User login
The latest migraine therapies – some you might not know about
This transcript has been edited for clarity.
Matthew F. Watto, MD: Welcome back to The Curbsiders. I’m Dr. Matthew Watto, here with my very good friend, Dr. Paul Williams. It’s time to talk about headaches. We did a great recent podcast on migraines, Headache Update: Making Migraines Less Painful with Dr. Kevin Weber. One of the quotes from that episode that stayed with me was when he said, “I tell my patients to think about migraine as an irritable old miser set in their ways, and your brain is set in its ways. It doesn’t like changes in routine. It doesn’t like lack of sleep, it doesn’t like being hungry, it doesn’t like being thirsty, and it doesn’t like changes in the weather.” That’s a reminder of the good, old-fashioned primary care tips for taking care of headache.
Paul N. Williams, MD: That’s right. Conservative supportive management goes by the wayside because we focus on the medications. But I thought that was a really nice way to start the episode.
Dr. Watto: I asked him about cervicogenic headaches, which I guess you have to diagnose by giving a cervical steroid injection and see if the patient feels better, but he said he doesn’t do this. This is expert opinion territory. He asks his patients with chronic headache about cervical neck pain, because if they have it, he goes after it with physical therapy, which can help with the headaches. I thought that was a great pearl that I hadn’t heard before.
Give the audience a pearl from this great episode.
Dr. Williams: We talked about foundational treatments. We reviewed some of the abortive therapies and over-the-counter products. Some patients do quite well with acetaminophen or NSAIDs. We also talked about triptans, which are the standard medicines that we all know about. You can use those in combination, by the way. Patients can take their triptan with the NSAID that works best for them. They don’t have to be used one at a time, trying one and then trying the other one if the first one doesn’t help. Dr. Weber gave us practical guides in terms of which triptans he favors. He mentioned rizatriptan and naratriptan, which is one that I had not used with any frequency. I’ve seen rizatriptan a fair amount and that one seems to be covered by most insurances. He favors those two triptans.
He also reminded us that even though there is theoretical concern for serotonin toxicity because these are serotonergic and you’ll see these scary pop-ups in your electronic health record, that concern is almost purely theoretical. It hasn’t been borne out. They are really safe medications to use. But do use caution if you have a patient with known cardiovascular disease or cerebrovascular disease. We spent a fair amount of time talking about chest pressure as a common side effect. We also talked about some of the newer agents.
Dr. Watto: I wanted to add something about the triptans. Part of the reason he favors rizatriptan and naratriptan is that they are newer. He thinks they tend to have fewer side effects. But he did mention sumatriptan because it comes in the most different formulations. If patients have severe nausea, there is a subcutaneous version of sumatriptan and also an intranasal version.
The new kids on the block are the CGRP receptor antagonists, and they are available for preventive and abortive therapy. The abortive therapies are probably what people will be seeing most often in primary care – ubrogepant and rimegepant. Patients can take ubrogepant for abortive therapy and then repeat it if necessary. That’s similar to what patients are used to with the triptans. Rimegepant is taken once daily for abortive therapy or every other day as a preventive agent. Those are two of the agents that you might see patients taking. I’ve certainly started to see them.
There are also a whole bunch of monoclonal antibodies that affect the CGRP pathway. Those are given either once a month by subcutaneous injection or once every 3 months, and one is an infusion. They are pretty safe, and the big appeal is that they can be used in patients with cardiovascular disease. He also said that he has some patients who take them because triptans can cause the medication overuse side effect, but the CGRP receptor antagonists don’t. It’s an option for some patients to take the CGRP receptor antagonists on certain days for abortive therapy and then they can take the triptans the rest of the month.
Dr. Weber said that in his practice, these new drugs have really been great, which I can imagine, if you’re a specialist, patients have exhausted many of the typical therapies we offer in primary care.
Paul, bring us home here. What else should we tell the audience about? In primary care, what can we offer these patients?
Dr. Williams: A lot of the stuff we can offer works, by the way. It’s exciting to have fancy new medications to use, but you don’t even necessarily need to get to that point. We have a lot of medications that we can use for migraine prophylaxis, such as the beta-blockers and antihypertensives. Candesartan was a new one to me, an angiotensin receptor blocker that apparently has good evidence for migraine prophylaxis and Dr. Weber swears by it. We talked about some of the antiseizure medications, such as topiramate, which is probably the one with the most comfort in primary care. Some older folks may be using valproic acid or the tricyclic antidepressants (amitriptyline and nortriptyline) because people with migraine often will have comorbid anxiety or trouble sleeping, so I find that can sometimes be an effective medication or if they have comorbid neuropathic pain.
Another one that was new to me was venlafaxine as migraine prophylaxis. It’s not something I’d heard about before this episode. Certainly, for someone with chronic pain or a mood disorder that’s comorbid with migraines, it may be worth a shot. So there are options that we can exhaust first, and we may actually be doing our specialist friends a favor by trying one or two of these in advance, because then by the time the patient gets to the neurologist, it makes the prior authorization process much easier for the newer, fancier-pants medications that we’re all very excited about.
Dr. Watto: Paul, we’ve teased this fantastic podcast episode filled with so much more great stuff, so people should check out Headache Update: Making Migraines Less Painful with Dr. Kevin Weber.
Until next time, this has been another episode of The Curbsiders, bringing you a little knowledge food for your brain hole.
The Curbsiders is an internal medicine podcast, in which three board-certified internists interview experts on clinically important topics. In a collaboration with Medscape, the Curbsiders share clinical pearls and practice-changing knowledge from selected podcasts.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Matthew F. Watto, MD: Welcome back to The Curbsiders. I’m Dr. Matthew Watto, here with my very good friend, Dr. Paul Williams. It’s time to talk about headaches. We did a great recent podcast on migraines, Headache Update: Making Migraines Less Painful with Dr. Kevin Weber. One of the quotes from that episode that stayed with me was when he said, “I tell my patients to think about migraine as an irritable old miser set in their ways, and your brain is set in its ways. It doesn’t like changes in routine. It doesn’t like lack of sleep, it doesn’t like being hungry, it doesn’t like being thirsty, and it doesn’t like changes in the weather.” That’s a reminder of the good, old-fashioned primary care tips for taking care of headache.
Paul N. Williams, MD: That’s right. Conservative supportive management goes by the wayside because we focus on the medications. But I thought that was a really nice way to start the episode.
Dr. Watto: I asked him about cervicogenic headaches, which I guess you have to diagnose by giving a cervical steroid injection and see if the patient feels better, but he said he doesn’t do this. This is expert opinion territory. He asks his patients with chronic headache about cervical neck pain, because if they have it, he goes after it with physical therapy, which can help with the headaches. I thought that was a great pearl that I hadn’t heard before.
Give the audience a pearl from this great episode.
Dr. Williams: We talked about foundational treatments. We reviewed some of the abortive therapies and over-the-counter products. Some patients do quite well with acetaminophen or NSAIDs. We also talked about triptans, which are the standard medicines that we all know about. You can use those in combination, by the way. Patients can take their triptan with the NSAID that works best for them. They don’t have to be used one at a time, trying one and then trying the other one if the first one doesn’t help. Dr. Weber gave us practical guides in terms of which triptans he favors. He mentioned rizatriptan and naratriptan, which is one that I had not used with any frequency. I’ve seen rizatriptan a fair amount and that one seems to be covered by most insurances. He favors those two triptans.
He also reminded us that even though there is theoretical concern for serotonin toxicity because these are serotonergic and you’ll see these scary pop-ups in your electronic health record, that concern is almost purely theoretical. It hasn’t been borne out. They are really safe medications to use. But do use caution if you have a patient with known cardiovascular disease or cerebrovascular disease. We spent a fair amount of time talking about chest pressure as a common side effect. We also talked about some of the newer agents.
Dr. Watto: I wanted to add something about the triptans. Part of the reason he favors rizatriptan and naratriptan is that they are newer. He thinks they tend to have fewer side effects. But he did mention sumatriptan because it comes in the most different formulations. If patients have severe nausea, there is a subcutaneous version of sumatriptan and also an intranasal version.
The new kids on the block are the CGRP receptor antagonists, and they are available for preventive and abortive therapy. The abortive therapies are probably what people will be seeing most often in primary care – ubrogepant and rimegepant. Patients can take ubrogepant for abortive therapy and then repeat it if necessary. That’s similar to what patients are used to with the triptans. Rimegepant is taken once daily for abortive therapy or every other day as a preventive agent. Those are two of the agents that you might see patients taking. I’ve certainly started to see them.
There are also a whole bunch of monoclonal antibodies that affect the CGRP pathway. Those are given either once a month by subcutaneous injection or once every 3 months, and one is an infusion. They are pretty safe, and the big appeal is that they can be used in patients with cardiovascular disease. He also said that he has some patients who take them because triptans can cause the medication overuse side effect, but the CGRP receptor antagonists don’t. It’s an option for some patients to take the CGRP receptor antagonists on certain days for abortive therapy and then they can take the triptans the rest of the month.
Dr. Weber said that in his practice, these new drugs have really been great, which I can imagine, if you’re a specialist, patients have exhausted many of the typical therapies we offer in primary care.
Paul, bring us home here. What else should we tell the audience about? In primary care, what can we offer these patients?
Dr. Williams: A lot of the stuff we can offer works, by the way. It’s exciting to have fancy new medications to use, but you don’t even necessarily need to get to that point. We have a lot of medications that we can use for migraine prophylaxis, such as the beta-blockers and antihypertensives. Candesartan was a new one to me, an angiotensin receptor blocker that apparently has good evidence for migraine prophylaxis and Dr. Weber swears by it. We talked about some of the antiseizure medications, such as topiramate, which is probably the one with the most comfort in primary care. Some older folks may be using valproic acid or the tricyclic antidepressants (amitriptyline and nortriptyline) because people with migraine often will have comorbid anxiety or trouble sleeping, so I find that can sometimes be an effective medication or if they have comorbid neuropathic pain.
Another one that was new to me was venlafaxine as migraine prophylaxis. It’s not something I’d heard about before this episode. Certainly, for someone with chronic pain or a mood disorder that’s comorbid with migraines, it may be worth a shot. So there are options that we can exhaust first, and we may actually be doing our specialist friends a favor by trying one or two of these in advance, because then by the time the patient gets to the neurologist, it makes the prior authorization process much easier for the newer, fancier-pants medications that we’re all very excited about.
Dr. Watto: Paul, we’ve teased this fantastic podcast episode filled with so much more great stuff, so people should check out Headache Update: Making Migraines Less Painful with Dr. Kevin Weber.
Until next time, this has been another episode of The Curbsiders, bringing you a little knowledge food for your brain hole.
The Curbsiders is an internal medicine podcast, in which three board-certified internists interview experts on clinically important topics. In a collaboration with Medscape, the Curbsiders share clinical pearls and practice-changing knowledge from selected podcasts.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Matthew F. Watto, MD: Welcome back to The Curbsiders. I’m Dr. Matthew Watto, here with my very good friend, Dr. Paul Williams. It’s time to talk about headaches. We did a great recent podcast on migraines, Headache Update: Making Migraines Less Painful with Dr. Kevin Weber. One of the quotes from that episode that stayed with me was when he said, “I tell my patients to think about migraine as an irritable old miser set in their ways, and your brain is set in its ways. It doesn’t like changes in routine. It doesn’t like lack of sleep, it doesn’t like being hungry, it doesn’t like being thirsty, and it doesn’t like changes in the weather.” That’s a reminder of the good, old-fashioned primary care tips for taking care of headache.
Paul N. Williams, MD: That’s right. Conservative supportive management goes by the wayside because we focus on the medications. But I thought that was a really nice way to start the episode.
Dr. Watto: I asked him about cervicogenic headaches, which I guess you have to diagnose by giving a cervical steroid injection and see if the patient feels better, but he said he doesn’t do this. This is expert opinion territory. He asks his patients with chronic headache about cervical neck pain, because if they have it, he goes after it with physical therapy, which can help with the headaches. I thought that was a great pearl that I hadn’t heard before.
Give the audience a pearl from this great episode.
Dr. Williams: We talked about foundational treatments. We reviewed some of the abortive therapies and over-the-counter products. Some patients do quite well with acetaminophen or NSAIDs. We also talked about triptans, which are the standard medicines that we all know about. You can use those in combination, by the way. Patients can take their triptan with the NSAID that works best for them. They don’t have to be used one at a time, trying one and then trying the other one if the first one doesn’t help. Dr. Weber gave us practical guides in terms of which triptans he favors. He mentioned rizatriptan and naratriptan, which is one that I had not used with any frequency. I’ve seen rizatriptan a fair amount and that one seems to be covered by most insurances. He favors those two triptans.
He also reminded us that even though there is theoretical concern for serotonin toxicity because these are serotonergic and you’ll see these scary pop-ups in your electronic health record, that concern is almost purely theoretical. It hasn’t been borne out. They are really safe medications to use. But do use caution if you have a patient with known cardiovascular disease or cerebrovascular disease. We spent a fair amount of time talking about chest pressure as a common side effect. We also talked about some of the newer agents.
Dr. Watto: I wanted to add something about the triptans. Part of the reason he favors rizatriptan and naratriptan is that they are newer. He thinks they tend to have fewer side effects. But he did mention sumatriptan because it comes in the most different formulations. If patients have severe nausea, there is a subcutaneous version of sumatriptan and also an intranasal version.
The new kids on the block are the CGRP receptor antagonists, and they are available for preventive and abortive therapy. The abortive therapies are probably what people will be seeing most often in primary care – ubrogepant and rimegepant. Patients can take ubrogepant for abortive therapy and then repeat it if necessary. That’s similar to what patients are used to with the triptans. Rimegepant is taken once daily for abortive therapy or every other day as a preventive agent. Those are two of the agents that you might see patients taking. I’ve certainly started to see them.
There are also a whole bunch of monoclonal antibodies that affect the CGRP pathway. Those are given either once a month by subcutaneous injection or once every 3 months, and one is an infusion. They are pretty safe, and the big appeal is that they can be used in patients with cardiovascular disease. He also said that he has some patients who take them because triptans can cause the medication overuse side effect, but the CGRP receptor antagonists don’t. It’s an option for some patients to take the CGRP receptor antagonists on certain days for abortive therapy and then they can take the triptans the rest of the month.
Dr. Weber said that in his practice, these new drugs have really been great, which I can imagine, if you’re a specialist, patients have exhausted many of the typical therapies we offer in primary care.
Paul, bring us home here. What else should we tell the audience about? In primary care, what can we offer these patients?
Dr. Williams: A lot of the stuff we can offer works, by the way. It’s exciting to have fancy new medications to use, but you don’t even necessarily need to get to that point. We have a lot of medications that we can use for migraine prophylaxis, such as the beta-blockers and antihypertensives. Candesartan was a new one to me, an angiotensin receptor blocker that apparently has good evidence for migraine prophylaxis and Dr. Weber swears by it. We talked about some of the antiseizure medications, such as topiramate, which is probably the one with the most comfort in primary care. Some older folks may be using valproic acid or the tricyclic antidepressants (amitriptyline and nortriptyline) because people with migraine often will have comorbid anxiety or trouble sleeping, so I find that can sometimes be an effective medication or if they have comorbid neuropathic pain.
Another one that was new to me was venlafaxine as migraine prophylaxis. It’s not something I’d heard about before this episode. Certainly, for someone with chronic pain or a mood disorder that’s comorbid with migraines, it may be worth a shot. So there are options that we can exhaust first, and we may actually be doing our specialist friends a favor by trying one or two of these in advance, because then by the time the patient gets to the neurologist, it makes the prior authorization process much easier for the newer, fancier-pants medications that we’re all very excited about.
Dr. Watto: Paul, we’ve teased this fantastic podcast episode filled with so much more great stuff, so people should check out Headache Update: Making Migraines Less Painful with Dr. Kevin Weber.
Until next time, this has been another episode of The Curbsiders, bringing you a little knowledge food for your brain hole.
The Curbsiders is an internal medicine podcast, in which three board-certified internists interview experts on clinically important topics. In a collaboration with Medscape, the Curbsiders share clinical pearls and practice-changing knowledge from selected podcasts.
A version of this article first appeared on Medscape.com.
Criminal profiles of medical murderers
Today’s health care professionals run the very real risk of being sued. This is especially true when a patient dies unexpectedly. But many times, doctors find that they’re defending themselves against very serious charges, such as murder and attempted murder.
In Mexico, a physician can be wrongfully accused of such crimes, as was Azucena Calvillo, MD, last year in Durango. The case drew much media attention, and the accusations were so implausible and ridiculous that the charges were dropped and the case was dismissed.
There are instances in which the authorities create a circuslike atmosphere by making farcical and false accusations against healthcare professionals. Still, there are medical murderers – and these killers are among the most difficult to identify. As John E. Douglas put it, “Medical murderers (physicians, nurses, elder care workers) can have a long list of victims, longer than other kinds of serial killers.” Ted Bundy, one of the most written-about serial killers, confessed to 30 murders. The cases discussed below involve from 60 to 200.
Mr. Douglas was a special agent with the United States Federal Bureau of Investigation. He is the author of Mindhunter, a nonfiction crime book in which he recounts the early days of the FBI’s Behavioral Science Unit and how he and his colleagues began to study the criminal profiles of serial killers. The book has been adapted into a Netflix TV series of the same name.
He is also one of the authors of Crime Classification Manual: A Standard System for Investigating and Classifying Violent Crime. In this book, there are descriptions of criminal profiles of medical murderers.
According to the authors, Each type is associated with a different motive. In the former, the murderers believe that they’re alleviating the patient’s suffering; in the latter, the murderers create a medical emergency so that they can play the hero in what they know will be an unsuccessful attempt to save the patient’s life.
Pseudo-mercy homicide
An example of pseudo-mercy homicide is the infamous case of Harold Shipman, MD, who was convicted of killing 15 people, although an investigation found that more than 200 persons, and possibly as many as 250, died at his hands. In Prescription for Murder: The True Story of Dr. Harold Frederick Shipman, biographer Brian Whittle writes that the general practitioner is England’s (if not the world’s) most prolific serial killer. Dr. Shipman is the only physician in that country’s history to have been convicted of killing his patients.
His modus operandi? Injecting morphine. Most of his victims were elderly women. And though unconfirmed, his youngest victim may have been only 4 years old. It was the death of 81-year-old Kathleen Grundy that led to the physician’s arrest. Her family became extremely suspicious when they learned that her will named Dr. Shipman as the beneficiary of her entire estate.
He always denied being involved in the murders, for which authorities have yet to determine a motive. The speculation is that he enjoyed watching people die. Almost none of the cases attributed to Dr. Shipman involved a critically ill individual with a life-threatening condition. Therefore, his acts were not real acts of mercy. He would make a house call to carry out a routine visit. Once in the patient’s home, he would inject a lethal dose of morphine. Sometimes, relatives and physicians alike would be struck by the strange turn of events.
In 2004, Dr. Shipman committed suicide in prison. His case led to numerous changes to British law with respect to the use of controlled substances, the issuance of death certificates, and the procedure for reporting healthcare staff suspected of engaging in illegal activities. Biographer Whittle concluded, “It is very unlikely that the world will ever see another physician as unrelentingly wicked as Dr. Shipman.”
Pseudo-hero homicide
The pseudo-hero creates serious situations, generally by administering drugs, and then tries to save the patient. Mr. Douglas presents a terrifying case study: Genene Jones, a nurse known as the “Angel of Death.”
Many of Ms. Jones’ colleagues considered her an excellent nurse, an expert at handling unexpected emergencies. If a child died while she was on duty, she would sometimes accompany their body to the morgue. She would even sing children’s songs to their lifeless body. When people started to question the number of deaths that were occurring during her shifts, the staff stood up for Ms. Jones, saying that it was because she took on the most serious cases.
Ms. Jones was found out when a vial of succinylcholine went missing. After it was located, a physician, who had been suspicious of the nurse, noticed that there were two puncture holes in the stopper. None of the staff could offer any explanation. A few days before this event, that same physician had left a healthy 15-month-old girl in Jones’ care. Within a few minutes, the child was showing signs of paralysis and started to have seizures. It appears that Ms. Jones had used succinylcholine to make it appear that the children were sick or were experiencing some sort of emergency so that she could then attempt to save them, and they could die in her arms.
This case highlights the need for mortality review committees and for proper statistical analysis to discern trends in deaths and complications among patients. Genene Jones was convicted of killing the 15-month-old girl and was sentenced to 99 years in prison. Authorities suspect that the nurse was responsible for the deaths of up to 60 children.
A new criminal profile?
Through the podcast and subsequent TV series Dr. Death, many people have come to know of a more recent medical murderer: Christopher Duntsch, MD, PhD. The Texas neurosurgeon killed at least two patients, and his actions left several others with adverse outcomes and serious injuries.
These acts occurred during surgical procedures. Witnesses said that the deaths and injuries were the result of unprecedented, egregious negligence, as though the operations had been performed by someone who had never been trained in the specialty. This is something that resonates very strongly for those who are aware of what’s going on in Mexico, where it’s well known that many physicians who lack specialty training perform operations (mainly cosmetic surgery). No doubt cases such as Dr. Duntsch’s are more frequent in Mexico.
What makes the situation in the United States involving Christopher Duntsch so astonishing is that it resulted from a perfect storm of a physician whom some colleagues described as a “sociopath” and legal loopholes in the country’s healthcare system. Apparently, during his residency, Dr. Duntsch never developed the skills necessary to perform operations. He spent more time carrying out research and engaging in other activities than in participating in the operating room. This is a case that calls into question the way specialists are trained, as it seems that what matters is not how much time they’re spending inside the hospital but what they’re doing and learning there.
Dr. Duntsch’s license was suspended and then permanently revoked. He is currently serving a life sentence. Through the podcast or the TV series, one comes to realize that it’s not easy to catch medical murderers. They are among the most difficult to identify – serial killers who commit numerous homicides before they are captured. Reading about the case of Christopher Duntsch, one might ask, What’s his criminal profile: pseudo-hero? Pseudo-mercy? It is hard to say. Maybe his is a different kind of profile – one that will open a new chapter in the books on medical murderers.
Dr. Sarmiento studied medicine and did his residency in anatomic pathology, internal medicine, and clinical hematology. He went on to study at Central University City Campus Law School, National Autonomous University of Mexico. He now runs a law firm that, among other things, advises physicians on matters of civil liability, administrative processes, and the legal implications of practicing medicine.
This article was translated from the Medscape Spanish edition.
Today’s health care professionals run the very real risk of being sued. This is especially true when a patient dies unexpectedly. But many times, doctors find that they’re defending themselves against very serious charges, such as murder and attempted murder.
In Mexico, a physician can be wrongfully accused of such crimes, as was Azucena Calvillo, MD, last year in Durango. The case drew much media attention, and the accusations were so implausible and ridiculous that the charges were dropped and the case was dismissed.
There are instances in which the authorities create a circuslike atmosphere by making farcical and false accusations against healthcare professionals. Still, there are medical murderers – and these killers are among the most difficult to identify. As John E. Douglas put it, “Medical murderers (physicians, nurses, elder care workers) can have a long list of victims, longer than other kinds of serial killers.” Ted Bundy, one of the most written-about serial killers, confessed to 30 murders. The cases discussed below involve from 60 to 200.
Mr. Douglas was a special agent with the United States Federal Bureau of Investigation. He is the author of Mindhunter, a nonfiction crime book in which he recounts the early days of the FBI’s Behavioral Science Unit and how he and his colleagues began to study the criminal profiles of serial killers. The book has been adapted into a Netflix TV series of the same name.
He is also one of the authors of Crime Classification Manual: A Standard System for Investigating and Classifying Violent Crime. In this book, there are descriptions of criminal profiles of medical murderers.
According to the authors, Each type is associated with a different motive. In the former, the murderers believe that they’re alleviating the patient’s suffering; in the latter, the murderers create a medical emergency so that they can play the hero in what they know will be an unsuccessful attempt to save the patient’s life.
Pseudo-mercy homicide
An example of pseudo-mercy homicide is the infamous case of Harold Shipman, MD, who was convicted of killing 15 people, although an investigation found that more than 200 persons, and possibly as many as 250, died at his hands. In Prescription for Murder: The True Story of Dr. Harold Frederick Shipman, biographer Brian Whittle writes that the general practitioner is England’s (if not the world’s) most prolific serial killer. Dr. Shipman is the only physician in that country’s history to have been convicted of killing his patients.
His modus operandi? Injecting morphine. Most of his victims were elderly women. And though unconfirmed, his youngest victim may have been only 4 years old. It was the death of 81-year-old Kathleen Grundy that led to the physician’s arrest. Her family became extremely suspicious when they learned that her will named Dr. Shipman as the beneficiary of her entire estate.
He always denied being involved in the murders, for which authorities have yet to determine a motive. The speculation is that he enjoyed watching people die. Almost none of the cases attributed to Dr. Shipman involved a critically ill individual with a life-threatening condition. Therefore, his acts were not real acts of mercy. He would make a house call to carry out a routine visit. Once in the patient’s home, he would inject a lethal dose of morphine. Sometimes, relatives and physicians alike would be struck by the strange turn of events.
In 2004, Dr. Shipman committed suicide in prison. His case led to numerous changes to British law with respect to the use of controlled substances, the issuance of death certificates, and the procedure for reporting healthcare staff suspected of engaging in illegal activities. Biographer Whittle concluded, “It is very unlikely that the world will ever see another physician as unrelentingly wicked as Dr. Shipman.”
Pseudo-hero homicide
The pseudo-hero creates serious situations, generally by administering drugs, and then tries to save the patient. Mr. Douglas presents a terrifying case study: Genene Jones, a nurse known as the “Angel of Death.”
Many of Ms. Jones’ colleagues considered her an excellent nurse, an expert at handling unexpected emergencies. If a child died while she was on duty, she would sometimes accompany their body to the morgue. She would even sing children’s songs to their lifeless body. When people started to question the number of deaths that were occurring during her shifts, the staff stood up for Ms. Jones, saying that it was because she took on the most serious cases.
Ms. Jones was found out when a vial of succinylcholine went missing. After it was located, a physician, who had been suspicious of the nurse, noticed that there were two puncture holes in the stopper. None of the staff could offer any explanation. A few days before this event, that same physician had left a healthy 15-month-old girl in Jones’ care. Within a few minutes, the child was showing signs of paralysis and started to have seizures. It appears that Ms. Jones had used succinylcholine to make it appear that the children were sick or were experiencing some sort of emergency so that she could then attempt to save them, and they could die in her arms.
This case highlights the need for mortality review committees and for proper statistical analysis to discern trends in deaths and complications among patients. Genene Jones was convicted of killing the 15-month-old girl and was sentenced to 99 years in prison. Authorities suspect that the nurse was responsible for the deaths of up to 60 children.
A new criminal profile?
Through the podcast and subsequent TV series Dr. Death, many people have come to know of a more recent medical murderer: Christopher Duntsch, MD, PhD. The Texas neurosurgeon killed at least two patients, and his actions left several others with adverse outcomes and serious injuries.
These acts occurred during surgical procedures. Witnesses said that the deaths and injuries were the result of unprecedented, egregious negligence, as though the operations had been performed by someone who had never been trained in the specialty. This is something that resonates very strongly for those who are aware of what’s going on in Mexico, where it’s well known that many physicians who lack specialty training perform operations (mainly cosmetic surgery). No doubt cases such as Dr. Duntsch’s are more frequent in Mexico.
What makes the situation in the United States involving Christopher Duntsch so astonishing is that it resulted from a perfect storm of a physician whom some colleagues described as a “sociopath” and legal loopholes in the country’s healthcare system. Apparently, during his residency, Dr. Duntsch never developed the skills necessary to perform operations. He spent more time carrying out research and engaging in other activities than in participating in the operating room. This is a case that calls into question the way specialists are trained, as it seems that what matters is not how much time they’re spending inside the hospital but what they’re doing and learning there.
Dr. Duntsch’s license was suspended and then permanently revoked. He is currently serving a life sentence. Through the podcast or the TV series, one comes to realize that it’s not easy to catch medical murderers. They are among the most difficult to identify – serial killers who commit numerous homicides before they are captured. Reading about the case of Christopher Duntsch, one might ask, What’s his criminal profile: pseudo-hero? Pseudo-mercy? It is hard to say. Maybe his is a different kind of profile – one that will open a new chapter in the books on medical murderers.
Dr. Sarmiento studied medicine and did his residency in anatomic pathology, internal medicine, and clinical hematology. He went on to study at Central University City Campus Law School, National Autonomous University of Mexico. He now runs a law firm that, among other things, advises physicians on matters of civil liability, administrative processes, and the legal implications of practicing medicine.
This article was translated from the Medscape Spanish edition.
Today’s health care professionals run the very real risk of being sued. This is especially true when a patient dies unexpectedly. But many times, doctors find that they’re defending themselves against very serious charges, such as murder and attempted murder.
In Mexico, a physician can be wrongfully accused of such crimes, as was Azucena Calvillo, MD, last year in Durango. The case drew much media attention, and the accusations were so implausible and ridiculous that the charges were dropped and the case was dismissed.
There are instances in which the authorities create a circuslike atmosphere by making farcical and false accusations against healthcare professionals. Still, there are medical murderers – and these killers are among the most difficult to identify. As John E. Douglas put it, “Medical murderers (physicians, nurses, elder care workers) can have a long list of victims, longer than other kinds of serial killers.” Ted Bundy, one of the most written-about serial killers, confessed to 30 murders. The cases discussed below involve from 60 to 200.
Mr. Douglas was a special agent with the United States Federal Bureau of Investigation. He is the author of Mindhunter, a nonfiction crime book in which he recounts the early days of the FBI’s Behavioral Science Unit and how he and his colleagues began to study the criminal profiles of serial killers. The book has been adapted into a Netflix TV series of the same name.
He is also one of the authors of Crime Classification Manual: A Standard System for Investigating and Classifying Violent Crime. In this book, there are descriptions of criminal profiles of medical murderers.
According to the authors, Each type is associated with a different motive. In the former, the murderers believe that they’re alleviating the patient’s suffering; in the latter, the murderers create a medical emergency so that they can play the hero in what they know will be an unsuccessful attempt to save the patient’s life.
Pseudo-mercy homicide
An example of pseudo-mercy homicide is the infamous case of Harold Shipman, MD, who was convicted of killing 15 people, although an investigation found that more than 200 persons, and possibly as many as 250, died at his hands. In Prescription for Murder: The True Story of Dr. Harold Frederick Shipman, biographer Brian Whittle writes that the general practitioner is England’s (if not the world’s) most prolific serial killer. Dr. Shipman is the only physician in that country’s history to have been convicted of killing his patients.
His modus operandi? Injecting morphine. Most of his victims were elderly women. And though unconfirmed, his youngest victim may have been only 4 years old. It was the death of 81-year-old Kathleen Grundy that led to the physician’s arrest. Her family became extremely suspicious when they learned that her will named Dr. Shipman as the beneficiary of her entire estate.
He always denied being involved in the murders, for which authorities have yet to determine a motive. The speculation is that he enjoyed watching people die. Almost none of the cases attributed to Dr. Shipman involved a critically ill individual with a life-threatening condition. Therefore, his acts were not real acts of mercy. He would make a house call to carry out a routine visit. Once in the patient’s home, he would inject a lethal dose of morphine. Sometimes, relatives and physicians alike would be struck by the strange turn of events.
In 2004, Dr. Shipman committed suicide in prison. His case led to numerous changes to British law with respect to the use of controlled substances, the issuance of death certificates, and the procedure for reporting healthcare staff suspected of engaging in illegal activities. Biographer Whittle concluded, “It is very unlikely that the world will ever see another physician as unrelentingly wicked as Dr. Shipman.”
Pseudo-hero homicide
The pseudo-hero creates serious situations, generally by administering drugs, and then tries to save the patient. Mr. Douglas presents a terrifying case study: Genene Jones, a nurse known as the “Angel of Death.”
Many of Ms. Jones’ colleagues considered her an excellent nurse, an expert at handling unexpected emergencies. If a child died while she was on duty, she would sometimes accompany their body to the morgue. She would even sing children’s songs to their lifeless body. When people started to question the number of deaths that were occurring during her shifts, the staff stood up for Ms. Jones, saying that it was because she took on the most serious cases.
Ms. Jones was found out when a vial of succinylcholine went missing. After it was located, a physician, who had been suspicious of the nurse, noticed that there were two puncture holes in the stopper. None of the staff could offer any explanation. A few days before this event, that same physician had left a healthy 15-month-old girl in Jones’ care. Within a few minutes, the child was showing signs of paralysis and started to have seizures. It appears that Ms. Jones had used succinylcholine to make it appear that the children were sick or were experiencing some sort of emergency so that she could then attempt to save them, and they could die in her arms.
This case highlights the need for mortality review committees and for proper statistical analysis to discern trends in deaths and complications among patients. Genene Jones was convicted of killing the 15-month-old girl and was sentenced to 99 years in prison. Authorities suspect that the nurse was responsible for the deaths of up to 60 children.
A new criminal profile?
Through the podcast and subsequent TV series Dr. Death, many people have come to know of a more recent medical murderer: Christopher Duntsch, MD, PhD. The Texas neurosurgeon killed at least two patients, and his actions left several others with adverse outcomes and serious injuries.
These acts occurred during surgical procedures. Witnesses said that the deaths and injuries were the result of unprecedented, egregious negligence, as though the operations had been performed by someone who had never been trained in the specialty. This is something that resonates very strongly for those who are aware of what’s going on in Mexico, where it’s well known that many physicians who lack specialty training perform operations (mainly cosmetic surgery). No doubt cases such as Dr. Duntsch’s are more frequent in Mexico.
What makes the situation in the United States involving Christopher Duntsch so astonishing is that it resulted from a perfect storm of a physician whom some colleagues described as a “sociopath” and legal loopholes in the country’s healthcare system. Apparently, during his residency, Dr. Duntsch never developed the skills necessary to perform operations. He spent more time carrying out research and engaging in other activities than in participating in the operating room. This is a case that calls into question the way specialists are trained, as it seems that what matters is not how much time they’re spending inside the hospital but what they’re doing and learning there.
Dr. Duntsch’s license was suspended and then permanently revoked. He is currently serving a life sentence. Through the podcast or the TV series, one comes to realize that it’s not easy to catch medical murderers. They are among the most difficult to identify – serial killers who commit numerous homicides before they are captured. Reading about the case of Christopher Duntsch, one might ask, What’s his criminal profile: pseudo-hero? Pseudo-mercy? It is hard to say. Maybe his is a different kind of profile – one that will open a new chapter in the books on medical murderers.
Dr. Sarmiento studied medicine and did his residency in anatomic pathology, internal medicine, and clinical hematology. He went on to study at Central University City Campus Law School, National Autonomous University of Mexico. He now runs a law firm that, among other things, advises physicians on matters of civil liability, administrative processes, and the legal implications of practicing medicine.
This article was translated from the Medscape Spanish edition.
Caring for the aging transgender patient
The elderly transgender population is rapidly expanding and remains significantly overlooked. Although emerging evidence provides some guidance for medical and surgical treatment for transgender youth, there is still a paucity of research directed at the management of gender-diverse elders.
To a large extent, the challenges that transgender elders face are no different from those experienced by the general elder population. Irrespective of gender identity, patients begin to undergo cognitive and physical changes, encounter difficulties with activities of daily living, suffer the loss of social networks and friends, and face end-of-life issues.1 Attributes that contribute to successful aging in the general population include good health, social engagement and support, and having a positive outlook on life.1 Yet, stigma surrounding gender identity and sexual orientation continues to negatively affect elder transgender people.
Many members of the LGBTQIA+ population have higher rates of obesity, sedentary lifestyle, smoking, cardiovascular disease, substance abuse, depression, suicide, and intimate partner violence than the general same-age cohort.2 Compared with lesbian, gay, and bisexual elders of age-matched cohorts, transgender elders have significantly poorer overall physical health, disability, depressive symptoms, and perceived stress.2

Rates of sexually transmitted infections are also rising in the aging general population and increased by 30% between 2014 and 2017.2 There have been no current studies examining these rates in the LGBTQIA+ population. As providers interact more frequently with these patients, it’s not only essential to screen for conditions such as diabetes, lipid disorders, and sexually transmitted infections, but also to evaluate current gender-affirming hormone therapy (GAHT) regimens and order appropriate screening tests.
Hormonal therapy for transfeminine patients should be continued as patients age. One of the biggest concerns providers have in continuing hormone therapy is the development of cardiovascular disease (CVD) and increasing thromboembolic risk, both of which tend to occur naturally as patients age. Overall, studies on the prevalence of CVD or stroke in gender-diverse individuals indicate an elevated risk independent of GAHT.3 While the overall rates of thromboembolic events are low in transfeminine populations, estrogen therapy does confer an increased risk. However, most transgender women who have experienced cardiac events or stroke were over the age of 50, had one or more CVD risk factors, or were using synthetic estrogens.3
How these studies affect screening is unclear. Current guidelines recommend using tailored risk-based calculators, which take into consideration the patient’s sex assigned at birth, hormone regimen, length of hormone usage, and additional modifiable risk factors, such as diabetes, obesity, and smoking.3 For transfeminine patients who want to continue GAHT but either develop a venous thromboembolism on estrogen or have increased risk for VTE, providers should consider transitioning them to a transdermal application. Patients who stay on GAHT should be counseled accordingly on the heightened risk of VTE recurrence. It is not unreasonable to consider life-long anticoagulation for patients who remain on estrogen therapy after a VTE.4
While exogenous estrogen exposure is one risk factor for the development of breast cancer in cisgender females, the role of GAHT in breast cancer in transgender women is ambiguous. Therefore, breast screening guidelines should follow current recommendations for cisgender female patients with some caveats. The provider must also take into consideration current estrogen dosage, the age at which hormones were initiated, and whether a patient has undergone an augmentation mammaplasty.3
Both estrogen and testosterone play an important role in bone formation and health. Patients who undergo either medical or surgical interventions that alter sex hormone production, such as GAHT, orchiectomy, or androgen blockade, may be at elevated risk for osteoporosis. Providers should take a thorough medical history to determine patients who may be at risk for osteoporosis and treat them accordingly. Overall, GAHT has a positive effect on bone mineral density. Conversely, gonadectomy, particularly if a patient is not taking GAHT, can decrease bone density. Generally, transgender women, like cisgender women, should undergo DEXA scans starting at the age of 65, with earlier screening considered if they have undergone an orchiectomy and are not currently taking GAHT.3
There is no evidence that GAHT or surgery increases the rate of prostate cancer. Providers should note that the prostate is not removed at the time of gender-affirming surgery and that malignancy or benign prostatic hypertrophy can still occur. The U.S. Preventive Services Task Force recommends that clinicians have a discussion with cisgender men between the ages of 55 and 69 about the risks and benefits of prostate-specific antigen (PSA) screening.5 For cisgender men aged 70 and older, the USPSTF recommends against PSA-based screening.5 If digital examination of the prostate is warranted for transfeminine patients, the examination is performed through the neovaginal canal.
Caring for elderly transgender patients is complex. Even though evidence guiding the management of elderly transgender patients is improving, there are still not enough definitive long-term data on this dynamic demographic. Like clinical approaches with hormonal or surgical treatments, caring for transgender elders is also multidisciplinary. Providers should be prepared to work with social workers, geriatric care physicians, endocrinologists, surgeons, and other relevant specialists to assist with potential knowledge gaps. The goals for the aging transgender population are the same as those for cisgender patients – preventing preventable diseases and reducing overall mortality so our patients can enjoy their golden years.
Dr. Brandt is an ob.gyn. and fellowship-trained gender-affirming surgeon in West Reading, Pa. Contact her at [email protected].
References
1. Carroll L. Psychiatr Clin N Am. 2017;40:127-40.
2. Selix NW et al. Clinical care of the aging LGBT population. J Nurse Pract. 2020;16(7):349-54.
3. World Professional Association for Transgender Health. Standards of care for the health of transgender and gender diverse people. 2022;8th version.
4. Shatzel JJ et al. Am J Hematol. 2017;92(2):204-8.
5. Wolf-Gould CS and Wolf-Gould CH. Primary and preventative care for transgender patients. In: Ferrando CA, ed. Comprehensive Care of the Transgender Patient. Philadelphia: Elsevier, 2020, p. 114-30.
The elderly transgender population is rapidly expanding and remains significantly overlooked. Although emerging evidence provides some guidance for medical and surgical treatment for transgender youth, there is still a paucity of research directed at the management of gender-diverse elders.
To a large extent, the challenges that transgender elders face are no different from those experienced by the general elder population. Irrespective of gender identity, patients begin to undergo cognitive and physical changes, encounter difficulties with activities of daily living, suffer the loss of social networks and friends, and face end-of-life issues.1 Attributes that contribute to successful aging in the general population include good health, social engagement and support, and having a positive outlook on life.1 Yet, stigma surrounding gender identity and sexual orientation continues to negatively affect elder transgender people.
Many members of the LGBTQIA+ population have higher rates of obesity, sedentary lifestyle, smoking, cardiovascular disease, substance abuse, depression, suicide, and intimate partner violence than the general same-age cohort.2 Compared with lesbian, gay, and bisexual elders of age-matched cohorts, transgender elders have significantly poorer overall physical health, disability, depressive symptoms, and perceived stress.2
Rates of sexually transmitted infections are also rising in the aging general population and increased by 30% between 2014 and 2017.2 There have been no current studies examining these rates in the LGBTQIA+ population. As providers interact more frequently with these patients, it’s not only essential to screen for conditions such as diabetes, lipid disorders, and sexually transmitted infections, but also to evaluate current gender-affirming hormone therapy (GAHT) regimens and order appropriate screening tests.
Hormonal therapy for transfeminine patients should be continued as patients age. One of the biggest concerns providers have in continuing hormone therapy is the development of cardiovascular disease (CVD) and increasing thromboembolic risk, both of which tend to occur naturally as patients age. Overall, studies on the prevalence of CVD or stroke in gender-diverse individuals indicate an elevated risk independent of GAHT.3 While the overall rates of thromboembolic events are low in transfeminine populations, estrogen therapy does confer an increased risk. However, most transgender women who have experienced cardiac events or stroke were over the age of 50, had one or more CVD risk factors, or were using synthetic estrogens.3
How these studies affect screening is unclear. Current guidelines recommend using tailored risk-based calculators, which take into consideration the patient’s sex assigned at birth, hormone regimen, length of hormone usage, and additional modifiable risk factors, such as diabetes, obesity, and smoking.3 For transfeminine patients who want to continue GAHT but either develop a venous thromboembolism on estrogen or have increased risk for VTE, providers should consider transitioning them to a transdermal application. Patients who stay on GAHT should be counseled accordingly on the heightened risk of VTE recurrence. It is not unreasonable to consider life-long anticoagulation for patients who remain on estrogen therapy after a VTE.4
While exogenous estrogen exposure is one risk factor for the development of breast cancer in cisgender females, the role of GAHT in breast cancer in transgender women is ambiguous. Therefore, breast screening guidelines should follow current recommendations for cisgender female patients with some caveats. The provider must also take into consideration current estrogen dosage, the age at which hormones were initiated, and whether a patient has undergone an augmentation mammaplasty.3
Both estrogen and testosterone play an important role in bone formation and health. Patients who undergo either medical or surgical interventions that alter sex hormone production, such as GAHT, orchiectomy, or androgen blockade, may be at elevated risk for osteoporosis. Providers should take a thorough medical history to determine patients who may be at risk for osteoporosis and treat them accordingly. Overall, GAHT has a positive effect on bone mineral density. Conversely, gonadectomy, particularly if a patient is not taking GAHT, can decrease bone density. Generally, transgender women, like cisgender women, should undergo DEXA scans starting at the age of 65, with earlier screening considered if they have undergone an orchiectomy and are not currently taking GAHT.3
There is no evidence that GAHT or surgery increases the rate of prostate cancer. Providers should note that the prostate is not removed at the time of gender-affirming surgery and that malignancy or benign prostatic hypertrophy can still occur. The U.S. Preventive Services Task Force recommends that clinicians have a discussion with cisgender men between the ages of 55 and 69 about the risks and benefits of prostate-specific antigen (PSA) screening.5 For cisgender men aged 70 and older, the USPSTF recommends against PSA-based screening.5 If digital examination of the prostate is warranted for transfeminine patients, the examination is performed through the neovaginal canal.
Caring for elderly transgender patients is complex. Even though evidence guiding the management of elderly transgender patients is improving, there are still not enough definitive long-term data on this dynamic demographic. Like clinical approaches with hormonal or surgical treatments, caring for transgender elders is also multidisciplinary. Providers should be prepared to work with social workers, geriatric care physicians, endocrinologists, surgeons, and other relevant specialists to assist with potential knowledge gaps. The goals for the aging transgender population are the same as those for cisgender patients – preventing preventable diseases and reducing overall mortality so our patients can enjoy their golden years.
Dr. Brandt is an ob.gyn. and fellowship-trained gender-affirming surgeon in West Reading, Pa. Contact her at [email protected].
References
1. Carroll L. Psychiatr Clin N Am. 2017;40:127-40.
2. Selix NW et al. Clinical care of the aging LGBT population. J Nurse Pract. 2020;16(7):349-54.
3. World Professional Association for Transgender Health. Standards of care for the health of transgender and gender diverse people. 2022;8th version.
4. Shatzel JJ et al. Am J Hematol. 2017;92(2):204-8.
5. Wolf-Gould CS and Wolf-Gould CH. Primary and preventative care for transgender patients. In: Ferrando CA, ed. Comprehensive Care of the Transgender Patient. Philadelphia: Elsevier, 2020, p. 114-30.
The elderly transgender population is rapidly expanding and remains significantly overlooked. Although emerging evidence provides some guidance for medical and surgical treatment for transgender youth, there is still a paucity of research directed at the management of gender-diverse elders.
To a large extent, the challenges that transgender elders face are no different from those experienced by the general elder population. Irrespective of gender identity, patients begin to undergo cognitive and physical changes, encounter difficulties with activities of daily living, suffer the loss of social networks and friends, and face end-of-life issues.1 Attributes that contribute to successful aging in the general population include good health, social engagement and support, and having a positive outlook on life.1 Yet, stigma surrounding gender identity and sexual orientation continues to negatively affect elder transgender people.
Many members of the LGBTQIA+ population have higher rates of obesity, sedentary lifestyle, smoking, cardiovascular disease, substance abuse, depression, suicide, and intimate partner violence than the general same-age cohort.2 Compared with lesbian, gay, and bisexual elders of age-matched cohorts, transgender elders have significantly poorer overall physical health, disability, depressive symptoms, and perceived stress.2
Rates of sexually transmitted infections are also rising in the aging general population and increased by 30% between 2014 and 2017.2 There have been no current studies examining these rates in the LGBTQIA+ population. As providers interact more frequently with these patients, it’s not only essential to screen for conditions such as diabetes, lipid disorders, and sexually transmitted infections, but also to evaluate current gender-affirming hormone therapy (GAHT) regimens and order appropriate screening tests.
Hormonal therapy for transfeminine patients should be continued as patients age. One of the biggest concerns providers have in continuing hormone therapy is the development of cardiovascular disease (CVD) and increasing thromboembolic risk, both of which tend to occur naturally as patients age. Overall, studies on the prevalence of CVD or stroke in gender-diverse individuals indicate an elevated risk independent of GAHT.3 While the overall rates of thromboembolic events are low in transfeminine populations, estrogen therapy does confer an increased risk. However, most transgender women who have experienced cardiac events or stroke were over the age of 50, had one or more CVD risk factors, or were using synthetic estrogens.3
How these studies affect screening is unclear. Current guidelines recommend using tailored risk-based calculators, which take into consideration the patient’s sex assigned at birth, hormone regimen, length of hormone usage, and additional modifiable risk factors, such as diabetes, obesity, and smoking.3 For transfeminine patients who want to continue GAHT but either develop a venous thromboembolism on estrogen or have increased risk for VTE, providers should consider transitioning them to a transdermal application. Patients who stay on GAHT should be counseled accordingly on the heightened risk of VTE recurrence. It is not unreasonable to consider life-long anticoagulation for patients who remain on estrogen therapy after a VTE.4
While exogenous estrogen exposure is one risk factor for the development of breast cancer in cisgender females, the role of GAHT in breast cancer in transgender women is ambiguous. Therefore, breast screening guidelines should follow current recommendations for cisgender female patients with some caveats. The provider must also take into consideration current estrogen dosage, the age at which hormones were initiated, and whether a patient has undergone an augmentation mammaplasty.3
Both estrogen and testosterone play an important role in bone formation and health. Patients who undergo either medical or surgical interventions that alter sex hormone production, such as GAHT, orchiectomy, or androgen blockade, may be at elevated risk for osteoporosis. Providers should take a thorough medical history to determine patients who may be at risk for osteoporosis and treat them accordingly. Overall, GAHT has a positive effect on bone mineral density. Conversely, gonadectomy, particularly if a patient is not taking GAHT, can decrease bone density. Generally, transgender women, like cisgender women, should undergo DEXA scans starting at the age of 65, with earlier screening considered if they have undergone an orchiectomy and are not currently taking GAHT.3
There is no evidence that GAHT or surgery increases the rate of prostate cancer. Providers should note that the prostate is not removed at the time of gender-affirming surgery and that malignancy or benign prostatic hypertrophy can still occur. The U.S. Preventive Services Task Force recommends that clinicians have a discussion with cisgender men between the ages of 55 and 69 about the risks and benefits of prostate-specific antigen (PSA) screening.5 For cisgender men aged 70 and older, the USPSTF recommends against PSA-based screening.5 If digital examination of the prostate is warranted for transfeminine patients, the examination is performed through the neovaginal canal.
Caring for elderly transgender patients is complex. Even though evidence guiding the management of elderly transgender patients is improving, there are still not enough definitive long-term data on this dynamic demographic. Like clinical approaches with hormonal or surgical treatments, caring for transgender elders is also multidisciplinary. Providers should be prepared to work with social workers, geriatric care physicians, endocrinologists, surgeons, and other relevant specialists to assist with potential knowledge gaps. The goals for the aging transgender population are the same as those for cisgender patients – preventing preventable diseases and reducing overall mortality so our patients can enjoy their golden years.
Dr. Brandt is an ob.gyn. and fellowship-trained gender-affirming surgeon in West Reading, Pa. Contact her at [email protected].
References
1. Carroll L. Psychiatr Clin N Am. 2017;40:127-40.
2. Selix NW et al. Clinical care of the aging LGBT population. J Nurse Pract. 2020;16(7):349-54.
3. World Professional Association for Transgender Health. Standards of care for the health of transgender and gender diverse people. 2022;8th version.
4. Shatzel JJ et al. Am J Hematol. 2017;92(2):204-8.
5. Wolf-Gould CS and Wolf-Gould CH. Primary and preventative care for transgender patients. In: Ferrando CA, ed. Comprehensive Care of the Transgender Patient. Philadelphia: Elsevier, 2020, p. 114-30.
Global Initiative for Chronic Obstructive Lung Disease guidelines 2022: Management and treatment
In the United States and around the globe, chronic obstructive pulmonary disease (COPD) remains one of the leading causes of death. In addition to new diagnostic guidelines, the Global Initiative for Chronic Obstructive Lung Disease 2022 Report, or GOLD report, sets forth recommendations for management and treatment.
According to the GOLD report, initial management of COPD should aim at reducing exposure to risk factors such as smoking or other chemical exposures. In addition to medications, stable COPD patients should be evaluated for inhaler technique, adherence to prescribed therapies, smoking status, and continued exposure to other risk factors. Also, physical activity should be advised and pulmonary rehabilitation should be considered. Spirometry should be performed annually.

These guidelines offer very practical advice but often are difficult to implement in clinical practice. Everyone knows smoking is harmful and quitting provides huge health benefits, not only regarding COPD. However, nicotine is very addictive, and most smokers cannot just quit. Many need smoking cessation aids and counseling. Additionally, some smokers just don’t want to quit. Regarding workplace exposures, it often is not easy for someone just to change their job. Many are afraid to speak because they are afraid of losing their jobs. Everyone, not just patients with COPD, can benefit from increased physical activity, and all doctors know how difficult it is to motivate patients to do this.
The decision to initiate medications should be based on an individual patient’s symptoms and risk of exacerbations. In general, long-acting bronchodilators, including long-acting beta agonists (LABA) and long-acting muscarinic antagonists (LAMA), are preferred except when immediate relief of dyspnea is needed, and then short-acting bronchodilators should be used. Either a single long-acting or dual long-acting bronchodilator can be initiated. If a patient continues to have dyspnea on a single long-acting bronchodilator, treatment should be switched to a dual therapy.
In general, inhaled corticosteroids (ICS) are not recommended for stable COPD patients. If a patient has exacerbations despite appropriate treatment with LABAs, an ICS may be added to the LABA, the GOLD guidelines say. Oral corticosteroids are not recommended for long-term use. PDE4 inhibitors should be considered in patents with severe to very severe airflow obstruction, chronic bronchitis, and exacerbations. Macrolide antibiotics, especially azithromycin, can be considered in acute exacerbations. There is no evidence to support the use of antitussives and mucolytics are advised in only certain patients. Inhaled bronchodilators are advised over oral ones and theophylline is recommended when long-acting bronchodilators are unavailable or unaffordable.
In clinical practice, I see many patients treated based on symptomatology with spirometry testing not being done. This may help control many symptoms, but unless my patient has an accurate diagnosis, I won’t know if my patient is receiving the correct treatment.
It is important to keep in mind that COPD is a progressive disease and without appropriate treatment and monitoring, it will just get worse, and this is most likely to be irreversible.
Medications and treatment goals for patients with COPD
Patients with alpha-1 antitrypsin deficiency may benefit from the addition of alpha-1 antitrypsin augmentation therapy, the new guidelines say. In patients with severe disease experiencing dyspnea, oral and parental opioids can be considered. Medications that are used to treat primary pulmonary hypertension are not advised to treat pulmonary hypertension secondary to COPD.
The treatment goals of COPD should be to decrease severity of symptoms, reduce the occurrence of exacerbations, and improve exercise tolerance. Peripheral eosinophil counts can be used to guide the use of ICS to prevent exacerbations. However, the best predictor of exacerbations is previous exacerbations. Frequent exacerbations are defined as two or more annually. Additionally, deteriorating airflow is correlated with increased risk of exacerbations, hospitalizations, and death. Forced expiratory volume in 1 second (FEV1) alone lacks precision to predict exacerbations or death.
Vaccines and pulmonary rehabilitation recommended
The Centers for Disease Control and Prevention and World Health Organization recommend several vaccines for stable patients with COPD. Influenza vaccine was shown to reduce serious complications in COPD patients. Pneumococcal vaccines (PCV13 and PPSV23) reduced the likelihood of COPD exacerbations. The COVID-19 vaccine also has been effective at reducing hospitalizations, in particular ICU admissions, and death in patients with COPD. The CDC also recommends TdaP and Zoster vaccines.
An acute exacerbation of COPD occurs when a patient experiences worsening of respiratory symptoms that requires additional treatment, according to the updated GOLD guidelines. They are usually associated with increased airway inflammation, mucous productions, and trapping of gases. They are often triggered by viral infections, but bacterial and environment factors play a role as well. Less commonly, fungi such as Aspergillus can be observed as well. COPD exacerbations contribute to overall progression of the disease.
In patients with hypoxemia, supplemental oxygen should be titrated to a target O2 saturation of 88%-92%. It is important to follow blood gases to be sure adequate oxygenation is taking place while at the same time avoiding carbon dioxide retention and/or worsening acidosis. In patients with severe exacerbations whose dyspnea does not respond to initial emergency therapy, ICU admission is warranted. Other factors indicating the need for ICU admission include mental status changes, persistent or worsening hypoxemia, severe or worsening respiratory acidosis, the need for mechanical ventilation, and hemodynamic instability. Following an acute exacerbation, steps to prevent further exacerbations should be initiated.
Systemic glucocorticoids are indicated during acute exacerbations. They have been shown to hasten recovery time and improve functioning of the lungs as well as oxygenation. It is recommended to give prednisone 40 mg per day for 5 days. Antibiotics should be used in exacerbations if patients have dyspnea, sputum production, and purulence of the sputum or require mechanical ventilation. The choice of which antibiotic to use should be based on local bacterial resistance.
Pulmonary rehabilitation is an important component of COPD management. It incorporates exercise, education, and self-management aimed to change behavior and improve conditioning. The benefits of rehab have been shown to be considerable. The optimal length is 6-8 weeks. Palliative and end-of-life care are also very important factors to consider when treating COPD patients, according to the GOLD guidelines.
COPD is a very common disease and cause of mortality seen by family physicians. The GOLD report is an extensive document providing very clear guidelines and evidence to support these guidelines in every level of the treatment of COPD patients. As primary care doctors, we are often the first to treat patients with COPD and it is important to know the latest guidelines.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at [email protected].
In the United States and around the globe, chronic obstructive pulmonary disease (COPD) remains one of the leading causes of death. In addition to new diagnostic guidelines, the Global Initiative for Chronic Obstructive Lung Disease 2022 Report, or GOLD report, sets forth recommendations for management and treatment.
According to the GOLD report, initial management of COPD should aim at reducing exposure to risk factors such as smoking or other chemical exposures. In addition to medications, stable COPD patients should be evaluated for inhaler technique, adherence to prescribed therapies, smoking status, and continued exposure to other risk factors. Also, physical activity should be advised and pulmonary rehabilitation should be considered. Spirometry should be performed annually.
These guidelines offer very practical advice but often are difficult to implement in clinical practice. Everyone knows smoking is harmful and quitting provides huge health benefits, not only regarding COPD. However, nicotine is very addictive, and most smokers cannot just quit. Many need smoking cessation aids and counseling. Additionally, some smokers just don’t want to quit. Regarding workplace exposures, it often is not easy for someone just to change their job. Many are afraid to speak because they are afraid of losing their jobs. Everyone, not just patients with COPD, can benefit from increased physical activity, and all doctors know how difficult it is to motivate patients to do this.
The decision to initiate medications should be based on an individual patient’s symptoms and risk of exacerbations. In general, long-acting bronchodilators, including long-acting beta agonists (LABA) and long-acting muscarinic antagonists (LAMA), are preferred except when immediate relief of dyspnea is needed, and then short-acting bronchodilators should be used. Either a single long-acting or dual long-acting bronchodilator can be initiated. If a patient continues to have dyspnea on a single long-acting bronchodilator, treatment should be switched to a dual therapy.
In general, inhaled corticosteroids (ICS) are not recommended for stable COPD patients. If a patient has exacerbations despite appropriate treatment with LABAs, an ICS may be added to the LABA, the GOLD guidelines say. Oral corticosteroids are not recommended for long-term use. PDE4 inhibitors should be considered in patents with severe to very severe airflow obstruction, chronic bronchitis, and exacerbations. Macrolide antibiotics, especially azithromycin, can be considered in acute exacerbations. There is no evidence to support the use of antitussives and mucolytics are advised in only certain patients. Inhaled bronchodilators are advised over oral ones and theophylline is recommended when long-acting bronchodilators are unavailable or unaffordable.
In clinical practice, I see many patients treated based on symptomatology with spirometry testing not being done. This may help control many symptoms, but unless my patient has an accurate diagnosis, I won’t know if my patient is receiving the correct treatment.
It is important to keep in mind that COPD is a progressive disease and without appropriate treatment and monitoring, it will just get worse, and this is most likely to be irreversible.
Medications and treatment goals for patients with COPD
Patients with alpha-1 antitrypsin deficiency may benefit from the addition of alpha-1 antitrypsin augmentation therapy, the new guidelines say. In patients with severe disease experiencing dyspnea, oral and parental opioids can be considered. Medications that are used to treat primary pulmonary hypertension are not advised to treat pulmonary hypertension secondary to COPD.
The treatment goals of COPD should be to decrease severity of symptoms, reduce the occurrence of exacerbations, and improve exercise tolerance. Peripheral eosinophil counts can be used to guide the use of ICS to prevent exacerbations. However, the best predictor of exacerbations is previous exacerbations. Frequent exacerbations are defined as two or more annually. Additionally, deteriorating airflow is correlated with increased risk of exacerbations, hospitalizations, and death. Forced expiratory volume in 1 second (FEV1) alone lacks precision to predict exacerbations or death.
Vaccines and pulmonary rehabilitation recommended
The Centers for Disease Control and Prevention and World Health Organization recommend several vaccines for stable patients with COPD. Influenza vaccine was shown to reduce serious complications in COPD patients. Pneumococcal vaccines (PCV13 and PPSV23) reduced the likelihood of COPD exacerbations. The COVID-19 vaccine also has been effective at reducing hospitalizations, in particular ICU admissions, and death in patients with COPD. The CDC also recommends TdaP and Zoster vaccines.
An acute exacerbation of COPD occurs when a patient experiences worsening of respiratory symptoms that requires additional treatment, according to the updated GOLD guidelines. They are usually associated with increased airway inflammation, mucous productions, and trapping of gases. They are often triggered by viral infections, but bacterial and environment factors play a role as well. Less commonly, fungi such as Aspergillus can be observed as well. COPD exacerbations contribute to overall progression of the disease.
In patients with hypoxemia, supplemental oxygen should be titrated to a target O2 saturation of 88%-92%. It is important to follow blood gases to be sure adequate oxygenation is taking place while at the same time avoiding carbon dioxide retention and/or worsening acidosis. In patients with severe exacerbations whose dyspnea does not respond to initial emergency therapy, ICU admission is warranted. Other factors indicating the need for ICU admission include mental status changes, persistent or worsening hypoxemia, severe or worsening respiratory acidosis, the need for mechanical ventilation, and hemodynamic instability. Following an acute exacerbation, steps to prevent further exacerbations should be initiated.
Systemic glucocorticoids are indicated during acute exacerbations. They have been shown to hasten recovery time and improve functioning of the lungs as well as oxygenation. It is recommended to give prednisone 40 mg per day for 5 days. Antibiotics should be used in exacerbations if patients have dyspnea, sputum production, and purulence of the sputum or require mechanical ventilation. The choice of which antibiotic to use should be based on local bacterial resistance.
Pulmonary rehabilitation is an important component of COPD management. It incorporates exercise, education, and self-management aimed to change behavior and improve conditioning. The benefits of rehab have been shown to be considerable. The optimal length is 6-8 weeks. Palliative and end-of-life care are also very important factors to consider when treating COPD patients, according to the GOLD guidelines.
COPD is a very common disease and cause of mortality seen by family physicians. The GOLD report is an extensive document providing very clear guidelines and evidence to support these guidelines in every level of the treatment of COPD patients. As primary care doctors, we are often the first to treat patients with COPD and it is important to know the latest guidelines.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at [email protected].
In the United States and around the globe, chronic obstructive pulmonary disease (COPD) remains one of the leading causes of death. In addition to new diagnostic guidelines, the Global Initiative for Chronic Obstructive Lung Disease 2022 Report, or GOLD report, sets forth recommendations for management and treatment.
According to the GOLD report, initial management of COPD should aim at reducing exposure to risk factors such as smoking or other chemical exposures. In addition to medications, stable COPD patients should be evaluated for inhaler technique, adherence to prescribed therapies, smoking status, and continued exposure to other risk factors. Also, physical activity should be advised and pulmonary rehabilitation should be considered. Spirometry should be performed annually.
These guidelines offer very practical advice but often are difficult to implement in clinical practice. Everyone knows smoking is harmful and quitting provides huge health benefits, not only regarding COPD. However, nicotine is very addictive, and most smokers cannot just quit. Many need smoking cessation aids and counseling. Additionally, some smokers just don’t want to quit. Regarding workplace exposures, it often is not easy for someone just to change their job. Many are afraid to speak because they are afraid of losing their jobs. Everyone, not just patients with COPD, can benefit from increased physical activity, and all doctors know how difficult it is to motivate patients to do this.
The decision to initiate medications should be based on an individual patient’s symptoms and risk of exacerbations. In general, long-acting bronchodilators, including long-acting beta agonists (LABA) and long-acting muscarinic antagonists (LAMA), are preferred except when immediate relief of dyspnea is needed, and then short-acting bronchodilators should be used. Either a single long-acting or dual long-acting bronchodilator can be initiated. If a patient continues to have dyspnea on a single long-acting bronchodilator, treatment should be switched to a dual therapy.
In general, inhaled corticosteroids (ICS) are not recommended for stable COPD patients. If a patient has exacerbations despite appropriate treatment with LABAs, an ICS may be added to the LABA, the GOLD guidelines say. Oral corticosteroids are not recommended for long-term use. PDE4 inhibitors should be considered in patents with severe to very severe airflow obstruction, chronic bronchitis, and exacerbations. Macrolide antibiotics, especially azithromycin, can be considered in acute exacerbations. There is no evidence to support the use of antitussives and mucolytics are advised in only certain patients. Inhaled bronchodilators are advised over oral ones and theophylline is recommended when long-acting bronchodilators are unavailable or unaffordable.
In clinical practice, I see many patients treated based on symptomatology with spirometry testing not being done. This may help control many symptoms, but unless my patient has an accurate diagnosis, I won’t know if my patient is receiving the correct treatment.
It is important to keep in mind that COPD is a progressive disease and without appropriate treatment and monitoring, it will just get worse, and this is most likely to be irreversible.
Medications and treatment goals for patients with COPD
Patients with alpha-1 antitrypsin deficiency may benefit from the addition of alpha-1 antitrypsin augmentation therapy, the new guidelines say. In patients with severe disease experiencing dyspnea, oral and parental opioids can be considered. Medications that are used to treat primary pulmonary hypertension are not advised to treat pulmonary hypertension secondary to COPD.
The treatment goals of COPD should be to decrease severity of symptoms, reduce the occurrence of exacerbations, and improve exercise tolerance. Peripheral eosinophil counts can be used to guide the use of ICS to prevent exacerbations. However, the best predictor of exacerbations is previous exacerbations. Frequent exacerbations are defined as two or more annually. Additionally, deteriorating airflow is correlated with increased risk of exacerbations, hospitalizations, and death. Forced expiratory volume in 1 second (FEV1) alone lacks precision to predict exacerbations or death.
Vaccines and pulmonary rehabilitation recommended
The Centers for Disease Control and Prevention and World Health Organization recommend several vaccines for stable patients with COPD. Influenza vaccine was shown to reduce serious complications in COPD patients. Pneumococcal vaccines (PCV13 and PPSV23) reduced the likelihood of COPD exacerbations. The COVID-19 vaccine also has been effective at reducing hospitalizations, in particular ICU admissions, and death in patients with COPD. The CDC also recommends TdaP and Zoster vaccines.
An acute exacerbation of COPD occurs when a patient experiences worsening of respiratory symptoms that requires additional treatment, according to the updated GOLD guidelines. They are usually associated with increased airway inflammation, mucous productions, and trapping of gases. They are often triggered by viral infections, but bacterial and environment factors play a role as well. Less commonly, fungi such as Aspergillus can be observed as well. COPD exacerbations contribute to overall progression of the disease.
In patients with hypoxemia, supplemental oxygen should be titrated to a target O2 saturation of 88%-92%. It is important to follow blood gases to be sure adequate oxygenation is taking place while at the same time avoiding carbon dioxide retention and/or worsening acidosis. In patients with severe exacerbations whose dyspnea does not respond to initial emergency therapy, ICU admission is warranted. Other factors indicating the need for ICU admission include mental status changes, persistent or worsening hypoxemia, severe or worsening respiratory acidosis, the need for mechanical ventilation, and hemodynamic instability. Following an acute exacerbation, steps to prevent further exacerbations should be initiated.
Systemic glucocorticoids are indicated during acute exacerbations. They have been shown to hasten recovery time and improve functioning of the lungs as well as oxygenation. It is recommended to give prednisone 40 mg per day for 5 days. Antibiotics should be used in exacerbations if patients have dyspnea, sputum production, and purulence of the sputum or require mechanical ventilation. The choice of which antibiotic to use should be based on local bacterial resistance.
Pulmonary rehabilitation is an important component of COPD management. It incorporates exercise, education, and self-management aimed to change behavior and improve conditioning. The benefits of rehab have been shown to be considerable. The optimal length is 6-8 weeks. Palliative and end-of-life care are also very important factors to consider when treating COPD patients, according to the GOLD guidelines.
COPD is a very common disease and cause of mortality seen by family physicians. The GOLD report is an extensive document providing very clear guidelines and evidence to support these guidelines in every level of the treatment of COPD patients. As primary care doctors, we are often the first to treat patients with COPD and it is important to know the latest guidelines.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at [email protected].
Germline genetic testing: Why it matters and where we are failing
Historically, the role of genetic testing has been to identify familial cancer syndromes and initiate cascade testing. If a germline pathogenic variant is found in an individual, cascade testing involves genetic counseling and testing of blood relatives, starting with those closest in relation to the proband, to identify other family members at high hereditary cancer risk. Once testing identifies those family members at higher cancer risk, these individuals can be referred for risk-reducing procedures. They can undergo screening tests starting at an earlier age and/or increased frequency to help prevent invasive cancer or diagnose it at an earlier stage.
Genetic testing can also inform prognosis. While women with a BRCA1 or BRCA2 mutation are at higher risk of developing ovarian cancer compared with the baseline population, the presence of a germline BRCA mutation has been shown to confer improved survival compared with no BRCA mutation (BRCA wild type). However, more recent data have shown that when long-term survival was analyzed, the prognostic benefit seen in patients with a germline BRCA mutation was lost. The initial survival advantage seen in this population may be related to increased sensitivity to treatment. There appears to be improved response to platinum therapy, which is the standard of care for upfront treatment, in germline BRCA mutation carriers.

Most recently, genetic testing has been used to guide treatment decisions in gynecologic cancers. In 2014, the first poly ADP-ribose polymerase (PARP) inhibitor, olaparib, received Food and Drug Administration approval for the treatment of recurrent ovarian cancer in the presence of a germline BRCA mutation. Now there are multiple PARP inhibitors that have FDA approval for ovarian cancer treatment, some as frontline treatment.
Previous data indicate that 13%-18% of women with ovarian cancer have a germline BRCA mutation that places them at increased risk of hereditary ovarian cancer.1 Current guidelines from the American Society of Clinical Oncology, the U.S. Preventive Services Task Force, the National Comprehensive Cancer Network, the Society of Gynecologic Oncology (SGO), and the American College of Obstetricians and Gynecologists recommend universal genetic counseling and testing for patients diagnosed with epithelial ovarian cancer. Despite these guidelines, rates of referral for genetic counseling and completion of genetic testing are low.
There has been improvement for both referrals and testing since the publication of the 2014 SGO clinical practice statement on genetic testing for ovarian cancer patients, which recommended that all women, even those without any significant family history, should receive genetic counseling and be offered genetic testing.2 When including only studies that collected data after the publication of the 2014 SGO clinical practice statement on genetic testing, a recent systematic review found that 64% of patients were referred for genetic counseling and 63% underwent testing.3
Clinical interventions to target genetic evaluation appear to improve uptake of both counseling and testing. These interventions include using telemedicine to deliver genetic counseling services, mainstreaming (counseling and testing are provided in an oncology clinic by nongenetics specialists), having a genetic counselor within the clinic, and performing reflex testing. With limited numbers of genetic counselors (and even further limited numbers of cancer-specific genetic counselors),4 referral for genetic counseling before testing is often challenging and may not be feasible. There is continued need for strategies to help overcome the barrier to accessing genetic counseling.
While the data are limited, there appear to be significant disparities in rates of genetic testing. Genetic counseling and testing were completed by White (43% and 40%) patients more frequently than by either Black (24% and 26%) or Asian (23% and 14%) patients.4 Uninsured patients were about half as likely (23% vs. 47%) to complete genetic testing as were those with private insurance.4
Genetic testing is an important tool to help identify individuals and families at risk of having hereditary cancer syndromes. This identification allows us to prevent many cancers and identify others while still early stage, significantly decreasing the health care and financial burden on our society and improving outcomes for patients. While we have seen improvement in rates of referral for genetic counseling and testing, we are still falling short. Given the shortage of genetic counselors, it is imperative that we find solutions to ensure continued and improved access to genetic testing for our patients.
Dr. Tucker is assistant professor of gynecologic oncology at the University of North Carolina at Chapel Hill.
References
1. Norquist BM et al. JAMA Oncol. 2016;2(4):482-90.
2. SGO Clinical Practice Statement. 2014 Oct 1.
3. Lin J et al. Gynecol Oncol. 2021;162(2):506-16.
4. American Society of Clinical Oncology. J Oncol Pract. 2016 Apr;12(4):339-83.
Historically, the role of genetic testing has been to identify familial cancer syndromes and initiate cascade testing. If a germline pathogenic variant is found in an individual, cascade testing involves genetic counseling and testing of blood relatives, starting with those closest in relation to the proband, to identify other family members at high hereditary cancer risk. Once testing identifies those family members at higher cancer risk, these individuals can be referred for risk-reducing procedures. They can undergo screening tests starting at an earlier age and/or increased frequency to help prevent invasive cancer or diagnose it at an earlier stage.
Genetic testing can also inform prognosis. While women with a BRCA1 or BRCA2 mutation are at higher risk of developing ovarian cancer compared with the baseline population, the presence of a germline BRCA mutation has been shown to confer improved survival compared with no BRCA mutation (BRCA wild type). However, more recent data have shown that when long-term survival was analyzed, the prognostic benefit seen in patients with a germline BRCA mutation was lost. The initial survival advantage seen in this population may be related to increased sensitivity to treatment. There appears to be improved response to platinum therapy, which is the standard of care for upfront treatment, in germline BRCA mutation carriers.
Most recently, genetic testing has been used to guide treatment decisions in gynecologic cancers. In 2014, the first poly ADP-ribose polymerase (PARP) inhibitor, olaparib, received Food and Drug Administration approval for the treatment of recurrent ovarian cancer in the presence of a germline BRCA mutation. Now there are multiple PARP inhibitors that have FDA approval for ovarian cancer treatment, some as frontline treatment.
Previous data indicate that 13%-18% of women with ovarian cancer have a germline BRCA mutation that places them at increased risk of hereditary ovarian cancer.1 Current guidelines from the American Society of Clinical Oncology, the U.S. Preventive Services Task Force, the National Comprehensive Cancer Network, the Society of Gynecologic Oncology (SGO), and the American College of Obstetricians and Gynecologists recommend universal genetic counseling and testing for patients diagnosed with epithelial ovarian cancer. Despite these guidelines, rates of referral for genetic counseling and completion of genetic testing are low.
There has been improvement for both referrals and testing since the publication of the 2014 SGO clinical practice statement on genetic testing for ovarian cancer patients, which recommended that all women, even those without any significant family history, should receive genetic counseling and be offered genetic testing.2 When including only studies that collected data after the publication of the 2014 SGO clinical practice statement on genetic testing, a recent systematic review found that 64% of patients were referred for genetic counseling and 63% underwent testing.3
Clinical interventions to target genetic evaluation appear to improve uptake of both counseling and testing. These interventions include using telemedicine to deliver genetic counseling services, mainstreaming (counseling and testing are provided in an oncology clinic by nongenetics specialists), having a genetic counselor within the clinic, and performing reflex testing. With limited numbers of genetic counselors (and even further limited numbers of cancer-specific genetic counselors),4 referral for genetic counseling before testing is often challenging and may not be feasible. There is continued need for strategies to help overcome the barrier to accessing genetic counseling.
While the data are limited, there appear to be significant disparities in rates of genetic testing. Genetic counseling and testing were completed by White (43% and 40%) patients more frequently than by either Black (24% and 26%) or Asian (23% and 14%) patients.4 Uninsured patients were about half as likely (23% vs. 47%) to complete genetic testing as were those with private insurance.4
Genetic testing is an important tool to help identify individuals and families at risk of having hereditary cancer syndromes. This identification allows us to prevent many cancers and identify others while still early stage, significantly decreasing the health care and financial burden on our society and improving outcomes for patients. While we have seen improvement in rates of referral for genetic counseling and testing, we are still falling short. Given the shortage of genetic counselors, it is imperative that we find solutions to ensure continued and improved access to genetic testing for our patients.
Dr. Tucker is assistant professor of gynecologic oncology at the University of North Carolina at Chapel Hill.
References
1. Norquist BM et al. JAMA Oncol. 2016;2(4):482-90.
2. SGO Clinical Practice Statement. 2014 Oct 1.
3. Lin J et al. Gynecol Oncol. 2021;162(2):506-16.
4. American Society of Clinical Oncology. J Oncol Pract. 2016 Apr;12(4):339-83.
Historically, the role of genetic testing has been to identify familial cancer syndromes and initiate cascade testing. If a germline pathogenic variant is found in an individual, cascade testing involves genetic counseling and testing of blood relatives, starting with those closest in relation to the proband, to identify other family members at high hereditary cancer risk. Once testing identifies those family members at higher cancer risk, these individuals can be referred for risk-reducing procedures. They can undergo screening tests starting at an earlier age and/or increased frequency to help prevent invasive cancer or diagnose it at an earlier stage.
Genetic testing can also inform prognosis. While women with a BRCA1 or BRCA2 mutation are at higher risk of developing ovarian cancer compared with the baseline population, the presence of a germline BRCA mutation has been shown to confer improved survival compared with no BRCA mutation (BRCA wild type). However, more recent data have shown that when long-term survival was analyzed, the prognostic benefit seen in patients with a germline BRCA mutation was lost. The initial survival advantage seen in this population may be related to increased sensitivity to treatment. There appears to be improved response to platinum therapy, which is the standard of care for upfront treatment, in germline BRCA mutation carriers.
Most recently, genetic testing has been used to guide treatment decisions in gynecologic cancers. In 2014, the first poly ADP-ribose polymerase (PARP) inhibitor, olaparib, received Food and Drug Administration approval for the treatment of recurrent ovarian cancer in the presence of a germline BRCA mutation. Now there are multiple PARP inhibitors that have FDA approval for ovarian cancer treatment, some as frontline treatment.
Previous data indicate that 13%-18% of women with ovarian cancer have a germline BRCA mutation that places them at increased risk of hereditary ovarian cancer.1 Current guidelines from the American Society of Clinical Oncology, the U.S. Preventive Services Task Force, the National Comprehensive Cancer Network, the Society of Gynecologic Oncology (SGO), and the American College of Obstetricians and Gynecologists recommend universal genetic counseling and testing for patients diagnosed with epithelial ovarian cancer. Despite these guidelines, rates of referral for genetic counseling and completion of genetic testing are low.
There has been improvement for both referrals and testing since the publication of the 2014 SGO clinical practice statement on genetic testing for ovarian cancer patients, which recommended that all women, even those without any significant family history, should receive genetic counseling and be offered genetic testing.2 When including only studies that collected data after the publication of the 2014 SGO clinical practice statement on genetic testing, a recent systematic review found that 64% of patients were referred for genetic counseling and 63% underwent testing.3
Clinical interventions to target genetic evaluation appear to improve uptake of both counseling and testing. These interventions include using telemedicine to deliver genetic counseling services, mainstreaming (counseling and testing are provided in an oncology clinic by nongenetics specialists), having a genetic counselor within the clinic, and performing reflex testing. With limited numbers of genetic counselors (and even further limited numbers of cancer-specific genetic counselors),4 referral for genetic counseling before testing is often challenging and may not be feasible. There is continued need for strategies to help overcome the barrier to accessing genetic counseling.
While the data are limited, there appear to be significant disparities in rates of genetic testing. Genetic counseling and testing were completed by White (43% and 40%) patients more frequently than by either Black (24% and 26%) or Asian (23% and 14%) patients.4 Uninsured patients were about half as likely (23% vs. 47%) to complete genetic testing as were those with private insurance.4
Genetic testing is an important tool to help identify individuals and families at risk of having hereditary cancer syndromes. This identification allows us to prevent many cancers and identify others while still early stage, significantly decreasing the health care and financial burden on our society and improving outcomes for patients. While we have seen improvement in rates of referral for genetic counseling and testing, we are still falling short. Given the shortage of genetic counselors, it is imperative that we find solutions to ensure continued and improved access to genetic testing for our patients.
Dr. Tucker is assistant professor of gynecologic oncology at the University of North Carolina at Chapel Hill.
References
1. Norquist BM et al. JAMA Oncol. 2016;2(4):482-90.
2. SGO Clinical Practice Statement. 2014 Oct 1.
3. Lin J et al. Gynecol Oncol. 2021;162(2):506-16.
4. American Society of Clinical Oncology. J Oncol Pract. 2016 Apr;12(4):339-83.
Rules for performing research with children
The road to hell is paved with good intentions – especially true in clinical research. A Food and Drug Administration press release notes, “Historically, children were not included in clinical trials because of a misperception that excluding them from research was in fact protecting them. This resulted in many FDA-approved, licensed, cleared, or authorized drugs, biological products, and medical devices lacking pediatric-specific labeling information.” In an effort to improve on this situation, the FDA published in September 2022 a proposed new draft guidance on performing research with children that is open for public comment for 3 months.

There is a long history of government attempts to promote research and development for the benefit of society. Sometimes government succeeds and sometimes not. For instance, when the U.S. federal government funded scientific research in the 1960s, it sought to increase the common good by promulgating those discoveries. The government insisted that all federally funded research be in the public domain. The funding produced a spectacular number of technological advancements that have enriched society. However, a decade later, the government concluded that too many good research ideas were never developed into beneficial products because without the ability to patent the results, the costs and risks of product development were not profitable for industry. By the late 1970s, new laws were enacted to enable universities and their faculty to patent the results of government-funded research and share in any wealth created.
Pharmaceutical research in the 1970s and 1980s was mostly performed on men in order to reduce the risk of giving treatments of unknown safety to pregnant women. The unintended consequence was that the new drugs frequently were less effective for women. This was particularly true for cardiac medications for which lifestyle risk factors differed between the sexes.
Similarly, children were often excluded from research because of the unknown risks of new drugs on growing bodies and brains. Children were also seen as a vulnerable population for whom informed consent was problematic. The result of these well-intentioned restrictions was the creation of new products that did not have pediatric dosing recommendations, pediatric safety assessments, or approval for pediatric indications. To remediate these deficiencies, in 1997 and 2007 the FDA offered a 6-month extension on patent protection as motivation for companies to develop those pediatric recommendations. Alas, those laws were primarily used to extend the profitability of blockbuster products rather than truly benefit children.
Over the past 4 decades, pediatric ethicists proposed and refined rules to govern research on children. The Common Rule used by institutional review boards (IRBs) to protect human research subjects was expanded with guidelines covering children. The new draft guidance is the latest iteration of this effort. Nothing in the 14 pages of draft regulation appears revolutionary to me. The ideas are tweaks, based on theory and experience, of principles agreed upon 30 years ago. Finding the optimal social moral contract involves some empirical assessment of praxis and effectiveness.
I am loathe to summarize this new document, which itself is a summary of a vast body of literature, that supports the Code of Federal Regulations Title 21 Part 50 and 45 CFR Part 46. The draft document is well organized and I recommend it as an excellent primer for the area of pediatric research ethics if the subject is new to you. I also recommend it as required reading for anyone serving on an IRB.
IRBs usually review and approve any research on people. Generally, the selection of people for research should be done equitably. However, children should not be enrolled unless it is necessary to answer an important question relevant to children. For the past 2 decades, there has been an emphasis on obtaining the assent of the child as well as informed consent by the parents.
An important determination is whether the research is likely to help that particular child or whether it is aimed at advancing general knowledge. If there is no prospect of direct benefit, research is still permissible but more restricted for safety and comfort reasons. Next is determining whether the research carries only minimal risk or a minor increase over minimal risk. The draft defines and provides anchor examples of these situations. For instance, oral placebos and single blood draws are typically minimal risk. Multiple injections and blood draws over a year fall into the second category. One MRI is minimal risk but a minor increase in risk if it involves sedation or contrast.
I strongly support the ideals expressed in these guidelines. They represent the best blend of intentions and practical experience. They will become the law of the land. In ethics, there is merit in striving to do things properly, orderly, and enforceably.
The cynic in me sees two weaknesses in the stated approach. First, the volume of harm to children occurring during organized clinical research is extremely small. The greater harms come from off-label use, nonsystematic research, and the ignorance resulting from a lack of research. Second, my observation in all endeavors of morality is, “Raise the bar high enough and people walk under it.”
Dr. Powell is a retired pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at [email protected].
The road to hell is paved with good intentions – especially true in clinical research. A Food and Drug Administration press release notes, “Historically, children were not included in clinical trials because of a misperception that excluding them from research was in fact protecting them. This resulted in many FDA-approved, licensed, cleared, or authorized drugs, biological products, and medical devices lacking pediatric-specific labeling information.” In an effort to improve on this situation, the FDA published in September 2022 a proposed new draft guidance on performing research with children that is open for public comment for 3 months.
There is a long history of government attempts to promote research and development for the benefit of society. Sometimes government succeeds and sometimes not. For instance, when the U.S. federal government funded scientific research in the 1960s, it sought to increase the common good by promulgating those discoveries. The government insisted that all federally funded research be in the public domain. The funding produced a spectacular number of technological advancements that have enriched society. However, a decade later, the government concluded that too many good research ideas were never developed into beneficial products because without the ability to patent the results, the costs and risks of product development were not profitable for industry. By the late 1970s, new laws were enacted to enable universities and their faculty to patent the results of government-funded research and share in any wealth created.
Pharmaceutical research in the 1970s and 1980s was mostly performed on men in order to reduce the risk of giving treatments of unknown safety to pregnant women. The unintended consequence was that the new drugs frequently were less effective for women. This was particularly true for cardiac medications for which lifestyle risk factors differed between the sexes.
Similarly, children were often excluded from research because of the unknown risks of new drugs on growing bodies and brains. Children were also seen as a vulnerable population for whom informed consent was problematic. The result of these well-intentioned restrictions was the creation of new products that did not have pediatric dosing recommendations, pediatric safety assessments, or approval for pediatric indications. To remediate these deficiencies, in 1997 and 2007 the FDA offered a 6-month extension on patent protection as motivation for companies to develop those pediatric recommendations. Alas, those laws were primarily used to extend the profitability of blockbuster products rather than truly benefit children.
Over the past 4 decades, pediatric ethicists proposed and refined rules to govern research on children. The Common Rule used by institutional review boards (IRBs) to protect human research subjects was expanded with guidelines covering children. The new draft guidance is the latest iteration of this effort. Nothing in the 14 pages of draft regulation appears revolutionary to me. The ideas are tweaks, based on theory and experience, of principles agreed upon 30 years ago. Finding the optimal social moral contract involves some empirical assessment of praxis and effectiveness.
I am loathe to summarize this new document, which itself is a summary of a vast body of literature, that supports the Code of Federal Regulations Title 21 Part 50 and 45 CFR Part 46. The draft document is well organized and I recommend it as an excellent primer for the area of pediatric research ethics if the subject is new to you. I also recommend it as required reading for anyone serving on an IRB.
IRBs usually review and approve any research on people. Generally, the selection of people for research should be done equitably. However, children should not be enrolled unless it is necessary to answer an important question relevant to children. For the past 2 decades, there has been an emphasis on obtaining the assent of the child as well as informed consent by the parents.
An important determination is whether the research is likely to help that particular child or whether it is aimed at advancing general knowledge. If there is no prospect of direct benefit, research is still permissible but more restricted for safety and comfort reasons. Next is determining whether the research carries only minimal risk or a minor increase over minimal risk. The draft defines and provides anchor examples of these situations. For instance, oral placebos and single blood draws are typically minimal risk. Multiple injections and blood draws over a year fall into the second category. One MRI is minimal risk but a minor increase in risk if it involves sedation or contrast.
I strongly support the ideals expressed in these guidelines. They represent the best blend of intentions and practical experience. They will become the law of the land. In ethics, there is merit in striving to do things properly, orderly, and enforceably.
The cynic in me sees two weaknesses in the stated approach. First, the volume of harm to children occurring during organized clinical research is extremely small. The greater harms come from off-label use, nonsystematic research, and the ignorance resulting from a lack of research. Second, my observation in all endeavors of morality is, “Raise the bar high enough and people walk under it.”
Dr. Powell is a retired pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at [email protected].
The road to hell is paved with good intentions – especially true in clinical research. A Food and Drug Administration press release notes, “Historically, children were not included in clinical trials because of a misperception that excluding them from research was in fact protecting them. This resulted in many FDA-approved, licensed, cleared, or authorized drugs, biological products, and medical devices lacking pediatric-specific labeling information.” In an effort to improve on this situation, the FDA published in September 2022 a proposed new draft guidance on performing research with children that is open for public comment for 3 months.
There is a long history of government attempts to promote research and development for the benefit of society. Sometimes government succeeds and sometimes not. For instance, when the U.S. federal government funded scientific research in the 1960s, it sought to increase the common good by promulgating those discoveries. The government insisted that all federally funded research be in the public domain. The funding produced a spectacular number of technological advancements that have enriched society. However, a decade later, the government concluded that too many good research ideas were never developed into beneficial products because without the ability to patent the results, the costs and risks of product development were not profitable for industry. By the late 1970s, new laws were enacted to enable universities and their faculty to patent the results of government-funded research and share in any wealth created.
Pharmaceutical research in the 1970s and 1980s was mostly performed on men in order to reduce the risk of giving treatments of unknown safety to pregnant women. The unintended consequence was that the new drugs frequently were less effective for women. This was particularly true for cardiac medications for which lifestyle risk factors differed between the sexes.
Similarly, children were often excluded from research because of the unknown risks of new drugs on growing bodies and brains. Children were also seen as a vulnerable population for whom informed consent was problematic. The result of these well-intentioned restrictions was the creation of new products that did not have pediatric dosing recommendations, pediatric safety assessments, or approval for pediatric indications. To remediate these deficiencies, in 1997 and 2007 the FDA offered a 6-month extension on patent protection as motivation for companies to develop those pediatric recommendations. Alas, those laws were primarily used to extend the profitability of blockbuster products rather than truly benefit children.
Over the past 4 decades, pediatric ethicists proposed and refined rules to govern research on children. The Common Rule used by institutional review boards (IRBs) to protect human research subjects was expanded with guidelines covering children. The new draft guidance is the latest iteration of this effort. Nothing in the 14 pages of draft regulation appears revolutionary to me. The ideas are tweaks, based on theory and experience, of principles agreed upon 30 years ago. Finding the optimal social moral contract involves some empirical assessment of praxis and effectiveness.
I am loathe to summarize this new document, which itself is a summary of a vast body of literature, that supports the Code of Federal Regulations Title 21 Part 50 and 45 CFR Part 46. The draft document is well organized and I recommend it as an excellent primer for the area of pediatric research ethics if the subject is new to you. I also recommend it as required reading for anyone serving on an IRB.
IRBs usually review and approve any research on people. Generally, the selection of people for research should be done equitably. However, children should not be enrolled unless it is necessary to answer an important question relevant to children. For the past 2 decades, there has been an emphasis on obtaining the assent of the child as well as informed consent by the parents.
An important determination is whether the research is likely to help that particular child or whether it is aimed at advancing general knowledge. If there is no prospect of direct benefit, research is still permissible but more restricted for safety and comfort reasons. Next is determining whether the research carries only minimal risk or a minor increase over minimal risk. The draft defines and provides anchor examples of these situations. For instance, oral placebos and single blood draws are typically minimal risk. Multiple injections and blood draws over a year fall into the second category. One MRI is minimal risk but a minor increase in risk if it involves sedation or contrast.
I strongly support the ideals expressed in these guidelines. They represent the best blend of intentions and practical experience. They will become the law of the land. In ethics, there is merit in striving to do things properly, orderly, and enforceably.
The cynic in me sees two weaknesses in the stated approach. First, the volume of harm to children occurring during organized clinical research is extremely small. The greater harms come from off-label use, nonsystematic research, and the ignorance resulting from a lack of research. Second, my observation in all endeavors of morality is, “Raise the bar high enough and people walk under it.”
Dr. Powell is a retired pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at [email protected].
Why the 5-day isolation period for COVID makes no sense
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
One of the more baffling decisions the CDC made during this pandemic was when they reduced the duration of isolation after a positive COVID test from 10 days to 5 days and did not require a negative antigen test to end isolation.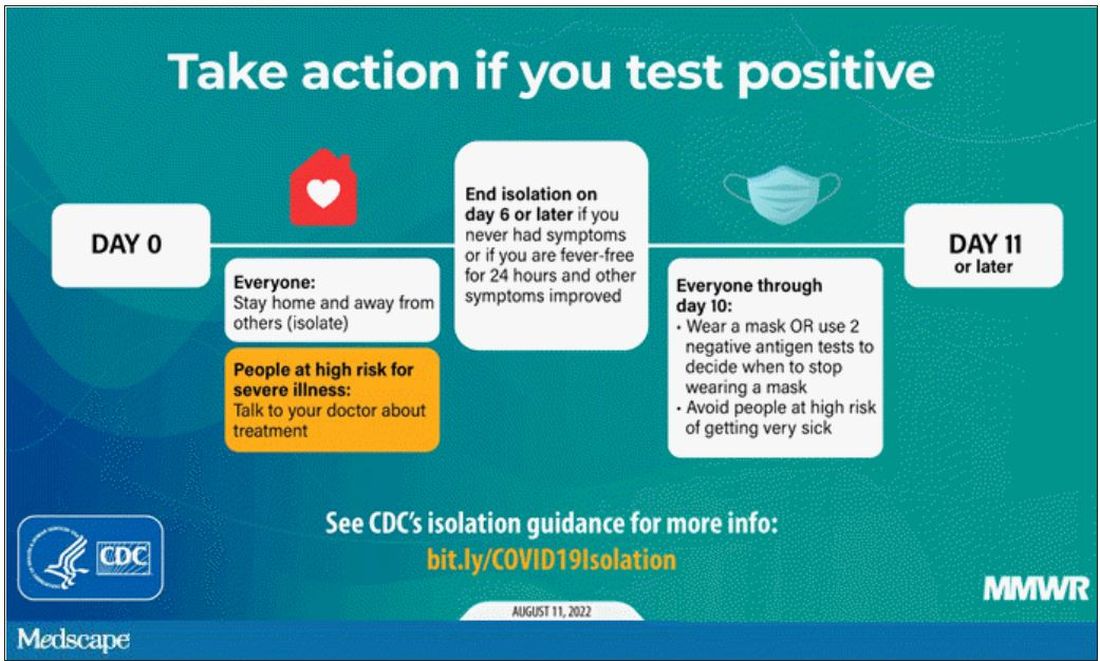
Multiple studies had suggested, after all, that positive antigen tests, while not perfect, were a decent proxy for infectivity. And if the purpose of isolation is to keep other community members safe, why not use a readily available test to know when it might be safe to go out in public again?
Also, 5 days just wasn’t that much time. Many individuals are symptomatic long after that point. Many people test positive long after that point. What exactly is the point of the 5-day isolation period?
We got some hard numbers this week to show just how good (or bad) an arbitrary-seeming 5-day isolation period is, thanks to this study from JAMA Network Open, which gives us a low-end estimate for the proportion of people who remain positive on antigen tests, which is to say infectious, after an isolation period.
This study estimates the low end of postisolation infectivity because of the study population: student athletes at an NCAA Division I school, which may or may not be Stanford. These athletes tested positive for COVID after having at least one dose of vaccine from January to May 2022. School protocol was to put the students in isolation for 7 days, at which time they could “test out” with a negative antigen test.
Put simply, these were healthy people. They were young. They were athletes. They were vaccinated. If anyone is going to have a brief, easy COVID course, it would be them. And they are doing at least a week of isolation, not 5 days.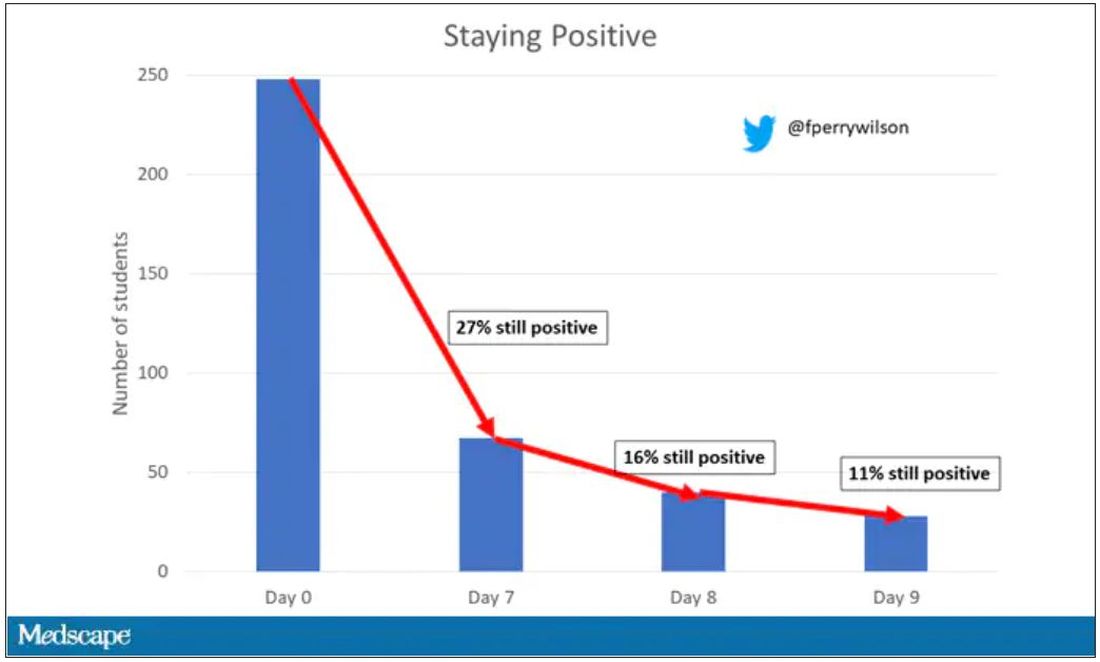
So – isolation for 7 days. Antigen testing on day 7. How many still tested positive? Of 248 individuals tested, 67 (27%) tested positive. One in four.
More than half of those positive on day 7 tested positive on day 8, and more than half of those tested positive again on day 9. By day 10, they were released from isolation without further testing.
So, right there .
There were some predictors of prolonged positivity.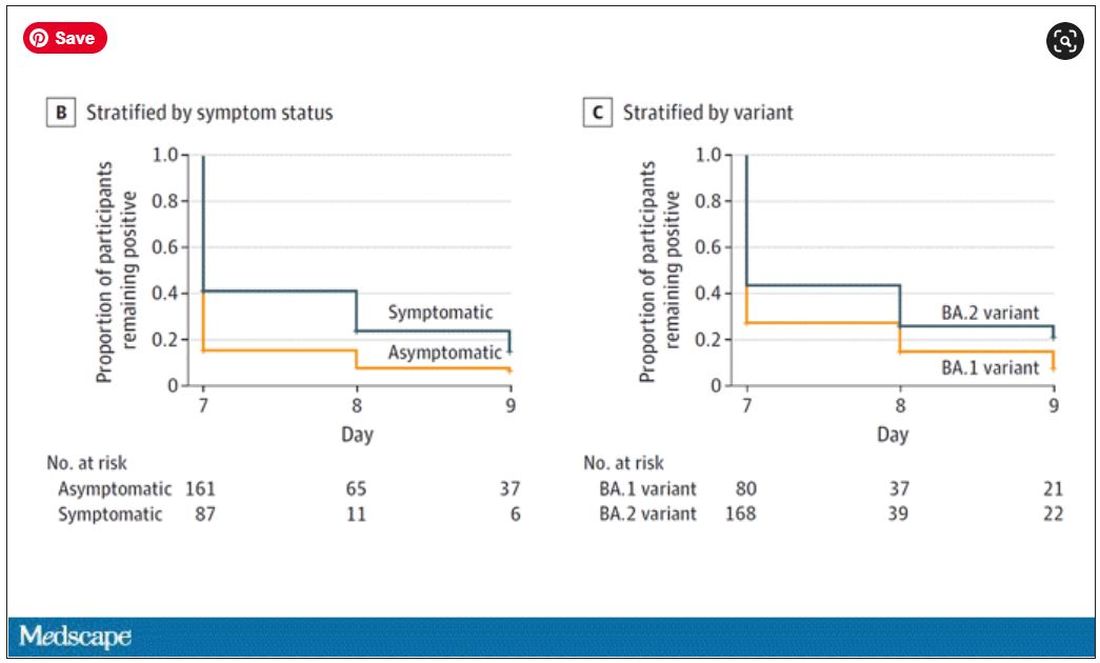
Symptomatic athletes were much more likely to test positive than asymptomatic athletes.
And the particular variant seemed to matter as well. In this time period, BA.1 and BA.2 were dominant, and it was pretty clear that BA.2 persisted longer than BA.1.
This brings me back to my original question: What is the point of the 5-day isolation period? On the basis of this study, you could imagine a guideline based on symptoms: Stay home until you feel better. You could imagine a guideline based on testing: Stay home until you test negative. A guideline based on time alone just doesn’t comport with the data. The benefit of policies based on symptoms or testing are obvious; some people would be out of isolation even before 5 days. But the downside, of course, is that some people would be stuck in isolation for much longer.
Maybe we should just say it. At this point, you could even imagine there being no recommendation at all – no isolation period. Like, you just stay home if you feel like you should stay home. I’m not entirely sure that such a policy would necessarily result in a greater number of infectious people out in the community.
In any case, as the arbitrariness of this particular 5-day isolation policy becomes more clear, the policy itself may be living on borrowed time.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and on Medscape. He tweets @fperrywilson and hosts a repository of his communication work at www.methodsman.com. He disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
One of the more baffling decisions the CDC made during this pandemic was when they reduced the duration of isolation after a positive COVID test from 10 days to 5 days and did not require a negative antigen test to end isolation.
Multiple studies had suggested, after all, that positive antigen tests, while not perfect, were a decent proxy for infectivity. And if the purpose of isolation is to keep other community members safe, why not use a readily available test to know when it might be safe to go out in public again?
Also, 5 days just wasn’t that much time. Many individuals are symptomatic long after that point. Many people test positive long after that point. What exactly is the point of the 5-day isolation period?
We got some hard numbers this week to show just how good (or bad) an arbitrary-seeming 5-day isolation period is, thanks to this study from JAMA Network Open, which gives us a low-end estimate for the proportion of people who remain positive on antigen tests, which is to say infectious, after an isolation period.
This study estimates the low end of postisolation infectivity because of the study population: student athletes at an NCAA Division I school, which may or may not be Stanford. These athletes tested positive for COVID after having at least one dose of vaccine from January to May 2022. School protocol was to put the students in isolation for 7 days, at which time they could “test out” with a negative antigen test.
Put simply, these were healthy people. They were young. They were athletes. They were vaccinated. If anyone is going to have a brief, easy COVID course, it would be them. And they are doing at least a week of isolation, not 5 days.
So – isolation for 7 days. Antigen testing on day 7. How many still tested positive? Of 248 individuals tested, 67 (27%) tested positive. One in four.
More than half of those positive on day 7 tested positive on day 8, and more than half of those tested positive again on day 9. By day 10, they were released from isolation without further testing.
So, right there .
There were some predictors of prolonged positivity.
Symptomatic athletes were much more likely to test positive than asymptomatic athletes.
And the particular variant seemed to matter as well. In this time period, BA.1 and BA.2 were dominant, and it was pretty clear that BA.2 persisted longer than BA.1.
This brings me back to my original question: What is the point of the 5-day isolation period? On the basis of this study, you could imagine a guideline based on symptoms: Stay home until you feel better. You could imagine a guideline based on testing: Stay home until you test negative. A guideline based on time alone just doesn’t comport with the data. The benefit of policies based on symptoms or testing are obvious; some people would be out of isolation even before 5 days. But the downside, of course, is that some people would be stuck in isolation for much longer.
Maybe we should just say it. At this point, you could even imagine there being no recommendation at all – no isolation period. Like, you just stay home if you feel like you should stay home. I’m not entirely sure that such a policy would necessarily result in a greater number of infectious people out in the community.
In any case, as the arbitrariness of this particular 5-day isolation policy becomes more clear, the policy itself may be living on borrowed time.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and on Medscape. He tweets @fperrywilson and hosts a repository of his communication work at www.methodsman.com. He disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
One of the more baffling decisions the CDC made during this pandemic was when they reduced the duration of isolation after a positive COVID test from 10 days to 5 days and did not require a negative antigen test to end isolation.
Multiple studies had suggested, after all, that positive antigen tests, while not perfect, were a decent proxy for infectivity. And if the purpose of isolation is to keep other community members safe, why not use a readily available test to know when it might be safe to go out in public again?
Also, 5 days just wasn’t that much time. Many individuals are symptomatic long after that point. Many people test positive long after that point. What exactly is the point of the 5-day isolation period?
We got some hard numbers this week to show just how good (or bad) an arbitrary-seeming 5-day isolation period is, thanks to this study from JAMA Network Open, which gives us a low-end estimate for the proportion of people who remain positive on antigen tests, which is to say infectious, after an isolation period.
This study estimates the low end of postisolation infectivity because of the study population: student athletes at an NCAA Division I school, which may or may not be Stanford. These athletes tested positive for COVID after having at least one dose of vaccine from January to May 2022. School protocol was to put the students in isolation for 7 days, at which time they could “test out” with a negative antigen test.
Put simply, these were healthy people. They were young. They were athletes. They were vaccinated. If anyone is going to have a brief, easy COVID course, it would be them. And they are doing at least a week of isolation, not 5 days.
So – isolation for 7 days. Antigen testing on day 7. How many still tested positive? Of 248 individuals tested, 67 (27%) tested positive. One in four.
More than half of those positive on day 7 tested positive on day 8, and more than half of those tested positive again on day 9. By day 10, they were released from isolation without further testing.
So, right there .
There were some predictors of prolonged positivity.
Symptomatic athletes were much more likely to test positive than asymptomatic athletes.
And the particular variant seemed to matter as well. In this time period, BA.1 and BA.2 were dominant, and it was pretty clear that BA.2 persisted longer than BA.1.
This brings me back to my original question: What is the point of the 5-day isolation period? On the basis of this study, you could imagine a guideline based on symptoms: Stay home until you feel better. You could imagine a guideline based on testing: Stay home until you test negative. A guideline based on time alone just doesn’t comport with the data. The benefit of policies based on symptoms or testing are obvious; some people would be out of isolation even before 5 days. But the downside, of course, is that some people would be stuck in isolation for much longer.
Maybe we should just say it. At this point, you could even imagine there being no recommendation at all – no isolation period. Like, you just stay home if you feel like you should stay home. I’m not entirely sure that such a policy would necessarily result in a greater number of infectious people out in the community.
In any case, as the arbitrariness of this particular 5-day isolation policy becomes more clear, the policy itself may be living on borrowed time.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and on Medscape. He tweets @fperrywilson and hosts a repository of his communication work at www.methodsman.com. He disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
How to remain apolitical with patients
It is assumed that psychiatrists in general, but particularly in academia, are progressive liberals. There is evidence to support this idea, with a survey finding that more than three-quarters of U.S. psychiatrists are registered Democrats.1

Other corroborating factors to our field’s progressive tendency include the publication of pseudo-political books like “The Dangerous Case of Donald Trump: 27 Psychiatrists and Mental Health Experts Assess a President” – without a well-known equivalent on the other side.
Additionally, psychiatry has in the recent past, rightfully spent significant effort examining the disproportional trauma faced by patients with underprivileged backgrounds, which is often seen as a political position. The American Psychiatric Association has itself taken a stance on the national debate about abortion to warn against the psychiatric consequences of the Dobbs v. Jackson Supreme Court decision despite the clear political statement it makes.

We understand a likely rationale for psychiatry’s liberal tendency. Most psychiatrists support political objectives that provide resources for the treatment of the severely mentally ill. In general, the psychosocial consequences of mental illness place a downward economic pressure on our patients that leads to poverty and its associated traumas that then tend to feedback to worsen the severity of the illness itself. It is thus natural for psychiatry to promote political causes such as progressivism that focus on the needs of economically and socially struggling communities. If one posits a natural role for psychiatry in promoting the interests of patients, then it is a short leap to psychiatry promoting the political causes of the underprivileged, often in the form of endorsing the Democratic party.
As a result, a proportion of patients come into psychiatric treatment with expectations that their providers will negatively judge them and possibly punish their conservative beliefs or Republican political affiliation. Herein lies a question – “Is psychiatry willing to make 46.9% of Americans uncomfortable?” How should psychiatry address the 46.9% of Americans who voted Republican during the 2020 presidential election? In our desire to support the disadvantaged, how political are we willing to get and at what cost? While we cannot speak for the field as a whole, it is our concern that a vast percentage of Americans feel alienated from talking to us, which is particularly problematic in a field based on mutual trust and understanding.
This problem may be particularly palpable to us, as we are psychiatrists in a large metropolitan area of California who often treat specialty populations like veterans and law enforcement. In one study, law enforcement officers were found to be twice as likely to be Republicans as civilians.2 Michael McHale, the president of the National Association of Police Organizations, spoke at the 2020 Republican Party’s national convention as documented in an article titled “Union leader tells Republican convention why cops back Trump.”3 Similarly, about 60% of veterans identify as Republicans.4
Within the first few sessions, when patients are most vulnerable and sensitive to the perception of being judged, we commonly get asked questions to test our political beliefs. Some patients will display clothing that suggests a political affiliation; those wardrobe arrangements are, at times, an attempt at testing our knowledge of their in-group. While a bright-red cap with a reminder to keep the United States “great” in capital letters may be an overt invitation to address the topic, other patients may have a small symbol of a rattlesnake to test our ability to recognize the “Don’t Tread on Me” Gadsden flag.
Alternatively, other patients will ask our opinion, or bring up news topics, to share their concerns and/or examine our response and reactions. We remember, in particular, a patient who subtly asked if they needed to be vaccinated to attend therapy visits in person as a leading statement into their conservative political beliefs. It is a reminder that many patients fear how we will judge them or where we will draw the line – “Is there something I, the patient, can say that will make him dislike me?”
While the concept of making all patients comfortable may feel abstract or trivial to some, the consequences can be very real. We remember a patient with severe depression and occasional suicidality, who required many months of treatment for him to reveal that he owned a gun. His conservative beliefs made him very resistant to discuss gun ownership with someone who is presumably liberal and has the power to restrict such ownership. However, after a frank discussion that our concerns about his gun were not constitutional or political but medical, the patient agreed to relinquish his gun, at least temporarily, a likely more important intervention than many in psychiatry.
The ramifications are also wider than most imagine. In California, a particularly liberal state, many consistently and reliably liberal patients have some conservative beliefs. Those beliefs are often closeted: a Democratic mother who doesn’t think her 3-year-old daughter should wear a mask in school; a Democratic woman who questioned the veracity of Amber Heard during the Johnny Depp defamation trial and feels guilty about her prior dedication to the #MeToo movement.
Patients may feel torn about those beliefs and may be apprehensive to discuss them despite a nagging need to express or examine them in a place without judgment.
that we attempted to highlight in this article. In particular, a vast proportion of Americans may feel alienated from treatment or may refuse to divulge clinically relevant information, and a large number of patients may enter psychiatric treatment with concerns that they will be judged.
Psychiatry is founded on the honest exchange of thoughts and feelings between patients and providers without the fear of harsh judgment and intellectual retaliation. Psychiatrists would be wise to consider those factors and their repercussions when choosing to take political positions and setting a frame of care with their patients.
Dr. Lehman is a professor of psychiatry at the University of California, San Diego. He is codirector of all acute and intensive psychiatric treatment at the Veterans Affairs Medical Center in San Diego, where he practices clinical psychiatry. He has no conflicts of interest. Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. He has no conflicts of interest.
References
1. Sanger-Katz M. Your surgeon is probably a Republican, your psychiatrist probably a Democrat. New York Times. 2016 Oct 6.
2. Ba B et al. Who are the police? Descriptive representation in the coercive arm of government. 2022 Mar 21.
3. Rainey J. Union leader tells Republican convention why cops back Trump. Los Angeles Times. 2020 Aug 26.
4. Igielnik R et al. Trump draws stronger support from veterans than from the public on leadership of U.S. military. Pew Research Center. 2019 July 10.
It is assumed that psychiatrists in general, but particularly in academia, are progressive liberals. There is evidence to support this idea, with a survey finding that more than three-quarters of U.S. psychiatrists are registered Democrats.1
Other corroborating factors to our field’s progressive tendency include the publication of pseudo-political books like “The Dangerous Case of Donald Trump: 27 Psychiatrists and Mental Health Experts Assess a President” – without a well-known equivalent on the other side.
Additionally, psychiatry has in the recent past, rightfully spent significant effort examining the disproportional trauma faced by patients with underprivileged backgrounds, which is often seen as a political position. The American Psychiatric Association has itself taken a stance on the national debate about abortion to warn against the psychiatric consequences of the Dobbs v. Jackson Supreme Court decision despite the clear political statement it makes.
We understand a likely rationale for psychiatry’s liberal tendency. Most psychiatrists support political objectives that provide resources for the treatment of the severely mentally ill. In general, the psychosocial consequences of mental illness place a downward economic pressure on our patients that leads to poverty and its associated traumas that then tend to feedback to worsen the severity of the illness itself. It is thus natural for psychiatry to promote political causes such as progressivism that focus on the needs of economically and socially struggling communities. If one posits a natural role for psychiatry in promoting the interests of patients, then it is a short leap to psychiatry promoting the political causes of the underprivileged, often in the form of endorsing the Democratic party.
As a result, a proportion of patients come into psychiatric treatment with expectations that their providers will negatively judge them and possibly punish their conservative beliefs or Republican political affiliation. Herein lies a question – “Is psychiatry willing to make 46.9% of Americans uncomfortable?” How should psychiatry address the 46.9% of Americans who voted Republican during the 2020 presidential election? In our desire to support the disadvantaged, how political are we willing to get and at what cost? While we cannot speak for the field as a whole, it is our concern that a vast percentage of Americans feel alienated from talking to us, which is particularly problematic in a field based on mutual trust and understanding.
This problem may be particularly palpable to us, as we are psychiatrists in a large metropolitan area of California who often treat specialty populations like veterans and law enforcement. In one study, law enforcement officers were found to be twice as likely to be Republicans as civilians.2 Michael McHale, the president of the National Association of Police Organizations, spoke at the 2020 Republican Party’s national convention as documented in an article titled “Union leader tells Republican convention why cops back Trump.”3 Similarly, about 60% of veterans identify as Republicans.4
Within the first few sessions, when patients are most vulnerable and sensitive to the perception of being judged, we commonly get asked questions to test our political beliefs. Some patients will display clothing that suggests a political affiliation; those wardrobe arrangements are, at times, an attempt at testing our knowledge of their in-group. While a bright-red cap with a reminder to keep the United States “great” in capital letters may be an overt invitation to address the topic, other patients may have a small symbol of a rattlesnake to test our ability to recognize the “Don’t Tread on Me” Gadsden flag.
Alternatively, other patients will ask our opinion, or bring up news topics, to share their concerns and/or examine our response and reactions. We remember, in particular, a patient who subtly asked if they needed to be vaccinated to attend therapy visits in person as a leading statement into their conservative political beliefs. It is a reminder that many patients fear how we will judge them or where we will draw the line – “Is there something I, the patient, can say that will make him dislike me?”
While the concept of making all patients comfortable may feel abstract or trivial to some, the consequences can be very real. We remember a patient with severe depression and occasional suicidality, who required many months of treatment for him to reveal that he owned a gun. His conservative beliefs made him very resistant to discuss gun ownership with someone who is presumably liberal and has the power to restrict such ownership. However, after a frank discussion that our concerns about his gun were not constitutional or political but medical, the patient agreed to relinquish his gun, at least temporarily, a likely more important intervention than many in psychiatry.
The ramifications are also wider than most imagine. In California, a particularly liberal state, many consistently and reliably liberal patients have some conservative beliefs. Those beliefs are often closeted: a Democratic mother who doesn’t think her 3-year-old daughter should wear a mask in school; a Democratic woman who questioned the veracity of Amber Heard during the Johnny Depp defamation trial and feels guilty about her prior dedication to the #MeToo movement.
Patients may feel torn about those beliefs and may be apprehensive to discuss them despite a nagging need to express or examine them in a place without judgment.
that we attempted to highlight in this article. In particular, a vast proportion of Americans may feel alienated from treatment or may refuse to divulge clinically relevant information, and a large number of patients may enter psychiatric treatment with concerns that they will be judged.
Psychiatry is founded on the honest exchange of thoughts and feelings between patients and providers without the fear of harsh judgment and intellectual retaliation. Psychiatrists would be wise to consider those factors and their repercussions when choosing to take political positions and setting a frame of care with their patients.
Dr. Lehman is a professor of psychiatry at the University of California, San Diego. He is codirector of all acute and intensive psychiatric treatment at the Veterans Affairs Medical Center in San Diego, where he practices clinical psychiatry. He has no conflicts of interest. Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. He has no conflicts of interest.
References
1. Sanger-Katz M. Your surgeon is probably a Republican, your psychiatrist probably a Democrat. New York Times. 2016 Oct 6.
2. Ba B et al. Who are the police? Descriptive representation in the coercive arm of government. 2022 Mar 21.
3. Rainey J. Union leader tells Republican convention why cops back Trump. Los Angeles Times. 2020 Aug 26.
4. Igielnik R et al. Trump draws stronger support from veterans than from the public on leadership of U.S. military. Pew Research Center. 2019 July 10.
It is assumed that psychiatrists in general, but particularly in academia, are progressive liberals. There is evidence to support this idea, with a survey finding that more than three-quarters of U.S. psychiatrists are registered Democrats.1
Other corroborating factors to our field’s progressive tendency include the publication of pseudo-political books like “The Dangerous Case of Donald Trump: 27 Psychiatrists and Mental Health Experts Assess a President” – without a well-known equivalent on the other side.
Additionally, psychiatry has in the recent past, rightfully spent significant effort examining the disproportional trauma faced by patients with underprivileged backgrounds, which is often seen as a political position. The American Psychiatric Association has itself taken a stance on the national debate about abortion to warn against the psychiatric consequences of the Dobbs v. Jackson Supreme Court decision despite the clear political statement it makes.
We understand a likely rationale for psychiatry’s liberal tendency. Most psychiatrists support political objectives that provide resources for the treatment of the severely mentally ill. In general, the psychosocial consequences of mental illness place a downward economic pressure on our patients that leads to poverty and its associated traumas that then tend to feedback to worsen the severity of the illness itself. It is thus natural for psychiatry to promote political causes such as progressivism that focus on the needs of economically and socially struggling communities. If one posits a natural role for psychiatry in promoting the interests of patients, then it is a short leap to psychiatry promoting the political causes of the underprivileged, often in the form of endorsing the Democratic party.
As a result, a proportion of patients come into psychiatric treatment with expectations that their providers will negatively judge them and possibly punish their conservative beliefs or Republican political affiliation. Herein lies a question – “Is psychiatry willing to make 46.9% of Americans uncomfortable?” How should psychiatry address the 46.9% of Americans who voted Republican during the 2020 presidential election? In our desire to support the disadvantaged, how political are we willing to get and at what cost? While we cannot speak for the field as a whole, it is our concern that a vast percentage of Americans feel alienated from talking to us, which is particularly problematic in a field based on mutual trust and understanding.
This problem may be particularly palpable to us, as we are psychiatrists in a large metropolitan area of California who often treat specialty populations like veterans and law enforcement. In one study, law enforcement officers were found to be twice as likely to be Republicans as civilians.2 Michael McHale, the president of the National Association of Police Organizations, spoke at the 2020 Republican Party’s national convention as documented in an article titled “Union leader tells Republican convention why cops back Trump.”3 Similarly, about 60% of veterans identify as Republicans.4
Within the first few sessions, when patients are most vulnerable and sensitive to the perception of being judged, we commonly get asked questions to test our political beliefs. Some patients will display clothing that suggests a political affiliation; those wardrobe arrangements are, at times, an attempt at testing our knowledge of their in-group. While a bright-red cap with a reminder to keep the United States “great” in capital letters may be an overt invitation to address the topic, other patients may have a small symbol of a rattlesnake to test our ability to recognize the “Don’t Tread on Me” Gadsden flag.
Alternatively, other patients will ask our opinion, or bring up news topics, to share their concerns and/or examine our response and reactions. We remember, in particular, a patient who subtly asked if they needed to be vaccinated to attend therapy visits in person as a leading statement into their conservative political beliefs. It is a reminder that many patients fear how we will judge them or where we will draw the line – “Is there something I, the patient, can say that will make him dislike me?”
While the concept of making all patients comfortable may feel abstract or trivial to some, the consequences can be very real. We remember a patient with severe depression and occasional suicidality, who required many months of treatment for him to reveal that he owned a gun. His conservative beliefs made him very resistant to discuss gun ownership with someone who is presumably liberal and has the power to restrict such ownership. However, after a frank discussion that our concerns about his gun were not constitutional or political but medical, the patient agreed to relinquish his gun, at least temporarily, a likely more important intervention than many in psychiatry.
The ramifications are also wider than most imagine. In California, a particularly liberal state, many consistently and reliably liberal patients have some conservative beliefs. Those beliefs are often closeted: a Democratic mother who doesn’t think her 3-year-old daughter should wear a mask in school; a Democratic woman who questioned the veracity of Amber Heard during the Johnny Depp defamation trial and feels guilty about her prior dedication to the #MeToo movement.
Patients may feel torn about those beliefs and may be apprehensive to discuss them despite a nagging need to express or examine them in a place without judgment.
that we attempted to highlight in this article. In particular, a vast proportion of Americans may feel alienated from treatment or may refuse to divulge clinically relevant information, and a large number of patients may enter psychiatric treatment with concerns that they will be judged.
Psychiatry is founded on the honest exchange of thoughts and feelings between patients and providers without the fear of harsh judgment and intellectual retaliation. Psychiatrists would be wise to consider those factors and their repercussions when choosing to take political positions and setting a frame of care with their patients.
Dr. Lehman is a professor of psychiatry at the University of California, San Diego. He is codirector of all acute and intensive psychiatric treatment at the Veterans Affairs Medical Center in San Diego, where he practices clinical psychiatry. He has no conflicts of interest. Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. He has no conflicts of interest.
References
1. Sanger-Katz M. Your surgeon is probably a Republican, your psychiatrist probably a Democrat. New York Times. 2016 Oct 6.
2. Ba B et al. Who are the police? Descriptive representation in the coercive arm of government. 2022 Mar 21.
3. Rainey J. Union leader tells Republican convention why cops back Trump. Los Angeles Times. 2020 Aug 26.
4. Igielnik R et al. Trump draws stronger support from veterans than from the public on leadership of U.S. military. Pew Research Center. 2019 July 10.
Vision loss may be a risk with PRP facial injections
A systematic review was recently conducted by Wu and colleagues examining the risk of blindness associated with platelet-rich plasma (PRP) injection. In dermatology, PRP is used more commonly now than 5 years ago to promote hair growth with injections on the scalp, as an adjunct to microneedling procedures, and sometimes – in a similar way to facial fillers – to improve volume loss, and skin tone and texture (particularly to the tear trough region).
Total unilateral blindness occurred in all cases. In one of the seven reported cases, the patient experienced recovery of vision after 3 months, but with some residual deficits noted on the ophthalmologist examination. In this case, the patient was evaluated and treated by an ophthalmologist within 3 hours of symptom onset.

In addition, four cases were reported from Venezuela, one from the United States, one from the United Kingdom, and one from Malaysia. Similar to reports of blindness with facial fillers, the most common injection site reported with this adverse effect was the glabella (five cases);
Other reports involved injections of the forehead (two), followed by the nasolabial fold (one), lateral canthus (one), and temporomandibular joint (one). Two of the seven patients received injections at more than one site, resulting in the total number of injections reported (10) being higher than the number of patients.
The risk of blindness is inherent with deep injection into a vessel that anastomoses with the blood supply to the eye. No mention was made as to whether PRP or platelet-rich fibrin was used. Other details are lacking from the original articles as to injection technique and whether or not cannula injection was used. No treatment was attempted in four of seven cases.
As plasma is native to the arteries and dissolves in the blood stream naturally, the mechanism as to why retinal artery occlusion or blindness would occur is not completely clear. One theory is that it is volume related and results from the speed of injection, causing a large rapid bolus that temporarily occludes or compresses an involved vessel.
Another theory is that damage to the vessel results from the injection itself or injection technique, leading to a clotting cascade and clot of the involved vessel with subsequent retrograde flow or blockade of the retinal artery. But if this were the case, we would expect to hear about more cases of clots leading to vascular occlusion or skin necrosis, which does not typically occur or we do not hear about.
Details about proper collection materials and technique or mixing with some other materials are also unknown in these cases, thus leaving the possibility that a more occlusive material may have been injected, as opposed to the fluid-like composition of the typical PRP preparation.With regards to risk with scalp PRP injection, the frontal scalp does receive blood supply from the supratrochlear artery that anastomoses with the angular artery of the face – both of which anastomose with the retinal artery (where occlusion would occur via back flow). The scalp tributaries are small and far enough away from the retina at that point that risk of back flow the to retinal artery should be minimal. Additionally, no reports of vascular occlusion from PRP scalp injection leading to skin necrosis have ever been reported. Of note, this is also not a risk that has been reported with the use of PRP with microneedling procedures, where PRP is placed on top of the skin before, during and after microneedling.
Anything that occludes the blood supply to the eye, whether it be fat, filler, or PRP, has an inherent risk of blindness. As there is no reversal agent or designated treatment for PRP occlusion, care must be taken to minimize risk, including awareness of anatomy and avoidance of injection into high risk areas, and cannula use where appropriate. Gentle, slow, low-volume administration, and when possible, use of a retrograde injection technique, may also be helpful.
Dr. Wesley and Lily Talakoub, MD, are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Wesley. Write to them at [email protected]. They had no relevant disclosures.
A systematic review was recently conducted by Wu and colleagues examining the risk of blindness associated with platelet-rich plasma (PRP) injection. In dermatology, PRP is used more commonly now than 5 years ago to promote hair growth with injections on the scalp, as an adjunct to microneedling procedures, and sometimes – in a similar way to facial fillers – to improve volume loss, and skin tone and texture (particularly to the tear trough region).
Total unilateral blindness occurred in all cases. In one of the seven reported cases, the patient experienced recovery of vision after 3 months, but with some residual deficits noted on the ophthalmologist examination. In this case, the patient was evaluated and treated by an ophthalmologist within 3 hours of symptom onset.
In addition, four cases were reported from Venezuela, one from the United States, one from the United Kingdom, and one from Malaysia. Similar to reports of blindness with facial fillers, the most common injection site reported with this adverse effect was the glabella (five cases);
Other reports involved injections of the forehead (two), followed by the nasolabial fold (one), lateral canthus (one), and temporomandibular joint (one). Two of the seven patients received injections at more than one site, resulting in the total number of injections reported (10) being higher than the number of patients.
The risk of blindness is inherent with deep injection into a vessel that anastomoses with the blood supply to the eye. No mention was made as to whether PRP or platelet-rich fibrin was used. Other details are lacking from the original articles as to injection technique and whether or not cannula injection was used. No treatment was attempted in four of seven cases.
As plasma is native to the arteries and dissolves in the blood stream naturally, the mechanism as to why retinal artery occlusion or blindness would occur is not completely clear. One theory is that it is volume related and results from the speed of injection, causing a large rapid bolus that temporarily occludes or compresses an involved vessel.
Another theory is that damage to the vessel results from the injection itself or injection technique, leading to a clotting cascade and clot of the involved vessel with subsequent retrograde flow or blockade of the retinal artery. But if this were the case, we would expect to hear about more cases of clots leading to vascular occlusion or skin necrosis, which does not typically occur or we do not hear about.
Details about proper collection materials and technique or mixing with some other materials are also unknown in these cases, thus leaving the possibility that a more occlusive material may have been injected, as opposed to the fluid-like composition of the typical PRP preparation.With regards to risk with scalp PRP injection, the frontal scalp does receive blood supply from the supratrochlear artery that anastomoses with the angular artery of the face – both of which anastomose with the retinal artery (where occlusion would occur via back flow). The scalp tributaries are small and far enough away from the retina at that point that risk of back flow the to retinal artery should be minimal. Additionally, no reports of vascular occlusion from PRP scalp injection leading to skin necrosis have ever been reported. Of note, this is also not a risk that has been reported with the use of PRP with microneedling procedures, where PRP is placed on top of the skin before, during and after microneedling.
Anything that occludes the blood supply to the eye, whether it be fat, filler, or PRP, has an inherent risk of blindness. As there is no reversal agent or designated treatment for PRP occlusion, care must be taken to minimize risk, including awareness of anatomy and avoidance of injection into high risk areas, and cannula use where appropriate. Gentle, slow, low-volume administration, and when possible, use of a retrograde injection technique, may also be helpful.
Dr. Wesley and Lily Talakoub, MD, are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Wesley. Write to them at [email protected]. They had no relevant disclosures.
A systematic review was recently conducted by Wu and colleagues examining the risk of blindness associated with platelet-rich plasma (PRP) injection. In dermatology, PRP is used more commonly now than 5 years ago to promote hair growth with injections on the scalp, as an adjunct to microneedling procedures, and sometimes – in a similar way to facial fillers – to improve volume loss, and skin tone and texture (particularly to the tear trough region).
Total unilateral blindness occurred in all cases. In one of the seven reported cases, the patient experienced recovery of vision after 3 months, but with some residual deficits noted on the ophthalmologist examination. In this case, the patient was evaluated and treated by an ophthalmologist within 3 hours of symptom onset.
In addition, four cases were reported from Venezuela, one from the United States, one from the United Kingdom, and one from Malaysia. Similar to reports of blindness with facial fillers, the most common injection site reported with this adverse effect was the glabella (five cases);
Other reports involved injections of the forehead (two), followed by the nasolabial fold (one), lateral canthus (one), and temporomandibular joint (one). Two of the seven patients received injections at more than one site, resulting in the total number of injections reported (10) being higher than the number of patients.
The risk of blindness is inherent with deep injection into a vessel that anastomoses with the blood supply to the eye. No mention was made as to whether PRP or platelet-rich fibrin was used. Other details are lacking from the original articles as to injection technique and whether or not cannula injection was used. No treatment was attempted in four of seven cases.
As plasma is native to the arteries and dissolves in the blood stream naturally, the mechanism as to why retinal artery occlusion or blindness would occur is not completely clear. One theory is that it is volume related and results from the speed of injection, causing a large rapid bolus that temporarily occludes or compresses an involved vessel.
Another theory is that damage to the vessel results from the injection itself or injection technique, leading to a clotting cascade and clot of the involved vessel with subsequent retrograde flow or blockade of the retinal artery. But if this were the case, we would expect to hear about more cases of clots leading to vascular occlusion or skin necrosis, which does not typically occur or we do not hear about.
Details about proper collection materials and technique or mixing with some other materials are also unknown in these cases, thus leaving the possibility that a more occlusive material may have been injected, as opposed to the fluid-like composition of the typical PRP preparation.With regards to risk with scalp PRP injection, the frontal scalp does receive blood supply from the supratrochlear artery that anastomoses with the angular artery of the face – both of which anastomose with the retinal artery (where occlusion would occur via back flow). The scalp tributaries are small and far enough away from the retina at that point that risk of back flow the to retinal artery should be minimal. Additionally, no reports of vascular occlusion from PRP scalp injection leading to skin necrosis have ever been reported. Of note, this is also not a risk that has been reported with the use of PRP with microneedling procedures, where PRP is placed on top of the skin before, during and after microneedling.
Anything that occludes the blood supply to the eye, whether it be fat, filler, or PRP, has an inherent risk of blindness. As there is no reversal agent or designated treatment for PRP occlusion, care must be taken to minimize risk, including awareness of anatomy and avoidance of injection into high risk areas, and cannula use where appropriate. Gentle, slow, low-volume administration, and when possible, use of a retrograde injection technique, may also be helpful.
Dr. Wesley and Lily Talakoub, MD, are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Wesley. Write to them at [email protected]. They had no relevant disclosures.