Robert J. Kreitman, MD
Hairy cell leukemia (HCL) is an indolent, low-grade B-cell lymphoid malignancy that typically presents with fatigue, pancytopenia, and splenomegaly.1,2 It is a rare disease, with an estimated 1,200 new cases of HCL diagnosed annually in the United States.1 Demographically, HCL is a disease of older adults (median age at diagnosis, 58 years), and is more commonly found in men than women and in White individuals compared with other ethnic or racial backgrounds.3,4 Environmental or occupational exposure to toxic substances, pesticides, ionizing radiation, and petroleum products may be linked to increased risk for HCL development.1,4
Pathophysiology
HCL develops from activated, mature memory B-cells that, in most cases, have the acquired mutation in BRAF V600E, which is present in 80% to 90% of patients with classic HCL.1,3,5 BRAF is an integral part of the RAS-BRAF-MEK-ERK cellular pathway that transmits growth factor signals from the cell surface to the nucleus to regulate cell growth and proliferation.6 Mutated BRAF V600E continuously activates BRAF kinase and downstream signaling, resulting in enhanced HCL cell survival and unchecked proliferation.3
Variant HCL (HCLv) is a separate, more virulent disease that lacks BRAF V600E mutation and CD25 expression on flow cytometry.1,7-9 Patients with HCLv have a worse prognosis and poor responses to front-line purine analogs, and a higher proportion of these patients carry the unmutated immunoglobulin heavy chain variable (IGHV) gene (54% vs 17% in HCL).1,10,11 About 30% to 50% have wild-type BRAF and activating mutations in MAP2K1, which encodes aberrant MEK downstream of BRAF.10,12
Most patients with HCL have somatic mutations in the IGHV gene.3,13,14 Patients with unmutated IGHV4-34 and wildtype BRAF have an aggressive form of the disease, even if the HCL cells express CD25 as in classic HCL.1,15 HCL in patients with unmutated IGHV is often refractory to purine analogs and these patients have poor prognosis and rapid progression.16 Other identified mutations include CDKN1B in HCL and MAP2K1 and CCNC3 in HCLv.2
Signs and Symptoms
In many cases, HCL is asymptomatic, and diagnosed when pancytopenia, monocytopenia, and leukopenia are discovered on unrelated blood work.2,3,11 Monocytopenia is a specific presentation of HCL, but not HCLv.11 Typical systemic symptoms include unexplained weight loss and extreme fatigue (80%).1,3 Other symptoms can include fever, recurrent infections, night sweats, splenomegaly and related pain or abdominal fullness, hepatomegaly, and bleeding or bruising due to thrombocytopenia.1,3 Splenomegaly is associated with advanced disease.11
Up to 30% of patients may present with autoimmune disorders such as vasculitis or psoriasis. Although skin involvement is rare with HCL, 10% to 12% of patients will have dermatologic symptoms either due to recurrent infection or autoimmune reactions.1,2 Skin reactions include localized or generalized maculopapular rash, pyoderma gangrenosum (which may be severe), and recurrent bacterial or viral skin infections.17
Diagnosis
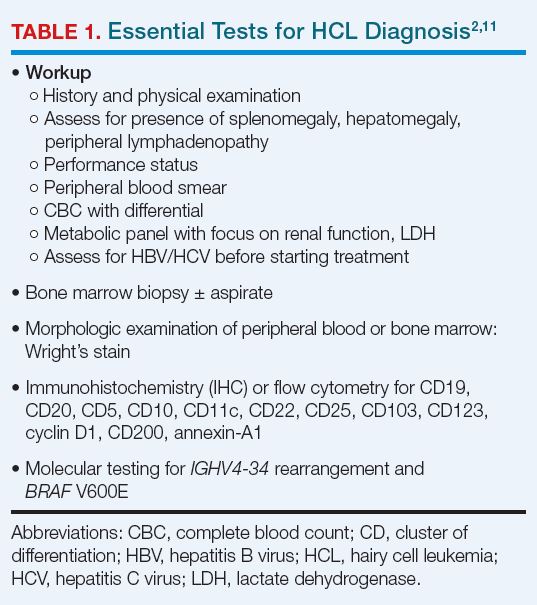
After complete history and physical examination, a diagnosis of HCL is usually made based on flow cytometry for immunophenotyping and molecular testing for BRAF V600E (Table 1).2,17
Table 1. Essential Tests for HCL Diagnosis
Disease-related fibrosis may impede bone marrow aspiration, and trephine biopsy should be done to make the diagnosis.11 On morphologic examination, HCL cells are small- to medium-sized, with round, oval, or indented, well-defined nuclei. Cytoplasm is pale blue, and cells have small cytoplasmic projections (Figure 1).2,18
Figure 1. Typical Appearance of Hairy Cell Leukemia
On flow cytometry, HCL is positive for B-cell antigens (CD19, CD20, CD22), as well as antigens specific to the disease (CD11c, CD25, CD103, CD123), and by immunohistochemistry (IHC) for cyclin D1 and annexin-A1. CD20, CD123, and CD200 are bright in HCL. The presence of T-cell marker CD103 on B-cells indicates HCL.1-3 HCLv, in contrast, is positive for CD11c and CD103, but usually negative for CD25, CD123, and annexin-A1.2,19
BRAF V600E mutation can be identified using droplet digital polymerase chain reaction (PCR), next-generation molecular sequencing, or IHC with a VE1 stain.3,11 IHC for CD20, annexin-1, and VE1 establish the diagnosis, but also are useful in determining the extent to which leukemic cells have infiltrated bone marrow.11
Differential diagnosis of HCL includes HCL variants, splenic marginal zone lymphoma, and splenic diffuse red pulp small B-cell lymphoma.7,11
Indications for Treatment and Criteria for Response
Over time, about 90% of patients with HCL will require treatment. However, not all such patients will require urgent or immediate treatment, and some can be managed with observation and close monitoring.1,11 The indications for initiating treatment generally are systemic symptoms and significant pancytopenia (Table 2).2,11
Table 3. Indications for Treatment of HCL
The optimal response with treatment of HCL is complete response (CR) without minimal residual disease (MRD-free), which minimizes the risk for relapse.1,11 Hematologic and molecular response is assessed using peripheral blood samples; physical examination, ultrasound, computed tomography, or magnetic resonance imaging is used to determine response in lymph nodes, spleen, or liver.1 MRD-free is defined by the absence of HCL cells by the chosen method (IHC, flow cytometry, or PCR).20 Bone marrow aspirate flow cytometry is the most sensitive standard test for MRD detection.1Table 3 summarizes response criteria for HCL.2,11
Table 3. Indications for Treatment of HCL
Initial Treatment of HCL
The purine nucleoside analogs (PNAs) cladribine (± rituximab) and pentostatin are widely recommended for initial treatment.1,2,11 As monotherapy, cladribine and pentostatin are considered similarly effective, with CR in 70% to 90% of patients and durations of response > 10 years.1 Adding the anti-CD20 monoclonal antibody rituximab in 8 weekly doses starting the first day of front-line cladribine (CDAR) improves remission, MRD-free rates, and duration of response (94% MRD-free at 96 months), with minimal added toxicity.21 Rituximab is often added 4 weeks after cladribine, which offers more convenience, an equally high CR rate of 100%, and a 76% MRD-free rate at 3 months.11 Bone marrow biopsy should be delayed for 4 to 6 months to allow a full response to develop with cladribine.1,11
Daily (intravenous or subcutaneous) and weekly cladribine are equally safe and effective.2,11 Pentostatin is administered intravenously every 2 weeks for 3 to 6 months, allowing time for hematologic recovery between doses.1,11 Patient factors to consider when choosing treatment include baseline neutropenia, patient preference, and comorbidities.
Toxicities of PNAs include neutropenia and fever, which typically occur during the first month of treatment and are more frequent in patients with baseline severe neutropenia; T-cell recovery may take years.1 CDAR is associated with higher transient thrombocytopenia, but faster platelet and neutrophil recovery at 4 weeks than cladribine alone.21 Both therapies are immunosuppressive. Patients should be evaluated for existing infections and watched for new infections during treatment. Control of active infection prior to treatment initiation is required.11,23
Patients with confirmed BRAF V600E mutation are candidates for vemurafenib if they are unable to tolerate a PNA, have an active infection, or would like effective vaccinations.2,23-25
Treatment at Relapse
At suspected HCL relapse, patients should be evaluated to determine whether cytopenia is due to recurrent disease or lingering effects from prior treatment. Use of successive flow cytometry over time can clarify whether symptoms are related to disease and need interventional treatment, or will resolve with additional time.1
Patients who have an HCL relapse after initial therapy with cladribine or pentostatin may be candidates for re-treatment with the same or alternate PNA plus rituximab.2 Rituximab monotherapy has been used for patients unable to tolerate PNA but yields CR rates as low as 13%.26 Repeated courses of PNA therapy yield lower rates and durations of response with each course.1,2
For patients with primary refractory disease (less than CR with initial therapy) or relapse within 2 years of initial therapy, treatment with the BRAF V600E inhibitor vemurafenib off-label, with or without rituximab, is an option.2,5 In HCL, vemurafenib for patients with relapsed or refractory disease achieved CR in 35% and 42% in 2 small trials (N = 54). Relapse-free survival among people with CR was 19 months in 1 of the trials.27 Vemurafenib plus rituximab achieved CR in 87% of patients with relapsed or refractory HCL, and an MRD-free CR rate of 57%. Among patients with CR, 85% were relapse-free at a median follow-up of 34 months.5 Treatment with vemurafenib is not myelotoxic—an advantage for HCL patients. Adverse effects with vemurafenib are often manageable with dose reductions, if needed. A specific concern with vemurafenib is the potential development of secondary skin cancers.5,27,28
Novel Targeted Options and Recommended Use
Promising alternatives for patients with relapsed or refractory HCL include combined BRAF and MEK inhibitors and the Bruton tyrosine kinase (BTK) inhibitor ibrutinib. The concept of BRAF/MEK inhibition was validated in studies with BRAF-mutated melanoma, in which dabrafenib plus trametinib (the MEK inhibitor) improved overall survival (OS) with less toxicity and better quality of life than vemurafenib.1,29 In a phase 2 trial in HCL, dabrafenib monotherapy demonstrated an overall response rate (ORR) of 80%, including 30% CR.30 In a subsequent phase 2 trial, dabrafenib combined with trametinib was evaluated in refractory or late relapsed HCL. Among 55 enrolled patients, objective response rate was 89%, including 65.5% CR. Nine of 36 patients with CR were MRD-free. Among responding patients, duration of response was 97.7% at 24 months.31 The most common grade ≥ 3 toxicities were hyperglycemia, pyrexia, neutropenia, and pneumonia. Secondary skin cancers were seen in about 5% of patients.31
BRAF/MEK inhibitor combinations in HCL offer effective therapy with less myelosuppression than PNAs, making them useful for patients with or at risk for infection.23 Their use in HCL is off-label, as they currently are approved for treatment of BRAF-mutated melanoma and some other tumors.32 A study of encorafenib (a BRAF inhibitor) combined with binimetinib (a MEK inhibitor) is ongoing (Table 4).32
Table 4. Currently Recruiting Clinical Trials Specifically for HCL
Ibrutinib interrupts B-cell receptor signaling to stop tumor cell growth. In a phase 2 trial, patients with relapsed or refractory HCL or HCLv were treated with once-daily oral ibrutinib. Best ORR was 54% (19% CR; 3% MRD-free). Despite the low CR rate, 3-year progression-free survival with ibrutinib was 73% and OS was 85%. Treatment was well-tolerated; cytopenia (including 22% grade ≥ 3 thrombocytopenia and neutropenia) and diarrhea were frequent toxicities.33
Moxetumomab pasudotox is a novel CD22-targeted antibody fused with protein toxin that interrupts protein synthesis in tumor cells.1 As treatment, it was studied in a phase 3 trial of relapsed HCL in heavily pretreated patients, and achieved a CR rate of 41%, including 36% durable CR.34 Although FDA-approved for relapsed or refractory HCL, the drug is being discontinued due to business decisions, not safety or efficacy concerns.2 It is notable that many types of B-cell lymphoma also express CD22.35
Enrollment in a clinical trial to study possible treatment advances is recommended by the National Comprehensive Cancer Network (NCCN) at first and subsequent relapses of HCL for appropriate patients.2 Figure 2 summarizes an approach to treatment choice and sequencing for patients with HCL.
Figure 2. Standard & Investigational Treatment of HCL/HCLv
Supportive Care
Patients being treated for HCL should have supportive care to manage adverse effects of their disease. Such care includes prophylaxis against herpes virus if CD4+ T cells < 200 cells/μL and other prophylactic vaccinations to hepatitis B virus, COVID-19 and Influenza. Patients with neutropeni may require broad-spectrum antibacterial prophylaxis or neutrophil growth factors if neutropenic fever develops. Blood product support is recommended if needed.2 Assessment of anti-COVID-19 antibodies is recommended to optimize immunity, particularly prior to beginning anti-CD20 antibody therapy like rituximab.23
Unmet Needs
Despite improvements in response and survival with newer therapies, not all patients with HCL benefit from these advances. Unmet needs are finding optimal treatment for patients with HCLv, despite some success with MEK inhibitors, and for patients with BRAF mutations other than V600E, who have few options beyond PNAs and rituximab.
Kreitman RJ, Arons E. Diagnosis and treatment of hairy cell leukemia as the COVID-19 pandemic continues. Blood Rev. 2022;51:100888. doi:10.1016/j.blre.2021.100888
Janus A, Robak T. Hairy cell leukemia. In: Li W, ed. Leukemia [Internet]. Brisbane: Exon Publications; 2022:chap3. Accessed February 16, 2023. doi:10.36255/exon-publications-leukemia-hairy-cell-leukemia
Tadmor T, Polliack A. Epidemiology and environmental risk in hairy cell leukemia. Best Pract Res Clin Haematol. 2015;28(4):175-179. doi:10.1016/j.beha.2015.10.014
Tiacci E, De Carolis L, Simonetti E, et al. Vemurafenib plus rituximab in refractory or relapsed hairy-cell leukemia. N Engl J Med. 2021;384(19):1810-1823. doi:10.1056/NEJMoa20312986
Falini B, Martelli MP, Tiacci E. BRAF V600E mutation in hairy cell leukemia: from bench to bedside. Blood. 2016;128(15):1918-1927. doi:10.1182/blood-2016-07-418434
Matutes E. Diagnostic and therapeutic challenges in hairy cell leukemia-variant: where are we in 2021? Expert Rev Hematol. 2021;14(4):355-363. doi:10.1080/17474086.2021.1908121
Cawley JC, Burns GF, Hayhoe FG. A chronic lymphoproliferative disorder with distinctive features: a distinct variant of hairy-cell leukaemia. Leuk Res. 1980;4(6):547-559. doi:10.1016/0145-2126(80)90066-1
Xi L, Arons E, Navarro W, et al. Both variant and IGHV4-34-expressing hairy cell leukemia lack the BRAF V600E mutation. Blood. 2012;119(14):3330-3332. doi:10.1182/blood-2011-09-379339
Durham BH, Getta B, Dietrich S, et al. Genomic analysis of hairy cell leukemia identifies novel recurrent genetic alterations. Blood. 2017;130(14):1644-1648. doi:10.1182/blood-2017-01-76510711
Grever MR, Abdel-Wahab O, Andritsos LA, et al. Consensus guidelines for the diagnosis and management of patients with hairy cell leukemia. Blood. 2017;129(5):553-560. doi:10.1182/blood-2016-01-689422
Waterfall JJ, Arons E, Walker RL, et al. High prevalence of MAP2K1 mutations in variant and IGHV4-34-expressing hairy-cell leukemias. Nat Genet. 2014;46(1):8-10. doi:10.1038/ng.2828
Arons E, Sunshine J, Suntum T, Kreitman RJ. Somatic hypermutation and VH gene usage in hairy cell leukaemia. Br J Haematol. 2006;133(5):504-512. doi:10.1111/j.1365-2141.2006.06066.x
Arons E, Roth L, Sapolsky J, Suntum T, Stetler-Stevenson M, Kreitman RJ. Evidence of canonical somatic hypermutation in hairy cell leukemia. Blood. 2011;117(18):4844-4851. doi:10.1182/blood-2010-11-316737
Arons E, Suntum T, Stetler-Stevenson M, Kreitman RJ. VH4-34+ hairy cell leukemia, a new variant with poor prognosis despite standard therapy. Blood. 2009;114(21):4687-4695. doi:10.1182/blood-2009-01-201731
Forconi F, Sozzi E, Cencini E, et al. Hairy cell leukemias with unmutated IGHV genes define the minor subset refractory to single-agent cladribine and with more aggressive behavior. Blood. 2009;114(21):4696-4702. doi:10.1182/blood-2009-03-212449
Robak E, Jesionek-Kupnicka D, Robak T. Skin changes in hairy cell leukemia. Ann Hematol. 2021;100(3):615-625. doi:10.1007/s00277-020-04349-z
Falini B, Tiacci E, Liso A, et al. Simple diagnostic assay for hairy cell leukaemia by immunocytochemical detection of annexin A1 (ANXA1). Lancet. 2004;363(9424): 1869-1870. doi:10.1016/S0140-6736(04)16356-3
Robak T, Robak P. Measurable residual disease in hairy cell leukemia: technical considerations and clinical significance. Front Oncol. 2022;12:976374. doi:10.3389/fonc.2022.976374
Chihara D, Arons E, Stetler-Stevenson M, et al. Randomized phase II study of first-line cladribine with concurrent or delayed rituximab in patients with hairy cell leukemia. J Clin Oncol. 2020;38(14):1527-1538. doi:10.1200/JCO.19.02250
Chihara D, Kantarjian H, O’Brien S, et al. Long-term durable remission by cladribine followed by rituximab in patients with hairy cell leukaemia: update of a phase II trial. Br J Haematol. 2016;174(5):760-766. doi:10.1111/bjh.14129
Grever M, Andritsos L, Banerji V, et al. Hairy cell leukemia and COVID-19 adaptation of treatment guidelines. Leukemia. 2021;35(7):1864-1872. doi:10.1038/s41375-021-01257-7
Konrat J, Rösler W, Roiss M, et al. BRAF inhibitor treatment of classical hairy cell leukemia allows successful vaccination against SARS-CoV-2. Ann Hematol. 2023;102(2):403-406. doi:10.1007/s00277-022-05026-z
Park JH, Shukla M, Salcedo JM, et al. First-line chemo-free therapy with the BRAF inhibitor vemurafenib combined with obinutuzumab is effective in patients with HCL. Blood. 2019;134(suppl 1):Abstract 3998. https://doi.org/10.1182/blood-2019-124478
Nieva J, Bethel K, Saven A. Phase 2 study of rituximab in the treatment of cladribine-failed patients with hairy cell leukemia. Blood. 2003;102(3):810-813. doi:10.1182/blood-2003-01-0014
Tiacci E, Park JH, De Carolis L, et al. Targeting mutant BRAF in relapsed or refractory hairy-cell leukemia. N Engl J Med. 2015;373(18):1733-1747. doi:10.1056/NEJMoa1506583
Maitre E, Paillassa J, Troussard X. Novel targeted treatments in hairy cell leukemia and other hairy cell-like disorders. Front Oncol. 2022;12:1068981. doi:10.3389/fonc.2022.1068981
Grob JJ, Amonkar MM, Karaszewska B, et al. Comparison of dabrafenib and trametinib combination therapy with vemurafenib monotherapy on health-related quality of life in patients with unresectable or metastatic cutaneous BRAF Val600-mutation-positive melanoma (COMBI-v): results of a phase 3, open-label, randomised trial. Lancet Oncol. 2015;16(13):1389-1398. doi:10.1016/S1470-2045(15)00087-X
Tiacci E, De Carolis L, Simonetti E, et al. Safety and efficacy of the BRAF inhibitor dabrafenib in relapsed or refractory hairy cell leukemia: a pilot phase-2 clinical trial. Leukemia. 2021;35(11):3314-3318. doi:10.1038/s41375-021-01210-8
Kreitman RJ, Moreau P, Ravandi F, et al. Dabrafenib plus trametinib in patients with relapsed/refractory BRAF V600E mutation-positive hairy cell leukemia. Blood. 2023;141(9):996-1006. doi:10.1182/blood.2021013658
Adashek JJ, Menta AK, Reddy NK, Desai AP, Roszik J, Subbiah V. Tissue agnostic activity of BRAF plus MEK inhibitor in BRAF V600E-mutated tumors. Mol Cancer Ther. 2022;21(6):871-878. doi:10.1158/1535-7163.MCT-21-0950
Rogers KA, Andritsos LA, Wei L, et al. Phase 2 study of ibrutinib in classic and variant hairy cell leukemia. Blood. 2021;137(25):3473-3483. doi:10.1182/blood.2020009688
Kreitman RJ, Dearden C, Zinzani PL, et al; Study 1053 investigators. Moxetumomab pasudotox in heavily pre-treated patients with relapsed/refractory hairy cell leukemia (HCL): long-term follow-up from the pivotal trial. J Hematol Oncol. 2021;14(1):35. doi:10.1186/s13045-020-01004-y
Leonard JP, Goldenberg DM. Preclinical and clinical evaluation of epratuzumab (anti-CD22 IgG) in B-cell malignancies. Oncogene. 2007;26(25):3704-3713. doi:10.1038/sj.onc.1210370
Author and Disclosure Information
Robert J. Kreitman, MD Senior Investigator National Cancer Institute National Institutes of Health Bethesda, MD
Robert J. Kreitman, MD, has disclosed the following relevant financial relationships:
Coinventor on the NIH patent for Moxetumomab Pasudotox.
Receives research support and/or investigation drugs for trials from AstraZeneca, Pfizer, Novartis, Teva, and Genentech.
Dr. Robert J. Kreitman contributed to this article in his personal capacity. The views expressed are his own and do not necessarily represent tthe views of the National Institutes of Health or the United States Government.
Robert J. Kreitman, MD Senior Investigator National Cancer Institute National Institutes of Health Bethesda, MD
Robert J. Kreitman, MD, has disclosed the following relevant financial relationships:
Coinventor on the NIH patent for Moxetumomab Pasudotox.
Receives research support and/or investigation drugs for trials from AstraZeneca, Pfizer, Novartis, Teva, and Genentech.
Dr. Robert J. Kreitman contributed to this article in his personal capacity. The views expressed are his own and do not necessarily represent tthe views of the National Institutes of Health or the United States Government.
Author and Disclosure Information
Robert J. Kreitman, MD Senior Investigator National Cancer Institute National Institutes of Health Bethesda, MD
Robert J. Kreitman, MD, has disclosed the following relevant financial relationships:
Coinventor on the NIH patent for Moxetumomab Pasudotox.
Receives research support and/or investigation drugs for trials from AstraZeneca, Pfizer, Novartis, Teva, and Genentech.
Dr. Robert J. Kreitman contributed to this article in his personal capacity. The views expressed are his own and do not necessarily represent tthe views of the National Institutes of Health or the United States Government.
Robert J. Kreitman, MD
Hairy cell leukemia (HCL) is an indolent, low-grade B-cell lymphoid malignancy that typically presents with fatigue, pancytopenia, and splenomegaly.1,2 It is a rare disease, with an estimated 1,200 new cases of HCL diagnosed annually in the United States.1 Demographically, HCL is a disease of older adults (median age at diagnosis, 58 years), and is more commonly found in men than women and in White individuals compared with other ethnic or racial backgrounds.3,4 Environmental or occupational exposure to toxic substances, pesticides, ionizing radiation, and petroleum products may be linked to increased risk for HCL development.1,4
Pathophysiology
HCL develops from activated, mature memory B-cells that, in most cases, have the acquired mutation in BRAF V600E, which is present in 80% to 90% of patients with classic HCL.1,3,5 BRAF is an integral part of the RAS-BRAF-MEK-ERK cellular pathway that transmits growth factor signals from the cell surface to the nucleus to regulate cell growth and proliferation.6 Mutated BRAF V600E continuously activates BRAF kinase and downstream signaling, resulting in enhanced HCL cell survival and unchecked proliferation.3
Variant HCL (HCLv) is a separate, more virulent disease that lacks BRAF V600E mutation and CD25 expression on flow cytometry.1,7-9 Patients with HCLv have a worse prognosis and poor responses to front-line purine analogs, and a higher proportion of these patients carry the unmutated immunoglobulin heavy chain variable (IGHV) gene (54% vs 17% in HCL).1,10,11 About 30% to 50% have wild-type BRAF and activating mutations in MAP2K1, which encodes aberrant MEK downstream of BRAF.10,12
Most patients with HCL have somatic mutations in the IGHV gene.3,13,14 Patients with unmutated IGHV4-34 and wildtype BRAF have an aggressive form of the disease, even if the HCL cells express CD25 as in classic HCL.1,15 HCL in patients with unmutated IGHV is often refractory to purine analogs and these patients have poor prognosis and rapid progression.16 Other identified mutations include CDKN1B in HCL and MAP2K1 and CCNC3 in HCLv.2
Signs and Symptoms
In many cases, HCL is asymptomatic, and diagnosed when pancytopenia, monocytopenia, and leukopenia are discovered on unrelated blood work.2,3,11 Monocytopenia is a specific presentation of HCL, but not HCLv.11 Typical systemic symptoms include unexplained weight loss and extreme fatigue (80%).1,3 Other symptoms can include fever, recurrent infections, night sweats, splenomegaly and related pain or abdominal fullness, hepatomegaly, and bleeding or bruising due to thrombocytopenia.1,3 Splenomegaly is associated with advanced disease.11
Up to 30% of patients may present with autoimmune disorders such as vasculitis or psoriasis. Although skin involvement is rare with HCL, 10% to 12% of patients will have dermatologic symptoms either due to recurrent infection or autoimmune reactions.1,2 Skin reactions include localized or generalized maculopapular rash, pyoderma gangrenosum (which may be severe), and recurrent bacterial or viral skin infections.17
Diagnosis
After complete history and physical examination, a diagnosis of HCL is usually made based on flow cytometry for immunophenotyping and molecular testing for BRAF V600E (Table 1).2,17
Table 1. Essential Tests for HCL Diagnosis
Disease-related fibrosis may impede bone marrow aspiration, and trephine biopsy should be done to make the diagnosis.11 On morphologic examination, HCL cells are small- to medium-sized, with round, oval, or indented, well-defined nuclei. Cytoplasm is pale blue, and cells have small cytoplasmic projections (Figure 1).2,18
Figure 1. Typical Appearance of Hairy Cell Leukemia
On flow cytometry, HCL is positive for B-cell antigens (CD19, CD20, CD22), as well as antigens specific to the disease (CD11c, CD25, CD103, CD123), and by immunohistochemistry (IHC) for cyclin D1 and annexin-A1. CD20, CD123, and CD200 are bright in HCL. The presence of T-cell marker CD103 on B-cells indicates HCL.1-3 HCLv, in contrast, is positive for CD11c and CD103, but usually negative for CD25, CD123, and annexin-A1.2,19
BRAF V600E mutation can be identified using droplet digital polymerase chain reaction (PCR), next-generation molecular sequencing, or IHC with a VE1 stain.3,11 IHC for CD20, annexin-1, and VE1 establish the diagnosis, but also are useful in determining the extent to which leukemic cells have infiltrated bone marrow.11
Differential diagnosis of HCL includes HCL variants, splenic marginal zone lymphoma, and splenic diffuse red pulp small B-cell lymphoma.7,11
Indications for Treatment and Criteria for Response
Over time, about 90% of patients with HCL will require treatment. However, not all such patients will require urgent or immediate treatment, and some can be managed with observation and close monitoring.1,11 The indications for initiating treatment generally are systemic symptoms and significant pancytopenia (Table 2).2,11
Table 3. Indications for Treatment of HCL
The optimal response with treatment of HCL is complete response (CR) without minimal residual disease (MRD-free), which minimizes the risk for relapse.1,11 Hematologic and molecular response is assessed using peripheral blood samples; physical examination, ultrasound, computed tomography, or magnetic resonance imaging is used to determine response in lymph nodes, spleen, or liver.1 MRD-free is defined by the absence of HCL cells by the chosen method (IHC, flow cytometry, or PCR).20 Bone marrow aspirate flow cytometry is the most sensitive standard test for MRD detection.1Table 3 summarizes response criteria for HCL.2,11
Table 3. Indications for Treatment of HCL
Initial Treatment of HCL
The purine nucleoside analogs (PNAs) cladribine (± rituximab) and pentostatin are widely recommended for initial treatment.1,2,11 As monotherapy, cladribine and pentostatin are considered similarly effective, with CR in 70% to 90% of patients and durations of response > 10 years.1 Adding the anti-CD20 monoclonal antibody rituximab in 8 weekly doses starting the first day of front-line cladribine (CDAR) improves remission, MRD-free rates, and duration of response (94% MRD-free at 96 months), with minimal added toxicity.21 Rituximab is often added 4 weeks after cladribine, which offers more convenience, an equally high CR rate of 100%, and a 76% MRD-free rate at 3 months.11 Bone marrow biopsy should be delayed for 4 to 6 months to allow a full response to develop with cladribine.1,11
Daily (intravenous or subcutaneous) and weekly cladribine are equally safe and effective.2,11 Pentostatin is administered intravenously every 2 weeks for 3 to 6 months, allowing time for hematologic recovery between doses.1,11 Patient factors to consider when choosing treatment include baseline neutropenia, patient preference, and comorbidities.
Toxicities of PNAs include neutropenia and fever, which typically occur during the first month of treatment and are more frequent in patients with baseline severe neutropenia; T-cell recovery may take years.1 CDAR is associated with higher transient thrombocytopenia, but faster platelet and neutrophil recovery at 4 weeks than cladribine alone.21 Both therapies are immunosuppressive. Patients should be evaluated for existing infections and watched for new infections during treatment. Control of active infection prior to treatment initiation is required.11,23
Patients with confirmed BRAF V600E mutation are candidates for vemurafenib if they are unable to tolerate a PNA, have an active infection, or would like effective vaccinations.2,23-25
Treatment at Relapse
At suspected HCL relapse, patients should be evaluated to determine whether cytopenia is due to recurrent disease or lingering effects from prior treatment. Use of successive flow cytometry over time can clarify whether symptoms are related to disease and need interventional treatment, or will resolve with additional time.1
Patients who have an HCL relapse after initial therapy with cladribine or pentostatin may be candidates for re-treatment with the same or alternate PNA plus rituximab.2 Rituximab monotherapy has been used for patients unable to tolerate PNA but yields CR rates as low as 13%.26 Repeated courses of PNA therapy yield lower rates and durations of response with each course.1,2
For patients with primary refractory disease (less than CR with initial therapy) or relapse within 2 years of initial therapy, treatment with the BRAF V600E inhibitor vemurafenib off-label, with or without rituximab, is an option.2,5 In HCL, vemurafenib for patients with relapsed or refractory disease achieved CR in 35% and 42% in 2 small trials (N = 54). Relapse-free survival among people with CR was 19 months in 1 of the trials.27 Vemurafenib plus rituximab achieved CR in 87% of patients with relapsed or refractory HCL, and an MRD-free CR rate of 57%. Among patients with CR, 85% were relapse-free at a median follow-up of 34 months.5 Treatment with vemurafenib is not myelotoxic—an advantage for HCL patients. Adverse effects with vemurafenib are often manageable with dose reductions, if needed. A specific concern with vemurafenib is the potential development of secondary skin cancers.5,27,28
Novel Targeted Options and Recommended Use
Promising alternatives for patients with relapsed or refractory HCL include combined BRAF and MEK inhibitors and the Bruton tyrosine kinase (BTK) inhibitor ibrutinib. The concept of BRAF/MEK inhibition was validated in studies with BRAF-mutated melanoma, in which dabrafenib plus trametinib (the MEK inhibitor) improved overall survival (OS) with less toxicity and better quality of life than vemurafenib.1,29 In a phase 2 trial in HCL, dabrafenib monotherapy demonstrated an overall response rate (ORR) of 80%, including 30% CR.30 In a subsequent phase 2 trial, dabrafenib combined with trametinib was evaluated in refractory or late relapsed HCL. Among 55 enrolled patients, objective response rate was 89%, including 65.5% CR. Nine of 36 patients with CR were MRD-free. Among responding patients, duration of response was 97.7% at 24 months.31 The most common grade ≥ 3 toxicities were hyperglycemia, pyrexia, neutropenia, and pneumonia. Secondary skin cancers were seen in about 5% of patients.31
BRAF/MEK inhibitor combinations in HCL offer effective therapy with less myelosuppression than PNAs, making them useful for patients with or at risk for infection.23 Their use in HCL is off-label, as they currently are approved for treatment of BRAF-mutated melanoma and some other tumors.32 A study of encorafenib (a BRAF inhibitor) combined with binimetinib (a MEK inhibitor) is ongoing (Table 4).32
Table 4. Currently Recruiting Clinical Trials Specifically for HCL
Ibrutinib interrupts B-cell receptor signaling to stop tumor cell growth. In a phase 2 trial, patients with relapsed or refractory HCL or HCLv were treated with once-daily oral ibrutinib. Best ORR was 54% (19% CR; 3% MRD-free). Despite the low CR rate, 3-year progression-free survival with ibrutinib was 73% and OS was 85%. Treatment was well-tolerated; cytopenia (including 22% grade ≥ 3 thrombocytopenia and neutropenia) and diarrhea were frequent toxicities.33
Moxetumomab pasudotox is a novel CD22-targeted antibody fused with protein toxin that interrupts protein synthesis in tumor cells.1 As treatment, it was studied in a phase 3 trial of relapsed HCL in heavily pretreated patients, and achieved a CR rate of 41%, including 36% durable CR.34 Although FDA-approved for relapsed or refractory HCL, the drug is being discontinued due to business decisions, not safety or efficacy concerns.2 It is notable that many types of B-cell lymphoma also express CD22.35
Enrollment in a clinical trial to study possible treatment advances is recommended by the National Comprehensive Cancer Network (NCCN) at first and subsequent relapses of HCL for appropriate patients.2 Figure 2 summarizes an approach to treatment choice and sequencing for patients with HCL.
Figure 2. Standard & Investigational Treatment of HCL/HCLv
Supportive Care
Patients being treated for HCL should have supportive care to manage adverse effects of their disease. Such care includes prophylaxis against herpes virus if CD4+ T cells < 200 cells/μL and other prophylactic vaccinations to hepatitis B virus, COVID-19 and Influenza. Patients with neutropeni may require broad-spectrum antibacterial prophylaxis or neutrophil growth factors if neutropenic fever develops. Blood product support is recommended if needed.2 Assessment of anti-COVID-19 antibodies is recommended to optimize immunity, particularly prior to beginning anti-CD20 antibody therapy like rituximab.23
Unmet Needs
Despite improvements in response and survival with newer therapies, not all patients with HCL benefit from these advances. Unmet needs are finding optimal treatment for patients with HCLv, despite some success with MEK inhibitors, and for patients with BRAF mutations other than V600E, who have few options beyond PNAs and rituximab.
Robert J. Kreitman, MD
Hairy cell leukemia (HCL) is an indolent, low-grade B-cell lymphoid malignancy that typically presents with fatigue, pancytopenia, and splenomegaly.1,2 It is a rare disease, with an estimated 1,200 new cases of HCL diagnosed annually in the United States.1 Demographically, HCL is a disease of older adults (median age at diagnosis, 58 years), and is more commonly found in men than women and in White individuals compared with other ethnic or racial backgrounds.3,4 Environmental or occupational exposure to toxic substances, pesticides, ionizing radiation, and petroleum products may be linked to increased risk for HCL development.1,4
Pathophysiology
HCL develops from activated, mature memory B-cells that, in most cases, have the acquired mutation in BRAF V600E, which is present in 80% to 90% of patients with classic HCL.1,3,5 BRAF is an integral part of the RAS-BRAF-MEK-ERK cellular pathway that transmits growth factor signals from the cell surface to the nucleus to regulate cell growth and proliferation.6 Mutated BRAF V600E continuously activates BRAF kinase and downstream signaling, resulting in enhanced HCL cell survival and unchecked proliferation.3
Variant HCL (HCLv) is a separate, more virulent disease that lacks BRAF V600E mutation and CD25 expression on flow cytometry.1,7-9 Patients with HCLv have a worse prognosis and poor responses to front-line purine analogs, and a higher proportion of these patients carry the unmutated immunoglobulin heavy chain variable (IGHV) gene (54% vs 17% in HCL).1,10,11 About 30% to 50% have wild-type BRAF and activating mutations in MAP2K1, which encodes aberrant MEK downstream of BRAF.10,12
Most patients with HCL have somatic mutations in the IGHV gene.3,13,14 Patients with unmutated IGHV4-34 and wildtype BRAF have an aggressive form of the disease, even if the HCL cells express CD25 as in classic HCL.1,15 HCL in patients with unmutated IGHV is often refractory to purine analogs and these patients have poor prognosis and rapid progression.16 Other identified mutations include CDKN1B in HCL and MAP2K1 and CCNC3 in HCLv.2
Signs and Symptoms
In many cases, HCL is asymptomatic, and diagnosed when pancytopenia, monocytopenia, and leukopenia are discovered on unrelated blood work.2,3,11 Monocytopenia is a specific presentation of HCL, but not HCLv.11 Typical systemic symptoms include unexplained weight loss and extreme fatigue (80%).1,3 Other symptoms can include fever, recurrent infections, night sweats, splenomegaly and related pain or abdominal fullness, hepatomegaly, and bleeding or bruising due to thrombocytopenia.1,3 Splenomegaly is associated with advanced disease.11
Up to 30% of patients may present with autoimmune disorders such as vasculitis or psoriasis. Although skin involvement is rare with HCL, 10% to 12% of patients will have dermatologic symptoms either due to recurrent infection or autoimmune reactions.1,2 Skin reactions include localized or generalized maculopapular rash, pyoderma gangrenosum (which may be severe), and recurrent bacterial or viral skin infections.17
Diagnosis
After complete history and physical examination, a diagnosis of HCL is usually made based on flow cytometry for immunophenotyping and molecular testing for BRAF V600E (Table 1).2,17
Table 1. Essential Tests for HCL Diagnosis
Disease-related fibrosis may impede bone marrow aspiration, and trephine biopsy should be done to make the diagnosis.11 On morphologic examination, HCL cells are small- to medium-sized, with round, oval, or indented, well-defined nuclei. Cytoplasm is pale blue, and cells have small cytoplasmic projections (Figure 1).2,18
Figure 1. Typical Appearance of Hairy Cell Leukemia
On flow cytometry, HCL is positive for B-cell antigens (CD19, CD20, CD22), as well as antigens specific to the disease (CD11c, CD25, CD103, CD123), and by immunohistochemistry (IHC) for cyclin D1 and annexin-A1. CD20, CD123, and CD200 are bright in HCL. The presence of T-cell marker CD103 on B-cells indicates HCL.1-3 HCLv, in contrast, is positive for CD11c and CD103, but usually negative for CD25, CD123, and annexin-A1.2,19
BRAF V600E mutation can be identified using droplet digital polymerase chain reaction (PCR), next-generation molecular sequencing, or IHC with a VE1 stain.3,11 IHC for CD20, annexin-1, and VE1 establish the diagnosis, but also are useful in determining the extent to which leukemic cells have infiltrated bone marrow.11
Differential diagnosis of HCL includes HCL variants, splenic marginal zone lymphoma, and splenic diffuse red pulp small B-cell lymphoma.7,11
Indications for Treatment and Criteria for Response
Over time, about 90% of patients with HCL will require treatment. However, not all such patients will require urgent or immediate treatment, and some can be managed with observation and close monitoring.1,11 The indications for initiating treatment generally are systemic symptoms and significant pancytopenia (Table 2).2,11
Table 3. Indications for Treatment of HCL
The optimal response with treatment of HCL is complete response (CR) without minimal residual disease (MRD-free), which minimizes the risk for relapse.1,11 Hematologic and molecular response is assessed using peripheral blood samples; physical examination, ultrasound, computed tomography, or magnetic resonance imaging is used to determine response in lymph nodes, spleen, or liver.1 MRD-free is defined by the absence of HCL cells by the chosen method (IHC, flow cytometry, or PCR).20 Bone marrow aspirate flow cytometry is the most sensitive standard test for MRD detection.1Table 3 summarizes response criteria for HCL.2,11
Table 3. Indications for Treatment of HCL
Initial Treatment of HCL
The purine nucleoside analogs (PNAs) cladribine (± rituximab) and pentostatin are widely recommended for initial treatment.1,2,11 As monotherapy, cladribine and pentostatin are considered similarly effective, with CR in 70% to 90% of patients and durations of response > 10 years.1 Adding the anti-CD20 monoclonal antibody rituximab in 8 weekly doses starting the first day of front-line cladribine (CDAR) improves remission, MRD-free rates, and duration of response (94% MRD-free at 96 months), with minimal added toxicity.21 Rituximab is often added 4 weeks after cladribine, which offers more convenience, an equally high CR rate of 100%, and a 76% MRD-free rate at 3 months.11 Bone marrow biopsy should be delayed for 4 to 6 months to allow a full response to develop with cladribine.1,11
Daily (intravenous or subcutaneous) and weekly cladribine are equally safe and effective.2,11 Pentostatin is administered intravenously every 2 weeks for 3 to 6 months, allowing time for hematologic recovery between doses.1,11 Patient factors to consider when choosing treatment include baseline neutropenia, patient preference, and comorbidities.
Toxicities of PNAs include neutropenia and fever, which typically occur during the first month of treatment and are more frequent in patients with baseline severe neutropenia; T-cell recovery may take years.1 CDAR is associated with higher transient thrombocytopenia, but faster platelet and neutrophil recovery at 4 weeks than cladribine alone.21 Both therapies are immunosuppressive. Patients should be evaluated for existing infections and watched for new infections during treatment. Control of active infection prior to treatment initiation is required.11,23
Patients with confirmed BRAF V600E mutation are candidates for vemurafenib if they are unable to tolerate a PNA, have an active infection, or would like effective vaccinations.2,23-25
Treatment at Relapse
At suspected HCL relapse, patients should be evaluated to determine whether cytopenia is due to recurrent disease or lingering effects from prior treatment. Use of successive flow cytometry over time can clarify whether symptoms are related to disease and need interventional treatment, or will resolve with additional time.1
Patients who have an HCL relapse after initial therapy with cladribine or pentostatin may be candidates for re-treatment with the same or alternate PNA plus rituximab.2 Rituximab monotherapy has been used for patients unable to tolerate PNA but yields CR rates as low as 13%.26 Repeated courses of PNA therapy yield lower rates and durations of response with each course.1,2
For patients with primary refractory disease (less than CR with initial therapy) or relapse within 2 years of initial therapy, treatment with the BRAF V600E inhibitor vemurafenib off-label, with or without rituximab, is an option.2,5 In HCL, vemurafenib for patients with relapsed or refractory disease achieved CR in 35% and 42% in 2 small trials (N = 54). Relapse-free survival among people with CR was 19 months in 1 of the trials.27 Vemurafenib plus rituximab achieved CR in 87% of patients with relapsed or refractory HCL, and an MRD-free CR rate of 57%. Among patients with CR, 85% were relapse-free at a median follow-up of 34 months.5 Treatment with vemurafenib is not myelotoxic—an advantage for HCL patients. Adverse effects with vemurafenib are often manageable with dose reductions, if needed. A specific concern with vemurafenib is the potential development of secondary skin cancers.5,27,28
Novel Targeted Options and Recommended Use
Promising alternatives for patients with relapsed or refractory HCL include combined BRAF and MEK inhibitors and the Bruton tyrosine kinase (BTK) inhibitor ibrutinib. The concept of BRAF/MEK inhibition was validated in studies with BRAF-mutated melanoma, in which dabrafenib plus trametinib (the MEK inhibitor) improved overall survival (OS) with less toxicity and better quality of life than vemurafenib.1,29 In a phase 2 trial in HCL, dabrafenib monotherapy demonstrated an overall response rate (ORR) of 80%, including 30% CR.30 In a subsequent phase 2 trial, dabrafenib combined with trametinib was evaluated in refractory or late relapsed HCL. Among 55 enrolled patients, objective response rate was 89%, including 65.5% CR. Nine of 36 patients with CR were MRD-free. Among responding patients, duration of response was 97.7% at 24 months.31 The most common grade ≥ 3 toxicities were hyperglycemia, pyrexia, neutropenia, and pneumonia. Secondary skin cancers were seen in about 5% of patients.31
BRAF/MEK inhibitor combinations in HCL offer effective therapy with less myelosuppression than PNAs, making them useful for patients with or at risk for infection.23 Their use in HCL is off-label, as they currently are approved for treatment of BRAF-mutated melanoma and some other tumors.32 A study of encorafenib (a BRAF inhibitor) combined with binimetinib (a MEK inhibitor) is ongoing (Table 4).32
Table 4. Currently Recruiting Clinical Trials Specifically for HCL
Ibrutinib interrupts B-cell receptor signaling to stop tumor cell growth. In a phase 2 trial, patients with relapsed or refractory HCL or HCLv were treated with once-daily oral ibrutinib. Best ORR was 54% (19% CR; 3% MRD-free). Despite the low CR rate, 3-year progression-free survival with ibrutinib was 73% and OS was 85%. Treatment was well-tolerated; cytopenia (including 22% grade ≥ 3 thrombocytopenia and neutropenia) and diarrhea were frequent toxicities.33
Moxetumomab pasudotox is a novel CD22-targeted antibody fused with protein toxin that interrupts protein synthesis in tumor cells.1 As treatment, it was studied in a phase 3 trial of relapsed HCL in heavily pretreated patients, and achieved a CR rate of 41%, including 36% durable CR.34 Although FDA-approved for relapsed or refractory HCL, the drug is being discontinued due to business decisions, not safety or efficacy concerns.2 It is notable that many types of B-cell lymphoma also express CD22.35
Enrollment in a clinical trial to study possible treatment advances is recommended by the National Comprehensive Cancer Network (NCCN) at first and subsequent relapses of HCL for appropriate patients.2 Figure 2 summarizes an approach to treatment choice and sequencing for patients with HCL.
Figure 2. Standard & Investigational Treatment of HCL/HCLv
Supportive Care
Patients being treated for HCL should have supportive care to manage adverse effects of their disease. Such care includes prophylaxis against herpes virus if CD4+ T cells < 200 cells/μL and other prophylactic vaccinations to hepatitis B virus, COVID-19 and Influenza. Patients with neutropeni may require broad-spectrum antibacterial prophylaxis or neutrophil growth factors if neutropenic fever develops. Blood product support is recommended if needed.2 Assessment of anti-COVID-19 antibodies is recommended to optimize immunity, particularly prior to beginning anti-CD20 antibody therapy like rituximab.23
Unmet Needs
Despite improvements in response and survival with newer therapies, not all patients with HCL benefit from these advances. Unmet needs are finding optimal treatment for patients with HCLv, despite some success with MEK inhibitors, and for patients with BRAF mutations other than V600E, who have few options beyond PNAs and rituximab.
Kreitman RJ, Arons E. Diagnosis and treatment of hairy cell leukemia as the COVID-19 pandemic continues. Blood Rev. 2022;51:100888. doi:10.1016/j.blre.2021.100888
Janus A, Robak T. Hairy cell leukemia. In: Li W, ed. Leukemia [Internet]. Brisbane: Exon Publications; 2022:chap3. Accessed February 16, 2023. doi:10.36255/exon-publications-leukemia-hairy-cell-leukemia
Tadmor T, Polliack A. Epidemiology and environmental risk in hairy cell leukemia. Best Pract Res Clin Haematol. 2015;28(4):175-179. doi:10.1016/j.beha.2015.10.014
Tiacci E, De Carolis L, Simonetti E, et al. Vemurafenib plus rituximab in refractory or relapsed hairy-cell leukemia. N Engl J Med. 2021;384(19):1810-1823. doi:10.1056/NEJMoa20312986
Falini B, Martelli MP, Tiacci E. BRAF V600E mutation in hairy cell leukemia: from bench to bedside. Blood. 2016;128(15):1918-1927. doi:10.1182/blood-2016-07-418434
Matutes E. Diagnostic and therapeutic challenges in hairy cell leukemia-variant: where are we in 2021? Expert Rev Hematol. 2021;14(4):355-363. doi:10.1080/17474086.2021.1908121
Cawley JC, Burns GF, Hayhoe FG. A chronic lymphoproliferative disorder with distinctive features: a distinct variant of hairy-cell leukaemia. Leuk Res. 1980;4(6):547-559. doi:10.1016/0145-2126(80)90066-1
Xi L, Arons E, Navarro W, et al. Both variant and IGHV4-34-expressing hairy cell leukemia lack the BRAF V600E mutation. Blood. 2012;119(14):3330-3332. doi:10.1182/blood-2011-09-379339
Durham BH, Getta B, Dietrich S, et al. Genomic analysis of hairy cell leukemia identifies novel recurrent genetic alterations. Blood. 2017;130(14):1644-1648. doi:10.1182/blood-2017-01-76510711
Grever MR, Abdel-Wahab O, Andritsos LA, et al. Consensus guidelines for the diagnosis and management of patients with hairy cell leukemia. Blood. 2017;129(5):553-560. doi:10.1182/blood-2016-01-689422
Waterfall JJ, Arons E, Walker RL, et al. High prevalence of MAP2K1 mutations in variant and IGHV4-34-expressing hairy-cell leukemias. Nat Genet. 2014;46(1):8-10. doi:10.1038/ng.2828
Arons E, Sunshine J, Suntum T, Kreitman RJ. Somatic hypermutation and VH gene usage in hairy cell leukaemia. Br J Haematol. 2006;133(5):504-512. doi:10.1111/j.1365-2141.2006.06066.x
Arons E, Roth L, Sapolsky J, Suntum T, Stetler-Stevenson M, Kreitman RJ. Evidence of canonical somatic hypermutation in hairy cell leukemia. Blood. 2011;117(18):4844-4851. doi:10.1182/blood-2010-11-316737
Arons E, Suntum T, Stetler-Stevenson M, Kreitman RJ. VH4-34+ hairy cell leukemia, a new variant with poor prognosis despite standard therapy. Blood. 2009;114(21):4687-4695. doi:10.1182/blood-2009-01-201731
Forconi F, Sozzi E, Cencini E, et al. Hairy cell leukemias with unmutated IGHV genes define the minor subset refractory to single-agent cladribine and with more aggressive behavior. Blood. 2009;114(21):4696-4702. doi:10.1182/blood-2009-03-212449
Robak E, Jesionek-Kupnicka D, Robak T. Skin changes in hairy cell leukemia. Ann Hematol. 2021;100(3):615-625. doi:10.1007/s00277-020-04349-z
Falini B, Tiacci E, Liso A, et al. Simple diagnostic assay for hairy cell leukaemia by immunocytochemical detection of annexin A1 (ANXA1). Lancet. 2004;363(9424): 1869-1870. doi:10.1016/S0140-6736(04)16356-3
Robak T, Robak P. Measurable residual disease in hairy cell leukemia: technical considerations and clinical significance. Front Oncol. 2022;12:976374. doi:10.3389/fonc.2022.976374
Chihara D, Arons E, Stetler-Stevenson M, et al. Randomized phase II study of first-line cladribine with concurrent or delayed rituximab in patients with hairy cell leukemia. J Clin Oncol. 2020;38(14):1527-1538. doi:10.1200/JCO.19.02250
Chihara D, Kantarjian H, O’Brien S, et al. Long-term durable remission by cladribine followed by rituximab in patients with hairy cell leukaemia: update of a phase II trial. Br J Haematol. 2016;174(5):760-766. doi:10.1111/bjh.14129
Grever M, Andritsos L, Banerji V, et al. Hairy cell leukemia and COVID-19 adaptation of treatment guidelines. Leukemia. 2021;35(7):1864-1872. doi:10.1038/s41375-021-01257-7
Konrat J, Rösler W, Roiss M, et al. BRAF inhibitor treatment of classical hairy cell leukemia allows successful vaccination against SARS-CoV-2. Ann Hematol. 2023;102(2):403-406. doi:10.1007/s00277-022-05026-z
Park JH, Shukla M, Salcedo JM, et al. First-line chemo-free therapy with the BRAF inhibitor vemurafenib combined with obinutuzumab is effective in patients with HCL. Blood. 2019;134(suppl 1):Abstract 3998. https://doi.org/10.1182/blood-2019-124478
Nieva J, Bethel K, Saven A. Phase 2 study of rituximab in the treatment of cladribine-failed patients with hairy cell leukemia. Blood. 2003;102(3):810-813. doi:10.1182/blood-2003-01-0014
Tiacci E, Park JH, De Carolis L, et al. Targeting mutant BRAF in relapsed or refractory hairy-cell leukemia. N Engl J Med. 2015;373(18):1733-1747. doi:10.1056/NEJMoa1506583
Maitre E, Paillassa J, Troussard X. Novel targeted treatments in hairy cell leukemia and other hairy cell-like disorders. Front Oncol. 2022;12:1068981. doi:10.3389/fonc.2022.1068981
Grob JJ, Amonkar MM, Karaszewska B, et al. Comparison of dabrafenib and trametinib combination therapy with vemurafenib monotherapy on health-related quality of life in patients with unresectable or metastatic cutaneous BRAF Val600-mutation-positive melanoma (COMBI-v): results of a phase 3, open-label, randomised trial. Lancet Oncol. 2015;16(13):1389-1398. doi:10.1016/S1470-2045(15)00087-X
Tiacci E, De Carolis L, Simonetti E, et al. Safety and efficacy of the BRAF inhibitor dabrafenib in relapsed or refractory hairy cell leukemia: a pilot phase-2 clinical trial. Leukemia. 2021;35(11):3314-3318. doi:10.1038/s41375-021-01210-8
Kreitman RJ, Moreau P, Ravandi F, et al. Dabrafenib plus trametinib in patients with relapsed/refractory BRAF V600E mutation-positive hairy cell leukemia. Blood. 2023;141(9):996-1006. doi:10.1182/blood.2021013658
Adashek JJ, Menta AK, Reddy NK, Desai AP, Roszik J, Subbiah V. Tissue agnostic activity of BRAF plus MEK inhibitor in BRAF V600E-mutated tumors. Mol Cancer Ther. 2022;21(6):871-878. doi:10.1158/1535-7163.MCT-21-0950
Rogers KA, Andritsos LA, Wei L, et al. Phase 2 study of ibrutinib in classic and variant hairy cell leukemia. Blood. 2021;137(25):3473-3483. doi:10.1182/blood.2020009688
Kreitman RJ, Dearden C, Zinzani PL, et al; Study 1053 investigators. Moxetumomab pasudotox in heavily pre-treated patients with relapsed/refractory hairy cell leukemia (HCL): long-term follow-up from the pivotal trial. J Hematol Oncol. 2021;14(1):35. doi:10.1186/s13045-020-01004-y
Leonard JP, Goldenberg DM. Preclinical and clinical evaluation of epratuzumab (anti-CD22 IgG) in B-cell malignancies. Oncogene. 2007;26(25):3704-3713. doi:10.1038/sj.onc.1210370
References
Kreitman RJ, Arons E. Diagnosis and treatment of hairy cell leukemia as the COVID-19 pandemic continues. Blood Rev. 2022;51:100888. doi:10.1016/j.blre.2021.100888
Janus A, Robak T. Hairy cell leukemia. In: Li W, ed. Leukemia [Internet]. Brisbane: Exon Publications; 2022:chap3. Accessed February 16, 2023. doi:10.36255/exon-publications-leukemia-hairy-cell-leukemia
Tadmor T, Polliack A. Epidemiology and environmental risk in hairy cell leukemia. Best Pract Res Clin Haematol. 2015;28(4):175-179. doi:10.1016/j.beha.2015.10.014
Tiacci E, De Carolis L, Simonetti E, et al. Vemurafenib plus rituximab in refractory or relapsed hairy-cell leukemia. N Engl J Med. 2021;384(19):1810-1823. doi:10.1056/NEJMoa20312986
Falini B, Martelli MP, Tiacci E. BRAF V600E mutation in hairy cell leukemia: from bench to bedside. Blood. 2016;128(15):1918-1927. doi:10.1182/blood-2016-07-418434
Matutes E. Diagnostic and therapeutic challenges in hairy cell leukemia-variant: where are we in 2021? Expert Rev Hematol. 2021;14(4):355-363. doi:10.1080/17474086.2021.1908121
Cawley JC, Burns GF, Hayhoe FG. A chronic lymphoproliferative disorder with distinctive features: a distinct variant of hairy-cell leukaemia. Leuk Res. 1980;4(6):547-559. doi:10.1016/0145-2126(80)90066-1
Xi L, Arons E, Navarro W, et al. Both variant and IGHV4-34-expressing hairy cell leukemia lack the BRAF V600E mutation. Blood. 2012;119(14):3330-3332. doi:10.1182/blood-2011-09-379339
Durham BH, Getta B, Dietrich S, et al. Genomic analysis of hairy cell leukemia identifies novel recurrent genetic alterations. Blood. 2017;130(14):1644-1648. doi:10.1182/blood-2017-01-76510711
Grever MR, Abdel-Wahab O, Andritsos LA, et al. Consensus guidelines for the diagnosis and management of patients with hairy cell leukemia. Blood. 2017;129(5):553-560. doi:10.1182/blood-2016-01-689422
Waterfall JJ, Arons E, Walker RL, et al. High prevalence of MAP2K1 mutations in variant and IGHV4-34-expressing hairy-cell leukemias. Nat Genet. 2014;46(1):8-10. doi:10.1038/ng.2828
Arons E, Sunshine J, Suntum T, Kreitman RJ. Somatic hypermutation and VH gene usage in hairy cell leukaemia. Br J Haematol. 2006;133(5):504-512. doi:10.1111/j.1365-2141.2006.06066.x
Arons E, Roth L, Sapolsky J, Suntum T, Stetler-Stevenson M, Kreitman RJ. Evidence of canonical somatic hypermutation in hairy cell leukemia. Blood. 2011;117(18):4844-4851. doi:10.1182/blood-2010-11-316737
Arons E, Suntum T, Stetler-Stevenson M, Kreitman RJ. VH4-34+ hairy cell leukemia, a new variant with poor prognosis despite standard therapy. Blood. 2009;114(21):4687-4695. doi:10.1182/blood-2009-01-201731
Forconi F, Sozzi E, Cencini E, et al. Hairy cell leukemias with unmutated IGHV genes define the minor subset refractory to single-agent cladribine and with more aggressive behavior. Blood. 2009;114(21):4696-4702. doi:10.1182/blood-2009-03-212449
Robak E, Jesionek-Kupnicka D, Robak T. Skin changes in hairy cell leukemia. Ann Hematol. 2021;100(3):615-625. doi:10.1007/s00277-020-04349-z
Falini B, Tiacci E, Liso A, et al. Simple diagnostic assay for hairy cell leukaemia by immunocytochemical detection of annexin A1 (ANXA1). Lancet. 2004;363(9424): 1869-1870. doi:10.1016/S0140-6736(04)16356-3
Robak T, Robak P. Measurable residual disease in hairy cell leukemia: technical considerations and clinical significance. Front Oncol. 2022;12:976374. doi:10.3389/fonc.2022.976374
Chihara D, Arons E, Stetler-Stevenson M, et al. Randomized phase II study of first-line cladribine with concurrent or delayed rituximab in patients with hairy cell leukemia. J Clin Oncol. 2020;38(14):1527-1538. doi:10.1200/JCO.19.02250
Chihara D, Kantarjian H, O’Brien S, et al. Long-term durable remission by cladribine followed by rituximab in patients with hairy cell leukaemia: update of a phase II trial. Br J Haematol. 2016;174(5):760-766. doi:10.1111/bjh.14129
Grever M, Andritsos L, Banerji V, et al. Hairy cell leukemia and COVID-19 adaptation of treatment guidelines. Leukemia. 2021;35(7):1864-1872. doi:10.1038/s41375-021-01257-7
Konrat J, Rösler W, Roiss M, et al. BRAF inhibitor treatment of classical hairy cell leukemia allows successful vaccination against SARS-CoV-2. Ann Hematol. 2023;102(2):403-406. doi:10.1007/s00277-022-05026-z
Park JH, Shukla M, Salcedo JM, et al. First-line chemo-free therapy with the BRAF inhibitor vemurafenib combined with obinutuzumab is effective in patients with HCL. Blood. 2019;134(suppl 1):Abstract 3998. https://doi.org/10.1182/blood-2019-124478
Nieva J, Bethel K, Saven A. Phase 2 study of rituximab in the treatment of cladribine-failed patients with hairy cell leukemia. Blood. 2003;102(3):810-813. doi:10.1182/blood-2003-01-0014
Tiacci E, Park JH, De Carolis L, et al. Targeting mutant BRAF in relapsed or refractory hairy-cell leukemia. N Engl J Med. 2015;373(18):1733-1747. doi:10.1056/NEJMoa1506583
Maitre E, Paillassa J, Troussard X. Novel targeted treatments in hairy cell leukemia and other hairy cell-like disorders. Front Oncol. 2022;12:1068981. doi:10.3389/fonc.2022.1068981
Grob JJ, Amonkar MM, Karaszewska B, et al. Comparison of dabrafenib and trametinib combination therapy with vemurafenib monotherapy on health-related quality of life in patients with unresectable or metastatic cutaneous BRAF Val600-mutation-positive melanoma (COMBI-v): results of a phase 3, open-label, randomised trial. Lancet Oncol. 2015;16(13):1389-1398. doi:10.1016/S1470-2045(15)00087-X
Tiacci E, De Carolis L, Simonetti E, et al. Safety and efficacy of the BRAF inhibitor dabrafenib in relapsed or refractory hairy cell leukemia: a pilot phase-2 clinical trial. Leukemia. 2021;35(11):3314-3318. doi:10.1038/s41375-021-01210-8
Kreitman RJ, Moreau P, Ravandi F, et al. Dabrafenib plus trametinib in patients with relapsed/refractory BRAF V600E mutation-positive hairy cell leukemia. Blood. 2023;141(9):996-1006. doi:10.1182/blood.2021013658
Adashek JJ, Menta AK, Reddy NK, Desai AP, Roszik J, Subbiah V. Tissue agnostic activity of BRAF plus MEK inhibitor in BRAF V600E-mutated tumors. Mol Cancer Ther. 2022;21(6):871-878. doi:10.1158/1535-7163.MCT-21-0950
Rogers KA, Andritsos LA, Wei L, et al. Phase 2 study of ibrutinib in classic and variant hairy cell leukemia. Blood. 2021;137(25):3473-3483. doi:10.1182/blood.2020009688
Kreitman RJ, Dearden C, Zinzani PL, et al; Study 1053 investigators. Moxetumomab pasudotox in heavily pre-treated patients with relapsed/refractory hairy cell leukemia (HCL): long-term follow-up from the pivotal trial. J Hematol Oncol. 2021;14(1):35. doi:10.1186/s13045-020-01004-y
Leonard JP, Goldenberg DM. Preclinical and clinical evaluation of epratuzumab (anti-CD22 IgG) in B-cell malignancies. Oncogene. 2007;26(25):3704-3713. doi:10.1038/sj.onc.1210370
Liang Cheng, MD
Approximately 1% of adult neoplasms and 5% of all urologic cancers are testicular cancer (TC).1 In the United States, 9190 new cases have been estimated for 2023.1 Testicular germ cell tumors (GCTs) comprise 90% to 95% of all TCs and are grouped into seminomas, nonseminomatous GCTs (NSGCTs), and mixed histology GCTs.1 NSGCTs tend to be more aggressive and are more common in younger men (15-40 years old), whereas seminomas are slower growing and generally develop later in a patient’s life.2,3
Mortality from TC has been decreasing since the 1970s due to cisplatin-based chemotherapy regimens2,3; TC is among the most curable of solid neoplasms, with a 5-year relative survival rate of 95%.2-4 Thus, the focus of research has shifted from optimizing treatments for improved survival to decreasing treatment-related, long-term adverse events (AEs).5
New Modifications in Risk Assessment and Prognostication
The widely accepted risk stratification model in use today was first developed in 1997 by the International Germ Cell Cancer Collaborative Group (IGCCCG) after studying data on patients with seminoma and NSGCTs.6 The original classification categorized metastatic NSGCTs as having good, intermediate, or poor prognosis based on levels of alpha-fetoprotein (AFP), human chorionic gonadotropin (hCG), lactate dehydrogenase (LDH), and the presence of nonpulmonary visceral metastases (NPVM). Primary mediastinal NSGCTs were classified as having poor prognosis regardless of the other factors.6 Metastatic seminoma GCTs were categorized as having good or intermediate prognosis based on the occurrence of brain, liver, or bone metastasis.7
Using contemporary data from more than 12,000 patients with metastatic GCTs who received either cisplatin or etoposide, the IGCCCG model was updated in 2021. For seminoma GCTs, 5-year progression-free survival (PFS) and 5-year overall survival (OS) were extended for both good and intermediate prognostic groups.7 LDH remained the most significant prognostic factor for determining good prognosis however, patients with LDH above 2.5× upper limit of normal (ULN) before chemotherapy had worse survival probabilities than patients with LDH at 2.5× ULN or lower. The survival probabilities for patients with otherwise good prognosis with LDH of more than 2.5× ULN were like those for patients with intermediate prognosis.7 Thus, using LDH of more than 2.5× ULN has revealed a subgroup with significantly worse outcomes within the “good” prognostic group.7,8
For NSGCTs, 5-year PFS rates did not differ from the original IGCCCG for good and intermediate prognostic groups; however, the 2021 update revealed an improved PFS for the poor prognostic group. The 2021 update also demonstrated that 5-year OS rates improved for each group, and further confirmed that the 2 most important prognostic factors for NSGCT were the presence of NPVM and the presence of a mediastinal primary tumor. The update added 2 new adverse prognostic variables: age and metastases. Risk of progression increases 25% with every decade-of-life increase, and 66% with the presence of lung metastases. The LDH groups were reduced to a single cutoff at 2.5× ULN for NSGCTs.8
Primary and Subsequent Treatments for TC
Guideline-directed first-line and subsequent treatments for seminomas and NSGCTs have been developed by several organizations, including the National Comprehensive Cancer Network, IGCCCG, and the American Urological Association (see Figure 1 and 2). An analysis of the most used treatments was performed using the National Cancer Database.2 Most patients underwent orchiectomy without chemotherapy or radiation for both stage I seminomas (78%) and NSGCTs (57%). For stage II and III seminomas, most patients underwent surgery with chemotherapy (66% and 68%, respectively). Nearly half of patients with stage II NSGCTs were treated with surgery and chemotherapy (49%), and a third were treated with retroperitoneal lymph node dissection (RPLND) in addition to surgery and chemotherapy. Surgery with chemotherapy was used for 55% of stage III NSGCTs; other treatments included surgery combined with chemotherapy and RPLND (19%), and chemotherapy with or without radiation (20%).2 However, nearly 30% of patients with TC do not receive guideline-directed therapy, including inappropriate imaging and overtreatment; and nonguideline–directed therapy has been independently associated with risk of relapse.12,13
Figure 1. First-line and Subsequent Treatment of Seminomas
Figure 2. First-line and Subsequent Treatment of Non-Seminomas
TC Survivorship
The trend of improved OS after treatment for metastatic GCTs highlights a need to focus on survivorship. The 10-year survival rate for TC post-treatment is 95%.14 Latest estimates suggest there are more than 300,000 TC survivors in the United States,2 accounting for approximately 4% of all US male cancer survivors.14 With longer-term survival, however, comes the risk for long-term complications from cancer treatments. For example, circulating platinum has been detected in the plasma of men up to 28 years after undergoing cisplatin-based chemotherapy for TC.15 Increasing levels of residual serum platinum have also been shown to correlate with severity of neurotoxicity between 5 and 20 years after treatment.16
A significant concern with cancer treatment is the development of second malignant neoplasms (SMNs).14,17 The relative risk of the development of SMNs depends on whetherradiation therapy or chemotherapy, or both, was used as the primary treatment. Patients who received either radiation therapy or chemotherapy are at increased risk for leukemia and solid cancers, including gastrointestinal cancers. For patients treated with cisplatin, a significant dose-response relationship between cumulative dose and leukemic risk has been reported.14
Other concerns are increased non-TC mortality and SMN mortality. Hellesnes et al examined cause-specific, non-TC mortality using a population-based cohort in Norway.18 They determined that the overall 25-year, non-TC mortality risk was 13.7% (95% CI, 12.5-14.9) for patients who previously had TC vs 11.3% for patients who never had TC. The highest mortality rates were reported for patients who had radiation (19%) or platinum-based chemotherapy plus radiation (18.4%); the lowest mortality rate was reported for patients who had received platinum-based chemotherapy only (9.5%). Patients with the highest non-TC mortality risk were fewer than 20 years post-cancer diagnosis. Non-TC mortality excess ranged from 23% to 40% for patients with a prior TC diagnosis, and a significant 1.43- to 3.24-fold increase in SMN mortality emerged after treatment with platinum-based chemotherapy or radiation therapy, or both.19 Awareness of the increased premature mortality risk is crucial for both TC survivors and their care providers.18
Quality of life for TC survivors appears to be affected by the presence of long-term treatment-related AEs.18 The relative risk of developing cardiovascular disease increases after treatment with chemotherapy. Raynaud phenomenon resulting from bleomycin-induced vascular damage developed within 4 to 12 months after chemotherapy for 18.7% to 39% of TC survivors.14,19 Bleomycin may also cause pulmonary toxicity. Pulmonary surgery, tobacco use of ≥ 20 pack-years, and a cumulative cisplatin dose of > 850 mg are risk factors for late bleomycin-associated pulmonary toxicity.14
Other late-developing toxicities resulting from cisplatin treatment include ototoxicity, neurotoxicity, nephrotoxicity, chronic fatigue, and hypogonadism.14,19 Nearly 1 in 5 North American survivors treated with cisplatin reported severe-to-profound hearing loss within a median of 4.3 years. The extent of hearing loss has been directly associated with the increase in cumulative cisplatin dose. Peripheral neurotoxicity after cisplatin-based chemotherapy is reported to be as high as 40%.14 Chronic cancer-related fatigue can range from 15% to 27%, and has been associated with peripheral neuropathy, low testosterone levels, low physical activity, anxiety, and depression. Post-treatment hypogonadism ranges from 11% to 16%.14,17,20,21
Psychosocial issues are also of concern. Mild-to-moderate psychological distress with diagnosis and survivorship has been reported.17 Anxiety and depression are higher in TC survivors than in the general population. Variables associated with clinically significant anxiety include younger age and shorter time from diagnosis; whereas feeling helpless/hopeless, having less social support, having a higher number of physical symptoms, and having children are factors associated with higher levels of depression. A moderate-to-high level of fear of recurrence has also been reported.17
Recent Clinical Trials in Stage II Disease
Stage II disease has been the focus of current research to reduce treatment-related toxicities and limit longer-term complications. While few phase 3 clinical trials are ongoing (see Table), the results of several phase 2 trials have been reported recently.22-24
Table. Ongoing Interventional Phase 3 Clinical Trials Involving Testicular Cancer
PRIMETEST was a single-arm, single-center, phase 2 study examining the efficacy and surgical safety of primary RPLND for stage II disease.22 Participants underwent either open or robot-assisted unilateral RPLND for stage IIA or B seminoma. No adjuvant treatment was permitted. Of the 33 participants, 9 presented initially with clinical stage II disease (27%) and 24 (73%) had recurrence during active surveillance. Five of the 24 had 1 cycle of carboplatin prior to progressing to stage II. With a median follow-up of 32 months, the study did not meet its primary endpoint of PFS at 36 months. After 32 months, 10 recurrences (30%) were detected, yielding a PFS rate of 70%. All 10 patients with recurrence received chemotherapy and were alive without evidence of disease at the time of publication. This study demonstrates that RPLND may be appropriate for select patients; however, criteria for selecting patients to receive only RPLND need to be clearly defined.22
The SEMS (surgery in early metastatic seminoma) trial was a single-arm, international, phase 2 study of RPLND as first-line treatment for early metastatic seminoma with isolated retroperitoneal lymphadenopathy between 1 and 3 cm (stage II).23 With a median follow-up of 24 months, OS was 100% and 2-year recurrence-free survival was 87%. Recurrence rate was 18% (10 recurrences) with a median time to recurrence of 8 months. Short-term complications occurred in 7 patients (13%), and no patients reported long-term complications. The authors suggested that RPLND is a therapeutic option for first-line treatment in early metastatic seminoma.23
SAKK 01/10 was a single-arm, international, phase 2 study examining the de-escalation of treatment to potentially avoid toxic effects for patients with either stage IIA or stage IIB seminoma.24 Treatment included carboplatin (area under the curve [AUC] 7 mg/mL/min) followed 3 weeks later with involvednode radiotherapy (30 Gy in 15 fractions for stage IIA and 36 Gy in 18 fractions for stage IIB). The study did not meet its primary endpoint of PFS of 95% at 3 years. Grade ≥ 3 treatment-related AEs (TRAEs) included neutropenia (4%), thrombocytopenia (3%), and vomiting (1%). No treatment-related deaths and no late TRAEs were reported. One case of transient creatinine increase was reported as a serious AE, and second primary tumors were reported in 4 participants. Although the primary endpoint was not met, long-term AEs continue to be recorded for potentially up to 20 years. The favorable efficacy and toxicity profile observed in the deescalation combination treatment warrants further study.24
Emerging Trends and Future Directions for TC Treatment
Although the outlook for most newly diagnosed patients with TC is promising, especially for those diagnosed with early-stage disease and good prognosis advanced disease, treatment challenges remain. Between 10% and 20% of patients will have a relapse of TC after initially achieving a complete remission. Most patients will have a relapse within 2 years of initial treatment, but a small subgroup will have a relapse more than 5 years after therapy. Most recurrences occur in the retroperitoneum and lungs and require definitive therapy using chemotherapy and surgical resection.21
Patients with platinum-refractory disease may still achiev long-term remission with salvage therapy of surgery, conventional-dose chemotherapy, or high-dose chemotherapy with autologous stem cell transplantation; however, these treatments will fail for some patients, resulting in poor prognosis. Targeted therapy for TC has not produced meaningful benefits for this population with refractory disease, and the optimal treatment for this group of patients with TC remains to be determined.21
Although current guidelines recommend determining the levels of AFP, hCG, and LDH for clinical staging, treatment monitoring, and follow-up, limitations exist with their usage.9 The assays for these markers have low sensitivity and lack specificity; about half of all GCTs express only 1 of the 3 biomarkers, and seminomas lack AFP expression.7,25,26 Further research is needed on LDH. An emerging group of patients with LDH below 2.5× ULN may be candidates for de-escalatio strategies to reduce treatment burden, while inferior outcomes remain for patients with either good prognosis seminoma and elevated LDH, or intermediate prognosis seminoma.7
Other biomarkers, such as miRNA371a-3p and PD-L1, are being investigated; miRNA371a-3p has been shown to have prognostic significance. The results of this assay can be informative for both seminomas and NSGCTs.26 However, the protocol for quantification and implementation still needs to be determined.27
Chovanec M, Cheng L. Advances in diagnosis and treatment of testicular cancer. BMJ. 2022;379:e070499. doi:10.1136/bmj-2022-070499
Gaddam SJ, Chesnut GT. Testicle cancer. StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2022. Updated October 16, 2022. Accessed March 13, 2023. https://www.ncbi.nlm.nih.gov/books/NBK563159/
Yang H, Obiora D, Tomaszewski JJ. Outcomes and expanding indications for robotic retroperitoneal lymph node dissection for testicular cancer. Transl Androl Urol. 2021;10(5):2188-2194. doi:10.21037/tau.2020.03.14
International Germ Cell Cancer Collaborative Group. International germ cell consensus classification: a prognostic factor-based staging system for metastatic germ cell cancers. J Clin Oncol. 1997;15(2):594-603. doi:10.1200/JCO.1997.15.2.594
Beyer J, Collette L, Sauvé N, et al. Survival and new prognosticators in metastatic seminoma: results from the IGCCCG-Update Consortium. J Clin Oncol. 2021;39(14):1553-1562. doi:10.1200/JCO.20.03292
Gillessen S, Sauvé N, Collette L, et al. Predicting outcomes in men with metastatic nonseminomatous germ cell tumors (NSGCT): results from the IGCCCG Update Consortium. J Clin Oncol. 2021;39(14):1563-1574. doi:10.1200/JCO.20.03296
Gilligan T, Lin DW, Aggarwal R, et al. Testicular cancer, version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2019;17(12):1529-1554. doi:10.6004/jnccn.2019.0058
Heinzelbecker J, Schmidt S, Lackner J, et al. Therapy of clinical stage IIa and IIb seminoma: a systematic review. World J Urol. 2022;40(12):2829-2841. doi:10.1007/s00345-021-03873-5
Oldenburg J, Berney DM, Bokemeyer C, et al. Testicular seminoma and nonseminoma: ESMA-EURACAN Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022;33(4):362-375. doi:10.1016/j.annonc.2022.01.002
Wymer KM, Pearce SM, Harris KT, Pierorazio PM, Daneshmand S, Eggener SE. Adherence to National Comprehensive Cancer Network® guidelines for testicular cancer. J Urol. 2017;197(3 pt 1):684-689. doi:10.1016/j.juro.2016.09.073
Saoud RM, Andolfi C, Aizen J, et al. Impact of non-guideline-directed care on quality of life in testicular cancer survivors. Eur Urol Focus. 2021;7(5):1137-1142. doi:10.1016/j.euf.2020.10.005
Guo CC, Czerniak B. Somatic-type malignancies in testicular germ cell tumors. Hum Pathol. 2022;127:123-135.
Sprauten M, Darrah TH, Peterson DR, et al. Impact of long-term serum platinum concentrations on neuro- and ototoxicity in cisplatin-treated survivors of testicular cancer. J Clin Oncol. 2012;30(3):300-307. doi:10.1200/JCO.2011.37.4025
Shrem NS, Wood L, Hamilton RJ, et al. Testicular cancer survivorship: long-term toxicity and management. Can Urol Assoc J. 2022;16(8):257-272. doi:10.5489/cuaj.8009
Hellesnes R, Myklebust TA, Fosså SD, et al. Testicular cancer in the cisplatin era: causes of death and mortality rates in a population-based cohort. J Clin Oncol. 2021;39(32):3561-3573. doi:10.1200/JCO.21.00637
Mercieca-Bebber R, Naher SK, Rincones O, Smith AB, Stockler MR. Patient-reported outcomes associated with treatments for testicular cancer: a systematic review. Patient Relat Outcome Meas. 2021;12:129-171. doi:10.2147/PROM.S242754
Sprauten M, Haugnes HS, Brydøy M, et al. Chronic fatigue in 812 testicular cancer survivors during long-term follow-up: increasing prevalence and risk factors. Ann Oncol. 2015;26(10):2133-2140. doi:10.1093/annonc/mdv328
King J, Adra N, Einhorn LH. Testicular cancer: biology to bedside. Cancer Res. 2021;81(21):5369-5376. doi:10.1158/0008-5472.CAN-21-1452
Hiester A, Che Y, Lusch A, et al. Phase 2 single-arm trial of primary retroperitoneal lymph node dissection in patients with seminomatous testicular germ cell tumors with clinical stage IIA/B (PRIMETEST). Eur Urol. 2022;S0302-2838(22)02775-0. doi:10.1016/j.eururo.2022.10.021
Daneshmand S, Cary C, Masterson TA, et al. SEMS trial: result of a prospective, multi-institutional phase II clinical trial of surgery in early metastatic seminoma. J Clin Oncol. 2021;39(6 suppl):Abstract 375. doi:10.1200JCO.2021.39.6_suppl.375
Papachristofilou A, Bedke J, Hayoz S, et al. Single-dose carboplatin followed by involved-node radiotherapy for stage IIA and stage IIB seminoma (SAKK 01/10): a single-arm, multicentre, phase 2 trial. Lancet Oncol. 2022;23(11):1441-1450. doi:10.1016/S1470-2045(22)00564-2
Dieckmann KP, Richter-Simonsen H, Kulejewski M, et al. Testicular germ-cell tumours: a descriptive analysis of clinical characteristics at first presentation. Urol Int. 2018;100(4):409-419. doi:10.1159/000488284
Murray MJ, Huddart RA, Coleman N. The present and future of serum diagnostic tests for testicular germ cell tumours. Nat Rev Urol. 2016;13(12):715-725. doi:10.1038/nrurol.2016.170
Author and Disclosure Information
Liang Cheng, MD Professor and Vice Chair for Translational Research Director of Anatomic and Molecular Pathology Department of Pathology and Laboratory Medicine Brown University Warren Alpert Medical School, Lifespan Academic Medical Center Legorreta Cancer Center at Brown University Providence, RI
Liang Cheng, MD, has disclosed no relevant financial relationships.
Liang Cheng, MD Professor and Vice Chair for Translational Research Director of Anatomic and Molecular Pathology Department of Pathology and Laboratory Medicine Brown University Warren Alpert Medical School, Lifespan Academic Medical Center Legorreta Cancer Center at Brown University Providence, RI
Liang Cheng, MD, has disclosed no relevant financial relationships.
Author and Disclosure Information
Liang Cheng, MD Professor and Vice Chair for Translational Research Director of Anatomic and Molecular Pathology Department of Pathology and Laboratory Medicine Brown University Warren Alpert Medical School, Lifespan Academic Medical Center Legorreta Cancer Center at Brown University Providence, RI
Liang Cheng, MD, has disclosed no relevant financial relationships.
Liang Cheng, MD
Approximately 1% of adult neoplasms and 5% of all urologic cancers are testicular cancer (TC).1 In the United States, 9190 new cases have been estimated for 2023.1 Testicular germ cell tumors (GCTs) comprise 90% to 95% of all TCs and are grouped into seminomas, nonseminomatous GCTs (NSGCTs), and mixed histology GCTs.1 NSGCTs tend to be more aggressive and are more common in younger men (15-40 years old), whereas seminomas are slower growing and generally develop later in a patient’s life.2,3
Mortality from TC has been decreasing since the 1970s due to cisplatin-based chemotherapy regimens2,3; TC is among the most curable of solid neoplasms, with a 5-year relative survival rate of 95%.2-4 Thus, the focus of research has shifted from optimizing treatments for improved survival to decreasing treatment-related, long-term adverse events (AEs).5
New Modifications in Risk Assessment and Prognostication
The widely accepted risk stratification model in use today was first developed in 1997 by the International Germ Cell Cancer Collaborative Group (IGCCCG) after studying data on patients with seminoma and NSGCTs.6 The original classification categorized metastatic NSGCTs as having good, intermediate, or poor prognosis based on levels of alpha-fetoprotein (AFP), human chorionic gonadotropin (hCG), lactate dehydrogenase (LDH), and the presence of nonpulmonary visceral metastases (NPVM). Primary mediastinal NSGCTs were classified as having poor prognosis regardless of the other factors.6 Metastatic seminoma GCTs were categorized as having good or intermediate prognosis based on the occurrence of brain, liver, or bone metastasis.7
Using contemporary data from more than 12,000 patients with metastatic GCTs who received either cisplatin or etoposide, the IGCCCG model was updated in 2021. For seminoma GCTs, 5-year progression-free survival (PFS) and 5-year overall survival (OS) were extended for both good and intermediate prognostic groups.7 LDH remained the most significant prognostic factor for determining good prognosis however, patients with LDH above 2.5× upper limit of normal (ULN) before chemotherapy had worse survival probabilities than patients with LDH at 2.5× ULN or lower. The survival probabilities for patients with otherwise good prognosis with LDH of more than 2.5× ULN were like those for patients with intermediate prognosis.7 Thus, using LDH of more than 2.5× ULN has revealed a subgroup with significantly worse outcomes within the “good” prognostic group.7,8
For NSGCTs, 5-year PFS rates did not differ from the original IGCCCG for good and intermediate prognostic groups; however, the 2021 update revealed an improved PFS for the poor prognostic group. The 2021 update also demonstrated that 5-year OS rates improved for each group, and further confirmed that the 2 most important prognostic factors for NSGCT were the presence of NPVM and the presence of a mediastinal primary tumor. The update added 2 new adverse prognostic variables: age and metastases. Risk of progression increases 25% with every decade-of-life increase, and 66% with the presence of lung metastases. The LDH groups were reduced to a single cutoff at 2.5× ULN for NSGCTs.8
Primary and Subsequent Treatments for TC
Guideline-directed first-line and subsequent treatments for seminomas and NSGCTs have been developed by several organizations, including the National Comprehensive Cancer Network, IGCCCG, and the American Urological Association (see Figure 1 and 2). An analysis of the most used treatments was performed using the National Cancer Database.2 Most patients underwent orchiectomy without chemotherapy or radiation for both stage I seminomas (78%) and NSGCTs (57%). For stage II and III seminomas, most patients underwent surgery with chemotherapy (66% and 68%, respectively). Nearly half of patients with stage II NSGCTs were treated with surgery and chemotherapy (49%), and a third were treated with retroperitoneal lymph node dissection (RPLND) in addition to surgery and chemotherapy. Surgery with chemotherapy was used for 55% of stage III NSGCTs; other treatments included surgery combined with chemotherapy and RPLND (19%), and chemotherapy with or without radiation (20%).2 However, nearly 30% of patients with TC do not receive guideline-directed therapy, including inappropriate imaging and overtreatment; and nonguideline–directed therapy has been independently associated with risk of relapse.12,13
Figure 1. First-line and Subsequent Treatment of Seminomas
Figure 2. First-line and Subsequent Treatment of Non-Seminomas
TC Survivorship
The trend of improved OS after treatment for metastatic GCTs highlights a need to focus on survivorship. The 10-year survival rate for TC post-treatment is 95%.14 Latest estimates suggest there are more than 300,000 TC survivors in the United States,2 accounting for approximately 4% of all US male cancer survivors.14 With longer-term survival, however, comes the risk for long-term complications from cancer treatments. For example, circulating platinum has been detected in the plasma of men up to 28 years after undergoing cisplatin-based chemotherapy for TC.15 Increasing levels of residual serum platinum have also been shown to correlate with severity of neurotoxicity between 5 and 20 years after treatment.16
A significant concern with cancer treatment is the development of second malignant neoplasms (SMNs).14,17 The relative risk of the development of SMNs depends on whetherradiation therapy or chemotherapy, or both, was used as the primary treatment. Patients who received either radiation therapy or chemotherapy are at increased risk for leukemia and solid cancers, including gastrointestinal cancers. For patients treated with cisplatin, a significant dose-response relationship between cumulative dose and leukemic risk has been reported.14
Other concerns are increased non-TC mortality and SMN mortality. Hellesnes et al examined cause-specific, non-TC mortality using a population-based cohort in Norway.18 They determined that the overall 25-year, non-TC mortality risk was 13.7% (95% CI, 12.5-14.9) for patients who previously had TC vs 11.3% for patients who never had TC. The highest mortality rates were reported for patients who had radiation (19%) or platinum-based chemotherapy plus radiation (18.4%); the lowest mortality rate was reported for patients who had received platinum-based chemotherapy only (9.5%). Patients with the highest non-TC mortality risk were fewer than 20 years post-cancer diagnosis. Non-TC mortality excess ranged from 23% to 40% for patients with a prior TC diagnosis, and a significant 1.43- to 3.24-fold increase in SMN mortality emerged after treatment with platinum-based chemotherapy or radiation therapy, or both.19 Awareness of the increased premature mortality risk is crucial for both TC survivors and their care providers.18
Quality of life for TC survivors appears to be affected by the presence of long-term treatment-related AEs.18 The relative risk of developing cardiovascular disease increases after treatment with chemotherapy. Raynaud phenomenon resulting from bleomycin-induced vascular damage developed within 4 to 12 months after chemotherapy for 18.7% to 39% of TC survivors.14,19 Bleomycin may also cause pulmonary toxicity. Pulmonary surgery, tobacco use of ≥ 20 pack-years, and a cumulative cisplatin dose of > 850 mg are risk factors for late bleomycin-associated pulmonary toxicity.14
Other late-developing toxicities resulting from cisplatin treatment include ototoxicity, neurotoxicity, nephrotoxicity, chronic fatigue, and hypogonadism.14,19 Nearly 1 in 5 North American survivors treated with cisplatin reported severe-to-profound hearing loss within a median of 4.3 years. The extent of hearing loss has been directly associated with the increase in cumulative cisplatin dose. Peripheral neurotoxicity after cisplatin-based chemotherapy is reported to be as high as 40%.14 Chronic cancer-related fatigue can range from 15% to 27%, and has been associated with peripheral neuropathy, low testosterone levels, low physical activity, anxiety, and depression. Post-treatment hypogonadism ranges from 11% to 16%.14,17,20,21
Psychosocial issues are also of concern. Mild-to-moderate psychological distress with diagnosis and survivorship has been reported.17 Anxiety and depression are higher in TC survivors than in the general population. Variables associated with clinically significant anxiety include younger age and shorter time from diagnosis; whereas feeling helpless/hopeless, having less social support, having a higher number of physical symptoms, and having children are factors associated with higher levels of depression. A moderate-to-high level of fear of recurrence has also been reported.17
Recent Clinical Trials in Stage II Disease
Stage II disease has been the focus of current research to reduce treatment-related toxicities and limit longer-term complications. While few phase 3 clinical trials are ongoing (see Table), the results of several phase 2 trials have been reported recently.22-24
Table. Ongoing Interventional Phase 3 Clinical Trials Involving Testicular Cancer
PRIMETEST was a single-arm, single-center, phase 2 study examining the efficacy and surgical safety of primary RPLND for stage II disease.22 Participants underwent either open or robot-assisted unilateral RPLND for stage IIA or B seminoma. No adjuvant treatment was permitted. Of the 33 participants, 9 presented initially with clinical stage II disease (27%) and 24 (73%) had recurrence during active surveillance. Five of the 24 had 1 cycle of carboplatin prior to progressing to stage II. With a median follow-up of 32 months, the study did not meet its primary endpoint of PFS at 36 months. After 32 months, 10 recurrences (30%) were detected, yielding a PFS rate of 70%. All 10 patients with recurrence received chemotherapy and were alive without evidence of disease at the time of publication. This study demonstrates that RPLND may be appropriate for select patients; however, criteria for selecting patients to receive only RPLND need to be clearly defined.22
The SEMS (surgery in early metastatic seminoma) trial was a single-arm, international, phase 2 study of RPLND as first-line treatment for early metastatic seminoma with isolated retroperitoneal lymphadenopathy between 1 and 3 cm (stage II).23 With a median follow-up of 24 months, OS was 100% and 2-year recurrence-free survival was 87%. Recurrence rate was 18% (10 recurrences) with a median time to recurrence of 8 months. Short-term complications occurred in 7 patients (13%), and no patients reported long-term complications. The authors suggested that RPLND is a therapeutic option for first-line treatment in early metastatic seminoma.23
SAKK 01/10 was a single-arm, international, phase 2 study examining the de-escalation of treatment to potentially avoid toxic effects for patients with either stage IIA or stage IIB seminoma.24 Treatment included carboplatin (area under the curve [AUC] 7 mg/mL/min) followed 3 weeks later with involvednode radiotherapy (30 Gy in 15 fractions for stage IIA and 36 Gy in 18 fractions for stage IIB). The study did not meet its primary endpoint of PFS of 95% at 3 years. Grade ≥ 3 treatment-related AEs (TRAEs) included neutropenia (4%), thrombocytopenia (3%), and vomiting (1%). No treatment-related deaths and no late TRAEs were reported. One case of transient creatinine increase was reported as a serious AE, and second primary tumors were reported in 4 participants. Although the primary endpoint was not met, long-term AEs continue to be recorded for potentially up to 20 years. The favorable efficacy and toxicity profile observed in the deescalation combination treatment warrants further study.24
Emerging Trends and Future Directions for TC Treatment
Although the outlook for most newly diagnosed patients with TC is promising, especially for those diagnosed with early-stage disease and good prognosis advanced disease, treatment challenges remain. Between 10% and 20% of patients will have a relapse of TC after initially achieving a complete remission. Most patients will have a relapse within 2 years of initial treatment, but a small subgroup will have a relapse more than 5 years after therapy. Most recurrences occur in the retroperitoneum and lungs and require definitive therapy using chemotherapy and surgical resection.21
Patients with platinum-refractory disease may still achiev long-term remission with salvage therapy of surgery, conventional-dose chemotherapy, or high-dose chemotherapy with autologous stem cell transplantation; however, these treatments will fail for some patients, resulting in poor prognosis. Targeted therapy for TC has not produced meaningful benefits for this population with refractory disease, and the optimal treatment for this group of patients with TC remains to be determined.21
Although current guidelines recommend determining the levels of AFP, hCG, and LDH for clinical staging, treatment monitoring, and follow-up, limitations exist with their usage.9 The assays for these markers have low sensitivity and lack specificity; about half of all GCTs express only 1 of the 3 biomarkers, and seminomas lack AFP expression.7,25,26 Further research is needed on LDH. An emerging group of patients with LDH below 2.5× ULN may be candidates for de-escalatio strategies to reduce treatment burden, while inferior outcomes remain for patients with either good prognosis seminoma and elevated LDH, or intermediate prognosis seminoma.7
Other biomarkers, such as miRNA371a-3p and PD-L1, are being investigated; miRNA371a-3p has been shown to have prognostic significance. The results of this assay can be informative for both seminomas and NSGCTs.26 However, the protocol for quantification and implementation still needs to be determined.27
Liang Cheng, MD
Approximately 1% of adult neoplasms and 5% of all urologic cancers are testicular cancer (TC).1 In the United States, 9190 new cases have been estimated for 2023.1 Testicular germ cell tumors (GCTs) comprise 90% to 95% of all TCs and are grouped into seminomas, nonseminomatous GCTs (NSGCTs), and mixed histology GCTs.1 NSGCTs tend to be more aggressive and are more common in younger men (15-40 years old), whereas seminomas are slower growing and generally develop later in a patient’s life.2,3
Mortality from TC has been decreasing since the 1970s due to cisplatin-based chemotherapy regimens2,3; TC is among the most curable of solid neoplasms, with a 5-year relative survival rate of 95%.2-4 Thus, the focus of research has shifted from optimizing treatments for improved survival to decreasing treatment-related, long-term adverse events (AEs).5
New Modifications in Risk Assessment and Prognostication
The widely accepted risk stratification model in use today was first developed in 1997 by the International Germ Cell Cancer Collaborative Group (IGCCCG) after studying data on patients with seminoma and NSGCTs.6 The original classification categorized metastatic NSGCTs as having good, intermediate, or poor prognosis based on levels of alpha-fetoprotein (AFP), human chorionic gonadotropin (hCG), lactate dehydrogenase (LDH), and the presence of nonpulmonary visceral metastases (NPVM). Primary mediastinal NSGCTs were classified as having poor prognosis regardless of the other factors.6 Metastatic seminoma GCTs were categorized as having good or intermediate prognosis based on the occurrence of brain, liver, or bone metastasis.7
Using contemporary data from more than 12,000 patients with metastatic GCTs who received either cisplatin or etoposide, the IGCCCG model was updated in 2021. For seminoma GCTs, 5-year progression-free survival (PFS) and 5-year overall survival (OS) were extended for both good and intermediate prognostic groups.7 LDH remained the most significant prognostic factor for determining good prognosis however, patients with LDH above 2.5× upper limit of normal (ULN) before chemotherapy had worse survival probabilities than patients with LDH at 2.5× ULN or lower. The survival probabilities for patients with otherwise good prognosis with LDH of more than 2.5× ULN were like those for patients with intermediate prognosis.7 Thus, using LDH of more than 2.5× ULN has revealed a subgroup with significantly worse outcomes within the “good” prognostic group.7,8
For NSGCTs, 5-year PFS rates did not differ from the original IGCCCG for good and intermediate prognostic groups; however, the 2021 update revealed an improved PFS for the poor prognostic group. The 2021 update also demonstrated that 5-year OS rates improved for each group, and further confirmed that the 2 most important prognostic factors for NSGCT were the presence of NPVM and the presence of a mediastinal primary tumor. The update added 2 new adverse prognostic variables: age and metastases. Risk of progression increases 25% with every decade-of-life increase, and 66% with the presence of lung metastases. The LDH groups were reduced to a single cutoff at 2.5× ULN for NSGCTs.8
Primary and Subsequent Treatments for TC
Guideline-directed first-line and subsequent treatments for seminomas and NSGCTs have been developed by several organizations, including the National Comprehensive Cancer Network, IGCCCG, and the American Urological Association (see Figure 1 and 2). An analysis of the most used treatments was performed using the National Cancer Database.2 Most patients underwent orchiectomy without chemotherapy or radiation for both stage I seminomas (78%) and NSGCTs (57%). For stage II and III seminomas, most patients underwent surgery with chemotherapy (66% and 68%, respectively). Nearly half of patients with stage II NSGCTs were treated with surgery and chemotherapy (49%), and a third were treated with retroperitoneal lymph node dissection (RPLND) in addition to surgery and chemotherapy. Surgery with chemotherapy was used for 55% of stage III NSGCTs; other treatments included surgery combined with chemotherapy and RPLND (19%), and chemotherapy with or without radiation (20%).2 However, nearly 30% of patients with TC do not receive guideline-directed therapy, including inappropriate imaging and overtreatment; and nonguideline–directed therapy has been independently associated with risk of relapse.12,13
Figure 1. First-line and Subsequent Treatment of Seminomas
Figure 2. First-line and Subsequent Treatment of Non-Seminomas
TC Survivorship
The trend of improved OS after treatment for metastatic GCTs highlights a need to focus on survivorship. The 10-year survival rate for TC post-treatment is 95%.14 Latest estimates suggest there are more than 300,000 TC survivors in the United States,2 accounting for approximately 4% of all US male cancer survivors.14 With longer-term survival, however, comes the risk for long-term complications from cancer treatments. For example, circulating platinum has been detected in the plasma of men up to 28 years after undergoing cisplatin-based chemotherapy for TC.15 Increasing levels of residual serum platinum have also been shown to correlate with severity of neurotoxicity between 5 and 20 years after treatment.16
A significant concern with cancer treatment is the development of second malignant neoplasms (SMNs).14,17 The relative risk of the development of SMNs depends on whetherradiation therapy or chemotherapy, or both, was used as the primary treatment. Patients who received either radiation therapy or chemotherapy are at increased risk for leukemia and solid cancers, including gastrointestinal cancers. For patients treated with cisplatin, a significant dose-response relationship between cumulative dose and leukemic risk has been reported.14
Other concerns are increased non-TC mortality and SMN mortality. Hellesnes et al examined cause-specific, non-TC mortality using a population-based cohort in Norway.18 They determined that the overall 25-year, non-TC mortality risk was 13.7% (95% CI, 12.5-14.9) for patients who previously had TC vs 11.3% for patients who never had TC. The highest mortality rates were reported for patients who had radiation (19%) or platinum-based chemotherapy plus radiation (18.4%); the lowest mortality rate was reported for patients who had received platinum-based chemotherapy only (9.5%). Patients with the highest non-TC mortality risk were fewer than 20 years post-cancer diagnosis. Non-TC mortality excess ranged from 23% to 40% for patients with a prior TC diagnosis, and a significant 1.43- to 3.24-fold increase in SMN mortality emerged after treatment with platinum-based chemotherapy or radiation therapy, or both.19 Awareness of the increased premature mortality risk is crucial for both TC survivors and their care providers.18
Quality of life for TC survivors appears to be affected by the presence of long-term treatment-related AEs.18 The relative risk of developing cardiovascular disease increases after treatment with chemotherapy. Raynaud phenomenon resulting from bleomycin-induced vascular damage developed within 4 to 12 months after chemotherapy for 18.7% to 39% of TC survivors.14,19 Bleomycin may also cause pulmonary toxicity. Pulmonary surgery, tobacco use of ≥ 20 pack-years, and a cumulative cisplatin dose of > 850 mg are risk factors for late bleomycin-associated pulmonary toxicity.14
Other late-developing toxicities resulting from cisplatin treatment include ototoxicity, neurotoxicity, nephrotoxicity, chronic fatigue, and hypogonadism.14,19 Nearly 1 in 5 North American survivors treated with cisplatin reported severe-to-profound hearing loss within a median of 4.3 years. The extent of hearing loss has been directly associated with the increase in cumulative cisplatin dose. Peripheral neurotoxicity after cisplatin-based chemotherapy is reported to be as high as 40%.14 Chronic cancer-related fatigue can range from 15% to 27%, and has been associated with peripheral neuropathy, low testosterone levels, low physical activity, anxiety, and depression. Post-treatment hypogonadism ranges from 11% to 16%.14,17,20,21
Psychosocial issues are also of concern. Mild-to-moderate psychological distress with diagnosis and survivorship has been reported.17 Anxiety and depression are higher in TC survivors than in the general population. Variables associated with clinically significant anxiety include younger age and shorter time from diagnosis; whereas feeling helpless/hopeless, having less social support, having a higher number of physical symptoms, and having children are factors associated with higher levels of depression. A moderate-to-high level of fear of recurrence has also been reported.17
Recent Clinical Trials in Stage II Disease
Stage II disease has been the focus of current research to reduce treatment-related toxicities and limit longer-term complications. While few phase 3 clinical trials are ongoing (see Table), the results of several phase 2 trials have been reported recently.22-24
Table. Ongoing Interventional Phase 3 Clinical Trials Involving Testicular Cancer
PRIMETEST was a single-arm, single-center, phase 2 study examining the efficacy and surgical safety of primary RPLND for stage II disease.22 Participants underwent either open or robot-assisted unilateral RPLND for stage IIA or B seminoma. No adjuvant treatment was permitted. Of the 33 participants, 9 presented initially with clinical stage II disease (27%) and 24 (73%) had recurrence during active surveillance. Five of the 24 had 1 cycle of carboplatin prior to progressing to stage II. With a median follow-up of 32 months, the study did not meet its primary endpoint of PFS at 36 months. After 32 months, 10 recurrences (30%) were detected, yielding a PFS rate of 70%. All 10 patients with recurrence received chemotherapy and were alive without evidence of disease at the time of publication. This study demonstrates that RPLND may be appropriate for select patients; however, criteria for selecting patients to receive only RPLND need to be clearly defined.22
The SEMS (surgery in early metastatic seminoma) trial was a single-arm, international, phase 2 study of RPLND as first-line treatment for early metastatic seminoma with isolated retroperitoneal lymphadenopathy between 1 and 3 cm (stage II).23 With a median follow-up of 24 months, OS was 100% and 2-year recurrence-free survival was 87%. Recurrence rate was 18% (10 recurrences) with a median time to recurrence of 8 months. Short-term complications occurred in 7 patients (13%), and no patients reported long-term complications. The authors suggested that RPLND is a therapeutic option for first-line treatment in early metastatic seminoma.23
SAKK 01/10 was a single-arm, international, phase 2 study examining the de-escalation of treatment to potentially avoid toxic effects for patients with either stage IIA or stage IIB seminoma.24 Treatment included carboplatin (area under the curve [AUC] 7 mg/mL/min) followed 3 weeks later with involvednode radiotherapy (30 Gy in 15 fractions for stage IIA and 36 Gy in 18 fractions for stage IIB). The study did not meet its primary endpoint of PFS of 95% at 3 years. Grade ≥ 3 treatment-related AEs (TRAEs) included neutropenia (4%), thrombocytopenia (3%), and vomiting (1%). No treatment-related deaths and no late TRAEs were reported. One case of transient creatinine increase was reported as a serious AE, and second primary tumors were reported in 4 participants. Although the primary endpoint was not met, long-term AEs continue to be recorded for potentially up to 20 years. The favorable efficacy and toxicity profile observed in the deescalation combination treatment warrants further study.24
Emerging Trends and Future Directions for TC Treatment
Although the outlook for most newly diagnosed patients with TC is promising, especially for those diagnosed with early-stage disease and good prognosis advanced disease, treatment challenges remain. Between 10% and 20% of patients will have a relapse of TC after initially achieving a complete remission. Most patients will have a relapse within 2 years of initial treatment, but a small subgroup will have a relapse more than 5 years after therapy. Most recurrences occur in the retroperitoneum and lungs and require definitive therapy using chemotherapy and surgical resection.21
Patients with platinum-refractory disease may still achiev long-term remission with salvage therapy of surgery, conventional-dose chemotherapy, or high-dose chemotherapy with autologous stem cell transplantation; however, these treatments will fail for some patients, resulting in poor prognosis. Targeted therapy for TC has not produced meaningful benefits for this population with refractory disease, and the optimal treatment for this group of patients with TC remains to be determined.21
Although current guidelines recommend determining the levels of AFP, hCG, and LDH for clinical staging, treatment monitoring, and follow-up, limitations exist with their usage.9 The assays for these markers have low sensitivity and lack specificity; about half of all GCTs express only 1 of the 3 biomarkers, and seminomas lack AFP expression.7,25,26 Further research is needed on LDH. An emerging group of patients with LDH below 2.5× ULN may be candidates for de-escalatio strategies to reduce treatment burden, while inferior outcomes remain for patients with either good prognosis seminoma and elevated LDH, or intermediate prognosis seminoma.7
Other biomarkers, such as miRNA371a-3p and PD-L1, are being investigated; miRNA371a-3p has been shown to have prognostic significance. The results of this assay can be informative for both seminomas and NSGCTs.26 However, the protocol for quantification and implementation still needs to be determined.27
Chovanec M, Cheng L. Advances in diagnosis and treatment of testicular cancer. BMJ. 2022;379:e070499. doi:10.1136/bmj-2022-070499
Gaddam SJ, Chesnut GT. Testicle cancer. StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2022. Updated October 16, 2022. Accessed March 13, 2023. https://www.ncbi.nlm.nih.gov/books/NBK563159/
Yang H, Obiora D, Tomaszewski JJ. Outcomes and expanding indications for robotic retroperitoneal lymph node dissection for testicular cancer. Transl Androl Urol. 2021;10(5):2188-2194. doi:10.21037/tau.2020.03.14
International Germ Cell Cancer Collaborative Group. International germ cell consensus classification: a prognostic factor-based staging system for metastatic germ cell cancers. J Clin Oncol. 1997;15(2):594-603. doi:10.1200/JCO.1997.15.2.594
Beyer J, Collette L, Sauvé N, et al. Survival and new prognosticators in metastatic seminoma: results from the IGCCCG-Update Consortium. J Clin Oncol. 2021;39(14):1553-1562. doi:10.1200/JCO.20.03292
Gillessen S, Sauvé N, Collette L, et al. Predicting outcomes in men with metastatic nonseminomatous germ cell tumors (NSGCT): results from the IGCCCG Update Consortium. J Clin Oncol. 2021;39(14):1563-1574. doi:10.1200/JCO.20.03296
Gilligan T, Lin DW, Aggarwal R, et al. Testicular cancer, version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2019;17(12):1529-1554. doi:10.6004/jnccn.2019.0058
Heinzelbecker J, Schmidt S, Lackner J, et al. Therapy of clinical stage IIa and IIb seminoma: a systematic review. World J Urol. 2022;40(12):2829-2841. doi:10.1007/s00345-021-03873-5
Oldenburg J, Berney DM, Bokemeyer C, et al. Testicular seminoma and nonseminoma: ESMA-EURACAN Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022;33(4):362-375. doi:10.1016/j.annonc.2022.01.002
Wymer KM, Pearce SM, Harris KT, Pierorazio PM, Daneshmand S, Eggener SE. Adherence to National Comprehensive Cancer Network® guidelines for testicular cancer. J Urol. 2017;197(3 pt 1):684-689. doi:10.1016/j.juro.2016.09.073
Saoud RM, Andolfi C, Aizen J, et al. Impact of non-guideline-directed care on quality of life in testicular cancer survivors. Eur Urol Focus. 2021;7(5):1137-1142. doi:10.1016/j.euf.2020.10.005
Guo CC, Czerniak B. Somatic-type malignancies in testicular germ cell tumors. Hum Pathol. 2022;127:123-135.
Sprauten M, Darrah TH, Peterson DR, et al. Impact of long-term serum platinum concentrations on neuro- and ototoxicity in cisplatin-treated survivors of testicular cancer. J Clin Oncol. 2012;30(3):300-307. doi:10.1200/JCO.2011.37.4025
Shrem NS, Wood L, Hamilton RJ, et al. Testicular cancer survivorship: long-term toxicity and management. Can Urol Assoc J. 2022;16(8):257-272. doi:10.5489/cuaj.8009
Hellesnes R, Myklebust TA, Fosså SD, et al. Testicular cancer in the cisplatin era: causes of death and mortality rates in a population-based cohort. J Clin Oncol. 2021;39(32):3561-3573. doi:10.1200/JCO.21.00637
Mercieca-Bebber R, Naher SK, Rincones O, Smith AB, Stockler MR. Patient-reported outcomes associated with treatments for testicular cancer: a systematic review. Patient Relat Outcome Meas. 2021;12:129-171. doi:10.2147/PROM.S242754
Sprauten M, Haugnes HS, Brydøy M, et al. Chronic fatigue in 812 testicular cancer survivors during long-term follow-up: increasing prevalence and risk factors. Ann Oncol. 2015;26(10):2133-2140. doi:10.1093/annonc/mdv328
King J, Adra N, Einhorn LH. Testicular cancer: biology to bedside. Cancer Res. 2021;81(21):5369-5376. doi:10.1158/0008-5472.CAN-21-1452
Hiester A, Che Y, Lusch A, et al. Phase 2 single-arm trial of primary retroperitoneal lymph node dissection in patients with seminomatous testicular germ cell tumors with clinical stage IIA/B (PRIMETEST). Eur Urol. 2022;S0302-2838(22)02775-0. doi:10.1016/j.eururo.2022.10.021
Daneshmand S, Cary C, Masterson TA, et al. SEMS trial: result of a prospective, multi-institutional phase II clinical trial of surgery in early metastatic seminoma. J Clin Oncol. 2021;39(6 suppl):Abstract 375. doi:10.1200JCO.2021.39.6_suppl.375
Papachristofilou A, Bedke J, Hayoz S, et al. Single-dose carboplatin followed by involved-node radiotherapy for stage IIA and stage IIB seminoma (SAKK 01/10): a single-arm, multicentre, phase 2 trial. Lancet Oncol. 2022;23(11):1441-1450. doi:10.1016/S1470-2045(22)00564-2
Dieckmann KP, Richter-Simonsen H, Kulejewski M, et al. Testicular germ-cell tumours: a descriptive analysis of clinical characteristics at first presentation. Urol Int. 2018;100(4):409-419. doi:10.1159/000488284
Murray MJ, Huddart RA, Coleman N. The present and future of serum diagnostic tests for testicular germ cell tumours. Nat Rev Urol. 2016;13(12):715-725. doi:10.1038/nrurol.2016.170
References
Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17-48. doi:10.3322/caac.21763
Chovanec M, Cheng L. Advances in diagnosis and treatment of testicular cancer. BMJ. 2022;379:e070499. doi:10.1136/bmj-2022-070499
Gaddam SJ, Chesnut GT. Testicle cancer. StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2022. Updated October 16, 2022. Accessed March 13, 2023. https://www.ncbi.nlm.nih.gov/books/NBK563159/
Yang H, Obiora D, Tomaszewski JJ. Outcomes and expanding indications for robotic retroperitoneal lymph node dissection for testicular cancer. Transl Androl Urol. 2021;10(5):2188-2194. doi:10.21037/tau.2020.03.14
International Germ Cell Cancer Collaborative Group. International germ cell consensus classification: a prognostic factor-based staging system for metastatic germ cell cancers. J Clin Oncol. 1997;15(2):594-603. doi:10.1200/JCO.1997.15.2.594
Beyer J, Collette L, Sauvé N, et al. Survival and new prognosticators in metastatic seminoma: results from the IGCCCG-Update Consortium. J Clin Oncol. 2021;39(14):1553-1562. doi:10.1200/JCO.20.03292
Gillessen S, Sauvé N, Collette L, et al. Predicting outcomes in men with metastatic nonseminomatous germ cell tumors (NSGCT): results from the IGCCCG Update Consortium. J Clin Oncol. 2021;39(14):1563-1574. doi:10.1200/JCO.20.03296
Gilligan T, Lin DW, Aggarwal R, et al. Testicular cancer, version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2019;17(12):1529-1554. doi:10.6004/jnccn.2019.0058
Heinzelbecker J, Schmidt S, Lackner J, et al. Therapy of clinical stage IIa and IIb seminoma: a systematic review. World J Urol. 2022;40(12):2829-2841. doi:10.1007/s00345-021-03873-5
Oldenburg J, Berney DM, Bokemeyer C, et al. Testicular seminoma and nonseminoma: ESMA-EURACAN Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022;33(4):362-375. doi:10.1016/j.annonc.2022.01.002
Wymer KM, Pearce SM, Harris KT, Pierorazio PM, Daneshmand S, Eggener SE. Adherence to National Comprehensive Cancer Network® guidelines for testicular cancer. J Urol. 2017;197(3 pt 1):684-689. doi:10.1016/j.juro.2016.09.073
Saoud RM, Andolfi C, Aizen J, et al. Impact of non-guideline-directed care on quality of life in testicular cancer survivors. Eur Urol Focus. 2021;7(5):1137-1142. doi:10.1016/j.euf.2020.10.005
Guo CC, Czerniak B. Somatic-type malignancies in testicular germ cell tumors. Hum Pathol. 2022;127:123-135.
Sprauten M, Darrah TH, Peterson DR, et al. Impact of long-term serum platinum concentrations on neuro- and ototoxicity in cisplatin-treated survivors of testicular cancer. J Clin Oncol. 2012;30(3):300-307. doi:10.1200/JCO.2011.37.4025
Shrem NS, Wood L, Hamilton RJ, et al. Testicular cancer survivorship: long-term toxicity and management. Can Urol Assoc J. 2022;16(8):257-272. doi:10.5489/cuaj.8009
Hellesnes R, Myklebust TA, Fosså SD, et al. Testicular cancer in the cisplatin era: causes of death and mortality rates in a population-based cohort. J Clin Oncol. 2021;39(32):3561-3573. doi:10.1200/JCO.21.00637
Mercieca-Bebber R, Naher SK, Rincones O, Smith AB, Stockler MR. Patient-reported outcomes associated with treatments for testicular cancer: a systematic review. Patient Relat Outcome Meas. 2021;12:129-171. doi:10.2147/PROM.S242754
Sprauten M, Haugnes HS, Brydøy M, et al. Chronic fatigue in 812 testicular cancer survivors during long-term follow-up: increasing prevalence and risk factors. Ann Oncol. 2015;26(10):2133-2140. doi:10.1093/annonc/mdv328
King J, Adra N, Einhorn LH. Testicular cancer: biology to bedside. Cancer Res. 2021;81(21):5369-5376. doi:10.1158/0008-5472.CAN-21-1452
Hiester A, Che Y, Lusch A, et al. Phase 2 single-arm trial of primary retroperitoneal lymph node dissection in patients with seminomatous testicular germ cell tumors with clinical stage IIA/B (PRIMETEST). Eur Urol. 2022;S0302-2838(22)02775-0. doi:10.1016/j.eururo.2022.10.021
Daneshmand S, Cary C, Masterson TA, et al. SEMS trial: result of a prospective, multi-institutional phase II clinical trial of surgery in early metastatic seminoma. J Clin Oncol. 2021;39(6 suppl):Abstract 375. doi:10.1200JCO.2021.39.6_suppl.375
Papachristofilou A, Bedke J, Hayoz S, et al. Single-dose carboplatin followed by involved-node radiotherapy for stage IIA and stage IIB seminoma (SAKK 01/10): a single-arm, multicentre, phase 2 trial. Lancet Oncol. 2022;23(11):1441-1450. doi:10.1016/S1470-2045(22)00564-2
Dieckmann KP, Richter-Simonsen H, Kulejewski M, et al. Testicular germ-cell tumours: a descriptive analysis of clinical characteristics at first presentation. Urol Int. 2018;100(4):409-419. doi:10.1159/000488284
Murray MJ, Huddart RA, Coleman N. The present and future of serum diagnostic tests for testicular germ cell tumours. Nat Rev Urol. 2016;13(12):715-725. doi:10.1038/nrurol.2016.170
Jason K. Sicklick, MD, FACS
Gastrointestinal stromal tumor (GIST) was recognized as a distinct tumor type in the late 1990s.1 Advances in treatment have expanded since the 2001 US Food and Drug Administration (FDA) approval of imatinib, the first tyrosine kinase inhibitor (TKI).2 In 2023, there are now 5 FDA-approved agents for GIST, and 4 additional agents have been approved (tumor agnostic) for patients whose cancer harbors specific genomic alterations (neurotrophic tyrosine receptor kinase [NTRK] fusions3,4 or BRAF V600E mutations5). According to the National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology, several other drugs (ie, in addition to those specifically approved for GIST) are listed as “useful in certain circumstances.”6
Since the early 2000s, new discoveries about GIST genomics have contributed to better, more targeted treatments. Some genomic mutations have been linked to specific gut regions,7 which may further help guide therapy as well.
GIST: What Is It, Who Gets It, and How Is It Diagnosed?
What, How Many, Where?
Even though GIST is considered rare—representing less than 1% of gastrointestinal tumors8—it is the most common sarcoma, which is a family of mesenchymal neoplasms. GISTs are thought to arise from the interstitial cells of Cajal, or the pacemaker cells of the gut that control peristalsis. In the United States, the incidence of GIST is roughly 4,000 to 6,000 new cases diagnosed per year, with most cases found in the stomach (60%) or small intestine (35%). Other gut regions in which GISTs may be identified include the rectum and esophagus.8
Although asymptomatic tumors are often discovered incidentally, GISTs that originate in the stomach—the most common primary tumor site—may present with nonspecific subjective symptoms such as pain, nausea, loss of appetite, early satiety, or bloating.9 Symptoms may vary according to tumor location (eg, stomach vs rectum vs esophagus), size, and pattern of growth. More objective signs could include anemia related to gastrointestinal bleeding, weight loss, or a palpable mass.9
Who?
Most cases of GIST occur in patients later in life, with a median age of 64 years at diagnosis. A slight predominance of men has been noted, along with African American and Asian individuals affected somewhat more frequently than White or Hispanic populations.10 GIST is rare in children and adolescents, and the symptoms and pathology differ from those in most adults.9 Previously age was considered a determining factor in the differences in GIST, with cases in children classified as “pediatric-type” GIST or “wild-type” GIST. These cases generally present in the stomach, are more likely to include lymph node involvement, and can also spread to the liver and abdominal lining. Importantly, they are usually not associated with the tyrosine-protein kinase (KIT) or platelet-derived growth factor receptor alpha (PDGFRA) gene mutations found in most adults.9 About 80% of these cases have hereditary mutations of the succinate dehydrogenase (SDH) enzyme complex. Because some adult cases of GIST share the distinct characteristics found in most pediatric cases, distinguishing them based on age, rather than on the specific genetic characteristics of the tumor, is unwarranted.9
How?
When GIST is suspected or when symptoms mandate further investigation, coordination among colleagues in imaging, gastroenterology, pathology, surgery, and oncology is critical for accurate diagnosis, staging, and treatment. Abdominal imaging may be ordered using modalities such as ultrasound, computed tomography, magnetic resonance imaging, and, occasionally, positron emission tomography.11 Endoscopic ultrasound is useful to identify and biopsy lesions in the stomach or rectum, as these tumors arise below the lining of the stomach or rectum. GIST diagnosis can be confirmed by biopsy during endoscopic ultrasound, which is the preferred approach, or by percutaneous biopsy when endoscopic biopsy is not feasible or safe.11
According to the European Society for Medical Oncology (ESMO) and European Reference Group for Rare Adult Solid Cancers (EURACAN) Clinical Practice Guidelines, the “standard approach to tumors ≥ 2 cm in size is excision, because they are associated with a higher risk of progression if confirmed as GIST. If there is an abdominal nodule not amenable to endoscopic assessment, laparoscopic or laparotomic excision is the standard approach.”11
Genetic Mutations
A diagnosis of GIST is made based on the combination of the clinical scenario, the tumor’s anatomic location, immunohistochemistry patterns, and molecular features.12 Research has shown that genetic mutations in the KIT, PDGFRA, or SDH genes are present in most cases of GIST (70-80%,13 10%,12 and less than 10% of cases12,14 respectively) and their presence can be used for diagnosis. A growing number of rarer mutations have also been discovered,13 meaning that gene-based diagnosis of GIST is becoming increasingly sensitive. In addition, antigens on the surface of cancer cells can help classify them as GIST. For example, researchers have discovered that most GIST cells have the marker CD117, the protein product of the KIT gene that is commonly mutated in GIST, on their surfaces. A different marker, DOG1 (ie, Discovered On GIST 1), is also present on the vast majority of GISTs, but not unanimously overlapping with CD117. A tumor that is positive for both CD117 and DOG1 has a high probability (> 97%) of being GIST.15
Next-generation sequencing (NGS) is considered the best tool for determining both germline and somatic mutations in patients with GIST, and NGS is recommended by both the NCCN6 and the ESMO11 for individualizing systemic therapy. Despite these recommendations, most patients do not undergo genetic testing, both in the United States16 and internationally.17 Several barriers to genetic testing have been cited, predominately inadequate tissue and high cost. However, a study demonstrated that costs of up to $3,730 for genetic testing were ultimately cost-effective for tailoring therapy with first-line imatinib for patients with newly diagnosed metastatic GIST.18 Moreover, genetic testing also should be strongly considered for patients with nonmetastatic disease in whom systemic therapy is being considered.
Increasing evidence has emerged that gastric GIST mutations are related to tumor location within the gastrointestinal tract (Figure).7 The anatomic location of the GIST may provide clues for clinical decision-making and may guide selective confirmatory genomic testing when access to testing is limited.
Proximal gastric GISTs are overwhelmingly KIT exon 11 mutant, whereas distal stomach tumors display non-KIT genomic diversity (PDGFRA, as well as germline [or inherited] SDHx mutant and SDHC epimutations). In contrast, tumors that arise in the small intestine (eg, duodenum, jejunum, and ileum) are associated with gene fusions and germline NF1, as well as mutations in KIT exons 11 and 9. Colon and rectal tumors are likely to be KIT-related, whereas those found in the duodenal-jejunal flexure (also called the ligament of Treitz) correlate with rarer mutations, such as BRAF V600E and somatic (nonhereditary NF1) in addition to germline NF, as well as KIT.
Treatment of GIST
Surgery
Surgery remains the main treatment for localized GIST, especially if the tumor is discovered at an early stage. Unfortunately, up to a quarter of patients present with metastatic disease at diagnosis. The goal of surgery is to resect the tumor with histologically negative margins. Every effort should be made to avoid rupturing the tumor capsule during resection. Studies have shown that laparoscopic resection is feasible and safe for gastric GISTs and is less invasive than traditional open surgery, with similar oncological outcomes.19
Debulking surgery is sometimes considered for patients with metastatic disease, especially for patients who demonstrate sensitivity to TKI and whose disease has not yet progressed.20,21 Other interventions, such as microwave ablation or transhepatic arterial embolization, are sometimes used to control hepatic metastases.
Systemic Therapies
Whether systemic therapy is being considered in the neoadjuvant (preoperative), adjuvant (postoperative), or advanced disease setting, mutations in GIST determine the likelihood of treatment success. Both NCCN6 and ESMO11 strongly encourage use of mutational analyses and genetic testing for patients with GIST before systemic therapy is initiated.
In some cases of locally advanced GIST, tumors may be situated in particularly challenging anatomic locations(eg, esophagus, duodenum, rectum) or may require a highly morbid, multivisceral resection. In such situations, neoadjuvant treatment with imatinib,22,23 if deemed appropriate per mutational profiling, should be considered.
Patients who are determined to be at high risk for recurrence after surgery, based on tumor size, mitotic index determined by pathologist review of dividing cells, tumor location, and tumor rupture, may be eligible for adjuvant treatment with imatinib.24 Although the ideal duration of adjuvant therapy is not yet known, the current standard is at least 3 years,25 but many practitioners advocate for lifelong therapy.
Imatinib.Because chemotherapy was ineffective against GIST, prognosis was dismal for patients diagnosed with advanced disease before the approval of imatinib in the early 2000s.2 A selective TKI, imatinib targets the KIT and PDGFRA receptor kinases, and most patients experience clinical benefit,26 at least initially. Unfortunately, many tumors eventually develop resistance, and discontinuation of imatinib is associated with a risk for disease progression.27
Sunitinib. The emergence of resistance to imatinib spurred the search for second-line agents that might be useful after disease progression. Another TKI, sunitinib, which has both antitumor and antiangiogenic activity, was approved in 2006 for management of advanced imatinib-resistant GIST.28 Knowledge of a tumor’s driver mutation(s) can help optimize use of sunitinib.29
Regorafenib. In 2013, the FDA approved regorafenib, another TKI, as a third-line agent for patients with advanced GIST that is refractory to imatinib and sunitinib.30 Regorafenib exerts its activity against multiple targets, including VEGFR1-3, TIE2 (ie, antiangiogenic activity), PDGFR-β, FGFR (ie, stromal targets), and KIT, RET, and RAF (ie, oncogenic targets). As with other TKIs, common adverse effects associated with regorafenib treatment include hypertension, hand-foot skin reaction, rash, diarrhea, and fatigue.
Larotrectinib/entrectinib. The FDA approved larotrectinib31 (2018) and entrectinib32 (2019) as the first tumor-agnostic agents, whose use is based on the presence of specific genomic alteration, in this case NTRK. If a tumor, including a GIST, harbors a specific, albeit rare, gene fusion, it may be considered for treatment with one of these small-molecule TRK family inhibitors. Although these agents are not specifically indicated for GIST, some subjects enrolled in the trials had GIST harboring the target NTRK gene fusion and their tumors responded to treatment.
Ripretinib. FDA-approved in 2020,33 ripretinib is a novel TKI indicated for adult patients with advanced GIST who have received prior treatment with 3 or more kinase inhibitors, including imatinib. A phase 3 trial demonstrated improved progression-free and overall survival when ripretinib was compared with placebo in patients who had disease progression after treatment with imatinib, sunitinib, or regorafenib.34 Ripretinib is now being investigated in the second-line setting in selected patients with KIT mutations.
Avapritinib. Cases of GIST with PDGFRA D842V-mutant tumors often demonstrate primary resistance to imatinib and sunitinib. In 2020, avapritinib, a selective TKI that targets both KIT and PDGFRA, was approved35 for treatment of patients with unresectable or metastatic GIST harboring a PDGFRA exon 18 mutation, including D842V mutations. However, it is noteworthy that many of the non-D842V mutations in PDGFRA respond to imatinib.
Dabrafenib/trametinib. In 2022, the FDA issued an approval for treatment based on a driver mutation rather than tumor type. Acknowledging that a BRAF mutation—specifically a V600E mutation—appears to be a critical target in several cancers, the FDA granted accelerated approval for the use of dabrafenib plus trametinib in adults and children 6 years of age and older with unresectable or metastatic solid tumors with BRAF V600E mutation who have progressed following prior treatment and have no satisfactory alternative treatment options.36
Researchers have studied additional TKIs in the setting of unresectable, metastatic disease due to the varied genomic landscape of GIST. The NCCN Guidelines include evidence of some benefit for agents such as dasatinib, cabozantinib, everolimus (plus a TKI), nilotinib, pazopanib, and sorafenib “in certain circumstances.”6
The Future of GIST
The most critical step toward optimal treatment decision-making when a patient has been diagnosed with GIST is identification of physicians with expertise in the care of patients with GIST. With increasing knowledge of genomic variations in GIST, patient care has become less prescripted and much more personalized. To that end, determination of the tumor’s genetic mutational profile is critical to guiding treatment. Although factors such as cost, availability/accessibility, and insufficient tissue continue to represent substantial obstacles, pursing this information may be the most important way that clinicians can advocate for their patients. Moreover, now that the anatomic location of GIST has been linked to specific driver mutations, the ability to select and refine treatments may improve significantly.
Likewise, in view of the increasing complexity and multidisciplinary management of patients with GIST, efficient coordination is paramount among surgical and medical oncologists, as well as radiologists, gastroenterologists, and pathologists.
Miettinen M, Virolainen M, Maarit-Sarlomo-Rikala. Gastrointestinal stromal tumors—value of CD34 antigen in their identification and separation from true leiomyomas and schwannomas. Am J Surg Pathol. 1995;19(2):207-216. doi:10.1097/00000478-199502000-00009
Dagher R, Cohen M, Williams G, et al. Approval summary: imatinib mesylate in the treatment of metastatic and/or unresectable malignant gastrointestinal stromal tumors. Clin Cancer Res. 2002;8(10):3034-3038. PMID:12374669
Sharma AK, de la Torre J, IJzerman NS, et al. Location of gastrointestinal stromal tumor (GIST) in the stomach predicts tumor mutation profile and drug sensitivity. Clin Cancer Res. 2021;27(19):5334-5342. doi:10.1158/1078-0432.CCR-21-1221
Ma GL, Murphy JD, Martinez ME, Sicklick JK. Epidemiology of gastrointestinal stromal tumors in the era of histology codes: results of a population-based study. Cancer Epidemiol Biomarkers Prev. 2014;24(1):298-302. doi:10.1158/1055-9965.EPI-14-1002
Casali PG, Abecassis N, Aro HT, et al. Gastrointestinal stromal tumours: ESMOEURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29(suppl 4):iv68-iv78. doi:10.1093/annonc/mdy095
Kelly CM, Sainz LG, Chi P. The management of metastatic GIST: current standard and investigational therapeutics. J Hematol Oncol. 2021;14(1):2. doi:10.1186/s13045-020-01026-6
Shi E, Chmielecki J, Tang CM, et al. FGR1 and NTRK3 actionable alterations in “wild-type” gastrointestinal stromal tumors. J Translat Med. 2016;14(1):339. doi:10.1186/s12967-016-1075-6
Bannon AE, Klug LR, Corless CL, Heinrich MC. Using molecular diagnostic testing to personalize the treatment of patients with gastrointestinal stromal tumors. Expert Rev Mol Diagn. 2017;17(5):445-457. doi:10.1080/14737159.2017.1308826
Wu CE, Tzen CY, Wang SY, Yeh CN. Clinical diagnosis of gastrointestinal stromal tumor (GIST): from the molecular genetic point of view. Cancers (Basel). 2019;11(5):679. doi:10.3390/cancers11050679
Florindez J, Trent J. Low frequency of mutation testing in the United States: an analysis of 3866 GIST patients. Am J Clin Oncol. 2020;43(4):270-278. doi:10.1097/COC.0000000000000659
Verschoor AJ, Bovée JVMG, Overbeek LIH, PALGA group; Hogendoorn PCW, Gelderblom H. The incidence, mutational status, risk classification and referral pattern of gastrointestinal stromal tumours in the Netherlands: a nationwide pathology registry (PALGA) study. Virchows Arch. 2018;472(2):221-229. doi:10.1007/s00428-017-2285-x
Banerjee S, Kumar A, Lopez N, et al. Cost-effectiveness analysis of genetic testing and tailored first-line therapy for patients with metastatic gastrointestinal stromal tumors. JAMA Netw Open. 2020;3(9):e2013565. doi:10.1001/jamanetworkopen.2020.1356519
Chen K, Zhou YC, Mou YP, Xu XW, Jin WW, Ajoodhea H. Systematic review and meta-analysis of safety and efficacy of laparoscopic resection of gastrointestinal stromal tumors of the stomach. Surg Endosc. 2015;29:355-367. doi:10.1007/s00464-014-3676-6
Fairweather M, Balachandran VP, Li GZ, et al. Cytoreductive surgery for metastatic gastrointestinal stromal tumors treated with tyrosine kinase inhibitors: a 2-institutional analysis. Ann Surg. 2018;268(2):296-302. doi:10.1097/SLA.0000000000002281
Bauer S, Rutkowski P, Hohenberger P, et al. Long-term follow-up of patients with GIST undergoing metastasectomy in the era of imatinib—analysis of prognostic factors (EORTC-STBSG collaborative study). Eur J Surg Oncol. 2014;40(4):412-419. doi:10.1016/j.ejso.2013.12.020
Rutkowski P, Gronchi A, Hohenberger P, et al. Neoadjuvant imatinib in locally advanced gastrointestinal stromal tumors (GIST): the EORTC STBSG experience. Ann Surg Oncol. 2013;20(9):2937-2943. doi:10.1245/s10434-013-3013-7
Cavnar MJ, Seier K, Gönen M, et al. Prognostic factors after neoadjuvant imatinib for newly diagnosed primary gastrointestinal stromal tumor. J Gastrointest Surg. 2021;25(7):1828-1836. doi:10.1007/s11605-020-04843-9
Joensuu H. Risk stratification of patients diagnosed with gastrointestinal stromal tumor. Hum Pathol. 2008;39(10):1411-1419. doi:10.1016/j.humpath.2008.06.025
Joensuu H, Eriksson M, Sundby Hall K, et al. Survival outcomes associated with 3 years vs 1 year of adjuvant imatinib for patients with high-risk gastrointestinal stromal tumors: an analysis of a randomized clinical trial after 10-year follow-up. JAMA Oncol. 2020;6(8):1241-1246. doi:10.1001/jamaoncol.2020.2091
Heinrich MC, Rankin C, Blanke CD, et al. Correlation of long-term results of imatinib in advanced gastrointestinal stromal tumors with next-generation sequencing results: analysis of phase 3 SWOG Intergroup Trial S0033. JAMA Oncol. 2017;3(7):944-952. doi:10.1001/jamaoncol.2016.6728
Le Cesne A, Ray-Coquard I, Bui BN, et al. Discontinuation of imatinib in patients with advanced gastrointestinal stromal tumours after 3 years of treatment: an open-label multicentre randomised phase 3 trial. Lancet Oncol. 2020;11(10):942-949. doi:10.1016/S1470-2045(10)70222-9
Demetri GD, van Oosterom AT, Garrett CR, et al. Efficacy and safety of sunitinib in patients with advanced gastrointestinal stromal tumour after failure of imatinib: a randomised controlled trial. Lancet. 2006;368(9544):1329-1338. doi:10.1016/S0140-6736(06)69446-4
Heinrich MC, Maki RG, Corless CL, et al. Primary and secondary kinase genotypes correlate with the biological and clinical activity of sunitinib in imatinib-resistant gastrointestinal stromal tumor. J Clin Oncol. 2008;26(33):5352-5359. doi:10.1200/JCO.2007.15.7461
Crona DJ, Keisler MD, Walko CM. Regorafenib: a novel multitargeted tyrosine kinase inhibitor for colorectal and gastrointestinal stromal tumors. Ann Pharmacother. 2013;47(12):1685-1696. doi:10.1177/1060028013509792
Drilon A, Laetsch TW, Kummar S, et al. Efficacy of larotrectinib in TRK fusion-positive cancers in adults and children. N Engl J Med. 2018;378(8):731-739. doi:10.1056/NEJMoa1714448
Doebele RC, Drilon A, Paz-Ares L, et al. Entrectinib in patients with advanced or metastatic NTRK fusion-positive solid tumours: integrated analysis of three phase 1-2 trials. Lancet Oncol. 2020;21(2):271-282. doi:10.1016/S1470-2045(19)30691-6
Jason K. Sicklick, MD, FACS Professor of Surgery, Division of Surgical Oncology Adjunct Professor, Department of Pharmacology, UC San Diego School of Medicine Executive Vice Chair of Research, Department of Surgery Associate Program Director, General Surgery Residency Program Leader, Sarcoma Disease Team, Moores Cancer Center, UC San Diego Health Co-Leader, Structural and Functional Genomics Program, Moores Cancer Center La Jolla, CA
Jason K. Sicklick, MD, has disclosed the following relevant financial relationships:
Receives consultant fees from Deciphera; Aadi and Ground Rounds
Serves as a consultant for CureMatch
Received speakers fees from Deciphera; La-Hoffman Roche; Foundation Medicine; Merck; QED; Daiichi Sankyo
Jason K. Sicklick, MD, FACS Professor of Surgery, Division of Surgical Oncology Adjunct Professor, Department of Pharmacology, UC San Diego School of Medicine Executive Vice Chair of Research, Department of Surgery Associate Program Director, General Surgery Residency Program Leader, Sarcoma Disease Team, Moores Cancer Center, UC San Diego Health Co-Leader, Structural and Functional Genomics Program, Moores Cancer Center La Jolla, CA
Jason K. Sicklick, MD, has disclosed the following relevant financial relationships:
Receives consultant fees from Deciphera; Aadi and Ground Rounds
Serves as a consultant for CureMatch
Received speakers fees from Deciphera; La-Hoffman Roche; Foundation Medicine; Merck; QED; Daiichi Sankyo
Owns stock in Personalis
Author and Disclosure Information
Jason K. Sicklick, MD, FACS Professor of Surgery, Division of Surgical Oncology Adjunct Professor, Department of Pharmacology, UC San Diego School of Medicine Executive Vice Chair of Research, Department of Surgery Associate Program Director, General Surgery Residency Program Leader, Sarcoma Disease Team, Moores Cancer Center, UC San Diego Health Co-Leader, Structural and Functional Genomics Program, Moores Cancer Center La Jolla, CA
Jason K. Sicklick, MD, has disclosed the following relevant financial relationships:
Receives consultant fees from Deciphera; Aadi and Ground Rounds
Serves as a consultant for CureMatch
Received speakers fees from Deciphera; La-Hoffman Roche; Foundation Medicine; Merck; QED; Daiichi Sankyo
Owns stock in Personalis
Jason K. Sicklick, MD, FACS
Gastrointestinal stromal tumor (GIST) was recognized as a distinct tumor type in the late 1990s.1 Advances in treatment have expanded since the 2001 US Food and Drug Administration (FDA) approval of imatinib, the first tyrosine kinase inhibitor (TKI).2 In 2023, there are now 5 FDA-approved agents for GIST, and 4 additional agents have been approved (tumor agnostic) for patients whose cancer harbors specific genomic alterations (neurotrophic tyrosine receptor kinase [NTRK] fusions3,4 or BRAF V600E mutations5). According to the National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology, several other drugs (ie, in addition to those specifically approved for GIST) are listed as “useful in certain circumstances.”6
Since the early 2000s, new discoveries about GIST genomics have contributed to better, more targeted treatments. Some genomic mutations have been linked to specific gut regions,7 which may further help guide therapy as well.
GIST: What Is It, Who Gets It, and How Is It Diagnosed?
What, How Many, Where?
Even though GIST is considered rare—representing less than 1% of gastrointestinal tumors8—it is the most common sarcoma, which is a family of mesenchymal neoplasms. GISTs are thought to arise from the interstitial cells of Cajal, or the pacemaker cells of the gut that control peristalsis. In the United States, the incidence of GIST is roughly 4,000 to 6,000 new cases diagnosed per year, with most cases found in the stomach (60%) or small intestine (35%). Other gut regions in which GISTs may be identified include the rectum and esophagus.8
Although asymptomatic tumors are often discovered incidentally, GISTs that originate in the stomach—the most common primary tumor site—may present with nonspecific subjective symptoms such as pain, nausea, loss of appetite, early satiety, or bloating.9 Symptoms may vary according to tumor location (eg, stomach vs rectum vs esophagus), size, and pattern of growth. More objective signs could include anemia related to gastrointestinal bleeding, weight loss, or a palpable mass.9
Who?
Most cases of GIST occur in patients later in life, with a median age of 64 years at diagnosis. A slight predominance of men has been noted, along with African American and Asian individuals affected somewhat more frequently than White or Hispanic populations.10 GIST is rare in children and adolescents, and the symptoms and pathology differ from those in most adults.9 Previously age was considered a determining factor in the differences in GIST, with cases in children classified as “pediatric-type” GIST or “wild-type” GIST. These cases generally present in the stomach, are more likely to include lymph node involvement, and can also spread to the liver and abdominal lining. Importantly, they are usually not associated with the tyrosine-protein kinase (KIT) or platelet-derived growth factor receptor alpha (PDGFRA) gene mutations found in most adults.9 About 80% of these cases have hereditary mutations of the succinate dehydrogenase (SDH) enzyme complex. Because some adult cases of GIST share the distinct characteristics found in most pediatric cases, distinguishing them based on age, rather than on the specific genetic characteristics of the tumor, is unwarranted.9
How?
When GIST is suspected or when symptoms mandate further investigation, coordination among colleagues in imaging, gastroenterology, pathology, surgery, and oncology is critical for accurate diagnosis, staging, and treatment. Abdominal imaging may be ordered using modalities such as ultrasound, computed tomography, magnetic resonance imaging, and, occasionally, positron emission tomography.11 Endoscopic ultrasound is useful to identify and biopsy lesions in the stomach or rectum, as these tumors arise below the lining of the stomach or rectum. GIST diagnosis can be confirmed by biopsy during endoscopic ultrasound, which is the preferred approach, or by percutaneous biopsy when endoscopic biopsy is not feasible or safe.11
According to the European Society for Medical Oncology (ESMO) and European Reference Group for Rare Adult Solid Cancers (EURACAN) Clinical Practice Guidelines, the “standard approach to tumors ≥ 2 cm in size is excision, because they are associated with a higher risk of progression if confirmed as GIST. If there is an abdominal nodule not amenable to endoscopic assessment, laparoscopic or laparotomic excision is the standard approach.”11
Genetic Mutations
A diagnosis of GIST is made based on the combination of the clinical scenario, the tumor’s anatomic location, immunohistochemistry patterns, and molecular features.12 Research has shown that genetic mutations in the KIT, PDGFRA, or SDH genes are present in most cases of GIST (70-80%,13 10%,12 and less than 10% of cases12,14 respectively) and their presence can be used for diagnosis. A growing number of rarer mutations have also been discovered,13 meaning that gene-based diagnosis of GIST is becoming increasingly sensitive. In addition, antigens on the surface of cancer cells can help classify them as GIST. For example, researchers have discovered that most GIST cells have the marker CD117, the protein product of the KIT gene that is commonly mutated in GIST, on their surfaces. A different marker, DOG1 (ie, Discovered On GIST 1), is also present on the vast majority of GISTs, but not unanimously overlapping with CD117. A tumor that is positive for both CD117 and DOG1 has a high probability (> 97%) of being GIST.15
Next-generation sequencing (NGS) is considered the best tool for determining both germline and somatic mutations in patients with GIST, and NGS is recommended by both the NCCN6 and the ESMO11 for individualizing systemic therapy. Despite these recommendations, most patients do not undergo genetic testing, both in the United States16 and internationally.17 Several barriers to genetic testing have been cited, predominately inadequate tissue and high cost. However, a study demonstrated that costs of up to $3,730 for genetic testing were ultimately cost-effective for tailoring therapy with first-line imatinib for patients with newly diagnosed metastatic GIST.18 Moreover, genetic testing also should be strongly considered for patients with nonmetastatic disease in whom systemic therapy is being considered.
Increasing evidence has emerged that gastric GIST mutations are related to tumor location within the gastrointestinal tract (Figure).7 The anatomic location of the GIST may provide clues for clinical decision-making and may guide selective confirmatory genomic testing when access to testing is limited.
Proximal gastric GISTs are overwhelmingly KIT exon 11 mutant, whereas distal stomach tumors display non-KIT genomic diversity (PDGFRA, as well as germline [or inherited] SDHx mutant and SDHC epimutations). In contrast, tumors that arise in the small intestine (eg, duodenum, jejunum, and ileum) are associated with gene fusions and germline NF1, as well as mutations in KIT exons 11 and 9. Colon and rectal tumors are likely to be KIT-related, whereas those found in the duodenal-jejunal flexure (also called the ligament of Treitz) correlate with rarer mutations, such as BRAF V600E and somatic (nonhereditary NF1) in addition to germline NF, as well as KIT.
Treatment of GIST
Surgery
Surgery remains the main treatment for localized GIST, especially if the tumor is discovered at an early stage. Unfortunately, up to a quarter of patients present with metastatic disease at diagnosis. The goal of surgery is to resect the tumor with histologically negative margins. Every effort should be made to avoid rupturing the tumor capsule during resection. Studies have shown that laparoscopic resection is feasible and safe for gastric GISTs and is less invasive than traditional open surgery, with similar oncological outcomes.19
Debulking surgery is sometimes considered for patients with metastatic disease, especially for patients who demonstrate sensitivity to TKI and whose disease has not yet progressed.20,21 Other interventions, such as microwave ablation or transhepatic arterial embolization, are sometimes used to control hepatic metastases.
Systemic Therapies
Whether systemic therapy is being considered in the neoadjuvant (preoperative), adjuvant (postoperative), or advanced disease setting, mutations in GIST determine the likelihood of treatment success. Both NCCN6 and ESMO11 strongly encourage use of mutational analyses and genetic testing for patients with GIST before systemic therapy is initiated.
In some cases of locally advanced GIST, tumors may be situated in particularly challenging anatomic locations(eg, esophagus, duodenum, rectum) or may require a highly morbid, multivisceral resection. In such situations, neoadjuvant treatment with imatinib,22,23 if deemed appropriate per mutational profiling, should be considered.
Patients who are determined to be at high risk for recurrence after surgery, based on tumor size, mitotic index determined by pathologist review of dividing cells, tumor location, and tumor rupture, may be eligible for adjuvant treatment with imatinib.24 Although the ideal duration of adjuvant therapy is not yet known, the current standard is at least 3 years,25 but many practitioners advocate for lifelong therapy.
Imatinib.Because chemotherapy was ineffective against GIST, prognosis was dismal for patients diagnosed with advanced disease before the approval of imatinib in the early 2000s.2 A selective TKI, imatinib targets the KIT and PDGFRA receptor kinases, and most patients experience clinical benefit,26 at least initially. Unfortunately, many tumors eventually develop resistance, and discontinuation of imatinib is associated with a risk for disease progression.27
Sunitinib. The emergence of resistance to imatinib spurred the search for second-line agents that might be useful after disease progression. Another TKI, sunitinib, which has both antitumor and antiangiogenic activity, was approved in 2006 for management of advanced imatinib-resistant GIST.28 Knowledge of a tumor’s driver mutation(s) can help optimize use of sunitinib.29
Regorafenib. In 2013, the FDA approved regorafenib, another TKI, as a third-line agent for patients with advanced GIST that is refractory to imatinib and sunitinib.30 Regorafenib exerts its activity against multiple targets, including VEGFR1-3, TIE2 (ie, antiangiogenic activity), PDGFR-β, FGFR (ie, stromal targets), and KIT, RET, and RAF (ie, oncogenic targets). As with other TKIs, common adverse effects associated with regorafenib treatment include hypertension, hand-foot skin reaction, rash, diarrhea, and fatigue.
Larotrectinib/entrectinib. The FDA approved larotrectinib31 (2018) and entrectinib32 (2019) as the first tumor-agnostic agents, whose use is based on the presence of specific genomic alteration, in this case NTRK. If a tumor, including a GIST, harbors a specific, albeit rare, gene fusion, it may be considered for treatment with one of these small-molecule TRK family inhibitors. Although these agents are not specifically indicated for GIST, some subjects enrolled in the trials had GIST harboring the target NTRK gene fusion and their tumors responded to treatment.
Ripretinib. FDA-approved in 2020,33 ripretinib is a novel TKI indicated for adult patients with advanced GIST who have received prior treatment with 3 or more kinase inhibitors, including imatinib. A phase 3 trial demonstrated improved progression-free and overall survival when ripretinib was compared with placebo in patients who had disease progression after treatment with imatinib, sunitinib, or regorafenib.34 Ripretinib is now being investigated in the second-line setting in selected patients with KIT mutations.
Avapritinib. Cases of GIST with PDGFRA D842V-mutant tumors often demonstrate primary resistance to imatinib and sunitinib. In 2020, avapritinib, a selective TKI that targets both KIT and PDGFRA, was approved35 for treatment of patients with unresectable or metastatic GIST harboring a PDGFRA exon 18 mutation, including D842V mutations. However, it is noteworthy that many of the non-D842V mutations in PDGFRA respond to imatinib.
Dabrafenib/trametinib. In 2022, the FDA issued an approval for treatment based on a driver mutation rather than tumor type. Acknowledging that a BRAF mutation—specifically a V600E mutation—appears to be a critical target in several cancers, the FDA granted accelerated approval for the use of dabrafenib plus trametinib in adults and children 6 years of age and older with unresectable or metastatic solid tumors with BRAF V600E mutation who have progressed following prior treatment and have no satisfactory alternative treatment options.36
Researchers have studied additional TKIs in the setting of unresectable, metastatic disease due to the varied genomic landscape of GIST. The NCCN Guidelines include evidence of some benefit for agents such as dasatinib, cabozantinib, everolimus (plus a TKI), nilotinib, pazopanib, and sorafenib “in certain circumstances.”6
The Future of GIST
The most critical step toward optimal treatment decision-making when a patient has been diagnosed with GIST is identification of physicians with expertise in the care of patients with GIST. With increasing knowledge of genomic variations in GIST, patient care has become less prescripted and much more personalized. To that end, determination of the tumor’s genetic mutational profile is critical to guiding treatment. Although factors such as cost, availability/accessibility, and insufficient tissue continue to represent substantial obstacles, pursing this information may be the most important way that clinicians can advocate for their patients. Moreover, now that the anatomic location of GIST has been linked to specific driver mutations, the ability to select and refine treatments may improve significantly.
Likewise, in view of the increasing complexity and multidisciplinary management of patients with GIST, efficient coordination is paramount among surgical and medical oncologists, as well as radiologists, gastroenterologists, and pathologists.
Jason K. Sicklick, MD, FACS
Gastrointestinal stromal tumor (GIST) was recognized as a distinct tumor type in the late 1990s.1 Advances in treatment have expanded since the 2001 US Food and Drug Administration (FDA) approval of imatinib, the first tyrosine kinase inhibitor (TKI).2 In 2023, there are now 5 FDA-approved agents for GIST, and 4 additional agents have been approved (tumor agnostic) for patients whose cancer harbors specific genomic alterations (neurotrophic tyrosine receptor kinase [NTRK] fusions3,4 or BRAF V600E mutations5). According to the National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology, several other drugs (ie, in addition to those specifically approved for GIST) are listed as “useful in certain circumstances.”6
Since the early 2000s, new discoveries about GIST genomics have contributed to better, more targeted treatments. Some genomic mutations have been linked to specific gut regions,7 which may further help guide therapy as well.
GIST: What Is It, Who Gets It, and How Is It Diagnosed?
What, How Many, Where?
Even though GIST is considered rare—representing less than 1% of gastrointestinal tumors8—it is the most common sarcoma, which is a family of mesenchymal neoplasms. GISTs are thought to arise from the interstitial cells of Cajal, or the pacemaker cells of the gut that control peristalsis. In the United States, the incidence of GIST is roughly 4,000 to 6,000 new cases diagnosed per year, with most cases found in the stomach (60%) or small intestine (35%). Other gut regions in which GISTs may be identified include the rectum and esophagus.8
Although asymptomatic tumors are often discovered incidentally, GISTs that originate in the stomach—the most common primary tumor site—may present with nonspecific subjective symptoms such as pain, nausea, loss of appetite, early satiety, or bloating.9 Symptoms may vary according to tumor location (eg, stomach vs rectum vs esophagus), size, and pattern of growth. More objective signs could include anemia related to gastrointestinal bleeding, weight loss, or a palpable mass.9
Who?
Most cases of GIST occur in patients later in life, with a median age of 64 years at diagnosis. A slight predominance of men has been noted, along with African American and Asian individuals affected somewhat more frequently than White or Hispanic populations.10 GIST is rare in children and adolescents, and the symptoms and pathology differ from those in most adults.9 Previously age was considered a determining factor in the differences in GIST, with cases in children classified as “pediatric-type” GIST or “wild-type” GIST. These cases generally present in the stomach, are more likely to include lymph node involvement, and can also spread to the liver and abdominal lining. Importantly, they are usually not associated with the tyrosine-protein kinase (KIT) or platelet-derived growth factor receptor alpha (PDGFRA) gene mutations found in most adults.9 About 80% of these cases have hereditary mutations of the succinate dehydrogenase (SDH) enzyme complex. Because some adult cases of GIST share the distinct characteristics found in most pediatric cases, distinguishing them based on age, rather than on the specific genetic characteristics of the tumor, is unwarranted.9
How?
When GIST is suspected or when symptoms mandate further investigation, coordination among colleagues in imaging, gastroenterology, pathology, surgery, and oncology is critical for accurate diagnosis, staging, and treatment. Abdominal imaging may be ordered using modalities such as ultrasound, computed tomography, magnetic resonance imaging, and, occasionally, positron emission tomography.11 Endoscopic ultrasound is useful to identify and biopsy lesions in the stomach or rectum, as these tumors arise below the lining of the stomach or rectum. GIST diagnosis can be confirmed by biopsy during endoscopic ultrasound, which is the preferred approach, or by percutaneous biopsy when endoscopic biopsy is not feasible or safe.11
According to the European Society for Medical Oncology (ESMO) and European Reference Group for Rare Adult Solid Cancers (EURACAN) Clinical Practice Guidelines, the “standard approach to tumors ≥ 2 cm in size is excision, because they are associated with a higher risk of progression if confirmed as GIST. If there is an abdominal nodule not amenable to endoscopic assessment, laparoscopic or laparotomic excision is the standard approach.”11
Genetic Mutations
A diagnosis of GIST is made based on the combination of the clinical scenario, the tumor’s anatomic location, immunohistochemistry patterns, and molecular features.12 Research has shown that genetic mutations in the KIT, PDGFRA, or SDH genes are present in most cases of GIST (70-80%,13 10%,12 and less than 10% of cases12,14 respectively) and their presence can be used for diagnosis. A growing number of rarer mutations have also been discovered,13 meaning that gene-based diagnosis of GIST is becoming increasingly sensitive. In addition, antigens on the surface of cancer cells can help classify them as GIST. For example, researchers have discovered that most GIST cells have the marker CD117, the protein product of the KIT gene that is commonly mutated in GIST, on their surfaces. A different marker, DOG1 (ie, Discovered On GIST 1), is also present on the vast majority of GISTs, but not unanimously overlapping with CD117. A tumor that is positive for both CD117 and DOG1 has a high probability (> 97%) of being GIST.15
Next-generation sequencing (NGS) is considered the best tool for determining both germline and somatic mutations in patients with GIST, and NGS is recommended by both the NCCN6 and the ESMO11 for individualizing systemic therapy. Despite these recommendations, most patients do not undergo genetic testing, both in the United States16 and internationally.17 Several barriers to genetic testing have been cited, predominately inadequate tissue and high cost. However, a study demonstrated that costs of up to $3,730 for genetic testing were ultimately cost-effective for tailoring therapy with first-line imatinib for patients with newly diagnosed metastatic GIST.18 Moreover, genetic testing also should be strongly considered for patients with nonmetastatic disease in whom systemic therapy is being considered.
Increasing evidence has emerged that gastric GIST mutations are related to tumor location within the gastrointestinal tract (Figure).7 The anatomic location of the GIST may provide clues for clinical decision-making and may guide selective confirmatory genomic testing when access to testing is limited.
Proximal gastric GISTs are overwhelmingly KIT exon 11 mutant, whereas distal stomach tumors display non-KIT genomic diversity (PDGFRA, as well as germline [or inherited] SDHx mutant and SDHC epimutations). In contrast, tumors that arise in the small intestine (eg, duodenum, jejunum, and ileum) are associated with gene fusions and germline NF1, as well as mutations in KIT exons 11 and 9. Colon and rectal tumors are likely to be KIT-related, whereas those found in the duodenal-jejunal flexure (also called the ligament of Treitz) correlate with rarer mutations, such as BRAF V600E and somatic (nonhereditary NF1) in addition to germline NF, as well as KIT.
Treatment of GIST
Surgery
Surgery remains the main treatment for localized GIST, especially if the tumor is discovered at an early stage. Unfortunately, up to a quarter of patients present with metastatic disease at diagnosis. The goal of surgery is to resect the tumor with histologically negative margins. Every effort should be made to avoid rupturing the tumor capsule during resection. Studies have shown that laparoscopic resection is feasible and safe for gastric GISTs and is less invasive than traditional open surgery, with similar oncological outcomes.19
Debulking surgery is sometimes considered for patients with metastatic disease, especially for patients who demonstrate sensitivity to TKI and whose disease has not yet progressed.20,21 Other interventions, such as microwave ablation or transhepatic arterial embolization, are sometimes used to control hepatic metastases.
Systemic Therapies
Whether systemic therapy is being considered in the neoadjuvant (preoperative), adjuvant (postoperative), or advanced disease setting, mutations in GIST determine the likelihood of treatment success. Both NCCN6 and ESMO11 strongly encourage use of mutational analyses and genetic testing for patients with GIST before systemic therapy is initiated.
In some cases of locally advanced GIST, tumors may be situated in particularly challenging anatomic locations(eg, esophagus, duodenum, rectum) or may require a highly morbid, multivisceral resection. In such situations, neoadjuvant treatment with imatinib,22,23 if deemed appropriate per mutational profiling, should be considered.
Patients who are determined to be at high risk for recurrence after surgery, based on tumor size, mitotic index determined by pathologist review of dividing cells, tumor location, and tumor rupture, may be eligible for adjuvant treatment with imatinib.24 Although the ideal duration of adjuvant therapy is not yet known, the current standard is at least 3 years,25 but many practitioners advocate for lifelong therapy.
Imatinib.Because chemotherapy was ineffective against GIST, prognosis was dismal for patients diagnosed with advanced disease before the approval of imatinib in the early 2000s.2 A selective TKI, imatinib targets the KIT and PDGFRA receptor kinases, and most patients experience clinical benefit,26 at least initially. Unfortunately, many tumors eventually develop resistance, and discontinuation of imatinib is associated with a risk for disease progression.27
Sunitinib. The emergence of resistance to imatinib spurred the search for second-line agents that might be useful after disease progression. Another TKI, sunitinib, which has both antitumor and antiangiogenic activity, was approved in 2006 for management of advanced imatinib-resistant GIST.28 Knowledge of a tumor’s driver mutation(s) can help optimize use of sunitinib.29
Regorafenib. In 2013, the FDA approved regorafenib, another TKI, as a third-line agent for patients with advanced GIST that is refractory to imatinib and sunitinib.30 Regorafenib exerts its activity against multiple targets, including VEGFR1-3, TIE2 (ie, antiangiogenic activity), PDGFR-β, FGFR (ie, stromal targets), and KIT, RET, and RAF (ie, oncogenic targets). As with other TKIs, common adverse effects associated with regorafenib treatment include hypertension, hand-foot skin reaction, rash, diarrhea, and fatigue.
Larotrectinib/entrectinib. The FDA approved larotrectinib31 (2018) and entrectinib32 (2019) as the first tumor-agnostic agents, whose use is based on the presence of specific genomic alteration, in this case NTRK. If a tumor, including a GIST, harbors a specific, albeit rare, gene fusion, it may be considered for treatment with one of these small-molecule TRK family inhibitors. Although these agents are not specifically indicated for GIST, some subjects enrolled in the trials had GIST harboring the target NTRK gene fusion and their tumors responded to treatment.
Ripretinib. FDA-approved in 2020,33 ripretinib is a novel TKI indicated for adult patients with advanced GIST who have received prior treatment with 3 or more kinase inhibitors, including imatinib. A phase 3 trial demonstrated improved progression-free and overall survival when ripretinib was compared with placebo in patients who had disease progression after treatment with imatinib, sunitinib, or regorafenib.34 Ripretinib is now being investigated in the second-line setting in selected patients with KIT mutations.
Avapritinib. Cases of GIST with PDGFRA D842V-mutant tumors often demonstrate primary resistance to imatinib and sunitinib. In 2020, avapritinib, a selective TKI that targets both KIT and PDGFRA, was approved35 for treatment of patients with unresectable or metastatic GIST harboring a PDGFRA exon 18 mutation, including D842V mutations. However, it is noteworthy that many of the non-D842V mutations in PDGFRA respond to imatinib.
Dabrafenib/trametinib. In 2022, the FDA issued an approval for treatment based on a driver mutation rather than tumor type. Acknowledging that a BRAF mutation—specifically a V600E mutation—appears to be a critical target in several cancers, the FDA granted accelerated approval for the use of dabrafenib plus trametinib in adults and children 6 years of age and older with unresectable or metastatic solid tumors with BRAF V600E mutation who have progressed following prior treatment and have no satisfactory alternative treatment options.36
Researchers have studied additional TKIs in the setting of unresectable, metastatic disease due to the varied genomic landscape of GIST. The NCCN Guidelines include evidence of some benefit for agents such as dasatinib, cabozantinib, everolimus (plus a TKI), nilotinib, pazopanib, and sorafenib “in certain circumstances.”6
The Future of GIST
The most critical step toward optimal treatment decision-making when a patient has been diagnosed with GIST is identification of physicians with expertise in the care of patients with GIST. With increasing knowledge of genomic variations in GIST, patient care has become less prescripted and much more personalized. To that end, determination of the tumor’s genetic mutational profile is critical to guiding treatment. Although factors such as cost, availability/accessibility, and insufficient tissue continue to represent substantial obstacles, pursing this information may be the most important way that clinicians can advocate for their patients. Moreover, now that the anatomic location of GIST has been linked to specific driver mutations, the ability to select and refine treatments may improve significantly.
Likewise, in view of the increasing complexity and multidisciplinary management of patients with GIST, efficient coordination is paramount among surgical and medical oncologists, as well as radiologists, gastroenterologists, and pathologists.
Miettinen M, Virolainen M, Maarit-Sarlomo-Rikala. Gastrointestinal stromal tumors—value of CD34 antigen in their identification and separation from true leiomyomas and schwannomas. Am J Surg Pathol. 1995;19(2):207-216. doi:10.1097/00000478-199502000-00009
Dagher R, Cohen M, Williams G, et al. Approval summary: imatinib mesylate in the treatment of metastatic and/or unresectable malignant gastrointestinal stromal tumors. Clin Cancer Res. 2002;8(10):3034-3038. PMID:12374669
Sharma AK, de la Torre J, IJzerman NS, et al. Location of gastrointestinal stromal tumor (GIST) in the stomach predicts tumor mutation profile and drug sensitivity. Clin Cancer Res. 2021;27(19):5334-5342. doi:10.1158/1078-0432.CCR-21-1221
Ma GL, Murphy JD, Martinez ME, Sicklick JK. Epidemiology of gastrointestinal stromal tumors in the era of histology codes: results of a population-based study. Cancer Epidemiol Biomarkers Prev. 2014;24(1):298-302. doi:10.1158/1055-9965.EPI-14-1002
Casali PG, Abecassis N, Aro HT, et al. Gastrointestinal stromal tumours: ESMOEURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29(suppl 4):iv68-iv78. doi:10.1093/annonc/mdy095
Kelly CM, Sainz LG, Chi P. The management of metastatic GIST: current standard and investigational therapeutics. J Hematol Oncol. 2021;14(1):2. doi:10.1186/s13045-020-01026-6
Shi E, Chmielecki J, Tang CM, et al. FGR1 and NTRK3 actionable alterations in “wild-type” gastrointestinal stromal tumors. J Translat Med. 2016;14(1):339. doi:10.1186/s12967-016-1075-6
Bannon AE, Klug LR, Corless CL, Heinrich MC. Using molecular diagnostic testing to personalize the treatment of patients with gastrointestinal stromal tumors. Expert Rev Mol Diagn. 2017;17(5):445-457. doi:10.1080/14737159.2017.1308826
Wu CE, Tzen CY, Wang SY, Yeh CN. Clinical diagnosis of gastrointestinal stromal tumor (GIST): from the molecular genetic point of view. Cancers (Basel). 2019;11(5):679. doi:10.3390/cancers11050679
Florindez J, Trent J. Low frequency of mutation testing in the United States: an analysis of 3866 GIST patients. Am J Clin Oncol. 2020;43(4):270-278. doi:10.1097/COC.0000000000000659
Verschoor AJ, Bovée JVMG, Overbeek LIH, PALGA group; Hogendoorn PCW, Gelderblom H. The incidence, mutational status, risk classification and referral pattern of gastrointestinal stromal tumours in the Netherlands: a nationwide pathology registry (PALGA) study. Virchows Arch. 2018;472(2):221-229. doi:10.1007/s00428-017-2285-x
Banerjee S, Kumar A, Lopez N, et al. Cost-effectiveness analysis of genetic testing and tailored first-line therapy for patients with metastatic gastrointestinal stromal tumors. JAMA Netw Open. 2020;3(9):e2013565. doi:10.1001/jamanetworkopen.2020.1356519
Chen K, Zhou YC, Mou YP, Xu XW, Jin WW, Ajoodhea H. Systematic review and meta-analysis of safety and efficacy of laparoscopic resection of gastrointestinal stromal tumors of the stomach. Surg Endosc. 2015;29:355-367. doi:10.1007/s00464-014-3676-6
Fairweather M, Balachandran VP, Li GZ, et al. Cytoreductive surgery for metastatic gastrointestinal stromal tumors treated with tyrosine kinase inhibitors: a 2-institutional analysis. Ann Surg. 2018;268(2):296-302. doi:10.1097/SLA.0000000000002281
Bauer S, Rutkowski P, Hohenberger P, et al. Long-term follow-up of patients with GIST undergoing metastasectomy in the era of imatinib—analysis of prognostic factors (EORTC-STBSG collaborative study). Eur J Surg Oncol. 2014;40(4):412-419. doi:10.1016/j.ejso.2013.12.020
Rutkowski P, Gronchi A, Hohenberger P, et al. Neoadjuvant imatinib in locally advanced gastrointestinal stromal tumors (GIST): the EORTC STBSG experience. Ann Surg Oncol. 2013;20(9):2937-2943. doi:10.1245/s10434-013-3013-7
Cavnar MJ, Seier K, Gönen M, et al. Prognostic factors after neoadjuvant imatinib for newly diagnosed primary gastrointestinal stromal tumor. J Gastrointest Surg. 2021;25(7):1828-1836. doi:10.1007/s11605-020-04843-9
Joensuu H. Risk stratification of patients diagnosed with gastrointestinal stromal tumor. Hum Pathol. 2008;39(10):1411-1419. doi:10.1016/j.humpath.2008.06.025
Joensuu H, Eriksson M, Sundby Hall K, et al. Survival outcomes associated with 3 years vs 1 year of adjuvant imatinib for patients with high-risk gastrointestinal stromal tumors: an analysis of a randomized clinical trial after 10-year follow-up. JAMA Oncol. 2020;6(8):1241-1246. doi:10.1001/jamaoncol.2020.2091
Heinrich MC, Rankin C, Blanke CD, et al. Correlation of long-term results of imatinib in advanced gastrointestinal stromal tumors with next-generation sequencing results: analysis of phase 3 SWOG Intergroup Trial S0033. JAMA Oncol. 2017;3(7):944-952. doi:10.1001/jamaoncol.2016.6728
Le Cesne A, Ray-Coquard I, Bui BN, et al. Discontinuation of imatinib in patients with advanced gastrointestinal stromal tumours after 3 years of treatment: an open-label multicentre randomised phase 3 trial. Lancet Oncol. 2020;11(10):942-949. doi:10.1016/S1470-2045(10)70222-9
Demetri GD, van Oosterom AT, Garrett CR, et al. Efficacy and safety of sunitinib in patients with advanced gastrointestinal stromal tumour after failure of imatinib: a randomised controlled trial. Lancet. 2006;368(9544):1329-1338. doi:10.1016/S0140-6736(06)69446-4
Heinrich MC, Maki RG, Corless CL, et al. Primary and secondary kinase genotypes correlate with the biological and clinical activity of sunitinib in imatinib-resistant gastrointestinal stromal tumor. J Clin Oncol. 2008;26(33):5352-5359. doi:10.1200/JCO.2007.15.7461
Crona DJ, Keisler MD, Walko CM. Regorafenib: a novel multitargeted tyrosine kinase inhibitor for colorectal and gastrointestinal stromal tumors. Ann Pharmacother. 2013;47(12):1685-1696. doi:10.1177/1060028013509792
Drilon A, Laetsch TW, Kummar S, et al. Efficacy of larotrectinib in TRK fusion-positive cancers in adults and children. N Engl J Med. 2018;378(8):731-739. doi:10.1056/NEJMoa1714448
Doebele RC, Drilon A, Paz-Ares L, et al. Entrectinib in patients with advanced or metastatic NTRK fusion-positive solid tumours: integrated analysis of three phase 1-2 trials. Lancet Oncol. 2020;21(2):271-282. doi:10.1016/S1470-2045(19)30691-6
Miettinen M, Virolainen M, Maarit-Sarlomo-Rikala. Gastrointestinal stromal tumors—value of CD34 antigen in their identification and separation from true leiomyomas and schwannomas. Am J Surg Pathol. 1995;19(2):207-216. doi:10.1097/00000478-199502000-00009
Dagher R, Cohen M, Williams G, et al. Approval summary: imatinib mesylate in the treatment of metastatic and/or unresectable malignant gastrointestinal stromal tumors. Clin Cancer Res. 2002;8(10):3034-3038. PMID:12374669
Sharma AK, de la Torre J, IJzerman NS, et al. Location of gastrointestinal stromal tumor (GIST) in the stomach predicts tumor mutation profile and drug sensitivity. Clin Cancer Res. 2021;27(19):5334-5342. doi:10.1158/1078-0432.CCR-21-1221
Ma GL, Murphy JD, Martinez ME, Sicklick JK. Epidemiology of gastrointestinal stromal tumors in the era of histology codes: results of a population-based study. Cancer Epidemiol Biomarkers Prev. 2014;24(1):298-302. doi:10.1158/1055-9965.EPI-14-1002
Casali PG, Abecassis N, Aro HT, et al. Gastrointestinal stromal tumours: ESMOEURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29(suppl 4):iv68-iv78. doi:10.1093/annonc/mdy095
Kelly CM, Sainz LG, Chi P. The management of metastatic GIST: current standard and investigational therapeutics. J Hematol Oncol. 2021;14(1):2. doi:10.1186/s13045-020-01026-6
Shi E, Chmielecki J, Tang CM, et al. FGR1 and NTRK3 actionable alterations in “wild-type” gastrointestinal stromal tumors. J Translat Med. 2016;14(1):339. doi:10.1186/s12967-016-1075-6
Bannon AE, Klug LR, Corless CL, Heinrich MC. Using molecular diagnostic testing to personalize the treatment of patients with gastrointestinal stromal tumors. Expert Rev Mol Diagn. 2017;17(5):445-457. doi:10.1080/14737159.2017.1308826
Wu CE, Tzen CY, Wang SY, Yeh CN. Clinical diagnosis of gastrointestinal stromal tumor (GIST): from the molecular genetic point of view. Cancers (Basel). 2019;11(5):679. doi:10.3390/cancers11050679
Florindez J, Trent J. Low frequency of mutation testing in the United States: an analysis of 3866 GIST patients. Am J Clin Oncol. 2020;43(4):270-278. doi:10.1097/COC.0000000000000659
Verschoor AJ, Bovée JVMG, Overbeek LIH, PALGA group; Hogendoorn PCW, Gelderblom H. The incidence, mutational status, risk classification and referral pattern of gastrointestinal stromal tumours in the Netherlands: a nationwide pathology registry (PALGA) study. Virchows Arch. 2018;472(2):221-229. doi:10.1007/s00428-017-2285-x
Banerjee S, Kumar A, Lopez N, et al. Cost-effectiveness analysis of genetic testing and tailored first-line therapy for patients with metastatic gastrointestinal stromal tumors. JAMA Netw Open. 2020;3(9):e2013565. doi:10.1001/jamanetworkopen.2020.1356519
Chen K, Zhou YC, Mou YP, Xu XW, Jin WW, Ajoodhea H. Systematic review and meta-analysis of safety and efficacy of laparoscopic resection of gastrointestinal stromal tumors of the stomach. Surg Endosc. 2015;29:355-367. doi:10.1007/s00464-014-3676-6
Fairweather M, Balachandran VP, Li GZ, et al. Cytoreductive surgery for metastatic gastrointestinal stromal tumors treated with tyrosine kinase inhibitors: a 2-institutional analysis. Ann Surg. 2018;268(2):296-302. doi:10.1097/SLA.0000000000002281
Bauer S, Rutkowski P, Hohenberger P, et al. Long-term follow-up of patients with GIST undergoing metastasectomy in the era of imatinib—analysis of prognostic factors (EORTC-STBSG collaborative study). Eur J Surg Oncol. 2014;40(4):412-419. doi:10.1016/j.ejso.2013.12.020
Rutkowski P, Gronchi A, Hohenberger P, et al. Neoadjuvant imatinib in locally advanced gastrointestinal stromal tumors (GIST): the EORTC STBSG experience. Ann Surg Oncol. 2013;20(9):2937-2943. doi:10.1245/s10434-013-3013-7
Cavnar MJ, Seier K, Gönen M, et al. Prognostic factors after neoadjuvant imatinib for newly diagnosed primary gastrointestinal stromal tumor. J Gastrointest Surg. 2021;25(7):1828-1836. doi:10.1007/s11605-020-04843-9
Joensuu H. Risk stratification of patients diagnosed with gastrointestinal stromal tumor. Hum Pathol. 2008;39(10):1411-1419. doi:10.1016/j.humpath.2008.06.025
Joensuu H, Eriksson M, Sundby Hall K, et al. Survival outcomes associated with 3 years vs 1 year of adjuvant imatinib for patients with high-risk gastrointestinal stromal tumors: an analysis of a randomized clinical trial after 10-year follow-up. JAMA Oncol. 2020;6(8):1241-1246. doi:10.1001/jamaoncol.2020.2091
Heinrich MC, Rankin C, Blanke CD, et al. Correlation of long-term results of imatinib in advanced gastrointestinal stromal tumors with next-generation sequencing results: analysis of phase 3 SWOG Intergroup Trial S0033. JAMA Oncol. 2017;3(7):944-952. doi:10.1001/jamaoncol.2016.6728
Le Cesne A, Ray-Coquard I, Bui BN, et al. Discontinuation of imatinib in patients with advanced gastrointestinal stromal tumours after 3 years of treatment: an open-label multicentre randomised phase 3 trial. Lancet Oncol. 2020;11(10):942-949. doi:10.1016/S1470-2045(10)70222-9
Demetri GD, van Oosterom AT, Garrett CR, et al. Efficacy and safety of sunitinib in patients with advanced gastrointestinal stromal tumour after failure of imatinib: a randomised controlled trial. Lancet. 2006;368(9544):1329-1338. doi:10.1016/S0140-6736(06)69446-4
Heinrich MC, Maki RG, Corless CL, et al. Primary and secondary kinase genotypes correlate with the biological and clinical activity of sunitinib in imatinib-resistant gastrointestinal stromal tumor. J Clin Oncol. 2008;26(33):5352-5359. doi:10.1200/JCO.2007.15.7461
Crona DJ, Keisler MD, Walko CM. Regorafenib: a novel multitargeted tyrosine kinase inhibitor for colorectal and gastrointestinal stromal tumors. Ann Pharmacother. 2013;47(12):1685-1696. doi:10.1177/1060028013509792
Drilon A, Laetsch TW, Kummar S, et al. Efficacy of larotrectinib in TRK fusion-positive cancers in adults and children. N Engl J Med. 2018;378(8):731-739. doi:10.1056/NEJMoa1714448
Doebele RC, Drilon A, Paz-Ares L, et al. Entrectinib in patients with advanced or metastatic NTRK fusion-positive solid tumours: integrated analysis of three phase 1-2 trials. Lancet Oncol. 2020;21(2):271-282. doi:10.1016/S1470-2045(19)30691-6
Rajwanth Veluswamy, MD, MSCR
Adenosquamous carcinoma (ASC) of the lung is a rare, biphasic type of non-small cell lung cancer (NSCLC) that accounts for 2% to 4% of all lung cancers.1 According to the World Health Organization (WHO) classification, the composition of ASC includes both adenocarcinoma (AC) and squamous cell carcinoma (SCC) histologies, with each subtype comprising at least 10% of the tumor.2 As with other lung cancers, the average age at ASC diagnosis is about 70 years of age, it affects more men than women, and most patients are current or former smokers.3,4 Despite these similarities, mounting evidence suggests that the molecular and genomic features of ASC are unique and they remain poorly understood.5-8
Perhaps owing to the distinct genomics of these tumors, ASC of the lung is reported to be relatively aggressive compared to typical AC and SCC tumors. Studies indicate that ASCs at diagnosis have higher rates of lymph node invasion, metastasize rapidly, and carry a generally poor prognosis. Accordingly, the overall survival (OS) of patients with these tumors is relatively short compared to other NSCLC subtypes.2,3,8-10 In a 2022 population-based study of the SEER database, 5-year postsurgical survival rates for early-stage cancers were reportedly 65% for ASC vs 69% for SCC P=0.003 and 77% for AC P<0.001.3 While it is clear that underlying biology driving ASC differs from more typical NSCLC subtypes, there is a lack of effective treatment options specific to ASC and a paucity of clinical research available to support therapeutic decisions for patients with ASC histology. Current management of NSCLC is based primarily on the stage of the tumor, and clinical features of the patient. In a more personalized era of targeted treatments, tumor histology is used only to predict the presence of actionable mutations in adenocarcinomas.7,8 However, optimal treatment strategies for ASC remain a significant unmet need in lung cancer.
Diagnosis: Complex but Critically Important
Given the mixed histologies that characterize ASC of the lung, intratumoral heterogeneity often hinders and may delay diagnosis. Studies suggest that ASC is misdiagnosed as AC or SCC in at least half of biopsies prior to surgical pathology confirming an ASC diagnosis.11 In one retrospective study, nearly all ASC cases (98%) were either misdiagnosed or undiagnosed preoperatively.12 What’s more is that different types of biopsy samples may yield different results. One case report of a patient eventually diagnosed with ASC described 3 different results on workup: SCC on bronchial lavage and bronchial biopsy, AC on immunohistochemistry, and NSCLC undifferentiated on pleural effusion cytology.13 While a diagnosis can be made using biopsy and cytology samples, a definitive diagnosis may require larger samples (ie, several core biopsies or complete surgical resections) to fully evaluate all components of the tumor lesion.
Comprehensively evaluating entire tumor specimens can aid in further characterization ASC of the lung. ASCs may be sub-classified according to the proportions of AC and SCC histology components present. Tumors with either AC or SCC components comprising at least 60% of the tumor are referred to as AC- or SCC-predominant ASC, respectively. Those with a more even split of AC and SCC histologies (40% to 60% of each) are referred to as structure-balanced ASC and have been reported to have a better prognosis than either of the more imbalanced subtypes.9,14
Adding to the complexity of diagnosing ASC of the lung is its unclear histologic origin and the transitional nature of these tumors over time. Some studies have pointed to possible precursor lesions, including AC with squamous metaplasia, collision tumor, and high-grade mucoepidermoid tumors.15 Reports have also shown that the molecular and histological features of the primary tumor can differ from that of metastases/recurrences.16,17 In one case report, a patient with a resected ASC harboring an epidermal growth factor receptor (EGFR)-sensitizing mutation recurred several months later as SCC in the brain with the same EGFR mutation. A later recurrence in the lung was diagnosed as an AC and had the same EGFR mutation.16 In this example, if only the SCC component had been diagnosed, molecular testing would likely have never been ordered and the potentially actionable EGFR mutation would have been left undetected. Therefore, careful and accurate diagnosis of ASC is critically important in guiding testing for driver mutations, as well as in informing treatment choices in ASC.
Genomics
Studies indicate that ASC of the lung exhibits genomic features of both AC and SCC, with standard immunohistochemical profiles represented in each component. As expected, TTF1 positivity is common in the AC component while p63 and CK5/6 are expressed in the SCC component.18 However, evidence also indicates that ASC of the lung is a distinct entity rather than being a simple hybrid of AC and SCC histologies. That is, despite the seemingly dichotomous nature of ASC, this type of tumor is thought to have unique molecular and genomic features that have not yet been fully identified.5-8
While the genomics of AC and SCC of the lung have been well studied, the inherent intratumoral heterogeneity that defines ASC, together with its relative rarity, complicates its analysis. There is a paucity of data available, but several groups have conducted molecular testing to better understand the genotype of ASC and potentially discover predictors about prognosis and treatment. To date, most studies on ASC lung samples have been small, and while some groups have reported overlapping results, other findings contrast with one another. In one of the most recent and comprehensive studies published on the topic, Wang et al. used next-generation sequencing (NGS) to identify a wide range of somatic mutations in 124 Chinese patients with ASC of the lung, including TP53 (66.9%), CDKN2A (21%), TERT (21%), and LRP1B (18.5%).6 Importantly, they found high rates of EGFR mutations (54.8%), of which 45.6% were EGFR 19del, 38.2% were EGFR L858R and 29.4% were EGFR amplifications.
Notably, not all studies have found such a strikingly increased rate of EGFR mutations in ASC versus AC of the lung.19 Other actionable mutations were found in the analysis by Wang and colleagues, including ALK and ROS1 fusions. Regarding known predictors of immunogenicity in these tumors, a subset of patients were associated with high tumor mutational burden (TMB), which was correlated with mutations in ARID2, BRCA1, and KEAP1. Immunohistochemical analyses demonstrated half of patients were positive for PD-L1 (≥ 1% tumor proportion score [TPS]).6 Interestingly, another study showed that PD-L1 expression in ASC differed between SCC (30% to 40%) and AC (11% to 15%) components.20
Actionable mutation rates (ie, EGFR, ALK) in AC are known to vary between Asian and White patients, a finding that seems to be similar in ASC of the lung as well, although it is less clear given the limited sample size of ASC studies. Vassella et al. performed NGS and fluorescence in situ hybridization (FISH) on ASC samples from 16 White patients and found that 30% had EGFR mutations, while Tochigi et al reported an EGFR mutation rate of 13% in a study of 23 Western patients.5,12,21 In their analysis, Vassella and colleagues also found a high rate of mutations in the PI3K pathway (25%), but no KRAS mutations, which are the most common molecular driver in typical AC (30%), and thus supporting the notion that ASC has its own molecular genomic profile, distinct from AC or SCC.5,21 Also of interest in this study was the finding that classifier miR-205 expression was intermediate between that of classical AC and SCC, suggesting that ASC of the lung may alternatively represent a transitional stage between these tumor types rather than an unrelated entity.5 These findings, along with others that have been reported on the genomic landscape of ASC, have advanced our understanding of the underlying biology of this malignancy, but also highlight the unmet need for more research to improve our ability to personalize treatment for ASCs.
Treatment
Owing to the heterogeneity of ASC of the lung, as well as its complex and incompletely characterized genomic landscape, treating patients with these tumors is challenging. In general, stage-based treatment approaches are used to manage ASC. The current treatment paradigm of all NSCLC has dramatically changed in recent years, with increasing incorporation of targeted treatments and immunotherapies across all stages and histologic types. Considering ASCs are composed of glandular cell components, they can contain substantial levels of relevant actionable driver mutations as described above. Therefore, if ASC is diagnosed or if a SCC has a glandular component,molecular testing is recommended and supported by guidelines, even on surgical specimens where EGFR may be targeted as adjuvant treatment.23 However, while targeting actionable mutations and the PD1/PDL1 axis has been studied extensively in AC and SCC in all stages, the impact of these markers in ASC is unknown because patients with this histologic subtype are frequently excluded from clinical trials.
For patients with ASC and actionable mutations, EGFR inhibitors have been perhaps the best-studied targeted therapies. EGFR inhibitors have yielded responses in ASC, but the benefit has been highly variable in small case series and generally inferior to outcomes in patients with AC alone.19 Ongoing clinical trials are aiming to better understand the effects of EGFR inhibitors in ASC. As one example, first-line almonertinib is being compared to paclitaxel/carboplatin in the phase 2 ARISE clinical trial, which is specifically enrolling patients with EGFR mutation-positive locally advanced or metastatic pulmonary ASC (Clinicaltrials.gov NCT04354961). Most other reported studies are case studies or retrospective in nature.
Given that outcomes are usually reported from single patients or a group of only a few patients, contradictory findings are not uncommon. For example, crizotinib, a multi-kinase inhibitor approved for the treatment of advanced or metastatic ALK-positive and ROS1-positive NSCLC, was reported to have a clinical response in an ASC in a patient with recurrent ALK-positive disease which lasted for just over one year.24 However, the response to second-line crizotinib in a case report of female non-smoking patient with ROS1-positive ASC was only 4 months.25 Newer, more specific kinase inhibitors are currently in clinical practice and trials of ALK and ROS1 NSCLCs; however, their efficacy is ASC remains unclear.
In the absence of driver mutations, the optimal choice of chemotherapy (often given with immunotherapy) for neo-/adjuvant therapy or for metastatic disease has not yet been identified. While the AC component might typically be treated with pemetrexed plus a platinum agent, the SCC component may be better treated with taxane plus a platinum agent.23 Especially in cases where neither histologic subtype is predominant, it can be difficult to decide which combination may be suitable for an individual patient. Whether the relative proportion of AC and SCC components affect treatment outcomes is not yet known. Outcomes of pemetrexed-based chemotherapy have been reported in a case study of 2 patients with relapsed disease harboring ALK and ROS1 mutations, pemetrexed alone or as part of a combination regimen (with pembrolizumab and carboplatin) was able to maintain stable disease for at least a year.26
While immune checkpoint inhibitors, either as monotherapy or in combination with chemotherapy, are currently recommended for patients with NSCLC23, few studies have reported outcomes of patients with ASC specifically. One recent real-world analysis by Li et al. evaluated the effect of immunotherapy in 46 patients with ASC, of which 18 (39%) did not contain actionable driver mutations and 18 (39%) had unknown mutational status.27 In this study, 28% of the overall cohort responded to checkpoint inhibitors, the median progression-free survival was 6 months, and the median OS was 24.7 months. Notably, similar efficacy was observed in the 20 patients receiving immunotherapy monotherapy vs 26 patients who received combination immunotherapy plus chemotherapy.27 Among 4 patients with EGFR mutations, 2 received immunotherapy monotherapy and progressed immediately compared to the other 2 receiving combination immunotherapy with chemotherapy achieving disease control and improved OS (18 months).
As exemplified by the select few cases summarized above, conventional treatments used in NSCLC have achieved only modest responses in ASC, most with a shorter response duration. The lack of specific treatment strategies for ASC, based on our understanding of underlying tumor biology, limits optimal treatment outcomes for this increasingly common diagnosis. Novel therapies are sorely needed. A consensus should be developed to either study novel treatments specifically in this subtype or allow for the incorporation of ASCs into future NSCLC clinical trials.
Ruffini E, Rena O, Oliaro A, Filosso PL, Bongiovanni M, Arslanian A, Papalia E, Maggi G. Lung tumors with mixed histologic pattern. Clinico-pathologic characteristics and prognostic significance. Eur J Cardiothorac Surg. 2002; 22:701–707. doi:10.1016/s1010-7940(02)00481-5
Almonertinib versus paclitaxel plus carboplatin as first-line treatment in patients with EGFR mutation positive locally advanced or metastatic pulmonary adenosquamous carcinoma (ARISE). ClinicalTrials.gov website. Accessed March 7, 2023. https://clinicaltrials.gov/ct2/show/NCT0435496
Maeda H, Matsumura A, Kawabata T, et al. Adenosquamous carcinoma of the lung: surgical results as compared with squamous cell and adeno¬carcinoma cases. Eur J Cardiothorac Surg. 2012;41:357–361. doi:10.1016/j.ejcts.2011.05.050
Wang T, Zhou J, Wang Y, et al. Clinicopathological characteristics and prognosis of resectable lung adenosquamous carcinoma: a population-based study of the SEER database. Jpn J Clin Oncol. 2022;52:1191-1200. doi:10.1093/jjco/hyac096
Vassella E, Langsch S, Dettmer MS, et al. Molecular profiling of lung adenosquamous carcinoma: a hybrid or genuine type? Oncotarget. 2015;6:23905-23916. doi:10.18632/oncotarget.4163
Wang H, Liu J, Zhu S, et al. Comprehensive analyses of genomic features and mutational signatures in adenosquamous carcinoma of the lung. Front Oncol. 2022;12:945843. doi:10.3389/fonc.2022.945843
Li C, Lu H. Adenosquamous carcinoma of the lung. Onco Targets Ther. 2018;11:4829-4835. doi:10.2147/OTT.S164574
Wang J, Wang Y, Tong M, Pan H, Li D. Research progress of the clinicopathologic features of lung adenosquamous carcinoma. Onco Targets Ther. 2018;11:7011-7017. doi:10.2147/OTT.S179904
Gawrychowski J, Brulinski K, Malinowski E, Papla B. Prognosis and survival after radical resection of primary adenosquamous lung carcinoma. Eur J Cardiothorac Surg. 2005; 27:686–692. doi:10.1016/j.ejcts.2004.12.030
Cooke DT, Nguyen DV, Yang Y, Chen SL, Yu C, Calhoun RF. Survival comparison of adenosquamous, squamous cell, and adenocarcinoma of the lung after lobectomy. Annal Thorac Surg. 2010; 90:943–948. doi:10.1016/j.athoracsur.2010.05.025
Damadoglu E, Aybatli A, Yalçinsoy M, et al. Adenosquamous carcinoma of the lung (an analysis of 13 cases). Tuberk Toraks. 2005;53:161–166. https://pubmed.ncbi.nlm.nih.gov/16100653/
Mordant P, Grand B, Cazes A, et al. Adenosquamous carcinoma of the lung: surgical management, pathologic characteristics, and prognostic implications. Ann Thorac Surg. 2013;95:1189–1195. doi:10.1016/j.athoracsur.2012.12.037
Shelton DA, Rana DN, Holbrook M, Taylor P, Bailey S. Adenosquamous carcinoma of the lung diagnosed by cytology? A diagnostic dilemma. Diagn Cytopathol. 2012;40:830–833. doi:10.1002/dc.21664
Zhao H, Yang H, Yao F, et al. Improved survival associated with a balanced structure between adenomatous and squamous components in patients with adenosquamous carcinoma of the lung. Eur J Surg Oncol. 2016;42:1699–1706. doi:10.1016/j.ejso.2016.05.009
Shimizu J,Oda M,Hayashi Y,Nonomura A,Watanabe YA. Clinicopathological Study of resected cases of adenosquamous carcinoma of the lung. Chest. 1996; 109: 989-994. doi:10.1378/chest.109.4.989
Burkart J, Shilo K, Zhao W, Ozkan E, Ajam A, Otterson GA. Metastatic squamous cell carcinoma component from an adenosquamous carcinoma of the lung with Identical epidermal growth factor receptor mutations. Case Rep Pulmonol. 2015;2015:283875. doi:10.1155/2015/283875
Du C, Li Z, Wang Z, Wang L, Tian YU. Stereotactic aspiration combined with gamma knife radiosurgery for the treatment of cystic brainstem metastasis originating from lung adenosquamous carcinoma: A case report. Oncol Lett. 2015;9:1607–1613. doi:10.3892/ol.2015.2968
Mukhopadhyay S, Katzenstein ALA. Subclassification of non-small cell lung carcinomas lacking morphologic differentiation on biopsy specimens: Utility of an immuno-histochemical panel containing TTF-1, napsin A, p63, and CK5/6. Am J Surg Pathol. 2011; 35:15–25. doi:10.1097/PAS.0b013e3182036d05
Song X, Wang Z. Clinical efficacy evaluation of tyrosine kinase inhibitors for nonadenocarcinoma lung cancer patients harboring EGFR-sensitizing mutations. Onco Targets Ther. 2017;10:3119-3122. doi:10.2147/OTT.S134523
Shi X, Wu S, Sun J, Liu Y, Zeng X, Liang Z. PD-L1 expression in lung adenosquamous carcinomas compared with the more common variants of non-small cell lung cancer. Sci Rep. 2017;7:46209. doi:10.1038/srep46209
Cancer Genome Atlas Research N. Comprehensive molec¬ular profiling of lung adenocarcinoma. Nature. 2014; 511:543–550. doi:10.1038/nature13385
Tochigi N, Dacic S, Nikiforova M, Cieply KM, Yousem SA. Adenosquamous carcinoma of the lung: a microdissection study of KRAS and EGFR mutational and amplification status in a western patient population. Am J Clin Pathol. 2011; 135:783–789. doi:10.1309/AJCP08IQZAOGYLFL
National Comprehensive Cancer Network®. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Non-small cell lung cancer. Version 2.2023. February 17, 2023. https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf. Accessed March 7, 2023.
Chaft JE, Rekhtman N, Ladanyi M, Riely GJ. ALK-rearranged lung cancer: adenosquamous lung cancer masquerading as pure squamous carcinoma. J Thorac Oncol. 2012;7:768–769. doi:10.1097/JTO.0b013e31824c9485
Cheng Y, Yang J, Wang D, Yan D. ROS1 fusion lung adenosquamous carcinoma patient with short-term clinical benefit after crizotinib treatment: a case report. Ann Transl Med. 2022;10:157. doi:10.21037/atm-21-6754
Patil J, Nie Y, Aisner DL, Camidge DR. Case report: significant clinical benefit from pemetrexed-based therapy in ROS-1 and ALK-rearranged lung cancer with adenosquamous histology. Front Oncol. 2022;11:788245. doi:10.3389/fonc.2021.788245
Li C, Zheng X, Li P, et al. Heterogeneity of tumor immune microenvironment and real-world analysis of immunotherapy efficacy in lung adenosquamous carcinoma. Front Immunol. 2022;13:944812. doi:10.3389/fimmu.2022.944812
Author and Disclosure Information
Rajwanth Veluswamy, MD, MSCR Assistant Professor of Medicine, Hematology and Medical Oncology Icahn School of Medicine at Mount Sinai New York, NY
Rajwanth R. Veluswamy, MD, MSCR, has disclosed the following relevant financial relationships:
Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: AstraZeneca; Boehringer Ingelheim; Merus; Novocure; Merck; Regeneron; Beigene; G1 Therapeutics; Novartis; BerGenBio.
Serve(d) as a speaker or a member of a speakers bureau for: AstraZeneca
Received research grant from: Bristol-Myers Squibb; Onconova; AstraZeneca; Boehringer Ingelheim
Rajwanth Veluswamy, MD, MSCR Assistant Professor of Medicine, Hematology and Medical Oncology Icahn School of Medicine at Mount Sinai New York, NY
Rajwanth R. Veluswamy, MD, MSCR, has disclosed the following relevant financial relationships:
Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: AstraZeneca; Boehringer Ingelheim; Merus; Novocure; Merck; Regeneron; Beigene; G1 Therapeutics; Novartis; BerGenBio.
Serve(d) as a speaker or a member of a speakers bureau for: AstraZeneca
Received research grant from: Bristol-Myers Squibb; Onconova; AstraZeneca; Boehringer Ingelheim
Author and Disclosure Information
Rajwanth Veluswamy, MD, MSCR Assistant Professor of Medicine, Hematology and Medical Oncology Icahn School of Medicine at Mount Sinai New York, NY
Rajwanth R. Veluswamy, MD, MSCR, has disclosed the following relevant financial relationships:
Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: AstraZeneca; Boehringer Ingelheim; Merus; Novocure; Merck; Regeneron; Beigene; G1 Therapeutics; Novartis; BerGenBio.
Serve(d) as a speaker or a member of a speakers bureau for: AstraZeneca
Received research grant from: Bristol-Myers Squibb; Onconova; AstraZeneca; Boehringer Ingelheim
Rajwanth Veluswamy, MD, MSCR
Adenosquamous carcinoma (ASC) of the lung is a rare, biphasic type of non-small cell lung cancer (NSCLC) that accounts for 2% to 4% of all lung cancers.1 According to the World Health Organization (WHO) classification, the composition of ASC includes both adenocarcinoma (AC) and squamous cell carcinoma (SCC) histologies, with each subtype comprising at least 10% of the tumor.2 As with other lung cancers, the average age at ASC diagnosis is about 70 years of age, it affects more men than women, and most patients are current or former smokers.3,4 Despite these similarities, mounting evidence suggests that the molecular and genomic features of ASC are unique and they remain poorly understood.5-8
Perhaps owing to the distinct genomics of these tumors, ASC of the lung is reported to be relatively aggressive compared to typical AC and SCC tumors. Studies indicate that ASCs at diagnosis have higher rates of lymph node invasion, metastasize rapidly, and carry a generally poor prognosis. Accordingly, the overall survival (OS) of patients with these tumors is relatively short compared to other NSCLC subtypes.2,3,8-10 In a 2022 population-based study of the SEER database, 5-year postsurgical survival rates for early-stage cancers were reportedly 65% for ASC vs 69% for SCC P=0.003 and 77% for AC P<0.001.3 While it is clear that underlying biology driving ASC differs from more typical NSCLC subtypes, there is a lack of effective treatment options specific to ASC and a paucity of clinical research available to support therapeutic decisions for patients with ASC histology. Current management of NSCLC is based primarily on the stage of the tumor, and clinical features of the patient. In a more personalized era of targeted treatments, tumor histology is used only to predict the presence of actionable mutations in adenocarcinomas.7,8 However, optimal treatment strategies for ASC remain a significant unmet need in lung cancer.
Diagnosis: Complex but Critically Important
Given the mixed histologies that characterize ASC of the lung, intratumoral heterogeneity often hinders and may delay diagnosis. Studies suggest that ASC is misdiagnosed as AC or SCC in at least half of biopsies prior to surgical pathology confirming an ASC diagnosis.11 In one retrospective study, nearly all ASC cases (98%) were either misdiagnosed or undiagnosed preoperatively.12 What’s more is that different types of biopsy samples may yield different results. One case report of a patient eventually diagnosed with ASC described 3 different results on workup: SCC on bronchial lavage and bronchial biopsy, AC on immunohistochemistry, and NSCLC undifferentiated on pleural effusion cytology.13 While a diagnosis can be made using biopsy and cytology samples, a definitive diagnosis may require larger samples (ie, several core biopsies or complete surgical resections) to fully evaluate all components of the tumor lesion.
Comprehensively evaluating entire tumor specimens can aid in further characterization ASC of the lung. ASCs may be sub-classified according to the proportions of AC and SCC histology components present. Tumors with either AC or SCC components comprising at least 60% of the tumor are referred to as AC- or SCC-predominant ASC, respectively. Those with a more even split of AC and SCC histologies (40% to 60% of each) are referred to as structure-balanced ASC and have been reported to have a better prognosis than either of the more imbalanced subtypes.9,14
Adding to the complexity of diagnosing ASC of the lung is its unclear histologic origin and the transitional nature of these tumors over time. Some studies have pointed to possible precursor lesions, including AC with squamous metaplasia, collision tumor, and high-grade mucoepidermoid tumors.15 Reports have also shown that the molecular and histological features of the primary tumor can differ from that of metastases/recurrences.16,17 In one case report, a patient with a resected ASC harboring an epidermal growth factor receptor (EGFR)-sensitizing mutation recurred several months later as SCC in the brain with the same EGFR mutation. A later recurrence in the lung was diagnosed as an AC and had the same EGFR mutation.16 In this example, if only the SCC component had been diagnosed, molecular testing would likely have never been ordered and the potentially actionable EGFR mutation would have been left undetected. Therefore, careful and accurate diagnosis of ASC is critically important in guiding testing for driver mutations, as well as in informing treatment choices in ASC.
Genomics
Studies indicate that ASC of the lung exhibits genomic features of both AC and SCC, with standard immunohistochemical profiles represented in each component. As expected, TTF1 positivity is common in the AC component while p63 and CK5/6 are expressed in the SCC component.18 However, evidence also indicates that ASC of the lung is a distinct entity rather than being a simple hybrid of AC and SCC histologies. That is, despite the seemingly dichotomous nature of ASC, this type of tumor is thought to have unique molecular and genomic features that have not yet been fully identified.5-8
While the genomics of AC and SCC of the lung have been well studied, the inherent intratumoral heterogeneity that defines ASC, together with its relative rarity, complicates its analysis. There is a paucity of data available, but several groups have conducted molecular testing to better understand the genotype of ASC and potentially discover predictors about prognosis and treatment. To date, most studies on ASC lung samples have been small, and while some groups have reported overlapping results, other findings contrast with one another. In one of the most recent and comprehensive studies published on the topic, Wang et al. used next-generation sequencing (NGS) to identify a wide range of somatic mutations in 124 Chinese patients with ASC of the lung, including TP53 (66.9%), CDKN2A (21%), TERT (21%), and LRP1B (18.5%).6 Importantly, they found high rates of EGFR mutations (54.8%), of which 45.6% were EGFR 19del, 38.2% were EGFR L858R and 29.4% were EGFR amplifications.
Notably, not all studies have found such a strikingly increased rate of EGFR mutations in ASC versus AC of the lung.19 Other actionable mutations were found in the analysis by Wang and colleagues, including ALK and ROS1 fusions. Regarding known predictors of immunogenicity in these tumors, a subset of patients were associated with high tumor mutational burden (TMB), which was correlated with mutations in ARID2, BRCA1, and KEAP1. Immunohistochemical analyses demonstrated half of patients were positive for PD-L1 (≥ 1% tumor proportion score [TPS]).6 Interestingly, another study showed that PD-L1 expression in ASC differed between SCC (30% to 40%) and AC (11% to 15%) components.20
Actionable mutation rates (ie, EGFR, ALK) in AC are known to vary between Asian and White patients, a finding that seems to be similar in ASC of the lung as well, although it is less clear given the limited sample size of ASC studies. Vassella et al. performed NGS and fluorescence in situ hybridization (FISH) on ASC samples from 16 White patients and found that 30% had EGFR mutations, while Tochigi et al reported an EGFR mutation rate of 13% in a study of 23 Western patients.5,12,21 In their analysis, Vassella and colleagues also found a high rate of mutations in the PI3K pathway (25%), but no KRAS mutations, which are the most common molecular driver in typical AC (30%), and thus supporting the notion that ASC has its own molecular genomic profile, distinct from AC or SCC.5,21 Also of interest in this study was the finding that classifier miR-205 expression was intermediate between that of classical AC and SCC, suggesting that ASC of the lung may alternatively represent a transitional stage between these tumor types rather than an unrelated entity.5 These findings, along with others that have been reported on the genomic landscape of ASC, have advanced our understanding of the underlying biology of this malignancy, but also highlight the unmet need for more research to improve our ability to personalize treatment for ASCs.
Treatment
Owing to the heterogeneity of ASC of the lung, as well as its complex and incompletely characterized genomic landscape, treating patients with these tumors is challenging. In general, stage-based treatment approaches are used to manage ASC. The current treatment paradigm of all NSCLC has dramatically changed in recent years, with increasing incorporation of targeted treatments and immunotherapies across all stages and histologic types. Considering ASCs are composed of glandular cell components, they can contain substantial levels of relevant actionable driver mutations as described above. Therefore, if ASC is diagnosed or if a SCC has a glandular component,molecular testing is recommended and supported by guidelines, even on surgical specimens where EGFR may be targeted as adjuvant treatment.23 However, while targeting actionable mutations and the PD1/PDL1 axis has been studied extensively in AC and SCC in all stages, the impact of these markers in ASC is unknown because patients with this histologic subtype are frequently excluded from clinical trials.
For patients with ASC and actionable mutations, EGFR inhibitors have been perhaps the best-studied targeted therapies. EGFR inhibitors have yielded responses in ASC, but the benefit has been highly variable in small case series and generally inferior to outcomes in patients with AC alone.19 Ongoing clinical trials are aiming to better understand the effects of EGFR inhibitors in ASC. As one example, first-line almonertinib is being compared to paclitaxel/carboplatin in the phase 2 ARISE clinical trial, which is specifically enrolling patients with EGFR mutation-positive locally advanced or metastatic pulmonary ASC (Clinicaltrials.gov NCT04354961). Most other reported studies are case studies or retrospective in nature.
Given that outcomes are usually reported from single patients or a group of only a few patients, contradictory findings are not uncommon. For example, crizotinib, a multi-kinase inhibitor approved for the treatment of advanced or metastatic ALK-positive and ROS1-positive NSCLC, was reported to have a clinical response in an ASC in a patient with recurrent ALK-positive disease which lasted for just over one year.24 However, the response to second-line crizotinib in a case report of female non-smoking patient with ROS1-positive ASC was only 4 months.25 Newer, more specific kinase inhibitors are currently in clinical practice and trials of ALK and ROS1 NSCLCs; however, their efficacy is ASC remains unclear.
In the absence of driver mutations, the optimal choice of chemotherapy (often given with immunotherapy) for neo-/adjuvant therapy or for metastatic disease has not yet been identified. While the AC component might typically be treated with pemetrexed plus a platinum agent, the SCC component may be better treated with taxane plus a platinum agent.23 Especially in cases where neither histologic subtype is predominant, it can be difficult to decide which combination may be suitable for an individual patient. Whether the relative proportion of AC and SCC components affect treatment outcomes is not yet known. Outcomes of pemetrexed-based chemotherapy have been reported in a case study of 2 patients with relapsed disease harboring ALK and ROS1 mutations, pemetrexed alone or as part of a combination regimen (with pembrolizumab and carboplatin) was able to maintain stable disease for at least a year.26
While immune checkpoint inhibitors, either as monotherapy or in combination with chemotherapy, are currently recommended for patients with NSCLC23, few studies have reported outcomes of patients with ASC specifically. One recent real-world analysis by Li et al. evaluated the effect of immunotherapy in 46 patients with ASC, of which 18 (39%) did not contain actionable driver mutations and 18 (39%) had unknown mutational status.27 In this study, 28% of the overall cohort responded to checkpoint inhibitors, the median progression-free survival was 6 months, and the median OS was 24.7 months. Notably, similar efficacy was observed in the 20 patients receiving immunotherapy monotherapy vs 26 patients who received combination immunotherapy plus chemotherapy.27 Among 4 patients with EGFR mutations, 2 received immunotherapy monotherapy and progressed immediately compared to the other 2 receiving combination immunotherapy with chemotherapy achieving disease control and improved OS (18 months).
As exemplified by the select few cases summarized above, conventional treatments used in NSCLC have achieved only modest responses in ASC, most with a shorter response duration. The lack of specific treatment strategies for ASC, based on our understanding of underlying tumor biology, limits optimal treatment outcomes for this increasingly common diagnosis. Novel therapies are sorely needed. A consensus should be developed to either study novel treatments specifically in this subtype or allow for the incorporation of ASCs into future NSCLC clinical trials.
Rajwanth Veluswamy, MD, MSCR
Adenosquamous carcinoma (ASC) of the lung is a rare, biphasic type of non-small cell lung cancer (NSCLC) that accounts for 2% to 4% of all lung cancers.1 According to the World Health Organization (WHO) classification, the composition of ASC includes both adenocarcinoma (AC) and squamous cell carcinoma (SCC) histologies, with each subtype comprising at least 10% of the tumor.2 As with other lung cancers, the average age at ASC diagnosis is about 70 years of age, it affects more men than women, and most patients are current or former smokers.3,4 Despite these similarities, mounting evidence suggests that the molecular and genomic features of ASC are unique and they remain poorly understood.5-8
Perhaps owing to the distinct genomics of these tumors, ASC of the lung is reported to be relatively aggressive compared to typical AC and SCC tumors. Studies indicate that ASCs at diagnosis have higher rates of lymph node invasion, metastasize rapidly, and carry a generally poor prognosis. Accordingly, the overall survival (OS) of patients with these tumors is relatively short compared to other NSCLC subtypes.2,3,8-10 In a 2022 population-based study of the SEER database, 5-year postsurgical survival rates for early-stage cancers were reportedly 65% for ASC vs 69% for SCC P=0.003 and 77% for AC P<0.001.3 While it is clear that underlying biology driving ASC differs from more typical NSCLC subtypes, there is a lack of effective treatment options specific to ASC and a paucity of clinical research available to support therapeutic decisions for patients with ASC histology. Current management of NSCLC is based primarily on the stage of the tumor, and clinical features of the patient. In a more personalized era of targeted treatments, tumor histology is used only to predict the presence of actionable mutations in adenocarcinomas.7,8 However, optimal treatment strategies for ASC remain a significant unmet need in lung cancer.
Diagnosis: Complex but Critically Important
Given the mixed histologies that characterize ASC of the lung, intratumoral heterogeneity often hinders and may delay diagnosis. Studies suggest that ASC is misdiagnosed as AC or SCC in at least half of biopsies prior to surgical pathology confirming an ASC diagnosis.11 In one retrospective study, nearly all ASC cases (98%) were either misdiagnosed or undiagnosed preoperatively.12 What’s more is that different types of biopsy samples may yield different results. One case report of a patient eventually diagnosed with ASC described 3 different results on workup: SCC on bronchial lavage and bronchial biopsy, AC on immunohistochemistry, and NSCLC undifferentiated on pleural effusion cytology.13 While a diagnosis can be made using biopsy and cytology samples, a definitive diagnosis may require larger samples (ie, several core biopsies or complete surgical resections) to fully evaluate all components of the tumor lesion.
Comprehensively evaluating entire tumor specimens can aid in further characterization ASC of the lung. ASCs may be sub-classified according to the proportions of AC and SCC histology components present. Tumors with either AC or SCC components comprising at least 60% of the tumor are referred to as AC- or SCC-predominant ASC, respectively. Those with a more even split of AC and SCC histologies (40% to 60% of each) are referred to as structure-balanced ASC and have been reported to have a better prognosis than either of the more imbalanced subtypes.9,14
Adding to the complexity of diagnosing ASC of the lung is its unclear histologic origin and the transitional nature of these tumors over time. Some studies have pointed to possible precursor lesions, including AC with squamous metaplasia, collision tumor, and high-grade mucoepidermoid tumors.15 Reports have also shown that the molecular and histological features of the primary tumor can differ from that of metastases/recurrences.16,17 In one case report, a patient with a resected ASC harboring an epidermal growth factor receptor (EGFR)-sensitizing mutation recurred several months later as SCC in the brain with the same EGFR mutation. A later recurrence in the lung was diagnosed as an AC and had the same EGFR mutation.16 In this example, if only the SCC component had been diagnosed, molecular testing would likely have never been ordered and the potentially actionable EGFR mutation would have been left undetected. Therefore, careful and accurate diagnosis of ASC is critically important in guiding testing for driver mutations, as well as in informing treatment choices in ASC.
Genomics
Studies indicate that ASC of the lung exhibits genomic features of both AC and SCC, with standard immunohistochemical profiles represented in each component. As expected, TTF1 positivity is common in the AC component while p63 and CK5/6 are expressed in the SCC component.18 However, evidence also indicates that ASC of the lung is a distinct entity rather than being a simple hybrid of AC and SCC histologies. That is, despite the seemingly dichotomous nature of ASC, this type of tumor is thought to have unique molecular and genomic features that have not yet been fully identified.5-8
While the genomics of AC and SCC of the lung have been well studied, the inherent intratumoral heterogeneity that defines ASC, together with its relative rarity, complicates its analysis. There is a paucity of data available, but several groups have conducted molecular testing to better understand the genotype of ASC and potentially discover predictors about prognosis and treatment. To date, most studies on ASC lung samples have been small, and while some groups have reported overlapping results, other findings contrast with one another. In one of the most recent and comprehensive studies published on the topic, Wang et al. used next-generation sequencing (NGS) to identify a wide range of somatic mutations in 124 Chinese patients with ASC of the lung, including TP53 (66.9%), CDKN2A (21%), TERT (21%), and LRP1B (18.5%).6 Importantly, they found high rates of EGFR mutations (54.8%), of which 45.6% were EGFR 19del, 38.2% were EGFR L858R and 29.4% were EGFR amplifications.
Notably, not all studies have found such a strikingly increased rate of EGFR mutations in ASC versus AC of the lung.19 Other actionable mutations were found in the analysis by Wang and colleagues, including ALK and ROS1 fusions. Regarding known predictors of immunogenicity in these tumors, a subset of patients were associated with high tumor mutational burden (TMB), which was correlated with mutations in ARID2, BRCA1, and KEAP1. Immunohistochemical analyses demonstrated half of patients were positive for PD-L1 (≥ 1% tumor proportion score [TPS]).6 Interestingly, another study showed that PD-L1 expression in ASC differed between SCC (30% to 40%) and AC (11% to 15%) components.20
Actionable mutation rates (ie, EGFR, ALK) in AC are known to vary between Asian and White patients, a finding that seems to be similar in ASC of the lung as well, although it is less clear given the limited sample size of ASC studies. Vassella et al. performed NGS and fluorescence in situ hybridization (FISH) on ASC samples from 16 White patients and found that 30% had EGFR mutations, while Tochigi et al reported an EGFR mutation rate of 13% in a study of 23 Western patients.5,12,21 In their analysis, Vassella and colleagues also found a high rate of mutations in the PI3K pathway (25%), but no KRAS mutations, which are the most common molecular driver in typical AC (30%), and thus supporting the notion that ASC has its own molecular genomic profile, distinct from AC or SCC.5,21 Also of interest in this study was the finding that classifier miR-205 expression was intermediate between that of classical AC and SCC, suggesting that ASC of the lung may alternatively represent a transitional stage between these tumor types rather than an unrelated entity.5 These findings, along with others that have been reported on the genomic landscape of ASC, have advanced our understanding of the underlying biology of this malignancy, but also highlight the unmet need for more research to improve our ability to personalize treatment for ASCs.
Treatment
Owing to the heterogeneity of ASC of the lung, as well as its complex and incompletely characterized genomic landscape, treating patients with these tumors is challenging. In general, stage-based treatment approaches are used to manage ASC. The current treatment paradigm of all NSCLC has dramatically changed in recent years, with increasing incorporation of targeted treatments and immunotherapies across all stages and histologic types. Considering ASCs are composed of glandular cell components, they can contain substantial levels of relevant actionable driver mutations as described above. Therefore, if ASC is diagnosed or if a SCC has a glandular component,molecular testing is recommended and supported by guidelines, even on surgical specimens where EGFR may be targeted as adjuvant treatment.23 However, while targeting actionable mutations and the PD1/PDL1 axis has been studied extensively in AC and SCC in all stages, the impact of these markers in ASC is unknown because patients with this histologic subtype are frequently excluded from clinical trials.
For patients with ASC and actionable mutations, EGFR inhibitors have been perhaps the best-studied targeted therapies. EGFR inhibitors have yielded responses in ASC, but the benefit has been highly variable in small case series and generally inferior to outcomes in patients with AC alone.19 Ongoing clinical trials are aiming to better understand the effects of EGFR inhibitors in ASC. As one example, first-line almonertinib is being compared to paclitaxel/carboplatin in the phase 2 ARISE clinical trial, which is specifically enrolling patients with EGFR mutation-positive locally advanced or metastatic pulmonary ASC (Clinicaltrials.gov NCT04354961). Most other reported studies are case studies or retrospective in nature.
Given that outcomes are usually reported from single patients or a group of only a few patients, contradictory findings are not uncommon. For example, crizotinib, a multi-kinase inhibitor approved for the treatment of advanced or metastatic ALK-positive and ROS1-positive NSCLC, was reported to have a clinical response in an ASC in a patient with recurrent ALK-positive disease which lasted for just over one year.24 However, the response to second-line crizotinib in a case report of female non-smoking patient with ROS1-positive ASC was only 4 months.25 Newer, more specific kinase inhibitors are currently in clinical practice and trials of ALK and ROS1 NSCLCs; however, their efficacy is ASC remains unclear.
In the absence of driver mutations, the optimal choice of chemotherapy (often given with immunotherapy) for neo-/adjuvant therapy or for metastatic disease has not yet been identified. While the AC component might typically be treated with pemetrexed plus a platinum agent, the SCC component may be better treated with taxane plus a platinum agent.23 Especially in cases where neither histologic subtype is predominant, it can be difficult to decide which combination may be suitable for an individual patient. Whether the relative proportion of AC and SCC components affect treatment outcomes is not yet known. Outcomes of pemetrexed-based chemotherapy have been reported in a case study of 2 patients with relapsed disease harboring ALK and ROS1 mutations, pemetrexed alone or as part of a combination regimen (with pembrolizumab and carboplatin) was able to maintain stable disease for at least a year.26
While immune checkpoint inhibitors, either as monotherapy or in combination with chemotherapy, are currently recommended for patients with NSCLC23, few studies have reported outcomes of patients with ASC specifically. One recent real-world analysis by Li et al. evaluated the effect of immunotherapy in 46 patients with ASC, of which 18 (39%) did not contain actionable driver mutations and 18 (39%) had unknown mutational status.27 In this study, 28% of the overall cohort responded to checkpoint inhibitors, the median progression-free survival was 6 months, and the median OS was 24.7 months. Notably, similar efficacy was observed in the 20 patients receiving immunotherapy monotherapy vs 26 patients who received combination immunotherapy plus chemotherapy.27 Among 4 patients with EGFR mutations, 2 received immunotherapy monotherapy and progressed immediately compared to the other 2 receiving combination immunotherapy with chemotherapy achieving disease control and improved OS (18 months).
As exemplified by the select few cases summarized above, conventional treatments used in NSCLC have achieved only modest responses in ASC, most with a shorter response duration. The lack of specific treatment strategies for ASC, based on our understanding of underlying tumor biology, limits optimal treatment outcomes for this increasingly common diagnosis. Novel therapies are sorely needed. A consensus should be developed to either study novel treatments specifically in this subtype or allow for the incorporation of ASCs into future NSCLC clinical trials.
Ruffini E, Rena O, Oliaro A, Filosso PL, Bongiovanni M, Arslanian A, Papalia E, Maggi G. Lung tumors with mixed histologic pattern. Clinico-pathologic characteristics and prognostic significance. Eur J Cardiothorac Surg. 2002; 22:701–707. doi:10.1016/s1010-7940(02)00481-5
Almonertinib versus paclitaxel plus carboplatin as first-line treatment in patients with EGFR mutation positive locally advanced or metastatic pulmonary adenosquamous carcinoma (ARISE). ClinicalTrials.gov website. Accessed March 7, 2023. https://clinicaltrials.gov/ct2/show/NCT0435496
Maeda H, Matsumura A, Kawabata T, et al. Adenosquamous carcinoma of the lung: surgical results as compared with squamous cell and adeno¬carcinoma cases. Eur J Cardiothorac Surg. 2012;41:357–361. doi:10.1016/j.ejcts.2011.05.050
Wang T, Zhou J, Wang Y, et al. Clinicopathological characteristics and prognosis of resectable lung adenosquamous carcinoma: a population-based study of the SEER database. Jpn J Clin Oncol. 2022;52:1191-1200. doi:10.1093/jjco/hyac096
Vassella E, Langsch S, Dettmer MS, et al. Molecular profiling of lung adenosquamous carcinoma: a hybrid or genuine type? Oncotarget. 2015;6:23905-23916. doi:10.18632/oncotarget.4163
Wang H, Liu J, Zhu S, et al. Comprehensive analyses of genomic features and mutational signatures in adenosquamous carcinoma of the lung. Front Oncol. 2022;12:945843. doi:10.3389/fonc.2022.945843
Li C, Lu H. Adenosquamous carcinoma of the lung. Onco Targets Ther. 2018;11:4829-4835. doi:10.2147/OTT.S164574
Wang J, Wang Y, Tong M, Pan H, Li D. Research progress of the clinicopathologic features of lung adenosquamous carcinoma. Onco Targets Ther. 2018;11:7011-7017. doi:10.2147/OTT.S179904
Gawrychowski J, Brulinski K, Malinowski E, Papla B. Prognosis and survival after radical resection of primary adenosquamous lung carcinoma. Eur J Cardiothorac Surg. 2005; 27:686–692. doi:10.1016/j.ejcts.2004.12.030
Cooke DT, Nguyen DV, Yang Y, Chen SL, Yu C, Calhoun RF. Survival comparison of adenosquamous, squamous cell, and adenocarcinoma of the lung after lobectomy. Annal Thorac Surg. 2010; 90:943–948. doi:10.1016/j.athoracsur.2010.05.025
Damadoglu E, Aybatli A, Yalçinsoy M, et al. Adenosquamous carcinoma of the lung (an analysis of 13 cases). Tuberk Toraks. 2005;53:161–166. https://pubmed.ncbi.nlm.nih.gov/16100653/
Mordant P, Grand B, Cazes A, et al. Adenosquamous carcinoma of the lung: surgical management, pathologic characteristics, and prognostic implications. Ann Thorac Surg. 2013;95:1189–1195. doi:10.1016/j.athoracsur.2012.12.037
Shelton DA, Rana DN, Holbrook M, Taylor P, Bailey S. Adenosquamous carcinoma of the lung diagnosed by cytology? A diagnostic dilemma. Diagn Cytopathol. 2012;40:830–833. doi:10.1002/dc.21664
Zhao H, Yang H, Yao F, et al. Improved survival associated with a balanced structure between adenomatous and squamous components in patients with adenosquamous carcinoma of the lung. Eur J Surg Oncol. 2016;42:1699–1706. doi:10.1016/j.ejso.2016.05.009
Shimizu J,Oda M,Hayashi Y,Nonomura A,Watanabe YA. Clinicopathological Study of resected cases of adenosquamous carcinoma of the lung. Chest. 1996; 109: 989-994. doi:10.1378/chest.109.4.989
Burkart J, Shilo K, Zhao W, Ozkan E, Ajam A, Otterson GA. Metastatic squamous cell carcinoma component from an adenosquamous carcinoma of the lung with Identical epidermal growth factor receptor mutations. Case Rep Pulmonol. 2015;2015:283875. doi:10.1155/2015/283875
Du C, Li Z, Wang Z, Wang L, Tian YU. Stereotactic aspiration combined with gamma knife radiosurgery for the treatment of cystic brainstem metastasis originating from lung adenosquamous carcinoma: A case report. Oncol Lett. 2015;9:1607–1613. doi:10.3892/ol.2015.2968
Mukhopadhyay S, Katzenstein ALA. Subclassification of non-small cell lung carcinomas lacking morphologic differentiation on biopsy specimens: Utility of an immuno-histochemical panel containing TTF-1, napsin A, p63, and CK5/6. Am J Surg Pathol. 2011; 35:15–25. doi:10.1097/PAS.0b013e3182036d05
Song X, Wang Z. Clinical efficacy evaluation of tyrosine kinase inhibitors for nonadenocarcinoma lung cancer patients harboring EGFR-sensitizing mutations. Onco Targets Ther. 2017;10:3119-3122. doi:10.2147/OTT.S134523
Shi X, Wu S, Sun J, Liu Y, Zeng X, Liang Z. PD-L1 expression in lung adenosquamous carcinomas compared with the more common variants of non-small cell lung cancer. Sci Rep. 2017;7:46209. doi:10.1038/srep46209
Cancer Genome Atlas Research N. Comprehensive molec¬ular profiling of lung adenocarcinoma. Nature. 2014; 511:543–550. doi:10.1038/nature13385
Tochigi N, Dacic S, Nikiforova M, Cieply KM, Yousem SA. Adenosquamous carcinoma of the lung: a microdissection study of KRAS and EGFR mutational and amplification status in a western patient population. Am J Clin Pathol. 2011; 135:783–789. doi:10.1309/AJCP08IQZAOGYLFL
National Comprehensive Cancer Network®. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Non-small cell lung cancer. Version 2.2023. February 17, 2023. https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf. Accessed March 7, 2023.
Chaft JE, Rekhtman N, Ladanyi M, Riely GJ. ALK-rearranged lung cancer: adenosquamous lung cancer masquerading as pure squamous carcinoma. J Thorac Oncol. 2012;7:768–769. doi:10.1097/JTO.0b013e31824c9485
Cheng Y, Yang J, Wang D, Yan D. ROS1 fusion lung adenosquamous carcinoma patient with short-term clinical benefit after crizotinib treatment: a case report. Ann Transl Med. 2022;10:157. doi:10.21037/atm-21-6754
Patil J, Nie Y, Aisner DL, Camidge DR. Case report: significant clinical benefit from pemetrexed-based therapy in ROS-1 and ALK-rearranged lung cancer with adenosquamous histology. Front Oncol. 2022;11:788245. doi:10.3389/fonc.2021.788245
Li C, Zheng X, Li P, et al. Heterogeneity of tumor immune microenvironment and real-world analysis of immunotherapy efficacy in lung adenosquamous carcinoma. Front Immunol. 2022;13:944812. doi:10.3389/fimmu.2022.944812
References
Ruffini E, Rena O, Oliaro A, Filosso PL, Bongiovanni M, Arslanian A, Papalia E, Maggi G. Lung tumors with mixed histologic pattern. Clinico-pathologic characteristics and prognostic significance. Eur J Cardiothorac Surg. 2002; 22:701–707. doi:10.1016/s1010-7940(02)00481-5
Almonertinib versus paclitaxel plus carboplatin as first-line treatment in patients with EGFR mutation positive locally advanced or metastatic pulmonary adenosquamous carcinoma (ARISE). ClinicalTrials.gov website. Accessed March 7, 2023. https://clinicaltrials.gov/ct2/show/NCT0435496
Maeda H, Matsumura A, Kawabata T, et al. Adenosquamous carcinoma of the lung: surgical results as compared with squamous cell and adeno¬carcinoma cases. Eur J Cardiothorac Surg. 2012;41:357–361. doi:10.1016/j.ejcts.2011.05.050
Wang T, Zhou J, Wang Y, et al. Clinicopathological characteristics and prognosis of resectable lung adenosquamous carcinoma: a population-based study of the SEER database. Jpn J Clin Oncol. 2022;52:1191-1200. doi:10.1093/jjco/hyac096
Vassella E, Langsch S, Dettmer MS, et al. Molecular profiling of lung adenosquamous carcinoma: a hybrid or genuine type? Oncotarget. 2015;6:23905-23916. doi:10.18632/oncotarget.4163
Wang H, Liu J, Zhu S, et al. Comprehensive analyses of genomic features and mutational signatures in adenosquamous carcinoma of the lung. Front Oncol. 2022;12:945843. doi:10.3389/fonc.2022.945843
Li C, Lu H. Adenosquamous carcinoma of the lung. Onco Targets Ther. 2018;11:4829-4835. doi:10.2147/OTT.S164574
Wang J, Wang Y, Tong M, Pan H, Li D. Research progress of the clinicopathologic features of lung adenosquamous carcinoma. Onco Targets Ther. 2018;11:7011-7017. doi:10.2147/OTT.S179904
Gawrychowski J, Brulinski K, Malinowski E, Papla B. Prognosis and survival after radical resection of primary adenosquamous lung carcinoma. Eur J Cardiothorac Surg. 2005; 27:686–692. doi:10.1016/j.ejcts.2004.12.030
Cooke DT, Nguyen DV, Yang Y, Chen SL, Yu C, Calhoun RF. Survival comparison of adenosquamous, squamous cell, and adenocarcinoma of the lung after lobectomy. Annal Thorac Surg. 2010; 90:943–948. doi:10.1016/j.athoracsur.2010.05.025
Damadoglu E, Aybatli A, Yalçinsoy M, et al. Adenosquamous carcinoma of the lung (an analysis of 13 cases). Tuberk Toraks. 2005;53:161–166. https://pubmed.ncbi.nlm.nih.gov/16100653/
Mordant P, Grand B, Cazes A, et al. Adenosquamous carcinoma of the lung: surgical management, pathologic characteristics, and prognostic implications. Ann Thorac Surg. 2013;95:1189–1195. doi:10.1016/j.athoracsur.2012.12.037
Shelton DA, Rana DN, Holbrook M, Taylor P, Bailey S. Adenosquamous carcinoma of the lung diagnosed by cytology? A diagnostic dilemma. Diagn Cytopathol. 2012;40:830–833. doi:10.1002/dc.21664
Zhao H, Yang H, Yao F, et al. Improved survival associated with a balanced structure between adenomatous and squamous components in patients with adenosquamous carcinoma of the lung. Eur J Surg Oncol. 2016;42:1699–1706. doi:10.1016/j.ejso.2016.05.009
Shimizu J,Oda M,Hayashi Y,Nonomura A,Watanabe YA. Clinicopathological Study of resected cases of adenosquamous carcinoma of the lung. Chest. 1996; 109: 989-994. doi:10.1378/chest.109.4.989
Burkart J, Shilo K, Zhao W, Ozkan E, Ajam A, Otterson GA. Metastatic squamous cell carcinoma component from an adenosquamous carcinoma of the lung with Identical epidermal growth factor receptor mutations. Case Rep Pulmonol. 2015;2015:283875. doi:10.1155/2015/283875
Du C, Li Z, Wang Z, Wang L, Tian YU. Stereotactic aspiration combined with gamma knife radiosurgery for the treatment of cystic brainstem metastasis originating from lung adenosquamous carcinoma: A case report. Oncol Lett. 2015;9:1607–1613. doi:10.3892/ol.2015.2968
Mukhopadhyay S, Katzenstein ALA. Subclassification of non-small cell lung carcinomas lacking morphologic differentiation on biopsy specimens: Utility of an immuno-histochemical panel containing TTF-1, napsin A, p63, and CK5/6. Am J Surg Pathol. 2011; 35:15–25. doi:10.1097/PAS.0b013e3182036d05
Song X, Wang Z. Clinical efficacy evaluation of tyrosine kinase inhibitors for nonadenocarcinoma lung cancer patients harboring EGFR-sensitizing mutations. Onco Targets Ther. 2017;10:3119-3122. doi:10.2147/OTT.S134523
Shi X, Wu S, Sun J, Liu Y, Zeng X, Liang Z. PD-L1 expression in lung adenosquamous carcinomas compared with the more common variants of non-small cell lung cancer. Sci Rep. 2017;7:46209. doi:10.1038/srep46209
Cancer Genome Atlas Research N. Comprehensive molec¬ular profiling of lung adenocarcinoma. Nature. 2014; 511:543–550. doi:10.1038/nature13385
Tochigi N, Dacic S, Nikiforova M, Cieply KM, Yousem SA. Adenosquamous carcinoma of the lung: a microdissection study of KRAS and EGFR mutational and amplification status in a western patient population. Am J Clin Pathol. 2011; 135:783–789. doi:10.1309/AJCP08IQZAOGYLFL
National Comprehensive Cancer Network®. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Non-small cell lung cancer. Version 2.2023. February 17, 2023. https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf. Accessed March 7, 2023.
Chaft JE, Rekhtman N, Ladanyi M, Riely GJ. ALK-rearranged lung cancer: adenosquamous lung cancer masquerading as pure squamous carcinoma. J Thorac Oncol. 2012;7:768–769. doi:10.1097/JTO.0b013e31824c9485
Cheng Y, Yang J, Wang D, Yan D. ROS1 fusion lung adenosquamous carcinoma patient with short-term clinical benefit after crizotinib treatment: a case report. Ann Transl Med. 2022;10:157. doi:10.21037/atm-21-6754
Patil J, Nie Y, Aisner DL, Camidge DR. Case report: significant clinical benefit from pemetrexed-based therapy in ROS-1 and ALK-rearranged lung cancer with adenosquamous histology. Front Oncol. 2022;11:788245. doi:10.3389/fonc.2021.788245
Li C, Zheng X, Li P, et al. Heterogeneity of tumor immune microenvironment and real-world analysis of immunotherapy efficacy in lung adenosquamous carcinoma. Front Immunol. 2022;13:944812. doi:10.3389/fimmu.2022.944812
Health care providers are missing opportunities to give medical treatment to high-risk individuals hospitalized for alcohol use disorder (AUD), a national analysis of Medicare beneficiaries reported.
Increasing such patients’ access to psychiatric care and addiction medicine, as well as encouraging medication prescribing by generalists and nonaddiction specialists, are remedial strategies recommended by lead author Eden Y. Bernstein, MD, of the division of general internal medicine at Massachusetts General Hospital and Harvard Medical School, both in Boston, and colleagues.
“Hospitalizations for alcohol use disorder are common,” Dr. Bernstein said in an interview. “Our work shows they represent an underutilized opportunity to engage patients with appropriate treatment, including initiation of medications for alcohol use disorder.”
There is a pressing need for such treatment strategies since 29 million U.S. adults have AUD, and alcohol contributes to more than 140,000 deaths annually, the authors noted.
Rarely initiated either at hospital discharge or during follow-up care, medical therapy for AUD was more likely to be provided to younger patients and those involved with psychiatric care or addiction medicine, Dr. Bernstein’s group reported in Annals of Internal Medicine.Hospital admissions, they argued, give patients more access to clinicians and social workers and the vulnerability experienced during hospitalization may motivate behavioral change.
National study
The cohort included 28,601 AUD hospitalizations for 20,401 unique Medicare patients from 2015 to 2017. About 30% of admissions were for women and about 72% for non-Hispanic Blacks. Discharge initiation of medication for AUD was defined as a pharmacy claim for naltrexone, acamprosate, or disulfiram from the day before discharge to 2 days after.
Overall, just 206 patients (0.7%) initiated medication for AUD within 2 days of discharge and 364 (1.3%) started it within 30 days. Among those discharged with a primary diagnosis of AUD, only 70 (2.3%) started medical therapy within 2 days.
The most predictive demographic factor for discharge medication for AUD was younger age: 18-39 years versus 75 years and older (adjusted odds ratio, 3.87; 95% confidence interval, 1.34-11.16).
Initiation of medication for AUD should involve a long-term treatment plan, according to Dr. Bernstein’s group, and if that is not feasible during hospitalization, patients should be referred for outpatient treatment.
An accompanying editorial agrees that the results offer strong evidence of a missed opportunity to address AUD at a potential flexion point. “Hospitalization is a critical touch point for identifying and treating AUD,” wrote Michael F. Mayo-Smith, MD, MPH, of White River Junction (Vt.) VA Medical Center, and Geisel School of Medicine at Dartmouth, Hanover, N.H., and David Lawrence, MD, of the VA Greater Los Angeles Healthcare System and the University of California, Los Angeles.
An intentional discharge protocol can be effective, they noted, as evidenced by a 2014 report in which this approach increased medication-assisted treatment from 0% to 64% in tandem with a decrease in all-cause, 30-day readmission rates.
“There is also growing interest in inpatient addiction consultation services, which have shown [medication] for AUD treatment initiation rates of up to 70% as well as improved engagement in posthospital treatment,” Dr. Mayo-Smith and Dr. Lawrence wrote.
Minority populations need particular attention, they added. “Unfortunately, the availability of evidence-based treatments for AUD does not by itself lead to improved care. We need strategies for widespread adoption so that patients can realize the benefits of these treatments.”
Dr. Bernstein reported funding support from a National Research Service Award and the Massachusetts General Hospital division of general internal medicine; he disclosed fees from Alosa Health. One coauthor was supported by the Agency for Healthcare Research and Quality. Another was supported by the National Institute on Aging and reported relationships with the American College of Cardiology, Boston OIAC Pepper Center, American Heart Association, and US Deprescribing Research Network. Dr. Mayo-Smith disclosed no competing interests. Dr. Lawrence reported fees related to presentations at DDW 2023 and the California Society of Addiction Medicine 2022.
Health care providers are missing opportunities to give medical treatment to high-risk individuals hospitalized for alcohol use disorder (AUD), a national analysis of Medicare beneficiaries reported.
Increasing such patients’ access to psychiatric care and addiction medicine, as well as encouraging medication prescribing by generalists and nonaddiction specialists, are remedial strategies recommended by lead author Eden Y. Bernstein, MD, of the division of general internal medicine at Massachusetts General Hospital and Harvard Medical School, both in Boston, and colleagues.
“Hospitalizations for alcohol use disorder are common,” Dr. Bernstein said in an interview. “Our work shows they represent an underutilized opportunity to engage patients with appropriate treatment, including initiation of medications for alcohol use disorder.”
There is a pressing need for such treatment strategies since 29 million U.S. adults have AUD, and alcohol contributes to more than 140,000 deaths annually, the authors noted.
Rarely initiated either at hospital discharge or during follow-up care, medical therapy for AUD was more likely to be provided to younger patients and those involved with psychiatric care or addiction medicine, Dr. Bernstein’s group reported in Annals of Internal Medicine.Hospital admissions, they argued, give patients more access to clinicians and social workers and the vulnerability experienced during hospitalization may motivate behavioral change.
National study
The cohort included 28,601 AUD hospitalizations for 20,401 unique Medicare patients from 2015 to 2017. About 30% of admissions were for women and about 72% for non-Hispanic Blacks. Discharge initiation of medication for AUD was defined as a pharmacy claim for naltrexone, acamprosate, or disulfiram from the day before discharge to 2 days after.
Overall, just 206 patients (0.7%) initiated medication for AUD within 2 days of discharge and 364 (1.3%) started it within 30 days. Among those discharged with a primary diagnosis of AUD, only 70 (2.3%) started medical therapy within 2 days.
The most predictive demographic factor for discharge medication for AUD was younger age: 18-39 years versus 75 years and older (adjusted odds ratio, 3.87; 95% confidence interval, 1.34-11.16).
Initiation of medication for AUD should involve a long-term treatment plan, according to Dr. Bernstein’s group, and if that is not feasible during hospitalization, patients should be referred for outpatient treatment.
An accompanying editorial agrees that the results offer strong evidence of a missed opportunity to address AUD at a potential flexion point. “Hospitalization is a critical touch point for identifying and treating AUD,” wrote Michael F. Mayo-Smith, MD, MPH, of White River Junction (Vt.) VA Medical Center, and Geisel School of Medicine at Dartmouth, Hanover, N.H., and David Lawrence, MD, of the VA Greater Los Angeles Healthcare System and the University of California, Los Angeles.
An intentional discharge protocol can be effective, they noted, as evidenced by a 2014 report in which this approach increased medication-assisted treatment from 0% to 64% in tandem with a decrease in all-cause, 30-day readmission rates.
“There is also growing interest in inpatient addiction consultation services, which have shown [medication] for AUD treatment initiation rates of up to 70% as well as improved engagement in posthospital treatment,” Dr. Mayo-Smith and Dr. Lawrence wrote.
Minority populations need particular attention, they added. “Unfortunately, the availability of evidence-based treatments for AUD does not by itself lead to improved care. We need strategies for widespread adoption so that patients can realize the benefits of these treatments.”
Dr. Bernstein reported funding support from a National Research Service Award and the Massachusetts General Hospital division of general internal medicine; he disclosed fees from Alosa Health. One coauthor was supported by the Agency for Healthcare Research and Quality. Another was supported by the National Institute on Aging and reported relationships with the American College of Cardiology, Boston OIAC Pepper Center, American Heart Association, and US Deprescribing Research Network. Dr. Mayo-Smith disclosed no competing interests. Dr. Lawrence reported fees related to presentations at DDW 2023 and the California Society of Addiction Medicine 2022.
Health care providers are missing opportunities to give medical treatment to high-risk individuals hospitalized for alcohol use disorder (AUD), a national analysis of Medicare beneficiaries reported.
Increasing such patients’ access to psychiatric care and addiction medicine, as well as encouraging medication prescribing by generalists and nonaddiction specialists, are remedial strategies recommended by lead author Eden Y. Bernstein, MD, of the division of general internal medicine at Massachusetts General Hospital and Harvard Medical School, both in Boston, and colleagues.
“Hospitalizations for alcohol use disorder are common,” Dr. Bernstein said in an interview. “Our work shows they represent an underutilized opportunity to engage patients with appropriate treatment, including initiation of medications for alcohol use disorder.”
There is a pressing need for such treatment strategies since 29 million U.S. adults have AUD, and alcohol contributes to more than 140,000 deaths annually, the authors noted.
Rarely initiated either at hospital discharge or during follow-up care, medical therapy for AUD was more likely to be provided to younger patients and those involved with psychiatric care or addiction medicine, Dr. Bernstein’s group reported in Annals of Internal Medicine.Hospital admissions, they argued, give patients more access to clinicians and social workers and the vulnerability experienced during hospitalization may motivate behavioral change.
National study
The cohort included 28,601 AUD hospitalizations for 20,401 unique Medicare patients from 2015 to 2017. About 30% of admissions were for women and about 72% for non-Hispanic Blacks. Discharge initiation of medication for AUD was defined as a pharmacy claim for naltrexone, acamprosate, or disulfiram from the day before discharge to 2 days after.
Overall, just 206 patients (0.7%) initiated medication for AUD within 2 days of discharge and 364 (1.3%) started it within 30 days. Among those discharged with a primary diagnosis of AUD, only 70 (2.3%) started medical therapy within 2 days.
The most predictive demographic factor for discharge medication for AUD was younger age: 18-39 years versus 75 years and older (adjusted odds ratio, 3.87; 95% confidence interval, 1.34-11.16).
Initiation of medication for AUD should involve a long-term treatment plan, according to Dr. Bernstein’s group, and if that is not feasible during hospitalization, patients should be referred for outpatient treatment.
An accompanying editorial agrees that the results offer strong evidence of a missed opportunity to address AUD at a potential flexion point. “Hospitalization is a critical touch point for identifying and treating AUD,” wrote Michael F. Mayo-Smith, MD, MPH, of White River Junction (Vt.) VA Medical Center, and Geisel School of Medicine at Dartmouth, Hanover, N.H., and David Lawrence, MD, of the VA Greater Los Angeles Healthcare System and the University of California, Los Angeles.
An intentional discharge protocol can be effective, they noted, as evidenced by a 2014 report in which this approach increased medication-assisted treatment from 0% to 64% in tandem with a decrease in all-cause, 30-day readmission rates.
“There is also growing interest in inpatient addiction consultation services, which have shown [medication] for AUD treatment initiation rates of up to 70% as well as improved engagement in posthospital treatment,” Dr. Mayo-Smith and Dr. Lawrence wrote.
Minority populations need particular attention, they added. “Unfortunately, the availability of evidence-based treatments for AUD does not by itself lead to improved care. We need strategies for widespread adoption so that patients can realize the benefits of these treatments.”
Dr. Bernstein reported funding support from a National Research Service Award and the Massachusetts General Hospital division of general internal medicine; he disclosed fees from Alosa Health. One coauthor was supported by the Agency for Healthcare Research and Quality. Another was supported by the National Institute on Aging and reported relationships with the American College of Cardiology, Boston OIAC Pepper Center, American Heart Association, and US Deprescribing Research Network. Dr. Mayo-Smith disclosed no competing interests. Dr. Lawrence reported fees related to presentations at DDW 2023 and the California Society of Addiction Medicine 2022.
Ronny Drapkin, MD, PhD
The field of ovarian cancer has experienced a paradigm shift; ovarian cancer is now known to most often arise from the fallopian tubes.1 The ovaries can act as a magnet for tumor cells that may originate elsewhere in the body. Moreover, it has been found that relatively simple risk-reducing interventions may virtually eliminate progression to invasive disease in the ovaries.1 These types of discoveries—and others—are igniting new research into novel approaches to improving outcomes for patients with ovarian cancer.
Incidence and Mortality
By 2040, the number of women diagnosed with ovarian cancer annually worldwide is expected to increase by 100% in low Human Development Index (HDI) countries, and by 19-28% in high HDI countries.2 The causes of this increasing incidence are likely to be multifactorial, including both hereditary and modifiable risk factors.3 In addition to increasing population size, the growing prevalence of obesity, estrogen exposures, and nulliparity are particularly pertinent as potential causes of the rising incidence of ovarian cancer in younger women. The number of ovarian cancer-related deaths is also projected to rise from about 200,000 to nearly 314,000 annually, an increase of over 50% from 2020.2,4 Although outcomes in developed regions and nations continue to improve somewhat, 5-year survival rates range from 36% to 46%.5 These outcomes are nevertheless dismal when compared with 5-year survival rates from other cancer types, such as breast cancer, which are approaching 90%.6
Principal Histotypes
The principal histotypes in ovarian cancer are epithelial in origin and include high-grade serous carcinoma, clear-cell carcinoma, endometrioid carcinoma, low-grade serous carcinoma, and mucinous carcinoma. Other rarer types are nonepithelial, ie, arising from stromal or germ cell lines.7 Incidence rates appear to be affected over time by trends such as birth rates, use of combination oral contraceptives, and menopausal hormone therapy.8Figure 1 shows that most ovarian cancers—approximately 70%—are high-grade serous carcinoma, although in Asian countries clear cell and endometrioid carcinomas comprise a higher proportion.9
Figure 1.Major Histotypes in Ovarian Cancer Most ovarian cancers are epithelial carcinomas. High-grade serous carcinoma is the most common, whereas the other subtypes represent 10% or fewer cases each.9
Into the Fallopian Tube
One of the most salient and dramatic discoveries of the last 2 decades has been the finding that high-grade, clear-cell, and endometrioid tumors appear to arise from tissues not normally present in the ovary.1 As a result of risk-reducing efforts to prevent serous cancers in women with genetic predisposition to develop ovarian cancer (ie, those with BRCA1 or BRCA2 mutations), it became increasingly clear that many early cancers arose in the fallopian tube,10-12 with the distal portion—the fimbria—as the most common site of origin.13-16
Figure 2 depicts the female reproductive tract, including the location of the fimbria compared with the ovaries. Moreover, lesions observed in the fallopian tube fimbria—serous tubal intraepithelial carcinomas (STICs)—were identified as precursors of ovarian cancer, with a window of 7 years between development of STIC and the beginning of an ovarian cancer.14,16
Figure 2. Serous Tubal Intraepithelial Carcinomas Lesions that develop in the fallopian tube fimbria, called serous tubal intraepithelial carcinomas (STICs), have been identified as precursors of ovarian cancer.
Early Detection
Early, localized ovarian cancer is asymptomatic; by the time a patient presents with symptoms, even with nonspecific abdominal complaints, the disease is almost invariably advanced. The concept of early detection has improved both the rate of cancer diagnoses and outcomes for some malignancies, such as cervical, colorectal, breast, and lung cancers,17 but this strategy is yet to be effectively applied in ovarian cancer. A large, population-based study, for instance, yielded negative results when multimodal screening (using both measurement of CA125 blood levels and transvaginal ultrasound imaging) failed to improve survival, even though such screening was able to detect lower stage disease.18 Emerging technologies, such as liquid biopsies and uterine lavage, which seek to detect potential biomarkers (new types of blood tests) of ovarian cancer at an early stage and closer to the site of tumor origin, are being investigated and refined but are not yet ready for clinical use, particularly at the population level for screening.19
Risk-Reducing Interventions
Use of oral contraceptives has been associated with a significant reduction in risk for ovarian cancer, but the potential risks (eg, increased risk for breast cancer, increased risk for venous thromboembolism) preclude its universal recommendation.20-22 Simple removal of the fallopian tube, salpingectomy, was proposed as a potential intervention to “intercept” the progression of a STIC to cancer. Researchers recently compared simple salpingectomy with salpingo-oophorectomy as a risk-reduction procedure in carriers of BRCA 1/2 pathogenic variants after they had completed childbearing.23
These investigators proposed that later removal of the ovaries would delay menopause and would contribute to fewer/less severe symptoms, such as hot flashes, disturbed sleep, and sexual issues, as well as maintain or improve overall quality of life. The hypothesis was supported by results, which showed that patients had better menopause-related quality of life after salpingectomy than after salpingo-oophorectomy, regardless of the use of hormone replacement therapy.23 The oncologic safety of this approach was subsequently demonstrated by other studies that showed a significantly lower incidence of ovarian cancers in women who had undergone opportunistic salpingectomy.22,24,25
An international prospective trial, TUBA-WISPII, is now underway to test the hypothesis that postponement of oophorectomy after salpingectomy is non-inferior to standard salpingo-oophorectomy in terms of ovarian cancer risk for patients at high risk.26
Treatment
First-Line Therapy Currently, there are no durable curative therapies for ovarian cancer once advanced disease has been diagnosed.
Surgery plus platinum-based chemotherapy. Most patients, even those diagnosed with advanced disease, are treated initially with debulking surgery, ideally by a gynecologic oncologist, and adjuvant chemotherapy. Most ovarian carcinomas are initially platinum-sensitive, but resistance and disease recurrence are almost inevitable. According to the National Comprehensive Cancer Network (NCCN) guidelines for ovarian cancer,27 preferred chemotherapy regimens include paclitaxel and carboplatin with or without bevacizumab, docetaxel and carboplatin, or carboplatin and liposomal doxorubicin. Numerous other regimens, combinations, and agents are included in the guidelines to help providers customize treatment plans.
Neoadjuvant vs adjuvant regimens. Neoadjuvant chemotherapy has been used for other malignancies to gauge sensitivity to systemic treatments and to improve surgical margins.28 Thus far, though, outcomes in ovarian cancer have been similar whether patients were given neoadjuvant or adjuvant treatment in the perioperative period. Individualizing these decisions based on ability to surgically resect, patient age, tumor histology, disease stage, and performance status is recommended.29
Intraperitoneal chemotherapy. Other approaches have been explored to reduce risk for micrometastases after surgery. Hyperthermic intraperitoneal chemotherapy,32 for instance, administered immediately after cytoreductive surgery was studied as a technique that might prevent some of the risks and adverse effects associated with intraperitoneal chemotherapy.31 Results showed some improvement in progression-free survival and overall survival in a subgroup of patients who underwent interval cytoreductive surgery after neoadjuvant therapy, but no differences were observed for the larger population with advanced epithelial ovarian cancer. Adverse reactions to intraperitoneal chemotherapy were also observed.
Angiogenesis inhibition. Tumors need energy and oxygen to grow. Angiogenesis is the process of new blood vessel formation that provides the tumor with nutrients. Blocking angiogenesis can thwart tumor growth and improve patient outcomes. Bevacizumab is an antiangiogenic agent that has been extensively studied for 2 decades for many cancers including ovarian carcinoma. The NCCN guidelines note that bevacizumab may be considered as part of a first-line regimen with platinum agents, as maintenance in patients with wild-type or unknown BRCA mutation status and a good response to first-line therapy, or in combination with a poly (ADP-ribose) polymerase (PARP) inhibitor in eligible patients.27
PARP inhibitors. Approximately half of all high-grade serous ovarian carcinomas exhibit some defect in the ability to repair DNA damage using the homologous recombination (HR) pathway. These tumors include those with mutations in the BRCA1, BRCA2, and other HR genes. Defects in HR make tumors more dependent on back-up DNA repair systems, including the activity of PARP. PARP inhibitors were developed to specifically target HR-deficient tumors. To date, 3 PARP inhibitors have been approved for use in ovarian cancer—olaparib, rucaparib, and niraparib. Their use has expanded from later-line use in patients with BRCA1/2-mutated tumors to include frontline maintenance regimens for women with high-grade serous and high-grade endometrioid carcinomas, as well as women with recurrent disease.32 Numerous clinical trials are ongoing to develop next-generation PARP inhibitors and to explore their efficacy in combination with chemotherapy and other targeted agents.
Resistance and Disease Progression: Second-Line and Subsequent Treatment
A number of second-line and subsequent systemic treatment regimens may be considered when primary platinum-based chemotherapy and/or maintenance are no longer effective.33,34 As emphasized by the NCCN, a clinical trial is always an appropriate option, depending on eligibility, and sometimes a second cytoreductive surgery35,36 may be considered for patients who experience radiographic and/or clinical relapse after a long disease-free interval (6+ months). Each line of treatment is associated with progressively lower response rates and shorter durations of response. According to the NCCN guidelines, as patient performance status decreases and the toxicities of each line of therapy accumulate, assessment for palliative care should be considered and discussed.27
Investigational Approaches
With the high mortality rate associated with ovarian cancer, the challenges of detecting the disease at its early stages, and the lack of therapies that can significantly extend progression-free and overall survival in patients with advanced disease, many investigators are focused on novel treatment approaches. Preclinical observations, for instance, showing synergy between ataxia telangiectasia and RAD3-related (ATR) kinase inhibitors and PARP inhibitors led researchers to initiate a phase 2 study of olaparib plus ceralasertib (an ATR inhibitor) in patients with recurrent, platinum-resistant epithelial ovarian cancer.37 No objective responses were noted, but some signals of activity were seen among patients with BRCA1 mutations.
Due to success in other malignancies, immunotherapy is also being explored. Although some promising signals were reported at 6 months when nivolumab, a PD-1 (programmed cell death protein 1) inhibitor, and ipilimumab, a cytotoxic T-lymphocyte-associated antigen 4 antibody, were combined to treat patients with platinum-resistant epithelial ovarian cancer; final results are not yet available.38
Ovarian cancer is sometimes characterized as immunologically “cold.” This description means that immune cells, especially T cells, are not able to enter the tumor and destroy the cancer cells. It also means that these tumors are not as responsive to immune-based treatments. Therefore, some researchers are examining novel alternative immunotherapy strategies, such as chimeric antigen receptor T-cell (CAR-T) therapy.39 When a CAR T-cell encounters a tumor antigen, the CAR T-cell becomes activated. Activated CAR T-cells multiply, signal to other immune cells, and ultimately kill the tumor cells. Although CAR T-cell therapy has been tremendously successful in hematologic malignancies, to date, the benefits in solid tumors have been modest.39 However, there is significant enthusiasm for novel tumor antigens that can be targeted by CAR-T therapy, including mesothelin, folate receptor, Claudin-6, B7-H3, B7-H4, HER2, CD47, and L1-CAM, among others.40
Other investigational strategies include a p53 vaccine that would enhance the patient’s immunologic response to abnormal proteins produced by a mutated p53 gene, which is the most common finding in ovarian tumors.
Although researchers are investigating many approaches to treating advanced ovarian cancer, one strategy that has been pursued in other cancer settings—development of antibody-drug conjugates (ADCs)41—has seen promising results. In the late fall of 2022, the US Food and Drug Administration granted accelerated approval for mirvetuximab soravtansine-gynx for use in patients with a specific type of type of tumor (folate receptor alpha [FRα]-positive) when platinum resistance emerges.42 A companion diagnostic assay was also approved for selecting patients with FRα-positive disease. Several other clinical trials are investigating the efficacy of targeting other ovarian tumor antigens using the ADC approach. These targets include NaPi2b, mesothelin, B7-H4, Claudin-6, and Trop-2.43,44
Progress to Come
Progress in ovarian cancer will be made through a multipronged approach that includes interventions that may proactively “intercept” the development of cancer (eg, salpingectomy for women planning to have other simple gynecologic procedures after childbearing is complete). Although prophylactic surgeries are often undertaken by individuals at high risk for ovarian cancer because of genetic findings, such as BRCA1/2 abnormalities, even women with normal risk may consider when planning tubal ligation, removing their tubes, and other routine procedures. A substantial number of malignant tumors, and associated morbidity and mortality, may be thwarted as a result. The question of whether to treat when a STIC is detected remains to be answered.
The search for better methods of early detection continues, as local therapies for early-stage disease are invariably more effective than treatments in the advanced and/or metastatic setting.
Finally, as with certain other malignancies, even in the advanced setting, effective, often targeted, treatments can significantly prolong both progression-free and overall survival, transforming an often-lethal disease into a chronic one that allows patients to enjoy a better life expectancy with good quality of life.
Karnezis AN, Cho KR, Gilks CB, Pearce CL, Huntsman DG. The disparate origins of ovarian cancers: pathogenesis and prevention strategies. Nat Rev Cancer. 2017;17(1):65-74. doi:10.1038/nrc.2016.113
Cabasag CJ, Fagan PJ, Ferlay J, et al. Ovarian cancer today and tomorrow: A global assessment by world region and Human Development Index using GLOBOCAN 2020. Int J Cancer. 2022;151(9):1535-1541. doi:10.1002/ijc.34002
Huang J, Chan WC, Ngai CH, et al. Worldwide burden, risk factors, and temporal trends of ovarian cancer: a global study. Cancers (Basel). 2022;14(9):2230. doi:10.3390/cancers14092230
Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17-48. doi:10.3322/caac.21763
Phung MT, Pearce CL, Meza R, Jeon J. Trends of ovarian cancer incidence by histotype and race/ethnicity in the United States 1992–2019. Cancer Res Commun. 2023;3(1):1-8. doi:10.1158/2767-9764.CRC-22-0410
Coburn SB, Bray F, Sherman ME, Trabert B. International patterns and trends in ovarian cancer incidence, overall and by histologic subtype. Int J Cancer. 2017;140(11):2451-2460. doi:10.1002/ijc.30676
Kroeger PT Jr, Drapkin R. Pathogenesis and heterogeneity of ovarian cancer. Curr Obstet Gynecol. 2017;29(1):26-34. doi:10.1097/GCO.0000000000000340
Shih lM, Wang Y, Wang TL. The origin of ovarian cancer species and precancerous landscape. Am J Pathol. 2021;191(1):26-39. doi:10.1016/j.ajpath.2020.09.006
Meserve EEK, Brouwer J, Crum CP. Serous tubal intraepithelial neoplasia: the concept and its application. Mod Pathol. 2017;30(5):710-721. doi:10.1038/modpathol.2016.23
Crum CP, Drapkin R, Kindelberger D, Medeiros F, Miron A, Lee Y. Lessons from BRCA: the tubal fimbria emerges as an origin for pelvic serous cancer. Clin Med Res. 2007;5(1):35-44. doi:10.3121/cmr.2007.702
Wu RC, Wang P, Lin SF, et al. Genomic landscape and evolutionary trajectories of ovarian cancer precursor lesions. J Pathol. 2019;248(1):41-50. doi:10.1002/path.5219
Eckert MA, Pan S, Hernandez KM, et al. Genomics of ovarian cancer progression reveals diverse metastatic trajectories including intraepithelial metastasis to the fallopian tube. Cancer Discov. 2016;6(12):1342-1351. doi:10.1158/2159-8290.CD-16-0607
Labidi-Galy SI, Papp E, Hallberg D, et al. High grade serous ovarian carcinomas originate in the fallopian tube. Nat Comm. 2017;8(1):1093. doi:10.1038/s41467-017-00962-1
Menon U, Gentry-Maharaj A, Burnell M, et al. Ovarian cancer population screening and mortality after long-term follow-up in the UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS): a randomised controlled trial. Lancet. 2021;397(10290):2182-2193. doi:10.1016/S0140-6736(21)00731-5
Žilovic D, Ciurliene R, Sabaliauskaite R, Jarmalaitė S. Future screening prospects for ovarian cancer. Cancers (Basel). 2021;13(15):3840. doi:10.3390/cancers1315384
Michels KA, Pfeiffer RM, Brinton LA, Trabert B. Modification of the associations between duration of oral contraceptive use and ovarian, endometrial, breast, and colorectal cancers. JAMA Oncol. 2018;4(4):516-521. doi:10.1001/jamaoncol.2017.4942
Havrilesky LJ, Moorman PG, Lowery WJ, et al. Oral contraceptive pills as primary prevention for ovarian cancer: a systematic review and meta-analysis. Obstet Gynecol. 2013;122(1):139-147. doi:10.1097/AOG.0b013e318291c235
Kotsopoulos J, Narod SA. Prophylactic salpingectomy for the prevention of ovarian cancer: who should we target? Int J Cancer. 2020;147(5):1245-1251. doi:10.1002/ijc.32916
Steenbeek MP, Harmsen MG, Hoogerbrugge N, et al. Association of salpingectomy with delayed oophorectomy versus salpingo-oophorectomy with quality of life in BRCA 1/2 pathogenic variant carriers. A nonrandomized controlled trial. JAMA Oncol. 2021;7(8):1203-1212. doi:10.1001/jamaoncol.2021.1590
Hanley GE, Pearce CL, Talhouk A, et al. Outcomes from opportunistic salpingectomy for ovarian cancer prevention. JAMA Netw Open. 2022;5(2):e2147343. doi:10.1001/jamanetworkopen.2021.47343
Steenbeek MP, van Bommel MHD, intHout J, et al. TUBectomy with delayed oophorectomy as an alternative to risk-reducing salpingo-oophorectomy in high-risk women to assess the safety of prevention: the TUBA-WISP II study protocol [published online ahead of print, 2023 Apr 12]. Int J Gynecol Cancer. 2023;ijgc-2023-004377. doi:10.1136/ijgc-2023-004377
National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: Ovarian cancer including fallopian tube cancer and primary peritoneal cancer. Version 1.2023. December 22, 2022. Accessed May 8, 2023. https://www.nccn.org/professionals/physician_gls/pdf/ovarian.pdf
Chawla A, Hunt KK, Mittendorf EA. Surgical considerations in patients receiving neoadjuvant systemic therapy. Future Oncol. 2012;8(3):239-250. doi:10.2217/fon.12.12
Coleridge SL, Bryant A, Kehoe S, Morrison J. Neoadjuvant chemotherapy before surgery versus surgery followed by chemotherapy for initial treatment in advanced ovarian epithelial cancer. Cochrane Database Syst Rev. 2021;7(7):CD005343. doi:10.1002/14651858.CD005343.pub6
Lim MC, Chang SJ, Park B, et al; HIPEC for Ovarian Cancer Collaborators. Survival after hyperthermic intraperitoneal chemotherapy and primary or interval cytoreductive surgery in ovarian cancer: a randomized clinical trial. JAMA Surg. 2022;157(5):374-383. doi:10.1001/jamasurg.2022.0143
Walker JL, Brady MF, Wenzel L, et al. Randomized trial of intravenous versus intraperitoneal chemotherapy plus bevacizumab in advanced ovarian carcinoma: an NRG Oncology/Gynecologic Oncology Group study. J Clin Oncol. 2019;37(16):1380-1390. doi:10.1200/JCO.18.01568
Konstantinopoulos PA, Lheureux S, Moore KN. PARP inhibitors for ovarian cancer: current indications, future combinations, and novel assets in development to target DNA damage repair. Am Soc Clin Oncol Educ Book. 2020;40:1-16. doi:10.1200/EDBK_288015
Markman M. Pharmaceutical management of ovarian cancer: current status. Drugs. 2019;79(11):1231-1239. doi:10.1007/s40265-019-01158-1
Bristow RE, Puri I, Chi DS. Cytoreductive surgery for recurrent ovarian cancer: a meta-analysis. Gynecol Oncol. 2009;112(1):265-274. doi:10.1016/j.ygyno.2008.08.033
de Bree E, Michelakis D, Anagnostopoulou E. The current role of secondary cytoreductive surgery for recurrent ovarian cancer. Front Oncol. 2022;12:1029976. doi:10.3389/fonc.2022.1029976
Shah PD, Wethington SL, Pagan C, et al. Combination ATR and PARP inhibitor (CAPRI): a phase 2 study of ceralasertib plus olaparib in patients with recurrent, platinum-resistant epithelial ovarian cancer. Gynecol Oncol. 2021;163(2): 246-253. doi:10.1016/j.ygyno.2021.08.024
Borella F, Ghisoni E, Giannone G, et al. Immune checkpoint inhibitors in epithelial ovarian cancer: an overview on efficacy and future perspectives. Diagnostics (Basel). 2020;10(3):146. doi:10.3390/diagnostics10030146
Wu JWY, Dand S, Doig L, et al. T-cell receptor therapy in the treatment of ovarian cancer: a mini review. Front Immunol. 2021;12:672502. doi:10.3389/fimmu.2021.672502
Benard E, Casey NP, Inderberg EM, Wälchli S. SJI 2020 special issue: a catalogue of ovarian cancer targets for CAR therapy. Scand J Immunol. 2020;92(4):e12917 doi:10.1111/sji.12917
Martín-Sabroso C, Lozza I, Torres-Suárez AI, Fraguas-Sánchez AI. Antibodyantineoplastic conjugates in gynecological malignancies: current status and future perspectives. Pharmaceutics. 2021;13(10):1705. doi:10.3390/pharmaceutics13101705
Tolcher A, Hamilton E, Coleman RL. The evolving landscape of antibody-drug conjugates in gynecologic cancers. Cancer Treat Rev. 2023;116:102546. doi:10.1016/j.ctrv.2023.102546
Banerjee S, Drapkin R, Richarson DL, Birrer M. Targeting NaPi2b in ovarian cancer. Cancer Treat Rev. 2023;112:102489. doi:10.1016/j.ctrv.2022.102489
Author and Disclosure Information
Ronny Drapkin, MD, PhD Franklin Payne Associate Professor of Pathology Department of Obstetrics and Gynecology University of Pennsylvania Perelman School of Medicine; Director, Ovarian Cancer Research Center Department of Obstetrics and Gynecology Hospital of the University of Pennsylvania Philadelphia, PA
Ronny Drapkin, MD, PhD, has disclosed the following relevant financial relationships: Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: Repare Therapeutics (scientific advisory board); VOC Health Inc (advisor). Received income in an amount equal to or greater than $250 from: Repare Therapeutics (scientific advisory board).
Ronny Drapkin, MD, PhD Franklin Payne Associate Professor of Pathology Department of Obstetrics and Gynecology University of Pennsylvania Perelman School of Medicine; Director, Ovarian Cancer Research Center Department of Obstetrics and Gynecology Hospital of the University of Pennsylvania Philadelphia, PA
Ronny Drapkin, MD, PhD, has disclosed the following relevant financial relationships: Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: Repare Therapeutics (scientific advisory board); VOC Health Inc (advisor). Received income in an amount equal to or greater than $250 from: Repare Therapeutics (scientific advisory board).
Author and Disclosure Information
Ronny Drapkin, MD, PhD Franklin Payne Associate Professor of Pathology Department of Obstetrics and Gynecology University of Pennsylvania Perelman School of Medicine; Director, Ovarian Cancer Research Center Department of Obstetrics and Gynecology Hospital of the University of Pennsylvania Philadelphia, PA
Ronny Drapkin, MD, PhD, has disclosed the following relevant financial relationships: Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: Repare Therapeutics (scientific advisory board); VOC Health Inc (advisor). Received income in an amount equal to or greater than $250 from: Repare Therapeutics (scientific advisory board).
Ronny Drapkin, MD, PhD
The field of ovarian cancer has experienced a paradigm shift; ovarian cancer is now known to most often arise from the fallopian tubes.1 The ovaries can act as a magnet for tumor cells that may originate elsewhere in the body. Moreover, it has been found that relatively simple risk-reducing interventions may virtually eliminate progression to invasive disease in the ovaries.1 These types of discoveries—and others—are igniting new research into novel approaches to improving outcomes for patients with ovarian cancer.
Incidence and Mortality
By 2040, the number of women diagnosed with ovarian cancer annually worldwide is expected to increase by 100% in low Human Development Index (HDI) countries, and by 19-28% in high HDI countries.2 The causes of this increasing incidence are likely to be multifactorial, including both hereditary and modifiable risk factors.3 In addition to increasing population size, the growing prevalence of obesity, estrogen exposures, and nulliparity are particularly pertinent as potential causes of the rising incidence of ovarian cancer in younger women. The number of ovarian cancer-related deaths is also projected to rise from about 200,000 to nearly 314,000 annually, an increase of over 50% from 2020.2,4 Although outcomes in developed regions and nations continue to improve somewhat, 5-year survival rates range from 36% to 46%.5 These outcomes are nevertheless dismal when compared with 5-year survival rates from other cancer types, such as breast cancer, which are approaching 90%.6
Principal Histotypes
The principal histotypes in ovarian cancer are epithelial in origin and include high-grade serous carcinoma, clear-cell carcinoma, endometrioid carcinoma, low-grade serous carcinoma, and mucinous carcinoma. Other rarer types are nonepithelial, ie, arising from stromal or germ cell lines.7 Incidence rates appear to be affected over time by trends such as birth rates, use of combination oral contraceptives, and menopausal hormone therapy.8Figure 1 shows that most ovarian cancers—approximately 70%—are high-grade serous carcinoma, although in Asian countries clear cell and endometrioid carcinomas comprise a higher proportion.9
Figure 1.Major Histotypes in Ovarian Cancer Most ovarian cancers are epithelial carcinomas. High-grade serous carcinoma is the most common, whereas the other subtypes represent 10% or fewer cases each.9
Into the Fallopian Tube
One of the most salient and dramatic discoveries of the last 2 decades has been the finding that high-grade, clear-cell, and endometrioid tumors appear to arise from tissues not normally present in the ovary.1 As a result of risk-reducing efforts to prevent serous cancers in women with genetic predisposition to develop ovarian cancer (ie, those with BRCA1 or BRCA2 mutations), it became increasingly clear that many early cancers arose in the fallopian tube,10-12 with the distal portion—the fimbria—as the most common site of origin.13-16
Figure 2 depicts the female reproductive tract, including the location of the fimbria compared with the ovaries. Moreover, lesions observed in the fallopian tube fimbria—serous tubal intraepithelial carcinomas (STICs)—were identified as precursors of ovarian cancer, with a window of 7 years between development of STIC and the beginning of an ovarian cancer.14,16
Figure 2. Serous Tubal Intraepithelial Carcinomas Lesions that develop in the fallopian tube fimbria, called serous tubal intraepithelial carcinomas (STICs), have been identified as precursors of ovarian cancer.
Early Detection
Early, localized ovarian cancer is asymptomatic; by the time a patient presents with symptoms, even with nonspecific abdominal complaints, the disease is almost invariably advanced. The concept of early detection has improved both the rate of cancer diagnoses and outcomes for some malignancies, such as cervical, colorectal, breast, and lung cancers,17 but this strategy is yet to be effectively applied in ovarian cancer. A large, population-based study, for instance, yielded negative results when multimodal screening (using both measurement of CA125 blood levels and transvaginal ultrasound imaging) failed to improve survival, even though such screening was able to detect lower stage disease.18 Emerging technologies, such as liquid biopsies and uterine lavage, which seek to detect potential biomarkers (new types of blood tests) of ovarian cancer at an early stage and closer to the site of tumor origin, are being investigated and refined but are not yet ready for clinical use, particularly at the population level for screening.19
Risk-Reducing Interventions
Use of oral contraceptives has been associated with a significant reduction in risk for ovarian cancer, but the potential risks (eg, increased risk for breast cancer, increased risk for venous thromboembolism) preclude its universal recommendation.20-22 Simple removal of the fallopian tube, salpingectomy, was proposed as a potential intervention to “intercept” the progression of a STIC to cancer. Researchers recently compared simple salpingectomy with salpingo-oophorectomy as a risk-reduction procedure in carriers of BRCA 1/2 pathogenic variants after they had completed childbearing.23
These investigators proposed that later removal of the ovaries would delay menopause and would contribute to fewer/less severe symptoms, such as hot flashes, disturbed sleep, and sexual issues, as well as maintain or improve overall quality of life. The hypothesis was supported by results, which showed that patients had better menopause-related quality of life after salpingectomy than after salpingo-oophorectomy, regardless of the use of hormone replacement therapy.23 The oncologic safety of this approach was subsequently demonstrated by other studies that showed a significantly lower incidence of ovarian cancers in women who had undergone opportunistic salpingectomy.22,24,25
An international prospective trial, TUBA-WISPII, is now underway to test the hypothesis that postponement of oophorectomy after salpingectomy is non-inferior to standard salpingo-oophorectomy in terms of ovarian cancer risk for patients at high risk.26
Treatment
First-Line Therapy Currently, there are no durable curative therapies for ovarian cancer once advanced disease has been diagnosed.
Surgery plus platinum-based chemotherapy. Most patients, even those diagnosed with advanced disease, are treated initially with debulking surgery, ideally by a gynecologic oncologist, and adjuvant chemotherapy. Most ovarian carcinomas are initially platinum-sensitive, but resistance and disease recurrence are almost inevitable. According to the National Comprehensive Cancer Network (NCCN) guidelines for ovarian cancer,27 preferred chemotherapy regimens include paclitaxel and carboplatin with or without bevacizumab, docetaxel and carboplatin, or carboplatin and liposomal doxorubicin. Numerous other regimens, combinations, and agents are included in the guidelines to help providers customize treatment plans.
Neoadjuvant vs adjuvant regimens. Neoadjuvant chemotherapy has been used for other malignancies to gauge sensitivity to systemic treatments and to improve surgical margins.28 Thus far, though, outcomes in ovarian cancer have been similar whether patients were given neoadjuvant or adjuvant treatment in the perioperative period. Individualizing these decisions based on ability to surgically resect, patient age, tumor histology, disease stage, and performance status is recommended.29
Intraperitoneal chemotherapy. Other approaches have been explored to reduce risk for micrometastases after surgery. Hyperthermic intraperitoneal chemotherapy,32 for instance, administered immediately after cytoreductive surgery was studied as a technique that might prevent some of the risks and adverse effects associated with intraperitoneal chemotherapy.31 Results showed some improvement in progression-free survival and overall survival in a subgroup of patients who underwent interval cytoreductive surgery after neoadjuvant therapy, but no differences were observed for the larger population with advanced epithelial ovarian cancer. Adverse reactions to intraperitoneal chemotherapy were also observed.
Angiogenesis inhibition. Tumors need energy and oxygen to grow. Angiogenesis is the process of new blood vessel formation that provides the tumor with nutrients. Blocking angiogenesis can thwart tumor growth and improve patient outcomes. Bevacizumab is an antiangiogenic agent that has been extensively studied for 2 decades for many cancers including ovarian carcinoma. The NCCN guidelines note that bevacizumab may be considered as part of a first-line regimen with platinum agents, as maintenance in patients with wild-type or unknown BRCA mutation status and a good response to first-line therapy, or in combination with a poly (ADP-ribose) polymerase (PARP) inhibitor in eligible patients.27
PARP inhibitors. Approximately half of all high-grade serous ovarian carcinomas exhibit some defect in the ability to repair DNA damage using the homologous recombination (HR) pathway. These tumors include those with mutations in the BRCA1, BRCA2, and other HR genes. Defects in HR make tumors more dependent on back-up DNA repair systems, including the activity of PARP. PARP inhibitors were developed to specifically target HR-deficient tumors. To date, 3 PARP inhibitors have been approved for use in ovarian cancer—olaparib, rucaparib, and niraparib. Their use has expanded from later-line use in patients with BRCA1/2-mutated tumors to include frontline maintenance regimens for women with high-grade serous and high-grade endometrioid carcinomas, as well as women with recurrent disease.32 Numerous clinical trials are ongoing to develop next-generation PARP inhibitors and to explore their efficacy in combination with chemotherapy and other targeted agents.
Resistance and Disease Progression: Second-Line and Subsequent Treatment
A number of second-line and subsequent systemic treatment regimens may be considered when primary platinum-based chemotherapy and/or maintenance are no longer effective.33,34 As emphasized by the NCCN, a clinical trial is always an appropriate option, depending on eligibility, and sometimes a second cytoreductive surgery35,36 may be considered for patients who experience radiographic and/or clinical relapse after a long disease-free interval (6+ months). Each line of treatment is associated with progressively lower response rates and shorter durations of response. According to the NCCN guidelines, as patient performance status decreases and the toxicities of each line of therapy accumulate, assessment for palliative care should be considered and discussed.27
Investigational Approaches
With the high mortality rate associated with ovarian cancer, the challenges of detecting the disease at its early stages, and the lack of therapies that can significantly extend progression-free and overall survival in patients with advanced disease, many investigators are focused on novel treatment approaches. Preclinical observations, for instance, showing synergy between ataxia telangiectasia and RAD3-related (ATR) kinase inhibitors and PARP inhibitors led researchers to initiate a phase 2 study of olaparib plus ceralasertib (an ATR inhibitor) in patients with recurrent, platinum-resistant epithelial ovarian cancer.37 No objective responses were noted, but some signals of activity were seen among patients with BRCA1 mutations.
Due to success in other malignancies, immunotherapy is also being explored. Although some promising signals were reported at 6 months when nivolumab, a PD-1 (programmed cell death protein 1) inhibitor, and ipilimumab, a cytotoxic T-lymphocyte-associated antigen 4 antibody, were combined to treat patients with platinum-resistant epithelial ovarian cancer; final results are not yet available.38
Ovarian cancer is sometimes characterized as immunologically “cold.” This description means that immune cells, especially T cells, are not able to enter the tumor and destroy the cancer cells. It also means that these tumors are not as responsive to immune-based treatments. Therefore, some researchers are examining novel alternative immunotherapy strategies, such as chimeric antigen receptor T-cell (CAR-T) therapy.39 When a CAR T-cell encounters a tumor antigen, the CAR T-cell becomes activated. Activated CAR T-cells multiply, signal to other immune cells, and ultimately kill the tumor cells. Although CAR T-cell therapy has been tremendously successful in hematologic malignancies, to date, the benefits in solid tumors have been modest.39 However, there is significant enthusiasm for novel tumor antigens that can be targeted by CAR-T therapy, including mesothelin, folate receptor, Claudin-6, B7-H3, B7-H4, HER2, CD47, and L1-CAM, among others.40
Other investigational strategies include a p53 vaccine that would enhance the patient’s immunologic response to abnormal proteins produced by a mutated p53 gene, which is the most common finding in ovarian tumors.
Although researchers are investigating many approaches to treating advanced ovarian cancer, one strategy that has been pursued in other cancer settings—development of antibody-drug conjugates (ADCs)41—has seen promising results. In the late fall of 2022, the US Food and Drug Administration granted accelerated approval for mirvetuximab soravtansine-gynx for use in patients with a specific type of type of tumor (folate receptor alpha [FRα]-positive) when platinum resistance emerges.42 A companion diagnostic assay was also approved for selecting patients with FRα-positive disease. Several other clinical trials are investigating the efficacy of targeting other ovarian tumor antigens using the ADC approach. These targets include NaPi2b, mesothelin, B7-H4, Claudin-6, and Trop-2.43,44
Progress to Come
Progress in ovarian cancer will be made through a multipronged approach that includes interventions that may proactively “intercept” the development of cancer (eg, salpingectomy for women planning to have other simple gynecologic procedures after childbearing is complete). Although prophylactic surgeries are often undertaken by individuals at high risk for ovarian cancer because of genetic findings, such as BRCA1/2 abnormalities, even women with normal risk may consider when planning tubal ligation, removing their tubes, and other routine procedures. A substantial number of malignant tumors, and associated morbidity and mortality, may be thwarted as a result. The question of whether to treat when a STIC is detected remains to be answered.
The search for better methods of early detection continues, as local therapies for early-stage disease are invariably more effective than treatments in the advanced and/or metastatic setting.
Finally, as with certain other malignancies, even in the advanced setting, effective, often targeted, treatments can significantly prolong both progression-free and overall survival, transforming an often-lethal disease into a chronic one that allows patients to enjoy a better life expectancy with good quality of life.
Ronny Drapkin, MD, PhD
The field of ovarian cancer has experienced a paradigm shift; ovarian cancer is now known to most often arise from the fallopian tubes.1 The ovaries can act as a magnet for tumor cells that may originate elsewhere in the body. Moreover, it has been found that relatively simple risk-reducing interventions may virtually eliminate progression to invasive disease in the ovaries.1 These types of discoveries—and others—are igniting new research into novel approaches to improving outcomes for patients with ovarian cancer.
Incidence and Mortality
By 2040, the number of women diagnosed with ovarian cancer annually worldwide is expected to increase by 100% in low Human Development Index (HDI) countries, and by 19-28% in high HDI countries.2 The causes of this increasing incidence are likely to be multifactorial, including both hereditary and modifiable risk factors.3 In addition to increasing population size, the growing prevalence of obesity, estrogen exposures, and nulliparity are particularly pertinent as potential causes of the rising incidence of ovarian cancer in younger women. The number of ovarian cancer-related deaths is also projected to rise from about 200,000 to nearly 314,000 annually, an increase of over 50% from 2020.2,4 Although outcomes in developed regions and nations continue to improve somewhat, 5-year survival rates range from 36% to 46%.5 These outcomes are nevertheless dismal when compared with 5-year survival rates from other cancer types, such as breast cancer, which are approaching 90%.6
Principal Histotypes
The principal histotypes in ovarian cancer are epithelial in origin and include high-grade serous carcinoma, clear-cell carcinoma, endometrioid carcinoma, low-grade serous carcinoma, and mucinous carcinoma. Other rarer types are nonepithelial, ie, arising from stromal or germ cell lines.7 Incidence rates appear to be affected over time by trends such as birth rates, use of combination oral contraceptives, and menopausal hormone therapy.8Figure 1 shows that most ovarian cancers—approximately 70%—are high-grade serous carcinoma, although in Asian countries clear cell and endometrioid carcinomas comprise a higher proportion.9
Figure 1.Major Histotypes in Ovarian Cancer Most ovarian cancers are epithelial carcinomas. High-grade serous carcinoma is the most common, whereas the other subtypes represent 10% or fewer cases each.9
Into the Fallopian Tube
One of the most salient and dramatic discoveries of the last 2 decades has been the finding that high-grade, clear-cell, and endometrioid tumors appear to arise from tissues not normally present in the ovary.1 As a result of risk-reducing efforts to prevent serous cancers in women with genetic predisposition to develop ovarian cancer (ie, those with BRCA1 or BRCA2 mutations), it became increasingly clear that many early cancers arose in the fallopian tube,10-12 with the distal portion—the fimbria—as the most common site of origin.13-16
Figure 2 depicts the female reproductive tract, including the location of the fimbria compared with the ovaries. Moreover, lesions observed in the fallopian tube fimbria—serous tubal intraepithelial carcinomas (STICs)—were identified as precursors of ovarian cancer, with a window of 7 years between development of STIC and the beginning of an ovarian cancer.14,16
Figure 2. Serous Tubal Intraepithelial Carcinomas Lesions that develop in the fallopian tube fimbria, called serous tubal intraepithelial carcinomas (STICs), have been identified as precursors of ovarian cancer.
Early Detection
Early, localized ovarian cancer is asymptomatic; by the time a patient presents with symptoms, even with nonspecific abdominal complaints, the disease is almost invariably advanced. The concept of early detection has improved both the rate of cancer diagnoses and outcomes for some malignancies, such as cervical, colorectal, breast, and lung cancers,17 but this strategy is yet to be effectively applied in ovarian cancer. A large, population-based study, for instance, yielded negative results when multimodal screening (using both measurement of CA125 blood levels and transvaginal ultrasound imaging) failed to improve survival, even though such screening was able to detect lower stage disease.18 Emerging technologies, such as liquid biopsies and uterine lavage, which seek to detect potential biomarkers (new types of blood tests) of ovarian cancer at an early stage and closer to the site of tumor origin, are being investigated and refined but are not yet ready for clinical use, particularly at the population level for screening.19
Risk-Reducing Interventions
Use of oral contraceptives has been associated with a significant reduction in risk for ovarian cancer, but the potential risks (eg, increased risk for breast cancer, increased risk for venous thromboembolism) preclude its universal recommendation.20-22 Simple removal of the fallopian tube, salpingectomy, was proposed as a potential intervention to “intercept” the progression of a STIC to cancer. Researchers recently compared simple salpingectomy with salpingo-oophorectomy as a risk-reduction procedure in carriers of BRCA 1/2 pathogenic variants after they had completed childbearing.23
These investigators proposed that later removal of the ovaries would delay menopause and would contribute to fewer/less severe symptoms, such as hot flashes, disturbed sleep, and sexual issues, as well as maintain or improve overall quality of life. The hypothesis was supported by results, which showed that patients had better menopause-related quality of life after salpingectomy than after salpingo-oophorectomy, regardless of the use of hormone replacement therapy.23 The oncologic safety of this approach was subsequently demonstrated by other studies that showed a significantly lower incidence of ovarian cancers in women who had undergone opportunistic salpingectomy.22,24,25
An international prospective trial, TUBA-WISPII, is now underway to test the hypothesis that postponement of oophorectomy after salpingectomy is non-inferior to standard salpingo-oophorectomy in terms of ovarian cancer risk for patients at high risk.26
Treatment
First-Line Therapy Currently, there are no durable curative therapies for ovarian cancer once advanced disease has been diagnosed.
Surgery plus platinum-based chemotherapy. Most patients, even those diagnosed with advanced disease, are treated initially with debulking surgery, ideally by a gynecologic oncologist, and adjuvant chemotherapy. Most ovarian carcinomas are initially platinum-sensitive, but resistance and disease recurrence are almost inevitable. According to the National Comprehensive Cancer Network (NCCN) guidelines for ovarian cancer,27 preferred chemotherapy regimens include paclitaxel and carboplatin with or without bevacizumab, docetaxel and carboplatin, or carboplatin and liposomal doxorubicin. Numerous other regimens, combinations, and agents are included in the guidelines to help providers customize treatment plans.
Neoadjuvant vs adjuvant regimens. Neoadjuvant chemotherapy has been used for other malignancies to gauge sensitivity to systemic treatments and to improve surgical margins.28 Thus far, though, outcomes in ovarian cancer have been similar whether patients were given neoadjuvant or adjuvant treatment in the perioperative period. Individualizing these decisions based on ability to surgically resect, patient age, tumor histology, disease stage, and performance status is recommended.29
Intraperitoneal chemotherapy. Other approaches have been explored to reduce risk for micrometastases after surgery. Hyperthermic intraperitoneal chemotherapy,32 for instance, administered immediately after cytoreductive surgery was studied as a technique that might prevent some of the risks and adverse effects associated with intraperitoneal chemotherapy.31 Results showed some improvement in progression-free survival and overall survival in a subgroup of patients who underwent interval cytoreductive surgery after neoadjuvant therapy, but no differences were observed for the larger population with advanced epithelial ovarian cancer. Adverse reactions to intraperitoneal chemotherapy were also observed.
Angiogenesis inhibition. Tumors need energy and oxygen to grow. Angiogenesis is the process of new blood vessel formation that provides the tumor with nutrients. Blocking angiogenesis can thwart tumor growth and improve patient outcomes. Bevacizumab is an antiangiogenic agent that has been extensively studied for 2 decades for many cancers including ovarian carcinoma. The NCCN guidelines note that bevacizumab may be considered as part of a first-line regimen with platinum agents, as maintenance in patients with wild-type or unknown BRCA mutation status and a good response to first-line therapy, or in combination with a poly (ADP-ribose) polymerase (PARP) inhibitor in eligible patients.27
PARP inhibitors. Approximately half of all high-grade serous ovarian carcinomas exhibit some defect in the ability to repair DNA damage using the homologous recombination (HR) pathway. These tumors include those with mutations in the BRCA1, BRCA2, and other HR genes. Defects in HR make tumors more dependent on back-up DNA repair systems, including the activity of PARP. PARP inhibitors were developed to specifically target HR-deficient tumors. To date, 3 PARP inhibitors have been approved for use in ovarian cancer—olaparib, rucaparib, and niraparib. Their use has expanded from later-line use in patients with BRCA1/2-mutated tumors to include frontline maintenance regimens for women with high-grade serous and high-grade endometrioid carcinomas, as well as women with recurrent disease.32 Numerous clinical trials are ongoing to develop next-generation PARP inhibitors and to explore their efficacy in combination with chemotherapy and other targeted agents.
Resistance and Disease Progression: Second-Line and Subsequent Treatment
A number of second-line and subsequent systemic treatment regimens may be considered when primary platinum-based chemotherapy and/or maintenance are no longer effective.33,34 As emphasized by the NCCN, a clinical trial is always an appropriate option, depending on eligibility, and sometimes a second cytoreductive surgery35,36 may be considered for patients who experience radiographic and/or clinical relapse after a long disease-free interval (6+ months). Each line of treatment is associated with progressively lower response rates and shorter durations of response. According to the NCCN guidelines, as patient performance status decreases and the toxicities of each line of therapy accumulate, assessment for palliative care should be considered and discussed.27
Investigational Approaches
With the high mortality rate associated with ovarian cancer, the challenges of detecting the disease at its early stages, and the lack of therapies that can significantly extend progression-free and overall survival in patients with advanced disease, many investigators are focused on novel treatment approaches. Preclinical observations, for instance, showing synergy between ataxia telangiectasia and RAD3-related (ATR) kinase inhibitors and PARP inhibitors led researchers to initiate a phase 2 study of olaparib plus ceralasertib (an ATR inhibitor) in patients with recurrent, platinum-resistant epithelial ovarian cancer.37 No objective responses were noted, but some signals of activity were seen among patients with BRCA1 mutations.
Due to success in other malignancies, immunotherapy is also being explored. Although some promising signals were reported at 6 months when nivolumab, a PD-1 (programmed cell death protein 1) inhibitor, and ipilimumab, a cytotoxic T-lymphocyte-associated antigen 4 antibody, were combined to treat patients with platinum-resistant epithelial ovarian cancer; final results are not yet available.38
Ovarian cancer is sometimes characterized as immunologically “cold.” This description means that immune cells, especially T cells, are not able to enter the tumor and destroy the cancer cells. It also means that these tumors are not as responsive to immune-based treatments. Therefore, some researchers are examining novel alternative immunotherapy strategies, such as chimeric antigen receptor T-cell (CAR-T) therapy.39 When a CAR T-cell encounters a tumor antigen, the CAR T-cell becomes activated. Activated CAR T-cells multiply, signal to other immune cells, and ultimately kill the tumor cells. Although CAR T-cell therapy has been tremendously successful in hematologic malignancies, to date, the benefits in solid tumors have been modest.39 However, there is significant enthusiasm for novel tumor antigens that can be targeted by CAR-T therapy, including mesothelin, folate receptor, Claudin-6, B7-H3, B7-H4, HER2, CD47, and L1-CAM, among others.40
Other investigational strategies include a p53 vaccine that would enhance the patient’s immunologic response to abnormal proteins produced by a mutated p53 gene, which is the most common finding in ovarian tumors.
Although researchers are investigating many approaches to treating advanced ovarian cancer, one strategy that has been pursued in other cancer settings—development of antibody-drug conjugates (ADCs)41—has seen promising results. In the late fall of 2022, the US Food and Drug Administration granted accelerated approval for mirvetuximab soravtansine-gynx for use in patients with a specific type of type of tumor (folate receptor alpha [FRα]-positive) when platinum resistance emerges.42 A companion diagnostic assay was also approved for selecting patients with FRα-positive disease. Several other clinical trials are investigating the efficacy of targeting other ovarian tumor antigens using the ADC approach. These targets include NaPi2b, mesothelin, B7-H4, Claudin-6, and Trop-2.43,44
Progress to Come
Progress in ovarian cancer will be made through a multipronged approach that includes interventions that may proactively “intercept” the development of cancer (eg, salpingectomy for women planning to have other simple gynecologic procedures after childbearing is complete). Although prophylactic surgeries are often undertaken by individuals at high risk for ovarian cancer because of genetic findings, such as BRCA1/2 abnormalities, even women with normal risk may consider when planning tubal ligation, removing their tubes, and other routine procedures. A substantial number of malignant tumors, and associated morbidity and mortality, may be thwarted as a result. The question of whether to treat when a STIC is detected remains to be answered.
The search for better methods of early detection continues, as local therapies for early-stage disease are invariably more effective than treatments in the advanced and/or metastatic setting.
Finally, as with certain other malignancies, even in the advanced setting, effective, often targeted, treatments can significantly prolong both progression-free and overall survival, transforming an often-lethal disease into a chronic one that allows patients to enjoy a better life expectancy with good quality of life.
Karnezis AN, Cho KR, Gilks CB, Pearce CL, Huntsman DG. The disparate origins of ovarian cancers: pathogenesis and prevention strategies. Nat Rev Cancer. 2017;17(1):65-74. doi:10.1038/nrc.2016.113
Cabasag CJ, Fagan PJ, Ferlay J, et al. Ovarian cancer today and tomorrow: A global assessment by world region and Human Development Index using GLOBOCAN 2020. Int J Cancer. 2022;151(9):1535-1541. doi:10.1002/ijc.34002
Huang J, Chan WC, Ngai CH, et al. Worldwide burden, risk factors, and temporal trends of ovarian cancer: a global study. Cancers (Basel). 2022;14(9):2230. doi:10.3390/cancers14092230
Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17-48. doi:10.3322/caac.21763
Phung MT, Pearce CL, Meza R, Jeon J. Trends of ovarian cancer incidence by histotype and race/ethnicity in the United States 1992–2019. Cancer Res Commun. 2023;3(1):1-8. doi:10.1158/2767-9764.CRC-22-0410
Coburn SB, Bray F, Sherman ME, Trabert B. International patterns and trends in ovarian cancer incidence, overall and by histologic subtype. Int J Cancer. 2017;140(11):2451-2460. doi:10.1002/ijc.30676
Kroeger PT Jr, Drapkin R. Pathogenesis and heterogeneity of ovarian cancer. Curr Obstet Gynecol. 2017;29(1):26-34. doi:10.1097/GCO.0000000000000340
Shih lM, Wang Y, Wang TL. The origin of ovarian cancer species and precancerous landscape. Am J Pathol. 2021;191(1):26-39. doi:10.1016/j.ajpath.2020.09.006
Meserve EEK, Brouwer J, Crum CP. Serous tubal intraepithelial neoplasia: the concept and its application. Mod Pathol. 2017;30(5):710-721. doi:10.1038/modpathol.2016.23
Crum CP, Drapkin R, Kindelberger D, Medeiros F, Miron A, Lee Y. Lessons from BRCA: the tubal fimbria emerges as an origin for pelvic serous cancer. Clin Med Res. 2007;5(1):35-44. doi:10.3121/cmr.2007.702
Wu RC, Wang P, Lin SF, et al. Genomic landscape and evolutionary trajectories of ovarian cancer precursor lesions. J Pathol. 2019;248(1):41-50. doi:10.1002/path.5219
Eckert MA, Pan S, Hernandez KM, et al. Genomics of ovarian cancer progression reveals diverse metastatic trajectories including intraepithelial metastasis to the fallopian tube. Cancer Discov. 2016;6(12):1342-1351. doi:10.1158/2159-8290.CD-16-0607
Labidi-Galy SI, Papp E, Hallberg D, et al. High grade serous ovarian carcinomas originate in the fallopian tube. Nat Comm. 2017;8(1):1093. doi:10.1038/s41467-017-00962-1
Menon U, Gentry-Maharaj A, Burnell M, et al. Ovarian cancer population screening and mortality after long-term follow-up in the UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS): a randomised controlled trial. Lancet. 2021;397(10290):2182-2193. doi:10.1016/S0140-6736(21)00731-5
Žilovic D, Ciurliene R, Sabaliauskaite R, Jarmalaitė S. Future screening prospects for ovarian cancer. Cancers (Basel). 2021;13(15):3840. doi:10.3390/cancers1315384
Michels KA, Pfeiffer RM, Brinton LA, Trabert B. Modification of the associations between duration of oral contraceptive use and ovarian, endometrial, breast, and colorectal cancers. JAMA Oncol. 2018;4(4):516-521. doi:10.1001/jamaoncol.2017.4942
Havrilesky LJ, Moorman PG, Lowery WJ, et al. Oral contraceptive pills as primary prevention for ovarian cancer: a systematic review and meta-analysis. Obstet Gynecol. 2013;122(1):139-147. doi:10.1097/AOG.0b013e318291c235
Kotsopoulos J, Narod SA. Prophylactic salpingectomy for the prevention of ovarian cancer: who should we target? Int J Cancer. 2020;147(5):1245-1251. doi:10.1002/ijc.32916
Steenbeek MP, Harmsen MG, Hoogerbrugge N, et al. Association of salpingectomy with delayed oophorectomy versus salpingo-oophorectomy with quality of life in BRCA 1/2 pathogenic variant carriers. A nonrandomized controlled trial. JAMA Oncol. 2021;7(8):1203-1212. doi:10.1001/jamaoncol.2021.1590
Hanley GE, Pearce CL, Talhouk A, et al. Outcomes from opportunistic salpingectomy for ovarian cancer prevention. JAMA Netw Open. 2022;5(2):e2147343. doi:10.1001/jamanetworkopen.2021.47343
Steenbeek MP, van Bommel MHD, intHout J, et al. TUBectomy with delayed oophorectomy as an alternative to risk-reducing salpingo-oophorectomy in high-risk women to assess the safety of prevention: the TUBA-WISP II study protocol [published online ahead of print, 2023 Apr 12]. Int J Gynecol Cancer. 2023;ijgc-2023-004377. doi:10.1136/ijgc-2023-004377
National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: Ovarian cancer including fallopian tube cancer and primary peritoneal cancer. Version 1.2023. December 22, 2022. Accessed May 8, 2023. https://www.nccn.org/professionals/physician_gls/pdf/ovarian.pdf
Chawla A, Hunt KK, Mittendorf EA. Surgical considerations in patients receiving neoadjuvant systemic therapy. Future Oncol. 2012;8(3):239-250. doi:10.2217/fon.12.12
Coleridge SL, Bryant A, Kehoe S, Morrison J. Neoadjuvant chemotherapy before surgery versus surgery followed by chemotherapy for initial treatment in advanced ovarian epithelial cancer. Cochrane Database Syst Rev. 2021;7(7):CD005343. doi:10.1002/14651858.CD005343.pub6
Lim MC, Chang SJ, Park B, et al; HIPEC for Ovarian Cancer Collaborators. Survival after hyperthermic intraperitoneal chemotherapy and primary or interval cytoreductive surgery in ovarian cancer: a randomized clinical trial. JAMA Surg. 2022;157(5):374-383. doi:10.1001/jamasurg.2022.0143
Walker JL, Brady MF, Wenzel L, et al. Randomized trial of intravenous versus intraperitoneal chemotherapy plus bevacizumab in advanced ovarian carcinoma: an NRG Oncology/Gynecologic Oncology Group study. J Clin Oncol. 2019;37(16):1380-1390. doi:10.1200/JCO.18.01568
Konstantinopoulos PA, Lheureux S, Moore KN. PARP inhibitors for ovarian cancer: current indications, future combinations, and novel assets in development to target DNA damage repair. Am Soc Clin Oncol Educ Book. 2020;40:1-16. doi:10.1200/EDBK_288015
Markman M. Pharmaceutical management of ovarian cancer: current status. Drugs. 2019;79(11):1231-1239. doi:10.1007/s40265-019-01158-1
Bristow RE, Puri I, Chi DS. Cytoreductive surgery for recurrent ovarian cancer: a meta-analysis. Gynecol Oncol. 2009;112(1):265-274. doi:10.1016/j.ygyno.2008.08.033
de Bree E, Michelakis D, Anagnostopoulou E. The current role of secondary cytoreductive surgery for recurrent ovarian cancer. Front Oncol. 2022;12:1029976. doi:10.3389/fonc.2022.1029976
Shah PD, Wethington SL, Pagan C, et al. Combination ATR and PARP inhibitor (CAPRI): a phase 2 study of ceralasertib plus olaparib in patients with recurrent, platinum-resistant epithelial ovarian cancer. Gynecol Oncol. 2021;163(2): 246-253. doi:10.1016/j.ygyno.2021.08.024
Borella F, Ghisoni E, Giannone G, et al. Immune checkpoint inhibitors in epithelial ovarian cancer: an overview on efficacy and future perspectives. Diagnostics (Basel). 2020;10(3):146. doi:10.3390/diagnostics10030146
Wu JWY, Dand S, Doig L, et al. T-cell receptor therapy in the treatment of ovarian cancer: a mini review. Front Immunol. 2021;12:672502. doi:10.3389/fimmu.2021.672502
Benard E, Casey NP, Inderberg EM, Wälchli S. SJI 2020 special issue: a catalogue of ovarian cancer targets for CAR therapy. Scand J Immunol. 2020;92(4):e12917 doi:10.1111/sji.12917
Martín-Sabroso C, Lozza I, Torres-Suárez AI, Fraguas-Sánchez AI. Antibodyantineoplastic conjugates in gynecological malignancies: current status and future perspectives. Pharmaceutics. 2021;13(10):1705. doi:10.3390/pharmaceutics13101705
Tolcher A, Hamilton E, Coleman RL. The evolving landscape of antibody-drug conjugates in gynecologic cancers. Cancer Treat Rev. 2023;116:102546. doi:10.1016/j.ctrv.2023.102546
Banerjee S, Drapkin R, Richarson DL, Birrer M. Targeting NaPi2b in ovarian cancer. Cancer Treat Rev. 2023;112:102489. doi:10.1016/j.ctrv.2022.102489
References
Karnezis AN, Cho KR, Gilks CB, Pearce CL, Huntsman DG. The disparate origins of ovarian cancers: pathogenesis and prevention strategies. Nat Rev Cancer. 2017;17(1):65-74. doi:10.1038/nrc.2016.113
Cabasag CJ, Fagan PJ, Ferlay J, et al. Ovarian cancer today and tomorrow: A global assessment by world region and Human Development Index using GLOBOCAN 2020. Int J Cancer. 2022;151(9):1535-1541. doi:10.1002/ijc.34002
Huang J, Chan WC, Ngai CH, et al. Worldwide burden, risk factors, and temporal trends of ovarian cancer: a global study. Cancers (Basel). 2022;14(9):2230. doi:10.3390/cancers14092230
Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17-48. doi:10.3322/caac.21763
Phung MT, Pearce CL, Meza R, Jeon J. Trends of ovarian cancer incidence by histotype and race/ethnicity in the United States 1992–2019. Cancer Res Commun. 2023;3(1):1-8. doi:10.1158/2767-9764.CRC-22-0410
Coburn SB, Bray F, Sherman ME, Trabert B. International patterns and trends in ovarian cancer incidence, overall and by histologic subtype. Int J Cancer. 2017;140(11):2451-2460. doi:10.1002/ijc.30676
Kroeger PT Jr, Drapkin R. Pathogenesis and heterogeneity of ovarian cancer. Curr Obstet Gynecol. 2017;29(1):26-34. doi:10.1097/GCO.0000000000000340
Shih lM, Wang Y, Wang TL. The origin of ovarian cancer species and precancerous landscape. Am J Pathol. 2021;191(1):26-39. doi:10.1016/j.ajpath.2020.09.006
Meserve EEK, Brouwer J, Crum CP. Serous tubal intraepithelial neoplasia: the concept and its application. Mod Pathol. 2017;30(5):710-721. doi:10.1038/modpathol.2016.23
Crum CP, Drapkin R, Kindelberger D, Medeiros F, Miron A, Lee Y. Lessons from BRCA: the tubal fimbria emerges as an origin for pelvic serous cancer. Clin Med Res. 2007;5(1):35-44. doi:10.3121/cmr.2007.702
Wu RC, Wang P, Lin SF, et al. Genomic landscape and evolutionary trajectories of ovarian cancer precursor lesions. J Pathol. 2019;248(1):41-50. doi:10.1002/path.5219
Eckert MA, Pan S, Hernandez KM, et al. Genomics of ovarian cancer progression reveals diverse metastatic trajectories including intraepithelial metastasis to the fallopian tube. Cancer Discov. 2016;6(12):1342-1351. doi:10.1158/2159-8290.CD-16-0607
Labidi-Galy SI, Papp E, Hallberg D, et al. High grade serous ovarian carcinomas originate in the fallopian tube. Nat Comm. 2017;8(1):1093. doi:10.1038/s41467-017-00962-1
Menon U, Gentry-Maharaj A, Burnell M, et al. Ovarian cancer population screening and mortality after long-term follow-up in the UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS): a randomised controlled trial. Lancet. 2021;397(10290):2182-2193. doi:10.1016/S0140-6736(21)00731-5
Žilovic D, Ciurliene R, Sabaliauskaite R, Jarmalaitė S. Future screening prospects for ovarian cancer. Cancers (Basel). 2021;13(15):3840. doi:10.3390/cancers1315384
Michels KA, Pfeiffer RM, Brinton LA, Trabert B. Modification of the associations between duration of oral contraceptive use and ovarian, endometrial, breast, and colorectal cancers. JAMA Oncol. 2018;4(4):516-521. doi:10.1001/jamaoncol.2017.4942
Havrilesky LJ, Moorman PG, Lowery WJ, et al. Oral contraceptive pills as primary prevention for ovarian cancer: a systematic review and meta-analysis. Obstet Gynecol. 2013;122(1):139-147. doi:10.1097/AOG.0b013e318291c235
Kotsopoulos J, Narod SA. Prophylactic salpingectomy for the prevention of ovarian cancer: who should we target? Int J Cancer. 2020;147(5):1245-1251. doi:10.1002/ijc.32916
Steenbeek MP, Harmsen MG, Hoogerbrugge N, et al. Association of salpingectomy with delayed oophorectomy versus salpingo-oophorectomy with quality of life in BRCA 1/2 pathogenic variant carriers. A nonrandomized controlled trial. JAMA Oncol. 2021;7(8):1203-1212. doi:10.1001/jamaoncol.2021.1590
Hanley GE, Pearce CL, Talhouk A, et al. Outcomes from opportunistic salpingectomy for ovarian cancer prevention. JAMA Netw Open. 2022;5(2):e2147343. doi:10.1001/jamanetworkopen.2021.47343
Steenbeek MP, van Bommel MHD, intHout J, et al. TUBectomy with delayed oophorectomy as an alternative to risk-reducing salpingo-oophorectomy in high-risk women to assess the safety of prevention: the TUBA-WISP II study protocol [published online ahead of print, 2023 Apr 12]. Int J Gynecol Cancer. 2023;ijgc-2023-004377. doi:10.1136/ijgc-2023-004377
National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: Ovarian cancer including fallopian tube cancer and primary peritoneal cancer. Version 1.2023. December 22, 2022. Accessed May 8, 2023. https://www.nccn.org/professionals/physician_gls/pdf/ovarian.pdf
Chawla A, Hunt KK, Mittendorf EA. Surgical considerations in patients receiving neoadjuvant systemic therapy. Future Oncol. 2012;8(3):239-250. doi:10.2217/fon.12.12
Coleridge SL, Bryant A, Kehoe S, Morrison J. Neoadjuvant chemotherapy before surgery versus surgery followed by chemotherapy for initial treatment in advanced ovarian epithelial cancer. Cochrane Database Syst Rev. 2021;7(7):CD005343. doi:10.1002/14651858.CD005343.pub6
Lim MC, Chang SJ, Park B, et al; HIPEC for Ovarian Cancer Collaborators. Survival after hyperthermic intraperitoneal chemotherapy and primary or interval cytoreductive surgery in ovarian cancer: a randomized clinical trial. JAMA Surg. 2022;157(5):374-383. doi:10.1001/jamasurg.2022.0143
Walker JL, Brady MF, Wenzel L, et al. Randomized trial of intravenous versus intraperitoneal chemotherapy plus bevacizumab in advanced ovarian carcinoma: an NRG Oncology/Gynecologic Oncology Group study. J Clin Oncol. 2019;37(16):1380-1390. doi:10.1200/JCO.18.01568
Konstantinopoulos PA, Lheureux S, Moore KN. PARP inhibitors for ovarian cancer: current indications, future combinations, and novel assets in development to target DNA damage repair. Am Soc Clin Oncol Educ Book. 2020;40:1-16. doi:10.1200/EDBK_288015
Markman M. Pharmaceutical management of ovarian cancer: current status. Drugs. 2019;79(11):1231-1239. doi:10.1007/s40265-019-01158-1
Bristow RE, Puri I, Chi DS. Cytoreductive surgery for recurrent ovarian cancer: a meta-analysis. Gynecol Oncol. 2009;112(1):265-274. doi:10.1016/j.ygyno.2008.08.033
de Bree E, Michelakis D, Anagnostopoulou E. The current role of secondary cytoreductive surgery for recurrent ovarian cancer. Front Oncol. 2022;12:1029976. doi:10.3389/fonc.2022.1029976
Shah PD, Wethington SL, Pagan C, et al. Combination ATR and PARP inhibitor (CAPRI): a phase 2 study of ceralasertib plus olaparib in patients with recurrent, platinum-resistant epithelial ovarian cancer. Gynecol Oncol. 2021;163(2): 246-253. doi:10.1016/j.ygyno.2021.08.024
Borella F, Ghisoni E, Giannone G, et al. Immune checkpoint inhibitors in epithelial ovarian cancer: an overview on efficacy and future perspectives. Diagnostics (Basel). 2020;10(3):146. doi:10.3390/diagnostics10030146
Wu JWY, Dand S, Doig L, et al. T-cell receptor therapy in the treatment of ovarian cancer: a mini review. Front Immunol. 2021;12:672502. doi:10.3389/fimmu.2021.672502
Benard E, Casey NP, Inderberg EM, Wälchli S. SJI 2020 special issue: a catalogue of ovarian cancer targets for CAR therapy. Scand J Immunol. 2020;92(4):e12917 doi:10.1111/sji.12917
Martín-Sabroso C, Lozza I, Torres-Suárez AI, Fraguas-Sánchez AI. Antibodyantineoplastic conjugates in gynecological malignancies: current status and future perspectives. Pharmaceutics. 2021;13(10):1705. doi:10.3390/pharmaceutics13101705
Tolcher A, Hamilton E, Coleman RL. The evolving landscape of antibody-drug conjugates in gynecologic cancers. Cancer Treat Rev. 2023;116:102546. doi:10.1016/j.ctrv.2023.102546
Banerjee S, Drapkin R, Richarson DL, Birrer M. Targeting NaPi2b in ovarian cancer. Cancer Treat Rev. 2023;112:102489. doi:10.1016/j.ctrv.2022.102489
Among women with angina without obstructive coronary artery disease (ANOCA), mental stress induced a greater degree of myocardial ischemia than among those without ANOCA, new results show.
Further analysis in the small study suggested that mental stress–induced myocardial ischemia (MSIMI) was not statistically related to coronary microvascular dysfunction (CMD).
“Since the findings do not support a correlation between MSIMI and CMD, which has been a widely accepted mechanistic explanation of ANOCA, routine mental stress testing in patients with ANOCA seems necessary,” researchers led by Qingshan Geng, MD, PhD, of Shenzhen People’s Hospital, Guangdong, China, conclude in a report published online in the Journal of the American College of Cardiology.
Dr. Geng said in an interview that the use of virtual reality devices to administer mental stress tests “ensures standardized experimental procedures, with each participant receiving an objectively equivalent level of stress load.
“The immersive experience provided by VR lowers the environmental requirements for the test,” he noted. “Furthermore, the application of VR reduces the workload of personnel responsible for inducing mental stress, simplifying the experimental process.”
The team also developed a mobile app that enables remote monitoring of participants’ visual experiences during PET/CT scans and facilitates communication, he added.
Mental stress testing and meds?
Both ANOCA and MSIMI in patients with coronary artery disease disproportionately affect women and are associated with poor cardiovascular prognosis, the researchers write.
“However, the role of MSIMI and the exact influence of mental stress in ANOCA have not previously been studied,” they point out.
For this investigation, 84 women with ANOCA and 42 age-matched controls underwent three mental stress challenges delivered via VR.
Tests included mental arithmetic, making a public speech describing a recent emotionally upsetting event, and a task-modified Stroop test, in which participants were asked to say the color in which the word appears, not the color that the word names. For example, if the word “yellow” appears in blue type, blue would be the correct answer.
An adenosine stress test was given 5-8 minutes after the mental stress challenges started, and cardiac PET/CT was used to examine myocardial blood flow and perfusion.
The investigators report that women with ANOCA had a much higher rate of MSIMI (42.9%), compared with control participants (one patient; 2.4%). They also had a higher proportion of coronary microvascular dysfunction (CMD; 24.6% vs. 8.6%), but the occurrence of MSIMI and CMD was not related, the authors note.
Consistent with previous studies, “we observed that CMD is more prevalent in ANOCA women than the age-matched healthy individuals. MSIMI rate, however, was notably higher than the rate of CMD in our female ANOCA population,” they write. “The lack of a significant association between MSIMI and CMD indicates the mechanisms of MSIMI cannot be well explained by the adenosine-induced CMD.”
Dr. Geng suggested that ANOCA patients may benefit from treatment with escitalopram.
“Compelling evidence” from the REMIT randomized, placebo-controlled trial validates the efficacy of the drug as an MSIMI treatment, he said.
Sample size too small?
Asked for comment on the findings, Viola Vaccarino, MD, PhD, Wilton Looney Distinguished Professor of Cardiovascular Research at Emory University’s Rollins School of Public Health and a professor in the university’s School of Medicine, Atlanta, said she disagreed with several aspects of this study and the investigators’ conclusions.
Although the study suggests that MSIMI is prevalent among women with ANOCA, “the sample size was too small to make any definite conclusions,” she said in an interview.
“In fact,” she said, “I do not agree with the authors’ conclusions that MSIMI and CMD were not related, based on the data presented, even though the P value was not significant.”
In addition, more research is needed before screening can be recommended, she said. “The effectiveness of this testing modality in this population should be demonstrated first.”
Furthermore, she added, “an established treatment for MSIMI has yet to be tested in large, controlled trials, which limits the potential clinical benefit that may result from this [screening] test.”
For now, to ameliorate potential MSIMI in women with ANOCA, Dr. Vaccarino recommends behavioral modalities or stress-reduction management techniques, including biofeedback, meditation, breathing exercises, and “just plain regular physical activity,” rather than the use of psychotropic medications.
Dr. Vaccarino’s team has a study underway that builds on earlier work involving more than 900 participants, which showed that MSIMI was significantly associated with an increased risk of cardiovascular death or nonfatal myocardial infarction (hazard ratio, 2.5).
The ongoing study, which investigates the link between emotional stress and heart disease in men and women, should be completed in about 3 years, she said.
Microvascular disease or spasm?
Leslie Cho, MD, chair of the American College of Cardiology’s Cardiovascular Disease in Women Committee, director of the Cleveland Clinic’s Women’s Cardiovascular Center, and professor of medicine at Cleveland Clinic Lerner School of Medicine and Case Western Reserve Medical School, commented on the mental stress–heart connection and mental stress testing for this article.
A “very big flaw” of the JACC study, she said, is that although PET testing can detect microvascular disease, it cannot detect microvascular spasm.
PET can show the coronary flow reserve, “which is a nice way to assess microvascular dysfunction,” she acknowledged, “but it really can’t tell microvascular spasm, because adenosine works in a different pathway than acetylcholine – and I think it’s important for people to have the right diagnosis.
“We do physiologic testing to distinguish the two conditions,” she noted. “We do the gold standard, which is the cath lab.”
“The problem with women with chest pain for years is that they get a stress test, they get a cath, and everything’s normal. Then they get blown off as anxious or whatever.”
Clinicians should conduct the gold standard workup – provocative physiologic testing – for these women who continue to have chest pain when results of other tests are negative, she said. “The test used to be very cumbersome, but today, we have systems that make it super easy to use and to distinguish microvascular disease and microvascular spasm.”
Importantly, she added, physiologic testing should be performed when women are off therapy – something that doesn’t always happen in the clinic.
Regarding treatment, she added, “if you’re having emotional stress, the answer is not another medicine. The answer is cognitive-behavioral therapy or another behavioral intervention to overcome anxiety.”
Tune in and advocate
What can clinicians do for women with ANOCA after testing reveals no significant coronary artery disease or microvascular spasms?
“Very often, it’s a matter of the doctor listening and responding to the patient,” Johanna Contreras, MD, a cardiologist at Mount Sinai Hospital, New York, said in an intereview.
In her practice, Dr. Contreras sees highly stressed women on a daily basis. Many of her patients are women from diverse racial/ethnic groups, often of lower socioeconomic status, who are heads of households, work more than one job, and experience other major stressors.
“My message to clinicians is: don’t give up on a woman just because you looked at the arteries and couldn’t find anything specific. If she keeps coming back with the same symptom, it’s important to address it,” she said. “Maybe it isn’t the symptom. Maybe she needs to talk about her situation, about the physiological and psychosocial factors contributing to the symptom that a test alone won’t reveal.”
Regarding cardiovascular spasms that are identified through physiologic testing, she said, “I don’t know that medications such as SSRIs [selective serotonin reuptake inhibitors] are going to change anything. But many things can be changed by listening or helping the patient to stop and think about her mental health.”
Following up with a referral to a therapist can help, she said; “Take away the mental health stigma by telling the patient that the referral is simply to help her cope.”
Dr. Contreras urges clinicians to be advocates for such patients. If an insurance company says it will cover only three therapy sessions, “tell them that three appointments are not enough” to address multiple issues.
“If we invest money in helping patients identify and cope with these issues, we are likely to get better long-term outcomes, rather than having that woman come into the emergency department with chest pain over and over and doing 20,000 tests that are going to show exactly the same thing,” Dr. Contreras concluded.
Dr. Geng’s study was supported by the High-Level Hospital Construction Project of Guangdong Provincial People’s Hospital, by a grant from Guangdong Provincial Bureau of Traditional Chinese Medicine, and by a grant from Guangdong Medical Science and Technology Research Foundation. The authors, Dr. Vaccarino, Dr. Contreras, and Dr. Cho report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Among women with angina without obstructive coronary artery disease (ANOCA), mental stress induced a greater degree of myocardial ischemia than among those without ANOCA, new results show.
Further analysis in the small study suggested that mental stress–induced myocardial ischemia (MSIMI) was not statistically related to coronary microvascular dysfunction (CMD).
“Since the findings do not support a correlation between MSIMI and CMD, which has been a widely accepted mechanistic explanation of ANOCA, routine mental stress testing in patients with ANOCA seems necessary,” researchers led by Qingshan Geng, MD, PhD, of Shenzhen People’s Hospital, Guangdong, China, conclude in a report published online in the Journal of the American College of Cardiology.
Dr. Geng said in an interview that the use of virtual reality devices to administer mental stress tests “ensures standardized experimental procedures, with each participant receiving an objectively equivalent level of stress load.
“The immersive experience provided by VR lowers the environmental requirements for the test,” he noted. “Furthermore, the application of VR reduces the workload of personnel responsible for inducing mental stress, simplifying the experimental process.”
The team also developed a mobile app that enables remote monitoring of participants’ visual experiences during PET/CT scans and facilitates communication, he added.
Mental stress testing and meds?
Both ANOCA and MSIMI in patients with coronary artery disease disproportionately affect women and are associated with poor cardiovascular prognosis, the researchers write.
“However, the role of MSIMI and the exact influence of mental stress in ANOCA have not previously been studied,” they point out.
For this investigation, 84 women with ANOCA and 42 age-matched controls underwent three mental stress challenges delivered via VR.
Tests included mental arithmetic, making a public speech describing a recent emotionally upsetting event, and a task-modified Stroop test, in which participants were asked to say the color in which the word appears, not the color that the word names. For example, if the word “yellow” appears in blue type, blue would be the correct answer.
An adenosine stress test was given 5-8 minutes after the mental stress challenges started, and cardiac PET/CT was used to examine myocardial blood flow and perfusion.
The investigators report that women with ANOCA had a much higher rate of MSIMI (42.9%), compared with control participants (one patient; 2.4%). They also had a higher proportion of coronary microvascular dysfunction (CMD; 24.6% vs. 8.6%), but the occurrence of MSIMI and CMD was not related, the authors note.
Consistent with previous studies, “we observed that CMD is more prevalent in ANOCA women than the age-matched healthy individuals. MSIMI rate, however, was notably higher than the rate of CMD in our female ANOCA population,” they write. “The lack of a significant association between MSIMI and CMD indicates the mechanisms of MSIMI cannot be well explained by the adenosine-induced CMD.”
Dr. Geng suggested that ANOCA patients may benefit from treatment with escitalopram.
“Compelling evidence” from the REMIT randomized, placebo-controlled trial validates the efficacy of the drug as an MSIMI treatment, he said.
Sample size too small?
Asked for comment on the findings, Viola Vaccarino, MD, PhD, Wilton Looney Distinguished Professor of Cardiovascular Research at Emory University’s Rollins School of Public Health and a professor in the university’s School of Medicine, Atlanta, said she disagreed with several aspects of this study and the investigators’ conclusions.
Although the study suggests that MSIMI is prevalent among women with ANOCA, “the sample size was too small to make any definite conclusions,” she said in an interview.
“In fact,” she said, “I do not agree with the authors’ conclusions that MSIMI and CMD were not related, based on the data presented, even though the P value was not significant.”
In addition, more research is needed before screening can be recommended, she said. “The effectiveness of this testing modality in this population should be demonstrated first.”
Furthermore, she added, “an established treatment for MSIMI has yet to be tested in large, controlled trials, which limits the potential clinical benefit that may result from this [screening] test.”
For now, to ameliorate potential MSIMI in women with ANOCA, Dr. Vaccarino recommends behavioral modalities or stress-reduction management techniques, including biofeedback, meditation, breathing exercises, and “just plain regular physical activity,” rather than the use of psychotropic medications.
Dr. Vaccarino’s team has a study underway that builds on earlier work involving more than 900 participants, which showed that MSIMI was significantly associated with an increased risk of cardiovascular death or nonfatal myocardial infarction (hazard ratio, 2.5).
The ongoing study, which investigates the link between emotional stress and heart disease in men and women, should be completed in about 3 years, she said.
Microvascular disease or spasm?
Leslie Cho, MD, chair of the American College of Cardiology’s Cardiovascular Disease in Women Committee, director of the Cleveland Clinic’s Women’s Cardiovascular Center, and professor of medicine at Cleveland Clinic Lerner School of Medicine and Case Western Reserve Medical School, commented on the mental stress–heart connection and mental stress testing for this article.
A “very big flaw” of the JACC study, she said, is that although PET testing can detect microvascular disease, it cannot detect microvascular spasm.
PET can show the coronary flow reserve, “which is a nice way to assess microvascular dysfunction,” she acknowledged, “but it really can’t tell microvascular spasm, because adenosine works in a different pathway than acetylcholine – and I think it’s important for people to have the right diagnosis.
“We do physiologic testing to distinguish the two conditions,” she noted. “We do the gold standard, which is the cath lab.”
“The problem with women with chest pain for years is that they get a stress test, they get a cath, and everything’s normal. Then they get blown off as anxious or whatever.”
Clinicians should conduct the gold standard workup – provocative physiologic testing – for these women who continue to have chest pain when results of other tests are negative, she said. “The test used to be very cumbersome, but today, we have systems that make it super easy to use and to distinguish microvascular disease and microvascular spasm.”
Importantly, she added, physiologic testing should be performed when women are off therapy – something that doesn’t always happen in the clinic.
Regarding treatment, she added, “if you’re having emotional stress, the answer is not another medicine. The answer is cognitive-behavioral therapy or another behavioral intervention to overcome anxiety.”
Tune in and advocate
What can clinicians do for women with ANOCA after testing reveals no significant coronary artery disease or microvascular spasms?
“Very often, it’s a matter of the doctor listening and responding to the patient,” Johanna Contreras, MD, a cardiologist at Mount Sinai Hospital, New York, said in an intereview.
In her practice, Dr. Contreras sees highly stressed women on a daily basis. Many of her patients are women from diverse racial/ethnic groups, often of lower socioeconomic status, who are heads of households, work more than one job, and experience other major stressors.
“My message to clinicians is: don’t give up on a woman just because you looked at the arteries and couldn’t find anything specific. If she keeps coming back with the same symptom, it’s important to address it,” she said. “Maybe it isn’t the symptom. Maybe she needs to talk about her situation, about the physiological and psychosocial factors contributing to the symptom that a test alone won’t reveal.”
Regarding cardiovascular spasms that are identified through physiologic testing, she said, “I don’t know that medications such as SSRIs [selective serotonin reuptake inhibitors] are going to change anything. But many things can be changed by listening or helping the patient to stop and think about her mental health.”
Following up with a referral to a therapist can help, she said; “Take away the mental health stigma by telling the patient that the referral is simply to help her cope.”
Dr. Contreras urges clinicians to be advocates for such patients. If an insurance company says it will cover only three therapy sessions, “tell them that three appointments are not enough” to address multiple issues.
“If we invest money in helping patients identify and cope with these issues, we are likely to get better long-term outcomes, rather than having that woman come into the emergency department with chest pain over and over and doing 20,000 tests that are going to show exactly the same thing,” Dr. Contreras concluded.
Dr. Geng’s study was supported by the High-Level Hospital Construction Project of Guangdong Provincial People’s Hospital, by a grant from Guangdong Provincial Bureau of Traditional Chinese Medicine, and by a grant from Guangdong Medical Science and Technology Research Foundation. The authors, Dr. Vaccarino, Dr. Contreras, and Dr. Cho report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Among women with angina without obstructive coronary artery disease (ANOCA), mental stress induced a greater degree of myocardial ischemia than among those without ANOCA, new results show.
Further analysis in the small study suggested that mental stress–induced myocardial ischemia (MSIMI) was not statistically related to coronary microvascular dysfunction (CMD).
“Since the findings do not support a correlation between MSIMI and CMD, which has been a widely accepted mechanistic explanation of ANOCA, routine mental stress testing in patients with ANOCA seems necessary,” researchers led by Qingshan Geng, MD, PhD, of Shenzhen People’s Hospital, Guangdong, China, conclude in a report published online in the Journal of the American College of Cardiology.
Dr. Geng said in an interview that the use of virtual reality devices to administer mental stress tests “ensures standardized experimental procedures, with each participant receiving an objectively equivalent level of stress load.
“The immersive experience provided by VR lowers the environmental requirements for the test,” he noted. “Furthermore, the application of VR reduces the workload of personnel responsible for inducing mental stress, simplifying the experimental process.”
The team also developed a mobile app that enables remote monitoring of participants’ visual experiences during PET/CT scans and facilitates communication, he added.
Mental stress testing and meds?
Both ANOCA and MSIMI in patients with coronary artery disease disproportionately affect women and are associated with poor cardiovascular prognosis, the researchers write.
“However, the role of MSIMI and the exact influence of mental stress in ANOCA have not previously been studied,” they point out.
For this investigation, 84 women with ANOCA and 42 age-matched controls underwent three mental stress challenges delivered via VR.
Tests included mental arithmetic, making a public speech describing a recent emotionally upsetting event, and a task-modified Stroop test, in which participants were asked to say the color in which the word appears, not the color that the word names. For example, if the word “yellow” appears in blue type, blue would be the correct answer.
An adenosine stress test was given 5-8 minutes after the mental stress challenges started, and cardiac PET/CT was used to examine myocardial blood flow and perfusion.
The investigators report that women with ANOCA had a much higher rate of MSIMI (42.9%), compared with control participants (one patient; 2.4%). They also had a higher proportion of coronary microvascular dysfunction (CMD; 24.6% vs. 8.6%), but the occurrence of MSIMI and CMD was not related, the authors note.
Consistent with previous studies, “we observed that CMD is more prevalent in ANOCA women than the age-matched healthy individuals. MSIMI rate, however, was notably higher than the rate of CMD in our female ANOCA population,” they write. “The lack of a significant association between MSIMI and CMD indicates the mechanisms of MSIMI cannot be well explained by the adenosine-induced CMD.”
Dr. Geng suggested that ANOCA patients may benefit from treatment with escitalopram.
“Compelling evidence” from the REMIT randomized, placebo-controlled trial validates the efficacy of the drug as an MSIMI treatment, he said.
Sample size too small?
Asked for comment on the findings, Viola Vaccarino, MD, PhD, Wilton Looney Distinguished Professor of Cardiovascular Research at Emory University’s Rollins School of Public Health and a professor in the university’s School of Medicine, Atlanta, said she disagreed with several aspects of this study and the investigators’ conclusions.
Although the study suggests that MSIMI is prevalent among women with ANOCA, “the sample size was too small to make any definite conclusions,” she said in an interview.
“In fact,” she said, “I do not agree with the authors’ conclusions that MSIMI and CMD were not related, based on the data presented, even though the P value was not significant.”
In addition, more research is needed before screening can be recommended, she said. “The effectiveness of this testing modality in this population should be demonstrated first.”
Furthermore, she added, “an established treatment for MSIMI has yet to be tested in large, controlled trials, which limits the potential clinical benefit that may result from this [screening] test.”
For now, to ameliorate potential MSIMI in women with ANOCA, Dr. Vaccarino recommends behavioral modalities or stress-reduction management techniques, including biofeedback, meditation, breathing exercises, and “just plain regular physical activity,” rather than the use of psychotropic medications.
Dr. Vaccarino’s team has a study underway that builds on earlier work involving more than 900 participants, which showed that MSIMI was significantly associated with an increased risk of cardiovascular death or nonfatal myocardial infarction (hazard ratio, 2.5).
The ongoing study, which investigates the link between emotional stress and heart disease in men and women, should be completed in about 3 years, she said.
Microvascular disease or spasm?
Leslie Cho, MD, chair of the American College of Cardiology’s Cardiovascular Disease in Women Committee, director of the Cleveland Clinic’s Women’s Cardiovascular Center, and professor of medicine at Cleveland Clinic Lerner School of Medicine and Case Western Reserve Medical School, commented on the mental stress–heart connection and mental stress testing for this article.
A “very big flaw” of the JACC study, she said, is that although PET testing can detect microvascular disease, it cannot detect microvascular spasm.
PET can show the coronary flow reserve, “which is a nice way to assess microvascular dysfunction,” she acknowledged, “but it really can’t tell microvascular spasm, because adenosine works in a different pathway than acetylcholine – and I think it’s important for people to have the right diagnosis.
“We do physiologic testing to distinguish the two conditions,” she noted. “We do the gold standard, which is the cath lab.”
“The problem with women with chest pain for years is that they get a stress test, they get a cath, and everything’s normal. Then they get blown off as anxious or whatever.”
Clinicians should conduct the gold standard workup – provocative physiologic testing – for these women who continue to have chest pain when results of other tests are negative, she said. “The test used to be very cumbersome, but today, we have systems that make it super easy to use and to distinguish microvascular disease and microvascular spasm.”
Importantly, she added, physiologic testing should be performed when women are off therapy – something that doesn’t always happen in the clinic.
Regarding treatment, she added, “if you’re having emotional stress, the answer is not another medicine. The answer is cognitive-behavioral therapy or another behavioral intervention to overcome anxiety.”
Tune in and advocate
What can clinicians do for women with ANOCA after testing reveals no significant coronary artery disease or microvascular spasms?
“Very often, it’s a matter of the doctor listening and responding to the patient,” Johanna Contreras, MD, a cardiologist at Mount Sinai Hospital, New York, said in an intereview.
In her practice, Dr. Contreras sees highly stressed women on a daily basis. Many of her patients are women from diverse racial/ethnic groups, often of lower socioeconomic status, who are heads of households, work more than one job, and experience other major stressors.
“My message to clinicians is: don’t give up on a woman just because you looked at the arteries and couldn’t find anything specific. If she keeps coming back with the same symptom, it’s important to address it,” she said. “Maybe it isn’t the symptom. Maybe she needs to talk about her situation, about the physiological and psychosocial factors contributing to the symptom that a test alone won’t reveal.”
Regarding cardiovascular spasms that are identified through physiologic testing, she said, “I don’t know that medications such as SSRIs [selective serotonin reuptake inhibitors] are going to change anything. But many things can be changed by listening or helping the patient to stop and think about her mental health.”
Following up with a referral to a therapist can help, she said; “Take away the mental health stigma by telling the patient that the referral is simply to help her cope.”
Dr. Contreras urges clinicians to be advocates for such patients. If an insurance company says it will cover only three therapy sessions, “tell them that three appointments are not enough” to address multiple issues.
“If we invest money in helping patients identify and cope with these issues, we are likely to get better long-term outcomes, rather than having that woman come into the emergency department with chest pain over and over and doing 20,000 tests that are going to show exactly the same thing,” Dr. Contreras concluded.
Dr. Geng’s study was supported by the High-Level Hospital Construction Project of Guangdong Provincial People’s Hospital, by a grant from Guangdong Provincial Bureau of Traditional Chinese Medicine, and by a grant from Guangdong Medical Science and Technology Research Foundation. The authors, Dr. Vaccarino, Dr. Contreras, and Dr. Cho report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
VIENNA – An algorithm, the Steatosis-Associated Fibrosis Estimator (SAFE), was developed to detect clinically significant fibrosis in patients with nonalcoholic fatty liver disease (NAFLD). It is effective at detecting chronic liver disease from all causes with or without NAFLD in the general population, according the results of a U.S. population-based study. The algorithm was designed for use in primary care to help slow the steep rise in liver disease burden.
On the basis of the SAFE score, 61.3% of participants were at low risk for clinically significant fibrosis; 11.2% were at high risk; and 27.5% were at intermediate risk. Upon validation, very few of the low-risk participants had liver fibrosis, while nearly a third of those with a high-risk score had clinically significant fibrosis. In addition, a high percentage of the patients with high-risk SAFE scores had viral hepatitis and elevations in ferritin level.
“This is the first time that there has been a test that provides a score to detect low-risk liver disease in primary care,” said Ray Kim, MD, from Stanford (Calif.) University, senior investigator, who was speaking to this news organization at the annual International Liver Congress sponsored by the European Association for the Study of the Liver
“Primary care doctors currently detect liver disease through a serendipitous abnormal finding on ultrasound or blood tests that detect elevated transaminases, and then the patient is referred to a hepatologist, who figures out what is really going on,” said Dr. Kim.
“This approach is limited, so we need to get SAFE into primary care so these doctors can automatically calculate their scores, and if the patient is over 100 [high risk of chronic liver disease], then they need help [referral to a hepatologist].”
Liver deaths sharply rising
Public health data show that more people are dying of liver disease today than previously. Deaths in the United States have doubled over the past 20 years, said Dr. Kim. “If our mission is to help these patients and prevent death, [things are] moving in the wrong direction.”
He stressed that in order to change the direction, “primary care doctors need to engage with the issue and have appropriate tools to identify people with liver disease.”
Most often, the reason for this rise in deaths is that cases are being diagnosed at advanced stages of disease in which reversibility is limited, he added. “We want to move upstream where people might have early-stage disease and where we can intervene and make a difference.”
In an effort to help earlier detection of liver disease, the SAFE score was developed and validated by Dr. Kim and his colleagues to detect clinically significant (greater than stage 2) fibrosis in patients with NAFLD in primary care. The score is based upon age, body mass index, diabetes, platelet level, aspartate and alanine aminotransferase levels, and globulin level. A score of less than zero signifies that a patient is at low risk for liver fibrosis, while a score greater than 100 signifies a high risk of fibrosis. A score between 0 and 99 denotes intermediate risk of fibrosis.
“Unlike other noninvasive tests that detect advanced fibrosis, this one detects early-stage fibrosis. We’ve shown that the SAFE estimator is better than all other blood-based markers,” explained Dr. Kim.
Applying SAFE to the general population
In the study presented here at EASL, Dr. Kim aimed to expand the horizon for SAFE testing to the U.S. general population and to assess whether SAFE was effective in screening for chronic liver disease regardless of steatosis of the liver.
Together with first author Nakia Chung, MD, also from Stanford University, Dr. Kim applied the SAFE score to data from 7,156 participants of the National Health and Nutrition Examination Survey (NHANES) for 2017-2020. NHANES is representative of the noninstitutionalized, civilian population of the United States. It includes broad demographic, clinical, and laboratory data, including transient elastography data. FibroScans were first used in 2017, so the investigators had 3 years of FibroScan data with which to validate the score.
The researchers extrapolated the NHANES sample data to the U.S. population. They found that the proportion of adults with steatosis (CAP score > 274 dB/m) and significant fibrosis (LSM > 8.0 kPa) was 42.7% (95% confidence interval, 41.0%- 44.3%) and 8.9% (7.6%-10.2%), respectively. In addition, 11.3% (10.2%-12.5%) of the adult U.S. population demonstrated a significant amount of alcohol use, 2.3% (1.4%-3.3%) showed evidence of hepatitis B or C, and 5.4% (4.6%-6.2%) had elevated serum ferritin levels.
The researchers then stratified the patients according to previously defined SAFE tiers of low, intermediate, and high risk and projected findings to the U.S. general population.
“When we applied our score to the general population, we found multiple abnormalities in the high-risk groups [SAFE >100] having Fibroscan data that are consistent with stage 2 or higher fibrosis regardless of etiology, “Dr. Kim pointed out.
Results also showed that very few patients with SAFE less than 0 had liver fibrosis (4% among those with liver stiffness measure [LSM] > 8kPa, and 0.8% with LSM > 12kPa). Among those with SAFE > 100, nearly a third (31.5%) had LSM of > 8kPa, and 16.5% had LSM > 12kPa.
In addition to fibrosis, liver abnormalities were common among patients with SAFE greater than 100, including steatosis (68.0%), viral hepatitis (7.0%), and abnormal ferritin levels (12.9%); 10.8% of these patients used alcohol.
“Right now, some patients are referred, but on examination and FibroScan, they might actually be okay, so it it’s a waste of time and money for everyone. We can preempt all of this by doing a blood test and focusing on those people who really need a scan,” said Dr. Kim.
The researcher is now working with primary care colleagues to help further develop and integrate SAFE into the primary care setting.
Fibrosis score in patients with metabolic dysfunction
Also presenting at the same session on population health was Willem Pieter Brouwer, MD, PhD, from Erasmus University Medical Center, Rotterdam, the Netherlands. He reported results of a validation study of a new risk score – the Metabolic Dysfunction-Associated Fibrosis–5 (MAF-5) score – for use for people with metabolic dysfunction who are recommended for screening for liver fibrosis.
“We believe the MAF-5 score may be a good alternative to the FIB-4 [a liver fibrosis biomarker] for use in the referral pathway for liver health evaluation,” remarked Dr. Brouwer. “The clinical practice guidelines recommend using FIB-4 scores, but these have a poor-moderate performance in the population setting.
“We developed and validated our score in a population of 5,500 from the NHANES 2017-2020 cycle and validated the score in populations from Rotterdam, which is a cohort of elderly participants, and in fibrosis among patients with biopsy-proven NAFLD from Colombia and Belgium,” he explained.
He also validated the score against different existing scoring systems and different methods of measuring liver stiffness and validated it for prognostic use to predict all-cause mortality in the NHANES III cohort.
Dr. Brouwer removed age as a factor of his new MAF-5 score; the score is thus stable for patients of all ages and is suitable for detecting liver disease in younger patients. “This is very important because these patients are currently underserved and have the most years of life to win.”
Referring to the SAFE score discussed by Dr. Kim, as well as other scores, he said, “The FIB-4, SAFE, and NFS [NAFLD fibrosis score] all include age in the scores, which causes problems and limitations in aging populations, as more and more patients will be referred due to an increasing score. Hence, the elderly are mostly all referred for liver checkups.”
Dr. Kim and Dr. Brouwer have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
VIENNA – An algorithm, the Steatosis-Associated Fibrosis Estimator (SAFE), was developed to detect clinically significant fibrosis in patients with nonalcoholic fatty liver disease (NAFLD). It is effective at detecting chronic liver disease from all causes with or without NAFLD in the general population, according the results of a U.S. population-based study. The algorithm was designed for use in primary care to help slow the steep rise in liver disease burden.
On the basis of the SAFE score, 61.3% of participants were at low risk for clinically significant fibrosis; 11.2% were at high risk; and 27.5% were at intermediate risk. Upon validation, very few of the low-risk participants had liver fibrosis, while nearly a third of those with a high-risk score had clinically significant fibrosis. In addition, a high percentage of the patients with high-risk SAFE scores had viral hepatitis and elevations in ferritin level.
“This is the first time that there has been a test that provides a score to detect low-risk liver disease in primary care,” said Ray Kim, MD, from Stanford (Calif.) University, senior investigator, who was speaking to this news organization at the annual International Liver Congress sponsored by the European Association for the Study of the Liver
“Primary care doctors currently detect liver disease through a serendipitous abnormal finding on ultrasound or blood tests that detect elevated transaminases, and then the patient is referred to a hepatologist, who figures out what is really going on,” said Dr. Kim.
“This approach is limited, so we need to get SAFE into primary care so these doctors can automatically calculate their scores, and if the patient is over 100 [high risk of chronic liver disease], then they need help [referral to a hepatologist].”
Liver deaths sharply rising
Public health data show that more people are dying of liver disease today than previously. Deaths in the United States have doubled over the past 20 years, said Dr. Kim. “If our mission is to help these patients and prevent death, [things are] moving in the wrong direction.”
He stressed that in order to change the direction, “primary care doctors need to engage with the issue and have appropriate tools to identify people with liver disease.”
Most often, the reason for this rise in deaths is that cases are being diagnosed at advanced stages of disease in which reversibility is limited, he added. “We want to move upstream where people might have early-stage disease and where we can intervene and make a difference.”
In an effort to help earlier detection of liver disease, the SAFE score was developed and validated by Dr. Kim and his colleagues to detect clinically significant (greater than stage 2) fibrosis in patients with NAFLD in primary care. The score is based upon age, body mass index, diabetes, platelet level, aspartate and alanine aminotransferase levels, and globulin level. A score of less than zero signifies that a patient is at low risk for liver fibrosis, while a score greater than 100 signifies a high risk of fibrosis. A score between 0 and 99 denotes intermediate risk of fibrosis.
“Unlike other noninvasive tests that detect advanced fibrosis, this one detects early-stage fibrosis. We’ve shown that the SAFE estimator is better than all other blood-based markers,” explained Dr. Kim.
Applying SAFE to the general population
In the study presented here at EASL, Dr. Kim aimed to expand the horizon for SAFE testing to the U.S. general population and to assess whether SAFE was effective in screening for chronic liver disease regardless of steatosis of the liver.
Together with first author Nakia Chung, MD, also from Stanford University, Dr. Kim applied the SAFE score to data from 7,156 participants of the National Health and Nutrition Examination Survey (NHANES) for 2017-2020. NHANES is representative of the noninstitutionalized, civilian population of the United States. It includes broad demographic, clinical, and laboratory data, including transient elastography data. FibroScans were first used in 2017, so the investigators had 3 years of FibroScan data with which to validate the score.
The researchers extrapolated the NHANES sample data to the U.S. population. They found that the proportion of adults with steatosis (CAP score > 274 dB/m) and significant fibrosis (LSM > 8.0 kPa) was 42.7% (95% confidence interval, 41.0%- 44.3%) and 8.9% (7.6%-10.2%), respectively. In addition, 11.3% (10.2%-12.5%) of the adult U.S. population demonstrated a significant amount of alcohol use, 2.3% (1.4%-3.3%) showed evidence of hepatitis B or C, and 5.4% (4.6%-6.2%) had elevated serum ferritin levels.
The researchers then stratified the patients according to previously defined SAFE tiers of low, intermediate, and high risk and projected findings to the U.S. general population.
“When we applied our score to the general population, we found multiple abnormalities in the high-risk groups [SAFE >100] having Fibroscan data that are consistent with stage 2 or higher fibrosis regardless of etiology, “Dr. Kim pointed out.
Results also showed that very few patients with SAFE less than 0 had liver fibrosis (4% among those with liver stiffness measure [LSM] > 8kPa, and 0.8% with LSM > 12kPa). Among those with SAFE > 100, nearly a third (31.5%) had LSM of > 8kPa, and 16.5% had LSM > 12kPa.
In addition to fibrosis, liver abnormalities were common among patients with SAFE greater than 100, including steatosis (68.0%), viral hepatitis (7.0%), and abnormal ferritin levels (12.9%); 10.8% of these patients used alcohol.
“Right now, some patients are referred, but on examination and FibroScan, they might actually be okay, so it it’s a waste of time and money for everyone. We can preempt all of this by doing a blood test and focusing on those people who really need a scan,” said Dr. Kim.
The researcher is now working with primary care colleagues to help further develop and integrate SAFE into the primary care setting.
Fibrosis score in patients with metabolic dysfunction
Also presenting at the same session on population health was Willem Pieter Brouwer, MD, PhD, from Erasmus University Medical Center, Rotterdam, the Netherlands. He reported results of a validation study of a new risk score – the Metabolic Dysfunction-Associated Fibrosis–5 (MAF-5) score – for use for people with metabolic dysfunction who are recommended for screening for liver fibrosis.
“We believe the MAF-5 score may be a good alternative to the FIB-4 [a liver fibrosis biomarker] for use in the referral pathway for liver health evaluation,” remarked Dr. Brouwer. “The clinical practice guidelines recommend using FIB-4 scores, but these have a poor-moderate performance in the population setting.
“We developed and validated our score in a population of 5,500 from the NHANES 2017-2020 cycle and validated the score in populations from Rotterdam, which is a cohort of elderly participants, and in fibrosis among patients with biopsy-proven NAFLD from Colombia and Belgium,” he explained.
He also validated the score against different existing scoring systems and different methods of measuring liver stiffness and validated it for prognostic use to predict all-cause mortality in the NHANES III cohort.
Dr. Brouwer removed age as a factor of his new MAF-5 score; the score is thus stable for patients of all ages and is suitable for detecting liver disease in younger patients. “This is very important because these patients are currently underserved and have the most years of life to win.”
Referring to the SAFE score discussed by Dr. Kim, as well as other scores, he said, “The FIB-4, SAFE, and NFS [NAFLD fibrosis score] all include age in the scores, which causes problems and limitations in aging populations, as more and more patients will be referred due to an increasing score. Hence, the elderly are mostly all referred for liver checkups.”
Dr. Kim and Dr. Brouwer have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
VIENNA – An algorithm, the Steatosis-Associated Fibrosis Estimator (SAFE), was developed to detect clinically significant fibrosis in patients with nonalcoholic fatty liver disease (NAFLD). It is effective at detecting chronic liver disease from all causes with or without NAFLD in the general population, according the results of a U.S. population-based study. The algorithm was designed for use in primary care to help slow the steep rise in liver disease burden.
On the basis of the SAFE score, 61.3% of participants were at low risk for clinically significant fibrosis; 11.2% were at high risk; and 27.5% were at intermediate risk. Upon validation, very few of the low-risk participants had liver fibrosis, while nearly a third of those with a high-risk score had clinically significant fibrosis. In addition, a high percentage of the patients with high-risk SAFE scores had viral hepatitis and elevations in ferritin level.
“This is the first time that there has been a test that provides a score to detect low-risk liver disease in primary care,” said Ray Kim, MD, from Stanford (Calif.) University, senior investigator, who was speaking to this news organization at the annual International Liver Congress sponsored by the European Association for the Study of the Liver
“Primary care doctors currently detect liver disease through a serendipitous abnormal finding on ultrasound or blood tests that detect elevated transaminases, and then the patient is referred to a hepatologist, who figures out what is really going on,” said Dr. Kim.
“This approach is limited, so we need to get SAFE into primary care so these doctors can automatically calculate their scores, and if the patient is over 100 [high risk of chronic liver disease], then they need help [referral to a hepatologist].”
Liver deaths sharply rising
Public health data show that more people are dying of liver disease today than previously. Deaths in the United States have doubled over the past 20 years, said Dr. Kim. “If our mission is to help these patients and prevent death, [things are] moving in the wrong direction.”
He stressed that in order to change the direction, “primary care doctors need to engage with the issue and have appropriate tools to identify people with liver disease.”
Most often, the reason for this rise in deaths is that cases are being diagnosed at advanced stages of disease in which reversibility is limited, he added. “We want to move upstream where people might have early-stage disease and where we can intervene and make a difference.”
In an effort to help earlier detection of liver disease, the SAFE score was developed and validated by Dr. Kim and his colleagues to detect clinically significant (greater than stage 2) fibrosis in patients with NAFLD in primary care. The score is based upon age, body mass index, diabetes, platelet level, aspartate and alanine aminotransferase levels, and globulin level. A score of less than zero signifies that a patient is at low risk for liver fibrosis, while a score greater than 100 signifies a high risk of fibrosis. A score between 0 and 99 denotes intermediate risk of fibrosis.
“Unlike other noninvasive tests that detect advanced fibrosis, this one detects early-stage fibrosis. We’ve shown that the SAFE estimator is better than all other blood-based markers,” explained Dr. Kim.
Applying SAFE to the general population
In the study presented here at EASL, Dr. Kim aimed to expand the horizon for SAFE testing to the U.S. general population and to assess whether SAFE was effective in screening for chronic liver disease regardless of steatosis of the liver.
Together with first author Nakia Chung, MD, also from Stanford University, Dr. Kim applied the SAFE score to data from 7,156 participants of the National Health and Nutrition Examination Survey (NHANES) for 2017-2020. NHANES is representative of the noninstitutionalized, civilian population of the United States. It includes broad demographic, clinical, and laboratory data, including transient elastography data. FibroScans were first used in 2017, so the investigators had 3 years of FibroScan data with which to validate the score.
The researchers extrapolated the NHANES sample data to the U.S. population. They found that the proportion of adults with steatosis (CAP score > 274 dB/m) and significant fibrosis (LSM > 8.0 kPa) was 42.7% (95% confidence interval, 41.0%- 44.3%) and 8.9% (7.6%-10.2%), respectively. In addition, 11.3% (10.2%-12.5%) of the adult U.S. population demonstrated a significant amount of alcohol use, 2.3% (1.4%-3.3%) showed evidence of hepatitis B or C, and 5.4% (4.6%-6.2%) had elevated serum ferritin levels.
The researchers then stratified the patients according to previously defined SAFE tiers of low, intermediate, and high risk and projected findings to the U.S. general population.
“When we applied our score to the general population, we found multiple abnormalities in the high-risk groups [SAFE >100] having Fibroscan data that are consistent with stage 2 or higher fibrosis regardless of etiology, “Dr. Kim pointed out.
Results also showed that very few patients with SAFE less than 0 had liver fibrosis (4% among those with liver stiffness measure [LSM] > 8kPa, and 0.8% with LSM > 12kPa). Among those with SAFE > 100, nearly a third (31.5%) had LSM of > 8kPa, and 16.5% had LSM > 12kPa.
In addition to fibrosis, liver abnormalities were common among patients with SAFE greater than 100, including steatosis (68.0%), viral hepatitis (7.0%), and abnormal ferritin levels (12.9%); 10.8% of these patients used alcohol.
“Right now, some patients are referred, but on examination and FibroScan, they might actually be okay, so it it’s a waste of time and money for everyone. We can preempt all of this by doing a blood test and focusing on those people who really need a scan,” said Dr. Kim.
The researcher is now working with primary care colleagues to help further develop and integrate SAFE into the primary care setting.
Fibrosis score in patients with metabolic dysfunction
Also presenting at the same session on population health was Willem Pieter Brouwer, MD, PhD, from Erasmus University Medical Center, Rotterdam, the Netherlands. He reported results of a validation study of a new risk score – the Metabolic Dysfunction-Associated Fibrosis–5 (MAF-5) score – for use for people with metabolic dysfunction who are recommended for screening for liver fibrosis.
“We believe the MAF-5 score may be a good alternative to the FIB-4 [a liver fibrosis biomarker] for use in the referral pathway for liver health evaluation,” remarked Dr. Brouwer. “The clinical practice guidelines recommend using FIB-4 scores, but these have a poor-moderate performance in the population setting.
“We developed and validated our score in a population of 5,500 from the NHANES 2017-2020 cycle and validated the score in populations from Rotterdam, which is a cohort of elderly participants, and in fibrosis among patients with biopsy-proven NAFLD from Colombia and Belgium,” he explained.
He also validated the score against different existing scoring systems and different methods of measuring liver stiffness and validated it for prognostic use to predict all-cause mortality in the NHANES III cohort.
Dr. Brouwer removed age as a factor of his new MAF-5 score; the score is thus stable for patients of all ages and is suitable for detecting liver disease in younger patients. “This is very important because these patients are currently underserved and have the most years of life to win.”
Referring to the SAFE score discussed by Dr. Kim, as well as other scores, he said, “The FIB-4, SAFE, and NFS [NAFLD fibrosis score] all include age in the scores, which causes problems and limitations in aging populations, as more and more patients will be referred due to an increasing score. Hence, the elderly are mostly all referred for liver checkups.”
Dr. Kim and Dr. Brouwer have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
CHICAGO – Treatment of hyperthyroidism with surgery or radioactive iodine significantly extends survival, compared with antithyroid medication, while surgery raises the risk for obesity, new data from a large cohort study suggest.
“I think this is something we need to take into our discussions with patients because treatment for hyperthyroidism is very much individualized decision-making ... The effects on mortality are not usually one of the factors we discuss there. But now, we have strong data from a very large cohort of patients indicating that this is something that does need to be discussed,” lead author Kristien Boelaert, MD, who is the current president of the British Thyroid Association, said in an interview.
Dr. Boelaert presented the findings of the EGRET (Weight Changes, Cardio-Metabolic Risks and Mortality in Patients With Hyperthyroidism) study at the Annual Meeting of the Endocrine Society.
Other notable findings from EGRET were that the patients on antithyroid medication were thinner than expected, suggesting undertreatment, and that no differences were found for major adverse cardiac events (MACE) across the treatment options, leaving unexplained the reasons for the increased mortality in the medicated group.
Asked to comment, session moderator Spyridoula Maraka, MD, said: “I think this is very important work because so far when we counsel our patients about the different treatment modalities we focus more on risk for recurrence and other short-term outcomes.”
“But these data give us a bigger perspective on mortality and cardiovascular outcomes ... We haven’t had such good quality data to accurately counsel our patients,” added Dr. Maraka, of the University of Arkansas for Medical Sciences, Little Rock.
Mortality higher for medication-treated, but why?
“Hyperthyroidism or an overactive thyroid gland is common, affecting up to 3% of the population, and is associated with long-term adverse cardiac and metabolic consequences. The optimal treatment choice remains unclear,” explained Dr. Boelaert, professor of endocrinology at the University of Birmingham, England, outlining the reasons they conducted the EGRET study.
The study population was 55,318 patients (77% women) with newly diagnosed hyperthyroidism identified from a U.K. population-based primary care electronic health record database. Of those, 77.8% were treated with antithyroid medication, 14.6% with radioactive iodine, and 7.8% with surgery (total or hemithyroidectomy). The health records were linked with national mortality data and Health Survey England data on body mass index (BMI) for comparison.
Dr. Boelaert noted that the trial design “is the best we have” because a randomized clinical trial comparing hyperthyroid treatments would be extremely difficult given the need to individualize therapy and the impossibility of blinding. On the other hand, with the current study, “it’s certainly the largest patient group we’ve looked at.”
Over an average 12.1 years of follow-up, the proportion of patients who died was 14.1% in the medication group, 18.7% of those who had radioiodine therapy, and 9.2% of those who underwent surgery.
Compared with the number who would have been expected to die based on the general background population, the likelihood of reduced life expectancy for the treated groups was increased 2.10-fold for radioiodine, 2.13-fold for surgery, and 2.71-fold for medication. All were significantly higher than the general population (P < .0001).
After further adjustment for multiple confounders, mortality risk was reduced in patients treated with radioiodine (by 13%) or surgery (by 20%), compared with those treated with antithyroid medication, both significant reductions (P < .0001).
After exclusion of the 3.9% with baseline cardiovascular disease, MACE (defined as cardiovascular death or hospitalization for stroke or myocardial infarction) occurred in 9.9%, 13.4%, and 8.0% of the medication, radioiodine, and surgery groups, respectively.
After adjustments, there were no differences in MACE, compared with medications, with hazard ratios of 1.00 (P = .94) for radioactive iodine and 0.97 for surgery (P = .61).
“We were expecting to see a reduction in cardiovascular events, as previous studies suggest that radioactive iodine patients have fewer cardiovascular deaths. We did not see that but our protocol wasn’t set up to get every single specific cause of death. That will require further ongoing analysis,” said Dr. Boelaert.
Weight gain: Worth it for longer life
Compared with the background population, thyroidectomy was associated with an increased likelihood of developing obesity (BMI > 30 kg/m2) in both men (odds ratio, 1.56; P < .001), and women (OR, 1.27; P < .001), while radioiodine increased obesity risk in women (OR, 1.12; P < .001) but not in men (OR, 1.03; P = .55).
Among the women, those treated with antithyroid medications had an average 0.28 kg/m2 lower BMI, compared with the background population, and those treated with surgery had a 0.83 kg/m2 higher BMI. Both differences were significant (P < .001).
The BMI differences were not significant for radioactive iodine in women and for medications and radioactive iodine in men, although the men treated surgically also had a significantly higher BMI (1.09 kg/m2; P < .001).
“The patients on antithyroid drugs were lighter than we would expect. I think that’s ongoing hyperthyroidism. I strongly believe that ... to get rid of hyperthyroidism you have to make patients hypothyroid ... It’s really important that you get good control,” Dr. Boelaert commented.
Dr. Maraka, who is also endocrine section chief of the Arkansas Veteran’s Healthcare System, Little Rock, commented: “[Dr. Boelaert’s] concern is that the patients on antithyroid drugs are not adequately controlled, and we know very well that uncontrolled hyperthyroidism is associated with increased mortality and increased cardiovascular outcomes. This suggests that if patients are on antithyroid medications, they should at least be monitored very well.”
Regarding the possible cause of the increased mortality, if not cardiovascular, Dr. Maraka also pointed out that typically once antithyroid medications are stopped, about half of patients will stay in remission and the other half will return to hyperthyroidism.
“It might be that this kind of ‘yo-yo’ is what’s actually leading to the increased mortality, compared to patients who had definitive treatment and this problem was taken care of. This is speculation but it might be what we’re seeing,” Dr. Maraka observed.
The BMI differences worked out to a weight gain with surgery of approximately 2.1 kg (4.6 lb) for a woman with a height of 160 cm and 2.4 kg for 170 cm. Among men, those differences were 3.2 kg and 3.5 kg for heights of 170 cm and 190 cm, respectively.
Dr. Boelaert said, “I think we should discuss this with patients. They will say they don’t want to get fat, but the absolute weight gain is ... not that much.”
“I personally think that 2 kg is not a big price to pay to live longer. I hope that’s what we’ll be telling our patients in clinic in the next few years after we get this published.”
Dr. Boelaert and Dr. Maraka have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
CHICAGO – Treatment of hyperthyroidism with surgery or radioactive iodine significantly extends survival, compared with antithyroid medication, while surgery raises the risk for obesity, new data from a large cohort study suggest.
“I think this is something we need to take into our discussions with patients because treatment for hyperthyroidism is very much individualized decision-making ... The effects on mortality are not usually one of the factors we discuss there. But now, we have strong data from a very large cohort of patients indicating that this is something that does need to be discussed,” lead author Kristien Boelaert, MD, who is the current president of the British Thyroid Association, said in an interview.
Dr. Boelaert presented the findings of the EGRET (Weight Changes, Cardio-Metabolic Risks and Mortality in Patients With Hyperthyroidism) study at the Annual Meeting of the Endocrine Society.
Other notable findings from EGRET were that the patients on antithyroid medication were thinner than expected, suggesting undertreatment, and that no differences were found for major adverse cardiac events (MACE) across the treatment options, leaving unexplained the reasons for the increased mortality in the medicated group.
Asked to comment, session moderator Spyridoula Maraka, MD, said: “I think this is very important work because so far when we counsel our patients about the different treatment modalities we focus more on risk for recurrence and other short-term outcomes.”
“But these data give us a bigger perspective on mortality and cardiovascular outcomes ... We haven’t had such good quality data to accurately counsel our patients,” added Dr. Maraka, of the University of Arkansas for Medical Sciences, Little Rock.
Mortality higher for medication-treated, but why?
“Hyperthyroidism or an overactive thyroid gland is common, affecting up to 3% of the population, and is associated with long-term adverse cardiac and metabolic consequences. The optimal treatment choice remains unclear,” explained Dr. Boelaert, professor of endocrinology at the University of Birmingham, England, outlining the reasons they conducted the EGRET study.
The study population was 55,318 patients (77% women) with newly diagnosed hyperthyroidism identified from a U.K. population-based primary care electronic health record database. Of those, 77.8% were treated with antithyroid medication, 14.6% with radioactive iodine, and 7.8% with surgery (total or hemithyroidectomy). The health records were linked with national mortality data and Health Survey England data on body mass index (BMI) for comparison.
Dr. Boelaert noted that the trial design “is the best we have” because a randomized clinical trial comparing hyperthyroid treatments would be extremely difficult given the need to individualize therapy and the impossibility of blinding. On the other hand, with the current study, “it’s certainly the largest patient group we’ve looked at.”
Over an average 12.1 years of follow-up, the proportion of patients who died was 14.1% in the medication group, 18.7% of those who had radioiodine therapy, and 9.2% of those who underwent surgery.
Compared with the number who would have been expected to die based on the general background population, the likelihood of reduced life expectancy for the treated groups was increased 2.10-fold for radioiodine, 2.13-fold for surgery, and 2.71-fold for medication. All were significantly higher than the general population (P < .0001).
After further adjustment for multiple confounders, mortality risk was reduced in patients treated with radioiodine (by 13%) or surgery (by 20%), compared with those treated with antithyroid medication, both significant reductions (P < .0001).
After exclusion of the 3.9% with baseline cardiovascular disease, MACE (defined as cardiovascular death or hospitalization for stroke or myocardial infarction) occurred in 9.9%, 13.4%, and 8.0% of the medication, radioiodine, and surgery groups, respectively.
After adjustments, there were no differences in MACE, compared with medications, with hazard ratios of 1.00 (P = .94) for radioactive iodine and 0.97 for surgery (P = .61).
“We were expecting to see a reduction in cardiovascular events, as previous studies suggest that radioactive iodine patients have fewer cardiovascular deaths. We did not see that but our protocol wasn’t set up to get every single specific cause of death. That will require further ongoing analysis,” said Dr. Boelaert.
Weight gain: Worth it for longer life
Compared with the background population, thyroidectomy was associated with an increased likelihood of developing obesity (BMI > 30 kg/m2) in both men (odds ratio, 1.56; P < .001), and women (OR, 1.27; P < .001), while radioiodine increased obesity risk in women (OR, 1.12; P < .001) but not in men (OR, 1.03; P = .55).
Among the women, those treated with antithyroid medications had an average 0.28 kg/m2 lower BMI, compared with the background population, and those treated with surgery had a 0.83 kg/m2 higher BMI. Both differences were significant (P < .001).
The BMI differences were not significant for radioactive iodine in women and for medications and radioactive iodine in men, although the men treated surgically also had a significantly higher BMI (1.09 kg/m2; P < .001).
“The patients on antithyroid drugs were lighter than we would expect. I think that’s ongoing hyperthyroidism. I strongly believe that ... to get rid of hyperthyroidism you have to make patients hypothyroid ... It’s really important that you get good control,” Dr. Boelaert commented.
Dr. Maraka, who is also endocrine section chief of the Arkansas Veteran’s Healthcare System, Little Rock, commented: “[Dr. Boelaert’s] concern is that the patients on antithyroid drugs are not adequately controlled, and we know very well that uncontrolled hyperthyroidism is associated with increased mortality and increased cardiovascular outcomes. This suggests that if patients are on antithyroid medications, they should at least be monitored very well.”
Regarding the possible cause of the increased mortality, if not cardiovascular, Dr. Maraka also pointed out that typically once antithyroid medications are stopped, about half of patients will stay in remission and the other half will return to hyperthyroidism.
“It might be that this kind of ‘yo-yo’ is what’s actually leading to the increased mortality, compared to patients who had definitive treatment and this problem was taken care of. This is speculation but it might be what we’re seeing,” Dr. Maraka observed.
The BMI differences worked out to a weight gain with surgery of approximately 2.1 kg (4.6 lb) for a woman with a height of 160 cm and 2.4 kg for 170 cm. Among men, those differences were 3.2 kg and 3.5 kg for heights of 170 cm and 190 cm, respectively.
Dr. Boelaert said, “I think we should discuss this with patients. They will say they don’t want to get fat, but the absolute weight gain is ... not that much.”
“I personally think that 2 kg is not a big price to pay to live longer. I hope that’s what we’ll be telling our patients in clinic in the next few years after we get this published.”
Dr. Boelaert and Dr. Maraka have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
CHICAGO – Treatment of hyperthyroidism with surgery or radioactive iodine significantly extends survival, compared with antithyroid medication, while surgery raises the risk for obesity, new data from a large cohort study suggest.
“I think this is something we need to take into our discussions with patients because treatment for hyperthyroidism is very much individualized decision-making ... The effects on mortality are not usually one of the factors we discuss there. But now, we have strong data from a very large cohort of patients indicating that this is something that does need to be discussed,” lead author Kristien Boelaert, MD, who is the current president of the British Thyroid Association, said in an interview.
Dr. Boelaert presented the findings of the EGRET (Weight Changes, Cardio-Metabolic Risks and Mortality in Patients With Hyperthyroidism) study at the Annual Meeting of the Endocrine Society.
Other notable findings from EGRET were that the patients on antithyroid medication were thinner than expected, suggesting undertreatment, and that no differences were found for major adverse cardiac events (MACE) across the treatment options, leaving unexplained the reasons for the increased mortality in the medicated group.
Asked to comment, session moderator Spyridoula Maraka, MD, said: “I think this is very important work because so far when we counsel our patients about the different treatment modalities we focus more on risk for recurrence and other short-term outcomes.”
“But these data give us a bigger perspective on mortality and cardiovascular outcomes ... We haven’t had such good quality data to accurately counsel our patients,” added Dr. Maraka, of the University of Arkansas for Medical Sciences, Little Rock.
Mortality higher for medication-treated, but why?
“Hyperthyroidism or an overactive thyroid gland is common, affecting up to 3% of the population, and is associated with long-term adverse cardiac and metabolic consequences. The optimal treatment choice remains unclear,” explained Dr. Boelaert, professor of endocrinology at the University of Birmingham, England, outlining the reasons they conducted the EGRET study.
The study population was 55,318 patients (77% women) with newly diagnosed hyperthyroidism identified from a U.K. population-based primary care electronic health record database. Of those, 77.8% were treated with antithyroid medication, 14.6% with radioactive iodine, and 7.8% with surgery (total or hemithyroidectomy). The health records were linked with national mortality data and Health Survey England data on body mass index (BMI) for comparison.
Dr. Boelaert noted that the trial design “is the best we have” because a randomized clinical trial comparing hyperthyroid treatments would be extremely difficult given the need to individualize therapy and the impossibility of blinding. On the other hand, with the current study, “it’s certainly the largest patient group we’ve looked at.”
Over an average 12.1 years of follow-up, the proportion of patients who died was 14.1% in the medication group, 18.7% of those who had radioiodine therapy, and 9.2% of those who underwent surgery.
Compared with the number who would have been expected to die based on the general background population, the likelihood of reduced life expectancy for the treated groups was increased 2.10-fold for radioiodine, 2.13-fold for surgery, and 2.71-fold for medication. All were significantly higher than the general population (P < .0001).
After further adjustment for multiple confounders, mortality risk was reduced in patients treated with radioiodine (by 13%) or surgery (by 20%), compared with those treated with antithyroid medication, both significant reductions (P < .0001).
After exclusion of the 3.9% with baseline cardiovascular disease, MACE (defined as cardiovascular death or hospitalization for stroke or myocardial infarction) occurred in 9.9%, 13.4%, and 8.0% of the medication, radioiodine, and surgery groups, respectively.
After adjustments, there were no differences in MACE, compared with medications, with hazard ratios of 1.00 (P = .94) for radioactive iodine and 0.97 for surgery (P = .61).
“We were expecting to see a reduction in cardiovascular events, as previous studies suggest that radioactive iodine patients have fewer cardiovascular deaths. We did not see that but our protocol wasn’t set up to get every single specific cause of death. That will require further ongoing analysis,” said Dr. Boelaert.
Weight gain: Worth it for longer life
Compared with the background population, thyroidectomy was associated with an increased likelihood of developing obesity (BMI > 30 kg/m2) in both men (odds ratio, 1.56; P < .001), and women (OR, 1.27; P < .001), while radioiodine increased obesity risk in women (OR, 1.12; P < .001) but not in men (OR, 1.03; P = .55).
Among the women, those treated with antithyroid medications had an average 0.28 kg/m2 lower BMI, compared with the background population, and those treated with surgery had a 0.83 kg/m2 higher BMI. Both differences were significant (P < .001).
The BMI differences were not significant for radioactive iodine in women and for medications and radioactive iodine in men, although the men treated surgically also had a significantly higher BMI (1.09 kg/m2; P < .001).
“The patients on antithyroid drugs were lighter than we would expect. I think that’s ongoing hyperthyroidism. I strongly believe that ... to get rid of hyperthyroidism you have to make patients hypothyroid ... It’s really important that you get good control,” Dr. Boelaert commented.
Dr. Maraka, who is also endocrine section chief of the Arkansas Veteran’s Healthcare System, Little Rock, commented: “[Dr. Boelaert’s] concern is that the patients on antithyroid drugs are not adequately controlled, and we know very well that uncontrolled hyperthyroidism is associated with increased mortality and increased cardiovascular outcomes. This suggests that if patients are on antithyroid medications, they should at least be monitored very well.”
Regarding the possible cause of the increased mortality, if not cardiovascular, Dr. Maraka also pointed out that typically once antithyroid medications are stopped, about half of patients will stay in remission and the other half will return to hyperthyroidism.
“It might be that this kind of ‘yo-yo’ is what’s actually leading to the increased mortality, compared to patients who had definitive treatment and this problem was taken care of. This is speculation but it might be what we’re seeing,” Dr. Maraka observed.
The BMI differences worked out to a weight gain with surgery of approximately 2.1 kg (4.6 lb) for a woman with a height of 160 cm and 2.4 kg for 170 cm. Among men, those differences were 3.2 kg and 3.5 kg for heights of 170 cm and 190 cm, respectively.
Dr. Boelaert said, “I think we should discuss this with patients. They will say they don’t want to get fat, but the absolute weight gain is ... not that much.”
“I personally think that 2 kg is not a big price to pay to live longer. I hope that’s what we’ll be telling our patients in clinic in the next few years after we get this published.”
Dr. Boelaert and Dr. Maraka have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN DIEGO – Children with type 2 diabetes face a strikingly high complication rate as they age into young adulthood, with an 80% incidence of at least one vascular complication during up to 15 years of follow-up, show findings from the TODAY prospective, longitudinal study of 699 U.S. children newly diagnosed with type 2 diabetes.
Arterial stiffness and worsened cardiac function often appear in these children within 2-5 years of diagnosis and seem driven in part by the development of hypertension and worsening hemoglobin A1c levels, said Rachelle G. Gandica, MD, at the annual scientific sessions of the American Diabetes Association.
Indeed, an A1c greater than 6.2% at study entry generally predicts these children will fail treatment and is a red flag, said Dr. Gandica. “I teach fellows this all the time, that if a child’s A1c is above 6.2% they will fail, and you have to watch for that,” she noted.
Mitchel L. Zoler/Medscape
Dr. Rachelle G. Gandica
The results from the Treatment Options for Type 2 Diabetes in Adolescents and Youth (TODAY) study showed, for example, an overall cardiovascular event rate of 3.7/1,000 patient-years in a population that had just reached an average age of 26 years old, with type 2 diabetes diagnosed for an average of more than 13 years.
During follow-up, there were six cases of congestive heart failure, four myocardial infarctions, four strokes, and three cases of coronary artery disease in the cohort. Hypertension ballooned from a prevalence of 19% at study entry to 68% by the end of follow-up.
Dr. Gandica called these and other findings “sobering details” that document the toll type 2 diabetes takes on children, who averaged 14 years old at the time they entered the study – when their diabetes had been diagnosed for an average of about 8 months – and then underwent an average 12.6 years of follow-up.
Investigators also found:
After more than 12 years of type 2 diabetes, 49% of the cohort had developed diabetic retinopathy, with 3.5% having macular edema.
Kidney damage (diabetic nephropathy) affected 8% of the cohort at entry, and then increased to a prevalence of 55% after up to 14 years of follow-up.
Among the 452 girls who entered the study, 141 (31%) later became pregnant, with a total of 260 pregnancies. A quarter of the pregnancies resulted in preterm deliveries (43% went to term), 25% resulted in miscarriage or fetal demise, with the remaining 8% having elective terminations or unknown outcomes.
Complications in neonates were common, including hypoglycemia (29%), respiratory disorder (19%), and cardiac issues (10%).
Dire prognosis a reason to aggressively treat these patients
It has become apparent from this and other studies in youth with type 2 diabetes that the difference in outcomes between youth and adults is stark and could indicate that type 2 diabetes in childhood or adolescence likely has a different underlying pathology and natural history, with a more aggressive disease course.
The dire prognosis is therefore a reason to aggressively treat these patients with antidiabetic medications from drug classes with proven cardiovascular disease protection, specifically sodium-glucose cotransporter 2 (SGLT2) inhibitors and glucagonlike peptide-1 (GLP-1) agonists, said Dr. Gandica, a pediatric endocrinologist at Columbia University Medical Center in New York.
“It’s fair to say we now more aggressively use [these agents] in children,” she said in an interview, and noted the very recent approval, just last week, by the U.S. Food and Drug Administration of the SGLT2 inhibitor empagliflozin (Jardiance, Boehringer Ingelheim/Lilly) for children as young as 10 years.
“I look forward to prescribing empagliflozin to children with type 2 diabetes to lower their blood pressure and get additional cardiovascular disease benefits,” Dr. Gandica said.
Other newer type 2 diabetes medications approved for U.S. children in the past few years include the once-weekly injectable GLP-1 agonist exenatide extended release (Bydureon/Bydureon BCise, AstraZeneca) for children with type 2 diabetes aged 10 and older, in 2021, and the daily injectable GLP-1 agonist liraglutide (Victoza, Novo Nordisk) in 2019.
A1c spike heralds treatment failure: ‘Watch for that’
TODAY enrolled 699 children with type 2 diabetes for an average of 8 months since diagnosis at 16 U.S. sites starting in 2004. The protocol began with a run-in phase of up to 6 months, when participating children came off any preexisting antidiabetes medications and then began a metformin-only regimen to bring A1c below 8.0%. If achieved, patients were eligible to continue to randomization.
Participants were randomized to one of three treatment groups: metformin alone, metformin plus lifestyle interventions, or metformin plus rosiglitazone (Avandia, GSK). The primary endpoint was the incidence of treatment failure, defined as A1c that rose back above 8.0% for at least 6 months or persistent metabolic decompensation during initial follow-up, for an average of just under 4 years.
The results showed that only metformin plus rosiglitazone significantly surpassed metformin alone for preventing treatment failure, reported in 2012 in the New England Journal of Medicine
More recent reports on findings from longer-term follow-up have appeared in several journals, including the cardiovascular disease results, reported in 2021 also in the New England Journal of Medicine.
Another key finding from TODAY is the importance of A1c as a risk marker for impending treatment failure. Study findingsshow that an A1c of 6.2% or higher when children entered the study best predicted loss of glycemic control during follow-up. Also, a rise in A1c of at least 0.5 percentage points was significantly associated with loss of glycemic control within the following 3-6 months.
That’s an important message for clinicians, Dr. Gandica concluded.
TODAY and TODAY2 received no commercial funding. Dr. Gandica has reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
SAN DIEGO – Children with type 2 diabetes face a strikingly high complication rate as they age into young adulthood, with an 80% incidence of at least one vascular complication during up to 15 years of follow-up, show findings from the TODAY prospective, longitudinal study of 699 U.S. children newly diagnosed with type 2 diabetes.
Arterial stiffness and worsened cardiac function often appear in these children within 2-5 years of diagnosis and seem driven in part by the development of hypertension and worsening hemoglobin A1c levels, said Rachelle G. Gandica, MD, at the annual scientific sessions of the American Diabetes Association.
Indeed, an A1c greater than 6.2% at study entry generally predicts these children will fail treatment and is a red flag, said Dr. Gandica. “I teach fellows this all the time, that if a child’s A1c is above 6.2% they will fail, and you have to watch for that,” she noted.
Mitchel L. Zoler/Medscape
Dr. Rachelle G. Gandica
The results from the Treatment Options for Type 2 Diabetes in Adolescents and Youth (TODAY) study showed, for example, an overall cardiovascular event rate of 3.7/1,000 patient-years in a population that had just reached an average age of 26 years old, with type 2 diabetes diagnosed for an average of more than 13 years.
During follow-up, there were six cases of congestive heart failure, four myocardial infarctions, four strokes, and three cases of coronary artery disease in the cohort. Hypertension ballooned from a prevalence of 19% at study entry to 68% by the end of follow-up.
Dr. Gandica called these and other findings “sobering details” that document the toll type 2 diabetes takes on children, who averaged 14 years old at the time they entered the study – when their diabetes had been diagnosed for an average of about 8 months – and then underwent an average 12.6 years of follow-up.
Investigators also found:
After more than 12 years of type 2 diabetes, 49% of the cohort had developed diabetic retinopathy, with 3.5% having macular edema.
Kidney damage (diabetic nephropathy) affected 8% of the cohort at entry, and then increased to a prevalence of 55% after up to 14 years of follow-up.
Among the 452 girls who entered the study, 141 (31%) later became pregnant, with a total of 260 pregnancies. A quarter of the pregnancies resulted in preterm deliveries (43% went to term), 25% resulted in miscarriage or fetal demise, with the remaining 8% having elective terminations or unknown outcomes.
Complications in neonates were common, including hypoglycemia (29%), respiratory disorder (19%), and cardiac issues (10%).
Dire prognosis a reason to aggressively treat these patients
It has become apparent from this and other studies in youth with type 2 diabetes that the difference in outcomes between youth and adults is stark and could indicate that type 2 diabetes in childhood or adolescence likely has a different underlying pathology and natural history, with a more aggressive disease course.
The dire prognosis is therefore a reason to aggressively treat these patients with antidiabetic medications from drug classes with proven cardiovascular disease protection, specifically sodium-glucose cotransporter 2 (SGLT2) inhibitors and glucagonlike peptide-1 (GLP-1) agonists, said Dr. Gandica, a pediatric endocrinologist at Columbia University Medical Center in New York.
“It’s fair to say we now more aggressively use [these agents] in children,” she said in an interview, and noted the very recent approval, just last week, by the U.S. Food and Drug Administration of the SGLT2 inhibitor empagliflozin (Jardiance, Boehringer Ingelheim/Lilly) for children as young as 10 years.
“I look forward to prescribing empagliflozin to children with type 2 diabetes to lower their blood pressure and get additional cardiovascular disease benefits,” Dr. Gandica said.
Other newer type 2 diabetes medications approved for U.S. children in the past few years include the once-weekly injectable GLP-1 agonist exenatide extended release (Bydureon/Bydureon BCise, AstraZeneca) for children with type 2 diabetes aged 10 and older, in 2021, and the daily injectable GLP-1 agonist liraglutide (Victoza, Novo Nordisk) in 2019.
A1c spike heralds treatment failure: ‘Watch for that’
TODAY enrolled 699 children with type 2 diabetes for an average of 8 months since diagnosis at 16 U.S. sites starting in 2004. The protocol began with a run-in phase of up to 6 months, when participating children came off any preexisting antidiabetes medications and then began a metformin-only regimen to bring A1c below 8.0%. If achieved, patients were eligible to continue to randomization.
Participants were randomized to one of three treatment groups: metformin alone, metformin plus lifestyle interventions, or metformin plus rosiglitazone (Avandia, GSK). The primary endpoint was the incidence of treatment failure, defined as A1c that rose back above 8.0% for at least 6 months or persistent metabolic decompensation during initial follow-up, for an average of just under 4 years.
The results showed that only metformin plus rosiglitazone significantly surpassed metformin alone for preventing treatment failure, reported in 2012 in the New England Journal of Medicine
More recent reports on findings from longer-term follow-up have appeared in several journals, including the cardiovascular disease results, reported in 2021 also in the New England Journal of Medicine.
Another key finding from TODAY is the importance of A1c as a risk marker for impending treatment failure. Study findingsshow that an A1c of 6.2% or higher when children entered the study best predicted loss of glycemic control during follow-up. Also, a rise in A1c of at least 0.5 percentage points was significantly associated with loss of glycemic control within the following 3-6 months.
That’s an important message for clinicians, Dr. Gandica concluded.
TODAY and TODAY2 received no commercial funding. Dr. Gandica has reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
SAN DIEGO – Children with type 2 diabetes face a strikingly high complication rate as they age into young adulthood, with an 80% incidence of at least one vascular complication during up to 15 years of follow-up, show findings from the TODAY prospective, longitudinal study of 699 U.S. children newly diagnosed with type 2 diabetes.
Arterial stiffness and worsened cardiac function often appear in these children within 2-5 years of diagnosis and seem driven in part by the development of hypertension and worsening hemoglobin A1c levels, said Rachelle G. Gandica, MD, at the annual scientific sessions of the American Diabetes Association.
Indeed, an A1c greater than 6.2% at study entry generally predicts these children will fail treatment and is a red flag, said Dr. Gandica. “I teach fellows this all the time, that if a child’s A1c is above 6.2% they will fail, and you have to watch for that,” she noted.
Mitchel L. Zoler/Medscape
Dr. Rachelle G. Gandica
The results from the Treatment Options for Type 2 Diabetes in Adolescents and Youth (TODAY) study showed, for example, an overall cardiovascular event rate of 3.7/1,000 patient-years in a population that had just reached an average age of 26 years old, with type 2 diabetes diagnosed for an average of more than 13 years.
During follow-up, there were six cases of congestive heart failure, four myocardial infarctions, four strokes, and three cases of coronary artery disease in the cohort. Hypertension ballooned from a prevalence of 19% at study entry to 68% by the end of follow-up.
Dr. Gandica called these and other findings “sobering details” that document the toll type 2 diabetes takes on children, who averaged 14 years old at the time they entered the study – when their diabetes had been diagnosed for an average of about 8 months – and then underwent an average 12.6 years of follow-up.
Investigators also found:
After more than 12 years of type 2 diabetes, 49% of the cohort had developed diabetic retinopathy, with 3.5% having macular edema.
Kidney damage (diabetic nephropathy) affected 8% of the cohort at entry, and then increased to a prevalence of 55% after up to 14 years of follow-up.
Among the 452 girls who entered the study, 141 (31%) later became pregnant, with a total of 260 pregnancies. A quarter of the pregnancies resulted in preterm deliveries (43% went to term), 25% resulted in miscarriage or fetal demise, with the remaining 8% having elective terminations or unknown outcomes.
Complications in neonates were common, including hypoglycemia (29%), respiratory disorder (19%), and cardiac issues (10%).
Dire prognosis a reason to aggressively treat these patients
It has become apparent from this and other studies in youth with type 2 diabetes that the difference in outcomes between youth and adults is stark and could indicate that type 2 diabetes in childhood or adolescence likely has a different underlying pathology and natural history, with a more aggressive disease course.
The dire prognosis is therefore a reason to aggressively treat these patients with antidiabetic medications from drug classes with proven cardiovascular disease protection, specifically sodium-glucose cotransporter 2 (SGLT2) inhibitors and glucagonlike peptide-1 (GLP-1) agonists, said Dr. Gandica, a pediatric endocrinologist at Columbia University Medical Center in New York.
“It’s fair to say we now more aggressively use [these agents] in children,” she said in an interview, and noted the very recent approval, just last week, by the U.S. Food and Drug Administration of the SGLT2 inhibitor empagliflozin (Jardiance, Boehringer Ingelheim/Lilly) for children as young as 10 years.
“I look forward to prescribing empagliflozin to children with type 2 diabetes to lower their blood pressure and get additional cardiovascular disease benefits,” Dr. Gandica said.
Other newer type 2 diabetes medications approved for U.S. children in the past few years include the once-weekly injectable GLP-1 agonist exenatide extended release (Bydureon/Bydureon BCise, AstraZeneca) for children with type 2 diabetes aged 10 and older, in 2021, and the daily injectable GLP-1 agonist liraglutide (Victoza, Novo Nordisk) in 2019.
A1c spike heralds treatment failure: ‘Watch for that’
TODAY enrolled 699 children with type 2 diabetes for an average of 8 months since diagnosis at 16 U.S. sites starting in 2004. The protocol began with a run-in phase of up to 6 months, when participating children came off any preexisting antidiabetes medications and then began a metformin-only regimen to bring A1c below 8.0%. If achieved, patients were eligible to continue to randomization.
Participants were randomized to one of three treatment groups: metformin alone, metformin plus lifestyle interventions, or metformin plus rosiglitazone (Avandia, GSK). The primary endpoint was the incidence of treatment failure, defined as A1c that rose back above 8.0% for at least 6 months or persistent metabolic decompensation during initial follow-up, for an average of just under 4 years.
The results showed that only metformin plus rosiglitazone significantly surpassed metformin alone for preventing treatment failure, reported in 2012 in the New England Journal of Medicine
More recent reports on findings from longer-term follow-up have appeared in several journals, including the cardiovascular disease results, reported in 2021 also in the New England Journal of Medicine.
Another key finding from TODAY is the importance of A1c as a risk marker for impending treatment failure. Study findingsshow that an A1c of 6.2% or higher when children entered the study best predicted loss of glycemic control during follow-up. Also, a rise in A1c of at least 0.5 percentage points was significantly associated with loss of glycemic control within the following 3-6 months.
That’s an important message for clinicians, Dr. Gandica concluded.
TODAY and TODAY2 received no commercial funding. Dr. Gandica has reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.