User login
Metabolic monitoring of antipsychotic meds
Introduction
The use of antipsychotic medications has become more common in children and adolescents over the past 2 decades (Arch Gen Psychiatry. 2012 Dec;69[12]:1247-56). Whether or not one agrees that the trend in prescribing these agents is problematic (and I do), often the prescription and monitoring of antipsychotic medication falls to the primary care clinician who may have concerns about how to manage them. Here, we present a case to illustrate just such an issue.
Case summary
James is a 17-year-old young man with a diagnosis of bipolar disorder made earlier this year after an inpatient day at a local hospital. James had a history of attention-deficit/hyperactivity disorder (ADHD) growing up, but also had a strong family history of bipolar disorder. He began having increasing difficulty during the summer after his junior year, and then had a clear manic episode with elation and grandiosity that necessitated the hospitalization. During the relatively short stay on the psychiatric unit, he was placed on lithium carbonate and risperidone to treat the mania, which did respond. Although it was recommended that he follow up with a child and adolescent psychiatrist, through a series of happenstances he missed two appointments for an intake. He is now only able to get a new intake that is 4 months off.

You have continued to prescribe for him, waiting for what always seemed to be an imminent appointment. But now he comes to the office for a follow-up visit that can no longer wait. His mood symptoms are actually doing quite well. However, you have always known James to have a relatively thin build in the 25th percentile for weight and the 75th percentile for height. Now (is it possible?) 6 months after starting the risperidone and lithium, he returns to the office in the 50th percentile for weight and remains in the 75th percentile for height. There is nothing else noted to be concerning on physical or mental status examination, but you wonder what should be done for monitoring of his weight, should you be doing it, and whether there are other metabolic parameters that you should be measuring?
Case discussion
Regardless of your stance on pediatric bipolar disorder and the treatments for it, James has been placed on medications that need to be monitored. While it appears that James will, eventually, have a prescriber who can monitor his medication for side effects, it is incumbent on all of his providers to make sure that monitoring is occurring. Recent studies have demonstrated that guidelines for monitoring of antipsychotic use are not consistently being adhered to. For example, Rettew et al. (Pediatrics. 2015 Apr;135[4]:658-65) recently reported that metabolic monitoring that included laboratory tests was reported in only 57.2% of cases where an antipsychotic was prescribed.
Children and adolescents placed on these agents should be monitored in a number of ways. First, height and weight should be taken at baseline and at follow-up visits – at least every 6 months. The American Academy of Child and Adolescent Psychiatry practice parameters state that “consideration of weight management interventions and increased regularity of blood glucose and lipid levels should be implemented if [atypical antipsychotic agent]–induced weight gain exceeds 90th percentile body mass index (BMI) for age, or a change of five BMI units in those youths who were obese at the beginning of treatment.” Fasting blood sugar, fasting triglyceride, and cholesterol panels should be done at baseline and at approximately 6-month intervals. Screening for dystonic movements with an Abnormal Involuntary Movement Scale (AIMS) should be done at 6-month intervals. In the case of risperidone, if there are any questions about gynecomastia, galactorrhea, and/or sexual dysfunction, a prolactin level should be considered. Certain other antipsychotics require specific monitoring (for example, ECG for prolonged QT interval for ziprasidone, CBC for clozapine, and an eye exam for quetiapine).
The most important kinds of monitoring are for dose and efficacy. While the antipsychotic medications may have a role, they are not a panacea and do carry longer-term risks of metabolic problems and obesity, among others. If it is possible to provide interventions to reduce the dose or duration of use, that is preferable. If not, it’s best to work with the psychiatrist (if available) to determine who will perform the monitoring and how often it will be done to stave off metabolic problems as early as possible.
Dr. Althoff is associate professor of psychiatry, psychology, and pediatrics at the University of Vermont, Burlington. He is director of the division of behavioral genetics and conducts research on the development of self-regulation in children. Dr. Althoff receives no funding from pharmaceutical companies or industry. He has grant funding from the National Institute of General Medical Sciences and the Klingenstein Third Generation Foundation and is employed, in part, by the nonprofit Research Center for Children, Youth, and Families that develops the Child Behavior Checklist and associated instruments. E-mail him at [email protected].
Introduction
The use of antipsychotic medications has become more common in children and adolescents over the past 2 decades (Arch Gen Psychiatry. 2012 Dec;69[12]:1247-56). Whether or not one agrees that the trend in prescribing these agents is problematic (and I do), often the prescription and monitoring of antipsychotic medication falls to the primary care clinician who may have concerns about how to manage them. Here, we present a case to illustrate just such an issue.
Case summary
James is a 17-year-old young man with a diagnosis of bipolar disorder made earlier this year after an inpatient day at a local hospital. James had a history of attention-deficit/hyperactivity disorder (ADHD) growing up, but also had a strong family history of bipolar disorder. He began having increasing difficulty during the summer after his junior year, and then had a clear manic episode with elation and grandiosity that necessitated the hospitalization. During the relatively short stay on the psychiatric unit, he was placed on lithium carbonate and risperidone to treat the mania, which did respond. Although it was recommended that he follow up with a child and adolescent psychiatrist, through a series of happenstances he missed two appointments for an intake. He is now only able to get a new intake that is 4 months off.
You have continued to prescribe for him, waiting for what always seemed to be an imminent appointment. But now he comes to the office for a follow-up visit that can no longer wait. His mood symptoms are actually doing quite well. However, you have always known James to have a relatively thin build in the 25th percentile for weight and the 75th percentile for height. Now (is it possible?) 6 months after starting the risperidone and lithium, he returns to the office in the 50th percentile for weight and remains in the 75th percentile for height. There is nothing else noted to be concerning on physical or mental status examination, but you wonder what should be done for monitoring of his weight, should you be doing it, and whether there are other metabolic parameters that you should be measuring?
Case discussion
Regardless of your stance on pediatric bipolar disorder and the treatments for it, James has been placed on medications that need to be monitored. While it appears that James will, eventually, have a prescriber who can monitor his medication for side effects, it is incumbent on all of his providers to make sure that monitoring is occurring. Recent studies have demonstrated that guidelines for monitoring of antipsychotic use are not consistently being adhered to. For example, Rettew et al. (Pediatrics. 2015 Apr;135[4]:658-65) recently reported that metabolic monitoring that included laboratory tests was reported in only 57.2% of cases where an antipsychotic was prescribed.
Children and adolescents placed on these agents should be monitored in a number of ways. First, height and weight should be taken at baseline and at follow-up visits – at least every 6 months. The American Academy of Child and Adolescent Psychiatry practice parameters state that “consideration of weight management interventions and increased regularity of blood glucose and lipid levels should be implemented if [atypical antipsychotic agent]–induced weight gain exceeds 90th percentile body mass index (BMI) for age, or a change of five BMI units in those youths who were obese at the beginning of treatment.” Fasting blood sugar, fasting triglyceride, and cholesterol panels should be done at baseline and at approximately 6-month intervals. Screening for dystonic movements with an Abnormal Involuntary Movement Scale (AIMS) should be done at 6-month intervals. In the case of risperidone, if there are any questions about gynecomastia, galactorrhea, and/or sexual dysfunction, a prolactin level should be considered. Certain other antipsychotics require specific monitoring (for example, ECG for prolonged QT interval for ziprasidone, CBC for clozapine, and an eye exam for quetiapine).
The most important kinds of monitoring are for dose and efficacy. While the antipsychotic medications may have a role, they are not a panacea and do carry longer-term risks of metabolic problems and obesity, among others. If it is possible to provide interventions to reduce the dose or duration of use, that is preferable. If not, it’s best to work with the psychiatrist (if available) to determine who will perform the monitoring and how often it will be done to stave off metabolic problems as early as possible.
Dr. Althoff is associate professor of psychiatry, psychology, and pediatrics at the University of Vermont, Burlington. He is director of the division of behavioral genetics and conducts research on the development of self-regulation in children. Dr. Althoff receives no funding from pharmaceutical companies or industry. He has grant funding from the National Institute of General Medical Sciences and the Klingenstein Third Generation Foundation and is employed, in part, by the nonprofit Research Center for Children, Youth, and Families that develops the Child Behavior Checklist and associated instruments. E-mail him at [email protected].
Introduction
The use of antipsychotic medications has become more common in children and adolescents over the past 2 decades (Arch Gen Psychiatry. 2012 Dec;69[12]:1247-56). Whether or not one agrees that the trend in prescribing these agents is problematic (and I do), often the prescription and monitoring of antipsychotic medication falls to the primary care clinician who may have concerns about how to manage them. Here, we present a case to illustrate just such an issue.
Case summary
James is a 17-year-old young man with a diagnosis of bipolar disorder made earlier this year after an inpatient day at a local hospital. James had a history of attention-deficit/hyperactivity disorder (ADHD) growing up, but also had a strong family history of bipolar disorder. He began having increasing difficulty during the summer after his junior year, and then had a clear manic episode with elation and grandiosity that necessitated the hospitalization. During the relatively short stay on the psychiatric unit, he was placed on lithium carbonate and risperidone to treat the mania, which did respond. Although it was recommended that he follow up with a child and adolescent psychiatrist, through a series of happenstances he missed two appointments for an intake. He is now only able to get a new intake that is 4 months off.
You have continued to prescribe for him, waiting for what always seemed to be an imminent appointment. But now he comes to the office for a follow-up visit that can no longer wait. His mood symptoms are actually doing quite well. However, you have always known James to have a relatively thin build in the 25th percentile for weight and the 75th percentile for height. Now (is it possible?) 6 months after starting the risperidone and lithium, he returns to the office in the 50th percentile for weight and remains in the 75th percentile for height. There is nothing else noted to be concerning on physical or mental status examination, but you wonder what should be done for monitoring of his weight, should you be doing it, and whether there are other metabolic parameters that you should be measuring?
Case discussion
Regardless of your stance on pediatric bipolar disorder and the treatments for it, James has been placed on medications that need to be monitored. While it appears that James will, eventually, have a prescriber who can monitor his medication for side effects, it is incumbent on all of his providers to make sure that monitoring is occurring. Recent studies have demonstrated that guidelines for monitoring of antipsychotic use are not consistently being adhered to. For example, Rettew et al. (Pediatrics. 2015 Apr;135[4]:658-65) recently reported that metabolic monitoring that included laboratory tests was reported in only 57.2% of cases where an antipsychotic was prescribed.
Children and adolescents placed on these agents should be monitored in a number of ways. First, height and weight should be taken at baseline and at follow-up visits – at least every 6 months. The American Academy of Child and Adolescent Psychiatry practice parameters state that “consideration of weight management interventions and increased regularity of blood glucose and lipid levels should be implemented if [atypical antipsychotic agent]–induced weight gain exceeds 90th percentile body mass index (BMI) for age, or a change of five BMI units in those youths who were obese at the beginning of treatment.” Fasting blood sugar, fasting triglyceride, and cholesterol panels should be done at baseline and at approximately 6-month intervals. Screening for dystonic movements with an Abnormal Involuntary Movement Scale (AIMS) should be done at 6-month intervals. In the case of risperidone, if there are any questions about gynecomastia, galactorrhea, and/or sexual dysfunction, a prolactin level should be considered. Certain other antipsychotics require specific monitoring (for example, ECG for prolonged QT interval for ziprasidone, CBC for clozapine, and an eye exam for quetiapine).
The most important kinds of monitoring are for dose and efficacy. While the antipsychotic medications may have a role, they are not a panacea and do carry longer-term risks of metabolic problems and obesity, among others. If it is possible to provide interventions to reduce the dose or duration of use, that is preferable. If not, it’s best to work with the psychiatrist (if available) to determine who will perform the monitoring and how often it will be done to stave off metabolic problems as early as possible.
Dr. Althoff is associate professor of psychiatry, psychology, and pediatrics at the University of Vermont, Burlington. He is director of the division of behavioral genetics and conducts research on the development of self-regulation in children. Dr. Althoff receives no funding from pharmaceutical companies or industry. He has grant funding from the National Institute of General Medical Sciences and the Klingenstein Third Generation Foundation and is employed, in part, by the nonprofit Research Center for Children, Youth, and Families that develops the Child Behavior Checklist and associated instruments. E-mail him at [email protected].

Reflections on My VA Experience and Why I See the Proverbial Glass as Half Full
Veterans Health Administration (VA) hospitals have received notoriety due to episodes of misdiagnosis, poor management, and negligent care described in many recent reports and news articles.1-3 While veterans are appropriately the primary focus of these investigative reports, physicians are also challenged in this setting, as they often meet resistance when advocating for patients and attempting to improve a flawed system.2 Although my residency training includes 6 months at a VA hospital mired in controversy, the hospital has played a critical role in my training.3
Despite my many frustrations with the VA and the daily stresses incurred because of barriers impeding the timing and quality of care, I have several reasons to see the glass as “half full” when reflecting on my experiences as an orthopedic surgery resident at a VA medical center. This editorial will focus on the most important of these reasons—the special opportunity and pride associated with caring for veterans and these patients’ extremely appreciative nature.
The VA is one of the largest integrated health care systems in the United States, offering both inpatient and outpatient care to eligible veterans. Although eligibility has historically been based on military service–related medical conditions, disability, and financial need, reforms from 1996 to 2002 expanded enrollment to veteran populations previously deemed ineligible for VA care.4,5 Despite this, studies suggest that some uninsured veterans do not seek VA care, even when eligible for VA coverage. This troubling notion is further complicated by research suggesting that veterans who use the VA for all of their health care are more likely to be from poor, less-educated, and minority populations, and are more likely to report fair or poor health and seek more disability days.6
Such disheartening realities can mask the most important attributes of VA patients, which pertain to their selfless commitment to our country. Orthopedic surgery residents must appreciate these attributes as well as the tremendous need for musculoskeletal care in this setting, as musculoskeletal conditions are some of the most common reasons for patient visits at the VA.7 Although combat-related high-energy blast injuries and the reconstructive procedures used to treat them have received a lot of attention, it is the more common musculoskeletal disorders that are most responsible for the tremendous burden of musculoskeletal disease in the VA. In a study by Dominick and colleagues,8 veterans had significantly greater odds of reporting doctor-diagnosed arthritis compared with nonveterans. Furthermore, veterans are also more vulnerable to overuse injuries, a finding attributed to the intense physical activity associated with military training and service.9
The busy orthopedic surgery clinic at my VA hospital is a fulfilling experience and a reminder of the large demand for musculoskeletal care. However, it is the patient population that makes it most gratifying. Most of the veterans seeking care are appreciative, regularly expressing their gratitude. They view me and the other residents as their physicians, not simply as doctors in training, like so many other non-VA patients do. Despite the fact that VA patients sometimes have to wait several hours to be seen in clinic and several months for surgery, I have never been subjected to their inevitable disdain or frustration. This is true in even the most trying and infuriating times, such as when an operation is cancelled on the day of surgery for reasons that many surgeons in non-VA hospitals would consider trivial. And even when witness to my visible irritation with the VA system, the veterans remain respectful and understanding; if they ever share similar feelings, they most certainly never voice them to me.
I cannot refute the notion that the VA must change and that the veterans deserve an improved health care system. However, this editorial is not written as a call to action. Instead, I hope it helps to humanize the patients of the VA, serving as a reminder to residents and other providers that the VA is a unique and extraordinary opportunity to give back and say thank you to veterans.
This editorial is dedicated to CPT David Huskie, USAR (Ret.), a veteran of Operation Desert Storm and orthopedic nurse at my VA hospital. It was he who first reminded me, and the other orthopedic residents, of the importance of our time at the VA. The Figure depicts the letter he gives to orthopedic residents at our program, along with a pewter coin, after their first VA rotation.
1. Pearson M. The VA’s troubled history. Cable News Network (CNN) website. http://www.cnn.com/2014/05/23/politics/va-scandals-timeline. Updated May 30, 2014. Accessed August 28, 2015.
2. Scherz H. Doctors’ war stories from VA hospitals. The Wall Street Journal website. http://www.wsj.com/articles/hal-scherz-doctors-war-stories-from-va-hospitals-1401233147. Published May 27, 2014. Accessed August 28, 2015.
3. Riviello V. Nurse exposes VA hospital: stolen drugs, tortured veterans. New York Post website. http://nypost.com/2014/07/12/nurse-exposes-va-hospital-stolen-drugs-tortured-veterans. Published July 12, 2014. Accessed August 28, 2015.
4. Enrollment—provision of hospital and outpatient care to veterans—VA. Proposed rule. Fed Regist. 1998;63(132):37299-37307.
5. US Department of Veterans Affairs, Veterans Health Administration, Office of Assistant Deputy Under Secretary for Health for Policy and Planning. 2003 Survey of Veteran Enrollees’ Health and Reliance Upon VA With Selected Comparisons to the 1999 and 2002 Surveys. US Department of Veterans Affairs website. www.va.gov/healthpolicyplanning/Docs/SOE2003_Report.pdf. Published December 2004. Accessed August 28, 2015.
6. Nelson KM, Starkebaum GA, Reiber GE. Veterans using and uninsured veterans not using Veterans Affairs (VA) health care. Public Health Rep. 2007;122(1):93-100.
7. Wasserman GM, Martin BL, Hyams KC, Merrill BR, Oaks HG, McAdoo HA. A survey of outpatient visits in a United States Army forward unit during Operation Desert Shield. Mil Med. 1997;162(6):374-379.
8. Dominick KL, Golightly YM, Jackson GL. Arthritis prevalence and symptoms among US non-veterans, veterans, and veterans receiving Department of Veterans Affairs Healthcare. J Rheumatol. 2006;33(2):348-354.
9. West SG. Rheumatic disorders during Operation Desert Storm. Arthritis Rheum. 1993;36(10):1487-1488.
Veterans Health Administration (VA) hospitals have received notoriety due to episodes of misdiagnosis, poor management, and negligent care described in many recent reports and news articles.1-3 While veterans are appropriately the primary focus of these investigative reports, physicians are also challenged in this setting, as they often meet resistance when advocating for patients and attempting to improve a flawed system.2 Although my residency training includes 6 months at a VA hospital mired in controversy, the hospital has played a critical role in my training.3
Despite my many frustrations with the VA and the daily stresses incurred because of barriers impeding the timing and quality of care, I have several reasons to see the glass as “half full” when reflecting on my experiences as an orthopedic surgery resident at a VA medical center. This editorial will focus on the most important of these reasons—the special opportunity and pride associated with caring for veterans and these patients’ extremely appreciative nature.
The VA is one of the largest integrated health care systems in the United States, offering both inpatient and outpatient care to eligible veterans. Although eligibility has historically been based on military service–related medical conditions, disability, and financial need, reforms from 1996 to 2002 expanded enrollment to veteran populations previously deemed ineligible for VA care.4,5 Despite this, studies suggest that some uninsured veterans do not seek VA care, even when eligible for VA coverage. This troubling notion is further complicated by research suggesting that veterans who use the VA for all of their health care are more likely to be from poor, less-educated, and minority populations, and are more likely to report fair or poor health and seek more disability days.6
Such disheartening realities can mask the most important attributes of VA patients, which pertain to their selfless commitment to our country. Orthopedic surgery residents must appreciate these attributes as well as the tremendous need for musculoskeletal care in this setting, as musculoskeletal conditions are some of the most common reasons for patient visits at the VA.7 Although combat-related high-energy blast injuries and the reconstructive procedures used to treat them have received a lot of attention, it is the more common musculoskeletal disorders that are most responsible for the tremendous burden of musculoskeletal disease in the VA. In a study by Dominick and colleagues,8 veterans had significantly greater odds of reporting doctor-diagnosed arthritis compared with nonveterans. Furthermore, veterans are also more vulnerable to overuse injuries, a finding attributed to the intense physical activity associated with military training and service.9
The busy orthopedic surgery clinic at my VA hospital is a fulfilling experience and a reminder of the large demand for musculoskeletal care. However, it is the patient population that makes it most gratifying. Most of the veterans seeking care are appreciative, regularly expressing their gratitude. They view me and the other residents as their physicians, not simply as doctors in training, like so many other non-VA patients do. Despite the fact that VA patients sometimes have to wait several hours to be seen in clinic and several months for surgery, I have never been subjected to their inevitable disdain or frustration. This is true in even the most trying and infuriating times, such as when an operation is cancelled on the day of surgery for reasons that many surgeons in non-VA hospitals would consider trivial. And even when witness to my visible irritation with the VA system, the veterans remain respectful and understanding; if they ever share similar feelings, they most certainly never voice them to me.
I cannot refute the notion that the VA must change and that the veterans deserve an improved health care system. However, this editorial is not written as a call to action. Instead, I hope it helps to humanize the patients of the VA, serving as a reminder to residents and other providers that the VA is a unique and extraordinary opportunity to give back and say thank you to veterans.
This editorial is dedicated to CPT David Huskie, USAR (Ret.), a veteran of Operation Desert Storm and orthopedic nurse at my VA hospital. It was he who first reminded me, and the other orthopedic residents, of the importance of our time at the VA. The Figure depicts the letter he gives to orthopedic residents at our program, along with a pewter coin, after their first VA rotation.
Veterans Health Administration (VA) hospitals have received notoriety due to episodes of misdiagnosis, poor management, and negligent care described in many recent reports and news articles.1-3 While veterans are appropriately the primary focus of these investigative reports, physicians are also challenged in this setting, as they often meet resistance when advocating for patients and attempting to improve a flawed system.2 Although my residency training includes 6 months at a VA hospital mired in controversy, the hospital has played a critical role in my training.3
Despite my many frustrations with the VA and the daily stresses incurred because of barriers impeding the timing and quality of care, I have several reasons to see the glass as “half full” when reflecting on my experiences as an orthopedic surgery resident at a VA medical center. This editorial will focus on the most important of these reasons—the special opportunity and pride associated with caring for veterans and these patients’ extremely appreciative nature.
The VA is one of the largest integrated health care systems in the United States, offering both inpatient and outpatient care to eligible veterans. Although eligibility has historically been based on military service–related medical conditions, disability, and financial need, reforms from 1996 to 2002 expanded enrollment to veteran populations previously deemed ineligible for VA care.4,5 Despite this, studies suggest that some uninsured veterans do not seek VA care, even when eligible for VA coverage. This troubling notion is further complicated by research suggesting that veterans who use the VA for all of their health care are more likely to be from poor, less-educated, and minority populations, and are more likely to report fair or poor health and seek more disability days.6
Such disheartening realities can mask the most important attributes of VA patients, which pertain to their selfless commitment to our country. Orthopedic surgery residents must appreciate these attributes as well as the tremendous need for musculoskeletal care in this setting, as musculoskeletal conditions are some of the most common reasons for patient visits at the VA.7 Although combat-related high-energy blast injuries and the reconstructive procedures used to treat them have received a lot of attention, it is the more common musculoskeletal disorders that are most responsible for the tremendous burden of musculoskeletal disease in the VA. In a study by Dominick and colleagues,8 veterans had significantly greater odds of reporting doctor-diagnosed arthritis compared with nonveterans. Furthermore, veterans are also more vulnerable to overuse injuries, a finding attributed to the intense physical activity associated with military training and service.9
The busy orthopedic surgery clinic at my VA hospital is a fulfilling experience and a reminder of the large demand for musculoskeletal care. However, it is the patient population that makes it most gratifying. Most of the veterans seeking care are appreciative, regularly expressing their gratitude. They view me and the other residents as their physicians, not simply as doctors in training, like so many other non-VA patients do. Despite the fact that VA patients sometimes have to wait several hours to be seen in clinic and several months for surgery, I have never been subjected to their inevitable disdain or frustration. This is true in even the most trying and infuriating times, such as when an operation is cancelled on the day of surgery for reasons that many surgeons in non-VA hospitals would consider trivial. And even when witness to my visible irritation with the VA system, the veterans remain respectful and understanding; if they ever share similar feelings, they most certainly never voice them to me.
I cannot refute the notion that the VA must change and that the veterans deserve an improved health care system. However, this editorial is not written as a call to action. Instead, I hope it helps to humanize the patients of the VA, serving as a reminder to residents and other providers that the VA is a unique and extraordinary opportunity to give back and say thank you to veterans.
This editorial is dedicated to CPT David Huskie, USAR (Ret.), a veteran of Operation Desert Storm and orthopedic nurse at my VA hospital. It was he who first reminded me, and the other orthopedic residents, of the importance of our time at the VA. The Figure depicts the letter he gives to orthopedic residents at our program, along with a pewter coin, after their first VA rotation.
1. Pearson M. The VA’s troubled history. Cable News Network (CNN) website. http://www.cnn.com/2014/05/23/politics/va-scandals-timeline. Updated May 30, 2014. Accessed August 28, 2015.
2. Scherz H. Doctors’ war stories from VA hospitals. The Wall Street Journal website. http://www.wsj.com/articles/hal-scherz-doctors-war-stories-from-va-hospitals-1401233147. Published May 27, 2014. Accessed August 28, 2015.
3. Riviello V. Nurse exposes VA hospital: stolen drugs, tortured veterans. New York Post website. http://nypost.com/2014/07/12/nurse-exposes-va-hospital-stolen-drugs-tortured-veterans. Published July 12, 2014. Accessed August 28, 2015.
4. Enrollment—provision of hospital and outpatient care to veterans—VA. Proposed rule. Fed Regist. 1998;63(132):37299-37307.
5. US Department of Veterans Affairs, Veterans Health Administration, Office of Assistant Deputy Under Secretary for Health for Policy and Planning. 2003 Survey of Veteran Enrollees’ Health and Reliance Upon VA With Selected Comparisons to the 1999 and 2002 Surveys. US Department of Veterans Affairs website. www.va.gov/healthpolicyplanning/Docs/SOE2003_Report.pdf. Published December 2004. Accessed August 28, 2015.
6. Nelson KM, Starkebaum GA, Reiber GE. Veterans using and uninsured veterans not using Veterans Affairs (VA) health care. Public Health Rep. 2007;122(1):93-100.
7. Wasserman GM, Martin BL, Hyams KC, Merrill BR, Oaks HG, McAdoo HA. A survey of outpatient visits in a United States Army forward unit during Operation Desert Shield. Mil Med. 1997;162(6):374-379.
8. Dominick KL, Golightly YM, Jackson GL. Arthritis prevalence and symptoms among US non-veterans, veterans, and veterans receiving Department of Veterans Affairs Healthcare. J Rheumatol. 2006;33(2):348-354.
9. West SG. Rheumatic disorders during Operation Desert Storm. Arthritis Rheum. 1993;36(10):1487-1488.
1. Pearson M. The VA’s troubled history. Cable News Network (CNN) website. http://www.cnn.com/2014/05/23/politics/va-scandals-timeline. Updated May 30, 2014. Accessed August 28, 2015.
2. Scherz H. Doctors’ war stories from VA hospitals. The Wall Street Journal website. http://www.wsj.com/articles/hal-scherz-doctors-war-stories-from-va-hospitals-1401233147. Published May 27, 2014. Accessed August 28, 2015.
3. Riviello V. Nurse exposes VA hospital: stolen drugs, tortured veterans. New York Post website. http://nypost.com/2014/07/12/nurse-exposes-va-hospital-stolen-drugs-tortured-veterans. Published July 12, 2014. Accessed August 28, 2015.
4. Enrollment—provision of hospital and outpatient care to veterans—VA. Proposed rule. Fed Regist. 1998;63(132):37299-37307.
5. US Department of Veterans Affairs, Veterans Health Administration, Office of Assistant Deputy Under Secretary for Health for Policy and Planning. 2003 Survey of Veteran Enrollees’ Health and Reliance Upon VA With Selected Comparisons to the 1999 and 2002 Surveys. US Department of Veterans Affairs website. www.va.gov/healthpolicyplanning/Docs/SOE2003_Report.pdf. Published December 2004. Accessed August 28, 2015.
6. Nelson KM, Starkebaum GA, Reiber GE. Veterans using and uninsured veterans not using Veterans Affairs (VA) health care. Public Health Rep. 2007;122(1):93-100.
7. Wasserman GM, Martin BL, Hyams KC, Merrill BR, Oaks HG, McAdoo HA. A survey of outpatient visits in a United States Army forward unit during Operation Desert Shield. Mil Med. 1997;162(6):374-379.
8. Dominick KL, Golightly YM, Jackson GL. Arthritis prevalence and symptoms among US non-veterans, veterans, and veterans receiving Department of Veterans Affairs Healthcare. J Rheumatol. 2006;33(2):348-354.
9. West SG. Rheumatic disorders during Operation Desert Storm. Arthritis Rheum. 1993;36(10):1487-1488.

ACS Surgery News September issue digital version is available
The September issue of ACS Surgery News is available online -- use the mobile app to download or view as a pdf.
This month's issue features news about intragastric balloons now approved by the FDA, commentary by Dr. Mark Weissler on the rich variety of learning and networking opportunities at the upcoming Clinical Congress, and an update on the implications of a recent court ruling on the number of lawsuits brought against doctors.
The September issue of ACS Surgery News is available online -- use the mobile app to download or view as a pdf.
This month's issue features news about intragastric balloons now approved by the FDA, commentary by Dr. Mark Weissler on the rich variety of learning and networking opportunities at the upcoming Clinical Congress, and an update on the implications of a recent court ruling on the number of lawsuits brought against doctors.
The September issue of ACS Surgery News is available online -- use the mobile app to download or view as a pdf.
This month's issue features news about intragastric balloons now approved by the FDA, commentary by Dr. Mark Weissler on the rich variety of learning and networking opportunities at the upcoming Clinical Congress, and an update on the implications of a recent court ruling on the number of lawsuits brought against doctors.
Bullying
Back to school brings, as it does every year, an increased focus on school issues. Parents and children may feel uncomfortable discussing many of these concerns or may not realize that their pediatrician can be a source of help and support. One topic in particular, bullying, is an important and difficult issue that affects a large number of children and adolescents, yet unfortunately, often goes undetected.
More than half of teens have been either the victims or perpetrators of some type of bullying; for one in five, this takes the form of actual physical bullying or violence. Bullying can happen to anyone, from any socioeconomic status, in any school or neighborhood. Even children who are seemingly well adjusted and “popular” at school can be victimized. The dramatic increase in technology use, smartphones and social media only increases the vulnerability of youth to bullying – cyberbullying can be incredibly damaging and difficult to detect and address.

Pediatric providers can help in many ways. First, don’t hesitate to bring up the issue of bullying during well visits or sports physicals when discussing school performance or school readiness. While I admit – given the large range of topics that need to be covered – I don’t discuss this at every visit, I often do ask about friendships at school and have a low threshold for bringing up the issue of bullying with families.
Second, be alert to possible signs that your patients may be bullied. Nonspecific symptoms – such as headaches, stomach pains, fatigue, or behavior or mood changes – can be manifestations of the distress associated with being bullied. When evaluating children for these concerns, it is important to take a detailed history that includes potential psychosocial stressors or changes, such as bullying. Equally as important is to approach this history-taking in a culturally sensitive and trauma-informed way and to recognize that your patients may not immediately disclose concerns. However, by demonstrating that you are a trusted source of support, you can open the door for future conversations.
Lastly, be prepared to respond in a nonthreatening and nonjudgmental way when concerns arise. These are very challenging situations, and it is important to engage families – and the child or teen – in the best way to address them. Youth may feel a great loss of control in the bullying relationship, and thus, to avoid further trauma, it is critically important for their family and professionals to give them as much control as possible in dealing with it. Of course, there are times when the child’s safety could be compromised, and more directive intervention is needed, but even in those situations the provider and family can help by being open and communicative.
Typically, other support systems will also need to be involved – for example, the school (if that is where the bullying is taking place) or trained mental health providers. Families may need help thinking about the best way to approach or initiate these discussions, especially as they themselves may be angry or in denial. Providers can even serve as a resource to schools and communities in thinking about the best way to prevent and address bullying, either in individual situations or more generally. The U.S. Department of Health & Human Services offers comprehensive resources to providers and families faced with the issue of bullying (www.stopbullying.gov).
As partners with the family, patient, and community, pediatric providers can play an important role in preventing and addressing bullying, which can have a lifelong impact on the health of a child.
Dr. Beers is assistant professor of pediatrics at Children’s National Medical Center and the George Washington University Medical Center, both in Washington.
Back to school brings, as it does every year, an increased focus on school issues. Parents and children may feel uncomfortable discussing many of these concerns or may not realize that their pediatrician can be a source of help and support. One topic in particular, bullying, is an important and difficult issue that affects a large number of children and adolescents, yet unfortunately, often goes undetected.
More than half of teens have been either the victims or perpetrators of some type of bullying; for one in five, this takes the form of actual physical bullying or violence. Bullying can happen to anyone, from any socioeconomic status, in any school or neighborhood. Even children who are seemingly well adjusted and “popular” at school can be victimized. The dramatic increase in technology use, smartphones and social media only increases the vulnerability of youth to bullying – cyberbullying can be incredibly damaging and difficult to detect and address.
Pediatric providers can help in many ways. First, don’t hesitate to bring up the issue of bullying during well visits or sports physicals when discussing school performance or school readiness. While I admit – given the large range of topics that need to be covered – I don’t discuss this at every visit, I often do ask about friendships at school and have a low threshold for bringing up the issue of bullying with families.
Second, be alert to possible signs that your patients may be bullied. Nonspecific symptoms – such as headaches, stomach pains, fatigue, or behavior or mood changes – can be manifestations of the distress associated with being bullied. When evaluating children for these concerns, it is important to take a detailed history that includes potential psychosocial stressors or changes, such as bullying. Equally as important is to approach this history-taking in a culturally sensitive and trauma-informed way and to recognize that your patients may not immediately disclose concerns. However, by demonstrating that you are a trusted source of support, you can open the door for future conversations.
Lastly, be prepared to respond in a nonthreatening and nonjudgmental way when concerns arise. These are very challenging situations, and it is important to engage families – and the child or teen – in the best way to address them. Youth may feel a great loss of control in the bullying relationship, and thus, to avoid further trauma, it is critically important for their family and professionals to give them as much control as possible in dealing with it. Of course, there are times when the child’s safety could be compromised, and more directive intervention is needed, but even in those situations the provider and family can help by being open and communicative.
Typically, other support systems will also need to be involved – for example, the school (if that is where the bullying is taking place) or trained mental health providers. Families may need help thinking about the best way to approach or initiate these discussions, especially as they themselves may be angry or in denial. Providers can even serve as a resource to schools and communities in thinking about the best way to prevent and address bullying, either in individual situations or more generally. The U.S. Department of Health & Human Services offers comprehensive resources to providers and families faced with the issue of bullying (www.stopbullying.gov).
As partners with the family, patient, and community, pediatric providers can play an important role in preventing and addressing bullying, which can have a lifelong impact on the health of a child.
Dr. Beers is assistant professor of pediatrics at Children’s National Medical Center and the George Washington University Medical Center, both in Washington.
Back to school brings, as it does every year, an increased focus on school issues. Parents and children may feel uncomfortable discussing many of these concerns or may not realize that their pediatrician can be a source of help and support. One topic in particular, bullying, is an important and difficult issue that affects a large number of children and adolescents, yet unfortunately, often goes undetected.
More than half of teens have been either the victims or perpetrators of some type of bullying; for one in five, this takes the form of actual physical bullying or violence. Bullying can happen to anyone, from any socioeconomic status, in any school or neighborhood. Even children who are seemingly well adjusted and “popular” at school can be victimized. The dramatic increase in technology use, smartphones and social media only increases the vulnerability of youth to bullying – cyberbullying can be incredibly damaging and difficult to detect and address.
Pediatric providers can help in many ways. First, don’t hesitate to bring up the issue of bullying during well visits or sports physicals when discussing school performance or school readiness. While I admit – given the large range of topics that need to be covered – I don’t discuss this at every visit, I often do ask about friendships at school and have a low threshold for bringing up the issue of bullying with families.
Second, be alert to possible signs that your patients may be bullied. Nonspecific symptoms – such as headaches, stomach pains, fatigue, or behavior or mood changes – can be manifestations of the distress associated with being bullied. When evaluating children for these concerns, it is important to take a detailed history that includes potential psychosocial stressors or changes, such as bullying. Equally as important is to approach this history-taking in a culturally sensitive and trauma-informed way and to recognize that your patients may not immediately disclose concerns. However, by demonstrating that you are a trusted source of support, you can open the door for future conversations.
Lastly, be prepared to respond in a nonthreatening and nonjudgmental way when concerns arise. These are very challenging situations, and it is important to engage families – and the child or teen – in the best way to address them. Youth may feel a great loss of control in the bullying relationship, and thus, to avoid further trauma, it is critically important for their family and professionals to give them as much control as possible in dealing with it. Of course, there are times when the child’s safety could be compromised, and more directive intervention is needed, but even in those situations the provider and family can help by being open and communicative.
Typically, other support systems will also need to be involved – for example, the school (if that is where the bullying is taking place) or trained mental health providers. Families may need help thinking about the best way to approach or initiate these discussions, especially as they themselves may be angry or in denial. Providers can even serve as a resource to schools and communities in thinking about the best way to prevent and address bullying, either in individual situations or more generally. The U.S. Department of Health & Human Services offers comprehensive resources to providers and families faced with the issue of bullying (www.stopbullying.gov).
As partners with the family, patient, and community, pediatric providers can play an important role in preventing and addressing bullying, which can have a lifelong impact on the health of a child.
Dr. Beers is assistant professor of pediatrics at Children’s National Medical Center and the George Washington University Medical Center, both in Washington.

Big changes in practice, but none for the better
Dr. Nasrallah’s approach to psychiatry, especially to the real problems confronting us, is both professionally astute and realistic.
I have been in practice for more than 60 years and have seen tremendous changes—none for the better— in the intrusion of insurance tyranny and government overregulation. Dr. Nasrallah’s comments about obstacles created from the system, regardless of so-called “parity,” hit the mark. The insurance companies control everything by setting fees so low and documentation requirements so high that there is little time to focus on the dynamics of the patient population. Unqualified people are deciding whether or not the medications we prescribe will be paid for.
To illustrate what I think of some of the changes, here is what I have observed:
• Electroconvulsive therapy for severe depression has been “rediscovered,” but for decades those of us who used it selectively, with good results, were considered to be practicing quackery.
• Dr. Nasrallah’s recent article on development of immediate treatment plans for a patient given a diagnosis of schizophrenia (Current Psychiatry. 2015;14(5):32-34,36-40,42 [http://bit.ly/1GLGtrZ]) reminds me of a time when it was thought that you couldn’t diagnose schizophrenia until symptoms had been present for 6 months. (Had they ever heard of the work of Eugen Bleuler?)
• At a national meeting 20 years ago, I raised the question of why every other specialty of medicine stressed early diagnosis and treatment but psychiatry did not—and, instead, was doing the opposite. The speaker did not have the courtesy to answer my question.
Keep up the good work! We need people such as Dr. Nasrallah to educate the public about how government and insurance companies are destroying our specialty.
Dr. Nasrallah’s approach to psychiatry, especially to the real problems confronting us, is both professionally astute and realistic.
I have been in practice for more than 60 years and have seen tremendous changes—none for the better— in the intrusion of insurance tyranny and government overregulation. Dr. Nasrallah’s comments about obstacles created from the system, regardless of so-called “parity,” hit the mark. The insurance companies control everything by setting fees so low and documentation requirements so high that there is little time to focus on the dynamics of the patient population. Unqualified people are deciding whether or not the medications we prescribe will be paid for.
To illustrate what I think of some of the changes, here is what I have observed:
• Electroconvulsive therapy for severe depression has been “rediscovered,” but for decades those of us who used it selectively, with good results, were considered to be practicing quackery.
• Dr. Nasrallah’s recent article on development of immediate treatment plans for a patient given a diagnosis of schizophrenia (Current Psychiatry. 2015;14(5):32-34,36-40,42 [http://bit.ly/1GLGtrZ]) reminds me of a time when it was thought that you couldn’t diagnose schizophrenia until symptoms had been present for 6 months. (Had they ever heard of the work of Eugen Bleuler?)
• At a national meeting 20 years ago, I raised the question of why every other specialty of medicine stressed early diagnosis and treatment but psychiatry did not—and, instead, was doing the opposite. The speaker did not have the courtesy to answer my question.
Keep up the good work! We need people such as Dr. Nasrallah to educate the public about how government and insurance companies are destroying our specialty.
Dr. Nasrallah’s approach to psychiatry, especially to the real problems confronting us, is both professionally astute and realistic.
I have been in practice for more than 60 years and have seen tremendous changes—none for the better— in the intrusion of insurance tyranny and government overregulation. Dr. Nasrallah’s comments about obstacles created from the system, regardless of so-called “parity,” hit the mark. The insurance companies control everything by setting fees so low and documentation requirements so high that there is little time to focus on the dynamics of the patient population. Unqualified people are deciding whether or not the medications we prescribe will be paid for.
To illustrate what I think of some of the changes, here is what I have observed:
• Electroconvulsive therapy for severe depression has been “rediscovered,” but for decades those of us who used it selectively, with good results, were considered to be practicing quackery.
• Dr. Nasrallah’s recent article on development of immediate treatment plans for a patient given a diagnosis of schizophrenia (Current Psychiatry. 2015;14(5):32-34,36-40,42 [http://bit.ly/1GLGtrZ]) reminds me of a time when it was thought that you couldn’t diagnose schizophrenia until symptoms had been present for 6 months. (Had they ever heard of the work of Eugen Bleuler?)
• At a national meeting 20 years ago, I raised the question of why every other specialty of medicine stressed early diagnosis and treatment but psychiatry did not—and, instead, was doing the opposite. The speaker did not have the courtesy to answer my question.
Keep up the good work! We need people such as Dr. Nasrallah to educate the public about how government and insurance companies are destroying our specialty.
A nod to a ‘psychiatry great’
In his recent editorial, “Is there only 1 neurobiologic psychiatric disorder, with different clinical expressions?” (Current Psychiatry. 2015;14(7):10-12 [http://bit.ly/1INCvxw]), Dr. Nasrallah presents convincing evidence for such a conclusion. However, he did not mention that a somewhat similar concept was established by one of psychiatry’s greats, Karl Menninger, MD, more than 50 years ago. I’m referring to Menninger’s unitary concept of mental illness, espoused in his book, The Vital Balance.1 Dr. Menninger was, of course, founder of the Menninger Clinic in Topeka, Kansas, which now thrives in Houston, Texas, at Baylor College of Medicine. Like Freud, who predicted that advances in viewing the brain will someday help us understand it better than he could at the time, Dr. Menninger perhaps was ahead of his time in his perspective on mental illness.
We should appreciate Dr. Nasrallah for putting together the research that provides an updated, somewhat revised view of Dr. Menninger’s theory.
Reference
1. Menninger K. The vital balance. New York, NY: Viking; 1963.
In his recent editorial, “Is there only 1 neurobiologic psychiatric disorder, with different clinical expressions?” (Current Psychiatry. 2015;14(7):10-12 [http://bit.ly/1INCvxw]), Dr. Nasrallah presents convincing evidence for such a conclusion. However, he did not mention that a somewhat similar concept was established by one of psychiatry’s greats, Karl Menninger, MD, more than 50 years ago. I’m referring to Menninger’s unitary concept of mental illness, espoused in his book, The Vital Balance.1 Dr. Menninger was, of course, founder of the Menninger Clinic in Topeka, Kansas, which now thrives in Houston, Texas, at Baylor College of Medicine. Like Freud, who predicted that advances in viewing the brain will someday help us understand it better than he could at the time, Dr. Menninger perhaps was ahead of his time in his perspective on mental illness.
We should appreciate Dr. Nasrallah for putting together the research that provides an updated, somewhat revised view of Dr. Menninger’s theory.
In his recent editorial, “Is there only 1 neurobiologic psychiatric disorder, with different clinical expressions?” (Current Psychiatry. 2015;14(7):10-12 [http://bit.ly/1INCvxw]), Dr. Nasrallah presents convincing evidence for such a conclusion. However, he did not mention that a somewhat similar concept was established by one of psychiatry’s greats, Karl Menninger, MD, more than 50 years ago. I’m referring to Menninger’s unitary concept of mental illness, espoused in his book, The Vital Balance.1 Dr. Menninger was, of course, founder of the Menninger Clinic in Topeka, Kansas, which now thrives in Houston, Texas, at Baylor College of Medicine. Like Freud, who predicted that advances in viewing the brain will someday help us understand it better than he could at the time, Dr. Menninger perhaps was ahead of his time in his perspective on mental illness.
We should appreciate Dr. Nasrallah for putting together the research that provides an updated, somewhat revised view of Dr. Menninger’s theory.
Reference
1. Menninger K. The vital balance. New York, NY: Viking; 1963.
Reference
1. Menninger K. The vital balance. New York, NY: Viking; 1963.
‘Appreciate the editorials’
I appreciate Dr. Nasrallah’s editorial on the so-called abdominal brain (Current Psychiatry. 2015;14(5):10- 11 [http://bit.ly/1PcxFNP]). Current Psychiatry is a journal with useful reports of advances, reviews, and opinion of research and treatment in our specialty. The selections and editing are always pertinent and thoughtful.
I appreciate Dr. Nasrallah’s editorial on the so-called abdominal brain (Current Psychiatry. 2015;14(5):10- 11 [http://bit.ly/1PcxFNP]). Current Psychiatry is a journal with useful reports of advances, reviews, and opinion of research and treatment in our specialty. The selections and editing are always pertinent and thoughtful.
I appreciate Dr. Nasrallah’s editorial on the so-called abdominal brain (Current Psychiatry. 2015;14(5):10- 11 [http://bit.ly/1PcxFNP]). Current Psychiatry is a journal with useful reports of advances, reviews, and opinion of research and treatment in our specialty. The selections and editing are always pertinent and thoughtful.
Practical approaches to promoting brain health
More than once in his Current Psychiatry essays, Henry A. Nasrallah, MD, has stressed the seismic paradigmatic shifts in our understanding of mental illness and brain disease. He has highlighted the critical significance of processes of neurogenesis and neuroinflammation, yet little has been offered to practitioners in terms of practical approaches to promoting the brain health that he encourages.
Two of the most potent modalities for maintaining brain wellness and facilitating ongoing neurogenesis and synaptogenesis are exercise and nutrition—specifically, high-intensity interval training and a diet heavily, if not entirely, plant-based. The neuroprotective capabilities of mindfulness practice and its impact on prefrontal cortical regions also are relevant.
In society at large, it strikes me that physicians have not fared any better than the general population when it comes to maintaining a healthy diet and engaging in physical exercise. I encourage Dr. Nasrallah to continue addressing these themes, and to remind his audience of physicians to “heal thyself.”
More than once in his Current Psychiatry essays, Henry A. Nasrallah, MD, has stressed the seismic paradigmatic shifts in our understanding of mental illness and brain disease. He has highlighted the critical significance of processes of neurogenesis and neuroinflammation, yet little has been offered to practitioners in terms of practical approaches to promoting the brain health that he encourages.
Two of the most potent modalities for maintaining brain wellness and facilitating ongoing neurogenesis and synaptogenesis are exercise and nutrition—specifically, high-intensity interval training and a diet heavily, if not entirely, plant-based. The neuroprotective capabilities of mindfulness practice and its impact on prefrontal cortical regions also are relevant.
In society at large, it strikes me that physicians have not fared any better than the general population when it comes to maintaining a healthy diet and engaging in physical exercise. I encourage Dr. Nasrallah to continue addressing these themes, and to remind his audience of physicians to “heal thyself.”
More than once in his Current Psychiatry essays, Henry A. Nasrallah, MD, has stressed the seismic paradigmatic shifts in our understanding of mental illness and brain disease. He has highlighted the critical significance of processes of neurogenesis and neuroinflammation, yet little has been offered to practitioners in terms of practical approaches to promoting the brain health that he encourages.
Two of the most potent modalities for maintaining brain wellness and facilitating ongoing neurogenesis and synaptogenesis are exercise and nutrition—specifically, high-intensity interval training and a diet heavily, if not entirely, plant-based. The neuroprotective capabilities of mindfulness practice and its impact on prefrontal cortical regions also are relevant.
In society at large, it strikes me that physicians have not fared any better than the general population when it comes to maintaining a healthy diet and engaging in physical exercise. I encourage Dr. Nasrallah to continue addressing these themes, and to remind his audience of physicians to “heal thyself.”
Billing audits: The bane of a small practice
The photo you see below is a reasonably thick pile of paper, roughly 2 inches high. It’s certainly not as bad as some charts I’ve seen, especially at the VA, but still a lot of pages.
What is it?
This is, believe it or not, the stacked copies of charts we had to print in the last 30 days to fax to insurance companies for billing audits. Yeah – just the last 30 days.
Mind you, to date I don’t have any sort of actual complaints or charges against me for fraudulent billing. If anything, I tend to underbill for fear of risking the ire of insurance companies.
On one level, I understand it. The news is replete with stories of physicians who made fraudulent insurance claims, and the insurance companies want to make sure others are playing fair. Just like security cameras and magnetic tags at retailers, they’re doing what they can to avoid losses. I get that.
On the other hand, this irritates me, and it is a pain in the butt. Someone here has to print up the requested notes, organize them, fill out the accompanying forms, and fax them back. I also have to sign each note in the pile. For the number of charts they typically want, this process takes about 30-45 minutes. Then we fax them, and a 100-plus-page document ties up your office fax for a while. Incoming and outgoing faxes, such as medication refills, get put on hold. Overall, it takes maybe an hour of staff time to do this, not to mention the cost of paper and ink used.
About 25% of the time the company calls us after a few days to say they never got them (even though we have a confirmation). For this reason, we always hold onto the print-out for a month so we don’t have to start over again. Then it all has to be shredded.
In a large practice, I’m sure there are dedicated medical records staff members for this. But in my small solo world it means that someone has to let phones go to voicemail, dictations get delayed, and other work piles up, just so the insurance red tape gets done. Then we have to catch up on the more routine issues of patient care.
I can’t really refuse to send them, either. Doing so, in the insurance company’s mind, would be an admission of guilt that I never saw the patient and my claim is bogus. Then they’ll withhold payment, or ask for a refund.
This is, regrettably, a case where a few bad apples – docs filing bogus claims – have spoiled the entire barrel. Now we’re all guilty of fraud until proven innocent by sending these records. Isn’t that the reverse of the American justice system’s ideal?
I also wonder if there’s an intentional drudgery factor here. By making me do something that’s irritatingly time-wasting, is an insurance plan hoping I’ll drop them because I’m sick of this process? Does having fewer contracted neurologists work out to their benefit? It certainly isn’t to the patient’s advantage.
I don’t have an easy answer. I don’t like the wrench these requests throw into the office routine, but I also know that fraud surveillance is a necessary evil. I just wish there was a less time-consuming way of doing it.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
The photo you see below is a reasonably thick pile of paper, roughly 2 inches high. It’s certainly not as bad as some charts I’ve seen, especially at the VA, but still a lot of pages.
What is it?
This is, believe it or not, the stacked copies of charts we had to print in the last 30 days to fax to insurance companies for billing audits. Yeah – just the last 30 days.
Mind you, to date I don’t have any sort of actual complaints or charges against me for fraudulent billing. If anything, I tend to underbill for fear of risking the ire of insurance companies.
On one level, I understand it. The news is replete with stories of physicians who made fraudulent insurance claims, and the insurance companies want to make sure others are playing fair. Just like security cameras and magnetic tags at retailers, they’re doing what they can to avoid losses. I get that.
On the other hand, this irritates me, and it is a pain in the butt. Someone here has to print up the requested notes, organize them, fill out the accompanying forms, and fax them back. I also have to sign each note in the pile. For the number of charts they typically want, this process takes about 30-45 minutes. Then we fax them, and a 100-plus-page document ties up your office fax for a while. Incoming and outgoing faxes, such as medication refills, get put on hold. Overall, it takes maybe an hour of staff time to do this, not to mention the cost of paper and ink used.
About 25% of the time the company calls us after a few days to say they never got them (even though we have a confirmation). For this reason, we always hold onto the print-out for a month so we don’t have to start over again. Then it all has to be shredded.
In a large practice, I’m sure there are dedicated medical records staff members for this. But in my small solo world it means that someone has to let phones go to voicemail, dictations get delayed, and other work piles up, just so the insurance red tape gets done. Then we have to catch up on the more routine issues of patient care.
I can’t really refuse to send them, either. Doing so, in the insurance company’s mind, would be an admission of guilt that I never saw the patient and my claim is bogus. Then they’ll withhold payment, or ask for a refund.
This is, regrettably, a case where a few bad apples – docs filing bogus claims – have spoiled the entire barrel. Now we’re all guilty of fraud until proven innocent by sending these records. Isn’t that the reverse of the American justice system’s ideal?
I also wonder if there’s an intentional drudgery factor here. By making me do something that’s irritatingly time-wasting, is an insurance plan hoping I’ll drop them because I’m sick of this process? Does having fewer contracted neurologists work out to their benefit? It certainly isn’t to the patient’s advantage.
I don’t have an easy answer. I don’t like the wrench these requests throw into the office routine, but I also know that fraud surveillance is a necessary evil. I just wish there was a less time-consuming way of doing it.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
The photo you see below is a reasonably thick pile of paper, roughly 2 inches high. It’s certainly not as bad as some charts I’ve seen, especially at the VA, but still a lot of pages.
What is it?
This is, believe it or not, the stacked copies of charts we had to print in the last 30 days to fax to insurance companies for billing audits. Yeah – just the last 30 days.
Mind you, to date I don’t have any sort of actual complaints or charges against me for fraudulent billing. If anything, I tend to underbill for fear of risking the ire of insurance companies.
On one level, I understand it. The news is replete with stories of physicians who made fraudulent insurance claims, and the insurance companies want to make sure others are playing fair. Just like security cameras and magnetic tags at retailers, they’re doing what they can to avoid losses. I get that.
On the other hand, this irritates me, and it is a pain in the butt. Someone here has to print up the requested notes, organize them, fill out the accompanying forms, and fax them back. I also have to sign each note in the pile. For the number of charts they typically want, this process takes about 30-45 minutes. Then we fax them, and a 100-plus-page document ties up your office fax for a while. Incoming and outgoing faxes, such as medication refills, get put on hold. Overall, it takes maybe an hour of staff time to do this, not to mention the cost of paper and ink used.
About 25% of the time the company calls us after a few days to say they never got them (even though we have a confirmation). For this reason, we always hold onto the print-out for a month so we don’t have to start over again. Then it all has to be shredded.
In a large practice, I’m sure there are dedicated medical records staff members for this. But in my small solo world it means that someone has to let phones go to voicemail, dictations get delayed, and other work piles up, just so the insurance red tape gets done. Then we have to catch up on the more routine issues of patient care.
I can’t really refuse to send them, either. Doing so, in the insurance company’s mind, would be an admission of guilt that I never saw the patient and my claim is bogus. Then they’ll withhold payment, or ask for a refund.
This is, regrettably, a case where a few bad apples – docs filing bogus claims – have spoiled the entire barrel. Now we’re all guilty of fraud until proven innocent by sending these records. Isn’t that the reverse of the American justice system’s ideal?
I also wonder if there’s an intentional drudgery factor here. By making me do something that’s irritatingly time-wasting, is an insurance plan hoping I’ll drop them because I’m sick of this process? Does having fewer contracted neurologists work out to their benefit? It certainly isn’t to the patient’s advantage.
I don’t have an easy answer. I don’t like the wrench these requests throw into the office routine, but I also know that fraud surveillance is a necessary evil. I just wish there was a less time-consuming way of doing it.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Infection prevention
Not a long ago, I received a call from a friend working in a local pediatric clinic. One of her partners had just seen a young child with an unusual rash. The diagnosis? Crusted scabies.
Sarcoptes scabiei var. hominis, the mite that causes typical scabies, also causes crusted or Norwegian scabies. These terms refer to severe infestations that occur in individuals who are immune compromised or debilitated. The rash is characterized by vesicles and thick crusts and may or may not be itchy. Because patients with crusted scabies can be infested with as many as 2 million mites, transmission from very brief skin-to-skin contact is possible, and outbreaks have occurred in health care facilities and other institutional settings.

That was the reason for my friend’s call. “What do we do for the doctors and nurses in the clinic who saw the patient?” she wanted to know.
“Everyone wore gloves, right?” I asked. There was silence on the other end of the phone.
After a quick consultation with our health department, every health care provider (HCP) who touched the patient without gloves was treated preemptively with topical permethrin. None went on to develop scabies. The experience prompted me to think about the challenges of infection prevention in ambulatory care.
Both the American Academy of Pediatrics (AAP Committee on Infectious Diseases, “Infection prevention and control in pediatric ambulatory settings,” Pediatrics 2007;20[3]:650-65) and the Centers for Disease Control and Prevention (Guide to Infection Prevention for Outpatient Settings: Minimum Expectations for Safe Care) have published recommendations for infection prevention in outpatient settings. Both organizations emphasize the importance of standard precautions. According to the CDC, standard precautions “are the minimum infection prevention practices that apply to all patient care, regardless of suspected or confirmed infection status of the patient, in any setting where health care is delivered.” They are designed to protect HCPs, as well as prevent us from spreading infections among patients. Standard precautions include:
• Hand hygiene.
• Use of personal protective equipment (gloves, gowns, masks).
• Safe injection practices.
• Safe handling of potentially contaminated equipment or surfaces in the patient environment.
• Respiratory hygiene/cough etiquette.
Some of these elements are likely second nature to office-based pediatricians. Hands must be cleaned before and after every patient encounter or an encounter with the patient’s immediate environment. “Cover your cough” signs have become ubiquitous in ambulatory care waiting rooms, even as we acknowledge the difficulties associated with expecting toddlers to wear masks or use a tissue to contain their coughs and sneezes.
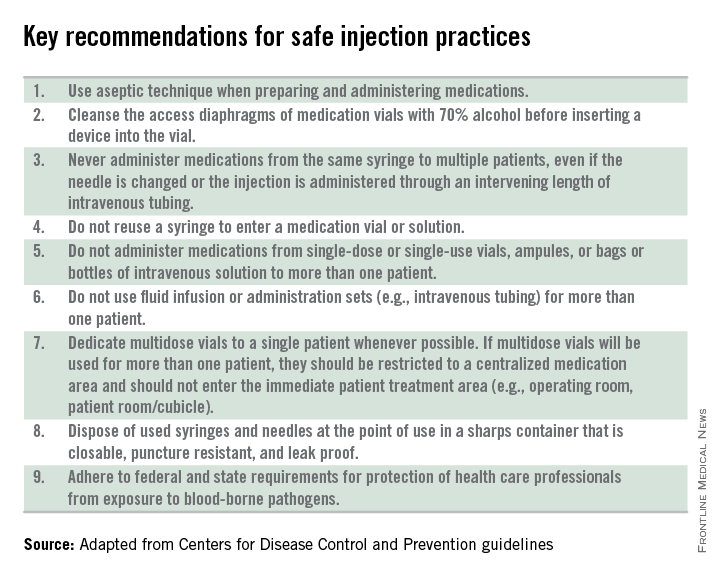
Other elements of standard precautions may receive increased attention because the consequences of noncompliance are perceived to be dangerous or severe. For example, we know that failure to reliably employ safe injection practices (see table) has resulted in transmission of blood-borne pathogens, including hepatitis B and C, in ambulatory settings.
In my experience, the use of personal protective equipment (PPE) in the ambulatory setting is the element of standard precautions that is the least understood and perhaps the most underutilized. It’s certainly easier in the inpatient setting, where we use transmission-based precautions, and colorful isolation signs instruct us to put on gown and gloves when we visit the patient with viral gastroenteritis, or gown, gloves, and mask for the child with acute viral respiratory tract infection. In the office, we expect the HCP to anticipate what kind of contact with blood or body fluids is likely and choose PPE accordingly.
Of course, anticipation can be tricky. Gowns, for example, are only required during procedures or activities when contact with blood and body fluids is likely. In routine office-based care, these sorts of procedures are uncommon. Incision and drainage of an abscess is one example of a procedure that might warrant protection of one’s clothing with a gown. Conversely, the need for a mask might arise several times a day, as these are worn to protect the mouth, nose, and eyes “during procedures that are likely to generate splashes or sprays of blood or other body fluids.” Examination of a coughing patient is a common “procedure” likely to results in sprays of saliva. Use of a mask can protect the examiner from potential exposures to Bordetella pertussis, Mycoplasma pneumoniae, and a host of respiratory viruses.
While the AAP has been careful to point out that gloves are not needed for the routine care of well children, they should be used when “there is the potential to contact blood, body fluids, mucous membranes, nonintact skin, or potentially infectious material.” In our world, potentially infectious material might include a cluster of vesicles thought to be herpes simplex, the honey-crusted lesions of impetigo, or the weeping, crusted rash of Norwegian scabies.
My own office had a powerful reminder about the importance of standard precautions last year when we were referred a young infant with recurrent fevers and a mostly dry, peeling rash. As we learned in medical school, the mucocutanous lesions of congenital syphilis can be highly contagious. In accordance with AAP recommendations, all HCPs who examined this child without the protection of gloves underwent serologic testing for syphilis. Fortunately, there were no transmissions!
Published data about infectious disease exposures and the transmission of infectious diseases in the outpatient setting, either from patients to health care workers or among patients, are largely limited to outbreak or case reports. A 1991 review identified 53 reports of infectious disease transmission in outpatient settings between 1961 and 1990 (JAMA 1991;265(18): 2377-81). Transmission occurred in medical and dental offices, clinics, emergency departments, ophthalmology offices, and alternative care settings that included chiropractic clinics and an acupuncture practice. A variety of pathogens were involved, including measles, adenovirus, hepatitis B, atypical mycobacteria, and Streptococcus pyogenes. The authors concluded that many of the outbreaks and episodes of transmission could have been prevented “if existing infection control guidelines,” including what we now consider standard precautions, had been utilized. Many reports published in the intervening 25 years have come to similar conclusions.
So why don’t HCPs yet follow standard precautions, including appropriate use of PPE? The reasons are complex and multifactorial. We’re all busy and lack of time is a common complaint. Gowns, gloves, masks, and alcohol hand gel aren’t always readily available. Some HCPs may not be knowledgeable about the elements of standard precautions while others may not understand the risks to themselves and their patients associated with nonadherence. Finally, some organizations have not established clear expectations related to infection prevention and compliance with AAP and CDC recommendations.
Several years ago, at the very beginning of the H1N1 influenza epidemic, a colleague of mine working in a pediatric practice saw a patient complaining of fever, lethargy, and myalgia. Not surprisingly, the patient’s rapid influenza test was positive. My colleague recalls that she was handed the result before she ever walked into the room – without any PPE – to see the patient.
“This was different than my usual routine at the hospital,” she told me. The expectation at the hospital was gown, gloves, and masks for any patient with influenza or influenzalike illness. At the office though, there was no such expectation, and providers did not routinely wear masks, even when seeing patients with respiratory symptoms. My colleague wasn’t reckless or rebellious. She was simply conforming to the culture in that office, and following the behavioral cues of more senior physicians in the practice. Subsequently, she developed severe influenza infection requiring a prolonged hospital stay.
It’s time to change the culture. As a first step, perform a quick audit in the office, using the AAP’s “Infection prevention and control in pediatric ambulatory settings” as a guide.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Kosair Children’s Hospital, also in Louisville. She had no relevant financial disclosures.
Not a long ago, I received a call from a friend working in a local pediatric clinic. One of her partners had just seen a young child with an unusual rash. The diagnosis? Crusted scabies.
Sarcoptes scabiei var. hominis, the mite that causes typical scabies, also causes crusted or Norwegian scabies. These terms refer to severe infestations that occur in individuals who are immune compromised or debilitated. The rash is characterized by vesicles and thick crusts and may or may not be itchy. Because patients with crusted scabies can be infested with as many as 2 million mites, transmission from very brief skin-to-skin contact is possible, and outbreaks have occurred in health care facilities and other institutional settings.
That was the reason for my friend’s call. “What do we do for the doctors and nurses in the clinic who saw the patient?” she wanted to know.
“Everyone wore gloves, right?” I asked. There was silence on the other end of the phone.
After a quick consultation with our health department, every health care provider (HCP) who touched the patient without gloves was treated preemptively with topical permethrin. None went on to develop scabies. The experience prompted me to think about the challenges of infection prevention in ambulatory care.
Both the American Academy of Pediatrics (AAP Committee on Infectious Diseases, “Infection prevention and control in pediatric ambulatory settings,” Pediatrics 2007;20[3]:650-65) and the Centers for Disease Control and Prevention (Guide to Infection Prevention for Outpatient Settings: Minimum Expectations for Safe Care) have published recommendations for infection prevention in outpatient settings. Both organizations emphasize the importance of standard precautions. According to the CDC, standard precautions “are the minimum infection prevention practices that apply to all patient care, regardless of suspected or confirmed infection status of the patient, in any setting where health care is delivered.” They are designed to protect HCPs, as well as prevent us from spreading infections among patients. Standard precautions include:
• Hand hygiene.
• Use of personal protective equipment (gloves, gowns, masks).
• Safe injection practices.
• Safe handling of potentially contaminated equipment or surfaces in the patient environment.
• Respiratory hygiene/cough etiquette.
Some of these elements are likely second nature to office-based pediatricians. Hands must be cleaned before and after every patient encounter or an encounter with the patient’s immediate environment. “Cover your cough” signs have become ubiquitous in ambulatory care waiting rooms, even as we acknowledge the difficulties associated with expecting toddlers to wear masks or use a tissue to contain their coughs and sneezes.
Other elements of standard precautions may receive increased attention because the consequences of noncompliance are perceived to be dangerous or severe. For example, we know that failure to reliably employ safe injection practices (see table) has resulted in transmission of blood-borne pathogens, including hepatitis B and C, in ambulatory settings.
In my experience, the use of personal protective equipment (PPE) in the ambulatory setting is the element of standard precautions that is the least understood and perhaps the most underutilized. It’s certainly easier in the inpatient setting, where we use transmission-based precautions, and colorful isolation signs instruct us to put on gown and gloves when we visit the patient with viral gastroenteritis, or gown, gloves, and mask for the child with acute viral respiratory tract infection. In the office, we expect the HCP to anticipate what kind of contact with blood or body fluids is likely and choose PPE accordingly.
Of course, anticipation can be tricky. Gowns, for example, are only required during procedures or activities when contact with blood and body fluids is likely. In routine office-based care, these sorts of procedures are uncommon. Incision and drainage of an abscess is one example of a procedure that might warrant protection of one’s clothing with a gown. Conversely, the need for a mask might arise several times a day, as these are worn to protect the mouth, nose, and eyes “during procedures that are likely to generate splashes or sprays of blood or other body fluids.” Examination of a coughing patient is a common “procedure” likely to results in sprays of saliva. Use of a mask can protect the examiner from potential exposures to Bordetella pertussis, Mycoplasma pneumoniae, and a host of respiratory viruses.
While the AAP has been careful to point out that gloves are not needed for the routine care of well children, they should be used when “there is the potential to contact blood, body fluids, mucous membranes, nonintact skin, or potentially infectious material.” In our world, potentially infectious material might include a cluster of vesicles thought to be herpes simplex, the honey-crusted lesions of impetigo, or the weeping, crusted rash of Norwegian scabies.
My own office had a powerful reminder about the importance of standard precautions last year when we were referred a young infant with recurrent fevers and a mostly dry, peeling rash. As we learned in medical school, the mucocutanous lesions of congenital syphilis can be highly contagious. In accordance with AAP recommendations, all HCPs who examined this child without the protection of gloves underwent serologic testing for syphilis. Fortunately, there were no transmissions!
Published data about infectious disease exposures and the transmission of infectious diseases in the outpatient setting, either from patients to health care workers or among patients, are largely limited to outbreak or case reports. A 1991 review identified 53 reports of infectious disease transmission in outpatient settings between 1961 and 1990 (JAMA 1991;265(18): 2377-81). Transmission occurred in medical and dental offices, clinics, emergency departments, ophthalmology offices, and alternative care settings that included chiropractic clinics and an acupuncture practice. A variety of pathogens were involved, including measles, adenovirus, hepatitis B, atypical mycobacteria, and Streptococcus pyogenes. The authors concluded that many of the outbreaks and episodes of transmission could have been prevented “if existing infection control guidelines,” including what we now consider standard precautions, had been utilized. Many reports published in the intervening 25 years have come to similar conclusions.
So why don’t HCPs yet follow standard precautions, including appropriate use of PPE? The reasons are complex and multifactorial. We’re all busy and lack of time is a common complaint. Gowns, gloves, masks, and alcohol hand gel aren’t always readily available. Some HCPs may not be knowledgeable about the elements of standard precautions while others may not understand the risks to themselves and their patients associated with nonadherence. Finally, some organizations have not established clear expectations related to infection prevention and compliance with AAP and CDC recommendations.
Several years ago, at the very beginning of the H1N1 influenza epidemic, a colleague of mine working in a pediatric practice saw a patient complaining of fever, lethargy, and myalgia. Not surprisingly, the patient’s rapid influenza test was positive. My colleague recalls that she was handed the result before she ever walked into the room – without any PPE – to see the patient.
“This was different than my usual routine at the hospital,” she told me. The expectation at the hospital was gown, gloves, and masks for any patient with influenza or influenzalike illness. At the office though, there was no such expectation, and providers did not routinely wear masks, even when seeing patients with respiratory symptoms. My colleague wasn’t reckless or rebellious. She was simply conforming to the culture in that office, and following the behavioral cues of more senior physicians in the practice. Subsequently, she developed severe influenza infection requiring a prolonged hospital stay.
It’s time to change the culture. As a first step, perform a quick audit in the office, using the AAP’s “Infection prevention and control in pediatric ambulatory settings” as a guide.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Kosair Children’s Hospital, also in Louisville. She had no relevant financial disclosures.
Not a long ago, I received a call from a friend working in a local pediatric clinic. One of her partners had just seen a young child with an unusual rash. The diagnosis? Crusted scabies.
Sarcoptes scabiei var. hominis, the mite that causes typical scabies, also causes crusted or Norwegian scabies. These terms refer to severe infestations that occur in individuals who are immune compromised or debilitated. The rash is characterized by vesicles and thick crusts and may or may not be itchy. Because patients with crusted scabies can be infested with as many as 2 million mites, transmission from very brief skin-to-skin contact is possible, and outbreaks have occurred in health care facilities and other institutional settings.
That was the reason for my friend’s call. “What do we do for the doctors and nurses in the clinic who saw the patient?” she wanted to know.
“Everyone wore gloves, right?” I asked. There was silence on the other end of the phone.
After a quick consultation with our health department, every health care provider (HCP) who touched the patient without gloves was treated preemptively with topical permethrin. None went on to develop scabies. The experience prompted me to think about the challenges of infection prevention in ambulatory care.
Both the American Academy of Pediatrics (AAP Committee on Infectious Diseases, “Infection prevention and control in pediatric ambulatory settings,” Pediatrics 2007;20[3]:650-65) and the Centers for Disease Control and Prevention (Guide to Infection Prevention for Outpatient Settings: Minimum Expectations for Safe Care) have published recommendations for infection prevention in outpatient settings. Both organizations emphasize the importance of standard precautions. According to the CDC, standard precautions “are the minimum infection prevention practices that apply to all patient care, regardless of suspected or confirmed infection status of the patient, in any setting where health care is delivered.” They are designed to protect HCPs, as well as prevent us from spreading infections among patients. Standard precautions include:
• Hand hygiene.
• Use of personal protective equipment (gloves, gowns, masks).
• Safe injection practices.
• Safe handling of potentially contaminated equipment or surfaces in the patient environment.
• Respiratory hygiene/cough etiquette.
Some of these elements are likely second nature to office-based pediatricians. Hands must be cleaned before and after every patient encounter or an encounter with the patient’s immediate environment. “Cover your cough” signs have become ubiquitous in ambulatory care waiting rooms, even as we acknowledge the difficulties associated with expecting toddlers to wear masks or use a tissue to contain their coughs and sneezes.
Other elements of standard precautions may receive increased attention because the consequences of noncompliance are perceived to be dangerous or severe. For example, we know that failure to reliably employ safe injection practices (see table) has resulted in transmission of blood-borne pathogens, including hepatitis B and C, in ambulatory settings.
In my experience, the use of personal protective equipment (PPE) in the ambulatory setting is the element of standard precautions that is the least understood and perhaps the most underutilized. It’s certainly easier in the inpatient setting, where we use transmission-based precautions, and colorful isolation signs instruct us to put on gown and gloves when we visit the patient with viral gastroenteritis, or gown, gloves, and mask for the child with acute viral respiratory tract infection. In the office, we expect the HCP to anticipate what kind of contact with blood or body fluids is likely and choose PPE accordingly.
Of course, anticipation can be tricky. Gowns, for example, are only required during procedures or activities when contact with blood and body fluids is likely. In routine office-based care, these sorts of procedures are uncommon. Incision and drainage of an abscess is one example of a procedure that might warrant protection of one’s clothing with a gown. Conversely, the need for a mask might arise several times a day, as these are worn to protect the mouth, nose, and eyes “during procedures that are likely to generate splashes or sprays of blood or other body fluids.” Examination of a coughing patient is a common “procedure” likely to results in sprays of saliva. Use of a mask can protect the examiner from potential exposures to Bordetella pertussis, Mycoplasma pneumoniae, and a host of respiratory viruses.
While the AAP has been careful to point out that gloves are not needed for the routine care of well children, they should be used when “there is the potential to contact blood, body fluids, mucous membranes, nonintact skin, or potentially infectious material.” In our world, potentially infectious material might include a cluster of vesicles thought to be herpes simplex, the honey-crusted lesions of impetigo, or the weeping, crusted rash of Norwegian scabies.
My own office had a powerful reminder about the importance of standard precautions last year when we were referred a young infant with recurrent fevers and a mostly dry, peeling rash. As we learned in medical school, the mucocutanous lesions of congenital syphilis can be highly contagious. In accordance with AAP recommendations, all HCPs who examined this child without the protection of gloves underwent serologic testing for syphilis. Fortunately, there were no transmissions!
Published data about infectious disease exposures and the transmission of infectious diseases in the outpatient setting, either from patients to health care workers or among patients, are largely limited to outbreak or case reports. A 1991 review identified 53 reports of infectious disease transmission in outpatient settings between 1961 and 1990 (JAMA 1991;265(18): 2377-81). Transmission occurred in medical and dental offices, clinics, emergency departments, ophthalmology offices, and alternative care settings that included chiropractic clinics and an acupuncture practice. A variety of pathogens were involved, including measles, adenovirus, hepatitis B, atypical mycobacteria, and Streptococcus pyogenes. The authors concluded that many of the outbreaks and episodes of transmission could have been prevented “if existing infection control guidelines,” including what we now consider standard precautions, had been utilized. Many reports published in the intervening 25 years have come to similar conclusions.
So why don’t HCPs yet follow standard precautions, including appropriate use of PPE? The reasons are complex and multifactorial. We’re all busy and lack of time is a common complaint. Gowns, gloves, masks, and alcohol hand gel aren’t always readily available. Some HCPs may not be knowledgeable about the elements of standard precautions while others may not understand the risks to themselves and their patients associated with nonadherence. Finally, some organizations have not established clear expectations related to infection prevention and compliance with AAP and CDC recommendations.
Several years ago, at the very beginning of the H1N1 influenza epidemic, a colleague of mine working in a pediatric practice saw a patient complaining of fever, lethargy, and myalgia. Not surprisingly, the patient’s rapid influenza test was positive. My colleague recalls that she was handed the result before she ever walked into the room – without any PPE – to see the patient.
“This was different than my usual routine at the hospital,” she told me. The expectation at the hospital was gown, gloves, and masks for any patient with influenza or influenzalike illness. At the office though, there was no such expectation, and providers did not routinely wear masks, even when seeing patients with respiratory symptoms. My colleague wasn’t reckless or rebellious. She was simply conforming to the culture in that office, and following the behavioral cues of more senior physicians in the practice. Subsequently, she developed severe influenza infection requiring a prolonged hospital stay.
It’s time to change the culture. As a first step, perform a quick audit in the office, using the AAP’s “Infection prevention and control in pediatric ambulatory settings” as a guide.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Kosair Children’s Hospital, also in Louisville. She had no relevant financial disclosures.
