User login
Psoas Abscess: A Diagnostic Dilemma
Infection Prevention in Total Knee and Total Hip Arthroplasties
Bites and Stings

Hymenoptera
The order Hymenoptera of the phylum Arthropoda can be divided into three subgroups that are medically relevant: (1) Apidae (Apids), which include the honeybee and bumblebee; (2) Vespidae, (Vespids) which include yellow jackets, hornets and wasps; and (3) Formicidae (ants).6
Bees and Wasps
The main allergens in Apid venom are phospholipase A2, hyaluronidase, and melittin. Melittin, the main component, is a membrane active polypeptide that causes degranulation of basophils and mast cells. The allergens in Vespid venom are phospholipase, hyaluronidase, and antigen 5. As all Hymenoptera share some of these components, cross-sensitization may occur and individuals may be allergic to more than one species.7

Occasionally after multiple stings, patients present with symptoms of a systemic toxic reaction. This is often seen in an Africanized bee attack. These so-called “killer bees” are hybrids of African bees that escaped from laboratories in Brazil in the 1950s and spread northward; they are found in most of the warmer US states. Their venom is not more toxic than that of any other bee, but Africanized honeybees are more aggressive and respond to a perceived threat in far greater numbers. The reaction that results from multiple stings is systemic and may resemble anaphylaxis. Common symptoms include nausea, vomiting, and diarrhea, as well as lightheadedness and syncope. Interestingly, urticaria and bronchospasm are not universally present, even though respiratory failure and cardiac arrest may occur. Other symptoms include renal failure with acute tubular necrosis, myoglobinuria or hemoglobinuria, hepatic failure, and disseminated intravascular coagulation (DIC).10,11 In addition, there have been reports of unusual reactions such as vasculitis, nephrosis, neuritis, encephalitis, and serum sickness. Late-appearing symptoms usually start several days to weeks after a sting and tend last for a prolonged period of time. Serum sickness tends to appear 5 to 14 days after exposure and consists of fever, malaise, headache, urticaria, lymphadenopathy, and polyarthritis.12 Of note, patients who have venom-induced serum sickness may be at risk for anaphylaxis after subsequent stings and may therefore be suitable candidates for venom immunotherapy.13
Anaphylaxis
The definition of anaphylaxis is not universally agreed upon. The American Academy of Allergy, Asthma and Immunology defines anaphylaxis as a serious allergic response that often involves swelling, hives, hypotension and, in severe cases, shock. A major difference between anaphylaxis and other allergic reactions is that anaphylaxis typically involves more than one body system.14 The clinical features of anaphylaxis from insect stings are the same as those from other causes, typically generalized urticaria, facial flushing, and angioedema. Abdominal cramping, nausea, vomiting, and diarrhea are also seen. Life-threatening symptoms include stridor, circulatory collapse with shock, and bronchospasm. Symptoms usually begin 10 to 20 minutes after a sting, and almost all will develop within 6 hours. Interestingly, symptoms may recur 8 to 12 hours after the initial reaction.15-18
Management
Immediate removal of the bee stinger is the most important principle as it precludes any further venom transfer. Traditional teaching recommended scraping the stinger out to avoid squeezing remaining venom into the tissues; however, involuntary muscle contractions of the gland continue after the stinger detaches, and the venom is quickly exhausted. Thus, immediate removal of the stinger is crucial, though the method of removal is now thought irrelevant.19
The mainstay of therapy for serious reactions is intramuscular (IM) epinephrine. The initial dosing is 0.3 to 0.5 mg (0.3 to 0.5 mL of 1:1000 concentration) in adults, and 0.01 mg/kg in children (maximum 0.3 mg). The injection should be IM and not subcutaneous, as IM dosing provides higher and more consistent and rapid peak blood epinephrine levels.20 Concomitant intravenous (IV) administration of standard antihistamines, often diphenhydramine 1 mg/kg (generally 25-50 mg) and histamine-2 receptor antagonists (typically ranitidine 50 mg) are also recommended. The administration of steroids (methylprednisolone 125 mg IV or prednisone 60 mg orally) is traditionally recommended and thought to help potentiate the effect of other interventional measures.20 Bronchospasm, if present, is treated with nebulized β-agonists (albuterol). Hypotension may develop and requires significant crystalloid infusion—often several liters. If hypotension persists despite adequate fluid replacement, vasopressor therapy is recommended.
If a patient does not respond to initial treatment and cardiovascular (CV) collapse is evident, IV infusion of epinephrine should be initiated. Epinephrine, 100 mcg (0.1 mg) IV, should be given as a 1:100,000 dilution. This can be done by placing epinephrine, 0.1 mg (0.1 mL of the 1:1000 dilution), in 10 mL of normal saline solution and infusing it over 5 to 10 minutes (a rate of 1 to 2 mL/min). If the patient is refractory to the initial bolus, then an epinephrine infusion can be started by placing epinephrine, 1 mg (1.0 mL of the 1:1000 dilution), in 500 mL of 5% dextrose in water or NS and administering at a rate of 1 to 4 mcg per minute (0.5 to 2 mL/min), titrating to effect.20 Antivenins have been studied for treatment, but none are commercially available at this time.21 Patients with anaphylaxis associated with severe signs and symptoms, including any evidence of CV collapse, should be admitted to the hospital for aggressive therapy and monitoring. Persons with mild-to-moderate reactions should be observed for 4 to 6 hours to monitor for late occurring symptoms. Outpatient therapy with antihistamines, oral steroids, and a prescription for an epinephrine auto-injector—including training on proper administration prior to discharge—are strongly recommended.22 Follow-up with an allergist is also indicated in patients with significant reactions, as skin testing and immunotherapy may be beneficial to prevent anaphylaxis during future exposures.
Ants

Fire ant venom is composed of an insoluble alkaloid, and crossreactivity with the venom of other Hymenopteras species does exist. Stings generally result in a papule, which evolves into a sterile pustule. Localized necrosis, scarring, and secondary infection can occur. Systemic reactions with angioedema and urticaria have been documented, which can sometimes lead to fatalities.24
Treatment
Treatment of fire ant stings begin and end with local wound care. If the reaction is systemic, a treatment plan similar to that outlined in the treatment section for bees and wasps is indicated.
Araneae
The order Araneae of the phylum Arthropoda includes over 34,000 species of spiders divided into 105 families. Of those, only half a dozen are medically relevant and only three are commonly encountered in the United States. These include Loxosceles (most notably, the brown recluse spider), Tegeneria (mainly the hobo brown spider) and Latrodectus (includes the black widow spider). True spiders have a worldwide distribution and tend to thrive in heavily populated areas, resulting in many biting episodes per year. Data from the AAPPC’s most recent annual report listed 9,255 single spider-bite exposures in 2012, with one associated death.3
Spiders are carnivores and use venom to paralyze their prey. They are generally not a threat to humans as their fangs are too small to penetrate human skin, and the amount of venom injected is too small to produce toxicity. Thus, reactions resulting from a spider bite are typically limited to a localized reaction. Fortunately, most bites only require supportive medical therapy.
Loxosceles
Loxosceles are present worldwide, but L reclusa (the “brown recluse spider”) accounts for a significant number of envenomations in the United States. The AAPCC’s 2012 data notes 1,365 cases of exposure to the brown recluse spider with 510 of those victims seeking medical care.3 In many instances, clinicians attribute necrotic bites to the brown recluse spider, however, confirmation is often lacking. Loxosceles are nocturnal, and they are found both indoors and outdoors—mostly in dark and dry areas such as basements, closets, and woodpiles. These spiders are shy, but may bite when threatened. Their venom contains enzymes, including hyaluronidase and sphingomyelinase. Though rare, wounds can become necrotic due to neutrophil activation, platelet aggregation, and thrombosis.25 The most common reaction to a Loxosceles bite is a mild painless erythematous lesion that becomes firm and generally heals over several days to weeks. In severe reactions, erythema, edema, and pruritus initially develop, followed within 24 to 72 hours by a hemorrhagic bulla surrounded by blanched skin. This leads to the “red, white, and blue sign” (ie, erythema, blanching, and ecchymosis). Infrequently, the ecchymotic area becomes necrotic and ulcerates in 3 to 5 days. The differential diagnoses should include necrotizing fasciitis, erythema chronicum migrans (from Borrelia-infected tick bites), and anthrax. Ulcerated lesions may result in significant cosmetic defect. Healing may take up to 2 weeks, and skin grafting is occasionally required.26

Treatment begins with the usual supportive measures, including analgesia, ice, elevation, and a light compression dressing. Antibiotics are not indicated, unless there are signs of secondary infection. Serial evaluation for wound checks should be arranged. If ulceration develops, surgical debridement may be required. The vast majority of bites heal with supportive care alone, and aggressive medical therapy is usually not warranted.27Patients with systemic manifestations should be admitted to the hospital for further care. There is no evidence-based literature to guide therapy. Many therapies have been tried with variable results and there remains no definitive standard of care.
Treatment regimens include antihistamines, antivenin, colchicine, dapsone, hyperbaric oxygen, cyproheptadine, surgical excision, and steroids.28 Dapsone continues to be widely advocated worldwide despite its known adverse effects—most notably hemolysis and methemoglobinemia. Antivenin administration has shown some promise in animal models, but its efficacy in humans is still unclear.29
Tegenaria
The Tegenaria agrestis or hobo spider is a native of Europe and central Asia and is only found in the northwest part of the United States. It is considered aggressive and tends to bite even with only mild provocation. The clinical presentation, inclusive of systemic reactions, is similar to that of the brown recluse spider. Similarly, there is no proven treatment. Surgical wound resection and skin grafting should be considered and is at times required.
Latrodectus.
Latrodectus, also known as widow spiders, are found worldwide. Five species are commonly found in the United States, but the black widow is the most well known. Only three of the species are actually black. Other varieties are typically brown or red. However, almost all Latrodectus spiders have a characteristic orange-red hourglass-shaped marking (Figure 3). Widow spiders aggressively defend their webs, and are most often found in woodpiles, basements, garages, and sheds. Most bites occur in the warmer months, between April and October.

Latrodectus antivenin is very effective, often resolving symptoms rapidly and reducing the duration of illness—even when administered up to 90 hours postenvenomation.32 This antivenin is derived from horse serum, and hypersensitivity reactions are possible. One death from anaphylaxis has been reported in the United States after antivenin was given undiluted via IV push; however, slow administration of diluted antivenin is considered safe.33
Diptera
The order Diptera of the phylum Arthropoda includes over 240,000 species. Among those, the mosquitoes and flies are the most medically relevant.
Mosquitoes
An actual mosquito bite itself causes minimal trauma and is not usually felt by the victim. However, the local anesthetic that is injected into the wound at the time of the attack causes local tissue damage. Mosquito bites can lead to both immediate and delayed reactions. Typical immediate reactions are of short duration and include edema, erythema, and pruritus. More severe reactions are extremely rare and consist of skin necrosis. Delayed skin reactions are fairly common, but tend to last longer, persisting for days or even weeks. Treatment is symptomatic, usually with antihistamines and NSAIDS.
Patients can acquire an allergy to mosquito saliva over time and develop increasingly pronounced edematous and pruritic lesions with subsequent bites. They can also experience fever, malaise, generalized edema, as well as severe nausea and vomiting.
Systemic or anaphylactic reactions are not known to occur. Instead, the greatest danger occurs with the transmission of life-threatening diseases. Malaria, yellow fever, dengue hemorrhagic fever, and different types of equine encephalitis are all transmitted by mosquito bites. One interesting newcomer to the United States is the West Nile virus (WNV), which has spread rapidly since its introduction in 2003. Over 1,850 cases were reported in 22 different states over the initial 8 months. Acute symptoms are mild in the majority of patients, but a small minority can experience fatal disease. Neurological symptoms include tumor, myoclonus, and Parkinsonism. An irreversible poliomyelitis-like syndrome may also develop. In addition to WNV, St Louis encephalitis and equine encephalitis also remain important pathogens in the United States.34 Prevention of bites is crucial and includes the use of pyrethroid-impregnated mosquito netting, repellents, and oral malaria prophylaxis. N,N-diethyl-3-methylbenzamide (DEET) remains the most effective mosquito repellent.35 Although toxic reactions are rare, they do occur and anaphylaxis has been reported. 36,37
Flies
Flies are blood-sucking insects that feed by stabbing and piercing their victim’s skin. Their bites always cause some degree of pain and pruritus. Allergic reactions are possible, though not as severe as those produced by Hymenoptera venom. Treatment is largely symptomatic with ice, oral antihistamine, analgesics. and topical or oral steroids as needed. Secondary bite infection is a concern and antibiotics are sometimes necessary.
Shiponaptera
The order Shinoptera includes fleas and lice. All produce very similar lesions, making diagnosis difficult. One concern with these bites is the development of secondary infections, especially in children. The skin should be washed with soap and water. Calamine, cool soaks, and oral or topical antihistamine may all be helpful to reduce symptoms.
Fleas
With fleas, as with mosquitoes, there is additionally a concern for transmission of life-threatening diseases. Fleas transmit bubonic plague, endemic typhus, brucellosis, melioidosis, and erysipeloid. Fortunately, effective oral and injectable formulations for both dogs and cats are now available to control fleas on most family pets.
Lice
Hemiptera

Lepidoptera
The order Lepidoptera includes butterflies and moths and their caterpillars. Symptoms that result from contact with this class of insects are referred to as lepidopterism. Caterpillars have hair or spines for protection, which are also sometimes connected to a venom gland. Contact with these spines usually causes localized skin irritation and pruritus. Megalopyge opercularis, also known as the “puss caterpillar,” is mainly found in the southeastern United States and accounts for the majority of envenomation cases in this country. Intense local burning pain is typical at the site of contact and is followed by a grid-like pattern of hemorrhagic papules, which appear 2 to 3 hours after exposure and may last for several days. Regional lymphadenopathy is common. Other symptoms include headache, fever, hypotension, and convulsions. No deaths have ever been reported.
As there is no antivenin available for lepidopterism, treatment is mostly supportive. If spines are visible following contact, they should be removed with adhesive tape. Antihistamines and steroids may be used for symptom control. In patients with hypotension, IV fluids and IV epinephrine may be required.43
Coleoptera
The order Coleoptera includes a large number of beetles, though clinically significant envenomation occurs only with blister beetles. There are over 1,500 species of blister beetles worldwide, approximately 2,002 of which are in the United States. The blister beetle responsible for most of the medically significant envenomations is Cantharis vesicatoria—also known as “Spanish fly.” Of note, the Spanish fly is not naturally found in the United States.

Cantharidin-containing substances are sometimes used medicinally in wart removal preparations and are also sold for their purported aphrodisiac effects (the associated vascular congestion and urethral inflammation are interpreted as enhanced sexuality). Transdermal absorption or ingestion may lead to systemic toxicity with severe vomiting, hematemesis, abdominal pain, diarrhea, hematuria, renal failure, etc. Death has been reported after large ingestions.
Treatment is largely supportive. The skin should be irrigated thoroughly after exposure, followed by local wound care. Patients who present after ingestion should be admitted to the hospital for further treatment and care.47
Conclusion
Knowledge of a vast array of stinging insects and spiders is important for any clinician, but the appropriate evaluation and treatment of bites and envenomations are crucial for EPs. Most exposures can be treated with supportive care, while others require in-depth knowledge and clinical expertise.
Dr Deljoui is a former resident, department of emergency medicine, Eastern Virginia Medical School, Norfolk; and current critical care fellow, University of Maryland, Baltimore.
Dr Knapp is an associate professor and residency program director, department of emergency medicine, Eastern Virginia Medical School, Norfolk.
- White J. Bites and stings from venomous animals: a global overview. The Drug Monit. 2000;22(1):65-68.
- Oten EJ. Venomous animal injuries. In: Marx JA, Hockberger RS, Walls RM, et al, eds. Rosen’s Emergency Medicine: Concepts and Clinical Practice. Vol 1. 8th ed. Philadelphia, PA: Elsevier Saunders; 2014:794-807.
- Mowry JB, Spyker DA, Cantilena LR Jr, Bailey JE, Ford M. 2012 Annual Report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 30th Annual Report. Clin Toxicol (Phila). 2013;51(10):949-1229. doi:10.3109/15563650.2013.863906. https://aapcc.s3.amazonaws.com/pdfs/annual_reports/2012_NPDS_Annual_Report.pdf. Accessed April 2, 2014.
- Liberman P, Camargo CA, Bohike K, et al. Epidemiology of anaphylaxis: findings of the American College of Allergy, Asthma and Immunology Epidemiology of Anaphylaxis Working Group. Ann Allergy Asthma Immunol. 2006;97(5):596-602.
- Barnard JH. Studies of 400 Hymenoptera sting deaths in the United States. J Allergy Clin Immunol. 1973;52(5):259-264.
- Frazier CA. Insect Allergy: Allergic and Toxic Reactions to Insects and Other Arthropods. 2nd Ed. St Louis, MO: WH Green; 1987:421.
- King TP, Spangfort MD. Structure and biology of stinging insect venom allergens. Int Arch Allergy Immunol. 2000;123(2):99-106.
- Antonicelli L, Bilo MB, Bonifazi F. Epidemiology of Hymenoptera allergy. Curr Opin Allergy Clin Immunol.2002;2(4);341-346.
- Mauriello PM, Barde SH. Natural history of large local reactions from stinging insects. J Allergy Clin Immunol. 1984;74(4 Pt 1):494-498.
- Díaz-Sánchez CL, Lifshitz-Guinzberg A, Ignacio-Ibarra G, Halabe-Cherem J, Quinones-Galvan A. Survival after massive (>2,000) Africanized honey bee stings. Arch Intern Med. 1998;158(8):925-927.
- Elston DM. Life-threatening stings, bites, infestations and parasitic diseases. Clin Dermatol. 2005;23(2):164-170.
- Lazoglu AH1, Boglioli LR, Taff ML, Rosenbluth M, Macris NT. Serum sickness reaction following multiple insect stings. Ann Allergy Asthma Immunol. 1995;75(6 Pt 1):522-524.
- Reisman RE, Livingston A. Late-onset allergic reactions, including serum sickness, after insect stings. J Allergy Clin Immunol. 1989;84(3);331-337.
- Anaphylaxis. American Academy of Allergy, Asthma & Immunology Web site. http://www.aaaai.org/conditions-and-treatments/conditions-a-to-zsearch/anaphylaxis.aspx. Accessed April 2, 2014.
- Brown H, Benton HS. Allergy to the Hymenoptera. V. Clinical study of 400 patients. Arch Intern Med. 1970;125(4):665-669.
- Frazier CA. Allergic reactions to insect stings: a review of 180 cases. South Med J. 1964;57;1023-1034.
- Mueller HL. Further experiences with severe allergic reactions to insect stings. N Engl J Med. 1959;161:374-377.
- Lockey RF, Turkeltaub PC, Baird-Warren IA, et al. The Hymenoptera venom study I, 1979-1982: demographics and history-sting data. J Allergy Clin Immunol. 1988;82(3 Pt 1):370-381.
- Schneir AB, Clark RF. Bites and stings. In: Tintinalli JE, Stapczynski JS, Ma OJ, Cline DM, Cydulka RK, Meckler GD, eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 7th ed. New York, NY: McGraw-Hill; 2011:chap120;585-596.
- Rowe BH, Gaeta T. Anaphylaxis, acute allergic reactions, and angioedema. In: Tintinalli JE, Stapczynski JS, Ma OJ, Cline DM, Cydulka RK, Meckler GD, eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 7th ed. New York, NY: McGraw-Hill; 2011:chap 6;52-54.
- Jones RG1, Corteling RL, Bhogal G, Landon J. A novel Fab-based antivenom for the treatment of mass bee attacks. Am J Trop Med Hyg. 1999;61(3):361-366.
- National Institutes of Health, US Department of Health and Human Services, National Insitute of Allergy and Infectious Diseases. Guidelines for the Diagnosis and Management of Food Allergy in the United States. Summary of the NIAID-Sponsored Expert Panel Report. Bethesda, MD: National Institutes of Health; 2010. NIH Publication No. 11-7700. http://www.niaid.nih.gov/topics/foodAllergy/clinical/Documents/FAGuidelinesExecSummary.pdf. Accessed April 2, 2014.
- Kemp SF, deShazo RD, Moffitt JE, Williams DF, Buhner WA 2nd. Expanding habitat of the imported fire ant (Solenopsis invicta): a public health concern. J Allergy Clin Immunol. 2000;105(4):683-691.
- Fernández-Meléndez S, Miranda A, García-González JJ, Barber D, Lombardero M. Anaphylaxis caused by imported red fire ant stings in Málaga, Spain. J Investig Allergol Immunol. 2007;17(1):48,49.
- Swanson DL. Bites of brown recluse spiders and suspected necrotic arachnidism. N Engl J Med. 2005;352(7):700-707.
- Saucier JR. Arachnid envenomation. Emerg Med Clin North Am. 2004;22(2):405-422.
- Wright SW, Wrenn KD, Murray L, Seger D. Clinical presentation and outcome of brown recluse spider bite. Ann Emerg Med. 1997;30(1):28-32.
- Phillips S, Kohn M, Baker D, et al. Therapy of brown spider envenomation: a controlled trial of hyperbaric oxygen, dapsone, and cyproheptadine. Ann Emerg Med. 1995;25(3):363-368.
- Pauli I, Puka J, Gubert IC, Minozzo JC. The efficacy of antivenom in loxoscelism treatment. Toxicon. 2006;48(2):123-127.
- Ushkaryov YA, Volynski KE, Ashton AC. The multiple actions of black widow spider toxins and their selective use in neurosecretion studies. Toxicon. 2004;43(5):527-542.
- Clark RF, Wethern-Kestner S, Vance MV, Gerkin R. Clinical presentation and treatment of black widow spider envenomation: a review of 163 cases. Ann Emerg Med. 1992;21(7):782-787.
- O’Malley GF, Dart RC, Kuffner EF. Successful treatment of latrodectism with antivenom after 90 hours. N Engl J Med. 1999;340(8):657.
- Clark RF. The safety and efficacy of antivenin Latrodectus mactans. J Toxicol Clin Toxicol. 2001;39(2):125-127.
- Sejvar JJ, Haddad MB, Tierney BC. Neurologic manifestations and outcome of West Nile virus infection [published correction appears in JAMA. 2003;290(10):1318]. JAMA. 2003;290(4):511-515.
- Brown M, Herbert AA. Insect repellents: an overview. J Am Acad Dermatol. 1997;36(2 Pt 1):243-249.
- Fradin MS. Mosquitoes and mosquito repellents: a clinician’s quide. Ann Intern Med. 1998;128(11):931-940.
- Miller JD. Anaphylaxis associated with insect repellent. N Engl J Med. 1982;307(21):1341,1342.
- Spach DH, Kanter AS, Dougherty MJ, et al. Bartonella (Rochalimaea) quintana bacteremia in inner-city patients with chronic alcoholism. N Engl J Med. 1995;332(7): 424-428.
- Jackson LA, Spach DH, Kippen DA, et al. Seroprevalence to Bartonella quintana among patients at a community clinic in downtown Seattle. J Infect Dis. 1996;173(4):1023-1026.
- Sundnes KO. Epidemic of louse-borne relapsing fever in Ethiopia. Lancet. 1993;342(8881):1213-1215.
- Vetter R. Kissing bugs (Triatoma) and the skin. Dermatol Online J. 2001;7(1):6. http://escholarship.org/uc/item/59k2m8wt. Accessed April 2, 2014.
- Stucki A, Ludwig R. Images in clinical medicine. Bedbug bites. N Engl J Med. 2008; 359:10)1047.
- Kuspis DA, Rawlins JE, Krenzelok EP. Human exposures to stinging caterpillars: Lophocampa caryae exposures. Am J Emerg Med. 2001;19(5):396-398.
- Moed L, Shwayder TA, 0.Chang MW. Cantharidin revisited: a blistering defense of an ancient medicine. Arch Dermatol. 2001;137(10):1357-1360.
Hymenoptera
The order Hymenoptera of the phylum Arthropoda can be divided into three subgroups that are medically relevant: (1) Apidae (Apids), which include the honeybee and bumblebee; (2) Vespidae, (Vespids) which include yellow jackets, hornets and wasps; and (3) Formicidae (ants).6
Bees and Wasps
The main allergens in Apid venom are phospholipase A2, hyaluronidase, and melittin. Melittin, the main component, is a membrane active polypeptide that causes degranulation of basophils and mast cells. The allergens in Vespid venom are phospholipase, hyaluronidase, and antigen 5. As all Hymenoptera share some of these components, cross-sensitization may occur and individuals may be allergic to more than one species.7
Occasionally after multiple stings, patients present with symptoms of a systemic toxic reaction. This is often seen in an Africanized bee attack. These so-called “killer bees” are hybrids of African bees that escaped from laboratories in Brazil in the 1950s and spread northward; they are found in most of the warmer US states. Their venom is not more toxic than that of any other bee, but Africanized honeybees are more aggressive and respond to a perceived threat in far greater numbers. The reaction that results from multiple stings is systemic and may resemble anaphylaxis. Common symptoms include nausea, vomiting, and diarrhea, as well as lightheadedness and syncope. Interestingly, urticaria and bronchospasm are not universally present, even though respiratory failure and cardiac arrest may occur. Other symptoms include renal failure with acute tubular necrosis, myoglobinuria or hemoglobinuria, hepatic failure, and disseminated intravascular coagulation (DIC).10,11 In addition, there have been reports of unusual reactions such as vasculitis, nephrosis, neuritis, encephalitis, and serum sickness. Late-appearing symptoms usually start several days to weeks after a sting and tend last for a prolonged period of time. Serum sickness tends to appear 5 to 14 days after exposure and consists of fever, malaise, headache, urticaria, lymphadenopathy, and polyarthritis.12 Of note, patients who have venom-induced serum sickness may be at risk for anaphylaxis after subsequent stings and may therefore be suitable candidates for venom immunotherapy.13
Anaphylaxis
The definition of anaphylaxis is not universally agreed upon. The American Academy of Allergy, Asthma and Immunology defines anaphylaxis as a serious allergic response that often involves swelling, hives, hypotension and, in severe cases, shock. A major difference between anaphylaxis and other allergic reactions is that anaphylaxis typically involves more than one body system.14 The clinical features of anaphylaxis from insect stings are the same as those from other causes, typically generalized urticaria, facial flushing, and angioedema. Abdominal cramping, nausea, vomiting, and diarrhea are also seen. Life-threatening symptoms include stridor, circulatory collapse with shock, and bronchospasm. Symptoms usually begin 10 to 20 minutes after a sting, and almost all will develop within 6 hours. Interestingly, symptoms may recur 8 to 12 hours after the initial reaction.15-18
Management
Immediate removal of the bee stinger is the most important principle as it precludes any further venom transfer. Traditional teaching recommended scraping the stinger out to avoid squeezing remaining venom into the tissues; however, involuntary muscle contractions of the gland continue after the stinger detaches, and the venom is quickly exhausted. Thus, immediate removal of the stinger is crucial, though the method of removal is now thought irrelevant.19
The mainstay of therapy for serious reactions is intramuscular (IM) epinephrine. The initial dosing is 0.3 to 0.5 mg (0.3 to 0.5 mL of 1:1000 concentration) in adults, and 0.01 mg/kg in children (maximum 0.3 mg). The injection should be IM and not subcutaneous, as IM dosing provides higher and more consistent and rapid peak blood epinephrine levels.20 Concomitant intravenous (IV) administration of standard antihistamines, often diphenhydramine 1 mg/kg (generally 25-50 mg) and histamine-2 receptor antagonists (typically ranitidine 50 mg) are also recommended. The administration of steroids (methylprednisolone 125 mg IV or prednisone 60 mg orally) is traditionally recommended and thought to help potentiate the effect of other interventional measures.20 Bronchospasm, if present, is treated with nebulized β-agonists (albuterol). Hypotension may develop and requires significant crystalloid infusion—often several liters. If hypotension persists despite adequate fluid replacement, vasopressor therapy is recommended.
If a patient does not respond to initial treatment and cardiovascular (CV) collapse is evident, IV infusion of epinephrine should be initiated. Epinephrine, 100 mcg (0.1 mg) IV, should be given as a 1:100,000 dilution. This can be done by placing epinephrine, 0.1 mg (0.1 mL of the 1:1000 dilution), in 10 mL of normal saline solution and infusing it over 5 to 10 minutes (a rate of 1 to 2 mL/min). If the patient is refractory to the initial bolus, then an epinephrine infusion can be started by placing epinephrine, 1 mg (1.0 mL of the 1:1000 dilution), in 500 mL of 5% dextrose in water or NS and administering at a rate of 1 to 4 mcg per minute (0.5 to 2 mL/min), titrating to effect.20 Antivenins have been studied for treatment, but none are commercially available at this time.21 Patients with anaphylaxis associated with severe signs and symptoms, including any evidence of CV collapse, should be admitted to the hospital for aggressive therapy and monitoring. Persons with mild-to-moderate reactions should be observed for 4 to 6 hours to monitor for late occurring symptoms. Outpatient therapy with antihistamines, oral steroids, and a prescription for an epinephrine auto-injector—including training on proper administration prior to discharge—are strongly recommended.22 Follow-up with an allergist is also indicated in patients with significant reactions, as skin testing and immunotherapy may be beneficial to prevent anaphylaxis during future exposures.
Ants
Fire ant venom is composed of an insoluble alkaloid, and crossreactivity with the venom of other Hymenopteras species does exist. Stings generally result in a papule, which evolves into a sterile pustule. Localized necrosis, scarring, and secondary infection can occur. Systemic reactions with angioedema and urticaria have been documented, which can sometimes lead to fatalities.24
Treatment
Treatment of fire ant stings begin and end with local wound care. If the reaction is systemic, a treatment plan similar to that outlined in the treatment section for bees and wasps is indicated.
Araneae
The order Araneae of the phylum Arthropoda includes over 34,000 species of spiders divided into 105 families. Of those, only half a dozen are medically relevant and only three are commonly encountered in the United States. These include Loxosceles (most notably, the brown recluse spider), Tegeneria (mainly the hobo brown spider) and Latrodectus (includes the black widow spider). True spiders have a worldwide distribution and tend to thrive in heavily populated areas, resulting in many biting episodes per year. Data from the AAPPC’s most recent annual report listed 9,255 single spider-bite exposures in 2012, with one associated death.3
Spiders are carnivores and use venom to paralyze their prey. They are generally not a threat to humans as their fangs are too small to penetrate human skin, and the amount of venom injected is too small to produce toxicity. Thus, reactions resulting from a spider bite are typically limited to a localized reaction. Fortunately, most bites only require supportive medical therapy.
Loxosceles
Loxosceles are present worldwide, but L reclusa (the “brown recluse spider”) accounts for a significant number of envenomations in the United States. The AAPCC’s 2012 data notes 1,365 cases of exposure to the brown recluse spider with 510 of those victims seeking medical care.3 In many instances, clinicians attribute necrotic bites to the brown recluse spider, however, confirmation is often lacking. Loxosceles are nocturnal, and they are found both indoors and outdoors—mostly in dark and dry areas such as basements, closets, and woodpiles. These spiders are shy, but may bite when threatened. Their venom contains enzymes, including hyaluronidase and sphingomyelinase. Though rare, wounds can become necrotic due to neutrophil activation, platelet aggregation, and thrombosis.25 The most common reaction to a Loxosceles bite is a mild painless erythematous lesion that becomes firm and generally heals over several days to weeks. In severe reactions, erythema, edema, and pruritus initially develop, followed within 24 to 72 hours by a hemorrhagic bulla surrounded by blanched skin. This leads to the “red, white, and blue sign” (ie, erythema, blanching, and ecchymosis). Infrequently, the ecchymotic area becomes necrotic and ulcerates in 3 to 5 days. The differential diagnoses should include necrotizing fasciitis, erythema chronicum migrans (from Borrelia-infected tick bites), and anthrax. Ulcerated lesions may result in significant cosmetic defect. Healing may take up to 2 weeks, and skin grafting is occasionally required.26
Treatment begins with the usual supportive measures, including analgesia, ice, elevation, and a light compression dressing. Antibiotics are not indicated, unless there are signs of secondary infection. Serial evaluation for wound checks should be arranged. If ulceration develops, surgical debridement may be required. The vast majority of bites heal with supportive care alone, and aggressive medical therapy is usually not warranted.27Patients with systemic manifestations should be admitted to the hospital for further care. There is no evidence-based literature to guide therapy. Many therapies have been tried with variable results and there remains no definitive standard of care.
Treatment regimens include antihistamines, antivenin, colchicine, dapsone, hyperbaric oxygen, cyproheptadine, surgical excision, and steroids.28 Dapsone continues to be widely advocated worldwide despite its known adverse effects—most notably hemolysis and methemoglobinemia. Antivenin administration has shown some promise in animal models, but its efficacy in humans is still unclear.29
Tegenaria
The Tegenaria agrestis or hobo spider is a native of Europe and central Asia and is only found in the northwest part of the United States. It is considered aggressive and tends to bite even with only mild provocation. The clinical presentation, inclusive of systemic reactions, is similar to that of the brown recluse spider. Similarly, there is no proven treatment. Surgical wound resection and skin grafting should be considered and is at times required.
Latrodectus.
Latrodectus, also known as widow spiders, are found worldwide. Five species are commonly found in the United States, but the black widow is the most well known. Only three of the species are actually black. Other varieties are typically brown or red. However, almost all Latrodectus spiders have a characteristic orange-red hourglass-shaped marking (Figure 3). Widow spiders aggressively defend their webs, and are most often found in woodpiles, basements, garages, and sheds. Most bites occur in the warmer months, between April and October.
Latrodectus antivenin is very effective, often resolving symptoms rapidly and reducing the duration of illness—even when administered up to 90 hours postenvenomation.32 This antivenin is derived from horse serum, and hypersensitivity reactions are possible. One death from anaphylaxis has been reported in the United States after antivenin was given undiluted via IV push; however, slow administration of diluted antivenin is considered safe.33
Diptera
The order Diptera of the phylum Arthropoda includes over 240,000 species. Among those, the mosquitoes and flies are the most medically relevant.
Mosquitoes
An actual mosquito bite itself causes minimal trauma and is not usually felt by the victim. However, the local anesthetic that is injected into the wound at the time of the attack causes local tissue damage. Mosquito bites can lead to both immediate and delayed reactions. Typical immediate reactions are of short duration and include edema, erythema, and pruritus. More severe reactions are extremely rare and consist of skin necrosis. Delayed skin reactions are fairly common, but tend to last longer, persisting for days or even weeks. Treatment is symptomatic, usually with antihistamines and NSAIDS.
Patients can acquire an allergy to mosquito saliva over time and develop increasingly pronounced edematous and pruritic lesions with subsequent bites. They can also experience fever, malaise, generalized edema, as well as severe nausea and vomiting.
Systemic or anaphylactic reactions are not known to occur. Instead, the greatest danger occurs with the transmission of life-threatening diseases. Malaria, yellow fever, dengue hemorrhagic fever, and different types of equine encephalitis are all transmitted by mosquito bites. One interesting newcomer to the United States is the West Nile virus (WNV), which has spread rapidly since its introduction in 2003. Over 1,850 cases were reported in 22 different states over the initial 8 months. Acute symptoms are mild in the majority of patients, but a small minority can experience fatal disease. Neurological symptoms include tumor, myoclonus, and Parkinsonism. An irreversible poliomyelitis-like syndrome may also develop. In addition to WNV, St Louis encephalitis and equine encephalitis also remain important pathogens in the United States.34 Prevention of bites is crucial and includes the use of pyrethroid-impregnated mosquito netting, repellents, and oral malaria prophylaxis. N,N-diethyl-3-methylbenzamide (DEET) remains the most effective mosquito repellent.35 Although toxic reactions are rare, they do occur and anaphylaxis has been reported. 36,37
Flies
Flies are blood-sucking insects that feed by stabbing and piercing their victim’s skin. Their bites always cause some degree of pain and pruritus. Allergic reactions are possible, though not as severe as those produced by Hymenoptera venom. Treatment is largely symptomatic with ice, oral antihistamine, analgesics. and topical or oral steroids as needed. Secondary bite infection is a concern and antibiotics are sometimes necessary.
Shiponaptera
The order Shinoptera includes fleas and lice. All produce very similar lesions, making diagnosis difficult. One concern with these bites is the development of secondary infections, especially in children. The skin should be washed with soap and water. Calamine, cool soaks, and oral or topical antihistamine may all be helpful to reduce symptoms.
Fleas
With fleas, as with mosquitoes, there is additionally a concern for transmission of life-threatening diseases. Fleas transmit bubonic plague, endemic typhus, brucellosis, melioidosis, and erysipeloid. Fortunately, effective oral and injectable formulations for both dogs and cats are now available to control fleas on most family pets.
Lice
Hemiptera
Lepidoptera
The order Lepidoptera includes butterflies and moths and their caterpillars. Symptoms that result from contact with this class of insects are referred to as lepidopterism. Caterpillars have hair or spines for protection, which are also sometimes connected to a venom gland. Contact with these spines usually causes localized skin irritation and pruritus. Megalopyge opercularis, also known as the “puss caterpillar,” is mainly found in the southeastern United States and accounts for the majority of envenomation cases in this country. Intense local burning pain is typical at the site of contact and is followed by a grid-like pattern of hemorrhagic papules, which appear 2 to 3 hours after exposure and may last for several days. Regional lymphadenopathy is common. Other symptoms include headache, fever, hypotension, and convulsions. No deaths have ever been reported.
As there is no antivenin available for lepidopterism, treatment is mostly supportive. If spines are visible following contact, they should be removed with adhesive tape. Antihistamines and steroids may be used for symptom control. In patients with hypotension, IV fluids and IV epinephrine may be required.43
Coleoptera
The order Coleoptera includes a large number of beetles, though clinically significant envenomation occurs only with blister beetles. There are over 1,500 species of blister beetles worldwide, approximately 2,002 of which are in the United States. The blister beetle responsible for most of the medically significant envenomations is Cantharis vesicatoria—also known as “Spanish fly.” Of note, the Spanish fly is not naturally found in the United States.
Cantharidin-containing substances are sometimes used medicinally in wart removal preparations and are also sold for their purported aphrodisiac effects (the associated vascular congestion and urethral inflammation are interpreted as enhanced sexuality). Transdermal absorption or ingestion may lead to systemic toxicity with severe vomiting, hematemesis, abdominal pain, diarrhea, hematuria, renal failure, etc. Death has been reported after large ingestions.
Treatment is largely supportive. The skin should be irrigated thoroughly after exposure, followed by local wound care. Patients who present after ingestion should be admitted to the hospital for further treatment and care.47
Conclusion
Knowledge of a vast array of stinging insects and spiders is important for any clinician, but the appropriate evaluation and treatment of bites and envenomations are crucial for EPs. Most exposures can be treated with supportive care, while others require in-depth knowledge and clinical expertise.
Dr Deljoui is a former resident, department of emergency medicine, Eastern Virginia Medical School, Norfolk; and current critical care fellow, University of Maryland, Baltimore.
Dr Knapp is an associate professor and residency program director, department of emergency medicine, Eastern Virginia Medical School, Norfolk.
Hymenoptera
The order Hymenoptera of the phylum Arthropoda can be divided into three subgroups that are medically relevant: (1) Apidae (Apids), which include the honeybee and bumblebee; (2) Vespidae, (Vespids) which include yellow jackets, hornets and wasps; and (3) Formicidae (ants).6
Bees and Wasps
The main allergens in Apid venom are phospholipase A2, hyaluronidase, and melittin. Melittin, the main component, is a membrane active polypeptide that causes degranulation of basophils and mast cells. The allergens in Vespid venom are phospholipase, hyaluronidase, and antigen 5. As all Hymenoptera share some of these components, cross-sensitization may occur and individuals may be allergic to more than one species.7
Occasionally after multiple stings, patients present with symptoms of a systemic toxic reaction. This is often seen in an Africanized bee attack. These so-called “killer bees” are hybrids of African bees that escaped from laboratories in Brazil in the 1950s and spread northward; they are found in most of the warmer US states. Their venom is not more toxic than that of any other bee, but Africanized honeybees are more aggressive and respond to a perceived threat in far greater numbers. The reaction that results from multiple stings is systemic and may resemble anaphylaxis. Common symptoms include nausea, vomiting, and diarrhea, as well as lightheadedness and syncope. Interestingly, urticaria and bronchospasm are not universally present, even though respiratory failure and cardiac arrest may occur. Other symptoms include renal failure with acute tubular necrosis, myoglobinuria or hemoglobinuria, hepatic failure, and disseminated intravascular coagulation (DIC).10,11 In addition, there have been reports of unusual reactions such as vasculitis, nephrosis, neuritis, encephalitis, and serum sickness. Late-appearing symptoms usually start several days to weeks after a sting and tend last for a prolonged period of time. Serum sickness tends to appear 5 to 14 days after exposure and consists of fever, malaise, headache, urticaria, lymphadenopathy, and polyarthritis.12 Of note, patients who have venom-induced serum sickness may be at risk for anaphylaxis after subsequent stings and may therefore be suitable candidates for venom immunotherapy.13
Anaphylaxis
The definition of anaphylaxis is not universally agreed upon. The American Academy of Allergy, Asthma and Immunology defines anaphylaxis as a serious allergic response that often involves swelling, hives, hypotension and, in severe cases, shock. A major difference between anaphylaxis and other allergic reactions is that anaphylaxis typically involves more than one body system.14 The clinical features of anaphylaxis from insect stings are the same as those from other causes, typically generalized urticaria, facial flushing, and angioedema. Abdominal cramping, nausea, vomiting, and diarrhea are also seen. Life-threatening symptoms include stridor, circulatory collapse with shock, and bronchospasm. Symptoms usually begin 10 to 20 minutes after a sting, and almost all will develop within 6 hours. Interestingly, symptoms may recur 8 to 12 hours after the initial reaction.15-18
Management
Immediate removal of the bee stinger is the most important principle as it precludes any further venom transfer. Traditional teaching recommended scraping the stinger out to avoid squeezing remaining venom into the tissues; however, involuntary muscle contractions of the gland continue after the stinger detaches, and the venom is quickly exhausted. Thus, immediate removal of the stinger is crucial, though the method of removal is now thought irrelevant.19
The mainstay of therapy for serious reactions is intramuscular (IM) epinephrine. The initial dosing is 0.3 to 0.5 mg (0.3 to 0.5 mL of 1:1000 concentration) in adults, and 0.01 mg/kg in children (maximum 0.3 mg). The injection should be IM and not subcutaneous, as IM dosing provides higher and more consistent and rapid peak blood epinephrine levels.20 Concomitant intravenous (IV) administration of standard antihistamines, often diphenhydramine 1 mg/kg (generally 25-50 mg) and histamine-2 receptor antagonists (typically ranitidine 50 mg) are also recommended. The administration of steroids (methylprednisolone 125 mg IV or prednisone 60 mg orally) is traditionally recommended and thought to help potentiate the effect of other interventional measures.20 Bronchospasm, if present, is treated with nebulized β-agonists (albuterol). Hypotension may develop and requires significant crystalloid infusion—often several liters. If hypotension persists despite adequate fluid replacement, vasopressor therapy is recommended.
If a patient does not respond to initial treatment and cardiovascular (CV) collapse is evident, IV infusion of epinephrine should be initiated. Epinephrine, 100 mcg (0.1 mg) IV, should be given as a 1:100,000 dilution. This can be done by placing epinephrine, 0.1 mg (0.1 mL of the 1:1000 dilution), in 10 mL of normal saline solution and infusing it over 5 to 10 minutes (a rate of 1 to 2 mL/min). If the patient is refractory to the initial bolus, then an epinephrine infusion can be started by placing epinephrine, 1 mg (1.0 mL of the 1:1000 dilution), in 500 mL of 5% dextrose in water or NS and administering at a rate of 1 to 4 mcg per minute (0.5 to 2 mL/min), titrating to effect.20 Antivenins have been studied for treatment, but none are commercially available at this time.21 Patients with anaphylaxis associated with severe signs and symptoms, including any evidence of CV collapse, should be admitted to the hospital for aggressive therapy and monitoring. Persons with mild-to-moderate reactions should be observed for 4 to 6 hours to monitor for late occurring symptoms. Outpatient therapy with antihistamines, oral steroids, and a prescription for an epinephrine auto-injector—including training on proper administration prior to discharge—are strongly recommended.22 Follow-up with an allergist is also indicated in patients with significant reactions, as skin testing and immunotherapy may be beneficial to prevent anaphylaxis during future exposures.
Ants
Fire ant venom is composed of an insoluble alkaloid, and crossreactivity with the venom of other Hymenopteras species does exist. Stings generally result in a papule, which evolves into a sterile pustule. Localized necrosis, scarring, and secondary infection can occur. Systemic reactions with angioedema and urticaria have been documented, which can sometimes lead to fatalities.24
Treatment
Treatment of fire ant stings begin and end with local wound care. If the reaction is systemic, a treatment plan similar to that outlined in the treatment section for bees and wasps is indicated.
Araneae
The order Araneae of the phylum Arthropoda includes over 34,000 species of spiders divided into 105 families. Of those, only half a dozen are medically relevant and only three are commonly encountered in the United States. These include Loxosceles (most notably, the brown recluse spider), Tegeneria (mainly the hobo brown spider) and Latrodectus (includes the black widow spider). True spiders have a worldwide distribution and tend to thrive in heavily populated areas, resulting in many biting episodes per year. Data from the AAPPC’s most recent annual report listed 9,255 single spider-bite exposures in 2012, with one associated death.3
Spiders are carnivores and use venom to paralyze their prey. They are generally not a threat to humans as their fangs are too small to penetrate human skin, and the amount of venom injected is too small to produce toxicity. Thus, reactions resulting from a spider bite are typically limited to a localized reaction. Fortunately, most bites only require supportive medical therapy.
Loxosceles
Loxosceles are present worldwide, but L reclusa (the “brown recluse spider”) accounts for a significant number of envenomations in the United States. The AAPCC’s 2012 data notes 1,365 cases of exposure to the brown recluse spider with 510 of those victims seeking medical care.3 In many instances, clinicians attribute necrotic bites to the brown recluse spider, however, confirmation is often lacking. Loxosceles are nocturnal, and they are found both indoors and outdoors—mostly in dark and dry areas such as basements, closets, and woodpiles. These spiders are shy, but may bite when threatened. Their venom contains enzymes, including hyaluronidase and sphingomyelinase. Though rare, wounds can become necrotic due to neutrophil activation, platelet aggregation, and thrombosis.25 The most common reaction to a Loxosceles bite is a mild painless erythematous lesion that becomes firm and generally heals over several days to weeks. In severe reactions, erythema, edema, and pruritus initially develop, followed within 24 to 72 hours by a hemorrhagic bulla surrounded by blanched skin. This leads to the “red, white, and blue sign” (ie, erythema, blanching, and ecchymosis). Infrequently, the ecchymotic area becomes necrotic and ulcerates in 3 to 5 days. The differential diagnoses should include necrotizing fasciitis, erythema chronicum migrans (from Borrelia-infected tick bites), and anthrax. Ulcerated lesions may result in significant cosmetic defect. Healing may take up to 2 weeks, and skin grafting is occasionally required.26
Treatment begins with the usual supportive measures, including analgesia, ice, elevation, and a light compression dressing. Antibiotics are not indicated, unless there are signs of secondary infection. Serial evaluation for wound checks should be arranged. If ulceration develops, surgical debridement may be required. The vast majority of bites heal with supportive care alone, and aggressive medical therapy is usually not warranted.27Patients with systemic manifestations should be admitted to the hospital for further care. There is no evidence-based literature to guide therapy. Many therapies have been tried with variable results and there remains no definitive standard of care.
Treatment regimens include antihistamines, antivenin, colchicine, dapsone, hyperbaric oxygen, cyproheptadine, surgical excision, and steroids.28 Dapsone continues to be widely advocated worldwide despite its known adverse effects—most notably hemolysis and methemoglobinemia. Antivenin administration has shown some promise in animal models, but its efficacy in humans is still unclear.29
Tegenaria
The Tegenaria agrestis or hobo spider is a native of Europe and central Asia and is only found in the northwest part of the United States. It is considered aggressive and tends to bite even with only mild provocation. The clinical presentation, inclusive of systemic reactions, is similar to that of the brown recluse spider. Similarly, there is no proven treatment. Surgical wound resection and skin grafting should be considered and is at times required.
Latrodectus.
Latrodectus, also known as widow spiders, are found worldwide. Five species are commonly found in the United States, but the black widow is the most well known. Only three of the species are actually black. Other varieties are typically brown or red. However, almost all Latrodectus spiders have a characteristic orange-red hourglass-shaped marking (Figure 3). Widow spiders aggressively defend their webs, and are most often found in woodpiles, basements, garages, and sheds. Most bites occur in the warmer months, between April and October.
Latrodectus antivenin is very effective, often resolving symptoms rapidly and reducing the duration of illness—even when administered up to 90 hours postenvenomation.32 This antivenin is derived from horse serum, and hypersensitivity reactions are possible. One death from anaphylaxis has been reported in the United States after antivenin was given undiluted via IV push; however, slow administration of diluted antivenin is considered safe.33
Diptera
The order Diptera of the phylum Arthropoda includes over 240,000 species. Among those, the mosquitoes and flies are the most medically relevant.
Mosquitoes
An actual mosquito bite itself causes minimal trauma and is not usually felt by the victim. However, the local anesthetic that is injected into the wound at the time of the attack causes local tissue damage. Mosquito bites can lead to both immediate and delayed reactions. Typical immediate reactions are of short duration and include edema, erythema, and pruritus. More severe reactions are extremely rare and consist of skin necrosis. Delayed skin reactions are fairly common, but tend to last longer, persisting for days or even weeks. Treatment is symptomatic, usually with antihistamines and NSAIDS.
Patients can acquire an allergy to mosquito saliva over time and develop increasingly pronounced edematous and pruritic lesions with subsequent bites. They can also experience fever, malaise, generalized edema, as well as severe nausea and vomiting.
Systemic or anaphylactic reactions are not known to occur. Instead, the greatest danger occurs with the transmission of life-threatening diseases. Malaria, yellow fever, dengue hemorrhagic fever, and different types of equine encephalitis are all transmitted by mosquito bites. One interesting newcomer to the United States is the West Nile virus (WNV), which has spread rapidly since its introduction in 2003. Over 1,850 cases were reported in 22 different states over the initial 8 months. Acute symptoms are mild in the majority of patients, but a small minority can experience fatal disease. Neurological symptoms include tumor, myoclonus, and Parkinsonism. An irreversible poliomyelitis-like syndrome may also develop. In addition to WNV, St Louis encephalitis and equine encephalitis also remain important pathogens in the United States.34 Prevention of bites is crucial and includes the use of pyrethroid-impregnated mosquito netting, repellents, and oral malaria prophylaxis. N,N-diethyl-3-methylbenzamide (DEET) remains the most effective mosquito repellent.35 Although toxic reactions are rare, they do occur and anaphylaxis has been reported. 36,37
Flies
Flies are blood-sucking insects that feed by stabbing and piercing their victim’s skin. Their bites always cause some degree of pain and pruritus. Allergic reactions are possible, though not as severe as those produced by Hymenoptera venom. Treatment is largely symptomatic with ice, oral antihistamine, analgesics. and topical or oral steroids as needed. Secondary bite infection is a concern and antibiotics are sometimes necessary.
Shiponaptera
The order Shinoptera includes fleas and lice. All produce very similar lesions, making diagnosis difficult. One concern with these bites is the development of secondary infections, especially in children. The skin should be washed with soap and water. Calamine, cool soaks, and oral or topical antihistamine may all be helpful to reduce symptoms.
Fleas
With fleas, as with mosquitoes, there is additionally a concern for transmission of life-threatening diseases. Fleas transmit bubonic plague, endemic typhus, brucellosis, melioidosis, and erysipeloid. Fortunately, effective oral and injectable formulations for both dogs and cats are now available to control fleas on most family pets.
Lice
Hemiptera
Lepidoptera
The order Lepidoptera includes butterflies and moths and their caterpillars. Symptoms that result from contact with this class of insects are referred to as lepidopterism. Caterpillars have hair or spines for protection, which are also sometimes connected to a venom gland. Contact with these spines usually causes localized skin irritation and pruritus. Megalopyge opercularis, also known as the “puss caterpillar,” is mainly found in the southeastern United States and accounts for the majority of envenomation cases in this country. Intense local burning pain is typical at the site of contact and is followed by a grid-like pattern of hemorrhagic papules, which appear 2 to 3 hours after exposure and may last for several days. Regional lymphadenopathy is common. Other symptoms include headache, fever, hypotension, and convulsions. No deaths have ever been reported.
As there is no antivenin available for lepidopterism, treatment is mostly supportive. If spines are visible following contact, they should be removed with adhesive tape. Antihistamines and steroids may be used for symptom control. In patients with hypotension, IV fluids and IV epinephrine may be required.43
Coleoptera
The order Coleoptera includes a large number of beetles, though clinically significant envenomation occurs only with blister beetles. There are over 1,500 species of blister beetles worldwide, approximately 2,002 of which are in the United States. The blister beetle responsible for most of the medically significant envenomations is Cantharis vesicatoria—also known as “Spanish fly.” Of note, the Spanish fly is not naturally found in the United States.
Cantharidin-containing substances are sometimes used medicinally in wart removal preparations and are also sold for their purported aphrodisiac effects (the associated vascular congestion and urethral inflammation are interpreted as enhanced sexuality). Transdermal absorption or ingestion may lead to systemic toxicity with severe vomiting, hematemesis, abdominal pain, diarrhea, hematuria, renal failure, etc. Death has been reported after large ingestions.
Treatment is largely supportive. The skin should be irrigated thoroughly after exposure, followed by local wound care. Patients who present after ingestion should be admitted to the hospital for further treatment and care.47
Conclusion
Knowledge of a vast array of stinging insects and spiders is important for any clinician, but the appropriate evaluation and treatment of bites and envenomations are crucial for EPs. Most exposures can be treated with supportive care, while others require in-depth knowledge and clinical expertise.
Dr Deljoui is a former resident, department of emergency medicine, Eastern Virginia Medical School, Norfolk; and current critical care fellow, University of Maryland, Baltimore.
Dr Knapp is an associate professor and residency program director, department of emergency medicine, Eastern Virginia Medical School, Norfolk.
- White J. Bites and stings from venomous animals: a global overview. The Drug Monit. 2000;22(1):65-68.
- Oten EJ. Venomous animal injuries. In: Marx JA, Hockberger RS, Walls RM, et al, eds. Rosen’s Emergency Medicine: Concepts and Clinical Practice. Vol 1. 8th ed. Philadelphia, PA: Elsevier Saunders; 2014:794-807.
- Mowry JB, Spyker DA, Cantilena LR Jr, Bailey JE, Ford M. 2012 Annual Report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 30th Annual Report. Clin Toxicol (Phila). 2013;51(10):949-1229. doi:10.3109/15563650.2013.863906. https://aapcc.s3.amazonaws.com/pdfs/annual_reports/2012_NPDS_Annual_Report.pdf. Accessed April 2, 2014.
- Liberman P, Camargo CA, Bohike K, et al. Epidemiology of anaphylaxis: findings of the American College of Allergy, Asthma and Immunology Epidemiology of Anaphylaxis Working Group. Ann Allergy Asthma Immunol. 2006;97(5):596-602.
- Barnard JH. Studies of 400 Hymenoptera sting deaths in the United States. J Allergy Clin Immunol. 1973;52(5):259-264.
- Frazier CA. Insect Allergy: Allergic and Toxic Reactions to Insects and Other Arthropods. 2nd Ed. St Louis, MO: WH Green; 1987:421.
- King TP, Spangfort MD. Structure and biology of stinging insect venom allergens. Int Arch Allergy Immunol. 2000;123(2):99-106.
- Antonicelli L, Bilo MB, Bonifazi F. Epidemiology of Hymenoptera allergy. Curr Opin Allergy Clin Immunol.2002;2(4);341-346.
- Mauriello PM, Barde SH. Natural history of large local reactions from stinging insects. J Allergy Clin Immunol. 1984;74(4 Pt 1):494-498.
- Díaz-Sánchez CL, Lifshitz-Guinzberg A, Ignacio-Ibarra G, Halabe-Cherem J, Quinones-Galvan A. Survival after massive (>2,000) Africanized honey bee stings. Arch Intern Med. 1998;158(8):925-927.
- Elston DM. Life-threatening stings, bites, infestations and parasitic diseases. Clin Dermatol. 2005;23(2):164-170.
- Lazoglu AH1, Boglioli LR, Taff ML, Rosenbluth M, Macris NT. Serum sickness reaction following multiple insect stings. Ann Allergy Asthma Immunol. 1995;75(6 Pt 1):522-524.
- Reisman RE, Livingston A. Late-onset allergic reactions, including serum sickness, after insect stings. J Allergy Clin Immunol. 1989;84(3);331-337.
- Anaphylaxis. American Academy of Allergy, Asthma & Immunology Web site. http://www.aaaai.org/conditions-and-treatments/conditions-a-to-zsearch/anaphylaxis.aspx. Accessed April 2, 2014.
- Brown H, Benton HS. Allergy to the Hymenoptera. V. Clinical study of 400 patients. Arch Intern Med. 1970;125(4):665-669.
- Frazier CA. Allergic reactions to insect stings: a review of 180 cases. South Med J. 1964;57;1023-1034.
- Mueller HL. Further experiences with severe allergic reactions to insect stings. N Engl J Med. 1959;161:374-377.
- Lockey RF, Turkeltaub PC, Baird-Warren IA, et al. The Hymenoptera venom study I, 1979-1982: demographics and history-sting data. J Allergy Clin Immunol. 1988;82(3 Pt 1):370-381.
- Schneir AB, Clark RF. Bites and stings. In: Tintinalli JE, Stapczynski JS, Ma OJ, Cline DM, Cydulka RK, Meckler GD, eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 7th ed. New York, NY: McGraw-Hill; 2011:chap120;585-596.
- Rowe BH, Gaeta T. Anaphylaxis, acute allergic reactions, and angioedema. In: Tintinalli JE, Stapczynski JS, Ma OJ, Cline DM, Cydulka RK, Meckler GD, eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 7th ed. New York, NY: McGraw-Hill; 2011:chap 6;52-54.
- Jones RG1, Corteling RL, Bhogal G, Landon J. A novel Fab-based antivenom for the treatment of mass bee attacks. Am J Trop Med Hyg. 1999;61(3):361-366.
- National Institutes of Health, US Department of Health and Human Services, National Insitute of Allergy and Infectious Diseases. Guidelines for the Diagnosis and Management of Food Allergy in the United States. Summary of the NIAID-Sponsored Expert Panel Report. Bethesda, MD: National Institutes of Health; 2010. NIH Publication No. 11-7700. http://www.niaid.nih.gov/topics/foodAllergy/clinical/Documents/FAGuidelinesExecSummary.pdf. Accessed April 2, 2014.
- Kemp SF, deShazo RD, Moffitt JE, Williams DF, Buhner WA 2nd. Expanding habitat of the imported fire ant (Solenopsis invicta): a public health concern. J Allergy Clin Immunol. 2000;105(4):683-691.
- Fernández-Meléndez S, Miranda A, García-González JJ, Barber D, Lombardero M. Anaphylaxis caused by imported red fire ant stings in Málaga, Spain. J Investig Allergol Immunol. 2007;17(1):48,49.
- Swanson DL. Bites of brown recluse spiders and suspected necrotic arachnidism. N Engl J Med. 2005;352(7):700-707.
- Saucier JR. Arachnid envenomation. Emerg Med Clin North Am. 2004;22(2):405-422.
- Wright SW, Wrenn KD, Murray L, Seger D. Clinical presentation and outcome of brown recluse spider bite. Ann Emerg Med. 1997;30(1):28-32.
- Phillips S, Kohn M, Baker D, et al. Therapy of brown spider envenomation: a controlled trial of hyperbaric oxygen, dapsone, and cyproheptadine. Ann Emerg Med. 1995;25(3):363-368.
- Pauli I, Puka J, Gubert IC, Minozzo JC. The efficacy of antivenom in loxoscelism treatment. Toxicon. 2006;48(2):123-127.
- Ushkaryov YA, Volynski KE, Ashton AC. The multiple actions of black widow spider toxins and their selective use in neurosecretion studies. Toxicon. 2004;43(5):527-542.
- Clark RF, Wethern-Kestner S, Vance MV, Gerkin R. Clinical presentation and treatment of black widow spider envenomation: a review of 163 cases. Ann Emerg Med. 1992;21(7):782-787.
- O’Malley GF, Dart RC, Kuffner EF. Successful treatment of latrodectism with antivenom after 90 hours. N Engl J Med. 1999;340(8):657.
- Clark RF. The safety and efficacy of antivenin Latrodectus mactans. J Toxicol Clin Toxicol. 2001;39(2):125-127.
- Sejvar JJ, Haddad MB, Tierney BC. Neurologic manifestations and outcome of West Nile virus infection [published correction appears in JAMA. 2003;290(10):1318]. JAMA. 2003;290(4):511-515.
- Brown M, Herbert AA. Insect repellents: an overview. J Am Acad Dermatol. 1997;36(2 Pt 1):243-249.
- Fradin MS. Mosquitoes and mosquito repellents: a clinician’s quide. Ann Intern Med. 1998;128(11):931-940.
- Miller JD. Anaphylaxis associated with insect repellent. N Engl J Med. 1982;307(21):1341,1342.
- Spach DH, Kanter AS, Dougherty MJ, et al. Bartonella (Rochalimaea) quintana bacteremia in inner-city patients with chronic alcoholism. N Engl J Med. 1995;332(7): 424-428.
- Jackson LA, Spach DH, Kippen DA, et al. Seroprevalence to Bartonella quintana among patients at a community clinic in downtown Seattle. J Infect Dis. 1996;173(4):1023-1026.
- Sundnes KO. Epidemic of louse-borne relapsing fever in Ethiopia. Lancet. 1993;342(8881):1213-1215.
- Vetter R. Kissing bugs (Triatoma) and the skin. Dermatol Online J. 2001;7(1):6. http://escholarship.org/uc/item/59k2m8wt. Accessed April 2, 2014.
- Stucki A, Ludwig R. Images in clinical medicine. Bedbug bites. N Engl J Med. 2008; 359:10)1047.
- Kuspis DA, Rawlins JE, Krenzelok EP. Human exposures to stinging caterpillars: Lophocampa caryae exposures. Am J Emerg Med. 2001;19(5):396-398.
- Moed L, Shwayder TA, 0.Chang MW. Cantharidin revisited: a blistering defense of an ancient medicine. Arch Dermatol. 2001;137(10):1357-1360.
- White J. Bites and stings from venomous animals: a global overview. The Drug Monit. 2000;22(1):65-68.
- Oten EJ. Venomous animal injuries. In: Marx JA, Hockberger RS, Walls RM, et al, eds. Rosen’s Emergency Medicine: Concepts and Clinical Practice. Vol 1. 8th ed. Philadelphia, PA: Elsevier Saunders; 2014:794-807.
- Mowry JB, Spyker DA, Cantilena LR Jr, Bailey JE, Ford M. 2012 Annual Report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 30th Annual Report. Clin Toxicol (Phila). 2013;51(10):949-1229. doi:10.3109/15563650.2013.863906. https://aapcc.s3.amazonaws.com/pdfs/annual_reports/2012_NPDS_Annual_Report.pdf. Accessed April 2, 2014.
- Liberman P, Camargo CA, Bohike K, et al. Epidemiology of anaphylaxis: findings of the American College of Allergy, Asthma and Immunology Epidemiology of Anaphylaxis Working Group. Ann Allergy Asthma Immunol. 2006;97(5):596-602.
- Barnard JH. Studies of 400 Hymenoptera sting deaths in the United States. J Allergy Clin Immunol. 1973;52(5):259-264.
- Frazier CA. Insect Allergy: Allergic and Toxic Reactions to Insects and Other Arthropods. 2nd Ed. St Louis, MO: WH Green; 1987:421.
- King TP, Spangfort MD. Structure and biology of stinging insect venom allergens. Int Arch Allergy Immunol. 2000;123(2):99-106.
- Antonicelli L, Bilo MB, Bonifazi F. Epidemiology of Hymenoptera allergy. Curr Opin Allergy Clin Immunol.2002;2(4);341-346.
- Mauriello PM, Barde SH. Natural history of large local reactions from stinging insects. J Allergy Clin Immunol. 1984;74(4 Pt 1):494-498.
- Díaz-Sánchez CL, Lifshitz-Guinzberg A, Ignacio-Ibarra G, Halabe-Cherem J, Quinones-Galvan A. Survival after massive (>2,000) Africanized honey bee stings. Arch Intern Med. 1998;158(8):925-927.
- Elston DM. Life-threatening stings, bites, infestations and parasitic diseases. Clin Dermatol. 2005;23(2):164-170.
- Lazoglu AH1, Boglioli LR, Taff ML, Rosenbluth M, Macris NT. Serum sickness reaction following multiple insect stings. Ann Allergy Asthma Immunol. 1995;75(6 Pt 1):522-524.
- Reisman RE, Livingston A. Late-onset allergic reactions, including serum sickness, after insect stings. J Allergy Clin Immunol. 1989;84(3);331-337.
- Anaphylaxis. American Academy of Allergy, Asthma & Immunology Web site. http://www.aaaai.org/conditions-and-treatments/conditions-a-to-zsearch/anaphylaxis.aspx. Accessed April 2, 2014.
- Brown H, Benton HS. Allergy to the Hymenoptera. V. Clinical study of 400 patients. Arch Intern Med. 1970;125(4):665-669.
- Frazier CA. Allergic reactions to insect stings: a review of 180 cases. South Med J. 1964;57;1023-1034.
- Mueller HL. Further experiences with severe allergic reactions to insect stings. N Engl J Med. 1959;161:374-377.
- Lockey RF, Turkeltaub PC, Baird-Warren IA, et al. The Hymenoptera venom study I, 1979-1982: demographics and history-sting data. J Allergy Clin Immunol. 1988;82(3 Pt 1):370-381.
- Schneir AB, Clark RF. Bites and stings. In: Tintinalli JE, Stapczynski JS, Ma OJ, Cline DM, Cydulka RK, Meckler GD, eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 7th ed. New York, NY: McGraw-Hill; 2011:chap120;585-596.
- Rowe BH, Gaeta T. Anaphylaxis, acute allergic reactions, and angioedema. In: Tintinalli JE, Stapczynski JS, Ma OJ, Cline DM, Cydulka RK, Meckler GD, eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 7th ed. New York, NY: McGraw-Hill; 2011:chap 6;52-54.
- Jones RG1, Corteling RL, Bhogal G, Landon J. A novel Fab-based antivenom for the treatment of mass bee attacks. Am J Trop Med Hyg. 1999;61(3):361-366.
- National Institutes of Health, US Department of Health and Human Services, National Insitute of Allergy and Infectious Diseases. Guidelines for the Diagnosis and Management of Food Allergy in the United States. Summary of the NIAID-Sponsored Expert Panel Report. Bethesda, MD: National Institutes of Health; 2010. NIH Publication No. 11-7700. http://www.niaid.nih.gov/topics/foodAllergy/clinical/Documents/FAGuidelinesExecSummary.pdf. Accessed April 2, 2014.
- Kemp SF, deShazo RD, Moffitt JE, Williams DF, Buhner WA 2nd. Expanding habitat of the imported fire ant (Solenopsis invicta): a public health concern. J Allergy Clin Immunol. 2000;105(4):683-691.
- Fernández-Meléndez S, Miranda A, García-González JJ, Barber D, Lombardero M. Anaphylaxis caused by imported red fire ant stings in Málaga, Spain. J Investig Allergol Immunol. 2007;17(1):48,49.
- Swanson DL. Bites of brown recluse spiders and suspected necrotic arachnidism. N Engl J Med. 2005;352(7):700-707.
- Saucier JR. Arachnid envenomation. Emerg Med Clin North Am. 2004;22(2):405-422.
- Wright SW, Wrenn KD, Murray L, Seger D. Clinical presentation and outcome of brown recluse spider bite. Ann Emerg Med. 1997;30(1):28-32.
- Phillips S, Kohn M, Baker D, et al. Therapy of brown spider envenomation: a controlled trial of hyperbaric oxygen, dapsone, and cyproheptadine. Ann Emerg Med. 1995;25(3):363-368.
- Pauli I, Puka J, Gubert IC, Minozzo JC. The efficacy of antivenom in loxoscelism treatment. Toxicon. 2006;48(2):123-127.
- Ushkaryov YA, Volynski KE, Ashton AC. The multiple actions of black widow spider toxins and their selective use in neurosecretion studies. Toxicon. 2004;43(5):527-542.
- Clark RF, Wethern-Kestner S, Vance MV, Gerkin R. Clinical presentation and treatment of black widow spider envenomation: a review of 163 cases. Ann Emerg Med. 1992;21(7):782-787.
- O’Malley GF, Dart RC, Kuffner EF. Successful treatment of latrodectism with antivenom after 90 hours. N Engl J Med. 1999;340(8):657.
- Clark RF. The safety and efficacy of antivenin Latrodectus mactans. J Toxicol Clin Toxicol. 2001;39(2):125-127.
- Sejvar JJ, Haddad MB, Tierney BC. Neurologic manifestations and outcome of West Nile virus infection [published correction appears in JAMA. 2003;290(10):1318]. JAMA. 2003;290(4):511-515.
- Brown M, Herbert AA. Insect repellents: an overview. J Am Acad Dermatol. 1997;36(2 Pt 1):243-249.
- Fradin MS. Mosquitoes and mosquito repellents: a clinician’s quide. Ann Intern Med. 1998;128(11):931-940.
- Miller JD. Anaphylaxis associated with insect repellent. N Engl J Med. 1982;307(21):1341,1342.
- Spach DH, Kanter AS, Dougherty MJ, et al. Bartonella (Rochalimaea) quintana bacteremia in inner-city patients with chronic alcoholism. N Engl J Med. 1995;332(7): 424-428.
- Jackson LA, Spach DH, Kippen DA, et al. Seroprevalence to Bartonella quintana among patients at a community clinic in downtown Seattle. J Infect Dis. 1996;173(4):1023-1026.
- Sundnes KO. Epidemic of louse-borne relapsing fever in Ethiopia. Lancet. 1993;342(8881):1213-1215.
- Vetter R. Kissing bugs (Triatoma) and the skin. Dermatol Online J. 2001;7(1):6. http://escholarship.org/uc/item/59k2m8wt. Accessed April 2, 2014.
- Stucki A, Ludwig R. Images in clinical medicine. Bedbug bites. N Engl J Med. 2008; 359:10)1047.
- Kuspis DA, Rawlins JE, Krenzelok EP. Human exposures to stinging caterpillars: Lophocampa caryae exposures. Am J Emerg Med. 2001;19(5):396-398.
- Moed L, Shwayder TA, 0.Chang MW. Cantharidin revisited: a blistering defense of an ancient medicine. Arch Dermatol. 2001;137(10):1357-1360.

Nurse-Driven Protocol Reduces HAIs in Burn Patients
The Burn Center of Shands Hospital at University of Florida Health in Gainesville admits about 500 burn patients every year. Using standard prevention “care bundles,” the multidisciplinary team caring for patients with thermal injuries brought down the rates of hospital-acquired infections (HAIs) and burn-wound infections, but they had not been able to eliminate them.
Noting that previous research in nonthermal injuries had suggested that daily bathing with chlorhexidine gluconate (CHG) reduces bloodstream infections and vancomycin-resistant enterococci, the burn team developed a study to evaluate this protocol in preventing HAIs in patients with thermal injuries. Researchers from Shands Hospital, University of Florida Health and the University of Florida College of Medicine, both in Gainesville; and Geisinger Health System in Danville, Pennsylvania, conducted the study. They say that, to their knowledge, this is the first study to evaluate CHG baths for burn patients, a group at high risk for infections. At first, they were concerned that CHG, which is not recommended for use on mucous membranes, might further injure compromised skin but decided significant benefits would result if the protocol worked.
Standard procedures and care bundles were not changed, but the bathing protocol for adults with thermal injuries was switched from twice daily with soap and water to twice daily with 0.9% CHG solution. This concentration is similar to that found in commercial wipes, the researchers say, and significantly more than the concentration found to be useful in surgical wounds. The diluted CHG solution was used on the patient’s entire body except the face and eyes. The only protocol change was to not allow the CHG solution to dry before rinsing. They also used appropriate analgesia, since this was a bedside “mini-debridement.”
The 17-month trial included 203 patients in the pretrial group and 277 in the posttrial group. The median burn area was 25% of the total body surface area. At baseline, the rates of HAI were ventilator-associated pneumonia (VAP), 2.2 cases; catheter-associated urinary tract infection (CAUTI), 2.7 cases; and central line–associated bloodstream infection (CLABSI), 1.4 cases.
Using the CHG solution lowered the HAI rate to nearly zero. Over the first 17 months, no VAPs, CAUTIs, or CLABSIs were reported. From the start of the study in February 2011 through June 2013, those results were sustained, apart from 1 case of CAUTI. No integumentary complications were associated with the use of the CHG solution.
Source
Popp JA, Layon AJ, Nappo R, Richards WT, Mozingo DW. Am J Infect Contr. 2014;42(2):129-132.
doi: 10.1016/j.ajic.2013.08.015.
The Burn Center of Shands Hospital at University of Florida Health in Gainesville admits about 500 burn patients every year. Using standard prevention “care bundles,” the multidisciplinary team caring for patients with thermal injuries brought down the rates of hospital-acquired infections (HAIs) and burn-wound infections, but they had not been able to eliminate them.
Noting that previous research in nonthermal injuries had suggested that daily bathing with chlorhexidine gluconate (CHG) reduces bloodstream infections and vancomycin-resistant enterococci, the burn team developed a study to evaluate this protocol in preventing HAIs in patients with thermal injuries. Researchers from Shands Hospital, University of Florida Health and the University of Florida College of Medicine, both in Gainesville; and Geisinger Health System in Danville, Pennsylvania, conducted the study. They say that, to their knowledge, this is the first study to evaluate CHG baths for burn patients, a group at high risk for infections. At first, they were concerned that CHG, which is not recommended for use on mucous membranes, might further injure compromised skin but decided significant benefits would result if the protocol worked.
Standard procedures and care bundles were not changed, but the bathing protocol for adults with thermal injuries was switched from twice daily with soap and water to twice daily with 0.9% CHG solution. This concentration is similar to that found in commercial wipes, the researchers say, and significantly more than the concentration found to be useful in surgical wounds. The diluted CHG solution was used on the patient’s entire body except the face and eyes. The only protocol change was to not allow the CHG solution to dry before rinsing. They also used appropriate analgesia, since this was a bedside “mini-debridement.”
The 17-month trial included 203 patients in the pretrial group and 277 in the posttrial group. The median burn area was 25% of the total body surface area. At baseline, the rates of HAI were ventilator-associated pneumonia (VAP), 2.2 cases; catheter-associated urinary tract infection (CAUTI), 2.7 cases; and central line–associated bloodstream infection (CLABSI), 1.4 cases.
Using the CHG solution lowered the HAI rate to nearly zero. Over the first 17 months, no VAPs, CAUTIs, or CLABSIs were reported. From the start of the study in February 2011 through June 2013, those results were sustained, apart from 1 case of CAUTI. No integumentary complications were associated with the use of the CHG solution.
Source
Popp JA, Layon AJ, Nappo R, Richards WT, Mozingo DW. Am J Infect Contr. 2014;42(2):129-132.
doi: 10.1016/j.ajic.2013.08.015.
The Burn Center of Shands Hospital at University of Florida Health in Gainesville admits about 500 burn patients every year. Using standard prevention “care bundles,” the multidisciplinary team caring for patients with thermal injuries brought down the rates of hospital-acquired infections (HAIs) and burn-wound infections, but they had not been able to eliminate them.
Noting that previous research in nonthermal injuries had suggested that daily bathing with chlorhexidine gluconate (CHG) reduces bloodstream infections and vancomycin-resistant enterococci, the burn team developed a study to evaluate this protocol in preventing HAIs in patients with thermal injuries. Researchers from Shands Hospital, University of Florida Health and the University of Florida College of Medicine, both in Gainesville; and Geisinger Health System in Danville, Pennsylvania, conducted the study. They say that, to their knowledge, this is the first study to evaluate CHG baths for burn patients, a group at high risk for infections. At first, they were concerned that CHG, which is not recommended for use on mucous membranes, might further injure compromised skin but decided significant benefits would result if the protocol worked.
Standard procedures and care bundles were not changed, but the bathing protocol for adults with thermal injuries was switched from twice daily with soap and water to twice daily with 0.9% CHG solution. This concentration is similar to that found in commercial wipes, the researchers say, and significantly more than the concentration found to be useful in surgical wounds. The diluted CHG solution was used on the patient’s entire body except the face and eyes. The only protocol change was to not allow the CHG solution to dry before rinsing. They also used appropriate analgesia, since this was a bedside “mini-debridement.”
The 17-month trial included 203 patients in the pretrial group and 277 in the posttrial group. The median burn area was 25% of the total body surface area. At baseline, the rates of HAI were ventilator-associated pneumonia (VAP), 2.2 cases; catheter-associated urinary tract infection (CAUTI), 2.7 cases; and central line–associated bloodstream infection (CLABSI), 1.4 cases.
Using the CHG solution lowered the HAI rate to nearly zero. Over the first 17 months, no VAPs, CAUTIs, or CLABSIs were reported. From the start of the study in February 2011 through June 2013, those results were sustained, apart from 1 case of CAUTI. No integumentary complications were associated with the use of the CHG solution.
Source
Popp JA, Layon AJ, Nappo R, Richards WT, Mozingo DW. Am J Infect Contr. 2014;42(2):129-132.
doi: 10.1016/j.ajic.2013.08.015.
Arthroscopic Treatment of Femoroacetabular Impingement
2014 Update on minimally invasive gynecology
CASE: POSTMENSTRUAL BLEEDING, HISTORY OF CESAREAN DELIVERIES
A 36-year-old woman (G3P3) reports prolonged and postmenstrual bleeding. Her cycles are regular, every 28 to 30 days, and are associated with ovulatory symptoms. She bleeds for 8 to 10 days with each cycle, having heavy bleeding on cycle day 2 requiring use of super tampons every 3 hours. Beginning on day 5 of the cycle, the blood becomes much darker and scant requiring a small pad, which she changes twice daily. Often, she experiences dark bleeding with physical activity—specifically, running—usually several days after her cycle has ended. She is otherwise healthy and uses no medications. She uses condoms for contraception. She has had a prior vaginal delivery followed by two cesarean sections. Physical examination is normal.
What is causing this patient’s abnormal bleeding pattern?
From 1996 to 2009, the total US cesarean delivery rate increased steadily from 20.7% to 32.9% and has remained stable at 32.8% through 2012.1 With 3,952,841 registered births in 2012, the number of operative procedures performed annually approximates 1.3 million.2 This means, potentially, that one-third of pregnant American women will undergo cesarean delivery annually, translating into an increasing prevalence of long-term sequelae of this surgery.
An increasingly recognized etiology of AUB
One long-term complication of cesarean delivery, not often discussed, is the presence of a defect within the uterine scar that is directly associated with a type of abnormal uterine bleeding (AUB) referred to as postmenstrual bleeding. Stewart first reported this post–cesarean delivery phenomenon in 1975.3 It is postulated that the cesarean scar defect (CSD)4 forms a pocket, which holds the menstrual effluent, allowing bleeding to occur after regular menstrual cycle bleeding has concluded. Often, remnant menstrual blood is extruded slowly over several days, and is generally dark brown, indicating old blood. Physical activity sometimes can initiate expulsion of the old blood even after the regular cycle has ceased (FIGURE 1).
As early as 1995, Morris reported the histopathologic changes within the cesarean scar in a series of 51 hysterectomy specimens with scar present for 2 to 15 years. His findings included distortion and widening of the lower uterine segment (75%), congested endometrium above the scar recess (61%), marked lymphocytic infiltration (65%), capillary dilation (65%), residual suture material with foreign body giant cell reaction (92%), fragmentation and breakdown of the endometrium of the scar (37%), and iatrogenic adenomyosis confined to the scar (28%). Morris concluded that in addition to AUB, these scar abnormalities could give rise to clinical symptoms such as pelvic pain, dyspareunia, and dysmenorrhea.5 It also has been suggested that otherwise unexplained infertility is associated with anatomic and physiologic changes seen with CSD.6 A recent review article published by Tower summarized additional clinical outcomes of CSD, such as ectopic pregnancy and increased surgical risks for such gynecologic procedures as uterine evacuation in the nonpregnant or postpartum state, hysterectomy, endometrial ablation, and intrauterine device placement.4
The CSD generally is described as a triangular or circular sonographically anechoic area in the myometrium of the anterior lower uterine segment or cervix at the site of a previous cesarean section. In nonpregnant patients, the defect is best evaluated with contrast infusion sonography (CIS), such as saline infusion or gel infusion, versus transvaginal ultrasound (TVUS) alone (FIGURE 2).4,7,8 However, the precise dimensions and definition of the scar defect vary among investigators.4,6,7,8,10
The reported prevalence of CSD has varied in the literature and appears to depend on the modality of diagnosis and the population studied. For instance, van der Voet and colleagues reported that in random populations of women who had undergone cesarean delivery, the defect was evident in 24% to 69% of women evaluated with transvaginal noncontrast ultrasound; the defect was evident in 56% to 78% of women evaluated with transvaginal contrast sonography.8
The scar defect also has been identified with magnetic resonance imaging (MRI) and found to be equal in sensitivity to TVUS.9,10 When identified hysteroscopically, a definitive out-pouching is visualized in the lower uterine segment, where the defect has been termed an “isthmocele.”6 Hysteroscopically, the defect also is visualized commonly within the cervical canal, indicating that cesarean incisions often are made through cervical tissue at the time of delivery (FIGURE 3, VIDEO 1, VIDEO 2 [see below]). Not all women with CSD report bleeding abnormalities, but it appears that the deeper and wider the defect, the more likely a woman is to present with postmenstrual AUB.7 According to the International Federation of Gynecology and Obstetrics (FIGO) Classification of AUB, CSD-associated postmenstrual bleeding falls into the “iatrogenic” category in the PALM-COIEN pneumonic.11
Related article: Dr. Garcia discusses the FIGO classification and the PALM-COEIN pneumonic in Update: Minimally invasive gynecology (April 2013)
![]()
![]()
A pair of studies shed light on CSD
Two recent European publications by van der Voet and colleagues addressed CSD and its association with AUB. These studies refer to CSD as the “niche” within the cesarean scar, but for the purpose of this article, I will use the term CSD. The first is a prospective cohort study, in which the authors addressed the definition, diagnosis, and prevalence of a defect within the cesarean scar and reported the incidence of associated AUB.7 The second publication is a systematic review which includes a critical investigation of minimally invasive therapy for CSD-related AUB.8 Both publications provide current clinical insight into the evaluation and management of AUB associated with CSD.
Related articles:
• Update on abnormal uterine bleeding Malcolm G. Munro, MD (March 2014)
• Update on Technology Barbara S. Levy, MD (September 2013)
• STOP performing dilation and curettage for the evaluation of abnormal uterine bleeding Amy Garcia, MD (Stop/Start, June 2013)
THE NICHE IN THE SCAR
van der Voet LF, Bij de Vaate AM, Veersema S, Brolmann HAM, Huirne JAF. Long-term complications of caesarean section. The niche in the scar: A prospective cohort study on niche prevalence and its relation to abnormal uterine bleeding. BJOG. 2014;121(2):236–244.
Most studies reporting the prevalence of cesarean delivery–associated postmenstrual bleeding are based on populations of women who were symptomatic with AUB, thus infusing a potential referral bias into these prevalence estimates. In contrast, this study by van der Voet and colleagues utilizes a prospective cohort design, making it the only study to date to enroll a random cohort of patients immediately after having undergone cesarean delivery.
Details of the study
The purpose of the study was to evaluate the prevalence of CSD formation in the cesarean scar at 6 to 12 weeks after cesarean delivery with TVUS and gel infusion study (GIS) in 197 women. The uterus was closed in two layers for four women and in one layer for all others.
The cohort was followed with menstruation questionnaires at 6 to 12 weeks, 6 months, and 12 months after surgery. The questionnaire response rate at 12 months for those women who had both TVUS and GIS evaluation of the scar was 73%. Data analysis accounted for confounding factors such as breastfeeding and amenorrhea, use of hormonal contraception, use of a levonorgestrel intrauterine system (LNG-IUS) as well as a body mass index (BMI) of at least 25 kg/m2.
Consistent with previous studies showing the superiority of saline-infused studies over TVUS for CSD identification,4 van der Voet and colleagues found that GIS was more sensitive than TVUS in diagnosing CSD (64.5% vs 49.6%, respectively). The percentage of women with CSD who had undergone two cesarean deliveries was 68.2%, while the percentage with CSD who had undergone three cesarean deliveries was 77.8%.
Data analysis correlated postmenstrual bleeding with the following CSD characteristics:
- depth and width of the defect
- residual myometrial thickness to the serosal surface of the uterus
- ratio of residual myometrium divided by the adjacent normal myometrial thickness.
Those women who had a ratio of residual myometrium to adjacent normal myometrium of less than 0.5 were more likely to report postmenstrual bleeding than those with a ratio greater than 0.5 (odds ratio, 6.1; 95% confidence interval, 1.74–21.63). The investigators stated that 1 out of 3 women with CSD identified by GIS reported postmenstrual bleeding, compared with 1 out of 10 women without identifiable CSD.
Study takeaways have merit
In summary, despite the small cohort of 197 women and the relatively short observation period of 1 year, these data collected by van der Voet and colleagues enable the gynecologist to begin to more fully understand the potential impact of cesarean section and the probability of AUB following an abdominal delivery. Applying these study statistics to the number of cesarean sections performed annually in the United States translates to nearly 280,000 women yearly who may experience postmenstrual bleeding related to a defect in the cesarean section scar.
Prospective cohort studies with longer follow-up periods are needed to assess the longer-term risks of CSD-related bleeding. As the authors suggest, perhaps the possibility of post–cesarean section AUB should be considered as part of the informed consent process for cesarean delivery.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
• Contrast infusion sonography has better sensitivity than TVUS at identification of the scar defect.
• About 64.5% of women are predicted to have scar defects after one cesarean delivery.
• The incidence of scar defects increases with increasing number of cesarean deliveries.
• One of three women with CSD is predicted to experience postmenstrual bleeding.
• Women with deeper and wider defects are more likely to experience postmenstrual bleeding.
• Post–cesarean section AUB is a probable occurrence in approximately 20% of all cesarean deliveries. Perhaps this information should be considered part of the informed consent process for cesarean delivery.
MINIMALLY INVASIVE THERAPY FOR GYNECOLOGIC SYMPTOMS
van der Voet LF, Vervoort AJ, Veersema S, Bij de Vatte AJ, Brolmann HAM, Huirne JAF. Minimally invasive therapy for gynaecological symptoms related to a niche in the caesarean scar: A systematic review. BJOG. 2014;121(2):145-156.
CSD-related bleeding issues may not respond to hormonal management and are frequently underdiagnosed. This scenario often leads to hysterectomy. Because there are women who desire uterine preservation, van der Voet and colleagues sought to evaluate the results of nonhysterectomy treatments of CSD-related AUB. They limited this systematic review to include only published studies that were randomized controlled trials, cohort studies, case-control studies, and case series of at least five patients.
Additionally, they included only studies that reported on conservative therapies (hysteroscopic resection, laparoscopic repair, abdominal repair, vaginal repair, endometrial ablation, LNG-IUS, or medical management) as well as at least one of the following outcomes: AUB, pain relief, sexual function, quality of life, surgical outcome, anatomic reconstruction, fertility or pregnancy outcome. Of 1,629 publications that were screened, 12 ultimately met inclusion criteria for the review. The studies, 11 of which were peer reviewed and 1 abstract, were published between 1996 and 2013 and reported on a total of 455 women with postcesarean AUB.
Weaknesses of the study
The most poignant statements made by the investigators pertain to the methodologic quality of the included articles. No study met requisite quality criteria. A clear definition of outcomes, including standardized measurements, was lacking in most studies. Most of the studies reviewed did not report CSD measurements, and only one study provided an objective reproducible method of CSD measurement. Few studies reported AUB symptom evaluation methodology, and no study used validated questionnaires. In the majority of studies, methods of posttreatment outcome measurements either were not reported or differed from pretreatment evaluation methods, potentiating verification bias. Because their literature review yielded primarily small case series publications that reported positive effects of interventions, and because of a lack of large RCT and prospective cohort trials, little could be gleaned regarding the viability of treatment interventions for CSD-related AUB.
Only three studies provided sufficient data to be included in a meta-analysis. The number of days of bleeding was reduced with hysteroscopic defect resection by 2 to 4 days in two studies, and in one study, vaginal repair decreased days of bleeding by 4 to 7 days. Only one study with laparoscopic repair compared CSD characteristics before and after surgery. Residual myometrial thickness increased for laparoscopic repair to greater than 8.3 mm; however, it is not known if this will make a clinical difference in the risk of scar dehiscence or improved functionality of the lower uterine segment.
Two studies reported on the laparoscopic repair of scar defects in asymptomatic patients, which is not recommended by these investigators. It is not known what ramifications hysteroscopic resection of the scar will have for the risk of uterine rupture, malplacentation or cervical incompetence for women who conceive after hysteroscopic repair.
Meaningful conclusions are lacking
Despite the high success rates reported by investigators of various surgical intervention case series involving hysteroscopic resection, vaginal repair, or laparoscopic repair, van der Voet and colleagues ultimately state that the methodologies of these studies do not allow meaningful conclusions to be drawn regarding the effectiveness of any of these interventions. Consequently, the authors recommend that the outcomes of their meta-analysis be scrutinized. They also point out that the LNG-IUS has proven benefit for AUB and yet has not been studied in the treatment of AUB associated with a CSD.
They finally propose that women who are symptomatic be treated with oral contraceptives unless immediate fertility is desired, or by expectant management without intervention. While their primary focus was to assess AUB, given the stated shortcomings of the included studies and lack of long-term follow-up, the authors also warn against hysteroscopic, laparoscopic, or vaginal repair for fertility, as the risk to pregnancy or delivery after these therapies is unknown.
CASE RESOLVED
Suspecting a cesarean scar defect, you perform a saline infusion sonography and diagnose a 14 mm x 19 mm anechoic region within the scar, with no other intracavitary abnormalities found. You first reassure the patient that this is a benign finding and inform her why she likely is experiencing this type of bleeding pattern. After an informed discussion with you regarding the risks and benefits of possible surgical or nonsurgical options for management, she chooses to use oral contraceptive pills in a continuous fashion.
CONCLUSION
Consider a history of cesarean section in the evaluation of AUB, and be cognizant of the prevalence of CSD with cesarean delivery and the association of postmenstrual bleeding with CSD.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
• A critical systematic review of available data suggests that there is not enough clinical evidence to support surgical intervention for the treatment of CSD for women symptomatic with AUB.
• Recommended nonhysterectomy treatments for AUB associated with CSD include oral contraceptives or expectant management.
• Surgical treatment should be limited to the research environment in the form of RCT to assess the long-term outcomes of intervention.
• An RCT of the LNG-IUS for the treatment of AUB associated with CSD is needed.
Acknowledgments
The author would like to thank Andrew Brill, MD, Lee Sloan-Garcia, MD, and William Parker, MD, for their thoughtful review of this manuscript.
We want to hear from you!
Share your thoughts on this article or on any topic relevant to ObGyns and women’s health practitioners. Tell us which topics you’d like to see covered in future issues, and what challenges you face in daily practice. We will consider publishing your letter and in a future issue. Send your letter to: [email protected] Please include the city and state in which you practice. Stay in touch! Your feedback is important to us!
- Osterman MJK, Martin JA. Primary cesarean delivery rates, by state: Results from the revised birth certificate, 2006-2012. Natl Vital Stat Rep. 2014;63(1):1–11.
- Martin JA, Hamilton BE, Osterman MJK, Curtin SC, Mathews TJ. Births: Final data for 2012. Natl Vital Stat Rep. 2013;62(9). Hyattsville, MD: National Center for Health Statistics. http://www.cdc.gov/nchs/data/nvsr/nvsr62/nvsr62_09.pdf. Accessed March 19, 2014.
- Stewart KS, Evans TW. Recurrent bleeding from the lower segment scar – a late complication of Caesarean section. Br J Obstet Gynaecol. 1975;82(8):682–686.
- Tower AM, Frishman GN. Cesarean scar defects: An underrecognized cause of abnormal uterine bleeding and other gynecologic complications. J Minim Invasive Gynecol. 2013;20(5):562–572.
- Morris H. Surgical pathology of the lower uterine segment cesarean section scar: Is the scar a source of clinical symptoms? Intl J Gynecol Pathol. 1995;14(1):16–20.
- Gubbini G, Centini G, Nascetti D, et al. Surgical hysteroscopic treatment of cesarean-induced isthmocele in restoring fertility: Prospective study. J Minim Invasive Gynecol. 2011;18(2):234–237.
- van der Voet LF, Bijde Vaate AM, Veersema S, Brolmann HA, Huirne JA. Long-term complications of caesarean section. The niche in the scar: A prospective cohort study on niche prevalence and its relation to abnormal uterine bleeding. BJOG. 2014;121(2):236–244.
- van der Voet LF, Vervoort AJ, Veersema S, Bijde Vatte AJ, Brolmann HA, Huirne JA. Minimally invasive therapy for gynaecological symptoms related to a niche in the caesarean scar: A systematic review. BJOG. 2014;121(2):145–156.
- Maldjian C, Adam R, Maldjian J, Smith R. MRI appearance of the pelvis in the post cesarean-section patient. Magn Reson Imaging. 1999;17(2):223–227.
- Marotta ML, Donnez J, Squifflet J, Jadoul P, Darii N, Donnez O. Laparoscopic repair of post-Cesarean section uterine scar defects diagnosed in nonpregnant women. J Minim Invasive Gynecol. 2013;20(3):386–391.
- Munro MG, Critchley HO, Broder MS, Fraser IS; FIGO Working Group on Menstrual Disorders. FIGO classification system (PALM-COIEN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. Int J Gynaecol Obstet. 2011;113(1):3–13.

Amy Garcia, MD, is Director, Center for Women’s Surgery and Garcia Institute for Hysteroscopic Training, Albuquerque, and Clinical Assistant Professor, Department of Obstetrics and Gynecology, University of New Mexico School of Medicine, Albuquerque. Dr. Garcia serves on the OBG Management Board of Editors.
Dr. Garcia reports that she receives grant or research support from Hologic, Inc. She is a consultant to Bayer, Boston Scientific, Channel Medsystems, Ethicon, Hologic, IOGYN, Karl Storz Endoscopy, Minerva Surgical, and Smith & Nephew. She is a speaker for Ethicon.
Amy Garcia, MD, is Director, Center for Women’s Surgery and Garcia Institute for Hysteroscopic Training, Albuquerque, and Clinical Assistant Professor, Department of Obstetrics and Gynecology, University of New Mexico School of Medicine, Albuquerque. Dr. Garcia serves on the OBG Management Board of Editors.
Dr. Garcia reports that she receives grant or research support from Hologic, Inc. She is a consultant to Bayer, Boston Scientific, Channel Medsystems, Ethicon, Hologic, IOGYN, Karl Storz Endoscopy, Minerva Surgical, and Smith & Nephew. She is a speaker for Ethicon.
Amy Garcia, MD, is Director, Center for Women’s Surgery and Garcia Institute for Hysteroscopic Training, Albuquerque, and Clinical Assistant Professor, Department of Obstetrics and Gynecology, University of New Mexico School of Medicine, Albuquerque. Dr. Garcia serves on the OBG Management Board of Editors.
Dr. Garcia reports that she receives grant or research support from Hologic, Inc. She is a consultant to Bayer, Boston Scientific, Channel Medsystems, Ethicon, Hologic, IOGYN, Karl Storz Endoscopy, Minerva Surgical, and Smith & Nephew. She is a speaker for Ethicon.
CASE: POSTMENSTRUAL BLEEDING, HISTORY OF CESAREAN DELIVERIES
A 36-year-old woman (G3P3) reports prolonged and postmenstrual bleeding. Her cycles are regular, every 28 to 30 days, and are associated with ovulatory symptoms. She bleeds for 8 to 10 days with each cycle, having heavy bleeding on cycle day 2 requiring use of super tampons every 3 hours. Beginning on day 5 of the cycle, the blood becomes much darker and scant requiring a small pad, which she changes twice daily. Often, she experiences dark bleeding with physical activity—specifically, running—usually several days after her cycle has ended. She is otherwise healthy and uses no medications. She uses condoms for contraception. She has had a prior vaginal delivery followed by two cesarean sections. Physical examination is normal.
What is causing this patient’s abnormal bleeding pattern?
From 1996 to 2009, the total US cesarean delivery rate increased steadily from 20.7% to 32.9% and has remained stable at 32.8% through 2012.1 With 3,952,841 registered births in 2012, the number of operative procedures performed annually approximates 1.3 million.2 This means, potentially, that one-third of pregnant American women will undergo cesarean delivery annually, translating into an increasing prevalence of long-term sequelae of this surgery.
An increasingly recognized etiology of AUB
One long-term complication of cesarean delivery, not often discussed, is the presence of a defect within the uterine scar that is directly associated with a type of abnormal uterine bleeding (AUB) referred to as postmenstrual bleeding. Stewart first reported this post–cesarean delivery phenomenon in 1975.3 It is postulated that the cesarean scar defect (CSD)4 forms a pocket, which holds the menstrual effluent, allowing bleeding to occur after regular menstrual cycle bleeding has concluded. Often, remnant menstrual blood is extruded slowly over several days, and is generally dark brown, indicating old blood. Physical activity sometimes can initiate expulsion of the old blood even after the regular cycle has ceased (FIGURE 1).
As early as 1995, Morris reported the histopathologic changes within the cesarean scar in a series of 51 hysterectomy specimens with scar present for 2 to 15 years. His findings included distortion and widening of the lower uterine segment (75%), congested endometrium above the scar recess (61%), marked lymphocytic infiltration (65%), capillary dilation (65%), residual suture material with foreign body giant cell reaction (92%), fragmentation and breakdown of the endometrium of the scar (37%), and iatrogenic adenomyosis confined to the scar (28%). Morris concluded that in addition to AUB, these scar abnormalities could give rise to clinical symptoms such as pelvic pain, dyspareunia, and dysmenorrhea.5 It also has been suggested that otherwise unexplained infertility is associated with anatomic and physiologic changes seen with CSD.6 A recent review article published by Tower summarized additional clinical outcomes of CSD, such as ectopic pregnancy and increased surgical risks for such gynecologic procedures as uterine evacuation in the nonpregnant or postpartum state, hysterectomy, endometrial ablation, and intrauterine device placement.4
The CSD generally is described as a triangular or circular sonographically anechoic area in the myometrium of the anterior lower uterine segment or cervix at the site of a previous cesarean section. In nonpregnant patients, the defect is best evaluated with contrast infusion sonography (CIS), such as saline infusion or gel infusion, versus transvaginal ultrasound (TVUS) alone (FIGURE 2).4,7,8 However, the precise dimensions and definition of the scar defect vary among investigators.4,6,7,8,10
The reported prevalence of CSD has varied in the literature and appears to depend on the modality of diagnosis and the population studied. For instance, van der Voet and colleagues reported that in random populations of women who had undergone cesarean delivery, the defect was evident in 24% to 69% of women evaluated with transvaginal noncontrast ultrasound; the defect was evident in 56% to 78% of women evaluated with transvaginal contrast sonography.8
The scar defect also has been identified with magnetic resonance imaging (MRI) and found to be equal in sensitivity to TVUS.9,10 When identified hysteroscopically, a definitive out-pouching is visualized in the lower uterine segment, where the defect has been termed an “isthmocele.”6 Hysteroscopically, the defect also is visualized commonly within the cervical canal, indicating that cesarean incisions often are made through cervical tissue at the time of delivery (FIGURE 3, VIDEO 1, VIDEO 2 [see below]). Not all women with CSD report bleeding abnormalities, but it appears that the deeper and wider the defect, the more likely a woman is to present with postmenstrual AUB.7 According to the International Federation of Gynecology and Obstetrics (FIGO) Classification of AUB, CSD-associated postmenstrual bleeding falls into the “iatrogenic” category in the PALM-COIEN pneumonic.11
Related article: Dr. Garcia discusses the FIGO classification and the PALM-COEIN pneumonic in Update: Minimally invasive gynecology (April 2013)
![]()
![]()
A pair of studies shed light on CSD
Two recent European publications by van der Voet and colleagues addressed CSD and its association with AUB. These studies refer to CSD as the “niche” within the cesarean scar, but for the purpose of this article, I will use the term CSD. The first is a prospective cohort study, in which the authors addressed the definition, diagnosis, and prevalence of a defect within the cesarean scar and reported the incidence of associated AUB.7 The second publication is a systematic review which includes a critical investigation of minimally invasive therapy for CSD-related AUB.8 Both publications provide current clinical insight into the evaluation and management of AUB associated with CSD.
Related articles:
• Update on abnormal uterine bleeding Malcolm G. Munro, MD (March 2014)
• Update on Technology Barbara S. Levy, MD (September 2013)
• STOP performing dilation and curettage for the evaluation of abnormal uterine bleeding Amy Garcia, MD (Stop/Start, June 2013)
THE NICHE IN THE SCAR
van der Voet LF, Bij de Vaate AM, Veersema S, Brolmann HAM, Huirne JAF. Long-term complications of caesarean section. The niche in the scar: A prospective cohort study on niche prevalence and its relation to abnormal uterine bleeding. BJOG. 2014;121(2):236–244.
Most studies reporting the prevalence of cesarean delivery–associated postmenstrual bleeding are based on populations of women who were symptomatic with AUB, thus infusing a potential referral bias into these prevalence estimates. In contrast, this study by van der Voet and colleagues utilizes a prospective cohort design, making it the only study to date to enroll a random cohort of patients immediately after having undergone cesarean delivery.
Details of the study
The purpose of the study was to evaluate the prevalence of CSD formation in the cesarean scar at 6 to 12 weeks after cesarean delivery with TVUS and gel infusion study (GIS) in 197 women. The uterus was closed in two layers for four women and in one layer for all others.
The cohort was followed with menstruation questionnaires at 6 to 12 weeks, 6 months, and 12 months after surgery. The questionnaire response rate at 12 months for those women who had both TVUS and GIS evaluation of the scar was 73%. Data analysis accounted for confounding factors such as breastfeeding and amenorrhea, use of hormonal contraception, use of a levonorgestrel intrauterine system (LNG-IUS) as well as a body mass index (BMI) of at least 25 kg/m2.
Consistent with previous studies showing the superiority of saline-infused studies over TVUS for CSD identification,4 van der Voet and colleagues found that GIS was more sensitive than TVUS in diagnosing CSD (64.5% vs 49.6%, respectively). The percentage of women with CSD who had undergone two cesarean deliveries was 68.2%, while the percentage with CSD who had undergone three cesarean deliveries was 77.8%.
Data analysis correlated postmenstrual bleeding with the following CSD characteristics:
- depth and width of the defect
- residual myometrial thickness to the serosal surface of the uterus
- ratio of residual myometrium divided by the adjacent normal myometrial thickness.
Those women who had a ratio of residual myometrium to adjacent normal myometrium of less than 0.5 were more likely to report postmenstrual bleeding than those with a ratio greater than 0.5 (odds ratio, 6.1; 95% confidence interval, 1.74–21.63). The investigators stated that 1 out of 3 women with CSD identified by GIS reported postmenstrual bleeding, compared with 1 out of 10 women without identifiable CSD.
Study takeaways have merit
In summary, despite the small cohort of 197 women and the relatively short observation period of 1 year, these data collected by van der Voet and colleagues enable the gynecologist to begin to more fully understand the potential impact of cesarean section and the probability of AUB following an abdominal delivery. Applying these study statistics to the number of cesarean sections performed annually in the United States translates to nearly 280,000 women yearly who may experience postmenstrual bleeding related to a defect in the cesarean section scar.
Prospective cohort studies with longer follow-up periods are needed to assess the longer-term risks of CSD-related bleeding. As the authors suggest, perhaps the possibility of post–cesarean section AUB should be considered as part of the informed consent process for cesarean delivery.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
• Contrast infusion sonography has better sensitivity than TVUS at identification of the scar defect.
• About 64.5% of women are predicted to have scar defects after one cesarean delivery.
• The incidence of scar defects increases with increasing number of cesarean deliveries.
• One of three women with CSD is predicted to experience postmenstrual bleeding.
• Women with deeper and wider defects are more likely to experience postmenstrual bleeding.
• Post–cesarean section AUB is a probable occurrence in approximately 20% of all cesarean deliveries. Perhaps this information should be considered part of the informed consent process for cesarean delivery.
MINIMALLY INVASIVE THERAPY FOR GYNECOLOGIC SYMPTOMS
van der Voet LF, Vervoort AJ, Veersema S, Bij de Vatte AJ, Brolmann HAM, Huirne JAF. Minimally invasive therapy for gynaecological symptoms related to a niche in the caesarean scar: A systematic review. BJOG. 2014;121(2):145-156.
CSD-related bleeding issues may not respond to hormonal management and are frequently underdiagnosed. This scenario often leads to hysterectomy. Because there are women who desire uterine preservation, van der Voet and colleagues sought to evaluate the results of nonhysterectomy treatments of CSD-related AUB. They limited this systematic review to include only published studies that were randomized controlled trials, cohort studies, case-control studies, and case series of at least five patients.
Additionally, they included only studies that reported on conservative therapies (hysteroscopic resection, laparoscopic repair, abdominal repair, vaginal repair, endometrial ablation, LNG-IUS, or medical management) as well as at least one of the following outcomes: AUB, pain relief, sexual function, quality of life, surgical outcome, anatomic reconstruction, fertility or pregnancy outcome. Of 1,629 publications that were screened, 12 ultimately met inclusion criteria for the review. The studies, 11 of which were peer reviewed and 1 abstract, were published between 1996 and 2013 and reported on a total of 455 women with postcesarean AUB.
Weaknesses of the study
The most poignant statements made by the investigators pertain to the methodologic quality of the included articles. No study met requisite quality criteria. A clear definition of outcomes, including standardized measurements, was lacking in most studies. Most of the studies reviewed did not report CSD measurements, and only one study provided an objective reproducible method of CSD measurement. Few studies reported AUB symptom evaluation methodology, and no study used validated questionnaires. In the majority of studies, methods of posttreatment outcome measurements either were not reported or differed from pretreatment evaluation methods, potentiating verification bias. Because their literature review yielded primarily small case series publications that reported positive effects of interventions, and because of a lack of large RCT and prospective cohort trials, little could be gleaned regarding the viability of treatment interventions for CSD-related AUB.
Only three studies provided sufficient data to be included in a meta-analysis. The number of days of bleeding was reduced with hysteroscopic defect resection by 2 to 4 days in two studies, and in one study, vaginal repair decreased days of bleeding by 4 to 7 days. Only one study with laparoscopic repair compared CSD characteristics before and after surgery. Residual myometrial thickness increased for laparoscopic repair to greater than 8.3 mm; however, it is not known if this will make a clinical difference in the risk of scar dehiscence or improved functionality of the lower uterine segment.
Two studies reported on the laparoscopic repair of scar defects in asymptomatic patients, which is not recommended by these investigators. It is not known what ramifications hysteroscopic resection of the scar will have for the risk of uterine rupture, malplacentation or cervical incompetence for women who conceive after hysteroscopic repair.
Meaningful conclusions are lacking
Despite the high success rates reported by investigators of various surgical intervention case series involving hysteroscopic resection, vaginal repair, or laparoscopic repair, van der Voet and colleagues ultimately state that the methodologies of these studies do not allow meaningful conclusions to be drawn regarding the effectiveness of any of these interventions. Consequently, the authors recommend that the outcomes of their meta-analysis be scrutinized. They also point out that the LNG-IUS has proven benefit for AUB and yet has not been studied in the treatment of AUB associated with a CSD.
They finally propose that women who are symptomatic be treated with oral contraceptives unless immediate fertility is desired, or by expectant management without intervention. While their primary focus was to assess AUB, given the stated shortcomings of the included studies and lack of long-term follow-up, the authors also warn against hysteroscopic, laparoscopic, or vaginal repair for fertility, as the risk to pregnancy or delivery after these therapies is unknown.
CASE RESOLVED
Suspecting a cesarean scar defect, you perform a saline infusion sonography and diagnose a 14 mm x 19 mm anechoic region within the scar, with no other intracavitary abnormalities found. You first reassure the patient that this is a benign finding and inform her why she likely is experiencing this type of bleeding pattern. After an informed discussion with you regarding the risks and benefits of possible surgical or nonsurgical options for management, she chooses to use oral contraceptive pills in a continuous fashion.
CONCLUSION
Consider a history of cesarean section in the evaluation of AUB, and be cognizant of the prevalence of CSD with cesarean delivery and the association of postmenstrual bleeding with CSD.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
• A critical systematic review of available data suggests that there is not enough clinical evidence to support surgical intervention for the treatment of CSD for women symptomatic with AUB.
• Recommended nonhysterectomy treatments for AUB associated with CSD include oral contraceptives or expectant management.
• Surgical treatment should be limited to the research environment in the form of RCT to assess the long-term outcomes of intervention.
• An RCT of the LNG-IUS for the treatment of AUB associated with CSD is needed.
Acknowledgments
The author would like to thank Andrew Brill, MD, Lee Sloan-Garcia, MD, and William Parker, MD, for their thoughtful review of this manuscript.
We want to hear from you!
Share your thoughts on this article or on any topic relevant to ObGyns and women’s health practitioners. Tell us which topics you’d like to see covered in future issues, and what challenges you face in daily practice. We will consider publishing your letter and in a future issue. Send your letter to: [email protected] Please include the city and state in which you practice. Stay in touch! Your feedback is important to us!
CASE: POSTMENSTRUAL BLEEDING, HISTORY OF CESAREAN DELIVERIES
A 36-year-old woman (G3P3) reports prolonged and postmenstrual bleeding. Her cycles are regular, every 28 to 30 days, and are associated with ovulatory symptoms. She bleeds for 8 to 10 days with each cycle, having heavy bleeding on cycle day 2 requiring use of super tampons every 3 hours. Beginning on day 5 of the cycle, the blood becomes much darker and scant requiring a small pad, which she changes twice daily. Often, she experiences dark bleeding with physical activity—specifically, running—usually several days after her cycle has ended. She is otherwise healthy and uses no medications. She uses condoms for contraception. She has had a prior vaginal delivery followed by two cesarean sections. Physical examination is normal.
What is causing this patient’s abnormal bleeding pattern?
From 1996 to 2009, the total US cesarean delivery rate increased steadily from 20.7% to 32.9% and has remained stable at 32.8% through 2012.1 With 3,952,841 registered births in 2012, the number of operative procedures performed annually approximates 1.3 million.2 This means, potentially, that one-third of pregnant American women will undergo cesarean delivery annually, translating into an increasing prevalence of long-term sequelae of this surgery.
An increasingly recognized etiology of AUB
One long-term complication of cesarean delivery, not often discussed, is the presence of a defect within the uterine scar that is directly associated with a type of abnormal uterine bleeding (AUB) referred to as postmenstrual bleeding. Stewart first reported this post–cesarean delivery phenomenon in 1975.3 It is postulated that the cesarean scar defect (CSD)4 forms a pocket, which holds the menstrual effluent, allowing bleeding to occur after regular menstrual cycle bleeding has concluded. Often, remnant menstrual blood is extruded slowly over several days, and is generally dark brown, indicating old blood. Physical activity sometimes can initiate expulsion of the old blood even after the regular cycle has ceased (FIGURE 1).
As early as 1995, Morris reported the histopathologic changes within the cesarean scar in a series of 51 hysterectomy specimens with scar present for 2 to 15 years. His findings included distortion and widening of the lower uterine segment (75%), congested endometrium above the scar recess (61%), marked lymphocytic infiltration (65%), capillary dilation (65%), residual suture material with foreign body giant cell reaction (92%), fragmentation and breakdown of the endometrium of the scar (37%), and iatrogenic adenomyosis confined to the scar (28%). Morris concluded that in addition to AUB, these scar abnormalities could give rise to clinical symptoms such as pelvic pain, dyspareunia, and dysmenorrhea.5 It also has been suggested that otherwise unexplained infertility is associated with anatomic and physiologic changes seen with CSD.6 A recent review article published by Tower summarized additional clinical outcomes of CSD, such as ectopic pregnancy and increased surgical risks for such gynecologic procedures as uterine evacuation in the nonpregnant or postpartum state, hysterectomy, endometrial ablation, and intrauterine device placement.4
The CSD generally is described as a triangular or circular sonographically anechoic area in the myometrium of the anterior lower uterine segment or cervix at the site of a previous cesarean section. In nonpregnant patients, the defect is best evaluated with contrast infusion sonography (CIS), such as saline infusion or gel infusion, versus transvaginal ultrasound (TVUS) alone (FIGURE 2).4,7,8 However, the precise dimensions and definition of the scar defect vary among investigators.4,6,7,8,10
The reported prevalence of CSD has varied in the literature and appears to depend on the modality of diagnosis and the population studied. For instance, van der Voet and colleagues reported that in random populations of women who had undergone cesarean delivery, the defect was evident in 24% to 69% of women evaluated with transvaginal noncontrast ultrasound; the defect was evident in 56% to 78% of women evaluated with transvaginal contrast sonography.8
The scar defect also has been identified with magnetic resonance imaging (MRI) and found to be equal in sensitivity to TVUS.9,10 When identified hysteroscopically, a definitive out-pouching is visualized in the lower uterine segment, where the defect has been termed an “isthmocele.”6 Hysteroscopically, the defect also is visualized commonly within the cervical canal, indicating that cesarean incisions often are made through cervical tissue at the time of delivery (FIGURE 3, VIDEO 1, VIDEO 2 [see below]). Not all women with CSD report bleeding abnormalities, but it appears that the deeper and wider the defect, the more likely a woman is to present with postmenstrual AUB.7 According to the International Federation of Gynecology and Obstetrics (FIGO) Classification of AUB, CSD-associated postmenstrual bleeding falls into the “iatrogenic” category in the PALM-COIEN pneumonic.11
Related article: Dr. Garcia discusses the FIGO classification and the PALM-COEIN pneumonic in Update: Minimally invasive gynecology (April 2013)
![]()
![]()
A pair of studies shed light on CSD
Two recent European publications by van der Voet and colleagues addressed CSD and its association with AUB. These studies refer to CSD as the “niche” within the cesarean scar, but for the purpose of this article, I will use the term CSD. The first is a prospective cohort study, in which the authors addressed the definition, diagnosis, and prevalence of a defect within the cesarean scar and reported the incidence of associated AUB.7 The second publication is a systematic review which includes a critical investigation of minimally invasive therapy for CSD-related AUB.8 Both publications provide current clinical insight into the evaluation and management of AUB associated with CSD.
Related articles:
• Update on abnormal uterine bleeding Malcolm G. Munro, MD (March 2014)
• Update on Technology Barbara S. Levy, MD (September 2013)
• STOP performing dilation and curettage for the evaluation of abnormal uterine bleeding Amy Garcia, MD (Stop/Start, June 2013)
THE NICHE IN THE SCAR
van der Voet LF, Bij de Vaate AM, Veersema S, Brolmann HAM, Huirne JAF. Long-term complications of caesarean section. The niche in the scar: A prospective cohort study on niche prevalence and its relation to abnormal uterine bleeding. BJOG. 2014;121(2):236–244.
Most studies reporting the prevalence of cesarean delivery–associated postmenstrual bleeding are based on populations of women who were symptomatic with AUB, thus infusing a potential referral bias into these prevalence estimates. In contrast, this study by van der Voet and colleagues utilizes a prospective cohort design, making it the only study to date to enroll a random cohort of patients immediately after having undergone cesarean delivery.
Details of the study
The purpose of the study was to evaluate the prevalence of CSD formation in the cesarean scar at 6 to 12 weeks after cesarean delivery with TVUS and gel infusion study (GIS) in 197 women. The uterus was closed in two layers for four women and in one layer for all others.
The cohort was followed with menstruation questionnaires at 6 to 12 weeks, 6 months, and 12 months after surgery. The questionnaire response rate at 12 months for those women who had both TVUS and GIS evaluation of the scar was 73%. Data analysis accounted for confounding factors such as breastfeeding and amenorrhea, use of hormonal contraception, use of a levonorgestrel intrauterine system (LNG-IUS) as well as a body mass index (BMI) of at least 25 kg/m2.
Consistent with previous studies showing the superiority of saline-infused studies over TVUS for CSD identification,4 van der Voet and colleagues found that GIS was more sensitive than TVUS in diagnosing CSD (64.5% vs 49.6%, respectively). The percentage of women with CSD who had undergone two cesarean deliveries was 68.2%, while the percentage with CSD who had undergone three cesarean deliveries was 77.8%.
Data analysis correlated postmenstrual bleeding with the following CSD characteristics:
- depth and width of the defect
- residual myometrial thickness to the serosal surface of the uterus
- ratio of residual myometrium divided by the adjacent normal myometrial thickness.
Those women who had a ratio of residual myometrium to adjacent normal myometrium of less than 0.5 were more likely to report postmenstrual bleeding than those with a ratio greater than 0.5 (odds ratio, 6.1; 95% confidence interval, 1.74–21.63). The investigators stated that 1 out of 3 women with CSD identified by GIS reported postmenstrual bleeding, compared with 1 out of 10 women without identifiable CSD.
Study takeaways have merit
In summary, despite the small cohort of 197 women and the relatively short observation period of 1 year, these data collected by van der Voet and colleagues enable the gynecologist to begin to more fully understand the potential impact of cesarean section and the probability of AUB following an abdominal delivery. Applying these study statistics to the number of cesarean sections performed annually in the United States translates to nearly 280,000 women yearly who may experience postmenstrual bleeding related to a defect in the cesarean section scar.
Prospective cohort studies with longer follow-up periods are needed to assess the longer-term risks of CSD-related bleeding. As the authors suggest, perhaps the possibility of post–cesarean section AUB should be considered as part of the informed consent process for cesarean delivery.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
• Contrast infusion sonography has better sensitivity than TVUS at identification of the scar defect.
• About 64.5% of women are predicted to have scar defects after one cesarean delivery.
• The incidence of scar defects increases with increasing number of cesarean deliveries.
• One of three women with CSD is predicted to experience postmenstrual bleeding.
• Women with deeper and wider defects are more likely to experience postmenstrual bleeding.
• Post–cesarean section AUB is a probable occurrence in approximately 20% of all cesarean deliveries. Perhaps this information should be considered part of the informed consent process for cesarean delivery.
MINIMALLY INVASIVE THERAPY FOR GYNECOLOGIC SYMPTOMS
van der Voet LF, Vervoort AJ, Veersema S, Bij de Vatte AJ, Brolmann HAM, Huirne JAF. Minimally invasive therapy for gynaecological symptoms related to a niche in the caesarean scar: A systematic review. BJOG. 2014;121(2):145-156.
CSD-related bleeding issues may not respond to hormonal management and are frequently underdiagnosed. This scenario often leads to hysterectomy. Because there are women who desire uterine preservation, van der Voet and colleagues sought to evaluate the results of nonhysterectomy treatments of CSD-related AUB. They limited this systematic review to include only published studies that were randomized controlled trials, cohort studies, case-control studies, and case series of at least five patients.
Additionally, they included only studies that reported on conservative therapies (hysteroscopic resection, laparoscopic repair, abdominal repair, vaginal repair, endometrial ablation, LNG-IUS, or medical management) as well as at least one of the following outcomes: AUB, pain relief, sexual function, quality of life, surgical outcome, anatomic reconstruction, fertility or pregnancy outcome. Of 1,629 publications that were screened, 12 ultimately met inclusion criteria for the review. The studies, 11 of which were peer reviewed and 1 abstract, were published between 1996 and 2013 and reported on a total of 455 women with postcesarean AUB.
Weaknesses of the study
The most poignant statements made by the investigators pertain to the methodologic quality of the included articles. No study met requisite quality criteria. A clear definition of outcomes, including standardized measurements, was lacking in most studies. Most of the studies reviewed did not report CSD measurements, and only one study provided an objective reproducible method of CSD measurement. Few studies reported AUB symptom evaluation methodology, and no study used validated questionnaires. In the majority of studies, methods of posttreatment outcome measurements either were not reported or differed from pretreatment evaluation methods, potentiating verification bias. Because their literature review yielded primarily small case series publications that reported positive effects of interventions, and because of a lack of large RCT and prospective cohort trials, little could be gleaned regarding the viability of treatment interventions for CSD-related AUB.
Only three studies provided sufficient data to be included in a meta-analysis. The number of days of bleeding was reduced with hysteroscopic defect resection by 2 to 4 days in two studies, and in one study, vaginal repair decreased days of bleeding by 4 to 7 days. Only one study with laparoscopic repair compared CSD characteristics before and after surgery. Residual myometrial thickness increased for laparoscopic repair to greater than 8.3 mm; however, it is not known if this will make a clinical difference in the risk of scar dehiscence or improved functionality of the lower uterine segment.
Two studies reported on the laparoscopic repair of scar defects in asymptomatic patients, which is not recommended by these investigators. It is not known what ramifications hysteroscopic resection of the scar will have for the risk of uterine rupture, malplacentation or cervical incompetence for women who conceive after hysteroscopic repair.
Meaningful conclusions are lacking
Despite the high success rates reported by investigators of various surgical intervention case series involving hysteroscopic resection, vaginal repair, or laparoscopic repair, van der Voet and colleagues ultimately state that the methodologies of these studies do not allow meaningful conclusions to be drawn regarding the effectiveness of any of these interventions. Consequently, the authors recommend that the outcomes of their meta-analysis be scrutinized. They also point out that the LNG-IUS has proven benefit for AUB and yet has not been studied in the treatment of AUB associated with a CSD.
They finally propose that women who are symptomatic be treated with oral contraceptives unless immediate fertility is desired, or by expectant management without intervention. While their primary focus was to assess AUB, given the stated shortcomings of the included studies and lack of long-term follow-up, the authors also warn against hysteroscopic, laparoscopic, or vaginal repair for fertility, as the risk to pregnancy or delivery after these therapies is unknown.
CASE RESOLVED
Suspecting a cesarean scar defect, you perform a saline infusion sonography and diagnose a 14 mm x 19 mm anechoic region within the scar, with no other intracavitary abnormalities found. You first reassure the patient that this is a benign finding and inform her why she likely is experiencing this type of bleeding pattern. After an informed discussion with you regarding the risks and benefits of possible surgical or nonsurgical options for management, she chooses to use oral contraceptive pills in a continuous fashion.
CONCLUSION
Consider a history of cesarean section in the evaluation of AUB, and be cognizant of the prevalence of CSD with cesarean delivery and the association of postmenstrual bleeding with CSD.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
• A critical systematic review of available data suggests that there is not enough clinical evidence to support surgical intervention for the treatment of CSD for women symptomatic with AUB.
• Recommended nonhysterectomy treatments for AUB associated with CSD include oral contraceptives or expectant management.
• Surgical treatment should be limited to the research environment in the form of RCT to assess the long-term outcomes of intervention.
• An RCT of the LNG-IUS for the treatment of AUB associated with CSD is needed.
Acknowledgments
The author would like to thank Andrew Brill, MD, Lee Sloan-Garcia, MD, and William Parker, MD, for their thoughtful review of this manuscript.
We want to hear from you!
Share your thoughts on this article or on any topic relevant to ObGyns and women’s health practitioners. Tell us which topics you’d like to see covered in future issues, and what challenges you face in daily practice. We will consider publishing your letter and in a future issue. Send your letter to: [email protected] Please include the city and state in which you practice. Stay in touch! Your feedback is important to us!
- Osterman MJK, Martin JA. Primary cesarean delivery rates, by state: Results from the revised birth certificate, 2006-2012. Natl Vital Stat Rep. 2014;63(1):1–11.
- Martin JA, Hamilton BE, Osterman MJK, Curtin SC, Mathews TJ. Births: Final data for 2012. Natl Vital Stat Rep. 2013;62(9). Hyattsville, MD: National Center for Health Statistics. http://www.cdc.gov/nchs/data/nvsr/nvsr62/nvsr62_09.pdf. Accessed March 19, 2014.
- Stewart KS, Evans TW. Recurrent bleeding from the lower segment scar – a late complication of Caesarean section. Br J Obstet Gynaecol. 1975;82(8):682–686.
- Tower AM, Frishman GN. Cesarean scar defects: An underrecognized cause of abnormal uterine bleeding and other gynecologic complications. J Minim Invasive Gynecol. 2013;20(5):562–572.
- Morris H. Surgical pathology of the lower uterine segment cesarean section scar: Is the scar a source of clinical symptoms? Intl J Gynecol Pathol. 1995;14(1):16–20.
- Gubbini G, Centini G, Nascetti D, et al. Surgical hysteroscopic treatment of cesarean-induced isthmocele in restoring fertility: Prospective study. J Minim Invasive Gynecol. 2011;18(2):234–237.
- van der Voet LF, Bijde Vaate AM, Veersema S, Brolmann HA, Huirne JA. Long-term complications of caesarean section. The niche in the scar: A prospective cohort study on niche prevalence and its relation to abnormal uterine bleeding. BJOG. 2014;121(2):236–244.
- van der Voet LF, Vervoort AJ, Veersema S, Bijde Vatte AJ, Brolmann HA, Huirne JA. Minimally invasive therapy for gynaecological symptoms related to a niche in the caesarean scar: A systematic review. BJOG. 2014;121(2):145–156.
- Maldjian C, Adam R, Maldjian J, Smith R. MRI appearance of the pelvis in the post cesarean-section patient. Magn Reson Imaging. 1999;17(2):223–227.
- Marotta ML, Donnez J, Squifflet J, Jadoul P, Darii N, Donnez O. Laparoscopic repair of post-Cesarean section uterine scar defects diagnosed in nonpregnant women. J Minim Invasive Gynecol. 2013;20(3):386–391.
- Munro MG, Critchley HO, Broder MS, Fraser IS; FIGO Working Group on Menstrual Disorders. FIGO classification system (PALM-COIEN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. Int J Gynaecol Obstet. 2011;113(1):3–13.
- Osterman MJK, Martin JA. Primary cesarean delivery rates, by state: Results from the revised birth certificate, 2006-2012. Natl Vital Stat Rep. 2014;63(1):1–11.
- Martin JA, Hamilton BE, Osterman MJK, Curtin SC, Mathews TJ. Births: Final data for 2012. Natl Vital Stat Rep. 2013;62(9). Hyattsville, MD: National Center for Health Statistics. http://www.cdc.gov/nchs/data/nvsr/nvsr62/nvsr62_09.pdf. Accessed March 19, 2014.
- Stewart KS, Evans TW. Recurrent bleeding from the lower segment scar – a late complication of Caesarean section. Br J Obstet Gynaecol. 1975;82(8):682–686.
- Tower AM, Frishman GN. Cesarean scar defects: An underrecognized cause of abnormal uterine bleeding and other gynecologic complications. J Minim Invasive Gynecol. 2013;20(5):562–572.
- Morris H. Surgical pathology of the lower uterine segment cesarean section scar: Is the scar a source of clinical symptoms? Intl J Gynecol Pathol. 1995;14(1):16–20.
- Gubbini G, Centini G, Nascetti D, et al. Surgical hysteroscopic treatment of cesarean-induced isthmocele in restoring fertility: Prospective study. J Minim Invasive Gynecol. 2011;18(2):234–237.
- van der Voet LF, Bijde Vaate AM, Veersema S, Brolmann HA, Huirne JA. Long-term complications of caesarean section. The niche in the scar: A prospective cohort study on niche prevalence and its relation to abnormal uterine bleeding. BJOG. 2014;121(2):236–244.
- van der Voet LF, Vervoort AJ, Veersema S, Bijde Vatte AJ, Brolmann HA, Huirne JA. Minimally invasive therapy for gynaecological symptoms related to a niche in the caesarean scar: A systematic review. BJOG. 2014;121(2):145–156.
- Maldjian C, Adam R, Maldjian J, Smith R. MRI appearance of the pelvis in the post cesarean-section patient. Magn Reson Imaging. 1999;17(2):223–227.
- Marotta ML, Donnez J, Squifflet J, Jadoul P, Darii N, Donnez O. Laparoscopic repair of post-Cesarean section uterine scar defects diagnosed in nonpregnant women. J Minim Invasive Gynecol. 2013;20(3):386–391.
- Munro MG, Critchley HO, Broder MS, Fraser IS; FIGO Working Group on Menstrual Disorders. FIGO classification system (PALM-COIEN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. Int J Gynaecol Obstet. 2011;113(1):3–13.
CESAREAN SCAR DEFECT DIAGNOSED WITH HYSTEROSCOPY
![]()
![]()
Videos courtesy of Amy Garcia, MD
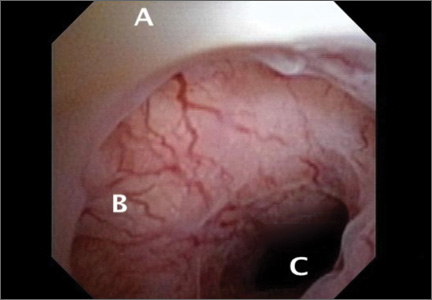
Unusual Case of Chest and Left Arm Pain
A 37-year-old white man presented to his primary care provider’s office for follow-up after a visit to the emergency department (ED). He had been evaluated at a local ED a week earlier for atypical chest pain and left arm pain. At the ED, blood work was done, along with an ECG, chest x-ray, and chest CT scan, but the results of these evaluations were not available during his initial primary care visit. On discharge from the ED, he was told that his heart was not the cause of his pain and that he should follow up with his primary care provider.
In the office, the patient reported that for the past several months he had been experiencing pain in his left arm when doing heavy or continuous physical labor; he noted that his job as a laborer required vigorous activity. Rest seemed to make his pain go away. He denied pain in the right arm or being awakened by the pain at night. Review of systems was unremarkable, and medical and surgical history was negative.
On physical exam, inspection of his torso and upper and lower extremities did not reveal any apparent abnormalities. Left shoulder and neck exams were normal. Cardiac auscultation was unremarkable, but palpation of the left upper extremity revealed neither a brachial, radial, nor ulnar pulse. Pulses in his right upper extremity were within normal limits. No bruits were appreciated over the carotids or either subclavian artery. Basic Doppler ultrasound over the left upper extremity at the brachial, radial, and ulnar sites showed symmetrical Doppler sounds. The remainder of his exam was unremarkable.
The patient’s ED documents and imaging results were received later in the day, after his office visit. The ECG, blood work results, and chest x-ray were normal. The chest CT results showed no evidence of pulmonary embolism. The radiologist did note mild narrowing at the left subclavian artery secondary to nonspecific surrounding soft tissue, which was noted to possibly represent intramural hemorrhage or atherosclerotic changes. No intimal flap was identified.
Because the diagnosis remained unclear, the patient was asked to bring the disc containing his chest CT images to the office. The radiologist, who was informed about the patient’s history and exam findings by phone, reviewed the CT images and felt there were changes surrounding the three branches off the aortic arch suggestive of inflammation, in addition to the stenosis at the left subclavian artery (see Figure 1 and Figure 2).
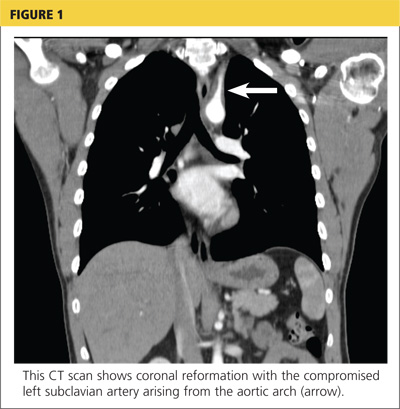
Based on the radiologist’s interpretation, additional lab tests were ordered. A complete blood count, comprehensive metabolic panel, prothrombin time/partial thromboplastin time, and lipid panel all yielded results within normal limits. Erythrocyte sedimentation rate (ESR) was 12 mm/h (reference range, 0 to 15 mm/h) and C-reactive protein (CRP) level was 4.9 mg/dL (reference range, 0.1 to 4.9 mg/dL). These laboratory results were essentially unremarkable, and therefore made his diagnosis more elusive.
The patient was referred to a vascular surgeon because of his immediate symptoms. The surgeon performed a thoracic outlet study in which Doppler waveform analysis of the left brachial, radial, and ulnar arteries of the thoracic outlet were analyzed during range-of-motion testing. Results suggested the possibility of thoracic outlet syndrome involving the left upper extremity, with significant baseline arterial insufficiency. A CT angiogram showed critical stenosis of the left subclavian artery and arterial wall thickening. Inflammatory changes were noted as well, and concern for “an inflammatory vasculitis” was described on the CT angiogram. The patient underwent left carotid-to-axillary bypass grafting, after which his left arm pain improved.
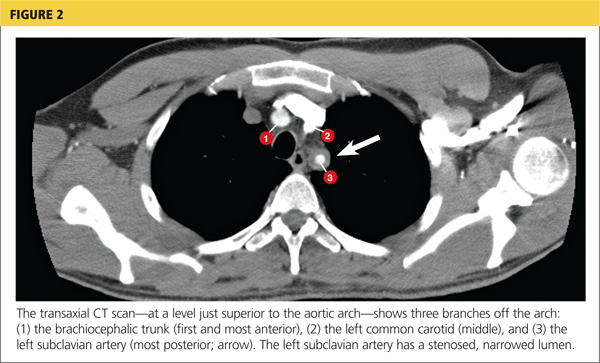
Following surgery, the patient returned to the primary care office for evaluation. Although the surgery was successful, the diagnosis was still not clear, requiring additional medical evaluation. The physical exam showed normal pulses in his left upper extremity. Lab tests revealed an elevated ESR of 54 mm/h and a CRP level of 4 mg/dL (reference range, 0.1 to 0.8 mg/dL; a different lab testing site was used, which accounts for the different reference range). In light of the patient’s lab test results, premature arterial vascular disease, and imaging studies suggesting inflammation, Takayasu arteritis (TA) was arrived at as a working diagnosis.
The patient was referred to a rheumatologist, who ordered a repeat ESR and CRP, antineutrophil cytoplasmic antibodies, and a magnetic resonance angiography study of the right brachial artery and major aortic branches to rule out other types of arteritis. Based on the test results, the patient was diagnosed with TA. He was placed on high-dose corticosteroid therapy (prednisone 60 mg/d). Methotrexate 10 mg/wk po was added three months after initiation of the prednisone.
Since being diagnosed with TA, the patient has presented with complaints related to the adverse effects of high-dose corticosteroids (ie, insomnia, weight gain, elevated blood pressure).
Continued on the next page >>
DISCUSSION
The first description of TA is credited to Japanese ophthalmologist Mikito Takayasu, who in 1908 described a wreathlike arteriovenous anastomosis around the optic disc of a 21-year-old woman who had experienced acute vision loss.1-3 Much earlier, in 1761, Italian anatomist Giovanni Battista Morgagni described large-vessel aneurysms and stenosis on a postmortem exam of a 40-year-old woman.2,4 However, TA was not formally labeled a disease until 1975.
TA is a chronic large vessel vasculitis of unknown origin, mainly involving the aorta and its primary branches: the left common carotid, brachiocephalic, and left subclavian arteries. Ongoing inflammation of affected vessels causes fibrotic changes, stenosis, and eventual occlusion and may lead to aneurysm formation.5,6 TA is rare, with an annual incidence in North America of 2.6 cases per million population.6 It occurs most frequently in Asian countries but has been reported in a wide range of ethnic groups.5,7 TA has been characterized as a disease of young women: Between 80% and 97% of patients are women,6,8 and the average age at diagnosis is 25 to 30.8-10
The process of vascular injury in TA begins with inflammation in the vasa vasorum of the aortic vessels. This inflammation, thought to be triggered by an as-yet-unknown antigen, leads to an initial inflammatory cellular infiltration of the aortic media and adventitia; the infiltrate is comprised predominantly of macrophages and T cells.5,9 Inflammatory infiltration causes myointimal proliferation, thickening of the blood vessel wall, and eventual luminal stenosis.5 Cytokines, interleukin 6, interferon , and other chemokines released by infiltrating inflammatory cells within the injured tissue also contribute to the inflammatory response and tissue damage.5,11
Histologically, granulomatous inflammation and giant cells are found in the media.12,13 Destruction of the elastic lamina and the muscular media results in the aneurysmal dilation seen in TA, while dense scarring and continued inflammation of the arterial vasculature results in arterial stenosis.12
Continued on the next page >>
CLINICAL PRESENTATION
Presentation of TA varies widely and can range from asymptomatic disease identified by pulse deficits or impalpable pulses to severe neurologic impairment. The early or prepulseless phase of TA is characterized by inflammatory changes.14 Signs and symptoms are frequently vague and nonspecific, particularly in this early phase, when fatigue, weight loss, and low-grade fever may be seen.12 Headache is another common symptom at the time of disease onset.5
In the later or chronic phase of the disease, individuals will begin to demonstrate signs and symptoms of vascular insufficiency.14 More common physical signs reflect the underlying arterial occlusive disease and include diminished or absent arterial pulses, asymmetrical arm blood pressures, bruits, extremity claudication, and hypertension.5,9,10 Hypertension, generally reflecting renal artery stenosis,10 is present in approximately 40% of cases in the United States and Europe.5,7,15 Neurologic features secondary to hypertension or ischemia affect more than half of patients; in addition to headache, these may include dizziness, syncope, vertigo, transient ischemic attack, and stroke.5
TA can also present with eye, lung, and skin manifestations; however, these features are less common. Although ocular involvement, including amaurosis fugax, has been reported in up to 26% of patients in TA series,5,7,16 permanent loss of vision in North American patients is uncommon.5,7 Pulmonary involvement affecting the large- or medium-sized pulmonary arteries has been reported to occur in approximately 55% of cases5; however, there is uncertainty regarding the prevalence of angiographically demonstrated pulmonary artery involvement, as studies have reported rates ranging from 14.3% to 70%.9,17-20 Pulmonary involvement is often asymptomatic, but features can include dyspnea, cough, and chest pain.5 Skin lesions are seen in up to 28% of cases, most commonly erythema nodosum, erythema induratum, tuberculoidlike eruptions, pyoderma gangrenosum, and cutaneous signs of necrotizing or granulomatous vasculitis.5,21
Continued on the next page >>
DIAGNOSIS
The American College of Rheumatology (ACR) has developed classification criteria for the diagnosis of TA.22 The presence of three or more of the six criteria (age of onset ≤ 40, claudication of the extremities, decreased brachial artery pulse, > 10 mm Hg difference in systolic blood pressure between the arms, bruit over subclavian arteries or aorta, and arteriographic abnormalities) yields a sensitivity of 90.5% and a specificity of 97.8%. Although the ACR classification remains the most widely applied for TA, a limitation of its diagnostic criteria is its failure to distinguish patients with early nonocclusive disease.23
In 1988, the Ishikawa classification criteria were developed, with a modified version subsequently published in 1996.23 Considered superior to the original Ishikawa and ACR criteria based on its application in 106 patients with angiographically proven TA, the modified version has a reported sensitivity and specificity of 92.5% and 95%, respectively.23
With the modified Ishikawa diagnostic criteria, the presence of two major or one major and two or four minor criteria suggests a high probability of TA. The three major criteria consist of lesions of the left mid-subclavian artery and the right mid-subclavian artery and characteristic signs and symptoms of at least 1 mo duration. The 10 minor criteria are high ESR (> 20 mm/h); carotid artery tenderness; hypertension; aortic regurgitation or annuloaortic ectasia; and lesions of pulmonary artery, left mid-common carotid, distal brachiocephalic trunk, descending thoracic aorta, abdominal aorta, and coronary artery.
The diagnosis of TA is based on recognition of clinical findings suggestive of large-vessel vasculitis. Imaging of the arterial tree with CT, MRI, or angiography also demonstrates findings consistent with TA, typically including early-onset vascular wall thickening/enhancement.24 Late imaging studies may reveal arterial stenoses, occlusions, and aneurysms.
Several types of imaging modalities have been used in the diagnosis and management of TA, each with strengths and limitations. Traditional angiography is invasive and requires an arterial puncture. Large doses of radiation are used, exposing the patient to iodinated contrast material, which may be dangerous in patients with poor renal function. However, the primary advantage of traditional angiography is that it allows for interventions such as stent placement and/or angioplasty to be performed.24 Findings on angiography often include long, smooth, tapered stenoses ranging from mild to severe or frank occlusions, as well as collateral vessels or the subclavian steal phenomenon.24
CT imaging is very useful for assessing thickening of the arterial wall. In early TA disease, evaluation of vessel wall thickness may be identified prior to frank stenosis of the artery(s).24 The spectrum of findings on CT angiography includes stenoses; occlusions; aneurysms; and concentric arterial wall thickening affecting the aorta and its branches, the pulmonary arteries, and occasionally the coronary arteries.24
MRI does not require the use of iodinated contrast, nor is there radiation exposure. MRI also has the advantage of evaluating arterial wall thickening, which is often present prior to stenosis (similar to CT imaging).24 Findings of TA on MRI include mural thrombi, signal alterations within and surrounding inflamed vessels, fusiform vascular dilation, thickened aortic valvular cusps, multifocal stenoses, and concentric thickening of the aortic wall.24
Laboratory testing is neither specific nor sensitive. Hoffman and Ahmed studied multiple serologic tests and found that no test reliably distinguishes between patients with active TA and healthy volunteers.25 Increases in the acute phase reactants (ESR and CRP) support the presence of an underlying inflammatory process, and these laboratory tests may be useful in disease monitoring. The ESR and CRP often do not correlate with systemic symptoms or disease progression but are used in conjunction with the clinical exam and serial imaging to gauge treatment success and to monitor disease progression.5,25 Biopsy material typically is not available in the initial diagnosis of TA, but histologic examination at the time of a surgery or procedure is often undertaken to confirm the diagnosis.5
The differential diagnosis of TA includes connective tissue diseases associated with the formation of multiple aneurysms, such as Marfan syndrome and Ehlers-Danlos syndrome.5 However, these diseases do not manifest with large vessel stenosis, the hallmark of TA. Infections known to cause aneurysms of the aorta should also be considered; these include bacterial, fungal, syphilitic, mycotic, and mycobacterial pathogens.5 Blood cultures are used to rule out bacterial agents. Rapid plasma reagin (RPR) and venereal disease research laboratory tests (VDRL) will identify a syphilitic etiology. Fungal cultures or fungal serology will help to rule out a mycotic pathogen.
Autoimmune diseases that can mimic TA include Behçet’s disease, Cogan syndrome, the spondyloarthropathies, and systemic lupus erythematosus. These diseases are not associated with stenosis of large vessels, which differentiates them from TA.5 Giant cell (temporal) arteritis (GCA) may present very similarly to TA, as both diseases affect large arteries.12 The table provides distinguishing features of TA and GCA.26
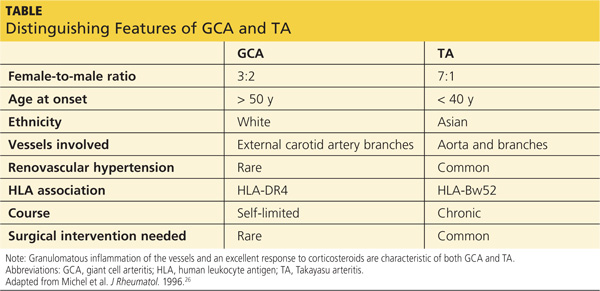
Continued on the next page >>
TREATMENT
Active phase TA is initially treated with high-dose glucocorticoid therapy (prednisone or methylprednisolone). Typical prednisone doses are 0.5 to 1 mg/kg/d.5 Clinical improvement is seen in almost all patients with glucocorticoid therapy,6,10,23 but relapse is common when prednisone is tapered to less than 20 mg/d.5 The corticosteroid dose is gradually tapered depending on patient response. Common side effects of corticosteroids may include weight gain, elevations in blood glucose, insomnia, increased infection risk, osteoporosis, and slowing of wound healing.
Because nearly half of all patients treated with glucocorticoids alone demonstrate chronic active disease, immunosuppressive therapies are almost always used concomitantly.27 Immune-suppressing drugs that may be used include methotrexate (15 to 25 mg/wk), azathioprine (2 mg/kg/d), and cyclophosphamide (1 to 2 mg/kg/d orally).5,28 Tumor necrosis factor (TNF)–blocking agents used to treat TA include etanercept, infliximab, or adalimumab.28,29 Adverse effects associated with immunosuppressive therapies and TNF-blocking agents include an increased risk for infection(s) and malignancy, bone marrow suppression, and hepatitis B reactivation. Although data are limited on anti-TNF agents, this class of drug has shown promise when used in conjunction with corticosteroids.28
In one open-label study by Hoffman and colleagues, remission rates with methotrexate plus steroids were 81%. Relapse occurred in 44% of study participants when the steroid dose was tapered or decreased to near discontinuation.27 More recently, in an uncontrolled study series involving 15 TA patients from India who were treated with azathioprine plus steroids, remission was achieved following 12 weeks of therapy. Angiographically, there was no progression of arterial disease after one year.30
Surgical and endovascular procedures used to return blood flow in stenotic or occluded vessels include synthetic or autologous vessel bypass, endarterectomy, and percutaneous transluminal angioplasty.5 When aortic insufficiency is present, aortic root replacement or repair is undertaken.5 These procedures are performed by vascular or cardiovascular surgeons and interventional radiologists. Rheumatologists are the medical specialists most involved in the direct care and management of TA patients. Cardiologists are sometimes consulted as well.
Continued on the next page >>
PROGNOSIS
Disability is common in TA. In a National Institutes of Health cohort study, 74% of TA patients reported experiencing functional effects from their disease, and 47% were fully disabled.2,8 In their retrospective review of 107 cases of TA, Lupi-Herrera and colleagues reported a 14% mortality rate.31 Half the deaths in this study were attributed to congestive heart failure (CHF). A cohort study in India that included 88 patients with TA reported cumulative 5- and 10-year survival rates of 91% and 84%, respectively. Of the 10 deaths in this cohort, four were due to CHF.2,32
CONCLUSION
Signs and symptoms of rheumatologic diseases such as TA are often vague, and diagnosis may prove difficult and elusive. Repeat office visits at short intervals may prove to be helpful in making the diagnosis. Referral for radiology and/or rheumatology consultation (face-to-face, if possible) is often necessary.
In cases such as this, completing a personal review of documents and test results done elsewhere, particularly ED/inpatient hospital data, is necessary; relying on the patient’s word that “they told me everything was fine” is insufficient. Clinicians should implement a system that works best for obtaining test results and other documents, follow their instincts, and if the correct diagnosis is not arrived at immediately, keep looking.
References >>
REFERENCES
1. Takayasu M. A case with peculiar changes of the retinal central vessels. Acta Soc Ophthalmol Jpn. 1908;12:554-555.
2. Maksimowicz-McKinnon K, Hoffman GS. Takayasu arteritis: what is the long-term prognosis? Rheum Dis Clin North Am. 2007;33:777-786.
3. Numano F. The story of Takayasu arteritis. Rheumatology. 2002;41:103-106.
4. Morgagni GB. De sedibus et causis morborum per anatomen indagatis.
(Letter 30).1761. Article 12.
5. Hernandez-Rodriguez J, Maksimowicz-McKinnon K, Hoffman GS. Takayasu’s arteritis. In: Carey WD, ed. Current Clinical Medicine. 2nd ed. Philadelphia: Saunders Elsevier; 2010:1195-1199.
6. Hall S, Barr W, Lie JT, et al. Takayasu arteritis. A study of 32 North American patients. Medicine (Baltimore). 1985;64:89-99.
7. Maksimowicz-McKinnon K, Clark TM, Hoffman GS. Limitations of therapy and a guarded prognosis in an American cohort of Takayasu arteritis patients. Arthritis Rheum. 2007;56:1000-1009.
8. Kerr GS, Hallahan CW, Giordano J, et al. Takayasu arteritis. Ann Intern Med. 1994:120:919-929.
9. Gornik HL, Creager MA. Aortic diseases: aortitis. Circulation. 2008;117:
3039-3051.
10. Mwipatayi BP, Jeffery PC, Beningfield SJ, et al. Takayasu arteritis: clinical features and management: report of 272 cases. ANZ J Surg. 2005;75:110-117.
11. Noris M. Pathogenesis of Takayasu’s arteritis. J Nephrol. 2001;14:506-513.
12. Hunder GG, Stone JH, Ramirez MP. Clinical features and diagnosis of Takayasu arteritis (2013). www.uptodate.com/contents/clinical-features-and-
diagnosis-of-takayasu-arteritis. Accessed March 24, 2014.
13. Nasu T. Takayasu’s truncoarteritis. Pulseless disease or aortitis syndrome. Acta Pathol Jpn. 1982;32 (suppl 1):117.
14. Johnston SL, Lock RJ, Gompels MM. Takayasu arteritis: a review. J Clin Pathol. 2002;55:481-486.
15. Vanoli M, Daina E, Salvarani C, et al. Takayasu’s arteritis: a study of 104 Italian patients. Arthritis Rheum. 2005;53:100-107.
16. Chun YS, Park SJ, Chung H, Lee J. The clinical and ocular manifestations of Takayasu’s arteritis. Retina. 2001;21:132-140.
17. Liu YQ, Jin BL, Ling J. Pulmonary artery involvement in aortoarteritis: an angiographic study. Cardiovasc Intervent Radiol. 1994;17:2-6.
18. Yamada I, Shibuya H, Matsubara O, et al. Pulmonary artery disease in Takayasu’s arteritis: angiographic findings. AJR Am J Roentgenol. 1992;159:
263-269.
19. Sharma S, Kamalakar T, Rajani M, et al. The incidence and patterns of pulmonary artery involvement in Takayasu’s arteritis. Clin Radiol. 1990;42:177-181.
20. He NS, Liu F, Wu EH, et al. Pulmonary artery involvement in aorto-arteritis: an analysis of DSA. Chin Med J (Engl). 1990;103:666-672.
21. Werfel T, Kuipers JG, Zeidler H, et al. Cutaneous manifestations of Takayasu arteritis. Acta Derm Venereol. 1996;76:496-497.
22. Arend WP, Michel BA, Bloch DA, et al. The American College of Rheumatology 1990 criteria for the classification of Takayasu arteritis. Arthritis Rheum. 1990;33:1129-1134.
23. Andrews J, Mason JC. Takayasu’s arteritis—recent advances in imaging offer promise. Rheumatology (Oxford). 2007;46:6-15.
24. Gotway MB, Araoz PA, Macedo TA, et al. Imaging findings in Takayasu’s arteritis. AJR Am J Roentgenol. 2005;184:1945-1950.
25. Hoffman GS, Ahmed AE. Surrogate markers of disease activity in patients with Takayasu arteritis. A preliminary report from The International Network for the Study of the Systemic Vasculitides (INSSYS). Int J Cardiol. 1998;66 (suppl 1):S191-S194.
26. Michel BA, Arend WP, Hunder GG. Clinical differentiation between giant cell (temporal) arteritis and Takayasu’s arteritis. J Rheumatol. 1996;23:106-111.
27. Hoffman GS, Leavitt RY, Kerr GS, et al. Treatment of glucocorticoid-resistant or relapsing Takayasu arteritis with methotrexate. Arthritis Rheum. 1994;37:578-582.
28. Hunder GG, Stone JH, Ramirez MP. Treatment of Takayasu arteritis (2013). www.uptodate.com/contents/treatment-of-takayasu-arteritis. Accessed March 24, 2014.
29. Schmidt J, Kerman TA, Bacani AK, et al. Tumor necrosis factor inhibitors in patients with Takayasu arteritis: experience from a referral center with long-term followup. Arthritis Care Res (Hoboken). 2012;64:1079-1083.
30. Valsakumar AK, Valappil UC, Jorapur V, et al. Role of immunosuppressive therapy on clinical, immunological, and angiographic outcome in active Takayasu’s arteritis. J Rheumatol. 2003;30:1793-1798.
31. Lupi-Herrera E, Sanchez-Torres G, Marcushamer J, et al. Takayasu’s arteritis: clinical study of 107 cases. Am Heart J. 1977;93:94-103.
32. Subramanyan R, Joy J, Balakrishnan KG. Natural history of aortoarteritis (Takayasu’s disease). Circulation. 1989;80:429-437.
A 37-year-old white man presented to his primary care provider’s office for follow-up after a visit to the emergency department (ED). He had been evaluated at a local ED a week earlier for atypical chest pain and left arm pain. At the ED, blood work was done, along with an ECG, chest x-ray, and chest CT scan, but the results of these evaluations were not available during his initial primary care visit. On discharge from the ED, he was told that his heart was not the cause of his pain and that he should follow up with his primary care provider.
In the office, the patient reported that for the past several months he had been experiencing pain in his left arm when doing heavy or continuous physical labor; he noted that his job as a laborer required vigorous activity. Rest seemed to make his pain go away. He denied pain in the right arm or being awakened by the pain at night. Review of systems was unremarkable, and medical and surgical history was negative.
On physical exam, inspection of his torso and upper and lower extremities did not reveal any apparent abnormalities. Left shoulder and neck exams were normal. Cardiac auscultation was unremarkable, but palpation of the left upper extremity revealed neither a brachial, radial, nor ulnar pulse. Pulses in his right upper extremity were within normal limits. No bruits were appreciated over the carotids or either subclavian artery. Basic Doppler ultrasound over the left upper extremity at the brachial, radial, and ulnar sites showed symmetrical Doppler sounds. The remainder of his exam was unremarkable.
The patient’s ED documents and imaging results were received later in the day, after his office visit. The ECG, blood work results, and chest x-ray were normal. The chest CT results showed no evidence of pulmonary embolism. The radiologist did note mild narrowing at the left subclavian artery secondary to nonspecific surrounding soft tissue, which was noted to possibly represent intramural hemorrhage or atherosclerotic changes. No intimal flap was identified.
Because the diagnosis remained unclear, the patient was asked to bring the disc containing his chest CT images to the office. The radiologist, who was informed about the patient’s history and exam findings by phone, reviewed the CT images and felt there were changes surrounding the three branches off the aortic arch suggestive of inflammation, in addition to the stenosis at the left subclavian artery (see Figure 1 and Figure 2).
Based on the radiologist’s interpretation, additional lab tests were ordered. A complete blood count, comprehensive metabolic panel, prothrombin time/partial thromboplastin time, and lipid panel all yielded results within normal limits. Erythrocyte sedimentation rate (ESR) was 12 mm/h (reference range, 0 to 15 mm/h) and C-reactive protein (CRP) level was 4.9 mg/dL (reference range, 0.1 to 4.9 mg/dL). These laboratory results were essentially unremarkable, and therefore made his diagnosis more elusive.
The patient was referred to a vascular surgeon because of his immediate symptoms. The surgeon performed a thoracic outlet study in which Doppler waveform analysis of the left brachial, radial, and ulnar arteries of the thoracic outlet were analyzed during range-of-motion testing. Results suggested the possibility of thoracic outlet syndrome involving the left upper extremity, with significant baseline arterial insufficiency. A CT angiogram showed critical stenosis of the left subclavian artery and arterial wall thickening. Inflammatory changes were noted as well, and concern for “an inflammatory vasculitis” was described on the CT angiogram. The patient underwent left carotid-to-axillary bypass grafting, after which his left arm pain improved.
Following surgery, the patient returned to the primary care office for evaluation. Although the surgery was successful, the diagnosis was still not clear, requiring additional medical evaluation. The physical exam showed normal pulses in his left upper extremity. Lab tests revealed an elevated ESR of 54 mm/h and a CRP level of 4 mg/dL (reference range, 0.1 to 0.8 mg/dL; a different lab testing site was used, which accounts for the different reference range). In light of the patient’s lab test results, premature arterial vascular disease, and imaging studies suggesting inflammation, Takayasu arteritis (TA) was arrived at as a working diagnosis.
The patient was referred to a rheumatologist, who ordered a repeat ESR and CRP, antineutrophil cytoplasmic antibodies, and a magnetic resonance angiography study of the right brachial artery and major aortic branches to rule out other types of arteritis. Based on the test results, the patient was diagnosed with TA. He was placed on high-dose corticosteroid therapy (prednisone 60 mg/d). Methotrexate 10 mg/wk po was added three months after initiation of the prednisone.
Since being diagnosed with TA, the patient has presented with complaints related to the adverse effects of high-dose corticosteroids (ie, insomnia, weight gain, elevated blood pressure).
Continued on the next page >>
DISCUSSION
The first description of TA is credited to Japanese ophthalmologist Mikito Takayasu, who in 1908 described a wreathlike arteriovenous anastomosis around the optic disc of a 21-year-old woman who had experienced acute vision loss.1-3 Much earlier, in 1761, Italian anatomist Giovanni Battista Morgagni described large-vessel aneurysms and stenosis on a postmortem exam of a 40-year-old woman.2,4 However, TA was not formally labeled a disease until 1975.
TA is a chronic large vessel vasculitis of unknown origin, mainly involving the aorta and its primary branches: the left common carotid, brachiocephalic, and left subclavian arteries. Ongoing inflammation of affected vessels causes fibrotic changes, stenosis, and eventual occlusion and may lead to aneurysm formation.5,6 TA is rare, with an annual incidence in North America of 2.6 cases per million population.6 It occurs most frequently in Asian countries but has been reported in a wide range of ethnic groups.5,7 TA has been characterized as a disease of young women: Between 80% and 97% of patients are women,6,8 and the average age at diagnosis is 25 to 30.8-10
The process of vascular injury in TA begins with inflammation in the vasa vasorum of the aortic vessels. This inflammation, thought to be triggered by an as-yet-unknown antigen, leads to an initial inflammatory cellular infiltration of the aortic media and adventitia; the infiltrate is comprised predominantly of macrophages and T cells.5,9 Inflammatory infiltration causes myointimal proliferation, thickening of the blood vessel wall, and eventual luminal stenosis.5 Cytokines, interleukin 6, interferon , and other chemokines released by infiltrating inflammatory cells within the injured tissue also contribute to the inflammatory response and tissue damage.5,11
Histologically, granulomatous inflammation and giant cells are found in the media.12,13 Destruction of the elastic lamina and the muscular media results in the aneurysmal dilation seen in TA, while dense scarring and continued inflammation of the arterial vasculature results in arterial stenosis.12
Continued on the next page >>
CLINICAL PRESENTATION
Presentation of TA varies widely and can range from asymptomatic disease identified by pulse deficits or impalpable pulses to severe neurologic impairment. The early or prepulseless phase of TA is characterized by inflammatory changes.14 Signs and symptoms are frequently vague and nonspecific, particularly in this early phase, when fatigue, weight loss, and low-grade fever may be seen.12 Headache is another common symptom at the time of disease onset.5
In the later or chronic phase of the disease, individuals will begin to demonstrate signs and symptoms of vascular insufficiency.14 More common physical signs reflect the underlying arterial occlusive disease and include diminished or absent arterial pulses, asymmetrical arm blood pressures, bruits, extremity claudication, and hypertension.5,9,10 Hypertension, generally reflecting renal artery stenosis,10 is present in approximately 40% of cases in the United States and Europe.5,7,15 Neurologic features secondary to hypertension or ischemia affect more than half of patients; in addition to headache, these may include dizziness, syncope, vertigo, transient ischemic attack, and stroke.5
TA can also present with eye, lung, and skin manifestations; however, these features are less common. Although ocular involvement, including amaurosis fugax, has been reported in up to 26% of patients in TA series,5,7,16 permanent loss of vision in North American patients is uncommon.5,7 Pulmonary involvement affecting the large- or medium-sized pulmonary arteries has been reported to occur in approximately 55% of cases5; however, there is uncertainty regarding the prevalence of angiographically demonstrated pulmonary artery involvement, as studies have reported rates ranging from 14.3% to 70%.9,17-20 Pulmonary involvement is often asymptomatic, but features can include dyspnea, cough, and chest pain.5 Skin lesions are seen in up to 28% of cases, most commonly erythema nodosum, erythema induratum, tuberculoidlike eruptions, pyoderma gangrenosum, and cutaneous signs of necrotizing or granulomatous vasculitis.5,21
Continued on the next page >>
DIAGNOSIS
The American College of Rheumatology (ACR) has developed classification criteria for the diagnosis of TA.22 The presence of three or more of the six criteria (age of onset ≤ 40, claudication of the extremities, decreased brachial artery pulse, > 10 mm Hg difference in systolic blood pressure between the arms, bruit over subclavian arteries or aorta, and arteriographic abnormalities) yields a sensitivity of 90.5% and a specificity of 97.8%. Although the ACR classification remains the most widely applied for TA, a limitation of its diagnostic criteria is its failure to distinguish patients with early nonocclusive disease.23
In 1988, the Ishikawa classification criteria were developed, with a modified version subsequently published in 1996.23 Considered superior to the original Ishikawa and ACR criteria based on its application in 106 patients with angiographically proven TA, the modified version has a reported sensitivity and specificity of 92.5% and 95%, respectively.23
With the modified Ishikawa diagnostic criteria, the presence of two major or one major and two or four minor criteria suggests a high probability of TA. The three major criteria consist of lesions of the left mid-subclavian artery and the right mid-subclavian artery and characteristic signs and symptoms of at least 1 mo duration. The 10 minor criteria are high ESR (> 20 mm/h); carotid artery tenderness; hypertension; aortic regurgitation or annuloaortic ectasia; and lesions of pulmonary artery, left mid-common carotid, distal brachiocephalic trunk, descending thoracic aorta, abdominal aorta, and coronary artery.
The diagnosis of TA is based on recognition of clinical findings suggestive of large-vessel vasculitis. Imaging of the arterial tree with CT, MRI, or angiography also demonstrates findings consistent with TA, typically including early-onset vascular wall thickening/enhancement.24 Late imaging studies may reveal arterial stenoses, occlusions, and aneurysms.
Several types of imaging modalities have been used in the diagnosis and management of TA, each with strengths and limitations. Traditional angiography is invasive and requires an arterial puncture. Large doses of radiation are used, exposing the patient to iodinated contrast material, which may be dangerous in patients with poor renal function. However, the primary advantage of traditional angiography is that it allows for interventions such as stent placement and/or angioplasty to be performed.24 Findings on angiography often include long, smooth, tapered stenoses ranging from mild to severe or frank occlusions, as well as collateral vessels or the subclavian steal phenomenon.24
CT imaging is very useful for assessing thickening of the arterial wall. In early TA disease, evaluation of vessel wall thickness may be identified prior to frank stenosis of the artery(s).24 The spectrum of findings on CT angiography includes stenoses; occlusions; aneurysms; and concentric arterial wall thickening affecting the aorta and its branches, the pulmonary arteries, and occasionally the coronary arteries.24
MRI does not require the use of iodinated contrast, nor is there radiation exposure. MRI also has the advantage of evaluating arterial wall thickening, which is often present prior to stenosis (similar to CT imaging).24 Findings of TA on MRI include mural thrombi, signal alterations within and surrounding inflamed vessels, fusiform vascular dilation, thickened aortic valvular cusps, multifocal stenoses, and concentric thickening of the aortic wall.24
Laboratory testing is neither specific nor sensitive. Hoffman and Ahmed studied multiple serologic tests and found that no test reliably distinguishes between patients with active TA and healthy volunteers.25 Increases in the acute phase reactants (ESR and CRP) support the presence of an underlying inflammatory process, and these laboratory tests may be useful in disease monitoring. The ESR and CRP often do not correlate with systemic symptoms or disease progression but are used in conjunction with the clinical exam and serial imaging to gauge treatment success and to monitor disease progression.5,25 Biopsy material typically is not available in the initial diagnosis of TA, but histologic examination at the time of a surgery or procedure is often undertaken to confirm the diagnosis.5
The differential diagnosis of TA includes connective tissue diseases associated with the formation of multiple aneurysms, such as Marfan syndrome and Ehlers-Danlos syndrome.5 However, these diseases do not manifest with large vessel stenosis, the hallmark of TA. Infections known to cause aneurysms of the aorta should also be considered; these include bacterial, fungal, syphilitic, mycotic, and mycobacterial pathogens.5 Blood cultures are used to rule out bacterial agents. Rapid plasma reagin (RPR) and venereal disease research laboratory tests (VDRL) will identify a syphilitic etiology. Fungal cultures or fungal serology will help to rule out a mycotic pathogen.
Autoimmune diseases that can mimic TA include Behçet’s disease, Cogan syndrome, the spondyloarthropathies, and systemic lupus erythematosus. These diseases are not associated with stenosis of large vessels, which differentiates them from TA.5 Giant cell (temporal) arteritis (GCA) may present very similarly to TA, as both diseases affect large arteries.12 The table provides distinguishing features of TA and GCA.26
Continued on the next page >>
TREATMENT
Active phase TA is initially treated with high-dose glucocorticoid therapy (prednisone or methylprednisolone). Typical prednisone doses are 0.5 to 1 mg/kg/d.5 Clinical improvement is seen in almost all patients with glucocorticoid therapy,6,10,23 but relapse is common when prednisone is tapered to less than 20 mg/d.5 The corticosteroid dose is gradually tapered depending on patient response. Common side effects of corticosteroids may include weight gain, elevations in blood glucose, insomnia, increased infection risk, osteoporosis, and slowing of wound healing.
Because nearly half of all patients treated with glucocorticoids alone demonstrate chronic active disease, immunosuppressive therapies are almost always used concomitantly.27 Immune-suppressing drugs that may be used include methotrexate (15 to 25 mg/wk), azathioprine (2 mg/kg/d), and cyclophosphamide (1 to 2 mg/kg/d orally).5,28 Tumor necrosis factor (TNF)–blocking agents used to treat TA include etanercept, infliximab, or adalimumab.28,29 Adverse effects associated with immunosuppressive therapies and TNF-blocking agents include an increased risk for infection(s) and malignancy, bone marrow suppression, and hepatitis B reactivation. Although data are limited on anti-TNF agents, this class of drug has shown promise when used in conjunction with corticosteroids.28
In one open-label study by Hoffman and colleagues, remission rates with methotrexate plus steroids were 81%. Relapse occurred in 44% of study participants when the steroid dose was tapered or decreased to near discontinuation.27 More recently, in an uncontrolled study series involving 15 TA patients from India who were treated with azathioprine plus steroids, remission was achieved following 12 weeks of therapy. Angiographically, there was no progression of arterial disease after one year.30
Surgical and endovascular procedures used to return blood flow in stenotic or occluded vessels include synthetic or autologous vessel bypass, endarterectomy, and percutaneous transluminal angioplasty.5 When aortic insufficiency is present, aortic root replacement or repair is undertaken.5 These procedures are performed by vascular or cardiovascular surgeons and interventional radiologists. Rheumatologists are the medical specialists most involved in the direct care and management of TA patients. Cardiologists are sometimes consulted as well.
Continued on the next page >>
PROGNOSIS
Disability is common in TA. In a National Institutes of Health cohort study, 74% of TA patients reported experiencing functional effects from their disease, and 47% were fully disabled.2,8 In their retrospective review of 107 cases of TA, Lupi-Herrera and colleagues reported a 14% mortality rate.31 Half the deaths in this study were attributed to congestive heart failure (CHF). A cohort study in India that included 88 patients with TA reported cumulative 5- and 10-year survival rates of 91% and 84%, respectively. Of the 10 deaths in this cohort, four were due to CHF.2,32
CONCLUSION
Signs and symptoms of rheumatologic diseases such as TA are often vague, and diagnosis may prove difficult and elusive. Repeat office visits at short intervals may prove to be helpful in making the diagnosis. Referral for radiology and/or rheumatology consultation (face-to-face, if possible) is often necessary.
In cases such as this, completing a personal review of documents and test results done elsewhere, particularly ED/inpatient hospital data, is necessary; relying on the patient’s word that “they told me everything was fine” is insufficient. Clinicians should implement a system that works best for obtaining test results and other documents, follow their instincts, and if the correct diagnosis is not arrived at immediately, keep looking.
References >>
REFERENCES
1. Takayasu M. A case with peculiar changes of the retinal central vessels. Acta Soc Ophthalmol Jpn. 1908;12:554-555.
2. Maksimowicz-McKinnon K, Hoffman GS. Takayasu arteritis: what is the long-term prognosis? Rheum Dis Clin North Am. 2007;33:777-786.
3. Numano F. The story of Takayasu arteritis. Rheumatology. 2002;41:103-106.
4. Morgagni GB. De sedibus et causis morborum per anatomen indagatis.
(Letter 30).1761. Article 12.
5. Hernandez-Rodriguez J, Maksimowicz-McKinnon K, Hoffman GS. Takayasu’s arteritis. In: Carey WD, ed. Current Clinical Medicine. 2nd ed. Philadelphia: Saunders Elsevier; 2010:1195-1199.
6. Hall S, Barr W, Lie JT, et al. Takayasu arteritis. A study of 32 North American patients. Medicine (Baltimore). 1985;64:89-99.
7. Maksimowicz-McKinnon K, Clark TM, Hoffman GS. Limitations of therapy and a guarded prognosis in an American cohort of Takayasu arteritis patients. Arthritis Rheum. 2007;56:1000-1009.
8. Kerr GS, Hallahan CW, Giordano J, et al. Takayasu arteritis. Ann Intern Med. 1994:120:919-929.
9. Gornik HL, Creager MA. Aortic diseases: aortitis. Circulation. 2008;117:
3039-3051.
10. Mwipatayi BP, Jeffery PC, Beningfield SJ, et al. Takayasu arteritis: clinical features and management: report of 272 cases. ANZ J Surg. 2005;75:110-117.
11. Noris M. Pathogenesis of Takayasu’s arteritis. J Nephrol. 2001;14:506-513.
12. Hunder GG, Stone JH, Ramirez MP. Clinical features and diagnosis of Takayasu arteritis (2013). www.uptodate.com/contents/clinical-features-and-
diagnosis-of-takayasu-arteritis. Accessed March 24, 2014.
13. Nasu T. Takayasu’s truncoarteritis. Pulseless disease or aortitis syndrome. Acta Pathol Jpn. 1982;32 (suppl 1):117.
14. Johnston SL, Lock RJ, Gompels MM. Takayasu arteritis: a review. J Clin Pathol. 2002;55:481-486.
15. Vanoli M, Daina E, Salvarani C, et al. Takayasu’s arteritis: a study of 104 Italian patients. Arthritis Rheum. 2005;53:100-107.
16. Chun YS, Park SJ, Chung H, Lee J. The clinical and ocular manifestations of Takayasu’s arteritis. Retina. 2001;21:132-140.
17. Liu YQ, Jin BL, Ling J. Pulmonary artery involvement in aortoarteritis: an angiographic study. Cardiovasc Intervent Radiol. 1994;17:2-6.
18. Yamada I, Shibuya H, Matsubara O, et al. Pulmonary artery disease in Takayasu’s arteritis: angiographic findings. AJR Am J Roentgenol. 1992;159:
263-269.
19. Sharma S, Kamalakar T, Rajani M, et al. The incidence and patterns of pulmonary artery involvement in Takayasu’s arteritis. Clin Radiol. 1990;42:177-181.
20. He NS, Liu F, Wu EH, et al. Pulmonary artery involvement in aorto-arteritis: an analysis of DSA. Chin Med J (Engl). 1990;103:666-672.
21. Werfel T, Kuipers JG, Zeidler H, et al. Cutaneous manifestations of Takayasu arteritis. Acta Derm Venereol. 1996;76:496-497.
22. Arend WP, Michel BA, Bloch DA, et al. The American College of Rheumatology 1990 criteria for the classification of Takayasu arteritis. Arthritis Rheum. 1990;33:1129-1134.
23. Andrews J, Mason JC. Takayasu’s arteritis—recent advances in imaging offer promise. Rheumatology (Oxford). 2007;46:6-15.
24. Gotway MB, Araoz PA, Macedo TA, et al. Imaging findings in Takayasu’s arteritis. AJR Am J Roentgenol. 2005;184:1945-1950.
25. Hoffman GS, Ahmed AE. Surrogate markers of disease activity in patients with Takayasu arteritis. A preliminary report from The International Network for the Study of the Systemic Vasculitides (INSSYS). Int J Cardiol. 1998;66 (suppl 1):S191-S194.
26. Michel BA, Arend WP, Hunder GG. Clinical differentiation between giant cell (temporal) arteritis and Takayasu’s arteritis. J Rheumatol. 1996;23:106-111.
27. Hoffman GS, Leavitt RY, Kerr GS, et al. Treatment of glucocorticoid-resistant or relapsing Takayasu arteritis with methotrexate. Arthritis Rheum. 1994;37:578-582.
28. Hunder GG, Stone JH, Ramirez MP. Treatment of Takayasu arteritis (2013). www.uptodate.com/contents/treatment-of-takayasu-arteritis. Accessed March 24, 2014.
29. Schmidt J, Kerman TA, Bacani AK, et al. Tumor necrosis factor inhibitors in patients with Takayasu arteritis: experience from a referral center with long-term followup. Arthritis Care Res (Hoboken). 2012;64:1079-1083.
30. Valsakumar AK, Valappil UC, Jorapur V, et al. Role of immunosuppressive therapy on clinical, immunological, and angiographic outcome in active Takayasu’s arteritis. J Rheumatol. 2003;30:1793-1798.
31. Lupi-Herrera E, Sanchez-Torres G, Marcushamer J, et al. Takayasu’s arteritis: clinical study of 107 cases. Am Heart J. 1977;93:94-103.
32. Subramanyan R, Joy J, Balakrishnan KG. Natural history of aortoarteritis (Takayasu’s disease). Circulation. 1989;80:429-437.
A 37-year-old white man presented to his primary care provider’s office for follow-up after a visit to the emergency department (ED). He had been evaluated at a local ED a week earlier for atypical chest pain and left arm pain. At the ED, blood work was done, along with an ECG, chest x-ray, and chest CT scan, but the results of these evaluations were not available during his initial primary care visit. On discharge from the ED, he was told that his heart was not the cause of his pain and that he should follow up with his primary care provider.
In the office, the patient reported that for the past several months he had been experiencing pain in his left arm when doing heavy or continuous physical labor; he noted that his job as a laborer required vigorous activity. Rest seemed to make his pain go away. He denied pain in the right arm or being awakened by the pain at night. Review of systems was unremarkable, and medical and surgical history was negative.
On physical exam, inspection of his torso and upper and lower extremities did not reveal any apparent abnormalities. Left shoulder and neck exams were normal. Cardiac auscultation was unremarkable, but palpation of the left upper extremity revealed neither a brachial, radial, nor ulnar pulse. Pulses in his right upper extremity were within normal limits. No bruits were appreciated over the carotids or either subclavian artery. Basic Doppler ultrasound over the left upper extremity at the brachial, radial, and ulnar sites showed symmetrical Doppler sounds. The remainder of his exam was unremarkable.
The patient’s ED documents and imaging results were received later in the day, after his office visit. The ECG, blood work results, and chest x-ray were normal. The chest CT results showed no evidence of pulmonary embolism. The radiologist did note mild narrowing at the left subclavian artery secondary to nonspecific surrounding soft tissue, which was noted to possibly represent intramural hemorrhage or atherosclerotic changes. No intimal flap was identified.
Because the diagnosis remained unclear, the patient was asked to bring the disc containing his chest CT images to the office. The radiologist, who was informed about the patient’s history and exam findings by phone, reviewed the CT images and felt there were changes surrounding the three branches off the aortic arch suggestive of inflammation, in addition to the stenosis at the left subclavian artery (see Figure 1 and Figure 2).
Based on the radiologist’s interpretation, additional lab tests were ordered. A complete blood count, comprehensive metabolic panel, prothrombin time/partial thromboplastin time, and lipid panel all yielded results within normal limits. Erythrocyte sedimentation rate (ESR) was 12 mm/h (reference range, 0 to 15 mm/h) and C-reactive protein (CRP) level was 4.9 mg/dL (reference range, 0.1 to 4.9 mg/dL). These laboratory results were essentially unremarkable, and therefore made his diagnosis more elusive.
The patient was referred to a vascular surgeon because of his immediate symptoms. The surgeon performed a thoracic outlet study in which Doppler waveform analysis of the left brachial, radial, and ulnar arteries of the thoracic outlet were analyzed during range-of-motion testing. Results suggested the possibility of thoracic outlet syndrome involving the left upper extremity, with significant baseline arterial insufficiency. A CT angiogram showed critical stenosis of the left subclavian artery and arterial wall thickening. Inflammatory changes were noted as well, and concern for “an inflammatory vasculitis” was described on the CT angiogram. The patient underwent left carotid-to-axillary bypass grafting, after which his left arm pain improved.
Following surgery, the patient returned to the primary care office for evaluation. Although the surgery was successful, the diagnosis was still not clear, requiring additional medical evaluation. The physical exam showed normal pulses in his left upper extremity. Lab tests revealed an elevated ESR of 54 mm/h and a CRP level of 4 mg/dL (reference range, 0.1 to 0.8 mg/dL; a different lab testing site was used, which accounts for the different reference range). In light of the patient’s lab test results, premature arterial vascular disease, and imaging studies suggesting inflammation, Takayasu arteritis (TA) was arrived at as a working diagnosis.
The patient was referred to a rheumatologist, who ordered a repeat ESR and CRP, antineutrophil cytoplasmic antibodies, and a magnetic resonance angiography study of the right brachial artery and major aortic branches to rule out other types of arteritis. Based on the test results, the patient was diagnosed with TA. He was placed on high-dose corticosteroid therapy (prednisone 60 mg/d). Methotrexate 10 mg/wk po was added three months after initiation of the prednisone.
Since being diagnosed with TA, the patient has presented with complaints related to the adverse effects of high-dose corticosteroids (ie, insomnia, weight gain, elevated blood pressure).
Continued on the next page >>
DISCUSSION
The first description of TA is credited to Japanese ophthalmologist Mikito Takayasu, who in 1908 described a wreathlike arteriovenous anastomosis around the optic disc of a 21-year-old woman who had experienced acute vision loss.1-3 Much earlier, in 1761, Italian anatomist Giovanni Battista Morgagni described large-vessel aneurysms and stenosis on a postmortem exam of a 40-year-old woman.2,4 However, TA was not formally labeled a disease until 1975.
TA is a chronic large vessel vasculitis of unknown origin, mainly involving the aorta and its primary branches: the left common carotid, brachiocephalic, and left subclavian arteries. Ongoing inflammation of affected vessels causes fibrotic changes, stenosis, and eventual occlusion and may lead to aneurysm formation.5,6 TA is rare, with an annual incidence in North America of 2.6 cases per million population.6 It occurs most frequently in Asian countries but has been reported in a wide range of ethnic groups.5,7 TA has been characterized as a disease of young women: Between 80% and 97% of patients are women,6,8 and the average age at diagnosis is 25 to 30.8-10
The process of vascular injury in TA begins with inflammation in the vasa vasorum of the aortic vessels. This inflammation, thought to be triggered by an as-yet-unknown antigen, leads to an initial inflammatory cellular infiltration of the aortic media and adventitia; the infiltrate is comprised predominantly of macrophages and T cells.5,9 Inflammatory infiltration causes myointimal proliferation, thickening of the blood vessel wall, and eventual luminal stenosis.5 Cytokines, interleukin 6, interferon , and other chemokines released by infiltrating inflammatory cells within the injured tissue also contribute to the inflammatory response and tissue damage.5,11
Histologically, granulomatous inflammation and giant cells are found in the media.12,13 Destruction of the elastic lamina and the muscular media results in the aneurysmal dilation seen in TA, while dense scarring and continued inflammation of the arterial vasculature results in arterial stenosis.12
Continued on the next page >>
CLINICAL PRESENTATION
Presentation of TA varies widely and can range from asymptomatic disease identified by pulse deficits or impalpable pulses to severe neurologic impairment. The early or prepulseless phase of TA is characterized by inflammatory changes.14 Signs and symptoms are frequently vague and nonspecific, particularly in this early phase, when fatigue, weight loss, and low-grade fever may be seen.12 Headache is another common symptom at the time of disease onset.5
In the later or chronic phase of the disease, individuals will begin to demonstrate signs and symptoms of vascular insufficiency.14 More common physical signs reflect the underlying arterial occlusive disease and include diminished or absent arterial pulses, asymmetrical arm blood pressures, bruits, extremity claudication, and hypertension.5,9,10 Hypertension, generally reflecting renal artery stenosis,10 is present in approximately 40% of cases in the United States and Europe.5,7,15 Neurologic features secondary to hypertension or ischemia affect more than half of patients; in addition to headache, these may include dizziness, syncope, vertigo, transient ischemic attack, and stroke.5
TA can also present with eye, lung, and skin manifestations; however, these features are less common. Although ocular involvement, including amaurosis fugax, has been reported in up to 26% of patients in TA series,5,7,16 permanent loss of vision in North American patients is uncommon.5,7 Pulmonary involvement affecting the large- or medium-sized pulmonary arteries has been reported to occur in approximately 55% of cases5; however, there is uncertainty regarding the prevalence of angiographically demonstrated pulmonary artery involvement, as studies have reported rates ranging from 14.3% to 70%.9,17-20 Pulmonary involvement is often asymptomatic, but features can include dyspnea, cough, and chest pain.5 Skin lesions are seen in up to 28% of cases, most commonly erythema nodosum, erythema induratum, tuberculoidlike eruptions, pyoderma gangrenosum, and cutaneous signs of necrotizing or granulomatous vasculitis.5,21
Continued on the next page >>
DIAGNOSIS
The American College of Rheumatology (ACR) has developed classification criteria for the diagnosis of TA.22 The presence of three or more of the six criteria (age of onset ≤ 40, claudication of the extremities, decreased brachial artery pulse, > 10 mm Hg difference in systolic blood pressure between the arms, bruit over subclavian arteries or aorta, and arteriographic abnormalities) yields a sensitivity of 90.5% and a specificity of 97.8%. Although the ACR classification remains the most widely applied for TA, a limitation of its diagnostic criteria is its failure to distinguish patients with early nonocclusive disease.23
In 1988, the Ishikawa classification criteria were developed, with a modified version subsequently published in 1996.23 Considered superior to the original Ishikawa and ACR criteria based on its application in 106 patients with angiographically proven TA, the modified version has a reported sensitivity and specificity of 92.5% and 95%, respectively.23
With the modified Ishikawa diagnostic criteria, the presence of two major or one major and two or four minor criteria suggests a high probability of TA. The three major criteria consist of lesions of the left mid-subclavian artery and the right mid-subclavian artery and characteristic signs and symptoms of at least 1 mo duration. The 10 minor criteria are high ESR (> 20 mm/h); carotid artery tenderness; hypertension; aortic regurgitation or annuloaortic ectasia; and lesions of pulmonary artery, left mid-common carotid, distal brachiocephalic trunk, descending thoracic aorta, abdominal aorta, and coronary artery.
The diagnosis of TA is based on recognition of clinical findings suggestive of large-vessel vasculitis. Imaging of the arterial tree with CT, MRI, or angiography also demonstrates findings consistent with TA, typically including early-onset vascular wall thickening/enhancement.24 Late imaging studies may reveal arterial stenoses, occlusions, and aneurysms.
Several types of imaging modalities have been used in the diagnosis and management of TA, each with strengths and limitations. Traditional angiography is invasive and requires an arterial puncture. Large doses of radiation are used, exposing the patient to iodinated contrast material, which may be dangerous in patients with poor renal function. However, the primary advantage of traditional angiography is that it allows for interventions such as stent placement and/or angioplasty to be performed.24 Findings on angiography often include long, smooth, tapered stenoses ranging from mild to severe or frank occlusions, as well as collateral vessels or the subclavian steal phenomenon.24
CT imaging is very useful for assessing thickening of the arterial wall. In early TA disease, evaluation of vessel wall thickness may be identified prior to frank stenosis of the artery(s).24 The spectrum of findings on CT angiography includes stenoses; occlusions; aneurysms; and concentric arterial wall thickening affecting the aorta and its branches, the pulmonary arteries, and occasionally the coronary arteries.24
MRI does not require the use of iodinated contrast, nor is there radiation exposure. MRI also has the advantage of evaluating arterial wall thickening, which is often present prior to stenosis (similar to CT imaging).24 Findings of TA on MRI include mural thrombi, signal alterations within and surrounding inflamed vessels, fusiform vascular dilation, thickened aortic valvular cusps, multifocal stenoses, and concentric thickening of the aortic wall.24
Laboratory testing is neither specific nor sensitive. Hoffman and Ahmed studied multiple serologic tests and found that no test reliably distinguishes between patients with active TA and healthy volunteers.25 Increases in the acute phase reactants (ESR and CRP) support the presence of an underlying inflammatory process, and these laboratory tests may be useful in disease monitoring. The ESR and CRP often do not correlate with systemic symptoms or disease progression but are used in conjunction with the clinical exam and serial imaging to gauge treatment success and to monitor disease progression.5,25 Biopsy material typically is not available in the initial diagnosis of TA, but histologic examination at the time of a surgery or procedure is often undertaken to confirm the diagnosis.5
The differential diagnosis of TA includes connective tissue diseases associated with the formation of multiple aneurysms, such as Marfan syndrome and Ehlers-Danlos syndrome.5 However, these diseases do not manifest with large vessel stenosis, the hallmark of TA. Infections known to cause aneurysms of the aorta should also be considered; these include bacterial, fungal, syphilitic, mycotic, and mycobacterial pathogens.5 Blood cultures are used to rule out bacterial agents. Rapid plasma reagin (RPR) and venereal disease research laboratory tests (VDRL) will identify a syphilitic etiology. Fungal cultures or fungal serology will help to rule out a mycotic pathogen.
Autoimmune diseases that can mimic TA include Behçet’s disease, Cogan syndrome, the spondyloarthropathies, and systemic lupus erythematosus. These diseases are not associated with stenosis of large vessels, which differentiates them from TA.5 Giant cell (temporal) arteritis (GCA) may present very similarly to TA, as both diseases affect large arteries.12 The table provides distinguishing features of TA and GCA.26
Continued on the next page >>
TREATMENT
Active phase TA is initially treated with high-dose glucocorticoid therapy (prednisone or methylprednisolone). Typical prednisone doses are 0.5 to 1 mg/kg/d.5 Clinical improvement is seen in almost all patients with glucocorticoid therapy,6,10,23 but relapse is common when prednisone is tapered to less than 20 mg/d.5 The corticosteroid dose is gradually tapered depending on patient response. Common side effects of corticosteroids may include weight gain, elevations in blood glucose, insomnia, increased infection risk, osteoporosis, and slowing of wound healing.
Because nearly half of all patients treated with glucocorticoids alone demonstrate chronic active disease, immunosuppressive therapies are almost always used concomitantly.27 Immune-suppressing drugs that may be used include methotrexate (15 to 25 mg/wk), azathioprine (2 mg/kg/d), and cyclophosphamide (1 to 2 mg/kg/d orally).5,28 Tumor necrosis factor (TNF)–blocking agents used to treat TA include etanercept, infliximab, or adalimumab.28,29 Adverse effects associated with immunosuppressive therapies and TNF-blocking agents include an increased risk for infection(s) and malignancy, bone marrow suppression, and hepatitis B reactivation. Although data are limited on anti-TNF agents, this class of drug has shown promise when used in conjunction with corticosteroids.28
In one open-label study by Hoffman and colleagues, remission rates with methotrexate plus steroids were 81%. Relapse occurred in 44% of study participants when the steroid dose was tapered or decreased to near discontinuation.27 More recently, in an uncontrolled study series involving 15 TA patients from India who were treated with azathioprine plus steroids, remission was achieved following 12 weeks of therapy. Angiographically, there was no progression of arterial disease after one year.30
Surgical and endovascular procedures used to return blood flow in stenotic or occluded vessels include synthetic or autologous vessel bypass, endarterectomy, and percutaneous transluminal angioplasty.5 When aortic insufficiency is present, aortic root replacement or repair is undertaken.5 These procedures are performed by vascular or cardiovascular surgeons and interventional radiologists. Rheumatologists are the medical specialists most involved in the direct care and management of TA patients. Cardiologists are sometimes consulted as well.
Continued on the next page >>
PROGNOSIS
Disability is common in TA. In a National Institutes of Health cohort study, 74% of TA patients reported experiencing functional effects from their disease, and 47% were fully disabled.2,8 In their retrospective review of 107 cases of TA, Lupi-Herrera and colleagues reported a 14% mortality rate.31 Half the deaths in this study were attributed to congestive heart failure (CHF). A cohort study in India that included 88 patients with TA reported cumulative 5- and 10-year survival rates of 91% and 84%, respectively. Of the 10 deaths in this cohort, four were due to CHF.2,32
CONCLUSION
Signs and symptoms of rheumatologic diseases such as TA are often vague, and diagnosis may prove difficult and elusive. Repeat office visits at short intervals may prove to be helpful in making the diagnosis. Referral for radiology and/or rheumatology consultation (face-to-face, if possible) is often necessary.
In cases such as this, completing a personal review of documents and test results done elsewhere, particularly ED/inpatient hospital data, is necessary; relying on the patient’s word that “they told me everything was fine” is insufficient. Clinicians should implement a system that works best for obtaining test results and other documents, follow their instincts, and if the correct diagnosis is not arrived at immediately, keep looking.
References >>
REFERENCES
1. Takayasu M. A case with peculiar changes of the retinal central vessels. Acta Soc Ophthalmol Jpn. 1908;12:554-555.
2. Maksimowicz-McKinnon K, Hoffman GS. Takayasu arteritis: what is the long-term prognosis? Rheum Dis Clin North Am. 2007;33:777-786.
3. Numano F. The story of Takayasu arteritis. Rheumatology. 2002;41:103-106.
4. Morgagni GB. De sedibus et causis morborum per anatomen indagatis.
(Letter 30).1761. Article 12.
5. Hernandez-Rodriguez J, Maksimowicz-McKinnon K, Hoffman GS. Takayasu’s arteritis. In: Carey WD, ed. Current Clinical Medicine. 2nd ed. Philadelphia: Saunders Elsevier; 2010:1195-1199.
6. Hall S, Barr W, Lie JT, et al. Takayasu arteritis. A study of 32 North American patients. Medicine (Baltimore). 1985;64:89-99.
7. Maksimowicz-McKinnon K, Clark TM, Hoffman GS. Limitations of therapy and a guarded prognosis in an American cohort of Takayasu arteritis patients. Arthritis Rheum. 2007;56:1000-1009.
8. Kerr GS, Hallahan CW, Giordano J, et al. Takayasu arteritis. Ann Intern Med. 1994:120:919-929.
9. Gornik HL, Creager MA. Aortic diseases: aortitis. Circulation. 2008;117:
3039-3051.
10. Mwipatayi BP, Jeffery PC, Beningfield SJ, et al. Takayasu arteritis: clinical features and management: report of 272 cases. ANZ J Surg. 2005;75:110-117.
11. Noris M. Pathogenesis of Takayasu’s arteritis. J Nephrol. 2001;14:506-513.
12. Hunder GG, Stone JH, Ramirez MP. Clinical features and diagnosis of Takayasu arteritis (2013). www.uptodate.com/contents/clinical-features-and-
diagnosis-of-takayasu-arteritis. Accessed March 24, 2014.
13. Nasu T. Takayasu’s truncoarteritis. Pulseless disease or aortitis syndrome. Acta Pathol Jpn. 1982;32 (suppl 1):117.
14. Johnston SL, Lock RJ, Gompels MM. Takayasu arteritis: a review. J Clin Pathol. 2002;55:481-486.
15. Vanoli M, Daina E, Salvarani C, et al. Takayasu’s arteritis: a study of 104 Italian patients. Arthritis Rheum. 2005;53:100-107.
16. Chun YS, Park SJ, Chung H, Lee J. The clinical and ocular manifestations of Takayasu’s arteritis. Retina. 2001;21:132-140.
17. Liu YQ, Jin BL, Ling J. Pulmonary artery involvement in aortoarteritis: an angiographic study. Cardiovasc Intervent Radiol. 1994;17:2-6.
18. Yamada I, Shibuya H, Matsubara O, et al. Pulmonary artery disease in Takayasu’s arteritis: angiographic findings. AJR Am J Roentgenol. 1992;159:
263-269.
19. Sharma S, Kamalakar T, Rajani M, et al. The incidence and patterns of pulmonary artery involvement in Takayasu’s arteritis. Clin Radiol. 1990;42:177-181.
20. He NS, Liu F, Wu EH, et al. Pulmonary artery involvement in aorto-arteritis: an analysis of DSA. Chin Med J (Engl). 1990;103:666-672.
21. Werfel T, Kuipers JG, Zeidler H, et al. Cutaneous manifestations of Takayasu arteritis. Acta Derm Venereol. 1996;76:496-497.
22. Arend WP, Michel BA, Bloch DA, et al. The American College of Rheumatology 1990 criteria for the classification of Takayasu arteritis. Arthritis Rheum. 1990;33:1129-1134.
23. Andrews J, Mason JC. Takayasu’s arteritis—recent advances in imaging offer promise. Rheumatology (Oxford). 2007;46:6-15.
24. Gotway MB, Araoz PA, Macedo TA, et al. Imaging findings in Takayasu’s arteritis. AJR Am J Roentgenol. 2005;184:1945-1950.
25. Hoffman GS, Ahmed AE. Surrogate markers of disease activity in patients with Takayasu arteritis. A preliminary report from The International Network for the Study of the Systemic Vasculitides (INSSYS). Int J Cardiol. 1998;66 (suppl 1):S191-S194.
26. Michel BA, Arend WP, Hunder GG. Clinical differentiation between giant cell (temporal) arteritis and Takayasu’s arteritis. J Rheumatol. 1996;23:106-111.
27. Hoffman GS, Leavitt RY, Kerr GS, et al. Treatment of glucocorticoid-resistant or relapsing Takayasu arteritis with methotrexate. Arthritis Rheum. 1994;37:578-582.
28. Hunder GG, Stone JH, Ramirez MP. Treatment of Takayasu arteritis (2013). www.uptodate.com/contents/treatment-of-takayasu-arteritis. Accessed March 24, 2014.
29. Schmidt J, Kerman TA, Bacani AK, et al. Tumor necrosis factor inhibitors in patients with Takayasu arteritis: experience from a referral center with long-term followup. Arthritis Care Res (Hoboken). 2012;64:1079-1083.
30. Valsakumar AK, Valappil UC, Jorapur V, et al. Role of immunosuppressive therapy on clinical, immunological, and angiographic outcome in active Takayasu’s arteritis. J Rheumatol. 2003;30:1793-1798.
31. Lupi-Herrera E, Sanchez-Torres G, Marcushamer J, et al. Takayasu’s arteritis: clinical study of 107 cases. Am Heart J. 1977;93:94-103.
32. Subramanyan R, Joy J, Balakrishnan KG. Natural history of aortoarteritis (Takayasu’s disease). Circulation. 1989;80:429-437.

Does screening mammography save lives?
When 25-year follow-up data from the Canadian National Breast Screening Study—published earlier this year—showed no benefit for annual mammography in women aged 40 to 59 years, the findings generated renewed debate about whether screening mammography actually saves lives.1
In that study, Miller and colleagues continued their follow-up of almost 90,000 women who had been randomly assigned to mammography (five annual screens) or no mammography from 1980 to 1985. Women aged 40 to 49 in the mammography arm and all women aged 50 to 69 underwent annual clinical breast examination (CBE). Women aged 40 to 49 in the control arm had a single CBE and continued usual care in the community. The main outcome measure was death from breast cancer.1
During the entire 25-year study, 3,250 women in the mammography arm were given a diagnosis of breast cancer, and 3,133 in the control arm received the same diagnosis. Of these, 500 and 505 women, respectively, died of the malignancy.
The overall hazard ratio for death from breast cancer in the mammography and control arms was 0.99 (95% confidence interval, 0.88–1.12). After 15 years of follow-up, 106 residual excess cancers (106/484; or 22%) were identified in the mammography arm and were attributed to “overdiagnosis.”1
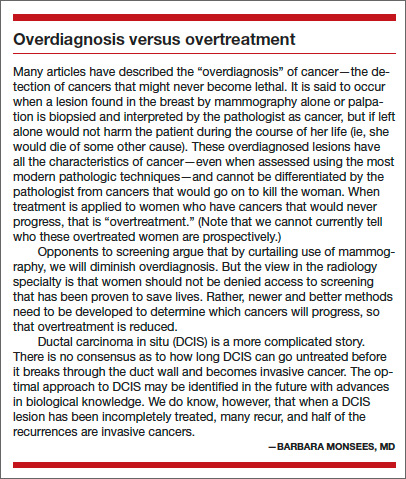
During the screening period the mean size of breast cancers identified was 1.91 cm and 2.10 cm in the mammography and control arms, respectively (P = .01), and 30.6% and 32.4% of tumors, respectively, were associated with positive lymph nodes (P = .53).
PROFESSIONAL SOCIETIES STICK BY THEIR GUIDELINES
Following publication of the Canadian findings, the American College of Obstetricians and Gynecologists (ACOG) reaffirmed its recommendation for women at average risk for breast cancer to initiate annual screening at age 40. In an announcement issued February 14, 2014, ACOG noted that it had “a number of concerns” with the Canadian study.2
Similarly, the American Cancer Society reiterated its own recommendation that women aged 40 and older undergo annual mammography and CBE for as long as they remain healthy.3
The American College of Radiology went a few steps further, calling the Canadian study “incredibly flawed and misleading.”4 Its guidelines call for annual mammography beginning at age 40.
The US Preventive Services Task Force (USPSTF) 2009 guidelines on breast cancer screening also stand, with biennial mammography beginning at age 50 for women at average risk for breast cancer.5
The Canadian Cancer Society also reaffirmed its recommendations for breast cancer screening following publication of the Canadian trial 25-year follow-up data—although its recommendations call for screening to begin at age 50 and to be repeated thereafter at 2- to 3-year intervals.6,7
In short, nothing has changed…yet. But the Canadian trial raises a number of questions about breast cancer screening—and the answers aren’t as clear-cut as you might imagine.
IS THE CANADIAN TRIAL CREDIBLE?
Results from earlier randomized, controlled trials have indicated that screening mammography reduces death from breast cancer.
“The Canadian study is an outlier,” says Barbara Monsees, MD, Ronald and Hanna Evens Professor of Women’s Health in the department of radiology at Washington University in St. Louis, Missouri.
“There is an overwhelming amount of evidence that tells us that screening mammography saves lives,” says Dr. Monsees. “This evidence includes other randomized trials, case-control studies, results of organized screening programs, and downward trends in breast cancer deaths where screening is used.”
Mark D. Pearlman, MD, also believes the body of evidence shows that screening mammography is effective. Dr. Pearlman is vice chair and service chief in the division of obstetrics and gynecology and professor of surgery and director of the breast fellowship in obstetrics and gynecology at the University of Michigan Health System in Ann Arbor, Michigan. He has been on the surgical staff of the Breast Care Center there since 1990, with expertise in the management of women with breast disease and increased genetic risks for breast and ovarian cancer.
The Canadian trial is “a reasonably done study,” he says, “but there are some concerns. First, it’s not a new study—it was initially published 22 years ago. This latest publication is just a continuation of following these women.”
“This study, along with seven other randomized, controlled trials, was considered by the USPSTF in formulating its 2009 recommendations. In that meta-analysis, which included women in their 40s, screening mammography had benefit in every decade of life of interest.8 That is the basis on which ACOG made its recommendation for women at average risk to start annual screening at age 40 and continue at least until age 70,” Dr. Pearlman says. “When the USPSTF considered this negative study, it realized that there is benefit for mammography despite this single trial.”
Related article: Which women are most likely to die from breast cancer—those screened annually starting at age 40, biennially starting at age 50, or not at all? Mark D. Pearlman, MD (Examining the Evidence, November 2013)
James Dickinson, MBBS, PhD, a family physician and member of the Canadian Task Force on Preventive Health Care (a forerunner of the USPSTF), which has published its own set of guidelines on breast cancer screening, has a different perspective. Dr. Dickinson teaches at the University of Calgary in Alberta.
“One of the tendencies—particularly in medicine driven by commercial interests—is that as soon as there is even the slightest hint that something is worthwhile, there’s a rush to have everybody do it and make lots of profit from it. People don’t wait for the evidence. They jump to assume guilt or innocence without even looking for the evidence.”
“I give all credit to the Canadian trial investigators,” Dr. Dickinson says. “The world had jumped ahead of them and just assumed that breast screening worked. But they kept looking. They set up a good trial to start with and then followed it through and helped us understand that things aren’t as good as we would like them to be.”
Andrew M. Kaunitz, MD, professor and vice chair of obstetrics and gynecology at the University of Florida–Jacksonville also believes that the Canadian study’s findings are reliable. Dr. Kaunitz serves on the OBG Management Board of Editors.
“As pointed out in an editorial accompanying the Canadian trial, this study’s findings of a lack of efficacy of screening mammograms are ‘strikingly similar’ to other recent studies assessing breast cancer screening.”9–11
“Further, mammograms are costly and associated with a high rate of false-positive findings,” Dr. Kaunitz says.
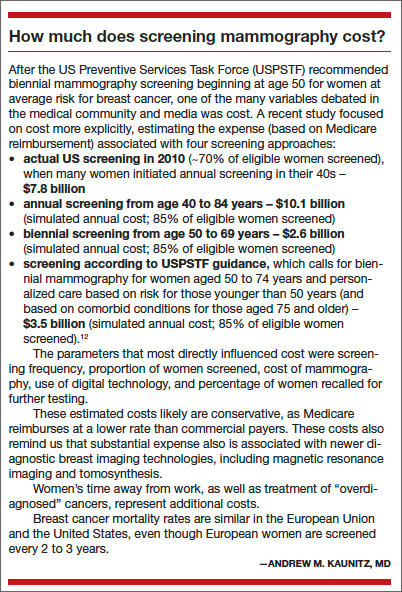
“Too many weak links”
Among the main criticisms of the Canadian trial is a claim of flawed methodology.
“The Canadian trial is an update of a flawed study that was previously discredited for good reasons,” says Dr. Monsees. “In short, the quality of the mammograms was poor, and the overall study design did not reflect a true randomization process.”
“For example, true randomization requires eligible patients to be randomly divided into two or more groups, without any knowledge of their specific conditions that might bias trial results,” Dr. Monsees explains. “In the most valid randomized trials, this was accomplished by invitation. Without knowing anything about the women, investigators randomly assigned them to a group invited to be screened and a group not invited. In this manner, two equal groups were produced, with no way to corrupt the randomization process.”
“In the Canadian National Breast Screening Study, in contrast, once the women volunteered, they were given a clinical breast examination, and women with breast lumps and large lymph nodes in their underarms were identified. This information was provided to study coordinators, who assigned women on open lists to the mammography group or the control group,” Dr. Monsees says.
“Those of us in the imaging field know that the quality of mammography is only as good as the weakest link in the imaging chain. This study had far too many weak links. These criticisms are not new; they were raised during and after the trial and remain valid today.”
Dr. Pearlman does not believe that the Canadian trial reflects modern breast cancer screening.
“There are things in the Canadian trial that differ from what we see in modern mammography,” he says. “In the Canadian trial, in women diagnosed with breast cancer, they noted whether there was a palpable mass in the area of cancer. In the Canadian trial the percentage of palpable masses was approximately 66%, and that’s very very different from what we see with modern mammography. In current practice, about 15% of breast cancers diagnosed by mammography are palpable. And so it appears that, for some reason, they were seeing more advanced breast cancers when they were screening by mammography.”
Another concern focuses on the technology used in the trial.
“It appears that the Canadian investigators pulled old machines into service for the trial,” Dr. Pearlman says.
In addition, more recent advances, such as digital mammography and tomosynthesis, were not available at the time of the Canadian trial.
“Overall, the Canadian trial appears to be looking at a different group of women than what we typically see in the United States in women diagnosed with breast cancer,” says Dr. Pearlman. “And if they were, then it makes sense that there would be no benefit in mortality, since they were detecting more advanced breast cancers in that population.”
Dr. Pearlman also points to other studies of screening mammography that have produced findings contrasting those of the Canadian trial.
“At least eight large observational trials, case-control studies, and randomized, controlled trials of screening mammography have been published and were later evaluated by meta-analysis.8 That analysis showed a 50% reduction in mortality in women who had screening mammography. In both randomized, controlled trials, it showed a decrease of about 15% in mortality. In practice, looking at large populations of women who died of breast cancer and comparing them to women who had breast cancer but didn’t die, there is a 50% increased likelihood of dying if you don’t have screening mammography. So looking in both directions—both prospectively and retrospectively—there appears to be a substantial benefit to undergoing routine screening mammography in reducing breast cancer mortality,” Dr. Pearlman says.
Dr. Dickinson asserts that criticisms of the Canadian National Breast Screening Study were disproved long ago.
“Many of those accusations were brought out very early in the course of the Canadian trial and investigated in great detail and rejected. After all, this trial was funded by a major research funding body in Canada. And when it was informed that it had funded a ‘fraudulent’ trial, it investigated and found that the findings actually were legitimate,” says Dr. Dickinson.
“I think that the people who are still bringing up those accusations are doing it primarily because the results don’t fit what they wanted. It’s attacking the messenger because they don’t like the results.”
WEIGHING BENEFITS AND HARMS
When the Canadian Task Force on Preventive Health Care formulated its guidelines on screening mammography, it considered the same body of evidence assessed by the USPSTF for its 2009 guidelines. Dr. Dickinson, a member of the Canadian Task Force, notes that the Canadian approach differed from the American approach in several distinct areas.
“We used the USPSTF literature search up to 2008 and then we did an updated search, looking for papers published up to that time. But there were no new trials published from 2008 to 2011,” he says.
“So we looked at the same data but used the GRADE scheme, which carefully separates the strength of the evidence from the strength of the recommendations. It’s a ‘newish’ way of evaluating evidence,” Dr. Dickinson says. “It’s different from the USPSTF approach, which involves a different scale.”
“We used to assess preventive measures purely on the basis of efficacy—if they worked, we’d recommend them. Now we look at the balance of benefits and the potential for causing harm. So it’s not just about whether an intervention works, but about whether it works more than it causes harm,” he says.
“That means that you can have statistically significant benefits that are fairly small and are outweighed by harms. So, while screening mammography can significantly reduce the risk of death from breast cancer by a small amount, our recommendation for it is very weak because, to achieve that benefit, you also incur a lot of harm,” Dr. Dickinson says.
Dr. Pearlman agrees that “mammography is not a perfect test, by any means.”
“It’s inconvenient, people get worried, it’s uncomfortable, and it isn’t perfectly sensitive,” he says. “It’s also somewhat nonspecific, which means that about 10% of women who don’t have breast cancer will be called back for additional images, and about 10% of that group will get called back for a biopsy that is not due to cancer.”
HOW WE COUNSEL OUR PATIENTS
Dr. Kaunitz says he is less likely to recommend annual mammography screening in the wake of the Canadian trial and other findings.
“For decades, we have marched to the drumbeat of ‘mammograms save lives,’” he says. “Annual screens have become an easy recommendation for us to make and, for our patients, the reassurance that accompanies a normal mammogram is comforting. Many patients will be perplexed by this new information; others may view it with suspicion. While we await updated guidance from professional societies, my approach is to encourage patients to follow the 2009 USPSTF guidelines, which recommend that screening start at age 50 in average-risk women and be repeated every 2 years.”
Related articles:
Biennial vs annual mammograpy: How I manage my patients Andrew M. Kaunitz, MD (Commentary, June 2013)
Best age to begin screening mammograms: How I manage my patients Andrew M. Kaunitz, MD (Commentary, November 2013)
Dr. Dickinson takes a similar approach. “I recommend that people be cautious about having screening, but I listen to their stories. Someone may say, ‘My sister had breast cancer and I want a mammogram.’ Overall, I don’t encourage people to undergo mammography unless they have a strong reason for doing so. I try to follow the latest [Canadian] guidelines because I feel they’re based on the best available evidence.”
In contrast, Dr. Pearlman advises his patients according to ACOG guidelines (guidelines that he formulated on ACOG’s behalf), which call for annual screening to begin at age 40.
Dr. Monsees counsels her patients similarly.
“The scientific evidence clearly shows that screening saves the most lives if average-risk women begin annual screening at the age of 40,” she says. “For high-risk women, our recommendations are tailored to each woman’s individual case and made in conjunction with the referring physician. For example, we often begin screening earlier or perform supplemental screening with breast magnetic resonance imaging for women who are at high risk due to prior chest wall radiation or a strong family history.”
“Others have argued against screening average-risk women in their 40s,” Dr. Monsees notes. “But if diagnosed with breast cancer, women in their 40s have more years of life to lose. More than 40% of the years of life lost to breast cancer are among women diagnosed in their 40s. Others also have argued that only high-risk women should be screened in their 40s or yearly after 50. However, that is problematic because more than 75% of women diagnosed with breast cancer each year are not at elevated risk. If you screen only high-risk women you will miss most breast cancers.”13–15
“Mammography screening has been proven to save lives,” Dr. Monsees says. “It can’t find every cancer, and it can’t find every cancer early enough to save all women. Nevertheless, screening should not be abandoned while we are awaiting better screening tests, better pathological markers to differentiate which tumors should be treated more aggressively, and the development of better therapies. The bottom line: Mammography saves lives now, and we should embrace it.”
Dr. Dickinson is more cautious.
“There isn’t a perfect answer,” he says. “That’s the sad thing.”
Related audiocast: Dr. JoAnn V. Pinkerton discusses how she screens patients at increased risk for breast cancer
ACOG's stance
Current ACOG guidelines recommend that annual screening mammography begin at age 40 for women at average risk for breast cancer. Women with an elevated risk of breast cancer require a more complex assessment and thorough counseling and may begin screening even before age 40 in some cases.
We want to hear from you!
Share your thoughts on this article or on any topic relevant to ObGyns and women’s health practitioners. Tell us which topics you’d like to see covered in future issues, and what challenges you face in daily practice. We will consider publishing your letter and in a future issue. Send your letter to: [email protected] Please include the city and state in which you practice. Stay in touch! Your feedback is important to us!
- Miller AB, Wall C, Baines CJ, Sun P, To T, Narod SA. Twenty-five year follow-up for breast cancer incidence and mortality of the Canadian National Breast Screening Study: randomised screening trial. BMJ. 2014;348:g366.
- ObGyns continue to recommend annual mammograms for women beginning at age 40. A look at the Canadian Trial Mammography Study. American College of Obstetricians and Gynecologists. https://www.acog.org/About_ACOG/News_Room/News_Releases/2011/Annual_Mammograms_Now_Recommended_for_Women_Beginning_at_Age_40. Published February 14, 2014. Accessed March 14, 2014.
- Simon S. Canadian study questions mammogram screening; findings unlike those of other studies. American Cancer Society. http://www.cancer.org/cancer/news/news/canadian -study-questions-mammogram-screening-findings-unlike-those-of-other-studies. Published February 12, 2014. Accessed March 14, 2014.
- BMJ article on breast cancer screening effectiveness incredibly flawed and misleading. American College of Radiology. http://www.acr.org/News-Publications/News/News-Articles/2014/ACR/BMJ-Article-on-Breast-Cancer-Screening-Effectiveness-Incredibly-Flawed-and-Misleading. Published February 12, 2014. Accessed March 14, 2014.
- US Preventive Services Task Force. Screening for breast cancer. http://www.uspreventiveservicestaskforce.org/uspstf /uspsbrca.htm. Published December 2009. Accessed March 14, 2014.
- Canadian Cancer Society’s perspective on new mammography study. Canadian Cancer Society. http://www.cancer.ca/en/about-us/for-media/media-releases/national/2014/mammography-study/?region=on. Published February 13, 2014. Accessed March 14, 2014.
- Canadian Task Force on Preventive Health Care. Recommendations on screening for breast cancer in average-risk women aged 40 to 74 years. CMAJ. 2011;183(17):1991–2001.
- Nickson C, Mason KE, English DR, Kavanagh AM. Mammographic screening and breast cancer mortality: a case-control study and meta-analysis. Cancer Epidemiol Biomarkers Prev. 2012;21(9):1479–1488.
- Kalager M, Adami H-O, Bretthauer M. Too much mammography. BMJ. 2014;348:g1403.
- Kalager M, Zelen M, Langmark F, Adami HO. Effect of screening mammography on breast cancer mortality in Norway. N Engl J Med. 2010;363(13):1203–1210.
- Autier P, Boniol M, Gavin A, Vatten LJ. Breast cancer mortality in neighbouring European countries with different levels of screening but similar access to treatment: trend analysis of WHO mortality database. BMJ. 2011;343:d4411.
- O’Donoghue C, Eklund M, Ozanne EM, Esserman LJ. Aggregate cost of mammography screening in the United States: comparison of current practice and advocated strategies. Ann Intern Med. 2014;160:145–153.
- American Cancer Society. What are the risk factors for breast cancer? January 31, 2014. http://www.cancer.org/cancer/breastcancer/detailedguide/breast-cancer-risk-factors. Accessed March 21, 2014.
- National Breast Cancer Coalition: The Breast Cancer Deadline 2020. Myth #8: Most women with breast cancer have a family history of the disease. http://www.breastcancerdeadline2020.org/breast-cancer-information/myths-and-truths/myth-8-most-women-with-bc-have-family-history.html. Accessed March 21, 2014.
- Berg WA. Benefits of screening mammography. JAMA. 2010;303(2):168–169.
- Woodworth KA. Breast imaging through the ages: a historical review and future outlook. eradimaging. September 6, 2011. http://www.eradimaging.com/site/article.cfm?ID=769#.UzAv79ySuMM. Accessed March 24, 2014.
When 25-year follow-up data from the Canadian National Breast Screening Study—published earlier this year—showed no benefit for annual mammography in women aged 40 to 59 years, the findings generated renewed debate about whether screening mammography actually saves lives.1
In that study, Miller and colleagues continued their follow-up of almost 90,000 women who had been randomly assigned to mammography (five annual screens) or no mammography from 1980 to 1985. Women aged 40 to 49 in the mammography arm and all women aged 50 to 69 underwent annual clinical breast examination (CBE). Women aged 40 to 49 in the control arm had a single CBE and continued usual care in the community. The main outcome measure was death from breast cancer.1
During the entire 25-year study, 3,250 women in the mammography arm were given a diagnosis of breast cancer, and 3,133 in the control arm received the same diagnosis. Of these, 500 and 505 women, respectively, died of the malignancy.
The overall hazard ratio for death from breast cancer in the mammography and control arms was 0.99 (95% confidence interval, 0.88–1.12). After 15 years of follow-up, 106 residual excess cancers (106/484; or 22%) were identified in the mammography arm and were attributed to “overdiagnosis.”1
During the screening period the mean size of breast cancers identified was 1.91 cm and 2.10 cm in the mammography and control arms, respectively (P = .01), and 30.6% and 32.4% of tumors, respectively, were associated with positive lymph nodes (P = .53).
PROFESSIONAL SOCIETIES STICK BY THEIR GUIDELINES
Following publication of the Canadian findings, the American College of Obstetricians and Gynecologists (ACOG) reaffirmed its recommendation for women at average risk for breast cancer to initiate annual screening at age 40. In an announcement issued February 14, 2014, ACOG noted that it had “a number of concerns” with the Canadian study.2
Similarly, the American Cancer Society reiterated its own recommendation that women aged 40 and older undergo annual mammography and CBE for as long as they remain healthy.3
The American College of Radiology went a few steps further, calling the Canadian study “incredibly flawed and misleading.”4 Its guidelines call for annual mammography beginning at age 40.
The US Preventive Services Task Force (USPSTF) 2009 guidelines on breast cancer screening also stand, with biennial mammography beginning at age 50 for women at average risk for breast cancer.5
The Canadian Cancer Society also reaffirmed its recommendations for breast cancer screening following publication of the Canadian trial 25-year follow-up data—although its recommendations call for screening to begin at age 50 and to be repeated thereafter at 2- to 3-year intervals.6,7
In short, nothing has changed…yet. But the Canadian trial raises a number of questions about breast cancer screening—and the answers aren’t as clear-cut as you might imagine.
IS THE CANADIAN TRIAL CREDIBLE?
Results from earlier randomized, controlled trials have indicated that screening mammography reduces death from breast cancer.
“The Canadian study is an outlier,” says Barbara Monsees, MD, Ronald and Hanna Evens Professor of Women’s Health in the department of radiology at Washington University in St. Louis, Missouri.
“There is an overwhelming amount of evidence that tells us that screening mammography saves lives,” says Dr. Monsees. “This evidence includes other randomized trials, case-control studies, results of organized screening programs, and downward trends in breast cancer deaths where screening is used.”
Mark D. Pearlman, MD, also believes the body of evidence shows that screening mammography is effective. Dr. Pearlman is vice chair and service chief in the division of obstetrics and gynecology and professor of surgery and director of the breast fellowship in obstetrics and gynecology at the University of Michigan Health System in Ann Arbor, Michigan. He has been on the surgical staff of the Breast Care Center there since 1990, with expertise in the management of women with breast disease and increased genetic risks for breast and ovarian cancer.
The Canadian trial is “a reasonably done study,” he says, “but there are some concerns. First, it’s not a new study—it was initially published 22 years ago. This latest publication is just a continuation of following these women.”
“This study, along with seven other randomized, controlled trials, was considered by the USPSTF in formulating its 2009 recommendations. In that meta-analysis, which included women in their 40s, screening mammography had benefit in every decade of life of interest.8 That is the basis on which ACOG made its recommendation for women at average risk to start annual screening at age 40 and continue at least until age 70,” Dr. Pearlman says. “When the USPSTF considered this negative study, it realized that there is benefit for mammography despite this single trial.”
Related article: Which women are most likely to die from breast cancer—those screened annually starting at age 40, biennially starting at age 50, or not at all? Mark D. Pearlman, MD (Examining the Evidence, November 2013)
James Dickinson, MBBS, PhD, a family physician and member of the Canadian Task Force on Preventive Health Care (a forerunner of the USPSTF), which has published its own set of guidelines on breast cancer screening, has a different perspective. Dr. Dickinson teaches at the University of Calgary in Alberta.
“One of the tendencies—particularly in medicine driven by commercial interests—is that as soon as there is even the slightest hint that something is worthwhile, there’s a rush to have everybody do it and make lots of profit from it. People don’t wait for the evidence. They jump to assume guilt or innocence without even looking for the evidence.”
“I give all credit to the Canadian trial investigators,” Dr. Dickinson says. “The world had jumped ahead of them and just assumed that breast screening worked. But they kept looking. They set up a good trial to start with and then followed it through and helped us understand that things aren’t as good as we would like them to be.”
Andrew M. Kaunitz, MD, professor and vice chair of obstetrics and gynecology at the University of Florida–Jacksonville also believes that the Canadian study’s findings are reliable. Dr. Kaunitz serves on the OBG Management Board of Editors.
“As pointed out in an editorial accompanying the Canadian trial, this study’s findings of a lack of efficacy of screening mammograms are ‘strikingly similar’ to other recent studies assessing breast cancer screening.”9–11
“Further, mammograms are costly and associated with a high rate of false-positive findings,” Dr. Kaunitz says.
“Too many weak links”
Among the main criticisms of the Canadian trial is a claim of flawed methodology.
“The Canadian trial is an update of a flawed study that was previously discredited for good reasons,” says Dr. Monsees. “In short, the quality of the mammograms was poor, and the overall study design did not reflect a true randomization process.”
“For example, true randomization requires eligible patients to be randomly divided into two or more groups, without any knowledge of their specific conditions that might bias trial results,” Dr. Monsees explains. “In the most valid randomized trials, this was accomplished by invitation. Without knowing anything about the women, investigators randomly assigned them to a group invited to be screened and a group not invited. In this manner, two equal groups were produced, with no way to corrupt the randomization process.”
“In the Canadian National Breast Screening Study, in contrast, once the women volunteered, they were given a clinical breast examination, and women with breast lumps and large lymph nodes in their underarms were identified. This information was provided to study coordinators, who assigned women on open lists to the mammography group or the control group,” Dr. Monsees says.
“Those of us in the imaging field know that the quality of mammography is only as good as the weakest link in the imaging chain. This study had far too many weak links. These criticisms are not new; they were raised during and after the trial and remain valid today.”
Dr. Pearlman does not believe that the Canadian trial reflects modern breast cancer screening.
“There are things in the Canadian trial that differ from what we see in modern mammography,” he says. “In the Canadian trial, in women diagnosed with breast cancer, they noted whether there was a palpable mass in the area of cancer. In the Canadian trial the percentage of palpable masses was approximately 66%, and that’s very very different from what we see with modern mammography. In current practice, about 15% of breast cancers diagnosed by mammography are palpable. And so it appears that, for some reason, they were seeing more advanced breast cancers when they were screening by mammography.”
Another concern focuses on the technology used in the trial.
“It appears that the Canadian investigators pulled old machines into service for the trial,” Dr. Pearlman says.
In addition, more recent advances, such as digital mammography and tomosynthesis, were not available at the time of the Canadian trial.
“Overall, the Canadian trial appears to be looking at a different group of women than what we typically see in the United States in women diagnosed with breast cancer,” says Dr. Pearlman. “And if they were, then it makes sense that there would be no benefit in mortality, since they were detecting more advanced breast cancers in that population.”
Dr. Pearlman also points to other studies of screening mammography that have produced findings contrasting those of the Canadian trial.
“At least eight large observational trials, case-control studies, and randomized, controlled trials of screening mammography have been published and were later evaluated by meta-analysis.8 That analysis showed a 50% reduction in mortality in women who had screening mammography. In both randomized, controlled trials, it showed a decrease of about 15% in mortality. In practice, looking at large populations of women who died of breast cancer and comparing them to women who had breast cancer but didn’t die, there is a 50% increased likelihood of dying if you don’t have screening mammography. So looking in both directions—both prospectively and retrospectively—there appears to be a substantial benefit to undergoing routine screening mammography in reducing breast cancer mortality,” Dr. Pearlman says.
Dr. Dickinson asserts that criticisms of the Canadian National Breast Screening Study were disproved long ago.
“Many of those accusations were brought out very early in the course of the Canadian trial and investigated in great detail and rejected. After all, this trial was funded by a major research funding body in Canada. And when it was informed that it had funded a ‘fraudulent’ trial, it investigated and found that the findings actually were legitimate,” says Dr. Dickinson.
“I think that the people who are still bringing up those accusations are doing it primarily because the results don’t fit what they wanted. It’s attacking the messenger because they don’t like the results.”
WEIGHING BENEFITS AND HARMS
When the Canadian Task Force on Preventive Health Care formulated its guidelines on screening mammography, it considered the same body of evidence assessed by the USPSTF for its 2009 guidelines. Dr. Dickinson, a member of the Canadian Task Force, notes that the Canadian approach differed from the American approach in several distinct areas.
“We used the USPSTF literature search up to 2008 and then we did an updated search, looking for papers published up to that time. But there were no new trials published from 2008 to 2011,” he says.
“So we looked at the same data but used the GRADE scheme, which carefully separates the strength of the evidence from the strength of the recommendations. It’s a ‘newish’ way of evaluating evidence,” Dr. Dickinson says. “It’s different from the USPSTF approach, which involves a different scale.”
“We used to assess preventive measures purely on the basis of efficacy—if they worked, we’d recommend them. Now we look at the balance of benefits and the potential for causing harm. So it’s not just about whether an intervention works, but about whether it works more than it causes harm,” he says.
“That means that you can have statistically significant benefits that are fairly small and are outweighed by harms. So, while screening mammography can significantly reduce the risk of death from breast cancer by a small amount, our recommendation for it is very weak because, to achieve that benefit, you also incur a lot of harm,” Dr. Dickinson says.
Dr. Pearlman agrees that “mammography is not a perfect test, by any means.”
“It’s inconvenient, people get worried, it’s uncomfortable, and it isn’t perfectly sensitive,” he says. “It’s also somewhat nonspecific, which means that about 10% of women who don’t have breast cancer will be called back for additional images, and about 10% of that group will get called back for a biopsy that is not due to cancer.”
HOW WE COUNSEL OUR PATIENTS
Dr. Kaunitz says he is less likely to recommend annual mammography screening in the wake of the Canadian trial and other findings.
“For decades, we have marched to the drumbeat of ‘mammograms save lives,’” he says. “Annual screens have become an easy recommendation for us to make and, for our patients, the reassurance that accompanies a normal mammogram is comforting. Many patients will be perplexed by this new information; others may view it with suspicion. While we await updated guidance from professional societies, my approach is to encourage patients to follow the 2009 USPSTF guidelines, which recommend that screening start at age 50 in average-risk women and be repeated every 2 years.”
Related articles:
Biennial vs annual mammograpy: How I manage my patients Andrew M. Kaunitz, MD (Commentary, June 2013)
Best age to begin screening mammograms: How I manage my patients Andrew M. Kaunitz, MD (Commentary, November 2013)
Dr. Dickinson takes a similar approach. “I recommend that people be cautious about having screening, but I listen to their stories. Someone may say, ‘My sister had breast cancer and I want a mammogram.’ Overall, I don’t encourage people to undergo mammography unless they have a strong reason for doing so. I try to follow the latest [Canadian] guidelines because I feel they’re based on the best available evidence.”
In contrast, Dr. Pearlman advises his patients according to ACOG guidelines (guidelines that he formulated on ACOG’s behalf), which call for annual screening to begin at age 40.
Dr. Monsees counsels her patients similarly.
“The scientific evidence clearly shows that screening saves the most lives if average-risk women begin annual screening at the age of 40,” she says. “For high-risk women, our recommendations are tailored to each woman’s individual case and made in conjunction with the referring physician. For example, we often begin screening earlier or perform supplemental screening with breast magnetic resonance imaging for women who are at high risk due to prior chest wall radiation or a strong family history.”
“Others have argued against screening average-risk women in their 40s,” Dr. Monsees notes. “But if diagnosed with breast cancer, women in their 40s have more years of life to lose. More than 40% of the years of life lost to breast cancer are among women diagnosed in their 40s. Others also have argued that only high-risk women should be screened in their 40s or yearly after 50. However, that is problematic because more than 75% of women diagnosed with breast cancer each year are not at elevated risk. If you screen only high-risk women you will miss most breast cancers.”13–15
“Mammography screening has been proven to save lives,” Dr. Monsees says. “It can’t find every cancer, and it can’t find every cancer early enough to save all women. Nevertheless, screening should not be abandoned while we are awaiting better screening tests, better pathological markers to differentiate which tumors should be treated more aggressively, and the development of better therapies. The bottom line: Mammography saves lives now, and we should embrace it.”
Dr. Dickinson is more cautious.
“There isn’t a perfect answer,” he says. “That’s the sad thing.”
Related audiocast: Dr. JoAnn V. Pinkerton discusses how she screens patients at increased risk for breast cancer
ACOG's stance
Current ACOG guidelines recommend that annual screening mammography begin at age 40 for women at average risk for breast cancer. Women with an elevated risk of breast cancer require a more complex assessment and thorough counseling and may begin screening even before age 40 in some cases.
We want to hear from you!
Share your thoughts on this article or on any topic relevant to ObGyns and women’s health practitioners. Tell us which topics you’d like to see covered in future issues, and what challenges you face in daily practice. We will consider publishing your letter and in a future issue. Send your letter to: [email protected] Please include the city and state in which you practice. Stay in touch! Your feedback is important to us!
When 25-year follow-up data from the Canadian National Breast Screening Study—published earlier this year—showed no benefit for annual mammography in women aged 40 to 59 years, the findings generated renewed debate about whether screening mammography actually saves lives.1
In that study, Miller and colleagues continued their follow-up of almost 90,000 women who had been randomly assigned to mammography (five annual screens) or no mammography from 1980 to 1985. Women aged 40 to 49 in the mammography arm and all women aged 50 to 69 underwent annual clinical breast examination (CBE). Women aged 40 to 49 in the control arm had a single CBE and continued usual care in the community. The main outcome measure was death from breast cancer.1
During the entire 25-year study, 3,250 women in the mammography arm were given a diagnosis of breast cancer, and 3,133 in the control arm received the same diagnosis. Of these, 500 and 505 women, respectively, died of the malignancy.
The overall hazard ratio for death from breast cancer in the mammography and control arms was 0.99 (95% confidence interval, 0.88–1.12). After 15 years of follow-up, 106 residual excess cancers (106/484; or 22%) were identified in the mammography arm and were attributed to “overdiagnosis.”1
During the screening period the mean size of breast cancers identified was 1.91 cm and 2.10 cm in the mammography and control arms, respectively (P = .01), and 30.6% and 32.4% of tumors, respectively, were associated with positive lymph nodes (P = .53).
PROFESSIONAL SOCIETIES STICK BY THEIR GUIDELINES
Following publication of the Canadian findings, the American College of Obstetricians and Gynecologists (ACOG) reaffirmed its recommendation for women at average risk for breast cancer to initiate annual screening at age 40. In an announcement issued February 14, 2014, ACOG noted that it had “a number of concerns” with the Canadian study.2
Similarly, the American Cancer Society reiterated its own recommendation that women aged 40 and older undergo annual mammography and CBE for as long as they remain healthy.3
The American College of Radiology went a few steps further, calling the Canadian study “incredibly flawed and misleading.”4 Its guidelines call for annual mammography beginning at age 40.
The US Preventive Services Task Force (USPSTF) 2009 guidelines on breast cancer screening also stand, with biennial mammography beginning at age 50 for women at average risk for breast cancer.5
The Canadian Cancer Society also reaffirmed its recommendations for breast cancer screening following publication of the Canadian trial 25-year follow-up data—although its recommendations call for screening to begin at age 50 and to be repeated thereafter at 2- to 3-year intervals.6,7
In short, nothing has changed…yet. But the Canadian trial raises a number of questions about breast cancer screening—and the answers aren’t as clear-cut as you might imagine.
IS THE CANADIAN TRIAL CREDIBLE?
Results from earlier randomized, controlled trials have indicated that screening mammography reduces death from breast cancer.
“The Canadian study is an outlier,” says Barbara Monsees, MD, Ronald and Hanna Evens Professor of Women’s Health in the department of radiology at Washington University in St. Louis, Missouri.
“There is an overwhelming amount of evidence that tells us that screening mammography saves lives,” says Dr. Monsees. “This evidence includes other randomized trials, case-control studies, results of organized screening programs, and downward trends in breast cancer deaths where screening is used.”
Mark D. Pearlman, MD, also believes the body of evidence shows that screening mammography is effective. Dr. Pearlman is vice chair and service chief in the division of obstetrics and gynecology and professor of surgery and director of the breast fellowship in obstetrics and gynecology at the University of Michigan Health System in Ann Arbor, Michigan. He has been on the surgical staff of the Breast Care Center there since 1990, with expertise in the management of women with breast disease and increased genetic risks for breast and ovarian cancer.
The Canadian trial is “a reasonably done study,” he says, “but there are some concerns. First, it’s not a new study—it was initially published 22 years ago. This latest publication is just a continuation of following these women.”
“This study, along with seven other randomized, controlled trials, was considered by the USPSTF in formulating its 2009 recommendations. In that meta-analysis, which included women in their 40s, screening mammography had benefit in every decade of life of interest.8 That is the basis on which ACOG made its recommendation for women at average risk to start annual screening at age 40 and continue at least until age 70,” Dr. Pearlman says. “When the USPSTF considered this negative study, it realized that there is benefit for mammography despite this single trial.”
Related article: Which women are most likely to die from breast cancer—those screened annually starting at age 40, biennially starting at age 50, or not at all? Mark D. Pearlman, MD (Examining the Evidence, November 2013)
James Dickinson, MBBS, PhD, a family physician and member of the Canadian Task Force on Preventive Health Care (a forerunner of the USPSTF), which has published its own set of guidelines on breast cancer screening, has a different perspective. Dr. Dickinson teaches at the University of Calgary in Alberta.
“One of the tendencies—particularly in medicine driven by commercial interests—is that as soon as there is even the slightest hint that something is worthwhile, there’s a rush to have everybody do it and make lots of profit from it. People don’t wait for the evidence. They jump to assume guilt or innocence without even looking for the evidence.”
“I give all credit to the Canadian trial investigators,” Dr. Dickinson says. “The world had jumped ahead of them and just assumed that breast screening worked. But they kept looking. They set up a good trial to start with and then followed it through and helped us understand that things aren’t as good as we would like them to be.”
Andrew M. Kaunitz, MD, professor and vice chair of obstetrics and gynecology at the University of Florida–Jacksonville also believes that the Canadian study’s findings are reliable. Dr. Kaunitz serves on the OBG Management Board of Editors.
“As pointed out in an editorial accompanying the Canadian trial, this study’s findings of a lack of efficacy of screening mammograms are ‘strikingly similar’ to other recent studies assessing breast cancer screening.”9–11
“Further, mammograms are costly and associated with a high rate of false-positive findings,” Dr. Kaunitz says.
“Too many weak links”
Among the main criticisms of the Canadian trial is a claim of flawed methodology.
“The Canadian trial is an update of a flawed study that was previously discredited for good reasons,” says Dr. Monsees. “In short, the quality of the mammograms was poor, and the overall study design did not reflect a true randomization process.”
“For example, true randomization requires eligible patients to be randomly divided into two or more groups, without any knowledge of their specific conditions that might bias trial results,” Dr. Monsees explains. “In the most valid randomized trials, this was accomplished by invitation. Without knowing anything about the women, investigators randomly assigned them to a group invited to be screened and a group not invited. In this manner, two equal groups were produced, with no way to corrupt the randomization process.”
“In the Canadian National Breast Screening Study, in contrast, once the women volunteered, they were given a clinical breast examination, and women with breast lumps and large lymph nodes in their underarms were identified. This information was provided to study coordinators, who assigned women on open lists to the mammography group or the control group,” Dr. Monsees says.
“Those of us in the imaging field know that the quality of mammography is only as good as the weakest link in the imaging chain. This study had far too many weak links. These criticisms are not new; they were raised during and after the trial and remain valid today.”
Dr. Pearlman does not believe that the Canadian trial reflects modern breast cancer screening.
“There are things in the Canadian trial that differ from what we see in modern mammography,” he says. “In the Canadian trial, in women diagnosed with breast cancer, they noted whether there was a palpable mass in the area of cancer. In the Canadian trial the percentage of palpable masses was approximately 66%, and that’s very very different from what we see with modern mammography. In current practice, about 15% of breast cancers diagnosed by mammography are palpable. And so it appears that, for some reason, they were seeing more advanced breast cancers when they were screening by mammography.”
Another concern focuses on the technology used in the trial.
“It appears that the Canadian investigators pulled old machines into service for the trial,” Dr. Pearlman says.
In addition, more recent advances, such as digital mammography and tomosynthesis, were not available at the time of the Canadian trial.
“Overall, the Canadian trial appears to be looking at a different group of women than what we typically see in the United States in women diagnosed with breast cancer,” says Dr. Pearlman. “And if they were, then it makes sense that there would be no benefit in mortality, since they were detecting more advanced breast cancers in that population.”
Dr. Pearlman also points to other studies of screening mammography that have produced findings contrasting those of the Canadian trial.
“At least eight large observational trials, case-control studies, and randomized, controlled trials of screening mammography have been published and were later evaluated by meta-analysis.8 That analysis showed a 50% reduction in mortality in women who had screening mammography. In both randomized, controlled trials, it showed a decrease of about 15% in mortality. In practice, looking at large populations of women who died of breast cancer and comparing them to women who had breast cancer but didn’t die, there is a 50% increased likelihood of dying if you don’t have screening mammography. So looking in both directions—both prospectively and retrospectively—there appears to be a substantial benefit to undergoing routine screening mammography in reducing breast cancer mortality,” Dr. Pearlman says.
Dr. Dickinson asserts that criticisms of the Canadian National Breast Screening Study were disproved long ago.
“Many of those accusations were brought out very early in the course of the Canadian trial and investigated in great detail and rejected. After all, this trial was funded by a major research funding body in Canada. And when it was informed that it had funded a ‘fraudulent’ trial, it investigated and found that the findings actually were legitimate,” says Dr. Dickinson.
“I think that the people who are still bringing up those accusations are doing it primarily because the results don’t fit what they wanted. It’s attacking the messenger because they don’t like the results.”
WEIGHING BENEFITS AND HARMS
When the Canadian Task Force on Preventive Health Care formulated its guidelines on screening mammography, it considered the same body of evidence assessed by the USPSTF for its 2009 guidelines. Dr. Dickinson, a member of the Canadian Task Force, notes that the Canadian approach differed from the American approach in several distinct areas.
“We used the USPSTF literature search up to 2008 and then we did an updated search, looking for papers published up to that time. But there were no new trials published from 2008 to 2011,” he says.
“So we looked at the same data but used the GRADE scheme, which carefully separates the strength of the evidence from the strength of the recommendations. It’s a ‘newish’ way of evaluating evidence,” Dr. Dickinson says. “It’s different from the USPSTF approach, which involves a different scale.”
“We used to assess preventive measures purely on the basis of efficacy—if they worked, we’d recommend them. Now we look at the balance of benefits and the potential for causing harm. So it’s not just about whether an intervention works, but about whether it works more than it causes harm,” he says.
“That means that you can have statistically significant benefits that are fairly small and are outweighed by harms. So, while screening mammography can significantly reduce the risk of death from breast cancer by a small amount, our recommendation for it is very weak because, to achieve that benefit, you also incur a lot of harm,” Dr. Dickinson says.
Dr. Pearlman agrees that “mammography is not a perfect test, by any means.”
“It’s inconvenient, people get worried, it’s uncomfortable, and it isn’t perfectly sensitive,” he says. “It’s also somewhat nonspecific, which means that about 10% of women who don’t have breast cancer will be called back for additional images, and about 10% of that group will get called back for a biopsy that is not due to cancer.”
HOW WE COUNSEL OUR PATIENTS
Dr. Kaunitz says he is less likely to recommend annual mammography screening in the wake of the Canadian trial and other findings.
“For decades, we have marched to the drumbeat of ‘mammograms save lives,’” he says. “Annual screens have become an easy recommendation for us to make and, for our patients, the reassurance that accompanies a normal mammogram is comforting. Many patients will be perplexed by this new information; others may view it with suspicion. While we await updated guidance from professional societies, my approach is to encourage patients to follow the 2009 USPSTF guidelines, which recommend that screening start at age 50 in average-risk women and be repeated every 2 years.”
Related articles:
Biennial vs annual mammograpy: How I manage my patients Andrew M. Kaunitz, MD (Commentary, June 2013)
Best age to begin screening mammograms: How I manage my patients Andrew M. Kaunitz, MD (Commentary, November 2013)
Dr. Dickinson takes a similar approach. “I recommend that people be cautious about having screening, but I listen to their stories. Someone may say, ‘My sister had breast cancer and I want a mammogram.’ Overall, I don’t encourage people to undergo mammography unless they have a strong reason for doing so. I try to follow the latest [Canadian] guidelines because I feel they’re based on the best available evidence.”
In contrast, Dr. Pearlman advises his patients according to ACOG guidelines (guidelines that he formulated on ACOG’s behalf), which call for annual screening to begin at age 40.
Dr. Monsees counsels her patients similarly.
“The scientific evidence clearly shows that screening saves the most lives if average-risk women begin annual screening at the age of 40,” she says. “For high-risk women, our recommendations are tailored to each woman’s individual case and made in conjunction with the referring physician. For example, we often begin screening earlier or perform supplemental screening with breast magnetic resonance imaging for women who are at high risk due to prior chest wall radiation or a strong family history.”
“Others have argued against screening average-risk women in their 40s,” Dr. Monsees notes. “But if diagnosed with breast cancer, women in their 40s have more years of life to lose. More than 40% of the years of life lost to breast cancer are among women diagnosed in their 40s. Others also have argued that only high-risk women should be screened in their 40s or yearly after 50. However, that is problematic because more than 75% of women diagnosed with breast cancer each year are not at elevated risk. If you screen only high-risk women you will miss most breast cancers.”13–15
“Mammography screening has been proven to save lives,” Dr. Monsees says. “It can’t find every cancer, and it can’t find every cancer early enough to save all women. Nevertheless, screening should not be abandoned while we are awaiting better screening tests, better pathological markers to differentiate which tumors should be treated more aggressively, and the development of better therapies. The bottom line: Mammography saves lives now, and we should embrace it.”
Dr. Dickinson is more cautious.
“There isn’t a perfect answer,” he says. “That’s the sad thing.”
Related audiocast: Dr. JoAnn V. Pinkerton discusses how she screens patients at increased risk for breast cancer
ACOG's stance
Current ACOG guidelines recommend that annual screening mammography begin at age 40 for women at average risk for breast cancer. Women with an elevated risk of breast cancer require a more complex assessment and thorough counseling and may begin screening even before age 40 in some cases.
We want to hear from you!
Share your thoughts on this article or on any topic relevant to ObGyns and women’s health practitioners. Tell us which topics you’d like to see covered in future issues, and what challenges you face in daily practice. We will consider publishing your letter and in a future issue. Send your letter to: [email protected] Please include the city and state in which you practice. Stay in touch! Your feedback is important to us!
- Miller AB, Wall C, Baines CJ, Sun P, To T, Narod SA. Twenty-five year follow-up for breast cancer incidence and mortality of the Canadian National Breast Screening Study: randomised screening trial. BMJ. 2014;348:g366.
- ObGyns continue to recommend annual mammograms for women beginning at age 40. A look at the Canadian Trial Mammography Study. American College of Obstetricians and Gynecologists. https://www.acog.org/About_ACOG/News_Room/News_Releases/2011/Annual_Mammograms_Now_Recommended_for_Women_Beginning_at_Age_40. Published February 14, 2014. Accessed March 14, 2014.
- Simon S. Canadian study questions mammogram screening; findings unlike those of other studies. American Cancer Society. http://www.cancer.org/cancer/news/news/canadian -study-questions-mammogram-screening-findings-unlike-those-of-other-studies. Published February 12, 2014. Accessed March 14, 2014.
- BMJ article on breast cancer screening effectiveness incredibly flawed and misleading. American College of Radiology. http://www.acr.org/News-Publications/News/News-Articles/2014/ACR/BMJ-Article-on-Breast-Cancer-Screening-Effectiveness-Incredibly-Flawed-and-Misleading. Published February 12, 2014. Accessed March 14, 2014.
- US Preventive Services Task Force. Screening for breast cancer. http://www.uspreventiveservicestaskforce.org/uspstf /uspsbrca.htm. Published December 2009. Accessed March 14, 2014.
- Canadian Cancer Society’s perspective on new mammography study. Canadian Cancer Society. http://www.cancer.ca/en/about-us/for-media/media-releases/national/2014/mammography-study/?region=on. Published February 13, 2014. Accessed March 14, 2014.
- Canadian Task Force on Preventive Health Care. Recommendations on screening for breast cancer in average-risk women aged 40 to 74 years. CMAJ. 2011;183(17):1991–2001.
- Nickson C, Mason KE, English DR, Kavanagh AM. Mammographic screening and breast cancer mortality: a case-control study and meta-analysis. Cancer Epidemiol Biomarkers Prev. 2012;21(9):1479–1488.
- Kalager M, Adami H-O, Bretthauer M. Too much mammography. BMJ. 2014;348:g1403.
- Kalager M, Zelen M, Langmark F, Adami HO. Effect of screening mammography on breast cancer mortality in Norway. N Engl J Med. 2010;363(13):1203–1210.
- Autier P, Boniol M, Gavin A, Vatten LJ. Breast cancer mortality in neighbouring European countries with different levels of screening but similar access to treatment: trend analysis of WHO mortality database. BMJ. 2011;343:d4411.
- O’Donoghue C, Eklund M, Ozanne EM, Esserman LJ. Aggregate cost of mammography screening in the United States: comparison of current practice and advocated strategies. Ann Intern Med. 2014;160:145–153.
- American Cancer Society. What are the risk factors for breast cancer? January 31, 2014. http://www.cancer.org/cancer/breastcancer/detailedguide/breast-cancer-risk-factors. Accessed March 21, 2014.
- National Breast Cancer Coalition: The Breast Cancer Deadline 2020. Myth #8: Most women with breast cancer have a family history of the disease. http://www.breastcancerdeadline2020.org/breast-cancer-information/myths-and-truths/myth-8-most-women-with-bc-have-family-history.html. Accessed March 21, 2014.
- Berg WA. Benefits of screening mammography. JAMA. 2010;303(2):168–169.
- Woodworth KA. Breast imaging through the ages: a historical review and future outlook. eradimaging. September 6, 2011. http://www.eradimaging.com/site/article.cfm?ID=769#.UzAv79ySuMM. Accessed March 24, 2014.
- Miller AB, Wall C, Baines CJ, Sun P, To T, Narod SA. Twenty-five year follow-up for breast cancer incidence and mortality of the Canadian National Breast Screening Study: randomised screening trial. BMJ. 2014;348:g366.
- ObGyns continue to recommend annual mammograms for women beginning at age 40. A look at the Canadian Trial Mammography Study. American College of Obstetricians and Gynecologists. https://www.acog.org/About_ACOG/News_Room/News_Releases/2011/Annual_Mammograms_Now_Recommended_for_Women_Beginning_at_Age_40. Published February 14, 2014. Accessed March 14, 2014.
- Simon S. Canadian study questions mammogram screening; findings unlike those of other studies. American Cancer Society. http://www.cancer.org/cancer/news/news/canadian -study-questions-mammogram-screening-findings-unlike-those-of-other-studies. Published February 12, 2014. Accessed March 14, 2014.
- BMJ article on breast cancer screening effectiveness incredibly flawed and misleading. American College of Radiology. http://www.acr.org/News-Publications/News/News-Articles/2014/ACR/BMJ-Article-on-Breast-Cancer-Screening-Effectiveness-Incredibly-Flawed-and-Misleading. Published February 12, 2014. Accessed March 14, 2014.
- US Preventive Services Task Force. Screening for breast cancer. http://www.uspreventiveservicestaskforce.org/uspstf /uspsbrca.htm. Published December 2009. Accessed March 14, 2014.
- Canadian Cancer Society’s perspective on new mammography study. Canadian Cancer Society. http://www.cancer.ca/en/about-us/for-media/media-releases/national/2014/mammography-study/?region=on. Published February 13, 2014. Accessed March 14, 2014.
- Canadian Task Force on Preventive Health Care. Recommendations on screening for breast cancer in average-risk women aged 40 to 74 years. CMAJ. 2011;183(17):1991–2001.
- Nickson C, Mason KE, English DR, Kavanagh AM. Mammographic screening and breast cancer mortality: a case-control study and meta-analysis. Cancer Epidemiol Biomarkers Prev. 2012;21(9):1479–1488.
- Kalager M, Adami H-O, Bretthauer M. Too much mammography. BMJ. 2014;348:g1403.
- Kalager M, Zelen M, Langmark F, Adami HO. Effect of screening mammography on breast cancer mortality in Norway. N Engl J Med. 2010;363(13):1203–1210.
- Autier P, Boniol M, Gavin A, Vatten LJ. Breast cancer mortality in neighbouring European countries with different levels of screening but similar access to treatment: trend analysis of WHO mortality database. BMJ. 2011;343:d4411.
- O’Donoghue C, Eklund M, Ozanne EM, Esserman LJ. Aggregate cost of mammography screening in the United States: comparison of current practice and advocated strategies. Ann Intern Med. 2014;160:145–153.
- American Cancer Society. What are the risk factors for breast cancer? January 31, 2014. http://www.cancer.org/cancer/breastcancer/detailedguide/breast-cancer-risk-factors. Accessed March 21, 2014.
- National Breast Cancer Coalition: The Breast Cancer Deadline 2020. Myth #8: Most women with breast cancer have a family history of the disease. http://www.breastcancerdeadline2020.org/breast-cancer-information/myths-and-truths/myth-8-most-women-with-bc-have-family-history.html. Accessed March 21, 2014.
- Berg WA. Benefits of screening mammography. JAMA. 2010;303(2):168–169.
- Woodworth KA. Breast imaging through the ages: a historical review and future outlook. eradimaging. September 6, 2011. http://www.eradimaging.com/site/article.cfm?ID=769#.UzAv79ySuMM. Accessed March 24, 2014.


Legal and Clinical Evolution of Veterans Health Administration Policy on Medical Marijuana
This conflict between state and federal law has been the subject of considerable discussion in the professional literature and popular media, even reaching the Supreme Court.3,4 Much less attention has been paid to the parallel, but in some ways even more complicated, ethical, legal, and policy dilemmas facing administrators and practitioners in the Veterans Health Administration (VHA). Federal law governs VA health care facilities and clinical practice, yet there are VA hospitals and clinics in every state that have passed medical marijuana legislation, and veterans are eligible to obtain medical marijuana as residents of their respective states.
This article examines the evolution of VA policy regarding the use of medical marijuana within the confines of federal law and the nature of the VA as a beneficiary system with a mission to provide comprehensive health care to veterans and the legal, clinical, and ethical issues these often opposing obligations present to VA practitioners.
Completion of State Medical Marijuana Forms
In 2008, the VA Office of the General Counsel (OGC) issued to VA physicians the first official directions regarding state medical marijuana programs.5 The ruling of the VA OGC pertained to state medical marijuana registration forms and was addressed to the Under Secretary for Health. The VHA had requested guidance on how VA staff should respond when patients ask them to fill out state forms used to access medical marijuana; specifically, whether VA physicians are permitted or required to complete state medical marijuana registration forms.
The VA OGC was further asked to address the legal issues involved when a VA physician is requested to complete such a form and whether completion of such a form could result in criminal action or other penalties against the physician.
The opinion of the VA OGC issued in a memorandum on May 21, 2008, held that “VA should not authorize the completion of forms seeking recommendation or opinions regarding participation in such a program. Applicable statutes and regulations do not require VA physicians to complete such forms.”5 In response to the first question posed, the VA OGC identified the legal issues involved in the completion of the forms, arguing that the CSA designated marijuana as a Schedule 1 drug, meaning it had no accepted medical use but does have high potential for abuse. The Schedule 1 classification carried with it penalties for the dispensing, manufacturing, distributing, and possession of marijuana that were the responsibility of the Drug Enforcement Agency (DEA) to enforce.
In response to the second question, the VA OGC held that if a VA physician did complete a form permitting a patient to participate in a state medical marijuana program, this could result in DEA action, including revocation of the physician’s registration to prescribe controlled substances, as well as possible criminal charges.6 The VA OGC cited several landmark medical marijuana cases as the background to its issued opinion.
The first case cited in the VA OGC’s opinion was Pearson v McCaffrey, a 2001 ruling pertaining to the U.S. District Court of the District of Columbia.7 Barry McCaffrey, then-director of the Office of National Drug Control Policy, Donna Shalala, the secretary for the U.S. Department of Health and Human Services, and Janet Reno, attorney general, promulgated a policy that allowed the federal government to prosecute or revoke the controlled substance registration of any physician who prescribed or, more relevant to the VA situation, recommended medical marijuana to patients.
Physicians and patients in states with medical marijuana laws sought an injunction against the federal government prohibiting them from initiating civil, criminal, or administrative actions against physicians who recommended and prescribed or patients who obtained and used medical marijuana. The court refused to enforce the injunction the plaintiffs filed against the policy, finding that the federal position did not violate the First Amendment rights of the plaintiffs and, more pertinent, that Congress did have the authority under the Commerce Clause to regulate medical marijuana as a matter of public health and safety.7
Article 1, section 8, clause 3 of the U.S. Constitution grants that the U.S. Congress has the authority “To regulate Commerce with foreign Nations, and among the several states, and with the Indian tribes.”8 The Commerce Clause is often at issue in cases where the scope of federal power toward the states is challenged. The Commerce Clause is especially relevant to the legal status of state medical marijuana laws examined here because it is cited as the legal authority for the CSA, and the CSA governs practitioner prescribing.9
At the same time, an injunction against enforcement was filed in the District Court for the Northern District of California. A group of patients and physicians again initiated the legal action; this time, they were successful in obtaining a permanent injunction of the policy: The court prohibited the federal government from revoking the controlled substance registration or investigating any physician who recommended medical marijuana on the basis of a sincere medical judgment. The Supreme Court declined to hear the case.10
The U.S. Supreme Court did accept the third case, Gonzales v Raich, which did not address whether the individual physician would be prosecuted for recommending a state medical marijuana program but instead whether the federal government possessed the authority under the Commerce Clause to regulate intrastate use of marijuana for medical purposes, including revoking physicians’ controlled substance licenses.
The facts of the Raich case and legal background leading to the Supreme Court decision are as follows: In 1996, California voters passed the Compassionate Use Act, making California the first state in the country to legalize the medical use of marijuana. The law conflicted with the classification of marijuana as a Schedule 1 drug. This conflict between state and federal law rendered the case highly relevant to the question of VA physicians’ completion of medical marijuana forms for patients in states where medical marijuana is legal. The DEA had acted in California, not against a physician’s prescribing authority but against a patient, Angel Raich, for possession of medical marijuana. The DEA agents confiscated the medical marijuana from the patient’s home. In response, a group of medical marijuana users sued the DEA and California Attorney General Roberto Gonzales in federal district court.11
Raich’s attorneys argued that the constitutional basis of the federal government’s power to regulate interstate commerce, which formed the legal claim of the CSA, overreached Congress’s Commerce Clause powers. The district court ruled in favor of the attorney general, but the Ninth Circuit Court of Appeals reversed the decision, ruling that the application of the CSA to the intrastate transactions involved in California’s medical marijuana program was unconstitutional. The Ninth Circuit Court ruling cited 2 important prior cases not involving medical marijuana that also limited the Commerce Clause, although not with reference to marijuana: U.S. v Lopez in 1995 and U.S. v Morrison in 2000.12,13
The Supreme Court agreed to hear the case in June 2004 and in a 6-3 decision ruled that the application of the CSA to intrastate cultivation and possession of marijuana for medical use does not exceed Congress’s power under the Commerce Clause. Supreme Court Justice John Paul Stevens wrote the majority opinion, arguing that the power of the Commerce Clause did extend to the regulation of a “class of activities” that had a substantial effect on interstate commerce. Because marijuana use, even for medical purposes, confined to a local area, such as a state, materially affected the supply and demand market for marijuana in the nation, the regulation of state use of marijuana was required to govern the interstate traffic of marijuana.11
The VA OGC opinion referenced these cases in its analysis of the question VHA providers raised regarding the completion of state medical marijuana forms, particularly those in states such as Colorado and New Mexico where completing forms is not equivalent to providing a prescription yet does constitute a medical recommendation for the use of marijuana.14 The OGC noted that recommendation is not a term of art contained within the CSA and that Pearson ruled that there was no salient distinction between a prescription and a recommendation, where a recommendation was necessary for a patient to be able to obtain medical marijuana, which is the requirement in most states.5
The VA OGC concluded, “While some states may provide for the use of medical marijuana, such programs are in violation of federal law.”5 In formulating its judgment, the VA OGC cited the Supremacy Clause as the key to all subsequent VHA directives regarding medical marijuana. “The Supremacy Clause is the most important guarantor of national union. It assures that the Constitution and federal laws and treaties take precedence over state law and binds all judges to adhere to that principle in their courts.”8
Quoting an informal communication from the Department of Justice (DOJ), the VA OGC warned that the DOJ “may seek civil or criminal penalties for federal physicians and practitioners who completed forms that either recommend the use of medical marijuana or forms that describe the patient’s physical condition in order to facilitate the patient’s procurement of medical marijuana pursuant to state law.”5
Local vs Federal Policy
By 2009, 15 states had passed legislation allowing the medical use of marijuana. Many VA hospitals and clinics continued to regard marijuana, whether prescribed or not, as an illicit drug that violated opioid contracts or agreements. The clinical justification for these denials or other treatment plan modifications was to ensure that veterans used marijuana safely, for example, through detecting and preventing drug interactions or impairment of driving ability.
A group called Veterans for Medical Marijuana Access, founded by veteran Michael Krawitz, was the most politically active among veterans’ organizations on the issue of medical marijuana. Astutely, Mr. Krawitz and other advocates did not aim to change federal law and the Supremacy Clause or the court’s interpretations of the Commerce Clause as it applied to medical marijuana. Instead, their strategy was to expand veterans’ access to state programs, and their tactic was to work directly with the VA to formulate a policy. Mr. Krawitz adroitly used the media to champion his cause.
On March 5, 2010, Krawitz received a letter from Col. Will A. Gunn of the VA OGC. Mr. Krawitz had written the VA OGC regarding the inequities in VA policy regarding the provision of opioid medications for pain management to veterans enrolled in state medical marijuana programs. Mr. Krawitz informed Col. Gunn that the directors of some facilities had issued policies explicitly stating that veterans who provide medical marijuana registration in accordance with state programs and who tested positive for the drug would not be considered in violation of opioid contracts. Mr. Krawitz asked for official confirmation that these local policies were valid. On July 6, 2010, Under Secretary for Health Dr. Robert Petzel wrote Mr. Krawitz a memorandum stating, “If a veteran obtains and uses medical marijuana in a manner consistent with state law, testing positive for marijuana would not preclude the veteran from receiving opioids for pain management in a Department of Veterans Affairs facility.”
Dr. Petzel also outlined what would become the clinical ethics principles VA would employ to manage the federal-state law conflict regarding medical marijuana. First, a patient must inform his provider of medical marijuana use to ensure safety. Second, opioid agreements must make a clear distinction between illegal drugs, including the recreational use of marijuana, and medical marijuana. Third, the practitioner has the discretion to make the opioid prescribing decision and must make that decision on clinical grounds. Fourth, the prescribing decision should be made on a case-by-case basis “based upon the provider’s judgment and the needs of the patient.”
Following these letters was a highly publicized article in The New York Times in which Principal Deputy Under Secretary for Health Dr. Robert L. Jesse confirmed the new policy.15 The article included comments from Mr. Krawitz on the change in VA’s approach to medical marijuana. The VHA codified these less formal communications in VHA Directive 2010-035 issued on July 22, 2010.16 This directive was rescinded and replaced in January 2011 by VHA Directive 2011-004, which remains in effect as of this article’s publication.17 The provisions of this directive titled “Access to Clinical Programs for Veterans Participating in State-Approved Medical Marijuana Programs” are summarized in the Table as practical guidance for federal practitioners.
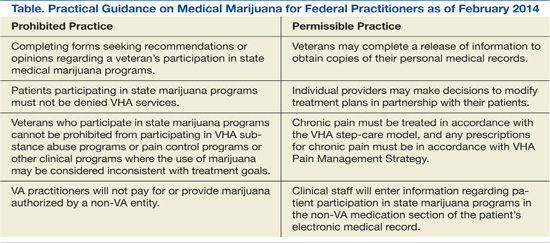
In contrast to the VA, the DoD has not revised its position that the use and possession of marijuana for any purpose is a violation of the Uniform Code of Military Justice.18 There is no indication that the DoD plans to change its ruling that military personnel who use or possess marijuana are subject to court martial, even in states where marijuana is available for therapeutic purposes.
Clinical Considerations
Concerns and questions from practitioners in the field about how to practically implement the opinion of VA OGC and VHA Directive 2010-035 led the Office of Patient Care Services (PCS) in August 2010 to issue clinical guidance that has significant ethical implications.2
Veterans who are certified to use medical marijuana should present evidence of their registration, often a medical marijuana card, to their VA provider. The provider is then advised to ask the patient to sign a release of information to enable the VA practitioner to speak to the non-VA counterpart who is prescribing the medical marijuana. This approach respects the patient’s confidentiality and obtains informed consent for coordinated treatment. One limitation of this guidance is that it does not advise the practitioner how to proceed if the patient refuses to sign the release. The VA confidentiality regulations regarding substance use information are the strictest of all federal privacy laws. Under 38 USC 7332, this information cannot be released without the explicit written consent of the veteran in order to prevent stigma and discrimination.19 The ethical objective of this communication between VA and community practitioners is nonmaleficence and thus is focused on “adherence monitoring, treatment effectiveness, safety, and impact on cognitive, emotional, social and physical functioning, and side-effects.”20
Clinicians at VA are expected to know the dosage, frequency, and form of marijuana prescribed and the medical condition for which it is approved. The directive identifies but does not officially recognize as clinical indications for the use of medical marijuana a number of medical conditions for which marijuana is commonly prescribed—glaucoma, chemotherapy-induced nausea, multiple sclerosis, epilepsy, and chronic pain—but it is the specific state laws that determine what medical and psychiatric conditions are approved for the use of medical marijuana.16,21 The PCS clearly states that it is the VA clinician, presumptively the primary care provider (PCP), who is responsible for and directs the patient’s care, just as with any consultant or provider outside VA auspices. Some clinicians find this arrangement problematic, in that they may be potentially liable for bad outcomes and may not refuse a clinically reasonable request for opioids for chronic pain, yet are unable to control the secondary prescribing of marijuana. Clinicians with political, scientific, or moral objections to any use of marijuana for medical purpose may have little recourse under the policy, as there is no indication that such objections would fall under a conscience clause.
The use of medical marijuana is an area of intense research and cultural controversy, and the empirical data to support ethical refusal by a clinician to care for a patient using medical marijuana is often difficult to separate from social attitudes and political positions.22 The VA practitioner has a duty to “adjust treatment plans to promote effective management of these conditions” for which the veteran is using medical marijuana, such as offering adjunctive medications for pain or counseling for substance use.2
The VA clinician in the service of integrated care is required to document all clinical information regarding medical marijuana, including entering the substance as a non-VA prescription in the Computerized Patient Record System. This requirement is essential to protect the veteran from having necessary and appropriate care restricted if the results of toxicology screens are positive for marijuana. One gap in the guidance is that VA clinicians have no ready means of distinguishing prescribed marijuana from illegal marijuana in a standard toxicology screen, and if the patient has a state medical marijuana registration, the clinician must assume the source is prescribed and not illicit. Since the federal practitioner cannot prescribe marijuana, there is even more uncertainty and concern regarding a positive result. Laws passed in 2013 in Colorado and Washington states, which make the recreational use of medical marijuana legal, render toxicology interpretation and medical decision-making even more complex.23
The practitioner is directed to counsel and educate the patient from a nonjudgmental and beneficence-based orientation, which fosters the patient’s autonomy and informed consent. The VA clinician’s discussion of the evidence-base for the health benefits and risks of marijuana should include criteria for a marijuana substance use disorder, emerging data on marijuana withdrawal syndrome and empirical treatment, and most important effective alternative treatments for the target symptoms or conditions for which marijuana is being used.2
Along with this general guidance for the appropriate treatment of patients who use medical marijuana, specific advice is proffered on the 2 most strongly impacted areas of clinical care: pain management and substance use disorders. Practitioners on the ground struggle to reconcile the conflict between state and federal law and policy on medical marijuana in these 2 key domains. Ethics consultation is advised as potentially helpful in resolving ethical dilemmas that arise in patient care.
Pain Management
The PCS articulates the ethical principles surrounding chronic pain treatment with a focus on opioid prescribing for veterans approved to use medical marijuana. A multimodal and stepped-care approach to pain management is endorsed that “should be based on principles of shared medical decision-making and patient autonomy.”2 In this context, veteran safety and minimizing risk to the public are high priorities. Decisions about the use of opioid analgesics need to balance the veteran’s right to pain management and veteran well-being. The informed consent discussion regarding the use of opioids and marijuana should encompass benefits and risks of each substance and its interaction, especially those related to psychomotor impairment, such as driving and memory deficits, which could affect daily functioning. Practitioners are strongly advised to cogently record the clinical evaluation and treatment rationale for prescribing opioids to patients who use medical marijuana.2
Substance Use Disorders
It is the position of the American Society of Addiction Medicine that medical marijuana is not clinically appropriate for patients with substance use disorders.24 The VA policy clearly states that no veteran participating in a state-approved program will be denied substance use treatment or stigmatized for their use of medical marijuana, which is paradoxically a substance of abuse that is illegal in many states outside of these programs. Veterans being treated for other substance use disorders may also develop a marijuana use disorder, even if the drug is medically prescribed, or may concurrently use both legal and recreational marijuana. Just as the principle of justice requires patients who use medical marijuana are not denied participation in substance use treatment, so must veterans who develop abuse of marijuana have equal access to treatment when the addiction risks outweigh the health benefits of marijuana. Central to fairness is the identification of alternative treatments for the conditions for which marijuana is prescribed.2 Unfortunately, diagnosing a marijuana use disorder in a patient using the drug for medical purposes is neither easy nor clear.
There may also be situations in which appropriate use of medical marijuana may interfere with recovery from other substances of abuse, such as benzodiazepines or alcohol, or contravene employment of the optimal therapies for comorbid medical or psychiatric conditions, for example, other sedating psychoactive medications. Medical marijuana use could in theory lead a patient or other patients in a program to relapse to the substance of choice, although preliminary evidence suggests this may not necessarily be the case.25
Self-medication with medical marijuana for symptoms other than those for which the drug is approved may become an obstacle to efficacious treatment of other psychiatric problems. For instance, a veteran being treated for depression with cognitive behavioral therapy (CBT) may find the apathy chronic marijuana often induces to be an obstacle to the homework and activation exercises used in CBT.2
Patient-Physician Partnership
The nature of VA as a beneficiary health care system precludes the organization from denying VA services to veterans participating in state medical marijuana programs. However, the system does allow providers to make decisions to modify treatment plans on clinical grounds so long as those modifications are made in partnership with patients in accordance with VA’s emphasis on shared decision-making in medical care.
It should be noted that despite this emphasis, the autonomy of both patient and physician is legally and administratively circumscribed. If a clinician’s independent reading of the medical literature and professional judgment regarding the patient’s specific clinical circumstances determine medical marijuana is clinically indicated, the clinician is not free to communicate this recommendation to the patient without risking criminal prosecution or institutional sanctions. These considerations may weigh heavily on practitioners who think that medical marijuana would benefit patients, especially in states where it is legally available.
Conversely, patients residing in states with medical marijuana laws who believe the substance would relieve their symptoms can seek out a community provider to assist them in obtaining registration. However, patients’ self-determination is limited in that they do not have the choice to have their PCP, who presumably is most familiar with their medical history, recommend or prescribe medical marijuana. Veterans also are not permitted to use VA pharmacy benefits to have VA pharmacists fill the prescription.
This is a clear statement of the limit of veteran entitlement: VA will not pay for medical marijuana. No exception is made if the veteran is using medical marijuana to treat service-connected injuries or illnesses. Directive 2010-035 (now rescinded) and the original VA OGC opinion assert that medical marijuana does not meet criteria as a core health benefit that VHA as an entitlement program must provide as an aspect of basic care.5,20 The justification for this exclusion is that non-Food and Drug Administration (FDA) approved drugs are not encompassed in the medical benefits package outside either an Investigational New Drug Application or compassionate use FDA provision. Veterans may experience this as a social justice issue and a violation of the VA fiduciary duty to its beneficiaries. A sharp demarcation is made between the private use and public possession of marijuana. Veterans who carry marijuana on VA property, even if they are certified to carry medical marijuana, will be prosecuted under CSA.
Conclusion
Studies estimate that 50% of veterans experience chronic pain, and nearly half of these patients receive prescription opioids.26 Conversely, up to 35% of VA patients are diagnosed with both substance use and mental health disorders.27
The one aspect of the controversy that stakeholders on the pro and con sides of the medical marijuana question agree on is the need for more empirical data.28 There is an urgent need for more study of the use of medical marijuana as a treatment for posttraumatic stress disorder, which is a qualifying health condition in a growing number of states.29
Along with federal law, it is federal agencies, including the DEA, FDA, and the National Institute on Drug Abuse, that may be the biggest obstacle to conducting this vital research.30 These regulatory obstacles must be removed before researchers can conduct the scientific studies needed to provide a factual foundation to inform what has too often been a political debate. Solid science grounding legal reform and shaping public policy toward medical marijuana may be the only means of resolving the ethical dilemmas that confront veterans daily and the VA clinicians committed to caring for them.31,32
In the interim, VA practitioners should be provided effective training in educating and counseling patients about the implications of VA policy regarding state-approved medical marijuana programs for their individual health care. Such a patient-centered approach represents the most ethically acceptable means of mediating the conflict between state and federal law regarding medical marijuana in its current stage of evolution.
Author disclosures
The author reports no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the author and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
References
1. State Medical Marijuana Laws. National Conference of State Legislators Website. http://www.ncsl.org/issues-research/health/state-medical-marijuana-laws.aspx. Updated January 2014. Accessed February 1, 2014.
2. Veterans Health Administration. Clinical Considerations Regarding Veteran Patients Who Participate in State-Approved Medical Marijuana Programs. Washington, DC: Department of Veterans Affairs; 2010.
3. The Associated Press. Supreme Court is set to consider medical marijuana. New York Times. November 28, 2004. http://www.nytimes.com/2004/11/28/politics/28marijuana.html?fta=y. Accessed February 5, 2014.
4. Dresser R. Irrational basis: The legal status of medical marijuana. Hastings Cent Rep. 2009;39(6):7-8.
5. Office of General Counsel. Opinion on State Medical Marijuana Registration Forms. Washington, DC: Department of Veterans Affairs; 2008. VAOPGCADV 9-2008.
6. Cohen PJ. Medical marijuana: The conflict between scientific evidence and political ideology. Part one of two. J Pain Palliat Care Pharmacother. 2009;23(1):4-25.
7. Pearson v McCaffrey, 139 F Supp 2d 772 (D DC 2001).
8. Constitution of the United States. United States Senate Website. http://www.senate.gov/civics/constitution_item/constitution.htm. Accessed January 22, 2012.
9. White BD. New York, NY: Informa Healthcare; 2007.
10. Conant v Walters, 309 F3d 629 (9th Cir 2002).
11. Gonzales v Raich, 545 US 1, 125 SCt, 2195 (2005).
12. United States v Lopez, 514 US 549, 115 SCt, 1624 (1995).
13. United States v Morrison, 529 US 598, 120 SCt, 1740 (2000).
14. The Lynn and Erin Compassionate Use Act, NMSA 1978 §26-2B (2007).
15. Frosch D. V.A. Easing rules for users of medical marijuana. New York Times. July 24, 2010:A1.
16. Medical Marijuana. Washington, DC: Dept of Veterans Affairs; 2010. VHA Directive 2010-035.
17. Access to Clinical Programs for Veterans Participating in State-Approved Marijuana Programs. Washington, DC: Dept of Veterans Affairs; 2011. VHA Directive 2011-004.
18. Uniform Code of Military Justice, 10 USC § 912A (2011).
19. Confidentiality of Certain Medical Records, 38 USC § 7332 (1991).
20. Petzel RA. Access to Clinical Programs for Veterans Participating in State-Approved Marijuana Programs. Washington, DC: Dept of Veterans Affairs; 2011. VHA Directive 2011-004.
21. Institute of Medicine. Marijuana and Medicine: Assessing the Science. Joy JE, Watson SJ Jr, Benson JA Jr, eds. Washington, DC: National Academy Press; 1999.
22. Charuvastra A, Friedmann PD, Stein MD. Physician attitudes regarding the prescription of medical marijuana. J Addict Dis. 2005;24(3):87-93.
23. Healy J. Up early and in line for a medical marijuana milestone in Colorado. New York Times. January 1, 2014:A1.
24. Public Policy Statement on Medical Marijuana. Chevy Chase, MD: American Society of Addiction Medicine; 2010.
25. Swartz R. Medical marijuana users in substance abuse treatment. Harm Reduct J. 2010;7:3.
26. Clark JD. Chronic pain prevalence and analgesic prescribing in a general medical population. J Pain Symptom Manage. 2002;23(2):131-137.
27. Petrakis IL, Rosenheck R, Desai R. Substance use comorbidity among veterans with posttraumatic stress disorder and other psychiatric illness. Am J Addict. 2011;20(3):185-189.
28. Medical Marijuana. ProCon.org Website. http://medicalmarijuana.procon.org. Updated February 3, 2014. Accessed February 5, 2014.
29. Busemeyer D. Cannabis catch-22. Santa Fe New Mexican. October 14, 2012:A1, A4-A5.
30. Harris G. Researchers find study of medical marijuana discouraged. New York Times. January 18, 2010:A14.
31. Cohen PJ. Medical marijuana: The conflict between scientific evidence and political ideology. Part two of two. J Pain Palliat Care Pharmacother. 2009;23(2):120-140.
32. Daigle L. Medical Marijuana. Bethesda, MD: American Society of Health-System Pharmacists; 2011.
This conflict between state and federal law has been the subject of considerable discussion in the professional literature and popular media, even reaching the Supreme Court.3,4 Much less attention has been paid to the parallel, but in some ways even more complicated, ethical, legal, and policy dilemmas facing administrators and practitioners in the Veterans Health Administration (VHA). Federal law governs VA health care facilities and clinical practice, yet there are VA hospitals and clinics in every state that have passed medical marijuana legislation, and veterans are eligible to obtain medical marijuana as residents of their respective states.
This article examines the evolution of VA policy regarding the use of medical marijuana within the confines of federal law and the nature of the VA as a beneficiary system with a mission to provide comprehensive health care to veterans and the legal, clinical, and ethical issues these often opposing obligations present to VA practitioners.
Completion of State Medical Marijuana Forms
In 2008, the VA Office of the General Counsel (OGC) issued to VA physicians the first official directions regarding state medical marijuana programs.5 The ruling of the VA OGC pertained to state medical marijuana registration forms and was addressed to the Under Secretary for Health. The VHA had requested guidance on how VA staff should respond when patients ask them to fill out state forms used to access medical marijuana; specifically, whether VA physicians are permitted or required to complete state medical marijuana registration forms.
The VA OGC was further asked to address the legal issues involved when a VA physician is requested to complete such a form and whether completion of such a form could result in criminal action or other penalties against the physician.
The opinion of the VA OGC issued in a memorandum on May 21, 2008, held that “VA should not authorize the completion of forms seeking recommendation or opinions regarding participation in such a program. Applicable statutes and regulations do not require VA physicians to complete such forms.”5 In response to the first question posed, the VA OGC identified the legal issues involved in the completion of the forms, arguing that the CSA designated marijuana as a Schedule 1 drug, meaning it had no accepted medical use but does have high potential for abuse. The Schedule 1 classification carried with it penalties for the dispensing, manufacturing, distributing, and possession of marijuana that were the responsibility of the Drug Enforcement Agency (DEA) to enforce.
In response to the second question, the VA OGC held that if a VA physician did complete a form permitting a patient to participate in a state medical marijuana program, this could result in DEA action, including revocation of the physician’s registration to prescribe controlled substances, as well as possible criminal charges.6 The VA OGC cited several landmark medical marijuana cases as the background to its issued opinion.
The first case cited in the VA OGC’s opinion was Pearson v McCaffrey, a 2001 ruling pertaining to the U.S. District Court of the District of Columbia.7 Barry McCaffrey, then-director of the Office of National Drug Control Policy, Donna Shalala, the secretary for the U.S. Department of Health and Human Services, and Janet Reno, attorney general, promulgated a policy that allowed the federal government to prosecute or revoke the controlled substance registration of any physician who prescribed or, more relevant to the VA situation, recommended medical marijuana to patients.
Physicians and patients in states with medical marijuana laws sought an injunction against the federal government prohibiting them from initiating civil, criminal, or administrative actions against physicians who recommended and prescribed or patients who obtained and used medical marijuana. The court refused to enforce the injunction the plaintiffs filed against the policy, finding that the federal position did not violate the First Amendment rights of the plaintiffs and, more pertinent, that Congress did have the authority under the Commerce Clause to regulate medical marijuana as a matter of public health and safety.7
Article 1, section 8, clause 3 of the U.S. Constitution grants that the U.S. Congress has the authority “To regulate Commerce with foreign Nations, and among the several states, and with the Indian tribes.”8 The Commerce Clause is often at issue in cases where the scope of federal power toward the states is challenged. The Commerce Clause is especially relevant to the legal status of state medical marijuana laws examined here because it is cited as the legal authority for the CSA, and the CSA governs practitioner prescribing.9
At the same time, an injunction against enforcement was filed in the District Court for the Northern District of California. A group of patients and physicians again initiated the legal action; this time, they were successful in obtaining a permanent injunction of the policy: The court prohibited the federal government from revoking the controlled substance registration or investigating any physician who recommended medical marijuana on the basis of a sincere medical judgment. The Supreme Court declined to hear the case.10
The U.S. Supreme Court did accept the third case, Gonzales v Raich, which did not address whether the individual physician would be prosecuted for recommending a state medical marijuana program but instead whether the federal government possessed the authority under the Commerce Clause to regulate intrastate use of marijuana for medical purposes, including revoking physicians’ controlled substance licenses.
The facts of the Raich case and legal background leading to the Supreme Court decision are as follows: In 1996, California voters passed the Compassionate Use Act, making California the first state in the country to legalize the medical use of marijuana. The law conflicted with the classification of marijuana as a Schedule 1 drug. This conflict between state and federal law rendered the case highly relevant to the question of VA physicians’ completion of medical marijuana forms for patients in states where medical marijuana is legal. The DEA had acted in California, not against a physician’s prescribing authority but against a patient, Angel Raich, for possession of medical marijuana. The DEA agents confiscated the medical marijuana from the patient’s home. In response, a group of medical marijuana users sued the DEA and California Attorney General Roberto Gonzales in federal district court.11
Raich’s attorneys argued that the constitutional basis of the federal government’s power to regulate interstate commerce, which formed the legal claim of the CSA, overreached Congress’s Commerce Clause powers. The district court ruled in favor of the attorney general, but the Ninth Circuit Court of Appeals reversed the decision, ruling that the application of the CSA to the intrastate transactions involved in California’s medical marijuana program was unconstitutional. The Ninth Circuit Court ruling cited 2 important prior cases not involving medical marijuana that also limited the Commerce Clause, although not with reference to marijuana: U.S. v Lopez in 1995 and U.S. v Morrison in 2000.12,13
The Supreme Court agreed to hear the case in June 2004 and in a 6-3 decision ruled that the application of the CSA to intrastate cultivation and possession of marijuana for medical use does not exceed Congress’s power under the Commerce Clause. Supreme Court Justice John Paul Stevens wrote the majority opinion, arguing that the power of the Commerce Clause did extend to the regulation of a “class of activities” that had a substantial effect on interstate commerce. Because marijuana use, even for medical purposes, confined to a local area, such as a state, materially affected the supply and demand market for marijuana in the nation, the regulation of state use of marijuana was required to govern the interstate traffic of marijuana.11
The VA OGC opinion referenced these cases in its analysis of the question VHA providers raised regarding the completion of state medical marijuana forms, particularly those in states such as Colorado and New Mexico where completing forms is not equivalent to providing a prescription yet does constitute a medical recommendation for the use of marijuana.14 The OGC noted that recommendation is not a term of art contained within the CSA and that Pearson ruled that there was no salient distinction between a prescription and a recommendation, where a recommendation was necessary for a patient to be able to obtain medical marijuana, which is the requirement in most states.5
The VA OGC concluded, “While some states may provide for the use of medical marijuana, such programs are in violation of federal law.”5 In formulating its judgment, the VA OGC cited the Supremacy Clause as the key to all subsequent VHA directives regarding medical marijuana. “The Supremacy Clause is the most important guarantor of national union. It assures that the Constitution and federal laws and treaties take precedence over state law and binds all judges to adhere to that principle in their courts.”8
Quoting an informal communication from the Department of Justice (DOJ), the VA OGC warned that the DOJ “may seek civil or criminal penalties for federal physicians and practitioners who completed forms that either recommend the use of medical marijuana or forms that describe the patient’s physical condition in order to facilitate the patient’s procurement of medical marijuana pursuant to state law.”5
Local vs Federal Policy
By 2009, 15 states had passed legislation allowing the medical use of marijuana. Many VA hospitals and clinics continued to regard marijuana, whether prescribed or not, as an illicit drug that violated opioid contracts or agreements. The clinical justification for these denials or other treatment plan modifications was to ensure that veterans used marijuana safely, for example, through detecting and preventing drug interactions or impairment of driving ability.
A group called Veterans for Medical Marijuana Access, founded by veteran Michael Krawitz, was the most politically active among veterans’ organizations on the issue of medical marijuana. Astutely, Mr. Krawitz and other advocates did not aim to change federal law and the Supremacy Clause or the court’s interpretations of the Commerce Clause as it applied to medical marijuana. Instead, their strategy was to expand veterans’ access to state programs, and their tactic was to work directly with the VA to formulate a policy. Mr. Krawitz adroitly used the media to champion his cause.
On March 5, 2010, Krawitz received a letter from Col. Will A. Gunn of the VA OGC. Mr. Krawitz had written the VA OGC regarding the inequities in VA policy regarding the provision of opioid medications for pain management to veterans enrolled in state medical marijuana programs. Mr. Krawitz informed Col. Gunn that the directors of some facilities had issued policies explicitly stating that veterans who provide medical marijuana registration in accordance with state programs and who tested positive for the drug would not be considered in violation of opioid contracts. Mr. Krawitz asked for official confirmation that these local policies were valid. On July 6, 2010, Under Secretary for Health Dr. Robert Petzel wrote Mr. Krawitz a memorandum stating, “If a veteran obtains and uses medical marijuana in a manner consistent with state law, testing positive for marijuana would not preclude the veteran from receiving opioids for pain management in a Department of Veterans Affairs facility.”
Dr. Petzel also outlined what would become the clinical ethics principles VA would employ to manage the federal-state law conflict regarding medical marijuana. First, a patient must inform his provider of medical marijuana use to ensure safety. Second, opioid agreements must make a clear distinction between illegal drugs, including the recreational use of marijuana, and medical marijuana. Third, the practitioner has the discretion to make the opioid prescribing decision and must make that decision on clinical grounds. Fourth, the prescribing decision should be made on a case-by-case basis “based upon the provider’s judgment and the needs of the patient.”
Following these letters was a highly publicized article in The New York Times in which Principal Deputy Under Secretary for Health Dr. Robert L. Jesse confirmed the new policy.15 The article included comments from Mr. Krawitz on the change in VA’s approach to medical marijuana. The VHA codified these less formal communications in VHA Directive 2010-035 issued on July 22, 2010.16 This directive was rescinded and replaced in January 2011 by VHA Directive 2011-004, which remains in effect as of this article’s publication.17 The provisions of this directive titled “Access to Clinical Programs for Veterans Participating in State-Approved Medical Marijuana Programs” are summarized in the Table as practical guidance for federal practitioners.
In contrast to the VA, the DoD has not revised its position that the use and possession of marijuana for any purpose is a violation of the Uniform Code of Military Justice.18 There is no indication that the DoD plans to change its ruling that military personnel who use or possess marijuana are subject to court martial, even in states where marijuana is available for therapeutic purposes.
Clinical Considerations
Concerns and questions from practitioners in the field about how to practically implement the opinion of VA OGC and VHA Directive 2010-035 led the Office of Patient Care Services (PCS) in August 2010 to issue clinical guidance that has significant ethical implications.2
Veterans who are certified to use medical marijuana should present evidence of their registration, often a medical marijuana card, to their VA provider. The provider is then advised to ask the patient to sign a release of information to enable the VA practitioner to speak to the non-VA counterpart who is prescribing the medical marijuana. This approach respects the patient’s confidentiality and obtains informed consent for coordinated treatment. One limitation of this guidance is that it does not advise the practitioner how to proceed if the patient refuses to sign the release. The VA confidentiality regulations regarding substance use information are the strictest of all federal privacy laws. Under 38 USC 7332, this information cannot be released without the explicit written consent of the veteran in order to prevent stigma and discrimination.19 The ethical objective of this communication between VA and community practitioners is nonmaleficence and thus is focused on “adherence monitoring, treatment effectiveness, safety, and impact on cognitive, emotional, social and physical functioning, and side-effects.”20
Clinicians at VA are expected to know the dosage, frequency, and form of marijuana prescribed and the medical condition for which it is approved. The directive identifies but does not officially recognize as clinical indications for the use of medical marijuana a number of medical conditions for which marijuana is commonly prescribed—glaucoma, chemotherapy-induced nausea, multiple sclerosis, epilepsy, and chronic pain—but it is the specific state laws that determine what medical and psychiatric conditions are approved for the use of medical marijuana.16,21 The PCS clearly states that it is the VA clinician, presumptively the primary care provider (PCP), who is responsible for and directs the patient’s care, just as with any consultant or provider outside VA auspices. Some clinicians find this arrangement problematic, in that they may be potentially liable for bad outcomes and may not refuse a clinically reasonable request for opioids for chronic pain, yet are unable to control the secondary prescribing of marijuana. Clinicians with political, scientific, or moral objections to any use of marijuana for medical purpose may have little recourse under the policy, as there is no indication that such objections would fall under a conscience clause.
The use of medical marijuana is an area of intense research and cultural controversy, and the empirical data to support ethical refusal by a clinician to care for a patient using medical marijuana is often difficult to separate from social attitudes and political positions.22 The VA practitioner has a duty to “adjust treatment plans to promote effective management of these conditions” for which the veteran is using medical marijuana, such as offering adjunctive medications for pain or counseling for substance use.2
The VA clinician in the service of integrated care is required to document all clinical information regarding medical marijuana, including entering the substance as a non-VA prescription in the Computerized Patient Record System. This requirement is essential to protect the veteran from having necessary and appropriate care restricted if the results of toxicology screens are positive for marijuana. One gap in the guidance is that VA clinicians have no ready means of distinguishing prescribed marijuana from illegal marijuana in a standard toxicology screen, and if the patient has a state medical marijuana registration, the clinician must assume the source is prescribed and not illicit. Since the federal practitioner cannot prescribe marijuana, there is even more uncertainty and concern regarding a positive result. Laws passed in 2013 in Colorado and Washington states, which make the recreational use of medical marijuana legal, render toxicology interpretation and medical decision-making even more complex.23
The practitioner is directed to counsel and educate the patient from a nonjudgmental and beneficence-based orientation, which fosters the patient’s autonomy and informed consent. The VA clinician’s discussion of the evidence-base for the health benefits and risks of marijuana should include criteria for a marijuana substance use disorder, emerging data on marijuana withdrawal syndrome and empirical treatment, and most important effective alternative treatments for the target symptoms or conditions for which marijuana is being used.2
Along with this general guidance for the appropriate treatment of patients who use medical marijuana, specific advice is proffered on the 2 most strongly impacted areas of clinical care: pain management and substance use disorders. Practitioners on the ground struggle to reconcile the conflict between state and federal law and policy on medical marijuana in these 2 key domains. Ethics consultation is advised as potentially helpful in resolving ethical dilemmas that arise in patient care.
Pain Management
The PCS articulates the ethical principles surrounding chronic pain treatment with a focus on opioid prescribing for veterans approved to use medical marijuana. A multimodal and stepped-care approach to pain management is endorsed that “should be based on principles of shared medical decision-making and patient autonomy.”2 In this context, veteran safety and minimizing risk to the public are high priorities. Decisions about the use of opioid analgesics need to balance the veteran’s right to pain management and veteran well-being. The informed consent discussion regarding the use of opioids and marijuana should encompass benefits and risks of each substance and its interaction, especially those related to psychomotor impairment, such as driving and memory deficits, which could affect daily functioning. Practitioners are strongly advised to cogently record the clinical evaluation and treatment rationale for prescribing opioids to patients who use medical marijuana.2
Substance Use Disorders
It is the position of the American Society of Addiction Medicine that medical marijuana is not clinically appropriate for patients with substance use disorders.24 The VA policy clearly states that no veteran participating in a state-approved program will be denied substance use treatment or stigmatized for their use of medical marijuana, which is paradoxically a substance of abuse that is illegal in many states outside of these programs. Veterans being treated for other substance use disorders may also develop a marijuana use disorder, even if the drug is medically prescribed, or may concurrently use both legal and recreational marijuana. Just as the principle of justice requires patients who use medical marijuana are not denied participation in substance use treatment, so must veterans who develop abuse of marijuana have equal access to treatment when the addiction risks outweigh the health benefits of marijuana. Central to fairness is the identification of alternative treatments for the conditions for which marijuana is prescribed.2 Unfortunately, diagnosing a marijuana use disorder in a patient using the drug for medical purposes is neither easy nor clear.
There may also be situations in which appropriate use of medical marijuana may interfere with recovery from other substances of abuse, such as benzodiazepines or alcohol, or contravene employment of the optimal therapies for comorbid medical or psychiatric conditions, for example, other sedating psychoactive medications. Medical marijuana use could in theory lead a patient or other patients in a program to relapse to the substance of choice, although preliminary evidence suggests this may not necessarily be the case.25
Self-medication with medical marijuana for symptoms other than those for which the drug is approved may become an obstacle to efficacious treatment of other psychiatric problems. For instance, a veteran being treated for depression with cognitive behavioral therapy (CBT) may find the apathy chronic marijuana often induces to be an obstacle to the homework and activation exercises used in CBT.2
Patient-Physician Partnership
The nature of VA as a beneficiary health care system precludes the organization from denying VA services to veterans participating in state medical marijuana programs. However, the system does allow providers to make decisions to modify treatment plans on clinical grounds so long as those modifications are made in partnership with patients in accordance with VA’s emphasis on shared decision-making in medical care.
It should be noted that despite this emphasis, the autonomy of both patient and physician is legally and administratively circumscribed. If a clinician’s independent reading of the medical literature and professional judgment regarding the patient’s specific clinical circumstances determine medical marijuana is clinically indicated, the clinician is not free to communicate this recommendation to the patient without risking criminal prosecution or institutional sanctions. These considerations may weigh heavily on practitioners who think that medical marijuana would benefit patients, especially in states where it is legally available.
Conversely, patients residing in states with medical marijuana laws who believe the substance would relieve their symptoms can seek out a community provider to assist them in obtaining registration. However, patients’ self-determination is limited in that they do not have the choice to have their PCP, who presumably is most familiar with their medical history, recommend or prescribe medical marijuana. Veterans also are not permitted to use VA pharmacy benefits to have VA pharmacists fill the prescription.
This is a clear statement of the limit of veteran entitlement: VA will not pay for medical marijuana. No exception is made if the veteran is using medical marijuana to treat service-connected injuries or illnesses. Directive 2010-035 (now rescinded) and the original VA OGC opinion assert that medical marijuana does not meet criteria as a core health benefit that VHA as an entitlement program must provide as an aspect of basic care.5,20 The justification for this exclusion is that non-Food and Drug Administration (FDA) approved drugs are not encompassed in the medical benefits package outside either an Investigational New Drug Application or compassionate use FDA provision. Veterans may experience this as a social justice issue and a violation of the VA fiduciary duty to its beneficiaries. A sharp demarcation is made between the private use and public possession of marijuana. Veterans who carry marijuana on VA property, even if they are certified to carry medical marijuana, will be prosecuted under CSA.
Conclusion
Studies estimate that 50% of veterans experience chronic pain, and nearly half of these patients receive prescription opioids.26 Conversely, up to 35% of VA patients are diagnosed with both substance use and mental health disorders.27
The one aspect of the controversy that stakeholders on the pro and con sides of the medical marijuana question agree on is the need for more empirical data.28 There is an urgent need for more study of the use of medical marijuana as a treatment for posttraumatic stress disorder, which is a qualifying health condition in a growing number of states.29
Along with federal law, it is federal agencies, including the DEA, FDA, and the National Institute on Drug Abuse, that may be the biggest obstacle to conducting this vital research.30 These regulatory obstacles must be removed before researchers can conduct the scientific studies needed to provide a factual foundation to inform what has too often been a political debate. Solid science grounding legal reform and shaping public policy toward medical marijuana may be the only means of resolving the ethical dilemmas that confront veterans daily and the VA clinicians committed to caring for them.31,32
In the interim, VA practitioners should be provided effective training in educating and counseling patients about the implications of VA policy regarding state-approved medical marijuana programs for their individual health care. Such a patient-centered approach represents the most ethically acceptable means of mediating the conflict between state and federal law regarding medical marijuana in its current stage of evolution.
Author disclosures
The author reports no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the author and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
References
1. State Medical Marijuana Laws. National Conference of State Legislators Website. http://www.ncsl.org/issues-research/health/state-medical-marijuana-laws.aspx. Updated January 2014. Accessed February 1, 2014.
2. Veterans Health Administration. Clinical Considerations Regarding Veteran Patients Who Participate in State-Approved Medical Marijuana Programs. Washington, DC: Department of Veterans Affairs; 2010.
3. The Associated Press. Supreme Court is set to consider medical marijuana. New York Times. November 28, 2004. http://www.nytimes.com/2004/11/28/politics/28marijuana.html?fta=y. Accessed February 5, 2014.
4. Dresser R. Irrational basis: The legal status of medical marijuana. Hastings Cent Rep. 2009;39(6):7-8.
5. Office of General Counsel. Opinion on State Medical Marijuana Registration Forms. Washington, DC: Department of Veterans Affairs; 2008. VAOPGCADV 9-2008.
6. Cohen PJ. Medical marijuana: The conflict between scientific evidence and political ideology. Part one of two. J Pain Palliat Care Pharmacother. 2009;23(1):4-25.
7. Pearson v McCaffrey, 139 F Supp 2d 772 (D DC 2001).
8. Constitution of the United States. United States Senate Website. http://www.senate.gov/civics/constitution_item/constitution.htm. Accessed January 22, 2012.
9. White BD. New York, NY: Informa Healthcare; 2007.
10. Conant v Walters, 309 F3d 629 (9th Cir 2002).
11. Gonzales v Raich, 545 US 1, 125 SCt, 2195 (2005).
12. United States v Lopez, 514 US 549, 115 SCt, 1624 (1995).
13. United States v Morrison, 529 US 598, 120 SCt, 1740 (2000).
14. The Lynn and Erin Compassionate Use Act, NMSA 1978 §26-2B (2007).
15. Frosch D. V.A. Easing rules for users of medical marijuana. New York Times. July 24, 2010:A1.
16. Medical Marijuana. Washington, DC: Dept of Veterans Affairs; 2010. VHA Directive 2010-035.
17. Access to Clinical Programs for Veterans Participating in State-Approved Marijuana Programs. Washington, DC: Dept of Veterans Affairs; 2011. VHA Directive 2011-004.
18. Uniform Code of Military Justice, 10 USC § 912A (2011).
19. Confidentiality of Certain Medical Records, 38 USC § 7332 (1991).
20. Petzel RA. Access to Clinical Programs for Veterans Participating in State-Approved Marijuana Programs. Washington, DC: Dept of Veterans Affairs; 2011. VHA Directive 2011-004.
21. Institute of Medicine. Marijuana and Medicine: Assessing the Science. Joy JE, Watson SJ Jr, Benson JA Jr, eds. Washington, DC: National Academy Press; 1999.
22. Charuvastra A, Friedmann PD, Stein MD. Physician attitudes regarding the prescription of medical marijuana. J Addict Dis. 2005;24(3):87-93.
23. Healy J. Up early and in line for a medical marijuana milestone in Colorado. New York Times. January 1, 2014:A1.
24. Public Policy Statement on Medical Marijuana. Chevy Chase, MD: American Society of Addiction Medicine; 2010.
25. Swartz R. Medical marijuana users in substance abuse treatment. Harm Reduct J. 2010;7:3.
26. Clark JD. Chronic pain prevalence and analgesic prescribing in a general medical population. J Pain Symptom Manage. 2002;23(2):131-137.
27. Petrakis IL, Rosenheck R, Desai R. Substance use comorbidity among veterans with posttraumatic stress disorder and other psychiatric illness. Am J Addict. 2011;20(3):185-189.
28. Medical Marijuana. ProCon.org Website. http://medicalmarijuana.procon.org. Updated February 3, 2014. Accessed February 5, 2014.
29. Busemeyer D. Cannabis catch-22. Santa Fe New Mexican. October 14, 2012:A1, A4-A5.
30. Harris G. Researchers find study of medical marijuana discouraged. New York Times. January 18, 2010:A14.
31. Cohen PJ. Medical marijuana: The conflict between scientific evidence and political ideology. Part two of two. J Pain Palliat Care Pharmacother. 2009;23(2):120-140.
32. Daigle L. Medical Marijuana. Bethesda, MD: American Society of Health-System Pharmacists; 2011.
This conflict between state and federal law has been the subject of considerable discussion in the professional literature and popular media, even reaching the Supreme Court.3,4 Much less attention has been paid to the parallel, but in some ways even more complicated, ethical, legal, and policy dilemmas facing administrators and practitioners in the Veterans Health Administration (VHA). Federal law governs VA health care facilities and clinical practice, yet there are VA hospitals and clinics in every state that have passed medical marijuana legislation, and veterans are eligible to obtain medical marijuana as residents of their respective states.
This article examines the evolution of VA policy regarding the use of medical marijuana within the confines of federal law and the nature of the VA as a beneficiary system with a mission to provide comprehensive health care to veterans and the legal, clinical, and ethical issues these often opposing obligations present to VA practitioners.
Completion of State Medical Marijuana Forms
In 2008, the VA Office of the General Counsel (OGC) issued to VA physicians the first official directions regarding state medical marijuana programs.5 The ruling of the VA OGC pertained to state medical marijuana registration forms and was addressed to the Under Secretary for Health. The VHA had requested guidance on how VA staff should respond when patients ask them to fill out state forms used to access medical marijuana; specifically, whether VA physicians are permitted or required to complete state medical marijuana registration forms.
The VA OGC was further asked to address the legal issues involved when a VA physician is requested to complete such a form and whether completion of such a form could result in criminal action or other penalties against the physician.
The opinion of the VA OGC issued in a memorandum on May 21, 2008, held that “VA should not authorize the completion of forms seeking recommendation or opinions regarding participation in such a program. Applicable statutes and regulations do not require VA physicians to complete such forms.”5 In response to the first question posed, the VA OGC identified the legal issues involved in the completion of the forms, arguing that the CSA designated marijuana as a Schedule 1 drug, meaning it had no accepted medical use but does have high potential for abuse. The Schedule 1 classification carried with it penalties for the dispensing, manufacturing, distributing, and possession of marijuana that were the responsibility of the Drug Enforcement Agency (DEA) to enforce.
In response to the second question, the VA OGC held that if a VA physician did complete a form permitting a patient to participate in a state medical marijuana program, this could result in DEA action, including revocation of the physician’s registration to prescribe controlled substances, as well as possible criminal charges.6 The VA OGC cited several landmark medical marijuana cases as the background to its issued opinion.
The first case cited in the VA OGC’s opinion was Pearson v McCaffrey, a 2001 ruling pertaining to the U.S. District Court of the District of Columbia.7 Barry McCaffrey, then-director of the Office of National Drug Control Policy, Donna Shalala, the secretary for the U.S. Department of Health and Human Services, and Janet Reno, attorney general, promulgated a policy that allowed the federal government to prosecute or revoke the controlled substance registration of any physician who prescribed or, more relevant to the VA situation, recommended medical marijuana to patients.
Physicians and patients in states with medical marijuana laws sought an injunction against the federal government prohibiting them from initiating civil, criminal, or administrative actions against physicians who recommended and prescribed or patients who obtained and used medical marijuana. The court refused to enforce the injunction the plaintiffs filed against the policy, finding that the federal position did not violate the First Amendment rights of the plaintiffs and, more pertinent, that Congress did have the authority under the Commerce Clause to regulate medical marijuana as a matter of public health and safety.7
Article 1, section 8, clause 3 of the U.S. Constitution grants that the U.S. Congress has the authority “To regulate Commerce with foreign Nations, and among the several states, and with the Indian tribes.”8 The Commerce Clause is often at issue in cases where the scope of federal power toward the states is challenged. The Commerce Clause is especially relevant to the legal status of state medical marijuana laws examined here because it is cited as the legal authority for the CSA, and the CSA governs practitioner prescribing.9
At the same time, an injunction against enforcement was filed in the District Court for the Northern District of California. A group of patients and physicians again initiated the legal action; this time, they were successful in obtaining a permanent injunction of the policy: The court prohibited the federal government from revoking the controlled substance registration or investigating any physician who recommended medical marijuana on the basis of a sincere medical judgment. The Supreme Court declined to hear the case.10
The U.S. Supreme Court did accept the third case, Gonzales v Raich, which did not address whether the individual physician would be prosecuted for recommending a state medical marijuana program but instead whether the federal government possessed the authority under the Commerce Clause to regulate intrastate use of marijuana for medical purposes, including revoking physicians’ controlled substance licenses.
The facts of the Raich case and legal background leading to the Supreme Court decision are as follows: In 1996, California voters passed the Compassionate Use Act, making California the first state in the country to legalize the medical use of marijuana. The law conflicted with the classification of marijuana as a Schedule 1 drug. This conflict between state and federal law rendered the case highly relevant to the question of VA physicians’ completion of medical marijuana forms for patients in states where medical marijuana is legal. The DEA had acted in California, not against a physician’s prescribing authority but against a patient, Angel Raich, for possession of medical marijuana. The DEA agents confiscated the medical marijuana from the patient’s home. In response, a group of medical marijuana users sued the DEA and California Attorney General Roberto Gonzales in federal district court.11
Raich’s attorneys argued that the constitutional basis of the federal government’s power to regulate interstate commerce, which formed the legal claim of the CSA, overreached Congress’s Commerce Clause powers. The district court ruled in favor of the attorney general, but the Ninth Circuit Court of Appeals reversed the decision, ruling that the application of the CSA to the intrastate transactions involved in California’s medical marijuana program was unconstitutional. The Ninth Circuit Court ruling cited 2 important prior cases not involving medical marijuana that also limited the Commerce Clause, although not with reference to marijuana: U.S. v Lopez in 1995 and U.S. v Morrison in 2000.12,13
The Supreme Court agreed to hear the case in June 2004 and in a 6-3 decision ruled that the application of the CSA to intrastate cultivation and possession of marijuana for medical use does not exceed Congress’s power under the Commerce Clause. Supreme Court Justice John Paul Stevens wrote the majority opinion, arguing that the power of the Commerce Clause did extend to the regulation of a “class of activities” that had a substantial effect on interstate commerce. Because marijuana use, even for medical purposes, confined to a local area, such as a state, materially affected the supply and demand market for marijuana in the nation, the regulation of state use of marijuana was required to govern the interstate traffic of marijuana.11
The VA OGC opinion referenced these cases in its analysis of the question VHA providers raised regarding the completion of state medical marijuana forms, particularly those in states such as Colorado and New Mexico where completing forms is not equivalent to providing a prescription yet does constitute a medical recommendation for the use of marijuana.14 The OGC noted that recommendation is not a term of art contained within the CSA and that Pearson ruled that there was no salient distinction between a prescription and a recommendation, where a recommendation was necessary for a patient to be able to obtain medical marijuana, which is the requirement in most states.5
The VA OGC concluded, “While some states may provide for the use of medical marijuana, such programs are in violation of federal law.”5 In formulating its judgment, the VA OGC cited the Supremacy Clause as the key to all subsequent VHA directives regarding medical marijuana. “The Supremacy Clause is the most important guarantor of national union. It assures that the Constitution and federal laws and treaties take precedence over state law and binds all judges to adhere to that principle in their courts.”8
Quoting an informal communication from the Department of Justice (DOJ), the VA OGC warned that the DOJ “may seek civil or criminal penalties for federal physicians and practitioners who completed forms that either recommend the use of medical marijuana or forms that describe the patient’s physical condition in order to facilitate the patient’s procurement of medical marijuana pursuant to state law.”5
Local vs Federal Policy
By 2009, 15 states had passed legislation allowing the medical use of marijuana. Many VA hospitals and clinics continued to regard marijuana, whether prescribed or not, as an illicit drug that violated opioid contracts or agreements. The clinical justification for these denials or other treatment plan modifications was to ensure that veterans used marijuana safely, for example, through detecting and preventing drug interactions or impairment of driving ability.
A group called Veterans for Medical Marijuana Access, founded by veteran Michael Krawitz, was the most politically active among veterans’ organizations on the issue of medical marijuana. Astutely, Mr. Krawitz and other advocates did not aim to change federal law and the Supremacy Clause or the court’s interpretations of the Commerce Clause as it applied to medical marijuana. Instead, their strategy was to expand veterans’ access to state programs, and their tactic was to work directly with the VA to formulate a policy. Mr. Krawitz adroitly used the media to champion his cause.
On March 5, 2010, Krawitz received a letter from Col. Will A. Gunn of the VA OGC. Mr. Krawitz had written the VA OGC regarding the inequities in VA policy regarding the provision of opioid medications for pain management to veterans enrolled in state medical marijuana programs. Mr. Krawitz informed Col. Gunn that the directors of some facilities had issued policies explicitly stating that veterans who provide medical marijuana registration in accordance with state programs and who tested positive for the drug would not be considered in violation of opioid contracts. Mr. Krawitz asked for official confirmation that these local policies were valid. On July 6, 2010, Under Secretary for Health Dr. Robert Petzel wrote Mr. Krawitz a memorandum stating, “If a veteran obtains and uses medical marijuana in a manner consistent with state law, testing positive for marijuana would not preclude the veteran from receiving opioids for pain management in a Department of Veterans Affairs facility.”
Dr. Petzel also outlined what would become the clinical ethics principles VA would employ to manage the federal-state law conflict regarding medical marijuana. First, a patient must inform his provider of medical marijuana use to ensure safety. Second, opioid agreements must make a clear distinction between illegal drugs, including the recreational use of marijuana, and medical marijuana. Third, the practitioner has the discretion to make the opioid prescribing decision and must make that decision on clinical grounds. Fourth, the prescribing decision should be made on a case-by-case basis “based upon the provider’s judgment and the needs of the patient.”
Following these letters was a highly publicized article in The New York Times in which Principal Deputy Under Secretary for Health Dr. Robert L. Jesse confirmed the new policy.15 The article included comments from Mr. Krawitz on the change in VA’s approach to medical marijuana. The VHA codified these less formal communications in VHA Directive 2010-035 issued on July 22, 2010.16 This directive was rescinded and replaced in January 2011 by VHA Directive 2011-004, which remains in effect as of this article’s publication.17 The provisions of this directive titled “Access to Clinical Programs for Veterans Participating in State-Approved Medical Marijuana Programs” are summarized in the Table as practical guidance for federal practitioners.
In contrast to the VA, the DoD has not revised its position that the use and possession of marijuana for any purpose is a violation of the Uniform Code of Military Justice.18 There is no indication that the DoD plans to change its ruling that military personnel who use or possess marijuana are subject to court martial, even in states where marijuana is available for therapeutic purposes.
Clinical Considerations
Concerns and questions from practitioners in the field about how to practically implement the opinion of VA OGC and VHA Directive 2010-035 led the Office of Patient Care Services (PCS) in August 2010 to issue clinical guidance that has significant ethical implications.2
Veterans who are certified to use medical marijuana should present evidence of their registration, often a medical marijuana card, to their VA provider. The provider is then advised to ask the patient to sign a release of information to enable the VA practitioner to speak to the non-VA counterpart who is prescribing the medical marijuana. This approach respects the patient’s confidentiality and obtains informed consent for coordinated treatment. One limitation of this guidance is that it does not advise the practitioner how to proceed if the patient refuses to sign the release. The VA confidentiality regulations regarding substance use information are the strictest of all federal privacy laws. Under 38 USC 7332, this information cannot be released without the explicit written consent of the veteran in order to prevent stigma and discrimination.19 The ethical objective of this communication between VA and community practitioners is nonmaleficence and thus is focused on “adherence monitoring, treatment effectiveness, safety, and impact on cognitive, emotional, social and physical functioning, and side-effects.”20
Clinicians at VA are expected to know the dosage, frequency, and form of marijuana prescribed and the medical condition for which it is approved. The directive identifies but does not officially recognize as clinical indications for the use of medical marijuana a number of medical conditions for which marijuana is commonly prescribed—glaucoma, chemotherapy-induced nausea, multiple sclerosis, epilepsy, and chronic pain—but it is the specific state laws that determine what medical and psychiatric conditions are approved for the use of medical marijuana.16,21 The PCS clearly states that it is the VA clinician, presumptively the primary care provider (PCP), who is responsible for and directs the patient’s care, just as with any consultant or provider outside VA auspices. Some clinicians find this arrangement problematic, in that they may be potentially liable for bad outcomes and may not refuse a clinically reasonable request for opioids for chronic pain, yet are unable to control the secondary prescribing of marijuana. Clinicians with political, scientific, or moral objections to any use of marijuana for medical purpose may have little recourse under the policy, as there is no indication that such objections would fall under a conscience clause.
The use of medical marijuana is an area of intense research and cultural controversy, and the empirical data to support ethical refusal by a clinician to care for a patient using medical marijuana is often difficult to separate from social attitudes and political positions.22 The VA practitioner has a duty to “adjust treatment plans to promote effective management of these conditions” for which the veteran is using medical marijuana, such as offering adjunctive medications for pain or counseling for substance use.2
The VA clinician in the service of integrated care is required to document all clinical information regarding medical marijuana, including entering the substance as a non-VA prescription in the Computerized Patient Record System. This requirement is essential to protect the veteran from having necessary and appropriate care restricted if the results of toxicology screens are positive for marijuana. One gap in the guidance is that VA clinicians have no ready means of distinguishing prescribed marijuana from illegal marijuana in a standard toxicology screen, and if the patient has a state medical marijuana registration, the clinician must assume the source is prescribed and not illicit. Since the federal practitioner cannot prescribe marijuana, there is even more uncertainty and concern regarding a positive result. Laws passed in 2013 in Colorado and Washington states, which make the recreational use of medical marijuana legal, render toxicology interpretation and medical decision-making even more complex.23
The practitioner is directed to counsel and educate the patient from a nonjudgmental and beneficence-based orientation, which fosters the patient’s autonomy and informed consent. The VA clinician’s discussion of the evidence-base for the health benefits and risks of marijuana should include criteria for a marijuana substance use disorder, emerging data on marijuana withdrawal syndrome and empirical treatment, and most important effective alternative treatments for the target symptoms or conditions for which marijuana is being used.2
Along with this general guidance for the appropriate treatment of patients who use medical marijuana, specific advice is proffered on the 2 most strongly impacted areas of clinical care: pain management and substance use disorders. Practitioners on the ground struggle to reconcile the conflict between state and federal law and policy on medical marijuana in these 2 key domains. Ethics consultation is advised as potentially helpful in resolving ethical dilemmas that arise in patient care.
Pain Management
The PCS articulates the ethical principles surrounding chronic pain treatment with a focus on opioid prescribing for veterans approved to use medical marijuana. A multimodal and stepped-care approach to pain management is endorsed that “should be based on principles of shared medical decision-making and patient autonomy.”2 In this context, veteran safety and minimizing risk to the public are high priorities. Decisions about the use of opioid analgesics need to balance the veteran’s right to pain management and veteran well-being. The informed consent discussion regarding the use of opioids and marijuana should encompass benefits and risks of each substance and its interaction, especially those related to psychomotor impairment, such as driving and memory deficits, which could affect daily functioning. Practitioners are strongly advised to cogently record the clinical evaluation and treatment rationale for prescribing opioids to patients who use medical marijuana.2
Substance Use Disorders
It is the position of the American Society of Addiction Medicine that medical marijuana is not clinically appropriate for patients with substance use disorders.24 The VA policy clearly states that no veteran participating in a state-approved program will be denied substance use treatment or stigmatized for their use of medical marijuana, which is paradoxically a substance of abuse that is illegal in many states outside of these programs. Veterans being treated for other substance use disorders may also develop a marijuana use disorder, even if the drug is medically prescribed, or may concurrently use both legal and recreational marijuana. Just as the principle of justice requires patients who use medical marijuana are not denied participation in substance use treatment, so must veterans who develop abuse of marijuana have equal access to treatment when the addiction risks outweigh the health benefits of marijuana. Central to fairness is the identification of alternative treatments for the conditions for which marijuana is prescribed.2 Unfortunately, diagnosing a marijuana use disorder in a patient using the drug for medical purposes is neither easy nor clear.
There may also be situations in which appropriate use of medical marijuana may interfere with recovery from other substances of abuse, such as benzodiazepines or alcohol, or contravene employment of the optimal therapies for comorbid medical or psychiatric conditions, for example, other sedating psychoactive medications. Medical marijuana use could in theory lead a patient or other patients in a program to relapse to the substance of choice, although preliminary evidence suggests this may not necessarily be the case.25
Self-medication with medical marijuana for symptoms other than those for which the drug is approved may become an obstacle to efficacious treatment of other psychiatric problems. For instance, a veteran being treated for depression with cognitive behavioral therapy (CBT) may find the apathy chronic marijuana often induces to be an obstacle to the homework and activation exercises used in CBT.2
Patient-Physician Partnership
The nature of VA as a beneficiary health care system precludes the organization from denying VA services to veterans participating in state medical marijuana programs. However, the system does allow providers to make decisions to modify treatment plans on clinical grounds so long as those modifications are made in partnership with patients in accordance with VA’s emphasis on shared decision-making in medical care.
It should be noted that despite this emphasis, the autonomy of both patient and physician is legally and administratively circumscribed. If a clinician’s independent reading of the medical literature and professional judgment regarding the patient’s specific clinical circumstances determine medical marijuana is clinically indicated, the clinician is not free to communicate this recommendation to the patient without risking criminal prosecution or institutional sanctions. These considerations may weigh heavily on practitioners who think that medical marijuana would benefit patients, especially in states where it is legally available.
Conversely, patients residing in states with medical marijuana laws who believe the substance would relieve their symptoms can seek out a community provider to assist them in obtaining registration. However, patients’ self-determination is limited in that they do not have the choice to have their PCP, who presumably is most familiar with their medical history, recommend or prescribe medical marijuana. Veterans also are not permitted to use VA pharmacy benefits to have VA pharmacists fill the prescription.
This is a clear statement of the limit of veteran entitlement: VA will not pay for medical marijuana. No exception is made if the veteran is using medical marijuana to treat service-connected injuries or illnesses. Directive 2010-035 (now rescinded) and the original VA OGC opinion assert that medical marijuana does not meet criteria as a core health benefit that VHA as an entitlement program must provide as an aspect of basic care.5,20 The justification for this exclusion is that non-Food and Drug Administration (FDA) approved drugs are not encompassed in the medical benefits package outside either an Investigational New Drug Application or compassionate use FDA provision. Veterans may experience this as a social justice issue and a violation of the VA fiduciary duty to its beneficiaries. A sharp demarcation is made between the private use and public possession of marijuana. Veterans who carry marijuana on VA property, even if they are certified to carry medical marijuana, will be prosecuted under CSA.
Conclusion
Studies estimate that 50% of veterans experience chronic pain, and nearly half of these patients receive prescription opioids.26 Conversely, up to 35% of VA patients are diagnosed with both substance use and mental health disorders.27
The one aspect of the controversy that stakeholders on the pro and con sides of the medical marijuana question agree on is the need for more empirical data.28 There is an urgent need for more study of the use of medical marijuana as a treatment for posttraumatic stress disorder, which is a qualifying health condition in a growing number of states.29
Along with federal law, it is federal agencies, including the DEA, FDA, and the National Institute on Drug Abuse, that may be the biggest obstacle to conducting this vital research.30 These regulatory obstacles must be removed before researchers can conduct the scientific studies needed to provide a factual foundation to inform what has too often been a political debate. Solid science grounding legal reform and shaping public policy toward medical marijuana may be the only means of resolving the ethical dilemmas that confront veterans daily and the VA clinicians committed to caring for them.31,32
In the interim, VA practitioners should be provided effective training in educating and counseling patients about the implications of VA policy regarding state-approved medical marijuana programs for their individual health care. Such a patient-centered approach represents the most ethically acceptable means of mediating the conflict between state and federal law regarding medical marijuana in its current stage of evolution.
Author disclosures
The author reports no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the author and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
References
1. State Medical Marijuana Laws. National Conference of State Legislators Website. http://www.ncsl.org/issues-research/health/state-medical-marijuana-laws.aspx. Updated January 2014. Accessed February 1, 2014.
2. Veterans Health Administration. Clinical Considerations Regarding Veteran Patients Who Participate in State-Approved Medical Marijuana Programs. Washington, DC: Department of Veterans Affairs; 2010.
3. The Associated Press. Supreme Court is set to consider medical marijuana. New York Times. November 28, 2004. http://www.nytimes.com/2004/11/28/politics/28marijuana.html?fta=y. Accessed February 5, 2014.
4. Dresser R. Irrational basis: The legal status of medical marijuana. Hastings Cent Rep. 2009;39(6):7-8.
5. Office of General Counsel. Opinion on State Medical Marijuana Registration Forms. Washington, DC: Department of Veterans Affairs; 2008. VAOPGCADV 9-2008.
6. Cohen PJ. Medical marijuana: The conflict between scientific evidence and political ideology. Part one of two. J Pain Palliat Care Pharmacother. 2009;23(1):4-25.
7. Pearson v McCaffrey, 139 F Supp 2d 772 (D DC 2001).
8. Constitution of the United States. United States Senate Website. http://www.senate.gov/civics/constitution_item/constitution.htm. Accessed January 22, 2012.
9. White BD. New York, NY: Informa Healthcare; 2007.
10. Conant v Walters, 309 F3d 629 (9th Cir 2002).
11. Gonzales v Raich, 545 US 1, 125 SCt, 2195 (2005).
12. United States v Lopez, 514 US 549, 115 SCt, 1624 (1995).
13. United States v Morrison, 529 US 598, 120 SCt, 1740 (2000).
14. The Lynn and Erin Compassionate Use Act, NMSA 1978 §26-2B (2007).
15. Frosch D. V.A. Easing rules for users of medical marijuana. New York Times. July 24, 2010:A1.
16. Medical Marijuana. Washington, DC: Dept of Veterans Affairs; 2010. VHA Directive 2010-035.
17. Access to Clinical Programs for Veterans Participating in State-Approved Marijuana Programs. Washington, DC: Dept of Veterans Affairs; 2011. VHA Directive 2011-004.
18. Uniform Code of Military Justice, 10 USC § 912A (2011).
19. Confidentiality of Certain Medical Records, 38 USC § 7332 (1991).
20. Petzel RA. Access to Clinical Programs for Veterans Participating in State-Approved Marijuana Programs. Washington, DC: Dept of Veterans Affairs; 2011. VHA Directive 2011-004.
21. Institute of Medicine. Marijuana and Medicine: Assessing the Science. Joy JE, Watson SJ Jr, Benson JA Jr, eds. Washington, DC: National Academy Press; 1999.
22. Charuvastra A, Friedmann PD, Stein MD. Physician attitudes regarding the prescription of medical marijuana. J Addict Dis. 2005;24(3):87-93.
23. Healy J. Up early and in line for a medical marijuana milestone in Colorado. New York Times. January 1, 2014:A1.
24. Public Policy Statement on Medical Marijuana. Chevy Chase, MD: American Society of Addiction Medicine; 2010.
25. Swartz R. Medical marijuana users in substance abuse treatment. Harm Reduct J. 2010;7:3.
26. Clark JD. Chronic pain prevalence and analgesic prescribing in a general medical population. J Pain Symptom Manage. 2002;23(2):131-137.
27. Petrakis IL, Rosenheck R, Desai R. Substance use comorbidity among veterans with posttraumatic stress disorder and other psychiatric illness. Am J Addict. 2011;20(3):185-189.
28. Medical Marijuana. ProCon.org Website. http://medicalmarijuana.procon.org. Updated February 3, 2014. Accessed February 5, 2014.
29. Busemeyer D. Cannabis catch-22. Santa Fe New Mexican. October 14, 2012:A1, A4-A5.
30. Harris G. Researchers find study of medical marijuana discouraged. New York Times. January 18, 2010:A14.
31. Cohen PJ. Medical marijuana: The conflict between scientific evidence and political ideology. Part two of two. J Pain Palliat Care Pharmacother. 2009;23(2):120-140.
32. Daigle L. Medical Marijuana. Bethesda, MD: American Society of Health-System Pharmacists; 2011.

Antibiotic Therapy and Bacterial Resistance in Patients With Spinal Cord Injury
Nosocomial urinary tract infections (UTIs) are often associated with significant morbidity, mortality, and health care costs.1,2 Patients with spinal cord injury (SCI) often have indwelling or intermittent urinary catheters and are prone to have asymptomatic bacteriuria and UTIs. As a result, they frequently receive antimicrobial therapy and have a higher prevalence of antibiotic resistant urinary tract isolates compared with patients without SCI.3-5 Unfortunately, data are lacking to provide guidance for optimal treatment and duration for UTIs in patients with SCI.
Many studies have evaluated patient propensity for development of antibiotic resistance in UTIs. Age > 65 years, use of a urinary catheter, previous hospitalization, and prior antimicrobial use have been identified as common risk factors.6-8 Waites and colleagues evaluated antimicrobial resistance of urinary tract organisms in outpatients with SCI and found that 33% of urinary cultures isolated multidrug-resistant microorganisms. The authors demonstrated a relationship between antimicrobial resistance and broad spectrum and prophylactic use of antibiotics.3,9
This study sought to determine the incidence of resistance acquisition by comparing susceptibility profiles of the same organisms isolated from the same patient in consecutive episodes of bacteriuria. Given that prior antimicrobial use was identified as a common risk factor for antibiotic resistance in previous reports, this study also sought to determine patterns of antibiotic use in patients with SCI at the VA North Texas Health Care System (VANTHCS) in Dallas, Texas, to evaluate whether any correlations between antibiotic use and resistance acquisition exist. A secondary objective included identification of other risk factors that may increase acquisition of resistance.
Study Design
This study was a retrospective chart review approved by the Institutional Review Board at the VANTHCS. Since computerized charting was available beginning July 2003, the VA Computerized Patient Record System was queried to identify male or female adult (aged ≥ 18 years) veterans admitted to the SCI inpatient unit between July 1, 2003, and December 31, 2009, for review. Patients who had an ICD-9 code consistent with paraplegia, tetraplegia, or quadriplegia and 2 consecutive urine cultures that isolated the same organism within 6 months of each other were included. Males with a diagnosis of epididymitis or prostatitis were excluded.
The following data were collected for analysis: gender, age, weight, height, American Spinal Injury Association (ASIA) Impairment Scale Grades (A-E), duration of hospitalization in the SCI unit, the presence and type of urinary catheter, microbiology and antibiotic regimen, past medical history, previous antibiotic history, comorbidities, and concomitant drug therapy. The presence and type of urinary catheter was determined by the primary investigator and verified by the physician who oversaw care of patients with SCI.
All antimicrobial sensitivity testing was performed via the Microscan (Microscan Systems, Inc., Renton, WA) automated testing system. Acquisition of antibiotic resistance was defined as an increase of at least 2 dilutions in the breakpoint or change on the susceptibility panel from Susceptible (S) to Resistant (R) on the repeat urine culture.
Analysis of Resistance
Continuous parameters were reported as mean (standard deviation [SD]), and discrete parameters were reported as a percentage. Analyses of variance (ANOVA) were computed to evaluate the difference in the mean of the continuous parameters. The Mann-Whitney U test replaced the ANOVA when a dependent variable was not normally distributed. Associations between pairs of discrete parameters were tested with the Pearson chi-square test. Logistic regression analyses were performed to determine the associations between potential risk factors (age, ASIA grade, antibiotic duration, class of antibiotic) and antibiotic resistance. The study alpha was α < .05. All analyses were performed with SPSS 20.0 for Windows.
Three hundred fifty-five veterans admitted to the SCI unit during the study period were initially identified. Of those, 269 did not meet inclusion criteria and were excluded. The most common reason for exclusion was absence of a second positive urine culture with isolation of the same organism. Other reasons for exclusion included no urine cultures completed while admitted to the SCI unit or no diagnosis of SCI.
A total of 86 subjects, mean aged 56.7 years (SD, 14.2), were included in the study. Subjects were primarily men (93%) with a mean body mass index of 25.5 (SD, 7). Most of the subjects were classified Complete on the ASIA scale, meaning no motor strength or sensation below their neurologic level of injury (ASIA A; 38.4%), followed by Sensory Incomplete (ASIA B; 25.6%), Motor Incomplete-Low Muscle Strength (ASIA C; 16.3%), Motor Incomplete-High Muscle Strength (ASIA D; 14%), and Normal (ASIA E; 1.2%).
Both groups (resistance and no resistance) had similar baseline characteristics, and no differences were found for the following characteristics: ASIA grade, length of stay (LOS), presence of or control of diabetes, and presence of an indwelling urinary catheter (Table 1). However, veterans in the resistance group were significantly older than those in the no resistance group (aged 61 years vs aged 54 years; P = .03) and spent more time housed in the SCI unit with a mean LOS of 141 days vs 84 days (P = .049). Urinary pathogens developed resistance in 32 patients (37.2%, resistance group), and 54 patients (62.8%, no resistance group) did not.
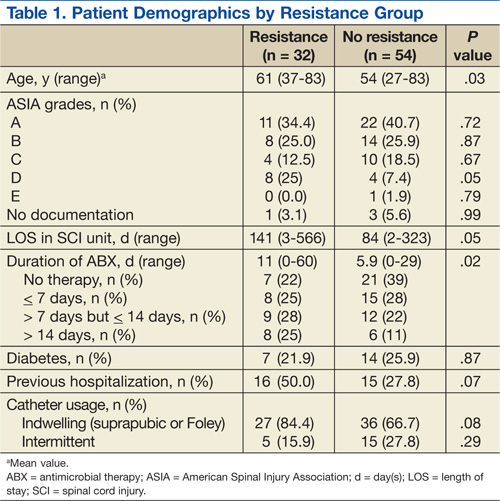
No significant differences in the types of organisms isolated were noted between the groups (Table 2). The most common pathogens isolated were Pseudomonas aeruginosa (24%), Enterococcus spp. (18%), Escherichia coli (17%), Proteus spp. (14%), Klebsiella spp. (7%), and Acinetobacter spp. (6%).
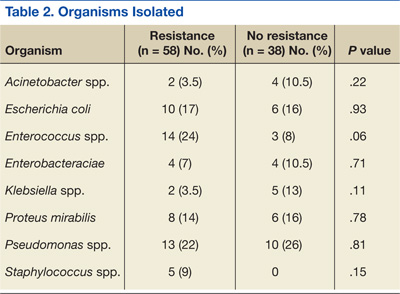
Thirty-six percent of the pathogens in the first cultures were not treated with any antibiotics, because they were considered as colonizers or contaminants. Only 61% of pathogens in the no resistance group vs 78% in the resistance group were exposed to antimicrobial treatment. In those veterans who were treated, antibiotic usage on the first urine culture was assessed to determine whether any relationship existed between receipt of a particular antimicrobial class and development of resistance. Fluoroquinolones were the most commonly prescribed antimicrobials in both the resistance and no resistance groups (Table 3).
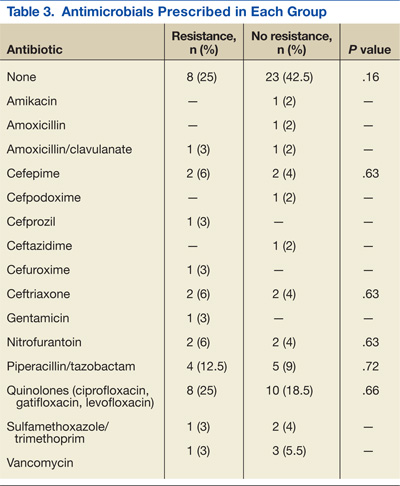
Four risk factors (ASIA grade, antibiotic treatment duration, prior use of a cephalosporin, and prior use of penicillin) were initially identified by logistic regression analyses as being associated with resistance development. Since veterans in the resistance group were significantly older than those in the no resistance group, the analysis was repeated with age as a covariate to independently assess the association between the risk factors and resistance. After controlling for age, no significant association between the ASIA grade and resistance was identified (adjusted odds ratio [OR], 1.03; 95% confidence interval [CI]: 0.66 – 1.6). Median duration of antibiotic treatment was 6 days in all patients, 3.5 days in the no resistance group, and 9 days in the resistance group. Longer duration of treatment significantly predicted resistance (adjusted OR, 1.07; P = .03; 95% CI: 1.01 – 1.03). For every additional day the patient was on an antibiotic, he or she was 7% more likely to develop resistance.
The incidence of resistant organisms after exposure to a cephalosporin was not statistically different between groups (adjusted OR, 1.74; P = .36; 95% CI: 1.0 – 1.2). In the resistance group, 28% of the antibiotics prescribed were cephalosporins (cefuroxime, ceftriaxone, ceftazidime, and cefepime), which were used for Proteus mirabilis, Escherichia coli, Klebsiella pneumoniae, and Pseudomonas aeruginosa. In the no resistance group, 17% of the antibiotics prescribed were cephalosporins (cefepime only) and were used for Proteus mirabilis.
Organisms treated with penicillin were significantly less likely to become resistant (adjusted OR, 0.26; P = .04; 95% CI: 0.07 - 0.96). In the resistance group, 16% of the antibiotics were penicillins (piperacillin/tazobactam), which were used for Escherichia coli, Enterococcus faecalis, Acinetobacter baumannii, Pseudomonas aeruginosa, and Klebsiella pneumoniae. In the no resistance group, 22% of the antibiotics were penicillins (amoxicillin, amoxicillin/clavulanate and piperacillin/tazobactam), which were used for Proteus mirabilis, Enterococcus faecalis, and Acinetobacter baumannii.
Discussion
Longer duration of treatment significantly increased resistance on the subsequent culture in this study. For every additional day the patient was on an antibiotic, he or she was 7% more likely to develop a resistance. However, the potential impact of using a given antibiotic class on the acquisition of resistance in patients with SCI who had a UTI was not demonstrated. Surprisingly, the use of a cephalosporin was not associated with an increased incidence of resistance in this study, which was inconsistent with the findings from other studies.10 Weber and colleagues evaluated nosocomial infections in the intensive care unit. The authors suggested that restriction on the use of third-generation cephalosporins might decrease antibiotic resistance, especially in extended spectrum beta-lactamase producing gram-negative bacilli.11
The difference in this study may be explained by the lower incidence of Escherichia coli and Klebsiella pneumoniae, which are known to exhibit inducible resistance on exposure to third-generation cephalosporins. Conversely, it was found that patients treated with a penicillin were significantly less likely to develop resistant organisms from subsequent cultures. The most common penicillin used in this study’s patient population was piperacillin/tazobactam.
For complicated UTIs including pyelonephritis, the European Association of Urology (EAU) guidelines for the management of urinary and male genital tract infections recommend treatment for 3 to 5 days after defervescence or control of complicating factors.12 These recommendations could lead to much shorter treatment durations than the traditional 14-day “standard” course often prescribed. One meta-analysis recommends a 5-day course for UTIs without fever in patients with SCI vs a 14-day course for patients with fever.13 Due to the lack of data, care often varies based on the patient’s clinical status, provider experience, and opinions. The Pannek study surveyed 16 centers that specialized in SCI care. When compared with the recommendations in the EAU guidelines, the study found providers in > 50% of the responding facilities overtreated UTIs.14
Limitations
This study has several limitations. First, the sample size was much smaller than expected. Of the 355 charts reviewed, only 86 met all the criteria to be included, which limited analysis. Additionally, given the retrospective nature of the study, it was impossible to determine provider rationale for the treatment. Since a diagnosis of UTI in patients with SCI often cannot be done with conventional methods due to lack of symptoms, many investigators have emphasized the use of quantitative urinalysis to differentiate true infection vs contamination.15-17
According to the National Institute on Disability and Rehabilitation Research consensus conference recommendations, the definition of significant bacteriuria will vary, depending on the method of bladder drainage.18 While this study reviewed microbiologic cultures and the type of patient’s urinary catheter, the method of bladder drainage in the context of quantitative urinalysis was not evaluated, which limited the interpretation of microbiologic data.
It was also impossible to determine whether bacteria were cleared by the initial treatment, leading to new bacterial strains with a multidrug resistance, or whether patients relapsed. While antibiotic selection was appropriate for antimicrobial coverage, this study was not designed to detect potential inadequacies in dosing, which could also affect resistance. Last, since no genetic evaluation of the microorganisms was done, the authors cannot be sure whether the microorganisms noted on the first urine culture were of the same genetic makeup as those identified in the second urine culture.
Conclusion
Optimal duration of therapy for treatment of UTIs in patients with SCI is unclear. Despite its limitations, the study suggests exposure to longer antibiotic treatment courses may lead to increased antimicrobial resistance in the urinary tract organisms in this patient population. Further investigation with a larger sample size is required to confirm these findings.
Author disclosures
Dr. Bedimo received research grant funding from Janssen Pharmaceuticals and Merck and Company. He also serves as an ad hoc scientific advisor for Viiv Healthcare, Gilead Science, and BMD Science. All other authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
References
1. Saint S, Lipsky BA. Preventing catheter-related bacteriuria: Should we? Can we? How? Arch Intern Med. 1999;159(8):800-808.
2. Laupland KB, Bagshaw SM, Gregson DB, Kirkpatrick AW, Ross T, Church DL. Intensive care unit-acquired urinary tract infections in a regional critical care system. Crit Care. 2005;9(2):R60-R65.
3. Girard R, Mazoyer MA, Plauchu MM, Rode G. High prevalence of nosocomial infections in rehabilitation units accounted for by urinary tract infections in patients with spinal cord injury. J Hosp Infect. 2006;62(4):473-479.
4. Cardenas DD, Hooton TM. Urinary tract infection in persons with spinal cord injury. Arch Phys Med Rehabil. 1995;76(3):272-280.
5. Salomon J, Gory A, Bernard L, Ruffion A, Denys P, Chartier-Kastler E. [Urinary tract infection and neurogenic bladder]. Prog Urol. 2007;17(3):448-453.
6. Ena J, Amador C, Martinez C, Ortiz de la Tabla V. Risk factors for acquisition of urinary tract infections caused by ciprofloxacin resistant Escherichia coli. J Urol. 1995;153(1):117-120.
7. Allen UD, MacDonald N, Fuite L, Chan F, Stephens D. Risk factors for resistance to “first-line” antimicrobials among urinary tract isolates of Escherichia coli in children. CMAJ. 1999;160(10):1436-1440.
8. De Mouy D, Cavallo JD, Armengaud M, et al. [Urinary tract infection in an urban population: Etiology and antibiotic sensitivity as a function of patient history]. Presse Med. 1999;28(30):1624-1628.
9. Waites KB, Chen Y, DeVivo MJ, Canupp KC, Moser SA. Antimicrobial resistance in gram-negative bacteria isolated from the urinary tract in community-residing persons with spinal cord injury. Arch Phys Med Rehabil. 2000;81(6):764-769.
10. Shah PS, Cannon JP, Sullivan CL, Nemchausky B, Pachucki CT. Controlling antimicrobial use and decreasing microbiological laboratory tests for urinary tract infections in spinal-cord-injury patients with chronic indwelling catheters. Am J Health Syst Pharm. 2005;62(1):74-77.
11. Weber DJ, Raasch R, Rutala WA. Nosocomial infections in the ICU: The growing importance of antibiotic-resistant pathogens. Chest. 1999;115(suppl 3):34S-41S.
12. Naber KG, Bergman B, Bishop MC, et al; Urinary Tract Infection (UTI) Working Group of the Health Care Office (HCO) of the European Association of Urology (EAU). EAU guidelines for the management of urinary and male genital tract infections. Urinary Tract Infection (UTI) Working Group of the Health Care Office (HCO) of the European Association of Urology (EAU). Eur Urol. 2001;40(5):576-588.
13. Everaert K, Lumen N, Kerckhaert W, Willaert P, van Driel M. Urinary tract infections in spinal cord injury: Prevention and treatment guidelines. Acta Clin Belg. 2009;64(4):335-340.
14. Pannek J. Treatment of urinary tract infection in persons with spinal cord injury: Guidelines, evidence, and clinical practice. A questionnaire-based survey and review of the literature. J Spinal Cord Med. 2011;34(1):11-15.
15. Musher DM, Thorsteinsson SB, Airola VM II. Quantitative urinalysis. Diagnosing urinary tract infection in men. JAMA. 1976;236(18):2069-2072.
16. Deresinski SC, Perkash I. Urinary tract infections in male spinal cord injured patients. Part two: Diagnostic value of symptoms and of quantitative urinalysis. J Am Paraplegia Soc. 1985;8(1):7-10.
17. Deresinski SC, Perkash I. Urinary tract infections in male spinal cord injured patients. Part one: Bacteriologic diagnosis. J Am Paraplegia Soc. 1985;8(1):4-6.
18. Garcia Leoni ME, Esclarin De Ruz A. Management of urinary tract infection in patients with spinal cord injuries. Clin Microbiol Infect. 2003;9(8):780-785.
Nosocomial urinary tract infections (UTIs) are often associated with significant morbidity, mortality, and health care costs.1,2 Patients with spinal cord injury (SCI) often have indwelling or intermittent urinary catheters and are prone to have asymptomatic bacteriuria and UTIs. As a result, they frequently receive antimicrobial therapy and have a higher prevalence of antibiotic resistant urinary tract isolates compared with patients without SCI.3-5 Unfortunately, data are lacking to provide guidance for optimal treatment and duration for UTIs in patients with SCI.
Many studies have evaluated patient propensity for development of antibiotic resistance in UTIs. Age > 65 years, use of a urinary catheter, previous hospitalization, and prior antimicrobial use have been identified as common risk factors.6-8 Waites and colleagues evaluated antimicrobial resistance of urinary tract organisms in outpatients with SCI and found that 33% of urinary cultures isolated multidrug-resistant microorganisms. The authors demonstrated a relationship between antimicrobial resistance and broad spectrum and prophylactic use of antibiotics.3,9
This study sought to determine the incidence of resistance acquisition by comparing susceptibility profiles of the same organisms isolated from the same patient in consecutive episodes of bacteriuria. Given that prior antimicrobial use was identified as a common risk factor for antibiotic resistance in previous reports, this study also sought to determine patterns of antibiotic use in patients with SCI at the VA North Texas Health Care System (VANTHCS) in Dallas, Texas, to evaluate whether any correlations between antibiotic use and resistance acquisition exist. A secondary objective included identification of other risk factors that may increase acquisition of resistance.
Study Design
This study was a retrospective chart review approved by the Institutional Review Board at the VANTHCS. Since computerized charting was available beginning July 2003, the VA Computerized Patient Record System was queried to identify male or female adult (aged ≥ 18 years) veterans admitted to the SCI inpatient unit between July 1, 2003, and December 31, 2009, for review. Patients who had an ICD-9 code consistent with paraplegia, tetraplegia, or quadriplegia and 2 consecutive urine cultures that isolated the same organism within 6 months of each other were included. Males with a diagnosis of epididymitis or prostatitis were excluded.
The following data were collected for analysis: gender, age, weight, height, American Spinal Injury Association (ASIA) Impairment Scale Grades (A-E), duration of hospitalization in the SCI unit, the presence and type of urinary catheter, microbiology and antibiotic regimen, past medical history, previous antibiotic history, comorbidities, and concomitant drug therapy. The presence and type of urinary catheter was determined by the primary investigator and verified by the physician who oversaw care of patients with SCI.
All antimicrobial sensitivity testing was performed via the Microscan (Microscan Systems, Inc., Renton, WA) automated testing system. Acquisition of antibiotic resistance was defined as an increase of at least 2 dilutions in the breakpoint or change on the susceptibility panel from Susceptible (S) to Resistant (R) on the repeat urine culture.
Analysis of Resistance
Continuous parameters were reported as mean (standard deviation [SD]), and discrete parameters were reported as a percentage. Analyses of variance (ANOVA) were computed to evaluate the difference in the mean of the continuous parameters. The Mann-Whitney U test replaced the ANOVA when a dependent variable was not normally distributed. Associations between pairs of discrete parameters were tested with the Pearson chi-square test. Logistic regression analyses were performed to determine the associations between potential risk factors (age, ASIA grade, antibiotic duration, class of antibiotic) and antibiotic resistance. The study alpha was α < .05. All analyses were performed with SPSS 20.0 for Windows.
Three hundred fifty-five veterans admitted to the SCI unit during the study period were initially identified. Of those, 269 did not meet inclusion criteria and were excluded. The most common reason for exclusion was absence of a second positive urine culture with isolation of the same organism. Other reasons for exclusion included no urine cultures completed while admitted to the SCI unit or no diagnosis of SCI.
A total of 86 subjects, mean aged 56.7 years (SD, 14.2), were included in the study. Subjects were primarily men (93%) with a mean body mass index of 25.5 (SD, 7). Most of the subjects were classified Complete on the ASIA scale, meaning no motor strength or sensation below their neurologic level of injury (ASIA A; 38.4%), followed by Sensory Incomplete (ASIA B; 25.6%), Motor Incomplete-Low Muscle Strength (ASIA C; 16.3%), Motor Incomplete-High Muscle Strength (ASIA D; 14%), and Normal (ASIA E; 1.2%).
Both groups (resistance and no resistance) had similar baseline characteristics, and no differences were found for the following characteristics: ASIA grade, length of stay (LOS), presence of or control of diabetes, and presence of an indwelling urinary catheter (Table 1). However, veterans in the resistance group were significantly older than those in the no resistance group (aged 61 years vs aged 54 years; P = .03) and spent more time housed in the SCI unit with a mean LOS of 141 days vs 84 days (P = .049). Urinary pathogens developed resistance in 32 patients (37.2%, resistance group), and 54 patients (62.8%, no resistance group) did not.
No significant differences in the types of organisms isolated were noted between the groups (Table 2). The most common pathogens isolated were Pseudomonas aeruginosa (24%), Enterococcus spp. (18%), Escherichia coli (17%), Proteus spp. (14%), Klebsiella spp. (7%), and Acinetobacter spp. (6%).
Thirty-six percent of the pathogens in the first cultures were not treated with any antibiotics, because they were considered as colonizers or contaminants. Only 61% of pathogens in the no resistance group vs 78% in the resistance group were exposed to antimicrobial treatment. In those veterans who were treated, antibiotic usage on the first urine culture was assessed to determine whether any relationship existed between receipt of a particular antimicrobial class and development of resistance. Fluoroquinolones were the most commonly prescribed antimicrobials in both the resistance and no resistance groups (Table 3).
Four risk factors (ASIA grade, antibiotic treatment duration, prior use of a cephalosporin, and prior use of penicillin) were initially identified by logistic regression analyses as being associated with resistance development. Since veterans in the resistance group were significantly older than those in the no resistance group, the analysis was repeated with age as a covariate to independently assess the association between the risk factors and resistance. After controlling for age, no significant association between the ASIA grade and resistance was identified (adjusted odds ratio [OR], 1.03; 95% confidence interval [CI]: 0.66 – 1.6). Median duration of antibiotic treatment was 6 days in all patients, 3.5 days in the no resistance group, and 9 days in the resistance group. Longer duration of treatment significantly predicted resistance (adjusted OR, 1.07; P = .03; 95% CI: 1.01 – 1.03). For every additional day the patient was on an antibiotic, he or she was 7% more likely to develop resistance.
The incidence of resistant organisms after exposure to a cephalosporin was not statistically different between groups (adjusted OR, 1.74; P = .36; 95% CI: 1.0 – 1.2). In the resistance group, 28% of the antibiotics prescribed were cephalosporins (cefuroxime, ceftriaxone, ceftazidime, and cefepime), which were used for Proteus mirabilis, Escherichia coli, Klebsiella pneumoniae, and Pseudomonas aeruginosa. In the no resistance group, 17% of the antibiotics prescribed were cephalosporins (cefepime only) and were used for Proteus mirabilis.
Organisms treated with penicillin were significantly less likely to become resistant (adjusted OR, 0.26; P = .04; 95% CI: 0.07 - 0.96). In the resistance group, 16% of the antibiotics were penicillins (piperacillin/tazobactam), which were used for Escherichia coli, Enterococcus faecalis, Acinetobacter baumannii, Pseudomonas aeruginosa, and Klebsiella pneumoniae. In the no resistance group, 22% of the antibiotics were penicillins (amoxicillin, amoxicillin/clavulanate and piperacillin/tazobactam), which were used for Proteus mirabilis, Enterococcus faecalis, and Acinetobacter baumannii.
Discussion
Longer duration of treatment significantly increased resistance on the subsequent culture in this study. For every additional day the patient was on an antibiotic, he or she was 7% more likely to develop a resistance. However, the potential impact of using a given antibiotic class on the acquisition of resistance in patients with SCI who had a UTI was not demonstrated. Surprisingly, the use of a cephalosporin was not associated with an increased incidence of resistance in this study, which was inconsistent with the findings from other studies.10 Weber and colleagues evaluated nosocomial infections in the intensive care unit. The authors suggested that restriction on the use of third-generation cephalosporins might decrease antibiotic resistance, especially in extended spectrum beta-lactamase producing gram-negative bacilli.11
The difference in this study may be explained by the lower incidence of Escherichia coli and Klebsiella pneumoniae, which are known to exhibit inducible resistance on exposure to third-generation cephalosporins. Conversely, it was found that patients treated with a penicillin were significantly less likely to develop resistant organisms from subsequent cultures. The most common penicillin used in this study’s patient population was piperacillin/tazobactam.
For complicated UTIs including pyelonephritis, the European Association of Urology (EAU) guidelines for the management of urinary and male genital tract infections recommend treatment for 3 to 5 days after defervescence or control of complicating factors.12 These recommendations could lead to much shorter treatment durations than the traditional 14-day “standard” course often prescribed. One meta-analysis recommends a 5-day course for UTIs without fever in patients with SCI vs a 14-day course for patients with fever.13 Due to the lack of data, care often varies based on the patient’s clinical status, provider experience, and opinions. The Pannek study surveyed 16 centers that specialized in SCI care. When compared with the recommendations in the EAU guidelines, the study found providers in > 50% of the responding facilities overtreated UTIs.14
Limitations
This study has several limitations. First, the sample size was much smaller than expected. Of the 355 charts reviewed, only 86 met all the criteria to be included, which limited analysis. Additionally, given the retrospective nature of the study, it was impossible to determine provider rationale for the treatment. Since a diagnosis of UTI in patients with SCI often cannot be done with conventional methods due to lack of symptoms, many investigators have emphasized the use of quantitative urinalysis to differentiate true infection vs contamination.15-17
According to the National Institute on Disability and Rehabilitation Research consensus conference recommendations, the definition of significant bacteriuria will vary, depending on the method of bladder drainage.18 While this study reviewed microbiologic cultures and the type of patient’s urinary catheter, the method of bladder drainage in the context of quantitative urinalysis was not evaluated, which limited the interpretation of microbiologic data.
It was also impossible to determine whether bacteria were cleared by the initial treatment, leading to new bacterial strains with a multidrug resistance, or whether patients relapsed. While antibiotic selection was appropriate for antimicrobial coverage, this study was not designed to detect potential inadequacies in dosing, which could also affect resistance. Last, since no genetic evaluation of the microorganisms was done, the authors cannot be sure whether the microorganisms noted on the first urine culture were of the same genetic makeup as those identified in the second urine culture.
Conclusion
Optimal duration of therapy for treatment of UTIs in patients with SCI is unclear. Despite its limitations, the study suggests exposure to longer antibiotic treatment courses may lead to increased antimicrobial resistance in the urinary tract organisms in this patient population. Further investigation with a larger sample size is required to confirm these findings.
Author disclosures
Dr. Bedimo received research grant funding from Janssen Pharmaceuticals and Merck and Company. He also serves as an ad hoc scientific advisor for Viiv Healthcare, Gilead Science, and BMD Science. All other authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
References
1. Saint S, Lipsky BA. Preventing catheter-related bacteriuria: Should we? Can we? How? Arch Intern Med. 1999;159(8):800-808.
2. Laupland KB, Bagshaw SM, Gregson DB, Kirkpatrick AW, Ross T, Church DL. Intensive care unit-acquired urinary tract infections in a regional critical care system. Crit Care. 2005;9(2):R60-R65.
3. Girard R, Mazoyer MA, Plauchu MM, Rode G. High prevalence of nosocomial infections in rehabilitation units accounted for by urinary tract infections in patients with spinal cord injury. J Hosp Infect. 2006;62(4):473-479.
4. Cardenas DD, Hooton TM. Urinary tract infection in persons with spinal cord injury. Arch Phys Med Rehabil. 1995;76(3):272-280.
5. Salomon J, Gory A, Bernard L, Ruffion A, Denys P, Chartier-Kastler E. [Urinary tract infection and neurogenic bladder]. Prog Urol. 2007;17(3):448-453.
6. Ena J, Amador C, Martinez C, Ortiz de la Tabla V. Risk factors for acquisition of urinary tract infections caused by ciprofloxacin resistant Escherichia coli. J Urol. 1995;153(1):117-120.
7. Allen UD, MacDonald N, Fuite L, Chan F, Stephens D. Risk factors for resistance to “first-line” antimicrobials among urinary tract isolates of Escherichia coli in children. CMAJ. 1999;160(10):1436-1440.
8. De Mouy D, Cavallo JD, Armengaud M, et al. [Urinary tract infection in an urban population: Etiology and antibiotic sensitivity as a function of patient history]. Presse Med. 1999;28(30):1624-1628.
9. Waites KB, Chen Y, DeVivo MJ, Canupp KC, Moser SA. Antimicrobial resistance in gram-negative bacteria isolated from the urinary tract in community-residing persons with spinal cord injury. Arch Phys Med Rehabil. 2000;81(6):764-769.
10. Shah PS, Cannon JP, Sullivan CL, Nemchausky B, Pachucki CT. Controlling antimicrobial use and decreasing microbiological laboratory tests for urinary tract infections in spinal-cord-injury patients with chronic indwelling catheters. Am J Health Syst Pharm. 2005;62(1):74-77.
11. Weber DJ, Raasch R, Rutala WA. Nosocomial infections in the ICU: The growing importance of antibiotic-resistant pathogens. Chest. 1999;115(suppl 3):34S-41S.
12. Naber KG, Bergman B, Bishop MC, et al; Urinary Tract Infection (UTI) Working Group of the Health Care Office (HCO) of the European Association of Urology (EAU). EAU guidelines for the management of urinary and male genital tract infections. Urinary Tract Infection (UTI) Working Group of the Health Care Office (HCO) of the European Association of Urology (EAU). Eur Urol. 2001;40(5):576-588.
13. Everaert K, Lumen N, Kerckhaert W, Willaert P, van Driel M. Urinary tract infections in spinal cord injury: Prevention and treatment guidelines. Acta Clin Belg. 2009;64(4):335-340.
14. Pannek J. Treatment of urinary tract infection in persons with spinal cord injury: Guidelines, evidence, and clinical practice. A questionnaire-based survey and review of the literature. J Spinal Cord Med. 2011;34(1):11-15.
15. Musher DM, Thorsteinsson SB, Airola VM II. Quantitative urinalysis. Diagnosing urinary tract infection in men. JAMA. 1976;236(18):2069-2072.
16. Deresinski SC, Perkash I. Urinary tract infections in male spinal cord injured patients. Part two: Diagnostic value of symptoms and of quantitative urinalysis. J Am Paraplegia Soc. 1985;8(1):7-10.
17. Deresinski SC, Perkash I. Urinary tract infections in male spinal cord injured patients. Part one: Bacteriologic diagnosis. J Am Paraplegia Soc. 1985;8(1):4-6.
18. Garcia Leoni ME, Esclarin De Ruz A. Management of urinary tract infection in patients with spinal cord injuries. Clin Microbiol Infect. 2003;9(8):780-785.
Nosocomial urinary tract infections (UTIs) are often associated with significant morbidity, mortality, and health care costs.1,2 Patients with spinal cord injury (SCI) often have indwelling or intermittent urinary catheters and are prone to have asymptomatic bacteriuria and UTIs. As a result, they frequently receive antimicrobial therapy and have a higher prevalence of antibiotic resistant urinary tract isolates compared with patients without SCI.3-5 Unfortunately, data are lacking to provide guidance for optimal treatment and duration for UTIs in patients with SCI.
Many studies have evaluated patient propensity for development of antibiotic resistance in UTIs. Age > 65 years, use of a urinary catheter, previous hospitalization, and prior antimicrobial use have been identified as common risk factors.6-8 Waites and colleagues evaluated antimicrobial resistance of urinary tract organisms in outpatients with SCI and found that 33% of urinary cultures isolated multidrug-resistant microorganisms. The authors demonstrated a relationship between antimicrobial resistance and broad spectrum and prophylactic use of antibiotics.3,9
This study sought to determine the incidence of resistance acquisition by comparing susceptibility profiles of the same organisms isolated from the same patient in consecutive episodes of bacteriuria. Given that prior antimicrobial use was identified as a common risk factor for antibiotic resistance in previous reports, this study also sought to determine patterns of antibiotic use in patients with SCI at the VA North Texas Health Care System (VANTHCS) in Dallas, Texas, to evaluate whether any correlations between antibiotic use and resistance acquisition exist. A secondary objective included identification of other risk factors that may increase acquisition of resistance.
Study Design
This study was a retrospective chart review approved by the Institutional Review Board at the VANTHCS. Since computerized charting was available beginning July 2003, the VA Computerized Patient Record System was queried to identify male or female adult (aged ≥ 18 years) veterans admitted to the SCI inpatient unit between July 1, 2003, and December 31, 2009, for review. Patients who had an ICD-9 code consistent with paraplegia, tetraplegia, or quadriplegia and 2 consecutive urine cultures that isolated the same organism within 6 months of each other were included. Males with a diagnosis of epididymitis or prostatitis were excluded.
The following data were collected for analysis: gender, age, weight, height, American Spinal Injury Association (ASIA) Impairment Scale Grades (A-E), duration of hospitalization in the SCI unit, the presence and type of urinary catheter, microbiology and antibiotic regimen, past medical history, previous antibiotic history, comorbidities, and concomitant drug therapy. The presence and type of urinary catheter was determined by the primary investigator and verified by the physician who oversaw care of patients with SCI.
All antimicrobial sensitivity testing was performed via the Microscan (Microscan Systems, Inc., Renton, WA) automated testing system. Acquisition of antibiotic resistance was defined as an increase of at least 2 dilutions in the breakpoint or change on the susceptibility panel from Susceptible (S) to Resistant (R) on the repeat urine culture.
Analysis of Resistance
Continuous parameters were reported as mean (standard deviation [SD]), and discrete parameters were reported as a percentage. Analyses of variance (ANOVA) were computed to evaluate the difference in the mean of the continuous parameters. The Mann-Whitney U test replaced the ANOVA when a dependent variable was not normally distributed. Associations between pairs of discrete parameters were tested with the Pearson chi-square test. Logistic regression analyses were performed to determine the associations between potential risk factors (age, ASIA grade, antibiotic duration, class of antibiotic) and antibiotic resistance. The study alpha was α < .05. All analyses were performed with SPSS 20.0 for Windows.
Three hundred fifty-five veterans admitted to the SCI unit during the study period were initially identified. Of those, 269 did not meet inclusion criteria and were excluded. The most common reason for exclusion was absence of a second positive urine culture with isolation of the same organism. Other reasons for exclusion included no urine cultures completed while admitted to the SCI unit or no diagnosis of SCI.
A total of 86 subjects, mean aged 56.7 years (SD, 14.2), were included in the study. Subjects were primarily men (93%) with a mean body mass index of 25.5 (SD, 7). Most of the subjects were classified Complete on the ASIA scale, meaning no motor strength or sensation below their neurologic level of injury (ASIA A; 38.4%), followed by Sensory Incomplete (ASIA B; 25.6%), Motor Incomplete-Low Muscle Strength (ASIA C; 16.3%), Motor Incomplete-High Muscle Strength (ASIA D; 14%), and Normal (ASIA E; 1.2%).
Both groups (resistance and no resistance) had similar baseline characteristics, and no differences were found for the following characteristics: ASIA grade, length of stay (LOS), presence of or control of diabetes, and presence of an indwelling urinary catheter (Table 1). However, veterans in the resistance group were significantly older than those in the no resistance group (aged 61 years vs aged 54 years; P = .03) and spent more time housed in the SCI unit with a mean LOS of 141 days vs 84 days (P = .049). Urinary pathogens developed resistance in 32 patients (37.2%, resistance group), and 54 patients (62.8%, no resistance group) did not.
No significant differences in the types of organisms isolated were noted between the groups (Table 2). The most common pathogens isolated were Pseudomonas aeruginosa (24%), Enterococcus spp. (18%), Escherichia coli (17%), Proteus spp. (14%), Klebsiella spp. (7%), and Acinetobacter spp. (6%).
Thirty-six percent of the pathogens in the first cultures were not treated with any antibiotics, because they were considered as colonizers or contaminants. Only 61% of pathogens in the no resistance group vs 78% in the resistance group were exposed to antimicrobial treatment. In those veterans who were treated, antibiotic usage on the first urine culture was assessed to determine whether any relationship existed between receipt of a particular antimicrobial class and development of resistance. Fluoroquinolones were the most commonly prescribed antimicrobials in both the resistance and no resistance groups (Table 3).
Four risk factors (ASIA grade, antibiotic treatment duration, prior use of a cephalosporin, and prior use of penicillin) were initially identified by logistic regression analyses as being associated with resistance development. Since veterans in the resistance group were significantly older than those in the no resistance group, the analysis was repeated with age as a covariate to independently assess the association between the risk factors and resistance. After controlling for age, no significant association between the ASIA grade and resistance was identified (adjusted odds ratio [OR], 1.03; 95% confidence interval [CI]: 0.66 – 1.6). Median duration of antibiotic treatment was 6 days in all patients, 3.5 days in the no resistance group, and 9 days in the resistance group. Longer duration of treatment significantly predicted resistance (adjusted OR, 1.07; P = .03; 95% CI: 1.01 – 1.03). For every additional day the patient was on an antibiotic, he or she was 7% more likely to develop resistance.
The incidence of resistant organisms after exposure to a cephalosporin was not statistically different between groups (adjusted OR, 1.74; P = .36; 95% CI: 1.0 – 1.2). In the resistance group, 28% of the antibiotics prescribed were cephalosporins (cefuroxime, ceftriaxone, ceftazidime, and cefepime), which were used for Proteus mirabilis, Escherichia coli, Klebsiella pneumoniae, and Pseudomonas aeruginosa. In the no resistance group, 17% of the antibiotics prescribed were cephalosporins (cefepime only) and were used for Proteus mirabilis.
Organisms treated with penicillin were significantly less likely to become resistant (adjusted OR, 0.26; P = .04; 95% CI: 0.07 - 0.96). In the resistance group, 16% of the antibiotics were penicillins (piperacillin/tazobactam), which were used for Escherichia coli, Enterococcus faecalis, Acinetobacter baumannii, Pseudomonas aeruginosa, and Klebsiella pneumoniae. In the no resistance group, 22% of the antibiotics were penicillins (amoxicillin, amoxicillin/clavulanate and piperacillin/tazobactam), which were used for Proteus mirabilis, Enterococcus faecalis, and Acinetobacter baumannii.
Discussion
Longer duration of treatment significantly increased resistance on the subsequent culture in this study. For every additional day the patient was on an antibiotic, he or she was 7% more likely to develop a resistance. However, the potential impact of using a given antibiotic class on the acquisition of resistance in patients with SCI who had a UTI was not demonstrated. Surprisingly, the use of a cephalosporin was not associated with an increased incidence of resistance in this study, which was inconsistent with the findings from other studies.10 Weber and colleagues evaluated nosocomial infections in the intensive care unit. The authors suggested that restriction on the use of third-generation cephalosporins might decrease antibiotic resistance, especially in extended spectrum beta-lactamase producing gram-negative bacilli.11
The difference in this study may be explained by the lower incidence of Escherichia coli and Klebsiella pneumoniae, which are known to exhibit inducible resistance on exposure to third-generation cephalosporins. Conversely, it was found that patients treated with a penicillin were significantly less likely to develop resistant organisms from subsequent cultures. The most common penicillin used in this study’s patient population was piperacillin/tazobactam.
For complicated UTIs including pyelonephritis, the European Association of Urology (EAU) guidelines for the management of urinary and male genital tract infections recommend treatment for 3 to 5 days after defervescence or control of complicating factors.12 These recommendations could lead to much shorter treatment durations than the traditional 14-day “standard” course often prescribed. One meta-analysis recommends a 5-day course for UTIs without fever in patients with SCI vs a 14-day course for patients with fever.13 Due to the lack of data, care often varies based on the patient’s clinical status, provider experience, and opinions. The Pannek study surveyed 16 centers that specialized in SCI care. When compared with the recommendations in the EAU guidelines, the study found providers in > 50% of the responding facilities overtreated UTIs.14
Limitations
This study has several limitations. First, the sample size was much smaller than expected. Of the 355 charts reviewed, only 86 met all the criteria to be included, which limited analysis. Additionally, given the retrospective nature of the study, it was impossible to determine provider rationale for the treatment. Since a diagnosis of UTI in patients with SCI often cannot be done with conventional methods due to lack of symptoms, many investigators have emphasized the use of quantitative urinalysis to differentiate true infection vs contamination.15-17
According to the National Institute on Disability and Rehabilitation Research consensus conference recommendations, the definition of significant bacteriuria will vary, depending on the method of bladder drainage.18 While this study reviewed microbiologic cultures and the type of patient’s urinary catheter, the method of bladder drainage in the context of quantitative urinalysis was not evaluated, which limited the interpretation of microbiologic data.
It was also impossible to determine whether bacteria were cleared by the initial treatment, leading to new bacterial strains with a multidrug resistance, or whether patients relapsed. While antibiotic selection was appropriate for antimicrobial coverage, this study was not designed to detect potential inadequacies in dosing, which could also affect resistance. Last, since no genetic evaluation of the microorganisms was done, the authors cannot be sure whether the microorganisms noted on the first urine culture were of the same genetic makeup as those identified in the second urine culture.
Conclusion
Optimal duration of therapy for treatment of UTIs in patients with SCI is unclear. Despite its limitations, the study suggests exposure to longer antibiotic treatment courses may lead to increased antimicrobial resistance in the urinary tract organisms in this patient population. Further investigation with a larger sample size is required to confirm these findings.
Author disclosures
Dr. Bedimo received research grant funding from Janssen Pharmaceuticals and Merck and Company. He also serves as an ad hoc scientific advisor for Viiv Healthcare, Gilead Science, and BMD Science. All other authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
References
1. Saint S, Lipsky BA. Preventing catheter-related bacteriuria: Should we? Can we? How? Arch Intern Med. 1999;159(8):800-808.
2. Laupland KB, Bagshaw SM, Gregson DB, Kirkpatrick AW, Ross T, Church DL. Intensive care unit-acquired urinary tract infections in a regional critical care system. Crit Care. 2005;9(2):R60-R65.
3. Girard R, Mazoyer MA, Plauchu MM, Rode G. High prevalence of nosocomial infections in rehabilitation units accounted for by urinary tract infections in patients with spinal cord injury. J Hosp Infect. 2006;62(4):473-479.
4. Cardenas DD, Hooton TM. Urinary tract infection in persons with spinal cord injury. Arch Phys Med Rehabil. 1995;76(3):272-280.
5. Salomon J, Gory A, Bernard L, Ruffion A, Denys P, Chartier-Kastler E. [Urinary tract infection and neurogenic bladder]. Prog Urol. 2007;17(3):448-453.
6. Ena J, Amador C, Martinez C, Ortiz de la Tabla V. Risk factors for acquisition of urinary tract infections caused by ciprofloxacin resistant Escherichia coli. J Urol. 1995;153(1):117-120.
7. Allen UD, MacDonald N, Fuite L, Chan F, Stephens D. Risk factors for resistance to “first-line” antimicrobials among urinary tract isolates of Escherichia coli in children. CMAJ. 1999;160(10):1436-1440.
8. De Mouy D, Cavallo JD, Armengaud M, et al. [Urinary tract infection in an urban population: Etiology and antibiotic sensitivity as a function of patient history]. Presse Med. 1999;28(30):1624-1628.
9. Waites KB, Chen Y, DeVivo MJ, Canupp KC, Moser SA. Antimicrobial resistance in gram-negative bacteria isolated from the urinary tract in community-residing persons with spinal cord injury. Arch Phys Med Rehabil. 2000;81(6):764-769.
10. Shah PS, Cannon JP, Sullivan CL, Nemchausky B, Pachucki CT. Controlling antimicrobial use and decreasing microbiological laboratory tests for urinary tract infections in spinal-cord-injury patients with chronic indwelling catheters. Am J Health Syst Pharm. 2005;62(1):74-77.
11. Weber DJ, Raasch R, Rutala WA. Nosocomial infections in the ICU: The growing importance of antibiotic-resistant pathogens. Chest. 1999;115(suppl 3):34S-41S.
12. Naber KG, Bergman B, Bishop MC, et al; Urinary Tract Infection (UTI) Working Group of the Health Care Office (HCO) of the European Association of Urology (EAU). EAU guidelines for the management of urinary and male genital tract infections. Urinary Tract Infection (UTI) Working Group of the Health Care Office (HCO) of the European Association of Urology (EAU). Eur Urol. 2001;40(5):576-588.
13. Everaert K, Lumen N, Kerckhaert W, Willaert P, van Driel M. Urinary tract infections in spinal cord injury: Prevention and treatment guidelines. Acta Clin Belg. 2009;64(4):335-340.
14. Pannek J. Treatment of urinary tract infection in persons with spinal cord injury: Guidelines, evidence, and clinical practice. A questionnaire-based survey and review of the literature. J Spinal Cord Med. 2011;34(1):11-15.
15. Musher DM, Thorsteinsson SB, Airola VM II. Quantitative urinalysis. Diagnosing urinary tract infection in men. JAMA. 1976;236(18):2069-2072.
16. Deresinski SC, Perkash I. Urinary tract infections in male spinal cord injured patients. Part two: Diagnostic value of symptoms and of quantitative urinalysis. J Am Paraplegia Soc. 1985;8(1):7-10.
17. Deresinski SC, Perkash I. Urinary tract infections in male spinal cord injured patients. Part one: Bacteriologic diagnosis. J Am Paraplegia Soc. 1985;8(1):4-6.
18. Garcia Leoni ME, Esclarin De Ruz A. Management of urinary tract infection in patients with spinal cord injuries. Clin Microbiol Infect. 2003;9(8):780-785.