User login
Weight Loss Modest With Primary Care Program
Enhanced brief lifestyle counseling by a primary care team helped about one-third of obese patients lose and keep off 5% or more of their baseline weight after 2 years, according to a study published online Nov. 14 in the New England Journal of Medicine and simultaneously presented at the annual meeting of the American Heart Association.
However, many of the patients during the study’s second year regained at least some of the lost weight, confirming "the problem of weight regain despite ongoing counseling for weight-loss maintenance," the study’s authors noted.
The intervention involved quarterly visits with a primary care physician, brief lifestyle coaching delivered monthly by a medical assistant, and the use of meal replacements or weight-loss medication.
The average weight loss of 4.7%, most of which was maintained for 2 years and was accompanied by improvements in some cardiovascular risk factors, was greater than that observed in other primary care trials, said Thomas A. Wadden, Ph.D., of the department of psychiatry at the University of Pennsylvania, Philadelphia, and his associates (N. Engl. J. Med. 2011 Nov. 14 [doi:10.1056/NEJMoa1109220]).
The results of the 2-year study of 390 obese patients demonstrate that "primary care physicians could help a considerable minority of obese persons achieve clinically meaningful weight loss, which they may not achieve if they were simply told to reduce their weight on their own," the investigators noted.
Dr. Wadden and his colleagues conducted the POWER-UP (Practice-based Opportunities for Weight Reduction trial at the University of Pennsylvania) study at three primary care practices in urban settings and three in suburban settings. A total of 30 primary care physicians took part.
The study enrolled 311 women and 79 men, with a mean age of 52 years, a mean body weight of 108 kg, and a mean body mass index of 39 kg/m2 at baseline. By patient self-report, approximately 59% were white, 38.5% were black, and 4.6% were Hispanic.
The study participants all had the same dietary and activity goals but were given different levels of support to achieve them.
All were instructed to gradually increase their physical activity to 180 min/wk. Those who weighed less than 113 kg were prescribed a diet of 1,200-1,500 kcal/day, while those who were heavier were prescribed 1,500-1,800 kcal/day.
A total of 130 patients were randomly assigned to receive usual care, which consisted of quarterly visits in which their primary care physician spent 5-7 minutes discussing the weight-loss information and reviewing any weight change.
Another 131 were randomly assigned to that same care plus brief lifestyle counseling, in which they spent 10-15 min/mo with a medical assistant, called a "lifestyle coach," who conducted a weigh-in, reviewed a diary of food intake, reviewed a physical activity diary, and delivered abbreviated lessons from the Diabetes Prevention Program.
Another 129 patients were randomly assigned to receive enhanced lifestyle counseling, which included that same intervention plus their choice of taking sibutramine, orlistat, or meal replacements under the guidance of the primary care physician. Sibutramine was withdrawn from the market during the trial, and patients in that group were switched to orlistat or meal replacements.
Patients taking meal replacements were instructed to substitute two meals and one snack every day with Slim-Fast shakes or meal bars for the first 4 months, and to replace one meal and one snack each day for the remainder of the study.
The primary outcome was weight loss at 2 years. Enhanced lifestyle counseling produced significantly greater weight loss (mean, 4.6 kg) than either lifestyle counseling (2.9 kg) or usual care (1.7 kg). Within the group receiving enhanced lifestyle counseling, there were no significant differences in weight loss among those taking meal replacements (67 patients), sibutramine (38 patients), or orlistat (24 patients).
The differences among the groups were first evident at 6 months, and maximal weight loss was achieved at 12 months. Between year 1 and year 2, however, most patients regained at least some of the weight they had lost.
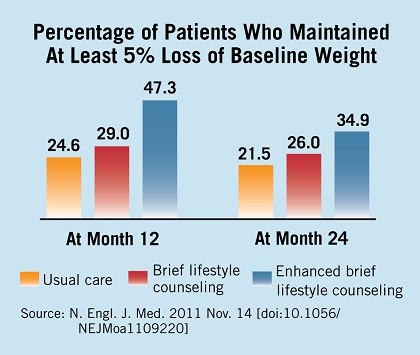
Secondary outcomes also were significantly better in the group that received enhanced lifestyle counseling than in the usual-care group, including the percentage of patients whose weight was at or below their baseline weight at 1 year (72.1% vs. 59.2%) and 2 years (67.4% vs. 53.1%); the percentages who lost 5% or more of their baseline weight at 1 year (47.3% vs. 24.6%) and 2 years (34.9% vs. 21.5%); and the percentages who lost 10% or more of their baseline weight at 1 year (25.6% vs. 3.9%) and 2 years (17.8% vs. 6.2%).
Patients who received enhanced lifestyle counseling showed significantly greater improvements in waist circumference, HDL cholesterol levels, and triglyceride levels, but not in LDL cholesterol levels or blood pressure.
There were 73 hospitalizations for severe adverse events, with no significant differences among the three study groups. Only three such events were deemed to be possibly related to the intervention: two cholecystectomies, and one case of syncope. In addition, sibutramine was discontinued in seven patients because of blood pressure elevation, tachycardia, or anxiety; and orlistat was discontinued in five patients because of gastrointestinal symptoms.
"Although our study has shown that primary care personnel can provide effective weight-management support, it has not addressed the more challenging question of who will pay for these or related weight-loss interventions," the researchers noted.
The National Heart, Lung, and Blood Institute funded the study. Dr. Wadden reported ties to Novo Nordisk, Orexigen, Vivus, Nutrisystem, Guilford Press, and the Cardiometabolic Support Network. His associates reported ties to numerous industry sources. Orlistat and Slim-Fast products were provided free of charge by the manufacturers, GlaxoSmithKline and Unilever.
Enhanced brief lifestyle counseling by a primary care team helped about one-third of obese patients lose and keep off 5% or more of their baseline weight after 2 years, according to a study published online Nov. 14 in the New England Journal of Medicine and simultaneously presented at the annual meeting of the American Heart Association.
However, many of the patients during the study’s second year regained at least some of the lost weight, confirming "the problem of weight regain despite ongoing counseling for weight-loss maintenance," the study’s authors noted.
The intervention involved quarterly visits with a primary care physician, brief lifestyle coaching delivered monthly by a medical assistant, and the use of meal replacements or weight-loss medication.
The average weight loss of 4.7%, most of which was maintained for 2 years and was accompanied by improvements in some cardiovascular risk factors, was greater than that observed in other primary care trials, said Thomas A. Wadden, Ph.D., of the department of psychiatry at the University of Pennsylvania, Philadelphia, and his associates (N. Engl. J. Med. 2011 Nov. 14 [doi:10.1056/NEJMoa1109220]).
The results of the 2-year study of 390 obese patients demonstrate that "primary care physicians could help a considerable minority of obese persons achieve clinically meaningful weight loss, which they may not achieve if they were simply told to reduce their weight on their own," the investigators noted.
Dr. Wadden and his colleagues conducted the POWER-UP (Practice-based Opportunities for Weight Reduction trial at the University of Pennsylvania) study at three primary care practices in urban settings and three in suburban settings. A total of 30 primary care physicians took part.
The study enrolled 311 women and 79 men, with a mean age of 52 years, a mean body weight of 108 kg, and a mean body mass index of 39 kg/m2 at baseline. By patient self-report, approximately 59% were white, 38.5% were black, and 4.6% were Hispanic.
The study participants all had the same dietary and activity goals but were given different levels of support to achieve them.
All were instructed to gradually increase their physical activity to 180 min/wk. Those who weighed less than 113 kg were prescribed a diet of 1,200-1,500 kcal/day, while those who were heavier were prescribed 1,500-1,800 kcal/day.
A total of 130 patients were randomly assigned to receive usual care, which consisted of quarterly visits in which their primary care physician spent 5-7 minutes discussing the weight-loss information and reviewing any weight change.
Another 131 were randomly assigned to that same care plus brief lifestyle counseling, in which they spent 10-15 min/mo with a medical assistant, called a "lifestyle coach," who conducted a weigh-in, reviewed a diary of food intake, reviewed a physical activity diary, and delivered abbreviated lessons from the Diabetes Prevention Program.
Another 129 patients were randomly assigned to receive enhanced lifestyle counseling, which included that same intervention plus their choice of taking sibutramine, orlistat, or meal replacements under the guidance of the primary care physician. Sibutramine was withdrawn from the market during the trial, and patients in that group were switched to orlistat or meal replacements.
Patients taking meal replacements were instructed to substitute two meals and one snack every day with Slim-Fast shakes or meal bars for the first 4 months, and to replace one meal and one snack each day for the remainder of the study.
The primary outcome was weight loss at 2 years. Enhanced lifestyle counseling produced significantly greater weight loss (mean, 4.6 kg) than either lifestyle counseling (2.9 kg) or usual care (1.7 kg). Within the group receiving enhanced lifestyle counseling, there were no significant differences in weight loss among those taking meal replacements (67 patients), sibutramine (38 patients), or orlistat (24 patients).
The differences among the groups were first evident at 6 months, and maximal weight loss was achieved at 12 months. Between year 1 and year 2, however, most patients regained at least some of the weight they had lost.
Secondary outcomes also were significantly better in the group that received enhanced lifestyle counseling than in the usual-care group, including the percentage of patients whose weight was at or below their baseline weight at 1 year (72.1% vs. 59.2%) and 2 years (67.4% vs. 53.1%); the percentages who lost 5% or more of their baseline weight at 1 year (47.3% vs. 24.6%) and 2 years (34.9% vs. 21.5%); and the percentages who lost 10% or more of their baseline weight at 1 year (25.6% vs. 3.9%) and 2 years (17.8% vs. 6.2%).
Patients who received enhanced lifestyle counseling showed significantly greater improvements in waist circumference, HDL cholesterol levels, and triglyceride levels, but not in LDL cholesterol levels or blood pressure.
There were 73 hospitalizations for severe adverse events, with no significant differences among the three study groups. Only three such events were deemed to be possibly related to the intervention: two cholecystectomies, and one case of syncope. In addition, sibutramine was discontinued in seven patients because of blood pressure elevation, tachycardia, or anxiety; and orlistat was discontinued in five patients because of gastrointestinal symptoms.
"Although our study has shown that primary care personnel can provide effective weight-management support, it has not addressed the more challenging question of who will pay for these or related weight-loss interventions," the researchers noted.
The National Heart, Lung, and Blood Institute funded the study. Dr. Wadden reported ties to Novo Nordisk, Orexigen, Vivus, Nutrisystem, Guilford Press, and the Cardiometabolic Support Network. His associates reported ties to numerous industry sources. Orlistat and Slim-Fast products were provided free of charge by the manufacturers, GlaxoSmithKline and Unilever.
Enhanced brief lifestyle counseling by a primary care team helped about one-third of obese patients lose and keep off 5% or more of their baseline weight after 2 years, according to a study published online Nov. 14 in the New England Journal of Medicine and simultaneously presented at the annual meeting of the American Heart Association.
However, many of the patients during the study’s second year regained at least some of the lost weight, confirming "the problem of weight regain despite ongoing counseling for weight-loss maintenance," the study’s authors noted.
The intervention involved quarterly visits with a primary care physician, brief lifestyle coaching delivered monthly by a medical assistant, and the use of meal replacements or weight-loss medication.
The average weight loss of 4.7%, most of which was maintained for 2 years and was accompanied by improvements in some cardiovascular risk factors, was greater than that observed in other primary care trials, said Thomas A. Wadden, Ph.D., of the department of psychiatry at the University of Pennsylvania, Philadelphia, and his associates (N. Engl. J. Med. 2011 Nov. 14 [doi:10.1056/NEJMoa1109220]).
The results of the 2-year study of 390 obese patients demonstrate that "primary care physicians could help a considerable minority of obese persons achieve clinically meaningful weight loss, which they may not achieve if they were simply told to reduce their weight on their own," the investigators noted.
Dr. Wadden and his colleagues conducted the POWER-UP (Practice-based Opportunities for Weight Reduction trial at the University of Pennsylvania) study at three primary care practices in urban settings and three in suburban settings. A total of 30 primary care physicians took part.
The study enrolled 311 women and 79 men, with a mean age of 52 years, a mean body weight of 108 kg, and a mean body mass index of 39 kg/m2 at baseline. By patient self-report, approximately 59% were white, 38.5% were black, and 4.6% were Hispanic.
The study participants all had the same dietary and activity goals but were given different levels of support to achieve them.
All were instructed to gradually increase their physical activity to 180 min/wk. Those who weighed less than 113 kg were prescribed a diet of 1,200-1,500 kcal/day, while those who were heavier were prescribed 1,500-1,800 kcal/day.
A total of 130 patients were randomly assigned to receive usual care, which consisted of quarterly visits in which their primary care physician spent 5-7 minutes discussing the weight-loss information and reviewing any weight change.
Another 131 were randomly assigned to that same care plus brief lifestyle counseling, in which they spent 10-15 min/mo with a medical assistant, called a "lifestyle coach," who conducted a weigh-in, reviewed a diary of food intake, reviewed a physical activity diary, and delivered abbreviated lessons from the Diabetes Prevention Program.
Another 129 patients were randomly assigned to receive enhanced lifestyle counseling, which included that same intervention plus their choice of taking sibutramine, orlistat, or meal replacements under the guidance of the primary care physician. Sibutramine was withdrawn from the market during the trial, and patients in that group were switched to orlistat or meal replacements.
Patients taking meal replacements were instructed to substitute two meals and one snack every day with Slim-Fast shakes or meal bars for the first 4 months, and to replace one meal and one snack each day for the remainder of the study.
The primary outcome was weight loss at 2 years. Enhanced lifestyle counseling produced significantly greater weight loss (mean, 4.6 kg) than either lifestyle counseling (2.9 kg) or usual care (1.7 kg). Within the group receiving enhanced lifestyle counseling, there were no significant differences in weight loss among those taking meal replacements (67 patients), sibutramine (38 patients), or orlistat (24 patients).
The differences among the groups were first evident at 6 months, and maximal weight loss was achieved at 12 months. Between year 1 and year 2, however, most patients regained at least some of the weight they had lost.
Secondary outcomes also were significantly better in the group that received enhanced lifestyle counseling than in the usual-care group, including the percentage of patients whose weight was at or below their baseline weight at 1 year (72.1% vs. 59.2%) and 2 years (67.4% vs. 53.1%); the percentages who lost 5% or more of their baseline weight at 1 year (47.3% vs. 24.6%) and 2 years (34.9% vs. 21.5%); and the percentages who lost 10% or more of their baseline weight at 1 year (25.6% vs. 3.9%) and 2 years (17.8% vs. 6.2%).
Patients who received enhanced lifestyle counseling showed significantly greater improvements in waist circumference, HDL cholesterol levels, and triglyceride levels, but not in LDL cholesterol levels or blood pressure.
There were 73 hospitalizations for severe adverse events, with no significant differences among the three study groups. Only three such events were deemed to be possibly related to the intervention: two cholecystectomies, and one case of syncope. In addition, sibutramine was discontinued in seven patients because of blood pressure elevation, tachycardia, or anxiety; and orlistat was discontinued in five patients because of gastrointestinal symptoms.
"Although our study has shown that primary care personnel can provide effective weight-management support, it has not addressed the more challenging question of who will pay for these or related weight-loss interventions," the researchers noted.
The National Heart, Lung, and Blood Institute funded the study. Dr. Wadden reported ties to Novo Nordisk, Orexigen, Vivus, Nutrisystem, Guilford Press, and the Cardiometabolic Support Network. His associates reported ties to numerous industry sources. Orlistat and Slim-Fast products were provided free of charge by the manufacturers, GlaxoSmithKline and Unilever.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: Enhanced lifestyle counseling produced significantly greater weight loss (mean, 4.6 kg) than did either brief lifestyle counseling (2.9 kg) or usual care (1.7 kg).
Data Source: A randomized clinical trial comparing weight loss in 390 obese patients after 2 years of usual care, brief lifestyle counseling, and enhanced lifestyle counseling delivered by a primary care physician and staff medical assistants.
Disclosures: The study was supported by the National Heart, Lung, and Blood Institute. Dr. Wadden reported ties to Novo Nordisk, Orexigen, Vivus, Nutrisystem, Guilford Press, and the Cardiometabolic Support Network. His associates reported ties to numerous industry sources. Orlistat and Slim-Fast products were provided free of charge by the manufacturers, GlaxoSmithKline and Unilever.
Novel Therapies Put Multiple Myeloma 'On the Ropes'
SAN FRANCISCO – A sweep of new agents are poised to deliver what could be a knock-out blow to multiple myeloma, according to the director of the myeloma program at the University of California, San Francisco.
Some are second- or third-generation agents in a mainstay class that appear to have less toxicity than and/or overcome resistance to their predecessors, Dr. Jeffrey L. Wolf said at the annual Oncology Congress here. Others come from classes not previously used in this disease.

"There is a rush to develop new drugs in myeloma," Dr. Wolf told attendees. "We [understand] some mechanisms that the disease seems to favor, so we can interfere with those."
The prospects, in turn, are excellent: "We have made such tremendous headway in myeloma, except for those exceptional cases with 17p deletions and some other adverse prognostic features," he said. "As a disease, it seems to be on the ropes."
A Less-Toxic Proteasome Inhibitor
The first-generation proteasome inhibitor bortezomib (Velcade) improves myeloma outcomes, but maximizing its benefit will require addressing the peripheral neuropathy that limits its use. Three strategies may lessen this toxicity without compromising efficacy, Dr. Wolf suggested: modestly reducing the standard dose, adjusting the schedule from twice to once weekly, and altering the route of administration from intravenous to subcutaneous.
For example, in patients with pretreated myeloma, giving bortezomib subcutaneously instead of intravenously results in an identical overall response rate of 52% (Lancet Oncol. 2011;12:431-40). But there are significant reductions in rates of peripheral neuropathy of any grade (38% vs. 53%) and grade 3 or higher (6% vs. 16%).
"Practically everybody that we see now at UCSF gets subcutaneous [bortezomib]," Dr. Wolf said. It’s a great way to go back and treat patients who maybe otherwise have stopped their therapy because of their neuropathy."
Carfilzomib, an investigational next-generation proteasome inhibitor in phase III trials, is showing good antimyeloma activity and a low rate of peripheral neuropathy. Among patients with pretreated, relapsed, or refractory disease, carfilzomib monotherapy achieved overall response rates of 42% to 53% in a bortezomib-naive group (ASCO 2011 annual meeting. Abstract 8026) and 21% in a bortezomib-exposed group (Haematologica 2010;95:452 Abstract 1099). Median time to progression was at least 8 months for both.
Dr. Wolf said that unpublished data suggest that the response rate was still 17% specifically among patients who had had progression on bortezomib, "so there appears to be some activity in patients who are already refractory to a prior proteasome inhibitor."
Meanwhile, the rates of grade 1/2 and grade 3 peripheral neuropathy were 6% and 1%, respectively. And only a single patient of the 155 had to stop treatment because of this adverse effect.
When carfilzomib is combined with lenalidomide-dexamethasone (the so-called CRd regimen), the overall response rate in patients with pretreated, relapsed, and refractory disease is 78%, and the rate of complete or near complete response is 24% (ASCO 2011 meeting. Abstract 8025).
And, in newly diagnosed myeloma, among 18 patients receiving eight cycles of CRd, the overall response rate was 100%, and the rate of stringent-complete, complete, or near-complete response was 61% (2011 International Myeloma Workshop. Poster P-253). "This is very, very exciting—I don’t think we’ve seen this in any other combination," Dr. Wolf commented. "But these are small numbers of patients; we still need to increase the numbers of patients studied with this combination."
Bortezomib and carfilzomib may soon have company from several investigational proteasome inhibitors available in oral formulations that have shown promise in preclinical testing or have advanced to clinical trials: CEP-18770 (Cephalon), ONX-0912 (Onyx), and MLN-9708 (Millenium).
A Third-Generation IMiD in Trials
Pomalidomide, a third-generation immunomodulatory drug (IMiD), coming after thalidomide (Thalomid), and lenalidomide (Revlimid), is also showing good antimyeloma activity in clinical trials, according to Dr. Wolf.
Among patients with pretreated myeloma, the rate of partial or better response when pomalidomide is combined with dexamethasone has ranged from 25% to 42%, depending on the trial and patient population. Adverse events are primarily hematologic.
And in patients who have previously received lenalidomide, the response rate is similar, at 35% (ASCO 2011 annual meeting. Abstract 8067). "So, as with carfilzomib, where there appear to be responses in patients who have prior resistance to bortezomib, it appears that pomalidomide can give us responses in patients who have already had resistance to lenalidomide," he said.
HDAC Inhibitors Show Activity
The histone deacetylase (HDAC) inhibitor vorinostat (Zolinza) is approved for treatment of lymphoma. But it is being tested in clinical trials for myeloma, in combination therapy, with promising results, according to Dr. Wolf. Overall response rates have ranged from 40% to 94%, depending on the patient population and combination.
Similarly, the HDAC inhibitor romidepsin (Istodax) is approved for lymphoma treatment but is also being studied for antimyeloma activity. And panobinostat, an investigational member of this drug class, is being evaluated as a component of combination therapy in phase II and III myeloma trials.
Monoclonal Antibodies Tested
Elotuzumab is an investigational monoclonal antibody directed against CS1, a glycoprotein that is highly expressed on the surface of plasma cells and implicated in myeloma pathogenesis.
In a phase I trial among patients with relapsed or refractory myeloma, the combination of elotuzumab with lenalidomide and low-dose dexamethasone yielded an overall response rate of 82% (ASCO 2011 meeting. Abstract 8076). The rate was 83% among the subset of patients whose disease was refractory to the most recent therapy and 95% among the subset of lenalidomide-naive patients.
The combination of elotuzumab with bortezomib has also been tested in patients with relapsed or refractory myeloma. But the overall response rate with this combination was less impressive, at 48% (ASH 2010 meeting. Abstract 3023).
Other Agents and Pathways
Several other agents are being eyed for roles in myeloma therapy as well. They include bendamustine (Treanda), an old drug initially revived for lymphoma treatment; aurora kinase inhibitors (for example, MLN-8237); and inhibitors of the mammalian target of rapamycin, or mTOR (for example, INK-128).
Additionally, there is considerable interest in agents that target fibroblast growth factor receptor 3 (FGFR3) for one subgroup. "In patients with the 4;14 translocation, FGFR3 is overexpressed," Dr. Wolf explained. "Finding an inhibitor for that or a direct antibody ... may be quite effective in those patients."
Investigators are also assessing the impact of targeting certain signaling pathways, such as the Jak/Stat pathway and the AKT pathway. For instance, a phase III trial is testing perifosine, an investigational AKT inhibitor, in combination therapy among patients with relapsed or refractory myeloma (NCT01002248).
The Oncology Congress is presented by Reed Medical Education. Reed Medical Education and this news organization are owned by Reed Elsevier Inc.
Dr. Wolf disclosed that he is on the speakers bureaus of Millenium, Celgene, and Ortho-Biotech, and is a consultant to and speaker for Onyx.
SAN FRANCISCO – A sweep of new agents are poised to deliver what could be a knock-out blow to multiple myeloma, according to the director of the myeloma program at the University of California, San Francisco.
Some are second- or third-generation agents in a mainstay class that appear to have less toxicity than and/or overcome resistance to their predecessors, Dr. Jeffrey L. Wolf said at the annual Oncology Congress here. Others come from classes not previously used in this disease.
"There is a rush to develop new drugs in myeloma," Dr. Wolf told attendees. "We [understand] some mechanisms that the disease seems to favor, so we can interfere with those."
The prospects, in turn, are excellent: "We have made such tremendous headway in myeloma, except for those exceptional cases with 17p deletions and some other adverse prognostic features," he said. "As a disease, it seems to be on the ropes."
A Less-Toxic Proteasome Inhibitor
The first-generation proteasome inhibitor bortezomib (Velcade) improves myeloma outcomes, but maximizing its benefit will require addressing the peripheral neuropathy that limits its use. Three strategies may lessen this toxicity without compromising efficacy, Dr. Wolf suggested: modestly reducing the standard dose, adjusting the schedule from twice to once weekly, and altering the route of administration from intravenous to subcutaneous.
For example, in patients with pretreated myeloma, giving bortezomib subcutaneously instead of intravenously results in an identical overall response rate of 52% (Lancet Oncol. 2011;12:431-40). But there are significant reductions in rates of peripheral neuropathy of any grade (38% vs. 53%) and grade 3 or higher (6% vs. 16%).
"Practically everybody that we see now at UCSF gets subcutaneous [bortezomib]," Dr. Wolf said. It’s a great way to go back and treat patients who maybe otherwise have stopped their therapy because of their neuropathy."
Carfilzomib, an investigational next-generation proteasome inhibitor in phase III trials, is showing good antimyeloma activity and a low rate of peripheral neuropathy. Among patients with pretreated, relapsed, or refractory disease, carfilzomib monotherapy achieved overall response rates of 42% to 53% in a bortezomib-naive group (ASCO 2011 annual meeting. Abstract 8026) and 21% in a bortezomib-exposed group (Haematologica 2010;95:452 Abstract 1099). Median time to progression was at least 8 months for both.
Dr. Wolf said that unpublished data suggest that the response rate was still 17% specifically among patients who had had progression on bortezomib, "so there appears to be some activity in patients who are already refractory to a prior proteasome inhibitor."
Meanwhile, the rates of grade 1/2 and grade 3 peripheral neuropathy were 6% and 1%, respectively. And only a single patient of the 155 had to stop treatment because of this adverse effect.
When carfilzomib is combined with lenalidomide-dexamethasone (the so-called CRd regimen), the overall response rate in patients with pretreated, relapsed, and refractory disease is 78%, and the rate of complete or near complete response is 24% (ASCO 2011 meeting. Abstract 8025).
And, in newly diagnosed myeloma, among 18 patients receiving eight cycles of CRd, the overall response rate was 100%, and the rate of stringent-complete, complete, or near-complete response was 61% (2011 International Myeloma Workshop. Poster P-253). "This is very, very exciting—I don’t think we’ve seen this in any other combination," Dr. Wolf commented. "But these are small numbers of patients; we still need to increase the numbers of patients studied with this combination."
Bortezomib and carfilzomib may soon have company from several investigational proteasome inhibitors available in oral formulations that have shown promise in preclinical testing or have advanced to clinical trials: CEP-18770 (Cephalon), ONX-0912 (Onyx), and MLN-9708 (Millenium).
A Third-Generation IMiD in Trials
Pomalidomide, a third-generation immunomodulatory drug (IMiD), coming after thalidomide (Thalomid), and lenalidomide (Revlimid), is also showing good antimyeloma activity in clinical trials, according to Dr. Wolf.
Among patients with pretreated myeloma, the rate of partial or better response when pomalidomide is combined with dexamethasone has ranged from 25% to 42%, depending on the trial and patient population. Adverse events are primarily hematologic.
And in patients who have previously received lenalidomide, the response rate is similar, at 35% (ASCO 2011 annual meeting. Abstract 8067). "So, as with carfilzomib, where there appear to be responses in patients who have prior resistance to bortezomib, it appears that pomalidomide can give us responses in patients who have already had resistance to lenalidomide," he said.
HDAC Inhibitors Show Activity
The histone deacetylase (HDAC) inhibitor vorinostat (Zolinza) is approved for treatment of lymphoma. But it is being tested in clinical trials for myeloma, in combination therapy, with promising results, according to Dr. Wolf. Overall response rates have ranged from 40% to 94%, depending on the patient population and combination.
Similarly, the HDAC inhibitor romidepsin (Istodax) is approved for lymphoma treatment but is also being studied for antimyeloma activity. And panobinostat, an investigational member of this drug class, is being evaluated as a component of combination therapy in phase II and III myeloma trials.
Monoclonal Antibodies Tested
Elotuzumab is an investigational monoclonal antibody directed against CS1, a glycoprotein that is highly expressed on the surface of plasma cells and implicated in myeloma pathogenesis.
In a phase I trial among patients with relapsed or refractory myeloma, the combination of elotuzumab with lenalidomide and low-dose dexamethasone yielded an overall response rate of 82% (ASCO 2011 meeting. Abstract 8076). The rate was 83% among the subset of patients whose disease was refractory to the most recent therapy and 95% among the subset of lenalidomide-naive patients.
The combination of elotuzumab with bortezomib has also been tested in patients with relapsed or refractory myeloma. But the overall response rate with this combination was less impressive, at 48% (ASH 2010 meeting. Abstract 3023).
Other Agents and Pathways
Several other agents are being eyed for roles in myeloma therapy as well. They include bendamustine (Treanda), an old drug initially revived for lymphoma treatment; aurora kinase inhibitors (for example, MLN-8237); and inhibitors of the mammalian target of rapamycin, or mTOR (for example, INK-128).
Additionally, there is considerable interest in agents that target fibroblast growth factor receptor 3 (FGFR3) for one subgroup. "In patients with the 4;14 translocation, FGFR3 is overexpressed," Dr. Wolf explained. "Finding an inhibitor for that or a direct antibody ... may be quite effective in those patients."
Investigators are also assessing the impact of targeting certain signaling pathways, such as the Jak/Stat pathway and the AKT pathway. For instance, a phase III trial is testing perifosine, an investigational AKT inhibitor, in combination therapy among patients with relapsed or refractory myeloma (NCT01002248).
The Oncology Congress is presented by Reed Medical Education. Reed Medical Education and this news organization are owned by Reed Elsevier Inc.
Dr. Wolf disclosed that he is on the speakers bureaus of Millenium, Celgene, and Ortho-Biotech, and is a consultant to and speaker for Onyx.
SAN FRANCISCO – A sweep of new agents are poised to deliver what could be a knock-out blow to multiple myeloma, according to the director of the myeloma program at the University of California, San Francisco.
Some are second- or third-generation agents in a mainstay class that appear to have less toxicity than and/or overcome resistance to their predecessors, Dr. Jeffrey L. Wolf said at the annual Oncology Congress here. Others come from classes not previously used in this disease.
"There is a rush to develop new drugs in myeloma," Dr. Wolf told attendees. "We [understand] some mechanisms that the disease seems to favor, so we can interfere with those."
The prospects, in turn, are excellent: "We have made such tremendous headway in myeloma, except for those exceptional cases with 17p deletions and some other adverse prognostic features," he said. "As a disease, it seems to be on the ropes."
A Less-Toxic Proteasome Inhibitor
The first-generation proteasome inhibitor bortezomib (Velcade) improves myeloma outcomes, but maximizing its benefit will require addressing the peripheral neuropathy that limits its use. Three strategies may lessen this toxicity without compromising efficacy, Dr. Wolf suggested: modestly reducing the standard dose, adjusting the schedule from twice to once weekly, and altering the route of administration from intravenous to subcutaneous.
For example, in patients with pretreated myeloma, giving bortezomib subcutaneously instead of intravenously results in an identical overall response rate of 52% (Lancet Oncol. 2011;12:431-40). But there are significant reductions in rates of peripheral neuropathy of any grade (38% vs. 53%) and grade 3 or higher (6% vs. 16%).
"Practically everybody that we see now at UCSF gets subcutaneous [bortezomib]," Dr. Wolf said. It’s a great way to go back and treat patients who maybe otherwise have stopped their therapy because of their neuropathy."
Carfilzomib, an investigational next-generation proteasome inhibitor in phase III trials, is showing good antimyeloma activity and a low rate of peripheral neuropathy. Among patients with pretreated, relapsed, or refractory disease, carfilzomib monotherapy achieved overall response rates of 42% to 53% in a bortezomib-naive group (ASCO 2011 annual meeting. Abstract 8026) and 21% in a bortezomib-exposed group (Haematologica 2010;95:452 Abstract 1099). Median time to progression was at least 8 months for both.
Dr. Wolf said that unpublished data suggest that the response rate was still 17% specifically among patients who had had progression on bortezomib, "so there appears to be some activity in patients who are already refractory to a prior proteasome inhibitor."
Meanwhile, the rates of grade 1/2 and grade 3 peripheral neuropathy were 6% and 1%, respectively. And only a single patient of the 155 had to stop treatment because of this adverse effect.
When carfilzomib is combined with lenalidomide-dexamethasone (the so-called CRd regimen), the overall response rate in patients with pretreated, relapsed, and refractory disease is 78%, and the rate of complete or near complete response is 24% (ASCO 2011 meeting. Abstract 8025).
And, in newly diagnosed myeloma, among 18 patients receiving eight cycles of CRd, the overall response rate was 100%, and the rate of stringent-complete, complete, or near-complete response was 61% (2011 International Myeloma Workshop. Poster P-253). "This is very, very exciting—I don’t think we’ve seen this in any other combination," Dr. Wolf commented. "But these are small numbers of patients; we still need to increase the numbers of patients studied with this combination."
Bortezomib and carfilzomib may soon have company from several investigational proteasome inhibitors available in oral formulations that have shown promise in preclinical testing or have advanced to clinical trials: CEP-18770 (Cephalon), ONX-0912 (Onyx), and MLN-9708 (Millenium).
A Third-Generation IMiD in Trials
Pomalidomide, a third-generation immunomodulatory drug (IMiD), coming after thalidomide (Thalomid), and lenalidomide (Revlimid), is also showing good antimyeloma activity in clinical trials, according to Dr. Wolf.
Among patients with pretreated myeloma, the rate of partial or better response when pomalidomide is combined with dexamethasone has ranged from 25% to 42%, depending on the trial and patient population. Adverse events are primarily hematologic.
And in patients who have previously received lenalidomide, the response rate is similar, at 35% (ASCO 2011 annual meeting. Abstract 8067). "So, as with carfilzomib, where there appear to be responses in patients who have prior resistance to bortezomib, it appears that pomalidomide can give us responses in patients who have already had resistance to lenalidomide," he said.
HDAC Inhibitors Show Activity
The histone deacetylase (HDAC) inhibitor vorinostat (Zolinza) is approved for treatment of lymphoma. But it is being tested in clinical trials for myeloma, in combination therapy, with promising results, according to Dr. Wolf. Overall response rates have ranged from 40% to 94%, depending on the patient population and combination.
Similarly, the HDAC inhibitor romidepsin (Istodax) is approved for lymphoma treatment but is also being studied for antimyeloma activity. And panobinostat, an investigational member of this drug class, is being evaluated as a component of combination therapy in phase II and III myeloma trials.
Monoclonal Antibodies Tested
Elotuzumab is an investigational monoclonal antibody directed against CS1, a glycoprotein that is highly expressed on the surface of plasma cells and implicated in myeloma pathogenesis.
In a phase I trial among patients with relapsed or refractory myeloma, the combination of elotuzumab with lenalidomide and low-dose dexamethasone yielded an overall response rate of 82% (ASCO 2011 meeting. Abstract 8076). The rate was 83% among the subset of patients whose disease was refractory to the most recent therapy and 95% among the subset of lenalidomide-naive patients.
The combination of elotuzumab with bortezomib has also been tested in patients with relapsed or refractory myeloma. But the overall response rate with this combination was less impressive, at 48% (ASH 2010 meeting. Abstract 3023).
Other Agents and Pathways
Several other agents are being eyed for roles in myeloma therapy as well. They include bendamustine (Treanda), an old drug initially revived for lymphoma treatment; aurora kinase inhibitors (for example, MLN-8237); and inhibitors of the mammalian target of rapamycin, or mTOR (for example, INK-128).
Additionally, there is considerable interest in agents that target fibroblast growth factor receptor 3 (FGFR3) for one subgroup. "In patients with the 4;14 translocation, FGFR3 is overexpressed," Dr. Wolf explained. "Finding an inhibitor for that or a direct antibody ... may be quite effective in those patients."
Investigators are also assessing the impact of targeting certain signaling pathways, such as the Jak/Stat pathway and the AKT pathway. For instance, a phase III trial is testing perifosine, an investigational AKT inhibitor, in combination therapy among patients with relapsed or refractory myeloma (NCT01002248).
The Oncology Congress is presented by Reed Medical Education. Reed Medical Education and this news organization are owned by Reed Elsevier Inc.
Dr. Wolf disclosed that he is on the speakers bureaus of Millenium, Celgene, and Ortho-Biotech, and is a consultant to and speaker for Onyx.
EXPERT ANALYSIS FROM THE ANNUAL ONCOLOGY CONGRESS
Partner with Pharmacy to Maximize Patient Care
You’re ready to discharge a patient, but you don’t know whether the medication you’ve ordered will be available in the outpatient setting. Who do you ask? Your pharmacy service will have the answers, and if you’ve established a collegial relationship with the pharmacists there, most likely you can get a quick answer via page, text, or phone call. But if you don’t have personal contact with your pharmacists, chances are the interchange will impersonal—and that could mean missing ou
“Pharmacists may be underutilized, especially if the range of clinical services they offer are not recognized,” notes Kristine Gleason, RPh, clinical quality leader at Northwestern Memorial Hospital in Chicago. “We can be an excellent resource for young hospitalists and clinicians, offering information on clinical dosing and monitoring of complex, high-risk medications.”
Pharmacists also can be valuable resources for medication reconciliation and patient counseling, Gleason says, adding that “our goal is to work collaboratively with our clinicians to help ensure patients receive evidence-based medication regimens that are safe and without error and that are tailored to each patient’s individualized characteristics.”
Benefits of Rounding
Interactions between hospital pharmacies and HM services vary by institution size and organization. Roberta Barber, PharmD, MPH, is assistant vice president of pharmacy for Virtua Health’s four hospital campuses in New Jersey. At Memorial Hospital, where Erik DeLue, MD, MBA, SFHM, first established a hospitalist program, pharmacists are present in the ICU units and participate in care-coordination rounds.
Barber is crafting policies to extend the decentralized pharmacist model to all of Virtua’s hospitals. Equipped with cordless phones and tablet computers, pharmacists will be able to round with the HM team without sacrificing availability to other physicians and hospital staff. In this way, she says, “physicians will be able to consult with pharmacists as they’re creating their treatment plans, and the pharmacist can intervene regarding potential problem orders right then and there.”
At the University of California at San Francisco Medical Center, clinical pharmacists in the general medicine division work closely with the nine medicine teams run by hospitalists. That means 24/7 availability by pager, participating in multidisciplinary rounds, and furnishing new physicians with a “contacts” card and an orientation guide to help hospitalists write better orders, says Vicki Ising Jue, PharmD.
The personal touch is appreciated. “If I am in the pharmacy making a call and not on the unit, it just makes the phone call so much easier if the caller happens to be someone I’ve worked with before,” says UCSF’s Alan Tan, PharmD.
View hundreds of HM opportunities at SHM's Career Center
The degree of communication with pharmacy services may depend on whether you’re working in a teaching hospital with a structured orientation program or starting out in a community hospital. No matter the setting, though, Gleason says the pharmacist’s mission stays the same.
“We’re all striving to get to the same goal: safe, effective and patient-centered care to achieve positive outcomes for our patients,” she says. “Partnering with pharmacists can really move all of us closer to that goal.”
Gretchen Henkel is a freelance writer based in California.
Be PROACTIVE
One excellent way to foster collaboration with your hospital pharmacists and gain a better understanding of the medication management services they can provide, Gleason says, is to visit the department. “Spend an hour with us, shadow us, come to a meeting, and understand what we do professionally,” she explains.
Barber agrees: “If your hospital doesn’t offer training on the range of pharmacy services, solicit that yourself. Orient yourself to pharmacy rules and regulations; familiarize yourself with your hospital’s formulary and the role of the P&T committee in placing drugs on the formulary.”—GH
You’re ready to discharge a patient, but you don’t know whether the medication you’ve ordered will be available in the outpatient setting. Who do you ask? Your pharmacy service will have the answers, and if you’ve established a collegial relationship with the pharmacists there, most likely you can get a quick answer via page, text, or phone call. But if you don’t have personal contact with your pharmacists, chances are the interchange will impersonal—and that could mean missing ou
“Pharmacists may be underutilized, especially if the range of clinical services they offer are not recognized,” notes Kristine Gleason, RPh, clinical quality leader at Northwestern Memorial Hospital in Chicago. “We can be an excellent resource for young hospitalists and clinicians, offering information on clinical dosing and monitoring of complex, high-risk medications.”
Pharmacists also can be valuable resources for medication reconciliation and patient counseling, Gleason says, adding that “our goal is to work collaboratively with our clinicians to help ensure patients receive evidence-based medication regimens that are safe and without error and that are tailored to each patient’s individualized characteristics.”
Benefits of Rounding
Interactions between hospital pharmacies and HM services vary by institution size and organization. Roberta Barber, PharmD, MPH, is assistant vice president of pharmacy for Virtua Health’s four hospital campuses in New Jersey. At Memorial Hospital, where Erik DeLue, MD, MBA, SFHM, first established a hospitalist program, pharmacists are present in the ICU units and participate in care-coordination rounds.
Barber is crafting policies to extend the decentralized pharmacist model to all of Virtua’s hospitals. Equipped with cordless phones and tablet computers, pharmacists will be able to round with the HM team without sacrificing availability to other physicians and hospital staff. In this way, she says, “physicians will be able to consult with pharmacists as they’re creating their treatment plans, and the pharmacist can intervene regarding potential problem orders right then and there.”
At the University of California at San Francisco Medical Center, clinical pharmacists in the general medicine division work closely with the nine medicine teams run by hospitalists. That means 24/7 availability by pager, participating in multidisciplinary rounds, and furnishing new physicians with a “contacts” card and an orientation guide to help hospitalists write better orders, says Vicki Ising Jue, PharmD.
The personal touch is appreciated. “If I am in the pharmacy making a call and not on the unit, it just makes the phone call so much easier if the caller happens to be someone I’ve worked with before,” says UCSF’s Alan Tan, PharmD.
View hundreds of HM opportunities at SHM's Career Center
The degree of communication with pharmacy services may depend on whether you’re working in a teaching hospital with a structured orientation program or starting out in a community hospital. No matter the setting, though, Gleason says the pharmacist’s mission stays the same.
“We’re all striving to get to the same goal: safe, effective and patient-centered care to achieve positive outcomes for our patients,” she says. “Partnering with pharmacists can really move all of us closer to that goal.”
Gretchen Henkel is a freelance writer based in California.
Be PROACTIVE
One excellent way to foster collaboration with your hospital pharmacists and gain a better understanding of the medication management services they can provide, Gleason says, is to visit the department. “Spend an hour with us, shadow us, come to a meeting, and understand what we do professionally,” she explains.
Barber agrees: “If your hospital doesn’t offer training on the range of pharmacy services, solicit that yourself. Orient yourself to pharmacy rules and regulations; familiarize yourself with your hospital’s formulary and the role of the P&T committee in placing drugs on the formulary.”—GH
You’re ready to discharge a patient, but you don’t know whether the medication you’ve ordered will be available in the outpatient setting. Who do you ask? Your pharmacy service will have the answers, and if you’ve established a collegial relationship with the pharmacists there, most likely you can get a quick answer via page, text, or phone call. But if you don’t have personal contact with your pharmacists, chances are the interchange will impersonal—and that could mean missing ou
“Pharmacists may be underutilized, especially if the range of clinical services they offer are not recognized,” notes Kristine Gleason, RPh, clinical quality leader at Northwestern Memorial Hospital in Chicago. “We can be an excellent resource for young hospitalists and clinicians, offering information on clinical dosing and monitoring of complex, high-risk medications.”
Pharmacists also can be valuable resources for medication reconciliation and patient counseling, Gleason says, adding that “our goal is to work collaboratively with our clinicians to help ensure patients receive evidence-based medication regimens that are safe and without error and that are tailored to each patient’s individualized characteristics.”
Benefits of Rounding
Interactions between hospital pharmacies and HM services vary by institution size and organization. Roberta Barber, PharmD, MPH, is assistant vice president of pharmacy for Virtua Health’s four hospital campuses in New Jersey. At Memorial Hospital, where Erik DeLue, MD, MBA, SFHM, first established a hospitalist program, pharmacists are present in the ICU units and participate in care-coordination rounds.
Barber is crafting policies to extend the decentralized pharmacist model to all of Virtua’s hospitals. Equipped with cordless phones and tablet computers, pharmacists will be able to round with the HM team without sacrificing availability to other physicians and hospital staff. In this way, she says, “physicians will be able to consult with pharmacists as they’re creating their treatment plans, and the pharmacist can intervene regarding potential problem orders right then and there.”
At the University of California at San Francisco Medical Center, clinical pharmacists in the general medicine division work closely with the nine medicine teams run by hospitalists. That means 24/7 availability by pager, participating in multidisciplinary rounds, and furnishing new physicians with a “contacts” card and an orientation guide to help hospitalists write better orders, says Vicki Ising Jue, PharmD.
The personal touch is appreciated. “If I am in the pharmacy making a call and not on the unit, it just makes the phone call so much easier if the caller happens to be someone I’ve worked with before,” says UCSF’s Alan Tan, PharmD.
View hundreds of HM opportunities at SHM's Career Center
The degree of communication with pharmacy services may depend on whether you’re working in a teaching hospital with a structured orientation program or starting out in a community hospital. No matter the setting, though, Gleason says the pharmacist’s mission stays the same.
“We’re all striving to get to the same goal: safe, effective and patient-centered care to achieve positive outcomes for our patients,” she says. “Partnering with pharmacists can really move all of us closer to that goal.”
Gretchen Henkel is a freelance writer based in California.
Be PROACTIVE
One excellent way to foster collaboration with your hospital pharmacists and gain a better understanding of the medication management services they can provide, Gleason says, is to visit the department. “Spend an hour with us, shadow us, come to a meeting, and understand what we do professionally,” she explains.
Barber agrees: “If your hospital doesn’t offer training on the range of pharmacy services, solicit that yourself. Orient yourself to pharmacy rules and regulations; familiarize yourself with your hospital’s formulary and the role of the P&T committee in placing drugs on the formulary.”—GH
Geriatric Assessment Predicts Overall Survival in AML
PARIS – Impaired physical and cognitive abilities are predictive of worse overall survival in elderly patients with acute myeloid leukemia, according to prospective study findings.
In a 74-patient trial, scores of less than 9 out of 12 on the Short Physical Performance Battery (SPPB) and less than 77 out of 100 on a Modified Mini-Mental State (3MS) exam were associated with a threefold increase in risk of death, compared with scores in patients who had no physical or cognitive difficulties.
The study’s findings could ultimately help determine which elderly patients with acute myeloid leukemia (AML) are fit enough to receive standard chemotherapy regimens for the disease, and which may require a different therapeutic approach. The results should currently be viewed as a "signal" of a possible worse prognosis, however, until further validation.

"Acute leukemia is probably one of the most dramatic examples of age-related outcome disparity in oncology," said study author Dr. Heidi D. Klepin, of Wake Forest University, Winston-Salem, N.C.
"Older patients consistently do much worse when diagnosed with disease than [do] young patients," Dr. Klepin said on Nov. 4 in an interview at the annual meeting of the International Society for Geriatric Oncology (also known as Société Internationale d’Oncologie Gériatrique).
While much research has focused on examining tumor biology in older and younger patients with AML, few studies have looked at differences in the capabilities of the patients themselves, such as increasing vulnerability or frailty in the geriatric population.
"There has been so little done in geriatric assessment in the leukemia population," Dr. Stuart M. Lichtman said in a separate interview.
Dr. Lichtman of Memorial-Sloan–Kettering Cancer Center, N.Y., who was not involved in the study and served as scientific committee chair of the meeting, said the findings were important because they suggest that general and relatively simple-to-measure parameters could provide valuable information to help clinical decision-making. The SPPB includes asking patients to perform a 4-meter timed walk, stand after being in a seated position, and show how well they balance while standing.
The objective of the study was to assess whether performing a geriatric assessment at the patient’s bedside could predict patient’s likely overall survival. All of the patients included in the trial were about to start induction chemotherapy for AML.
The geriatric assessment consisted of multiple tests to examine cognition (3MS), emotion (Center for Epidemiological Studies Depression Scale, Distress Thermometer), self-reported disability (Pepper Assessment Tool for Disability) and objective (SPPB) physical function, grip strength, and the Hematopoietic Cell Transplantation Comorbidity Index (HCT-CI).
The mean age of patients included in the study was 70 years, 56% was male and 78% had an Eastern Cooperative Group Oncology Performance Status (ECOG PS) score of 0-1. The majority (95%) had an intermediate or poor cytogenic profile. The median follow-up was 7.4 months.
At baseline, 30% of patients were identified as having some form of cognitive impairment, 39% had depressive symptoms, 42% were distressed, 41% had reduced instrumental activities of daily living (IADL), 50% had reduced objective physical function, and 42% had comorbidities.
After researchers adjusted for a host of potentially confounding factors, including age, gender, ECOG PS, and cytogenic risk group, among others, hazard ratios for overall survival were 3.4 for SPPB score less than 9 (P =.03) and 3.0 for a 3MS score less than 77 (P = .008).
"There has been so little done in geriatric assessment in the leukemia population."
Reduced self-reported IADL was also associated with worse overall survival (HR, 2.6), but only after adjusting for confounding factors. SPPB and 3MS were also predictive on univariate analysis.
These data suggest that a better assessment of physical function could provide valuable information about a patient’s likely outcome, "even in clinical practice right now," Dr. Klepin said.
"I think we can use this to improve how patients do with standard treatments, by just paying attention [to baseline parameters] and changing how we manage people," she said. "If we are aware of a problem, can we do things that would prevent that problem from putting a patient in the ICU?"
Dr. Klepin also noted that the information provided by the geriatric assessment could be used to inform and to help patents decide whether they want to be treated with standard chemotherapy or perhaps enter into an appropriate clinical trial of novel agents.
Preliminary data from the trial have been published in the Journal of the American Geriatrics Society (2011;59:1837-46).
The study was supported by the American Society of Hematology, Atlantic Philanthropies, the John A. Hartford Association, the Association of Specialty Professors, and the Pepper Center at Wake Forest University. Dr. Klepin and Dr. Lichtman did not report any conflicts of interest.
PARIS – Impaired physical and cognitive abilities are predictive of worse overall survival in elderly patients with acute myeloid leukemia, according to prospective study findings.
In a 74-patient trial, scores of less than 9 out of 12 on the Short Physical Performance Battery (SPPB) and less than 77 out of 100 on a Modified Mini-Mental State (3MS) exam were associated with a threefold increase in risk of death, compared with scores in patients who had no physical or cognitive difficulties.
The study’s findings could ultimately help determine which elderly patients with acute myeloid leukemia (AML) are fit enough to receive standard chemotherapy regimens for the disease, and which may require a different therapeutic approach. The results should currently be viewed as a "signal" of a possible worse prognosis, however, until further validation.
"Acute leukemia is probably one of the most dramatic examples of age-related outcome disparity in oncology," said study author Dr. Heidi D. Klepin, of Wake Forest University, Winston-Salem, N.C.
"Older patients consistently do much worse when diagnosed with disease than [do] young patients," Dr. Klepin said on Nov. 4 in an interview at the annual meeting of the International Society for Geriatric Oncology (also known as Société Internationale d’Oncologie Gériatrique).
While much research has focused on examining tumor biology in older and younger patients with AML, few studies have looked at differences in the capabilities of the patients themselves, such as increasing vulnerability or frailty in the geriatric population.
"There has been so little done in geriatric assessment in the leukemia population," Dr. Stuart M. Lichtman said in a separate interview.
Dr. Lichtman of Memorial-Sloan–Kettering Cancer Center, N.Y., who was not involved in the study and served as scientific committee chair of the meeting, said the findings were important because they suggest that general and relatively simple-to-measure parameters could provide valuable information to help clinical decision-making. The SPPB includes asking patients to perform a 4-meter timed walk, stand after being in a seated position, and show how well they balance while standing.
The objective of the study was to assess whether performing a geriatric assessment at the patient’s bedside could predict patient’s likely overall survival. All of the patients included in the trial were about to start induction chemotherapy for AML.
The geriatric assessment consisted of multiple tests to examine cognition (3MS), emotion (Center for Epidemiological Studies Depression Scale, Distress Thermometer), self-reported disability (Pepper Assessment Tool for Disability) and objective (SPPB) physical function, grip strength, and the Hematopoietic Cell Transplantation Comorbidity Index (HCT-CI).
The mean age of patients included in the study was 70 years, 56% was male and 78% had an Eastern Cooperative Group Oncology Performance Status (ECOG PS) score of 0-1. The majority (95%) had an intermediate or poor cytogenic profile. The median follow-up was 7.4 months.
At baseline, 30% of patients were identified as having some form of cognitive impairment, 39% had depressive symptoms, 42% were distressed, 41% had reduced instrumental activities of daily living (IADL), 50% had reduced objective physical function, and 42% had comorbidities.
After researchers adjusted for a host of potentially confounding factors, including age, gender, ECOG PS, and cytogenic risk group, among others, hazard ratios for overall survival were 3.4 for SPPB score less than 9 (P =.03) and 3.0 for a 3MS score less than 77 (P = .008).
"There has been so little done in geriatric assessment in the leukemia population."
Reduced self-reported IADL was also associated with worse overall survival (HR, 2.6), but only after adjusting for confounding factors. SPPB and 3MS were also predictive on univariate analysis.
These data suggest that a better assessment of physical function could provide valuable information about a patient’s likely outcome, "even in clinical practice right now," Dr. Klepin said.
"I think we can use this to improve how patients do with standard treatments, by just paying attention [to baseline parameters] and changing how we manage people," she said. "If we are aware of a problem, can we do things that would prevent that problem from putting a patient in the ICU?"
Dr. Klepin also noted that the information provided by the geriatric assessment could be used to inform and to help patents decide whether they want to be treated with standard chemotherapy or perhaps enter into an appropriate clinical trial of novel agents.
Preliminary data from the trial have been published in the Journal of the American Geriatrics Society (2011;59:1837-46).
The study was supported by the American Society of Hematology, Atlantic Philanthropies, the John A. Hartford Association, the Association of Specialty Professors, and the Pepper Center at Wake Forest University. Dr. Klepin and Dr. Lichtman did not report any conflicts of interest.
PARIS – Impaired physical and cognitive abilities are predictive of worse overall survival in elderly patients with acute myeloid leukemia, according to prospective study findings.
In a 74-patient trial, scores of less than 9 out of 12 on the Short Physical Performance Battery (SPPB) and less than 77 out of 100 on a Modified Mini-Mental State (3MS) exam were associated with a threefold increase in risk of death, compared with scores in patients who had no physical or cognitive difficulties.
The study’s findings could ultimately help determine which elderly patients with acute myeloid leukemia (AML) are fit enough to receive standard chemotherapy regimens for the disease, and which may require a different therapeutic approach. The results should currently be viewed as a "signal" of a possible worse prognosis, however, until further validation.
"Acute leukemia is probably one of the most dramatic examples of age-related outcome disparity in oncology," said study author Dr. Heidi D. Klepin, of Wake Forest University, Winston-Salem, N.C.
"Older patients consistently do much worse when diagnosed with disease than [do] young patients," Dr. Klepin said on Nov. 4 in an interview at the annual meeting of the International Society for Geriatric Oncology (also known as Société Internationale d’Oncologie Gériatrique).
While much research has focused on examining tumor biology in older and younger patients with AML, few studies have looked at differences in the capabilities of the patients themselves, such as increasing vulnerability or frailty in the geriatric population.
"There has been so little done in geriatric assessment in the leukemia population," Dr. Stuart M. Lichtman said in a separate interview.
Dr. Lichtman of Memorial-Sloan–Kettering Cancer Center, N.Y., who was not involved in the study and served as scientific committee chair of the meeting, said the findings were important because they suggest that general and relatively simple-to-measure parameters could provide valuable information to help clinical decision-making. The SPPB includes asking patients to perform a 4-meter timed walk, stand after being in a seated position, and show how well they balance while standing.
The objective of the study was to assess whether performing a geriatric assessment at the patient’s bedside could predict patient’s likely overall survival. All of the patients included in the trial were about to start induction chemotherapy for AML.
The geriatric assessment consisted of multiple tests to examine cognition (3MS), emotion (Center for Epidemiological Studies Depression Scale, Distress Thermometer), self-reported disability (Pepper Assessment Tool for Disability) and objective (SPPB) physical function, grip strength, and the Hematopoietic Cell Transplantation Comorbidity Index (HCT-CI).
The mean age of patients included in the study was 70 years, 56% was male and 78% had an Eastern Cooperative Group Oncology Performance Status (ECOG PS) score of 0-1. The majority (95%) had an intermediate or poor cytogenic profile. The median follow-up was 7.4 months.
At baseline, 30% of patients were identified as having some form of cognitive impairment, 39% had depressive symptoms, 42% were distressed, 41% had reduced instrumental activities of daily living (IADL), 50% had reduced objective physical function, and 42% had comorbidities.
After researchers adjusted for a host of potentially confounding factors, including age, gender, ECOG PS, and cytogenic risk group, among others, hazard ratios for overall survival were 3.4 for SPPB score less than 9 (P =.03) and 3.0 for a 3MS score less than 77 (P = .008).
"There has been so little done in geriatric assessment in the leukemia population."
Reduced self-reported IADL was also associated with worse overall survival (HR, 2.6), but only after adjusting for confounding factors. SPPB and 3MS were also predictive on univariate analysis.
These data suggest that a better assessment of physical function could provide valuable information about a patient’s likely outcome, "even in clinical practice right now," Dr. Klepin said.
"I think we can use this to improve how patients do with standard treatments, by just paying attention [to baseline parameters] and changing how we manage people," she said. "If we are aware of a problem, can we do things that would prevent that problem from putting a patient in the ICU?"
Dr. Klepin also noted that the information provided by the geriatric assessment could be used to inform and to help patents decide whether they want to be treated with standard chemotherapy or perhaps enter into an appropriate clinical trial of novel agents.
Preliminary data from the trial have been published in the Journal of the American Geriatrics Society (2011;59:1837-46).
The study was supported by the American Society of Hematology, Atlantic Philanthropies, the John A. Hartford Association, the Association of Specialty Professors, and the Pepper Center at Wake Forest University. Dr. Klepin and Dr. Lichtman did not report any conflicts of interest.
FROM THE ANNUAL MEETING OF THE INTERNATIONAL SOCIETY FOR GERIATRIC ONCOLOGY
Major Finding: Scores of less than 9 out of 12 on the Short Physical Performance Battery (SPPB) and less than 77 out of 100 on a Modified Mini-Mental State exam (3MS) were associated with a threefold increase in risk of death.
Data Source: Prospective trial of 74 elderly hospitalized patients undergoing induction chemotherapy for acute myeloid leukemia.
Disclosures: The study was supported by the American Society of Hematology, Atlantic Philanthropies, the John A. Hartford Association, the Association of Specialty Professors, and the Pepper Center at Wake Forest University. Dr. Klepin and Dr. Lichtman had no conflicts of interest.
A Grumpy Old Man
Ms Chen acutely worse, altered, please assist, room 522Beth, chirped my pager. Ever increasing time pressures meant that hospitalists were supervising rounds almost daily. I had sent my resident, Beth, and the rest of the team to round separately that day, to foster their independence. It looked like we would be meeting ahead of schedule.
I'd received a similar page 2 years earlier when I was a junior resident myself. From the beginning of internship, our faculty never hesitated to challenge us. I will never forget when one of the hospitalists who had just come across an unresponsive patient tapped me on the shoulder and casually asked, Hey, you wanna run a code? and will never forget my inadequacy or the specific assistance I required in those tense few minutes. He, and the ICU team that arrived, gave me every chance to lead, and supported me each time I hesitated.
In similar fashion, I had sent my intern, David, to admit a patient with suspected CHF. I received his urgent update shortly after our patient arrived on the cardiology floor: Mr Johnson dropping sats, please help, room 207. I jogged to the patient's room, where I found David, 3 nurses, 2 medical students, and in the center, Mr Johnson: lethargic, gray, cachectic, and making no effort to rise from the 40 degree incline of his hospital bed. Weak respirations fogged his non‐rebreather mask about 28 times a minute.
David offered a quick report: 74‐year‐old male, CAD, hypertension, dementia CHF exacerbation hypertensive to 190. I think he needs IV nitroglycerin and another 80 of lasix.
I was pleased to hear him commit to a diagnosis and plan, but after sitting Mr Johnson up for a quick exam, I couldn't agree. Are you sure? He sounds more junky than crackly. Neck veins are flat.
His EF is 25% and he's been here 3 times with CHF.
Well, that won't protect him from anything else. Mr Johnson slumped forward, accessory muscles firing weakly, and only half‐opened his eyes to a loud command and vigorous shake. Well, let's get the diagnosis later, what does he need, now?
Well, the lasix and the nitro
Assuming this is CHF, looking at him now, will that work fast enough to prevent intubation? David shook his head no. He's full code, right? Let's just call a code before he gets any worse. Anyone disagree? A nurse made the call, then guarded the door to turn away everyone but anesthesia and the MICU as they arrived.
So what do you think it is? David asked.
This doesn't smell like failure. He's not anxious, he's more obtunded than dyspneic. He looks hypercarbic. He doesn't have COPD?
Nah, just vomiting, then weaker, more confused, restless.
Maybe he aspirated. We'll see. So what do you want to have ready for anesthesia?
Um, meds. An IV. Chest X‐ray ready.
Good they bring the meds he's got an IV how about we pull the bed from the wall and raise it up, get some suction ready, take the headboard off? Nurses sprang into action.
If he's hypercarbic, shouldn't we bag him? David asked.
Good point, I said. David took the mask from the bag of emergency gear from the wall and started to fit it on Mr Johnson. It's a 2‐person job, if you want to hold the mask2 hands, good. A nurse began ventilations, and I added some cricoid pressure. Keeps us from inflating his stomach.
Seconds later, anesthesia arrived, and David provided a concise, organized summary. Mr Johnson was intubated and whisked without incident to the MICU, where bronchoscopy extracted several mucus plugs. He was soon extubated, and later recovered from a delirium which began with promethazine for nausea. It was the last year before the 80‐hour workweek regulations, and not once in the entire processfrom admission, to emergency on the ward, to initial MICU managementdid I or my fellow residents think to call an attending, although I'm sure we would have learned something, as I hadn't suspected a mucous plug. We weren't hiding anything. We were just taking care of our patient.
Two years later, it didn't seem odd that my junior resident called me for assistance with Ms Cheninitially. In room 522, much as I found Mr Johnson, I found Ms Chen: elderly, lethargic, gray, frail, laboring to breathe, rhythmically fogging a non‐rebreather mask 30 times a minute, only half‐opening her eyes to a vigorous shake. It was day 4 of her fifth hospitalization for bronchiectasis‐related respiratory failure within 2 months.
She just got a treatment but she still sounds awful, offered Beth. Indeed, Ms Chen's chest was gurgly and wheezy throughout. We put her on a non‐rebreather, but that hasn't helped.
I glanced at her monitor. Sat's 99%. What was she before?
96%.
So hypoxia isn't the problemwho's this? I asked, as transportation staff arrived.
Stat head CT for Chen, he replied.
I'm sorry, she can't go off the floor right now. Thanks for coming, I apologized, and sent him away. Beth, can you lay her flat or send her off the unit right now?
She's altered and I need to rule out stroke.
Let's talk about that later. I did a quick neuro exam as I spoke: Besides, she resists weak but equal; pupils and face symmetricshe's not focal. What's a more likely cause?
Metabolic? We can repeat her morning labs
Will they be different? Why is she here? What's her exam telling you?
Beth took in the scene before her, as Ms Chen struggled weakly to ventilate her lungs, and after a brief pause she had it worked out. She's hypercarbic. She needs an ABG. You think she plugged? She shook her head, and grasped Ms Chen's hand in her own. But she really hates suctioning.
Well, she's DNI, and without it, she could die. Beth agreed; we also called for noninvasive ventilation. But the team missed much of the action. The medical student missed the entire eventaside from attempting to summarize it from second‐hand reports for rounds the following day. I realized only later that her intern had been pushed to the back of the room for the critical decisions (much like the students during Mr Johnson's emergency), and headed out midway to attend a mandatory teaching sessionthe chief residents had begun taking attendance. The resident soon left for noon conference and afternoon clinic, enlisting me to write transfer orders and call the family. Finished with her other work, and under pressure to bank time against work hour limitations, which she was at risk of violating, the intern signed her pager over to me and left in the early afternoon, after sheepishly asking me if I wouldn't mind keeping an eye on our patient.
Later, a translator and I met with the Chens to comfort them and plan care for the family matriarch, having found a quiet solarium we could use, with summery views of the city and ocean in the distance to belie the grim topic of discussion.
What is your understanding of her lung problem right now?
Nay yeega jee um'jee huigor fai ho jing yeung?
What were her hopes and fears about her health?
Nay jee um'jee huigor see seung hai mai ho tai hoi?
My mind drifted during the Cantonese as I thought about how I use the unique teaching opportunities offered by wholly translated meetings. Never check the time. This body language says I am listening. I am speaking to them, not the translator. I make notes because families don't remember much after the C‐word, I would whisper to trainees while families conversed with translators. Now, as I began to discuss hospice philosophy, I felt acutely alone.
My team had missed most of a great hospital medicine experience: applying knowledge to manage a physiologic crisis; using communication skills to ease the resulting human crisis. Recently, to manage the latest set of work hour restrictions, our residency program withdrew from medicine consultation at 2 of 3 sites, and from the medicine wards at the hospital that serves most of our insured, geriatric, and oncology patients. The cost of this experiment to the overall residency experience is unknown. But cases like Ms Chen's remind me how much I missed being the primary doctor. I do not mind the new tasks I perform for my trainees. But I worry about what they are missing: sufficient responsibility for making key clinical decisions while protected by supervision on demand. I am glad my internship challenged meit prepared me for residency, moonlighting, and attending positions. Without a doubt, residency remains challenging, but it seems that the greatestor firstchallenge imposed on residents is now to beat the clock, not to become a well‐rounded, capable, independent physician.
That night, I complained to my spouse, then a psychiatry intern: We weren't giving our trainees the best preparation for a career in medicine the lengthy shift I spent managing a hypotensive crisis would be forbidden now my pre‐work hours interns were much happier than their work hours successors a 4‐year residency must be around the corner. The response I got was more bemused smile than grave concern. You don't think that's important? I asked.
Of course I do. It's just that with all this talk about the days of the giants, he said gently, you're starting to sound like a grumpy old man. We chuckled. He was right. I expect a lot from myself, my trainees, and every clinician. I'd figured I'd be worthy of the title at some point.
But at 30?
Ms Chen acutely worse, altered, please assist, room 522Beth, chirped my pager. Ever increasing time pressures meant that hospitalists were supervising rounds almost daily. I had sent my resident, Beth, and the rest of the team to round separately that day, to foster their independence. It looked like we would be meeting ahead of schedule.
I'd received a similar page 2 years earlier when I was a junior resident myself. From the beginning of internship, our faculty never hesitated to challenge us. I will never forget when one of the hospitalists who had just come across an unresponsive patient tapped me on the shoulder and casually asked, Hey, you wanna run a code? and will never forget my inadequacy or the specific assistance I required in those tense few minutes. He, and the ICU team that arrived, gave me every chance to lead, and supported me each time I hesitated.
In similar fashion, I had sent my intern, David, to admit a patient with suspected CHF. I received his urgent update shortly after our patient arrived on the cardiology floor: Mr Johnson dropping sats, please help, room 207. I jogged to the patient's room, where I found David, 3 nurses, 2 medical students, and in the center, Mr Johnson: lethargic, gray, cachectic, and making no effort to rise from the 40 degree incline of his hospital bed. Weak respirations fogged his non‐rebreather mask about 28 times a minute.
David offered a quick report: 74‐year‐old male, CAD, hypertension, dementia CHF exacerbation hypertensive to 190. I think he needs IV nitroglycerin and another 80 of lasix.
I was pleased to hear him commit to a diagnosis and plan, but after sitting Mr Johnson up for a quick exam, I couldn't agree. Are you sure? He sounds more junky than crackly. Neck veins are flat.
His EF is 25% and he's been here 3 times with CHF.
Well, that won't protect him from anything else. Mr Johnson slumped forward, accessory muscles firing weakly, and only half‐opened his eyes to a loud command and vigorous shake. Well, let's get the diagnosis later, what does he need, now?
Well, the lasix and the nitro
Assuming this is CHF, looking at him now, will that work fast enough to prevent intubation? David shook his head no. He's full code, right? Let's just call a code before he gets any worse. Anyone disagree? A nurse made the call, then guarded the door to turn away everyone but anesthesia and the MICU as they arrived.
So what do you think it is? David asked.
This doesn't smell like failure. He's not anxious, he's more obtunded than dyspneic. He looks hypercarbic. He doesn't have COPD?
Nah, just vomiting, then weaker, more confused, restless.
Maybe he aspirated. We'll see. So what do you want to have ready for anesthesia?
Um, meds. An IV. Chest X‐ray ready.
Good they bring the meds he's got an IV how about we pull the bed from the wall and raise it up, get some suction ready, take the headboard off? Nurses sprang into action.
If he's hypercarbic, shouldn't we bag him? David asked.
Good point, I said. David took the mask from the bag of emergency gear from the wall and started to fit it on Mr Johnson. It's a 2‐person job, if you want to hold the mask2 hands, good. A nurse began ventilations, and I added some cricoid pressure. Keeps us from inflating his stomach.
Seconds later, anesthesia arrived, and David provided a concise, organized summary. Mr Johnson was intubated and whisked without incident to the MICU, where bronchoscopy extracted several mucus plugs. He was soon extubated, and later recovered from a delirium which began with promethazine for nausea. It was the last year before the 80‐hour workweek regulations, and not once in the entire processfrom admission, to emergency on the ward, to initial MICU managementdid I or my fellow residents think to call an attending, although I'm sure we would have learned something, as I hadn't suspected a mucous plug. We weren't hiding anything. We were just taking care of our patient.
Two years later, it didn't seem odd that my junior resident called me for assistance with Ms Cheninitially. In room 522, much as I found Mr Johnson, I found Ms Chen: elderly, lethargic, gray, frail, laboring to breathe, rhythmically fogging a non‐rebreather mask 30 times a minute, only half‐opening her eyes to a vigorous shake. It was day 4 of her fifth hospitalization for bronchiectasis‐related respiratory failure within 2 months.
She just got a treatment but she still sounds awful, offered Beth. Indeed, Ms Chen's chest was gurgly and wheezy throughout. We put her on a non‐rebreather, but that hasn't helped.
I glanced at her monitor. Sat's 99%. What was she before?
96%.
So hypoxia isn't the problemwho's this? I asked, as transportation staff arrived.
Stat head CT for Chen, he replied.
I'm sorry, she can't go off the floor right now. Thanks for coming, I apologized, and sent him away. Beth, can you lay her flat or send her off the unit right now?
She's altered and I need to rule out stroke.
Let's talk about that later. I did a quick neuro exam as I spoke: Besides, she resists weak but equal; pupils and face symmetricshe's not focal. What's a more likely cause?
Metabolic? We can repeat her morning labs
Will they be different? Why is she here? What's her exam telling you?
Beth took in the scene before her, as Ms Chen struggled weakly to ventilate her lungs, and after a brief pause she had it worked out. She's hypercarbic. She needs an ABG. You think she plugged? She shook her head, and grasped Ms Chen's hand in her own. But she really hates suctioning.
Well, she's DNI, and without it, she could die. Beth agreed; we also called for noninvasive ventilation. But the team missed much of the action. The medical student missed the entire eventaside from attempting to summarize it from second‐hand reports for rounds the following day. I realized only later that her intern had been pushed to the back of the room for the critical decisions (much like the students during Mr Johnson's emergency), and headed out midway to attend a mandatory teaching sessionthe chief residents had begun taking attendance. The resident soon left for noon conference and afternoon clinic, enlisting me to write transfer orders and call the family. Finished with her other work, and under pressure to bank time against work hour limitations, which she was at risk of violating, the intern signed her pager over to me and left in the early afternoon, after sheepishly asking me if I wouldn't mind keeping an eye on our patient.
Later, a translator and I met with the Chens to comfort them and plan care for the family matriarch, having found a quiet solarium we could use, with summery views of the city and ocean in the distance to belie the grim topic of discussion.
What is your understanding of her lung problem right now?
Nay yeega jee um'jee huigor fai ho jing yeung?
What were her hopes and fears about her health?
Nay jee um'jee huigor see seung hai mai ho tai hoi?
My mind drifted during the Cantonese as I thought about how I use the unique teaching opportunities offered by wholly translated meetings. Never check the time. This body language says I am listening. I am speaking to them, not the translator. I make notes because families don't remember much after the C‐word, I would whisper to trainees while families conversed with translators. Now, as I began to discuss hospice philosophy, I felt acutely alone.
My team had missed most of a great hospital medicine experience: applying knowledge to manage a physiologic crisis; using communication skills to ease the resulting human crisis. Recently, to manage the latest set of work hour restrictions, our residency program withdrew from medicine consultation at 2 of 3 sites, and from the medicine wards at the hospital that serves most of our insured, geriatric, and oncology patients. The cost of this experiment to the overall residency experience is unknown. But cases like Ms Chen's remind me how much I missed being the primary doctor. I do not mind the new tasks I perform for my trainees. But I worry about what they are missing: sufficient responsibility for making key clinical decisions while protected by supervision on demand. I am glad my internship challenged meit prepared me for residency, moonlighting, and attending positions. Without a doubt, residency remains challenging, but it seems that the greatestor firstchallenge imposed on residents is now to beat the clock, not to become a well‐rounded, capable, independent physician.
That night, I complained to my spouse, then a psychiatry intern: We weren't giving our trainees the best preparation for a career in medicine the lengthy shift I spent managing a hypotensive crisis would be forbidden now my pre‐work hours interns were much happier than their work hours successors a 4‐year residency must be around the corner. The response I got was more bemused smile than grave concern. You don't think that's important? I asked.
Of course I do. It's just that with all this talk about the days of the giants, he said gently, you're starting to sound like a grumpy old man. We chuckled. He was right. I expect a lot from myself, my trainees, and every clinician. I'd figured I'd be worthy of the title at some point.
But at 30?
Ms Chen acutely worse, altered, please assist, room 522Beth, chirped my pager. Ever increasing time pressures meant that hospitalists were supervising rounds almost daily. I had sent my resident, Beth, and the rest of the team to round separately that day, to foster their independence. It looked like we would be meeting ahead of schedule.
I'd received a similar page 2 years earlier when I was a junior resident myself. From the beginning of internship, our faculty never hesitated to challenge us. I will never forget when one of the hospitalists who had just come across an unresponsive patient tapped me on the shoulder and casually asked, Hey, you wanna run a code? and will never forget my inadequacy or the specific assistance I required in those tense few minutes. He, and the ICU team that arrived, gave me every chance to lead, and supported me each time I hesitated.
In similar fashion, I had sent my intern, David, to admit a patient with suspected CHF. I received his urgent update shortly after our patient arrived on the cardiology floor: Mr Johnson dropping sats, please help, room 207. I jogged to the patient's room, where I found David, 3 nurses, 2 medical students, and in the center, Mr Johnson: lethargic, gray, cachectic, and making no effort to rise from the 40 degree incline of his hospital bed. Weak respirations fogged his non‐rebreather mask about 28 times a minute.
David offered a quick report: 74‐year‐old male, CAD, hypertension, dementia CHF exacerbation hypertensive to 190. I think he needs IV nitroglycerin and another 80 of lasix.
I was pleased to hear him commit to a diagnosis and plan, but after sitting Mr Johnson up for a quick exam, I couldn't agree. Are you sure? He sounds more junky than crackly. Neck veins are flat.
His EF is 25% and he's been here 3 times with CHF.
Well, that won't protect him from anything else. Mr Johnson slumped forward, accessory muscles firing weakly, and only half‐opened his eyes to a loud command and vigorous shake. Well, let's get the diagnosis later, what does he need, now?
Well, the lasix and the nitro
Assuming this is CHF, looking at him now, will that work fast enough to prevent intubation? David shook his head no. He's full code, right? Let's just call a code before he gets any worse. Anyone disagree? A nurse made the call, then guarded the door to turn away everyone but anesthesia and the MICU as they arrived.
So what do you think it is? David asked.
This doesn't smell like failure. He's not anxious, he's more obtunded than dyspneic. He looks hypercarbic. He doesn't have COPD?
Nah, just vomiting, then weaker, more confused, restless.
Maybe he aspirated. We'll see. So what do you want to have ready for anesthesia?
Um, meds. An IV. Chest X‐ray ready.
Good they bring the meds he's got an IV how about we pull the bed from the wall and raise it up, get some suction ready, take the headboard off? Nurses sprang into action.
If he's hypercarbic, shouldn't we bag him? David asked.
Good point, I said. David took the mask from the bag of emergency gear from the wall and started to fit it on Mr Johnson. It's a 2‐person job, if you want to hold the mask2 hands, good. A nurse began ventilations, and I added some cricoid pressure. Keeps us from inflating his stomach.
Seconds later, anesthesia arrived, and David provided a concise, organized summary. Mr Johnson was intubated and whisked without incident to the MICU, where bronchoscopy extracted several mucus plugs. He was soon extubated, and later recovered from a delirium which began with promethazine for nausea. It was the last year before the 80‐hour workweek regulations, and not once in the entire processfrom admission, to emergency on the ward, to initial MICU managementdid I or my fellow residents think to call an attending, although I'm sure we would have learned something, as I hadn't suspected a mucous plug. We weren't hiding anything. We were just taking care of our patient.
Two years later, it didn't seem odd that my junior resident called me for assistance with Ms Cheninitially. In room 522, much as I found Mr Johnson, I found Ms Chen: elderly, lethargic, gray, frail, laboring to breathe, rhythmically fogging a non‐rebreather mask 30 times a minute, only half‐opening her eyes to a vigorous shake. It was day 4 of her fifth hospitalization for bronchiectasis‐related respiratory failure within 2 months.
She just got a treatment but she still sounds awful, offered Beth. Indeed, Ms Chen's chest was gurgly and wheezy throughout. We put her on a non‐rebreather, but that hasn't helped.
I glanced at her monitor. Sat's 99%. What was she before?
96%.
So hypoxia isn't the problemwho's this? I asked, as transportation staff arrived.
Stat head CT for Chen, he replied.
I'm sorry, she can't go off the floor right now. Thanks for coming, I apologized, and sent him away. Beth, can you lay her flat or send her off the unit right now?
She's altered and I need to rule out stroke.
Let's talk about that later. I did a quick neuro exam as I spoke: Besides, she resists weak but equal; pupils and face symmetricshe's not focal. What's a more likely cause?
Metabolic? We can repeat her morning labs
Will they be different? Why is she here? What's her exam telling you?
Beth took in the scene before her, as Ms Chen struggled weakly to ventilate her lungs, and after a brief pause she had it worked out. She's hypercarbic. She needs an ABG. You think she plugged? She shook her head, and grasped Ms Chen's hand in her own. But she really hates suctioning.
Well, she's DNI, and without it, she could die. Beth agreed; we also called for noninvasive ventilation. But the team missed much of the action. The medical student missed the entire eventaside from attempting to summarize it from second‐hand reports for rounds the following day. I realized only later that her intern had been pushed to the back of the room for the critical decisions (much like the students during Mr Johnson's emergency), and headed out midway to attend a mandatory teaching sessionthe chief residents had begun taking attendance. The resident soon left for noon conference and afternoon clinic, enlisting me to write transfer orders and call the family. Finished with her other work, and under pressure to bank time against work hour limitations, which she was at risk of violating, the intern signed her pager over to me and left in the early afternoon, after sheepishly asking me if I wouldn't mind keeping an eye on our patient.
Later, a translator and I met with the Chens to comfort them and plan care for the family matriarch, having found a quiet solarium we could use, with summery views of the city and ocean in the distance to belie the grim topic of discussion.
What is your understanding of her lung problem right now?
Nay yeega jee um'jee huigor fai ho jing yeung?
What were her hopes and fears about her health?
Nay jee um'jee huigor see seung hai mai ho tai hoi?
My mind drifted during the Cantonese as I thought about how I use the unique teaching opportunities offered by wholly translated meetings. Never check the time. This body language says I am listening. I am speaking to them, not the translator. I make notes because families don't remember much after the C‐word, I would whisper to trainees while families conversed with translators. Now, as I began to discuss hospice philosophy, I felt acutely alone.
My team had missed most of a great hospital medicine experience: applying knowledge to manage a physiologic crisis; using communication skills to ease the resulting human crisis. Recently, to manage the latest set of work hour restrictions, our residency program withdrew from medicine consultation at 2 of 3 sites, and from the medicine wards at the hospital that serves most of our insured, geriatric, and oncology patients. The cost of this experiment to the overall residency experience is unknown. But cases like Ms Chen's remind me how much I missed being the primary doctor. I do not mind the new tasks I perform for my trainees. But I worry about what they are missing: sufficient responsibility for making key clinical decisions while protected by supervision on demand. I am glad my internship challenged meit prepared me for residency, moonlighting, and attending positions. Without a doubt, residency remains challenging, but it seems that the greatestor firstchallenge imposed on residents is now to beat the clock, not to become a well‐rounded, capable, independent physician.
That night, I complained to my spouse, then a psychiatry intern: We weren't giving our trainees the best preparation for a career in medicine the lengthy shift I spent managing a hypotensive crisis would be forbidden now my pre‐work hours interns were much happier than their work hours successors a 4‐year residency must be around the corner. The response I got was more bemused smile than grave concern. You don't think that's important? I asked.
Of course I do. It's just that with all this talk about the days of the giants, he said gently, you're starting to sound like a grumpy old man. We chuckled. He was right. I expect a lot from myself, my trainees, and every clinician. I'd figured I'd be worthy of the title at some point.
But at 30?
VRE Bacteremia Treatment With Linezolid or Daptomycin
Enterococci have been identified as a causative organism in approximately 10% of all nosocomial bloodstream infections (BSIs).1, 2 In 2006, the Infectious Diseases Society of America identified vancomycin‐ resistant Enterococcus faecium (VRE) as 1 of 6 microbes considered to be among the most dangerous due to high rates of resistance and a limited number of effective antimicrobials.3 E. faecium has exhibited high rates of glycopeptide resistance with as many as 60% of isolates from BSIs being resistant to vancomycin.2, 4 Due to increasing resistance to glycopeptides, vancomycin has become obsolete in the treatment of E. faecium infections.5
A limited number of antimicrobials are available for the treatment of infections due to VRE. Agents active in vitro are quinupristin‐dalfopristin, tigecycline, linezolid, and daptomycin. Quinupristin‐dalfopristin was one of the first agents approved for use in VRE infections; however, treatment with this agent has been limited because of mediocre clinical response rates, undesirable adverse effects, high cost, and insufficient E. faecalis activity.6, 7 Tigecycline is not an optimal antibiotic for the treatment of VRE bacteremia, because serum concentrations achieved after administration are inadequate to treat BSIs.7 In contrast, linezolid and daptomycin have evinced efficacy against VRE bacteremia, with reported microbiologic response rates of 85% and 80%, respectively.7, 8 One inherent difference between these antibiotics that may theoretically affect their use in immunocompromised patients is that linezolid is bacteriostatic, whereas daptomycin is bactericidal. It has been postulated that by using a bactericidal antibiotic such as daptomycin in the immunocompromised host, one may achieve superior clinical and microbiologic response rates.3, 7, 9, 10
Since the introduction of the oxazolidinone linezolid in 2000, widespread use has led to reports of linezolid‐resistant VRE as well as nosocomial transmission of linezolid‐resistant VRE in hospitals.4, 1114 Despite linezolid being a key antibiotic for the treatment of VRE infections over the last 10 years, development of resistance along with potential hematologic and neurologic toxicity during long‐term use remains a concern.7, 8 Although daptomycin is active against several resistant organisms, including VRE, the evidence supporting use of daptomycin for VRE BSI is limited to case reports or small case series.7, 9 Moreover, daptomycin has not received US Food and Drug Administration approval for the treatment of VRE infections,15 and emerging data regarding daptomycin‐nonsusceptible enterococci (Minimum Inhibitory Concentration, MIC >4 mg/L) highlight a new problem for this multidrug‐resistant pathogen.16, 17 Few studies in recent years have compared these 2 antibiotics in the treatment of VRE BSIs.4, 18, 19 Due to the high rates of vancomycin resistance reported at our institution and the ubiquitous use of linezolid and daptomycin in the treatment of VRE bacteremia, we chose to evaluate response rates for these antibiotics in an effort to add to previously published literature on this topic.
MATERIALS AND METHODS
Patient Selection
Methodist University Hospital (MUH) in Memphis, Tennessee, is part of a 7‐hospital system with 697 licensed beds. MUH is a tertiary teaching hospital with centers of excellence in neuroscience and transplantation. Patients admitted to MUH diagnosed with VRE bacteremia between January 1, 2004, and July 31, 2009, were identified by the microbiology laboratory. All patients who were 18 years of age, had 1 documented positive VRE blood culture, and received linezolid or daptomycin for 5 days were eligible. Patients were excluded if they were treated simultaneously with more than 1 agent active against VRE. This study was approved by the MUH Institutional Review Board. Of note, use of linezolid or daptomycin at MUH is restricted to an infectious disease physician or pulmonologist. Currently, there are no protocols at our institution for treating VRE infections.
Data Collection and Definitions
Cerner Millennium was used to collect all pertinent patient information. Patient records were reviewed to determine demographic data, comorbid illnesses, laboratory data (from admission to discharge), medications, and discharge status (home, long‐term care facility, or death). Comorbid illnesses evaluated included: chronic obstructive pulmonary disease, diabetes mellitus, malignancy (solid or hematologic), transplant (liver or kidney), end‐stage renal disease (ESRD) (hemodialysis or nonhemodialysis), cirrhosis, and endocarditis. ESRD and endocarditis were defined per chart diagnosis. Laboratory data collected included serum creatinine, creatine phosphokinase, absolute neutrophil count (neutropenia defined as absolute neutrophil count <1000), and number and site (intravenous line or peripheral blood draw) of positive VRE blood cultures. Other data collected were (1) time elapsed to adequate antibiotic coverage, which was defined as microbiologic documentation of an infection that was being effectively treated at the time of its identification, and (2) time to appropriate antibiotic coverage, which was defined as antimicrobial treatment selected for efficacy based on presumptive identification of the causative pathogen, the antimicrobial agent's spectrum of activity, and local microbial resistance patterns.20 Doses of daptomycin and linezolid used in patients with VRE bacteremia were also documented.
Clinical cure was defined as a resolution of signs and/or symptoms of infection (white blood cell count <10,000/mm3, bands <5%, heart rate <90 beats per minute, respiratory rate <20 breaths per minute, and maximum oral temperature <38C) after gram‐positive therapy was discontinued. The definition of microbiologic cure was lack of positive blood cultures for VRE at least 14 days after cessation of gram‐positive therapy. Microbiologic failure was defined as positive VRE blood cultures obtained on gram‐positive therapy necessitating a change in treatment. Recurrence was defined as VRE bacteremia within 30 days after discontinuation of gram‐positive therapy. Reinfection was defined as VRE bacteremia that appeared 30 days after completion of primary gram‐positive therapy.
All isolates were tested for susceptibility to linezolid using the MicroScan system, whereas daptomycin susceptibility patterns were obtained by either the Etest or MicroScan system. Of importance, our laboratory did not routinely report isolate susceptibility for daptomycin until 2008. Clinical Laboratory Standards Institute breakpoint guidelines were used to delineate minimum inhibitory concentrations for linezolid and daptomycin.
Outcomes
The primary objective was to determine the cure rate, both clinical and microbiologic, of VRE bacteremia with the use of linezolid and daptomycin. Secondary outcomes were rates of recurrence and reinfection as well as 30‐day mortality. Clinical and microbiologic response rates for subsets of the patient population that were deemed immunocompromised or at an increased risk for VRE infections (neutropenic, transplant, malignancy, and ESRD on hemodialysis) were also evaluated.
Statistical Analysis
Data were analyzed using SAS version 9.2 (SAS Inc, Cary, NC). Patients with categorical characteristics were compared using a chi‐square test or Fisher's exact test. Continuous data were analyzed using a Student t test and are expressed as the mean standard deviation. The mean duration of initial antibiotics, time to appropriate antibiotics, time to adequate antibiotic therapy, and LOS were all calculated for the linezolid and daptomycin group with a Student t test used to compare the differences. Multivariate logistic regression was used for the following outcomes: clinical cure, microbiologic cure, mortality, reinfection, and recurrence. For the interval variable, LOS, stepwise multiple regression was used to choose significant independent variables. P < 0.05 was considered statistically significant.
RESULTS
Patient Characteristics
Of the 361 patients identified with a positive VRE blood culture, 201 were included in the study. The remaining 160 patients were excluded for one of the following reasons: <5 days of therapy (n = 87), no documented gram‐positive therapy (n = 49), simultaneous gram‐positive therapy (n = 10), or insufficient data to evaluate response rates (n = 14). For the treatment of VRE bacteremia, 138 patients received linezolid and 63 patients received daptomycin. Demographics, comorbid illnesses, and patient characteristics are shown in Table 1. There was a statistically significant difference in the average age, with the linezolid group consisting of older patients. The daptomycin group had more patients with hematologic malignancies than the linezolid group (33% vs 14%; P = 0.0021) and more patients who received liver transplants (13% vs 4%; P = 0.0264).
| Linezolid (n = 138) | Daptomycin (n = 63) | P Value | |
|---|---|---|---|
| |||
| Average age, years, mean SD | 60 16 | 5315 | 0.0028 |
| Male, No. (%) | 59 (43) | 36 (57) | 0.0682 |
| Race, No. (%) | |||
| Caucasian | 34 (25) | 23 (37) | 0.1043 |
| African American | 103 (75) | 39 (62) | |
| Other | 1 (1) | 1 (2) | |
| COPD, No. (%) | 8 (6) | 2 (3) | 0.7277 |
| Diabetes mellitus, No. (%) | 61 (44) | 21 (33) | 0.1655 |
| Hemodialysis, No. (%) | 35 (25) | 17 (27) | 0.8627 |
| Malignancy, No. (%) | |||
| Solid organ | 26 (19) | 16 (25) | 0.3499 |
| Hematologic | 19 (14) | 21 (33) | 0.0021 |
| Transplant, No. (%) | |||
| Liver | 5 (4) | 8 (13) | 0.0264 |
| Kidney | 3 (2) | 0 | 0.5533 |
| Endocarditis,* No. (%) | 4 (3) | 3 (5) | 0.6801 |
| Species of VRE (%) | |||
| Enterococcus faecalis | 33 (24) | 10 (16) | 0.2658 |
| Enterococcus faecium | 105 (76) | 53 (84) | 0.2658 |
| Time to appropriate abx therapy, hours, mean SD | 12.4 26.9 | 818.8 | 0.1851 |
| Time to adequate abx therapy, days, mean SD | 2.3 1.8 | 1.81.5 | 0.0554 |
| Duration of initial abx, days, mean SD | 11.1 6.0 | 14.114.6 | 0.0401 |
| Abx before initial therapy, No. (%) | 85 (62) | 34 (54) | 0.3541 |
| Average dose, mg/kg, mean SD | NA | 6.11.5 | NA |
| Mortality, No. (%) | 25 (18) | 15 (24) | 0.3481 |
| LOS (days) | 37.527.7 | 40.827.9 | 0.4336 |
From the microbiology laboratory report of initial blood cultures, 78.6% of the isolates were noted as being E. faecium, with the remainder being E. faecalis (21.4%). One patient was classified as having linezolid‐resistant E. faecium (MIC >4 mg/L) upon repeat blood culture. Daptomycin MICs were obtained for 44 isolates using the Etest or MicroScan system; all isolates were susceptible with MICs ranging from 0.254 mg/L. As mentioned previously, our laboratory did not routinely report isolate susceptibility to daptomycin until 2008.
There were no statistically significant differences between the treatment groups with regard to time to appropriate or adequate antibiotic therapy (Table 1). However, there was a statistically significant difference in the mean duration of initial antibiotics between linezolid and daptomycin (11.1 days vs 14.1 days; P = 0.0401). Dosing strategies used in these patients were also evaluated. All linezolid patients received a dose of 600 mg every 12 hours by mouth or intravenously. The average dose of daptomycin was 6.1 mg/kg (range, 3.410.4 mg/kg; median, 6 mg/kg). The average LOS was 37 days for linezolid vs 40 days for daptomycin, which did not confer statistical significance. Overall mortality was 20%, occurring in 25 linezolid patients versus 15 daptomycin patients (P = 0.3481). The stepwise multiple regression analysis did not identify any statistically significant variables in patients treated with linezolid or daptomycin that affected any of the outcomes.
Outcomes and Analysis
As shown in Table 2, there were no statistically significant differences in clinical or microbiologic cure between the linezolid and daptomycin groups (74% vs 75% and 94% vs 94%, respectively). However, the linezolid group compared with the daptomycin group had fewer patients that developed a positive blood culture while on their initial antibiotic therapy (8% vs 22%; P = 0.0097). Follow‐up cultures were required to determine rates of recurrence and reinfection. Only 107/138 patients in the linezolid group and 51/63 patients in the daptomycin group had follow‐up cultures collected. Recurrence was documented in 3% of linezolid patients vs 12% of daptomycin patients (P = 0.0321). The odds ratio for developing a recurrent infection with daptomycin versus linezolid was 5.51 (95% confidence interval, 1.2524.28). Out of 6 patients that developed a recurrent VRE infection in the daptomycin group, 2 were prescribed doses <4 mg/kg with no reported MICs, and 2 patients received 6 mg/kg with reported MICs of 4 mg/L. No statistically significant difference existed for the rate of reinfection between linezolid and daptomycin (1% vs 6%; P = 0.0992).
| Linezolid (n = 138) | Daptomycin (n = 63) | P Value | |
|---|---|---|---|
| |||
| Patients with positive culture on G+ therapy | 11 (8) | 14 (22) | 0.0097 |
| Clinical cure | 102 (74) | 47 (75) | 1 |
| Microbiologic cure | 130 (94) | 59 (94) | 1 |
| Recurrence* | 3 (3) | 6 (12) | 0.0321 |
| Reinfection* | 1 (1) | 3 (6) | 0.0992 |
Table 3 provides information on subsets of the patient population deemed high‐risk for VRE infection or immunocompromised. There was no statistically significant difference between the 2 antibiotic groups in clinical or microbiologic cure. In the subsets of immunocompromised patients, there was no difference in recurrence or reinfection between the linezolid and daptomycin patients. Furthermore, all groups had similar LOS regardless of the antibiotic used to treat the VRE BSI. Moreover, there were no statistically significant differences in 30‐day mortality in these subsets of the population with regard to initial antibiotic choice. No significant independent variables were found between linezolid or daptomycin that affected any of the outcomes listed in Table 3.
| Neutropenia (%) | Hematologic Malignancy (%) | ESRD on Hemodialysis (%) | Liver Transplant (%) | |||||
|---|---|---|---|---|---|---|---|---|
| LZD (n = 16) | Dapto (n = 5) | LZD (n = 19) | Dapto (n = 21) | LZD (n = 35) | Dapto (n = 17) | LZD (n = 5) | Dapto (n = 8) | |
| ||||||||
| Clinical cure, No. (%) | 12 (75) | 5 (100) | 18 (95) | 17 (81) | 24 (69) | 12 (71) | 4 (80) | 3 (38) |
| Microbiologic cure,* No. (%) | 13 (81) | 5 (100) | 18 (95) | 20 (95) | 33 (94) | 16 (94) | 5 (100) | 8 (100) |
| Recurrence,* No. (%) | 2 (13) | 1 (20) | 1 (6) | 2 (11) | 0 | 2 (15) | 0 | 1 (14) |
| Reinfection,* No. (%) | 0 | 0 | 0 | 0 | 1 (4) | 2 (15) | 0 | 1 (14) |
| Mortality, No. (%) | 3 (19) | 1 (20) | 4 (21) | 3 (14) | 7 (20) | 4 (24) | 1 (20) | 4 (50) |
| LOS, days, meanSD | 57.422 | 39.412.4 | 47.626.2 | 4127.1 | 38.833.8 | 39.640.4 | 5034.5 | 73.338.8 |
DISCUSSION
Vergis et al21 reported that infections with VRE compared with vancomycin‐sensitive infections were associated with a higher rate of mortality and that the chosen antimicrobial therapy may play a pivotal role in the risk of death. Our retrospective study suggests that linezolid and daptomycin appear to be equally efficacious for the treatment of VRE BSIs. The results from our study for clinical and microbiologic cure rates for linezolid and daptomycin are similar to previously published data.7, 8 In accordance with previous studies,4 our data demonstrate that there is a higher rate of recurrence in patients treated with daptomycin. This finding may be explained by the fact that the daptomycin group was comprised of more complex patients with a greater disease burden versus the linezolid group; therefore, they were more susceptible to a recurrent VRE infection. In our study, patients who were treated with daptomycin were 5.5 times more likely to have a recurrent infection than linezolid‐treated patients. However, this finding must be scrutinized, because over half of the patients with recurrence either received an inappropriate dose or had high MICs to daptomycin.
Despite there being few clinical and microbiologic outcome data with daptomycin, our study proposes that a bactericidal antibiotic and a bacteriostatic antibiotic have comparable efficacy in the treatment of VRE BSIs. Previous literature has mainly comprised case studies or series that have evaluated clinical outcomes with daptomycin in the treatment of VRE BSIs. Gallagher et al7 reported the results of a retrospective case series of 30 patients with VRE bacteremia who were treated with daptomycin. In this study, microbiologic cure was achieved in 80% of patients, with clinical success in 59% of the patients. In 2009, Mave et al4 compared clinical outcomes between daptomycin and linezolid in the treatment of VRE bacteremia. Reported results demonstrated a microbiologic cure rate of 90% for daptomycin versus 88% for linezolid.4 Moreover, there were no differences in mortality between the groups in our study. In 2010, Crank et al18 reported no differences in mortality (in‐hospital) for hospitalized patients with VRE BSIs treated with linezolid or daptomycin. Our results seem to be consistent with what has been published previously concerning clinical outcomes associated with linezolid or daptomycin in the treatment of VRE BSI.
The average daptomycin dose received in our patients was 6.1 mg/kg with doses ranging from 3.410.4 mg/kg. The underdosing as well as higher MICs to daptomycin may have contributed to a higher rate of recurrence. Previous reports state that Enterococcus species may have higher MICs to daptomycin than Staphylococcus or Streptococcus species; consequently, higher doses may be needed to adequately treat enterococcal infections.7 In the aforementioned study by Gallagher et al,7 doses of daptomycin 6 mg/kg were associated with a positive clinical outcome in 81% of patients compared with 31% if the dose used was <6 mg/kg. Linezolid is dosed 600 mg every 12 hours by mouth or intravenously, with no variations. There have been no studies comparing the uniform dosing of linezolid to the weight‐based dosing of daptomycin and their effects on outcomes.
Patients particularly susceptible to VRE infections include those with neutropenia and/or cancer, patients receiving long‐term hemodialysis, and liver transplant recipients.3, 22, 23 Upon review of this immunocompromised population, we noted no statistically significant differences in overall outcomes. A study by Kraft et al.24 supports the findings in our study that both drugs appear useful in the treatment of VRE bacteremia in patients with hematologic malignancy. We did identify a difference, albeit nonsignificant, in LOS for daptomycin versus linezolid in patients with a history of liver transplantation. Again, the level of care that these patients needed compared with the general population may explain this difference. As mentioned previously, another pertinent factor would be the dose of daptomycin used in these patients, because the dose can affect clinical success. Because all of the other patients had a similar LOS, we cannot determine that the increased LOS seen in liver transplant patients treated with daptomycin was solely due to daptomycin use. The reason for the increased LOS seems to be multifactorial. In the neutropenic population, a difference in LOS was also recognized, but follow‐up complete blood count values were not collected for these patients to determine whether linezolid contributed to further bone marrow suppression leading to an increase in LOS. For both of these patient populations, the number of patients included is very small (n = 21 for neutropenia total, n = 13 for liver transplant total), which can lead to a high degree of variance.
This study has several limitations. This was a retrospective review; therefore, we had no control over the selection of therapy. This may be reflected in an apparent preferential use of daptomycin in immunocompromised patients. Furthermore, 62% of linezolid patients and 54% of daptomycin patients received an antibiotic before initial therapy that could have potentially altered response rates. Due to the paucity of documentation surrounding initial site of infection, some of the positive cultures may represent potential contamination, because VRE may contaminate skin.25 Contamination seems implausible, however, because patients were seen by an infectious disease physician and had at least 1 documented positive VRE blood culture. We chose arbitrary definitions for clinical cure, microbiologic cure, microbiologic failure, recurrence, and reinfection. Previous studies have used their own definitions leading to discrepancies in reporting. Another limitation was that follow‐up cultures were not obtained on all of the patients, which was needed to determine rates of recurrence, reinfection, and microbiologic cure. MICs to daptomycin were not reported in 30% of our patients, potentially altering the recurrence rate seen in the daptomycin‐treated patients. Because clinical cure was not documented in the chart, it was inferred from the laboratory values and vital sign information. One investigator analyzed all of the values and made the determination of clinical cure, allowing for a consistent approach to data review.
In the face of the imposing threat of a highly resistant organism such as VRE with a limited number of efficacious antibiotics, antimicrobial selection becomes increasingly important and is requisite to clinical and microbiological success. To our knowledge, this is one of the largest studies to date comparing the efficacy of linezolid with that of daptomycin in the treatment of VRE bacteremia. Both of these agents are effective for the treatment of VRE BSIs. Nevertheless, specific factors related to the medication (eg, dose, route of administration) as well as the patient (eg, comorbid conditions, acuity of illness) should be taken into consideration when selecting an initial antimicrobial agent. Because the treatment of VRE BSIs continues to be a challenge, larger prospective randomized controlled trials are needed to corroborate our results and determine the optimal therapy for this serious infection.
Acknowledgements
Disclosures: Michael S. Gelfand is on the speaker's bureau for Cubist and Pfizer.
- ,,,,,.Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study.Clin Infect Dis.2004;39:309–317.
- ,,, et al.Clinical practice guidelines for the management of intravascular catheter‐related infection: 2009 update by the Infectious Diseases Society of America.Clin Infect Dis.2009;49:1–45.
- ,,,,,.Bad bugs need drugs: an update on the development pipeline from the antimicrobial availability task force of the infectious diseases society of America.Clin Infect Dis.2006;42:657–668.
- ,,,.Vancomycin‐resistant enterococcal bacteraemia: is daptomycin as effective as linezolid?J Antimicrob Chemother.2009;64:175–180.
- ,,.Management of multidrug‐resistant enterococcal Infections.Clin Microbiol Infect.2010;16:555–562.
- ,,, et al.Treatment of vancomycin‐resistant Enterococcus faecium infections with quinupristin/dalfopristin.Clin Infect Dis.2001;33:1816–1823.
- ,,, et al.Daptomycin for vancomycin‐resistant enterococcol bacteremia: a retrospective case series of 30 patients.Pharmacotherapy.2009;29:792–799.
- ,,, et al.Safety, efficacy and pharmacokinetics of linezolid for treatment of resistant gram positive infections in cancer patients with neutropenia.Ann Oncol.2003;14:795–801.
- ,,,,.Daptomycin for the treatment of vancomycin resistant Enterococcus faecium bacteremia.Scand J Infect Dis.2003;38:290–292.
- ,.New antimicrobial agents for the treatment of gram positive bacterial infections.Clin Microbiol Infec.2008;14:411–420.
- ,.Emergence and management of drug‐resistant enterococcal infections.Expert Rev Anti Infect Ther.2008;6:637–655.
- ,,.Nosocomial spread of linezolid‐resistant, Vancomycin resistant Enterococcus faecium.N Engl J Med.2002;346:867–869.
- ,, et al.Nosocomial superinfections due to linezolid‐resitant Enterococcus faecalis: evidence for a gene dosage effect of linezolid MICs.Diagn Microbiol Infect Dis.2003;47:511–513.
- .Quinupristin‐dalfopristin and linezolid: evidence and opinion.Clin Infect Dis.2003;36:473–481.
- Cubicin (Daptomycin for injection) [package insert].Lexington, MA:Cubist Pharmaceuticals;2010.
- ,,,.Daptomycin nonsusceptible Enterococci: an emerging challenge for clinicians.Clin Infect Dis.2011;52:228–234.
- ,,,.A potential role for daptomycin in enterococcal infections: what is the evidence?J Antimicrob Chemother.2010;65:1126–1136.
- ,,, et al.Comparison of outcomes from daptomycin or linezolid for vancomycin‐resistant enterococcal bloodstream infection: a retrospective, multicenter, cohort study.Clin Ther.2010;32:1713–1719.
- ,,,,,.Observational study of the epidemiology and outcomes of vancomycin‐resistant Enterococcus bacteraemia treated with newer antimicrobial agents.Epidemiol Infect.2010;15:1–9.
- .Inadequate antimicrobial treatment: an important determinant of outcome for hospitalized patients.Clin Infect Dis.2000;31:S131–S138.
- ,,, et al.Determinants of vancomycin resistance and mortality rates in enterococcal bacteremia: a prospective multicenter study.Ann Intern Med.2001;135:484–492.
- ,,,,,.Vancomycin resistant enterococci among chronic hemodialysis patients: a prospective study of acquisition.Clin Infect Dis.2001;32:23–29.
- ,,, et al.A nationwide, multicenter, case control study comparing risk factors, treatment, and outcome for vancomycin resistant andsusceptible enterococcal bacteremia.Diagn Microbiol Infect Dis.2000;36:145–158.
- ,,,,.Outcomes of therapy: vancomycin‐resistant enterococcal bacteremia in hematology and bone marrow transplant patients [published online ahead of print November 26, 2010].Support Care Cancer. doi: 10.1007/s00520–010‐1038‐z.
- ,,, et al.Skin colonization with vancomycin‐resistant enterococci among hospitalized patients with bacteremia.Clin Infect Dis.1997;24:704–706.
Enterococci have been identified as a causative organism in approximately 10% of all nosocomial bloodstream infections (BSIs).1, 2 In 2006, the Infectious Diseases Society of America identified vancomycin‐ resistant Enterococcus faecium (VRE) as 1 of 6 microbes considered to be among the most dangerous due to high rates of resistance and a limited number of effective antimicrobials.3 E. faecium has exhibited high rates of glycopeptide resistance with as many as 60% of isolates from BSIs being resistant to vancomycin.2, 4 Due to increasing resistance to glycopeptides, vancomycin has become obsolete in the treatment of E. faecium infections.5
A limited number of antimicrobials are available for the treatment of infections due to VRE. Agents active in vitro are quinupristin‐dalfopristin, tigecycline, linezolid, and daptomycin. Quinupristin‐dalfopristin was one of the first agents approved for use in VRE infections; however, treatment with this agent has been limited because of mediocre clinical response rates, undesirable adverse effects, high cost, and insufficient E. faecalis activity.6, 7 Tigecycline is not an optimal antibiotic for the treatment of VRE bacteremia, because serum concentrations achieved after administration are inadequate to treat BSIs.7 In contrast, linezolid and daptomycin have evinced efficacy against VRE bacteremia, with reported microbiologic response rates of 85% and 80%, respectively.7, 8 One inherent difference between these antibiotics that may theoretically affect their use in immunocompromised patients is that linezolid is bacteriostatic, whereas daptomycin is bactericidal. It has been postulated that by using a bactericidal antibiotic such as daptomycin in the immunocompromised host, one may achieve superior clinical and microbiologic response rates.3, 7, 9, 10
Since the introduction of the oxazolidinone linezolid in 2000, widespread use has led to reports of linezolid‐resistant VRE as well as nosocomial transmission of linezolid‐resistant VRE in hospitals.4, 1114 Despite linezolid being a key antibiotic for the treatment of VRE infections over the last 10 years, development of resistance along with potential hematologic and neurologic toxicity during long‐term use remains a concern.7, 8 Although daptomycin is active against several resistant organisms, including VRE, the evidence supporting use of daptomycin for VRE BSI is limited to case reports or small case series.7, 9 Moreover, daptomycin has not received US Food and Drug Administration approval for the treatment of VRE infections,15 and emerging data regarding daptomycin‐nonsusceptible enterococci (Minimum Inhibitory Concentration, MIC >4 mg/L) highlight a new problem for this multidrug‐resistant pathogen.16, 17 Few studies in recent years have compared these 2 antibiotics in the treatment of VRE BSIs.4, 18, 19 Due to the high rates of vancomycin resistance reported at our institution and the ubiquitous use of linezolid and daptomycin in the treatment of VRE bacteremia, we chose to evaluate response rates for these antibiotics in an effort to add to previously published literature on this topic.
MATERIALS AND METHODS
Patient Selection
Methodist University Hospital (MUH) in Memphis, Tennessee, is part of a 7‐hospital system with 697 licensed beds. MUH is a tertiary teaching hospital with centers of excellence in neuroscience and transplantation. Patients admitted to MUH diagnosed with VRE bacteremia between January 1, 2004, and July 31, 2009, were identified by the microbiology laboratory. All patients who were 18 years of age, had 1 documented positive VRE blood culture, and received linezolid or daptomycin for 5 days were eligible. Patients were excluded if they were treated simultaneously with more than 1 agent active against VRE. This study was approved by the MUH Institutional Review Board. Of note, use of linezolid or daptomycin at MUH is restricted to an infectious disease physician or pulmonologist. Currently, there are no protocols at our institution for treating VRE infections.
Data Collection and Definitions
Cerner Millennium was used to collect all pertinent patient information. Patient records were reviewed to determine demographic data, comorbid illnesses, laboratory data (from admission to discharge), medications, and discharge status (home, long‐term care facility, or death). Comorbid illnesses evaluated included: chronic obstructive pulmonary disease, diabetes mellitus, malignancy (solid or hematologic), transplant (liver or kidney), end‐stage renal disease (ESRD) (hemodialysis or nonhemodialysis), cirrhosis, and endocarditis. ESRD and endocarditis were defined per chart diagnosis. Laboratory data collected included serum creatinine, creatine phosphokinase, absolute neutrophil count (neutropenia defined as absolute neutrophil count <1000), and number and site (intravenous line or peripheral blood draw) of positive VRE blood cultures. Other data collected were (1) time elapsed to adequate antibiotic coverage, which was defined as microbiologic documentation of an infection that was being effectively treated at the time of its identification, and (2) time to appropriate antibiotic coverage, which was defined as antimicrobial treatment selected for efficacy based on presumptive identification of the causative pathogen, the antimicrobial agent's spectrum of activity, and local microbial resistance patterns.20 Doses of daptomycin and linezolid used in patients with VRE bacteremia were also documented.
Clinical cure was defined as a resolution of signs and/or symptoms of infection (white blood cell count <10,000/mm3, bands <5%, heart rate <90 beats per minute, respiratory rate <20 breaths per minute, and maximum oral temperature <38C) after gram‐positive therapy was discontinued. The definition of microbiologic cure was lack of positive blood cultures for VRE at least 14 days after cessation of gram‐positive therapy. Microbiologic failure was defined as positive VRE blood cultures obtained on gram‐positive therapy necessitating a change in treatment. Recurrence was defined as VRE bacteremia within 30 days after discontinuation of gram‐positive therapy. Reinfection was defined as VRE bacteremia that appeared 30 days after completion of primary gram‐positive therapy.
All isolates were tested for susceptibility to linezolid using the MicroScan system, whereas daptomycin susceptibility patterns were obtained by either the Etest or MicroScan system. Of importance, our laboratory did not routinely report isolate susceptibility for daptomycin until 2008. Clinical Laboratory Standards Institute breakpoint guidelines were used to delineate minimum inhibitory concentrations for linezolid and daptomycin.
Outcomes
The primary objective was to determine the cure rate, both clinical and microbiologic, of VRE bacteremia with the use of linezolid and daptomycin. Secondary outcomes were rates of recurrence and reinfection as well as 30‐day mortality. Clinical and microbiologic response rates for subsets of the patient population that were deemed immunocompromised or at an increased risk for VRE infections (neutropenic, transplant, malignancy, and ESRD on hemodialysis) were also evaluated.
Statistical Analysis
Data were analyzed using SAS version 9.2 (SAS Inc, Cary, NC). Patients with categorical characteristics were compared using a chi‐square test or Fisher's exact test. Continuous data were analyzed using a Student t test and are expressed as the mean standard deviation. The mean duration of initial antibiotics, time to appropriate antibiotics, time to adequate antibiotic therapy, and LOS were all calculated for the linezolid and daptomycin group with a Student t test used to compare the differences. Multivariate logistic regression was used for the following outcomes: clinical cure, microbiologic cure, mortality, reinfection, and recurrence. For the interval variable, LOS, stepwise multiple regression was used to choose significant independent variables. P < 0.05 was considered statistically significant.
RESULTS
Patient Characteristics
Of the 361 patients identified with a positive VRE blood culture, 201 were included in the study. The remaining 160 patients were excluded for one of the following reasons: <5 days of therapy (n = 87), no documented gram‐positive therapy (n = 49), simultaneous gram‐positive therapy (n = 10), or insufficient data to evaluate response rates (n = 14). For the treatment of VRE bacteremia, 138 patients received linezolid and 63 patients received daptomycin. Demographics, comorbid illnesses, and patient characteristics are shown in Table 1. There was a statistically significant difference in the average age, with the linezolid group consisting of older patients. The daptomycin group had more patients with hematologic malignancies than the linezolid group (33% vs 14%; P = 0.0021) and more patients who received liver transplants (13% vs 4%; P = 0.0264).
| Linezolid (n = 138) | Daptomycin (n = 63) | P Value | |
|---|---|---|---|
| |||
| Average age, years, mean SD | 60 16 | 5315 | 0.0028 |
| Male, No. (%) | 59 (43) | 36 (57) | 0.0682 |
| Race, No. (%) | |||
| Caucasian | 34 (25) | 23 (37) | 0.1043 |
| African American | 103 (75) | 39 (62) | |
| Other | 1 (1) | 1 (2) | |
| COPD, No. (%) | 8 (6) | 2 (3) | 0.7277 |
| Diabetes mellitus, No. (%) | 61 (44) | 21 (33) | 0.1655 |
| Hemodialysis, No. (%) | 35 (25) | 17 (27) | 0.8627 |
| Malignancy, No. (%) | |||
| Solid organ | 26 (19) | 16 (25) | 0.3499 |
| Hematologic | 19 (14) | 21 (33) | 0.0021 |
| Transplant, No. (%) | |||
| Liver | 5 (4) | 8 (13) | 0.0264 |
| Kidney | 3 (2) | 0 | 0.5533 |
| Endocarditis,* No. (%) | 4 (3) | 3 (5) | 0.6801 |
| Species of VRE (%) | |||
| Enterococcus faecalis | 33 (24) | 10 (16) | 0.2658 |
| Enterococcus faecium | 105 (76) | 53 (84) | 0.2658 |
| Time to appropriate abx therapy, hours, mean SD | 12.4 26.9 | 818.8 | 0.1851 |
| Time to adequate abx therapy, days, mean SD | 2.3 1.8 | 1.81.5 | 0.0554 |
| Duration of initial abx, days, mean SD | 11.1 6.0 | 14.114.6 | 0.0401 |
| Abx before initial therapy, No. (%) | 85 (62) | 34 (54) | 0.3541 |
| Average dose, mg/kg, mean SD | NA | 6.11.5 | NA |
| Mortality, No. (%) | 25 (18) | 15 (24) | 0.3481 |
| LOS (days) | 37.527.7 | 40.827.9 | 0.4336 |
From the microbiology laboratory report of initial blood cultures, 78.6% of the isolates were noted as being E. faecium, with the remainder being E. faecalis (21.4%). One patient was classified as having linezolid‐resistant E. faecium (MIC >4 mg/L) upon repeat blood culture. Daptomycin MICs were obtained for 44 isolates using the Etest or MicroScan system; all isolates were susceptible with MICs ranging from 0.254 mg/L. As mentioned previously, our laboratory did not routinely report isolate susceptibility to daptomycin until 2008.
There were no statistically significant differences between the treatment groups with regard to time to appropriate or adequate antibiotic therapy (Table 1). However, there was a statistically significant difference in the mean duration of initial antibiotics between linezolid and daptomycin (11.1 days vs 14.1 days; P = 0.0401). Dosing strategies used in these patients were also evaluated. All linezolid patients received a dose of 600 mg every 12 hours by mouth or intravenously. The average dose of daptomycin was 6.1 mg/kg (range, 3.410.4 mg/kg; median, 6 mg/kg). The average LOS was 37 days for linezolid vs 40 days for daptomycin, which did not confer statistical significance. Overall mortality was 20%, occurring in 25 linezolid patients versus 15 daptomycin patients (P = 0.3481). The stepwise multiple regression analysis did not identify any statistically significant variables in patients treated with linezolid or daptomycin that affected any of the outcomes.
Outcomes and Analysis
As shown in Table 2, there were no statistically significant differences in clinical or microbiologic cure between the linezolid and daptomycin groups (74% vs 75% and 94% vs 94%, respectively). However, the linezolid group compared with the daptomycin group had fewer patients that developed a positive blood culture while on their initial antibiotic therapy (8% vs 22%; P = 0.0097). Follow‐up cultures were required to determine rates of recurrence and reinfection. Only 107/138 patients in the linezolid group and 51/63 patients in the daptomycin group had follow‐up cultures collected. Recurrence was documented in 3% of linezolid patients vs 12% of daptomycin patients (P = 0.0321). The odds ratio for developing a recurrent infection with daptomycin versus linezolid was 5.51 (95% confidence interval, 1.2524.28). Out of 6 patients that developed a recurrent VRE infection in the daptomycin group, 2 were prescribed doses <4 mg/kg with no reported MICs, and 2 patients received 6 mg/kg with reported MICs of 4 mg/L. No statistically significant difference existed for the rate of reinfection between linezolid and daptomycin (1% vs 6%; P = 0.0992).
| Linezolid (n = 138) | Daptomycin (n = 63) | P Value | |
|---|---|---|---|
| |||
| Patients with positive culture on G+ therapy | 11 (8) | 14 (22) | 0.0097 |
| Clinical cure | 102 (74) | 47 (75) | 1 |
| Microbiologic cure | 130 (94) | 59 (94) | 1 |
| Recurrence* | 3 (3) | 6 (12) | 0.0321 |
| Reinfection* | 1 (1) | 3 (6) | 0.0992 |
Table 3 provides information on subsets of the patient population deemed high‐risk for VRE infection or immunocompromised. There was no statistically significant difference between the 2 antibiotic groups in clinical or microbiologic cure. In the subsets of immunocompromised patients, there was no difference in recurrence or reinfection between the linezolid and daptomycin patients. Furthermore, all groups had similar LOS regardless of the antibiotic used to treat the VRE BSI. Moreover, there were no statistically significant differences in 30‐day mortality in these subsets of the population with regard to initial antibiotic choice. No significant independent variables were found between linezolid or daptomycin that affected any of the outcomes listed in Table 3.
| Neutropenia (%) | Hematologic Malignancy (%) | ESRD on Hemodialysis (%) | Liver Transplant (%) | |||||
|---|---|---|---|---|---|---|---|---|
| LZD (n = 16) | Dapto (n = 5) | LZD (n = 19) | Dapto (n = 21) | LZD (n = 35) | Dapto (n = 17) | LZD (n = 5) | Dapto (n = 8) | |
| ||||||||
| Clinical cure, No. (%) | 12 (75) | 5 (100) | 18 (95) | 17 (81) | 24 (69) | 12 (71) | 4 (80) | 3 (38) |
| Microbiologic cure,* No. (%) | 13 (81) | 5 (100) | 18 (95) | 20 (95) | 33 (94) | 16 (94) | 5 (100) | 8 (100) |
| Recurrence,* No. (%) | 2 (13) | 1 (20) | 1 (6) | 2 (11) | 0 | 2 (15) | 0 | 1 (14) |
| Reinfection,* No. (%) | 0 | 0 | 0 | 0 | 1 (4) | 2 (15) | 0 | 1 (14) |
| Mortality, No. (%) | 3 (19) | 1 (20) | 4 (21) | 3 (14) | 7 (20) | 4 (24) | 1 (20) | 4 (50) |
| LOS, days, meanSD | 57.422 | 39.412.4 | 47.626.2 | 4127.1 | 38.833.8 | 39.640.4 | 5034.5 | 73.338.8 |
DISCUSSION
Vergis et al21 reported that infections with VRE compared with vancomycin‐sensitive infections were associated with a higher rate of mortality and that the chosen antimicrobial therapy may play a pivotal role in the risk of death. Our retrospective study suggests that linezolid and daptomycin appear to be equally efficacious for the treatment of VRE BSIs. The results from our study for clinical and microbiologic cure rates for linezolid and daptomycin are similar to previously published data.7, 8 In accordance with previous studies,4 our data demonstrate that there is a higher rate of recurrence in patients treated with daptomycin. This finding may be explained by the fact that the daptomycin group was comprised of more complex patients with a greater disease burden versus the linezolid group; therefore, they were more susceptible to a recurrent VRE infection. In our study, patients who were treated with daptomycin were 5.5 times more likely to have a recurrent infection than linezolid‐treated patients. However, this finding must be scrutinized, because over half of the patients with recurrence either received an inappropriate dose or had high MICs to daptomycin.
Despite there being few clinical and microbiologic outcome data with daptomycin, our study proposes that a bactericidal antibiotic and a bacteriostatic antibiotic have comparable efficacy in the treatment of VRE BSIs. Previous literature has mainly comprised case studies or series that have evaluated clinical outcomes with daptomycin in the treatment of VRE BSIs. Gallagher et al7 reported the results of a retrospective case series of 30 patients with VRE bacteremia who were treated with daptomycin. In this study, microbiologic cure was achieved in 80% of patients, with clinical success in 59% of the patients. In 2009, Mave et al4 compared clinical outcomes between daptomycin and linezolid in the treatment of VRE bacteremia. Reported results demonstrated a microbiologic cure rate of 90% for daptomycin versus 88% for linezolid.4 Moreover, there were no differences in mortality between the groups in our study. In 2010, Crank et al18 reported no differences in mortality (in‐hospital) for hospitalized patients with VRE BSIs treated with linezolid or daptomycin. Our results seem to be consistent with what has been published previously concerning clinical outcomes associated with linezolid or daptomycin in the treatment of VRE BSI.
The average daptomycin dose received in our patients was 6.1 mg/kg with doses ranging from 3.410.4 mg/kg. The underdosing as well as higher MICs to daptomycin may have contributed to a higher rate of recurrence. Previous reports state that Enterococcus species may have higher MICs to daptomycin than Staphylococcus or Streptococcus species; consequently, higher doses may be needed to adequately treat enterococcal infections.7 In the aforementioned study by Gallagher et al,7 doses of daptomycin 6 mg/kg were associated with a positive clinical outcome in 81% of patients compared with 31% if the dose used was <6 mg/kg. Linezolid is dosed 600 mg every 12 hours by mouth or intravenously, with no variations. There have been no studies comparing the uniform dosing of linezolid to the weight‐based dosing of daptomycin and their effects on outcomes.
Patients particularly susceptible to VRE infections include those with neutropenia and/or cancer, patients receiving long‐term hemodialysis, and liver transplant recipients.3, 22, 23 Upon review of this immunocompromised population, we noted no statistically significant differences in overall outcomes. A study by Kraft et al.24 supports the findings in our study that both drugs appear useful in the treatment of VRE bacteremia in patients with hematologic malignancy. We did identify a difference, albeit nonsignificant, in LOS for daptomycin versus linezolid in patients with a history of liver transplantation. Again, the level of care that these patients needed compared with the general population may explain this difference. As mentioned previously, another pertinent factor would be the dose of daptomycin used in these patients, because the dose can affect clinical success. Because all of the other patients had a similar LOS, we cannot determine that the increased LOS seen in liver transplant patients treated with daptomycin was solely due to daptomycin use. The reason for the increased LOS seems to be multifactorial. In the neutropenic population, a difference in LOS was also recognized, but follow‐up complete blood count values were not collected for these patients to determine whether linezolid contributed to further bone marrow suppression leading to an increase in LOS. For both of these patient populations, the number of patients included is very small (n = 21 for neutropenia total, n = 13 for liver transplant total), which can lead to a high degree of variance.
This study has several limitations. This was a retrospective review; therefore, we had no control over the selection of therapy. This may be reflected in an apparent preferential use of daptomycin in immunocompromised patients. Furthermore, 62% of linezolid patients and 54% of daptomycin patients received an antibiotic before initial therapy that could have potentially altered response rates. Due to the paucity of documentation surrounding initial site of infection, some of the positive cultures may represent potential contamination, because VRE may contaminate skin.25 Contamination seems implausible, however, because patients were seen by an infectious disease physician and had at least 1 documented positive VRE blood culture. We chose arbitrary definitions for clinical cure, microbiologic cure, microbiologic failure, recurrence, and reinfection. Previous studies have used their own definitions leading to discrepancies in reporting. Another limitation was that follow‐up cultures were not obtained on all of the patients, which was needed to determine rates of recurrence, reinfection, and microbiologic cure. MICs to daptomycin were not reported in 30% of our patients, potentially altering the recurrence rate seen in the daptomycin‐treated patients. Because clinical cure was not documented in the chart, it was inferred from the laboratory values and vital sign information. One investigator analyzed all of the values and made the determination of clinical cure, allowing for a consistent approach to data review.
In the face of the imposing threat of a highly resistant organism such as VRE with a limited number of efficacious antibiotics, antimicrobial selection becomes increasingly important and is requisite to clinical and microbiological success. To our knowledge, this is one of the largest studies to date comparing the efficacy of linezolid with that of daptomycin in the treatment of VRE bacteremia. Both of these agents are effective for the treatment of VRE BSIs. Nevertheless, specific factors related to the medication (eg, dose, route of administration) as well as the patient (eg, comorbid conditions, acuity of illness) should be taken into consideration when selecting an initial antimicrobial agent. Because the treatment of VRE BSIs continues to be a challenge, larger prospective randomized controlled trials are needed to corroborate our results and determine the optimal therapy for this serious infection.
Acknowledgements
Disclosures: Michael S. Gelfand is on the speaker's bureau for Cubist and Pfizer.
Enterococci have been identified as a causative organism in approximately 10% of all nosocomial bloodstream infections (BSIs).1, 2 In 2006, the Infectious Diseases Society of America identified vancomycin‐ resistant Enterococcus faecium (VRE) as 1 of 6 microbes considered to be among the most dangerous due to high rates of resistance and a limited number of effective antimicrobials.3 E. faecium has exhibited high rates of glycopeptide resistance with as many as 60% of isolates from BSIs being resistant to vancomycin.2, 4 Due to increasing resistance to glycopeptides, vancomycin has become obsolete in the treatment of E. faecium infections.5
A limited number of antimicrobials are available for the treatment of infections due to VRE. Agents active in vitro are quinupristin‐dalfopristin, tigecycline, linezolid, and daptomycin. Quinupristin‐dalfopristin was one of the first agents approved for use in VRE infections; however, treatment with this agent has been limited because of mediocre clinical response rates, undesirable adverse effects, high cost, and insufficient E. faecalis activity.6, 7 Tigecycline is not an optimal antibiotic for the treatment of VRE bacteremia, because serum concentrations achieved after administration are inadequate to treat BSIs.7 In contrast, linezolid and daptomycin have evinced efficacy against VRE bacteremia, with reported microbiologic response rates of 85% and 80%, respectively.7, 8 One inherent difference between these antibiotics that may theoretically affect their use in immunocompromised patients is that linezolid is bacteriostatic, whereas daptomycin is bactericidal. It has been postulated that by using a bactericidal antibiotic such as daptomycin in the immunocompromised host, one may achieve superior clinical and microbiologic response rates.3, 7, 9, 10
Since the introduction of the oxazolidinone linezolid in 2000, widespread use has led to reports of linezolid‐resistant VRE as well as nosocomial transmission of linezolid‐resistant VRE in hospitals.4, 1114 Despite linezolid being a key antibiotic for the treatment of VRE infections over the last 10 years, development of resistance along with potential hematologic and neurologic toxicity during long‐term use remains a concern.7, 8 Although daptomycin is active against several resistant organisms, including VRE, the evidence supporting use of daptomycin for VRE BSI is limited to case reports or small case series.7, 9 Moreover, daptomycin has not received US Food and Drug Administration approval for the treatment of VRE infections,15 and emerging data regarding daptomycin‐nonsusceptible enterococci (Minimum Inhibitory Concentration, MIC >4 mg/L) highlight a new problem for this multidrug‐resistant pathogen.16, 17 Few studies in recent years have compared these 2 antibiotics in the treatment of VRE BSIs.4, 18, 19 Due to the high rates of vancomycin resistance reported at our institution and the ubiquitous use of linezolid and daptomycin in the treatment of VRE bacteremia, we chose to evaluate response rates for these antibiotics in an effort to add to previously published literature on this topic.
MATERIALS AND METHODS
Patient Selection
Methodist University Hospital (MUH) in Memphis, Tennessee, is part of a 7‐hospital system with 697 licensed beds. MUH is a tertiary teaching hospital with centers of excellence in neuroscience and transplantation. Patients admitted to MUH diagnosed with VRE bacteremia between January 1, 2004, and July 31, 2009, were identified by the microbiology laboratory. All patients who were 18 years of age, had 1 documented positive VRE blood culture, and received linezolid or daptomycin for 5 days were eligible. Patients were excluded if they were treated simultaneously with more than 1 agent active against VRE. This study was approved by the MUH Institutional Review Board. Of note, use of linezolid or daptomycin at MUH is restricted to an infectious disease physician or pulmonologist. Currently, there are no protocols at our institution for treating VRE infections.
Data Collection and Definitions
Cerner Millennium was used to collect all pertinent patient information. Patient records were reviewed to determine demographic data, comorbid illnesses, laboratory data (from admission to discharge), medications, and discharge status (home, long‐term care facility, or death). Comorbid illnesses evaluated included: chronic obstructive pulmonary disease, diabetes mellitus, malignancy (solid or hematologic), transplant (liver or kidney), end‐stage renal disease (ESRD) (hemodialysis or nonhemodialysis), cirrhosis, and endocarditis. ESRD and endocarditis were defined per chart diagnosis. Laboratory data collected included serum creatinine, creatine phosphokinase, absolute neutrophil count (neutropenia defined as absolute neutrophil count <1000), and number and site (intravenous line or peripheral blood draw) of positive VRE blood cultures. Other data collected were (1) time elapsed to adequate antibiotic coverage, which was defined as microbiologic documentation of an infection that was being effectively treated at the time of its identification, and (2) time to appropriate antibiotic coverage, which was defined as antimicrobial treatment selected for efficacy based on presumptive identification of the causative pathogen, the antimicrobial agent's spectrum of activity, and local microbial resistance patterns.20 Doses of daptomycin and linezolid used in patients with VRE bacteremia were also documented.
Clinical cure was defined as a resolution of signs and/or symptoms of infection (white blood cell count <10,000/mm3, bands <5%, heart rate <90 beats per minute, respiratory rate <20 breaths per minute, and maximum oral temperature <38C) after gram‐positive therapy was discontinued. The definition of microbiologic cure was lack of positive blood cultures for VRE at least 14 days after cessation of gram‐positive therapy. Microbiologic failure was defined as positive VRE blood cultures obtained on gram‐positive therapy necessitating a change in treatment. Recurrence was defined as VRE bacteremia within 30 days after discontinuation of gram‐positive therapy. Reinfection was defined as VRE bacteremia that appeared 30 days after completion of primary gram‐positive therapy.
All isolates were tested for susceptibility to linezolid using the MicroScan system, whereas daptomycin susceptibility patterns were obtained by either the Etest or MicroScan system. Of importance, our laboratory did not routinely report isolate susceptibility for daptomycin until 2008. Clinical Laboratory Standards Institute breakpoint guidelines were used to delineate minimum inhibitory concentrations for linezolid and daptomycin.
Outcomes
The primary objective was to determine the cure rate, both clinical and microbiologic, of VRE bacteremia with the use of linezolid and daptomycin. Secondary outcomes were rates of recurrence and reinfection as well as 30‐day mortality. Clinical and microbiologic response rates for subsets of the patient population that were deemed immunocompromised or at an increased risk for VRE infections (neutropenic, transplant, malignancy, and ESRD on hemodialysis) were also evaluated.
Statistical Analysis
Data were analyzed using SAS version 9.2 (SAS Inc, Cary, NC). Patients with categorical characteristics were compared using a chi‐square test or Fisher's exact test. Continuous data were analyzed using a Student t test and are expressed as the mean standard deviation. The mean duration of initial antibiotics, time to appropriate antibiotics, time to adequate antibiotic therapy, and LOS were all calculated for the linezolid and daptomycin group with a Student t test used to compare the differences. Multivariate logistic regression was used for the following outcomes: clinical cure, microbiologic cure, mortality, reinfection, and recurrence. For the interval variable, LOS, stepwise multiple regression was used to choose significant independent variables. P < 0.05 was considered statistically significant.
RESULTS
Patient Characteristics
Of the 361 patients identified with a positive VRE blood culture, 201 were included in the study. The remaining 160 patients were excluded for one of the following reasons: <5 days of therapy (n = 87), no documented gram‐positive therapy (n = 49), simultaneous gram‐positive therapy (n = 10), or insufficient data to evaluate response rates (n = 14). For the treatment of VRE bacteremia, 138 patients received linezolid and 63 patients received daptomycin. Demographics, comorbid illnesses, and patient characteristics are shown in Table 1. There was a statistically significant difference in the average age, with the linezolid group consisting of older patients. The daptomycin group had more patients with hematologic malignancies than the linezolid group (33% vs 14%; P = 0.0021) and more patients who received liver transplants (13% vs 4%; P = 0.0264).
| Linezolid (n = 138) | Daptomycin (n = 63) | P Value | |
|---|---|---|---|
| |||
| Average age, years, mean SD | 60 16 | 5315 | 0.0028 |
| Male, No. (%) | 59 (43) | 36 (57) | 0.0682 |
| Race, No. (%) | |||
| Caucasian | 34 (25) | 23 (37) | 0.1043 |
| African American | 103 (75) | 39 (62) | |
| Other | 1 (1) | 1 (2) | |
| COPD, No. (%) | 8 (6) | 2 (3) | 0.7277 |
| Diabetes mellitus, No. (%) | 61 (44) | 21 (33) | 0.1655 |
| Hemodialysis, No. (%) | 35 (25) | 17 (27) | 0.8627 |
| Malignancy, No. (%) | |||
| Solid organ | 26 (19) | 16 (25) | 0.3499 |
| Hematologic | 19 (14) | 21 (33) | 0.0021 |
| Transplant, No. (%) | |||
| Liver | 5 (4) | 8 (13) | 0.0264 |
| Kidney | 3 (2) | 0 | 0.5533 |
| Endocarditis,* No. (%) | 4 (3) | 3 (5) | 0.6801 |
| Species of VRE (%) | |||
| Enterococcus faecalis | 33 (24) | 10 (16) | 0.2658 |
| Enterococcus faecium | 105 (76) | 53 (84) | 0.2658 |
| Time to appropriate abx therapy, hours, mean SD | 12.4 26.9 | 818.8 | 0.1851 |
| Time to adequate abx therapy, days, mean SD | 2.3 1.8 | 1.81.5 | 0.0554 |
| Duration of initial abx, days, mean SD | 11.1 6.0 | 14.114.6 | 0.0401 |
| Abx before initial therapy, No. (%) | 85 (62) | 34 (54) | 0.3541 |
| Average dose, mg/kg, mean SD | NA | 6.11.5 | NA |
| Mortality, No. (%) | 25 (18) | 15 (24) | 0.3481 |
| LOS (days) | 37.527.7 | 40.827.9 | 0.4336 |
From the microbiology laboratory report of initial blood cultures, 78.6% of the isolates were noted as being E. faecium, with the remainder being E. faecalis (21.4%). One patient was classified as having linezolid‐resistant E. faecium (MIC >4 mg/L) upon repeat blood culture. Daptomycin MICs were obtained for 44 isolates using the Etest or MicroScan system; all isolates were susceptible with MICs ranging from 0.254 mg/L. As mentioned previously, our laboratory did not routinely report isolate susceptibility to daptomycin until 2008.
There were no statistically significant differences between the treatment groups with regard to time to appropriate or adequate antibiotic therapy (Table 1). However, there was a statistically significant difference in the mean duration of initial antibiotics between linezolid and daptomycin (11.1 days vs 14.1 days; P = 0.0401). Dosing strategies used in these patients were also evaluated. All linezolid patients received a dose of 600 mg every 12 hours by mouth or intravenously. The average dose of daptomycin was 6.1 mg/kg (range, 3.410.4 mg/kg; median, 6 mg/kg). The average LOS was 37 days for linezolid vs 40 days for daptomycin, which did not confer statistical significance. Overall mortality was 20%, occurring in 25 linezolid patients versus 15 daptomycin patients (P = 0.3481). The stepwise multiple regression analysis did not identify any statistically significant variables in patients treated with linezolid or daptomycin that affected any of the outcomes.
Outcomes and Analysis
As shown in Table 2, there were no statistically significant differences in clinical or microbiologic cure between the linezolid and daptomycin groups (74% vs 75% and 94% vs 94%, respectively). However, the linezolid group compared with the daptomycin group had fewer patients that developed a positive blood culture while on their initial antibiotic therapy (8% vs 22%; P = 0.0097). Follow‐up cultures were required to determine rates of recurrence and reinfection. Only 107/138 patients in the linezolid group and 51/63 patients in the daptomycin group had follow‐up cultures collected. Recurrence was documented in 3% of linezolid patients vs 12% of daptomycin patients (P = 0.0321). The odds ratio for developing a recurrent infection with daptomycin versus linezolid was 5.51 (95% confidence interval, 1.2524.28). Out of 6 patients that developed a recurrent VRE infection in the daptomycin group, 2 were prescribed doses <4 mg/kg with no reported MICs, and 2 patients received 6 mg/kg with reported MICs of 4 mg/L. No statistically significant difference existed for the rate of reinfection between linezolid and daptomycin (1% vs 6%; P = 0.0992).
| Linezolid (n = 138) | Daptomycin (n = 63) | P Value | |
|---|---|---|---|
| |||
| Patients with positive culture on G+ therapy | 11 (8) | 14 (22) | 0.0097 |
| Clinical cure | 102 (74) | 47 (75) | 1 |
| Microbiologic cure | 130 (94) | 59 (94) | 1 |
| Recurrence* | 3 (3) | 6 (12) | 0.0321 |
| Reinfection* | 1 (1) | 3 (6) | 0.0992 |
Table 3 provides information on subsets of the patient population deemed high‐risk for VRE infection or immunocompromised. There was no statistically significant difference between the 2 antibiotic groups in clinical or microbiologic cure. In the subsets of immunocompromised patients, there was no difference in recurrence or reinfection between the linezolid and daptomycin patients. Furthermore, all groups had similar LOS regardless of the antibiotic used to treat the VRE BSI. Moreover, there were no statistically significant differences in 30‐day mortality in these subsets of the population with regard to initial antibiotic choice. No significant independent variables were found between linezolid or daptomycin that affected any of the outcomes listed in Table 3.
| Neutropenia (%) | Hematologic Malignancy (%) | ESRD on Hemodialysis (%) | Liver Transplant (%) | |||||
|---|---|---|---|---|---|---|---|---|
| LZD (n = 16) | Dapto (n = 5) | LZD (n = 19) | Dapto (n = 21) | LZD (n = 35) | Dapto (n = 17) | LZD (n = 5) | Dapto (n = 8) | |
| ||||||||
| Clinical cure, No. (%) | 12 (75) | 5 (100) | 18 (95) | 17 (81) | 24 (69) | 12 (71) | 4 (80) | 3 (38) |
| Microbiologic cure,* No. (%) | 13 (81) | 5 (100) | 18 (95) | 20 (95) | 33 (94) | 16 (94) | 5 (100) | 8 (100) |
| Recurrence,* No. (%) | 2 (13) | 1 (20) | 1 (6) | 2 (11) | 0 | 2 (15) | 0 | 1 (14) |
| Reinfection,* No. (%) | 0 | 0 | 0 | 0 | 1 (4) | 2 (15) | 0 | 1 (14) |
| Mortality, No. (%) | 3 (19) | 1 (20) | 4 (21) | 3 (14) | 7 (20) | 4 (24) | 1 (20) | 4 (50) |
| LOS, days, meanSD | 57.422 | 39.412.4 | 47.626.2 | 4127.1 | 38.833.8 | 39.640.4 | 5034.5 | 73.338.8 |
DISCUSSION
Vergis et al21 reported that infections with VRE compared with vancomycin‐sensitive infections were associated with a higher rate of mortality and that the chosen antimicrobial therapy may play a pivotal role in the risk of death. Our retrospective study suggests that linezolid and daptomycin appear to be equally efficacious for the treatment of VRE BSIs. The results from our study for clinical and microbiologic cure rates for linezolid and daptomycin are similar to previously published data.7, 8 In accordance with previous studies,4 our data demonstrate that there is a higher rate of recurrence in patients treated with daptomycin. This finding may be explained by the fact that the daptomycin group was comprised of more complex patients with a greater disease burden versus the linezolid group; therefore, they were more susceptible to a recurrent VRE infection. In our study, patients who were treated with daptomycin were 5.5 times more likely to have a recurrent infection than linezolid‐treated patients. However, this finding must be scrutinized, because over half of the patients with recurrence either received an inappropriate dose or had high MICs to daptomycin.
Despite there being few clinical and microbiologic outcome data with daptomycin, our study proposes that a bactericidal antibiotic and a bacteriostatic antibiotic have comparable efficacy in the treatment of VRE BSIs. Previous literature has mainly comprised case studies or series that have evaluated clinical outcomes with daptomycin in the treatment of VRE BSIs. Gallagher et al7 reported the results of a retrospective case series of 30 patients with VRE bacteremia who were treated with daptomycin. In this study, microbiologic cure was achieved in 80% of patients, with clinical success in 59% of the patients. In 2009, Mave et al4 compared clinical outcomes between daptomycin and linezolid in the treatment of VRE bacteremia. Reported results demonstrated a microbiologic cure rate of 90% for daptomycin versus 88% for linezolid.4 Moreover, there were no differences in mortality between the groups in our study. In 2010, Crank et al18 reported no differences in mortality (in‐hospital) for hospitalized patients with VRE BSIs treated with linezolid or daptomycin. Our results seem to be consistent with what has been published previously concerning clinical outcomes associated with linezolid or daptomycin in the treatment of VRE BSI.
The average daptomycin dose received in our patients was 6.1 mg/kg with doses ranging from 3.410.4 mg/kg. The underdosing as well as higher MICs to daptomycin may have contributed to a higher rate of recurrence. Previous reports state that Enterococcus species may have higher MICs to daptomycin than Staphylococcus or Streptococcus species; consequently, higher doses may be needed to adequately treat enterococcal infections.7 In the aforementioned study by Gallagher et al,7 doses of daptomycin 6 mg/kg were associated with a positive clinical outcome in 81% of patients compared with 31% if the dose used was <6 mg/kg. Linezolid is dosed 600 mg every 12 hours by mouth or intravenously, with no variations. There have been no studies comparing the uniform dosing of linezolid to the weight‐based dosing of daptomycin and their effects on outcomes.
Patients particularly susceptible to VRE infections include those with neutropenia and/or cancer, patients receiving long‐term hemodialysis, and liver transplant recipients.3, 22, 23 Upon review of this immunocompromised population, we noted no statistically significant differences in overall outcomes. A study by Kraft et al.24 supports the findings in our study that both drugs appear useful in the treatment of VRE bacteremia in patients with hematologic malignancy. We did identify a difference, albeit nonsignificant, in LOS for daptomycin versus linezolid in patients with a history of liver transplantation. Again, the level of care that these patients needed compared with the general population may explain this difference. As mentioned previously, another pertinent factor would be the dose of daptomycin used in these patients, because the dose can affect clinical success. Because all of the other patients had a similar LOS, we cannot determine that the increased LOS seen in liver transplant patients treated with daptomycin was solely due to daptomycin use. The reason for the increased LOS seems to be multifactorial. In the neutropenic population, a difference in LOS was also recognized, but follow‐up complete blood count values were not collected for these patients to determine whether linezolid contributed to further bone marrow suppression leading to an increase in LOS. For both of these patient populations, the number of patients included is very small (n = 21 for neutropenia total, n = 13 for liver transplant total), which can lead to a high degree of variance.
This study has several limitations. This was a retrospective review; therefore, we had no control over the selection of therapy. This may be reflected in an apparent preferential use of daptomycin in immunocompromised patients. Furthermore, 62% of linezolid patients and 54% of daptomycin patients received an antibiotic before initial therapy that could have potentially altered response rates. Due to the paucity of documentation surrounding initial site of infection, some of the positive cultures may represent potential contamination, because VRE may contaminate skin.25 Contamination seems implausible, however, because patients were seen by an infectious disease physician and had at least 1 documented positive VRE blood culture. We chose arbitrary definitions for clinical cure, microbiologic cure, microbiologic failure, recurrence, and reinfection. Previous studies have used their own definitions leading to discrepancies in reporting. Another limitation was that follow‐up cultures were not obtained on all of the patients, which was needed to determine rates of recurrence, reinfection, and microbiologic cure. MICs to daptomycin were not reported in 30% of our patients, potentially altering the recurrence rate seen in the daptomycin‐treated patients. Because clinical cure was not documented in the chart, it was inferred from the laboratory values and vital sign information. One investigator analyzed all of the values and made the determination of clinical cure, allowing for a consistent approach to data review.
In the face of the imposing threat of a highly resistant organism such as VRE with a limited number of efficacious antibiotics, antimicrobial selection becomes increasingly important and is requisite to clinical and microbiological success. To our knowledge, this is one of the largest studies to date comparing the efficacy of linezolid with that of daptomycin in the treatment of VRE bacteremia. Both of these agents are effective for the treatment of VRE BSIs. Nevertheless, specific factors related to the medication (eg, dose, route of administration) as well as the patient (eg, comorbid conditions, acuity of illness) should be taken into consideration when selecting an initial antimicrobial agent. Because the treatment of VRE BSIs continues to be a challenge, larger prospective randomized controlled trials are needed to corroborate our results and determine the optimal therapy for this serious infection.
Acknowledgements
Disclosures: Michael S. Gelfand is on the speaker's bureau for Cubist and Pfizer.
- ,,,,,.Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study.Clin Infect Dis.2004;39:309–317.
- ,,, et al.Clinical practice guidelines for the management of intravascular catheter‐related infection: 2009 update by the Infectious Diseases Society of America.Clin Infect Dis.2009;49:1–45.
- ,,,,,.Bad bugs need drugs: an update on the development pipeline from the antimicrobial availability task force of the infectious diseases society of America.Clin Infect Dis.2006;42:657–668.
- ,,,.Vancomycin‐resistant enterococcal bacteraemia: is daptomycin as effective as linezolid?J Antimicrob Chemother.2009;64:175–180.
- ,,.Management of multidrug‐resistant enterococcal Infections.Clin Microbiol Infect.2010;16:555–562.
- ,,, et al.Treatment of vancomycin‐resistant Enterococcus faecium infections with quinupristin/dalfopristin.Clin Infect Dis.2001;33:1816–1823.
- ,,, et al.Daptomycin for vancomycin‐resistant enterococcol bacteremia: a retrospective case series of 30 patients.Pharmacotherapy.2009;29:792–799.
- ,,, et al.Safety, efficacy and pharmacokinetics of linezolid for treatment of resistant gram positive infections in cancer patients with neutropenia.Ann Oncol.2003;14:795–801.
- ,,,,.Daptomycin for the treatment of vancomycin resistant Enterococcus faecium bacteremia.Scand J Infect Dis.2003;38:290–292.
- ,.New antimicrobial agents for the treatment of gram positive bacterial infections.Clin Microbiol Infec.2008;14:411–420.
- ,.Emergence and management of drug‐resistant enterococcal infections.Expert Rev Anti Infect Ther.2008;6:637–655.
- ,,.Nosocomial spread of linezolid‐resistant, Vancomycin resistant Enterococcus faecium.N Engl J Med.2002;346:867–869.
- ,, et al.Nosocomial superinfections due to linezolid‐resitant Enterococcus faecalis: evidence for a gene dosage effect of linezolid MICs.Diagn Microbiol Infect Dis.2003;47:511–513.
- .Quinupristin‐dalfopristin and linezolid: evidence and opinion.Clin Infect Dis.2003;36:473–481.
- Cubicin (Daptomycin for injection) [package insert].Lexington, MA:Cubist Pharmaceuticals;2010.
- ,,,.Daptomycin nonsusceptible Enterococci: an emerging challenge for clinicians.Clin Infect Dis.2011;52:228–234.
- ,,,.A potential role for daptomycin in enterococcal infections: what is the evidence?J Antimicrob Chemother.2010;65:1126–1136.
- ,,, et al.Comparison of outcomes from daptomycin or linezolid for vancomycin‐resistant enterococcal bloodstream infection: a retrospective, multicenter, cohort study.Clin Ther.2010;32:1713–1719.
- ,,,,,.Observational study of the epidemiology and outcomes of vancomycin‐resistant Enterococcus bacteraemia treated with newer antimicrobial agents.Epidemiol Infect.2010;15:1–9.
- .Inadequate antimicrobial treatment: an important determinant of outcome for hospitalized patients.Clin Infect Dis.2000;31:S131–S138.
- ,,, et al.Determinants of vancomycin resistance and mortality rates in enterococcal bacteremia: a prospective multicenter study.Ann Intern Med.2001;135:484–492.
- ,,,,,.Vancomycin resistant enterococci among chronic hemodialysis patients: a prospective study of acquisition.Clin Infect Dis.2001;32:23–29.
- ,,, et al.A nationwide, multicenter, case control study comparing risk factors, treatment, and outcome for vancomycin resistant andsusceptible enterococcal bacteremia.Diagn Microbiol Infect Dis.2000;36:145–158.
- ,,,,.Outcomes of therapy: vancomycin‐resistant enterococcal bacteremia in hematology and bone marrow transplant patients [published online ahead of print November 26, 2010].Support Care Cancer. doi: 10.1007/s00520–010‐1038‐z.
- ,,, et al.Skin colonization with vancomycin‐resistant enterococci among hospitalized patients with bacteremia.Clin Infect Dis.1997;24:704–706.
- ,,,,,.Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study.Clin Infect Dis.2004;39:309–317.
- ,,, et al.Clinical practice guidelines for the management of intravascular catheter‐related infection: 2009 update by the Infectious Diseases Society of America.Clin Infect Dis.2009;49:1–45.
- ,,,,,.Bad bugs need drugs: an update on the development pipeline from the antimicrobial availability task force of the infectious diseases society of America.Clin Infect Dis.2006;42:657–668.
- ,,,.Vancomycin‐resistant enterococcal bacteraemia: is daptomycin as effective as linezolid?J Antimicrob Chemother.2009;64:175–180.
- ,,.Management of multidrug‐resistant enterococcal Infections.Clin Microbiol Infect.2010;16:555–562.
- ,,, et al.Treatment of vancomycin‐resistant Enterococcus faecium infections with quinupristin/dalfopristin.Clin Infect Dis.2001;33:1816–1823.
- ,,, et al.Daptomycin for vancomycin‐resistant enterococcol bacteremia: a retrospective case series of 30 patients.Pharmacotherapy.2009;29:792–799.
- ,,, et al.Safety, efficacy and pharmacokinetics of linezolid for treatment of resistant gram positive infections in cancer patients with neutropenia.Ann Oncol.2003;14:795–801.
- ,,,,.Daptomycin for the treatment of vancomycin resistant Enterococcus faecium bacteremia.Scand J Infect Dis.2003;38:290–292.
- ,.New antimicrobial agents for the treatment of gram positive bacterial infections.Clin Microbiol Infec.2008;14:411–420.
- ,.Emergence and management of drug‐resistant enterococcal infections.Expert Rev Anti Infect Ther.2008;6:637–655.
- ,,.Nosocomial spread of linezolid‐resistant, Vancomycin resistant Enterococcus faecium.N Engl J Med.2002;346:867–869.
- ,, et al.Nosocomial superinfections due to linezolid‐resitant Enterococcus faecalis: evidence for a gene dosage effect of linezolid MICs.Diagn Microbiol Infect Dis.2003;47:511–513.
- .Quinupristin‐dalfopristin and linezolid: evidence and opinion.Clin Infect Dis.2003;36:473–481.
- Cubicin (Daptomycin for injection) [package insert].Lexington, MA:Cubist Pharmaceuticals;2010.
- ,,,.Daptomycin nonsusceptible Enterococci: an emerging challenge for clinicians.Clin Infect Dis.2011;52:228–234.
- ,,,.A potential role for daptomycin in enterococcal infections: what is the evidence?J Antimicrob Chemother.2010;65:1126–1136.
- ,,, et al.Comparison of outcomes from daptomycin or linezolid for vancomycin‐resistant enterococcal bloodstream infection: a retrospective, multicenter, cohort study.Clin Ther.2010;32:1713–1719.
- ,,,,,.Observational study of the epidemiology and outcomes of vancomycin‐resistant Enterococcus bacteraemia treated with newer antimicrobial agents.Epidemiol Infect.2010;15:1–9.
- .Inadequate antimicrobial treatment: an important determinant of outcome for hospitalized patients.Clin Infect Dis.2000;31:S131–S138.
- ,,, et al.Determinants of vancomycin resistance and mortality rates in enterococcal bacteremia: a prospective multicenter study.Ann Intern Med.2001;135:484–492.
- ,,,,,.Vancomycin resistant enterococci among chronic hemodialysis patients: a prospective study of acquisition.Clin Infect Dis.2001;32:23–29.
- ,,, et al.A nationwide, multicenter, case control study comparing risk factors, treatment, and outcome for vancomycin resistant andsusceptible enterococcal bacteremia.Diagn Microbiol Infect Dis.2000;36:145–158.
- ,,,,.Outcomes of therapy: vancomycin‐resistant enterococcal bacteremia in hematology and bone marrow transplant patients [published online ahead of print November 26, 2010].Support Care Cancer. doi: 10.1007/s00520–010‐1038‐z.
- ,,, et al.Skin colonization with vancomycin‐resistant enterococci among hospitalized patients with bacteremia.Clin Infect Dis.1997;24:704–706.
Copyright © 2011 Society of Hospital Medicine
Report Finds U.S. Health Quality Stagnant
A recent report (PDF) from The Commonwealth Fund that suggests the quality and efficacy of the U.S. healthcare system has remained relatively static in the past three years has bright spots for HM, an academic hospitalist says.
Kedar Mate, MD, assistant professor of medicine with the division of hospital medicine at Weill Cornell Medical School in New York City, says the report, which was compiled before any of the facets of the Affordable Care Act were implemented, helps argue why hospitalists are poised to take the reins of those needed quality reforms.
"They're the natural leaders of this work moving forward from the physician perspective," says Dr. Mate, a faculty member at the Institute for Healthcare Improvement in Cambridge, Mass. "They have a strong role to play in shepherding and championing and really being the arms and legs of the quality and safety movement, in many ways. Not only leading it, but actually executing it."
The report released last month, "Why Not the Best? Results from the National Scorecard on U.S. Health System Performance, 2011," measures 42 indicators of healthcare quality, access, efficiency, equity, and healthy lives. In overall terms, the U.S. score has varied only slightly in the third national scorecard. And while the report cautions that year-to-year analyses of quality measures are not directly comparable because of changing categories, Dr. Mate notes there have been significant improvements in areas that HM and health system improvement efforts have targeted.
The study, for example, reports half of adults with high blood pressure had the condition under control in 2007-2008, up from 31% in 1999-2000. The data also show that the rate of controlled blood sugar levels in adults with diabetes ticked up to 86% in 2007-2008 from 79% in 1999-2000.
"Where we turn our attention, particularly with focused quality initiatives, we're seeing some measurable change," Dr. Mate says. "There's absolutely value in identifying and knowing where we are seeing benefits, because those ought to be built upon."
A recent report (PDF) from The Commonwealth Fund that suggests the quality and efficacy of the U.S. healthcare system has remained relatively static in the past three years has bright spots for HM, an academic hospitalist says.
Kedar Mate, MD, assistant professor of medicine with the division of hospital medicine at Weill Cornell Medical School in New York City, says the report, which was compiled before any of the facets of the Affordable Care Act were implemented, helps argue why hospitalists are poised to take the reins of those needed quality reforms.
"They're the natural leaders of this work moving forward from the physician perspective," says Dr. Mate, a faculty member at the Institute for Healthcare Improvement in Cambridge, Mass. "They have a strong role to play in shepherding and championing and really being the arms and legs of the quality and safety movement, in many ways. Not only leading it, but actually executing it."
The report released last month, "Why Not the Best? Results from the National Scorecard on U.S. Health System Performance, 2011," measures 42 indicators of healthcare quality, access, efficiency, equity, and healthy lives. In overall terms, the U.S. score has varied only slightly in the third national scorecard. And while the report cautions that year-to-year analyses of quality measures are not directly comparable because of changing categories, Dr. Mate notes there have been significant improvements in areas that HM and health system improvement efforts have targeted.
The study, for example, reports half of adults with high blood pressure had the condition under control in 2007-2008, up from 31% in 1999-2000. The data also show that the rate of controlled blood sugar levels in adults with diabetes ticked up to 86% in 2007-2008 from 79% in 1999-2000.
"Where we turn our attention, particularly with focused quality initiatives, we're seeing some measurable change," Dr. Mate says. "There's absolutely value in identifying and knowing where we are seeing benefits, because those ought to be built upon."
A recent report (PDF) from The Commonwealth Fund that suggests the quality and efficacy of the U.S. healthcare system has remained relatively static in the past three years has bright spots for HM, an academic hospitalist says.
Kedar Mate, MD, assistant professor of medicine with the division of hospital medicine at Weill Cornell Medical School in New York City, says the report, which was compiled before any of the facets of the Affordable Care Act were implemented, helps argue why hospitalists are poised to take the reins of those needed quality reforms.
"They're the natural leaders of this work moving forward from the physician perspective," says Dr. Mate, a faculty member at the Institute for Healthcare Improvement in Cambridge, Mass. "They have a strong role to play in shepherding and championing and really being the arms and legs of the quality and safety movement, in many ways. Not only leading it, but actually executing it."
The report released last month, "Why Not the Best? Results from the National Scorecard on U.S. Health System Performance, 2011," measures 42 indicators of healthcare quality, access, efficiency, equity, and healthy lives. In overall terms, the U.S. score has varied only slightly in the third national scorecard. And while the report cautions that year-to-year analyses of quality measures are not directly comparable because of changing categories, Dr. Mate notes there have been significant improvements in areas that HM and health system improvement efforts have targeted.
The study, for example, reports half of adults with high blood pressure had the condition under control in 2007-2008, up from 31% in 1999-2000. The data also show that the rate of controlled blood sugar levels in adults with diabetes ticked up to 86% in 2007-2008 from 79% in 1999-2000.
"Where we turn our attention, particularly with focused quality initiatives, we're seeing some measurable change," Dr. Mate says. "There's absolutely value in identifying and knowing where we are seeing benefits, because those ought to be built upon."
Church Coalition Helps Prevent Readmissions
A partnership with nearly 400 local churches is helping the seven-hospital Methodist Le Bonheur Healthcare System, based in Memphis, Tenn., return hospitalized patients to their communities with the support they need to manage such chronic conditions as congestive heart failure.
Preliminary research into the Congregational Health Network shows a 20% decrease in readmissions by participating patients, compared with matched controls, says Teresa Cutts, PhD, director of research for innovation for Methodist's Center of Excellence in Faith & Health.
But the program is more than just "outreach" from the health system to the churches, she adds. It also is "in-reach" from community partners to the health system and a true collaboration. "The clergy have a covenant; they have deep ownership of this network," she says.
Trained volunteer liaisons at each participating church are the bridge to the health system. Patients who are members of the network and who opt in at admission are connected to liaisons or other church volunteers, who then visit patients in the hospital and at their homes following discharge. Hospital-employed community care workers (called navigators) help coordinate these connections, supported by Methodist's electronic health record (EHR).
The network has 12,000 registered members. Approximately 1,100 volunteers have received training in such subjects as hospital visitation, hands-on aftercare, and mental health first aid. Larger goals, Dr. Cutts says, include pushing this support further upstream into preventive care, documenting outcomes, and incorporating more clinical issues into the volunteer training.
"We think it's time, and will really empower people," she says.
In September, health system representatives visited the White House to share the coalition's success story. For more information, contact Cutts at [email protected].
A partnership with nearly 400 local churches is helping the seven-hospital Methodist Le Bonheur Healthcare System, based in Memphis, Tenn., return hospitalized patients to their communities with the support they need to manage such chronic conditions as congestive heart failure.
Preliminary research into the Congregational Health Network shows a 20% decrease in readmissions by participating patients, compared with matched controls, says Teresa Cutts, PhD, director of research for innovation for Methodist's Center of Excellence in Faith & Health.
But the program is more than just "outreach" from the health system to the churches, she adds. It also is "in-reach" from community partners to the health system and a true collaboration. "The clergy have a covenant; they have deep ownership of this network," she says.
Trained volunteer liaisons at each participating church are the bridge to the health system. Patients who are members of the network and who opt in at admission are connected to liaisons or other church volunteers, who then visit patients in the hospital and at their homes following discharge. Hospital-employed community care workers (called navigators) help coordinate these connections, supported by Methodist's electronic health record (EHR).
The network has 12,000 registered members. Approximately 1,100 volunteers have received training in such subjects as hospital visitation, hands-on aftercare, and mental health first aid. Larger goals, Dr. Cutts says, include pushing this support further upstream into preventive care, documenting outcomes, and incorporating more clinical issues into the volunteer training.
"We think it's time, and will really empower people," she says.
In September, health system representatives visited the White House to share the coalition's success story. For more information, contact Cutts at [email protected].
A partnership with nearly 400 local churches is helping the seven-hospital Methodist Le Bonheur Healthcare System, based in Memphis, Tenn., return hospitalized patients to their communities with the support they need to manage such chronic conditions as congestive heart failure.
Preliminary research into the Congregational Health Network shows a 20% decrease in readmissions by participating patients, compared with matched controls, says Teresa Cutts, PhD, director of research for innovation for Methodist's Center of Excellence in Faith & Health.
But the program is more than just "outreach" from the health system to the churches, she adds. It also is "in-reach" from community partners to the health system and a true collaboration. "The clergy have a covenant; they have deep ownership of this network," she says.
Trained volunteer liaisons at each participating church are the bridge to the health system. Patients who are members of the network and who opt in at admission are connected to liaisons or other church volunteers, who then visit patients in the hospital and at their homes following discharge. Hospital-employed community care workers (called navigators) help coordinate these connections, supported by Methodist's electronic health record (EHR).
The network has 12,000 registered members. Approximately 1,100 volunteers have received training in such subjects as hospital visitation, hands-on aftercare, and mental health first aid. Larger goals, Dr. Cutts says, include pushing this support further upstream into preventive care, documenting outcomes, and incorporating more clinical issues into the volunteer training.
"We think it's time, and will really empower people," she says.
In September, health system representatives visited the White House to share the coalition's success story. For more information, contact Cutts at [email protected].
FDA: Trilipix May Not Cut Heart Attack Risk
Treatment with fenofibric acid "may not" lower the risk of myocardial infarction or stroke in patients treated with the cholesterol-lowering medication, information that is being added to the drug’s label, the Food and Drug Administration announced on Nov. 9.
The FDA statement and decision to make the labeling change are based on the agency’s review of the ACCORD (Action to Control Cardiovascular Risk in Diabetes) lipid trial, which showed no significant differences in the risk of major adverse cardiac events between patients treated with fenofibrate and simvastatin and those treated with simvastatin alone.
Data from the ACCORD lipid trial have been added to the drug label’s "Important Limitations of Use" and "Warnings and Precautions" sections, and to the medication guide given to patients with each prescription.
"Health care professionals should consider the benefits and risks of Trilipix when deciding to prescribe the drug to patients," the FDA cautioned in its statement, and physicians should encourage their patients to read the medication guide.
At a meeting of the FDA’s Endocrinologic and Metabolic Drugs Advisory Committee earlier this year, the panel was divided over how the ACCORD lipid results should affect the drugs labeling and the approved indication for use with a statin. Of the 13 panel members, 6 agreed that the main findings of ACCORD should be added to the drug’s label, while 4 said that the co-administration indication should be withdrawn. The remaining three panelists said that marketing should continue with no label changes.
Fenofibric acid, a peroxisome proliferator receptor-alpha activator marketed as Trilipix by Abbott Laboratories, was approved in 2008, for use with a statin to reduce triglycerides and increase HDL cholesterol in patients with mixed dyslipidemia and coronary heart disease or a CHD risk equivalent who are on optimal statin therapy to achieve their LDL cholesterol goal. It is also indicated as monotherapy to reduce triglycerides in patients with severe hypertriglyceridemia; as monotherapy to reduce elevated LDL cholesterol levels, total-C cholesterol, triglycerides, and apolipoprotein-B, and to increase HDL cholesterol levels in patients with primary hyperlipidemia or mixed dyslipidemia.
In the ACCORD lipid study, patients were treated with simvastatin for 4 weeks and were then randomized to continue treatment with simvastatin and placebo (2,753 patients) or simvastatin and fenofibrate (2,765 patients).
Over a mean follow-up of 4.7 years, the risk of major adverse cardiovascular events (nonfatal MI, nonfatal stroke, and death from cardiovascular disease) was 8% lower among patients on the combination, but the difference was not statistically significant. Among men, the risk was reduced by 18% among those on the combination, compared with those on simvastatin alone.
Among women, however, the risk of major adverse cardiovascular events was 38% greater among those on the combination, compared with those on placebo.
That gender effect was not seen in another large randomized controlled clinical trial comparing fenofibrate to placebo, so "the clinical significance of this subgroup finding is unclear," the FDA statement noted.
But "the study results also raised the hypothesis that a subgroup of patients with high triglycerides and low high-density lipoprotein cholesterol may experience some reduction in the risk of MACE [major adverse cardiovascular events] from the combination therapy vs. simvastatin monotherapy," the agency noted.
The FDA will require Abbott to conduct a randomized, double-blind, placebo-controlled clinical trial to evaluate whether combination treatment with fenofibrate plus a statin significantly reduces the rate of MACE in men and women who are at their LDL cholesterol goal on statin therapy but have residually high triglycerides and low HDL cholesterol.
Serious adverse events associated with Trilipix should be reported to the FDA’s MedWatch program online or at 800-332-1088.
Treatment with fenofibric acid "may not" lower the risk of myocardial infarction or stroke in patients treated with the cholesterol-lowering medication, information that is being added to the drug’s label, the Food and Drug Administration announced on Nov. 9.
The FDA statement and decision to make the labeling change are based on the agency’s review of the ACCORD (Action to Control Cardiovascular Risk in Diabetes) lipid trial, which showed no significant differences in the risk of major adverse cardiac events between patients treated with fenofibrate and simvastatin and those treated with simvastatin alone.
Data from the ACCORD lipid trial have been added to the drug label’s "Important Limitations of Use" and "Warnings and Precautions" sections, and to the medication guide given to patients with each prescription.
"Health care professionals should consider the benefits and risks of Trilipix when deciding to prescribe the drug to patients," the FDA cautioned in its statement, and physicians should encourage their patients to read the medication guide.
At a meeting of the FDA’s Endocrinologic and Metabolic Drugs Advisory Committee earlier this year, the panel was divided over how the ACCORD lipid results should affect the drugs labeling and the approved indication for use with a statin. Of the 13 panel members, 6 agreed that the main findings of ACCORD should be added to the drug’s label, while 4 said that the co-administration indication should be withdrawn. The remaining three panelists said that marketing should continue with no label changes.
Fenofibric acid, a peroxisome proliferator receptor-alpha activator marketed as Trilipix by Abbott Laboratories, was approved in 2008, for use with a statin to reduce triglycerides and increase HDL cholesterol in patients with mixed dyslipidemia and coronary heart disease or a CHD risk equivalent who are on optimal statin therapy to achieve their LDL cholesterol goal. It is also indicated as monotherapy to reduce triglycerides in patients with severe hypertriglyceridemia; as monotherapy to reduce elevated LDL cholesterol levels, total-C cholesterol, triglycerides, and apolipoprotein-B, and to increase HDL cholesterol levels in patients with primary hyperlipidemia or mixed dyslipidemia.
In the ACCORD lipid study, patients were treated with simvastatin for 4 weeks and were then randomized to continue treatment with simvastatin and placebo (2,753 patients) or simvastatin and fenofibrate (2,765 patients).
Over a mean follow-up of 4.7 years, the risk of major adverse cardiovascular events (nonfatal MI, nonfatal stroke, and death from cardiovascular disease) was 8% lower among patients on the combination, but the difference was not statistically significant. Among men, the risk was reduced by 18% among those on the combination, compared with those on simvastatin alone.
Among women, however, the risk of major adverse cardiovascular events was 38% greater among those on the combination, compared with those on placebo.
That gender effect was not seen in another large randomized controlled clinical trial comparing fenofibrate to placebo, so "the clinical significance of this subgroup finding is unclear," the FDA statement noted.
But "the study results also raised the hypothesis that a subgroup of patients with high triglycerides and low high-density lipoprotein cholesterol may experience some reduction in the risk of MACE [major adverse cardiovascular events] from the combination therapy vs. simvastatin monotherapy," the agency noted.
The FDA will require Abbott to conduct a randomized, double-blind, placebo-controlled clinical trial to evaluate whether combination treatment with fenofibrate plus a statin significantly reduces the rate of MACE in men and women who are at their LDL cholesterol goal on statin therapy but have residually high triglycerides and low HDL cholesterol.
Serious adverse events associated with Trilipix should be reported to the FDA’s MedWatch program online or at 800-332-1088.
Treatment with fenofibric acid "may not" lower the risk of myocardial infarction or stroke in patients treated with the cholesterol-lowering medication, information that is being added to the drug’s label, the Food and Drug Administration announced on Nov. 9.
The FDA statement and decision to make the labeling change are based on the agency’s review of the ACCORD (Action to Control Cardiovascular Risk in Diabetes) lipid trial, which showed no significant differences in the risk of major adverse cardiac events between patients treated with fenofibrate and simvastatin and those treated with simvastatin alone.
Data from the ACCORD lipid trial have been added to the drug label’s "Important Limitations of Use" and "Warnings and Precautions" sections, and to the medication guide given to patients with each prescription.
"Health care professionals should consider the benefits and risks of Trilipix when deciding to prescribe the drug to patients," the FDA cautioned in its statement, and physicians should encourage their patients to read the medication guide.
At a meeting of the FDA’s Endocrinologic and Metabolic Drugs Advisory Committee earlier this year, the panel was divided over how the ACCORD lipid results should affect the drugs labeling and the approved indication for use with a statin. Of the 13 panel members, 6 agreed that the main findings of ACCORD should be added to the drug’s label, while 4 said that the co-administration indication should be withdrawn. The remaining three panelists said that marketing should continue with no label changes.
Fenofibric acid, a peroxisome proliferator receptor-alpha activator marketed as Trilipix by Abbott Laboratories, was approved in 2008, for use with a statin to reduce triglycerides and increase HDL cholesterol in patients with mixed dyslipidemia and coronary heart disease or a CHD risk equivalent who are on optimal statin therapy to achieve their LDL cholesterol goal. It is also indicated as monotherapy to reduce triglycerides in patients with severe hypertriglyceridemia; as monotherapy to reduce elevated LDL cholesterol levels, total-C cholesterol, triglycerides, and apolipoprotein-B, and to increase HDL cholesterol levels in patients with primary hyperlipidemia or mixed dyslipidemia.
In the ACCORD lipid study, patients were treated with simvastatin for 4 weeks and were then randomized to continue treatment with simvastatin and placebo (2,753 patients) or simvastatin and fenofibrate (2,765 patients).
Over a mean follow-up of 4.7 years, the risk of major adverse cardiovascular events (nonfatal MI, nonfatal stroke, and death from cardiovascular disease) was 8% lower among patients on the combination, but the difference was not statistically significant. Among men, the risk was reduced by 18% among those on the combination, compared with those on simvastatin alone.
Among women, however, the risk of major adverse cardiovascular events was 38% greater among those on the combination, compared with those on placebo.
That gender effect was not seen in another large randomized controlled clinical trial comparing fenofibrate to placebo, so "the clinical significance of this subgroup finding is unclear," the FDA statement noted.
But "the study results also raised the hypothesis that a subgroup of patients with high triglycerides and low high-density lipoprotein cholesterol may experience some reduction in the risk of MACE [major adverse cardiovascular events] from the combination therapy vs. simvastatin monotherapy," the agency noted.
The FDA will require Abbott to conduct a randomized, double-blind, placebo-controlled clinical trial to evaluate whether combination treatment with fenofibrate plus a statin significantly reduces the rate of MACE in men and women who are at their LDL cholesterol goal on statin therapy but have residually high triglycerides and low HDL cholesterol.
Serious adverse events associated with Trilipix should be reported to the FDA’s MedWatch program online or at 800-332-1088.
FROM THE FOOD AND DRUG ADMINISTRATION
New Tool Improves Outcome Assessment in Pediatric Vasculitis
Overuse injuries are very common in children and teenagers, especially among kids who play sports throughout the year.
Although rare, primary systemic vasculitis in children is associated with significant mortality and morbidity when not properly treated. Optimal management of the group of multiorgan inflammatory conditions is hampered by the lack of evidence-based therapies. This shortage of data has been attributed, in part, to the absence of a standardized outcome measure for use in clinical trials, according to Dr. Pavla Dolezalova.
"Until recently, no standardized vasculitis activity assessment tool has been available for children, so some pediatric studies apply adult measures, such as the Birmingham Vasculitis Activity Score [BVAS]," she said. Further, although nonspecific inflammatory markers such as erythrocyte sedimentation rate or C-reactive protein can reflect systemic vasculitis disease activity, they do not distinguish it from infectious complications. Use of the global assessment of disease activity by the treating physician using the visual analog scale is of limited utility in clinical trials, she noted.
In an effort to facilitate more informative clinical trials of primary systemic vasculitis in children, Dr. Dolezalova of Charles University and General University Hospital in Prague, Czech Republic, and her colleagues have developed a quantitative clinical index of manifestations of active disease, called the Pediatric Vasculitis Activity Score (PVAS), which has been preliminarily validated as a useful clinical measure with good interobserver reliability (Pediatr. Rheumatol. Online J. 2011 [doi:10.1186/1546-0096-9-S1-P92]).
In this column, Dr. Dolezalova describes the need for the assessment tool as well as some of the development challenges.
Question: Why are outcome assessment tools used for adults with systemic vasculitis not ideal for measuring disease activity in children?
Dr. Dolezalova: Tools used in adults are not fully applicable in children for multiple reasons. Disease presentations and outcome of primary systemic vasculitides appear to be different in children. Among the most obvious differences between adult and pediatric variants of the disease are the developmental and growth aspects; differences in functional, educational, and social impacts of longstanding disease; different drug pharmacokinetics and toxicity profiles; and the absence of comorbidities in children.
Question: What specific features have been incorporated into the PVAS?
Dr. Dolezalova: The development of the pediatric-specific tool has been a result of an international collaborative effort of pediatric rheumatologists from the vasculitis working groups of PReS (Pediatric Rheumatology European Society) and CARRA (North American Childhood Arthritis & Rheumatology Research Alliance), with the help of the European Vasculitis Study Group (EUVAS). We adapted the Birmingham Vasculitis Activity Score (BVAS 2003), the most commonly used tool in adult vasculitis patients, into PVAS. It is a systematic clinical scoring system that identifies selected features of active vasculitis in nine organ systems. Based on the analysis of the most common systemic vasculitis presentations in children reported to the PReS/PRINTO (Pediatric Rheumatology International Trials Organization) vasculitis registry, eight pediatric-relevant items and their definitions were added to the original BVAS 2003 in the cutaneous, cardiovascular, and abdominal systems. Additionally, by consensus, the maximum score for each organ system was to remain unchanged to facilitate longitudinal congruity with the BVAS. Among the 56 BVAS 2003 items, we redefined 22 for pediatric use.
Question: What were some of the challenges involved in the development of this tool?
Dr. Dolezalova: At the beginning of the process, we had to decide which principal way to follow: whether to start developing a brand new, originally pediatric tool, or to explore the applicability of existing measures and rely on the expertise of our adult rheumatology colleagues. Having gone for the second option meant that we had to accept existing adult concepts of vasculitis activity and damage assessments. The next challenge we had to overcome was that of modifying definitions of individual disease signs and symptoms from the BVAS glossary to be appropriate for pediatric patients. We wanted them to remain compatible with their adult counterparts but also to reflect pediatric reality. Learning the training process of vasculitis activity assessment and undergoing it according to the principles set up by EUVAS had been a true challenge for all pediatricians involved in the PVAS development.
Question: How is the PVAS tool being validated?
Dr. Dolezalova: The PVAS validation has been a multistep process that is now in its final stage. During consensus meetings, content and face validity were established, resulting in minor modifications to the PVAS and its glossary. Scoring of the pediatric paper cases during the training process provided information on the tool’s feasibility. Prospective real-patient assessment, including duplicate assessments by two trained researchers and follow-up evaluation in newly diagnosed or relapsing patients, provided data on the tool’s reliability, responsiveness, and discriminative ability. Currently, analysis of the prospective multicenter data on the larger patient cohort is ongoing.
Interview by Diana Mahoney
Dr. Dolezalova is the national co-coordinator of PRINTO and chairperson of the PReS clinical affairs committee. She had no relevant financial disclosures.
Overuse injuries are very common in children and teenagers, especially among kids who play sports throughout the year.
Although rare, primary systemic vasculitis in children is associated with significant mortality and morbidity when not properly treated. Optimal management of the group of multiorgan inflammatory conditions is hampered by the lack of evidence-based therapies. This shortage of data has been attributed, in part, to the absence of a standardized outcome measure for use in clinical trials, according to Dr. Pavla Dolezalova.
"Until recently, no standardized vasculitis activity assessment tool has been available for children, so some pediatric studies apply adult measures, such as the Birmingham Vasculitis Activity Score [BVAS]," she said. Further, although nonspecific inflammatory markers such as erythrocyte sedimentation rate or C-reactive protein can reflect systemic vasculitis disease activity, they do not distinguish it from infectious complications. Use of the global assessment of disease activity by the treating physician using the visual analog scale is of limited utility in clinical trials, she noted.
In an effort to facilitate more informative clinical trials of primary systemic vasculitis in children, Dr. Dolezalova of Charles University and General University Hospital in Prague, Czech Republic, and her colleagues have developed a quantitative clinical index of manifestations of active disease, called the Pediatric Vasculitis Activity Score (PVAS), which has been preliminarily validated as a useful clinical measure with good interobserver reliability (Pediatr. Rheumatol. Online J. 2011 [doi:10.1186/1546-0096-9-S1-P92]).
In this column, Dr. Dolezalova describes the need for the assessment tool as well as some of the development challenges.
Question: Why are outcome assessment tools used for adults with systemic vasculitis not ideal for measuring disease activity in children?
Dr. Dolezalova: Tools used in adults are not fully applicable in children for multiple reasons. Disease presentations and outcome of primary systemic vasculitides appear to be different in children. Among the most obvious differences between adult and pediatric variants of the disease are the developmental and growth aspects; differences in functional, educational, and social impacts of longstanding disease; different drug pharmacokinetics and toxicity profiles; and the absence of comorbidities in children.
Question: What specific features have been incorporated into the PVAS?
Dr. Dolezalova: The development of the pediatric-specific tool has been a result of an international collaborative effort of pediatric rheumatologists from the vasculitis working groups of PReS (Pediatric Rheumatology European Society) and CARRA (North American Childhood Arthritis & Rheumatology Research Alliance), with the help of the European Vasculitis Study Group (EUVAS). We adapted the Birmingham Vasculitis Activity Score (BVAS 2003), the most commonly used tool in adult vasculitis patients, into PVAS. It is a systematic clinical scoring system that identifies selected features of active vasculitis in nine organ systems. Based on the analysis of the most common systemic vasculitis presentations in children reported to the PReS/PRINTO (Pediatric Rheumatology International Trials Organization) vasculitis registry, eight pediatric-relevant items and their definitions were added to the original BVAS 2003 in the cutaneous, cardiovascular, and abdominal systems. Additionally, by consensus, the maximum score for each organ system was to remain unchanged to facilitate longitudinal congruity with the BVAS. Among the 56 BVAS 2003 items, we redefined 22 for pediatric use.
Question: What were some of the challenges involved in the development of this tool?
Dr. Dolezalova: At the beginning of the process, we had to decide which principal way to follow: whether to start developing a brand new, originally pediatric tool, or to explore the applicability of existing measures and rely on the expertise of our adult rheumatology colleagues. Having gone for the second option meant that we had to accept existing adult concepts of vasculitis activity and damage assessments. The next challenge we had to overcome was that of modifying definitions of individual disease signs and symptoms from the BVAS glossary to be appropriate for pediatric patients. We wanted them to remain compatible with their adult counterparts but also to reflect pediatric reality. Learning the training process of vasculitis activity assessment and undergoing it according to the principles set up by EUVAS had been a true challenge for all pediatricians involved in the PVAS development.
Question: How is the PVAS tool being validated?
Dr. Dolezalova: The PVAS validation has been a multistep process that is now in its final stage. During consensus meetings, content and face validity were established, resulting in minor modifications to the PVAS and its glossary. Scoring of the pediatric paper cases during the training process provided information on the tool’s feasibility. Prospective real-patient assessment, including duplicate assessments by two trained researchers and follow-up evaluation in newly diagnosed or relapsing patients, provided data on the tool’s reliability, responsiveness, and discriminative ability. Currently, analysis of the prospective multicenter data on the larger patient cohort is ongoing.
Interview by Diana Mahoney
Dr. Dolezalova is the national co-coordinator of PRINTO and chairperson of the PReS clinical affairs committee. She had no relevant financial disclosures.
Overuse injuries are very common in children and teenagers, especially among kids who play sports throughout the year.
Although rare, primary systemic vasculitis in children is associated with significant mortality and morbidity when not properly treated. Optimal management of the group of multiorgan inflammatory conditions is hampered by the lack of evidence-based therapies. This shortage of data has been attributed, in part, to the absence of a standardized outcome measure for use in clinical trials, according to Dr. Pavla Dolezalova.
"Until recently, no standardized vasculitis activity assessment tool has been available for children, so some pediatric studies apply adult measures, such as the Birmingham Vasculitis Activity Score [BVAS]," she said. Further, although nonspecific inflammatory markers such as erythrocyte sedimentation rate or C-reactive protein can reflect systemic vasculitis disease activity, they do not distinguish it from infectious complications. Use of the global assessment of disease activity by the treating physician using the visual analog scale is of limited utility in clinical trials, she noted.
In an effort to facilitate more informative clinical trials of primary systemic vasculitis in children, Dr. Dolezalova of Charles University and General University Hospital in Prague, Czech Republic, and her colleagues have developed a quantitative clinical index of manifestations of active disease, called the Pediatric Vasculitis Activity Score (PVAS), which has been preliminarily validated as a useful clinical measure with good interobserver reliability (Pediatr. Rheumatol. Online J. 2011 [doi:10.1186/1546-0096-9-S1-P92]).
In this column, Dr. Dolezalova describes the need for the assessment tool as well as some of the development challenges.
Question: Why are outcome assessment tools used for adults with systemic vasculitis not ideal for measuring disease activity in children?
Dr. Dolezalova: Tools used in adults are not fully applicable in children for multiple reasons. Disease presentations and outcome of primary systemic vasculitides appear to be different in children. Among the most obvious differences between adult and pediatric variants of the disease are the developmental and growth aspects; differences in functional, educational, and social impacts of longstanding disease; different drug pharmacokinetics and toxicity profiles; and the absence of comorbidities in children.
Question: What specific features have been incorporated into the PVAS?
Dr. Dolezalova: The development of the pediatric-specific tool has been a result of an international collaborative effort of pediatric rheumatologists from the vasculitis working groups of PReS (Pediatric Rheumatology European Society) and CARRA (North American Childhood Arthritis & Rheumatology Research Alliance), with the help of the European Vasculitis Study Group (EUVAS). We adapted the Birmingham Vasculitis Activity Score (BVAS 2003), the most commonly used tool in adult vasculitis patients, into PVAS. It is a systematic clinical scoring system that identifies selected features of active vasculitis in nine organ systems. Based on the analysis of the most common systemic vasculitis presentations in children reported to the PReS/PRINTO (Pediatric Rheumatology International Trials Organization) vasculitis registry, eight pediatric-relevant items and their definitions were added to the original BVAS 2003 in the cutaneous, cardiovascular, and abdominal systems. Additionally, by consensus, the maximum score for each organ system was to remain unchanged to facilitate longitudinal congruity with the BVAS. Among the 56 BVAS 2003 items, we redefined 22 for pediatric use.
Question: What were some of the challenges involved in the development of this tool?
Dr. Dolezalova: At the beginning of the process, we had to decide which principal way to follow: whether to start developing a brand new, originally pediatric tool, or to explore the applicability of existing measures and rely on the expertise of our adult rheumatology colleagues. Having gone for the second option meant that we had to accept existing adult concepts of vasculitis activity and damage assessments. The next challenge we had to overcome was that of modifying definitions of individual disease signs and symptoms from the BVAS glossary to be appropriate for pediatric patients. We wanted them to remain compatible with their adult counterparts but also to reflect pediatric reality. Learning the training process of vasculitis activity assessment and undergoing it according to the principles set up by EUVAS had been a true challenge for all pediatricians involved in the PVAS development.
Question: How is the PVAS tool being validated?
Dr. Dolezalova: The PVAS validation has been a multistep process that is now in its final stage. During consensus meetings, content and face validity were established, resulting in minor modifications to the PVAS and its glossary. Scoring of the pediatric paper cases during the training process provided information on the tool’s feasibility. Prospective real-patient assessment, including duplicate assessments by two trained researchers and follow-up evaluation in newly diagnosed or relapsing patients, provided data on the tool’s reliability, responsiveness, and discriminative ability. Currently, analysis of the prospective multicenter data on the larger patient cohort is ongoing.
Interview by Diana Mahoney
Dr. Dolezalova is the national co-coordinator of PRINTO and chairperson of the PReS clinical affairs committee. She had no relevant financial disclosures.