User login
Save your breath
If you haven’t already stopped investing your limited supply of office time in fruitless attempts to convince vaccine-hesitant parents to immunize their children, a small study at the University of North Carolina Women’s Hospital in Chapel Hill might finally convince you it’s time to save your breath for other more achievable goals. In a survey of 171 parents, 72% reported that they already had settled on their vaccine preferences prior to pregnancy.
This was a limited survey and may not reflect the responses of a national sample of parents, but it is concerning in light of several other studies that paint a similar gloomy picture. One such study found that even when vaccine-denying parents were presented with educational materials that they acknowledged seemed valid, they continued to withhold vaccines by falling back on other arguments to support their views (“Effective Messages in Vaccine Promotion: A Randomized Trial” by Nyhan et al. [Pediatrics. 2014 Apr;133(4):e835-42]).

If a larger and more geographically diverse study continues to find that the die is cast well before pediatricians have gotten our chance to discuss vaccines with parents-to-be, we will need to rethink our strategies for dealing with vaccine refusers. For those pediatricians who already ask vaccine decliners to find another practice, this new study suggests that they could save themselves time and trouble by advertising their policy to the obstetricians in their communities. This proactive advertising would require some courage, but in the long run it probably makes economic sense.
However, for most pediatricians it may be better to wait in hopes that future research can determine exactly when and under what circumstances most vaccine decliners arrive at their unfortunate decisions. How often was it a philosophy that they inherited from their parents? How often did it reflect their religious views? How often did it evolve from something they heard in school? Junior high, high school, college? Was it a science class, or history, or philosophy?
Was it the result of some media story? TV? Print? Internet? If they can recall a particular show or website, what was it that made it sound so convincing? If it was an individual, was it a friend, celebrity, or a teacher?
A study this detailed would be time consuming and labor intensive, as it would be best done in face-to-face structured interviews by someone who could project a nonjudgmental aura. It would necessarily be retrospective. But it might yield some surprising and helpful information that could be used to target our attack on the epidemic of vaccine refusal.
We know that outbreaks of certain infectious diseases, smallpox being the prime example, do not respond to media blitzes and immunization campaigns. Epidemics will continue to roll along unchecked until a labor-intensive, boots-on-the-ground, door-to-door case-finding effort is undertaken. Vaccine refusal may be similar to smallpox. It appears to be unresponsive to mass media and educational initiatives. It may continue to plague us until we chase down its roots.
Whatever strategy we try next, it is clear that although most parents report that they consider pediatricians among their most trusted sources of health information for their children, we are failing to reach a segment of our target audience. We are too late, long after the die is cast.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
*This story was updated 1/28/2016.
If you haven’t already stopped investing your limited supply of office time in fruitless attempts to convince vaccine-hesitant parents to immunize their children, a small study at the University of North Carolina Women’s Hospital in Chapel Hill might finally convince you it’s time to save your breath for other more achievable goals. In a survey of 171 parents, 72% reported that they already had settled on their vaccine preferences prior to pregnancy.
This was a limited survey and may not reflect the responses of a national sample of parents, but it is concerning in light of several other studies that paint a similar gloomy picture. One such study found that even when vaccine-denying parents were presented with educational materials that they acknowledged seemed valid, they continued to withhold vaccines by falling back on other arguments to support their views (“Effective Messages in Vaccine Promotion: A Randomized Trial” by Nyhan et al. [Pediatrics. 2014 Apr;133(4):e835-42]).
If a larger and more geographically diverse study continues to find that the die is cast well before pediatricians have gotten our chance to discuss vaccines with parents-to-be, we will need to rethink our strategies for dealing with vaccine refusers. For those pediatricians who already ask vaccine decliners to find another practice, this new study suggests that they could save themselves time and trouble by advertising their policy to the obstetricians in their communities. This proactive advertising would require some courage, but in the long run it probably makes economic sense.
However, for most pediatricians it may be better to wait in hopes that future research can determine exactly when and under what circumstances most vaccine decliners arrive at their unfortunate decisions. How often was it a philosophy that they inherited from their parents? How often did it reflect their religious views? How often did it evolve from something they heard in school? Junior high, high school, college? Was it a science class, or history, or philosophy?
Was it the result of some media story? TV? Print? Internet? If they can recall a particular show or website, what was it that made it sound so convincing? If it was an individual, was it a friend, celebrity, or a teacher?
A study this detailed would be time consuming and labor intensive, as it would be best done in face-to-face structured interviews by someone who could project a nonjudgmental aura. It would necessarily be retrospective. But it might yield some surprising and helpful information that could be used to target our attack on the epidemic of vaccine refusal.
We know that outbreaks of certain infectious diseases, smallpox being the prime example, do not respond to media blitzes and immunization campaigns. Epidemics will continue to roll along unchecked until a labor-intensive, boots-on-the-ground, door-to-door case-finding effort is undertaken. Vaccine refusal may be similar to smallpox. It appears to be unresponsive to mass media and educational initiatives. It may continue to plague us until we chase down its roots.
Whatever strategy we try next, it is clear that although most parents report that they consider pediatricians among their most trusted sources of health information for their children, we are failing to reach a segment of our target audience. We are too late, long after the die is cast.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
*This story was updated 1/28/2016.
If you haven’t already stopped investing your limited supply of office time in fruitless attempts to convince vaccine-hesitant parents to immunize their children, a small study at the University of North Carolina Women’s Hospital in Chapel Hill might finally convince you it’s time to save your breath for other more achievable goals. In a survey of 171 parents, 72% reported that they already had settled on their vaccine preferences prior to pregnancy.
This was a limited survey and may not reflect the responses of a national sample of parents, but it is concerning in light of several other studies that paint a similar gloomy picture. One such study found that even when vaccine-denying parents were presented with educational materials that they acknowledged seemed valid, they continued to withhold vaccines by falling back on other arguments to support their views (“Effective Messages in Vaccine Promotion: A Randomized Trial” by Nyhan et al. [Pediatrics. 2014 Apr;133(4):e835-42]).
If a larger and more geographically diverse study continues to find that the die is cast well before pediatricians have gotten our chance to discuss vaccines with parents-to-be, we will need to rethink our strategies for dealing with vaccine refusers. For those pediatricians who already ask vaccine decliners to find another practice, this new study suggests that they could save themselves time and trouble by advertising their policy to the obstetricians in their communities. This proactive advertising would require some courage, but in the long run it probably makes economic sense.
However, for most pediatricians it may be better to wait in hopes that future research can determine exactly when and under what circumstances most vaccine decliners arrive at their unfortunate decisions. How often was it a philosophy that they inherited from their parents? How often did it reflect their religious views? How often did it evolve from something they heard in school? Junior high, high school, college? Was it a science class, or history, or philosophy?
Was it the result of some media story? TV? Print? Internet? If they can recall a particular show or website, what was it that made it sound so convincing? If it was an individual, was it a friend, celebrity, or a teacher?
A study this detailed would be time consuming and labor intensive, as it would be best done in face-to-face structured interviews by someone who could project a nonjudgmental aura. It would necessarily be retrospective. But it might yield some surprising and helpful information that could be used to target our attack on the epidemic of vaccine refusal.
We know that outbreaks of certain infectious diseases, smallpox being the prime example, do not respond to media blitzes and immunization campaigns. Epidemics will continue to roll along unchecked until a labor-intensive, boots-on-the-ground, door-to-door case-finding effort is undertaken. Vaccine refusal may be similar to smallpox. It appears to be unresponsive to mass media and educational initiatives. It may continue to plague us until we chase down its roots.
Whatever strategy we try next, it is clear that although most parents report that they consider pediatricians among their most trusted sources of health information for their children, we are failing to reach a segment of our target audience. We are too late, long after the die is cast.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
*This story was updated 1/28/2016.

Dr. Robert Spitzer: A personal tribute
Imagine that it is 1974, and you are given the following task: Create a modern system of cataloguing and organizing the vast and dark chaos of psychological suffering. If done well, it will become the official diagnostic manual for millions of mental health clinicians in the United States and in the world, for decades to come.
Here are your tools: a 1962 spiral bound manual of 150 pages (DSM-II), a small cadre of experts to serve as colleagues and assistants, and a scientific understanding of neurobiology so slim that it had barely reached its infancy.
This was the job assigned to young Robert Spitzer, then a faculty member at Columbia University. Dr. Spitzer had been tangentially involved in the creation of the DSM-II, and was offered chairmanship of the DSM-III – a job that was at that time considered fairly insignificant. But Dr. Spitzer took it on with relish, and to the surprise of the profession, transformed the DSM into the defining document of modern psychiatry. Robert L. Spitzer died on Christmas Day this past year at the age of 83.
Over the years, Dr. Spitzer has become a household name in psychiatry, a larger-than-life figure. He is thought of by many as the architect of modern psychiatry, but also as a brilliant and brash disrupter who expunged the word “neurosis” from our diagnostic vocabulary, who persuaded organized psychiatry that homosexuality was not a disease, and who laid the groundwork for a system of thinking about mental illness that has guided the field for the past 36 years.
The Bob Spitzer I met was far more approachable than the myth suggests. Ten years ago, I emailed him out of the blue, to request an interview for a book I was writing about the state of psychiatry. To my surprise, not only did he respond positively, but a few weeks later, in December 2007, he had arranged a limo to drive me from La Guardia Airport to his house in a suburb of New York a block away from the Hudson River.
Butterflies in my stomach at the prospect of meeting a living legend, I wheeled my luggage from the limo and knocked on the door, and Dr. Spitzer himself opened it. He was wearing an apron, greeted me with a big smile, and asked me how I liked my eggs. We soon sat down at a kitchen table bathed in sunlight from the windows overlooking his back yard, and we ate cheese omelets and sausages, as we talked about the DSM and his career.

Our conversation was wide ranging, but I’ll recount one interchange because it encapsulates Bob’s relentless honesty and thirst for the truth – both of which were key ingredients in his genius and his legacy.
I had always been curious about how the definition of depression was transformed from the vague “depressive neurosis” in the DSM-II (“This disorder is manifested by an excessive reaction of depression due to an internal conflict or to an identifiable event such as the loss of a love object or cherished possession”) to the precisely defined “major depressive disorder” in the DSM-III.
Bob described the DSM committee process, the long hours of reviewing the literature, and the field trials in which psychiatrists were recruited to test drive the committee’s proposed criteria in their patients. Much of this I had read about, both in the various versions of DSM and in the many articles that Bob and his colleagues had published.
But I had more questions – especially about depression.
“I now understand the process of how you gathered the data,” I said. “But exactly how did you decide on five criteria as being your minimum threshold for depression?”
He took a sip of orange juice and thought for a second. “It was just a consensus. We would ask clinicians and researchers: ‘How many symptoms do you think patients ought to have before you would give the diagnosis of depression?’ And we came up with the arbitrary number of five.”
“But why did you choose five and not four? Or why didn’t you choose six?”
He smiled impishly, looking me directly in the eyes. “Because four just seemed like not enough. And six seemed like too much.”
Even with the benefit of the field trials, Bob pointed out to me, “there is no sharp dividing line where you can confidently say, ‘This is the perfect number of symptoms to make a diagnosis.”
I remember being startled by his honesty. After all, over the years, critics have derided the DSM as being an arbitrary exercise in decision by committee. Bob’s answer, essentially, was, that’s right – but it’s the best we could do given the limitations of our scientific knowledge.
Our patients’ suffering is long, and our understanding of the brain is short. Bob Spitzer provided both psychiatrists and patients with an enduring language that creating meaningful landmarks – a coherent geography of pain. The language has been tweaked over the years, but the underlying classification method has stood the test of time.
Bob Spitzer left us the legacy of the DSM, but he left us so much more. Honesty, generosity, and an unquenchable passion for getting important things right – these are the qualities that I remember and hope to emulate whenever I think of him. That, and his delicious cheese omelets.
Dr. Carlat, a clinical associate professor of psychiatry at Tufts University, Boston, is editor in chief of The Carlat Psychiatry Report, a monthly newsletter on psychopharmacology. He is the author of “The Psychiatric Interview,” (LWW, 2011), and “Unhinged: The Trouble With Psychiatry – A Doctor’s Revelations About a Profession in Crisis,” (Free Press, 2010).
Imagine that it is 1974, and you are given the following task: Create a modern system of cataloguing and organizing the vast and dark chaos of psychological suffering. If done well, it will become the official diagnostic manual for millions of mental health clinicians in the United States and in the world, for decades to come.
Here are your tools: a 1962 spiral bound manual of 150 pages (DSM-II), a small cadre of experts to serve as colleagues and assistants, and a scientific understanding of neurobiology so slim that it had barely reached its infancy.
This was the job assigned to young Robert Spitzer, then a faculty member at Columbia University. Dr. Spitzer had been tangentially involved in the creation of the DSM-II, and was offered chairmanship of the DSM-III – a job that was at that time considered fairly insignificant. But Dr. Spitzer took it on with relish, and to the surprise of the profession, transformed the DSM into the defining document of modern psychiatry. Robert L. Spitzer died on Christmas Day this past year at the age of 83.
Over the years, Dr. Spitzer has become a household name in psychiatry, a larger-than-life figure. He is thought of by many as the architect of modern psychiatry, but also as a brilliant and brash disrupter who expunged the word “neurosis” from our diagnostic vocabulary, who persuaded organized psychiatry that homosexuality was not a disease, and who laid the groundwork for a system of thinking about mental illness that has guided the field for the past 36 years.
The Bob Spitzer I met was far more approachable than the myth suggests. Ten years ago, I emailed him out of the blue, to request an interview for a book I was writing about the state of psychiatry. To my surprise, not only did he respond positively, but a few weeks later, in December 2007, he had arranged a limo to drive me from La Guardia Airport to his house in a suburb of New York a block away from the Hudson River.
Butterflies in my stomach at the prospect of meeting a living legend, I wheeled my luggage from the limo and knocked on the door, and Dr. Spitzer himself opened it. He was wearing an apron, greeted me with a big smile, and asked me how I liked my eggs. We soon sat down at a kitchen table bathed in sunlight from the windows overlooking his back yard, and we ate cheese omelets and sausages, as we talked about the DSM and his career.
Our conversation was wide ranging, but I’ll recount one interchange because it encapsulates Bob’s relentless honesty and thirst for the truth – both of which were key ingredients in his genius and his legacy.
I had always been curious about how the definition of depression was transformed from the vague “depressive neurosis” in the DSM-II (“This disorder is manifested by an excessive reaction of depression due to an internal conflict or to an identifiable event such as the loss of a love object or cherished possession”) to the precisely defined “major depressive disorder” in the DSM-III.
Bob described the DSM committee process, the long hours of reviewing the literature, and the field trials in which psychiatrists were recruited to test drive the committee’s proposed criteria in their patients. Much of this I had read about, both in the various versions of DSM and in the many articles that Bob and his colleagues had published.
But I had more questions – especially about depression.
“I now understand the process of how you gathered the data,” I said. “But exactly how did you decide on five criteria as being your minimum threshold for depression?”
He took a sip of orange juice and thought for a second. “It was just a consensus. We would ask clinicians and researchers: ‘How many symptoms do you think patients ought to have before you would give the diagnosis of depression?’ And we came up with the arbitrary number of five.”
“But why did you choose five and not four? Or why didn’t you choose six?”
He smiled impishly, looking me directly in the eyes. “Because four just seemed like not enough. And six seemed like too much.”
Even with the benefit of the field trials, Bob pointed out to me, “there is no sharp dividing line where you can confidently say, ‘This is the perfect number of symptoms to make a diagnosis.”
I remember being startled by his honesty. After all, over the years, critics have derided the DSM as being an arbitrary exercise in decision by committee. Bob’s answer, essentially, was, that’s right – but it’s the best we could do given the limitations of our scientific knowledge.
Our patients’ suffering is long, and our understanding of the brain is short. Bob Spitzer provided both psychiatrists and patients with an enduring language that creating meaningful landmarks – a coherent geography of pain. The language has been tweaked over the years, but the underlying classification method has stood the test of time.
Bob Spitzer left us the legacy of the DSM, but he left us so much more. Honesty, generosity, and an unquenchable passion for getting important things right – these are the qualities that I remember and hope to emulate whenever I think of him. That, and his delicious cheese omelets.
Dr. Carlat, a clinical associate professor of psychiatry at Tufts University, Boston, is editor in chief of The Carlat Psychiatry Report, a monthly newsletter on psychopharmacology. He is the author of “The Psychiatric Interview,” (LWW, 2011), and “Unhinged: The Trouble With Psychiatry – A Doctor’s Revelations About a Profession in Crisis,” (Free Press, 2010).
Imagine that it is 1974, and you are given the following task: Create a modern system of cataloguing and organizing the vast and dark chaos of psychological suffering. If done well, it will become the official diagnostic manual for millions of mental health clinicians in the United States and in the world, for decades to come.
Here are your tools: a 1962 spiral bound manual of 150 pages (DSM-II), a small cadre of experts to serve as colleagues and assistants, and a scientific understanding of neurobiology so slim that it had barely reached its infancy.
This was the job assigned to young Robert Spitzer, then a faculty member at Columbia University. Dr. Spitzer had been tangentially involved in the creation of the DSM-II, and was offered chairmanship of the DSM-III – a job that was at that time considered fairly insignificant. But Dr. Spitzer took it on with relish, and to the surprise of the profession, transformed the DSM into the defining document of modern psychiatry. Robert L. Spitzer died on Christmas Day this past year at the age of 83.
Over the years, Dr. Spitzer has become a household name in psychiatry, a larger-than-life figure. He is thought of by many as the architect of modern psychiatry, but also as a brilliant and brash disrupter who expunged the word “neurosis” from our diagnostic vocabulary, who persuaded organized psychiatry that homosexuality was not a disease, and who laid the groundwork for a system of thinking about mental illness that has guided the field for the past 36 years.
The Bob Spitzer I met was far more approachable than the myth suggests. Ten years ago, I emailed him out of the blue, to request an interview for a book I was writing about the state of psychiatry. To my surprise, not only did he respond positively, but a few weeks later, in December 2007, he had arranged a limo to drive me from La Guardia Airport to his house in a suburb of New York a block away from the Hudson River.
Butterflies in my stomach at the prospect of meeting a living legend, I wheeled my luggage from the limo and knocked on the door, and Dr. Spitzer himself opened it. He was wearing an apron, greeted me with a big smile, and asked me how I liked my eggs. We soon sat down at a kitchen table bathed in sunlight from the windows overlooking his back yard, and we ate cheese omelets and sausages, as we talked about the DSM and his career.
Our conversation was wide ranging, but I’ll recount one interchange because it encapsulates Bob’s relentless honesty and thirst for the truth – both of which were key ingredients in his genius and his legacy.
I had always been curious about how the definition of depression was transformed from the vague “depressive neurosis” in the DSM-II (“This disorder is manifested by an excessive reaction of depression due to an internal conflict or to an identifiable event such as the loss of a love object or cherished possession”) to the precisely defined “major depressive disorder” in the DSM-III.
Bob described the DSM committee process, the long hours of reviewing the literature, and the field trials in which psychiatrists were recruited to test drive the committee’s proposed criteria in their patients. Much of this I had read about, both in the various versions of DSM and in the many articles that Bob and his colleagues had published.
But I had more questions – especially about depression.
“I now understand the process of how you gathered the data,” I said. “But exactly how did you decide on five criteria as being your minimum threshold for depression?”
He took a sip of orange juice and thought for a second. “It was just a consensus. We would ask clinicians and researchers: ‘How many symptoms do you think patients ought to have before you would give the diagnosis of depression?’ And we came up with the arbitrary number of five.”
“But why did you choose five and not four? Or why didn’t you choose six?”
He smiled impishly, looking me directly in the eyes. “Because four just seemed like not enough. And six seemed like too much.”
Even with the benefit of the field trials, Bob pointed out to me, “there is no sharp dividing line where you can confidently say, ‘This is the perfect number of symptoms to make a diagnosis.”
I remember being startled by his honesty. After all, over the years, critics have derided the DSM as being an arbitrary exercise in decision by committee. Bob’s answer, essentially, was, that’s right – but it’s the best we could do given the limitations of our scientific knowledge.
Our patients’ suffering is long, and our understanding of the brain is short. Bob Spitzer provided both psychiatrists and patients with an enduring language that creating meaningful landmarks – a coherent geography of pain. The language has been tweaked over the years, but the underlying classification method has stood the test of time.
Bob Spitzer left us the legacy of the DSM, but he left us so much more. Honesty, generosity, and an unquenchable passion for getting important things right – these are the qualities that I remember and hope to emulate whenever I think of him. That, and his delicious cheese omelets.
Dr. Carlat, a clinical associate professor of psychiatry at Tufts University, Boston, is editor in chief of The Carlat Psychiatry Report, a monthly newsletter on psychopharmacology. He is the author of “The Psychiatric Interview,” (LWW, 2011), and “Unhinged: The Trouble With Psychiatry – A Doctor’s Revelations About a Profession in Crisis,” (Free Press, 2010).
Topical Psoriasis Therapies and Unmet Patient Needs: The Importance of Optimizing Methotrexate
Although a wide variety of treatment modalities exist for the management of psoriasis, nontreatment, undertreatment, and treatment dissatisfaction represent key clinical challenges. Careful tailoring of therapeutic regimens to meet individual patient needs and priorities may therefore be critical to improving treatment adherence and clinical outcomes. Importantly, systemic therapies such as methotrexate (MTX) may be particularly useful for individualizing patient treatment regimens and appear to be underutilized components of treatment optimization.
A majority of psoriasis patients have mild to moderate disease and many are treated primarily with topical medications. Although these treatments generally are safe and effective, practical limitations (eg, formulation, ease of application) may affect patients’ treatment adherence and satisfaction even in the context of high efficacy. Systemic therapies, although associated with a distinct set of risks and treatment challenges, may enable patients to overcome many of these limitations, particularly in patients with moderate to severe disease or impaired quality of life as well as those with an inadequate response to or dissatisfaction with topical treatments.
Systemic Treatment Options
Among the systemic treatment options for psoriasis, biologic therapies often are most highly regarded due to their strong efficacy, although traditional systemic therapies such as MTX, cyclosporine, and acitretin remain important treatment options and have an extensive history in the treatment of psoriasis. In addition to typically being required by insurance companies prior to the initiation of biologic therapies, traditional systemic therapies also may be preferred by patients because of the options for oral and subcutaneous administration and their relatively low costs. Furthermore, systemic therapies may be critical in patients for whom biologic therapies are relatively contraindicated, such as those with an increased risk of infection, history of malignancy, or hypersensitivity to any of the product’s ingredients.
Among traditional systemic therapies, MTX is one of the most frequently used psoriasis treatment worldwide and can be highly effective for even severe cases. Importantly, MTX is a valuable component of combination treatments for psoriasis and is frequently coadministered with topical and biologic agents and phototherapy, suggesting that MTX may be a particularly useful option to consider when adjusting a patient’s treatment regimen.
Benefits of Subcutaneous Methotrexate Administration
Methotrexate can be delivered either orally or parenterally, contributing to its compatibility with a wide variety of psoriasis treatment regimens and patient preferences. Administration is predominantly oral in the United States, but parenteral MTX (most commonly delivered subcutaneously) can confer important benefits and is used regularly in countries outside of the United States.
An important advantage of subcutaneous versus oral MTX is greater bioavailability, particularly at higher doses. In studies of healthy volunteers or patients with rheumatoid arthritis, the bioavailability of MTX following oral administration appears to plateau at doses of 15 mg or higher,1 whereas that of subcutaneous MTX appears to increase linearly at a wide range of doses and exceeds that of oral MTX at each dose examined.1,2 A switch from oral to subcutaneous MTX may therefore benefit patients experiencing suboptimal disease control.
Another important benefit of subcutanoues versus oral MTX is the potential for reduced intensity of gastrointestinal adverse events.2,3 In a study of patients with rheumatoid arthritis, those who received subcutaneous MTX reported less severe nausea, vomiting, abdominal pain, and diarrhea than those who received oral MTX,3 which may improve treatment adherence and potentially enable patients to tolerate higher doses. Because gastrointestinal adverse events are a common cause of MTX treatment discontinuation, a switch from oral to subcutaneous MTX may be an important strategy to enable more patients to benefit from this treatment option.
Subcutaneous MTX presents some potential challenges, including patients’ fear of needles and difficulties with drawing and administering an accurate drug dose using a vial, needle, and syringe. However, recent developments in autoinjector technology have produced MTX injection devices that largely mitigate many of these challenges. Methotrexate autoinjectors allow for the accurate administration of prespecified doses, and patients generally find them easy to use.4 Furthermore, MTX autoinjectors have been associated with low levels of adminsitration-site pain (median pain score on a visual analog scale, 1.0/100 mm in one study4), and the concealment of a needle from view may potentially lessen needle phobia.
Role of Subcutaneous Methotrexate in Patient Care
The types of patients expected to benefit most from subcutaneous MTX include those with moderate to severe psoriasis and those who have experienced dissatisfaction with topical medications or phototherapy. The increased bioavailability of subcutaneous MTX as well as the reduced intensity of gastrointestinal adverse events compared with oral MTX may enable patients to achieve a greater clinical response, and the systemic route of administration may improve treatment adherence and patient satisfaction among those who are dissatisfied with topical treatment regimens. Notably, an additional benefit of optimizing MTX treatment may be the potential to prevent or delay progression to biologic therapies, which may be an important goal of both patients and physicians to prevent higher health care costs.
Another principal role of subcutaneous MTX is as a component of combination therapy with topicals or other systemic therapies for either long-term care or periodic treatment of disease flares. Methotrexate is a frequent component of combination therapies, and subcutaneous administration may be preferable for many patients, particularly those who are already accustomed to injectable therapies (eg, biologic agents) and those who regularly visit a physician who can perform the injections (eg, for regular phototherapy treatments). Interestingly, the coadministration of MTX may be especially valuable in the context of biologic therapies, as concomitant MTX is associated with a reduced incidence of antidrug antibodies and may therefore enhance or prolong responses to biologic agents.
Final Thoughts
Because subcutaneous MTX is infrequently used for the treatment of psoriasis in the United States, increased awareness of its unique advantages may provide new opportunities for patients to tailor treatment regimens to meet individual needs and preferences. Treatment optimization across a broad range of patient characteristics may be critical to improving adherence and satisfaction in psoriasis patients and may be considered a major therapeutic goal.
Acknowledgment
Medical writing assistance was provided by Anna Abt, PhD, of ETHOS Health Communications in Newtown, Pennsylvania, with financial support from LEO Pharma.
- Schiff MH, Jaffe JS, Freundlich B. Head-to-head, randomised, crossover study of oral versus subcutaneous methotrexate in patients with rheumatoid arthritis: drug-exposure limitations of oral methotrexate at doses ≥15 mg may be overcome with subcutaneous administration. Ann Rheum Dis. 2014;73:1549-1551.
- Pichlmeier U, Heuer KU. Subcutaneous administration of methotrexate with a prefilled autoinjector pen results in a higher relative bioavailability compared with oral administration of methotrexate. Clin Exp Rheumatol. 2014;32:563-571.
- Rutkowska-Sak L, Rell-Bakalarska M, Lisowska B. Oral vs. subcutaneous low-dose methotrexate treatment in reducing gastrointestinal side effects. Reumatologia. 2009;47:207-211.
- Freundlich B, Kivitz A, Jaffe JS. Nearly pain-free self-administration of subcutaneous methotrexate with an autoinjector: results of a phase 2 clinical trial in patients with rheumatoid arthritis who have functional limitations. J Clin Rheumatol. 2014;20:256-260.
Although a wide variety of treatment modalities exist for the management of psoriasis, nontreatment, undertreatment, and treatment dissatisfaction represent key clinical challenges. Careful tailoring of therapeutic regimens to meet individual patient needs and priorities may therefore be critical to improving treatment adherence and clinical outcomes. Importantly, systemic therapies such as methotrexate (MTX) may be particularly useful for individualizing patient treatment regimens and appear to be underutilized components of treatment optimization.
A majority of psoriasis patients have mild to moderate disease and many are treated primarily with topical medications. Although these treatments generally are safe and effective, practical limitations (eg, formulation, ease of application) may affect patients’ treatment adherence and satisfaction even in the context of high efficacy. Systemic therapies, although associated with a distinct set of risks and treatment challenges, may enable patients to overcome many of these limitations, particularly in patients with moderate to severe disease or impaired quality of life as well as those with an inadequate response to or dissatisfaction with topical treatments.
Systemic Treatment Options
Among the systemic treatment options for psoriasis, biologic therapies often are most highly regarded due to their strong efficacy, although traditional systemic therapies such as MTX, cyclosporine, and acitretin remain important treatment options and have an extensive history in the treatment of psoriasis. In addition to typically being required by insurance companies prior to the initiation of biologic therapies, traditional systemic therapies also may be preferred by patients because of the options for oral and subcutaneous administration and their relatively low costs. Furthermore, systemic therapies may be critical in patients for whom biologic therapies are relatively contraindicated, such as those with an increased risk of infection, history of malignancy, or hypersensitivity to any of the product’s ingredients.
Among traditional systemic therapies, MTX is one of the most frequently used psoriasis treatment worldwide and can be highly effective for even severe cases. Importantly, MTX is a valuable component of combination treatments for psoriasis and is frequently coadministered with topical and biologic agents and phototherapy, suggesting that MTX may be a particularly useful option to consider when adjusting a patient’s treatment regimen.
Benefits of Subcutaneous Methotrexate Administration
Methotrexate can be delivered either orally or parenterally, contributing to its compatibility with a wide variety of psoriasis treatment regimens and patient preferences. Administration is predominantly oral in the United States, but parenteral MTX (most commonly delivered subcutaneously) can confer important benefits and is used regularly in countries outside of the United States.
An important advantage of subcutaneous versus oral MTX is greater bioavailability, particularly at higher doses. In studies of healthy volunteers or patients with rheumatoid arthritis, the bioavailability of MTX following oral administration appears to plateau at doses of 15 mg or higher,1 whereas that of subcutaneous MTX appears to increase linearly at a wide range of doses and exceeds that of oral MTX at each dose examined.1,2 A switch from oral to subcutaneous MTX may therefore benefit patients experiencing suboptimal disease control.
Another important benefit of subcutanoues versus oral MTX is the potential for reduced intensity of gastrointestinal adverse events.2,3 In a study of patients with rheumatoid arthritis, those who received subcutaneous MTX reported less severe nausea, vomiting, abdominal pain, and diarrhea than those who received oral MTX,3 which may improve treatment adherence and potentially enable patients to tolerate higher doses. Because gastrointestinal adverse events are a common cause of MTX treatment discontinuation, a switch from oral to subcutaneous MTX may be an important strategy to enable more patients to benefit from this treatment option.
Subcutaneous MTX presents some potential challenges, including patients’ fear of needles and difficulties with drawing and administering an accurate drug dose using a vial, needle, and syringe. However, recent developments in autoinjector technology have produced MTX injection devices that largely mitigate many of these challenges. Methotrexate autoinjectors allow for the accurate administration of prespecified doses, and patients generally find them easy to use.4 Furthermore, MTX autoinjectors have been associated with low levels of adminsitration-site pain (median pain score on a visual analog scale, 1.0/100 mm in one study4), and the concealment of a needle from view may potentially lessen needle phobia.
Role of Subcutaneous Methotrexate in Patient Care
The types of patients expected to benefit most from subcutaneous MTX include those with moderate to severe psoriasis and those who have experienced dissatisfaction with topical medications or phototherapy. The increased bioavailability of subcutaneous MTX as well as the reduced intensity of gastrointestinal adverse events compared with oral MTX may enable patients to achieve a greater clinical response, and the systemic route of administration may improve treatment adherence and patient satisfaction among those who are dissatisfied with topical treatment regimens. Notably, an additional benefit of optimizing MTX treatment may be the potential to prevent or delay progression to biologic therapies, which may be an important goal of both patients and physicians to prevent higher health care costs.
Another principal role of subcutaneous MTX is as a component of combination therapy with topicals or other systemic therapies for either long-term care or periodic treatment of disease flares. Methotrexate is a frequent component of combination therapies, and subcutaneous administration may be preferable for many patients, particularly those who are already accustomed to injectable therapies (eg, biologic agents) and those who regularly visit a physician who can perform the injections (eg, for regular phototherapy treatments). Interestingly, the coadministration of MTX may be especially valuable in the context of biologic therapies, as concomitant MTX is associated with a reduced incidence of antidrug antibodies and may therefore enhance or prolong responses to biologic agents.
Final Thoughts
Because subcutaneous MTX is infrequently used for the treatment of psoriasis in the United States, increased awareness of its unique advantages may provide new opportunities for patients to tailor treatment regimens to meet individual needs and preferences. Treatment optimization across a broad range of patient characteristics may be critical to improving adherence and satisfaction in psoriasis patients and may be considered a major therapeutic goal.
Acknowledgment
Medical writing assistance was provided by Anna Abt, PhD, of ETHOS Health Communications in Newtown, Pennsylvania, with financial support from LEO Pharma.
Although a wide variety of treatment modalities exist for the management of psoriasis, nontreatment, undertreatment, and treatment dissatisfaction represent key clinical challenges. Careful tailoring of therapeutic regimens to meet individual patient needs and priorities may therefore be critical to improving treatment adherence and clinical outcomes. Importantly, systemic therapies such as methotrexate (MTX) may be particularly useful for individualizing patient treatment regimens and appear to be underutilized components of treatment optimization.
A majority of psoriasis patients have mild to moderate disease and many are treated primarily with topical medications. Although these treatments generally are safe and effective, practical limitations (eg, formulation, ease of application) may affect patients’ treatment adherence and satisfaction even in the context of high efficacy. Systemic therapies, although associated with a distinct set of risks and treatment challenges, may enable patients to overcome many of these limitations, particularly in patients with moderate to severe disease or impaired quality of life as well as those with an inadequate response to or dissatisfaction with topical treatments.
Systemic Treatment Options
Among the systemic treatment options for psoriasis, biologic therapies often are most highly regarded due to their strong efficacy, although traditional systemic therapies such as MTX, cyclosporine, and acitretin remain important treatment options and have an extensive history in the treatment of psoriasis. In addition to typically being required by insurance companies prior to the initiation of biologic therapies, traditional systemic therapies also may be preferred by patients because of the options for oral and subcutaneous administration and their relatively low costs. Furthermore, systemic therapies may be critical in patients for whom biologic therapies are relatively contraindicated, such as those with an increased risk of infection, history of malignancy, or hypersensitivity to any of the product’s ingredients.
Among traditional systemic therapies, MTX is one of the most frequently used psoriasis treatment worldwide and can be highly effective for even severe cases. Importantly, MTX is a valuable component of combination treatments for psoriasis and is frequently coadministered with topical and biologic agents and phototherapy, suggesting that MTX may be a particularly useful option to consider when adjusting a patient’s treatment regimen.
Benefits of Subcutaneous Methotrexate Administration
Methotrexate can be delivered either orally or parenterally, contributing to its compatibility with a wide variety of psoriasis treatment regimens and patient preferences. Administration is predominantly oral in the United States, but parenteral MTX (most commonly delivered subcutaneously) can confer important benefits and is used regularly in countries outside of the United States.
An important advantage of subcutaneous versus oral MTX is greater bioavailability, particularly at higher doses. In studies of healthy volunteers or patients with rheumatoid arthritis, the bioavailability of MTX following oral administration appears to plateau at doses of 15 mg or higher,1 whereas that of subcutaneous MTX appears to increase linearly at a wide range of doses and exceeds that of oral MTX at each dose examined.1,2 A switch from oral to subcutaneous MTX may therefore benefit patients experiencing suboptimal disease control.
Another important benefit of subcutanoues versus oral MTX is the potential for reduced intensity of gastrointestinal adverse events.2,3 In a study of patients with rheumatoid arthritis, those who received subcutaneous MTX reported less severe nausea, vomiting, abdominal pain, and diarrhea than those who received oral MTX,3 which may improve treatment adherence and potentially enable patients to tolerate higher doses. Because gastrointestinal adverse events are a common cause of MTX treatment discontinuation, a switch from oral to subcutaneous MTX may be an important strategy to enable more patients to benefit from this treatment option.
Subcutaneous MTX presents some potential challenges, including patients’ fear of needles and difficulties with drawing and administering an accurate drug dose using a vial, needle, and syringe. However, recent developments in autoinjector technology have produced MTX injection devices that largely mitigate many of these challenges. Methotrexate autoinjectors allow for the accurate administration of prespecified doses, and patients generally find them easy to use.4 Furthermore, MTX autoinjectors have been associated with low levels of adminsitration-site pain (median pain score on a visual analog scale, 1.0/100 mm in one study4), and the concealment of a needle from view may potentially lessen needle phobia.
Role of Subcutaneous Methotrexate in Patient Care
The types of patients expected to benefit most from subcutaneous MTX include those with moderate to severe psoriasis and those who have experienced dissatisfaction with topical medications or phototherapy. The increased bioavailability of subcutaneous MTX as well as the reduced intensity of gastrointestinal adverse events compared with oral MTX may enable patients to achieve a greater clinical response, and the systemic route of administration may improve treatment adherence and patient satisfaction among those who are dissatisfied with topical treatment regimens. Notably, an additional benefit of optimizing MTX treatment may be the potential to prevent or delay progression to biologic therapies, which may be an important goal of both patients and physicians to prevent higher health care costs.
Another principal role of subcutaneous MTX is as a component of combination therapy with topicals or other systemic therapies for either long-term care or periodic treatment of disease flares. Methotrexate is a frequent component of combination therapies, and subcutaneous administration may be preferable for many patients, particularly those who are already accustomed to injectable therapies (eg, biologic agents) and those who regularly visit a physician who can perform the injections (eg, for regular phototherapy treatments). Interestingly, the coadministration of MTX may be especially valuable in the context of biologic therapies, as concomitant MTX is associated with a reduced incidence of antidrug antibodies and may therefore enhance or prolong responses to biologic agents.
Final Thoughts
Because subcutaneous MTX is infrequently used for the treatment of psoriasis in the United States, increased awareness of its unique advantages may provide new opportunities for patients to tailor treatment regimens to meet individual needs and preferences. Treatment optimization across a broad range of patient characteristics may be critical to improving adherence and satisfaction in psoriasis patients and may be considered a major therapeutic goal.
Acknowledgment
Medical writing assistance was provided by Anna Abt, PhD, of ETHOS Health Communications in Newtown, Pennsylvania, with financial support from LEO Pharma.
- Schiff MH, Jaffe JS, Freundlich B. Head-to-head, randomised, crossover study of oral versus subcutaneous methotrexate in patients with rheumatoid arthritis: drug-exposure limitations of oral methotrexate at doses ≥15 mg may be overcome with subcutaneous administration. Ann Rheum Dis. 2014;73:1549-1551.
- Pichlmeier U, Heuer KU. Subcutaneous administration of methotrexate with a prefilled autoinjector pen results in a higher relative bioavailability compared with oral administration of methotrexate. Clin Exp Rheumatol. 2014;32:563-571.
- Rutkowska-Sak L, Rell-Bakalarska M, Lisowska B. Oral vs. subcutaneous low-dose methotrexate treatment in reducing gastrointestinal side effects. Reumatologia. 2009;47:207-211.
- Freundlich B, Kivitz A, Jaffe JS. Nearly pain-free self-administration of subcutaneous methotrexate with an autoinjector: results of a phase 2 clinical trial in patients with rheumatoid arthritis who have functional limitations. J Clin Rheumatol. 2014;20:256-260.
- Schiff MH, Jaffe JS, Freundlich B. Head-to-head, randomised, crossover study of oral versus subcutaneous methotrexate in patients with rheumatoid arthritis: drug-exposure limitations of oral methotrexate at doses ≥15 mg may be overcome with subcutaneous administration. Ann Rheum Dis. 2014;73:1549-1551.
- Pichlmeier U, Heuer KU. Subcutaneous administration of methotrexate with a prefilled autoinjector pen results in a higher relative bioavailability compared with oral administration of methotrexate. Clin Exp Rheumatol. 2014;32:563-571.
- Rutkowska-Sak L, Rell-Bakalarska M, Lisowska B. Oral vs. subcutaneous low-dose methotrexate treatment in reducing gastrointestinal side effects. Reumatologia. 2009;47:207-211.
- Freundlich B, Kivitz A, Jaffe JS. Nearly pain-free self-administration of subcutaneous methotrexate with an autoinjector: results of a phase 2 clinical trial in patients with rheumatoid arthritis who have functional limitations. J Clin Rheumatol. 2014;20:256-260.

Direct-to-Consumer Pharmaceutical Advertising
The American Medical Association (AMA) recently adopted a new policy supporting a ban on direct-to-consumer pharmaceutical advertising (DTCPA) of prescription drugs and medical devices in an effort to make prescription drugs more affordable.1 Dr. Patrice A. Harris, MD, MA, chair-elect of the AMA Board of Trustees, stated that the vote “reflects concerns among physicians about the negative impact of commercially-driven promotions, and the role that marketing costs play in fueling escalating drug prices.” She added, “[it] also inflates demand for new and more expensive drugs, even when these drugs may not be appropriate.”1
The United States and New Zealand are the only 2 countries that allow DTCPA that includes product claims.1 There are 3 basic types of DTCPA, all of which are regulated by the US Food and Drug Administration (FDA): (1) help-seeking advertisements, which provide information about a disease but do not recommend specific drugs or devices; (2) reminder advertisements, which mention specific drugs and provide some information (eg, strength, dosage form, price) but do not mention the indication or make efficacy claims; and (3) product claim advertisements, which are the most common type and mention drug names, indications, and efficacy and/or safety data.2
The FDA’s Division of Drug Marketing, Advertising, and Communications is responsible for regulating DTCPA. The FDA has had authority to approve pharmaceutical products in the United States since 1938 and has regulated labeling and advertising of these products since 1962. In 1969, the FDA issued regulations stipulating that drug advertisements should not be false or misleading and should provide information about risks and benefits, facts about the uses of the drug, and a list of all risks in the product’s labeling. At that time, drug advertisements were directed at health care providers—not the general public—and were mainly found in medical journals and other print sources aimed directly as physicians.
When a number of pharmaceutical manufacturers ran direct-to-consumer advertisements in print and broadcast media, the FDA had to consider how to regulate a new area of advertising. In 1985, the FDA issued a notice claiming regulatory jurisdiction over DTCPA. Believing that DTCPA was beneficial to the general health of consumers, the FDA gradually eased its regulations in recognition of the prohibitive time and expense that the older rules required. Advertisers now only had to list major risks rather than all risks and direct consumers to sources of further information.
In 1980, total spending on DTCPA by industry was $12 million; this figure reached $1.2 billion by 1998, topped out at $5 billion in 2006 and 2007, and dropped to $4.5 billion in 2009.2 Today, most DTCPA spending goes toward television commercials, with the average American viewer watching as many as 9 drug advertisements per day; however, spending on Internet advertising is increasing since the return on investment in that medium is greater.
Is DTCPA beneficial or detrimental to the health of US consumers and, specifically, to patients with skin disease? Unfortunately, there are no quick answers. In a review by Ventola,2 data showed that DTCPA informs, educates, and empowers patients and encourages them to seek medical care as well as to make appointments with their doctors to discuss conditions they had not previously discussed. Data also showed that DTCPA strengthens patients’ relationships with health care providers and improves patient compliance with treatments. Importantly, DTCPA has been shown to reduce underdiagnosis and undertreatment of medical conditions and removes the stigma associated with certain diseases. Finally, DTCPA also has been shown to encourage product competition and lower drug prices.2
In contrast, data also have shown that DTCPA can lead to patient misinformation and may damage the patient-physician relationship.2 Many advertisements may overemphasize a drug’s benefits while downplaying associated risks, while others may promote an unnecessary fear of side effects. These advertisements have been criticized for causing beliefs about diseases in patients that lead to overutilization of drugs and inappropriate prescribing. Some fear DTCPA may promote new drugs before their safety profiles are fully known, which may be particularly true for first-in-class drugs. Finally, DTCPA may increase the cost of drugs in general, not only because of the amount spent on the advertisements themselves, but also because DTCPAs promote copycat drugs that do not offer any increased benefit over older and cheaper medications.
How does all of this relate to dermatology? In the last few years, we have seen the development of drugs (eg, psoriasis treatments) that offer real improvement for patients who only had access to minimally effective therapies in the past. The research pipeline is full of agents for other diseases for which we lack adequate treatments, such as atopic eczema and certain forms of skin cancer. Additionally, for patients with diseases like psoriasis and eczema who may have given up on dermatologists to provide adequate treatments, DTCPAs may give them hope and renewed interest in seeking our help.
It comes as no surprise to dermatologists and their patients that the costs for drugs used to treat dermatologic diseases have skyrocketed. Rosenberg and Rosenberg3 recently evaluated the cost of 19 dermatologic drugs from 2009 to 2015 and noted increases ranging from 60% to 1698%, the majority of which may be passed on directly to our patients.
Ultimately, there are no easy answers. Hopefully, studies evaluating the pros and cons of DTCPAs—specifically for dermatology patients—that can help dermatologists make rational decisions about how to best serve our patients in a cost-efficient manner will be forthcoming. For the time being, it is unlikely that DTCPA will be banned in the United States, as such action would surely lead to claims of unconstitutional infringement on free speech. Nevertheless, increased oversight and more stringent regulations might improve the acceptability of such advertising to those that oppose DTCPA.
- AMA calls for ban on direct to consumer advertising of prescription drugs and medical devices [press release]. Atlanta, GA: American Medical Association; November 17, 2105.
- Ventola CL. Direct-to-consumer pharmaceutical advertising: therapeutic or toxic? P T. 2011;36:669-684.
- Rosenberg ME, Rosenberg SP. Changes in retail prices of prescription dermatologic drugs from 2009 to 2015 [published online November 25, 2015]. JAMA Dermatol. doi: 10.1001/jamadermatol.2015.3897.
The American Medical Association (AMA) recently adopted a new policy supporting a ban on direct-to-consumer pharmaceutical advertising (DTCPA) of prescription drugs and medical devices in an effort to make prescription drugs more affordable.1 Dr. Patrice A. Harris, MD, MA, chair-elect of the AMA Board of Trustees, stated that the vote “reflects concerns among physicians about the negative impact of commercially-driven promotions, and the role that marketing costs play in fueling escalating drug prices.” She added, “[it] also inflates demand for new and more expensive drugs, even when these drugs may not be appropriate.”1
The United States and New Zealand are the only 2 countries that allow DTCPA that includes product claims.1 There are 3 basic types of DTCPA, all of which are regulated by the US Food and Drug Administration (FDA): (1) help-seeking advertisements, which provide information about a disease but do not recommend specific drugs or devices; (2) reminder advertisements, which mention specific drugs and provide some information (eg, strength, dosage form, price) but do not mention the indication or make efficacy claims; and (3) product claim advertisements, which are the most common type and mention drug names, indications, and efficacy and/or safety data.2
The FDA’s Division of Drug Marketing, Advertising, and Communications is responsible for regulating DTCPA. The FDA has had authority to approve pharmaceutical products in the United States since 1938 and has regulated labeling and advertising of these products since 1962. In 1969, the FDA issued regulations stipulating that drug advertisements should not be false or misleading and should provide information about risks and benefits, facts about the uses of the drug, and a list of all risks in the product’s labeling. At that time, drug advertisements were directed at health care providers—not the general public—and were mainly found in medical journals and other print sources aimed directly as physicians.
When a number of pharmaceutical manufacturers ran direct-to-consumer advertisements in print and broadcast media, the FDA had to consider how to regulate a new area of advertising. In 1985, the FDA issued a notice claiming regulatory jurisdiction over DTCPA. Believing that DTCPA was beneficial to the general health of consumers, the FDA gradually eased its regulations in recognition of the prohibitive time and expense that the older rules required. Advertisers now only had to list major risks rather than all risks and direct consumers to sources of further information.
In 1980, total spending on DTCPA by industry was $12 million; this figure reached $1.2 billion by 1998, topped out at $5 billion in 2006 and 2007, and dropped to $4.5 billion in 2009.2 Today, most DTCPA spending goes toward television commercials, with the average American viewer watching as many as 9 drug advertisements per day; however, spending on Internet advertising is increasing since the return on investment in that medium is greater.
Is DTCPA beneficial or detrimental to the health of US consumers and, specifically, to patients with skin disease? Unfortunately, there are no quick answers. In a review by Ventola,2 data showed that DTCPA informs, educates, and empowers patients and encourages them to seek medical care as well as to make appointments with their doctors to discuss conditions they had not previously discussed. Data also showed that DTCPA strengthens patients’ relationships with health care providers and improves patient compliance with treatments. Importantly, DTCPA has been shown to reduce underdiagnosis and undertreatment of medical conditions and removes the stigma associated with certain diseases. Finally, DTCPA also has been shown to encourage product competition and lower drug prices.2
In contrast, data also have shown that DTCPA can lead to patient misinformation and may damage the patient-physician relationship.2 Many advertisements may overemphasize a drug’s benefits while downplaying associated risks, while others may promote an unnecessary fear of side effects. These advertisements have been criticized for causing beliefs about diseases in patients that lead to overutilization of drugs and inappropriate prescribing. Some fear DTCPA may promote new drugs before their safety profiles are fully known, which may be particularly true for first-in-class drugs. Finally, DTCPA may increase the cost of drugs in general, not only because of the amount spent on the advertisements themselves, but also because DTCPAs promote copycat drugs that do not offer any increased benefit over older and cheaper medications.
How does all of this relate to dermatology? In the last few years, we have seen the development of drugs (eg, psoriasis treatments) that offer real improvement for patients who only had access to minimally effective therapies in the past. The research pipeline is full of agents for other diseases for which we lack adequate treatments, such as atopic eczema and certain forms of skin cancer. Additionally, for patients with diseases like psoriasis and eczema who may have given up on dermatologists to provide adequate treatments, DTCPAs may give them hope and renewed interest in seeking our help.
It comes as no surprise to dermatologists and their patients that the costs for drugs used to treat dermatologic diseases have skyrocketed. Rosenberg and Rosenberg3 recently evaluated the cost of 19 dermatologic drugs from 2009 to 2015 and noted increases ranging from 60% to 1698%, the majority of which may be passed on directly to our patients.
Ultimately, there are no easy answers. Hopefully, studies evaluating the pros and cons of DTCPAs—specifically for dermatology patients—that can help dermatologists make rational decisions about how to best serve our patients in a cost-efficient manner will be forthcoming. For the time being, it is unlikely that DTCPA will be banned in the United States, as such action would surely lead to claims of unconstitutional infringement on free speech. Nevertheless, increased oversight and more stringent regulations might improve the acceptability of such advertising to those that oppose DTCPA.
The American Medical Association (AMA) recently adopted a new policy supporting a ban on direct-to-consumer pharmaceutical advertising (DTCPA) of prescription drugs and medical devices in an effort to make prescription drugs more affordable.1 Dr. Patrice A. Harris, MD, MA, chair-elect of the AMA Board of Trustees, stated that the vote “reflects concerns among physicians about the negative impact of commercially-driven promotions, and the role that marketing costs play in fueling escalating drug prices.” She added, “[it] also inflates demand for new and more expensive drugs, even when these drugs may not be appropriate.”1
The United States and New Zealand are the only 2 countries that allow DTCPA that includes product claims.1 There are 3 basic types of DTCPA, all of which are regulated by the US Food and Drug Administration (FDA): (1) help-seeking advertisements, which provide information about a disease but do not recommend specific drugs or devices; (2) reminder advertisements, which mention specific drugs and provide some information (eg, strength, dosage form, price) but do not mention the indication or make efficacy claims; and (3) product claim advertisements, which are the most common type and mention drug names, indications, and efficacy and/or safety data.2
The FDA’s Division of Drug Marketing, Advertising, and Communications is responsible for regulating DTCPA. The FDA has had authority to approve pharmaceutical products in the United States since 1938 and has regulated labeling and advertising of these products since 1962. In 1969, the FDA issued regulations stipulating that drug advertisements should not be false or misleading and should provide information about risks and benefits, facts about the uses of the drug, and a list of all risks in the product’s labeling. At that time, drug advertisements were directed at health care providers—not the general public—and were mainly found in medical journals and other print sources aimed directly as physicians.
When a number of pharmaceutical manufacturers ran direct-to-consumer advertisements in print and broadcast media, the FDA had to consider how to regulate a new area of advertising. In 1985, the FDA issued a notice claiming regulatory jurisdiction over DTCPA. Believing that DTCPA was beneficial to the general health of consumers, the FDA gradually eased its regulations in recognition of the prohibitive time and expense that the older rules required. Advertisers now only had to list major risks rather than all risks and direct consumers to sources of further information.
In 1980, total spending on DTCPA by industry was $12 million; this figure reached $1.2 billion by 1998, topped out at $5 billion in 2006 and 2007, and dropped to $4.5 billion in 2009.2 Today, most DTCPA spending goes toward television commercials, with the average American viewer watching as many as 9 drug advertisements per day; however, spending on Internet advertising is increasing since the return on investment in that medium is greater.
Is DTCPA beneficial or detrimental to the health of US consumers and, specifically, to patients with skin disease? Unfortunately, there are no quick answers. In a review by Ventola,2 data showed that DTCPA informs, educates, and empowers patients and encourages them to seek medical care as well as to make appointments with their doctors to discuss conditions they had not previously discussed. Data also showed that DTCPA strengthens patients’ relationships with health care providers and improves patient compliance with treatments. Importantly, DTCPA has been shown to reduce underdiagnosis and undertreatment of medical conditions and removes the stigma associated with certain diseases. Finally, DTCPA also has been shown to encourage product competition and lower drug prices.2
In contrast, data also have shown that DTCPA can lead to patient misinformation and may damage the patient-physician relationship.2 Many advertisements may overemphasize a drug’s benefits while downplaying associated risks, while others may promote an unnecessary fear of side effects. These advertisements have been criticized for causing beliefs about diseases in patients that lead to overutilization of drugs and inappropriate prescribing. Some fear DTCPA may promote new drugs before their safety profiles are fully known, which may be particularly true for first-in-class drugs. Finally, DTCPA may increase the cost of drugs in general, not only because of the amount spent on the advertisements themselves, but also because DTCPAs promote copycat drugs that do not offer any increased benefit over older and cheaper medications.
How does all of this relate to dermatology? In the last few years, we have seen the development of drugs (eg, psoriasis treatments) that offer real improvement for patients who only had access to minimally effective therapies in the past. The research pipeline is full of agents for other diseases for which we lack adequate treatments, such as atopic eczema and certain forms of skin cancer. Additionally, for patients with diseases like psoriasis and eczema who may have given up on dermatologists to provide adequate treatments, DTCPAs may give them hope and renewed interest in seeking our help.
It comes as no surprise to dermatologists and their patients that the costs for drugs used to treat dermatologic diseases have skyrocketed. Rosenberg and Rosenberg3 recently evaluated the cost of 19 dermatologic drugs from 2009 to 2015 and noted increases ranging from 60% to 1698%, the majority of which may be passed on directly to our patients.
Ultimately, there are no easy answers. Hopefully, studies evaluating the pros and cons of DTCPAs—specifically for dermatology patients—that can help dermatologists make rational decisions about how to best serve our patients in a cost-efficient manner will be forthcoming. For the time being, it is unlikely that DTCPA will be banned in the United States, as such action would surely lead to claims of unconstitutional infringement on free speech. Nevertheless, increased oversight and more stringent regulations might improve the acceptability of such advertising to those that oppose DTCPA.
- AMA calls for ban on direct to consumer advertising of prescription drugs and medical devices [press release]. Atlanta, GA: American Medical Association; November 17, 2105.
- Ventola CL. Direct-to-consumer pharmaceutical advertising: therapeutic or toxic? P T. 2011;36:669-684.
- Rosenberg ME, Rosenberg SP. Changes in retail prices of prescription dermatologic drugs from 2009 to 2015 [published online November 25, 2015]. JAMA Dermatol. doi: 10.1001/jamadermatol.2015.3897.
- AMA calls for ban on direct to consumer advertising of prescription drugs and medical devices [press release]. Atlanta, GA: American Medical Association; November 17, 2105.
- Ventola CL. Direct-to-consumer pharmaceutical advertising: therapeutic or toxic? P T. 2011;36:669-684.
- Rosenberg ME, Rosenberg SP. Changes in retail prices of prescription dermatologic drugs from 2009 to 2015 [published online November 25, 2015]. JAMA Dermatol. doi: 10.1001/jamadermatol.2015.3897.

50 years of ob.gyn.: Embracing the ‘voice of the woman’
I hadn’t originally planned to be an obstetrician-gynecologist; in fact, I trained as an internist for 2 years. But as I became more exposed to the real-life experience of medical care, I realized that ob.gyn. would allow me to take care of women in all facets of their lives, from family planning to childbirth to endocrine problems and even depression.
Having joined the American College of Obstetricians and Gynecologists in 1965, my tenure as an ob.gyn. has spanned almost the exact length of this 50th anniversary retrospective of Ob.Gyn.News. But in my experience, those early days of my practice were actually the turning point for our specialty.
I’m an observer, not a historian. But I can’t imagine that any other specialty was more impacted by societal change in the mid-1960s than ours.

For one thing, when I was training, we were an overwhelmingly male group of residents who were learning about how to take care of women. Our commitment was not in question, but our ability to truly connect with women was certainly underdeveloped.
I’m gratified now to see that the demographics of ob.gyn. have changed, because they should. Without disrespecting my male ob.gyn. brethren, I was pleased to see that more than 80% of ob.gyn. trainees are now women. Importantly, many of them are learning now from female ob.gyns. This foretells a future in which connections between patient and physician are as strong as they should be.
Moreover, ob.gyn. trainees today have the highest proportions of African American and Hispanic trainees compared with any other specialty. We are doing a better job of representing, within our ranks, the women whom we treat. This continues to bolster our relationships, and in no other field is a trusting, intimate relationship as important as in ours.
Of course, the mid-1960s also heralded dramatic changes within reproductive health. Women were beginning to dip their toes into being able to control their own fertility and, in so doing, to prevent pregnancy. This also gave us the opportunity to focus on a woman’s greater well-being, helping her to address her own health before becoming pregnant. It pivoted the role of the ob.gyn. and charted us on a course to being, for many women, their primary point of care. And it gave women educational, professional, and economic opportunities the likes of which had never existed before.
Outside of fertility planning, we also began to make inroads in obstetric care – and to make some mistakes. The 1960s heralded some developments that we still embrace, but we also began a path toward dependence on technology and overinvasive care that we are trying to step away from today.
And, we had difficult conversations then that we have now. The more things change, the more they stay the same.
One of the most exciting, and essential, changes that I have seen since I began my career is the voice of the woman in ob.gyn. care. We speak with our patients. We screen them for depression and for intimate partner violence. We discuss their lives and whether they are using the birth control that is best for them. We try to reflect their own preferences in our approach to their labor and delivery. We missed an opportunity to do this in the past, to discuss a woman’s social history. We know now that there is more to a woman’s well-being than whether she smokes and drinks.
It makes sense that our specialty has changed, because we are the only specialty dedicated to women, and the last 50 years have brought about intense societal change for women.
We still have further to go. We can be slow to evolve, and we constantly face challenges that other specialties don’t confront. But I believe that the same dedication to women that inspired me to go into ob.gyn. 50 years ago is the same inspiration that is leading today’s trainees to do the same.
Dr. Pion is a clinical professor at the UCLA School of Medicine. He has served on the faculty of the University of Washington and the University of Hawaii, and worked for more than 25 years in the development and production of TV and radio programming on health care. He is a fellow of the American College of Obstetricians and Gynecologists.
I hadn’t originally planned to be an obstetrician-gynecologist; in fact, I trained as an internist for 2 years. But as I became more exposed to the real-life experience of medical care, I realized that ob.gyn. would allow me to take care of women in all facets of their lives, from family planning to childbirth to endocrine problems and even depression.
Having joined the American College of Obstetricians and Gynecologists in 1965, my tenure as an ob.gyn. has spanned almost the exact length of this 50th anniversary retrospective of Ob.Gyn.News. But in my experience, those early days of my practice were actually the turning point for our specialty.
I’m an observer, not a historian. But I can’t imagine that any other specialty was more impacted by societal change in the mid-1960s than ours.
For one thing, when I was training, we were an overwhelmingly male group of residents who were learning about how to take care of women. Our commitment was not in question, but our ability to truly connect with women was certainly underdeveloped.
I’m gratified now to see that the demographics of ob.gyn. have changed, because they should. Without disrespecting my male ob.gyn. brethren, I was pleased to see that more than 80% of ob.gyn. trainees are now women. Importantly, many of them are learning now from female ob.gyns. This foretells a future in which connections between patient and physician are as strong as they should be.
Moreover, ob.gyn. trainees today have the highest proportions of African American and Hispanic trainees compared with any other specialty. We are doing a better job of representing, within our ranks, the women whom we treat. This continues to bolster our relationships, and in no other field is a trusting, intimate relationship as important as in ours.
Of course, the mid-1960s also heralded dramatic changes within reproductive health. Women were beginning to dip their toes into being able to control their own fertility and, in so doing, to prevent pregnancy. This also gave us the opportunity to focus on a woman’s greater well-being, helping her to address her own health before becoming pregnant. It pivoted the role of the ob.gyn. and charted us on a course to being, for many women, their primary point of care. And it gave women educational, professional, and economic opportunities the likes of which had never existed before.
Outside of fertility planning, we also began to make inroads in obstetric care – and to make some mistakes. The 1960s heralded some developments that we still embrace, but we also began a path toward dependence on technology and overinvasive care that we are trying to step away from today.
And, we had difficult conversations then that we have now. The more things change, the more they stay the same.
One of the most exciting, and essential, changes that I have seen since I began my career is the voice of the woman in ob.gyn. care. We speak with our patients. We screen them for depression and for intimate partner violence. We discuss their lives and whether they are using the birth control that is best for them. We try to reflect their own preferences in our approach to their labor and delivery. We missed an opportunity to do this in the past, to discuss a woman’s social history. We know now that there is more to a woman’s well-being than whether she smokes and drinks.
It makes sense that our specialty has changed, because we are the only specialty dedicated to women, and the last 50 years have brought about intense societal change for women.
We still have further to go. We can be slow to evolve, and we constantly face challenges that other specialties don’t confront. But I believe that the same dedication to women that inspired me to go into ob.gyn. 50 years ago is the same inspiration that is leading today’s trainees to do the same.
Dr. Pion is a clinical professor at the UCLA School of Medicine. He has served on the faculty of the University of Washington and the University of Hawaii, and worked for more than 25 years in the development and production of TV and radio programming on health care. He is a fellow of the American College of Obstetricians and Gynecologists.
I hadn’t originally planned to be an obstetrician-gynecologist; in fact, I trained as an internist for 2 years. But as I became more exposed to the real-life experience of medical care, I realized that ob.gyn. would allow me to take care of women in all facets of their lives, from family planning to childbirth to endocrine problems and even depression.
Having joined the American College of Obstetricians and Gynecologists in 1965, my tenure as an ob.gyn. has spanned almost the exact length of this 50th anniversary retrospective of Ob.Gyn.News. But in my experience, those early days of my practice were actually the turning point for our specialty.
I’m an observer, not a historian. But I can’t imagine that any other specialty was more impacted by societal change in the mid-1960s than ours.
For one thing, when I was training, we were an overwhelmingly male group of residents who were learning about how to take care of women. Our commitment was not in question, but our ability to truly connect with women was certainly underdeveloped.
I’m gratified now to see that the demographics of ob.gyn. have changed, because they should. Without disrespecting my male ob.gyn. brethren, I was pleased to see that more than 80% of ob.gyn. trainees are now women. Importantly, many of them are learning now from female ob.gyns. This foretells a future in which connections between patient and physician are as strong as they should be.
Moreover, ob.gyn. trainees today have the highest proportions of African American and Hispanic trainees compared with any other specialty. We are doing a better job of representing, within our ranks, the women whom we treat. This continues to bolster our relationships, and in no other field is a trusting, intimate relationship as important as in ours.
Of course, the mid-1960s also heralded dramatic changes within reproductive health. Women were beginning to dip their toes into being able to control their own fertility and, in so doing, to prevent pregnancy. This also gave us the opportunity to focus on a woman’s greater well-being, helping her to address her own health before becoming pregnant. It pivoted the role of the ob.gyn. and charted us on a course to being, for many women, their primary point of care. And it gave women educational, professional, and economic opportunities the likes of which had never existed before.
Outside of fertility planning, we also began to make inroads in obstetric care – and to make some mistakes. The 1960s heralded some developments that we still embrace, but we also began a path toward dependence on technology and overinvasive care that we are trying to step away from today.
And, we had difficult conversations then that we have now. The more things change, the more they stay the same.
One of the most exciting, and essential, changes that I have seen since I began my career is the voice of the woman in ob.gyn. care. We speak with our patients. We screen them for depression and for intimate partner violence. We discuss their lives and whether they are using the birth control that is best for them. We try to reflect their own preferences in our approach to their labor and delivery. We missed an opportunity to do this in the past, to discuss a woman’s social history. We know now that there is more to a woman’s well-being than whether she smokes and drinks.
It makes sense that our specialty has changed, because we are the only specialty dedicated to women, and the last 50 years have brought about intense societal change for women.
We still have further to go. We can be slow to evolve, and we constantly face challenges that other specialties don’t confront. But I believe that the same dedication to women that inspired me to go into ob.gyn. 50 years ago is the same inspiration that is leading today’s trainees to do the same.
Dr. Pion is a clinical professor at the UCLA School of Medicine. He has served on the faculty of the University of Washington and the University of Hawaii, and worked for more than 25 years in the development and production of TV and radio programming on health care. He is a fellow of the American College of Obstetricians and Gynecologists.

Royal jelly
Used for centuries by humans for its health-promoting qualities, royal jelly is a yellowish, viscous secretion from the hypopharyngeal and mandibular glands of worker bees that nourishes bee larvae of all kinds (i.e., drones, workers, queens) after which it becomes the exclusive nourishment for queens throughout their development.1-3 A wide range of biologic activity has been attributed to royal jelly, including antitumor, antibacterial, anti-inflammatory, antioxidant, collagen production-promoting, immunomodulatory, and wound healing.3-8 Royal jelly is used in cosmetics, health tonics (particularly in Asia), dietary supplements, and beverages.2,9
Produced from pollen, royal jelly contains water, proteins (82%-90% of which are known as the major royal jelly proteins, with five primary members), lipids – including its primary unsaturated fatty acid, 10-hydroxy-2-decenoic acid (10-HDA) – sugars, carbohydrates, free amino acids, vitamins, and minerals.4,7,10 Many of the benefits to human health linked to royal jelly can be partly attributed to the activity of its lipids, particularly 10-HDA, which render the royal jelly emulsion highly acidic and impart antimicrobial properties.10 These and other constituents of royal jelly operate in ways that are thought to yield broad protection against skin aging and cancer development, modulation of the immune system, induction of neurogenesis, and alleviation of menopausal symptoms.1 This column will focus on recent studies pertaining to the topical use of royal jelly.

Wound healing
In 2008, Abdelatif et al. conducted a pilot study to determine the safety and effectiveness of a then-new ointment combining royal jelly and panthenol (Pedyphar) in 60 patients with limb-threatening diabetic foot infections. After 9 weeks of treatment and through 6 months of follow-up, 96% of subjects with full-thickness skin ulcers (Wagner grades 1 and 2) or deep tissue infection and suspected osteomyelitis (grade 3) responded well, with all grade 1 and 2 ulcers healing and 92% of grade 3 ulcers healing. All patients with gangrenous lesions (grades 4 and 5) healed after surgical excision, debridement, and conservative treatment with the royal jelly/panthenol product. The researchers called for more double-blind, randomized controlled studies to confirm their promising findings of the safety and efficacy of the royal jelly/panthenol combination.11
Two years later, Kim et al. treated freshly scratched normal human dermal fibroblasts with different concentrations of royal jelly (0.1 mg/mL, 1.0 mg/mL, or 5 mg/mL) for up to 48 hours. Fibroblast migration was found to have peaked at 24 hours after wound induction, with royal jelly significantly and dose-dependently accelerating the migration at the 8-hour mark. Royal jelly also influenced several fibroblast lipids involved in the wound healing process, with a decrease in cholesterol level and an increase in sphinganines.12
A small study with eight subjects was done in 2011 by Siavash et al. to evaluate the efficacy of topically applied royal jelly for diabetic foot ulcers. Seven of the eight ulcers treated healed, with a mean healing time of 41 days. The eighth ulcer improved, diminishing significantly in size. The researchers concluded that a royal jelly dressing is an effective alternative for treatment of diabetic foot ulcers.13 However, the same team conducted a double-blind, placebo-controlled clinical trial of topical royal jelly on diabetic foot ulcers in 25 patients (6 females, 19 males) and found no significant differences between 5% sterile topical royal jelly or placebo.6
Collagen production

A decade ago, Koya-Miyata et al. showed that royal jelly promotes collagen synthesis by skin fibroblasts in the presence of ascorbic acid-2-O-alpha-glucoside. They also showed that its primary fatty acid constituent, 10-HDA, facilitates the collagen production by fibroblasts treated with ascorbic acid-2-O-alpha-glucoside through activation of transforming growth factor-beta 1 production.5
Photoprotection
Park et al. measured the 10-HDA content of royal jelly in 2011 and studied its effects on UVB-induced skin photoaging in normal human dermal fibroblasts. The introduction of royal jelly (0.211% 10-HDA) promoted the production of procollagen type I and transforming growth factor (TGF)-beta-1 without affecting matrix metalloproteinase (MMP)-1 levels. The investigators concluded that the impact of royal jelly on collagen production positioned the bee product as a potential photoprotectant against UVB-induced photoaging.14 The next year, Park et al. observed that the production of type I collagen in the dorsal skin of ovariectomized Sprague-Dawley rats was enhanced by the dietary supplementation of 1% royal jelly extract. Although MMP-1 levels were unaffected, the investigators speculated that the effects on collagen synthesis alone were sufficient for royal jelly to provide anti-aging activity.4
In 2013, Zheng et al. found that 10-HDA significantly protected fibroblasts from UVA-induced cytotoxicity, reactive oxygen species, and cellular senescence. They also noted that 10-HDA inhibited the UVA-generated expression of MMP-1 and -3, and stimulated collagen production. Treatment with 10-HDA also reduced the activation of the c-Jun N-terminal kinase (JNK) and p38 mitogen-activated protein kinase (MAPK) pathways. The researchers concluded that this royal jelly fatty acid appears to be a promising agent for the prevention and treatment of cutaneous photoaging.8
Skin whitening
In 2011, Han et al. reported that royal jelly dose-dependently inhibited melanin biosynthesis in the B16F1 mouse melanocyte cell line by reducing tyrosinase activity. Royal jelly also lowered mRNA levels of tyrosinase. The investigators concluded that royal jelly may be a viable option in the skin-lightening arsenal.3
Safety
There are some reports of contact dermatitis from the use of topical royal jelly.15 Far more significant, while rare, adverse reactions have been linked to oral use of royal jelly, including acute asthma, anaphylaxis, and even death.2,16,17
Conclusion
Royal jelly is one of several bee products found to have beneficial health effects in humans. Various dermatologic applications of royal jelly have been employed in recent decades. More research is necessary, though, to determine just how useful this bee product may be for a range of cutaneous conditions.
References
1. J Med Food. 2013;16(2):96-102.
2. Biosci Biotechnol Biochem. 2013;77(4):789-95.
3. Am J Chin Med. 2011;39(6):1253-60.
4. J Med Food. 2012;15(6):568-75.
5. Biosci Biotechnol Biochem. 2004 Apr;68(4):767-73.
6. Int Wound J. 2015;12(2):137-42.
7. J Food Sci. 2008 Nov;73(9):R117-24.
8. J Eur Acad Dermatol. Venereol. 2013;27(10):1269-77.
9. Pharmacogn Mag. 2013;9(33):9-13.
11. J Wound Care. 2008;17(3):108-10.
12. Nutr Res Pract. 2010;4(5):362-8.
13. J Res Med Sci. 2011;16(7):904-9.
14. J Med Food. 2011;14(9):899-906.
15. Contact Dermatitis. 1983;9(6):452-5.
16. Trop Biomed. 2008;25(3):243-51.
17. J Dermatol. 2011;38(11):1079-81.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook, “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). She has contributed to the Cosmeceutical Critique column in Dermatology News since January 2001. Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera Biopharmaceuticals, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever.
Used for centuries by humans for its health-promoting qualities, royal jelly is a yellowish, viscous secretion from the hypopharyngeal and mandibular glands of worker bees that nourishes bee larvae of all kinds (i.e., drones, workers, queens) after which it becomes the exclusive nourishment for queens throughout their development.1-3 A wide range of biologic activity has been attributed to royal jelly, including antitumor, antibacterial, anti-inflammatory, antioxidant, collagen production-promoting, immunomodulatory, and wound healing.3-8 Royal jelly is used in cosmetics, health tonics (particularly in Asia), dietary supplements, and beverages.2,9
Produced from pollen, royal jelly contains water, proteins (82%-90% of which are known as the major royal jelly proteins, with five primary members), lipids – including its primary unsaturated fatty acid, 10-hydroxy-2-decenoic acid (10-HDA) – sugars, carbohydrates, free amino acids, vitamins, and minerals.4,7,10 Many of the benefits to human health linked to royal jelly can be partly attributed to the activity of its lipids, particularly 10-HDA, which render the royal jelly emulsion highly acidic and impart antimicrobial properties.10 These and other constituents of royal jelly operate in ways that are thought to yield broad protection against skin aging and cancer development, modulation of the immune system, induction of neurogenesis, and alleviation of menopausal symptoms.1 This column will focus on recent studies pertaining to the topical use of royal jelly.
Wound healing
In 2008, Abdelatif et al. conducted a pilot study to determine the safety and effectiveness of a then-new ointment combining royal jelly and panthenol (Pedyphar) in 60 patients with limb-threatening diabetic foot infections. After 9 weeks of treatment and through 6 months of follow-up, 96% of subjects with full-thickness skin ulcers (Wagner grades 1 and 2) or deep tissue infection and suspected osteomyelitis (grade 3) responded well, with all grade 1 and 2 ulcers healing and 92% of grade 3 ulcers healing. All patients with gangrenous lesions (grades 4 and 5) healed after surgical excision, debridement, and conservative treatment with the royal jelly/panthenol product. The researchers called for more double-blind, randomized controlled studies to confirm their promising findings of the safety and efficacy of the royal jelly/panthenol combination.11
Two years later, Kim et al. treated freshly scratched normal human dermal fibroblasts with different concentrations of royal jelly (0.1 mg/mL, 1.0 mg/mL, or 5 mg/mL) for up to 48 hours. Fibroblast migration was found to have peaked at 24 hours after wound induction, with royal jelly significantly and dose-dependently accelerating the migration at the 8-hour mark. Royal jelly also influenced several fibroblast lipids involved in the wound healing process, with a decrease in cholesterol level and an increase in sphinganines.12
A small study with eight subjects was done in 2011 by Siavash et al. to evaluate the efficacy of topically applied royal jelly for diabetic foot ulcers. Seven of the eight ulcers treated healed, with a mean healing time of 41 days. The eighth ulcer improved, diminishing significantly in size. The researchers concluded that a royal jelly dressing is an effective alternative for treatment of diabetic foot ulcers.13 However, the same team conducted a double-blind, placebo-controlled clinical trial of topical royal jelly on diabetic foot ulcers in 25 patients (6 females, 19 males) and found no significant differences between 5% sterile topical royal jelly or placebo.6
Collagen production
A decade ago, Koya-Miyata et al. showed that royal jelly promotes collagen synthesis by skin fibroblasts in the presence of ascorbic acid-2-O-alpha-glucoside. They also showed that its primary fatty acid constituent, 10-HDA, facilitates the collagen production by fibroblasts treated with ascorbic acid-2-O-alpha-glucoside through activation of transforming growth factor-beta 1 production.5
Photoprotection
Park et al. measured the 10-HDA content of royal jelly in 2011 and studied its effects on UVB-induced skin photoaging in normal human dermal fibroblasts. The introduction of royal jelly (0.211% 10-HDA) promoted the production of procollagen type I and transforming growth factor (TGF)-beta-1 without affecting matrix metalloproteinase (MMP)-1 levels. The investigators concluded that the impact of royal jelly on collagen production positioned the bee product as a potential photoprotectant against UVB-induced photoaging.14 The next year, Park et al. observed that the production of type I collagen in the dorsal skin of ovariectomized Sprague-Dawley rats was enhanced by the dietary supplementation of 1% royal jelly extract. Although MMP-1 levels were unaffected, the investigators speculated that the effects on collagen synthesis alone were sufficient for royal jelly to provide anti-aging activity.4
In 2013, Zheng et al. found that 10-HDA significantly protected fibroblasts from UVA-induced cytotoxicity, reactive oxygen species, and cellular senescence. They also noted that 10-HDA inhibited the UVA-generated expression of MMP-1 and -3, and stimulated collagen production. Treatment with 10-HDA also reduced the activation of the c-Jun N-terminal kinase (JNK) and p38 mitogen-activated protein kinase (MAPK) pathways. The researchers concluded that this royal jelly fatty acid appears to be a promising agent for the prevention and treatment of cutaneous photoaging.8
Skin whitening
In 2011, Han et al. reported that royal jelly dose-dependently inhibited melanin biosynthesis in the B16F1 mouse melanocyte cell line by reducing tyrosinase activity. Royal jelly also lowered mRNA levels of tyrosinase. The investigators concluded that royal jelly may be a viable option in the skin-lightening arsenal.3
Safety
There are some reports of contact dermatitis from the use of topical royal jelly.15 Far more significant, while rare, adverse reactions have been linked to oral use of royal jelly, including acute asthma, anaphylaxis, and even death.2,16,17
Conclusion
Royal jelly is one of several bee products found to have beneficial health effects in humans. Various dermatologic applications of royal jelly have been employed in recent decades. More research is necessary, though, to determine just how useful this bee product may be for a range of cutaneous conditions.
References
1. J Med Food. 2013;16(2):96-102.
2. Biosci Biotechnol Biochem. 2013;77(4):789-95.
3. Am J Chin Med. 2011;39(6):1253-60.
4. J Med Food. 2012;15(6):568-75.
5. Biosci Biotechnol Biochem. 2004 Apr;68(4):767-73.
6. Int Wound J. 2015;12(2):137-42.
7. J Food Sci. 2008 Nov;73(9):R117-24.
8. J Eur Acad Dermatol. Venereol. 2013;27(10):1269-77.
9. Pharmacogn Mag. 2013;9(33):9-13.
11. J Wound Care. 2008;17(3):108-10.
12. Nutr Res Pract. 2010;4(5):362-8.
13. J Res Med Sci. 2011;16(7):904-9.
14. J Med Food. 2011;14(9):899-906.
15. Contact Dermatitis. 1983;9(6):452-5.
16. Trop Biomed. 2008;25(3):243-51.
17. J Dermatol. 2011;38(11):1079-81.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook, “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). She has contributed to the Cosmeceutical Critique column in Dermatology News since January 2001. Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera Biopharmaceuticals, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever.
Used for centuries by humans for its health-promoting qualities, royal jelly is a yellowish, viscous secretion from the hypopharyngeal and mandibular glands of worker bees that nourishes bee larvae of all kinds (i.e., drones, workers, queens) after which it becomes the exclusive nourishment for queens throughout their development.1-3 A wide range of biologic activity has been attributed to royal jelly, including antitumor, antibacterial, anti-inflammatory, antioxidant, collagen production-promoting, immunomodulatory, and wound healing.3-8 Royal jelly is used in cosmetics, health tonics (particularly in Asia), dietary supplements, and beverages.2,9
Produced from pollen, royal jelly contains water, proteins (82%-90% of which are known as the major royal jelly proteins, with five primary members), lipids – including its primary unsaturated fatty acid, 10-hydroxy-2-decenoic acid (10-HDA) – sugars, carbohydrates, free amino acids, vitamins, and minerals.4,7,10 Many of the benefits to human health linked to royal jelly can be partly attributed to the activity of its lipids, particularly 10-HDA, which render the royal jelly emulsion highly acidic and impart antimicrobial properties.10 These and other constituents of royal jelly operate in ways that are thought to yield broad protection against skin aging and cancer development, modulation of the immune system, induction of neurogenesis, and alleviation of menopausal symptoms.1 This column will focus on recent studies pertaining to the topical use of royal jelly.
Wound healing
In 2008, Abdelatif et al. conducted a pilot study to determine the safety and effectiveness of a then-new ointment combining royal jelly and panthenol (Pedyphar) in 60 patients with limb-threatening diabetic foot infections. After 9 weeks of treatment and through 6 months of follow-up, 96% of subjects with full-thickness skin ulcers (Wagner grades 1 and 2) or deep tissue infection and suspected osteomyelitis (grade 3) responded well, with all grade 1 and 2 ulcers healing and 92% of grade 3 ulcers healing. All patients with gangrenous lesions (grades 4 and 5) healed after surgical excision, debridement, and conservative treatment with the royal jelly/panthenol product. The researchers called for more double-blind, randomized controlled studies to confirm their promising findings of the safety and efficacy of the royal jelly/panthenol combination.11
Two years later, Kim et al. treated freshly scratched normal human dermal fibroblasts with different concentrations of royal jelly (0.1 mg/mL, 1.0 mg/mL, or 5 mg/mL) for up to 48 hours. Fibroblast migration was found to have peaked at 24 hours after wound induction, with royal jelly significantly and dose-dependently accelerating the migration at the 8-hour mark. Royal jelly also influenced several fibroblast lipids involved in the wound healing process, with a decrease in cholesterol level and an increase in sphinganines.12
A small study with eight subjects was done in 2011 by Siavash et al. to evaluate the efficacy of topically applied royal jelly for diabetic foot ulcers. Seven of the eight ulcers treated healed, with a mean healing time of 41 days. The eighth ulcer improved, diminishing significantly in size. The researchers concluded that a royal jelly dressing is an effective alternative for treatment of diabetic foot ulcers.13 However, the same team conducted a double-blind, placebo-controlled clinical trial of topical royal jelly on diabetic foot ulcers in 25 patients (6 females, 19 males) and found no significant differences between 5% sterile topical royal jelly or placebo.6
Collagen production
A decade ago, Koya-Miyata et al. showed that royal jelly promotes collagen synthesis by skin fibroblasts in the presence of ascorbic acid-2-O-alpha-glucoside. They also showed that its primary fatty acid constituent, 10-HDA, facilitates the collagen production by fibroblasts treated with ascorbic acid-2-O-alpha-glucoside through activation of transforming growth factor-beta 1 production.5
Photoprotection
Park et al. measured the 10-HDA content of royal jelly in 2011 and studied its effects on UVB-induced skin photoaging in normal human dermal fibroblasts. The introduction of royal jelly (0.211% 10-HDA) promoted the production of procollagen type I and transforming growth factor (TGF)-beta-1 without affecting matrix metalloproteinase (MMP)-1 levels. The investigators concluded that the impact of royal jelly on collagen production positioned the bee product as a potential photoprotectant against UVB-induced photoaging.14 The next year, Park et al. observed that the production of type I collagen in the dorsal skin of ovariectomized Sprague-Dawley rats was enhanced by the dietary supplementation of 1% royal jelly extract. Although MMP-1 levels were unaffected, the investigators speculated that the effects on collagen synthesis alone were sufficient for royal jelly to provide anti-aging activity.4
In 2013, Zheng et al. found that 10-HDA significantly protected fibroblasts from UVA-induced cytotoxicity, reactive oxygen species, and cellular senescence. They also noted that 10-HDA inhibited the UVA-generated expression of MMP-1 and -3, and stimulated collagen production. Treatment with 10-HDA also reduced the activation of the c-Jun N-terminal kinase (JNK) and p38 mitogen-activated protein kinase (MAPK) pathways. The researchers concluded that this royal jelly fatty acid appears to be a promising agent for the prevention and treatment of cutaneous photoaging.8
Skin whitening
In 2011, Han et al. reported that royal jelly dose-dependently inhibited melanin biosynthesis in the B16F1 mouse melanocyte cell line by reducing tyrosinase activity. Royal jelly also lowered mRNA levels of tyrosinase. The investigators concluded that royal jelly may be a viable option in the skin-lightening arsenal.3
Safety
There are some reports of contact dermatitis from the use of topical royal jelly.15 Far more significant, while rare, adverse reactions have been linked to oral use of royal jelly, including acute asthma, anaphylaxis, and even death.2,16,17
Conclusion
Royal jelly is one of several bee products found to have beneficial health effects in humans. Various dermatologic applications of royal jelly have been employed in recent decades. More research is necessary, though, to determine just how useful this bee product may be for a range of cutaneous conditions.
References
1. J Med Food. 2013;16(2):96-102.
2. Biosci Biotechnol Biochem. 2013;77(4):789-95.
3. Am J Chin Med. 2011;39(6):1253-60.
4. J Med Food. 2012;15(6):568-75.
5. Biosci Biotechnol Biochem. 2004 Apr;68(4):767-73.
6. Int Wound J. 2015;12(2):137-42.
7. J Food Sci. 2008 Nov;73(9):R117-24.
8. J Eur Acad Dermatol. Venereol. 2013;27(10):1269-77.
9. Pharmacogn Mag. 2013;9(33):9-13.
11. J Wound Care. 2008;17(3):108-10.
12. Nutr Res Pract. 2010;4(5):362-8.
13. J Res Med Sci. 2011;16(7):904-9.
14. J Med Food. 2011;14(9):899-906.
15. Contact Dermatitis. 1983;9(6):452-5.
16. Trop Biomed. 2008;25(3):243-51.
17. J Dermatol. 2011;38(11):1079-81.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook, “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). She has contributed to the Cosmeceutical Critique column in Dermatology News since January 2001. Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera Biopharmaceuticals, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever.

Definitive Fixation of Hand and Wrist Fractures in the Emergency Department
A mentor—now in his 60s—related his experiences as a resident. On call as a second-year resident, he would often be alone at a busy trauma center with no backup. When a case came in, he would quickly read about it in the library, then manage it in the emergency department (ED) if possible, or, if necessary, take the patient to the operating room (OR).
In the era of improved patient care, increased supervision, and decreased autonomy, this is not the reality anymore.1 In theory, more reliable patient care is the result; however, the pendulum may have swung too far.
There are a number of injuries that are amenable to definitive fixation in the ED, but not as limited an array of injuries as we have perhaps grown accustomed to. Hand injuries are among the most common orthopedic injuries seen in the ED, with fractures of the metacarpals and phalanges constituting nearly one-half of all hand injuries.2 The authors recently attended an excellent instructional course lecture on “The Lost and Found Art of Percutaneous Pinning in the Hand and Wrist” at the annual conference of the American Academy of Orthopaedic Surgeons.3 The presenters itemized a comprehensive list of fractures and simple dislocations of the hand, which could be simply, safely, effectively, and definitively managed through percutaneous pinning techniques. A significant number of unstable fractures of the phalanges and metacarpals can be treated in the ED under mini–C-arm fluoroscopy without an admission and trip to the OR.3,4 Most phalangeal and metacarpal fractures are nondisplaced or minimally displaced and stable, and can often be handled with a combination of closed reduction, buddy-taping, and splinting.5 The indications for percutaneous versus internal fixation depend on a number of factors, including bone quality, degree of comminution, quality of the soft-tissue envelope, articular involvement, acuity of presentation, and goals for motion.6,7
Many simple injury patterns involving unstable fractures or dislocations may be definitively managed in the ED with percutaneous pinning (eg, injuries that are unstable with closed reduction alone but that do not necessitate soft-tissue dissection). These include but are not limited to bony mallet injuries, unstable transverse or oblique fractures or fracture-dislocations of the phalanges and metacarpals, carpometacarpal fracture- dislocations, and underlying fractures that need protection of nail-bed repairs, soft-tissue flaps, or extensor tendon injuries (Figures 1, 2).7,8 The techniques for specific fracture types are beyond the scope of this article but are readily available.5,6
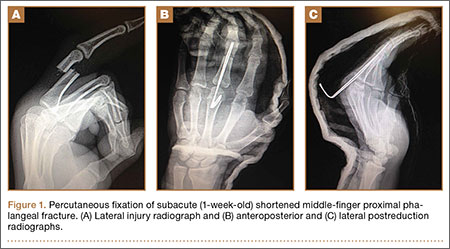
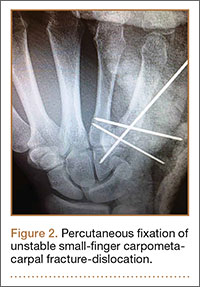
There are certain situations that undoubtedly warrant surgery in the OR, such as neurovascular injury necessitating microvascular repair, flexor tendon laceration, severely comminuted or segmental fractures, irreducible dislocations, and fractures with severe soft-tissue injury or contamination not amenable to primary irrigation, débridement, and closure at bedside.4,7,8
You might ask, “Why would one treat an operative injury in the ED and not formally in the OR?,” and we submit that there are a number of reasons.
First, and most important, with increasing health care costs and decreasing reimbursements, physicians are faced with providing safe but economical care. Percutaneous Kirschner wire (K-wire) fixation is dramatically more cost-effective when performed in the ED than in the OR. The cost of a procedure performed in either setting is similarly dependent on a variety of factors, generally including complexity of the patient or procedure, costs of supplies and pharmacologic agents, fixed versus variable overhead costs, and the professional fees of providers and ancillary personnel.9,10
While the patient is not charged per hour in the ED, it is estimated that ORs in the United States cost, on average, $62 per minute, ranging from as low as $22 to as high as $133 per minute.9 Additionally, the number of personnel involved in running an OR exceeds those for a similar procedure performed in the ED, considering (at a minimum) the orthopedic surgeon, anesthesiologist, scrub and radiology technicians, and nursing personnel required before, during, and after an operation.
While analgesia and procedural sedation can be performed similarly in either setting, it is our experience that patients are managed much more often in the ED with local anesthesia under direct care of only the orthopedic provider, whereas intravenous sedation and general anesthesia are far more commonly implemented in the OR. There are exceptions for pediatric patients or those who are unable to tolerate the procedure under only local anesthesia. Local anesthesia or even intravenous conscious sedation entails less risk as well as lower associated drug costs.11
The difference in risk is especially true for sicker patients undergoing minimally invasive procedures.11 Although administration of adequate procedural analgesia grows increasingly difficult the more proximal the injury, the hand and the fingers are easily and reliably anesthetized with well-placed wrist or digital blocks, with infrequent complications.12 Application of a lidocaine/bupivacaine mixture provides up to 6 to 8 hours of analgesia. A small tourniquet alternative, such as the finger of a sterile glove or phlebotomy tourniquet, applied to the base of the finger or the wrist additionally provides a relatively bloodless field and effectively acts as a Bier block.
Percutaneous pins are much more forgiving than rigid internal fixation. If the initial placement of a pin is unsatisfactory, the pin can be reinserted at little cost.12 Conversely, it may not be possible to reposition a misplaced screw or screw with inadequate purchase and still maintain adequate fixation. While percutaneous pin fixation is not as rigid as screw fixation, the degree of stability provided is adequate for the small forces affecting the hand in most cases. Accordingly, there is a very low incidence of fibrous union or nonunion.13,14 With an increasing appreciation of soft-tissue handling over the past few decades, another significant advantage of K-wire fixation is the obviation of soft-tissue dissection, preserving the biology to maximize healing and minimize adverse sequelae.12 Percutaneous fixation has been shown to achieve functional outcomes comparable to open reduction with internal fixation of operative phalangeal and metacarpal fractures, without soft-tissue disruption, scarring, or implant irritation, and with minimal risk of infection.3,13,15,16 Ultimate range of motion after percutaneous fixation is comparable, if not superior, to that of internal fixation, despite the initial advantage of rigid internal fixation secondary to decreased scarring and lack of indwelling hardware.16,17
While the risk of infection, perhaps the primary concern with percutaneous fixation, has been cited as high as 7%, osteomyelitis is exceedingly rare (<0.5%).3,13,14 Furthermore, pins are often left in place for 3 to 6 weeks, and infection has been found to occur most often at a mean of 10 weeks.7,13 Infection can also be mitigated by intelligent pin placement, relief of residual tension, and splint immobilization.4,15 Pin loosening has similarly been reported in up to 4% of cases in large retrospective studies, occurring at an average of 8 weeks, by which time most pins would have been extricated.13 Other complications related to impaling adjacent neurovascular or tendinous structures have also been cited but are rare.13 A 12-month prospective study of 75 patients specifically evaluating the outcomes after closed reduction with percutaneous fixation of unstable hand fractures in the ED reported only 6 complications at final follow-up.4 Complications were all minor, with no cases of nonunion, delayed union, malunion, pin-tract infection, pyarthrosis, or cellulitis, even in the setting of open fractures. Three patients required revision in the OR for pin migration, initial malreduction, and bone loss in the setting of comminution, respectively. The authors credited their low complication rate to supplementary immobilization.
In conclusion, many unstable simple fractures and dislocations of the hand and wrist can be safely and effectively treated in the ED. While it may seem daunting for a junior resident who is unfamiliar with percutaneous techniques, the authors advocate learning from a more senior mentor. The only additional training required is an understanding of how to apply this skill set in a different setting.
1. Levine WN, Spang RC 3rd. ACGME duty hour requirements: perceptions and impact on resident training and patient care. J Am Acad Orthop Surg. 2014;22(9):535-544.
2. Chung KC, Spilson SV. The frequency and epidemiology of hand and forearm fractures in the United States. J Hand Surg Am. 2001;26(5):908-915.
3. Catalano LW 3rd, Glickel SZ, Strauch RJ, Barron AO. The lost and found art of percutaneous pinning in the hand and wrist. Instructional Course Lectures. Annual Meeting of the American Academy of Orthopaedic Surgeons; March 24, 2015; Las Vegas, NV.
4. Starker I, Eaton RG. Kirschner wire placement in the emergency room. Is there a risk? J Hand Surg Br. 1995;20(4):535-538.
5. Meals C, Meals R. Hand fractures: a review of current treatment strategies. J Hand Surg Am. 2013;38(5):1021-1031.
6. Henry MH. Fractures of the proximal phalanx and metacarpals in the hand: preferred methods of stabilization. J Am Acad Orthop Surg. 2008;16(10):586-595.
7. Klein DM, Belsole RJ. Percutaneous treatment of carpal, metacarpal, and phalangeal injuries. Clin Orthop Relat Res. 2000;(375):116-125.
8. Bernstein ML, Chung KC. Hand fractures and their management: an international view. Injury. 2006;37(11):1043-1048.
9. Macario A. What does one minute of operating room time cost? J Clin Anesth. 2010;22(4):233-236.
10. Williams RM. The costs of visits to emergency departments. N Engl J Med. 1996;334(10):642-646.
11. Bodenham AR, Howell SJ. General anesthesia vs local anaesthesia: an ongoing story. Br J Anaesth. 2009;103(6):785-789.
12. Stern PJ. Management of fractures of the hand over the last 25 years. J Hand Surg Am. 2000;25(5):817-823.
13. Botte MJ, Davis JL, Rose BA, et al. Complications of smooth pin fixation of fractures and dislocations in the hand and wrist. Clin Orthop Relat Res. 1992;(276):194-201.
14. Wray RC Jr, Glunk R. Treatment of delayed union, nonunion, and malunion of the phalanges of the hand. Ann Plast Surg. 1989;22(1):14-18.
15. Hsu LP, Schwartz EG, Kalainov DM, Chen F, Makowiec RL. Complications of K-wire fixation in procedures involving the hand and wrist. J Hand Surg Am. 2011;36(4):610-616.
16. Stem PJ, Wieser MJ, Reilly DG. Complications of plate fixation in the hand skeleton. Clin Orthop Relat Res. 1987;(214):59-65.
17. Page SM, Stern PJ. Complications and range of motion following plate fixation of metacarpal and phalangeal fractures. J Hand Surg Am. 1998;23(5):827-832.
A mentor—now in his 60s—related his experiences as a resident. On call as a second-year resident, he would often be alone at a busy trauma center with no backup. When a case came in, he would quickly read about it in the library, then manage it in the emergency department (ED) if possible, or, if necessary, take the patient to the operating room (OR).
In the era of improved patient care, increased supervision, and decreased autonomy, this is not the reality anymore.1 In theory, more reliable patient care is the result; however, the pendulum may have swung too far.
There are a number of injuries that are amenable to definitive fixation in the ED, but not as limited an array of injuries as we have perhaps grown accustomed to. Hand injuries are among the most common orthopedic injuries seen in the ED, with fractures of the metacarpals and phalanges constituting nearly one-half of all hand injuries.2 The authors recently attended an excellent instructional course lecture on “The Lost and Found Art of Percutaneous Pinning in the Hand and Wrist” at the annual conference of the American Academy of Orthopaedic Surgeons.3 The presenters itemized a comprehensive list of fractures and simple dislocations of the hand, which could be simply, safely, effectively, and definitively managed through percutaneous pinning techniques. A significant number of unstable fractures of the phalanges and metacarpals can be treated in the ED under mini–C-arm fluoroscopy without an admission and trip to the OR.3,4 Most phalangeal and metacarpal fractures are nondisplaced or minimally displaced and stable, and can often be handled with a combination of closed reduction, buddy-taping, and splinting.5 The indications for percutaneous versus internal fixation depend on a number of factors, including bone quality, degree of comminution, quality of the soft-tissue envelope, articular involvement, acuity of presentation, and goals for motion.6,7
Many simple injury patterns involving unstable fractures or dislocations may be definitively managed in the ED with percutaneous pinning (eg, injuries that are unstable with closed reduction alone but that do not necessitate soft-tissue dissection). These include but are not limited to bony mallet injuries, unstable transverse or oblique fractures or fracture-dislocations of the phalanges and metacarpals, carpometacarpal fracture- dislocations, and underlying fractures that need protection of nail-bed repairs, soft-tissue flaps, or extensor tendon injuries (Figures 1, 2).7,8 The techniques for specific fracture types are beyond the scope of this article but are readily available.5,6
There are certain situations that undoubtedly warrant surgery in the OR, such as neurovascular injury necessitating microvascular repair, flexor tendon laceration, severely comminuted or segmental fractures, irreducible dislocations, and fractures with severe soft-tissue injury or contamination not amenable to primary irrigation, débridement, and closure at bedside.4,7,8
You might ask, “Why would one treat an operative injury in the ED and not formally in the OR?,” and we submit that there are a number of reasons.
First, and most important, with increasing health care costs and decreasing reimbursements, physicians are faced with providing safe but economical care. Percutaneous Kirschner wire (K-wire) fixation is dramatically more cost-effective when performed in the ED than in the OR. The cost of a procedure performed in either setting is similarly dependent on a variety of factors, generally including complexity of the patient or procedure, costs of supplies and pharmacologic agents, fixed versus variable overhead costs, and the professional fees of providers and ancillary personnel.9,10
While the patient is not charged per hour in the ED, it is estimated that ORs in the United States cost, on average, $62 per minute, ranging from as low as $22 to as high as $133 per minute.9 Additionally, the number of personnel involved in running an OR exceeds those for a similar procedure performed in the ED, considering (at a minimum) the orthopedic surgeon, anesthesiologist, scrub and radiology technicians, and nursing personnel required before, during, and after an operation.
While analgesia and procedural sedation can be performed similarly in either setting, it is our experience that patients are managed much more often in the ED with local anesthesia under direct care of only the orthopedic provider, whereas intravenous sedation and general anesthesia are far more commonly implemented in the OR. There are exceptions for pediatric patients or those who are unable to tolerate the procedure under only local anesthesia. Local anesthesia or even intravenous conscious sedation entails less risk as well as lower associated drug costs.11
The difference in risk is especially true for sicker patients undergoing minimally invasive procedures.11 Although administration of adequate procedural analgesia grows increasingly difficult the more proximal the injury, the hand and the fingers are easily and reliably anesthetized with well-placed wrist or digital blocks, with infrequent complications.12 Application of a lidocaine/bupivacaine mixture provides up to 6 to 8 hours of analgesia. A small tourniquet alternative, such as the finger of a sterile glove or phlebotomy tourniquet, applied to the base of the finger or the wrist additionally provides a relatively bloodless field and effectively acts as a Bier block.
Percutaneous pins are much more forgiving than rigid internal fixation. If the initial placement of a pin is unsatisfactory, the pin can be reinserted at little cost.12 Conversely, it may not be possible to reposition a misplaced screw or screw with inadequate purchase and still maintain adequate fixation. While percutaneous pin fixation is not as rigid as screw fixation, the degree of stability provided is adequate for the small forces affecting the hand in most cases. Accordingly, there is a very low incidence of fibrous union or nonunion.13,14 With an increasing appreciation of soft-tissue handling over the past few decades, another significant advantage of K-wire fixation is the obviation of soft-tissue dissection, preserving the biology to maximize healing and minimize adverse sequelae.12 Percutaneous fixation has been shown to achieve functional outcomes comparable to open reduction with internal fixation of operative phalangeal and metacarpal fractures, without soft-tissue disruption, scarring, or implant irritation, and with minimal risk of infection.3,13,15,16 Ultimate range of motion after percutaneous fixation is comparable, if not superior, to that of internal fixation, despite the initial advantage of rigid internal fixation secondary to decreased scarring and lack of indwelling hardware.16,17
While the risk of infection, perhaps the primary concern with percutaneous fixation, has been cited as high as 7%, osteomyelitis is exceedingly rare (<0.5%).3,13,14 Furthermore, pins are often left in place for 3 to 6 weeks, and infection has been found to occur most often at a mean of 10 weeks.7,13 Infection can also be mitigated by intelligent pin placement, relief of residual tension, and splint immobilization.4,15 Pin loosening has similarly been reported in up to 4% of cases in large retrospective studies, occurring at an average of 8 weeks, by which time most pins would have been extricated.13 Other complications related to impaling adjacent neurovascular or tendinous structures have also been cited but are rare.13 A 12-month prospective study of 75 patients specifically evaluating the outcomes after closed reduction with percutaneous fixation of unstable hand fractures in the ED reported only 6 complications at final follow-up.4 Complications were all minor, with no cases of nonunion, delayed union, malunion, pin-tract infection, pyarthrosis, or cellulitis, even in the setting of open fractures. Three patients required revision in the OR for pin migration, initial malreduction, and bone loss in the setting of comminution, respectively. The authors credited their low complication rate to supplementary immobilization.
In conclusion, many unstable simple fractures and dislocations of the hand and wrist can be safely and effectively treated in the ED. While it may seem daunting for a junior resident who is unfamiliar with percutaneous techniques, the authors advocate learning from a more senior mentor. The only additional training required is an understanding of how to apply this skill set in a different setting.
A mentor—now in his 60s—related his experiences as a resident. On call as a second-year resident, he would often be alone at a busy trauma center with no backup. When a case came in, he would quickly read about it in the library, then manage it in the emergency department (ED) if possible, or, if necessary, take the patient to the operating room (OR).
In the era of improved patient care, increased supervision, and decreased autonomy, this is not the reality anymore.1 In theory, more reliable patient care is the result; however, the pendulum may have swung too far.
There are a number of injuries that are amenable to definitive fixation in the ED, but not as limited an array of injuries as we have perhaps grown accustomed to. Hand injuries are among the most common orthopedic injuries seen in the ED, with fractures of the metacarpals and phalanges constituting nearly one-half of all hand injuries.2 The authors recently attended an excellent instructional course lecture on “The Lost and Found Art of Percutaneous Pinning in the Hand and Wrist” at the annual conference of the American Academy of Orthopaedic Surgeons.3 The presenters itemized a comprehensive list of fractures and simple dislocations of the hand, which could be simply, safely, effectively, and definitively managed through percutaneous pinning techniques. A significant number of unstable fractures of the phalanges and metacarpals can be treated in the ED under mini–C-arm fluoroscopy without an admission and trip to the OR.3,4 Most phalangeal and metacarpal fractures are nondisplaced or minimally displaced and stable, and can often be handled with a combination of closed reduction, buddy-taping, and splinting.5 The indications for percutaneous versus internal fixation depend on a number of factors, including bone quality, degree of comminution, quality of the soft-tissue envelope, articular involvement, acuity of presentation, and goals for motion.6,7
Many simple injury patterns involving unstable fractures or dislocations may be definitively managed in the ED with percutaneous pinning (eg, injuries that are unstable with closed reduction alone but that do not necessitate soft-tissue dissection). These include but are not limited to bony mallet injuries, unstable transverse or oblique fractures or fracture-dislocations of the phalanges and metacarpals, carpometacarpal fracture- dislocations, and underlying fractures that need protection of nail-bed repairs, soft-tissue flaps, or extensor tendon injuries (Figures 1, 2).7,8 The techniques for specific fracture types are beyond the scope of this article but are readily available.5,6
There are certain situations that undoubtedly warrant surgery in the OR, such as neurovascular injury necessitating microvascular repair, flexor tendon laceration, severely comminuted or segmental fractures, irreducible dislocations, and fractures with severe soft-tissue injury or contamination not amenable to primary irrigation, débridement, and closure at bedside.4,7,8
You might ask, “Why would one treat an operative injury in the ED and not formally in the OR?,” and we submit that there are a number of reasons.
First, and most important, with increasing health care costs and decreasing reimbursements, physicians are faced with providing safe but economical care. Percutaneous Kirschner wire (K-wire) fixation is dramatically more cost-effective when performed in the ED than in the OR. The cost of a procedure performed in either setting is similarly dependent on a variety of factors, generally including complexity of the patient or procedure, costs of supplies and pharmacologic agents, fixed versus variable overhead costs, and the professional fees of providers and ancillary personnel.9,10
While the patient is not charged per hour in the ED, it is estimated that ORs in the United States cost, on average, $62 per minute, ranging from as low as $22 to as high as $133 per minute.9 Additionally, the number of personnel involved in running an OR exceeds those for a similar procedure performed in the ED, considering (at a minimum) the orthopedic surgeon, anesthesiologist, scrub and radiology technicians, and nursing personnel required before, during, and after an operation.
While analgesia and procedural sedation can be performed similarly in either setting, it is our experience that patients are managed much more often in the ED with local anesthesia under direct care of only the orthopedic provider, whereas intravenous sedation and general anesthesia are far more commonly implemented in the OR. There are exceptions for pediatric patients or those who are unable to tolerate the procedure under only local anesthesia. Local anesthesia or even intravenous conscious sedation entails less risk as well as lower associated drug costs.11
The difference in risk is especially true for sicker patients undergoing minimally invasive procedures.11 Although administration of adequate procedural analgesia grows increasingly difficult the more proximal the injury, the hand and the fingers are easily and reliably anesthetized with well-placed wrist or digital blocks, with infrequent complications.12 Application of a lidocaine/bupivacaine mixture provides up to 6 to 8 hours of analgesia. A small tourniquet alternative, such as the finger of a sterile glove or phlebotomy tourniquet, applied to the base of the finger or the wrist additionally provides a relatively bloodless field and effectively acts as a Bier block.
Percutaneous pins are much more forgiving than rigid internal fixation. If the initial placement of a pin is unsatisfactory, the pin can be reinserted at little cost.12 Conversely, it may not be possible to reposition a misplaced screw or screw with inadequate purchase and still maintain adequate fixation. While percutaneous pin fixation is not as rigid as screw fixation, the degree of stability provided is adequate for the small forces affecting the hand in most cases. Accordingly, there is a very low incidence of fibrous union or nonunion.13,14 With an increasing appreciation of soft-tissue handling over the past few decades, another significant advantage of K-wire fixation is the obviation of soft-tissue dissection, preserving the biology to maximize healing and minimize adverse sequelae.12 Percutaneous fixation has been shown to achieve functional outcomes comparable to open reduction with internal fixation of operative phalangeal and metacarpal fractures, without soft-tissue disruption, scarring, or implant irritation, and with minimal risk of infection.3,13,15,16 Ultimate range of motion after percutaneous fixation is comparable, if not superior, to that of internal fixation, despite the initial advantage of rigid internal fixation secondary to decreased scarring and lack of indwelling hardware.16,17
While the risk of infection, perhaps the primary concern with percutaneous fixation, has been cited as high as 7%, osteomyelitis is exceedingly rare (<0.5%).3,13,14 Furthermore, pins are often left in place for 3 to 6 weeks, and infection has been found to occur most often at a mean of 10 weeks.7,13 Infection can also be mitigated by intelligent pin placement, relief of residual tension, and splint immobilization.4,15 Pin loosening has similarly been reported in up to 4% of cases in large retrospective studies, occurring at an average of 8 weeks, by which time most pins would have been extricated.13 Other complications related to impaling adjacent neurovascular or tendinous structures have also been cited but are rare.13 A 12-month prospective study of 75 patients specifically evaluating the outcomes after closed reduction with percutaneous fixation of unstable hand fractures in the ED reported only 6 complications at final follow-up.4 Complications were all minor, with no cases of nonunion, delayed union, malunion, pin-tract infection, pyarthrosis, or cellulitis, even in the setting of open fractures. Three patients required revision in the OR for pin migration, initial malreduction, and bone loss in the setting of comminution, respectively. The authors credited their low complication rate to supplementary immobilization.
In conclusion, many unstable simple fractures and dislocations of the hand and wrist can be safely and effectively treated in the ED. While it may seem daunting for a junior resident who is unfamiliar with percutaneous techniques, the authors advocate learning from a more senior mentor. The only additional training required is an understanding of how to apply this skill set in a different setting.
1. Levine WN, Spang RC 3rd. ACGME duty hour requirements: perceptions and impact on resident training and patient care. J Am Acad Orthop Surg. 2014;22(9):535-544.
2. Chung KC, Spilson SV. The frequency and epidemiology of hand and forearm fractures in the United States. J Hand Surg Am. 2001;26(5):908-915.
3. Catalano LW 3rd, Glickel SZ, Strauch RJ, Barron AO. The lost and found art of percutaneous pinning in the hand and wrist. Instructional Course Lectures. Annual Meeting of the American Academy of Orthopaedic Surgeons; March 24, 2015; Las Vegas, NV.
4. Starker I, Eaton RG. Kirschner wire placement in the emergency room. Is there a risk? J Hand Surg Br. 1995;20(4):535-538.
5. Meals C, Meals R. Hand fractures: a review of current treatment strategies. J Hand Surg Am. 2013;38(5):1021-1031.
6. Henry MH. Fractures of the proximal phalanx and metacarpals in the hand: preferred methods of stabilization. J Am Acad Orthop Surg. 2008;16(10):586-595.
7. Klein DM, Belsole RJ. Percutaneous treatment of carpal, metacarpal, and phalangeal injuries. Clin Orthop Relat Res. 2000;(375):116-125.
8. Bernstein ML, Chung KC. Hand fractures and their management: an international view. Injury. 2006;37(11):1043-1048.
9. Macario A. What does one minute of operating room time cost? J Clin Anesth. 2010;22(4):233-236.
10. Williams RM. The costs of visits to emergency departments. N Engl J Med. 1996;334(10):642-646.
11. Bodenham AR, Howell SJ. General anesthesia vs local anaesthesia: an ongoing story. Br J Anaesth. 2009;103(6):785-789.
12. Stern PJ. Management of fractures of the hand over the last 25 years. J Hand Surg Am. 2000;25(5):817-823.
13. Botte MJ, Davis JL, Rose BA, et al. Complications of smooth pin fixation of fractures and dislocations in the hand and wrist. Clin Orthop Relat Res. 1992;(276):194-201.
14. Wray RC Jr, Glunk R. Treatment of delayed union, nonunion, and malunion of the phalanges of the hand. Ann Plast Surg. 1989;22(1):14-18.
15. Hsu LP, Schwartz EG, Kalainov DM, Chen F, Makowiec RL. Complications of K-wire fixation in procedures involving the hand and wrist. J Hand Surg Am. 2011;36(4):610-616.
16. Stem PJ, Wieser MJ, Reilly DG. Complications of plate fixation in the hand skeleton. Clin Orthop Relat Res. 1987;(214):59-65.
17. Page SM, Stern PJ. Complications and range of motion following plate fixation of metacarpal and phalangeal fractures. J Hand Surg Am. 1998;23(5):827-832.
1. Levine WN, Spang RC 3rd. ACGME duty hour requirements: perceptions and impact on resident training and patient care. J Am Acad Orthop Surg. 2014;22(9):535-544.
2. Chung KC, Spilson SV. The frequency and epidemiology of hand and forearm fractures in the United States. J Hand Surg Am. 2001;26(5):908-915.
3. Catalano LW 3rd, Glickel SZ, Strauch RJ, Barron AO. The lost and found art of percutaneous pinning in the hand and wrist. Instructional Course Lectures. Annual Meeting of the American Academy of Orthopaedic Surgeons; March 24, 2015; Las Vegas, NV.
4. Starker I, Eaton RG. Kirschner wire placement in the emergency room. Is there a risk? J Hand Surg Br. 1995;20(4):535-538.
5. Meals C, Meals R. Hand fractures: a review of current treatment strategies. J Hand Surg Am. 2013;38(5):1021-1031.
6. Henry MH. Fractures of the proximal phalanx and metacarpals in the hand: preferred methods of stabilization. J Am Acad Orthop Surg. 2008;16(10):586-595.
7. Klein DM, Belsole RJ. Percutaneous treatment of carpal, metacarpal, and phalangeal injuries. Clin Orthop Relat Res. 2000;(375):116-125.
8. Bernstein ML, Chung KC. Hand fractures and their management: an international view. Injury. 2006;37(11):1043-1048.
9. Macario A. What does one minute of operating room time cost? J Clin Anesth. 2010;22(4):233-236.
10. Williams RM. The costs of visits to emergency departments. N Engl J Med. 1996;334(10):642-646.
11. Bodenham AR, Howell SJ. General anesthesia vs local anaesthesia: an ongoing story. Br J Anaesth. 2009;103(6):785-789.
12. Stern PJ. Management of fractures of the hand over the last 25 years. J Hand Surg Am. 2000;25(5):817-823.
13. Botte MJ, Davis JL, Rose BA, et al. Complications of smooth pin fixation of fractures and dislocations in the hand and wrist. Clin Orthop Relat Res. 1992;(276):194-201.
14. Wray RC Jr, Glunk R. Treatment of delayed union, nonunion, and malunion of the phalanges of the hand. Ann Plast Surg. 1989;22(1):14-18.
15. Hsu LP, Schwartz EG, Kalainov DM, Chen F, Makowiec RL. Complications of K-wire fixation in procedures involving the hand and wrist. J Hand Surg Am. 2011;36(4):610-616.
16. Stem PJ, Wieser MJ, Reilly DG. Complications of plate fixation in the hand skeleton. Clin Orthop Relat Res. 1987;(214):59-65.
17. Page SM, Stern PJ. Complications and range of motion following plate fixation of metacarpal and phalangeal fractures. J Hand Surg Am. 1998;23(5):827-832.

A Perfect Storm: The current climate in breast cancer
This is the first installment of a five-part monthly series that will discuss the pathologic, genomic, and clinical factors that contribute to the racial survival disparity in breast cancer. The series, which is adapted from an article that originally appeared in CA: A Cancer Journal for Clinicians,1 a journal of the American Cancer Society, will also review exciting and innovative interventions to close this survival gap. This month’s column reviews the scope of this important health care issue.
The National Cancer Institute’s (NCI) Surveillance, Epidemiology, and End Results Program (SEER) has estimated that 231,840 new cases of female breast cancer will be diagnosed in 2015, representing 14% of all new cancer cases among women. The NCI also has estimated 40,290 deaths from breast cancer, representing 6.8% of all cancer deaths among women.2 Breast cancer is the second leading cause of cancer death among women after lung cancer. It is well known that there has historically been a significant racial divide in breast cancer incidence (rate of new occurrences of breast cancer) and mortality (death) rates. Caucasian women were more likely to be diagnosed with breast cancer, but African American women were more likely to die from it.
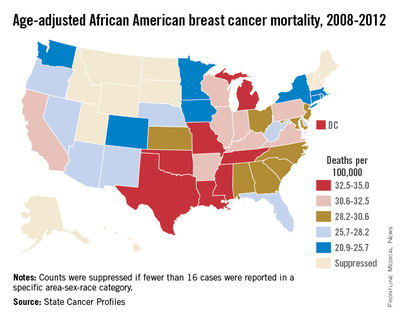
However, in a recently released study by DeSantis et al. this incidence trend no longer holds, and in 2012 there was a convergence of breast cancer incidence rates at 135 cases per 100,000 women for both Caucasian and African American women.3 In addition, this recent analysis revealed that the mortality disparity between African American and Caucasian women has continued to increase, with a death rate 42% higher in African American than in Caucasian women in 2012. While overall improvements in therapy have led to a decrease in breast cancer death rates in the United States since 1990, the decreases in death rates began earlier and have been larger in proportionate terms for Caucasians than for African Americans.4,5 According to SEER data from 1975 to 2011, Caucasian women had a 23% increase in breast cancer incidence and a 34% decrease in mortality, whereas African American women experienced a 35% increase in incidence and a 2% increase in mortality.6
Beyond national statistics and on a more-local level, several studies have explored regional variations in breast cancer mortality by race. One such study analyzed mortality data from the National Center for Health Statistics from 1975 to 2004.5 The researchers discovered that trends in breast cancer death rates varied widely by region. While breast cancer death rates in Caucasian women decreased in all 50 states, among African American women in 37 states analyzed, breast cancer death rates increased in 2 states, were level in 24 states, and decreased in only 11 states. Many of the states in which African American breast cancer death rates were level or rising were in the South and Midwest.

There are also differences in age and stage at diagnosis between African American and Caucasian women. Although the overall incidence of breast cancer has been historically higher in Caucasians, the incidence profile changes when the data are looked at by age. Among African American women with breast cancer, 33% are diagnosed at an age younger than 50 years, compared with 21.9% among Caucasian women.7
In women younger than 35 years, the incidence of breast cancer in African Americans is 1.4-2.0 times that of Caucasians.8 In addition, African American women present with more advanced-stage disease. Again, using the SEER program and examining data from 2005-2011, 62% of Caucasians had localized disease (cancer confined to the breast and potentially curable) versus 53% of African Americans. In all, 5% of Caucasians had distant disease (cancer outside the breast and treatable but not curable), compared with 9% of African Americans.9 A recent study in JAMA of 373,563 women with breast cancer during 2004-2011 found that African American women were less likely to be diagnosed with stage I breast cancer than were non-Hispanic white women across all age groups (non-Hispanic white women, 50.8%; African American women, 37.0%).10
The researchers examined further those women with small breast cancers (breast tumors ≤ 2 cm) and the percentages of nodal metastases (cancer in the lymph nodes) and distant metastases (cancer outside the breast) by race/ethnicity. The authors found that an African American woman with a small-sized breast tumor was more likely to present with lymph node metastases and distant metastases. Significantly, African American women were also more likely to die of breast cancer with small-sized tumors than were non-Hispanic white women.
These differences in age and stage highlight important differences in tumor biology, genomics, and patterns of care that contribute to the disparity in breast cancer survival between Caucasian and African American women. The February installment of this column will explore tumor biology – the first element in the perfect storm.
Other installments of this column can be found in the Related Content box.
1. Daly B, Olopade OI: A perfect storm: How tumor biology, genomics, and health care delivery patterns collide to create a racial survival disparity in breast cancer and proposed interventions for change. CA Cancer J Clin. 65:221-38, 2015.
2. National Cancer Institute. Surveillance, Epidemiology, and End Results (SEER) Program Stat fact sheets: Breast cancer. Surveillance, Epidemiology, and End Results Program. http://seer.cancer.gov/statfacts/html/breast.html. Accessed Nov. 20, 2015.
3. DeSantis C, Fedewa S, Goding Sauer A, et al., Breast cancer statistics, 2015: Convergence of incidence rates between black and white women. CA: A Cancer Journal for Clinicians. doi: 10.3322/caac.21320
4. DeLancey JO, Thun MJ, Jemal A, et al.: Recent trends in Black-White disparities in cancer mortality. Cancer Epidemiol Biomarkers Prev. 17:2908-12, 2008.
5. DeSantis C, Jemal A, Ward E, et al.: Temporal trends in breast cancer mortality by state and race. Cancer Causes Control. 19:537-45, 2008.
6. Howlander N NA, Krapcho M, et al. eds.: SEER Cancer Statistics Review, 1975-2011, 2014.
7. Clarke CA, West DW, Edwards BK, et al.: Existing data on breast cancer in African-American women: what we know and what we need to know. Cancer. 97:211-21, 2003.
8. Marie Swanson G, Haslam SZ, Azzouz F: Breast cancer among young African-American women: a summary of data and literature and of issues discussed during the Summit Meeting on Breast Cancer Among African American Women, Washington, DC, September 8-10, 2000. Cancer. 97:273-9, 2003.
9. National Cancer Institute. SEER Cancer Statistics Review, 1975-2012. http://seer.cancer.gov/csr/1975_2012/results_single/sect_04_table.13.pdf. Accessed, Nov. 20, 2015.
10. Iqbal J, Ginsburg O, Rochon PA, et al: Differences in breast cancer stage at diagnosis and cancer-specific survival by race and ethnicity in the United States. JAMA 313:165-73, 2015.

Bobby Daly, MD, MBA, is the chief fellow in the section of hematology/oncology at the University of Chicago Medicine. His clinical focus is breast and thoracic oncology, and his research focus is health services. Specifically, Dr. Daly researches disparities in oncology care delivery, oncology health care utilization, aggressive end-of-life oncology care, and oncology payment models. He received his MD and MBA from Harvard Medical School and Harvard Business School, both in Boston, and a BA in Economics and History from Stanford (Calif.) University. He was the recipient of the Dean’s Award at Harvard Medical and Business Schools.

Olufunmilayo Olopade, MD, FACP, OON, is the Walter L. Palmer Distinguished Service Professor of Medicine and Human Genetics, and director, Center for Global Health at the University of Chicago. She is adopting emerging high throughput genomic and informatics strategies to identify genetic and nongenetic risk factors for breast cancer in order to implement precision health care in diverse populations. This innovative approach has the potential to improve the quality of care and reduce costs while saving more lives.
Disclosures: Dr. Olopade serves on the Medical Advisory Board for CancerIQ. Dr. Daly serves as a director of Quadrant Holdings Corporation and receives compensation from this entity. Frontline Medical Communications is a subsidiary of Quadrant Holdings Corporation.
Published in conjunction with Susan G. Komen®.
This is the first installment of a five-part monthly series that will discuss the pathologic, genomic, and clinical factors that contribute to the racial survival disparity in breast cancer. The series, which is adapted from an article that originally appeared in CA: A Cancer Journal for Clinicians,1 a journal of the American Cancer Society, will also review exciting and innovative interventions to close this survival gap. This month’s column reviews the scope of this important health care issue.
The National Cancer Institute’s (NCI) Surveillance, Epidemiology, and End Results Program (SEER) has estimated that 231,840 new cases of female breast cancer will be diagnosed in 2015, representing 14% of all new cancer cases among women. The NCI also has estimated 40,290 deaths from breast cancer, representing 6.8% of all cancer deaths among women.2 Breast cancer is the second leading cause of cancer death among women after lung cancer. It is well known that there has historically been a significant racial divide in breast cancer incidence (rate of new occurrences of breast cancer) and mortality (death) rates. Caucasian women were more likely to be diagnosed with breast cancer, but African American women were more likely to die from it.
However, in a recently released study by DeSantis et al. this incidence trend no longer holds, and in 2012 there was a convergence of breast cancer incidence rates at 135 cases per 100,000 women for both Caucasian and African American women.3 In addition, this recent analysis revealed that the mortality disparity between African American and Caucasian women has continued to increase, with a death rate 42% higher in African American than in Caucasian women in 2012. While overall improvements in therapy have led to a decrease in breast cancer death rates in the United States since 1990, the decreases in death rates began earlier and have been larger in proportionate terms for Caucasians than for African Americans.4,5 According to SEER data from 1975 to 2011, Caucasian women had a 23% increase in breast cancer incidence and a 34% decrease in mortality, whereas African American women experienced a 35% increase in incidence and a 2% increase in mortality.6
Beyond national statistics and on a more-local level, several studies have explored regional variations in breast cancer mortality by race. One such study analyzed mortality data from the National Center for Health Statistics from 1975 to 2004.5 The researchers discovered that trends in breast cancer death rates varied widely by region. While breast cancer death rates in Caucasian women decreased in all 50 states, among African American women in 37 states analyzed, breast cancer death rates increased in 2 states, were level in 24 states, and decreased in only 11 states. Many of the states in which African American breast cancer death rates were level or rising were in the South and Midwest.
There are also differences in age and stage at diagnosis between African American and Caucasian women. Although the overall incidence of breast cancer has been historically higher in Caucasians, the incidence profile changes when the data are looked at by age. Among African American women with breast cancer, 33% are diagnosed at an age younger than 50 years, compared with 21.9% among Caucasian women.7
In women younger than 35 years, the incidence of breast cancer in African Americans is 1.4-2.0 times that of Caucasians.8 In addition, African American women present with more advanced-stage disease. Again, using the SEER program and examining data from 2005-2011, 62% of Caucasians had localized disease (cancer confined to the breast and potentially curable) versus 53% of African Americans. In all, 5% of Caucasians had distant disease (cancer outside the breast and treatable but not curable), compared with 9% of African Americans.9 A recent study in JAMA of 373,563 women with breast cancer during 2004-2011 found that African American women were less likely to be diagnosed with stage I breast cancer than were non-Hispanic white women across all age groups (non-Hispanic white women, 50.8%; African American women, 37.0%).10
The researchers examined further those women with small breast cancers (breast tumors ≤ 2 cm) and the percentages of nodal metastases (cancer in the lymph nodes) and distant metastases (cancer outside the breast) by race/ethnicity. The authors found that an African American woman with a small-sized breast tumor was more likely to present with lymph node metastases and distant metastases. Significantly, African American women were also more likely to die of breast cancer with small-sized tumors than were non-Hispanic white women.
These differences in age and stage highlight important differences in tumor biology, genomics, and patterns of care that contribute to the disparity in breast cancer survival between Caucasian and African American women. The February installment of this column will explore tumor biology – the first element in the perfect storm.
Other installments of this column can be found in the Related Content box.
1. Daly B, Olopade OI: A perfect storm: How tumor biology, genomics, and health care delivery patterns collide to create a racial survival disparity in breast cancer and proposed interventions for change. CA Cancer J Clin. 65:221-38, 2015.
2. National Cancer Institute. Surveillance, Epidemiology, and End Results (SEER) Program Stat fact sheets: Breast cancer. Surveillance, Epidemiology, and End Results Program. http://seer.cancer.gov/statfacts/html/breast.html. Accessed Nov. 20, 2015.
3. DeSantis C, Fedewa S, Goding Sauer A, et al., Breast cancer statistics, 2015: Convergence of incidence rates between black and white women. CA: A Cancer Journal for Clinicians. doi: 10.3322/caac.21320
4. DeLancey JO, Thun MJ, Jemal A, et al.: Recent trends in Black-White disparities in cancer mortality. Cancer Epidemiol Biomarkers Prev. 17:2908-12, 2008.
5. DeSantis C, Jemal A, Ward E, et al.: Temporal trends in breast cancer mortality by state and race. Cancer Causes Control. 19:537-45, 2008.
6. Howlander N NA, Krapcho M, et al. eds.: SEER Cancer Statistics Review, 1975-2011, 2014.
7. Clarke CA, West DW, Edwards BK, et al.: Existing data on breast cancer in African-American women: what we know and what we need to know. Cancer. 97:211-21, 2003.
8. Marie Swanson G, Haslam SZ, Azzouz F: Breast cancer among young African-American women: a summary of data and literature and of issues discussed during the Summit Meeting on Breast Cancer Among African American Women, Washington, DC, September 8-10, 2000. Cancer. 97:273-9, 2003.
9. National Cancer Institute. SEER Cancer Statistics Review, 1975-2012. http://seer.cancer.gov/csr/1975_2012/results_single/sect_04_table.13.pdf. Accessed, Nov. 20, 2015.
10. Iqbal J, Ginsburg O, Rochon PA, et al: Differences in breast cancer stage at diagnosis and cancer-specific survival by race and ethnicity in the United States. JAMA 313:165-73, 2015.
Bobby Daly, MD, MBA, is the chief fellow in the section of hematology/oncology at the University of Chicago Medicine. His clinical focus is breast and thoracic oncology, and his research focus is health services. Specifically, Dr. Daly researches disparities in oncology care delivery, oncology health care utilization, aggressive end-of-life oncology care, and oncology payment models. He received his MD and MBA from Harvard Medical School and Harvard Business School, both in Boston, and a BA in Economics and History from Stanford (Calif.) University. He was the recipient of the Dean’s Award at Harvard Medical and Business Schools.
Olufunmilayo Olopade, MD, FACP, OON, is the Walter L. Palmer Distinguished Service Professor of Medicine and Human Genetics, and director, Center for Global Health at the University of Chicago. She is adopting emerging high throughput genomic and informatics strategies to identify genetic and nongenetic risk factors for breast cancer in order to implement precision health care in diverse populations. This innovative approach has the potential to improve the quality of care and reduce costs while saving more lives.
Disclosures: Dr. Olopade serves on the Medical Advisory Board for CancerIQ. Dr. Daly serves as a director of Quadrant Holdings Corporation and receives compensation from this entity. Frontline Medical Communications is a subsidiary of Quadrant Holdings Corporation.
Published in conjunction with Susan G. Komen®.
This is the first installment of a five-part monthly series that will discuss the pathologic, genomic, and clinical factors that contribute to the racial survival disparity in breast cancer. The series, which is adapted from an article that originally appeared in CA: A Cancer Journal for Clinicians,1 a journal of the American Cancer Society, will also review exciting and innovative interventions to close this survival gap. This month’s column reviews the scope of this important health care issue.
The National Cancer Institute’s (NCI) Surveillance, Epidemiology, and End Results Program (SEER) has estimated that 231,840 new cases of female breast cancer will be diagnosed in 2015, representing 14% of all new cancer cases among women. The NCI also has estimated 40,290 deaths from breast cancer, representing 6.8% of all cancer deaths among women.2 Breast cancer is the second leading cause of cancer death among women after lung cancer. It is well known that there has historically been a significant racial divide in breast cancer incidence (rate of new occurrences of breast cancer) and mortality (death) rates. Caucasian women were more likely to be diagnosed with breast cancer, but African American women were more likely to die from it.
However, in a recently released study by DeSantis et al. this incidence trend no longer holds, and in 2012 there was a convergence of breast cancer incidence rates at 135 cases per 100,000 women for both Caucasian and African American women.3 In addition, this recent analysis revealed that the mortality disparity between African American and Caucasian women has continued to increase, with a death rate 42% higher in African American than in Caucasian women in 2012. While overall improvements in therapy have led to a decrease in breast cancer death rates in the United States since 1990, the decreases in death rates began earlier and have been larger in proportionate terms for Caucasians than for African Americans.4,5 According to SEER data from 1975 to 2011, Caucasian women had a 23% increase in breast cancer incidence and a 34% decrease in mortality, whereas African American women experienced a 35% increase in incidence and a 2% increase in mortality.6
Beyond national statistics and on a more-local level, several studies have explored regional variations in breast cancer mortality by race. One such study analyzed mortality data from the National Center for Health Statistics from 1975 to 2004.5 The researchers discovered that trends in breast cancer death rates varied widely by region. While breast cancer death rates in Caucasian women decreased in all 50 states, among African American women in 37 states analyzed, breast cancer death rates increased in 2 states, were level in 24 states, and decreased in only 11 states. Many of the states in which African American breast cancer death rates were level or rising were in the South and Midwest.
There are also differences in age and stage at diagnosis between African American and Caucasian women. Although the overall incidence of breast cancer has been historically higher in Caucasians, the incidence profile changes when the data are looked at by age. Among African American women with breast cancer, 33% are diagnosed at an age younger than 50 years, compared with 21.9% among Caucasian women.7
In women younger than 35 years, the incidence of breast cancer in African Americans is 1.4-2.0 times that of Caucasians.8 In addition, African American women present with more advanced-stage disease. Again, using the SEER program and examining data from 2005-2011, 62% of Caucasians had localized disease (cancer confined to the breast and potentially curable) versus 53% of African Americans. In all, 5% of Caucasians had distant disease (cancer outside the breast and treatable but not curable), compared with 9% of African Americans.9 A recent study in JAMA of 373,563 women with breast cancer during 2004-2011 found that African American women were less likely to be diagnosed with stage I breast cancer than were non-Hispanic white women across all age groups (non-Hispanic white women, 50.8%; African American women, 37.0%).10
The researchers examined further those women with small breast cancers (breast tumors ≤ 2 cm) and the percentages of nodal metastases (cancer in the lymph nodes) and distant metastases (cancer outside the breast) by race/ethnicity. The authors found that an African American woman with a small-sized breast tumor was more likely to present with lymph node metastases and distant metastases. Significantly, African American women were also more likely to die of breast cancer with small-sized tumors than were non-Hispanic white women.
These differences in age and stage highlight important differences in tumor biology, genomics, and patterns of care that contribute to the disparity in breast cancer survival between Caucasian and African American women. The February installment of this column will explore tumor biology – the first element in the perfect storm.
Other installments of this column can be found in the Related Content box.
1. Daly B, Olopade OI: A perfect storm: How tumor biology, genomics, and health care delivery patterns collide to create a racial survival disparity in breast cancer and proposed interventions for change. CA Cancer J Clin. 65:221-38, 2015.
2. National Cancer Institute. Surveillance, Epidemiology, and End Results (SEER) Program Stat fact sheets: Breast cancer. Surveillance, Epidemiology, and End Results Program. http://seer.cancer.gov/statfacts/html/breast.html. Accessed Nov. 20, 2015.
3. DeSantis C, Fedewa S, Goding Sauer A, et al., Breast cancer statistics, 2015: Convergence of incidence rates between black and white women. CA: A Cancer Journal for Clinicians. doi: 10.3322/caac.21320
4. DeLancey JO, Thun MJ, Jemal A, et al.: Recent trends in Black-White disparities in cancer mortality. Cancer Epidemiol Biomarkers Prev. 17:2908-12, 2008.
5. DeSantis C, Jemal A, Ward E, et al.: Temporal trends in breast cancer mortality by state and race. Cancer Causes Control. 19:537-45, 2008.
6. Howlander N NA, Krapcho M, et al. eds.: SEER Cancer Statistics Review, 1975-2011, 2014.
7. Clarke CA, West DW, Edwards BK, et al.: Existing data on breast cancer in African-American women: what we know and what we need to know. Cancer. 97:211-21, 2003.
8. Marie Swanson G, Haslam SZ, Azzouz F: Breast cancer among young African-American women: a summary of data and literature and of issues discussed during the Summit Meeting on Breast Cancer Among African American Women, Washington, DC, September 8-10, 2000. Cancer. 97:273-9, 2003.
9. National Cancer Institute. SEER Cancer Statistics Review, 1975-2012. http://seer.cancer.gov/csr/1975_2012/results_single/sect_04_table.13.pdf. Accessed, Nov. 20, 2015.
10. Iqbal J, Ginsburg O, Rochon PA, et al: Differences in breast cancer stage at diagnosis and cancer-specific survival by race and ethnicity in the United States. JAMA 313:165-73, 2015.
Bobby Daly, MD, MBA, is the chief fellow in the section of hematology/oncology at the University of Chicago Medicine. His clinical focus is breast and thoracic oncology, and his research focus is health services. Specifically, Dr. Daly researches disparities in oncology care delivery, oncology health care utilization, aggressive end-of-life oncology care, and oncology payment models. He received his MD and MBA from Harvard Medical School and Harvard Business School, both in Boston, and a BA in Economics and History from Stanford (Calif.) University. He was the recipient of the Dean’s Award at Harvard Medical and Business Schools.
Olufunmilayo Olopade, MD, FACP, OON, is the Walter L. Palmer Distinguished Service Professor of Medicine and Human Genetics, and director, Center for Global Health at the University of Chicago. She is adopting emerging high throughput genomic and informatics strategies to identify genetic and nongenetic risk factors for breast cancer in order to implement precision health care in diverse populations. This innovative approach has the potential to improve the quality of care and reduce costs while saving more lives.
Disclosures: Dr. Olopade serves on the Medical Advisory Board for CancerIQ. Dr. Daly serves as a director of Quadrant Holdings Corporation and receives compensation from this entity. Frontline Medical Communications is a subsidiary of Quadrant Holdings Corporation.
Published in conjunction with Susan G. Komen®.

The Right Choice? Kindness and Surgical Ethics: Reflections on a Friend and Mentor
As I sit down to write this column, I reflect on the news that my mentor and friend, Norman W. Thompson, M.D, FACS, passed away yesterday. I had the good fortune to spend 1 year as an endocrine surgery fellow with Dr. Thompson at the University of Michigan in 1995-96. That year was certainly the most significant of my training in terms of defining my professional life as an endocrine surgeon. However, as I think back on my time with Dr. Thompson, I am struck by how much more I learned from him than how to take out a thyroid or a parathyroid or manage multiple endocrine neoplasia.
Dr. Thompson was an excellent technical surgeon, and he would have had a tremendous career helping thousands of patients if that was all that he had done. However, he was much more than an excellent technician. He was also a great doctor. In order for a surgeon to be a great doctor, it is necessary to be technically excellent, but that alone is not sufficient. I believe that what makes a surgeon a great doctor is the combination of technical mastery with outstanding interpersonal skills and ethically sound clinical judgment. Dr. Thompson had all of that, and he was exceptionally kind.

Kindness is not a word that we commonly use in describing surgeons today. In an era of surgeons being pressured to see more patients and generate more RVUs [relative value units], it is unusual to hear kindness mentioned as an essential attribute of a great surgeon. However, Dr. Thompson’s kindness was immediately apparent to all who spent time with him. He treated each patient as a unique individual. In addition, he treated his trainees and his colleagues in Ann Arbor and around the world with respect and incredible humility. He was generous with his time and was always approachable no matter how inexperienced the surgeon asking him a question. Dr. Thompson was kind to all of us and made us feel that he valued spending time with us.
What does kindness have to do with a column that traditionally focuses on ethical issues in the practice of surgery? Although acting with kindness is not the same as acting in an ethical manner, I believe that there is more overlap of the terms than we often imagine. The kind surgeon is the one who treats people – whether they are patients or colleagues – as though they matter. The ethical surgeon respects the patient’s wishes and acts to benefit the patient as much as possible in all circumstances. I am certain that I have met ethical surgeons who were not kind, but I have met very few kind surgeons who are not ethical.
As someone who has spent significant time and energy in the last 19 years as a surgery faculty member trying to teach ethics, I am also struck by a clear truth. Actions always speak louder than words. It may be valuable to talk about the ethical principles that may come to play in a particularly difficult surgical case. Defining the competing interests and assessing the patient’s wishes are important components of the ethical practice of surgery. However, no amount of discussion of these issues can substitute for the value of behavior. Treating patients and colleagues with kindness and respect is modeling the behaviors of an ethical surgeon – perhaps learned from a wise and thoughtful mentor.
Dr. Thompson was an excellent role model for me and so many others in how he treated patients and everyone around him. As I see patients and perform surgery, I still hear myself saying many of the same things that he said many years ago. His genuine expressions of optimism before difficult operations, honesty in communicating, and sadness when things did not go well were tremendous examples to me of how a great doctor treats those around him. These lessons that I learned from Dr. Thompson have influenced my practice significantly, and I am grateful for the opportunity to try to model them on a daily basis.
Although I remain convinced that formal curricula in ethics and professionalism remain important in the education of today’s surgeons, it is valuable to remember the impact that the behaviors of those we respect have on us. Perhaps we surgeons more than other physicians are molded by the people who train us, but there is no question that the ethical behaviors of our teachers and mentors will have a greater impact than any lecture or manuscript. I want to acknowledge and commemorate the kindness and ethical behaviors that Dr. Thompson modeled daily for all who were fortunate enough to work with him.
Dr. Angelos is an ACS Fellow; the Linda Kohler Anderson Professor of Surgery and Surgical Ethics; chief, endocrine surgery; and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
As I sit down to write this column, I reflect on the news that my mentor and friend, Norman W. Thompson, M.D, FACS, passed away yesterday. I had the good fortune to spend 1 year as an endocrine surgery fellow with Dr. Thompson at the University of Michigan in 1995-96. That year was certainly the most significant of my training in terms of defining my professional life as an endocrine surgeon. However, as I think back on my time with Dr. Thompson, I am struck by how much more I learned from him than how to take out a thyroid or a parathyroid or manage multiple endocrine neoplasia.
Dr. Thompson was an excellent technical surgeon, and he would have had a tremendous career helping thousands of patients if that was all that he had done. However, he was much more than an excellent technician. He was also a great doctor. In order for a surgeon to be a great doctor, it is necessary to be technically excellent, but that alone is not sufficient. I believe that what makes a surgeon a great doctor is the combination of technical mastery with outstanding interpersonal skills and ethically sound clinical judgment. Dr. Thompson had all of that, and he was exceptionally kind.
Kindness is not a word that we commonly use in describing surgeons today. In an era of surgeons being pressured to see more patients and generate more RVUs [relative value units], it is unusual to hear kindness mentioned as an essential attribute of a great surgeon. However, Dr. Thompson’s kindness was immediately apparent to all who spent time with him. He treated each patient as a unique individual. In addition, he treated his trainees and his colleagues in Ann Arbor and around the world with respect and incredible humility. He was generous with his time and was always approachable no matter how inexperienced the surgeon asking him a question. Dr. Thompson was kind to all of us and made us feel that he valued spending time with us.
What does kindness have to do with a column that traditionally focuses on ethical issues in the practice of surgery? Although acting with kindness is not the same as acting in an ethical manner, I believe that there is more overlap of the terms than we often imagine. The kind surgeon is the one who treats people – whether they are patients or colleagues – as though they matter. The ethical surgeon respects the patient’s wishes and acts to benefit the patient as much as possible in all circumstances. I am certain that I have met ethical surgeons who were not kind, but I have met very few kind surgeons who are not ethical.
As someone who has spent significant time and energy in the last 19 years as a surgery faculty member trying to teach ethics, I am also struck by a clear truth. Actions always speak louder than words. It may be valuable to talk about the ethical principles that may come to play in a particularly difficult surgical case. Defining the competing interests and assessing the patient’s wishes are important components of the ethical practice of surgery. However, no amount of discussion of these issues can substitute for the value of behavior. Treating patients and colleagues with kindness and respect is modeling the behaviors of an ethical surgeon – perhaps learned from a wise and thoughtful mentor.
Dr. Thompson was an excellent role model for me and so many others in how he treated patients and everyone around him. As I see patients and perform surgery, I still hear myself saying many of the same things that he said many years ago. His genuine expressions of optimism before difficult operations, honesty in communicating, and sadness when things did not go well were tremendous examples to me of how a great doctor treats those around him. These lessons that I learned from Dr. Thompson have influenced my practice significantly, and I am grateful for the opportunity to try to model them on a daily basis.
Although I remain convinced that formal curricula in ethics and professionalism remain important in the education of today’s surgeons, it is valuable to remember the impact that the behaviors of those we respect have on us. Perhaps we surgeons more than other physicians are molded by the people who train us, but there is no question that the ethical behaviors of our teachers and mentors will have a greater impact than any lecture or manuscript. I want to acknowledge and commemorate the kindness and ethical behaviors that Dr. Thompson modeled daily for all who were fortunate enough to work with him.
Dr. Angelos is an ACS Fellow; the Linda Kohler Anderson Professor of Surgery and Surgical Ethics; chief, endocrine surgery; and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
As I sit down to write this column, I reflect on the news that my mentor and friend, Norman W. Thompson, M.D, FACS, passed away yesterday. I had the good fortune to spend 1 year as an endocrine surgery fellow with Dr. Thompson at the University of Michigan in 1995-96. That year was certainly the most significant of my training in terms of defining my professional life as an endocrine surgeon. However, as I think back on my time with Dr. Thompson, I am struck by how much more I learned from him than how to take out a thyroid or a parathyroid or manage multiple endocrine neoplasia.
Dr. Thompson was an excellent technical surgeon, and he would have had a tremendous career helping thousands of patients if that was all that he had done. However, he was much more than an excellent technician. He was also a great doctor. In order for a surgeon to be a great doctor, it is necessary to be technically excellent, but that alone is not sufficient. I believe that what makes a surgeon a great doctor is the combination of technical mastery with outstanding interpersonal skills and ethically sound clinical judgment. Dr. Thompson had all of that, and he was exceptionally kind.
Kindness is not a word that we commonly use in describing surgeons today. In an era of surgeons being pressured to see more patients and generate more RVUs [relative value units], it is unusual to hear kindness mentioned as an essential attribute of a great surgeon. However, Dr. Thompson’s kindness was immediately apparent to all who spent time with him. He treated each patient as a unique individual. In addition, he treated his trainees and his colleagues in Ann Arbor and around the world with respect and incredible humility. He was generous with his time and was always approachable no matter how inexperienced the surgeon asking him a question. Dr. Thompson was kind to all of us and made us feel that he valued spending time with us.
What does kindness have to do with a column that traditionally focuses on ethical issues in the practice of surgery? Although acting with kindness is not the same as acting in an ethical manner, I believe that there is more overlap of the terms than we often imagine. The kind surgeon is the one who treats people – whether they are patients or colleagues – as though they matter. The ethical surgeon respects the patient’s wishes and acts to benefit the patient as much as possible in all circumstances. I am certain that I have met ethical surgeons who were not kind, but I have met very few kind surgeons who are not ethical.
As someone who has spent significant time and energy in the last 19 years as a surgery faculty member trying to teach ethics, I am also struck by a clear truth. Actions always speak louder than words. It may be valuable to talk about the ethical principles that may come to play in a particularly difficult surgical case. Defining the competing interests and assessing the patient’s wishes are important components of the ethical practice of surgery. However, no amount of discussion of these issues can substitute for the value of behavior. Treating patients and colleagues with kindness and respect is modeling the behaviors of an ethical surgeon – perhaps learned from a wise and thoughtful mentor.
Dr. Thompson was an excellent role model for me and so many others in how he treated patients and everyone around him. As I see patients and perform surgery, I still hear myself saying many of the same things that he said many years ago. His genuine expressions of optimism before difficult operations, honesty in communicating, and sadness when things did not go well were tremendous examples to me of how a great doctor treats those around him. These lessons that I learned from Dr. Thompson have influenced my practice significantly, and I am grateful for the opportunity to try to model them on a daily basis.
Although I remain convinced that formal curricula in ethics and professionalism remain important in the education of today’s surgeons, it is valuable to remember the impact that the behaviors of those we respect have on us. Perhaps we surgeons more than other physicians are molded by the people who train us, but there is no question that the ethical behaviors of our teachers and mentors will have a greater impact than any lecture or manuscript. I want to acknowledge and commemorate the kindness and ethical behaviors that Dr. Thompson modeled daily for all who were fortunate enough to work with him.
Dr. Angelos is an ACS Fellow; the Linda Kohler Anderson Professor of Surgery and Surgical Ethics; chief, endocrine surgery; and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.

Screening Mammography: Debates, Guidelines, Issues
The screening mammography debate has been rekindled by the American Cancer Society’s updated guideline released in October 2015. Surgeons are now looking at yet another iteration of the optimal surveillance schedule aimed at reducing breast cancer mortality.
Nearly all breast cancer patients undergo surgery as at least one component of their care through diagnostic biopsy and/or definitive locoregional management, and many women are referred to surgeons for evaluation as well as follow-up for a variety of benign breast problems. The discussion of breast cancer screening with patients can be complicated by the many guidelines with conflicting recommendations, not to mention patient fears triggered by incompletely informed or simplistic media coverage. Surgeons are therefore obliged to remain knowledgeable regarding the status and rationale for breast cancer screening guidelines that have been developed by our colleagues in the American Cancer Society as well as other organizations.

Context of the updated guideline
The American Cancer Society and the American College of Surgeons have historically advocated in favor of annual screening mammography for average-risk women in the United States beginning at age 40 years (https://goo.gl/4W92EI). In 2009, the United States Preventive Services Task Force (USPSTF) published a recommendation that women delay initiation of screening mammography until reaching age 50, with follow-up studies performed biennially thereafter. This USPSTF guideline has remain unchanged as of 2015 (http://goo.gl/RYYWEP). Other medical societies and institutions have established their own guidelines.
The updated American Cancer Society guideline now recommends that average-risk women initiate annual mammography at age 45, but advocates in favor of availability of annual mammography beginning at age 40; the updated guideline also indicates that women can transition to biennial mammography at age 55, but should have access to continued annual mammography in accordance with personal preferences and after consideration of risks and benefits (JAMA. 2015;314[15]:1599-614).
The updated guideline can basically be interpreted as a more relaxed version of the prior guideline, which featured a straightforward mandate for average-risk women to undergo annual screening mammography beginning at age 40 years. However, the increased complexity of the more flexible guideline has generated legitimate concerns regarding the potential for confusion and misinterpretation.
Updated guideline rationale and empirical basis
The Society commissioned a systematic review to evaluate the benefits and harms of mammographic screening as well as clinical breast examination, based upon randomized clinical trials, and observational and modeling studies (JAMA. 2015;314[15]: 1615-34).
The Society then convened their Guideline Development Group (GDG) and GDG Breast Subgroup to interpret the systematic review for the purpose of drafting the breast cancer screening update. This process was further guided by a panel of External Expert Advisors. Mortality reductions were analyzed in the context of population-based breast cancer incidence rates by 5-year age increments.
Not surprisingly, the overall review confirmed the findings of several published studies that screening mammography in women aged 40-79 reduces breast cancer mortality rates by 20%-50%, with extent of benefit varying by age, as well as study design (randomized clinical trial versus observational). Since breast cancer incidence rates increase substantially among women by age (incidence rates per 100,000 population for women 35-39; 40-44; 45-49; 50-54; and 55-59 reported as 59.5; 122.5; 188.6; 224.0; and 266.4, respectively), the likelihood of a mammogram detecting a true cancer clearly increases with age. The American Cancer Society GDG Breast Subgroup balanced the mortality reductions and population-based incidence rates against the risks of mammography “harms” (defined as needing to be recalled for additional testing via imaging and/or biopsy).
The quality of evidence for estimating risk of “overdiagnosis” (detecting a breast cancer that was not destined to be biologically significant or life threatening) was deemed to be insufficient and so this controversial metric was omitted from the final analysis. However, data regarding the general tendency for breast cancers to have more favorable biologic features (and therefore presumed to be more indolent) in older-aged women were taken into account with regard to recommendations for age-based screening intervals.
Upon review of the above incidence and mortality-related issues, the Society generated their age- and interval-based mammography screening recommendations. The recommendations were stratified as either “strong” (defined as a screening practice that “most” patients should follow, and one that could be reasonably used as a “quality criterion or performance indicator”) or “qualified” (defined as a screening practice that is reasonable for the “majority” of patients, but encouraging a balanced discussion of possible alternatives and informed decision making). The recommendations for average-risk women are summarized as follows:
• Strong Recommendation: Women should initiate screening mammography at age 45 years.
• Qualified Recommendation: Screening mammography should be performed annually between ages 45 and 54 years.
• Qualified Recommendation: Women should have the opportunity to undergo annual screening mammography between ages 40 and 44 years.
• Qualified Recommendation: Women aged 55 and older should transition to biennial screening mammography but they should have the opportunity to continue annual screening.
• Qualified Recommendation: Women should continue screening mammography until they no longer have a life expectancy of at least 10 years.
The updated American Cancer Society screening mammography guideline therefore continues to support availability of annual screening mammography for average-risk women beginning at age 40 years and continuing for as long as life expectancy supports the benefit of undergoing treatment for a screen-detected breast cancer. However, in acknowledging the increasing risk of breast cancer with age and the increased prevalence of biologically favorable breast cancers among older versus younger women, the Society stresses that screening mammography is a must by the time a woman reaches age 45, and that she can safely consider transitioning from annual to biennial screening at age 55.
Other components of the updated guideline:
While the mammography component of the breast cancer screening guidelines have provoked the most substantial discussion, they have also addressed other screening practices, and these are summarized as follows:
• Qualified Recommendation: Clinical breast examination is not recommended for breast cancer screening among average-risk women at any age.
• Not addressed in the update, and therefore not changed from prior American Cancer Society recommendation: Breast self-examination is not recommended for average-risk women at any age.
Additional issues in the screening mammography debate
While the American Cancer Society and other organizations attempt to synthesize and interpret the existing data regarding the benefits and risks of various screening practices, clinicians must also consider several public health issues when deciding upon their own screening recommendation practices:
• Disparities and variation in breast cancer patterns associated with racial/ethnic identity: Although white American women have historically had higher population-based incidence rates of breast cancer, compared with African American women, incidence rates have risen among African Americans, and 2012 data indicate comparable rates for both groups. Furthermore, breast cancer outcome disparities have worsened, with breast cancer mortality rates 42% higher for African Americans (CA Cancer J Clin. 2015 Oct 29. doi: 10.3322/caac.21320 [Epub ahead of print]). African American women have a twofold higher population-based incidence rate of the biologically more aggressive triple-negative breast cancers at all ages, and the rates among African American women in their forties is higher than those among white American women in their fifties (Cancer. 2011;117[12]:2747-53; J Natl Cancer Inst. 2015;107[6]: djv048). Prevalence of breast cancer in the premenopausal age range is also higher among African American patients. Delayed initiation of breast cancer screening, and more prolonged intervals between screenings is therefore likely to have a disproportionate impact on the breast cancer burden of the African American population.
• Demographics of the American female population: While overall population-based incidence rates of breast cancer have been stable among American women younger than age 45 years, U.S. Census data reveal 10 million more women in the 20-45 years age range for 2010, compared with 1980. The absolute number of breast cancer patients belonging to this young age category has therefore increased (JAMA Oncol. 2015;1[7]:877-8).
• Scenarios that are not relevant for routine screening recommendations: Clinicians must continue to aggressively counsel patients regarding the importance of overall breast health awareness. The development of a new breast mass, inflammatory skin changes, and/or bloody nipple discharge should prompt immediate medical attention regardless of the result and timing of the most recent mammogram. Furthermore, women facing increased risk of breast cancer because of family history, chest wall irradiation in adolescence/early adulthood, and high-risk breast biopsy pathology (atypia, lobular carcinoma in situ) are candidates for more intense surveillance such as breast MRI in addition to mammography. The most appropriate management of women with increased risk based upon mammographic density remains unclear. Lastly but extremely importantly, American-based breast cancer screening recommendations do not apply to low- and middle-income countries where screening mammography is not widely available. Clinical breast examination and breast self-examination may play a different role in the breast cancer burden of these populations.
Dr. Newman is an ACS Fellow, Director of the Breast Oncology Program, Multi-Hospital Henry Ford Health System, Detroit, and founding Medical Director, Henry Ford Health System International Center for the Study of Breast Cancer Subtypes. Dr. Newman has acted as a volunteer advisor to the American Cancer Society.
The screening mammography debate has been rekindled by the American Cancer Society’s updated guideline released in October 2015. Surgeons are now looking at yet another iteration of the optimal surveillance schedule aimed at reducing breast cancer mortality.
Nearly all breast cancer patients undergo surgery as at least one component of their care through diagnostic biopsy and/or definitive locoregional management, and many women are referred to surgeons for evaluation as well as follow-up for a variety of benign breast problems. The discussion of breast cancer screening with patients can be complicated by the many guidelines with conflicting recommendations, not to mention patient fears triggered by incompletely informed or simplistic media coverage. Surgeons are therefore obliged to remain knowledgeable regarding the status and rationale for breast cancer screening guidelines that have been developed by our colleagues in the American Cancer Society as well as other organizations.
Context of the updated guideline
The American Cancer Society and the American College of Surgeons have historically advocated in favor of annual screening mammography for average-risk women in the United States beginning at age 40 years (https://goo.gl/4W92EI). In 2009, the United States Preventive Services Task Force (USPSTF) published a recommendation that women delay initiation of screening mammography until reaching age 50, with follow-up studies performed biennially thereafter. This USPSTF guideline has remain unchanged as of 2015 (http://goo.gl/RYYWEP). Other medical societies and institutions have established their own guidelines.
The updated American Cancer Society guideline now recommends that average-risk women initiate annual mammography at age 45, but advocates in favor of availability of annual mammography beginning at age 40; the updated guideline also indicates that women can transition to biennial mammography at age 55, but should have access to continued annual mammography in accordance with personal preferences and after consideration of risks and benefits (JAMA. 2015;314[15]:1599-614).
The updated guideline can basically be interpreted as a more relaxed version of the prior guideline, which featured a straightforward mandate for average-risk women to undergo annual screening mammography beginning at age 40 years. However, the increased complexity of the more flexible guideline has generated legitimate concerns regarding the potential for confusion and misinterpretation.
Updated guideline rationale and empirical basis
The Society commissioned a systematic review to evaluate the benefits and harms of mammographic screening as well as clinical breast examination, based upon randomized clinical trials, and observational and modeling studies (JAMA. 2015;314[15]: 1615-34).
The Society then convened their Guideline Development Group (GDG) and GDG Breast Subgroup to interpret the systematic review for the purpose of drafting the breast cancer screening update. This process was further guided by a panel of External Expert Advisors. Mortality reductions were analyzed in the context of population-based breast cancer incidence rates by 5-year age increments.
Not surprisingly, the overall review confirmed the findings of several published studies that screening mammography in women aged 40-79 reduces breast cancer mortality rates by 20%-50%, with extent of benefit varying by age, as well as study design (randomized clinical trial versus observational). Since breast cancer incidence rates increase substantially among women by age (incidence rates per 100,000 population for women 35-39; 40-44; 45-49; 50-54; and 55-59 reported as 59.5; 122.5; 188.6; 224.0; and 266.4, respectively), the likelihood of a mammogram detecting a true cancer clearly increases with age. The American Cancer Society GDG Breast Subgroup balanced the mortality reductions and population-based incidence rates against the risks of mammography “harms” (defined as needing to be recalled for additional testing via imaging and/or biopsy).
The quality of evidence for estimating risk of “overdiagnosis” (detecting a breast cancer that was not destined to be biologically significant or life threatening) was deemed to be insufficient and so this controversial metric was omitted from the final analysis. However, data regarding the general tendency for breast cancers to have more favorable biologic features (and therefore presumed to be more indolent) in older-aged women were taken into account with regard to recommendations for age-based screening intervals.
Upon review of the above incidence and mortality-related issues, the Society generated their age- and interval-based mammography screening recommendations. The recommendations were stratified as either “strong” (defined as a screening practice that “most” patients should follow, and one that could be reasonably used as a “quality criterion or performance indicator”) or “qualified” (defined as a screening practice that is reasonable for the “majority” of patients, but encouraging a balanced discussion of possible alternatives and informed decision making). The recommendations for average-risk women are summarized as follows:
• Strong Recommendation: Women should initiate screening mammography at age 45 years.
• Qualified Recommendation: Screening mammography should be performed annually between ages 45 and 54 years.
• Qualified Recommendation: Women should have the opportunity to undergo annual screening mammography between ages 40 and 44 years.
• Qualified Recommendation: Women aged 55 and older should transition to biennial screening mammography but they should have the opportunity to continue annual screening.
• Qualified Recommendation: Women should continue screening mammography until they no longer have a life expectancy of at least 10 years.
The updated American Cancer Society screening mammography guideline therefore continues to support availability of annual screening mammography for average-risk women beginning at age 40 years and continuing for as long as life expectancy supports the benefit of undergoing treatment for a screen-detected breast cancer. However, in acknowledging the increasing risk of breast cancer with age and the increased prevalence of biologically favorable breast cancers among older versus younger women, the Society stresses that screening mammography is a must by the time a woman reaches age 45, and that she can safely consider transitioning from annual to biennial screening at age 55.
Other components of the updated guideline:
While the mammography component of the breast cancer screening guidelines have provoked the most substantial discussion, they have also addressed other screening practices, and these are summarized as follows:
• Qualified Recommendation: Clinical breast examination is not recommended for breast cancer screening among average-risk women at any age.
• Not addressed in the update, and therefore not changed from prior American Cancer Society recommendation: Breast self-examination is not recommended for average-risk women at any age.
Additional issues in the screening mammography debate
While the American Cancer Society and other organizations attempt to synthesize and interpret the existing data regarding the benefits and risks of various screening practices, clinicians must also consider several public health issues when deciding upon their own screening recommendation practices:
• Disparities and variation in breast cancer patterns associated with racial/ethnic identity: Although white American women have historically had higher population-based incidence rates of breast cancer, compared with African American women, incidence rates have risen among African Americans, and 2012 data indicate comparable rates for both groups. Furthermore, breast cancer outcome disparities have worsened, with breast cancer mortality rates 42% higher for African Americans (CA Cancer J Clin. 2015 Oct 29. doi: 10.3322/caac.21320 [Epub ahead of print]). African American women have a twofold higher population-based incidence rate of the biologically more aggressive triple-negative breast cancers at all ages, and the rates among African American women in their forties is higher than those among white American women in their fifties (Cancer. 2011;117[12]:2747-53; J Natl Cancer Inst. 2015;107[6]: djv048). Prevalence of breast cancer in the premenopausal age range is also higher among African American patients. Delayed initiation of breast cancer screening, and more prolonged intervals between screenings is therefore likely to have a disproportionate impact on the breast cancer burden of the African American population.
• Demographics of the American female population: While overall population-based incidence rates of breast cancer have been stable among American women younger than age 45 years, U.S. Census data reveal 10 million more women in the 20-45 years age range for 2010, compared with 1980. The absolute number of breast cancer patients belonging to this young age category has therefore increased (JAMA Oncol. 2015;1[7]:877-8).
• Scenarios that are not relevant for routine screening recommendations: Clinicians must continue to aggressively counsel patients regarding the importance of overall breast health awareness. The development of a new breast mass, inflammatory skin changes, and/or bloody nipple discharge should prompt immediate medical attention regardless of the result and timing of the most recent mammogram. Furthermore, women facing increased risk of breast cancer because of family history, chest wall irradiation in adolescence/early adulthood, and high-risk breast biopsy pathology (atypia, lobular carcinoma in situ) are candidates for more intense surveillance such as breast MRI in addition to mammography. The most appropriate management of women with increased risk based upon mammographic density remains unclear. Lastly but extremely importantly, American-based breast cancer screening recommendations do not apply to low- and middle-income countries where screening mammography is not widely available. Clinical breast examination and breast self-examination may play a different role in the breast cancer burden of these populations.
Dr. Newman is an ACS Fellow, Director of the Breast Oncology Program, Multi-Hospital Henry Ford Health System, Detroit, and founding Medical Director, Henry Ford Health System International Center for the Study of Breast Cancer Subtypes. Dr. Newman has acted as a volunteer advisor to the American Cancer Society.
The screening mammography debate has been rekindled by the American Cancer Society’s updated guideline released in October 2015. Surgeons are now looking at yet another iteration of the optimal surveillance schedule aimed at reducing breast cancer mortality.
Nearly all breast cancer patients undergo surgery as at least one component of their care through diagnostic biopsy and/or definitive locoregional management, and many women are referred to surgeons for evaluation as well as follow-up for a variety of benign breast problems. The discussion of breast cancer screening with patients can be complicated by the many guidelines with conflicting recommendations, not to mention patient fears triggered by incompletely informed or simplistic media coverage. Surgeons are therefore obliged to remain knowledgeable regarding the status and rationale for breast cancer screening guidelines that have been developed by our colleagues in the American Cancer Society as well as other organizations.
Context of the updated guideline
The American Cancer Society and the American College of Surgeons have historically advocated in favor of annual screening mammography for average-risk women in the United States beginning at age 40 years (https://goo.gl/4W92EI). In 2009, the United States Preventive Services Task Force (USPSTF) published a recommendation that women delay initiation of screening mammography until reaching age 50, with follow-up studies performed biennially thereafter. This USPSTF guideline has remain unchanged as of 2015 (http://goo.gl/RYYWEP). Other medical societies and institutions have established their own guidelines.
The updated American Cancer Society guideline now recommends that average-risk women initiate annual mammography at age 45, but advocates in favor of availability of annual mammography beginning at age 40; the updated guideline also indicates that women can transition to biennial mammography at age 55, but should have access to continued annual mammography in accordance with personal preferences and after consideration of risks and benefits (JAMA. 2015;314[15]:1599-614).
The updated guideline can basically be interpreted as a more relaxed version of the prior guideline, which featured a straightforward mandate for average-risk women to undergo annual screening mammography beginning at age 40 years. However, the increased complexity of the more flexible guideline has generated legitimate concerns regarding the potential for confusion and misinterpretation.
Updated guideline rationale and empirical basis
The Society commissioned a systematic review to evaluate the benefits and harms of mammographic screening as well as clinical breast examination, based upon randomized clinical trials, and observational and modeling studies (JAMA. 2015;314[15]: 1615-34).
The Society then convened their Guideline Development Group (GDG) and GDG Breast Subgroup to interpret the systematic review for the purpose of drafting the breast cancer screening update. This process was further guided by a panel of External Expert Advisors. Mortality reductions were analyzed in the context of population-based breast cancer incidence rates by 5-year age increments.
Not surprisingly, the overall review confirmed the findings of several published studies that screening mammography in women aged 40-79 reduces breast cancer mortality rates by 20%-50%, with extent of benefit varying by age, as well as study design (randomized clinical trial versus observational). Since breast cancer incidence rates increase substantially among women by age (incidence rates per 100,000 population for women 35-39; 40-44; 45-49; 50-54; and 55-59 reported as 59.5; 122.5; 188.6; 224.0; and 266.4, respectively), the likelihood of a mammogram detecting a true cancer clearly increases with age. The American Cancer Society GDG Breast Subgroup balanced the mortality reductions and population-based incidence rates against the risks of mammography “harms” (defined as needing to be recalled for additional testing via imaging and/or biopsy).
The quality of evidence for estimating risk of “overdiagnosis” (detecting a breast cancer that was not destined to be biologically significant or life threatening) was deemed to be insufficient and so this controversial metric was omitted from the final analysis. However, data regarding the general tendency for breast cancers to have more favorable biologic features (and therefore presumed to be more indolent) in older-aged women were taken into account with regard to recommendations for age-based screening intervals.
Upon review of the above incidence and mortality-related issues, the Society generated their age- and interval-based mammography screening recommendations. The recommendations were stratified as either “strong” (defined as a screening practice that “most” patients should follow, and one that could be reasonably used as a “quality criterion or performance indicator”) or “qualified” (defined as a screening practice that is reasonable for the “majority” of patients, but encouraging a balanced discussion of possible alternatives and informed decision making). The recommendations for average-risk women are summarized as follows:
• Strong Recommendation: Women should initiate screening mammography at age 45 years.
• Qualified Recommendation: Screening mammography should be performed annually between ages 45 and 54 years.
• Qualified Recommendation: Women should have the opportunity to undergo annual screening mammography between ages 40 and 44 years.
• Qualified Recommendation: Women aged 55 and older should transition to biennial screening mammography but they should have the opportunity to continue annual screening.
• Qualified Recommendation: Women should continue screening mammography until they no longer have a life expectancy of at least 10 years.
The updated American Cancer Society screening mammography guideline therefore continues to support availability of annual screening mammography for average-risk women beginning at age 40 years and continuing for as long as life expectancy supports the benefit of undergoing treatment for a screen-detected breast cancer. However, in acknowledging the increasing risk of breast cancer with age and the increased prevalence of biologically favorable breast cancers among older versus younger women, the Society stresses that screening mammography is a must by the time a woman reaches age 45, and that she can safely consider transitioning from annual to biennial screening at age 55.
Other components of the updated guideline:
While the mammography component of the breast cancer screening guidelines have provoked the most substantial discussion, they have also addressed other screening practices, and these are summarized as follows:
• Qualified Recommendation: Clinical breast examination is not recommended for breast cancer screening among average-risk women at any age.
• Not addressed in the update, and therefore not changed from prior American Cancer Society recommendation: Breast self-examination is not recommended for average-risk women at any age.
Additional issues in the screening mammography debate
While the American Cancer Society and other organizations attempt to synthesize and interpret the existing data regarding the benefits and risks of various screening practices, clinicians must also consider several public health issues when deciding upon their own screening recommendation practices:
• Disparities and variation in breast cancer patterns associated with racial/ethnic identity: Although white American women have historically had higher population-based incidence rates of breast cancer, compared with African American women, incidence rates have risen among African Americans, and 2012 data indicate comparable rates for both groups. Furthermore, breast cancer outcome disparities have worsened, with breast cancer mortality rates 42% higher for African Americans (CA Cancer J Clin. 2015 Oct 29. doi: 10.3322/caac.21320 [Epub ahead of print]). African American women have a twofold higher population-based incidence rate of the biologically more aggressive triple-negative breast cancers at all ages, and the rates among African American women in their forties is higher than those among white American women in their fifties (Cancer. 2011;117[12]:2747-53; J Natl Cancer Inst. 2015;107[6]: djv048). Prevalence of breast cancer in the premenopausal age range is also higher among African American patients. Delayed initiation of breast cancer screening, and more prolonged intervals between screenings is therefore likely to have a disproportionate impact on the breast cancer burden of the African American population.
• Demographics of the American female population: While overall population-based incidence rates of breast cancer have been stable among American women younger than age 45 years, U.S. Census data reveal 10 million more women in the 20-45 years age range for 2010, compared with 1980. The absolute number of breast cancer patients belonging to this young age category has therefore increased (JAMA Oncol. 2015;1[7]:877-8).
• Scenarios that are not relevant for routine screening recommendations: Clinicians must continue to aggressively counsel patients regarding the importance of overall breast health awareness. The development of a new breast mass, inflammatory skin changes, and/or bloody nipple discharge should prompt immediate medical attention regardless of the result and timing of the most recent mammogram. Furthermore, women facing increased risk of breast cancer because of family history, chest wall irradiation in adolescence/early adulthood, and high-risk breast biopsy pathology (atypia, lobular carcinoma in situ) are candidates for more intense surveillance such as breast MRI in addition to mammography. The most appropriate management of women with increased risk based upon mammographic density remains unclear. Lastly but extremely importantly, American-based breast cancer screening recommendations do not apply to low- and middle-income countries where screening mammography is not widely available. Clinical breast examination and breast self-examination may play a different role in the breast cancer burden of these populations.
Dr. Newman is an ACS Fellow, Director of the Breast Oncology Program, Multi-Hospital Henry Ford Health System, Detroit, and founding Medical Director, Henry Ford Health System International Center for the Study of Breast Cancer Subtypes. Dr. Newman has acted as a volunteer advisor to the American Cancer Society.
