User login
Should you dismiss that patient?
After a recent column about the dilemma of dealing with patients who refuse to be vaccinated against COVID-19, several readers raised the
Contrary to what seems to be the popular opinion, there are no statutory laws that I am aware of that directly apply to patient dismissal, beyond the obvious ones prohibiting discrimination that I’ve discussed many times. The more realistic concern is leaving yourself vulnerable to civil litigation – usually charges of abandonment.

Criteria will vary by region, jurisdiction, and practice. Since there are no hard and fast rules, your reasons for dismissal should be determined in advance, written out, and included in your practice manual. Once you have laid down your rules, follow them. Exceptions should be rare and made only under extraordinary circumstances.
Most patients are dismissed because of interpersonal conflicts between physician or staff members. Usually, that involves noncompliance with a reasonable treatment plan (including vaccinations), but there are other valid reasons. These include threats of violence, inappropriate sexual advances, providing false or misleading medical history, demands for inappropriate treatments or medications, and repeated failure to keep appointments or pay bills. And most ethics experts agree that you can dismiss someone who insists on treatment outside your area of expertise, or at a location other than your private office.
Even when circumstances warrant, dismissal should be a last resort. As with most interpersonal conflicts, your best option is usually reconciliation. Sit down with the patient, explain your concerns, and discuss what must be done if your doctor-patient relationship is to continue. Often, such patients are not aware (or willing to admit) that they are violating your office policies. Honest communication will often save such relationships. But be sure to make it clear that failure to address the problems you have outlined will result in dismissal from your practice. Document this conversation in detail in the patient’s chart, and follow up with a written communication reconfirming what you discussed.
If, despite your best (documented) efforts, the problems continue and dismissal becomes necessary, following a few generally accepted guidelines will help keep the process smooth and consequence free.
First, try to avoid dismissing a patient in the middle of a course of treatment. If that is unavoidable, you might want to contact your malpractice carrier and review the case with them prior to doing so.
Inform the patient, preferably by certified mail, of your decision. Spell out your reasons, with a reminder that these problems were discussed, and that a warning was issued and not heeded. If the patient belongs to a third-party health plan, be certain that you are acting within the stipulations of your contract with that plan, and inform the payer in writing of your action.
Once again, you must clearly document in the patient’s chart exactly how he or she violated your office policies. This will minimize grounds for charges of discrimination of any sort. Be especially diligent about this step if the patient has any known physical or mental disability.
Give the patient a reasonable amount of time (30 days is common) to find another physician, and mention that you will address any emergent problems within the scope of your specialty within that 30-day period. To minimize any potential allegations of abandonment, include a list of competent physicians in your area (without any guarantees) who might be willing to assume the patient’s care. Alternatively, you can list the phone number or website of a local medical society that they can contact to find a replacement. Offer to transfer medical records to the new physician upon receipt of written permission.
File a copy or scan of the letter, the certified delivery receipt, and the returned signature card in the patient’s chart. While the law states that a first-class letter, properly addressed and stamped, is presumed to have been delivered, you don’t want any question as to whether the patient received written notice of dismissal.
Forcibly ending a physician-patient relationship is a significant event that should not be undertaken lightly. Again, dismissal should be a rare occurrence, a last resort.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
After a recent column about the dilemma of dealing with patients who refuse to be vaccinated against COVID-19, several readers raised the
Contrary to what seems to be the popular opinion, there are no statutory laws that I am aware of that directly apply to patient dismissal, beyond the obvious ones prohibiting discrimination that I’ve discussed many times. The more realistic concern is leaving yourself vulnerable to civil litigation – usually charges of abandonment.
Criteria will vary by region, jurisdiction, and practice. Since there are no hard and fast rules, your reasons for dismissal should be determined in advance, written out, and included in your practice manual. Once you have laid down your rules, follow them. Exceptions should be rare and made only under extraordinary circumstances.
Most patients are dismissed because of interpersonal conflicts between physician or staff members. Usually, that involves noncompliance with a reasonable treatment plan (including vaccinations), but there are other valid reasons. These include threats of violence, inappropriate sexual advances, providing false or misleading medical history, demands for inappropriate treatments or medications, and repeated failure to keep appointments or pay bills. And most ethics experts agree that you can dismiss someone who insists on treatment outside your area of expertise, or at a location other than your private office.
Even when circumstances warrant, dismissal should be a last resort. As with most interpersonal conflicts, your best option is usually reconciliation. Sit down with the patient, explain your concerns, and discuss what must be done if your doctor-patient relationship is to continue. Often, such patients are not aware (or willing to admit) that they are violating your office policies. Honest communication will often save such relationships. But be sure to make it clear that failure to address the problems you have outlined will result in dismissal from your practice. Document this conversation in detail in the patient’s chart, and follow up with a written communication reconfirming what you discussed.
If, despite your best (documented) efforts, the problems continue and dismissal becomes necessary, following a few generally accepted guidelines will help keep the process smooth and consequence free.
First, try to avoid dismissing a patient in the middle of a course of treatment. If that is unavoidable, you might want to contact your malpractice carrier and review the case with them prior to doing so.
Inform the patient, preferably by certified mail, of your decision. Spell out your reasons, with a reminder that these problems were discussed, and that a warning was issued and not heeded. If the patient belongs to a third-party health plan, be certain that you are acting within the stipulations of your contract with that plan, and inform the payer in writing of your action.
Once again, you must clearly document in the patient’s chart exactly how he or she violated your office policies. This will minimize grounds for charges of discrimination of any sort. Be especially diligent about this step if the patient has any known physical or mental disability.
Give the patient a reasonable amount of time (30 days is common) to find another physician, and mention that you will address any emergent problems within the scope of your specialty within that 30-day period. To minimize any potential allegations of abandonment, include a list of competent physicians in your area (without any guarantees) who might be willing to assume the patient’s care. Alternatively, you can list the phone number or website of a local medical society that they can contact to find a replacement. Offer to transfer medical records to the new physician upon receipt of written permission.
File a copy or scan of the letter, the certified delivery receipt, and the returned signature card in the patient’s chart. While the law states that a first-class letter, properly addressed and stamped, is presumed to have been delivered, you don’t want any question as to whether the patient received written notice of dismissal.
Forcibly ending a physician-patient relationship is a significant event that should not be undertaken lightly. Again, dismissal should be a rare occurrence, a last resort.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
After a recent column about the dilemma of dealing with patients who refuse to be vaccinated against COVID-19, several readers raised the
Contrary to what seems to be the popular opinion, there are no statutory laws that I am aware of that directly apply to patient dismissal, beyond the obvious ones prohibiting discrimination that I’ve discussed many times. The more realistic concern is leaving yourself vulnerable to civil litigation – usually charges of abandonment.
Criteria will vary by region, jurisdiction, and practice. Since there are no hard and fast rules, your reasons for dismissal should be determined in advance, written out, and included in your practice manual. Once you have laid down your rules, follow them. Exceptions should be rare and made only under extraordinary circumstances.
Most patients are dismissed because of interpersonal conflicts between physician or staff members. Usually, that involves noncompliance with a reasonable treatment plan (including vaccinations), but there are other valid reasons. These include threats of violence, inappropriate sexual advances, providing false or misleading medical history, demands for inappropriate treatments or medications, and repeated failure to keep appointments or pay bills. And most ethics experts agree that you can dismiss someone who insists on treatment outside your area of expertise, or at a location other than your private office.
Even when circumstances warrant, dismissal should be a last resort. As with most interpersonal conflicts, your best option is usually reconciliation. Sit down with the patient, explain your concerns, and discuss what must be done if your doctor-patient relationship is to continue. Often, such patients are not aware (or willing to admit) that they are violating your office policies. Honest communication will often save such relationships. But be sure to make it clear that failure to address the problems you have outlined will result in dismissal from your practice. Document this conversation in detail in the patient’s chart, and follow up with a written communication reconfirming what you discussed.
If, despite your best (documented) efforts, the problems continue and dismissal becomes necessary, following a few generally accepted guidelines will help keep the process smooth and consequence free.
First, try to avoid dismissing a patient in the middle of a course of treatment. If that is unavoidable, you might want to contact your malpractice carrier and review the case with them prior to doing so.
Inform the patient, preferably by certified mail, of your decision. Spell out your reasons, with a reminder that these problems were discussed, and that a warning was issued and not heeded. If the patient belongs to a third-party health plan, be certain that you are acting within the stipulations of your contract with that plan, and inform the payer in writing of your action.
Once again, you must clearly document in the patient’s chart exactly how he or she violated your office policies. This will minimize grounds for charges of discrimination of any sort. Be especially diligent about this step if the patient has any known physical or mental disability.
Give the patient a reasonable amount of time (30 days is common) to find another physician, and mention that you will address any emergent problems within the scope of your specialty within that 30-day period. To minimize any potential allegations of abandonment, include a list of competent physicians in your area (without any guarantees) who might be willing to assume the patient’s care. Alternatively, you can list the phone number or website of a local medical society that they can contact to find a replacement. Offer to transfer medical records to the new physician upon receipt of written permission.
File a copy or scan of the letter, the certified delivery receipt, and the returned signature card in the patient’s chart. While the law states that a first-class letter, properly addressed and stamped, is presumed to have been delivered, you don’t want any question as to whether the patient received written notice of dismissal.
Forcibly ending a physician-patient relationship is a significant event that should not be undertaken lightly. Again, dismissal should be a rare occurrence, a last resort.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].

NPs, PAs say stop attacks and support health care colleagues
This commentary was submitted as a rebuttal to “PA name change bad for patients and the profession.”
To the Editor:
At a time when COVID-19 cases are climbing and health care workers are struggling to meet the needs of our nation’s healthcare system, the commentary by Rebekah Bernard, MD, divides health care providers and demeans the education, experience, and value of physician associates (PA) and nurse practitioners (NP) in our opinion.
The ill timing of this negative message is equally matched by her mischaracterization of the PA title change and PA efforts to eliminate outdated administrative barriers, as well as her baseless attack on NP education and clinical training.
Let us be clear about one thing: What patients really want and deserve is access to high-quality care delivered by the health care provider of their choice. Patients deserve health care providers who are committed to modern, integrated, and coordinated health care delivery, led by professionals who are dedicated to ensuring that everyone is practicing to the full extent of their education, clinical experience, and scope of practice. Patients deserve health care providers who respect each other and work together to embrace solutions that will improve health care for the future.
Decades of research confirm the high quality of PA- and NP-delivered health care. The evidence is in, and it is irrefutable: PA- and NP-delivered care is associated with improved access to care, lower health care costs, and fewer avoidable emergency room visits.
With regard to the PA title change, the fact is this: Changing the profession’s title does not change what PAs do or affect a PA’s scope of practice. The new title – physician associate – directly addresses the common misperception that PAs merely “assist” physicians. It is in the best interest of patients and the health care system for PAs to hold a professional title that ensures clarity about the work that PAs do.
For the sake of patients, we urge Bernard and her organization to stop continuously attacking other professions and focus on what really matters – providing access to safe, effective, equitable, high-quality care to all patients.
We are committed to patient-centered, coordinated health care, and we continue to work with like-minded physicians and other colleagues to make this a reality.
Ms. Orozco is president and chair of the board of directors for the American Academy of Physician Associates. Dr. Kapu is president of the American Association of Nurse Practitioners.
A version of this article first appeared on Medscape.com.
This commentary was submitted as a rebuttal to “PA name change bad for patients and the profession.”
To the Editor:
At a time when COVID-19 cases are climbing and health care workers are struggling to meet the needs of our nation’s healthcare system, the commentary by Rebekah Bernard, MD, divides health care providers and demeans the education, experience, and value of physician associates (PA) and nurse practitioners (NP) in our opinion.
The ill timing of this negative message is equally matched by her mischaracterization of the PA title change and PA efforts to eliminate outdated administrative barriers, as well as her baseless attack on NP education and clinical training.
Let us be clear about one thing: What patients really want and deserve is access to high-quality care delivered by the health care provider of their choice. Patients deserve health care providers who are committed to modern, integrated, and coordinated health care delivery, led by professionals who are dedicated to ensuring that everyone is practicing to the full extent of their education, clinical experience, and scope of practice. Patients deserve health care providers who respect each other and work together to embrace solutions that will improve health care for the future.
Decades of research confirm the high quality of PA- and NP-delivered health care. The evidence is in, and it is irrefutable: PA- and NP-delivered care is associated with improved access to care, lower health care costs, and fewer avoidable emergency room visits.
With regard to the PA title change, the fact is this: Changing the profession’s title does not change what PAs do or affect a PA’s scope of practice. The new title – physician associate – directly addresses the common misperception that PAs merely “assist” physicians. It is in the best interest of patients and the health care system for PAs to hold a professional title that ensures clarity about the work that PAs do.
For the sake of patients, we urge Bernard and her organization to stop continuously attacking other professions and focus on what really matters – providing access to safe, effective, equitable, high-quality care to all patients.
We are committed to patient-centered, coordinated health care, and we continue to work with like-minded physicians and other colleagues to make this a reality.
Ms. Orozco is president and chair of the board of directors for the American Academy of Physician Associates. Dr. Kapu is president of the American Association of Nurse Practitioners.
A version of this article first appeared on Medscape.com.
This commentary was submitted as a rebuttal to “PA name change bad for patients and the profession.”
To the Editor:
At a time when COVID-19 cases are climbing and health care workers are struggling to meet the needs of our nation’s healthcare system, the commentary by Rebekah Bernard, MD, divides health care providers and demeans the education, experience, and value of physician associates (PA) and nurse practitioners (NP) in our opinion.
The ill timing of this negative message is equally matched by her mischaracterization of the PA title change and PA efforts to eliminate outdated administrative barriers, as well as her baseless attack on NP education and clinical training.
Let us be clear about one thing: What patients really want and deserve is access to high-quality care delivered by the health care provider of their choice. Patients deserve health care providers who are committed to modern, integrated, and coordinated health care delivery, led by professionals who are dedicated to ensuring that everyone is practicing to the full extent of their education, clinical experience, and scope of practice. Patients deserve health care providers who respect each other and work together to embrace solutions that will improve health care for the future.
Decades of research confirm the high quality of PA- and NP-delivered health care. The evidence is in, and it is irrefutable: PA- and NP-delivered care is associated with improved access to care, lower health care costs, and fewer avoidable emergency room visits.
With regard to the PA title change, the fact is this: Changing the profession’s title does not change what PAs do or affect a PA’s scope of practice. The new title – physician associate – directly addresses the common misperception that PAs merely “assist” physicians. It is in the best interest of patients and the health care system for PAs to hold a professional title that ensures clarity about the work that PAs do.
For the sake of patients, we urge Bernard and her organization to stop continuously attacking other professions and focus on what really matters – providing access to safe, effective, equitable, high-quality care to all patients.
We are committed to patient-centered, coordinated health care, and we continue to work with like-minded physicians and other colleagues to make this a reality.
Ms. Orozco is president and chair of the board of directors for the American Academy of Physician Associates. Dr. Kapu is president of the American Association of Nurse Practitioners.
A version of this article first appeared on Medscape.com.
75-year-old White male presenting with progressive pruritus and a worsening rash
, although it can also be contracted through contaminated bedding and clothing. It can affect all races and ages.
Patients typically present with extremely pruritic, symmetric papules and excoriations. In nodular scabies, nodules and large papules are seen on exam. Thin lines in the skin called burrows may be present, especially in the webs between fingers. Female mites create burrows as they tunnel through the epidermis and lay eggs. The wrists, areola, waistline, and groin may all be involved, creating an imaginary circle between the areas described as the “circle of Hebra.” Penile and scrotal lesions are common in men.
Patients usually experience worse pruritus at night, which disturbs sleep. Crusted scabies is a severe form of scabies more often seen in those with immunocompromised immune systems. Clinically, thick crusted and scaly patches are present that are teeming with mites.
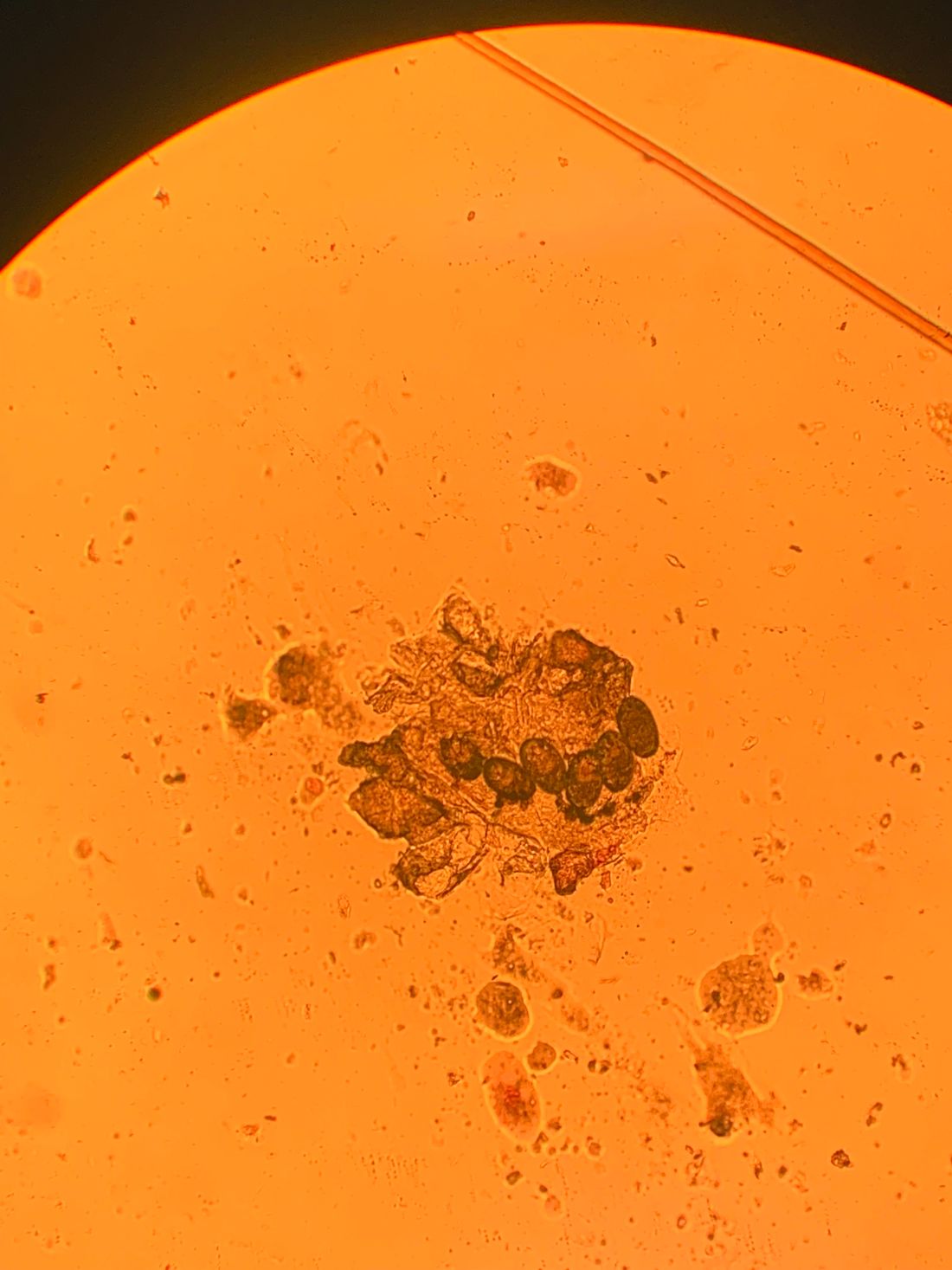
Diagnosis can be confirmed by performing a scabies prep, during which a burrow is scraped with a surgical blade. A drop of mineral oil is placed on the skin cells. The mite, ova, and feces can be visualized under the microscope. Wrists and hands usually have the highest yield for finding the parasites.

Topical treatments include permethrin 5% cream, lindane, benzyl benzoate, and crotamiton, and should be applied as two treatments a week apart. In the United States, permethrin is most commonly used. Ivermectin pills are used off label and are very effective and may be repeated for 1-2 weeks. All household contacts should be treated. Patients may still have pruritus for 2-4 weeks following treatment.
In this patient, a scabies prep was performed prior to performing repeat skin biopsies. Microscopic examination revealed ova, one mite, and feces. Treatment was initiated with ivermectin and permethrin.
Photos and case were submitted by Susannah Berke, MD, and Damon McClain, MD, Three Rivers Dermatology, Coraopolis, Pa.; and Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
, although it can also be contracted through contaminated bedding and clothing. It can affect all races and ages.
Patients typically present with extremely pruritic, symmetric papules and excoriations. In nodular scabies, nodules and large papules are seen on exam. Thin lines in the skin called burrows may be present, especially in the webs between fingers. Female mites create burrows as they tunnel through the epidermis and lay eggs. The wrists, areola, waistline, and groin may all be involved, creating an imaginary circle between the areas described as the “circle of Hebra.” Penile and scrotal lesions are common in men.
Patients usually experience worse pruritus at night, which disturbs sleep. Crusted scabies is a severe form of scabies more often seen in those with immunocompromised immune systems. Clinically, thick crusted and scaly patches are present that are teeming with mites.
Diagnosis can be confirmed by performing a scabies prep, during which a burrow is scraped with a surgical blade. A drop of mineral oil is placed on the skin cells. The mite, ova, and feces can be visualized under the microscope. Wrists and hands usually have the highest yield for finding the parasites.
Topical treatments include permethrin 5% cream, lindane, benzyl benzoate, and crotamiton, and should be applied as two treatments a week apart. In the United States, permethrin is most commonly used. Ivermectin pills are used off label and are very effective and may be repeated for 1-2 weeks. All household contacts should be treated. Patients may still have pruritus for 2-4 weeks following treatment.
In this patient, a scabies prep was performed prior to performing repeat skin biopsies. Microscopic examination revealed ova, one mite, and feces. Treatment was initiated with ivermectin and permethrin.
Photos and case were submitted by Susannah Berke, MD, and Damon McClain, MD, Three Rivers Dermatology, Coraopolis, Pa.; and Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
, although it can also be contracted through contaminated bedding and clothing. It can affect all races and ages.
Patients typically present with extremely pruritic, symmetric papules and excoriations. In nodular scabies, nodules and large papules are seen on exam. Thin lines in the skin called burrows may be present, especially in the webs between fingers. Female mites create burrows as they tunnel through the epidermis and lay eggs. The wrists, areola, waistline, and groin may all be involved, creating an imaginary circle between the areas described as the “circle of Hebra.” Penile and scrotal lesions are common in men.
Patients usually experience worse pruritus at night, which disturbs sleep. Crusted scabies is a severe form of scabies more often seen in those with immunocompromised immune systems. Clinically, thick crusted and scaly patches are present that are teeming with mites.
Diagnosis can be confirmed by performing a scabies prep, during which a burrow is scraped with a surgical blade. A drop of mineral oil is placed on the skin cells. The mite, ova, and feces can be visualized under the microscope. Wrists and hands usually have the highest yield for finding the parasites.
Topical treatments include permethrin 5% cream, lindane, benzyl benzoate, and crotamiton, and should be applied as two treatments a week apart. In the United States, permethrin is most commonly used. Ivermectin pills are used off label and are very effective and may be repeated for 1-2 weeks. All household contacts should be treated. Patients may still have pruritus for 2-4 weeks following treatment.
In this patient, a scabies prep was performed prior to performing repeat skin biopsies. Microscopic examination revealed ova, one mite, and feces. Treatment was initiated with ivermectin and permethrin.
Photos and case were submitted by Susannah Berke, MD, and Damon McClain, MD, Three Rivers Dermatology, Coraopolis, Pa.; and Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].

Lifestyle changes can lead to remission, but not a cure, in type 2 diabetes
Whenever I get a new patient with type 2 diabetes, who is generally on metformin, one of the very first questions they ask me is, “Can I get off my medication?” Everybody, it seems, who gets diabetes wants to not have diabetes.
So, what does this really mean? What does this mean to me as a clinician? And what does this mean to my patients? The American Diabetes Association recently came out with a consensus statement that defines and interprets the definition of remission in people with type 2 diabetes. Basically, if the hemoglobin A1c is less than 6.5% without diabetes medications for at least 3 months, that’s considered remission.
There are other considerations, such as metabolic surgery, that can lead to remission. But again, such patients should be 3 months post surgery and at least 3 months off diabetes medication. As for a lifestyle intervention, the authors state that remission really happens within about 6 months.

That leads me to wonder: What is remission? Remission really means temporary recovery, so it doesn’t mean a cure. Now, I’m not against curing diabetes. In fact, I’m all for it. But when somebody gets diabetes – and honestly, it doesn’t matter whether it’s type 1 or type 2 – the first thing I think of, and I think the first thing that my patients are taught, is how important it is to have a healthy lifestyle. This healthy lifestyle isn’t just for people with diabetes; it largely means the healthy lifestyle that all of us should follow, one where we eat fewer simple carbs, less processed food, more vegetables, more lean proteins and meats – all of the things that we know we should do. And all of the things that keep us healthy. To some degree, I don’t think you can ever get “remission” from diabetes, because if having diabetes points an individual toward having a healthier lifestyle, I think that’s great.
I think people should exercise more. When it comes to treating diabetes, exercise is key. When you think about obesity, we want to help people who are overweight or obese lose weight as part of their treatment for diabetes. And that doesn’t go away, either.
So, no, people who are diagnosed with diabetes don’t really go into remission if they keep their same old habits and don’t lose weight and don’t exercise. But many people with diabetes can get off medication if they do those things.
However, it’s not true for everybody, and I don’t want people to get unrealistic expectations because I think there are probably about a thousand different subtypes of type 2 diabetes. And I’ve definitely seen people who are lean with type 2 diabetes who don’t respond as well to a lifestyle intervention, or people who are more insulin deficient, who also need medication.
I think it’s really important to frame the expectation that, if remission means going back to the way it was before, when they didn’t have to think about what they ate or whether or not they exercised, that’s not going to happen. I think diabetes should really be a wake-up call that people need to be healthier in terms of their lifestyle habits.
The issue of medication is really an individual one, and I think we need to help patients look for what’s best for the individual, what their targets are, what their goals are. But we also have to think that diabetes isn’t just about glucose.
So remission in terms of the ADA’s definition looks at glucose, but I look at more than glucose. You have to look at lipids and blood pressure. And, as I mentioned earlier, you have to look at whether or not a person has preexisting cardiovascular disease or has the presence of microvascular complications that need to be screened for and treated.
I actually think that, in some ways, the diagnosis of diabetes is helpful simply because it helps put people on a better path to health. I don’t want people to think that remission means that they can go back to unhealthy habits. I really encourage all people to live a healthier lifestyle, and if it leads to improvements in glucose levels and getting off medication, I think that’s wonderful and a worthy goal. But remember, health and meeting one’s targets remain key in the treatment of type 2 diabetes.
Dr. Peters is a professor in the department of clinical medicine at the University of Southern California, Los Angeles. She reported serving on the advisory board or speakers’ bureau of Medscape and several pharmaceutical companies, and has received research support from Dexcom, MannKind, and AstraZeneca. This perspective and an accompanying video first appeared on Medscape.com.
Whenever I get a new patient with type 2 diabetes, who is generally on metformin, one of the very first questions they ask me is, “Can I get off my medication?” Everybody, it seems, who gets diabetes wants to not have diabetes.
So, what does this really mean? What does this mean to me as a clinician? And what does this mean to my patients? The American Diabetes Association recently came out with a consensus statement that defines and interprets the definition of remission in people with type 2 diabetes. Basically, if the hemoglobin A1c is less than 6.5% without diabetes medications for at least 3 months, that’s considered remission.
There are other considerations, such as metabolic surgery, that can lead to remission. But again, such patients should be 3 months post surgery and at least 3 months off diabetes medication. As for a lifestyle intervention, the authors state that remission really happens within about 6 months.
That leads me to wonder: What is remission? Remission really means temporary recovery, so it doesn’t mean a cure. Now, I’m not against curing diabetes. In fact, I’m all for it. But when somebody gets diabetes – and honestly, it doesn’t matter whether it’s type 1 or type 2 – the first thing I think of, and I think the first thing that my patients are taught, is how important it is to have a healthy lifestyle. This healthy lifestyle isn’t just for people with diabetes; it largely means the healthy lifestyle that all of us should follow, one where we eat fewer simple carbs, less processed food, more vegetables, more lean proteins and meats – all of the things that we know we should do. And all of the things that keep us healthy. To some degree, I don’t think you can ever get “remission” from diabetes, because if having diabetes points an individual toward having a healthier lifestyle, I think that’s great.
I think people should exercise more. When it comes to treating diabetes, exercise is key. When you think about obesity, we want to help people who are overweight or obese lose weight as part of their treatment for diabetes. And that doesn’t go away, either.
So, no, people who are diagnosed with diabetes don’t really go into remission if they keep their same old habits and don’t lose weight and don’t exercise. But many people with diabetes can get off medication if they do those things.
However, it’s not true for everybody, and I don’t want people to get unrealistic expectations because I think there are probably about a thousand different subtypes of type 2 diabetes. And I’ve definitely seen people who are lean with type 2 diabetes who don’t respond as well to a lifestyle intervention, or people who are more insulin deficient, who also need medication.
I think it’s really important to frame the expectation that, if remission means going back to the way it was before, when they didn’t have to think about what they ate or whether or not they exercised, that’s not going to happen. I think diabetes should really be a wake-up call that people need to be healthier in terms of their lifestyle habits.
The issue of medication is really an individual one, and I think we need to help patients look for what’s best for the individual, what their targets are, what their goals are. But we also have to think that diabetes isn’t just about glucose.
So remission in terms of the ADA’s definition looks at glucose, but I look at more than glucose. You have to look at lipids and blood pressure. And, as I mentioned earlier, you have to look at whether or not a person has preexisting cardiovascular disease or has the presence of microvascular complications that need to be screened for and treated.
I actually think that, in some ways, the diagnosis of diabetes is helpful simply because it helps put people on a better path to health. I don’t want people to think that remission means that they can go back to unhealthy habits. I really encourage all people to live a healthier lifestyle, and if it leads to improvements in glucose levels and getting off medication, I think that’s wonderful and a worthy goal. But remember, health and meeting one’s targets remain key in the treatment of type 2 diabetes.
Dr. Peters is a professor in the department of clinical medicine at the University of Southern California, Los Angeles. She reported serving on the advisory board or speakers’ bureau of Medscape and several pharmaceutical companies, and has received research support from Dexcom, MannKind, and AstraZeneca. This perspective and an accompanying video first appeared on Medscape.com.
Whenever I get a new patient with type 2 diabetes, who is generally on metformin, one of the very first questions they ask me is, “Can I get off my medication?” Everybody, it seems, who gets diabetes wants to not have diabetes.
So, what does this really mean? What does this mean to me as a clinician? And what does this mean to my patients? The American Diabetes Association recently came out with a consensus statement that defines and interprets the definition of remission in people with type 2 diabetes. Basically, if the hemoglobin A1c is less than 6.5% without diabetes medications for at least 3 months, that’s considered remission.
There are other considerations, such as metabolic surgery, that can lead to remission. But again, such patients should be 3 months post surgery and at least 3 months off diabetes medication. As for a lifestyle intervention, the authors state that remission really happens within about 6 months.
That leads me to wonder: What is remission? Remission really means temporary recovery, so it doesn’t mean a cure. Now, I’m not against curing diabetes. In fact, I’m all for it. But when somebody gets diabetes – and honestly, it doesn’t matter whether it’s type 1 or type 2 – the first thing I think of, and I think the first thing that my patients are taught, is how important it is to have a healthy lifestyle. This healthy lifestyle isn’t just for people with diabetes; it largely means the healthy lifestyle that all of us should follow, one where we eat fewer simple carbs, less processed food, more vegetables, more lean proteins and meats – all of the things that we know we should do. And all of the things that keep us healthy. To some degree, I don’t think you can ever get “remission” from diabetes, because if having diabetes points an individual toward having a healthier lifestyle, I think that’s great.
I think people should exercise more. When it comes to treating diabetes, exercise is key. When you think about obesity, we want to help people who are overweight or obese lose weight as part of their treatment for diabetes. And that doesn’t go away, either.
So, no, people who are diagnosed with diabetes don’t really go into remission if they keep their same old habits and don’t lose weight and don’t exercise. But many people with diabetes can get off medication if they do those things.
However, it’s not true for everybody, and I don’t want people to get unrealistic expectations because I think there are probably about a thousand different subtypes of type 2 diabetes. And I’ve definitely seen people who are lean with type 2 diabetes who don’t respond as well to a lifestyle intervention, or people who are more insulin deficient, who also need medication.
I think it’s really important to frame the expectation that, if remission means going back to the way it was before, when they didn’t have to think about what they ate or whether or not they exercised, that’s not going to happen. I think diabetes should really be a wake-up call that people need to be healthier in terms of their lifestyle habits.
The issue of medication is really an individual one, and I think we need to help patients look for what’s best for the individual, what their targets are, what their goals are. But we also have to think that diabetes isn’t just about glucose.
So remission in terms of the ADA’s definition looks at glucose, but I look at more than glucose. You have to look at lipids and blood pressure. And, as I mentioned earlier, you have to look at whether or not a person has preexisting cardiovascular disease or has the presence of microvascular complications that need to be screened for and treated.
I actually think that, in some ways, the diagnosis of diabetes is helpful simply because it helps put people on a better path to health. I don’t want people to think that remission means that they can go back to unhealthy habits. I really encourage all people to live a healthier lifestyle, and if it leads to improvements in glucose levels and getting off medication, I think that’s wonderful and a worthy goal. But remember, health and meeting one’s targets remain key in the treatment of type 2 diabetes.
Dr. Peters is a professor in the department of clinical medicine at the University of Southern California, Los Angeles. She reported serving on the advisory board or speakers’ bureau of Medscape and several pharmaceutical companies, and has received research support from Dexcom, MannKind, and AstraZeneca. This perspective and an accompanying video first appeared on Medscape.com.
The limits of education
For more than a decade, studies on the dubious value of education in the face of vaccine refusal and hesitancy have been accumulating. But, too often, the research has been ignored by folks who believe that they can teach the “misinformed” into dropping their resistance. Among some circles education ranks right up there with apple pie and motherhood as one of the pillars of Americana. Those wedded to the education mantra may acknowledge that teaching and preaching hasn’t worked well in the past. But, they may claim it’s because we haven’t done enough of it or hit the right buttons. The notion that if we can just share the facts with the uninformed everything will be fine is a myth that obviously is going to die slowly.

In a recent op-ed piece in the New York Times two physicians at Harvard Medical School reported on their study of about three-quarters of a million children who were eligible to receive HPV vaccines (2021 Dec 21. “Facts alone aren’t going to win over the unvaccinated. This might,” Anupam B. Jena and Christopher M. Worsham). The researchers found that children whose mothers had been diagnosed with cervical cancer were no more likely to be immunized than those children whose mothers had not had the disease. Who could be better informed about risks and hazards of contracting HPV than women with cervical cancer? If the facts won’t motivate, where does that leave us?
Those of you born before 1960 may remember or at least have heard about a television show called “Truth or Consequences.” It was a silly farce of a game show which has no bearing on our nation’s crisis of widespread vaccine refusal. However, buried in its title is the answer. If the truth isn’t convincing the resistors, then the obvious choice is consequences.
I hope that you have discovered that same strategy when counseling parents of misbehaving children. Talk is cheap and often ineffective. Explaining the error of his ways to a child who probably already knows what he is doing wrong is a waste of everyone’s time and unpleasant for those within earshot. At some point, sooner better than later, it’s time to say there is going to be a consequence for this misbehavior – going home from the playground, spending a few minutes in time-out, removing a privilege, etc. If consequences are chosen well and instituted with a minimum of idle threats, they work.
And, we are beginning to see it work in the face of pandemic shot refusal. Here in Maine the governor mandated that all health care workers be vaccinated. There was plenty of gnashing of teeth and threats of mass job walk offs. And, there were a few hospital workers who quit, but in the end it worked.
The trick is choosing consequences that have some teeth and make sense. Clearly, some folks who have read about the consequences of not getting vaccinated and may have even lost family members to the disease don’t see those losses as significant consequences for whatever reason. The threat of losing a job is likely to get their attention.
Threats must be carried out even though they may be disruptive in the short term. The good thing about well-crafted mandates is that they can be a win-win for everyone. The vaccine resisters don’t need to admit they were wrong. “Those shots are B.S., but the governor made me do it.” The problem is finding leaders who understand that education has its limits and who have the courage to create and administer the consequences.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
For more than a decade, studies on the dubious value of education in the face of vaccine refusal and hesitancy have been accumulating. But, too often, the research has been ignored by folks who believe that they can teach the “misinformed” into dropping their resistance. Among some circles education ranks right up there with apple pie and motherhood as one of the pillars of Americana. Those wedded to the education mantra may acknowledge that teaching and preaching hasn’t worked well in the past. But, they may claim it’s because we haven’t done enough of it or hit the right buttons. The notion that if we can just share the facts with the uninformed everything will be fine is a myth that obviously is going to die slowly.
In a recent op-ed piece in the New York Times two physicians at Harvard Medical School reported on their study of about three-quarters of a million children who were eligible to receive HPV vaccines (2021 Dec 21. “Facts alone aren’t going to win over the unvaccinated. This might,” Anupam B. Jena and Christopher M. Worsham). The researchers found that children whose mothers had been diagnosed with cervical cancer were no more likely to be immunized than those children whose mothers had not had the disease. Who could be better informed about risks and hazards of contracting HPV than women with cervical cancer? If the facts won’t motivate, where does that leave us?
Those of you born before 1960 may remember or at least have heard about a television show called “Truth or Consequences.” It was a silly farce of a game show which has no bearing on our nation’s crisis of widespread vaccine refusal. However, buried in its title is the answer. If the truth isn’t convincing the resistors, then the obvious choice is consequences.
I hope that you have discovered that same strategy when counseling parents of misbehaving children. Talk is cheap and often ineffective. Explaining the error of his ways to a child who probably already knows what he is doing wrong is a waste of everyone’s time and unpleasant for those within earshot. At some point, sooner better than later, it’s time to say there is going to be a consequence for this misbehavior – going home from the playground, spending a few minutes in time-out, removing a privilege, etc. If consequences are chosen well and instituted with a minimum of idle threats, they work.
And, we are beginning to see it work in the face of pandemic shot refusal. Here in Maine the governor mandated that all health care workers be vaccinated. There was plenty of gnashing of teeth and threats of mass job walk offs. And, there were a few hospital workers who quit, but in the end it worked.
The trick is choosing consequences that have some teeth and make sense. Clearly, some folks who have read about the consequences of not getting vaccinated and may have even lost family members to the disease don’t see those losses as significant consequences for whatever reason. The threat of losing a job is likely to get their attention.
Threats must be carried out even though they may be disruptive in the short term. The good thing about well-crafted mandates is that they can be a win-win for everyone. The vaccine resisters don’t need to admit they were wrong. “Those shots are B.S., but the governor made me do it.” The problem is finding leaders who understand that education has its limits and who have the courage to create and administer the consequences.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
For more than a decade, studies on the dubious value of education in the face of vaccine refusal and hesitancy have been accumulating. But, too often, the research has been ignored by folks who believe that they can teach the “misinformed” into dropping their resistance. Among some circles education ranks right up there with apple pie and motherhood as one of the pillars of Americana. Those wedded to the education mantra may acknowledge that teaching and preaching hasn’t worked well in the past. But, they may claim it’s because we haven’t done enough of it or hit the right buttons. The notion that if we can just share the facts with the uninformed everything will be fine is a myth that obviously is going to die slowly.
In a recent op-ed piece in the New York Times two physicians at Harvard Medical School reported on their study of about three-quarters of a million children who were eligible to receive HPV vaccines (2021 Dec 21. “Facts alone aren’t going to win over the unvaccinated. This might,” Anupam B. Jena and Christopher M. Worsham). The researchers found that children whose mothers had been diagnosed with cervical cancer were no more likely to be immunized than those children whose mothers had not had the disease. Who could be better informed about risks and hazards of contracting HPV than women with cervical cancer? If the facts won’t motivate, where does that leave us?
Those of you born before 1960 may remember or at least have heard about a television show called “Truth or Consequences.” It was a silly farce of a game show which has no bearing on our nation’s crisis of widespread vaccine refusal. However, buried in its title is the answer. If the truth isn’t convincing the resistors, then the obvious choice is consequences.
I hope that you have discovered that same strategy when counseling parents of misbehaving children. Talk is cheap and often ineffective. Explaining the error of his ways to a child who probably already knows what he is doing wrong is a waste of everyone’s time and unpleasant for those within earshot. At some point, sooner better than later, it’s time to say there is going to be a consequence for this misbehavior – going home from the playground, spending a few minutes in time-out, removing a privilege, etc. If consequences are chosen well and instituted with a minimum of idle threats, they work.
And, we are beginning to see it work in the face of pandemic shot refusal. Here in Maine the governor mandated that all health care workers be vaccinated. There was plenty of gnashing of teeth and threats of mass job walk offs. And, there were a few hospital workers who quit, but in the end it worked.
The trick is choosing consequences that have some teeth and make sense. Clearly, some folks who have read about the consequences of not getting vaccinated and may have even lost family members to the disease don’t see those losses as significant consequences for whatever reason. The threat of losing a job is likely to get their attention.
Threats must be carried out even though they may be disruptive in the short term. The good thing about well-crafted mandates is that they can be a win-win for everyone. The vaccine resisters don’t need to admit they were wrong. “Those shots are B.S., but the governor made me do it.” The problem is finding leaders who understand that education has its limits and who have the courage to create and administer the consequences.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
What is the diagnosis?
Hidradenitis suppurativa (HS) is a chronic inflammatory skin condition that is becoming more recognized in children. It has a variable presentation, most commonly presenting as painful, recurrent cysts, abscesses, nodules, and/or pustules in classic locations with associated scarring and sinus tract formation.
The majority of patients present with bilateral lesions found most commonly in the axillae and inguinal folds.1 There are myriad other potential sites of involvement including the inframammary folds, inner thighs, buttocks, and groin.1 Diagnosis is made based on history and physical exam. There is a standard severity classification scheme called the Hurley score, which stratifies disease severity based on the presence of sinus tracts and extent of disease.1 HS is associated with comorbid conditions such as obesity, overweight, acne, and inflammatory bowel and joint disease.2 This painful, persistent condition is well documented to have a negative impact on quality of life in adult patients, and similar impairment has been found in pediatric patients.3,4

HS may be increasing in pediatric and adolescent patients, with recent studies showing onset coinciding most commonly with the onset of puberty.1,2 There is often a period of several years between symptom onset and diagnosis.1 A recent editorial highlighted the disparities that exist in HS, with disease more common in Black children and limited information about disease prevalence in Hispanic children.5
What’s the treatment plan?
HS is a difficult disease to treat, with few patients achieving remission and a significant proportion of patients with treatment-refractory disease.1 There are limited studies of HS treatment in pediatric patients. Topical and systemic antibiotic therapy are mainstays of HS treatment, with tetracyclines and a combination of clindamycin plus rifampin commonly used in adults and children alike. Topical therapies including topical antibiotics and antibacterial solutions are frequently used as adjunctive therapy.6 Adalimumab, a tumor necrosis factor receptor blocker, has been Food and Drug Administration approved for HS for ages 12 and up and is currently the only FDA-approved medication for HS in pediatric patients. Our patient was started on 100 mg doxycycline twice daily, with short-dose topical corticosteroids for symptom management of the most inflamed lesions.
What’s on the differential?
Acne conglobata
Acne conglobata is an uncommon, severe variant of acne vulgaris which arise in patients with a history of acne vulgaris and presents with comedones, cysts, abscesses, and scarring with possible drainage of pus. Lesions can present diffusely on the face, back, and body, including in the axillae, groin, and buttocks, and as such can be confused with HS.7
However, in contrast with HS, patients with acne conglobata will also develop disease in non–apocrine gland–bearing skin. This patient’s lack of preceding acne and restriction of lesions to the axillae, inguinal folds, and buttocks makes acne conglobata less likely.

Epidermal inclusion cyst
Epidermal inclusion cyst (EIC) is a common cutaneous cyst, presenting as a well-circumscribed nodule(s) with a central punctum. If not excised, lesions can sometimes become infected and painful.8 In contrast with HS, EIC presents only uncommonly as multiple lesions arising in different areas, and spontaneous drainage is uncommon. Our patient’s development of multiple draining lesions makes this diagnosis unlikely.
Furunculosis
Furunculosis is a common bacterial infection of the skin, presenting with inflammatory nodules or pustules centered around the hair follicle. Lesions may commonly present at sites of skin trauma and are found most frequently on the extremities.9 Though furunculosis lesions may drain pus and can coalesce to form larger “carbuncles,” our patient’s presence of significant scarring and lack of extremity involvement makes HS more likely.
Recurrent MRSA abscesses
Methicillin-resistant Staphylococcus aureus skin and soft-tissue infections are not uncommon in the pediatric population, with presentation of infection ranging from cellulitis to fluid-containing abscesses.10 Recurrent abscesses may be seen in MRSA infection, however in this patient the presence of draining, scarring lesions in multiple locations typical for HS over time is more consistent with a diagnosis of HS.
Dr. Eichenfield is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego, and Rady Children’s Hospital, San Diego. Ms. Appiah is a pediatric dermatology research associate in the division of pediatric and adolescent dermatology at the University of California, San Diego, and Rady Children’s Hospital. Dr. Eichenfield and Ms. Appiah have no relevant financial disclosures.
References
1. Liy-Wong C et al. JAMA Dermatol. 2021;157(4):385-91.
2. Choi E et al. J Am Acad Dermatol. 2022;86(1):140-7.
3. Machado MO et al. JAMA Dermatol. 2019;155(8):939-45.
4. McAndrew R et al. J Am Acad Dermatol. 2021;84(3):829-30.
5. Kirby JS and Zaenglein AL. JAMA Dermatol. 2021;157(4):379-80.
6. Alikhan A et al. J Am Acad Dermatol. 2019;81(1):91-101.
7. Greydanus DE et al. Dis Mon. 2021;67(4):101103.
8. Weir CB, St. Hilaire NJ. Epidermal Inclusion Cyst, in “StatPearls.” Treasure Island, Fla: StatPearls Publishing, 2021.
9. Atanaskova N and Tomecki KJ. Dermatol Clin. 2010;28(3):479-87.
10. Papastefan ST et al. J Surg Res. 2019;242:70-7.
Hidradenitis suppurativa (HS) is a chronic inflammatory skin condition that is becoming more recognized in children. It has a variable presentation, most commonly presenting as painful, recurrent cysts, abscesses, nodules, and/or pustules in classic locations with associated scarring and sinus tract formation.
The majority of patients present with bilateral lesions found most commonly in the axillae and inguinal folds.1 There are myriad other potential sites of involvement including the inframammary folds, inner thighs, buttocks, and groin.1 Diagnosis is made based on history and physical exam. There is a standard severity classification scheme called the Hurley score, which stratifies disease severity based on the presence of sinus tracts and extent of disease.1 HS is associated with comorbid conditions such as obesity, overweight, acne, and inflammatory bowel and joint disease.2 This painful, persistent condition is well documented to have a negative impact on quality of life in adult patients, and similar impairment has been found in pediatric patients.3,4
HS may be increasing in pediatric and adolescent patients, with recent studies showing onset coinciding most commonly with the onset of puberty.1,2 There is often a period of several years between symptom onset and diagnosis.1 A recent editorial highlighted the disparities that exist in HS, with disease more common in Black children and limited information about disease prevalence in Hispanic children.5
What’s the treatment plan?
HS is a difficult disease to treat, with few patients achieving remission and a significant proportion of patients with treatment-refractory disease.1 There are limited studies of HS treatment in pediatric patients. Topical and systemic antibiotic therapy are mainstays of HS treatment, with tetracyclines and a combination of clindamycin plus rifampin commonly used in adults and children alike. Topical therapies including topical antibiotics and antibacterial solutions are frequently used as adjunctive therapy.6 Adalimumab, a tumor necrosis factor receptor blocker, has been Food and Drug Administration approved for HS for ages 12 and up and is currently the only FDA-approved medication for HS in pediatric patients. Our patient was started on 100 mg doxycycline twice daily, with short-dose topical corticosteroids for symptom management of the most inflamed lesions.
What’s on the differential?
Acne conglobata
Acne conglobata is an uncommon, severe variant of acne vulgaris which arise in patients with a history of acne vulgaris and presents with comedones, cysts, abscesses, and scarring with possible drainage of pus. Lesions can present diffusely on the face, back, and body, including in the axillae, groin, and buttocks, and as such can be confused with HS.7
However, in contrast with HS, patients with acne conglobata will also develop disease in non–apocrine gland–bearing skin. This patient’s lack of preceding acne and restriction of lesions to the axillae, inguinal folds, and buttocks makes acne conglobata less likely.
Epidermal inclusion cyst
Epidermal inclusion cyst (EIC) is a common cutaneous cyst, presenting as a well-circumscribed nodule(s) with a central punctum. If not excised, lesions can sometimes become infected and painful.8 In contrast with HS, EIC presents only uncommonly as multiple lesions arising in different areas, and spontaneous drainage is uncommon. Our patient’s development of multiple draining lesions makes this diagnosis unlikely.
Furunculosis
Furunculosis is a common bacterial infection of the skin, presenting with inflammatory nodules or pustules centered around the hair follicle. Lesions may commonly present at sites of skin trauma and are found most frequently on the extremities.9 Though furunculosis lesions may drain pus and can coalesce to form larger “carbuncles,” our patient’s presence of significant scarring and lack of extremity involvement makes HS more likely.
Recurrent MRSA abscesses
Methicillin-resistant Staphylococcus aureus skin and soft-tissue infections are not uncommon in the pediatric population, with presentation of infection ranging from cellulitis to fluid-containing abscesses.10 Recurrent abscesses may be seen in MRSA infection, however in this patient the presence of draining, scarring lesions in multiple locations typical for HS over time is more consistent with a diagnosis of HS.
Dr. Eichenfield is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego, and Rady Children’s Hospital, San Diego. Ms. Appiah is a pediatric dermatology research associate in the division of pediatric and adolescent dermatology at the University of California, San Diego, and Rady Children’s Hospital. Dr. Eichenfield and Ms. Appiah have no relevant financial disclosures.
References
1. Liy-Wong C et al. JAMA Dermatol. 2021;157(4):385-91.
2. Choi E et al. J Am Acad Dermatol. 2022;86(1):140-7.
3. Machado MO et al. JAMA Dermatol. 2019;155(8):939-45.
4. McAndrew R et al. J Am Acad Dermatol. 2021;84(3):829-30.
5. Kirby JS and Zaenglein AL. JAMA Dermatol. 2021;157(4):379-80.
6. Alikhan A et al. J Am Acad Dermatol. 2019;81(1):91-101.
7. Greydanus DE et al. Dis Mon. 2021;67(4):101103.
8. Weir CB, St. Hilaire NJ. Epidermal Inclusion Cyst, in “StatPearls.” Treasure Island, Fla: StatPearls Publishing, 2021.
9. Atanaskova N and Tomecki KJ. Dermatol Clin. 2010;28(3):479-87.
10. Papastefan ST et al. J Surg Res. 2019;242:70-7.
Hidradenitis suppurativa (HS) is a chronic inflammatory skin condition that is becoming more recognized in children. It has a variable presentation, most commonly presenting as painful, recurrent cysts, abscesses, nodules, and/or pustules in classic locations with associated scarring and sinus tract formation.
The majority of patients present with bilateral lesions found most commonly in the axillae and inguinal folds.1 There are myriad other potential sites of involvement including the inframammary folds, inner thighs, buttocks, and groin.1 Diagnosis is made based on history and physical exam. There is a standard severity classification scheme called the Hurley score, which stratifies disease severity based on the presence of sinus tracts and extent of disease.1 HS is associated with comorbid conditions such as obesity, overweight, acne, and inflammatory bowel and joint disease.2 This painful, persistent condition is well documented to have a negative impact on quality of life in adult patients, and similar impairment has been found in pediatric patients.3,4
HS may be increasing in pediatric and adolescent patients, with recent studies showing onset coinciding most commonly with the onset of puberty.1,2 There is often a period of several years between symptom onset and diagnosis.1 A recent editorial highlighted the disparities that exist in HS, with disease more common in Black children and limited information about disease prevalence in Hispanic children.5
What’s the treatment plan?
HS is a difficult disease to treat, with few patients achieving remission and a significant proportion of patients with treatment-refractory disease.1 There are limited studies of HS treatment in pediatric patients. Topical and systemic antibiotic therapy are mainstays of HS treatment, with tetracyclines and a combination of clindamycin plus rifampin commonly used in adults and children alike. Topical therapies including topical antibiotics and antibacterial solutions are frequently used as adjunctive therapy.6 Adalimumab, a tumor necrosis factor receptor blocker, has been Food and Drug Administration approved for HS for ages 12 and up and is currently the only FDA-approved medication for HS in pediatric patients. Our patient was started on 100 mg doxycycline twice daily, with short-dose topical corticosteroids for symptom management of the most inflamed lesions.
What’s on the differential?
Acne conglobata
Acne conglobata is an uncommon, severe variant of acne vulgaris which arise in patients with a history of acne vulgaris and presents with comedones, cysts, abscesses, and scarring with possible drainage of pus. Lesions can present diffusely on the face, back, and body, including in the axillae, groin, and buttocks, and as such can be confused with HS.7
However, in contrast with HS, patients with acne conglobata will also develop disease in non–apocrine gland–bearing skin. This patient’s lack of preceding acne and restriction of lesions to the axillae, inguinal folds, and buttocks makes acne conglobata less likely.
Epidermal inclusion cyst
Epidermal inclusion cyst (EIC) is a common cutaneous cyst, presenting as a well-circumscribed nodule(s) with a central punctum. If not excised, lesions can sometimes become infected and painful.8 In contrast with HS, EIC presents only uncommonly as multiple lesions arising in different areas, and spontaneous drainage is uncommon. Our patient’s development of multiple draining lesions makes this diagnosis unlikely.
Furunculosis
Furunculosis is a common bacterial infection of the skin, presenting with inflammatory nodules or pustules centered around the hair follicle. Lesions may commonly present at sites of skin trauma and are found most frequently on the extremities.9 Though furunculosis lesions may drain pus and can coalesce to form larger “carbuncles,” our patient’s presence of significant scarring and lack of extremity involvement makes HS more likely.
Recurrent MRSA abscesses
Methicillin-resistant Staphylococcus aureus skin and soft-tissue infections are not uncommon in the pediatric population, with presentation of infection ranging from cellulitis to fluid-containing abscesses.10 Recurrent abscesses may be seen in MRSA infection, however in this patient the presence of draining, scarring lesions in multiple locations typical for HS over time is more consistent with a diagnosis of HS.
Dr. Eichenfield is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego, and Rady Children’s Hospital, San Diego. Ms. Appiah is a pediatric dermatology research associate in the division of pediatric and adolescent dermatology at the University of California, San Diego, and Rady Children’s Hospital. Dr. Eichenfield and Ms. Appiah have no relevant financial disclosures.
References
1. Liy-Wong C et al. JAMA Dermatol. 2021;157(4):385-91.
2. Choi E et al. J Am Acad Dermatol. 2022;86(1):140-7.
3. Machado MO et al. JAMA Dermatol. 2019;155(8):939-45.
4. McAndrew R et al. J Am Acad Dermatol. 2021;84(3):829-30.
5. Kirby JS and Zaenglein AL. JAMA Dermatol. 2021;157(4):379-80.
6. Alikhan A et al. J Am Acad Dermatol. 2019;81(1):91-101.
7. Greydanus DE et al. Dis Mon. 2021;67(4):101103.
8. Weir CB, St. Hilaire NJ. Epidermal Inclusion Cyst, in “StatPearls.” Treasure Island, Fla: StatPearls Publishing, 2021.
9. Atanaskova N and Tomecki KJ. Dermatol Clin. 2010;28(3):479-87.
10. Papastefan ST et al. J Surg Res. 2019;242:70-7.


Prior authorization abuse: It’s time for health insurance CEOs and their proxies to cease and desist the practice once and for all!
Before reading this editorial and concluding that the author (me) has lost his grip on reality, I would ask that you consider the facts I provide below and the ramifications incurred by your patients and practices, due to the misbehaviors adopted by the health insurance industry.
- Two of the most common issues discussed in today’s health care environment are revenue generation and provider/staff burnout.
While these issues are impacted by several factors, one of the most common denominators is increasing administrative workloads driven by non–revenue-generating activities. Consider this:
- A recent American Medical Association survey pointed out that during the course of the average workweek, a physician completes an average of 37 prior authorization requests. Physicians and their staff spend an average of 16.4 hours per week completing prior authorization requirements for patient medicines, procedures, and medical services that they may need.1
- While physicians report that about 65% of prior authorizations take only 1 day, they report that 26% take 3 or more days.2
The potential significance of the generated delays
While this may not seem like a long time (other than the impact it has on staff workload), consider the impact this can have on the patient if the medication being requested is: PrEP, the morning after pill, or other contraceptives? The consequences of the delay or denial could be a lifetime living with HIV, or an unintended pregnancy. This is to say nothing on the larger impact to family, partners, and the potential social stigma faced by all.
Beyond the personal costs and costs within your practice associated with the additional workload, consider the financial costs. The average cost to complete a prior authorization remains the single highest cost for the health care industry at $13.40 per manual transaction, and $7.19 per partially electronic web portal transaction,3 meaning that if I did only one prescription per week, I probably would not mind, but at $13.40 per prior authorization, this burden amounts to millions, actually $767 million by recent estimates.3 Additionally, if you factor in the number of denials and potential follow-ups, this creates a significant amount of waste and spending.
Ultimately, in my experience, I have found that most prior authorizations are simply unnecessary. Here, I’ve picked key examples from just my own recent experiences:
- My patient was denied access to a particular birth control pill she had been on successfully before, and my office was told she needed to try and fail on 5 different generic pills before she could be approved. However, the Affordable Care Act’s (ACA; aka Obamacare) Contraceptive Mandate requires coverage of all contraceptives determined to be most appropriate between a patient and their provider (see below).
- A menopausal patient was denied coverage twice (electronically) for generic micronized progesterone, and I was asked to write a letter of appeal because the insurance company wanted me to use medroxyprogesterone acetate instead. Polling my nearby retail independent pharmacy, the total cost difference per year was $19.96 savings/year ($47.01 ‒ $27.05 = $19.96). My pharmacist did note it could have been a different amount at a large chain pharmacy. Really? I had to write a letter, following two denials, to save less than $20, for a full year!
- A 78-year-old patient using Prolia for severe osteoporosis and preexisting fractures was delayed in getting her next Prolia injection due to a prior authorization snafu. She ended up with multiple additional fractures, a well-described effect of the increase in bone turnover when stopping or delaying this medication. She is now disabled.
- A 94-year-old patient was sent an email reminder to get the medical practice to authorize a refill of ileostomy bags. The email went to spam, and the patient ran out of bags prior to a holiday weekend. I got them in 2 days on Amazon Prime. But who emails a 94-year-old? And ileostomy bags! When does anyone stop needing ileostomy bags?
- I requested a prior authorization for Orilissa (clearly off label) because a severely progestogen-sensitive patient (augmented depression) with severe premenstrual dysphoric disorder requiring hospitalization was thought by her psychiatrist to be better off without menstrual periods. I completed the proper paperwork, two electronic appeals, and a letter of explanation including available references on the use of gonadotropin-releasing hormone analogues for such patients. I was then told I would need to have a peer-to-peer discussion, so I filled out that paperwork, which clearly noted that I am a board-certified reproductive endocrinologist. I got a phone call a few days later by a pleasant, young-sounding pediatric rheumatologist. Our interaction did not go well for him. This was not peer-to-peer!
Let us be clear, prior authorizations have nothing to do with patient care. In fact, they are solely about the money. We in ObGyn have mostly inexpensive and generic products, but even that fact has not lowered the excessive burden of the prior authorization process. In the case of contraception, whether you like the ACA or not it is the law, and it contains specific provisions regarding contraception. With the goals of providing broad access to patients and incentives to developers for new and novel contraceptive methods, these provisions require insurers to cover, without cost-sharing, women’s preventive services including the full range of FDA-approved contraceptives (currently 18 different method categories), and additional methods identified by the FDA as they become available. Further, providers must have an easily accessible, transparent, and sufficiently expedient exceptions process that is not unduly burdensome on the individual or a provider (or other individuals acting as a patient’s authorized representative).
And while I can regale you with chapter and verse and citations of the legal precedent and language, it boils down to this:
- The AMA reported that medical practices spend an average of 2 business days a week per physician to comply with health plans’ inefficient and overused prior-authorization protocols.4 To keep up with the administrative burden, 2 out of 5 physicians (40%) employ staff members who work exclusively on tasks associated with prior authorization.4
- About 86% of practices reported an increased burden of prior authorizations in the last 5 years.5
Continue to: What is to be done?
What is to be done?
I do have suggested solutions. Given the insurance industry’s complete lack of progress in voluntarily reducing the burdens of prior authorizations agreed to in their consensus statement with the AMA, American Hospital Association, America’s Health Insurance Plans, American Pharmacists Association, Blue Cross Blue Shield Association, and the Medical Group Management Association, I say, why not fine them? The AMA is calling on Congress to pass legislation that would codify much of the agreement, in which the above parties had already agreed that reforms were needed to reduce prior authorization burdens and enhance patient-centered care.6
A good model for enforcement via fines could be based on the old “incident to” rules of Medicare. These state that a physician needs to be “in the space” when advanced practice nurses or physician assistants see Medicare recipients. If they are not actually “in the space” they are subject to a fine. As a completely theoretical example, let’s say the claim was for $100. The practitioner would have to pay it back plus triple that amount in damages, or $400. They can also be fined up to $11,000 per claim and kick you out of Medicare and Medicaid. Take my example of Prolia from above…a single shot of Prolia is about $1,000. The insurer would theoretically have to pay $14,000/claim (the claim + triple damages + $11,000) if it was determined that the prior authorization was unnecessary. Seems about right to me. Or we could just sit the health insurance CEOs and their proxies in the corner on 2-foot-tall plastic Little Tikes® chairs for a “timeout” (dunce cap optional), like the outset of the article says.
Until the detrimental prior authorization process is challenged at all levels, we will continue to see and feel the effects of the harm it causes. Being able to drive change through advocacy and education is the best way we as clinicians can impact not just the future of health care but provide for the daily care of our patients who depend on and trust us to provide for their medical needs. We must be the impactors of change for ourselves, colleagues, staff, and profession if we are to really make advancements into the future.
Oh…and health insurance CEOs and their proxies, to get out of their “time-out” would still be entitled to one phone call to beg forgiveness from their mommies/daddies, priest/ rabbi/pastor, psychologist/psychiatrist/mystic healer, etc., but alas, the average wait time is an hour, and if anyone answers the phone, they have a grade school education used in following an irrelevant algorithm. ●
- Corder JC. Streamlining the insurance prior authorization debacle. Mo Med. 2018;115:312-314.
- Prior authorization hurdles have led to serious adverse events. American Medical Association website. February 5, 2019. https://www.ama-assn .org/press-center/press-releases/prior-author ization-hurdles-have-led-serious-adverse -events. Accessed November 29, 2021.
- Council for Affordable Quality Healthcare. 2020 CAQH INDEX. https://www.caqh.org/sites /default/files/explorations/index/2020-caqh -index.pdf. Accessed November 22, 2021.
- Most physicians had little relief from prior authorization as COVID cases soared. American Medical Association website. April 7, 2021. https:// www.ama-assn.org/press-center/press-releases /most-physicians-had-little-relief-prior-author ization-covid-cases. Accessed November 29, 2021.
- Robeznieks A. 1 in 4 doctors say prior authorization has led to a serious adverse event. American Medical Association website. February 5, 2019. https://www .ama-assn.org/practice-management/sustainability /1-4-doctors-say-prior-authorization-has-led-serious -adverse. Accessed November 29, 2021.
- Physicians call on Congress to address prior authorization reform. American Medical Association website. May 14, 2021. https://www .ama-assn.org/press-center/press-releases /physicians-call-congress-address-prior-author ization-reform. Accessed November 29, 2021.

James A. Simon, MD
Dr. Simon is Clinical Professor, Department of Obstetrics and Gynecology, George Washington University, and Medical Director, IntimMedicine® Specialists, Washington, DC.
Dr. Simon reports receiving grant/research support from: AbbVie, Inc.; Bayer Healthcare LLC.; Dare´ Bioscience; Ipsen; Myovant Sciences; ObsEva SA; Sebela Pharmaceuticals Inc.; and Viveve Medical; being a consultant/advisory board member for: Bayer HealthCare Pharmaceuticals Inc.; Besins Healthcare; California Institute of Integral Studies (CIIS); Camargo Pharmaceutical Services, LLC; Covance Inc.; Dare´ Bioscience; DEKA M.E.L.A S.r.l.; Femasys Inc.; KaNDy/NeRRe Therapeutics Ltd.; Madorra Pty Ltd.; Mitsubishi Tanabe Pharma Development America, Inc.; QUE Oncology Pty; Limited; Sebela Pharmaceuticals, Inc.; Sprout Pharmaceuticals, Inc.; and Vella Bioscience Inc.; serving on the speaker’s bureaus of: Mayne Pharma, Inc.; Myovant Sciences, Inc.; Pfizer Inc. (New York, NY); Pharmavite LLC.; and TherapeuticsMD; and being a stockholder (direct purchase) in: Sermonix Pharmaceuticals.
James A. Simon, MD
Dr. Simon is Clinical Professor, Department of Obstetrics and Gynecology, George Washington University, and Medical Director, IntimMedicine® Specialists, Washington, DC.
Dr. Simon reports receiving grant/research support from: AbbVie, Inc.; Bayer Healthcare LLC.; Dare´ Bioscience; Ipsen; Myovant Sciences; ObsEva SA; Sebela Pharmaceuticals Inc.; and Viveve Medical; being a consultant/advisory board member for: Bayer HealthCare Pharmaceuticals Inc.; Besins Healthcare; California Institute of Integral Studies (CIIS); Camargo Pharmaceutical Services, LLC; Covance Inc.; Dare´ Bioscience; DEKA M.E.L.A S.r.l.; Femasys Inc.; KaNDy/NeRRe Therapeutics Ltd.; Madorra Pty Ltd.; Mitsubishi Tanabe Pharma Development America, Inc.; QUE Oncology Pty; Limited; Sebela Pharmaceuticals, Inc.; Sprout Pharmaceuticals, Inc.; and Vella Bioscience Inc.; serving on the speaker’s bureaus of: Mayne Pharma, Inc.; Myovant Sciences, Inc.; Pfizer Inc. (New York, NY); Pharmavite LLC.; and TherapeuticsMD; and being a stockholder (direct purchase) in: Sermonix Pharmaceuticals.
James A. Simon, MD
Dr. Simon is Clinical Professor, Department of Obstetrics and Gynecology, George Washington University, and Medical Director, IntimMedicine® Specialists, Washington, DC.
Dr. Simon reports receiving grant/research support from: AbbVie, Inc.; Bayer Healthcare LLC.; Dare´ Bioscience; Ipsen; Myovant Sciences; ObsEva SA; Sebela Pharmaceuticals Inc.; and Viveve Medical; being a consultant/advisory board member for: Bayer HealthCare Pharmaceuticals Inc.; Besins Healthcare; California Institute of Integral Studies (CIIS); Camargo Pharmaceutical Services, LLC; Covance Inc.; Dare´ Bioscience; DEKA M.E.L.A S.r.l.; Femasys Inc.; KaNDy/NeRRe Therapeutics Ltd.; Madorra Pty Ltd.; Mitsubishi Tanabe Pharma Development America, Inc.; QUE Oncology Pty; Limited; Sebela Pharmaceuticals, Inc.; Sprout Pharmaceuticals, Inc.; and Vella Bioscience Inc.; serving on the speaker’s bureaus of: Mayne Pharma, Inc.; Myovant Sciences, Inc.; Pfizer Inc. (New York, NY); Pharmavite LLC.; and TherapeuticsMD; and being a stockholder (direct purchase) in: Sermonix Pharmaceuticals.
Before reading this editorial and concluding that the author (me) has lost his grip on reality, I would ask that you consider the facts I provide below and the ramifications incurred by your patients and practices, due to the misbehaviors adopted by the health insurance industry.
- Two of the most common issues discussed in today’s health care environment are revenue generation and provider/staff burnout.
While these issues are impacted by several factors, one of the most common denominators is increasing administrative workloads driven by non–revenue-generating activities. Consider this:
- A recent American Medical Association survey pointed out that during the course of the average workweek, a physician completes an average of 37 prior authorization requests. Physicians and their staff spend an average of 16.4 hours per week completing prior authorization requirements for patient medicines, procedures, and medical services that they may need.1
- While physicians report that about 65% of prior authorizations take only 1 day, they report that 26% take 3 or more days.2
The potential significance of the generated delays
While this may not seem like a long time (other than the impact it has on staff workload), consider the impact this can have on the patient if the medication being requested is: PrEP, the morning after pill, or other contraceptives? The consequences of the delay or denial could be a lifetime living with HIV, or an unintended pregnancy. This is to say nothing on the larger impact to family, partners, and the potential social stigma faced by all.
Beyond the personal costs and costs within your practice associated with the additional workload, consider the financial costs. The average cost to complete a prior authorization remains the single highest cost for the health care industry at $13.40 per manual transaction, and $7.19 per partially electronic web portal transaction,3 meaning that if I did only one prescription per week, I probably would not mind, but at $13.40 per prior authorization, this burden amounts to millions, actually $767 million by recent estimates.3 Additionally, if you factor in the number of denials and potential follow-ups, this creates a significant amount of waste and spending.
Ultimately, in my experience, I have found that most prior authorizations are simply unnecessary. Here, I’ve picked key examples from just my own recent experiences:
- My patient was denied access to a particular birth control pill she had been on successfully before, and my office was told she needed to try and fail on 5 different generic pills before she could be approved. However, the Affordable Care Act’s (ACA; aka Obamacare) Contraceptive Mandate requires coverage of all contraceptives determined to be most appropriate between a patient and their provider (see below).
- A menopausal patient was denied coverage twice (electronically) for generic micronized progesterone, and I was asked to write a letter of appeal because the insurance company wanted me to use medroxyprogesterone acetate instead. Polling my nearby retail independent pharmacy, the total cost difference per year was $19.96 savings/year ($47.01 ‒ $27.05 = $19.96). My pharmacist did note it could have been a different amount at a large chain pharmacy. Really? I had to write a letter, following two denials, to save less than $20, for a full year!
- A 78-year-old patient using Prolia for severe osteoporosis and preexisting fractures was delayed in getting her next Prolia injection due to a prior authorization snafu. She ended up with multiple additional fractures, a well-described effect of the increase in bone turnover when stopping or delaying this medication. She is now disabled.
- A 94-year-old patient was sent an email reminder to get the medical practice to authorize a refill of ileostomy bags. The email went to spam, and the patient ran out of bags prior to a holiday weekend. I got them in 2 days on Amazon Prime. But who emails a 94-year-old? And ileostomy bags! When does anyone stop needing ileostomy bags?
- I requested a prior authorization for Orilissa (clearly off label) because a severely progestogen-sensitive patient (augmented depression) with severe premenstrual dysphoric disorder requiring hospitalization was thought by her psychiatrist to be better off without menstrual periods. I completed the proper paperwork, two electronic appeals, and a letter of explanation including available references on the use of gonadotropin-releasing hormone analogues for such patients. I was then told I would need to have a peer-to-peer discussion, so I filled out that paperwork, which clearly noted that I am a board-certified reproductive endocrinologist. I got a phone call a few days later by a pleasant, young-sounding pediatric rheumatologist. Our interaction did not go well for him. This was not peer-to-peer!
Let us be clear, prior authorizations have nothing to do with patient care. In fact, they are solely about the money. We in ObGyn have mostly inexpensive and generic products, but even that fact has not lowered the excessive burden of the prior authorization process. In the case of contraception, whether you like the ACA or not it is the law, and it contains specific provisions regarding contraception. With the goals of providing broad access to patients and incentives to developers for new and novel contraceptive methods, these provisions require insurers to cover, without cost-sharing, women’s preventive services including the full range of FDA-approved contraceptives (currently 18 different method categories), and additional methods identified by the FDA as they become available. Further, providers must have an easily accessible, transparent, and sufficiently expedient exceptions process that is not unduly burdensome on the individual or a provider (or other individuals acting as a patient’s authorized representative).
And while I can regale you with chapter and verse and citations of the legal precedent and language, it boils down to this:
- The AMA reported that medical practices spend an average of 2 business days a week per physician to comply with health plans’ inefficient and overused prior-authorization protocols.4 To keep up with the administrative burden, 2 out of 5 physicians (40%) employ staff members who work exclusively on tasks associated with prior authorization.4
- About 86% of practices reported an increased burden of prior authorizations in the last 5 years.5
Continue to: What is to be done?
What is to be done?
I do have suggested solutions. Given the insurance industry’s complete lack of progress in voluntarily reducing the burdens of prior authorizations agreed to in their consensus statement with the AMA, American Hospital Association, America’s Health Insurance Plans, American Pharmacists Association, Blue Cross Blue Shield Association, and the Medical Group Management Association, I say, why not fine them? The AMA is calling on Congress to pass legislation that would codify much of the agreement, in which the above parties had already agreed that reforms were needed to reduce prior authorization burdens and enhance patient-centered care.6
A good model for enforcement via fines could be based on the old “incident to” rules of Medicare. These state that a physician needs to be “in the space” when advanced practice nurses or physician assistants see Medicare recipients. If they are not actually “in the space” they are subject to a fine. As a completely theoretical example, let’s say the claim was for $100. The practitioner would have to pay it back plus triple that amount in damages, or $400. They can also be fined up to $11,000 per claim and kick you out of Medicare and Medicaid. Take my example of Prolia from above…a single shot of Prolia is about $1,000. The insurer would theoretically have to pay $14,000/claim (the claim + triple damages + $11,000) if it was determined that the prior authorization was unnecessary. Seems about right to me. Or we could just sit the health insurance CEOs and their proxies in the corner on 2-foot-tall plastic Little Tikes® chairs for a “timeout” (dunce cap optional), like the outset of the article says.
Until the detrimental prior authorization process is challenged at all levels, we will continue to see and feel the effects of the harm it causes. Being able to drive change through advocacy and education is the best way we as clinicians can impact not just the future of health care but provide for the daily care of our patients who depend on and trust us to provide for their medical needs. We must be the impactors of change for ourselves, colleagues, staff, and profession if we are to really make advancements into the future.
Oh…and health insurance CEOs and their proxies, to get out of their “time-out” would still be entitled to one phone call to beg forgiveness from their mommies/daddies, priest/ rabbi/pastor, psychologist/psychiatrist/mystic healer, etc., but alas, the average wait time is an hour, and if anyone answers the phone, they have a grade school education used in following an irrelevant algorithm. ●
Before reading this editorial and concluding that the author (me) has lost his grip on reality, I would ask that you consider the facts I provide below and the ramifications incurred by your patients and practices, due to the misbehaviors adopted by the health insurance industry.
- Two of the most common issues discussed in today’s health care environment are revenue generation and provider/staff burnout.
While these issues are impacted by several factors, one of the most common denominators is increasing administrative workloads driven by non–revenue-generating activities. Consider this:
- A recent American Medical Association survey pointed out that during the course of the average workweek, a physician completes an average of 37 prior authorization requests. Physicians and their staff spend an average of 16.4 hours per week completing prior authorization requirements for patient medicines, procedures, and medical services that they may need.1
- While physicians report that about 65% of prior authorizations take only 1 day, they report that 26% take 3 or more days.2
The potential significance of the generated delays
While this may not seem like a long time (other than the impact it has on staff workload), consider the impact this can have on the patient if the medication being requested is: PrEP, the morning after pill, or other contraceptives? The consequences of the delay or denial could be a lifetime living with HIV, or an unintended pregnancy. This is to say nothing on the larger impact to family, partners, and the potential social stigma faced by all.
Beyond the personal costs and costs within your practice associated with the additional workload, consider the financial costs. The average cost to complete a prior authorization remains the single highest cost for the health care industry at $13.40 per manual transaction, and $7.19 per partially electronic web portal transaction,3 meaning that if I did only one prescription per week, I probably would not mind, but at $13.40 per prior authorization, this burden amounts to millions, actually $767 million by recent estimates.3 Additionally, if you factor in the number of denials and potential follow-ups, this creates a significant amount of waste and spending.
Ultimately, in my experience, I have found that most prior authorizations are simply unnecessary. Here, I’ve picked key examples from just my own recent experiences:
- My patient was denied access to a particular birth control pill she had been on successfully before, and my office was told she needed to try and fail on 5 different generic pills before she could be approved. However, the Affordable Care Act’s (ACA; aka Obamacare) Contraceptive Mandate requires coverage of all contraceptives determined to be most appropriate between a patient and their provider (see below).
- A menopausal patient was denied coverage twice (electronically) for generic micronized progesterone, and I was asked to write a letter of appeal because the insurance company wanted me to use medroxyprogesterone acetate instead. Polling my nearby retail independent pharmacy, the total cost difference per year was $19.96 savings/year ($47.01 ‒ $27.05 = $19.96). My pharmacist did note it could have been a different amount at a large chain pharmacy. Really? I had to write a letter, following two denials, to save less than $20, for a full year!
- A 78-year-old patient using Prolia for severe osteoporosis and preexisting fractures was delayed in getting her next Prolia injection due to a prior authorization snafu. She ended up with multiple additional fractures, a well-described effect of the increase in bone turnover when stopping or delaying this medication. She is now disabled.
- A 94-year-old patient was sent an email reminder to get the medical practice to authorize a refill of ileostomy bags. The email went to spam, and the patient ran out of bags prior to a holiday weekend. I got them in 2 days on Amazon Prime. But who emails a 94-year-old? And ileostomy bags! When does anyone stop needing ileostomy bags?
- I requested a prior authorization for Orilissa (clearly off label) because a severely progestogen-sensitive patient (augmented depression) with severe premenstrual dysphoric disorder requiring hospitalization was thought by her psychiatrist to be better off without menstrual periods. I completed the proper paperwork, two electronic appeals, and a letter of explanation including available references on the use of gonadotropin-releasing hormone analogues for such patients. I was then told I would need to have a peer-to-peer discussion, so I filled out that paperwork, which clearly noted that I am a board-certified reproductive endocrinologist. I got a phone call a few days later by a pleasant, young-sounding pediatric rheumatologist. Our interaction did not go well for him. This was not peer-to-peer!
Let us be clear, prior authorizations have nothing to do with patient care. In fact, they are solely about the money. We in ObGyn have mostly inexpensive and generic products, but even that fact has not lowered the excessive burden of the prior authorization process. In the case of contraception, whether you like the ACA or not it is the law, and it contains specific provisions regarding contraception. With the goals of providing broad access to patients and incentives to developers for new and novel contraceptive methods, these provisions require insurers to cover, without cost-sharing, women’s preventive services including the full range of FDA-approved contraceptives (currently 18 different method categories), and additional methods identified by the FDA as they become available. Further, providers must have an easily accessible, transparent, and sufficiently expedient exceptions process that is not unduly burdensome on the individual or a provider (or other individuals acting as a patient’s authorized representative).
And while I can regale you with chapter and verse and citations of the legal precedent and language, it boils down to this:
- The AMA reported that medical practices spend an average of 2 business days a week per physician to comply with health plans’ inefficient and overused prior-authorization protocols.4 To keep up with the administrative burden, 2 out of 5 physicians (40%) employ staff members who work exclusively on tasks associated with prior authorization.4
- About 86% of practices reported an increased burden of prior authorizations in the last 5 years.5
Continue to: What is to be done?
What is to be done?
I do have suggested solutions. Given the insurance industry’s complete lack of progress in voluntarily reducing the burdens of prior authorizations agreed to in their consensus statement with the AMA, American Hospital Association, America’s Health Insurance Plans, American Pharmacists Association, Blue Cross Blue Shield Association, and the Medical Group Management Association, I say, why not fine them? The AMA is calling on Congress to pass legislation that would codify much of the agreement, in which the above parties had already agreed that reforms were needed to reduce prior authorization burdens and enhance patient-centered care.6
A good model for enforcement via fines could be based on the old “incident to” rules of Medicare. These state that a physician needs to be “in the space” when advanced practice nurses or physician assistants see Medicare recipients. If they are not actually “in the space” they are subject to a fine. As a completely theoretical example, let’s say the claim was for $100. The practitioner would have to pay it back plus triple that amount in damages, or $400. They can also be fined up to $11,000 per claim and kick you out of Medicare and Medicaid. Take my example of Prolia from above…a single shot of Prolia is about $1,000. The insurer would theoretically have to pay $14,000/claim (the claim + triple damages + $11,000) if it was determined that the prior authorization was unnecessary. Seems about right to me. Or we could just sit the health insurance CEOs and their proxies in the corner on 2-foot-tall plastic Little Tikes® chairs for a “timeout” (dunce cap optional), like the outset of the article says.
Until the detrimental prior authorization process is challenged at all levels, we will continue to see and feel the effects of the harm it causes. Being able to drive change through advocacy and education is the best way we as clinicians can impact not just the future of health care but provide for the daily care of our patients who depend on and trust us to provide for their medical needs. We must be the impactors of change for ourselves, colleagues, staff, and profession if we are to really make advancements into the future.
Oh…and health insurance CEOs and their proxies, to get out of their “time-out” would still be entitled to one phone call to beg forgiveness from their mommies/daddies, priest/ rabbi/pastor, psychologist/psychiatrist/mystic healer, etc., but alas, the average wait time is an hour, and if anyone answers the phone, they have a grade school education used in following an irrelevant algorithm. ●
- Corder JC. Streamlining the insurance prior authorization debacle. Mo Med. 2018;115:312-314.
- Prior authorization hurdles have led to serious adverse events. American Medical Association website. February 5, 2019. https://www.ama-assn .org/press-center/press-releases/prior-author ization-hurdles-have-led-serious-adverse -events. Accessed November 29, 2021.
- Council for Affordable Quality Healthcare. 2020 CAQH INDEX. https://www.caqh.org/sites /default/files/explorations/index/2020-caqh -index.pdf. Accessed November 22, 2021.
- Most physicians had little relief from prior authorization as COVID cases soared. American Medical Association website. April 7, 2021. https:// www.ama-assn.org/press-center/press-releases /most-physicians-had-little-relief-prior-author ization-covid-cases. Accessed November 29, 2021.
- Robeznieks A. 1 in 4 doctors say prior authorization has led to a serious adverse event. American Medical Association website. February 5, 2019. https://www .ama-assn.org/practice-management/sustainability /1-4-doctors-say-prior-authorization-has-led-serious -adverse. Accessed November 29, 2021.
- Physicians call on Congress to address prior authorization reform. American Medical Association website. May 14, 2021. https://www .ama-assn.org/press-center/press-releases /physicians-call-congress-address-prior-author ization-reform. Accessed November 29, 2021.
- Corder JC. Streamlining the insurance prior authorization debacle. Mo Med. 2018;115:312-314.
- Prior authorization hurdles have led to serious adverse events. American Medical Association website. February 5, 2019. https://www.ama-assn .org/press-center/press-releases/prior-author ization-hurdles-have-led-serious-adverse -events. Accessed November 29, 2021.
- Council for Affordable Quality Healthcare. 2020 CAQH INDEX. https://www.caqh.org/sites /default/files/explorations/index/2020-caqh -index.pdf. Accessed November 22, 2021.
- Most physicians had little relief from prior authorization as COVID cases soared. American Medical Association website. April 7, 2021. https:// www.ama-assn.org/press-center/press-releases /most-physicians-had-little-relief-prior-author ization-covid-cases. Accessed November 29, 2021.
- Robeznieks A. 1 in 4 doctors say prior authorization has led to a serious adverse event. American Medical Association website. February 5, 2019. https://www .ama-assn.org/practice-management/sustainability /1-4-doctors-say-prior-authorization-has-led-serious -adverse. Accessed November 29, 2021.
- Physicians call on Congress to address prior authorization reform. American Medical Association website. May 14, 2021. https://www .ama-assn.org/press-center/press-releases /physicians-call-congress-address-prior-author ization-reform. Accessed November 29, 2021.

Physician as trusted counselor
Pediatricians play many roles as they fulfill their duties and responsibilities. Among these is the role of trusted counselor.
A pediatrician is a risk manager. Not the risk manager at a brokerage firm assessing financial risks. Not the hospital lawyer providing legal advice to minimize lawsuits against the hospital. The pediatrician, as risk manager, is a fiduciary, confidant, partner, and guide for parents seeking to protect and maximize the health of their children.

The practice of pediatrics deals with many low-probability, high-impact threats. This begins before birth. The obstetrician has already ordered a litany of prenatal screens, blood tests, and ultrasounds. Many of these have a positive predictive value of less than 20%. That means the alarming positive results are wrong more than 80% of the time. Tests done purportedly to reassure the parents are likely to falsely terrify them. This devilish process continues immediately after birth. The newborns are subjected to a wide variety of screening tests that they must pass before being stamped USDA Prime baby. Early in my career, a thorough newborn physical exam was the key means of identifying problems. Modern medicine employs a wide variety of blood tests, a hearing screen, a pulse ox check, and a transcutaneous bilirubin test before discharge. It is a gauntlet that few escape unscathed. Even the totally normal infant is going to flunk a handful of these screens. Then the nursery doctor is ready to erect additional hoops to jump through. Too big or too small? You need glucose checks. Breech presentation? A hip ultrasound. Too long in labor? Blood tests. Too pale or too ruddy? Blood tests. Not acting quite right? Temperature too high? Temperature too low? Too irritable? Too lethargic? Baby, you’ve hit the jackpot for extra blood tests, an app to estimate the risk of early-onset sepsis, and maybe a trip to the NICU.
Many of these protocols have poor positive predictive value results that are not easy to explain to lay people. The ideas are not easily taught to medical students. Those results can be even harder to communicate to new parents with health care careers. A little knowledge goes a long ways toward long, sleepless nights of worrying even though the baby is just fine. Even cute. Snuggly. A good baby! Parents, hug your baby! Feed the baby! Let the professional do most of the worrying.
What does a professional worrier offer? First, a comprehension of the science. The professional understands sensitivity and specificity, false-positive rates, prevalence, and positive predictive value. Second, particular knowledge of the various tests involved, including the confirmatory tests and the risk-benefit of treatment. Third, experienced clinical judgment that knows that lotteries are bad investments even though two people are splitting a $600 million lottery win this week. Most people don’t emotionally cope with small risks. Fourth, the ability to do values clarification. There is not a one-size-fits-all bedside approach in pediatrics. Parents have differing expectations, differing levels of risk aversion, and different methods for handling anxiety. First-time parents may be very risk intolerant with their baby. Some people deal with fear by seeking more information. Others are looking for evidence that the expert physician is committed to compassionately providing whatever is best for their child.
How has medicine evolved recently? I will highlight four items. First, as described earlier, there has been a large increase in the number of these screens that will be failed. Typical office practice continues the methodology with well child exams and developmental screening. Second, many screens have been introduced that have very low positive predictive value. This leads to many anxious parents who will benefit from pediatricians with the bedside manner to guide the parents and their precious baby through this maze of scientific interventions. The science is difficult enough to master during training. It takes more time to learn the art of counseling parents, listening to their concerns, and earning their trust. That art is practiced in face-to-face encounters with the parents. The classic approach to residency training limits the opportunity to observe and mentor the knowledge, skills, and empathy of a good bedside manner.
A third evolution, more recent, has been the widespread pollution of scientific knowledge with misinformation and disinformation through social media. I addressed that issue in my columns in January and March 2019.
Fourth, most recently, I believe the pandemic has emphasized to the public that nothing in life is totally risk free. Extreme efforts to reduce risk produce unwanted consequences. There is a window of opportunity here to work with parents and patients to build relationships that help people to assess risks and make more rational and beneficial choices. For example, when is the risk of meningitis in a febrile young infant low enough to manage at home? The risk will never be zero. But admission to the hospital “just in case” is not risk free either. People are acutely aware of that right now.
Health care professionals can position themselves as the trusted source of health information specific to a particular person’s situation. Health care professionals can be competent, committed, and compassionate listeners to what really worries people. In this way, we manage risk. This role also involves addressing the mental health crisis causing so much suicide and addiction. Severe problems should be referred to specialists, but I anticipate in the near future that most pediatricians will require more skills dealing with risk and anxiety rather than microbes.
Dr. Powell is a retired pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at [email protected].
Pediatricians play many roles as they fulfill their duties and responsibilities. Among these is the role of trusted counselor.
A pediatrician is a risk manager. Not the risk manager at a brokerage firm assessing financial risks. Not the hospital lawyer providing legal advice to minimize lawsuits against the hospital. The pediatrician, as risk manager, is a fiduciary, confidant, partner, and guide for parents seeking to protect and maximize the health of their children.
The practice of pediatrics deals with many low-probability, high-impact threats. This begins before birth. The obstetrician has already ordered a litany of prenatal screens, blood tests, and ultrasounds. Many of these have a positive predictive value of less than 20%. That means the alarming positive results are wrong more than 80% of the time. Tests done purportedly to reassure the parents are likely to falsely terrify them. This devilish process continues immediately after birth. The newborns are subjected to a wide variety of screening tests that they must pass before being stamped USDA Prime baby. Early in my career, a thorough newborn physical exam was the key means of identifying problems. Modern medicine employs a wide variety of blood tests, a hearing screen, a pulse ox check, and a transcutaneous bilirubin test before discharge. It is a gauntlet that few escape unscathed. Even the totally normal infant is going to flunk a handful of these screens. Then the nursery doctor is ready to erect additional hoops to jump through. Too big or too small? You need glucose checks. Breech presentation? A hip ultrasound. Too long in labor? Blood tests. Too pale or too ruddy? Blood tests. Not acting quite right? Temperature too high? Temperature too low? Too irritable? Too lethargic? Baby, you’ve hit the jackpot for extra blood tests, an app to estimate the risk of early-onset sepsis, and maybe a trip to the NICU.
Many of these protocols have poor positive predictive value results that are not easy to explain to lay people. The ideas are not easily taught to medical students. Those results can be even harder to communicate to new parents with health care careers. A little knowledge goes a long ways toward long, sleepless nights of worrying even though the baby is just fine. Even cute. Snuggly. A good baby! Parents, hug your baby! Feed the baby! Let the professional do most of the worrying.
What does a professional worrier offer? First, a comprehension of the science. The professional understands sensitivity and specificity, false-positive rates, prevalence, and positive predictive value. Second, particular knowledge of the various tests involved, including the confirmatory tests and the risk-benefit of treatment. Third, experienced clinical judgment that knows that lotteries are bad investments even though two people are splitting a $600 million lottery win this week. Most people don’t emotionally cope with small risks. Fourth, the ability to do values clarification. There is not a one-size-fits-all bedside approach in pediatrics. Parents have differing expectations, differing levels of risk aversion, and different methods for handling anxiety. First-time parents may be very risk intolerant with their baby. Some people deal with fear by seeking more information. Others are looking for evidence that the expert physician is committed to compassionately providing whatever is best for their child.
How has medicine evolved recently? I will highlight four items. First, as described earlier, there has been a large increase in the number of these screens that will be failed. Typical office practice continues the methodology with well child exams and developmental screening. Second, many screens have been introduced that have very low positive predictive value. This leads to many anxious parents who will benefit from pediatricians with the bedside manner to guide the parents and their precious baby through this maze of scientific interventions. The science is difficult enough to master during training. It takes more time to learn the art of counseling parents, listening to their concerns, and earning their trust. That art is practiced in face-to-face encounters with the parents. The classic approach to residency training limits the opportunity to observe and mentor the knowledge, skills, and empathy of a good bedside manner.
A third evolution, more recent, has been the widespread pollution of scientific knowledge with misinformation and disinformation through social media. I addressed that issue in my columns in January and March 2019.
Fourth, most recently, I believe the pandemic has emphasized to the public that nothing in life is totally risk free. Extreme efforts to reduce risk produce unwanted consequences. There is a window of opportunity here to work with parents and patients to build relationships that help people to assess risks and make more rational and beneficial choices. For example, when is the risk of meningitis in a febrile young infant low enough to manage at home? The risk will never be zero. But admission to the hospital “just in case” is not risk free either. People are acutely aware of that right now.
Health care professionals can position themselves as the trusted source of health information specific to a particular person’s situation. Health care professionals can be competent, committed, and compassionate listeners to what really worries people. In this way, we manage risk. This role also involves addressing the mental health crisis causing so much suicide and addiction. Severe problems should be referred to specialists, but I anticipate in the near future that most pediatricians will require more skills dealing with risk and anxiety rather than microbes.
Dr. Powell is a retired pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at [email protected].
Pediatricians play many roles as they fulfill their duties and responsibilities. Among these is the role of trusted counselor.
A pediatrician is a risk manager. Not the risk manager at a brokerage firm assessing financial risks. Not the hospital lawyer providing legal advice to minimize lawsuits against the hospital. The pediatrician, as risk manager, is a fiduciary, confidant, partner, and guide for parents seeking to protect and maximize the health of their children.
The practice of pediatrics deals with many low-probability, high-impact threats. This begins before birth. The obstetrician has already ordered a litany of prenatal screens, blood tests, and ultrasounds. Many of these have a positive predictive value of less than 20%. That means the alarming positive results are wrong more than 80% of the time. Tests done purportedly to reassure the parents are likely to falsely terrify them. This devilish process continues immediately after birth. The newborns are subjected to a wide variety of screening tests that they must pass before being stamped USDA Prime baby. Early in my career, a thorough newborn physical exam was the key means of identifying problems. Modern medicine employs a wide variety of blood tests, a hearing screen, a pulse ox check, and a transcutaneous bilirubin test before discharge. It is a gauntlet that few escape unscathed. Even the totally normal infant is going to flunk a handful of these screens. Then the nursery doctor is ready to erect additional hoops to jump through. Too big or too small? You need glucose checks. Breech presentation? A hip ultrasound. Too long in labor? Blood tests. Too pale or too ruddy? Blood tests. Not acting quite right? Temperature too high? Temperature too low? Too irritable? Too lethargic? Baby, you’ve hit the jackpot for extra blood tests, an app to estimate the risk of early-onset sepsis, and maybe a trip to the NICU.
Many of these protocols have poor positive predictive value results that are not easy to explain to lay people. The ideas are not easily taught to medical students. Those results can be even harder to communicate to new parents with health care careers. A little knowledge goes a long ways toward long, sleepless nights of worrying even though the baby is just fine. Even cute. Snuggly. A good baby! Parents, hug your baby! Feed the baby! Let the professional do most of the worrying.
What does a professional worrier offer? First, a comprehension of the science. The professional understands sensitivity and specificity, false-positive rates, prevalence, and positive predictive value. Second, particular knowledge of the various tests involved, including the confirmatory tests and the risk-benefit of treatment. Third, experienced clinical judgment that knows that lotteries are bad investments even though two people are splitting a $600 million lottery win this week. Most people don’t emotionally cope with small risks. Fourth, the ability to do values clarification. There is not a one-size-fits-all bedside approach in pediatrics. Parents have differing expectations, differing levels of risk aversion, and different methods for handling anxiety. First-time parents may be very risk intolerant with their baby. Some people deal with fear by seeking more information. Others are looking for evidence that the expert physician is committed to compassionately providing whatever is best for their child.
How has medicine evolved recently? I will highlight four items. First, as described earlier, there has been a large increase in the number of these screens that will be failed. Typical office practice continues the methodology with well child exams and developmental screening. Second, many screens have been introduced that have very low positive predictive value. This leads to many anxious parents who will benefit from pediatricians with the bedside manner to guide the parents and their precious baby through this maze of scientific interventions. The science is difficult enough to master during training. It takes more time to learn the art of counseling parents, listening to their concerns, and earning their trust. That art is practiced in face-to-face encounters with the parents. The classic approach to residency training limits the opportunity to observe and mentor the knowledge, skills, and empathy of a good bedside manner.
A third evolution, more recent, has been the widespread pollution of scientific knowledge with misinformation and disinformation through social media. I addressed that issue in my columns in January and March 2019.
Fourth, most recently, I believe the pandemic has emphasized to the public that nothing in life is totally risk free. Extreme efforts to reduce risk produce unwanted consequences. There is a window of opportunity here to work with parents and patients to build relationships that help people to assess risks and make more rational and beneficial choices. For example, when is the risk of meningitis in a febrile young infant low enough to manage at home? The risk will never be zero. But admission to the hospital “just in case” is not risk free either. People are acutely aware of that right now.
Health care professionals can position themselves as the trusted source of health information specific to a particular person’s situation. Health care professionals can be competent, committed, and compassionate listeners to what really worries people. In this way, we manage risk. This role also involves addressing the mental health crisis causing so much suicide and addiction. Severe problems should be referred to specialists, but I anticipate in the near future that most pediatricians will require more skills dealing with risk and anxiety rather than microbes.
Dr. Powell is a retired pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at [email protected].
Pediatric depression and parents
In October of 2021, the American Academy of Child and Adolescent Psychiatry, the American Academy of Pediatrics, and the Children’s Hospital Association jointly declared a National State of Emergency in Children’s Mental Health and called on policy makers to address a host of challenges that have impeded access to effective mental health care for youth.
In November, we wrote about how pediatricians may increase their use of screening for adolescent depression and initiate treatment when appropriate.

Now we complement that piece with guidance you may offer the parents of your depressed adolescent patients. Adolescent depression is a common pediatric disorder, especially in the COVID-19 era when so many relationships and activities have been limited or cut off. With treatment, most adolescents recover. Accepting that it may be taking longer to find a therapist, you can make treatment recommendations, support the teenager and parents, address safety concerns and, if the depression is of moderate or more serious severity, start medications. Parents are your natural partners as they are concerned about their children’s health and safety and eager for guidance on how to best support their recovery.

Adolescence is a time in which parents transition to more of a consulting than a controlling posture with their children, but illness calls for a shift toward setting rules and routines that will support health and healing. Prepare both the teenager (in a 1:1 discussion) and parents for this temporary shift, and for some teenagers, expect resistance. Depression will make the teenager more unhappy and irritable. It also causes withdrawal, by sapping energy and making one feel unwelcome at activities, believing his or her presence will be a burden to others. Treatment includes something called “behavioral activation,” or continuous nudging, to keep the patient involved in social, intellectual, and physical activities. Parents (and siblings) are the keys to this behavioral activation, whether nudging to participate in a board game or a walk. Reassure parents they should not take it personally when their teen resists, and not be discouraged if they fail sometimes. Their focus is on calmly, warmly, and repeatedly prompting their children with nudges toward these routines and activities. They should be ready to remind them why they are “nagging,” framing these efforts explicitly as supporting recovery from depression. If possible, applying these rules to everyone at home will help. They need to avoid being drawn into conflict, focusing instead on staying connected to their teens. Their task is to keep planning and cajoling, giving their children multiple opportunities to participate, pushing back against depression’s gravitational pull for total withdrawal.
Sleep
One of the most important thing parents can do for their depressed adolescents is to support their healthy restful sleep. During adolescence, the timing of sleep naturally shifts later, and the need for restful sleep increases. Working against the demands of homework, extracurricular activities, and social connections, sleep often suffers during adolescence. Further sleep disruptions, including difficulty falling asleep and frequent awakening during sleep or in the early morning, are typical of depression. Restful sleep is instrumental to recovery, and parents need to help their depressed teens set good sleep habits. This includes setting a time for bed that is realistic and consistent and turning off screens 30 minutes before lights out. A soothing, consistent bedtime routine, including a hot shower and reading in bed, is a powerful cue for sleep. Getting daily exercise and avoiding a heavy meal and caffeine in the hours before bed supports both falling and staying asleep. Having light reading near bed (magazines or comics) instead of screens can provide a way to pass 30 minutes if they wake up during the night (ideally reading out of bed), one that will not make it harder for them to go back to sleep. Finally, teens should not be allowed to spend all day in bed or nap in the afternoon. This may be the hardest task for parents, as adolescents naturally treat their beds like their center of operations and depression lowers their energy and initiative. If parents set these rules and routines for all members of the family, it can improve the chances that their depressed adolescents may begin to return to healthy sleep.
Exercise
Vigorous exercise (for 20 minutes three times weekly) is as effective as SSRIs in treating mild to moderate depression. Even in severe depression, exercise may accelerate recovery and certainly contributes to returning to restful sleep and a feeling of improved energy. Inviting their depressed teens to join them on a trip to the gym may seem like a fool’s errand to parents, but they should prioritize getting their children moving. Don’t offer choices or ask what activity they would like to do. Most invitations will be met with “no, thanks” (or probably something less polite). Instead, initiate simple activities and then cajole the children with “let’s go!” They should use loving persistence to get them out the door. Parents are the experts on their children and will know if there is an activity that they are more likely to enjoy. Make any activities group ones, easy to start and not too long. They could initiate family walks or bike rides in their neighborhood. If it helps, they can blame you, “these are doctor’s orders!” This approach of warm persistence should be applied across the board, helping their depressed teens participate in mealtimes and other activities. Prepare parents that this can feel unnatural, if they have been letting their healthy teenagers have more space and independence and less time in family activities.
Social connections
Behavioral activation includes keeping a depressed teen engaged in social activities. Friendships are a potent motivator in the lives of healthy adolescents. If depressed teens can stay connected to close friends, it is a powerful force for recovery. Find out if their friends know about their depression, whom do they trust to tell about it? Help them find comfortable language to speak about their depression with trusted friends. Parents can use their behavioral activation strategies to prompt their teenagers to participate in social activities. If texting, video chatting, or social media platforms are how they stay connected with close friends, support their use of these platforms. But be mindful that social media promotes social comparison over connection, and depression sets them up to feel less than others even without assistance. Parents should support real time with their friends in small groups, for short periods during the time of day when they have the most energy.
Safety
Suicide is the second leading cause of death for adolescents in the United States, and the rate of attempted and completed suicide in adolescents has been steadily climbing over the past decade according to the CDC. The rate is higher in older adolescents, though thankfully relatively uncommon (about 1 in 10,000 a year), and, although we know risk factors, no one has been able to predict reliably the risk for an individual teenager at a point in time. In a clinically referred sample, 85% of depressed adolescents will have suicidal ideation and 32% will make a suicide attempt. The risk is higher in those adolescents with more than one psychiatric diagnosis and with a history of impulsive behaviors, substance abuse, prior suicide attempts, and a family history of suicide. It is important that parents hear that asking about suicidal thoughts will not cause them. On the contrary, preserving open communication and a warm relationship is very protective. Adolescent suicide attempts are likely to be impulsive, so helping the family to consider ways to “put up obstacles” that would slow down any possible attempt is an effective way to improve safety. Ask your patients about suicidal thoughts, plans, and what keeps them safe. Find out if they worry about sharing these thoughts with their parents and why. Ask if there are ways their parents can check on them that “aren’t too annoying.” Determine if there are guns in the home, and if so, are they safely stored (locked, separate from ammunition)? More than 50% of completed adolescent suicides involve firearms, so this question is critical. What about access to medications that could be dangerous in overdose in your home or a relative’s home they may visit? Discussing these facts with your patients and their parents together will make it easier for them to continue the conversation outside of your office and can make an enormous difference in their recovery.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at [email protected].
Reference
Kovacs M et al. J Am Acad Child Adolesc Psychiatry. 1993 Jan;32(1):8-20.
In October of 2021, the American Academy of Child and Adolescent Psychiatry, the American Academy of Pediatrics, and the Children’s Hospital Association jointly declared a National State of Emergency in Children’s Mental Health and called on policy makers to address a host of challenges that have impeded access to effective mental health care for youth.
In November, we wrote about how pediatricians may increase their use of screening for adolescent depression and initiate treatment when appropriate.
Now we complement that piece with guidance you may offer the parents of your depressed adolescent patients. Adolescent depression is a common pediatric disorder, especially in the COVID-19 era when so many relationships and activities have been limited or cut off. With treatment, most adolescents recover. Accepting that it may be taking longer to find a therapist, you can make treatment recommendations, support the teenager and parents, address safety concerns and, if the depression is of moderate or more serious severity, start medications. Parents are your natural partners as they are concerned about their children’s health and safety and eager for guidance on how to best support their recovery.
Adolescence is a time in which parents transition to more of a consulting than a controlling posture with their children, but illness calls for a shift toward setting rules and routines that will support health and healing. Prepare both the teenager (in a 1:1 discussion) and parents for this temporary shift, and for some teenagers, expect resistance. Depression will make the teenager more unhappy and irritable. It also causes withdrawal, by sapping energy and making one feel unwelcome at activities, believing his or her presence will be a burden to others. Treatment includes something called “behavioral activation,” or continuous nudging, to keep the patient involved in social, intellectual, and physical activities. Parents (and siblings) are the keys to this behavioral activation, whether nudging to participate in a board game or a walk. Reassure parents they should not take it personally when their teen resists, and not be discouraged if they fail sometimes. Their focus is on calmly, warmly, and repeatedly prompting their children with nudges toward these routines and activities. They should be ready to remind them why they are “nagging,” framing these efforts explicitly as supporting recovery from depression. If possible, applying these rules to everyone at home will help. They need to avoid being drawn into conflict, focusing instead on staying connected to their teens. Their task is to keep planning and cajoling, giving their children multiple opportunities to participate, pushing back against depression’s gravitational pull for total withdrawal.
Sleep
One of the most important thing parents can do for their depressed adolescents is to support their healthy restful sleep. During adolescence, the timing of sleep naturally shifts later, and the need for restful sleep increases. Working against the demands of homework, extracurricular activities, and social connections, sleep often suffers during adolescence. Further sleep disruptions, including difficulty falling asleep and frequent awakening during sleep or in the early morning, are typical of depression. Restful sleep is instrumental to recovery, and parents need to help their depressed teens set good sleep habits. This includes setting a time for bed that is realistic and consistent and turning off screens 30 minutes before lights out. A soothing, consistent bedtime routine, including a hot shower and reading in bed, is a powerful cue for sleep. Getting daily exercise and avoiding a heavy meal and caffeine in the hours before bed supports both falling and staying asleep. Having light reading near bed (magazines or comics) instead of screens can provide a way to pass 30 minutes if they wake up during the night (ideally reading out of bed), one that will not make it harder for them to go back to sleep. Finally, teens should not be allowed to spend all day in bed or nap in the afternoon. This may be the hardest task for parents, as adolescents naturally treat their beds like their center of operations and depression lowers their energy and initiative. If parents set these rules and routines for all members of the family, it can improve the chances that their depressed adolescents may begin to return to healthy sleep.
Exercise
Vigorous exercise (for 20 minutes three times weekly) is as effective as SSRIs in treating mild to moderate depression. Even in severe depression, exercise may accelerate recovery and certainly contributes to returning to restful sleep and a feeling of improved energy. Inviting their depressed teens to join them on a trip to the gym may seem like a fool’s errand to parents, but they should prioritize getting their children moving. Don’t offer choices or ask what activity they would like to do. Most invitations will be met with “no, thanks” (or probably something less polite). Instead, initiate simple activities and then cajole the children with “let’s go!” They should use loving persistence to get them out the door. Parents are the experts on their children and will know if there is an activity that they are more likely to enjoy. Make any activities group ones, easy to start and not too long. They could initiate family walks or bike rides in their neighborhood. If it helps, they can blame you, “these are doctor’s orders!” This approach of warm persistence should be applied across the board, helping their depressed teens participate in mealtimes and other activities. Prepare parents that this can feel unnatural, if they have been letting their healthy teenagers have more space and independence and less time in family activities.
Social connections
Behavioral activation includes keeping a depressed teen engaged in social activities. Friendships are a potent motivator in the lives of healthy adolescents. If depressed teens can stay connected to close friends, it is a powerful force for recovery. Find out if their friends know about their depression, whom do they trust to tell about it? Help them find comfortable language to speak about their depression with trusted friends. Parents can use their behavioral activation strategies to prompt their teenagers to participate in social activities. If texting, video chatting, or social media platforms are how they stay connected with close friends, support their use of these platforms. But be mindful that social media promotes social comparison over connection, and depression sets them up to feel less than others even without assistance. Parents should support real time with their friends in small groups, for short periods during the time of day when they have the most energy.
Safety
Suicide is the second leading cause of death for adolescents in the United States, and the rate of attempted and completed suicide in adolescents has been steadily climbing over the past decade according to the CDC. The rate is higher in older adolescents, though thankfully relatively uncommon (about 1 in 10,000 a year), and, although we know risk factors, no one has been able to predict reliably the risk for an individual teenager at a point in time. In a clinically referred sample, 85% of depressed adolescents will have suicidal ideation and 32% will make a suicide attempt. The risk is higher in those adolescents with more than one psychiatric diagnosis and with a history of impulsive behaviors, substance abuse, prior suicide attempts, and a family history of suicide. It is important that parents hear that asking about suicidal thoughts will not cause them. On the contrary, preserving open communication and a warm relationship is very protective. Adolescent suicide attempts are likely to be impulsive, so helping the family to consider ways to “put up obstacles” that would slow down any possible attempt is an effective way to improve safety. Ask your patients about suicidal thoughts, plans, and what keeps them safe. Find out if they worry about sharing these thoughts with their parents and why. Ask if there are ways their parents can check on them that “aren’t too annoying.” Determine if there are guns in the home, and if so, are they safely stored (locked, separate from ammunition)? More than 50% of completed adolescent suicides involve firearms, so this question is critical. What about access to medications that could be dangerous in overdose in your home or a relative’s home they may visit? Discussing these facts with your patients and their parents together will make it easier for them to continue the conversation outside of your office and can make an enormous difference in their recovery.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at [email protected].
Reference
Kovacs M et al. J Am Acad Child Adolesc Psychiatry. 1993 Jan;32(1):8-20.
In October of 2021, the American Academy of Child and Adolescent Psychiatry, the American Academy of Pediatrics, and the Children’s Hospital Association jointly declared a National State of Emergency in Children’s Mental Health and called on policy makers to address a host of challenges that have impeded access to effective mental health care for youth.
In November, we wrote about how pediatricians may increase their use of screening for adolescent depression and initiate treatment when appropriate.
Now we complement that piece with guidance you may offer the parents of your depressed adolescent patients. Adolescent depression is a common pediatric disorder, especially in the COVID-19 era when so many relationships and activities have been limited or cut off. With treatment, most adolescents recover. Accepting that it may be taking longer to find a therapist, you can make treatment recommendations, support the teenager and parents, address safety concerns and, if the depression is of moderate or more serious severity, start medications. Parents are your natural partners as they are concerned about their children’s health and safety and eager for guidance on how to best support their recovery.
Adolescence is a time in which parents transition to more of a consulting than a controlling posture with their children, but illness calls for a shift toward setting rules and routines that will support health and healing. Prepare both the teenager (in a 1:1 discussion) and parents for this temporary shift, and for some teenagers, expect resistance. Depression will make the teenager more unhappy and irritable. It also causes withdrawal, by sapping energy and making one feel unwelcome at activities, believing his or her presence will be a burden to others. Treatment includes something called “behavioral activation,” or continuous nudging, to keep the patient involved in social, intellectual, and physical activities. Parents (and siblings) are the keys to this behavioral activation, whether nudging to participate in a board game or a walk. Reassure parents they should not take it personally when their teen resists, and not be discouraged if they fail sometimes. Their focus is on calmly, warmly, and repeatedly prompting their children with nudges toward these routines and activities. They should be ready to remind them why they are “nagging,” framing these efforts explicitly as supporting recovery from depression. If possible, applying these rules to everyone at home will help. They need to avoid being drawn into conflict, focusing instead on staying connected to their teens. Their task is to keep planning and cajoling, giving their children multiple opportunities to participate, pushing back against depression’s gravitational pull for total withdrawal.
Sleep
One of the most important thing parents can do for their depressed adolescents is to support their healthy restful sleep. During adolescence, the timing of sleep naturally shifts later, and the need for restful sleep increases. Working against the demands of homework, extracurricular activities, and social connections, sleep often suffers during adolescence. Further sleep disruptions, including difficulty falling asleep and frequent awakening during sleep or in the early morning, are typical of depression. Restful sleep is instrumental to recovery, and parents need to help their depressed teens set good sleep habits. This includes setting a time for bed that is realistic and consistent and turning off screens 30 minutes before lights out. A soothing, consistent bedtime routine, including a hot shower and reading in bed, is a powerful cue for sleep. Getting daily exercise and avoiding a heavy meal and caffeine in the hours before bed supports both falling and staying asleep. Having light reading near bed (magazines or comics) instead of screens can provide a way to pass 30 minutes if they wake up during the night (ideally reading out of bed), one that will not make it harder for them to go back to sleep. Finally, teens should not be allowed to spend all day in bed or nap in the afternoon. This may be the hardest task for parents, as adolescents naturally treat their beds like their center of operations and depression lowers their energy and initiative. If parents set these rules and routines for all members of the family, it can improve the chances that their depressed adolescents may begin to return to healthy sleep.
Exercise
Vigorous exercise (for 20 minutes three times weekly) is as effective as SSRIs in treating mild to moderate depression. Even in severe depression, exercise may accelerate recovery and certainly contributes to returning to restful sleep and a feeling of improved energy. Inviting their depressed teens to join them on a trip to the gym may seem like a fool’s errand to parents, but they should prioritize getting their children moving. Don’t offer choices or ask what activity they would like to do. Most invitations will be met with “no, thanks” (or probably something less polite). Instead, initiate simple activities and then cajole the children with “let’s go!” They should use loving persistence to get them out the door. Parents are the experts on their children and will know if there is an activity that they are more likely to enjoy. Make any activities group ones, easy to start and not too long. They could initiate family walks or bike rides in their neighborhood. If it helps, they can blame you, “these are doctor’s orders!” This approach of warm persistence should be applied across the board, helping their depressed teens participate in mealtimes and other activities. Prepare parents that this can feel unnatural, if they have been letting their healthy teenagers have more space and independence and less time in family activities.
Social connections
Behavioral activation includes keeping a depressed teen engaged in social activities. Friendships are a potent motivator in the lives of healthy adolescents. If depressed teens can stay connected to close friends, it is a powerful force for recovery. Find out if their friends know about their depression, whom do they trust to tell about it? Help them find comfortable language to speak about their depression with trusted friends. Parents can use their behavioral activation strategies to prompt their teenagers to participate in social activities. If texting, video chatting, or social media platforms are how they stay connected with close friends, support their use of these platforms. But be mindful that social media promotes social comparison over connection, and depression sets them up to feel less than others even without assistance. Parents should support real time with their friends in small groups, for short periods during the time of day when they have the most energy.
Safety
Suicide is the second leading cause of death for adolescents in the United States, and the rate of attempted and completed suicide in adolescents has been steadily climbing over the past decade according to the CDC. The rate is higher in older adolescents, though thankfully relatively uncommon (about 1 in 10,000 a year), and, although we know risk factors, no one has been able to predict reliably the risk for an individual teenager at a point in time. In a clinically referred sample, 85% of depressed adolescents will have suicidal ideation and 32% will make a suicide attempt. The risk is higher in those adolescents with more than one psychiatric diagnosis and with a history of impulsive behaviors, substance abuse, prior suicide attempts, and a family history of suicide. It is important that parents hear that asking about suicidal thoughts will not cause them. On the contrary, preserving open communication and a warm relationship is very protective. Adolescent suicide attempts are likely to be impulsive, so helping the family to consider ways to “put up obstacles” that would slow down any possible attempt is an effective way to improve safety. Ask your patients about suicidal thoughts, plans, and what keeps them safe. Find out if they worry about sharing these thoughts with their parents and why. Ask if there are ways their parents can check on them that “aren’t too annoying.” Determine if there are guns in the home, and if so, are they safely stored (locked, separate from ammunition)? More than 50% of completed adolescent suicides involve firearms, so this question is critical. What about access to medications that could be dangerous in overdose in your home or a relative’s home they may visit? Discussing these facts with your patients and their parents together will make it easier for them to continue the conversation outside of your office and can make an enormous difference in their recovery.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at [email protected].
Reference
Kovacs M et al. J Am Acad Child Adolesc Psychiatry. 1993 Jan;32(1):8-20.
The etiology of acute otitis media in young children in recent years
Since the COVID-19 pandemic began, pediatricians have been seeing fewer cases of all respiratory illnesses, including acute otitis media (AOM). However, as I prepare this column, an uptick has commenced and likely will continue in an upward trajectory as we emerge from the pandemic into an endemic coronavirus era. Our group in Rochester, N.Y., has continued prospective studies of AOM throughout the pandemic. We found that nasopharyngeal colonization by Streptococcus pneumoniae (pneumococcus), Haemophilus influenzae, and Moraxella catarrhalis remained prevalent in our study cohort of children aged 6-36 months. However, with all the precautions of masking, social distancing, hand washing, and quick exclusion from day care when illness occurred, the frequency of detecting these common otopathogens decreased, as one might expect.1
Leading up to the pandemic, we had an abundance of data to characterize AOM etiology and found that the cause of AOM continues to change following the introduction of the 13-valent pneumococcal conjugate vaccine (PCV13, Prevnar 13). Our most recent report on otopathogen distribution and antibiotic susceptibility covered the years 2015-2019.2 A total of 589 children were enrolled prospectively and we collected 495 middle ear fluid samples (MEF) from 319 AOM cases using tympanocentesis. The frequency of isolates was H. influenzae (34%), pneumococcus (24%), and M. catarrhalis (15%). Beta-lactamase–positive H. influenzae strains were identified among 49% of the isolates, rendering them resistant to amoxicillin. PCV13 serotypes were infrequently isolated. However, we did isolate vaccine types (VTs) in some children from MEF, notably serotypes 19F, 19A, and 3. Non-PCV13 pneumococcus serotypes 35B, 23B, and 15B/C emerged as the most common serotypes. Amoxicillin resistance was identified among 25% of pneumococcal strains. Out of 16 antibiotics tested, 9 (56%) showed a significant increase in nonsusceptibility among pneumococcal isolates. 100% of M. catarrhalis isolates were beta-lactamase producers and therefore resistant to amoxicillin.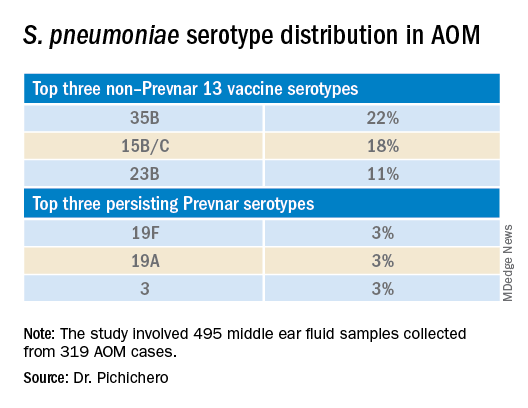
PCV13 has resulted in a decline in both invasive and noninvasive pneumococcal infections caused by strains expressing the 13 capsular serotypes included in the vaccine. However, the emergence of replacement serotypes occurred after introduction of PCV73,4 and continues to occur during the PCV13 era, as shown from the results presented here. Non-PCV13 serotypes accounted for more than 90% of MEF isolates during 2015-2019, with 35B, 21 and 23B being the most commonly isolated. Other emergent serotypes of potential importance were nonvaccine serotypes 15A, 15B, 15C, 23A and 11A. This is highly relevant because forthcoming higher-valency PCVs – PCV15 (manufactured by Merck) and PCV20 (manufactured by Pfizer) will not include many of the dominant capsular serotypes of pneumococcus strains causing AOM. Consequently, the impact of higher-valency PCVs on AOM will not be as great as was observed with the introduction of PCV7 or PCV13.
Of special interest, 22% of pneumococcus isolates from MEF were serotype 35B, making it the most prevalent. Recently we reported a significant rise in antibiotic nonsusceptibility in Spn isolates, contributed mainly by serotype 35B5 and we have been studying how 35B strains transitioned from commensal to otopathogen in children.6 Because serotype 35B strains are increasingly prevalent and often antibiotic resistant, absence of this serotype from PCV15 and PCV20 is cause for concern.

The frequency of isolation of H. influenzae and M. catarrhalis has remained stable across the PCV13 era as the No. 1 and No. 3 pathogens. Similarly, the production of beta-lactamase among strains causing AOM has remained stable at close to 50% and 100%, respectively. Use of amoxicillin, either high dose or standard dose, would not be expected to kill these bacteria.
Our study design has limitations. The population is derived from a predominantly middle-class, suburban population of children in upstate New York and may not be representative of other types of populations in the United States. The children are 6-36 months old, the age when most AOM occurs. MEF samples that were culture negative for bacteria were not further tested by polymerase chain reaction methods.
Dr. Pichichero is a specialist in pediatric infectious diseases, Center for Infectious Diseases and Immunology, and director of the Research Institute, at Rochester (N.Y.) General Hospital. He has no conflicts of interest to declare.
References
1. Kaur R et al. Front Pediatr. 2021;9:722483.
2. Kaur R et al. Euro J Clin Microbiol Infect Dis. 2021;41:37-44
3. Pelton SI et al. Pediatr Infect Disease J. 2004;23:1015-22.
4. Farrell DJ et al. Pediatr Infect Disease J. 2007;26:123-8..
5. Kaur R et al. Clin Infect Dis 2021;72(5):797-805.
6. Fuji N et al. Front Cell Infect Microbiol. 2021;11:744742.
Since the COVID-19 pandemic began, pediatricians have been seeing fewer cases of all respiratory illnesses, including acute otitis media (AOM). However, as I prepare this column, an uptick has commenced and likely will continue in an upward trajectory as we emerge from the pandemic into an endemic coronavirus era. Our group in Rochester, N.Y., has continued prospective studies of AOM throughout the pandemic. We found that nasopharyngeal colonization by Streptococcus pneumoniae (pneumococcus), Haemophilus influenzae, and Moraxella catarrhalis remained prevalent in our study cohort of children aged 6-36 months. However, with all the precautions of masking, social distancing, hand washing, and quick exclusion from day care when illness occurred, the frequency of detecting these common otopathogens decreased, as one might expect.1
Leading up to the pandemic, we had an abundance of data to characterize AOM etiology and found that the cause of AOM continues to change following the introduction of the 13-valent pneumococcal conjugate vaccine (PCV13, Prevnar 13). Our most recent report on otopathogen distribution and antibiotic susceptibility covered the years 2015-2019.2 A total of 589 children were enrolled prospectively and we collected 495 middle ear fluid samples (MEF) from 319 AOM cases using tympanocentesis. The frequency of isolates was H. influenzae (34%), pneumococcus (24%), and M. catarrhalis (15%). Beta-lactamase–positive H. influenzae strains were identified among 49% of the isolates, rendering them resistant to amoxicillin. PCV13 serotypes were infrequently isolated. However, we did isolate vaccine types (VTs) in some children from MEF, notably serotypes 19F, 19A, and 3. Non-PCV13 pneumococcus serotypes 35B, 23B, and 15B/C emerged as the most common serotypes. Amoxicillin resistance was identified among 25% of pneumococcal strains. Out of 16 antibiotics tested, 9 (56%) showed a significant increase in nonsusceptibility among pneumococcal isolates. 100% of M. catarrhalis isolates were beta-lactamase producers and therefore resistant to amoxicillin.
PCV13 has resulted in a decline in both invasive and noninvasive pneumococcal infections caused by strains expressing the 13 capsular serotypes included in the vaccine. However, the emergence of replacement serotypes occurred after introduction of PCV73,4 and continues to occur during the PCV13 era, as shown from the results presented here. Non-PCV13 serotypes accounted for more than 90% of MEF isolates during 2015-2019, with 35B, 21 and 23B being the most commonly isolated. Other emergent serotypes of potential importance were nonvaccine serotypes 15A, 15B, 15C, 23A and 11A. This is highly relevant because forthcoming higher-valency PCVs – PCV15 (manufactured by Merck) and PCV20 (manufactured by Pfizer) will not include many of the dominant capsular serotypes of pneumococcus strains causing AOM. Consequently, the impact of higher-valency PCVs on AOM will not be as great as was observed with the introduction of PCV7 or PCV13.
Of special interest, 22% of pneumococcus isolates from MEF were serotype 35B, making it the most prevalent. Recently we reported a significant rise in antibiotic nonsusceptibility in Spn isolates, contributed mainly by serotype 35B5 and we have been studying how 35B strains transitioned from commensal to otopathogen in children.6 Because serotype 35B strains are increasingly prevalent and often antibiotic resistant, absence of this serotype from PCV15 and PCV20 is cause for concern.
The frequency of isolation of H. influenzae and M. catarrhalis has remained stable across the PCV13 era as the No. 1 and No. 3 pathogens. Similarly, the production of beta-lactamase among strains causing AOM has remained stable at close to 50% and 100%, respectively. Use of amoxicillin, either high dose or standard dose, would not be expected to kill these bacteria.
Our study design has limitations. The population is derived from a predominantly middle-class, suburban population of children in upstate New York and may not be representative of other types of populations in the United States. The children are 6-36 months old, the age when most AOM occurs. MEF samples that were culture negative for bacteria were not further tested by polymerase chain reaction methods.
Dr. Pichichero is a specialist in pediatric infectious diseases, Center for Infectious Diseases and Immunology, and director of the Research Institute, at Rochester (N.Y.) General Hospital. He has no conflicts of interest to declare.
References
1. Kaur R et al. Front Pediatr. 2021;9:722483.
2. Kaur R et al. Euro J Clin Microbiol Infect Dis. 2021;41:37-44
3. Pelton SI et al. Pediatr Infect Disease J. 2004;23:1015-22.
4. Farrell DJ et al. Pediatr Infect Disease J. 2007;26:123-8..
5. Kaur R et al. Clin Infect Dis 2021;72(5):797-805.
6. Fuji N et al. Front Cell Infect Microbiol. 2021;11:744742.
Since the COVID-19 pandemic began, pediatricians have been seeing fewer cases of all respiratory illnesses, including acute otitis media (AOM). However, as I prepare this column, an uptick has commenced and likely will continue in an upward trajectory as we emerge from the pandemic into an endemic coronavirus era. Our group in Rochester, N.Y., has continued prospective studies of AOM throughout the pandemic. We found that nasopharyngeal colonization by Streptococcus pneumoniae (pneumococcus), Haemophilus influenzae, and Moraxella catarrhalis remained prevalent in our study cohort of children aged 6-36 months. However, with all the precautions of masking, social distancing, hand washing, and quick exclusion from day care when illness occurred, the frequency of detecting these common otopathogens decreased, as one might expect.1
Leading up to the pandemic, we had an abundance of data to characterize AOM etiology and found that the cause of AOM continues to change following the introduction of the 13-valent pneumococcal conjugate vaccine (PCV13, Prevnar 13). Our most recent report on otopathogen distribution and antibiotic susceptibility covered the years 2015-2019.2 A total of 589 children were enrolled prospectively and we collected 495 middle ear fluid samples (MEF) from 319 AOM cases using tympanocentesis. The frequency of isolates was H. influenzae (34%), pneumococcus (24%), and M. catarrhalis (15%). Beta-lactamase–positive H. influenzae strains were identified among 49% of the isolates, rendering them resistant to amoxicillin. PCV13 serotypes were infrequently isolated. However, we did isolate vaccine types (VTs) in some children from MEF, notably serotypes 19F, 19A, and 3. Non-PCV13 pneumococcus serotypes 35B, 23B, and 15B/C emerged as the most common serotypes. Amoxicillin resistance was identified among 25% of pneumococcal strains. Out of 16 antibiotics tested, 9 (56%) showed a significant increase in nonsusceptibility among pneumococcal isolates. 100% of M. catarrhalis isolates were beta-lactamase producers and therefore resistant to amoxicillin.
PCV13 has resulted in a decline in both invasive and noninvasive pneumococcal infections caused by strains expressing the 13 capsular serotypes included in the vaccine. However, the emergence of replacement serotypes occurred after introduction of PCV73,4 and continues to occur during the PCV13 era, as shown from the results presented here. Non-PCV13 serotypes accounted for more than 90% of MEF isolates during 2015-2019, with 35B, 21 and 23B being the most commonly isolated. Other emergent serotypes of potential importance were nonvaccine serotypes 15A, 15B, 15C, 23A and 11A. This is highly relevant because forthcoming higher-valency PCVs – PCV15 (manufactured by Merck) and PCV20 (manufactured by Pfizer) will not include many of the dominant capsular serotypes of pneumococcus strains causing AOM. Consequently, the impact of higher-valency PCVs on AOM will not be as great as was observed with the introduction of PCV7 or PCV13.
Of special interest, 22% of pneumococcus isolates from MEF were serotype 35B, making it the most prevalent. Recently we reported a significant rise in antibiotic nonsusceptibility in Spn isolates, contributed mainly by serotype 35B5 and we have been studying how 35B strains transitioned from commensal to otopathogen in children.6 Because serotype 35B strains are increasingly prevalent and often antibiotic resistant, absence of this serotype from PCV15 and PCV20 is cause for concern.
The frequency of isolation of H. influenzae and M. catarrhalis has remained stable across the PCV13 era as the No. 1 and No. 3 pathogens. Similarly, the production of beta-lactamase among strains causing AOM has remained stable at close to 50% and 100%, respectively. Use of amoxicillin, either high dose or standard dose, would not be expected to kill these bacteria.
Our study design has limitations. The population is derived from a predominantly middle-class, suburban population of children in upstate New York and may not be representative of other types of populations in the United States. The children are 6-36 months old, the age when most AOM occurs. MEF samples that were culture negative for bacteria were not further tested by polymerase chain reaction methods.
Dr. Pichichero is a specialist in pediatric infectious diseases, Center for Infectious Diseases and Immunology, and director of the Research Institute, at Rochester (N.Y.) General Hospital. He has no conflicts of interest to declare.
References
1. Kaur R et al. Front Pediatr. 2021;9:722483.
2. Kaur R et al. Euro J Clin Microbiol Infect Dis. 2021;41:37-44
3. Pelton SI et al. Pediatr Infect Disease J. 2004;23:1015-22.
4. Farrell DJ et al. Pediatr Infect Disease J. 2007;26:123-8..
5. Kaur R et al. Clin Infect Dis 2021;72(5):797-805.
6. Fuji N et al. Front Cell Infect Microbiol. 2021;11:744742.