User login
In the Literature: The latest research you need to know
In This Edition
Literature At A Glance
A guide to this month’s studies
- Procalcitonin to guide antimicrobial use in ICU patients
- Platelet reactivity and event rates after PCI
- Conservative treatment of necrotizing pancreatitis
- Use of MRI to diagnose Takotsubo cardiomyopathy
- Rates of inadvertent medication discontinuation after hospitalization
- Role of history and physical exam in diagnosing medical illness
- Red-cell distribution width and rates of mortality
Procalcitonin-Guided Therapy Decreases Antimicrobial Duration in ICU Patients
Clinical question: Can utilization of serum procalcitonin (PCT) levels safely reduce antimicrobial exposure in ICU patients?
Background: Serum PCT levels are elevated in bacterial infections and sepsis and have been used in some settings to guide antimicrobial therapy. Randomized controlled trials have demonstrated reduction of antibiotic use with PCT measurement. This systematic review assessed the safety and effectiveness of PCT measurements in reducing antimicrobial exposure in ICU patients.
Study design: Systematic review.
Setting: Adult medical and surgical ICUs.
Synopsis: A search of MEDLINE and EMBASE yielded 1,018 publications related to PCT, critically ill patients, and antimicrobial therapy. Six randomized controlled trials involving 1,476 patients were reviewed. The duration of antimicrobial use was significantly decreased in all five studies that evaluated treatment duration. The remaining study only assessed the impact of PCT on initiation of antimicrobial therapy and did not demonstrate decreased antimicrobial exposure. Compared with the control group, patients randomized to PCT-guided therapy had relative reductions in duration of first antibiotic course by 21%, down to 38%, and decreases in days of antimicrobial therapy per 1,000 ICU patient days by 20%, down to 23%. PCT intervention also was associated with a 23% to 37% increase in days alive without antimicrobial therapy during the first 28 days. The length of ICU stay was significantly decreased in two studies but was not significantly different in the other studies. There were no significant differences in rates of mortality, infection relapse, or days free of mechanical ventilation.
Bottom line: PCT guidance reduced antimicrobial exposure of ICU patients without increasing rates of mortality or infection relapse.
Citation: Agarwal R, Schwartz DN. Procalcitonin to guide duration of antimicrobial therapy in intensive care units: a systematic review. Clin Infect Dis. 2011;53:379-387.
High Residual Platelet Reactivity Increases Risk of Cardiovascular Events among Patients with Acute Coronary Syndromes Undergoing PCI
Clinical question: Is high residual platelet reactivity (HRPR) in patients receiving clopidogrel associated with increased risk of ischemic events after percutaneous coronary intervention (PCI)?
Background: Studies have demonstrated an increased risk of cardiovascular events associated with HRPR in patients receiving clopidogrel while undergoing PCI. However, these studies have used a variety of platelet function tests, and thresholds for positive tests have not been established. In addition, these studies have enrolled heterogeneous populations with short-term follow-up and few have included patients with acute coronary syndromes (ACSs).
Study design: Prospective cohort study.
Setting: Cardiology service of a referral center in Italy.
Synopsis: This study included 1,789 consecutive patients with ACS undergoing PCI. Patients were given 325 mg aspirin and a 600-mg loading dose of clopidogrel on admission, followed by a daily maintenance dose of aspirin 325 mg and clopidogrel 75 mg for at least six months. Platelet reactivity was measured using adenosine diphosphate (ADP) testing, and those with HRPR (≥70% platelet aggregation) were given increased dosing of clopidogrel or switched to ticlopidine using ADP test guidance. At two-year follow-up, patients with HRPR experienced an increased composite endpoint of cardiac death, myocardial infarction, urgent coronary revascularization, and stroke with a combined event rate of 14.6% in patients with HRPR and 8.7% in patients with low residual platelet reactivity (95% CI, 1.6%-11.1%; P=0.003). Stent thrombosis was also higher in HRPR patients (absolute risk increase 3.2%; 95% CI, 0.4%-6.7%; P=0.01).
This study is nonrandomized, and residual unmeasured confounding cannot be excluded. In addition, use of non-antiplatelet drugs and adherence to recommended drugs might have influenced outcomes.
Bottom line: HRPR is associated with increased risk of ischemic events in patients with ACS receiving antiplatelet agents after PCI.
Citation: Parodi G, Marcucci R, Valenti R, et al. High residual platelet reactivity after clopidogrel loading and long-term cardiovascular events among patients with acute coronary syndromes undergoing PCI. JAMA. 2011;306:1215-1223.
Conservative Treatment of Necrotizing Pancreatitis Is Associated with Improved Outcomes
Clinical question: What are the outcomes of conservative and interventional management of necrotizing pancreatitis?
Background: Open necrosectomy was historically the treatment of choice for necrotizing pancreatitis, but, currently, pancreatic necrosis is only managed invasively when complicated by infection. Other changes in management over time have included a shift in the timing of intervention and the use of minimally invasive techniques. Existing studies do not reflect these changes in practice patterns and have been limited by small sample sizes or the exclusion of important subgroups of patients.
Study design: Prospective cohort study.
Setting: Twenty-one Dutch hospitals.
Synopsis: This study included 639 patients with acute necrotizing pancreatitis confirmed by imaging. Overall mortality was 15%. Conservative treatment was performed in 62% of the patients with a mortality of 7%; however, patients with organ failure (pulmonary, circulatory, and/or renal) who received conservative therapy had a mortality rate of 37%. Intervention (percutaneous drainage, video-assisted retroperitoneal debridement, endoscopic transluminal necrosectomy, laparotomy) in patients with suspected or confirmed infected pancreatic necrosis was performed on 38% of the patients with associated mortality of 27%. Interventions performed within the first 14 days of hospitalization resulted in a 56% mortality rate, whereas interventions performed after Day 29 resulted in a 15% mortality rate (P<0.001). Patients with organ failure experienced significantly greater mortality compared with patients with no organ failure (35% vs. 2%; P<0.001). Primary percutaneous drainage was associated with fewer complications than was primary necrosectomy (42% vs. 64%; P=0.003).
This study was nonrandomized, and final decisions regarding management were left to the treating physician. Notably, while there was no significant difference in APACHE II scores between the conservative and intervention groups, intervention patients had more severe pancreatic disease and scored higher on other measures of disease severity.
Bottom line: Patients with necrotizing pancreatitis can frequently be managed conservatively, though the presence of organ failure and parenchymal necrosis confer poorer prognosis. When intervention is indicated, postponing intervention and utilizing minimally invasive techniques decrease morbidity and mortality.
Citation: Van Santvoort HC, Bakker OJ, Bollen TL, et al. A conservative and minimally invasive approach to necrotizing pancreatitis improves outcome. Gastroenterology. 2011;141:1254-1263.
Cardiac MRI Complements Clinical Findings in Diagnosis of Stress Cardiomyopathy
Clinical question: What are the clinical features and cardiovascular MRI findings in patients with stress (Takotsubo) cardiomyopathy?
Background: Stress cardiomyopathy (SC) is characterized by acute and profound reversible left ventricular dysfunction that is thought to result from increased sympathetic activity related to emotional and/or physical stress. Prior studies evaluating the clinical features of SC were limited by small sample sizes and single-center enrollment, and cardiac MRI use in SC has not been well studied.
Study design: Prospective cohort study.
Setting: Seven North American and European tertiary-care centers.
Synopsis: This study enrolled 256 patients who met diagnostic criteria for SC according to Mayo criteria. Postmenopausal women were most commonly affected; only 11% of participants were men and 8% were women younger than 50 years old. An identifiable stressor was found in 71% of the patients. Clinical presentation was notable for symptoms of acute coronary syndrome (ACS) in 88% of patients, abnormal electrocardiogram in 87%, and elevated troponin T in 90%. Coronary angiography was normal in three-fourths of patients, and no patients had features of acute plaque rupture. Typical apical ballooning was seen on left ventriculography in 82% of patients.
Cardiac MRI findings included severe left ventricular dysfunction in a noncoronary distribution, myocardial edema in areas of regional wall abnormalities, absence of high signal areas in late gadolinium enhancement (e.g., absence of necrosis/fibrosis), and increased early gadolinium uptake (i.e. early inflammation). Repeat cardiac MRI four weeks after initial diagnosis showed near or complete resolution of imaging findings.
Bottom line: Stress cardiomyopathy typically presents like ACS, usually affects postmenopausal women, is often preceded by a stressful event, and is characterized by cardiac MRI findings of regional wall motion abnormalities, reversible myocardial injury, and the absence of fibrosis. Cardiac MRI may be valuable in diagnosing SC in patients who present without the classic clinical features.
Citation: Eitel I, von Knobelsdorff-Brenkenhoff F, Bernhardt P, et al. Clinical characteristics and cardiovascular magnetic resonance findings in stress (Takotsubo) cardiomyopathy. JAMA. 2011;306:277-286.
Increased Risk of Potentially Inadvertent Medication Discontinuation Following Acute-Care Hospitalization
Clinical question: Are medications for chronic diseases inadvertently discontinued after acute-care hospitalization, and is this risk increased in patients who had an ICU stay?
Background: Transitions of care are associated with medical errors. Two such transitions are a shift from the ICU to floor setting and from the inpatient to outpatient setting. Medications for chronic diseases might be held during hospitalization for a variety of reasons, and medication errors may occur if these drugs are not restarted when the acute problem resolves or the patient is discharged from the hospital.
Study design: Population-based cohort study.
Setting: Ontario, Canada.
Synopsis: Using four separate databases, administrative records were reviewed for 396,380 patients aged >65 years who were continuous users of at least one of five evidence-based medication groups for common chronic diseases. Medications included statins, antiplatelet/anticoagulant agents, levothyroxine, respiratory inhalers, and gastric acid suppressants. The primary outcome was potentially unintentional medication discontinuation (measured by failure to renew the prescription at 90 days) for hospitalized versus nonhospitalized patients. All medication groups had statistically significant adjusted odds ratios ranging from 1.18 (95% CI, 1.14-1.23) for discontinuation of levothyroxine to 1.86 (95% CI, 1.77-1.97) for discontinuation of antiplatelet/anticoagulant medications. Treatment in an ICU further increased this risk compared with nonhospitalized patients, and increased the risk for medication discontinuation in four of the five medication groups when compared with patients hospitalized without ICU treatment.
Important study limitations include the lack of appropriate clinical details to classify medication discontinuation as unintentional and the inability of administrative data to prove causality. This study highlights the importance of medication reconciliation and calls attention to inadvertent medication discontinuation during care transitions (see “Reconciliation Act,”).
Bottom line: Patients discharged from the hospital, particularly after ICU treatment, have a higher risk of discontinuation of long-term medications for chronic medical problems when compared with nonhospitalized patients.
Citation: Bell CM, Brener SS, Gunraj N, et al. Association of ICU or hospital admission with unintentional discontinuation of medications for chronic diseases. JAMA. 2011;306:840-847.
Clinical Exam Remains Valuable in the Diagnosis of Patients Admitted to a Medicine Service
Clinical question: Is a clinical exam useful in the diagnosis of newly admitted patients to a general medicine service?
Background: The clinical exam, which comprises the history and physical examination, has long been described as essential to the diagnosis of illness. However, the literature supporting this claim is limited to the ambulatory setting. There has not been evaluation of the clinical exam as a diagnostic tool in the hospital setting, where more advanced testing is readily available.
Study design: Retrospective chart review.
Setting: Urban academic medical center.
Synopsis: The study included 442 adult patients consecutively admitted from the emergency department to the general medicine service who were separately assessed by one senior resident (SR) and one experienced hospital physician (HP) not involved with the case. The SR and HP each made an initial diagnosis and documented the most helpful component(s) in arriving at that diagnosis. Outcomes included comparison of the SR and HP’s admission diagnosis with the discharge diagnosis, and the diagnostic value of the various components of the clinical exam and initial studies.
Compared with the discharge diagnosis, the SR’s initial diagnosis was correct in 80.1% of cases, while the HP was correct in 84.4%. The patient’s history was the most important element in the initial assessment, independently influencing approximately 20% of the correct diagnoses for both physicians. Approximately 60% of correct diagnoses were established using the history and/or physical, and more than 90% were made using a combination of history, physical exam, and/or basic tests (admission labs, electrocardiogram, chest X-ray).
The generalizability of these results is limited by the retrospective, single-center study design, involvement of only one resident physician, and the lack of information regarding number of experienced clinicians and types of diagnoses.
Bottom line: Among patients admitted to a general medicine service, the most powerful tool in obtaining an accurate diagnosis was the combination of a patient’s history and a physical exam.
Citation: Paley L, Zornitzki T, Cohen J, et al. Utility of clinical examination in the diagnosis of emergency department patients admitted to the department of medicine of an academic hospital. Arch Intern Med. 2011;171:1394-1396.
RDW Predicts All-Cause Mortality and Bloodstream Infection in ICU Patients
Clinical question: Among patients admitted to the ICU, is red blood cell distribution width (RDW) a reliable indicator of mortality?
Background: The RDW is an inexpensive test that is commonly included in routine laboratory studies. It has been associated with multiple disease processes and found to be a strong predictor of mortality in the general adult population. However, there has been limited study of the association between RDW and outcomes in critically ill patients.
Study design: Observational cohort study.
Setting: Urban tertiary-care academic medical center.
Synopsis: Data from 51,413 adult patients who received critical care between 1997 and 2007 were obtained from a computerized registry and evaluated for the primary outcome of 30-day mortality after critical-care initiation. Secondary outcomes included 90-day, 365-day, and in-hospital mortality, as well as bloodstream infection. Logistic regression examined both primary and secondary outcomes in association with pre-established RDW quintiles. After multivariable adjustment, RDW was found to be associated with mortality at 30, 90, and 365 days, in addition to in-hospital mortality. The highest RDW quintile (RDW >15.8%) had an adjusted OR of 2.61 (95% CI, 2.37-2.86; P<0.001) for the primary outcome, with similar risk for secondary outcomes of mortality. A subgroup of 18,525 patients with blood culture data was analyzed and an adjusted OR of 1.44 was found in the highest RDW quintile for the secondary outcome of bloodstream infection.
Bottom line: Red blood cell distribution width is a strong independent predictor of all-cause mortality and bloodstream infection in patients receiving intensive care.
Citation: Bazick HS, Chang D, Mahadevappa K, Gibbons FK, Christopher KB. Red cell distribution width and all-cause mortality in critically ill patients. Crit Care Med. 2011;39:1913-1921.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Procalcitonin to guide antimicrobial use in ICU patients
- Platelet reactivity and event rates after PCI
- Conservative treatment of necrotizing pancreatitis
- Use of MRI to diagnose Takotsubo cardiomyopathy
- Rates of inadvertent medication discontinuation after hospitalization
- Role of history and physical exam in diagnosing medical illness
- Red-cell distribution width and rates of mortality
Procalcitonin-Guided Therapy Decreases Antimicrobial Duration in ICU Patients
Clinical question: Can utilization of serum procalcitonin (PCT) levels safely reduce antimicrobial exposure in ICU patients?
Background: Serum PCT levels are elevated in bacterial infections and sepsis and have been used in some settings to guide antimicrobial therapy. Randomized controlled trials have demonstrated reduction of antibiotic use with PCT measurement. This systematic review assessed the safety and effectiveness of PCT measurements in reducing antimicrobial exposure in ICU patients.
Study design: Systematic review.
Setting: Adult medical and surgical ICUs.
Synopsis: A search of MEDLINE and EMBASE yielded 1,018 publications related to PCT, critically ill patients, and antimicrobial therapy. Six randomized controlled trials involving 1,476 patients were reviewed. The duration of antimicrobial use was significantly decreased in all five studies that evaluated treatment duration. The remaining study only assessed the impact of PCT on initiation of antimicrobial therapy and did not demonstrate decreased antimicrobial exposure. Compared with the control group, patients randomized to PCT-guided therapy had relative reductions in duration of first antibiotic course by 21%, down to 38%, and decreases in days of antimicrobial therapy per 1,000 ICU patient days by 20%, down to 23%. PCT intervention also was associated with a 23% to 37% increase in days alive without antimicrobial therapy during the first 28 days. The length of ICU stay was significantly decreased in two studies but was not significantly different in the other studies. There were no significant differences in rates of mortality, infection relapse, or days free of mechanical ventilation.
Bottom line: PCT guidance reduced antimicrobial exposure of ICU patients without increasing rates of mortality or infection relapse.
Citation: Agarwal R, Schwartz DN. Procalcitonin to guide duration of antimicrobial therapy in intensive care units: a systematic review. Clin Infect Dis. 2011;53:379-387.
High Residual Platelet Reactivity Increases Risk of Cardiovascular Events among Patients with Acute Coronary Syndromes Undergoing PCI
Clinical question: Is high residual platelet reactivity (HRPR) in patients receiving clopidogrel associated with increased risk of ischemic events after percutaneous coronary intervention (PCI)?
Background: Studies have demonstrated an increased risk of cardiovascular events associated with HRPR in patients receiving clopidogrel while undergoing PCI. However, these studies have used a variety of platelet function tests, and thresholds for positive tests have not been established. In addition, these studies have enrolled heterogeneous populations with short-term follow-up and few have included patients with acute coronary syndromes (ACSs).
Study design: Prospective cohort study.
Setting: Cardiology service of a referral center in Italy.
Synopsis: This study included 1,789 consecutive patients with ACS undergoing PCI. Patients were given 325 mg aspirin and a 600-mg loading dose of clopidogrel on admission, followed by a daily maintenance dose of aspirin 325 mg and clopidogrel 75 mg for at least six months. Platelet reactivity was measured using adenosine diphosphate (ADP) testing, and those with HRPR (≥70% platelet aggregation) were given increased dosing of clopidogrel or switched to ticlopidine using ADP test guidance. At two-year follow-up, patients with HRPR experienced an increased composite endpoint of cardiac death, myocardial infarction, urgent coronary revascularization, and stroke with a combined event rate of 14.6% in patients with HRPR and 8.7% in patients with low residual platelet reactivity (95% CI, 1.6%-11.1%; P=0.003). Stent thrombosis was also higher in HRPR patients (absolute risk increase 3.2%; 95% CI, 0.4%-6.7%; P=0.01).
This study is nonrandomized, and residual unmeasured confounding cannot be excluded. In addition, use of non-antiplatelet drugs and adherence to recommended drugs might have influenced outcomes.
Bottom line: HRPR is associated with increased risk of ischemic events in patients with ACS receiving antiplatelet agents after PCI.
Citation: Parodi G, Marcucci R, Valenti R, et al. High residual platelet reactivity after clopidogrel loading and long-term cardiovascular events among patients with acute coronary syndromes undergoing PCI. JAMA. 2011;306:1215-1223.
Conservative Treatment of Necrotizing Pancreatitis Is Associated with Improved Outcomes
Clinical question: What are the outcomes of conservative and interventional management of necrotizing pancreatitis?
Background: Open necrosectomy was historically the treatment of choice for necrotizing pancreatitis, but, currently, pancreatic necrosis is only managed invasively when complicated by infection. Other changes in management over time have included a shift in the timing of intervention and the use of minimally invasive techniques. Existing studies do not reflect these changes in practice patterns and have been limited by small sample sizes or the exclusion of important subgroups of patients.
Study design: Prospective cohort study.
Setting: Twenty-one Dutch hospitals.
Synopsis: This study included 639 patients with acute necrotizing pancreatitis confirmed by imaging. Overall mortality was 15%. Conservative treatment was performed in 62% of the patients with a mortality of 7%; however, patients with organ failure (pulmonary, circulatory, and/or renal) who received conservative therapy had a mortality rate of 37%. Intervention (percutaneous drainage, video-assisted retroperitoneal debridement, endoscopic transluminal necrosectomy, laparotomy) in patients with suspected or confirmed infected pancreatic necrosis was performed on 38% of the patients with associated mortality of 27%. Interventions performed within the first 14 days of hospitalization resulted in a 56% mortality rate, whereas interventions performed after Day 29 resulted in a 15% mortality rate (P<0.001). Patients with organ failure experienced significantly greater mortality compared with patients with no organ failure (35% vs. 2%; P<0.001). Primary percutaneous drainage was associated with fewer complications than was primary necrosectomy (42% vs. 64%; P=0.003).
This study was nonrandomized, and final decisions regarding management were left to the treating physician. Notably, while there was no significant difference in APACHE II scores between the conservative and intervention groups, intervention patients had more severe pancreatic disease and scored higher on other measures of disease severity.
Bottom line: Patients with necrotizing pancreatitis can frequently be managed conservatively, though the presence of organ failure and parenchymal necrosis confer poorer prognosis. When intervention is indicated, postponing intervention and utilizing minimally invasive techniques decrease morbidity and mortality.
Citation: Van Santvoort HC, Bakker OJ, Bollen TL, et al. A conservative and minimally invasive approach to necrotizing pancreatitis improves outcome. Gastroenterology. 2011;141:1254-1263.
Cardiac MRI Complements Clinical Findings in Diagnosis of Stress Cardiomyopathy
Clinical question: What are the clinical features and cardiovascular MRI findings in patients with stress (Takotsubo) cardiomyopathy?
Background: Stress cardiomyopathy (SC) is characterized by acute and profound reversible left ventricular dysfunction that is thought to result from increased sympathetic activity related to emotional and/or physical stress. Prior studies evaluating the clinical features of SC were limited by small sample sizes and single-center enrollment, and cardiac MRI use in SC has not been well studied.
Study design: Prospective cohort study.
Setting: Seven North American and European tertiary-care centers.
Synopsis: This study enrolled 256 patients who met diagnostic criteria for SC according to Mayo criteria. Postmenopausal women were most commonly affected; only 11% of participants were men and 8% were women younger than 50 years old. An identifiable stressor was found in 71% of the patients. Clinical presentation was notable for symptoms of acute coronary syndrome (ACS) in 88% of patients, abnormal electrocardiogram in 87%, and elevated troponin T in 90%. Coronary angiography was normal in three-fourths of patients, and no patients had features of acute plaque rupture. Typical apical ballooning was seen on left ventriculography in 82% of patients.
Cardiac MRI findings included severe left ventricular dysfunction in a noncoronary distribution, myocardial edema in areas of regional wall abnormalities, absence of high signal areas in late gadolinium enhancement (e.g., absence of necrosis/fibrosis), and increased early gadolinium uptake (i.e. early inflammation). Repeat cardiac MRI four weeks after initial diagnosis showed near or complete resolution of imaging findings.
Bottom line: Stress cardiomyopathy typically presents like ACS, usually affects postmenopausal women, is often preceded by a stressful event, and is characterized by cardiac MRI findings of regional wall motion abnormalities, reversible myocardial injury, and the absence of fibrosis. Cardiac MRI may be valuable in diagnosing SC in patients who present without the classic clinical features.
Citation: Eitel I, von Knobelsdorff-Brenkenhoff F, Bernhardt P, et al. Clinical characteristics and cardiovascular magnetic resonance findings in stress (Takotsubo) cardiomyopathy. JAMA. 2011;306:277-286.
Increased Risk of Potentially Inadvertent Medication Discontinuation Following Acute-Care Hospitalization
Clinical question: Are medications for chronic diseases inadvertently discontinued after acute-care hospitalization, and is this risk increased in patients who had an ICU stay?
Background: Transitions of care are associated with medical errors. Two such transitions are a shift from the ICU to floor setting and from the inpatient to outpatient setting. Medications for chronic diseases might be held during hospitalization for a variety of reasons, and medication errors may occur if these drugs are not restarted when the acute problem resolves or the patient is discharged from the hospital.
Study design: Population-based cohort study.
Setting: Ontario, Canada.
Synopsis: Using four separate databases, administrative records were reviewed for 396,380 patients aged >65 years who were continuous users of at least one of five evidence-based medication groups for common chronic diseases. Medications included statins, antiplatelet/anticoagulant agents, levothyroxine, respiratory inhalers, and gastric acid suppressants. The primary outcome was potentially unintentional medication discontinuation (measured by failure to renew the prescription at 90 days) for hospitalized versus nonhospitalized patients. All medication groups had statistically significant adjusted odds ratios ranging from 1.18 (95% CI, 1.14-1.23) for discontinuation of levothyroxine to 1.86 (95% CI, 1.77-1.97) for discontinuation of antiplatelet/anticoagulant medications. Treatment in an ICU further increased this risk compared with nonhospitalized patients, and increased the risk for medication discontinuation in four of the five medication groups when compared with patients hospitalized without ICU treatment.
Important study limitations include the lack of appropriate clinical details to classify medication discontinuation as unintentional and the inability of administrative data to prove causality. This study highlights the importance of medication reconciliation and calls attention to inadvertent medication discontinuation during care transitions (see “Reconciliation Act,”).
Bottom line: Patients discharged from the hospital, particularly after ICU treatment, have a higher risk of discontinuation of long-term medications for chronic medical problems when compared with nonhospitalized patients.
Citation: Bell CM, Brener SS, Gunraj N, et al. Association of ICU or hospital admission with unintentional discontinuation of medications for chronic diseases. JAMA. 2011;306:840-847.
Clinical Exam Remains Valuable in the Diagnosis of Patients Admitted to a Medicine Service
Clinical question: Is a clinical exam useful in the diagnosis of newly admitted patients to a general medicine service?
Background: The clinical exam, which comprises the history and physical examination, has long been described as essential to the diagnosis of illness. However, the literature supporting this claim is limited to the ambulatory setting. There has not been evaluation of the clinical exam as a diagnostic tool in the hospital setting, where more advanced testing is readily available.
Study design: Retrospective chart review.
Setting: Urban academic medical center.
Synopsis: The study included 442 adult patients consecutively admitted from the emergency department to the general medicine service who were separately assessed by one senior resident (SR) and one experienced hospital physician (HP) not involved with the case. The SR and HP each made an initial diagnosis and documented the most helpful component(s) in arriving at that diagnosis. Outcomes included comparison of the SR and HP’s admission diagnosis with the discharge diagnosis, and the diagnostic value of the various components of the clinical exam and initial studies.
Compared with the discharge diagnosis, the SR’s initial diagnosis was correct in 80.1% of cases, while the HP was correct in 84.4%. The patient’s history was the most important element in the initial assessment, independently influencing approximately 20% of the correct diagnoses for both physicians. Approximately 60% of correct diagnoses were established using the history and/or physical, and more than 90% were made using a combination of history, physical exam, and/or basic tests (admission labs, electrocardiogram, chest X-ray).
The generalizability of these results is limited by the retrospective, single-center study design, involvement of only one resident physician, and the lack of information regarding number of experienced clinicians and types of diagnoses.
Bottom line: Among patients admitted to a general medicine service, the most powerful tool in obtaining an accurate diagnosis was the combination of a patient’s history and a physical exam.
Citation: Paley L, Zornitzki T, Cohen J, et al. Utility of clinical examination in the diagnosis of emergency department patients admitted to the department of medicine of an academic hospital. Arch Intern Med. 2011;171:1394-1396.
RDW Predicts All-Cause Mortality and Bloodstream Infection in ICU Patients
Clinical question: Among patients admitted to the ICU, is red blood cell distribution width (RDW) a reliable indicator of mortality?
Background: The RDW is an inexpensive test that is commonly included in routine laboratory studies. It has been associated with multiple disease processes and found to be a strong predictor of mortality in the general adult population. However, there has been limited study of the association between RDW and outcomes in critically ill patients.
Study design: Observational cohort study.
Setting: Urban tertiary-care academic medical center.
Synopsis: Data from 51,413 adult patients who received critical care between 1997 and 2007 were obtained from a computerized registry and evaluated for the primary outcome of 30-day mortality after critical-care initiation. Secondary outcomes included 90-day, 365-day, and in-hospital mortality, as well as bloodstream infection. Logistic regression examined both primary and secondary outcomes in association with pre-established RDW quintiles. After multivariable adjustment, RDW was found to be associated with mortality at 30, 90, and 365 days, in addition to in-hospital mortality. The highest RDW quintile (RDW >15.8%) had an adjusted OR of 2.61 (95% CI, 2.37-2.86; P<0.001) for the primary outcome, with similar risk for secondary outcomes of mortality. A subgroup of 18,525 patients with blood culture data was analyzed and an adjusted OR of 1.44 was found in the highest RDW quintile for the secondary outcome of bloodstream infection.
Bottom line: Red blood cell distribution width is a strong independent predictor of all-cause mortality and bloodstream infection in patients receiving intensive care.
Citation: Bazick HS, Chang D, Mahadevappa K, Gibbons FK, Christopher KB. Red cell distribution width and all-cause mortality in critically ill patients. Crit Care Med. 2011;39:1913-1921.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Procalcitonin to guide antimicrobial use in ICU patients
- Platelet reactivity and event rates after PCI
- Conservative treatment of necrotizing pancreatitis
- Use of MRI to diagnose Takotsubo cardiomyopathy
- Rates of inadvertent medication discontinuation after hospitalization
- Role of history and physical exam in diagnosing medical illness
- Red-cell distribution width and rates of mortality
Procalcitonin-Guided Therapy Decreases Antimicrobial Duration in ICU Patients
Clinical question: Can utilization of serum procalcitonin (PCT) levels safely reduce antimicrobial exposure in ICU patients?
Background: Serum PCT levels are elevated in bacterial infections and sepsis and have been used in some settings to guide antimicrobial therapy. Randomized controlled trials have demonstrated reduction of antibiotic use with PCT measurement. This systematic review assessed the safety and effectiveness of PCT measurements in reducing antimicrobial exposure in ICU patients.
Study design: Systematic review.
Setting: Adult medical and surgical ICUs.
Synopsis: A search of MEDLINE and EMBASE yielded 1,018 publications related to PCT, critically ill patients, and antimicrobial therapy. Six randomized controlled trials involving 1,476 patients were reviewed. The duration of antimicrobial use was significantly decreased in all five studies that evaluated treatment duration. The remaining study only assessed the impact of PCT on initiation of antimicrobial therapy and did not demonstrate decreased antimicrobial exposure. Compared with the control group, patients randomized to PCT-guided therapy had relative reductions in duration of first antibiotic course by 21%, down to 38%, and decreases in days of antimicrobial therapy per 1,000 ICU patient days by 20%, down to 23%. PCT intervention also was associated with a 23% to 37% increase in days alive without antimicrobial therapy during the first 28 days. The length of ICU stay was significantly decreased in two studies but was not significantly different in the other studies. There were no significant differences in rates of mortality, infection relapse, or days free of mechanical ventilation.
Bottom line: PCT guidance reduced antimicrobial exposure of ICU patients without increasing rates of mortality or infection relapse.
Citation: Agarwal R, Schwartz DN. Procalcitonin to guide duration of antimicrobial therapy in intensive care units: a systematic review. Clin Infect Dis. 2011;53:379-387.
High Residual Platelet Reactivity Increases Risk of Cardiovascular Events among Patients with Acute Coronary Syndromes Undergoing PCI
Clinical question: Is high residual platelet reactivity (HRPR) in patients receiving clopidogrel associated with increased risk of ischemic events after percutaneous coronary intervention (PCI)?
Background: Studies have demonstrated an increased risk of cardiovascular events associated with HRPR in patients receiving clopidogrel while undergoing PCI. However, these studies have used a variety of platelet function tests, and thresholds for positive tests have not been established. In addition, these studies have enrolled heterogeneous populations with short-term follow-up and few have included patients with acute coronary syndromes (ACSs).
Study design: Prospective cohort study.
Setting: Cardiology service of a referral center in Italy.
Synopsis: This study included 1,789 consecutive patients with ACS undergoing PCI. Patients were given 325 mg aspirin and a 600-mg loading dose of clopidogrel on admission, followed by a daily maintenance dose of aspirin 325 mg and clopidogrel 75 mg for at least six months. Platelet reactivity was measured using adenosine diphosphate (ADP) testing, and those with HRPR (≥70% platelet aggregation) were given increased dosing of clopidogrel or switched to ticlopidine using ADP test guidance. At two-year follow-up, patients with HRPR experienced an increased composite endpoint of cardiac death, myocardial infarction, urgent coronary revascularization, and stroke with a combined event rate of 14.6% in patients with HRPR and 8.7% in patients with low residual platelet reactivity (95% CI, 1.6%-11.1%; P=0.003). Stent thrombosis was also higher in HRPR patients (absolute risk increase 3.2%; 95% CI, 0.4%-6.7%; P=0.01).
This study is nonrandomized, and residual unmeasured confounding cannot be excluded. In addition, use of non-antiplatelet drugs and adherence to recommended drugs might have influenced outcomes.
Bottom line: HRPR is associated with increased risk of ischemic events in patients with ACS receiving antiplatelet agents after PCI.
Citation: Parodi G, Marcucci R, Valenti R, et al. High residual platelet reactivity after clopidogrel loading and long-term cardiovascular events among patients with acute coronary syndromes undergoing PCI. JAMA. 2011;306:1215-1223.
Conservative Treatment of Necrotizing Pancreatitis Is Associated with Improved Outcomes
Clinical question: What are the outcomes of conservative and interventional management of necrotizing pancreatitis?
Background: Open necrosectomy was historically the treatment of choice for necrotizing pancreatitis, but, currently, pancreatic necrosis is only managed invasively when complicated by infection. Other changes in management over time have included a shift in the timing of intervention and the use of minimally invasive techniques. Existing studies do not reflect these changes in practice patterns and have been limited by small sample sizes or the exclusion of important subgroups of patients.
Study design: Prospective cohort study.
Setting: Twenty-one Dutch hospitals.
Synopsis: This study included 639 patients with acute necrotizing pancreatitis confirmed by imaging. Overall mortality was 15%. Conservative treatment was performed in 62% of the patients with a mortality of 7%; however, patients with organ failure (pulmonary, circulatory, and/or renal) who received conservative therapy had a mortality rate of 37%. Intervention (percutaneous drainage, video-assisted retroperitoneal debridement, endoscopic transluminal necrosectomy, laparotomy) in patients with suspected or confirmed infected pancreatic necrosis was performed on 38% of the patients with associated mortality of 27%. Interventions performed within the first 14 days of hospitalization resulted in a 56% mortality rate, whereas interventions performed after Day 29 resulted in a 15% mortality rate (P<0.001). Patients with organ failure experienced significantly greater mortality compared with patients with no organ failure (35% vs. 2%; P<0.001). Primary percutaneous drainage was associated with fewer complications than was primary necrosectomy (42% vs. 64%; P=0.003).
This study was nonrandomized, and final decisions regarding management were left to the treating physician. Notably, while there was no significant difference in APACHE II scores between the conservative and intervention groups, intervention patients had more severe pancreatic disease and scored higher on other measures of disease severity.
Bottom line: Patients with necrotizing pancreatitis can frequently be managed conservatively, though the presence of organ failure and parenchymal necrosis confer poorer prognosis. When intervention is indicated, postponing intervention and utilizing minimally invasive techniques decrease morbidity and mortality.
Citation: Van Santvoort HC, Bakker OJ, Bollen TL, et al. A conservative and minimally invasive approach to necrotizing pancreatitis improves outcome. Gastroenterology. 2011;141:1254-1263.
Cardiac MRI Complements Clinical Findings in Diagnosis of Stress Cardiomyopathy
Clinical question: What are the clinical features and cardiovascular MRI findings in patients with stress (Takotsubo) cardiomyopathy?
Background: Stress cardiomyopathy (SC) is characterized by acute and profound reversible left ventricular dysfunction that is thought to result from increased sympathetic activity related to emotional and/or physical stress. Prior studies evaluating the clinical features of SC were limited by small sample sizes and single-center enrollment, and cardiac MRI use in SC has not been well studied.
Study design: Prospective cohort study.
Setting: Seven North American and European tertiary-care centers.
Synopsis: This study enrolled 256 patients who met diagnostic criteria for SC according to Mayo criteria. Postmenopausal women were most commonly affected; only 11% of participants were men and 8% were women younger than 50 years old. An identifiable stressor was found in 71% of the patients. Clinical presentation was notable for symptoms of acute coronary syndrome (ACS) in 88% of patients, abnormal electrocardiogram in 87%, and elevated troponin T in 90%. Coronary angiography was normal in three-fourths of patients, and no patients had features of acute plaque rupture. Typical apical ballooning was seen on left ventriculography in 82% of patients.
Cardiac MRI findings included severe left ventricular dysfunction in a noncoronary distribution, myocardial edema in areas of regional wall abnormalities, absence of high signal areas in late gadolinium enhancement (e.g., absence of necrosis/fibrosis), and increased early gadolinium uptake (i.e. early inflammation). Repeat cardiac MRI four weeks after initial diagnosis showed near or complete resolution of imaging findings.
Bottom line: Stress cardiomyopathy typically presents like ACS, usually affects postmenopausal women, is often preceded by a stressful event, and is characterized by cardiac MRI findings of regional wall motion abnormalities, reversible myocardial injury, and the absence of fibrosis. Cardiac MRI may be valuable in diagnosing SC in patients who present without the classic clinical features.
Citation: Eitel I, von Knobelsdorff-Brenkenhoff F, Bernhardt P, et al. Clinical characteristics and cardiovascular magnetic resonance findings in stress (Takotsubo) cardiomyopathy. JAMA. 2011;306:277-286.
Increased Risk of Potentially Inadvertent Medication Discontinuation Following Acute-Care Hospitalization
Clinical question: Are medications for chronic diseases inadvertently discontinued after acute-care hospitalization, and is this risk increased in patients who had an ICU stay?
Background: Transitions of care are associated with medical errors. Two such transitions are a shift from the ICU to floor setting and from the inpatient to outpatient setting. Medications for chronic diseases might be held during hospitalization for a variety of reasons, and medication errors may occur if these drugs are not restarted when the acute problem resolves or the patient is discharged from the hospital.
Study design: Population-based cohort study.
Setting: Ontario, Canada.
Synopsis: Using four separate databases, administrative records were reviewed for 396,380 patients aged >65 years who were continuous users of at least one of five evidence-based medication groups for common chronic diseases. Medications included statins, antiplatelet/anticoagulant agents, levothyroxine, respiratory inhalers, and gastric acid suppressants. The primary outcome was potentially unintentional medication discontinuation (measured by failure to renew the prescription at 90 days) for hospitalized versus nonhospitalized patients. All medication groups had statistically significant adjusted odds ratios ranging from 1.18 (95% CI, 1.14-1.23) for discontinuation of levothyroxine to 1.86 (95% CI, 1.77-1.97) for discontinuation of antiplatelet/anticoagulant medications. Treatment in an ICU further increased this risk compared with nonhospitalized patients, and increased the risk for medication discontinuation in four of the five medication groups when compared with patients hospitalized without ICU treatment.
Important study limitations include the lack of appropriate clinical details to classify medication discontinuation as unintentional and the inability of administrative data to prove causality. This study highlights the importance of medication reconciliation and calls attention to inadvertent medication discontinuation during care transitions (see “Reconciliation Act,”).
Bottom line: Patients discharged from the hospital, particularly after ICU treatment, have a higher risk of discontinuation of long-term medications for chronic medical problems when compared with nonhospitalized patients.
Citation: Bell CM, Brener SS, Gunraj N, et al. Association of ICU or hospital admission with unintentional discontinuation of medications for chronic diseases. JAMA. 2011;306:840-847.
Clinical Exam Remains Valuable in the Diagnosis of Patients Admitted to a Medicine Service
Clinical question: Is a clinical exam useful in the diagnosis of newly admitted patients to a general medicine service?
Background: The clinical exam, which comprises the history and physical examination, has long been described as essential to the diagnosis of illness. However, the literature supporting this claim is limited to the ambulatory setting. There has not been evaluation of the clinical exam as a diagnostic tool in the hospital setting, where more advanced testing is readily available.
Study design: Retrospective chart review.
Setting: Urban academic medical center.
Synopsis: The study included 442 adult patients consecutively admitted from the emergency department to the general medicine service who were separately assessed by one senior resident (SR) and one experienced hospital physician (HP) not involved with the case. The SR and HP each made an initial diagnosis and documented the most helpful component(s) in arriving at that diagnosis. Outcomes included comparison of the SR and HP’s admission diagnosis with the discharge diagnosis, and the diagnostic value of the various components of the clinical exam and initial studies.
Compared with the discharge diagnosis, the SR’s initial diagnosis was correct in 80.1% of cases, while the HP was correct in 84.4%. The patient’s history was the most important element in the initial assessment, independently influencing approximately 20% of the correct diagnoses for both physicians. Approximately 60% of correct diagnoses were established using the history and/or physical, and more than 90% were made using a combination of history, physical exam, and/or basic tests (admission labs, electrocardiogram, chest X-ray).
The generalizability of these results is limited by the retrospective, single-center study design, involvement of only one resident physician, and the lack of information regarding number of experienced clinicians and types of diagnoses.
Bottom line: Among patients admitted to a general medicine service, the most powerful tool in obtaining an accurate diagnosis was the combination of a patient’s history and a physical exam.
Citation: Paley L, Zornitzki T, Cohen J, et al. Utility of clinical examination in the diagnosis of emergency department patients admitted to the department of medicine of an academic hospital. Arch Intern Med. 2011;171:1394-1396.
RDW Predicts All-Cause Mortality and Bloodstream Infection in ICU Patients
Clinical question: Among patients admitted to the ICU, is red blood cell distribution width (RDW) a reliable indicator of mortality?
Background: The RDW is an inexpensive test that is commonly included in routine laboratory studies. It has been associated with multiple disease processes and found to be a strong predictor of mortality in the general adult population. However, there has been limited study of the association between RDW and outcomes in critically ill patients.
Study design: Observational cohort study.
Setting: Urban tertiary-care academic medical center.
Synopsis: Data from 51,413 adult patients who received critical care between 1997 and 2007 were obtained from a computerized registry and evaluated for the primary outcome of 30-day mortality after critical-care initiation. Secondary outcomes included 90-day, 365-day, and in-hospital mortality, as well as bloodstream infection. Logistic regression examined both primary and secondary outcomes in association with pre-established RDW quintiles. After multivariable adjustment, RDW was found to be associated with mortality at 30, 90, and 365 days, in addition to in-hospital mortality. The highest RDW quintile (RDW >15.8%) had an adjusted OR of 2.61 (95% CI, 2.37-2.86; P<0.001) for the primary outcome, with similar risk for secondary outcomes of mortality. A subgroup of 18,525 patients with blood culture data was analyzed and an adjusted OR of 1.44 was found in the highest RDW quintile for the secondary outcome of bloodstream infection.
Bottom line: Red blood cell distribution width is a strong independent predictor of all-cause mortality and bloodstream infection in patients receiving intensive care.
Citation: Bazick HS, Chang D, Mahadevappa K, Gibbons FK, Christopher KB. Red cell distribution width and all-cause mortality in critically ill patients. Crit Care Med. 2011;39:1913-1921.
Network Connection
Education and training always will be a major draw for hospitalists attending SHM’s annual meetings, but hospitalists who let their day end after the last educational session are missing some of the meeting’s biggest opportunities for professional growth, according to conference veterans.
Networking, whether in between sessions, on the exhibit floor, at receptions, or after hours, can be a powerful career development tool, according to Jeff Glasheen, MD, SFHM, HM12 course director, and Michael Pistoria, DO, FACP, SFHM, course director for HM13.
“Hospitalists who haven’t attended an SHM annual meeting before are going to be pleasantly surprised by the accessibility and friendliness of faculty and other leaders in the field,” Dr. Pistoria says. “Networking opportunities will be everywhere at HM12. Smart hospitalists will take advantage of them to make connections, find resources, and advance their careers.”
Dr. Pistoria also points to SHM’s special-interest groups as easy ways to quickly find hospitalists with similar interests and establish professional networks.
The impact of networking at the annual meeting extends beyond individual interests, Dr. Glasheen says. Savvy networkers can impact the entire specialty, but they need to show up.
“This is our chance to influence the society—both big ‘S’ and small ‘s.’ And you can’t do that on your couch at home,” he says. “If you care about your field, be at the meeting learning with others, meeting colleagues, and influencing the direction of the field. This field is still new enough, small enough, and undifferentiated enough that you can influence its direction. Your odds of doing that are enhanced with the more people you meet.”
—Michael Pistoria, DO, FACP, SFHM, HM13 course director
Staying true to the “connect” and “collaborate” themes, HM12 will provide unprecedented opportunities to network with other hospitalists from across the country, including new breaks, receptions, and the special-interest groups.
As in years past, the most resourceful hospitalists will find even more informal opportunities, such as time between sessions and unwinding after a full day of meetings. Dr. Pistoria says the after-hours sessions pay off in the form of a support structure that he can rely on for professional advice.
“I remember the relationships that are developed and nurtured during time networking,” he says. “Those same relationships then help me when I am faced with an issue at my institution. I’ve now got built-in ‘consultants’—friends at other institutions that I can email and ask, ‘What are you doing about …’”
He also finds the networking personally rewarding, bridging the gap from professional colleagues to personal friends. “Those hours are where I’ve developed the friendships that I have with other SHM members,” he says.
Brendon Shank is associate vice president of communications for SHM.
Education and training always will be a major draw for hospitalists attending SHM’s annual meetings, but hospitalists who let their day end after the last educational session are missing some of the meeting’s biggest opportunities for professional growth, according to conference veterans.
Networking, whether in between sessions, on the exhibit floor, at receptions, or after hours, can be a powerful career development tool, according to Jeff Glasheen, MD, SFHM, HM12 course director, and Michael Pistoria, DO, FACP, SFHM, course director for HM13.
“Hospitalists who haven’t attended an SHM annual meeting before are going to be pleasantly surprised by the accessibility and friendliness of faculty and other leaders in the field,” Dr. Pistoria says. “Networking opportunities will be everywhere at HM12. Smart hospitalists will take advantage of them to make connections, find resources, and advance their careers.”
Dr. Pistoria also points to SHM’s special-interest groups as easy ways to quickly find hospitalists with similar interests and establish professional networks.
The impact of networking at the annual meeting extends beyond individual interests, Dr. Glasheen says. Savvy networkers can impact the entire specialty, but they need to show up.
“This is our chance to influence the society—both big ‘S’ and small ‘s.’ And you can’t do that on your couch at home,” he says. “If you care about your field, be at the meeting learning with others, meeting colleagues, and influencing the direction of the field. This field is still new enough, small enough, and undifferentiated enough that you can influence its direction. Your odds of doing that are enhanced with the more people you meet.”
—Michael Pistoria, DO, FACP, SFHM, HM13 course director
Staying true to the “connect” and “collaborate” themes, HM12 will provide unprecedented opportunities to network with other hospitalists from across the country, including new breaks, receptions, and the special-interest groups.
As in years past, the most resourceful hospitalists will find even more informal opportunities, such as time between sessions and unwinding after a full day of meetings. Dr. Pistoria says the after-hours sessions pay off in the form of a support structure that he can rely on for professional advice.
“I remember the relationships that are developed and nurtured during time networking,” he says. “Those same relationships then help me when I am faced with an issue at my institution. I’ve now got built-in ‘consultants’—friends at other institutions that I can email and ask, ‘What are you doing about …’”
He also finds the networking personally rewarding, bridging the gap from professional colleagues to personal friends. “Those hours are where I’ve developed the friendships that I have with other SHM members,” he says.
Brendon Shank is associate vice president of communications for SHM.
Education and training always will be a major draw for hospitalists attending SHM’s annual meetings, but hospitalists who let their day end after the last educational session are missing some of the meeting’s biggest opportunities for professional growth, according to conference veterans.
Networking, whether in between sessions, on the exhibit floor, at receptions, or after hours, can be a powerful career development tool, according to Jeff Glasheen, MD, SFHM, HM12 course director, and Michael Pistoria, DO, FACP, SFHM, course director for HM13.
“Hospitalists who haven’t attended an SHM annual meeting before are going to be pleasantly surprised by the accessibility and friendliness of faculty and other leaders in the field,” Dr. Pistoria says. “Networking opportunities will be everywhere at HM12. Smart hospitalists will take advantage of them to make connections, find resources, and advance their careers.”
Dr. Pistoria also points to SHM’s special-interest groups as easy ways to quickly find hospitalists with similar interests and establish professional networks.
The impact of networking at the annual meeting extends beyond individual interests, Dr. Glasheen says. Savvy networkers can impact the entire specialty, but they need to show up.
“This is our chance to influence the society—both big ‘S’ and small ‘s.’ And you can’t do that on your couch at home,” he says. “If you care about your field, be at the meeting learning with others, meeting colleagues, and influencing the direction of the field. This field is still new enough, small enough, and undifferentiated enough that you can influence its direction. Your odds of doing that are enhanced with the more people you meet.”
—Michael Pistoria, DO, FACP, SFHM, HM13 course director
Staying true to the “connect” and “collaborate” themes, HM12 will provide unprecedented opportunities to network with other hospitalists from across the country, including new breaks, receptions, and the special-interest groups.
As in years past, the most resourceful hospitalists will find even more informal opportunities, such as time between sessions and unwinding after a full day of meetings. Dr. Pistoria says the after-hours sessions pay off in the form of a support structure that he can rely on for professional advice.
“I remember the relationships that are developed and nurtured during time networking,” he says. “Those same relationships then help me when I am faced with an issue at my institution. I’ve now got built-in ‘consultants’—friends at other institutions that I can email and ask, ‘What are you doing about …’”
He also finds the networking personally rewarding, bridging the gap from professional colleagues to personal friends. “Those hours are where I’ve developed the friendships that I have with other SHM members,” he says.
Brendon Shank is associate vice president of communications for SHM.
Policy Corner: An Inside Look at the Most Pressing Policy Issues
In early November, the Institute of Medicine (IOM) released a report on the current status of health information technology (HIT). Although the report was developed at the request of the Office of the National Coordinator (ONC), the arm within the Department of Health and Human Services (HHS) responsible for promoting the use of HIT, not everything in the report was positive—and could leave the impression that HIT is not quite as successful as some think.
The report recommends that the ONC should work with the private and public sectors to make comparative user experiences across vendors publicly available.
Many hospitalists have developed significant expertise with HIT, played significant roles in its effective implementation and use, and are acutely aware of implementation pitfalls. This practical experience could be very helpful in working with the ONC to develop solutions. It is for this reason that hospitalists should reach out to the ONC and offer their expertise instead of waiting for the ONC to act.
The report, “Patient Safety and Health IT: Building Safer Systems for Better Care,” did praise HIT’s potential for eventual cost savings and increased patient safety but stopped short of being a ringing endorsement of the pace HM is taking toward implementation initiatives, such as meaningful use. An overall theme of the report is that greater oversight of HIT is needed to protect patients from potential medical errors associated with its use.
A few of the recommendations given by the IOM to achieve a greater level of safety range from the establishment of a mechanism for vendors and users to report health IT-related deaths, injuries, or unsafe conditions to possible FDA regulation of the systems themselves.
Information-sharing and reporting in a nonpunitive environment, as recommended by the IOM, would go a long way when it comes to remedying or avoiding IT-related problems, and hospitalists probably have some ideas about how this could be done.
Unfortunately, IT vendor contracts often prevent the open sharing of information, so working toward doing away with such contract terms might be a worthy step before making a push toward overall FDA regulation and the unintended consequences that may come with it.
At first glance, FDA regulation seems like the easiest solution because the FDA can theoretically control every aspect of what might go wrong with HIT, but at what cost would such regulation come? FDA approval can be long, complicated and expensive. The whole process could result in cutting-edge technology becoming outdated by the time approval is granted or innovations being overlooked entirely because of a negative cost-benefit analysis. Furthermore, the expense associated with FDA approval could in turn increase the cost of already costly electronic health records (EHR).
Despite the myriad problems that can arise if implementation moves too fast, HIT holds promise and has shown success when done well.
SHM is currently working to position hospitalists as a resource for the ONC, so hospitalists with expertise in this area should not hesitate to come forward with ideas on how to make HIT work better and more safely. HIT is not going to go away, so the best option is to help make it better.
In early November, the Institute of Medicine (IOM) released a report on the current status of health information technology (HIT). Although the report was developed at the request of the Office of the National Coordinator (ONC), the arm within the Department of Health and Human Services (HHS) responsible for promoting the use of HIT, not everything in the report was positive—and could leave the impression that HIT is not quite as successful as some think.
The report recommends that the ONC should work with the private and public sectors to make comparative user experiences across vendors publicly available.
Many hospitalists have developed significant expertise with HIT, played significant roles in its effective implementation and use, and are acutely aware of implementation pitfalls. This practical experience could be very helpful in working with the ONC to develop solutions. It is for this reason that hospitalists should reach out to the ONC and offer their expertise instead of waiting for the ONC to act.
The report, “Patient Safety and Health IT: Building Safer Systems for Better Care,” did praise HIT’s potential for eventual cost savings and increased patient safety but stopped short of being a ringing endorsement of the pace HM is taking toward implementation initiatives, such as meaningful use. An overall theme of the report is that greater oversight of HIT is needed to protect patients from potential medical errors associated with its use.
A few of the recommendations given by the IOM to achieve a greater level of safety range from the establishment of a mechanism for vendors and users to report health IT-related deaths, injuries, or unsafe conditions to possible FDA regulation of the systems themselves.
Information-sharing and reporting in a nonpunitive environment, as recommended by the IOM, would go a long way when it comes to remedying or avoiding IT-related problems, and hospitalists probably have some ideas about how this could be done.
Unfortunately, IT vendor contracts often prevent the open sharing of information, so working toward doing away with such contract terms might be a worthy step before making a push toward overall FDA regulation and the unintended consequences that may come with it.
At first glance, FDA regulation seems like the easiest solution because the FDA can theoretically control every aspect of what might go wrong with HIT, but at what cost would such regulation come? FDA approval can be long, complicated and expensive. The whole process could result in cutting-edge technology becoming outdated by the time approval is granted or innovations being overlooked entirely because of a negative cost-benefit analysis. Furthermore, the expense associated with FDA approval could in turn increase the cost of already costly electronic health records (EHR).
Despite the myriad problems that can arise if implementation moves too fast, HIT holds promise and has shown success when done well.
SHM is currently working to position hospitalists as a resource for the ONC, so hospitalists with expertise in this area should not hesitate to come forward with ideas on how to make HIT work better and more safely. HIT is not going to go away, so the best option is to help make it better.
In early November, the Institute of Medicine (IOM) released a report on the current status of health information technology (HIT). Although the report was developed at the request of the Office of the National Coordinator (ONC), the arm within the Department of Health and Human Services (HHS) responsible for promoting the use of HIT, not everything in the report was positive—and could leave the impression that HIT is not quite as successful as some think.
The report recommends that the ONC should work with the private and public sectors to make comparative user experiences across vendors publicly available.
Many hospitalists have developed significant expertise with HIT, played significant roles in its effective implementation and use, and are acutely aware of implementation pitfalls. This practical experience could be very helpful in working with the ONC to develop solutions. It is for this reason that hospitalists should reach out to the ONC and offer their expertise instead of waiting for the ONC to act.
The report, “Patient Safety and Health IT: Building Safer Systems for Better Care,” did praise HIT’s potential for eventual cost savings and increased patient safety but stopped short of being a ringing endorsement of the pace HM is taking toward implementation initiatives, such as meaningful use. An overall theme of the report is that greater oversight of HIT is needed to protect patients from potential medical errors associated with its use.
A few of the recommendations given by the IOM to achieve a greater level of safety range from the establishment of a mechanism for vendors and users to report health IT-related deaths, injuries, or unsafe conditions to possible FDA regulation of the systems themselves.
Information-sharing and reporting in a nonpunitive environment, as recommended by the IOM, would go a long way when it comes to remedying or avoiding IT-related problems, and hospitalists probably have some ideas about how this could be done.
Unfortunately, IT vendor contracts often prevent the open sharing of information, so working toward doing away with such contract terms might be a worthy step before making a push toward overall FDA regulation and the unintended consequences that may come with it.
At first glance, FDA regulation seems like the easiest solution because the FDA can theoretically control every aspect of what might go wrong with HIT, but at what cost would such regulation come? FDA approval can be long, complicated and expensive. The whole process could result in cutting-edge technology becoming outdated by the time approval is granted or innovations being overlooked entirely because of a negative cost-benefit analysis. Furthermore, the expense associated with FDA approval could in turn increase the cost of already costly electronic health records (EHR).
Despite the myriad problems that can arise if implementation moves too fast, HIT holds promise and has shown success when done well.
SHM is currently working to position hospitalists as a resource for the ONC, so hospitalists with expertise in this area should not hesitate to come forward with ideas on how to make HIT work better and more safely. HIT is not going to go away, so the best option is to help make it better.
CODE-H: Optimize Revenue with Improved Coding Education
Documentation and coding are facts of life for every HM group. Yet almost every group knows that it could be doing better, according to Barb Pierce, CCS-P, ACS-EM, of Barb Pierce Coding and Consulting Inc.
“Despite being a highly structured system, effective coding still depends on the acumen and experience of the people doing the coding,” she says. “No hospitalist will get it perfect every time, but everyone can improve through training. And that training can improve the practice’s bottom line.”
The challenges of coding optimization are getting more and more difficult as changes in government reimbursements impact both documentation and coding requirements. The financial and compliance imperatives to code accurately—even as these requirements shift—are the major driver behind SHM’s new remote learning series, CODE-H.
Short for “Coding Optimally by Documenting Effectively for Hospitalists,” CODE-H can improve the confidence that practice leaders and administrators have in their documentation and coding efforts through a comprehensive, eight-month program that includes webinars and a variety of other support resources. Six expert-led webinars will cover basic and more nuanced issues of documentation, coding, and compliance, including:
- Basics of E&M Coding for Hospitalists, Part 1 and Part 2
- Coding for Hospitalists’ Expanding Scope of Services
- Staying Out of Trouble
- Integrating Physician Billing & Hospital DRG Assurance
- Optimizing Performance and Compliance
Subscribers also receive exclusive access to an online learning community, pre- and post-webinar tests to evaluate learning, a library of additional resources, and CME or CEU credits, pending approval.
The program kicks off Feb. 1 with the first webinar, led by Pierce, the series course director. She is a veteran faculty member for SHM’s one-day coding pre-course. The remote learning series, which runs through Aug. 29, is offered as a site-based subscription for up to 10 individuals from the same HM group for $1,200. Additional participants from the same practice can be registered for a modest additional fee.
“Practice groups continue to lose tens of thousands of dollars through inappropriate documentation and coding,” says Leslie Flores, MHA, a partner in Nelson Flores Hospital Medicine Consultants and SHM’s senior advisor for practice management. “Investing in CODE-H is a way to recoup some of those losses and is a great value. A practice can provide eight months of coding education and support for 10 people for about the same cost as sending a single doctor to SHM’s all-day coding course.”
Visit www.hospitalmedicine.org/codeh to subscribe.
Documentation and coding are facts of life for every HM group. Yet almost every group knows that it could be doing better, according to Barb Pierce, CCS-P, ACS-EM, of Barb Pierce Coding and Consulting Inc.
“Despite being a highly structured system, effective coding still depends on the acumen and experience of the people doing the coding,” she says. “No hospitalist will get it perfect every time, but everyone can improve through training. And that training can improve the practice’s bottom line.”
The challenges of coding optimization are getting more and more difficult as changes in government reimbursements impact both documentation and coding requirements. The financial and compliance imperatives to code accurately—even as these requirements shift—are the major driver behind SHM’s new remote learning series, CODE-H.
Short for “Coding Optimally by Documenting Effectively for Hospitalists,” CODE-H can improve the confidence that practice leaders and administrators have in their documentation and coding efforts through a comprehensive, eight-month program that includes webinars and a variety of other support resources. Six expert-led webinars will cover basic and more nuanced issues of documentation, coding, and compliance, including:
- Basics of E&M Coding for Hospitalists, Part 1 and Part 2
- Coding for Hospitalists’ Expanding Scope of Services
- Staying Out of Trouble
- Integrating Physician Billing & Hospital DRG Assurance
- Optimizing Performance and Compliance
Subscribers also receive exclusive access to an online learning community, pre- and post-webinar tests to evaluate learning, a library of additional resources, and CME or CEU credits, pending approval.
The program kicks off Feb. 1 with the first webinar, led by Pierce, the series course director. She is a veteran faculty member for SHM’s one-day coding pre-course. The remote learning series, which runs through Aug. 29, is offered as a site-based subscription for up to 10 individuals from the same HM group for $1,200. Additional participants from the same practice can be registered for a modest additional fee.
“Practice groups continue to lose tens of thousands of dollars through inappropriate documentation and coding,” says Leslie Flores, MHA, a partner in Nelson Flores Hospital Medicine Consultants and SHM’s senior advisor for practice management. “Investing in CODE-H is a way to recoup some of those losses and is a great value. A practice can provide eight months of coding education and support for 10 people for about the same cost as sending a single doctor to SHM’s all-day coding course.”
Visit www.hospitalmedicine.org/codeh to subscribe.
Documentation and coding are facts of life for every HM group. Yet almost every group knows that it could be doing better, according to Barb Pierce, CCS-P, ACS-EM, of Barb Pierce Coding and Consulting Inc.
“Despite being a highly structured system, effective coding still depends on the acumen and experience of the people doing the coding,” she says. “No hospitalist will get it perfect every time, but everyone can improve through training. And that training can improve the practice’s bottom line.”
The challenges of coding optimization are getting more and more difficult as changes in government reimbursements impact both documentation and coding requirements. The financial and compliance imperatives to code accurately—even as these requirements shift—are the major driver behind SHM’s new remote learning series, CODE-H.
Short for “Coding Optimally by Documenting Effectively for Hospitalists,” CODE-H can improve the confidence that practice leaders and administrators have in their documentation and coding efforts through a comprehensive, eight-month program that includes webinars and a variety of other support resources. Six expert-led webinars will cover basic and more nuanced issues of documentation, coding, and compliance, including:
- Basics of E&M Coding for Hospitalists, Part 1 and Part 2
- Coding for Hospitalists’ Expanding Scope of Services
- Staying Out of Trouble
- Integrating Physician Billing & Hospital DRG Assurance
- Optimizing Performance and Compliance
Subscribers also receive exclusive access to an online learning community, pre- and post-webinar tests to evaluate learning, a library of additional resources, and CME or CEU credits, pending approval.
The program kicks off Feb. 1 with the first webinar, led by Pierce, the series course director. She is a veteran faculty member for SHM’s one-day coding pre-course. The remote learning series, which runs through Aug. 29, is offered as a site-based subscription for up to 10 individuals from the same HM group for $1,200. Additional participants from the same practice can be registered for a modest additional fee.
“Practice groups continue to lose tens of thousands of dollars through inappropriate documentation and coding,” says Leslie Flores, MHA, a partner in Nelson Flores Hospital Medicine Consultants and SHM’s senior advisor for practice management. “Investing in CODE-H is a way to recoup some of those losses and is a great value. A practice can provide eight months of coding education and support for 10 people for about the same cost as sending a single doctor to SHM’s all-day coding course.”
Visit www.hospitalmedicine.org/codeh to subscribe.
Survey Insights: Peeking under the Hood of Academic HM
The 2011 State of Hospital Medicine report offers some tantalizing insights into the operation of academic hospital medicine practices and how they compare with their nonacademic peers. Some results are not surprising, such as the fact that academic hospital medicine groups tend to be larger than nonacademic groups, and that compensation and clinical-FTE-adjusted productivity both tend to be lower for academic hospitalists. Interestingly, turnover rates were about the same in academic and nonacademic practices.
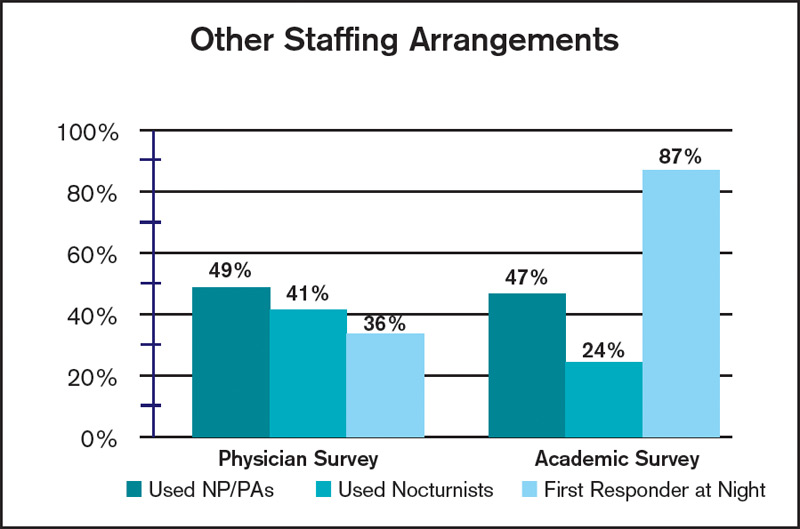
Among the more unexpected findings, however, is that academic HM practices tend to employ a higher proportion of women (44%) than nonacademic practices (35%). In addition, academic practices employed a wider range of staffing models, with only 43% of practices using shift-based staffing, compared with 78% of nonacademic respondents. Similarly, only 47% of academic groups provided on-site coverage at night, compared with 81% of nonacademic groups.
Additional differences between the way academic and nonacademic HM groups staff their programs are shown in the table, “Other Staffing Arrangements.” While the use of nurse practitioners and physician assistants (PA) was similar for academic and nonacademic practices, academic groups were much less likely to utilize nocturnists, and far more likely to have a nonphysician first responder at night (resident, nonphysician provider/PA, or other) than nonacademic groups.
It will be interesting to follow these trends over time. Because of new resident work-hour limits that went into effect in July, SHM Practice Analysis Committee (PAC) member Andrew White, MD, expects that there will be very few places that continue to use residents to cross-cover at night. “I suspect most academic centers have or will hire nocturnists,” he says, “but we’ll see.”
On the other hand, PAC member Scarlett Blue, RN, believes that continued growth in HM, coupled with a competitive job market, could result in increased use of nonphysician first responders at night—and in general. “Hospital medicine group leaders who are looking for alternative ways to meet the supply-demand conundrum may find a blended physician-NP/PA team to be one such answer,” she says.
Finally, the clinical services provided by academic HM groups vary from their nonacademic counterparts in some other important ways. Only 25% of academic practices provide care for ICU patients, compared with 78% of nonacademic practices, while 75% of academic groups perform procedures, compared with only 52% of nonacademic groups. And while the overwhelming majority of both academic and nonacademic practices provide surgical comanagement, academic practices were more than twice as likely to provide comanagement for medical subspecialty patients (45%, compared with 20% for nonacademic practices).
PAC member Troy Ahlstrom, MD, explains, tongue-in-cheek, that “academic hospitalists don’t do procedures because they have oodles of residents, fellows, and interventional radiologists to do them instead, and academics do more medical comanagement because the subspecialist who only does Waldenstrom’s macroglobulinemia probably doesn’t do diabetes.”
Whatever the reason, there are meaningful differences between academic and nonacademic HM practices that bear watching over time. You can help us identify and track these differences by ensuring that your group participates in SHM’s annual State of Hospital Medicine survey, launching this month.
The 2011 State of Hospital Medicine report offers some tantalizing insights into the operation of academic hospital medicine practices and how they compare with their nonacademic peers. Some results are not surprising, such as the fact that academic hospital medicine groups tend to be larger than nonacademic groups, and that compensation and clinical-FTE-adjusted productivity both tend to be lower for academic hospitalists. Interestingly, turnover rates were about the same in academic and nonacademic practices.
Among the more unexpected findings, however, is that academic HM practices tend to employ a higher proportion of women (44%) than nonacademic practices (35%). In addition, academic practices employed a wider range of staffing models, with only 43% of practices using shift-based staffing, compared with 78% of nonacademic respondents. Similarly, only 47% of academic groups provided on-site coverage at night, compared with 81% of nonacademic groups.
Additional differences between the way academic and nonacademic HM groups staff their programs are shown in the table, “Other Staffing Arrangements.” While the use of nurse practitioners and physician assistants (PA) was similar for academic and nonacademic practices, academic groups were much less likely to utilize nocturnists, and far more likely to have a nonphysician first responder at night (resident, nonphysician provider/PA, or other) than nonacademic groups.
It will be interesting to follow these trends over time. Because of new resident work-hour limits that went into effect in July, SHM Practice Analysis Committee (PAC) member Andrew White, MD, expects that there will be very few places that continue to use residents to cross-cover at night. “I suspect most academic centers have or will hire nocturnists,” he says, “but we’ll see.”
On the other hand, PAC member Scarlett Blue, RN, believes that continued growth in HM, coupled with a competitive job market, could result in increased use of nonphysician first responders at night—and in general. “Hospital medicine group leaders who are looking for alternative ways to meet the supply-demand conundrum may find a blended physician-NP/PA team to be one such answer,” she says.
Finally, the clinical services provided by academic HM groups vary from their nonacademic counterparts in some other important ways. Only 25% of academic practices provide care for ICU patients, compared with 78% of nonacademic practices, while 75% of academic groups perform procedures, compared with only 52% of nonacademic groups. And while the overwhelming majority of both academic and nonacademic practices provide surgical comanagement, academic practices were more than twice as likely to provide comanagement for medical subspecialty patients (45%, compared with 20% for nonacademic practices).
PAC member Troy Ahlstrom, MD, explains, tongue-in-cheek, that “academic hospitalists don’t do procedures because they have oodles of residents, fellows, and interventional radiologists to do them instead, and academics do more medical comanagement because the subspecialist who only does Waldenstrom’s macroglobulinemia probably doesn’t do diabetes.”
Whatever the reason, there are meaningful differences between academic and nonacademic HM practices that bear watching over time. You can help us identify and track these differences by ensuring that your group participates in SHM’s annual State of Hospital Medicine survey, launching this month.
The 2011 State of Hospital Medicine report offers some tantalizing insights into the operation of academic hospital medicine practices and how they compare with their nonacademic peers. Some results are not surprising, such as the fact that academic hospital medicine groups tend to be larger than nonacademic groups, and that compensation and clinical-FTE-adjusted productivity both tend to be lower for academic hospitalists. Interestingly, turnover rates were about the same in academic and nonacademic practices.
Among the more unexpected findings, however, is that academic HM practices tend to employ a higher proportion of women (44%) than nonacademic practices (35%). In addition, academic practices employed a wider range of staffing models, with only 43% of practices using shift-based staffing, compared with 78% of nonacademic respondents. Similarly, only 47% of academic groups provided on-site coverage at night, compared with 81% of nonacademic groups.
Additional differences between the way academic and nonacademic HM groups staff their programs are shown in the table, “Other Staffing Arrangements.” While the use of nurse practitioners and physician assistants (PA) was similar for academic and nonacademic practices, academic groups were much less likely to utilize nocturnists, and far more likely to have a nonphysician first responder at night (resident, nonphysician provider/PA, or other) than nonacademic groups.
It will be interesting to follow these trends over time. Because of new resident work-hour limits that went into effect in July, SHM Practice Analysis Committee (PAC) member Andrew White, MD, expects that there will be very few places that continue to use residents to cross-cover at night. “I suspect most academic centers have or will hire nocturnists,” he says, “but we’ll see.”
On the other hand, PAC member Scarlett Blue, RN, believes that continued growth in HM, coupled with a competitive job market, could result in increased use of nonphysician first responders at night—and in general. “Hospital medicine group leaders who are looking for alternative ways to meet the supply-demand conundrum may find a blended physician-NP/PA team to be one such answer,” she says.
Finally, the clinical services provided by academic HM groups vary from their nonacademic counterparts in some other important ways. Only 25% of academic practices provide care for ICU patients, compared with 78% of nonacademic practices, while 75% of academic groups perform procedures, compared with only 52% of nonacademic groups. And while the overwhelming majority of both academic and nonacademic practices provide surgical comanagement, academic practices were more than twice as likely to provide comanagement for medical subspecialty patients (45%, compared with 20% for nonacademic practices).
PAC member Troy Ahlstrom, MD, explains, tongue-in-cheek, that “academic hospitalists don’t do procedures because they have oodles of residents, fellows, and interventional radiologists to do them instead, and academics do more medical comanagement because the subspecialist who only does Waldenstrom’s macroglobulinemia probably doesn’t do diabetes.”
Whatever the reason, there are meaningful differences between academic and nonacademic HM practices that bear watching over time. You can help us identify and track these differences by ensuring that your group participates in SHM’s annual State of Hospital Medicine survey, launching this month.
HM on the Move

Robert Wachter, MD, MHM, has been named a 2012 Fulbright Scholar. Dr. Wachter is professor and associate chairman of the Department of Medicine at the University of California at San Francisco. He will study patient safety with Charles Vincent, director of the Imperial Centre for Patient Safety and Service Quality and the Clinical Safety Research Unit at Imperial College, London.
Trustees at Bamberg County Hospital in South Carolina have honored Maggie Shatilla, MD, for her service to the hospital. Dr. Shatilla was recognized for her “outstanding leadership” and her “valuable and memorable humanitarian services” to the hospital and its patients. Dr. Shatilla served in the hospitalist position until October, when the board voted to end the HM program.
Jeffrey Sperring, MD, has been named president and chief executive officer of Riley Hospital for Children at Indiana University Health. Dr. Sperring joined IU Health in 2002 and has served as chief medical officer of Riley at IU Health since 2009. Marilyn Cox has been serving as interim president and CEO and will now return to her role as chief nursing officer and senior vice president for nursing and patient care services.
Gunjana Bhandari, MD, has been selected as medical director of Michigan-based Bronson Internal Medicine Hospital Specialists, a new hospitalist program at Bronson Battle Creek hospital.

Bert Puckett Wall, MD, has been named a winner of one of TeamHealth’s 2011 Medical Director of the Year awards. Dr. Wall is medical director of the hospital medi medicine program at Upson Regional Medical Center in Thomaston, Ga. Dr. Wall is one of 10 individuals honored for excellence in physician leadership.
Robert Wachter, MD, MHM, has been named a 2012 Fulbright Scholar. Dr. Wachter is professor and associate chairman of the Department of Medicine at the University of California at San Francisco. He will study patient safety with Charles Vincent, director of the Imperial Centre for Patient Safety and Service Quality and the Clinical Safety Research Unit at Imperial College, London.
Trustees at Bamberg County Hospital in South Carolina have honored Maggie Shatilla, MD, for her service to the hospital. Dr. Shatilla was recognized for her “outstanding leadership” and her “valuable and memorable humanitarian services” to the hospital and its patients. Dr. Shatilla served in the hospitalist position until October, when the board voted to end the HM program.
Jeffrey Sperring, MD, has been named president and chief executive officer of Riley Hospital for Children at Indiana University Health. Dr. Sperring joined IU Health in 2002 and has served as chief medical officer of Riley at IU Health since 2009. Marilyn Cox has been serving as interim president and CEO and will now return to her role as chief nursing officer and senior vice president for nursing and patient care services.
Gunjana Bhandari, MD, has been selected as medical director of Michigan-based Bronson Internal Medicine Hospital Specialists, a new hospitalist program at Bronson Battle Creek hospital.
Bert Puckett Wall, MD, has been named a winner of one of TeamHealth’s 2011 Medical Director of the Year awards. Dr. Wall is medical director of the hospital medi medicine program at Upson Regional Medical Center in Thomaston, Ga. Dr. Wall is one of 10 individuals honored for excellence in physician leadership.
Robert Wachter, MD, MHM, has been named a 2012 Fulbright Scholar. Dr. Wachter is professor and associate chairman of the Department of Medicine at the University of California at San Francisco. He will study patient safety with Charles Vincent, director of the Imperial Centre for Patient Safety and Service Quality and the Clinical Safety Research Unit at Imperial College, London.
Trustees at Bamberg County Hospital in South Carolina have honored Maggie Shatilla, MD, for her service to the hospital. Dr. Shatilla was recognized for her “outstanding leadership” and her “valuable and memorable humanitarian services” to the hospital and its patients. Dr. Shatilla served in the hospitalist position until October, when the board voted to end the HM program.
Jeffrey Sperring, MD, has been named president and chief executive officer of Riley Hospital for Children at Indiana University Health. Dr. Sperring joined IU Health in 2002 and has served as chief medical officer of Riley at IU Health since 2009. Marilyn Cox has been serving as interim president and CEO and will now return to her role as chief nursing officer and senior vice president for nursing and patient care services.
Gunjana Bhandari, MD, has been selected as medical director of Michigan-based Bronson Internal Medicine Hospital Specialists, a new hospitalist program at Bronson Battle Creek hospital.
Bert Puckett Wall, MD, has been named a winner of one of TeamHealth’s 2011 Medical Director of the Year awards. Dr. Wall is medical director of the hospital medi medicine program at Upson Regional Medical Center in Thomaston, Ga. Dr. Wall is one of 10 individuals honored for excellence in physician leadership.
Pediatric Readmissions Differ from Adult Readmissions

Clinical question: What is the epidemiology of 15-day readmissions to a children’s hospital?
Background: Readmissions are a common event in the adult population. Given the national focus on accountable care across the continuum, the Centers for Medicare & Medicaid Services (CMS) has devoted increasing attention to readmissions as a reportable quality metric in certain conditions and a target for improvement. Recommendations for pediatric patients are currently not available, primarily due to limited evidence.
Study design: Retrospective chart review.
Setting: Tertiary-care children’s hospital.
Synopsis: Of the 30,188 admissions over a two-year period, 2,546 (8.4%) resulted in readmission within 15 days. There were a total of 1,435 individual patients who were readmitted, for an average readmission rate of 1.8 per patient. Oncology patients represented the most likely group of patients to be readmitted (13.9%) and had the most number of readmissions per patient (4.1). Children with acute infectious disease, newborns, and patients with neurologic diseases represented 11.4%, 11.1%, and 10% of the readmitted patients, respectively.
Children with short-bowel syndrome and biliary atresia had a high number of readmissions per patient: 3.9 and 3.8, respectively. The majority of readmissions were unplanned (79.4%) and occurred in patients with an underlying chronic condition (78%). Readmissions 7 days from discharge accounted for 59.5% of the total, with the remaining 40.5% occurring between eight and 15 days of discharge.
This study provides one of the more comprehensive pictures of readmissions to a children’s hospital. Although the data are limited by an inability to account for readmissions to and from other facilities, they nonetheless clearly differentiate pediatric readmissions from those in an adult population.
Bottom line: Pediatric readmissions are quantitatively and qualitatively different from adult readmissions.
Citation: Gay JC, Hain PD, Grantham JA, Saville BR. Epidemiology of 15-day readmissions to a children’s hospital. Pediatrics. 2011;127:e1-e8.
Clinical question: What is the epidemiology of 15-day readmissions to a children’s hospital?
Background: Readmissions are a common event in the adult population. Given the national focus on accountable care across the continuum, the Centers for Medicare & Medicaid Services (CMS) has devoted increasing attention to readmissions as a reportable quality metric in certain conditions and a target for improvement. Recommendations for pediatric patients are currently not available, primarily due to limited evidence.
Study design: Retrospective chart review.
Setting: Tertiary-care children’s hospital.
Synopsis: Of the 30,188 admissions over a two-year period, 2,546 (8.4%) resulted in readmission within 15 days. There were a total of 1,435 individual patients who were readmitted, for an average readmission rate of 1.8 per patient. Oncology patients represented the most likely group of patients to be readmitted (13.9%) and had the most number of readmissions per patient (4.1). Children with acute infectious disease, newborns, and patients with neurologic diseases represented 11.4%, 11.1%, and 10% of the readmitted patients, respectively.
Children with short-bowel syndrome and biliary atresia had a high number of readmissions per patient: 3.9 and 3.8, respectively. The majority of readmissions were unplanned (79.4%) and occurred in patients with an underlying chronic condition (78%). Readmissions 7 days from discharge accounted for 59.5% of the total, with the remaining 40.5% occurring between eight and 15 days of discharge.
This study provides one of the more comprehensive pictures of readmissions to a children’s hospital. Although the data are limited by an inability to account for readmissions to and from other facilities, they nonetheless clearly differentiate pediatric readmissions from those in an adult population.
Bottom line: Pediatric readmissions are quantitatively and qualitatively different from adult readmissions.
Citation: Gay JC, Hain PD, Grantham JA, Saville BR. Epidemiology of 15-day readmissions to a children’s hospital. Pediatrics. 2011;127:e1-e8.
Clinical question: What is the epidemiology of 15-day readmissions to a children’s hospital?
Background: Readmissions are a common event in the adult population. Given the national focus on accountable care across the continuum, the Centers for Medicare & Medicaid Services (CMS) has devoted increasing attention to readmissions as a reportable quality metric in certain conditions and a target for improvement. Recommendations for pediatric patients are currently not available, primarily due to limited evidence.
Study design: Retrospective chart review.
Setting: Tertiary-care children’s hospital.
Synopsis: Of the 30,188 admissions over a two-year period, 2,546 (8.4%) resulted in readmission within 15 days. There were a total of 1,435 individual patients who were readmitted, for an average readmission rate of 1.8 per patient. Oncology patients represented the most likely group of patients to be readmitted (13.9%) and had the most number of readmissions per patient (4.1). Children with acute infectious disease, newborns, and patients with neurologic diseases represented 11.4%, 11.1%, and 10% of the readmitted patients, respectively.
Children with short-bowel syndrome and biliary atresia had a high number of readmissions per patient: 3.9 and 3.8, respectively. The majority of readmissions were unplanned (79.4%) and occurred in patients with an underlying chronic condition (78%). Readmissions 7 days from discharge accounted for 59.5% of the total, with the remaining 40.5% occurring between eight and 15 days of discharge.
This study provides one of the more comprehensive pictures of readmissions to a children’s hospital. Although the data are limited by an inability to account for readmissions to and from other facilities, they nonetheless clearly differentiate pediatric readmissions from those in an adult population.
Bottom line: Pediatric readmissions are quantitatively and qualitatively different from adult readmissions.
Citation: Gay JC, Hain PD, Grantham JA, Saville BR. Epidemiology of 15-day readmissions to a children’s hospital. Pediatrics. 2011;127:e1-e8.
Pediatric Potential

Dan Hale, MD, FAAP, started to seriously consider a career in medicine while in college. A summer job as a camp counselor helped convince him he’d found his calling.
“I realized how much I enjoyed spending time with children,” says Dr. Hale, who began his two-year Team Hospitalist term in May. “Everything is new for them, and they bring the joy of life to everything they do. That’s when I really began thinking about pediatrics.”
After residency, he joined the staff at Intermed Pediatrics in Portland, Maine. He split his time seeing patients in the office and in the hospital. Within three years, he made the transition to HM.
“Once I was exposed to hospitals, I knew that’s where I wanted to be,” says Dr. Hale, a pediatric hospitalist with Floating Hospital for Children at Tufts Medical Center in Boston and medical director of Floating’s pediatric hospitalist program at Lawrence (Mass.) General Hospital.
“I’ve really enjoyed being a part of this new field of pediatric hospital medicine,” he adds. “There is humongous potential for change, and I’m excited about what those of us in the hospital can do to improve healthcare.”
Floating Hospital has outreach programs at four community hospitals. How do those programs work?
If a child is very sick and requires a pediatric intensive care unit, they go to Boston to the Floating Hospital PICU. But because pediatric hospitalists from Floating staff these four other sites 24 hours a day, there is always someone there to see these patients in hopes of keeping them in their own community.
What is the biggest advantage of those affiliations?
In pediatric medicine, even more than adult medicine, it’s a family affair. It’s a big deal if a family has to drive over an hour into the city to get a child medical care. It can be a foreign environment and families have to find a place to stay. Floating’s philosophy is to provide optimal care for pediatric patients wherever they are. It’s a very unique solution to modern healthcare.
What types of care can Lawrence General provide now that it couldn’t prior to its affiliation with Floating Hospital?
Asthma and bronchiolitis are very common pediatric illnesses in winter, and they require very close monitoring. The hospitalists’ presence helps us keep those patients in the community hospital.
Can you quantify how many more patients are at Lawrence General?
Since starting the program in January, we decreased transfers for common pediatric conditions by 50%—from 10 pediatric transfers a month, on average, to about five per month.
Each community hospital’s pediatric HM program has its own medical director. Do you work with each other?
We work very closely together. Because every hospital is different, we learn from each other. We see what works and what doesn’t work at each site, and we build on that.
Can you give an example of how that network has improved the quality of care?
We have an asthma protocol developed by Floating Hospital for Children, and it was instituted at one of the community sites. It worked so well, we adopted a similar program at Lawrence General. It’s a perfect example of tailoring something that works well at one hospital to fit your patients’ needs rather than reinventing the wheel.
Did you have to overcome any obstacles when the affiliation launched?
The biggest hurdle was earning the trust of the nurses, the referring pediatricians, and the patients themselves. We started family-centered rounds, where we meet with every patient, their family, and the nurse to come up with a daily care plan. Slowly, by taking excellent care of every one of those patients and communicating at every single admission with the primary-care physician (PCP), we earned the trust of everyone.
Do you think these types of affiliations will become more common?
Yes. It’s truly a win-win situation. Lawrence General wins because they’re keeping more patients in the community. The patients win because they are close to home. Tufts Medical Center wins because it’s more involved in the community.
How pleased are PCPs in the community?
It’s definitely a win for them, too. If there is someone in their office that requires hospitalization, they can call the hospitalist and refer the patient directly to the pediatric inpatient unit, so there’s no going to the emergency room and no wait time. Also, if a pediatrician can refer to a hospitalist, they’re not leaving their office early to go see someone at the hospital. If they know their patient is getting really good care at the hospital, they can focus on delivering better, more efficient care in their practice.
Do you have to take a different approach to care because you are treating children?
The biggest difference is that you have two patients, the child and their family, so you have to spend more time explaining everything you do. No. 2, because you’re treating a child, you have to make sure you respect them by communicating with them and examining them in a nonthreatening way. The best part is, you’re required to have fun every day.
What is the biggest challenge pediatric hospitalists face?
The standardizing of care is new to our field, but it’s very important. Protocols and guidelines are still in development. I think it’s off to a good start, but there are still many new ways of thinking.
What is your biggest professional reward?
Because we’re a new field, the reward is seeing our field grow every year in terms of the number of pediatric hospitalists. Another is what we’re doing at Lawrence General, and seeing how our field keeps expanding and improving pediatric care in hospitals across the country. To have a job I can go to that’s so enjoyable, and at the end of every day I’m helping a smiling child, that makes it all worthwhile.
Mark Leiser is a freelance writer based in New Jersey.
Dan Hale, MD, FAAP, started to seriously consider a career in medicine while in college. A summer job as a camp counselor helped convince him he’d found his calling.
“I realized how much I enjoyed spending time with children,” says Dr. Hale, who began his two-year Team Hospitalist term in May. “Everything is new for them, and they bring the joy of life to everything they do. That’s when I really began thinking about pediatrics.”
After residency, he joined the staff at Intermed Pediatrics in Portland, Maine. He split his time seeing patients in the office and in the hospital. Within three years, he made the transition to HM.
“Once I was exposed to hospitals, I knew that’s where I wanted to be,” says Dr. Hale, a pediatric hospitalist with Floating Hospital for Children at Tufts Medical Center in Boston and medical director of Floating’s pediatric hospitalist program at Lawrence (Mass.) General Hospital.
“I’ve really enjoyed being a part of this new field of pediatric hospital medicine,” he adds. “There is humongous potential for change, and I’m excited about what those of us in the hospital can do to improve healthcare.”
Floating Hospital has outreach programs at four community hospitals. How do those programs work?
If a child is very sick and requires a pediatric intensive care unit, they go to Boston to the Floating Hospital PICU. But because pediatric hospitalists from Floating staff these four other sites 24 hours a day, there is always someone there to see these patients in hopes of keeping them in their own community.
What is the biggest advantage of those affiliations?
In pediatric medicine, even more than adult medicine, it’s a family affair. It’s a big deal if a family has to drive over an hour into the city to get a child medical care. It can be a foreign environment and families have to find a place to stay. Floating’s philosophy is to provide optimal care for pediatric patients wherever they are. It’s a very unique solution to modern healthcare.
What types of care can Lawrence General provide now that it couldn’t prior to its affiliation with Floating Hospital?
Asthma and bronchiolitis are very common pediatric illnesses in winter, and they require very close monitoring. The hospitalists’ presence helps us keep those patients in the community hospital.
Can you quantify how many more patients are at Lawrence General?
Since starting the program in January, we decreased transfers for common pediatric conditions by 50%—from 10 pediatric transfers a month, on average, to about five per month.
Each community hospital’s pediatric HM program has its own medical director. Do you work with each other?
We work very closely together. Because every hospital is different, we learn from each other. We see what works and what doesn’t work at each site, and we build on that.
Can you give an example of how that network has improved the quality of care?
We have an asthma protocol developed by Floating Hospital for Children, and it was instituted at one of the community sites. It worked so well, we adopted a similar program at Lawrence General. It’s a perfect example of tailoring something that works well at one hospital to fit your patients’ needs rather than reinventing the wheel.
Did you have to overcome any obstacles when the affiliation launched?
The biggest hurdle was earning the trust of the nurses, the referring pediatricians, and the patients themselves. We started family-centered rounds, where we meet with every patient, their family, and the nurse to come up with a daily care plan. Slowly, by taking excellent care of every one of those patients and communicating at every single admission with the primary-care physician (PCP), we earned the trust of everyone.
Do you think these types of affiliations will become more common?
Yes. It’s truly a win-win situation. Lawrence General wins because they’re keeping more patients in the community. The patients win because they are close to home. Tufts Medical Center wins because it’s more involved in the community.
How pleased are PCPs in the community?
It’s definitely a win for them, too. If there is someone in their office that requires hospitalization, they can call the hospitalist and refer the patient directly to the pediatric inpatient unit, so there’s no going to the emergency room and no wait time. Also, if a pediatrician can refer to a hospitalist, they’re not leaving their office early to go see someone at the hospital. If they know their patient is getting really good care at the hospital, they can focus on delivering better, more efficient care in their practice.
Do you have to take a different approach to care because you are treating children?
The biggest difference is that you have two patients, the child and their family, so you have to spend more time explaining everything you do. No. 2, because you’re treating a child, you have to make sure you respect them by communicating with them and examining them in a nonthreatening way. The best part is, you’re required to have fun every day.
What is the biggest challenge pediatric hospitalists face?
The standardizing of care is new to our field, but it’s very important. Protocols and guidelines are still in development. I think it’s off to a good start, but there are still many new ways of thinking.
What is your biggest professional reward?
Because we’re a new field, the reward is seeing our field grow every year in terms of the number of pediatric hospitalists. Another is what we’re doing at Lawrence General, and seeing how our field keeps expanding and improving pediatric care in hospitals across the country. To have a job I can go to that’s so enjoyable, and at the end of every day I’m helping a smiling child, that makes it all worthwhile.
Mark Leiser is a freelance writer based in New Jersey.
Dan Hale, MD, FAAP, started to seriously consider a career in medicine while in college. A summer job as a camp counselor helped convince him he’d found his calling.
“I realized how much I enjoyed spending time with children,” says Dr. Hale, who began his two-year Team Hospitalist term in May. “Everything is new for them, and they bring the joy of life to everything they do. That’s when I really began thinking about pediatrics.”
After residency, he joined the staff at Intermed Pediatrics in Portland, Maine. He split his time seeing patients in the office and in the hospital. Within three years, he made the transition to HM.
“Once I was exposed to hospitals, I knew that’s where I wanted to be,” says Dr. Hale, a pediatric hospitalist with Floating Hospital for Children at Tufts Medical Center in Boston and medical director of Floating’s pediatric hospitalist program at Lawrence (Mass.) General Hospital.
“I’ve really enjoyed being a part of this new field of pediatric hospital medicine,” he adds. “There is humongous potential for change, and I’m excited about what those of us in the hospital can do to improve healthcare.”
Floating Hospital has outreach programs at four community hospitals. How do those programs work?
If a child is very sick and requires a pediatric intensive care unit, they go to Boston to the Floating Hospital PICU. But because pediatric hospitalists from Floating staff these four other sites 24 hours a day, there is always someone there to see these patients in hopes of keeping them in their own community.
What is the biggest advantage of those affiliations?
In pediatric medicine, even more than adult medicine, it’s a family affair. It’s a big deal if a family has to drive over an hour into the city to get a child medical care. It can be a foreign environment and families have to find a place to stay. Floating’s philosophy is to provide optimal care for pediatric patients wherever they are. It’s a very unique solution to modern healthcare.
What types of care can Lawrence General provide now that it couldn’t prior to its affiliation with Floating Hospital?
Asthma and bronchiolitis are very common pediatric illnesses in winter, and they require very close monitoring. The hospitalists’ presence helps us keep those patients in the community hospital.
Can you quantify how many more patients are at Lawrence General?
Since starting the program in January, we decreased transfers for common pediatric conditions by 50%—from 10 pediatric transfers a month, on average, to about five per month.
Each community hospital’s pediatric HM program has its own medical director. Do you work with each other?
We work very closely together. Because every hospital is different, we learn from each other. We see what works and what doesn’t work at each site, and we build on that.
Can you give an example of how that network has improved the quality of care?
We have an asthma protocol developed by Floating Hospital for Children, and it was instituted at one of the community sites. It worked so well, we adopted a similar program at Lawrence General. It’s a perfect example of tailoring something that works well at one hospital to fit your patients’ needs rather than reinventing the wheel.
Did you have to overcome any obstacles when the affiliation launched?
The biggest hurdle was earning the trust of the nurses, the referring pediatricians, and the patients themselves. We started family-centered rounds, where we meet with every patient, their family, and the nurse to come up with a daily care plan. Slowly, by taking excellent care of every one of those patients and communicating at every single admission with the primary-care physician (PCP), we earned the trust of everyone.
Do you think these types of affiliations will become more common?
Yes. It’s truly a win-win situation. Lawrence General wins because they’re keeping more patients in the community. The patients win because they are close to home. Tufts Medical Center wins because it’s more involved in the community.
How pleased are PCPs in the community?
It’s definitely a win for them, too. If there is someone in their office that requires hospitalization, they can call the hospitalist and refer the patient directly to the pediatric inpatient unit, so there’s no going to the emergency room and no wait time. Also, if a pediatrician can refer to a hospitalist, they’re not leaving their office early to go see someone at the hospital. If they know their patient is getting really good care at the hospital, they can focus on delivering better, more efficient care in their practice.
Do you have to take a different approach to care because you are treating children?
The biggest difference is that you have two patients, the child and their family, so you have to spend more time explaining everything you do. No. 2, because you’re treating a child, you have to make sure you respect them by communicating with them and examining them in a nonthreatening way. The best part is, you’re required to have fun every day.
What is the biggest challenge pediatric hospitalists face?
The standardizing of care is new to our field, but it’s very important. Protocols and guidelines are still in development. I think it’s off to a good start, but there are still many new ways of thinking.
What is your biggest professional reward?
Because we’re a new field, the reward is seeing our field grow every year in terms of the number of pediatric hospitalists. Another is what we’re doing at Lawrence General, and seeing how our field keeps expanding and improving pediatric care in hospitals across the country. To have a job I can go to that’s so enjoyable, and at the end of every day I’m helping a smiling child, that makes it all worthwhile.
Mark Leiser is a freelance writer based in New Jersey.
Life in the Gap
This year will be a pivotal one in the brave new world of healthcare reform. While fee-for-service and volume-based reimbursement will not disappear, most would concede that those programs’ days are numbered, as public and private payors inexorably migrate to value-based payment mechanisms that hold physicians and hospitals increasingly accountable for more coordinated, safer, higher-quality, and more efficient care.
The Centers for Medicare & Medicaid Services (CMS) is busy putting more provider skin in the game as its shifts from volume to value. It has ramped up its Hospital Value-Based Purchasing Plan (VBP) by adding a third performance domain—quality outcome metrics—to the existing domains of core measure care processes and patient satisfaction scores. VBP will penalize hospitals for preventable readmissions. Armed with a new innovation center established by the Affordable Care Act, CMS is accelerating its experiments with such care and reimbursement models as bundled payments, accountable-care organizations (ACOs), and medical homes. Can it be very long before invitations for provider participation become subpoenas?
While the brunt of value-based reimbursement incentives have so far been directed at hospitals, “At what point will this shift begin putting the practicing physician at risk?” asks Sean Muldoon, MD, MPH, FCCP, FACPM, senior vice president and chief medical officer of Louisville, Ky.-based Kindred Healthcare’s hospital division.
“We’re living in a time of great uncertainty—from the economic, regulatory, and legislative standpoints—and we have to make the best decisions based on what we currently believe is coming,” says Ron Greeno, MD, FCCP, MHM, chief medical officer of Cogent HMG and chair of SHM’s Public Policy Committee.
As change un-folds, some see great opportunity. “Hospitalists are in an enviable position as drivers of change,” says David B. Nash, MD, MBA, professor of health policy and dean of Thomas Jefferson University’s School of Population Health in Philadelphia. “As frontline troops of hospital-based care, they are going to play a critical role in ensuring the most efficient patient stay possible to help hospitals survive under new reimbursement models.”
Evolving Environment
Confidence that HM is well-positioned to drive value is especially welcome as the field looks back on 15 years of its existence in a soul-searching appraisal of just how much value it has driven thus far. The evidence is mixed. The profession’s clearest documented success has been preventing delays in patient discharge. That achievement has yet to be buttressed by clear evidence of concomitant gains in quality attributable to hospitalist care.
In fact, a widely publicized study in the Annals of Internal Medicine this year has caused a good deal of hand-wringing, as it suggests that HM-driven efficiency improvements may simply be attributable to shifting costs elsewhere because their patients tend to have higher readmission rates.1
That finding highlights a defining challenge of healthcare reform: how to achieve better value (quality per unit cost) within a care delivery and payment infrastructure that still pays for fragmented care. That infrastructure is trying to achieve the integration that is needed—both in the hospital and post-discharge, with preventive and acute care, at the individual patient and population levels.
“We’re being asked to prepare for an entirely different system, one which cares for populations of patients and tries to keep them out of the hospital,” Dr. Greeno says, “but our payment encourages just the opposite.”
Transitioning to value-based models while still functioning largely in a volume-based, fee-for-service environment is much like having one foot on the dock and one foot on a boat that is leaving the dock. That’s how the American Hospital Association put it in a report it released in September, “Hospitals and Care Systems of the Future.” Providers are struggling to navigate “life in the gap” between a volume-based “first curve” environment that inadequately rewards innovation and a “second curve” environment in which reimbursement is integrally tied to delivering coordinated care that demonstrates value, the AHA notes, using terminology coined by healthcare futurist Ian Morrison.
Navigation
Hospitalists will need to seize collaborative opportunities with hospitals to develop strategies to navigate this “life in the gap” during the transition to value-based reimbursement models of the second curve. As Jeff Glasheen, MD, SFHM, physician editor of The Hospitalist, provocatively wrote in his September 2011 column: “We must improve the quality of care to levels that, if necessary, Medicare would happily pay more for. This must be our singular goal” (see “Fiddling As HM Burns,” The Hospitalist). Assuming that money will follow quality, hospitals should be willing to invest in hospitalist-led processes and safety improvement activities, which likely will be the standard of care tomorrow, even if they do not turn a profit today.
Hospitalists will be the “effector arm” of crucial care-management practices under new payment models, Dr. Nash predicts. He says HM should focus on helping to make the model work—for example, championing evidence-based protocols and approved drug formularies, eliminating wasteful tests, and promoting better medication reconciliation and care transitions (see “Reconciliation Act,”).“Because they are on-site full-time, hospitalists are in the cat-bird seat to teach other attending physicians about the importance of reading from the same hymnal on these best practices,” he adds.
Dr. Greeno agrees reform needs to be cost-effective as well as patient-focused.
“The pressure on hospitalists to demonstrate our value has never been higher,” he says, urging hospitalists to pay particular attention to key features of reform to which they are already accountable, such as improving patient satisfaction and promoting evidence-based interventions that prevent readmissions and hospital-acquired conditions (see “Priorities in an Age of Reform,” left).
Dr. Greeno notes that SHM’s advocacy activities have been ramped up significantly to stay on top of reform developments—and ensure that policymakers hear hospitalists’ voices. “If we want to have a positive impact, we must track these changes, understand them, influence them, implement them, and make them successful,” he says. “That’s the challenge our field faces. There’s no physician organization that knows more about what goes on in a hospital than we do, and we will help policymakers and hospitals to make intelligent decisions.”
Chris Guadagnino is a freelance medical writer based in Philadelphia.
Reference
This year will be a pivotal one in the brave new world of healthcare reform. While fee-for-service and volume-based reimbursement will not disappear, most would concede that those programs’ days are numbered, as public and private payors inexorably migrate to value-based payment mechanisms that hold physicians and hospitals increasingly accountable for more coordinated, safer, higher-quality, and more efficient care.
The Centers for Medicare & Medicaid Services (CMS) is busy putting more provider skin in the game as its shifts from volume to value. It has ramped up its Hospital Value-Based Purchasing Plan (VBP) by adding a third performance domain—quality outcome metrics—to the existing domains of core measure care processes and patient satisfaction scores. VBP will penalize hospitals for preventable readmissions. Armed with a new innovation center established by the Affordable Care Act, CMS is accelerating its experiments with such care and reimbursement models as bundled payments, accountable-care organizations (ACOs), and medical homes. Can it be very long before invitations for provider participation become subpoenas?
While the brunt of value-based reimbursement incentives have so far been directed at hospitals, “At what point will this shift begin putting the practicing physician at risk?” asks Sean Muldoon, MD, MPH, FCCP, FACPM, senior vice president and chief medical officer of Louisville, Ky.-based Kindred Healthcare’s hospital division.
“We’re living in a time of great uncertainty—from the economic, regulatory, and legislative standpoints—and we have to make the best decisions based on what we currently believe is coming,” says Ron Greeno, MD, FCCP, MHM, chief medical officer of Cogent HMG and chair of SHM’s Public Policy Committee.
As change un-folds, some see great opportunity. “Hospitalists are in an enviable position as drivers of change,” says David B. Nash, MD, MBA, professor of health policy and dean of Thomas Jefferson University’s School of Population Health in Philadelphia. “As frontline troops of hospital-based care, they are going to play a critical role in ensuring the most efficient patient stay possible to help hospitals survive under new reimbursement models.”
Evolving Environment
Confidence that HM is well-positioned to drive value is especially welcome as the field looks back on 15 years of its existence in a soul-searching appraisal of just how much value it has driven thus far. The evidence is mixed. The profession’s clearest documented success has been preventing delays in patient discharge. That achievement has yet to be buttressed by clear evidence of concomitant gains in quality attributable to hospitalist care.
In fact, a widely publicized study in the Annals of Internal Medicine this year has caused a good deal of hand-wringing, as it suggests that HM-driven efficiency improvements may simply be attributable to shifting costs elsewhere because their patients tend to have higher readmission rates.1
That finding highlights a defining challenge of healthcare reform: how to achieve better value (quality per unit cost) within a care delivery and payment infrastructure that still pays for fragmented care. That infrastructure is trying to achieve the integration that is needed—both in the hospital and post-discharge, with preventive and acute care, at the individual patient and population levels.
“We’re being asked to prepare for an entirely different system, one which cares for populations of patients and tries to keep them out of the hospital,” Dr. Greeno says, “but our payment encourages just the opposite.”
Transitioning to value-based models while still functioning largely in a volume-based, fee-for-service environment is much like having one foot on the dock and one foot on a boat that is leaving the dock. That’s how the American Hospital Association put it in a report it released in September, “Hospitals and Care Systems of the Future.” Providers are struggling to navigate “life in the gap” between a volume-based “first curve” environment that inadequately rewards innovation and a “second curve” environment in which reimbursement is integrally tied to delivering coordinated care that demonstrates value, the AHA notes, using terminology coined by healthcare futurist Ian Morrison.
Navigation
Hospitalists will need to seize collaborative opportunities with hospitals to develop strategies to navigate this “life in the gap” during the transition to value-based reimbursement models of the second curve. As Jeff Glasheen, MD, SFHM, physician editor of The Hospitalist, provocatively wrote in his September 2011 column: “We must improve the quality of care to levels that, if necessary, Medicare would happily pay more for. This must be our singular goal” (see “Fiddling As HM Burns,” The Hospitalist). Assuming that money will follow quality, hospitals should be willing to invest in hospitalist-led processes and safety improvement activities, which likely will be the standard of care tomorrow, even if they do not turn a profit today.
Hospitalists will be the “effector arm” of crucial care-management practices under new payment models, Dr. Nash predicts. He says HM should focus on helping to make the model work—for example, championing evidence-based protocols and approved drug formularies, eliminating wasteful tests, and promoting better medication reconciliation and care transitions (see “Reconciliation Act,”).“Because they are on-site full-time, hospitalists are in the cat-bird seat to teach other attending physicians about the importance of reading from the same hymnal on these best practices,” he adds.
Dr. Greeno agrees reform needs to be cost-effective as well as patient-focused.
“The pressure on hospitalists to demonstrate our value has never been higher,” he says, urging hospitalists to pay particular attention to key features of reform to which they are already accountable, such as improving patient satisfaction and promoting evidence-based interventions that prevent readmissions and hospital-acquired conditions (see “Priorities in an Age of Reform,” left).
Dr. Greeno notes that SHM’s advocacy activities have been ramped up significantly to stay on top of reform developments—and ensure that policymakers hear hospitalists’ voices. “If we want to have a positive impact, we must track these changes, understand them, influence them, implement them, and make them successful,” he says. “That’s the challenge our field faces. There’s no physician organization that knows more about what goes on in a hospital than we do, and we will help policymakers and hospitals to make intelligent decisions.”
Chris Guadagnino is a freelance medical writer based in Philadelphia.
Reference
This year will be a pivotal one in the brave new world of healthcare reform. While fee-for-service and volume-based reimbursement will not disappear, most would concede that those programs’ days are numbered, as public and private payors inexorably migrate to value-based payment mechanisms that hold physicians and hospitals increasingly accountable for more coordinated, safer, higher-quality, and more efficient care.
The Centers for Medicare & Medicaid Services (CMS) is busy putting more provider skin in the game as its shifts from volume to value. It has ramped up its Hospital Value-Based Purchasing Plan (VBP) by adding a third performance domain—quality outcome metrics—to the existing domains of core measure care processes and patient satisfaction scores. VBP will penalize hospitals for preventable readmissions. Armed with a new innovation center established by the Affordable Care Act, CMS is accelerating its experiments with such care and reimbursement models as bundled payments, accountable-care organizations (ACOs), and medical homes. Can it be very long before invitations for provider participation become subpoenas?
While the brunt of value-based reimbursement incentives have so far been directed at hospitals, “At what point will this shift begin putting the practicing physician at risk?” asks Sean Muldoon, MD, MPH, FCCP, FACPM, senior vice president and chief medical officer of Louisville, Ky.-based Kindred Healthcare’s hospital division.
“We’re living in a time of great uncertainty—from the economic, regulatory, and legislative standpoints—and we have to make the best decisions based on what we currently believe is coming,” says Ron Greeno, MD, FCCP, MHM, chief medical officer of Cogent HMG and chair of SHM’s Public Policy Committee.
As change un-folds, some see great opportunity. “Hospitalists are in an enviable position as drivers of change,” says David B. Nash, MD, MBA, professor of health policy and dean of Thomas Jefferson University’s School of Population Health in Philadelphia. “As frontline troops of hospital-based care, they are going to play a critical role in ensuring the most efficient patient stay possible to help hospitals survive under new reimbursement models.”
Evolving Environment
Confidence that HM is well-positioned to drive value is especially welcome as the field looks back on 15 years of its existence in a soul-searching appraisal of just how much value it has driven thus far. The evidence is mixed. The profession’s clearest documented success has been preventing delays in patient discharge. That achievement has yet to be buttressed by clear evidence of concomitant gains in quality attributable to hospitalist care.
In fact, a widely publicized study in the Annals of Internal Medicine this year has caused a good deal of hand-wringing, as it suggests that HM-driven efficiency improvements may simply be attributable to shifting costs elsewhere because their patients tend to have higher readmission rates.1
That finding highlights a defining challenge of healthcare reform: how to achieve better value (quality per unit cost) within a care delivery and payment infrastructure that still pays for fragmented care. That infrastructure is trying to achieve the integration that is needed—both in the hospital and post-discharge, with preventive and acute care, at the individual patient and population levels.
“We’re being asked to prepare for an entirely different system, one which cares for populations of patients and tries to keep them out of the hospital,” Dr. Greeno says, “but our payment encourages just the opposite.”
Transitioning to value-based models while still functioning largely in a volume-based, fee-for-service environment is much like having one foot on the dock and one foot on a boat that is leaving the dock. That’s how the American Hospital Association put it in a report it released in September, “Hospitals and Care Systems of the Future.” Providers are struggling to navigate “life in the gap” between a volume-based “first curve” environment that inadequately rewards innovation and a “second curve” environment in which reimbursement is integrally tied to delivering coordinated care that demonstrates value, the AHA notes, using terminology coined by healthcare futurist Ian Morrison.
Navigation
Hospitalists will need to seize collaborative opportunities with hospitals to develop strategies to navigate this “life in the gap” during the transition to value-based reimbursement models of the second curve. As Jeff Glasheen, MD, SFHM, physician editor of The Hospitalist, provocatively wrote in his September 2011 column: “We must improve the quality of care to levels that, if necessary, Medicare would happily pay more for. This must be our singular goal” (see “Fiddling As HM Burns,” The Hospitalist). Assuming that money will follow quality, hospitals should be willing to invest in hospitalist-led processes and safety improvement activities, which likely will be the standard of care tomorrow, even if they do not turn a profit today.
Hospitalists will be the “effector arm” of crucial care-management practices under new payment models, Dr. Nash predicts. He says HM should focus on helping to make the model work—for example, championing evidence-based protocols and approved drug formularies, eliminating wasteful tests, and promoting better medication reconciliation and care transitions (see “Reconciliation Act,”).“Because they are on-site full-time, hospitalists are in the cat-bird seat to teach other attending physicians about the importance of reading from the same hymnal on these best practices,” he adds.
Dr. Greeno agrees reform needs to be cost-effective as well as patient-focused.
“The pressure on hospitalists to demonstrate our value has never been higher,” he says, urging hospitalists to pay particular attention to key features of reform to which they are already accountable, such as improving patient satisfaction and promoting evidence-based interventions that prevent readmissions and hospital-acquired conditions (see “Priorities in an Age of Reform,” left).
Dr. Greeno notes that SHM’s advocacy activities have been ramped up significantly to stay on top of reform developments—and ensure that policymakers hear hospitalists’ voices. “If we want to have a positive impact, we must track these changes, understand them, influence them, implement them, and make them successful,” he says. “That’s the challenge our field faces. There’s no physician organization that knows more about what goes on in a hospital than we do, and we will help policymakers and hospitals to make intelligent decisions.”
Chris Guadagnino is a freelance medical writer based in Philadelphia.
Reference
Proactive Approaches Can Mitigate Dangerous Transitions into Hospitals
A recent study of care transitions for nursing home residents with advanced cognitive impairments (N Engl J Med. 2011; 365:1212-1221) finds that transitions into the hospital can be burdensome, with such negative outcomes as medical errors and hospital-acquired infections, but have limited clinical benefit for some patients, such as those with dementia and other impairments. One in 5 nursing home residents had at least one burdensome transition in the last 90 days of life, researchers found, and some experienced repeated hospitalizations.
Hospitals may not be able to prevent nursing home residents who are nearing the end of life from turning up in their EDs, says study coauthor Joan Teno, MD, from Brown University in Providence, R.I. But physicians and other members of the care team might help to stave off repeat visits by engaging in frank discussions with the patient (and/or patients’ family) about the course of a disease and goals of care. A referral to hospice or for a palliative-care consultation might be appropriate, or the patient could be sent back to long-term care with a “do not rehospitalize” order. In some cases, she adds, these conversations happen in the ED without an admission, and are facilitated by a palliative-care team.
“We have this assumption that hospitalization is a good thing. But hospitals can be dangerous places for some elderly patients,” Dr. Teno says.
A more proactive response could be to identify the nursing homes that transfer the majority of cognitively impaired patients and meet with them to talk about appropriate transfers, how to treat such conditions as pneumonia in place, and the use of advance directives and POLST (physician orders for life-sustaining treatment: www.ohsu.edu/polst/).
A recent study of care transitions for nursing home residents with advanced cognitive impairments (N Engl J Med. 2011; 365:1212-1221) finds that transitions into the hospital can be burdensome, with such negative outcomes as medical errors and hospital-acquired infections, but have limited clinical benefit for some patients, such as those with dementia and other impairments. One in 5 nursing home residents had at least one burdensome transition in the last 90 days of life, researchers found, and some experienced repeated hospitalizations.
Hospitals may not be able to prevent nursing home residents who are nearing the end of life from turning up in their EDs, says study coauthor Joan Teno, MD, from Brown University in Providence, R.I. But physicians and other members of the care team might help to stave off repeat visits by engaging in frank discussions with the patient (and/or patients’ family) about the course of a disease and goals of care. A referral to hospice or for a palliative-care consultation might be appropriate, or the patient could be sent back to long-term care with a “do not rehospitalize” order. In some cases, she adds, these conversations happen in the ED without an admission, and are facilitated by a palliative-care team.
“We have this assumption that hospitalization is a good thing. But hospitals can be dangerous places for some elderly patients,” Dr. Teno says.
A more proactive response could be to identify the nursing homes that transfer the majority of cognitively impaired patients and meet with them to talk about appropriate transfers, how to treat such conditions as pneumonia in place, and the use of advance directives and POLST (physician orders for life-sustaining treatment: www.ohsu.edu/polst/).
A recent study of care transitions for nursing home residents with advanced cognitive impairments (N Engl J Med. 2011; 365:1212-1221) finds that transitions into the hospital can be burdensome, with such negative outcomes as medical errors and hospital-acquired infections, but have limited clinical benefit for some patients, such as those with dementia and other impairments. One in 5 nursing home residents had at least one burdensome transition in the last 90 days of life, researchers found, and some experienced repeated hospitalizations.
Hospitals may not be able to prevent nursing home residents who are nearing the end of life from turning up in their EDs, says study coauthor Joan Teno, MD, from Brown University in Providence, R.I. But physicians and other members of the care team might help to stave off repeat visits by engaging in frank discussions with the patient (and/or patients’ family) about the course of a disease and goals of care. A referral to hospice or for a palliative-care consultation might be appropriate, or the patient could be sent back to long-term care with a “do not rehospitalize” order. In some cases, she adds, these conversations happen in the ED without an admission, and are facilitated by a palliative-care team.
“We have this assumption that hospitalization is a good thing. But hospitals can be dangerous places for some elderly patients,” Dr. Teno says.
A more proactive response could be to identify the nursing homes that transfer the majority of cognitively impaired patients and meet with them to talk about appropriate transfers, how to treat such conditions as pneumonia in place, and the use of advance directives and POLST (physician orders for life-sustaining treatment: www.ohsu.edu/polst/).