review of these important variables is warranted to assess the degree to which division- or practice-level quality improvement interventions can affect provider and patient behavior change and enhance patient safety.
CORRESPONDENCE
Robin E. Canada, MD, Medical Arts Building, Suite 102, 38th and Market Sts, Philadelphia, PA 19104; [email protected]
Acknowledgement
The authors gratefully acknowledge Judy Shea, PhD and Joanna Starrels, MD, who provided valuable comments in the development of this manuscript.
1. Lin JJ, Alfandre D, Moore C. Physician attitudes toward opioid prescribing for patients with persistent noncancer pain. Clin J Pain. 2007;23:799-803.
2. Hughes A, Sathe N, Spagnola K. (2009). State estimates of substance use from the 2006-2007 National Surveys on Drug Use and Health. Rockville, MD: Office of Applied Studies, Substance Abuse and Mental Health Services Administration; 2009. NSDUH Series H-35, HHS Publication No. SMA 09-4362.
3. Centers for Disease Control and Prevention (CDC). CDC grand rounds: prescription drug overdoses - a US epidemic. MMWR Morb Mortal Wkly Rep. 2012;61:10-13.
4. Washington State Department of Health- Medical Quality Assurance Commission. Rule-Making Order CR-103. University of Washington Web site. Available at: http://depts.washington.edu/anesth/education/forms/pain/WAC-Rules-CR-103P.pdf. Accessed February 1, 2012.
5. Leverence RR, Williams RL, Potter M, et al. Chronic non-cancer pain: a siren for primary care—a report from the PRImary Care MultiEthnic Network (PRIME Net). J Am Board Fam Med. 2011;24:551-561.
6. Green CR, Wheeler JR, LaPorte F, et al. How well is chronic pain managed? Who does it well? Pain Med. 2002;3:56-65.
7. Webster BS, Cifuentes M, Verma S, et al. Geographic variation in opioid prescribing for acute, work-related, low back pain and associated factors: a multilevel analysis. Am J Ind Med. 2009;52:162-171.
8. Gunderson EW, Coffin PO, Chang N, et al. The interface between substance abuse and chronic pain management in primary care: a curriculum for medical residents. Subst Abus. 2009;30:253-260.
9. Manchikanti L, Manchukonda R, Pampati V, et al. Does random urine drug testing reduce illicit drug use in chronic pain patients receiving opioids? Pain Physician. 2006;9:123-129.
10. Starrels JL, Becker WC, Alford DP, et al. Systematic review: treatment agreements and urine drug testing to reduce opioid misuse in patients with chronic pain. Ann Intern Med. 2010;152:712-720.
11. Starrels JL, Becker WC, Weiner MG, et al. Low use of opioid risk reduction strategies in primary care even for high risk patients with chronic pain. J Gen Intern Med. 2011;26:958-964.
12. Webster LR, Webster RM. Predicting aberrant behaviors in opioid- treated patients: preliminary validation of the Opioid Risk Tool. Pain Med. 2005;6:432-442.
13. Watson H, Maclaren W, Kerr S. Staff attitudes toward working with drug users: development of the Drug Problems Perceptions Questionnaire. Addiction. 2007;102:206-215.
14. Okie S. A flood of opioids, a rising tide of deaths. N Engl J Med. 2010;363:1981-1985.
ABSTRACT
Purpose Primary care physicians are at the center of a national prescription opioid epidemic, with little training or knowledge about the management of patients on opioids for chronic noncancer pain (CNCP). We developed an electronic medical record (EMR)-based protocol and educational intervention to standardize documentation and management of patients prescribed opioids by primary care providers. Our objective was to evaluate provider adherence to this protocol, attitudes toward the management of these patients, and knowledge of opioid prescribing.
Methods We trained providers and select staff from 3 primary care practices at the Division of General Internal Medicine at the University of Pennsylvania in the use of a protocol for managing patients taking opioids for CNCP. The following served as measures of protocol adherence: 1) the provider used a standard diagnosis (chronic pain, ICD-9 code 338.29A) in the problem list, 2) the provider ordered at least one urine drug screen (UDS) for the patient in the past year, and 3) the patient came in for at least one office visit every 6 months. We assessed physician and staff attitudes and knowledge with pre- and post-intervention surveys. Adherence to the protocol was linked to a monetary incentive.
Results Provider adherence to the protocol significantly improved measured outcomes. The number of UDSs ordered increased by 145%, and the diagnosis of chronic pain on the problem list increased by 424%. There was a statistically significant improvement in providers’ role adequacy, role support, and job satisfaction/role-related self-esteem when working with patients taking opioids. In addition, provider knowledge of proper management of these patients improved significantly. Eighty-nine percent of our physicians attained the monetary incentive.
Conclusions We developed a quality improvement intervention that addressed the need for better regulation of opioid prescribing, resulted in increased adherence to best-practice guidelines, and improved provider knowledge and attitudes.
Primary care physicians often express dissatisfaction with their competency in treating patients with opioids,1 and at our institution, this includes residents and faculty, as well. Their concern, combined with apprehension about patient safety and the potential for addiction, can hinder appropriate opioid management.1 We asked: Could a protocol that structures the intervention improve physician competence and performance in prescribing opioids and reduce patient risk?
Physician concerns are well-founded. Nonmedical use of prescription opioids is second only to smoking marijuana in the illicit use of drugs in the United States.2 Since 2003, more overdose deaths have involved opioid analgesics than heroin and cocaine combined, leading the Centers for Disease Control and Prevention to declare in 2012 that the problem was a “national epidemic.”3 The Washington State Medical Quality Assurance Commission now mandates extensive patient evaluation and documentation, the use of a Controlled Medication Agreement (CMA), and specific education requirements for physicians prescribing long-acting or high-dose opioids.4
Necessary adjustments going forward. As the nation moves toward more regulated prescribing of opioids, physicians will need to develop a consistent approach to this complicated task. Primary care doctors must be at the center of this effort, as they generate most opioid prescriptions for the treatment of CNCP. Currently, providers vary widely in their management of this condition,5-7 and recommended corrective steps include increased education8 and improved adherence to national guidelines. Our contention—and the basis of our study—was that a clinical protocol for opioid prescribing could improve the care that physicians and staff were providing to CNCP patients, as well as improve the satisfaction that clinicians felt in providing this care.
Our protocol intervention. Prior to our protocol intervention, no guidelines existed for managing patients on long-term opioid therapy in the clinical practices of the University of Pennsylvania Division of General Internal Medicine. Our providers, too, varied widely in their prescribing and management. Though regular urine drug screening is known to improve detection of opioid misuse and decrease the problem in patients treated for CNCP,9,10 a study reviewing opioid prescribing practices in our clinics from 2004 to 2007 showed that physicians ordered UDSs for only 8% of patients.11 Furthermore, only half of patients (49.8%) had regular office visits—even those at high risk for opioid misuse.11
|
Based on expert opinion and national best-practice guidelines, we created a division-wide quality improvement intervention for opioid prescribing. The protocol required standardized evaluation and documentation of a patient’s pain history and treatment plan, and the use of a UDS and a CMA, which is known to decrease emergency room visits and improve physician satisfaction, respectively.9,10 We trained attending physicians and staff on the protocol, and they in turn taught residents at their practice sites. The goal of this study was to determine whether this initiative would result in adherence to the protocol and improve provider and staff knowledge and satisfaction with management of patients prescribed opioids for CNCP.
METHODS
The intervention consisted of (1) the development of an EMR-based protocol to standardize documentation and management of patients with CNCP taking opioids; (2) instruction on using the protocol and on key components of opioid management; (3) collection of data; and (4) a monetary incentive for attending physicians to adhere to the protocol. We measured the impact of this intervention by assessing physician compliance with the protocol, provider satisfaction, and knowledge.
Protocol and process
We developed a division-wide protocol for managing primary-care patients with CNCP taking opioids, based on national guidelines, expert input, best practice data, and EMR capabilities (EpicCare Ambulatory Medical Record, version Summer 2009).
Health system experts from anesthesia, pain management, and psychiatry met regularly with our monthly workgroup to review the latest literature on UDSs and CMAs, and to assess best practices researched by the Center for Evidence Based Practice at our institution. We trained providers on the following steps:
• select patients who are taking opioids for CNCP (ie, receiving >2 opioid prescriptions in the 6 months prior to the intervention for a nonlimited pain condition)
• risk stratify these patients using the Opioid Risk Tool12
• follow high-risk patients monthly; low-to-moderate-risk patients every 3 to 6 months
• use a standard diagnosis (chronic pain, ICD-9 code 338.29A) in the EMR problem list
• complete a standardized EMR “smart set” documenting evaluation and management in the overview section of the EMR’s chronic pain diagnosis module (TABLE 1)
• complete a CMA
• order a UDS at regular intervals (at least one per year; every 1-3 months in high-risk patients)
• designate one provider (in the EMR) to be responsible for opioid prescribing. Medical residents were encouraged to specify a “Continuity Attending” to maintain continuity of care when they were not in clinic.
Educational intervention
The principal investigator conducted 4 training sessions that were available to all attending physicians and staff, to review the protocol as well as information on best practices in opioid prescribing. One session was a Quality Improvement Grand Rounds for the division, and 3 sessions were open presentations within each participating practice. During all sessions, we taught the protocol, provided instruction on riskstratifying patients, reviewed the definition and prevalence of chronic pain, described the national opioid problem, detailed the components of proper documentation, and explained how to interpret and manage UDS results.
We trained categorical internal medicine interns for 1 hour during their mandatory clinical lecture series. Primary care track residents received 4 hours of training as part of their regular educational program.
Ongoing education for attending physicians occurred at 4 bimonthly opioid management case conferences, where difficult cases were presented to a rotating panel of experts from pain medicine, addiction psychiatry, and primary care. We held regular noon conferences on opioid management for residents.
Monetary incentive for physicians
Our division further aided our efforts by offering a monetary incentive ($1500) to attending physicians who achieved all 3 of the following measures of adherence with at least 80% of their chronic pain patients: at least one UDS in the past year, an office visit at least every 6 months, and a chronic pain diagnosis on the problem list in the EMR.
Data feedback
We gave providers a list of their patients receiving >2 opioid prescriptions over 6 months, and were able to exclude those patients treated for a limited pain condition. For the remainder of patients, physicians received quarterly individual reports on their adherence to the protocol.
Study population
Three internal medicine clinical practices of the University of Pennsylvania in Philadelphia took part in this initiative. We included all attending providers at these practices in the analysis assessing adherence to the protocol. Those who consented and completed a survey were included in the survey analysis. Providers were attending physicians and nurse practitioners. In Practice 1, primary care track residents are fully integrated into the practice and were included in the survey as their extended training was timed with our intervention. We did not survey residents at the other practices due to their variable schedules and inability to train as a group.
Staff included registered nurses, licensed practical nurses, medical assistants, and patient service representatives. Because nurses and medical assistants are responsible for medication refills, they received education specifically about this intervention. The remaining staff also received instruction, as they have personal interactions with patients at the provider visit, and thus their attitudes were important to measure. Participants completed surveys at the time of the educational sessions and again 9 months following implementation of the intervention. This was a one-year intervention, with 3 initial months of teaching; the study period therefore lasted 9 months. Since surveys were anonymous, we could not link results to specific individuals. However, we provided post-intervention surveys only to those who reported completing the initial survey.
Survey design and administration
The provider survey contained an attitude component and a knowledge component (TABLE 2). The attitude component consisted of 6 items taken from the Drug Problems Perceptions Questionnaire,13 to address role adequacy, support, and self-esteem, as well as job satisfaction (the words “drug users” were replaced with “patients on [chronic] opioids”). We created an additional 3 items to further explore these domains (items 1-3). Three additional items addressed provider access to EMR specific tools (items 10-12).
The knowledge survey consisted of multiple choice questions created by the study team, and it reflected best practice guidelines for opioid management for CNCP and knowledge of protocol elements. Items included the definition of chronic pain, opioid medications not included on the UDS, interpretation of UDS results, addiction risk, intervals for office visits for patients on chronic opioid therapy, and pain medication dose escalation.
The staff survey included similar attitude components and a modified knowledge portion regarding which patients should have a CMA, where to document a CMA in the EMR, addiction risk, intervals for office visits, and how to handle early prescription refill requests.
Evaluation and statistical analysis
To assess the impact of the intervention, we chose 2 measures of physician adherence with the protocol (UDS and chronic pain diagnosis) because of our ability to access these measures within our approved protocol.
Individual attitude survey questions were compared using paired t-tests. We averaged knowledge test scores, and also used the paired t-test to compare pre- and posttest averages. We used Stata 11.2 (StataCorp LP, 2009) to analyze survey data.
This study was sponsored by the Matthew Slap Research Award and approved by the University of Pennsylvania Institutional Review Board.
RESULTS
Practice demographics
The 3 practices are located within the same zip code, a few city blocks from one another. Despite geographic proximity of the practices, their populations differ racially and ethnically as well as in neighborhood income distributions (TABLE 3). In all 3 practices, the total number of patients prescribed >2 opioid medications declined during the year-long study period. Practice 3 had the sharpest decline in the number of patients prescribed chronic opioids, likely due to provider turnover during the study period. Practices 1 and 2 had the highest adherence to guidelines. The marked variability in adoption of guidelines likely reflects a number of factors: the difference in baseline opioid prescribing (highest in Practice 3), the presence of physician champions in Practices 1 and 2, and more intensive training of the primary care residents in Practice 1.
Protocol adherence
We measured provider adherence to the protocol by comparing data from the year before the intervention to the year following the start of the intervention for the number of UDSs ordered, the number of chronic pain diagnoses on patients’ EMR problem lists, and the number of office visits with CNCP patients. UDSs ordered increased by 145% across all 3 practices, with the largest improvement seen in Practice 1 (430%; P<.05). Documentation of a chronic pain diagnosis in the EMR problem list increased by 424% across practices, with the largest improvement seen again in Practice 1 (918%, P<.05) (TABLE 4). Based on this performance, 24 of 27 (89%) full time physicians qualified for the financial incentive. We chose not to include the third measure (number of office visits) for analysis, as we discovered that >90% of patients were seen at least every 6 months before the intervention.
Survey results
Before the protocol training, we surveyed 26 providers and 33 staff members. Nine months after the initiation of the protocol, 25 providers and 26 staff were again surveyed. Surveys were anonymous so we were unable to link knowledge gains to individuals.
Providers exhibited statistically significant improvement of attitude for role adequacy (item 5), role support (item 6), job satisfaction/role-related self-esteem (item 9), and access to EMR-specific tools (items 10-12) (TABLE 2). In addition, the knowledge test score increased by 15% (P<.05) in the postintervention survey.
Staff surveys showed statistically significant improvement of attitude for job satisfaction/role-related self-esteem. There was no improvement in knowledge for staff, which is likely due to variability in training.
DISCUSSION
More than 40% of opioid prescriptions in the United States are written by primary care physicians.14 Therefore, interventions that enhance provider knowledge, institute best practices, and support role-related self-esteem in opioid management are vital to our profession.
Through a straightforward protocol, we greatly increased the number of UDSs ordered (145%) and documentation of chronic pain on the problem list (424%). By increasing adherence to best practice standards, we believe this protocol will lead to improved management of patients with CNCP by providing objective urine data to guide a treatment plan, patient education with the CMA, and a documented evaluation and care plan.
In addition to fostering adherence to the protocol, our multicomponent intervention resulted in marked improvement of provider and staff attitudes toward patients taking opioids for CNCP (TABLE 2). Participants’ satisfaction in working with these patients improved significantly (27%), as did their confidence in knowing whom to ask for help with management (43%). After this intervention, physicians reported a nonstatistically significant but large reductions in the perception that patients on opioids create stress for the office (-20%), and that patients on opioids make their job harder (-18%). Knowledge about chronic opioid prescribing also improved significantly for providers (15%).
At all practices, the number of patients receiving opioids decreased, likely due to the protocol intervention.
Previous studies have shown low adoption of best practices in opioid management without a structured intervention.10 Our findings suggest that a multicomponent quality improvement intervention that combines education, financial incentive, and a structured protocol can positively impact provider and staff attitudes and adherence to best practices in caring for patients with CNCP taking opioid medications. We believe that similar interventions could be adapted by other primary care clinics with a comparable favorable impact on physician behavior, attitudes, and knowledge.
Limitations
Our findings may not apply to nonacademic practices, as we required training and the use of an EMR. Additionally, our urban patient populations may not be generalizable to rural, suburban, or other populations in the management of patients taking prescription opioids. Further, the monetary incentive, which was included in a yearly incentive package at our institution, may not be feasible at other sites.
We did not design this study to allow for practice-level comparisons or to assess patient level variables. Analysis of patient data on safety, aberrant behavior, abnormal UDS results, and the impact of the intervention on these outcomes was outside of the scope of this study. We were unable to determine whether physician turnover, particularly high in one practice, could be linked to the results.
Providers often neglected to indicate their level of training on surveys, and we were therefore unable to compare adherence and knowledge between residents and attending physicians. Additionally, we lacked approval to search individual charts to completely investigate the components of our protocol (for example, completion of a CMA or UDS). Lastly, we did not design the study to control for confounders on a provider level (such as age, gender, and years of experience). A more comprehensive review of these important variables is warranted to assess the degree to which division- or practice-level quality improvement interventions can affect provider and patient behavior change and enhance patient safety.
CORRESPONDENCE
Robin E. Canada, MD, Medical Arts Building, Suite 102, 38th and Market Sts, Philadelphia, PA 19104; [email protected]
Acknowledgement
The authors gratefully acknowledge Judy Shea, PhD and Joanna Starrels, MD, who provided valuable comments in the development of this manuscript.
ABSTRACT
Purpose Primary care physicians are at the center of a national prescription opioid epidemic, with little training or knowledge about the management of patients on opioids for chronic noncancer pain (CNCP). We developed an electronic medical record (EMR)-based protocol and educational intervention to standardize documentation and management of patients prescribed opioids by primary care providers. Our objective was to evaluate provider adherence to this protocol, attitudes toward the management of these patients, and knowledge of opioid prescribing.
Methods We trained providers and select staff from 3 primary care practices at the Division of General Internal Medicine at the University of Pennsylvania in the use of a protocol for managing patients taking opioids for CNCP. The following served as measures of protocol adherence: 1) the provider used a standard diagnosis (chronic pain, ICD-9 code 338.29A) in the problem list, 2) the provider ordered at least one urine drug screen (UDS) for the patient in the past year, and 3) the patient came in for at least one office visit every 6 months. We assessed physician and staff attitudes and knowledge with pre- and post-intervention surveys. Adherence to the protocol was linked to a monetary incentive.
Results Provider adherence to the protocol significantly improved measured outcomes. The number of UDSs ordered increased by 145%, and the diagnosis of chronic pain on the problem list increased by 424%. There was a statistically significant improvement in providers’ role adequacy, role support, and job satisfaction/role-related self-esteem when working with patients taking opioids. In addition, provider knowledge of proper management of these patients improved significantly. Eighty-nine percent of our physicians attained the monetary incentive.
Conclusions We developed a quality improvement intervention that addressed the need for better regulation of opioid prescribing, resulted in increased adherence to best-practice guidelines, and improved provider knowledge and attitudes.
Primary care physicians often express dissatisfaction with their competency in treating patients with opioids,1 and at our institution, this includes residents and faculty, as well. Their concern, combined with apprehension about patient safety and the potential for addiction, can hinder appropriate opioid management.1 We asked: Could a protocol that structures the intervention improve physician competence and performance in prescribing opioids and reduce patient risk?
Physician concerns are well-founded. Nonmedical use of prescription opioids is second only to smoking marijuana in the illicit use of drugs in the United States.2 Since 2003, more overdose deaths have involved opioid analgesics than heroin and cocaine combined, leading the Centers for Disease Control and Prevention to declare in 2012 that the problem was a “national epidemic.”3 The Washington State Medical Quality Assurance Commission now mandates extensive patient evaluation and documentation, the use of a Controlled Medication Agreement (CMA), and specific education requirements for physicians prescribing long-acting or high-dose opioids.4
Necessary adjustments going forward. As the nation moves toward more regulated prescribing of opioids, physicians will need to develop a consistent approach to this complicated task. Primary care doctors must be at the center of this effort, as they generate most opioid prescriptions for the treatment of CNCP. Currently, providers vary widely in their management of this condition,5-7 and recommended corrective steps include increased education8 and improved adherence to national guidelines. Our contention—and the basis of our study—was that a clinical protocol for opioid prescribing could improve the care that physicians and staff were providing to CNCP patients, as well as improve the satisfaction that clinicians felt in providing this care.
Our protocol intervention. Prior to our protocol intervention, no guidelines existed for managing patients on long-term opioid therapy in the clinical practices of the University of Pennsylvania Division of General Internal Medicine. Our providers, too, varied widely in their prescribing and management. Though regular urine drug screening is known to improve detection of opioid misuse and decrease the problem in patients treated for CNCP,9,10 a study reviewing opioid prescribing practices in our clinics from 2004 to 2007 showed that physicians ordered UDSs for only 8% of patients.11 Furthermore, only half of patients (49.8%) had regular office visits—even those at high risk for opioid misuse.11
|
Based on expert opinion and national best-practice guidelines, we created a division-wide quality improvement intervention for opioid prescribing. The protocol required standardized evaluation and documentation of a patient’s pain history and treatment plan, and the use of a UDS and a CMA, which is known to decrease emergency room visits and improve physician satisfaction, respectively.9,10 We trained attending physicians and staff on the protocol, and they in turn taught residents at their practice sites. The goal of this study was to determine whether this initiative would result in adherence to the protocol and improve provider and staff knowledge and satisfaction with management of patients prescribed opioids for CNCP.
METHODS
The intervention consisted of (1) the development of an EMR-based protocol to standardize documentation and management of patients with CNCP taking opioids; (2) instruction on using the protocol and on key components of opioid management; (3) collection of data; and (4) a monetary incentive for attending physicians to adhere to the protocol. We measured the impact of this intervention by assessing physician compliance with the protocol, provider satisfaction, and knowledge.
Protocol and process
We developed a division-wide protocol for managing primary-care patients with CNCP taking opioids, based on national guidelines, expert input, best practice data, and EMR capabilities (EpicCare Ambulatory Medical Record, version Summer 2009).
Health system experts from anesthesia, pain management, and psychiatry met regularly with our monthly workgroup to review the latest literature on UDSs and CMAs, and to assess best practices researched by the Center for Evidence Based Practice at our institution. We trained providers on the following steps:
• select patients who are taking opioids for CNCP (ie, receiving >2 opioid prescriptions in the 6 months prior to the intervention for a nonlimited pain condition)
• risk stratify these patients using the Opioid Risk Tool12
• follow high-risk patients monthly; low-to-moderate-risk patients every 3 to 6 months
• use a standard diagnosis (chronic pain, ICD-9 code 338.29A) in the EMR problem list
• complete a standardized EMR “smart set” documenting evaluation and management in the overview section of the EMR’s chronic pain diagnosis module (TABLE 1)
• complete a CMA
• order a UDS at regular intervals (at least one per year; every 1-3 months in high-risk patients)
• designate one provider (in the EMR) to be responsible for opioid prescribing. Medical residents were encouraged to specify a “Continuity Attending” to maintain continuity of care when they were not in clinic.
Educational intervention
The principal investigator conducted 4 training sessions that were available to all attending physicians and staff, to review the protocol as well as information on best practices in opioid prescribing. One session was a Quality Improvement Grand Rounds for the division, and 3 sessions were open presentations within each participating practice. During all sessions, we taught the protocol, provided instruction on riskstratifying patients, reviewed the definition and prevalence of chronic pain, described the national opioid problem, detailed the components of proper documentation, and explained how to interpret and manage UDS results.
We trained categorical internal medicine interns for 1 hour during their mandatory clinical lecture series. Primary care track residents received 4 hours of training as part of their regular educational program.
Ongoing education for attending physicians occurred at 4 bimonthly opioid management case conferences, where difficult cases were presented to a rotating panel of experts from pain medicine, addiction psychiatry, and primary care. We held regular noon conferences on opioid management for residents.
Monetary incentive for physicians
Our division further aided our efforts by offering a monetary incentive ($1500) to attending physicians who achieved all 3 of the following measures of adherence with at least 80% of their chronic pain patients: at least one UDS in the past year, an office visit at least every 6 months, and a chronic pain diagnosis on the problem list in the EMR.
Data feedback
We gave providers a list of their patients receiving >2 opioid prescriptions over 6 months, and were able to exclude those patients treated for a limited pain condition. For the remainder of patients, physicians received quarterly individual reports on their adherence to the protocol.
Study population
Three internal medicine clinical practices of the University of Pennsylvania in Philadelphia took part in this initiative. We included all attending providers at these practices in the analysis assessing adherence to the protocol. Those who consented and completed a survey were included in the survey analysis. Providers were attending physicians and nurse practitioners. In Practice 1, primary care track residents are fully integrated into the practice and were included in the survey as their extended training was timed with our intervention. We did not survey residents at the other practices due to their variable schedules and inability to train as a group.
Staff included registered nurses, licensed practical nurses, medical assistants, and patient service representatives. Because nurses and medical assistants are responsible for medication refills, they received education specifically about this intervention. The remaining staff also received instruction, as they have personal interactions with patients at the provider visit, and thus their attitudes were important to measure. Participants completed surveys at the time of the educational sessions and again 9 months following implementation of the intervention. This was a one-year intervention, with 3 initial months of teaching; the study period therefore lasted 9 months. Since surveys were anonymous, we could not link results to specific individuals. However, we provided post-intervention surveys only to those who reported completing the initial survey.
Survey design and administration
The provider survey contained an attitude component and a knowledge component (TABLE 2). The attitude component consisted of 6 items taken from the Drug Problems Perceptions Questionnaire,13 to address role adequacy, support, and self-esteem, as well as job satisfaction (the words “drug users” were replaced with “patients on [chronic] opioids”). We created an additional 3 items to further explore these domains (items 1-3). Three additional items addressed provider access to EMR specific tools (items 10-12).
The knowledge survey consisted of multiple choice questions created by the study team, and it reflected best practice guidelines for opioid management for CNCP and knowledge of protocol elements. Items included the definition of chronic pain, opioid medications not included on the UDS, interpretation of UDS results, addiction risk, intervals for office visits for patients on chronic opioid therapy, and pain medication dose escalation.
The staff survey included similar attitude components and a modified knowledge portion regarding which patients should have a CMA, where to document a CMA in the EMR, addiction risk, intervals for office visits, and how to handle early prescription refill requests.
Evaluation and statistical analysis
To assess the impact of the intervention, we chose 2 measures of physician adherence with the protocol (UDS and chronic pain diagnosis) because of our ability to access these measures within our approved protocol.
Individual attitude survey questions were compared using paired t-tests. We averaged knowledge test scores, and also used the paired t-test to compare pre- and posttest averages. We used Stata 11.2 (StataCorp LP, 2009) to analyze survey data.
This study was sponsored by the Matthew Slap Research Award and approved by the University of Pennsylvania Institutional Review Board.
RESULTS
Practice demographics
The 3 practices are located within the same zip code, a few city blocks from one another. Despite geographic proximity of the practices, their populations differ racially and ethnically as well as in neighborhood income distributions (TABLE 3). In all 3 practices, the total number of patients prescribed >2 opioid medications declined during the year-long study period. Practice 3 had the sharpest decline in the number of patients prescribed chronic opioids, likely due to provider turnover during the study period. Practices 1 and 2 had the highest adherence to guidelines. The marked variability in adoption of guidelines likely reflects a number of factors: the difference in baseline opioid prescribing (highest in Practice 3), the presence of physician champions in Practices 1 and 2, and more intensive training of the primary care residents in Practice 1.
Protocol adherence
We measured provider adherence to the protocol by comparing data from the year before the intervention to the year following the start of the intervention for the number of UDSs ordered, the number of chronic pain diagnoses on patients’ EMR problem lists, and the number of office visits with CNCP patients. UDSs ordered increased by 145% across all 3 practices, with the largest improvement seen in Practice 1 (430%; P<.05). Documentation of a chronic pain diagnosis in the EMR problem list increased by 424% across practices, with the largest improvement seen again in Practice 1 (918%, P<.05) (TABLE 4). Based on this performance, 24 of 27 (89%) full time physicians qualified for the financial incentive. We chose not to include the third measure (number of office visits) for analysis, as we discovered that >90% of patients were seen at least every 6 months before the intervention.
Survey results
Before the protocol training, we surveyed 26 providers and 33 staff members. Nine months after the initiation of the protocol, 25 providers and 26 staff were again surveyed. Surveys were anonymous so we were unable to link knowledge gains to individuals.
Providers exhibited statistically significant improvement of attitude for role adequacy (item 5), role support (item 6), job satisfaction/role-related self-esteem (item 9), and access to EMR-specific tools (items 10-12) (TABLE 2). In addition, the knowledge test score increased by 15% (P<.05) in the postintervention survey.
Staff surveys showed statistically significant improvement of attitude for job satisfaction/role-related self-esteem. There was no improvement in knowledge for staff, which is likely due to variability in training.
DISCUSSION
More than 40% of opioid prescriptions in the United States are written by primary care physicians.14 Therefore, interventions that enhance provider knowledge, institute best practices, and support role-related self-esteem in opioid management are vital to our profession.
Through a straightforward protocol, we greatly increased the number of UDSs ordered (145%) and documentation of chronic pain on the problem list (424%). By increasing adherence to best practice standards, we believe this protocol will lead to improved management of patients with CNCP by providing objective urine data to guide a treatment plan, patient education with the CMA, and a documented evaluation and care plan.
In addition to fostering adherence to the protocol, our multicomponent intervention resulted in marked improvement of provider and staff attitudes toward patients taking opioids for CNCP (TABLE 2). Participants’ satisfaction in working with these patients improved significantly (27%), as did their confidence in knowing whom to ask for help with management (43%). After this intervention, physicians reported a nonstatistically significant but large reductions in the perception that patients on opioids create stress for the office (-20%), and that patients on opioids make their job harder (-18%). Knowledge about chronic opioid prescribing also improved significantly for providers (15%).
At all practices, the number of patients receiving opioids decreased, likely due to the protocol intervention.
Previous studies have shown low adoption of best practices in opioid management without a structured intervention.10 Our findings suggest that a multicomponent quality improvement intervention that combines education, financial incentive, and a structured protocol can positively impact provider and staff attitudes and adherence to best practices in caring for patients with CNCP taking opioid medications. We believe that similar interventions could be adapted by other primary care clinics with a comparable favorable impact on physician behavior, attitudes, and knowledge.
Limitations
Our findings may not apply to nonacademic practices, as we required training and the use of an EMR. Additionally, our urban patient populations may not be generalizable to rural, suburban, or other populations in the management of patients taking prescription opioids. Further, the monetary incentive, which was included in a yearly incentive package at our institution, may not be feasible at other sites.
We did not design this study to allow for practice-level comparisons or to assess patient level variables. Analysis of patient data on safety, aberrant behavior, abnormal UDS results, and the impact of the intervention on these outcomes was outside of the scope of this study. We were unable to determine whether physician turnover, particularly high in one practice, could be linked to the results.
Providers often neglected to indicate their level of training on surveys, and we were therefore unable to compare adherence and knowledge between residents and attending physicians. Additionally, we lacked approval to search individual charts to completely investigate the components of our protocol (for example, completion of a CMA or UDS). Lastly, we did not design the study to control for confounders on a provider level (such as age, gender, and years of experience). A more comprehensive review of these important variables is warranted to assess the degree to which division- or practice-level quality improvement interventions can affect provider and patient behavior change and enhance patient safety.
CORRESPONDENCE
Robin E. Canada, MD, Medical Arts Building, Suite 102, 38th and Market Sts, Philadelphia, PA 19104; [email protected]
Acknowledgement
The authors gratefully acknowledge Judy Shea, PhD and Joanna Starrels, MD, who provided valuable comments in the development of this manuscript.
1. Lin JJ, Alfandre D, Moore C. Physician attitudes toward opioid prescribing for patients with persistent noncancer pain. Clin J Pain. 2007;23:799-803.
2. Hughes A, Sathe N, Spagnola K. (2009). State estimates of substance use from the 2006-2007 National Surveys on Drug Use and Health. Rockville, MD: Office of Applied Studies, Substance Abuse and Mental Health Services Administration; 2009. NSDUH Series H-35, HHS Publication No. SMA 09-4362.
3. Centers for Disease Control and Prevention (CDC). CDC grand rounds: prescription drug overdoses - a US epidemic. MMWR Morb Mortal Wkly Rep. 2012;61:10-13.
4. Washington State Department of Health- Medical Quality Assurance Commission. Rule-Making Order CR-103. University of Washington Web site. Available at: http://depts.washington.edu/anesth/education/forms/pain/WAC-Rules-CR-103P.pdf. Accessed February 1, 2012.
5. Leverence RR, Williams RL, Potter M, et al. Chronic non-cancer pain: a siren for primary care—a report from the PRImary Care MultiEthnic Network (PRIME Net). J Am Board Fam Med. 2011;24:551-561.
6. Green CR, Wheeler JR, LaPorte F, et al. How well is chronic pain managed? Who does it well? Pain Med. 2002;3:56-65.
7. Webster BS, Cifuentes M, Verma S, et al. Geographic variation in opioid prescribing for acute, work-related, low back pain and associated factors: a multilevel analysis. Am J Ind Med. 2009;52:162-171.
8. Gunderson EW, Coffin PO, Chang N, et al. The interface between substance abuse and chronic pain management in primary care: a curriculum for medical residents. Subst Abus. 2009;30:253-260.
9. Manchikanti L, Manchukonda R, Pampati V, et al. Does random urine drug testing reduce illicit drug use in chronic pain patients receiving opioids? Pain Physician. 2006;9:123-129.
10. Starrels JL, Becker WC, Alford DP, et al. Systematic review: treatment agreements and urine drug testing to reduce opioid misuse in patients with chronic pain. Ann Intern Med. 2010;152:712-720.
11. Starrels JL, Becker WC, Weiner MG, et al. Low use of opioid risk reduction strategies in primary care even for high risk patients with chronic pain. J Gen Intern Med. 2011;26:958-964.
12. Webster LR, Webster RM. Predicting aberrant behaviors in opioid- treated patients: preliminary validation of the Opioid Risk Tool. Pain Med. 2005;6:432-442.
13. Watson H, Maclaren W, Kerr S. Staff attitudes toward working with drug users: development of the Drug Problems Perceptions Questionnaire. Addiction. 2007;102:206-215.
14. Okie S. A flood of opioids, a rising tide of deaths. N Engl J Med. 2010;363:1981-1985.
1. Lin JJ, Alfandre D, Moore C. Physician attitudes toward opioid prescribing for patients with persistent noncancer pain. Clin J Pain. 2007;23:799-803.
2. Hughes A, Sathe N, Spagnola K. (2009). State estimates of substance use from the 2006-2007 National Surveys on Drug Use and Health. Rockville, MD: Office of Applied Studies, Substance Abuse and Mental Health Services Administration; 2009. NSDUH Series H-35, HHS Publication No. SMA 09-4362.
3. Centers for Disease Control and Prevention (CDC). CDC grand rounds: prescription drug overdoses - a US epidemic. MMWR Morb Mortal Wkly Rep. 2012;61:10-13.
4. Washington State Department of Health- Medical Quality Assurance Commission. Rule-Making Order CR-103. University of Washington Web site. Available at: http://depts.washington.edu/anesth/education/forms/pain/WAC-Rules-CR-103P.pdf. Accessed February 1, 2012.
5. Leverence RR, Williams RL, Potter M, et al. Chronic non-cancer pain: a siren for primary care—a report from the PRImary Care MultiEthnic Network (PRIME Net). J Am Board Fam Med. 2011;24:551-561.
6. Green CR, Wheeler JR, LaPorte F, et al. How well is chronic pain managed? Who does it well? Pain Med. 2002;3:56-65.
7. Webster BS, Cifuentes M, Verma S, et al. Geographic variation in opioid prescribing for acute, work-related, low back pain and associated factors: a multilevel analysis. Am J Ind Med. 2009;52:162-171.
8. Gunderson EW, Coffin PO, Chang N, et al. The interface between substance abuse and chronic pain management in primary care: a curriculum for medical residents. Subst Abus. 2009;30:253-260.
9. Manchikanti L, Manchukonda R, Pampati V, et al. Does random urine drug testing reduce illicit drug use in chronic pain patients receiving opioids? Pain Physician. 2006;9:123-129.
10. Starrels JL, Becker WC, Alford DP, et al. Systematic review: treatment agreements and urine drug testing to reduce opioid misuse in patients with chronic pain. Ann Intern Med. 2010;152:712-720.
11. Starrels JL, Becker WC, Weiner MG, et al. Low use of opioid risk reduction strategies in primary care even for high risk patients with chronic pain. J Gen Intern Med. 2011;26:958-964.
12. Webster LR, Webster RM. Predicting aberrant behaviors in opioid- treated patients: preliminary validation of the Opioid Risk Tool. Pain Med. 2005;6:432-442.
13. Watson H, Maclaren W, Kerr S. Staff attitudes toward working with drug users: development of the Drug Problems Perceptions Questionnaire. Addiction. 2007;102:206-215.
14. Okie S. A flood of opioids, a rising tide of deaths. N Engl J Med. 2010;363:1981-1985.

Teenager with shortness of breath and hypoxia
A 19-year-old male complaining of shortness of breath was transferred from our facility’s urgent care unit to our emergency department. He had a 2-week history of hemoptysis and vomiting, and over the previous week, he had developed mild hematemesis. His other symptoms included left thigh, flank, and upper quadrant pain; left chest pain exacerbated by exertion, light-headedness, and palpitations. He said that over the past 8 months, he’d been tired and lost some weight.
His blood pressure was 138/77 mm Hg, pulse was 142 beats per min, respiratory rate was 22 breaths per min, and oxygen saturation was 93% on room air. The physical exam revealed normal breath sounds and a diffusely tender abdomen. We ordered a chest X-ray (FIGURE).
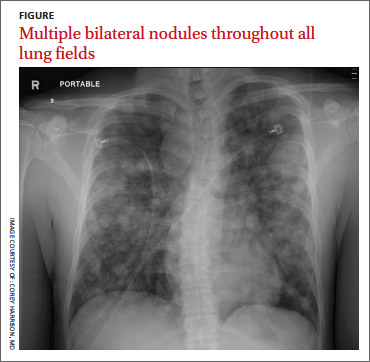
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Metastatic testicular cancer
The chest x-ray showed multiple bilateral discrete nodules throughout all of the lung fields. These findings, along with the age of the patient, prompted the radiologist to suspect metastatic testicular cancer. An examination of the patient’s scrotum revealed an 11-cm mass encompassing the patient’s left testicle. When asked about the mass, the patient acknowledged that it had been there for about 8 months.
A rare cancer seen in younger men
Although relatively uncommon, testicular cancer accounts for 1% to 2% of all tumors in men.1 If caught it is highly treatable.
Testicular cancer is classified into germ cell tumors (which our patient had) and sex cord-stromal tumors. Germ cell tumors are the most common malignancy in men ages 15 to 44 years, and have a 95% cure rate when identified early and promptly treated.2,3 Sex cordstromal tumors are more common in pediatric patients and are more often benign.2
Diagnosis usually is made clinically and pathologically at resection. Left untreated, testicular cancer spreads via the lymphatic system to the retroperitoneal lymph nodes and through the bloodstream to the lungs (predominantly),4 as well as to bone, the liver, and the brain. Metastatic testicular cancer to the lungs, liver, and retroperitoneum occurs in advanced disease and has a poor prognosis.4,5
Differential diagnosis includes pneumonia, septic emboli
The differential diagnosis includes atypical pneumonia, septic emboli (ie, endocarditis or Lemierre’s syndrome), or sarcoidosis. Patients with atypical pneumonia often present with a cough, fever, and malaise. Patients with septic emboli will have an x-ray that looks similar to that of our patient. Their signs and symptoms will include malaise, shortness of breath, hypoxia, tachycardia, and tachypnea. Risk factors and physical exam findings might include a history of intravenous drug abuse (endocarditis) or deep tissue neck infection (Lemierre’s syndrome). Sarcoidosis can be a challenging diagnosis without further study.
Successful treatment hinges on early detection
Treatment for testicular cancer often is successful if the condition is localized.
The choice of treatment depends on tumor type and stage. Options include orchiectomy, retroperitoneal lymph node dissection, chemotherapy, and radiation.2-5 After being diagnosed with testicular cancer 95% of patients live for 5 or more years.6 For localized testicular cancer, the 5-year survival rate is 99%.6
An eye toward prevention. The US Preventive Services Task Force recommends against screening with clinical examination or testicular self examination7; however, some clinicians support regular screening and self examinations.
When silence is deadly
Although physicians expect that patients will disclose obvious physical manifestations of disease, we know that this is not always the case. Patients often have barriers to care, including their own reluctance to share certain types of information with a provider.
Our patient. After we diagnosed metastatic testicular cancer in our patient, he was transferred to the medical intensive care unit. His overall clinical status declined and he died 14 days later.
1. Manecksha RP, Fitzpatrick JM. Epidemiology of testicular cancer. BJU Int. 2009;104(9 pt B):1329-1333.
2. Schultz KA, Schneider DT, Pashankar F, et al. Management of ovarian and testicular sex cord-stromal tumors in children and adolescents. J Pediatr Hematol Oncol. 2012;34 suppl 2:S55-S63.
3. Sohaib SA, Koh DM, Husband JE. The role of imaging in the diagnosis, staging, and management of testicular cancer. AJR Am J Roentgenol. 2008;191:387-395.
4. Viatori M. Testicular cancer. Semin Oncol Nurs. 2012;28:180-189.
5. Mannuel H, Mitikiri N, Khan M, et al. Testicular germ cell tumors: biology and clinical update. Curr Opin Oncol. 2012;24:266-271.
6. SEER Stat Fact Sheets: Testis Cancer. National Cancer Institute Web site. Available at: http://seer.cancer.gov/statfacts/html/testis.html. Accessed May 20, 2014.
7. Screening for testicular cancer. US Preventive Services Task Force Web site. Available at: http://www.uspreventiveservicestaskforce.org/uspstf10/testicular/testicuprs.htm. Accessed May 21, 2014.
A 19-year-old male complaining of shortness of breath was transferred from our facility’s urgent care unit to our emergency department. He had a 2-week history of hemoptysis and vomiting, and over the previous week, he had developed mild hematemesis. His other symptoms included left thigh, flank, and upper quadrant pain; left chest pain exacerbated by exertion, light-headedness, and palpitations. He said that over the past 8 months, he’d been tired and lost some weight.
His blood pressure was 138/77 mm Hg, pulse was 142 beats per min, respiratory rate was 22 breaths per min, and oxygen saturation was 93% on room air. The physical exam revealed normal breath sounds and a diffusely tender abdomen. We ordered a chest X-ray (FIGURE).
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Metastatic testicular cancer
The chest x-ray showed multiple bilateral discrete nodules throughout all of the lung fields. These findings, along with the age of the patient, prompted the radiologist to suspect metastatic testicular cancer. An examination of the patient’s scrotum revealed an 11-cm mass encompassing the patient’s left testicle. When asked about the mass, the patient acknowledged that it had been there for about 8 months.
A rare cancer seen in younger men
Although relatively uncommon, testicular cancer accounts for 1% to 2% of all tumors in men.1 If caught it is highly treatable.
Testicular cancer is classified into germ cell tumors (which our patient had) and sex cord-stromal tumors. Germ cell tumors are the most common malignancy in men ages 15 to 44 years, and have a 95% cure rate when identified early and promptly treated.2,3 Sex cordstromal tumors are more common in pediatric patients and are more often benign.2
Diagnosis usually is made clinically and pathologically at resection. Left untreated, testicular cancer spreads via the lymphatic system to the retroperitoneal lymph nodes and through the bloodstream to the lungs (predominantly),4 as well as to bone, the liver, and the brain. Metastatic testicular cancer to the lungs, liver, and retroperitoneum occurs in advanced disease and has a poor prognosis.4,5
Differential diagnosis includes pneumonia, septic emboli
The differential diagnosis includes atypical pneumonia, septic emboli (ie, endocarditis or Lemierre’s syndrome), or sarcoidosis. Patients with atypical pneumonia often present with a cough, fever, and malaise. Patients with septic emboli will have an x-ray that looks similar to that of our patient. Their signs and symptoms will include malaise, shortness of breath, hypoxia, tachycardia, and tachypnea. Risk factors and physical exam findings might include a history of intravenous drug abuse (endocarditis) or deep tissue neck infection (Lemierre’s syndrome). Sarcoidosis can be a challenging diagnosis without further study.
Successful treatment hinges on early detection
Treatment for testicular cancer often is successful if the condition is localized.
The choice of treatment depends on tumor type and stage. Options include orchiectomy, retroperitoneal lymph node dissection, chemotherapy, and radiation.2-5 After being diagnosed with testicular cancer 95% of patients live for 5 or more years.6 For localized testicular cancer, the 5-year survival rate is 99%.6
An eye toward prevention. The US Preventive Services Task Force recommends against screening with clinical examination or testicular self examination7; however, some clinicians support regular screening and self examinations.
When silence is deadly
Although physicians expect that patients will disclose obvious physical manifestations of disease, we know that this is not always the case. Patients often have barriers to care, including their own reluctance to share certain types of information with a provider.
Our patient. After we diagnosed metastatic testicular cancer in our patient, he was transferred to the medical intensive care unit. His overall clinical status declined and he died 14 days later.
A 19-year-old male complaining of shortness of breath was transferred from our facility’s urgent care unit to our emergency department. He had a 2-week history of hemoptysis and vomiting, and over the previous week, he had developed mild hematemesis. His other symptoms included left thigh, flank, and upper quadrant pain; left chest pain exacerbated by exertion, light-headedness, and palpitations. He said that over the past 8 months, he’d been tired and lost some weight.
His blood pressure was 138/77 mm Hg, pulse was 142 beats per min, respiratory rate was 22 breaths per min, and oxygen saturation was 93% on room air. The physical exam revealed normal breath sounds and a diffusely tender abdomen. We ordered a chest X-ray (FIGURE).
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Metastatic testicular cancer
The chest x-ray showed multiple bilateral discrete nodules throughout all of the lung fields. These findings, along with the age of the patient, prompted the radiologist to suspect metastatic testicular cancer. An examination of the patient’s scrotum revealed an 11-cm mass encompassing the patient’s left testicle. When asked about the mass, the patient acknowledged that it had been there for about 8 months.
A rare cancer seen in younger men
Although relatively uncommon, testicular cancer accounts for 1% to 2% of all tumors in men.1 If caught it is highly treatable.
Testicular cancer is classified into germ cell tumors (which our patient had) and sex cord-stromal tumors. Germ cell tumors are the most common malignancy in men ages 15 to 44 years, and have a 95% cure rate when identified early and promptly treated.2,3 Sex cordstromal tumors are more common in pediatric patients and are more often benign.2
Diagnosis usually is made clinically and pathologically at resection. Left untreated, testicular cancer spreads via the lymphatic system to the retroperitoneal lymph nodes and through the bloodstream to the lungs (predominantly),4 as well as to bone, the liver, and the brain. Metastatic testicular cancer to the lungs, liver, and retroperitoneum occurs in advanced disease and has a poor prognosis.4,5
Differential diagnosis includes pneumonia, septic emboli
The differential diagnosis includes atypical pneumonia, septic emboli (ie, endocarditis or Lemierre’s syndrome), or sarcoidosis. Patients with atypical pneumonia often present with a cough, fever, and malaise. Patients with septic emboli will have an x-ray that looks similar to that of our patient. Their signs and symptoms will include malaise, shortness of breath, hypoxia, tachycardia, and tachypnea. Risk factors and physical exam findings might include a history of intravenous drug abuse (endocarditis) or deep tissue neck infection (Lemierre’s syndrome). Sarcoidosis can be a challenging diagnosis without further study.
Successful treatment hinges on early detection
Treatment for testicular cancer often is successful if the condition is localized.
The choice of treatment depends on tumor type and stage. Options include orchiectomy, retroperitoneal lymph node dissection, chemotherapy, and radiation.2-5 After being diagnosed with testicular cancer 95% of patients live for 5 or more years.6 For localized testicular cancer, the 5-year survival rate is 99%.6
An eye toward prevention. The US Preventive Services Task Force recommends against screening with clinical examination or testicular self examination7; however, some clinicians support regular screening and self examinations.
When silence is deadly
Although physicians expect that patients will disclose obvious physical manifestations of disease, we know that this is not always the case. Patients often have barriers to care, including their own reluctance to share certain types of information with a provider.
Our patient. After we diagnosed metastatic testicular cancer in our patient, he was transferred to the medical intensive care unit. His overall clinical status declined and he died 14 days later.
1. Manecksha RP, Fitzpatrick JM. Epidemiology of testicular cancer. BJU Int. 2009;104(9 pt B):1329-1333.
2. Schultz KA, Schneider DT, Pashankar F, et al. Management of ovarian and testicular sex cord-stromal tumors in children and adolescents. J Pediatr Hematol Oncol. 2012;34 suppl 2:S55-S63.
3. Sohaib SA, Koh DM, Husband JE. The role of imaging in the diagnosis, staging, and management of testicular cancer. AJR Am J Roentgenol. 2008;191:387-395.
4. Viatori M. Testicular cancer. Semin Oncol Nurs. 2012;28:180-189.
5. Mannuel H, Mitikiri N, Khan M, et al. Testicular germ cell tumors: biology and clinical update. Curr Opin Oncol. 2012;24:266-271.
6. SEER Stat Fact Sheets: Testis Cancer. National Cancer Institute Web site. Available at: http://seer.cancer.gov/statfacts/html/testis.html. Accessed May 20, 2014.
7. Screening for testicular cancer. US Preventive Services Task Force Web site. Available at: http://www.uspreventiveservicestaskforce.org/uspstf10/testicular/testicuprs.htm. Accessed May 21, 2014.
1. Manecksha RP, Fitzpatrick JM. Epidemiology of testicular cancer. BJU Int. 2009;104(9 pt B):1329-1333.
2. Schultz KA, Schneider DT, Pashankar F, et al. Management of ovarian and testicular sex cord-stromal tumors in children and adolescents. J Pediatr Hematol Oncol. 2012;34 suppl 2:S55-S63.
3. Sohaib SA, Koh DM, Husband JE. The role of imaging in the diagnosis, staging, and management of testicular cancer. AJR Am J Roentgenol. 2008;191:387-395.
4. Viatori M. Testicular cancer. Semin Oncol Nurs. 2012;28:180-189.
5. Mannuel H, Mitikiri N, Khan M, et al. Testicular germ cell tumors: biology and clinical update. Curr Opin Oncol. 2012;24:266-271.
6. SEER Stat Fact Sheets: Testis Cancer. National Cancer Institute Web site. Available at: http://seer.cancer.gov/statfacts/html/testis.html. Accessed May 20, 2014.
7. Screening for testicular cancer. US Preventive Services Task Force Web site. Available at: http://www.uspreventiveservicestaskforce.org/uspstf10/testicular/testicuprs.htm. Accessed May 21, 2014.

Insulin before surgery
To the Editor: We appreciated the thoughtful 1-Minute Consult by Drs. Dobri and Lansang, “How should we manage insulin therapy before surgery?”1 We agree with them in regard to the benefits of perioperative control of blood glucose levels. However, we disagree in general with their assertion that the full dose of the patient’s home dose of basal insulin be administered while the patient is nil per os (NPO) before surgery, with a reduction to 75% of the home dose only if the patient has a history of hypoglycemia, a recommendation that did not differentiate between patients with type 1 and type 2 diabetes mellitus.
The RABBIT 2 Surgery trial,2 which showed superiority of basal-bolus insulin over sliding scale insulin in surgical patients with type 2 diabetes mellitus, also showed a surprisingly high rate of hypoglycemia—24 (23.1%) of 104 patients had blood glucose levels lower than 70 mg/dL, compared with a similar trial in nonsurgical patients in which 2 (3.1%) of 65 patients had a blood glucose level less than 60 mg/dL.3 The authors of the two studies explained2 that “differences in hypoglycemic events between the two trials could be in part explained by reduced nutritional intake in surgical patients…”
Although patients with well-controlled type 1 diabetes mellitus may tolerate their full dose of basal insulin while NPO, we contend that patients with type 2 diabetes mellitus should be prescribed a reduced dose of basal insulin while NPO, regardless of the dose distribution or the patient’s overall glycemic control. It is routine practice on our consult service to reduce the basal insulin dose in such patients by roughly half.
- Dobri GA, Lansang MC. How should we manage insulin therapy before surgery? Cleve Clin J Med 2013; 80:702–704.
- Umpierrez GE, Smiley D, Jacobs S, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes undergoing general surgery (RABBIT 2 surgery). Diabetes Care 2011; 34:256–261.
- Umpierrez GE, Smiley D, Zisman A, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes (RABBIT 2 trial). Diabetes Care 2007; 30:2181–2186.
To the Editor: We appreciated the thoughtful 1-Minute Consult by Drs. Dobri and Lansang, “How should we manage insulin therapy before surgery?”1 We agree with them in regard to the benefits of perioperative control of blood glucose levels. However, we disagree in general with their assertion that the full dose of the patient’s home dose of basal insulin be administered while the patient is nil per os (NPO) before surgery, with a reduction to 75% of the home dose only if the patient has a history of hypoglycemia, a recommendation that did not differentiate between patients with type 1 and type 2 diabetes mellitus.
The RABBIT 2 Surgery trial,2 which showed superiority of basal-bolus insulin over sliding scale insulin in surgical patients with type 2 diabetes mellitus, also showed a surprisingly high rate of hypoglycemia—24 (23.1%) of 104 patients had blood glucose levels lower than 70 mg/dL, compared with a similar trial in nonsurgical patients in which 2 (3.1%) of 65 patients had a blood glucose level less than 60 mg/dL.3 The authors of the two studies explained2 that “differences in hypoglycemic events between the two trials could be in part explained by reduced nutritional intake in surgical patients…”
Although patients with well-controlled type 1 diabetes mellitus may tolerate their full dose of basal insulin while NPO, we contend that patients with type 2 diabetes mellitus should be prescribed a reduced dose of basal insulin while NPO, regardless of the dose distribution or the patient’s overall glycemic control. It is routine practice on our consult service to reduce the basal insulin dose in such patients by roughly half.
To the Editor: We appreciated the thoughtful 1-Minute Consult by Drs. Dobri and Lansang, “How should we manage insulin therapy before surgery?”1 We agree with them in regard to the benefits of perioperative control of blood glucose levels. However, we disagree in general with their assertion that the full dose of the patient’s home dose of basal insulin be administered while the patient is nil per os (NPO) before surgery, with a reduction to 75% of the home dose only if the patient has a history of hypoglycemia, a recommendation that did not differentiate between patients with type 1 and type 2 diabetes mellitus.
The RABBIT 2 Surgery trial,2 which showed superiority of basal-bolus insulin over sliding scale insulin in surgical patients with type 2 diabetes mellitus, also showed a surprisingly high rate of hypoglycemia—24 (23.1%) of 104 patients had blood glucose levels lower than 70 mg/dL, compared with a similar trial in nonsurgical patients in which 2 (3.1%) of 65 patients had a blood glucose level less than 60 mg/dL.3 The authors of the two studies explained2 that “differences in hypoglycemic events between the two trials could be in part explained by reduced nutritional intake in surgical patients…”
Although patients with well-controlled type 1 diabetes mellitus may tolerate their full dose of basal insulin while NPO, we contend that patients with type 2 diabetes mellitus should be prescribed a reduced dose of basal insulin while NPO, regardless of the dose distribution or the patient’s overall glycemic control. It is routine practice on our consult service to reduce the basal insulin dose in such patients by roughly half.
- Dobri GA, Lansang MC. How should we manage insulin therapy before surgery? Cleve Clin J Med 2013; 80:702–704.
- Umpierrez GE, Smiley D, Jacobs S, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes undergoing general surgery (RABBIT 2 surgery). Diabetes Care 2011; 34:256–261.
- Umpierrez GE, Smiley D, Zisman A, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes (RABBIT 2 trial). Diabetes Care 2007; 30:2181–2186.
- Dobri GA, Lansang MC. How should we manage insulin therapy before surgery? Cleve Clin J Med 2013; 80:702–704.
- Umpierrez GE, Smiley D, Jacobs S, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes undergoing general surgery (RABBIT 2 surgery). Diabetes Care 2011; 34:256–261.
- Umpierrez GE, Smiley D, Zisman A, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes (RABBIT 2 trial). Diabetes Care 2007; 30:2181–2186.
In reply: Insulin before surgery
In Reply: We appreciate the kind words of Drs. Ditch and Moore, as well as their opinion.
Our article was intentionally brief—a 1-Minute Consult—and so could not cover all specific situations we encounter in clinical practice. We meant only to provide a general approach in this matter.
Quite often before surgery, patients receive less basal insulin than needed, or none at all, rather than too much. It has to be borne in mind that perioperative hyperglycemia—not just hypoglycemia—is linked with poor outcomes in cardiac1 and noncardiac surgery.2,3
Through our scenarios and suggestions, we have taken steps to err on the side of preventing hypoglycemia while averting hyperglycemia, at the same time making it easy to calculate the dose. In a scenario in which the basal insulin dose is about the same as the total of the prandial boluses, we have not yet seen evidence that raises concern for hypoglycemia, maybe because many of the patients with type 2 diabetes seen in our institution for surgery take, in addition to insulin, oral agents or noninsulin injections (which are appropriately withheld before surgery), and have suboptimal glycemic control on their home regimen. But if a physician has concerns for hypoglycemia, a dose reduction should be made.
There were some differences between the RABBIT 2 trial in medical patients4 and the RABBIT 2 Surgery trial5 that would make the results not completely comparable. In RABBIT 2, the medical patients included were on diet alone or any combination of oral antidiabetic agents (not on insulin), and they were started on a total daily dose of insulin of either 0.4 or 0.5 U/kg/day, depending on the glucose level. In RABBIT 2 Surgery, patients who were on insulin at home with a total daily dose of 0.4 U/kg or less were also included, and the starting daily dose of insulin was 0.5 U/kg (unless they were older or had a high serum creatinine).
In view of all the above, we agree with Drs. Ditch and Moore that if there is concern for hypoglycemia, the clinician should reduce the insulin dose in the manner that evidence from the local practice suggests, without causing undue hyperglycemia and postsurgical complications.
- Furnary AP, Gao G, Grunkemeier GL, et al. Continuous insulin infusion reduces mortality in patients with diabetes undergoing coronary artery bypass grafting. J Thorac Cardiovasc Surg 2003; 125:1007–1021.
- King JT, Goulet JL, Perkal MF, Rosenthal RA. Glycemic control and infections in patients with diabetes undergoing noncardiac surgery. Ann Surg 2011; 253:158–165.
- Frisch A, Chandra P, Smiley D, et al. Prevalence and clinical outcome of hyperglycemia in the perioperative period in noncardiac surgery. Diabetes Care 2010; 33:1783–1788.
- Umpierrez GE, Smiley D, Zisman A, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes (RABBIT 2 trial). Diabetes Care 2007; 30:2181–2186.
- Umpierrez GE, Smiley D, Jacobs S, Peng L, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes undergoing general surgery (RABBIT 2 surgery). Diabetes Care 2011; 34:256–261.
In Reply: We appreciate the kind words of Drs. Ditch and Moore, as well as their opinion.
Our article was intentionally brief—a 1-Minute Consult—and so could not cover all specific situations we encounter in clinical practice. We meant only to provide a general approach in this matter.
Quite often before surgery, patients receive less basal insulin than needed, or none at all, rather than too much. It has to be borne in mind that perioperative hyperglycemia—not just hypoglycemia—is linked with poor outcomes in cardiac1 and noncardiac surgery.2,3
Through our scenarios and suggestions, we have taken steps to err on the side of preventing hypoglycemia while averting hyperglycemia, at the same time making it easy to calculate the dose. In a scenario in which the basal insulin dose is about the same as the total of the prandial boluses, we have not yet seen evidence that raises concern for hypoglycemia, maybe because many of the patients with type 2 diabetes seen in our institution for surgery take, in addition to insulin, oral agents or noninsulin injections (which are appropriately withheld before surgery), and have suboptimal glycemic control on their home regimen. But if a physician has concerns for hypoglycemia, a dose reduction should be made.
There were some differences between the RABBIT 2 trial in medical patients4 and the RABBIT 2 Surgery trial5 that would make the results not completely comparable. In RABBIT 2, the medical patients included were on diet alone or any combination of oral antidiabetic agents (not on insulin), and they were started on a total daily dose of insulin of either 0.4 or 0.5 U/kg/day, depending on the glucose level. In RABBIT 2 Surgery, patients who were on insulin at home with a total daily dose of 0.4 U/kg or less were also included, and the starting daily dose of insulin was 0.5 U/kg (unless they were older or had a high serum creatinine).
In view of all the above, we agree with Drs. Ditch and Moore that if there is concern for hypoglycemia, the clinician should reduce the insulin dose in the manner that evidence from the local practice suggests, without causing undue hyperglycemia and postsurgical complications.
In Reply: We appreciate the kind words of Drs. Ditch and Moore, as well as their opinion.
Our article was intentionally brief—a 1-Minute Consult—and so could not cover all specific situations we encounter in clinical practice. We meant only to provide a general approach in this matter.
Quite often before surgery, patients receive less basal insulin than needed, or none at all, rather than too much. It has to be borne in mind that perioperative hyperglycemia—not just hypoglycemia—is linked with poor outcomes in cardiac1 and noncardiac surgery.2,3
Through our scenarios and suggestions, we have taken steps to err on the side of preventing hypoglycemia while averting hyperglycemia, at the same time making it easy to calculate the dose. In a scenario in which the basal insulin dose is about the same as the total of the prandial boluses, we have not yet seen evidence that raises concern for hypoglycemia, maybe because many of the patients with type 2 diabetes seen in our institution for surgery take, in addition to insulin, oral agents or noninsulin injections (which are appropriately withheld before surgery), and have suboptimal glycemic control on their home regimen. But if a physician has concerns for hypoglycemia, a dose reduction should be made.
There were some differences between the RABBIT 2 trial in medical patients4 and the RABBIT 2 Surgery trial5 that would make the results not completely comparable. In RABBIT 2, the medical patients included were on diet alone or any combination of oral antidiabetic agents (not on insulin), and they were started on a total daily dose of insulin of either 0.4 or 0.5 U/kg/day, depending on the glucose level. In RABBIT 2 Surgery, patients who were on insulin at home with a total daily dose of 0.4 U/kg or less were also included, and the starting daily dose of insulin was 0.5 U/kg (unless they were older or had a high serum creatinine).
In view of all the above, we agree with Drs. Ditch and Moore that if there is concern for hypoglycemia, the clinician should reduce the insulin dose in the manner that evidence from the local practice suggests, without causing undue hyperglycemia and postsurgical complications.
- Furnary AP, Gao G, Grunkemeier GL, et al. Continuous insulin infusion reduces mortality in patients with diabetes undergoing coronary artery bypass grafting. J Thorac Cardiovasc Surg 2003; 125:1007–1021.
- King JT, Goulet JL, Perkal MF, Rosenthal RA. Glycemic control and infections in patients with diabetes undergoing noncardiac surgery. Ann Surg 2011; 253:158–165.
- Frisch A, Chandra P, Smiley D, et al. Prevalence and clinical outcome of hyperglycemia in the perioperative period in noncardiac surgery. Diabetes Care 2010; 33:1783–1788.
- Umpierrez GE, Smiley D, Zisman A, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes (RABBIT 2 trial). Diabetes Care 2007; 30:2181–2186.
- Umpierrez GE, Smiley D, Jacobs S, Peng L, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes undergoing general surgery (RABBIT 2 surgery). Diabetes Care 2011; 34:256–261.
- Furnary AP, Gao G, Grunkemeier GL, et al. Continuous insulin infusion reduces mortality in patients with diabetes undergoing coronary artery bypass grafting. J Thorac Cardiovasc Surg 2003; 125:1007–1021.
- King JT, Goulet JL, Perkal MF, Rosenthal RA. Glycemic control and infections in patients with diabetes undergoing noncardiac surgery. Ann Surg 2011; 253:158–165.
- Frisch A, Chandra P, Smiley D, et al. Prevalence and clinical outcome of hyperglycemia in the perioperative period in noncardiac surgery. Diabetes Care 2010; 33:1783–1788.
- Umpierrez GE, Smiley D, Zisman A, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes (RABBIT 2 trial). Diabetes Care 2007; 30:2181–2186.
- Umpierrez GE, Smiley D, Jacobs S, Peng L, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes undergoing general surgery (RABBIT 2 surgery). Diabetes Care 2011; 34:256–261.